
Geldzaken in de praktijk Gerjoke Wilmink Rob Goedhart 20 april 2011.

Behandeling en nieuwste ontwikkelingen pancreascarcinoom
Hanneke Wilmink
Internist oncoloog, Amsterdam UMCGE masterclass 21-09-2018
Casus; heer O. 62 jaar
• Presentatie HA met bovenbuiksklachten
• VG: COPD
• Uiteindelijk: CTscan
• Pancreas corpus tumor met diffuse leverafwijkingen
• PA: adenocarcinoom
• Wat te doen?
• Behandelmogelijkheden?
• Winst chemotherapie?
• Verschillen tussen behandelmogelijkheden?
Original Article
FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer
Thierry Conroy, M.D., Françoise Desseigne, M.D., Marc Ychou, M.D., Ph.D., Olivier Bouché, M.D., Ph.D., Rosine Guimbaud, M.D., Ph.D., Yves Bécouarn, M.D., Antoine
Adenis, M.D., Ph.D., Jean-Luc Raoul, M.D., Ph.D., Sophie Gourgou-Bourgade, M.Sc., Christellede la Fouchardière, M.D., Jaafar Bennouna, M.D., Ph.D., Jean-Baptiste Bachet, M.D., Faiza
Khemissa-Akouz, M.D., Denis Péré-Vergé, M.D., Catherine Delbaldo, M.D., Eric Assenat, M.D., Ph.D., Bruno Chauffert, M.D., Ph.D., Pierre Michel, M.D., Ph.D., Christine Montoto-
Grillot, M.Chem., Michel Ducreux, M.D., Ph.D., for the Groupe Tumeurs Digestives of Unicancer and the PRODIGE Intergroup
N Engl J MedVolume 364(19):1817-1825
May 12, 2011


Discussie
• Toegenomen toxiciteit:
– weegt dat op tegen winst in niet curatieve setting?
– weten niets van graad 1-2 toxiciteit
• Representatieve patiënten populatie?
– WHO 0/1
– 60% corpus/ staart tumoren

Original Article
Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine
Daniel D. Von Hoff, M.D., Thomas Ervin, M.D., Francis P. Arena, M.D., E. Gabriela Chiorean, M.D., Jeffrey Infante, M.D., Malcolm Moore, M.D., Thomas Seay, M.D., Sergei A. Tjulandin, M.D., Wen Wee Ma, M.D.,
Mansoor N. Saleh, M.D., Marion Harris, M.D., Michele Reni, M.D., Scot Dowden, M.D., Daniel Laheru, M.D., Nathan Bahary, M.D., Ramesh K. Ramanathan, M.D., Josep Tabernero, M.D., Manuel Hidalgo, M.D., Ph.D.,
David Goldstein, M.D., Eric Van Cutsem, M.D., Xinyu Wei, Ph.D., Jose Iglesias, M.D., and Markus F. Renschler, M.D.
N Engl J MedVolume 369(18):1691-1703
October 31, 2013
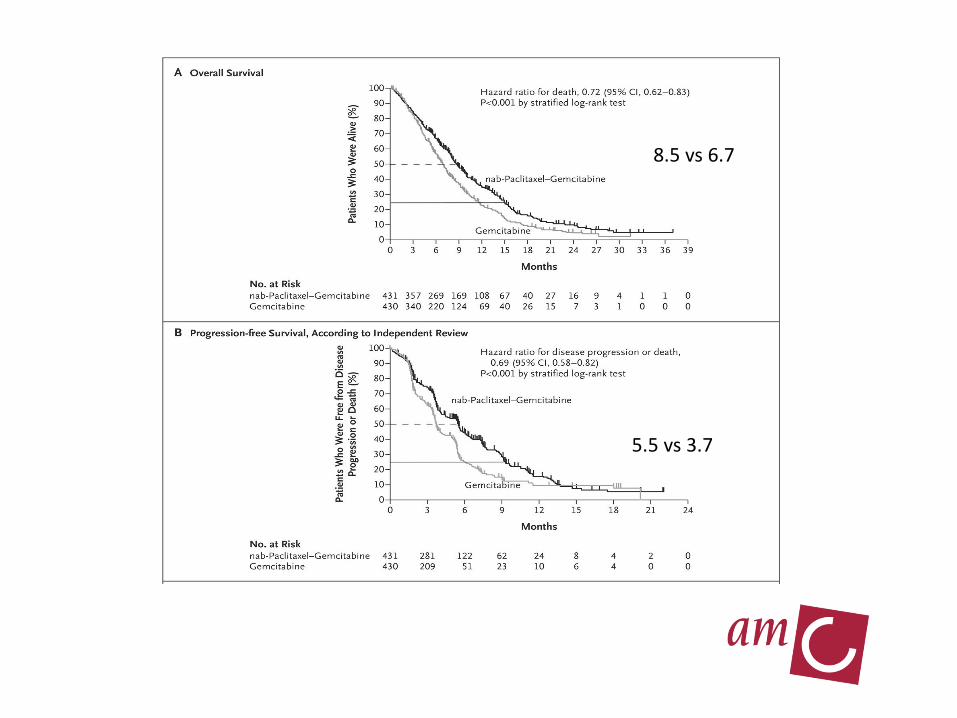
8.5 vs 6.7
5.5 vs 3.7

