Detectiemethoden voor medicatie- gerelateerde problemen maart... · Gestopte medicatie ICD-9...
28
© 2008 Universitair Ziekenhuis Gent 1 Detectiemethoden voor medicatie- gerelateerde problemen Hoe kunnen wij problemen detecteren om ze beter te voorkomen Hugo Robays UZGent 11 maart 2008
Transcript of Detectiemethoden voor medicatie- gerelateerde problemen maart... · Gestopte medicatie ICD-9...
© 2008 Universitair Ziekenhuis Gent 1
Detectiemethoden voor medicatie-gerelateerde problemen
Hoe kunnen wij problemen detecteren om ze beter te voorkome n
Hugo RobaysUZGent
11 maart 2008
22© 2008 Universitair Ziekenhuis Gent
overzicht
1. Terminologie en scoop2. Methodes
1. Exploratie1. Bronnen2. Tijdstip
3. Data-mining
2. Rapportering3. Observatie
3. Exit
33© 2008 Universitair Ziekenhuis Gent
TE
RM
INO
LOG
IE
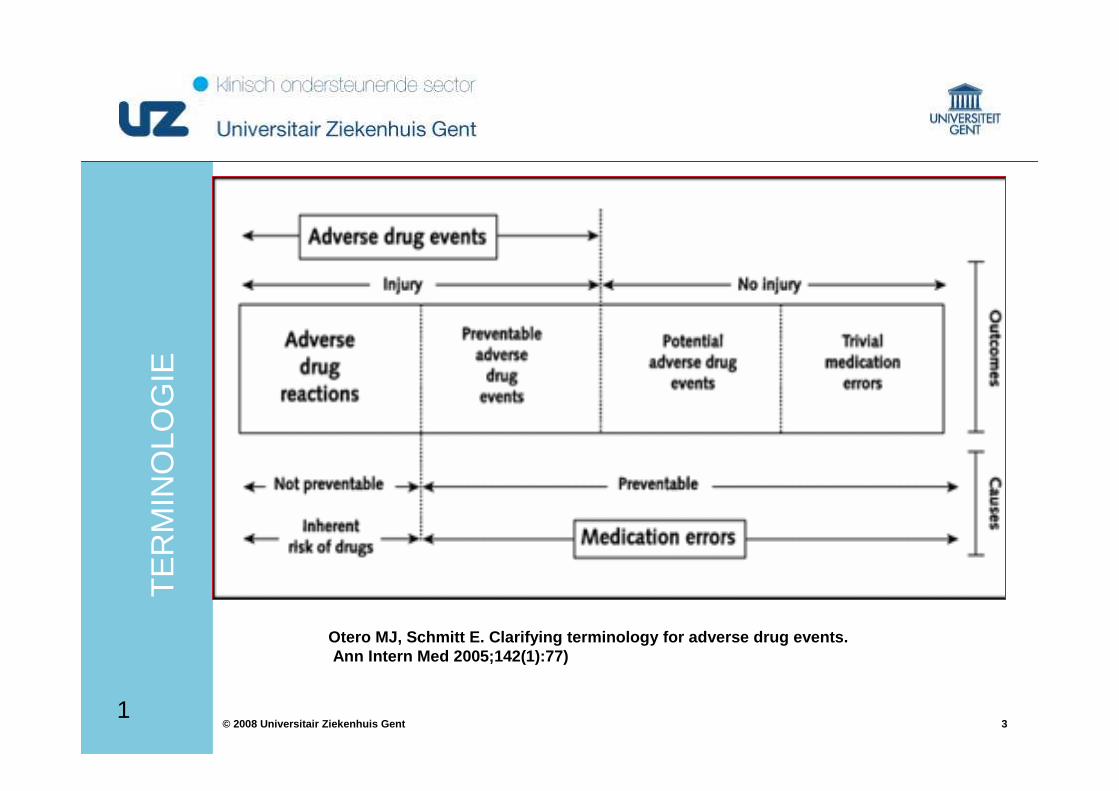
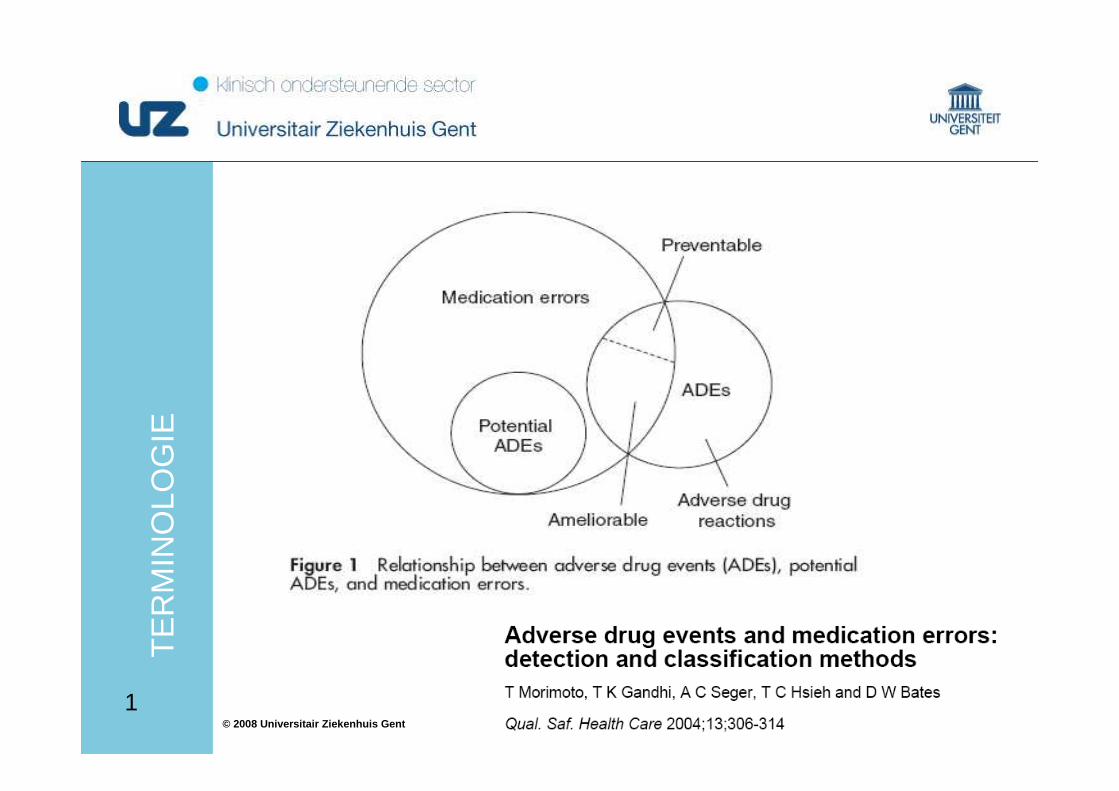
Otero MJ, Schmitt E. Clarifying terminology for adv erse drug events.Ann Intern Med 2005;142(1):77)
1
44© 2008 Universitair Ziekenhuis Gent
TE
RM
INO
LOG
IE
1
55© 2008 Universitair Ziekenhuis Gent
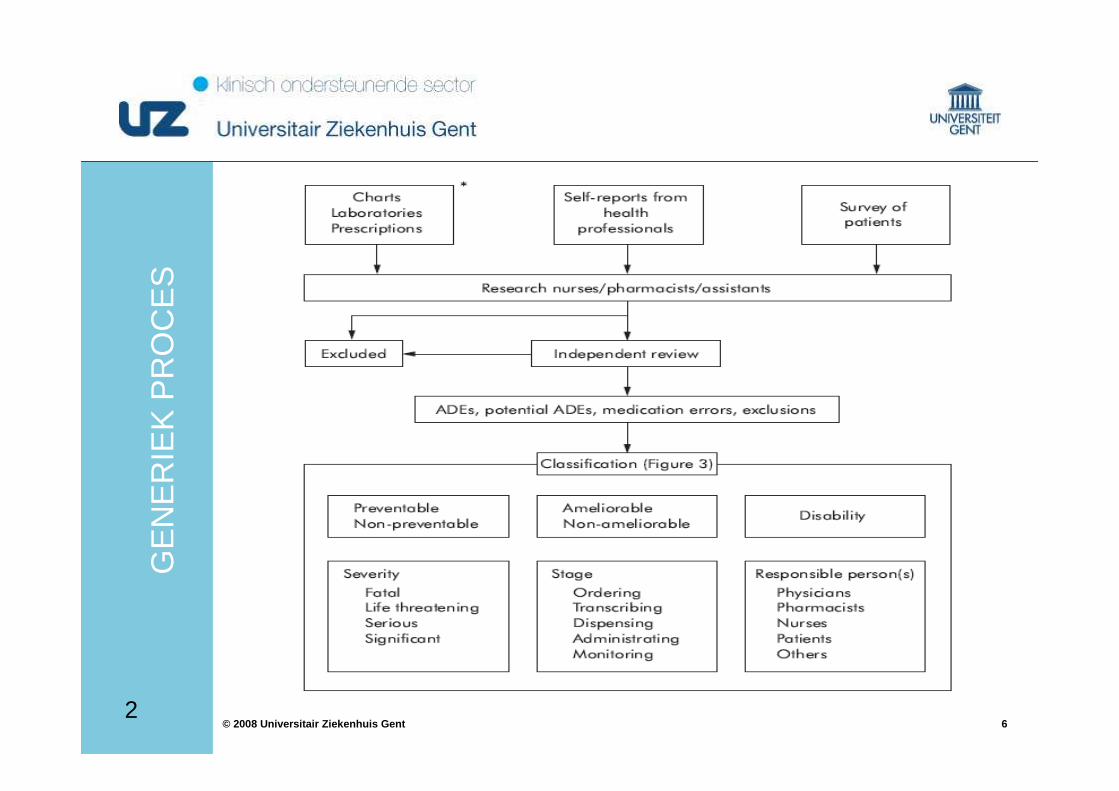
1. ExploratieVan praktijkdata (m.b.v. triggers)
2. RapporteringDoor zorgverstrekker, door patiënt
3. Observatie:Door zorgverstrekker of externe observator3
ME
TH
OD
ES
2
66© 2008 Universitair Ziekenhuis Gent
GE
NE
RIE
K P
RO
CE
S
2
77© 2008 Universitair Ziekenhuis Gent
