Anesthesie voor robotchirurgie, vrijdagochtendkrans · Ogen/IC pathologie glaucoom of andere...
37
Dr J Lauweryns Anesthesie voor robotchirurgie, vrijdagochtendkrans
Transcript of Anesthesie voor robotchirurgie, vrijdagochtendkrans · Ogen/IC pathologie glaucoom of andere...

Dr J Lauweryns
Anesthesie voor robotchirurgie, vrijdagochtendkrans

Indicaties voor robotchirurgie
• Hepato-biliaire-pancreas• Bovenbuik• Colorectale chirurgie• Urologie• Gynaecologie• Endocriene chirurgie, NKO

Principe van de ‘Da Vinci’• Telemanipulator
endoscopische instrumenten• Verschillende armen
camera• Bediening vanuit console door chirurg
• Assistent: retractor, suturen, irrigatie, suctie
• Voordeel robot tov laparoscopie: gecomputeriseerde elektromechanische controle: meer precisie en stabiliteit voor dissectie van kritische structurendriedimensioneel beeld

‘Da Vinci’ versus open prostatectomie
• Langere operatietijdVergelijkbare complicatieratio met verkorten van de hospitalisatieduur, minder bloedverlies en transfusie
• Lange termijn outcome? Vergelijkbare 3-jaar tumorvrije overleving
• Trend naar betere outcome qua continentie en potentie
Wilson T, Torrey R, Open versus robotic-assisted radical prostatectomy: which is better?, Current opinion in urology 2011, 21: 200-205

Kostprijs ‘Da Vinci’• Aankoop 1,2 miljoen dollar
• Jaarlijks Onderhoud 100 000 dollar
• Materiaal per patiënt 1500 dollar
Rekening houdend met minder lange hospitalisatie, minder transfusie, complicaties en operatieve tijd: meerkost van 150 dollar/patiënt
Wilson T, Torrey R, Open versus robotic-assisted radical prostatectomy: which is better?, Current opinion in urology 2011, 21: 200-205

Procedure• Anesthesie en installatie
• Laparoscopie met plaatsen trocars voor de camera en de werkkanalen
• ‘docken’ van de robot -> bij urgentie: ‘undocken’ noodzakelijk!
• Dissectie van de zenuwen, zaadblaasjes en prostaatresectie van de prostaat met achterlaten id caviteitvasthechten van de urethra aan de blaas: vesico-urethrale anastomoseplaatsen van perivesicale drain
• ‘undocken’ en verwijderen van prostaat door poort via zakje
• Bloedverlies 150-250ml, meer mogelijk

‘minimaal invasief’…• Snelle mobilisatie• Weinig pijn• Weinig complicaties zoals ileus,…• Weinig transfusie
maar: ‘maximaal invasief’ fysiologisch

