ZAT 10u10 Pulmonale Hypertensie Marion DELCROIX -...
51
Pneumologie 2012 Pulmonale hypertensie Prof M. Delcroix Prof M. Delcroix
Transcript of ZAT 10u10 Pulmonale Hypertensie Marion DELCROIX -...

Pneumologie 2012
Pulmonale hypertensie
Prof M. DelcroixProf M. Delcroix

Pulmonale vs systeemcirculatie
PAP 5 x < SAP
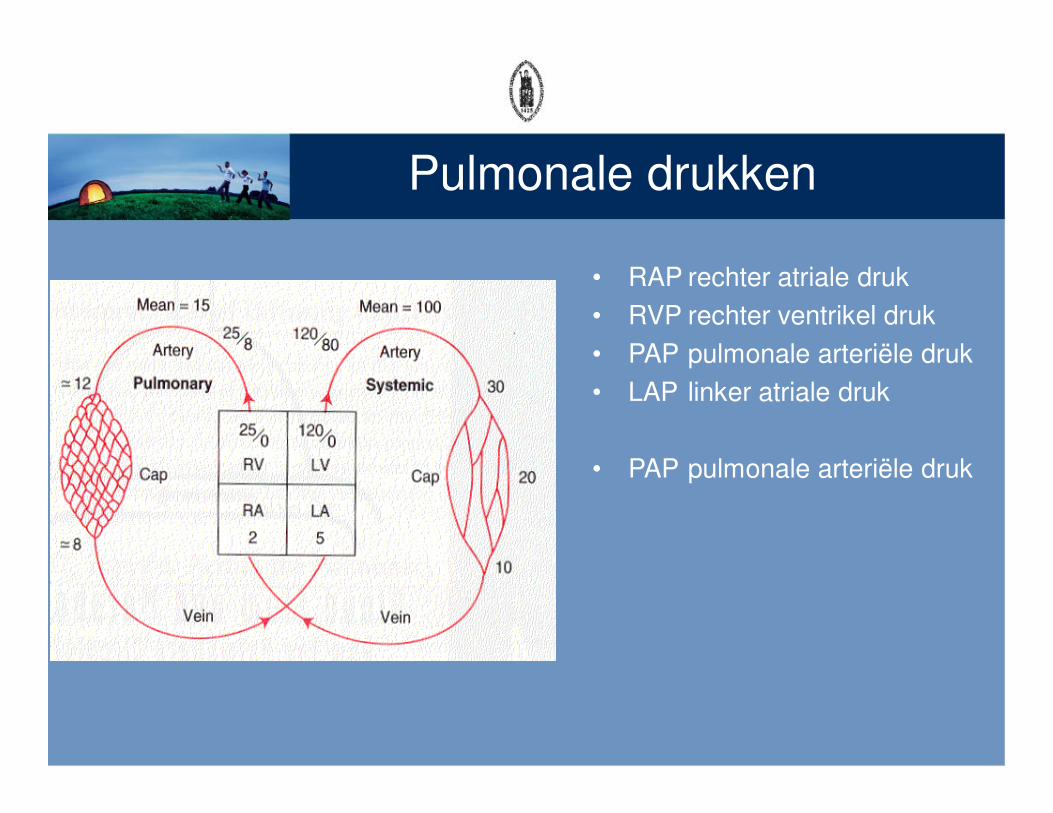
Pulmonale drukken
• RAP rechter atriale druk
• RVP rechter ventrikel druk
• PAP pulmonale arteriële druk
• LAP linker atriale druk
• PAP pulmonale arteriële druk
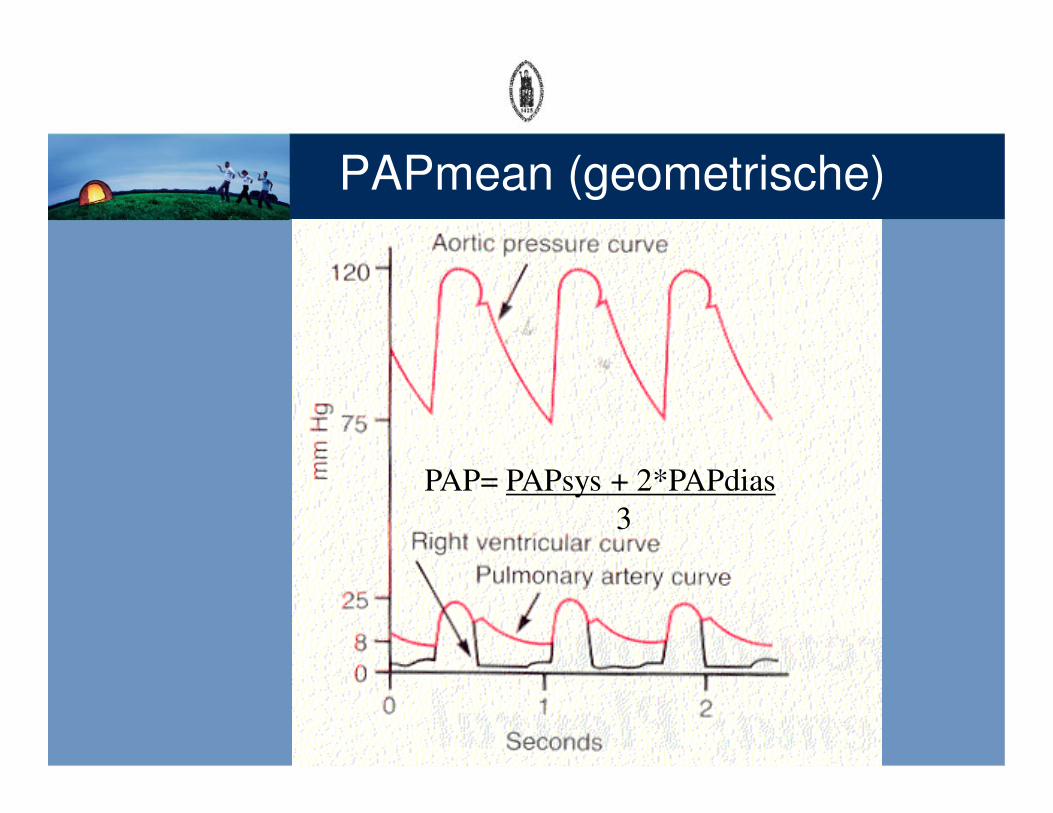
PAPmean (geometrische)
PAP= PAPsys + 2*PAPdias
3
Pulmonale vaatweerstand
• vaatweerstand = Pin-Pout stroom
• PVW = PAP-LAPCO
• PVW = 15 – 5 = 1.7 mmHg.L-1.min (WU)6 = 136 dyn.sec.cm-5 (*80)
• Wet van Poiseuille R = 8lη/π r4
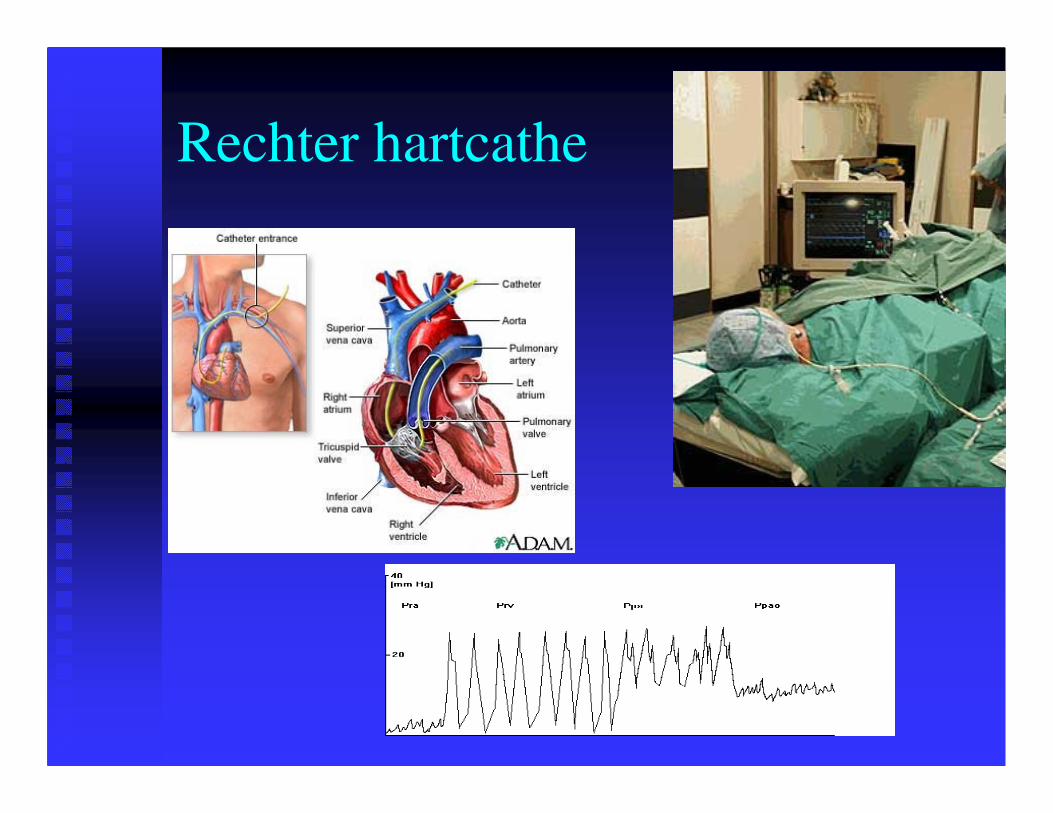
Rechter hartcathe
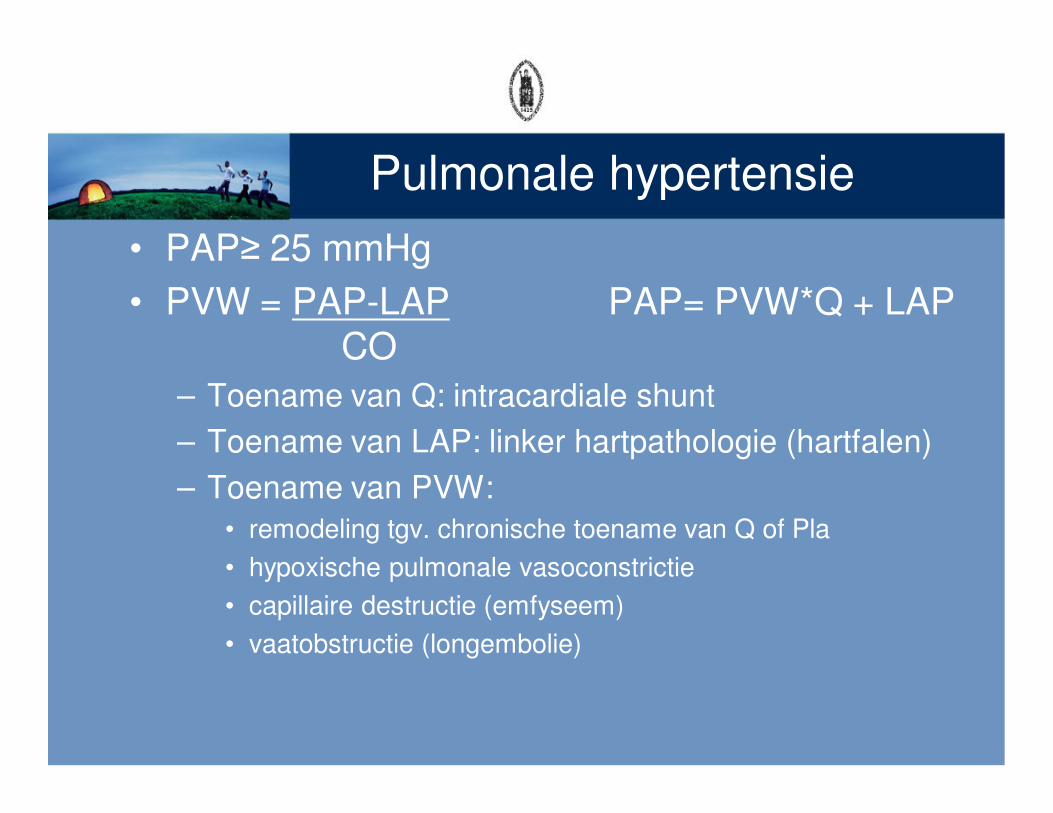
Pulmonale hypertensie
• PAP≥ 25 mmHg
• PVW = PAP-LAP PAP= PVW*Q + LAPCO
– Toename van Q: intracardiale shunt
– Toename van LAP: linker hartpathologie (hartfalen)
– Toename van PVW:
• remodeling tgv. chronische toename van Q of Pla
• hypoxische pulmonale vasoconstrictie
• capillaire destructie (emfyseem)
• vaatobstructie (longembolie)
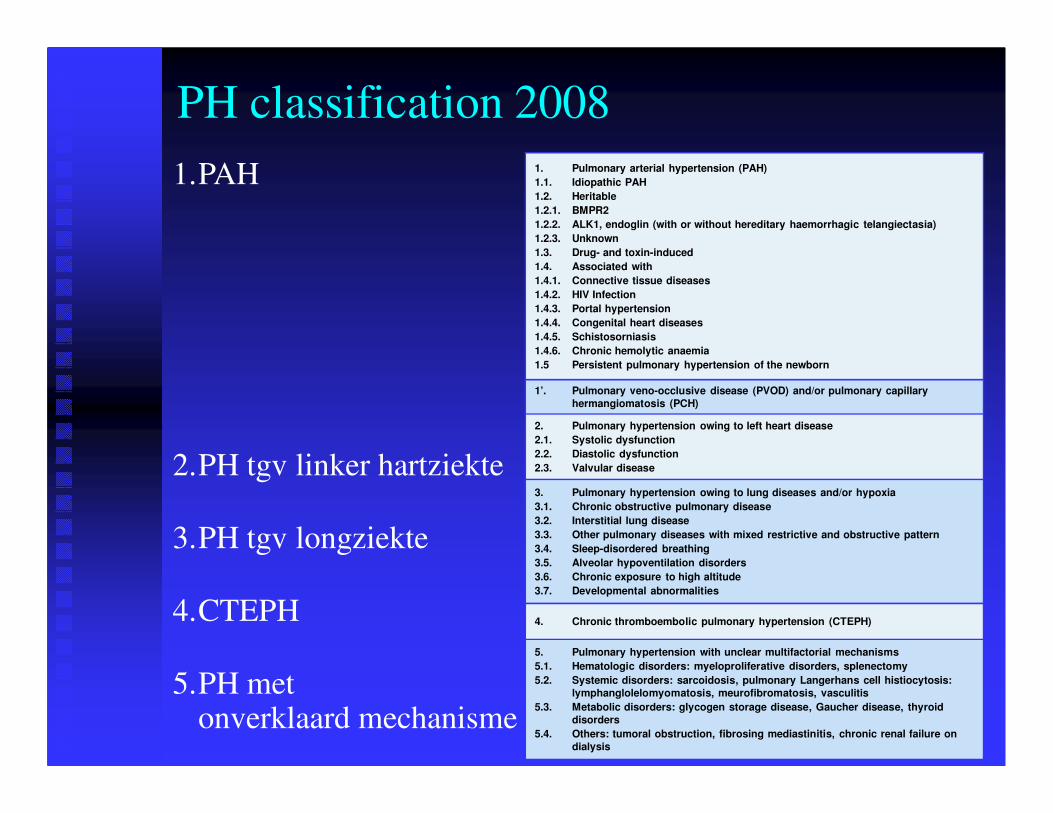
1. Pulmonary arterial hypertension (PAH)
1.1. Idiopathic PAH
1.2. Heritable
1.2.1. BMPR2
1.2.2. ALK1, endoglin (with or without hereditary haemorrhagic telangiectasia)
1.2.3. Unknown
1.3. Drug- and toxin-induced
1.4. Associated with
1.4.1. Connective tissue diseases
1.4.2. HIV Infection
1.4.3. Portal hypertension
1.4.4. Congenital heart diseases
1.4.5. Schistosorniasis
1.4.6. Chronic hemolytic anaemia
1.5 Persistent pulmonary hypertension of the newborn
1’. Pulmonary veno-occlusive disease (PVOD) and/or pulmonary capillary
hermangiomatosis (PCH)
