
Klinische manifestatie, etiologie, pathofysiologie, behandeling en … · - Tinnitus stabiele voor...
67
Cervicogene Tinnitus Klinische manifestatie, etiologie, pathofysiologie, behandeling en prognose
Transcript of Klinische manifestatie, etiologie, pathofysiologie, behandeling en … · - Tinnitus stabiele voor...

Cervicogene TinnitusKlinische manifestatie, etiologie, pathofysiologie, behandeling en prognose
1
Overzicht
• Somatische tinnitus
• Prevalentie
• Nek dysfunctie en tinnitus
• TMG dysfunctie en tinnitus
• Fysiotherapie behandeling
• Prognostische indicatoren
2
Somatische tinnitus
• Gerelateerd aan somatisch systeem
- CWK
- TMG
• Veranderen intensiteit / karakter
• Oorzaak tinnitus
3
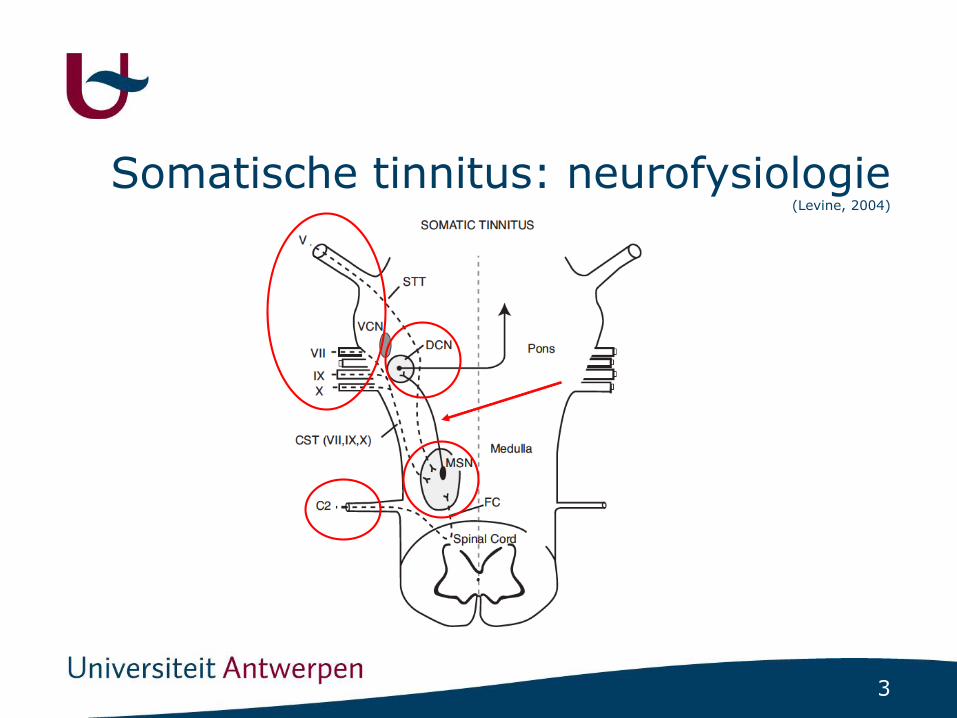
Somatische tinnitus: neurofysiologie(Levine, 2004)
4
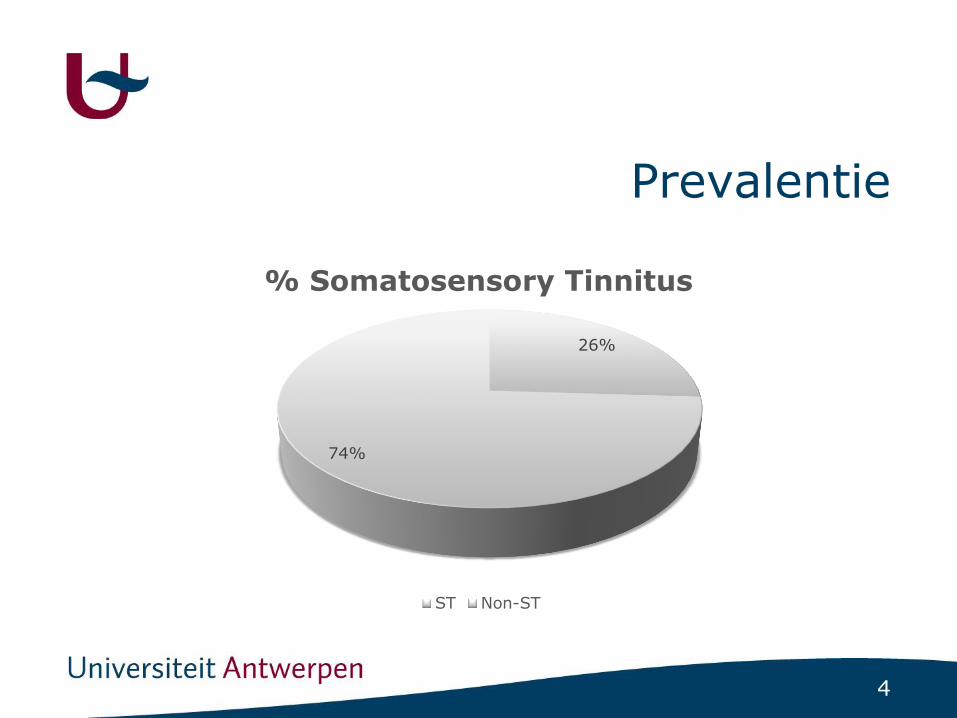
Prevalentie
26%
74%
% Somatosensory Tinnitus
ST Non-ST

5
Prevalentie
14
86
% Cervicogenic ST
ST Non-ST
6
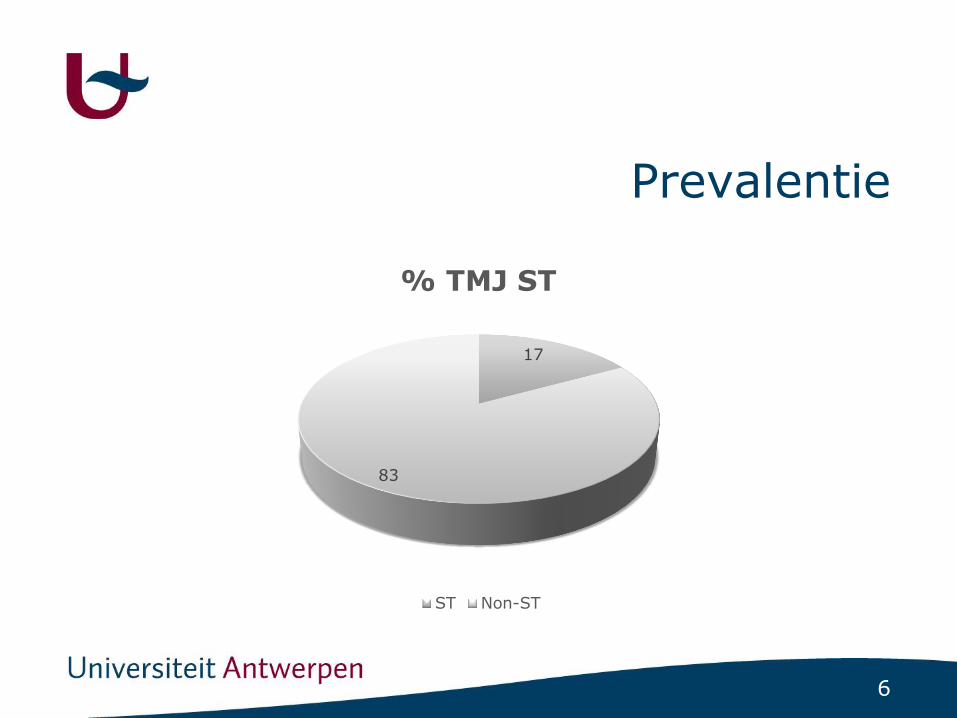
Prevalentie
17
83
% TMJ ST
ST Non-ST
7
Diagnostische criteria
• List of items, suggesting ST diagnosis
- The patient is able to modulate the tinnitus by voluntary movement of the head, neck, jaw or eyes
- The patient is able to modulate the tinnitus by somatic maneuvers
- Tinnitus is modulated by pressure on myofascial triggerpoints