Combinatie effecten van pneumoperitoneum en lithotomie met diepe trendelenburg 30-45°
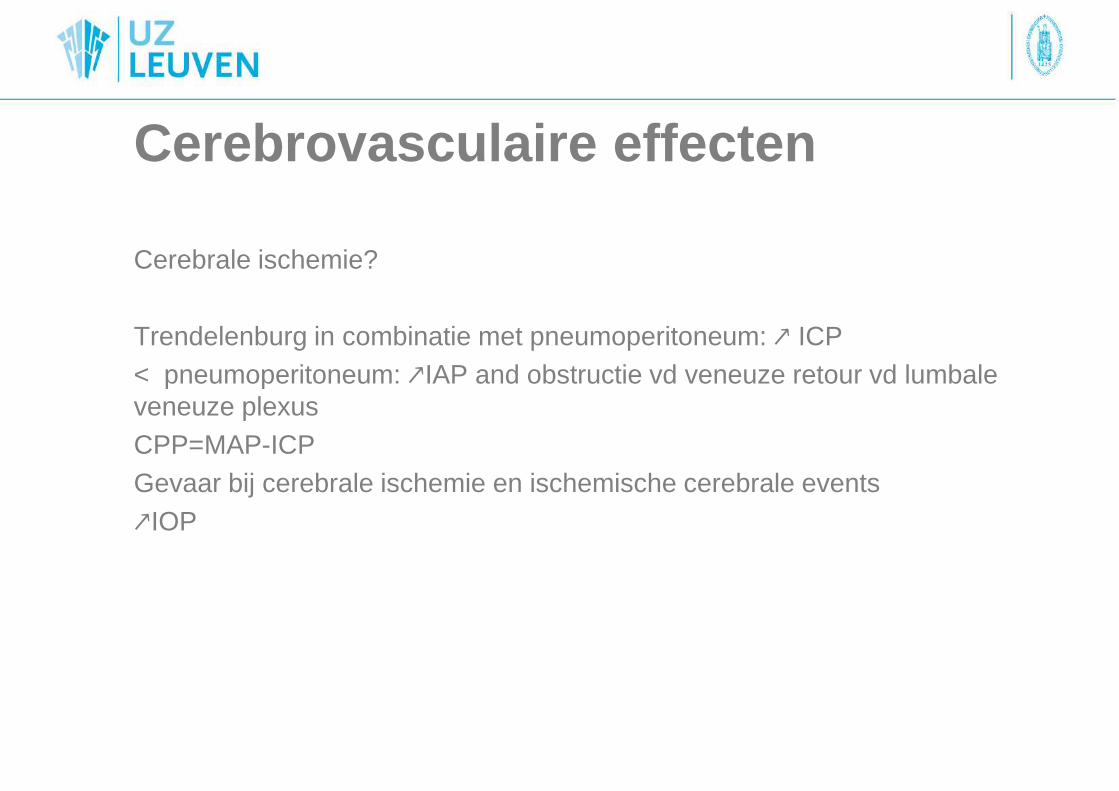
Cerebrovasculaire effecten
Cerebrale ischemie?
Trendelenburg in combinatie met pneumoperitoneum: ↗ ICP < pneumoperitoneum: ↗IAP and obstructie vd veneuze retour vd lumbale veneuze plexusCPP=MAP-ICPGevaar bij cerebrale ischemie en ischemische cerebrale events↗IOP

2
FIG. 1.
Effects of Neck Position and Head Elevation on Intracranial
Pressure in Anaesthetized Neurosurgical Patients:
Preliminary Results.
Mavrocordatos, P; Bissonnette, B; Ravussin, P
Journal of Neurosurgical Anesthesiology. 12(1):10-14,
January 2000.
FIG. 1. Fifteen head orientations with the table positioned
either horizontally, 30[degrees] head-up or 30[degrees]
head-down were studied. Each number represents the final
head and neck position and corresponds to: 1) head straight
in the axis of the body, 2) head angled at 45[degrees] to the
right, 3) head angled at 45[degrees] to the left, 4) head
rotated to the right, 5) head rotated to the left, 6) head
flexed straight, 7) head flexed and angled at 45[degrees] to
the right, 8) head flexed and angled at 45[degrees] to the
left, 9) head flexed and rotated to the right, 10) head flexed
and rotated to the left, 11) head extended straight, 12) head
extended and angled at 45[degrees] to the right, 13) head
extended and angled at 45[degrees] to the left, 14) head
extended and rotated to the right, and 15) head extended
and rotated to the left.

2
TABLE 1.
Effects of Neck Position and Head Elevation on Intracranial
Pressure in Anaesthetized Neurosurgical Patients:
Preliminary Results.
Mavrocordatos, P; Bissonnette, B; Ravussin, P
Journal of Neurosurgical Anesthesiology. 12(1):10-14,
January 2000.
TABLE 1. ICP (mean +/- SD) in each head and neck position
with the table in the three positions* P < .05 vs. the neutral
position (1) with the table horizontal.

Respiratoire effecten
Trendelenburg positie
◊ verplaatsing van het diafragma naar craniaal samen met mediastinum ◊toename in pulmonaire bloedflow, effect zwaartekracht op mediastinum ->↘ FRC, ↘ compliantie, ↗ atelectase ◊grote delen van de long onder niveau linker atrium zone 3 of 4 ->pulmonair oedeem, cave MS
Pneumoperitoneum
Effect op respiratoire mechanica
In combinatie met trendelenburg:
↘ compliantie, drukken ≤ 12mmHg(European association of endoscopic surgery) 50% ↗ piek en plateaudruk, risico barotrauma: ↘ Vt, ↗ RR, permissieve hypercapnie