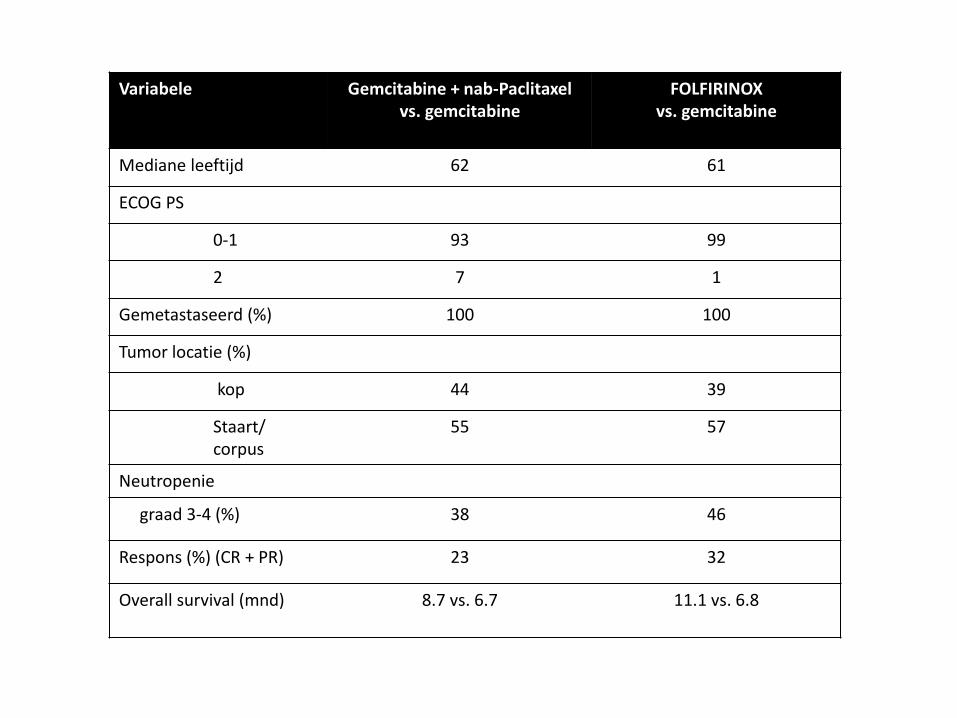
Variabele Gemcitabine + nab-Paclitaxelvs. gemcitabine
FOLFIRINOXvs. gemcitabine
Mediane leeftijd 62 61
ECOG PS
0-1 93 99
2 7 1
Gemetastaseerd (%) 100 100
Tumor locatie (%)
kop 44 39
Staart/ corpus
55 57
Neutropenie
graad 3-4 (%) 38 46
Respons (%) (CR + PR) 23 32
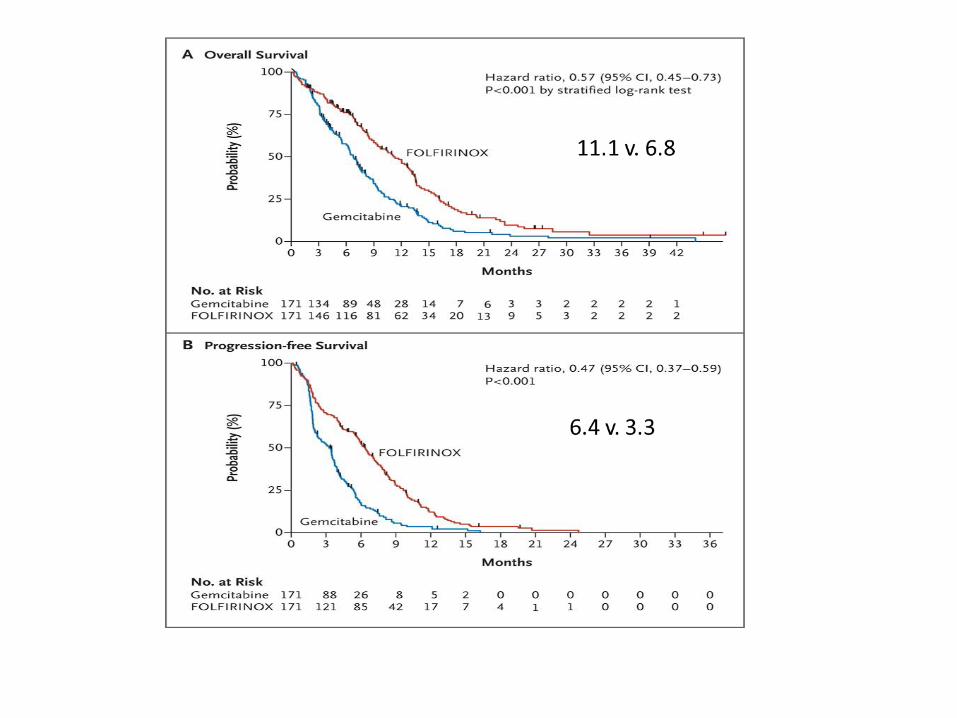
Overall survival (mnd) 8.7 vs. 6.7 11.1 vs. 6.8
• Er is vooruitgang geboekt afgelopen jaren
• 2 regimens overlevingsvoordeel t.o.v. gemcitabine
• 1-jaars overleving van 2% naar 40%
• Hoe nu vertalen/ ervaringen praktijk?
• Patiënten met gemetastaseerde ziekte

