spiral.imperial.ac.uk · Web viewThis manuscript describes the study design and rationale for the...
66
A Phase III study of triple therapy with budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler 320/18/9.6 μg and 160/18/9.6 μg using co-suspension delivery technology in moderate-to-very severe COPD: the ETHOS study protocol Klaus F Rabe a, *, Fernando J Martinez b , Gary T Ferguson c , Chen Wang d , Dave Singh e , Jadwiga A Wedzicha f , Roopa Trivedi g , Earl St Rose h , Shaila Ballal h , Julie McLaren i , Patrick Darken h , Colin Reisner h , Paul Dorinsky g a LungenClinic Grosshansdorf and Christian-Albrechts University Kiel, Airway Research Center North, Member of the German Center for Lung Research (DZL), Grosshansdorf, Germany b Joan and Sanford I. Weill Department of Medicine, Weill Cornell Medicine, New York, NY, USA c Pulmonary Research Institute of Southeast Michigan, Farmington Hills, MI, USA d National Clinical Research Centre for Respiratory Diseases, China-Japan Friendship Hospital, Beijing, China e Medicines Evaluation Unit, University of Manchester, Manchester University NHS Foundation Hospitals Trust, Manchester, UK f Respiratory Division, National Heart and Lung Institute, London, UK g AstraZeneca, Durham, NC, USA h AstraZeneca, Morristown, NJ, USA i AstraZeneca, Gaithersburg, MD, USA 1
Transcript of spiral.imperial.ac.uk · Web viewThis manuscript describes the study design and rationale for the...

A Phase III study of triple therapy with budesonide/glycopyrrolate/formoterol fumarate
metered dose inhaler 320/18/9.6 μg and 160/18/9.6 μg using co-suspension delivery technology in
moderate-to-very severe COPD: the ETHOS study protocol
Klaus F Rabea,*, Fernando J Martinezb, Gary T Fergusonc, Chen Wangd, Dave Singhe, Jadwiga A
Wedzichaf, Roopa Trivedig, Earl St Roseh, Shaila Ballalh, Julie McLareni, Patrick Darkenh,
Colin Reisnerh, Paul Dorinskyg
aLungenClinic Grosshansdorf and Christian-Albrechts University Kiel, Airway Research Center
North, Member of the German Center for Lung Research (DZL), Grosshansdorf, Germany
bJoan and Sanford I. Weill Department of Medicine, Weill Cornell Medicine, New York, NY, USA
cPulmonary Research Institute of Southeast Michigan, Farmington Hills, MI, USA
dNational Clinical Research Centre for Respiratory Diseases, China-Japan Friendship Hospital,
Beijing, China
eMedicines Evaluation Unit, University of Manchester, Manchester University NHS Foundation
Hospitals Trust, Manchester, UK
fRespiratory Division, National Heart and Lung Institute, London, UK
gAstraZeneca, Durham, NC, USA
hAstraZeneca, Morristown, NJ, USA
iAstraZeneca, Gaithersburg, MD, USA
*Corresponding author. Address: LungenClinic Grosshansdorf, Wöhrendamm 80, 22927
Großhansdorf, Germany. E-mail address: [email protected] (KF Rabe).
Word count: 3188
Tables/figures: 5/2
1

Abbreviations: AE, adverse event; AUC0–4, area under the curve from 0 to 4 h; BDI, Baseline Dyspnea
Index; BDP, beclometasone dipropionate; BFF, budesonide/formoterol fumarate;
BGF, budesonide/glycopyrrolate/formoterol fumarate; BID, twice daily; CAT, COPD Assessment
Test; COPD, chronic obstructive pulmonary disease; DPI, dry powder inhaler;
ECG, electrocardiogram; EXACT, Exacerbations of Chronic Pulmonary Disease Tool; FEV1, forced
expiratory volume in 1 s; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol;
FF/VI, fluticasone furoate/vilanterol; FVC, forced vital capacity; GFF, glycopyrrolate/formoterol
fumarate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HCRU, healthcare resource
utilization; ICS, inhaled corticosteroid; IND/GLY, indacaterol/glycopyrronium; LABA, long-acting
β2-agonist; LAMA, long-acting muscarinic antagonist; MCID, minimum clinically important
difference; MDI, metered dose inhaler; mITT, modified intent-to-treat; PFT, pulmonary function test;
PP, per-protocol; QD, once daily; QID, four times daily; SABA, short-acting β2-agonist; SAMA,
short-acting muscarinic antagonist; SD, standard deviation; SGRQ, St. George’s Respiratory
Questionnaire; TDI, Transition Dyspnea Index; UMEC/VI, umeclidinium/vilanterol.
2

Originality and clinical relevance statement
This manuscript describes the study design and rationale for the ETHOS study, a pivotal
Phase III study of budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler (BGF MDI),
one of three triple fixed-dose combinations that are in development or approved for the treatment of
chronic obstructive pulmonary disease (COPD). Studies thus far have shown that triple therapy can
improve lung function, symptoms, and reduce exacerbations versus dual therapies, with benefits
versus dual bronchodilators increasing at higher blood eosinophil levels. However, long-term inhaled
corticosteroid (ICS) use has been associated with potential safety concerns, although the risk of
adverse events may depend on the dose and duration of treatment, as well as the specific ICS used.
Further evidence is needed to identify which patients with COPD may benefit from ICS treatment,
and particularly whether a lower dose of ICS can still provide a benefit. With this in mind, the
ETHOS study will be the first to investigate a triple therapy with two doses of ICS (320 μg and
160 μg), in comparison to dual therapies. ETHOS enrolled patients with moderate-to-very severe
airflow obstruction (FEV1 < 65% predicted) who were symptomatic despite receiving ≥ 2 inhaled
maintenance therapies, and had a history of at least one COPD exacerbation in the previous year.
Furthermore, ETHOS is the first one-year triple therapy study to prospectively stratify randomization
by eosinophil count. These unique features of the study design will help clarify the appropriate role
for triple therapy in the management of COPD, and may provide support for the use of BGF MDI
with two doses of ICS, allowing for titration of COPD treatment to the lowest effective dose. Overall,
the findings are expected to help refine current treatment recommendations, with the ultimate goal of
improving outcomes and optimizing the benefit:risk ratio for patients with COPD.
3

ABSTRACT (250/250 words)
Background: Single inhaler triple therapies providing an inhaled corticosteroid, a long-acting
muscarinic antagonist, and a long-acting β2-agonist (ICS/LAMA/LABAs) are an emerging treatment
option for chronic obstructive pulmonary disease (COPD). Nevertheless, questions remain regarding
the optimal patient population for triple therapy as well as the benefit:risk ratio of ICS treatment.
Methods: ETHOS is an ongoing, randomized, double-blind, multicenter, parallel-group, 52-week
study in symptomatic patients with moderate-to-very severe COPD and a history of exacerbation(s) in
the previous year. Two doses of single inhaler triple therapy with
budesonide/glycopyrrolate/formoterol fumarate metered dose inhaler (BGF MDI 320/18/9.6 μg and
160/18/9.6 μg) will be compared to glycopyrrolate/formoterol fumarate (GFF) MDI 18/9.6 μg and
budesonide/formoterol fumarate (BFF) MDI 320/9.6 μg, all formulated using co-suspension delivery
technology. Outcomes include the rate of moderate/severe (primary endpoint) and severe COPD
exacerbations, symptoms, quality of life, and all-cause mortality. Sub-studies will assess lung function
and cardiovascular safety.
Study population: From June 2015-July 2018, 16,044 patients were screened and 8572 were
randomized. Preliminary baseline demographics show that 55.9% of patients had experienced ≥ 2
moderate/severe exacerbations in the previous year, 79.1% were receiving an ICS-containing
treatment at study entry, and 59.9% had blood eosinophil counts ≥ 150 cells/mm3.
Conclusions: ETHOS will provide data on exacerbations, patient-reported outcomes, mortality, and
safety in 8572 patients with moderate-to-very severe COPD receiving triple and dual fixed-dose
combinations. For the first time, ICS/LAMA/LABA triple therapy with two different doses of ICS
will be compared to dual ICS/LABA and LAMA/LABA therapies.
Clinical trial registration number: NCT02465567
Keywords (3–6): BGF MDI, Chronic obstructive pulmonary disease, Exacerbations, Inhaled
corticosteroid, Study protocol, Triple therapy
4