Evolution of the individual patient values (thin li nes) and the average value (thick line) of the end-tidal CO2 values (Pe ′co2), ventilatory plateau pressure (PPlat), TV, and pulmonary
compliance.
Kalmar A F et al. Br. J. Anaesth. 2010;104:433-439

The relationship between Paco2 and Pe ′co2.
Kalmar A F et al. Br. J. Anaesth. 2010;104:433-439

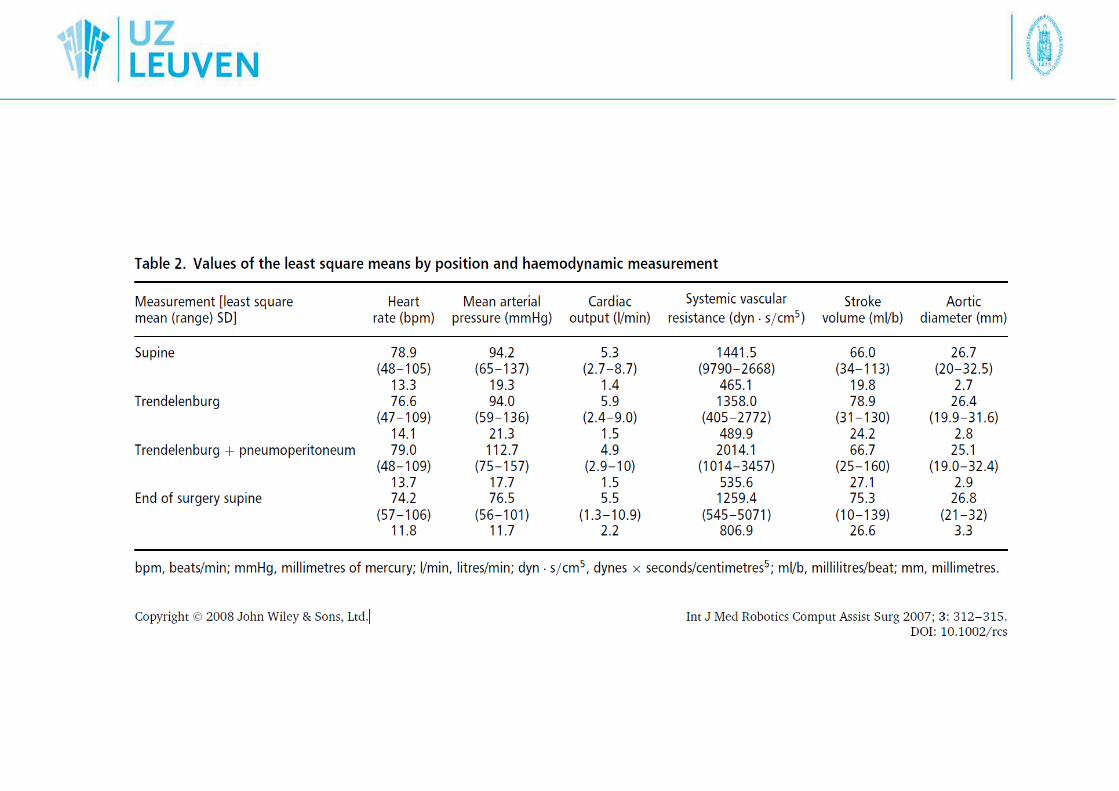
Cardiovasculair
Pneumoperitoneum
MAP↗25%, SVR↗20% (↗IAP zorgt voor compressie vd aorta en ↗afterload), HR ↗CVP, PAP mean, PCWP blijven =
Trendelenburg met pneumoperitoneum
MAP blijft 25%↗, SVR terug baseline CVP, PAP mean, PCWP allen X2 Strain op het hart ↗ tgv 2-3X ↗vullingsdrukken HR, SV, CO, SVO2 =, HR en CO ↗ onmiddellijk post-chirurgie
Bij patiënten met voldoende cardiale reserve, bij andere kan ↗ preload zorgen voor HFLestar M, Gunnarsson L, Lagerstrand L et al. Hemodynamic perturnbations during robot-assited laparoscopic prostatectomy in 45° Trendelenburg position. Anesth Analg2011;113:1069-75

