Principles of exercise: van de fitness naar het logopedielokaal€¦ · Principles of exercise: van...
45
Principles of exercise: van de fitness naar het logopedielokaal Gwen Van Nuffelen*° – Marc De Bodt*° – Cindy Guns – Leen Van den Steen Universitair Ziekenhuis Antwerpen , * UGent, ° Universiteit Antwerpen
Transcript of Principles of exercise: van de fitness naar het logopedielokaal€¦ · Principles of exercise: van...

Principles of exercise: van de fitness naar het logopedielokaal
Gwen Van Nuffelen*° – Marc De Bodt*° – Cindy Guns – Leen Van den Steen Universitair Ziekenhuis Antwerpen , * UGent, ° Universiteit Antwerpen

Slikrevalidatie is in beweging
Compensatie ! Revalidatie
• Meer mogelijkheden (nieuwe therapieën & toestellen): MDTP, EMST, IMST, IOPI, MOST, …
• Groeiende evidentie dat een bepaalde manier van revalideren, effectief kan zijn, zelfs bij chronische slikproblemen

Slikrevalidatie is in beweging
Integratie van de principes van • motor learning • cortical plasticiteit • ‘exercise’ of ‘strength training’
! hoe moet een trainings- of revalidatieprogramma eruit zien om resultaat te leveren? ! veel kennis hierover in fysische revalidatie &
sportwetenschappen Opm: overlap tussen de principes

Principles of exercise
Overload
Frequency
Intensity Specificity
Transference
Periodization
Reversibility
Recovery

Principles of exercise
Doel: zo effectief mogelijk verbeteren van • spierkracht & uithouding • uitvoering van neuromusculaire activiteiten: coördinatie,
timing, controle (cfr motor learning) Toepasbaar bij: • buikspieroefeningen • trainen van armspieren • … • lopen • fietsen • …

Principles of exercise: van de fitness naar het logopedielokaal
Principles of exercise… everywhere you look • fitness • sportwebsites - • maar ook …

Principles of exercise: van de fitness naar het logopedielokaal

Principles of exercise: van de fitness naar het logopedielokaal
accounting GET A BETTER GRADE. TRY LEARNSMART.
http://www.mcgrawhillconnect.comFITNESS AND WELLNESS
C H A P T E R 4 Muscular Strength and Endurance
LO O KI N G A H E A D… After reading this chapter, you should be able to: ■ Describe the basic physiology of muscles and explain
how strength training affects muscles ■ De! ne muscular strength and endurance, and
describe how they relate to wellness ■ Assess muscular strength and endurance ■ Apply the FITT principle to create a safe and
successful strength training program ■ Describe the effects of supplements and drugs that
are marketed to active people and athletes ■ Explain how to safely perform common strength training
exercises using free weights and weight machines
TEST YO U R KN OW LE D G E 1. For women, weight training typically results in which
of the following? a. bulky muscles b. signi! cant increases in body weight c. improved body image
2. To maximize strength gains, it is a good idea to hold your breath as you lift a weight. True or false?
3. Regular strength training is associated with which of the following bene! ts? a. denser bones b. reduced risk of heart disease c. improved body composition d. fewer injuries e. improved metabolic health f. Increased longevity
Answers 1. c. Because the vast majority of women have low levels of
testosterone, they do not develop large muscles or gain signi! cant amounts of weight in response to a moderate-intensity weight training program. Men have higher levels of testosterone, so they can build large muscles more easily.
2. False. Holding one’s breath while lifting weights can signi! cantly elevate blood pressure; it also reduces blood " ow to the heart and may cause faintness. You should breathe smoothly and normally while weight training. Some experts recommend that you exhale during the most dif! cult part of each exercise.
3. All six. Regular strength training has many bene! ts for both men and women.
IDK�����BFK��B��������LQGG����� ����������������30
The National Strength and Conditioning Association’s (NSCA)

