

Revalidatie voor PH-patiënten A. Vonk en M. Spruit.pdf · Conclusies •Inspanning is goed voor...
39
Revalidatie voor PH-patiënten Anton Vonk Noordegraaf Afd Longziekten VUMC& AMC Amsterdam Martijn Spruit CIRO Horn
Transcript of Revalidatie voor PH-patiënten A. Vonk en M. Spruit.pdf · Conclusies •Inspanning is goed voor...

Revalidatie voor PH-patiënten
Anton Vonk Noordegraaf
Afd Longziekten
VUMC& AMC Amsterdam
Martijn Spruit
CIRO
Horn
VROEGER: REVALIDATIE IS SLECHT
VOOR PATIËNTEN MET PULMONALE
HYPERTENSIE WANT HET
VEROORZAAKT OVERBELASTING
VAN HET HART
2
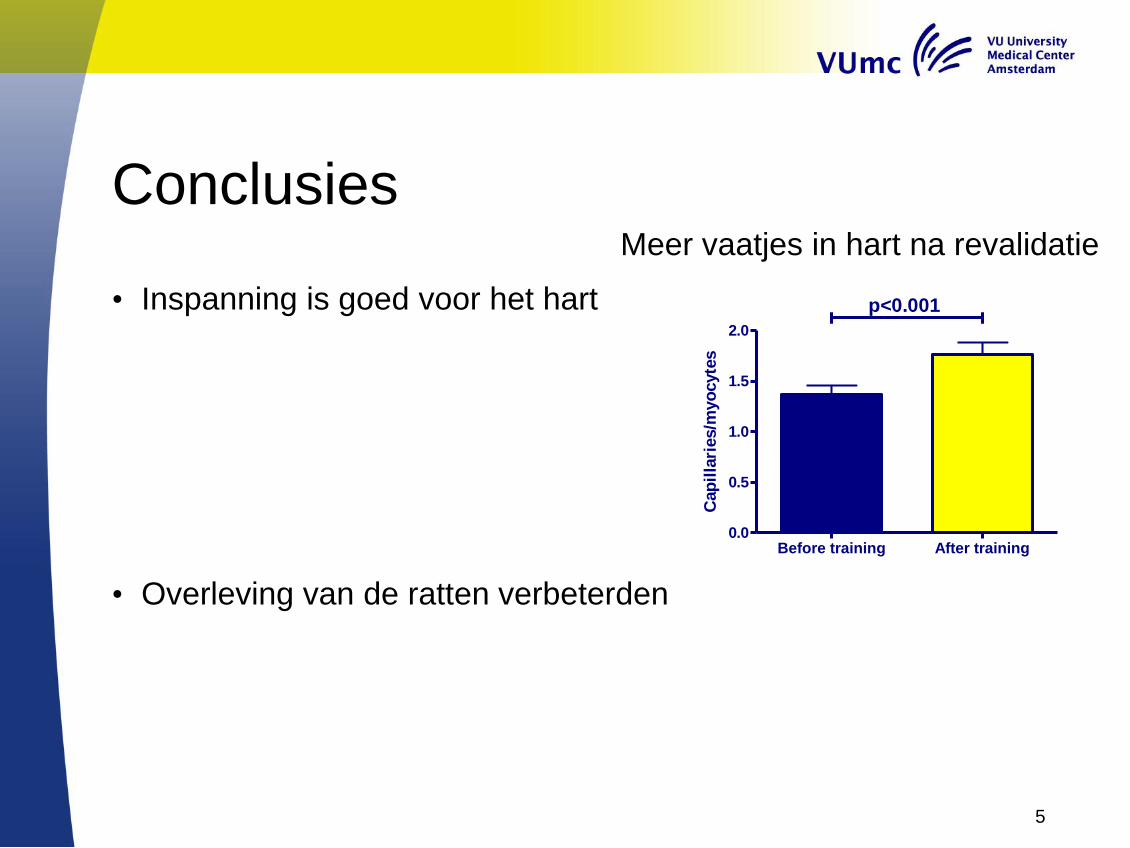
Conclusies
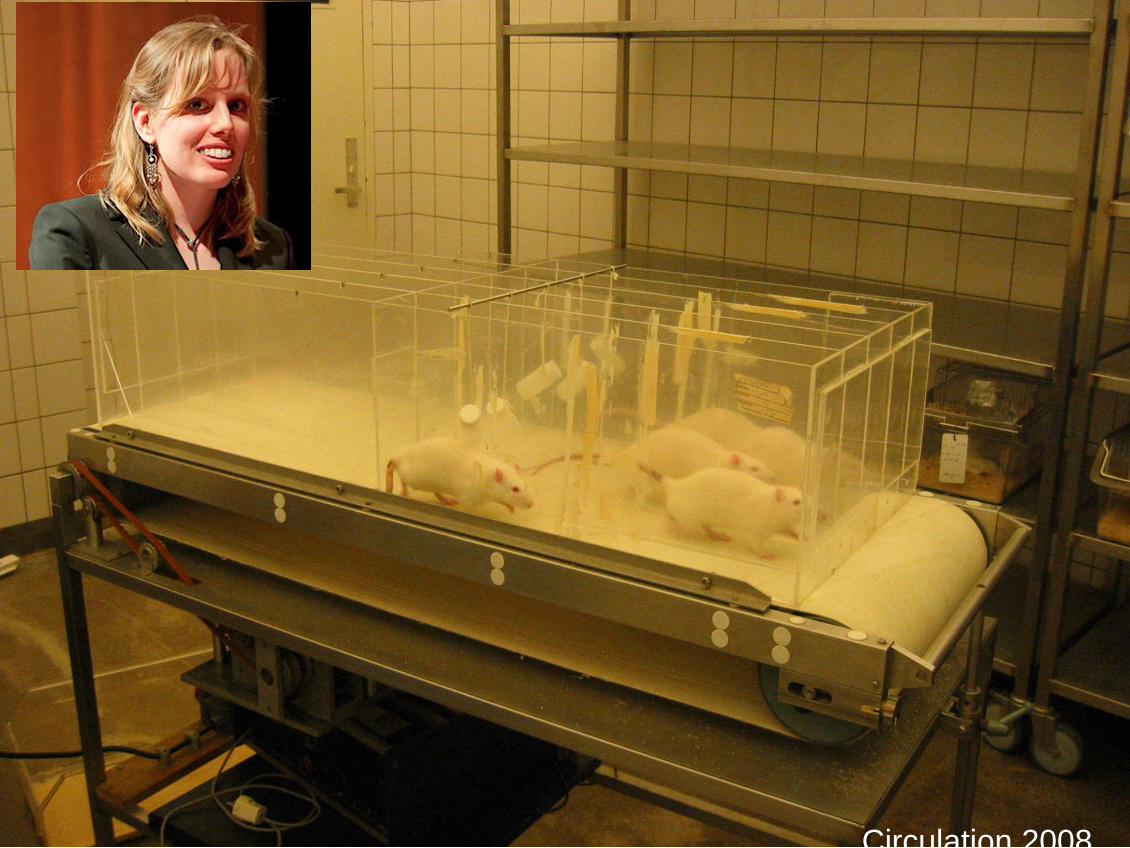
• Inspanning is goed voor het hart
• Overleving van de ratten verbeterden
5
Before training After training0.0
0.5
1.0
1.5
2.0
p<0.001
Cap
illa
ries/m
yo
cyte
s
Meer vaatjes in hart na revalidatie