Oorzakelijk verband en confounders
Patiënt: Risicofactoren als leeftijd, geslacht, ziekte en ernstgraad, comorbiditeit, nier en leverfunctie
Geneesmiddel:Dosis, duur, toxiciteit, frequentie, nieuw geneesmiddel?
WaarnemingVorige rapporten, tijdstip, ziekte-opflakkering, nieuw medisch probleem
88© 2008 Universitair Ziekenhuis Gent
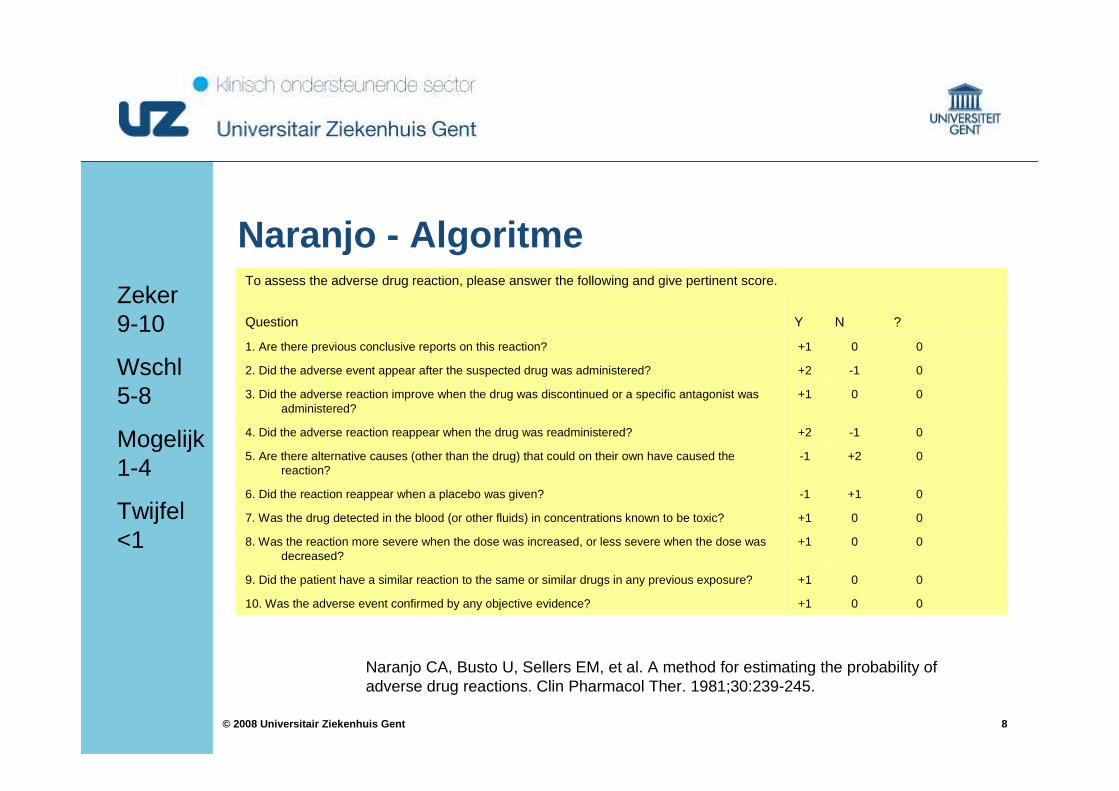
00+110. Was the adverse event confirmed by any objective evidence?
00+19. Did the patient have a similar reaction to the same or similar drugs in any previous exposure?
00+18. Was the reaction more severe when the dose was increased, or less severe when the dose was decreased?
00+17. Was the drug detected in the blood (or other fluids) in concentrations known to be toxic?
0+1-16. Did the reaction reappear when a placebo was given?
0+2-15. Are there alternative causes (other than the drug) that could on their own have caused the reaction?
0-1+24. Did the adverse reaction reappear when the drug was readministered?
00+13. Did the adverse reaction improve when the drug was discontinued or a specific antagonist was administered?
0-1+22. Did the adverse event appear after the suspected drug was administered?
00+11. Are there previous conclusive reports on this reaction?
?NYQuestion
To assess the adverse drug reaction, please answer the following and give pertinent score.
Naranjo - Algoritme
Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-245.
