VOL 1_n. 1_Spring 2001
29
Journal 1/01 01.05.01, 16:02 1
-
Upload
gingiasviladoconde -
Category
Documents
-
view
20 -
download
3
Transcript of VOL 1_n. 1_Spring 2001

Journal 1/01 01.05.01, 16:021

EWMA JOURNAL 2001 VOL 1 NO 12 EWMA JOURNAL 2001 VOL 1 NO 1 3
IntroductionA very warm welcome to the first edition of the EWMA
Journal. We hope that you will find this a useful resourceand that it will help you to keep in touch with some of the
developments in wound treatment and management that are occur-ring across Europe. We plan to produce two journals this year with apossible increase in the future. In addition to the paper based jour-nal you will find further information on our web site including in-formation in the five main European languages.
The European Wound Management Association (EWMA) hasbeen in existence for a decade. As we enter a new era in theAssociation’s history we are facing new challenges. One of the mostimportant is the need to ensure we have a truly European focus.This journal is one of a number of new initiatives, which seek toaddress these issues. The journal will bring together informationconcerning wound management across Europe.
We are seeking to work in close co-operation with existing woundmanagement societies as well as helping establish associations incountries, which as yet do not have this resource. This journal willprovide space for all wound healing and management organisationsin Europe who wish to publicise information concerning activitiesin their countries. All co-operating national associations will receivecopies of the journal to distribute free to their members.
In time, we hope this journal will draw together a rich wealth ofresources concerning wound management throughout Europe.We do encourage you to join EWMA and become involved in thisexciting development.
Christine MoffattEWMA President
The EWMA Journal
ISSN number: 1609-2759
Volume 1, No. 1. Spring, 2001
The Journal of
The European Wound Management Association
At present published twice a year
Legal Responsibility
Professor Christine Moffatt, EWMA President
Editorial Board
Michelle Briggs
Carol Dealey
Brian Gilchrist
Finn Gottrup
Deborah Hofman
E. Andrea Nelson
Peter Vowden
EWMA Homepage
www.ewma.org
For membership application, correspondence,
prospective publications contact:
EWMA Secretariat
PO Box 864
London SE1 8TT
United Kingdom
Tel: +44 207 848 3496
E-mail: [email protected]
Enquiries concerning advertising should be
addressed to:
Congress Consultants
Martensens Allé 8
DK 1828 - Frederiksberg C
Denmark.
Tel: +(45) 7020 0305
Fax (+45) 7020 0315
E-mail: [email protected]
Layout:
Birgitte Clematide and Claus Fenger
Printed by:
Kailow Tryk A/S, Denmark
Prices:
Distributed Free to Members of the European Wound
Management Association and members of Co-
operating Associations
Individual subscription: 7.50 €
Libraries and Institutions 25 €
The next issue will be published in November, 2001
Prospective material for publication must be with the
editors as soon as possible and in no case later than
July 31st. 2001
The contents of articles and letters in the EWMA
Journal do not necessarily reflect the opinions of the
Editors or the European Wound Management
Association.
The copyright of all published material and illustra-
tions is the property of The European Wound
Management Association. However, provided prior
written consent for their reproduction is obtained from
both the Author and EWMA via the Editorial Board of
the Journal, and proper acknowledgement made and
printed, such permission will normally be readily
granted.
Requests to reproduce material should state where
the material is to be published, and, if it is abstracted,
summarised, or abbreviated then the proposed new
text should be sent to the EWMA Journal Editor for
final approval.
EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 12
Madeleine Flanagan Peter Franks
Christine Moffatt, President
Carol Dealey George Cherry Michelle Briggs
Geoff Keye
Christina Lindholm
Peter Vowden,
President Elect
Deborah Hofman, Recorder E. Andrea Nelson, Treasurer Brian Gilchrist, Secretary
Joan-Enric Torra Bou Marco Romanelli
Finn Gottrup,
Immediate Past President
EWMA Council
For contact addresses, see www.ewma.org
Journal 1/01 01.05.01, 16:032-3

EWMA JOURNAL 2001 VOL 1 NO 1 5
[Coloplast Ad]
EWMA Strategy
I t is easy as we look back over the decadesince the association’s inception to becomeeither complacent or despondent concern-
ing the progress in wound treatment andmanagement throughout Europe. EWMAholds neither of these perspectives, recognisingthat there have been numerous developmentswithin the field of wound treatment and man-agement during this time, but that huge chal-lenges lie ahead of us. One of the major tasksof council in the last year has been to evaluatethe role and function of the association as anumbrella association, which seeks to promotedevelopments through co-operation withwound healing and management organisationsthroughout Europe. The thrust of our develop-ment programme is to deepen these relation-ships and seek to work effectively at developingboth a professional and political voice forwound management. It is our belief that in co-operation we can achieve these aims.
EUROPEAN WOUND MANAGEMENT
DEVELOPMENT PROGRAMME
EWMA JournalWe are delighted to be launching the first edi-tion of the EWMA Journal. The Journal willseek to publicise the work of EWMA, as well asacting as an important resource for woundtreatment and management. The journal is be-ing managed by an editorial board elected fromcouncil. The journal aims to provide space fornational wound management associations topublicise information and to highlight initia-tives occurring in Europe, including reviews ofother conferences and educational programmesavailable. Although our first edition will be inEnglish our desire in the future is to be able to
produce the journal in the main European lan-guages.
EWMA web siteOver the last year we have been developing theEWMA web site. Our vision is that this will bea premier web site for wound management. Acentral part of the development work at presentis linking the site directly to other relevant websites in the world. We want the site to be bothvisually attractive as well as accessible and pro-vide a rich resource of information to all whovisit it. We will be seeking in particular to linkwith national wound organisations. To fulfilour commitment as a European association weare seeking to translate as much information aspossible into the different European languages.Information from the journal, as well as confer-ence abstracts, will be made available on theweb site.
International ConferencesThe most important activity that EWMA hascarried out over the last decade has been organ-ising international conferences, which bring to-gether experts from around the world. This willcontinue to be an important part of the associa-tion’s activity. However our focus will now be todevelop international conferences in co-opera-tion with national wound organisations. Themodel for this was established in Sweden lastyear when over 700 delegates attended ourlatest conference. This journal contains a shortsummary of that event. This year we aredelighted to be visiting Dublin in a joint con-ference with the Wound Management Associa-tion of Ireland, and we will be reflecting on thedecade that has passed since EWMA was
Prof. Christine Moffat
Director of the Centre for
the Research and
Implementation of
Clinical Practice.
Thames Valley University
Project Director of the
largest United Kingdom
study in Leg Ulcer
Management.
EWMA President
Legal responsible for the
EWMA Journal
Founder and President of
the Leg Ulcer Forum
Co-editor of
worldwidewounds
Journal 1/01 01.05.01, 16:034-5

EWMA JOURNAL 2001 VOL 1 NO 16
[ConvatecAd]
formed in Cardiff in 1991. The con-ferences will continue to provide animportant platform for the presenta-tion of new research and develop-ments in the field. We will be de-veloping the conferences to incorpo-rate more time for networking ofthe wound healing and managementorganisations and will be using theseopportunities for developing otherprojects such as our educational pro-grammes.
We are delighted to report that in2002 our conference will be held inGranada in partnership withGNEUAPP, the Spanish ChronicWound and Pressure Ulcer AdvisoryPanel. We are expecting around1500 to attend, so we suggest youbook now! Future conference possi-bilities include Eastern Europe aswell as a return to the United King-dom. We are also considering othertypes of conference activity includ-ing smaller meetings with more spe-
EDUCATIONAL INITIATIVES
Educational DevelopmentProgrammeOne of the most important objec-tives of EWMA is to facilitatemulti-professional education inwound treatment and managementacross Europe. An exciting initiativeis underway to develop a curricu-lum for wound education that isendorsed by representatives of allthe European countries, and is trulymulti-professional in nature. Wehope to develop, by consensus, anagreed standard against which exist-ing educational programmes can beaccredited. In addition we want toidentify all the wound managementeducational initiatives and materialswithin Europe in order to provide acentral resource for those seekingtraining opportunities. By agreeingsuch standards we may be able toinfluence the educational standardson wound treatment and manage-ment throughout Europe.
Co operation withother associationsThe development of working co-operations with other wound heal-ing and management organisationsin Europe is well under way.
The focus of this work is tofoster relationships through thedevelopment of co-operativeprojects. Participating nationalwound healing and managementorganisations will be provided withcopies of the EWMA journal fordistribution to members and willreceive a number of other benefits.Each wound management associa-tion will be provided space withinthe journal to publicise their ownactivities. Other incentives will in-clude a number of free registrationsat EWMA conferences and priorityin initiatives such as joint meetings.
In return the associations will un-dertake initiatives such as comple-tion of questionnaires that EMWAdevelop and participation in jointbids to funding agencies such as theEuropean Commission when theyarise.
Eastern Europe InitiativeEWMA is particularly concerned toprovide assistance to countries with-in Eastern Europe. Our first projectis with Slovenia who is currentlyworking to establish a multi profes-sional wound management associa-tion. Representatives from EWMAvisited Ljubjana recently and we arecurrently establishing joint projectstogether. In this journal you willfind a focus on Slovenia and theprojects that we are commencingtogether. In the near future we areplanning to visit other EasternEuropean countries to establish asimilar relationship. We are deeplyconcerned to offer practical helpwherever possible within Europe.
Corporate SponsorsWe are deeply indebted to thefinancial support of our corporatesponsors who are helping us achievethese aims. Do join with us if youalso have a passion for woundmanagement and feel that youcould contribute to the work of theassociation. The different pro-grammes that we are now runningoffer opportunities whatever yourbackground. Help us to raise theprofile of wound management andplace it firmly on the Europeanhealth management agenda. ■
cialised topics of interest. Thesetypes of initiatives may be increas-ingly important as we seek to co-operate with other associations witha more specialised focus.
Journal 1/01 01.05.01, 16:036-7

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 18 9
CURRICULUM DEVELOPMENT
Following consultation with thecountry panels which will hopefullyrepresent the views of local and na-tional wound healing organisationsa curriculum will be developedwhich will concisely describe theaims, learning outcomes, content,teaching and assessment strategy forwound healing/management pro-grammes. It is envisaged that someareas will opt for short programmes,whilst others will implement longercourses which are likely to be de-pendant on the availability of localresources.
The flexibility of this approach sup-ports EWMA’s overall aim of imple-menting a wound healing/manage-ment educational framework thatcan accommodate national varia-tions in health care provision. It isenvisaged that this will providegreater opportunity for host institu-tions and organisations to adapt thecurriculum framework in ways thatthey consider most appropriate.Host institutions will need to definethe relevant target audience for anyeducational initiative and will beexpected to negotiate in advance thespecific content of each curriculumunit. It is envisaged that the curricu-lum will act as a menu describingcompulsory and elective content sothat local educational providers candevise a programme to reflect localrequirements.
In the future the curriculum has thepotential to be extended, but it isenvisaged that initially a small core
Chair: Madeleine Flanagan, Principal
Lecturer, University of Hertfordshire, UK
Co-chair: Finn Gottrup, Director, Copen-
hagen Wound Healing Center, Denmark
BACKGROUND
Over the years the European Wound Manage-ment Association has received many requests forassistance with the development of educationalinitiatives to improve wound care. As a result ofdevelopment of improved wound healing andmanagement techniques substantial improve-ments in the care of patients with wounds hasoccurred increasing the need for education that isdesigned to facilitate clinical decision-making andcollaborative practice.
GENERAL AIM
The aim of the EWMA Educational Develop-ment Project is to:
Produce a flexible, framework for the delivery ofeducation focussing on wound healing/managementacross Europe accommodating national variations inhealth care provision to raise the profile of wound carein a variety of health care settings.
It is envisaged that the EWMA EducationalDevelopment Project will produce a frameworkthat will support a structured range of practicedevelopment support services for countries wish-ing to raise awareness of best practice in woundcare including study days, scientific meetings/con-ferences, courses, protocol development, guidelineimplementation, formation of interest groups.
This project is based on the premise that that theacquisition of knowledge and skills gained froma rigorous educational framework is an effectivemethod of facilitating change in clinical practice.It is acknowledged that it is neither desirable norpossible to achieve uniform standardisation of oneeducational approach across Europe.
GENERAL PROJECT OBJECTIVES
■ Foster collaboration between wound healinggroups/organisations across Europe.
■ Develop a wound healing/managementcurricular framework to raise the profile ofwound care across Europe
■ Development of a quality assurance processin the form of a benchmarking standard forwound care education.
■ Development of a mechanism for endorse-ment of existing wound healing/manage-ment educational programmes acrossEurope.
■ Commissioning of new EWMA educationalmaterial
SPECIFIC PROJECT OBJECTIVES
■ Create inter-disciplinary panels of woundhealing/management specialists from eachcountry in Europe to develop internationalconsensus.
■ Conduct a needs analysis to facilitate thedevelopment of a national profile that pro-vides insight into the particular educationalrequirements of individual European coun-tries.
■ Identify current provision of wound healing/management programmes in different Euro-pean countries which could form the basisof an international directory.
■ Development of inter-disciplinary pro-gramme specifications to describe key learn-ing outcomes for basic and advanced woundhealing/management courses.
■ Formulate learning outcomes and flexibleassessment strategies for the core knowledgeand practical skills identified by the consen-sus groups.
■ Review existing educational resources (com-mercial and institutional) that could be usedto supplement educational activities.
■ Develop an audit tool to evaluate the suita-bility of the local environment to supportthe planned educational initiative.
European Wound Management Association
Educational DevelopmentProject
group of modules relevant across awide variety of health care settingswill be developed and piloted. Thesuccess of this ambitious project de-pends entirely on your support. Ifyou would like to participate in anyway in the project please contactEWMA via email at MadeleineFlanagan at [email protected] Finn Gottrup at
[email protected] or by re-turning the reply slip above. Cur-rently we are particularly keen tomake contact with individual prac-titioners who would be willing toparticipate in the formation of amultidisciplinary wound healing/management panel of specialists.
■
Madeleine Flanagan
MSc, BSc (Hons)
Nursing, Dip Nursing
RGN, Principal Lecturer,
Div. of Post-Registration
Nursing, University of
Hertfordshire, UK.
Certification Education,
Scheme Leader for BSc
(Hons) Tissue Viability,
MSc Advancing Practice
in Tissue Viability.
Editorial Advisor for the
Journal of Wound Care
and Journal of Tissue
Viability.
European Education Development Project
I would like to represent ________________________ (insert country name)
as a participant of the consultative panel for the
European Education Development Project.
Surname
First name(s)
Professional group M Doctor M Nurse M Therapist M Other
Please state
Title
Institution/Department
Work address
Postal code City
Country
Tel: Fax:
E-mail:
M I do not have access to E-mail
Address for correspondence (if different from above)
Please photocopy this form and distribute to interest colleagues.
Congress Consultants
Martensens Allé 8
DK-1828 Frederiksberg C
Denmark
Tel (int.): +45 7020 0305
Fax (int.): +45 7020 0315
E-mail: [email protected]
www.congress-consult.com
Return to
Prof. Finn Gottrup
MD, DMSci
Professor of Wound
Healing and Surgery,
and Director of
Copenhagen Wound
Healing Center,
Bispebjerg University
Hospital, Copenhagen,
Denmark
Specialist in General
Surgery and Surgical
Gastroenterology.
Assoc. Prof of Anatomy,
University of Aarhus.
Chair of Copenhagen
Wound Healing Center,
University of
Copenhagen.
EWMA Immediate Past
President
Council Member of the
EPUAP.
President of DSFS.
President of ETRS
1998-99
Journal 1/01 01.05.01, 16:038-9

EWMA JOURNAL 2001 VOL 1 NO 1 11
[Mölnlycke Ad]
Wound Management in Slovenia
By Christine Moffatt,EWMA president
SLOVENIA
The former Yugoslavian Republic,Slovenia is a small but very beautifulcountry in the southern part ofCentral Europe. With the Alps tothe Northwest and access to theMediterranean Sea to the SouthwestSlovenia has a unique countrysidewith an amazing diversity of land-scapes raging from high mountainsto green hills and wide plains. Thedistinctive geographic diversity in- fluences the Slovenian weather giv-
ing it a mixture of Continental,Alpine, and Mediterranean climates.
Slovenia became independent in1991 after the collapse of the Yugo-slav federation, making it one of theyoungest European countries. Witha population of roughly two million,Slovenia is a fairly small countrywith an active, small, but very capa-ble and highly qualified labourforce. Furthermore Slovenia has awell-developed infrastructure and anextensive social welfare system. In1994 there were 219 physicians,577.7 hospital beds and 53 dentistsfor every 100,000 inhabitants.
SLOVENIAN HEALTH AND
WOUND MANAGEMENT
The University Medical CentreLjubljana with is 2,734 beds and2,476 nurses is the Slovenian capi-tals main hospital, housing a largeaccident and emergency departmentand a central intensive care unit.
The overall aim of the nursingservice is to provide standardisednursing care that is accessible, effi-cient, goal oriented and tailored tothe patients’ needs. In order to pre-vent complication and secure thesafety of the patients all proceduresand equipment must conform to
documented professional standards.Goal setting is used to define theprocedures and documentation ofall activities. This ensures continuityof care and provides the basis for theevaluation of results. Furthermore amultidisciplinary approach to care isemployed.
In the field of pressure ulcer pro-phylaxis and management of chron-ic wounds the following standardprocedures are applied:
On the basis of a request submit-ted by the clinical department, aspecialist nurse visits the patient atthe agreed time, usually on the sameday. The Waterlow Score is used forassessing the patient’s risk of devel-oping a pressure ulcer.
Together with the patient’s nurseand the patient, the specialist nurseprepares a suitable preventive pro-gramme and nursing plan.
Both nurses monitor the efficien-cy of the programme.
When necessary, they enlist thehelp of physicians and other healthcare professionals.
This model of care should give effi-cient pressure ulcer prophylaxis; in-crease the satisfaction and involve-ment of the patients as well as en-
SLOVENIA IN SHORT
Official Name:Republic of Slovenia
Government:Parliamentary DemocraticRepublic
Area:20.256 square kilometres
Population:1.927.593 (July 2000 est.)
Language:Slovenian
Capital:Ljubljana (Pop: 330.000)
Important cities:MariborCeljeKranjKoper
Currency:Slovenian Tolar (SIT)
GDP per capita:USD 9.161 (1997)USD 9.878 (1998)USD 10.078 (1999)
Labour force:857.400
Unemployment:7,1% (1997 est.)
Journal 1/01 01.05.01, 16:0310-11

