FYSIOTHERAPIE NA CUFF REPAIR 20-03-2012... · MUSCULAIRE VERANDERING MUSCULAIRE DISBALANS woensdag...
38
FYSIOTHERAPIE NA CUFF REPAIR RYCHARD H. GERYSZEWSKI FYSIOTHERAPEUT woensdag 21 maart 12
Transcript of FYSIOTHERAPIE NA CUFF REPAIR 20-03-2012... · MUSCULAIRE VERANDERING MUSCULAIRE DISBALANS woensdag...

FYSIOTHERAPIE NA
CUFF REPAIR
RYCHARD H. GERYSZEWSKI FYSIOTHERAPEUT
woensdag 21 maart 12

EVOLUTIE FYSIOTHERAPIE
• Oorlog en Poliomyelitis; testen Fs, ROM behouden, Fs oefenen
• Hersenen en ruggenmerg; eigen inzicht
• Australië en N. Zeeland; ROM en pijn, Cyriax; oorzaak gericht
• Musculoskeletaal; locomotor systeem, adequate beweging
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Het kinesiopathologisch model van Shirley A. Sahrmann
Optimale functie
woensdag 21 maart 12

NIET GEBALANCEERDE MUSCULAIRE VERANDERING
MUSCULAIRE DISBALANS
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Afwijkendneurologisch of radiologisch
functioneel beperkt
herhaald specifieke-gewrichtsbeweging
-houding
beperkingen van componenten of
- interacties
bewegings- beperkingen
syndromen van bewegings-beperkingen
Het kinesiopathologisch model van Shirley A. Sahrmann
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Het kinesiopathologisch model van Shirley A. Sahrmann
Optimale functie
woensdag 21 maart 12

BLBK145-Gross February 13, 2009 20:34
18 Basic Concepts of Physical Examination Chapter 2
Figure 2.2 Normal posterior view.
Figure 2.3 Calcaneal valgus deformity.
(a)
(b)
Figure 2.4 Genu varum (a) and valgum (b) deformities.
BLBK145-Gross February 13, 2009 20:34
24 Basic Concepts of Physical Examination Chapter 2
sternocleidomastoid
Figure 2.17 Torticollis.
2
Figure 2.18 Normal lateral view.
on Feiss’ line (from the medial malleolus to the firstmetatarsophalangeal joint). The knees should be from0 to 5 degrees of flexion. The hips should be in 0 de-grees of flexion. The pelvis should be aligned so thatthe anterior and posterior superior iliac spines are inthe same plane horizontally, creating a normal lordo-sis. The pelvis should not be rotated. The anterior su-perior iliac spine and pubic symphysis should be in thesame plane vertically. The normal posterior–anteriorpelvic angle is 30 degrees from the posterior supe-rior iliac spine to the pubic ramus. The spine shoulddemonstrate the normal anterior–posterior curves oflumbar lordosis, thoracic kyphosis, and cervical lor-dosis. The chest should have a smooth contour with-out any areas of depression or protrusion. The shoul-ders should be in proper alignment without beingprotracted or rounded. The head should be over theshoulders with the ear lobe on a vertical line withthe acromion process. Rocabado (unpublished data,1982) notes that the apex of the thoracic kyphosisshould not be more than 2 in. posterior to the deepestpoint of the cervical lordosis (Figure 2.18).
Possible Deviations from the Norm
Start by observing the patient’s feet. Note the me-dial longitudinal arch (Figure 2.19). You can observe
Feiss’s line
Figure 2.19 Normal medial longitudinal arch.
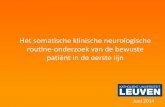
THORACALE WERVELKOLOM
woensdag 21 maart 12

