Clinical Study Impact of Dabigatran versus Phenprocoumon ...
Anticoagulantia en regionale anesthesie
prof. dr. Erik Vandermeulen
anesthesiologie
Anticoagulantia en LRA
– Orale-anticoagulantia
– Acetyl-salicylzuur, NSAIDS en Coxibs
– Directe Glycoproteïne IIb/IIIa antagonisten
– Ongefractioneerd heparine
– Laag-moleculair gewicht heparine
– Selectieve factor-Xa inhibitoren
– Directe trombine inhibitoren
Ongefractioneerd Heparine
• Heparine-antithrombine III complex
• Inhibitie van thrombine (=IIa), Xa, IXa, XIa,
en XIIa
• Xa /IIa inhibitie= 1:1
• Onderbreking van positieve feedback loops
via factor Va en VIIIa
Laag Moleculair Gewicht Heparine
(LMGH)
• Fragmenten van ongefractioneerd heparine
• LMGH/antithrombine III complex
• Xa /IIa inhibitie= 3/1 - 5/1
• Antistollend effect wordt uitgedrukt als anti-Xa activiteit (Choay-units)
Vitamine K-Antagonisten
• Vorming van deficiënte factoren II, VII, IX,
and X
– Complexeren van Ca2+ onmogelijk
• binding aan phospholipiden membraan wordt
bemoeilijkt
– Rechtstreeks effect op prothrombine activering
Incidentie van Bloeding in Aanwezigheid van
Risico Factoren
• Anticoagulantia/Stollingsstoornissen: 60-80%
• Bloederige punctie: 10-40%
– “Normale” incidentie: • 1-10% (Niet-zwanger)
• 18% (Zwanger)
– Invloed van ervaring, handigheid: • 0.5% in opleidingsziekenhuizen
• Moeilijke punctie: 27-36%
• Verwijdering van de epidurale catheter: 57%
Risico Factoren
• In 55 van de 64 gevallen (85%): minstens 1
• In 29 gevallen (37%):
minstens 2
• In 13 gevallen, spinaal hematoom ondanks
volgen van “accepted guidelines”
Diagnose van Spinale Bloedingen
• Eerste symptoom:
– Spierzwakte: 51%
– Rugpijn (gordelvormig): 39%
– Sensorisch deficiet: 22%
– Urinaire retentie: 6%
• Paraplegie in de volgende 15 ± 7h
• Diagnose:
– CT ± Myelografie
– NMR
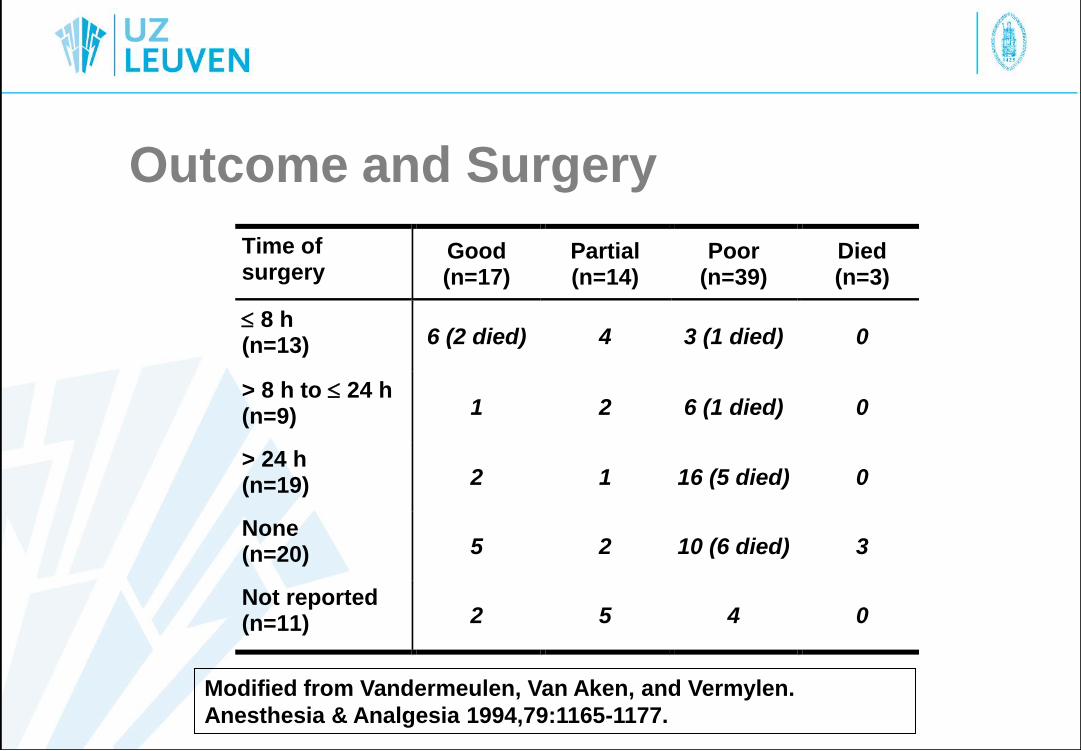
Outcome and Surgery
Time of surgery
Good (n=17)
Partial (n=14)
Poor (n=39)
Died (n=3)
8 h (n=13) 6 (2 died) 4 3 (1 died) 0
> 8 h to 24 h (n=9) 1 2 6 (1 died) 0
> 24 h (n=19) 2 1 16 (5 died) 0
None (n=20) 5 2 10 (6 died) 3
Not reported (n=11) 2 5 4 0
Modified from Vandermeulen, Van Aken, and Vermylen.
Anesthesia & Analgesia 1994,79:1165-1177.
Essentieel
• Strikte patiënten selectie
• Tijdsinterval punctie-anticoagulans
• Atraumatische techniek??
