case report banda aceh.docx
17
Case Report Primary MDR TB from Pleural fluid with Kidney Disorder Johannes Kevin Sinambela, Parluhutan Siaian Department of Pulmonoloy and Respiratory Medi!ine, "a!ulty of Medi!ine #niversitas Sumatera #tara, $a%i &dam Mali' (eneral $ospital &bstra' Latest statistic shows increasing number in new tuberculosis cases from 6,1 million cases in 2013 with the number of deaths from 2013 and 2014 remains constant around 1.5 million. In 2013, W! re"orted that 3.5# of $% cases globall& are estimated to become '() $%. '() $% cases are caused b& '. tuberculosis that resistant to at least two of the most "owerful first line anti $% drugs rifam"icin and isonia*id simultaneousl&, with or without other first line anti $% drugs. '() $% can be a "rimar& resistance, initial resistance and secondar& resi st ance. $he mana gement of '() $% cases can be more challenging and com"licated if there is im"aired renal function and increasing the ris+ of '() $% drug toicit&. - man aged 26 &ears came to the hos"ital with d &s"nea 1 wee+ before entering the hos"ital and worsening in 1 da&. e was diagnosed with right h&dro "neu motho ra because sus"ec t of $%. hest tube was inserted with W/(. $r eat ed wit h - $( cat ego r& I and ant ibi oti cs bas ed on cli nic al and radiolo gic al. 'ic robiological ea mination of s"utum was found an aer obic bac ter ia Acinetobacter baumannii , -% I negatie, -% II negatie, from the mi cr obiologi cal e aminat ion of "l eural fl ui d was found aerobi c bact er ia Enter obact er aero genes, -% I /cant& 5. $hen "r oc eed wi th ene "ert "leural fluid with "ositie '$% results )ifam"icin resistant. -$( categor& I was sto""ed and started with regimen of '() $% -$( a"reom&cin 50 mg 3 times wee+l&, 7&ra*inamide 1500 mg, Leofloacin 50 mg, &closerine 50 mg 3 times wee+l&, 8thionamide 500 mg, eer& da&. Keywords) MDR TB, TB drus to*i!ity, MDR TB reimen 1
-
Upload
gunawan-samosir -
Category
Documents
-
view
213 -
download
0
Transcript of case report banda aceh.docx

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 1/17
Case Report
Primary MDR TB from Pleural fluid with Kidney Disorder
Johannes Kevin Sinambela, Parluhutan Siaian
Department of Pulmonoloy and Respiratory Medi!ine,
"a!ulty of Medi!ine #niversitas Sumatera #tara,
$a%i &dam Mali' (eneral $ospital
&bstra'
Latest statistic shows increasing number in new tuberculosis cases from
6,1 million cases in 2013 with the number of deaths from 2013 and 2014
remains constant around 1.5 million. In 2013, W! re"orted that 3.5# of $%
cases globall& are estimated to become '() $%. '() $% cases are caused
b& '. tuberculosis that resistant to at least two of the most "owerful first line
anti $% drugs rifam"icin and isonia*id simultaneousl&, with or without other first
line anti $% drugs. '() $% can be a "rimar& resistance, initial resistance and
secondar& resistance. $he management of '() $% cases can be more
challenging and com"licated if there is im"aired renal function and increasing
the ris+ of '() $% drug toicit&.
- man aged 26 &ears came to the hos"ital with d&s"nea 1 wee+ before
entering the hos"ital and worsening in 1 da&. e was diagnosed with right
h&dro"neumothora because sus"ect of $%. hest tube was inserted with
W/(. $reated with -$( categor& I and antibiotics based on clinical and
radiological. 'icrobiological eamination of s"utum was found an aerobic
bacteria Acinetobacter baumannii , -% I negatie, -% II negatie, from the
microbiological eamination of "leural fluid was found aerobic bacteria
Enterobacter aerogenes, -% I /cant& 5. $hen "roceed with ene "ert
"leural fluid with "ositie '$% results )ifam"icin resistant. -$( categor& I was
sto""ed and started with regimen of '() $% -$( a"reom&cin 50 mg 3
times wee+l&, 7&ra*inamide 1500 mg, Leofloacin 50 mg, &closerine 50
mg 3 times wee+l&, 8thionamide 500 mg, eer& da&.
