Validiteit van werkplek beoordelingen door middel van ... · Validiteit van werkplek beoordelingen...
45
Validiteit van werkplek beoordelingen door middel van portfolio's Research Club UZA - 03.10.2012 Nele Michels prof. dr. Benedicte De Winter, prof. dr. Leo Bossaert, prof. dr. Luc Van Gaal
Transcript of Validiteit van werkplek beoordelingen door middel van ... · Validiteit van werkplek beoordelingen...

Validiteit van werkplek beoordelingen
door middel van portfolio's
Research Club UZA - 03.10.2012
Nele Michels prof. dr. Benedicte De Winter, prof. dr. Leo Bossaert, prof. dr. Luc Van Gaal
1
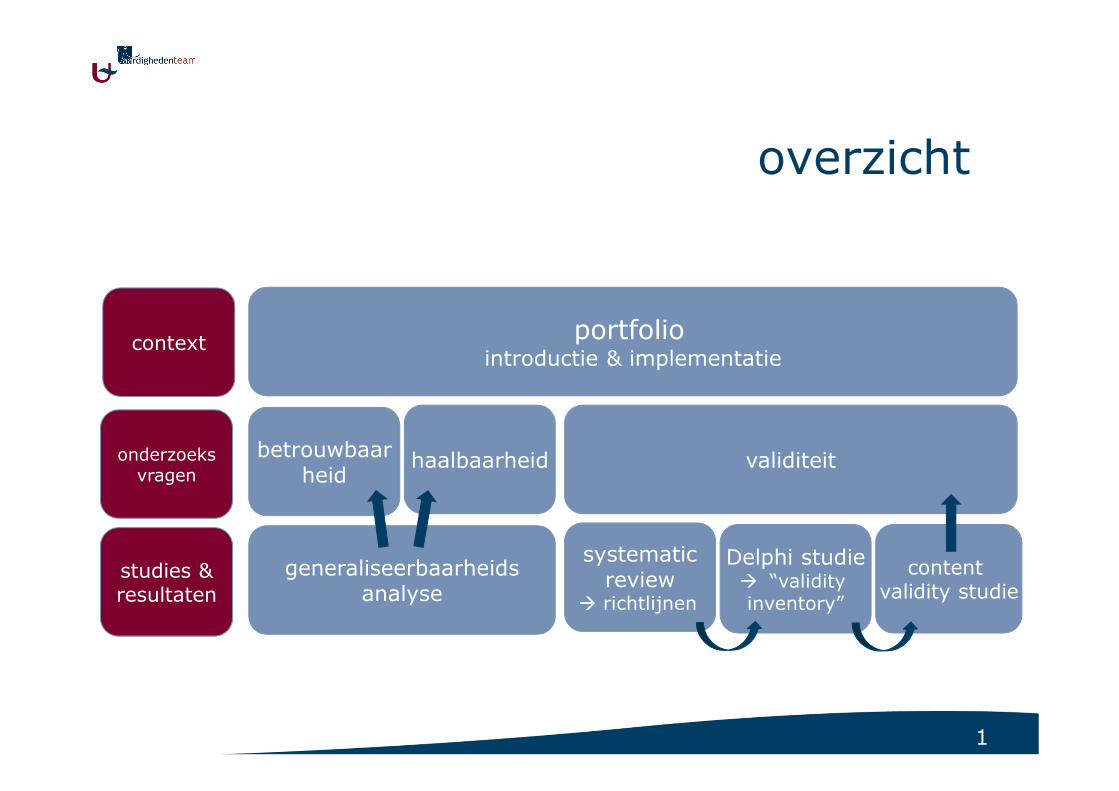
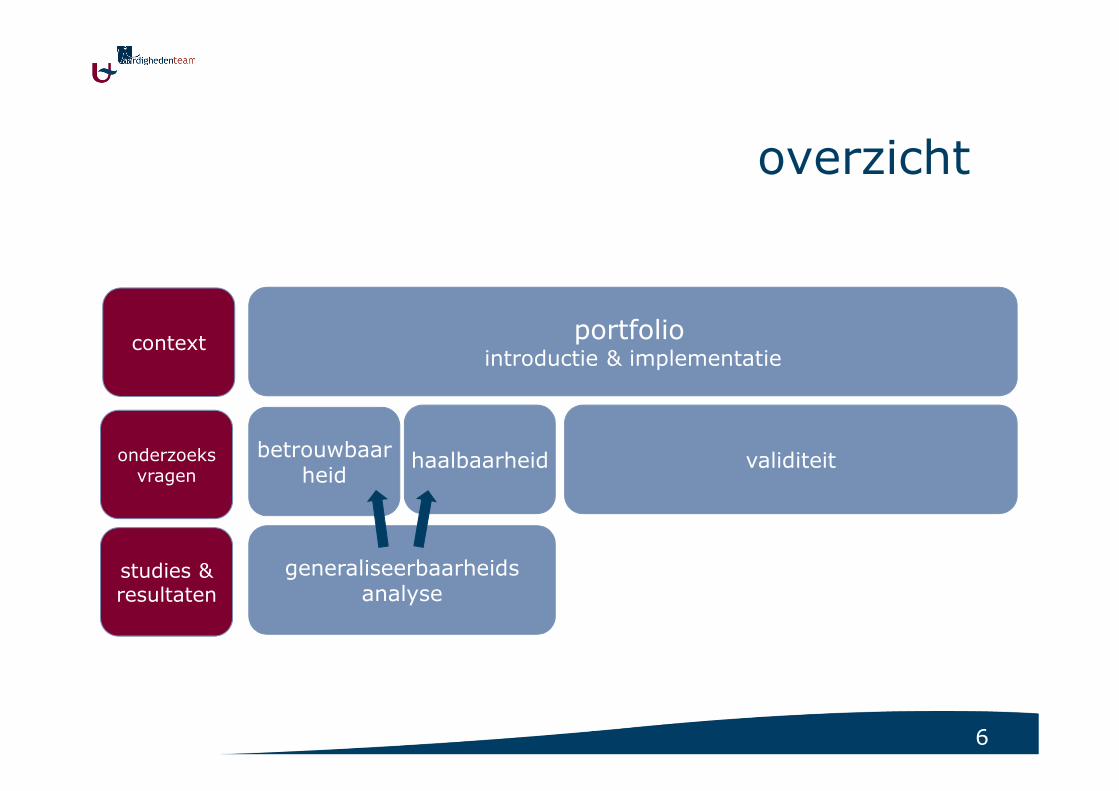
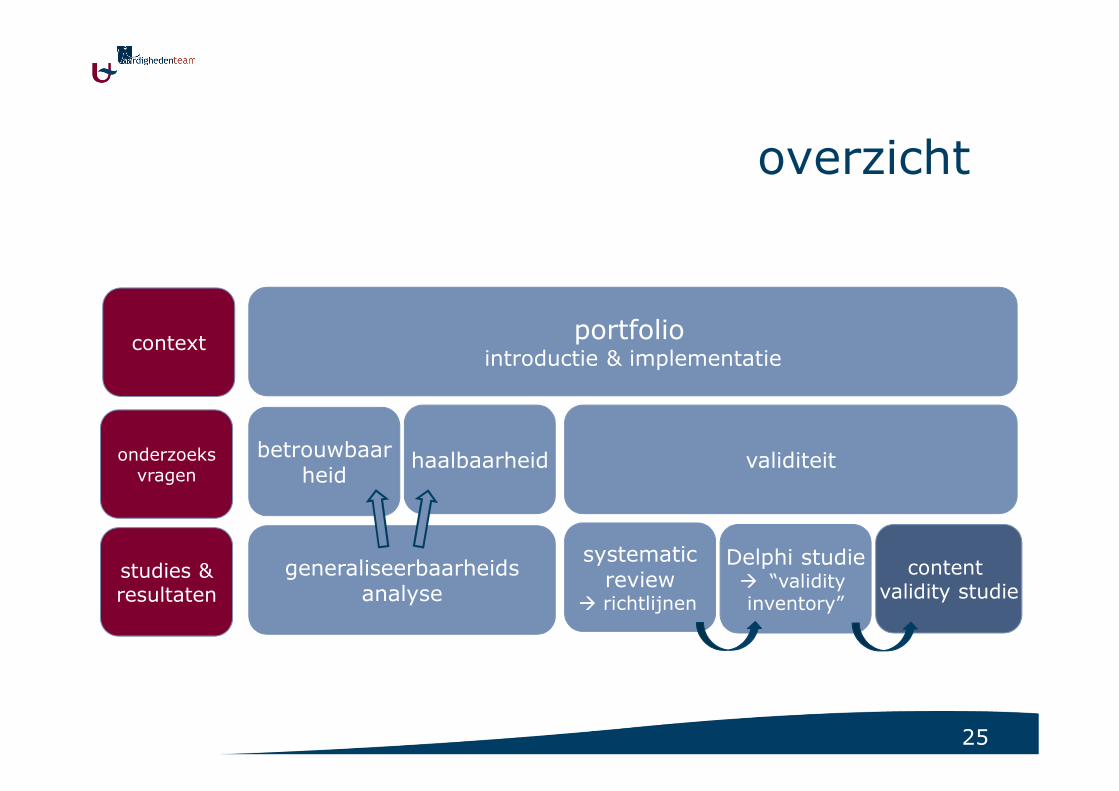
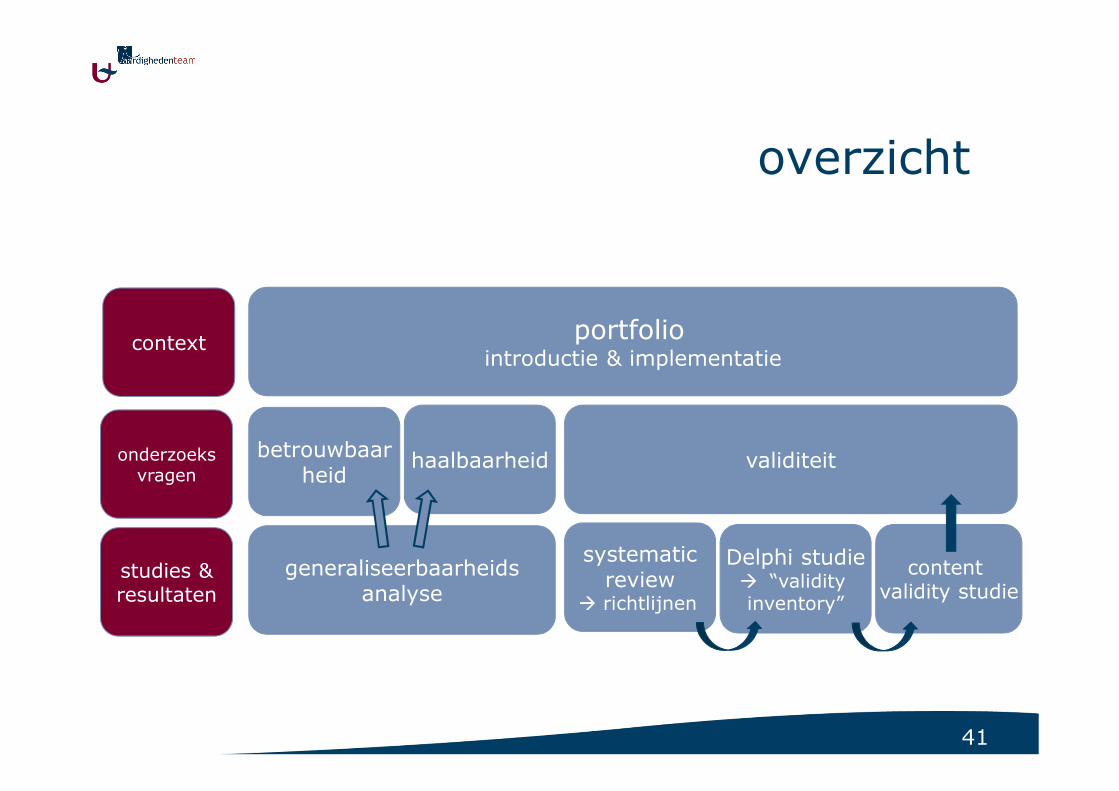
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
Delphi studie� “validityinventory”
content validity studie
context
onderzoeksvragen
studies &resultaten
systematicreview
� richtlijnen

2
ontwikkeling
- “zicht op (eigen) leren”
- bijsturen
begeleiding
beoordeling van competenties
- evaluatie van bereikte competenties
- evaluatie van ontwikkeling van competenties
portfolio - algemeen
lerendelerende
tutortutor
werkplekleren
feedback & follow up
werkplekleren
feedback & follow up
3
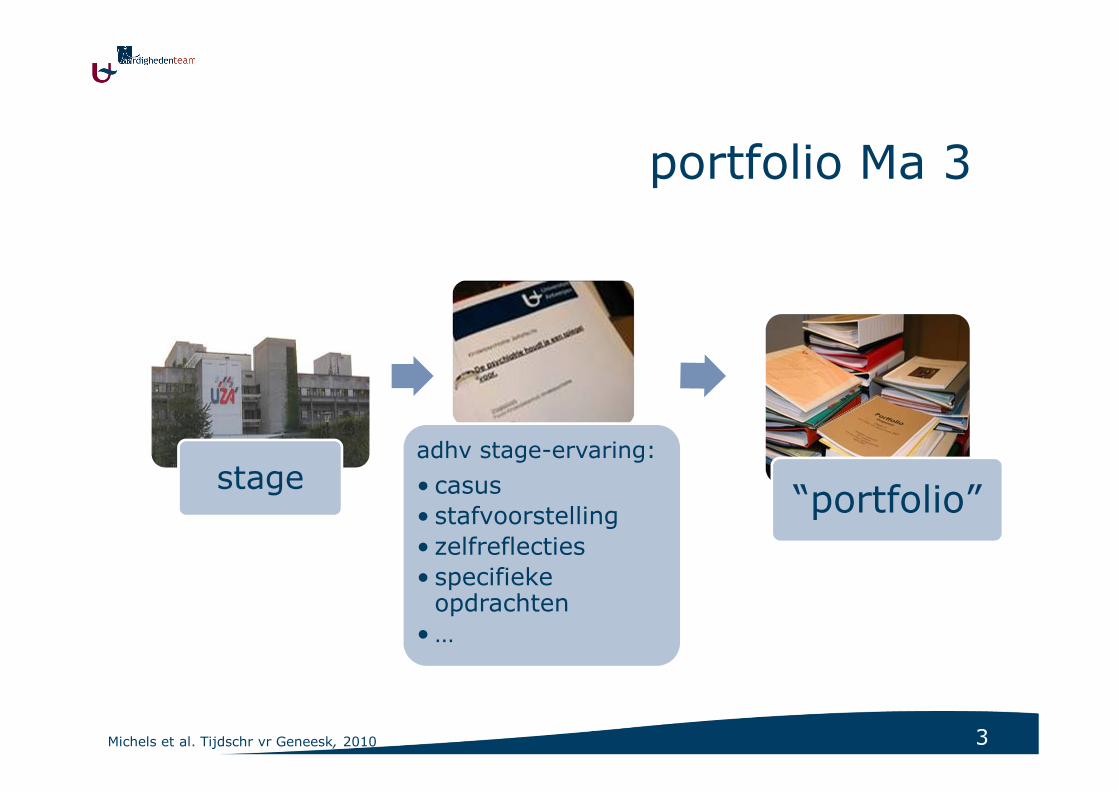
stageadhv stage-ervaring:
• casus
• stafvoorstelling
• zelfreflecties
• specifieke opdrachten
• …
“portfolio”
portfolio Ma 3
Michels et al. Tijdschr vr Geneesk, 2010
4
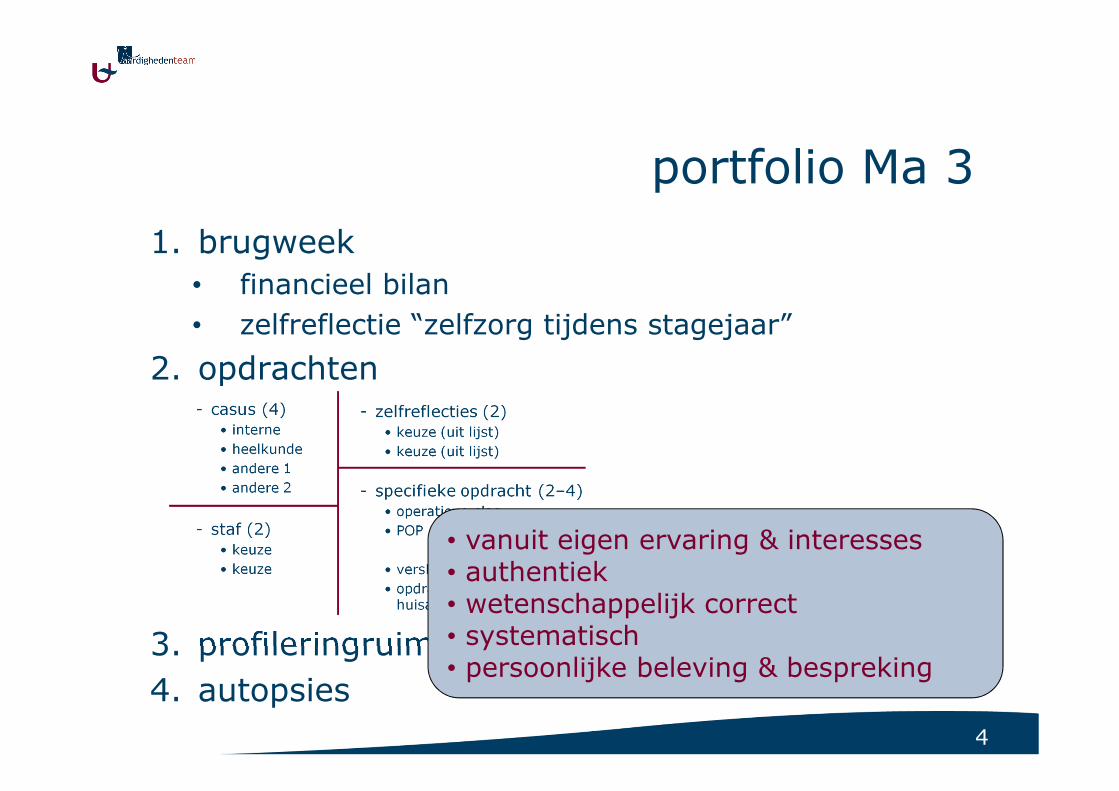
portfolio Ma 3
1. brugweek
• financieel bilan
• zelfreflectie “zelfzorg tijdens stagejaar”
2. opdrachten
3. profileringruimte
4. autopsies
• vanuit eigen ervaring & interesses• authentiek• wetenschappelijk correct• systematisch• persoonlijke beleving & bespreking
5
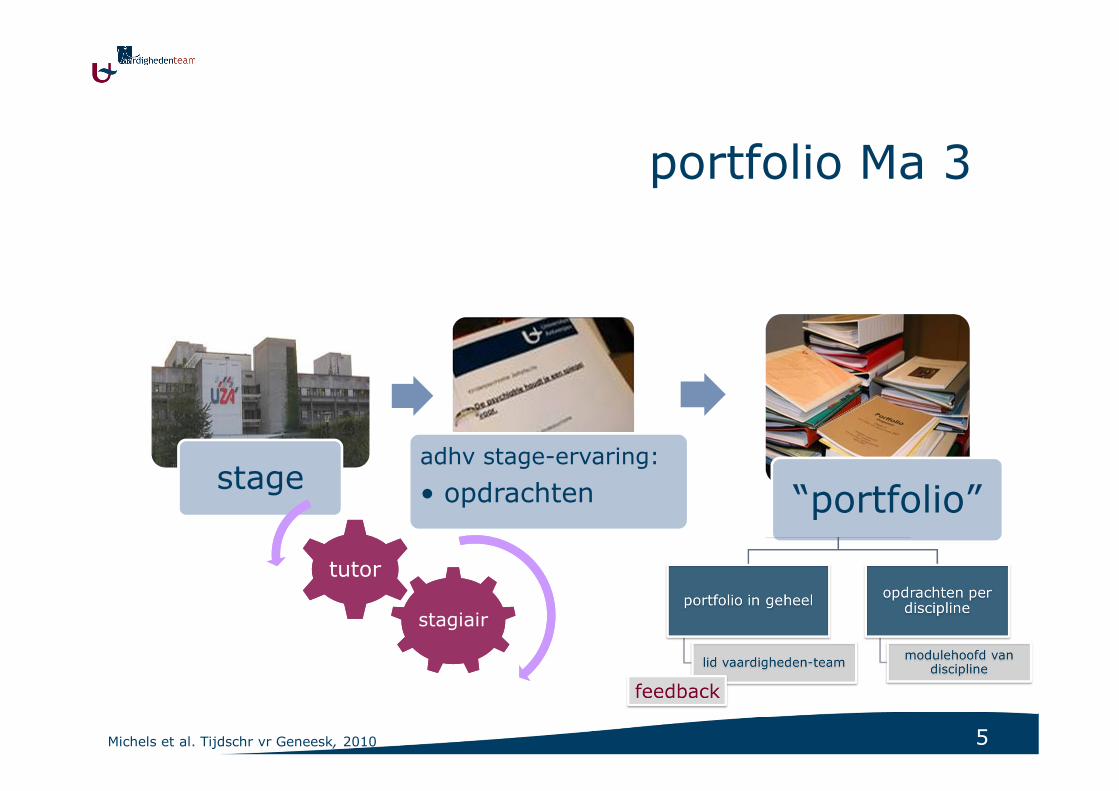
stageadhv stage-ervaring:
• opdrachten “portfolio”
portfolio Ma 3
stagiairstagiair
tutortutor
