Proefschrift Fahner
114
Experimental Studies on Glycerol Preserved Vascular Allografts Peter Fahner Experimental Studies on Glycerol Preserved Vascular Allografts Peter Fahner
-
Upload
nicole-nijhuis -
Category
Documents
-
view
230 -
download
3
description
Â
Transcript of Proefschrift Fahner

Experim
ental Stu
dies o
n G
lycerol Preserved
Vascu
lar Allo
grafts
Peter Fahn
er
Experimental Studies on Glycerol Preserved Vascular Allografts
Peter Fahner
UITNODIGING
voor het bijwonen van
de openbare verdediging
van het proefschrift
Experimental Studieson Glycerol Preserved
Vascular Allografts
op vrijdag 6 juni 2014
om 13.00 uur
in de Aula van de
Universiteit
van Amsterdam
Oude Lutherse Kerk
Singel 411, hoek Spui
1012 WN Amsterdam
Aansluitend receptie in de
naastgelegen
Tetterode Bibliotheek
Paranimfen:
Hanneke van Krimpen
André Janse
Peter [email protected]


Experimental studies
on glycerol preserved vascular allografts
Peter Jurriaan Fahner
Fahner.indd 1 5-5-2014 14:35:07

This study was performed at Department of Experimental Surgery in collaboration with
Department of Vascular Surgery of the Academic Medical Center (AMC), University of
Amsterdam, The Netherlands
Cover: Front: Stairwell Hotel Ohla, Barcelona, Spain
Back: AMC/ Inst. voor Wetenschappelijk Onderzoek, Amsterdam,
The Netherlands
Printed by: Gildeprint, Enschede, The Netherlands
ISBN: 9789461086815
Printing of this thesis was financially supported by
University of Amsterdam, The Netherlands
Glaxo Smith Kline, Zeist, The Netherlands
Fahner.indd 2 5-5-2014 14:35:07

Experimental studies
on glycerol preserved vascular allografts
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof. dr. D.C. van den Boom
ten overstaan van een door het college voor promoties
ingestelde commissie
in het openbaar te verdedigen in de Aula van de Universiteit
op vrijdag 6 juni 2014 om 13.00 uur
door
Peter Jurriaan Fahner
geboren te Angguruk, Indonesië
Fahner.indd 3 5-5-2014 14:35:07

Promotores: Prof. dr. D.A. Legemate
Prof. dr. T.M. van Gulik
Copromotor: Dr. M.M. Idu
Overige leden: Prof. dr. E.T. van Bavel
Dr. M. Heger
Prof. dr. B.A.J.M. de Mol
Dr. J.I. Rotmans
Prof. dr. B.H. Walpoth
Prof. dr. C.J.A.M. Zeebregts
Faculteit der Geneeskunde
Fahner.indd 4 5-5-2014 14:35:07

In memory of my father Dr. Chr. Fahner
In memory of my father in law F. Janse
Fahner.indd 5 5-5-2014 14:35:07

Fahner.indd 6 5-5-2014 14:35:07

CONTENTS
Contents
Chapter 1 General introduction and outline of the thesis 9
Chapter 2 Systematic review of preservation methods and clinical outcome of
infrainguinal vascular allografts 23
J Vasc Surg 2006;44:518-24
Chapter 3 Morphological and functional alterations in glycerol preserved rat aortic
allografts 39
Int J Art Org 2004;27:979-89
Chapter 4 Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta 57
Eur Surg Res 2009;42:78-86
Chapter 5 Comparison of preserved vascular allografts using glycerol and University
of Wisconsin solution in a goat carotid artery transplantation model 77
Eur Surg Res 2012;48:64-72
Chapter 6 Summary and conclusions
Samenvatting en conclusies 95
Chapter 7 General discussion and future perspectives 101
Dankwoord 107
Curriculum Vitae 111
Fahner.indd 7 5-5-2014 14:35:07

Fahner.indd 8 5-5-2014 14:35:07

1General introduction and outline of the thesis
Fahner.indd 9 5-5-2014 14:35:07

10 | Chapter 1
Introduction
The experiments described in this thesis focus on the applicability of glycerol preservation of
vascular allografts as an alternative to the existing vascular preservation methods and synthetic
conduits in peripheral arterial revascularization. As the synthetic prosthesis performs well in
central arterial reconstructions, the long term results in small caliber reconstructions of less than
6 mm are disappointing. Despite advances in secondary prevention, medical treatment, and
interventional technology (1;2), the incidence of peripheral arterial disease requiring vascular
reconstructions is increasing (3;4). Therefore we need to further pursue the development of a
durable patent vascular graft for peripheral vascular reconstructions.
Due to the limited results of the small diameter synthetic grafts, the focus for a vascular graft
has widened to biological allografts. Two obstacles in the development of a suitable biologic
vascular graft are the thrombogenicity of the graft lumen and the immunogenicity of the
transplanted structure. Furthermore, the vascular graft should have compliance characteristics
comparable to the native vessel. It is thought that preserved biological grafts could serve as a
scaffold for autologous cells including endothelial cells, vascular smooth muscle cells (SMC) and
fibroblasts to repopulate the graft, thereby improving its biocompatibility.
As an alternative to allografts, the use of xenografts such as the bovine venous graft has been
explored, however with disappointing long-term results in peripheral arterial reconstruction (5;6).
Allografts therefore are considered more suitable for reconstructive purposes.
Biological scaffolds have the advantage of possessing an extra cellular matrix which expresses
signaling components essential for cell adhesion, migration, proliferation and differentiation of
ingrowing recipient cells (7). Preservation of the collagen and elastin scaffold ensure retention of
tensile strength, and the glycosaminoglycans play a crucial role in endothelial cell adhesion and
proliferation, inhibition of SMC proliferation and migration in addition to their antithrombotic
properties (8;9). It has been shown that the production of endothelial mediators involved in
coagulation homeostasis was significantly greater in human saphenous vein endothelial cells
grown on biological matrices compared to those grown on polytetrafluoroethylene (PTFE) (10).
Another advantage of biological vascular grafts compared to synthetic conduits is the greater
resistance to infections. In a small-intestinal, submucosal biological scaffold used as an iliac patch
both infection and aneurysm formation were significantly lower as compared to PTFE patches
(11). The process of remodeling and earlier development of vasa vasora in biological scaffolds
enable a more rapid and effective recruitment of circulating immune system components,
thereby preventing graft infection (12). The early formation of a confluent endothelium layer
prevents formation of thrombi and disturbs bacterial adherence and, therefore, establishment
of infection (13).
Fahner.indd 10 5-5-2014 14:35:07

General introduction and outline of the thesis | 11
1The aims of the studies in this thesis were 1) to find evidence based on clinical studies in
literature for use of the best alternative vascular allograft in peripheral reconstructions 2) to
establish a standard method for glycerol preservation of arterial allografts and 3) to investigate
graft patency, morphological alterations and functionality of glycerol preserved allografts in two
animal models.
Historical perspective of vascular transplantation
The first records of arterial and venous transplantation were probably the reconstructions
performed during World War I when battle victims provided a readily accessible source of
vascular allografts (14). While initially autologous veins and arteries were employed in vascular
reconstructions, in the late 1940s a shift to allogeneic sources began with the work of Hufnagel
and Gross et al (15-17). Human arterial allografts, harvested at autopsies and sterilized by cobalt
irradiation, were used in reconstructions for thoracic aorta coarctations. In 1951, abdominal
aortic surgery was performed by Oudot when an aortic allograft was used for an occluded aortic
bifurcation. In that same period, Dubost et al replaced an abdominal aortic aneurysm by an
allograft (18;19). In the mid- 1950s, arterial allografts were frequently used after vascular graft
banks had been established (20). Initial enthusiasm for these grafts diminished, however, as
degeneration and graft failure were increasingly observed (21). After the addition of a synthetic
mesh around vascular allografts, these vascular grafts became the preferred material for vascular
reconstructions in the second half of the twentieth century (22-24). It was recognized that fresh
allografts suffered of a strong immune response, and, therefore, research focused on different
preservation methods to diminish rapid rejection and dissolution. Different preservation methods
were examined in the past decades using formalin, alcohol, ethylene oxide, betapropriolactone,
irradiation and freeze drying (17;25-31).
The above mentioned studies mainly dealt with vascular grafts for central reconstructions.
After the introduction of prosthetic vascular grafts made of PTFE and Dacron, showing good
results in aortic repair, the need for vascular allografts for central reconstructions diminished.
Nowadays, a few indications exist for the use of allografts in central reconstructions such as in
prolonged antibiotic resistant prosthetic graft infections.
For reconstructions of small and intermediate caliber arteries the use of autologous vein as
primary choice is generally accepted. Nevertheless, even autologous vein has its shortcomings
in that it is not always available, it may be diseased, and it requires additional time and surgical
dissection for preparation. Furthermore, the vein obviously can be inadequate in terms of length
or luminal diameter for use in a lower-limb revascularization procedure. Therefore, alternative
Fahner.indd 11 5-5-2014 14:35:07

12 | Chapter 1
biological resources have been explored as a potentially useful alternative for substitution of
small and intermediate caliber arteries.
Preservation methods of vascular allografts
Several methods have been explored for preservation of vascular allografts. The most commonly
used methods comprising treatment with gutaraldehyde, cold storage, cryopreservation and
lyophilization, are described below. Glycerol preservation is subsequently introduced as a
potential alternative for arterial allograft preservation.
Glutaraldehyde stabilized umbilical cord vein
Glutaraldehyde has been used to preserve human umbilical vein grafts, harvested after delivery.
These umbilical vein grafts (Biograft, Bio Vascular, Inc. St Paul, MN) consisted of veins tanned
with glutaraldehyde as described by Dardik. The conduit is supported by a polyester (Dacron)
mesh placed around the vein, sterilized and stored in 50% alcohol.
The use of fresh umbilical vein as a vascular graft was first attempted in the 1950s and 1960s
(32-34). In the following years, complications as early thrombosis, necrosis, microabcesses and
cellular infiltration hampered initial success of the vein graft. Based on studies by Rosenberg
et al and Carpentier et al (35;36), glutaraldehyde tanning of the umbilical vein was adopted
and applied in both animal and clinical studies (37-40). The aldehyde tanning process resulted
in cross-linkage of protein moieties in the vessel wall, especially the collagenous components,
which in turn increased tensile strength of the vessel wall and at the same time, sterilized the
tissue (41).
Cold storage
Cold storage, i.e. hypothermic preservation, is the standard method for preservation of solid
organ grafts. Vessels harvested during multi-organ donation are likewise stored and used when
reconstructive procedures are necessary to revascularize the graft in the recipient. Procured
arterial and venous segments are rinsed in saline and placed in a preservation medium such as
University of Wisconsin solution (UW). The usual storage temperature is 40C.
Experiences in liver and kidney transplant surgery show that arteries supplying organ
transplants rarely become thrombosed or aneurysmatic (42). Endothelial coverage of the
lumen of the transplanted vessel probably improves long-term patency as seen in autologous
and alloplastic bypass grafts (43-45). Although this concept seems promising when applied in
peripheral revascularization using arterial allografts even under immunosuppressive regimen,
graft rejection may still lead to graft occlusion. Prager et al reached a primary patency rate of
Fahner.indd 12 5-5-2014 14:35:07

General introduction and outline of the thesis | 13
154% after one year in a study of 13 patients in which immunosuppression was used in fresh
arterial homografts in peripheral arterial reconstructions (46). The experimental evaluation of
allogeneic vein transplantation began with the experiments of Alexis Carrel who transplanted
jugular vein allografts in the thoracic aorta in dogs (47). After follow-up of 2 years and 2 months,
the vein maintained the same size, but the vessel wall was replaced with connective tissue.
Since that time, numerous experimental and clinical studies have been performed to evaluate
transplantation of venous allografts (48-56). The immunologic basis for graft occlusion in fresh
cold-stored veins was supported by the study of Schwartz et al who demonstrated the antigenicity
of canine allograft veins (57). Degenerative changes occur first in the adventitia and the adjacent
media, but viable muscle cells were still identified 119 days after allografting. Graft failure usually
results from vessel occlusion, which is presumably due to the combined effect of fibrotic stenosis
of the vessel and thrombosis. Thrombosis is a prominent feature in graft rejection.
Cryopreservation
Cryopreservation is a technique used to preserve vascular allografts by cooling the tissue to
temperatures far below 00C. Using cryoprotectants, the tissue is gradually cooled to temperatures
of -70 0C with a rate of -2 0C/min. Finally, the tissue is rapidly cooled to -196 0C.
Early reports on the clinical use of cryopreserved veins indicated results inferior to autologous
vein grafts with patency rates of 25% to 33% after a follow-up to 20 months and 66% after
12 months in the aortacoronary position (58-63).
These poor patency rates are probably due to several causes. Carpenter and Tomaszewski have
demonstrated a sustained immunogenic activity in cryopreserved venous allografts and suggested
that the rejection response may contribute to venous graft failure (64;65). Loss of functional
endothelial lining in cryopreserved venous allografts has also been indicated as a cause of graft
failure. It has been estimated that cryopreservation yields preservation rates of approximately
50% - 80% of intact endothelial cells (66). These cells have decreased thrombomodulin activity
and decreased nitric oxide production resulting in impaired anticoagulative function (67).
Therefore, anticoagulation therapy would probably improve allograft patency. Posner et al
combined an anticoagulation protocol with moderate immunosuppressive therapy and obtained
improved patencies but on the other hand, had substantial complications with pseudo-aneurysm
formation and hemorrhage (68).
Arterial allografts were used for revascularization in peripheral reconstructions in the early
1950s (69;70). These consisted of large and medium-sized cadaveric arteries, but initial results
were discouraging. Subsequent advances in the design of synthetic prostheses led to the disuse
of these allografts. Recent improvements in organ harvesting methods, along with progress in
cryobiology, has however, renewed interest in the use of arterial allografts (71). Rigorous control
of the curve of cooling and the use of a penetrating cryoprotectant such as dimethylsulfoxide for
Fahner.indd 13 5-5-2014 14:35:08