• Ervaren anesthetist
• Minimaal motor block
• Neurologische monitoring
• Waakzaamheid en achterdocht
• Agressieve diagnostische en therapeutische
benadering
Bloedingsneiging?
• Steeds bloedingsanamnese
– Nabloeden bij tandarts, mineure traumata,
vorige ingrepen
– Spontane ecchymosen
• Klinisch onderzoek
– Petechiae, ecchymosen
Richtlijnen
• Preoperatief gebruik van orale anticoagulantia, thrombolytica en therapeutische heparinisering – Alternatieve anesthesie techniek (AA?)
– Alternatief: • Stop anticoagulantia
– Wacht tot normalisering betrokken stollingsparameters
• Therapeutische heparinisering na EA of SA – Punctie minstens 60 min voor heparine
– Volgen stollingstijden (ACT, aPTT max. X 2)
– Catheter uit: slechts na gedocumenteerde normalisering van ACT/aPTT
Aspirine en NSAIDs, Coxibs
• Geneesmiddel- bloedingsanamnese
– Geen bijzondere voorzorgen
Thiënopyridines
• Indirecte glycoproteine IIb-IIIa
antagonisten (via ADP)
– Clopidogrel (Plavix®): 7 dagen STOP
– Ticlopidine (Ticlid®): 10 dagen STOP
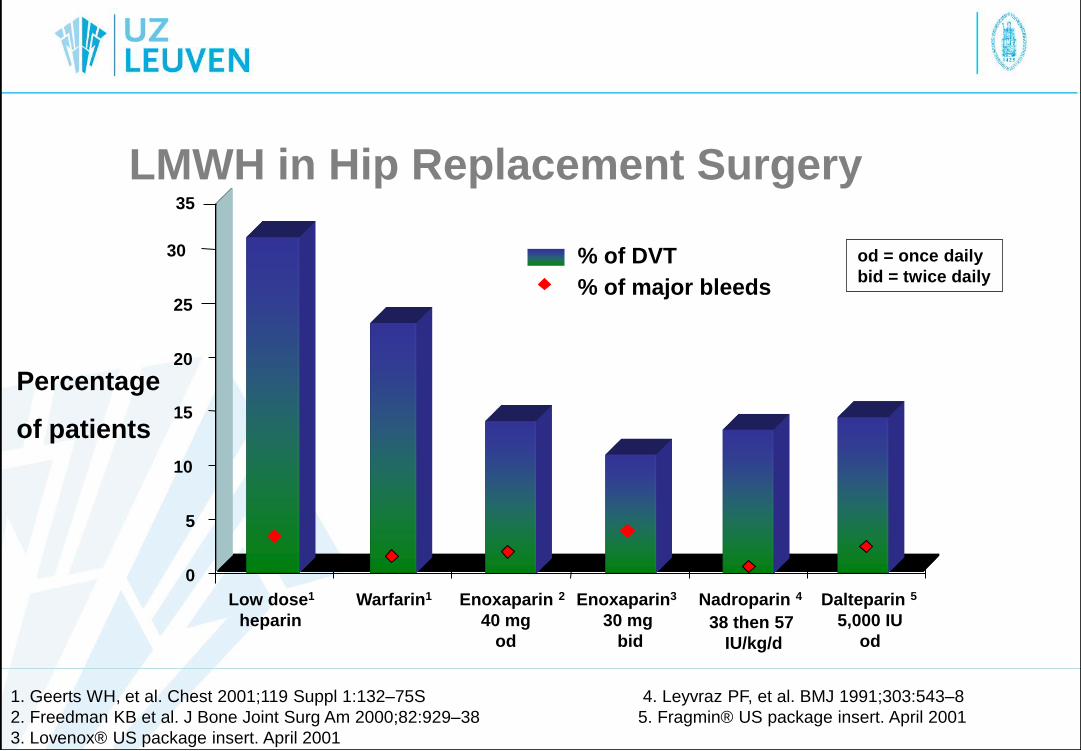
LMWH in Hip Replacement Surgery
1. Geerts WH, et al. Chest 2001;119 Suppl 1:132–75S 4. Leyvraz PF, et al. BMJ 1991;303:543–8
2. Freedman KB et al. J Bone Joint Surg Am 2000;82:929–38 5. Fragmin® US package insert. April 2001
3. Lovenox® US package insert. April 2001
38 then 57
IU/kg/d
0
5
10
15
20
25
30
35
Low dose1
heparin
Warfarin1 Enoxaparin 2
40 mg
od
Enoxaparin3
30 mg
bid
Nadroparin 4 Dalteparin 5
5,000 IU
od
% of DVT
% of major bleeds
od = once daily
bid = twice daily
Percentage
of patients
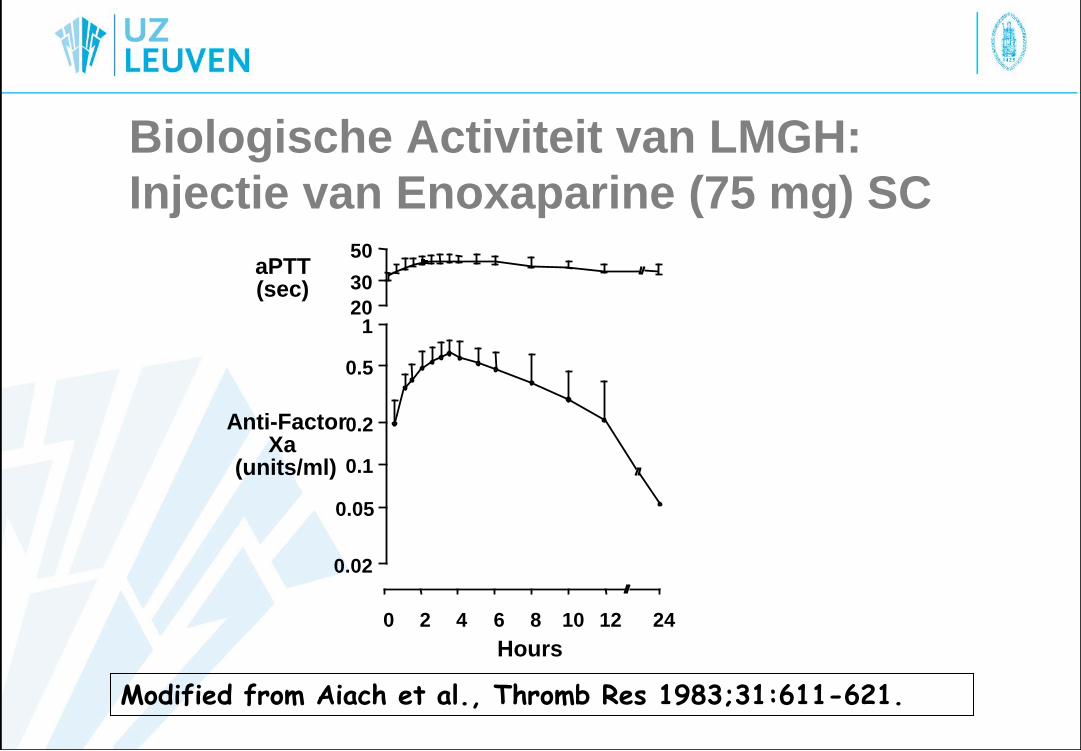
Biologische Activiteit van LMGH:
Injectie van Enoxaparine (75 mg) SC
Modified from Aiach et al., Thromb Res 1983;31:611-621.
