
DE DIAGNOSE IS NIET ALTIJD EENDUIDIG: OCCULTE MPN … · Pathophysiologie outflow block...
21
24/11/2015 1 DE DIAGNOSE IS NIET ALTIJD EENDUIDIG: OCCULTE MPN EN SPLANCHNISCHE THROMBOSE (CASUISTIEK) Wim Laleman MD PhD Dienst Maag-,Darm en Leverziekten Sectie Lever- en Biliopancreatische aandoeningen [email protected] DIAGNOSE MPN … BEGINT VAAK NIET BIJ DE HE MATOLOOG MAAR WEL HE P ATOLOOG
-
Upload
truonghuong -
Category
Documents
-
view
214 -
download
0
Transcript of DE DIAGNOSE IS NIET ALTIJD EENDUIDIG: OCCULTE MPN … · Pathophysiologie outflow block...
24/11/2015
1
DE DIAGNOSE IS NIET ALTIJD
EENDUIDIG: OCCULTE MPN EN
SPLANCHNISCHE THROMBOSE
(CASUISTIEK)
Wim Laleman MD PhDDienst Maag-,Darm en Leverziekten
Sectie Lever- en Biliopancreatische aandoeningen
DIAGNOSE MPN …
BEGINT VAAK NIET BIJ DE
HEMATOLOOG MAAR WEL
HEPATOLOOG
24/11/2015
2
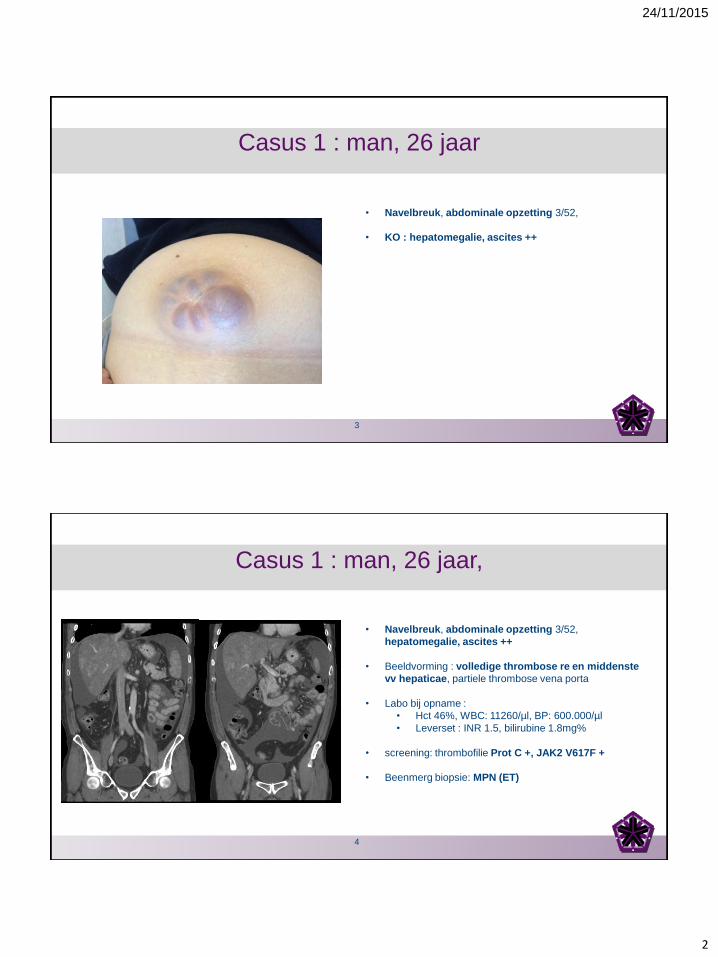
Casus 1 : man, 26 jaar
• Navelbreuk, abdominale opzetting 3/52,
• KO : hepatomegalie, ascites ++
3
Casus 1 : man, 26 jaar,
• Navelbreuk, abdominale opzetting 3/52,
hepatomegalie, ascites ++
• Beeldvorming : volledige thrombose re en middenste
vv hepaticae, partiele thrombose vena porta
• Labo bij opname :
• Hct 46%, WBC: 11260/µl, BP: 600.000/µl
• Leverset : INR 1.5, bilirubine 1.8mg%
• screening: thrombofilie Prot C +, JAK2 V617F +
• Beenmerg biopsie: MPN (ET)
4
24/11/2015
3
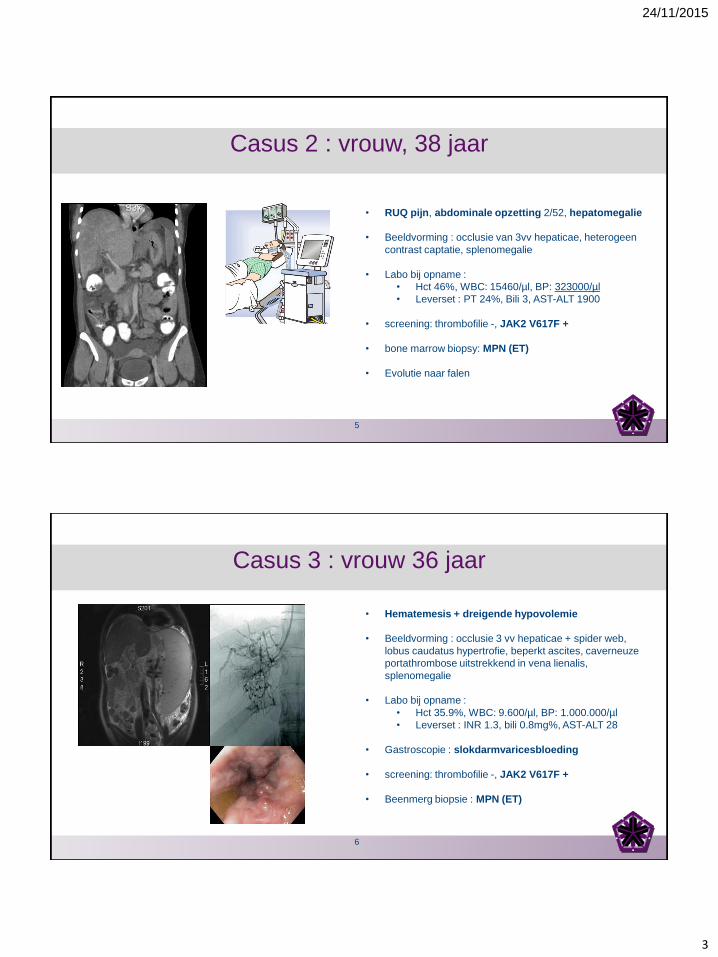
Casus 2 : vrouw, 38 jaar
• RUQ pijn, abdominale opzetting 2/52, hepatomegalie
• Beeldvorming : occlusie van 3vv hepaticae, heterogeen
contrast captatie, splenomegalie
• Labo bij opname :
• Hct 46%, WBC: 15460/µl, BP: 323000/µl
• Leverset : PT 24%, Bili 3, AST-ALT 1900
• screening: thrombofilie -, JAK2 V617F +