14 | Chapter 1
partial preservation of cellular viability greatly improved the success of cryopreservation. Clinical
studies of cryopreserved cadaveric arteries in infrageniculate reconstructions showed patencies
of 42% - 68% during 1 - 2 years of follow-up (72-74).
Although some authors found almost the same features of rejection for fresh and
cryopreserved allografts, others suggest that cryopreservation may decrease antigenicity of
arterial allografts (75;76). The prevention of rejection in cryopreserved allografts, however,
remains a challenge. Even though the use of immunosuppressive drugs could maintain structural
integrity of cryopreserved allografts, long-term immunosuppression does not seem a desirable
option in patients with critical leg ischemia (77;78).
Lyophylization
Since it is generally accepted that extracellular ice formation presents a hazard for biopreservation
by freezing of multicellular tissues, a major focus was set on developing low-temperature
preservation techniques that avoid ice crystallization.
Lyophilization has shown to be an effective technique to provide preservation of a number of
cells including monocytes, ova, early embryos and pancreatic islets. Cryoprotectants are added,
and the tissue is fast-cooled stepwise to temperatures around -100 ºC and then more slowly to
the final temperature between -135 ºC and -160 ºC via vapor nitrogen storage. Re-warming of
the tissue before transplantation is performed in a similar manner; slowly to -100 ºC and then
rapidly to 0 ºC.
Greater saphenous veins obtained from multi organ donations and preserved through
lyophylization were thought to be an attractive source of venous allografts for arterial
reconstructions (79;80). The freeze-drying process diminished immunogenicity and maintained
structural integrity (81-84). Despite the lack of antigenicity and satisfactory early graft patency
observed in animal studies, these results could not be reproduced in infrainguinal arterial
reconstructions using lyophilized saphenous allografts in humans (85).
Marrangoni et al introduced freeze-drying for preservation of arterial allografts in a clinical
study (86). Although the incidence of aneurysm development was relatively low, intimal
hyperplasia was observed. There are still controversies that make one hesitate to launch clinical
trials with lyophilized arterial allografts.
Glycerol preservation
Glycerol preservation of human amnion
Preservation of human amnion in 85% glycerol at 40C for over a year was performed as an
effective biological dressing in treatment of skin burns in rats. Microscopic examination of
Fahner.indd 14 5-5-2014 14:35:08

General introduction and outline of the thesis | 15
1preserved amnion revealed the maintenance of structural integrity comparable to that of fresh
amnion. No immunological rejection was observed with the use of glycerol-preserved amnion
on partial-thickness wounds in clinical cases (87). These observations encouraged further studies
on glycerol preservation of connective tissue structures.
Glycerol preservation of skin allografts
Glycerol preservation of skin was first implemented by Basile in 1982 (88) in a study of glycerol
preserved porcine skin. In 1984, the Dutch Skin Bank, later re-named Euro Skin Bank in 1992,
performed an extensive amount of research on glycerol preservation of skin allografts (89;90).
In the last twenty years, this skin bank delivered large quantities of glycerolized allografts to
burn centers throughout Europe. Clinical experiences at numerous burn centers proved the
effectiveness of glycerol preserved allografts as a temporary coverage in burn injuries and as
biological closure of various skin defects (91-93). The mechanism of glycerol preservation is
based on dehydratation of tissues by physically replacing most of the intracellular water while
maintaining the cell’s ionic concentration and preserving tissue by protecting cell integrity (94).
Advantages of glycerol preservation
I) Immunological
Glycerol preservation, by removing all cellular elements, results in a non-viable tissue matrix
which is considered less antigenic and less liable to rejection than cryopreserved or fresh skin
allografts (95).
II) Compliance
For optimal prolonged graft function, it appears to be important to have comparable compliance
of graft material and native vessel in preventing intimal hyperplasia, graft occlusion and aneurysm
formation (96-101). Compliance mismatch as a cause of intimal hyperplasia and graft failure may
still play an important role in failure of peripheral vascular grafting. This may cause excessive
stretching of SMC’s resulting in their proliferation (102). Abbot et al (103) demonstrated the effect
of compliance mismatch on graft patency in both arterial segments treated with glutaraldehyde
and untreated segments. Patency rates of the treated, less compliant segments were significantly
lower. The relevance of compliance match is also demonstrated by the substantial differences in
10 year patency rates between vein grafts (30-50%) and internal mammary artery grafts (80-
90%) used for coronary bypasses (104;105).
III) Antimicrobial properties
Previous experiments of storage of skin allografts in glycerol shows antiviral properties of glycerol
preservation dependent on concentration, time and temperature (106;107).
Fahner.indd 15 5-5-2014 14:35:08

16 | Chapter 1
IV) Storage duration
In comparison with other methods of tissue preservation, glycerolization has proven to be a
relatively simple and inexpensive procedure. Furthermore, it was able to store skin tissue for
periods up to 5 years while maintaining the morphological and structural integrity of the skin
(108).
Outline of the thesis
In the last decades, different methods have been used for vascular allograft preservation. The
most important preservation methods of venous and arterial allografts have been applied in
clinical trials. These include cryopreservation, cold storage, lyophilization and glutaraldehyde
preservation of vascular grafts. Chapter 2 offers a systematic review of the literature from 1966
to 2004 of clinical studies in which vascular allografts were used for infrainguinal reconstruction.
The goal of this review was to find evidence for the preservation of vascular allografts showing
the best long term patencies without aneurysmal changes. It was concluded that no systematic
review of randomized controlled trials of different allograft preservation methods had been
performed. Therefore, the evidence for the best alternative to autologous vein could only be
based on single randomized trials.
A great deal of research has been performed on the preservation of skin allografts for
the treatment of patients with extensive burn wounds when autologous tissue is lacking for
complete wound coverage. These studies convincingly demonstrated the superiority of glycerol
preservation compared to other methods for skin allograft preservation including glutaraldehyde
tanning, lyophilization, cold storage and cryopreservation. These results warranted research
on potential application of glycerol preservation in vascular allografts. Since the biomechanical
alterations of vascular tissue after glycerol preservation and the optimal glycerol preservation
protocol for preservation of vascular allografts were not established, experimental studies were
developed to investigate breaking strength, bursting pressure and functional alterations after
glycerol preservation in rat aorta segments. These experiments are described in chapter 3.
After having proved that glycerol preserved allografts could resist physiological blood
pressure, these allografts were tested in an infrarenal, rat aorta transplantation model as
described in chapter 4. The feasibility of implantation of a glycerol preserved allograft was
thereby examined in an animal model. Glycerol preserved aortic allografts of donor rats were
implanted in 18 recipients. Another group of 18 rats received an autotransplantation of the infra
renal aorta as controls. Graft surveillance with duplex sonography was performed on a regular
basis, and angiographic images were produced before harvesting the grafts after a follow-up
period of 3 months.
Fahner.indd 16 5-5-2014 14:35:08

General introduction and outline of the thesis | 17
1After the application of glycerol preserved allografts was shown to be feasible in a small-
animal transplantation model, these results needed to be evaluated in a large animal model to
enable extrapolation to the clinical setting. Chapter 5 discusses experiments performed in the
goat carotid artery transplantation model. The experiments consisted of three animal groups.
Firstly, carotid allografts preserved in University of Wisconsin (UW) solution were transplanted
bilaterally. In the second group, glycerol preserved allografts were used as bilateral interposition
grafts in the common carotid artery. The third group was considered to represent the golden
standard of autologous vein grafting. The jugular vein was used for unilateral autotransplantation.
A summary of the studies described in this thesis is provided in chapter 6. This thesis is
concluded with a general discussion and future perspectives in chapter 7.
Fahner.indd 17 5-5-2014 14:35:08

18 | Chapter 1
Reference List
(1) Babapulle MN, Joseph L, Belisle P, Brophy JM, Eisenberg MJ. A hierarchical Bayesian meta-analysis of randomised clinical trials of drug-eluting stents. Lancet 2004 Aug 14;364(9434):583-91.
(2) Wilt TJ, Bloomfield HE, MacDonald R, Nelson D, Rutks I, Ho M, et al. Effectiveness of statin therapy in adults with coronary heart disease. Arch Intern Med 2004 Jul 12;164(13):1427-36.
(3) Ansell D, Feest T, Byrne C, Ahmad A. UK Renal Registry: The Sixth Annual Report. Bristol; 2003.
(4) Fowkes FG, Housley E, Cawood EH, Macintyre CC, Ruckley CV, Prescott RJ. Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol 1991 Jun;20(2):384-92.
(5) Kovalic AJ, Beattie DK, Davies AH. Outcome of ProCol, a bovine mesenteric vein graft, in infrainguinal reconstruction. Eur J Vasc Endovasc Surg 2002 Dec;24(6):533-4.
(6) Schmidli J, Savolainen H, Heller G, Widmer MK, Then-Schlagau U, Baumgartner I, et al. Bovine mesenteric vein graft (ProCol) in critical limb ischaemia with tissue loss and infection. Eur J Vasc Endovasc Surg 2004 Mar;27(3):251-3.
(7) Wang X, Lin P, Yao Q, Chen C. Development of small-diameter vascular grafts. World J Surg 2007 Apr;31(4):682-9.
(8) Bingley JA, Hayward IP, Campbell JH, Campbell GR. Arterial heparan sulfate proteoglycans inhibit vascular smooth muscle cell proliferation and phenotype change in vitro and neointimal formation in vivo. J Vasc Surg 1998 Aug;28(2):308-18.
(9) Wight TN. Cell biology of arterial proteoglycans. Arteriosclerosis 1989 Jan;9(1):1-20.
(10) Gillis C, Bengtsson L, Wilman B, Haegerstrand A. Secretion of prostacyclin, tissue plasminogen activator and its inhibitor by cultured adult human endothelial cells grown on different matrices. Eur J Vasc Endovasc Surg 1996 Feb;11(2):127-33.
(11) Jernigan TW, Croce MA, Cagiannos C, Shell DH, Handorf CR, Fabian TC. Small intestinal submucosa for vascular reconstruction in the presence of gastrointestinal contamination. Ann Surg 2004 May;239(5):733-8.
(12) Lantz GC, Badylak SF, Hiles MC, Coffey AC, Geddes LA, Kokini K, et al. Small intestinal submucosa as a vascular graft: a review. J Invest Surg 1993 May;6(3):297-310.
(13) Rosenman JE, Kempczinski RF, Berlatzky Y, Pearce WH, Ramalanjaona GR, Bjornson HS. Bacterial adherence to endothelial-seeded polytetrafluoroethylene grafts. Surgery 1985 Oct;98(4):816-23.
(14) Jeger E. Zur technik der blutgefassnaht. Beitr Klin Chir 97, 553-559. 1915.
(15) Gross RE, Hurwitt ES, Bill AHea. Preliminary observations on the use of the human arterial grafts in the treatment of certain cardiovascular defects. N Engl J Med 1948;239:578-91.
(16) Gross RE, Bill AH, Peirce EC. Methods for preservation and transplantation of arterial grafts: Observations on arterial grafts in dogs: Report on transplantation of preserved arterial grafts in nine human cases. Surg Gynecol Obstet 1949;88:689-701.
(17) Hufnagel CA. Preserved homologous arterial transplants. Bull Am Coll Surg 1947;32:321-323.
(18) Dubost C, Allary M, Oeconomos N. Resection of an aneurysm of the abdominal aorta: reestablishment of the continuity by a preserved human arterial graft, with result after five months. AMA Arch Surg 1952 Mar;64(3):405-8.
(19) Oudet J, Beaconsfield P. Thromboses of the aortic bifurcation treated by resection and homograft replacement. Arch Surg 1953;66:365-74.
(20) Dardik H, Greisler H. History of prosthetic grafts. Semin Vasc Surg 1999 Mar;12(1):1-7.
(21) Crawford ES, De Bakey ME, Morris GC, Jr., Garrett E. Evaluation of late failures after reconstructive operations for occlusive lesions of the aorta and iliac, femoral, and popliteal arteries. Surgery 1960 Jan;47:79-104.
Fahner.indd 18 5-5-2014 14:35:08

General introduction and outline of the thesis | 19
1(22) Fisher B, Wilde R, Engstrom P, Fisher ER. Experimental reconstruction of the aortic bifurcation. Surgery
1956 Jun;39(6):940-9.
(23) Kremer K. [Problems of free vascular transplantation; methods to preserve grafts.]. Zentralbl Chir 1953;78(44):1857-67.
(24) Shumacker HB, Jr., Freeman LW, Hutchings LM, Radigan L. Studies in vascular repair. VI. Further observations on the growth of anastomoses and free vascular transplants in growing animals. Angiology 1951 Aug;2(4):263-9.
(25) Hyatt GW, Turner TC, Bassett CA, Pate JW, Sawyer PN. New methods for preserving bone, skin and blood vessels. Postgrad Med 1952 Sep;12(3):239-54.
(26) Pate JW, Sawyer PN, Deterling RA, Jr., Blunt JW, Parshley MS. Early results in the experimental use of freeze dried arterial grafts. Surg Forum 1953;(38th Congress):147-51.
(27) Creech O, Jr., De Bakey ME, Cooley DA, Self MM. Preparation and use of freeze-dried arterial homografts. Ann Surg 1954 Jul;140(1):35-43.
(28) Deterling RA, Jr., Coleman CC, Jr., Parshley M. A preliminary report on experimental studies of the frozen homologous aortic graft. NY Med 1950 Jul 5;6(13):19-20.
(29) Eastcott HHG, Hufnagel CA. The preservation of arterial grafts by freezing. Surg Forum, 1950;269-274.
(30) Pierce EC, Rheinlander HF, Moritz AR, Gross RE, Merrille K. Transplantation of aortic segments fixed in 4 percent neutral formalin. Am J Surg 1949;78:311-316.
(31) Szilagi DE, Overhulse PR, Shonnard CP, Logrippo GA. The sterilization of human arterial homografts with beta-propriolactone. Surg Forum 1954:5:244-252.
(32) Nabseth DC, Wilson JT, Tan B, McDonough EF, Jr., Wiener J, Child CG. Fetal arterial heterografts. Arch Surg 1960 Dec;81:929-33.
(33) Nzola J, Palmer TH, Welch CS. Long femoral and ilio-femoral grafts. Surg Forum 1951;243-6.
(34) Yong NK, Eiseman B. The experimental use of heterologous umbilical vein grafts as aortic substitutes. Singapore Med J 1962 Mar;3:52-7.
(35) Carpentier A, Blondeau P, Laurens P, Mancel P, Laurent D, Dubost C. [Replacement of mitral and tricuspid valves by heterografts]. Ann Chir Thorac Cardiovasc 1968 Jan;7(1):33-8.
(36) Rosenberg N, Martinez A, Sawyer PN, Wesolowski SA, Postlethwait RW, Dillon ML, Jr. Tanned collagen arterial prosthesis of bovine carotid origin in man. Preliminary studies of enzyme-treated heterografts. Ann Surg 1966 Aug;164(2):247-56.
(37) Baier RE, Akers CK, Perimutter S, Dardik H, Dardik I, Wodka M. Processed human umbilical cord veins for vascular reconstructive surgery. Trans Am Soc Artif Intern Organs 1976;22:514-26.
(38) Dardik H, Ibrahim IM, Dardik I. Modified and unmodified umbilical vein allografts and xenografts as arterial substitutes: morphologic assessment. Surg Forum 1975;26:286-7.
(39) Dardik HD, Ibrahim IM, Sprayregen S, Dardik II. Clinical experience with modified human umbilical cord vein for arterial bypass. Surgery 1976 Jun;79(6):618-24.
(40) Dardik II, Dardik H. The fate of human umbilical cord vessels used as interposition arterial grafts in the baboon. Surg Gynecol Obstet 1975 Apr;140(4):567-71.
(41) Wengerter K, Dardik H. Biological vascular grafts. In: Dardik H, editor. Graft Materials in Vascular Surgery. Miami: Symposia Specialists, Inc.; 1978, p. 46-51.
(42) Burkey SH, Vazquez MA, Valentine RJ. De novo renal artery aneurysm presenting 6 years after transplantation: a complication of recurrent arterial stenosis? J Vasc Surg 2000 Aug;32(2):388-91.
(43) LoGerfo FW, Quist WC, Cantelmo NL, Haudenschild CC. Integrity of vein grafts as a function of initial intimal and medial preservation. Circulation 1983 Sep;68(3 Pt 2):II117-II124.
Fahner.indd 19 5-5-2014 14:35:08

