Spirometrie in de Huisartspraktijk -...
88
Spirometrie in de Huisartspraktijk Johan Buffels, MD, PhD Jan Degryse, MD, PhD
Transcript of Spirometrie in de Huisartspraktijk -...
Spirometrie in de
Huisartspraktijk
Johan Buffels, MD, PhD
Jan Degryse, MD, PhD
Spirometrie in huisartspraktijk
• Indicaties voor “office spirometry”
• Voorwaarden voor kwaliteit
• Mogelijke hinderpalen?
• Zelf uitvoeren of andere mogelijkheden?
5 10 15
2
4
6
8
Time (s)
Vo
lum
e (L
)
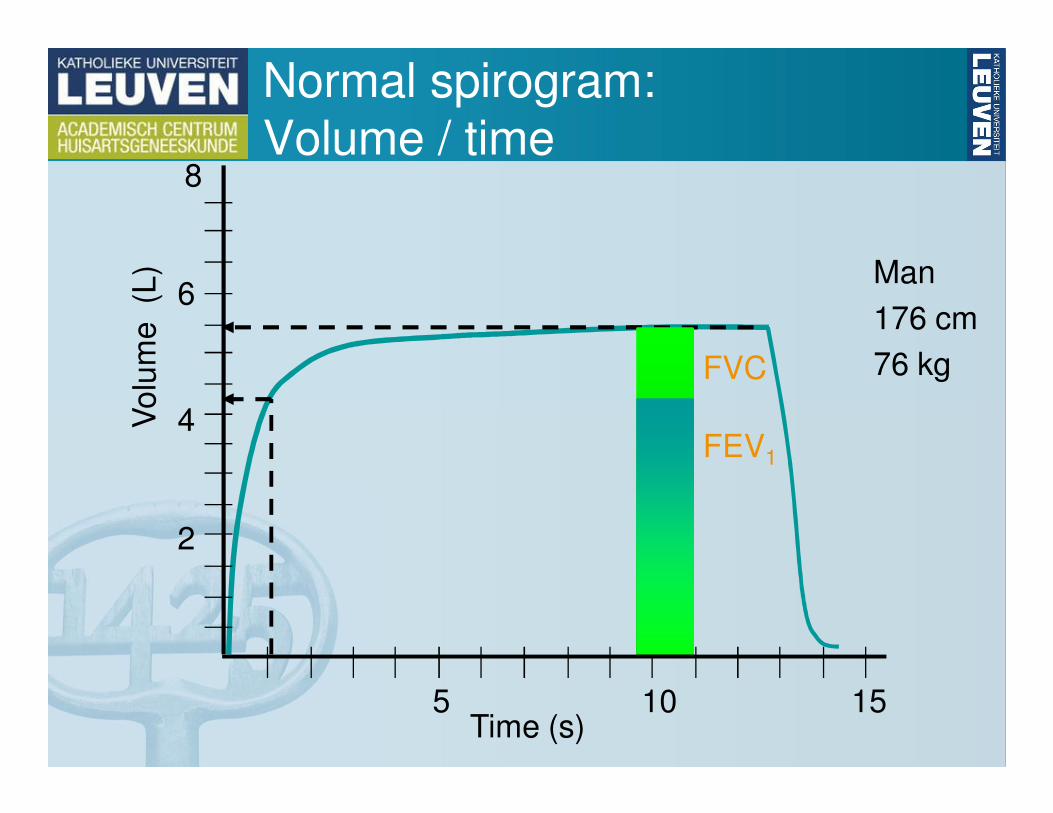
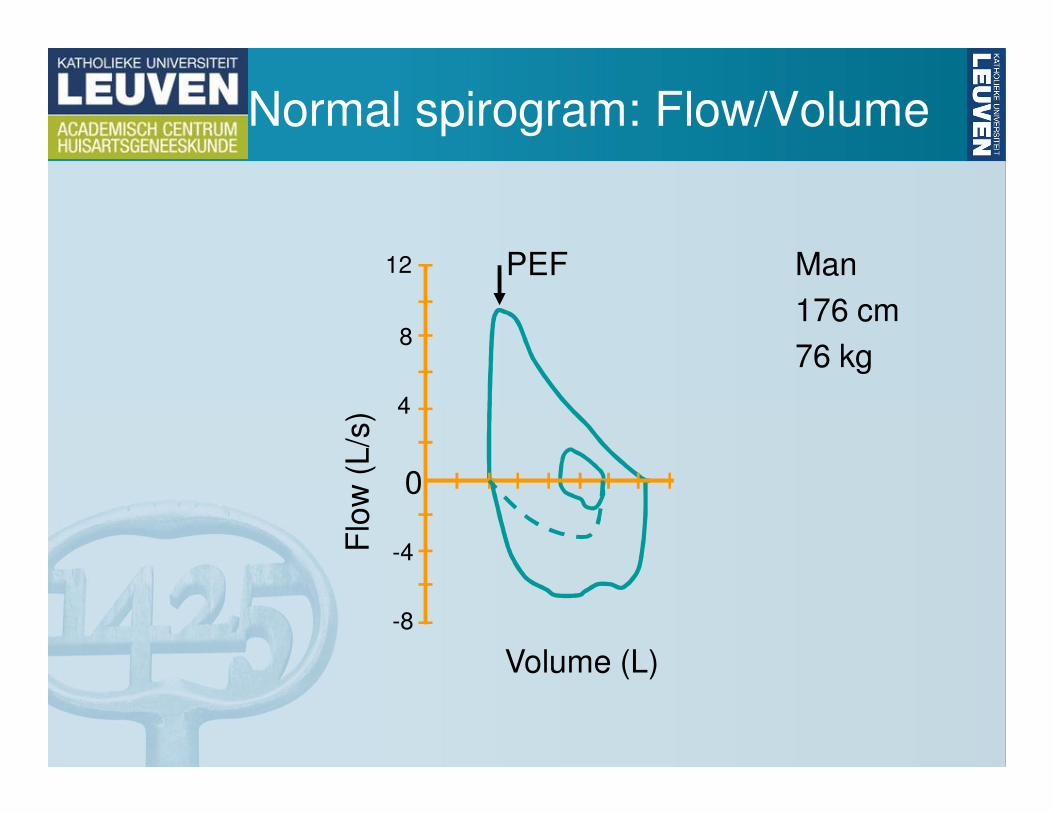
Normal spirogram:
Volume / time
Man
176 cm
76 kgFVC
FEV1
0
-4
-8
4
8
12
Flo
w (
L/s
)
PEF
Normal spirogram: Flow/Volume
Man
176 cm
76 kg
Volume (L)
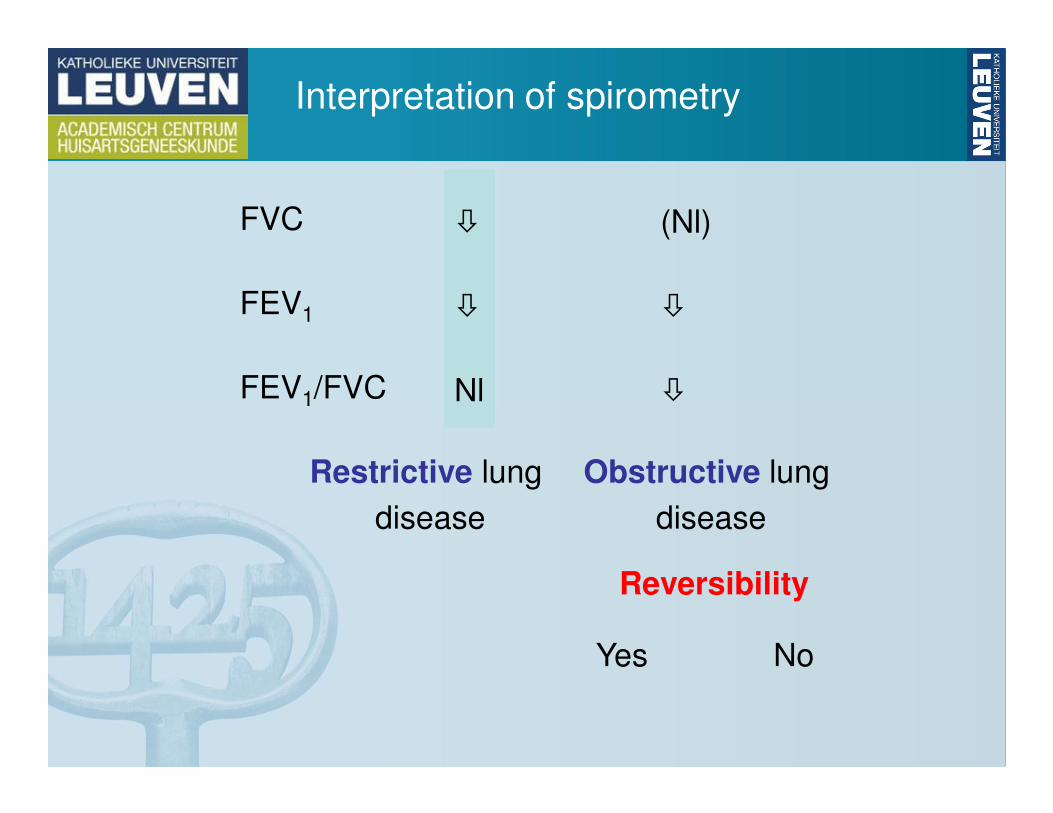
Interpretation of spirometry
FVC
FEV1
FEV1/FVC
�
�
Nl
(Nl)
�
�
Restrictive lung
disease
Obstructive lung
disease
Reversibility
Yes No
Spirometrie in huisartspraktijk
• Indicaties voor “office spirometry”
• Voorwaarden voor kwaliteit
• Mogelijke hinderpalen?
• Zelf uitvoeren of andere mogelijkheden?
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?

Mortality and FEV1
0
0,5
1
1,5
2
<73 73-87 88-96 97-107 >107
Men
Women
FEV1 (%pred)
Ad
juste
d o
dd
s r
atio
of d
ea
th
(all
ca
use
s)
Screening
• Population-based
• Man in the street
• May not have symptoms
• May be a smoker
• No reimbursement
Case Finding
• Individual patients
• Person visiting a doctor
• Respiratory symptoms
• Has COPD risk factors
• Covered by insurance
Screening vs Case finding
P. Enright et al. Respiratory Care 2003
Voorwaarden voor Screening
• Hoge prevalentie van en ernstige morbiditeit door de aandoening in de doelpopulatie
• Eenvoudige en goedkope test zonder ernstige neveneffecten
• Test met hoge sensitiviteit en specificiteit (weinig vals + en vals -)
• Opsporing in een vroeg stadium is zinvol: er bestaat een goede behandeling voor de op te sporen aandoening
Wilson, Proc R Soc Med 1971, Marshall, CMAJ 1996
Voorwaarden voor Screening
• Hoge prevalentie van en ernstige morbiditeit door de aandoening in de doelpopulatie
• Eenvoudige en goedkope test zonder ernstige neveneffecten
• Test met hoge sensitiviteit en specificiteit (weinig vals + en vals -) Probleem bij astma!
• Opsporing in een vroeg stadium is zinvol: er bestaat een goede behandeling voor de op te sporen aandoening
Wilson, Proc R Soc Med 1971, Marshall, CMAJ 1996
Voorwaarden voor Screening
• Hoge prevalentie van en ernstige morbiditeit door de aandoening in de doelpopulatie
• Eenvoudige en goedkope test zonder ernstige neveneffecten
• Test met hoge sensitiviteit en specificiteit (weinig vals + en vals -) Probleem bij astma!
• Opsporing in een vroeg stadium is zinvol: er bestaat een goede behandeling voor de op te sporen aandoening. Probleem bij COPD!
Wilson, Proc R Soc Med 1971, Marshall, CMAJ 1996
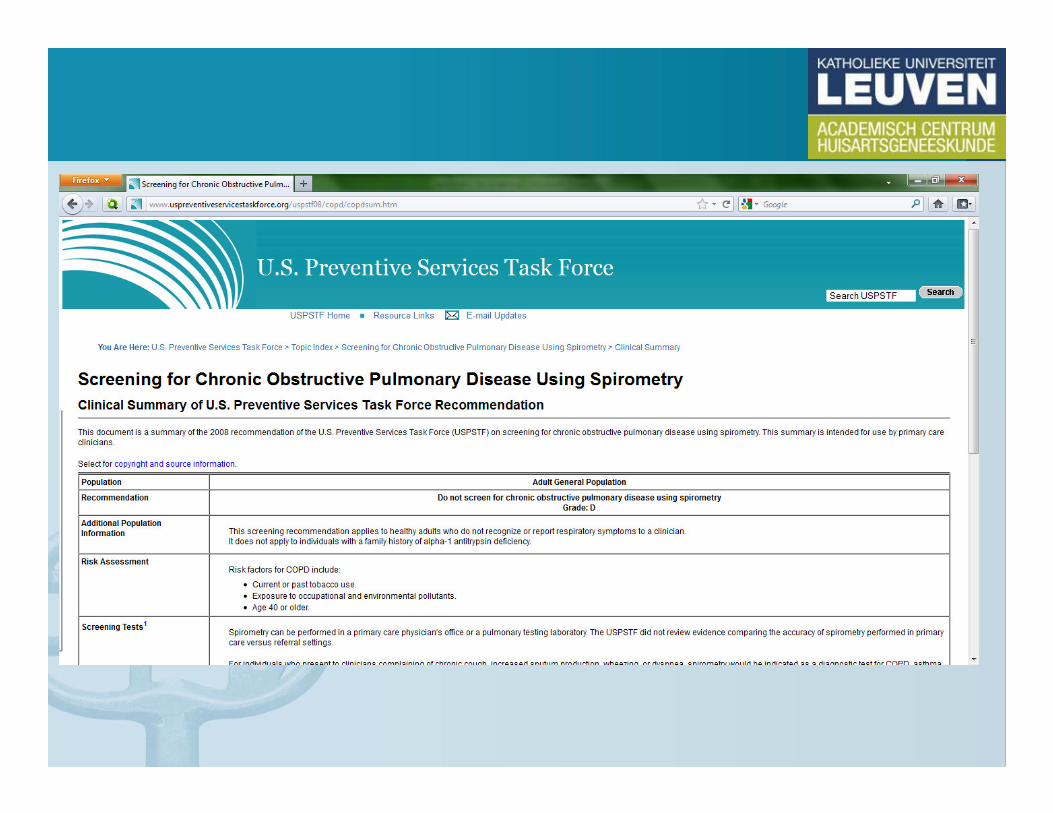
Screening for COPD? (USPSTF)
• Screening for COPD would theoretically benefit adults with a high probability of severe airflow obstruction who
might benefit from inhaled therapies.
• However, even in groups with the greatest prevalence
of airflow obstruction, hundreds of patients would need
to be screened with spirometry to defer 1 exacerbation.
• Although an unknown proportion of patients who
present with clinical symptoms of an exacerbation does
not receive a COPD diagnosis, the incremental benefit of early detection over clinical diagnosis for the
remainder of patients would, at most, be a deferral of
the first exacerbation.
Screening for COPD? (USPSTF)
• Good evidence indicates that history and clinical examination are not accurate predictors of airflow
limitation.
• Fair evidence indicates that fewer than 10% of those
identified by screening spirometry have severe or very
severe COPD, using current diagnostic criteria.
• All individuals with COPD, including those with mild or
moderate illness, would benefit from smoking cessation
and annual influenza vaccination
• No studies have examined whether performing spirometry increases influenza vaccination rates.
• Spirometry and smoking cessation: ???
Can spirometry enhance smoking cessation?
