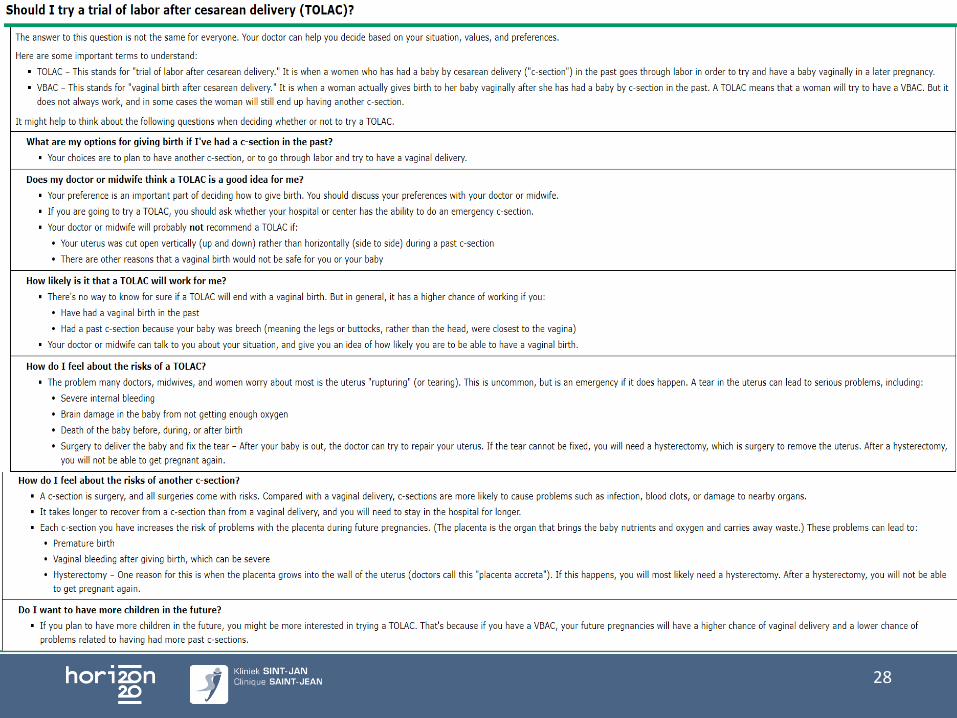
Vaginale partus na sectio - FPS Public Health · Indeling Introductie Wie is kandidaat Antenatale...
60
Vaginale partus na sectio Dr. Priska TIJDHOF Kliniek Sint-Jan te Brussel 12 dec 2017
Transcript of Vaginale partus na sectio - FPS Public Health · Indeling Introductie Wie is kandidaat Antenatale...

Vaginale partus na sectio
Dr. Priska TIJDHOF
Kliniek Sint-Jan te Brussel
12 dec 2017

Interactief
Ziekenhuizen zonder VBAC?
Na 2 sectio’s VBAC?
2
Indeling
Introductie
Wie is kandidaat
Antenatale counselling
• Risico’s
• Voordelen / Nadelen
Beleid arbeid / partus
Toekomst / Take home messages
3
Introductie
Sectiopercentage
België 20,5% 2015 (13-32%)
NL 16,4% 2013 Cyprus 52% Italië 38% 2014
< 1960: once a C/S, always C/S
SPE: 30% met sectio in VG bevalt vaginaal, TOLAC 69,5% vaginaal
4
Craigin, 1916, SPE, CBS NL,
Definities
TOLAC Trial of labor after cesarean
VBAC Vaginal birth after cesarean
ERCS Elective repeat cesarean section (Planned)
Uterusdehiscentie: defect uterusspier met intacte serosa
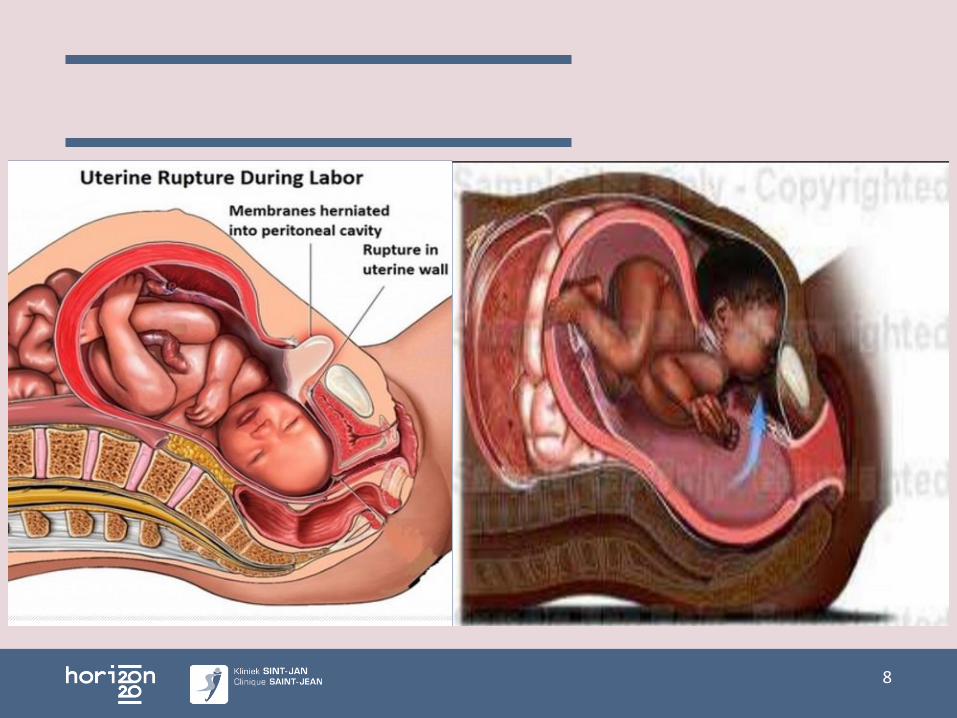
Uterusruptuur: open verbinding tussen uterusholte - buikholte
5
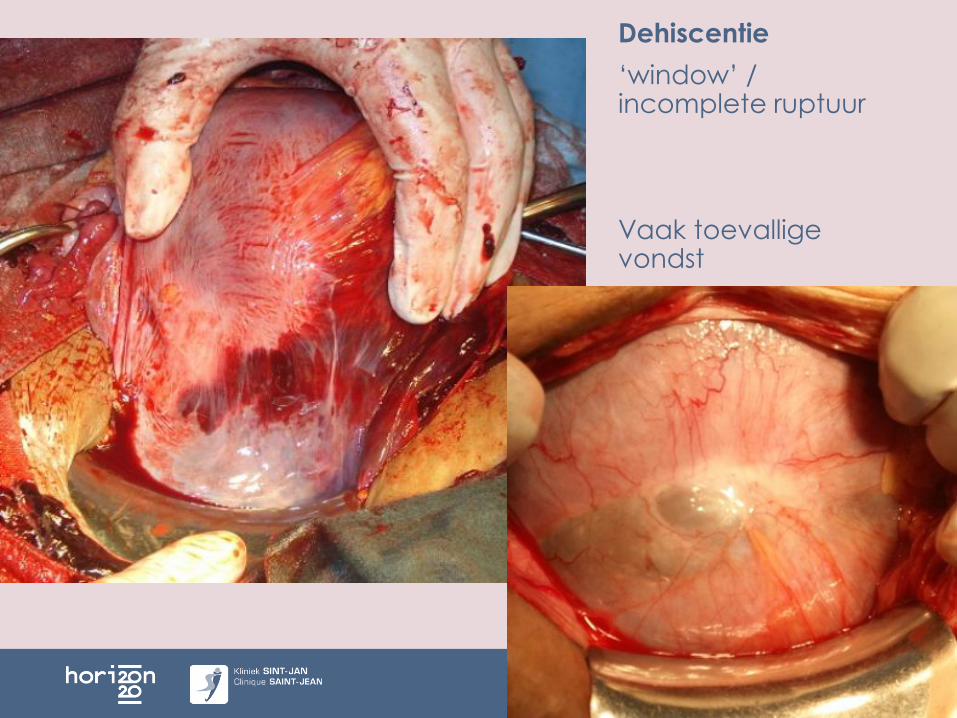
Dehiscentie
‘window’ / incomplete ruptuur
Vaak toevallige vondst
6
7
8
9
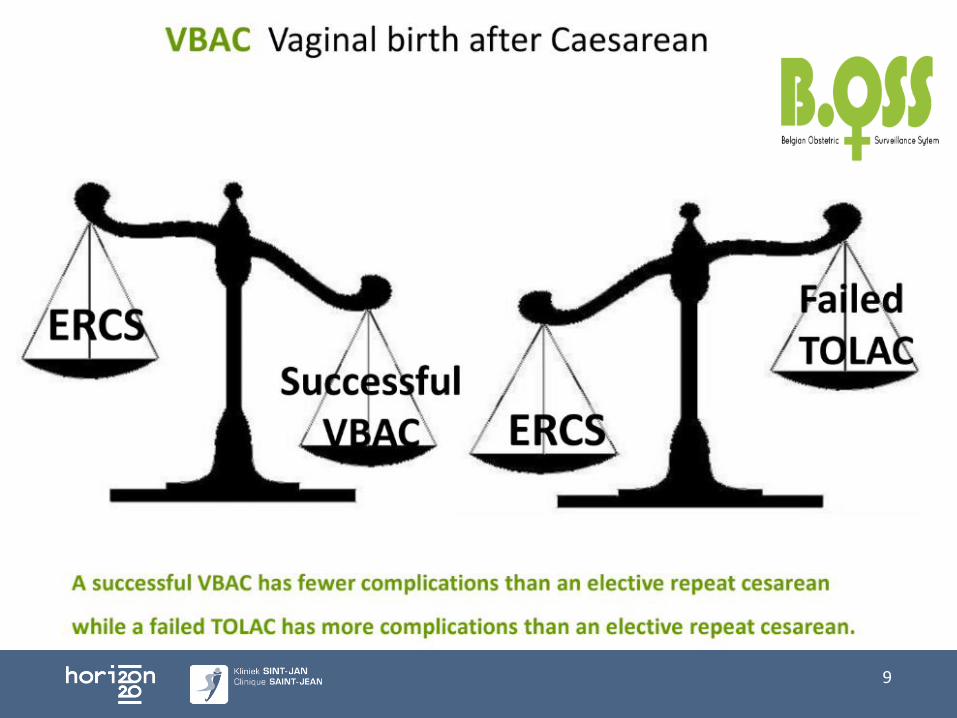
VBAC minste complicaties
Electieve sectio geen ruptuur, operatieve complicaties
