Dr. Frederic Baekelandt –Frederic.Baekelandt@stlucas · Robot vs Open Cystectomie 1....
57
Dr. Frederic Baekelandt – [email protected]
Transcript of Dr. Frederic Baekelandt –Frederic.Baekelandt@stlucas · Robot vs Open Cystectomie 1....

Dr. Frederic Baekelandt – [email protected]

Robot vs Open cystectomieBij spier-invasieve blaaskanker

Robot vs OpenCystectomie
1. Spier-Invasieve blaaskanker
2. Operatietechniek
3. Peri-operatieve zorg en nazorg
Indeling van de presentatie

Spier-Invasieve blaaskankerMIBC (MUSCLE INVASIVE BLADDER CANCER)
DE INDICATIE VOOR CYSTECTOMIE

EpidemiologieHoogste incidentie Europa in België:
◦ Man: 31/100.000 personen per jaar (vs. 19/100.000)
◦ Vrouw: 6/100.000 personen per jaar (vs 4/100.000)
25% is spier-invasief
Roken: oorzaak 1 op 2 bij mannen
Chemicaliën: 1 op 5
◦ rubber, verf, leder, aromatische amines
Radiotherapie: Externe en Brachytherapie
Schistosomiasis (600miljoen mensen blootgesteld)
A Dichotomy between the Risk and Incidence of Urothelial Cancers among Black and White Men: APopulation-Based Study
3 of 8
TCC, 56 had SCC, and only 14 had an AC. For the totalnumber of ureter cancer cases, 6,080 were White and only294 were Black. There were 6,762 men with renal pelviscancer; of these, 6,288 had TCC, 100 had SCC, and only 29had an AC. For the total number of renal pelvis cancersevaluated, there were a total of 3,961 White cases along withonly 125 Black cases. Generally these trends held true foreach histological type of bladder cancer. Table 1 providesthe rates for each group and anatomic site. For cases ofmalignant tumors of the urinary bladder, the mean age was65 for Black men and 67 for White men.
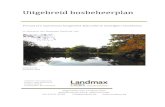
TrendsFrom 1973 through 2007, rates for TCC of the urinarybladder in White men were significantly higher than forBlack men (Figure 1). Overall, the average age-adjustedTCC incidence for Whites was 20 cases per 100,000 men.The average incidence rate for Blacks in the same periodwas 10.7 cases per 100,000 men. The difference in ratesbetween Blacks and Whites was more pronounced amongmen than among women (Data not shown).
Figure 1
Age-Adjusted Incidence Rates for TCC of the UrinaryBladder by Year of Diagnosis Among Men (SEER,1973-2007)
Comparatively, the trend for incidence rates of TCC of therenal pelvis was evaluated to determine if any congruencyexisted. Figure 2 shows that White men consistently hadhigher rates in comparison to Black men similar to the trendin the urinary bladder. However, due to the limited numberof cases, there is considerable variation seen in the trend.Rates for TCC of the ureter (Figure 3) show a similarpattern.
Figure 2
Age-Adjusted Incidence Rates for TCC of the Renal Pelvisby Year of Diagnosis Among Men (SEER, 1973-2007)
Figure 3
Age-Adjusted Incidence Rates for TCC of the Ureter byYear of Diagnosis Among Men (SEER, 1973-2007)
Age Frequency PatternsAge frequency plots are seen in Figure 4 for TCC of thebladder for Black and White men. Age frequency plots forTCC of the bladder, ureter, and renal pelvis are shown inFigure 5. Data from both groups were combined because ofthe limited number of cases of TCC of the ureter and renalpelvis in Blacks. The results reveal congruence in the agefrequency distribution of tumor development even thoughTCC of the bladder is significantly more common in Whitemen.

DiagnostiekAnamnese:
◦ Pijnloze macroscopische hematurie◦ Onverklaarde urgency, frequency
Klinisch onderzoek◦ Palpatie vaginaal en rectaal: Invasie rectum? Bekkenbodem?
Beeldvorming◦ Echografie bekken/nieren◦ CT abdomen met IVP; MRI
Urine onderzoek◦ Cytologie: gevoelig bij Cis en Hooggradige tumoren

DiagnostiekCystoscopie
◦ Bespreek Locatie, grootte, aantal en uitzicht◦ Solied, gesteeld, oppervlakkig spreidend◦ Photodynamische diagnostiek (PDD)
Transurethrale resectie van de blaas (TURB)◦ = BIOPSIE!◦ Ook biopsiename van de onderliggende spierwand: spierinvasief?
Her-TURB◦ Bij hooggradige niet spierinvasieve tumoren (33-53% residu!)◦ Biopsie urethra prostatica zo nodig

StagingAPO: Spierinvasief urotheelcelcarcinoom
Lokale staging:◦ MRI abdomen vs CT abdomen (+IVP!)◦ CT zeer goed bij evaluatie vetinfilatratie rondom blaas◦ MRI rol bij evaluatie van effect van neo-adj Chemo
Klier staging◦ Geen rol voor PET: MRI of CT, beide lage sensitiviteit (grootte)
Metastase staging◦ MRI of CT: long, lever◦ Bot en hersen meta’s zeldzaam: MRI voorkeur

Behandeling MIBCStandaardbehandeling = CystectomieIndicatiestelling

Spierinvasieve TumorenReseceerbare tumoren: cT2-4a N0M0 Tumoren
Niet reseceerbare tumoren (T4b, N+, M+): Palliatieve cystectomie◦ Pijn/dysurie◦ Fistels◦ Bloedverlies◦ Obstructie

Niet-spierinvasieve tumorenHooggradige niet-spierinvasieve blaastumoren
◦ =GEVAARLIJKE ZIEKTE!!◦ Upstaging na her-TURB in 10-20%◦ Kans op progressie na blaasspoelingen: 19,3% na 5 jaar
◦ Lagere CSS bij progressie (35% vs 50%)
◦ Risicofactoren: Carcinoma in situ, multiple, recidieven, grootte
Indicaties nonMIBC:◦ Hoog risico Hooggradige niet-spierinvasieve blaastumoren◦ Therapie falende niet-spierinvasieve blaastumoren