• bone marrow biopsy: MPN (ET)
• Evolutie naar falen
5
Casus 3 : vrouw 36 jaar
• Hematemesis + dreigende hypovolemie
• Beeldvorming : occlusie 3 vv hepaticae + spider web,
lobus caudatus hypertrofie, beperkt ascites, caverneuze
portathrombose uitstrekkend in vena lienalis,
splenomegalie
• Labo bij opname :
• Hct 35.9%, WBC: 9.600/µl, BP: 1.000.000/µl
• Leverset : INR 1.3, bili 0.8mg%, AST-ALT 28
• Gastroscopie : slokdarmvaricesbloeding
• screening: thrombofilie -, JAK2 V617F +
• Beenmerg biopsie : MPN (ET)
6
24/11/2015
4
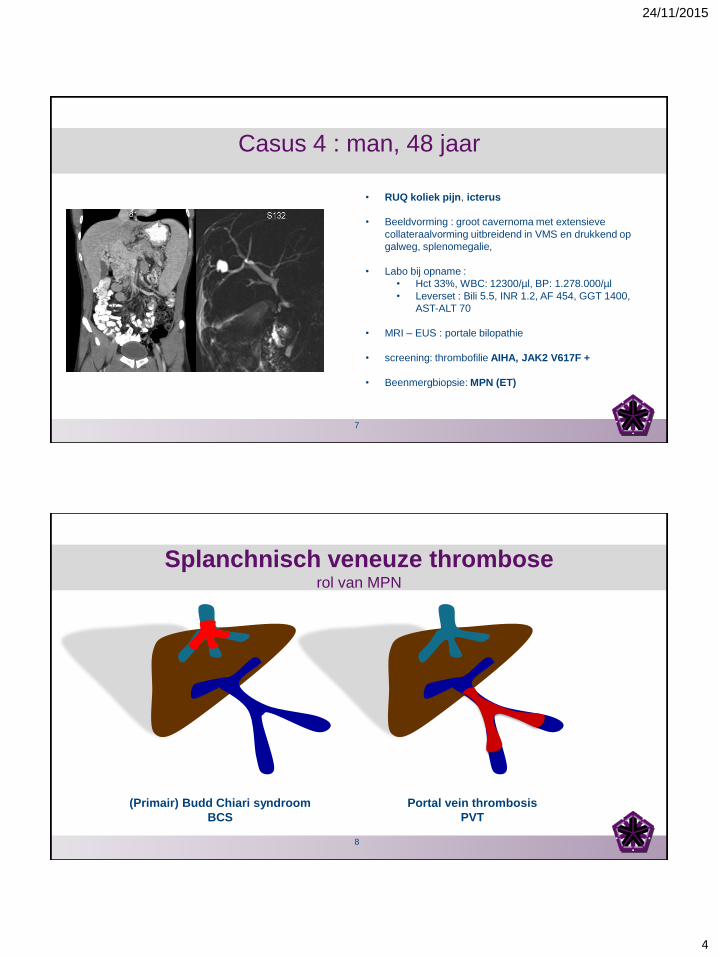
Casus 4 : man, 48 jaar
• RUQ koliek pijn, icterus
• Beeldvorming : groot cavernoma met extensieve
collateraalvorming uitbreidend in VMS en drukkend op
galweg, splenomegalie,
• Labo bij opname :
• Hct 33%, WBC: 12300/µl, BP: 1.278.000/µl
• Leverset : Bili 5.5, INR 1.2, AF 454, GGT 1400,
AST-ALT 70
• MRI – EUS : portale bilopathie
• screening: thrombofilie AIHA, JAK2 V617F +
• Beenmergbiopsie: MPN (ET)
7
Portal vein thrombosis
PVT
(Primair) Budd Chiari syndroom
BCS
Splanchnisch veneuze thromboserol van MPN
8
24/11/2015
5
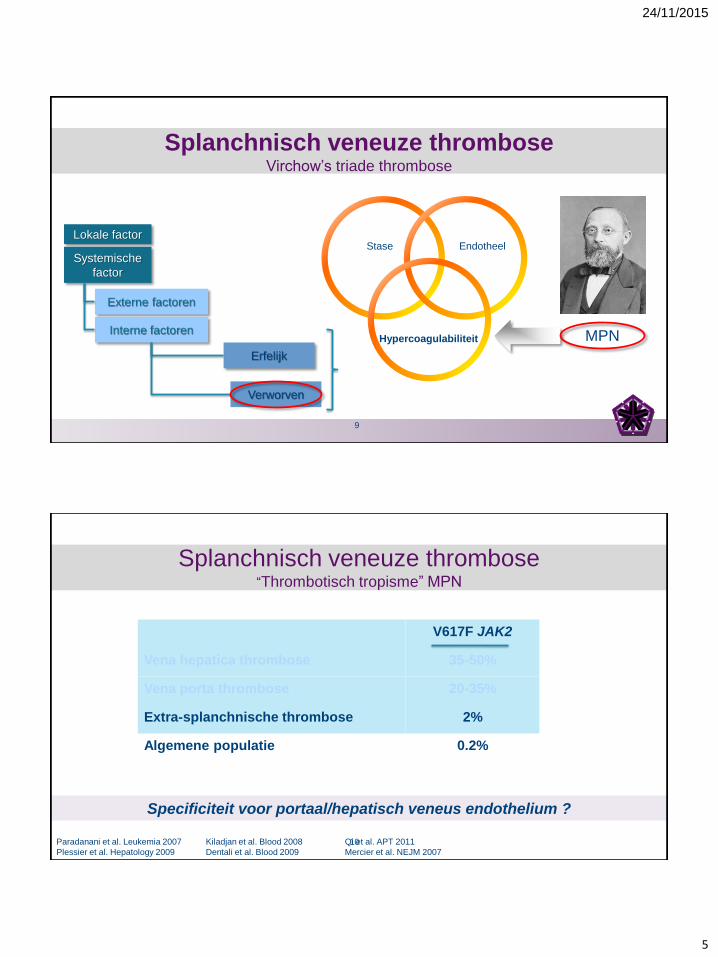
Stase Endotheel
Hypercoagulabiliteit
Splanchnisch veneuze thromboseVirchow’s triade thrombose
MPN
Lokale factor
Systemische
factor
Externe factoren
Interne factoren
Erfelijk
Verworven
9
Splanchnisch veneuze thrombose“Thrombotisch tropisme” MPN
V617F JAK2
Vena hepatica thrombose 35-50%
Vena porta thrombose 20-35%
Extra-splanchnische thrombose 2%
Algemene populatie 0.2%
Paradanani et al. Leukemia 2007
Plessier et al. Hepatology 2009
Kiladjan et al. Blood 2008
Dentali et al. Blood 2009
Qi et al. APT 2011
Mercier et al. NEJM 2007
Specificiteit voor portaal/hepatisch veneus endothelium ?