20 | Chapter 1
(44) Meinhart JG, Deutsch M, Fischlein T, Howanietz N, Froschl A, Zilla P. Clinical autologous in vitro endothelialization of 153 infrainguinal ePTFE grafts. Ann Thorac Surg 2001 May;71(5 Suppl):S327-S331.
(45) Zilla P, von OU, Deutsch M. The endothelium: a key to the future. J Card Surg 1993 Jan;8(1):32-60.
(46) Prager M, Holzenbein T, Aslim E, Domenig C, Muhlbacher F, Kretschmer G. Fresh arterial homograft transplantation: a novel concept for critical limb ischaemia. Eur J Vasc Endovasc Surg 2002 Oct;24(4):314-21.
(47) Carrel A. Ultimate result of aortic transplantation. Exp Med 1912;15:389.
(48) Barner HB, DeWeese JA, Schenk EA. Fresh and frozen homologous venous grafts for arterial repair. Angiology 1966 Jun;17(6):389-401.
(49) Jesseph JE, Jones TW, Sauvage LR, Kanar EA, Nyhus LM, Harkins HN. Five year observations on unsupported fresh venous grafts of the aorta in dogs. Surg Gynecol Obstet 1958 Nov;107(5):623-30.
(50) Nabatoff RA, Touroff AS, Gross M. Four year studies concerning the fate of experimental vena cava autografts used to bridge aortic defects. Surg Gynecol Obstet 1955 Jul;101(1):20-4.
(51) Sauvage LR, Harkins HN. Experimental vascular grafts: an evaluation relating to types, means of preservation, and methods of suture in the growing pig. Surgery 1953 Apr;33(4):587-635.
(52) Schloss G, Shumacker HB, Jr. The use of free vascular transplants for bridging arterial defects; an historical review with particular reference to histological observations. Yale J Biol Med 1950 Jan;22(3):273-90.
(53) Shumacker HB, Jr., Freeman LW, Hutchings LM, Radigan L. Studies in vascular repair. VI. Further observations on the growth of anastomoses and free vascular transplants in growing animals. Angiology 1951 Aug;2(4):263-9.
(54) Sugiura A. An experimental study on the vasa vasorum of the venous graft used in arterial replacement. Jpn Circ J 1968 May;32(5):727-44.
(55) Williamson CS, Mann FC. Functional survival of autogenous and homogenous transplants of blood vessels: Experimental study. Arch Surg 1947;54:529.
(56) Streinchenberger R, Barjoud H, Adeleine P, Larese A, Nemoz C, Chatelard P, et al. Venous allografts preserved at 4 degrees C for infrainguinal bypass: long-term results from 170 procedures. Ann Vasc Surg 2000 Nov;14(6):553-60.
(57) Schwartz SI, Kutner FR, Neistadt A, Barner H, Resnicoff S, Vaughan J. Antigenicity of homografted veins. Surgery 1967 Mar;61(3):471-7.
(58) Laub GW, Muralidharan S, Clancy R, Eldredge WJ, Chen C, Adkins MS, et al. Cryopreserved allograft veins as alternative coronary artery bypass conduits: early phase results. Ann Thorac Surg 1992 Nov;54(5):826-31.
(59) Martin RS, Edwards WH, Mulhern JLJ, Hurwitz RL, Decker M, Jenkins JM. Cryopreserved saphenous vein allografts for femoral-tibial and femoral-popliteal bypass: early results and observations. 1990.
(60) Ochsner JL, Lawson JD, Eskind SJ, Mills NL, DeCamp PT. Homologous veins as an arterial substitute: long-term results. J Vasc Surg 1984 Mar;1(2):306-13.
(61) Sellke FW, Meng RL, Rossi NP. Cryopreserved saphenous vein homografts for femoral-distal vascular reconstruction. J Cardiovasc Surg (Torino) 1989 Sep;30(5):838-42.
(62) Stephen M, Sheil AG, Wong J. Allograft vein arterial bypass. Arch Surg 1978 May;113(5):591-3.
(63) Tice DA, Zerbino V. Clinical experience with preserved human allografts for vascular reconstruction. Surgery 1972 Aug;72(2):260-7.
(64) Carpenter JP, Tomaszewski JE. Immunosuppression for human saphenous vein allograft bypass surgery: a prospective randomized trial. J Vasc Surg 1997 Jul;26(1):32-42.
(65) Carpenter JP, Tomaszewski JE. Human saphenous vein allograft bypass grafts: immune response. J Vasc Surg 1998 Mar;27(3):492-9.
Fahner.indd 20 5-5-2014 14:35:08

General introduction and outline of the thesis | 21
1(66) Bambang LS, Mazzucotelli JP, Moczar M, Beaujean F, Loisance D. Effects of cryopreservation on
the proliferation and anticoagulant activity of human saphenous vein endothelial cells. J Thorac Cardiovasc Surg 1995 Oct:998-1004.
(67) Bilfinger TV, Hartman AR, Liu Y, Magazine HI, Stefano GB. Cryopreserved veins in myocardial revascularization: possible mechanism for their increased failure. Ann Thorac Surg 1997 Apr;63(4): 1063-9.
(68) Posner MP, Makhoul RG, Altman M, Kimball P, Cohen N, Sobel M, et al. Early results of infrageniculate arterial reconstruction using cryopreserved homograft saphenous conduit (CADVEIN) and combination low-dose systemic immunosuppression. J Am Coll Surg 1996 Sep;183(3):208-16.
(69) De Bakey ME. Les greffes d’aorte. In: Fontaine R, Dubost C, editors. Les Greffes Vasculaires. Paris: Presse Universitaire de France; 1954, p. 264-5.
(70) Oudot J. Vascular grafting in thromboses of the aortic bifurcation. Presse Med 1951 Feb 21;59(12): 234-6.
(71) Gournier JP, Adham M, Favre JP, Raba M, Bancel B, Lepetit JC, et al. Cryopreserved arterial homografts: preliminary study. Ann Vasc Surg 1993 Nov;7(6):503-11.
(72) Alonso M, Segura RJ, Prada C, Caeiro S, Cachaldora JA, Diaz E, et al. Cryopreserved arterial homografts: preliminary results in infrageniculate arterial reconstructions. Ann Vasc Surg 1999 May;13(3):261-7.
(73) Castier Y, Leseche G, Palombi T, Petit MD, Cerceau O. Early experience with cryopreserved arterial allografts in below-knee revascularization for limb salvage. Am J Surg 1999 Mar;177(3):197-202.
(74) Gournier JP, Favre JP, Gay JL, Barral X. Cryopreserved arterial allografts for limb salvage in the absence of suitable saphenous vein: two-year results in 20 cases. Ann Vasc Surg 1995;9 Suppl:S7-14.
(75) Motomura N, Imakita M, Yutani C, Takamoto S, Kitoh Y, Tsuji T, et al. Chronic rejection in cryopreserved aortic allografts. Transplant Proc 1995 Jun;27(3):2105-6.
(76) Nataf P, Guettier C, Bourbon A, Nappi F, Lima L, Dorent R, et al. Influence of arterial allograft preparation techniques on chronic vascular rejection: a histological study. Transplant Proc 1996 Oct;28(5):2890-2.
(77) Callow AD. Arterial homografts. Eur J Vasc Endovasc Surg 1996 Oct;12(3):272-81.
(78) da Gama AD, Sarmento C, Vieira T, do Carmo GX. The use of arterial allografts for vascular reconstruction in patients receiving immunosuppression for organ transplantation. J Vasc Surg 1994 Aug;20(2):271-8.
(79) Foster JH, Lance EM, Scott HW, Jr. Experience with ethylene oxide treated freeze-dry arterial homografts in 110 consecutive patients. Ann Surg 1958 Aug;148(2):230-8.
(80) Goldman MH, Strong DM, Brickley-Parsons D, Floering DA, Gawith K, French D. Lyophilized veins as vascular substitutes. Transplant Proc 1979 Jun;11(2):1510-1.
(81) Goldman MH, Floering DA, French DR, Gawith KE, Forgey JD, Strong DM. Lyophilized veins as arterial interposition allografts. Cryobiology 1981 Jun;18(3):306-12.
(82) Merrill RH, McLeod CG, Jr., Jarstfer BS. The use of lyophilized vein grafts in vascular access for chronic hemodialysis. Artif Organs 1979 Aug;3(3):245-8.
(83) Reeves TR, Cezeaux JL, Sackman JE, Cassada DC, Freeman MB, Stevens SL, et al. Mechanical characteristics of lyophilized human saphenous vein valves. J Vasc Surg 1997 Nov;26(5):823-8.
(84) Wrede SS, Staudacher M, Weissenhofer W, Wetzstein R. Lyophilized veins studied by scanning electron microscopy. Eur Surg Res 1975;7(2):120-8.
(85) Timaran CH, Stevens SL, Freeman MB, Goldman MH. Infrainguinal bypass grafting using lyophilized saphenous vein allografts for limb salvage. Cardiovasc Surg 2002 Aug;10(4):315-9.
(86) Marrangoni AG, Cecchini LP. Homotransplantation of arterial segments preserved by the freeze-drying method. Ann Surg 1951 Dec;134(6):977-83.
(87) Maral T, Borman H, Arslan H, Demirhan B, Akinbingol G, Haberal M. Effectiveness of human amnion preserved long-term in glycerol as a temporary biological dressing. Burns 1999 Nov;25(7):625-35.
Fahner.indd 21 5-5-2014 14:35:08

22 | Chapter 1
(88) Basile AR. A comparative study of glycerinized and lyophilized porcine skin in dressings for third-degree burns. Plast Reconstr Surg 1982 Jun;69(6):969-74.
(89) Hoekstra MJ, Kreis RW, du Pont JS. History of the Euro Skin Bank: the innovation of preservation technologies. Burns 1994;20 Suppl 1:S43-S47.
(90) Kreis RW, Hoekstra MJ, Mackie DP, Vloemans AF, Hermans RP. Historical appraisal of the use of skin allografts in the treatment of extensive full skin thickness burns at the Red Cross Hospital Burns Centre, Beverwijk, The Netherlands. Burns 1992;18 Suppl 2:S19-S22.
(91) Kreis RW, Vloemans AF, Hoekstra MJ, Mackie DP, Hermans RP. The use of non-viable glycerol-preserved cadaver skin combined with widely expanded autografts in the treatment of extensive third-degree burns. J Trauma 1989 Jan;29(1):51-4.
(92) Hussmann J, Russell RC, Kucan JO, Hebebrand D, Bradley T, Steinau HU. Use of glycerolized human allografts as temporary (and permanent) cover in adults and children. Burns 1994;20 Suppl 1:S61-S65.
(93) Teepe RG, Kreis RW, Koebrugge EJ, Kempenaar JA, Vloemans AF, Hermans RP, et al. The use of cultured autologous epidermis in the treatment of extensive burn wounds. J Trauma 1990 Mar;30(3):269-75.
(94) Van Baare J, Ligtvoet EE, Middelkoop E. Microbiological evaluation of glycerolized cadaveric donor skin Transplantation 1998 Apr 15;65(7):966-70.
(95) Richters CD, Hoekstra MJ, van BJ, du Pont JS, Kamperdijk EW. Immunogenicity of glycerol-preserved human cadaver skin in vitro. J Burn Care Rehabil 1997 May;18(3):228-33.
(96) Berglund JD, Mohseni MM, Nerem RM, Sambanis A. A biological hybrid model for collagen-based tissue engineered vascular constructs. Biomaterials 2003 Mar;24(7):1241-54.
(97) Nerem RM. Atherogenesis: hemodynamics, vascular geometry, and the endothelium. Biorheology 1984;21(4):565-9.
(98) Nerem RM. Hemodynamics and the vascular endothelium. J Biomech Eng 1993 Nov;115(4B):510-4.
(99) Nerem RM. Role of mechanics in vascular tissue engineering. Biorheology 2003;40(1-3):281-7.
(100) Perktold K, Leuprecht A, Prosi M, Berk T, Czerny M, Trubel W, et al. Fluid dynamics, wall mechanics, and oxygen transfer in peripheral bypass anastomoses. Ann Biomed Eng 2002 Apr;30(4):447-60.
(101) Ziegler T, Nerem RM. Tissue engineering a blood vessel: regulation of vascular biology by mechanical stresses. J Cell Biochem 1994 Oct;56(2):204-9.
(102) Yow KH, Ingram J, Korossis SA, Ingham E, Homer-Vanniasinkam S. Tissue engineering of vascular conduits. Br J Surg 2006 Jun;93(6):652-61.
(103) Abbott WM, Megerman J, Hasson JE, L’Italien G, Warnock DF. Effect of compliance mismatch on vascular graft patency. J Vasc Surg 1987 Feb;5(2):376-82.
(104) Canver CC. Conduit options in coronary artery bypass surgery. Chest 1995 Oct;108(4):1150-5.
(105) Lytle BW. Prolonging patency--choosing coronary bypass grafts. N Engl J Med 2004 Nov 25;351(22):2262-4.
(106) Marshall L, Ghosh MM, Boyce SG, MacNeil S, Freedlander E, Kudesia G. Effect of glycerol on intracellular virus survival: implications for the clinical use of glycerol-preserved cadaver skin. Burns 1995 Aug;21(5):356-61.
(107) Van Baare J, Buitenwerf J, Hoekstra MJ, du Pont JS. Virucidal effect of glycerol as used in donor skin preservation. Burns 1994;20 Suppl 1:S77-S80.
(108) Richters CD, Hoekstra MJ, van Baare J, du Pont JS, Kamperdijk EW. Morphology of glycerol-preserved human cadaver skin. Burns 1996 Mar;22(2):113-6.
Fahner.indd 22 5-5-2014 14:35:08