Neo-adjuvante chemotherapieBij reseceerbare N0M0 ziekte, FITTE PATIENT!
Pre-operatief: ◦ weinig micrometastases, betere tolerantie◦ Tot doel: pT0 resectie, of pN0 resectie of neg SV
Weinig effect op morbiditeit post-operatief
Cisplatin combinatie therapie (vb MVAC, Gem-Cis)
Resultaat:◦ Na 5 jaar: 8% survival benefit (11% bij cT3 groep)1
◦ Na 10 jaar: 36% survival ipv 30%◦ Minder meta’s op afstand, geen voordeel voor lokale controle◦ Meer downstaging door NAC2
1. Nordic I, Nordic II, and BA06 30894 trial2. MP34-15: A EUROPEAN MULTICENTRE REPORT ON CURRENT NEOADJUVANT CHEMOTHERAPY ADMINISTRATION RATES IN ROBOT-ASSISTED RADICAL CYSTECTOMY PATIENTS AND THE IMPACT ON
PATHOLOGICAL STAGING, Collins et al.
Matthew Perry, Rami Issa, London, United Kingdom; Tommy Nyberg,Stockholm, Sweden; Martin Schumacher, Aarau, Switzerland;Carl Wijburg, Arnhem, Netherlands; A. Erdem Canda, Ankara, Turkey;Mevlana Balbay, Istanbul, Turkey; Karel Decaestecker, Ghent, Belgium;Christian Schwentner, Arnulf Stenzl, Tuebingen, Germany;Sebastian Edeling, Sasa Pokupik, Hanover, Germany;Ferderiek D’Hondt, Alexandre Mottrie, Aalst, Belgium; Peter Wiklund,Stockholm, Sweden
INTRODUCTION AND OBJECTIVES: Neoadjuvant chemo-therapy is considered the standard of care in patients with muscle-invasive bladder cancer (MIBC) and has been shown to confer overallsurvival advantages of 5% in RCTs. Data on neoadjuvant chemotherapy(NAC) administration rates in patients undergoing robot-assisted radicalcystectomy (RARC) is limited, ranging from 0 to 31% in the publishedliterature. We report administration rates of NAC from amulti-institutionalEuropean database focusing on the centres performing totally intra-corporeal RARC. Reporting the effect of NAC on down-staging and up-staging rates from clinical staging (cT) to the pathological specimen (pT).
METHODS: Retrospective review of the prospectively populatedmulti-institutional database identified 717 patients at 9 different In-stitutions (6 countries), with a minimum of 12 months follow-up, who un-derwent RARC for non-metastatic bladder cancer with curative intentbetween Dec 2003 and March 2015. Clinical stage was assigned basedon a combination of specimen pathology from TURBT, EUA and imagingstudies.Cisplatin basedNACwas offered to patientswith cT2-cT4, takinginto account patient performance status. Clinical staging, pathologicstaging and survival data at the latest follow-up were collected.
RESULTS: Median age was 68 years, 78% were men. 95.2% ofpatients had TCC. 532 (74.2%) patients were alive at the time of theanalysis. The median follow-up time for patients was 31 months (IQR 20-46). 465 patients (65%) had cT2-T4 TCC. In this series 25.3% of patientsreceived NAC. See table 1 for upstaging and down-staging related toNAC. PSM rates were associated with upstaging (p<0.001). On multi-variable analysis NAC was associated with down-staging in all patientsOR 3.46 95% CI 2.34-5.13 p<0.001 and this effect increased in patientswithnon-organconfineddiseaseOR5.4595%CI2.15-13.8p<0.001. The5-yearCSS,OSandRFSwere69.9%,66.1%and66.3%respectively.Onmultivariable analysis, pathological non-organ confined versus organconfineddiseasewas found to impactCSS,OSandRFS (HR4.4, 3.8 and3.8 respectively).
CONCLUSIONS: NAC was associated with downstaging ofMIBC. Increasing NAC administration rates would likely further improveoncological outcomes.
Source of Funding: None
MP34-16COULD ADJUVANT CHEMOTHERAPY HAVETHERAPEUTIC BENEFIT AFTER NEOADJUVANTCHEMOTHERAPY IN PATIENTS WITH EQUAL TO ORGREATER THAN PT3 MUSCLE INVASIVE BLADDERCANCER?
Minami Omura*, Eiji Kikuchi, Koichiro Ogihara, Kyohei Hakozaki,Keishiro Fukumoto, Tokyo, Japan; Go Kaneko, Yasumasa Miyazaki,Kanagawa, Japan; Nobuyuki Tanaka, Suguru Shirotake,Kunimitsu Kanai, Saitama, Japan; Kazuhiro Matsumoto,Hirohiko Nagata, Akira Miyajima, Mototsugu Oya, Tokyo, Japan
INTRODUCTION AND OBJECTIVES: Neoadjuvant chemo-therapy (NAC) has been associated with improved prognosis in muscleinvasive bladder carcinoma (MIBC) patients. However, the therapeuticeffect of adjuvant chemotherapy (AC) following NAC remains unknown.
METHODS: We retrospectively identified 576 patients whowere treated by radical cystectomy for MIBC at our 7 institutions be-tween 2007 and 2014. Among them, 196 patients with MIBC that wasequal to or greater than pT3 were included in the present analysis. Wecompared the clinical characteristics and outcomes between MIBCpatients with and without AC.
RESULTS: Overall, 65 patients (33.2%) were treated by AC.The mean age of the patients with AC (AC group) was 65.9 years, whichwas significantly lower than that in their counterparts (73.7 years,p<0.001). The AC group had a higher incidence of pathological lymphnode positive and concomitant CIS than their counterparts (p¼0.002,p¼0.018, respectively). The 5-year overall survival rate for the AC groupwas 46.0%, which was significantly higher than their counterparts(31.2%, p¼0.03). Multivariate analysis revealed that the absence of AC(hazard ratio: HR, 1.93, p¼0.015) was an independent indicator fordeath in addition to lymphovascular invasion (HR, 2.06, p¼0.002) andpathological lymph node positive (HR, 1.9, p¼0.011). In the subgroup ofpatients without NAC (N¼139), 43 patients (30.9%) were treated by AC.The mean age of patients in the AC group was 65.3 years, which wassignificantly lower than that in their counterparts (74.9 years, p<0.001).The AC group had a higher incidence of pathological lymph nodepositive than their counterparts (p¼0.006). The 5-year overall survivalrate for the AC group was 47.5%, which was significantly higher thanthat in their counterparts (29.4%, p¼0.015). Multivariate analysisrevealed that the absence of AC (hazard ratio: HR, 2.16, p¼0.028) wasan independent indicator for death in addition to pathological lymphnode positive (HR, 1.98, p¼0.025). In the subgroup of patients withNAC (N¼57), 22 patients (38.6%) were treated by AC. The 5-yearoverall survival rate for the AC group (40.2%) was not significantlyhigher than that in their counterparts (36.0%, p¼0.932).
CONCLUSIONS: In MIBC patients with a pathological stageequal to or greater than pT3, AC seems to be associated with a betterprognosis. However, our data does not support the addition of AC topatients previously treated with NAC.
Source of Funding: none
MP34-17PROGNOSTIC SIGNIFICANCE OF SERUMg-GLUTAMYLTRANSFERASE IN ADVANCED UROTHELIALCARCINOMA PATIENTS
Hiroshi Fukushima*, Yasukazu Nakanishi, Madoka Kataoka,Ken-ichi Tobisu, Fumitaka Koga, Tokyo, Japan
INTRODUCTION AND OBJECTIVES: g-glutamyltransferase(GGT), which is expressed in various human cancer cells, is known as amembrane-bound enzyme playing a protective role from oxidativestress. Recent studies indicated that GGT can also exert pro-oxidanteffects at the membrane surface and the extracellular microenviron-ment, contributing to the regulation of proliferative/apoptotic balance,the acquisition of chemo-resistance, and cancer progression. Here, we
Vol. 197, No. 4S, Supplement, Saturday, May 13, 2017 THE JOURNAL OF UROLOGY! e433

