

Preventie van chronificatie van postoperatieve pijn
97
Preventie van chronificatie van postoperatieve pijn Dr De Coster Olivier Anesthesist Algoloog AZDelta UZBrussel
Transcript of Preventie van chronificatie van postoperatieve pijn

Preventie van chronificatie van postoperatieve pijn
Dr De Coster Olivier
Anesthesist Algoloog
AZDelta
UZBrussel

Situering : is het een probleem ?
- of maken we ons zorgen om niets ?- is onze inspanning nuttig ?



Duidelijk een belangrijk probleem !
• Dus preventie belangrijk om menselijk en financieel leed te voorkomen.
• CPSP : • 10-20% in alle patiënten
• 1-2% erge CPSP
• 35% na thoractomie
• 20% na TKP
• 10% na THP

70% van CPS voorspeld door volgende factoren :
-leeftijd
-type heelkunde
-fysische en mentale gezondheid
-preoperatieve pijn ( in operatie gebeid OF elders)
probeer 5 risocofactoren op te sporen
1. Emotionele stress
2. Preoperatieve pijn in operatief gebied
3. Andere chronische pijn
4. Erger dan verwachte postoperatieve pijn
5. Comorbiditeit stress symtomen = angst, verstoorde slaap
Prediction of CPSP

• Preventie :een groepswerk van iedereen
artsen ( chirurgie en anesthesie )verplegingkinéapotheekpsychologenMAT’s patiënten

Basis = probleem opsporen
Pijnbehandeling is één van de basis patiëntenrechten
DUS iedere patiënt heeft recht op
- bevraging ivm pijn
- therapie ivm pijn
Pijncontrole = basisrecht

- Vermijden van chronificatie van pijn
- Dus minder pijnproblemen later ?
- Rol van opiaten perop beleid & sedatie beleid
- Rol van perop beleid
- Opsporen red en yellow flag
- Red flags
- Yellow flags
Goede pijncontrole = preventieve geneeskunde

Risico factoren

Risico factoren

Noteer
Organiseer
Structureer
maw pijnbevraging en pijn observatie ALTIJD bevragen
= alle andere parameters
Maar hou het praktisch en vergader niet te veel = patiënten zitten niet in de vergaderruimte
Meten = weten

In tijden van JCI
niet alleen naar cijfertjes kijken
vermijd cijfers als excuus
nadenken helpt
verschil gelaatsuitdrukking –NRS/VAS
onrust = pijn ? Of volle blaas ? Of delier …..
Maar niet altijd

Uniformisatie pijnbeleid is nodig
1ste stap = meten – bevragen naast al de andere parameters

1ste stap pijnbevraging : hoe ?
VAS NRS
GVS PAINAD
PACSLAC
DOLOPLUS
BPSCPOT
POKIS
SMILEY
MPQ
Oswestry
RDG
Waddell