10
24/11/2015
6
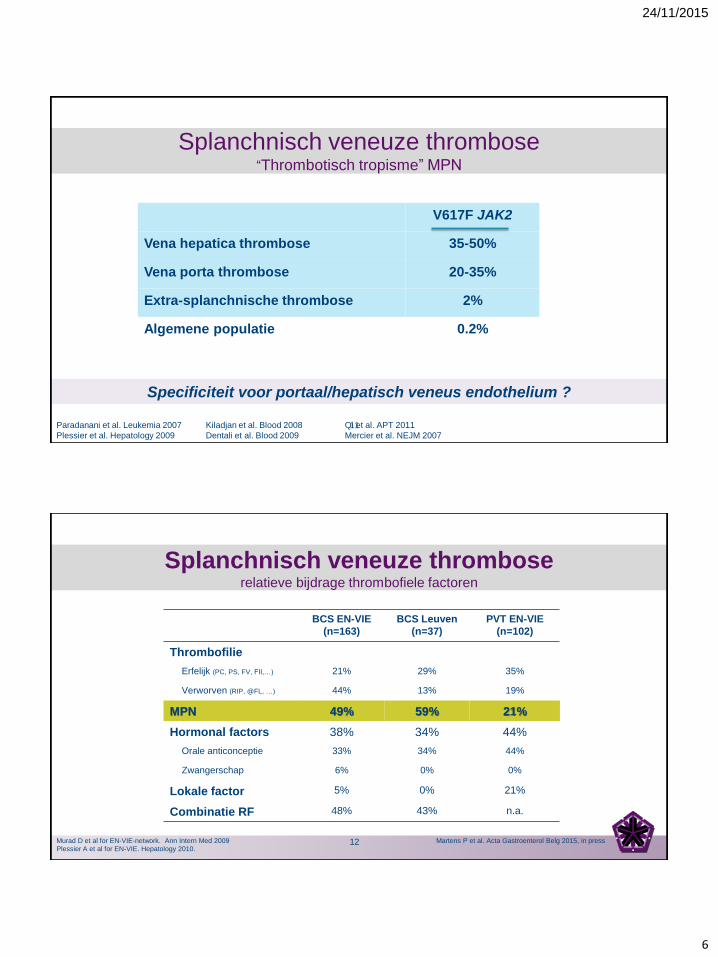
Splanchnisch veneuze thrombose“Thrombotisch tropisme” MPN
V617F JAK2
Vena hepatica thrombose 35-50%
Vena porta thrombose 20-35%
Extra-splanchnische thrombose 2%
Algemene populatie 0.2%
Paradanani et al. Leukemia 2007
Plessier et al. Hepatology 2009
Kiladjan et al. Blood 2008
Dentali et al. Blood 2009
Qi et al. APT 2011
Mercier et al. NEJM 2007
Specificiteit voor portaal/hepatisch veneus endothelium ?
11
Splanchnisch veneuze thromboserelatieve bijdrage thrombofiele factoren
Murad D et al for EN-VIE-network. Ann Intern Med 2009
Plessier A et al for EN-VIE. Hepatology 2010.
BCS EN-VIE
(n=163)
BCS Leuven
(n=37)
PVT EN-VIE
(n=102)
Thrombofilie
Erfelijk (PC, PS, FV, FII,…) 21% 29% 35%
Verworven (RIP, @FL, …) 44% 13% 19%
MPN 49% 59% 21%
Hormonal factors 38% 34% 44%
Orale anticonceptie 33% 34% 44%
Zwangerschap 6% 0% 0%
Lokale factor 5% 0% 21%
Combinatie RF 48% 43% n.a.
Martens P et al. Acta Gastroenterol Belg 2015, in press12
24/11/2015
7
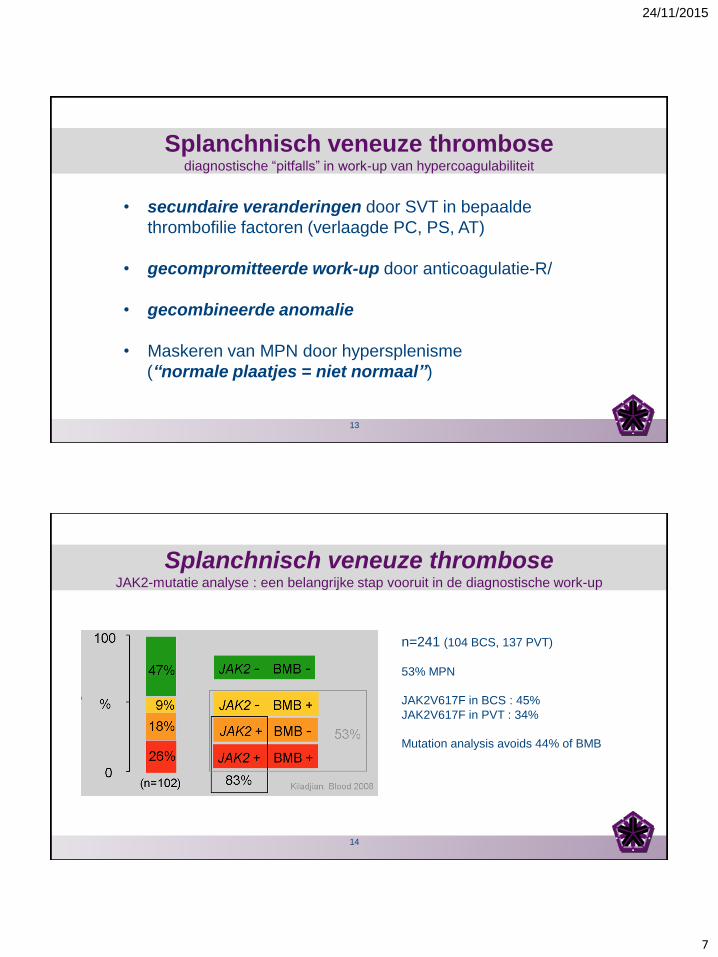
Splanchnisch veneuze thrombosediagnostische “pitfalls” in work-up van hypercoagulabiliteit
• secundaire veranderingen door SVT in bepaalde