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 112 13
ELIGIBILITY
Awards are only open to current full membersof the European Wound Management Associa-tion (EWMA)
SCOPE
There are three types of Awards:
■ EWMA / SSL Research Award:32,000 € available
■ EWMA / SSL Education Award:8,000 € available
■ EWMA travel award:4,800 € available
Awards are made to individuals, and ‘hosted’by an institution nominated by the Awardholder.It is expected that the award will commencebefore December 31st, 2001.
RESEARCH AWARDS
Funding will normally cover:
■ Salary support (including superannuationand national insurance), with increments,based on an appropriate point for the indi-vidual on the relevant pay scale
■ Up to 3,200 € per annum contribution toresearch expenses
■ The research Award will not cover over-heads or capital grants
■ The agreed term of the Award should pro-vide for the preparation of a final report
Note that the Council will interpret the term‘research’ in the broadest possible sense, so thatit might include e.g. the undertaking of a sys-tematic review.
EDUCATION AWARDS
Funding will normally cover:■ Expenses incurred while following a course
in wound care/ a course in which woundcare is a major component. These are likelyto include purchasing books, photocopying,travel and subsistence for attending a placeof study away from home.
■ The Award will not cover course fees, over-heads or replacement costs, or the cost ofattending a conference
■ The agreed term of the award should pro-vide for the preparation of the final report
TRAVEL AWARDS
Funding will normally cover:■ Cost of standard class travel, via the most
economical route, to agreed venues.■ Subsistence during travel and visit at agreed
venue(s). The rate allowed will be based onUK Civil Service Rates (2001), unless this isinappropriate, in which case the rate will beagreed before the travel commences.
■ The agreed term of the award should pro-vide for the preparation of the final report
SUBMITTING AN APPLICATION
For further information on application proce-dures please refer to the EWMA website atwww.ewma.org
EWMA GRANTS AND AWARDS, 2001
PO Box 864, London SE1 8TT
Registered Charity No. 1042404
Grants andAwards, 2001hance the nurses’ own education,
satisfaction and self-esteem derivedfrom their work.
As in any other field, knowledge andinformation are essential for furtherprogress and development. The suc-cess of this work depends on consci-entious notification of all new casesof pressure ulcers, consistent use of
to become the Slovenian WoundManagement Association. Togetherwith multidisciplinary wound heal-ing experts form all over Sloveniathe three EWMA council membershad a general discussion about theirdifferent experiences and the chal-lenges of wound management inSlovenia. Following the initial dis-cussions smaller groups whereformed to identified potential areasof co-operation between the newSlovenian Wound ManagementGroup and EWMA. Three generalareas of co-operation were identi-fied:
The first was education and com-munication which include the fol-lowing ideas:
■ Education for nurses■ Training on finding the evidence
to underpin clinical decisionmaking
■ Build on previous successes ofsharing the protocols of care,documentation and start sharingthe protocols of primary studiesto enable multi-centre and mul-ti-national trials to take place,e.g. to undertake cost-effective-ness analyses (to convince insur-ers)
■ Share and establish standards forassessing wounds (e.g. a portfolioof data for comparing healingrates)
■ Enable pain assessment inwound care
■ Provide seamless care of wounds(e.g. communicating acrosshealth care settings)
The second area of co-operation wasresearch where discussion focusedon Slovenian involvement in pan-
European research such as clinicaltrials and epidemiology research.
The third area discussed was the useof EWMA’s experiences in the pro-cess of forming a Slovenian WoundManagement Association. The needfor a multidisciplinary associationrepresenting all centres and all pro-fessional groups related to woundmanagement was identified. It wasrecognised that EWMA could helpSlovenia start up the association bysharing their experience in, forexample, constitutional set-up,accounts, awards and conferenceorganisation. Furthermore it was feltthat exchange programmes could beestablished which would benefitfrom the strong involvement ofplastic surgeons and burns specialistsin Slovenia, the existing care path-way for malignant wounds and thepresence of medical angiologists.Other areas of co-operation mightbe the establishment of both practi-cal and theoretical workshops andthe translation of EWMA materialinto Slovenian.
Three months later, on the 22nd ofFebruary 2001, a second meetingwas held and the Slovenian WoundManagement Association (SWMA)was officially formed. A great dealwas settled at this meeting. First adraft of the constitution of SWMAwas drawn up together with an over-view of the potential sponsor possi-bilities. Secondly, co-operation be-tween EWMA and SWMA wasformally agreed. The co-operationwill, as a starting point, include thefollowing areas: Education, EWMAJournal and EWMA CurriculumQuestionnaires. Finally severalprojects where initiated, amongthese European Union funding, costefficiency and price comparisons. ■
preventive measures in keeping withvalid standards, and maintenance ofdetailed records. Audit of results hasallowed the introduction of moreexpensive but more efficient dress-ings. A thorough staff educationprogramme, incorporating differentworkshops with follow up writtenassessments at six months, supportsthis. So far the programme has cov-ered pressure ulcer prevention, eval-uation, the appearance and cleans-ing of wounds, the use of pressurerelieving equipment and care of thechronic wound.
Being aware of a general need fortraining in pressure ulcer preventionthe education programme has beenextended to nurses working in otherhealth care institutions such as nurs-ing homes and the communityhealth services.
SLOVENIAN WOUND
MANAGEMENT ASSOCIATION
(SWMA)
On the 10th of November 2000EWMA President Christine Mof-fatt, Andrea Nelson and GeorgeCherry represented EWMA at theinaugural meeting of what was later
Journal 1/01 01.05.01, 16:0312-13

EWMA JOURNAL 2001 VOL 1 NO 1 15
[Smith+NephewAd]
SUMMARY
Zinc oxide is a common ingredient in bandagesfor wound management. Experimental studieshave demonstrated beneficial effects of topicalzinc oxide on the restoration of epitheliumduring wound repair by as yet unknown mecha-nisms of action. In this study, zinc oxide wasfound to up-regulate one growth factor (insulin-like growth factor-I) and matrix metalloprotein-ase activity several fold in standardised porcinewounds. These findings indicate that zinc oxidepromotes epithelialisation by enhancing endo-genous growth factors and enzymes important forepithelial proliferation and migration.
INTRODUCTION
Zinc is an essential trace element for developmentand growth. More than 300 enzymes are depend-ent on zinc for activity such as matrix metallopro-teinases (MMPs), and DNA and RNA polymer-ases1,2. Zinc fingers belong to an even largergroup of zinc-containing proteins.1-3 These zincprotrusions are found predominately in transcrip-tion factors that interact with the promoter re-gion of DNA before a segment is transcribed intoRNA coding for growth factors.3
Zinc Oxideaugments endogenous expression of insulin-likegrowth factor-I (IGF-I) and activates matrixmetalloproteinases (MMPs) in wounds
The crucial role of zinc in these biological andbiochemical systems can explain the retardedwound repair response seen in zinc deficientpatients and normalization of the wound healingmechanisms with zinc therapy.4 However, thereis limited evidence for using zinc enterally unlessthe patient is truly zinc deficient.
Zinc is more commonly used as zinc oxide invarious topical preparations to treat skin lesions.5
In contrast to zinc given orally, zinc administeredtopically appears to be beneficial regardless of zincstatus.6 The increased demand for zinc duringwound repair is satisfied for prolonged periods byzinc oxide administered to the wound site.6,7
When applied locally, zinc oxide is solubilizedslowly and supraphysiological concentrations ofionic zinc (an elevation of about 4-5 times) areachieved at the wound site over an extendedperiod.8 We have demonstrated a stimulatoryaction of zinc oxide on the healing of leg ulcerscompared with placebo in a double-blind, ran-domized controlled clinical trial.9 Beneficial heal-ing effects of topical zinc oxide have also been con-firmed repeatedly in skin wounds of variousdepths in zinc-sufficient pigs. Specifically, zincoxide accelerates re-epithelialisation by yet un-known mechanisms.6 The polypeptide growthfactor IGF-I is crucial for epidermis homeostasisand the zinc-dependent MMPs are required foroptimal epithelial migration.10-12 Our aims wereto examine the effect of zinc oxide on endogenousIGF-I levels and MMP activation in wounds indomestic pigs on zinc-sufficient diets.
MATERIALS AND METHODS
Animal wound model and treatmentsTwelve full-thickness cutaneous wounds (4.4 cmx 2.2 cm, 4-6 mm deep) were made on anaesthe-
Magnus S. Ågren1, Henrik H. Steenfos2 Peter Tarnow3 and John-Olov Jansson3
1 Copenhagen Wound Healing Center,
Bispebjerg Hospital,
Copenhagen, Denmark
2 Department of Plastic Surgery,
Rigshospitalet,
Copenhagen, Denmark
3 Sahlgrenska Hospital,
Gothenburg, Sweden
Dr Magnus Ågren
Associate professor in
experimental pathology,
University of Linköping,
Sweden.
Executive director of
Aagren Dermaconsulting
ApS
Correspondence to:
Dr. Magnus Ågren
Bispebjerg Hospital
Copenhagen Wound
Healing Center
Bispebjerg Bakke 23
DK-2400 Denmark
Tel: +45 49 19 28 25
Fax: +45 49 19 28 25
aagrendermaconsulting@
yahoo.com
PAPERS PRESENTED AT EWMA STOCKHOLM 2000
Journal 1/01 01.05.01, 16:0314-15

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 116 17
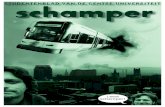
Figure 3. Matrix metalloproteinase (MMP) activity in wound tissue homoge-
nates treated without (control, open bars) or with 4 mg/ml zinc oxide (ZnO,
filled bars) ex vivo at 37°C for 18 hours. Active MMP represents activities
obtained with incubations carried out in the absence of the MMP activator
APMA (aminophenylmercuric acetate). Total MMP denotes activities ob-
tained in the presence of APMA. Zinc oxide increased significantly (p < 0.05)
both active and total MMP activity13. Results are given as mean ± sem.
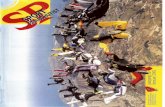
Figure 2. Effect of topical zinc oxide (filled circles) compared with the vehicle
alone (open circles) on the rate of closure of full-thickness skin wounds (4.4
cm x 2.2 cm) in domestic pigs. The non-epithelialized wound area was sig-
nificantly (p < 0.01) smaller in zinc oxide-treated wounds compared with
vehicle-treated wounds on post-operative day 1110. Results are given as
mean ± sem.
tised domestic pigs. On each pig the six wounds on theright side were treated with zinc oxide and the six woundson the left side with the control dressing. Zinc oxide (0.3mg zinc/cm2 or 17 mg zinc/g) was bound to a 100% cot-ton gauze dressing with polyvinylpyrrolidone.5 The con-trol dressings contained polyvinylpyrrolidone only. Thedressings were covered with separate adhesive polyurethanefilm dressings (Tegaderm®, 3M, St. Paul, MN, USA).Sterile saline (1.5 ml) was injected into the dressings witha needle on a syringe. The dressings were changed everytwo to three days. The investigator was unaware of whichgroup the samples came from when measuring woundareas and IGF-I mRNA.
Wound area measurementsThe outline of the epithelial front was drawn on a sterileplastic sheet and the non-epithelialised area measured byplanimetry.
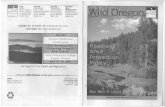
IGF mRNA assayGranulation tissue for analysis of IGF-I mRNA concen-tration was obtained with a 6-mm punch biopsy from thecentre of the wounds (Figure 1). The extraction of nucleicacids and hybridisation RNAase protection/solution reac-tions were carried out as described earlier by Tarnow et al.10
Activation of endogenous MMPsAn assay that utilises the present collagen in wound tissueas substrate for the endogenous MMPs was applied.13
Briefly, homogenates of control-treated wound tissue wereincubated ex vivo with zinc oxide (4 mg/ml) or without,and the amount of collagen degradation products releasedinto the incubation medium measured indirectly as hy-droxyproline.
Statistical analysesStudent’s t-test was applied to the data, given as mean ±sem. p < 0.05 was chosen as level significance.
RESULTS
Wound healingThe changes in wound area for zinc-treated and vehicle-treated wounds are depicted in Figure 2. A beneficial ef-fect on wound closure of topical zinc oxide became ap-parent after the wound cavities were filled with granula-tion tissue to the level of surrounding normal skin on day7 enabling epithelialisation from wound edges .7 The non-epithelialized area of the wounds, expressed as percentageof initial wound area, treated with zinc oxide (22.7 ± 1.3%,mean ± sem) was significantly (p < 0.01) smaller than con-trol-treated wounds (42.9 ± 5.0%) day 11 (Figure 2).
IGF-I mRNA levelsElevated levels (p < 0.05) of IGF-I mRNA were found inzinc oxide-treated (1.7 ± 0.2 amol/µmol DNA) comparedwith control-treated (1.0 ± 0.1 amol/µmol DNA) woundson day 4 but no significant differences between the twogroups were found from day 4 onwards.
Activation of MMPsZinc oxide added to wound tissue homogenates increased(p < 0.05) the activity of both active and latent MMPsabout 5-fold compared with control-treated wound tissuehomogenates (Figure 3).
DISCUSSION
In the present experimental study, locally applied zincoxide promoted epithelialisation of standardized full-thick-ness skin wounds confirming previous results in a partial-thickness wound model in pigs.6 Apart from zinc’smoderate anti-bacterial, anti-inflammatory and cytopro-tective activities,14-17 our biochemical and cellular findingscan possibly explain zinc’s mechanisms of action on epi-thelialisation of cutaneous wounds. Zinc oxide activatedendogenous zinc-dependent matrix metalloproteinases,which may facilitate keratinocyte migration. Furthermore,zinc oxide augmented endogenous expression of onegrowth factor insulin-like growth factor-I (IGF-I) ingranulation tissue. Recent in vitro work, where zinc en-hanced epithelial migration due to up-regulation of IGF-I specifically in fibroblasts, supports the hypothesis thatzinc promotes wound healing by increasing endogenousgrowth factors.18 In addition, other cell culture studies
Figure 1. Full-thickness skin wound on the back of pig on post-operative day
4. Note tissue defects in wound where biopsies of granulation tissue were
taken.
showed synergistic effects of zinc and IGF-I in NIH 3T3fibroblasts.19 Baroni et al.20 added zinc oxide to humandermal fibroblasts and observed increased secretion offibroblast growth factor (FGF) suggesting that zinc ingranulating wounds is also possibly capable of up-regulat-ing growth factors other than IGF-I. Hansson21 found thatzinc ions up to 1 mM mimicked the action of growthfactors by enhancing enzyme-dependent intracellularmitogenic signal pathways in Swiss 3T3 fibroblasts.
Topical zinc also appeared to promote healing of smalland acute skin wounds in humans.22,23 Work in ourlaboratory is in progress to elucidate the action of topicalzinc oxide on acute wounds healing by secondary intentionin humans.
Our study indicates that apart from being an essential traceelement, zinc exerts beneficial pharmacological actions onwound healing when applied locally as zinc oxide. Oralzinc merely corrects a nutritional deficit. Increased endo-genous expression of IGF-I and activation of MMPs mayexplain the stimulatory action of zinc oxide on resurfac-ing of wounds. ■
REFERENCES
1. Vallee, B.L., Coleman, J.E. & Auld, D.S. Zinc fingers, zinc clusters, and zinc twists in
DANN-binding protein domains. Proc. Natl. Acad. Sci. USA 1991, 88, 999-1003
2. Vallee, B.L. & Auld, D.S. New perspectives on zinc biochemistry: co-catalytic sites in multi-
zinc enzymes. Biochemistry 1993, 32, 6493-6500
3. Rhodes, D. & Klug, A. Zinc fingers. Sci. Am. 1993, 268, 32-39
4. Wilkinson, E.A.J. & Hawke, C.I. Does oral zinc aid the healing of chronic leg ulcers? Arch.
Dermatol. 1998, 134, 1556-1560
5. Ågren, M.S. Studies on zinc in wound healing. Acta Derm. Venereol. Suppl. (Stockh.)
1990, 154, 1-36
6. Ågren, M.S., Chvapil, M. & Franzén, L. Enhancement of re-epithelialization with topical
zinc oxide in porcine partial-thickness wounds. J. Surg. Res. 1991, 50, 101-105
7. Ågren, M.S., Franzén, L. & Chvapil, M. Effects on wound healing of zinc oxide in a hy-
drocolloid dressing. J. Am. Acad. Dermatol. 1993, 29, 221-227
8. Ågren, M.S., Krusell, M. & Franzén, L. Release and absorption of zinc from zinc oxide
and zinc sulfate in open wounds. Acta Derm. Venereol. (Stockh.) 1991, 71, 330-333
9. Strömberg, H.-E. & Ågren, M.S. Topical zinc oxide treatment improves arterial and ve-
nous leg ulcers. Br. J. Dermatol. 1984, 111, 461-468
10. Tarnow, P., Ågren, M., Steenfos, H. & Jansson, J.O. Topical zinc oxide treatment increas-
es endogenous gene expression of insulin-like growth factor-1 (IGF-1) in granulation
tissue from porcine wounds. Scand. J. Plast. Reconstr. Surg. Hand. Surg. 1994, 28, 255-
259
11. Mirastschijski, U., Karsdal, M., Steenfos, H.H. & Ågren, M.S. Influence of matrix metal-
loproteinse (MMPs) inhibitors on MMP expression and epithelialization in a human ex
vivo skin wound model. Eur. Surg. Res. 2000, 32 (suppl. 1), 2-3 (abstract)
12. Ågren, M.S. Matrix metalloproteinases (MMPs) are required for re-epithelialization of
cutaneous wounds. Arch. Dermatol. Res. 1999, 291, 583-590
13. Ågren, M.S. Zinc oxide increases degradation of collagen in necrotic wound tissue. Br.
J. Dermatol. 1993, 129, 221 (letter)
14. Ågren, M.S., Söderberg, T.A., Reuterving, C.O., Hallmans, G. & Tengrup, I. Effect of
topical zinc oxide on bacterial growth and inflammation in full-thickness skin wounds in
normal and diabetic rats. Eur. J. Surg. 1991, 157, 97-101
15. Söderberg, T., Ågren, M., Tengrup, I., Hallmans, G. & Banck, G. The effects of an oc-
clusive zinc medicated dressing on the bacterial flora in excised wounds in the rat. In-
fection 1989, 17, 81-85
16. Guéniche, A., Viac, J., Lizard, G., Charveron, M. & Schmitt, D. Protective effect of zinc
on keratinocyte activation markers induced by interferon or nickel. Acta Derm. Venere-
ol. (Stockh.) 1995, 75, 19-23
17. Johansson, A., Sunzel, B., Holm, S.E., Söderberg, T. & Gref, R. Antimicrobial screening
of zinc in the absence or presence of oleoresins and various resin acids. APMIS 1995,
103, 1-9
18. Watanabe, S., Wang, X.E., Hirose, M., et al. Insulin-like growth factor I plays a role in
gastric wound healing: evidence using a zinc derivative, polaprezinc, and an in vitro rabbit
wound repair model. Aliment Pharmacol. Ther. 1998, 12, 1131-1138
19. Huang, J.-S., Mukherjee, J.J., Chung, T., Crilly, K.S. & Kiss, Z. Extracellular calcium stim-
ulates DANN synthesis in synergism with zinc, insulin and insulin-like growth factor I in
fibroblasts. Eur. J. Biochem. 1999, 266, 943-951
20. Baroni, A, Perfetto, B, Buttini, G., Catalanotti, P., Gorga, F. & Tufano, M.A: Topical
amikacin formulation induces fibroblast growth factor and cytokine release from human
dermal fibroblasts. Arch. Dermatol. Res. 1999, 291, 296-299
21. Hannson, A. Extracellular zinc ions induces mitogen-activated protein kinase activity and
protein tyrosine phosphorylation in bombesin-sensitive Swiss 3T3 fibroblasts. Arch. Bio-
chem. Biophys. 1996, 328, 233-238
22. Tronnier, H. Experimentelle studie zur epithelisierung. Z. Hautkr. 1975, 50, 925-929
23. Greenway, S.E., Filler, L.E. & Greenway, F.L. Topical insulin in wound healing: a ran-
domised, double-blind, placebo-controlled trial. J. Wound Care 1999, 8, 526-528
Journal 1/01 01.05.01, 16:0416-17

