veneus en arterieel access 2015-2016 - UZ Leuven · Measuring central venous pressure lat 2 CETL...
113
Dr. Johan De Coster Dienst Anesthesiologie UZ Gasthuisberg Veneus en arterieel access
Transcript of veneus en arterieel access 2015-2016 - UZ Leuven · Measuring central venous pressure lat 2 CETL...
Dr. Johan De CosterDienst AnesthesiologieUZ Gasthuisberg
Veneus en arterieel access
➡Perifeer infuus➡Drukmonitoring➡Centraal veneuze catheter ➡Arteriële catheter➡Swan Ganz catheter
➡Perifeer infuus
Techniek:➡ onthaar de huid met een clipper➡ ontsmet de handen met alcogel➡ leg alle materiaal klaar➡ leg garrot aan➡ ontsmet de handen met alcogel➡ ontsmet de huid met choorhexidine 0,5 in alcohol 70%➡ trek niet-steriele handschoenen aan (bescherm jezelf)➡ prik op steriele manier➡ sluit infuus aan
Perifeer infuus
bron: Dienst Ziekenhuishygiëne UZ Leuven
Techniek:➡ onthaar de huid met een clipper: scheermesje beschadigt
de huid
Perifeer infuus
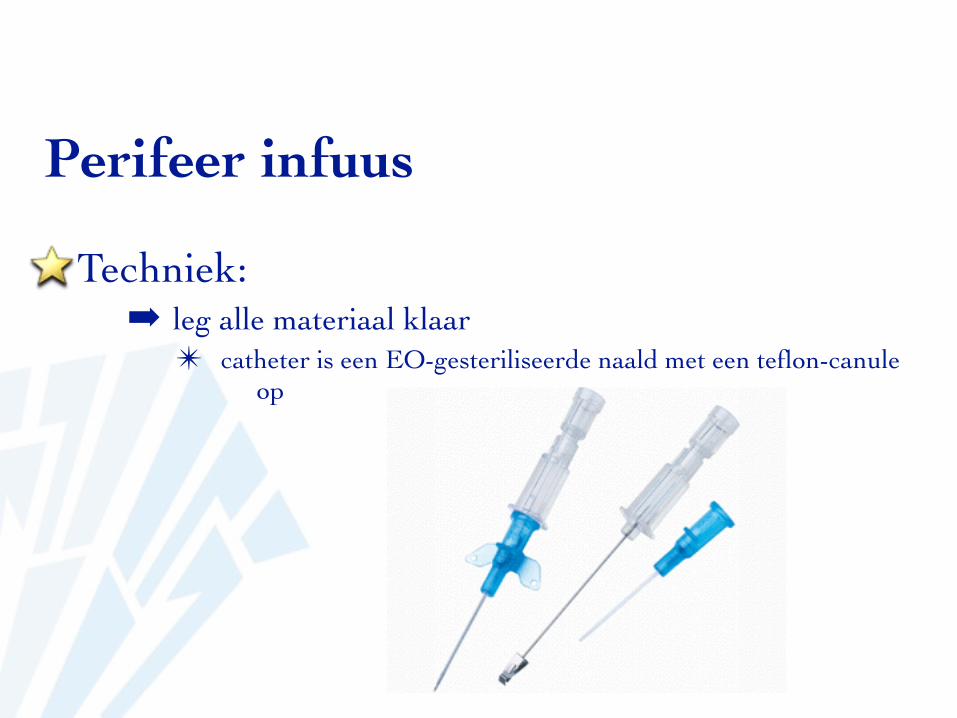
Techniek:➡ leg alle materiaal klaar
✴ catheter is een EO-gesteriliseerde naald met een teflon-canule op
Perifeer infuus
bepaalt debiet
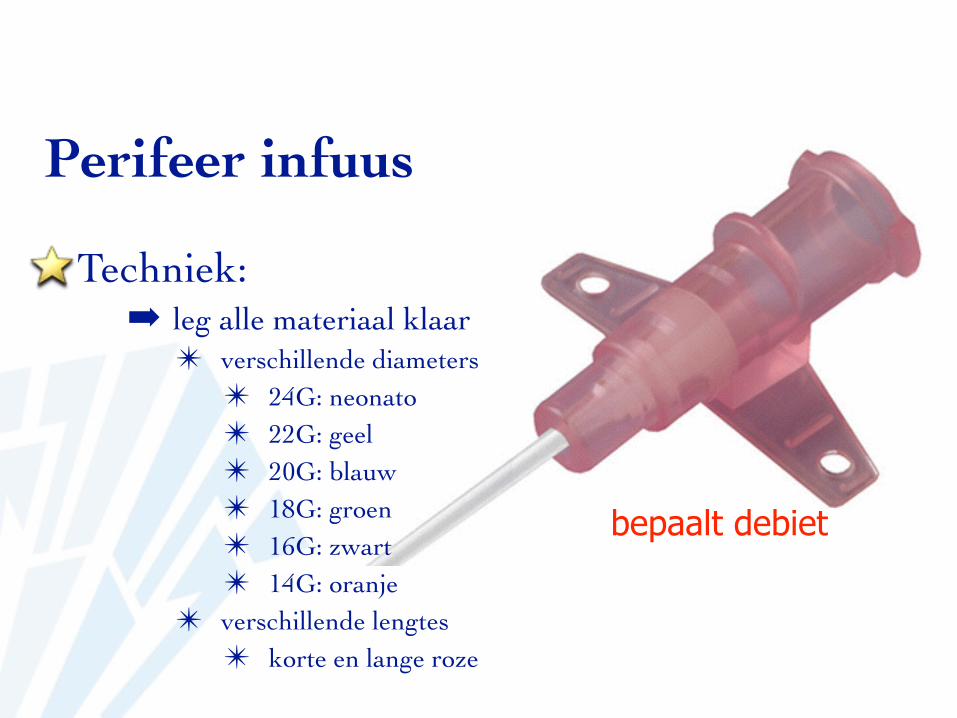
Techniek:➡ leg alle materiaal klaar
✴ verschillende diameters✴ 24G: neonato✴ 22G: geel✴ 20G: blauw✴ 18G: groen✴ 16G: zwart✴ 14G: oranje
✴ verschillende lengtes✴ korte en lange roze
bepaalt debiet
Perifeer infuus
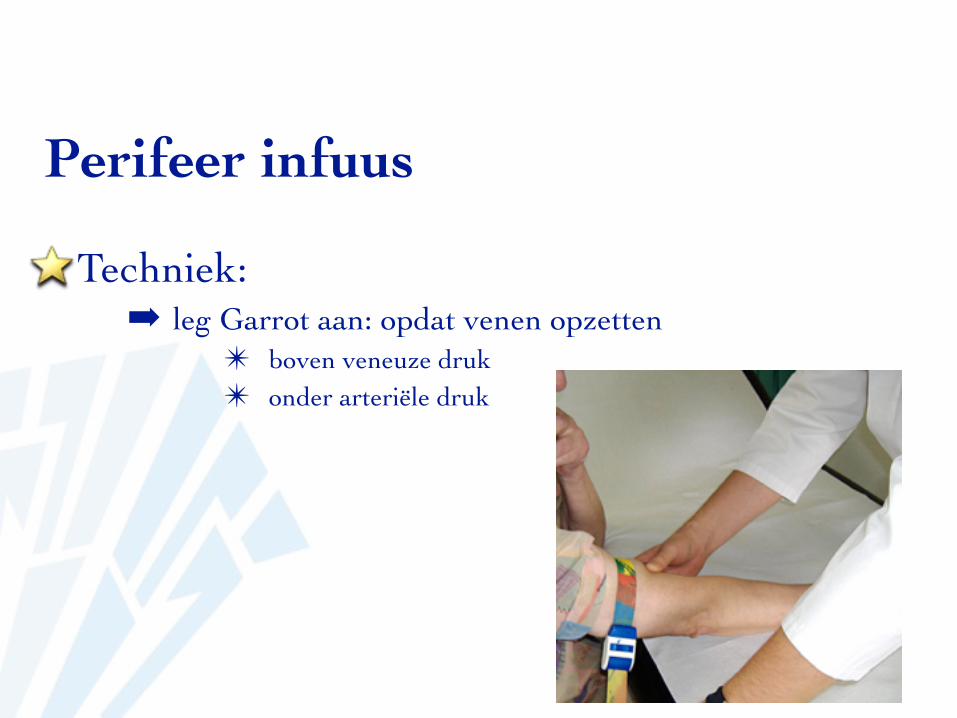
Techniek:➡ leg Garrot aan: opdat venen opzetten
✴ boven veneuze druk✴ onder arteriële druk
Perifeer infuus
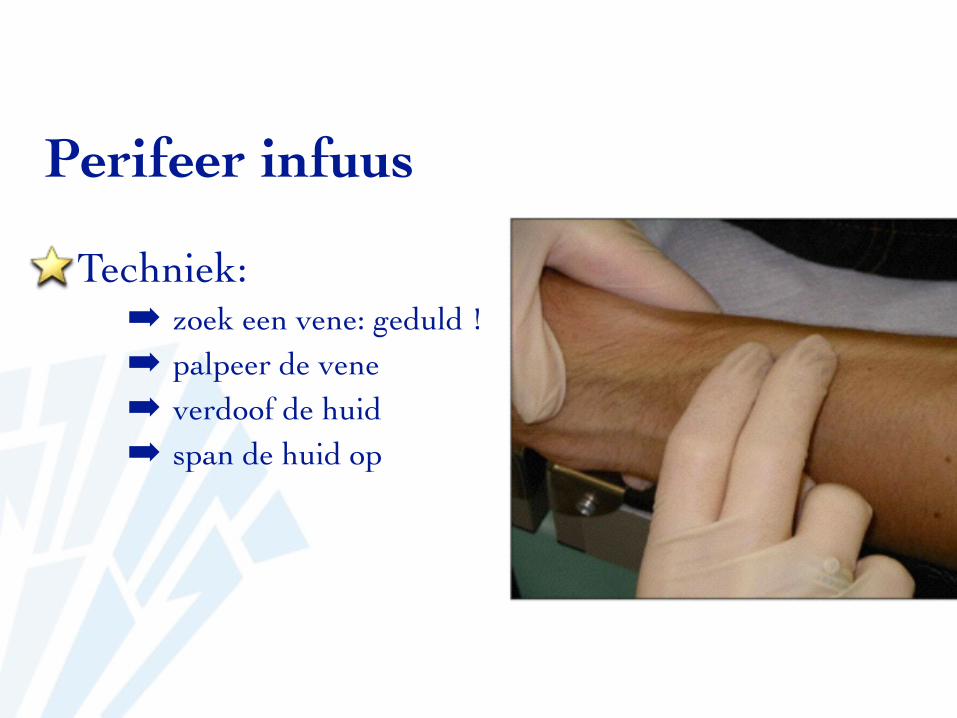
Techniek:➡ zoek een vene: geduld !!➡ palpeer de vene➡ verdoof de huid➡ span de huid op
Perifeer infuus
Perifeer infuus
Techniek:➡ bevel naar boven➡ prik aan en schuif aan tot de kamer vult;
➡ voldoende diep➡ ondiep: naald te paard, teflon nog niet in vene ==> schuift niet op➡ te diep: doorprikken van de vene
Perifeer infuus
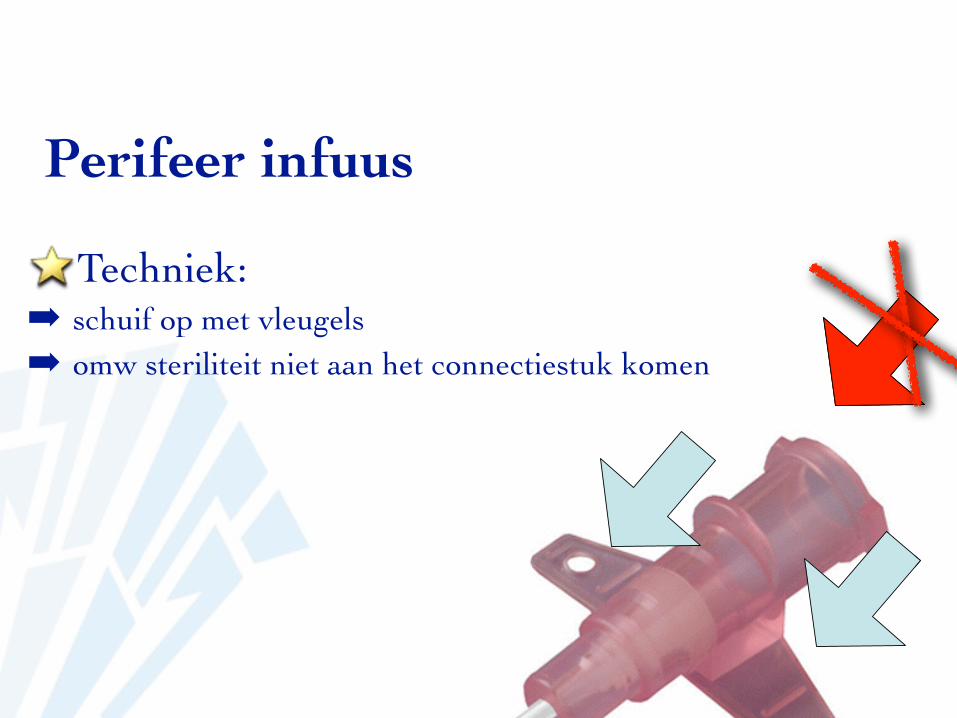
Techniek:➡ schuif op met vleugels➡ omw steriliteit niet aan het connectiestuk komen
Perifeer infuus
Techniek:➡ sluit aan➡ verwijder bloed➡ maak verband➡ trek handschoenen uit en gebruik alcogel
Perifeer infuus
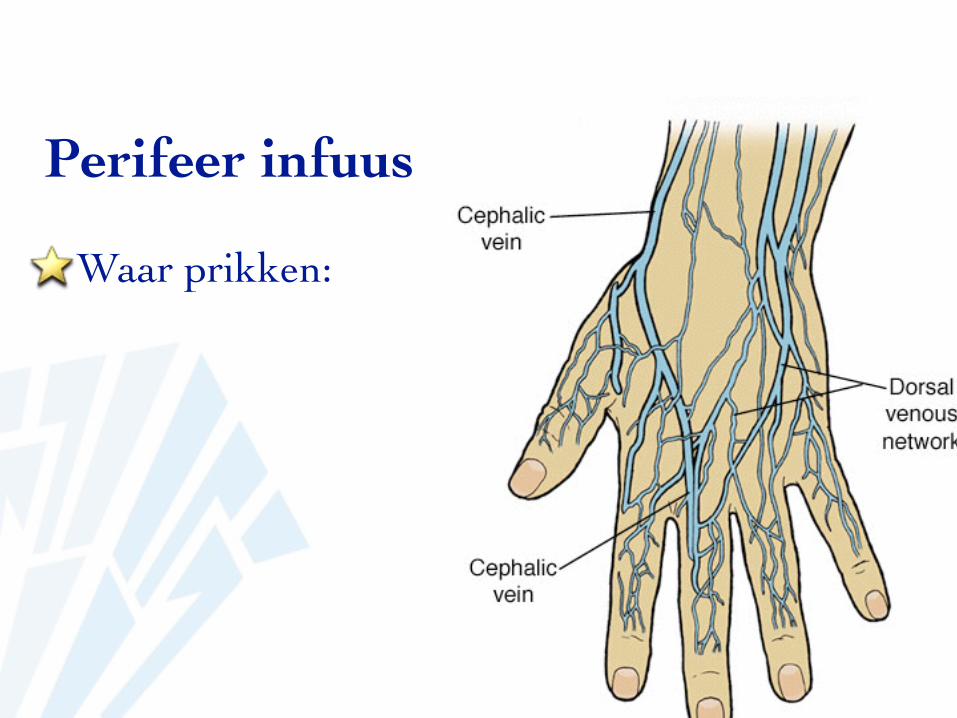
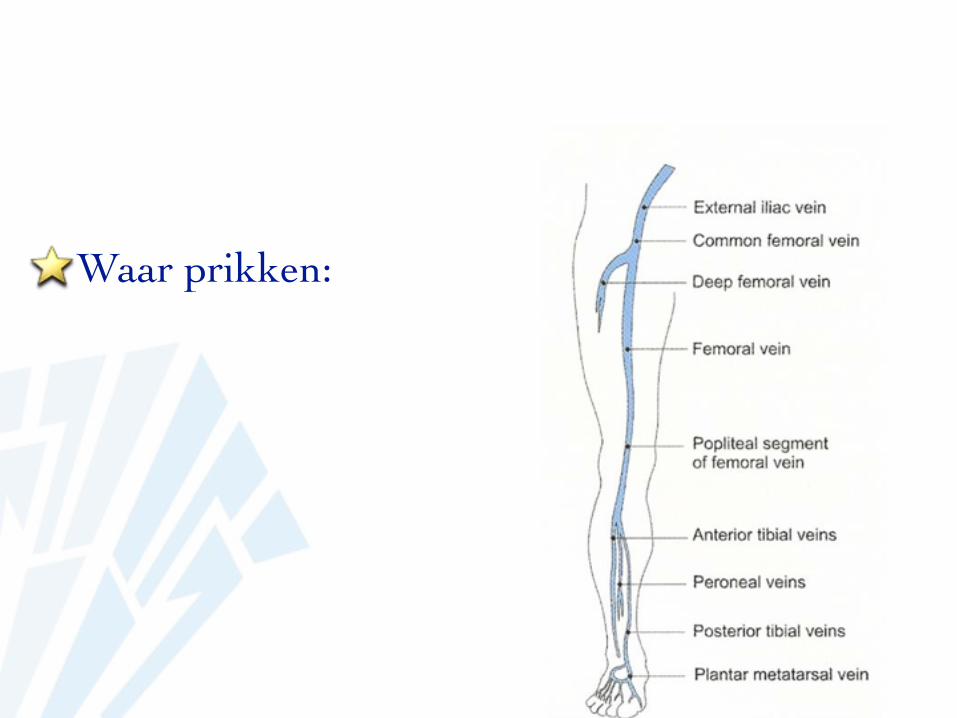
Waar prikken:
Perifeer infuus
Waar prikken:
Perifeer infuus
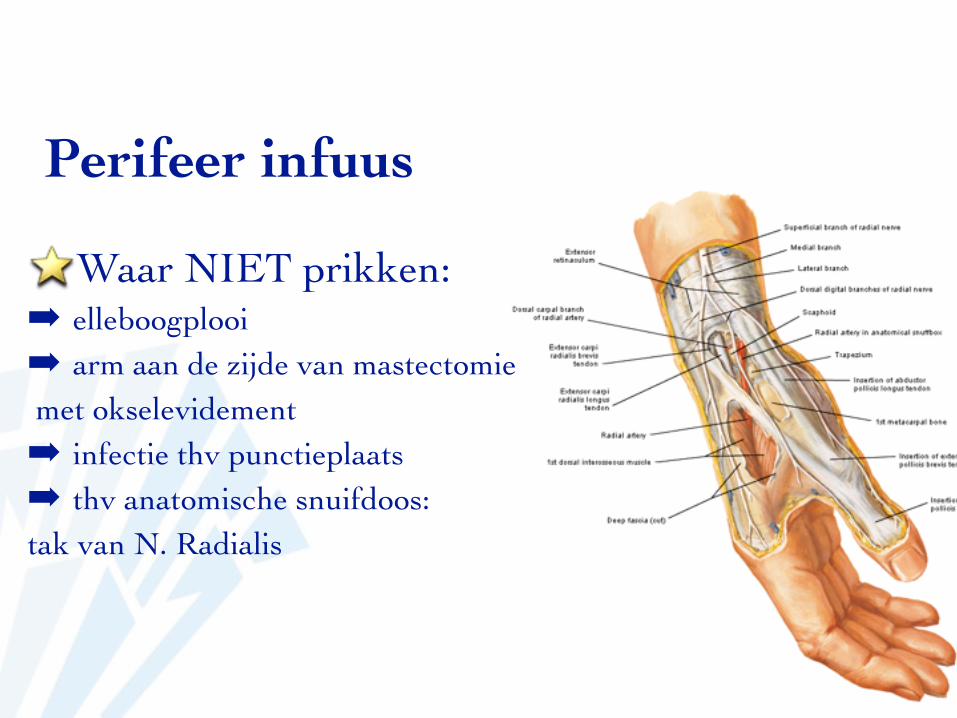
Waar NIET prikken:➡ elleboogplooi➡ arm aan de zijde van mastectomie met okselevidement➡ infectie thv punctieplaats➡ thv anatomische snuifdoos: tak van N. Radialis
Perifeer infuus
complicaties➡ hematoom➡ bloedverlies➡ paraveneus infuus➡ infectie
Perifeer infuus
problemen➡ weinig oppervlakkige venen ➡ angst: collaps van de vene➡ koude: vasoconstrictie➡ obesitas
Perifeer infuus
echo-guided
http://www.youtube.com/watch?v=fie9DI8lV3M
Perifeer infuus
wat mag er niet via perifeer infuus:➡ diprivan 2%➡ KCL in hoge dosis: vene-irritatief➡ cytostatica➡ vancomycine➡ bij voorkeur geen vaso-actieve drips
Perifeer infuus
video procedurehttp://www.youtube.com/watch?v=BiWstgS7hWw
Perifeer infuus: alternatief
intratracheale toediening van medicatie➡ tijdens reanimatie en geen access
intraosseuze toediening bij kinderen➡ bij kleine kinderen➡ in urgente situaties
Perifeer infuus: alternatief
diepe veneuze catheterkorte ingrepen: evt overwegen geen infuus te
plaatsen ???