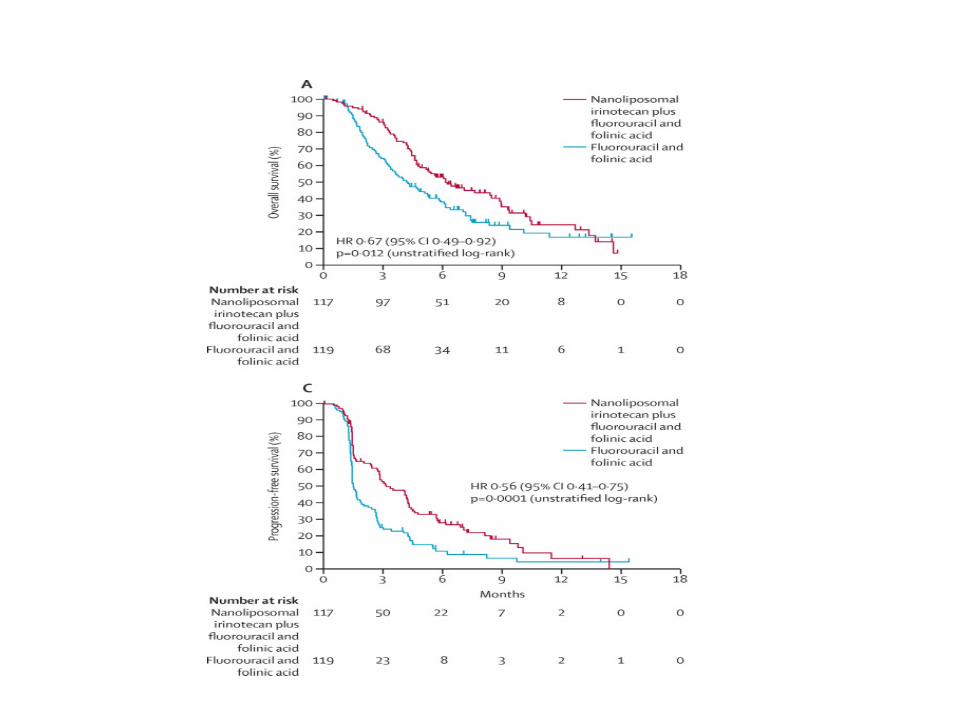
Lancet 2016; 387: 545–57

Hoe nu verder?
• Targeted therapie voor genetische subgroepen
• Immunotherapie
• Depletie stroma
• Specifieke inhibitors van belangrijke signaaltransductie routes
• ??
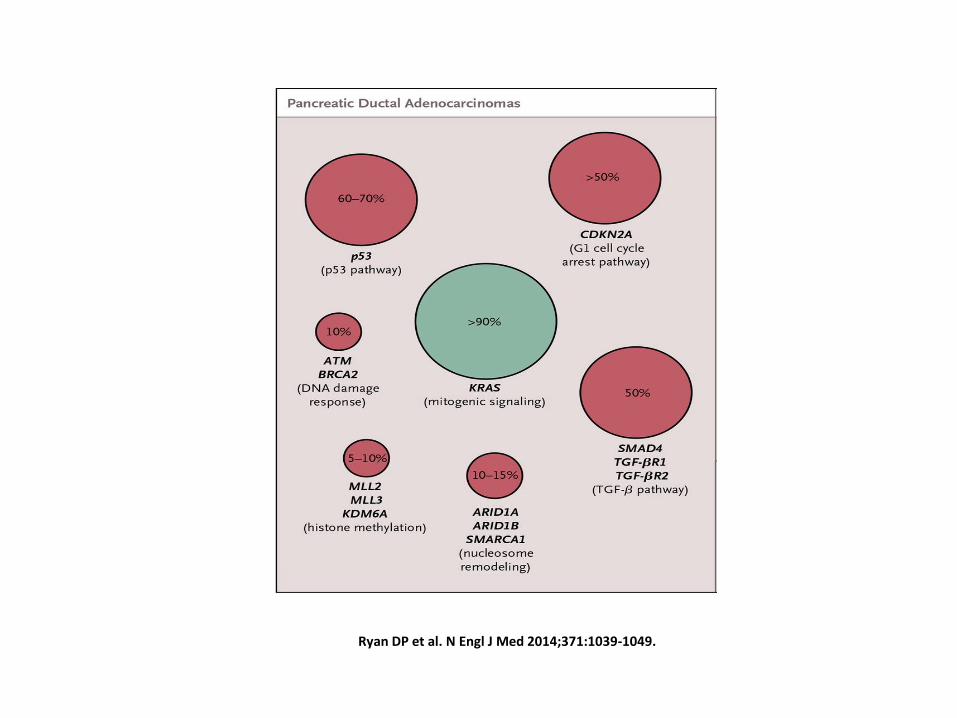
Approximate Frequencies of Mutations in Patients with Pancreatic Ductal Adenocarcinomas and Mucinous Neoplasms.
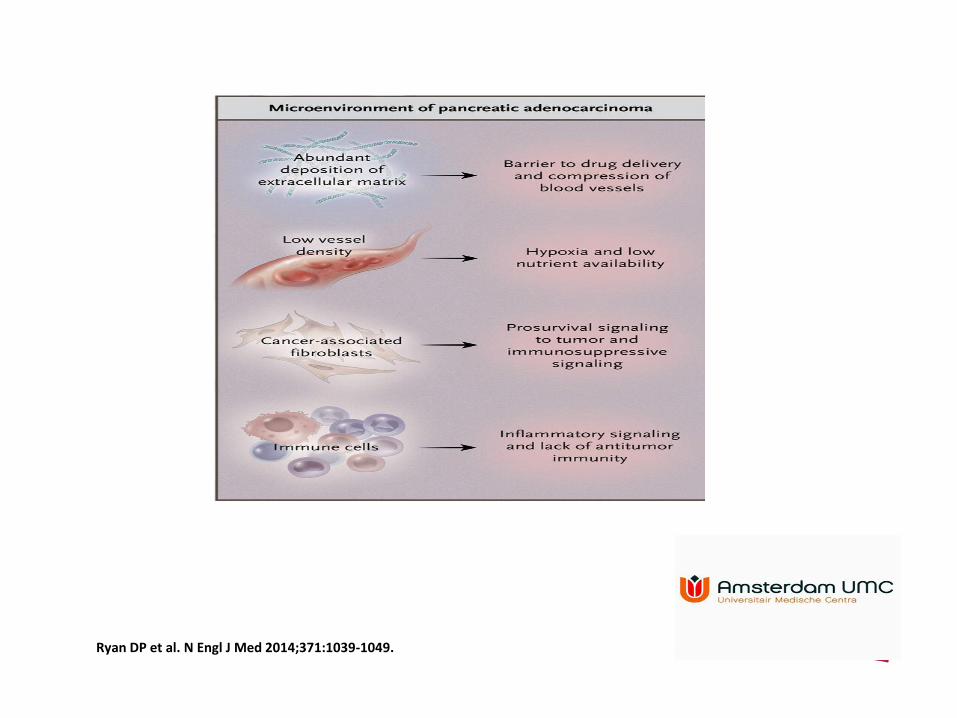
Ryan DP et al. N Engl J Med 2014;371:1039-1049.