2Systematic review of preservation methods and
clinical outcome of infrainguinal vascular allografts
P.J. Fahner, M.M. Idu, T.M. van Gulik, D.A. Legemate
J Vasc Surg 2006;44:518-24
Department of SurgeryAcademic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
Fahner.indd 23 5-5-2014 14:35:08

24 | Chapter 2
Abstract
Objective. We systematically reviewed clinical studies on the use of venous and arterial allografts
for infrainguinal revascularization in the absence of suitable autologous vein. We attempted to
find evidence for the best infrainguinal vascular allograft by a systematic review of the available
literature.
Methods. An electronic search of the Medline, Embase and Cochrane databases was employed
to determine key-articles from studies on the different types of vascular allograft used in
infrainguinal reconstruction from 1966 to 2004. Articles were independently reviewed using
previously defined inclusion and exclusion criteria. Study results were gathered with cumulative
primary patency as most important endpoint. Secondary end points were major complications,
graft disintegration, and major limb loss. Quantitative analysis was performed on the prospective
randomized trials and linear regression analysis was performed on cumulative primary patency.
Fontaine’s classification system was applied.
Results. No systematic review of randomized controlled trials (RCT) was found. Five RCTs,
three prospective cohort or case series and fifteen retrospective case series with 3837 vascular
allografts were found. Methods of allograft preservation were cryopreservation (CP) (5 studies),
cold storage (CS) (3 studies) and glutaraldehyde preservation (GA) (15 studies). One-year
cumulative primary patency rates were 13-79% for CP, 63-80% for CS and 40-91% for GA. The
weighted mean one-year cumulative primary graft patency rate was 41% for CP, 71% for CS and
70% for GA allografts. Four randomized trials on femoropopliteal bypasses demonstrated higher
patency rates of glutaraldehyde-preserved human umbilical veins than in PTFE-grafts. Statistical
heterogeneity between studies (I2 = 91.4%) was too high to perform a formal meta-analysis.
The rate of major limb loss was 20-58% for CP, 10-69% for CS and 0-65% for GA and the
percentage of graft disintegration was 2-6% for CP, 4-15% for CS and 0-11% for GA.
Conclusions. A firm conclusion could not be made because there were no studies available in
which direct comparison was performed between different preservation methods of vascular
allografts. In addition, heterogeneity of the individual studies hampered direct comparison of
different types of vascular allografts. However, the overall graft performance of glutaraldehyde-
preserved human umbilical vein allografts may be superior to that of other vascular allografts.
Fahner.indd 24 5-5-2014 14:35:08

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 25
2
Introduction
Autologous vein is the conduit of choice in patients who need a bypass for critical lower leg
ischemia. However, suitable autologous veins may be of inferior quality or absent as a result
of prior use. Alternatives include prosthetic grafts (Polytetrafluoroethylene [PTFE] and Dacron
[DuPont, Wilmington, Del]) or vascular allografts. Prosthetic vascular grafts have disappointing
patency rates of approximately 30% at 5 years in distal reconstructions and cannot prevent limb
loss in many patients with critical lower limb ischemia (1).
Transplantation of a vascular allograft is an attractive alternative in patients with no suitable
autologous vein. The technique of vascular transplantation was introduced by Carrel and Guthrie
in their classical studies of 1908 (2). In the mid-19th century, studies reported that large-caliber
vascular allografts could result in graft disruption, calcification and occlusion. As a consequence
large-caliber allografts were abandoned in favor of prosthetic grafts, which performed
satisfactorily in non-infected operative fields. Currently, the large majority of allografts are used
in infrainguinal vascular reconstructions.
Transplantation of blood vessels requires a suitable graft preservation method. Improvements
in tissue preservation techniques allow a considerable number of blood vessels of different
lengths and diameters to be stored and used whenever necessary (3). Over the past two decades
this has lead to a renewed interest in vascular allograft transplantation of small caliber grafts
(< 6 mm) for peripheral vascular reconstructions.
The aim of this systematic review was to evaluate the results of clinical studies in which
vascular allografts were used in the management of patients needing an infra inguinal bypass
operation and to find evidence for the best vascular preservation technique.
Methods
Inclusion and exclusion criteria
Clinical studies of patients with vascular allografts for infra-inguinal arterial obstructive disease
(acute and chronic) were included. In accordance with the recommendations of the Ad Hoc
Committee for Reporting Standards of the Society for Vascular Surgery of North America, only
series of at least 40 procedures were included (4;5). Requirements were that the donor vessels be
either arterial or venous segments and that the method of preservation of the allograft should be
mentioned. The arterial donor vessels had to be taken from the iliac or femoropopliteal arteries,
and the venous donor vessels had to be taken from the saphenous vein or human umbilical vein
(HUV).
Fahner.indd 25 5-5-2014 14:35:08

26 | Chapter 2
For inclusion, information on patency, location of the anastomosis, and length of follow-up
period had to be retrievable. Patency rates had to be based on objective findings and had to
have been demonstrated by an accepted vascular imaging technique such as duplex scanning,
arteriography or magnetic resonance imaging. Composite conduits were excluded. However,
we did include the Biograft® (Meadox Medicals, Oakland, NY) – an HUV allograft externally
reinforced by Dacron mesh – because there is no contact between the luminal blood flow and
the prosthetic material. Studies on xenografts were excluded, as were studies that included
reconstructions for aneurysmal disease, access for hemodialysis, or vascular trauma.
Cumulative primary graft patency was the primary endpoint. Secondary endpoints were
major complications, and major limb loss. Major limb loss was defined as a below-knee or more
proximal amputation.
Search strategy
Two authors (P.J.F and M.M.I) independently undertook an electronic search of Medline (January
1966 to January 2004), Embase (January 1988 to December 2003), the Cochrane Clinical
Trials Register, and the Cochrane Database of Systematic Reviews. No language restrictions
were enforced, and a manual cross-reference search of key articles was performed to identify
additional relevant articles. The following keywords and Medical Subject Heading terms were
used: peripheral arterial occlusive disease, peripheral ischemic disease, critical limb ischemia,
infra-inguinal repair, arterial reconstruction, vascular reconstruction, transplantation, arterial
graft, venous graft, arterial homograft, vein homograft, arterial allograft, venous allograft,
autologous vein, patency, limb salvage, reoperation, redo, amputation, fresh, cold storage, 40C,
cryopreservation, lyophilization and glutaraldehyde. The search commands were combined with
the maximally sensitive qualifying string for randomized controlled trials as defined by the UK
Cochrane Centre (6). The keywords and Medical Subject Heading terms were combined with
different suffixes to define the best fit for the search question.
Data collection
Extracting of patient data and graft characteristics and deciding wether the studies met the
inclusion criteria were performed independently by two authors (P.J.F and M.M.I). Patency data,
as primary outcome, were collected at 1, 6, 12 months and 2-3 years after surgery. The checklists
of three working groups on reporting standards served as guidelines to ensure that all relevant
data were gathered from the articles. These groups were the Meta-analysis Of Observational
Studies in Epidemiology Group (7), the Quality of Reporting of Meta-analyses Group (8) and the
Consolidated Standards of Reporting Trials (9).
Fahner.indd 26 5-5-2014 14:35:08

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 27
2
Statistical analysis
Quantitative data from the four prospective randomized controlled trials were entered into
Cochrane RevMan 4.2.7 software (The Cochrane Collaboration, Oxford, England) and analyzed
with MetaView. If statistical heterogeneity (I2) less than 60%, meta-analysis was planned (10).
The weighted mean was calculated for one-year and two- three year cumulative primary graft
patency for the non-randomized cohort studies. Weighted means were calculated by multiplying
the outcome concerned by the number of allografts included in each single study. These results
were added up and divided by the total number of allografts in the relevant allograft preservation
group.
Linear regression analysis was performed on the cumulative primary patency rates of all studies
after 24 months, and the percentage included patients with Fontaine stage II limb ischemia. The
Pearson correlation coefficient was calculated by use of SPSS 6.2 software (SPSS Inc, Chicago, Ill).
Results
Studies included
A total of 1260 publications were found. They were all screened by title to see whether they
matched the inclusion criteria. If the relevance of an article was unclear, the abstract was read
and information on patients, type of bypass surgery and graft type was collected. This search
yielded 81 articles that were then reviewed in detail on inclusion and exclusion criteria. A final set
of 23 key articles was obtained (11-33).
No systematic review of RCTs on vascular allograft preservation methods was retrieved.
Four RCTs, were retrieved that compared vascular allografts with alternative conduit material
for peripheral vascular bypass surgery. These trials compared HUV allografts with PTFE and
autologous vein grafts (29;30;32;33), and they provided the highest level of evidence available
for the comparison of the HUV allograft and prosthetic bypass (level Ib according to the Level
of Evidence and Grades of Recommendation as provided by the National Health Service Centre
for Evidence-Based Medicine). One RCT concerning venous allografts looked at the effect of
immunosuppressive therapy on graft patency (13). Three studies were prospective cohort or case
series, and the remaining studies were retrospective case series containing level IV evidence.
Studies excluded
If patient series were published more than once due to prolonged follow-up, only the article
with the longest follow-up was reviewed. Four review articles dealing with synthetic grafts,
xenografts and the financial aspects of vascular disease were excluded.
Fahner.indd 27 5-5-2014 14:35:08

28 | Chapter 2
If identical studies from the same institution were reported by different authors, they were
included only once. Two articles on lyophilization were excluded because of small study groups.
Studies on peripheral arterial reconstructions using vascular allografts in combination with
non-allograft material were also excluded. One Japanese and one Czech article were excluded
because of translation complications.
Vascular allograft preservation methods.
Three vascular allograft preservation methods were used in the selected studies: cryopreservation,
cold storage and glutaraldehyde preservation. Cryopreservation was used for both arterial (15)
and venous (11-14) allograft preservation. In all cases cryopreservation was performed in a
dimethyl sulfoxide containing solution by using a programmable control-rate freezer. Storage
temperatures ranged from –120ºC to –196ºC. Most grafts were obtained from Cryolife,
Inc (Kennesaw, Ga) and had an outer diameter of more than 3.5 mm. The storage, thawing,
and handling protocols provided by Cryolife have been established during the last two decades.
Cold storage was used in three studies, and all of these were on venous allografts that were
harvested during varicose vein surgery (16-18). Diameters ranged from 6 to 9 mm, and lengths
from 30 to 65 cm. The grafts were stored at 4ºC in a saline solution containing antibiotics
(chloromycetin and amphotericin). The veins were examined under aseptic conditions for wall
quality and diameter measurement and were ready for use after 10 to 21 days.
All articles about glutaraldehyde vascular allograft preservation were studies in which the
HUV was used as a conduit. These grafts (Biograft, Meadox Medicals, Oakland, NJ, or Bio-
Vascular Inc., St. Paul, Minn.) were manually prepared, tanned with glutaraldehyde, and
covered with a polyester Dacron mesh. Storage was performed in 50% aqueous ethanol. Just
before implantation, grafts underwent a rinse procedure. In most studies the glutaraldehyde
preservation protocol itself was not described in detail.
Baseline and outcome characteristics
Table 1 describes the baseline characteristics of the 23 key articles. The publication year of
the studies ranged from 1968 to 2002. Fifteen of these studies (68%) were published after
1990. A total of 3263 patients with 3837 vascular allografts were included in this systematic
review. Critical limb ischemia (CLI; Fontaine III-IV) was the indication for vascular reconstruction
in 78% (2927/3762) of the vascular allografts. The distal anastomosis was located crurally in
38% (1340/3527) and in the popliteal region in 57% (2034/3592) of the procedures. Crural
locations included the tibial, peroneal and pedal arteries. A popliteal anastomosis was defined as
being either above the knee or below the knee.
Fahner.indd 28 5-5-2014 14:35:08

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 29
2
Table 1. General characteristics of included studies of arterial and venous infrainguinal allografts
Study Year Inclusion period
No. grafts
Critical ischemia
Crural anastomosis
Anti- coagulation
Study design
Cryopreservation venous allografts
Brockbank (11) 1992 1985-1990 75 NR 39 % NR retrosp case serie
Martin (12) 1994 1987-1993 115 80 % 88 % AP or AC retrosp case serie
Carpenter (13) 1997 2 year 40 100 % 93 % AP prosp RCT
Farber(14) 2003 1992-2002 240 89 % 65 % AP or AC retrosp case serie
Cryopreservation arterial allografts
Branchereau (15) 2000 1991-1997 165* 100% 79 % AP and/or AC
retrosp case serie
Cold storage venous allografts
Reedt Dortland (16)
1991 1984-1989 156 67 % 33 % AC retrosp case serie
Rebane (17) 1997 1978-1993 107 100 % 63 % AC retrosp case serie
De Leersnijder (18)
1992 1982-1989 100 41 % NR AC (26%) retrosp case serie
Glutar aldehyde venous allografts (HUV)
Dardik (19) 1988 1975-1985 907 94 % 36 % NR retrosp case serie
Dardik (20) 1995 1985-1993 167 89 % 51 % NR retrosp case serie
Dardik (21) 2002 1990-2000 283 89 % 61 % AC prosp case serie
Robison (22) 1983 1976-1981 99 91 % 79 % BK NR retrosp case serie
Hirsch (23) 1984 5 year 133 63 % 0 % NR retrosp case serie
Boontje (24) 1986 1978-1984 257 26 % 38 % NR retrosp case serie
Jarrett (25) 1989 1977-1986 211 73 % 0 % NR retrosp case serie
Batt (26) 1990 1978-1987 105 95 % 50 % AC retrosp case serie
Sato (27) 1995 1977-1993 111 31 % NR NR retrosp case serie
Comparison HUV with other conduits
Weisel (28) 1981 1976-1979 66 68 % 18 % NR prosp cohort study
Eickhoff (29) 1987 1980-1981 50 81 % 0 % NR prosp RCT
McCollum (30) 1991- 1984-1981 87 73 % 0 % AP prosp RCT
Johnson (31) 1991 NR 55 85 % 25 % NR prospect case serie
Johnson (32) 2000 1983-1988 261 68 % 0 % AP prosp RCT
Aalders (33) 1992 1983-1984 47 23 % 0 % AC prosp RCT
NR = Not reported, retrosp = retrospective, CS = case serie, AP = antiplatelet therapy (aspirin and/ or clopridogrel), AC = anitcoagulant therapy (warfarin), CHS = prospective cohort study, BK = below knee prosp RCT = prospective randomized clinical trial, * = study included 45 grafts preserved by cold storage.
Fahner.indd 29 5-5-2014 14:35:08

