Informant Assessment of Geriatric Delirium Scale
16
Informant Assessment of Geriatric Delirium Scale I-AGED Recognition of delirium in geriatric patients by means of a caregiver based scale 8th Annual Meeting European Delirium Association 2013 Hanneke F.M. Rhodius- Meester Slotervaart Hospital, Amsterdam, the Netherlands EGM 4(2013):73-7
Transcript of Informant Assessment of Geriatric Delirium Scale
Informant Assessment of Geriatric Delirium Scale
I-AGED
Recognition of delirium in geriatric patients by
means of a caregiver based scale
8th Annual Meeting European Delirium Association 2013 Hanneke F.M. Rhodius- Meester
Slotervaart Hospital, Amsterdam, the Netherlands EGM 4(2013):73-7
Simple!
Even in dementia!
Reliable!
One observation!
Fast!
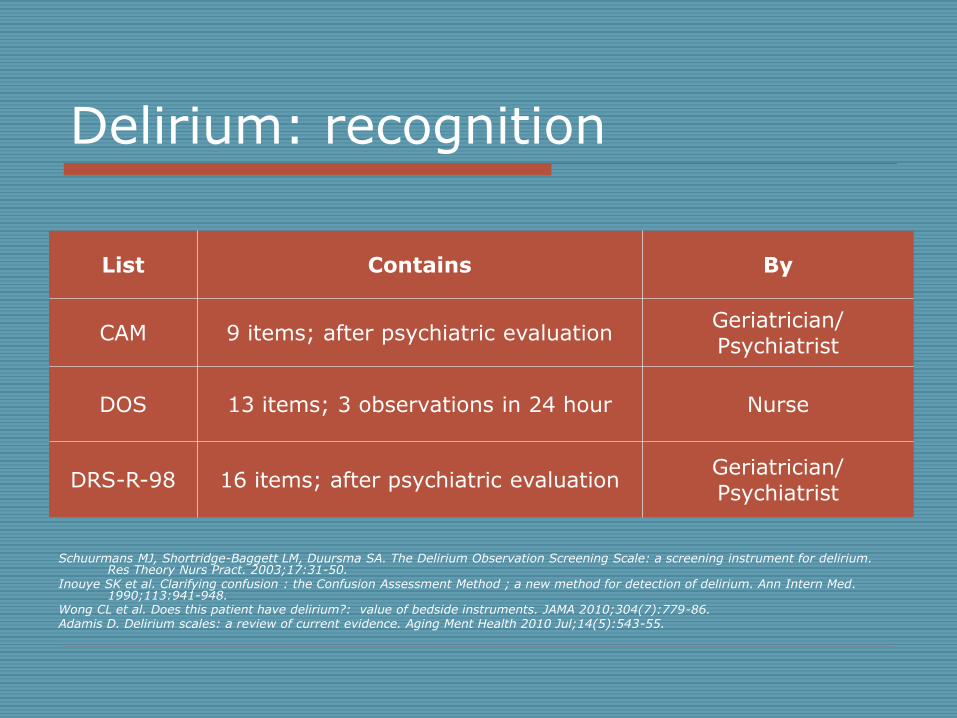
Delirium: recognition
Schuurmans MJ, Shortridge-Baggett LM, Duursma SA. The Delirium Observation Screening Scale: a screening instrument for delirium.
Res Theory Nurs Pract. 2003;17:31-50. Inouye SK et al. Clarifying confusion : the Confusion Assessment Method ; a new method for detection of delirium. Ann Intern Med.
1990;113:941-948. Wong CL et al. Does this patient have delirium?: value of bedside instruments. JAMA 2010;304(7):779-86. Adamis D. Delirium scales: a review of current evidence. Aging Ment Health 2010 Jul;14(5):543-55.
List Contains By
CAM 9 items; after psychiatric evaluation Geriatrician/
Psychiatrist
DOS 13 items; 3 observations in 24 hour Nurse
DRS-R-98 16 items; after psychiatric evaluation Geriatrician/
Psychiatrist
Aim
To develop a questionnaire for caregivers to recognize delirium
in geriatric patients.