Keywords) MDR TB, TB drus to*i!ity, MDR TB reimen
1

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 2/17
+TR-D#CT+-
In 2013, 6,1 million tuberculosis $% cases were re"orted to world
health organi*ation W!6. !f these, 5, million were "eo"le newl&
diagnosed and another 0,4 million were alread& on tr eatment. $he si
countries that stand out as haing the largest number of incident cases in
2013 were India 2.0 million92.3 million, hina 0.: million91.1 million,
;igeria 340 000<==0 000, 7a+istan 30 000<650 000, Indonesia 410
000<520 000 and /outh -frica 410 000<520 000.1
loball&, 3,5# of new and 20,5# of "reiousl& tr eated $% cases were
estimated to hae had multi drug resistant tuberculosis '()>$% in 2013.
$his translates into an estimated 4=0 000 "eo"le haing deelo"ed '()>$% in
2013. !n aerage, an estimated :,0# of "atients with '()> $% had
etensiel& drug resistant $% ()>$%. If all notified $% "atients 6,1 million,
new and "reiousl& treated had been tested for drug resistance in 2013, an
estimated 300.000 cases of '()>$% would hae been detected, more than
half of these in thr ee countries alone? India, hina and the )ussian
eder ation.1
Laborator& confirmation of $% and drug resistance is +e& to ensuring
that indiiduals with $% signs and s&m"toms are correctl& diagnosed and
treated. In 2013, 5=# of the 4,: million "ulmonar& $% "atients notified globall&
were bacteriologicall& confirmed ia a W!>recommended test, including
ra"id tests such as "ert '$%@)I.1
C&S. R.P-RT
- 26>&ear>old man came to -dam 'ali+ eneral os"ital at 2 th ebruar&
2016 with com"laints of shorthness of breath, since 1 wea+ and worsening in 1
da& before admitted to the hos"ital. Whee*e not found, histor& of whee*e not
found. ough since 1 month, "roductie cough, blood& cough not found, histor&
of blod& cough not found. /ub febril feer was found in 1 month, night sweat
found, loss of a""etite found, lose of weight 2 +g in one month. istor& of anti
tuberculosis drugs not found.
2
8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 3/17
Aital signs showed alert, blood "ressure was 100@60 mmg, "ulse rate
was :2 times@minute, res"irator& rate was 36 times@minute, tem"erature was
36,
℃
. er bod& weigth was 52 +g, her bod& height was 163 cm. !n
"h&sical eamination found dela&ed moement at the right hemithora . !n
auscultation, breath sounds were diminissed at the right hemithora and no
additional sound in the both lung. Laborator& findings increasing in leu+oc&tes.
7atient diagnose with right "&o"neumothora due to tuberculosis and "erform
chest tube at the emergenc& de"artment.
In the in"atient unit, microbiological eamination of "leural fluid and
"leural fluid microbiolog& were "rocessed. -waiting the results of eamination,
"atient was gien categor& 1 -$( based on clinical and radiological. !n the
net da& microbiological eamination of s"utum was found ancinetobacter
aerobic bacteria baumannii, sensitie to mero"enem. -% 1 negatie, -% 2
negatie. rom the results of microbiological s"utum, "atient was gien
antibiotics mero"enem 1 g @ = hours.
rom the results of microbiological eamination of "leural fluid , aerobic
bacteria 8nterobacter aerogenes 8/%L B was found and -% 1 scant& 5,
"atient was gien the addition of the antibiotic ami+acin of 1 g @ da&, gentamicin
=0 mg @ 12 hours, metronida*ole 500 mg @ = hours and ste"tomisin 1 g @ da&.
ene"ert "leural fluid eamination with a "ositie result of '$% )I>resistant.