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 118 19
1 Department of Wound Healing,
Dermatology, Churchill Hospital,
Oxford, United Kingdom
SUMMARY
Malignancy is often missed as a cause of non-healing leg ulcers. A retrospective survey wasundertaken of the underlying aetiology of allpatients referred to our nurse led leg ulcer clinic,over a twelve month period (01.01.99–01.01.2000), in order to identify the number ofpatients with malignant or pre-malignant changesas a possible cause of their non-healing leg ulcer.There were 245 referrals and 8 (3%) patients werediagnosed from biopsy as having previously un-diagnosed malignant or pre-malignant changes intheir lower limb; 4 patients with Bowen’s disease;3 with basal cell carcinoma and 1 with squamouscell carcinoma. Although malignancy in leg ulcer-ation is rare it should be considered in venous legulcers that are not responding to conventionaltherapy.
INTRODUCTION
Direct referrals to our nurse led leg ulcer clinic aretaken from general practitioners, communitynurses and hospital medical staff. The majority ofreferrals are new patients with a few re-referrals.All patients are seen and assessed by one of thespecialist nurses and a dermatologist is availablefor consultation during the assessment if requestedby the specialist nurse. Following patient assess-ment a biopsy from the leg ulcer is undertaken forhistological examination to confirm diagnosiswhere malignancy or pre-malignancy is suspect-ed. Malignancy is thought to be rare in chronicleg ulcers.1 Squamous cell carcinoma (SCC) is themost commonly reported malignancy in chronicleg ulceration.2 However some authors have
Malignancy andPre-malignancy inLeg Ulceration
found basal cell carcinoma (BCC) to be an impor-tant cause of non-healing leg ulcers.3 4
The aim of this study was to determine thenumber of patients referred to our clinic over atwelve month period diagnosed with malignant orpre-malignant changes as a possible cause of theirnon-healing leg ulcerations.
METHODS
A retrospective survey was undertaken of our pa-tient records for a twelve month period fromJanuary 1st 1999 to January 1st 2000. Medicalrecords and histology reports were examined ofpatients where malignancy or pre-malignancy wassuspected. A summary of the clinical findings wasrecorded including diagnosis of the type ofmalignancy and subsequent treatment.
RESULTS
A total of 245 patients were referred to the clinicduring the study period. Eight (3%) patients,7 female and 1 male were diagnosed from biopsywith malignant or pre-malignant changes in theirlower limb. (Table 1).
Squamous cell carcinoma (SCC)An 84 year old female patient with long standingvenous ulceration of more than 20 years wasdiagnosed with SCC. The patient had one episodeof ulcer healing for a brief period followed by re-currence 7 years prior to the diagnosis of mal-ignancy. SCC’s have a verrucous appearance andthe area of concern in this patient’s deterioratingleg ulcer was ‘cauliflower-like’ in appearance.5
This lady has declined any kind of surgery.
Bowen’s diseaseThere were 4 female patients, meanage 79.3 years, diagnosed with Bo-wen’s disease. Mean ulcer durationwas 2.4 years (range 8 months –4 years). Bowen’s disease is a form ofintra-epidermal Squamous cell carci-noma seen clinically as an erythema-tous plaque with an irregular borderand surface scaling.6 (Fig. 1) Onepatient was treated with curettage,one with excision and two prescribedfluorouracil, applied topically as a 5%cream.
Basal cell carcinoma (BCC)There were 3 patients, one male twofemale, mean age 87.3 years, dia-gnosed with BCC. Mean ulcer dura-tion was 2.7 years (range 2-4 years).BCC is a slow growing, locally inva-sive epidermal skin tumour arisingfrom basal cells of the epidermis andits appendages. 7 BCC’s are mainlyfound on sun exposed sites. 8 Clini-cal presentation is variable and maybe seen as thin pink scaling plaqueswith slightly raised margins; subcuta-neous nodules; or ulceration.9 (Fig. 2)The three patients diagnosed withBCC were treated by excision of thetumour.
DISCUSSION
Malignancy should be considered inpatients with long standing leg ulcer-ation. Several authors recommendbiopsy of all non-healing leg ulcersafter 3 months.3.4.10
It has been suggested that one biopsymay not be adequate for diagnosisand this should be repeated if theulcer continues to deteriorate.2 In ourstudy 7 patients (3 BCC; 3 Bowen’sdisease; 1 SCC) had received contin-uous treatment to their non-healingleg ulcer for over 2 years before refer-ral was made to the clinic. Continueduse of inappropriate treatment hasvast implications for health careresources, particularly in terms ofnursing time and pharmacy costs.
The discomfort and distress to thepatient also remains an important fac-tor, especially if it is avoidable and inthe case of an SCC delay in diagno-sis can be dangerous. Nurses aremainly responsible for the treatmentand management of patients withchronic leg ulcers; therefore it is essen-tial that they are able to recognisewhen to involve other professionals.
CONCLUSION
Malignancy should be considered invenous leg ulcers that are atypical,deteriorating or not responding toconventional therapy after 3 months.■
REFERENCES1 Ryan T.J. ; Willkinson D.S. Disease of the veins and ar-
teries: leg ulcers. In: Rook A., Wilkinson D.S., Ebling
F.J.G. (eds) Textbook of dermatology 4th edition. Black-
well, London. 1986
2 Baldursson B., Sigurgeirsson B., Lindelöf B. Leg ulcers
and Squamous cell carcinoma. An Epidemiological
study and review of the literature. Acta Dermato Vener-
eol (Stockholm) 1993, 73: 171-174
3 Phillips T.J., Salman S.M. Rogers G.S. Non healing leg
ulcers: A manifestation of basal cell carcinoma. Jour-
nal of the American Academy of Dermatology 1991,
25: 47-49
4 Walkden V., Black M. Basal cell carcinomatous chang-
es on the lower leg: an association with chronic venous
stasis British Journal of Dermatology 1981, 105 Supple-
ment 19, 9-10
5 Sneddon I.B. Church R.E. Practical Dermatology Third
Edition. Arnold London 1976
6 Cox N.H., Eedy D.J., Morton C.A. Guidelines for man-
agement of Bowen’s disease. British Journal of Derma-
tology 1999, 141: 633-641
7 Telfer N.R., Colver G.B., Bowers P.W. Guidelines for
management of basal cell carcinoma. British Journal of
Dermatology 1999, 141: 415-423
8 Marks R. Skin Cancer In: Marks R. Sun Damaged Skin.
Martin Dunits Ltd. London 1992
9 Pollack S.V., Golsen J.B., Sheretz E.F., Jegasothy B.V.
The biology of basal cell carcinoma: a review of the lit-
erature. Journal of the American Academy of Derma-
tology 1982,7(5): 569-575
10 Ackroyd J.S., Young A.E. Ulcers that do not heal. Brit-
ish Medical Journal 1983, 286: 207-208
Janice Cameron
Mphil, RGN
Wound Healing
Institute, Dept. of
Dermatology, Churchill
Hospital, Oxford, UK
Specialist nurse in
chronic wounds and
skin management.
Nurse 1998 award for
wound care
Deborah Hofman
RGN, BA Hons, Dip.
Nurse, FETC,Lic.Ac.
Senior Research Nurse
Involved in work for the
RCN Pressure Ulcer
Guidelines
EWMA Recorder.
Trustee for the
European Pressure
Ulcer Advisory Panel
Janice Cameron,1 Deborah Hofman,1 George Cherry1
Correspondence to:
Janice Cameron,
Wound Healing Institute,
Dept. of Dermatology,
Churchill Hospital,
Oxford,UK
Table 1Sex Age Ulcer Position Duration DiagnosisM 88 tibial crest 2 years BCCF 99 tibial crest 4 years BCCF 75 tibial crest 2 years BCCF 74 gaiter; medial aspect 8 months Bowen’sF 87 gaiter; medial aspect 3 years Bowen’sF 70 gaiter; medial aspect 4 years Bowen’sF 86 gaiter; lateral aspect 2 years Bowen’sF 84 gaiter, lateral aspect 7 years (recurrent) SCC
Figure 1 Figure 2
PAPERS PRESENTED AT EWMA STOCKHOLM 2000
Journal 1/01 01.05.01, 16:0418-19

EWMA JOURNAL 2001 VOL 1 NO 1 21
[SSL Ad]SUMMARY
The aim was to illuminate elderly people’s expe-riences of living with venous leg ulcer. Data in thisstudy was collected through individual interviewswith 15 people with venous leg ulcers. Interviewswere used to allow people the freedom to narratetheir situation and experience of living with ve-nous leg ulcer. Data was analysed by means of thephenomenological-hermeneutic approach. Theresults show that elderly people with venous legulcer struggle against the illness and can be regard-ed as existing in a tension between on the onehand imprisonment in the body, bandage andhome, on the other hand hope of freedom froma burdensome body. The relation between expe-riences of the body and the environment haschanged. The elderly try to find ways to managepain, an uncomfortable bandage and a disobedi-ent body, which are obstacles to the pursuit ofactivities of everyday life and relationships withothers in social life. They hope for complete heal-ing despite slow wound healing. The study showsthe importance of recognising the elderly peoples’perceptions of their leg ulcers and the impact ofthese perceptions on well-being. Nurses can there-by anticipate problems and provide more sensitivecare.
INTRODUCTION
There is growing awareness of the importance ofpatients’ perspectives. Most research in manage-ment of leg ulcer ration has examined the effec-tiveness of treatment. A few phenomenologicalstudies (1-3) from the perspective of a patient witha leg ulcer have reported experience of pain, disa-bility and worry about healing. The authors arguethat a reflective inquiry, using a qualitativemethodology, would be required to gain furtherunderstanding of the individual’s everyday expe-rience of chronic leg ulcer.
Leg ulcers are clearly a serious problem forelderly people. It is a necessity to recognise theneeds and the situation of the person who has adisease and feels ill (4-5). The central and start-ing point in clinical caring science is the individ-ual’s experiences of illness (6).
Research illustrating individuals’ subjective ex-periences of venous leg ulcers is rare. Walshe (3)concluded that further research is needed con-cerning people with long-term ulceration, for thepurpose of developing a clearer understanding ofhow the elderly experience it. A limited under-standing of how the illness is experienced by theindividual may result in an inappropriate responseto that person’s needs. It is important that thetreatment offered should be based on research,which facilitates better understanding. The aim ofthe study was to illuminate the meaning of elder-ly people’s experiences of living with venous legulcer in order to get a nuanced understanding ofwhat it is liked to live an ulcer.
METHODS
Fifteen people were interviewed. The interviewswith the elderly focused on the experience ofliving with venous leg ulcer and began with a ‘trig-ger’ question, ‘What’s it like to live with a legulcer?’ The participants were guided by a dialogueto speak as freely as possibly and to narrate theirexperiences by giving concrete examples fromdaily life.
The sample consisted of twelve women andthree men and with a mean age of 79.4. All par-
Elderly People’s Experiences
Britt Ebbeskog,1,2 S-L Ekman1,2
1 Department of Clinical Neuroscience,
Centre for Elderly Care Research,
Karolinska Institute,
Stockholm, Sweden,2 Department of Science and Health,
Blekinge Institute of Technology,
Karlskrona, Sweden
The Meaning of Living with Venous Leg Ulcer
Britt Ebbeskog
RNT
Doctorial Candidate.
Associate Professor,
Ersta Sköndal
University College,
Department of Nursing,
Sweden.
Correspondence to:
Britt Ebbeskog,
Centre for Elderly Care
Research,
Huddinge University
Hospital,
M98,
S-141 86 Stockholm,
Sweden
Tel: +46 8 58 58 68 69
Fax: +46 8 58 58 68 65
E-mail:
britt.ebbeskog@
neurotec.ki.se
PAPERS PRESENTED AT EWMA STOCKHOLM 2000
Journal 1/01 01.05.01, 16:0420-21