OperatietechniekenDOEL – OPEN - ROBOTISCH

Doel - ManVerwijderen van:
◦ Blaas◦ Prostaat◦ +/- urethra afhankelijk van biopt urethra prostatica en localisatie tumor◦ Zaadblaasjes◦ Distale ureters (+/- Vriescoupes)◦ Lymfadenectomie
>80% van N+ heeft ook M+ (autopsiestudies)Betere oncologische outcomeTemplate onduidelijk
◦ Zenuwsparende ingreep

Doel - VrouwVerwijderen van:
◦ Blaas◦ Uterus◦ Urethra volledig◦ Vagina voorwand◦ Distale ureters (+/- Vriescoupes)◦ Lymfadenectomie

Morbiditeit en mortaliteitMortaliteit
◦ 30 dagen: 1.2-3.2% ◦ 90 dagen: 2.3-8.0%
Morbiditeit◦ 90 dagen: 58%
◦ Relatie met derivatie (Neoblaas>Bricker)

SurvivalRFS: Recurrence free survival, 5 jaar: 58%
CSS: Cancer specific survival, 5 jaar: 62-66%
OS: Overall Survival◦ 5 jaar: 66%◦ 10 jaar: 43%
TNM specifiek, RFS, 5 jaar:◦ pT1: 76%◦ pT2: 74%◦ pT3: 52%◦ pT4: 36%
ONCOLOGICAL OUTCOMES OF TOTALLY INTRACORPOREAL ROBOT-ASSISTED RADICAL CYSTECTOMY: RESULTS FROM THE ERUS SCIENTIFIC WORKING GROUP. Collins et al.

Herval717 RARC pt
RFS: Recurrence Free Survival
◦ Na 3 maand: 95.9%
◦ Na 12 maand: 80.2%
◦ Na 24 maand: 74.6%
80% hervalt binnen 2 jaar
Bot, long, lever, lymfeklieren
◦ 0,7% peritoneale carcinomatose, NOT UNUSUAL!
◦ 0,3% Porthole: Extractie dmv endobag!!
Early Recurrence Patterns Following Totally Intracorporeal Robot-assisted Radical Cystectomy: Results from the EAU Robotic Urology Section (ERUS) Scientific Working Group. Collins et al.

Herval717 RARC pt
RFS: Recurrence Free Survival at ◦ Na 3 maand: 95.9%◦ Na 12 maand: 80.2%◦ Na 24 maand: 74.6%
Afhankelijk van APO◦ Organ confined &N0 &M0◦ Non-Organ confined, N1, M1
Early Recurrence Patterns Following Totally Intracorporeal Robot-assisted Radical Cystectomy: Results from the EAU Robotic Urology Section (ERUS) Scientific Working Group. Collins et al.

Herval717 RARC pt
Afhankelijk van APO
Early Recurrence Patterns Following Totally Intracorporeal Robot-assisted Radical Cystectomy: Results from the EAU Robotic Urology Section (ERUS) Scientific Working Group. Collins et al.

Robot vs OpenGrootste meta analyse tot nog toe
Gelijkwaardige oncologische outcome◦ Nguyen: Geen toename in recurrence post-op na RARC
Gelijkwaardige complicatieratio en mortaliteit◦ Gemiddeld 50% in beide!
Robot laparoscopische cystectomie◦ Kortere hospitalisatie◦ Graad van complicaties minder ernstig◦ Minder bloedverlies en transfusienood
Open cystectomie◦ Kortere operatietijd

Complicaties na intracorporiële RARCMulticenter 621pt RARC met intracorporiële derivatie (Bricker/Neoblaas)
55% complicaties 1e 90d post-op◦ 32% Laaggradig (1-2 Clavien Dindo)
◦ 23,5% Hooggradig (3-4 Clavien-Dindo)
49% Infectieuze complicaties
19% Gastro-intestinaal
15% Genito-urinair
¼ heropnames binnen de 30d na operatie
Neoblaas aanleg en ASA-score predictors voor kans op complicatie
PD39-03 COMPLICATIONS AFTER TOTALLY INTRACORPOREAL ROBOT-ASSISTED RADICAL CYSTECTOMY: RESULTS FROM THE EUROPEAN ASSOCIATION OF UROLOGY ROBOTIC UROLOGY SECTION
(ERUS) SCIENTIFIC WORKING GROUP. Hosseini et al.