groter risico op placenta praevia / accreta, adhesies
Failed TOLAC hoogste risico complicaties
Niet kosten-effectief
Moeilijkheid: WIE MAG TOLAC
Studies moeilijk: outcome partus ipv geplande manier
10
Grootste risico TOLAC
Ruptuur
1/200 (0,5% na 1 sectio)
1,5% na 2 sectio’s
ERCS 0,02%
0,02% intacte uterus (multipara)
Gevolg:
Ernstige neonatale morbiditeit 6-8%
Neonatale sterfte 5%
Hysterectomie 14-30%
Maternele sterfte 0,21%
11
Guise Obs Gyn 2010, Kaczmarczyk BJOG 2007, Holmgren Obst Gynecol 2012
Indeling
Introductie
Wie is kandidaat
Antenatale counselling
• Risico’s
• Voordelen / Nadelen
Beleid arbeid / partus
Toekomst
12
‘Ideale kandidaat’
Gemiddeld 70% slaagkans
1 Voorgaande sectio
Hoofdligging
Voorgaande vaginale partus of VBAC (80%-90%)
Spontane arbeid
Indicatie 1° C/S
• 75% foetale malpresentatie
• 60% foetaal lijden
• 54% CPD
13
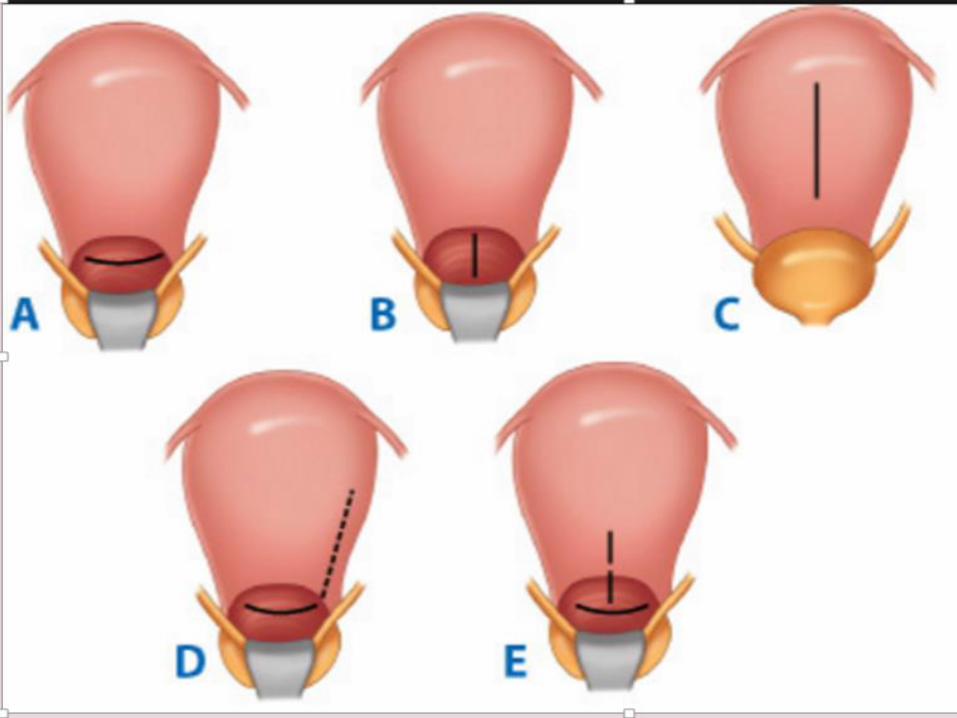
Absolute contra-indicaties
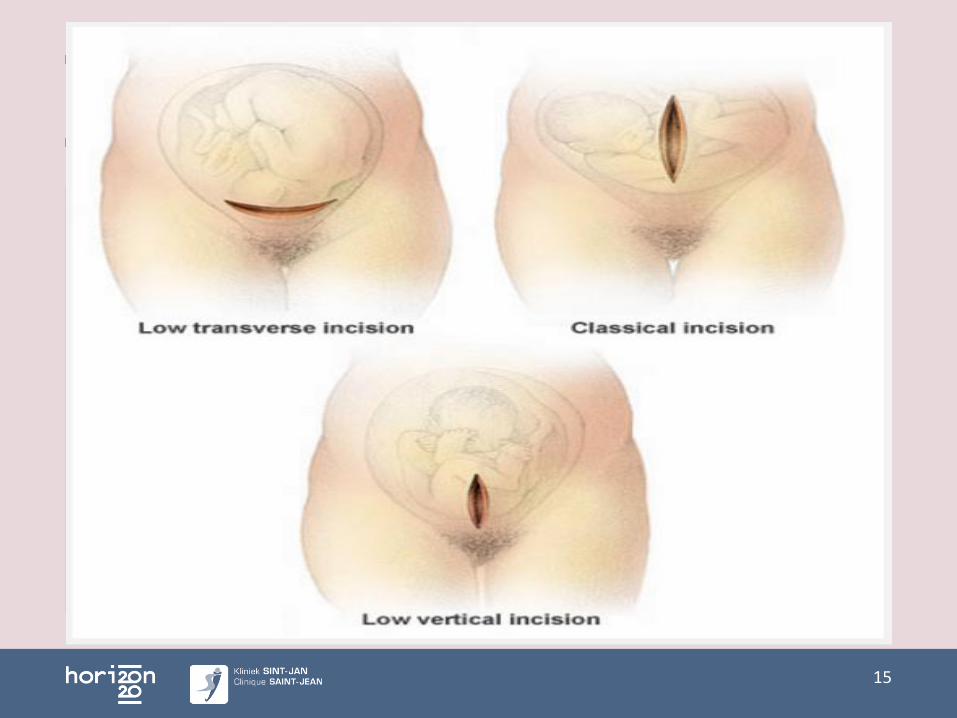
Voorgaande ruptuur (LUS 6% bij KT’s, HUS tot 30%)¹
Klassieke incisie (9%)
≥ 3 sectio’s (%?) ³
Contra-indicatie vaginale partus
14
¹Tita NEJM 2009, Chiossi Obs Gyn 2013, Chibber J Mat F Neonat Med2010 ²Turner 2005, Guise 2005,
15
16
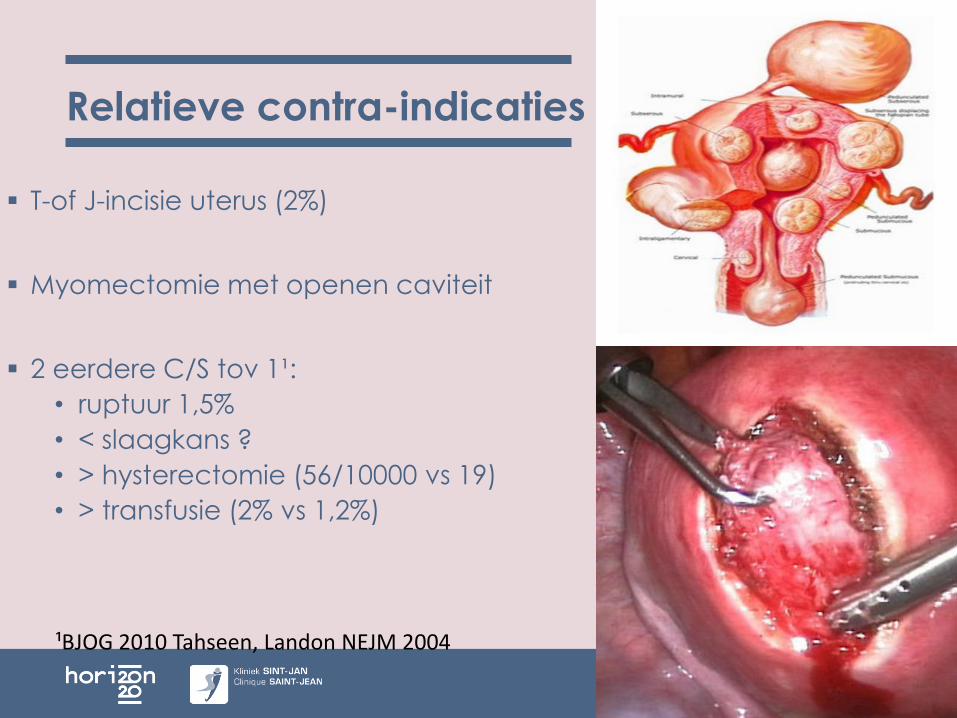
Relatieve contra-indicaties
T-of J-incisie uterus (2%)
Myomectomie met openen caviteit
2 eerdere C/S tov 1¹:
• ruptuur 1,5%
• < slaagkans ?