Perifeer infuus: opm
EO !!!!latex-vrij (cave bruine Garrot : latex)

Perifeer infuus: tips and tricks
geduld !!!garrot correcte manier aangelegdkies juiste venekies juiste dikte catheter
afh van veneafh van ingreep
zorg dat teflon in de vene (te paard)
➡drukmonitoring
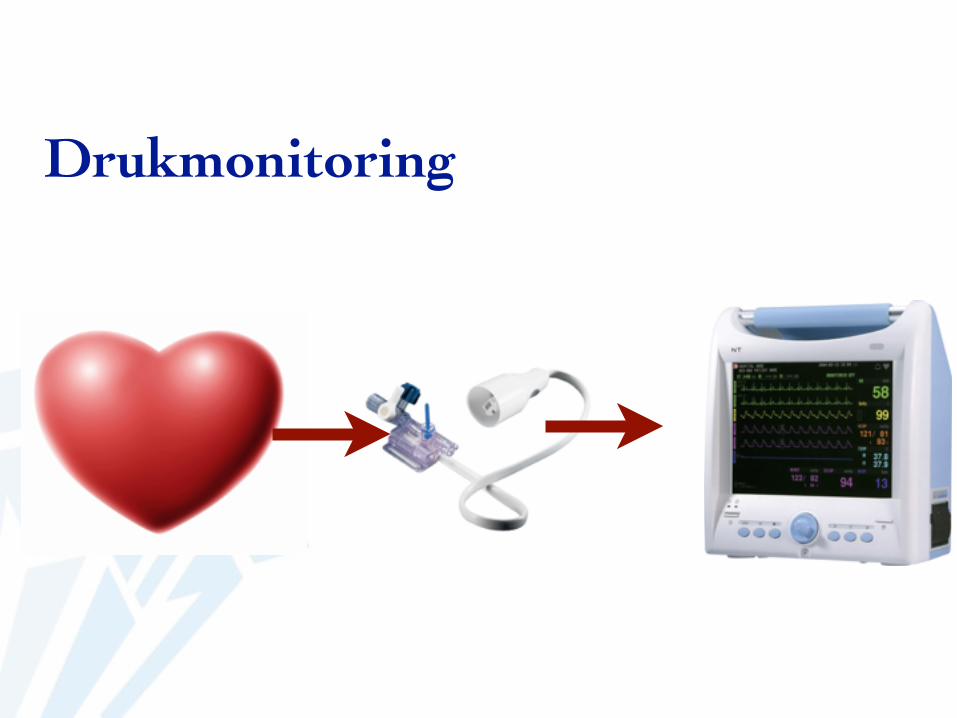
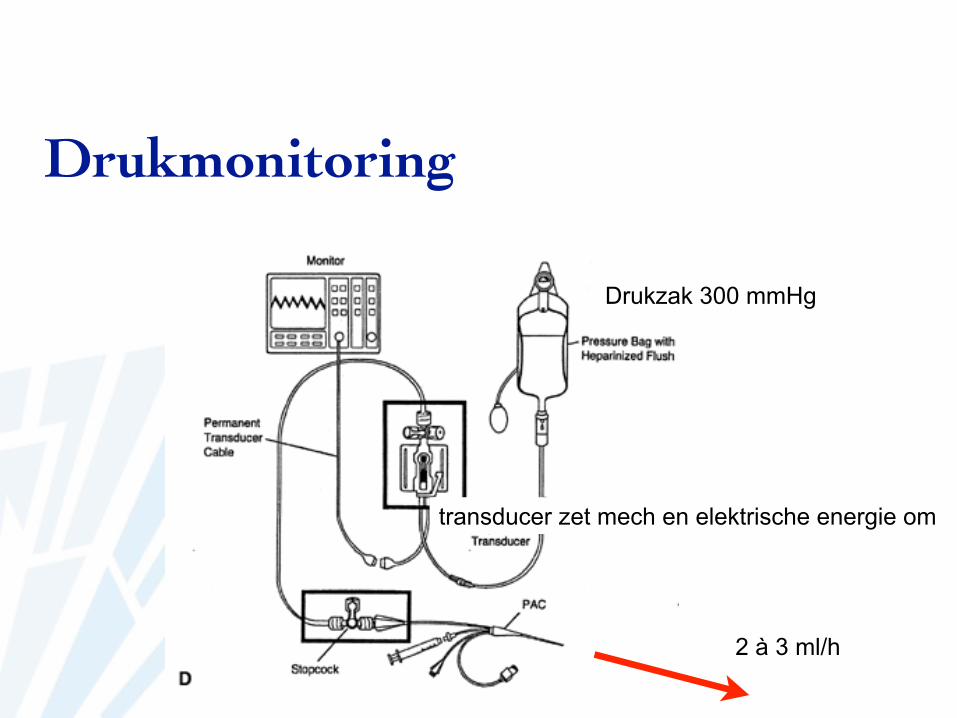
Drukmonitoring
Drukmonitoring
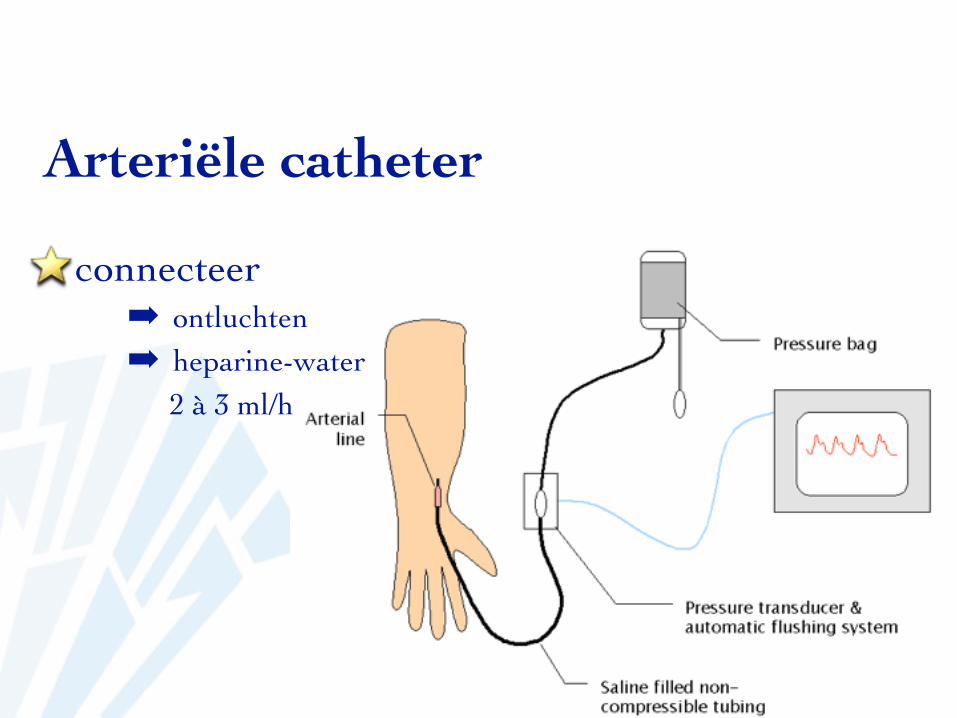
Drukzak 300 mmHg
transducer zet mech en elektrische energie om
2 à 3 ml/h
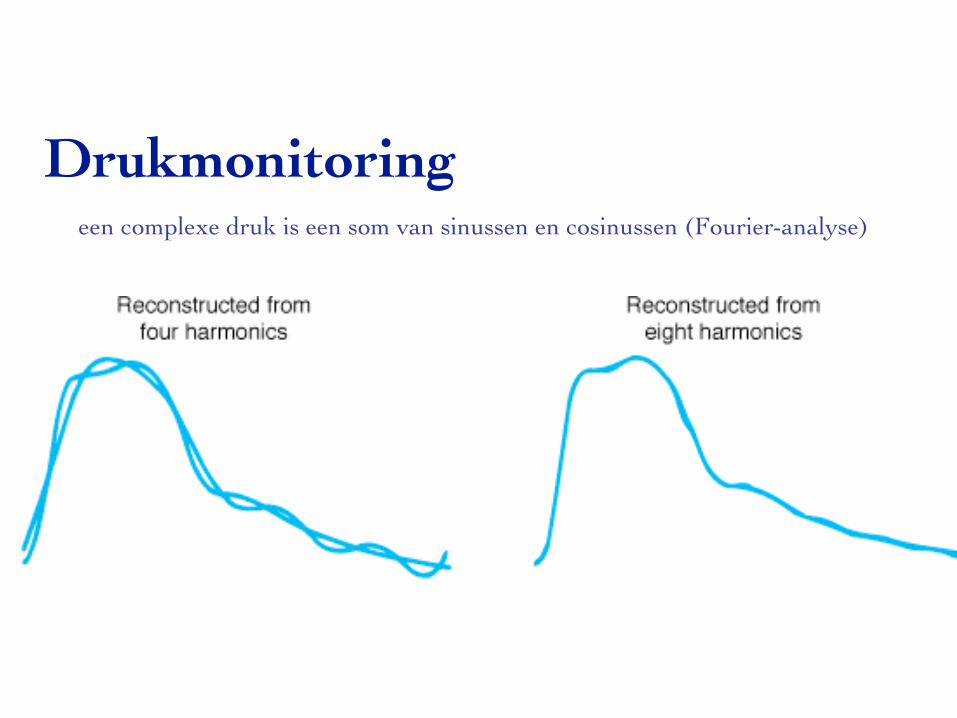
Drukmonitoringeen complexe druk is een som van sinussen en cosinussen (Fourier-analyse)
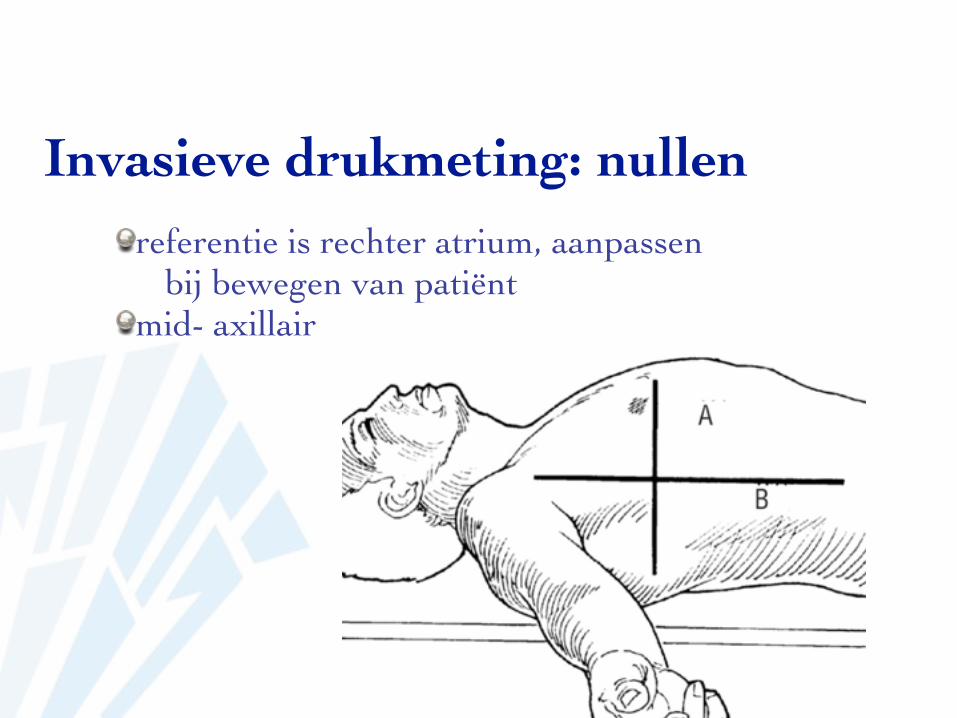
Invasieve drukmeting: nullenreferentie is rechter atrium, aanpassen
bij bewegen van patiëntmid- axillair
5 cm
Invasieve drukmeting: zittendcerebrale arteriële druk: plaatsen van
de transducer thv oor = circulus van willis
0-waarde beinvloed na verloop van tijd door temperatuur: regelmatig hernullen
Invasieve drukmeting: hernullen
➡CVD
Centraal veneuze catheter
indicaties:➡ monitoring CVD➡ infusie caustische stoffen (KCl)➡ infusie TPN➡ aspiratie van luchtembool➡ transveneuze pacing➡ infuus bij slecht veneus access
Centraal veneuze catheter
types:➡ klassieke diepe catheter: seldinger techniek:
➡ catheter over een guide-wire➡ opschuif-catheter
➡ catheter door naald➡ PICC-catheter
➡ catheter door naald
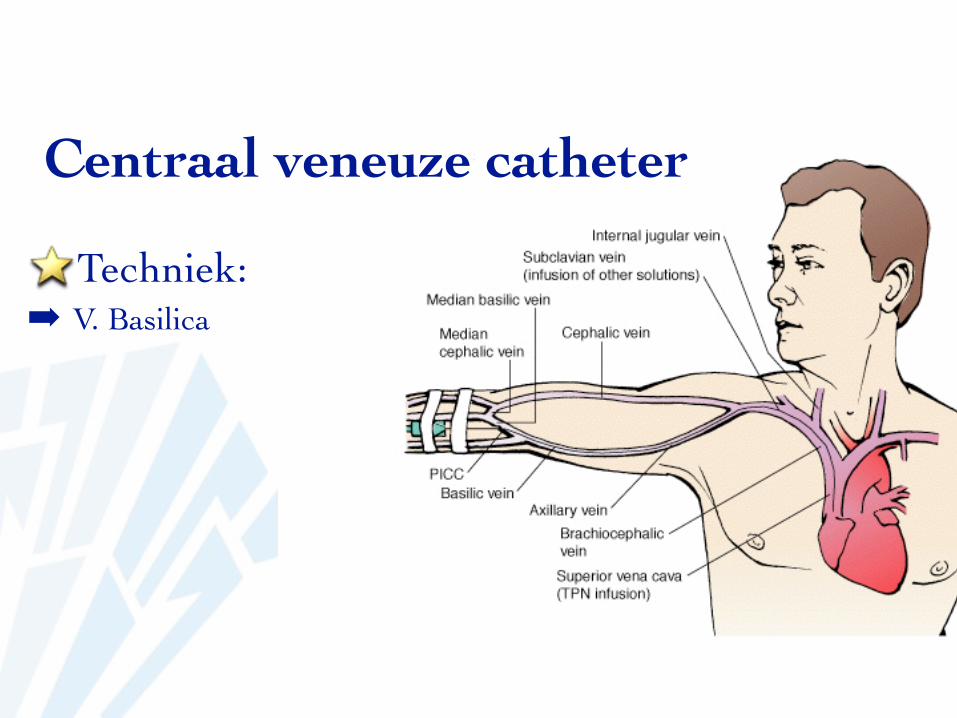
Centraal veneuze catheterLocaties:
➡ V. Subclaviacomfort, weinig besmettingsrisicopneumothorax
➡ V. Basilicacomfort, weinig besmettingsrisicogeen pneumothorax, soms nt intrathoracaal tot VCS (geen CVD-
meting)➡ V. Jugularis Interna
makkelijk af te duwen, gemakkelijk om te prikkenminder comfort, onmogelijk bij halskraag, moeilijk bij obese
patiënten
Centraal veneuze catheter
Locaties:➡ V. Jugularis externa
makkelijk af te duwen, moeilijk om te prikken, guide kan moeilijk opschuiven
minder comfort➡ V. Femoralis
besmettingsrisicogeen pneumothorax, nt intrathoracaal (geen CVD-meting)
Centraal veneuze catheter
Techniek:➡ Trendlenburg
vermijdt lucht-aspiratiestuwen van de venen