2. Pulmonary hypertension owing to left heart disease
2.1. Systolic dysfunction
2.2. Diastolic dysfunction
2.3. Valvular disease
3. Pulmonary hypertension owing to lung diseases and/or hypoxia
3.1. Chronic obstructive pulmonary disease
3.2. Interstitial lung disease
3.3. Other pulmonary diseases with mixed restrictive and obstructive pattern
3.4. Sleep-disordered breathing
3.5. Alveolar hypoventilation disorders
3.6. Chronic exposure to high altitude
3.7. Developmental abnormalities
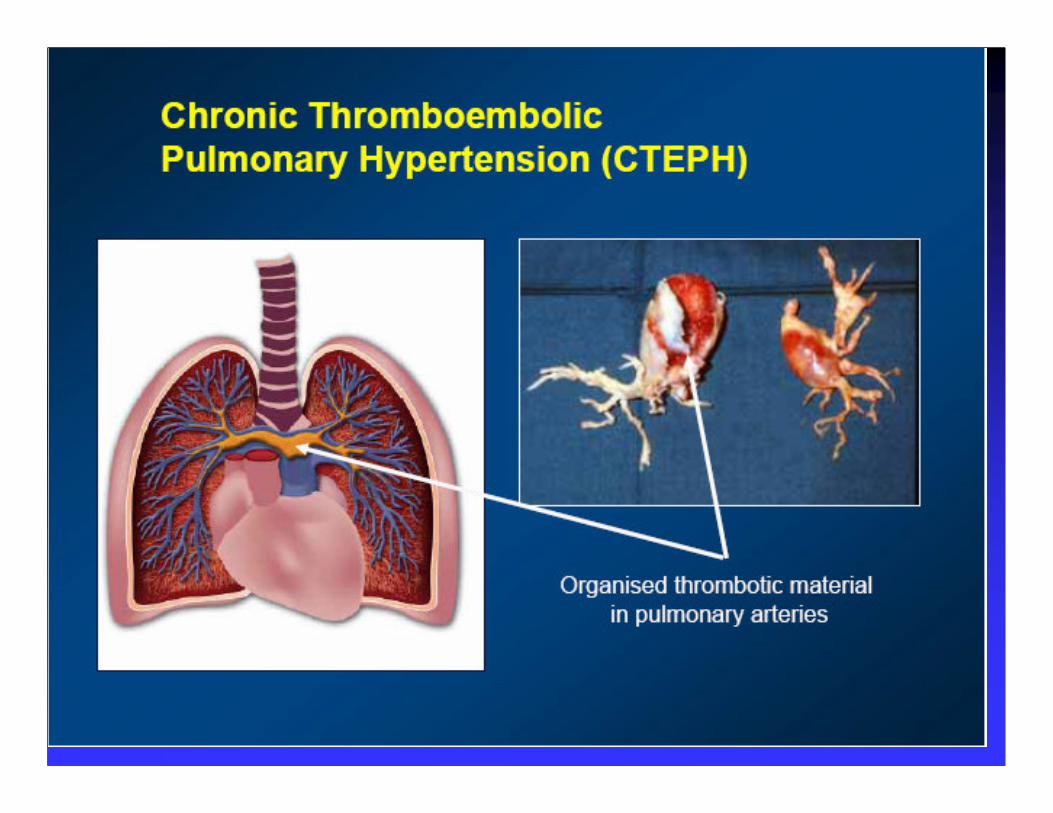
4. Chronic thromboembolic pulmonary hypertension (CTEPH)
5. Pulmonary hypertension with unclear multifactorial mechanisms
5.1. Hematologic disorders: myeloproliferative disorders, splenectomy
5.2. Systemic disorders: sarcoidosis, pulmonary Langerhans cell histiocytosis:
lymphanglolelomyomatosis, meurofibromatosis, vasculitis
5.3. Metabolic disorders: glycogen storage disease, Gaucher disease, thyroid
disorders
5.4. Others: tumoral obstruction, fibrosing mediastinitis, chronic renal failure on
dialysis
1.PAH
2.PH tgv linker hartziekte
3.PH tgv longziekte
4.CTEPH
5.PH met onverklaard mechanisme
PH classification 2008

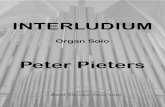
Hoe ontstaat PAH (1)?
�� de oppervlakkige laag van de oppervlakkige laag van
de vaten (het de vaten (het endotheelendotheel) )
wordt beschadigdwordt beschadigd
�� de de spiervezelsspiervezels in de wand in de wand
van de vaten prolifererenvan de vaten prolifereren
�� de de bloedplaatjesbloedplaatjes kleven kleven
aan de beschadigde aan de beschadigde
binnenkant van de vatenbinnenkant van de vaten
Progressieve afsluiting van de haarvatenProgressieve afsluiting van de haarvaten
REMODELING

Overbelasting van rechter hart
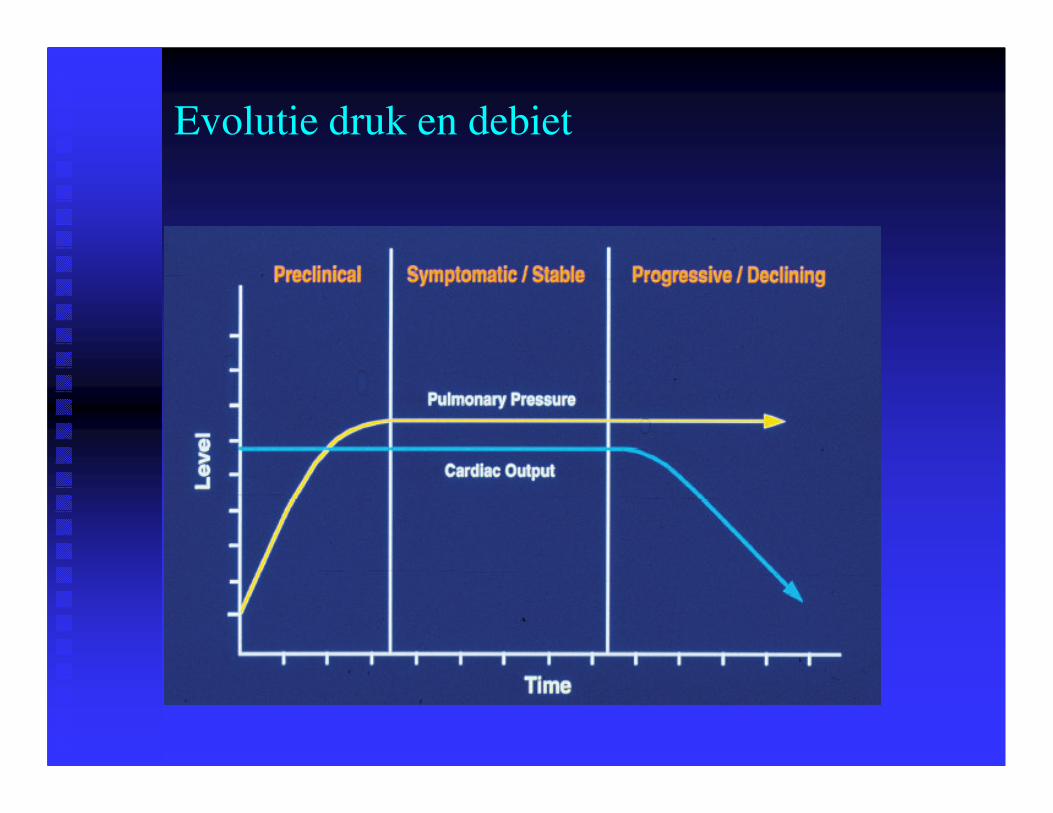
Evolutie druk en debiet
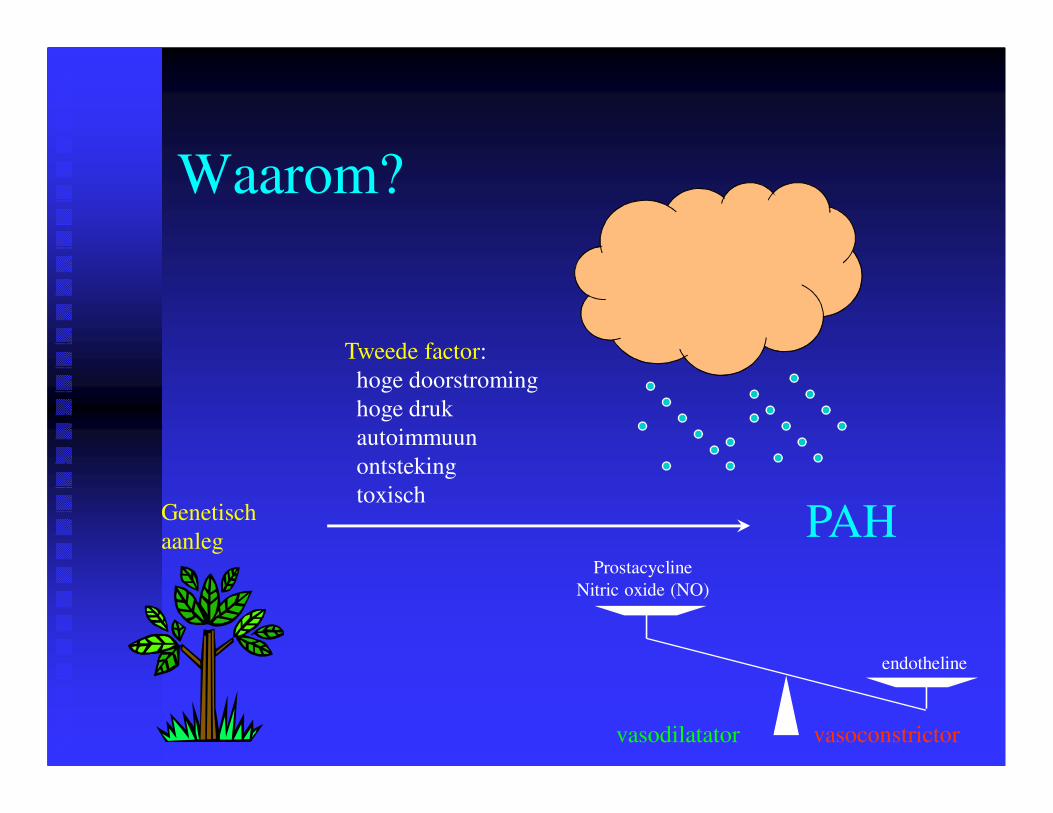
Waarom?