0 2 4 6 8 10 12 24
Hours
0.02
0.05
0.1
0.2
0.5
1 20
30
50
Anti-Factor Xa
(units/ml)
aPTT (sec)
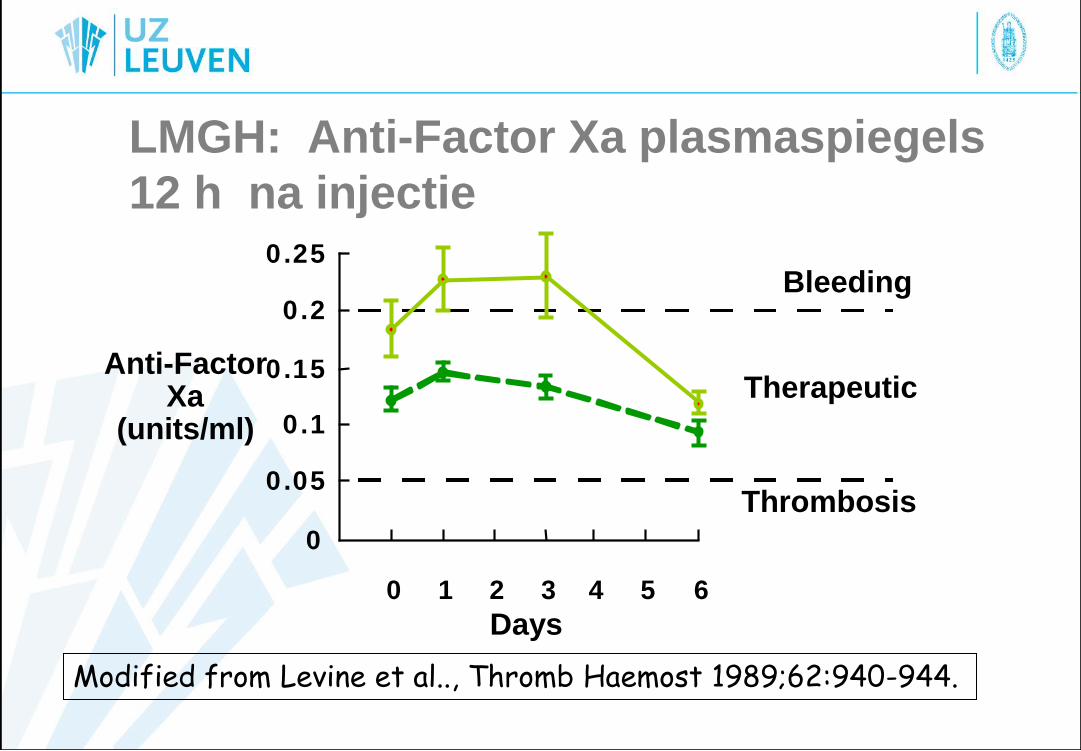
LMGH: Anti-Factor Xa plasmaspiegels
12 h na injectie
Modified from Levine et al.., Thromb Haemost 1989;62:940-944.
0 1 2 3 4 5 6
Anti-Factor Xa
(units/ml)
0
0 . 0 5
0 . 1
0 . 1 5
0 . 2
0 . 2 5
Days
Thrombosis
Therapeutic
Bleeding
Enoxaparine in de V.S.
• Op de markt sinds Mei 1993
• 16 spinale hematomen na EA en/of SA in 44
maanden
• R/ Enoxaparine 30 mg SC 1 h postop.,
Enoxaparine 30 mg SC / 12 h
(Data from Horlocker and Heit. Anesth
Analg 1997: 85, 874-885.)
Enoxaparine in Europe
• Op de markt sinds 1987
• 7 spinal hematomen na EA en/of SA in 10
jaren
• R/ Enoxaparine 20-40 mg SC 12 h preop.,
Enoxaparine 20-40 mg SC / 24 h
(Data from Horlocker and Heit. Anesth
Analg 1997: 85,874-885.)