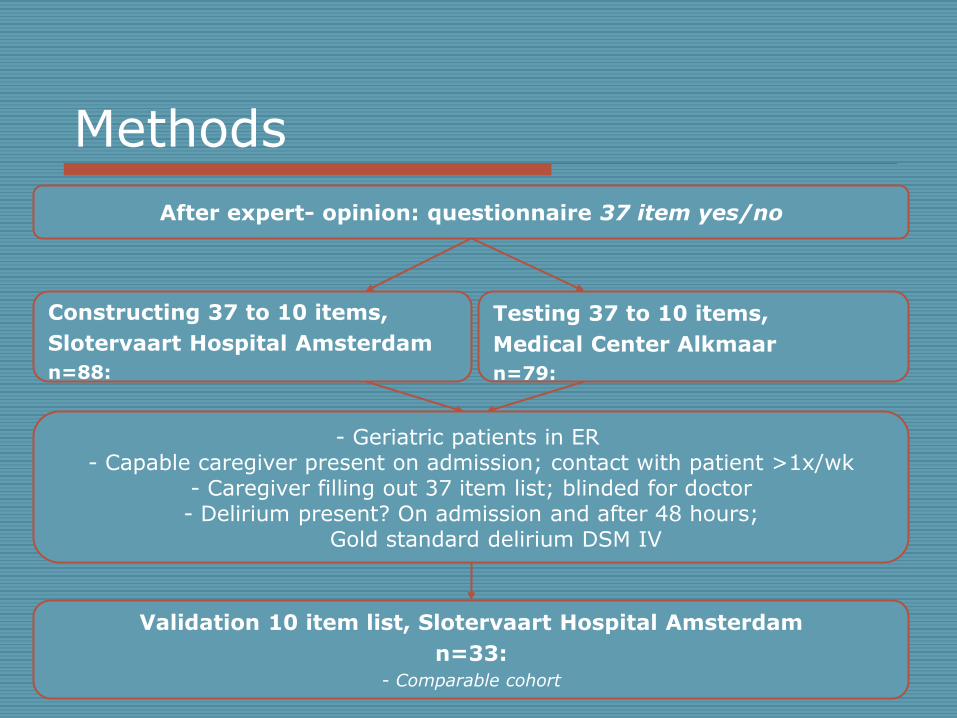
Methods
After expert- opinion: questionnaire 37 item yes/no
Constructing 37 to 10 items,
Slotervaart Hospital Amsterdam
n=88:
Testing 37 to 10 items,
Medical Center Alkmaar
n=79:
Validation 10 item list, Slotervaart Hospital Amsterdam
n=33: - Comparable cohort
- Geriatric patients in ER - Capable caregiver present on admission; contact with patient >1x/wk
- Caregiver filling out 37 item list; blinded for doctor - Delirium present? On admission and after 48 hours;
Gold standard delirium DSM IV
Data analysis
SPSS version 16.0 for Windows
From 37 to 10 items: - Chi squared test - Cronbach’s alpha - Factor analysis
Sensitivity and specificity final 10 item questionnaire
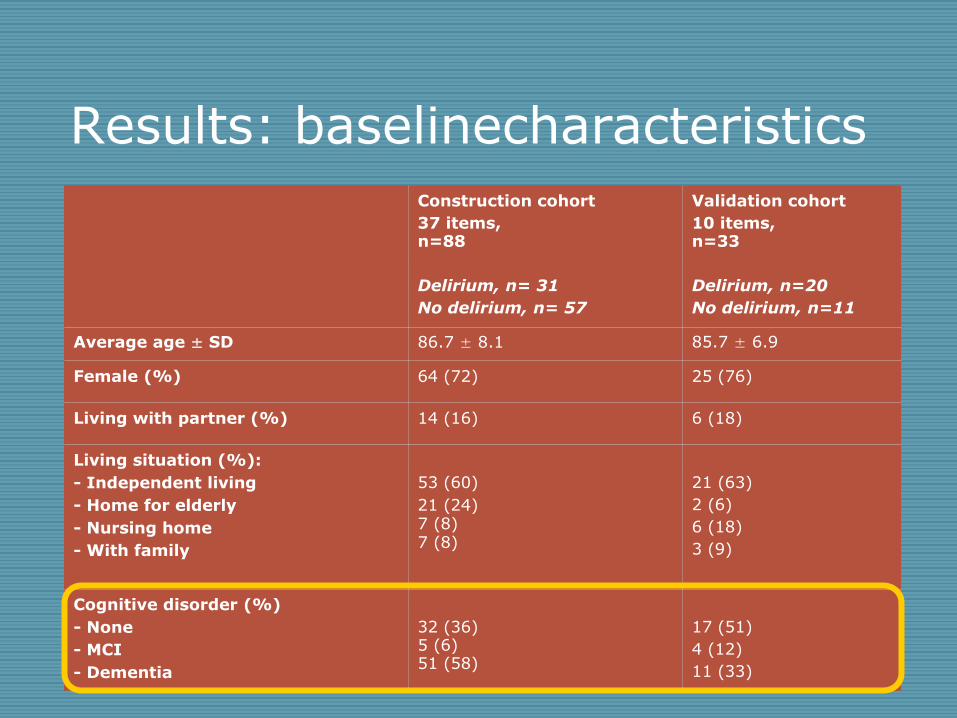
Results: baselinecharacteristics
Construction cohort
37 items, n=88