Genetisch
aanleg
Tweede factor:
hoge doorstroming
hoge druk
autoimmuun
ontsteking
toxisch
PAH
vasodilatator vasoconstrictor
Prostacycline
Nitric oxide (NO)
endotheline

Bindweefselziekten
�� SclerodermieSclerodermie
�� LupusLupus
�� ……

Sclerodermie
CREST

Aangeboren hartziekten
�� Atriaal septaal defect (ASD)Atriaal septaal defect (ASD)
�� Ventriculair septaal defect (VSD)Ventriculair septaal defect (VSD)
�� Open ductus Botalli (PDA: patent ductus Open ductus Botalli (PDA: patent ductus
arteriosus)arteriosus)
�� Meer complexeMeer complexe
��……

ASD

VSD
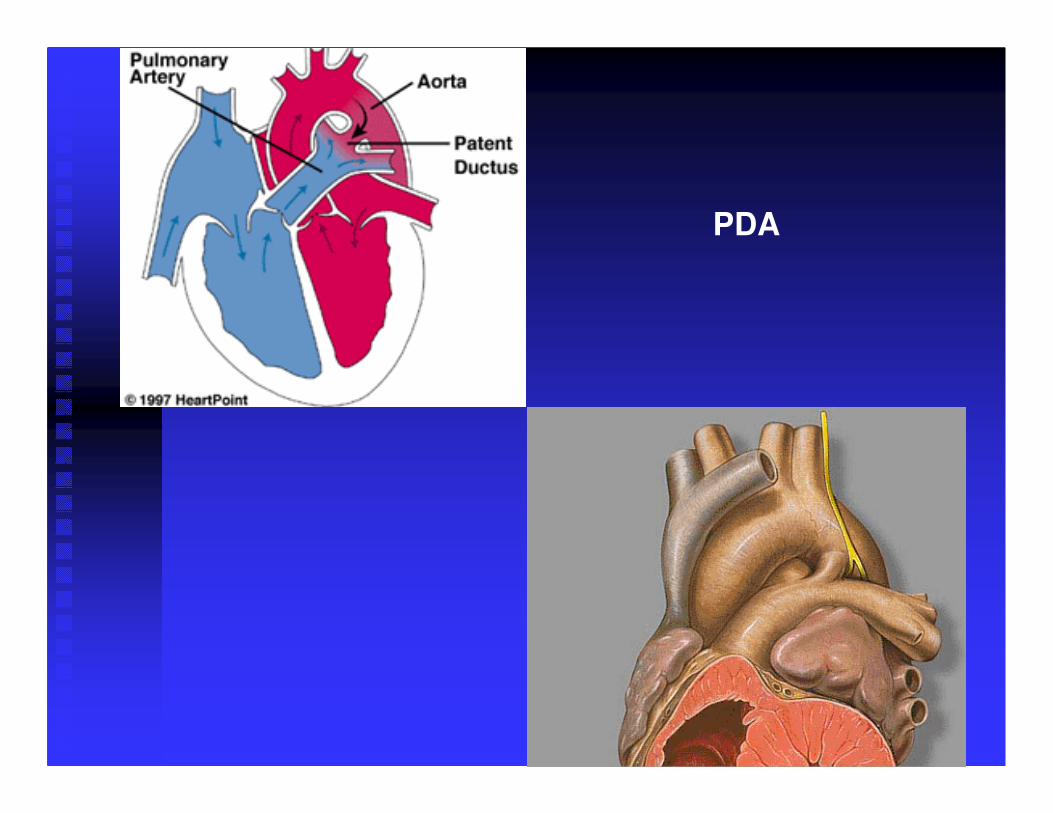
PDA
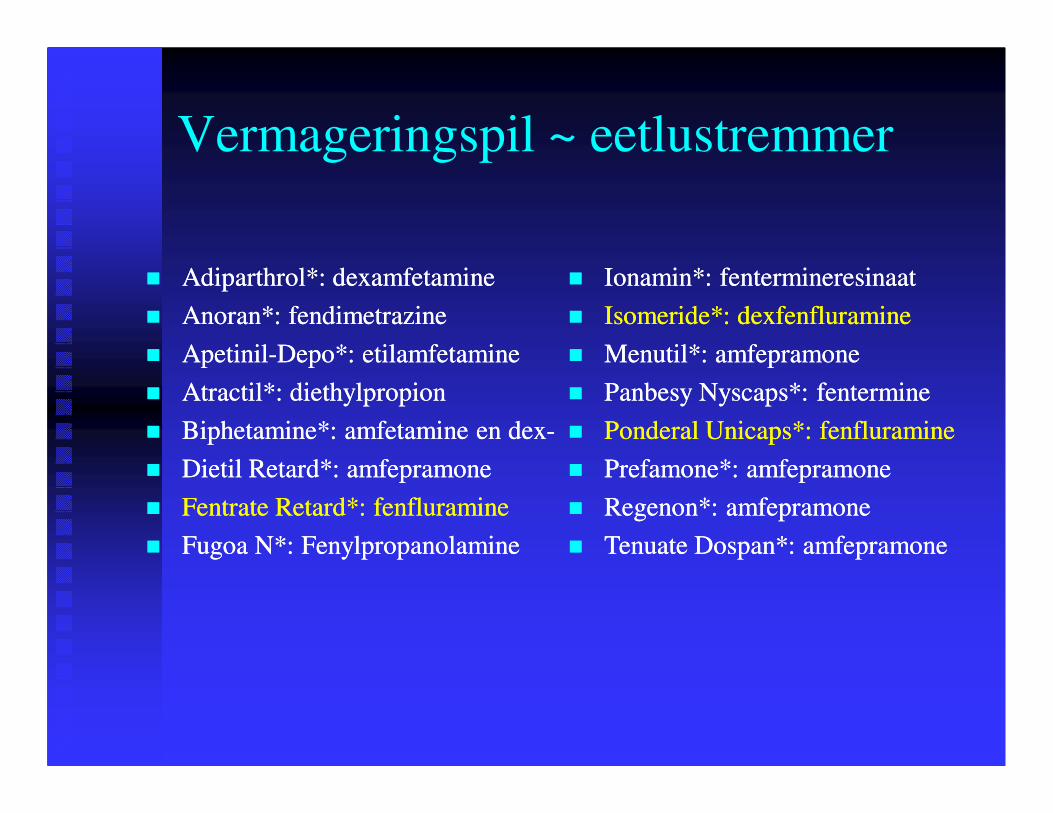
Vermageringspil ~ eetlustremmer
�� Adiparthrol*: dexamfetamineAdiparthrol*: dexamfetamine
�� Anoran*: fendimetrazineAnoran*: fendimetrazine
�� ApetinilApetinil--Depo*: etilamfetamineDepo*: etilamfetamine
�� Atractil*: diethylpropionAtractil*: diethylpropion
�� Biphetamine*: amfetamine en dexBiphetamine*: amfetamine en dex--
�� Dietil Retard*: amfepramoneDietil Retard*: amfepramone
�� Fentrate Retard*: fenfluramineFentrate Retard*: fenfluramine
�� Fugoa N*: FenylpropanolamineFugoa N*: Fenylpropanolamine
�� Ionamin*: fentermineresinaatIonamin*: fentermineresinaat
�� Isomeride*: dexfenfluramineIsomeride*: dexfenfluramine
�� Menutil*: amfepramoneMenutil*: amfepramone
�� Panbesy Nyscaps*: fenterminePanbesy Nyscaps*: fentermine
�� Ponderal Unicaps*: fenfluraminePonderal Unicaps*: fenfluramine
�� Prefamone*: amfepramonePrefamone*: amfepramone
�� Regenon*: amfepramoneRegenon*: amfepramone
�� Tenuate Dospan*: amfepramoneTenuate Dospan*: amfepramone
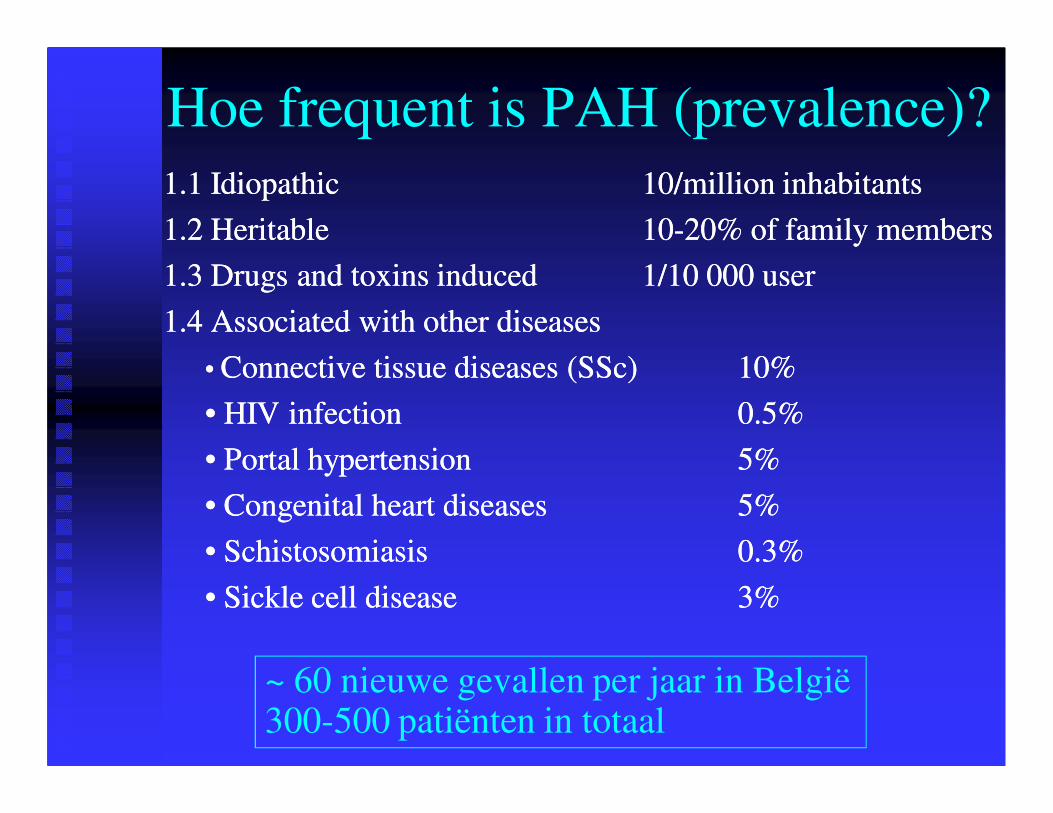
Hoe frequent is PAH (prevalence)?