Identificatie subgroepen

Single-center, single platform gene expression subtyping AMC

Approximate Frequencies of Mutations in Patients with Pancreatic Ductal Adenocarcinomas and Mucinous Neoplasms.
Ryan DP et al. N Engl J Med 2014;371:1039-1049.
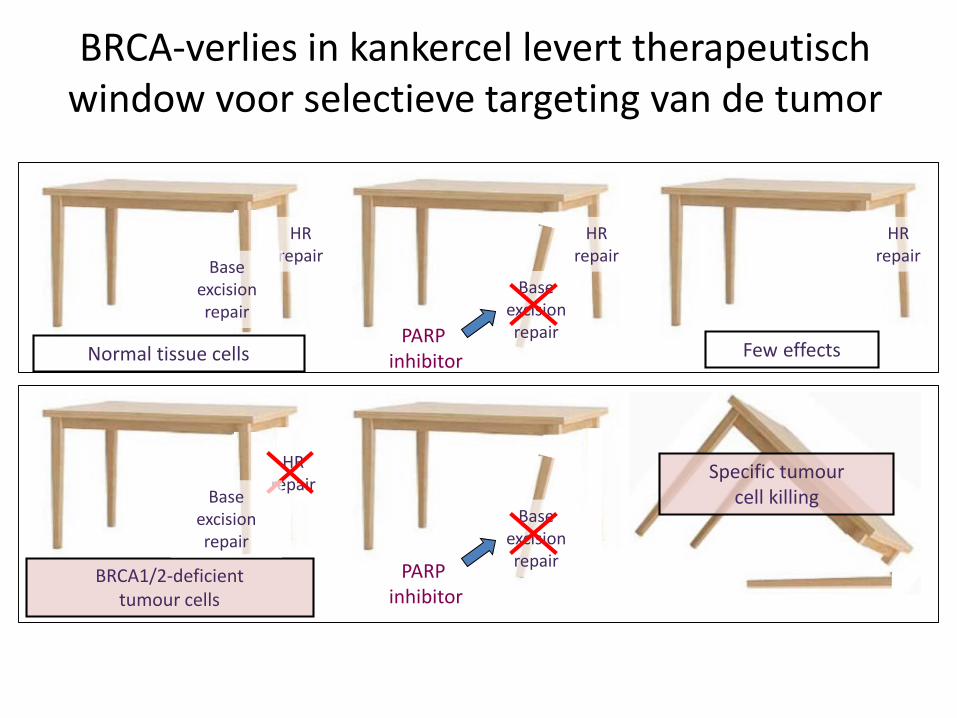
BRCA-verlies in kankercel levert therapeutisch window voor selectieve targeting van de tumor
HR repair
Base excision repair
HR repair
HR repair
Base excision repairPARP
inhibitor
Base excision repair
PARPinhibitor
HR repair
Normal tissue cells
BRCA1/2-deficient tumour cells
Few effects
Specific tumour cell killingBase
excision repair

POLO studie
Patients with:
metastatic gBRCAm
pancreatic cancer:
1-On a 1st line Rx
platinum regimen
2-Have not
progressed at time
of randomization
3- After at least 16
weeks of Rx with a
Platinum but need
not still be on plat
Olaparib 300
mg bid tablet
Placebo
3:2
Progress
by
RECIST:
Resume
Chemo
Study is double blindedSCREEN
FOR
gBRCA
RANDOMIZE
Progress by
local
standard:Treatment
according to local standard
N=145
Ryan DP et al. N Engl J Med 2014;371:1039-1049.