• Smokers with documented airflow obstruction have higher odds for smoking cessation(Bednarek, Thorax 2006)
• If randomized allocation to spirometry or not there is no significant difference in smoking cessation rate (Buffels, Respir Med 2006)
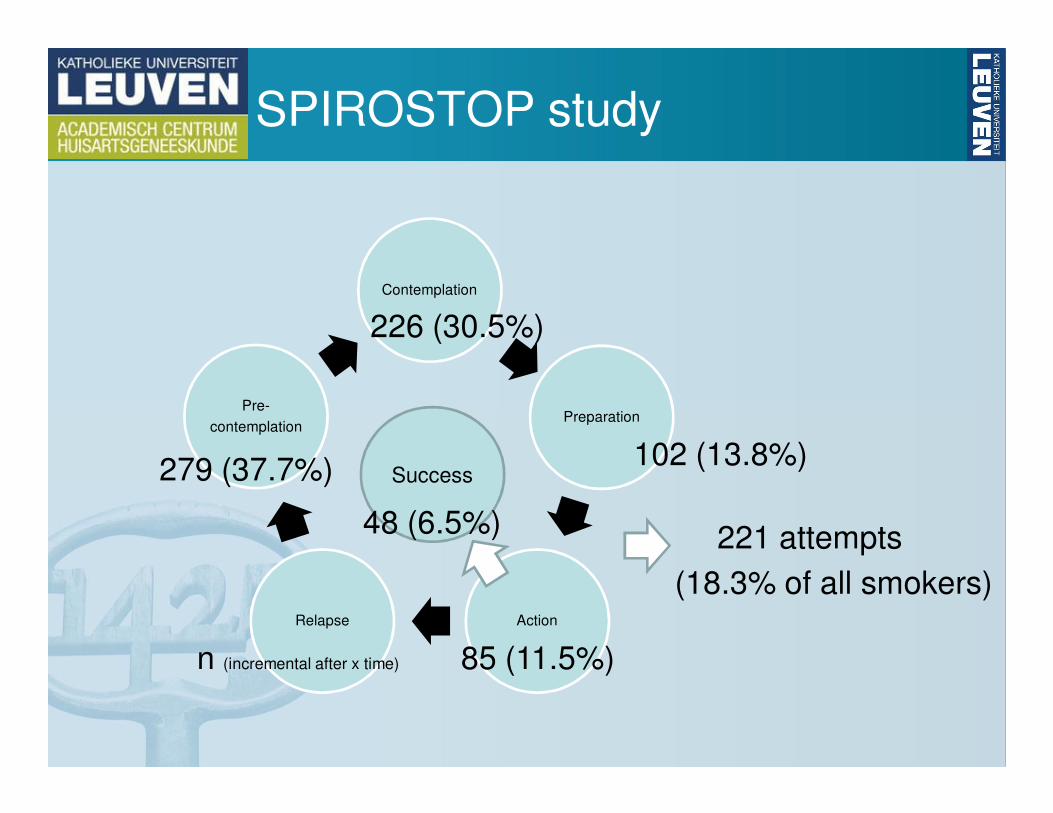
SPIROSTOP study
Contemplation
Preparation
ActionRelapse
Pre-
contemplation
Success102 (13.8%)
85 (11.5%)
48 (6.5%)
n (incremental after x time)
226 (30.5%)
279 (37.7%)
221 attempts
(18.3% of all smokers)
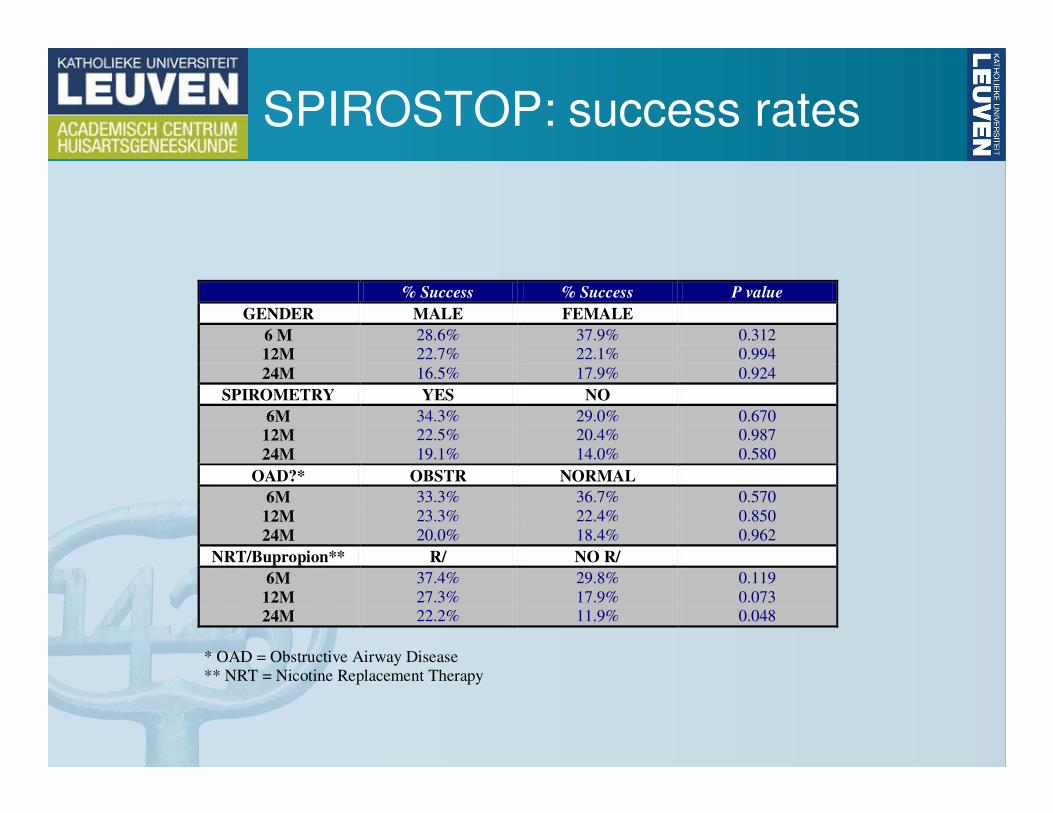
SPIROSTOP: success rates
% Success % Success P value
GENDER MALE FEMALE
6 M 28.6% 37.9% 0.312
12M 22.7% 22.1% 0.994
24M 16.5% 17.9% 0.924
SPIROMETRY YES NO
6M 34.3% 29.0% 0.670
12M 22.5% 20.4% 0.987
24M 19.1% 14.0% 0.580
OAD?* OBSTR NORMAL
6M 33.3% 36.7% 0.570
12M 23.3% 22.4% 0.850
24M 20.0% 18.4% 0.962
NRT/Bupropion** R/ NO R/
6M 37.4% 29.8% 0.119
12M 27.3% 17.9% 0.073
24M 22.2% 11.9% 0.048
* OAD = Obstructive Airway Disease ** NRT = Nicotine Replacement Therapy
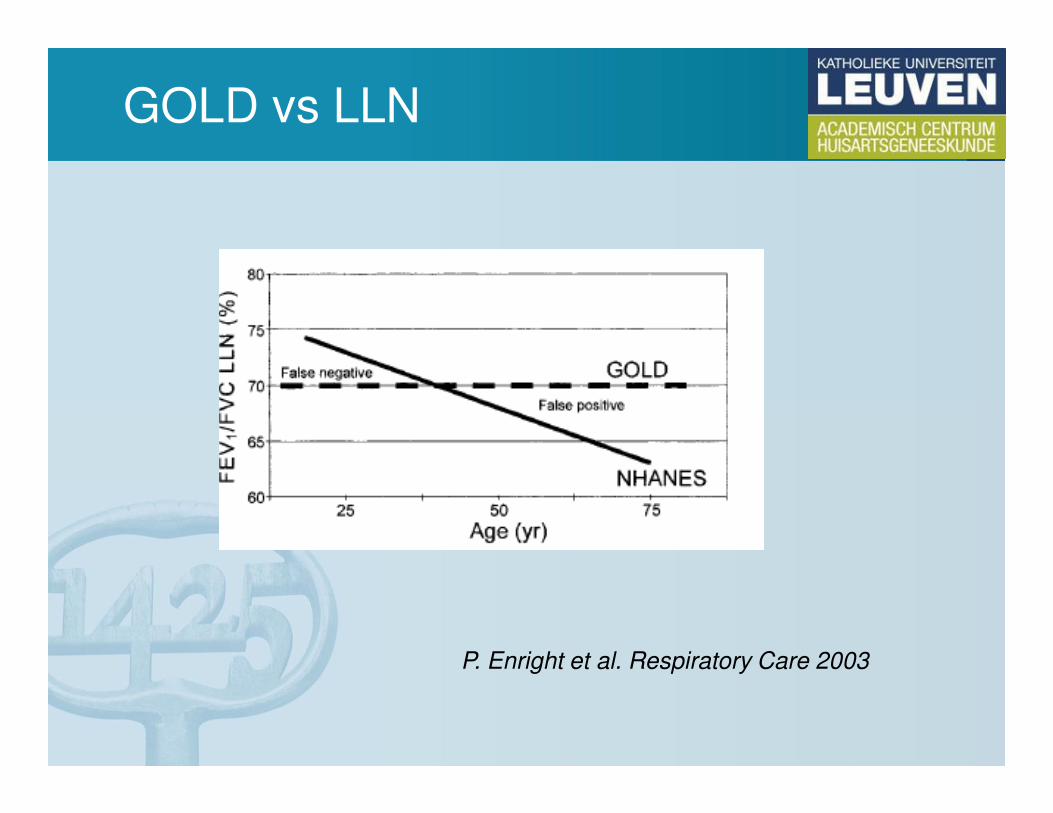
GOLD vs LLN
P. Enright et al. Respiratory Care 2003
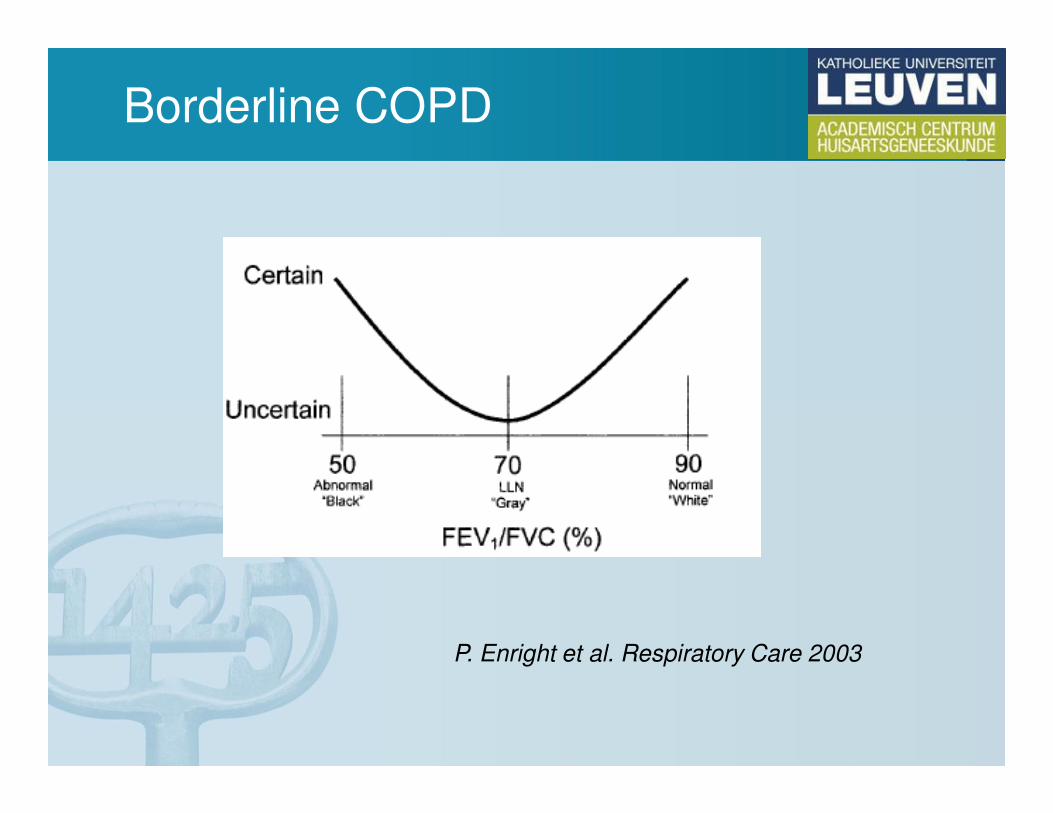
Borderline COPD
P. Enright et al. Respiratory Care 2003
So… no screening for COPD??
• Some indications that the message after spirometry matters: ELA (estimated lung age) Parkes, BMJ 2008
• No strict evidence for effects of early pharmacotherapyon the deterioration of lung function in COPD, but some
indications
• We do NOT screen for COPD: we screen for obstructive airway disease
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?
Vermoeden van COPD
• Chronische hoest
• Chronische productie van sputum
• Blootstelling aan risico’s– Tabaksrook
– Professionele irritantia
• Dyspnee, met 4 kenmerken:– Progressief (verslecht met de tijd)
– Persisterend (dagelijks aanwezig)
– Slechter met inspanning
– Slechter bij surinfectie
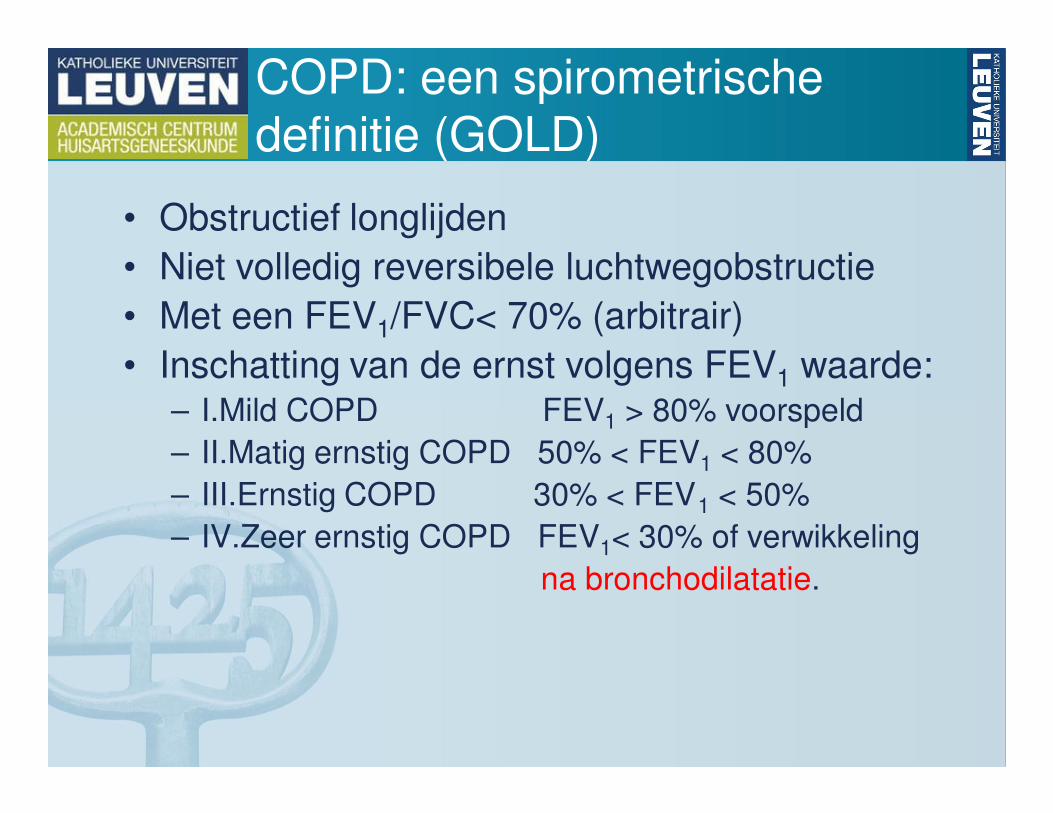
COPD: een spirometrische
definitie (GOLD)
• Obstructief longlijden
• Niet volledig reversibele luchtwegobstructie
• Met een FEV1/FVC< 70% (arbitrair)
• Inschatting van de ernst volgens FEV1 waarde:– I.Mild COPD FEV1 > 80% voorspeld
– II.Matig ernstig COPD 50% < FEV1 < 80%
– III.Ernstig COPD 30% < FEV1 < 50%
– IV.Zeer ernstig COPD FEV1< 30% of verwikkeling
na bronchodilatatie.
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?
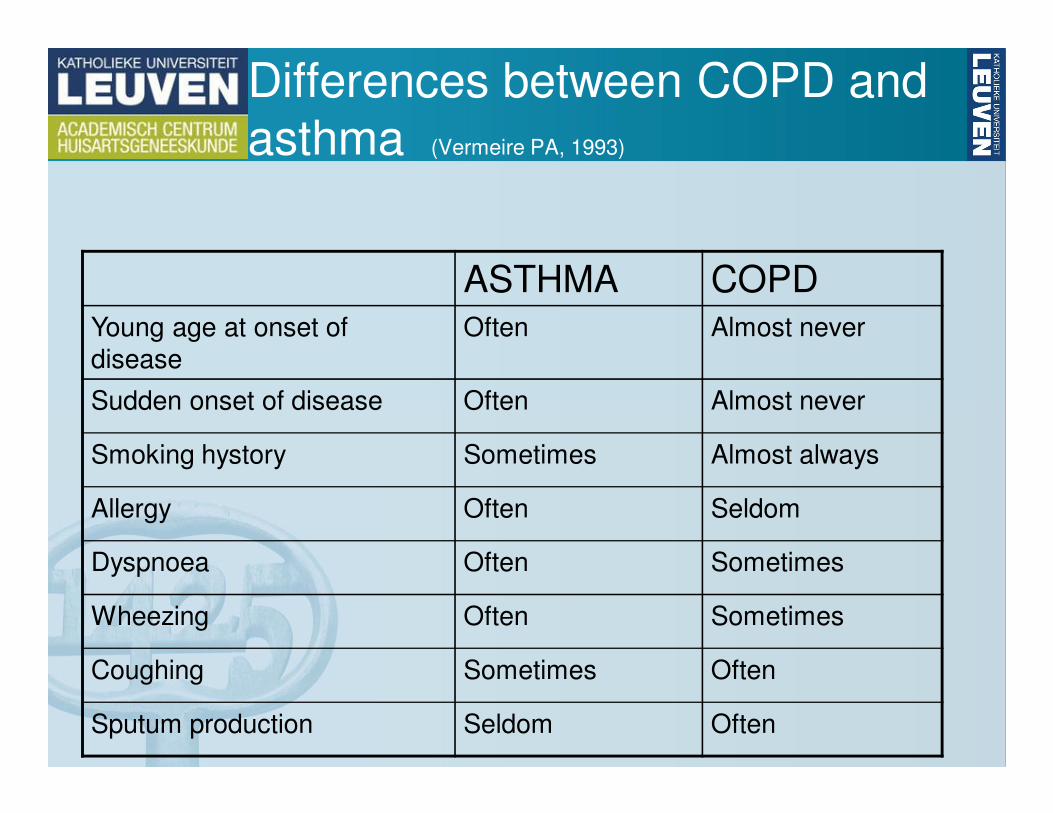
Differences between COPD and
asthma (Vermeire PA, 1993)
ASTHMA COPDYoung age at onset of
disease
Often Almost never
Sudden onset of disease Often Almost never
Smoking hystory Sometimes Almost always
Allergy Often Seldom
Dyspnoea Often Sometimes
Wheezing Often Sometimes
Coughing Sometimes Often
Sputum production Seldom Often
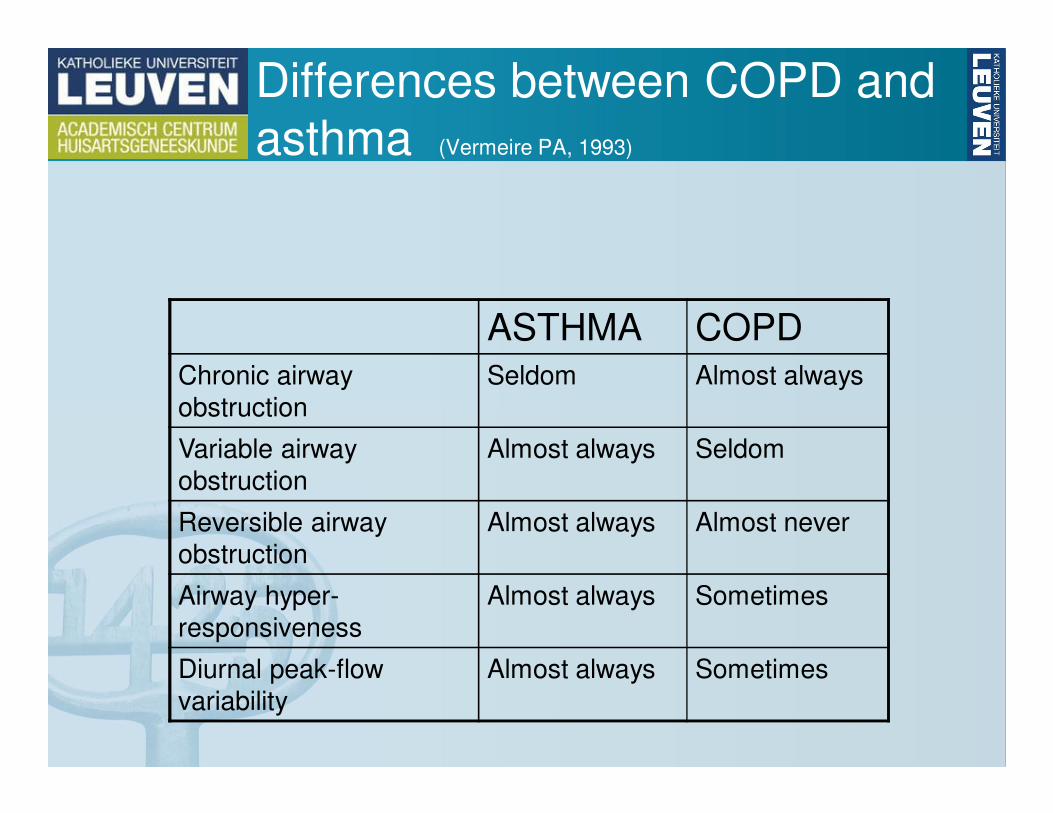
Differences between COPD and
asthma (Vermeire PA, 1993)
ASTHMA COPDChronic airway
obstruction
Seldom Almost always
Variable airway
obstruction
Almost always Seldom
Reversible airway
obstruction
Almost always Almost never
Airway hyper-
responsiveness
Almost always Sometimes
Diurnal peak-flow
variability
Almost always Sometimes
• What is the diagnostic accuracy for asthma
and COPD of subsequent diagnostic steps
in a population older than 40 years with
probable obstructive airway disease?