Delirium, n= 31
No delirium, n= 57
Validation cohort
10 items, n=33
Delirium, n=20
No delirium, n=11
Average age ± SD 86.7 ± 8.1 85.7 ± 6.9
Female (%) 64 (72) 25 (76)
Living with partner (%) 14 (16) 6 (18)
Living situation (%):
- Independent living
- Home for elderly
- Nursing home
- With family
53 (60)
21 (24) 7 (8) 7 (8)
21 (63)
2 (6)
6 (18)
3 (9)
Cognitive disorder (%)
- None
- MCI
- Dementia
32 (36) 5 (6) 51 (58)
17 (51)
4 (12)
11 (33)
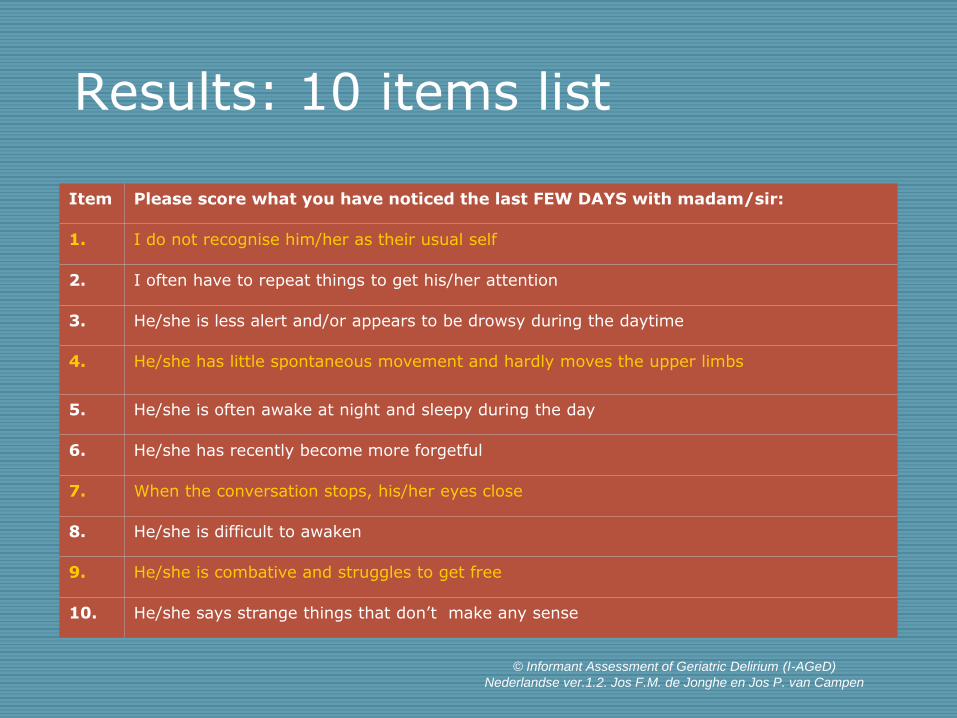
Results: 10 items list
Item Please score what you have noticed the last FEW DAYS with madam/sir:
1. I do not recognise him/her as their usual self
2. I often have to repeat things to get his/her attention
3. He/she is less alert and/or appears to be drowsy during the daytime
4. He/she has little spontaneous movement and hardly moves the upper limbs