Keep it simple

Keep it human
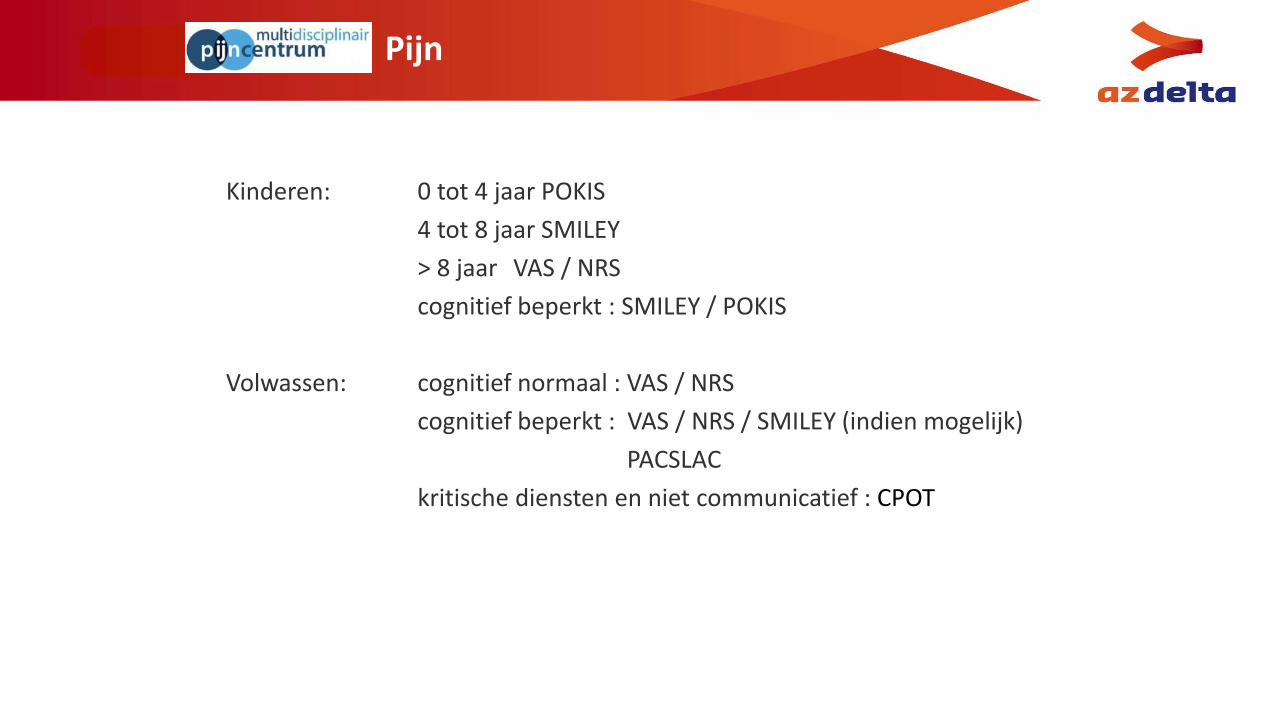
Pijn
Kinderen: 0 tot 4 jaar POKIS
4 tot 8 jaar SMILEY
> 8 jaar VAS / NRS
cognitief beperkt : SMILEY / POKIS
Volwassen: cognitief normaal : VAS / NRS
cognitief beperkt : VAS / NRS / SMILEY (indien mogelijk)
PACSLAC
kritische diensten en niet communicatief : CPOT

PACSLAC

PAINAID 0 1 2 score
Ademhaling NormaalIncidentele moeizame ademhalingKorte periode van hyperventilatie
Luidruchtige moeizame ademhalingLange periode van hyperventilatieChyene-Stokes ademhaling
Onrustgeluiden GeenIncidenteel kreunen of kermenZacht spreken met een negatieve of afkeurende toon
Herhaaldelijk angstig uitroepenLuid kreunen of kermenHuilen
GezichtsuitdrukkingGlimlachend of nietszeggend (neutraal, ontspannen)
DroevigBangFronsen
Grimas
Lichaamstaal OntspannenGespannenOverstuur op en neer stappen, ijsberen, zenuwachtig bewegen
Verstard, gebalde vuisten, opgetrokken knieënWegtrekken of wegduwen, uithalen
Troostbaarheid Niet nodig om te troostenAfgeleid of gerustgesteld door stem of aanraking
Onmogelijkheid te troosten, af te leiden of gerust te stellen
PAINAD of PAIN ASSESMENT IN ADVANCED DEMENTIA SCALE



Pijnbeoordeling bij de kritisch zieke patient
1.Chanques G, Sebbane M, Barbotte E, Viel E, Eledjam JJ, Jaber S. A prospective study of pain at rest: incidence and characteristics of an unrecognized symptom in surgical and trauma versus medical intensive care unit patients. Anesthesiology. 2007;107(5):858-860.
2. Puntillo KA, White C, Morris AB, et al. Patients’ perceptions and responses to procedural pain: results from Thunder Project II. Am J Crit Care. 2001;10(4):238-251.
Patiënten op ICU:
pijn bij rust : 30%
pijn tijdens verzorging : > 50%
Situering probleem

Sedatie niet gelijk aan pijnstilling
extreem : curare is geen pijnstiller ( oa critical illnesspolyneuropathy)

Pijnbeoordeling bij de kritisch zieke patient
On(der)behandelde pijn:
CV stelsel: tachycardie, hypertensie, cardiac output ↑
O2 verbruik ↑
AH stelsel: oppervlakkiger ademen , hypoventilatie, atelectase, infectie
O2 aanbod ↓
Stolling: abnormale stollingsneiging: DVT, longembolen
GI stelsel: vertraagde maag-darm transit
Neuro-humoraal
Immuniteit: immuunrespons ↓
Evolutie naar chronische pijn
3. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet 2006;367(9522):1618-1625.
4. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North America. 2005;23(1):21-36.
5. Dunwoody CJ, Krenzischek DA, Pasero C, Rathmell JP, Polomano RC. Assessment, physiological monitoring, and consequences of inadequately treated acute pain. J Perianesth Nurs. 2008:23(suppl 1), S15-S27.
Situering probleem : reden pijnstilling

observeer

Betrek de omgeving en familie

Spoed

Pijn : een urgentie ?