-nti>tuberculosis drugs and antibiotics was sto""ed and laborator& eamination
was "rocessed, eleated renal function was found from the laborator&
eamination. 7atient was consulted to the ;e"hrolog& diision before starting
the treatment of '() $%. (iagnosis from ;e"hrolog& diision is drug induced
acute tubulointerstinal ne"hritis dd -CI stadium inDur&.
7atient get her '()>$% regimen adDusted with her renal function
creatinine clearance was 10,53 ml@minute? ca"reom&cin inDection 50 mg
three times "er wee+ I', "ira*inamide tablet 1500 mg three times "er wee+
7!, leofloacin ca"let 50 mg three times "er wee+ 7!, ethionamide tablet
500 mg once dail& 7!, c&closerine ca"sul 500 mg three times "er wee+ 7!,
3

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 4/17
and "&ridoine tablet 100 mg once dail& 7!. 7atient was discharged on 04
-"ril 2016, and controlled to "ol&clinic of '()>$%
igure 1. hest >ra& on 03 ebruar& 2016 showed hidro"neumothora on
right lung
igure 2. hest >ra& on 05 ebruar& 2016 showed hidro"neumothora on
right lung with chest tube inserted.
4

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 5/17
D+SC#SS+-
(rug>resistant tuberculosis ()>$% is a t&"e of $% that has deelo"ed a
genetic mutations such that a certain drug or drugs is no longer effectie
against the bacteria. ()>$% is confirmed through laborator& tests that
demonstrate growth in>itro of infecting isolates of '&cobacterium tuberculosis
in the "resence of one or more anti>$% drugs. %& definition, there are fie
different categories of drug resistance, namel&?
• 'ono>resistance? )esistance to one anti>$% drug.
• 7ol&>resistance? )esistance to more than one anti>$% drug, other than
isonia*id and rifam"icin.
•
'ultidrug>resistant $% '()>$%? )esistance to at least isonia*id andrifam"icin, the two most "otent anti>$% agents.
• )ifam"icin>resistant $% ))>$%? )esistance to rifam"icin detected
using "henot&"ic or genot&"ic methods, with or without resistance to
other anti>$% drugs. It includes an& resistance to rifam"icin, including
mono>resistance, multi>drug resistance and "ol&>resistance.
• 8tensiel& drug>resistant $% ()>$%? '()>$%, "lus resistance to at
least one of the fluoroEuinolones, and at least one of three inDectable
second>line drugs ca"reom&cin, +anam&cin and ami+acin. 2,3,11
7atients sus"ected of '()>$% is li+el&?
1. 7ulmonar& $% cases with treatment failure on categor& 2, as eidenced
b& "reious medical record and medical histor&.
2. 7ulmonar& $% "atients with s"utum eamination results remain "ositie
after additional 1 month of intensie "hase with categor& 2.
3. $% "atients eer treated in non>(!$/ facilities, including those that
receied second>line -$$ as Euinolones and +anam&cin.
4. 7ulmonar& $% "atients who was failed on categor& 1 treatment.
5. 7ulmonar& $% "atients with s"utum eamination results remained
"ositie after additional 1 month of intensie "hase with categor& 1.
6. ase of rela"se "ulmonar& $%.
. $% "atients who returned after default @ loss to follow u" on treatment of
categor& 1 or categor& 2.
5

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 6/17
=. /us"ected tuberculosis with com"laints, who lies closel& to the
confirmed '() $% "atients, including health care on dut& in the '()>
$% ward.
:. $%>IA. 3,4,11
)esistance to anti>$% treatment are diided into ?
1 7rimar& resistance is when the "atient had neer receied treatment or
had receied treatment -$$ is less than 1 month.2 $he initial resistance is not +nown whether the "atient had no "reious
histor& of treatment -$$ or not.3 /econdar& resistance is when a "atient has had a histor& of at least 1
month.4
In this "atient is classified into 7rimar& resistance categor&.
