GIANT HYPERTROPHIC GASTRITIS
2
1012 GIANT HYPERTROPHIC GASTRITIS SIR,-Giant hypertrophic gastritis is generally con- sidered a benign condition : Dr. Williams (April 7) suggests that an extensive resection through healthy tissue, as for carcinoma, is unnecessary, and Mr. Park (May 19) advocates resection of part of the affected mucosa. Penetration of the muscularis mucosae by epithelial elements was not mentioned by Menetrier 1 or by Spriggs 2 but has been described as occurring in giant hypertrophic gastritis by a number of subsequent writers including Dr. Williams. Grime and Whitehead’s 3 case is cited as evidence that giant hypertrophic gastritis is a benign condition, since their patient was well 13 months after incomplete removal of the affected stomach ; but this stomach showed no submucosal penetration. Maimon et awl. describe submucosal penetration in three of their six cases, stating that " it does not suggest neoplasm ; it’is equivalent to the type of herniation commonly seen in the secondarily contracted gall bladder producing the gland spaces which are called crypts of Rokitansky." On the other hand Brunn and Pearl 5 say that the only certain sign of malignancy is the invasion by the epithelium through the muscularis mucosae ; describing Fig. I-Stomach wall. Compare hypertrophied portion with normal on left. cases of the allied and often associated condition of multiple gastric polyposis, they found evidence of carci- noma in 12% and, in a later paper,6 in 19 out of 37 cases. Histologists are accustomed to regard invasion of the submucosal stroma by epithelial elements as a major 1. Menetrier, P. Arch. Physiol. norm. path. 1888, 1, 32, 236. 2. Spriggs, E. I. Quart. J. med. 1943, 12, 1. 3. Grime, R. T., Whitehead. R. Brit. J. Surg. 1951, 39, 244. 4. Maimon, S. N., Bartlett, J. P., Humphreys, E. M., Palmer, W. L. Gastroenterology, 1947, 8, 397. 5. Brunn, H., Pearl, F. Surg. Gynec. Obstet. 1926, 43, 559. 6. Pear], F. L., Brunn, H. Ibid, 1943, 76, 257. Fig. 2--Section of hypertrophied stomach wall (x 5). criterion of malignancy in the large intestine. The following case raises the question of whether it should not be so regarded in the stomach : A man of 57 years came to hospital with epigastric and left subcostal pain, of 4 months’ duration, unrelated to meals, posture, or exercise but relieved by milk. Each night he had severe pain lasting 15 minutes, and all day he had an ache. He had nausea but had not vomited, and he had been constipated for 7 weeks. Haemoglobin 113%. Histamine test-meal : free acid, mucus, but no blood. Barium meal suggestive of gastric carcinoma. At laparotomy, by Mr. G. 0. Jelly, the stomach wall was found to be greatly thickened, and was recognised as an example of giant hypertrophic gastritis ; but at the ca’liae axis there was what appeared to be a carcinomatous lymph-node. No other site of’ primary carcinoma could be found, so a total gastrectomy was performed. The mucosa, over an area 16 X 13 cm. in the fundus, was much hypertrophied and thrown into rugse 1.5 cm. across and 2’J cm. high, resembling cerebral convolu- tions (fig. 1). ). The mucosa was everywhere freely mobile over the muscle. No polypi were present. There was no evidence of past or present ulceration. On histological examination the affected mucosa is greatly thickened but maintains the normal architecture and cytology (fig. 2). Dilated, irregularly shaped acini, lined by regular well-differentiated mucus-secreting columnar epithelium, are present in the lower levels of the mucosa and penetrate extensively through the muscularis mueosse into the sub- mucosal layer (fig. 3). Everywhere the epithelium remains regular and cytologically benign (fig. 4). There is a chronic inflammatory infiltrate by plasma-cells, lymphocytes, and some eosinophils in the lamina propria and submucosal layer. Fig. 3-Low power showing extensive invas[on of submucosal layer without invasion of muscle wall (x 20). Fig. 4-High power showing benign appear- ance of invading epithelial elements (X 70). Fig. S- Lymph-node secondary (X 70).
Transcript of GIANT HYPERTROPHIC GASTRITIS

1012
GIANT HYPERTROPHIC GASTRITIS
SIR,-Giant hypertrophic gastritis is generally con-
sidered a benign condition : Dr. Williams (April 7)suggests that an extensive resection through healthytissue, as for carcinoma, is unnecessary, and Mr. Park
(May 19) advocates resection of part of the affectedmucosa.
Penetration of the muscularis mucosae by epithelialelements was not mentioned by Menetrier 1 or by Spriggs 2but has been described as occurring in giant hypertrophicgastritis by a number of subsequent writers includingDr. Williams. Grime and Whitehead’s 3 case is cited asevidence that giant hypertrophic gastritis is a benigncondition, since their patient was well 13 months afterincomplete removal of the affected stomach ; but thisstomach showed no submucosal penetration. Maimonet awl. describe submucosal penetration in three of theirsix cases, stating that " it does not suggest neoplasm ;it’is equivalent to the type of herniation commonly seenin the secondarily contracted gall bladder producing thegland spaces which are called crypts of Rokitansky."On the other hand Brunn and Pearl 5 say that the only
certain sign of malignancy is the invasion by the
epithelium through the muscularis mucosae ; describing
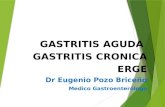
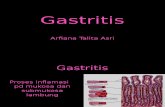
Fig. I-Stomach wall. Compare hypertrophied portion with normal on left.
cases of the allied and often associated condition of
multiple gastric polyposis, they found evidence of carci-noma in 12% and, in a later paper,6 in 19 out of 37 cases.
Histologists are accustomed to regard invasion of thesubmucosal stroma by epithelial elements as a major
1. Menetrier, P. Arch. Physiol. norm. path. 1888, 1, 32, 236.2. Spriggs, E. I. Quart. J. med. 1943, 12, 1.3. Grime, R. T., Whitehead. R. Brit. J. Surg. 1951, 39, 244.4. Maimon, S. N., Bartlett, J. P., Humphreys, E. M., Palmer, W. L.
Gastroenterology, 1947, 8, 397.5. Brunn, H., Pearl, F. Surg. Gynec. Obstet. 1926, 43, 559.6. Pear], F. L., Brunn, H. Ibid, 1943, 76, 257.
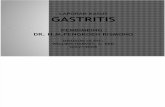
Fig. 2--Section of hypertrophied stomach wall (x 5).
criterion of malignancy in the large intestine. The
following case raises the question of whether it shouldnot be so regarded in the stomach :A man of 57 years came to hospital with epigastric and left
subcostal pain, of 4 months’ duration, unrelated to meals,posture, or exercise but relieved by milk. Each night he hadsevere pain lasting 15 minutes, and all day he had an ache.He had nausea but had not vomited, and he had been
constipated for 7 weeks. Haemoglobin 113%. Histaminetest-meal : free acid, mucus, but no blood.Barium meal suggestive of gastric carcinoma.At laparotomy, by Mr. G. 0. Jelly, the
stomach wall was found to be greatlythickened, and was recognised as an exampleof giant hypertrophic gastritis ; but atthe ca’liae axis there was what appearedto be a carcinomatous lymph-node. No othersite of’ primary carcinoma could be found,so a total gastrectomy was performed.The mucosa, over an area 16 X 13 cm.
in the fundus, was much hypertrophiedand thrown into rugse 1.5 cm. across and2’J cm. high, resembling cerebral convolu-tions (fig. 1). ). The mucosa was everywherefreely mobile over the muscle. No polypi
were present. There was no evidence of past or presentulceration.On histological examination the affected mucosa is greatly
thickened but maintains the normal architecture and cytology(fig. 2). Dilated, irregularly shaped acini, lined by regularwell-differentiated mucus-secreting columnar epithelium, arepresent in the lower levels of the mucosa and penetrateextensively through the muscularis mueosse into the sub-mucosal layer (fig. 3). Everywhere the epithelium remainsregular and cytologically benign (fig. 4). There is a chronicinflammatory infiltrate by plasma-cells, lymphocytes, andsome eosinophils in the lamina propria and submucosal layer.
Fig. 3-Low power showing extensive invas[onof submucosal layer without invasion of musclewall (x 20).
Fig. 4-High power showing benign appear-ance of invading epithelial elements (X 70).
Fig. S- Lymph-node secondary (X 70).

1013
Three lymph-nodes from the lesser curvature show sinuscatarrh but no evidence of malignancy. The coeliac lymph-node and adjacent connective and adipose tissue contain
mucus-secreting carcinoma, some of which is similar to, butless well differentiated than, the submucosal elements in thestomach, and some of which is poorly differentiated (fig. 5).The patient was well when last seen two months after theoperation.
I hope to follow this case in order to verify that there isno other primary from which this secondary deposit couldhave been derived. Meanwhile, in view of the histologicalsimilarity between the better-differentiated elements inthe lymph-node secondary and the submucosal elements,and the fact that no other primary was noted at the timeof operation, it must be assumed that the carcinomaoriginated in the stomach.
This case suggests that giant hypertrophic gastritismay not always be as benign as it is assumed to be, andthat penetration of the submucosa by epithelial elements,however benign in appearance, should be regarded withgrave susnicion.
ROGER GILLETTAncoats Hospital,Manchester, 4.
1. Dieckmann, W. J., Davies, M. E. Amer. J. Obstet. Gynec. 1933,25, 623.
2. Alvarez, H., Caldeyro, R. Surg. Gynec. Obstet. 1950, 91, 1.3. Serr, D. M., Sachs, L., Danon, M. Bull. Res. Coun. Israel, 1955,
5B, 137.4. Sachs, L., Serr, D. M., Danon, M. Science, 1956, 123, 548.5. Sachs, L., Serr, D. M., Danon, M. Brit. med. J. (in the press).6. Renwick, J. H., Lawler, S. D. Ann. Eugen., Lond. 1955, 19, 312.7. Goodall, H. B., Hendry, D. W. W., Lawler, S. D., Stephen, S. A.
Ibid, 1953, 17, 272.8. Race, R. R., Sanger, R. Blood Groups in Man. Oxford, 1954.
ANTENATAL IDENTIFICATION OF HEREDITARYDISORDERS
LEO SACHSMATHILDE DANON.
Weizmann Institute of Science,Rehovoth, Israel.
SiR,łSince amniotic-fluid cells can be obtained fromthe 12th week of pregnancy 1 2 and the fluid has beenshown to contain well-preserved cells from the 12th weekand possibly even earlier,3-5 the most obvious clinicalvalue of using these cells for antenatal diagnosis wouldbe in certain cases of sex-linked abnormalities. Dr.Edwards’s comments (April 28) on antenatal detectionof hereditary disorders raise the interesting point of usingamniotic-fluid cells for other purposes, such as thedetection of fcetal antigens.The actual detection of foetal antigens can lead directly
to early identification of incompatibility during preg-nancy, and this may be especially valuable in certaincases where the father is heterozygous. It may also beuseful in the field of preventive medicine, in cases ofhereditary abnormalities that are genetically linked to anantigen. For this latter purpose it is insufficient to havethe type of linkage that has been found with the nail-patella genes, s since this is a linkage with the ABO groupas a whole. It is necessary to have a close linkage,preferably without any crossing-over, between a heredi-tary abnormality and a particular antigen-e.g., the
antigen for B within the ABO group. The type of linkageto seek is that found between elliptocytosis and a specificRh combination, where in one family the gene for ovalcells always goes with the antigen constitution cDE. Inthis case there is complete linkage and no crossing-over.
In a list compiled in 1954,8 of 28 characters that hadbeen examined for linkage with blood-group genes, only1 shows positive evidence for linkage. But, as Race andSanger pointed out,8 this should not discourage furtherinvestigation since there are now available many moreantigenic markers than could be used in most of theearlier studies. It is therefore desirable that anyonecollecting material on human genetics should specificallytest for this type of evidence.
It may be predicted that, with an increase in our know-ledge of the genetics of man, there will be an increase inthe use of amniotic-fluid cells, and possibly even of otherconstituents of the fluid.
HORMONES AND BREAST CANCER
A. T. SANDISON.
his provocative letter last week Dr. Loeserstates that seaweed was used in Ancient Egypt as atherapeutic agent but wrongly makes the implicitassumption that this was a rational measure.
It is now generally appreciated that Egyptian medicinecomprised a curious admixture of largely empirical therapyand a strong element of magic, employing not only oral andwritten formulae but amulets and similar talismanic objects.The materia medica of Egypt included rather extraordinarysubstances and it is not surprising that seaweed should havebeen included.
It has also been suggested that in Classical Greece burntseaweed was administered in the treatment of goitre. Itcannot seriously be claimed, however, that either in Egyptor in Greece was iodine deliberately used as a rational thera-peutic agent, any more than it can be said that Leucippus,Democritus, or Lucretius really anticipated the modernatomic theory based on experimental evidence.
Edible seaweed or dulse has been utilised as a food inScotland and Ireland, and it would be interesting toknow whether there is folk-lore belief in its therapeuticapplication. A small breed of Orkney sheep is said tosubsist largely on seaweed and is claimed to have a highmutton-iodine content. It would be of further interestto know whether this diet has any effect on endocrine
relationship in these animals.Glasgow, S.1. A. T. SANDISOX.
SiR,-Dr. Loeser is to be congratulated on his letter.In view of your leading article of May 12, there can beno doubt that there is urgent need for reappraisal of thetreatment of advanced cancer. The surgical procedureshave become so radical that in many cases the cure, or
palliation, must be considered far worse than the disease.Adrenalectomy and hypophysectomy, the latest arrivalsin the field, offer magnificant opportunities for theexercise of a high degree of surgical skill, but it would bea brave family doctor who would actually advise a patientto undergo such operations. More and more, attentionmust turn to the endocrine control of advanced carci-noma, in preference to mutilating surgical procedures, andsome attempt must be made to collect the observationsand work of independent observers, such as Dr. Loeser,in this field.
All work on the endocrinotherapy of cancer is based on anattempt to modify the hormone environment of the tumourby injection or ingestion of hormones, or by deprivation ofhormones by thyroidectomy, oophorectomy, adrenalectomy,castration, or hypophysectomy. It would appear that thesuccess or otherwise of such methods of endocrinotherapydepends on the effect of the technique employed on theinternal balance of the pituitary. There is considerableevidence to show that the cause of cancer is a hypophysealdysfunction, or hyperfunction of the thyrotrophic centre
{the eosinophil cells), with a relative hypofunction of thegonadotrophic centre (the basophil cells). This hypothesisexplains the success of Dr. Loeser’s treatment by thyroid,just as it explains the success or failure of other hormonetreatments. -
The administration of small doses of thyroid extract overa long period will diminish the thyroid secretion and thesecretion of thyrotrophic hormones, and so enable the pituitarydysfunction to be temporarily corrected. There is a danger,however, that the effect of this administration of thyroid willwear off, and that the original imbalance will be restored, ashappens in massive testosterone therapy. We all have experi-ence of the patient with carcinoma of the breast whosesecondaries disappear completely with testosterone for two orthree years, and then return with speedily fatal results.As well as attempting to modify the pituitary state by
exogenous hormones, attention must be turned to modifyingthe production of endogenous hormones. This can best bedone by the application of short waves to the pituitary andgonads, although it is possible that future methods of treat-ment will be by radioactive isotopes. A combination of theadministration of exogenous hormones and short-waveirradiations on some inoperable cases, in my practice, has