Pijn = vitale parameter
Meten = weten
Behandel volgens protokol
maar wijk af waar nodig
Gebruik de aangepaste meetschalen
Access a free educational video to learn more about using the CPOT in the ICU at http://pointers.audiovideoweb.com/stcasx/il83win10115/CPOT2011-WMV.wmv/play.asx. Funded and created by Kaiser Permanente Northern California Nursing Research.
Samenvattend

Type anesthesie : belang ?AA met/zonder opiaten ? OFA locoregionale anesthesie ?

Central sensitization
Richebé, Simonnet 2005

Chronic pain with remifentanil
Br J anaesth 2013

Administered during anesthesia: “the more- the better” ? Or less is more ?

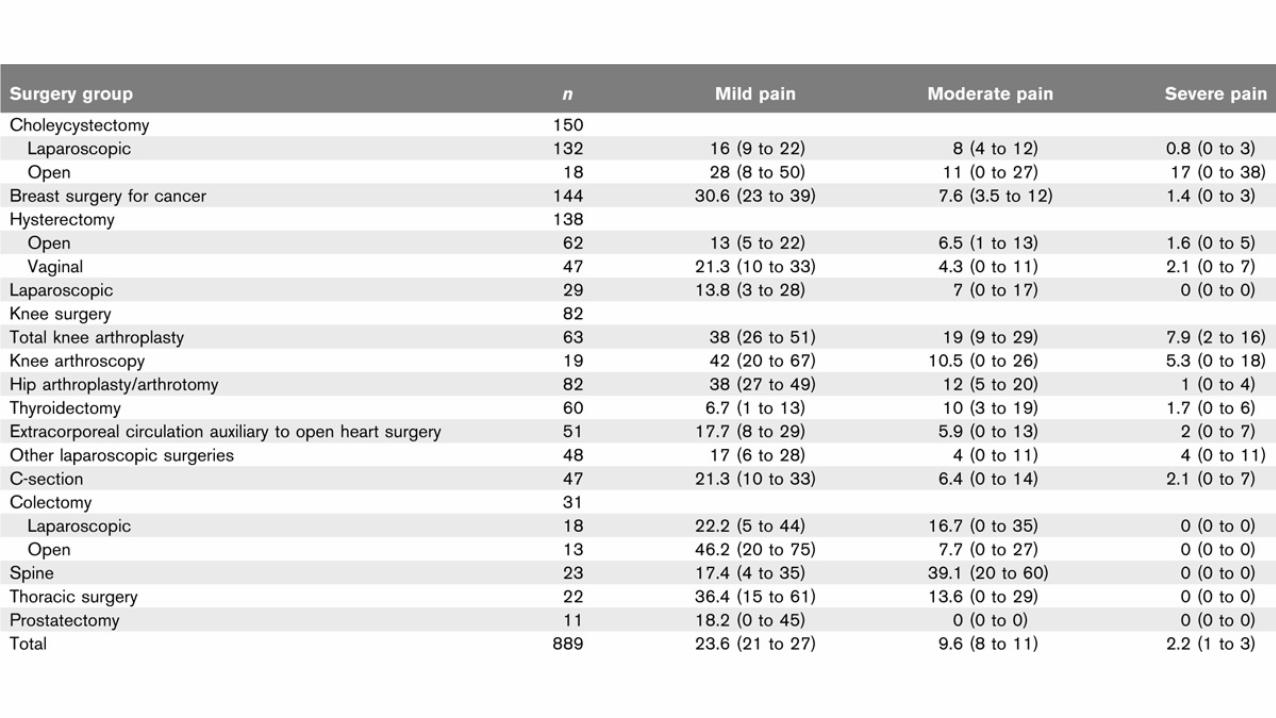
Predictive factors of severe postoperative pain in the PACU
Aubrun, Anesth Analg 2008

Is « Opioid-free » anesthesia possibleduring major thoracic surgery?