BLBK145-Gross February 13, 2009 20:34
25Chapter 2 Basic Concepts of Physical Examination
Figure 2.20 Genu recurvatum deformity.
Feiss’ line and determine if a pes planus (Figure 2.11)or cavus is present. Note the alignment of the knee.The lateral view gives you the easiest way to note aknee flexion contracture or genu recurvatum (Figure2.20).
Note the relative position of the anterior and poste-rior superior iliac spines. If the anterior superior iliacspine is higher, it could indicate a posterior pelvictilt or a posterior rotation of the innominate bone. Aposterior pelvic tilt will cause a decrease in the lum-bar lordosis or a flat back (Figure 2.21). Is a swayback present (Figure 2.22)? If the posterior superioriliac spine is relatively higher, this could indicate ananterior pelvic tilt or an anterior rotation of the in-nominate bone. An anterior pelvic tilt will cause anincrease in the lumbar lordosis.
Observe the trunk. The lateral view allows you toobserve the anterior and posterior curves. Does thepatient present with a rounded (Figure 2.6) or a flat-tened thoracic kyphosis? Is a Dowager’s hump present(Figure 2.23)?
Note the position of the shoulders. Does the pa-tient present with anteriorly displaced rounded shoul-ders (Figure 2.24)? Where are the upper extremitiesin relation to the trunk? Observe the head and neck.
Figure 2.21 Flat back deformity.
Figure 2.22 Sway back deformity.
BLBK145-Gross February 13, 2009 20:34
20 Basic Concepts of Physical Examination Chapter 2
Figure 2.6 Rounded thoracic kyphosis.
X
X is more than two inches
Figure 2.7 Abducted scapula.
Figure 2.8 Winged scapula.
Observe the position of the head and neck. Is thehead in a forward, rotated, or laterally flexed posture?Can the patient hold the head up against gravity?
Anterior View
Normal
The feet should show 8–10 degrees of toeing out.There should be a normal medial longitudinal archthat is symmetrical bilaterally. The navicular tuberos-ity should be located on Feiss’ line (see p. 385, Fig-ures 2.19, 13.7) (from the medial malleolus to thefirst metatarsophalangeal joint). The tibias shouldbe straight without bowing or torsion. The kneesshould show 13–18 degrees of valgus (normal Q an-gle) (see Figures 12.9, 12.12). The patellae shouldpoint straight ahead. The fibular heads should be ofequal height. The pelvis should be of equal height onboth sides. The anterior superior iliac spines shouldbe level bilaterally. The spine should be straight with-out any lateral curves. Although the spine is not di-rectly visible from this view, you can surmise curvesby observing the anterior trunk and the pattern inwhich the hair grows. The rib cage should be sym-metrical without any protrusion or depression of theribs or sternum. The shoulders should be of equal
THORACALE WERVELKOLOM
Kyfose Scoliose vlak
BLBK145-Gross February 13, 2009 20:34
19Chapter 2 Basic Concepts of Physical Examination
Figure 2.5 Scoliosis.
Note the alignment of the hip joint. Increased flex-ion may be present secondary to a hip flexion con-tracture (see pp. 324, 327, Figure 11.66). To confirmthis, a Thomas test would have to be performed to testfor hip flexor length. Is there excessive medial or lat-eral rotation? Check the relative heights of the greatertrochanters. A difference in height may be secondaryto a structural difference in the length of the femur.
Check the pelvis. Place your hands on the iliac crestsand observe their relative heights. If one is higher thanthe other, it may be secondary to a pelvic torsion,a structural anomaly, or a structural or functionalshort leg. Place your hands on the posterior superioriliac crests and note their relative location. A changein height may be secondary to a pelvic rotation, asacroiliac dysfunction, or a leg length discrepancy.
Observe the spine. First pay attention to the soft tis-sue. Are there any areas of muscle guarding or spasm?These may be secondary to a facilitated segment orsurrounding an area of dysfunction. Note any differ-ences in the skinfolds. This will allow you to bettervisualize lateral curves and spinal rotations. Note thealignment of the spinous processes. Is the back instraight alignment or does the patient present witha scoliosis (Figure 2.5) or kyphosis (Figure 2.6)? If
scoliosis is present, note the rib cage, the degree of ro-tation, and the presence of any lateral humps. Is theresymmetrical rib expansion both anteriorly/posteriorlyand laterally? Is a lateral shift present? Is the patientable to stand in the erect position or is he or she for-ward or laterally flexed?
Observe the scapulae. Are they equidistant fromthe spine? Are they of equal height? Are they overlyabducted or adducted (Figure 2.7)? Is one side winged(Figure 2.8)? This may be secondary to weaknessof the serratus anterior muscle or long thoracicnerve palsy. Is a Sprengel’s deformity present (Figure2.9)? Note the muscle bellies of the infraspinatus,supraspinatus, and teres major and minor musclesover the scapula. Is there an area of atrophy?Disuse atrophy may occur in the supraspinatus orinfraspinatus following a rotator cuff injury. Note therelative shoulder heights and position. Pay attentionto the upper trapezius and note any hypertrophy oratrophy. Note the upper extremities. Does the patientposition both arms in the same manner? Is one armheld farther away from the trunk or in either moreinternal or external rotation? This can be secondaryto muscle shortening and imbalances or fascialrestrictions.
woensdag 21 maart 12