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 122 23
despair. The painful wound controlstheir existence and everything seemshopeless. Pain was described as some-thing which they had to deal with,telling themselves that when thewound was aching it was healing.When the pain got too much to bearthey regularly took painkillers. A fewdescribed their existence in terms ofthe number of painkillers taken. Someavoided taking painkillers. They saidthat putting their leg in different po-sitions and doing massage could re-lieve the pain for a while. Pain reliefwas described as giving a feeling ofhappiness. The dressing pushed andscraped against the wound and causeddiscomfort. They took off the band-age to get rid of the discomfort. Theyfelt a moment of freedom when thewound and the leg were in the air.
They reduced the distance walked,changed when pain from the woundincreased, and the running, uncom-fortable wound also gave an uneasyfeeling that something bad might hap-pen. The dressing could come loose,which would be embarrassing. To dis-tract themselves from the pain andavoid thoughts of the leg ulcer, theytried to maintain their interests. Somesaid that they thought it was impor-tant for their well-being and the heal-ing to maintain their daily habits.
Struggle between hope and despairwith regard to a lengthyhealing processHope of healing was often mentioned.Hope for the future was still there de-spite the slow healing process. Theelderly people felt the signals fromtheir body which indicated that thewound was beginning to heal. Somewere hopeful and looking forward toa healed wound. They expressed joy atthe thought of getting rid of the ulcerand the dressing. But there was a con-
stant worry that the wound wouldstart to run, which gave them a needto repeatedly check up on its appear-ance. They took off the bandage andexamined the wound by squeezing itand then they cleaned it. There was in-security as to whether the wound wasgoing to stay healed.
Some reflected on earlier eventsand remember their bodily discom-forts like pain. A few were angry andsad that they have caused themselvesthis leg ulcer and spoke about howunfair their existence has been. Reflec-tions on the leg ulcer disease causethem to blame themselves and feelfrustrated, and they lose their self-con-fidence. But in the midst of their de-spair they are nevertheless hopeful thatsoon the wound will be healed.
Comprehensive understandingThe comprehensive understanding re-veals that elderly persons with venousleg ulcer are greatly influenced by theillness experience. Living with chronicleg ulceration as described by theelderly can be understood as a dialec-tical ongoing process between twoopposite poles. On the one hand thereis the sense of altered body image, ofbeing imprisoned in the body, disrup-tion of the body, which leads tochange in social life. One the otherhand there is hope of being cured andachieving freedom from a burden-some body from managing the expe-rience of a painful wound and of dis-ability restricting everyday living.
The elderly people’s experiences ofliving with venous leg ulcer indicatedthat the meaning of living with suchan ulcer can be understood as a dialec-tical relationship between on the onehand the experience of imprisonmentin the body, the bandage and thehome, on the other hand achievingfreedom from a disobedient body.
The results of the present studyindicate that nursing care should in-
ticipants had a verified diagnosis ofvenous insufficiency and the currentulcers had been present from fourmonths to two and a half years. Elevenparticipants had recurrent ulcers.
To analyse the text, a phenomeno-logical hermeneutical method waschosen. This method is inspired byRicœur’s philosophy (7). The analysiscomprised three steps: naïve reading,structural analysis and comprehensiveunderstanding. The first step was anaïve reading of each transcribed in-terview. The texts were reflected uponin order to get at the meaning of thestudied phenomena. This reading wasformulated as a preliminary under-standing that provided the directionfor the structural analysis. This anal-ysis aimed at explaining the text. Thetexts are reviewed in order to identifymeaningful connections. This was aprocess that entailed going back andforth between formulated meaningsand sub-themes and themes that werecreated, changed shape or disappeareduntil all this meanings were capturedin final sub-themes and themes. Thethird step an interpretation of the textsas a whole, where the preliminary un-derstanding and the structural analy-sis were brought together into a new,comprehensive understanding of themeaning of the studied phenomena.
RESULTS
Preliminary understandingThe preliminary understanding of theelderly people’s experience of livingwith venous leg ulceration involvesawareness of their sense of hopeless-ness due to the lengthiness of the heal-ing process, attention to wound pain,awareness of body image change andchange in social life. This preliminaryunderstanding providing further di-rection for the next step, the structuralanalysis.
Structural analysisIn the structural analysis, four themeswere identified: emotional conse-quences of altered body image, livinga restricted daily life, achievement ofwell-being to manage emotion in con-nection with a painful wound andbandage discomfort, and the strugglebetween hope and despair with regardto a lengthy healing process.
Emotional consequences ofaltered body imageThe participants in the study de-scribed the wound on the leg as if itconstituted a defective body part. Thewound was scary to look at and theyfelt uncomfortable about being con-stantly reminded of it. They describeda feeling of not having control overtheir body. The elderly people wereworried that the ulcer could sudden-ly start to run, which could cause pusto leak out from the bandage. A feel-ing of being controlled by the bodyled to a sense of powerlessness.
The bandage around the leg gavesome of the interviewed participantsa feeling of being imprisoned. Theyfelt it like armour around the body.The leg was described as something inthe way. The women could cover it upby wearing trousers, when they didnot want to show others that they hada bandaged leg. Going to public bath-ing-places was avoided because theyfelt that they could not show theirwound in public. It was shameful toshow that you had a leg ulcer and abandaged leg.
A few had adjusted themselves toa life with a leg ulcer and the risk thatit could come back. They saw their lifeas inevitably involving a wound ontheir leg, and accepted themselves aspeople with leg ulcers.
Living a restricted lifeThe elderly people had problems find-ing suitable shoes that fitted the band-aged foot. Old worn-out shoes werecut so as to make them fit. When itrained or snowed the possibility of go-ing out was limited, which narrowedsocial contact. Lack of suitable shoesand the risk that the dressing wouldget wet limited daily walks that theywere used to. The length of the walkwas limited by the fact that theyshould not subject the leg ulcer to anystrain. The social contact changedbecause of the reduced activity out-doors.
They were worried that taking afootbath and washing their bodiesevery day would cause the bandage toget wet or spoilt, disturbing the heal-ing. Some missed their daily routinesand body care. The pain interruptedsleep, which caused the hours of theday to be disturbed. Energy andstrength was limited. Tiredness duringthe day made it necessary to take arest, especially when there was dis-charge from the leg ulcer. The con-stant reminder of tiredness meant thatthe women no longer had the strengthto tidy their home as they used to.
Their social contact changed be-cause the elderly people decided tolimit themselves. They did not wantto subject those close to them to therunning ulcer, the bandage and thedressing. Relationships with friendsbecome narrowed to just the closestones. The only people they had theenergy to keep in contact with weretheir closest friends and their children.
Achievement of well-being inconnection with a painfulwound and bandageWhen pain is present, this takes a cen-tral place in the elderly peoples’ lives.They are sad, angry and cry in their
REFERENCES
1. Chase SK, Melloni M, Savage A. A forever healing: The
lived experience of venous ulcer disease. Journal of
Vascular Nursing 1997; XV (2): 73-78.
2. Bland M. Challenging the myths: The lived experience
of chronic leg ulcers. Nursing Praxis in New Zealand
1995; March 10, (1): 49.
3. Walshe C. Living with a venous leg ulcer: a descriptive
study of patients’ experiences. Journal of Advanced
Nursing 1995; 22: 1092-1100.
4. Watson J. Postmodernism and knowledge development
in nursing. Nursing Science Quarterly 1995; 8, (2): 60-
64.
5. Benner P, Wrubel J. The primacy of caring: Stress and
coping in health and illness. California: Addison-Wes-
ley Publishing Company, 1989: pp. 1-26, 53-54.
6. Eriksson K. 1997. Understanding the world of the pa-
tient, the suffering human being: The new clinical par-
adigm from nursing to caring. Advanced Practice Nurs-
ing Quarterly 1997; 3, (1): 8-13.
7. Ricoeur, P. Interpretation theory: Discourse and the sur-
plus of meaning. Texas: Christian University Press, Fort
Worth, 1976.
clude assessment of the body experi-ence and preventive action to restorehope and confidence for elderly peo-ples regarding wound healing.
ACKNOWLEDGEMENTS
We should like to thank the Depart-ment of Nursing, Ersta Sköndal Uni-versity College, the Committee ofCaring Sciences at Karolinska Insti-tute, Department of Science andHealth, Blekinge Institute of Techno-logy, the Board of Johanniterorden inSweden and the Municipal PensionInstitute, for financial support duringthe study. The authors are grateful tothe patients, district nurses and Mar-gareta Grauers for their co-operation.
■
Journal 1/01 01.05.01, 16:0422-23

EWMA JOURNAL 2001 VOL 1 NO 1 25
Peter J Franks
INTRODUCTION
The term ‘Cost effectiveness’ has becomepart of health services language to justi-fy the use of particular products and
health care systems. Despite its frequent use thereis often little objective evidence of true ‘cost ef-fectiveness’ of different products and proceduresin wound management. In this article we will de-scribe what is meant by the different cost terms,together with common misuses of the terms.
Whilst it is known that wound care treatmentand prevention consume large quantities of re-sources in terms of disposables, equipment andnursing time, there is still little objective evalua-tion of the economic burden of wound care onthe health services. Moreover, the health servicecosts may inadequately describe the total cost ofcare, as this burden falls increasingly outside theformal health services, and on to patients andtheir families. In addition, the assessment of costburden of disease does not describe the completeevaluation. Costs cannot be examined in isola-tion, but there must also be some measure ofhealth gain. Cost effectiveness is therefore a bal-ance between input (resources) and output (ef-fectiveness). The best treatments are low cost perunit of health gain, but it is important to appre-ciate that the cheapest option is not necessarilythe most cost effective.
Measuring the cost burden of woundsWhen we think of the economic burden of a dis-ease it is tempting to examine the costs of pro-viding the health services to patients sufferingfrom the disease in question. However, this maybe a very limited view of cost. Social appraisalrequires that costs not only related to the healthservice should be considered, but also costs to thepatient and their family, and the cost of the dis-
ease to society. Costs may be divided into ‘direct’costs of treating the patient and the ‘indirect’ costto society. Typically, direct costs would includehealth service costs as well as costs of drugs andtravel associated with the health care. Converse-ly, indirect costs would be derived from estimatesof lost production by the patient or family mem-bers caused by the disease, losses to society causedby the patient being unable to function to theirpotential, and quality of life issues, particularlyproblems associated with pain, poor mobility,discomfort and distress.
Which Measure of Effectiveness?In studies of acute life threatening disease surviv-al would be the accepted measure of effectiveness.However, when dealing with chronic (generally)non-life threatening diseases we must considerwhat our best outcome measure will be. In gen-eral, clinical measures of effectiveness are preferredsince these are of direct relevance to the clinician.In wound management one may consider the fol-lowing outcomes
■ Change in wound area■ Change in the severity of the wound■ Subjective improvement in wound■ Wound free days■ Complete wound healing
(clinical cure)
The latter of these is most commonly used out-come since it provides a hard (irrefutable) endpoint for clinical studies. However, it does haveits limitations, since it assumes that complete ul-cer healing is the only outcome of value to the pa-tient. Thus, an ulcer that reduces in size dramat-ically, or leads to lower perceived pain but does notheal, is still considered a treatment failure. In ad-dition, clinical cure may be poorly correlated withthe patients perceived health. This has led re-searchers to investigate the role of health related
What do we mean by
Cost EffectiveWound Care?
Prof. Peter J. Franks
Co-director of the Centre
for Research &
Implementation of
Clinical Practice, Thames
Valley University, UK.
Human Biologist,
doctoral thesis in Human
Physiology.
Postgraduate
qualifications in statistics
and epidemiology.
EWMA Council
member
Correspondence to:
Prof. Peter J Franks
Thames Valley University
Centre For Research and
Implementation of
Clinical Practice
Wolfson Institute of
Health Sciences
32-38 Uxbridge Road
GB-W5 2BS
London
United Kingdom
Tel: +44 181 280 5020
Fax: +44 181 280 5020
[Cook Ad]
Journal 1/01 01.05.01, 16:0424-25

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 126 27
value. Thus, one QALY in a child isequivalent to that for someone agedover 85 years. However, this is a pop-ular method of analysis for healtheconomists, with many policy deci-sions on health being made with theiruse.
Limitations of economicevaluationsEconomic evaluations have becomeincreasingly more important with theimprovements in technology, andmuch greater expectations of healthcare by the population, it must be ac-knowledged that these studies may belimited. As previously mentioned,evaluations of outcome are critical, yetthe methods used to quantify out-comes are frequently less than ideal. Itis also impossible to make all decisionsbased purely on cost and cost effec-tiveness arguments, as this excludesthe wishes of the consumers of healthcare who may wish to influence thetype of health care given and help setthe health care agenda. Clearly costand cost effectiveness arguments aloneare insufficient to fulfil the broaderaims of health services demanded bythe public.
Much of the evidence behind eco-nomic evaluations of wounds revolvesaround the evaluation of products,and in particular comparisons be-tween products that are used in simi-lar circumstances. There are a pletho-ra of studies that have looked at com-parisons of dressings, bandages, beds,mattresses and seating cushions, oftenwith soft end points, and frequentlywith serious design flaws. These stud-ies may be used by companies to mar-ket their products, with very little hardevidence to support their use over andabove other (often cheaper) products.In the systematic review of pressureulcer treatments it was recommended
that economic analysis should accom-pany any further randomised trials ofpressure relieving equipment [1].They stated that if purchasers were toconsider high tech ‘expensive’ pressureequipment they should do so, only inthe context of a randomised clinicaltrial.
In this paper we have outlined themethods used in economic evaluationof wound management, and high-lighted the drawbacks and limitationsof each method. While cost effective-ness is clearly the most clinicianfriendly method, there is a clear issueon the best measure of effectiveness.Cost utility analysis has many attrac-tions, particularly in its holistic ap-proach to the patient, but it is not easyto use and its interpretation remainscontroversial. While authors are keento point out the economic cost ofwound management to the healthservices, there is often little evidenceon how these costs were derived.Moreover, the direct current costs ofwound management are just a part ofthe overall equation. Most studies failto appreciate the importance of thepatients and families in the treatmentprocess, and the indirect cost ofwound care that leads to lower pro-ductivity for society.
Clearly the health care agenda is ina state of flux. There are clear differ-ences in the way health care is deliv-ered in the countries of Europe. All arebattling with ever increasing costs ofhealth care, with increases in newtechnologies, and greater expectationsfrom the public. Within this environ-ment it is essential to provide quality‘effective’ care. While earlier dischargefrom hospital reduces in-patient stays,this may lead to longer and more in-tensive care within the communitysetting, either through formal or in-
formal carers. To evaluate the full im-pact of a new system of care it is essen-tial to determine all costs to the healthservices, the individual and society.The literature would suggest that wehave a long way to go before cost ef-fective wound care becomes a reality.There is a clear need to evaluate thecurrent treatments for pressure ulcertreatment and prevention, not onlywith regard to effectiveness, but alsoto assess the cost effectiveness of treat-ment. Unlike pharmaceuticals, med-ical devices do not need to be evalu-ated in clinical trials prior to theirlaunch on to the health care market.There is a clear need to evaluate thecurrent procedures for wound treat-ment and prevention, not only withregard to effectiveness, but also to as-sess the cost effectiveness of treatment.■
REFERENCES1. Cullum N Deeks J Fletcher A et al. The prevention and
treatment of pressure sores. Effective Health Care Bul-
letin 1995; 2: 1. Edinburgh. Churchill Livingstone
quality of life (HRQoL) in determin-ing outcomes of treatment.
METHODS OF COST
ANALYSIS
Because the need to balance cost witheffectiveness different types of eco-nomic appraisals have been proposed.The choice of method will be depend-ent on the expectations of the treat-ment outcome. In the following sec-tions we will outline the major costevaluation methods.
Cost minimization: This term is usedto describe studies where the out-comes of treatment are expected to bethe same, but the costs are likely todiffer. This type of analysis becomesmore important for the introductionof new therapies where the treatmentis already highly effective. An examplemight be a comparison of hernia re-pair performed laparoscopically or bythe conventional open procedure. Inthis analysis the outcome is the same(hernia repaired) but the costs of treat-ment may vary considerably.
Cost effectiveness: Whilst cost min-imisation may be useful in situationswhere the outcome is expected to beidentical, frequently there is a balancebetween the effectiveness of a treat-ment and the cost of each procedure.There are four possible outcomeswhen introducing a new procedureinto medical practice.
■ Outcome is better, cost is lower. Thisis the ideal situation, since by imple-menting the new procedure this im-proves the outcome and reduces cost.This new technique should be adopt-ed.■ Outcome is poorer, cost is higher.This situation is the worst possible,since not only is the new technique
more expensive, but it gives pooreroutcome. The new technique shouldbe discarded immediately.■ Outcome is better, cost is higher. Thisis a complicated problem since thepatients have improved but at extracost.■ Outcome is poorer, cost is lower. Aswith the previous outcome, a decisionhas to be made about the relative re-ductions in outcome, and the appro-priate level of spending reduction.
Cost effectiveness studies are designedto evaluate the latter two models ofcare. In these analyses it is importantthat the outcome is the same for bothtreatment groups.
Cost benefit: While cost effectivenessstudies rely on the outcomes of treat-ment being the same, there may bemultiple outcomes of interest, some ofwhich may show benefit, others thatmay not. Clearly, to evaluate the over-all relative benefits of each treatmentone must relate all outcomes to onecommon value. The common valuemost frequently used is that of a mon-etary unit. All outcomes, be theywound free years, medical complica-tions avoided or improvements in so-cial functioning are converted into amonetary equivalent. The analysisthat uses both the costs and conse-quences (outcomes) of treatment inmonetary terms are called cost bene-fit studies. Most studies referred to ascost benefit studies are actually costeffectiveness studies!
Cost Utility Analysis: Early evalua-tion of treatment effectiveness re-volved around the survival of patientsfrom life threatening diseases. Howev-er, the shift in focus from infectious tochronic diseases required a re-evalua-
tion of the appropriate outcomes oftreatment. Whilst quantity of life wasimportant, quality of life was also seento be as important, and led to the de-velopment of quality of life tools toevaluate this. Utilities are values thatare placed on health states that includedeath (zero) and 1 (perfect health).The principle depends on the trade offbetween quality of life and survival. Itmakes the assumption that years ofperfect health can be traded off forlonger periods of poorer health. Thus,one year of perfect health is equivalentto a health utility of 0.5 over twoyears. Utilities can have negative val-ues that reflect health states that areconsidered to be worse than death. Anexample of this may be intractablepain, unrelieved by medication. Thevalues of these utilities are derivedfrom population studies where partic-ipants are asked to rate certain diseasestates to evaluate their potential worthon this scale. The utilities derived atdifferent stages in a patient’s life (ordisease) may then be multiplied by theyears of life within each state to derivea single index that incorporates bothquality and quantity of life (the socalled QALY, or quality adjusted lifeyear). This has the advantage of pro-ducing a single outcome measure thatcan be used in economic assessment.The use of QALYs has many advan-tages in health economics since it al-lows for comparisons not only acrossdifferent medical interventions for thesame disease, but also between dis-eases. However, their use remains con-troversial and emotive, particularlywith respect to the evaluating the rel-ative benefits of high cost life savingsurgery to low cost interventions thatmay help many people. There mayalso be issues in relation to the as-sumption that all life has the same
Cost Effectiveness Panel
Prof. Peter Franks is alsochairing a EWMA OpinionPanel on cost effectivenessand clinical outcome forreimbursement purposes.
Other members of the panelare Prof. Nick Bosanquet,London University, and Prof.John Posnett, York University.
For more information seenext issue of the EWMAJournal.
Journal 1/01 01.05.01, 16:0426-27