1. Introduction
Triple fixed-dose combination therapies providing an inhaled corticosteroid (ICS), a long-
acting muscarinic antagonist (LAMA), and a long-acting β2-agonist (LABA) in a single inhaler are a
recent addition to the range of available treatment options for chronic obstructive pulmonary disease
(COPD) [1-5]. Studies investigating the efficacy of triple fixed-dose ICS/LAMA/LABA therapies
have found benefits on lung function, quality of life, and exacerbation rates versus dual
LAMA/LABA [4-6] and ICS/LABA therapies [1, 4, 6].
Nevertheless, the efficacy benefits of ICS therapy were called into question by the results of
one large study which reported that dual long-acting bronchodilator therapy was superior to
ICS/LABA therapy for the prevention of COPD exacerbations in patients with high exacerbation risk
[7]. Furthermore, stepping down from triple therapy to LAMA/LABA did not increase the overall risk
of exacerbations in two studies that enrolled patients with either ≤ 1 [8] or ≥ 1 [9] exacerbations in the
previous year, though increased exacerbations were detected in subgroups of patients with high blood
eosinophil levels [8, 10]. These findings, in addition to other recent studies showing that higher
eosinophil levels predict a greater treatment response to ICS-containing therapies versus
bronchodilator-only treatments [3-5, 11, 12], have led to new recommendations regarding eosinophils
in the 2019 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report [13]. Clinicians
are now encouraged to use blood eosinophil counts to guide treatment decisions for patients with
exacerbations, with triple therapy recommended for those who experience persistent exacerbations on
LAMA/LABA (if eosinophil counts are ≥ 100 cells/mm3) or ICS/LABA therapy [13].
Questions also remain regarding the benefit:risk ratio of ICS therapy due to the potential for
an increased risk of steroid-associated adverse events, including pneumonia [13, 14]. However, the
risk of pneumonia associated with ICS therapy may differ according to dose, duration of treatment,
and potentially the specific compound used [15, 16], in addition to demographic and clinical
characteristics such as prior exacerbation history, age, body mass index, and degree of airflow
limitation [17, 18]. Further investigation of patient responses to ICS-containing therapies, taking into
account modifying factors such as symptom burden, exacerbation history, pneumonia risk, and
5

eosinophil levels, will allow clinicians to identify those patients who are most likely to benefit from
triple fixed-dose combination maintenance treatments for COPD [19].
BGF MDI is a triple fixed-dose combination therapy of budesonide (ICS), glycopyrrolate
(LAMA), and formoterol fumarate (LABA), delivered via metered dose inhaler (MDI) using co-
suspension delivery technology. The first pivotal Phase III study, KRONOS, assessed the efficacy and
safety of BGF MDI 320/18/9.6 μg (equivalent to budesonide/glycopyrronium/formoterol fumarate
dihydrate 320/14.4/10 µg) in patients with COPD over 24 weeks compared to its corresponding
LAMA/LABA (glycopyrrolate/formoterol fumarate [GFF] MDI) and ICS/LABA
(budesonide/formoterol fumarate [BFF] MDI) therapies, as well as open-label budesonide/formoterol
dry powder inhaler (Symbicort® Turbuhaler®) [6]. Patients in KRONOS were required to be
symptomatic (COPD assessment test [CAT] score ≥ 10), but a history of exacerbations in the prior
year was not an entry requirement. BGF MDI showed benefits on lung function, symptoms, and
exacerbations versus both dual therapies, and had a safety profile comparable to LAMA/LABA and
ICS/LABA therapies, with a similar incidence of pneumonia observed across groups [6].
The potential to use a lower dose of budesonide in COPD maintenance therapy, while still
maintaining the benefits of ICS treatment, has been previously examined in a Phase III, 24-week dual-
therapy study, TELOS, which demonstrated that two doses of BFF MDI (320/9.6 μg and 160/9.6 μg)
both reduced the rate of moderate or severe COPD exacerbations (by 37% and 28%, respectively)
versus formoterol fumarate MDI 9.6 μg, with no evidence of a dose response for safety [20].
Given the findings of KRONOS and TELOS, it is important to assess the relative efficacy of
different doses of ICS in triple therapy with BGF MDI, when administered over a longer study period
in a population of patients at high risk of exacerbations. In ETHOS, we will evaluate the efficacy and
safety of two doses of BGF MDI (320/18/9.6 μg and 160/18/9.6 μg), relative to BFF MDI and
GFF MDI, over 52 weeks in symptomatic patients with moderate-to-very severe COPD and a
documented history of exacerbation(s) in the prior year. Among studies of ICS/LAMA/LABA triple
therapies, ETHOS will be the first to assess two different doses of ICS, and the first 52-week study to
stratify randomization by eosinophil levels. These unique features of the study design will help
6

provide evidence needed to optimize the benefit:risk ratio of triple therapy relative to dual
combination therapies in the management of COPD.
2. Material and methods
2.1. Study design and population
ETHOS (NCT02465567) is a randomized, double-blind, multicenter, parallel-group, 52-week
study conducted in patients with moderate-to-very severe COPD [21]. The study aims to assess the
effect of two doses of BGF MDI relative to BFF MDI and GFF MDI on the rate of moderate or severe
COPD exacerbations (primary objective), as well as symptoms, quality of life, and all-cause mortality
(secondary objectives). In addition, subsets of patients at designated study sites have participated in
sub-studies assessing lung function (4-h pulmonary function testing) and cardiovascular safety (24-h
Holter monitoring). Key inclusion and exclusion criteria are shown in Table 1 (full details are
provided in the supplementary material). Notably, enrollment in ETHOS required ≥ 1 moderate or
severe COPD exacerbation in the previous 12 months (if post-bronchodilator forced expiratory
volume in 1 s [FEV1] was < 50% predicted normal [i.e. severe or very severe airflow obstruction]); or,
for patients with FEV1 ≥ 50% predicted normal (i.e. moderate airflow obstruction), ≥ 2 moderate or
≥ 1 severe exacerbation(s) were required. Exacerbations were classified as moderate if they required
treatment with systemic corticosteroids and/or antibiotics for at least 3 days (or a single depot
injectable dose of corticosteroids), and as severe if they resulted in hospitalization. All moderate or
severe exacerbations were documented by the investigator using an electronic case report form.
Patients have been randomized 1:1:1:1 using an interactive web response system to receive
twice-daily BGF MDI 320/18/9.6 μg, BGF MDI 160/18/9.6 μg, BFF MDI 320/9.6 μg, or GFF MDI
18/9.6 μg. Randomization was stratified by exacerbation history (1 or ≥ 2 moderate or severe
exacerbations), post-bronchodilator FEV1 (25% to < 50% or 50% to < 65% predicted), blood
eosinophil count (< 150 or ≥ 150 cells/mm3), and country.
7

Inclusion criteria
Male/female, 40–80 years of age
Established clinical history of COPD with post-bronchodilator FEV1/FVC ratio < 0.70 and
FEV1 < 65% predicted normal
Current or former smokers with a smoking history of ≥ 10 pack-years
CAT score ≥ 10
On ≥ 2 inhaled maintenance therapies for COPD for ≥ 6 weeks prior to screening (could
include scheduled SABA and/or SAMA)
History of moderate or severe COPD exacerbations in the 12 months prior to screening
o If post-bronchodilator FEV1 < 50% of predicted normal: ≥ 1 moderate or severe
o If post-bronchodilator FEV1 ≥ 50% of predicted normal: ≥ 2 moderate or
≥ 1 severe
Exclusion criteria
Significant diseases or conditions other than COPD, including cardiac, respiratory,
neurological, renal, and endocrine disorders
Current diagnosis of asthma
COPD resulting from alpha-1 antitrypsin deficiency
Acute worsening of COPD in the 6 weeks prior to screening resulting in treatment with
oral corticosteroids or antibiotics
Failure to meet criteria for spirometry acceptability and repeatability
4-h PFT sub-study
Failure to meet criteria for spirometry baseline stability
24-h Holter monitoring sub-study
Current pacemaker/defibrillator device, or clinically significant abnormal baseline Holter
monitor findings
Table 1
Key inclusion/exclusion criteria.
CAT: COPD assessment test, COPD: chronic obstructive pulmonary disease, FEV1: forced expiratory
volume in 1 s, FVC: forced vital capacity, PFT: pulmonary function test, SABA: short-acting β2-
agonist, SAMA: short-acting muscarinic antagonist.
Full inclusion and exclusion criteria are provided in the supplementary material.
8

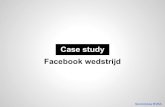
Fig. 1. ETHOS study design.
BFF: budesonide/formoterol fumarate, BGF: budesonide/glycopyrrolate/formoterol fumarate,
BID: twice daily, COPD: chronic obstructive pulmonary disease, GFF: glycopyrrolate/formoterol
fumarate, MDI: metered dose inhaler, SABA: short-acting β2-agonist, SAMA: short-acting muscarinic
antagonist.aThe screening period of 1–4 weeks could be extended to a maximum of 10 weeks if a patient
experienced a COPD exacerbation, in order to allow for treatment and recovery. bReversibility to a SABA (for classification) and a SAMA (for characterization) will be tested at
Visit 2 and 3, respectively.
Key study procedures including screening assessments and endpoint evaluations are shown in
Table 2. All patients completed a screening period of 1 to 4 weeks between Visit 1 and Visit 4
(randomization; Fig. 1). The screening period could be extended to a maximum of 10 weeks if a
patient experienced a COPD exacerbation, in order to allow for treatment, recovery, and a washout
period for any oral corticosteroid treatment. At Visit 1, the patients’ existing COPD maintenance
medications were adjusted as follows for the remainder of the screening period: all LAMA, LABA,
and LAMA/LABA therapies were discontinued; patients receiving an ICS/LABA discontinued the
ICS/LABA, but continued to receive the ICS component as monotherapy; all patients received open-
label ipratropium bromide four times daily, as well as albuterol sulfate for rescue use throughout the
screening period. Ipratropium bromide and ICS monotherapy were stopped at randomization while
albuterol sulfate was permitted for rescue use throughout the study.
9