• > hysterectomie (56/10000 vs 19)
• > transfusie (2% vs 1,2%)
17
¹BJOG 2010 Tahseen, Landon NEJM 2004
Wat verlaagt kans geslaagde VBAC
Geen voorgaande vag partus
Inductie
BMI >30
>40 jr
<155cm
>41w
>4000g (of > GG index)
Spoedsectio foetaal lijden (60%) / failed induction, < 8cm, 54% CPD, preterme sectio
< 1,5 jr interdelivery interval
Voorgaande onsuccesvolle instrumentatie (61%)
Bevallen in streekZH, zonder assistenten
18

Indeling
Introductie
Wie is kandidaat
Antenatale counselling
• Risico’s
• Voordelen / Nadelen
Beleid arbeid / partus
Toekomst
19

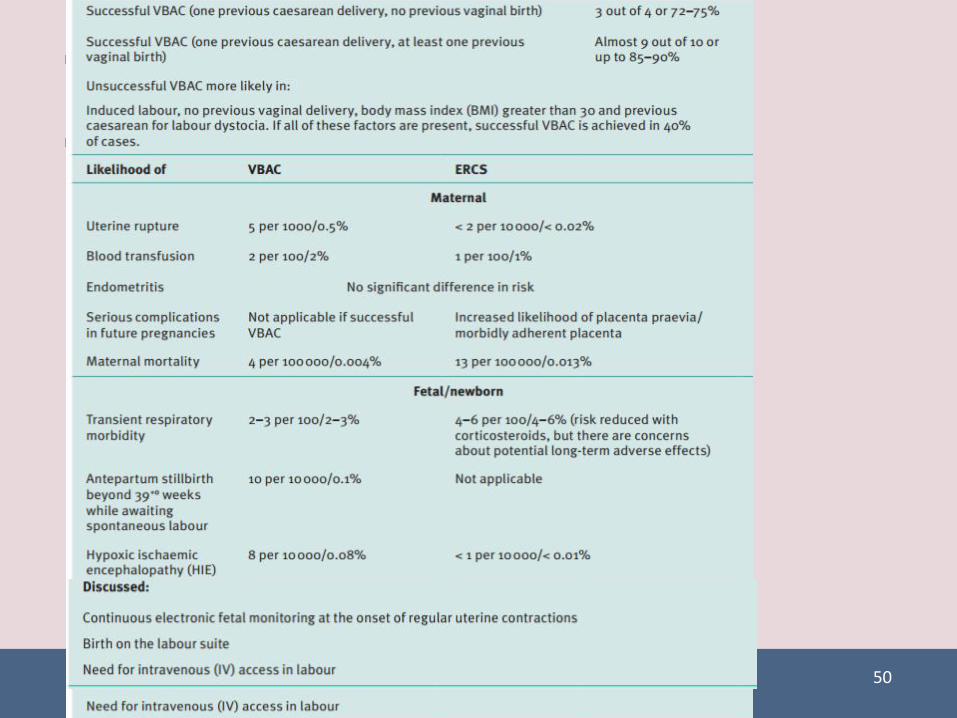
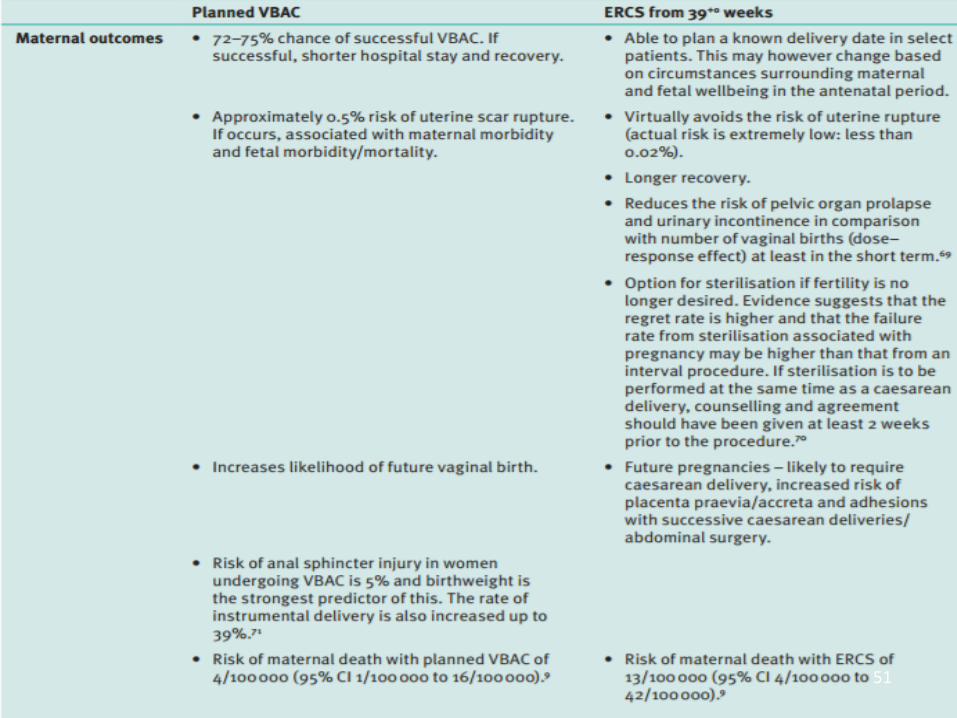
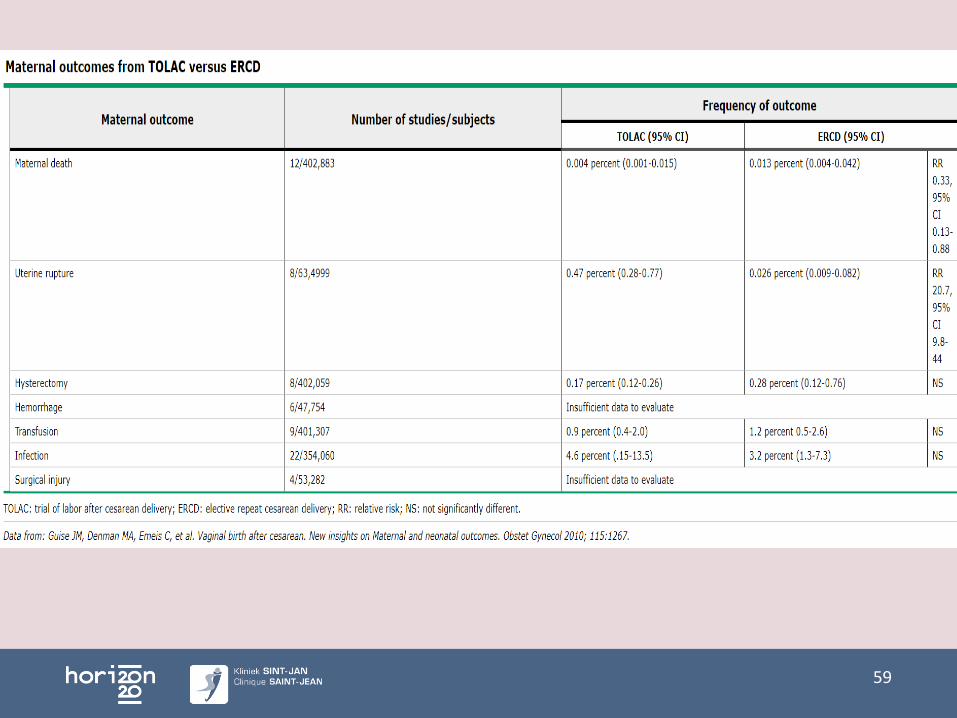
Geplande VBAC – Maternele uitkomst
20
Materneleoutcome
Geplande VBAC Electieve sectio
Succeskans 70% Planning
<Hospit, herstel sneller > Hospit, langer herstel
Ruptuur 0,5% Ruptuur 0,02%
Groot gezin Sterilisatie
> Kans vaginale partus nadien
Sectio nadien
> Complicaties nadien
- Plac praevia/acc, adhesies
Perineum, instrumentatie Perineum intact
Maternele † 4/10000 Maternele †13/10000
Gefaalde TOLAC: >> complics
Bloedtransfusie 2% Bloedtransfusie 1%

Geplande VBAC – Maternele uitkomst
21
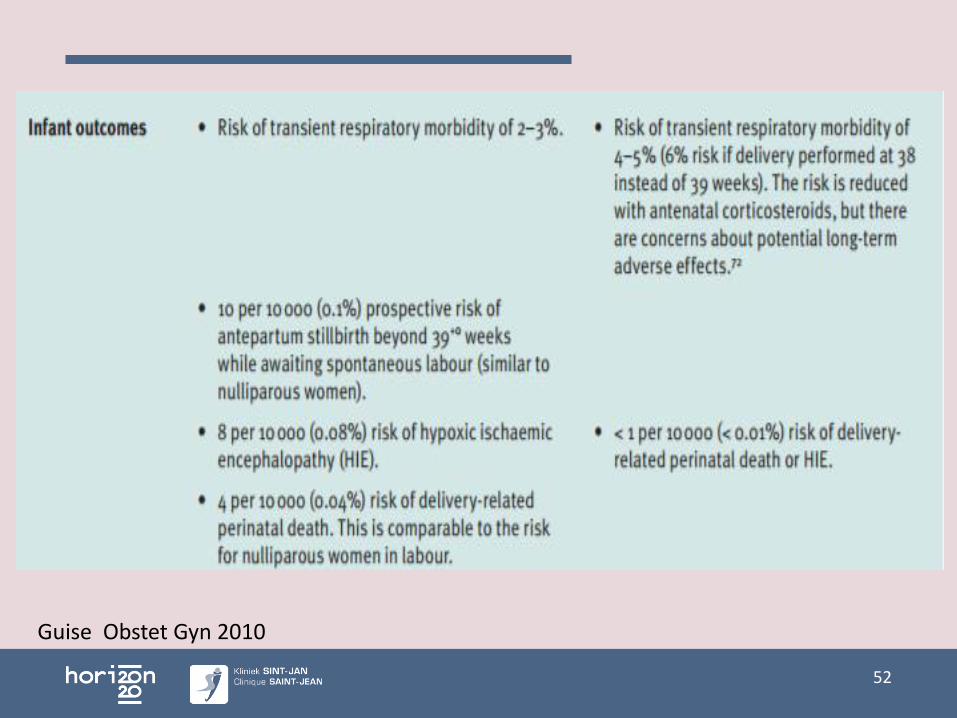
Neonatale outcome
Geplande VBAC Electieve sectio
Transiente respiratoire morbiditeit 2-3%- Transiente tachypnee 2%- Respiratoir distress
syndrome 0,05%
1,5% 39w, afh van timing
- 5%- 0,5%