Buffels, Respiration 2011
DIDASCO2: Inclusion
• 50 patients with probable OAD• (taking bronchodilators or wheezing)
• Diagnostic opinion:• Asthma
• COPD
• Asthma AND COPD
• Other OAD
• No OAD
• I don’t know
• Rate of certainty (ranging from 1 to 5)
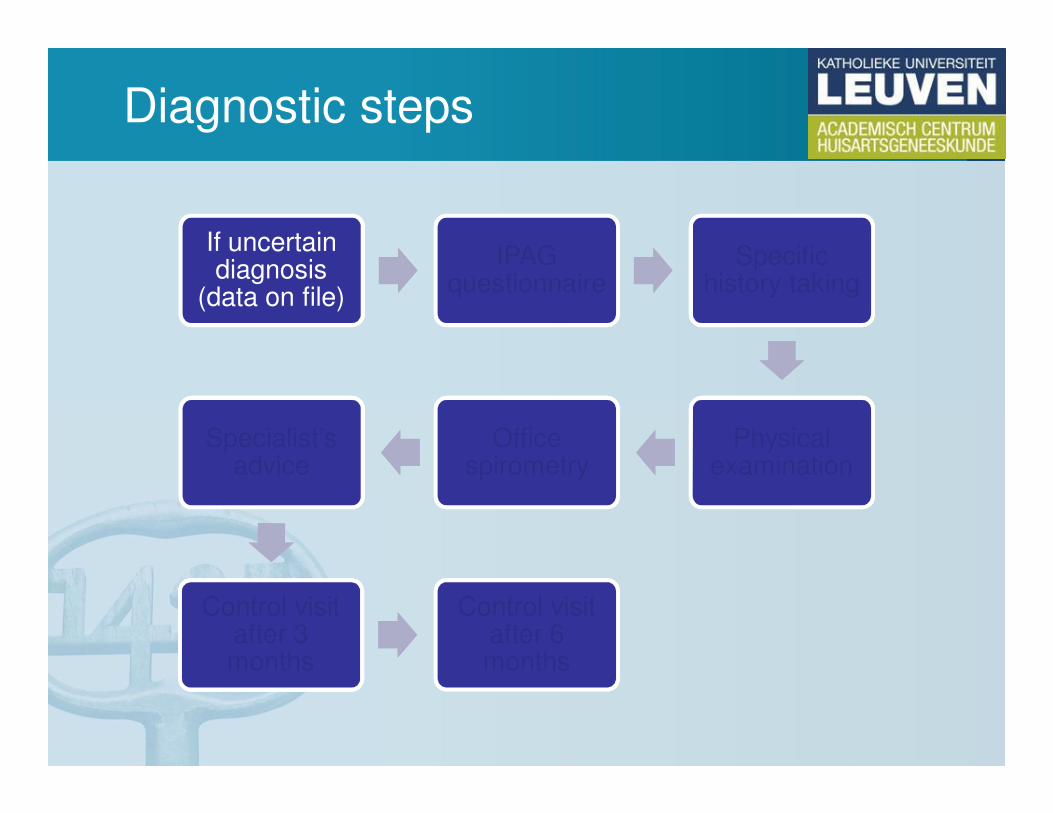
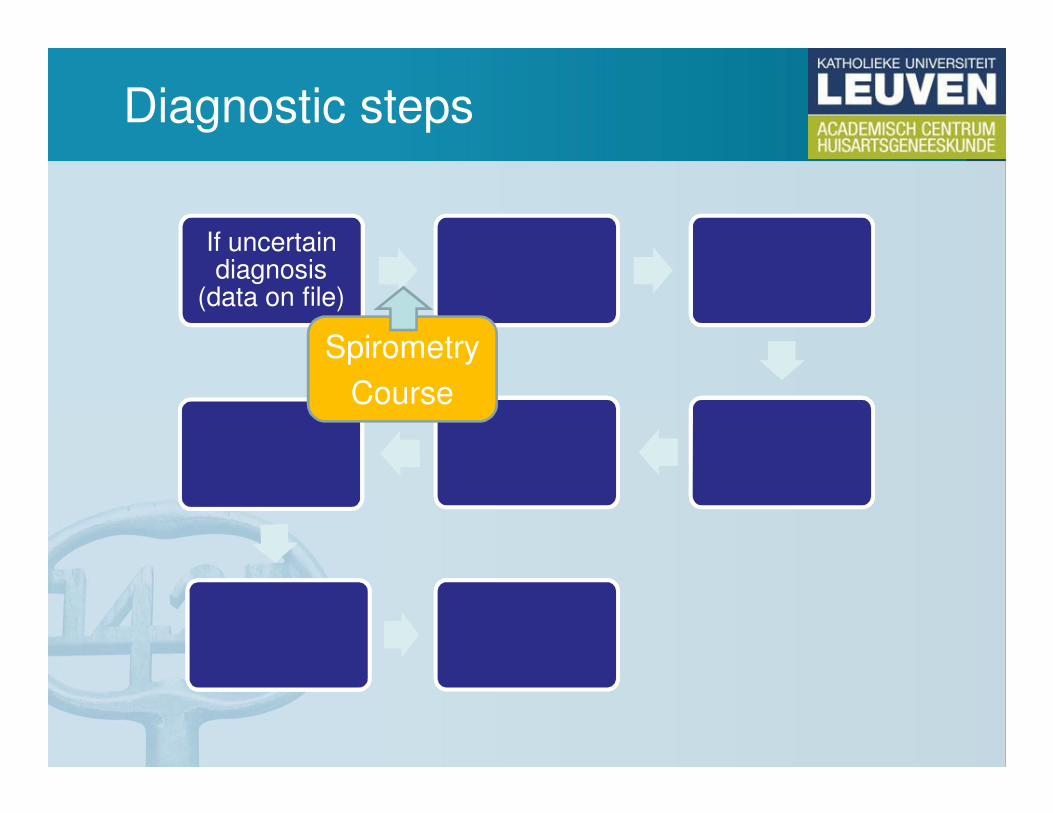
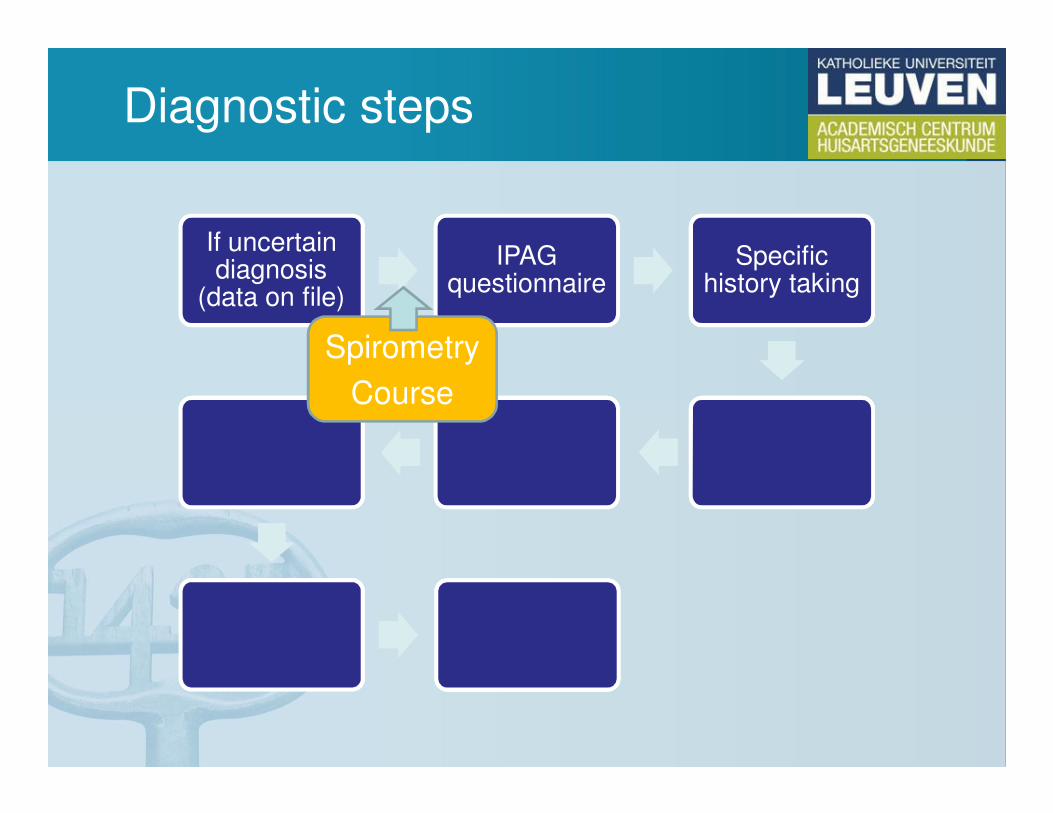
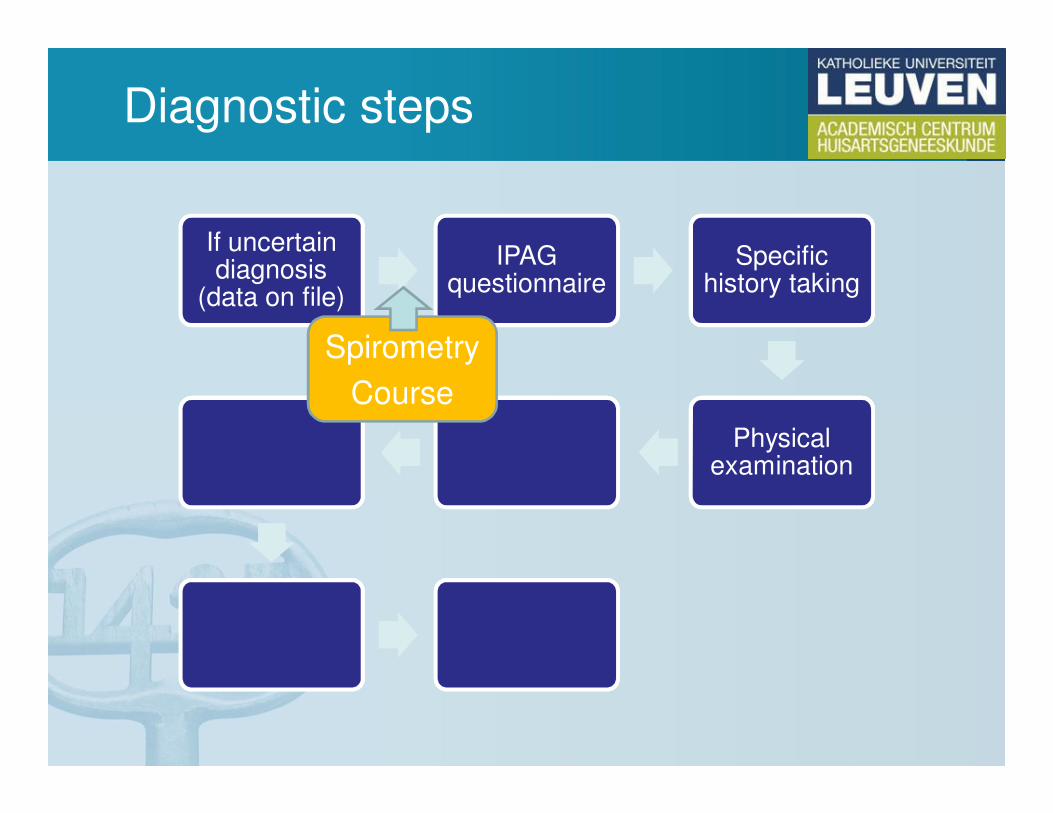
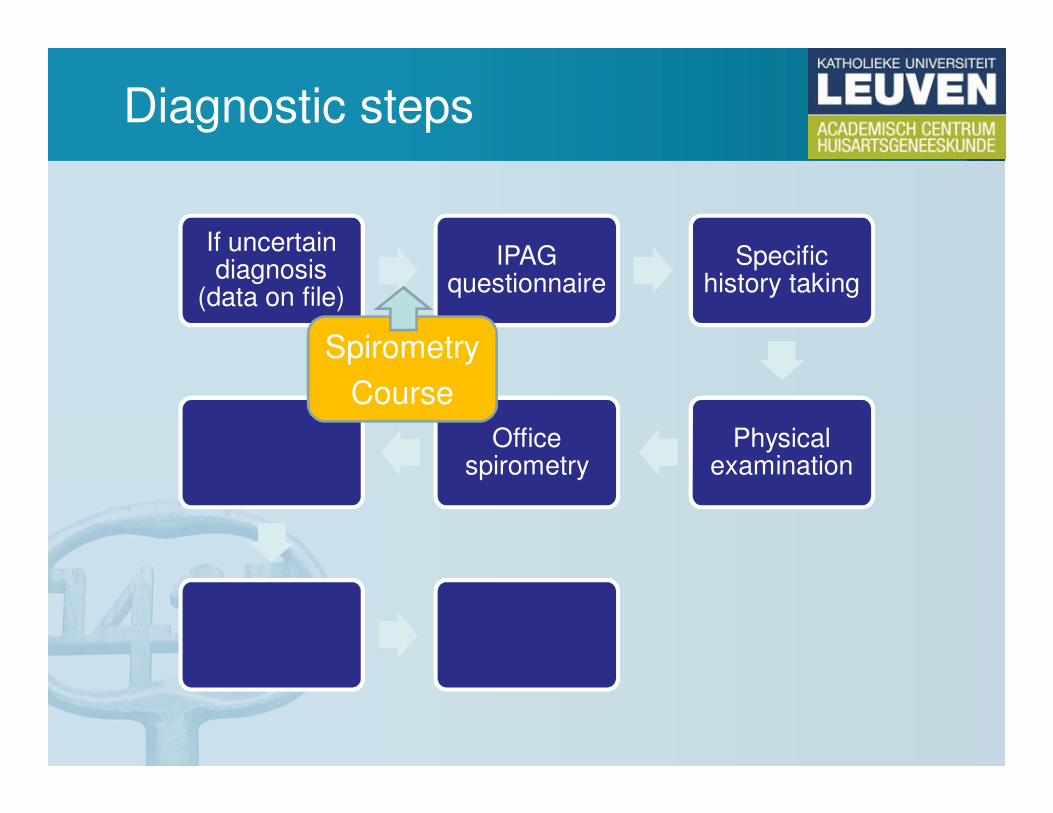
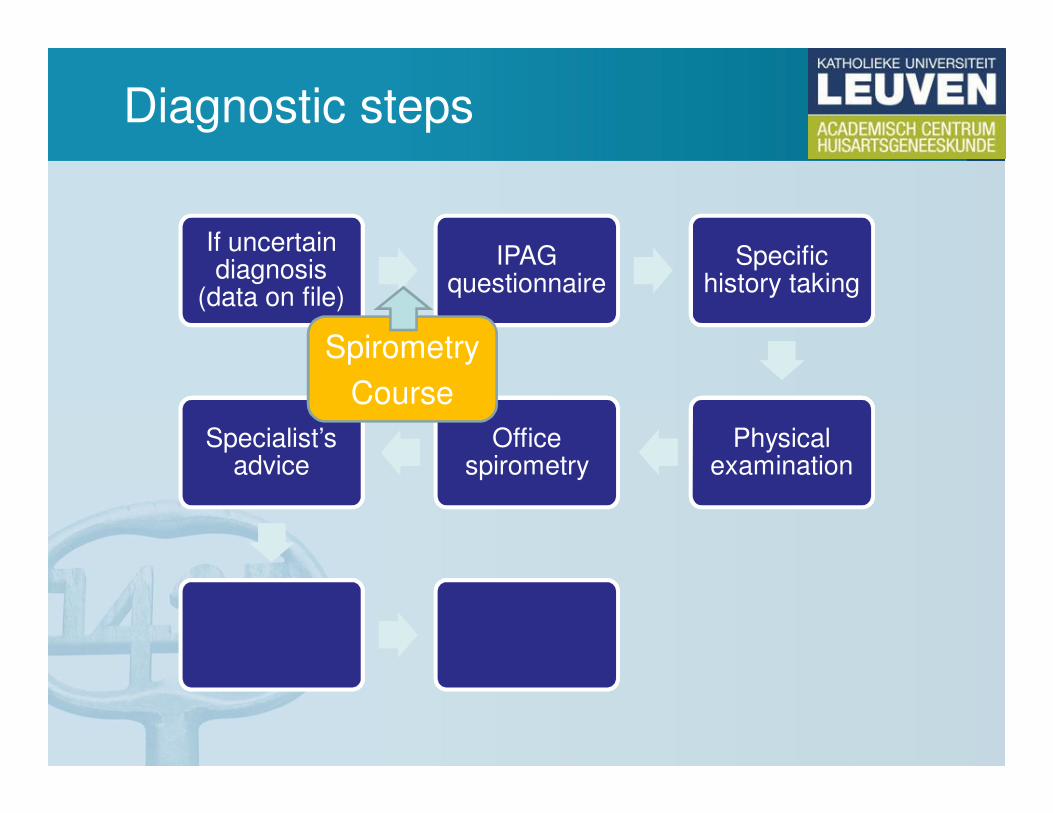
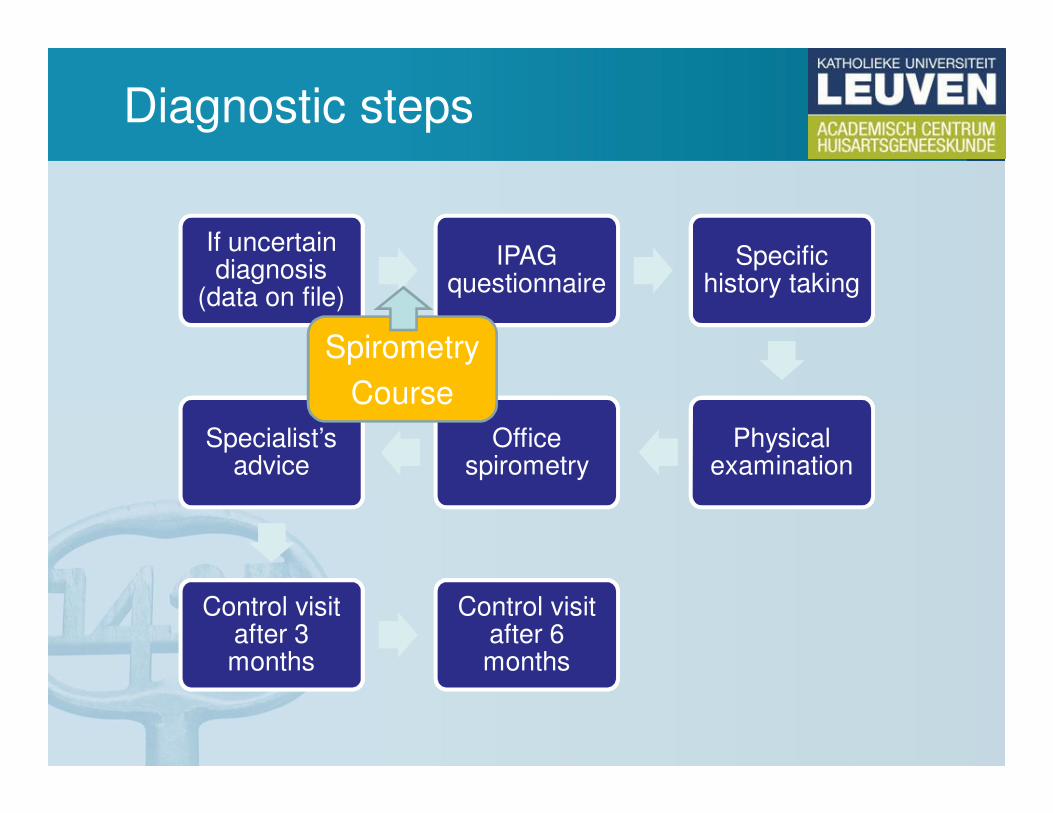
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
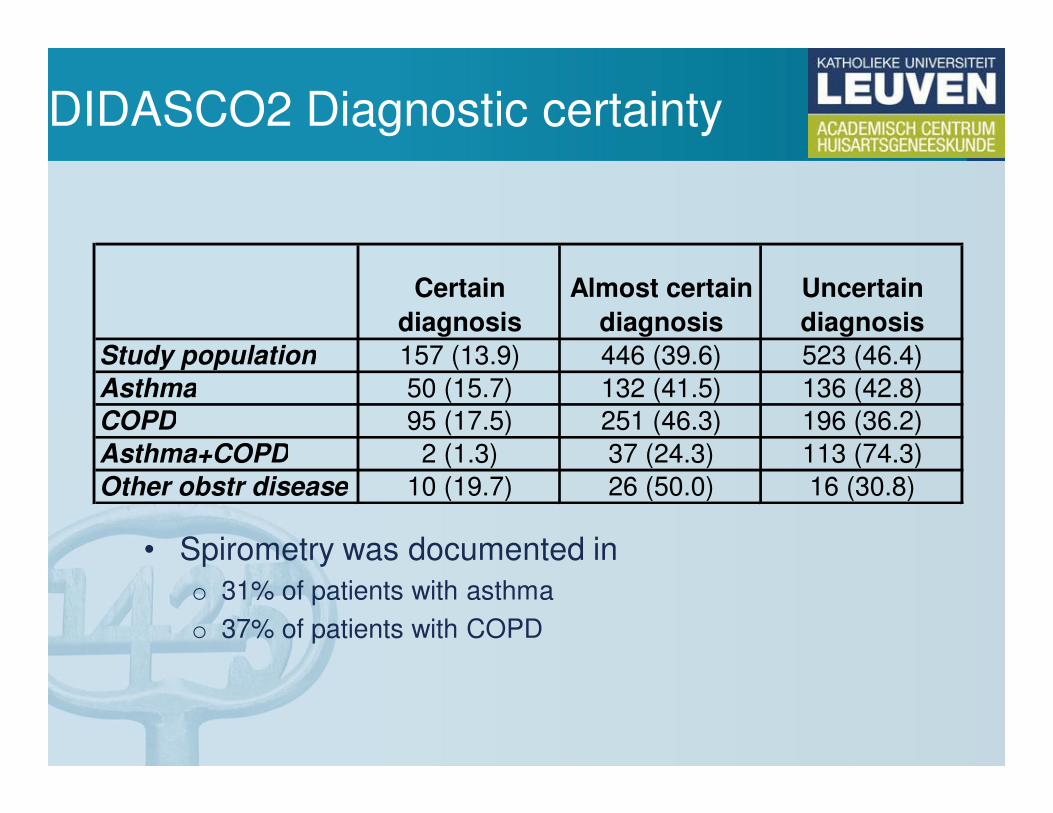
DIDASCO2 Diagnostic certainty
• Spirometry was documented in
o 31% of patients with asthma
o 37% of patients with COPD
Certain
diagnosis
Almost certain
diagnosis
Uncertain
diagnosis
Study population 157 (13.9) 446 (39.6) 523 (46.4)
Asthma 50 (15.7) 132 (41.5) 136 (42.8)
COPD 95 (17.5) 251 (46.3) 196 (36.2)
Asthma+COPD 2 (1.3) 37 (24.3) 113 (74.3)