The International Journal of Sports Physical Therapy | Volume 6, Number 3 | September 2011 | Page 241
ABSTRACTBackground and Purpose: Rehabilitation and strength and conditioning are often seen as two separate entities in athletic injury recovery. Traditionally an athlete progresses from the rehabilitation environment under the care of a physical therapist and/or athletic trainer to the strength and conditioning coach for specific return to sport training. These two facets of return to sport are often considered to have separate goals. Initial goals of each are often different due to the timing of their implementation encompassing different stages of post-injury recovery. The initial focus of post injury rehabilitation includes alleviation of dysfunction, enhancement of tissue healing, and provision of a sys-tematic progression of range-of-motion and strength. During the return to function phases, specific return to play goals are paramount. Understanding of specific principles and program parameters is necessary when designing and implementing an athlete’s rehabilitation program. Communication and collaboration amongst all individuals caring for the athlete is a must. The purpose of this review is to outline the current evidence supporting utilization of train-ing principles in athletic rehabilitation, as well as provide suggested implementation of such principles throughout different phases of a proposed rehabilitation program.
Evidence Acquisition: The following electronic databases were used to identify research relevant to this clinical com-mentary: MEDLINE (from 1950–June 2011) and CINAHL (1982–June 2011), for all relevant journal articles written in English. Additional references were accrued by independent searching of references from relevant articles.
Results: Currently evidence is lacking in the integration of strength and conditioning principles into the rehabilita-tion program for the injured athlete. Numerous methods are suggested for possible utilization by the clinician in prac-tice to improve strength, power, speed, endurance, and metabolic capacity.
Conclusion: Despite abundance of information on the implementation of training principles in the strength and con-ditioning field, investigation regarding the use of these principles in a properly designed rehabilitation program is lacking.
Keywords: periodization, program design, rehabilitation, strength, training
1 Duke University Medical Center, Durham, North Carolina, USA
2 Providence Medical Center, Kansas City, Kansas, USANo grant support or statement of the Institutional Review
Board approval.
IJSP
T CLINICAL COMMENTARYINTEGRATION OF STRENGTH AND CONDITIONING PRINCIPLES INTO A REHABILITATION PROGRAMMichael P. Reiman, PT, DPT, OCS, SCS, ATC, FAAOMPT, CSCS1
Daniel S. Lorenz, DPT, PT, ATC/L, CSCS2
CORRESPONDING AUTHORMichael P. Reiman, PT, DPT, SCS, OCS, ATC, FAAOMPT, CSCSDuke University Medical CenterDepartment of Community and Family MedicineDoctor of Physical Therapy DivisionDUMC 104002Durham, NC 27710 (USA)Phone: (919) 668-3014Fax: (919) 684-1846Email: [email protected]
The International Journal of Sports Physical Therapy | Volume 6, Number 3 | September 2011 | Page 241
ABSTRACTBackground and Purpose: Rehabilitation and strength and conditioning are often seen as two separate entities in athletic injury recovery. Traditionally an athlete progresses from the rehabilitation environment under the care of a physical therapist and/or athletic trainer to the strength and conditioning coach for specific return to sport training. These two facets of return to sport are often considered to have separate goals. Initial goals of each are often different due to the timing of their implementation encompassing different stages of post-injury recovery. The initial focus of post injury rehabilitation includes alleviation of dysfunction, enhancement of tissue healing, and provision of a sys-tematic progression of range-of-motion and strength. During the return to function phases, specific return to play goals are paramount. Understanding of specific principles and program parameters is necessary when designing and implementing an athlete’s rehabilitation program. Communication and collaboration amongst all individuals caring for the athlete is a must. The purpose of this review is to outline the current evidence supporting utilization of train-ing principles in athletic rehabilitation, as well as provide suggested implementation of such principles throughout different phases of a proposed rehabilitation program.
Evidence Acquisition: The following electronic databases were used to identify research relevant to this clinical com-mentary: MEDLINE (from 1950–June 2011) and CINAHL (1982–June 2011), for all relevant journal articles written in English. Additional references were accrued by independent searching of references from relevant articles.
Results: Currently evidence is lacking in the integration of strength and conditioning principles into the rehabilita-tion program for the injured athlete. Numerous methods are suggested for possible utilization by the clinician in prac-tice to improve strength, power, speed, endurance, and metabolic capacity.
Conclusion: Despite abundance of information on the implementation of training principles in the strength and con-ditioning field, investigation regarding the use of these principles in a properly designed rehabilitation program is lacking.
Keywords: periodization, program design, rehabilitation, strength, training
1 Duke University Medical Center, Durham, North Carolina, USA
2 Providence Medical Center, Kansas City, Kansas, USANo grant support or statement of the Institutional Review
Board approval.
IJSP
T CLINICAL COMMENTARYINTEGRATION OF STRENGTH AND CONDITIONING PRINCIPLES INTO A REHABILITATION PROGRAMMichael P. Reiman, PT, DPT, OCS, SCS, ATC, FAAOMPT, CSCS1
Daniel S. Lorenz, DPT, PT, ATC/L, CSCS2
CORRESPONDING AUTHORMichael P. Reiman, PT, DPT, SCS, OCS, ATC, FAAOMPT, CSCSDuke University Medical CenterDepartment of Community and Family MedicineDoctor of Physical Therapy DivisionDUMC 104002Durham, NC 27710 (USA)Phone: (919) 668-3014Fax: (919) 684-1846Email: [email protected]
Principles of exercise: van de fitness naar het logopedielokaal

Principles of exercise: van de fitness naar het logopedielokaal
through sound, progressive, mission-specific physical training for indi-viduals and units.
Principles of Exercise
Adherence to certain basic exerciseprinciples is important for developingan effective program. The principlesof exercise apply to everyone at alllevels of physical training, from theOlympic-caliber athlete to the week-end jogger. They also apply to fitnesstraining for military personnel.
These basic principles of exercisemust be followed:
Factors for a successful training program are Frequency, Intensity, Time, and Type; "FITT".
●
●
e
●
●
●
Regularity. To achieve a trainingeffect, a person must exercise often. One should strive to exerciseeach of the first four fitness com-ponents at least three times a week.Infrequent exercise can do moreharm than good. Regularity isalso important in resting, sleeping,and following a good diet.Progression. The intensity (howhard) and/or duration (how long)of exercise must gradually in-crease to improve the level of fit-ness.Balance. To be effective, a pro-gram should include activities thataddress all the fitness compo-nents, since overemphasizing anyone of them may hurt the others.Variety. Providing a variety of ac-tivities reduces boredom and in-creases motivation and progress.Specificity. Training must begeared toward specific goals. Forexample, soldiers become betterrunners if their training empha-sizes running. Although swim-ming is great exercise, it does notimprove a 2-mile-run time asmuch as a running program does.Recovery. A hard day of trainingfor a given component of fitnessshould be followed by an easiertraining day or rest day for thatcomponent and/or muscle group(s)to help permit recovery. Another
●
way to allow recovery is to alternatethe muscle groups exercised everyother day, especially when trainingfor strength and/or muscle endur-ance.Overload. The work load of eachexercise session must exceed thenormal demands placed on the bodyin order to bring about a trainingeffect.
FITT Factors
Certain factors must be part of anyfitness training program for it to besuccessful. These factors are Fre-quency, Intensity, Time, and Type.The acronym FITT makes it easier toremember them. (See Figure 1- 1.)
FREQUENCY
Army Regulation 350-15 specifiesthat vigorous physical fitness trainingwill be conducted 3 to 5 times perweek. For optimal results, command-ers must strive to conduct 5 days ofphysical training per week. Ideally, atleast three exercise sessions for CRfitness, muscle endurance, musclestrength, and flexibility should beperformed each week to improve fit-ness levels. Thus, for example, toobtain maximum gains in muscularstrength, soldiers should have at leastthree strength-training sessions perweek. Three physical activity periodsa week, however, with only one sessioneach of cardiorespiratory, strength,and flexibility training will not im-prove any of these three components.
With some planning, a training pro-gram for the average soldier can bedeveloped which provides fairly equalemphasis on all the components ofphysical fitness. The following train-ing program serves as an example.
In the first week, Monday, Wednes-day, and Friday are devoted to CRfitness, and Tuesday and Thursday aredevoted to muscle endurance andstrength. During the second week, the
1-4