Na 39w 0,1% risico MIU (cfrP0)
0,08% hypoxischeischemische encephalopathie,60% door ruptuur
<0,01% HIE
0,04% partus gebondenperinatale †, 1/3 door ruptuur
¹Smith, Jama 2002 ²Bahtiyar AJOG 2006, Tita NEJM 2009

22
Peripartum hysterectomie bij 4e C/S 1/406e 1/11
Silver, Obstet Gyn, 2006 Solheim 2011,
ERCS / VBAC
ERCS: Respiratoire morbiditeit ~ zw duur
• 37w 11%
• 38w 6%
• 39w 1,5%
Plan best maken <36w
10% spontane arbeid <39w
Plan indien spontane arbeid
23
Tita NEJM 2009
100,000 vrouwen à terme ondergaan TOLAC ipvERCS
• -9 Maternele mortaliteit
• +650 uteriene rupturen
• +50 neonatale sterfte
• 1/200 ruptuur
• 1/750 TOLAC perinatale sterfte
24
¹ L
Counselling - Inductie
25% voorgaande sectio medische indicatie voor inductie
Ruptuur: 0,5% spt arbeid,
> mechanisch
> inductie met synto
> augmentatie synto
> PG ¹
Inductie /optimalisatie: ruptuur x 2-3, falen TOLAC x1,5
Succesvolle TOLAC 91% vag p - BS ≥6, 77% <6
69% gn vag p - BS ≥6, 45% <6
25
Grobman, Obstet Gyn 2007, N=33.699
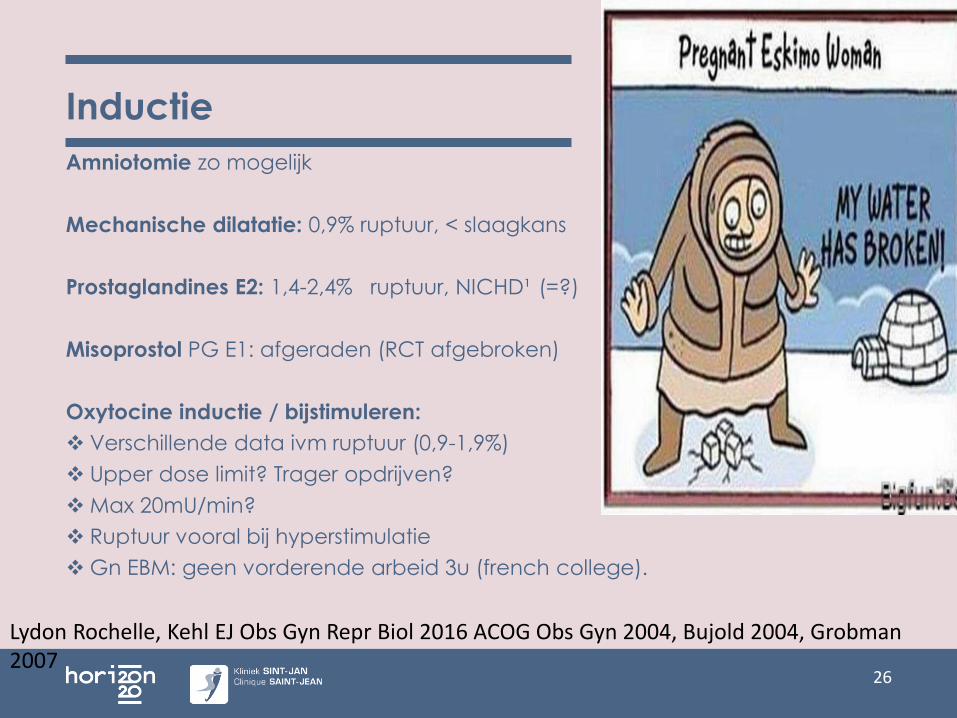
Inductie
Amniotomie zo mogelijk
Mechanische dilatatie: 0,9% ruptuur, < slaagkans
Prostaglandines E2: 1,4-2,4% ruptuur, NICHD¹ (=?)
Misoprostol PG E1: afgeraden (RCT afgebroken)
Oxytocine inductie / bijstimuleren:
Verschillende data ivm ruptuur (0,9-1,9%)
Upper dose limit? Trager opdrijven?
Max 20mU/min?
Ruptuur vooral bij hyperstimulatie
Gn EBM: geen vorderende arbeid 3u (french college).