)a"id drug susce"tibilit& testing (/$ of isonia*id and rifam"icin or of
rifam"icin alone is recommended oer conentional testing or no testing at the
time of diagnosis of $%, subDect to aailable resources. or the "ur"oses of the
recommendation, the grou" considered a ra"id test as one "roiding a
diagnosis of resistance to isonia*id and rifam"icin or rifam"icin alone within two
da&s of s"ecimen testing. !nl& molecular tests can detect resistance so fast, of
which two technologies 9 line "robe assa& and "ert '$%@)I 9 are currentl&
recommended for used b& W!. onentional (/$ of cultured m&cobacteria
t&"icall& "roides results within 193 months. 2,10
Reimen for MDR/TB
6

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 7/17
)egimen for '()>$% com"rises of 6 drugs > Canam&cin, Leofloacin,
8thionamide, 7&ra*inamide, 8thambutol and &closerine during the Intensie
7hase and 4 drugs Leofloacin, 8thionamide, 8thambutol and &closerine
during the ontinuation 7hase.5 $hese drugs hae man& side effects, "ractical
treatment longer, and the cost ma& be 100 times larger than the first line.6
$he current regimen for '()>$% is a standardi*ed treatment, the& are?3,
6Cm>8to>Lf>s>F8 @ 128to>Lf>s>F8
$able 1. -ntituberculosis agents
Duration of manaement
'()>$% treatment reEuires a longer time for 1=>24 months after culture
conersion. onersion culture is? a microsco"ic eamination of s"utum and
culture 2 times in a row with a distance of 30>da& eamination, was negatie.
onsists of two "hases, the intensie and continuation "hase. $he intensie
"hase is the "hase of giing inDections with at least 6 months or 4 months after
culture conersion. If at the end of the eight month conersion has not occurred
then called treatment failure. In continuation "hase, -$( were gien without
7

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 8/17
inDections after com"leting the intensie "hase. !ne month of treatment is
when the "atients receied 2= doses of medication. (uration of intensie "hase
treatment is b& the formula? a B 4 months, where GaH is? first month conersion
achieed. (uration of treatment intensie B continuation "hase follow the
formula? a B 1= months.3
$able 2. (oses of antituberculosis drugs adDusted to bod& weigth for treatment
of '()>$%=
-$(%!( W8I$
J 33 +g 33 9 50 +g 51 9 0 +g K0 +g
7&ra*inamide
tablet, 500mg
30>40
mg@+g@da&
1000>150 mg 150>2000 mg 2000>2500 mg
8thambutol
tablet, 400mg
25
mg@+g@da&
=00>1200 mg 1200>1600 mg 1600>2000 mg
Canam&cin
ial, 1000mg
15>20
mg@+g@da&
500>50 mg 1000 mg 1000 mg
a"reom&cin
ial, 1000mg
15>20
mg@+g@da&
500>50 mg 1000 mg 1000 mg
Leofloacin
a"let, 250mg
50 mg@da& 50 mg 50 mg 50>1000 mg
&closerine
ca"sul, 250mg
15>20
mg@+g@da&
500 mg 50 mg 50>1000 mg
8thionamide
tablet, 250 mg
15>20
mg@+g@da&
500 mg 50 mg 50>1000 mg
7-/
granules, 4 gr
150
mg@+g@da&
= gr = gr = gr
.valuation of Treatment
-ssessment of treatment res"onse is a microsco"ic eamination of
s"utum conersion and culture. ulture results can be obtained after 2 months.
$he main ealuation in "atients with '()>$% are? =
8

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 9/17
1. /"utum eamination eer& month in the intensie "hase and eer& 2
months in the continuation "hase.2. /"utum culture eer& month in the intensie "hase and eer& 2 months
in the continuation "hase.3. (rug sensitiit& test before treatment and in cases that are e"ected to
e"erience treatment failure.
8aluation su""orting '()>$% "atients are?=
1. linical assessments including weight2. -ssessment immediatel& if an& side effects3. hec+ the leels of "otassium and creatinine throughout the "atient
receied an inDection +anam&cin and ca"reom&cin4. 8amination of $/ $h&roid /timulating ormone is "erformed eer& 6
months and if there are signs of h&"oth&roid.