Other obstr disease 10 (19.7) 26 (50.0) 16 (30.8)
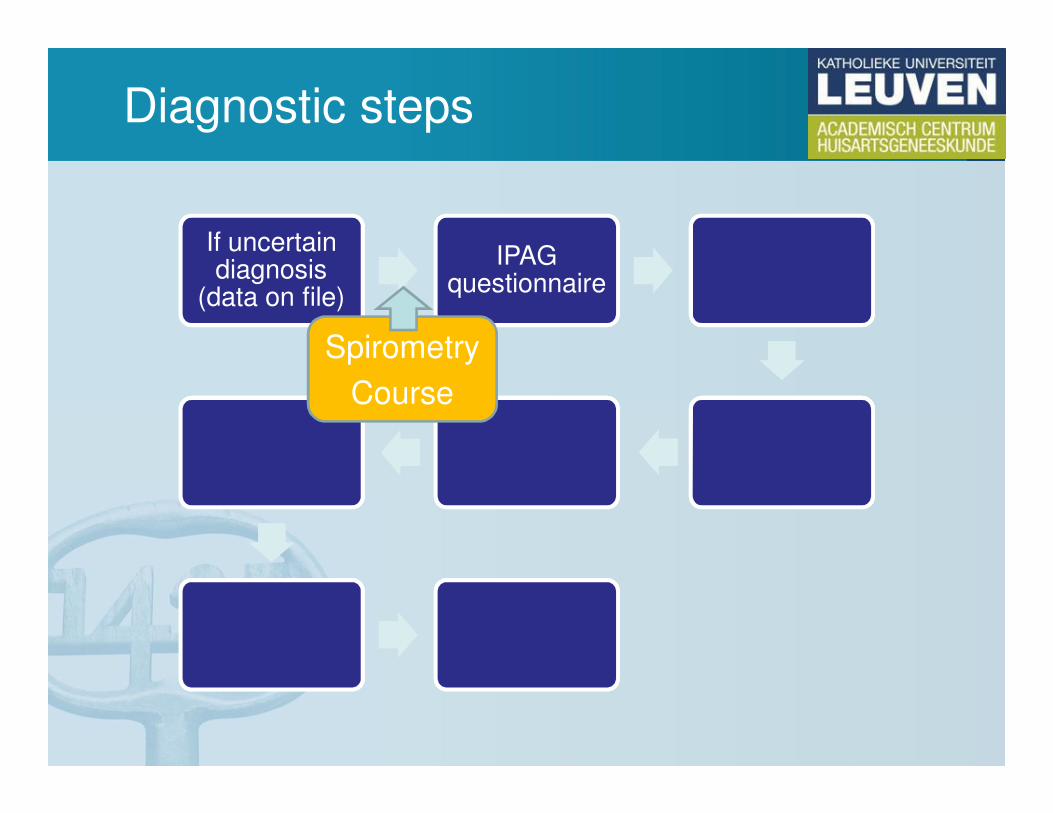
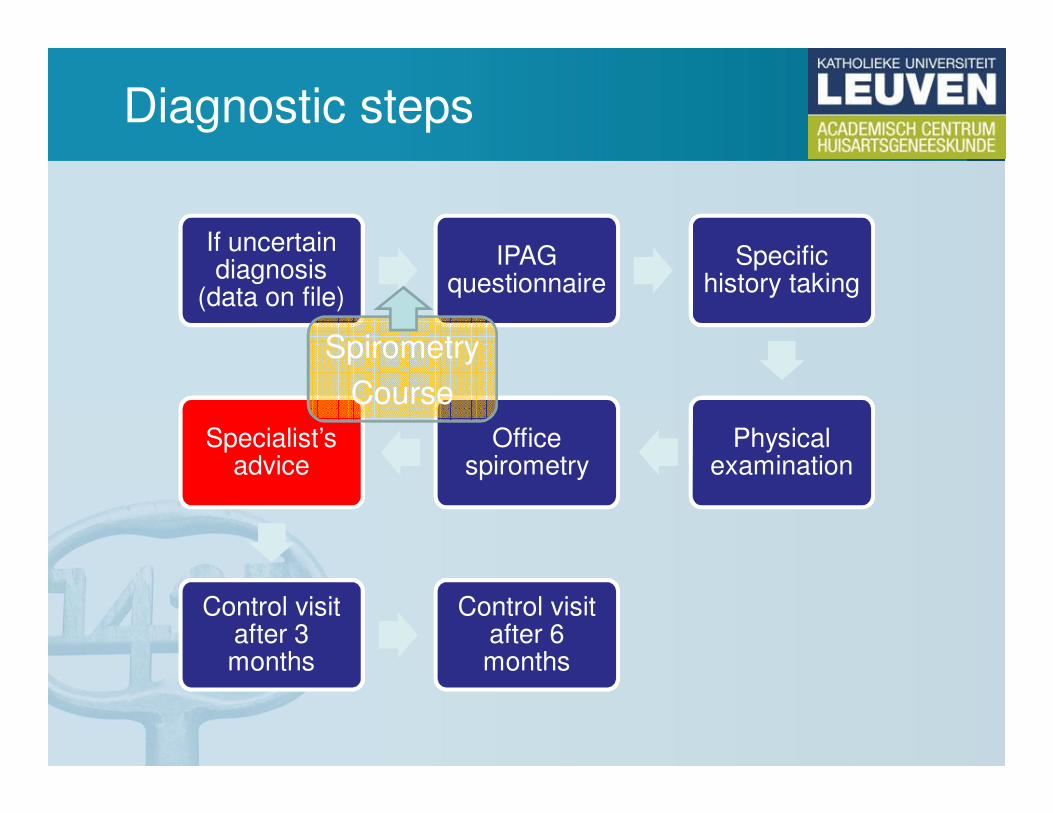
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
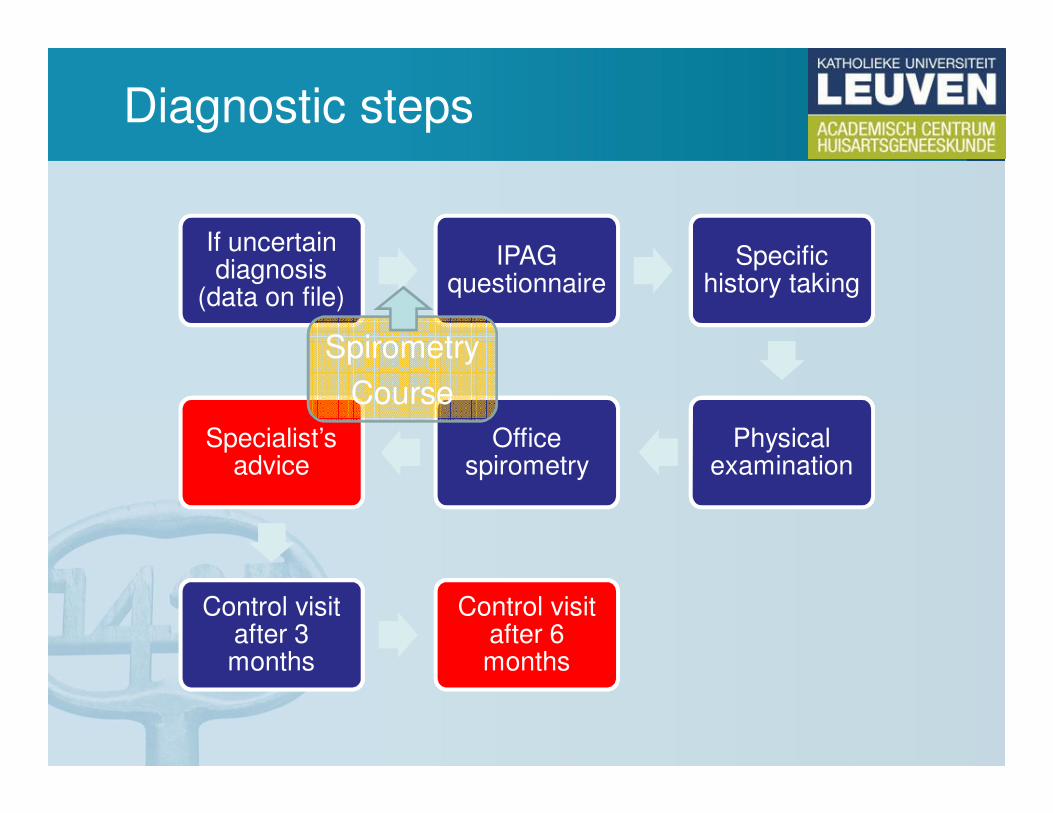
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
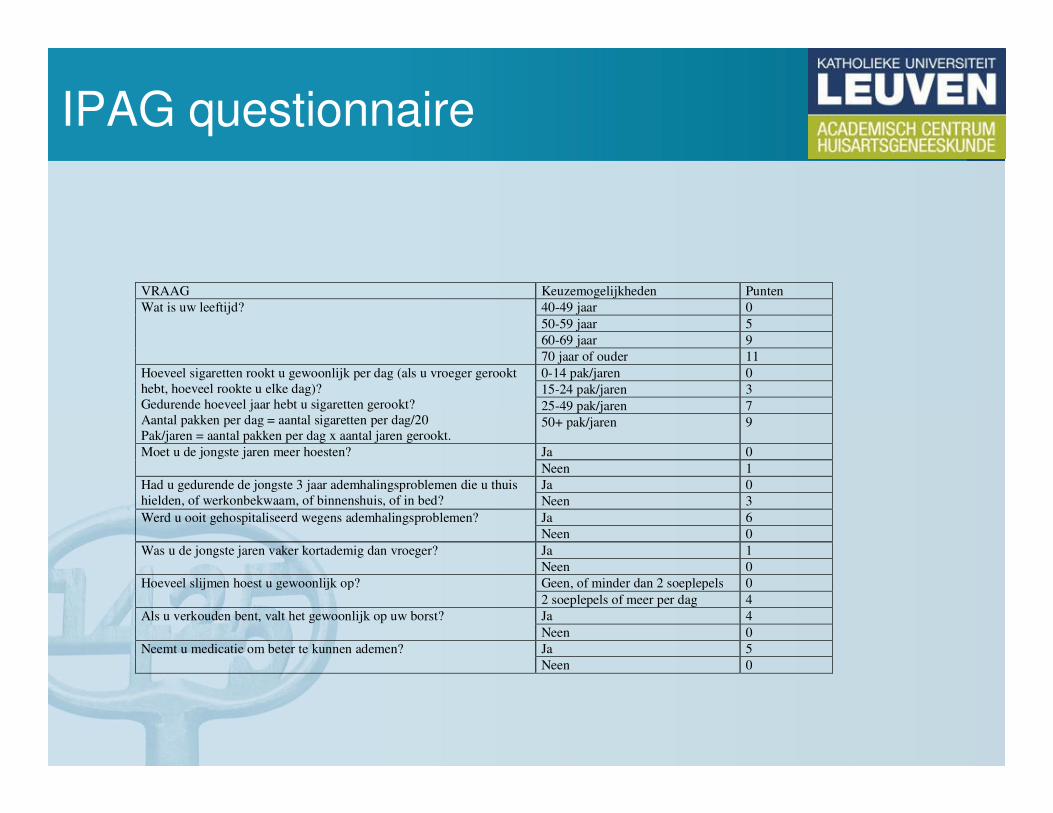
IPAG questionnaire
VRAAG Keuzemogelijkheden Punten
Wat is uw leeftijd? 40-49 jaar 0
50-59 jaar 5
60-69 jaar 9
70 jaar of ouder 11
Hoeveel sigaretten rookt u gewoonlijk per dag (als u vroeger gerookt
hebt, hoeveel rookte u elke dag)?
Gedurende hoeveel jaar hebt u sigaretten gerookt?
Aantal pakken per dag = aantal sigaretten per dag/20
Pak/jaren = aantal pakken per dag x aantal jaren gerookt.
0-14 pak/jaren 0
15-24 pak/jaren 3
25-49 pak/jaren 7
50+ pak/jaren 9
Moet u de jongste jaren meer hoesten? Ja 0
Neen 1
Had u gedurende de jongste 3 jaar ademhalingsproblemen die u thuis
hielden, of werkonbekwaam, of binnenshuis, of in bed?