Cardiovasculair
↘bloedflow organen abdominale caviteit
↘renale, portale, splanchnische flow
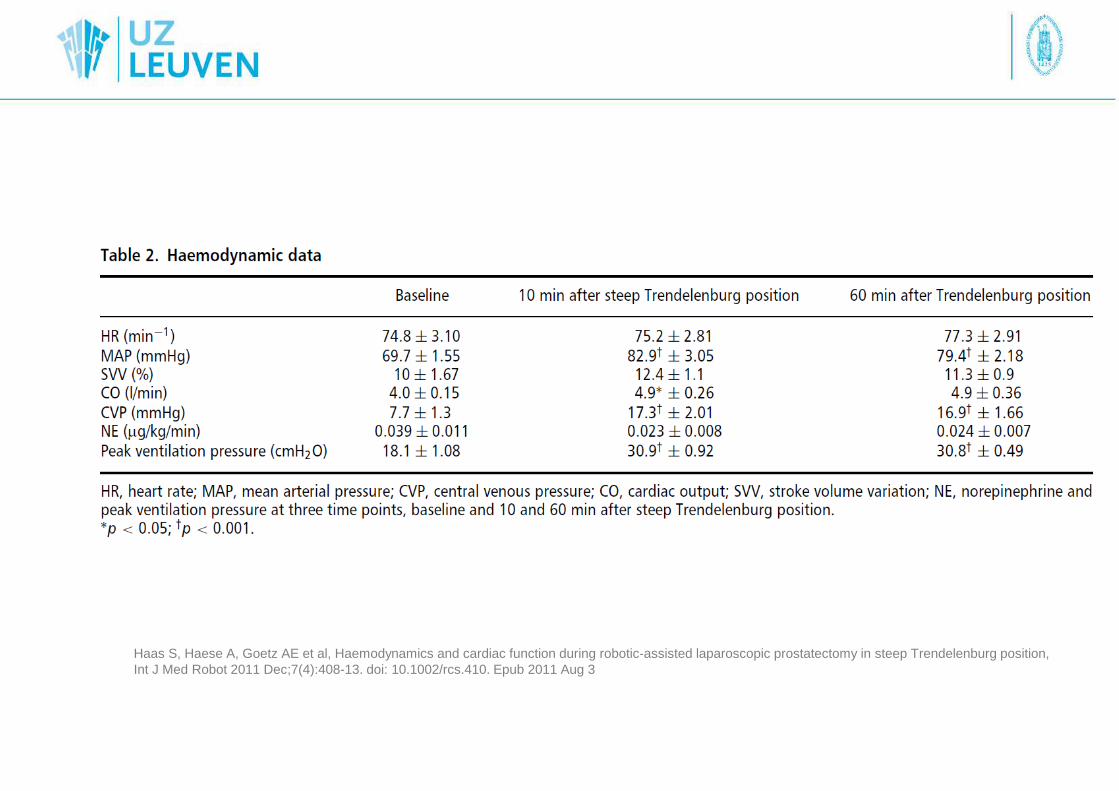
Haas S, Haese A, Goetz AE et al, Haemodynamics and cardiac function during robotic-assisted laparoscopic prostatectomy in steep Trendelenburg position, Int J Med Robot 2011 Dec;7(4):408-13. doi: 10.1002/rcs.410. Epub 2011 Aug 3
Endocrien systeem
↗CatecholaminesActivatie van RAA systeem->↗Vasopressine

Verwikkelingen van pneumoperitoneum• Subcutaan emfyseem: frekwent
Risicofactoren:
CO2 ≥ 50mmHg6 of meer operatiepoortenOperatietijd > 200minOudere patiënten
GevolgenSoms weinigPneumothorax, pneumomediastinum, pneumopericard (prefasciaal)->beademing postoperatief tot zakken CO2 (verhinderen verhoogde WOB) (thoraxdrain bij pneu)

Verwikkelingen van het pneumoperitoneum• Luchtembool
klinische presentatie ~ grootte, hoeveelheidPlotse cardiovasculaire collaps zonder duidelijke andere oorzaakDaling van de CO2
• CO2 embool
2 momenten: insufflatie, dissectie van het diepe dorsale veneuze complex+ : CO2 zeer bloedoplosbaar, minder effect dan vergelijkbaar luchtembool, subklinisch