8
Diagnostische criteria
• List of items, suggesting ST diagnosis
- Tinnitus and neck or jaw pain complaints appeared simultaneously
- Tinnitus and neck/jaw pain symptoms aggravate simultaneously
- Tinnitus is preceded by a head or neck trauma
- Tinnitus increases during bad postures
- Tinnitus pitch and/or loudness and/or location are reported to vary
- In case of unilateral tinnitus, the audiogram does not account for unilateral tinnitus
9
Diagnostische criteria
• List of items, suggesting ST diagnosis
- Tinnitus is accompanied by frequent pain in de cervical spine, head or shoulder girdle
- Tinnitus is accompanied by the presence of pressure tender myofascial trigger points
- Tinnitus is accompanied by increased muscle tension in the suboccipital muscles
- Tinnitus is accompanied by muscular tension in the extensor muscles of the cervical spine
- Tinnitus is accompanied by teeth clenching or bruxism
- Tinnitus is accompanied by temporomandibular disorders
- Tinnitus is accompanied by dental diseases
10
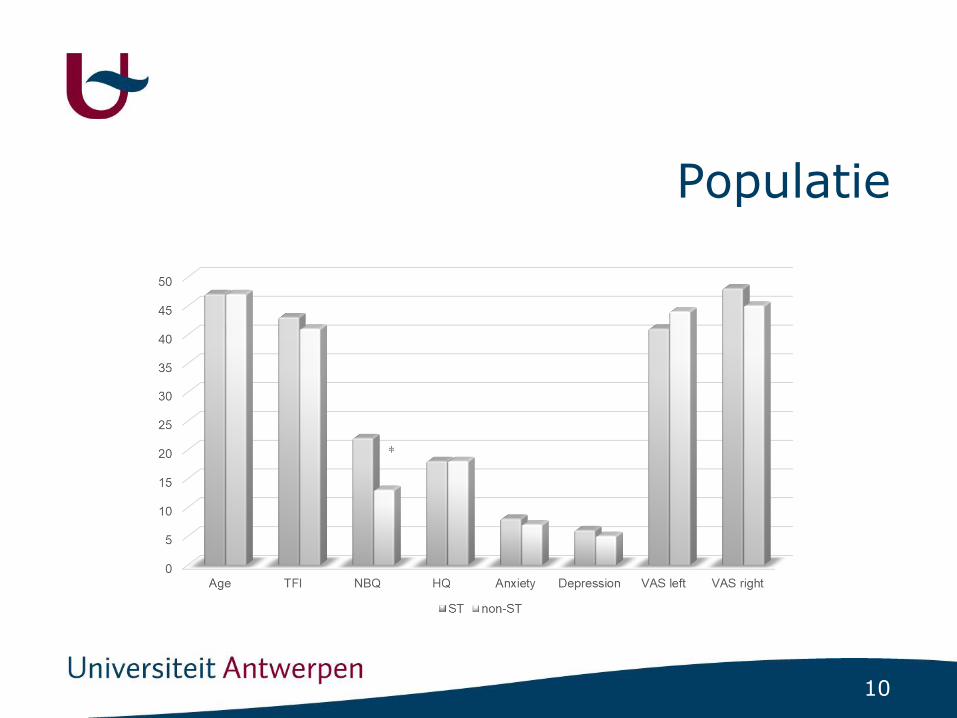
Populatie
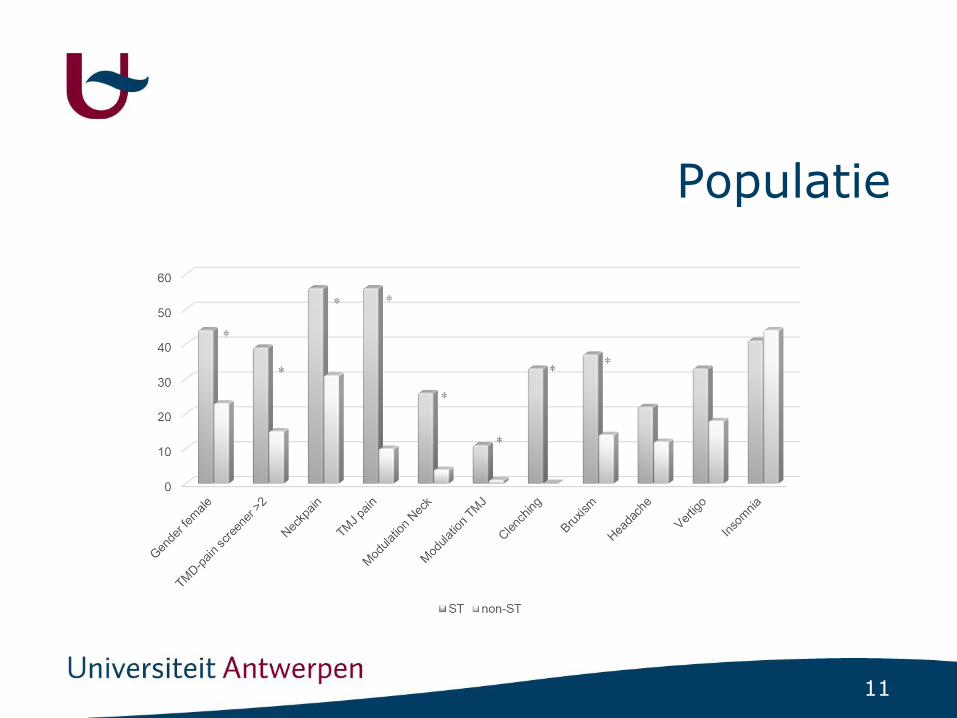
11
Populatie

12
Populatie
13
Neck dysfunctie en tinnitus
• Setting:- Tertiaire tinnitus kliniek UZA
• Patiënten:- Inclusie: chronische subjectieve tinnitus (> 3 months)
- Exclusie:
• Z. v. Menière
• Middenoor aandoeningen
• Intra craniële pathologie
• CWK operaties
• WAD
• TMD
14
Neck dysfunctie en tinnitus
• Onderzoek:
• Cervicogene Somatische Tinnitus (CST): predominant: Gelijktijding ontstaan/toenamenekpijn en tinnitus

15
CWK dysfunctie en tinnitus
• Nekonderzoek:- Neck Bournemouth Questionnaire (NBQ)
- Klinische manuele nektesten
- Therapeut en patient geblindeerd voor KNO diagnose
16
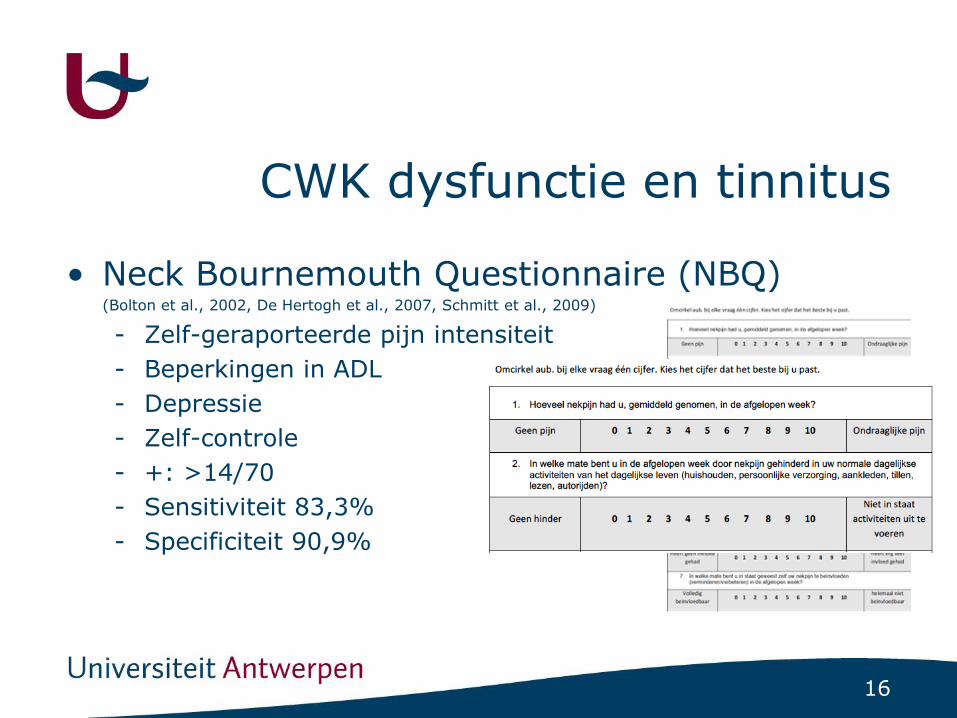
CWK dysfunctie en tinnitus
• Neck Bournemouth Questionnaire (NBQ) (Bolton et al., 2002, De Hertogh et al., 2007, Schmitt et al., 2009)
- Zelf-geraporteerde pijn intensiteit
- Beperkingen in ADL
- Depressie
- Zelf-controle
- +: >14/70
- Sensitiviteit 83,3%
- Specificiteit 90,9%