Multicenter Nederlandse revalidatie studie
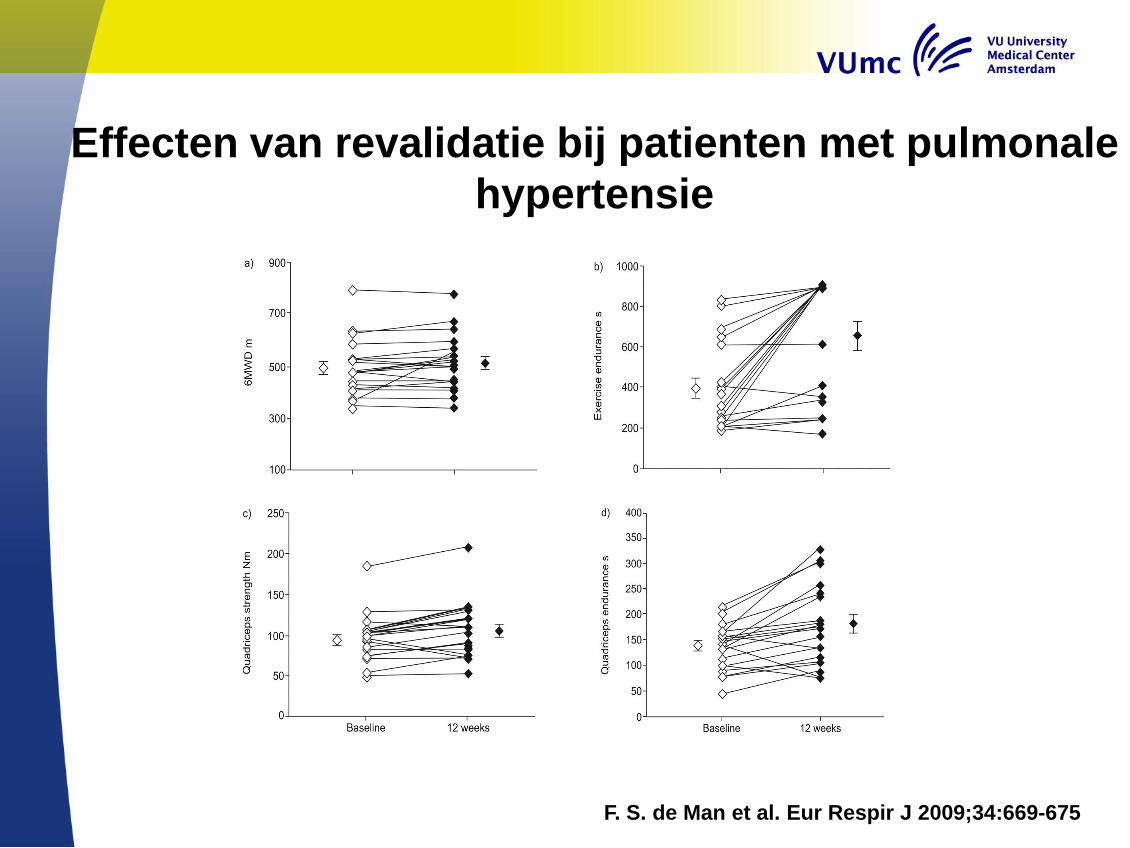
Effecten van revalidatie bij patienten met pulmonale
hypertensie
F. S. de Man et al. Eur Respir J 2009;34:669-675
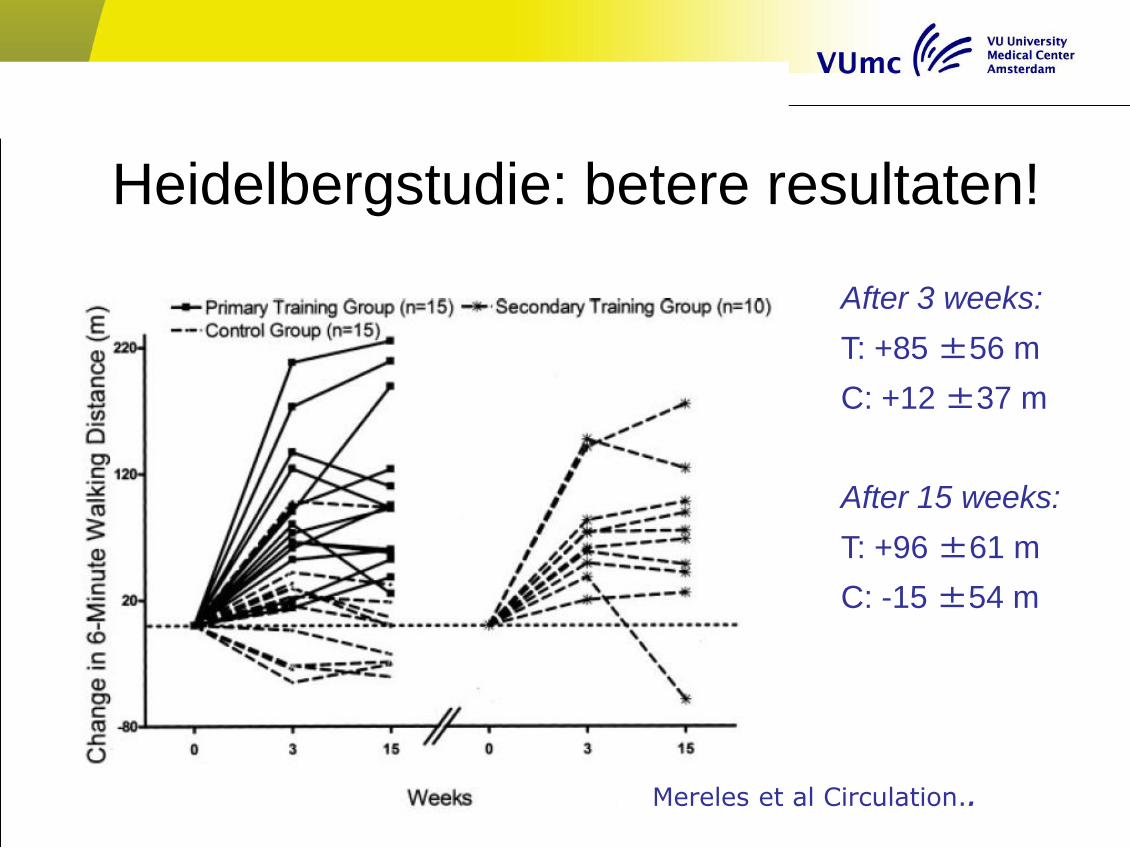
Heidelbergstudie: betere resultaten!
After 3 weeks:
T: +85 ±56 m
C: +12 ±37 m
After 15 weeks:
T: +96 ±61 m
C: -15 ±54 m
Mereles et al Circulation..