&dverse Rea!tions to Se!ond/line &nti/Tuber!ulosis Drus
$he timel& and intensie monitoring for, and management of, aderse
effects caused b& second>line drugs are essential com"onents of '()>$%
control "rogrammes. 7oor management of aderse effects increases the ris+ of
default or irregular adherence to treatment, and ma& result in death or
"ermanent morbidit&.5 $reatment for '()>$% reEuires the use of second>line
drugs /L(s. $he freEuenc& of aderse drug effects among '()>$% "atients
treated with /L(s is much higher than that among new "atients treated with
L(s.:
$able 3. ommon aderse effects of second>line drugs 5,,:
9

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 10/17
Manaement of &dverse Dru Rea!tions
$he +e& "rinci"les in the management of aderse drug effects in '()>
$% treatment are?:
1. If minor aderse effects occur, be su""ortie, consider administration of
ancillar& drugs and reassure "atients.2. In case of maDor aderse effects that are life>threatening or can
"otentiall& cause damage to ital organs, identif& and discontinue the
offending drugs.
Renal To*i!ity
7rior to starting treatment, all "atients will hae renal function ealuated.
(uring treatment of '()>$%, if the "atients "resents with s&m"toms and@or
signs of renal im"airment oliguria, anuria, "uffiness of face, "edal oedema,
all the drugs should be withheld, renal function tests should be done and, if
reEuired, o"inion of ne"hrologist should be sought. )e>introduction of drugs
will be underta+en b& the ()>$% entre committee in consultation
with a ne"hrologist, along with freEuent monitoring of renal "arameters.
ommon offending drug is an aminogl&coside.5
10
8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 11/17
(uring treatment, blood urea and serum creatinine should be done
eer& month for the first three months after treatment initiation and then eer&
three months thereafter whilst inDection Canam&cin is being administered.
/ilent renal toicit& ma& be "ic+ed u" b& these routine follow>u"
biochemical eaminations. If at an& time, the blood urea or serum
creatinine becomes abnormal, treatment should be withheld and further
management decided u"on in consultation with the ()>$% entre committee.5
MDR/TB Treatment in Spe!ial Situations
/ome s"ecial situations can ma+e the treatment of '()>$% more
com"le, but it can nonetheless be successful. $he following are the common
s"ecial situations to be considered during the treatment of '()>$% "atients?5,,:
• 7regnanc&
• %reastfeeding
• ontrace"tion
• hildren
• (iabetes mellitus
• )enal insufficienc&
• Lier disorders
• /ei*ure disorders
• 7s&chiatric illnesses
• /ubstance de"endence
• IA>infected "atient
Renal +nsuffi!ien!y
)enal insufficienc& due to longstanding $% disease itself, "reious use
of aminogl&cosides or concurrent renal disease is not uncommon. reat care
should be ta+en in the administration of second>line drugs in "atients with
renal im"airment. onsideration needs to be ta+en that '()>$% "atients
reEuire aminogl&cosides for 6 months or more. !ther drugs, which also
might reEuire dose or interal adDustment in "resence of mild to moderate
renal im"airment, are? 8thambutol, uinolones, &closerine and 7-/.
In the "resence of seere renal im"airment man& other drugs ma& also
reEuire adDustments. 2,5,4
11

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 12/17
In '()>$% "atients, blood urea and serum creatinine should be
monitored "rior to treatment initiation, monthl& for three months after
treatment initiation and then eer& three months whilst inDection Canam&cin
is being administered. In "atients with mild renal im"airment, the dose of
aminogl&cosides ma& be reduced. In the "resence of seere renal failure, the
aminogl&coside thera"& should be discontinued and re"laced with
other "otent non> ne"hrotoic antituberculosis drugs.5
Manaement of MDR/TB in Renal Dysfun!tion
)enal d&sfunction ma& lead to decreased immunit& and also to an
at&"ical $% "resentation. )enal d&sfunction occurs freEuentl& in (', and the
aforementioned com"lications ma& oerla". ;onetheless, the main "roblem
related to renal failure is that drug leels in the blood might remain high as the
+idne&s are unable to adeEuatel& Mlter them. (rug leels ma& increase to toic
leels, leading to worsening of the renal condition and the li+elihood of other
toicities. In addition, aminogl&cosides hae aderse effects on +idne& function.