Slikken:
" neuromusculaire activiteit " vereist spierkracht " vereist uithouding van de betrokken spieren " vereist coördinatie, timing, … ! principles of exercise lijken toepasbaar en zinvol ! misschien moeten logopedisten meer denken zoals een
fitnesscoach en kinesist Maar: ander type spieren
Principles of exercise: van de fitness naar het logopedielokaal

Principles of exercise: van de fitness naar het logopedielokaal
Review
Strength-Training Exercise in Dysphagia Rehabilitation: Principles,Procedures, and Directions for Future Research
Lori M. Burkhead, PhD,1,3, Christine M. Sapienza, PhD,2,3 and John C. Rosenbek, PhD1,3
1Department of Communicative Disorders, University of Florida, Gainesville, Florida, USA; 2Department of Communication Sciences andDisorders, University of Florida, Gainesville, Florida, USA; and 3Brain Rehabilitation Research Center of Excellence, Malcom Randall VAMedical Center, Gainesville, Florida, USA
Abstract. Dysphagia rehabilitation, historically, hasfocused a great deal on various compensations duringswallowing to prevent aspiration and/or improvesafety and e!ciency. Exercise, in general, has been apart of the dysphagia rehabilitation landscape.However, heightened discussions in the field regard-ing best practices for exercise training, particularlystrengthening, raise more questions than answers.The intent of this paper is to (1) explore the over-riding principles of neuromuscular plasticity withregard to strength training, (2) evaluate how currentexercise-training interventions in dysphagia rehabili-tation correspond to these principles, and (3) postu-late directions for future study of normal and disor-dered swallowing and determine how to incorporatethese principles into dysphagia rehabilitation.
Key words: Deglutition — Deglutition disorders —Dysphagia — Swallowing — Exercise — Strength-ening — Muscle.
Dysphagia is a pervasive and potentially life-threat-ening condition that can emerge from a variety ofdisturbances a"ecting neural, motor, and/or sensorysystems that underlie swallowing function. Publishedreports indicate a high incidence and prevalence ofdysphagia among neurologically impaired individuals
[1–4], those with head and neck cancer [5–8], andthose with tracheostomy and/or ventilator depen-dency without neurologic/structural disturbancesthat would otherwise precipitate dysphagia [9–12].Regardless of etiology, the potential health risks thatcan stem from dysphagia are great and include in-creased likelihood for malnutrition, pulmonaryinfection [13], and death [14].
Dysphagia can negatively impact medicalrecovery, resulting in longer hospitalizations and anincreased need for long-term care [15]. Aspirationpneumonia, a common sequela of dysphagia, isassociated with a significant risk for morbidity andmortality [16]. It has been reported that in the eight-year period from 1991 to 1998, the number of patientshospitalized for aspiration pneumonia increased by93.5%, making it the second most common reason forhospitalization [17]. Identifying more e"ective meth-ods of diagnosis and treatment has been designated asa top priority in rehabilitation research [18] in order toimprove the health and quality of life and decreasefatalities in those with dysphagia.
Historically, research has focused largely onthe use of compensatory maneuvers while swallowingto prevent aspiration. Postural compensations suchas manipulating the head, oral structures, and/orbody position [19, 24] have been beneficial to this end.Altering viscosity, volume, and consistency of foodand liquid has also proven successful for improvingsafety and e!ciency of oral intake [19, 25, 26]. Inaddition to the use of compensations, a variety ofexercise regimens have been proposed to improveswallowing ability by targeting range of motion [27],
Correspondence to: Lori M. Burkhead, PhD, Department ofOtolaryngology, Division of Laryngology, Medical College ofGeorgia, 1120 15th Street, Suite BP 4109, Augusta, GA, 30912-4060, USA; E-mail: [email protected]
Dysphagia 22:251–265 (2007)DOI: 10.1007/s00455-006-9074-z
Review
Strength-Training Exercise in Dysphagia Rehabilitation: Principles,Procedures, and Directions for Future Research
Lori M. Burkhead, PhD,1,3, Christine M. Sapienza, PhD,2,3 and John C. Rosenbek, PhD1,3
1Department of Communicative Disorders, University of Florida, Gainesville, Florida, USA; 2Department of Communication Sciences andDisorders, University of Florida, Gainesville, Florida, USA; and 3Brain Rehabilitation Research Center of Excellence, Malcom Randall VAMedical Center, Gainesville, Florida, USA
Abstract. Dysphagia rehabilitation, historically, hasfocused a great deal on various compensations duringswallowing to prevent aspiration and/or improvesafety and e!ciency. Exercise, in general, has been apart of the dysphagia rehabilitation landscape.However, heightened discussions in the field regard-ing best practices for exercise training, particularlystrengthening, raise more questions than answers.The intent of this paper is to (1) explore the over-riding principles of neuromuscular plasticity withregard to strength training, (2) evaluate how currentexercise-training interventions in dysphagia rehabili-tation correspond to these principles, and (3) postu-late directions for future study of normal and disor-dered swallowing and determine how to incorporatethese principles into dysphagia rehabilitation.
Key words: Deglutition — Deglutition disorders —Dysphagia — Swallowing — Exercise — Strength-ening — Muscle.
Dysphagia is a pervasive and potentially life-threat-ening condition that can emerge from a variety ofdisturbances a"ecting neural, motor, and/or sensorysystems that underlie swallowing function. Publishedreports indicate a high incidence and prevalence ofdysphagia among neurologically impaired individuals
[1–4], those with head and neck cancer [5–8], andthose with tracheostomy and/or ventilator depen-dency without neurologic/structural disturbancesthat would otherwise precipitate dysphagia [9–12].Regardless of etiology, the potential health risks thatcan stem from dysphagia are great and include in-creased likelihood for malnutrition, pulmonaryinfection [13], and death [14].
