Intoxicaties - ForumIG · 2018. 3. 26. · Epidemiologie • In de VS: 2.4 miljoen cases van...
87
Intoxicaties Jasper Callemeyn - Benjamin Heymans Dr. P. Vanbrabant
Transcript of Intoxicaties - ForumIG · 2018. 3. 26. · Epidemiologie • In de VS: 2.4 miljoen cases van...
-
Intoxicaties
Jasper Callemeyn - Benjamin Heymans
Dr. P. Vanbrabant
-
Epidemiologie
• In de VS: 2.4 miljoen cases van niet-intentionele intoxicaties in 2008
• 51.9% bij kinderen; slechts 2% van de mortaliteit
• 0.07% kans op fatale intoxicatie
• 90.5% intoxicatie met 1 substantie-> analgetica of sedativa (31.9%)
Stetka, et al. 2011
-
Epidemiologie: jaarverslag VS - 2016
Gummin et al., Clin Toxicol 2017
-
Epidemiologie: VS België
Oproepen Antigifcentrum
Jaarrapport Antigifcentrum 2016
-
Epidemiologie: VS België
Oproepen Antigifcentrum
Jaarrapport Antigifcentrum 2016
-
Help! Mijn patiënt
heeft zich
geïntoxiceerd
-
STAP 1 - Anamnese en klinisch onderzoek
• Geneesmiddelenanamnese: > 50% niet correct (Wright N., et al.1980)
• Klinisch onderzoek = sleutel!
>
1. Vitale parameters
2. Mentale status
3. Pupilgrootte
4. Peristaltiek
5. Reflexen/spier
6. Huid (kleur, textuur, …)
-> indeling in toxidromen
Monte A, et al. (2015)
-
Casus 1: 37-jarige, bewusteloze vrouw
37-jarige patiënt wordt bewusteloos
binnengebracht op de dienst
spoedgevallen. Voorgeschiedenis
van infertiliteit waarvoor
vruchtbaarheidsbehandelingen.
Parameters: HF 100/min, BD:
130/80 mmHg, ademhaling: 10/min,
T: 36.8°C.
Neurologisch: diepe coma,
bilaterale miose, doch licht reactief,
urineretentie en afwezigheid van
reflexen, GCS 3/15. Huid: normaal
Alcohol en paracetamol: negatief
Kakkar A, Kumar S. 2013
Welk toxidroom?
A) Opioïd
B) Anti-Cholinerg
C) Sedatief/Hypnotica
D) Cholinerg
E) Serotonine
-
Toxidromen – Sedativa/hypnotica
1. Vitale parameters
Hypotermie/bradypnee
hypotensie/bradycardie
2. Mentale status
Anxiolyse, coma
3. Pupilgrootte
GEEN miosis
4. Peristaltiek
GEEN duidelijk effect
5. Reflexen/ spier
Hypotonie
6. Huid
Geen veranderingen
Basismedicalkey.com
-
Toxidromen – Opioïd
1. Vitale parameters
Bradypnee/hypotensie/ bradycardie
2. Mentale status
Gedaald -> coma
3. Pupilgrootte
Miosis
4. Peristaltiek
Afwezig
5. Reflexen/spier
Hyporeflexie
6. Huid
Bleek/ Cyanose
Mussenhealth.us
• Methadone: QT-verlenging
• Tramadol: serotoninesyndroom, epileptische aanval
• Pethidine: weinig miose, epileptische aanval
-
Toxidromen – Alfa- en beta-receptor agonist
Beatylab.nl
Cocaïne, amfetamine, cafeïne, pseudo-efedrine
-
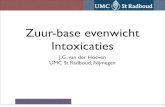
Hiramatsu, et al. Kerrigan, et al (2005).
Fatal caffeine overdose: Two case reports
Sarah Kerrigan* , Tania Lindsey
New Mexico Department of Health, Scientific Laboratory Division, Toxicology Bureau,
P.O. Box 4700, Albuquerque, NM 87196-4700, USA
Available online 2 June 2005
Abstract
Caffeineisamild central nervousstimulant that occursnaturally incoffeebeans, cocoabeansand tealeaves. In largedoses, it
can beprofoundly toxic, resulting in arrhythmia, tachycardia, vomiting, convulsions, comaand death. Theaveragecup of coffee
or tea in the United States is reported to contain between 40 and 150 mg caffeine although specialty coffees may contain much
higher doses. Over-the-counter supplements that areused tocombat fatiguetypically contain100–200 mgcaffeineper tablet and
doses of 32–200 mg are included in a variety of prescription drug mixtures.