17
Omcirkel aub. bij elke vraag één cijfer. Kies het cijfer dat het beste bij u past.
1. Hoeveel nekpijn had u, gemiddeld genomen, in de afgelopen week?
Geen pijn 0 1 2 3 4 5 6 7 8 9 10 Ondraaglijke pijn
2. In welke mate bent u in de afgelopen week door nekpijn gehinderd in uw normale dagelijkse activiteiten van het dagelijkse leven (huishouden, persoonlijke verzorging, aankleden, tillen, lezen, autorijden)?
Geen hinder 0 1 2 3 4 5 6 7 8 9 10
Niet in staat
activiteiten uit te
voeren
3. In welke mate bent u in de afgelopen week door nekpijn gehinderd in uw vrije tijd, bij sociale en gezinsactiviteiten?
Geen Hinder 0 1 2 3 4 5 6 7 8 9 10
Niet in staat
activiteiten uit te
voeren
4. Hoe gespannen (onrustig, nerveus, angstig, prikkelbaar, moeite met concentreren/ontspannen) bent u in de afgelopen week geweest?
Niet gespannen 0 1 2 3 4 5 6 7 8 9 10 Zeer gespannen
5. Hoe depressief (somber, neerslachtig, in de put, ongelukkig) bent u geweest in de afgelopen week?
Niet depressief 0 1 2 3 4 5 6 7 8 9 10 Zeer depressief
6. In welke mate heeft uw werk in de afgelopen week (binnen- en buitenshuis) invloed gehad op uw nekpijn?
Heeft geen invloed
gehad 0 1 2 3 4 5 6 7 8 9 10
Heeft erg veel
invloed gehad
7. In welke mate bent u in staat geweest zelf uw nekpijn te beïnvloeden (verminderen/verbeteren) in de afgelopen week?
Volledig
beïnvloedbaar 0 1 2 3 4 5 6 7 8 9 10
helemaal niet
beïnvloedbaar

18
CWK dysfunctie en tinnitus
• Nekonderzoek:- Manual rotation test
• Passieve rotatie
• C0-C2 and C2-C7
• ROM (normaal/hypo/hyper)
• Eindgevoel (normaal/hard/zacht/leeg)
• Pijnprovocatie (VAS > 2cm)
19
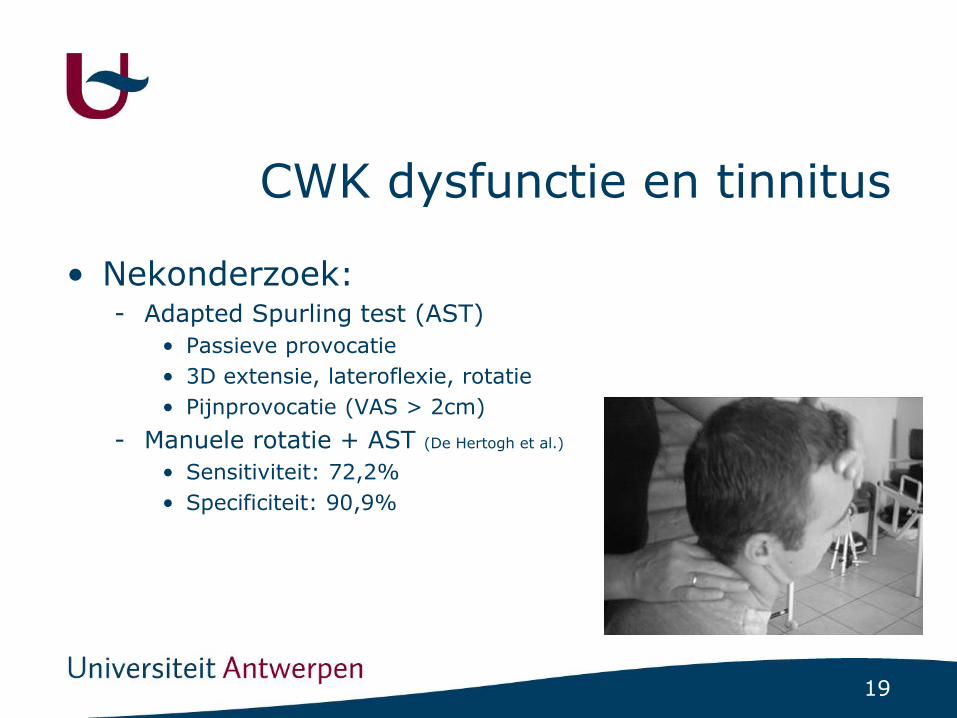
CWK dysfunctie en tinnitus
• Nekonderzoek:- Adapted Spurling test (AST)
• Passieve provocatie
• 3D extensie, lateroflexie, rotatie
• Pijnprovocatie (VAS > 2cm)
- Manuele rotatie + AST (De Hertogh et al.)
• Sensitiviteit: 72,2%
• Specificiteit: 90,9%
20
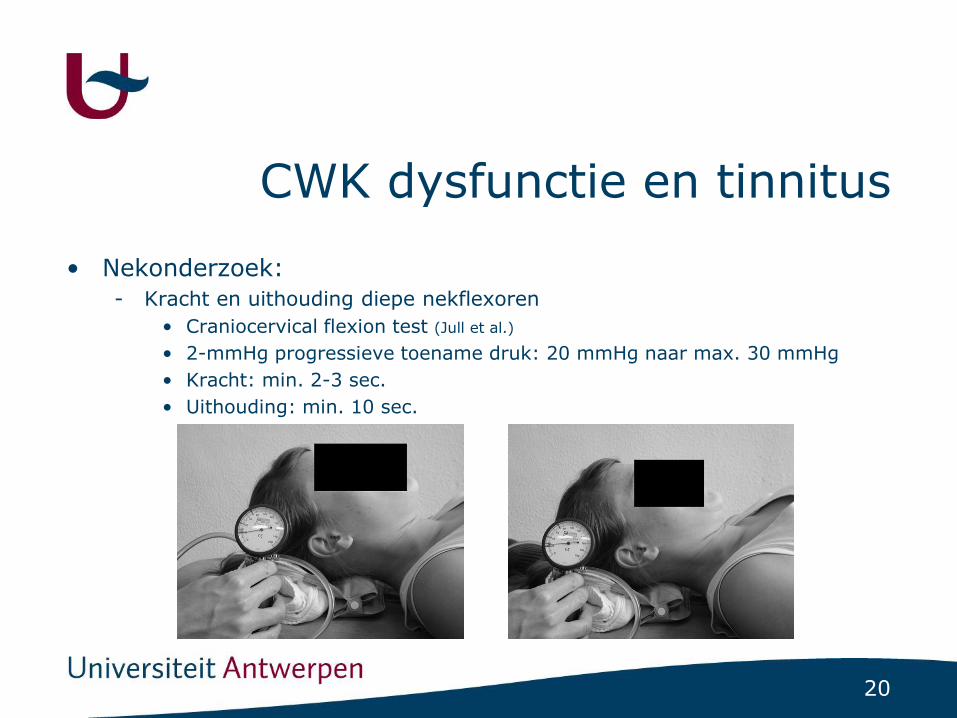
CWK dysfunctie en tinnitus
• Nekonderzoek:
- Kracht en uithouding diepe nekflexoren
• Craniocervical flexion test (Jull et al.)
• 2-mmHg progressieve toename druk: 20 mmHg naar max. 30 mmHg
• Kracht: min. 2-3 sec.
• Uithouding: min. 10 sec.

