Afscheids symposium Christina van der Feltz- Cornelis ... · DSM-III-R diagnosis of major...
48
Personalised Psychiatry Afscheids symposium Christina van der Feltz- Cornelis Tilburg 14 februari 2019 Aartjan TF Beekman Dpt Psychiatrie Amsterdam UMC, loc VUmc en GGZinGeest Amsterdam
Transcript of Afscheids symposium Christina van der Feltz- Cornelis ... · DSM-III-R diagnosis of major...

Personalised Psychiatry
Afscheids symposium Christina van der Feltz- Cornelis
Tilburg 14 februari 2019
Aartjan TF Beekman
Dpt Psychiatrie Amsterdam UMC, loc VUmc
en GGZinGeest Amsterdam

Over persoonlijk en persoonlijkheid gesproken…
• Een vrouw met koninklijke allure….

Over persoonlijk en persoonlijkheid gesproken…
• En gewoon een hele goede onderzoeker

Over persoonlijk en persoonlijkheid gesproken…
• En iemand waar je plezier mee kan beleven
Disclosures
• None, except being strongly biased in favour of personalisedmedicine

Where is health care going ?
• Preventive Medicine
• Precision Medicine
• Personalised Medicine


Precision Medicine
• Treatments targeted towards select groups within and across diagnostic categories
• Based on mechanism of action and effectiveness
• Revolutionizes diagnosis and treatment


Promises Precision Medicine (1)
• Improve precision allocation treatment
• Prevent exposition patients to treatments that do not work
• Speed-up recovery
• Bolster aspecific prognostic factors (optimism)
• Reduce damage due to side effects
• Huge improvement cost/benefit ratio’s health care

Promises Precision Medicine(2)
• Guide diagnosis towards etiology, development disorder and treatment effect
• Scientific model that is more likely to help discovering mechanisms for etiology and treatment response
• Radical change design experimental studies (RCTs)
Promises Personalised Medicine (3)
• Guide interaction patient towards shared decision making

Q: Do we have a case for Personalised Psychiatry?
• Focus on depression
• Is personalised approach necessary and helpful?
• Are sufficient data in place?
• Which steps should we take first

Diagnosis does not predict outcome(Spijker et al, Br J Psychiatry 2002: 202-213)
duration(months)
3020100
pro
port
ion s
till
in
epis
ode
1,2
1,0
,8
,6
,4
,2
0,0 censored
• 50% recovered < 3 mnths
• 20% duration > 1 year
Fig. 1 Survival curve of a cohort (n=250) with newly originated (first
or recurrent) major depressive episodes in the general population

J Clinical Psychiatry 2010,
1300-1306

• NNT antidepressants chronic depression
• NNT response = 6
• NNT remission = 7
• NNT chronic depression = 7,7
• Effect size d = 0,23
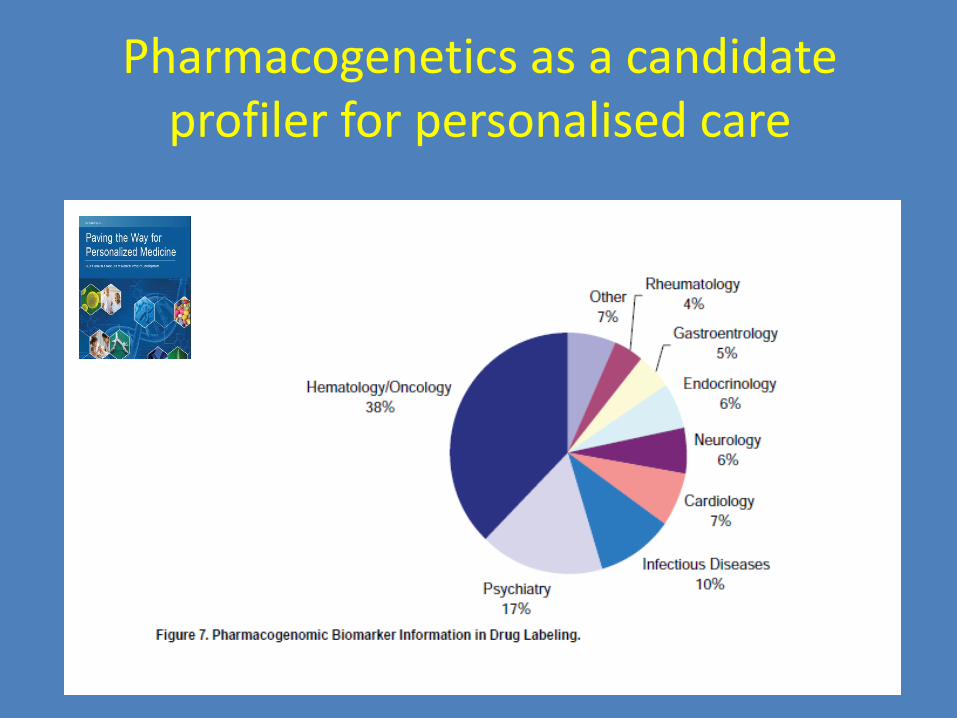
Pharmacogenetics as a candidate profiler for personalised care