➡ goede positionering➡ aseptisch
muts, masker, chirurgische handontsmetting, schortontsmetten Hibitane of Joodalcoholafdekprocedure
➡ voldoende lokale anesthesie bij wakkere patiënt
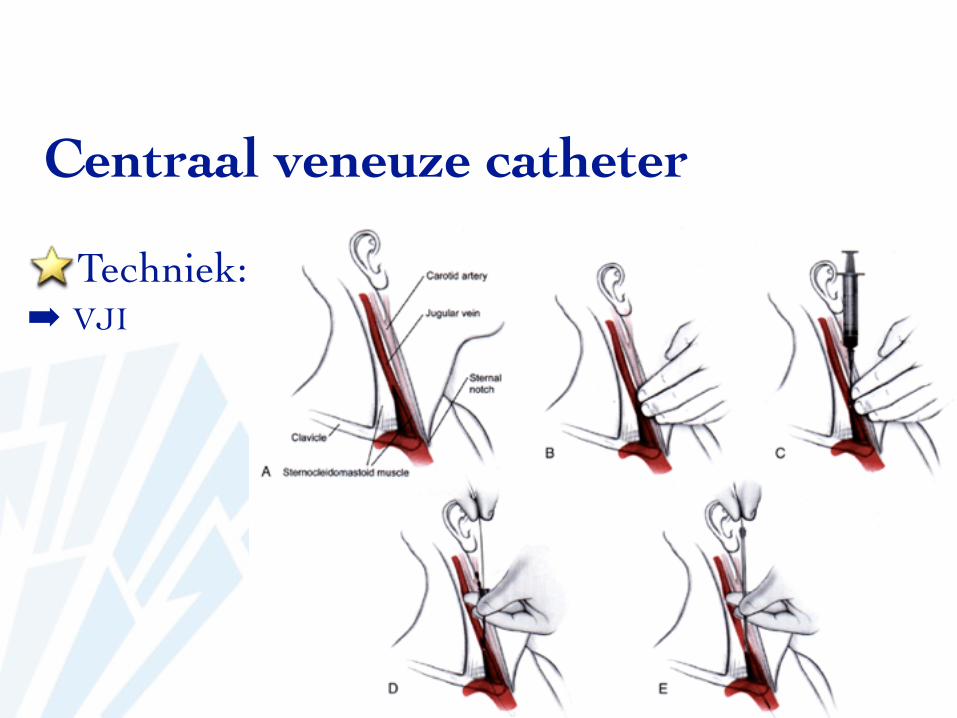
Centraal veneuze catheter
Techniek:➡ VJI
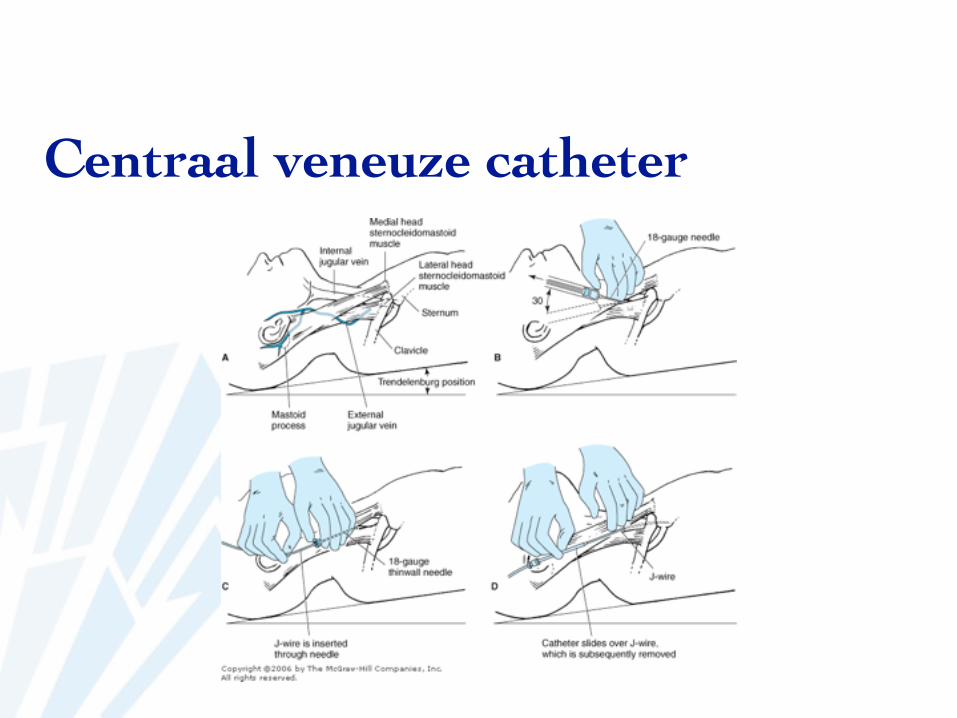
Centraal veneuze catheter
Centraal veneuze catheter
Techniek:➡ VJI
halve afstand mastoid -incisura sternum * palperen van de A. Carotis - prikken naast carotis
prikken onder hoek van 30° richting tepellijn met groene naaldprikken met dikke naaldinschuiven wiredilateren huidopschuiven catheterfixeren - vasthechten - verband
http://www.youtube.com/watch?v=QHiuYc22pfE
Centraal veneuze catheter
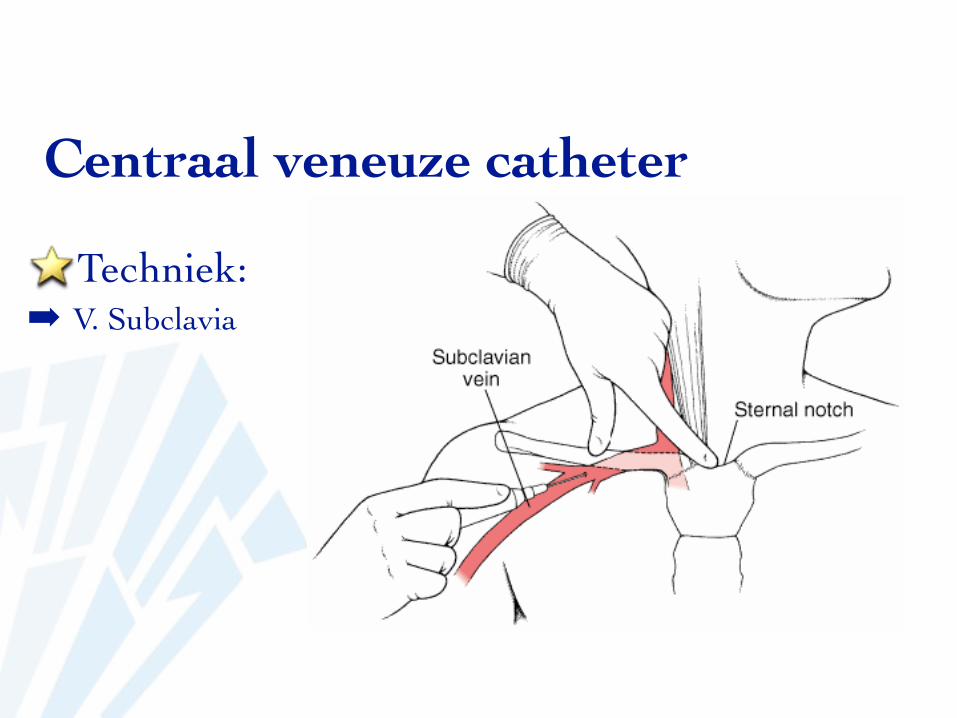
Techniek:➡ V. Subclavia
Centraal veneuze catheter
Techniek:➡ V. Subclavia
buitenste 1/3-overgang middenste 1/3Ongeveer 1 cm onder claviculatik tegen clavicula (periost = pijn)prikken quasi parallel met de huid richting incisura vh sternum met groene
naaldprikken met dikke naaldinschuiven wiredilateren huidopschuiven catheterfixeren - vasthechten - verband
Centraal veneuze catheter
Techniek:➡ V. Subclavia
hoofd in neutrale positie, misschien richting naald gedraaid om opschuiven naar v jugularis te vermijden
arm langs het lichaam, soms evt tractie op de arm
http://www.youtube.com/watch?v=A_Vlxz9KcBg
Centraal veneuze catheter
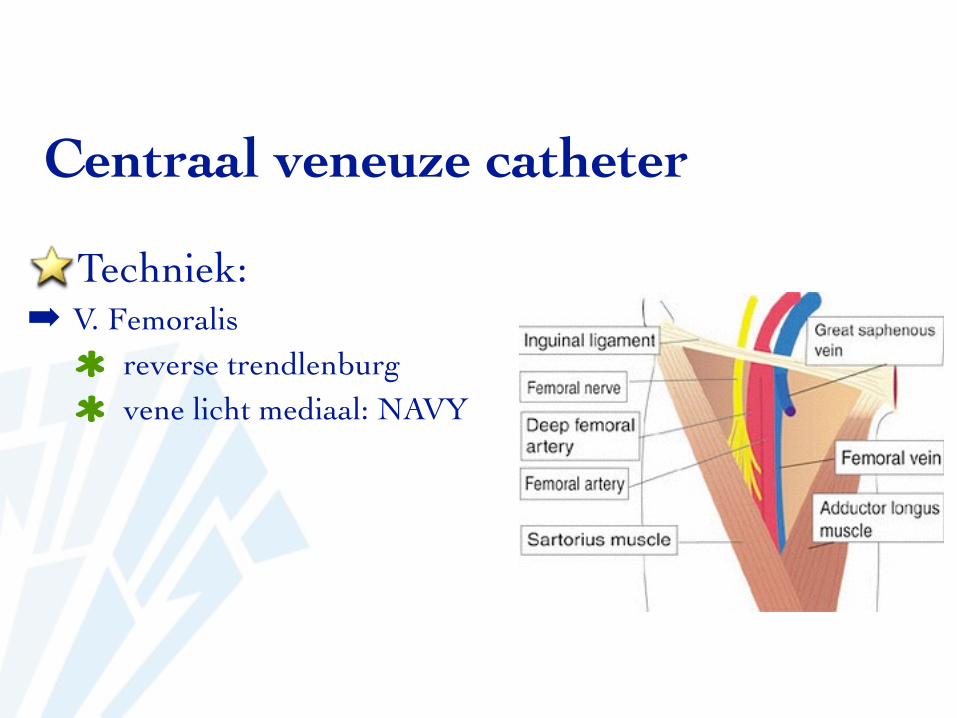
Techniek:➡ V. Femoralis
reverse trendlenburgvene licht mediaal: NAVY
Centraal veneuze catheter
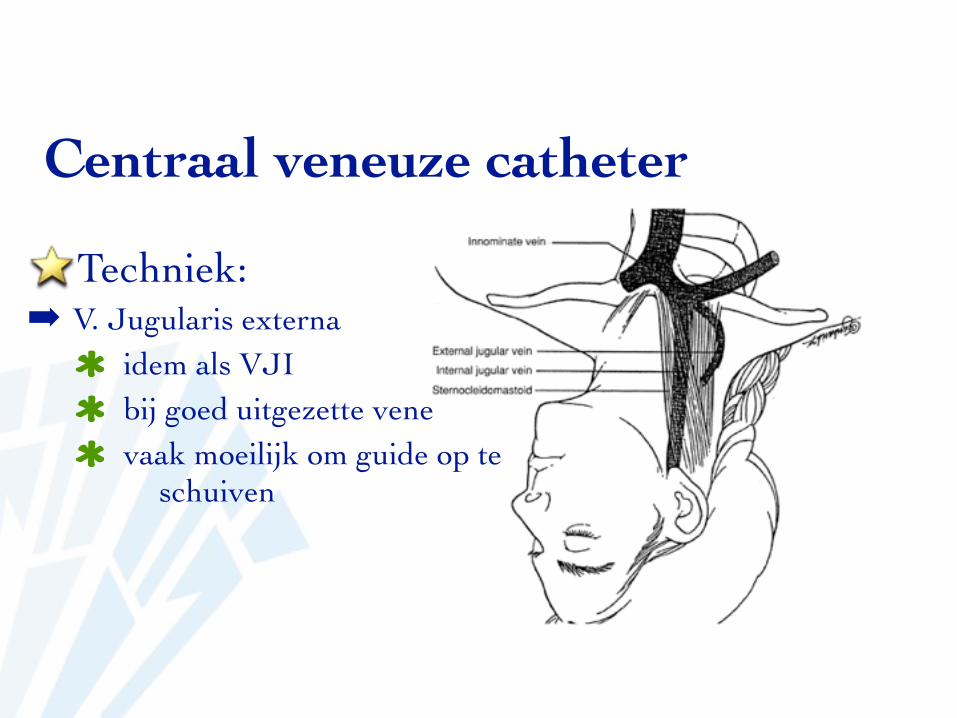
Techniek:➡ V. Jugularis externa
idem als VJIbij goed uitgezette venevaak moeilijk om guide op te
schuiven
Centraal veneuze catheter
Techniek:➡ V. Basilica
opschuifcathetersteriele no touch techniek
Centraal veneuze catheter
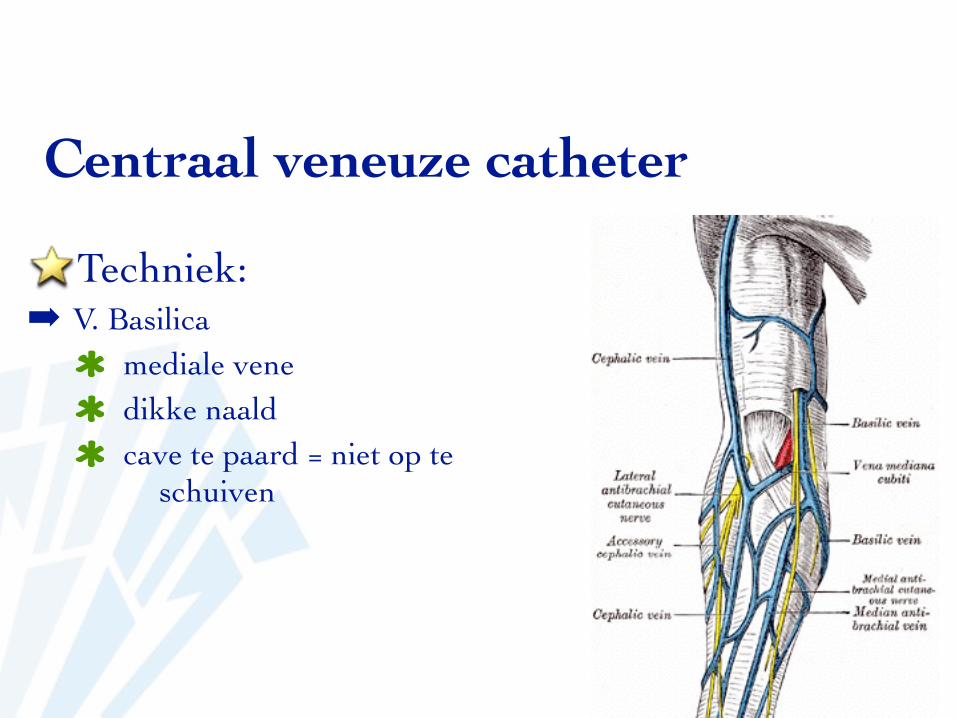
Techniek:➡ V. Basilica
mediale venedikke naaldcave te paard = niet op te
schuiven
Techniek:➡ V. Basilica
Centraal veneuze catheter
Centraal veneuze catheter
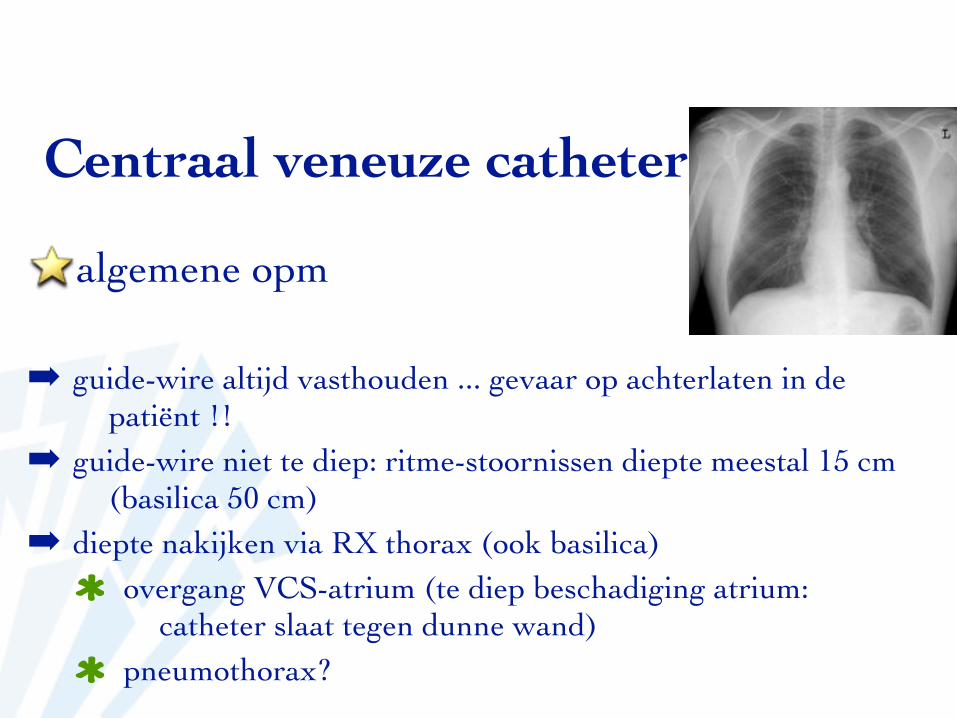
algemene opm
➡ guide-wire altijd vasthouden ... gevaar op achterlaten in de patiënt !!