RARC: Real life data
Eur Urol Suppl 2016; 15(7):227
PE10 Neobladder versus ileal conduit in Robot-Assisted Radical Cystectomy (RARC): Results from a high-volume academic centre
Decaestecker K., Vanmarsnille T., Vandamme E., Poelaert F.
Ghent University Hospital, Dept. of Urology, Ghent, Belgium
INTRODUCTION & OBJECTIVES: To reduce the morbidity of Radical Cystectomy, RARC has gained interest. A totally intracorporeal technique has possible advantages, but is challenging certainly regarding neobladder reconstruction. We report the results of a single surgeon experience with RARC.
MATERIAL & METHODS: Since 2013 patients undergoing RARC at Ghent University Hospital are prospectively registered (EC 2013/874). A standardized care pathway is implemented and operation is performed by a single surgeon. Analysis of this prospective database is performed using SPSS v23.
RESULTS: 72 patients, with at least 3 months follow-up, underwent RARC with ileal conduit (n=40) or neobladder (n=32). Median follow up was 10.5 months. An overview of patient, tumor and surgery characteristics is given in table 1.
Characteristics Total (n=72) Ileal conduit (n=40) Neobladder (n=32) p-value
Patient
Age [mean (95%CI)] 68 (65–70) 71 (68 – 74) 63 (61 – 66) <0.001
Male gender [n (%)] 56 (77.8) 29 (72.5) 27 (84.8) 0.228
BMI [median (range)] 26 (17–36) 26 (19 – 36) 26 (17 – 32) 0.211
Charlson Comorbidity Index [median (range)] 5 (3 – 12) 6 (3 – 12) 4 (3 – 10) 0.007
Treatments/tumor
Neoadjuvant chemotherapy [n (%)] 18 (25.0) 9 (22.5) 9 (28.1) 0.584
BCG therapy [n (%)] 19 (26.4) 11 (27.5) 8 (25.0) 0.811
T stage 0.767
≤ pT1 [n (%)] 30 (41.7) 15 (37.5) 15 (46.9)
pT2 [n (%)] 12 (16.7) 8 (20.0) 4 (12.5)
pT3 [n (%)] 22 (30.6) 12 (30.0) 10 (31.3)
pT4 [n (%)] 8 (11.8) 5 (12.5) 3 (9.4)
pN+ [n (%)] 24 (34.7) 15 (39.5) 9 (29.0) 0.365
Operation
Intracorporeal [n (%)] 64 (88.9) 33 (87.5) 29 (90.6) 0.675
Nerve sparing [n (%)] 27 (37.9) 2 (5.6) 25 (78.2) <0.001
Node yield [median (range)] 17 (5 – 33) 16 (7 – 33) 18 (5 – 32) 0.225
Positive margins [n (%)] 2 (2.8) 1 (2.5) 1 (3.1) 0.873
Bloodloss [ml, median (range)] 250 (5 – 1000)
250 (5 – 850)
250 (50 – 1000)
0.270
Operation time [min, median (range)] 420 (240 – 720)
365 (270 – 600)
525 (240 – 720)
<0.001
Hospitalisation [days, median (range)] 11 (5 – 36) 10 (5 – 36) 11 (6 – 29) 0.154
Follow-up
Follow-up [months, median (range)] 10.5 (1 – 28) 6.5 (1 – 28) 12 (1 – 28) 0.106
Clavien Dindo < 30 days 0.072
Eur Urol Suppl 2016; 15(7):227
PE10 Neobladder versus ileal conduit in Robot-Assisted Radical Cystectomy (RARC): Results from a high-volume academic centre
Decaestecker K., Vanmarsnille T., Vandamme E., Poelaert F.
Ghent University Hospital, Dept. of Urology, Ghent, Belgium
INTRODUCTION & OBJECTIVES: To reduce the morbidity of Radical Cystectomy, RARC has gained interest. A totally intracorporeal technique has possible advantages, but is challenging certainly regarding neobladder reconstruction. We report the results of a single surgeon experience with RARC.
MATERIAL & METHODS: Since 2013 patients undergoing RARC at Ghent University Hospital are prospectively registered (EC 2013/874). A standardized care pathway is implemented and operation is performed by a single surgeon. Analysis of this prospective database is performed using SPSS v23.
RESULTS: 72 patients, with at least 3 months follow-up, underwent RARC with ileal conduit (n=40) or neobladder (n=32). Median follow up was 10.5 months. An overview of patient, tumor and surgery characteristics is given in table 1.
Characteristics Total (n=72) Ileal conduit (n=40) Neobladder (n=32) p-value
Patient
Age [mean (95%CI)] 68 (65–70) 71 (68 – 74) 63 (61 – 66) <0.001
Male gender [n (%)] 56 (77.8) 29 (72.5) 27 (84.8) 0.228
BMI [median (range)] 26 (17–36) 26 (19 – 36) 26 (17 – 32) 0.211
Charlson Comorbidity Index [median (range)] 5 (3 – 12) 6 (3 – 12) 4 (3 – 10) 0.007
Treatments/tumor
Neoadjuvant chemotherapy [n (%)] 18 (25.0) 9 (22.5) 9 (28.1) 0.584
BCG therapy [n (%)] 19 (26.4) 11 (27.5) 8 (25.0) 0.811
T stage 0.767
≤ pT1 [n (%)] 30 (41.7) 15 (37.5) 15 (46.9)
pT2 [n (%)] 12 (16.7) 8 (20.0) 4 (12.5)
pT3 [n (%)] 22 (30.6) 12 (30.0) 10 (31.3)
pT4 [n (%)] 8 (11.8) 5 (12.5) 3 (9.4)
pN+ [n (%)] 24 (34.7) 15 (39.5) 9 (29.0) 0.365
Operation
Intracorporeal [n (%)] 64 (88.9) 33 (87.5) 29 (90.6) 0.675
Nerve sparing [n (%)] 27 (37.9) 2 (5.6) 25 (78.2) <0.001
Node yield [median (range)] 17 (5 – 33) 16 (7 – 33) 18 (5 – 32) 0.225
Positive margins [n (%)] 2 (2.8) 1 (2.5) 1 (3.1) 0.873
Bloodloss [ml, median (range)] 250 (5 – 1000)
250 (5 – 850)
250 (50 – 1000)
0.270
Operation time [min, median (range)] 420 (240 – 720)
365 (270 – 600)
525 (240 – 720)
<0.001
Hospitalisation [days, median (range)] 11 (5 – 36) 10 (5 – 36) 11 (6 – 29) 0.154
Follow-up
Follow-up [months, median (range)] 10.5 (1 – 28) 6.5 (1 – 28) 12 (1 – 28) 0.106
Clavien Dindo < 30 days 0.072
Eur Urol Suppl 2016; 15(7):227
PE10 Neobladder versus ileal conduit in Robot-Assisted Radical Cystectomy (RARC): Results from a high-volume academic centre
Decaestecker K., Vanmarsnille T., Vandamme E., Poelaert F.
Ghent University Hospital, Dept. of Urology, Ghent, Belgium
INTRODUCTION & OBJECTIVES: To reduce the morbidity of Radical Cystectomy, RARC has gained interest. A totally intracorporeal technique has possible advantages, but is challenging certainly regarding neobladder reconstruction. We report the results of a single surgeon experience with RARC.
MATERIAL & METHODS: Since 2013 patients undergoing RARC at Ghent University Hospital are prospectively registered (EC 2013/874). A standardized care pathway is implemented and operation is performed by a single surgeon. Analysis of this prospective database is performed using SPSS v23.
RESULTS: 72 patients, with at least 3 months follow-up, underwent RARC with ileal conduit (n=40) or neobladder (n=32). Median follow up was 10.5 months. An overview of patient, tumor and surgery characteristics is given in table 1.
Characteristics Total (n=72) Ileal conduit (n=40) Neobladder (n=32) p-value
Patient
Age [mean (95%CI)] 68 (65–70) 71 (68 – 74) 63 (61 – 66) <0.001
Male gender [n (%)] 56 (77.8) 29 (72.5) 27 (84.8) 0.228
BMI [median (range)] 26 (17–36) 26 (19 – 36) 26 (17 – 32) 0.211
Charlson Comorbidity Index [median (range)] 5 (3 – 12) 6 (3 – 12) 4 (3 – 10) 0.007
Treatments/tumor
Neoadjuvant chemotherapy [n (%)] 18 (25.0) 9 (22.5) 9 (28.1) 0.584
BCG therapy [n (%)] 19 (26.4) 11 (27.5) 8 (25.0) 0.811
T stage 0.767
≤ pT1 [n (%)] 30 (41.7) 15 (37.5) 15 (46.9)
pT2 [n (%)] 12 (16.7) 8 (20.0) 4 (12.5)
pT3 [n (%)] 22 (30.6) 12 (30.0) 10 (31.3)
pT4 [n (%)] 8 (11.8) 5 (12.5) 3 (9.4)
pN+ [n (%)] 24 (34.7) 15 (39.5) 9 (29.0) 0.365
Operation
Intracorporeal [n (%)] 64 (88.9) 33 (87.5) 29 (90.6) 0.675
Nerve sparing [n (%)] 27 (37.9) 2 (5.6) 25 (78.2) <0.001
Node yield [median (range)] 17 (5 – 33) 16 (7 – 33) 18 (5 – 32) 0.225
Positive margins [n (%)] 2 (2.8) 1 (2.5) 1 (3.1) 0.873
Bloodloss [ml, median (range)] 250 (5 – 1000)
250 (5 – 850)
250 (50 – 1000)
0.270
Operation time [min, median (range)] 420 (240 – 720)
365 (270 – 600)
525 (240 – 720)
<0.001
Hospitalisation [days, median (range)] 11 (5 – 36) 10 (5 – 36) 11 (6 – 29) 0.154
Follow-up
Follow-up [months, median (range)] 10.5 (1 – 28) 6.5 (1 – 28) 12 (1 – 28) 0.106
Clavien Dindo < 30 days 0.072
Eur Urol Suppl 2016; 15(7):227
PE10 Neobladder versus ileal conduit in Robot-Assisted Radical Cystectomy (RARC): Results from a high-volume academic centre
Decaestecker K., Vanmarsnille T., Vandamme E., Poelaert F.
Ghent University Hospital, Dept. of Urology, Ghent, Belgium
INTRODUCTION & OBJECTIVES: To reduce the morbidity of Radical Cystectomy, RARC has gained interest. A totally intracorporeal technique has possible advantages, but is challenging certainly regarding neobladder reconstruction. We report the results of a single surgeon experience with RARC.
MATERIAL & METHODS: Since 2013 patients undergoing RARC at Ghent University Hospital are prospectively registered (EC 2013/874). A standardized care pathway is implemented and operation is performed by a single surgeon. Analysis of this prospective database is performed using SPSS v23.
RESULTS: 72 patients, with at least 3 months follow-up, underwent RARC with ileal conduit (n=40) or neobladder (n=32). Median follow up was 10.5 months. An overview of patient, tumor and surgery characteristics is given in table 1.
Characteristics Total (n=72) Ileal conduit (n=40) Neobladder (n=32) p-value
Patient
Age [mean (95%CI)] 68 (65–70) 71 (68 – 74) 63 (61 – 66) <0.001
Male gender [n (%)] 56 (77.8) 29 (72.5) 27 (84.8) 0.228
BMI [median (range)] 26 (17–36) 26 (19 – 36) 26 (17 – 32) 0.211
Charlson Comorbidity Index [median (range)] 5 (3 – 12) 6 (3 – 12) 4 (3 – 10) 0.007
Treatments/tumor
Neoadjuvant chemotherapy [n (%)] 18 (25.0) 9 (22.5) 9 (28.1) 0.584
BCG therapy [n (%)] 19 (26.4) 11 (27.5) 8 (25.0) 0.811
T stage 0.767
≤ pT1 [n (%)] 30 (41.7) 15 (37.5) 15 (46.9)
pT2 [n (%)] 12 (16.7) 8 (20.0) 4 (12.5)
pT3 [n (%)] 22 (30.6) 12 (30.0) 10 (31.3)
pT4 [n (%)] 8 (11.8) 5 (12.5) 3 (9.4)
pN+ [n (%)] 24 (34.7) 15 (39.5) 9 (29.0) 0.365
Operation
Intracorporeal [n (%)] 64 (88.9) 33 (87.5) 29 (90.6) 0.675
Nerve sparing [n (%)] 27 (37.9) 2 (5.6) 25 (78.2) <0.001
Node yield [median (range)] 17 (5 – 33) 16 (7 – 33) 18 (5 – 32) 0.225
Positive margins [n (%)] 2 (2.8) 1 (2.5) 1 (3.1) 0.873
Bloodloss [ml, median (range)] 250 (5 – 1000)
250 (5 – 850)
250 (50 – 1000)
0.270
Operation time [min, median (range)] 420 (240 – 720)
365 (270 – 600)
525 (240 – 720)
<0.001
Hospitalisation [days, median (range)] 11 (5 – 36) 10 (5 – 36) 11 (6 – 29) 0.154
Follow-up
Follow-up [months, median (range)] 10.5 (1 – 28) 6.5 (1 – 28) 12 (1 – 28) 0.106
Clavien Dindo < 30 days 0.072