30 | Chapter 2
Most studies were retrospective case series. Of the prospective series five were RCTs, two were
case series and one was a cohort study. The only RCT performed on cryo-preserved allografts
was that of Carpenter et al (13) which, after vascular allograft implantation, randomized patients
to either immunosuppressive therapy with azathioprine (17 patients) or no immunosuppressive
therapy (23 patients). The overall cumulative primary graft patency rate at 12 months was 13%,
and there was no significant difference between the groups. Four RCTs were retrieved on studies
in which HUV allografts were compared with other conduits in femoropopliteal bypasses. Eickhoff
et al (29) published a multicenter trial comparing HUV and PTFE-grafts. They demonstrated a
1 year cumulative primary patency rate of 74% for the HUV grafts compared with 55% for the
PTFE grafts (81% CLI). Aalders et al (33) reported a study of above-knee femoropopliteal bypass
grafts only (23% CLI) in which the 6 year cumulative primary patency rates of PTFE and HUV
grafts were 38% and 71% respectively. Johnson et al (32) compared above-knee femoropopliteal
bypasses using autologous saphenous vein, PTFE and HUV. The cumulative primary patency rates
after 5 years were 73%, 39% and 53% respectively. McCollum et al (30) compared HUV grafts
with PTFE grafts (CLI 73%). The 1 year cumulative primary patency rates in this study were 68%
for HUV and 61% for PTFE.
Table 2 describes the clinical outcomes of the allografts in the 23 key articles. The data on
graft patency were extracted directly from the text or graphs. Only five articles had follow-
up periods of longer than five years. The 1 year cumulative primary patency of cryopreserved
venous allografts ranged from 13% to 79%. There was only one key article on cryopreserved
arterial allografts, with a reported 1 year cumulative primary patency of 49%. Key articles on
cold storage as a method of vascular preservation concerned venous allografts only. The 1 year
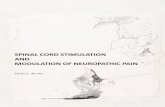
0 10 20 30 40 50 60 70 80 900
25
50
75
100
% patients with Fontaine stage II
Gra
ft p
aten
cy
Figure Plot of linear regression analysis of number of patients with Fontaine stage II and overall 2 year cumulative primary graft patency rate of all included studies. Pearson correlation coefficient = 0.58, (P = 0.01).
Fahner.indd 30 5-5-2014 14:35:09

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 31
2
Table 2. Clinical characteristics of allografts and patient outcomes
Study Cum prim (sec) patency Mortality 30d
Major comp
Majorlimb loss
Graft desint
1m 6m 1y 2-3y
Cryopreservation venous allografts
Brockbank (11) 94 87 79 79 NR NR NR NR
Martin (12) - 59(59) 37(40) 19(28) 0 % 0 % 27 % 2 %
Carpenter (13) - - 13 - 3 % 15 % 58 % 3 %
Farber (14) 83(83) 50(52) 30(30) 18(20) 6 % 11 % 33 % 4 %
Cryopreservation arterial allograftsBranchereau (15) 83(90) - 49(60) 35(42) 3 % 1 % 20 % 6 %
Weighted mean one-year cum prim patency
41
Cold storage venous allograftsReedt Dortland (16)
- 89 80 62 NR 4 % 10 % 15 %
Rebane (17) (83) - (65) (38) 4 % 1 % 69 % 4 %
De Leersnijder (18) - 79 63 46 4 % NR 15 % 15 %
Weighted mean one-year cum prim patency
71
Glutar aldehyde venous allograftsDardik 1988 (19) 83 67 59 43 NR 4 % 35 % 2 %
Dardik 1995 (20) (86) (84) (80) (65) NR 4 % 38 % 3 %
Dardik 2002 (21) - - 84(87) 67(74) NR 3 % 35 % 0.4 %
Robison (22) 86 69 64 43 2 % NR 29 % NR
Hirsch (23) 91 81 73 69 7 % 2 % NR 2 %
Boontje (24) 96 - 86 70 1 % NR NR 1 %
Jarrett (25) 90(85) 83(78) 78(70) 63(59) 1 % 6 % 10 % NR
Batt (26) 61 - 42 33 6 % 7 % 65 % 8 %
Sato (27) 94 87 86 79 NR 1 % NR 10 %
Comparison HUV with other conduitsWeisel (28) 70 49 40 36 5 % NR NR NR
Eickhoff (29) - 78 75 53 NR 0 % 4 % 0 %
McCollum (30) - 78 68 57 NR 1 % 14 % NR
Johnson 1991 (31) - - 63 49 NR NR 5 % 7 %
Johnson 2000 (32) - 77 74 64 1 % 3 % 10 % 0.4 %
Aalders (33) - 96 (96) 91 (92) 86 (89) 0 % 0 % 0 % 11 %
Weighted mean one-year cum prim patency
70
Cum prim (sec) patency = cumulative primary (secondary) patency, 30d = 30 days, comp = major complications, disint = disintegration, NR = Not reported
Fahner.indd 31 5-5-2014 14:35:09

32 | Chapter 2
cumulative primary patency of cold-stored venous allografts ranged from 63% to 80% and for
glutaraldehyde preserved venous allografts, it ranged from 40% to 91%. The weighted mean
1 year and 2-3 year cumulative primary graft patency rate was 41% and 31% for cryopreserved
allografts, 71% and 51% for cold-stored allografts, and 70% and 56% for glutaraldehyde
allografts, respectively.
Postoperative follow-up information on 30-day postoperative mortality, major complications,
major limb loss, and graft disintegration was collected. Postoperative mortality was not reported
in 9 of the key-articles. The overall postoperative mortality in the remaining 14 articles was
2.9% (51/1744). Major complications such as infection requiring graft removal, hemorrhage that
necessitated reoperation, and non-graft-related complications such as myocardial infarction,
pulmonary embolism, stroke, deep venous thrombosis, and gastro-intestinal hemorrhage. The
reported incidences of major complications were between 0% and 15%. Major limb loss occurred
in 0-69% of the patients after graft implantation. Graft disintegration (aneurysm formation or
graft rupture) was not reported in 5 of the 23 key articles but occurred in 0-15% of grafts.
In the analysis of the four RCTs concerning HUV allografts versus PTFE and saphenous vein, the
weighted mean difference could not be calculated in two RCTs because the standard deviation
was not reported. Statistical heterogeneity (I2) was 91.4%. This was far above the accepted
maximum level of 60% for performing a meta-analysis; therefore, it was not appropriate to
perform a meta-analysis.
A significant positive correlation existed between the percentage of patients with Fontaine
stage II disease and the 2 year cumulative primary graft patency (Fig). The Pearson correlation
coefficient was 0.58, significant at the 0.01 level.
Discussion
In this review we included 23 studies in which 3 different methods of vascular allograft
preservation were used. Because 15 of the 23 studies were retrospective case series, the level of
evidence of most studies in this review was low, and, as a consequence, results are susceptible
to bias. We tried to minimize bias by using objective criteria for important outcome parameters
and did not impose any restrictions on the language of publication in the initial search. Because
of the heterogeneity in various clinical factors, such as indication for operation, level of distal
anastomosis, anticoagulation use, and high statistical heterogeneity, it was not appropriate to
perform an overall meta-analysis of the studies.
The reported incidences of major complications were relatively low (0-15%). Two studies on
cryopreserved venous allografts (13;14) showed the highest major complication rates to be 11%
and 15% (Table 2). This is reflected by the high mean age and large number of patients with
Fahner.indd 32 5-5-2014 14:35:09

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 33
2
substantial renal dysfunction in the series of Farber et al (14) and the high percentage of CLI
(100%) and previous peripheral bypass procedures shown in the series of Carpenter et al (13).
In most series (12/21), the distal anastomosis was situated in the infrapopliteal or cruropedal
artery in more than 50% of cases. Reported major limb loss varied widely from 0-69% and was
highest in cold storage venous allografts described by Rebane et al (17).
Albers et al (1) performed a meta-analysis on 43 studies of PTFE bypass grafts to infrapopliteal
arteries and reported a pooled estimate of foot preservation of 66% after 3 years follow-up. Of
the studies in our review, 67% (12/18) reported a higher percentage of foot preservation. In
another meta-analysis, Albers et al (34) reviewed 33 studies of patients with an infrapopliteal
allograft bypass, and the pooled 1 year foot preservation rate was between 70% and 80%.
If a patient with limb ischemia needs a bypass to the popliteal artery, the most suitable type of
graft to use is still open to debate. In The Cochrane Review, Mamode and Scott (35) were unable
to demonstrate any clear evidence in support of the use of a particular type of graft at this level.
Yet a recent randomized trial clearly favored autologous saphenous vein over PTFE grafts (36).
If a patient needs a crural bypass the Transatlantic Inter-Society Consensus Working Group (37)
recommend the use of good-quality autologous vein to construct the bypass. They based their
findings on evidence from a meta-analysis by Hunink et al (38), with 5-year primary patency rates
for infrageniculate reconstructions of 66% for autologous vein and 33% for PTFE. Whether the
addition of a distal cuff in PTFE grafts or a distal arteriovenous fistula will ultimately result in an
improved patency of infrainguinal PTFE grafts is still to be defined (39-41).
Fifteen of the 23 series included looked at venous allografts preserved in glutaraldehyde
(HUV), and the highest patency rates were reported in this group (range 33-89%). With the
exception of Brockbank et al (11), studies in which cryopreserved venous allografts were used
reported the lowest patency rates. Because of the high percentage of patients lost to follow-up
(92% after 2 years), the results of this study should be interpreted cautiously. No studies that
included different types of allografts or graft preservation methods were available, so direct
comparison between various vascular allografts or preservation techniques was not possible.
Because of heterogeneity among studies, as reflected in differing levels of preoperative
critical ischemia, percentages of crural anastomosis, and differences in number of patients
lost to follow-up, it can be argued that weighted mean cumulative primary patency rate is
inappropriate for comparing the results of the different allografts. However, comparison of
patency rates is essential when deciding which allograft to use. Because the patency rate is
an important characteristic of graft function, the weighted mean primary patency used in this
review is currently the best approach when comparing the results of these allografts with the
data available in the literature.
Graft disintegration is a particular problem in cold-stored venous allografts. The degree of
antigenicity of the vascular allograft plays a role in the process of biodegradation, as shown in
Fahner.indd 33 5-5-2014 14:35:09

34 | Chapter 2
reconstructions with bovine heterografts. The preservation technique is important in diminishing
the rejection response to the allograft. It has been shown that the glutaraldehyde molecule
masks the histocompatibility antigen sites on vascular tissue (21), and it has been suggested that
cryopreservation decreases the acceptor immunological response against venous allografts (42).
This probably explains the lower biodegradation rate of glutaraldehyde and cryopreserved
vascular allografts in comparison with cold-stored grafts.
Tissue matching and immunosuppressive therapy are important issues in vascular
transplantation. Most studies in our review report the results of allotransplantations performed
without ABO blood type matching. The role of tissue matching on the function of vascular
allografts is still to be defined. Only one study randomized for immunosuppressive therapy (13),
and it was demonstrated that immunosuppression had no effect on the patency of cryopreserved
allografts. It has been demonstrated that cryopreserved and cold-stored allografts retain cell-
surface structures such as the major histocompatibility complex that are involved in the process
of allograft rejection.
The ideal vascular allograft should have a high graft patency rate, a low graft disintegration
rate, need no imunnosuppressive therapy, be available off the shelf in different diameters and
lengths, and be able to be stored for long periods. This systematic review addressed the various
aspects of vascular allografts. Because of recent advances in preservation of vascular allografts
for use in clinical vascular surgery, their results needs to be compared with those described in
this systematic review (43, 44).
In conclusion, this systematic review assessed the results of studies on infrainguinal vascular
allografts. Different allograft preservation methods were compared, and it was demonstrated that
heterogeneity among studies was high and excluded a formal meta-analysis. A firm conclusion
could not be made because there were no studies available in which direct comparison was
performed between different preservation methods of vascular allografs. However, this review
revealed that patency rates for infrainguinal reconstructions performed by using allografts were
satisfactory. If the results of major complications, limb loss, and graft disintegration were also
taken into account, glutaraldehyde preservation of HUV allografts seemed superior to the other
methods of vascular allograft preservation.
Acknowledgement
We are grateful to Dr D. Th. Ubbink for assistance in statistical and meta-analysis.
Fahner.indd 34 5-5-2014 14:35:09

