multidisciplinaire therapie nieuwe ontwikkelingen therapie nieuwe ontwikkelingen Roy Lalisang,...
51
Het gevorderd ovariumcarcinoom multidisciplinaire therapie nieuwe ontwikkelingen Roy Lalisang, internist-oncoloog Het ovariumcarcinoom, 10 november 2016 1
Transcript of multidisciplinaire therapie nieuwe ontwikkelingen therapie nieuwe ontwikkelingen Roy Lalisang,...
Het gevorderd ovariumcarcinoom multidisciplinaire therapie
nieuwe ontwikkelingen
Roy Lalisang, internist-oncoloog
Het ovariumcarcinoom, 10 november 2016 1
(potentiële) belangenverstrengeling Geen
Voor bijeenkomst mogelijk relevante
relaties met bedrijven Geen
Sponsoring of onderzoeksgeld
Honorarium of andere (financiële)
vergoeding
Aandeelhouder
Andere relatie, namelijk …
Astra Zeneca
Merck, Roche
Geen
Geen
Disclosure belangen
Onderwerpen
• Primaire behandeling
– De standaard: Primaire debulking chirurgie (PDS) + CT
– Controverse:
• Primaire debulking chirurgie (PDS) + CT
• Neo-adjuvante chemotherapie (NACT) + Interval debulking chirurgie (IDS)
• Behandeling van het recidief
– Onderhouds PARPi en angiogenese remmers
Het ovariumcarcinoom, 10 november 2016 3
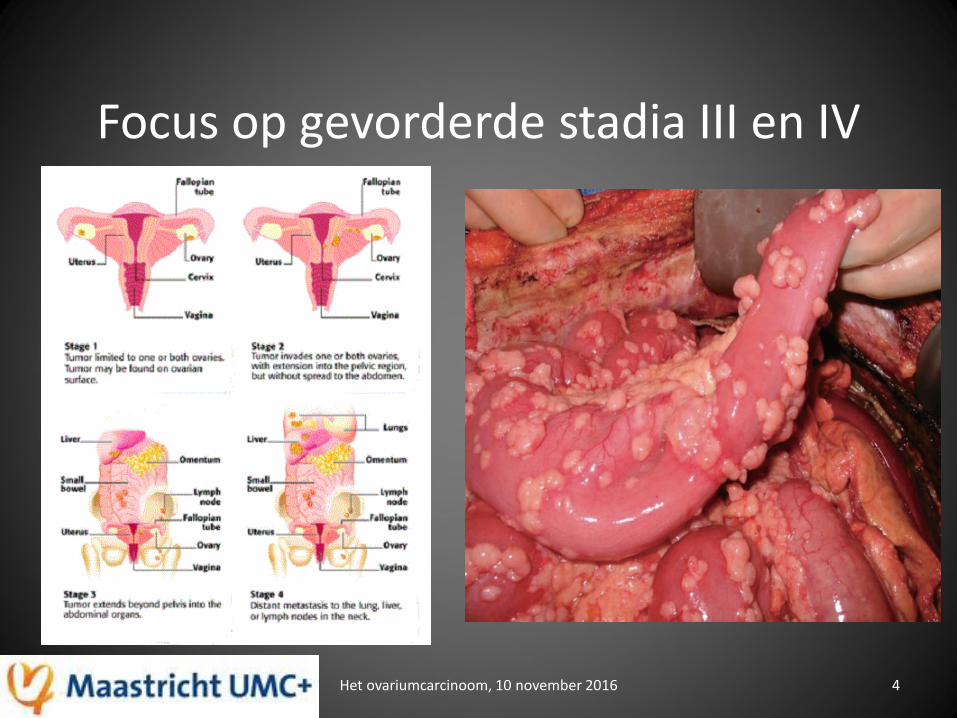
Focus op gevorderde stadia III en IV
Het ovariumcarcinoom, 10 november 2016 4
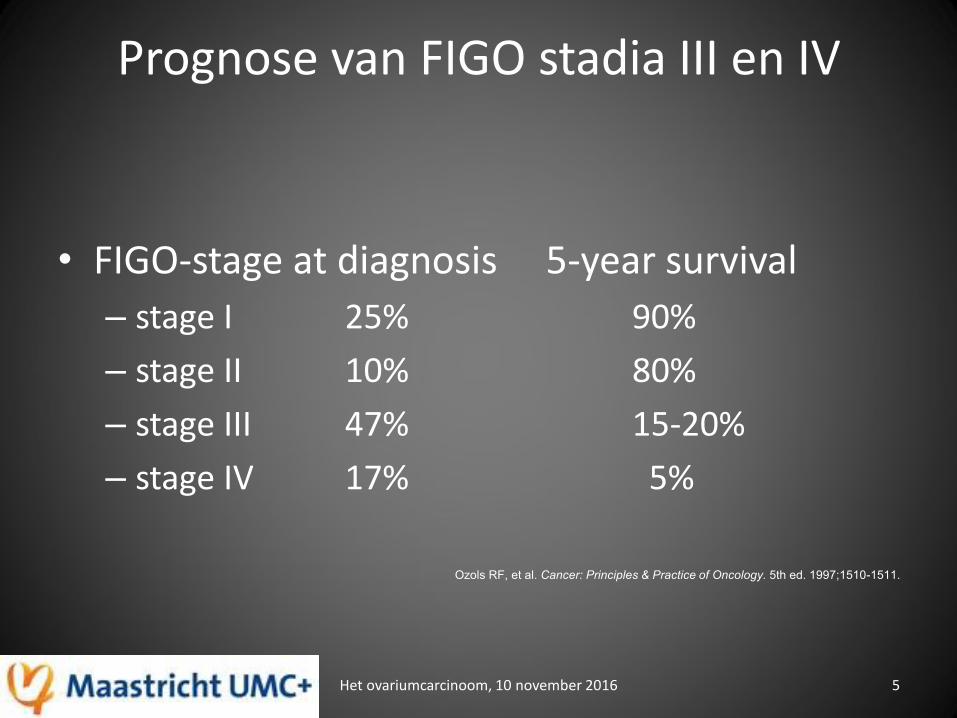
Prognose van FIGO stadia III en IV
Het ovariumcarcinoom, 10 november 2016 5
• FIGO-stage at diagnosis 5-year survival
– stage I 25% 90%
– stage II 10% 80%
– stage III 47% 15-20%
– stage IV 17% 5%
Ozols RF, et al. Cancer: Principles & Practice of Oncology. 5th ed. 1997;1510-1511.
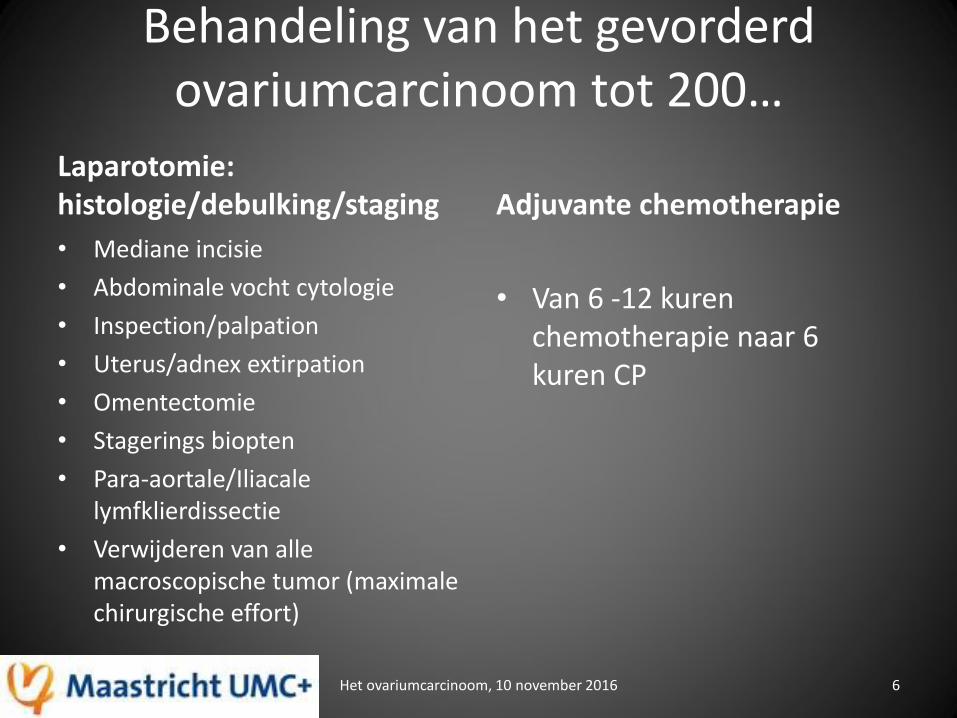
Behandeling van het gevorderd ovariumcarcinoom tot 200…
Laparotomie: histologie/debulking/staging
• Mediane incisie
• Abdominale vocht cytologie
• Inspection/palpation
• Uterus/adnex extirpation
• Omentectomie
• Stagerings biopten
• Para-aortale/Iliacale lymfklierdissectie
• Verwijderen van alle macroscopische tumor (maximale chirurgische effort)
Adjuvante chemotherapie
• Van 6 -12 kuren chemotherapie naar 6 kuren CP
Het ovariumcarcinoom, 10 november 2016 6
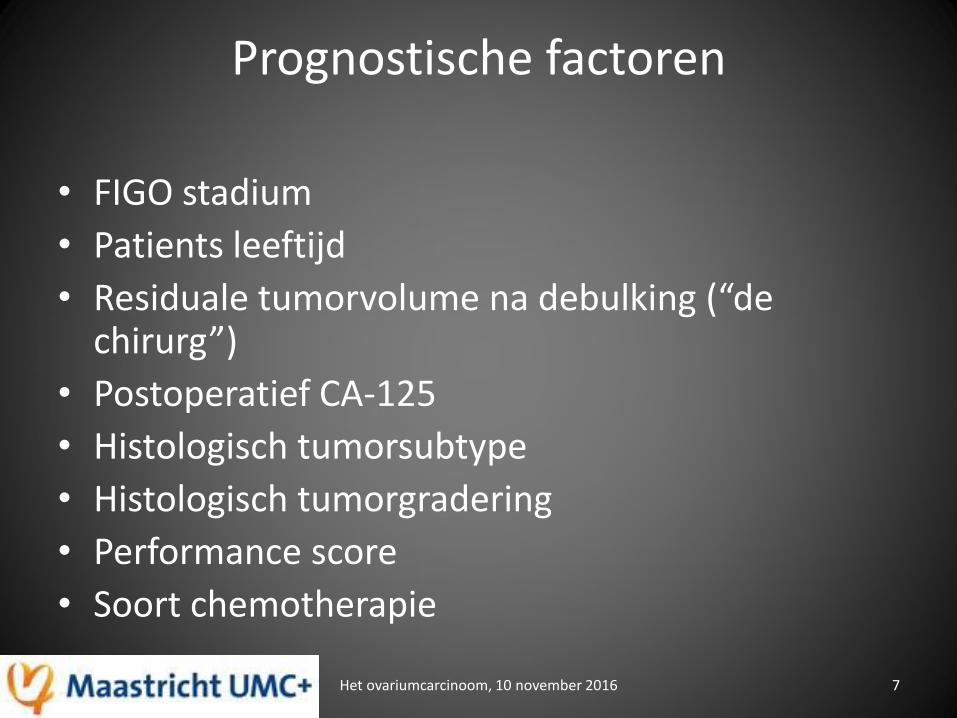
Prognostische factoren
• FIGO stadium
• Patients leeftijd
• Residuale tumorvolume na debulking (“de chirurg”)
• Postoperatief CA-125
• Histologisch tumorsubtype
• Histologisch tumorgradering
• Performance score
• Soort chemotherapie
Het ovariumcarcinoom, 10 november 2016 7
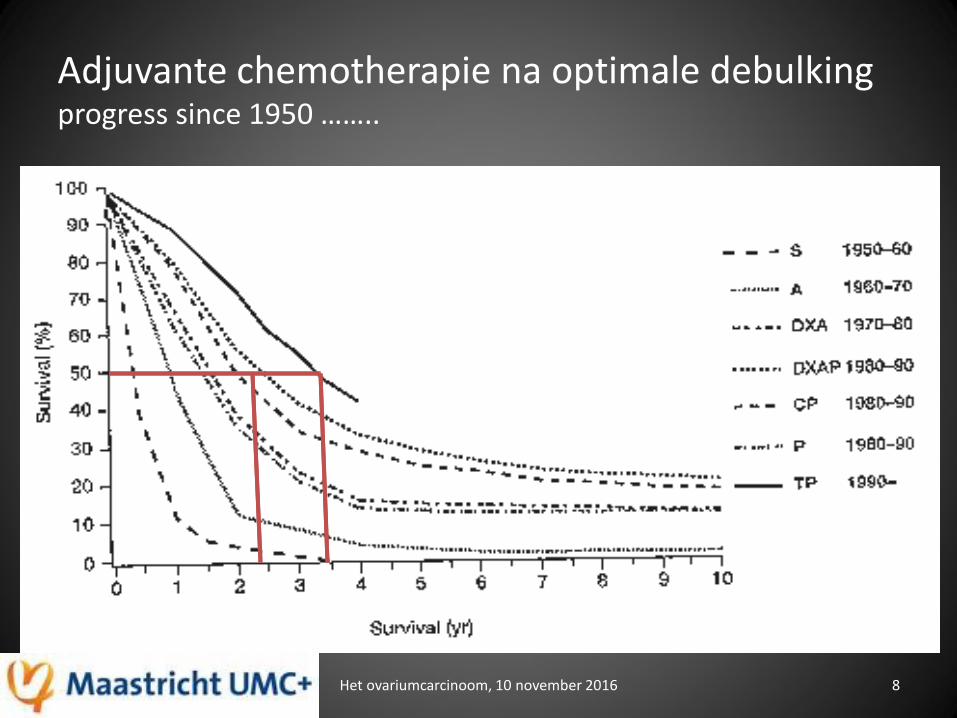
Adjuvante chemotherapie na optimale debulking progress since 1950 ……..