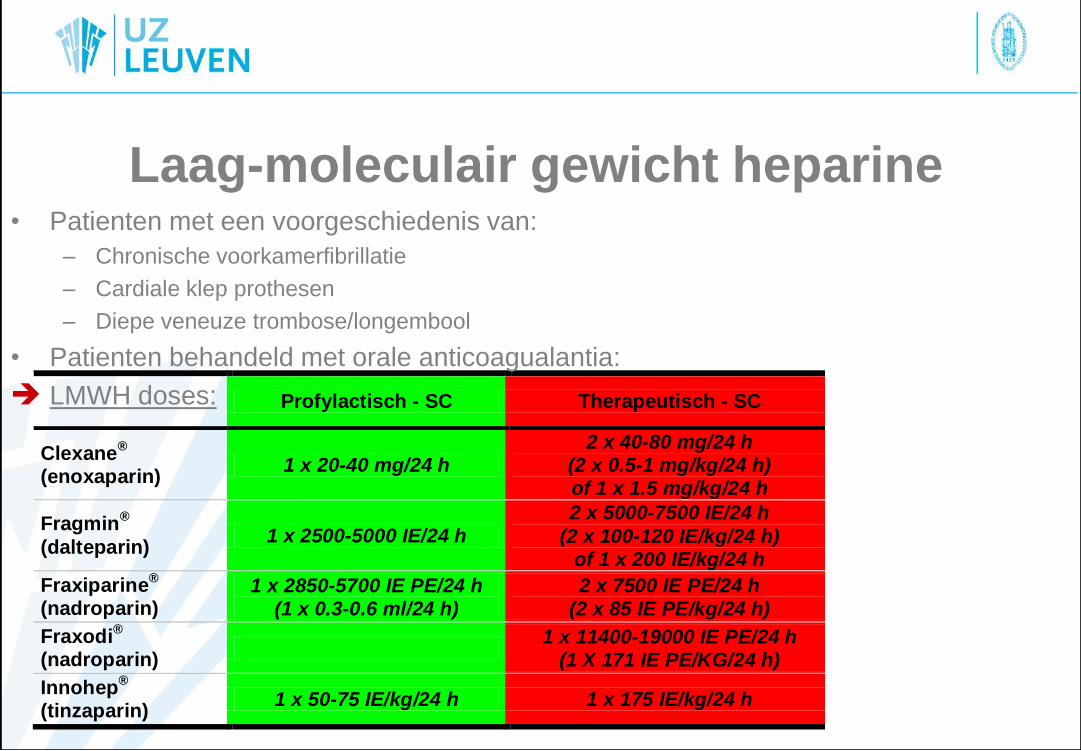
Laag-moleculair gewicht heparine
Profylactisch - SC Therapeutisch - SC
Clexane®
(enoxaparin) 1 x 20-40 mg/24 h
2 x 40-80 mg/24 h (2 x 0.5-1 mg/kg/24 h) of 1 x 1.5 mg/kg/24 h
Fragmin®
(dalteparin) 1 x 2500-5000 IE/24 h
2 x 5000-7500 IE/24 h
(2 x 100-120 IE/kg/24 h) of 1 x 200 IE/kg/24 h
Fraxiparine®
(nadroparin) 1 x 2850-5700 IE PE/24 h
(1 x 0.3-0.6 ml/24 h) 2 x 7500 IE PE/24 h
(2 x 85 IE PE/kg/24 h)
Fraxodi®
(nadroparin)
1 x 11400-19000 IE PE/24 h (1 X 171 IE PE/KG/24 h)
Innohep®
(tinzaparin) 1 x 50-75 IE/kg/24 h 1 x 175 IE/kg/24 h
• Patienten met een voorgeschiedenis van:
– Chronische voorkamerfibrillatie
– Cardiale klep prothesen
– Diepe veneuze trombose/longembool
• Patienten behandeld met orale anticoagualantia:
LMWH doses:
Prophylactisch gebruik van LMWH
• Plaatsen of verwijderen van epidurale
en/of spinale naald/catheter • 10 - 12 h na de laatste dosis (=avond
voorafgaand aan de operatie)
• volgende dosis =>4 h na verwijderen van
catheter
(Half)Therapeutisch gebruik van
LMWH – Plaatsen of verwijderen van epidurale en/of
spinale naald/catheter
• => 24h na de laatste dosis (=laatste dosis op
ochtend van dag voorafgaand aan de
operatiedag)
• voor de volgende dosis =>4 h na verwijderen van
catheter
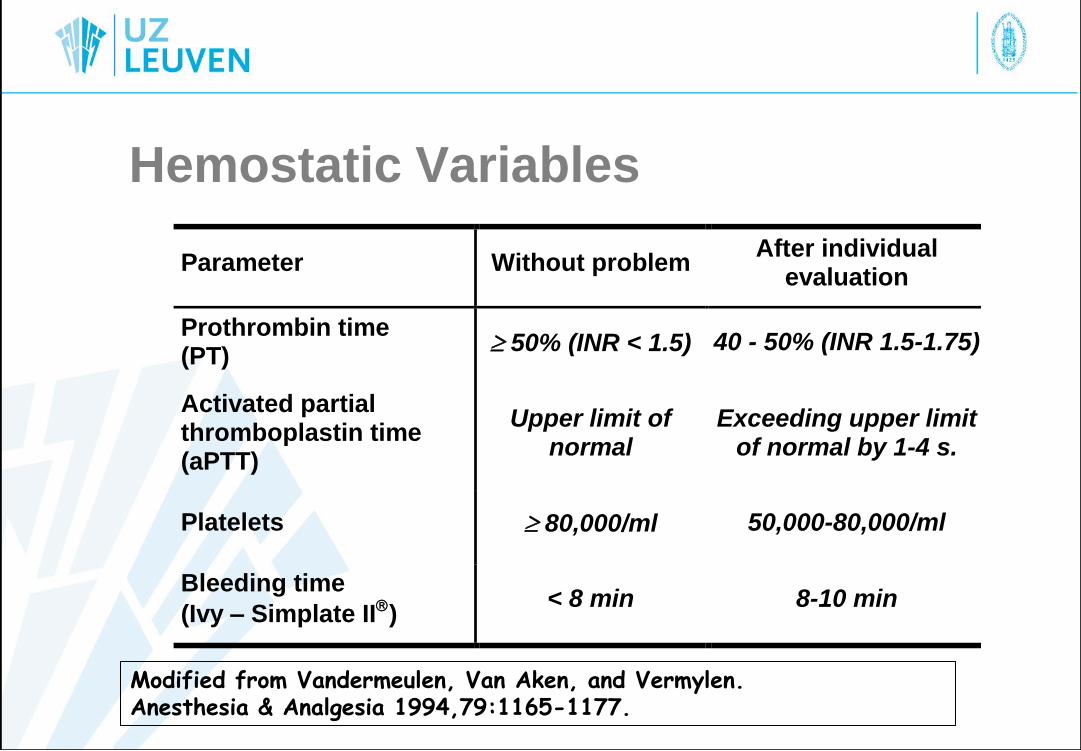
Hemostatic Variables
Parameter Without problem After individual
evaluation
Prothrombin time (PT)
50% (INR < 1.5) 40 - 50% (INR 1.5-1.75)
Activated partial thromboplastin time (aPTT)
Upper limit of normal
Exceeding upper limit of normal by 1-4 s.