➡ guide-wire niet te diep: ritme-stoornissen diepte meestal 15 cm (basilica 50 cm)
➡ diepte nakijken via RX thorax (ook basilica)overgang VCS-atrium (te diep beschadiging atrium:
catheter slaat tegen dunne wand)pneumothorax?
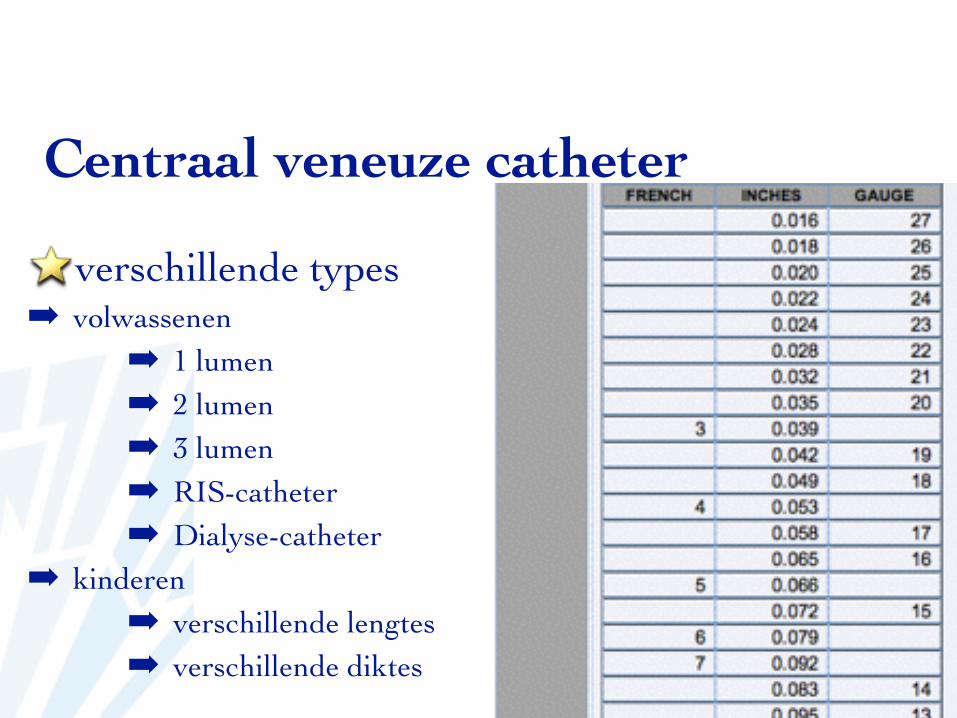
verschillende types➡ volwassenen
➡ 1 lumen➡ 2 lumen➡ 3 lumen➡ RIS-catheter➡ Dialyse-catheter
➡ kinderen➡ verschillende lengtes➡ verschillende diktes
Centraal veneuze catheter
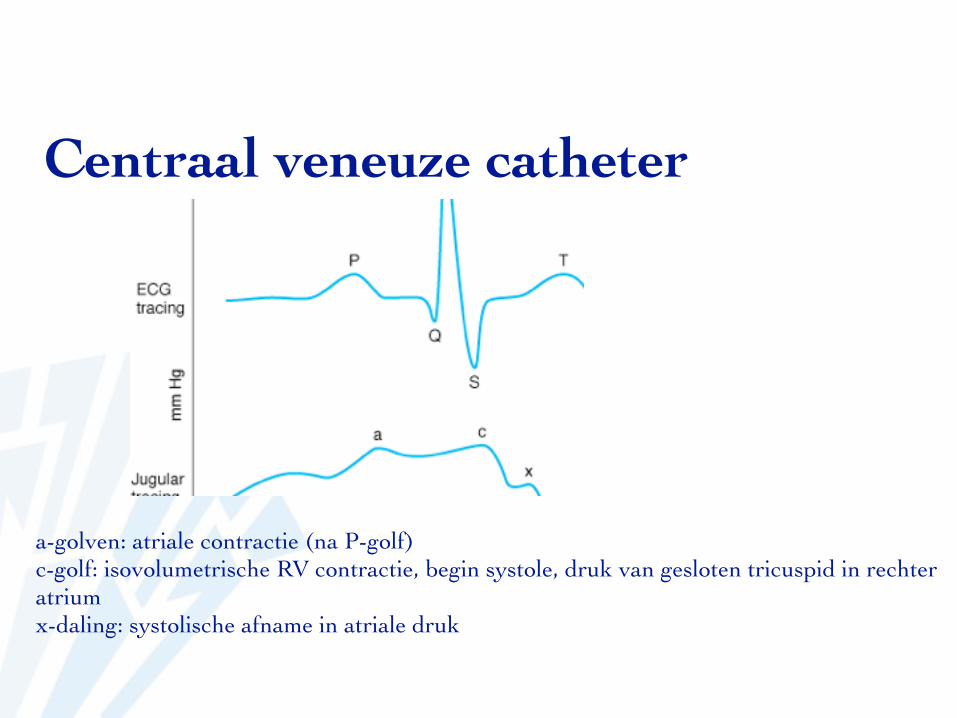
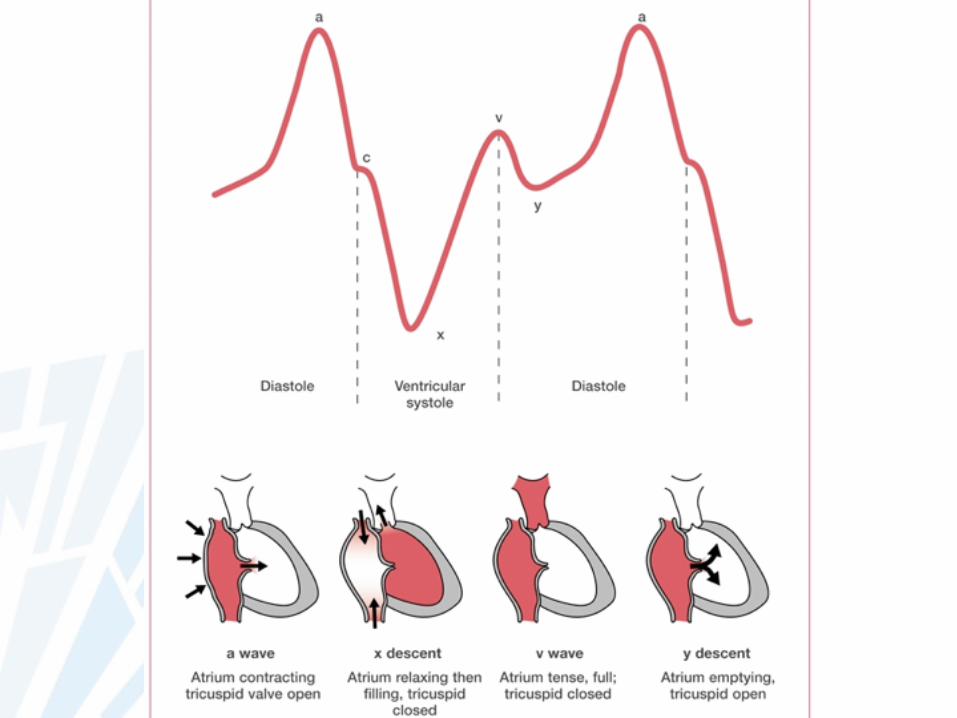
a-golven: atriale contractie (na P-golf)c-golf: isovolumetrische RV contractie, begin systole, druk van gesloten tricuspid in rechter atriumx-daling: systolische afname in atriale druk
Centraal veneuze catheter
Geeft een idee van de vullingsstatus bij gezonde patiënten
CVP ~ right atrial pressure ~ right ventricular end diastolic volume (preload )
Centraal veneuze catheter
Toename CVD■ Overvulling■ geforceerde expiratie■ Spanningspneumothorax■ hartfalen■ pleura-uitstorting■ afgenomen cardiac output■ Tamponade■ mechanische ventilatie en PEEP
Afname CVD■ Hypovolemia■ Diepe inhalatie■ Distributieve shock
Centraal veneuze catheter
■ Vullingsstatus■ dorst?■ tachycadie■ diurese, kleur urine■ bloeddruk, curve, pulsus■ cvd■ ...
Centraal veneuze catheter
Centraal veneuze catheter• Grote a-golf: door een grotere contractie van de atria
• PS, AS, MS, TS• Canon A golven: bij ritmestoornissen: contractie tegen gesloten Tc-klep: atriale
tachycardie of VK-flutter• Geen a-golf: bij VKF• Grote v-golf: : verhoogde atriale druk bij TI• X-afname: bij acute tamponade• Y-afname: bij trage chronische tamponade
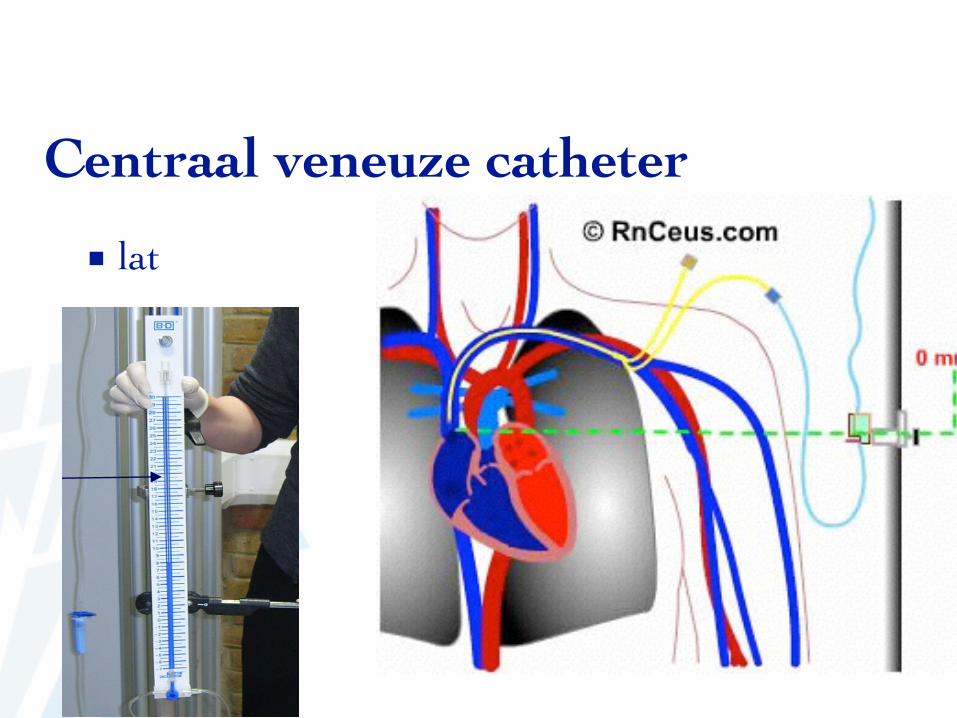
■ latMeasuring central venous pressure 2
CETL 2008
CVP is measured using an indwelling central venous catheter (CVC) and a pressure manometer or transducer. Both methods are reliable when used correctly.Wards generally use manometers.
Equipment: manometers
Accident and Emergency departments, High Dependency areas and Intensive Care units use transducers for measuring CVPs.