Procedures
52-week treatment periodFollow-
up callScreeningV4
(Rand)V5 V6 V7 V8 V9 V10 V11 V12 V13 V14
V1 V2 V3
Week -4 to 0 (variable) 0 4 8 12 16 20 24 28 36 44 52 54
In-clinic X X X X X X X X X
Telephone contact X X X X X X
Informed consent, demographics,
medical/surgical history,
eDiary training, chest imaging
X
Spirometry X X X
Eligibility criteria, inhalation
device and dose indicator trainingX X X X
Smoking status, vital signs X X X X X X X X X
Prior/concomitant medications,
AEs, COPD exacerbationsX X X X X X X X X X X X X X X
CAT X X
12-lead ECG, clinical laboratory
testingaX X X X X
Study-drug dispensing, pregnancy X X X X X X X
10

test
Physical examination,
eDiary dispensing/collection,
adjust COPD medications
X X
Reversibility testing X X
eDiary reviewb X X X X X X X X
24-h Holter monitoring X X
Study-drug administration and
collection, BDI/TDI, SGRQ,
spirometry (PFT sub-study)c
X X X X X X
Verify continued eligibility X X X X X
HCRU X X X X X X X X X X X
Vital status check X
Table 2
Study procedures.
AE: adverse event, BDI/TDI: Baseline Dyspnea Index/Transition Dyspnea Index, CAT: COPD assessment test, COPD: chronic obstructive pulmonary
disease, ECG: electrocardiogram, eDiary: electronic diary, EXACT: Exacerbations of Chronic Pulmonary Disease Tool, HCRU: healthcare resource
utilization, PFT: pulmonary function test, Rand: randomization, SGRQ: St. George’s Respiratory Questionnaire, V: visit.aincluding blood eosinophilsbPatients will be asked to maintain a daily record of their study-drug dosing and rescue-medication use. EXACT will be reviewed at each visit as part of the
subject diary review.
11

cSpirometry assessments for patients participating in the 4-h PFT sub-study will be conducted at 60 min and 30 min prior to study-drug administration and at
5 min (Visit 4 only), 15, and 30 min; and 1, 2, and 4 h after study-drug administration.
12

Primary and secondary study endpoints as well as the primary sub-study endpoints are shown
in Table 3. Safety is being assessed via adverse-event monitoring, 12-lead electrocardiograms, clinical
laboratory testing, and vital-sign measurements. In addition to efficacy and safety endpoints,
healthcare resource utilization is also being evaluated.
The study is being conducted in accordance with Good Clinical Practice, including the
Declaration of Helsinki and applicable regulatory requirements. The protocol and informed consent
form have been approved by the appropriate institutional review boards or independent ethics
committees. All patients provided written informed consent prior to screening.
Primary endpoint
Rate of moderate or severe COPD exacerbations (efficacy estimand)
Secondary endpoints
Rate of moderate or severe COPD exacerbations (attributable estimand)
Time to first moderate or severe COPD exacerbation
Change from baseline in average daily rescue albuterol sulfate use over 24 weeks
TDI focal score over 24 weeks (ex-US only)
Change from baseline in EXACT total score over 52 weeks (ex-US only)
Change from baseline in SGRQ total score over 24 weeks (ex-US only)
Percentage of patients achieving a MCID of ≥ 4 units in SGRQ total score at Week 24 (US only)
Time to death (all cause)
Rate of severe COPD exacerbations
Primary sub-study endpoints
4-h PFT
Change from baseline in morning pre-dose trough FEV1 at Week 24 (US) and over 24 weeks
(ex-US) for the comparison of BGF MDI 320/18/9.6 μg versus GFF MDI 18/9.6 μg
FEV1 AUC0–4 at Week 24 (US) and over 24 weeks (ex-US) for the comparison of BGF MDI
320/18/9.6 μg versus BFF MDI 320/9.6 μg
24-h Holter monitoring
Change from baseline in mean heart rate averaged over 24 h
Table 3
Key study endpoints.
13

AUC0–4: area under the curve from 0 to 4 h, BFF: budesonide/formoterol fumarate,
BGF: budesonide/glycopyrrolate/formoterol fumarate, COPD: chronic obstructive pulmonary disease,
EXACT: Exacerbations of Chronic Pulmonary Disease Tool, FEV1: forced expiratory volume in 1 s,
GFF: glycopyrrolate/formoterol fumarate, MCID: minimum clinically important difference,
MDI: metered dose inhaler, PFT: pulmonary function test, SGRQ: St. George’s Respiratory
Questionnaire, TDI: Transition Dyspnea Index.
Endpoints that differ between approaches (US vs ex-US) are indicated in parentheses.
All endpoints to include the following comparisons unless otherwise indicated: BGF MDI 320/18/9.6
μg versus GFF MDI 18/9.6 μg, BGF MDI 320/18/9.6 μg versus BFF MDI 320/9.6 μg, BGF MDI
160/18/9.6 μg versus GFF MDI 18/9.6 μg, and BGF MDI 160/18/9.6 μg versus BFF MDI 320/9.6 μg
(all for superiority with the exception of BGF MDI 160/18/9.6 μg MDI to BFF MDI 320/9.6 μg,
which will be for non-inferiority first, followed by superiority).
2.2. Statistical analysis
A sample size of approximately 8400 patients was selected to provide 93% power to detect a
15% reduction in the rate of moderate or severe COPD exacerbations for BGF MDI 320/18/9.6 μg
compared to both GFF MDI and BFF MDI (96% power for each comparison), with Type I error
controlled at a one-sided alpha level of 0.025. This sample size reflects assumptions for parameter
estimates that were updated following a pre-specified blinded sample size re-estimation, which
resulted in an increase of 400 patients (100 per treatment arm) from the original 8000 based on an
interim assessment of the underlying rate of moderate or severe COPD exacerbations and prediction
of the negative binomial shape parameter. The updated estimates assume an average treatment
exposure of 0.83 years and yearly moderate or severe exacerbation rates of 1.142, 1.210, 1.344, and
1.344 for BGF MDI 320/18/9.6 μg, BGF MDI 160/18/9.6 μg, and GFF MDI, and BFF MDI,
respectively.
14

The primary estimand of interest is the efficacy estimand, i.e. the effect of the randomized
treatments in all patients assuming continuation of randomized treatments for the duration of the
study, regardless of actual compliance. This estimand will be assessed via analyses of the primary and
secondary endpoints (for superiority) in the modified intent-to-treat (mITT) population, containing all
post-randomization data obtained prior to discontinuation from treatment. A secondary analysis of the
primary endpoint will be performed (also using the mITT population) to estimate the attributable
estimand, i.e. the effect of treatment in patients that is attributable to the randomized treatment, by
unfavorably imputing missing data that are attributable to lack of efficacy or tolerability. An
additional estimand of interest is the treatment policy estimand, which is the effect of randomized
treatment over the study period regardless of whether randomized treatment is continued, and is
estimated by also including the data collected post-treatment discontinuation. Finally, the per-protocol
(PP) estimand will assess the effect of treatment on patients who are compliant with the protocol
(i.e. no major protocol deviations), including the use of randomized medication. The PP estimand will
use the PP population, which consists of all patients with post-randomization data obtained prior to
any major protocol deviations, and will be the primary estimand of interest for the non-inferiority
analyses of BGF 160/18/9.6 μg (lower ICS dose) versus BFF MDI 320/9.6 μg (higher ICS dose). The
safety population will include the same patients as the mITT population, analyzed according to
treatment received rather than randomized.
15

The rate of moderate or severe COPD exacerbations (primary endpoint) will be analyzed
using negative binomial regression, with exacerbations considered separate events when there are
> 7 days between the end date of the earlier event and the start date of the later event. The start date of
a moderate or severe exacerbation is defined as the first day of prescribed treatment with a systemic
corticosteroid or antibiotic, hospitalization, or date of death; the end date is defined as the end of
treatment or the end of hospitalization, whichever is later. Time at risk of experiencing an
exacerbation will be used as an offset variable in the model, and time during an exacerbation, or in the
7 days following an exacerbation, will not be included in its calculation. Treatments will be compared
adjusting for baseline post-bronchodilator % predicted FEV1, baseline exacerbation history, baseline
blood eosinophil count (logarithmically transformed and obtained from the mean of non-missing
values measured at screening [Visit 1] and at randomization [Visit 4]), region, and ICS use at
screening.
Treatment comparisons will be made in the following order, and for superiority: BGF MDI
320/18/9.6 μg versus GFF MDI, BGF MDI 320/18/9.6 μg versus BFF MDI, BGF MDI 160/18/9.6 μg
versus GFF MDI, and BGF MDI 160/18/9.6 μg versus BFF MDI (this comparison will be made for
non-inferiority first followed by superiority). For the primary endpoint, non-inferiority will be
declared based on a margin of 0.1, i.e. if the 95% confidence interval for the rate ratio is under 1.1.
These four treatment comparisons will be made for the efficacy estimand first, followed by the
attributable estimand before testing can proceed to the secondary efficacy variables for each
comparison of interest. Analyses by pre-specified subgroups, including exacerbation history and
eosinophil levels, will also be performed. In addition, nonparametric regression will be used to
evaluate the benefit of budesonide treatment relative to blood eosinophil levels (as a continuous
variable).
A pre-specified interim efficacy analysis was conducted following the blinded sample size re-
estimation, at which an independent Data Monitoring Committee reviewed unblinded efficacy data.
As the pre-specified stopping criteria for unequivocal efficacy and clarity regarding budesonide dose
were not met, the study will continue until all patients complete their final study visit.
16