Zeker 9-10
Wschl 5-8
Mogelijk 1-4
Twijfel <1
99© 2008 Universitair Ziekenhuis Gent
prak
tijkd
ata
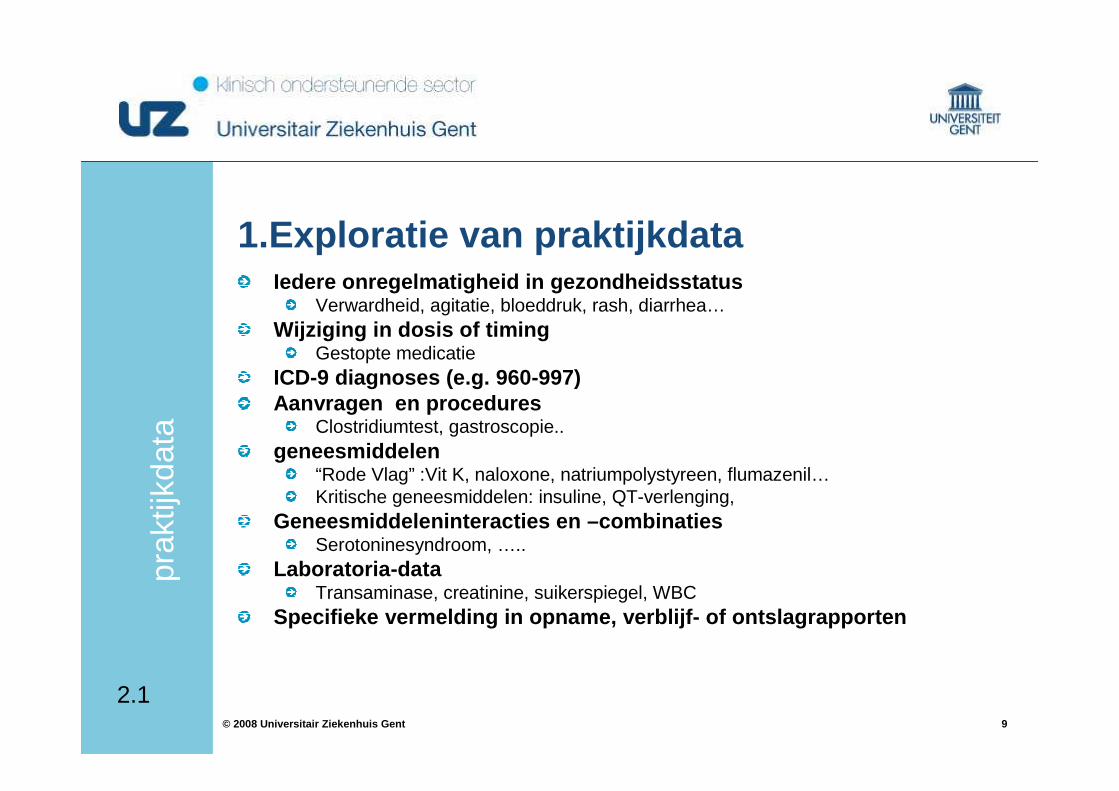
1.Exploratie van praktijkdataIedere onregelmatigheid in gezondheidsstatus
Verwardheid, agitatie, bloeddruk, rash, diarrhea…Wijziging in dosis of timing
Gestopte medicatieICD-9 diagnoses (e.g. 960-997)Aanvragen en procedures
Clostridiumtest, gastroscopie..geneesmiddelen
“Rode Vlag” :Vit K, naloxone, natriumpolystyreen, flumazenil…Kritische geneesmiddelen: insuline, QT-verlenging,
Geneesmiddeleninteracties en –combinatiesSerotoninesyndroom, …..
Laboratoria-dataTransaminase, creatinine, suikerspiegel, WBC
Specifieke vermelding in opname, verblijf- of ontsla grapporten
2.1
1010© 2008 Universitair Ziekenhuis Gent
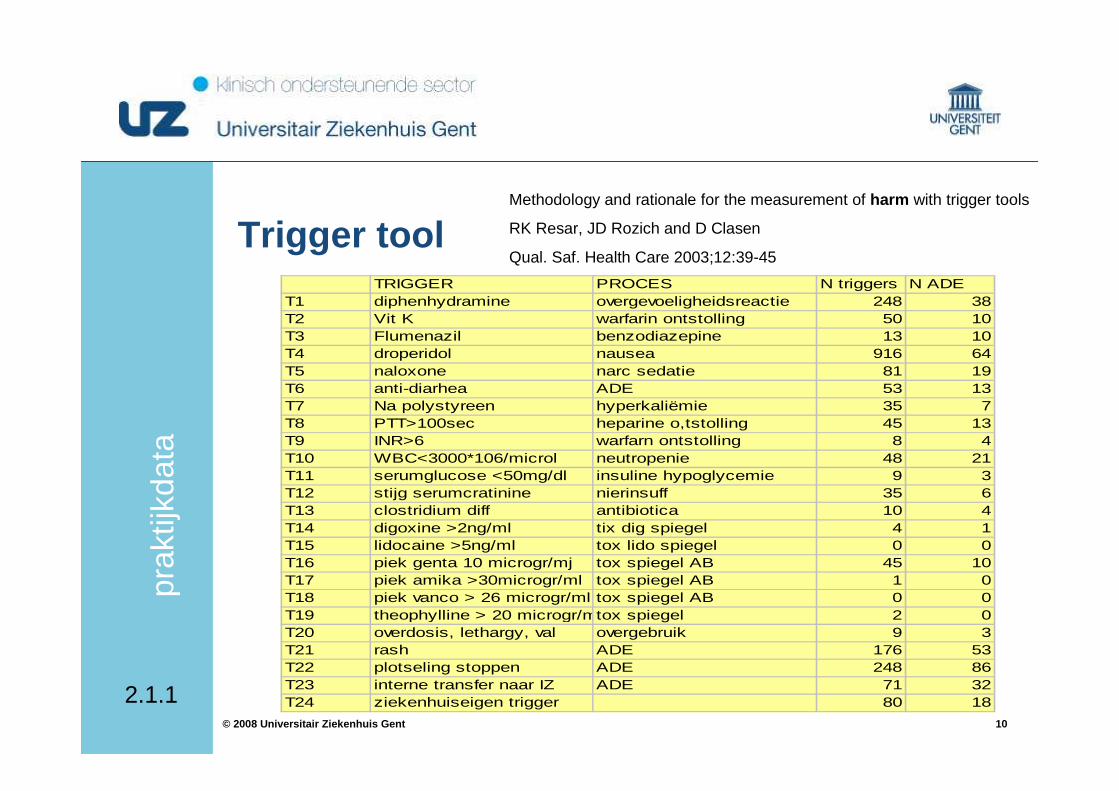
Trigger tool
prak
tijkd
ata
Methodology and rationale for the measurement of harm with trigger tools
RK Resar, JD Rozich and D Clasen
Qual. Saf. Health Care 2003;12:39-45
TRIGGER PROCES N triggers N ADET1 diphenhydramine overgevoeligheidsreactie 248 38T2 Vit K warfarin ontstolling 50 10T3 Flumenazil benzodiazepine 13 10T4 droperidol nausea 916 64T5 naloxone narc sedatie 81 19T6 anti-diarhea ADE 53 13T7 Na polystyreen hyperkaliëmie 35 7T8 PTT>100sec heparine o,tstolling 45 13T9 INR>6 warfarn ontstolling 8 4T10 WBC<3000*106/microl neutropenie 48 21T11 serumglucose <50mg/dl insuline hypoglycemie 9 3T12 stijg serumcratinine nierinsuff 35 6T13 clostridium diff antibiotica 10 4T14 digoxine >2ng/ml tix dig spiegel 4 1T15 lidocaine >5ng/ml tox lido spiegel 0 0T16 piek genta 10 microgr/mj tox spiegel AB 45 10T17 piek amika >30microgr/ml tox spiegel AB 1 0T18 piek vanco > 26 microgr/ml tox spiegel AB 0 0T19 theophylline > 20 microgr/mltox spiegel 2 0T20 overdosis, lethargy, val overgebruik 9 3T21 rash ADE 176 53T22 plotseling stoppen ADE 248 86T23 interne transfer naar IZ ADE 71 32T24 ziekenhuiseigen trigger 80 182.1.1
1111© 2008 Universitair Ziekenhuis Gent
Wel
ke m
etho
de
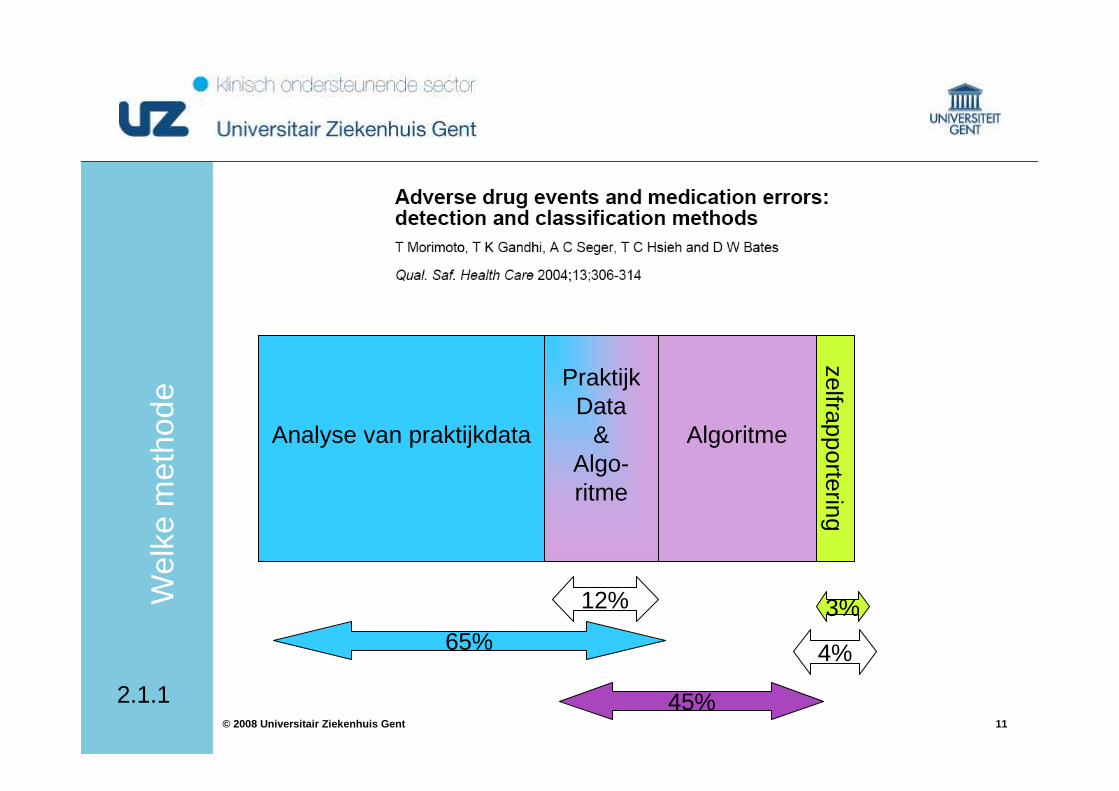
Analyse van praktijkdata
PraktijkData
&Algo-ritme
Algoritme
zelfrapportering
12%
65%
45%
3%
4%
2.1.1
1212© 2008 Universitair Ziekenhuis Gent