Equipment: transducers
Transduced CVP waveform
Insertion sites
CVC insertion sites include:
• Internal jugular vein
• Subclavian vein
• Femoral vein
Centraal veneuze catheter
■ conversie mmHg en cm H2O
1 mmHg = 1.36 cmH2O
Centraal veneuze catheter
Centraal veneuze catheter
problemen:➡ infectie➡ lucht- of thrombus-embool➡ ritmestoornissen (tip)➡ hematoom➡ pneumothorax➡ hemothorax➡ hydrothorax➡ chylothorax
contra-indicaties:➡ absoluut:
➡ VCS-syndroom➡ relatief
➡ infectie thv punctieplaats➡ stollingsstoornissen➡ recente pacemaker-leads➡ ipsilaterale carotis-endarterectomie
Centraal veneuze catheter
Centraal veneuze catheter
echo-guided access➡ minder puncteren
➡ comfort neemt toe➡ minder kans op arteriële punctie
➡ real-time bekijken tijdens prikken➡ http://www.youtube.com/watch?v=mrbmQxDalis
Centraal veneuze catheter
problemen:➡ perforatie hart➡ harttamponade➡ letsels aan nabijgelegen zenuwen en arteries➡ embool➡ thombus
➡Arteriële catheter
Arteriële catheter
indicaties:➡ anticipatie van grote fluid-shifts➡ intracraniële HK➡ trauma➡ gekende cardiovasc pathologie of cardiale HK➡ anticipatie van bloeddrukschomelingen➡ indicatie tot perop hypotensie➡ bloedgas-bepalingen➡ niet-invasieve bloeddrukmeting niet mogelijk/onbetrouwbaar:
obesitas
Arteriële catheter
contra-indicaties:➡ Raynaud➡ Bevloeiing zonder collaterale flow

Arteriële catheter
waar:➡ A Radialis➡ (A. Ulnaris)➡ A Brachialis➡ A. Axillaris➡ A. Femoralis➡ A. Dorsalis pedis
Arteriële catheter
waar:➡ A Radialis➡ (A. Ulnaris): tortues, dieper
niet indien ipsilateraleRadialis geprobeerd
Arteriële catheter
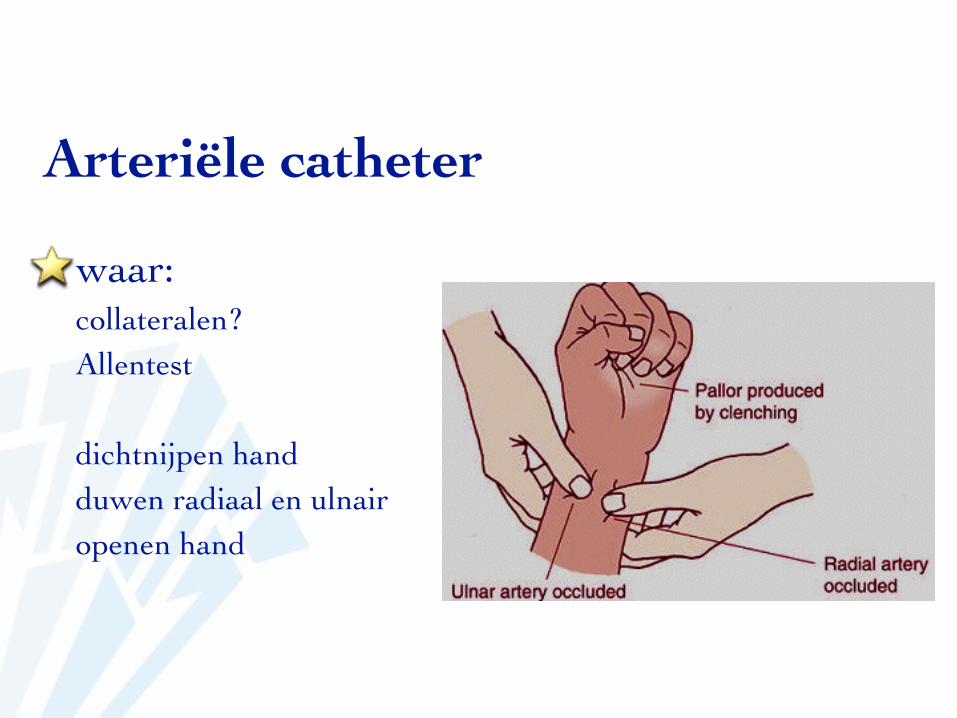
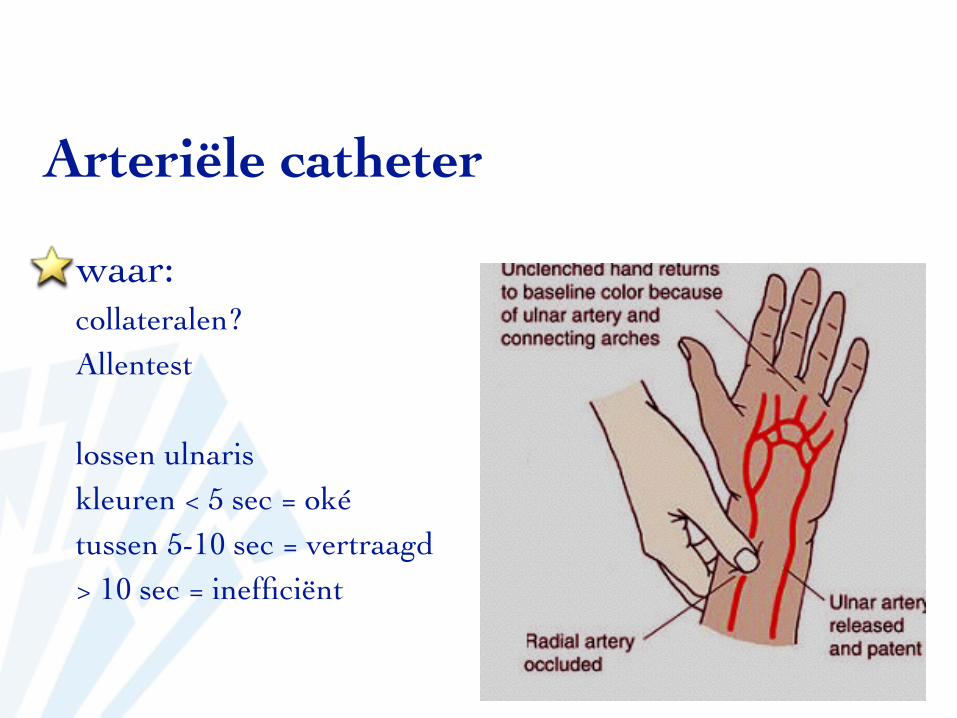
waar:collateralen?Allentest
dichtnijpen handduwen radiaal en ulnairopenen hand
Arteriële catheter
waar:collateralen?Allentest
lossen ulnariskleuren < 5 sec = okétussen 5-10 sec = vertraagd> 10 sec = inefficiënt
Arteriële catheter
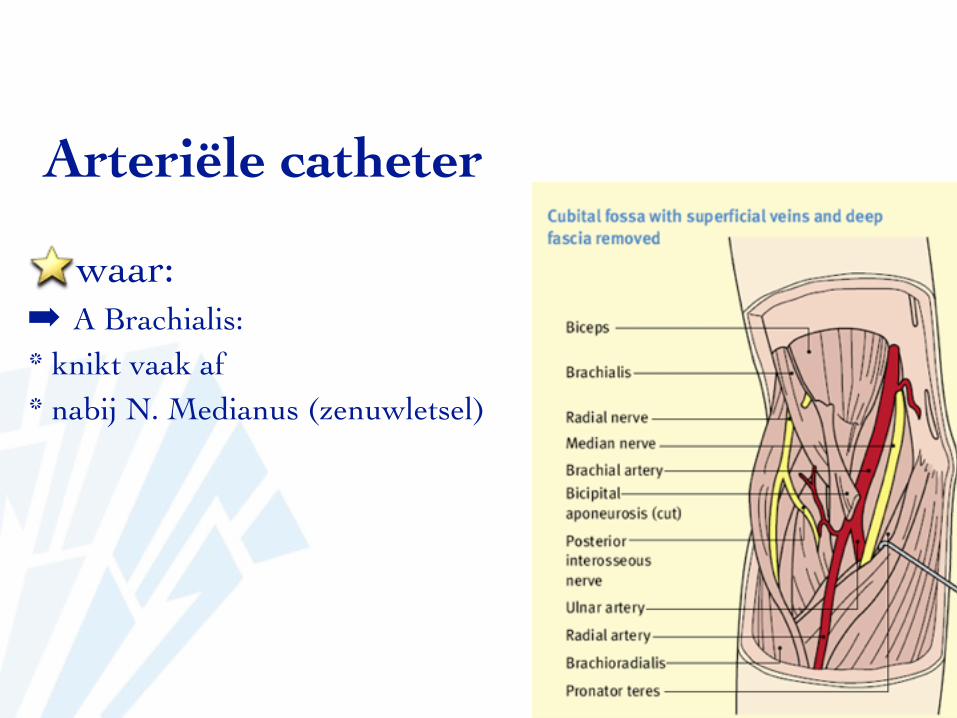
waar:➡ A Brachialis: * knikt vaak af* nabij N. Medianus (zenuwletsel)
Arteriële catheter
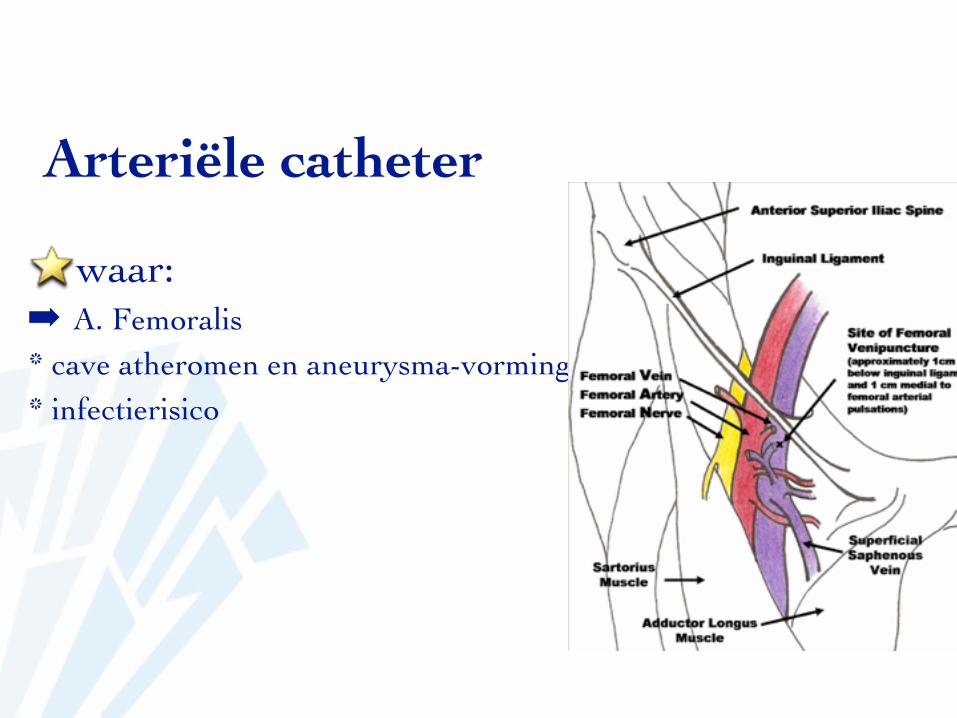
