A. Andres Bsn 4
15
PREPARED A. ANDRES BSN 4
Transcript of A. Andres Bsn 4

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 1/15
PREPARED
A. ANDRES BSN 4

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 2/15
Appendix

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 3/15
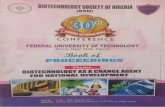
Appendix The appendix is a small, finger-like
appendage about 10 cm (4in) long
that is attached to the cecum justbelow the ileocecal valve.
Long appendix fills with food and
empties regularly into the cecumbecause it empties inefficiently and itslumen is small, the appendix is proneto obstruction and is particularly

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 4/15

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 5/15
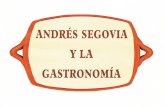
Pathophysiology The appendix become inflamed and
edematous as a result of either becomingkinked or occluded by a fecalith, tumor, orforeign body.
The inflammatory process increasesintraluminal pressure, initiating a
progressively severe, generalized or upperabdominal pain that become localized in theright lower quadrant of the abdomen withina few hours.

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 6/15
Clinical ManifestationVague epigastric or periumbilical pain progresses
to lower quadrant pain and usually accompanied bya low-grade fever and nausea and sometimes by
vomiting.Loss of appetite is common.
Local tenderness is elicited at McBurney’s pointwhen pressure is applied.
Rebound tenderness maybe present. The extent of tenderness and muscle spasm and
the existence of constipation and diarrhea dependnot so much of the severity of the appendeceal

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 7/15
If the appendix curls around behind the cecum,pain and tenderness maybe felt in the lumbarregion.
If its tip in the pelvis, this signs maybe elicitedonly on rectal examination
Rovsing’s sign maybe elicited by palpating thelower quadrant; this paradoxically cues pain tobe felt in the right lower quadrant.
Constipation can also occur with an acute
process such as appendicitis. Laxativesadministered in this instance may produceperforation of inflamed appendix.
In general, a laxative or cathartic should never

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 8/15
Assessment and
complete physical examination
Laboratory and X-ray findings.
The complete blood cell count demonstratesand elevated white blood cell count.
Leukocytes count may exceed 10,000cell/mm3
Neutrophil count may exceed 75%.Abdominal X-ray films, ultrasound studies, and
CT scan may reveal a right lower quadrantdensity or localized distension of the bowel.

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 9/15
COMPLICATIONS The major complication of appendicitis is
perforation of the appendix, which can lead toperitonitis or an abscess. The incidence of
perforation is 10% to 32%. The incidence is higher in young children and
elderly. Perforation generally occurs 24 hoursafter the onset of pain. Symptoms include a
fever of 37.7oC or higher, a toxic appearance,and continued abdominal pain or tenderness.

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 10/15
MEDICAL
Surgery is indicated if appendicitis isdiagnosed. To correct or prevent fluid andelectrolyte imbalance and dehydration, anti-
biotics and intravenous fluids are administereduntil surgery is performed. Analgesics can beadministered after the diagnosis is made.
Appendectomy (surgical removal of appendix)
is performed as soon as possible to decreasethe risk of perforation. It may be performedunder a general or spinal anesthetic with a lowabdominal incision or by laparoscopy.

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 11/15
NURSING MANAGEMENT:
Relieving pain
Preventing fluid volumedeficitReducing anxiety
Maintaining skin integrityAttainting optimal nutrition

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 12/15
NURSINGNURSINGINTERVENTIONINTERVENTION

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 13/15
Preoperative CareAdministered Intravenous Fluids
(IV)Administer opioid analgesics
The client should not receivelaxatives or enema.
Prepare for surgery and

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 14/15
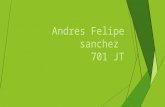
Operative ProceduresAppendectomy – is the removal of
inflamed appendix.
Most uncomplicated appendectomies
today are done via laparoscopy

8/14/2019 A. Andres Bsn 4
http://slidepdf.com/reader/full/a-andres-bsn-4 15/15
Postoperative CareIf peritonitis was present, a nasogastric
(NG) tube is placed to decompress thestomach and prevent abdominal distension.
IV antibiotics are typically prescribed if peritonitis is present.
Opioid analgesics are administered for pain
as neededMost client can return to usual activities in
1 to 2 weeks.