Cystectomy
©
2 0 0 9 T H E A U T H O R S
7 2 8
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
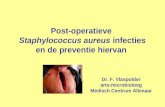
SPECIFIC PATIENT POSITIONING
Figure 1(a)
It is important that all elements of the patient set-up are consistent and reproducible to avoid plexus lesions or compartment syndrome. The patient is placed supine on the operating table. The head and shoulders are in contact with an anatomical pillow.
After general anaesthesia is induced, the patient’s arms are tucked at the sides and the legs are placed in boots. They are gently separated to facilitate docking of the robot, which is positioned between the legs. The knees are flexed to facilitate docking of the robotic arms. It is imperative that the table is orientated correctly to allow a maximal Trendelenburg position.
A metallic bar is placed just over the patient’s head and shoulders, without interfering with the endotracheal tube. This is useful in protecting the patient’s head from the robotic camera and arms. Great care is taken to adequately pad and support the patient to avoid neuromuscular injury.
During the first part of the procedure, the patient is maintained in a steep Trendelenburg position (
>
20
°
), while a normal position is required during reconstruction. The entire procedure is performed using a DaVinci-S HD System.
Under general anaesthesia, the patient is placed supine, with a nasogastric tube and Foley urethral catheter in place. In patients where no neobladder is planned, an en-bloc cystoprostatourethrectomy is performed. To do so, the urethra is freed first through a small scrotal incision up to the bulbar urethra. After completing the RC, the urethra is taken out en bloc, together with the whole specimen. Subsequently, the ports are placed.
Figure 1(b)
First, a 12-mm port is placed 3–5 cm above the umbilicus, depending on the length of the patient; an 8-mm port is placed at the umbilicus level on the left pararectal line, the other 8 mm port is placed on the right side where the stoma sign was made, a 5-mm port at the right side between the optic and the 8 mm port, a 12-mm port 3 cm up from the iliac crest on the right side, and an extra 8 mm port symmetrically on the left side. During RC the patient is placed in a steep Trendelenburg position.
12 mm8 mm 5 mm
b
a
Surgery Illustrated – Surgical Atlas Robotic radical cystectomy in the male. Buffi et al.