waar:➡ A. Femoralis* cave atheromen en aneurysma-vorming* infectierisico
Arteriële catheter
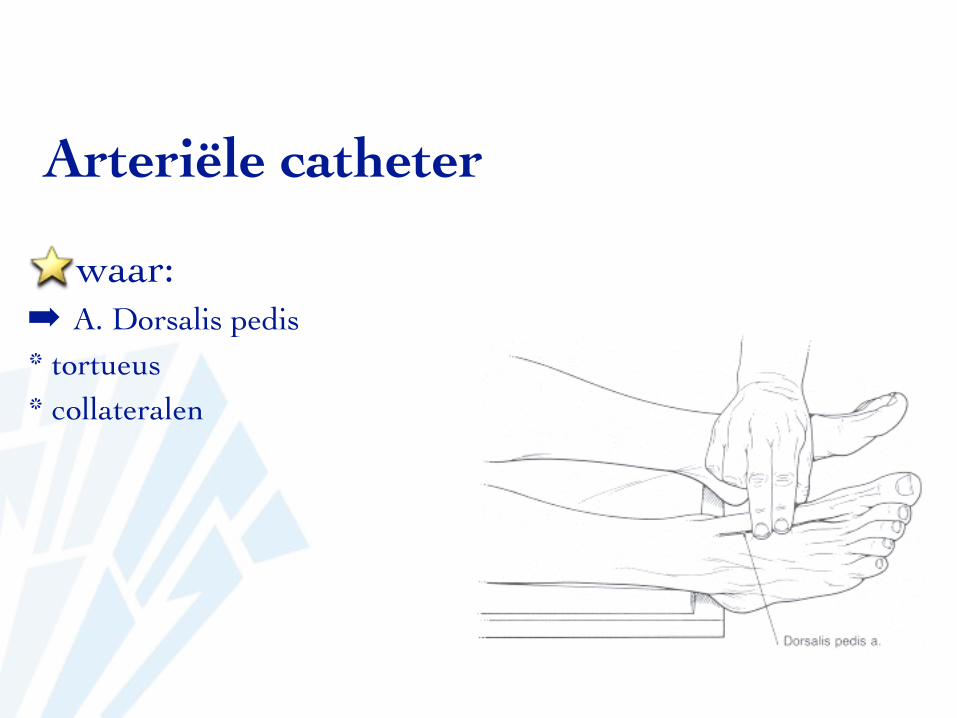
waar:➡ A. Dorsalis pedis* tortueus* collateralen
Arteriële catheter
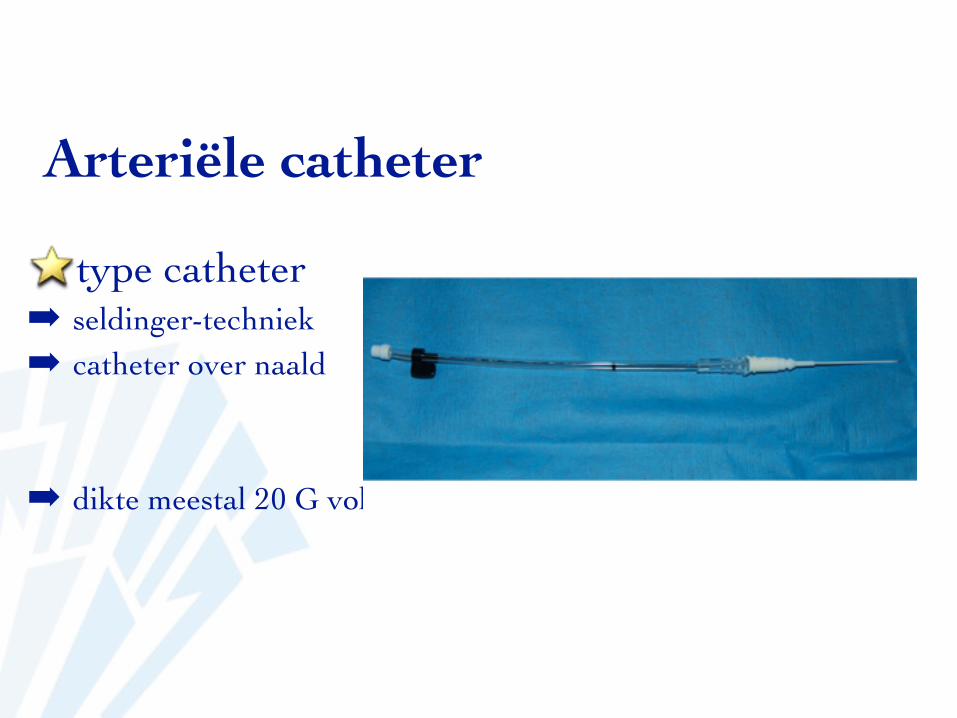
type catheter➡ seldinger-techniek➡ catheter over naald
➡ dikte meestal 20 G volw
Arteriële catheter
techniek➡ onthaar de huid met een clipper➡ ontsmet de handen met alcogel➡ leg alle materiaal klaar➡ ontsmet de handen met alcogel➡ ontsmet de huid met choorhexidine 0,5 in alcohol 70%➡ verdoof huid➡ trek steriele handschoenen aan+ veld of NO touch techniek➡ prik op steriele manier➡ sluit aan➡ maak verband
Arteriële catheter
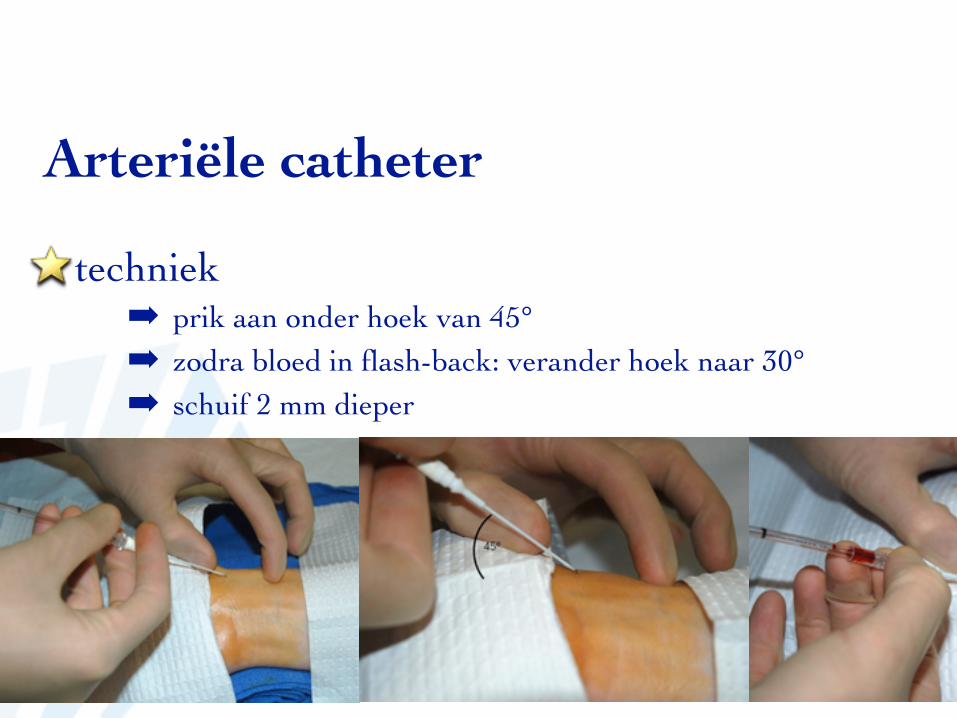
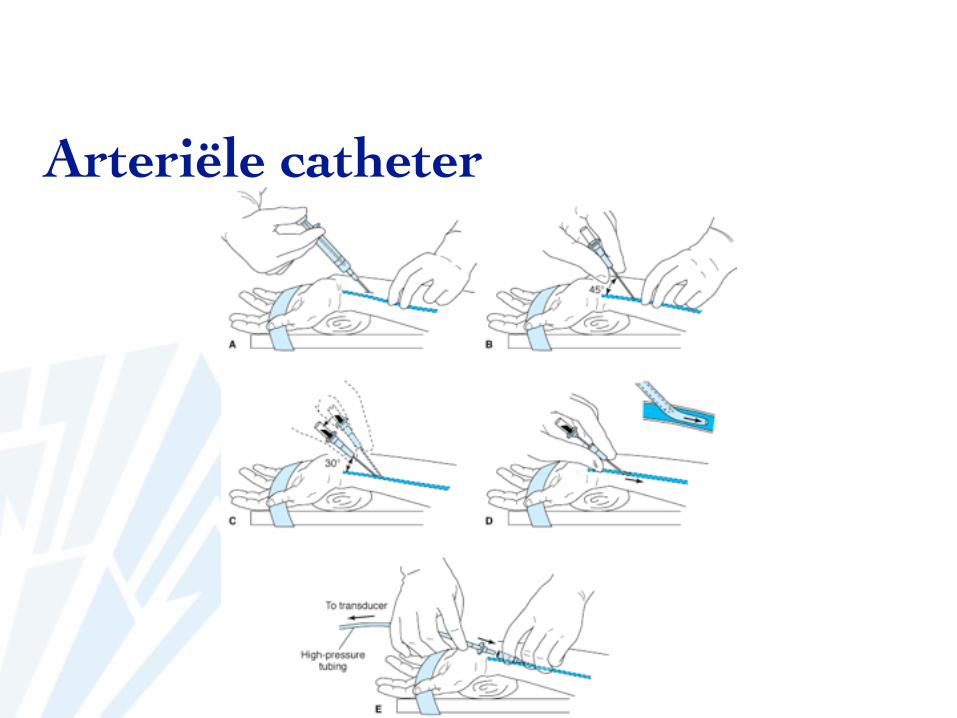
techniek➡ prik aan onder hoek van 45°➡ zodra bloed in flash-back: verander hoek naar 30°➡ schuif 2 mm dieper
Arteriële catheter

Arteriële catheter
http://www.youtube.com/watch?v=8NOaEo_EdP0
Arteriële catheter
connecteer➡ ontluchten➡ heparine-water 2 à 3 ml/h
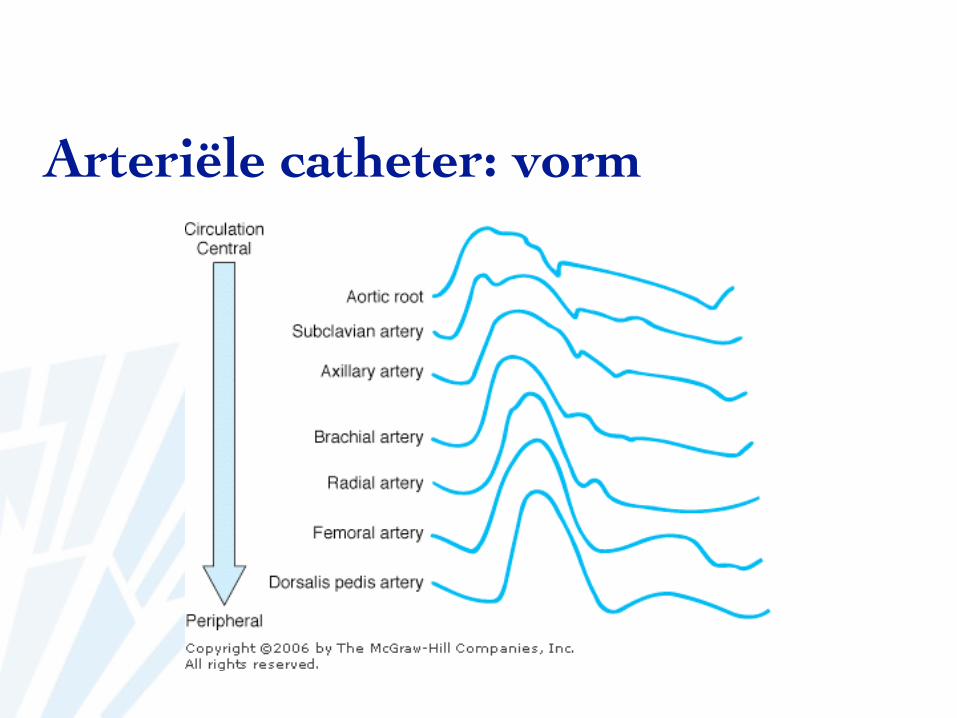
Arteriële catheter: vorm
verschil li en rechts: de hoogste druk is de werkelijke druk
Arteriële catheter
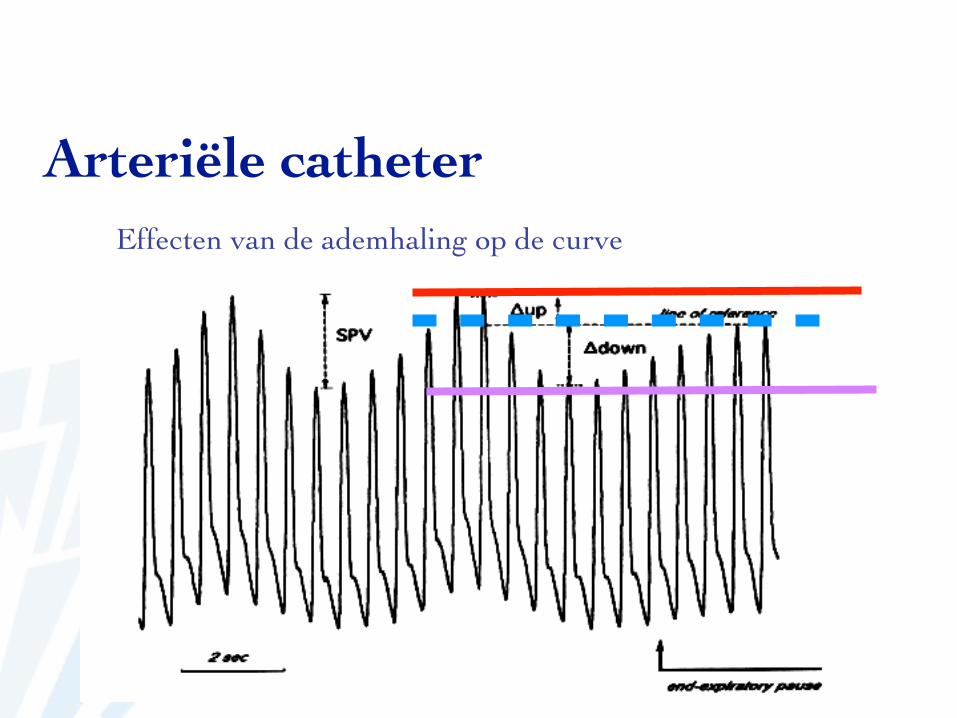
Effecten van de ademhaling op de curve
Arteriële catheter
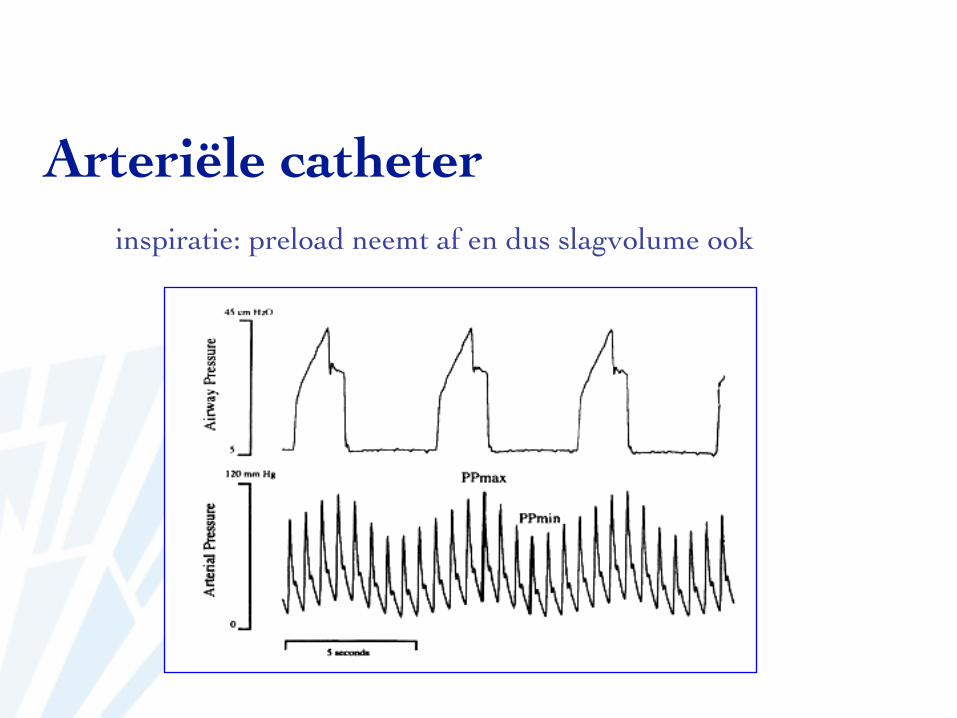
inspiratie: preload neemt af en dus slagvolume ook
Arteriële catheter
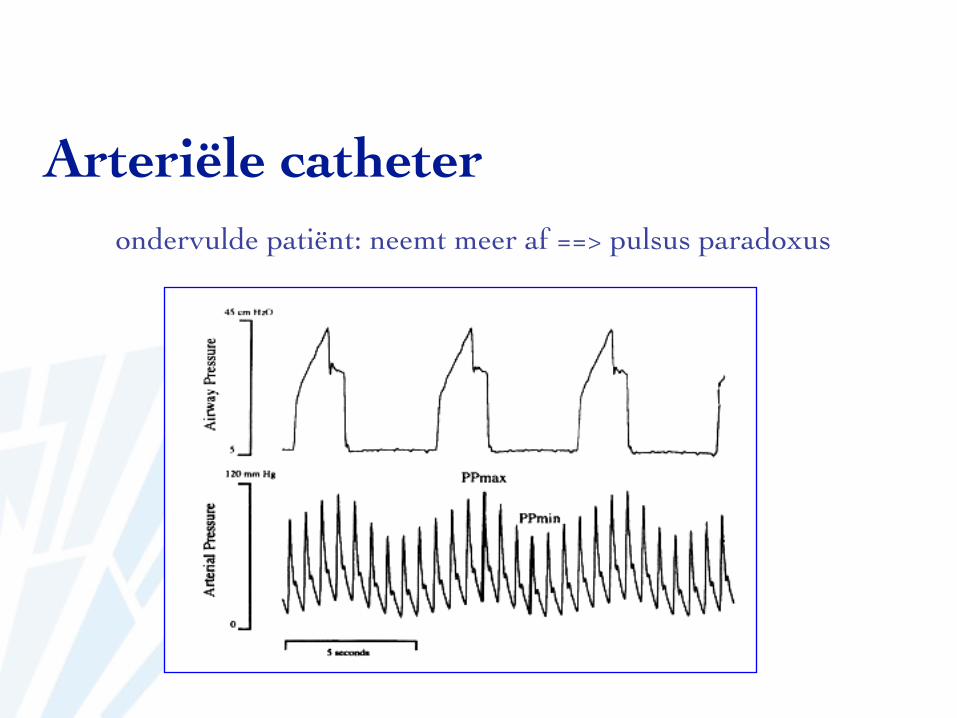
ondervulde patiënt: neemt meer af ==> pulsus paradoxus
Arteriële catheter
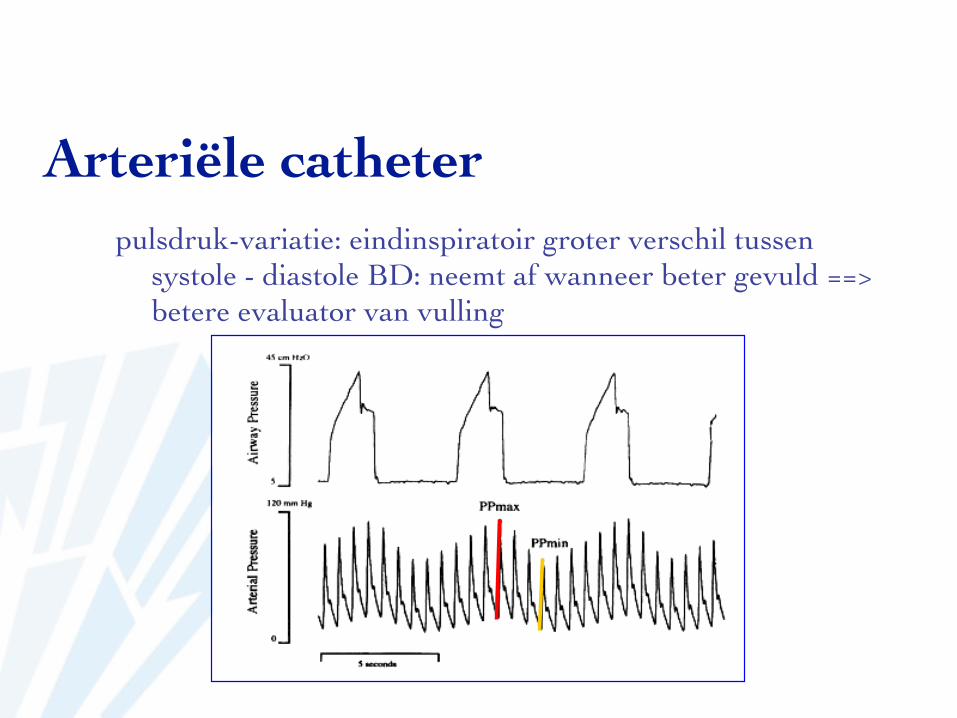
pulsdruk-variatie: eindinspiratoir groter verschil tussen systole - diastole BD: neemt af wanneer beter gevuld ==> betere evaluator van vulling
Arteriële catheter
Arteriële catheter
complicaties➡ hematoom➡ vasospasme➡ thrombose➡ lucht-embolisatie➡ necrose➡ zenuwletsel➡ medicatie-injectie➡ bloedverlies
Arteriële catheter
echogeleide punctie
Swan Ganz catheter
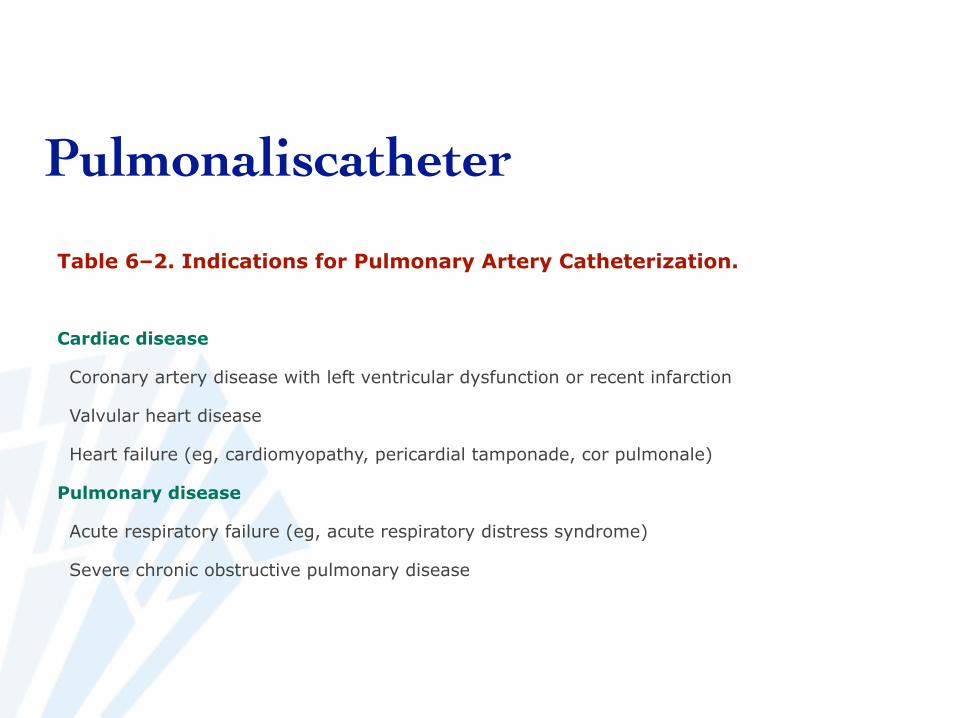
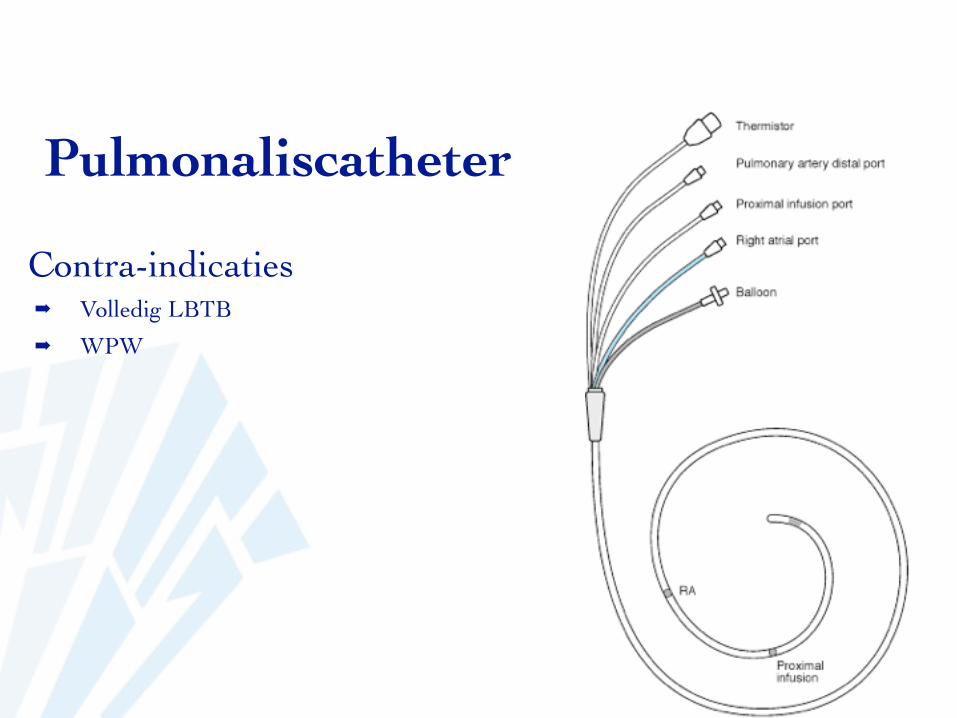
Pulmonaliscatheter
Table 6–2. Indications for Pulmonary Artery Catheterization.