Heidelbergconcept: aandacht voor
de hele mens!
9
Wens: Een revalidatietraject (intern)
opzetten zoals in Heidelberg
toegankelijk voor alle PAH patiënten
10
Wie betaalt?
Oplossing
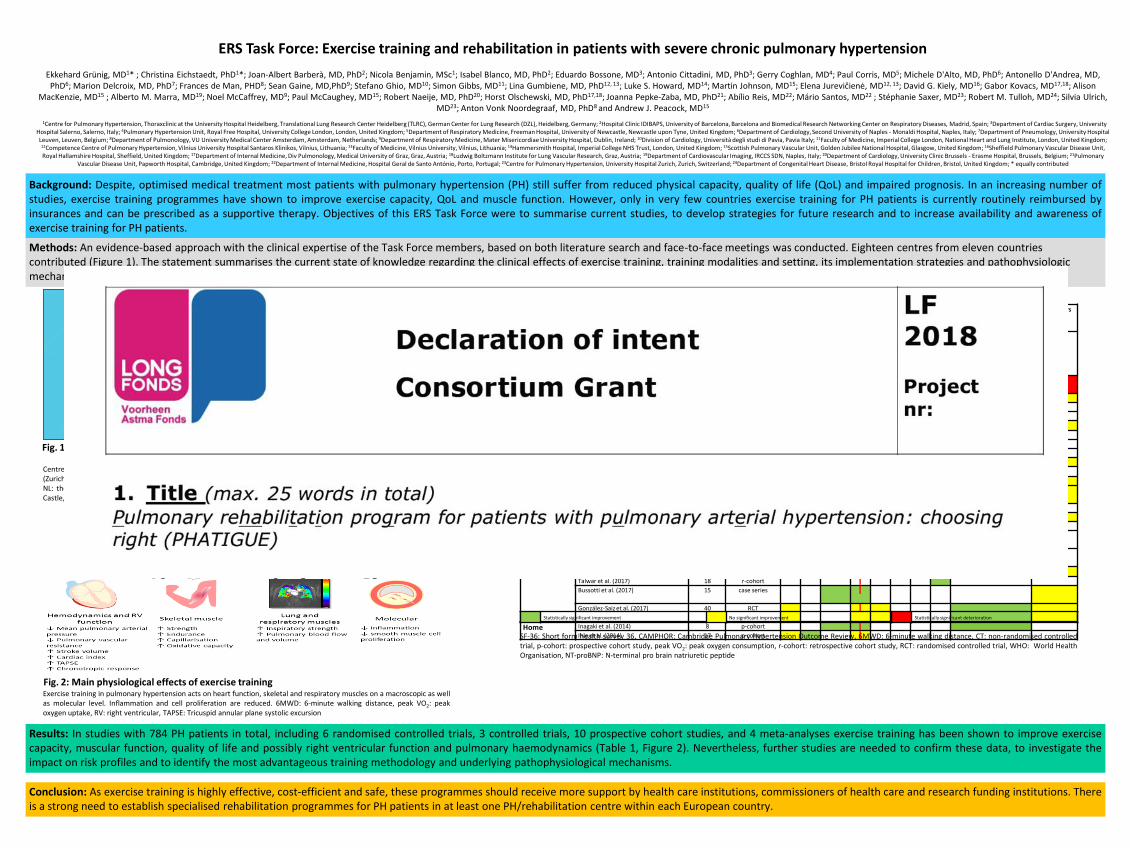
ERS Task Force: Exercise training and rehabilitation in patients with severe chronic pulmonary hypertension
Ekkehard Grünig, MD1* ; Christina Eichstaedt, PhD1*; Joan-Albert Barberà, MD, PhD2; Nicola Benjamin, MSc1; Isabel Blanco, MD, PhD2; Eduardo Bossone, MD3; Antonio Cittadini, MD, PhD3; Gerry Coghlan, MD4; Paul Corris, MD5; Michele D'Alto, MD, PhD6; Antonello D'Andrea, MD, PhD6; Marion Delcroix, MD, PhD7; Frances de Man, PHD8; Sean Gaine, MD,PhD9; Stefano Ghio, MD10; Simon Gibbs, MD11; Lina Gumbiene, MD, PhD12, 13; Luke S. Howard, MD14; Martin Johnson, MD15; Elena Jurevičienė, MD12, 13; David G. Kiely, MD16; Gabor Kovacs, MD17,18; Alison
MacKenzie, MD15 ; Alberto M. Marra, MD19; Noel McCaffrey, MD9; Paul McCaughey, MD15; Robert Naeije, MD, PhD20; Horst Olschewski, MD, PhD17,18; Joanna Pepke-Zaba, MD, PhD21; Abílio Reis, MD22; Mário Santos, MD22 ; Stéphanie Saxer, MD23; Robert M. Tulloh, MD24; Silvia Ulrich, MD23; Anton Vonk Noordegraaf, MD, PhD8 and Andrew J. Peacock, MD15
g
1Centre for Pulmonary Hypertension, Thoraxclinic at the University Hospital Heidelberg, Translational Lung Research Center Heidelberg (TLRC), German Center for Lung Research (DZL), Heidelberg, Germany; 2Hospital Clinic IDIBAPS, University of Barcelona, Barcelona and Biomedical Research Networking Center on Respiratory Diseases, Madrid, Spain; 3Department of Cardiac Surgery, University Hospital Salerno, Salerno, Italy; 4Pulmonary Hypertension Unit, Royal Free Hospital, University College London, London, United Kingdom; 5Department of Respiratory Medicine, Freeman Hospital, University of Newcastle, Newcastle upon Tyne, United Kingdom; 6Department of Cardiology, Second University of Naples - Monaldi Hospital, Naples, Italy; 7Department of Pneumology, University Hospital Leuven, Leuven, Belgium; 8Department of Pulmonology, VU University Medical Center Amsterdam, Amsterdam, Netherlands; 9Department of Respiratory Medicine, Mater Misericordiae University Hospital, Dublin, Ireland; 10Division of Cardiology, Università degli studi di Pavia, Pavia Italy; 11Faculty of Medicine, Imperial College London, National Heart and Lung Institute, London, United Kingdom;
12Competence Centre of Pulmonary Hypertension, Vilnius University Hospital Santaros Klinikos, Vilnius, Lithuania; 13Faculty of Medicine, Vilnius University, Vilnius, Lithuania; 14Hammersmith Hospital, Imperial College NHS Trust, London, United Kingdom; 15Scottish Pulmonary Vascular Unit, Golden Jubilee National Hospital, Glasgow, United Kingdom; 16Sheffield Pulmonary Vascular Disease Unit, Royal Hallamshire Hospital, Sheffield, United Kingdom; 17Department of Internal Medicine, Div Pulmonology, Medical University of Graz, Graz, Austria; 18Ludwig Boltzmann Institute for Lung Vascular Research, Graz, Austria; 19Department of Cardiovascular Imaging, IRCCS SDN, Naples, Italy; 20Department of Cardiology, University Clinic Brussels - Erasme Hospital, Brussels, Belgium; 21Pulmonary
Vascular Disease Unit, Papworth Hospital, Cambridge, United Kingdom; 22Department of Internal Medicine, Hospital Geral de Santo António, Porto, Portugal; 23Centre for Pulmonary Hypertension, University Hospital Zurich, Zurich, Switzerland; 24Department of Congenital Heart Disease, Bristol Royal Hospital for Children, Bristol, United Kingdom; * equally contributed
Results: In studies with 784 PH patients in total, including 6 randomised controlled trials, 3 controlled trials, 10 prospective cohort studies, and 4 meta-analyses exercise training has been shown to improve exercise capacity, muscular function, quality of life and possibly right ventricular function and pulmonary haemodynamics (Table 1, Figure 2). Nevertheless, further studies are needed to confirm these data, to investigate the impact on risk profiles and to identify the most advantageous training methodology and underlying pathophysiological mechanisms.