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 128 29
surgical wounds by using suction todrain excess fluid from wounds.
Objectives: To assess the effectivenessof topical negative pressure (TNP) intreating people with chronic woundsand to identify an optimum TNPregimen.
Search strategy: The CochraneWounds Group Specialised TrialsRegister was searched until July 2000.Experts in the field and relevant com-panies were contacted to enquireabout ongoing and recently complet-ed relevant trials. In addition citationswithin obtained papers were scruti-nised to identify additional studies.
Selection criteria: All randomisedcontrolled trials that evaluated the ef-fectiveness of TNP in treating chron-ic wounds were considered.
Data collection and analysis: Tworeviewers conducted eligibility for in-clusion, data extraction and details oftrial quality independently. A narra-tive synthesis of results was under-taken as only two small trials fulfilledthe selection criteria and they useddifferent outcome measures.
Main results: Two small trials with atotal of 34 participants evaluated theeffectiveness of TNP on chronicwound healing. Trial 1 consideredpatient with any type of chronicwound; Trial 2 considered patientswith diabetic foot ulcers only. The tri-als compared TNP (as open cell foamdressing with continuous suction) forthe first 48 hours with saline gauzedressings. Trial 1 reported a statistical-ly significant reduction in wound vol-ume at 6 weeks in favour of TNP. Trial 2 (continuous suction, followedby intermittent suction after 48 hours)reported a reduction in the number ofdays to healing and a reduction inwound surface area at 2 weeks in fa-vour of TNP, – although no statisticalanalysis was reported.
Reviewers’ conclusions: The twosmall trials provide weak evidence sug-gesting that TNP may be superior tosaline gauze dressings in healingchronic human wounds. However,due to the small sample sizes andmethodological limitations of thesetrials, the findings must be interpret-ed with extreme caution. The effect ofTNP on cost, quality of life, pain andcomfort was not reported. It was notpossible to determine which was theoptimum TNP regimen.
EXAMPLE 2
Beds, mattresses and cushions forpressure ulcer prevention andtreatment Cullum N, Deeks J,Sheldon TA, Song F, Fletcher AW
This review should be cited as: CullumN, Deeks J, Sheldon TA, Song F, Fletch-er AW. Beds, mattresses and cushions forpressure ulcer prevention and treatment(Cochrane Review). In: The CochraneLibrary, Issue 1, 2001. Oxford: UpdateSoftware.
A substantive amendment to this sys-tematic review was last made on 21January 2000. Cochrane reviews areregularly checked and updated ifnecessary.
Objectives: To assess the effectivenessof pressure relieving beds, mattressesand cushions (support surfaces) in theprevention and treatment of pressureulcers.
Search strategy: Searches of 19databases, hand searching of journals,conference proceedings, and biblio-graphies.
Selection criteria: Randomised con-trolled trials evaluating support surfac-es for the prevention or treatment ofpressure ulcers. There was no restric-tion on articles based on language orpublication status.
Data collection and analysis: Tworeviewers undertook data extractionand assessment of study quality inde-pendently. Trials with similar patients,comparisons, and outcomes werepooled. Where pooling was inappro-priate, trials are discussed in a narra-tive review.
MAIN RESULTS
Prevention: Twenty-nine RCTs ofsupport surfaces for pressure ulcer pre-vention were identified. Some highspecification foam mattresses weremore effective than ‘standard’ hospi-tal foam mattresses in moderate-highrisk patients. Pressure relieving mat-tresses in the operating theatre re-duced the incidence of pressure ulcerspost-operatively. The relative merits ofalternating and constant low pressure,and of the different alternating pres-sure devices are unclear. Seat cushionsand simple, constant low-pressuredevices have not been adequately eval-uated. Limited evidence suggests thatlow air loss beds reduce the incidenceof pressure ulcers in intensive care.
Treatment: Six RCTs of supportsurfaces for pressure ulcer treatmentwere identified. There is good evi-dence that air-fluidised and low airloss beds improve healing rates. Seatcushions have not been adequatelyevaluated. Two RCTs evaluated sur-faces for both prevention and treat-ment in the same trial.
REVIEWERS’ CONCLUSIONS
Prevention: There is good evidence ofthe effectiveness of high specificationfoam over standard hospital foam, andpressure relief in the operating theatre.
Treatment: There is good evidence ofthe effectiveness of air-fluidised andlow air loss devices as treatments.Overall, however, it is impossible todetermine the most effective surfacefor either prevention or treatment. ■
U sing research findings to make effectivedecisions about health care is a complexprocess. A comprehensive review of the
literature revealed a plethora of papers highlight-ing factors that impact on the effective use ofresearch. It is clear from these studies that thereare a number of barriers to research use.
These include issues such as:i lack of access to the large volume of research
informationii the need for good critical appraisal and li-
brary skillsiii lack of clarity in the presentation of research
findingsiv limited methods of dissemination within or-
ganisations
There are a number of initiatives to improve re-search access and utilisation. One such initiativeis the Cochrane Collaboration. This is an inter-national organisation involved in the productionof systematic reviews of clinical trial data to an-swer questions of effectiveness. The aim of the or-ganisation is to help people make informed choi-ces about health care interventions by conducting,maintaining and promoting access to systematicreviews of relevant research. The Collaboration ismade up of review groups with a specific subjectinterest. There are currently 50 groups contribut-ing to the work.
The Cochrane Wounds Group seeks to use pre-dominantly randomised controlled trial evidenceof the effects of interventions for the preventionand treatment of wounds and their complications.This includes interventions for the primary pre-vention of pressure ulcers, leg and foot ulcers;interventions to prevent complications ofwounds, e.g. surgical wound infection, scarring;and interventions to aid the healing of wounds(including burns) e.g. dressings, bandages, bedsand mattresses.
Only valid, objective outcomes such as pro-portion of wounds healing, healing rates, inci-
dence of wounds or infection are considered.Quality of life is included when reliable and validoutcome measures have been used.
Duplication of effort is avoided by liaison with theSkin, Injuries, Metabolic and Endocrine Disor-ders and Peripheral Vascular Disease Groups. TheCochrane Peripheral Vascular Disease Group con-ducts reviews in arterial and venous disease inwhich wound healing or incidence is not a prima-ry outcome measure. The Cochrane InjuriesGroup conducts reviews in the prevention ofburns and in the care of the burned patient. TheWounds Groups are maintaining 15 completedreviews and preparing 13 further reviews. Moreinformation can be obtained from contactingAndrea Nelson at the address. Abstracts of theCochrane Reviews are also available online atwww.cochrane.org
Examples of current abstracts are outlined below.
EXAMPLE 1
Topical negative pressure for treating chronicwoundsEvans D, Land L
This review should be cited as: Evans D, Land L.Topical negative pressure for treating chronic wounds(Cochrane Review). In: The Cochrane Library, Issue1, 2001. Oxford: Update Software.
A substantive amendment to this systematicreview was last made on 14 November 2000.Cochrane reviews are regularly checked andupdated if necessary.
Background: Chronic wounds mainly affect theelderly and those with multiple health problems.Despite the use of modern dressings, some ofthese wounds take a long time to heal, fail to heal,or recur, causing significant pain and discomfortto the person and cost to health services. Topicalnegative pressure is used to promote healing of
Using research in wound management decisions:
The Role of theCochrane Wounds Group
Michelle Briggs
RGN, MSC
Assistant Director,
Centre for the Analysis
of Nursing and
Professional Practice,
Leeds, UK
Chemistry Degree,
Nottingham University
Master in Nursing.
Currently part time PHD
student, studying the
Experienced Pain of
Leg Ulcer Patients.
Member of the
EWMA Council.
Co-Editor of the
EWMA Journal
Co-Editor of the
Cochrane Collaboration
Wound Group
Correspondence to:
Michelle Briggs,
CANP Meanwood
Park Hospital,
Tongue Lane LS6 4QB
Leeds
United Kingdom
Mbriggs@
allwoodley.u-net.com
or to:
E Andrea Nelson
Review Group
Co-ordinator,
Research Fellow Centre for
Evidence Based Nursing,
Dept. of Health Studies,
Univ. of York,
Genesis 6,
York YO105DQ
United Kingdom
Tel: +44 1904 434110
Fax: +44 1904 434102
E-mail: [email protected]
Michelle Briggs
Journal 1/01 01.05.01, 16:0428-29

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 130 31
[Pegasus ad]
Chris Lawrence has recently retired from theEWMA Council, having served as a membersince the foundation of the organization in
1991. Over the years he has made a significant contri-bution to the development of the Association, not leastas President from 1995-6.
I cannot resist starting with a personal anecdote. I firstmet Chris in 1986 when he was Director of the BurnsResearch Unit at Birmingham Accident Hospital. I wasa mere novice in Tissue Viability at the time and verythrilled to be meeting such an important person. Myfirst impression was that I had never seen a desk so piledhigh with paper. The second was bemusement when hedemonstrated the efficiency of a new smoke alarm (alsoon his desk) by blowing cigarette smoke into it !
On a more serious note, Chris brought with him to theAssociation, his considerable knowledge of microbio-logy and acute wounds and his keen scientific mind.This has been invaluable in stimulating debate at ourconferences, especially in relation to scientific papersand the ongoing discussions relating to infection.Chris has considerable experience of society constitu-tions which was of great value when we were establish-ing EWMA as first a society and then a charity. Latterly,Chris took on the thankless task of editor of the EWMAReporter.
So, thank you Chris for your contribution. We wish youwell in your retirement.
Carol Dealey, April 2001
■ Brown J, McElvenny D, NixonJ, Bainbridge J, Mason S. Somepractical issues in the design,monitoring and analysis of a se-quential randomized trial inpressure sore prevention. Statis-tics in Medicine.2000;19(24):3389-3400.
■ Cullum N, Deeks J, Sheldon TA,Song F, Fletcher AW. Beds, mat-tresses and cushions for pressuresore prevention and treatment(Cochrane Review). In: TheCochrane Library, Issue 4, 2000.Oxford: Update Software.
■ Flemming K, Cullum N. Thera-peutic ultrasound for pressuresores (Cochrane Review). In:The Cochrane Library, Issue 4,2000. Oxford: Update Software.
■ Flemming, K. Cullum, N. Elec-tromagnetic therapy for thetreatment of pressure sores(Cochrane Review). In: TheCochrane Library, Issue 4, 2000.Oxford: Update Software.
■ Kallianinen LK, Hirshberg J,Marchant B, Rees RS. Role ofplatelet-derived growth factor asan adjunct to surgery in themanagement of pressure ulcers.Plastic and Reconstructive Surgery.2000;106(6):1243-8.
■ Kuhn MA, Smith PD, Hill DP,Ko F, Meltzer DD, Vande BergJS, Robson MC. In vitro fibro-blast populated collagen latticesare not good models of in vivoclinical wound healing. WoundRepair and Regeneration.2000;8(4):270-6.
■ Land L, Evans D, Geary A, Tay-lor C. A clinical evaluation of analternating-pressure mattress re-placement system in hospital andresidential care settings. Journalof Tissue Viability 2000;10(1):6-11.
■ Nixon J, Brown J, McElvennyD, Mason S, Bond S. Prognosticfactors associated with pressuresore development in the immedi-ate post-operative period. Inter-national Journal of NursingStudies. 2000;37(4):279-89.
■ O’Meara SO, Cullum N, MajidM, Sheldon T. Systematic re-views of wound care manage-ment: (3) antimicrobial agentsfor chronic wounds; (4) diabeticfoot ulceration. Health Technolo-gy Assessment. 2000;4(21):1-237.
■ Robson MC, Hill DP, SmithPD, Wang X, Meyer-Siegler K,Ko F, VandeBerg JS, Payne WG,Ochs D, Robson LE. Sequentialcytokine therapy for pressure ul-cers: clinical and mechanistic re-sponse. Annals of Surgery.2000;231(4):600-11.
Research into Pressure Ulcers– Studies of effectiveness, diagnosis andprognosis during 2000
■ Anthony D, Reynolds T, RussellL. An investigation into the useof serum albumin in pressuresore prediction. Journal of Ad-vanced Nursing. 2000;32(2):359-65.
■ Byers PH, Carta SG, MayrovitzHN. Pressure ulcer research is-sues in surgical patients.Advances in Skin and WoundCare. 2000;13(3 Pt 1):115-21.
■ Ferrarin M, Andreoni G, PedottiA. Comparative biomechanicalevaluation of different wheel-chair seat cushions. Journal ofRehabilitation Research andDevelopment 2000;37(3):315-24.
■ Garber SL, Rintala DH, HartKA, Fuhrer MJ. Pressure ulcerrisk in spinal cord injury: predic-tors of ulcer status over 3 years.Archives of Physical Medicine andRehabilitation. 2000;81(4):465-71.
■ Kramer JD, Kearney M. Patient,wound, and treatment character-istics associated with healing inpressure ulcers. Advances in Skinand Wound Care 2000;13(1):17-24.
List compiled by E. Andrea Nelson
Questions of
effectiveness
Questions about
diagnosis/prognosis
Chris Lawrence:An Appreciation
Journal 1/01 01.05.01, 16:0430-31

EWMA JOURNAL 2001 VOL 1 NO 1 33
American Academy of Wound Management AAWM aawm.org USA
American Burn Association ABA ameriburn.org USA
Association for the Advancement of Wound Care AAWC aawc1.org USA
Australian Wound Management Association Inc. AWMA awma.com.au Australia
British Burn Association BBA – UK
European Burn Association EBA – Europe
European Pressure Ulcer Advisory Panel EPUAP epuap.org Europe
European Tissue Repair Society ETRS etrs.org Europe
Grupo ULCESUR ulcesur.com Spain
Hong Kong Council of Enterostomal Therapists H.K.C.E.T – Hong Kong
ICNA ICNA – Europe
Korean Association of Wound Ostomy Continence Nurses KAWCON – Korea
Mediterranean Burns Club – Southern Europe
National Decubitus Foundation NDF decubitus.org USA
National Pressure Ulcer Advisory Panel NPUAP npuap.org USA
Pediatric Tissue Society – Europe
PERSE PERSE – France
Società Italiana Riparazione Tissulate – Italy
Société Française et Francophone des Plaies et Cicatrisations SFFPC sffpc.org France
South Australian Wound Management Association SAWMA wound.sa.edu.au Australia
Tissue Viability Society TVS tvs.org.uk UK
Wound Care Institute, Inc. woundcare.org USA
Wound Care Society WCS woundcaresociety.org UK
Wound Care International, Inc. woundcareinternational.com USA
Wound Care Society of Thailand – Thailand
Wound Healer woundhealer.com USA
Wound Healing Society woundhealsoc.org USA
Wound Healing Society (Singapore) – Singapore
Wound, Ostomy and Continence Nurses Society WOCN wocn.org USA
Woundcare Consultant Society WCS wcs-nederland.nl Holland/Belgium
Organisations
Co-operating Organisations
Name Abbr. www. Country
Associação Portuguesa de Tratamento de Feridas – Portugal
Associazione Infermestica per lo Studio delle Lesioni Cutanee AISLeC aislec.it Italy
Associazione Italiana Ulcere Cutanee AIUC – Italy
Dansk Selskab for Sårheling DSFS dsfs.org Denmark
Deutsche Gesellschaft für Wundheilung und Wundbehandlung DGfW dgfw.de Germany
Finnish Wound Care Society FWCS – Finland
Grupo Nacional para el Asesoramiento en Úlceras por
Presion y Heridas Crónicas GNEAUPP gneaupp.org Spain
Leg Ulcer Forum LUF – UK
Lymphoedema Support Network LSN lymphoedema.org UK
Norsk Interessefaggruppe for Sårheling NIFS saar.dk/norsk.html Norway
Slovenian Wound Management Association SWMA – Slovenia
Svenskt Sårläkningssällskap SSS sarlakning.com Sweden
Wound Management Association of Ireland WMAI – Ireland
As a part of the new EWMAstrategy, we have within thelast year worked hard in an
attempt to create closer bonds be-tween the national wound healingand management organisations.
Through co-operating withEWMA the national organisationreceives a large number of benefitsincluding:
■ The members of the organisationregister as EWMA members atconferences
■ The members will receive theEWMA Journal
■ A quarter page or half a page inthe EWMA Journal for associa-tion data or national news
■ Link at EWMA web-site
■ Invitation for EWMAco-operating associationworkshop at to the annualEWMA conference
■ 1-2 free invitations for theannual EWMA Conference
■ Participate in the EuropeanCurriculum Group, developingguidelines for education withinthe Wound Management area
■ Co-operative status in relation toEWMA research funding
■ The organisation is free at anytime to co-operate with otherWound Management association
■ EWMA expects no financialobligations from the co-operating association
On the following pages you will finda presentation of some of the
European Co-operationorganisations which have agreed toco-operate with EWMA. Others willbe presented in the following issuesof the EWMA Journal.
We are very happy that so manywithin such a short time span haveagreed on the need for closer co-operation within Europe. We arealso convinced that the number willkeep rising, and that we all are wellon our way to create a truly Europe-an forum for the improvement ofwound management.
We hereby hope that more asso-ciations will se the opportunitiesand contact us, so that we can allbenefit from the synergy that is be-ing created around EWMA.
Christine Moffatt, EWMA President
[AdParkhouse]
Journal 1/01 01.05.01, 16:0432-33