26
Lydon Rochelle, Kehl EJ Obs Gyn Repr Biol 2016 ACOG Obs Gyn 2004, Bujold 2004, Grobman2007
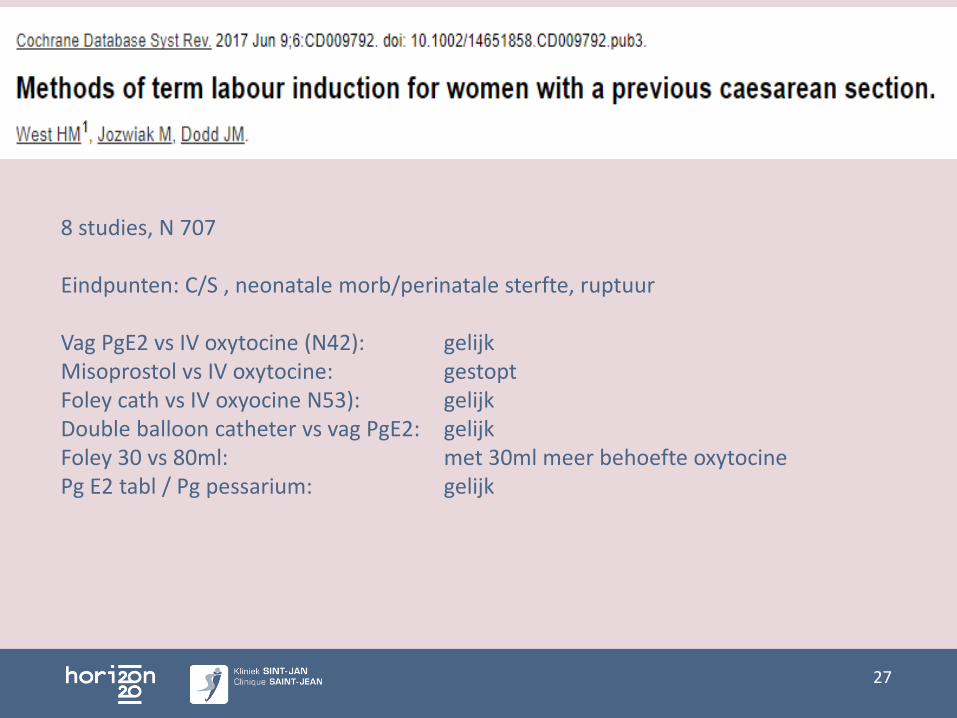
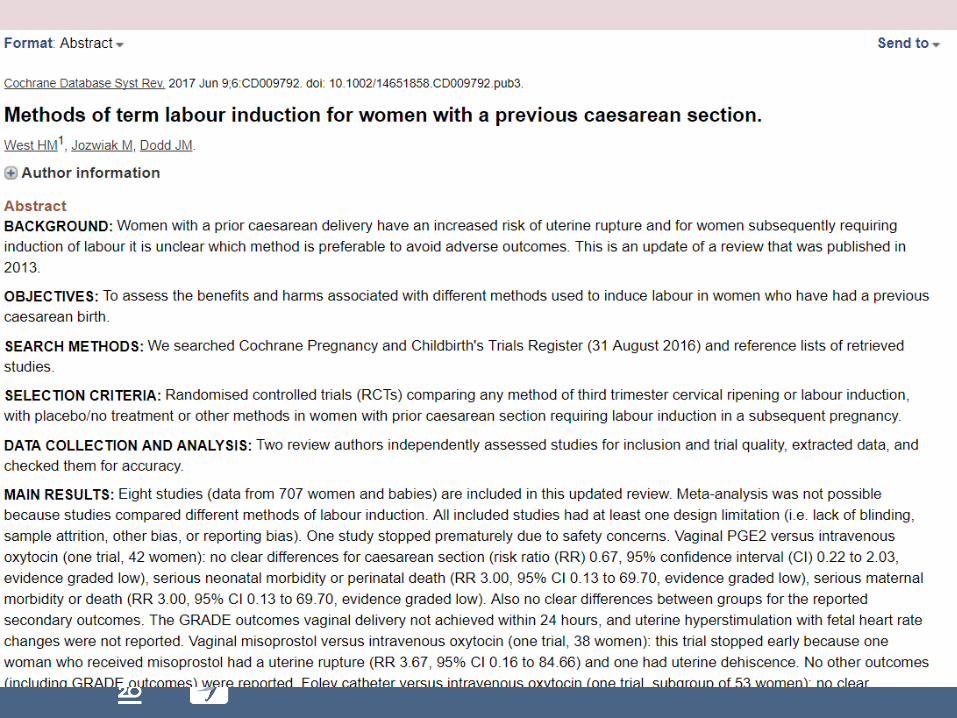
27
8 studies, N 707
Eindpunten: C/S , neonatale morb/perinatale sterfte, ruptuur
Vag PgE2 vs IV oxytocine (N42): gelijkMisoprostol vs IV oxytocine: gestoptFoley cath vs IV oxyocine N53): gelijkDouble balloon catheter vs vag PgE2: gelijkFoley 30 vs 80ml: met 30ml meer behoefte oxytocinePg E2 tabl / Pg pessarium: gelijk
28
Indeling
Introductie
Wie is kandidaat
Antenatale counselling
• Risico’s
• Voordelen / Nadelen
Beleid arbeid / partus
Toekomst
29
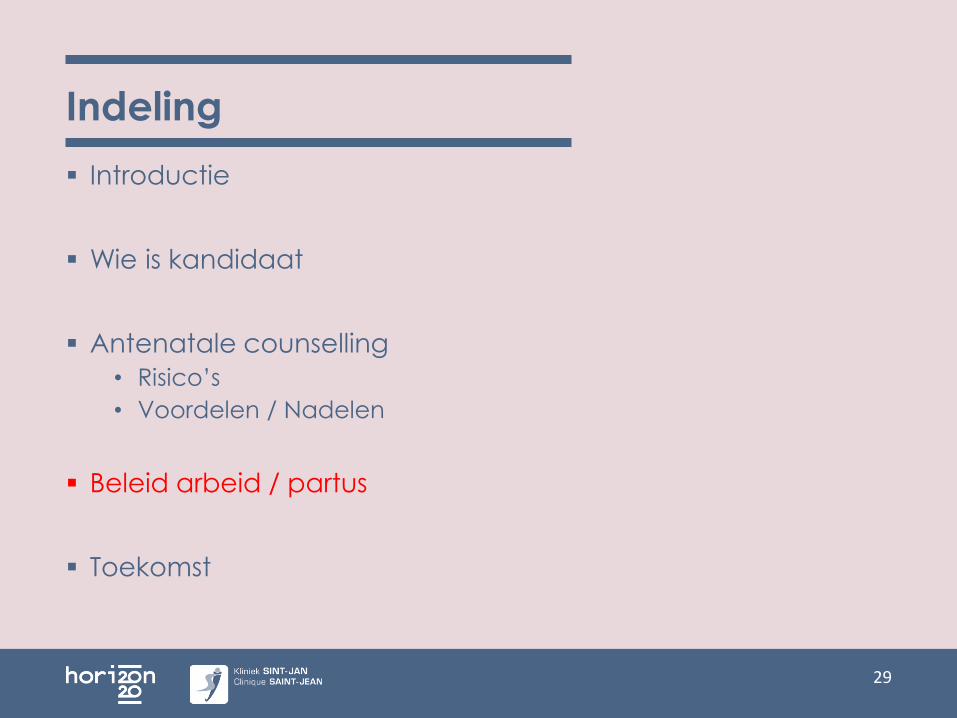
Intrapartum beleid VBAC
Continu CTG v/a actieve arbeid
IV-acces
Bloed bestellen
Peridurale verdoving mag
Regelmatige monitoring maternele S/
Regelmatig VT, partogram gelijk