Het ovariumcarcinoom, 10 november 2016 8
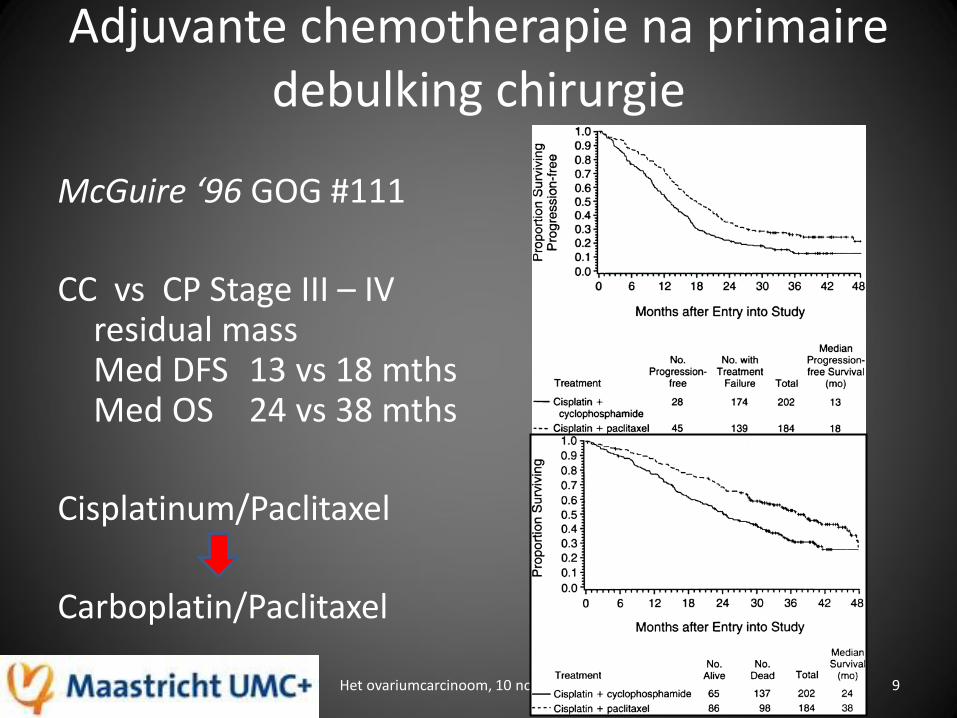
Adjuvante chemotherapie na primaire debulking chirurgie
McGuire ‘96 GOG #111
CC vs CP Stage III – IV residual mass Med DFS 13 vs 18 mths Med OS 24 vs 38 mths
Cisplatinum/Paclitaxel
Carboplatin/Paclitaxel
Het ovariumcarcinoom, 10 november 2016 9
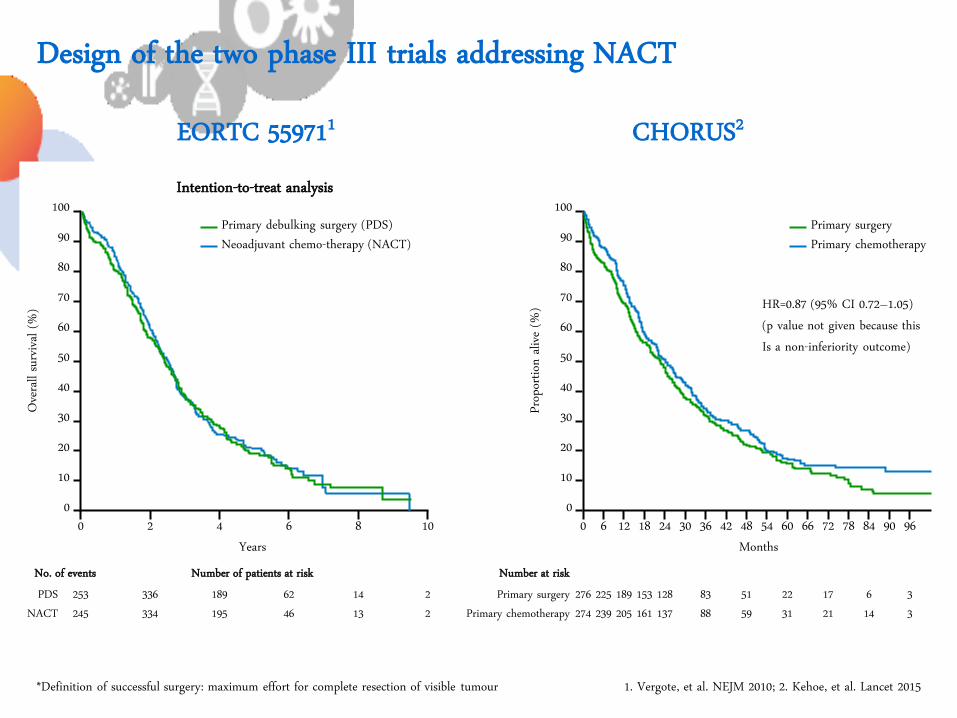
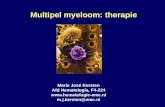
EORTC 559711 CHORUS2
Design of the two phase III trials addressing NACT
1. Vergote, et al. NEJM 2010; 2. Kehoe, et al. Lancet 2015 *Definition of successful surgery: maximum effort for complete resection of visible tumour
Randomise
Clinical FIGO stage III/IV ovarian cancer
+ CA125:CEA ratio >25
Primary surgery* followed by
chemotherapy
Neoadjuvant chemotherapy followed by surgery then chemotherapy
Biopsy/cytology PROVEN
Clinical FIGO stage III/IV ovarian cancer
+ CA125:CEA ratio >25
Primary surgery* followed by
chemotherapy
Neoadjuvant chemotherapy followed by surgery then chemotherapy
Biopsy/cytology
Randomise
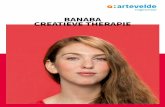
Intention-to-treat analysis
Years 0 8 6 4 2 10
Overa
ll surv
ival (
%)
100
90
80
70
60
40
30
20
10
0
50
Primary debulking surgery (PDS) Neoadjuvant chemo-therapy (NACT)
253 245
14 13
62 46
189 195
336 334
2 2
No. of events PDS
NACT
Number of patients at risk
HR=0.87 (95% CI 0.72–1.05) (p value not given because this Is a non-inferiority outcome)
0 24 18 12 6 Pro
portio
n aliv
e (%)
100
90
80
70
60
40
30
20
10
0
50
Primary surgery Primary chemotherapy
Primary surgery Primary chemotherapy
Number at risk
30 36 42 48 54 60 66 72 78 84 90 96
276 274
128 137
153 161
189 205
225 239
83 88
51 59
22 31
17 21
6 14
3 3
Months
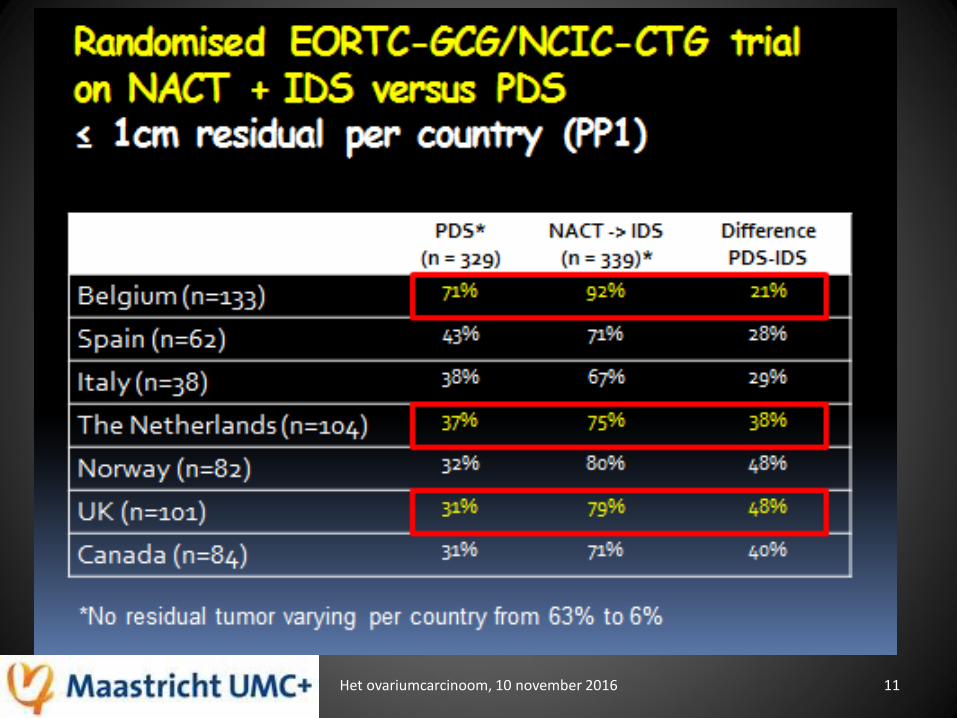
Het ovariumcarcinoom, 10 november 2016 11
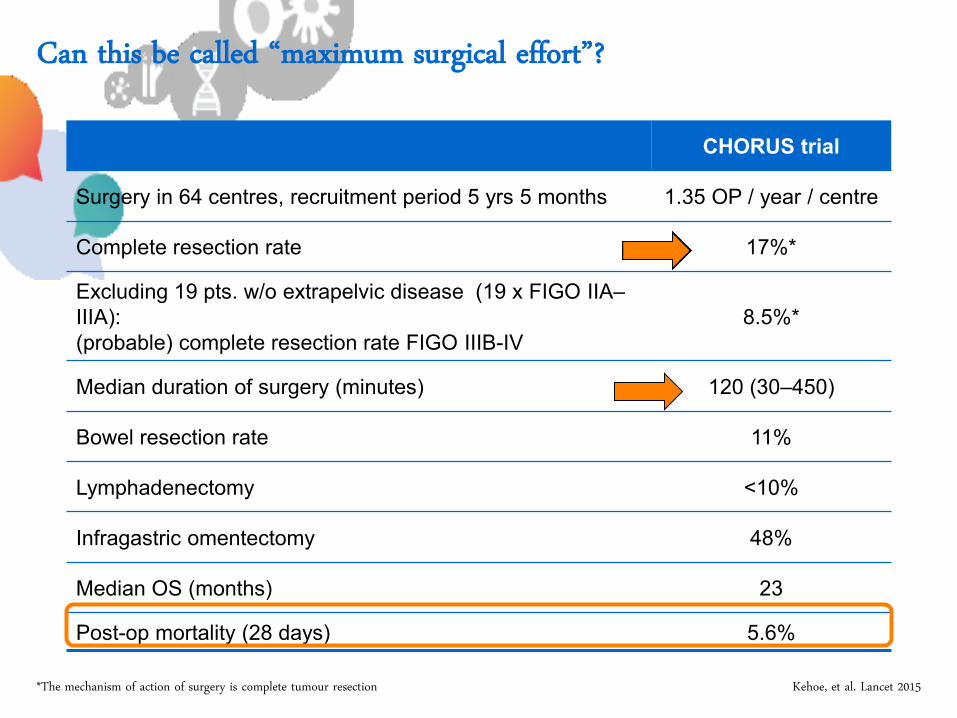
Can this be called “maximum surgical effort”?