21
CWK dysfunctie en tinnitus
• Nekonderzoek:- Actieve triggerpunten (Teachey et al.)
22
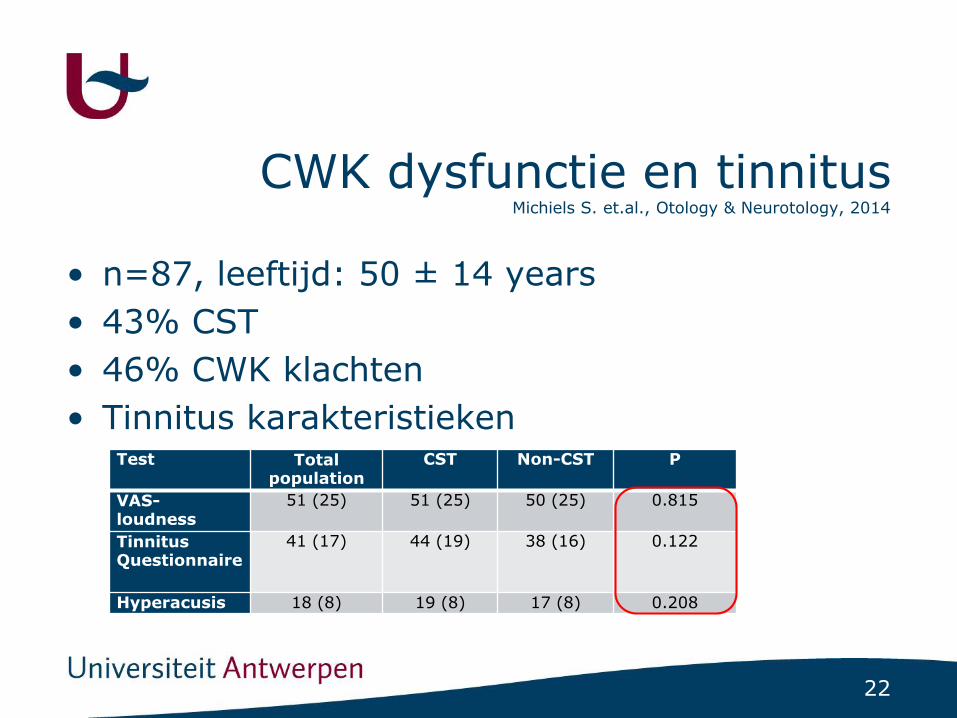
CWK dysfunctie en tinnitusMichiels S. et.al., Otology & Neurotology, 2014
• n=87, leeftijd: 50 ± 14 years
• 43% CST
• 46% CWK klachten
• Tinnitus karakteristiekenTest Total
populationCST Non-CST P
VAS-loudness
51 (25) 51 (25) 50 (25) 0.815
Tinnitus Questionnaire
41 (17) 44 (19) 38 (16) 0.122
Hyperacusis 18 (8) 19 (8) 17 (8) 0.208
23
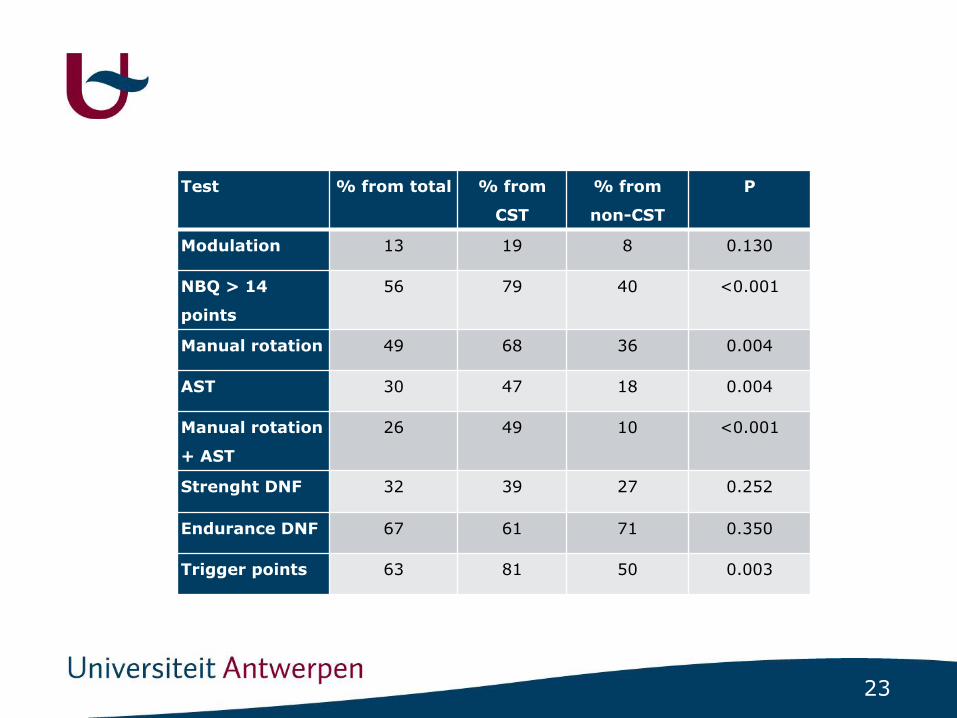
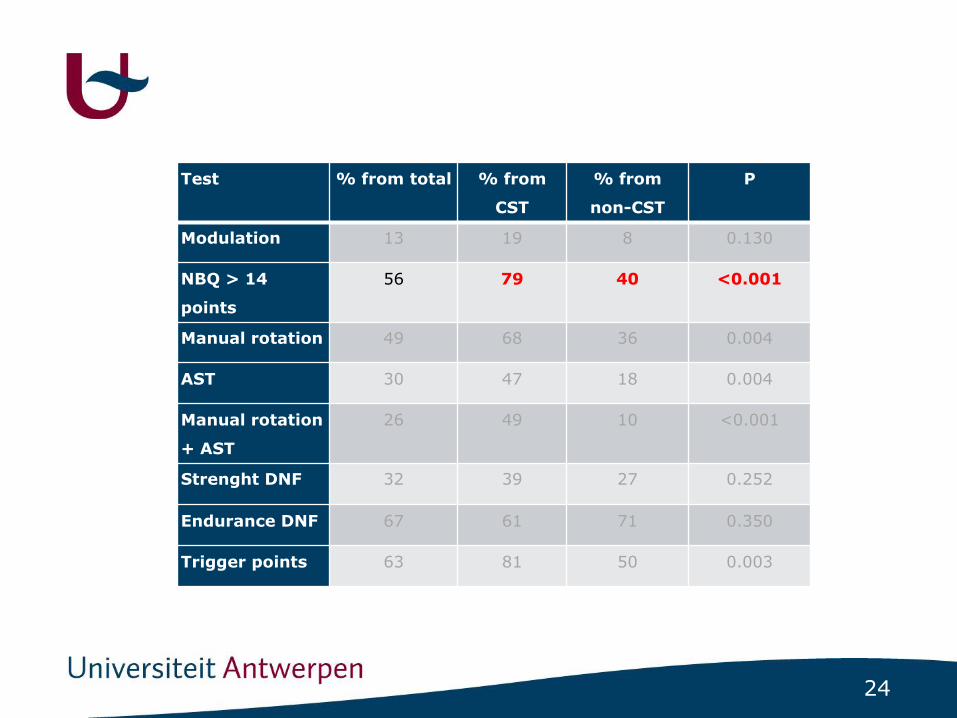
Test % from total % from
CST
% from
non-CST
P
Modulation 13 19 8 0.130
NBQ > 14
points
56 79 40 <0.001
Manual rotation 49 68 36 0.004
AST 30 47 18 0.004
Manual rotation
+ AST
26 49 10 <0.001
Strenght DNF 32 39 27 0.252
Endurance DNF 67 61 71 0.350
Trigger points 63 81 50 0.003
24
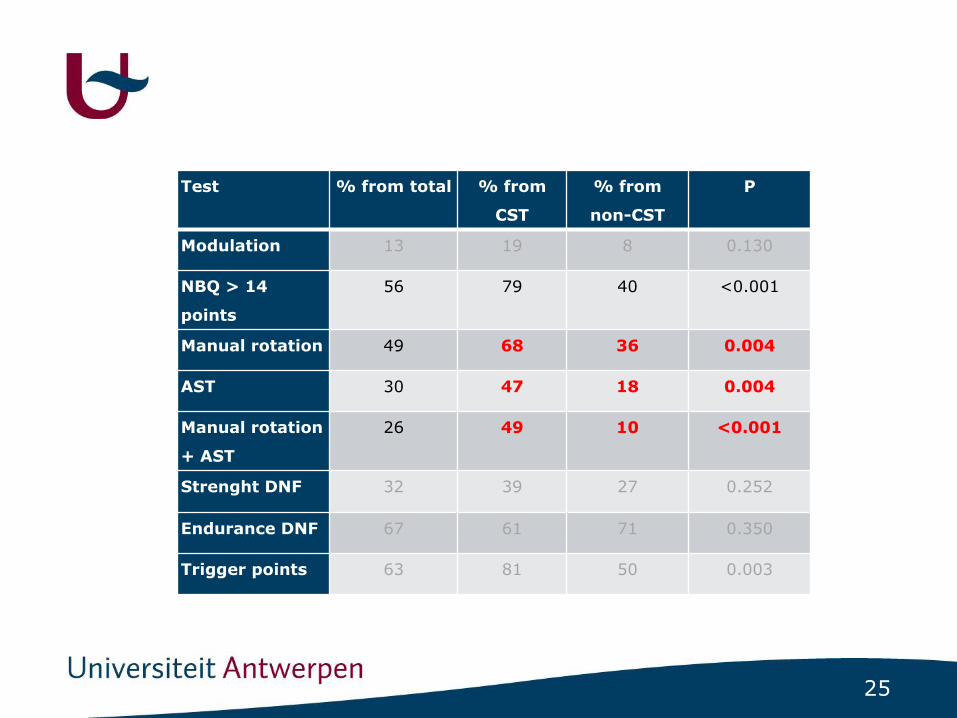
Test % from total % from
CST
% from
non-CST
P
Modulation 13 19 8 0.130
NBQ > 14
points
56 79 40 <0.001
Manual rotation 49 68 36 0.004
AST 30 47 18 0.004
Manual rotation
+ AST
26 49 10 <0.001
Strenght DNF 32 39 27 0.252
Endurance DNF 67 61 71 0.350
Trigger points 63 81 50 0.003
25
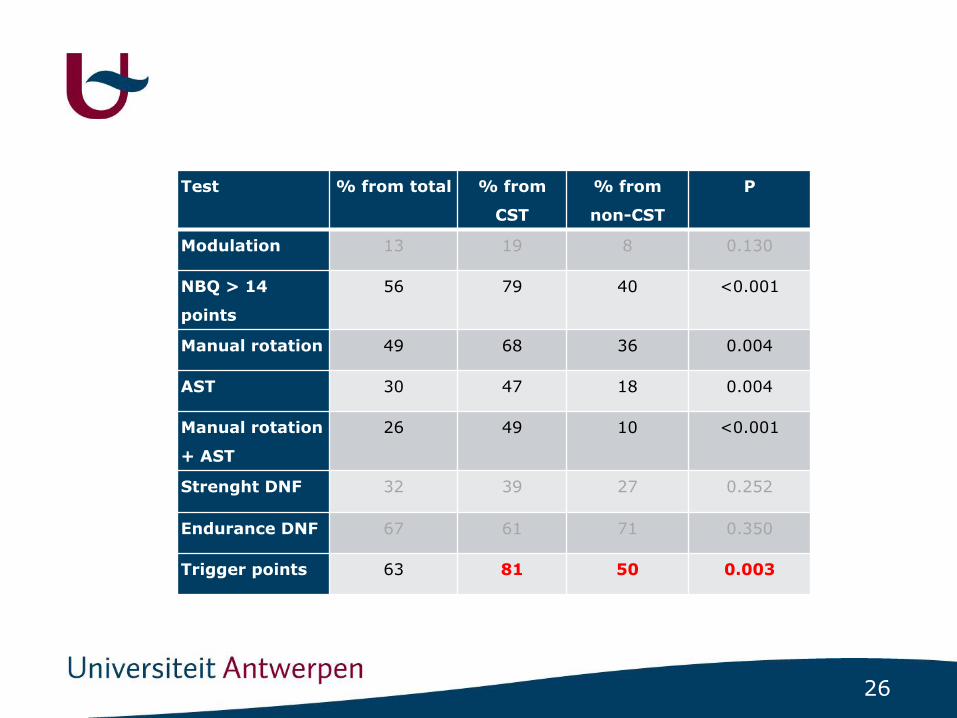
Test % from total % from
CST
% from
non-CST
P
Modulation 13 19 8 0.130
NBQ > 14
points
56 79 40 <0.001