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 134 35
The association has carried outepidemiology studies to examinethe size of the problem of chronicwounds in Italy. In 1984 the report-ed prevalence of pressure ulcers was8.6% rising in 1993 to 12.45% inthe 2288 patients examined. Thisdata was confirmed in 1996 when aprevalence of 13.98% was found in3296 patients, with 11.38% in2258 patients cared for in homecare.This study highlighted the problemsof correct use of wound care materi-als, and the organisation began tofocus on these issues. In 1998 in astudy involving 23 AISLeC mem-bers and 2665 patients an overallprevalence of chronic wounds was56.2%. Within this population24.84% suffered pressure ulcers,20.07% vascular lesions and11.29% lesions on the foot. Thislarge scale municipal study showedthe improper use of antibiotics andantiseptics. AISLeC have beenworking with thirty hospitals to im-plement protocols for assessmentand management and to revise thedrug tariff in relation to wound careproducts.
The organisation has worked withthe Italian Health Ministry usingthis data to intergrate the control ofpressure ulceration into the ItalianNational Health Program includinga major campaign through the mostimportant newspapers.
AISLeC was established in 1995 asa nursing organisation concernedwith wound healing problems andquality assurance initiatives for thispatient group. In 1998 the associa-tion became multidisciplinary wel-coming members from other profes-sional groups to ensure a truly glo-bal approach to care.
The association has been involvedin many quality assurance initiativesthroughout Italy since the organisa-tion began. The following are areport of the activities in this timeperiod.
■ 60 study days■ 76 courses (14 University) in-
volving 6600 nurses and somedoctors
■ Pressure ulcer epidemiology■ Winner of EWMA 1997 poster
prize■ Finalist at Quality Prize 1997
VRQ Italy■ Development and editing of in-
formation brochures for profes-sionals and care givers
■ Consultancy to Health Depart-ments and Professional Associa-tions
■ Training and consultancy forpharmaceutical and dressingcompanies
■ Contribution to pressure ulcertreatment guidelines circulation
Finnish Wound Care Society wasfounded 17.11.1995. Today the soci-ety has approximately 1500 individu-als and 24 corporate members. Fin-land has 5 million inhabitants.
The Society is a forum for multi-professional discussion and debateconcerning on wound care. The so-ciety also co-operates with nationalhealth authorities and through thisco-operation contributes to promo-tion of the development of woundcare in Finland.
The aims of the Society are
■ To promote multi-professionalco-operation by a holistic ap-proach to wound care
■ To promote good quality of careof the wound patients
■ To promote multidisciplinary re-search and experiments for thedevelopment of wound care
■ To promote professional educa-tion in the field of wound care
The activities of the Society
■ International co-operation withthe Wound Care Societies inNordic and European countries
■ Group travels to internationalwound care conferences
■ Scholarships for the participationin international conferences andresearch projects of wound care
■ Official Finnish translation andpublication of the internationalrecommendations for woundcare (eg. pressure ulcer preven-tion guidelines and pressure ulcertreatment guidelines of the Euro-pean Pressure Ulcer AdvisoryPanel).
■ Regional workshops and semi-nars on wound care. In 2001the main theme will be pressureulcers as a result of the PEPUSsurvey organized by EPUAP.
■ The journal HAAVA has beenpublished since 1998 quarterly.In the year 2001 the themes willbe Burn Care, National confer-ence of Wound Care, treatmentsof diabetic foot ulcers and infec-tions.
■ Annual National Wound CareConferences has been arrangedsince 1996. In 2001 the confer-ence theme has been AcuteWounds and the Care Path ofAmputation Patient.
The mail address is
PL BOX 1602201 EspooFinland
Tel + 358 9 412 5074Fax + 358 9 412 5074e-mail: [email protected]://pesonal.inet.fi/yhdistys/haava
AISLeCAssociazione
Infermestica per loStudio delle
Lesioni Cutanee
Italian CutaneousWounds
Association
Andrea Bellingeri, President
Battistino Paggi, Vice-President
Correspondence to:
AISLeC
Via Larer n 6
27100 Pavia
Italy
Tel: +39 382 422133
Fax: +39 382 523203
www.aislec.it
FWCSFinnish Wound
Care Society
Helvi Hietanen
Chairperson
Correspondence to:
PL BOX 16
02201 Espoo
Finland
Tel: +358 9 412 5074
Fax: + 358 9 412 5074
e-mail:[email protected]
http://personal.inet.fi/yhdistys/haava
Journal 1/01 01.05.01, 16:0434-35

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 136 37
Danish Wound Healing Societywas founded in 1992 by a groupof doctors and nurses interested inwound healing and management.At that time no functional woundhealing society existed in Scandina-via.
Aim: Danish Wound HealingSociety was founded in order to:1. Organize and co-ordinate con-
gresses and make joint meetingsin connection with other nation-al as well as international socie-ties with similar interests.
2. Increase and support educationand research in the area ofwound healing, especially relatedto types of wounds, epidemiolo-gy, pathogenesis, pathology, diag-nostic, prevention and treatmentof wounds with different aetio-logy.
3. Improve friendship and co-workbetween groups working inwound healing and wound care.
4. Work for a better collaborationbetween organisations, compa-nies and indivuals within alltypes of wound healing andwound care.
Organisation: The Society boardconsists of 8 board members(4 medical doctors and 4 nurses).
The Society has established twosubgroups.
The publishing group handles thepublishing of the journal of the So-ciety: ‘Sår’ (Wound). The journal ispublished quarterly and is free formembers of DWHS. Presently it hasalmost 2000 subscribers includingall of Scandinavia. Surveys as well asoriginal articles are published. Newliterature is reviewed and futuremeetings and congresses are an-nounced. In the journal it is alsopossible to debate all types of healthcare problems related to woundhealing and care.
The educational group takes care ofmeetings, workshops and congressesarranged by the Society.
DWHS is furthermore involved innational as well as internationalarrangements in cooperation withother societies.
The Leg Ulcer Forum (LUF),formed in 1993, was initially set upas a support network for all thosewhose had completed the EnglishNational Board Course (ENB) N18for nurses (The Management ofPatients with Leg Ulcers). It initiallyprovided a unique opportunity forformer course colleagues to shareexperiences and support each otheras they returned to their own clinicalenvironments. Often successfulindividuals would be the only spe-cifically trained nurse in their areaand yet their managers expectedthem to both organise and set uplocal leg ulcer services which had tobe seen to be clinically and costeffective.
As the availability of ENB N18courses has increased within theUnited Kingdom – as well as thenumber of nurses who have com-pleted the course – so has the natureof the LUF changed to reflect itsenvironments: clinical, political andsocial. Despite this, the aims of theforum have remained unchangedand are as highlighted below:
1. To promote a local network of re-sources for the benefit of patientssuffering from either ongoing legulcer or wound managementproblems, through the establish-ment of specialist services supportedby appropriately qualified staff –some of whom may be termed clini-cal nurse specialists/advanced practi-tioners.
2. To provide a forum for theadvancement of the education ofnurses and other health care profes-sionals involved in the treatment ofleg ulcers and related conditions.
3. Development of new branches ofthe Leg Ulcer Forum within UK.
4. To liase with similar and appro-priate organisations in other coun-tries in order to facilitate interna-tional affiliations.
The above can be summarised bythe current LUF philosophy, ‘Anational forum to advance clinicalpractice for the management of pa-tients with leg ulcers and associatedconditions through the educationand support of all relevant profes-sionals’. This philosophy was agreedby the forum executive, followingthe formal adoption by the LUFmembership of a working constitu-tion - at the Annual General Meet-ing held in 2000. Membership ofthe forum – open to all healthcareprofessionals who are actively in-volved with the management of pa-tients with leg ulcers or wounds –has always been and remains free,thanks both to the support of anumber of commercial sponsors aswell as the success of the Annual LegUlcer Forum Conference. However,it should be noted that membershave to actively renew each year byfilling in a simple renewal form.This ensures that the membershipremains ‘live’ - currently over 1000!Additionally members are given theopportunity to enter their details ona ‘live’ database with at present over150 entries. One of its aims is to en-sure that as patients move out of apractitioner’s area, they can be re-ferred to another apropriate servicewithout delay – providing continui-ty of care!
In recent years the LUF has de-veloped affiliations with the All IrishLUF, the British Lymphology Socie-ty (BLS), The Society of VascularNurses (SVN) and the Socity of Vas-cular Surgeons. One of the goals forthe LUF executive for the currentyear is to consolidate and further de-velop these links as well as fostertentative international links whichhave already been made with appro-priate organisations in Australia andCanada.
I look forward to correspondingwith you/welcoming you as a mem-ber of the Leg Ulcer Forum in thenot too distant future.
LUFThe Leg
UlcerForum
Mark Collier
Chairperson
Correspondence to:
Leg Ulcer Forum Secretariat
c/o PO Box 337
Hartford
Huntigdon
PE29 1FX
United Kingdom
Tel: +44 1480 456798
www.legulcerforum.com
Finn Gottrup
President
Correspondence to:
Niels Müller
Cypresvej 18
DK-3450 Allerød
Denmark
Tel: +45 4817 7025
Fax: +45 4817 7025
www.dsfs.org
DSFSDanish Wound
Healing Society
The latest issue of ‘Sår’
In 1994 the first meeting of EWMAoutside England was arranged inCopenhagen and supported byDWHS. In 1998 The EuropeanTissue Repair Society assembled al-most 1000 delegates in Copenha-gen, also supported by DWHS.We have also established a co-opera-tion with the European WoundManagement Association.
MembershipPersonal membership is open to allhealth care personal interested inwound healing and management,independent of nationality. Also nonhealth care personal active in re-search or other activities related towound healing and wound care canbecome members. Companies canbe sponsor members by paying asponsor fee each year. These mem-bers have advantages like specialmentioning in our journal and a cer-tain area of free exhibition at the an-nual Society congress.
Presently the Society has almost1000 members and 22 sponsors.The annual membership fee present-ly is 225 DKK (18£), which in-cludes 4 yearly issues of the journalSår.
Journal 1/01 01.05.01, 16:0436-37

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 138 39
NIFS means ‘spooky’ in Norwegian andis an abbreviation for ‘Norsk Interesse-faggruppe for Sårheling’ (NorwegianWound Healing Association). The aimof the organisation is to organise andcoordinate meetings and congresses re-lated to the subject area ‘Wounds’. TheAssociation also supports education andresearch within Wound Healing. NIFSis furthermore working actively to co-operate with and between organisa-tions, companies and individuals withinterest in Wound Healing.
NIFS has more than 500 members,spread all over Norway and consistingof nurses, doctors, orthopaedic thera-pists and -engineers, nursing assistentsand medical secretaries.
Healthcare, Wound Healing And SoreManagement in NorwayNorway is a lengthy country with rug-ged geographical conditions and 4.5million inhabitants. Although approxi-mately 1 million people live aroundOslo, the general settlement is very de-centralized. The geography is thereforea major factor in regards to the actualtreatment offered to the patients, but isalso of great importance in the runningof a national interest organisation. Nor-way has a very developed public healthcare system, and it is only in the majorcities one will find private clinics. With-in the Norwegian system the patientusually starts by contacting a generalpractitioner, who, if necessary, refers thepatient to a specialist or a hospital.Wounds are diagnosed and treated bysurgeons, orthopaedicians, dermatolo-gists and general practitioners. Chang-ing of dressings is however most oftendone locally at a doctor’s office or by ahome nurse. Chronic wounds is a lowstatus ailment in Norway, and the inter-est within the medical doctors concern-ing wound problems has until recentlybeen very small. Luckily things are be-ginning to improve, although thereprobably still are many patients receiv-ing inconsequent treatment for theirchronic wounds, because the under lay-ing problem has not been properly ad-dressed.
The Focus Areas of NIFSThe highest improvement potentialityis in increasing the knowledge ofwound diagnostics and to strengthenthe commitment amongst general prac-titioners to carry out the diagnostics.Besides there is a great need to educateand train the local health staff who haveto work with the practical wound treat-ment. NIFS sees the creation of inter-disciplinary forum for all connected tothe wound management environment,as its main objective. The first step hasbeen to organize an annual two-dayconference on wound aspects. Further-more we give assistance when interestgroups arrange seminars, i.e. the Ni-daros congress for general practitioners.
As chronic wounds are treated on alllevels in the health care system, involv-ing several specialities, communicationproblems often arise. The standard pro-cedures for the treatment of woundsand which speciality that should takecare of the patient can often vary withinthe same geographical area. Both thepatients and the public health budgetwould benefit greatly by having clearreference procedures and consequentwound treatment procedures. NIFS willcontinue to focus on this area. NIFS isalso working to develop wound journalsfor diabetes foot sores and other leg orfoot ulcers, which are to be used all overthe country.
NIFS is an ideological non-profit or-ganisation. Due to the limited time ofeveryone involved, we have in the firstperiod been forced to prioritise the con-solidation of the organisation inwards.We do however have a pleasant andclose co-operation with DSFS (DanishWound Healing Society), especiallyconcerning the editing of the magazineSÅR, which is distributed to all NIFSmembers. In the forthcoming period weintend to look more out towards Eu-rope, and EWMA will be a future part-ner in the process.
The last year has seen the formationof a new wound healing society inItaly.
The Associazione Italiana UlcereCutanee (AIUC – Italian CutaneousUlcer Association) was formed to af-front didactical and healthcarethemes in Italian wound care, withthe objective of promoting initia-tives regarding tissue repair and togroup together the interest ofhealthcare staff that work in woundcare.
Cutaneous ulcers in Italy are aproblem that regards around 1.5%of the population, a percentage onthe rise. A healthcare team made upof geriatricians, dermatologists, vas-cular surgeons, diabetologist andspecialised nursing staff carries outtreatment of these patients. TheAssociation has assumed a multi-disciplinary identity right from itsconception in order to represent aswidely as possible the variousmedical specialities involved in themanagement of skin ulcer patients.
The first annual AIUC confer-ence was held last November inRome, at the Istituto Dermopaticodell’ Immacolata (IDI), a dermato-logy hospital in the centre of Rome,which carries out a large amount ofday clinic and in-patient treatments.During the conference the ExecutiveCommittee, assembled in order toelect new representatives, determinethe terms of office for Committeemembers and decide the dates offuture conferences.
The main objectives of the Asso-ciation are aimed towards the im-provement of the training of medi-cal and nursing staff in the manage-ment of patients with skin ulcers,especially in the light of new etio-pathogenetic concepts of the variousdiseases involved and the develop-ment of new therapeutic techno-logies.
The Association also intends toextend working relationships withthe main international wound caresocieties and thus favour cultural ex-change. To further this end, Prof.Christine Moffatt, President of theEuropean Wound Management As-sociation and Prof. Keith Harding,President Elect of the European Tis-sue Repair Society, were invited tothe first annual AIUC conference.
The next national AIUC confer-ence will be held in Milan from the14th to the 16th November 2001and will be organized by ProfessorPiero Bonadeo.
AIUC Executive Committee
■ Prof. Giovani Micali, President■ Dr. Luca Chinni, President Elect■ Dr. Giorgio Guarnera, Secretary■ Dr. Massimo Papi, Treasurer■ Dr. Clemente Potenza, Relations
with Surgical Societies■ Dr. Elia Ricci, Relations with
national Health System■ Dr. Marco Romanelli, Relations
with Foreign Wound HealingSocieties
■ Mr. Battistino Paggi, Relationswith Nursing Sanitary System
■ Mr. Pierluigi Deriu, Relationswith Professional SanitaryDevelopment
NIFSNorsk InteresseFaggruppe for
Sårheling
Norwegian WoundHealing
Association
Theis Huldt-Nystrøm
Chairperson
Correspondence to:
NIFS Secretariat
Kirsti Gjønnes
Sårpoliklinikken
Buskerud Sentralsykehus
N-3004 Drammen
Tel: +47 3280 3339
Fax: +47 3280 3344
E-mail: [email protected]
Giovanni Micali
President
Correspondence to:
Marco Romanelli
University of Pisa
Dept. of Dermatology
Via Roma 67
I-56126 Pisa
Italy
Tel: +39 0 50 992436
Fax: +39 0 50 551124
E-mail: [email protected]
AssociazioneItaliana Ulcere
Cutanee
Italian Associationfor Cutaneous
Ulcers
Journal 1/01 01.05.01, 16:0538-39