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 35
2
Reference List
(1) Albers M, Battistella VM, Romiti M, Rodrigues AA, Pereira CA. Meta-analysis of polytetrafluoroethylene bypass grafts to infrapopliteal arteries. J Vasc Surg 2003 Jun;37(6):1263-9.
(2) Guthrie CC. Structural changes and survival of cells in transplanted bloodvessels. J Am Med Assoc 1908;50:1035-6.
(3) da Gama AD. The fate of arterial transplantation or the death of the microcosm. Leriche memorial lecture. Cardiovasc Surg 1999;7(7):671-80.
(4) Myers KA. Reporting standards and statistics for evaluating intervention. Cardiovasc Surg 1995 Oct;3(5):455-61.
(5) Rutherford RB, Becker GJ. Standards for evaluating and reporting the results of surgical and percutaneous therapy for peripheral arterial disease. J Vasc Interv Radiol 1991 May;2(2):169-74.
(6) Greenhalgh T. How to read a paper. The Medline database. BMJ 1997 Jul 19;315(7101):180-3.
(7) Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000 Apr 19;283(15):2008-12.
(8) Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM statement. Quality of Reporting of Meta-analyses. Lancet 1999 Nov 27;354(9193):1896-900.
(9) Moher D, Schulz KF, Altman D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. JAMA 2001 Apr 18;285(15):1987-91.
(10) Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003 Sep 6;327(7414):557-60.
(11) Brockbank KG, McNally RT, Walsh KA. Cryopreserved vein transplantation. J Card Surg 1992 Jun;7(2):170-6.
(12) Martin RS, III, Edwards WH, Mulherin JL, Jr., Edwards WH, Jr., Jenkins JM, Hoff SJ. Cryopreserved saphenous vein allografts for below-knee lower extremity revascularization. Ann Surg 1994 Jun;219(6):664-70.
(13) Carpenter JP, Tomaszewski JE. Immunosuppression for human saphenous vein allograft bypass surgery: a prospective randomized trial. J Vasc Surg 1997 Jul;26(1):32-42.
(14) Farber A, Major K, Wagner WH, Cohen JL, Cossman DV, Lauterbach SR, et al. Cryopreserved saphenous vein allografts in infrainguinal revascularization: analysis of 240 grafts. J Vasc Surg 2003 Jul;38(1):15-21.
(15) Branchereau A, Albertini JN, Magnan PE, Barral X, Favre JP, Guidicelli H, et al. Arterial allografts as a conduit for surgical reconstruction. Crit Ischemia 2000;10(3):71-5.
(16) Reedt Dortland RW, van Leeuwen MS, Steijling JJ, Theodorides T, van Vroonhoven TJ. Long-term results with vein homograft in femoro-distal arterial reconstructions. Eur J Vasc Surg 1991 Oct;5(5):557-64.
(17) Rebane E, Tikko H, Tunder E, Lepner U, Helberg A, Pulges A, et al. Venous allografts for infrainguinal vascular bypass. Cardiovasc Surg 1997 Feb;5(1):21-5.
(18) De Leersnijder D, Willocx P, Van Marck E, Vanmaele R. Venous homografts in infra-inguinal procedures: an eight years experience. J Cardiovasc Surg (Torino) 1992 Nov;33(6):633-40.
(19) Dardik H, Miller N, Dardik A, Ibrahim I, Sussman B, Berry SM, et al. A decade of experience with the glutaraldehyde-tanned human umbilical cord vein graft for revascularization of the lower limb. J Vasc Surg 1988 Feb;7(2):336-46.
(20) Dardik H. The second decade of experience with the umbilical vein graft for lower-limb revascularization. Cardiovasc Surg 1995 Jun;3(3):265-9.
Fahner.indd 35 5-5-2014 14:35:09

36 | Chapter 2
(21) Dardik H, Wengerter K, Qin F, Pangilinan A, Silvestri F, Wolodiger F, et al. Comparative decades of experience with glutaraldehyde-tanned human umbilical cord vein graft for lower limb revascularization: an analysis of 1275 cases. J Vasc Surg 2002 Jan;35(1):64-71.
(22) Robison JG, Brewster DC, Abbott WM, Darling RC. Femoropopliteal and tibioperoneal artery reconstruction using human umbilical vein. Arch Surg 1983 Sep;118(9):1039-42.
(23) Hirsch SA, Jarrett F. The use of stabilized human umbilical vein for femoropopliteal bypass. Experience with 133 operations with 5-year follow-up. Ann Surg 1984 Aug;200(2):147-52.
(24) Boontje AH. Angiographic assessment of biografts for femoropopliteal bypass. J Cardiovasc Surg (Torino) 1986 Mar;27(2):136-40.
(25) Jarrett F, Hirsch SA. Reoperation for complications of stabilized human umbilical vein grafts. Am J Surg 1989 Nov;158(5):438-42.
(26) Batt M, Gagliardi JM, Avril G, Guzman R, Guidoin R, Hassen-Khodja R, et al. Human umbilical vein grafts as infrainguinal bypasses: long-term clinical follow-up and pathological investigation of explanted grafts. Clin Invest Med 1990 Aug;13(4):155-64.
(27) Sato O, Okamoto H, Takagi A, Miyata T, Takayama Y. Biodegradation of glutaraldehyde-tanned human umbilical vein grafts. Surg Today 1995;25(10):901-5.
(28) Weisel RD, Johnston KW, Baird RJ, Drezner AD, Oates TK, Lipton IH. Comparison of conduits for leg revascularization. Surgery 1981 Jan;89(1):8-15.
(29) Eickhoff JH, Broome A, Ericsson BF, Buchardt Hansen HJ, Kordt KF, Mouritzen C, et al. Four years’ results of a prospective, randomized clinical trial comparing polytetrafluoroethylene and modified human umbilical vein for below-knee femoropopliteal bypass. J Vasc Surg 1987 Nov;6(5):506-11.
(30) McCollum C, Kenchington G, Alexander C, Franks PJ, Greenhalgh RM. PTFE or HUV for femoro-popliteal bypass: a multi-centre trial. Eur J Vasc Surg 1991 Aug;5(4):435-43.
(31) Johnson WC, Squires JW. Axillo-femoral (PTFE) and infrainguinal revascularization (PTFE and umbilical vein). Vascular Registry of the New England Society for Vascular Surgery. J Cardiovasc Surg (Torino) 1991 May;32(3):344-9.
(32) Johnson WC, Lee KK. A comparative evaluation of polytetrafluoroethylene, umbilical vein, and saphenous vein bypass grafts for femoral-popliteal above-knee revascularization: a prospective randomized Department of Veterans Affairs cooperative study. J Vasc Surg 2000 Aug;32(2):268-77.
(33) Aalders GJ, van Vroonhoven TJ. Polytetrafluoroethylene versus human umbilical vein in above-knee femoropopliteal bypass: six-year results of a randomized clinical trial. J Vasc Surg 1992 Dec;16(6):816-23.
(34) Albers M, Romiti M, Pereira CA, Antonini M, Wulkan M. Meta-analysis of allograft bypass grafting to infrapopliteal arteries. Eur J Vasc Endovasc Surg 2004 Nov;28(5):462-72.
(35) Mamode N, Scott RN. Graft type for femoro-popliteal bypass surgery. Cochrane Database Syst Rev 2000;(2):CD001487.
(36) Klinkert P, Schepers A, Burger DH, van Bockel JH, Breslau PJ. Vein versus polytetrafluoroethylene in above-knee femoropopliteal bypass grafting: five-year results of a randomized controlled trial. J Vasc Surg 2003 Jan;37(1):149-55.
(37) Management of peripheral arterial disease (PAD). TransAtlantic Inter-Society Consensus (TASC). Eur J Vasc Endovasc Surg 2000 Jun;19 Suppl A:Si-250.
(38) Hunink MG, Wong JB, Donaldson MC, Meyerovitz MF, Harrington DP. Patency results of percutaneous and surgical revascularization for femoropopliteal arterial disease. Med Decis Making 1994 Jan;14(1):71-81.
(39) Oderich GS, Panneton JM, Yagubyan M, Bower TC, Hofer J, Noel AA, et al. Comparison of precuffed and vein-cuffed expanded polytetrafluoroethylene grafts for infragenicular arterial reconstructions: a case-matched study. Ann Vasc Surg 2005; 19:49-55.
Fahner.indd 36 5-5-2014 14:35:09

Systematic review of preservation methods and clinical outcome of infrainguinal vascular allografts | 37
2
(40) Kreienberg PB Darling RC 3rd, Chang BB, Paty PS, Lloyd WE, Shah DM. Adjunctive techniques to improve patency of distal prosthetic bypass grafts: polytetrafluoroethylene with remote arteriovenous fistulae versus vein cuffs. J Vasc Surg 2000;31:696-701.
(41) Panneton JM, Hollier LH, Hofer JM. Multicenter randomized prospective trial comparing a pre-cuffed polytetrafluoroethylene graft to a vein cuffed polytetrafluoroethylene graft for infragenicular arterial bypass. Ann Vasc Surg 2004;18:199-206.
(42) Weber TR, Dent TL, Salles CA, Ramsburgh SR, Fonseca FP, Lindenauer SM. Cryopreservation of venous homografts. Surg Forum 1975;26:291-3
(43) Fahner PJ, Idu MM, Legemate DA, Vanbavel E, Borstlap J, Pfaffendorf M, et al. Morphological and functional alterations in glycerol preserved rat aortic allografts. Int J Artif Organs 2004;27:979-89.
(44) Martin ND, Schaner PJ, Tulenko TN, Shapiro IM, Dimatteo CA, Williams TK, et al. In vivo behavior of decellularized vein allograft. J Surg Res 2005;129:17-23.
Fahner.indd 37 5-5-2014 14:35:09

Fahner.indd 38 5-5-2014 14:35:09

3Morphological and functional alterations in
glycerol preserved rat aortic allografts
P.J. Fahner, MD 1, M.M. Idu*, MD, PhD 1, D.A. Legemate, MD, PhD 1, E. VanBavel, PhD2,J. Borstlap 1, M. Pfaffendorf, PhD
3, J. van Marle, PhD 4, T.M. van Gulik MD, PhD1
Department of Surgery and Surgical laboratory1, Department of Medical Physics 2, Department of Pharmacotherapy 3, Center for Microscopic Research 4 Academic
Medical Center, University of Amsterdam, Amsterdam, The Netherlands
Int J Art Org 2004;27:979-89
Fahner.indd 39 5-5-2014 14:35:09

40 | Chapter 3
Abstract
Glycerol preservation is an effective method for long-term preservation of skin allografts and has
a potential use in preserving arterial allografts. We evaluated the effect of glycerol concentration
and incubation period on vessel-wall integrity of rat aortic allografts. No significant differences
were measured in breaking strength (2.3 ± 0.3 N) and bursting pressure (223 ± 32 kPa) between
standard glycerolized and control segments
(1.7 ± 0.3 N, 226 ± 17 kPa). Isometric tension measurements showed complete lack of
functional contraction and relaxation capacity in allograft segments prepared according to all
preservation protocols. Morphologically, thickness of the vessel-wall media diminished after
preservation using low (30/50/75 %) or high (70/85/98 %) concentrations of glycerol, as
compared to control segments (i.e. 81 ± 2.4 μm, 95 ± 5.6 μm and 125 ± 3.5 μm, respectively).
Confocal microscopy and Fourier analysis demonstrated that vascular collagen and elastin bundle
orientation had remained unaltered. Electron microscopy showed defragmentation of luminal
endothelial cells.
In conclusion, glycerol preservation of rat aorta resulted in an acellular tissue matrix, which
maintained biomechanical integrity and extracellular matrix characteristics. The next step in the
investigation will be to test the concept of glycerol preservation of arterial allografts in a vascular
transplantation model.
Fahner.indd 40 5-5-2014 14:35:09

Morphological and functional alterations in glycerol preserved rat aortic allografts | 41
3
Introduction
Peripheral bypass surgery is usually the final therapeutic option for patients with extensive lower
limb arterial occlusive disease to prevent impending major limb loss. The autologous vein is
the material of choice for distal vascular reconstruction owing to its good long-term patency
(1). However, in about one-third of patients the autologous vein cannot be used because of
earlier harvesting or poor quality. Alternative materials such as synthetic grafts (Dacron,
Polytetrafluoroethyleen) and biological grafts (human umbilical vein) are commonly used as
peripheral arterial conduits. However, these alternative grafts are hampered by poor long-term
patency. Due to advanced preservation methods, vascular allotransplantation became an option
for patients who need a peripheral arterial reconstruction. In the past, different preservation
methods were developed for storage of vascular transplants and other biomaterials (2-5). Many of
these preservation methods were applied to and studied in skin allografts. Glycerol preservation,
relatively simple and cheap, proved to be a superior preservation method for skin grafts and is
currently the preservation technique of first choice for skin allograft preservation and storage
within the Euro Skin Bank in the Netherlands (6-9).
The main features of glycerol preservation of skin allografts are that the basic architecture
of the skin remains unaffected, glycerol is an effective antibacterial and antiviral agent, and it
diminishes glycerol diminishes antigenicity of the tissues used for transplantation (10-13). These
characteristics held promise for the preservation of vascular allografts and therefore we decided
to evaluate glycerol preservation of rat aortic vascular grafts. The aim of this study was two-fold:
(i) to determine the biomechanical properties and functional characteristics of rat aortic grafts
after preservation with different glycerol concentrations, and (ii) to assess possible morphological
alterations of rat aortic grafts after glycerol preservation.
Materials and methods
Glycerol-preservation protocol
Glycerol preservation was performed by successively immersing the grafts in solutions with
different glycerol concentrations using different incubation times. This preservation protocol was
based on the currently used standard protocol for preserving skin grafts by the Euro Skin Bank
(13). This glycerol-preservation protocol, which had been developed empirically, was extensively
tested and has now been used for many years. Briefly, the protocol consists of three aseptic
stages, i.e. the skin grafts are firstly immersed in a 50% concentrated glycerol solution for
4 hours at room temperature, then in a 70% glycerol solution for 3 hours at 33oC, and finally in
a 85% concentrated glycerol solution for another 3 hours at 33oC. After preservation the grafts
are stored at 4oC.
Fahner.indd 41 5-5-2014 14:35:09

42 | Chapter 3
Several experimental groups were studied. In the first group, the effects of storage on
biomechanical and morphological characteristics of the vessel wall were investigated (group
1A-C in Table Ι). In the second group, the effects of different glycerol concentrations were
examined (group 2A-C in Table Ι), and in the last group the influence of incubation time was
studied (group 3A-F in Table Ι). The incubation temperatures of all three stages of glycerolization
in all experimental groups were identical to the protocol used by the Euro Skin Bank. After
preservation, all glycerol-preserved grafts were cold-stored at 4 0C for 12 hours while remaining
immersed in their final glycerol solution until testing. Rat aorta segments tested immediately
after harvesting served as controls, and breaking strength was measured after incubation in
saline as well (group C1-2 in Table Ι).
Different glycerol concentrations were obtained by dilution of glycerol 98% (Genfarma Corp.
Maarssen, The Netherlands) with demiwater. To obtain a 0.9% NaCl concentration we added
0.45g of sodium chloride to 50 ml of glycerol solution.
Animals
Male Wistar rats (Charles Rivers, Maastricht, The Netherlands) weighing 240-290 g had a period
of acclimatization of at least five days before they were sacrificed by stunning and decapitation
for retrieval of the thoracic and abdominal aorta. The protocol was approved by the Animal
Ethics Committee of the University of Amsterdam, The Netherlands.
Biomechanical experiments
Breaking- strength experiments
Ring segments of 2 mm of descending thoracic aorta, devoid of intercostal arteries, were
harvested from eighteen rats. Each study group contained six aortic segments. The segments
were mounted on two metal hooks.
If a blood vessel is tested for a load-elongation curve, the internal structure of the tissue will
change with each cycle of loading and unloading. By repeated cycling, eventually a steady state is
reached, rendering the specimen into a preconditioned state (14). Therefore, in our experiments,
the tension-testing machine (Newport, Every Cedex, France) was loaded and unloaded ten times
up to 1 N. The segments were subsequently stretched at a constant speed of 0.1 mm/sec until
breaking. The load and deformation were continuously recorded on an X-Y recorder (Newport,
Every Cedex, France), and load-deformation curves were generated by computer software with
which the maximum strength at the breaking point, i.e. the maximum load, could be recorded.
Fahner.indd 42 5-5-2014 14:35:09