Manual rotation 49 68 36 0.004
AST 30 47 18 0.004
Manual rotation
+ AST
26 49 10 <0.001
Strenght DNF 32 39 27 0.252
Endurance DNF 67 61 71 0.350
Trigger points 63 81 50 0.003
26
Test % from total % from
CST
% from
non-CST
P
Modulation 13 19 8 0.130
NBQ > 14
points
56 79 40 <0.001
Manual rotation 49 68 36 0.004
AST 30 47 18 0.004
Manual rotation
+ AST
26 49 10 <0.001
Strenght DNF 32 39 27 0.252
Endurance DNF 67 61 71 0.350
Trigger points 63 81 50 0.003
27
TMG dysfunctie en tinnitus
• Setting:- Tertairy tinnitus clinic UZA
• Patients:- Inclusion:
• Chronic subjective tinnitus (> 3 months)
• Tinnitus attributed to TMD (ENT + dentist)
- Exclusion when suffering from:
• Meniere’s disease
• Middle ear pathology
• Intra cranial pathology
28
TMG dysfunctie en tinnitus
• Assessment:
• TMD related Somatic Tinnitus: predominant feature: temporal coincidence onset/increase TMD and tinnitus
29
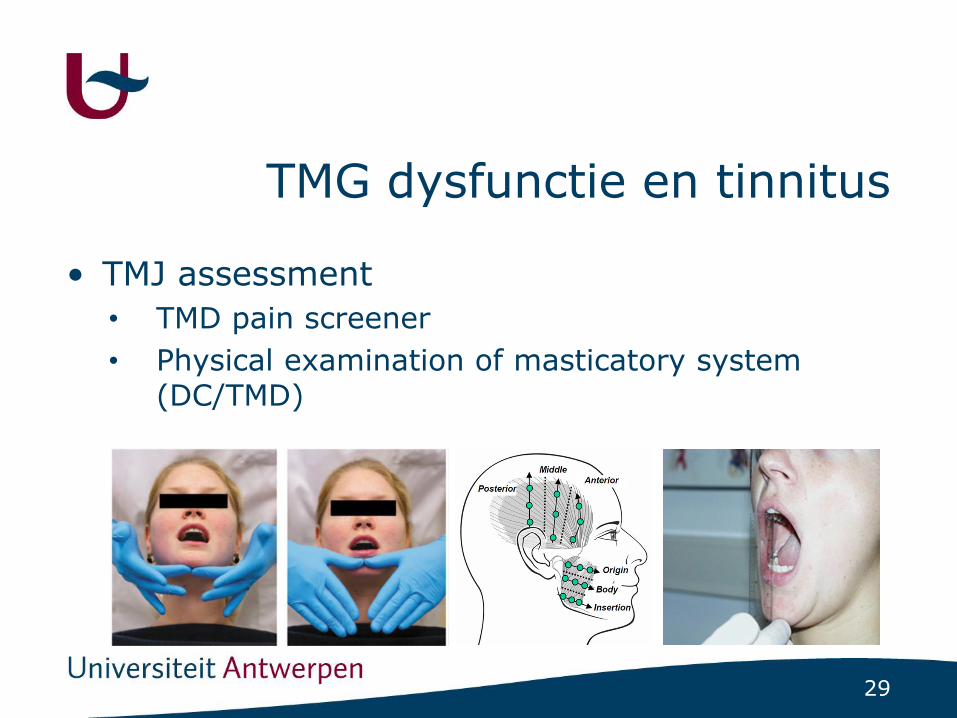
TMG dysfunctie en tinnitus
• TMJ assessment
• TMD pain screener
• Physical examination of masticatory system (DC/TMD)
30
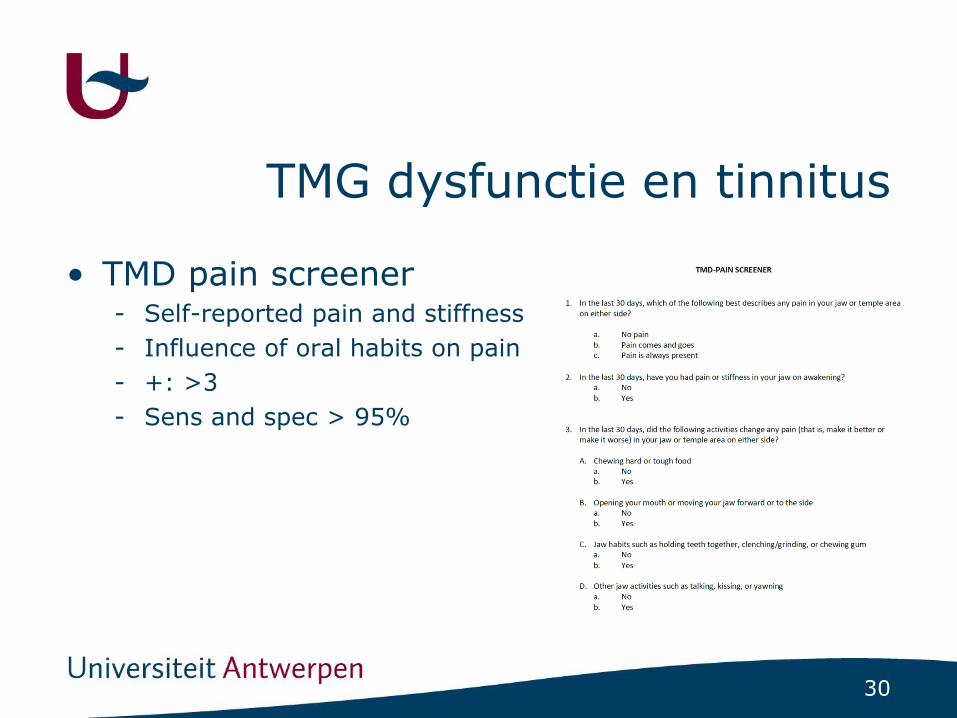
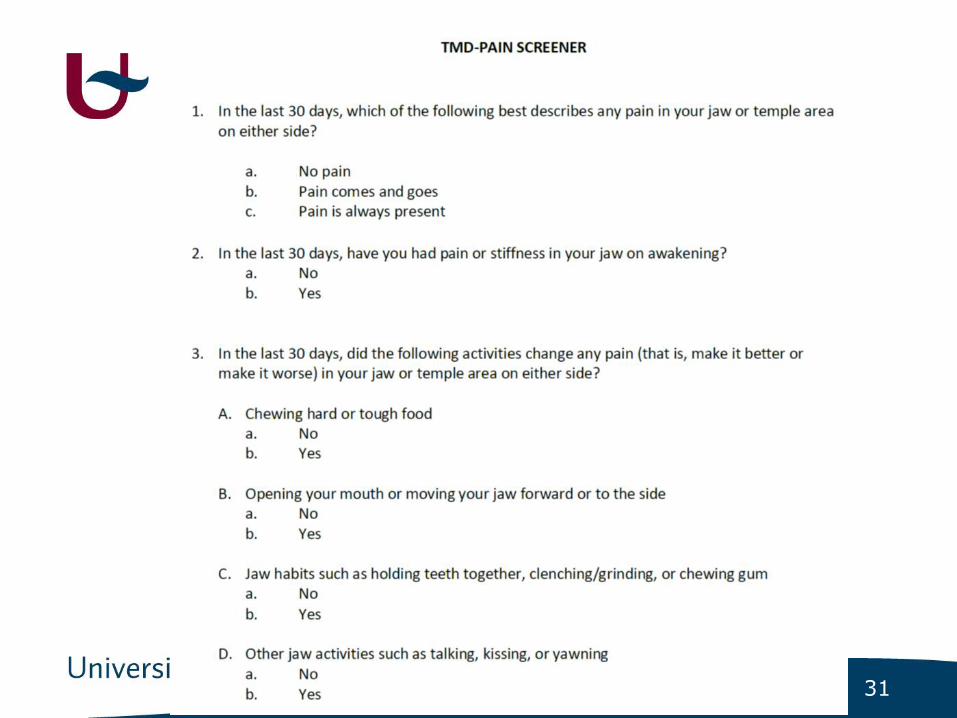
TMG dysfunctie en tinnitus
• TMD pain screener- Self-reported pain and stiffness
- Influence of oral habits on pain
- +: >3
- Sens and spec > 95%
31