3. Patient population
Enrollment and randomization were completed between June 30, 2015 and July 13, 2018,
with study completion expected in July 2019. In total, 16,044 patients were screened for participation
in ETHOS; of these, 8572 were randomized.
Preliminary baseline demographics for the safety population (n = 8539) are shown in Table 4
(treatment-group data remain blinded). At baseline, the majority of patients participating in ETHOS
had experienced ≥ 2 moderate or severe exacerbations in the previous 12 months (55.9%), and 21.2%
had experienced ≥ 1 severe exacerbation. Overall, 79.1% were receiving an ICS-containing treatment
at study entry. The mean (standard deviation) blood eosinophil count was 196.3 (132.9) cells/mm3,
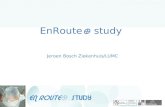
with 59.9% of patients having a count ≥ 150 cells/mm3 and 14.7% having ≥ 300 cells/mm3. The
baseline distribution of patients’ eosinophil levels is shown in Fig. 2.
All patients(N = 8539)
Mean age, years (SD) 64.7 (7.6)
Male, n (%) 5097 (59.7)
Race, n (%)WhiteAsianBlackAmerican Indian/Alaska NativeOther
7250 (84.9)651 (7.6)309 (3.6)140 (1.6)189 (2.2)
Mean body mass index, kg/m2 (SD) 27.5 (6.3)
Current smoker, n (%) 3508 (41.1)
Mean number of pack-years smokeda (SD) 47.7 (26.0)
Spirometric COPD severity, n (%)b
ModerateSevereVery severe
2437 (28.5)5169 (60.5)925 (10.8)
Mean COPD duration, years (SD) 8.3 (6.2)
17

COPD exacerbations in the past 12 months, n (%)c
0 moderate or severe1 moderate or severe≥ 2 moderate or severe≥ 1 severe
7 (0.1)3762 (44.1)4770 (55.9)1811 (21.2)
Blood eosinophil countd
nMean, cells/mm3 (SD)≥ 150 cells/mm3, n (%)≥ 300 cells/mm3, n (%)
8514196.3 (132.9)5109 (59.9)1252 (14.7)
Post-albuterol FEV1, % predicted nMean (SD)
851943.39 (10.34)
Reversibility to albuterold,e
nMean difference in FEV1 before and after albuterol, mL (SD)Reversible, n (%)
8500145.0 (151.4)2610 (30.6)
Use of ICS at screening, n (%) 6754 (79.1)
Mean CAT total score (SD) 19.6 (6.5)Table 4
Baseline demographics (safety population).
CAT: COPD Assessment Test, COPD: chronic obstructive pulmonary disease, FEV1: forced
expiratory volume in 1 s, ICS: inhaled corticosteroid, mITT: modified intent-to treat, SD: standard
deviation.aNumber of pack-years smoked = (number of cigarettes each day/20) x number of years smoked. bDefined by baseline post-bronchodilator FEV1 (moderate: 50% to 80% predicted normal; severe:
30% to <50% predicted normal; very severe: <30% predicted normal);13 note that the study only
enrolled patients with baseline post-bronchodilator FEV1 <65% predicted normal.cExacerbations were classified as moderate if they required treatment with systemic corticosteroids
and/or antibiotics for at least 3 days (or a single depot injectable dose of corticosteroids), and as
severe if they resulted in hospitalization. dmITT population. eReversible is defined as improvement in FEV1 post-albuterol administration compared with
pre-albuterol of ≥ 12% and ≥ 200 mL.
18

Fig. 2. Distribution of baseline eosinophil counts (mITT population).
mITT: modified intent-to-treat.
19

4. Discussion
20

The ETHOS study will provide important data comparing the effects of two doses of BGF
MDI (320/18/9.6 μg and 160/18/9.6 μg) with BFF MDI 320/9.6 μg and GFF MDI 18/9.6 μg on
moderate or severe COPD exacerbation rates over 52 weeks. A benefit of BGF MDI 320/18/9.6 μg
versus corresponding dual therapies on the rate of moderate or severe exacerbations has been shown
over 24 weeks in KRONOS, with a statistically significant and clinically meaningful improvement
versus GFF MDI and a numerical improvement versus BFF MDI [6]. A majority of the KRONOS
study population had not experienced an exacerbation in the year prior to study entry [6]. ETHOS will
determine whether similar benefits of BGF MDI are observed over a longer treatment period in a
larger population of patients at high risk of exacerbations, with adequate statistical power to detect
differences between BGF MDI and BFF MDI on the rate of moderate or severe COPD exacerbations.
21

ETHOS is the first study to include triple ICS/LAMA/LABA therapies with two different
doses of the ICS component, allowing an examination of the dose response of BGF MDI relative to
dual therapies. Studies of low/medium-dose ICS/LABA formulations have previously found
significant reductions in exacerbation rates versus LABA therapy alone [20, 22, 23]. ETHOS will
explore whether triple therapy with a lower dose of ICS could be an alternative treatment option for
patients with COPD by evaluating if BGF MDI 160/18/9.6 μg demonstrates comparable or better
efficacy versus a higher dose ICS/LABA (BFF MDI 320/9.6 μg) in reducing exacerbation rates while
also providing greater improvements in lung function. The availability of two BGF MDI formulations
would allow ICS treatment to be titrated to the lowest effective dose for individual patients based on
outcomes such as exacerbations. In addition, the two ICS doses will allow for an assessment of
possible interactions between ICS dose, eosinophil levels, and other modifying factors on treatment
response. Building on previous findings that eosinophils may be a useful biomarker of response to
ICS therapy [6, 11, 12, 24], randomization in ETHOS has been stratified by eosinophil count (from
values obtained prior to randomization); using pre-specified subgroups and visualizing relationships
with eosinophil count as a continuous variable in nonparametric regressions will help clarify the use
of this biomarker in COPD. This is especially important given recent updates to treatment
recommendations in the 2019 GOLD report, which now considers eosinophil counts in the initial and
follow-up treatment algorithms [13]. Eosinophil levels were assessed at several time points during the
study, and these measurements will allow for exploratory analyses of the consistency of eosinophil
levels over time across the treatment arms [25]. Overall, the unique features of ETHOS will provide
important data to inform the overall benefit:risk ratio of ICS treatment in COPD, enabling clinicians
to better identify patients who may be adequately managed without an ICS, or with a lower dose of
ICS, based on key background features including prior exacerbations and eosinophil levels.
As in previous studies that investigated the effect of fixed triple versus dual therapies on
exacerbation rates (IMPACT [4] and TRIBUTE [5]), all patients enrolled in ETHOS had a history of
exacerbation in the past year, and the majority had previous treatment with an ICS. However,
inclusion and exclusion criteria regarding the severity of airflow limitation, exacerbation history, and
22

prior medications, as well as the run-in treatments used, differ across studies (as summarized in
Table 5) [4, 5]. It should be noted that in TRIBUTE, any prior ICS use ceased at study entry, while in
IMPACT and ETHOS, patients on stable doses of ICS continued their treatment until the day prior to
randomization. Overall, these study-design differences will need to be considered when comparing
the results and subsequent analyses of these studies.
ETHOS will also provide additional data regarding the long-term safety of BGF MDI. Two
52-week extensions of the KRONOS study have been completed in the USA [26] and Japan [27] to
assess the safety and tolerability of BGF MDI compared to dual therapies. In US patients, BGF MDI
was found to be well tolerated over 52 weeks of treatment, with no evidence that the pattern or
frequency of adverse events changed appreciably with longer-term exposure [28]. In addition, BGF
MDI treatment did not have any clinically significant effects on bone mineral density or ocular safety
outcomes [28], which have been previously associated with long-term ICS use [29]. Results from the
Japanese safety extension study will also be published in 2019. ETHOS will provide safety data over
52 weeks in a substantially larger global population than the two completed extension studies, and
will characterize the safety profile of two doses of BGF MDI relative to both dual therapies in patients
with moderate-to-very severe COPD who had experienced at least one exacerbation in the previous
12 months (and > 50% of whom had reported ≥ 2 exacerbations during this time).
TRIBUTE [5]N = 1532
IMPACT [4]N = 10,355
ETHOS N = 8572
Treatmentsa
ICS/LAMA/LABA BDP/G/F MDI174/22/9.6 μg BID
FF/UMEC/VI DPI100/62.5/25 μg QD
BGF MDI 320/18/9.6 μg BID160/18/9.6 μg BID
LAMA/LABA IND/GLY DPI85/54 μg QD
UMEC/VI DPI62.5/25 μg QD
GFF MDI 18/9.6 μg BID
ICS/LABA – FF/VI DPI100/25 μg QD
BFF MDI 320/9.6 μg BID
Inclusion/exclusion criteria
23