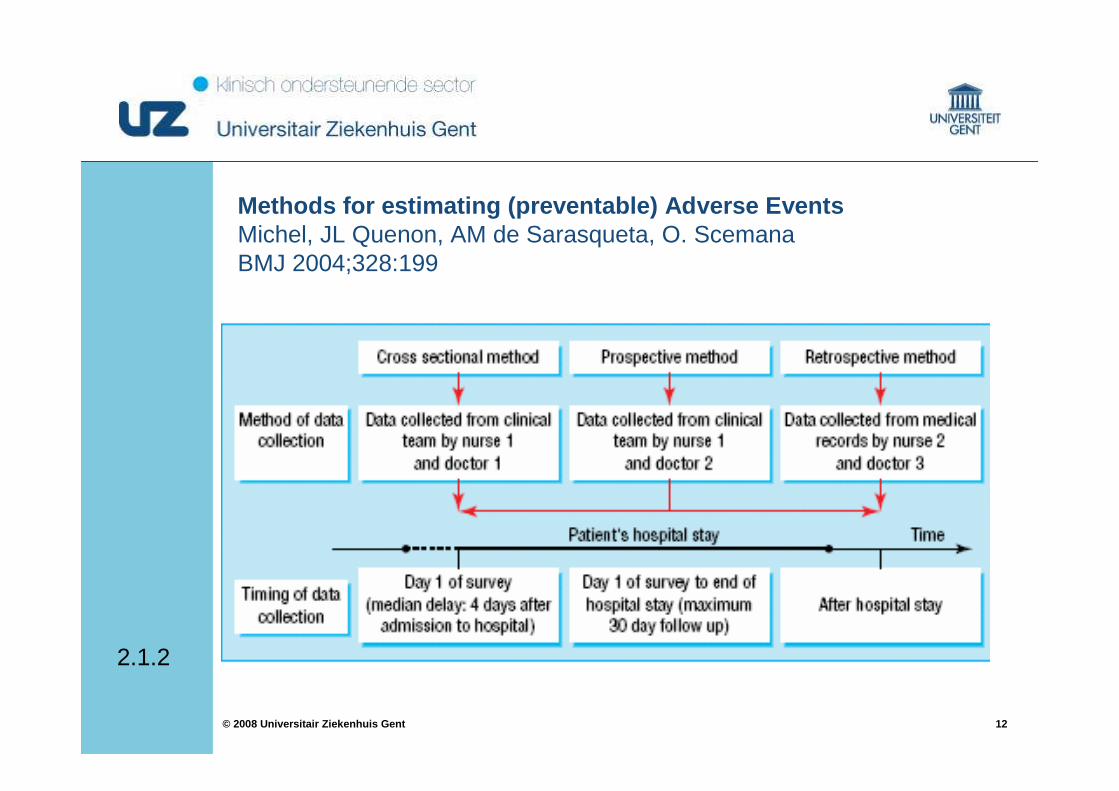
Methods for estimating (preventable) Adverse EventsMichel, JL Quenon, AM de Sarasqueta, O. ScemanaBMJ 2004;328:199
2.1.2
1313© 2008 Universitair Ziekenhuis Gent
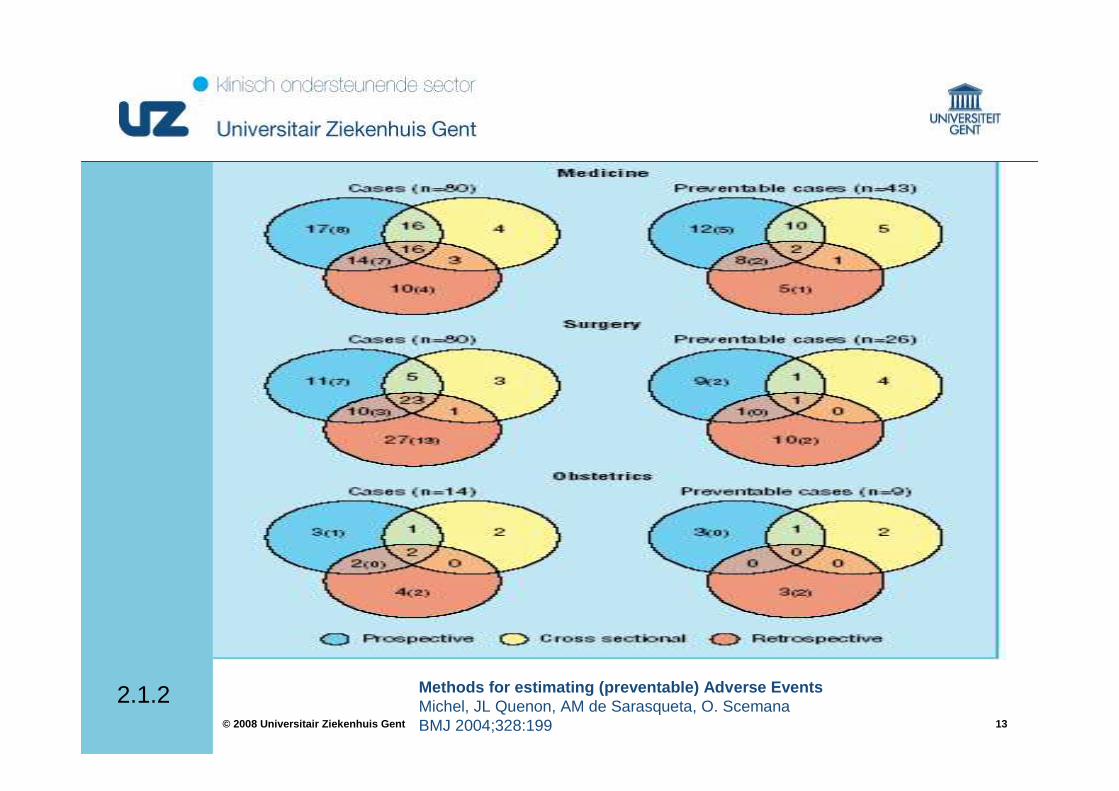
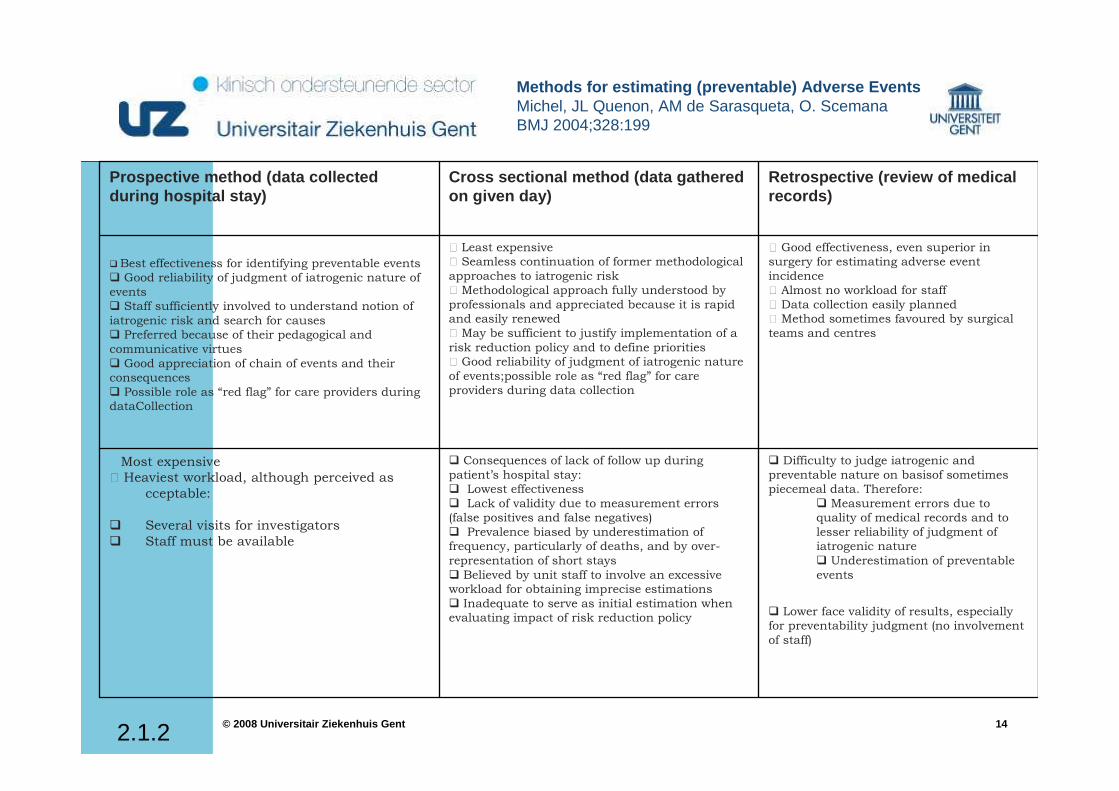
Methods for estimating (preventable) Adverse EventsMichel, JL Quenon, AM de Sarasqueta, O. ScemanaBMJ 2004;328:199
2.1.2
1414© 2008 Universitair Ziekenhuis Gent
� Difficulty to judge iatrogenic and
preventable nature on basisof sometimes
piecemeal data. Therefore:
� Measurement errors due to
quality of medical records and to
lesser reliability of judgment of
iatrogenic nature
� Underestimation of preventable
events
� Lower face validity of results, especially
for preventability judgment (no involvement
of staff)
� Consequences of lack of follow up during
patient’s hospital stay:
� Lowest effectiveness
� Lack of validity due to measurement errors
(false positives and false negatives)
� Prevalence biased by underestimation of
frequency, particularly of deaths, and by over-
representation of short stays
� Believed by unit staff to involve an excessive
workload for obtaining imprecise estimations
� Inadequate to serve as initial estimation when
evaluating impact of risk reduction policy
� Most expensive
+ Heaviest workload, although perceived as
cceptable:
� Several visits for investigators
� Staff must be available
+ Good effectiveness, even superior in
surgery for estimating adverse event
incidence
+ Almost no workload for staff
+ Data collection easily planned
+ Method sometimes favoured by surgical
teams and centres
+ Least expensive
+ Seamless continuation of former methodological
approaches to iatrogenic risk
+ Methodological approach fully understood by
professionals and appreciated because it is rapid
and easily renewed
+ May be sufficient to justify implementation of a
risk reduction policy and to define priorities
+ Good reliability of judgment of iatrogenic nature
of events;possible role as “red flag” for care
providers during data collection
� Best effectiveness for identifying preventable events