Platelets 80,000/ml 50,000-80,000/ml
Bleeding time
(Ivy – Simplate II) < 8 min 8-10 min
Modified from Vandermeulen, Van Aken, and Vermylen. Anesthesia & Analgesia 1994,79:1165-1177.
Selectieve Factor Xa Inhibitoren
Fondaparinux (Arixtra®):
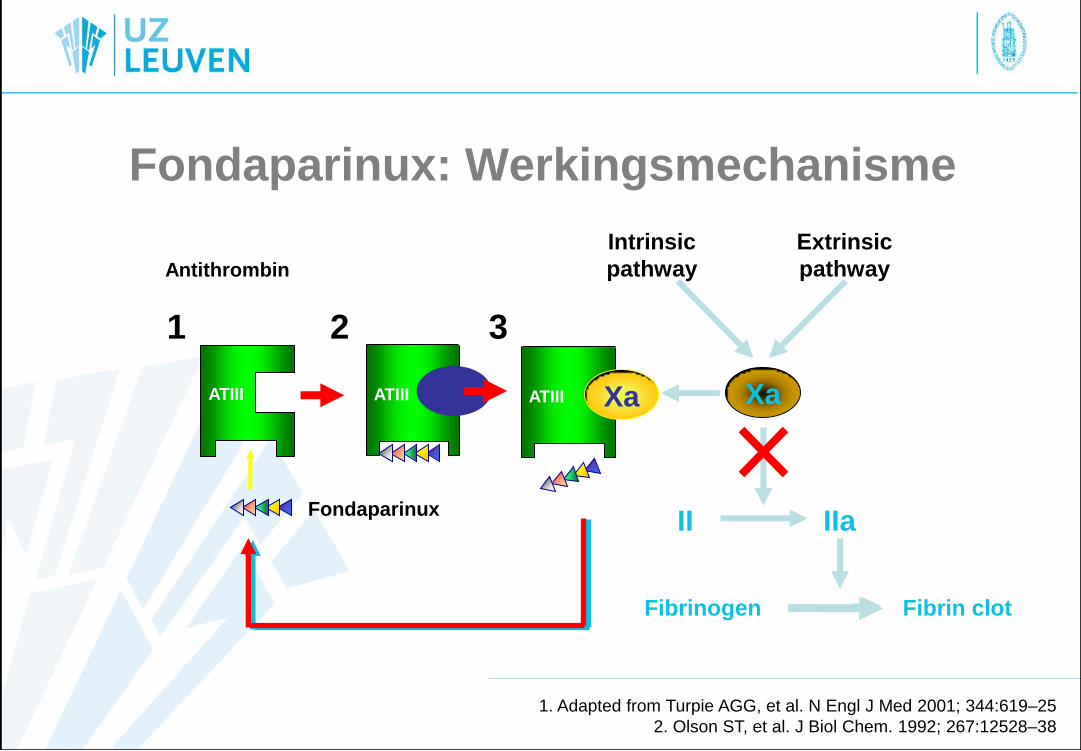
1. Adapted from Turpie AGG, et al. N Engl J Med 2001; 344:619–25
2. Olson ST, et al. J Biol Chem. 1992; 267:12528–38
IIa II
Fibrinogen Fibrin clot
Extrinsic
pathway
Intrinsic
pathway
3
ATIII Xa
1
ATIII ATIII
2
Fondaparinux
Xa
Fondaparinux: Werkingsmechanisme
Antithrombin
Selectieve Factor Xa Inhibitoren
• Fondaparinux
– Anti-thrombin gemedieerde inhibitie van factor Xa vorming
• Gebruikt in H.I.T. – maar recent 1 case report van HIT door fondaparinux
• t1/2: 18 h
• Dosering
– Start 6 – 12 h postoperatief
– Dosis interval: 24 h
– Preventie en behandeling van DVT en LE
• Superieur tov. LMWH, maar duurder +++
• Niet terugbetaald in België
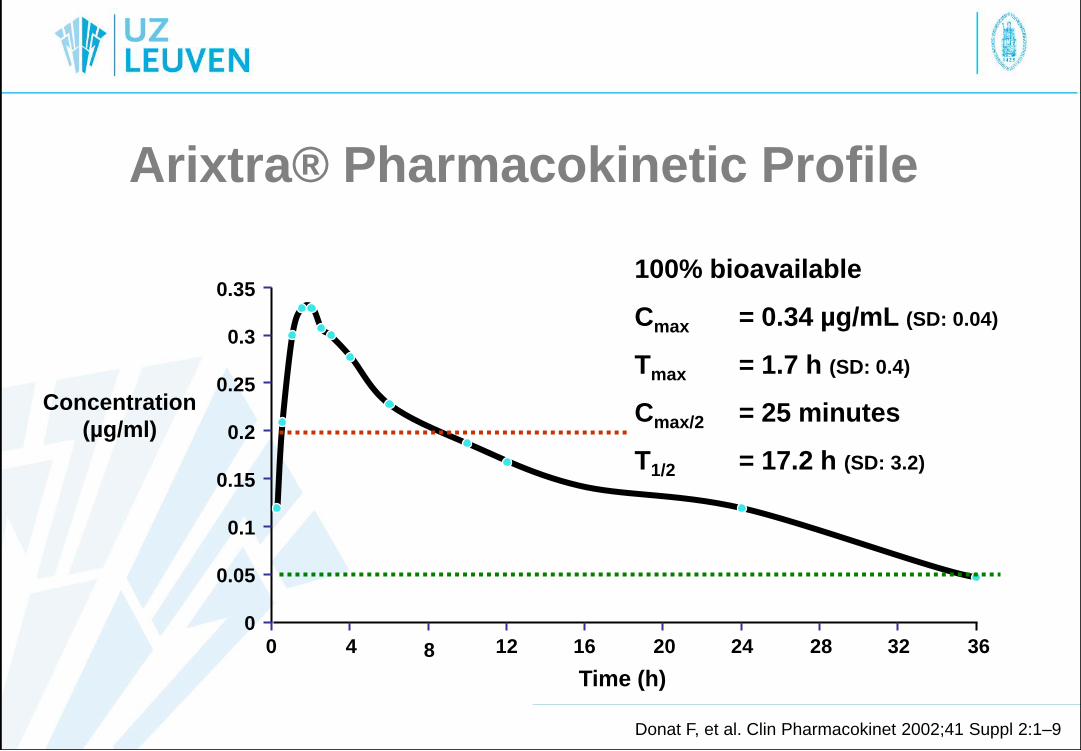
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Concentration
(µg/ml)
0 4 8 12 16 20 24 28 32 36
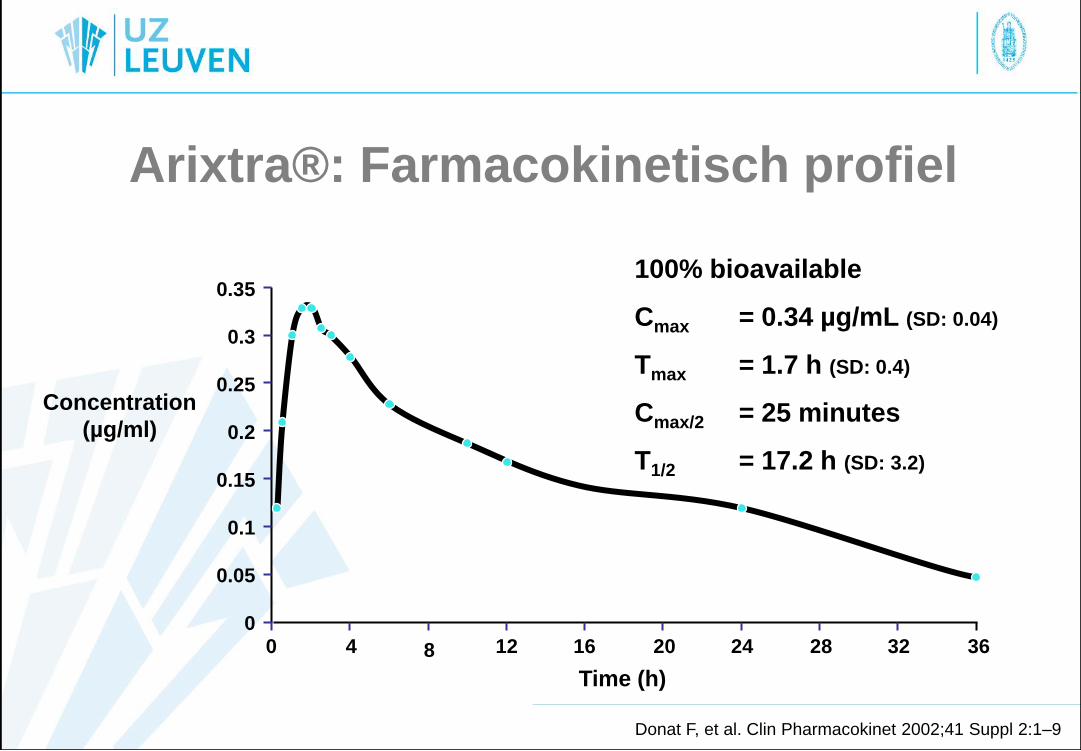
Donat F, et al. Clin Pharmacokinet 2002;41 Suppl 2:1–9
Time (h)
100% bioavailable
Cmax = 0.34 µg/mL (SD: 0.04)
Tmax = 1.7 h (SD: 0.4)
Cmax/2 = 25 minutes
T1/2 = 17.2 h (SD: 3.2)
Arixtra®: Farmacokinetisch profiel
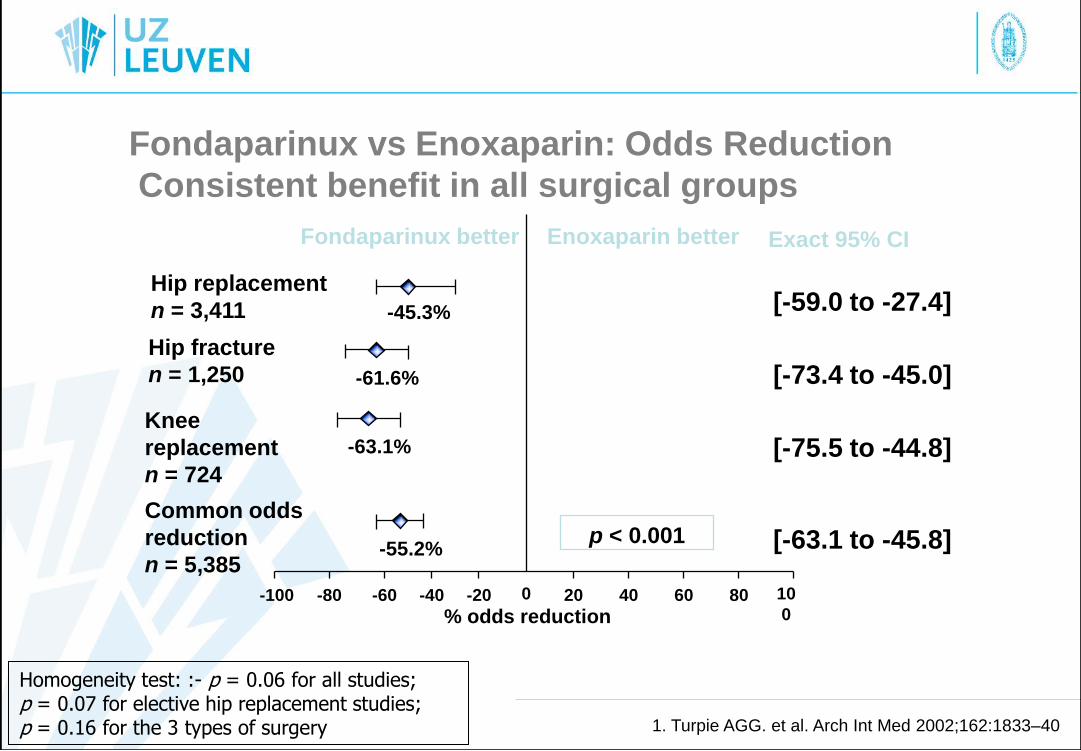
Hip replacement
n = 3,411
Hip fracture
n = 1,250
Knee
replacement
n = 724
Common odds
reduction
n = 5,385
% odds reduction
Fondaparinux better Enoxaparin better