Ja 0
Neen 3
Werd u ooit gehospitaliseerd wegens ademhalingsproblemen? Ja 6
Neen 0
Was u de jongste jaren vaker kortademig dan vroeger? Ja 1
Neen 0
Hoeveel slijmen hoest u gewoonlijk op? Geen, of minder dan 2 soeplepels 0
2 soeplepels of meer per dag 4
Als u verkouden bent, valt het gewoonlijk op uw borst? Ja 4
Neen 0
Neemt u medicatie om beter te kunnen ademen? Ja 5
Neen 0
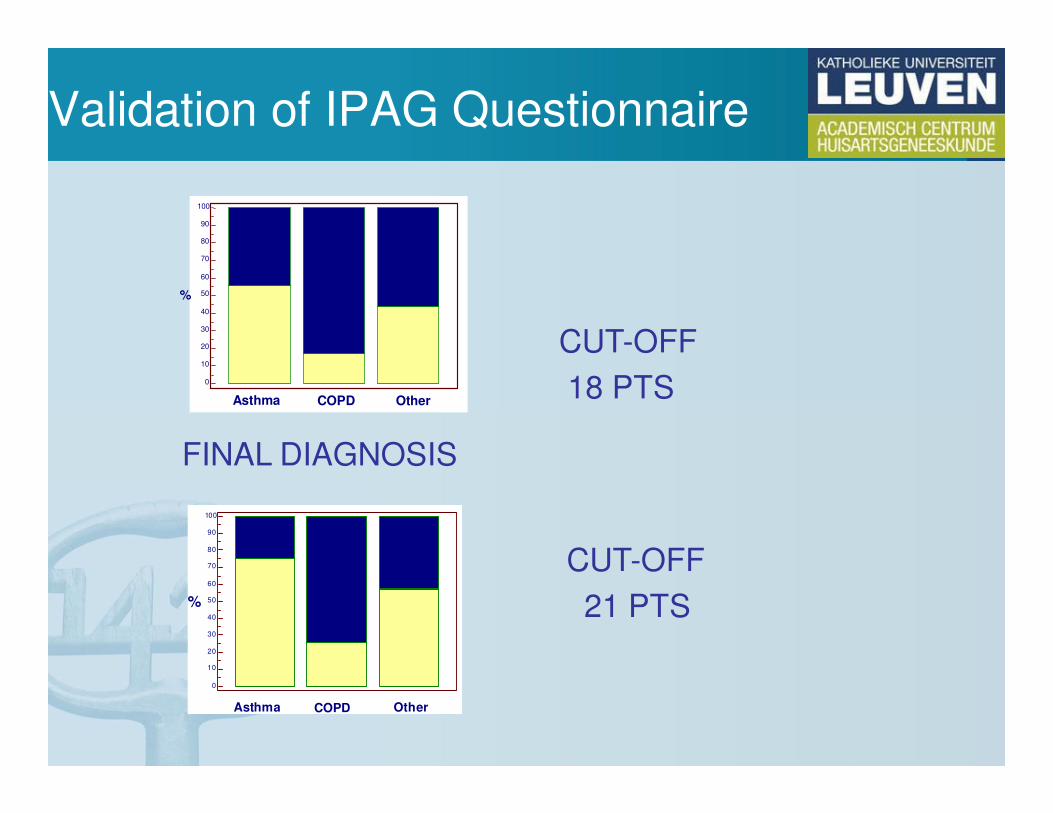
Validation of IPAG Questionnaire
100
90
80
70
60
50
40
30
20
10
0
%
Asthma COPD Other
100 90 80 70
60 50 40 30 20 10
0
%
Asthma COPD Other
CUT-OFF
18 PTS
CUT-OFF
21 PTS
FINAL DIAGNOSIS
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
Diagnostic steps
If uncertaindiagnosis
(data on file)
IPAG questionnaire
Specifichistory taking
Physicalexamination
Office spirometry
Specialist’sadvice
Control visitafter 3 months
Control visitafter 6 months
Spirometry
Course
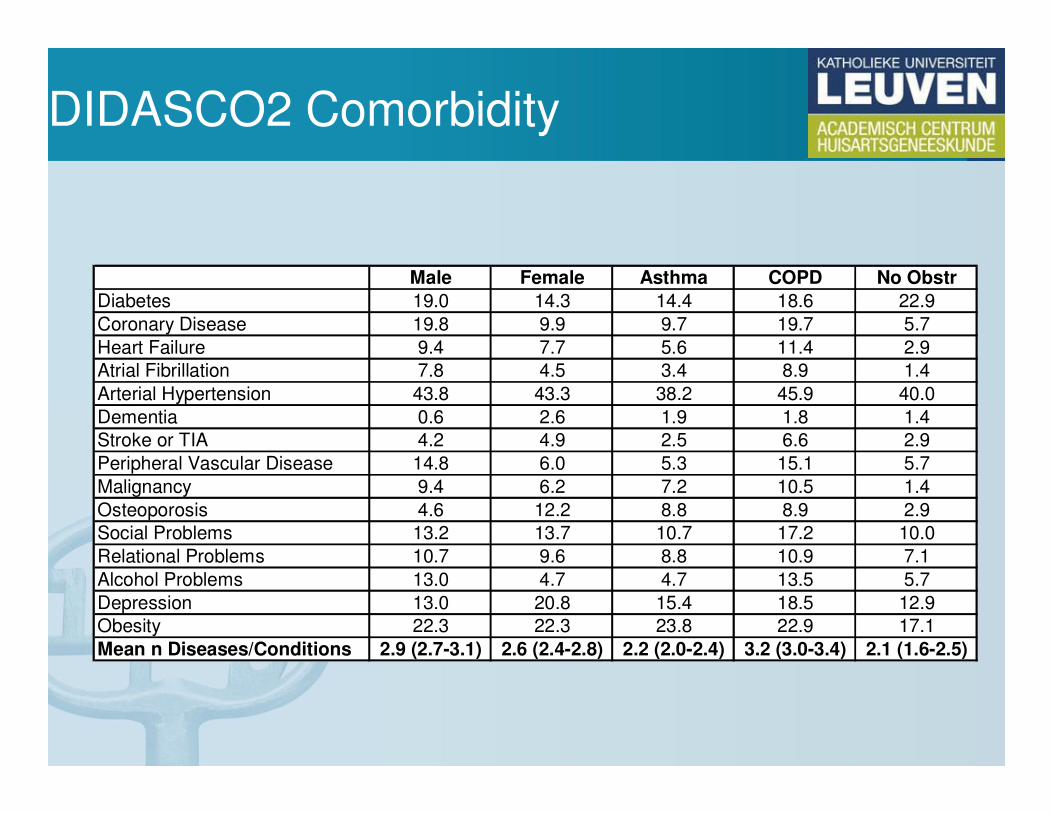
DIDASCO2 Comorbidity
Male Female Asthma COPD No Obstr
Diabetes 19.0 14.3 14.4 18.6 22.9
Coronary Disease 19.8 9.9 9.7 19.7 5.7
Heart Failure 9.4 7.7 5.6 11.4 2.9
Atrial Fibrillation 7.8 4.5 3.4 8.9 1.4
Arterial Hypertension 43.8 43.3 38.2 45.9 40.0
Dementia 0.6 2.6 1.9 1.8 1.4
Stroke or TIA 4.2 4.9 2.5 6.6 2.9
Peripheral Vascular Disease 14.8 6.0 5.3 15.1 5.7
Malignancy 9.4 6.2 7.2 10.5 1.4
Osteoporosis 4.6 12.2 8.8 8.9 2.9
Social Problems 13.2 13.7 10.7 17.2 10.0
Relational Problems 10.7 9.6 8.8 10.9 7.1
Alcohol Problems 13.0 4.7 4.7 13.5 5.7
Depression 13.0 20.8 15.4 18.5 12.9
Obesity 22.3 22.3 23.8 22.9 17.1
Mean n Diseases/Conditions 2.9 (2.7-3.1) 2.6 (2.4-2.8) 2.2 (2.0-2.4) 3.2 (3.0-3.4) 2.1 (1.6-2.5)
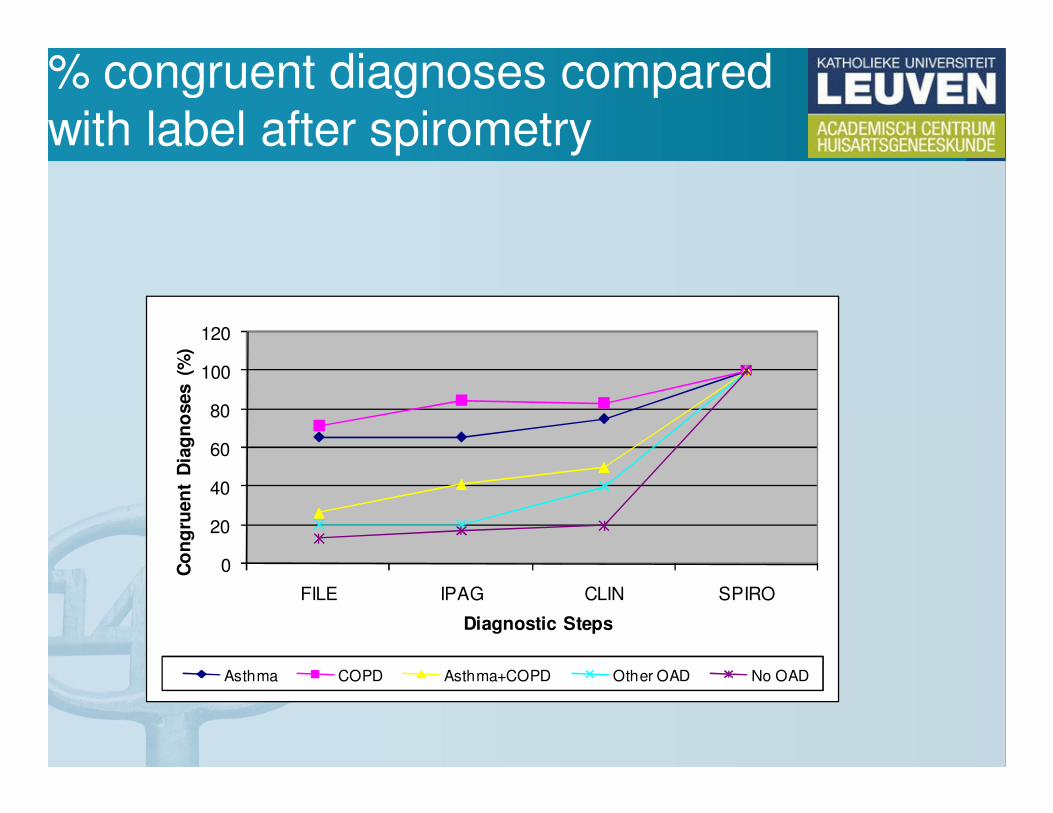
% congruent diagnoses comparedwith label after spirometry
0
20
40
60
80
100
120
FILE IPAG CLIN SPIRO
Co
ng
ruen
t D
iag
no
ses (
%)
Diagnostic Steps
Asthma COPD Asthma+COPD Other OAD No OAD
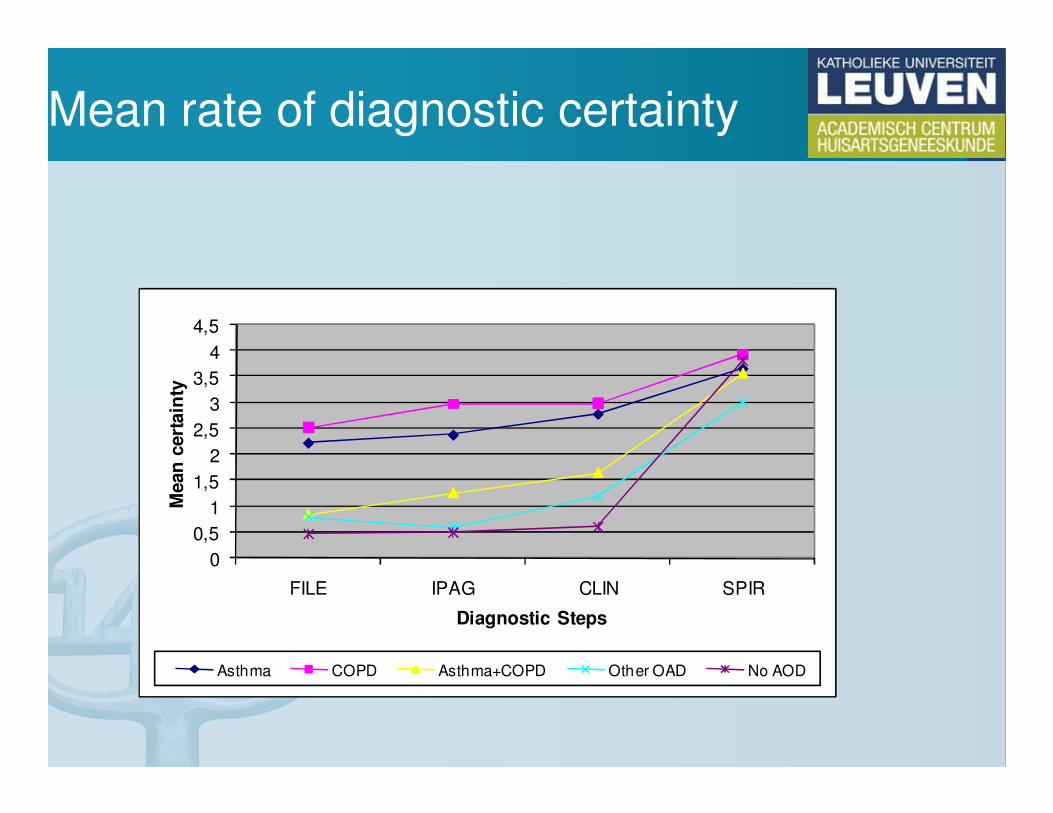
Mean rate of diagnostic certainty
0
0,5
1
1,5
2
2,5
3
3,5
4
4,5
FILE IPAG CLIN SPIR
Mean
cert
ain
ty
Diagnostic Steps
Asthma COPD Asthma+COPD Other OAD No AOD
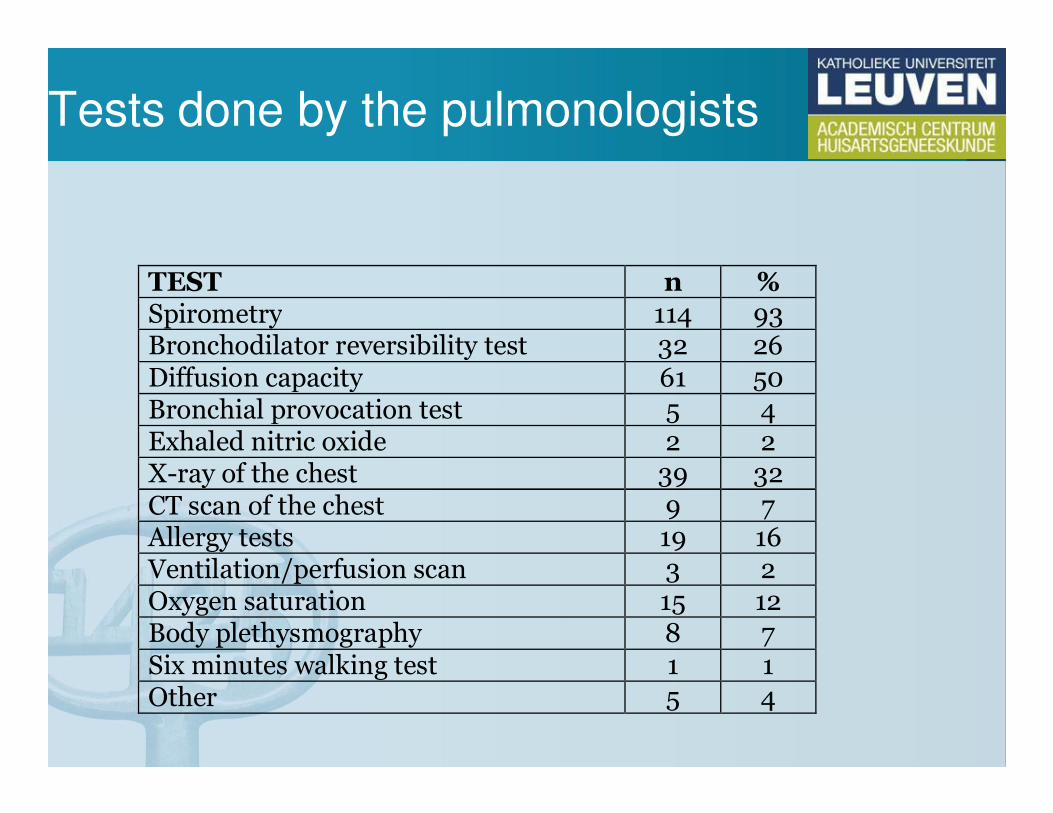
Tests done by the pulmonologists
TEST n %
Spirometry 114 93 Bronchodilator reversibility test 32 26 Diffusion capacity 61 50 Bronchial provocation test 5 4 Exhaled nitric oxide 2 2 X-ray of the chest 39 32 CT scan of the chest 9 7 Allergy tests 19 16 Ventilation/perfusion scan 3 2 Oxygen saturation 15 12 Body plethysmography 8 7 Six minutes walking test 1 1 Other 5 4
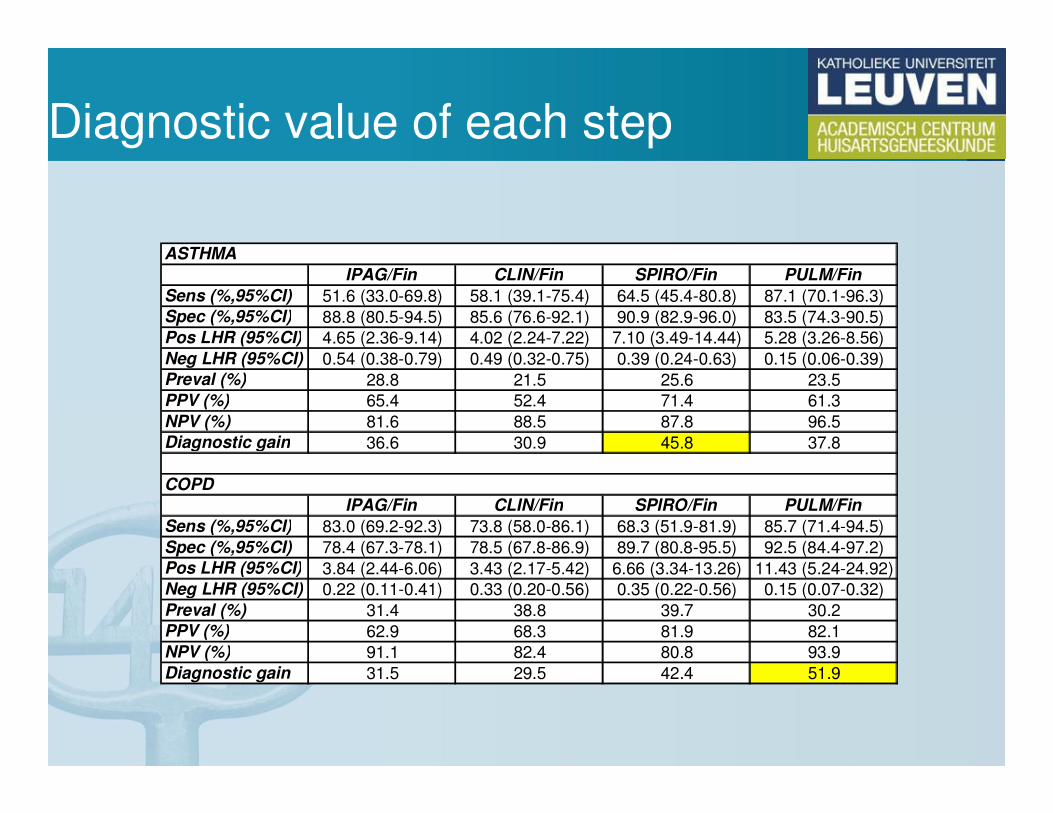
Diagnostic value of each step
ASTHMA
IPAG/Fin CLIN/Fin SPIRO/Fin PULM/Fin
Sens (%,95%CI) 51.6 (33.0-69.8) 58.1 (39.1-75.4) 64.5 (45.4-80.8) 87.1 (70.1-96.3)
Spec (%,95%CI) 88.8 (80.5-94.5) 85.6 (76.6-92.1) 90.9 (82.9-96.0) 83.5 (74.3-90.5)
Pos LHR (95%CI) 4.65 (2.36-9.14) 4.02 (2.24-7.22) 7.10 (3.49-14.44) 5.28 (3.26-8.56)
Neg LHR (95%CI) 0.54 (0.38-0.79) 0.49 (0.32-0.75) 0.39 (0.24-0.63) 0.15 (0.06-0.39)
Preval (%) 28.8 21.5 25.6 23.5
PPV (%) 65.4 52.4 71.4 61.3
NPV (%) 81.6 88.5 87.8 96.5
Diagnostic gain 36.6 30.9 45.8 37.8
COPD
IPAG/Fin CLIN/Fin SPIRO/Fin PULM/Fin
Sens (%,95%CI) 83.0 (69.2-92.3) 73.8 (58.0-86.1) 68.3 (51.9-81.9) 85.7 (71.4-94.5)
Spec (%,95%CI) 78.4 (67.3-78.1) 78.5 (67.8-86.9) 89.7 (80.8-95.5) 92.5 (84.4-97.2)
Pos LHR (95%CI) 3.84 (2.44-6.06) 3.43 (2.17-5.42) 6.66 (3.34-13.26) 11.43 (5.24-24.92)
Neg LHR (95%CI) 0.22 (0.11-0.41) 0.33 (0.20-0.56) 0.35 (0.22-0.56) 0.15 (0.07-0.32)
Preval (%) 31.4 38.8 39.7 30.2
PPV (%) 62.9 68.3 81.9 82.1
NPV (%) 91.1 82.4 80.8 93.9
Diagnostic gain 31.5 29.5 42.4 51.9
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?