Haller et al, Anesthesiology 2009

Marc De Kock, M.D. Ph.D.
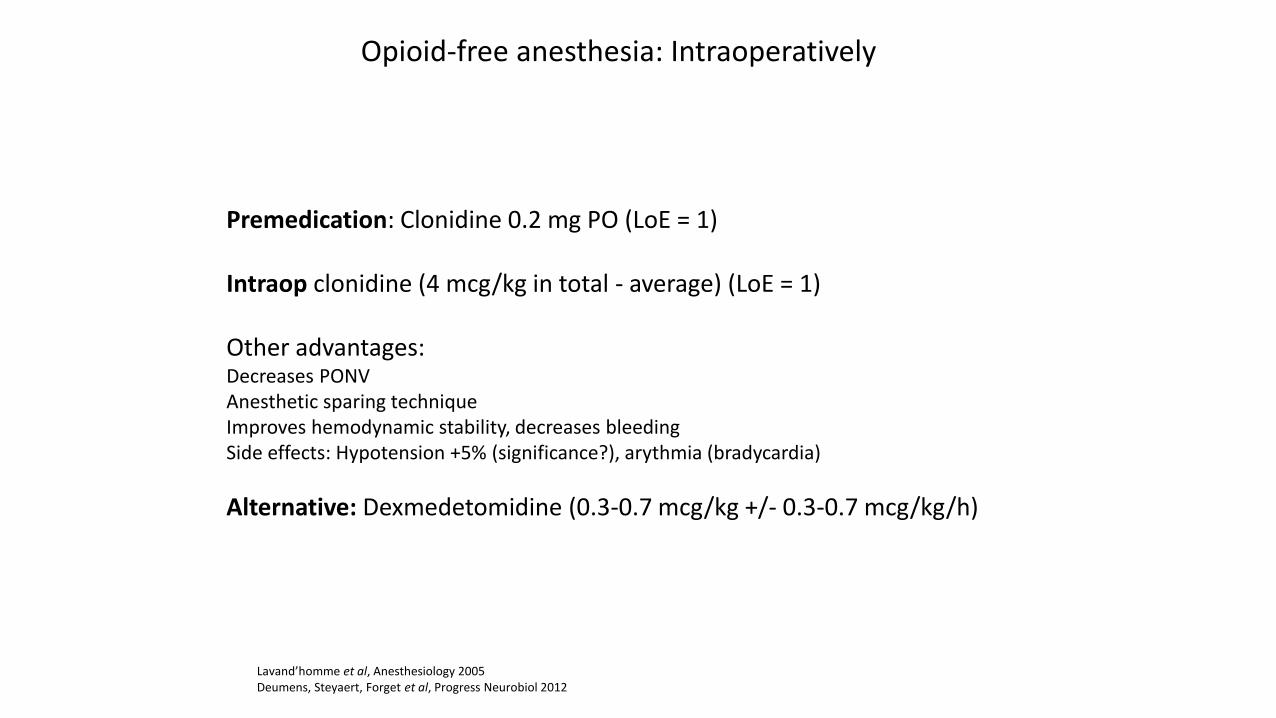
Opioid-free anesthesia: Intraoperatively
Premedication: Clonidine 0.2 mg PO (LoE = 1)
Intraop clonidine (4 mcg/kg in total - average) (LoE = 1)
Other advantages: Decreases PONVAnesthetic sparing techniqueImproves hemodynamic stability, decreases bleedingSide effects: Hypotension +5% (significance?), arythmia (bradycardia)
Alternative: Dexmedetomidine (0.3-0.7 mcg/kg +/- 0.3-0.7 mcg/kg/h)
Lavand’homme et al, Anesthesiology 2005Deumens, Steyaert, Forget et al, Progress Neurobiol 2012


Postoperative analgesic consumption
Sanchez, De Kock and Forget, J Clin Anesth 2017

Postoperative nausea and vomiting
Sanchez, De Kock and Forget, J Clin Anesth 2017

Hemodynamic stability (heart rate and mean arterial pressure)
Sanchez, De Kock and Forget, J Clin Anesth 2017