-100 -80 -60 -40 -20 20 0 40 60 80 10
0
-45.3%
-63.1%
-55.2%
[-59.0 to -27.4]
[-73.4 to -45.0]
[-75.5 to -44.8]
[-63.1 to -45.8]
-61.6%
Exact 95% CI
p < 0.001
Fondaparinux vs Enoxaparin: Odds Reduction
Consistent benefit in all surgical groups
Homogeneity test: :- p = 0.06 for all studies; p = 0.07 for elective hip replacement studies; p = 0.16 for the 3 types of surgery 1. Turpie AGG. et al. Arch Int Med 2002;162:1833–40
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Concentration
(µg/ml)
0 4 8 12 16 20 24 28 32 36
Donat F, et al. Clin Pharmacokinet 2002;41 Suppl 2:1–9
Time (h)
100% bioavailable
Cmax = 0.34 µg/mL (SD: 0.04)
Tmax = 1.7 h (SD: 0.4)
Cmax/2 = 25 minutes
T1/2 = 17.2 h (SD: 3.2)
Arixtra® Pharmacokinetic Profile
Fondaparinux en LRA
• Belgische guidelines
– Stop fondaparinux 36h voor punctie/catheter verwijderen
– Volgende dosis => 12 h na verwijdering van catheter
Directe Glycoproteïne IIb/IIIa
antagonisten • Indicatie: Acuut coronair syndroom
– Abciximab (Réopro®)
• Enkel IV
• Trombocytopenie (0.3-1%)
• 48 h (2 weken?)
– Eptifibatide (Integrilin®)
• Enkel IV
• Trombocytopenie mogelijk
• 24 h
– Tirofiban (Aggragstat®)
• Enkel IV
• Trombocytopenie mogelijk
• 24 h
Nieuwere producten
• Directe trombine inhibitoren
– Lepuridine (Refludan®)
• Geïndiceerd bij aan LMWH en bij HIT
– Min. 8-10 h na laatse dosis
– Min. 2-4 h voor de volgende dosis
– Anticoagualerend effect is meetbaar via ECT (Ecarin
Clotting Time) of aPTT (minder goed)
Nieuwe antitrombotica
• Directe trombine inhibitoren