thrombofilie factoren (verlaagde PC, PS, AT)
• gecompromitteerde work-up door anticoagulatie-R/
• gecombineerde anomalie
• Maskeren van MPN door hypersplenisme
(“normale plaatjes = niet normaal”)
13
Splanchnisch veneuze thrombose JAK2-mutatie analyse : een belangrijke stap vooruit in de diagnostische work-up
n=241 (104 BCS, 137 PVT)
53% MPN
JAK2V617F in BCS : 45%
JAK2V617F in PVT : 34%
Mutation analysis avoids 44% of BMB
14
24/11/2015
8
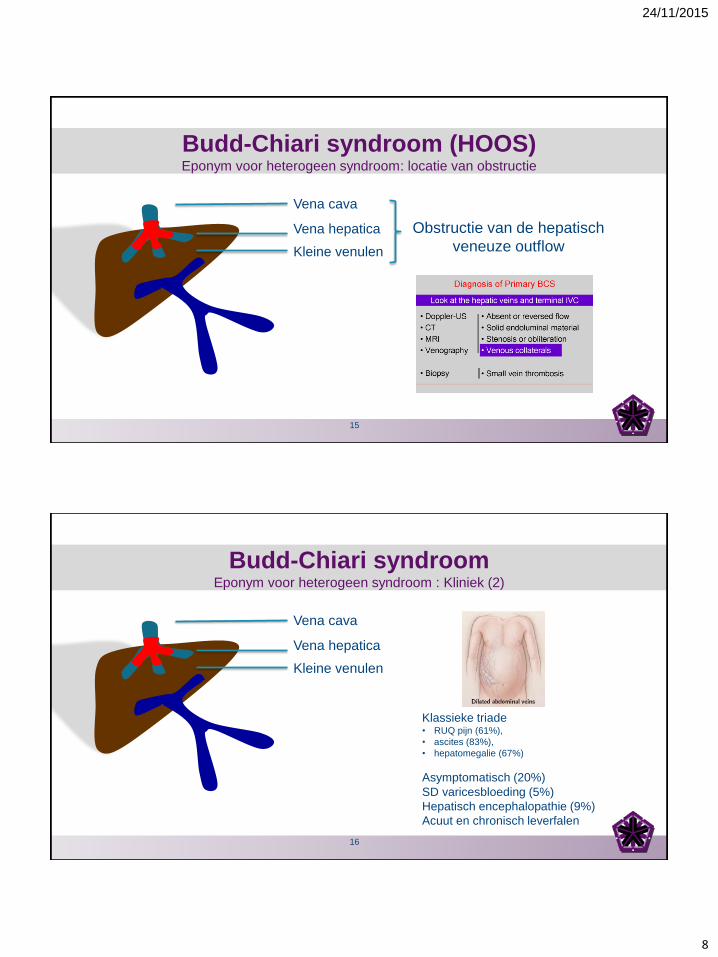
Budd-Chiari syndroom (HOOS)Eponym voor heterogeen syndroom: locatie van obstructie
Vena cava
Vena hepatica
Kleine venulen
Obstructie van de hepatisch
veneuze outflow
15
Vena cava
Vena hepatica
Kleine venulen
Klassieke triade• RUQ pijn (61%),
• ascites (83%),
• hepatomegalie (67%)
Asymptomatisch (20%)
SD varicesbloeding (5%)
Hepatisch encephalopathie (9%)
Acuut en chronisch leverfalen
Budd-Chiari syndroomEponym voor heterogeen syndroom : Kliniek (2)
16
24/11/2015
9
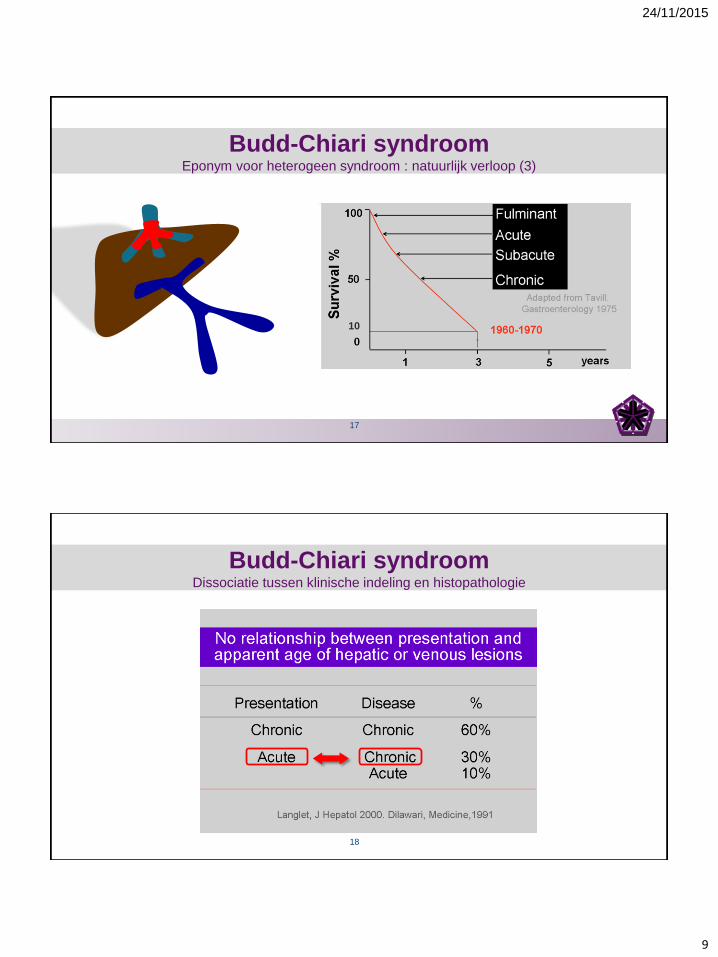
Budd-Chiari syndroomEponym voor heterogeen syndroom : natuurlijk verloop (3)
10
17
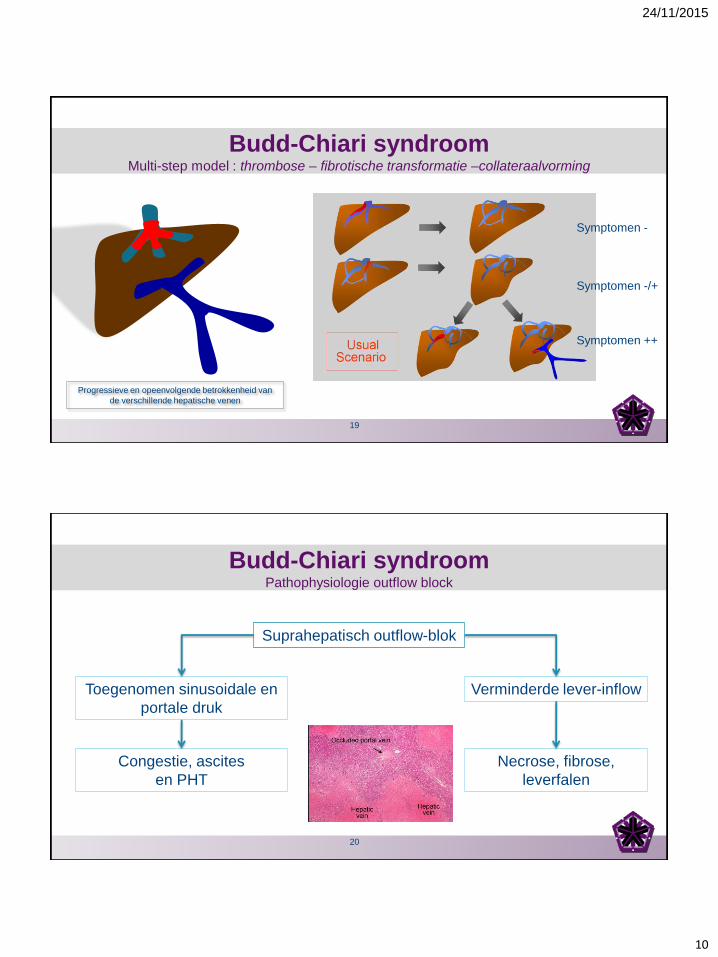
Budd-Chiari syndroomDissociatie tussen klinische indeling en histopathologie