Michels et al. Tijdschr vr Geneesk, 2010
6
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
context
onderzoeksvragen
studies &resultaten
7
validiteit?
� beoordelen we wat we “beogen” te beoordelen?
aantal manieren om naar validiteit te kijken:
1. “Trinitarian” point of view
2. “Messick’s” framework
3. “Kane’s” view
8
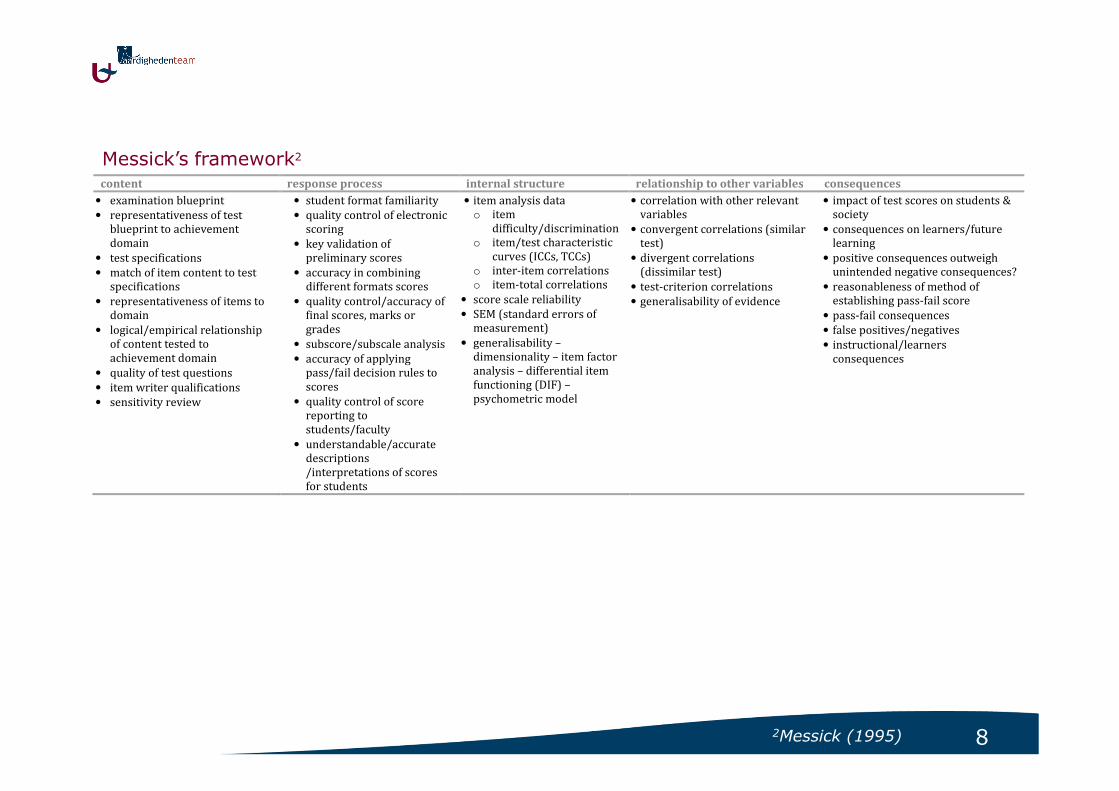
content response process internal structure relationship to other variables consequences
• examination blueprint
• representativeness of test
blueprint to achievement
domain
• test specifications
• match of item content to test
specifications
• representativeness of items to
domain
• logical/empirical relationship
of content tested to
achievement domain
• quality of test questions
• item writer qualifications
• sensitivity review
• student format familiarity
• quality control of electronic
scoring
• key validation of
preliminary scores
• accuracy in combining
different formats scores
• quality control/accuracy of
final scores, marks or
grades
• subscore/subscale analysis
• accuracy of applying
pass/fail decision rules to
scores
• quality control of score
reporting to
students/faculty
• understandable/accurate
descriptions
/interpretations of scores
for students
• item analysis data
o item
difficulty/discrimination
o item/test characteristic
curves (ICCs, TCCs)
o inter-item correlations
o item-total correlations
• score scale reliability
• SEM (standard errors of
measurement)
• generalisability –
dimensionality – item factor
analysis – differential item
functioning (DIF) –
psychometric model
• correlation with other relevant
variables
• convergent correlations (similar
test)
• divergent correlations
(dissimilar test)
• test-criterion correlations
• generalisability of evidence
• impact of test scores on students &
society
• consequences on learners/future
learning
• positive consequences outweigh
unintended negative consequences?