32
TMG dysfunctie en tinnitus
• Masticatory system Assessment:- Active movements
• Opening, closing, protrusion
• Concentric against manual resistance
• Isometric
33
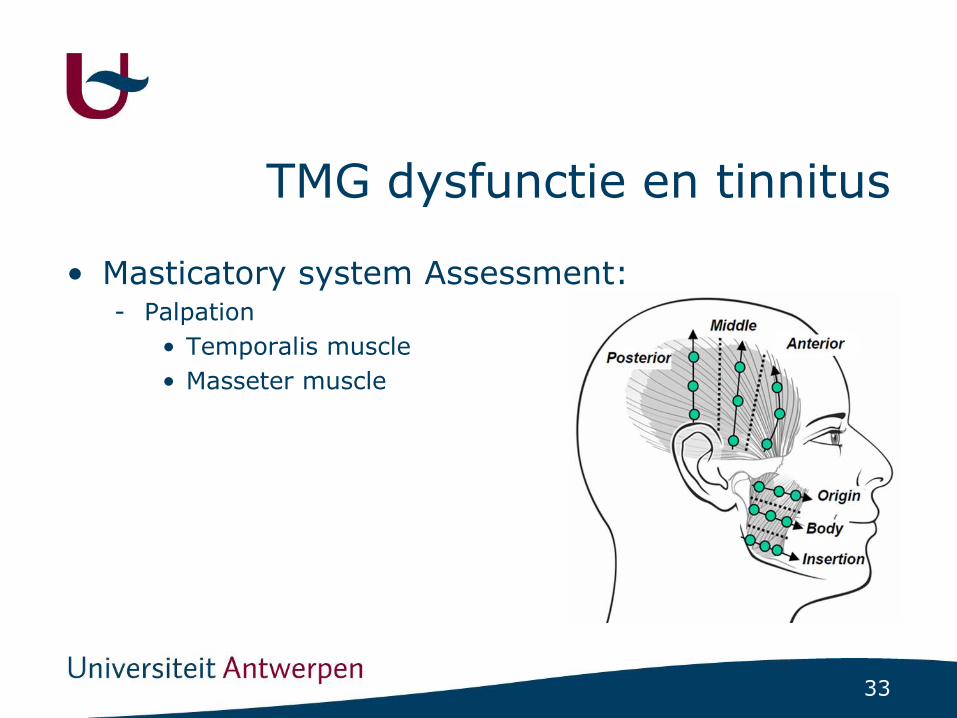
TMG dysfunctie en tinnitus
• Masticatory system Assessment:- Palpation
• Temporalis muscle
• Masseter muscle