Gas embolism detected by TOE during the transection of deepdorsal complex.
Hong J Y et al. Br. J. Anaesth. 2010;105:777-781
©
Verwikkelingen van de diepe trendelenburg
• Afglijden van de patiënt naar craniaal
• Faciaal, farygeaal, larygeaal oedeem
~ hoeveelheid toegediende vloeistof, reductie van de veneuze outflow vhhoofd door combinatie met pneumoperitoneum (hoge cuffdruk, traumatische intubatie, hypoalbuminemie)
Zo faciaal/conjunctivaal oedeem-> grote kans larygeaal oedeem:cufflek testen
• Migratie van de ETT: door trendelenburg: opwaartse migratie van de trachea, tube endobronchiaal (rol pneumoperitoneum en shift diafragma)

Verwikkelingen van de diepe trendelenburg• Oogafwijkingen
Cornea-abrasie
Ischemische opticusneuropathie: zeldenEén case report bij RALP: langdurige procedure, toediening veel vocht(veel bloedverlies) Weber ED, Colyer MH, Lesser MH et al. Posterior ischemic optic neuropathy after minimally invasive prostatectomy. J Neuro Ophtalmol 2007; 27:285-7
Andere risico’s• Beperkte toegang tot de patiënt
• Onverwachte viscerale schade of bloedverlies
• Zenuwschadeneuropathie van de n lingualis/buccalisperifere zenuwschade: incidentie 0,25%(vooral n medianus)brachiale plexus
• Hypothermie
Anesthesie• Preoperatieve evaluatie
Ogen/IC pathologie
glaucoom of andere pathologieGeen gekende associatie met ischemische opticusneuropathieBij twijfel: consult oftalmo
Luchtweg
Moeilijk?, kan erger worden PO bij oedeem

Anesthesie• Preoperatieve evaluatie
Pulmonair
COPD↔ hogere piekdrukkenEmfyseem: ruptuur bullae
Cardiaal
Coronair lijden, congestief hartfalen, hypertensie, kleplijdenoverweeg echocardio, stress testen bij zwaar cardiaal belaste patiënten

Anesthesie• Preoperatieve evaluatie
Documenteren van voorafbestaande perifere neurologische deficiets
Stolling?(weinig bloedverlies <-> moeilijk snelle controle), stoppen ontstollende medicatie iom cardio
Obesitas?
BMI>30 Kans op bemoeilijkte luchtwegMeer comorbiditeitIn ervaren handen

Dirk Meininger, Bernhard Zwissler, Christian Byhahn et al. Impact of Overweight and Pneumoperitoneum on Hemodynamics and Oxygenation during
Prolonged Laparoscopic Surgery, World J Surg (2006) 30: 520–526