Post-bronchodilatorFEV1 % predicted
< 50% < 80% < 65%
Moderate or severe exacerbations (last year)
≥ 1 ≥ 1 (if FEV1 < 50%);
≥ 2 (if FEV1 ≥ 50%)
≥ 1 (if FEV1 < 50%);
≥ 2 moderate / ≥ 1
severe (if FEV1 ≥ 50%)
Excluded patients on prior triple therapy
Yes No No
Run-in
Duration 2 weeks 2 weeks 1–4 weeksb
Maintenance treatment(s)
IND/GLY DPI85/54 μg
Patients’ own medications (LAMA, LABA, or ICS, alone or in combination)
Ipratropium bromide QID and patients’ own ICS (if on an ICS at screening)
Table 5
Studies assessing the rate of moderate or severe COPD exacerbations over 52 weeks with triple versus
dual fixed-dose combination therapies.
BDP/G/F: beclometasone dipropionate/glycopyrrolate/formoterol fumarate,
BFF: budesonide/formoterol fumarate, BGF: budesonide/glycopyrrolate/formoterol fumarate,
BID: twice daily, CAT: COPD Assessment Test, COPD: chronic obstructive pulmonary disease,
DPI: dry powder inhaler, FEV1: forced expiratory volume in 1 s, FF/UMEC/VI: fluticasone
furoate/umeclidinium/vilanterol, FF/VI: fluticasone furoate/vilanterol, FVC: forced vital capacity,
GFF: glycopyrrolate/formoterol fumarate, ICS: inhaled corticosteroid,
IND/GLY: indacaterol/glycopyrrolate, LABA: long-acting β2-agonist, LAMA: long-acting muscarinic
antagonist, MDI: metered dose inhaler, QD: once daily, QID: four times daily,
UMEC/VI: umeclidinium/vilanterol.
Note: all studies enrolled patients with a confirmed diagnosis of COPD who were symptomatic (CAT
score ≥ 10) and current/former smokers, with an FEV1/FVC ratio < 0.70. The use of rescue
medication (albuterol and/or terbutaline) was permitted throughout all three studies. aDoses represent the total amount per administered dose, which is the sum of two actuations for
BDP/G/F MDI, BGF MDI, GFF MDI, and BFF MDI. Doses are expressed as μg of glycopyrrolate
(glycopyrronium bromide) and formoterol fumarate. bCould be extended to a maximum of 10 weeks if a patient experienced a COPD exacerbation, in
order to allow for treatment and recovery.
5. Conclusions
The ETHOS study will investigate exacerbations, patient-reported outcomes, safety, and
24

mortality in a population of > 8500 symptomatic patients with moderate-to-very severe COPD
receiving triple and dual fixed-dose combination therapies. Sub-studies will also examine lung
function (in > 3000 patients) and cardiovascular safety (in > 700 patients). For the first time in a 52-
week study of triple therapy, randomization has been stratified by eosinophil count, and two different
ICS doses (320 μg and 160 μg) of ICS/LAMA/LABA triple therapy will be compared to
LAMA/LABA and ICS/LABA therapies. This may provide support for the use of triple therapies with
multiple ICS doses, increasing the versatility of prescribed treatments for COPD and allowing for
optimization of the benefit:risk profile for individual patients. Overall, the findings are expected to
add to the growing body of literature establishing an important role for single inhaler triple therapies,
thus helping to refine treatment recommendations with the ultimate goal of minimizing disease burden
and improving outcomes for patients with COPD.
25

Funding
The ETHOS study is supported by Pearl – a member of the AstraZeneca Group. The sponsor
was involved in the study design; the collection, analysis and interpretation of data; the writing of the
report; and in the decision to submit the article for publication.
Declarations of interest
KFR reports personal fees from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi
Pharmaceuticals, InterMune, Novartis, Sanofi, and Teva; and grants from the Ministry of Education
and Science, Germany, outside the submitted work. FJM reports grants from AstraZeneca during the
conduct of the study; personal fees and non-financial support from the American College of Chest
Physicians, AstraZeneca, Boehringer Ingelheim, Chiesi, Concert, Continuing Education, Genentech,
GlaxoSmithKline, Inova Fairfax Health System, Miller Communications, the National Association for
Continuing Education, Novartis, Pearl – a member of the AstraZeneca Group, PeerView
Communications, Prime Communications, the Puerto Rican Respiratory Society, Roche, Sunovion,
and Theravance; non-financial support from ProterixBio; personal fees from the American Thoracic
Society, Columbia University, Haymarket Communications, Integritas, inThought Research,
MD Magazine, Methodist Hospital Brooklyn, New York University, Unity, UpToDate,
WebMD/MedScape, and Western Connecticut Health Network; and grants from the National
Institutes of Health, outside the submitted work. GTF reports grants, personal fees, and non-financial
support from AstraZeneca during the conduct of the study; grants, personal fees, and non-financial
support from AstraZeneca, Boehringer Ingelheim, Novartis, Pearl – a member of the AstraZeneca
Group, and Sunovion; grants and personal fees from Theravance; and personal fees from Circassia,
GlaxoSmithKline, Innoviva, Mylan, and Verona, outside the submitted work. CW declares no
competing interests. DS reports receiving personal fees from Apellis, Cipla, Genentech, Peptinnovate,
and Skyepharma, and grants and personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi,
GlaxoSmithKline, Glenmark, Menarini, Merck, Mundipharma, Novartis, Pfizer, Pulmatrix, Teva,
Therevance, and Verona, outside the submitted work. JAW reports receiving research grants from
26

AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Johnson & Johnson, and Novartis, outside the
submitted work. RT, ESR, SB, JM, PDa, CR, and PDo are employees of AstraZeneca.
Acknowledgements
We thank all the patients, their families and the team of investigators, research nurses, and
operations staff involved in ETHOS. Medical writing support, under the direction of the authors, was
provided by Julia King, PhD, of CMC Connect, a division of McCann Health Medical
Communications Ltd, Glasgow, UK, which was funded by AstraZeneca, Cambridge, UK in
accordance with Good Publication Practice (GPP3) guidelines [30].
Data availability
Data underlying the findings described in this manuscript may be obtained in accordance with
AstraZeneca's data-sharing policy described at:
https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure
27

REFERENCES
[1] D. Singh, A. Papi, M. Corradi, I. Pavlišová, I. Montagna, C. Francisco, G. Cohuet, S. Vezzoli, M.
Scuri, J. Vestbo, Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist
therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group,
randomised controlled trial, Lancet (London, England) 388 (10048) (2016) 963-973.
[2] D.A. Lipson, H. Barnacle, R. Birk, N. Brealey, N. Locantore, D.A. Lomas, A. Ludwig-Sengpiel,
R. Mohindra, M. Tabberer, C.Q. Zhu, S.J. Pascoe, FULFIL trial: once-daily triple therapy for patients
with chronic obstructive pulmonary disease, Am J Respir Crit Care Med 196 (4) (2017) 438-446.
[3] J. Vestbo, A. Papi, M. Corradi, V. Blazhko, I. Montagna, C. Francisco, G. Cohuet, S. Vezzoli, M.
Scuri, D. Singh, Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist
therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group,
randomised controlled trial, Lancet (London, England) 389 (10082) (2017) 1919-1929.
[4] D.A. Lipson, F. Barnhart, N. Brealey, J. Brooks, G.J. Criner, N.C. Day, M.T. Dransfield, D.M.G.
Halpin, M.K. Han, C.E. Jones, S. Kilbride, P. Lange, D.A. Lomas, F.J. Martinez, D. Singh, M.
Tabberer, R.A. Wise, S.J. Pascoe, Once-daily single-inhaler triple versus dual therapy in patients with
COPD, N Engl J Med 378 (18) (2018) 1671-1680.
[5] A. Papi, J. Vestbo, L. Fabbri, M. Corradi, H. Prunier, G. Cohuet, A. Guasconi, I. Montagna, S.
Vezzoli, S. Petruzzelli, M. Scuri, N. Roche, D. Singh, Extrafine inhaled triple therapy versus dual
bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel
group, randomised controlled trial, Lancet (London, England) 391 (10125) (2018) 1076-1084.
[6] G.T. Ferguson, K.F. Rabe, F.J. Martinez, L.M. Fabbri, C. Wang, M. Ichinose, E. Bourne, S.
Ballal, P. Darken, K. DeAngelis, M. Aurivillius, P. Dorinsky, C. Reisner, Triple therapy with
budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual
therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group,
multicentre, phase 3 randomised controlled trial, The Lancet Respiratory medicine 6 (10) (2018) 747-
758.
[7] J.A. Wedzicha, D. Banerji, K.R. Chapman, J. Vestbo, N. Roche, R.T. Ayers, C. Thach, R. Fogel,
F. Patalano, C.F. Vogelmeier, Indacaterol-glycopyrronium versus salmeterol-fluticasone for COPD, N
Engl J Med 374 (23) (2016) 2222-2234.
28