1.1 Idiopathic1.1 Idiopathic 10/million inhabitants10/million inhabitants
1.2 Heritable 1.2 Heritable 1010--20% of family members20% of family members
1.3 Drugs and toxins induced 1.3 Drugs and toxins induced 1/10 000 user1/10 000 user
1.4 Associated with other diseases1.4 Associated with other diseases
• • Connective tissue diseases (SSc) Connective tissue diseases (SSc) 10%10%
• HIV infection • HIV infection 0.5%0.5%
• Portal hypertension• Portal hypertension 5%5%
• Congenital heart diseases• Congenital heart diseases 5%5%
• Schistosomiasis• Schistosomiasis 0.3%0.3%
• Sickle cell disease• Sickle cell disease 3%3%
~ 60 nieuwe gevallen per jaar in België300-500 patiënten in totaal

Hoe ontstaat PH tgv hartziekten (2)?
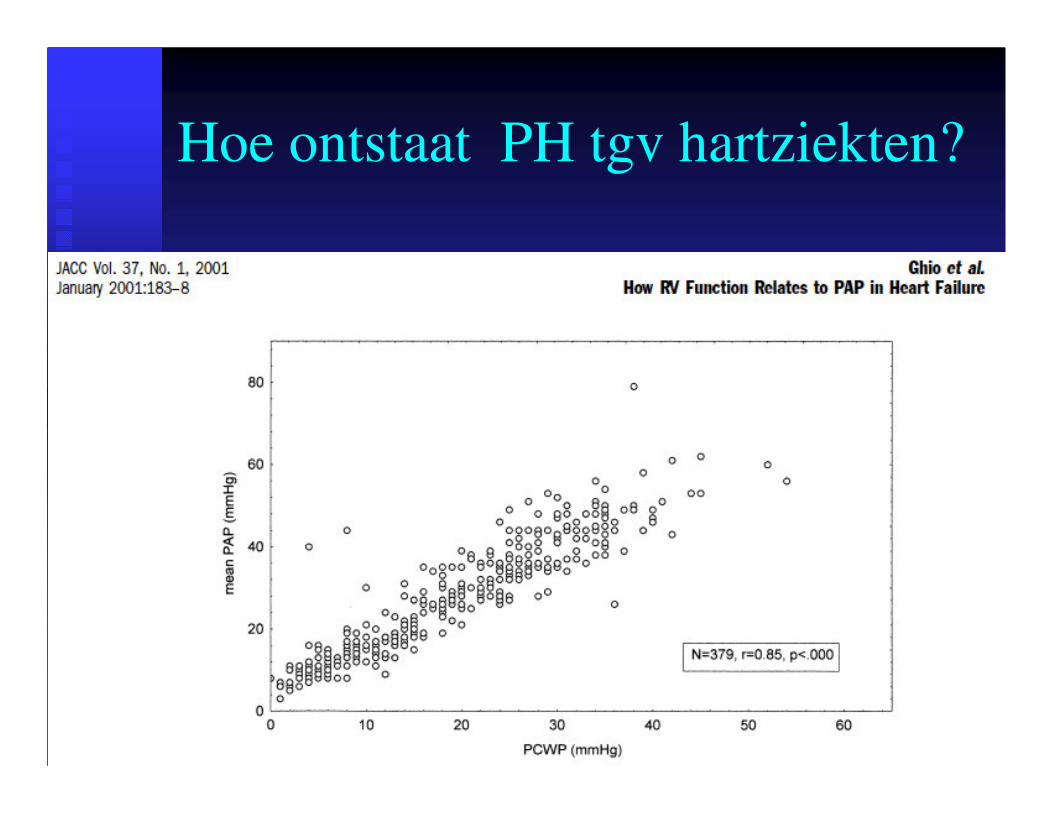
Hoe ontstaat PH tgv hartziekten?
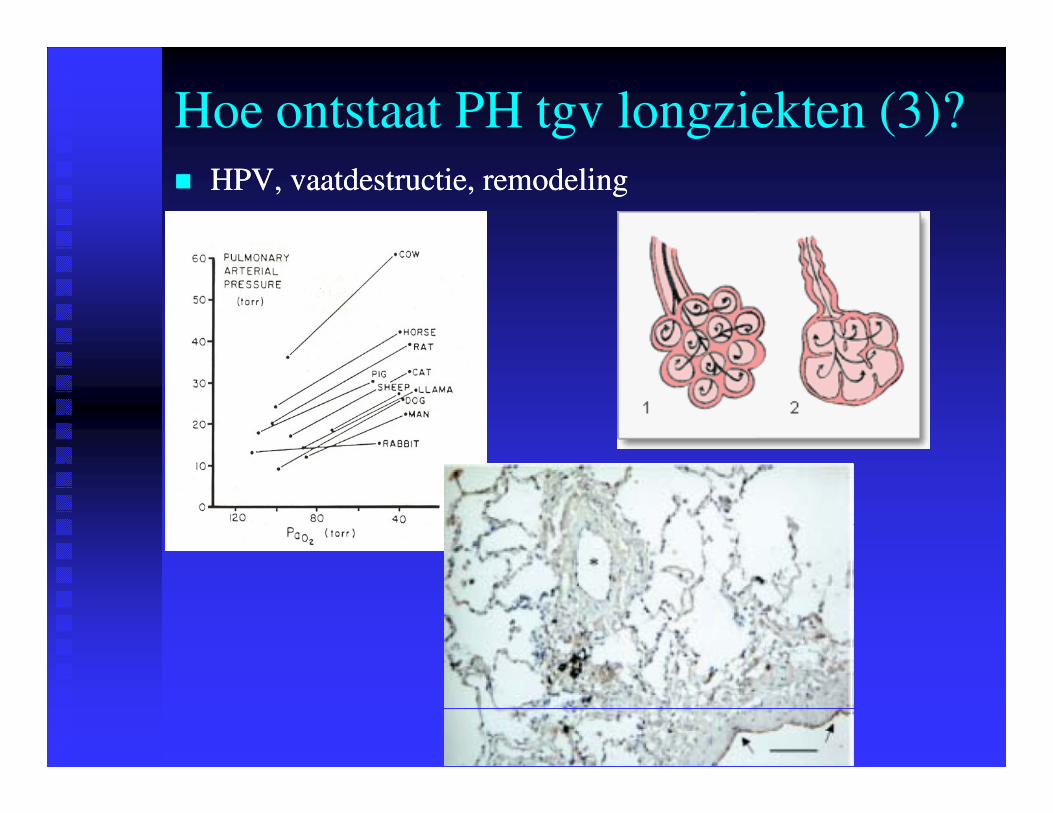
Hoe ontstaat PH tgv longziekten (3)?
�� HPV, vaatdestructie, remodelingHPV, vaatdestructie, remodeling
Hoe frequent is PH (prevalence)?
2. Tgv linker 2. Tgv linker hartziektenhartziekten
��26% 26% bijbij cardiomyopathie (cardiomyopathie (AbramsonAbramson 19921992))
��60% 60% bijbij systolischesystolische dysfunctiedysfunctie ((GhioGhio 20012001))
��80% 80% bijbij bewaardebewaarde LVEF (LVEF (LamLam 20092009))
3. Tgv 3. Tgv longziektenlongziekten
��30% 30% bijbij COPD COPD transplantkandidatentransplantkandidaten ((CutticaCuttica 20102010))
50.000 tot 100.000 patiënten in België
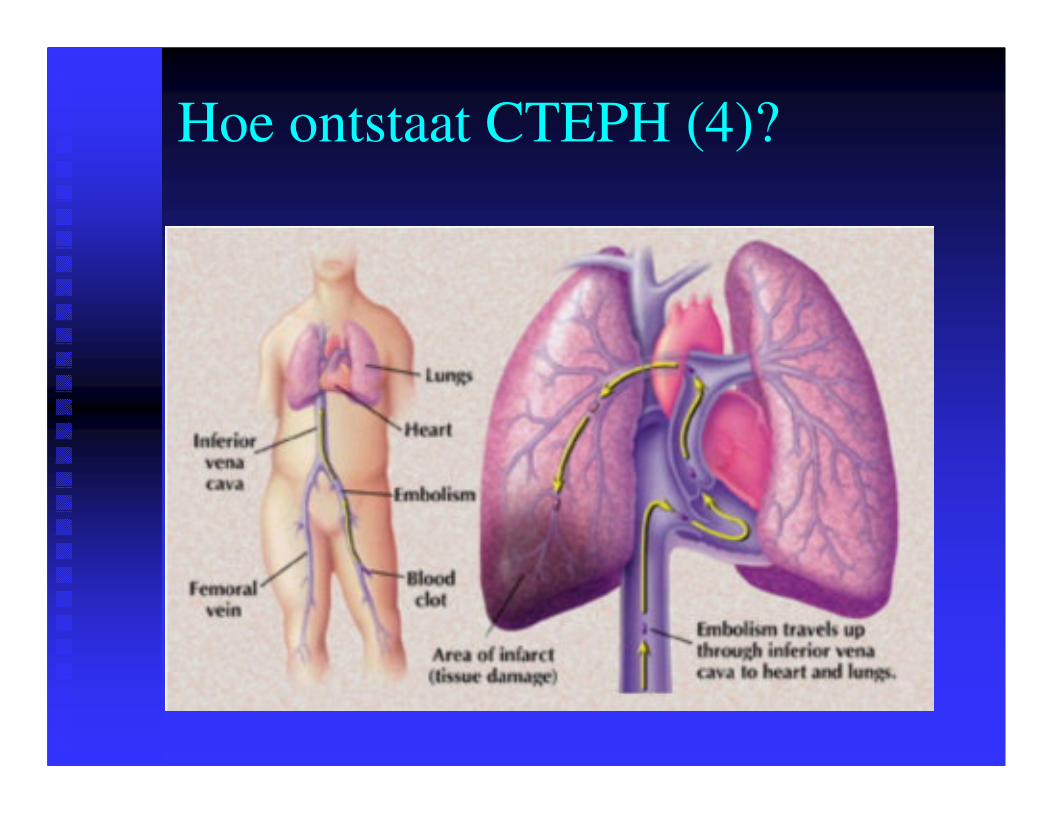
Hoe ontstaat CTEPH (4)?
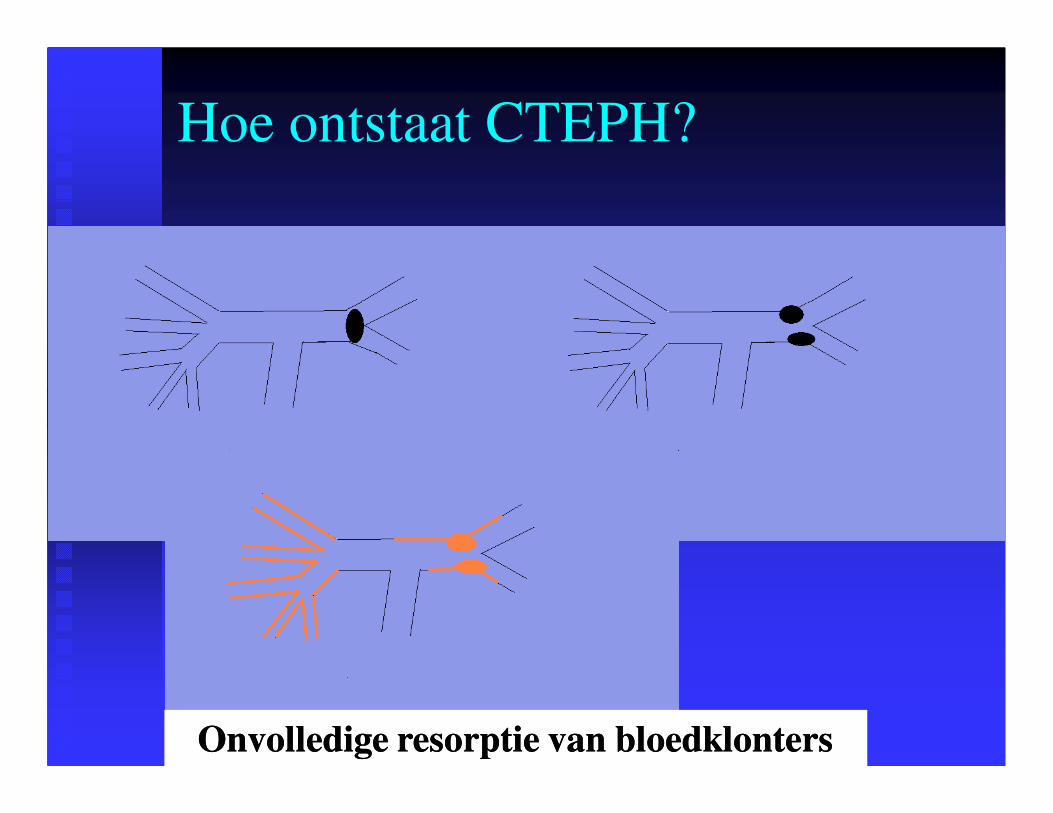
Hoe ontstaat CTEPH?