$enofoir $df, an -)A commonl& used concomitantl& with anti>$%
medications, can create renal toicit& es"eciall& in the deteriorating $% "atient
infected with IA. In cases of acute renal failure, consider sto""ing ne"hrotoic
medication. In a "atient with adanced IA, the combination of $df and m can
lead to an electrol&te wasting s&ndrome with life>threatening h&"o+alemia.:
(rugs should be sto""ed until the "atient recoers and "otassium
should be re"laced. 'ost anti>$% drug dosages will need to be adDusted in
"atients with renal d&sfunction and, wheneer "ossible, consultation with a
ne"hrologist is recommended. $he integrit& of the /L( regimen should be
maintained as much as "ossible to aoid com"romising the efMcac& of the anti>
$% treatment and death from $%. In the absence of a s"ecialist, one a""roach
recommended is shifting the dail& treatment to a thrice>wee+l& schedule while
monitoring renal function and "otassium.:
)enal insufficienc& caused b& longstanding $% infection itself or "reious
use of aminogl&cosides is not uncommon. reat care should be ta+en in the
administration of second>line drugs in "atients with renal insufficienc&, and the
12

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 13/17
dose and@or the interal between dosing should be adDusted according to $able
6. If aminogl&cosides hae to be sus"ended before three months of treatment
due to renal insufficienc&, add 7-/ to the treatment regimen. 2
$able 4. -dDustment of antituberculosis medication in renal insuf ficienc&4
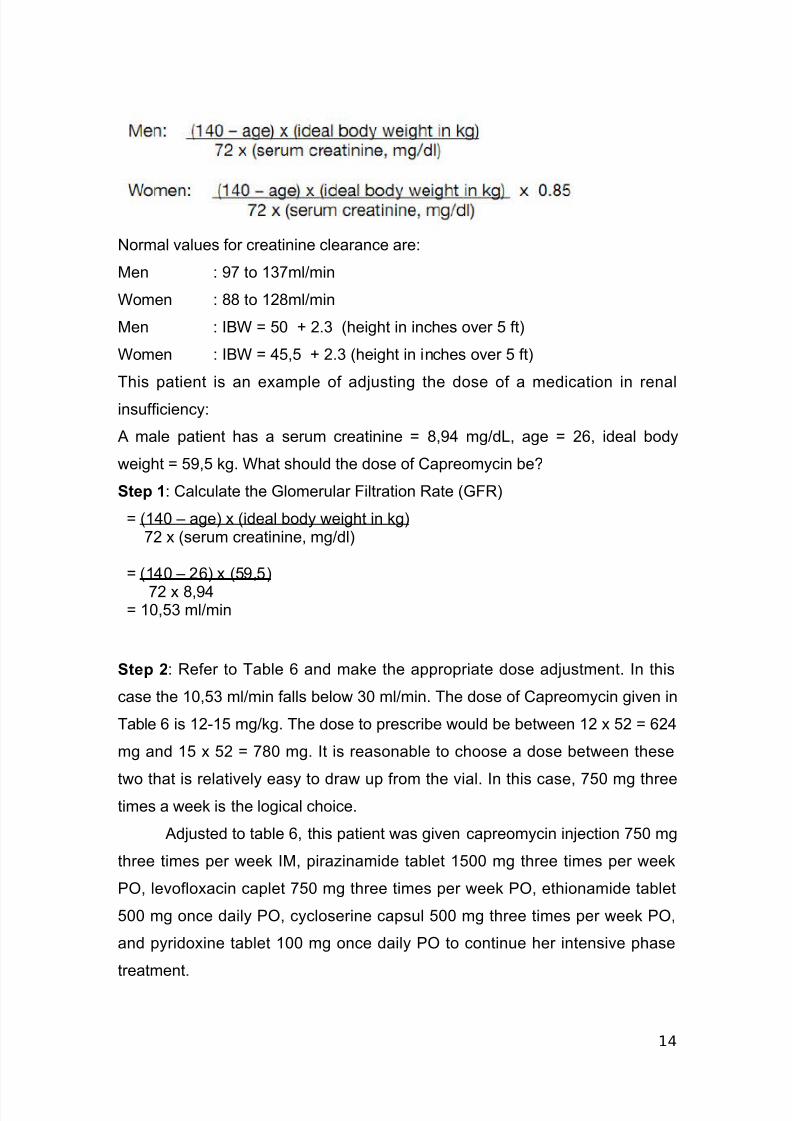
$he formula to calculate the creatinine clearance rI or the
glomerular filtration rate ) is as follows?10
8stimated lomerular iltration )ate )?