• reasonableness of method of
establishing pass-fail score
• pass-fail consequences
• false positives/negatives
• instructional/learners
consequences
Messick’s framework2
2Messick (1995)
9
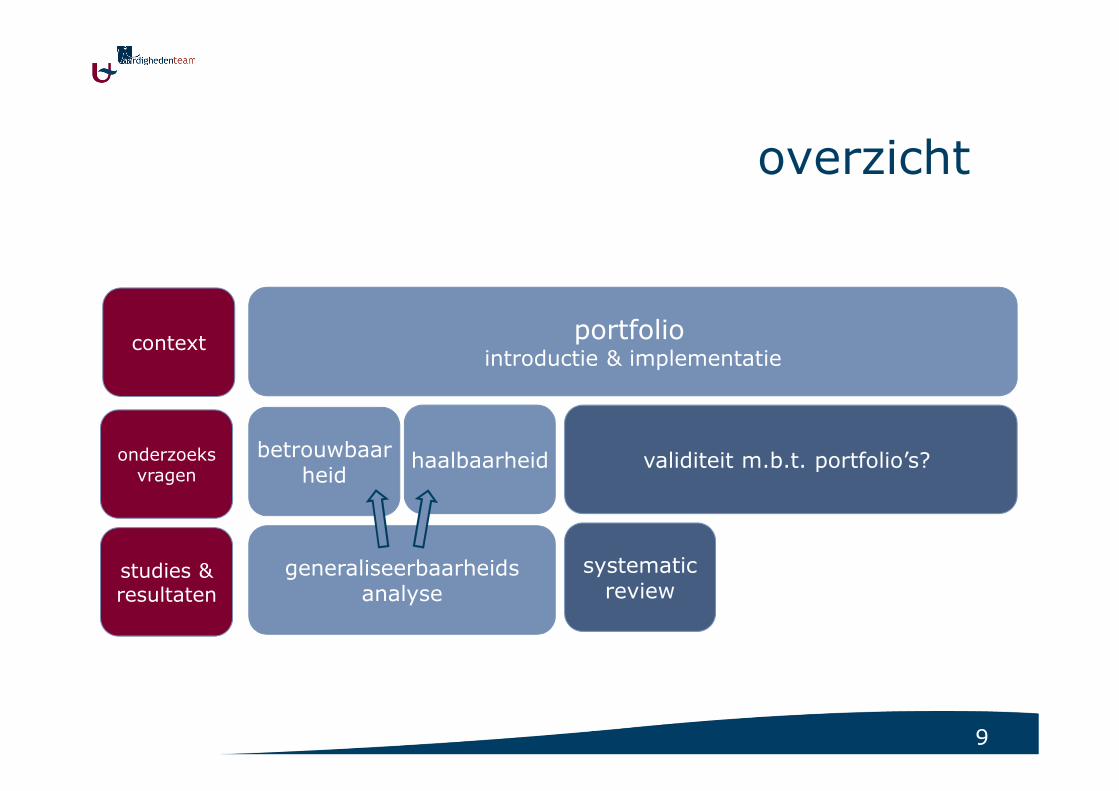
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit m.b.t. portfolio’s?
generaliseerbaarheidsanalyse
context
onderzoeksvragen
studies &resultaten
systematicreview

10Michels et al. Submitted/In revision
systematic review
• search Medline, Embase, ERIC - 1999-2010 / geen restrictie voor taal, geografie
- kwantitatieve & kwalitatieve studies, reviews, commentaren
- portfolio* – validity* – medical education*
142 titels & abstracts
19weerhouden �full reading
11weerhouden
8 niet weerhouden
123 niet weerhouden
inclusion criteria exclusion criteria
population - medical education : undergraduate,
postgraduate, CME
- nurse, dental education
education of other allied health professions or other
professions (teacher, manager, …)
study content validity investigation of portfolio
portfolio educational portfolio =
1. collection of evidence of student learning and
achievement
2. learning journals
logbook (tick box) = collection of single assignments
or activities
study design reporting empirical/evaluative data descriptive articles without empirical/evaluative data
data coding form
1. administration
please complete all sections
title article
author(s)
reviewer
2. relevance – inclusion/exclusion criteria
please complete all sections
1) portfolio: does it fit all of following definition?
a collection of evidence of student activity
outlining own learning experiences (e.g. patients seen, study subject covered, articles read)
involving intellectual processing (no logbook or thick box)
drawing together more than one item or type of evidence
reject if none is applicable
2) population (i.e. students)
medical school, undergraduate
medical school, postgraduate
continuing medical education
nurse education
dental education
reject if none is applicable
3) study content investigation of portfolio
validity is studied
validity is discussed
other psychometric aspects (e.g. reliability) are studied or discussed
if none then reject
reviewers preliminary decision:
inclusion
reserve, read for background context
exclusion
if the article is excluded do not complete the sections below
3. type of publication
journal article report editorial comment
4. study design
4) research design
comparative study (cohort) ( clinical trial) (RCT) (others)
type? ……………………………………………………………………………………………………….
descriptive study (non-comparative)
type? ……………………………………………………………………………………………………….
research study including data & statistical analysis (non-comparative)
(systematic) review
11
systematic review
• resultaten- beschrijving context:
Michels et al. Submitted/In revision
12
systematic review
Michels et al. Submitted/In revision
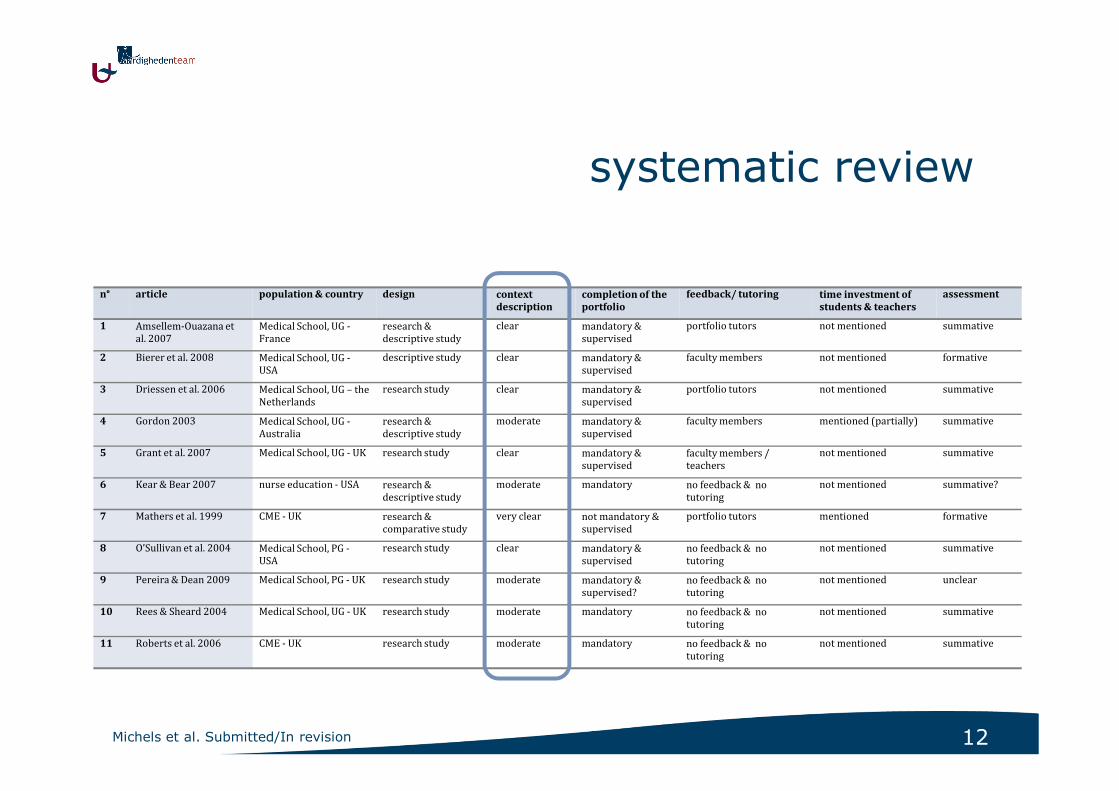
n° article population & country design context
description
completion of the
portfolio
feedback/ tutoring time investment of
students & teachers
assessment
1 Amsellem-Ouazana et
al. 2007
Medical School, UG -
France
research &
descriptive study
clear mandatory &
supervised
portfolio tutors not mentioned summative
2 Bierer et al. 2008 Medical School, UG -
USA
descriptive study clear mandatory &
supervised
faculty members not mentioned formative
3 Driessen et al. 2006 Medical School, UG – the
Netherlands
research study clear mandatory &
supervised
portfolio tutors not mentioned summative
4 Gordon 2003 Medical School, UG -
Australia
research &
descriptive study
moderate mandatory &
supervised
faculty members mentioned (partially) summative
5 Grant et al. 2007 Medical School, UG - UK research study clear mandatory &
supervised
faculty members /
teachers
not mentioned summative
6 Kear & Bear 2007 nurse education - USA research &
descriptive study
moderate mandatory no feedback & no
tutoring
not mentioned summative?