Onvolledige resorptie van bloedklonters Onvolledige resorptie van bloedklonters
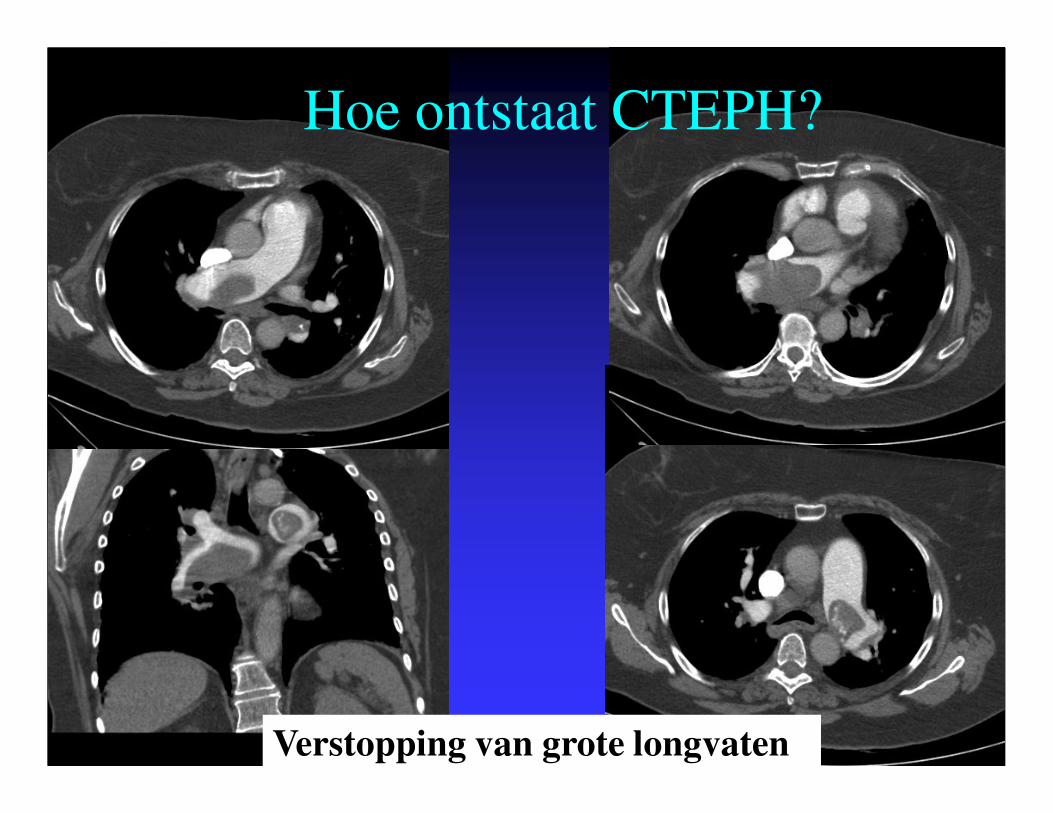
Hoe ontstaat CTEPH?
Verstopping van grote longvaten
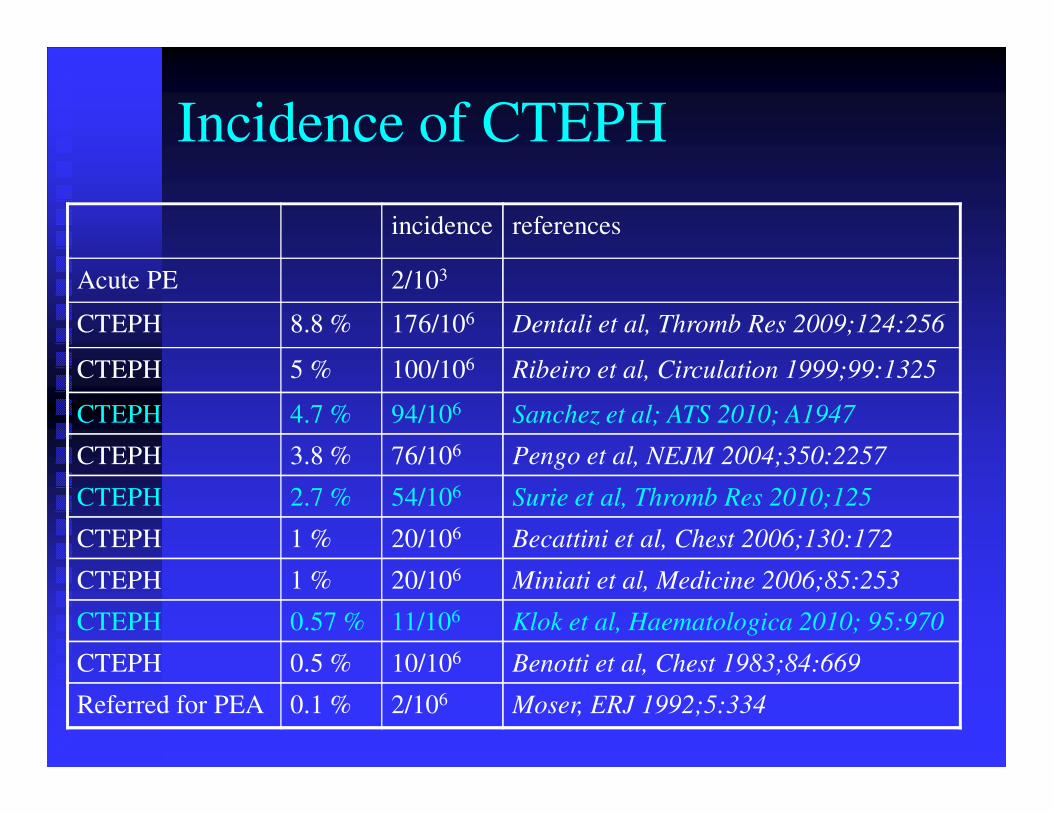
Incidence of CTEPH
incidence references
Acute PE 2/103
CTEPH 8.8 % 176/106 Dentali et al, Thromb Res 2009;124:256
CTEPH 5 % 100/106 Ribeiro et al, Circulation 1999;99:1325
CTEPH 4.7 % 94/106 Sanchez et al; ATS 2010; A1947
CTEPH 3.8 % 76/106 Pengo et al, NEJM 2004;350:2257
CTEPH 2.7 % 54/106 Surie et al, Thromb Res 2010;125
CTEPH 1 % 20/106 Becattini et al, Chest 2006;130:172
CTEPH 1 % 20/106 Miniati et al, Medicine 2006;85:253
CTEPH 0.57 % 11/106 Klok et al, Haematologica 2010; 95:970
CTEPH 0.5 % 10/106 Benotti et al, Chest 1983;84:669
Referred for PEA 0.1 % 2/106 Moser, ERJ 1992;5:334

Klachten
�� ~ 40 jaar (1~ 40 jaar (1--70)70)
�� niet specifiek en onopvallendniet specifiek en onopvallend
�� waardoor laattijdige diagnosewaardoor laattijdige diagnose
��±± 2 jaar na de eerste klachten2 jaar na de eerste klachten
�� Meest voorkomende klachten:Meest voorkomende klachten:�� kortademigheidkortademigheid 98%98%
�� vermoeidheidvermoeidheid 73%73%
�� thoracale pijnthoracale pijn 46%46%
�� syncopesyncope 41% 41%
�� oedemenoedemen 36%36%
�� hartkloppingenhartkloppingen 31%31%
�� RaynaudRaynaud 14%14%
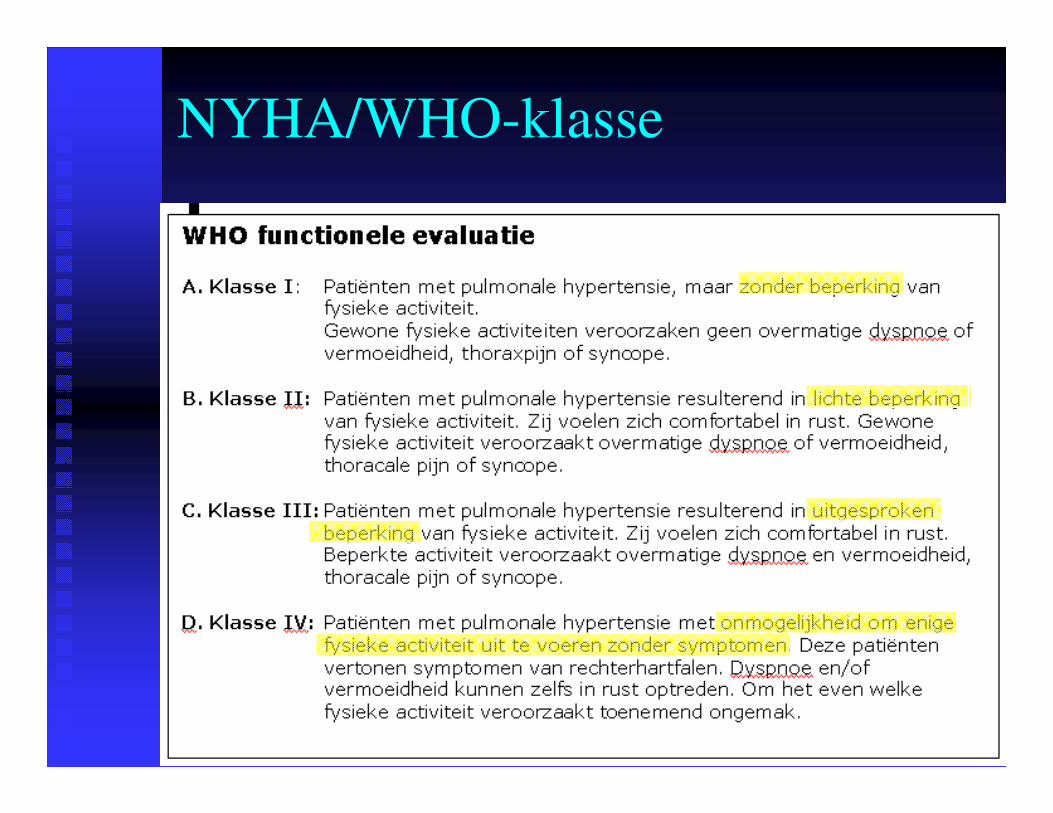
NYHA/WHO-klasse
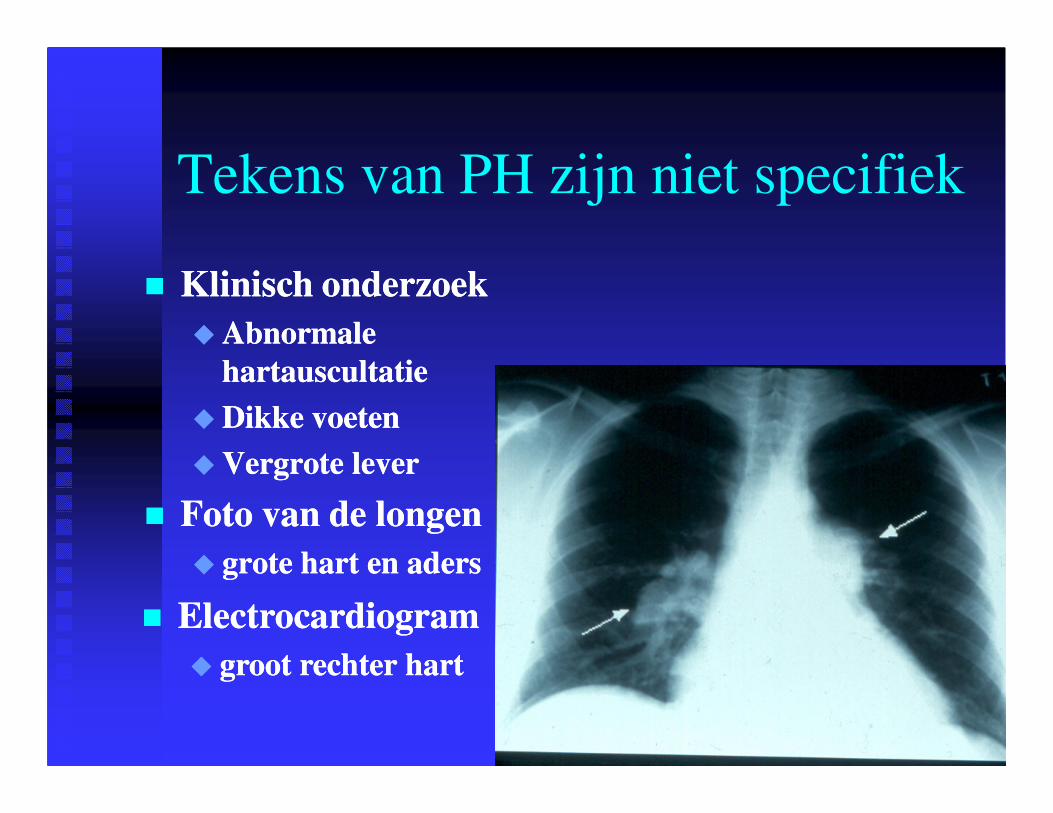
Tekens van PH zijn niet specifiek
�� Klinisch onderzoekKlinisch onderzoek
�� Abnormale Abnormale
hartauscultatiehartauscultatie
�� Dikke voetenDikke voeten
�� Vergrote leverVergrote lever
�� Foto van de longenFoto van de longen
�� grote hart en adersgrote hart en aders
