Het ECG van het sporthart - wikimedica.medica.be · Het ECG van het sporthart Prof. Dr. H....
23
1 Het ECG van het sporthart Prof. Dr. H. Heidbuchel Aanvullingen Elektrocardiografie 4e jaar Arts + Sportgeneeskunde UNIVERSITY OF F o u n d e d 1 4 2 5 De sport paradox De incidentie van plotse dood is omgekeerd evenredig met de dagelijkse fysieke activiteit en de “physical fitness” vs. Plotse dood komt meer voor tijdens fysieke activiteit en is 2.3 x hoger bij sporters dan bij sedentairen. Plotse dood en sport Onderliggend hartlijden • ≤35 jaar: (VS data) • >35j: 75% = ischemisch hartlijden HCM 38% Coronary Anomalies 19% CAD 2% Other 6% Tunneled LAD 5% Myocarditis 3% Dilated CM 3% AS 4% MVP 2% ARVD 3% Incr. Cardiac Mass 10% Ruptured Ao 5% Maron et al., JAMA 1996
Transcript of Het ECG van het sporthart - wikimedica.medica.be · Het ECG van het sporthart Prof. Dr. H....

1
Het ECG van het sporthart
Prof. Dr. H. Heidbuchel
Aanvullingen Elektrocardiografie 4e jaar Arts + Sportgeneeskunde
U N I V E R S I T Y O F!
F o u n d e d 1 4 2 5!
De sport paradox
De incidentie van plotse dood is omgekeerd evenredig met de dagelijkse fysieke activiteit en de “physical fitness” vs. Plotse dood komt meer voor tijdens fysieke activiteit en is 2.3 x hoger bij sporters dan bij sedentairen.
Plotse dood en sport Onderliggend hartlijden
• ≤35 jaar: (VS data)
• >35j: 75% = ischemisch hartlijden
HCM 38%
Coronary Anomalies
19%
CAD 2% Other
6% Tunneled LAD
5%
Myocarditis 3%
Dilated CM 3% AS
4% MVP 2%
ARVD 3%
Incr. Cardiac Mass 10%
Ruptured Ao 5%
Maron et al., JAMA 1996!

2
Screening to prevent sudden death
Screening in practice ESC/IOC Recommendation
• Basic screening – Personal and familial history (questionaires) – Physical examination – resting 12-lead ECG in all:
• first time at the age of 14-15y – not earlier:
• ECG can be confused with pediatric ECG changes • risk is low if younger
(no competitive sports; no developed substrate) • every 2 years, certainly if competitive athletes
1. Corrado et al, for the ESC Section on Sports Cardiology, Eur Heart J 2005
Probability to identify cardiac diseases by ECG or by history + physical examination
ECG Hx+PE • Hypertrophic cardiomyopathy up to 90% < 10% • ARVC 60-80% < 10% • Dilated cardiomyopathy 30-60% < 10% • Myocarditis 30-60% < 10% • Marfan’s syndrome < 10% > 90% • Valvular Disease < 10% > 90% • Long QT and Short QT syndrome > 80% zero • Brugada syndrome > 90% zero • Pre-excitation syndrome (WPW) > 90% zero • Congenital Coronary Artery Anomalies < 10% < 10%
Courtesy of Prof. Dr. A. Pelliccia

3
Sportbeoefening en het ECG Aanpassingen 1. toename van de vagus-activiteit. 2. afname van de autonome, intrinsieke activiteit van de
sinusknoop. 3. morfologische veranderingen, o.a. linker kamerhypertrofie.
– fysiologische aanpassingen – pathologische (tgv. doping; HOCM; ARVD; ...)
Interpretation of 12-lead ECG in athletes
ECG: Training-related vs. Uncommon
• Group 1: Training-related – i.e. physiological for athlete (and increasing with athletic level) – without increased cardiovascular risk – 3.4-12% in junior athletes4-5; 40-45% in elite athletes1-2
• Group 2: Uncommon, even in athletic population – potentially manifestation of pathology – 1.1 - 4 % 1-4 (much less related to athletic activity)
1. Pelliccia et al, Circ 2000; 2. Sharma et al, Br J Sports Med 1999; 3. Ma et al, J Sci Med Sport 2007; 4. Pelliccia et al, EuroPrevent2007; 5. Corrado et al, JAMA 2006