Evolutionary Psychiatry
• Interesting and necessary to understandpsychiatry … but …….
• Speculative and a lot of ‘borrelpraat’
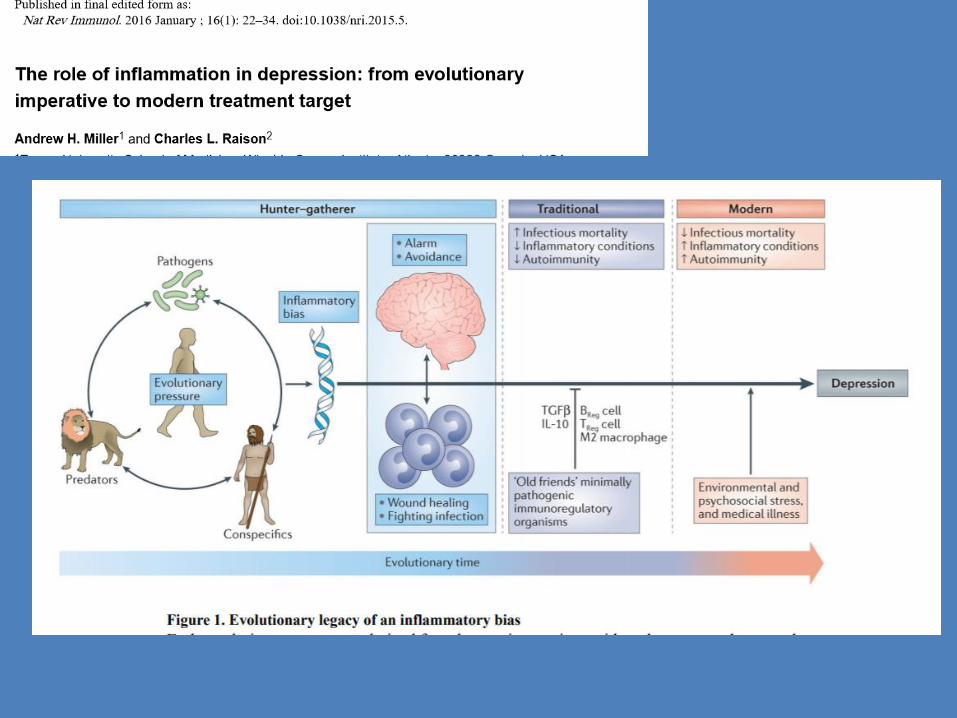

Pathogen host defense theorydepression (Miller & Raison)
• Immuun reaction varies, both due to geneticand (early life) environmental influences
• This is relevant for SOME patients depression
• And has cross-disorder relevance (anxiety,
psychosis)

• Meta-analysis 82 studies
• 3212 MDD vs 2798 controls
• Peripheral cytokines and chemokines

• Overall association MDD-INFL in place
• Much variation; weak associations
• Confounding (comorbidity, smoking)
• Explorative studies + many targets + peripheralmarkers + weak associaions + many statisticaltests…..

• Test hypothesis that markers for three basic pathophysiological systems are associated with the symptom profile of MDD

• NESDA - MDD
• Latent class analyses clinical characteristics
• Select two chronic MDD groups and test with healthy controls
• Severe, chronic melancholic dep (n=111)
• Severe, chronic atypical/immuno-metabolic dep (n=122)
• Normal controls (n=543)