�� ElectrocardiogramElectrocardiogram
�� groot rechter hartgroot rechter hart
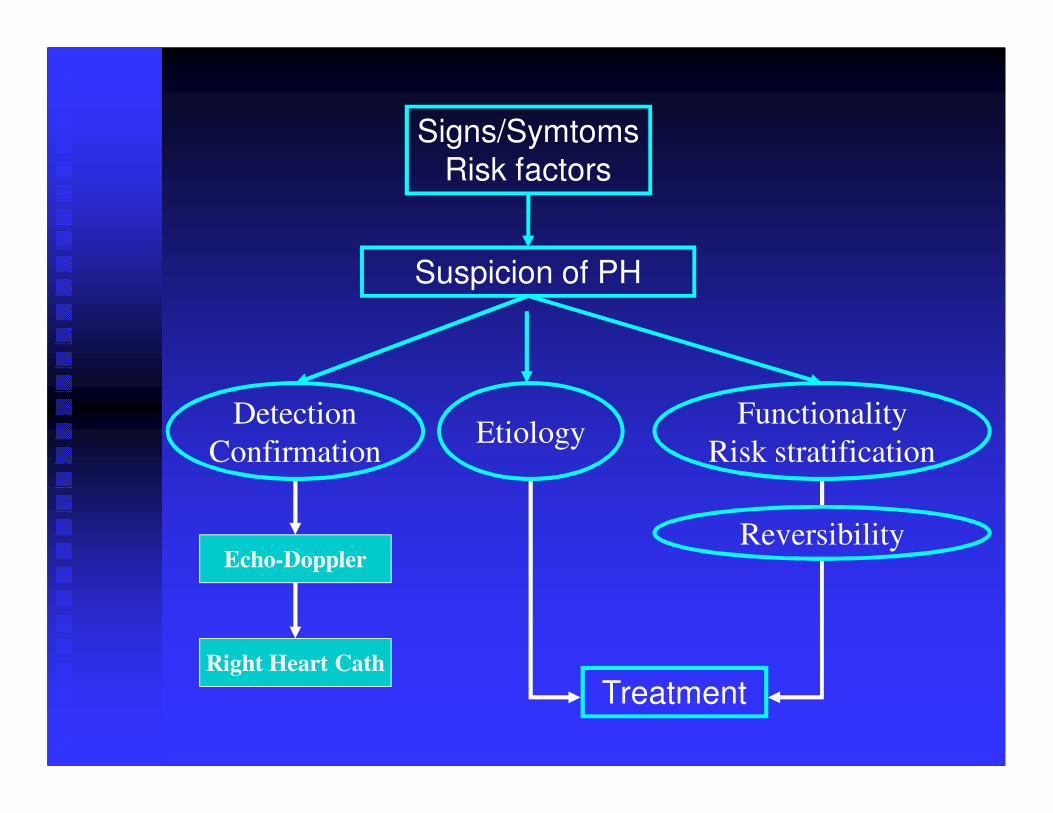
Signs/Symtoms
Risk factors
Suspicion of PH
Detection
ConfirmationEtiology
Functionality
Risk stratification
Echo-Doppler
Right Heart Cath
Treatment
Reversibility
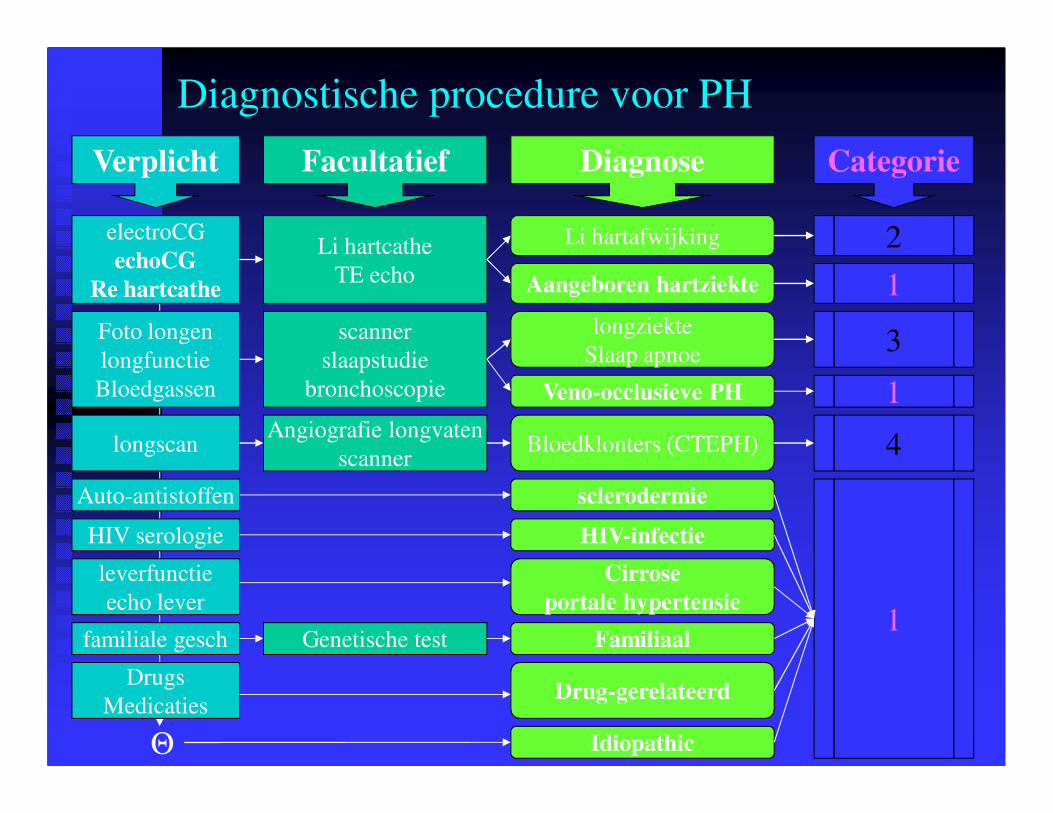
Diagnostische procedure voor PH
Verplicht Facultatief Diagnose Categorie
Foto longen
longfunctie
Bloedgassen
scanner
slaapstudie
bronchoscopie
longziekte
Slaap apnoe
Veno-occlusieve PH
3
1
electroCG
echoCG
Re hartcathe
Li hartafwijking 2Li hartcathe
TE echo Aangeboren hartziekte 1
Bloedklonters (CTEPH)longscanAngiografie longvaten
scanner4
Θ Idiopathic
1
leverfunctie
echo lever
familiale gesch
Drugs
Medicaties
Genetische test
sclerodermie
HIV-infectie
Familiaal
Drug-gerelateerd
Cirrose
portale hypertensie
HIV serologie
Auto-antistoffen
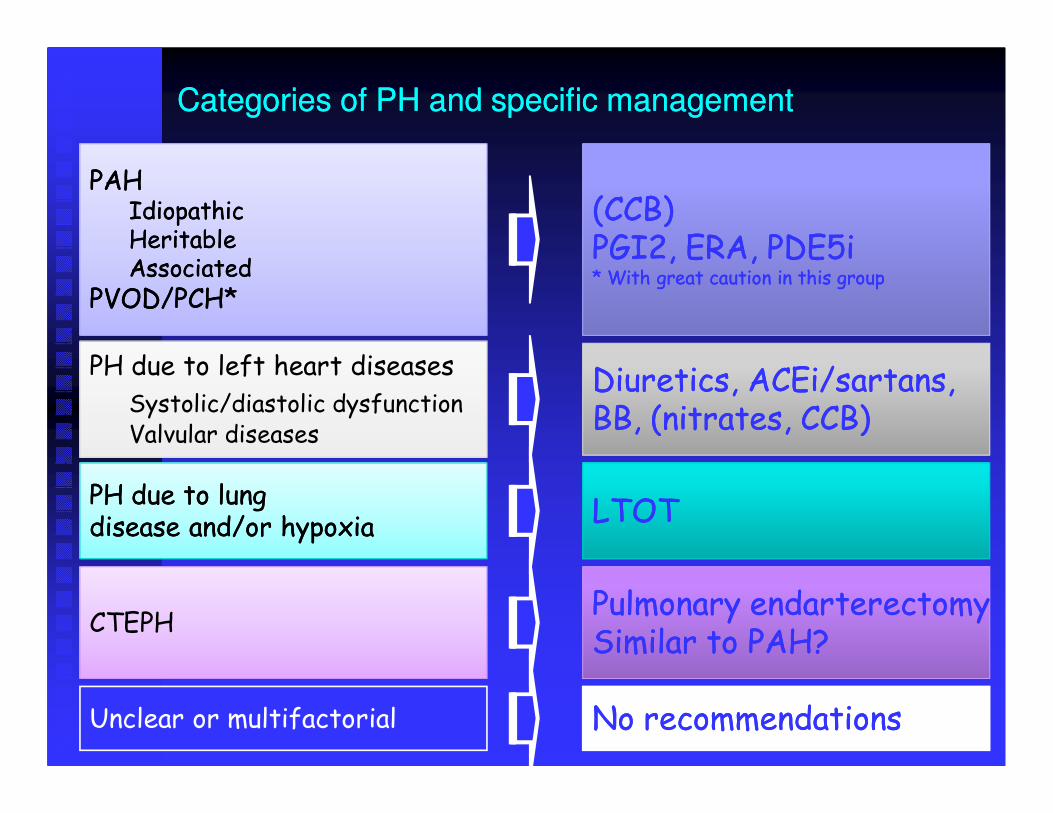
Categories of PH and specific managementCategories of PH and specific management
PAHPAHIdiopathicIdiopathicHeritableHeritableAssociatedAssociated
PVOD/PCH*PVOD/PCH*
PH due to left heart diseases
Systolic/diastolic dysfunctionValvular diseases
PH due to lung PH due to lung disease and/or hypoxiadisease and/or hypoxia
CTEPH
Unclear or multifactorial
(CCB)(CCB)PGI2, ERA, PDE5iPGI2, ERA, PDE5i* With great caution in this group* With great caution in this group
Diuretics, ACEi/sartans,Diuretics, ACEi/sartans,BB, (nitrates, CCB)BB, (nitrates, CCB)
LTOTLTOT
Pulmonary endarterectomyPulmonary endarterectomyPulmonary endarterectomyPulmonary endarterectomySimilar to PAH?Similar to PAH?
No recommendationsNo recommendations

Wat is de impact van PH?