Waarom spirometrie?
• Screening?
• Case finding?
• (Differentieel) diagnose?
• Evaluatie van exacerbaties?
• Follow-up therapie?
Spirometrie in huisartspraktijk
• Indicaties voor “office spirometry”
• Voorwaarden voor kwaliteit
• Mogelijke hinderpalen?
• Zelf uitvoeren of andere mogelijkheden?
Kwaliteit van « office spirometry »
• Kwaliteit van de toestellen
• Kwaliteit van de afname
• ATS/ERS criteria
• De invloed van training/retraining

Spirobank
Simplicity
SpiroPro
SpiroStar
Datospir 70
OneFlow

DatoSpir 120
MicroLoop
Pneumotrac
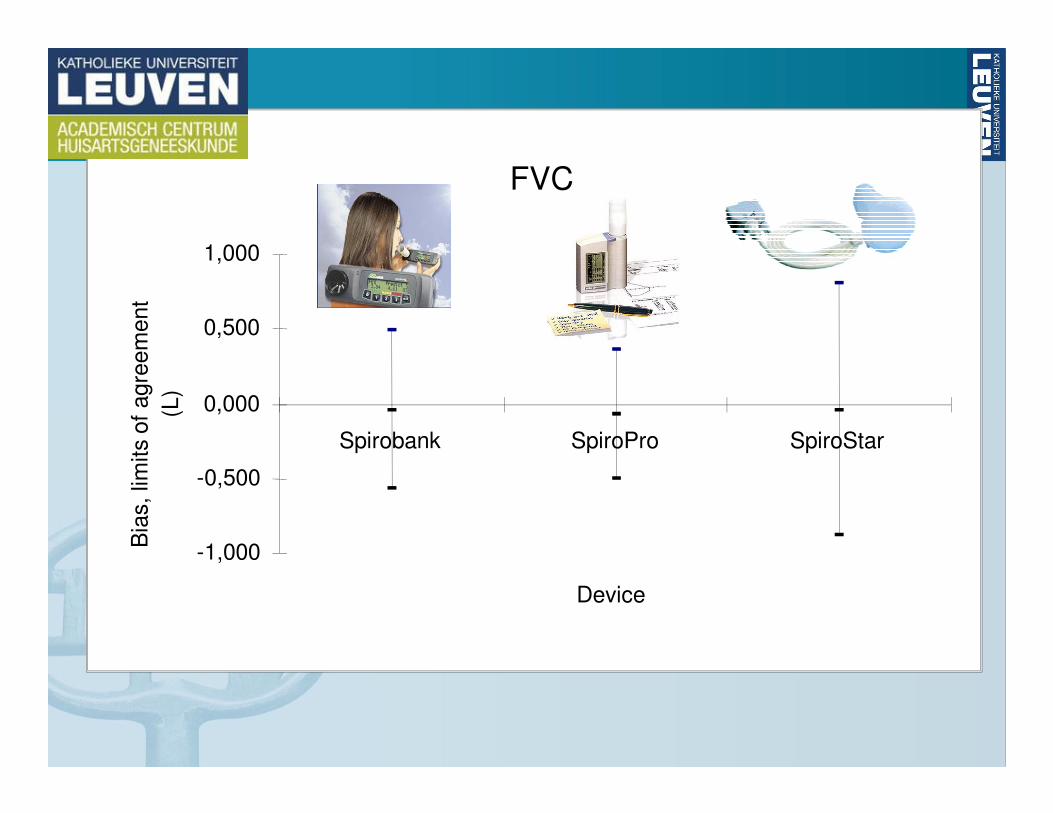
FVC
-1,000
-0,500
0,000
0,500
1,000
Spirobank SpiroPro SpiroStar
Device
Bia
s, lim
its o
f agre
em
ent
(L)
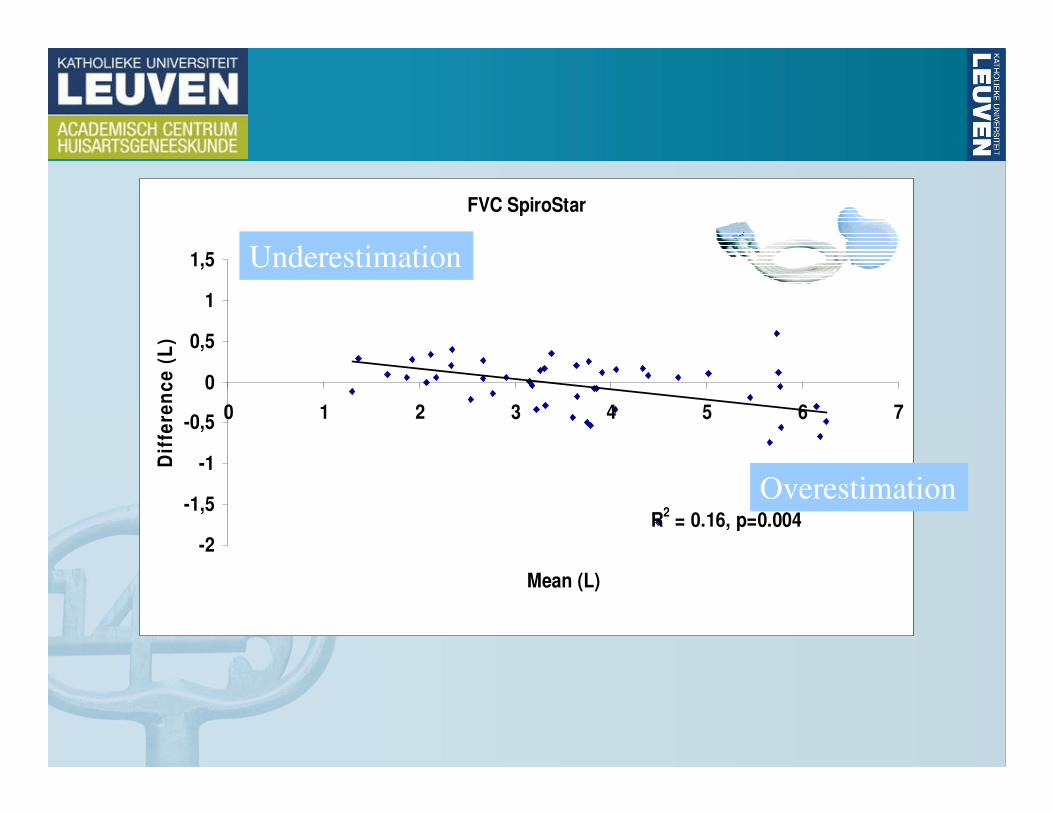
FVC SpiroStar
R2 = 0.16, p=0.004
-2
-1,5
-1
-0,5
0
0,5
1
1,5
0 1 2 3 4 5 6 7
Mean (L)
Dif
fere
nc
e (
L)
Underestimation
Overestimation
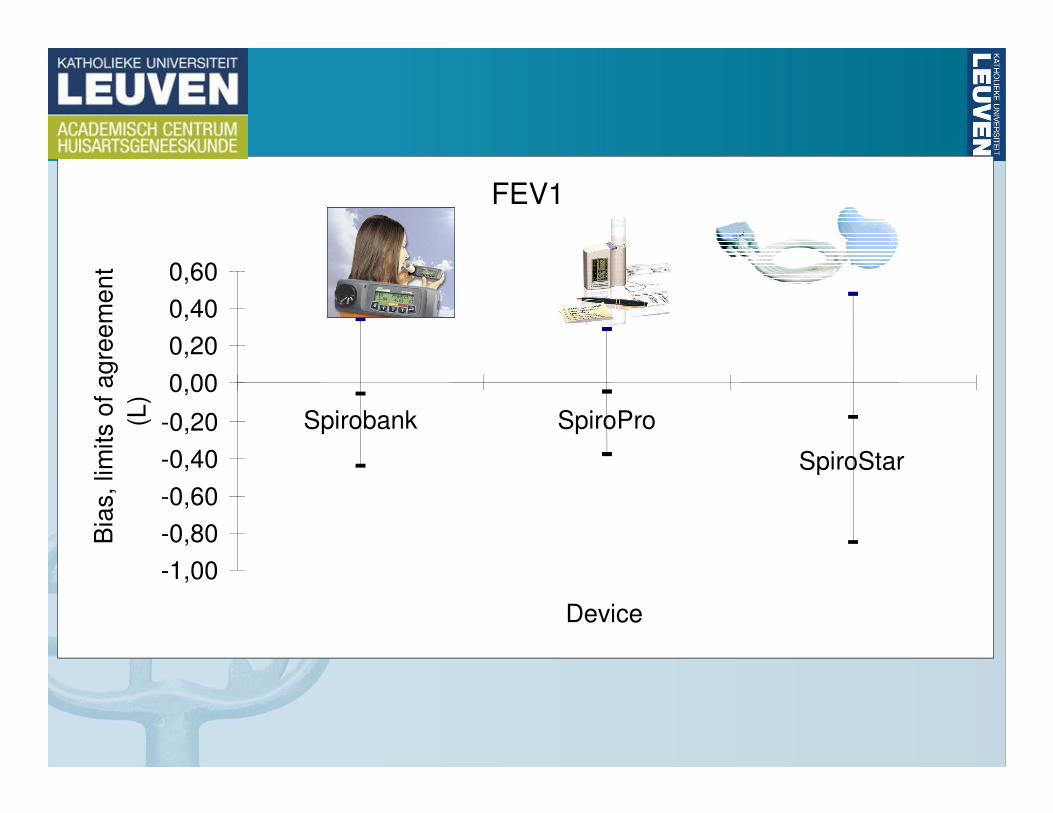
FEV1
-1,00
-0,80
-0,60
-0,40
-0,20
0,00
0,20
0,40
0,60
Spirobank SpiroPro
SpiroStar
Device
Bia
s, lim
its o
f a
gre
em
en
t
(L)
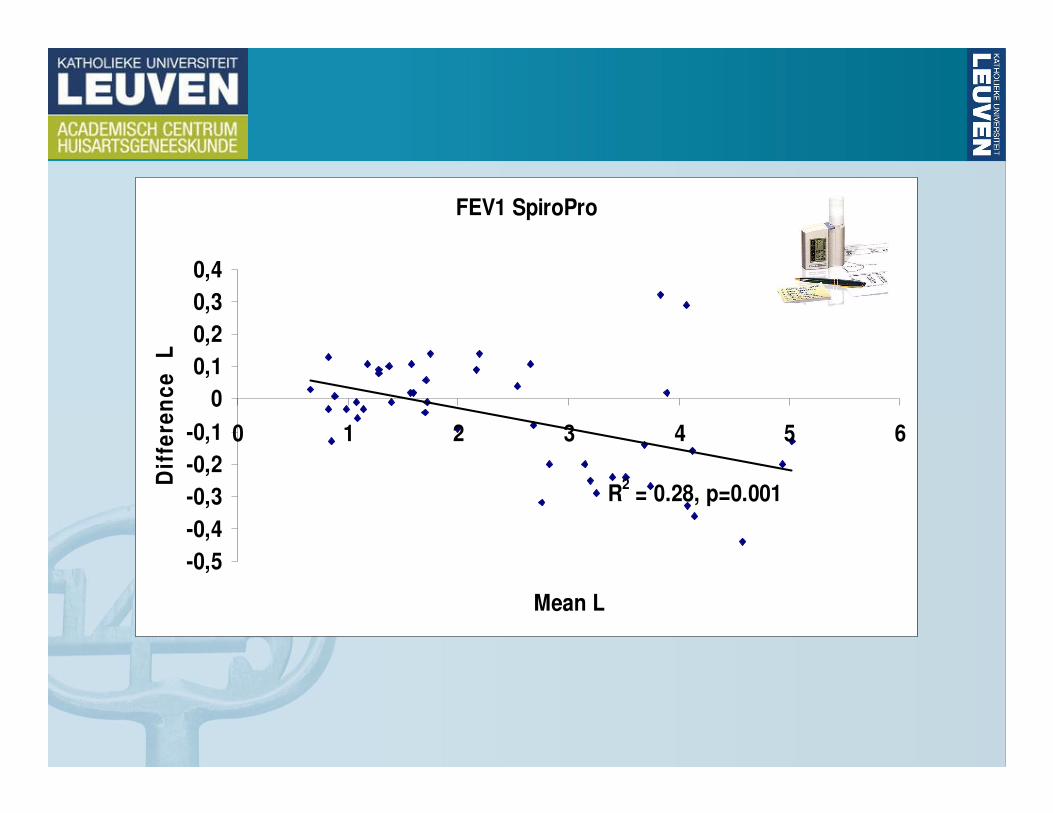
FEV1 SpiroPro
R2 = 0.28, p=0.001
-0,5
-0,4
-0,3
-0,2
-0,1
0
0,1
0,2
0,3
0,4
0 1 2 3 4 5 6
Mean L
Dif
fere
nc
e
L
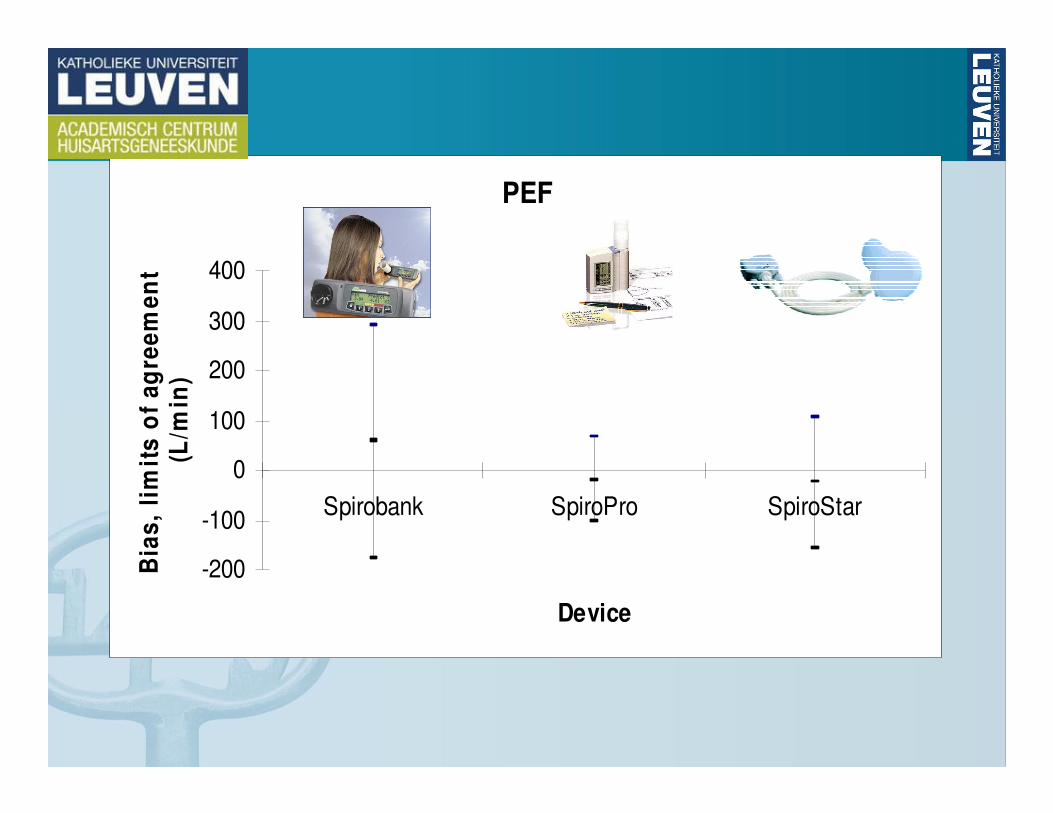
PEF
-200
-100
0
100
200
300
400
Spirobank SpiroPro SpiroStar
Device
Bia
s,
lim
its
of
ag
ree
me
nt
(L/m
in)
DIDASCO study
• What is the accuracy of spirometry performedwith the MIR Spirobank® spirometer?
• How accurately can trained primary care physicians perform spirometry by means of a portable electronic spirometer?