Dysphagia can negatively impact medicalrecovery, resulting in longer hospitalizations and anincreased need for long-term care [15]. Aspirationpneumonia, a common sequela of dysphagia, isassociated with a significant risk for morbidity andmortality [16]. It has been reported that in the eight-year period from 1991 to 1998, the number of patientshospitalized for aspiration pneumonia increased by93.5%, making it the second most common reason forhospitalization [17]. Identifying more e"ective meth-ods of diagnosis and treatment has been designated asa top priority in rehabilitation research [18] in order toimprove the health and quality of life and decreasefatalities in those with dysphagia.
Historically, research has focused largely onthe use of compensatory maneuvers while swallowingto prevent aspiration. Postural compensations suchas manipulating the head, oral structures, and/orbody position [19, 24] have been beneficial to this end.Altering viscosity, volume, and consistency of foodand liquid has also proven successful for improvingsafety and e!ciency of oral intake [19, 25, 26]. Inaddition to the use of compensations, a variety ofexercise regimens have been proposed to improveswallowing ability by targeting range of motion [27],
Correspondence to: Lori M. Burkhead, PhD, Department ofOtolaryngology, Division of Laryngology, Medical College ofGeorgia, 1120 15th Street, Suite BP 4109, Augusta, GA, 30912-4060, USA; E-mail: [email protected]
Dysphagia 22:251–265 (2007)DOI: 10.1007/s00455-006-9074-z
Review
Strength-Training Exercise in Dysphagia Rehabilitation: Principles,Procedures, and Directions for Future Research
Lori M. Burkhead, PhD,1,3, Christine M. Sapienza, PhD,2,3 and John C. Rosenbek, PhD1,3
1Department of Communicative Disorders, University of Florida, Gainesville, Florida, USA; 2Department of Communication Sciences andDisorders, University of Florida, Gainesville, Florida, USA; and 3Brain Rehabilitation Research Center of Excellence, Malcom Randall VAMedical Center, Gainesville, Florida, USA
Abstract. Dysphagia rehabilitation, historically, hasfocused a great deal on various compensations duringswallowing to prevent aspiration and/or improvesafety and e!ciency. Exercise, in general, has been apart of the dysphagia rehabilitation landscape.However, heightened discussions in the field regard-ing best practices for exercise training, particularlystrengthening, raise more questions than answers.The intent of this paper is to (1) explore the over-riding principles of neuromuscular plasticity withregard to strength training, (2) evaluate how currentexercise-training interventions in dysphagia rehabili-tation correspond to these principles, and (3) postu-late directions for future study of normal and disor-dered swallowing and determine how to incorporatethese principles into dysphagia rehabilitation.
Key words: Deglutition — Deglutition disorders —Dysphagia — Swallowing — Exercise — Strength-ening — Muscle.
Dysphagia is a pervasive and potentially life-threat-ening condition that can emerge from a variety ofdisturbances a"ecting neural, motor, and/or sensorysystems that underlie swallowing function. Publishedreports indicate a high incidence and prevalence ofdysphagia among neurologically impaired individuals
[1–4], those with head and neck cancer [5–8], andthose with tracheostomy and/or ventilator depen-dency without neurologic/structural disturbancesthat would otherwise precipitate dysphagia [9–12].Regardless of etiology, the potential health risks thatcan stem from dysphagia are great and include in-creased likelihood for malnutrition, pulmonaryinfection [13], and death [14].
Dysphagia can negatively impact medicalrecovery, resulting in longer hospitalizations and anincreased need for long-term care [15]. Aspirationpneumonia, a common sequela of dysphagia, isassociated with a significant risk for morbidity andmortality [16]. It has been reported that in the eight-year period from 1991 to 1998, the number of patientshospitalized for aspiration pneumonia increased by93.5%, making it the second most common reason forhospitalization [17]. Identifying more e"ective meth-ods of diagnosis and treatment has been designated asa top priority in rehabilitation research [18] in order toimprove the health and quality of life and decreasefatalities in those with dysphagia.
Historically, research has focused largely onthe use of compensatory maneuvers while swallowingto prevent aspiration. Postural compensations suchas manipulating the head, oral structures, and/orbody position [19, 24] have been beneficial to this end.Altering viscosity, volume, and consistency of foodand liquid has also proven successful for improvingsafety and e!ciency of oral intake [19, 25, 26]. Inaddition to the use of compensations, a variety ofexercise regimens have been proposed to improveswallowing ability by targeting range of motion [27],
Correspondence to: Lori M. Burkhead, PhD, Department ofOtolaryngology, Division of Laryngology, Medical College ofGeorgia, 1120 15th Street, Suite BP 4109, Augusta, GA, 30912-4060, USA; E-mail: [email protected]
Dysphagia 22:251–265 (2007)DOI: 10.1007/s00455-006-9074-z

Principles of exercise: van de fitness naar het logopedielokaal

Spierkracht
Type spiervezel Functie Activiteit
Type 1 – slow twitch traag, beperkte kracht, uithouding joggen Type 2 – fast twitch snel, grote kracht, snel vermoeid sprinten
Meeste spieren bevatten type 1 en 2 vezels; rekrutering afhankelijk van de activiteit

Spierkracht opbouwen
muscle learning hypertrophy
- toename van aantal motor units dat gerekruteerd wordt bij een activiteit
- motor unit = zenuw verbonden aan aantal spiervezels
- hoe meer units gerekruteerd, hoe meer kracht gegenereerd
- dikkere myofibrillen
- bij mensen waarschijnlijk geen hyperplasie = toename van aantal myofibrils
- wel hybride vezels
- hypertrofie vermoedelijk pas na 8 weken