Fatal caffeine overdoses in adults are relatively rare and require the ingestion of a large quantity of the drug, typically in
excess of 5 g. Over a period of approximately 12 months our office reported two cases of fatal caffeine intoxication. In thefirst
case, the femoral blood of a 39-year-old female with a history of intravenous drug use contained 192 mg/L caffeine. In the
second case, femoral blood from a29-year-old malewith ahistory of obesity and diabetes contained 567 mg/L caffeine. In both
cases, the cause of death was ruled as caffeine intoxication and the manner of death was accidental.
# 2005 Elsevier Ireland Ltd. All rights reserved.
Keywords: Caffeine; Intoxication; GCMS
1. Introduction
Caffeine (1,3,7-trimethylxanthine, guaranine) is a plant-
derived alkaloid and psychostimulant that is present in tea
leaves, coffee, cocoa beans and kola nuts. Caffeine, theo-
phylline, theobromineand paraxanthine areroutinely detect-
able in toxicological samples due to dietary exposure to
caffeine. The average cup of coffee or tea in the United
States isreported to contain between 40 and 150 mg caffeine
[1] although specialty coffees may contain much higher
doses [2]. Caffeine undergoes rapid absorption following
oral administration. A single130 mg oral dosein 36 subjects
produced peak plasma concentrations of 2.5–6.8 mg/L
(mean 4.0 mg/L) within 20–40 min [3]. Approximately,
90% of the caffeine in a cup of coffee is absorbed from
thestomach within 20 min with peak plasma concentrations
occurring approximately 40–60 min later.
Plasma/blood ratios of 0.93 have been reported and the
volumeof distribution is0.5 L/kg [4]. Thedrug iswidely dis-
tributed and undergoesplacental transfer, which isthereason
for limiting dietary intake of caffeine during pregnancy.
Caffeineundergoeshepaticmetabolism viaN-demethylation,
acetylation and oxidation. The CYP450 1A2 isoenzyme is
largely responsible for the N-demethylation of caffeine to
paraxanthine, the major metabolite. However, more than 25
metabolites have been identified and many are pharmacolo-
gically active. During elimination, approximately 85% of a
dose isexcreted in theurinewithin 48 h, with approximately
1% as unchanged drug [4]. Although the plasma half-life is
reportedtobe2–10 h(mean4 h) inadults[4], it may beaslong
as 4 days in neonates due to impaired metabolism [5].
Individuals may be exposed to caffeine via beverages,
food, over-the-counter drugs, prescription drugs, herbals or
dietary supplements. A dose of 50–200 mg is generally
www.elsevier.com/locate/forsciint
Forensic Science International 153 (2005) 67–69
* Corresponding author. Present address: P.O. Box 7429, Houston,
TX 77248-7429, USA. Tel.: +1 713 868 2440; fax: +1 713 868 2440.
E-mail address: [email protected] (S. Kerrigan).
0379-0738/$ – see front matter # 2005 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.forsciint.2005.04.016
106
-
Toxidromen – Alfa- en beta-receptor agonist
1. Vitale parametersTachycardie/Hypertensie/ Tachypneu
2. Mentale status
CNS excitatie/agitatie
3. Pupilgrootte
Gedilateerde pupillen (reactief)
4. Peristaltiek
Veel darmgeluiden
5. Reflexen/spier
Spierhyperreactiviteit
6. Huid
Diaphorese -> hypertermie
Urinedebiet blijft wel normaal anti-cholinergica
Pinterest.co.uk.
-
Toxidromen – Anti-cholinerg
1. Vitale parameters
Hypertermie/tachycardie
2. Mentale status
Delier, psychose, hallucinaties
3. Pupilgrootte
Mydriase
4. Peristaltiek
Gedaald
5. Reflexen/spier
Myoclonieën
6. Huid
Droge huid, flushing
I0.wp.com
Anti-histaminica, TCA,
anti-psychotica, …
-
Toxidromen – Cholinerg
1. Vitale parameters
Bradycardie (soms) Tachycardie
Hypotensie
2. Mentale status
Lethargie
3. Pupilgrootte
Miosis
4. Peristaltiek
Hyperperistaltiek
5. Reflexen/spier
Spierzwakte/fasciculaties
6. Huid
Zweten
+ toename van alle secreties: salivatie, lacrimatie, urineproductie, …
-
Toxidromen – Overige
Mussenhealth.us
• Serotonine syndroom
• Maligne neuroleptisch syndroom
• Sedativa/Hypnotica withdrawal syndroom
-
Sketchymedicine.com
-
Casus 2: 24 jarige vrouw met verwardheid
24-jarige vrouw wordt in midden
van de straat aangetroffen,
verward en met happerende
spraak.