BLBK145-Gross February 13, 2009 20:35
35Chapter 4 The Cervical Spine and Thoracic Spine
Hyoid boneThyroid cartilage
First cricoid ring
Carotid tubercle
Sternum
Trachea
C1C2
C6C7
T4
T2
Mastoid process
Superior nuchal line
Inion
Spinous processes
Mandible
Facet joint
C1 transverseprocess
Figure 4.1 Overview of the neck with anterior–posteriorrelationships.
clavicles and the sternum. An uneven contour may bepresent secondary to a healed fracture. Observe thescapulae and determine whether they are equidistantfrom the spine and are lying flat on the rib cage. Is asubluxation present at the glenohumeral joint and ifso, to what degree? Notice the size and contour of thedeltoid muscle and compare to the opposite deltoid.
Vertebraprominens (C7)
Spinous process of T1
Clavicle
Spine ofscapula
8th rib
7th rib
Rib angle
Inferior angleof scapula(T7 vertebra)
T2
T3
T7
Figure 4.2 Overview of the posterior thorax.
Temporalartery
Vertex of headTemporal bone
Parietal bone
Occipital bone
Mastoid process
Frontalbone
Orbit
Nasalbone
Maxilla
Zygoma
Parotidduct
Mandible
Parotidgland
Figure 4.3 Overview of the skull.
Sternocleidomastoidmuscle
Scalenemuscles
Figure 4.4 The sternocleidomastoid muscle acts both as acervical flexor and lateral rotator of the cervical spine. Thescaleni muscles act to bend the cervical spine laterally and alsoassist in flexion.
SCAPULA• T 2
• 7,5 cm afstand
• T 7
• plat op romp
• 30 graden frontale vlak
woensdag 21 maart 12

SCAPULA POSITIESForward Tilta) lev.scapulae en rhomb kortb) trap.pars desc verlengdc) serr.ant verlengd
Scapula bovenrand laaga) bovenrand lager dan T2b) angulus inf. lager dan T7c) pect.maj + latiss dorsi verkort
Scapula hooga) bovenrand C7b) trap.p.desc lev. scapulae } verkort rhomb
Adductie standa) margo medialis < 7.5 cm WKb) trap en rhomb verkortc) serratus verlengd
Abductie standa) margo medialis > 7,5 cm WKb) rotatie tov frontaal > 30 grad.c) glenoïd ant kijkt anteriord) stand humerus correct kom
Ang. Inf. komt losa) pect.min. kortb) korte biceps c. br. , delt en coracobrach.c) correctie scapula=> flexie elleboog
Depressie en ant. tilt Abductie en ant. tilt Winginga) margo med. los van thoraxb) serratus zwakte
Opwaartse rotatiea) ang. inferior opwaarts
literatuur Kibler en Cools
woensdag 21 maart 12

HUMERUS
• neutraal
• elleboogplooi “kijkt” voor
• Olecranon “ kijkt” achter
• 1/3 humeruskop voor acromion
woensdag 21 maart 12

HUMERUS POSITIES
naar anteriora) > 1/3 kop voor acr.
naar craniaalb) humerus migratie
abductiea) med. epicond weg van lijf en/of scapula naar mediorot/ depressie
endorotatiea) elb plooi mediaalb) olecranon lateraal
exorotatiea) zeldzaam tenzij icm scapula abductie
flexie&extensiea) trochl ant van proxb) trochl post v. prox
beiden irt scapula
woensdag 21 maart 12