4
Group 1: training-related ECG changes 3.4-12% in junior athletes3-5; 40-45% in elite athletes1-2
• Rhythm & Conduction – Sinus bradycardia and -arrhythmia
• wandering pacemaker, sinus arrest and/or SA block, junctional rhythm
– First degree AV block • intermittent Wenckebach type 2nd degree AV block
– Atrial ectopic beats
• Morphological – Notched QRS in V1 or incomplete RBBB – Isolated criteria for LVH (Sokolow-Lyon, Cornell, …)
• Repolarisation – Early repolarisation
1. Pelliccia et al, Circ 2000; 2. Sharma et al, Br J Sports Med 1999; 3. Pelliccia et al, EuroPrevent2007; 4. Corrado et al, JAMA 2006; 5. Pelliccia et al, Eur Heart J 2007
• Variable presence dependent on – gender (much less in women) – race (African/Caribbean) – level of fitness / sports – type of sports (high endurance)
• To be interpreted in light of – personal history (symptoms) – family history – physical examination
1. Pelliccia et al, Circ 2000; 2. Sharma et al, Br J Sports Med 1999; 3. Pelliccia et al, EuroPrevent2007; 4. Corrado et al, JAMA 2006; 5. Pelliccia et al, Eur Heart J 2007
Group 1: training-related ECG changes 3.4-12% in junior athletes3-5; 40-45% in elite athletes1-2
ECG findings vs. level of training
1. Pelliccia et al, Eur Heart J 2007; 2. Sharma et al, Br J Sports Med 1999; 3. Pelliccia et al, Circ 2000
Pelliccia et al, Eur Heart J 2007
1! 2! 3!

5
30 y old competitive cyclist
Sinus bradycardia: >50%; LVH voltage criteria: up to 40%
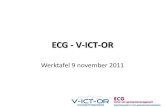
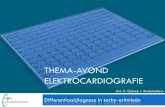
23 y old recreational jogger, cyclist, swimmer, soccer player, …
profound sinus arrhythmia; repetitive malaise while driving
23 y old recreational jogger, cyclist, swimmer, soccer player, …
exercise test, 100 W

6
14y old national swimmer asymptomatic
TTE & MRI normal
14y old national swimmer asymptomatic
TTE & MRI normal
45y old intensive recreational cyclist
asymptomatic pause at night; < 3 sec; first degree AV block

7
45y old intensive recreational cyclist
asymptomatic vagal surge (PP prolongation); PR after blok shorter than before block
45y old intensive recreational cyclist
exercise test, 50W normalisation with minor exercise
45y old intensive recreational cyclist
after 6m deconditioning

8
25 y old competitive cyclist
LVH voltage criteria: 40% in elite athletes; no path.Q, no repol., no LAH
! no TTE unless symptoms, family history and/or non-voltage ECG criteria !
24y old competitive amateur cyclist
rSr’ in V1, QRS ≤110ms: 20-50% DD RBBB: nog negative T-waves beyond V2; no reciprocal S in V6 and D1
21 y old competitive soccer player
Early repolarisation: 10-43%, more in younger athletes

9
Early repolarisation
Corrado et al, Eur Heart J 2010
Caucasian Black
Uncommon (potentially pathological) ECG 1.1 - 4.8 % of athletes
• Rhythm & Conduction – Complete bundle branch block – Left or right axis deviation / anterior or posterior hemiblock – Atrial flutter or fibrillation – Ventricular arrhythmias (ventricular extrasystoles?) – Preexcitation
• Morphological – LA hypertrophy – Pathological Q-waves
• Repolarisation – Long or short QTc – Brugada-ECG – ST-segment depression – Inverted T-waves in ≥2 consecutive leads
10-50% have disease!
Competitive soccer player, 4th league, 17y Screening; first ECG; fully asymptomatic

10
Latent preexcitation Unmasking by adenosine IV during SR
Courtesy of Dr. D. Koentges, Temse, Belgium
Baseline:
V1
V2
Adenosine 12 mg IV:
V1
V2
Preëxcitatie
Activatie tijdens sinusritme
18y old competitive cyclist
Negative T-waves are not aspecific!