Principles of exercise
Overload
Frequency
Intensity Specificity
Transference
Periodization
Reversibility
Recovery

Principles of exercise Name ________________________________________________ Date _________________ Class Period ___________
Fitness Zone Online Muscular Strength and Endurance 1
Copy
right
© b
y The
McG
raw-
Hill
Com
pani
es, I
nc. A
ll rig
hts r
eser
ved.
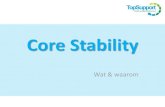
There are many considerations and variations for frequency, intensity, duration, and type when you consider muscular strength and endurance. Do you want to develop strength or muscular endurance? Do you want to use weights and machines, or do you want to use your own body weight, resistance bands, medicine balls, or other weighted equipment? How many reps or sets will you perform? Your personal goals will influence the FITT principle. Figure 4.2 illustrates the different categories of the FITT principle.
C04-03A
F
I
T
T
Frequency ofExercise
Intensity ofExercise
Time ofExercise
Type ofExercise
How Often
How Hard
–How many reps–How many sets–How much time between sets
Which Exercises
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Weight machines, free weights, resistance tubing, medicine ball, own bodyweight
2–3 days per weekFull-body workout of all 6 body areas48–72 hours of rest in-between workouts
4–5 days per week; often perform split workouts(example: Monday and Thursday, work chest,shoulders, triceps, abdominals; Tuesday and Friday,work back, legs, biceps)48–72 hours of rest in-between workouts
60%–70% of maximum strength
70%–90% of maximum strength
1–3 Sets8–12 repetitions
Endurance – 12–20+ Reps2–3 Sets
Strength – 2–6 Reps3–5 Sets
30 sec to 1 minute
30 sec to 1 minute
2 to 5 minutes
Note: Specificity Principle — you must work each muscle group to have strength gains in that particular part of the body.
FITT Principle for Muscular Strength and Endurance
Muscular Strength and Endurance—Activity 2
Name ________________________________________________ Date _________________ Class Period ___________
Fitness Zone Online Muscular Strength and Endurance 1
Copy
right
© b
y Th
e M
cGra
w-Hi
ll Co
mpa
nies
, Inc
. All
right
s re
serv
ed.
There are many considerations and variations for frequency, intensity, duration, and type when you consider muscular strength and endurance. Do you want to develop strength or muscular endurance? Do you want to use weights and machines, or do you want to use your own body weight, resistance bands, medicine balls, or other weighted equipment? How many reps or sets will you perform? Your personal goals will influence the FITT principle. Figure 4.2 illustrates the different categories of the FITT principle.
C04-03A
F
I
T
T
Frequency ofExercise
Intensity ofExercise
Time ofExercise
Type ofExercise
How Often
How Hard
–How many reps–How many sets–How much time between sets
Which Exercises
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Weight machines, free weights, resistance tubing, medicine ball, own bodyweight
2–3 days per weekFull-body workout of all 6 body areas48–72 hours of rest in-between workouts
4–5 days per week; often perform split workouts(example: Monday and Thursday, work chest,shoulders, triceps, abdominals; Tuesday and Friday,work back, legs, biceps)48–72 hours of rest in-between workouts
60%–70% of maximum strength
70%–90% of maximum strength
1–3 Sets8–12 repetitions
Endurance – 12–20+ Reps2–3 Sets
Strength – 2–6 Reps3–5 Sets
30 sec to 1 minute
30 sec to 1 minute
2 to 5 minutes
Note: Specificity Principle — you must work each muscle group to have strength gains in that particular part of the body.
FITT Principle for Muscular Strength and Endurance
Muscular Strength and Endurance—Activity 2
hoeveel x/week <> recovery
load, resistance <> overload

Frequency & recovery
Minimum: minstens 2x/week Maximum: niet consecutief of alterneren in spiergroepen anders kunnen de spieren niet met genoeg intensiteit werken & kans op pijn en blessures wordt groter (recovery)
Skeletspieren / fysische training
Previous authors have demonstrated insignificant differences in strength gains observed between training 1, 2, 3, or 5 days per week if the volume was kept constant. When near maximal resistances are used, more recovery time is advocated. Reiman et al. 2011

Frequency & recovery
Orale en faryngeale spieren/ logopedische revalidatie: geen idee Frequentie varieert: 2 – 5x / week • MDTP: 5x/week • Studies met bewezen positief effect op tongkracht
Study Participants N Exercise scheme
Robbins et al. 2007 Accident Vasculaire Cérébral (AVC)
10 3x/day; 3x/week;
Steele et al. 2013 Lésions cérébrale 6 2-3 x / week
Van Nuffelen et al. 2012
Carcinome tête et cou – dysphagie chronique
6 5x/week
Van Nuffelen et al. 2013
Maladies neuromusculaires
9 3-5x/week