18
24/11/2015
10
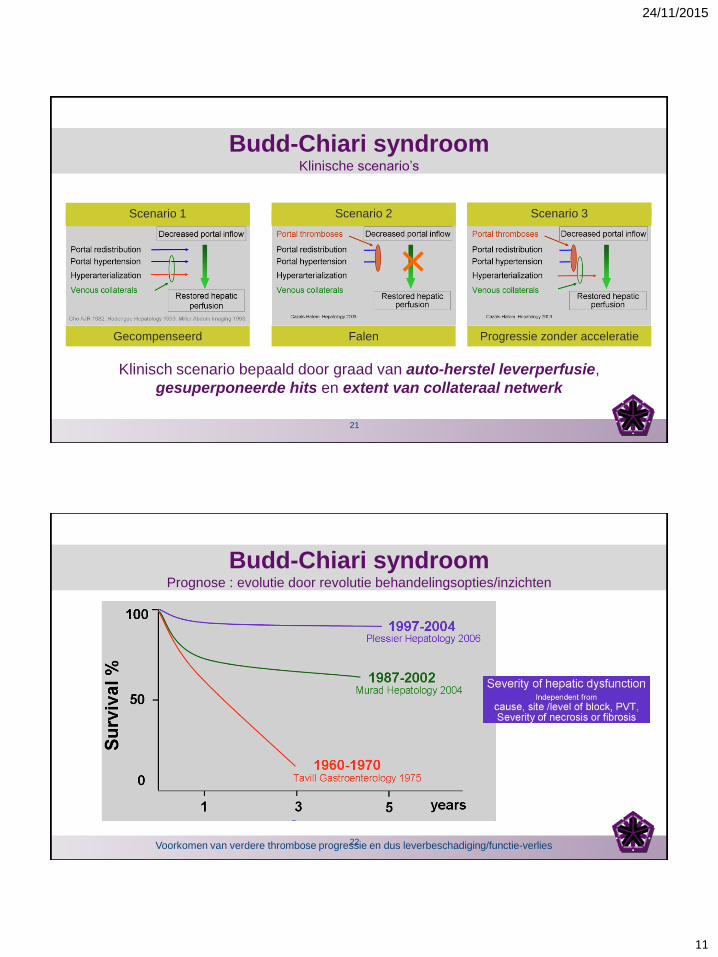
Budd-Chiari syndroomMulti-step model : thrombose – fibrotische transformatie –collateraalvorming
Symptomen -
Symptomen -/+
Symptomen ++
Progressieve en opeenvolgende betrokkenheid van
de verschillende hepatische venen
19
Budd-Chiari syndroomPathophysiologie outflow block
Suprahepatisch outflow-blok
Toegenomen sinusoidale en
portale druk
Congestie, ascites
en PHT
Verminderde lever-inflow
Necrose, fibrose,
leverfalen
20
24/11/2015
11
Budd-Chiari syndroomKlinische scenario’s
Klinisch scenario bepaald door graad van auto-herstel leverperfusie,
gesuperponeerde hits en extent van collateraal netwerk
Scenario 1 Scenario 2 Scenario 3
Gecompenseerd Falen Progressie zonder acceleratie
21
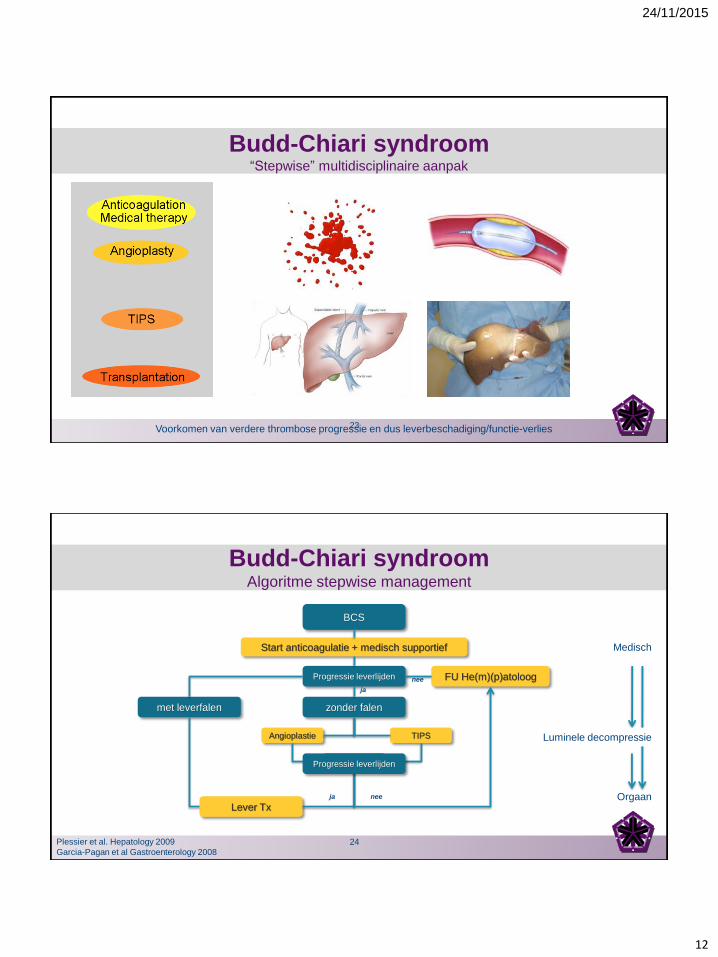
Budd-Chiari syndroomPrognose : evolutie door revolutie behandelingsopties/inzichten
Voorkomen van verdere thrombose progressie en dus leverbeschadiging/functie-verlies22
24/11/2015
12
Budd-Chiari syndroom“Stepwise” multidisciplinaire aanpak
Voorkomen van verdere thrombose progressie en dus leverbeschadiging/functie-verlies23
Budd-Chiari syndroomAlgoritme stepwise management