� Good reliability of judgment of iatrogenic nature of
events
� Staff sufficiently involved to understand notion of
iatrogenic risk and search for causes
� Preferred because of their pedagogical and
communicative virtues
� Good appreciation of chain of events and their
consequences
� Possible role as “red flag” for care providers during
dataCollection
Retrospective (review of medical records)
Cross sectional method (data gathered on given day)
Prospective method (data collected during hospital stay)
Methods for estimating (preventable) Adverse EventsMichel, JL Quenon, AM de Sarasqueta, O. ScemanaBMJ 2004;328:199
2.1.2
1515© 2008 Universitair Ziekenhuis Gent
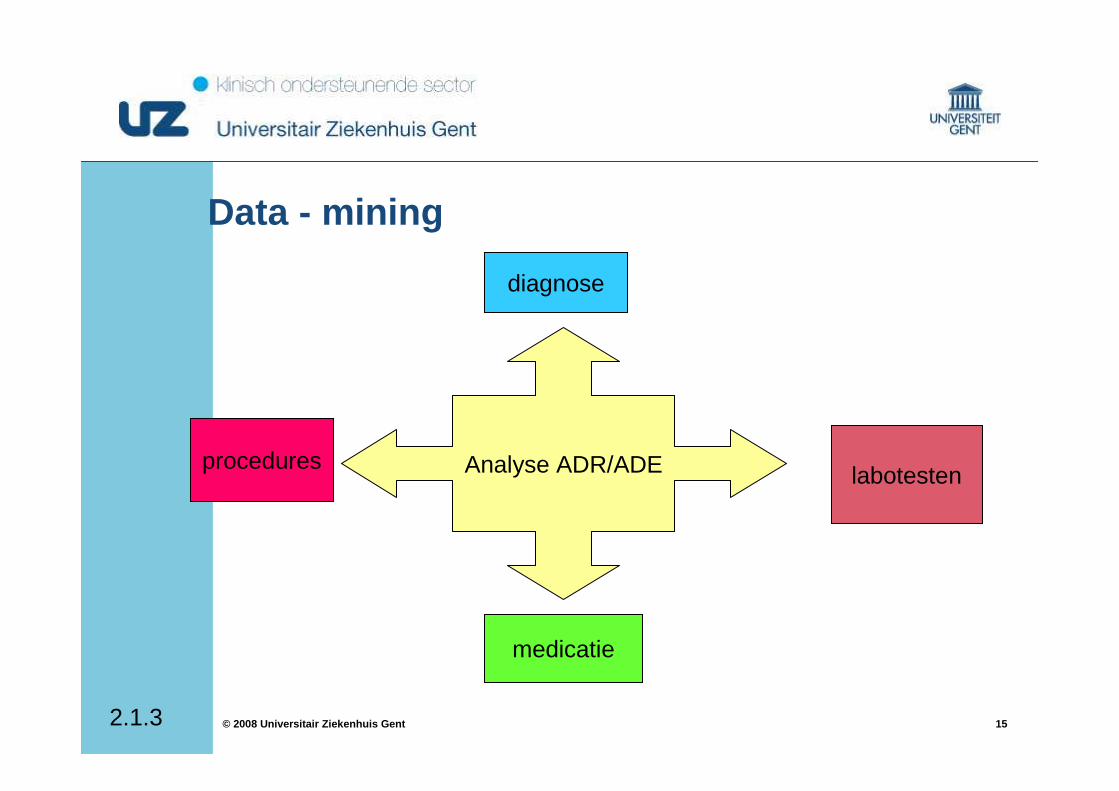
Data - mining
2.1.3
Analyse ADR/ADE labotesten
medicatie
diagnose
procedures
1616© 2008 Universitair Ziekenhuis Gent
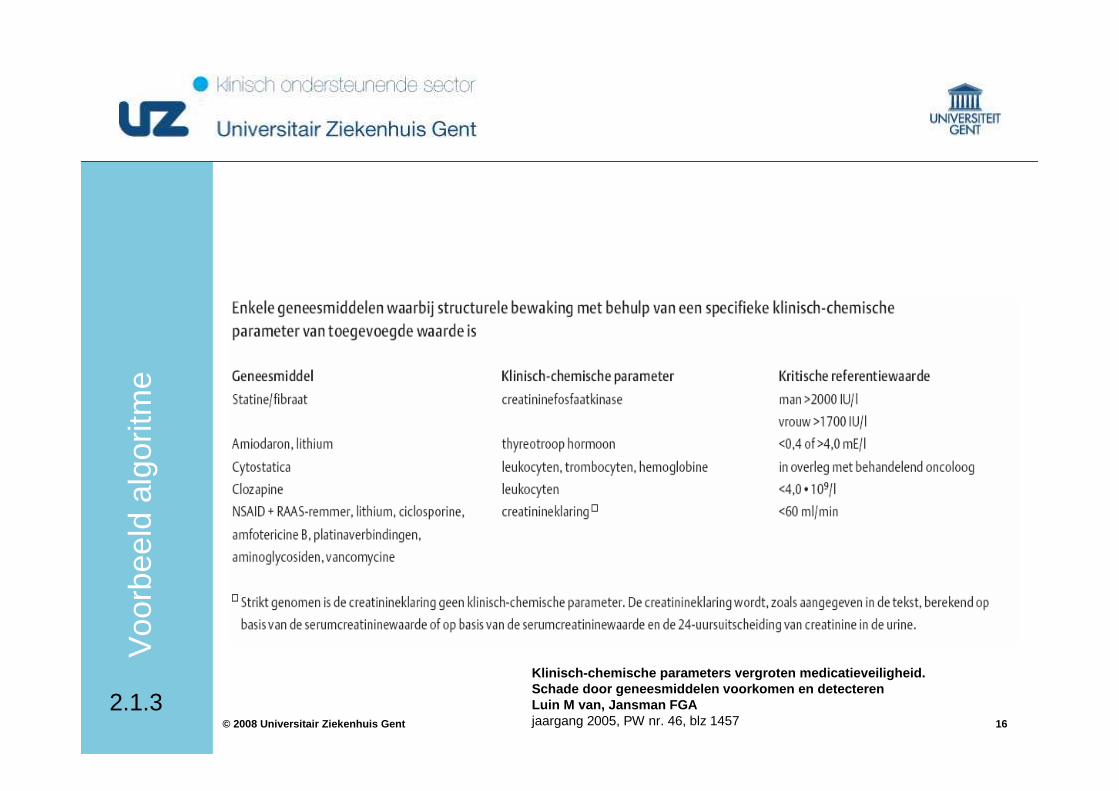
Klinisch-chemische parameters vergroten medicatieve iligheid. Schade door geneesmiddelen voorkomen en detecteren Luin M van, Jansman FGAjaargang 2005, PW nr. 46, blz 1457
2.1.3
Voo
rbee
ld a
lgor
itme
1717© 2008 Universitair Ziekenhuis Gent
Rap
port
erin
g do
or
zorg
vers
trek
ker
Onderrapportering doorGebrek aan cultuur & bewustmakingAansprakelijkheid
Declaratie aan verzekering voor beroepsaansprakelijkheid
Belangrijk != Expliciete vraag tot verandering
->terugkoppeling is vitaal
2. Rapportering
2.2
1818© 2008 Universitair Ziekenhuis Gent
1. Rapporteringscultuur: basis = vertrouwen2. Analyse van incidenten, bijna-incidenten
FONA : Faults or Near AccidentsFOBO : Fouten of bijna-fouten
3. Opzetten en meten van verbeteracties
“Without a detailed analysis of incidents and near misses, we have no way of knowing where the edge is until we fallover it” (J. Reason)
• fouten verwachten• personeel trainen om fouten te ontdekken en te vermijden• fouten en bijna-fouten bespreken• op fouten anticiperen• zoeken naar systeemverbeteringen
2.2
1919© 2008 Universitair Ziekenhuis Gent
Centrale meldpuntenVS: ISMP (www.ismp.org)Frankrijk: AAQTE - REEM (www.adiph.org/aaqte/)
UK: NHS - NPSA (www.npsa.nhs.uk)
FDA: MedwatchInitiatieven in Nederland (NVZA!), Spanje (ISMP),…