Parameters: HF 112/min, BD:
135/88mmHg,
ademhaling:12/min, T: 37.8
°C.
Neurologisch: mydriase
Huid: droge, flushed huid.
Reference.medscape.com
Welk toxidroom?
A) Opioïd
B) Anti-Cholinerg
C) Sedatief/Hypnotica
D) Cholinerg
E) Serotonine
-
STAP 2 – Labo en Urine
Urine: voor screening causaal agens
(+) Bevestigen/ uitsluiten van intoxicatie
(-) Vals negatieve/positieve resultaten
Vaak lang positief blijven
Verandering van acute beleid?
-
Erdman A, et al. 2015
Opzet: enkel snelle
urinescreening in specifieke
indicaties:
-Eerste psychose
-Respiratoir falen
-Hypotensie
-Coma
-Epilepsie
-Aritmie of verlengd QT
-Sympathomimetica
-Opioïden
-
Labo
• Algemene regel: tevens kwantificatie van paracetamol en ethanol
• Anion gap = ([Na+] + [K+]) − ([Cl−] + [HCO3 −])
Pas op voor:
1. Dilutie hyponatremie ikv hyperglycemie
2. Hypoalbuminemie Aggecorrigeerd = Aggemeten + 2.5 (4 – albumin)
-
Wikimedia commons
-
Labo
• Algemene regel: tevens kwantificatie van paracetamol en ethanol
• Anion gap = ([Na+] + [K+]) − ([Cl−] + [HCO −])
• Osmolar gap = gemeten osmolaliteit – berekende osmolaliteit.
-> Berekend: 2 Na (mEq/L) + (Urea [mg/dL])/2.8 +
(Glucose [mg/dL])/18 + (Ethanol [mg/dL])/3.7
-
STAP 3 – Supportieve maatregelen
• ABCDEFG- algoritme
- 10 % risico op aspiratie met
chemische pneumonitis als
gevolg.
DUS: Endotracheale intubatie als
1. Geen bescherming luchtweg
2. Respiratoir falen aanwezig
Marik PE, et al. (2001). Emergencypedia.com
-
STAP 4 – ADME en effect
• ADME
Absorptie
Distributie
Metabolisme
Eliminatie
• Effect
-> Antidota
creative-proteomics.com
-
Adsorptie
1. Actieve kool
- Voor volwassene: dosis van 25 à 100 gram
- Liefst binnen 1 uur na intoxicatie te geven
Uitzondering: als vertraagde afgifte/vertraagde maaglediging
Niet binden aan:
1. Zuren 2. Alcoholen 3. Alkali’s 4. Metalen: ijzer/lithium 5. Hydrocarbons
Nevenwerkingen:
I. Braken -> noodzaak van beschermde luchtweg
II. Abdominale opzetting
nootropedia.com
-
Factoren die meespelen in eventuele behandeling
met actieve kool.
Olson KR. 2010.
-
Adsorptie
1. Actieve kool
2. Polyethyleenglycol elektrolytenmengeling
- Doel: hele darm decontamineren door het fysiek uitdrijven van de gastro-
intestinale inhoud (tot anaal vocht helder is)
- Indicaties:
I. Als geen absorptie door actieve kool
II. Preparaten met vertraagde vrijzetting
- Contra-indicaties:
I. Ileus, darmperforatie
II. Hemodynamisch instabiliteit
III. Braken
IV. Onbeschermde luchtweg
-
Distributie en metabolisme
• DistributieToepassing: IV Lipid Emulsion
- Indicaties (experimenteel + case reports):
I Lokale anesthetica
II Bèta-blokkers
III Calcium kanaal blokkers
IV TCA
- Nevenwerkingen: vooral verstoring van verschillende labotests.