BCS
Progressie leverlijden
Start anticoagulatie + medisch supportief
FU He(m)(p)atoloog
met leverfalen
Lever Tx
zonder falen
Angioplastie TIPS
Progressie
ja
nee
ja nee
Progressie leverlijden
Medisch
Orgaan
Plessier et al. Hepatology 2009
Garcia-Pagan et al Gastroenterology 2008
Luminele decompressie
24
24/11/2015
13
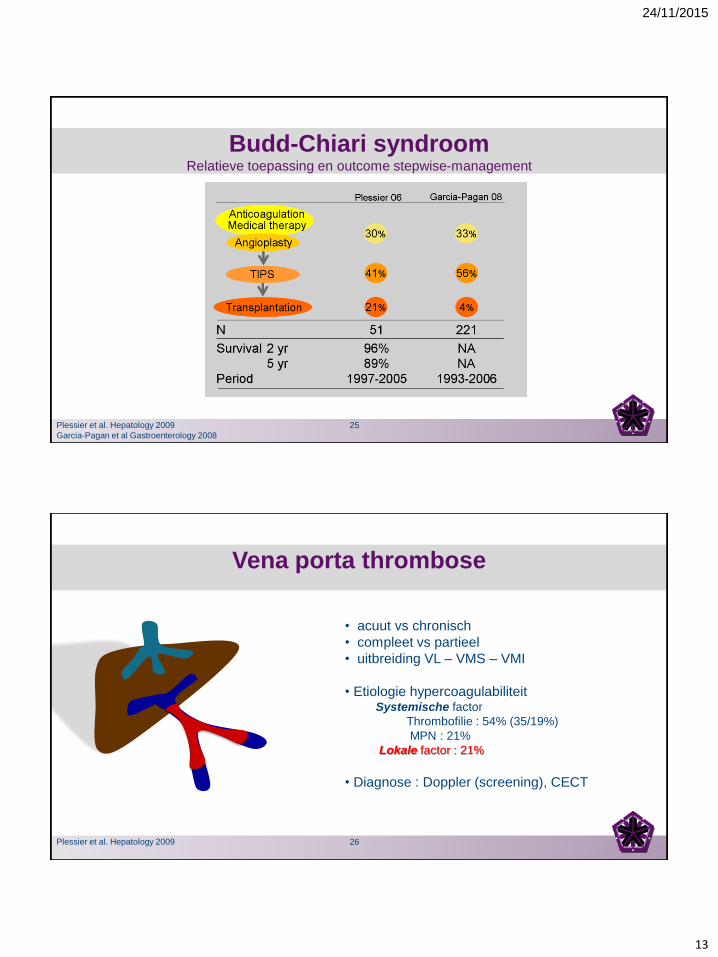
Budd-Chiari syndroomRelatieve toepassing en outcome stepwise-management
Plessier et al. Hepatology 2009
Garcia-Pagan et al Gastroenterology 2008
25
Vena porta thrombose
• acuut vs chronisch
• compleet vs partieel
• uitbreiding VL – VMS – VMI
• Etiologie hypercoagulabiliteitSystemische factor
Thrombofilie : 54% (35/19%)
MPN : 21%
Lokale factor : 21%
• Diagnose : Doppler (screening), CECT
Plessier et al. Hepatology 2009 26
24/11/2015
14
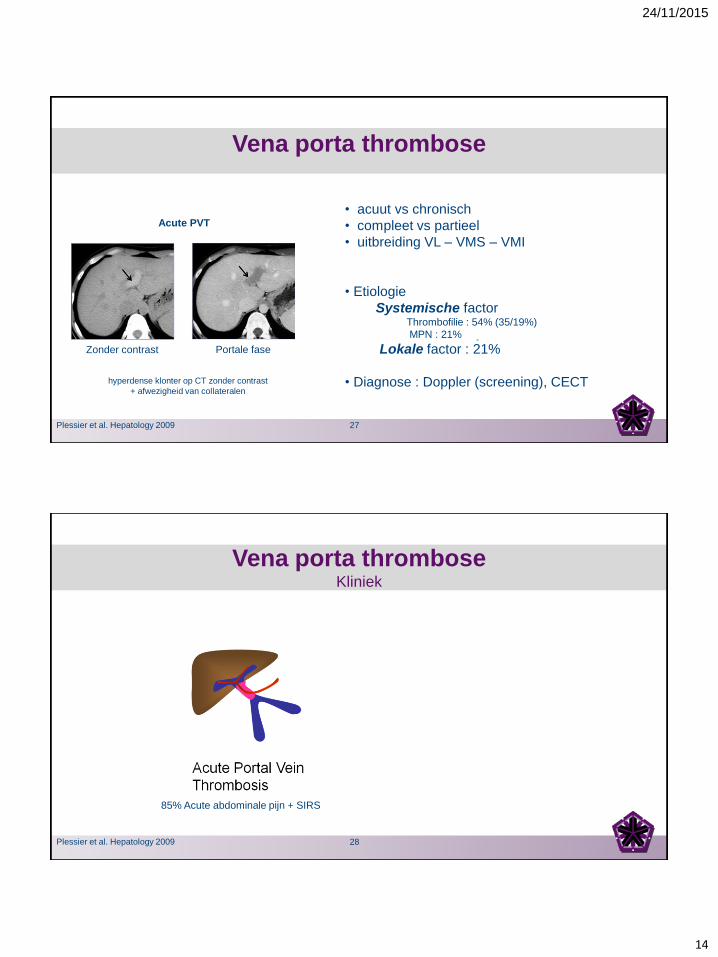
Vena porta thrombose
• acuut vs chronisch
• compleet vs partieel
• uitbreiding VL – VMS – VMI
• Etiologie
Systemische factorThrombofilie : 54% (35/19%)
MPN : 21%
Lokale factor : 21%
• Diagnose : Doppler (screening), CECT
Zonder contrast Portale fase
Acute PVT
Plessier et al. Hepatology 2009
hyperdense klonter op CT zonder contrast