Biological correlates immuno-metabolic and melancholic chronic depression – Cohen’s d
Mel vs Con Atyp vs Con Atyp vs Mel
Inf c-react protein
interleukin-6
TNF-a
=
=
=
0,29
0,30
0,30
0,39
0,40
0,42
Met
syn
BMI
waist circum
triglycerides
HDL cholesterol
RR
-0,25
=
=
=
=
0,78
0,63
0,31
-0,28
=
1,03
0,82
0,35
-0,28
=
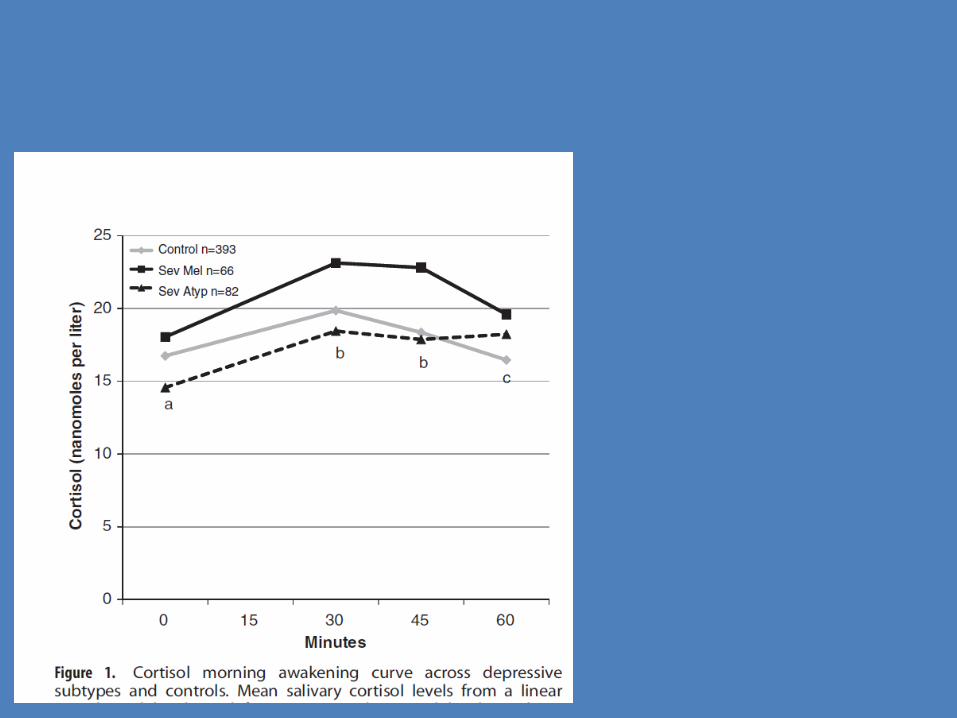
HPA AUC cortisol
diurn cort slope
0,45
0,34
=
-0,26
-0,59
-0,61

Patients with ‘immuno-metabolic depression’
• Older at first onset
• Obese or higher BMI
• More diabetes or abnormal GTT
• Higher risk cardiovascular problems
• Upregulated inflammation
• Higher risk chronic depression
• TCA: unfavorable lipid spectrum and upregulation inflammation
• Both SSRI en TCA probably < effect

Smith R.R. Medical Hypotheses 1991, 298-306.
The macrophage theory of depression.
Abstract
Excessive secretion of macrophage monokines is proposed as the cause of
depression.
Monokines when given to volunteers can produce the symptoms necessary for the
DSM-III-R diagnosis of major depressive episode. Interleukin-1 (IL-1) can provoke the
hormone abnormalities linked with depression. This theory provides an explanation for
the significant association of depression with coronary heart disease, rheumatoid
arthritis, stroke and other diseases with macrophage activation. The 3:1 female/male
incidence of depression ratio is accounted for by estrogen's ability to
activate macrophages. The extraordinary low rate of depression in Japan is consistent
with the suppressive effect of eicosapentanoic acid on macrophages. Fish oil is
proposed as a prophylaxis against depression and omega-6 fat as a promoter.
Infection, tissue damage, respiratory allergies and antigens found in food are some of
the possible causes of macrophage activation triggering depression.
• Statins: effects on lipids and inflammation
• 1 RCT: SSRI + statin better than SSRI solo
• SSRI’s en statins both commonly used
• Test: SSRI’s + statines better outcomes thanSSRI’s solo
• Observational study registers Denmark

Results

Comment
• Much room for bias
• But: very strong effect
• Interesting to test in MDD with metabolicsyndrome or upregulated inflammation

• GWAS: 135,458 cases and 344,901 controls
• 44 independent and significant loci.
VOL 50 | MAY 2018 | 668–681, Wray, N et al
Four key genes in more detail:
• OLFM4 and NEGR1 (associations obesity and BMI)
• RBFOX1 (chronic hypothalamic–pituitary–adrenal axis hyperactivation
• LRFN5 (presynaptic differentiation and neuroinflammation).

Data converge
• Genetics/GWAS: inflammation en obesitas
• Clinical epidemiology: metabolic-inflammatory depression
Back to personalised Psychiatry
• Will this lead to clinical profilers?
• And to new interventions?
• That are effective in SOME patients?
• In SPECIFIC stages depression?
• Under SPECIFIC circumstances…?
• Will this change Psychiatry?



Conclusions
• Personalising services = general trend
• This is a transactional proces, radicallychanging relationships actors
• Depends heavily on (big) data and digital transaction
• Personalised Health care = logical exponent
• Personalised Psychiatry = future
Conclusions
• Personalised Psychiatry is happening
• In all areas where services are provided
• Both in service-delivery
• And in research

Conclusions
• Much to be gained
• Revolutionises diagnosis, treatment and research
• In depression: data in place tot get started
• Clinical Staging and profiling helpful framework and something to get started with