Frequency, recovery & periodization Aspiration and swallowing in Parkinsondisease and rehabilitation with EMSTA randomized trial
M.S. Troche, PhDM.S. Okun, MDJ.C. Rosenbek, PhDN. Musson, MAH.H. Fernandez, MDR. Rodriguez, MDJ. Romrell, PA-CT. Pitts, PhDK.M. Wheeler-Hegland,
PhDC.M. Sapienza, PhD
ABSTRACT
Objective: Dysphagia is the main cause of aspiration pneumonia and death in Parkinson disease(PD) with no established restorative behavioral treatment to date. Reduced swallow safety maybe related to decreased elevation and excursion of the hyolaryngeal complex. Increased submen-tal muscle force generation has been associated with expiratory muscle strength training (EMST)and subsequent increases in hyolaryngeal complex movement provide a strong rationale for itsuse as a dysphagia treatment. The current study’s objective was to test the treatment outcome ofa 4-week device-driven EMST program on swallow safety and define the physiologic mechanismsthrough measures of swallow timing and hyoid displacement.
Methods: This was a randomized, blinded, sham-controlled EMST trial performed at an academiccenter. Sixty participants with PD completed EMST, 4 weeks, 5 days per week, for 20 minutesper day, using a calibrated or sham, handheld device. Measures of swallow function includingjudgments of swallow safety (penetration–aspiration [PA] scale scores), swallow timing, and hyoidmovement were made from videofluoroscopic images.
Results: No pretreatment group differences existed. The active treatment (EMST) group demon-strated improved swallow safety compared to the sham group as evidenced by improved PAscores. The EMST group demonstrated improvement of hyolaryngeal function during swallowing,findings not evident for the sham group.
Conclusions: EMST may be a restorative treatment for dysphagia in those with PD. The mecha-nism may be explained by improved hyolaryngeal complex movement.
Classification of evidence: This intervention study provides Class I evidence that swallow safety asdefined by PA score improved post EMST. Neurology® 2010;75:1912–1919
GLOSSARYCI ! confidence interval; EMST ! expiratory muscle strength training; MEP ! maximum expiratory pressure; PA ! penetra-tion–aspiration; PD ! Parkinson disease; SWAL-QOL ! Swallowing Quality of Life Questionnaire; UES ! upper esophagealsphincter; UF ! University of Florida Movement Disorders Center; VA ! Veterans Affairs.
Swallowing is a patterned sensorimotor process within a complex neural network involvingautomatic and volitional systems1-4 amenable to modification and adaptation. Accordingly,swallowing rehabilitation techniques aimed at restoration of function are gaining increasedinterest, particularly in populations like Parkinson disease (PD), where aspiration pneumonia isthe leading cause of death.5-10 This article presents results from the first blinded, randomizedplacebo-controlled clinical trial, testing the effects of a restorative treatment called expiratorymuscle strength training (EMST150, Aspire Products)11-17 for swallowing dysfunction in PD.EMST’s mechanistic underpinning is its ability to generate increased submental musculatureforce activation.15
Decreased elevation and excursion of the hyolaryngeal complex is considered one cause ofpenetration and aspiration.18-21 Submental muscle contraction elevates the hyolaryngealcomplex. EMST treatment produces significantly longer durations, higher peak amplitudes,
From the University of Florida (M.S.T., M.S.O., J.C.R., H.H.F., R.R., J.R., T.P., K.M.W.-H., C.M.S.), Gainesville; and Brain RehabilitationResearch Center (M.S.T., J.C.R., N.M., T.P., K.M.W.-H., C.M.S.), Malcom Randall VAMC Gainesville, Gainesville, FL.
Study funding: Supported by the VA Rehab R&D (B3721R to C.S.) and the Michael J. Fox Foundation (00056150).
Disclosure: Author disclosures are provided at the end of the article.
Address correspondence andreprint requests to Dr. Michelle S.Troche, PO Box 117420,University of Florida, Gainesville,FL [email protected]
1912 Copyright © 2010 by AAN Enterprises, Inc.

Intensity & overload
Krachttraining: weerstand/ belasting op het systeem
Principle of overload • exercises that do not force the neuromuscular system
beyond the level of usual activity will not elicit adaptations
• Progressive resistance: increase force-generating capacity ! increase load

Intensity & overload
Progressive resistance: rules based on large muscle groups
• load is a proportion of maximal force-generating capacity • i.e. a percentage of the 1-Repetion Maximum (1RM) • regelmatig opnieuw 1 RM bepalen ! progressie
• > 80 % better/faster outcome? needs investigation but some
suggest that this may lead to overuse injuries
Intensiteit richtlijnen Niveau Doel Functie 80 (-100) % 1RM high-intensity type II vezels kracht 40- 60 % 1 RM low - intensity type I vezels endurance

Intensity & overload
IOPI and EMST/IMST-devices allow for: determination of 1 RM practicing at a given % of the patient’s 1 RM

Intensity & overload
Tongkrachttraining: - Robbins et al 2007/2009: 60-80% 1 RM - Steele et al 2013: 25-85% 1 RM + MIP - UZA 1° schema: MIP
EMST: 75% 1 RM

Time of exercise
Name ________________________________________________ Date _________________ Class Period ___________
Fitness Zone Online Muscular Strength and Endurance 1
Copy
right
© b
y Th
e M
cGra
w-Hi
ll Co
mpa
nies
, Inc
. All
right
s re
serv
ed.
There are many considerations and variations for frequency, intensity, duration, and type when you consider muscular strength and endurance. Do you want to develop strength or muscular endurance? Do you want to use weights and machines, or do you want to use your own body weight, resistance bands, medicine balls, or other weighted equipment? How many reps or sets will you perform? Your personal goals will influence the FITT principle. Figure 4.2 illustrates the different categories of the FITT principle.
C04-03A
F
I
T
T
Frequency ofExercise
Intensity ofExercise
Time ofExercise
Type ofExercise
How Often
How Hard
–How many reps–How many sets–How much time between sets
Which Exercises
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Beginner
Intermediate toHigh
Weight machines, free weights, resistance tubing, medicine ball, own bodyweight
2–3 days per weekFull-body workout of all 6 body areas48–72 hours of rest in-between workouts
4–5 days per week; often perform split workouts(example: Monday and Thursday, work chest,shoulders, triceps, abdominals; Tuesday and Friday,work back, legs, biceps)48–72 hours of rest in-between workouts
60%–70% of maximum strength
70%–90% of maximum strength
1–3 Sets8–12 repetitions
Endurance – 12–20+ Reps2–3 Sets
Strength – 2–6 Reps3–5 Sets
30 sec to 1 minute
30 sec to 1 minute
2 to 5 minutes
Note: Specificity Principle — you must work each muscle group to have strength gains in that particular part of the body.
FITT Principle for Muscular Strength and Endurance
Muscular Strength and Endurance—Activity 2
Aantal reps / sessie: +/- 30 30 sec – 1 minuut rust tussen sets ? ook geldig voor orofaryngeale spieren

Time of exercise
EMST: 25 reps ; rustperiodes

Duur ?