Sanchez, De Kock and Forget, J Clin Anesth 2017
Prevention of shivering

Sanchez, De Kock and Forget, J Clin Anesth 2017
Recovery time

RCTs on the effect of clonidine vs. placebo
Reference Total N Clonidine Placebo Narcotic-Sparing Effect
Moghadam et al 160 80 80 p<0.0001 propofol
Ghosh et al 90 30 30 p<0.001 propofol
Morris et al 39 21 18 p<0.05 propofol
Laisalmi et al 30 15 15 p<0.05 alfentanil
Fehr et al 50 25 25 p<0.001 propofol / NS remifentanil
Goyagi et al 41 22 19 p=0.0013 propofol
Goyagi et al 39 19 20 p<0.05 propofol
Imai et al 80 40 20 p<0.01 propofol
Katoh et al 42 21 21 p<0.001 sevoflurane
Howie et al 54 28 26 p<0.04 sufentanil / p<0.01 sevoflurane
Singh et al 50 25 25 p<0.05 isoflurane
Oddly-Muhrbeck et al 68 30 30 p<0.04 propofol / p<0.01 sevoflurane
Taghipour et al 30 15 15 p<0.001 remifentanil
Marchal et al 40 19 21 p<0.001 isoflurane / p<0.001 fentanyl / NS propofol
Inomata et al 104 52 52 p=0.0001 sevoflurane
Kalajdzija et al 60 30 30 p<0.001 sevoflurane / NS fentanyl
Ellis et al 61 30 31 p<0.05 enflurane
Hamaya et al 57 38 19 p<0.05 isoflurane
NS = not statistically significant difference
Sanchez, De Kock and Forget, J Clin Anesth 2017

Opioid-free anesthesia: Intraoperatively
Thoracic epidural analgesia
The best analgesic and anti-hyperalgesic technique (LoE = 1)
Local anesthetics +/- clonidine (1 mcg/kg – 0,5-2 mcg/ml postop)
Side effects: Failure, dural puncture (0.5-1%), abcess, hematoma (<1/150,000)
Alternative: Patient-controlled morphine infusionSide effects: Nausea/vomiting, sedation, respiratory depression (1-10%)
Lavand’homme et al, Anesthesiology 2005Deumens, Steyaert, Forget et al, Progress Neurobiol 2012

Deumens, Steyaert, Forget et al, Progress Neurobiol 2012

Other techniques
De Kock et al, AAB 2012De Kock et al, Pain 2001
Deumens, Steyaert, Forget et al, Progress Neurobiol 2012Gobble et al, PRSJ 2014
Forget and Cata, 2017
Locoregional analgesia (central, peripheral blocks)The best analgesic and anti-hyperalgesic technique (LoE = 1) Local anesthetics +/- clonidine (1 mcg/kg – 0.5-2 mcg/ml postop)
Ketamine (low ‘anti-hyperalgesic’ doses) (0.5 mg/kg, bolus + infusion 0.25 mg/kg/h) Opioid sparing, decrease of chronic post-surgical pain (LoE = 1)Reduction of the variability of blood pressure (-8.4 mmgH; 95%CI[-15.1 to -1.8], P=0.0005).
Magnesium sulfate (40 mg/kg) (LoE = 1)Reduction of the variability of heart rate (-3.7 bpm; 95%CI[-6.5 to 0.9], P=0.01)
without lower blood pressure (+4.2 mmHg; 95%CI[-3.6 to +12.03], P=0.29).
IV lidocaine (in the absence of locoregional analgesia) (LoE = 2 to 3)
Non-steroidal anti-inflammatory drugsNo greater risk associated with bleeding, ketorolac including (LoE = 2)
Opioid-free anesthesia: Intraoperatively

Lois, De Kock, Forget. Submitted
21,463 patients receiving OFA
Matched-cohort retrospective study (n=521, laparoscopic hysterectomy)
- 118 receiving OFA during
- 403 controls
Results- OFA patients: clonidine (97%) and ketamine (95%)- Controls: sufentanil (mean±SD : 0.1±0.05 mcg/kg)- No difference of pain scores (4.5 [0-6] vs. 4 [0-5], P=0.74)- No other difference (including sedation scores, time in the PACU)
ConclusionsOFA is feasibleOFA is not associated with higher pain scores or longer PACU stayNo signal for specific immediate complications
Opioid-free anesthesia: Possible?

Therapie ?- kunnen we nog iets doen …..