KRITIEKE FACTORENontstaansmechanismea) traumatischb) geleidelijk progressief
weefselkwaliteita) weefselkwaliteit pees / spierb) bot kwaliteit
grootte & type scheura) absolute afmeting s/m/l/massief
b) aantal betrokken structurenc) crescent, U, L, retractie etc.
locatie van de scheur 1) geïsoleerde SSP 2) SSP en ISP3) subscapularisBurkhart et al 1992
integriteit overigena) ISP, TMi, Subscb) belang krachtkoppels
patiënt variabelena) activiteit; werk en sportb) motivatiec) ARBOd) roker - niet roker
besluit orthopeedconservatief versus operatief
bijkomende factorena) decompressieb) SLAP repairc) capsulaire ingreep
type ingreepa) arthroscopischb) mini-openc) open
fixatiea) hechting ankersb) single vs double rowc) suture bridge techniekPark et al 2008, Waltrip et al 2003,
revalidatie optiesa) revalidatie & supervisieb) revalidatie geen supervisie
woensdag 21 maart 12

CLASSIFICATIE VAN RUPTURENSIZE MATTERS
• small < 1 cm
• medium 1 - 3 cm
• large 3 - 5 cm
• massief > 5 cm
woensdag 21 maart 12

✴ Histologisch; degeneratief, metabolisch minder actief. Kannus, Josza, 1991 Histopathological changes preceding spontaneous rupture of a tendon.
✴ In tendinopathische en geruptureerde pezen is sprake van een reductie van type 1 collageen en een significante toename van type 3 collageen => afname van biologische en mechanische eigenschappen => afname van treksterkte.
Maffuli N, Ewen SW, Waterston SW, Reaper J, Barrass V, 2000, Tenocytes from ruptured and tendinopathic achillestendons produce greater quantities of type III collagen than tenocytes from normal Achilles tendons. an in vitro model of human tendon healing
✴ Rust; na 8 weken collageen afbraak >aanmaak. Nieuw gevormd collageen onvolgroeid en minder crosslinks en de treksterkte is laag.
Woo, Tkach, 1990, The cellulair and matrix respons of ligaments and tendons to mechanical injury.
Gamble, Edwards,Max et al.,1984, Enzymatic adaptation in ligaments during immobilization.
Consequenties voor revalidatie
woensdag 21 maart 12

De vezelstructuur van de pees is verstoord Blei, Nirschl, Grant, 1986, Achilles tendon: US diagnosis of pathologic conditions. Radiology; 159: 765 – 767.
Na ruptuur toont de pees oedemateus en verdikt. Fornage , 1986; Achilles Tendon: US examination. Radiology; 1959:759-764.
In de periode aansluitend op curatie breidt de zwelling van de peesuiteinden uit.
Karjalainen et al,1997, Magnetic resonance imaging during healing of surgically repaired achilles tendon
ruptures. Am J of Sports medicine, volume 25,no 2, 164 – 171.
De kans op re-ruptuur is groot, mede agv. gedesoriënteerde ingroei van het collageen. Kuwada , Schuberth , 1984, Evaluation of achilles tendon re-rupture J. Foot Surg.; 23: 340 – 343.
Consequenties voor revalidatie
woensdag 21 maart 12

Consequenties voor revalidatie
Major aim of physiotherapy, beyond the stage where treatment of specific symptoms may be the principal issue, is the restoration of optimal motor performance. It cannot be assumed that improvement in the presenting symptoms (pain, stifness) will necessarily generalize into improved functional activities.
Carr, Shepherd, 1995, Musculoskeletal Physiotherapy, blz 35
woensdag 21 maart 12

“Long after injury and immobilisation, muscle, tendon and ligament remain mechanically inferior to uninjured tissue. They tear at lower forces and they are capable of absorbing less energy before tearing”
Järvinen, Lehto, 1993, The effect of early mobilisation and immobilisation on the healing proces
following muscle injuries. Sports Med. 15, 78 – 89.
Whiting WC, Zernicke RF, 1998, Biomechanics of musculoskeletal injury, Human Kinetics
Woo SLY, Buckwalter JA, 1988, Injury and repair of the musculoskeletal soft tissues. Park IL: American Academy of orthopedic surgeons
Consequenties voor revalidatie
woensdag 21 maart 12