CHORUS trial
Surgery in 64 centres, recruitment period 5 yrs 5 months 1.35 OP / year / centre
Complete resection rate 17%*
Excluding 19 pts. w/o extrapelvic disease (19 x FIGO IIA–
IIIA):
(probable) complete resection rate FIGO IIIB-IV
8.5%*
Median duration of surgery (minutes) 120 (30–450)
Bowel resection rate 11%
Lymphadenectomy <10%
Infragastric omentectomy 48%
Median OS (months) 23
Post-op mortality (28 days) 5.6%
Kehoe, et al. Lancet 2015 *The mechanism of action of surgery is complete tumour resection
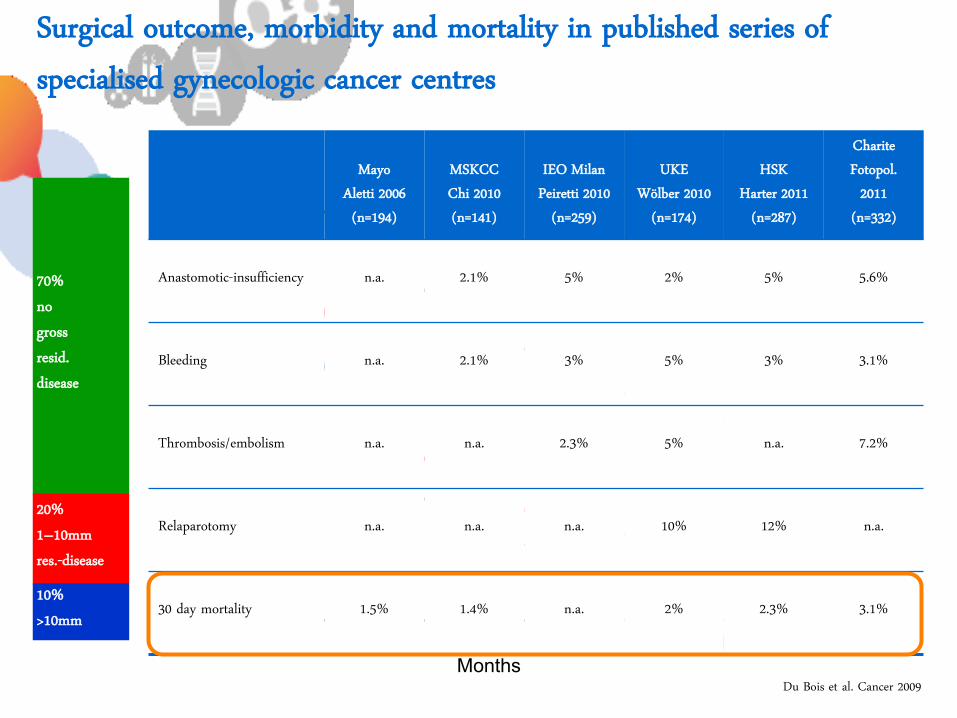
Surgical outcome, morbidity and mortality in published series of specialised gynecologic cancer centres
Du Bois et al. Cancer 2009
70% no gross resid. disease
70% no gross resid. disease
20% 1–10mm res.-disease
20% 1–10mm res.-disease 10% >10mm 10% >10mm
% O
ve
rall
su
rviv
al
100
75
50
25
0
0 12 24 36 48 60 72 84 96 108 120 130 144
0mm
1–10mm
>10mm
Months
Mayo Aletti 2006 (n=194)
MSKCC Chi 2010 (n=141)
IEO Milan Peiretti 2010
(n=259)
UKE Wölber 2010
(n=174)
HSK Harter 2011
(n=287)
Charite Fotopol.
2011 (n=332)
Anastomotic-insufficiency n.a. 2.1% 5% 2% 5% 5.6%
Bleeding n.a. 2.1% 3% 5% 3% 3.1%
Thrombosis/embolism n.a. n.a. 2.3% 5% n.a. 7.2%
Relaparotomy n.a. n.a. n.a. 10% 12% n.a.
30 day mortality 1.5% 1.4% n.a. 2% 2.3% 3.1%
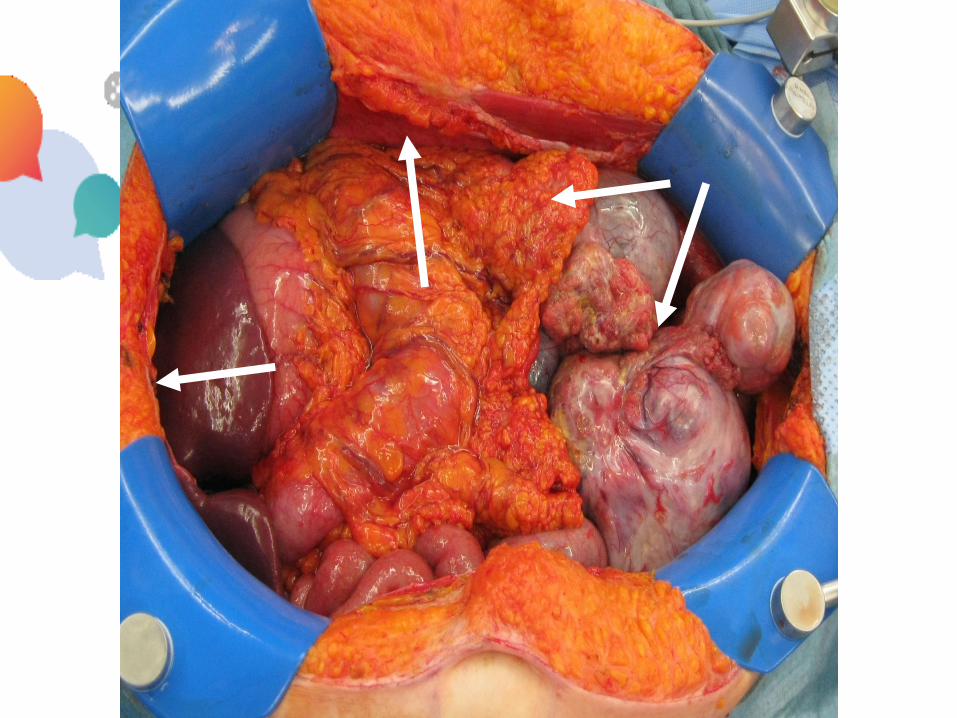
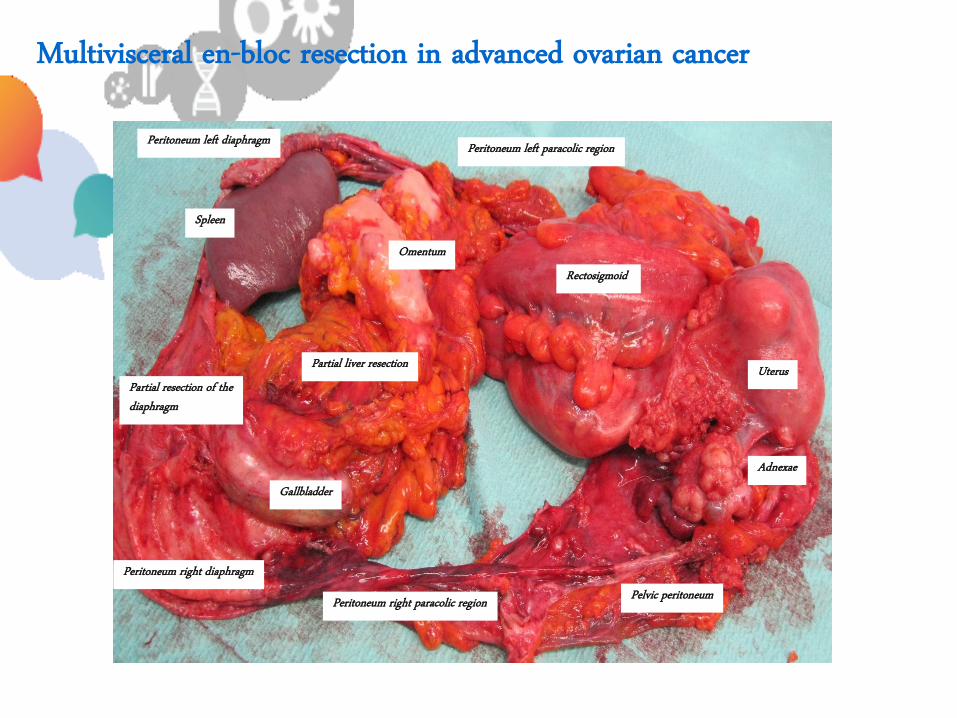
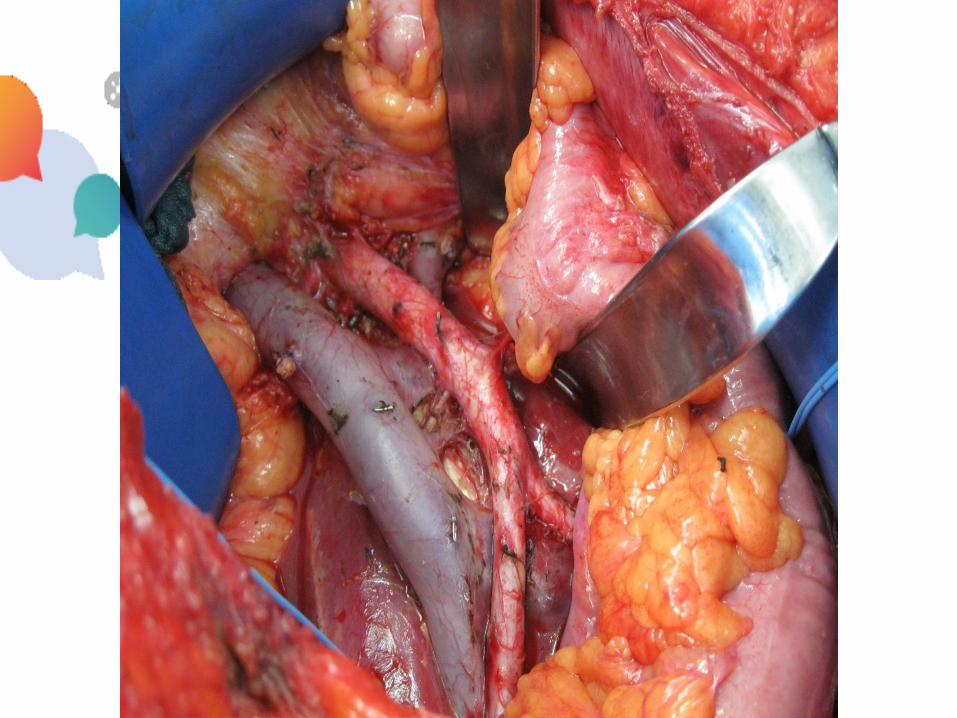
Multivisceral en-bloc resection in advanced ovarian cancer
Uterus
Rectosigmoid
Adnexae
Pelvic peritoneum Peritoneum right paracolic region
Peritoneum right diaphragm
Peritoneum left diaphragm
Gallbladder
Partial resection of the diaphragm
Partial liver resection
Omentum
Spleen
Peritoneum left paracolic region
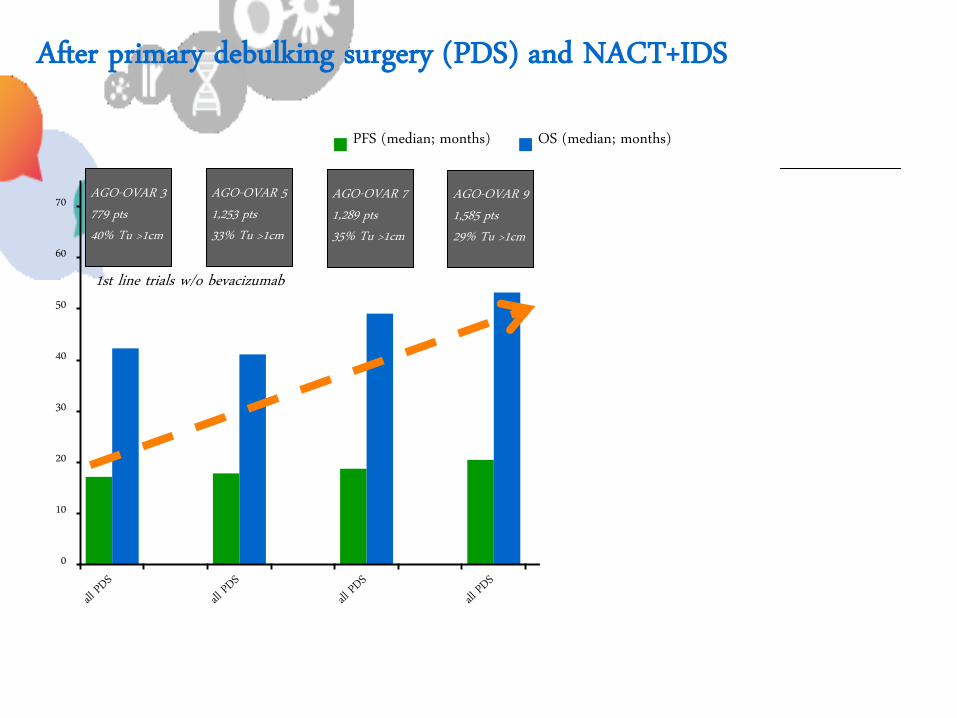
0
10
20
30
40
50
60
70
PFS (median; months) OS (median; months)
After primary debulking surgery (PDS) and NACT+IDS
1st line trials w/o bevacizumab
AGO-OVAR 3 779 pts 40% Tu >1cm
AGO-OVAR 5 1,253 pts 33% Tu >1cm
AGO-OVAR 7 1,289 pts 35% Tu >1cm