13
8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 14/17
;ormal alues for creatinine clearance are?
'en ? : to 13ml@min
Women ? == to 12=ml@min
'en ? I%W N 50 B 2.3 height in inches oer 5 ft
Women ? I%W N 45,5 B 2.3 height in inches oer 5 ft
$his "atient is an eam"le of adDusting the dose of a medication in renal
insufficienc&?
- male "atient has a serum creatinine N =,:4 mg@dL, age N 26, ideal bod&
weight N 5:,5 +g. What should the dose of a"reom&cin beO
Step 0? alculate the lomerular iltration )ate )
N 140 9 age ideal bod& weight in +g 2 serum creatinine, mg@dl
N 140 9 26 5:,5
2 =,:4 N 10,53 ml@min
Step 1? )efer to $able 6 and ma+e the a""ro"riate dose adDustment. In this
case the 10,53 ml@min falls below 30 ml@min. $he dose of a"reom&cin gien in
$able 6 is 12>15 mg@+g. $he dose to "rescribe would be between 12 52 N 624
mg and 15 52 N =0 mg. It is reasonable to choose a dose between these
two that is relatiel& eas& to draw u" from the ial. In this case, 50 mg threetimes a wee+ is the logical choice.
-dDusted to table 6, this "atient was gien ca"reom&cin inDection 50 mg
three times "er wee+ I', "ira*inamide tablet 1500 mg three times "er wee+
7!, leofloacin ca"let 50 mg three times "er wee+ 7!, ethionamide tablet
500 mg once dail& 7!, c&closerine ca"sul 500 mg three times "er wee+ 7!,
and "&ridoine tablet 100 mg once dail& 7! to continue her intensie "hase
treatment.
14

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 15/17
C-C2#S+-
ad been re"orted a 26>&ear>old man who was diagnosed with "rimer
'()>$% who suffered renal insufficienc& on the beginning intensie "hase
treatment. er '()>$% drugs had been adDusted in this "atients.
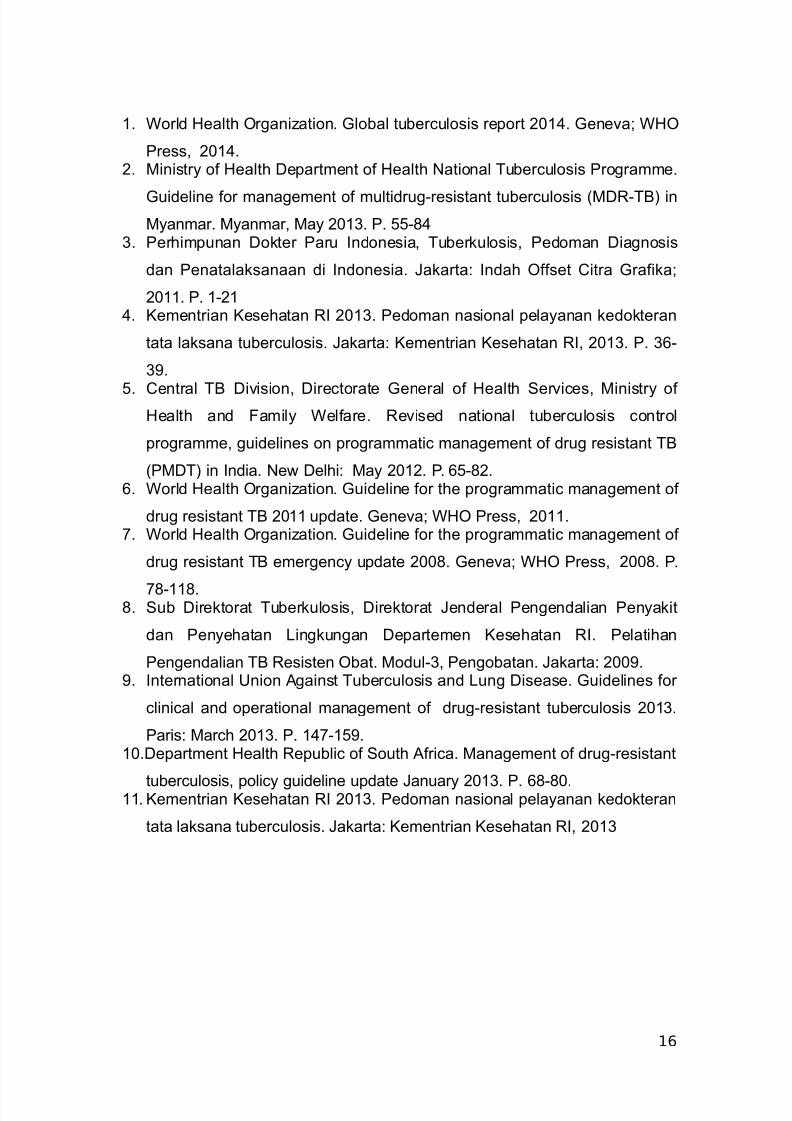
R.".R.C.S
15
8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 16/17