+ afwezigheid van collateralen
27
Vena porta thromboseKliniek
85% Acute abdominale pijn + SIRS
Plessier et al. Hepatology 2009 28
24/11/2015
15
Vena porta thromboseKliniek
Plessier et al. Hepatology 2009
Incidentie 2-20%
Acuut abdomen
MOF - RBPA
29
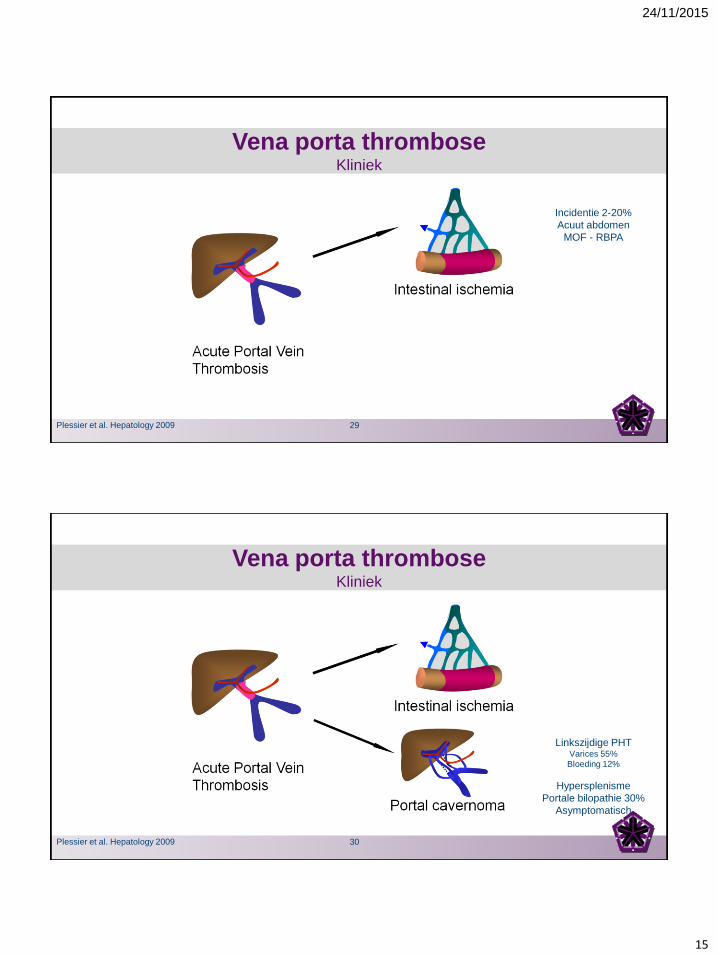
Vena porta thromboseKliniek
Plessier et al. Hepatology 2009
Linkszijdige PHT Varices 55%
Bloeding 12%
Hypersplenisme
Portale bilopathie 30%
Asymptomatisch
30
24/11/2015
16
ACUTE vena porta thromboseBeleid
Plessier et al. Hepatology 2010
1. Preventie van uitbreiding thrombose
(en dus darm-ischemie)
1. Bekomen van recanalisatie
Therapie-doel
Levenslang zo protrombotische conditie
31
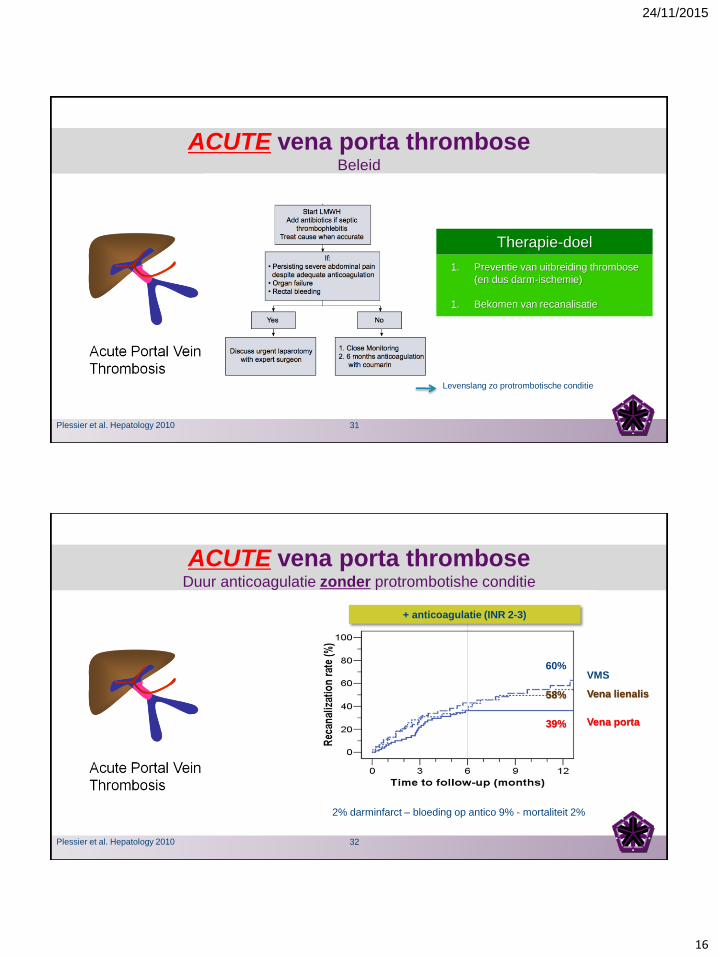
ACUTE vena porta thromboseDuur anticoagulatie zonder protrombotishe conditie
Plessier et al. Hepatology 2010
Vena porta
Vena lienalis
VMS
+ anticoagulatie (INR 2-3)
60%
58%
39%
2% darminfarct – bloeding op antico 9% - mortaliteit 2%
32
24/11/2015
17
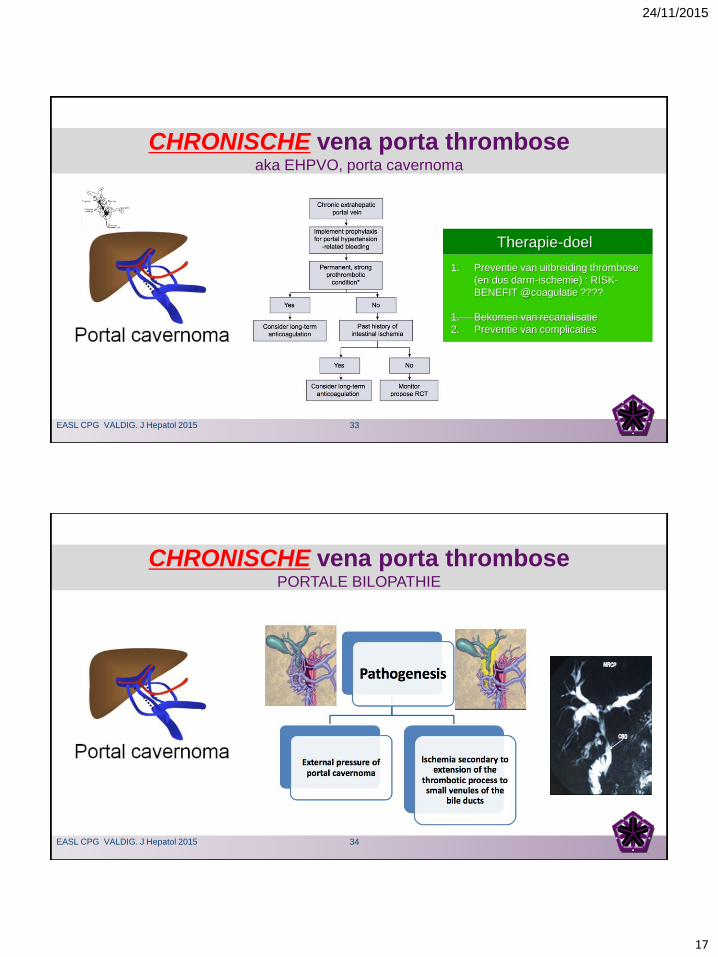
CHRONISCHE vena porta thromboseaka EHPVO, porta cavernoma
1. Preventie van uitbreiding thrombose
(en dus darm-ischemie) : RISK-
BENEFIT @coagulatie ????