Extended lymfadenectomy
Surgery Illustrated – Surgical Atlas Robotic radical cystectomy in the male. Buffi et al.
©
2 0 0 9 T H E A U T H O R S
7 3 4
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
Figure 7
The lymphadenectomy is started at the left side with lateral freeing of the iliac vessels and the lymphatic tissue. The vessels are pushed medially. Doing so, the obturator fossa is entered and its lymphatic tissue freed lateral from the pelvic wall. The obturator nerve is visualized.
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 3 5
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
Figure 8
The lymphadenectomy continues to the level of the aortic bifurcation. Artery and vein are skeletonized using the split-and-roll technique. All tissue lying over the promontory and sacrum is freed.
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 3 7
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
Figure 10
The superficial and deep obturator fossa are completely freed from all lymphatic and fatty tissue. One can see the external iliac vessels, obturator nerve and artery and hypogastric artery. This is the last stage of the lymphadenectomy. As the lymphadenectomy is performed caudally, all lymphatic tissue is left on the specimen.

Cystectomy
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 2 9
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
PROCEDURE
URETERIC ISOLATION
Figure 2
The goal of this step is to first mobilize the ureters from above the crossing of the iliac vessels up to the level of the bladder, then to ligate and transect them. The ureters are frequently identified just medial to the spermatic vessels or they can be found crossing over the iliac vessels. Ureteric dissection is carried out proximally as far as possible without disturbing its vasculature, and distally up to the level of the bladder.
©
2 0 0 9 T H E A U T H O R S
7 3 0
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
Figure 3
The ureters are ligated using a Hem-o-lok clip and transected. After transection, the ureters are released proximally and tucked into the upper quadrants, away from the pelvic dissection.
Surgery Illustrated – Surgical Atlas Robotic radical cystectomy in the male. Buffi et al.

Cystectomy
Surgery Illustrated – Surgical Atlas Robotic radical cystectomy in the male. Buffi et al.
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 3 1
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
RETROVESICAL DISSECTION
Figure 4
The aim of this dissection is to mobilize the posterior bladder and base of the prostate off the rectum. The posterior peritoneum is incised just above its reflection over the rectum, connecting the incision previously made for the ureteric dissection.
©
2 0 0 9 T H E A U T H O R S
7 3 2
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
DEVELOPING THE RECTOVESICAL SPACE
Figure 5
The seminal vesicles and vasa deferentia are freed, mainly bluntly. Medial vessels can be cauterized, lateral vessels are clipped and cut. Blunt dissection is used to develop the rectovesical cul-de-sac. Both seminal vesicles are lifted up and Denonvilliers’ fascia is incised. The back of the prostate is freed until its apex.
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 3 3
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
LATERAL DISSECTION
Figure 6
The goal of this step is to develop the space between the bladder and lateral pelvic side-walls. This will facilitate exposure and isolation of the bladder pedicles. Lateral incisions in the peritoneum are made bilaterally to develop the perivesical space. Incisions are made upwards from lateral to the medial umbilical ligaments and downwards to connect with the posterior peritoneal incisions made during the initial ureteric dissection. The line of incision travels parallel to the spermatic cord. It is important not to drop the bladder at this point. The urachal and medial umbilical attachments are left intact, to suspend the bladder. This will facilitate posterior access.
The perivesical space is developed distally up to the level of the endopelvic fascia and continues posteriorly towards the bladder pedicles. At this point, the lateral vascular pedicles of the bladder are readily visualized.

Cystectomy
Surgery Illustrated – Surgical Atlas Robotic radical cystectomy in the male. Buffi et al.
©
2 0 0 9 T H E A U T H O R S
7 3 8
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
SECURING THE BLADDER PEDICLES
Figure 11
An Endowrist robotic Gyrus radiofrequency device is used to coagulate the vascular pedicles of the bladder. Only the major vessels have to be clipped. The bladder pedicles are identified and isolated. The internal iliac arteries are followed downwards. The umbilical artery is secured with a clip at its origin and cut. Further distally, the upper vesical artery is encountered, clipped and cut. Smaller vessels and fatty tissue are coagulated using Gyrus. Larger vessels are clipped and cut.
©
2 0 0 9 T H E A U T H O R S
7 4 0
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
ANTERIOR DISSECTION
Figure 13
The aim of this dissection is to drop the bladder posteriorly, as is done in da Vinci prostatectomy, to gain access to the space of Retzius. The peritoneum is incised anteriorly through the medial umbilical ligaments and the urachus, just below the umbilicus. The bladder is dropped, as is done in da Vinci prostatectomy.

Cystectomy
©
2 0 0 9 T H E A U T H O R S
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
7 4 1
S U R G E R Y I L L U S T R A T E D – S U R G I C A L A T L A S
Figure 14
The endopelvic fascia is identified and incised bilaterally. The levator muscle fibres are gently pushed away from the lateral side of the bladder.
©
2 0 0 9 T H E A U T H O R S
7 4 2
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
DORSAL VENOUS COMPLEX (DVC) AND APICAL DISSECTION
Figure 15
The DVC is incised cold; to avoid venous bleeding, the intra-abdominal pressure is brought to 20 mmHg and the assistant is forbidden to aspirate. During incision of the DVC, two arteries are mostly encountered that are secured with monopolar coagulation. The anterior contour of the prostate is followed until the apex is reached. All periurethral tissue is cut to gain as much urethral length as possible. The DVC is now secured with a running suture of poliglecaprone 25 2/0 and the intra-abdominal pressure is lowered again.
©
2 0 0 9 T H E A U T H O R S
7 4 4
J O U R N A L C O M P I L A T I O N
©
2 0 0 9 B J U I N T E R N A T I O N A L
B U F F I
E T A L .
TRANSECTION OF THE URETHRA
Figure 17
The membranous urethra is now completely isolated. The catheter is withdrawn and a large Hem-o-lok clip is placed on the urethra just next to the apex of the prostate, to avoid possible urinary spillage that could be contaminated with tumour cells. The urethra is then cut. The specimen is put in a large Endocatch bag coming from the enlarged opening of the right lateral assistant port opening. The bag is closed and pushed in the upper abdomen until the end of the operation. It is then retrieved through a midline supra-umbilical incision.
Urinary diversion can then be performed intra- or extracorporeally. Two drains are placed in the pelvis.