�� PrognosePrognose
�� IIPPAAH H �� jonge volwassenen met een jonge volwassenen met een gemiddelde leeftijd gemiddelde leeftijd van van 40 jaar40 jaar
�� ook kinderenook kinderen
�� levensgevaarlijk met een levensgevaarlijk met een gemiddelde overleving gemiddelde overleving vanvan 2.2.88 jaar jaar
�� PAHPAH�� aangeboren hartafwijkingen: wat betere prognoseaangeboren hartafwijkingen: wat betere prognose
�� sclerodermie: wat slechtere prognosesclerodermie: wat slechtere prognose
�� PH tgv hartPH tgv hart-- en longziektenen longziekten�� Aanwezigheid van PH verslechtert prognose Aanwezigheid van PH verslechtert prognose
�� CTCTEPHEPH�� prognose afhankelijk van de pulmonale drukkenprognose afhankelijk van de pulmonale drukken
�� PpaPpa > > 5050 mmHgmmHg: 5 jaar: 5 jaar--overleving overleving 1010%%

Treatment algorythm (general measures)
ESC guidelines 2009
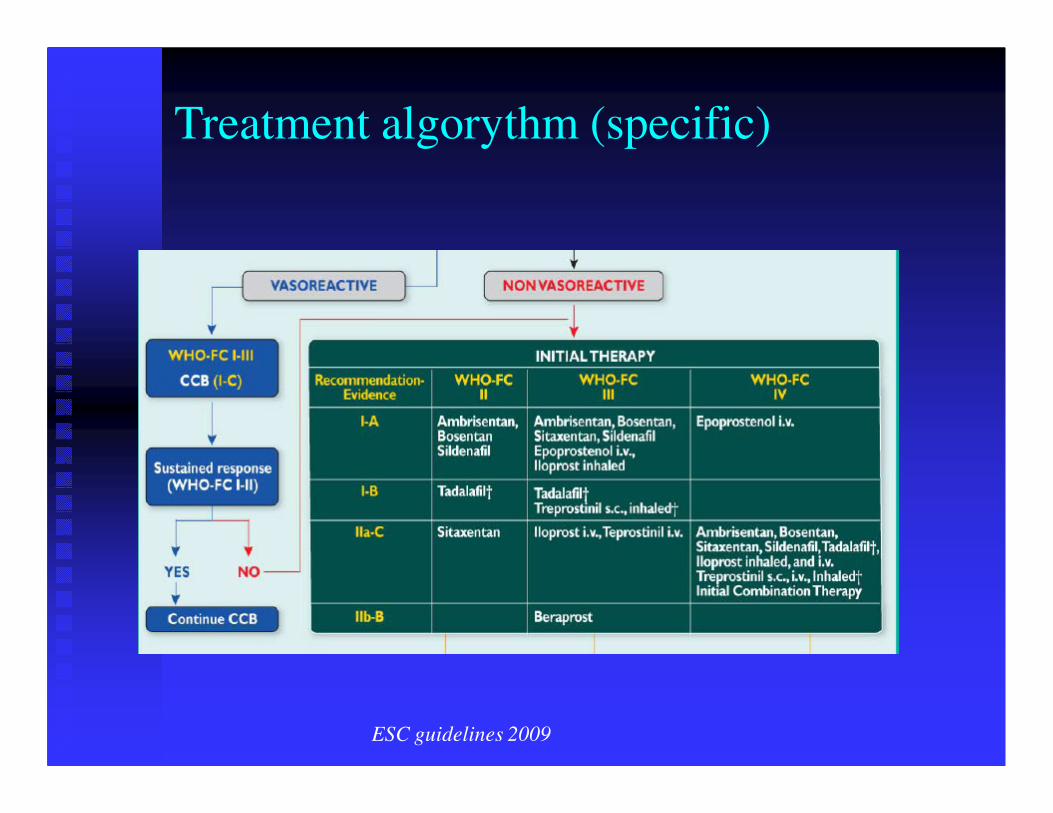
Treatment algorythm (specific)
ESC guidelines 2009
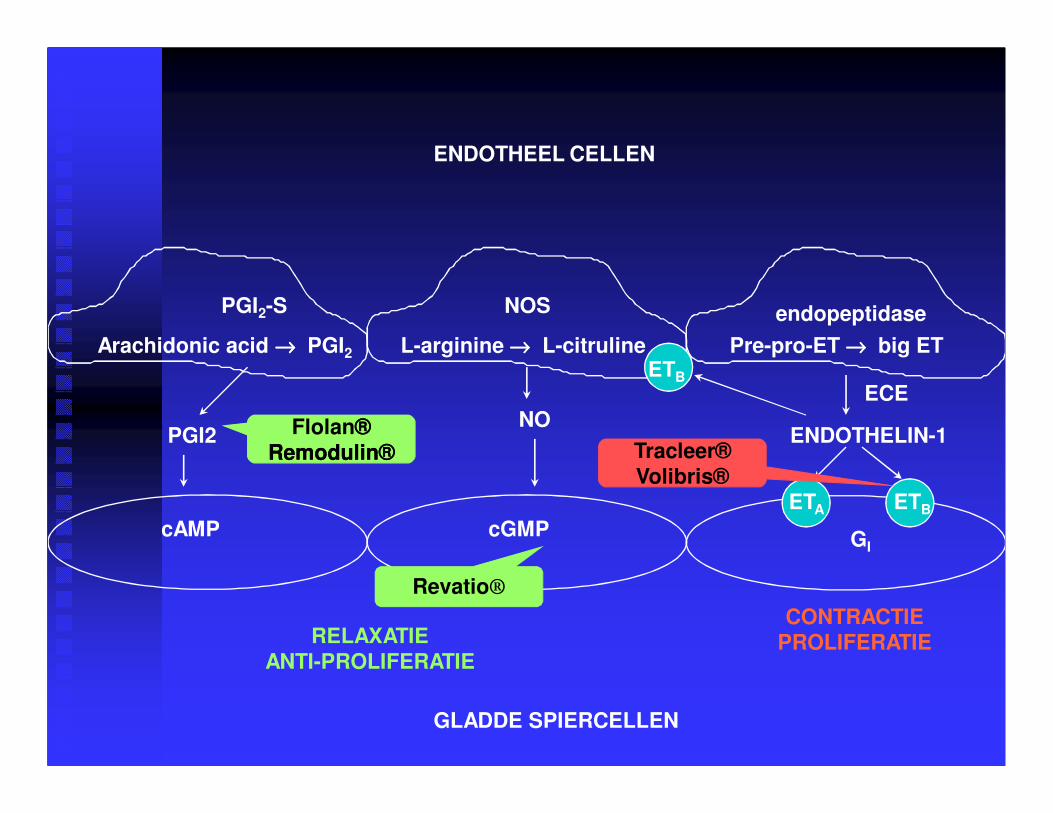
ENDOTHEEL CELLEN
GLADDE SPIERCELLEN
NOS
NO
cGMP
RELAXATIEANTI-PROLIFERATIE
PGI2
cAMP
ENDOTHELIN-1
CONTRACTIEPROLIFERATIE
ETA ETB
GI
Pre-pro-ET →→→→ big ET ETB
ECE
L-arginine →→→→ L-citruline Arachidonic acid →→→→ PGI2
PGI2-S
Flolan®®Remodulin®Remodulin®
Revatio®
Tracleer®Volibris®
endopeptidase
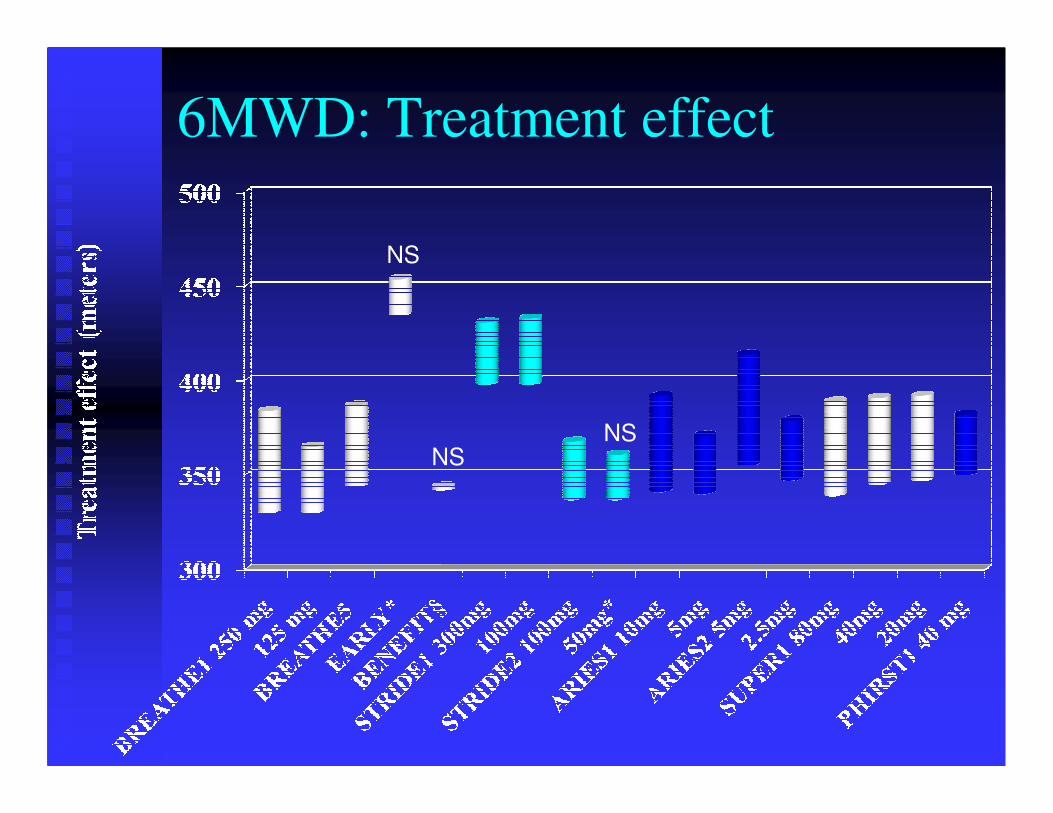
6MWD: Treatment effect
NS
NSNS
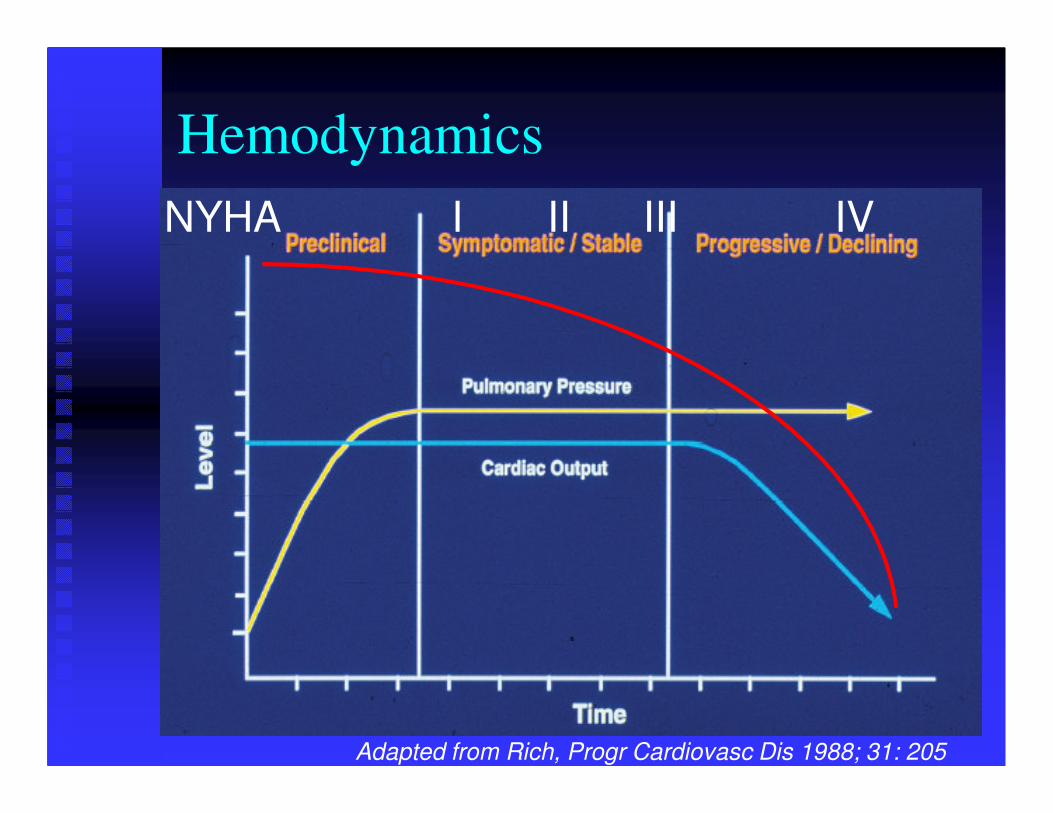
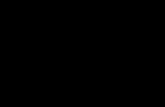
Hemodynamics
NYHA I II III IV
Adapted from Rich, Progr Cardiovasc Dis 1988; 31: 205