SHOULDER
Rotator cuff repair failure in vivo: a radiostereometricmeasurement study
Tobias K.A. Baring, MRCSa,b,*, Peter P.M. Cashman, PhDc, Peter Reilly, MSa,Roger J.H. Emery, MSa,b, Andrew A. Amis, DSc(Eng)b,d
aDepartment of Orthopaedic Surgery, St Mary’s Hospital, Imperial College London, London, UKbDepartment of Biosciences and Surgical Technology, St Mary’s Hospital, Imperial College London, London, UKcDepartment of Bioengineering, Imperial College London, London, UKdDepartment of Mechanical Engineering, Imperial College London, London, UK
Background: The prevalence of failure among repairs of the rotator cuff is well known, but very fewobjective data exist regarding either the scale or timing of this complication. The aim of this study wasto use a previously validated modified technique of roentgen stereophotogrammetric analysis to monitorthe behavior of the rotator cuff after repair to establish at what point failure may occur.Materials and methods: A series of 10 patients had metal beads and wire sutures embedded into thehumeral greater tuberosity and supraspinatus tendon, respectively, during open cuff repair procedures.Roentgen stereophotogrammetric analysis imaging of the repaired rotator cuffs was performed at set inter-vals during the first year after surgery.Results: The mean distance between the tendon and bone markers did not increase significantly betweenthe time of surgery and 3 to 4 weeks. There was then a significant increase of 7.0 mm in the distancebetween the tendon and bone markers, with the largest increase occurring between 3 to 4 weeks and 12to 14 weeks after surgery, as well as a further small but significant increase of 1.7 mm between 12 to14 weeks and 1 year. These results were compared with clinical examination and ultrasound findings.Conclusion: Most tendon marker movement was seen during the most intensive period of physiotherapy,in the second and third months after surgery. Significantly more movement was seen in the tendon markersof those patients in whom the repair failed.Level of evidence: Level I, Prospective Cohort, Prognosis Study.! 2011 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: Rotator cuff; failure; gap formation; RSA; repair; ultrasound
Monro14 first recorded a tear of the rotator cuff in 1778.Orthopaedic surgeons have now been attempting to repairsuch tears for over 100 years.3 Many studies have shown
a significant benefit from repair of the torn rotatorcuff.3,8,9,13 However, high rates of failure of rotator cuffrepairs have been reported with both open and arthroscopictechniques.8,13 There is still a high rate of satisfactionamong patients with failed repairs, most likely because ofthe pain-relieving benefits of the operation.8,13 Studies inthe past have looked at the mechanical causes of repairfailure,6,10,16 such as the strength of different suturingtechniques and the way in which sutures may cut through
Ethical approval was awarded by the Riverside Research Ethics Committee(RREC 3643).
*Reprint requests: Tobias K.A. Baring, MRCS, Department of Ortho-paedic Surgery, St Mary’s Hospital, London W2 1PG, England.
E-mail address: [email protected] (T.K.A. Baring).
J Shoulder Elbow Surg (2011) 20, 1194-1199
www.elsevier.com/locate/ymse
1058-2746/$ - see front matter ! 2011 Journal of Shoulder and Elbow Surgery Board of Trustees.doi:10.1016/j.jse.2011.04.010
SHOULDER
Rotator cuff repair failure in vivo: a radiostereometricmeasurement study
Tobias K.A. Baring, MRCSa,b,*, Peter P.M. Cashman, PhDc, Peter Reilly, MSa,Roger J.H. Emery, MSa,b, Andrew A. Amis, DSc(Eng)b,d
aDepartment of Orthopaedic Surgery, St Mary’s Hospital, Imperial College London, London, UKbDepartment of Biosciences and Surgical Technology, St Mary’s Hospital, Imperial College London, London, UKcDepartment of Bioengineering, Imperial College London, London, UKdDepartment of Mechanical Engineering, Imperial College London, London, UK
Background: The prevalence of failure among repairs of the rotator cuff is well known, but very fewobjective data exist regarding either the scale or timing of this complication. The aim of this study wasto use a previously validated modified technique of roentgen stereophotogrammetric analysis to monitorthe behavior of the rotator cuff after repair to establish at what point failure may occur.Materials and methods: A series of 10 patients had metal beads and wire sutures embedded into thehumeral greater tuberosity and supraspinatus tendon, respectively, during open cuff repair procedures.Roentgen stereophotogrammetric analysis imaging of the repaired rotator cuffs was performed at set inter-vals during the first year after surgery.Results: The mean distance between the tendon and bone markers did not increase significantly betweenthe time of surgery and 3 to 4 weeks. There was then a significant increase of 7.0 mm in the distancebetween the tendon and bone markers, with the largest increase occurring between 3 to 4 weeks and 12to 14 weeks after surgery, as well as a further small but significant increase of 1.7 mm between 12 to14 weeks and 1 year. These results were compared with clinical examination and ultrasound findings.Conclusion: Most tendon marker movement was seen during the most intensive period of physiotherapy,in the second and third months after surgery. Significantly more movement was seen in the tendon markersof those patients in whom the repair failed.Level of evidence: Level I, Prospective Cohort, Prognosis Study.! 2011 Journal of Shoulder and Elbow Surgery Board of Trustees.
Keywords: Rotator cuff; failure; gap formation; RSA; repair; ultrasound
Monro14 first recorded a tear of the rotator cuff in 1778.Orthopaedic surgeons have now been attempting to repairsuch tears for over 100 years.3 Many studies have shown
a significant benefit from repair of the torn rotatorcuff.3,8,9,13 However, high rates of failure of rotator cuffrepairs have been reported with both open and arthroscopictechniques.8,13 There is still a high rate of satisfactionamong patients with failed repairs, most likely because ofthe pain-relieving benefits of the operation.8,13 Studies inthe past have looked at the mechanical causes of repairfailure,6,10,16 such as the strength of different suturingtechniques and the way in which sutures may cut through
Ethical approval was awarded by the Riverside Research Ethics Committee(RREC 3643).
*Reprint requests: Tobias K.A. Baring, MRCS, Department of Ortho-paedic Surgery, St Mary’s Hospital, London W2 1PG, England.
E-mail address: [email protected] (T.K.A. Baring).
J Shoulder Elbow Surg (2011) 20, 1194-1199
www.elsevier.com/locate/ymse
1058-2746/$ - see front matter ! 2011 Journal of Shoulder and Elbow Surgery Board of Trustees.doi:10.1016/j.jse.2011.04.010
woensdag 21 maart 12