• MetabolismeSommige antidota: interferentie met metabolisme
Ozcan MS, et al. 2014
-
Eliminatie
• Achterliggende gedachte: sommige effecten treden pas op als zekere plasmaspiegels bereiken
• Methodes:1. Geforceerde diurese
2. Alkalinisatie van de urine
3. Multipele toedieningen van actieve kool
4. Extracorporele technieken
-
Eliminatie – Geforceerde diurese
• Stijging diurese door combinatie van intraveneus vocht en diuretica.
• Niet meer aanbevolen – reden:I. Risico op longoedeem
II. Grote kans op elektrolyentstoornissen
Mokhlesi B, et al. 2003
-
Eliminatie – Urine alkalinisatie
• Door toediening NaHCO3, zorgen dat urinaire pH > 7.5 (Salicylaten: pH > 8.5) -> ion trapping
• Indicatie:- Salicylaten
- Fenobarbital
- TCA
- Alcoholen
• Nevenwerkingen:I. Hypokaliëmie -> K-suppletie
II. Hypernatremie
III. Vochtoverbelasting
Mirrakhimov AE, et al. 2017
-
Eliminatie – Multipele toedieningen van
actieve kool
• Voor medicatie die enterohepatische recirculatie ondergaat.
• Dosis: 0.5 – 1 g/kg elke 4 uur
• Indicatie: ontwikkeling levensbedreigende complicaties na ingestie vanI. Carbamazepine
II. Dapsone
III. Fenobarbital
IV. Quinine
V. Theofyline
• Geen bewezen daling mortaliteit wel daling plasmaconcentratie
-
Eliminatie - Extracorporele technieken
• Hemodialyse
Voorwaarden:
I. Minimale eiwitbinding (< 80%)
II. Lage Vd (< 1 l/kg)
III. Laag gewicht (< 500 Daltons)
IV. Goed wateroplosbaar
• Hemofiltratie
Eventueel ook verwijdering stoffen:
- met een hoger moleculair gewicht
- vetoplosbare stoffen
Levine M, et al. 2011
-
Effect neutraliseren - antidota
-
Behandeling van de toxidromen
-
Sedativa/hypnotica• Supportieve maatregelen
• Actieve kool indien < 1 uur
• Benzodiazepines:
Flumazenil (niet aangeraden)
• Dosis: 0,2 mg IV, repeat bolus tot
totaal 3 mg
• Duur werking: 1-2 uur repeated
dose of continu
• Cave: verhoogd convulsierisico!
↑ bij TCA-gebruik, chronisch BZP-
gebruik
• Barbituraten:
Alkalinisatie urine minder reabsorptie
Multipele dosages actieve kool (MDAC)
Hemodialyse (fenobarbital > 100 mg/L)
Zhang et al., Drug Metab Dispos 2013
-
Specifieke behandeling opioïden
• Naloxone: toe te dienen vanaf tekens opioïdtoxiciteit (bradypneu, miose)
o Startdosis 0,2 à 0,4 mg IV herhalen tot max. 10 mg
o Duurtijd werking: 30-80 min
o Repeat bolus of continu aan 2/3 bolusdosis/uur
o Neveneffecten: niet-cardiogeen longoedeem, convulsies
-
Toxidromen – Alfa- en beta-receptor agonist
1. Benzodiazepine
-> bij agitatie, hypertensie, tremor en tachycardie
2. Passieve afkoeling
3. Labetalol of nitroprusside
4. IV Hydratatie
Goldstein S, Richards JR. Pubmed Central. 2017
-
Enkele specifieke
intoxicaties
-
Paracetamol
Epidemiologie
• Meest frequent medicamenteuze intoxicatie in V.S.
•± 50% gevallen acuut leverfalen in VS
• Optredend vanaf dosage > 75 mg/kg over 24 uur 5,25 g voor 70 kg
Farmacokinetiek
• Variabele tijd tot piek-plasma levels: 20 min. - 4 uur
• Distributievolume: 0,9 L/kg
• Halfwaarde tijd 2 uur – 12 uur (toenemend bij toxiciteit)
-
Pathogenese
Heard, N Engl J Med 2008 Hinson et al., Handb Exp Pharmacol 2010
-
Kliniek
Stadium Ontstaan Symptomen Labo
Preklinisch 0-24 uur Asymptomatisch
Nausea, braken,
abdominale pijn
= AST, ALT
=/↑ INR
Hepatische
schade
24-72 uur RUQ pijn ↑ AST, ALT
Leverfalen > 72 uur Icterus, hepatische
encefalopathie,
coagulopathie,
multi-orgaanfalen
↑↑ AST, ALT
↑ PT, bilirubine
lactaat, fosfaat
↓ pH, glucose
Hepatorenaal syndroom
Herstel > 120 uur Regressie Normalisatie
-
Initieel beleidAandachtspunten
o Chronologie
o Totaal ingenomen dosis?