5. He/she is often awake at night and sleepy during the day
6. He/she has recently become more forgetful
7. When the conversation stops, his/her eyes close
8. He/she is difficult to awaken
9. He/she is combative and struggles to get free
10. He/she says strange things that don’t make any sense
© Informant Assessment of Geriatric Delirium (I-AGeD)
Nederlandse ver.1.2. Jos F.M. de Jonghe en Jos P. van Campen
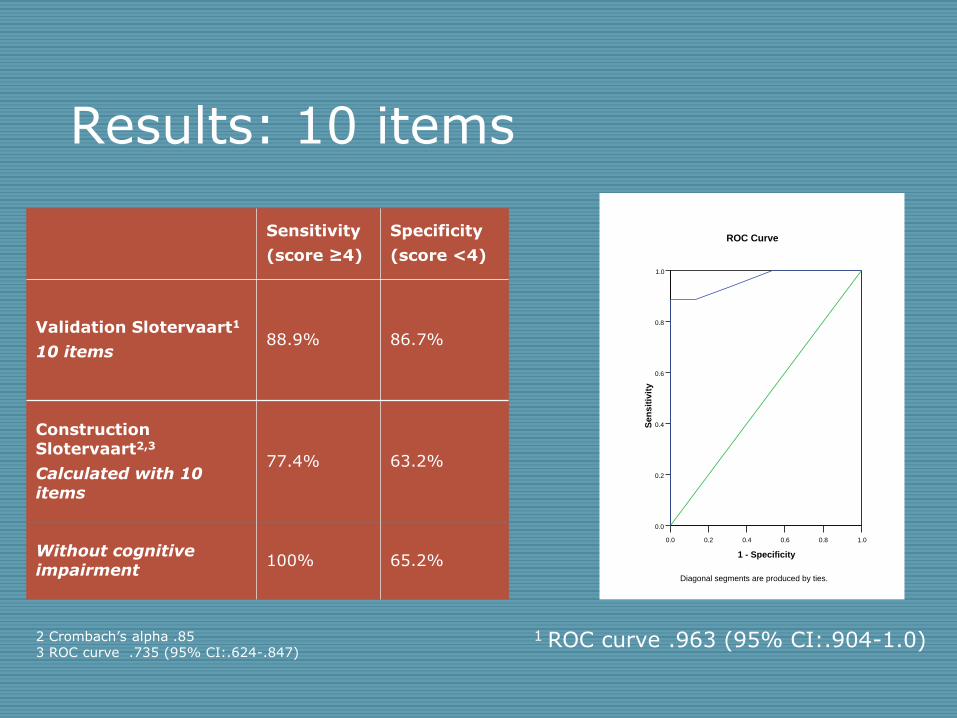
Results: 10 items
Sensitivity
(score ≥4)
Specificity
(score <4)
Validation Slotervaart1
10 items 88.9% 86.7%
Construction Slotervaart2,3
Calculated with 10 items
77.4%
63.2%
Without cognitive impairment
100% 65.2%
1 ROC curve .963 (95% CI:.904-1.0)
0.0 0.2 0.4 0.6 0.8 1.0
1 - Specificity
0.0
0.2
0.4
0.6
0.8
1.0
Sen
sit
ivit
y
Diagonal segments are produced by ties.