AGO-OVAR 9 1,585 pts 29% Tu >1cm
EORTC 718 pts PDS: 54% Tu >1cm NACT: 18% Tu >1cm
CHORUS 550 pts PDS: 61% Tu >1cm NACT: 25% Tu >1cm
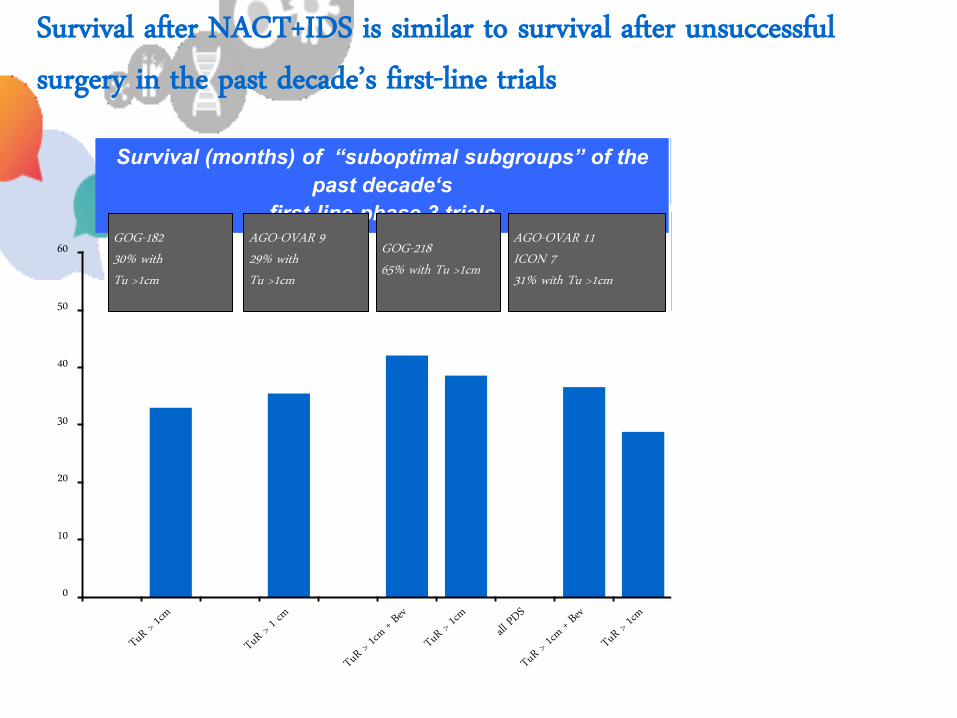
Survival (months) of “suboptimal subgroups” of the
past decade‘s
first-line phase 3 trials
Survival after NACT+IDS is similar to survival after unsuccessful surgery in the past decade’s first-line trials
0
10
20
30
40
50
60 GOG-182 30% with Tu >1cm
AGO-OVAR 9 29% with Tu >1cm
GOG-218 65% with Tu >1cm
AGO-OVAR 11 ICON 7 31% with Tu >1cm
EORTC NACT: all pts. only 18% Tu >1cm
CHORUS NACT: all pts. Only 25% Tu >1cm
All neoadjuvant patients
What we should aim for in a trial if we would like to answer this question…
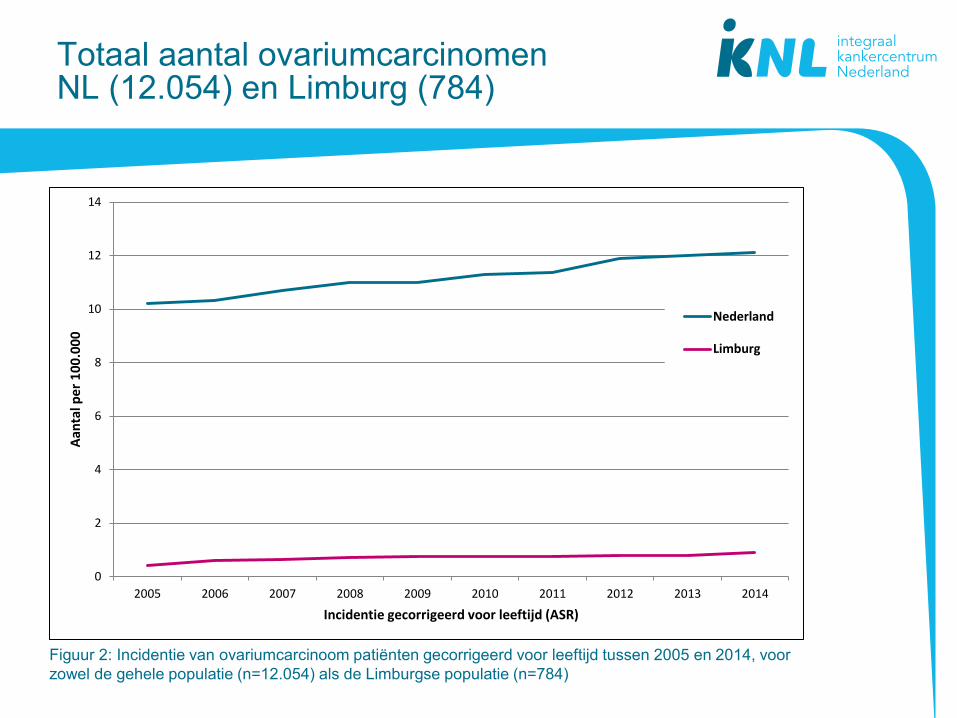
Totaal aantal ovariumcarcinomen NL (12.054) en Limburg (784)
Figuur 2: Incidentie van ovariumcarcinoom patiënten gecorrigeerd voor leeftijd tussen 2005 en 2014, voor
zowel de gehele populatie (n=12.054) als de Limburgse populatie (n=784)
0
2
4
6
8
10
12
14
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Aan
tal p
er 1
00
.00
0
Incidentie gecorrigeerd voor leeftijd (ASR)
Nederland
Limburg
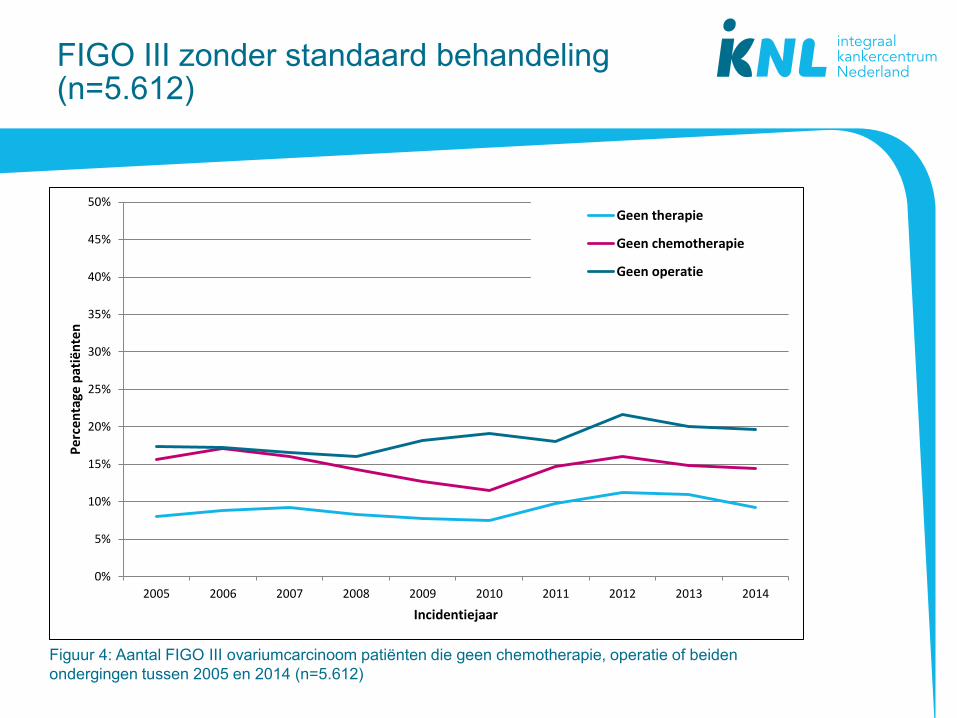
FIGO III zonder standaard behandeling (n=5.612)
Figuur 4: Aantal FIGO III ovariumcarcinoom patiënten die geen chemotherapie, operatie of beiden
ondergingen tussen 2005 en 2014 (n=5.612)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Per
cen
tage
pat
iën
ten
Incidentiejaar
Geen therapie
Geen chemotherapie
Geen operatie
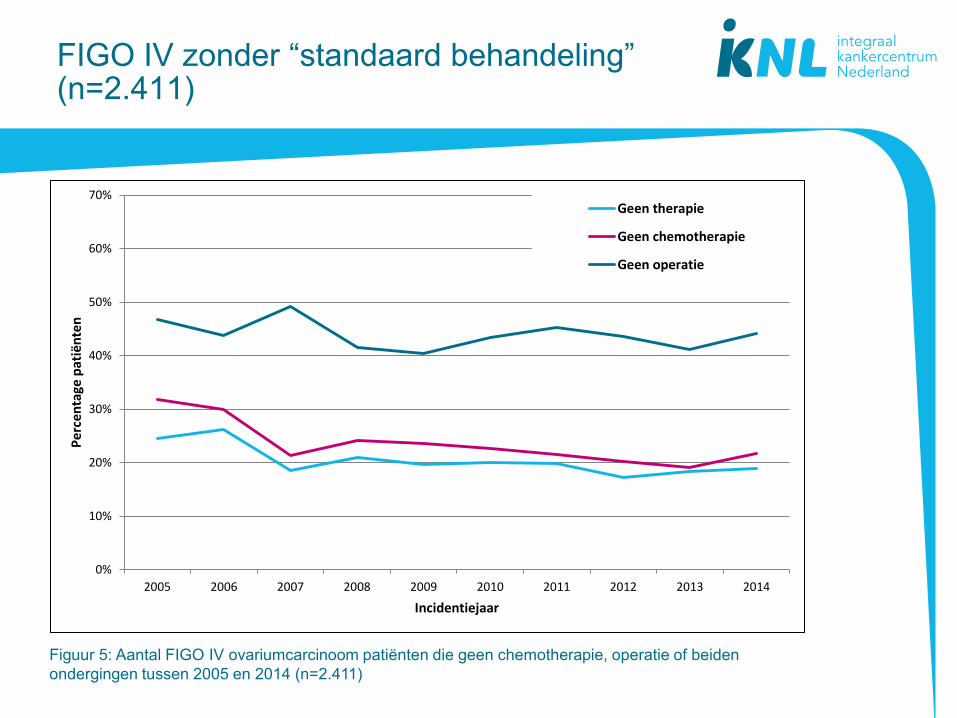
FIGO IV zonder “standaard behandeling” (n=2.411)
Figuur 5: Aantal FIGO IV ovariumcarcinoom patiënten die geen chemotherapie, operatie of beiden
ondergingen tussen 2005 en 2014 (n=2.411)
0%
10%
20%
30%
40%
50%
60%
70%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Geen therapie
Geen chemotherapie
Geen operatie
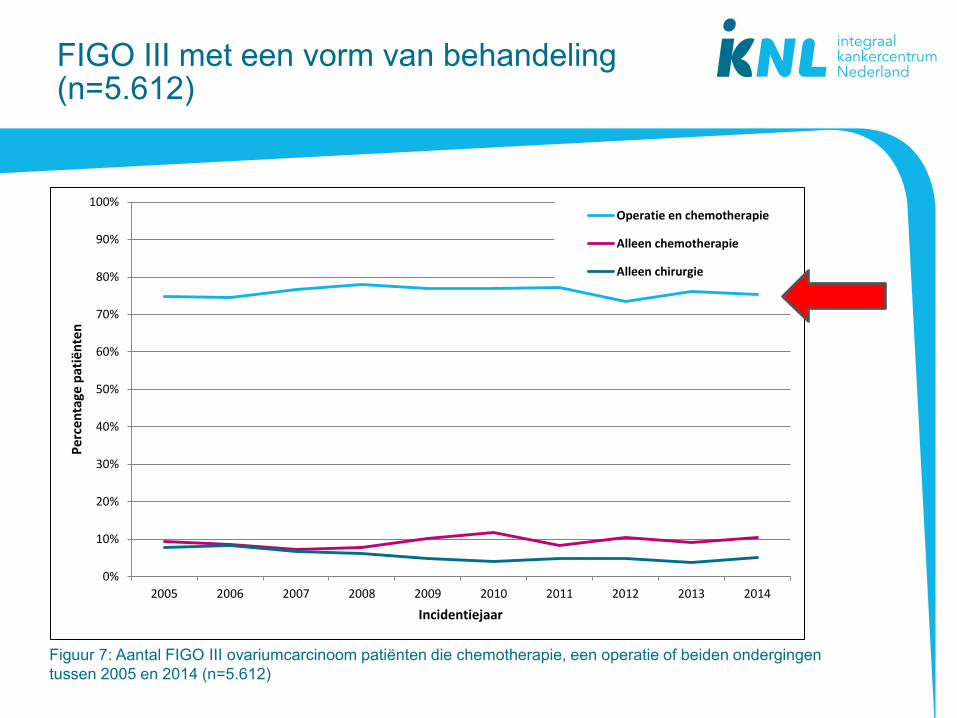
FIGO III met een vorm van behandeling (n=5.612)
Figuur 7: Aantal FIGO III ovariumcarcinoom patiënten die chemotherapie, een operatie of beiden ondergingen