Lokale meldpuntenVS: “risk comité” per ziekenhuisUK: NHS Trust ziekenhuizen: motivatie voor lokale rapportering
Initiatieven in Nederland (Zwolle, Delft,…), Spanje,...
2.2
2020© 2008 Universitair Ziekenhuis Gent
Het vermijdbare vermijden: beleidsnota
Het bevorderen van een cultuur van veiligheid als prioriteit, waarbij de nadruk ligt op een lerende cultuur en afgestapt wordt van een verwijt- en penalisatiecultuurHet informatief en actief betrekken van de patiënt/ fam ilie in het zorgproces om de veiligheid te verhogenHet ontwikkelen van meldsystemen voor het verzamelen van gestandaardiseerde informatie over aard en omvang v an vermijdbare schade Het systematisch analyseren van bestaande gegevensbronnen (systematische rapportering van incidenten en defecten, klachten van patiënten, klinische data bases…) Het informatief en actief betrekken van de patiënt/ fam ilie in het zorgproces om de veiligheid te verhogenHet creëren van een juridisch kader opdat meldsystemen optimaal kunnen funtioneren en de melder van het in cident beschermd wordt
Pat
iënt
veili
ghei
d:
bele
idsn
ota
2.2
2121© 2008 Universitair Ziekenhuis Gent
3. observatie
Prospectieve methodeVoornamelijk nuttig bij toedieningsfoutenDisguised ?Kan belangrijke systematische tekorkomingen aangevenInterne benchmarkExemplarisch voor discussie en mogelijke wijziging i n attitudeTijdsinvesteringRisico-analyse is mogelijk
(root-cause, bow-tie, failure mode and effect analysis)
obse
rvat
ie
2.3
2222© 2008 Universitair Ziekenhuis Gent
observatie
Continue registratie2x check, uitgifte
Periodische intensieve registratieProspectiefCross-sectioneel
Aan
pak
obse
rvat
ie
2.3
2323© 2008 Universitair Ziekenhuis Gent
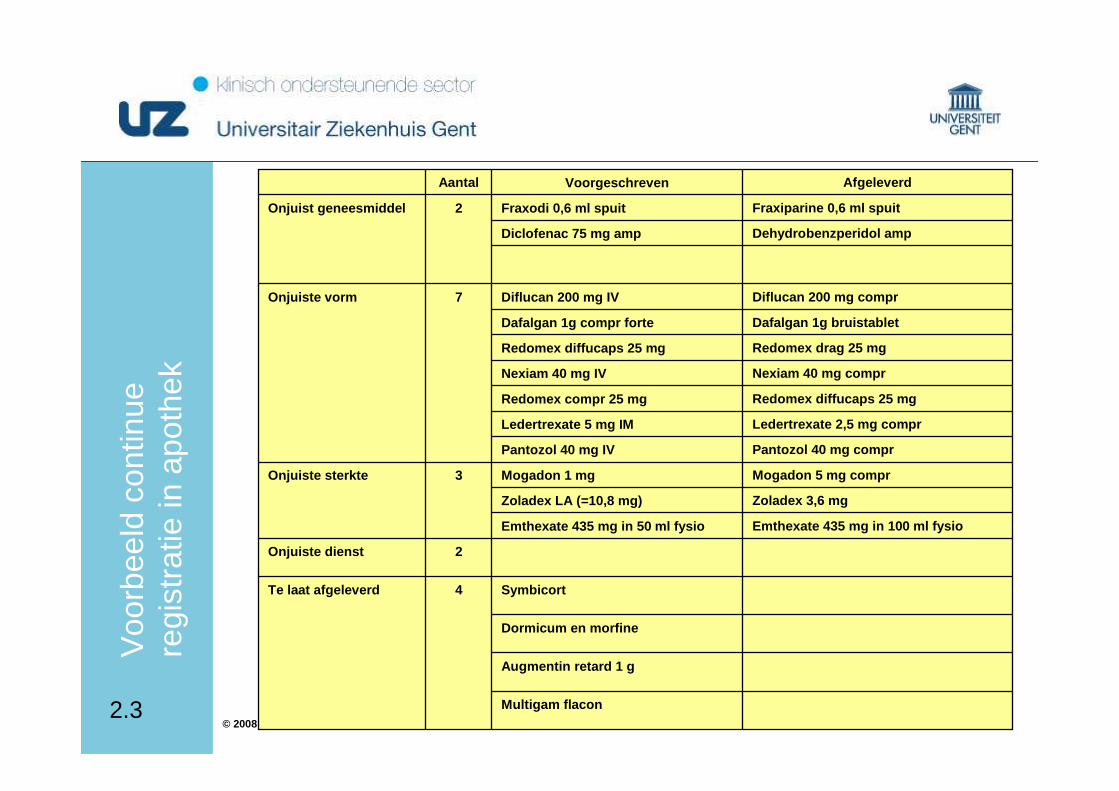
Multigam flacon
Augmentin retard 1 g
Dormicum en morfine
Symbicort4Te laat afgeleverd
2Onjuiste dienst
Emthexate 435 mg in 100 ml fysioEmthexate 435 mg in 50 ml fysio
Zoladex 3,6 mg Zoladex LA (=10,8 mg)
Mogadon 5 mg comprMogadon 1 mg3Onjuiste sterkte
Pantozol 40 mg comprPantozol 40 mg IV
Ledertrexate 2,5 mg comprLedertrexate 5 mg IM
Redomex diffucaps 25 mgRedomex compr 25 mg
Nexiam 40 mg comprNexiam 40 mg IV
Redomex drag 25 mgRedomex diffucaps 25 mg