Cardiac disease
Coronary artery disease with left ventricular dysfunction or recent infarction
Valvular heart disease
Heart failure (eg, cardiomyopathy, pericardial tamponade, cor pulmonale)
Pulmonary disease
Acute respiratory failure (eg, acute respiratory distress syndrome)
Severe chronic obstructive pulmonary disease
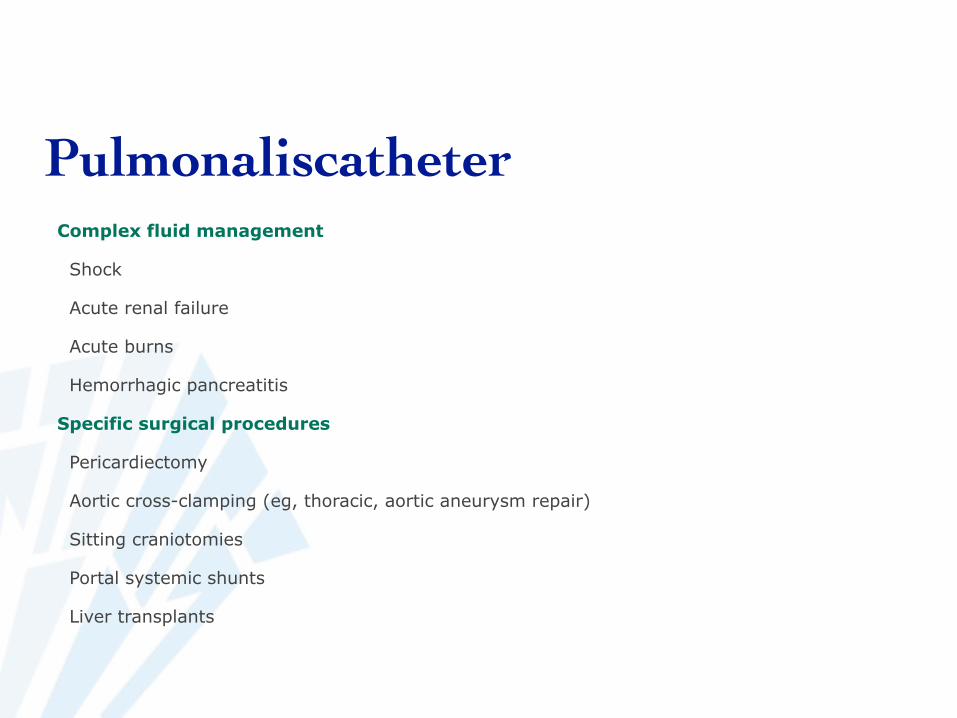
PulmonaliscatheterComplex fluid management
Shock
Acute renal failure
Acute burns
Hemorrhagic pancreatitis
Specific surgical procedures
Pericardiectomy
Aortic cross-clamping (eg, thoracic, aortic aneurysm repair)
Sitting craniotomies
Portal systemic shunts
Liver transplants
Pulmonaliscatheter
Contra-indicaties➡ Volledig LBTB➡ WPW
Pulmonaliscatheter
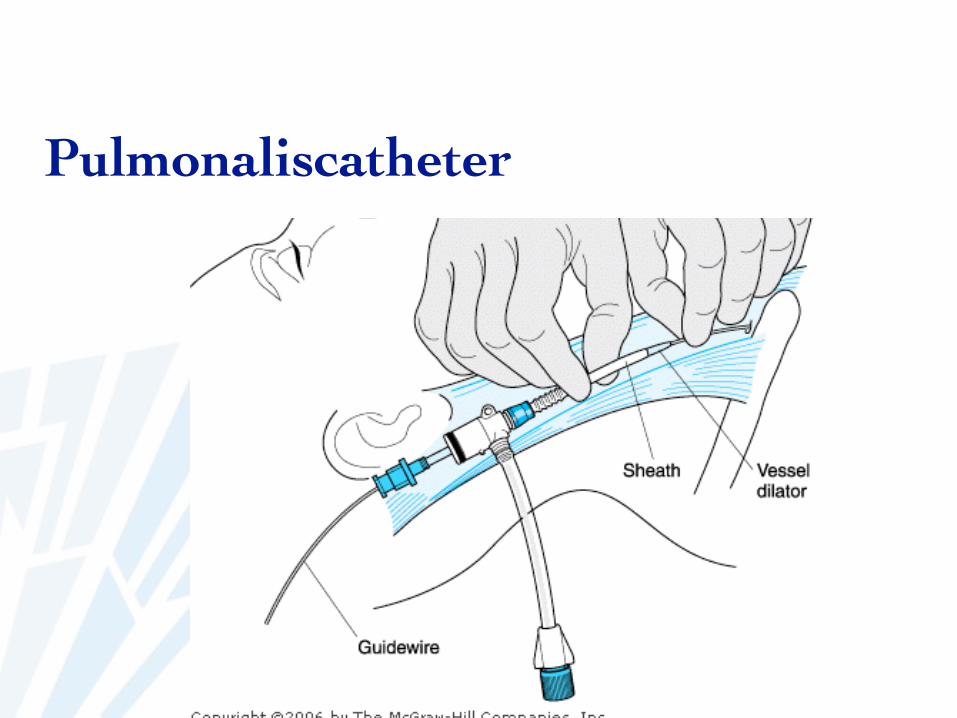
➡ Praktisch:➡ sheat is zeer dik:
➡ vergroot opening met optreknaald➡ schuif introducer op en verwijder tegelijk
stamper: anders risico op perforatie atrium, ventrikel
Pulmonaliscatheter
Pulmonaliscatheter
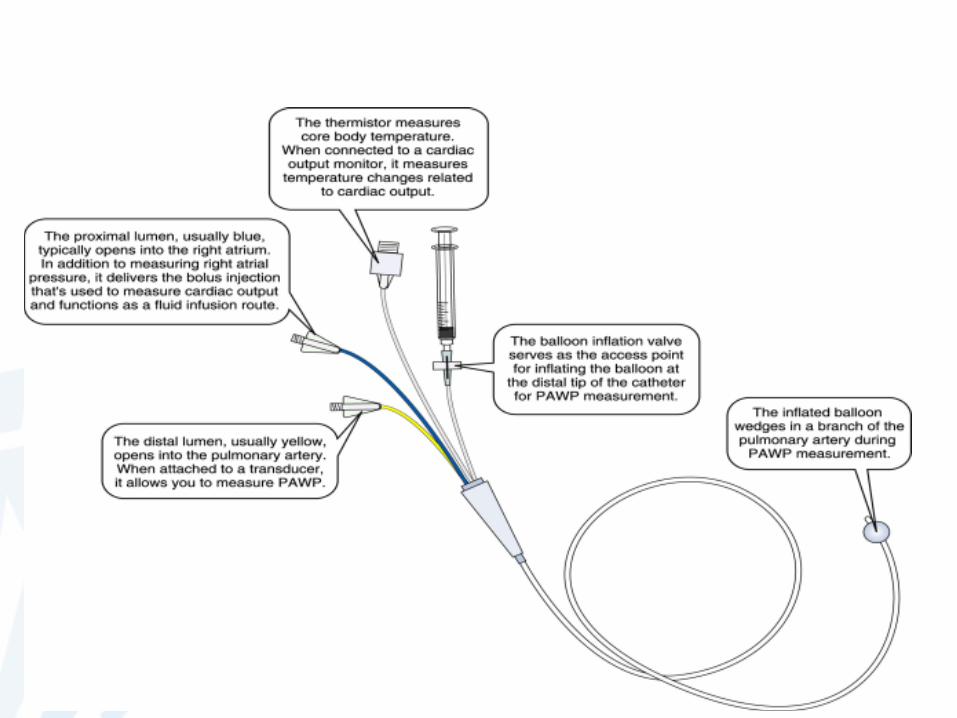
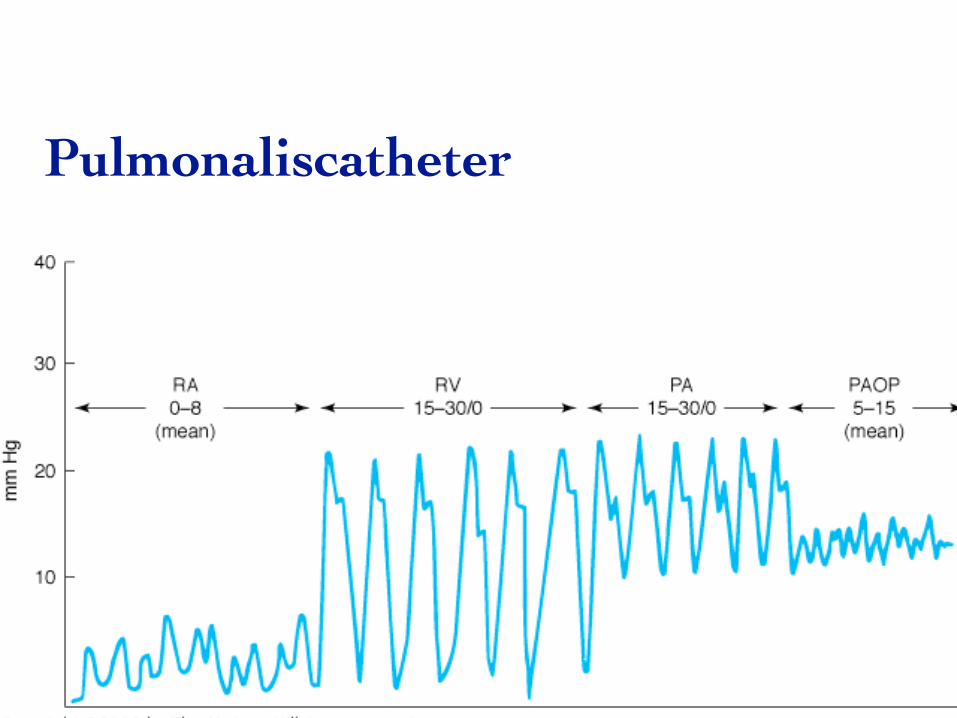
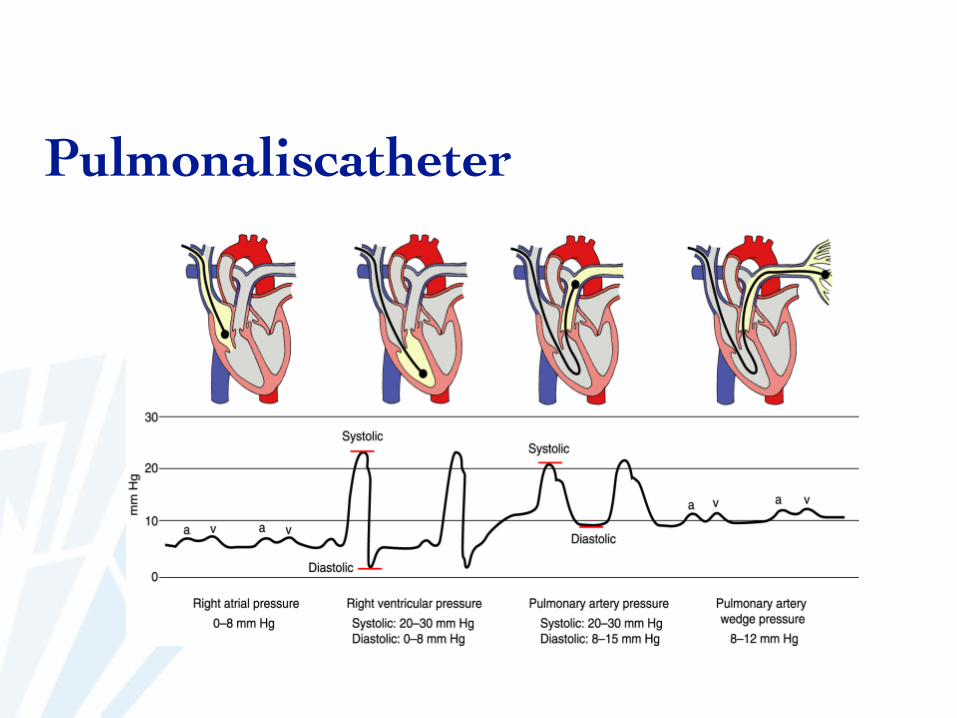
➡ Praktisch:➡ lumina ontluchten met fysiologisch➡ prikken TB ==> opschuiven antiTB➡ check ballon voor introductie➡ sleeve over catheter➡ opblazen ballon 1,5 cc na 15 à 20 cm (rechter
atrium)➡ meestal PAP-curve na 45 cm➡ in wedge plaatsen en dan ballon aflaten
Pulmonaliscatheter
Pulmonaliscatheter
Pulmonaliscatheter
➡ Aandachtspunten:➡ ballon steeds af➡ intermittent wedgen
➡ continue wedge ==> longinfarct➡ PAP-curve steeds opvolgen
Pulmonaliscatheter
➡ Complicaties:➡ idem CVD➡ ritmestoornissen➡ knoop
Pulmonaliscatheter
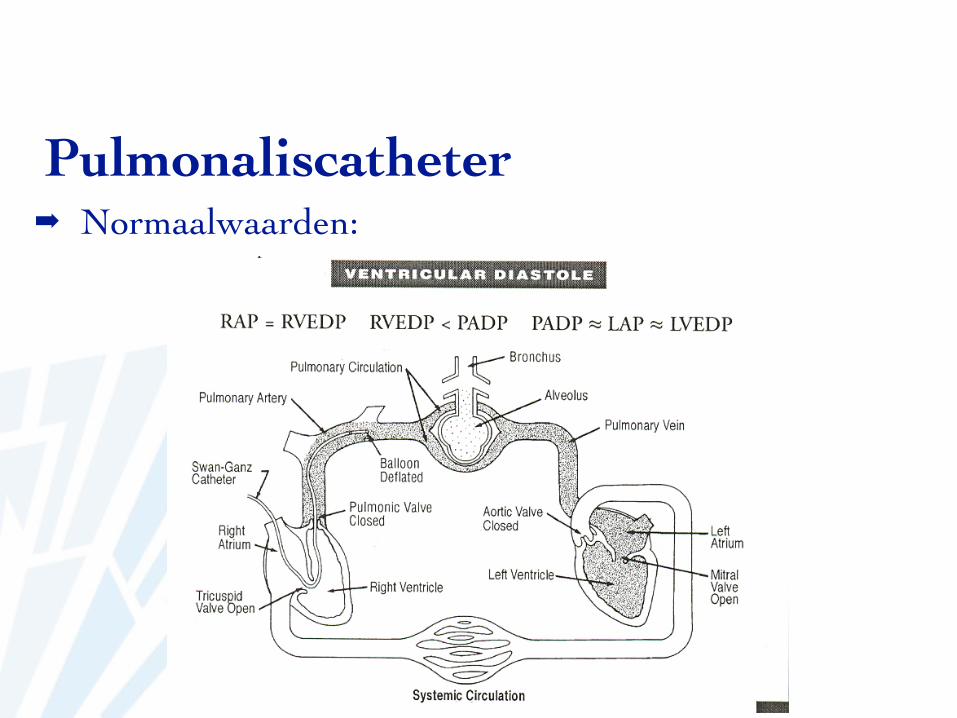
➡ Normaalwaarden:Pulmonaliscatheter
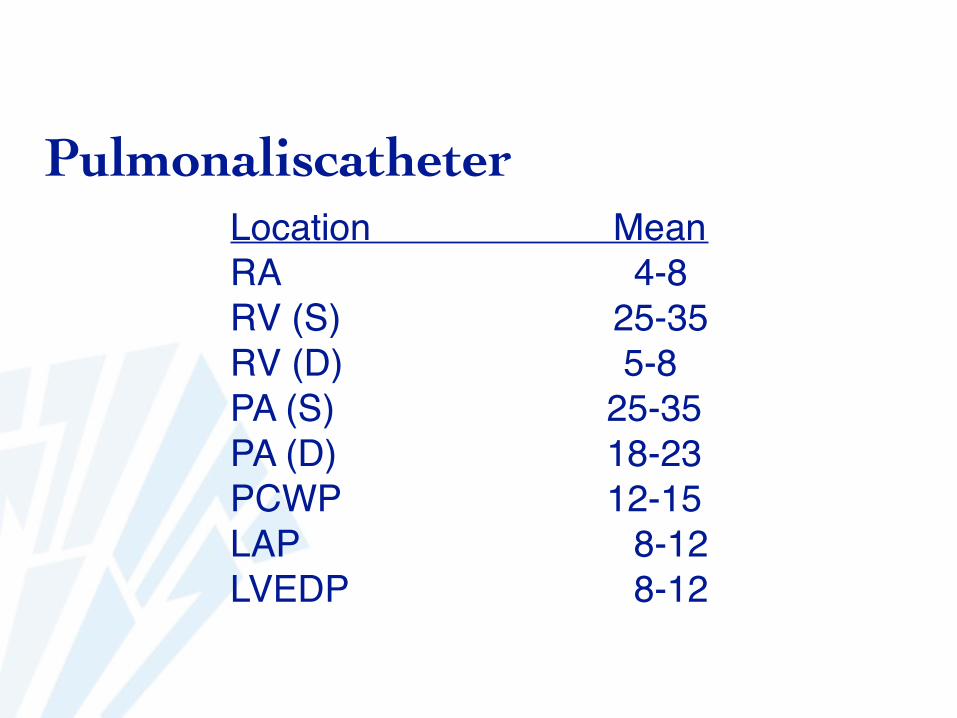
Location MeanRA 4-8RV (S) 25-35RV (D) 5-8PA (S) 25-35PA (D) 18-23PCWP 12-15LAP 8-12 LVEDP 8-12
Pulmonaliscatheter
Pulmonaliscatheter
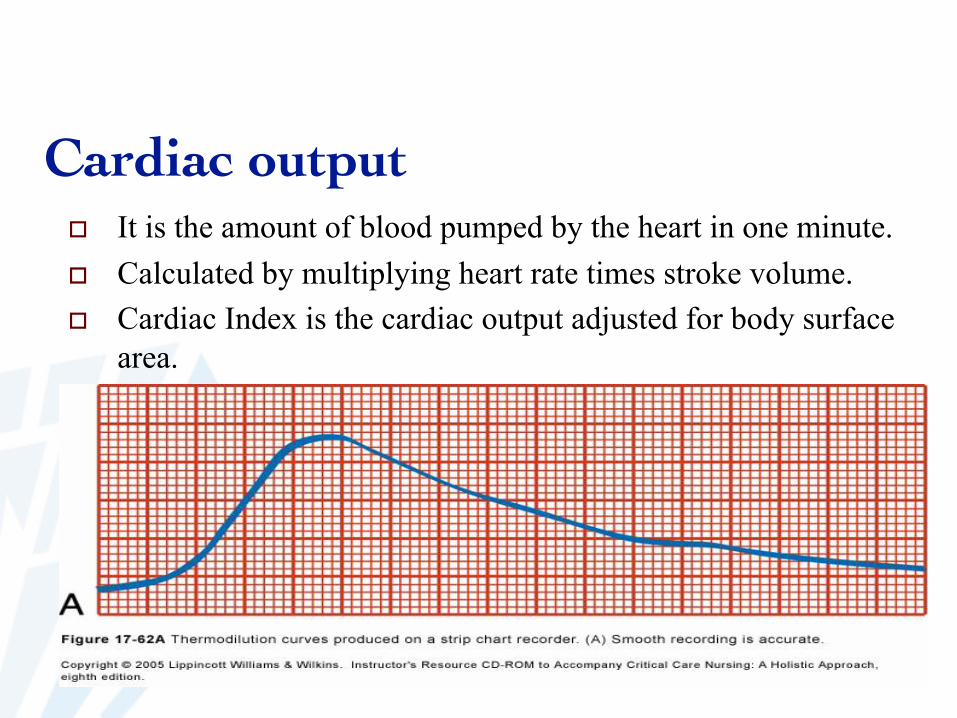
Cardiac output It is the amount of blood pumped by the heart in one minute.
Calculated by multiplying heart rate times stroke volume.
Cardiac Index is the cardiac output adjusted for body surface
area.