tussen 2005 en 2014 (n=5.612)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Operatie en chemotherapie
Alleen chemotherapie
Alleen chirurgie
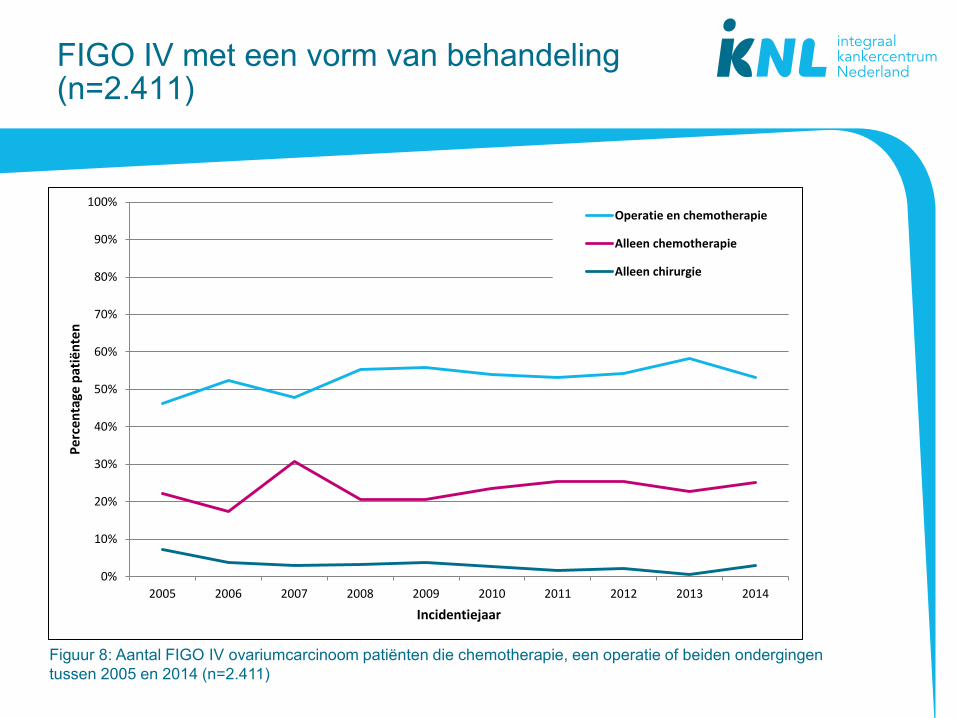
FIGO IV met een vorm van behandeling (n=2.411)
Figuur 8: Aantal FIGO IV ovariumcarcinoom patiënten die chemotherapie, een operatie of beiden ondergingen
tussen 2005 en 2014 (n=2.411)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Operatie en chemotherapie
Alleen chemotherapie
Alleen chirurgie
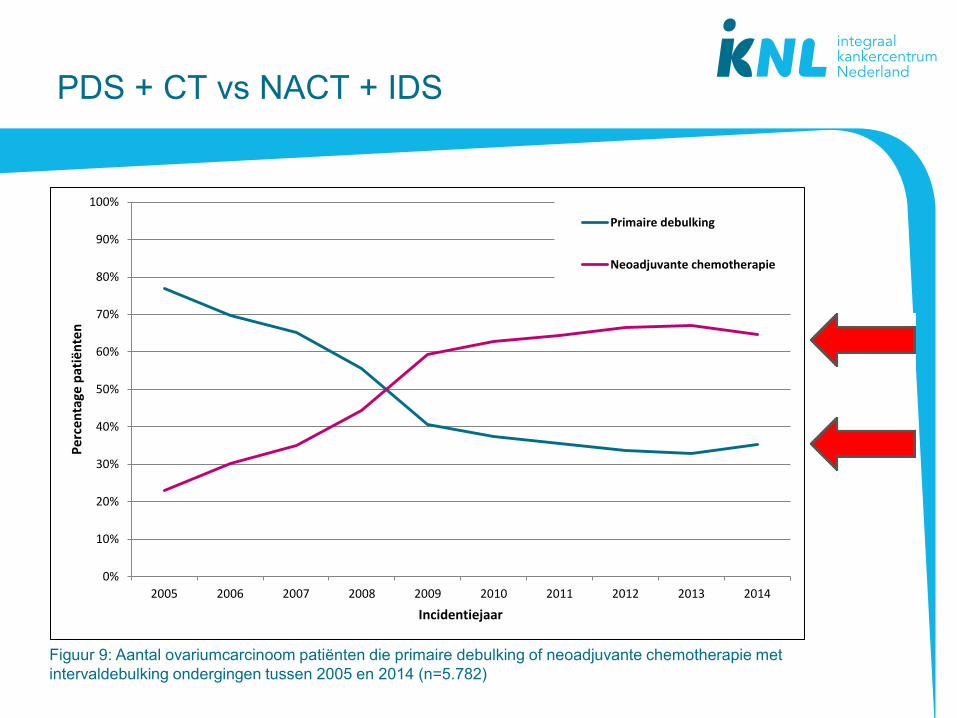
PDS + CT vs NACT + IDS
Figuur 9: Aantal ovariumcarcinoom patiënten die primaire debulking of neoadjuvante chemotherapie met
intervaldebulking ondergingen tussen 2005 en 2014 (n=5.782)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Primaire debulking
Neoadjuvante chemotherapie
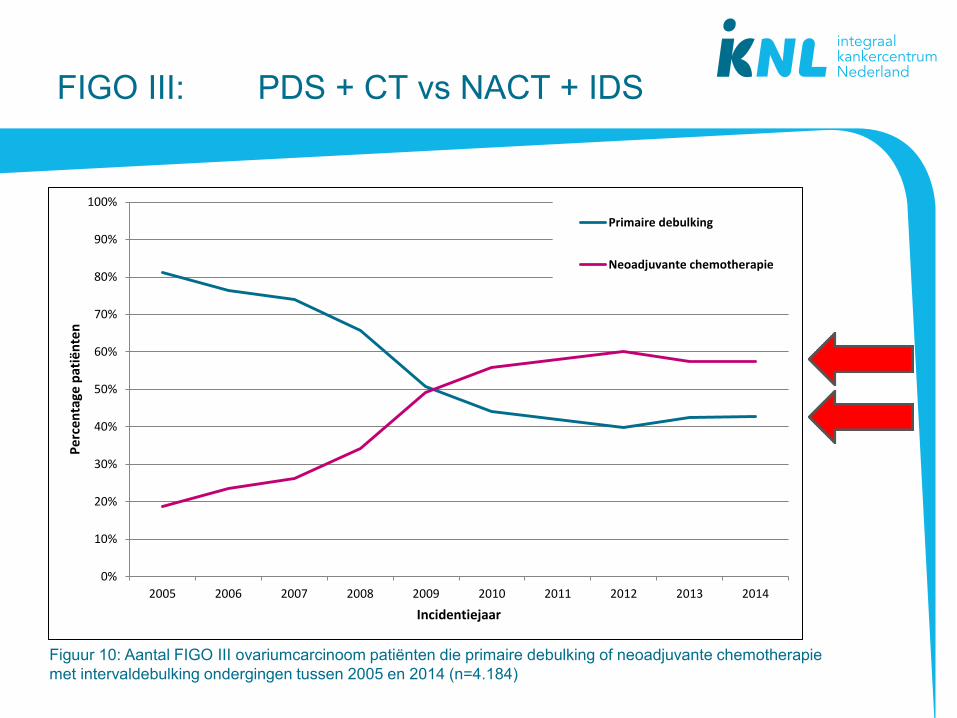
FIGO III: PDS + CT vs NACT + IDS
Figuur 10: Aantal FIGO III ovariumcarcinoom patiënten die primaire debulking of neoadjuvante chemotherapie
met intervaldebulking ondergingen tussen 2005 en 2014 (n=4.184)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Primaire debulking
Neoadjuvante chemotherapie
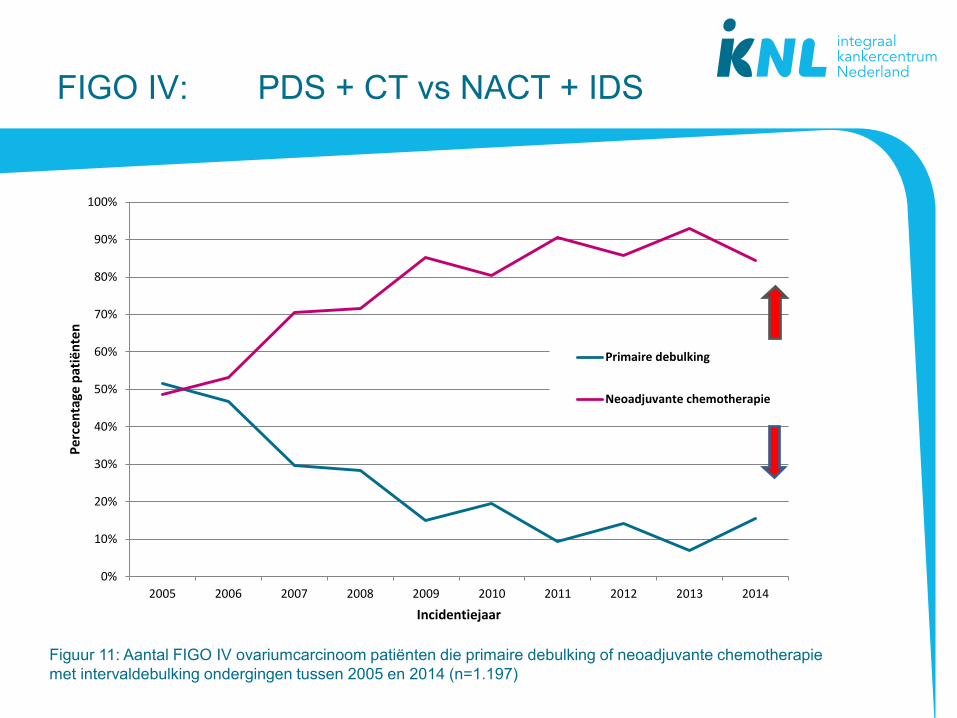
FIGO IV: PDS + CT vs NACT + IDS
Figuur 11: Aantal FIGO IV ovariumcarcinoom patiënten die primaire debulking of neoadjuvante chemotherapie
met intervaldebulking ondergingen tussen 2005 en 2014 (n=1.197)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Primaire debulking
Neoadjuvante chemotherapie
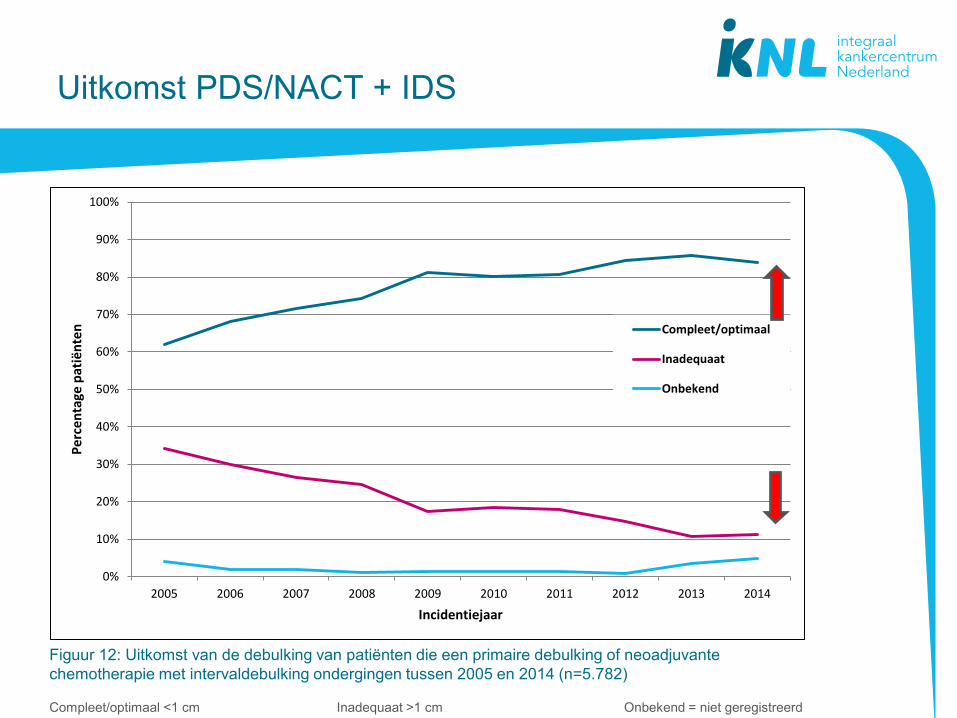
Uitkomst PDS/NACT + IDS
Figuur 12: Uitkomst van de debulking van patiënten die een primaire debulking of neoadjuvante
chemotherapie met intervaldebulking ondergingen tussen 2005 en 2014 (n=5.782)
Compleet/optimaal <1 cm Inadequaat >1 cm Onbekend = niet geregistreerd
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Compleet/optimaal
Inadequaat
Onbekend
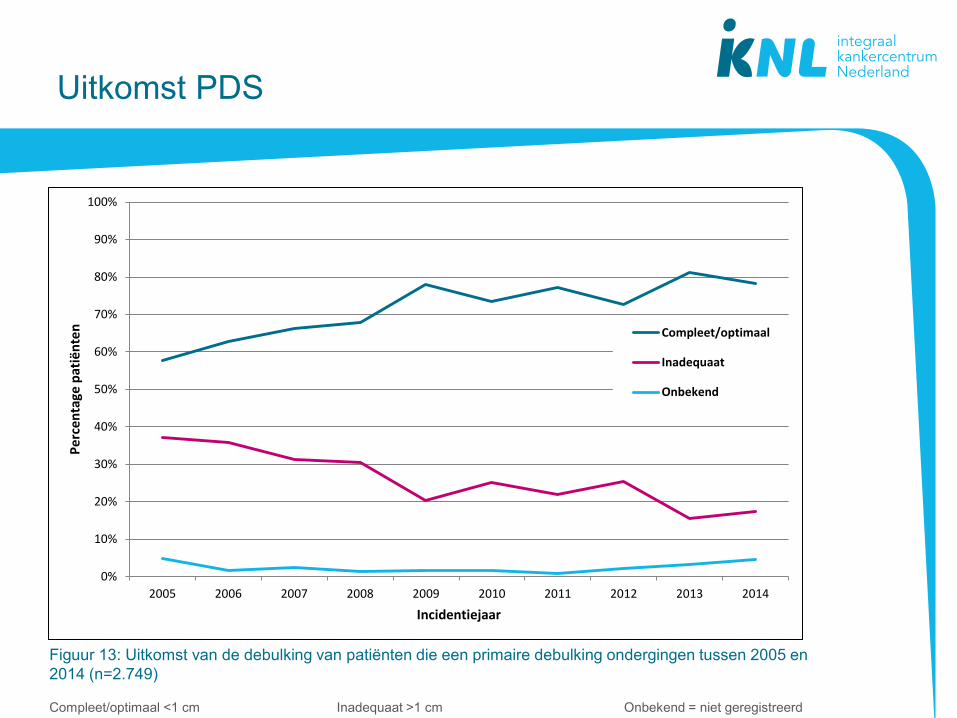
Uitkomst PDS
Figuur 13: Uitkomst van de debulking van patiënten die een primaire debulking ondergingen tussen 2005 en