34
TMG dysfunctie en tinnitus
• Masticatory system Assessment:- Mouth opening
35
TMG dysfunctie en tinnitus
36
37
TMG dysfunctie en tinnitus

38
TMG dysfunctie en tinnitus
39
Fysiotherapie en tinnitus
• Review (Michiels et al., Frontiers in Neuroscience, 2017)
- Effect PT op ernst tinnitus
- RCT’s en quasi-experimentele trials
- 6 studies geïncludeerd
• 4 CWK
• 2 TMG
40
Fysiotherapie en tinnitus
• Review (Michiels et al., Frontiers in Neuroscience, 2016)
- CWK
• Manipulaties, oefentherapie, triggerpunt behandeling
• + effect op tinnitus ernst
- TMG
• Opbeetplaat, oefentherapie
• + effect op tinnitus ernst en intensiteit

41
Fysiotherapie en tinnitus
• Review (Michiels et al., Frontiers in Neuroscience, 2016)
- Beperkingen
• Hoge risk of bias
- Randomizatie
- Blindering
• Heterogeniteit
- Populaties
- Behandeling
- Uitkomstmaten

42
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Setting
- Tertiaire tinnitus kliniek UZA
• Patiënten
- Ernstige chronische subjectieve tinnitus
- Tinnitus stabiele voor min. 3 maanden
- Nekklachten (NBQ > 14)
43
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Interventie
- Therapeuten
• MSc. PT + MT
• Getrained
• Guided referral
- Multimodale behandeling
• Manuele mobilizaties
• Oefentherapie
• Thuisoefeningen
44
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Interventie
- 12 sessies
- 30 min.
- 6 weken

45

46

47
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Uitkomstmaten
- Tinnitus Functional Index (TFI)
- Neck Bournemouth Questionnaire (NBQ)
- Klinische testen:
48
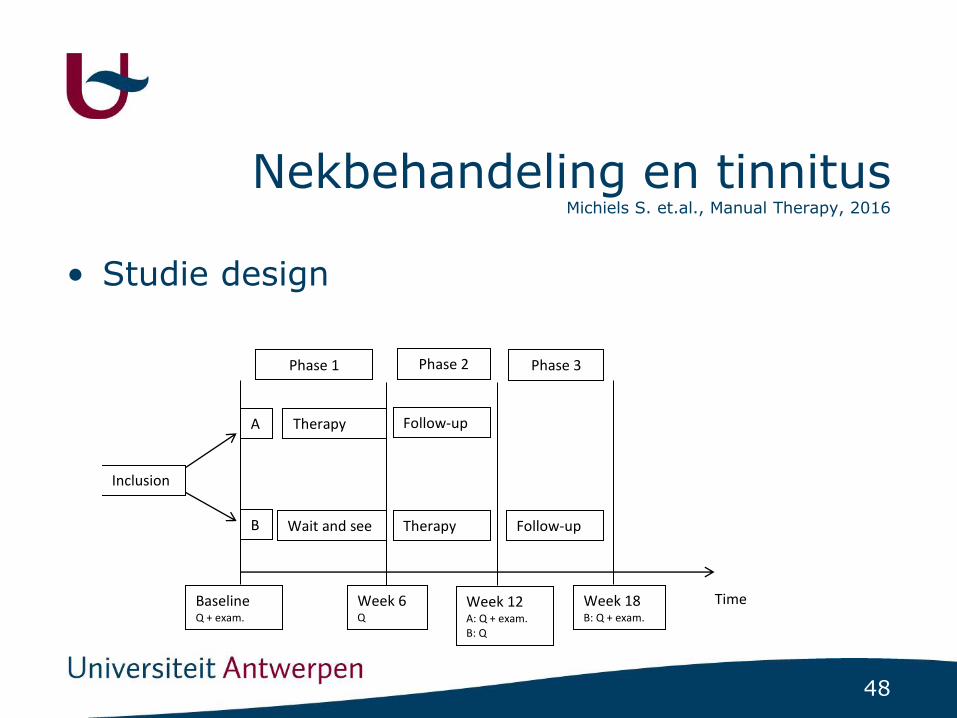
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Studie design 1
2
3
4
5
6
7
8
9
10
11
Inclusion
A
B
Time
Therapy
Wait and see
Baseline Q + exam.
Week 6 Q
Week 12 A: Q + exam. B: Q
Therapy
Follow-up
Follow-up
Week 18 B: Q + exam.
Phase 1 Phase 2 Phase 3

49
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
Assessed for eligibility (n=87)
Excluded
Not meeting inclusion criteria (n=32)
Declined to participate (n=4)
Other reasons (n=11)
Randomized (n=40)
Allocated the immediate-start group (n=20)
Received physical therapy (n=19)
Did not receive physical therapy (one patient never contacted the therapist) (n=1)
Allocated the delayed-start group (n=20)
Received physical therapy after 6 weeks wait and see (n=19)
Did not receive physical therapy after 6 weeks wait and see (one patient did not contact the therapist after the wait and see period) (n=1)
Follow-up (n=19) Follow-up (n=19)
Analyzed (n=19) Analyzed (n=19)
Enrollment
Allocation
Follow-up
Analysis

50
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• DemografischCharacteristic Immediate-start
group
Delayed-start
group
Total p
Number of subjects 20 20 40 1.00
Age (SD) 46(14) 52(12) 50(13) 0.26
TFI (SD) 50(23) 51(18) 51(21) 0.91
NBQ (SD) 37(10) 32(12) 35(11) 0.15
VAS tinnitus 6(2) 5(2) 5(2) 0.55
Hyperaccusis 20(9) 19(9) 19(9) 0.88
Manual rotation +
AST
68% 37% 53% 0.05
AST 74% 53% 63% 0.18
Trigger points 79% 84% 82% 0.68
Provocation of
tinnitus
11% 11% 11% 1.00
51
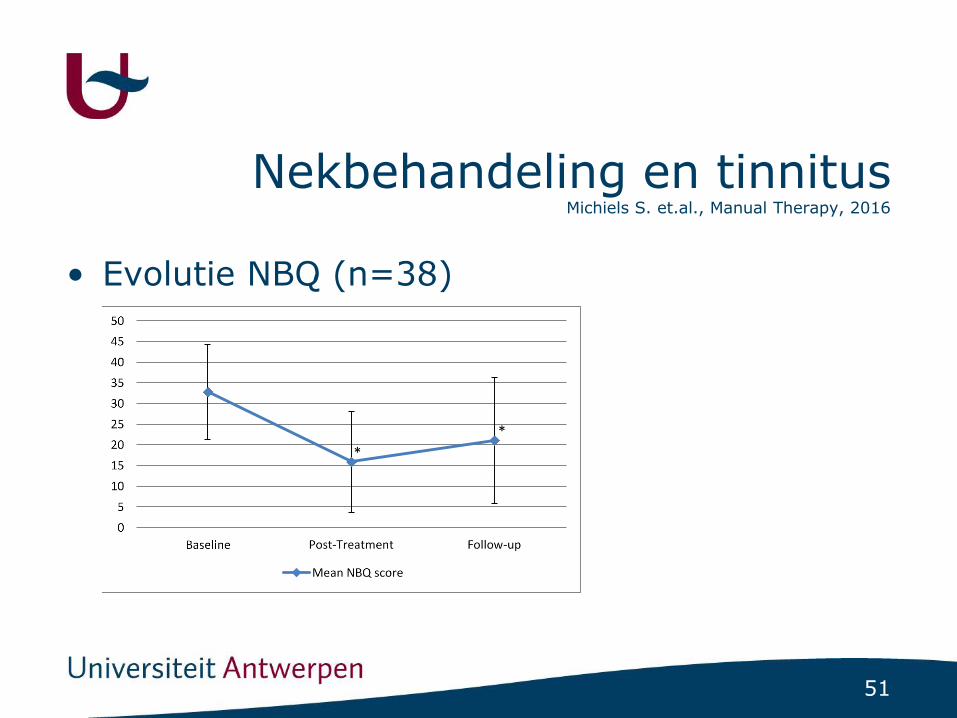
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Evolutie NBQ (n=38)
1
*
*

52
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Evolutie TFI (n=38)
1
15
25
35
45
55
65
75
Baseline Post-Treatment Follow-up
Mean TFI score
*