Cardiac output
Stewart-Hamilton formula
CO = Vol injected x (TB-TF)1.08K/ ? ? TB(t)dt • TB, TF = Blood and cold fluid temperature • ?? TB(t)dt = under-curve area • K = computational constants
Cardiac output
➡ CO = Slagvolume x hartfrequentie➡ SV = EDV – ESV➡ CI = CO / BSA
➡ Toegenomen: sepsis, inotropica➡ Afgenomen: hartfalen
Cardiac output
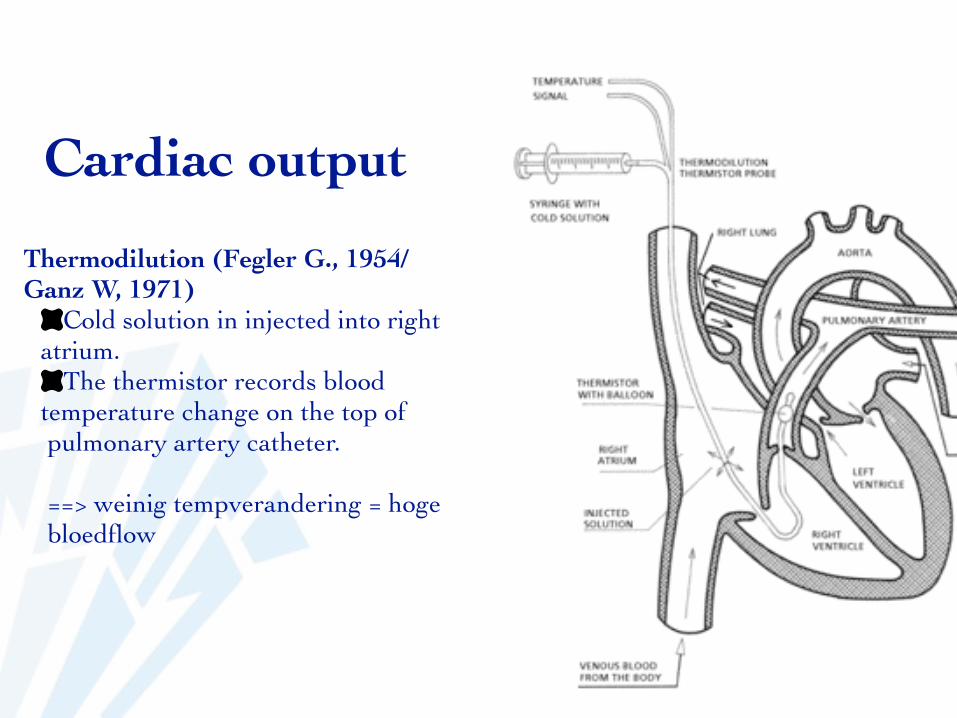
Thermodilution (Fegler G., 1954/Ganz W, 1971)
Cold solution in injected into right atrium.
The thermistor records blood temperature change on the top ofpulmonary artery catheter.
==> weinig tempverandering = hoge bloedflow
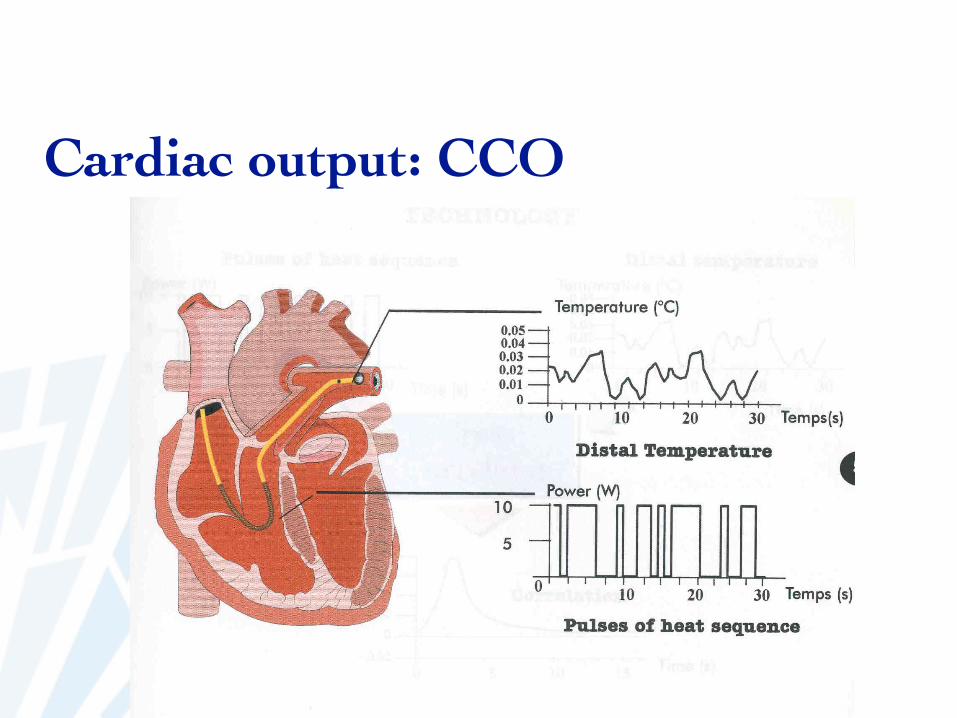
Cardiac output: CCO
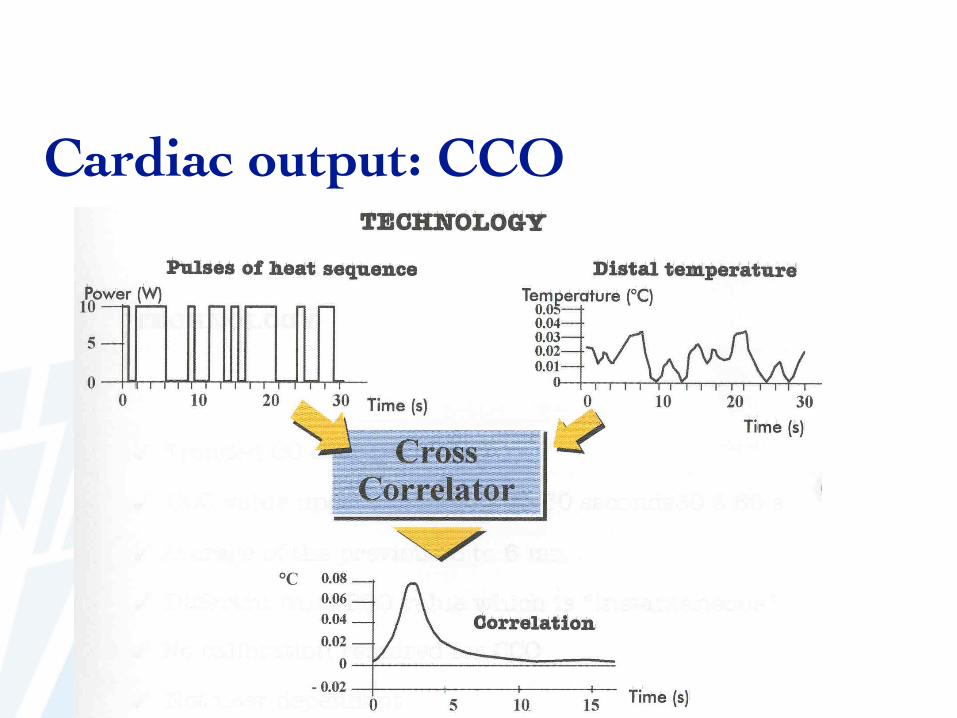
Cardiac output: CCO
Cardiac output: CCO
➡ Nadelen:➡ trage detectie van acute problemen (SvO2 = snelst)
➡ Voordelen:➡ cijfer: trend➡ niet-user-dependent➡ gemiddelde
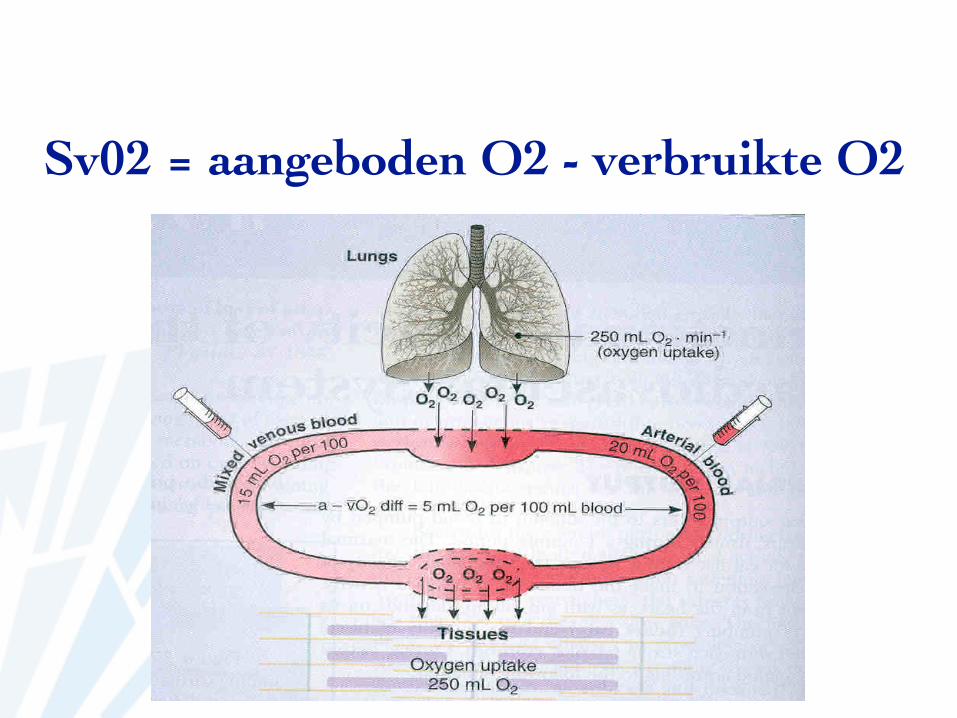
Sv02 = aangeboden O2 - verbruikte O2
Sv02 = aangeboden O2 - verbruikte O2
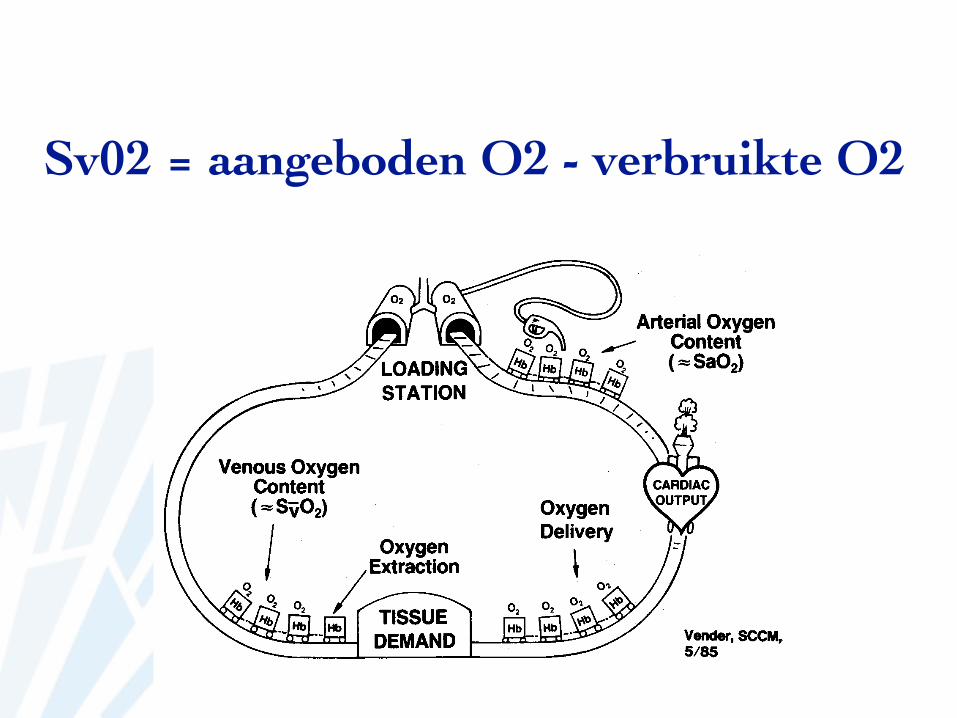
As the train progresses along the track, it stops at multipledepots. A portion of the product carried by the train isunloaded at each of these depots. The number of emptyboxcars represents the amount of product that has beenunloaded. Similarly, as blood flows from the left ventriclethrough the capillaries, oxygen is needed to meet themetabolic needs of the tissues. The difference between theamount of oxygen carried to the tissues (arterial oxygendelivery) and the amount of oxygen returned to the heart(venous oxygen delivery) indicates the total amount ofoxygen consumed by the tissues. (See Figure 9c.)
Those boxcars filled with oxygen as the train returns to theloading station represent the amount of product that wasnot used, and therefore, not unloaded at the depots. In thesame respect, mixed venous oxygen saturation reflects theamount of oxygen returning to the pulmonary capillaries,since it was not needed by the tissues to support metabolicfunction. (See Figure 9d.)
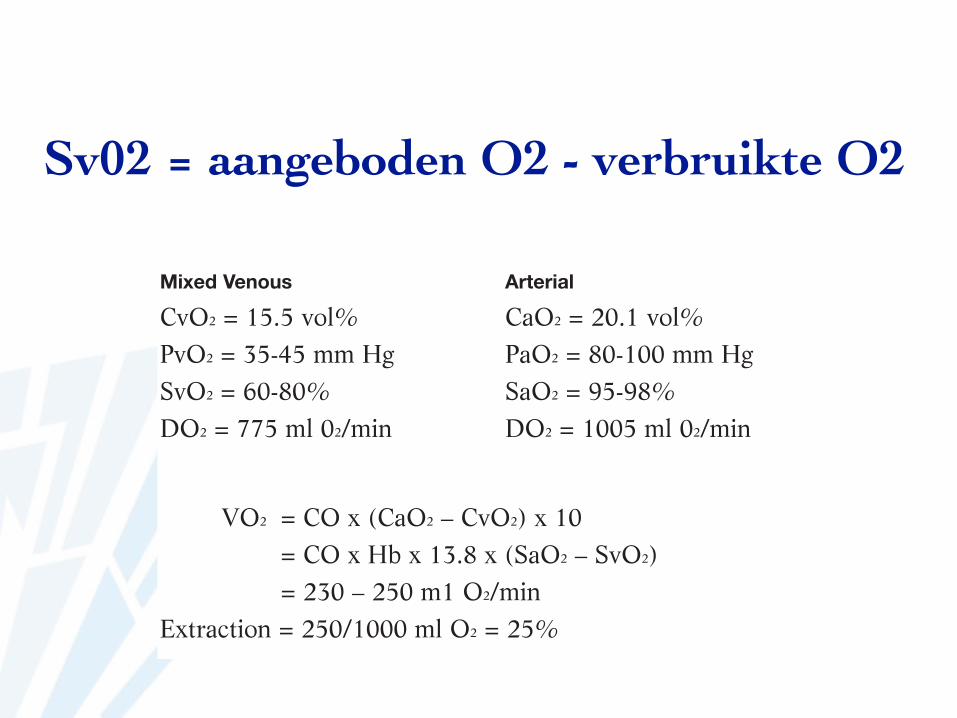
Mixed Venous Arterial
CvO2 = 15.5 vol% CaO2 = 20.1 vol%PvO2 = 35-45 mm Hg PaO2 = 80-100 mm HgSvO2 = 60-80% SaO2 = 95-98%DO2 = 775 ml 02/min DO2 = 1005 ml 02/min
VO2 = CO x (CaO2 – CvO2) x 10= CO x Hb x 13.8 x (SaO2 – SvO2)= 230 – 250 m1 O2/min
Extraction = 250/1000 ml O2 = 25%
7
Figure 9cDemand
Figure 9dMixed venous oxygen saturation
Table 1Normal values
Sv02 = aangeboden O2 - verbruikte O2
As the train progresses along the track, it stops at multipledepots. A portion of the product carried by the train isunloaded at each of these depots. The number of emptyboxcars represents the amount of product that has beenunloaded. Similarly, as blood flows from the left ventriclethrough the capillaries, oxygen is needed to meet themetabolic needs of the tissues. The difference between theamount of oxygen carried to the tissues (arterial oxygendelivery) and the amount of oxygen returned to the heart(venous oxygen delivery) indicates the total amount ofoxygen consumed by the tissues. (See Figure 9c.)
Those boxcars filled with oxygen as the train returns to theloading station represent the amount of product that wasnot used, and therefore, not unloaded at the depots. In thesame respect, mixed venous oxygen saturation reflects theamount of oxygen returning to the pulmonary capillaries,since it was not needed by the tissues to support metabolicfunction. (See Figure 9d.)
Mixed Venous Arterial
CvO2 = 15.5 vol% CaO2 = 20.1 vol%PvO2 = 35-45 mm Hg PaO2 = 80-100 mm HgSvO2 = 60-80% SaO2 = 95-98%DO2 = 775 ml 02/min DO2 = 1005 ml 02/min
VO2 = CO x (CaO2 – CvO2) x 10= CO x Hb x 13.8 x (SaO2 – SvO2)= 230 – 250 m1 O2/min
Extraction = 250/1000 ml O2 = 25%
7
Figure 9cDemand
Figure 9dMixed venous oxygen saturation
Table 1Normal values
Sv02: hoge waarde
Toegenomen O2 aanbod:Hoger FiO2
HyperoxieAfgenomen O2 vraag:
HypothermieAnesthesieFarmacologische paralyse
Sv02: lage waarde
Afgenomen O2 aanbod:Gedaald Hb: anemie, hemorraghieGedaald SaO2: hypoxieGedaald hartdebiet: hypovolemie, shock, arrhythmie
Toegenomen O2 vraag:HyperthermiePijnRillenConvulsies

Swan Ganz catheter
techniek➡ http://www.youtube.com/watch?v=YkKbg423vYM
curves:➡ http://www.youtube.com/watch?
v=7putxZN7ij4&feature=endscreen