2014 (n=2.749)
Compleet/optimaal <1 cm Inadequaat >1 cm Onbekend = niet geregistreerd
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Compleet/optimaal
Inadequaat
Onbekend
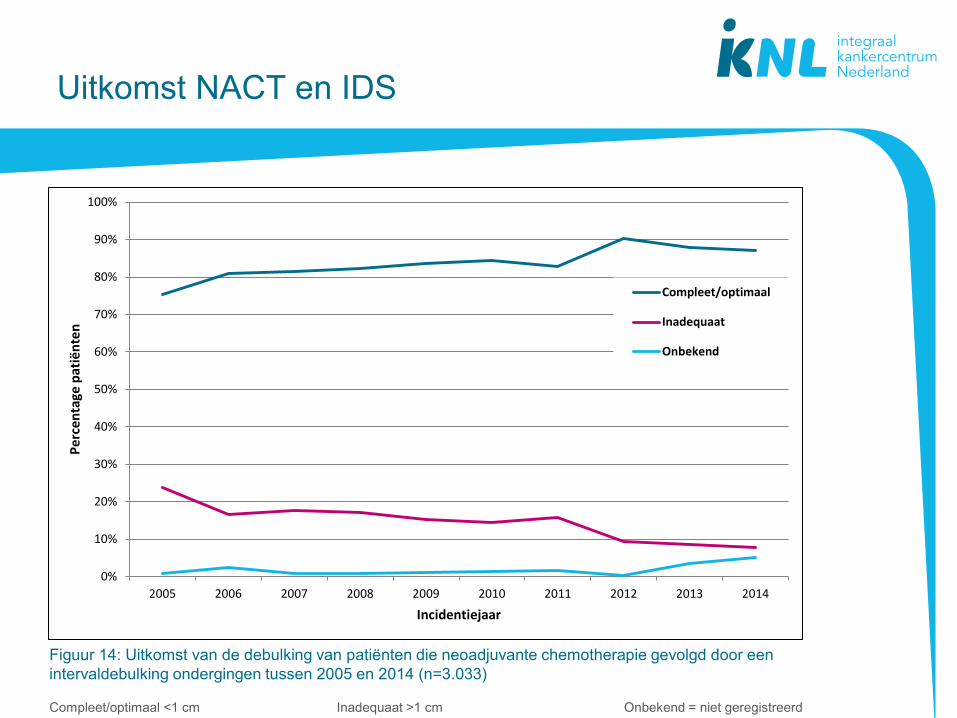
Uitkomst NACT en IDS
Figuur 14: Uitkomst van de debulking van patiënten die neoadjuvante chemotherapie gevolgd door een
intervaldebulking ondergingen tussen 2005 en 2014 (n=3.033)
Compleet/optimaal <1 cm Inadequaat >1 cm Onbekend = niet geregistreerd
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Pe
rcen
tage
pat
iën
ten
Incidentiejaar
Compleet/optimaal
Inadequaat
Onbekend
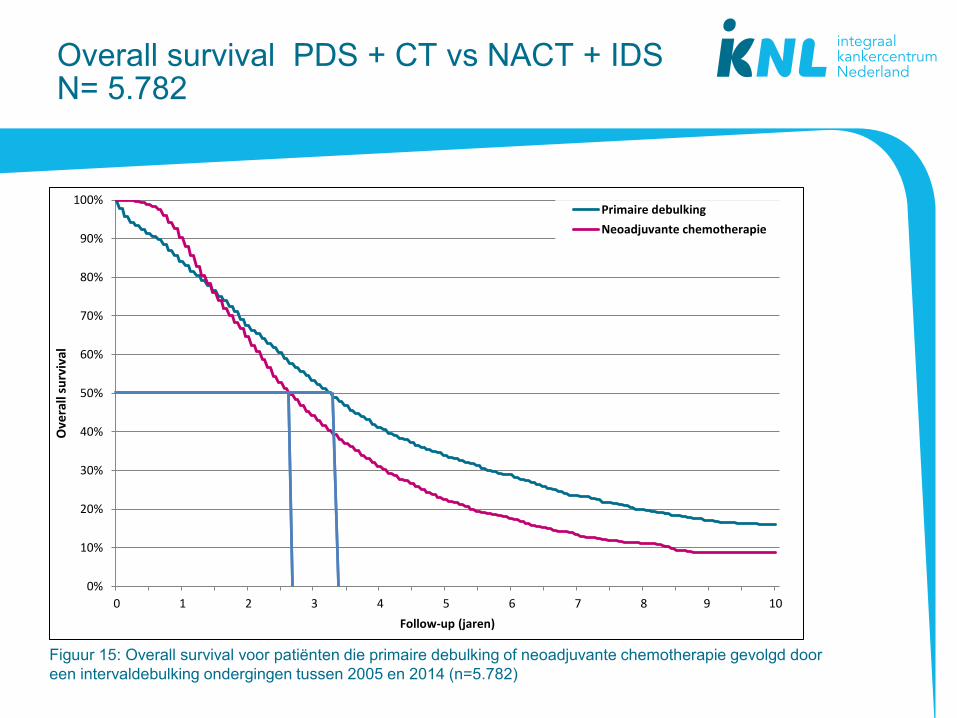
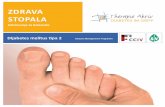
Overall survival PDS + CT vs NACT + IDS N= 5.782
Figuur 15: Overall survival voor patiënten die primaire debulking of neoadjuvante chemotherapie gevolgd door
een intervaldebulking ondergingen tussen 2005 en 2014 (n=5.782)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1 2 3 4 5 6 7 8 9 10
Ove
rall
surv
ival
Follow-up (jaren)
Primaire debulking
Neoadjuvante chemotherapie
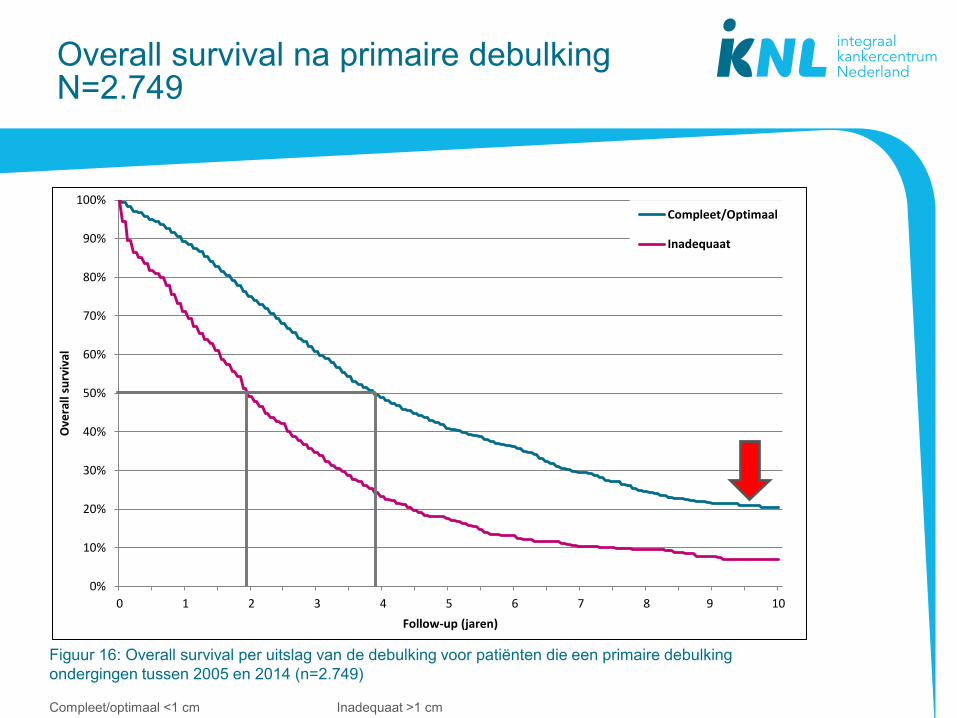
Overall survival na primaire debulking N=2.749
Figuur 16: Overall survival per uitslag van de debulking voor patiënten die een primaire debulking
ondergingen tussen 2005 en 2014 (n=2.749)
Compleet/optimaal <1 cm Inadequaat >1 cm
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1 2 3 4 5 6 7 8 9 10
Ove
rall
surv
ival
Follow-up (jaren)
Compleet/Optimaal
Inadequaat
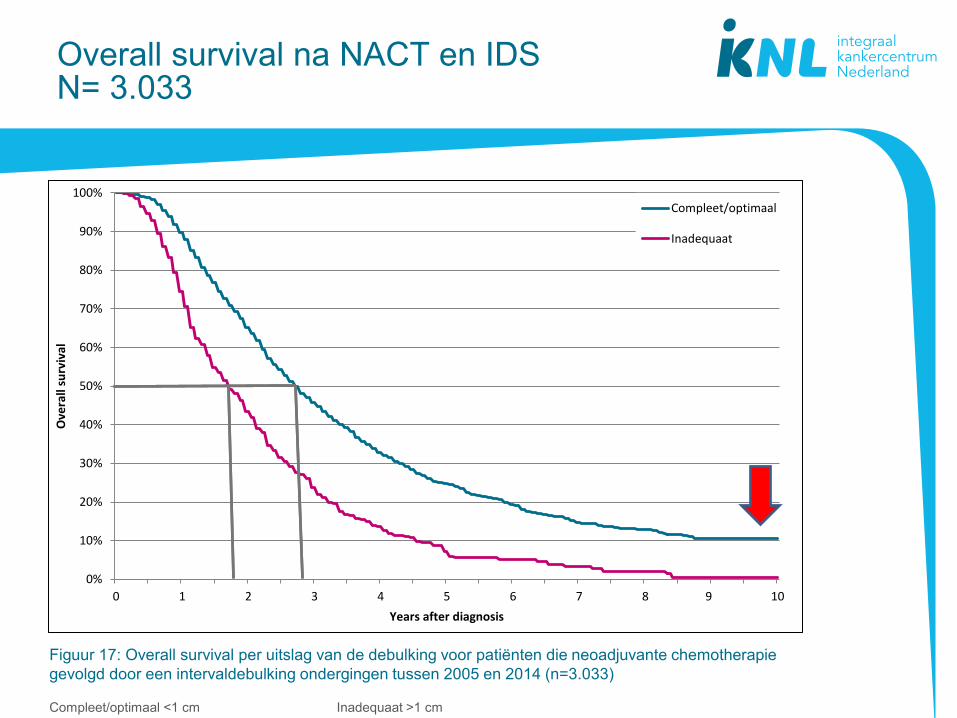
Overall survival na NACT en IDS N= 3.033
Figuur 17: Overall survival per uitslag van de debulking voor patiënten die neoadjuvante chemotherapie
gevolgd door een intervaldebulking ondergingen tussen 2005 en 2014 (n=3.033)
Compleet/optimaal <1 cm Inadequaat >1 cm
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 1 2 3 4 5 6 7 8 9 10
Ove
rall
surv
ival
Years after diagnosis
Compleet/optimaal
Inadequaat
Overgrote deel van de gevorderde ovariumcarcinoom recidiveert !!!
