





Talen
Pages
Wettelijk


Insight in Bipolar Disorder
Lynn Van Camp

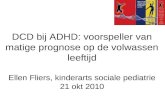
Polarity of Symptoms in Bipolar Disorder
Euthymia
Depression
Mania
Subsyndromaldepression
Depression
Hypomania
2
Bipolar I
Bipolar II

Prevalence: 2,8% 4,4% (Kessler, 2011)
Severe reduction in functional outcome: Quality of life
All-round functioning (IsHak, 2012)
Bipolar Disorder
3

Tohen et al. (2000)
Functional Recovery in Bipolar Disorder
4

Tohen et al. (2000)
Functional Recovery in Bipolar Disorder
5

Associations with Functioning
Neurocognition
Cognitive Insight
Symptoms
Social and Vocational
Functioning
Quality of Life
Clinical Insight
(Riggs et al., 2010)

1914 Joseph Babinski, Anosognosia
1934 Aubrey Lewis, The psychopathology of insight
1990 Anthony David, Multidimensional view on insight
History of insight

Anosognosia
The unawareness of patients of their paralyses after
a brain trauma.

Lewis, 1934
“the correct attitude to a morbid change in oneself, and moreover, the realization that the illness is mental”

Multidimensional view on insight, David, 1990

The awareness of the illness
Treatment compliance
Attribution of the symptoms to the disease
60 – 70% of the patients with bipolar disorder show a lack of insight! (Dias, 2008; Varga et al., 2006)
Clinical Insight
11

Research on clinical insight in bipolar disorder
Neurocognition
Social and Vocational
Functioning
Quality of Life
Clinical Insight
• Speed of Processing • Executive Functioning• Memory(Dias et al., 2008; van der Werf-Eldering et al., 2011; Varga et al., 2006; Yen et al., 2008)
(Yen et al., 2007)
(Dias et al., 2008)

Insight in symptoms
N= 412Amador et al., 1994

• Does not questions a person’s own interpretation
• It does not take into account important decision-making processes necessary in the understanding of the illness
• The consequences
• The view of others
• Different ideas regarding the illness
A more complete view of their illness creates a sense of ownership of the disorder, which could help the formation of autonomy
Shortcomings of Clinical Insight
14

• Adequate clinical insight <-> the full comprehension of the illness and all its complex consequences
• Superficial
• Has to hold metacognitive skills
• Awareness of misinterpretations
• Ability to correct these (Beck & Warman, 2004)
Shortcomings of Clinical Insight
15

Thus, “insight” should include
Recognition of which effect the illness has on: Mood
Actions
Thoughts
Interpretations
Beliefs
Shortcomings of Clinical Insight
16

“impairment of objectivity about cognitive distortions, loss of ability to put this into perspective, resistance to corrective information from others and overconfidence in conclusions” (p. 320-321)
Beck Cognitive Insight Scale (BCIS)
1. Self-reflectiveness: the capacity to reflect on our experiences
2. Self-certainty: dysfunctional decision-making, such as overconfidence in one’s judgments and jumping to conclusions
Cognitive Insight (Beck et al., 2004)
17

Cognitive Insight
• Individuals who are more self-reflective, have an increased ability to consider different perspectives and evaluate alternative hypotheses in order to make founded conclusions.
• Individuals who are too self-certain are excessively convinced of the accuracy of their own beliefs.
Therefore, cognitive insight both holds the ability to distance oneself from incorrect beliefs and includes the capacity to make an evaluation of interpretations using external feedback from others

Insight = Metacognition?
19
Patients show a lack of metacognitive capacities needed to correctly interpret the symptoms and effects of their disease

Metacognition in Bipolar Disorder
Van Camp et al., 2019

How to enhance insight or metacognition?
• Limit overly self-certain behaviour• Stimulate nuance in thinking• Promote self-reflective behavior
psycho-education (Jennings et al., 2002)
metacognitive training (Moritz & Woodward, 2007)
REFLEX (Pijnenborg et al., 2011)

How to enhance insight or metacognition?