Tumor HA as a Prognostic Biomarker: Accumulation Is Associated With Decreased Survival in Pancreas Cancer
Whatcott et al: Clin Cancer Res 2015, 21:3561-3568. HA staining by HABP. Scoring algorithm assessed percent staining and intensity
Retrospective Evaluation of Primary, Resectable Pancreatic Cancer Tissue for Survival by Tumor HA Level (N = 50)
10896847260483624
Time (months)
Pe
rce
nt
Surv
ival
120
0
10
20
30
40
50
60
70
80
90
100
Low HAHigh HA
HA-Low Median Survival: 24.3 months
HA-High Median Survival: 9.3 months
HR 2.6
p=0.037
Sunil R. Hingorani1, Andrea J. Bullock2, Tara E. Seery3, Lei Zheng4, Darren S. Sigal5, Paul S. Ritch6, Fadi Braiteh7, Mark M. Zalupski8, Nathan Bahary9, William P. Harris10, Jie Pu11, Carrie Aldrich11, Sihem Khelifa11, Wilson Wu12, Dimitrios Chondros12, Ping Jiang12, Andrew Hendifar13
1Fred Hutchinson Cancer Research Center, Seattle, WA, USA; 2Beth Israel Deaconess Medical Center, Boston, MA, USA; 3University of California – Irvine, Irvine,CA, USA; 4The Johns Hopkins University Hospital, Baltimore, MD, USA; 5Scripps Cancer Center, La Jolla, CA, USA; 6Froedtert Hospital and Medical College ofWisconsin, Milwaukee, WI, USA; 7Comprehensive Cancer Centers of Nevada, Las Vegas, NV, USA; 8University of Michigan, Ann Arbor, MI, USA; 9University ofPittsburgh Medical Center Cancer Pavilion, Pittsburgh, PA, USA; 10University of Washington, School of Medicine, Seattle, WA, USA; 11Ventana Medical Systems,Inc., Tucson, AZ, USA; 12Halozyme Therapeutics, San Diego, CA, USA; 13Samuel Oschin Cancer Center, Cedars-Sinai Medical Center, Los Angeles, CA, USA
HALO-202 PEGPH20 Improves PFS in Patients With Metastatic Pancreatic Ductal Adenocarcinoma: A Randomized Phase 2 Study in Combination With nab-Paclitaxel/Gemcitabine