[8] K.R. Chapman, J.R. Hurst, S.M. Frent, M. Larbig, R. Fogel, T. Guerin, D. Banerji, F. Patalano, P.
Goyal, P. Pfister, K. Kostikas, J.A. Wedzicha, Long-Term Triple Therapy De-escalation to
Indacaterol/Glycopyrronium in Patients with Chronic Obstructive Pulmonary Disease (SUNSET): A
Randomized, Double-Blind, Triple-Dummy Clinical Trial, Am J Respir Crit Care Med 198 (3) (2018)
329-339.
[9] H. Magnussen, B. Disse, R. Rodriguez-Roisin, A. Kirsten, H. Watz, K. Tetzlaff, L. Towse, H.
Finnigan, R. Dahl, M. Decramer, P. Chanez, E.F. Wouters, P.M. Calverley, Withdrawal of inhaled
glucocorticoids and exacerbations of COPD, N Engl J Med 371 (14) (2014) 1285-1294.
[10] H. Watz, K. Tetzlaff, E.F.M. Wouters, A. Kirsten, H. Magnussen, R. Rodriguez-Roisin, C.
Vogelmeier, L.M. Fabbri, P. Chanez, R. Dahl, B. Disse, H. Finnigan, P.M.A. Calverley, Blood
eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal
of inhaled corticosteroids: a post-hoc analysis of the WISDOM trial, The Lancet Respiratory medicine
4 (5) (2016) 390-398.
[11] M. Bafadhel, S. Peterson, M.A. De Blas, P.M. Calverley, S.I. Rennard, K. Richter, M. Fageras,
Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive
pulmonary disease: a post-hoc analysis of three randomised trials, The Lancet Respiratory medicine 6
(2) (2018) 117-126.
[12] S. Pascoe, N. Locantore, M.T. Dransfield, N.C. Barnes, I.D. Pavord, Blood eosinophil counts,
exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with
chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised
controlled trials, The Lancet Respiratory medicine 3 (6) (2015) 435-442.
[13] D. Singh, A. Agusti, A. Anzueto, P.J. Barnes, J. Bourbeau, B.R. Celli, G.J. Criner, P. Frith,
D.M.G. Halpin, M. Han, M.V. Lopez Varela, F. Martinez, M. Montes de Oca, A. Papi, I.D. Pavord,
N. Roche, D.D. Sin, R. Stockley, J. Vestbo, J.A. Wedzicha, C. Vogelmeier, Global Strategy for the
Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD Science
Committee Report 2019, Eur Respir J pii: 1900164. doi: 10.1183/13993003.00164-2019. [Epub ahead
of print] (2019).
[14] European Medicines Agency, Inhaled corticosteroids (ICS) containing medicinal products
indicated in the treatment of chronic obstructive pulmonary disease (COPD), 2016.
https://www.ema.europa.eu/en/documents/referral/inhaled-corticosteroids-article-31-referral-prac-
assessment-report_en.pdf. (Accessed 9 April 2019).
29

[15] S. Suissa, V. Patenaude, F. Lapi, P. Ernst, Inhaled corticosteroids in COPD and the risk of
serious pneumonia, Thorax 68 (11) (2013) 1029-1036.
[16] K.M. Kew, A. Seniukovich, Inhaled steroids and risk of pneumonia for chronic obstructive
pulmonary disease, Cochrane Database Syst Rev (3) (2014) CD010115.
[17] C. Crim, M.T. Dransfield, J. Bourbeau, P.W. Jones, N.A. Hanania, D.A. Mahler, J. Vestbo, A.
Wachtel, F.J. Martinez, F. Barnhart, S. Lettis, P.M. Calverley, Pneumonia risk with inhaled
fluticasone furoate and vilanterol compared with vilanterol alone in patients with COPD, Ann Am
Thorac Soc 12 (1) (2015) 27-34.
[18] D.D. Sin, D. Tashkin, X. Zhang, F. Radner, U. Sjobring, A. Thoren, P.M. Calverley, S.I.
Rennard, Budesonide and the risk of pneumonia: a meta-analysis of individual patient data, Lancet
(London, England) 374 (9691) (2009) 712-9.
[19] B. Lipworth, C.R. Kuo, S. Jabbal, Current appraisal of single inhaler triple therapy in COPD, Int
J Chron Obstruct Pulmon Dis 13 (2018) 3003–3009.
[20] G.T. Ferguson, A. Papi, A. Anzueto, E.M. Kerwin, C. Cappelletti, E.A. Duncan, J. Nyberg, P.
Dorinsky, Budesonide/formoterol MDI with co-suspension delivery technology in COPD: the TELOS
study, The European respiratory journal 52 (3) (2018) pii: 1801334.
[21] ClinicalTrials.gov, Study to Assess the Efficacy and Safety of PT010 Relative to PT003 and
PT009 in Subjects With Moderate to Very Severe COPD (Ethos), 2017.
https://clinicaltrials.gov/ct2/show/NCT02465567. (Accessed 9 April 2019).
[22] G.T. Ferguson, A. Anzueto, R. Fei, A. Emmett, K. Knobil, C. Kalberg, Effect of fluticasone
propionate/salmeterol (250/50 µg) or salmeterol (50 µg) on COPD exacerbations, Respir Med 102 (8)
(2008) 1099-1108.
[23] A. Anzueto, G.T. Ferguson , G. Feldman, K. Chinsky, A. Seibert, A. Emmett, K. Knobil, D.
O'Dell, C. Kalberg, G. Crater, Effect of fluticasone propionate/salmeterol (250/50) on COPD
exacerbations and impact on patient outcomes, Copd 6 (5) (2009) 320-329.
[24] G. Brusselle, I.D. Pavord, S. Landis, S. Pascoe, S. Lettis, N. Morjaria, N. Barnes, E. Hilton,
Blood eosinophil levels as a biomarker in COPD, Respir Med 138 (2018) 21-31.
[25] N.C. Barnes, R. Sharma, S. Lettis, P.M. Calverley, Blood eosinophils as a marker of response to
inhaled corticosteroids in COPD, The European respiratory journal 47 (5) (2016) 1374-82.
30

[26] ClinicalTrials.gov, Study to Assess the Safety and Tolerability of PT010, PT009 and PT003 in
Subjects With Moderate to Very Severe Chronic Obstructive Pulmonary Disease, 2018.
https://clinicaltrials.gov/ct2/show/NCT02536508. (Accessed 9 April 2019).
[27] ClinicalTrials.gov, Study to Assess the Safety and Efficacy of PT010, PT003, and PT009 in
Japanese Subjects With COPD Compared With Symbicort® Turbohaler®, 2017.
https://clinicaltrials.gov/ct2/show/NCT03262012. (Accessed 9 April 2019).
[28] E.M. Kerwin, G.T. Ferguson, M. Mo, K. DeAngelis, P. Dorinsky, Bone mineral density and
ocular safety after 52 weeks' treatment with budesonide/glycopyrrolate/formoterol fumarate metered
dose inhaler (BGF MDI) using co-suspension delivery technology in COPD, 2019.
https://www.abstractsonline.com/pp8/#!/5789/presentation/19649. (Accessed 9 April 2019).
[29] D. Price, B. Yawn, G. Brusselle, A. Rossi, Risk-to-benefit ratio of inhaled corticosteroids in
patients with COPD, Prim Care Respir J 22 (1) (2013) 92-100.
[30] W.P. Battisti, E. Wager, L. Baltzer, D. Bridges, A. Cairns, C.I. Carswell, L. Citrome, J.A. Gurr,
L.A. Mooney, B.J. Moore, T. Peña, C.H. Sanes-Miller, K. Veitch, K.L. Woolley, Y.E. Yarker, Good
publication practice for communicating company-sponsored medical research: GPP3, Ann Intern Med
163 (6) (2015) 461-464
31

Supplemental material
Methods
The ETHOS study is being conducted in the following countries: Argentina, Australia, Austria,
Belgium, Canada, Chile, China, Czech Republic, France, Germany, Hungary, Italy, Japan, Mexico,
the Netherlands, New Zealand, Peru, Poland, Russia, Serbia, South Africa, Spain, Sweden, Taiwan,
the United Kingdom and the United States of America.
Inclusion criteria
Each patient must meet the following criteria to be enrolled in this study:
1. Give their signed, written, informed consent to participate.
2. Are at least 40 years of age and no older than 80 years at Visit 1.
3. A female is eligible to enter and participate in the study if she is of:
a. Non-childbearing potential (i.e. physiologically incapable of becoming pregnant, including
any female who is 2 years post-menopausal)
b. Childbearing potential, has a negative serum pregnancy test at Visit 1, and agrees to an
acceptable contraceptive method used consistently and correctly (i.e. in accordance with the
approved product label and the instructions of the physician for the duration of the study –
from Visit 1 [screening] until 14 days after the final visit).
4. Have an established clinical history of chronic obstructive pulmonary disease (COPD) as
defined by the American Thoracic Society (ATS)/European Respiratory Society (ERS) [1] or
by locally applicable guidelines, e.g. Japanese Respiratory Society (JRS) Guidelines [2],
characterized by progressive airflow limitation associated with an abnormal inflammatory
response of the lungs to noxious particles or gases, primarily caused by cigarette smoking.
5. Tobacco use: Current or former smokers with a history of at least 10 pack-years of cigarette
smoking. [Number of pack-years = (number of cigarettes per day / 20) x number of years
32