7 Mathers et al. 1999 CME - UK research &
comparative study
very clear not mandatory &
supervised
portfolio tutors mentioned formative
8 O’Sullivan et al. 2004 Medical School, PG -
USA
research study clear mandatory &
supervised
no feedback & no
tutoring
not mentioned summative
9 Pereira & Dean 2009 Medical School, PG - UK research study moderate mandatory &
supervised?
no feedback & no
tutoring
not mentioned unclear
10 Rees & Sheard 2004 Medical School, UG - UK research study moderate mandatory no feedback & no
tutoring
not mentioned summative
11 Roberts et al. 2006 CME - UK research study moderate mandatory no feedback & no
tutoring
not mentioned summative
13
systematic review
• resultaten- beschrijving context: gemiddeld tot goed
- kwaliteit studies: laag tot gemiddeld
Michels et al. Submitted/In revision
14
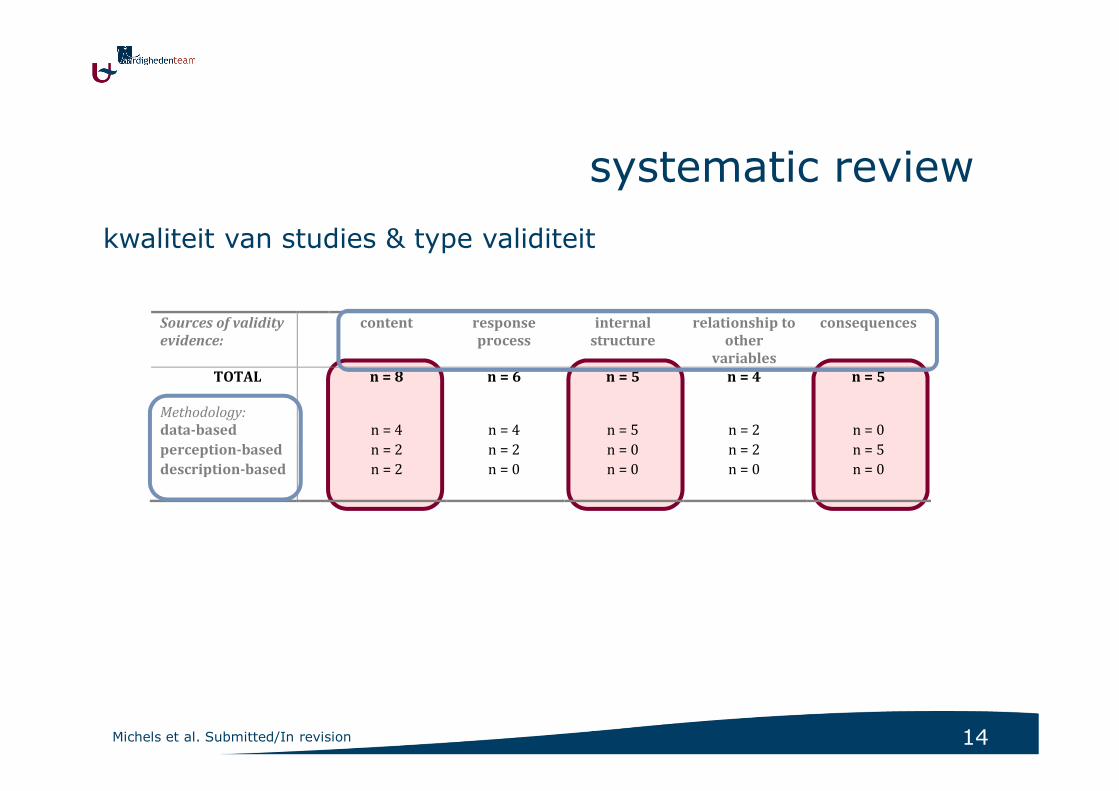
Sources of validity
evidence:
content response
process
internal
structure
relationship to
other
variables
consequences
TOTAL
Methodology:
n = 8 n = 6 n = 5 n = 4 n = 5
data-based n = 4 n = 4 n = 5 n = 2 n = 0
perception-based n = 2 n = 2 n = 0 n = 2 n = 5
description-based n = 2 n = 0 n = 0 n = 0 n = 0
systematic review
Michels et al. Submitted/In revision
kwaliteit van studies & type validiteit
15
systematic review
• resultaten- beschrijving context: gemiddeld tot goed
- kwaliteit studies: laag tot gemiddeld
- onderzoek validiteit
• geen tot weinig verwijzing naar bestaande “frameworks”
• meta-analyse niet mogelijk
= zeer divers, geen consensus
Michels et al. Submitted/In revision
16
systematic review
• conclusies
� minimale voorwaarden / richtlijnen
1. context
2. type validiteit? � vb. framework Messick
3. “evidence based” onderzoek opzetten
Michels et al. Submitted/In revision
17
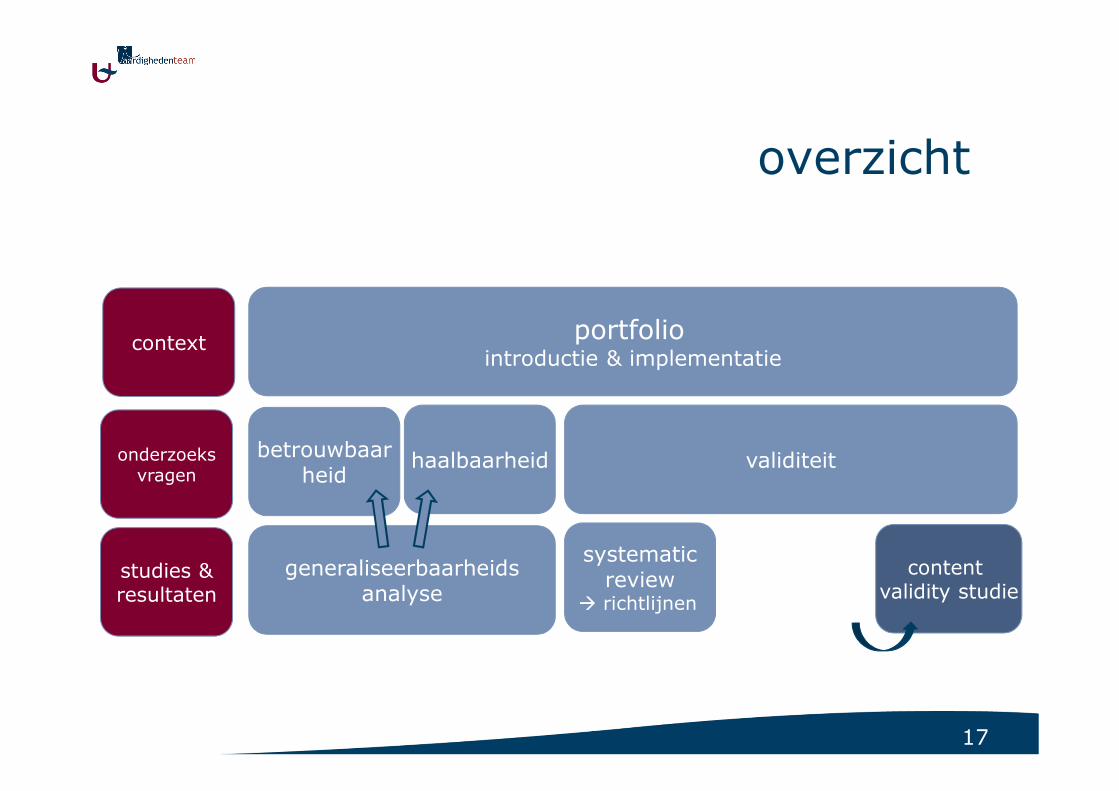
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
content validity studie
context
onderzoeksvragen
studies &resultaten
systematicreview
� richtlijnen
18
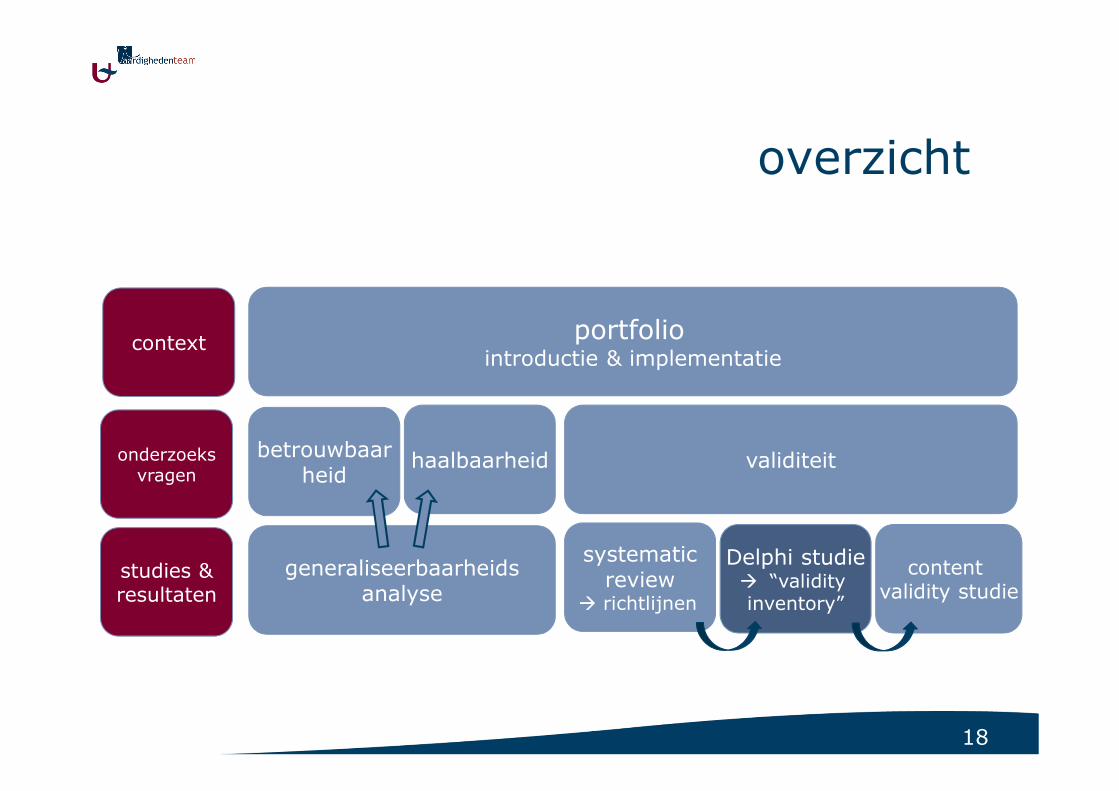
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
Delphi studie� “validityinventory”
content validity studie
context
onderzoeksvragen
studies &resultaten
systematicreview
� richtlijnen

19
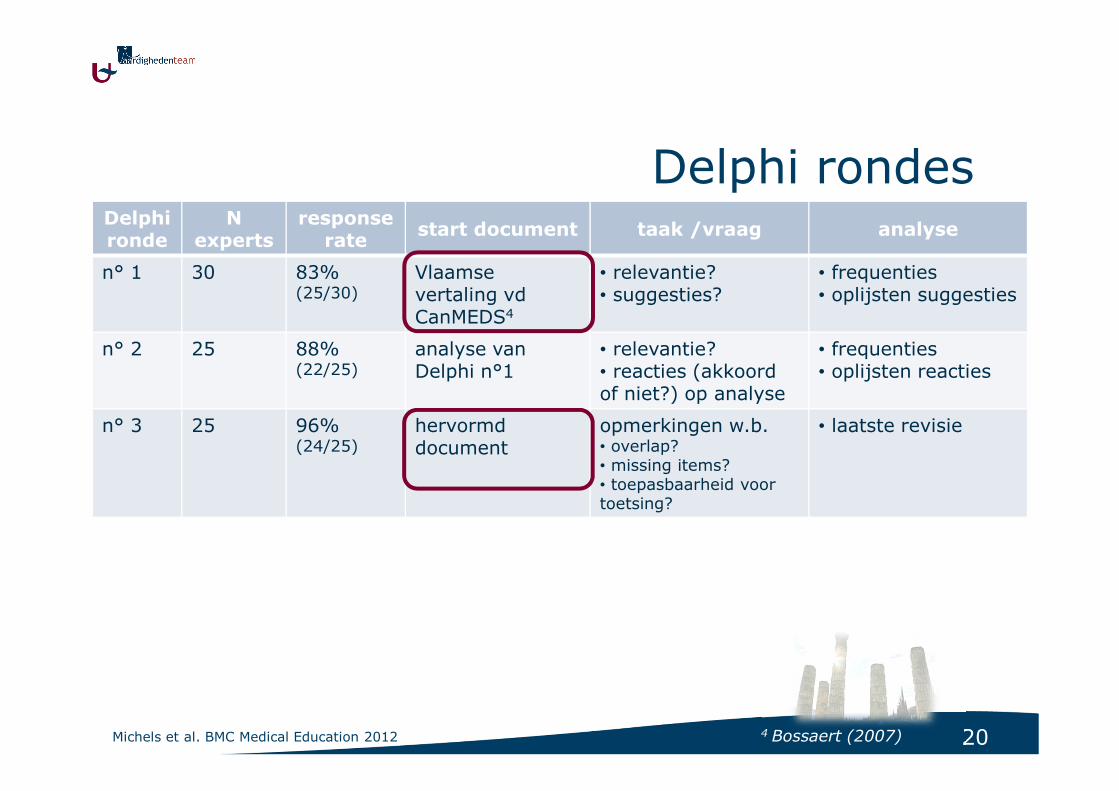
Delphi studie
• 30 experts
- onderwijskundigen (UA & extern)
- portfoliobeoordelaars
• per mail - anoniem
Michels et al. BMC Medical Education 2012
20
Delphi rondesDelphi ronde
Nexperts
response rate
start document taak /vraag analyse
n° 1 30 83% (25/30)
Vlaamse vertaling vdCanMEDS4
• relevantie? • suggesties?