Dafalgan 1g bruistabletDafalgan 1g compr forte
Diflucan 200 mg comprDiflucan 200 mg IV7Onjuiste vorm
Dehydrobenzperidol ampDiclofenac 75 mg amp
Fraxiparine 0,6 ml spuitFraxodi 0,6 ml spuit2Onjuist geneesmiddel
AfgeleverdVoorgeschrevenAantal
Voo
rbee
ld c
ontin
ue
regi
stra
tie in
apo
thek
2.3
2424© 2008 Universitair Ziekenhuis Gent
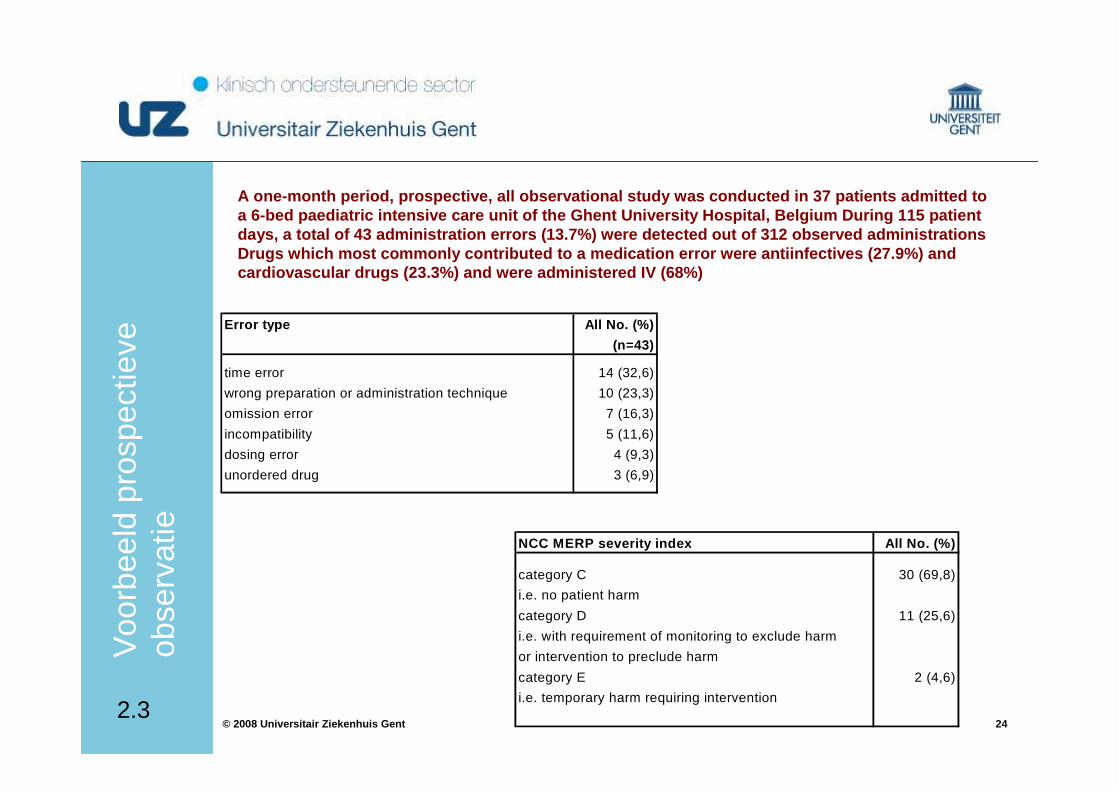
A one-month period, prospective, all observational study was conducted in 37 patients admitted to a 6-bed paediatric intensive care unit of the Ghent University Hospital, Belgium During 115 patient days, a total of 43 administration errors (13.7%) w ere detected out of 312 observed administrations Drugs which most commonly contributed to a medicati on error were antiinfectives (27.9%) and cardiovascular drugs (23.3%) and were administered IV (68%)
Error type All No. (%)
(n=43)
time error 14 (32,6)
wrong preparation or administration technique 10 (23,3)
omission error 7 (16,3)
incompatibility 5 (11,6)
dosing error 4 (9,3)
unordered drug 3 (6,9)
NCC MERP severity index All No. (%)
category C 30 (69,8)
i.e. no patient harm
category D 11 (25,6)
i.e. with requirement of monitoring to exclude harm
or intervention to preclude harm
category E 2 (4,6)
i.e. temporary harm requiring intervention
Voo
rbee
ld p
rosp
ectie
ve
obse
rvat
ie
2.3
2525© 2008 Universitair Ziekenhuis Gent
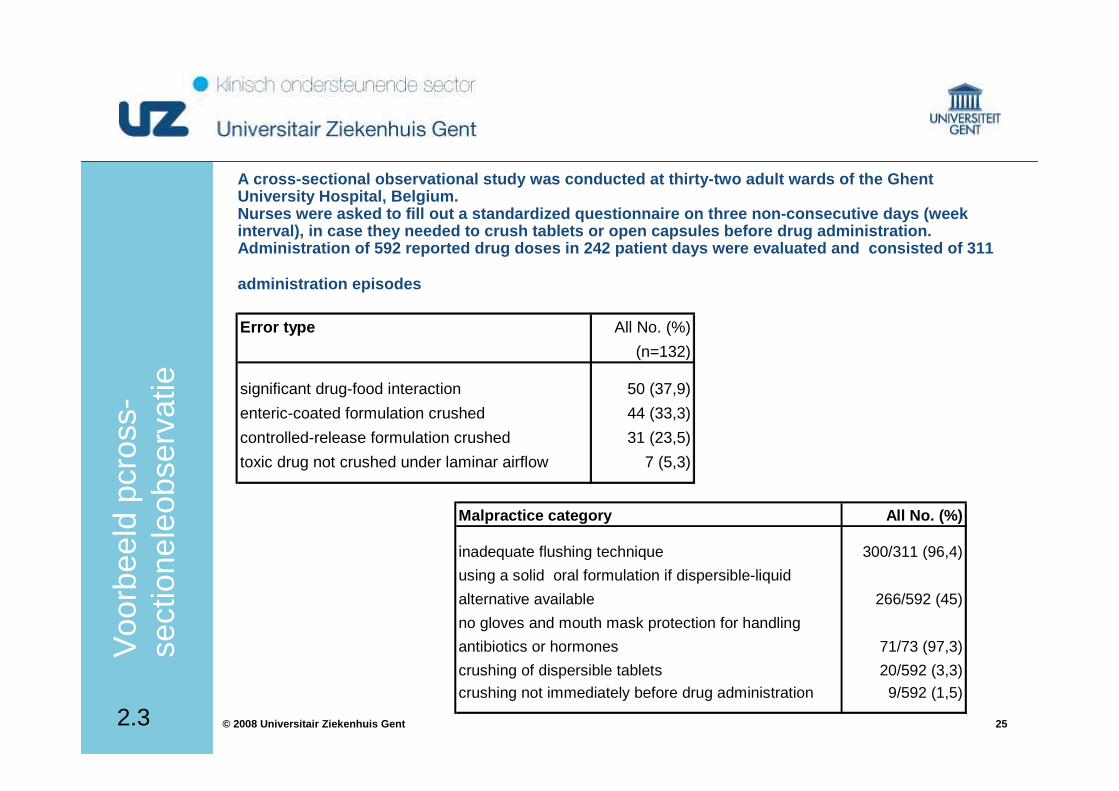
A cross-sectional observational study was conducted at thirty-two adult wards of the Ghent University Hospital, Belgium. Nurses were asked to fill out a standardized questi onnaire on three non-consecutive days (week interval), in case they needed to crush tablets or open capsules before drug administration. Administration of 592 reported drug doses in 242 pa tient days were evaluated and consisted of 311
administration episodes
Error type All No. (%)
(n=132)
significant drug-food interaction 50 (37,9)
enteric-coated formulation crushed 44 (33,3)
controlled-release formulation crushed 31 (23,5)
toxic drug not crushed under laminar airflow 7 (5,3)
Malpractice category All No. (%)
inadequate flushing technique 300/311 (96,4)