How to enhance insight or metacognition?
Focusing on the underpinnings of poor insight

How to enhance insight or metacognition?
Explanations of a lack of insight:
• Clinical model (Cuesta & Peralta, 1994)
primary symptom of the illness
• Psychological denial model (Moore et al., 1999)
coping strategy to protect against destress
• Neuropsychological model (Lysaker & Bell, 1994)
caused by deficits in neurocognitive functioning

Neuropsychological model
Neurocognitive problems
Inhibit enhancement of insight
e.g. memory problems
Problems in remembering symptoms of past episodes
Incapable to compare current and past symptoms
Limits insight in the disorder
Limits flexible and reflective thinking about the disorder

Cognitive Insight in Bipolar Disorder
• Speed of processing• Attention• Working memory• Learning• Executive functioning (Van Camp et al.,
2015; Van Camp et al., in review)
Neurocognition
Cognitive Insight

Metacognition in Bipolar Disorder
• Speed of processing• Attention• Working memory• Learning• Executive functioning (Van Camp et al.,
2019)Metacognition
Neurocognition

Neurocognitive functioning in bipolar disorder
(Van Camp et al., 2019)

Neurocognitive functioning in bipolar disorder
• It was assumed that cognitive impairments in bipolar disorder would disappear in times of euthymia (Deckersbach
et al., 2010).
• Recent studies point to neurocognitive impairments even when the mood of patients with bipolar disorder is stable (Bora et al., 2009; Robinson et al., 2006)
Impaired cognitive functioning seems a core feature of bipolar disorder.

Neurocognitive functioning in bipolar disorder
• 57.7% of the individuals with bipolar disorder have a cognitive impairment.
• Defined as scoring 1 standard deviation below healthy controls in at least two cognitive domains (Reichenberg et al., 2009)
• Research even shows a degenerative nature of cognition in bipolar disorder (Lewandowski et al., 2011; Nehra et al., 2006; Robinson & Ferrier, 2006).

Neurocognitive functioning in bipolar disorder
(Lewandowski et al., 2011)

Cognitive training in Bipolar Disorder
• To provide therapeutic treatment for these cognitive impairments, various research groups have developed cognitive remediation programs (Deckersbach et al., 2010; Torrent et al., 2013)
• These methods aim to improve neurocognitive functioning and reduce the limiting effects it has on functional outcome (Anaya et al., 2012).
• In schizophrenia and schizoaffective disorder durable effects on global cognition and functioning were found(McGurk et al., 2007; Wykes et al., 2010)

Cognitive training in Bipolar Disorder
In bipolar disorder, research is scarce:
• Demant et al., 2015
Study with randomized controlled design
No improvement in cognitive functioning after short training
Cognitive improvement when the training lasted longer than 12 weeks
• Deckersbach et al., 2010
Improvement in psychosocial and cognitive functioning

Cognitive training in Bipolar Disorder
In bipolar disorder, research is scarce:
• Torrent et al., 2013
Functional remediation training
Included cognitive training
Unable to detect improvement in cognition
Did find improvement in functional outcome

Cognitive training in Bipolar Disorder
Mixed results:
Generality of the applied cognitive training
Interventions do not address an individual’s specific needs
Cognitive training that specifically targets the neurocognitive weaknesses of individuals are more effective(Whitmer & Gotlib, 2012)
More specific and personalized cognitive training could be more beneficial for the improvement in cognitive and functional outcome(Franck et al., 2013; Preiss et al., 2013; Silverstein & Wilkniss, 2004)

How to enhance insight?
• To date, no research has reported the effect of cognitive training on insight
• It could be that insight increases when the specific neurocognitive correlates are trained.

Negative side effect to better cognitive insight

Negative side effect to better cognitive insight
Higher levels of cognitive insight are often associated with depressive mood.
This relationship seems to be mediated by self-stigma.
Research indicates that more insight is only correlated with higher depression rates when patients have stigmatizing beliefs about their psychiatric illness (Lysaker et al., 2005; Mak & Wu, 2006; Staring et al., 2009).
Highlights the importance to include the subject of stigma in a “top-down” training to enhance insight.

Future research
• Creation and validation of a top-down training that is specifically made to increase insight in bipolar disorder
• Neurocognitive / Functional Remediation Training
Tailored to an individuals specific needs
• How to capture the concept of (cognitive) insight
Valid questionnaire -> requires self-reflective capacities.

Thank you for your attention
Top Related