1. Bekomen van recanalisatie
2. Preventie van complicaties
Therapie-doel
EASL CPG VALDIG. J Hepatol 2015 33
CHRONISCHE vena porta thrombosePORTALE BILOPATHIE
EASL CPG VALDIG. J Hepatol 2015 34
24/11/2015
18
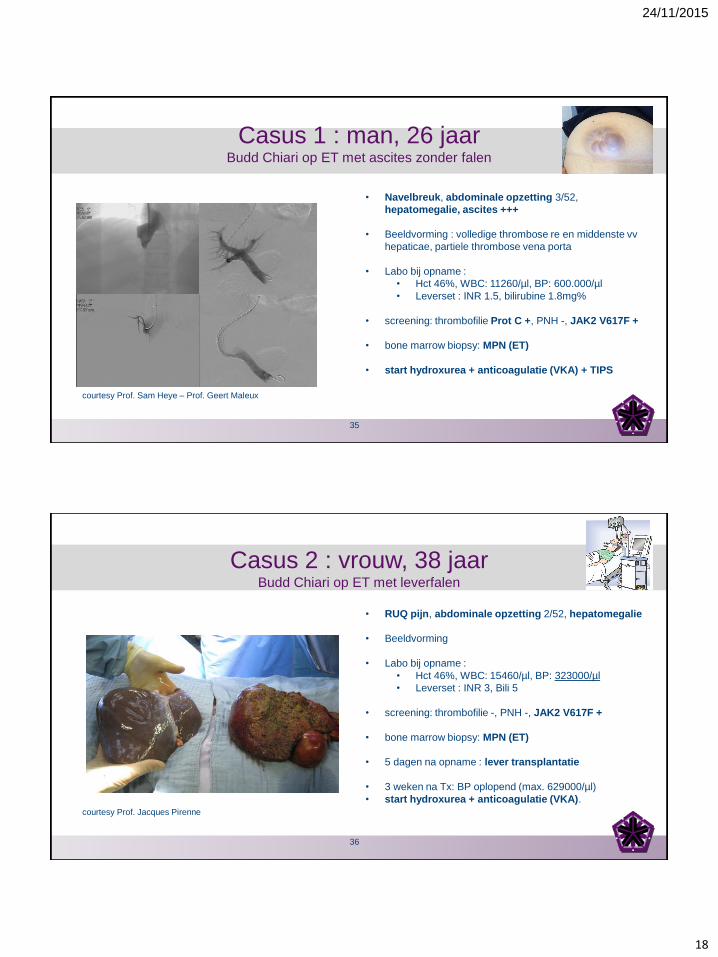
Casus 1 : man, 26 jaarBudd Chiari op ET met ascites zonder falen
• Navelbreuk, abdominale opzetting 3/52,
hepatomegalie, ascites +++
• Beeldvorming : volledige thrombose re en middenste vv
hepaticae, partiele thrombose vena porta
• Labo bij opname :
• Hct 46%, WBC: 11260/µl, BP: 600.000/µl
• Leverset : INR 1.5, bilirubine 1.8mg%
• screening: thrombofilie Prot C +, PNH -, JAK2 V617F +
• bone marrow biopsy: MPN (ET)
• start hydroxurea + anticoagulatie (VKA) + TIPS
courtesy Prof. Sam Heye – Prof. Geert Maleux
35
Casus 2 : vrouw, 38 jaarBudd Chiari op ET met leverfalen
• RUQ pijn, abdominale opzetting 2/52, hepatomegalie
• Beeldvorming
• Labo bij opname :
• Hct 46%, WBC: 15460/µl, BP: 323000/µl
• Leverset : INR 3, Bili 5
• screening: thrombofilie -, PNH -, JAK2 V617F +
• bone marrow biopsy: MPN (ET)
• 5 dagen na opname : lever transplantatie
• 3 weken na Tx: BP oplopend (max. 629000/µl)
• start hydroxurea + anticoagulatie (VKA).
courtesy Prof. Jacques Pirenne
36
24/11/2015
19
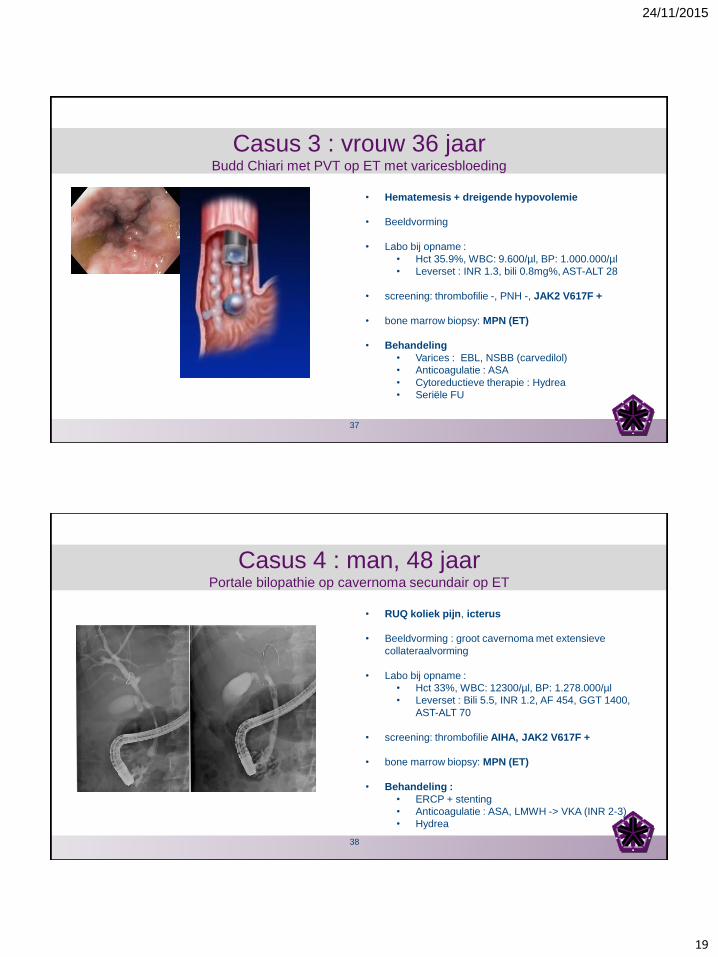
Casus 3 : vrouw 36 jaarBudd Chiari met PVT op ET met varicesbloeding
• Hematemesis + dreigende hypovolemie
• Beeldvorming
• Labo bij opname :
• Hct 35.9%, WBC: 9.600/µl, BP: 1.000.000/µl
• Leverset : INR 1.3, bili 0.8mg%, AST-ALT 28
• screening: thrombofilie -, PNH -, JAK2 V617F +
• bone marrow biopsy: MPN (ET)
• Behandeling
• Varices : EBL, NSBB (carvedilol)
• Anticoagulatie : ASA
• Cytoreductieve therapie : Hydrea
• Seriële FU
37
Casus 4 : man, 48 jaarPortale bilopathie op cavernoma secundair op ET
• RUQ koliek pijn, icterus
• Beeldvorming : groot cavernoma met extensieve
collateraalvorming
• Labo bij opname :
• Hct 33%, WBC: 12300/µl, BP: 1.278.000/µl
• Leverset : Bili 5.5, INR 1.2, AF 454, GGT 1400,
AST-ALT 70
• screening: thrombofilie AIHA, JAK2 V617F +
• bone marrow biopsy: MPN (ET)
• Behandeling :
• ERCP + stenting
• Anticoagulatie : ASA, LMWH -> VKA (INR 2-3)
• Hydrea
38
24/11/2015
20
• “blood disease”
• heterogeen qua kliniek, locatie en natuurlijk verloop
• gerelateerd in 20-50% tot MPN
• PHT complicaties en graad van leverinsufficiëntie
• Anticoagulatie altijd te overwegen + step-up beleid
CONCLUSIE
SPLANCHNISCH VENEUZE THROMBOSE
39
40
24/11/2015
21
41