Morphological and functional alterations in glycerol preserved rat aortic allografts | 43
3
Tab
le I.
Gly
cero
l inc
ubat
ion
prot
ocol
s an
d re
sult
s of
exp
erim
enta
l gro
ups.
Exp
erim
enta
lg
rou
pG
lyce
rol
con
cen
trat
ion
(%
)
Incu
bat
ion
tim
es (
h)
Bre
akin
gst
ren
gth
(N
)B
urs
tin
gp
ress
ure
(k
Pa)
Med
iath
ickn
ess
(μm
)
End
oth
elia
llin
ing
Ad
ven
titi
alco
mp
actn
ess
Cel
ln
ucl
eus
Ori
enta
tio
n in
dex
(%)
med
iaad
ven
titi
a
Biom
echa
nica
l exp
erim
ents
Mor
phol
ogic
al a
sses
smen
t
1 A
(ESB
)50
/70/
854
/3/3
2.29
(0.3
0)22
3.3
(31.
52)
117.
70
(11.
48)
inte
rmin
term
pykn
otic
54.
10 (3
.83)
78.2
0 (1
.43)
1 B
1 w
k st
orag
e)50
/70/
854
/3/3
2.6
4 (1
.12)
1 C
(3
m s
tora
ge)
50/7
0/85
4/3
/32.
28 (0
.42)
2 A
30/5
0/65
4/3
/32.
96 (0
.71)
232.
5 (4
5.81
)8
0.60
(2
.35)
lost
inte
rm/lo
wpy
knot
ic62
.96
(3.9
6)72
.41
(1.6
6)
2 B
40/
60/7
54
/3/3
1.81
(0.1
7)20
3.2
(11.
12)
2 C
50/7
0/85
4/3
/31.
79 (0
.17
204.
1 (2
8.01
)9
4.99
(5
.62)
lost
/inte
rmin
term
/low
pykn
otic
62.2
7 (2
.03)
78.2
0 (3
.26)
3 A
50/7
0/85
2/3
/32.
05 (0
.22)
3 B
50/7
0/85
6/3
/32.
14 (0
.27)
3 C
50/7
0/85
4/1
/31.
96 (0
.43)
3 D
50/7
0/85
4/6
/32.
29 (0
.27)
3 E
50/7
0/85
4/3
/11.
79 (0
.14)
3 F
50/7
0/85
4/3
/61.
90
(0.2
4)
C 1
fres
h0
1.70
(0.3
2)22
6.4
(17.
01)
125.
7 (3
.48)
com
plet
ehi
ghsp
arse
ch
rom
atin
55.3
4 (2
.94)
72.6
4 (3
.33)
C 2
salin
e4
/3/3
1.8
0 (0
.13)
Gro
up 1
= s
tand
ard
prot
ocol
, gro
up 2
= m
odifi
catio
n in
gly
cero
l con
cent
ratio
n, g
roup
3 =
mod
ifica
tion
in in
cuba
tion
time,
gro
up C
= c
ontr
ol, E
SB =
Eur
o Sk
in
Bank
, wk
= w
eek,
m =
mon
th, i
nter
m =
inte
rmed
iate
. Dat
a ar
e pr
esen
ted
as m
eans
(SEM
). (*
) p =
0.0
5 ve
rsus
con
trol
aft
er n
on-p
aram
etric
Man
n-W
hitn
ey te
st.
Fahner.indd 43 5-5-2014 14:35:09

44 | Chapter 3
Bursting-pressure experiments
Pilot study
A pilot experiment was performed to investigate if a significant difference existed in bursting
pressures between thoracic and abdominal aortic segments. Aortas from seven rats were
harvested proximally just below the thoracic arch and distally just above the bifurcation. Each
aorta was divided into five segments of one cm, three of them thoracic and two abdominal.
For the different thoracic and abdominal positions, the bursting pressures (n=6/ position) were
measured as described for the main study (Figure 1).
Main study
Segments of one cm of descending thoracic and abdominal aorta were harvested from sixteen
rats and randomly allocated to different experimental groups. In the first group (group 1A in
Table Ι), the Euro Skin Bank incubation protocol was tested and in the second group (group 2A-C
in Table Ι), the effect of incubation times was investigated. Fresh segments, which were tested
directly after harvesting, served as controls (group C1 in Table Ι). Each study group consisted of
three aortic segments.
The aortic segments were stretched to their original length in situ and fixed by two needle
tips. A 3 F balloon catheter (Le Maitre Vasc Inc., Bad Soden, Germany) was placed intraluminally
and connected to a pressure controller (Braun Medical, Melsungen, Germany) and a pressure
transducer (Baxter, Deerfield, Illinois, USA). The balloon catheter was inflated until the vessel wall
ruptured. The pressure transducer was linked to a computer for continuous registration of the
changes in pressure. A time/pressure curve was automatically generated. Pressure measurements
with the transducer were linear and reproducible for pressures up to 280 kPa.
thor 1 thor 2 thor 3 abd 1 abd 20
100
200
300
Anatomic position
Burs
ting
pres
sure
(kP
a)
Figure 1. Bursting-pressure results of a pilot experiment of unpreserved, sequential thoracic (thor) and abdominal (abd) aortic segments of seven rats. Bars represent means ± SEM.
Fahner.indd 44 5-5-2014 14:35:09

Morphological and functional alterations in glycerol preserved rat aortic allografts | 45
3
Viability testing, contraction and relaxation properties
Viability testing was performed on rat aortic segments preserved by two different glycerolization
protocols indicated as low and high protocol. The glycerol concentrations used for the low
protocol were 30%, 50% and 65%, and for the high protocol 70%, 85%, 98%. Incubation
periods, temperatures and storage times were the same as for group 1A in Table Ι. Fresh
segments, tested immediately after harvesting served as controls. To discriminate among effects
on viability induced by glycerol or incubation periods, temperatures and storage times, segments
preserved in saline for the same incubation periods, temperatures and storage times as the
glycerolization protocols, were also tested (Figure 2).
Aortic ring segments of three mm were vertically mounted between stainless-steel hooks
in a five-ml organ bath. Each study group consisted of six aortic rings. The upper hook was
attached to an isometric force transducer (Kyowa™, Tokyo, Japan) connected to a Power Lab/8s
data acquisition system (AD Instruments, Australia). The organ bath contained Tyrode’s solution
consisting of 124 mM NaCl, 4.0 mM KCl, 0.9 mM CaCl2, 1.1 mM MgCl2, 0.42 mM NaH2PO4,
24.9 mM NaHCO3 and 5.5 mM glucose. The solution was maintained at 37 °C and pH = 7.4 by
bubbling the solution with carbogen O2/CO2 (95:5).
The contraction ability of the aortic segments was tested by applying 100 μM L-phenylephrine,
an α1-adrenoceptor agonist. The relaxation capacity was measured in two functional pathways: a)
the endothelium-dependent pathway using methacholine (100 µM) to stimulate the endothelial
1.0e
-9
3.0e
-9
1.0e
-8
3.0e
-8
1.0e
- 7
3.0e
- 7
1.0e-
6
3.0e
-6-2.5
0.0
2.5
5.0
7.5
10.0freshNaCllow glycerolhigh glycerol
Na+- Nitroprusside concentration
Con
trac
tion
forc
e (m
N)
Figure 2. Viability tests, results of contraction and relaxation experiments. Control rat aortic ring segments tested immediately after harvesting (fresh) and segments stored in 0.9 % saline (NaCl) showed complete maintenance of relaxation capacity. Note the absence of endothelium-independent relaxation capacity of segments after both low and high glycerol concentration preservation protocols (see Materials and Methods). Bars represent means ± SEM.
Fahner.indd 45 5-5-2014 14:35:10

46 | Chapter 3
cell to release endothelium-derived relaxing factor (EDRF), and b) the endothelium-independent
pathway using Na+ -nitroprusside (100 µM), an NO-donor (15).
The initial resting tension was set at 10 mN and was adjusted throughout the experiment.
After 1 hour of equilibration, the ring segments were exposed to a high potassium concentration
(60 mM) for 10min to depolarise the cells, followed by contraction. When maximum contraction
had been reached, the segment was rinsed with Tyrode’s solution. The potassium contraction
was repeated twice with a 15-min interval. Afterwards, a dose-response curve was constructed
for L-phenylephrine (1.10-8 – 1.10-5 M) and methacholine (1.10-8 – 1.10-5 M) with a potassium
contraction, Tyrode’s rinsing, and a L-phenylephrine (1.10-6) contraction in between measurements.
To determine the endothelium-independent relaxation of the smooth-muscle cells, the NO-
donor Na+-nitroprusside (1.10-9 – 1.10-6 M) was added to the organ bath, after the potassium
contraction, Tyrode’s rinsing and the L-phenylephrine (1.10-6) contraction, in order to be able to
construct the dose-response curve.
Morphological assessment
Morphological assessment was performed in samples prepared according to the same
preservation protocols as for bursting-pressure experiments, corresponding to group 1A, 2A and
2C in Table Ι. Fresh segments served as controls (group C1 in Table Ι).
low intermed high control0
25
50
75
100media
adventitia
Glycerol concentration
Orie
ntat
ion
inde
x (%
)
Figure 3. Orientation index of the media extracellular matrix (media) and adventitial extracellular matrix (adventitia) of rat aortic segments preserved with low, intermediate or high glycerol concentration protocols. Fresh segments served as controls (control). Bars represent means ± SEM.
Fahner.indd 46 5-5-2014 14:35:10

Morphological and functional alterations in glycerol preserved rat aortic allografts | 47
3
Histology
Five-mm aortic ring segments were used, three specimens in each study group. After
preservation, the segments were fixed in 10% formaline solution (Mallinckrodt Baker, Deventer,
The Netherlands), dehydrated, and embedded in paraffin. Transverse sections (5 μm) were
stained with hematoxylin-eosin (HE), Elastin von Gieson, van Gieson, and picro sirius red, and
were mounted on slides for microscopic examination.
A Leica LB 30 S light microscope (Leica, Wetzlar, Germany) was used to view the slides. The
Qwin Image pro analysis software (version 2.6, Leica Imaging Systems Ltd., Cambridge, UK) was
used to measure elastin bundle width and distance between elastin bundles of the media, as
well as media thickness.
A scoring system was used to describe alterations in endothelial lining, adventitial compactness,
and features of cell nuclei as follows. Endothelial lining was scored as complete (all endothelial
cells attached to the media), intermediate (endothelial cells disconnected from the media for
less than 75%), or lost (endothelial cells disconnected from the media for more than 75%).
Compactness of the extracellular matrix of the tunica adventitia was graded as high (compact
collagen bundles), intermediate (low fragmentation of collagen bundles and loose matrix), or low
(high fragmentation of collagen bundles and loose matrix). The aspect of cell nuclei in intima,
media and adventitia was described as sparse chromatin (nuclei with low chromatin density) or
pyknotic (small nuclei with high chromatin density).
Extracellular matrix orientation
The same images as used for the assessment of bundle width and distance were used for matrix
orientation of measurements of the media and adventitia. Image analysis was done with the Fast
Fourier Transform (FFT) module of the same Qwin Image pro analysis software as used for the
histological measurements. To compare the elastin-bundle orientation and the collagen-bundle
orientation in the vessel wall after glycerol preservation with the same orientation in unpreserved
tissue, an orientation index was determined as described below.
Determination of orientation index
Images (512 * 512 pixels) were acquired with a Leica SP2 confocal system making use of the
fluorescent properties of eosin in the HE-stained histological slides: excitation 488 nm / detection
550-590 nm, using a 40* immersion objective and a pinhole setting corresponding with 1 Airy
disc. An orientation index was defined by dividing the short axis of the first-order maximum by
the long axis of the first-order maximum expressed as %. Consequently, a totally parallel structure
gives an orientation index close to zero, whereas as totally random orientation is represented by
an orientation index of 100%. This method was earlier described in detail for skin tissue (16;17).
Fahner.indd 47 5-5-2014 14:35:10

48 | Chapter 3
Each cross section of the aorta was scanned with the microscope to obtain four images (0°, 90°,
180°, 270°) of the media as well as of the adventitia.
Scanning electron microscopy
To examine the effect of glycerol preservation on the endothelial cell lining, scanning electron
microscopy was performed. Five-mm aortic segments were used, three specimens in each study
group.
The segments were rinsed in saline and fixed for 24 hours in McDowall fixative (4%
paraformaldehyde and 1% glutaraldehyde in 0.1M phosphate buffer). After fixation, the
segments were dehydrated in graded ethanols, placed in 1,1,1,3,3,3 hexamethyl disilazan (Merck-
Schuchardt), and dried at room temperature for 12 hours. Subsequently, they were mounted on
stubs with conductive carbon cement, sputter-coated with 20 nm gold-palladium, and scanned
with an electron microscope (Philips SEM 525 equipped with an Orion frame grabber) operated
at 10 kV and a spot size of 50 nm.
Statistical analysis
Continuous data are presented as means, and non-parametric statistical tests were used for
analysis: the Mann-Whitney test was used to determine differences between two unrelated
groups and the Kruskas-Wallis test was used to determine differences between more than
two unrelated groups. A difference with a p-value of 0.05 or less was considered a statistically
significant difference. The statistical analysis was performed with Statistical Package for the
Social Sciences version 11.01. for Windows ® (SPSS ®, Chicago, Illinois, USA).
Results
Biomechanical experiments
There were no significant differences (p = 0.27) in breaking-strength values measured in the
different glycerol-preserved experimental groups. There were also no significant differences
between the experimental and control groups (group C1-2 in Table Ι). The vessel wall ruptured
at a mean diameter of 17.4 (2.8) mm and 15.2 (2.2) mm in the glycerol-preserved groups and in
the control groups, respectively.
In the pilot study no significant differences (p = 0.31) were found among the mean bursting
pressures of the aortic segments of different locations (Figure 1). In the main study were no
significant differences (p = 0.84) within the glycerol-preserved experimental groups, the mean
bursting pressure tested being comparable to that of unpreserved grafts in the control group
(group C1 in Table Ι).
Fahner.indd 48 5-5-2014 14:35:10