o Risicostratificatie
• Alcoholgebruik (man > 21E/week, vrouw > 14E/week)
• Enzyme-inductoren (carbamazepine, fenytoïne)
• Glutathione depletie: malnutritie, HIV, eetstoornissen, mucoviscidose
Labo:
o serum paracetamol ten vroegste 4 uur na inname
o AST, ALT, gamma-GT, INR, glucose
o nierfunctie, ionogram
o bloedgas
Indien sufheid, overweeg overige intoxicaties!
-
Eenmalige overdosis
0-8 uur
< 1 à 2 uur: toedienen actieve kool
Paracetamolspiegel op 4 uur na inname
Behandeling met N-acetylcysteïne (NAC) i.f.v. Rumack-Matthew nomogram
-
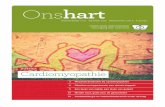
Prescot et al., Lancet 1971 Rumack & Matthew, Pediatrics 1975 Smilkstein et al., NEJM 1988
-
Rumack-Matthew nomogram
Wel
o Enkelvoudige inname
o Gekend tijdstip
Niet
o Tijdstip onduidelijk
o Tijdstip < 4 uur, > 24 uur
o Staggered inname
-
(N-)acetylcysteïne
Heard, N Engl J Med 2008
-
(N-)acetylcysteïne
Dosering
o IV: 150 mg/kg oplaaddosis – 15 à 60 minuten 50 mg/kg over 4 uur
100 mg/kg over 16 uur
o PO: 140 mg/kg oplaaddosis 70 mg/kg elke 4 uur, totaal 17 dosages
Neveneffecten:
o Oraal: nausea, braken
o Intraveneus: anafylaxis (5-15%)
• Voornamelijk in eerste 2 uren
• Frequenter bij lagere paracetamol levels
• Rash: verderzetten
• Flushing: antihistaminica
• Angio-oedeem, respiratoir: tijdelijk stoppen, anti-H2, CS,
adrenaline, verderzetten aan lagere snelheid na 1 uur
• Dilutionele hyponatriëmie
-
Eenmalige overdosis
0-8 uur
< 1 à 2 uur: actieve kool
Paracetamolspiegel op 4 uur na inname
Behandeling met N-acetylcysteïne (NAC) i.f.v. Rumack-Matthews nomogram
8-36 uur
Start NAC bij inname van toxische dosis
Verderzetten indien:
• AST, ALT↑• Paracetamol levels (< 24u: volgens nomogram, > 24u: vanaf detectie)
> 36 uur
Symptomatisch: start NAC
Asymptomatisch: start bij AST, ALT of detecteerbare spiegel
-
Beleid
http://www.antigifcentrum.be/sites/default/files/imce/APAP%20flowchart%20NL%20dec%202013.pdf
-
Overige gevallen
Herhaalde supratherapeutische inname= gedurende > 8 uur, dosis > 4g/24 uur
Vertraagde absorptie= extended release, co-intoxicatie opioïden, anticholinergica
-
Beleid
Monitoring: ICU
o Bloedname enkel indien > 8 uur interval tot behandeling
o Na beëindigen van schema: 100 mg/kg gedurende 16 uur indien
• Creatinine, INR, bicarbonaat, leverfunctiestoornissen niet persisterend
beter
• Detecteerbare paracetamolspiegel
op dag 2-3
-
HLN 06/2017
-
Casus 3
Welke biochemische bevindingen verwacht je bij deze
patiënte?