11
NMR Pathology
Histology
Arrhythmogenic RV Cardiomyopathy
Basso et al, Circulation 1996
Aritmogene Rechter Ventrikel Cardiomyopathie (ARVC)
Vrouw; 46j; gestopt door CSM: “SVT”

12
46 y old female volleybal player RVOT-VPB
Idiopathische RV Outflow Tract VT (RVOT-VT) ECG Karakteristieken
• Ventrikel-extrasystolen en/of VT: – LBTB patroon
• en doorgaans precordiale transitie in V3 of V4 – Hoge voltages in inferior afleidingen
• Totale R-golf amplitudo in inferior-afleidingen ≥ 40 mm – QS morfologie in aVL!
• ahw. conditio sine qua non...
• Sinusritme: – Geen negatieve T’s in de precordialen; – Geen late potentialen; – Focale aritmie ipv. reentry (cfr. Holter, cyclo, EFO, ...)
1: Callans DJ et al. PACE 19II; 2: Arruda M et al. PACE 19II
Negative T-waves right precordial leads
Corrado et al, Eur Heart J 2010
Early repolarisation (black athlete) ARVC

13
Jongen, 16j: een lokale zwemmer…
“Persisterend juveniel patroon van negatieve T-toppen in de precordialen”
16y old soccer player
Negative T waves (precordial / standard): <4%, even in elite athletes
(Note: more prevalent in black athletes, up to 11% (S. Sharma, oral comm.)
Hypertrofische Cardiomyopathie
Aritmieën tengevolge van - dispersie van depolarisatie en repolarisatie, - grotere spiermassa (en dus meer kans op reentry-circuits),
- ischemie tgv. vaat-afwijkingen en/of uitstroom-obstructie.

14
Deep negative T-waves in ≥3 leads In the absence of echocardiographic abnormalities
• Case control study1
– 81 cases vs. 229 matched controls with normal ECGs – average FU 9±7 years
• 5/81 cases (6%) developed a cardiomyopathy – 3 with HCM (after 12±5y), 1 ARVC, 1 DCM (after 9y) – 1 with sudden death (ARVC) and 1 aborted sudden death (HCM)
• vs. 0/229 controls (p = 0.001) – i.e.: absence of negative T-waves confers a good prognosis
• Note: in black athletes: 10% sedentary => 23% athletes – most often right precordial leads; cave if inferolateral!
1. Pelliccia et al, NEJM 2008
Man 25j, asymptomatisch Attest voor basketbalclub?
Broer en oom: plotse dood op 30-jarige leeftijd…
Brugada Syndroom
• Klinische presentatie: – Syncope tgv. nonsustained VT (niet noodzakelijk bij
inspanning) – Plotse dood tgv. VF
• ECG criteria: – Beeld van onvolledig rechter bundeltak blok met – ST-optrekking in de rechter precordialen en aVL
• In baseline of na toediening van een klasse-1 antiaritmicum • Koepelvormig (type 1) of zadelvormig (type 2)

15
Man, 35j, reanimatie:VF
28y old professional soccer player asymptomatic
SD during sleep of 35y old brother; aborted SD after exercise 25y old brother TTE and exercise test normal
Haissaguerre-teken
Jongen, 15j: "beste voetballer van ‘t dorp"

16
QT-interval in athletes
• QT interval is longer in athletes cf. bradycardia QTc is at upper limit of normal non-athlete distribution
• Ideal cut-off values at rest still under discussion: – normal = QTc ≤470 ms in men and QTc ≤480 ms in women1
– abnormal = QTc ≥500 ms; between 460-500 ms: look at family2
• Better to also include dynamic adaptation?: – after quickly standing (sinus tc): no QT shortening = abnormal3
– 4 min after exercise QTc ≥445 ms = abnormal4
1. Corrado et al, Eur Heart J 2010; 2. Basavarajaiah et al, Eur Heart J 2007; 3. Viskin et al, JACC 2010; 4. Sy et al, Circulaton 2011
ECG “Seattle criteria”: tools and training
• Online training modules via Br. J. Sports Medicine
• Other: “JS SportECG”
ECG “Seattle criteria”: tools and training
• Online training modules via Br. J. Sports Medicine
• Other: “JS SportECG”

17
35y, competitive, non-professional, cyclist asymptomatic
VPB on routine ECG: ±1%
VPB on a screening ECG
• Take even a single PVC seriously, especially when – concomitant repolarisation abnormalities – competitive (or high-intensity recreational) sports – endurance sports (with increased likelihood of performance-
enhancing drug use?)
• Tailor the work-up individually – combining imaging and electrophysiological tools
Plotse dood en sport Onderliggend hartlijden
• ≤35 jaar: (VS data)
• >35j: 75% = ischemisch hartlijden
HCM 38%
Coronary Anomalies
19%
CAD 2% Other
6% Tunneled LAD
5%
Myocarditis 3%
Dilated CM 3% AS
4% MVP 2%
ARVD 3%
Incr. Cardiac Mass 10%
Ruptured Ao 5%
Maron et al., JAMA 1996!