A SYSTEMATIC REVIEW OF REHABILITATION PROTOCOLS FOLLOWING ARTHROSCOPIC REPAIR OF ROTATOR CUFF
REPAIRSDONALDSON, WRIGHT, FUNK SECEC 2011
• “ there was insufficiënt evidence in any of the papers for the protocols or exercises advocated in the rehabilitaion programs ”
woensdag 21 maart 12

STANDARD SHOULDER PRACTICELEFTLEY , FUNK 2006
• schouderchirurgen
• 3 tot 6 weken immobiliseren
• weerstandstraining na 6 weken
• sportspecifieke training na 12 weken
• terugkeer sport 6-8 maanden
• fysiotherapeuten
• PROM & AROM week 1 “safe zone “
• gecontroleerde weerstand training week 2
• eindstandig weerstand 6-8 weken
• terugkeer sport na 3 maanden
woensdag 21 maart 12

REVALIDATIE NA ARTHROSCOPISCHE REPAIR
woensdag 21 maart 12

• weefsel ingroei
• ROM
• scapula en houding
• spieractiviteit / recrutering/ timing
• gedoseerd belasten TECHNIEK !!
• belast pijnvrij
• herstel functionele activiteit
SLEUTELS TOT SUCCES
1. McGann PD et al ( 1993) A kinematic and electromyographic study of shoulder rehabilitation exercises. Clin Orthop Rel Res 288(March); 179-188
2. Hintermeister RA et al (1998) Electromyographic Activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 26(2);210-220
3. Uhl T et al (2003) Shoulder Musculature activation during upper extremity weight bearing exercise. J Ortho Sports Phys Ther 33(3);109-117
4. Moseley JB et al (1992) EMG analysis of the scapular muscles during a shoulder rehabilitation program. 20(2); 128-134
woensdag 21 maart 12