1. Gedaalde pH, hoge osmolal gap
2. Normale pH, normale osmolal gap
3. Gedaald pH, normale osmolal gap
4. Normale pH, hoge osmolal gap
-
Ethyleenglycol
PropyleenglycolMethanol
Diethyleenglycol
Isopropanol Propyleenglycol
Diethyleenglycol
Methanol
-
Farmacokinetiek
Absorptie: peroraal > inhalatie > transcutaan (M, EG, IP)
Piekconcentratie: 30-90 minuten beperkte window
Wateroplosbaar + laagmoleculair + lage eiwitbinding dialyseerbaar
Kraut et al., Clin J Am Soc Nephrol, 2008
-
Pathogenese
Kraut et al., N Eng J Med 2018
-
Osmolar gap
Kraut et al., N Eng J Med 2018Kraut et al., Clin J Am Soc Nephrol, 2008
-
Alcohol Symptomen Incubatie Incubatie
+ ethanol
Laboratorium
Methanol Visusdaling
Fotofobie
Abdominale pijn
Pancreatitis
Stupor, coma
Putaminale
necrose
6-24 uur 72-96 uur High-anion gap metabole acidose
Gestegen osmolaire gap
Ethyleenglycol Stupor, cerebraal
oedeem
↓
Congestief
hartfalen
Myocarditis
↓
Acute
nierinsufficiëntie
12-24 uur 48-72 uur High-anion gap metabole acidose
Gestegen osmolaire gap
Urinaire calciumoxalaat
kristallen
Hypocalciëmie
Kliniek: verminderd bewustzijn orgaan dysfunctie
-
Kliniek: verminderd bewustzijn orgaan dysfunctie
Alcohol Symptomen Incubatie Incubatie
+ ethanol
Laboratorium
Diethyleenglycol Acute
tubulusnecrose
Abdominale pijn
Hepatitis
Pancreatitis
24-48 uur 48-72 uur High-anion gap metabole acidose
Lage of zelfs normale osmolaire
gap (hoogste moleculair gewicht)
Propyleenglycol Acute
tubulusnecrose
NG NG Lactaat-acidose (incl. D-lactaat)
Gestegen osmolaire gap
Isopropanol Abdominale pijn
Nausea, braken
Diarree
Hypotensie
2-5 uur NG Meestal geen high anion gap
acidose
Zeldzaam lactaatacidose
Gestegen osmolaire gap
-
Co-ingestie ethanol
-
Behandeling toxische alcoholen
Absorptie
Actieve kool niet mogelijk
Metabolisme
Ethanol, fomepizole
Thiamine, pyridoxine
Foliumzuur
Eliminatie
Alkalinisatie urine
Hemodialyse
Brent et al., N Engl J Med 2009
-
Kraut et al., N Eng J Med 2018
-
Ethanol Fomepizole
Oplaaddosis 600 mg/kg 15 mg/kg
Onderhoudsdosis 100-150 mg/kg/uur
Streef naar [EtOH]=100 mg/dl
10 mg/kg b.i.d. (0-48 uur)
15 mg/kg (> 48 uur)
Dosisaanpassing dialyse 250-360 mg/kg/uur Dosisinterval 6 uur
Neveneffecten CNS depressie
Lactaatacidose
Hoofdpijn
Nausea, braken
Duizeligheid
Voordelen Beschikbaarheid
Lage kostprijs
Hoge affiniteit
Geen ICU/seriële spiegels
Serum osmolaliteit
bruikbaar
Nadelen Hoge serumconcentraties
nodig
Depressie CNS
Opname IZ nodig
Seriële spiegels nodig
Kostprijs (€5000/48 uur)
Stopzetten indien methanol/ethyleenglycol < 20 mg/dl
-
The Guardian, 24 februari 2017
-
De Morgen, 7 maart 2018
-
Organofosfaten• Bron: pesticiden, zenuwgas
• Case fatality rate 10-20%
o Ontwikkelingslanden > industriële landen
o India 2010: 25288 doden, VS 2012: drie doden
• Farmacokinetiek
o Absorptie: ingestie, inhalatie, transdermaal
o Tijd tot piekconcentratie afhankelijk van inname
o Lipofiel
• Laboratorium
o Acetylcholinesterase-activiteit RBC < 80% LLN
o Urinaire metabolieten: para-nitrofenol, dialkylfosfaat
-