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 140 41
Wound care is nowadays an impor-tant and emergent challenge fornurses in Spain as the chronicwounds problem involves importantissues like quality of life of patients,cost for the National Health Serviceas well as important efforts forhealth care workers.
Nurses have an important role inthe wound management develop-ment, in collaboration with otherhealth care professionals, in order toachieve a holistic approach to theproblem of chronic wounds with theinvolvement of patients and theircaregivers.
The Spanish Health Care Systemis closely influenced by the improve-ment of the Primary Health CareNetwork, which has changed therole of the professionals in PrimaryHealth Care, specially the role ofnurses. Primary Health Care nursesare organised in Primary HealthCare Teams where they share a listof 2000-2500 persons older than 14years with a General Practitioner.These nurses are responsible for thecare of patients with leg ulcers, pres-sure ulcers and other chronicwounds in their offices in the Prima-ry Health Care Centre or in thehome of the patients. PrimaryHealth Care Centres use to haveguidelines for chronic wounds andthe Social Security reimburses thegreat majority of dressings (with aprescription signed by the GP).
In agreement with the philoso-phy of Primary Health Care, the ap-proach of chronic wounds is basedon their prevention and the involve-ment of family caregivers in self careactivities which include the treat-ment of the patients (specially in pa-tients with pressure ulcers at theirhomes). In a research done in 1995the amount of time spent by familycaregivers in the treatment at homeof patients with pressure ulcers wasestimated to 130 501 minutes everyyear (in a population of 66 patientswith pressure ulcers treated at theirhomes) in comparison with the 145
241 minutes spent by primaryhealth care nurses [3]. Although theSpanish National Health Service isemphasising home care activities,the main problem in this level pro-bably is the lack of prevention mate-rial (mattresses and overlays) fundedby the social security.
In the case of leg ulcers, there aresome recent experiences of settingup incipient community leg ulcerswith a comprehensive approach ofthe care of this type of patients thatincludes the assessment of patientsand the use of compressive therapyfor venous leg ulcers.
In hospitals and long term facili-ties there is a variety of approachesto the chronic wounds problem, buta great majority of settings are devel-oping local guidelines about preven-tion and treatment and are startingto invest in prevention equipment,although this type of material is notperceived as crucial in the budgets ofthe institutions.
In 1994, in order to highlight theimportance of the problem ofchronic wounds, and specially pres-sure ulcers, the ‘Grupo Nacionalpara el Estudio y Asesoramiento enÚlceras por Presión y HeridasCrónicas – GNEAUPP’ (SpanishPressure Ulcers and ChronicWounds Advisory Panel) was creat-ed. This is an interdisciplinary socie-ty with 1500 health care profession-als, most of them nurses. The aim ofthe GNEAUPP is to focus on thepromotion of evidence-based com-prehensive approaches for the pre-vention and treatment of chronicwounds involving different types ofdisciplines.
Every two years the GNEAUPPorganizes a national meeting aboutpressure ulcers and chronic woundsand is involved in other Europeanorganisations like the EuropeanPressure Ulcers Advisory Panel(EPUAP) and the European WoundManagement Association (EWMA).The GNEAUPP has publishedseveral guidelines:
■ The prevention of pressure ulcers■ The staging of pressure ulcers■ The treatment of pressure ulcers■ Obtaining samples from chronic
wounds■ Epidemiological indicators
GNEAUPP has funded several re-search projects about pressure ulcersand is developing a white reportabout pressure ulcers in Spain.
The GNEAUPP has its ownwebsite: www.gneaupp.org, it pro-duces a newsletter and publishes ascientific journal, Gerokomos-Hel-cos, in conjunction with the ‘Socie-dad Española de Enfermería Geriá-trica y Gerontológica’ (Spanish Geri-atric and Gerontologic Nursing So-ciety).
In 1999 the GNEAUPP made asurvey between their members thatmay be useful for describing someissues that concern to the problemof Chronic wounds in Spain in rela-tion with the professionals [5].
The evolution of both nursing andwound care in Spain has producedan increase of research activities infields like clinical, epidemiologicaland basic sciences. As an example ofthe research activity in pressure ul-cers and chronic wounds in ourcountry we can summarise the sub-jects of the 112 oral presentations
Method: Postal questionnaire sent to all members of the GNEAUPP.1434 questionnaires sent, 431 questionnaires (30%) answered.
Which is for you (in theory) the best option for treating pressure ulcers?Moist environment dressings: 79.1% Traditional dressings: 12.3%Both: 7% NA: 1.6%
Which option can you use in your institution for treating pressure ulcers?Both: 92.3% Only traditional dressings: 3.5%Only moist environment dressings: 3.2%
Do you need more education about pressure ulcers?Yes. 94.9% No: 4.6% NA: 0.5%
Have you done any research about pressure ulcers?Yes: 33.4% No: 65.4% NA: 1.2%
Do you use to review journals periodically that include papers aboutpressure ulcers?
Yes: 87.2% No: 12.5% NA: 0.2%
Questionnaire about pressure ulcers sent to all the members of the GNEAUPP [5]
term policies and targets for the Na-tional Health Service.
Subjects of the oral presentations and postersto the 3rd Symposium of the Spanish PressureUlcers and Chronic Wounds AdvisoryPanel, Logroño 7-11 April 2000 [6]:
■ Treatment of chronic wounds(dressings) (28)
■ Treatment of chronic wounds (15)■ Epidemiology of pressure ulcers (17)■ Special surfaces (5)■ Chronic wounds informatic records (4)■ Prevention of pressure ulcers (4)■ Pressure ulcers and quality of care (6)■ Treatment of chronic wounds
(guidelines) (6)■ Education in chronic wounds (4)■ Chronic wounds records (3)■ Pressure ulcers assessment (2)■ Caregivers (2)■ Risk assesment scales (2)■ Aetiology of pressure ulcers (2)■ Four layers bandage (2)■ Treatment of leg ulcers (2)■ Chronic wounds research practice (1)■ Cost of chronic wounds (1)■ Wounds in sportmen (1)■ Epidemiology of leg ulcers (1)■ Nutrition and pressure ulcers (1)
In brackets: number of abstracts
and posters accepted to the 3rd Sym-posium of the Spanish Pressure Ul-cers and Chronic Wounds AdvisoryPanel that was held in Logroño (LaRioja) last April and joined about1 000 professionals, the great majori-ty of them nurses, involved inchronic wounds.
In Spain there is no speciality ofwound healing, but some education-al activities, most of them in theframework of post-graduated nurs-ing educational activities in geriatric,community and surgical nursing, aredrawing the basis of a future post-graduate university wound healingcourse. There are also a lot of shortterm educational activities support-ed by wound care companies thatare collaborating, some times injoint activities with the GNEAUPP,in the education and support for allhealth care professionals involved inwound healing.
The future of wound healing inSpain is in close relations with theimportance of this problem for theNational Health Service. Some au-tonomous regions with responsibili-ties in health care like Cataloniahave included specific targets aboutchronic wounds (pressure ulcers anddiabetic feet) in their health maps[7]. These health maps are a basictool for establishing medium-long
GNEAUPPGrupo Nacionalpara el Estudio y
Asesoramiente enUlceras por Presión y
Heridas Crónicas
Spanish PressureUlcers and
Chronic WoundsAdvisory Panel
Javier Soldevilla
President
Correspondence to:
Joan Enric Torra Bou
Consord Sanitari De Terrassa
C/Citra De Torrebonica E-8227
Terrassa, Barcelona
Spain
Tel: +34 45 49 11 17 68
Fax: +34 45 49 11 17 07
E-mail: [email protected]
www.gneaupp.org
References
1 Soldevilla Agreda JJ, Tora i Bou J-E. Epidemiología de
las úlceras por presión en España. Estudio piloto en la
Comunidad Autónoma de la Rioja. Gerokomos/Helcos
1999; 10(2): 75-87
2 Torra i Bou JE, Pereira A, Camañes G. Epidemiología
de las Úlceras de Pierna en Atención Primaria. Libro
resumen de ponencias y comunicaciones del 1er Con-
greso Iberiomaericano de Enfermería Geriátrica y Ger-
ontológica. Logroño, 7-11 abril 2000. Convatec: Lo-
groño, 2000
3 Torra i Bou JE. Epidemiología y coste de la atención a
pacientes con úlceras por presión atendidos por enfer-
mería en el ámbito de atención primaria del Consorci
Sanitari de Terrassa. In: VII Premio a la investigación
en Enfermería (1996). Madrid: Knoll , 1997
4 Grupo Nacional para el Estudio y Asesoramiento en
Úlceras por Presión y Heridas Crónicas. Documentos
GNEAUPP, Abril 2000. Logroño: Grupo Nacional
para el Estudio y Asesoramiento en Úlceras por
Presión y Heridas Crónicas, 2000
5 Torra i Bou JE, Soldevilla Agreda JJ. Libro blanco de
las úlceras por presión en España. In: Libro resumen
de ponencias y comunicaciones del 1er Congreso Ibe-
riomaericano de Enfermería Geriátrica y Gerontológi-
ca. Logroño, 7-11 abril 2000. Convatec: Logroño,
2000
6 Libro resumen de ponencias y comunicaciones del 1er
Congreso Iberoamericano de Enfermería Geriátrica y
Gerontológica. Logroño, 7-11 abril 2000. Convatec:
Logroño, 2000
Journal 1/01 01.05.01, 16:0540-41

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 142 43
Short descriptionThe Wound Management Associa-tion of Ireland (WMAI) is organis-ing all categories of health area staff:doctors, nurses, therapists a.o. inboth Southern and Northern Ire-land.
WMAI objectives■ To create a multi-disciplinary ap-
proach to Wound Management■ To support education in evi-
dence based treatment■ To encourage research■ To arrange study days, work-
shops and conferences■ To improve quality of life of all
patients and especially for thosewith ‘hard to heal wounds’
■ To work for a higher profiling ofthe area and its importance tosociety.
WMAI has successfully been organ-ising conferences with participationfrom all over Ireland. The annualconference now alternates between
North and South Ireland. Last yearsconference in Belfast was attendedby more than 180 delegates.
WMAI has had great support fromIndustry and is very thankful for thekind support we are getting.
WMAI now have to increase theactivities and strengthen the effortwith respect to organisation promo-tion, memberships etc. We are look-ing very much forward to the co-operation with EWMA, and we aresure that this co-operation will helpboth organisations forward by giv-ing us the opportunity to learn fromeach other.
Title: The Foot in Diabetes (3rd Edition)Editors: Andrew J M Boulton, HenryConnor and Peter R CavanaghPublisher: John Wiley and Sons LtdPrice: RRP £50No of Pages: 373Illustrated: Yes
ISBN 0-471-48974-3
Foot lesions are one of the mostdevastating side effects of diabetes.‘The Foot in Diabetes’ has longbeen recognised as an invaluable textfor those striving to improve dia-betic foot care. This recent thirdedition includes new chapters thatbring extra ammunition to thecampaign.
In the 10 years that have passedsince the St Vincent Declarationthere have been many advances inthe care of diabetic feet, particularlyin the wealthy west. The diabeticfoot team is now an essential part ofevery diabetic service although theamputation rate still considerablyexceeds the St Vincent target.
The list of international con-tributors, which includes physicians,surgeons, nurses, radiologists andpodiatrists from both primary andsecondary care, highlights the needfor a collaborative approach in com-bating diabetic foot problems.
The introductory chapters in-clude an epidemiological and eco-nomic overview highlighting thesignificance of the problem. Thereare chapters covering clinical topicssuch as aetiopathogenesis, bio-mechanics, footwear, antimicrobial
therapy, dressings, radiology andsurgery that present research-basedevidence along with practice-basedexamples.
Useful new additional chapterscover psychological and behaviouralissues, new treatments and the log-istics of providing a diabetes footcare service.
The comprehensive nature ofthis text enables the clinician toidentify and implement best practicewhile developing a better under-standing of the roles of their col-laborative colleagues. The editorsacknowledge the significance ofeffective administration in deliveringclinical skills and several chapters aredevoted to the theory and practiceof service delivery.
The penultimate chapter describ-es the progress towards internationalconsensus and provides practicalguidelines for treatment, which arelikely to prove an extremely usefultool for improving diabetic footcare.
The editors conclude by identifyingthe path ahead. There are huge chal-lenges to be faced in less affluentparts of the world where the greatestincreases in prevalence are anticipat-ed. Improving diabetic foot careneeds to be a global collaboration.Systems of care should be efficientlyorganised to maximise the effective-ness of resources, further high quali-ty research is needed to informclinical practice, and patient educa-tion needs to be more than know-ledge transfer. ‘The Foot in Diabe-
tes’ will provide the reader withguidance for practice and food forthought.
Author:Una Adderley, BSc (Hons), BA(Hons), DN, RGN
Job Title:Research Nurse / District Nurse
Workplace:Dept of Health Studies, University ofYork / Scarborough and North EastYorkshire Healthcare Trust
Correspondence Address:Spring Farm, Cawton,York YO62 4LW, UKTel. +44 1653 628848
Book Review byE. Andrea Nelson
BookReviewWMAI
WoundManagement
Associationof Ireland
Bernadette Kerry
Chairperson
Correspondence to:
Ann Witherrow
Altnagelwin Hospital
Glen Shane Road
BT47 6SB
Londonderry
Northern Ireland
LYMPHOEDEMA
Do your patients suffer from this swelling of the limbs and body?
THE LYMPHOEDEMA
SUPPORT NETWORK
provides support and up-to-date information about lymphoedema topatients and health care professionals
For further information please contactThe Lymphoedema Support Network
LSNThe
LymphoedemaSupportNetwork
Correspondence to:
The Lymphoedema
Support Network
St. Luke’s Crypt
Sydney Street
London XW3 6NH
UK
Tel: +44 20 73514480
Fax: +44 20 7349 9809
E-mail: adminlsn@
lymphoedema.freeserve.co.uk
Website:
www.lymphoedema.org/lsn
Journal 1/01 01.05.01, 16:0542-43

EWMA JOURNAL 2001 VOL 1 NO 144
Conference Calendar
On the 17th to 19th of May 2001nurses, doctors, other specialists andcompanies from all over the worldwill join together in Dublin at the11th EWMA conference.
The EWMA conferences aresteadily growing in delegates, ab-stracts submitted and companies ex-hibiting.
Everything indicates that thisyear’s meeting will be as great a suc-cess as in the 10th EWMA confer-ence in Stockholm, Sweden 2000.
For more details please see theconference report in the next issue
The Dublin Conference
‘Back to the Future’of the EWMA Journal or visit theconference website at www.congress-consult.com/EWMA2001
[ActivaAd]
Conference 2001 Place Country
11th EWMA conference ‘Back to the Future’ May 17 - 19 Dublin Ireland
33rd Annual Wound, Ostomy and Continence Conference June 02 - 06 Portland, OR USA
Gordon Research Conference on Tissue Repair and Regeneration June 17 - 22 New London, NH USA
Satellite Meeting on Skin Immunology June 21 - 22 Stockholm Sweden
5. Kongress der DGfW June 21 - 23 Ulm Germany
European Cells & Materials June 25 - 28 Davos Switzerland
1er Congrès de I’International Academy on Nutrition and Aging June 29 - 30 Paris France
1er Congrès de I’European Union Geriatry Medicine Society Aug/Sept 30 - 01 Paris France
11th Annual Meeting of the ETRS Sept 05 - 08 Cardiff UK
14th World Congress of Union Internationale de Phlebologie Sept 09 - 14 Rome Italy
5th European Pressure Ulcer Advisory Panel Open Meeting Sept 27 - 30 Le Mans France
5th Annual Wound Care Congress for Rehabilitation Professionals Oct 25 - 27 Providence, RI USA
Achtste WCS Congres Nov 06 - 07 Utrecht Holland
1st Biennial Meeting of the European Tissue Engineering Society Nov 07 - 10 Freiburg Germany
Conference 2002 Place Country
4th Australian Wound Management Association Conference Mar 07 - 10 Adelaide Australia
Sår i 10 år Nordisk Jubilæumssymposium April 25 - 27 Helsingør Denmark
12th EWMA Conference May 23 - 25 Grenada Spain
20ème Congrès Mondial de Dermatologie July 01 - 05 Paris France
For links and further information, see www.ewma.org
Journal 1/01 01.05.01, 16:0544-45

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 146 47
Review ofStockholm Meeting
For some years now EWMAhave been holding meetingsthroughout mainland Europe
as well as in the UK (Copenhagen,Amsterdam, Madrid). Up until lastyear’s meeting in Stockholm theannual and in some years bi-annualconference had been held in con-junction with EMAP and the Jour-nal of Wound Care. The Conferencein Stockholm was EWMA’S firstattempt to ‘go it alone’ and by allaccounts the result was successful.A total of 729 participants attendedfrom 29 different countries.
A new departure was made by in-cluding veterinary surgeons in theconference and the case studies theypresented were of great interest,notably a young dog who had itsnose reconstructed following anaccident with a helicopter blade.
The programme was divided intothree days. The first day coveredphysiology of wound healing andgrowth factors. Professor Ferguson isable to make the subject of growthfactors not only accessible but also
amusing! He will be giving theopening lecture at the DublinConference.
The second day concentrated onsome of the issues involving thehealing of surgical wounds. Therewere presentations on wound clos-ure techniques, post operative infec-tion and scarring. There was also apresentation of some new workfrom The Copenhagen WoundHealing Centre on the detrimentaleffects of smoking on post-operativehealing. Yet another reason not tosmoke!
The third day concentrated onthe ever present problems of manag-ing chronic wounds and includedpresentations on fungating wounds,leg ulcers, pressure ulcers, diabeticfoot, nutrition, pressure relief andthe particular problem of woundhealing in the elderly population.Doctor Patricia Grocott presentedthe results of her PhD thesis onmanagement on fungating wounds.She will present more of her innova-tive work in Dublin this year.
There was a wide range of work-shops and seminars from which tochoose, running concurrently withoral presentations from non-invitedspeakers. Workshops included theever popular bandage and Dopplerworkshops, techniques for applyinglarvae, fistula management, traumat-ic wounds and skin care. There werealso seminars on pain management,and infected wounds.
A total of 113 abstracts were submit-ted of which 70 were accepted for oralpresentation and 37 for poster presen-tation.
These covered a wide range ofsubjects from the cutting edge ofwound healing, skin equivalents andtissue engineering, the variation incytokine levels in different types ofwounds to the reintroduction ofolder forms of wound management,larvae and honey.
A presentation on non-accidentalinjury to women by Gunn Heimerpromoted considerable interest anddebate. On the strength of this Dr.Heimer has been invited to speak atthe Dublin meeting this year but thepresentation has been extended toinclude discussion on the problemsof non-accidental injury to childrenand the elderly by experts in thesefields.
Each day began with a presenta-tion of case studies followed by ple-nary sessions, practical workshops,seminars and parallel presentations.
One of the adverse comments,which were mentioned in the evalu-ation forms, was the fact that therewere too many sessions to choose
from. This is a difficult criticism todeal with as time is limited (21/2
days) and there is an enormousamount of material that delegateswant included each year. It seems tous better to be spoilt for choice andthereby be encouraged to returnagain. Each year I am personallydisappointed in having had to miss a session on a subject in which I amparticularly interested.
However, overall the evaluationsof the conference by the delegateswere extremely positive Ratings forthe plenary sessions and workshopsvaried from 1.2 to 2.0 (1 being ex-cellent and 5 being bad)
The industry exhibition wasrepresented by 25 companies. It isalways a good opportunity for thoseinvolved in wound care to discussappropriate use of dressings, newproducts and to make contact withrepresentatives.
The social events were on thewhole very much enjoyed except bythe unfortunate delegates who wereon the boat, which broke downduring its trip through the Archipel-ago! However all delegates enjoyed
the opportunity of visiting the VasaMuseum and many made the mostof dancing after the conferencedinner.
This conference which was thefirst conference organized indepen-dently by EWMA has to be con-sidered a great success. We will,however, not allow ourselves torelax. EWMA is going through themost active period of it’s history andit is of vital importance to the futureaspects of the whole organizationthat we all make an even greatereffort to increase the level of theconferences and the work of theorganization.
EWMA 2000 was a good experi-ence, let’s work together to makefuture conferences even better. ■
Deborah HofmanEWMA recorder
Christina LindholmChairperson,Local OrganizingCommittee
Co-chairperson,Local Organizing
Committee Finn Gottrup
and EWMA presidentChristine Moffatt enjoying
the banquet.Foto Bo Jørgensen,
Sår, Denmark
Journal 1/01 01.05.01, 16:0546-47