• frequenties• oplijsten suggesties
n° 2 25 88% (22/25)
analyse van Delphi n°1
• relevantie? • reacties (akkoord of niet?) op analyse
• frequenties• oplijsten reacties
n° 3 25 96% (24/25)
hervormd document
opmerkingen w.b.• overlap?• missing items?• toepasbaarheid voor toetsing?
• laatste revisie
Michels et al. BMC Medical Education 2012 4 Bossaert (2007)
21
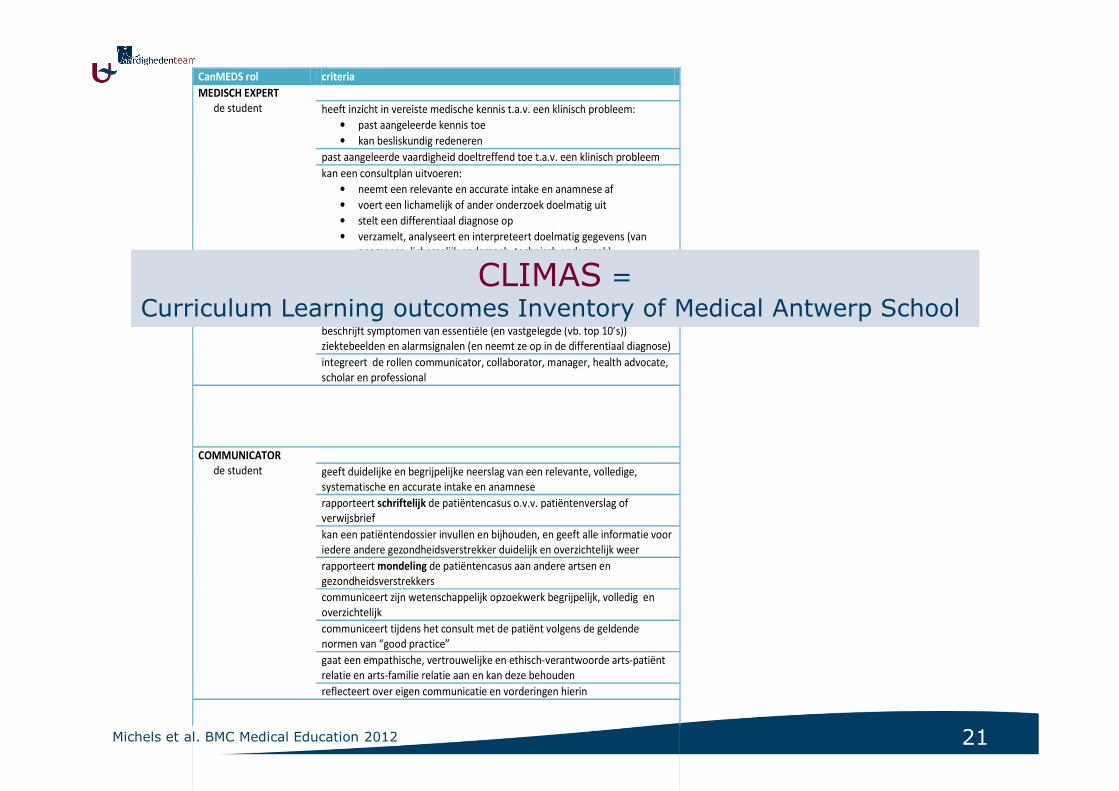
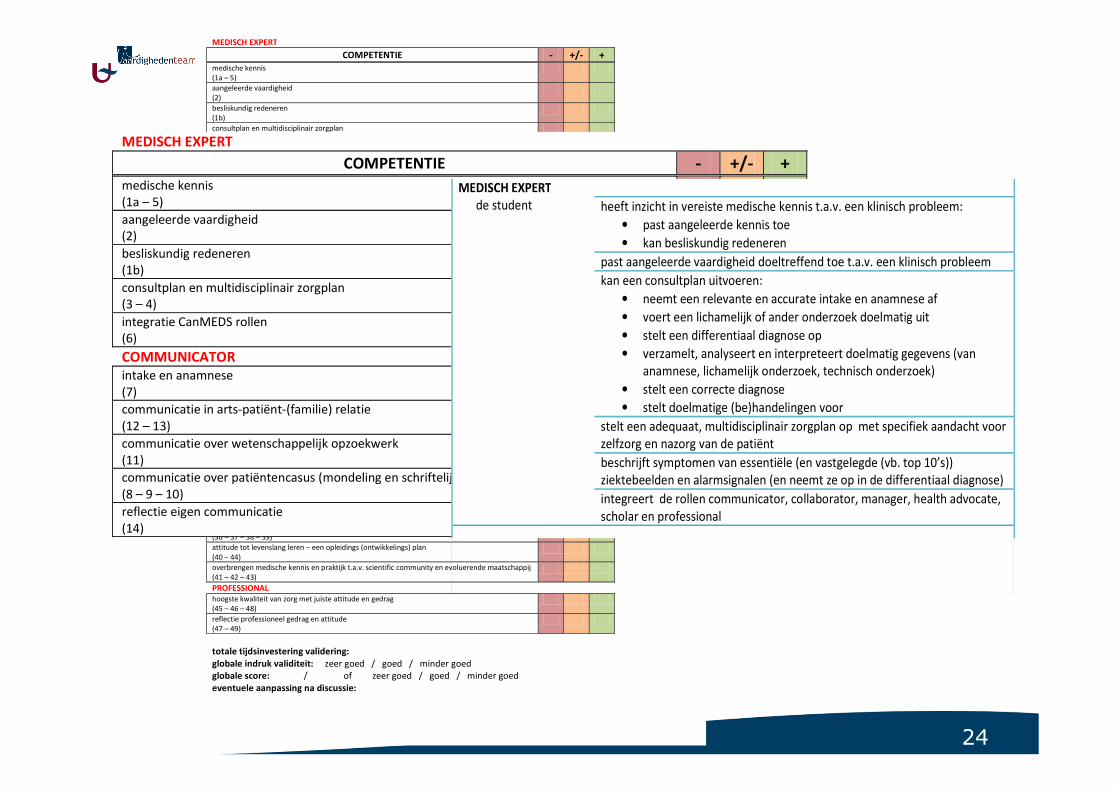
CanMEDS rol criteria
MEDISCH EXPERT
de student
heeft inzicht in vereiste medische kennis t.a.v. een klinisch probleem:
• past aangeleerde kennis toe
• kan besliskundig redeneren
past aangeleerde vaardigheid doeltreffend toe t.a.v. een klinisch probleem
kan een consultplan uitvoeren:
• neemt een relevante en accurate intake en anamnese af
• voert een lichamelijk of ander onderzoek doelmatig uit
• stelt een differentiaal diagnose op
• verzamelt, analyseert en interpreteert doelmatig gegevens (van
anamnese, lichamelijk onderzoek, technisch onderzoek)
• stelt een correcte diagnose
• stelt doelmatige (be)handelingen voor
stelt een adequaat, multidisciplinair zorgplan op met specifiek aandacht voor
zelfzorg en nazorg van de patiënt
beschrijft symptomen van essentiële (en vastgelegde (vb. top 10’s))
ziektebeelden en alarmsignalen (en neemt ze op in de differentiaal diagnose)
integreert de rollen communicator, collaborator, manager, health advocate,
scholar en professional
COMMUNICATOR
de student
geeft duidelijke en begrijpelijke neerslag van een relevante, volledige,
systematische en accurate intake en anamnese
rapporteert schriftelijk de patiëntencasus o.v.v. patiëntenverslag of
verwijsbrief
kan een patiëntendossier invullen en bijhouden, en geeft alle informatie voor
iedere andere gezondheidsverstrekker duidelijk en overzichtelijk weer
rapporteert mondeling de patiëntencasus aan andere artsen en
gezondheidsverstrekkers
communiceert zijn wetenschappelijk opzoekwerk begrijpelijk, volledig en
overzichtelijk
communiceert tijdens het consult met de patiënt volgens de geldende
normen van “good practice”
gaat een empathische, vertrouwelijke en ethisch-verantwoorde arts-patiënt
relatie en arts-familie relatie aan en kan deze behouden
reflecteert over eigen communicatie en vorderingen hierin
CLIMAS = Curriculum Learning outcomes Inventory of Medical Antwerp School
Michels et al. BMC Medical Education 2012
22
conclusie Delphi studie
• gevalideerde lijst van rollen en competenties die studenten moeten bereiken door te werken & te leren in de klinische setting (workplace based learning) en waarop ze getoetst kunnen worden
• cave “artificiële” fragmentatie van verschillende rollen en competenties
• geen praktische tool
Michels et al. BMC Medical Education 2012
23
extra Delphi ronde
• semi-gestructureerde interviews
• 10 Delphi experts � at random selectie
• tot saturatie (N=9)
Validity Inventory for Portfolio Assessment
“VIP-A”
24
VIP-A
MEDISCH EXPERT
COMPETENTIE - +/- + medische kennis
(1a – 5)
aangeleerde vaardigheid
(2)
besliskundig redeneren
(1b)
consultplan en multidisciplinair zorgplan
(3 – 4)
integratie CanMEDS rollen
(6)
COMMUNICATOR
intake en anamnese
(7)
communicatie in arts-patiënt-(familie) relatie
(12 – 13)
communicatie over wetenschappelijk opzoekwerk
(11)
communicatie over patiëntencasus (mondeling en schriftelijk)
(8 – 9 – 10)
reflectie eigen communicatie
(14)
COLLABORATOR
gepaste deelname in een team van zorgverstrekkers
(15 – 16 – 17)
(taken) teamwerk
(18)
reflectie werken in een team
(19)
MANAGER
reflectie zelfzorg en balans werk-persoonlijke ontwikkeling
(20)
prioriteiten, administratieve en organisatorische taken, informatietechnologie
(21 – 22 – 23 – 24)
gezondheidssysteem, inzicht in kosten en contractprocedures
(25 – 26 – 27)
HEALTH ADVOCATE
reflectie over aspecten die gezondheid beïnvloeden (biopsychosociaal en existentieel)
(28)
primaire en secundaire preventie, patiëntveiligheid
(29 – 30 – 31)
belangen van patiënt, begeleiding in gezondheidszorg
(32 – 33 – 34)
reflectie kritische incidenten
(35)
SCHOLAR wetenschappelijk denken en handelen
(36 – 37 – 38 – 39)
attitude tot levenslang leren – een opleidings (ontwikkelings) plan
(40 – 44)
overbrengen medische kennis en praktijk t.a.v. scientific community en evoluerende maatschappij
(41 – 42 – 43)
PROFESSIONAL hoogste kwaliteit van zorg met juiste attitude en gedrag
(45 – 46 – 48)
reflectie professioneel gedrag en attitude
(47 – 49)
totale tijdsinvestering validering:
globale indruk validiteit: zeer goed / goed / minder goed
globale score: / of zeer goed / goed / minder goed
eventuele aanpassing na discussie:
MEDISCH EXPERT
COMPETENTIE - +/- + medische kennis
(1a – 5)
aangeleerde vaardigheid
(2)
besliskundig redeneren
(1b)
consultplan en multidisciplinair zorgplan
(3 – 4)
integratie CanMEDS rollen
(6)
COMMUNICATOR
intake en anamnese
(7)
communicatie in arts-patiënt-(familie) relatie
(12 – 13)
communicatie over wetenschappelijk opzoekwerk
(11)
communicatie over patiëntencasus (mondeling en schriftelijk)
(8 – 9 – 10)
reflectie eigen communicatie
(14)
MEDISCH EXPERT
de student
heeft inzicht in vereiste medische kennis t.a.v. een klinisch probleem:
• past aangeleerde kennis toe
• kan besliskundig redeneren
past aangeleerde vaardigheid doeltreffend toe t.a.v. een klinisch probleem
kan een consultplan uitvoeren:
• neemt een relevante en accurate intake en anamnese af
• voert een lichamelijk of ander onderzoek doelmatig uit
• stelt een differentiaal diagnose op
• verzamelt, analyseert en interpreteert doelmatig gegevens (van
anamnese, lichamelijk onderzoek, technisch onderzoek)
• stelt een correcte diagnose
• stelt doelmatige (be)handelingen voor
stelt een adequaat, multidisciplinair zorgplan op met specifiek aandacht voor
zelfzorg en nazorg van de patiënt
beschrijft symptomen van essentiële (en vastgelegde (vb. top 10’s))
ziektebeelden en alarmsignalen (en neemt ze op in de differentiaal diagnose)
integreert de rollen communicator, collaborator, manager, health advocate,
scholar en professional
25
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
Delphi studie� “validityinventory”
content validity studie
context
onderzoeksvragen
studies &resultaten
systematicreview
� richtlijnen
26
content validity
• 120 portfolio’sUniversiteit Maastricht (N=40) – Universiteit Utrecht (N=40) – Universiteit Antwerpen (N=40)
• 3 beoordelaars, gepaard (3 sets):
Marijke Avonts, Griet Peeraer, Kris Ulenaers
onafhankelijke dubbel beoordeling
27
content validity
• 120 portfolio’sUniversiteit Maastricht (N=40) – Universiteit Utrecht (N=40) – Universiteit Antwerpen (N=40)
• 3 beoordelaars, gepaard (3 sets):
• verzamelen van context informatie
• VIP-A
- is mogelijk om over de competentie te oordelen d.m.v. portfolio? voldoende (+) / gedeeltelijk (+/-) / onvoldoende (-)
- welke opdrachten (portfolio inhoud) zorgen voor mogelijke beoordeling?