Degryse, Respiration 2012
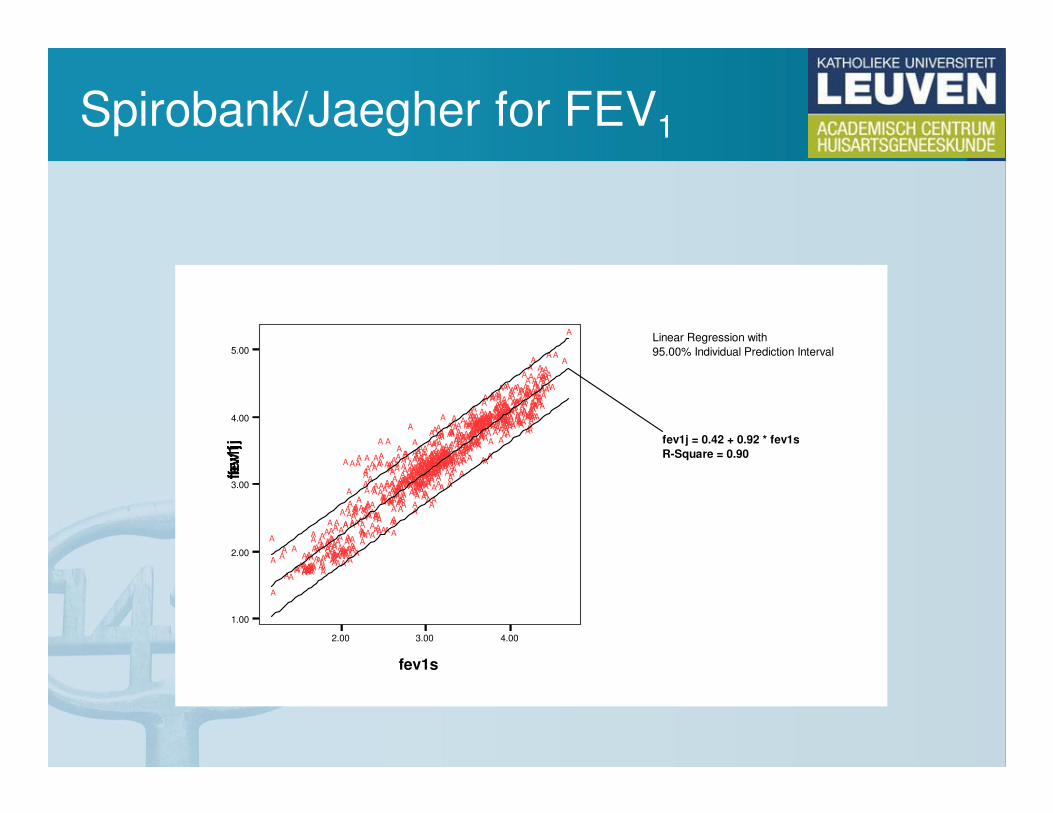
Spirobank/Jaegher for FEV1
Linear Regression with
95.00% Individual Prediction Interval
2.00 3.00 4.00
fev1s
1.00
2.00
3.00
4.00
5.00
fev1j
A
AAAA AA
AAA
AAA
AA
A
A
A
AA
A AAA
A
A
AA
A
AA
A
A
A
A
A
A
AAAA
AA A
A
A
A
AA
AAA
AAA
A A
A AA AAA
AAAA
AA A
A
AAA
A
AAAA AAA
AA
AA
AAAAAAA
AAA
AA
AA
A AAA
A
A
AA
A AAA
AA
AA
AAAA
AA
AA
AA
AA
AAAA
A
A
AA A
A
AAA
AA
A
AA
A
A AAAAA
A
A
AAAAA A
A
AA
A AAA
AA
AA
AA
AA
A
A
A A
A
A
AAA
A
AAA
AA
A A
AA
AAA
A A
A
A A
AAA
A
AAA
AAA
AA
A
A
AA
A
A
A
A
A A
A
A
A
AA
AA
AA
AA A
AA
A
AA
AAA
A
AAA
A AA AAA
A AA
A
AA
AA
AA
A
AAA AA
AAA
AA
AAAA
A
A
A
AA
A
A
A
A
A
AA AAA
AA
AA
AA
AA
AAA
AA
A
AA
A
AA
AA
AA
AA
A
A
AA
AAA A
A
A
AAA AA
AA A
AAAA
AA
AAA
A
A
AAAAAAA
AAAA
A
AA
A
AAA
A
AAAAA AA
AA
A
A
A A
AA
AAAAA
A
AA AAA
AA
AA
A
A
AA
AAAAA
A
A
A
A AA A
A
A
AAA
AA
AA
AAAAAAAAAAAAA
A
AA
AA
AA
AA
A
A
AA
A
A
A
AA
A
A
AA
AA
A
A
A
AA
AA AA AA
AAA
AAAA
A AAA
A
AAA
AAAA A
A
A
A
A
AA
AA
AA
AA
A
A
A
A
AA
A
AA
AA
A
A
AA
AA AAA AAA
AA AAAAAAAA
A AAAAAAAA
AA AAA
A
AAA
AAAAA
AA
AA
A
A
A
A
AA
A
A
A
A
A
A
A
A
A AA
AAA
AAA
AA
AA
AA A
AA
AAA
A
A AAAA A
A
AA
A
AAAAA
AA
AA
AA
AAA
AA
AA
A
A
AAA A
AA
AA
AAAAA A
AA
AA
AAAAA
AAA
AAAA
AA
A
A
AAA
A
AA
A
AA
A
A
AAAA
AA
A A
AAA
AA
A
AA
A AAAA
AAAAAAAA
A AA
AAA
AAA
A
AA
AAA
AAA
A
AA A
AAA
AA
A
A
A
A
AA
AA
A A
A
AA
AAA
AAA
AA
AA
AAAAA
AA
A AAA
AAAA
AA AA
AAA
AA
AA
AA
AA
AAA
AAAA
A
A
AAAA
A
AAA A
A
AA
AAA
A
A
AA
AAAAA A
A
A
A
AAA AA
AA
A
A AAAAAAAA
AAA
AAA
AAA
AA
A
AA
AAA
AAA
AAA
A
AA
AAAA
AAA
AAAAA AAAA
A A
A AAAAAAAA
A
A AA AAA
A
AAA
A
A
A
A
A
A
A
fev1j = 0.42 + 0.92 * fev1s
R-Square = 0.90
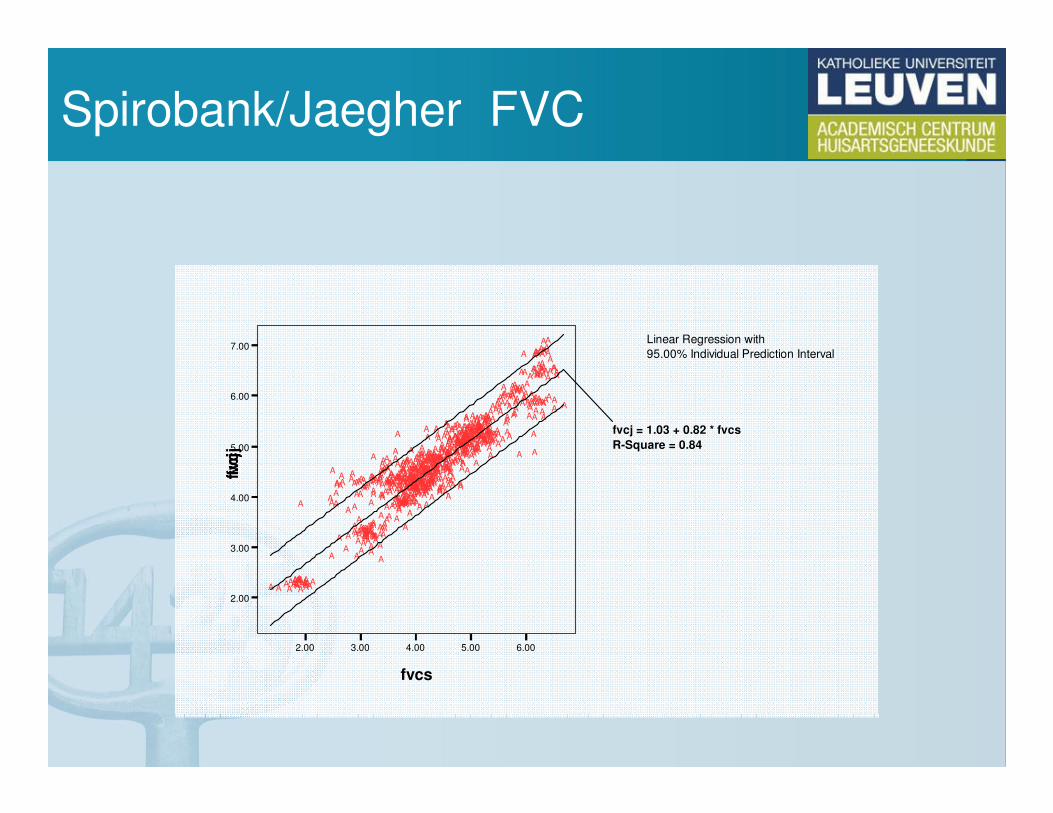
Spirobank/Jaegher FVC
Linear Regression with
95.00% Individual Prediction Interval
2.00 3.00 4.00 5.00 6.00
fvcs
2.00
3.00
4.00
5.00
6.00
7.00
fvc
j A
AA
AAAA
A
AA
AA
AAA
A
AAAAA
AA
A
A A
AA A
AA
A AA
AA A
A
A
AA AA AAA A
AA A
A
A A
A
A
A AAA
A A
A
A
AA
AA AAA AA
AA
AAA
AA A
AA
AA
A A
AAAAAAA AAA
AA
A
A
AA
AA
AAAAAAAAAA
AA AAAA
AAAAAAAAAA
AA
AA
AA
AAAA A
A
A
A
A
AAA A
AA AA
A
A AA
AA
AA AA
AAAA
AAA AAA
AA
AAA
A AA
A
AAA AAAAA
AA
AAA
A AA
AA
A
AA
A AAA A
AAA
A
A
AA
AAAA
A
A AA
A A
A
A
A
AA
AA
A
AA
AA
AAA
A AA
AA
A
AA
AA A
AA
A
AA A
AA
A A
A
AA
AA
A
A AAA
A AA
A AA
AAAA
AA
A
AA
AA
AA
AAA AAAA
AAAA
AAAAA
A
A
A
A
A
A
AAA
AA
AA AA
A
AA
A
AAA A
A AAA
A
A
AA
A
AAAA
AAA
AAA
A
AAAAA
AA
AAA
A AAA
AA
AAA
AAAA A
AAAAA A
AAA
A
AAAAAA
AAA
AA
A
AA
AA
A
AAAAAA A
AA
A
AAA
AAA
AA
AAAA
AAAAAAA
AAAA
AAA
A
A AA
AA
AAA
A
A
AA
AA
A
A A
AA
AAAA
AAAAAAA
AA
AAA AAAAA
AA
AAA
A AAAA AA AAA
A
A
A
A A
AAA
A
AAA
A
A
A
AA
A
AA
A
AA
A
AA A A AAA AA AAAAAAAAAAAA AA
AAAAAA
AA A
AA
A
AAA
A A
AAAA
AA
A
AA
A
A
AA
A
A
A
A
A
A
A
A
A AAAAA
AA
AAA
AA
AA A
A A
A
AAA
AAA
AA AA
AA
A
AAAA
AAA
AA
AAAA AAA
AA
A
AA AA AA
A
AA A A
AAA AA
A
AA
AAA
AA
AAA
AAA
AAA
A
A
AAA
A
A A
A
AAA A
AAAA
AAAA
AAA
AAA
AA
A AAAA
AAAAAAAA A A
A
AA
A
AAAAA A
A AA
A
AA A
AA AA A
AA
AA
AA
A
A
A
AAAA
A
AAAA
AA
AAA
AAAA A
AAAAAA AA
AAAAA
AA AA
A AA
AA
AA
AA
AA
A AA AA AA
A
A
AA AAA
AA AA
AAAAAA AA
AAA
AAAA
AAA
A AAAA
A
AAA
AAAAAA
AA
AA
A AAAAAAAAAA
AAAAAA
AAAA
AAAAA A A
AAAA
AAAAAAAAAAA
AAA
AAAAAAAA
AA AAAAAA
AA
AA
A
A
AA
fvcj = 1.03 + 0.82 * fvcs
R-Square = 0.84
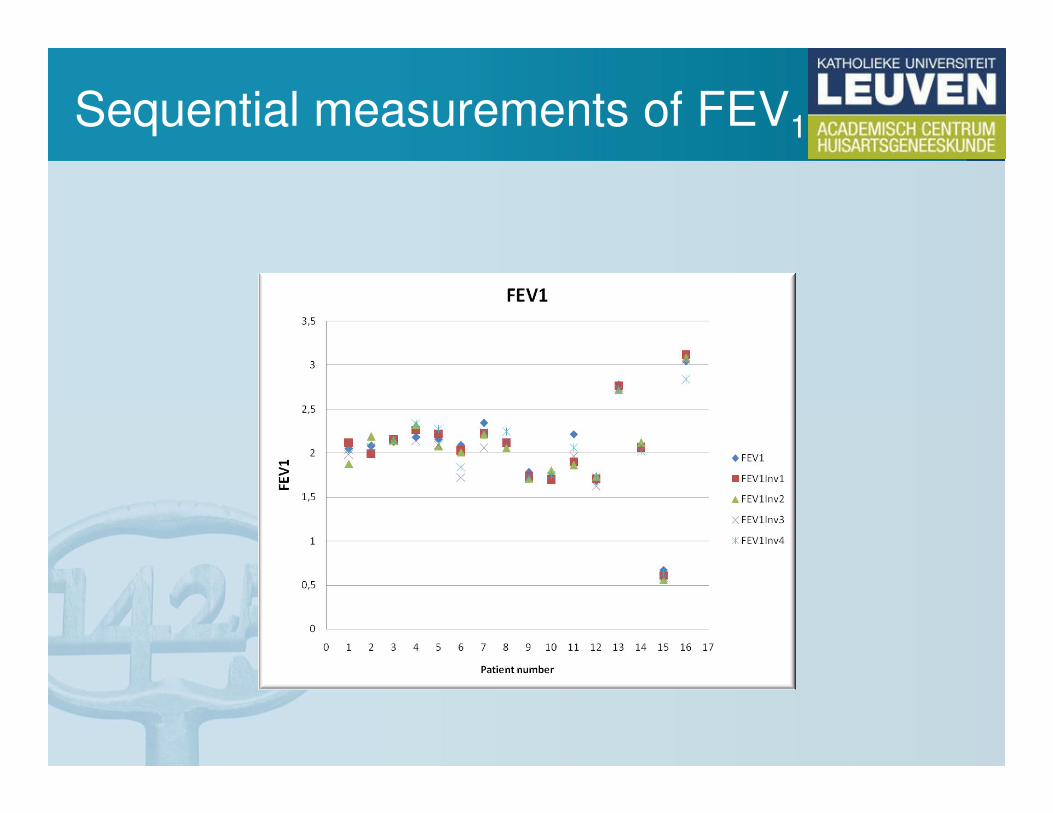
Sequential measurements of FEV1
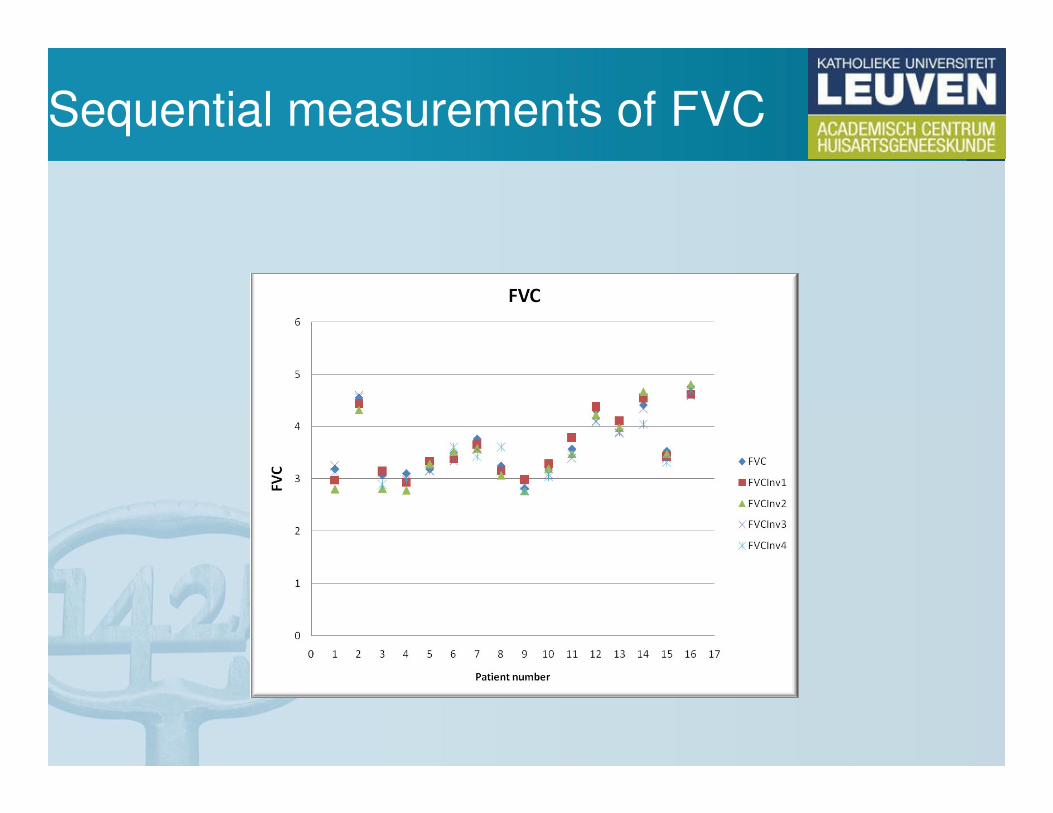
Sequential measurements of FVC
Acceptable spirometry (ATS)
• No artefacts– cough, glottis closure, abrubt ending, variable effort, leaks
• Fast start
• Expiratory time > 6 sec Or acceptable plateau
Volume / time
Acceptable spirometry (ATS)
• No artefacts– cough, glottis closure, abrubt ending, variable effort, leaks
• Fast start
• Expiratory time > 6 sec Or acceptable plateau
Volume / time
Acceptable spirometry (ATS)
• No artefacts– cough, glottis closure, abrubt ending, variable effort, leaks
• Fast start
• Expiratory time > 6 sec Or acceptable plateau
Volume / time
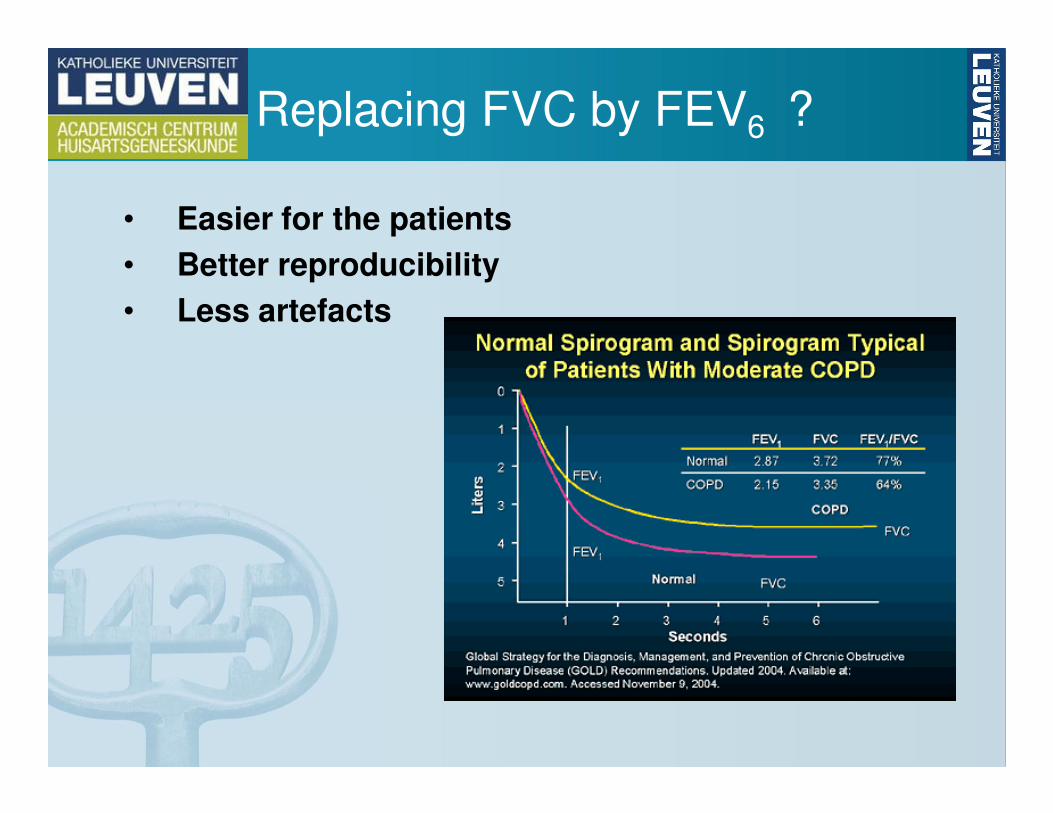
Replacing FVC by FEV6 ?