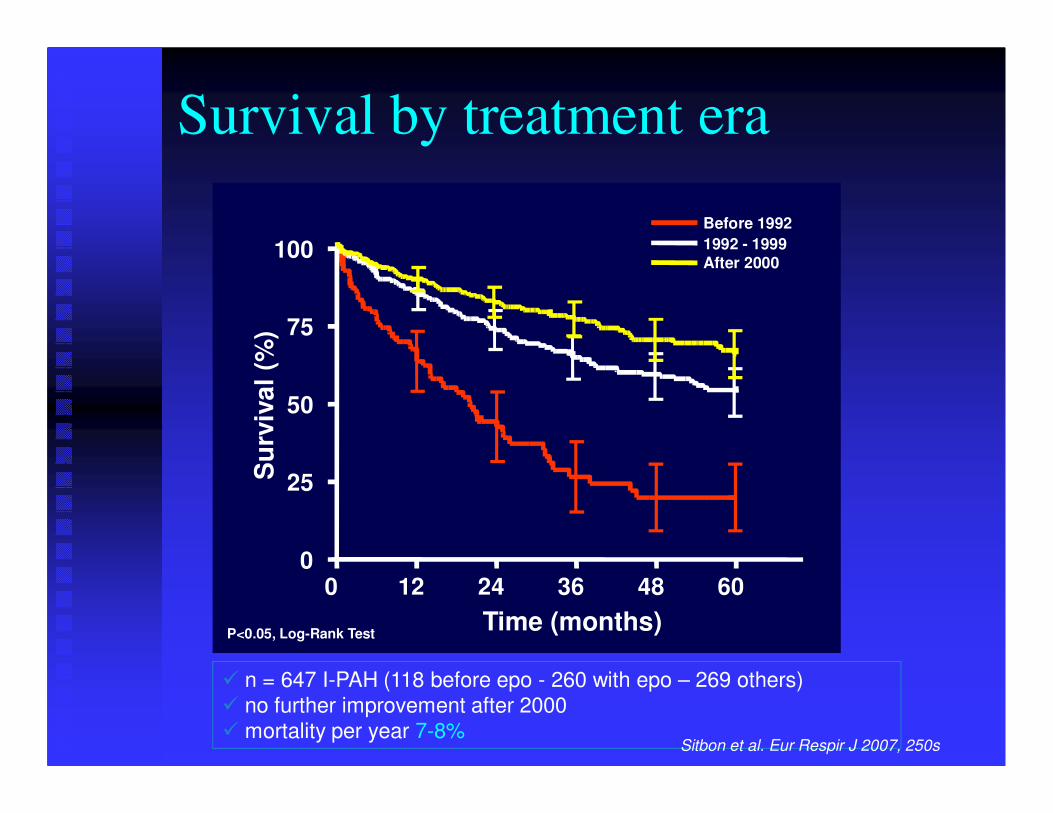
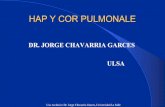
Survival by treatment era
0 12 24 36 48 600
25
50
75
100
Before 1992
1992 - 1999After 2000
Time (months)
Su
rviv
al
(%)
P<0.05, Log-Rank Test
� n = 647 I-PAH (118 before epo - 260 with epo – 269 others)� no further improvement after 2000� mortality per year 7-8%
Sitbon et al. Eur Respir J 2007, 250s
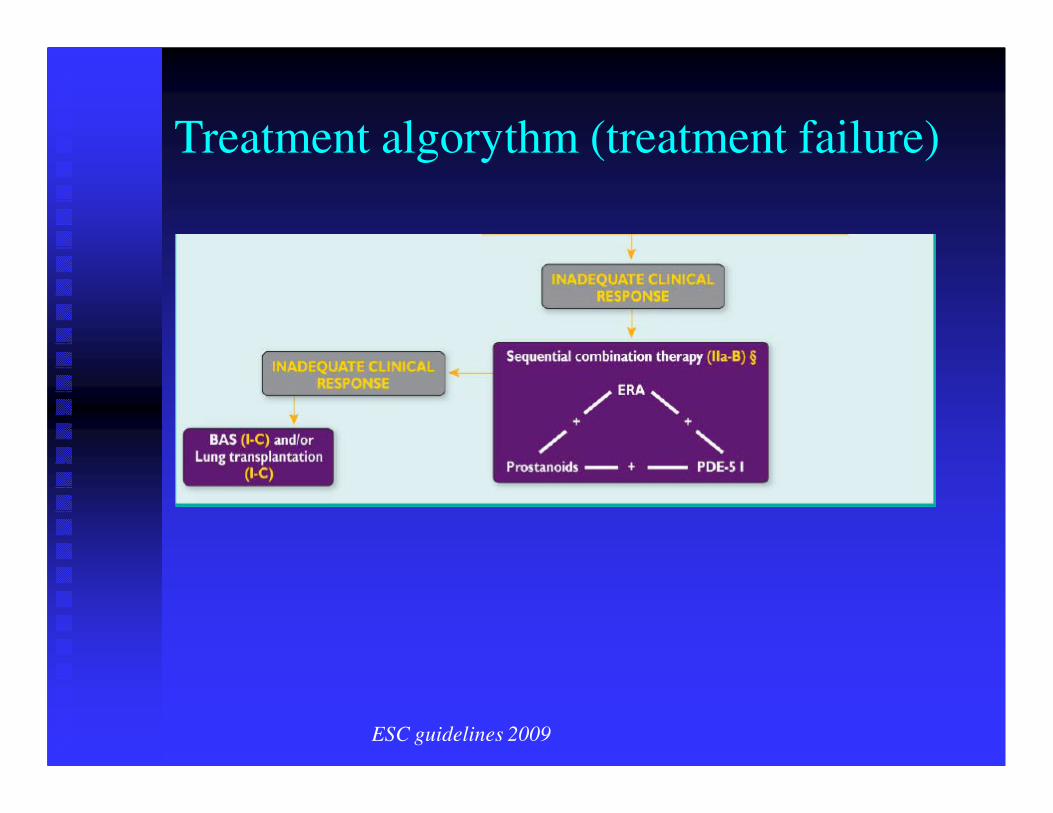
Treatment algorythm (treatment failure)
ESC guidelines 2009

Atriale septostomie
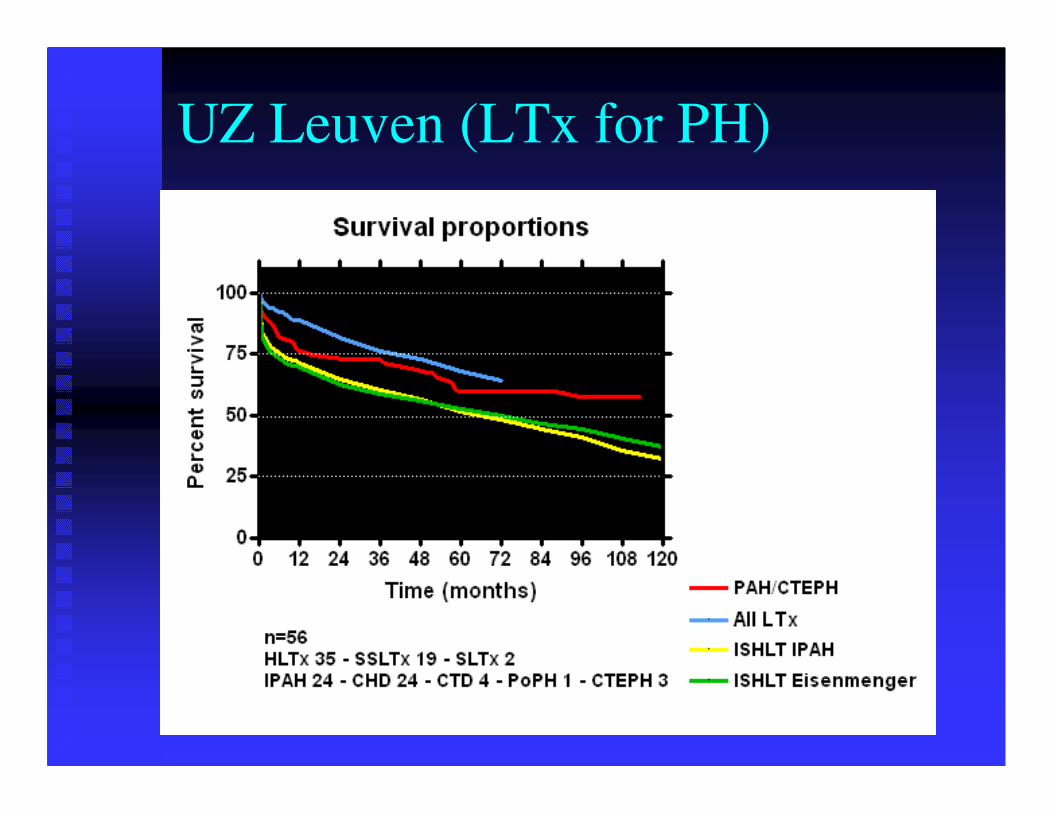
UZ Leuven (LTx for PH)
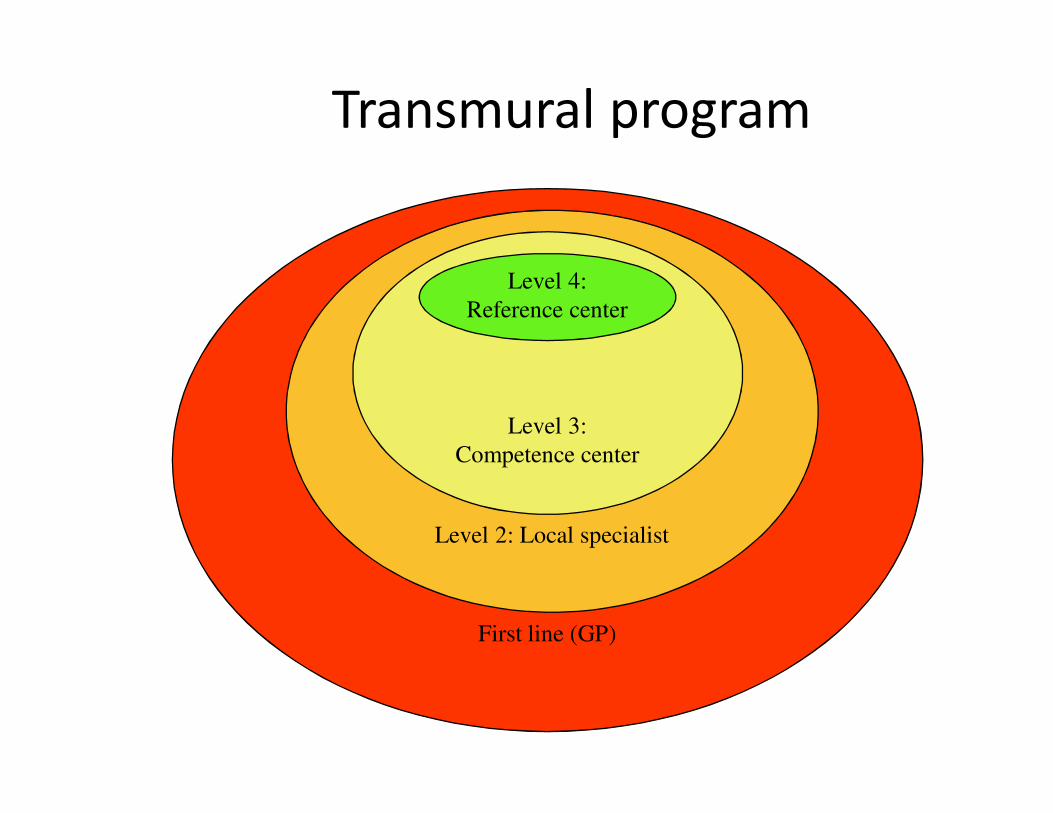
First line (GP)
Level 2: Local specialist
Level 3:
Competence center
Level 4:
Reference center
Transmural program
eerste lijn (huisartsen)
Niveau 3: tweede lijn
Niveau 2:
tweede en derde lijn
Niveau 1:
referentiecentrum
General practitioner
Detection of first symptoms
- dyspnea, …
Fine tuning of therapy
- OA
- Diuretics
Control of LFT for ERAs
Level 2: Local specialist
Diagnosis
Therapy for AE
- Holter for arrhythmias
- Emergency admissions
Oxygen reimbursement if needed
Level 3: Competence center
Confirmation of diagnosis
- Reversibility testing (NO)
First line therapy (oral drugs)
Combination therapy (PO)
Level 4: Reference center
� Offer all therapeutic approaches
� First line therapy (PO)
� Parenteral prostacyclines (NYHA III-IV)
� New drugs
� in trials, compassionate use, BSF-FSS
� oral PGI2, VIP, sGC, TKI
� Atrial septostomy
� (heart)-lung transplantation
� Pulmonary (thrombo)-endarterectomy