54
Acute en chronische pijn: implicatie voor behandling
Acute pijn Chronische pijn
...externe of interne lesie ...vaak onduidelijk link met eerste
evenement
...correlatie met stimulus / lesie
size
...geen meer correlatie tussen
lesie grootte en intensiteit
...gelocaliseerd ...een ziekte by its own
...warning systeem ...niet meer bruikbaar
...bio-psycho-sociale
behandeling wordt meer en meer
belangrijk

Farmacologische pijn behandeling
Opiaten(morphine, fentanyl)
-4000 Antidepressors(amitriptyline, duloxetine)
Jaren ‘60
Antiepileptics(gabapentine, pregabaline)
Jaren ‘90
NSAID(Acetylsalycilic zuur, ibuprofene)
1897
ParacetamolCannabinoïds,
capsaïcin
> 2010


Postoperatieve analgesie
StandardParacetamol 3-4 g/d +/- NSAID Diclofenac 75 mg 2x/d, ibuprofene 600 mg 3x/d of ketorolac 20-30 mg 3x/dDagen liever dan weken!Oppassen met oxicams (lange half-life en gastrische toxiciteit)
Moderate tot ernstige pijnTramadol 50 tot 100 mg (! Nausea risico)
Opiaten immediate release vs prolonged release
Andere mogelijgkhedenPatient-controlled (intraveneuze of locoregionale) analgesiaAdjuvants (clonidine, ketamine, IV lidocaine, gabapentinoids)

Central sensitization
HYPERALGESIE
ALLODYNIE

Basic notions : variabilityThe interactions: problem or solution?

Pijn transmissie
4. Perceptie, interpretatie
3. Spinal modulation
1. Peripheric detection
2. Axonal transmission
5. Descending inhibitory pathways

Pijn transmissie
1. Peripheric detection
Salic. zuur, NSAID, paracetamol

Pijn transmissie
2. Axonale transmission
Lokale anesthetica

Pijn transmissie
4. Perception, interpretation
3. Spinal modulation
5. Descending inhibitory pathways
OpioidsAntidepressiva
GABA modulators

Pijn transmissie

Opiaten en opioidsVan acute tot chronische pijn behandeling
Opioids

Opioids
• Krachtige analgetica – snel effect
• Verschillende niveaus (brein, spinal cord, periferie)
• Nadelen : nausea en braken, constipatie, sedatie, euforie, confusion, jeuk
• Intoxication/overdose : adem depressie, bradycardie, hypotensie
• Tolerance
• Ernstige afhankelijkheid fysisch en psychisch

Opioids in 2017
Morphine
Codeine
Buprenorphine (TemgesicR)
Fentanyl (DurogesicR)
Piritramide (DipidolorR)
Pethidine (DolantineR)
Pentazocine (FortalR)
Methadone (MephenonR)
Oxycodone (OxycontinR)
Hydromorphone (PalladoneR)
Step 2
Step 3
Morphine
Oxycodone
FentanylCodeine
Hydrocodone
Tilidine
Tramadol

Klinische visie
Opioids voor pijn behandeling
Efficaciteit (korte termijn)
Patches
Diversiteit
Constipatie, nausea, slaperigheid, jeuk
Interacties
Tolerantie/afhankelijkheid(vermindering van efficaciteit)

Mean N
um
ber
of P
ain
Events
0 14 28
0
4
12
16
20
24
42
Oxycodonen=151
Placebon=158
56 70 84Time [days]
Vondrackova D et al. J Pain 2008;9:1144–54
Vermindering van efficaciteit

Richebé et al, Ann Fr Anesth Réan 2005.
Opioid-induced hyperalgesia

Role of central sensitization
Zangh et al, Pain Medicine 2015.

Tramadol (1978)Twee farmaco activiteiten in
één molecule
TRAMADOLInhibition van de reuptake of
NA (en 5-HT)
O-DESMETHYL-TRAMADOLMetabolit :
Opioid agonist (intermediaire)

Anti-epilepticaVan acute tot chronische pijn behandeling
Anti-epileptica

Inhibition of the ions channels (cations)
Valproate
Phenytoine
Benzodiazepines
Gabapentine
Pregabaline
Ethosuximide
Lamotrigine
Felbamate
Carbamazepine

Chronische pijn : Modificaties van
TRANSMISSIE en modulatie van de pijn
Perifere amplificatie
Centrale amplificatieModificatie van de excitatoire ions channels expression (Na+
en Ca2+)

Anti-epileptica en pijn
Alle zouden we kunnen gebruiken……maar de nadelen zijn een significant probleem
Gabapentine (NeurontinR) ontwikkeld in 1983 (in 1996 tegen pijn)
Pregabaline (LyricaR) ontwikkeld in 1995, voor pijn behandeling
• Indicatie in chronische/neuropathische pijn behandeling
• Pregabaline : krachtiger
• Posologie als in epilepsie
• Constante farmacologie
• Specifiques voor Ca2+ voltage dependants channels, subunit 2: modulatie van de neurotransmitter liberation
Anti-epileptica