Organofosfaten - pathofysiologie
King et al., Emerg Med Clin N Am 2015 Cannard et al., J Neurol Sci 2006
-
Organofosfaten - kliniek
Muscarine Nicotine CZS
Defecatie Mydriase Centrale AH-depressie
Urine-incontinentie Tachycardie Hoofdpijn
Miosis Spierzwakte Duizeligheid
Bradycardie Hypertensie Convulsies
Bronchoconstrictie Fasciculatie Coma
Bronchorroe
Emesis
Lacrimatie
Salivatie
Intermediate syndrome: respiratoir falen, enkele dagen na cholinerge crisis
OP-induced delayed peripheral neuropathy: paresthesieën, parese, ataxie
-
Behandeling• Exposure: verwijderen kleren, wassen huid
• Atropine
o Competitieve inhibitor Musc-R
o Bolus 1 à 3 mg, verdubbeling elke 5 minuten
o Doel: verdwijnen bronchorree, HR > 80/min
o Onderhoudsdosis 10 à 20% oplaaddosis/uur
• Oximes (obidoxime, pralidoxime)
o Hydrolyse en reactivatie acetylcholinesterase
o Obidoxime: 250 mg IV (20 min) 750 mg/24 uur
• Benzodiazepines
o Indicatie: convulsies
o Diazepam 5 à 10 mg IV, elke 5 minuten tot couperen aanval
-
Tricyclische antidepressiva
Farmacokinetiek
Hoge EW-binding (tot 95%)
Groot distributievolume
Snelle GI absorptie
Lipofiel
Farmacodynamiek
Beperkte window AC
Geen hemodialyse
-
Cardiale toxiciteit
Sinustachycardie
Verbreed QRS
Verlengd QTc
R > 3 mm in aVR
Associatie QRS met convulsies (> 100 ms) en ventriculaire aritmieën (> 160 ms)
-
Behandeling
Hemodynamisch: intraveneus vocht, vasopressie
Cardiaal:
o Natriumbicarbonaat 1à2 mEQ/kg bolus 8,4%
250cc/uur
• Indicatie: verlengd QRS, ventriculaire
ritmestoornissen, hypotensie
• Doel: pH 7,5-7,55, stop bij normalisatie ECQ en
BP
o Lidocaïne, geen klasse 1a of 1c anti-arritmica
• Indicatie: refractair ritme ondanks bicarbonaat
en pH > 7,55
Neurologisch: benzodiazepines bij convulsies
-
Behandeling
-
Casus 4: 42-jarige man met amnesie en
incontinentie42- jarige man, amnesie,
hypotensie. Gevonden thuis in
semi-comateuze en incontinentie
toestand.
Parameters: aanvankelijk
hypotens/ tachycard. Saturatie
91%. GCS 7/15.
Aanwezigheid van
rhabdomyolyse, nierfalen,
neurologische uitval (dysartrie,
dwangblik naar boven, …),
cardiotoxiciteit
Bennetto L, et al. 2008
Welk toxidroom?
A) Alcohol
B) Sedatief/hypnotica
C) CO-intoxicatie
D) Maligne neuroleptisch syndroom
E) Intoxicatie met multipele
geneesmiddelen waaronder
tricyclische anti-depressiva.
-
CO-intoxicatie
-
Pathofysiologie
1. Vorming CO-Hb
2. Toename affiniteit vrije groepen
voor O2 (Haldane effect)
3. Binding overige heem-
bevattende proteïnes:
• Cytochroom c
(mitochondria)
• Trombocyten
• NO-productie
• Aggregatie met PMN
• Myoglobine
Voorbeschikking hart en CZS door
hoge metabole rate.
-
Symptomen
Guzman, Crit Care Clin 2012
• Geen duidelijk correlatie COHb met symptomen en prognose!
• Neuropsychologische sequellen (interval 2-40d): amnesie,
persoonlijkheid, parkinsonisme
• Chronische laaggradige blootstelling hoofdpijn/amnesie?
-
Symptomen
Kersrode verkleuring
Perifere vasodilatatie
Hoge O2-saturatie
Lokale ischemie
Lage sensitiviteit (1%)
Diagnostiek
Percutane saturatiemeting onbetrouwbaar!