Anesthesie• Preoperatieve evaluatie
‘relatieve contra-indicaties’ (UZ Leuven): worden relatiever naarmate ervaring toeneemt
1. Zwaar cardiaal belaste patiënten (echocardio)2. COPD3. Obesitas (BMI < 30)4. Leeftijd (<70j)5. Vroegere chirurgie in laag abdominale regio (lange dissectie waardoor
operatietijd toeneemt)
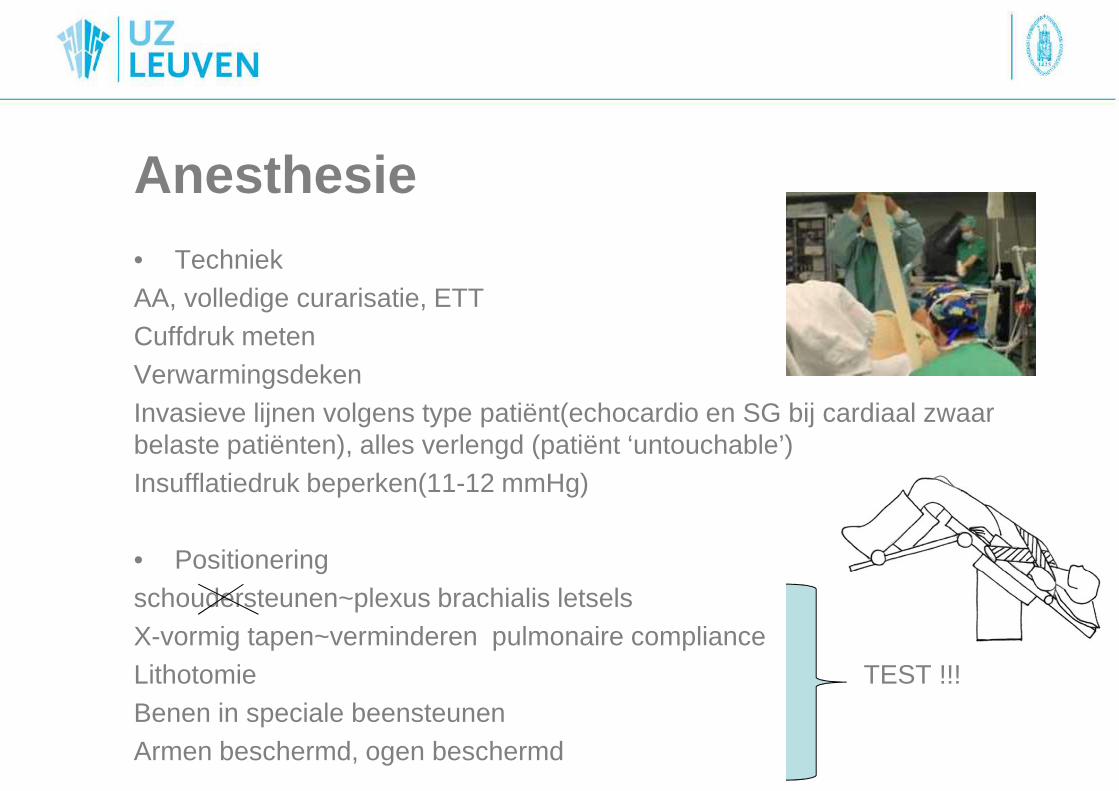
Anesthesie• TechniekAA, volledige curarisatie, ETTCuffdruk metenVerwarmingsdekenInvasieve lijnen volgens type patiënt(echocardio en SG bij cardiaal zwaar belaste patiënten), alles verlengd (patiënt ‘untouchable’)Insufflatiedruk beperken(11-12 mmHg)
• Positioneringschoudersteunen~plexus brachialis letselsX-vormig tapen~verminderen pulmonaire complianceLithotomie TEST !!!Benen in speciale beensteunenArmen beschermd, ogen beschermd

Anesthesie• Ventilatie
Pneumoperitoneum->↑IAP -> ↑luchtwegdrukProblemen bij obstructief, restrictief longlijden, reactieve LWTesten van verschillende beademingsmodi: IPPV, PCV, PC-VG(+ decelererende flow van PCV, controle van PaCO2 via volume garantie)