ROC Curve
2 Crombach’s alpha .85 3 ROC curve .735 (95% CI:.624-.847)
Simple!
Even in dementia!
Reliable!
One observation!
Fast!
I-AGeD
Future?
Further validation in relevant settings
Translation and testing abroad
Goal: improving recognition of delirium!
Interested? [email protected]

Acknowledgments:
Jos van Campen and staff Geriatric Medicine,
Slotervaart Hospital Amsterdam
Jos de Jonghe, Neuropsychology Medical Center Alkmaar
Barbara van Munster, Internal Medicine,
Academic Medical Centre, Amsterdam and Gelre Hospital, Apeldoorn
David Meagher, Psychiatry
University of Limerick, Ireland
Extra slides….
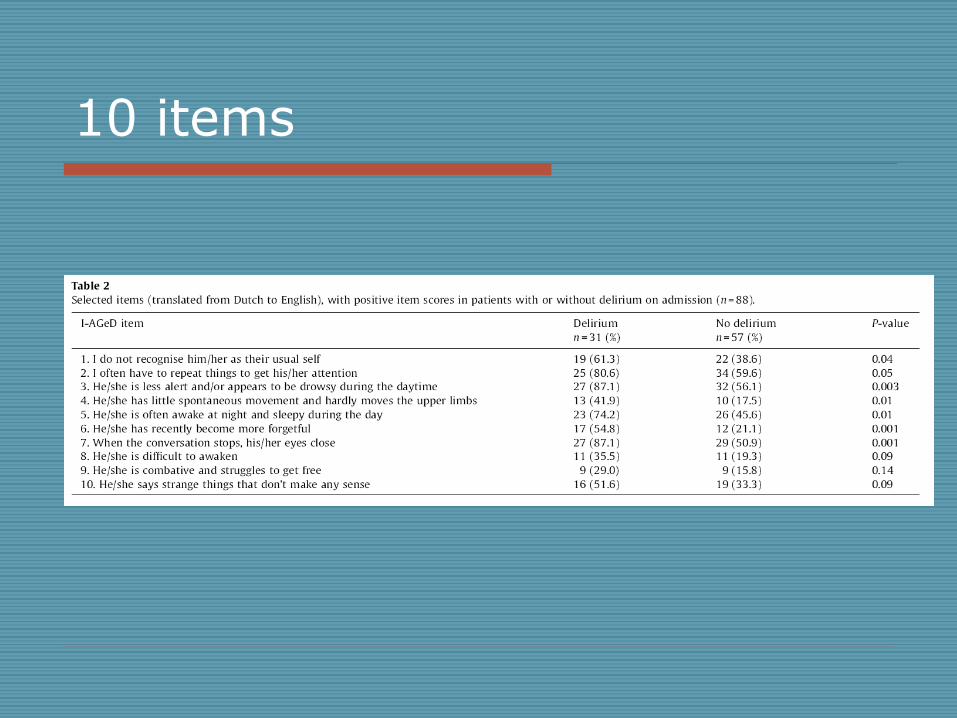
10 items
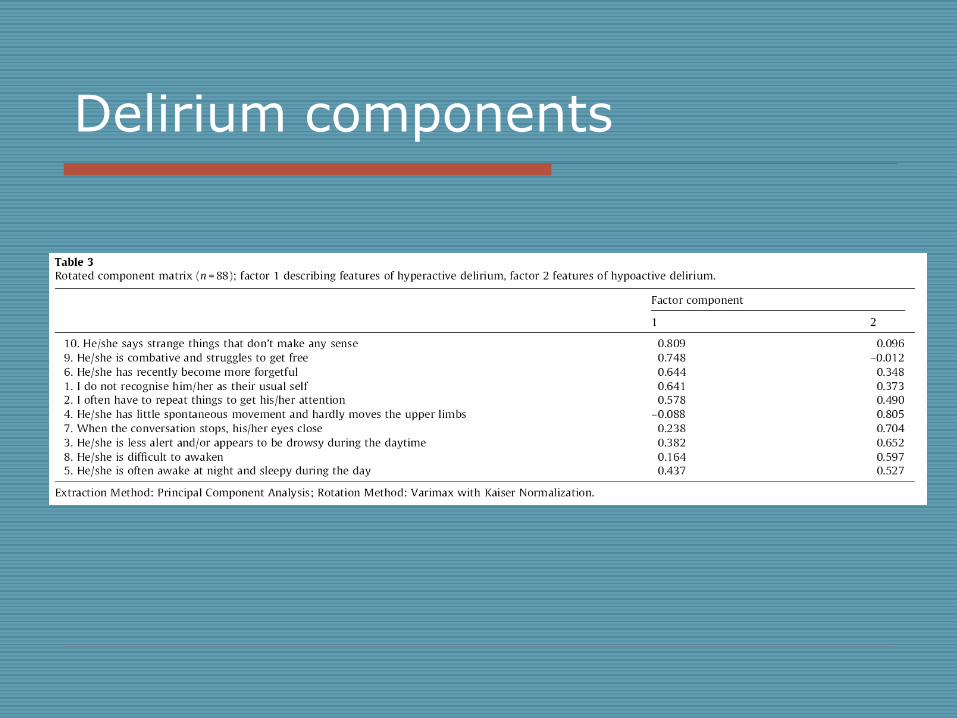
Delirium components
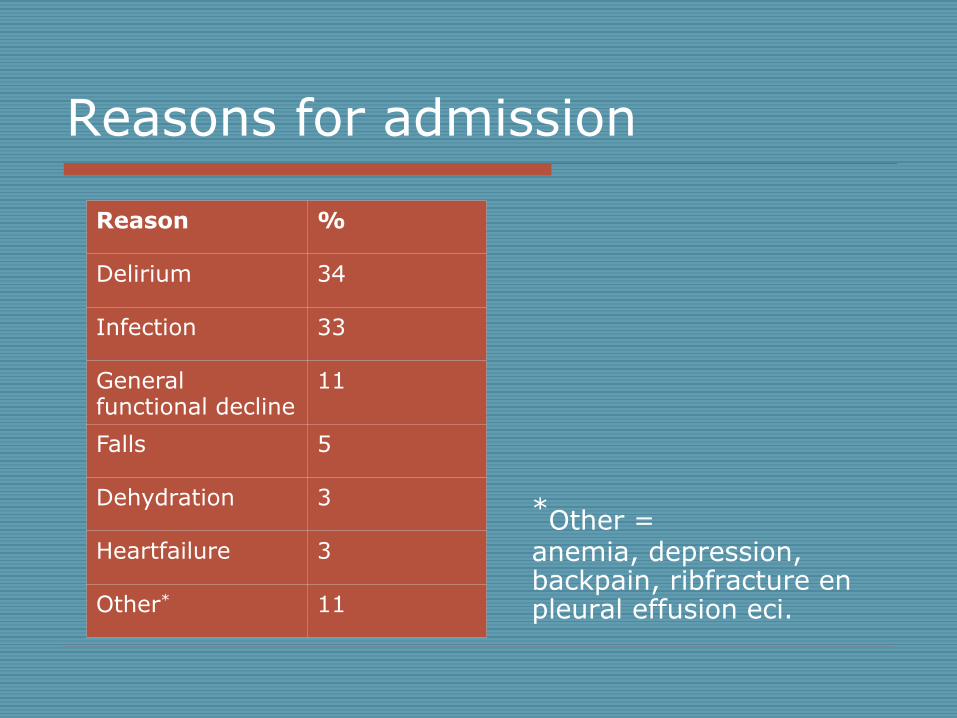
Reasons for admission
Reason %
Delirium 34
Infection 33
General functional decline
11
Falls 5
Dehydration 3
Heartfailure 3
Other* 11
*Other = anemia, depression, backpain, ribfracture en pleural effusion eci.