• Platinum gevoelig: >6 maanden ziektevrij
• Platinum resistent: <6 maanden ziektevrij
Het ovariumcarcinoom, 10 november 2016 34
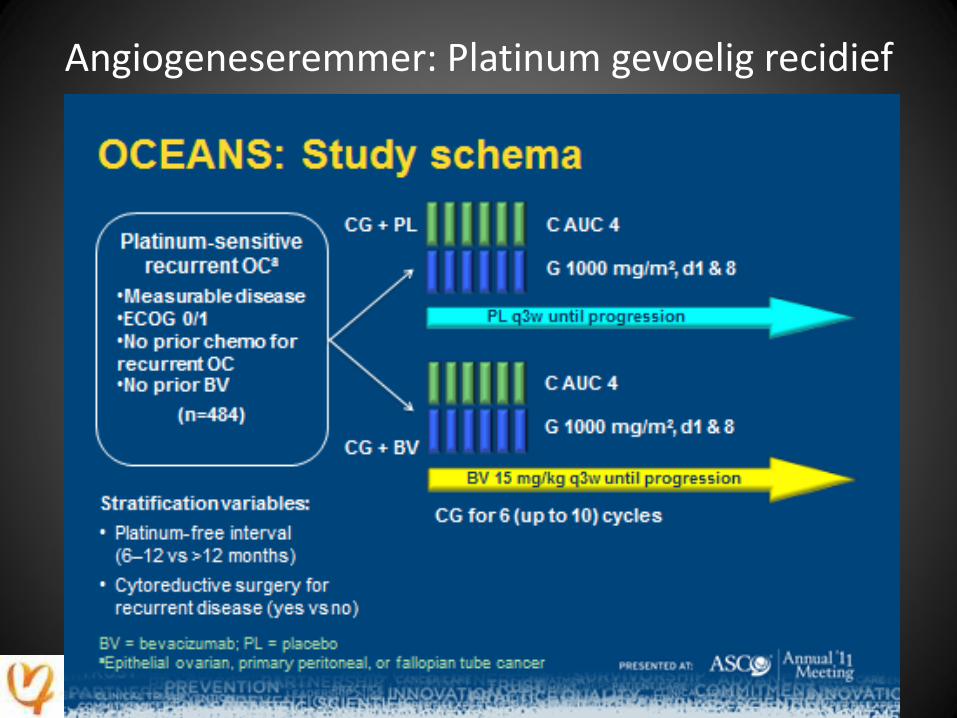
Angiogeneseremmer: Platinum gevoelig recidief
Het ovariumcarcinoom, 10 november 2016 35
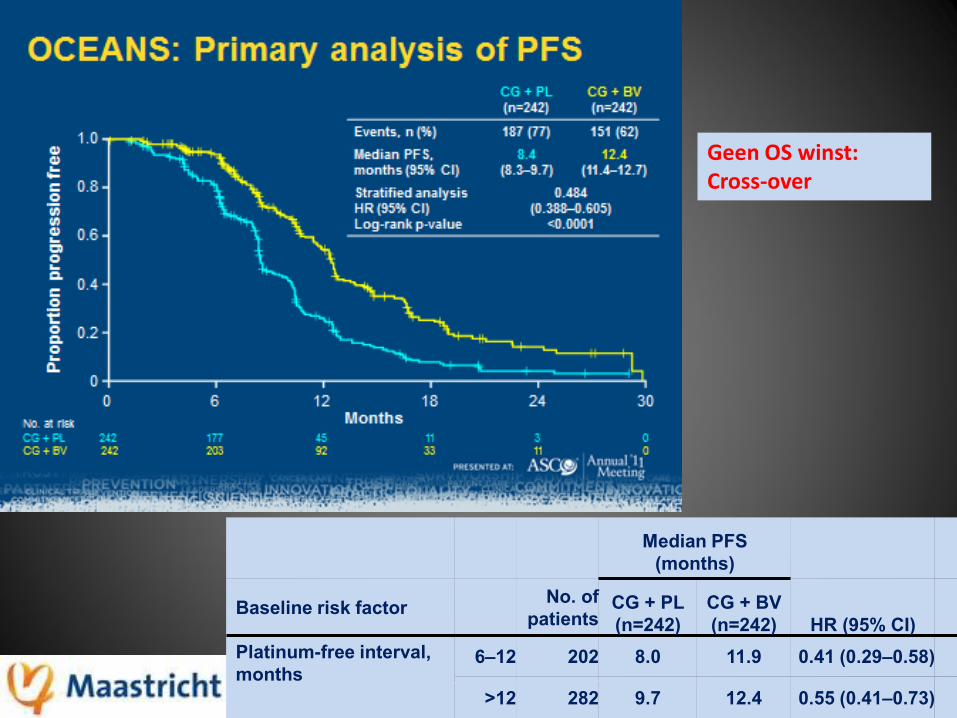
Het ovariumcarcinoom, 10 november 2016 36
Median PFS
(months)
Baseline risk factor No. of
patients CG + PL
(n=242)
CG + BV
(n=242) HR (95% CI)
Platinum-free interval,
months 6–12 202 8.0 11.9 0.41 (0.29–0.58)
>12 282 9.7 12.4 0.55 (0.41–0.73)
Geen OS winst: Cross-over

Angiogeneseremmer: Platinum resistent recidief
Aurelia studie
Weekly paclitaxel, pegylated liposomal doxorubicin or topotecan ± bevacizumab
Het ovariumcarcinoom, 10 november 2016 37
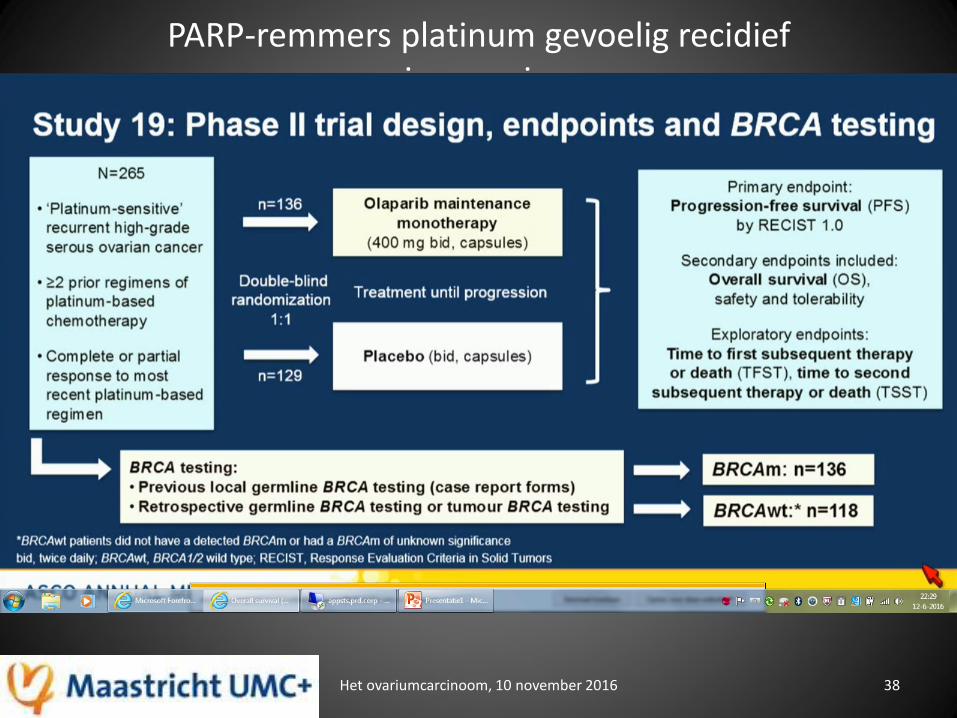
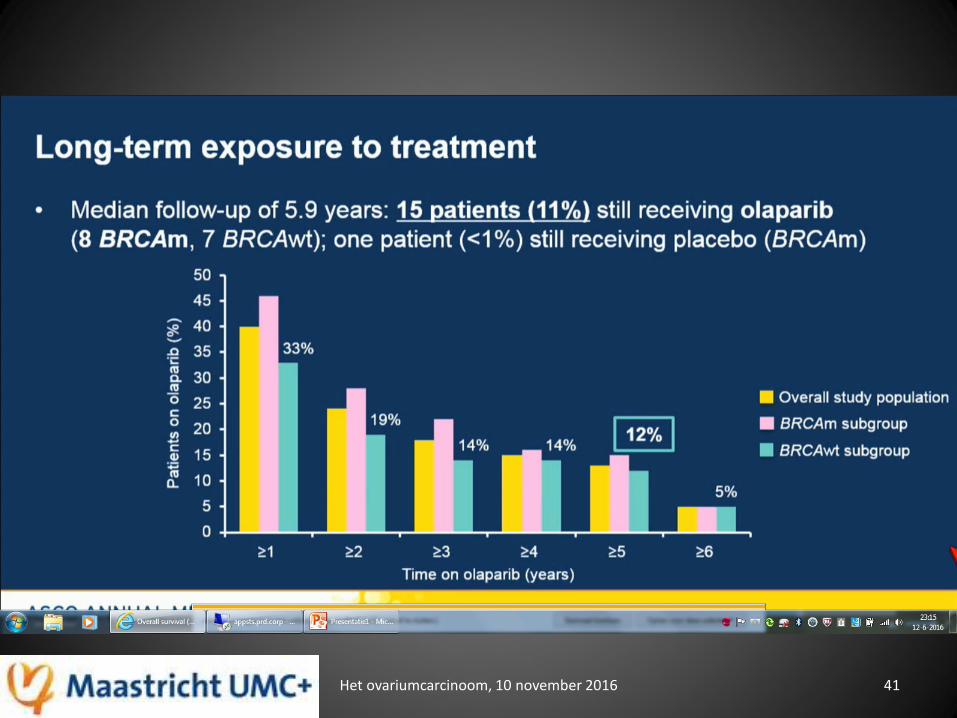
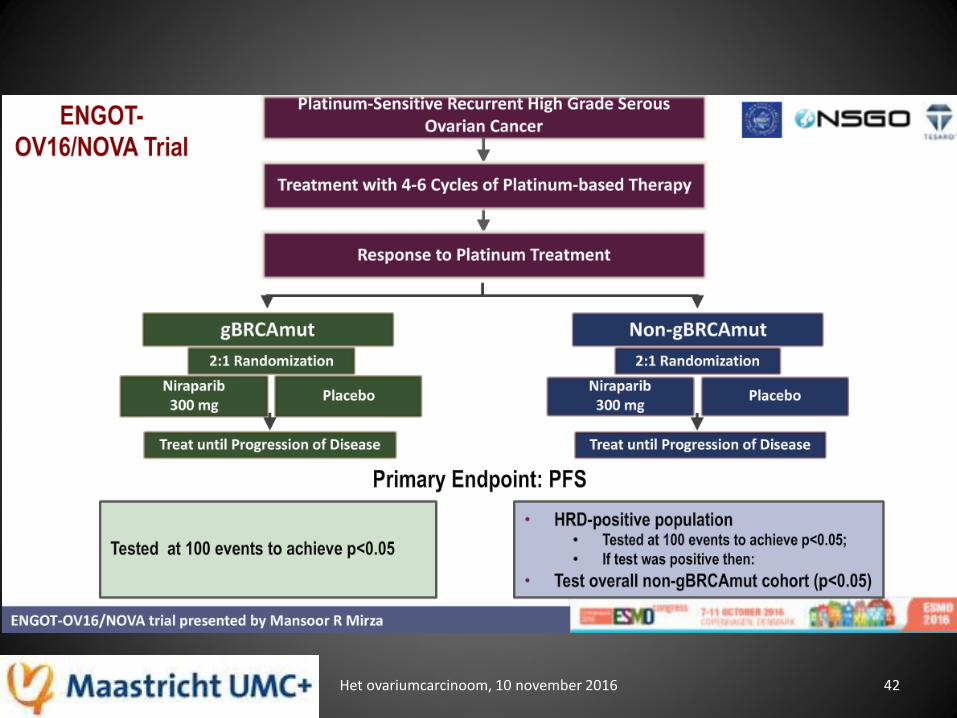
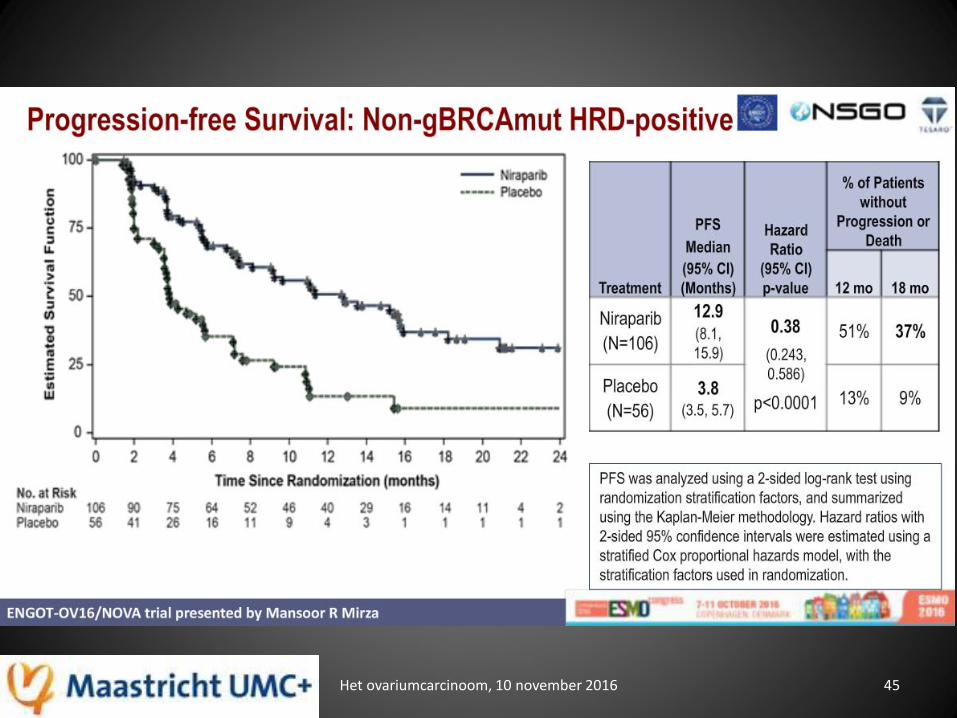
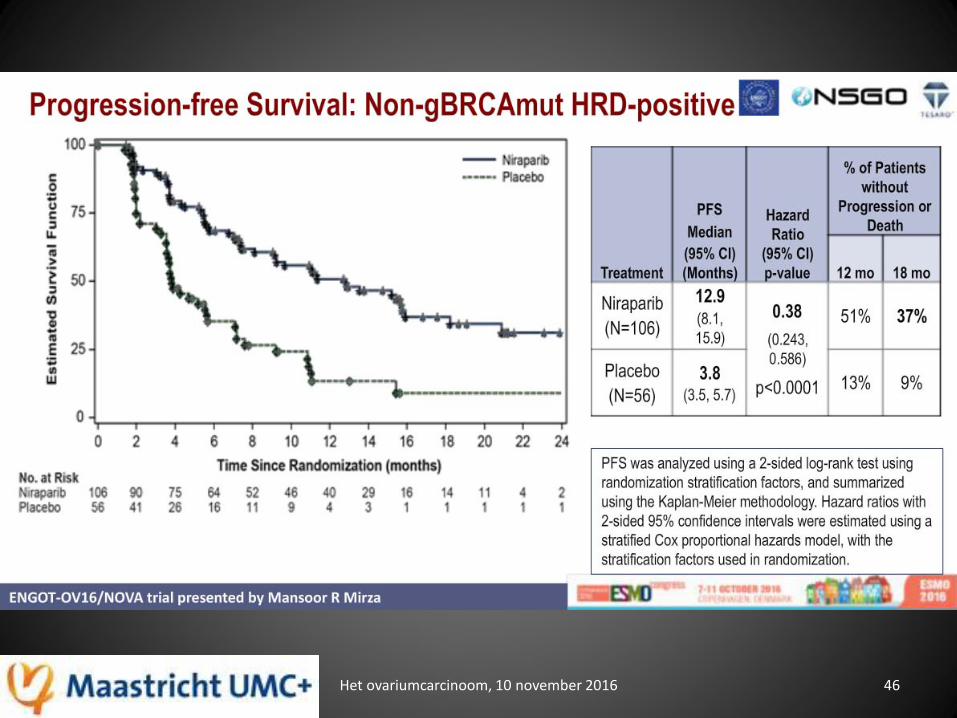
PARP-remmers platinum gevoelig recidief ovariumcarcinoom
Het ovariumcarcinoom, 10 november 2016 38
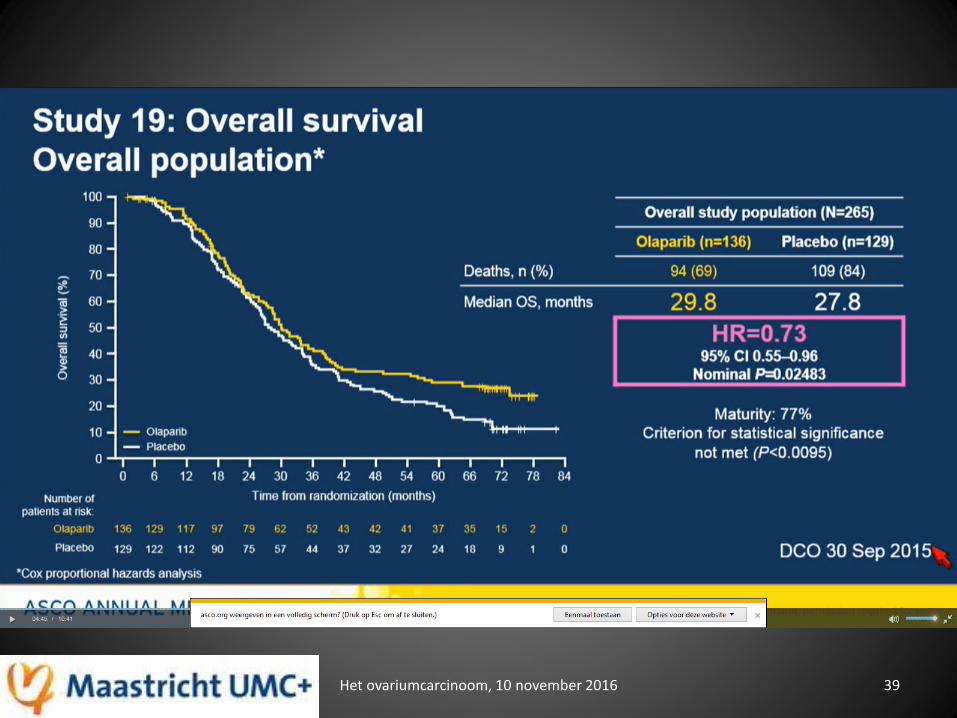
Het ovariumcarcinoom, 10 november 2016 39
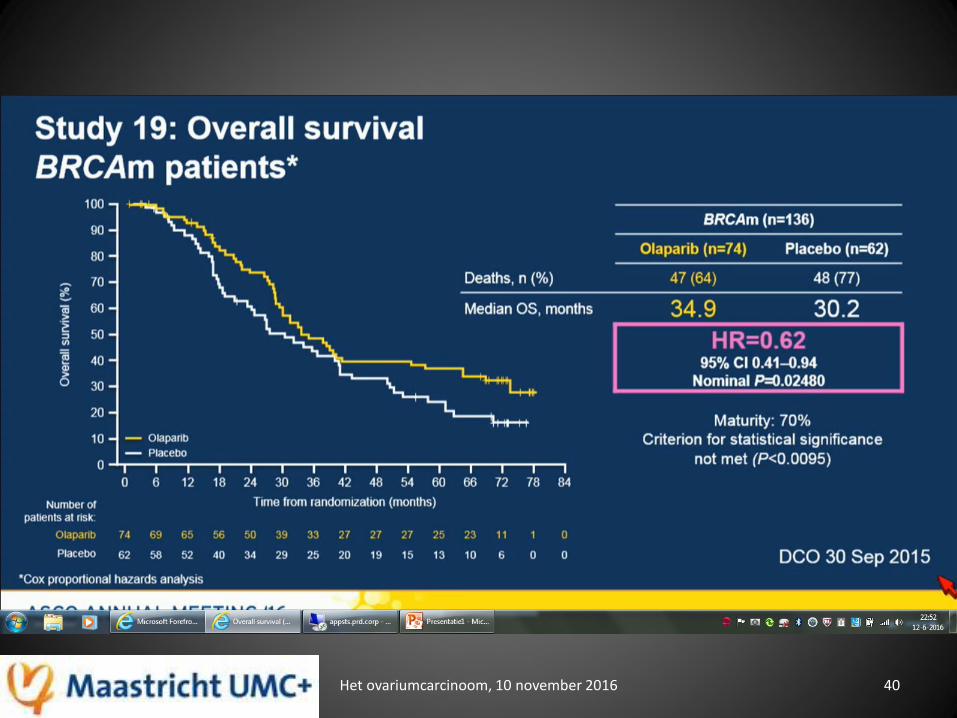
Het ovariumcarcinoom, 10 november 2016 40
Het ovariumcarcinoom, 10 november 2016 41
Het ovariumcarcinoom, 10 november 2016 42
Het ovariumcarcinoom, 10 november 2016 43