Morphological and functional alterations in glycerol preserved rat aortic allografts | 49
3
Viability testing: contraction and relaxation
The control segments showed a contraction capacity of 41% (9.23 N (±1.85) against 3.79 N
(±1.24)) after 12 hours of storage. Although the endothelium-dependent relaxation capacity
was absent, the endothelium-independent relaxation capacity was still complete (Figure 2).
The functional contraction capacity of the aortic segments preserved in glycerol was found
to be completely lost. The same was true for the endothelium-dependent and endothelium-
independent relaxation capacities (Figure 2).
Morphological assessment
Histology
The mean elastin-bundle width in the media in the control segments was 4.16 μm. There were
no significant differences (p = 0.56) between the mean elastin-bundle widths in the media in the
experimental groups, and there were no differences between the experimental groups and the
control group (see Materials and Methods).
The mean distances between elastin bundles in the media in the control segments was 9.25
μm. There were no significant differences (p = 0.63) between the mean elastin-bundle distances
in the media in the experimental groups, nor when this was compared to the control group.
The media thickness was significantly less in the segments preserved at low glycerol
concentrations (p = 0.05) and in those preserved at high glycerol concentrations (p = 0.05)
than in the control group (group C1 in Table Ι). For the segments incubated at intermediate
concentrations, no significant alterations were found in media thickness.
Endothelial lining, compactness of adventitia and nuclear aspects were assessed using the
scoring system described above. The endothelial lining of the aortic segments was invariably
lost after glycerol preservation. The adventitial compactness was diminished after glycerol
preservation and the cell nucleus of all glycerol-preserved cells were pyknotic (Table Ι). These
features demonstrate that after glycerol preservation, an extracellular tissue matrix without living
cells is all that is left.
Orientation Index
There were no significant differences (p = 0.21) in the orientation indices of the media within the
experimental groups, nor when these were compared to the index of the control group (group
C1 in Table Ι). There were no significant differences (p = 0.22) in the orientation indices of the
adventitia within the experimental groups, also not when these were compared to that of the
control group (Figure 3).
Fahner.indd 49 5-5-2014 14:35:10

50 | Chapter 3
Scanning electron microscopy
In the control segments, a confluent layer of endothelial cells was present (Figure 4a). The
segments preserved in glycerol showed a flattened layer of endothelial cell remnants with
defragmentation of cellular membranes (Figure 4b). Detachment of the intimal layer from the
internal elastic lamina was evident and fenestration of the intima was shown. These features
were more obvious in the segments preserved with the high glycerol concentrations than in the
segments preserved in low concentrations.
The layers of elastin, which tended to be arranged cylindrically around the lumen, were not
changed in any group.
Figure 4a. Electron micrograph of fresh rat aorta showing the luminal surface with a confluent layer of endothelial cells.
Figure 4b. Electron micrograph of rat aorta after preservation with high-concentration glycerol. Endothelial cells are flattened and partially detached from the underlying internal elastic lamina.
Discussion
For patients who need a peripheral vascular reconstrunction and who do not have an autologous
vein available, vascular transplantation is a reasonable alternative. To be able to prepare and store
appropriate biological grafts for a long time, an efficient preservation method is a prerequisite.
In the past, various methods of preserving arterial and venous grafts have been developed, such
as cryopreservation (18), glutaraldehyde tanning (19), lyophilization (20) and simple cold storage
(21). However, these methods did not result in successful vascular grafts for femorodistal bypass
grafting. Investigations of alternative preservation methods are, therefore, still ongoing.
Because the literature on glycerol preservation of arterial allografts was limited (22),
we decided to examine the alterations in vessel-wall function and architecture after glycerol
preservation of rat aorta arterial allografts.
Fahner.indd 50 5-5-2014 14:35:10

Morphological and functional alterations in glycerol preserved rat aortic allografts | 51
3
The incubation protocol for glycerol preservation from the Euro Skin Bank that we followed
is based on empirism. During years of development, the glycerol concentrations and incubation
periods were established. It was noted that high glycerol concentrations (85%) combined with
short incubation periods induced a quick dehydratation of skin grafts, resulting in a parchment-
like structure unsuitable for clinical use. Preservations starting with lower concentrations (50%)
proved to be more successful. In our present study this protocol was applied to vascular grafts
for the first time, and the influence was investigated of alterations in concentrations of glycerol
and incubation periods on vessel-wall characteristics.
Although most of the forces on a vessel are dilatational, vessels are also subject to longitudinal
stress.
We used the bursting-pressure test because the vessel wall is loaded in all directions, and this
test best represents the physiological situation. In addition, the breaking-strength experiments,
provide information about the diameter at which the vessel wall ruptures. Therefore, besides
bursting pressure, it is useful to measure longitudinal stress resistance as well (Table Ι).
Glycerol-preserved aortic allografts stored in glycerol at 4oC maintained tensile strength
up to 3 months after preservation, indicating that structural integrity of the vessel wall was
maintained. The breaking-strength values in our experiments were comparable to the control
values of 1.55 N in the study of Brüel et al (23) who investigated the role of cross-links in collagen
and elastin and their relation to mechanical stability in Wistar rats. As there were no significant
differences in tensile strength between the groups with different glycerol incubation periods
(group 3A-3F Table Ι), we continued to use the standard incubation times of the Euro Skin Bank.
Bursting-pressure measurements, often used for testing an anastomosis (24;25), are
classically performed by inflating the vessel through an intraluminal cannula after ligation of all
side branches (26-28). This method leads to a wide variation in results and has many confounding
factors, such as the presence of side branches and differences in vessel length. Therefore, we
used an intraluminally placed balloon catheter for determination of the bursting pressures. The
mean bursting pressures measured in this study were in the range of 203.2 kPa to 232.5 kPa,
corresponding to about 13 times the normal rat arterial systolic blood pressure. Since we could
not demonstrate a significant difference (p = 0.27) in the mean bursting pressures of the thoracic
and abdominal segments in our pilot study, we did not discriminate between these two locations
in the remaining part of the study. The biomechanical tests used in our study demonstrated
that glycerol preservation preserved the biomechanical characteristics of the rat aorta and we
could conclude that the extracellular matrix of the vessel wall was still able to withstand more
than physiological pressures after preservation according to the different glycerol preservation
protocols. Loss of extracellular matrix integrity may lead to serious complications, which was
illustrated by Noel et al (29) who reported 9% perianastomotic hemorrhage and graft rupture in
patients who had in situ aortic replacements with cryopreserved aortic allografts.
Fahner.indd 51 5-5-2014 14:35:10

52 | Chapter 3
We examined functional changes in the aortic segments in vitro using isometric tension
measurements. The experiments of Moriyama et al (30) showed a negative correlation between
the duration of warm ischemia in rat aortic tissue and cell viability. Segments of the thoracic aorta
were excised from rats at different postmortem intervals and the maximal contractile response of
freshly isolated arteries decreased to 50% after 6 to 8 hours of warm ischemia. Vischjager et al
(31) measured a 68% decrease in contractile responses of rat aortic segments after seven days of
preservation in University of Wisconsin preservation solution at 4 oC. Cryopreservation of vascular
grafts also influenced cell function (32). The relaxation capacity of human mesenteric artery
ring segments diminished to 29% after cryopreservation (33). We expected to find complete
absence of contraction and relaxation of the aortic segments after glycerol preservation because
of the known loss of viable cells in skin grafts after glycerol preservation. Although viable
endothelial cells play an important role in long-term graft performance by providing nutrition
to the fibroblasts in the vessel wall and by preventing thrombosis, enhanced endothelial viability
may, on the other hand, lead to increased antigenicity of the allograft after implantation
(34). The endothelial cell plays a central role in antigen presentation and is probably the most
immunogenic component of the vascular transplant (35). The low antigenic properties of a
glycerol-preserved skin allograft are probably due to the absence of viable cells. Although an
acellular matrix remained after glycerolization of rat aortic arteries, the structural architecture
of the vessel wall was unaffected. Preservation of only an acellular structure probably leads to
better graft function after implantation, because the endothelial and smooth muscle cells are
major causes of arterial graft rejection (36;37). The extracellular matrix, consisting of elastin and
collagen networks is obviously less immunogenic (38). Although the quality of endothelial and
smooth muscle cells is reduced after cryopreservation and cold storage, the remaining viable cells
still induce an immunological reaction. From this point of view, the absence of viable cells after
glycerol preservation is an advantage compared to other preservation methods.
The elastin bundle width and distance between bundles were measured to examine wether
the extracellular matrix was altered due to the glycerolization process. Alterations in the
extracellular matrix could have implications for the ingrowth of fibroblasts, smooth muscle cells
and endothelial cells (39).
The elastin bundle distances measured in our present study were similar to the results of
Berry et al (40) who found approximately 7.5 µm as mean distance between two elastic lamellae
in the aorta of adult rats. The results from our study confirm that the extracellular achitecture of
the vessel wall after glycerolization was preserved.
We used confocal laser scanning microscopy to analyse the orientation of the extracellular
matrix components after glycerol preservation. This technique was previously applied in our
institution to study collagen bundle architecture and orientation in normal and scar skin tissue.
The Fast Fourier Transformation is a mathematical method to calculate the periodicity and
Fahner.indd 52 5-5-2014 14:35:10

Morphological and functional alterations in glycerol preserved rat aortic allografts | 53
3
orientation of structures, e.g. collagen bundles, and can be represented as a power plot (41).
Fourier image analysis was shown to be a superior method to measure collagen orientation
compared to subjective histological evaluation (42). In our present study, we demonstrated that
glycerol preservation did not disturb the collagen bundle orientation in the extracellular matrix
in the rat aorta.
Due to the observed defragmentation of the endothelial cells, they were no longer able to
initiate any contraction or relaxation response, which was in accordance with the results of the
viability testing experiments. Futher experiments need to be performed in vivo to show whether
or not these endothelial cell remnants still induce any immunological reaction and how they may
have modified thrombogenicity of the luminal surface.
Conclusions
In this study, we demonstrated that glycerol preservation of rat aortic allografts resulted
in a nonviable structure that maintained the mechanical integrity and extracellular matrix
characteristics of fresh aorta segments. A significant decrease in media thickness was shown in
aorta segments after preservation in low (30/50/75 %) as well as high (70/85/98 %) concentrations
of glycerol, compared to intermediate (50/70/85 %) and control segments. Alterations in glycerol
concentration and incubation periods did not significantly influence breaking strength and
bursting-pressure. These results encourage us to test the concept of glycerol preservation of
arterial allografts in a vascular transplantation model.
Acknowledgements
The authors thank Ms M-J Mathy for excellent assistance with the isometric tension measurements
and Ms G. E. E. van Noppen for editorial comments.
Fahner.indd 53 5-5-2014 14:35:10

54 | Chapter 3
Reference List
(1) Johnson WC, Lee KK. A comparative evaluation of polytetrafluoroethylene, umbilical vein, and saphenous vein bypass grafts for femoral-popliteal above-knee revascularization: a prospective randomized Department of Veterans Affairs cooperative study. J Vasc Surg 2000; 32(2):268-277.
(2) Curtil A, Pegg DE, Wilson A. Freeze drying of cardiac valves in preparation for cellular repopulation. Cryobiology 1997; 34(1):13-22.
(3) Hu DJ, Basti S, Bryar PJ. Staining characteristics of preserved human amniotic membrane. Cornea 2003; 22(1):37-40.
(4) Feryha S, Ercan F, Arbak S. Scanning electron microscopic study of cold-stored small bowel: comparison of Euro-Collins and Lactated Ringer’s solutions. Dig Dis Sci 2003; 48(5):1006-1012.
(5) Debeer P, Decorte R, Delvaux S, Bellemans J. DNA analysis of a transplanted cryopreserved meniscal allograft. Arthroscopy 2000; 16(1):71-75.
(6) Basile AR. A comparative study of glycerinized and lyophilized porcine skin in dressings for third-degree burns. Plast Reconstr Surg 1982; 69(6):969-974.
(7) Burleson R, Eiseman B. Nature of the bond between partial-thickness skin and wound granulations. Surgery 1972; 72(2):315-322.
(8) Hoekstra MJ, Kreis RW, Du Pont JS. History of the Euro Skin Bank: the innovation of preservation technologies. Burns 1994; 20 Suppl 1:S43-S47.
(9) Martin B, Linwood FT. A study of the inhibitory concentrations of glycerine-sorbitol combinations on the growth of microorganisms. J Am Pharm Ass 1957; 46:217.
(10) Richters CD, Hoekstra MJ, van Baare J, du Pont JS, Kamperdijk EW. Morphology of glycerol-preserved human cadaver skin. Burns 1996; 22(2):113-116.
(11) van Baare J, Buitenwerf J, Hoekstra MJ, Du Pont JS. Virucidal effect of glycerol as used in donor skin preservation. Burns 1994; 20 Suppl 1:S77-S80.
(12) van Baare J, Cameron PU, Vardaxis N, Pagnon J, Reece J, Middelkoop E et al. The 1998 Lindberg Award. Comparison of glycerol preservation with cryopreservation methods on HIV-1 inactivation. J Burn Care Rehabil 1998; 19(6):494-500.
(13) van Baare J, Ligtvoet EE, Middelkoop E. Microbiological evaluation of glycerolized cadaveric donor skin. Transplantation 1998; 65(7):966-970.
(14) Fung yc. Collagen. In: Springer-Verlag, editor. Biomechanics Mechanical properties of living tissues. New York: 1990: 252-265.
(15) Vischjager M, Van Gulik TM, Kromhout JG, Van Marle J, Pfaffendorf M, Klopper PJ et al. Morphology and function of preserved microvascular arterial grafts: an experimental study in rats. Ann Vasc Surg 1997; 11(3):284-291.
(16) van Zuijlen PP, Lamme EN, van Galen MJ, van Marle J, