Presentatie seminariewerk 'Ernstige mondpathologie in de huisartspraktijk'
32
Ernstige mondpathologie in de huisartsenpraktijk: Pilootstudie De Grooff Suzanne Camerlynck Victor Cloet Dieter Promotor: Prof. Dr. J. Degryse
Transcript of Presentatie seminariewerk 'Ernstige mondpathologie in de huisartspraktijk'
Ernstige mondpathologie in de huisartsenpraktijk: Pilootstudie
De Grooff SuzanneCamerlynck VictorCloet Dieter
Promotor: Prof. Dr. J. Degryse

-> Conclusie van een studie van de Onafhankelijke Ziekenfondsen
WHO Global Burden of Oral Diseases
• 2 belangrijkste mondpathologieën
– Cariës
– Parodontitis
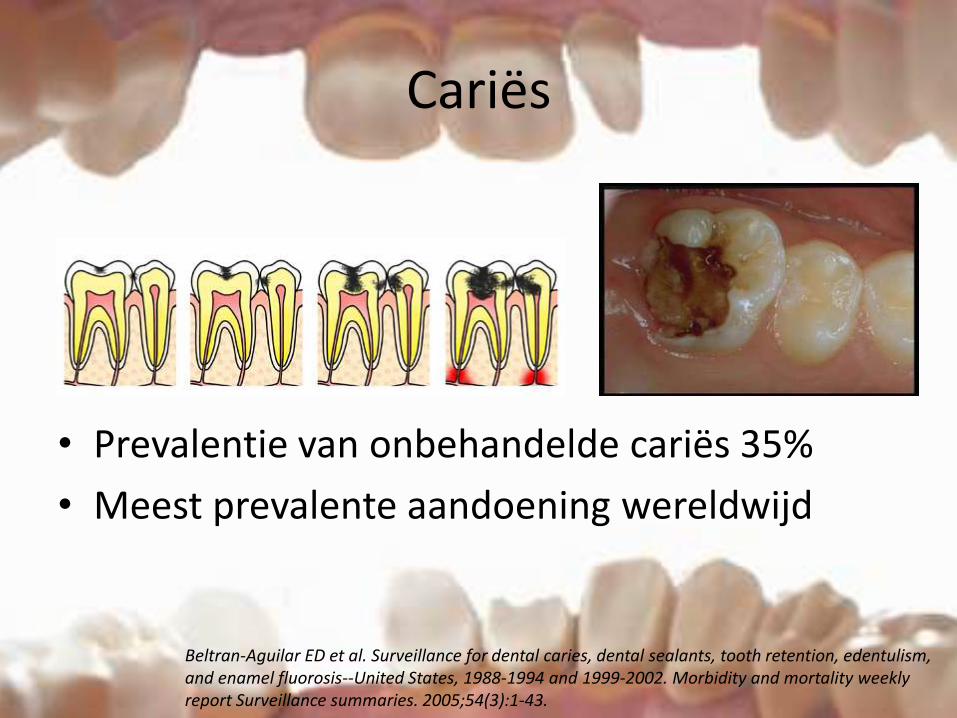
Cariës
• Prevalentie van onbehandelde cariës 35%
• Meest prevalente aandoening wereldwijd
Beltran-Aguilar ED et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis--United States, 1988-1994 and 1999-2002. Morbidity and mortality weeklyreport Surveillance summaries. 2005;54(3):1-43.
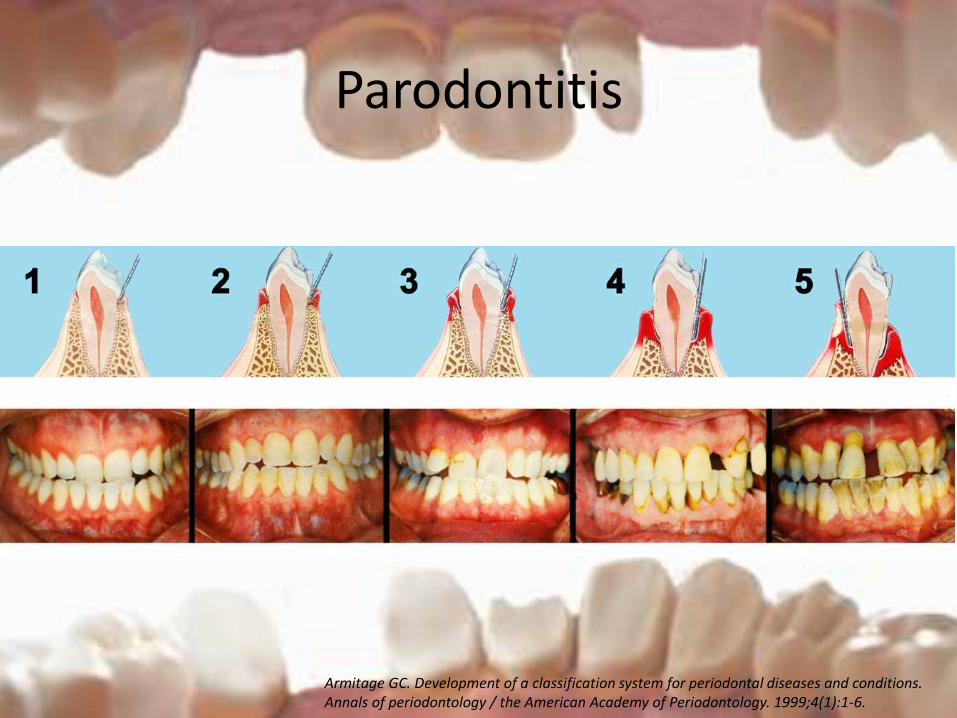
Parodontitis
Armitage GC. Development of a classification system for periodontal diseases and conditions. Annals of periodontology / the American Academy of Periodontology. 1999;4(1):1-6.
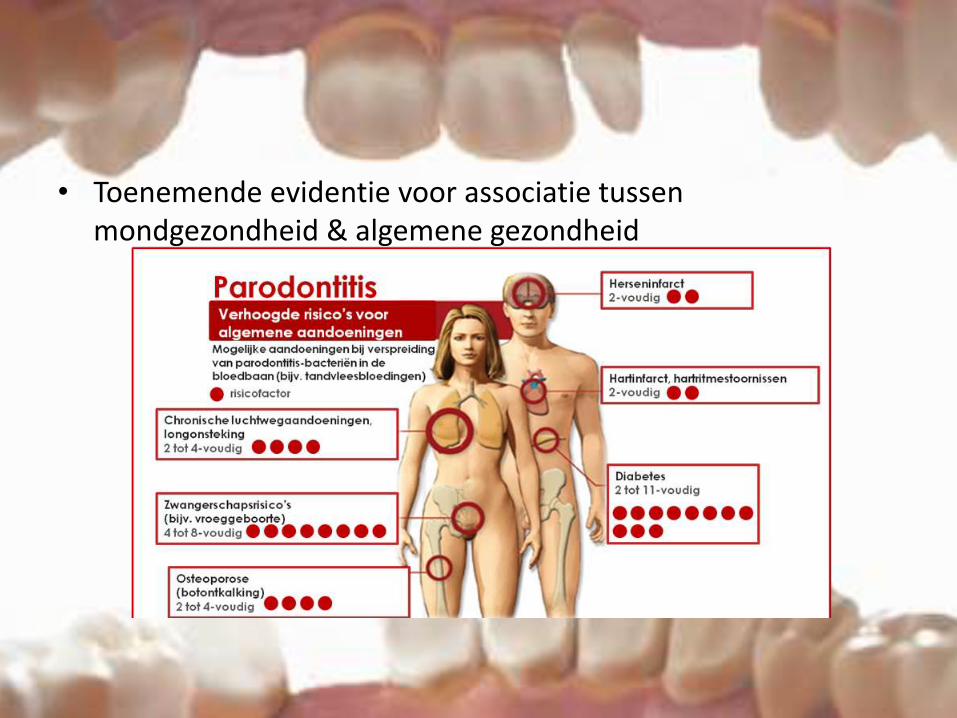
• Toenemende evidentie voor associatie tussen mondgezondheid & algemene gezondheid
Nochtans...

• Rol van de huisarts?
– Gegevens uit INTEGO databank (huisartsbezoek)
• Jaarlijkse contactgroep 84% (alle leeftijden)
• Boven 40 jaar bijna 90%
– Onderzoek RIZIV (2009-2010)
• 56 % minstens 3 contacten bij tandarts op periode 5 jaar
• 96% had jaarlijks minstens 1 contact met de huisarts
• Daarom deze pilootstudie!
– Onderzoeksvraag
• “Bij hoeveel personen die bij de huisarts langskomen, kan er een ernstige mondpathologie weerhouden worden?”– Ernstige Dentale pathologie
– Ernstig Parodontale pathologie
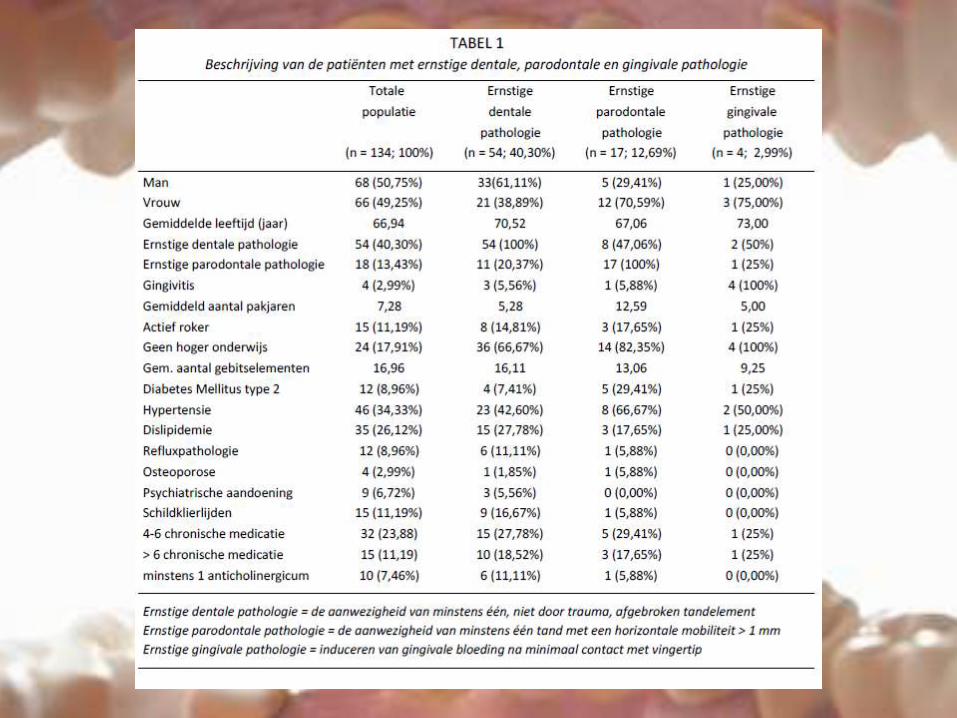
134 patiënten ≥ 40 jaar
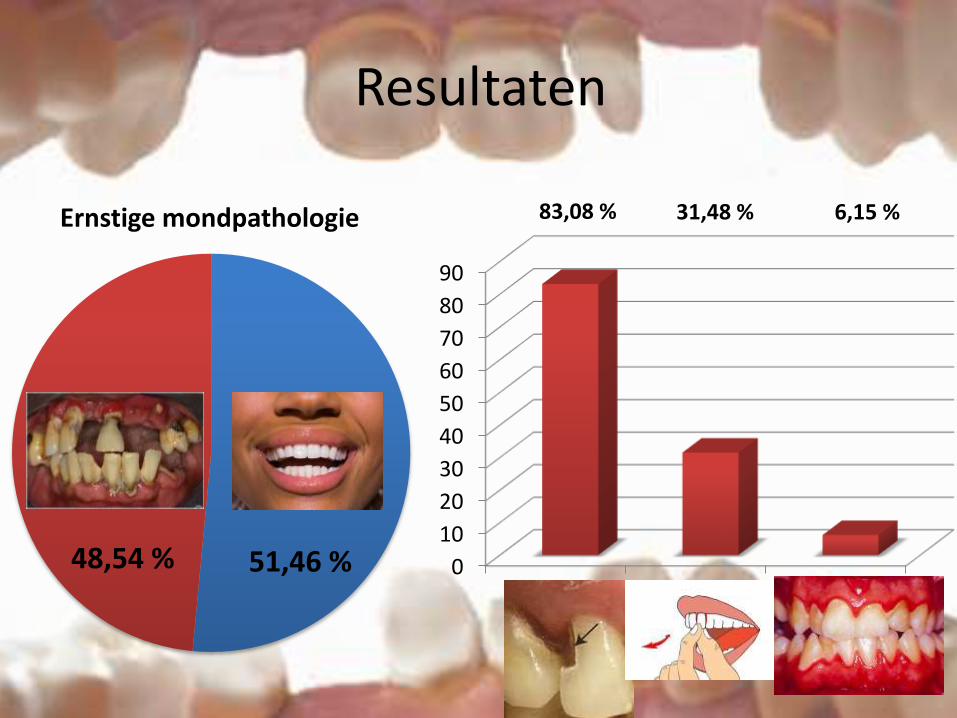
Ernstige mondpathologie
Resultaten
0
10
20
30
40
50
60
70
80
90
Ernstigedentale
pathologie
Ernstigeparodontalepathologie
Ernstigegingivitis
48,54 % 51,46 %
83,08 % 31,48 % 6,15 %

Achtergrondvariabelen
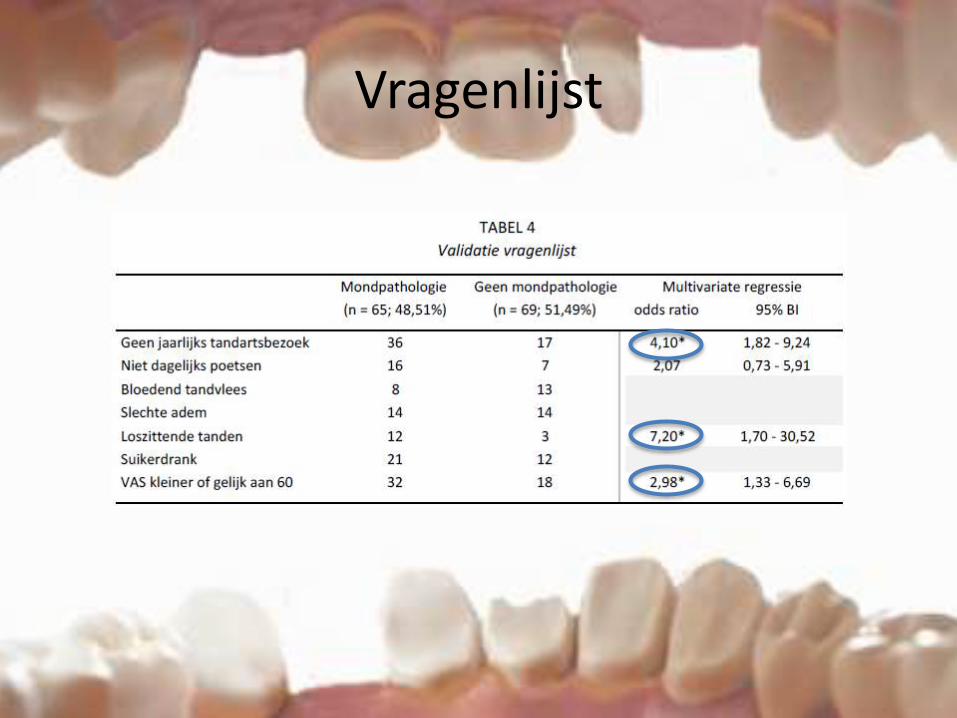
Vragenlijst
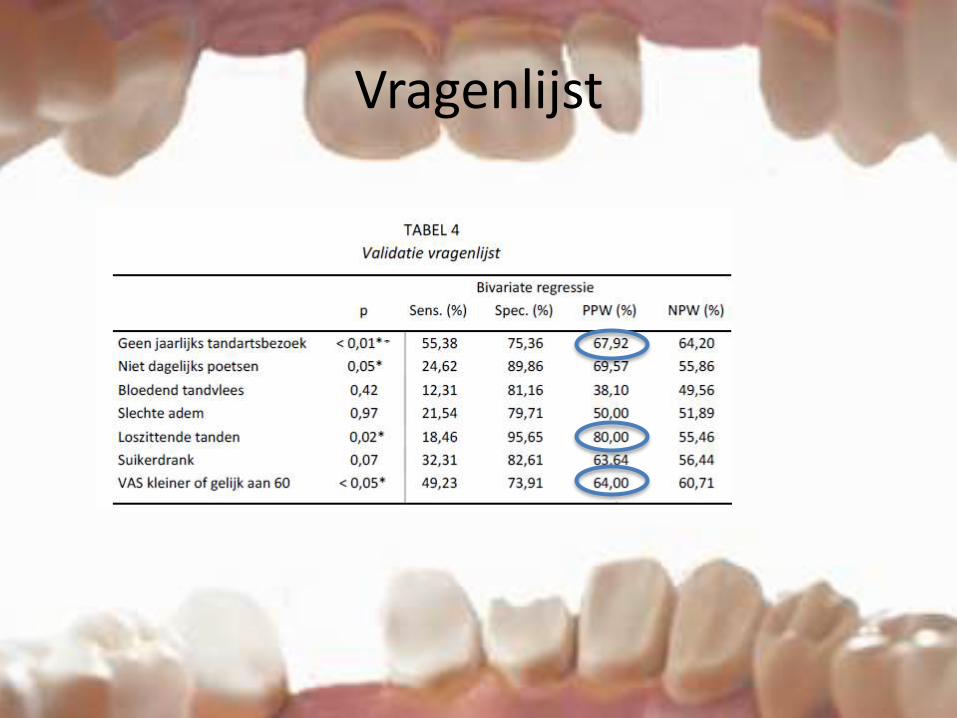
Vragenlijst

CONCLUSIE
• Pilootstudie: Opmerkelijke resultaten
• Associatie Mondgezondheid & Algemene Gezondheid
• Meer aandacht voor mondgezondheid– In het bijzonder bij:
• Ouderen
• Diabetici
• Zwangere vrouwen
• Rokers
• Suggesties
– Diabetici: jaarlijks tandartsbezoek
• NHG richtlijn
– Hoe mondgezondheid optimaliseren?
• Sensibiliseren huisartsen
• Sensibiliseren patiënten
– ‘ Preventieve mondgezondheid’ incorporeren in “GMD +”

Take to Clinic- Messages
Bedankt voor Uw aandacht!
• Deze presentatie is achter de kiezen!
– Zijn er nog vragen?
Referenties• Agnès l. de kostprijs van tandzorg voor de verlichte verzekering en voor de patiënt. brussel: landsbond van de onafhankelijke ziekenfondsen, 2012.
• Bottenberg P. DD, Vanden Abbeele A et al. Eindrapport project dataregistratie- en evaluatiesysteem mondgezondheid van de Belgische bevolking 2008-2010. In: Epidemiologie IC, editor. Brussel2011.
• D. C. parodontitis in relatie tot systemische aandoeningen. Leuven: Katholieke universiteit tandheelkunde; 2012.
• Weidlich P, Cimoes R, Pannuti CM, Oppermann RV. Association between periodontal diseases and systemic diseases. Brazilian oral research. 2008;22 Suppl 1:32-43.
• Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization. 2005;83(9):661-9.
• Campus G, Salem A, Uzzau S, Baldoni E, Tonolo G. Diabetes and periodontal disease: a case-control study. Journal of periodontology. 2005;76(3):418-25.
• Mealey BL. Diabetes and periodontal disease: two sides of a coin. Compendium of continuing education in dentistry. 2000;21(11):943-6, 8, 50, passim; quiz 56.
• Kiran M, Arpak N, Unsal E, Erdogan MF. The effect of improved periodontal health on metabolic control in type 2 diabetes mellitus. Journal of clinical periodontology. 2005;32(3):266-72.
• Marcenes W, Kassebaum NJ, Bernabe E, Flaxman A, Naghavi M, Lopez A, et al. Global burden of oral conditions in 1990-2010: a systematic analysis. Journal of dental research. 2013;92(7):592-7.
• Truyers C, Goderis G, Dewitte H, Vanden Akker M, Buntinx F. The Intego database: background, methods and basic results of a Flemish general practice-based continuous morbidity registration project. BMC medical informatics and decision making. 2014;14(1):48.
• Beltran-Aguilar ED, Barker LK, Canto MT, Dye BA, Gooch BF, Griffin SO, et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis--United States, 1988-1994 and 1999-2002. Morbidity and mortality weekly report Surveillance summaries. 2005;54(3):1-43.
• Carranza F, MG; Takei, HH; Carrana FA, . . Clinical Diagnosis. 9th Edition ed. Philadelphia: W.B. Saunders Company; 2002.
• Armitage GC. Development of a classification system for periodontal diseases and conditions. Annals of periodontology / the American Academy of Periodontology. 1999;4(1):1-6.
• Ronald I M. CDC health disparities and inequalities report Gina Thornton-Evans PE, Liang Wei et al., editor. United States2013. 129-35 p.
• Bank WOHD. Periodontal country profiles: WHO Oral Health Data Bank; 2005. Available from: http://www.dent.niigata-u.ac.jp/prevent/perio/perio.html.
• Baat Cd. Mondzorg voor ouderen in 2020. Ned Tijdschr Tandheelkd 2004. 2004;111:52-4.
• AFeilzer AJ DmRHBA. Praktijkboek tandheelkunde, bSL losbladige: Bohn Stafleu van Loghum mei 2009.
• Sakki T, Knuuttila M. Controlled study of the association of smoking with lactobacilli, mutans streptococci and yeasts in saliva. European journal of oral sciences. 1996;104(5-6):619-22• .• Wood B, Lieberman DE. Craniodental variation in Paranthropus boisei: a developmental and functional perspective. American journal of physical anthropology. 2001;116(1):13-25.
• Vellappally S, Fiala Z, Smejkalova J, Jacob V, Shriharsha P. Influence of tobacco use in dental caries development. Central European journal of public health. 2007;15(3):116-21.
• Warnakulasuriya S, Dietrich T, Bornstein MM, Casals Peidro E, Preshaw PM, Walter C, et al. Oral health risks of tobacco use and effects of cessation. International dental journal. 2010;60(1):7-30.
• Gomes BC, Renner RP. Periodontal considerations of the removable partial overdenture. Dental clinics of North America. 1990;34(4):653-68.•
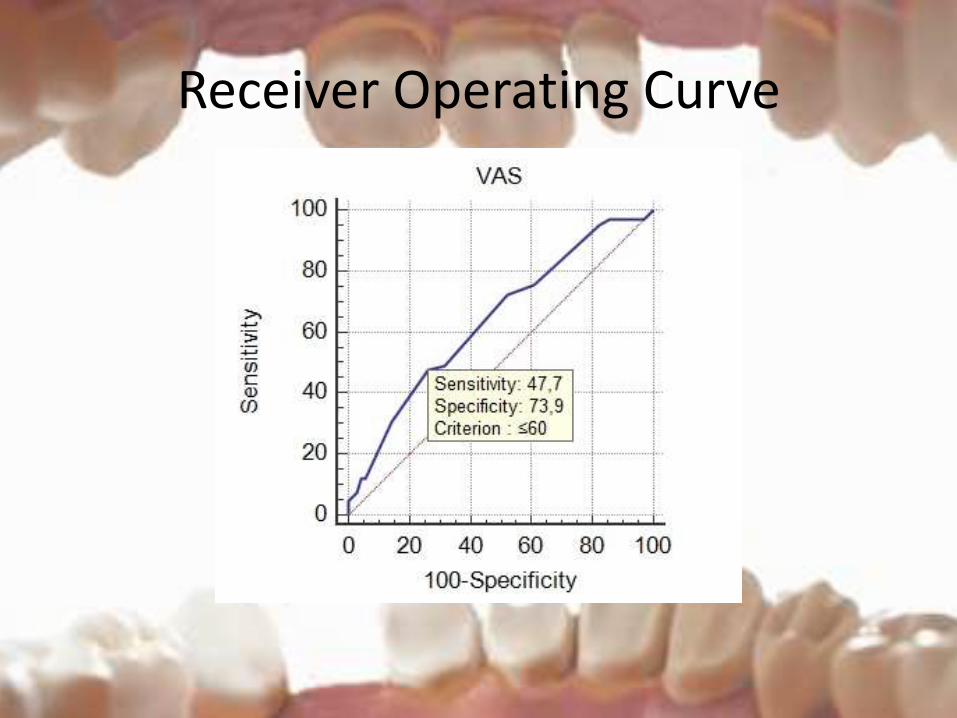
Receiver Operating Curve
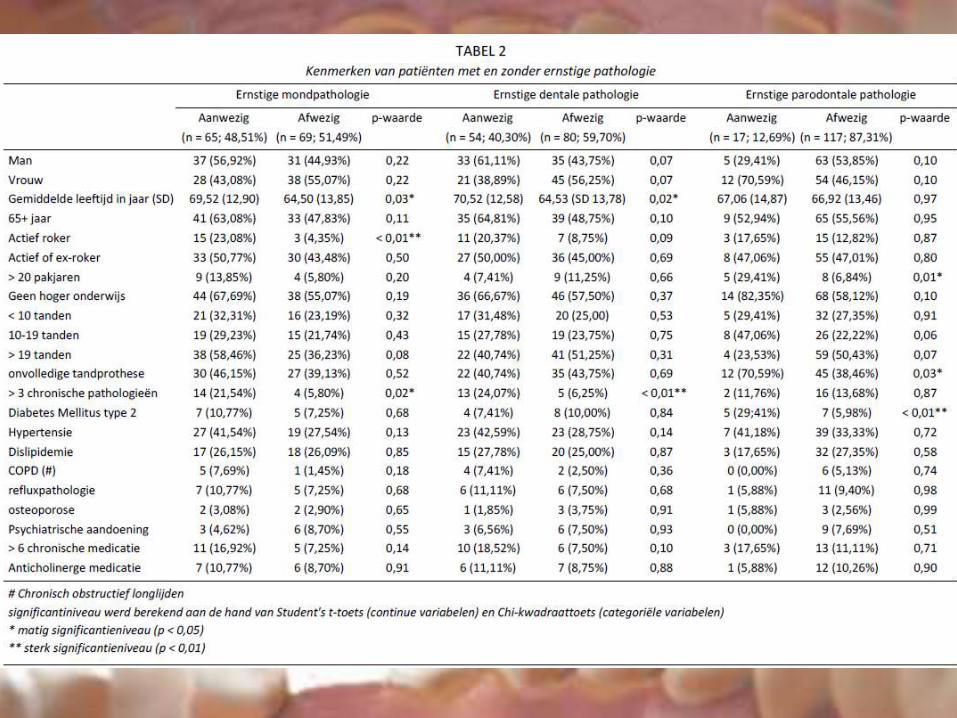
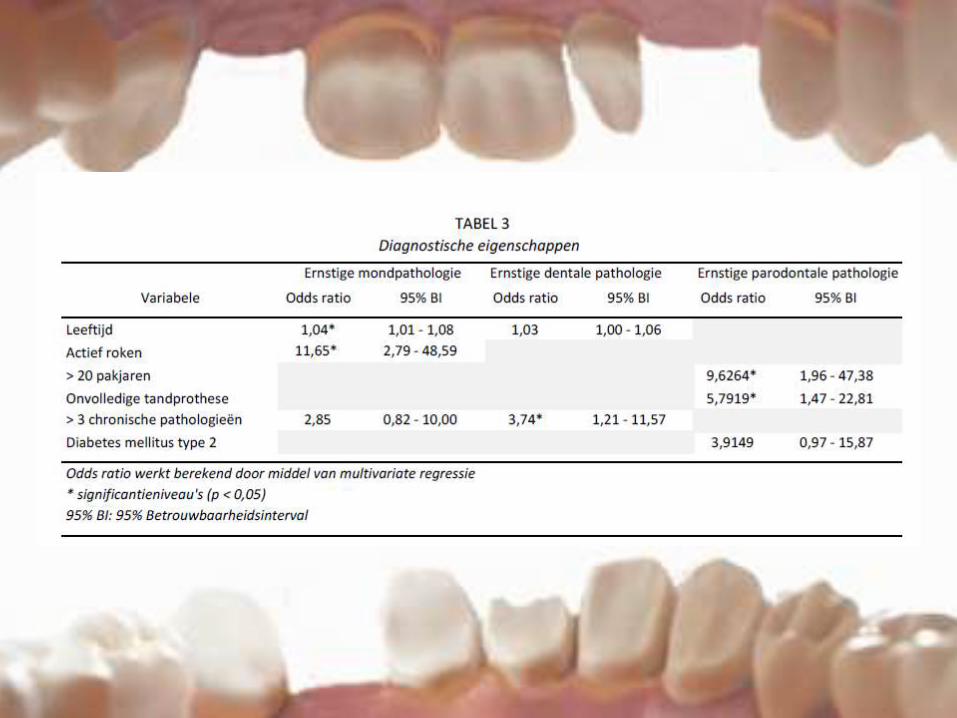
Leeftijd en mondpathologie
• Mondpathologie:gem hogere lftd dan zonder
– Literatuur:
• US onderzoek + WHO: mondpathologie met leeftijd
• hypothese:
– ouderen leven langer + meer gebitselementen
Roken en mondpathologie
• VG >= 20 PJ -> hogere kans op ernstige parodontale pathologie
• literatuur: rokers sneller parodontale pathologie dan niet-rokers
• lokale vasoconstrictie tandvlees
• later stadium bloedend tandvlees
• veranderingen in de microflora van de mond + afname speekselflow
Meer dan 3 chronische aandoeningen en dentale pathologie
• hypotheses
– multimorbiditeit verhoogt de kans op polyfarmacie -> verhoogde kans op droge mond
– Multimorbiditeit= zware last -> verslappen van aandacht voor preventieve mondzorg
Patiële gebitsprothese en parodontale pathologie
• studie + literatuur: parodontale aandoeningen bij gebitsprothese
• gebrek aan motivatie + minder frequente tandartsbezoeken