Cystectomy

Bricker Intracorporieel
©
2 0 1 0 T H E A U T H O R S
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
1 4 0 7
S U R G E R Y I L L U S T R A T E D
Figure 2
Isolation and transfer of the left ureter to the right side.
The left ureter is delivered to the right side under the sigmoid mesocolon using a Micro-France grasper.
©
2 0 1 0 T H E A U T H O R S
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
1 4 0 9
S U R G E R Y I L L U S T R A T E D
Figure 4
An
≈
12-cm segment of bowel is identified proximal to the ‘marionette’ suture (distal end of the conduit) and is held in place by the fourth-arm Cobra grasper. The hook cautery is used to incise the peritoneum of the bowel mesentery, after which the small mesenteric vessels are controlled using bipolar cautery or a stapler. The two mesenteric windows are created to isolate the ileal conduit.

Bricker Intracorporieel
©
2 0 1 0 T H E A U T H O R S
1 4 1 0
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
G U R U
E T A L .
Figure 5
Once adequate vascularity to the ileal conduit is ensured, a 45-mm Endo-GIA stapler is introduced through the 15 mm right assistant-port to divide the bowel lumen on both sides of the conduit. The ‘marionette’ is manoeuvred appropriately during this step.
©
2 0 1 0 T H E A U T H O R S
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
1 4 1 7
S U R G E R Y I L L U S T R A T E D
Figure 12
A skin incision is made in the suprapubic region and a 12-mm port is placed. The silk suture tagging the two bowel ends is held by the fourth arm. A laparoscopic 60-mm Endo-GIA stapler is passed through the suprapubic port into the enterotomies. After ensuring that the anti-mesenteric sides of the bowel are properly opposed, the stapler is fired and bowel continuity is re-established.

Bricker Intracorporieel
©
2 0 1 0 T H E A U T H O R S
1 4 1 8
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
G U R U
E T A L .
Figure 13
The two open bowel ends are held with the robotic arms and a second firing of the Endo-GIA stapler is performed transversely via the right assistant port. The peritoneal window can then be closed using 3-0 silk sutures, and reinforcement sutures can also be placed in the conduit. The 12-mm suprapubic port is used to remove the specimen through a Pfannenstiel incision. Specimen is removed via the vagina in female patients.
©
2 0 1 0 T H E A U T H O R S
1 4 1 2
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
G U R U
E T A L .
BOWEL WASHOUT AND SET-UP FOR ANASTOMOSIS
An electrosurgical J-hook is used to create a small opening in the distal (stomal) portion of the conduit for irrigation of the bowel contents. The ‘marionette’ is lowered to easily place a Foley catheter into the conduit. A 22 F catheter is introduced through the 15-mm right assistant-port, and fed into the conduit through this enterotomy using a Cardier grasper in the right hand after lowering the ‘marionette’ suture. The catheter balloon is inflated with 5 mL of sterile water to prevent spillage while irrigating, the catheter is then used to irrigate the bowel segment. Once the irrigant is clear, the balloon is deflated and the catheter is removed.
Figure 7
Uretero-ileal anastomosis
. Minimal proximal dissection and gentle handling of the ureter is crucial during uretero-ileal anastomosis. The distal end of the ureter (Hem-o-lock clip) is held in position using the fourth robotic arm Cobra grasper. The robotic scissor is used to partially transect and spatulate the distal end of the ureter. Scissors or an electrocautery hook is used to make two enterotomies in the proximal conduit segment on two opposite sides. The edges of the enterotomies are everted using interrupted 3-0 polyglactin 910 sutures. For the interrupted simple uretero-ileal anastomosis 4-0 polyglactin 910 or polydiaxonone is used.

Bricker Intracorporieel
©
2 0 1 0 T H E A U T H O R S
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
1 4 1 3
S U R G E R Y I L L U S T R A T E D
Figure 8
After half of the sutures have been placed, the ureteric stent is inserted. A metal laparoscopic suction tip is passed through the 15-mm assistant-side port, and the ‘marionette’ is lowered to align for easy passage through the conduit. The tip of the suction is gently guided through the entire conduit, starting at the previously made opening at the distal conduit for irrigation. A 90-cm, 8.5 F single-J ureteric stent with a guidewire is passed through the suction tip and fed into the ureteric opening while holding the metal suction tip in place using the left robotic arm. Once the single-J stent is positioned in the upper ureter, the suction tip is withdrawn while the robotic surgeon controls the stent with the guidewire. The guidewire is left in the stent to allow for easy identification of the stent inside the conduit.
©
2 0 1 0 T H E A U T H O R S
B J U I N T E R N A T I O N A L
©
2 0 1 0 B J U I N T E R N A T I O N A L
1 4 1 9
S U R G E R Y I L L U S T R A T E D
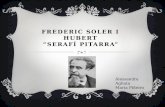
Figure 14
Creation of the stoma.
The marked stoma site is opened, and a cylinder of fat is removed A cruciate incision is made in the anterior rectus fascia, and a hemostat clamp is passed into the peritoneum. The distal end of the conduit and the stents are extracted using the ‘marionette’ suture and the stoma is fashioned according to the surgeon’s preferences.