53
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
• Evolutie TFI
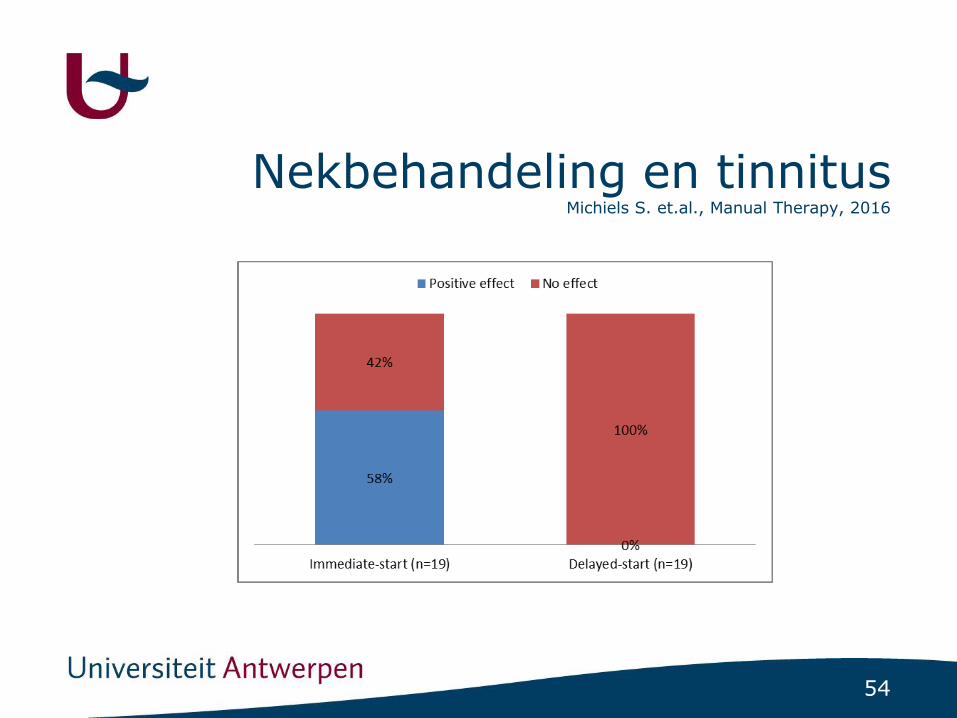
54
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016

55
Nekbehandeling en tinnitus Michiels S. et.al., Manual Therapy, 2016
Post Treatment Follow-up
Not improved Improved p Not improved Improved p
Change in TFI
+0.67 (4.78) -11.89 (21.43) 0.02* +2.42 (8.28) -16.89 (26.56) 0.001*
Change in NBQ
-15.19 (17.17) -18.32 (15.03) 0.57 -13.07 (18.28) -6.38 (24.63) 0.41
• Characteristics improved patients

56
• Potential prognostic indicators
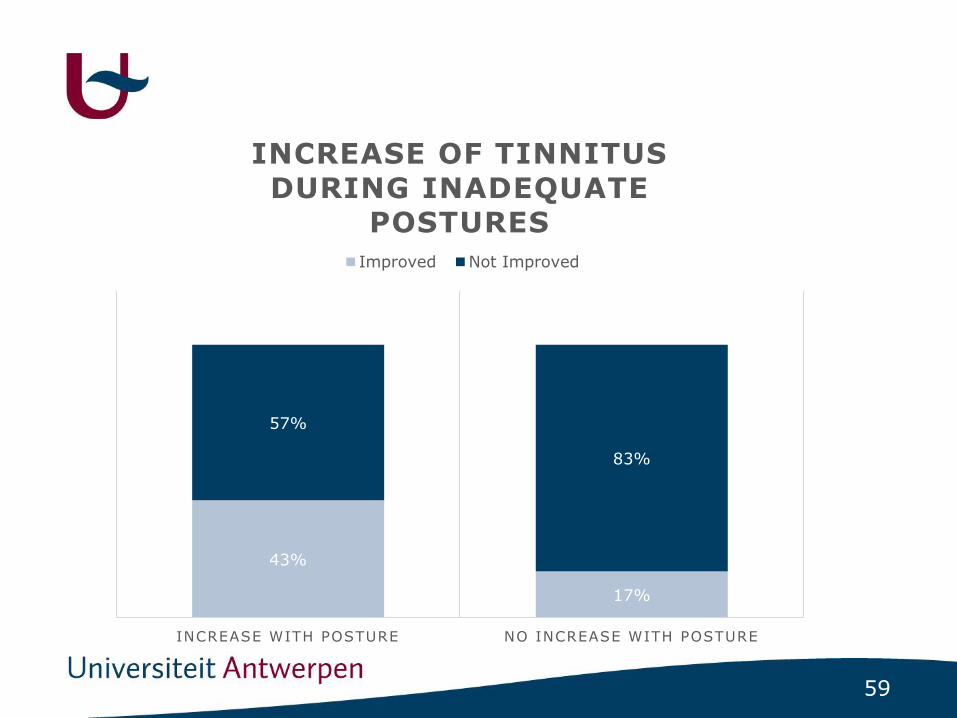
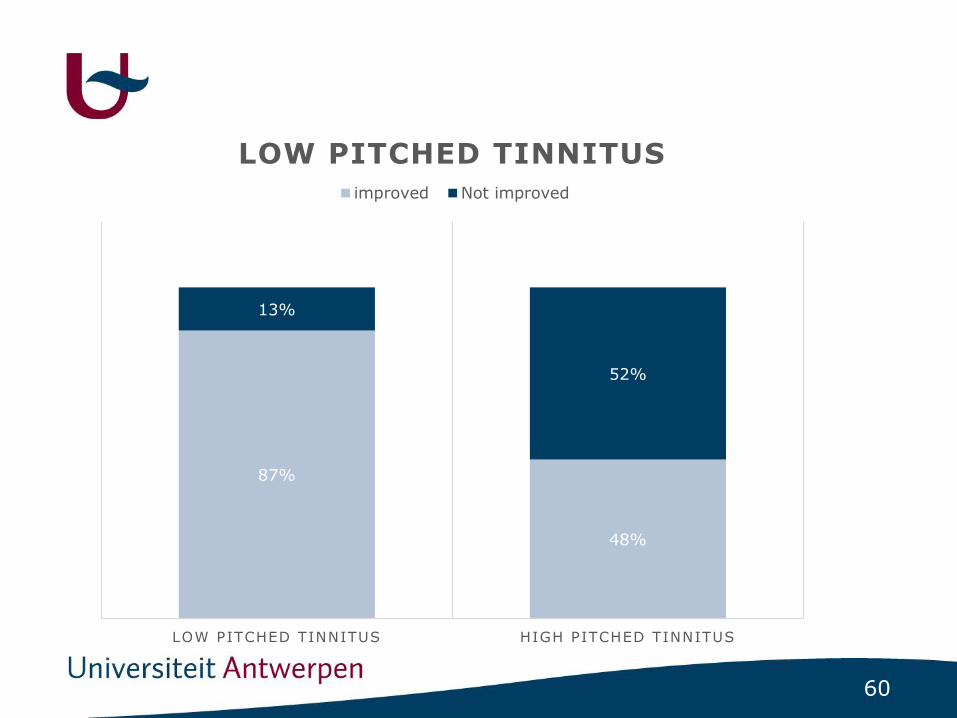
PrognoseMichiels S. et.al., Musculoskeletal Science and Practice, 2017
57
Prognose
Non-respondersResponders
38 Patients

58
65%
44%
35%
56%
CO-VARYING NON-CO-VARYING
CO-VARYING TINNITUS AND
NECK COMPLAINTS
Improved Not improved
59
43%
17%
57%
83%
INCREASE WITH POSTURE NO INCREASE WITH POSTURE
INCREASE OF TINNITUS
DURING INADEQUATE POSTURES
Improved Not Improved
60
87%
48%
13%
52%
LOW PITCHED TINNITUS HIGH PITCHED TINNITUS
LOW PITCHED TINNITUS
improved Not improved

61
PrognoseMichiels S. et.al., Musculoskeletal Science and Practice, 2017
• Prognostische indicatoren
- Co-variatie
- Low-pitched + toename tijdens houdingen

62
TMG behandeling en tinnitus
63
TMG dysfunctie en tinnitus
• Setting:- Tertairy tinnitus clinic UZA
• Patients:- Inclusion:
• Chronic subjective tinnitus (> 3 months)
• Tinnitus attributed to TMD (ENT + dentist)
- Exclusion when suffering from:
• Meniere’s disease
• Middle ear pathology
• Intra cranial pathology

64

65

66


