Duur ?
Study Participants N Method Exercise scheme
Lazarus et al. 2003
Adultes en bonne santé 31 IOPI & abaisse-langue
4 weeks
Clark et al. 2009
Adultes en bonne santé 39 Supressor linguale 9 weeks
Robbins et al. 2005 Personnes âgées (70-89 ans)
10 IOPI 8 weeks
Robbins et al. 2007 Accident Vasculaire Cérébral (AVC)
10 IOPI 8 weeks
Steele et al. 2013 Lésions cérébrale 6 IOPI 8-12 weken
Van Nuffelen et al. 2012
Carcinome tête et cou – dysphagie chronique
6 IOPI 4 weeks
Van Nuffelen et al. 2013
Maladies neuromusculaires 9 IOPI 4-8 weeks

EMST Aspiration and swallowing in Parkinsondisease and rehabilitation with EMSTA randomized trial
M.S. Troche, PhDM.S. Okun, MDJ.C. Rosenbek, PhDN. Musson, MAH.H. Fernandez, MDR. Rodriguez, MDJ. Romrell, PA-CT. Pitts, PhDK.M. Wheeler-Hegland,
PhDC.M. Sapienza, PhD
ABSTRACT
Objective: Dysphagia is the main cause of aspiration pneumonia and death in Parkinson disease(PD) with no established restorative behavioral treatment to date. Reduced swallow safety maybe related to decreased elevation and excursion of the hyolaryngeal complex. Increased submen-tal muscle force generation has been associated with expiratory muscle strength training (EMST)and subsequent increases in hyolaryngeal complex movement provide a strong rationale for itsuse as a dysphagia treatment. The current study’s objective was to test the treatment outcome ofa 4-week device-driven EMST program on swallow safety and define the physiologic mechanismsthrough measures of swallow timing and hyoid displacement.
Methods: This was a randomized, blinded, sham-controlled EMST trial performed at an academiccenter. Sixty participants with PD completed EMST, 4 weeks, 5 days per week, for 20 minutesper day, using a calibrated or sham, handheld device. Measures of swallow function includingjudgments of swallow safety (penetration–aspiration [PA] scale scores), swallow timing, and hyoidmovement were made from videofluoroscopic images.
Results: No pretreatment group differences existed. The active treatment (EMST) group demon-strated improved swallow safety compared to the sham group as evidenced by improved PAscores. The EMST group demonstrated improvement of hyolaryngeal function during swallowing,findings not evident for the sham group.
Conclusions: EMST may be a restorative treatment for dysphagia in those with PD. The mecha-nism may be explained by improved hyolaryngeal complex movement.
Classification of evidence: This intervention study provides Class I evidence that swallow safety asdefined by PA score improved post EMST. Neurology® 2010;75:1912–1919
GLOSSARYCI ! confidence interval; EMST ! expiratory muscle strength training; MEP ! maximum expiratory pressure; PA ! penetra-tion–aspiration; PD ! Parkinson disease; SWAL-QOL ! Swallowing Quality of Life Questionnaire; UES ! upper esophagealsphincter; UF ! University of Florida Movement Disorders Center; VA ! Veterans Affairs.
Swallowing is a patterned sensorimotor process within a complex neural network involvingautomatic and volitional systems1-4 amenable to modification and adaptation. Accordingly,swallowing rehabilitation techniques aimed at restoration of function are gaining increasedinterest, particularly in populations like Parkinson disease (PD), where aspiration pneumonia isthe leading cause of death.5-10 This article presents results from the first blinded, randomizedplacebo-controlled clinical trial, testing the effects of a restorative treatment called expiratorymuscle strength training (EMST150, Aspire Products)11-17 for swallowing dysfunction in PD.EMST’s mechanistic underpinning is its ability to generate increased submental musculatureforce activation.15
Decreased elevation and excursion of the hyolaryngeal complex is considered one cause ofpenetration and aspiration.18-21 Submental muscle contraction elevates the hyolaryngealcomplex. EMST treatment produces significantly longer durations, higher peak amplitudes,
From the University of Florida (M.S.T., M.S.O., J.C.R., H.H.F., R.R., J.R., T.P., K.M.W.-H., C.M.S.), Gainesville; and Brain RehabilitationResearch Center (M.S.T., J.C.R., N.M., T.P., K.M.W.-H., C.M.S.), Malcom Randall VAMC Gainesville, Gainesville, FL.
Study funding: Supported by the VA Rehab R&D (B3721R to C.S.) and the Michael J. Fox Foundation (00056150).
Disclosure: Author disclosures are provided at the end of the article.
Address correspondence andreprint requests to Dr. Michelle S.Troche, PO Box 117420,University of Florida, Gainesville,FL [email protected]
1912 Copyright © 2010 by AAN Enterprises, Inc.

Duur ?
Head-tilt-exercises 6 weken revalidatie ! significant verbeterde larynxelevatie en een toename van de UES-opening bij:
• oudere proefpersonen zonder dysfagie (Easterling et al. 2005 n=26; Shaker et al. 1997 n=31)
• dysfagiepatiënten (Shaker et al. 2002 n=27) 6 weken ! significante toename van de UES-opening alsook verminderde aspiratie na de slikact (Logemann et al 2009, 8 patiënten met orofaryngeale dysfagie)

Frequentie, tijd en intensiteit: conclusie
• Currently no knowledge on the ‘ideal’ volume of practice and load for oropharyngeal muscles
• No dose-dependent studies
• But: outcome studies indicate strength training requires: • multiple repetitions/session • multiple days/week • multiple weeks
• UZA: engagement van de patiënt voor minstens (4-) 8 weken ; 3-5x/week

Principles of exercise
Overload
Frequency
Intensity Specificity
Transference
Periodization
Reversibility
Recovery