Antiepileptica in pijn behandeling
Klinische visie
Efficaciteit
(inconstant)
Nadelen : slaperigheid, risico voor verkeersongeval!
Number needed to harm in favor…maar gerekend over 12 weken alleen !
Titratie over weken! Eliminatie via de nieren

Antidepressiva Van acute tot chronische pijn behandeling
Antidepressiva

Antidepressiva
Cerebral trunc
noradrenaline serotonine (5HT)
Alpha-2 5HT1,7 5HT2,3Spinal cord
Antidepressiva voor beter descending inhibitory
monoaminergic pathways
5HT NA
Sensoriele afferences
Ook: Clonidine, alpha2 adrénergic agonist

Antidepressiva
Antidepressiva voor beter descending inhibitory
monoaminergic pathways
5HT NA
Effect komt na weken…

Antidepressiva
Zelf als er een positieve indruk op depressieve affects verwacht is,,
Analgesic effect is onafhankelijk van de antidepressieve activiteit
Humor
Slapen
Pijn
Posologie voor analgesia < Posologie tegen depressie

Duloxétine
Belang van de serotonine in
pijnbehandeling !
Activiteit tegen noradrenaline en
serotonine reuptake
CYP enzymes

Antidepressiva in pijn
Amitriptyline (RedomexR) en andere tricyclics:
• Vaak gebruikt in chronishe pijn (<jaren ‘60); lage doses.
• Werkt goed maar grote inter-patiënten variabiliteit.
• Geen echte efficaciteit in acute pijn.
• Veel nadelen : anticholinercs (visual en cognitieve disorders, constipatie, sedatie, urine retentie - Prostatism, droge mond). Voorzichtigheid bij oude patienten.
• Cardiac toxicity.
Duloxetine (CymbaltaR) :
Sinds 1994 >< pijn sinds 2003
Efficacy/benefit als amitriptyline
Minder nadelen
SSRI (CipramilR, ProzacR, SeroxatR, …)
Weinig of geen benefit in pijn (behalve depressie)

Antidepressiva in pijn behandeling
Klinische visie
Minder nadelen
Weinig of geen titratie
Nadelen : slaperigheid, droge mond, prostatism
AmitriptylineHart conductie problem = CI
NauseaDuloxetine

Algoritme in praktijk
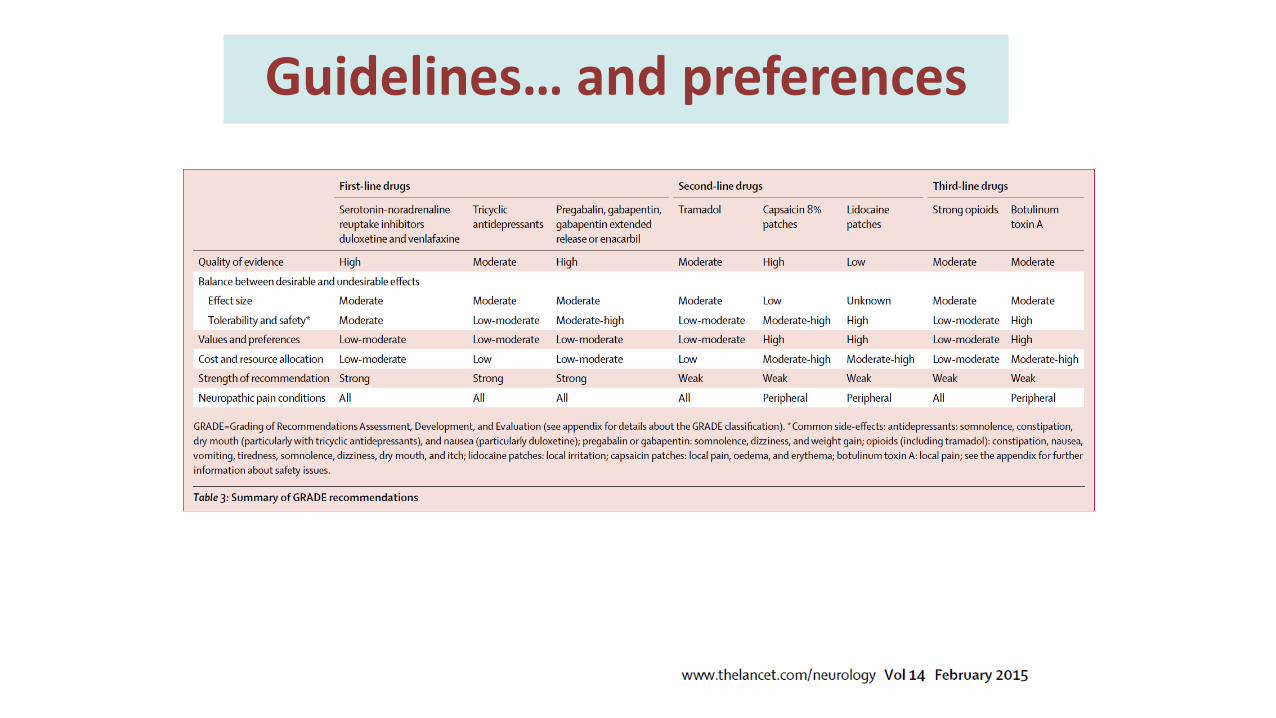
Guidelines… and preferences