28
• context
• doel van portfolio
• tutoring – feedback
• beoordeling
• portfolio inhoud
content validity
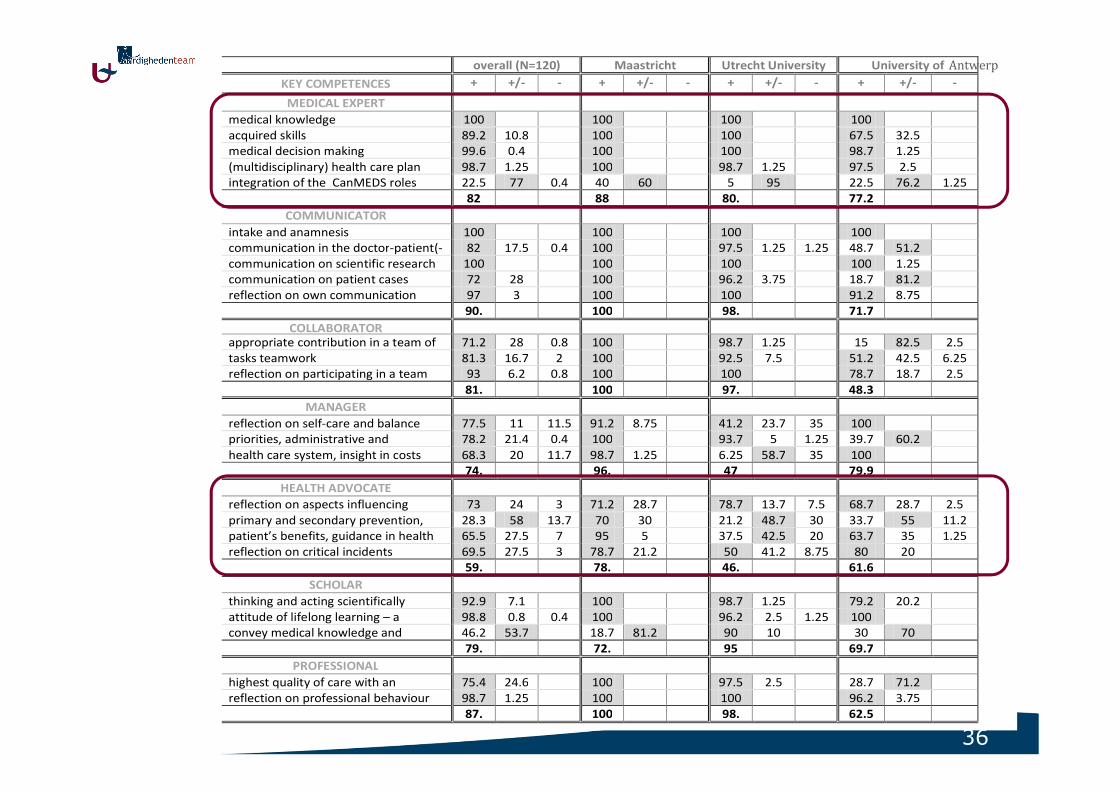
• resultaten
- context register
- frequentie analyse
29
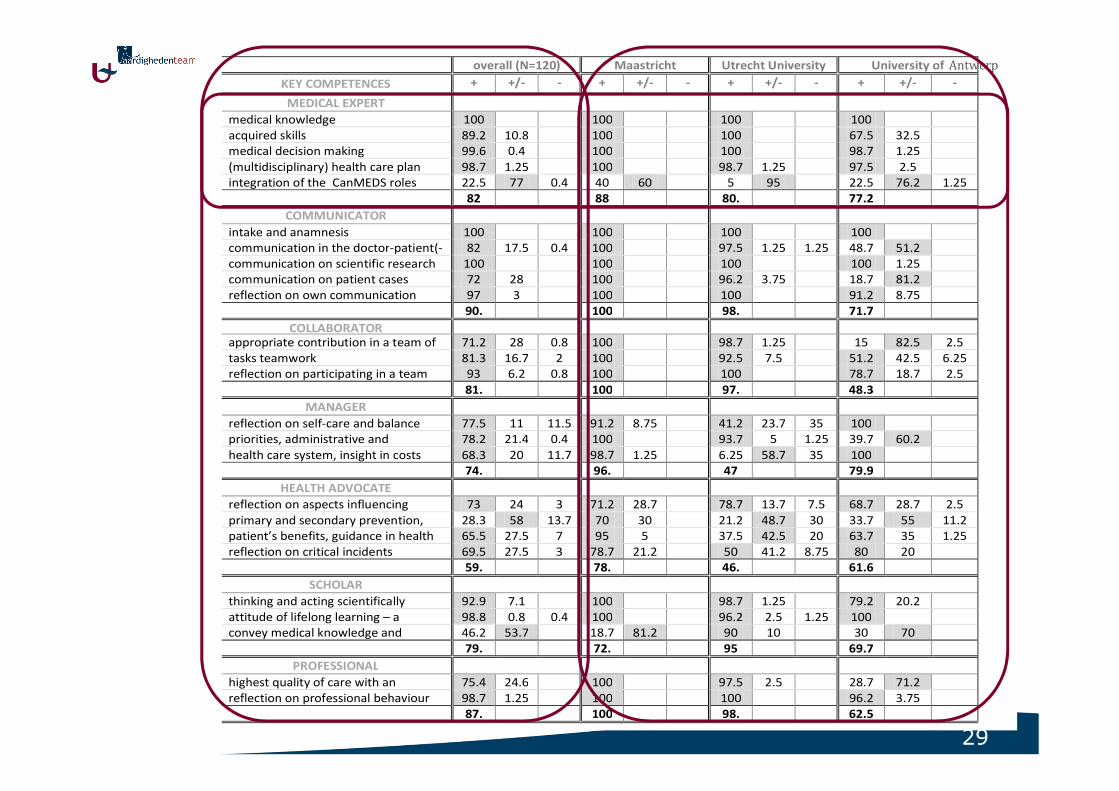
overall (N=120) Maastricht Utrecht University University of
KEY COMPETENCES + +/- - + +/- - + +/- - + +/- -
MEDICAL EXPERT
medical knowledge 100 100 100 100
acquired skills 89.2 10.8 100 100 67.5 32.5
medical decision making 99.6 0.4 100 100 98.7 1.25
(multidisciplinary) health care plan 98.7 1.25 100 98.7 1.25 97.5 2.5
integration of the CanMEDS roles 22.5 77 0.4 40 60 5 95 22.5 76.2 1.25
82 88 80. 77.2
COMMUNICATOR
intake and anamnesis 100 100 100 100
communication in the doctor-patient(- 82 17.5 0.4 100 97.5 1.25 1.25 48.7 51.2
communication on scientific research 100 100 100 100 1.25
communication on patient cases 72 28 100 96.2 3.75 18.7 81.2
reflection on own communication 97 3 100 100 91.2 8.75
90. 100 98. 71.7
COLLABORATOR appropriate contribution in a team of 71.2 28 0.8 100 98.7 1.25 15 82.5 2.5
tasks teamwork 81.3 16.7 2 100 92.5 7.5 51.2 42.5 6.25
reflection on participating in a team 93 6.2 0.8 100 100 78.7 18.7 2.5
81. 100 97. 48.3
MANAGER
reflection on self-care and balance 77.5 11 11.5 91.2 8.75 41.2 23.7 35 100
priorities, administrative and 78.2 21.4 0.4 100 93.7 5 1.25 39.7 60.2
health care system, insight in costs 68.3 20 11.7 98.7 1.25 6.25 58.7 35 100
74. 96. 47 79.9
HEALTH ADVOCATE
reflection on aspects influencing 73 24 3 71.2 28.7 78.7 13.7 7.5 68.7 28.7 2.5
primary and secondary prevention, 28.3 58 13.7 70 30 21.2 48.7 30 33.7 55 11.2
patient’s benefits, guidance in health 65.5 27.5 7 95 5 37.5 42.5 20 63.7 35 1.25
reflection on critical incidents 69.5 27.5 3 78.7 21.2 50 41.2 8.75 80 20
59. 78. 46. 61.6
SCHOLAR
thinking and acting scientifically 92.9 7.1 100 98.7 1.25 79.2 20.2
attitude of lifelong learning – a 98.8 0.8 0.4 100 96.2 2.5 1.25 100
convey medical knowledge and 46.2 53.7 18.7 81.2 90 10 30 70
79. 72. 95 69.7
PROFESSIONAL
highest quality of care with an 75.4 24.6 100 97.5 2.5 28.7 71.2
reflection on professional behaviour 98.7 1.25 100 100 96.2 3.75
87. 100 98. 62.5
Antwerp
30
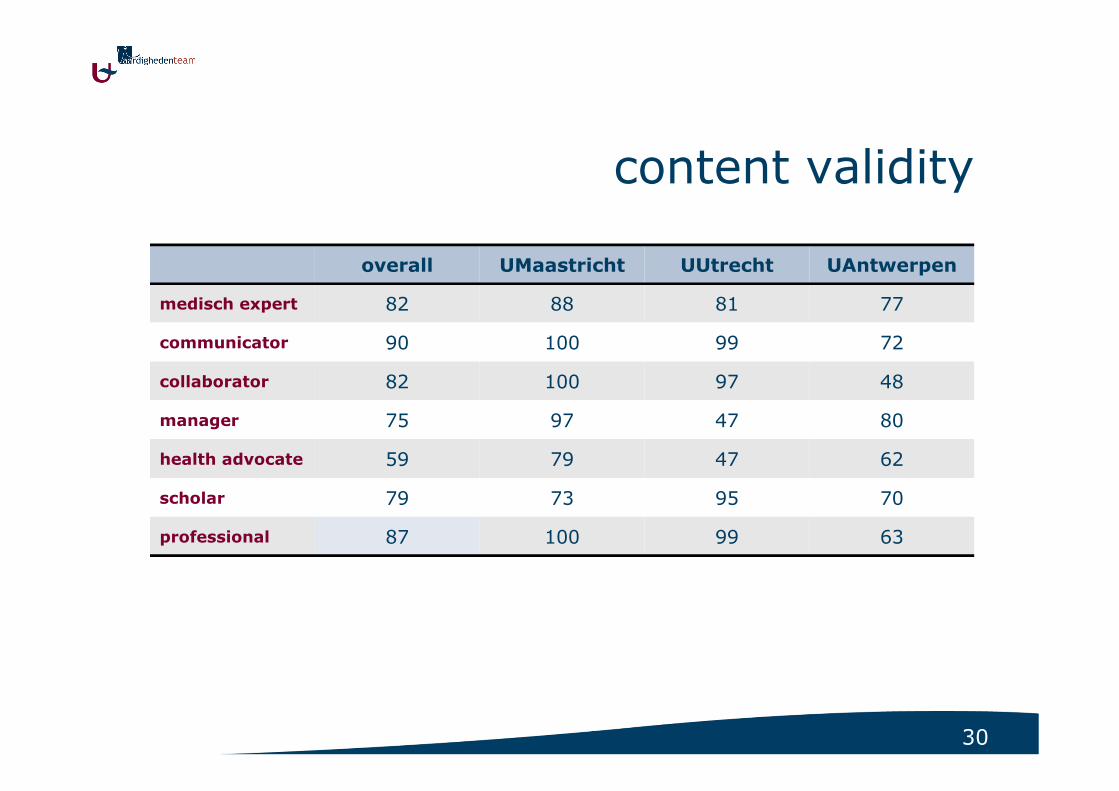
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
31
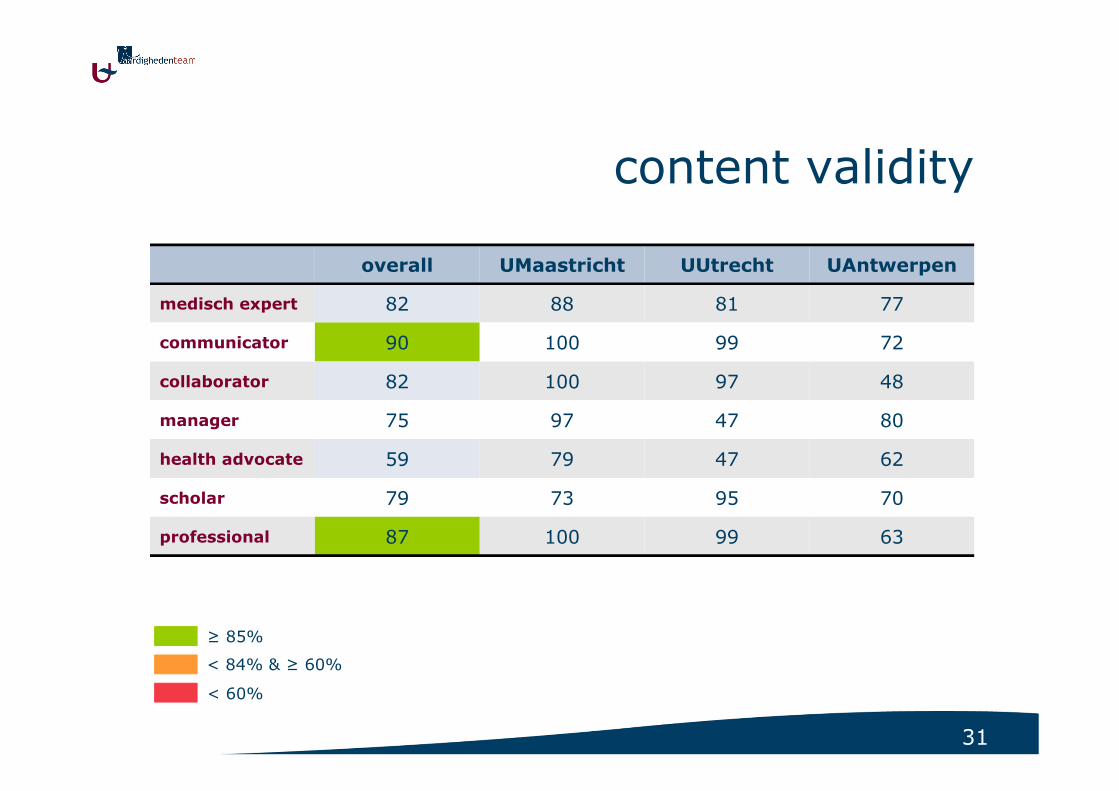
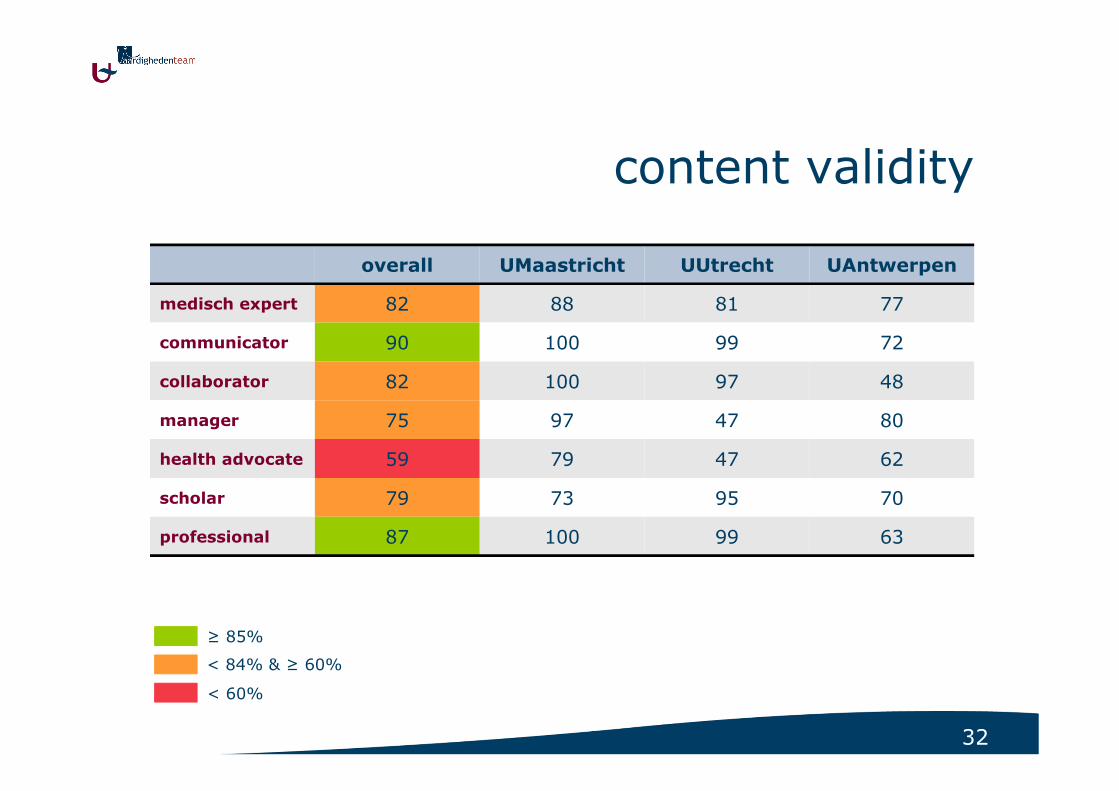
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
≥ 85%
< 84% & ≥ 60%
< 60%
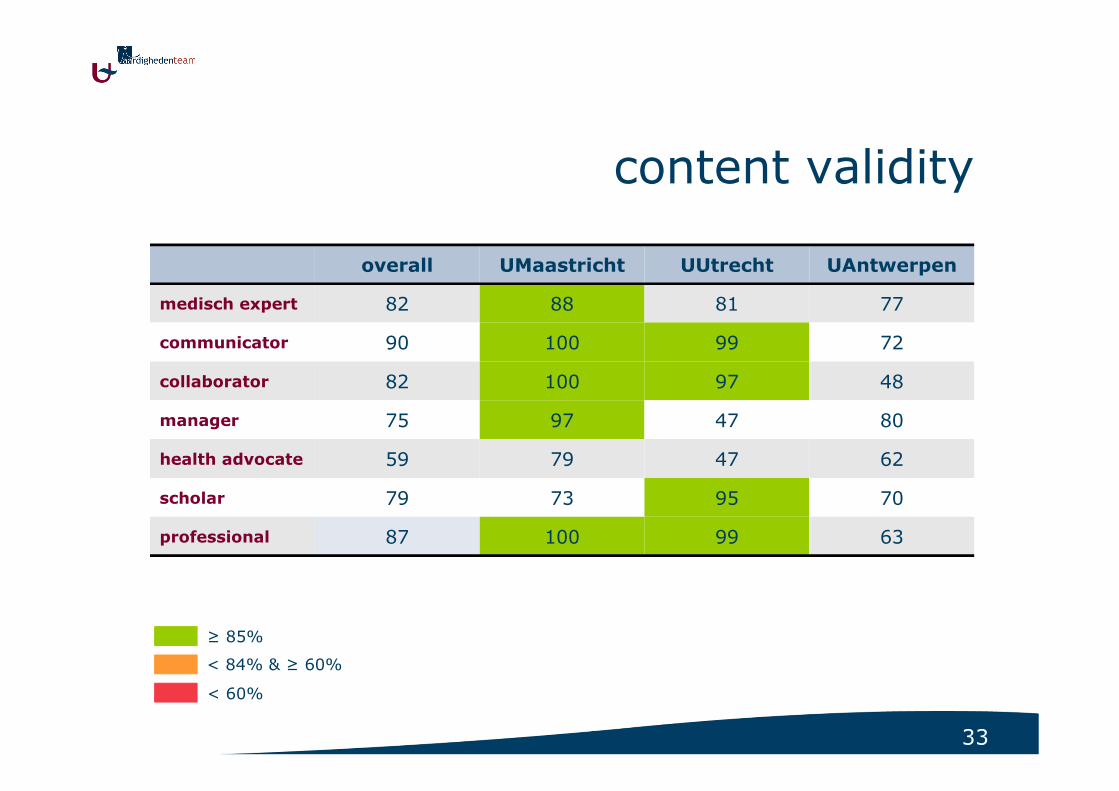
32
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