1. World ealth !rgani*ation. lobal tuberculosis re"ort 2014. eneaP W!
7ress, 2014.2. 'inistr& of ealth (e"artment of ealth ;ational $uberculosis 7rogramme.
uideline for management of multidrug>resistant tuberculosis '()>$% in
'&anmar. '&anmar, 'a& 2013. 7. 55>=43. 7erhim"unan (o+ter 7aru Indonesia, $uber+ulosis, 7edoman (iagnosis
dan 7enatala+sanaan di Indonesia. Qa+arta? Indah !ffset itra rafi+aP
2011. 7. 1>214. Cementrian Cesehatan )I 2013. 7edoman nasional "ela&anan +edo+teran
tata la+sana tuberculosis. Qa+arta? Cementrian Cesehatan )I, 2013. 7. 36>
3:.
5. entral $% (iision, (irectorate eneral of ealth /erices, 'inistr& of ealth and amil& Welfare. )eised national tuberculosis control
"rogramme, guidelines on "rogrammatic management of drug resistant $%
7'($ in India. ;ew (elhi? 'a& 2012. 7. 65>=2.6. World ealth !rgani*ation. uideline for the "rogrammatic management of
drug resistant $% 2011 u"date. eneaP W! 7ress, 2011.. World ealth !rgani*ation. uideline for the "rogrammatic management of
drug resistant $% emergenc& u"date 200=. eneaP W! 7ress, 200=. 7.
=>11=.=. /ub (ire+torat $uber+ulosis, (ire+torat Qenderal 7engendalian 7en&a+it
dan 7en&ehatan Ling+ungan (e"artemen Cesehatan )I. 7elatihan
7engendalian $% )esisten !bat. 'odul>3, 7engobatan. Qa+arta? 200:.:. International Rnion -gainst $uberculosis and Lung (isease. uidelines for
clinical and o"erational management of drug>resistant tuberculosis 2013.
7aris? 'arch 2013. 7. 14>15:.10.(e"artment ealth )e"ublic of /outh -frica. 'anagement of drug>resistant
tuberculosis, "olic& guideline u"date Qanuar& 2013. 7. 6=>=0.11. Cementrian Cesehatan )I 2013. 7edoman nasional "ela&anan +edo+teran
tata la+sana tuberculosis. Qa+arta? Cementrian Cesehatan )I, 2013
16

8/16/2019 case report banda aceh.docx
http://slidepdf.com/reader/full/case-report-banda-acehdocx 17/17