Primary Efficacy Endpoint: PFS
PAG (n = 166)
AG(n = 113)
Events 102 67
Median PFS, mo 6.0 5.3
HR (95% CI) 0.73 (0.53-0.99)
P value 0.045
100
90
80
70
60
50
40
30
20
10
0 2 4 6 8 10Study Duration (months)
12 14 16 18
166113
PAGAG
At Risk, n
10162
7942
5526
369
224
92
70
10
00
0
PAGAG
K-M
Est
imat
e o
fP
rogr
ess
ion
-Fre
e S
urv
ival
(%
)
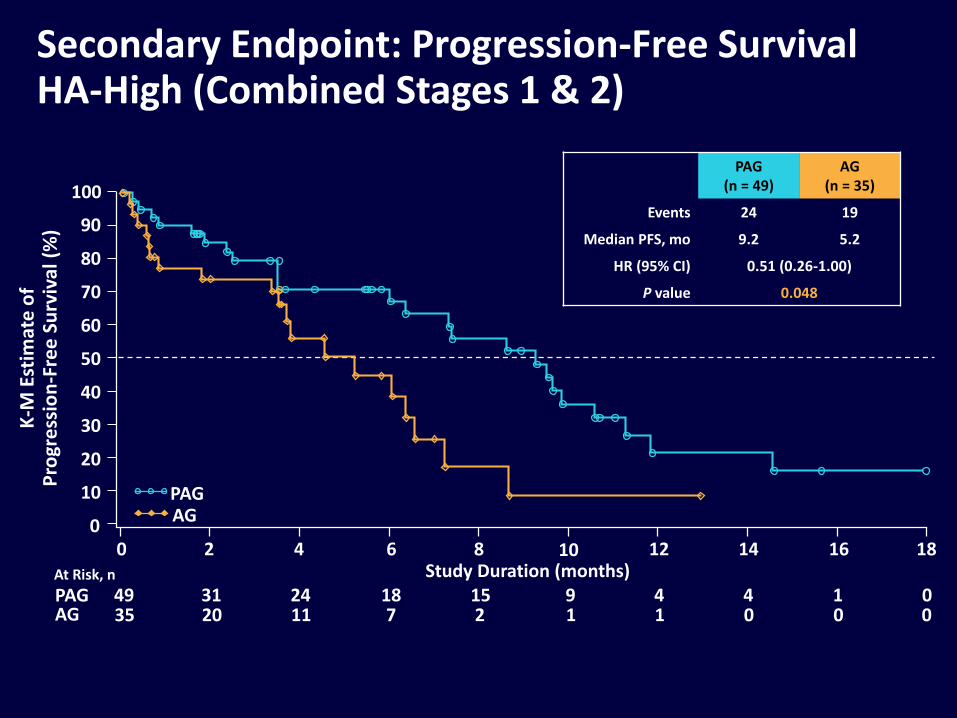
Secondary Endpoint: Progression-Free Survival HA-High (Combined Stages 1 & 2)
PAG(n = 49)
AG(n = 35)
Events 24 19
Median PFS, mo 9.2 5.2
HR (95% CI) 0.51 (0.26-1.00)
P value 0.048
18161412864
K-M
Est
imat
e o
fP
rogr
ess
ion
-Fre
e S
urv
ival
(%
)
20
0001127112035014491518243149PAG
AG
At Risk, n
100
90
80
70
60
50
40
30
20
10
0
PAGAG
10Study Duration (months)
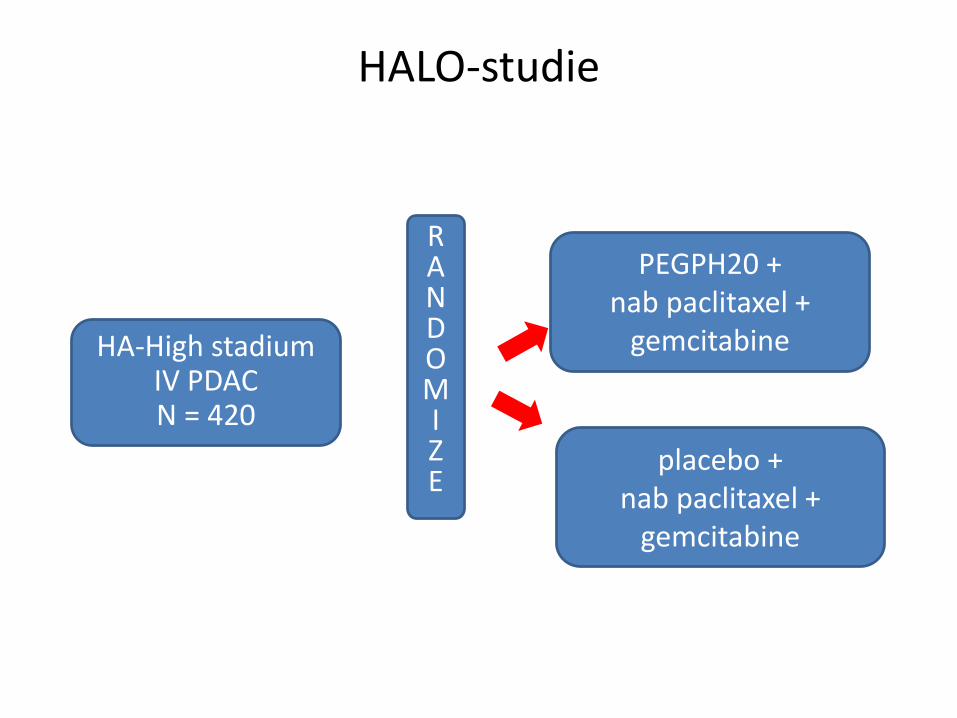
placebo +nab paclitaxel +
gemcitabine
HALO-studieMPACT Trial
HA-High stadiumIV PDACN = 420
PEGPH20 + nab paclitaxel +
gemcitabine
RANDOMIZE

Immune cell infiltrates during pancreatic tumor progression

Barriers voor imuuntherapie
• Lage mutational load (laag percentage neoantigenen)
• Immunosuppressieve micro-omgeving (desmoplastische reactie; macrofagen en MDSC)
• Relatief weinig T-cellen in omgeving tumor


• Patiënten met gemetastaseerde ziekte
• 40% patiënten lokaal gevorderde ziekte

Casus (2); heer P. 65 jaar
• Presentatie HA met bovenbuiksklachten
• VG: myocard infarct
• CTscan: pancreas kop tumor met uitgebreide vaatbetrokkenheid
• In MDO besproken: niet resectabel
• PA: adenocarcinoom

• Wat te doen?
• Behandelmogelijkheden?
• Winst chemotherapie?
• Lokale therapie?
• Verschillen tussen behandelmogelijkheden?
FOLFIRINOX bij LAPC?