using a solid oral formulation if dispersible-liquid
alternative available 266/592 (45)
no gloves and mouth mask protection for handling
antibiotics or hormones 71/73 (97,3)
crushing of dispersible tablets 20/592 (3,3)
crushing not immediately before drug administration 9/592 (1,5)
Voo
rbee
ld p
cros
s-se
ctio
nele
obse
rvat
ie
2.3
2626© 2008 Universitair Ziekenhuis Gent
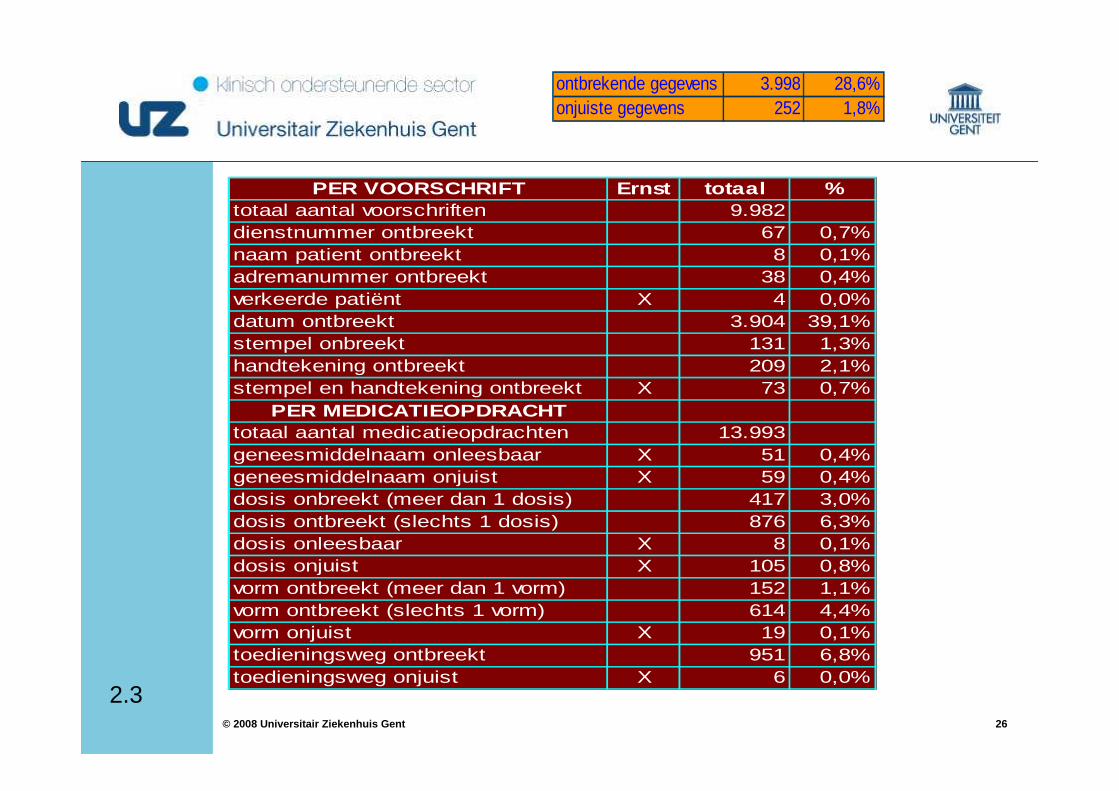
PER VOORSCHRIFT Ernst totaal %totaal aantal voorschriften 9.982dienstnummer ontbreekt 67 0,7%naam patient ontbreekt 8 0,1%adremanummer ontbreekt 38 0,4%verkeerde patiënt X 4 0,0%datum ontbreekt 3.904 39,1%stempel onbreekt 131 1,3%handtekening ontbreekt 209 2,1%stempel en handtekening ontbreekt X 73 0,7%
PER MEDICATIEOPDRACHTtotaal aantal medicatieopdrachten 13.993geneesmiddelnaam onleesbaar X 51 0,4%geneesmiddelnaam onjuist X 59 0,4%dosis onbreekt (meer dan 1 dosis) 417 3,0%dosis ontbreekt (slechts 1 dosis) 876 6,3%dosis onleesbaar X 8 0,1%dosis onjuist X 105 0,8%vorm ontbreekt (meer dan 1 vorm) 152 1,1%vorm ontbreekt (slechts 1 vorm) 614 4,4%vorm onjuist X 19 0,1%toedieningsweg ontbreekt 951 6,8%toedieningsweg onjuist X 6 0,0%
ontbrekende gegevens 3.998 28,6%onjuiste gegevens 252 1,8%
2.3
2727© 2008 Universitair Ziekenhuis Gent
Het vermijdbare vermijden: beleidsnota
Het ontwikkelen van opleidings- en bijscholingsprogramma’svoor alle zorgprofessionals en het management waari n patiëntveiligheid een vast onderdeel wordt, met inbegrip van de principes van klinische besluitvorming, risicobewus twording, risicocommunicatie, risicopreventie en het omgaan m et incidenten
Het aanmoedigen van de zorginstellingen, daarbij ge holpen door beleidsmakers en verzekeraars, om het risicobewustzijn te vergroten en om veiligheidsprogramma’s op te zetten
3
Tot
slo
t….
2828© 2008 Universitair Ziekenhuis Gent
“Weet jij welke weg ik moet volgen?”
vroeg de haas aan de uil.
“Dat hangt er van af waar je naar toe wilt”, antwoordde de uil.
“Dat weet ik niet precies”, zei de haas.
“Dan is iedere weg goed”, concludeerde de uil.(Vrij naar Lewis Carroll)
hoeveel keer staat kwaliteit van zorgop de agenda van de Raad van Bestuur?
Tot
slo
t….
3