smoked (e.g. 20 cigarettes per day for 10 years, or 10 cigarettes per day for 20 years represent
10 pack-years)].
6. COPD severity: An established clinical history of COPD and severity defined as:
At Visit 1, forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio must
be < 0.70 and FEV1 must be < 65% predicted normal value.
At Visit 2, post-bronchodilator FEV1/FVC ratio of < 0.70 and post-bronchodilator FEV1
must be ≥ 25% to < 65% predicted normal value.
At Visit 4, the average of the -60 min and -30 min pre-dose FEV1 assessments must be
< 65% predicted normal value. Note: This criterion applies to patients in the pulmonary
function test (PFT) sub-study only.
Note: All values calculated using the National Health and Nutrition Examination Survey III
reference equations (or reference norms applicable to other regions, e.g. for Japan, use JRS
reference equations [2])
Symptomatic (COPD assessment test score ≥ 10) at screening (Visit 1).
7. Required COPD maintenance therapy: All patients must have been on two or more inhaled
maintenance therapies for the management of their COPD for at least 6 weeks prior to
screening. Scheduled short-acting β2-agonists and/or short-acting muscarinic antagonists are
considered inhaled maintenance therapies.
8. History of exacerbations:
Patients with a post-bronchodilator FEV1 < 50% of predicted normal must have a
documented history of ≥ 1 moderate or severe COPD exacerbation in the 12 months
prior to screening (Visit 1).
Patients with a post-bronchodilator FEV1 ≥ 50% of predicted normal must have a
documented history of ≥ 2 moderate exacerbations or a documented history of ≥ 1 severe
COPD exacerbation in the 12 months prior to screening (Visit 1).
33

Note: Prior use of antibiotics and/or oral corticosteroids alone does not qualify as a COPD
exacerbation history unless the use was associated with treatment of worsening symptoms of
COPD (e.g. increased dyspnea, increased sputum volume, or a change in sputum purulence
[color]). Patient verbal reports are not acceptable.
Antibiotics or corticosteroids used for the treatment of upper respiratory infections with
no lower respiratory symptoms do not qualify for the treatment of COPD exacerbation.
9. Patient is willing and, in the opinion of the investigator, able to adjust current COPD therapy,
as required by the protocol.
10. Screening clinical laboratory tests must be acceptable to the investigator.
11. Screening electrocardiogram (ECG) must be acceptable to the investigator.
12. Chest X-ray or computed tomography (CT) scan of the chest/lungs within 6 months prior to
Visit 1 must be acceptable to the investigator. Patients who have a chest X-ray that reveals
clinically significant abnormalities not believed to be due to the presence of COPD should not
be included. A chest X-ray must be conducted if the most recent chest X-ray or CT scan are
more than 6 months old at the time of Visit 1, except in countries with restrictive radiology
assessment practice where only patients who have had an chest X-ray or CT scan (thorax)
performed outside of the study in the last 6 months are allowed to be enrolled. Alternatively,
in these countries, magnetic resonance imaging may be used instead of a CT scan or chest X-
ray as per local practice assessment.
13. Compliance: Patients must be willing to remain at the study center as required per protocol to
complete all visit assessments.
Exclusion criteria
Patients who meet any of the following criteria will be excluded from the study.
34

1. Significant diseases or conditions other than COPD, which, in the opinion of the investigator,
may put the patient at risk because of participation in the study or may influence either the
results of the study or the patient’s ability to participate in the study.
2. Women who are pregnant or lactating, or are planning to become pregnant during the course
of the study, or women of childbearing potential who are not using an acceptable method of
contraception.
3. Respiratory:
a. Asthma: Patients who, in the opinion of the investigator, have a current diagnosis of
asthma.
b. Alpha-1 antitrypsin deficiency: Patients who have alpha-1 antitrypsin deficiency as the
cause of COPD.
c. Other respiratory disorders: Patients who have other active pulmonary disease such as
active tuberculosis, lung cancer, significant bronchiectasis (high-resolution CT evidence
of bronchiectasis that causes repeated acute exacerbations), sarcoidosis, idiopathic
interstitial pulmonary fibrosis, primary pulmonary hypertension, or uncontrolled sleep
apnea (i.e. in the opinion of the investigator the severity of the disorder would impact the
conduct of the study). Note: Allergic rhinitis is not exclusionary.
d. Lung volume reduction: Patients who have undergone lung volume reduction surgery,
lobectomy, or bronchoscopic lung volume reduction (endobronchial blockers, airway
bypass, endobronchial valves, thermal vapor ablation, biological sealants, and airway
implants) within 6 months of Visit 1.
e. Hospitalization: Patients who have been hospitalized due to poorly controlled COPD
within 6 weeks prior to Visit 1 (screening) with less than a 4-week washout of
corticosteroids and/or antibiotics prior to Visit 1 (screening).
f. Poorly controlled COPD: Patients who have poorly controlled COPD, defined as acute
worsening of COPD that requires treatment with oral corticosteroids or antibiotics within
6 weeks prior to Visit 1 (screening) with less than a 4-week washout of corticosteroids
and/or antibiotics prior to Visit 1 (screening).
35

g. Lower respiratory tract infection: Patients who had lower respiratory tract infections that
required antibiotics within 6 weeks prior to Visit 1 (screening) with less than a 4-week
washout of antibiotics prior to Visit 1 (screening).
h. Other respiratory tract infections (e.g. upper respiratory tract infection) that have not
resolved at least 7 days prior to screening.
i. Chest X-ray (frontal and lateral) with suspicion of pneumonia or other
condition/abnormality that will require additional investigation/treatment, or put the
patient at risk because of participation in the study.
j. Risk factors for pneumonia: Immune suppression (e.g. human immunodeficiency virus),
severe neurological disorders affecting control of the upper airway or other risk factors
that, in the opinion of the investigator, would put the patient at substantial risk of
pneumonia.
k. Pneumonia not clinically resolved within 14 days of Visit 1.
l. Spirometry performance:
Acceptability: Patients who cannot perform acceptable spirometry (i.e. meet
ATS/ERS acceptability criteria).
Repeatability: Patients who cannot perform technically acceptable spirometry with
at least three acceptable flow-volume curves with two or more meeting ATS
repeatability criteria for FEV1 during at least one of the pre-bronchodilator
assessments at Visit 2 (-60 min or -30 min) and at the post-bronchodilator
assessment at Visit 2.
Note: Patients who have met all of the inclusion criteria, but have failed to meet
acceptability or repeatability criteria at Visit 1, may continue to Visit 2. Provided these
patients meet all spirometry criteria at Visit 2, including acceptability and repeatability,
they are eligible for inclusion in the main study but they are excluded from participating
in the PFT sub-study. Patients who fail to meet acceptability and repeatability criteria at
Visit 2 must be screen failed.
36

FEV1 baseline stability (for PFT sub-study only): Patients who cannot meet
protocol-specified baseline stability criteria. FEV1 baseline stability is defined as
the average of the -60 min and -30 min pre-dose FEV1 assessments at Visit 4 being
within ± 20% or 200 mL of the mean of the pre-bronchodilator FEV1 assessments
obtained at the two preceding visits (average of pre-dose FEV1 assessments
obtained at Visit 2 and Visit 3).
m. Oxygen: Patients receiving long-term-oxygen therapy or nocturnal oxygen therapy
required for > 15 h a day. Note: As-needed oxygen use is not exclusionary.
n. Patient use of any non-invasive positive pressure ventilation device. Note: Patients using
continuous positive airway pressure or bi-level positive airway pressure for sleep apnea
syndrome are allowed in the study if not used for ventilatory support.
o. Change in smoking status (i.e. start or stop smoking) or initiation of a smoking-cessation
program within 6 weeks of Visit 1 and throughout the screening period (Visit 1 to
Visit 4).
p. Pulmonary rehabilitation: Patients who have participated in the acute phase of a
pulmonary rehabilitation program within 4 weeks prior to Visit 1 (screening) or who are
scheduled to enter the acute phase of a pulmonary rehabilitation program during the
study. These patients will be allowed to rescreen after completion of the acute phase of
pulmonary rehabilitation. Patients who are in the maintenance phase of a pulmonary
rehabilitation program are not to be excluded.
q. Patients who have initiated or altered the dose regimen of intranasal corticosteroids,
intranasal antihistamines, or a combination thereof within 7 days prior to Visit 1 or
during the screening period (Visit 1 to Visit 4).
4. Cardiac disease:
a. Patients who have unstable ischemic heart disease, left ventricular failure, or documented
myocardial infarction within 6 months of enrollment. Patients with a recent history of
acute coronary syndrome, or who have undergone percutaneous coronary intervention or
coronary artery bypass graft within the past 3 months are to be excluded.
37