Conclusion: As exercise training is highly effective, cost-efficient and safe, these programmes should receive more support by health care institutions, commissioners of health care and research funding institutions. There is a strong need to establish specialised rehabilitation programmes for PH patients in at least one PH/rehabilitation centre within each European country.
Background: Despite, optimised medical treatment most patients with pulmonary hypertension (PH) still suffer from reduced physical capacity, quality of life (QoL) and impaired prognosis. In an increasing number of studies, exercise training programmes have shown to improve exercise capacity, QoL and muscle function. However, only in very few countries exercise training for PH patients is currently routinely reimbursed by insurances and can be prescribed as a supportive therapy. Objectives of this ERS Task Force were to summarise current studies, to develop strategies for future research and to increase availability and awareness of exercise training for PH patients.
Methods: An evidence-based approach with the clinical expertise of the Task Force members, based on both literature search and face-to-face meetings was conducted. Eighteen centres from eleven countries contributed (Figure 1). The statement summarises the current state of knowledge regarding the clinical effects of exercise training, training modalities and setting, its implementation strategies and pathophysiologic mechanisms in patients with PH.
Fig. 1: Participating countries in this Task Force having implemented the exercise training
Centres and participating countries in alphabetical order: AT: Austria (Graz), BE: Belgium (Brussels, Leuven), CH: Switzerland (Zurich), DE: Germany (Heidelberg), ES: Spain (Barcelona), IE: Ireland (Dublin), IT: Italy (Naples, Pavia), LT: Lithuania (Vilnius), NL: the Netherlands (Amsterdam), PT: Portugal (Porto), UK: United Kingdom (Glasgow, Bristol, Cambridge, London, New Castle, Sheffield).
Type Study n Design Quality of life Functional ability Peripheral muscle function Bio-markers
SF3
6
CA
MP
HO
R
Oth
er
qu
esti
on
nai
re
6MW
D
Pea
k V
O2
End
ura
nc
e WH
O
Cla
ss
Trea
dm
ill
spee
d
Mu
scle
stre
ngt
h
(NT-
pro
)-
BN
P
In-patient Becker-Grünig et al. (2013) 20 p-cohort
Grünig et al. (2012a) 183 p-cohort
Grünig et al. (2011) 58 p-cohort
Grünig et al. (2012b) 21 p-cohort
Nagel et al. (2012) 35 p-cohort
Kabitz et al. (2014) 7 p-cohort
Mereles et al. (2006) 30 RCT
Ley et al. (2013) 20 RCT
Ehlken et al. (2016) 87 RCT
Ehlken et al. (2014) 58 p-cohort
Fukui et al. (2016) 41 CT
Out-patient Martinez-Quintana et al. (2010) 8 CT
Raskin et al. (2014) 23 r-cohort
Fox et al. (2011) 22 CT
Chan et al. (2013) 23 RCT
Weinstein et al. (2013) 24 RCT
Mainguy et al. (2010) 5 case series
de Man et al. (2009) 19 p-cohort
Talwar et al. (2017) 18 r-cohort
Bussotti et al. (2017) 15 case series
González-Saiz et al. (2017) 40 RCT
Home Inagaki et al. (2014) 8 p-cohort
Ihle et al. (2014) 17 p-cohort
Table 1: Outcome measures for training programmes
Statistically significant improvement No significant improvement Statistically significant deterioration
SF-36: Short form health survey 36, CAMPHOR: Cambridge Pulmonary Hypertension Outcome Review, 6MWD: 6-minute walking distance, CT: non-randomised controlled trial, p-cohort: prospective cohort study, peak VO2: peak oxygen consumption, r-cohort: retrospective cohort study, RCT: randomised controlled trial, WHO: World Health Organisation, NT-proBNP: N-terminal pro brain natriuretic peptide
Fig. 2: Main physiological effects of exercise training Exercise training in pulmonary hypertension acts on heart function, skeletal and respiratory muscles on a macroscopic as well as molecular level. Inflammation and cell proliferation are reduced. 6MWD: 6-minute walking distance, peak VO2: peak oxygen uptake, RV: right ventricular, TAPSE: Tricuspid annular plane systolic excursion