Bricker Intracorporieel

Neoblaas intracorporieel
https://consultqd.clevelandclinic.org/robot-assisted-intracorporeal-ileal-neobladder-the-next-step-in-urinary-diversion/

Neoblaas intracorporieel

Neoblaas intracorporieel

Neoblaas intracorporieel

Neoblaas intracorporieel

Peri-operatieve zorgPRE – PER – POST OPERATIEF EN OPVOLGING

Pre-operatieve zorgAssessment – counseling - Voorbereiding

AssessmentCo-morbiditeit en leeftijd van de patiënt bepalend
◦ Operabiliteit◦ Keuze van derivatie: Neoblaas vs Bricker derivatie
◦ Geen Neoblaas bij >N1, geriatrische patiënt
◦ Zenuwsparende ingreep◦ Mogelijkheid Neo-adjuvante chemotherapie
Pre-operatief assessment – Geriatrisch assessment◦ Anesthesiologisch◦ Cardio-pulmonair◦ Nefrologisch◦ Nutriotionele status◦ Charlson Co-morbidity index

CounselingUroloog en Oncoloog
Oncologisch verpleegkundige◦ Oncologische uitleg diagnose◦ Uitleg peri-operatief verloop cystectomie
Psychologische bijstand
Stomaverpleegkundige◦ Uitleg stoma◦ Uitleg stomazorg, contactgegevens◦ Pre-operatieve localisatie stomaplaats
◦ Overnachting met stomazakje

Keuze van derivatieIleostoma
Nadelen◦ Mutilerend◦ Urineweginfecties: 50% op 15jr tijd◦ Stomaproblemen
◦ Lek◦ Stenose
Voordelen◦ Minder kans op peri-operatieve complicaties◦ Minder kans op long term complicaties vs Neoblaas: incontinentie, infectie, CIC

Keuze van derivatieNeoblaas: obv ileum
◦ Absolute contra-indicaties◦ Neurologische/psychiatrische aandoeningen◦ Korte levensverwachting (vaak dus ifv leeftijd, >80jr))◦ Lever- en nierfunctiestoornissen◦ Localisatie tumor thv urethra
◦ Relatieve contra-indicaties◦ Urethrastricturen◦ Incontinetie (mn stress incontinentie)◦ Bekkenradiotherapie
◦ Nadelen◦ Urineverlies: 10% overdag, 30% ‘s nachts◦ Metabole stoornissen◦ Nood tot CIC (vnl bij dames tot 62%!)

Keuze van derivatieIntracorporiële vs extracorporiële reconstructie
◦ Extracorporiële derivatie◦ Via minilaparotomie◦ Minder bloedverlies dan volledig open◦ MAAR: Geen winst in hospitalisatieduur, evenveel complicaties als bij open prodecure
◦ Intracorporiële derivatie◦ Derivatie volledig intra-abdominaal◦ Werkelijke winst in hospitalisatieduur◦ Minder complicaties dan bij open of extracorporieel
Is robotic radical cystectomy ready for prime time? Patel et al.

VoorbereidingEnhanced Recovery After Surgery
Vermindering van ileus van 22% naar 7,3%◦ Hospitaalduur verminderd met 30%◦ Tot 50% minder complicaties
Pre-, per- en postoperatief management
Multidisciplinair◦ Anesthesiologie◦ Chirurgie/Urologie◦ Verpleegkundigen◦ Kinesitherapeuten◦ Dietisten
Enhanced Recovery After Surgery protocols for radical cystectomy surgery: review of current evidence and local protocols. Maria C. Mir, et al.

Enhanced Recovery After Surgery

ERAS protocolPre-operatief:
◦ Goede counseling (impact op duur hospitalisatie!)
◦ Rookstop, alcohol intake verminderen
◦ Nazicht nutritionele status (20% slecht bij cystec)
◦ GEEN darmvoorbereiding
◦ Energiedrank pre-operatief
◦ Heldere vloeistoffen tot 2 u voor, 6u voor vast voedsel stop
◦ Kortwerkende anxiolytica pre-op
Enhanced Recovery After Surgery protocols for radical cystectomy surgery: review of current evidence and local protocols. Maria C. Mir, et al.
Enhanced Recovery After Robot-assisted Radical Cystectomy: EAU Robotic Urology Section Scientific Working Group Consensus View. Collins et al.

ERAS protocolPer-operatief:
◦ GEEN Epidurale pijnpomp◦ Vermijden van opioiden per en post-op◦ Vermijden hypothermie en hypoxemie◦ Streven naar euvolemie
◦ Vermijden hypo volemie maar ook overvulling◦ Goal Directed Fluid Therapy
◦ Antibioticaprofylaxe 2e of 3e genetratie cefalosporine ◦ Chloorhexedine in alcohol superieur◦ MINIMAAL INVASIEVE CHIRURGIE◦ INTRACORPORIELE DERIVATIE
◦ Minder 90d morbiditeit◦ Minder gastro-intestinale complicaties
Enhanced Recovery After Surgery protocols for radical cystectomy surgery: review of current evidence and local protocols. Maria C. Mir, et al.Enhanced Recovery After Robot-assisted Radical Cystectomy: EAU Robotic Urology Section Scientific Working Group Consensus View. Collins et al.

ERAS protocolPost-operatief:
◦ Geen nasogastrische tube
◦ Preventie PONV (Post-Op Nausea & Vomiting)
◦ Snelle mobilisatie◦ Opzitten asap, ten laatste dag 1
◦ Snelle orale voeding◦ Dag zelf: drinken toelaten, evt carbohydr
◦ Daags nadien: opklimmend
◦ Lichte voeding => normaal ASAP
◦ Gastro-intestinale stimulatie◦ Primeran systhematisch (of ander gastro-prokineticum)
◦ Kauwgom
◦ Thromboprofylaxe
Enhanced Recovery After Surgery protocols for radical cystectomy surgery: review of current evidence and local protocols. Maria C. Mir, et al.Enhanced Recovery After Robot-assisted Radical Cystectomy: EAU Robotic Urology Section Scientific Working Group Consensus View. Collins et al.

ERAS protocol
Enhanced Recovery After Robot-assisted Radical Cystectomy: EAU Robotic Urology Section Scientific Working Group Consensus View. Collins et al.

OntslagplanningOog voor sociale situatie van de patiënt
◦ Geriatrisch support team
◦ Sociale dienst: Thuiszorg optimaliseren
Patiënten Motivatie◦ Afspraken maken met pt
Patiënten Educatie (+ FAMILIE/MANTELZORG!)◦ Stomazorg
◦ Mogelijke complicaties na ontslag
◦ Counseling APO
Controle consultatie◦ 6 weken: DJ stent uit op raadpleging

Take Home MessagesRARC IS FEASEBLE !

Take home messages: RARCOncologisch en technisch veilig
◦ Gelijkwaardige resultaten naar CSS, snedevlakken, etc…◦ Geen toegenomen complicaties post-operatief◦ Eerder laaggradige complicaties
Minder bloedverlies, kortere hospitalisatie
Minimaal invasief, naukeuriger werken (ev zenuwsparend)
ENKEL te bereiken door multidisciplinaire samenwerking◦ Implementatie ERAS protocol◦ Minimaal invasieve chirugie◦ Counseling en opvolgen van de patiënt medisch en paramedisch
Hierdoor streven naar minder complicaties

Vragen?