Max 1u meepersen (consensus)
Elke 8u ranitidine?
Dringende sectio en neonatale resuscitatie mogelijk
<18 min? ¹
30
¹ Leung, 1993
31
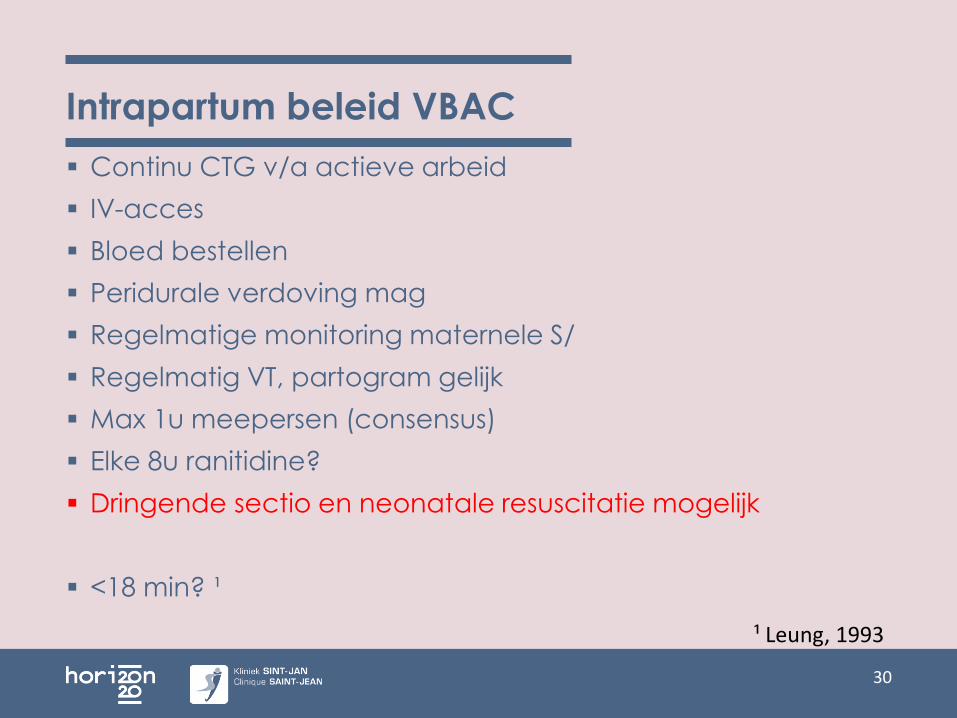
Symptomen ruptuur
Abnormaal CTG (70%)
Abdominale pijn, vooral tussen KT’s
Acute pijn litteken
Abnormaal vag bloedverlies / Hematurie
Afnemen KT’s (staircase sign)
Maternele tachycardie, hypotensie, shock, syncope
Geen voorliggend deel
Harttonen op andere plek
Verandering vorm abdomen
32
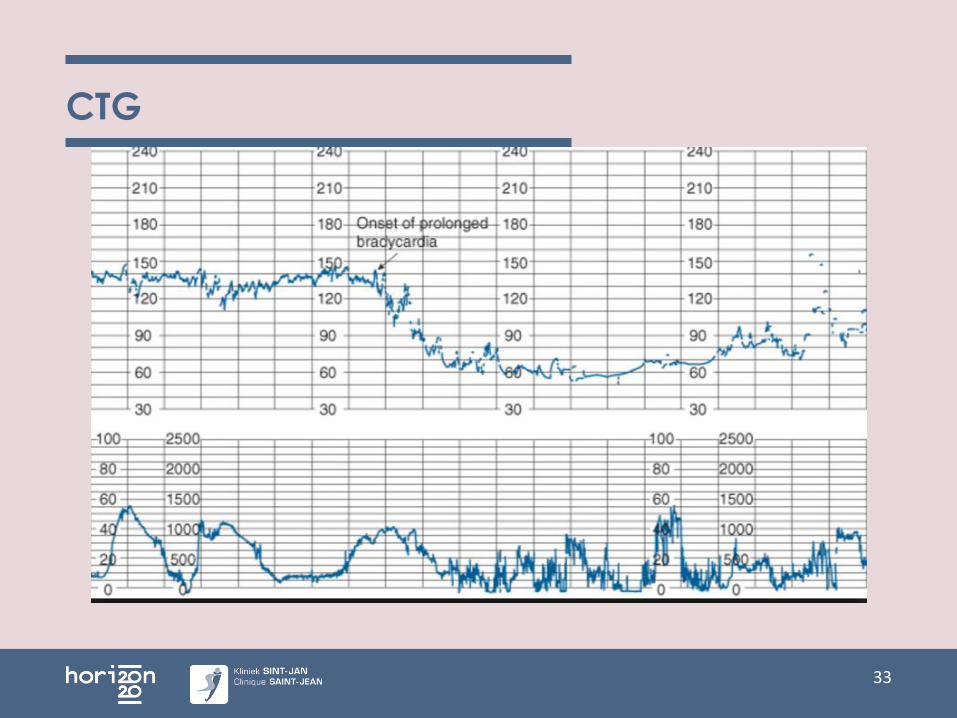
CTG
33
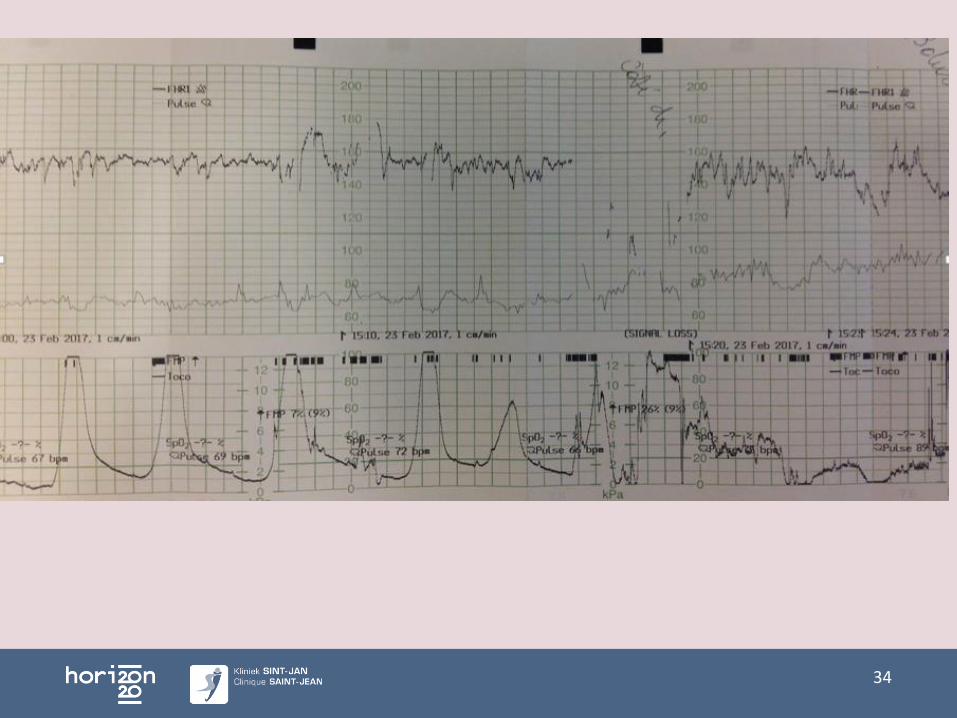
CTG
34
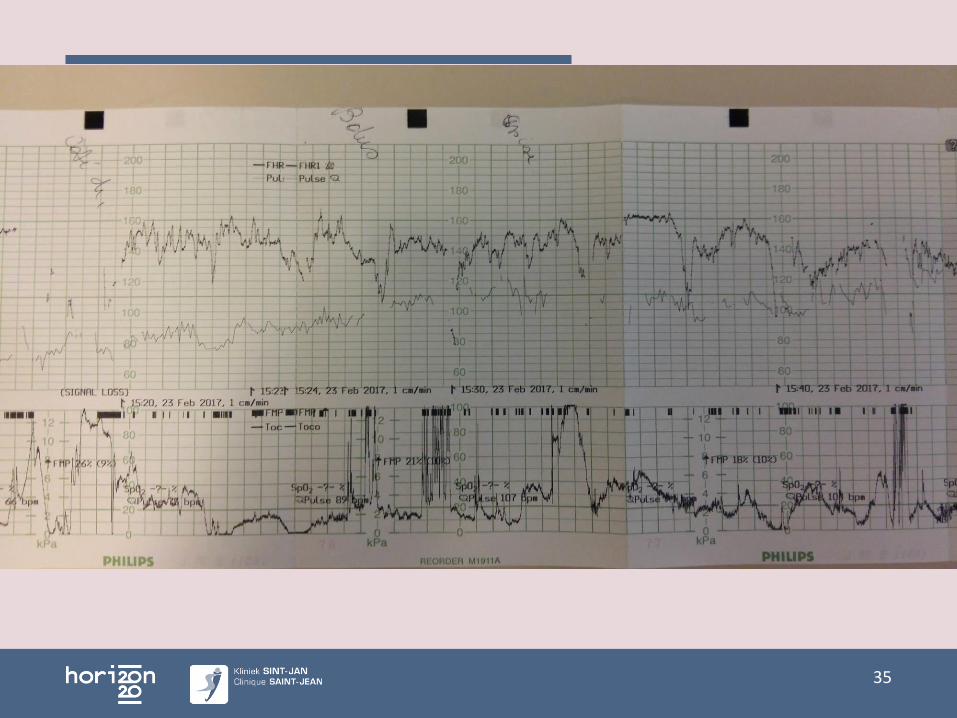
CTG
35
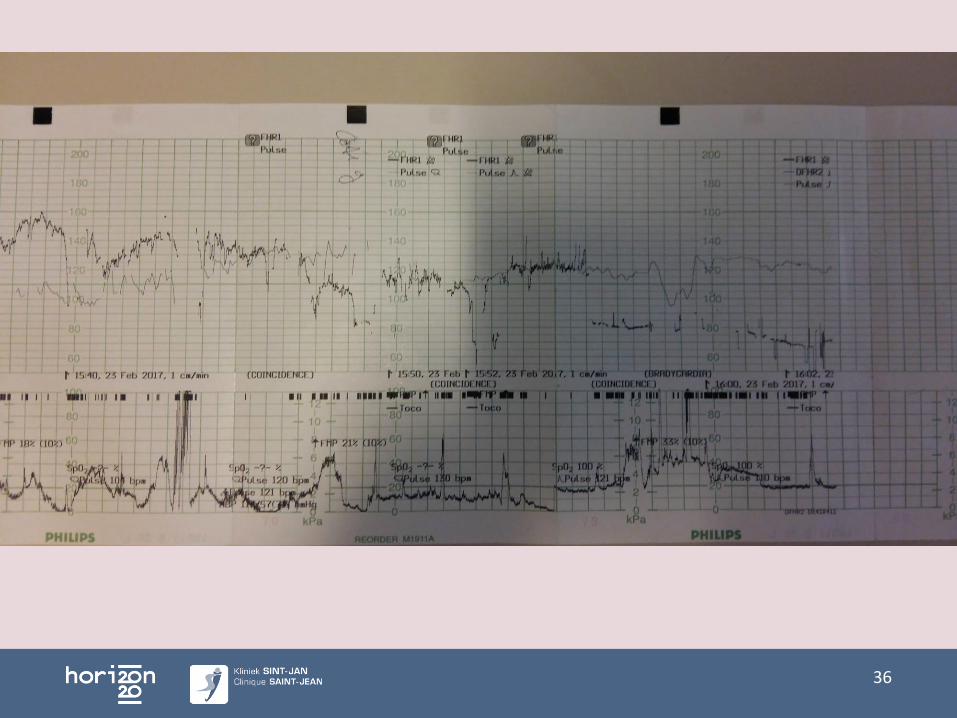
CTG
36
Wat vergroot risico ruptuur
Interdelivery interval <18 mnd (risico ruptuur x3)
Postterm
> 40 jr
BMI > 30
Inductie, Bishopscore <6
Macrosomie
Dun LUS (NPW >2,1mm, PPW <2,0 mm), meting niet zinvol¹.