• Easier for the patients
• Better reproducibility
• Less artefacts
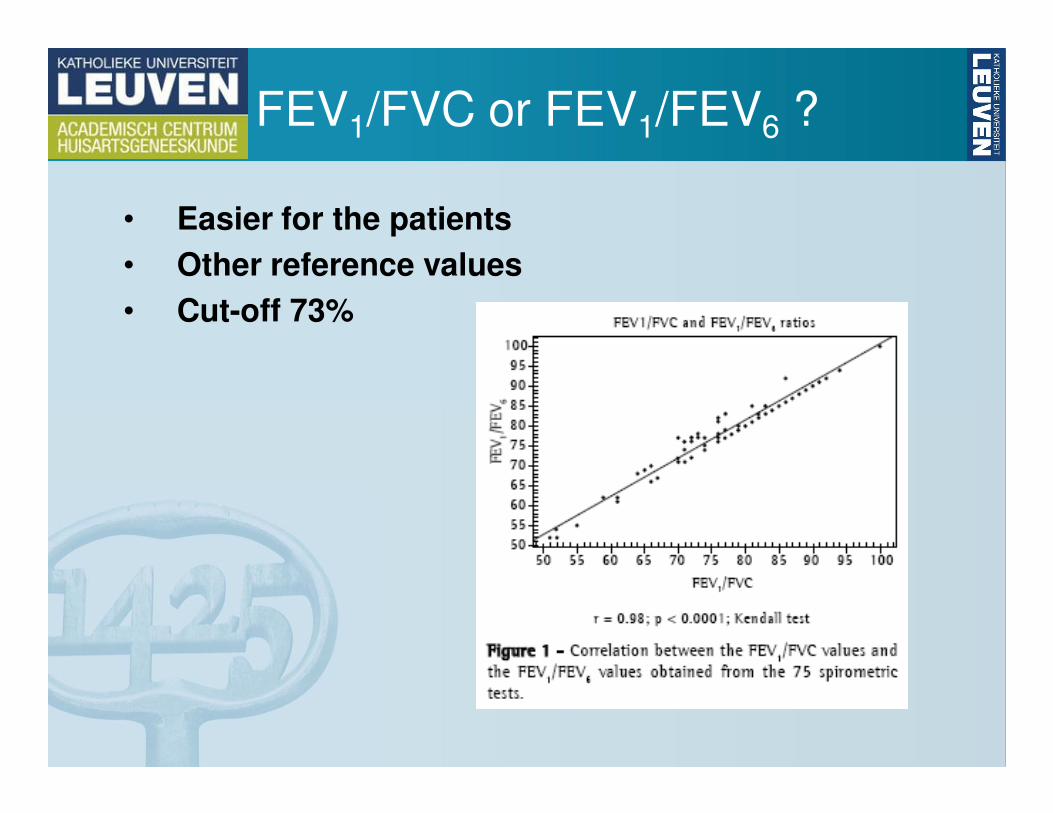
FEV1/FVC or FEV1/FEV6 ?
• Easier for the patients
• Other reference values
• Cut-off 73%

New screening tool?
Reproducibility
• Maximum 5% variability in technically
acceptable trials
• Maximum 150 ml ∆∆∆∆ for FEV1 and FVC
• Report highest FEV1 and FVC from acceptable
trials
• Up to 8 trials to be performed
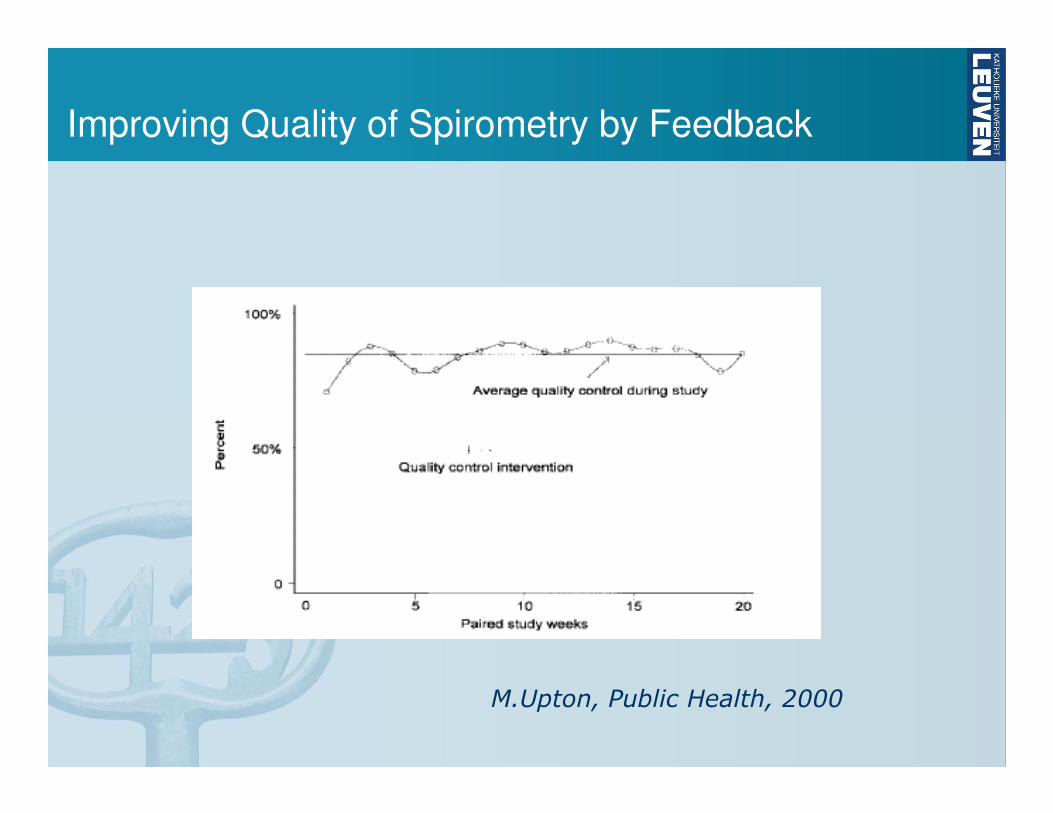
Improving Quality of Spirometry by Feedback
M.Upton, Public Health, 2000
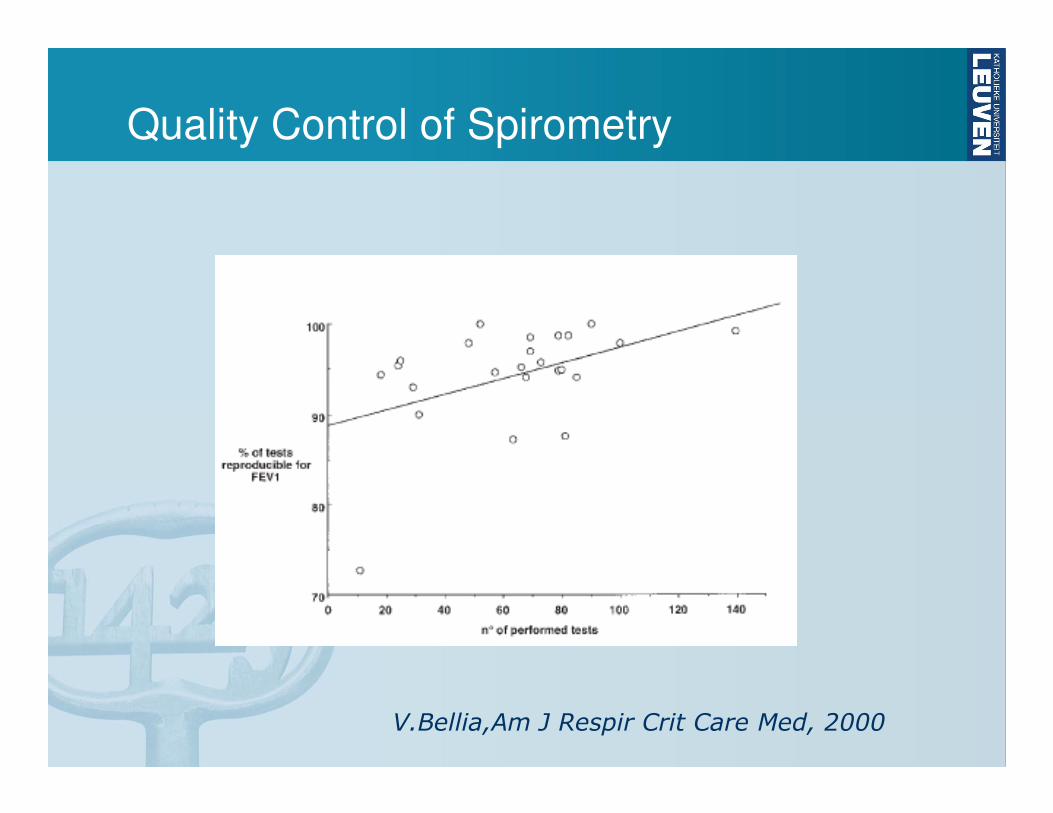
Quality Control of Spirometry
V.Bellia,Am J Respir Crit Care Med, 2000
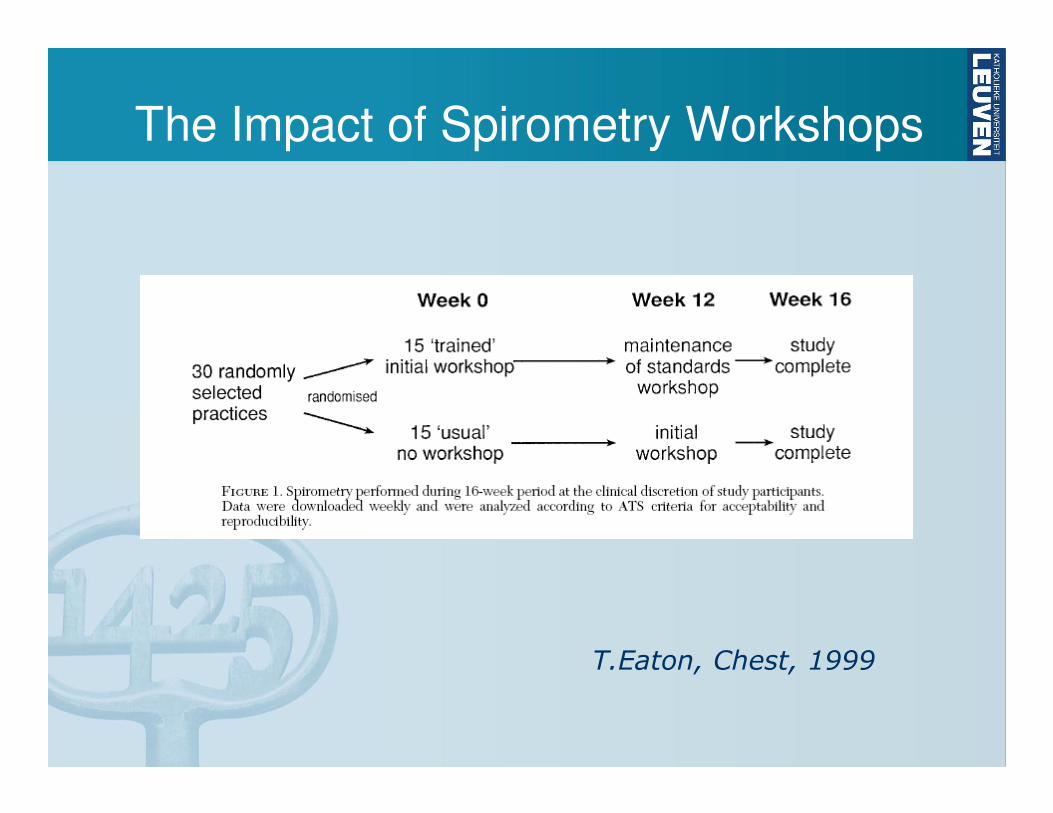
The Impact of Spirometry Workshops
T.Eaton, Chest, 1999
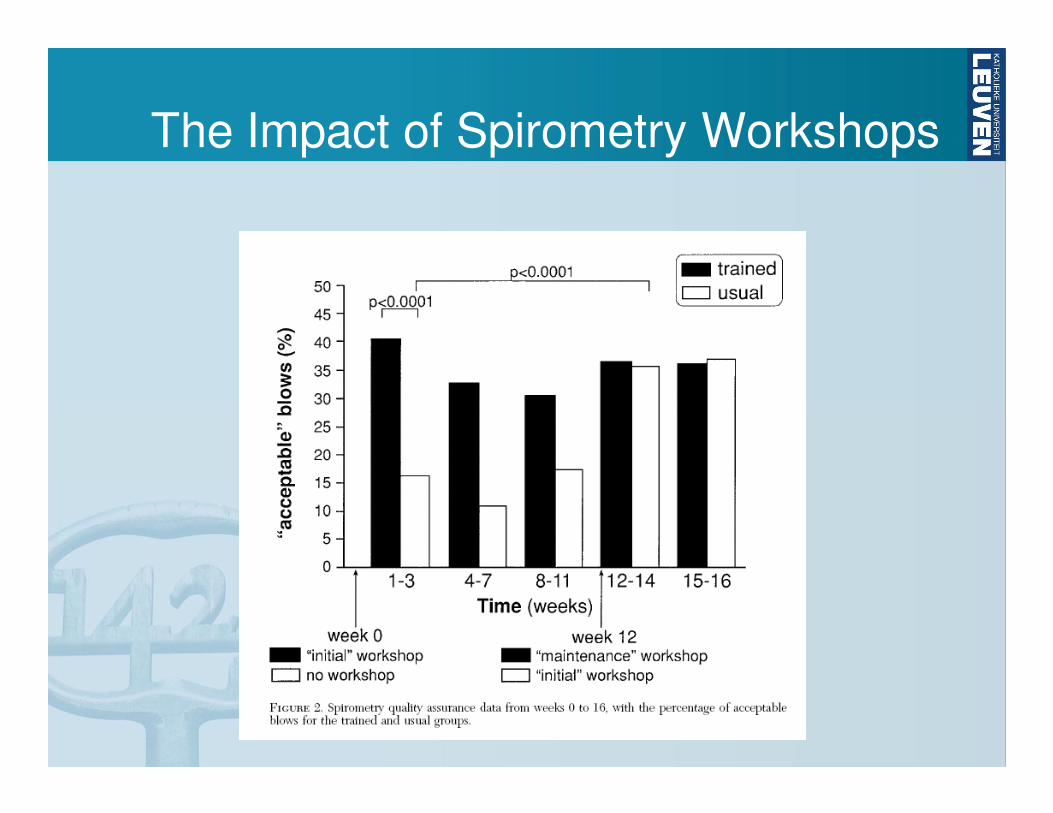
The Impact of Spirometry Workshops
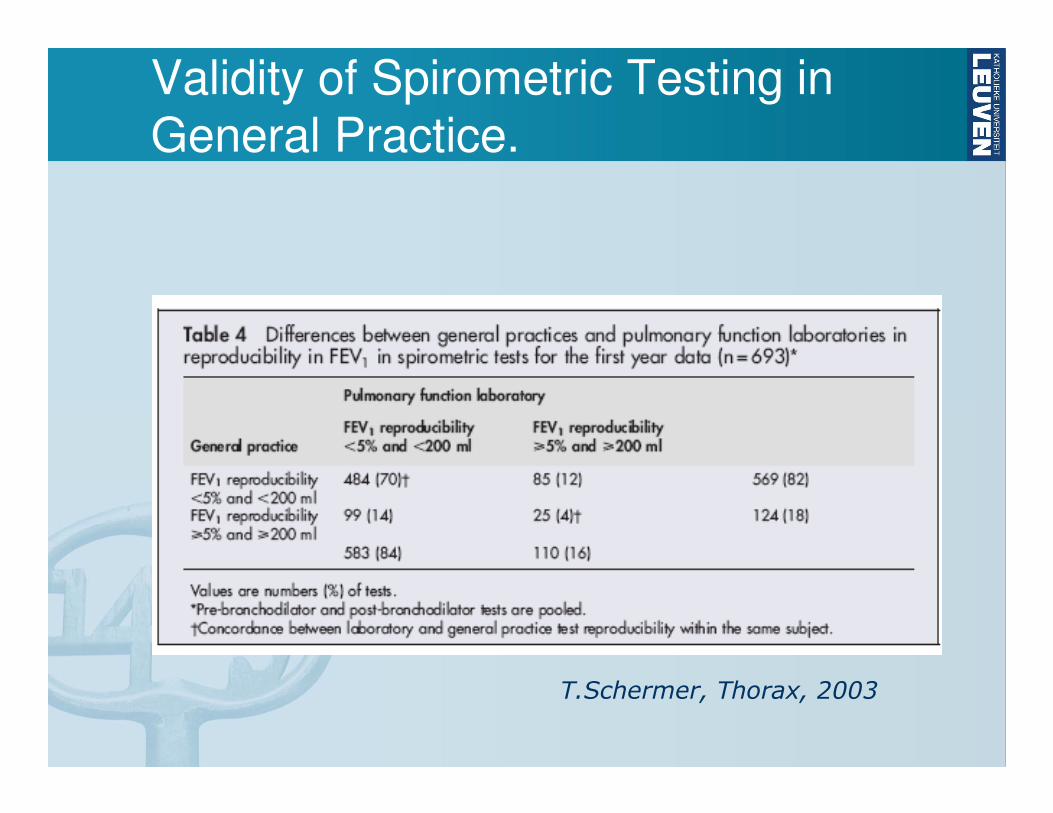
Validity of Spirometric Testing in
General Practice.
T.Schermer, Thorax, 2003
Spirometrie in huisartspraktijk
• Indicaties voor “office spirometry”
• Voorwaarden voor kwaliteit
• Mogelijke hinderpalen?
• Zelf uitvoeren of andere mogelijkheden?
Hinderpalen
• Onvoldoende competentie bij de huisarts
• Onvoldoende vergoeding voor de geleverde inspanning
• Geen zicht op indicaties
• Moeilijk in te plannen
• Onvoldoende mogelijkheden voor navorming
Spirometrie in huisartspraktijk
• Indicaties voor “office spirometry”
• Voorwaarden voor kwaliteit
• Mogelijke hinderpalen?
• Zelf uitvoeren of andere mogelijkheden?
Mogelijke alternatieven
• Uitvoering door praktijkassistente
• Uitvoering door “respiratory nurse”
• “MCH”?
• On line feedback?
• Open longfunctielab
• “Kaderhuisartsen”? “GPwSI”?
Criteria for referral
to a chest physician
• Discrepancy between the clinical findings and the spirometric values
• Arguments for an occupational factor in the ethiology of the airway obstruction
• A postbronchodilator FEV1 of <50% predicted
• COPD before the age of 50
• Doubt about a possible cardiac origin of the dyspnoea
• Arguments for malignancy
• Signs of restrictive lung disease
• Any atypical disease history
Thank you for
your attention!
Questions ??