Specificiteit
If you want to become a good swimmer, swim If you want to become a good runner, run
If you want to be become good in swallowing, swallow
Simply improving endurance or strength of a specific muscle group, is not necessarily enough for improved performance of a specific task ! McNeill Dysphagia Therapy Program (Crary & Mann)

Transference
BUT! we also know that isolated progressive strength-training can improve function (physical rehab)
in conjunction with or as precursor function training
in frail or decompensated individuals with significant weakness
! Can explain how exercises that are not swallowing-specific may improve swallowing function E.g. tongue strengthening exercises, EMST, LSVT, …

Specificity < > transference
Weinig geweten over geldigheid van het specificiteitsprincipe voor orofaryngeale spieren Enkele indicaties dat specificiteit geldt voor tongspieren maar ook dat transference mogelijk is

Specificity < > transference
Study Specificity Results Lazarus et al. 2003
Yes high resistance TSE • increased tongue strength • no impact on endurance
Clark et al. 2009
No
direction of TSE (protrusion, elevation, lateralization) • exercises for a specific direction result also in
an improvement of strength in the other directions
• no significant differences between methods!
Clark 2012 (Yes)
exercises for strength, endurance, power • significant differences in effect size

Specificity < > transference
Indications that TSE can improve functional swallowing - improvement of PAS (Robbins et al. 2005/2007; Steele et al. 2013) - reduction of pharyngeal residue (Robbins et al. 2005/2007)
- however: Steele et al. 2013: no improvement, even worsening

Principles of exercise
Overload
Frequency
Intensity Specificity
Transference
Periodization
Reversibility
Recovery

Reversibility
Use it or lose it

Reversibility
Disuse muscle atrophy: • Considerable muscle atrophy occurs in < 10 days of disuse (Wall et al. 2013)
Detraining: • Rugby spelers: opgebouwde spierkracht blijft behouden tot maximaal
3 weken van detraining (McMaster et al. 2013)
• MS-patiënten: spierkracht opgebouwd in 12 weken, is na 12 weken van detraining ook weer verdwenen (Medina-Perez et al 2014)

Reversibility
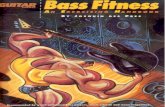
Tongue strength & detraining Effects of Directional Exercise on Lingual Strength. Clark HM et al. JSLHR, aug 2009 N = 39 healthy adults with normal IOPI-values training: 3 movements
elevation protrusion (tongue blade) lateralization (tongue blade) intensity: 7/7d, 30 reps (3*10)
scheme sequential: 3w elev – 3w protr – 3w later (30 reps) concurrent: 9w every movement (10 reps per movement)
control: ‘cheek press’

Reversibility
participants in the present study demonstrated only6% gains in lingual elevation strength, which was notonly less than gains noted by previous researchers butwas also considerably less than the gains demonstratedfor other lingual movements in this study. No immedi-ate explanation is available for this pattern of results.The training protocol in the present study dif-fered slightly from previous lingual training studies.Participants in theLazarus et al. (2003) study completedlingual exercise 5 days per week, whereas participantsin the Clark et al. (2004) study exercised 3 days perweek. In the present study, participants exercised everyday. It is possible that themuscles primarily responsiblefor lingual elevation (e.g., genioglossus, styloglossus) re-spond better to a lower-dose treatment protocol thanwas utilized in this experiment. Because measures ofprotrusion and lateralization strength were not obtainedin the earlier studies, it is unknown if similar dosage ef-fects exist for these exercises. Future research may re-veal differential dosage effects for individual articulatorsas well as different movements of single articulators.
Training SpecificityWehypothesized that training participants on a sin-
gle exercise would increase strength of all lingual move-ments and that the largest gains in strength would beobserved for the trainedmovement.Only the first of thesehypotheseswas supported by our findings.Although all ofthe exercises increased overall lingual strength equally,
none of the lingual strengthmeasureswere preferentiallyaffected by targeted exercise. In fact, for lingual protru-sion and lateralization, had the differential effects provenstatistically significant, the direction of the differenceswould not have been in the predicted direction. Our find-ings failed to provide evidence of training specificity forthe lingual movements targeted.
Our findings are consistent with the view that thebiomechanical properties of the lingualmusculaturemayallow these muscle groups to demonstrate training pat-terns atypical of other skeletal muscles with respect tospecificity. The present study provides explanatory powerfor the findings of other researchers demonstratingthat lingual strengthening improves swallowing function(Robbins et al., 2007). Although a number of studies havedemonstrated a relationship between lingual strengthand swallowing function (e.g., Clark, Henson, Barber,Stierwalt, & Sherrill, 2003; Reddy, Costarella, Grotz, &Canilang, 1990; Robinovitch, Herschler, & Romilly, 1991),Clark et al. (2003) found that strength ratings incorpo-rating tonguemovements in several directions, includingelevation, protrusion, and lateralization, better predictedoral phase swallowing function than did strength mea-sures obtained during lingual elevation alone. The currentfindings suggest that lingual protrusion and lateraliza-tionmay showgreater strengthgains in response to train-ing compared with lingual elevation. Thus, although theRobbins et al. (2007) study did not measure lingual pro-trusion and lateralization strength, we might speculatethat the strength of these movements also increased
Figure 9. Detraining effects. Lingual strength, averaged across all measures, significantly decreased during thedetraining period. Strength measures obtained at baseline and following detraining were not significantlydifferent.
1042 Journal of Speech, Language, and Hearing Research • Vol. 52 • 1034–1047 • August 2009

Krachttraining in slikrevalidatie

• slikrevalidatie = revalidatie van een neuromusculair systeem
• belangrijke component: verbeteren van spierkracht
• Principes van krachttraining ! evidentie dat die op zijn minst deels toepasbaar zijn
• FITT – principes
• Ideaal schema?
Take home messages

Try and fail but never fail to try
Vragen?