CIRO Horn
14 april 2018

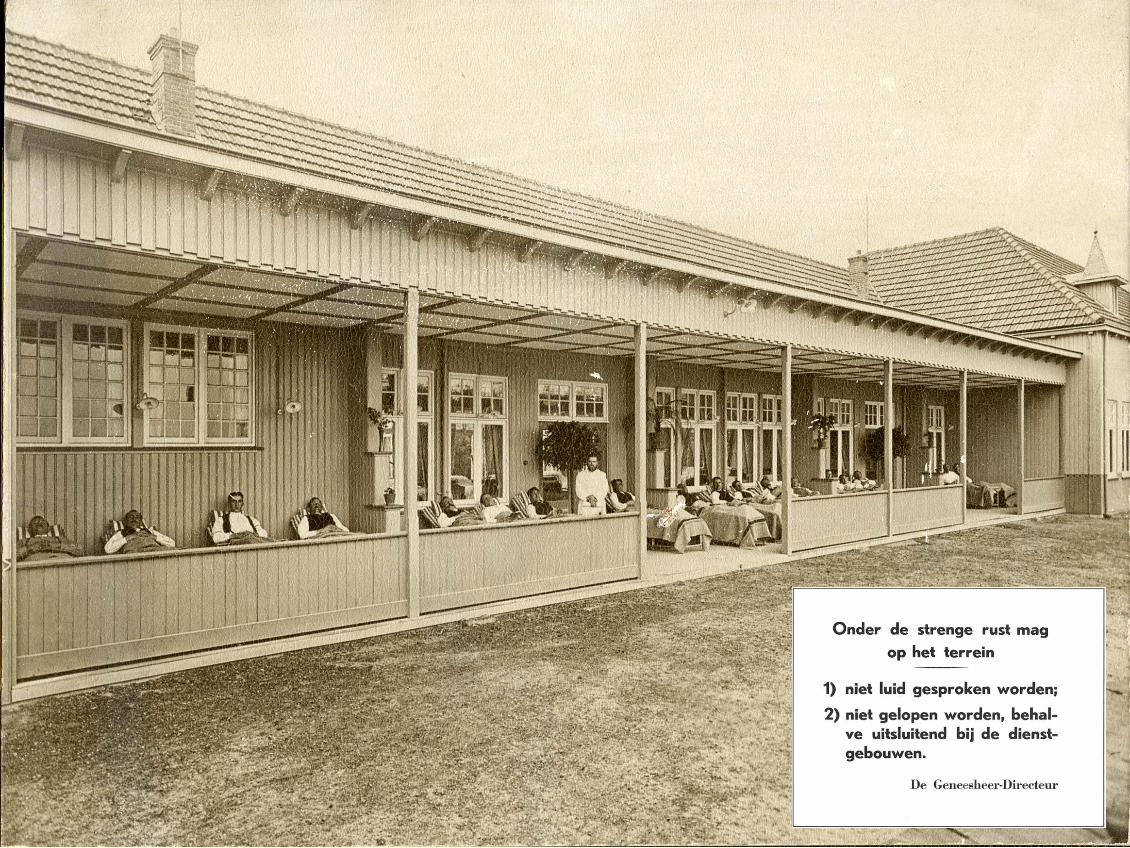
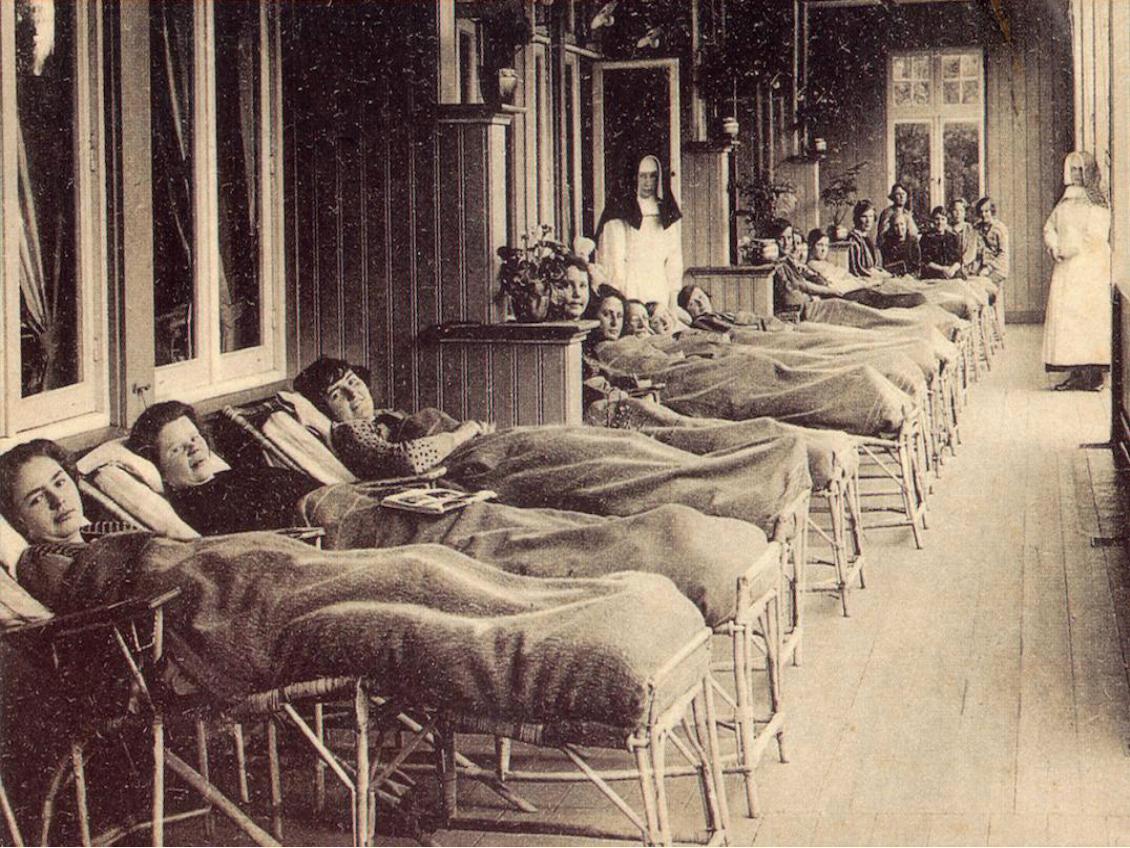
Geschiedenis van Hornerheide: 1935
Geschiedenis van Hornerheide: 1935
Sanatorium Hornerheide
1921
1968
Longkliniek Hornerheide
1985
De geschiedenis van CIRO
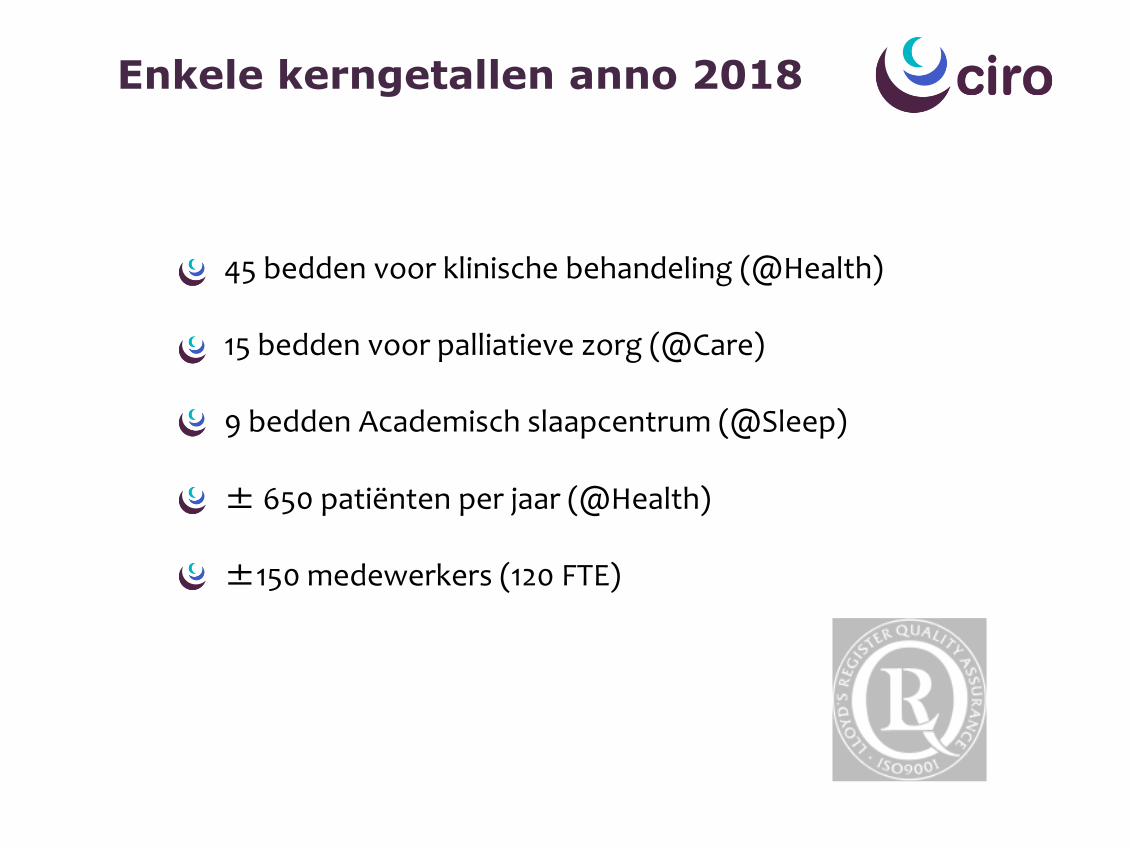
45 bedden voor klinische behandeling (@Health) 15 bedden voor palliatieve