Wondinfectie
Single layer closure
37
¹Rozenberg, Lancet 1996, Bujold AJOG 2009, Martins Ult Obs G 2009

38
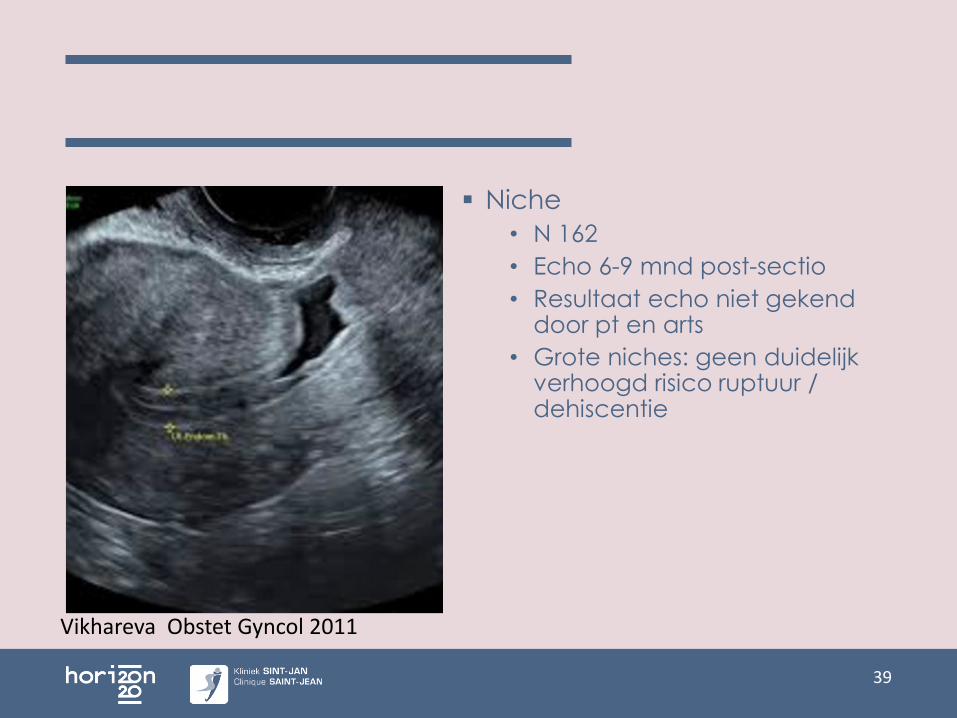
Niche
• N 162
• Echo 6-9 mnd post-sectio
• Resultaat echo niet gekend door pt en arts
• Grote niches: geen duidelijk verhoogd risico ruptuur / dehiscentie
39
Vikhareva Obstet Gyncol 2011
Succeskans
VBAC-scores
- Voor counselling
- Prenataal
- Bij opname
- Verschillende parameters
- https://mfmu.bsc.gwu.edu/PublicBSC/MFMU/VGBirthCalc/vagbirth.html
- https://www.mdcalc.com/vbac-risk-score-successful-vaginal-delivery-flamm-model (opname)
40
Grobman WA, National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU), Obs Gyn, 2007.
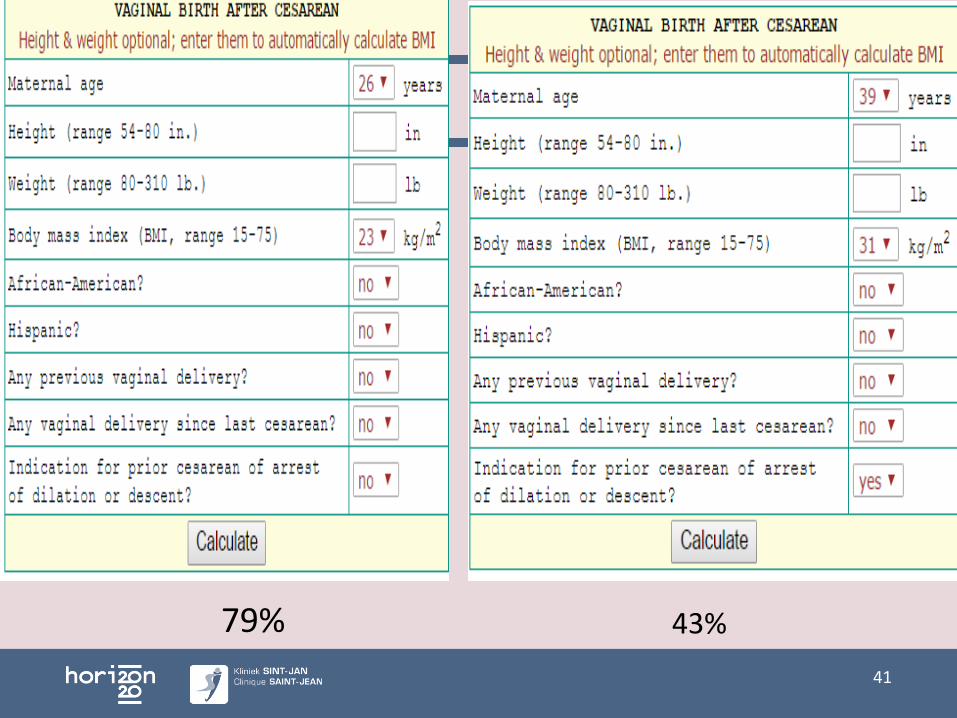
Introductie
41
79% 43%
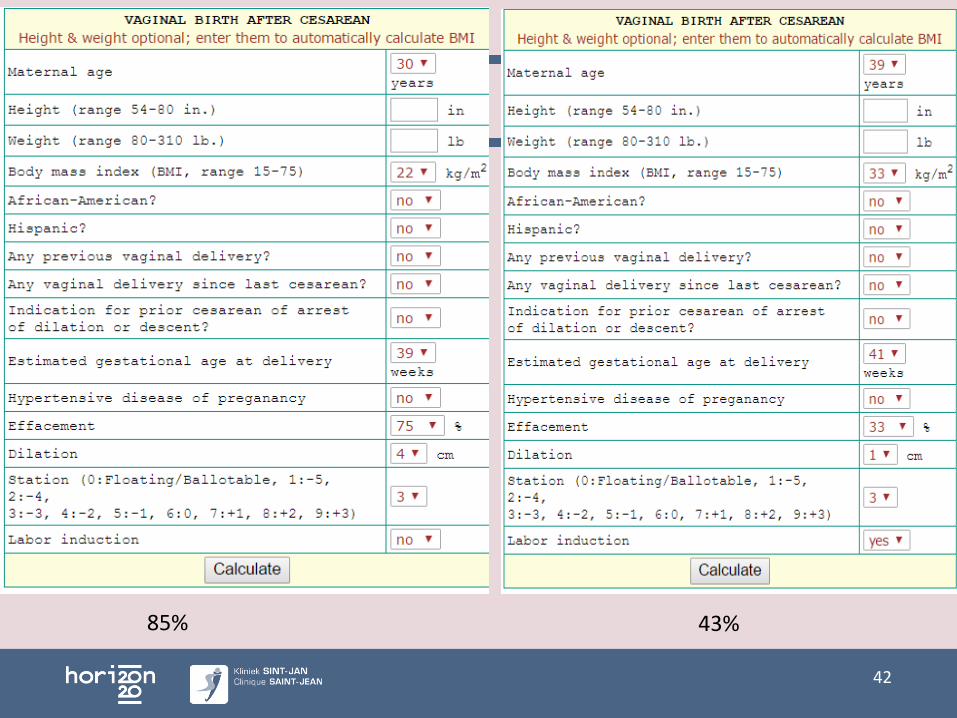
Introductie
42
85% 43%
Speciale omstandigheden
Preterm: = succeskans, < ruptuur¹²³
Twin: kleine studies, succeskans =?, risico ruptuur =
Macrosomie >4kg:• ruptuur 3,6%• Succesvolle VBAC <50% als gn voorgaande vag partus• Schouderdystocie, 3e/4e gr scheur
>BMI: < VBAC, > ruptuur
Antepartum MIU: VBAC succes 87%
>41w: >39w risico MIU bij voorgaande sectio x1,5-2 (0,11 vs 0,05%)
40 jr: Onafh factor MIU en onsuccesvolle VBAC
43
¹Durnwald AJOG 2005, Landon AJOG 2005, Ford AAJOG 2006, Obs Gyn 2016, Hibbard Obs Gyn2007
Toekomst
Beter inschatten slaagkans?
Betere voorspelling ruptuur: Waarde echo ikvruptuur
Partogram, timing interventies
Informed consent / protocol TOLAC
Nooit alles te voorspellen !
Rupturen zullen blijven komen
44
Protocol TOLAC
Vanuit de B.OSS werkgroep, met steun van het College Moeder en Kind.
Dit zal ter goedkeuring voorgelegd worden
• aan het College,
• aan VVOG en GGOLFB
• beroepsverenigingen voor vroedvrouwen: Vlaanderen, Bxl-Wallonia, nationaal.
45
46
Take-home messages
47
• Slaagkans 70%Na VBAC of vag partus: 85%
• Ruptuur 0,5%• Counselling patiënte• Cave inductie / optimalisatie• Goede follow-up arbeid en partus• Dringende sectio en neonatale resuscitatie
Proficiat
Bravo ziekenhuizen met BFHI –label
48
Vragen?