Bijkomende effect van opiaten : belang ?Wellicht effecten op
- immuniteit- carcinoomrecidief ?

Forget P, De Kock M, Ann Fr Anesth Réan 2009
Have well-known effects on the organism?
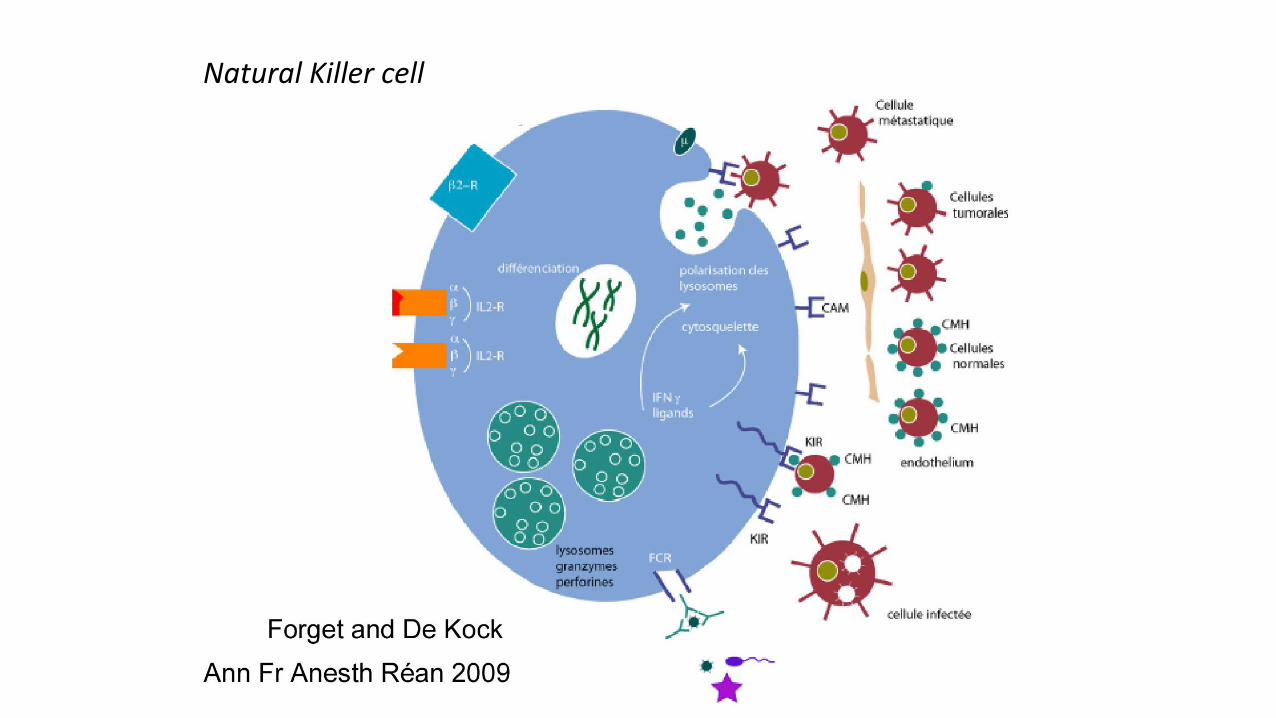
Natural Killer cell

Some concerns
Forget, Eur J Aanesth 2010

92
Increased expression by opioids

Cata, Cancer Medicine, 2014

ERAS : ook nuttig voor preventie ?
• = enhanced recovery after surgery• Nuttig voor herstel
• Psyche
• Kosten-baten



Dank u voor uw aandacht


