– Dabigatran (Pradaxa®) (t1/2=12-17 u, Tmax=2-4 u)
– ESA-guidelines 2010 • “Very limited experience with neuraxial blockade”
• “Extreme caution is recommended
• LRA gecontraindiceerd volgens fabrikant – In geval van “accidenteel” neuraxiaal block
» Verwijderen ≥ 34 u (36 u?) na laatste dosis
» Volgende dosis ≥ 4-6 u na verwijderen katheter
Direct thrombin inhibitors
• Dabigatran (Pradaxa®) in high dose – 220-300 mg oncedaily
• t1/2 =12-17 h
• Observe a 2 day delay between last dose and surgery with mild-moderate bleeding risk
• Observe a 3-4 day delay between last dose and surgery with high bleeding risk
• Substitution with LMWH?
• PT, anti- Xa assay for specific agent (under development)
• Next dose of rivaroxaban ≥6 h after CNB or manipulation/withdrawal of catheter
• Only applicable in patients with normal renal function
• CNB is contraindicated
BARA Guidelines 3rd Ed.
Nieuwe antitrombotica
• Factor Xa-inhibitoren
– Rivaroxaban (Xarelto®) (t1/2=7-11 u,
Tmax=1-2 u)
– ESA-guidelines 2010
• “Very limited experience with neuraxial blockade”
• “Extreme caution is recommended
– Geval van “accidenteel” neuraxiaal block
» Verwijderen ≥ 22 u (24 u?) na laatste dosis
» Volgende dosis ≥ 4-6 u na verwijderen katheter
Anti Xa agents
• Rivaroxaban (Xarelto®) in high dose – 1*20 mg once daily
• t1/2 =11-13 h
• Observe a 2 day delay between last dose and surgery with mild-moderate bleeding risk
• Observe a 3 day delay between last dose and surgery with high bleeding risk
• Substitution with LMWH?