18
Who can safely participate?
VPB AF
ICD
LQT
?
Recommendations
Two goals:
1. Prevent arrhythmias during exercise if underlying disease, and/or
2. Prevent development & progression of the underlying disease
• Balanced hypertrophy and dilatation of the four heart chambers1-5 – usually only regarded as marvelous adaptation – with only positive attributes.
• But: – Changes of the athlete’s heart may be involved in the
development of the arrhythmogenic substrate itself – on an atrial, nodal, and ventricular level
1. Fagard, Int J Sports Med 1996; 2. Fagard, Cardiol Clin 1997; 3. Pluim et al, Circulation 2000; 4. Scharhag et al, JACC 2002; 5. Perseghin et al, Am Heart J 2007
Athlete’s heart = Arrhythmic heart Athlete’s heart

19
Atrial fibrillation
• More and more studies: related to sports activity10
– Lone AF vs. general popul.4,5,8: 31-63% vs. 15% sports (p<0.05) – Athletes vs. general population1-3,6,7: x4 to x10 AF (1-4%/10y ?)
• Physician’s Health Study:11 – 16921 apparently healthy men; 12y FU; self-reported AF
1. Zehender, AHJ 1990; 2. Furlanello, JCE 1998; 3. Karjalainen, BMJ 1998; 4. Mont et al, EHJ 2002; 5. Elosua et al, Int J Cardiol 2006; 6. Molina, ESC 2005 (abstract); 7. Baldesberger, EHJ 2008;
8. Mont, Europace 2008; 9. Heidbuchel, Int J Cardiol 2006; 10. Mont, Europace 2009; 11. Aizer al, Am J Cardiol 2009
Lone atrial flutter Men, ≤65y, no SHD, no AF vs. controls
G. Claessen & H. Heidbuchel, Heart 2011
Recreational jogger ECG First Consultation

20
Recreational jogger ECG Visit-2: 1 month later
Recreational jogger Emergency admission
atrial flutter with 1-to-1 A-V conduction
The effect of an endurance event: RV dilates whilst the LV shrinks
La Gerche, Prior & Heidbuchel. Eur Heart J (2011)

21
Results: RV ejection fraction
La Gerche, Prior & Heidbuchel. Eur Heart J (2011)
*p<0.0001 † p=0.001
*
†
p = 0.05 for race duration
RV morphological changes Acute > Chronic ?
• Hypothesis:1-2
– Repeated RV insults may result in long-term RV dysfunction
1. Heidbuchel et al, Eur Heart J 2003; 2. Ector & Heidbuchel, Eur Heart J 2007
RV injury RV injury
RV injury Chronic RV remodelling
"Acquired ARVC" 1
RV morphological changes Acute > Chronic ?
• Facilitating factors?
1. Performance enhancing drugs?
2. Genetic predisposition?
• cf. ARVC (desmosomal mutations)1-2
3. Other … ?
1. Kirchhof et al, Circ 2006; 2. Sen-Chowdhry & McKenna, Circ Arrythm Electrophysiol 2010

22
Desmathlete trial Mutation findings
• 9 different heterozygous sequence variants in 10 patients – 7 novel - 2 previously known – 5 (in 6 patients, 12.8%) manifestly pathogenic
*: 1. Sen-Chowdhry et al, Circ 2007; 2. Dalal et al, Circ 2006; 3. Gerull et al, Nature Genetics 2004; 4. Pilichou et al, Circ 2006; 5. van Tintelen et al, Circ 2006; 6. den Haan et al, Circ Cardiovasc Genetics 2009; 7. Sen-Chowdhry et al, JACC 2007
p < 0.0005
Pulmonary vascular resistance
• 40 athletes & 15 non-athletes1
• Slope very reproducible through different patient groups2-3 1. Andre LaGerche, Heidbuchel, Prior. J Appl Physiol 2010; 2. Argiento, Naeije et al. Eur Resp J 2010;
3. Lewis, Semigran et al. Circ Heart Failure 2011
p = 0.71
RV vs. LV end-systolic wall stress Laplace equation: ESWS = P.r/2h
• 40 endurance athletes, 15 matched controls • TEE max exercise on semi-supine bicycle + radial artery catheter; CMR
1. LaGerche et al, Med Sci Sports Exerc 2010

23
Animal models?
• Rats, running 5d/w @85% of V02max for 16 weeks: But RV (not LV) fibrosis with myocyte disarray
Benito & Mont, Circ 2011
Accompanied by mRNA and protein expression of TGF-B1, fibronectin, MMP-2, TIMP1, collagen-I and -III, …
What happens to the RV during exercise?
– Exercise CMR – Invasive pressure
measures – Echo + bubbles