zorg (@Care) 9 bedden Academisch slaapcentrum (@Sleep) ± 650 patiënten per jaar (@Health) ±150 medewerkers (120 FTE)
Enkele kerngetallen anno 2018
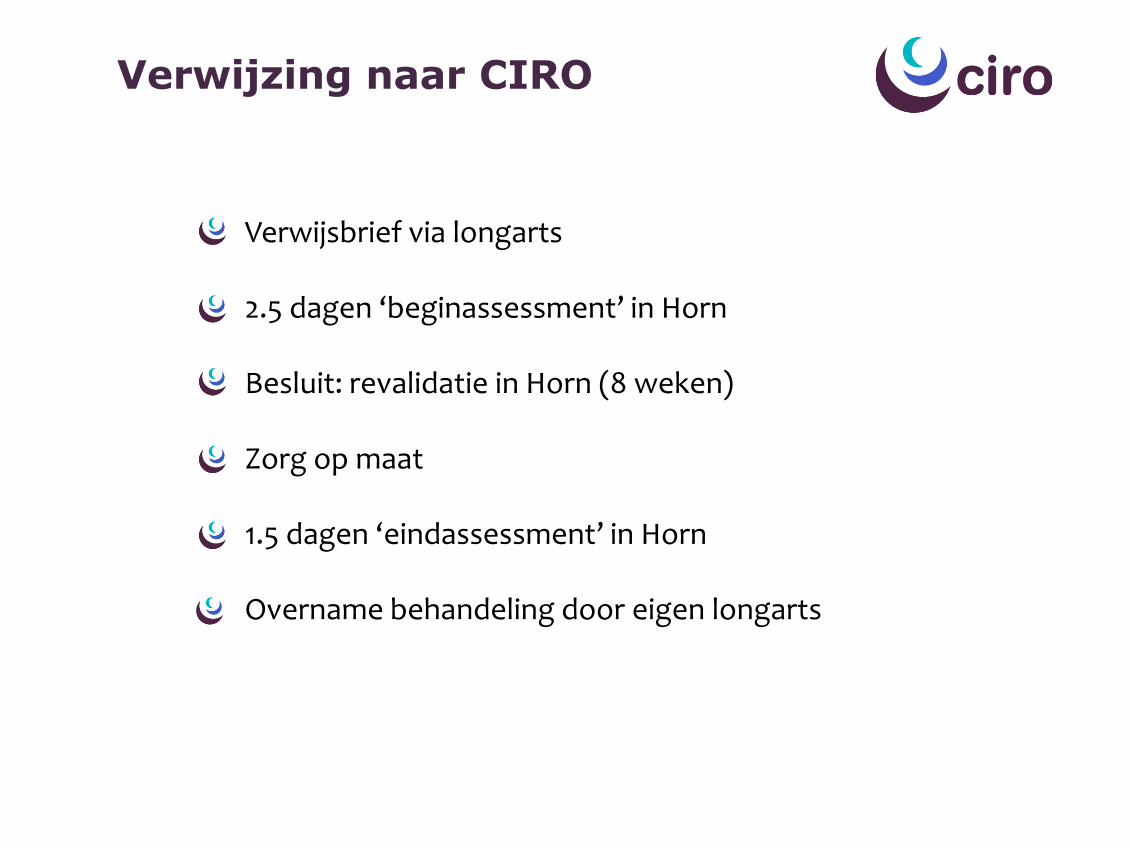
Verwijsbrief via longarts 2.5 dagen ‘beginassessment’ in Horn Besluit: revalidatie in Horn (8 weken) Zorg op maat 1.5 dagen ‘eindassessment’ in Horn Overname behandeling door eigen longarts
Verwijzing naar CIRO
Longrevalidatie is een gepersonaliseerde interventie (tenminste bestaande uit inspanningstraining, educatie en
gedragsverandering), gebaseerd op een uitgebreid beginonderzoek, gericht op de fysieke/psychologische
conditie van personen met een chronische longaandoening en op gezond gedrag op de langere termijn.
Spruit et al. AJRCCM 2013
Longrevalidatie