• Systematic review
– Overall survival
– Percentage resecties
– Adverse events/ dosis reducties/ aanvullende therapie?
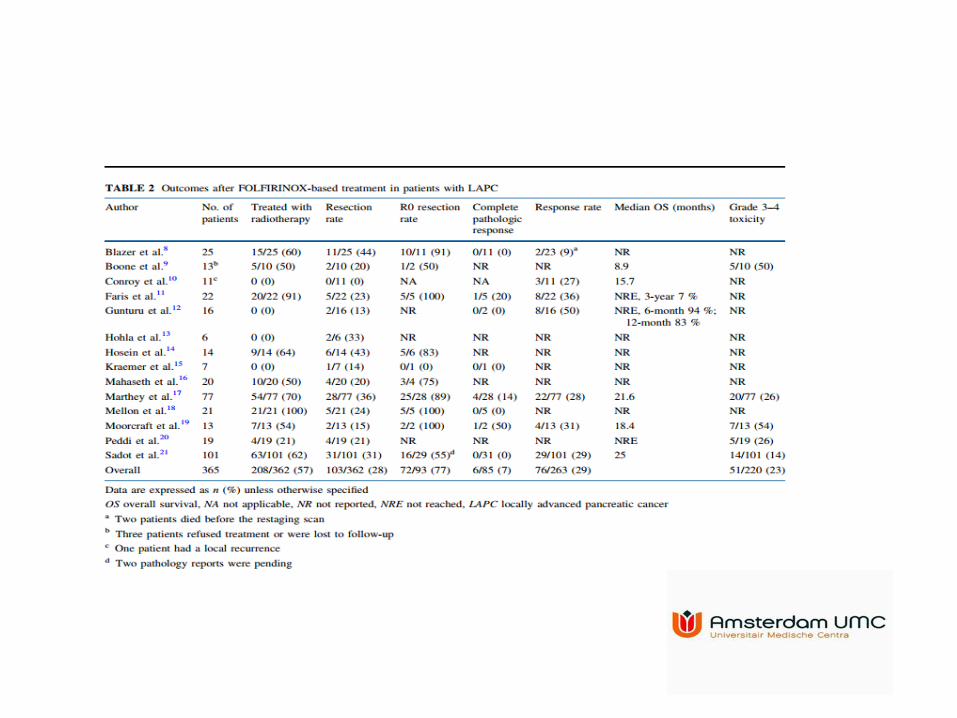
Conclusies
• Uitkomsten veelbelovend; mediane OS 24 maanden
• Toxiciteit graad 3-4 (voor zover gescoord): 23%
• Dosis reducties: 65%
• Percentage resecties: 25%
• Zeer heterogene groep, retrospectief!


Irreversibele electroporatie (IRE)
• Tot 6 electrodes rond tumor
• Hoog voltage electrische pulsen
• Cel dood door permeabel maken cel membraan
• Mediane OS 23 maanden1,2
1. Rombouts S., Vogel J. et al, BJS 2015; 2. Martin R. et al, Ann Surg Oncol2015
Behandeling 132 patiënten met LAPC
Chemotherapie (70%)
• 59/132 (45%) FOLFIRINOX
• 31/132 (23%) gemcitabine
Restagering: 45% niet-progressieve ziekte
• 43/59 (73%) na FOLFIRINOX
• 15/31 (48%) na gemcitabine
Exploratie: 11% resectie, 11% IRE

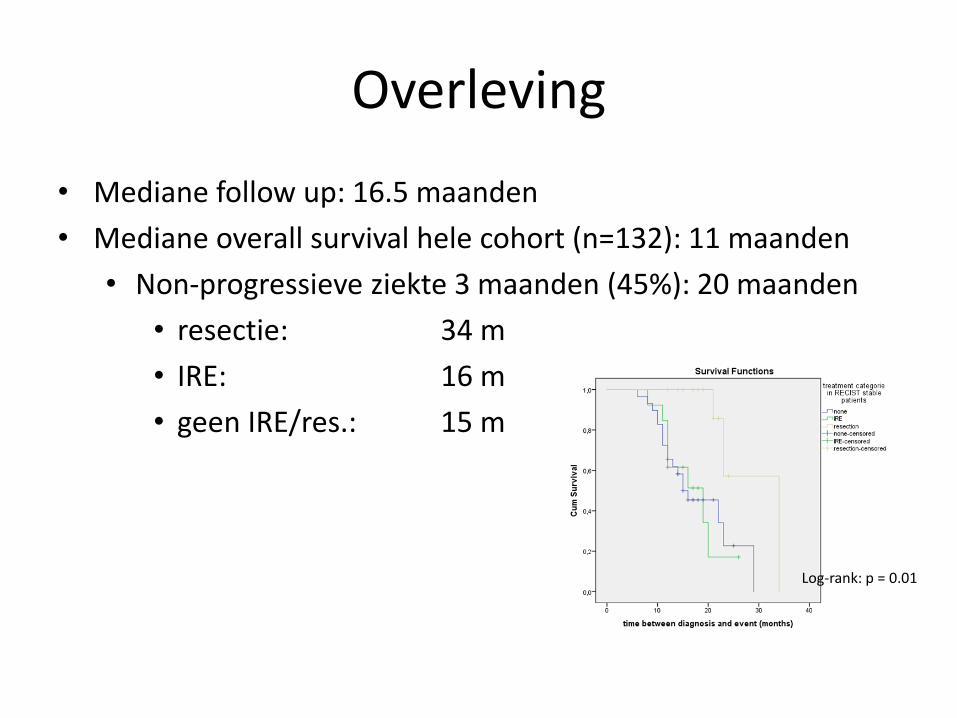
Overleving
• Mediane follow up: 16.5 maanden
• Mediane overall survival hele cohort (n=132): 11 maanden
• Non-progressieve ziekte 3 maanden (45%): 20 maanden
• resectie: 34 m
• IRE: 16 m
• geen IRE/res.: 15 m
Log-rank: p = 0.01