49
Introductie
50
Geplande VBAC – Maternele uitkomst
51
Geplande VBAC – Maternele uitkomst
52
Guise Obstet Gyn 2010

53
54
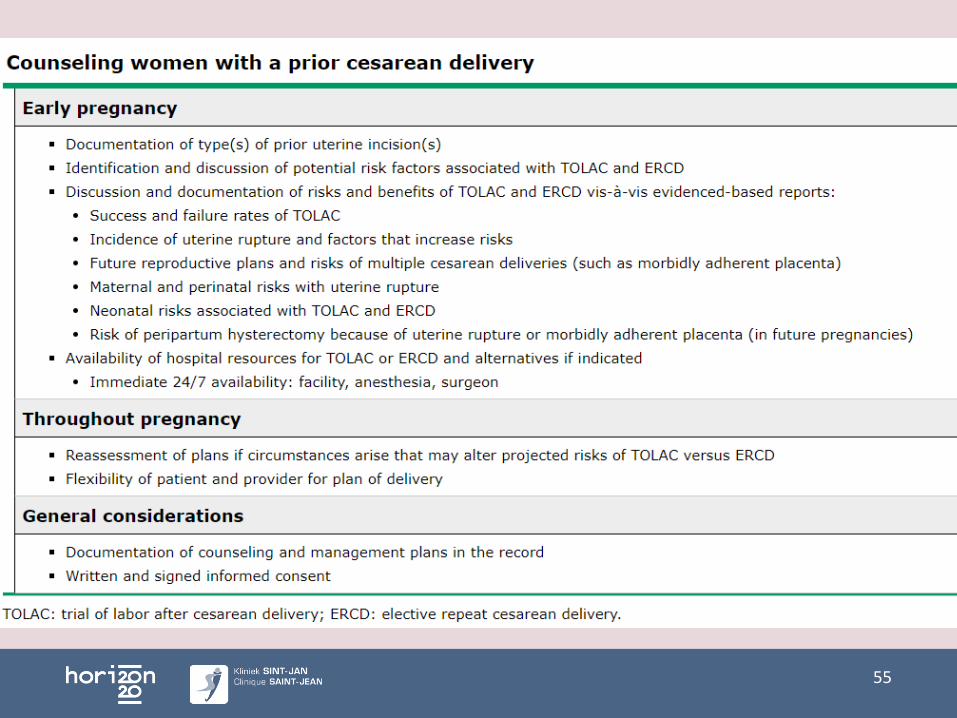
55
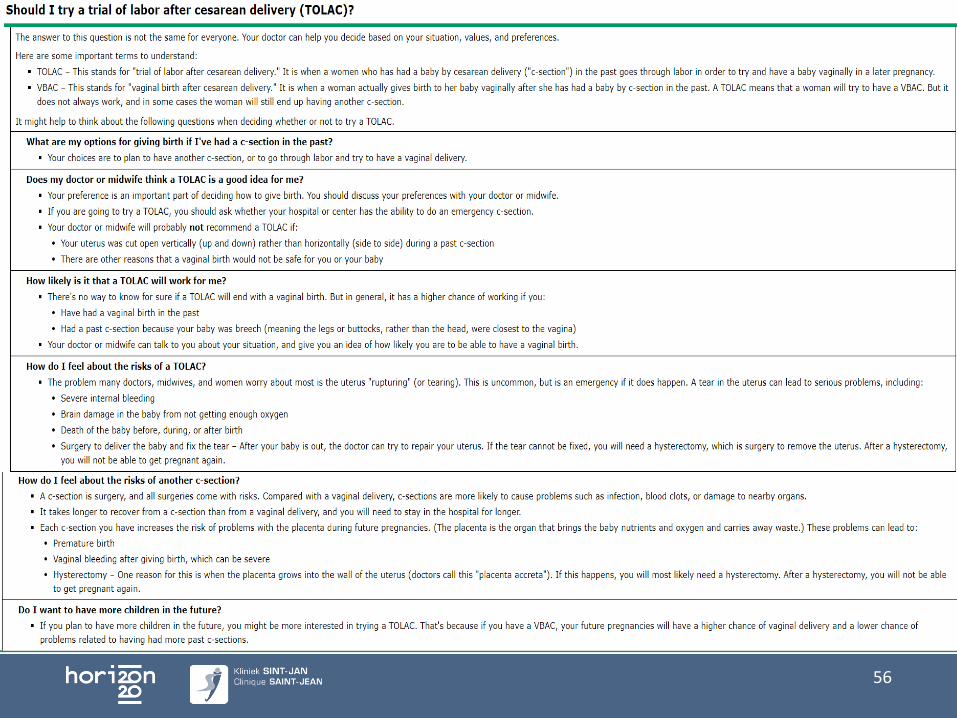
56
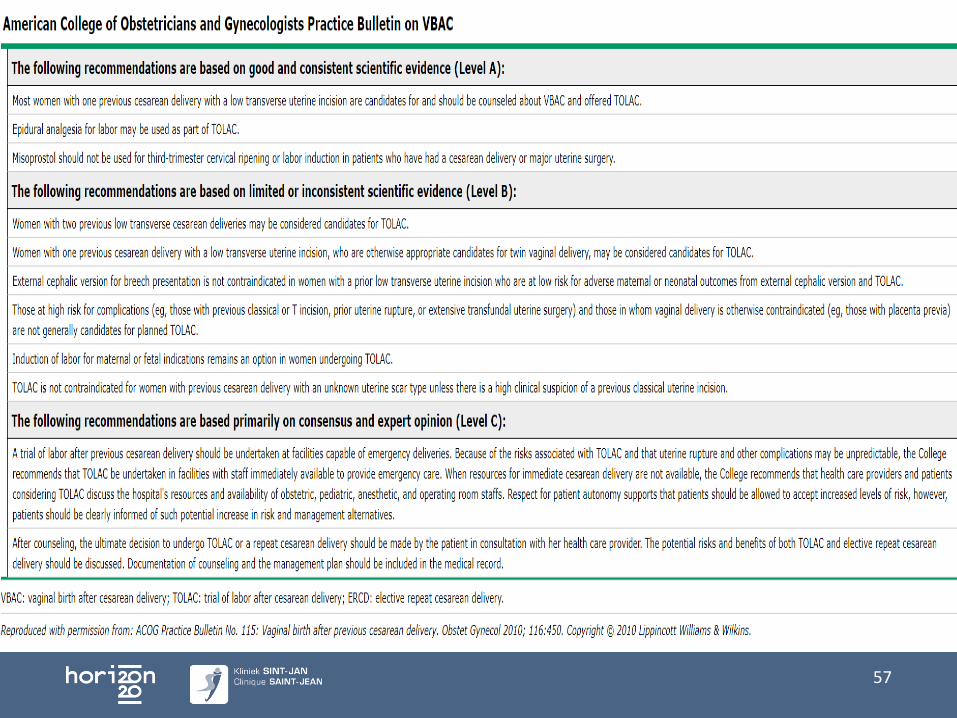
57
Voor 37w bespreken
• Kans op VBAC 70%
• Risico ruptuur 0,5% bij spt arbeid
• > Risico ruptuur bij stimulatie
• Voor- /Nadelen sectio
• Toekomstige kinderwens
• Risico placenta praevia / accreta
• Wat indien spt arbeid voor ERCS
58
59
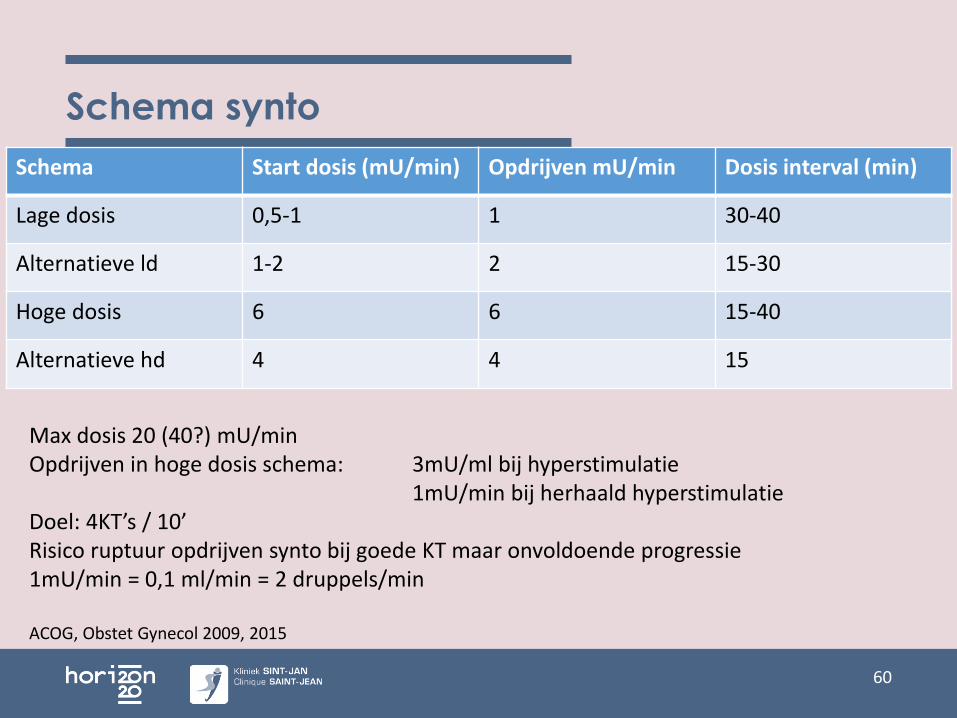
Schema synto
Schema Start dosis (mU/min) Opdrijven mU/min Dosis interval (min)
Lage dosis 0,5-1 1 30-40
Alternatieve ld 1-2 2 15-30
Hoge dosis 6 6 15-40
Alternatieve hd 4 4 15
60
Max dosis 20 (40?) mU/minOpdrijven in hoge dosis schema: 3mU/ml bij hyperstimulatie
1mU/min bij herhaald hyperstimulatieDoel: 4KT’s / 10’Risico ruptuur opdrijven synto bij goede KT maar onvoldoende progressie1mU/min = 0,1 ml/min = 2 druppels/min
ACOG, Obstet Gynecol 2009, 2015