• PT, anti- Xa assay for specific agent (under development)
• Next dose of rivaroxaban ≥6 h after CNB or manipulation/withdrawal of catheter
• CNB is contraindicated
BARA Guidelines 3rd Ed.

Anti Xa agents
• Apixaban (Eliquis®) in prophylactic dose – 2.5 mg twice daily (started postoperatively)
• t1/2=10-15 h
• Observe a ≥26-30 h between last dose of apixaban and CNB or manipulation/withdrawal of catheter
• PT, anti- Xa assay for specific agent (under development)
• Next dose of apixaban ≥6 h after CNB or manipulation/withdrawal of catheter
• Extreme caution is warranted as experience with NB is very limited
BARA Guidelines 3rd Ed.
Anti Xa agents
• Apixaban (Eliquis®) in high dose – 5 mg twice daily
• t1/2 =10-15 h
• Observe a 2 day delay between last dose and surgery with mild-moderate bleeding risk
• Observe a 3 day delay between last dose and surgery with high bleeding risk
• Substitution with LMWH?
• PT, anti- Xa assay for specific agent (under development)
• Next dose of rivaroxaban ≥6 h after CNB or manipulation/withdrawal of catheter
• CNB is contraindicated
BARA Guidelines 3rd Ed.
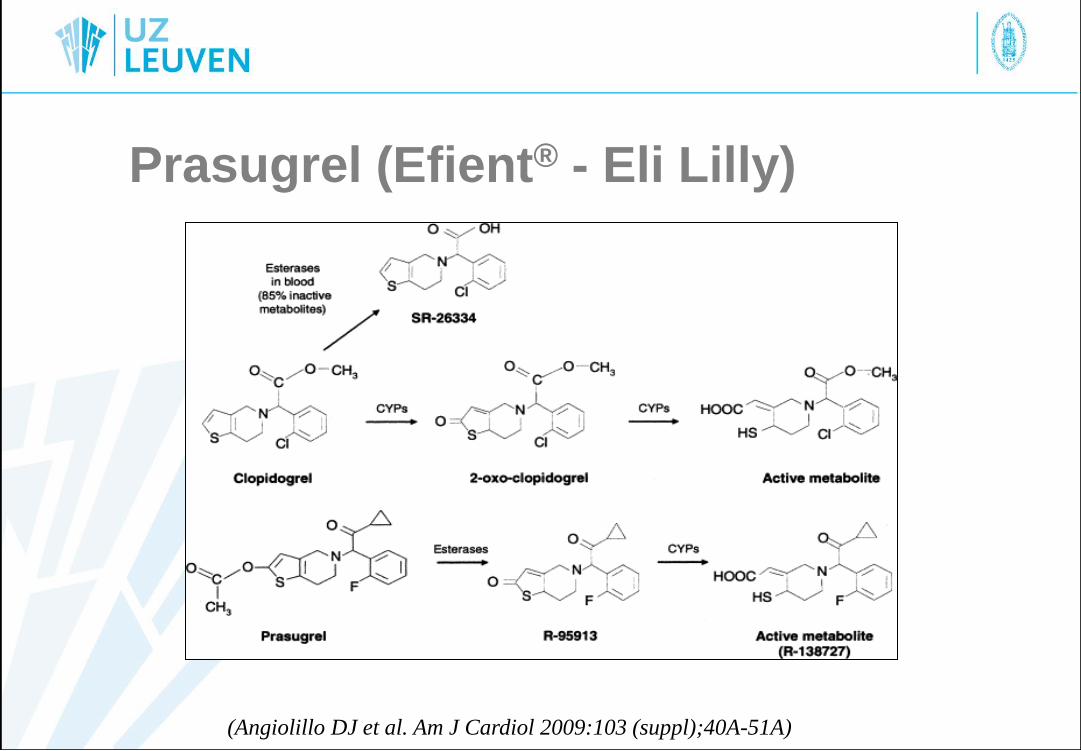
Prasugrel (Efient® - Eli Lilly)
(Angiolillo DJ et al. Am J Cardiol 2009:103 (suppl);40A-51A)
Nieuwe antitrombotica
• Thiënopyridines
– Prasugrel (Efient®) (t1/2=7.4 u, Tmax= < 60 min)
• Geen gegevens ivm. LRA gekend
• Antiplaatjes effect duurt 7-10 d
• Bijsluiter: Stop R/ ≥ 7d voor HK
• ESA guidelines 2010
» Punctie/insertie/verwijderen ≥ 7-10 d na laatste dosis
» Volgende dosis ≥ 6 u na verwijderen katheter
BARA Guidelines 3rd Ed.
Nieuwe antitrombotica
• Pyrimidines
– Ticagrelor (Brilique®) (t1/2=7-8 u, Tmax=60
min)
• Geen gegevens ivm. LRA gekend
• Antiplaatjes effect duurt 4.5-5 d
• Bijsluiter: Stop R/ ≥ 7d voor HK
• BARA guidelines 2011
» Punctie/insertie/verwijderen ≥ 7 d na laatste dosis
» Volgende dosis ≥ 6 u na verwijderen katheter
BARA Guidelines 3rd Ed.
Andere
• Stop 7d voor operatie
– Planten- kruidengeneeskunde
• Ginseng
• Ginkgo Biloba
• Look
• …
– Vitaminesupplementen
• Vitamine E
Aanbevolen Literatuur
• Vandermeulen E et al. Belgian guidelines concerning central
neural blockade in patients with drug-induced alteration of
coagulation: An Update. Acta Anaesthesiol Belg 2005:56;139-
146.
• Vandermeulen E, et al. Anticoagulants and Spinal-Epidural Anesthesia. Anesth Analg 1994;79:1165-1177.