≥ 85%
< 84% & ≥ 60%
< 60%
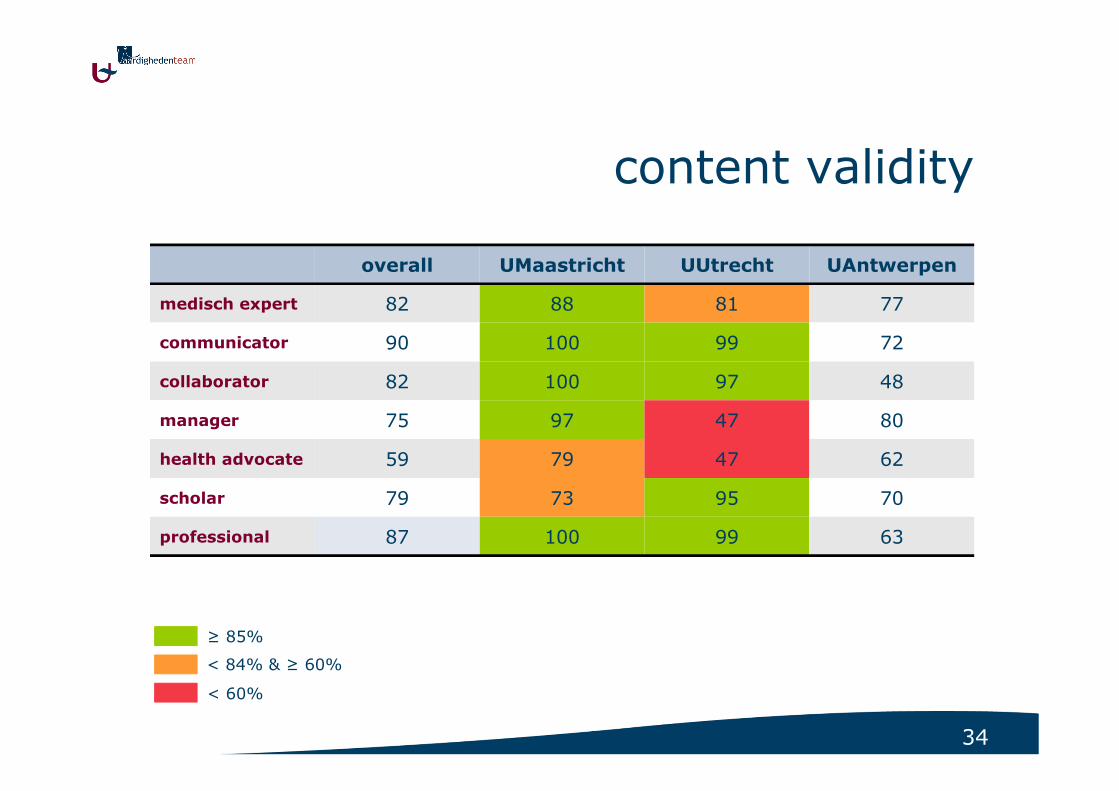
33
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
≥ 85%
< 84% & ≥ 60%
< 60%
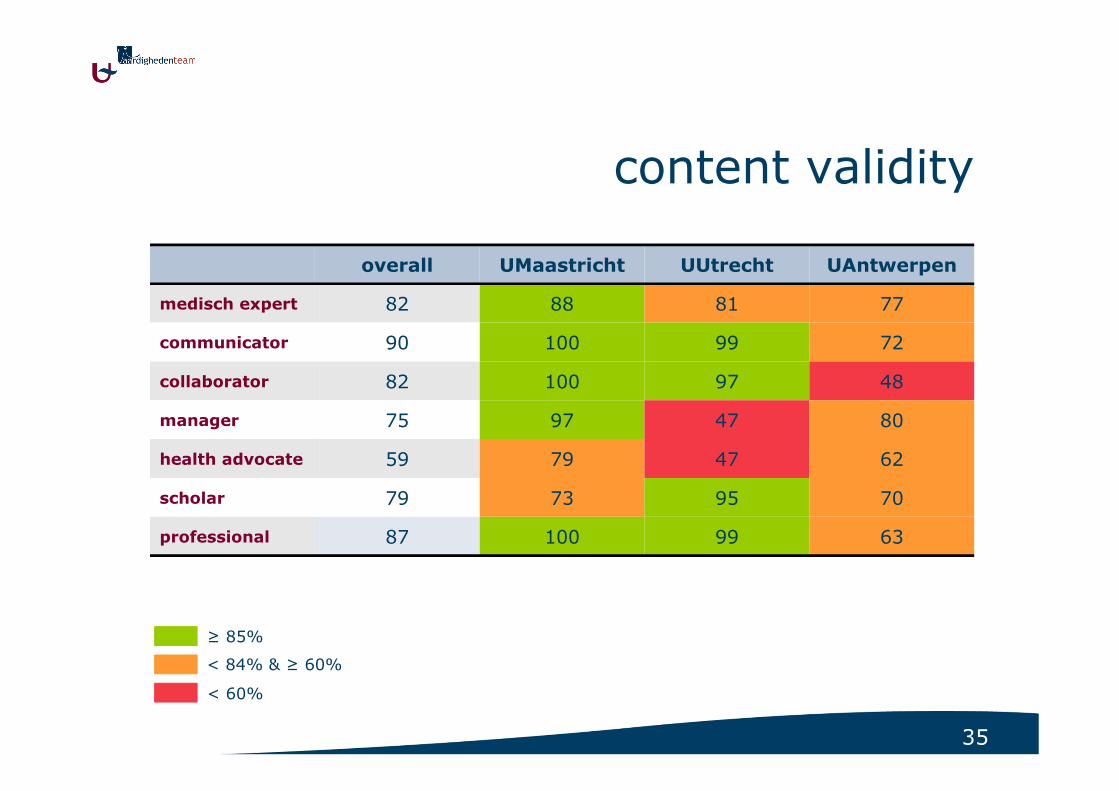
34
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
≥ 85%
< 84% & ≥ 60%
< 60%
35
content validity
overall UMaastricht UUtrecht UAntwerpen
medisch expert 82 88 81 77
communicator 90 100 99 72
collaborator 82 100 97 48
manager 75 97 47 80
health advocate 59 79 47 62
scholar 79 73 95 70
professional 87 100 99 63
≥ 85%
< 84% & ≥ 60%
< 60%
36
overall (N=120) Maastricht Utrecht University University of
KEY COMPETENCES + +/- - + +/- - + +/- - + +/- -
MEDICAL EXPERT
medical knowledge 100 100 100 100
acquired skills 89.2 10.8 100 100 67.5 32.5
medical decision making 99.6 0.4 100 100 98.7 1.25
(multidisciplinary) health care plan 98.7 1.25 100 98.7 1.25 97.5 2.5
integration of the CanMEDS roles 22.5 77 0.4 40 60 5 95 22.5 76.2 1.25
82 88 80. 77.2
COMMUNICATOR
intake and anamnesis 100 100 100 100
communication in the doctor-patient(- 82 17.5 0.4 100 97.5 1.25 1.25 48.7 51.2
communication on scientific research 100 100 100 100 1.25
communication on patient cases 72 28 100 96.2 3.75 18.7 81.2
reflection on own communication 97 3 100 100 91.2 8.75
90. 100 98. 71.7
COLLABORATOR appropriate contribution in a team of 71.2 28 0.8 100 98.7 1.25 15 82.5 2.5
tasks teamwork 81.3 16.7 2 100 92.5 7.5 51.2 42.5 6.25
reflection on participating in a team 93 6.2 0.8 100 100 78.7 18.7 2.5
81. 100 97. 48.3
MANAGER
reflection on self-care and balance 77.5 11 11.5 91.2 8.75 41.2 23.7 35 100
priorities, administrative and 78.2 21.4 0.4 100 93.7 5 1.25 39.7 60.2
health care system, insight in costs 68.3 20 11.7 98.7 1.25 6.25 58.7 35 100
74. 96. 47 79.9
HEALTH ADVOCATE
reflection on aspects influencing 73 24 3 71.2 28.7 78.7 13.7 7.5 68.7 28.7 2.5
primary and secondary prevention, 28.3 58 13.7 70 30 21.2 48.7 30 33.7 55 11.2
patient’s benefits, guidance in health 65.5 27.5 7 95 5 37.5 42.5 20 63.7 35 1.25
reflection on critical incidents 69.5 27.5 3 78.7 21.2 50 41.2 8.75 80 20
59. 78. 46. 61.6
SCHOLAR
thinking and acting scientifically 92.9 7.1 100 98.7 1.25 79.2 20.2
attitude of lifelong learning – a 98.8 0.8 0.4 100 96.2 2.5 1.25 100
convey medical knowledge and 46.2 53.7 18.7 81.2 90 10 30 70
79. 72. 95 69.7
PROFESSIONAL
highest quality of care with an 75.4 24.6 100 97.5 2.5 28.7 71.2
reflection on professional behaviour 98.7 1.25 100 100 96.2 3.75
87. 100 98. 62.5
Antwerp
37
content validity