SUCCES FALENA) INTEGRITEIT VAN HECHTING EN WEEFSELKWALITEIT
B) HERWINNEN VAN DYNAMISCHE STABILITEIT
woensdag 21 maart 12

AANDACHTS PUNTEN
beschermingROM
actief oefenenfunctionele activiteit
woensdag 21 maart 12

BESCHERMING
bescherm reparatie gebied“bevorder” weefsel herstelP- abductie 30-45 graden *
minder trek in scapulair vlakabductie en footprint contact
SLING 4 snel tot 8 traag weken
* Hatakeyama et al 2001
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Afwijkendneurologisch of radiologisch
functioneel beperkt
herhaald specifieke-gewrichtsbeweging
-houding
beperkingen van componenten of
- interacties
bewegings- beperkingen
syndromen van bewegings-beperkingen
Het kinesiopathologisch model van Shirley A. Sahrmann
woensdag 21 maart 12

WEEK 1 - 4BESCHERMING EN PROM
posturaal, scapulair.
abductie kussen 4 weken
PROM scapulaire vlak
Passief = FT *
PROM gunstig Trekkacht **
elleboog/hand ROM en actief
*Dockery et al 1998, ** Park JY et al 2008, Park MC 2007, Killian et al 2012
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Afwijkendneurologisch of radiologisch
functioneel beperkt
herhaald specifieke-gewrichtsbeweging
-houding
beperkingen van componenten of
- interacties
bewegings- beperkingen
syndromen van bewegings-beperkingen
Het kinesiopathologisch model van Shirley A. Sahrmann
woensdag 21 maart 12

WEEK 4 - 8PROM EN ACTIEF OEFENEN
Afbouw abductiekussen
passief full rom op geleide van pijn
geleid actief tot 90 graden pijnvrij
actief oefenen Fs nivo 3gesloten keten > open *
Propriocepsis ! **
* Kibler, Livingston, 2001 - Veeger, van der Helm , 2007** Edmonds 2003
woensdag 21 maart 12

woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Afwijkendneurologisch of radiologisch
functioneel beperkt
herhaald specifieke-gewrichtsbeweging
-houding
beperkingen van componenten of
- interacties
bewegings- beperkingen
syndromen van bewegings-beperkingen
Het kinesiopathologisch model van Shirley A. Sahrmann
woensdag 21 maart 12

WEEK 8 - 12ACTIEF OEFENEN
posturaal, scapulair, exo/endo, tonisch recruteren
actief full ROM zonder pijn
ER / ENDO PROM ER/IR @ 90 grd abductie scapulair vlak ER/IR @ 30/45 grd abductie scapulair vlakvervolg ER/IR @ 0 grd abductie weken later
BLBK145-Gross February 13, 2009 20:34
18 Basic Concepts of Physical Examination Chapter 2
Figure 2.2 Normal posterior view.
Figure 2.3 Calcaneal valgus deformity.
(a)
(b)
Figure 2.4 Genu varum (a) and valgum (b) deformities.
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Afwijkendneurologisch of radiologisch
functioneel beperkt
herhaald specifieke-gewrichtsbeweging
-houding
beperkingen van componenten of
- interacties
bewegings- beperkingen
syndromen van bewegings-beperkingen
Het kinesiopathologisch model van Shirley A. Sahrmann
woensdag 21 maart 12

VANAF WEEK 12ACTIEF OEFENEN EN FUNCTIONELE ACTIVITEITEN
passief full ROM actief full ROM
optimaliseren musculaire activiteit ADL gericht
optimaliseren techniek sportgericht
woensdag 21 maart 12

Basismusculoskeletaal
Modulatieneurologisch
Biomechanischstatiek dynamiek
Onderhoudhart long stofw.
Optimale functie
vanzelfsprekend ??
herwinnen dynamische stabiliteitverandering anatomie
weefselkwaliteitingroei
woensdag 21 maart 12

“....the biology of soft tissue and bone healing is paramount to the outcome and success of our practice”.
Lattermann, Fu, Gene therapy in orthopaedics. In; gene therapy and tissue engineering in orthopaedic and sports medicine. Huard, Fu (eds ), 2000, Birkhäuser Boston.
woensdag 21 maart 12

woensdag 21 maart 12