Voor de juiste uitkomst(en)
De juiste behandeling
For The Right Patien
Op het juiste moment
Voor de juiste patiënt(e)
Zorg op maat

Inzicht in beweeggedrag
Voedingssupplementen
Psychosociale begeleiding
Educatie
Zelfzorg / ADL training
Leefstijl coaching
Interval training
Duurtraining
Arbeidsreïntegratie
Krachttraining
Creatieve therapie
Ontspanningsoefeningen
Rookstop Beh. bijkomende aandoeningen
Meeloopdag familie ……
Programma op maat

Inzicht in beweeggedrag
Voedingssupplementen
Psychosociale begeleiding
Educatie
Zelfzorg / ADL training
Leefstijl coaching
Interval training
Duurtraining
Arbeidsreïntegratie
Krachttraining
Creatieve therapie
Ontspanningsoefeningen
Rookstop Beh. bijkomende aandoeningen
Meeloopdag familie ……
Programma op maat
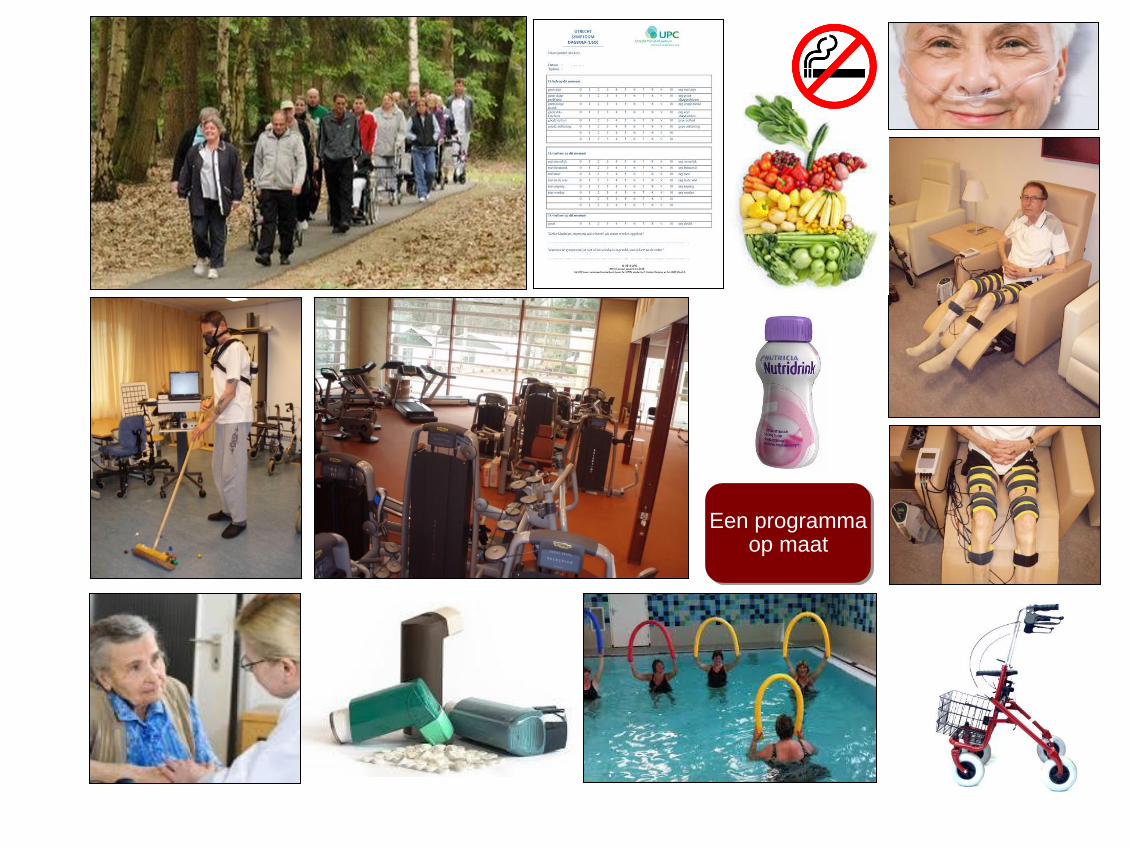
Een programma op maat

Interdisciplinair team

Afra: Specialist van haar eigen leven

Roy: Specialist van zijn eigen leven

Grenzen verleggen!
Resultaten
Vermindering van kortademigheid Toename inspanningsvermogen Afname zorgafhankelijkheid Toename kwaliteit van leven Afname somberheid en depressie Verbeterde lichaamssamenstelling Gezondere leefstijl Minder ziekenhuisopnames
Resultaten

PHATIGUE studie
N=45 8 weken leefstijl interventie door Chermaine Kwant (www.feads.nl) 8 weken klinische longrevalidatie in CIRO te Horn
Durf anders te zijn

Nabije toekomst