Het ovariumcarcinoom, 10 november 2016 44
Het ovariumcarcinoom, 10 november 2016 45
Het ovariumcarcinoom, 10 november 2016 46
Het ovariumcarcinoom, 10 november 2016 47
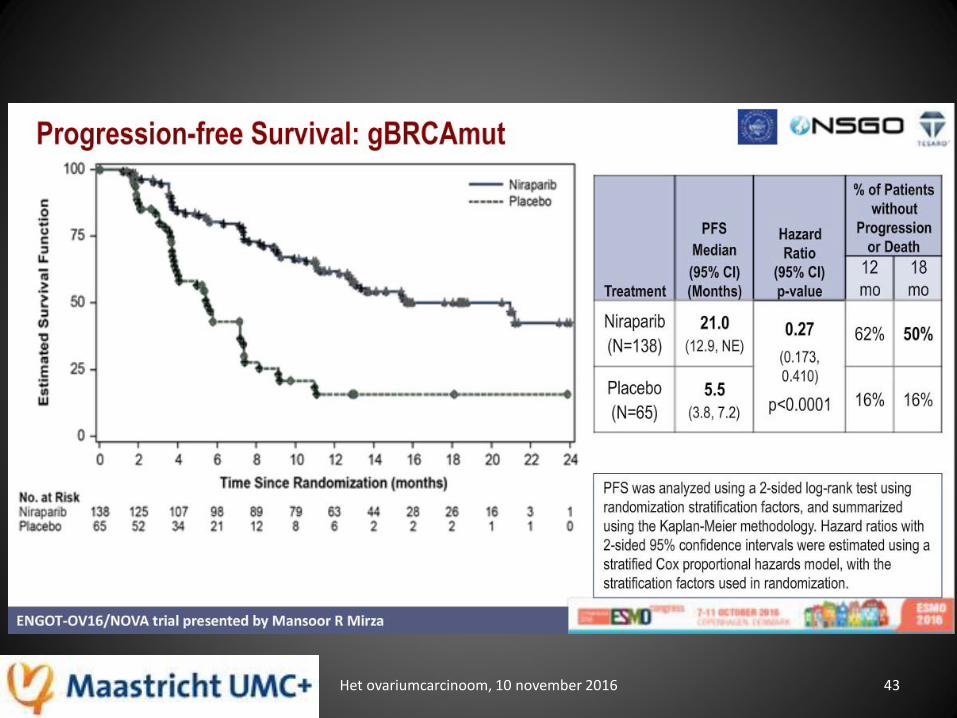
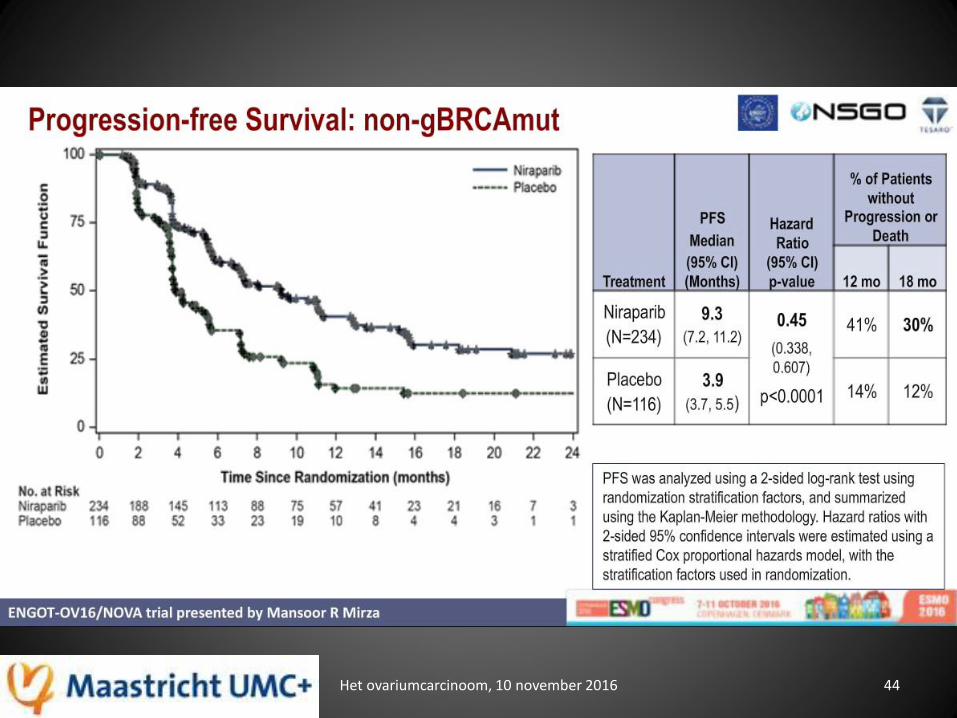
Conclusions Niraparib studie
• Niraparib geeft een verbeterde PFS in platinumgevoelig recidief ovariumcarcinoom ongeacht de BRCA of HRD mutatiestatus (HR 0.27 – 0.45)
• Iedere patiënt met platinum gevoelig recidief van hooggradig sereus ovarium die reageert op platinum chemotherapie is een potentiele kandidaat voor niraparib
Het ovariumcarcinoom, 10 november 2016 48
Algemene conclusies
• Primaire complete debulking, indien mogelijk, geeft de beste overlevingsresultaten!
• Hoe selecteer je de patiënten die in aanmerking komen voor primaire complete debulking?
• NACT en IDS is geen standaard behandeling!
• Onderhoudsbehandeling met targeted therapie (angiogeneseremmers of PARP remmers) geeft overlevingswinst, wie komt ervoor in aanmerking (selectie)?
• Immunotherapie met checkpoint inhibitors is in de onderzoekfase.
• De juiste selectie is de kwestie!
Het ovariumcarcinoom, 10 november 2016 49

Bronvermeldingen: • IKNL, NKR, Maite Timmermans
• Astra Zeneca
• Roche
• ASCO 2016, ESMO 2016, IGCS 2016
Het ovariumcarcinoom, 10 november 2016 50
Het ovariumcarcinoom, 10 november 2016 51