Randomized Controlled Trial
Pancreatic Locally advanced Irresectable Cancer Ablation
in the Netherlands
PELICAN trial
Randomized multicenter phase III study
Principal investigators:
Quintus Molenaar, HPB surgeon, University Medical Center Utrecht
Marc Besselink, HPB surgeon, Academic Medical Center Amsterdam
Hjalmar van Santvoort, HPB surgeon, St. Antonius Hospital, Nieuwegein
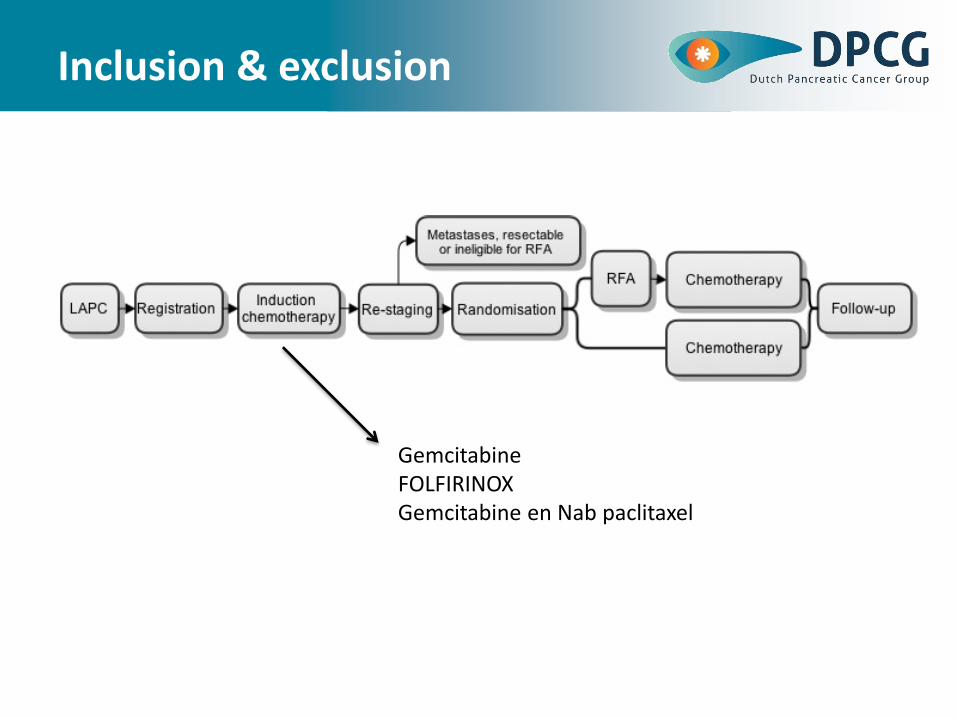
Inclusion & exclusion
GemcitabineFOLFIRINOXGemcitabine en Nab paclitaxel

Casus (3); merouw H. 61 jaar
• Presentatie HA met stille icterus
• VG: recent diabetes mellitus
• CTscan: pancreas kop tumor met beperkte vaatbetrokkenheid
• In MDO besproken: borderline resectabel

• Wat te doen?
• Behandelmogelijkheden?
• Winst chemotherapie?
• Resectie?

Rol neoadjuvante therapie?
• Pancreaskanker systemische ziekte
– Meerderheid occulte metastasen
– 30% niet resectabel
– 50% herstelt van operatie voor evt. adjuvantetherapie
– 5-jaars overleving alleen chirurgie < 10%

Voordelen
• Downstaging
• Selectie patiënten met gunstige tumor biologie
• Toename R0 resectie percentage
• 50% niet voldoende hersteld na operatie
Nadelen
• Multidisciplinaire benadering
• Pathologische bevestiging
• Behandeling biliaire obstructie
• Juiste stadiering?
• Dropout aanvankelijk operabele patiënten
• Geen bewijs en literatuur is beperkt
• Patiënten willen duidelijkheid….onmiddellijk

• Beste lange termijn overleving = chirurgie + chemo (radio) therapie
• Mediane overleving in 3 recente multicenter trials
– ESPAC-41 (730 pts in 92 centers in UK, Germany, France, Sweden, ) • 28 mnd adjuvant gem-cap [nb: gerandomiseerd na chirurgie]
– PRODIGE-242 (493 pts in 77 centers in France and Canada):• 54 mnd adjuvant mFOLFIRINOX [nb: gerandomiseerd na chirurgie]
– PREOPANC-13 (246 patients in 15 centers in the Netherlands; INTERIM)• 17 mnd met neoadj CRT in ALLE patienten, intention to treat• 42 mnd in gereserceerde patienten na neoad CRT

PREOPANC 2
Conclusies
• Prognose blijft slecht
• Nieuwe combinaties chemotherapie?
– Gemcitabine niet meer standaard
• FOLFIRINOX/ gemcitabine en nab paclitaxel: overlevingsvoordeel
– geselecteerde patiëntengroep
• Nieuwe middelen? Behandeling o.b.v. subtypen?
• Bij LAPC: FOLFIRINOX bij deel patiënten alsnog resectie
• Waarde lokaal ablatieve therapieën onduidelijk