Anesthesie• Vochtbeleid
Bloedverlies normaal beperkt, PC kruisenRestrictief vochtbeleid tot na vesico-urethrale anastomose<->visibiliteit operatieveld+ minder faciaal, pharyngeaal & laryngeaal oedeem
Opletten voor ‘te droge’ patiënt postoperatief
Oligurie tgv ↓ renale bloedflow & GFR bij laparoscopische proceduresMilde ↑ creat mog tov open procedure tijdens hospitalisatie, niet bij ontslag800ml pre-anastomose, 700-1200ml post-anastomose
Gainsburg D.M., Anesthetic concerns for robotic-assisted laparoscopic prostatectomy, Minerva Anesthesiol 2012; 78: 596-604
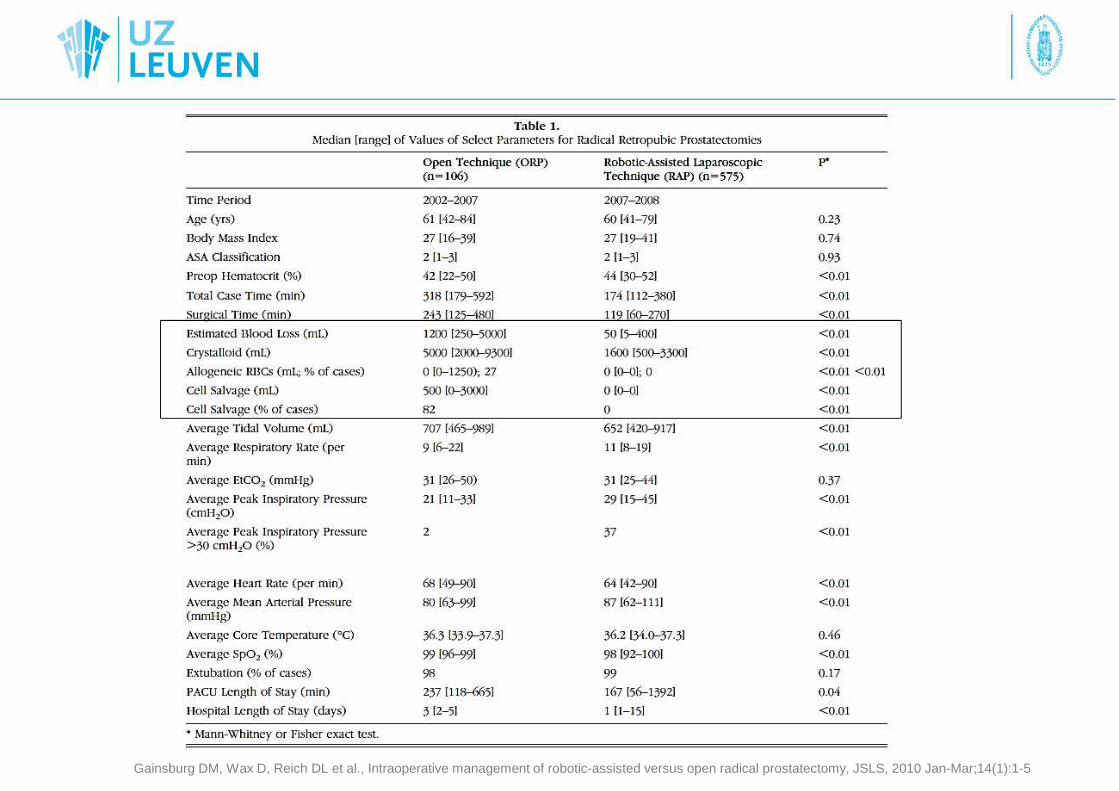
Gainsburg DM, Wax D, Reich DL et al., Intraoperative management of robotic-assisted versus open radical prostatectomy, JSLS, 2010 Jan-Mar;14(1):1-5

Anesthesie• Diep neuromusculair block
Inductie: sufenta, proprofol; onderhoud sufenta, sevo
Testen neuromusculair block(referentie) TOF aan 60mARocuronium 0.6mg/kg IVrocuroniumdrip: 0.5mg/kg/u IV, aanpassen volgens neuromusculair blockStreven naar een PTC van 1-2, stop drip bij sluiten
CI: NI
Decurarisatie met Sugammadex 4mg/kg IV (minstens PTC van 2)
(UZ Leuven)

Anesthesie• Ontwaken en extubatie
Extubatie in de zaal?~ duur ingreep~ faciaal, buccaal oedeem (cuff lek testen)~ comorbiditeit(~ residueel neuromusculair block)
Pijn: lokale infiltratie insteekpunten, klassiek schema(PFG, NSAIDS, Dipi, buscopan bij blaasspasmen)
Controle Hb
PAZA verblijf ~ 2u, ITE zelden
Referenties1. Gainsburg D.M. Anesthetic concerns for robotic-assisted laparoscopic radical prostatectomy, Minerva Anesthesiol 2012; 78: 596-604
2. Baltayian S. A brief review: anesthesia for robotic prostatectomy, J Robotic Surg 2008 2: 59-66
3. Lestar M, Gunnarsson L, Lagerstrand L et al. Hemodynamic perturnbations during robot-assited laparoscopic prostatectomy in 45° Trendelenburgposition. Anesth Analg 2011;113:1069-75
4. Wilson T, Torrey R, Open versus robotic-assisted radical prostatectomy: which is better?, Current opinion in urology 2011, 21: 200-205
5. Choi EM, Na S, Choi SH et al, Comparison of volume-controlled and pressure-controlled ventilation in steep Trendelenburg position fotr robt- assistedlaparoscopic radical prostatectomy, J Clin Anesth 2011 May;23(3):183-8
6. Phong S.V.N., KOH L.K.D. Anaesthesia for robotic-assisted radical prostatectomy: considerations for laparoscopy in Trendelenburg position, Anaesthesia and Intensive care, vol 35, No.2, april 2007