Arterieel bloedgas met bepaling COHb (> 3% niet-roker, > 10% roker)
Cardiale monitoring: ECG, laagdrempelig TTE, evt. angiografie
Labo: steeds CK-bepaling, (NT-proBNP)
-
Behandeling
• Normobare 100% zuurstoftherapie
o t1/2 5 uur 2,5 uur
o Duur: 24 uur (mineure symptomen), 72 uur (majeure symptomen)
• Hyperbare zuurstoftherapie
o t1/2 5 uur 30 minuten
o Anti-inflammatoire werking, ↓mitochondriale dysfunctie en ROS
o Indicatie:
• Ernstige cardiale/neurologische toxiciteit
• CO-concentratie > 25%
• Zwangere vrouwen (hoge affiniteit HbF)
-
Take home messages
• Aanpak
o Stap 1: herkenning toxidromen
o Stap 2: laboratoriumscreening
o Stap 3: ABCDEFG
o Stap 4: Overweeg antidota
• Toxicoscreening mag start supportieve therapie niet uitstellen
• Antigifcentrum: 070 245 245; http://www.antigifcentrum.be/
-
Referenties• Belgisch antigifcentrum
• Monte AA, Heard KJ, Hoppe JA, Vasiliou V, Gonzalez FJ. The accuracy of self-reported drug ingestion histories in emergency department patients. J Clin Pharmacol. 2015;55:33–38.
• Kellermann AL, Fihn SD, LoGerfo JP, et al. Impact of drug screen- ing in suspected overdose. Ann Emerg Med. 1987;16(11):1206-1216.
• Erdmann A, Werner D, et al. Focused use of drug screening in overdose patients increases impact on management. Swiss Med Wkly. 2015 Dec 28;145:w14242.
• Purssell RA, Pudek M, Brubacher J, Abu-Laban RB. Derivation and validation of a formula to calculate the contribution of ethanol to the osmolal gap. Ann Emerg Med. 2001;38:653-659.
• Marik PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med. 2001;344(9):665-671.
• Olson K. R. (2010). Activated charcoal for acute poisoning: one toxicologist’s journey. J. Med. Toxicol. 6 190–198.
• Ozcan M.S., Weinberg G. Intravenous lipid emulsion for the treatment of drug toxicity. J. Intensive Care Med. 2014;29(March–April (2)):59–70.
• Mokhlesi B, Leiken JB, Murray P, et al. Adult toxicology in critical care: part I: general approach to the intoxicated patient. Chest. 2003;123(2):577-592.
• .Mirrakhimov AE, Ayach T, Barbaryan A, Talari G, Chadha R, Gray A. The Role of Sodium Bicarbonate in the Management of Some Toxic Ingestions. Int J Nephrol. 2017;2017:7831358.
• Levine M, Brooks DE, Truitt CA, et al. Toxicology in the ICU: Part 1: general overview and approach to treatment. Chest. 2011;140:795–806.
• Gummin DD, Mowry JB, Spyker DA, Brooks DE, Fraser MO, Banner W. 2016 Annual Report of the American Association of Poison ControlCenters’ National Poison Data System (NPDS): 34th annual report. Clin Toxicol 2017;55(10):1072-1252.
• .Heard KJ. Acetylcysteine for acetaminophen poisoning. N Engl J Med 2008; 359:285-292.
• Prescott LF, Roscoe P, Wright N, Brown S. Plasma-paracetamol half-life and hepatic necrosis in patients with paracetamol overdose, Lancet 1971 Mar 13;1(7698):519-22.
• Rumack BH. Acetaminophen hepatotoxicity: the first 35 years. J Toxicol Clin Toxicol 2002;40(1):3–20.
-
Referenties (2)• Hodgman A, Garrard A. A review of acetaminophen poisoning. Crit Care Clin 2012(28): 499–516.
• Daly FF, O’Malley GF, Heard K, et al. Prospective evaluation of repeated supra- therapeutic acetaminophen (paracetamol) ingestion. Ann Emerg Med 2004; 44(4):393–8.
• Kraut JA, Mullins ME. Toxic alcohols. N Engl J Med 2018;378:270-80.
• Kraut JA, Kurtz I. Toxic alcohols: clinical features, diagnosis and management. Clin J Am Soc Nephrol 2008;3:208-225.
• Brent J. Fomepizole for Ethylene Glycol and Methanol Poisoning. N Engl J Med 2009;360: 2216-2223.
• Brooks DE, Levine M, O’Connor AD, French RN, Curry SC. Toxicology in the ICU: part 2: Specific Toxins. Chest 2011;140(4):1072-1085.
• King AM, Aaron CK. Organophosphate and carbamate poisoning Emerg Med Clin N Am 2015;33:133–151.
• Roberts DM, Aaron CK. Managing acute organophosphorus pesticide poisoning. BMJ 2007;334:629-34.
• Guzman JA. Carbon Monoxide Poisoning. Crit Care Clin 2012;28:537–548.