• resultaten
- context register
- frequentie analyse
- “inhoud” database
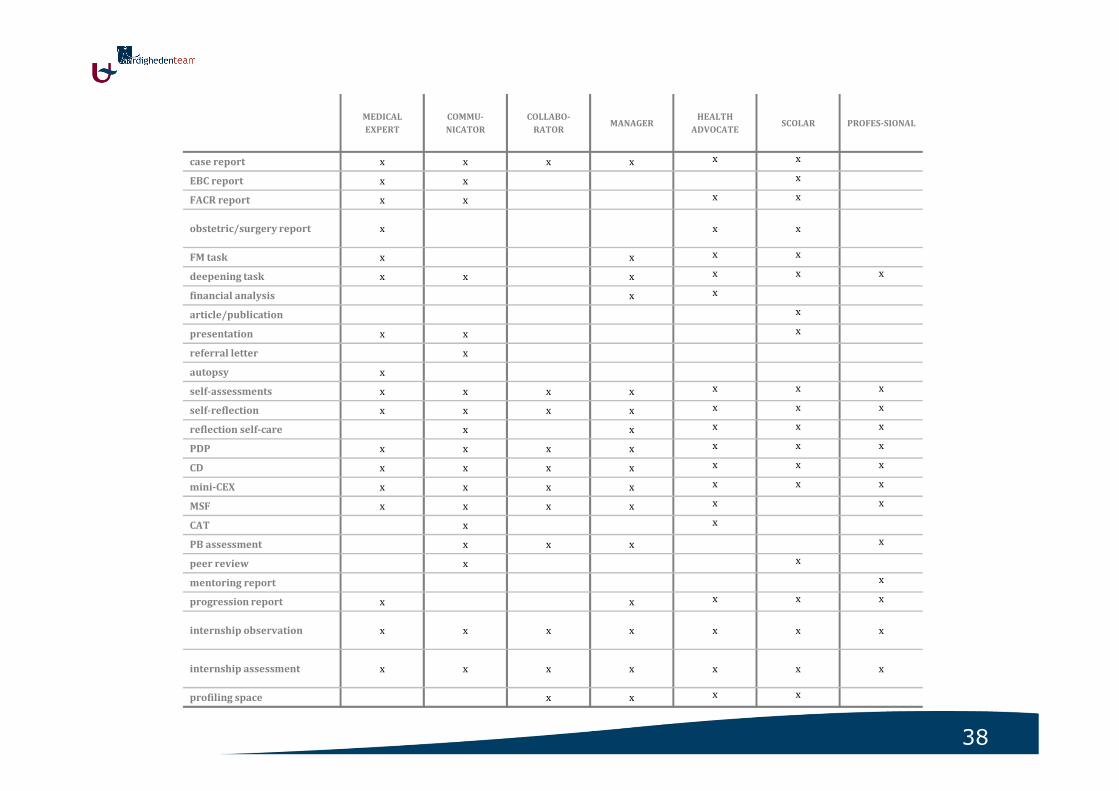
38
MEDICAL
EXPERT
COMMU-
NICATOR
COLLABO-
RATORMANAGER
HEALTH
ADVOCATESCOLAR PROFES-SIONAL
case report x x x x x x
EBC report x x x
FACR report x x x x
obstetric/surgery report x x x
FM task x x x x
deepening task x x x x x x
financial analysis x x
article/publication x
presentation x x x
referral letter x
autopsy x
self-assessments x x x x x x x
self-reflection x x x x x x x
reflection self-care x x x x x
PDP x x x x x x x
CD x x x x x x x
mini-CEX x x x x x x x
MSF x x x x x x
CAT x x
PB assessment x x x x
peer review x x
mentoring report x
progression report x x x x x
internship observation x x x x x x x
internship assessment x x x x x x x
profiling space x x x x
39
content validity
• resultaten
- context register
- frequentie analyse
- “inhoud” database
- validatie van VIP-A:
• inter beoordelaar betrouwbaarheid: Percentage Agreement
• agreement was hoog (>80% & <90%) tot zeer hoog (>90%)
health advocate role scoort minder (wel nog >60%)
40
content validity
• conclusie
- validatie VIP-A (“internal structure validity”)
- portfolio kan gebruikt worden om competenties te beoordelen
- “hoe content validity verbeteren?”
• duidelijke stellen van “doel” & blueprint
• expliciete link tussen competenties/rollen en portfolio opdracht
• content database
• portfolio & context: adequate procedures voor beoordeling & begeleiding
41
overzicht
portfoliointroductie & implementatie
betrouwbaarheid
haalbaarheid validiteit
generaliseerbaarheidsanalyse
Delphi studie� “validityinventory”
content validity studie
context
onderzoeksvragen
studies &resultaten
systematicreview
� richtlijnen
42
vervolg…
• CLIMAS & VIP-A
- andere doeleinden
- verder valideren
• validiteit:
- andere portfolio’s
- “consequences”
• portfolio verbeteren
- opdrachten ~ competenties
- “directe” beoordelingen, vb. KKB
- tutorship herbekijken
- “holistic assessment”
43
take home messages
• laat uw studenten & stagiairs actief stage lopen
• doel = werkplek leren
• betrek CLIMAS = skelet van waaruit u studenten kan begeleiden en beoordelen
• directe observaties: KKB
• zorg voor uiteenlopende ervaringen / patiënten
• bespreek mogelijke opdrachten tijdens stage bij u
• “tutor” rol: geef feedback en bespreek leernoden, leerplannen en progressie
44
als laatste
• dank aan
collega’s vaardighedenteam, portfoliobeoordelaars, reviewers, Delphi experts, validiteit beoordelaars, studenten, stagemeesters,…
• vragen of suggesties?