b. Patients with congestive heart failure (New York Heart Association Class III/IV).
c. Clinically significant abnormal ECG, defined as (but not limited to) any of the following:
Clinically significant conduction abnormalities (e.g. left bundle branch block,
Wolff-Parkinson-White syndrome, or evidence of second-degree [Mobitz Type II]
or third-degree atrioventricular block [unless a pacemaker or defibrillator has been
inserted]).
Clinically significant arrhythmias (e.g. atrial fibrillation with irregular ventricular
response, atrial flutter, ventricular tachycardia). Note: Atrial fibrillation that has
been clinically stable for at least 6 months and that has been appropriately treated
with anticoagulation and controlled with a rate control strategy (i.e. selective β-
blocker, calcium channel blocker, digoxin, or ablation therapy) for at least
6 months is allowed for inclusion. In such patients, if atrial fibrillation is present at
Visit 1, resting ventricular rate must be < 100 beats per min (bpm).
QT interval corrected for heart rate (using Fridericia’s formula; QTcF) ≥ 500
milliseconds (msec) in patients with QRS < 120 msec and QTcF ≥ 530 msec in
patients with QRS ≥ 120 msec.
Ventricular rate < 45 bpm.
ST-T wave abnormalities deemed to be clinically significant by the investigator.
Note: Patients with non-specific ST-T wave abnormalities that are not deemed
clinically significant (per investigator) are allowed.
Any other ECG abnormalities not listed above that, in the opinion of the
investigator, are clinically significant.
d. Patients who have clinically significant uncontrolled hypertension.
5. Neurological:
a. Patients with seizures requiring anticonvulsants within 12 months prior to Visit 1
(Screening). Note: Patients treated with anticonvulsant medication for 12 months or more
with no seizure events are eligible.
38

b. Patients taking selective serotonin reuptake inhibitors or serotonin-norepinephrine
reuptake inhibitors whose dose has not been stable for at least 4 weeks prior to Visit 1 or
is altered at any point during the screening period (Visit 1 to Visit 4), or exceeds the
maximum recommended dose.
c. Patients who have experienced a cerebrovascular accident within 6 months prior to
Visit 1.
6. Renal:
a. Patients with symptomatic prostatic hypertrophy that is clinically significant and not
adequately controlled with appropriate therapy in the opinion of the investigator. Patients
with a trans-urethral resection of prostate or full resection of the prostate within 6 months
prior to Visit 1 are excluded from the study.
b. Patients with bladder neck obstruction or urinary retention that is clinically significant in
the opinion of the investigator.
c. Patients with a calculated creatinine clearance ≤ 30 mL/min using the Chronic Kidney
Disease Epidemiology Collaboration formula [3] at Visit 1 and on repeat testing prior to
Visit 2.
Note: Patients with overactive bladder syndrome treated with oral anticholinergics who have
been on treatment for at least 1 month are allowed in the study.
7. Endocrine:
a. Patients who, in the opinion of the investigator, have uncontrolled hypo- or
hyperthyroidism, hypokalemia, or hyperadrenergic state.
b. Patients who, in the opinion of the investigator, have uncontrolled Type I or II diabetes.
8. Liver: Patients with abnormal liver function tests defined as aspartate transaminase, alanine
transaminase, or total bilirubin ≥ 1.5 times upper limit of normal at Visit 1 and on repeat
testing prior to Visit 2. Note: Chronic stable hepatitis B and C are acceptable if the patient
otherwise meets study entry criteria.
39

9. Cancer: Patients who have cancer that has not been in complete remission for at least 5 years.
Note: Patients with squamous cell carcinoma of the skin, basal cell carcinoma of the skin, or
localized prostate cancer are eligible if, in the opinion of the investigator, the condition has
been adequately worked up, is clinically controlled, and the patient’s participation in the study
would not represent a safety concern.
10. Glaucoma: Patients with a diagnosis of narrow-angle glaucoma, which, in the opinion of the
investigator, has not been adequately treated. All medications approved for control of
intraocular pressure are allowed, including topical ophthalmic non-selective β-blockers (such
as betaxolol, carteolol, levobunolol, metipranolol, and timolol), and prostaglandin analogs.
11. Drug allergy: Patients who have a history of hypersensitivity to β2-agonists, budesonide or
any other corticosteroid components, glycopyrronium or other muscarinic anticholinergics, or
any component of the metered dose inhaler (MDI).
12. Substance abuse: Patients who, in the opinion of the investigator, significantly abuse alcohol
or drugs.
13. Medication prior to spirometry: Patients who are medically unable to withhold their short-
acting bronchodilators for the 6-h period required prior to spirometry testing at each study
visit will be ineligible to participate in the PFT sub-study.
14. Prohibited medications: Patients who, in the opinion of the investigator, would be unable to
abstain from protocol-defined prohibited medications during the screening period and
treatment phases of this study.
15. Patients using any herbal inhalation and nebulizer products within 2 weeks prior to Visit 1
(screening) and do not agree to stop using them during the study-drug treatment.
Note: Nebulized products (e.g. albuterol/salbutamol, ipratropium) are acceptable, but require
a minimum of a 6-h washout prior to Visit 1 and must be discontinued at Visit 1 and
throughout the study.
16. Vaccinations: Patients who received a live attenuated vaccination within 7 days prior to
Visit 1 (screening).
40

17. Non-compliance: Patients unable to comply with study procedures including non-compliance
with diary completion (i.e. < 70% completion of diary assessments in the last 7 days
preceding Visit 4).
18. Affiliations with investigator site: Study investigators, sub-investigators, study coordinators,
employees of a participating investigator, or immediate family members of the
aforementioned are excluded from participation in this study.
19. Questionable validity of consent: Patients with a history of psychiatric disease, intellectual
deficiency, poor motivation, substance abuse (including drug and alcohol), or other conditions
that will limit the validity of informed consent to participate in the study.
20. Use of prohibited COPD medications following Visit 1 (see Supplemental Table S1).
21. Investigational drugs or devices: Treatment with an investigational study drug or device in
another clinical study within the last 30 days or five half-lives prior to Visit 1 (screening),
whichever is longer. Note: Participation in observational studies (i.e. studies that do not
require change to medication or an additional intervention) is not exclusionary.
22. Hand-to-breath coordination: Patients who require the use of a spacer device to compensate
for poor hand-to-breath coordination with a MDI. Note: Use of a nebulizer to deliver
maintenance COPD medications is prohibited throughout the study.
23. Previous participation: Patients who were previously enrolled in any budesonide/formoterol
fumarate MDI or budesonide/glycopyrrolate/formoterol fumarate MDI study conducted or
funded by the sponsor of this study.
41

24-h Holter monitoring sub-study exclusion criteria
Patients with a pacemaker or implantable cardioverter-defibrillator/cardiac resynchronization
therapy/cardiac resynchronization therapy-defibrillator devices will not be allowed into the Holter
monitor sub-study. Clinically significant abnormal findings during the baseline Holter monitor
recording are defined as (but not limited to) any of the following:
1. Average heart rate ≤ 40 bpm for any 1 h.
2. Atrioventricular block (second degree, Type 2, or third degree).
3. Sinus pause of:
2.5 s duration during daytime.
3.0 s duration during night-time.
4. Any episode of ventricular flutter and/or ventricular fibrillation.
5. Any episode of non-sustained ventricular tachycardia (VT) with symptoms of hypotension or
syncope or asymptomatic non-sustained VT > 15 ventricular premature beats in a row.
6. Sustained VT (> 30 s in duration).
7. Five or more episodes of non-sustained VT/24 h.
8. Greater than 500 ventricular premature beats/h.
REFERENCES
[1] B.R. Celli, W. MacNee, and ATS/ERS Task Force, Standards for the diagnosis and treatment of
patients with COPD: a summary of the ATS/ERS position paper, Eur Respir J 23 (6) (2004) 932-946.
[2] The Japanese Respiratory Society, Guidelines for the Diagnosis and Treatment of COPD, 4th
Edition, 2013. http://www.jrs.or.jp/. (Accessed 9 April 2019).
[3] A.S. Levey, L.A. Stevens, C.H. Schmid, Y.L. Zhang, A.F. Castro, 3rd, H.I. Feldman, J.W. Kusek,
P. Eggers, F. Van Lente, T. Greene, J. Coresh, CKD-EPI (Chronic Kidney Disease Epidemiology
Collaboration), A new equation to estimate glomerular filtration rate, Ann Intern Med 150 (9) (2009)
604-612.
42

Class of medication Minimum washout period prior to Visit 2
LAMAs Tiotropium: 14 days
Aclidinium: 7 days
Glycopyrronium: 7 days
Umeclidinium: 7 days
SAMAsa 6 h
LABAs (inhaled) 7 days (14 days for indacaterol and olodaterol)
Fixed combinations of LABA/LAMA 7 days (14 days for indacaterol/glycopyrronium and
olodaterol/tiotropium)
Fixed combinations of LABA/ICS 7 days
Fixed combinations of SABAs and SAMAs 6 h
SABAsb 6 h
Oral β-agonists 2 days
Theophylline (total daily dose
> 400 mg/day)c
7 days
Supplemental Table S1
Prohibited COPD medications and required washout periods prior to Visit 2.
COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid; LABA: long-acting β2-
agonist; LAMA: long-acting muscarinic antagonist; SABA: short-acting β2-agonist; SAMA: short-
acting muscarinic antagonists.
Note: Roflumilast (or any phosphodiesterase-4 inhibitor) is allowed provided the subject has been on
a stable dose of therapy for at least 2 months prior to randomization.aDiscontinue and use only sponsor-provided ipratropium bromide during screening. bDiscontinue and use only sponsor-provided rescue salbutamol throughout the study.cTheophylline (< 400 mg/day) is permitted provided the subject has been on a stable dose of therapy
for at least 4 weeks prior to randomization.
43