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 148 49
The fourth meeting of the European Pres-sure Ulcer Advisory Panel (EPUAP) washeld from 28th to 30th September, 2001
in Pisa, Italy. The convention center of the Uni-versity of Pisa provided the setting for this meet-ing which was attended by over 750 delegatesfrom Europe and United States. The conferencetheme was: ‘Pressure ulcers-technology in theNew Millennium. The scientific programme in-cluded several plenary lectures, workshops andfree paper presentations. For the first time in theshort history of EPUAP a simultaneous transla-tion was provided during the scientific pro-gramme, giving the over 350 italian delegates achance to listen to outstanding speakers from allover the world. As in the previous years the pro-gramme was coordinated by Prof. Gerry Bennett,the EPUAP recorder, who was able to realize anextremely well balanced and attracting list of newtopics in the field of pressure ulcers including:telemedicine, tissue engineering, cell biology, sup-port surface technology. Due to the large numberof oral presentations and in order to give to everyone the opportunity to attend the several work-shops which were repeated twice, the local organ-izers had to set up five parallel sessions everydayduring the conference for a total of over 1400 seatsavailable. A record number of posters (75) was dis-played in the exibition area and as a tradition inthe EPUAP organization, a final prize for bestposter presentation was given to the four nomi-nated groups coming from France, Spain, Italyand Belgium. The famous Techno-Cafè, an inter-active computerized area where delegates were
able to use PC’s to navigate into specific websites,was crowded during the break sessions. The Pres-idential address given by Prof. Jeen Haalboom onthe first day at the opening ceremony was an in-triguing and charming description of the relationsbetween the Leaning Tower of Pisa, a famous his-torical monument, and the pathogenesis of pres-sure ulcers. A delegation of the NPUAP from theUnited States attended the conference, confirm-ing the continuation of a long lasting cooperationbetween the EPUAP and the NPUAP. The socialprogramme offered the time to enjoy the Tuscandelicatessen in a warm and friendly atmosphere,looking at the magnificence of an ancient mon-astery on the first day or eating and dancing withlive music in a unique and famous Italian club onthe mediterranean coast. The city of Pisa with itsbeautiful monuments, churchs and the medioe-val centre, was the worthy corollary to this extraor-dinary conference. We would also like to empha-size the excellent work done at the EPUAP Busi-ness Office in Oxford, during the preparation ofthis meeting and we are looking forward for thenext EPUAP meeting in September this year in LeMans (France), where we will continue the grow-ing tradition of our leading society in the field ofpressure ulcers. ■
Dr. Marco Romanelli
The IVth European PressureUlcer Advisory Panel OpenMeeting28 - 30 September, 2000, Pisa, Italy
On behalf of EWMA, we are delightedto be sharing the opportunities ofthe joint Conference between
GNEAUPP and EWMA.
This conference is in line with the EWMAstrategy to develop the European perspectivesin Wound Healing and Wound Management.
The conference will be a highly innovativeconference with an important Spanish touch,referring the excellent work which is performedwithin Spanish wound management.
We are sure that the scientific programme will beenhanced by placing the conference in one of themost picturesque places in Europe and are look-ing forward to seeing you in Grenada, Spain in2002. ■
Christine Moffatt, EWMA PresidentFinn Gottrup, EWMA RecorderJavier Soldevilla, GNEUAPP PresidentJoan-Enric Torra Bou, Chairman of the LocalOrganizing Committee
Marco Romanelli
MD PhD
Italy
Consultant
Dermatologist at the
Dep. of Dermatology
Univ. of Pisa.
EWMA council member.
President elect and
founding member of the
EPUAP.
AIUC board member.
Dir. of the Wound
Healing Service at two
major hospitals.
Adjunct Assoc. Prof.,
Univ. of Miami, Florida.
Chairman of the Tissue
Repair School at the
Univ. of Pisa.
Correspondence to:
Epuap Business Office
Wound Healing Unit
Department of
Dermatology,
Churchill Hospital
Old Road, Hedington
Oxford 0X3 7LJ, UK
Tel: +44 1865 228269
Fax: +44 1865 228233
E-mail:
europeanpressure
ulceradvispanel@
compuserve.com
www.epuap.com
Grenada 2002
Journal 1/01 01.05.01, 16:0548-49

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 150 51
The First World Wound Heal-ing Congress was held inMelbourne in September
2000, and brought together woundhealing societies from around theworld. A total of 792 delegatesregistered for the Congress, withdelegates coming from 27 differentcountries. These included Australia,Austria, Belgium, Brazil, Canada,China, Denmark, France, Germany,Hong Kong, Hungary, India, Ireland,Italy, Japan, The Netherlands, NewZealand, Russia, Singapore, SlovakRepublic, South Africa, Sweden,Switzerland, Taiwan, Thailand, Uni-ted Kingdom, and United States ofAmerica. 520 of these came from thehost country, Australia, and 272 camefrom the international community.
The Congress commenced with aseries of workshops on the Sundaywhich related to the practical aspectsof wound management. These inclu-ded workshops on compressiontherapy, dressings, pressure ulcer pre-vention, non-invasive investigation,clinical research, wound documenta-tion, pressure off-loading, wound de-bridement, and information technol-ogy. These were coordinated mainlyby members of the Australian WoundManagement Association. However,valuable contributions were also madeby members of the international com-munity. In particular, Mike Leek andGeorge Cherry, who coordinated theinformation technology workshop,and Gerry Bennett who contributedto the pressure ulcer prevention work-shop. The formal conference opened
on Monday 11 September, with apresentation from Professor TomHunt on the development of the in-terest in wound healing. The differentwound healing societies who werecontributing in the World Congressalso gave brief presentations abouttheir societies. These included theAssociation for the Advancement ofWound Care, the Australian WoundManagement Association, the Cana-dian Association of Wound Care, theChinese Tissue Repair Society, theEuropean Pressure Ulcer AdvisoryPanel, the European Tissue RepairSociety, the European WoundManagement Association, the IndianSociety for Wound Management, LaSociété Française et Francophone desPlaies et Cicatrisations, the New Zea-land Wound Care Society, the Japa-nese Society for Wound Healing, theWound Healing Society (USA), andthe Wound Healing Society (Singa-pore).
The Congress then continuedwith two plenary sessions each day,each with a specific focus. In each ofthese sessions there were presentationsfrom basic scientific research, clinicalresearch, and practical clinical man-agement. The particular topics thatwere discussed in the plenary sessionswere burns and scars, the role of bac-teria in chronic wound healing, acutewounds, pressure ulcers, venous ul-cers, and diabetic foot ulcers. Thesesessions gave an opportunity for basicscientists, clinical researchers, and thepractical practising wound care clini-cians to gain a better appreciation of
First World Wound Healing CongressMelbourne, Australia, 10-13 September 2000
the work that their colleagues in theother disciplines are undertaking.
Two free paper sessions were heldeach day. In each of these there werefour concurrent rooms. Each of thesesessions had a room on basic science,one on clinical research, and one onclinical practice. The fourth room waseither a sponsored workshop or theYoung Investigator Awards. The freepaper sessions provided an opportuni-ty for the individual attendees to jointheir own discipline to discuss theirspecific areas of interest. A large rangeof topics were covered in the freepaper sessions. These included topicssuch as regulation of extra-cellularmatrix, wound healing regulation,cytokines and cell growth, patho-physiology of impaired healing,potential therapies, strategies for acutewounds, difficult wounds, assessingrisk, pressure ulcers, improving cur-rent practices, and new and old treat-ments.
Poster sessions were also runthroughout the Congress. The postersessions were separated into the disci-plines of basic research, clinical re-search, and clinical practice. An awardwas presented for each of these ses-sions. The Young Investigator Awardwas won by Sim Yeoh, a PhD studentat the University Department of Sur-gery in Fremantle Hospital.
Melbourne itself presented manydelights during the Congress. Therewas unfortunately some disruptionfrom the demonstrations associatedwith the World Economic Forumwhich was in the Crown Casino com-plex which was only approximately
Prof. Michael Stacey
Associate Professor of
Surgery, University of
Western Australia.
Vascular and General
Surgeon.
Inaugural president of
Australian Wound
Management
Association.
Co-Editor of Primary
Intention (Journal of
Australian Wound
Management
Association)
Editorial Board member
of: Wound Repair and
Regeneration and
Journal of Wound Care.
Correspondence to:
Fremantle Hospital,
Univ. Dep. of Surgery,
6160 Fremantle WA,
Australia
E-mail: mstacey@
cyllene.uwa.edu.au
500 metres from the Congress centre.This meant the cancellation of theoptional dinner which was scheduledfor the Monday evening. Tuesdaymorning started early with a Fun Runwhich had approximately 60 partici-pants, and the Congress Dinner wasan extremely enjoyable event whichsaw much merriment and dancing asthe night continued.
The Congress was well supportedby the Industry, and thanks go out tothem, as well as Intermedia, the Con-gress organisers, who did an outstand-ing job in managing the Congress.The Congress co-covenors wereGeoffrey Sussman and MichaelStacey, and the Chair of the Scienti-fic Programme, was Michael Stacey.
Another major event which oc-curred at the Congress was the forma-tion of The International Union ofWound Healing Societies. This inter-national union has a number of roles,one of which is to ensure that futureworld wound healing congresses are tobe held. The next World WoundHealing Congress will be held in Parisfrom 31 August to 4 September 2004,and the Convenor for that will be LucTeot. The International Union ofWound Healing Societies will distrib-ute an outline of its charter, and theareas of interest which a number ofworking parties intend to explorefrom an international perspective. TheChairman of the International Unionis Michael Stacey, and the DeputyChairman is Luc Teot. It is hoped thatthe next World Congress will contin-ue the success of the First WorldWound Healing Congress. ■
Journal 1/01 01.05.01, 16:0650-51

EWMA JOURNAL 2001 VOL 1 NO 152
Correspondence to:
Luc Teot
Hospital Lapeyronie
Burns Center
371 Av Doyen Giraud
F-34255 Montpellier
France
E-mail:
www.sffpc.org
5ème Conférence des Plaies etCicatrisations, Paris
A s the official annual meeting for theFrench WHS (Société Française desPlaies et Cicatrisations), the event has
become very popular as more than 3400 profes-sionals were present on the 14th, 15th and 16thof January, 2001.
The meeting was divided into four main parts:
■ The plenary sessions, in which importanttopics where addressed in order to give ageneral message based on validated data.Four plenary sessions were given duringthese three days, 90 minutes each. This year,we aborted ‘management of wounds’. Newwas: ‘palliative care’, ‘keratinisation’, andthe end of the process, ‘daily wound care’
■ The International Symposium, where inter-nationally famous speakers came and pre-sented new aspects in a designated field.This year, we had the chance to listen toChristine Moffatt, Keith Harding, LiorRosenberg, Finn Gottrup and Ralph Ger ina symposium on ‘alternative therapies’
■ The workshops where a tandem nurse-physician gave a practical interactive lessonon a specific topic. These two people areevaluated by the audience each year in orderto assess if change is necessary. 36 work-shops were given this year, covering thewhole field of wound healing, includingacute wounds, trauma, and burns
■ Innovative papers and posters were present-ed by the participants and the companies inconcurrent sessions. Two English speakingsessions were given using a simultaneoustranslation, and this event will from now onbe open to all English speaking participantscoming from outside France.
The success of this event was initiated five yearsago, and was mainly related to the fact thattransversality is very well accepted in France.More than 900 physicians were present at thisevent, coming from different medical fields, likegeriatry, dermatology, plastic surgery, ortho-pedic surgery, rehabilitation, endocrinology.Cohabitation and enthusiasm is common inwound healing, more pronounced in burns andgeriatrics in the public hospitals, but the com-plementarily is obvious and will lead to bettermanagement of the problems.
The French WHS is now a solid society, com-posed of 800 members, working in 10 commis-sions, disposing of a specific web site,www.sffpc.org
University Diplomas are open in Mont-pellier and Paris, forming each year more than120 experts (nurses, pharmacists, doctors), anda series of courses are given on the French terri-tory on a permanent basis.
The French WHS will be organizing thenext World Union of Wound Healing Societiesmeeting in Paris in August 2004. ■
Luc Teot
[KayMed Ad]
Journal 1/01 01.05.01, 16:0652-53

EWMA JOURNAL 2001 VOL 1 NO 1EWMA JOURNAL 2001 VOL 1 NO 154 55
Correspondence to:
ETRS Business Office
Wound Healing Unit
Department of
Dermatology,
Churchill Hospital
Old Road, Hedington
Oxford 0X3 7LJ, UK
Tel: +44 1865 228269
Fax: +44 1865 228233
www.etrs.org
The 10th Annual meeting of the
European Tissue Repair Society24-27th May, 2000, Brussels, Belgium
The International Conference Centre ofBrussels located at the foot of TheAtomium was the venue for this con-
ference. Wednesday afternoon Prof. Dr. MertonBernfield (Boston, USA) delivered the openinglecture with an interesting review on heparansulphate proteoglycans in the generation and inthe restoration of tissues. The following threedays of lectures emphasized on tissue repair as abroad theme, involving many organs, and thatclinicians and scientists of many different speci-alities have their own approaches to research it.
People from 25 countries attended the 153oral presentations on current knowledge and fu-ture applications concerning many aspects oftissue repair. Clinically oriented topics weregrouped around burns and other problemwounds, clinical studies on wound manage-ment, surgical issues, infection of wounds, newtreatment options. Practical themes encom-passed the setting up and organisation of a
wound centre, measuring and imaging tech-niques, legislation (especially concerning livingcells and organs). Reviewing the basic researchareas in tissue repair, people presented work inprogress on human and animal models, thebiology of acute and chronic wounds, mecha-nisms for remodelling of the matrix, its effectsin scarring, the action of growth factors andcytokines. There was much interest for angio-genesis, stem cells and gene therapy, and repairof tissues other than skin: bone, peri-odontalrepair, fetal healing.
Satellite symposia were organised in collabo-ration with ConvaTec highlighting hyaluronicacid in wound healing, and with Smith &Nephew on scarring.
The social evening in the Colonial Museum,sponsored by Jansen-Cilag, was lively andsplendid.
Mieke Flour,Chairperson of the Local Organizing Committee
EWMA was founded in 1991at a conference in Cardiff toaddress clinical and scientificissues associated with woundhealing represented by medical,nursing, scientific and pharma-ceutical interests.
The objectives agreed upon thenwas as follows:
■ To promote advancement ofeducation and research intoepidemiology, pathology,diagnosis, prevention andmanagement of wounds ofall aetiologies.
■ To hold conferences onaspects of wound manage-ment throughout Europe.
■ To provide grants and bursa-ries to EWMA members
■ To hold multi-centre, multi-disciplinary training courseson topical aspects of woundhealing.
EWMA has since worked to fulfilthese objectives and at the sametime searched for new ways tohelp the promotion of a trulyinternational forum for woundmanagement.
At present EWMA is enjoying anever increasing number of mem-bers; participants in the annualconferences; co-operating organi-sations; promising projects, and awarm support from the industry.
Ten years after the foundation, itis not too much to say that theEuropean Wound Manage-
ment Association truly has be-come the international forumenvisaged in Cardiff.
There are however still potentialfor improvements, and we hopethat many will join EWMA andthereby help the organisationand the whole wound manage-ment area.
EuropeanWound ManagementAssociation
Co-operation withSweden, Germany and Portugal
Latest news
■ Associação Portuguesade Tratamento de Feri-das (APTF)– Portuguese WoundHealing Society
President of APTF:Arminda CosteiraFax:+351 22 20 078 90
We are very pleased to an-nounce that the followingorganisations have chosento co-operate withEWMA.
■ Svenskt Sårläknings-sällskap (SSS)– Swedish WoundHealing Society
President of SSS:Harry BeitnerHudkliniken1Karolinska SjukhusetS-17176 StockholmSweden
■ Deutsche Gesellschaftfür Wundheilung undWundbehandlung(DGfW)– German WoundHealing Society
President of DGfW:Prof. Ralf Peter ThiedeDGfW e.V.Erlenbachstraße 19D-89155 ErbachGermany
Surname:
First name(s):
Profession:
Physician Surgeon Dietician
Nurse Pharmacist Other
Work Address:
Address for Correspondence (if different from above):
Tel:
Fax:
E-mail:
Membership application
Payment accepted in pound sterling only.
I enclose a cheque. Please indicate cheque no.:
Please make cheques payable to:European Wound Management Association
Or
Please debit my account:Credit Card type: (Delta, Master Card or Visa)Credit card no:
Expiry Date:
Exact name and initials on the credit card:
Please return formand enclose cheque to: EWMA
PO Box 864,London SE1 8TT,United Kingdom
Journal 1/01 01.05.01, 16:0654-55

3 President’s Introduction
5 The EWMA strategy
by Christine Moffatt
8 Educational development
by Madeleine Flanagan and
Prof. Finn Gottrup
11 The Slovenian Project
by Christine Moffatt
13 EWMA Grants
15 Zinc oxide augments in wounds
by Dr. Magnus Ågren
18 Malignancy and Pre-Malignancy
in Leg Ulceration
by Janice Cameron and
Deborah Hofman
21 The meaning of living with
venous leg ulcer
by Britt Ebbeskog
25 Cost-effectiveness in Wound
Management
by Prof. Peter Franks
28 The Cochrane Wounds Group
by Michelle Briggs
30 Pressure Sore References
by E. Andrea Nelson
32 The EWMA co-operation
34 FWCS – Finnish Wound
Care Society
35 AISLeC – The Italian
Wound Healing Society
36 LUF – The British
Leg Ulcer Forum
37 DSFS – The Danish
Wound Healing Society
38 NIFS – The Norwegian
Wound Healing Society
39 AIUC – The Italian
Wound Organisation
40 GNEAUPP – The Spanish
Wound Healing Society
42 WMAI – Wound Management
Association of Ireland
42 LSN – The Lymphoedema
Support Network
43 Book Review
by E. Andrea Nelson
44 Conference Calendar
46 EWMA 2000, Stockholm
48 EPUAP 2000, Pisa
49 EWMA 2002, Grenada
50 World Wound Healing
Conference 2000, Australia
52 WHS 2000, Paris
54 ETRS 2000, Brussels
55 EWMA Information
V OL 1 · N O 1 · 2 0 0 1
Journal 1/01 01.05.01, 16:0656