• Patiënten met gebitsprothese = risicogroep voor mondpathologie-> motiveren voor mondgezondheid
DM en parodontitis
• Studie + literatuur: DM ~ parodontitis
– NHG: jaarlijks mondonderzoek
– Diabetes- patiënten: baat bij goede mondhygiëne + frequente preventieve controles
• Pilootstudie: slechts 1/4 jaarlijks naar de tandarts
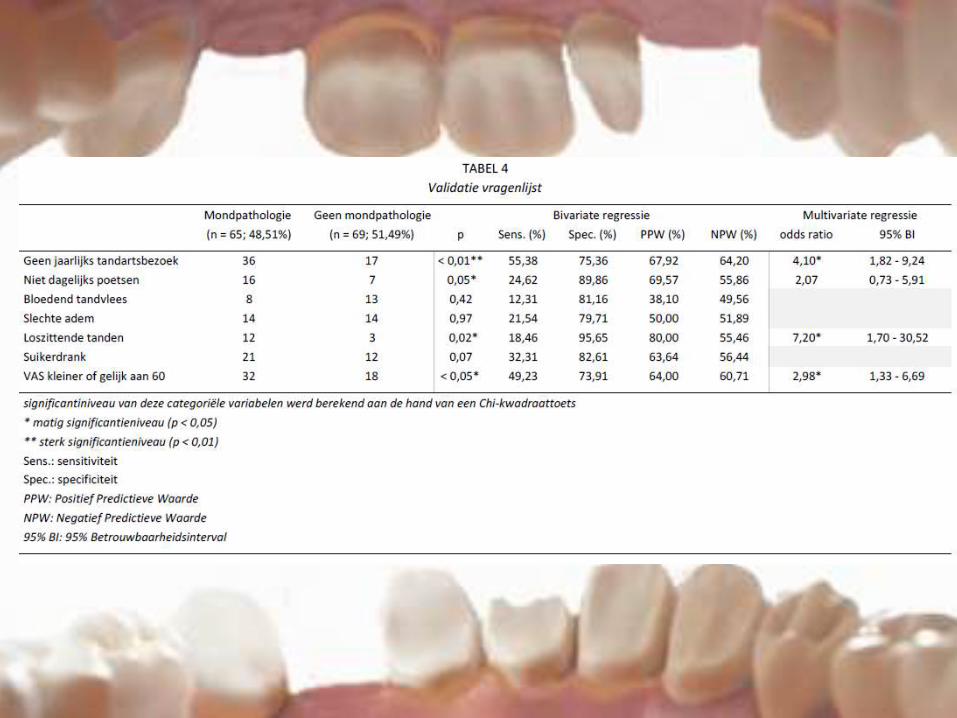
Geen jaarlijks tandartsbezoek
• pilootstudie: 39.6% vs Onafhankelijk Ziekenfonds: 70% niet jaarlijks naar de tandarts – Verklaringen
• Pilootstudie= kleine omvang + methode van verzamelen van gegevens
• eerlijkheid van patiënt?
• patiënten op vrijwillige basis
• de vraag: ‘Gaat u jaarlijks naar de tandarts?’
• alle personen in deze studie hebben een contact bij de HA -> HA ideaal geplaatst om te sensibiliseren
Gevoel van loszittende tanden + VAS < 60
• Stelling: goede zelfinschatting van mondgezondheid
• Reden uitstellen tandartsbezoek?– RIZIV: angst, geen klachten, geen tijd en financiële
problemen
• Vragenlijst= 1ste aanzet tot bewustwording
• bijkomend onderzoek– ïncorporeren in “GMD plus” -> preventief beleid
rond gezondheid van de patiënt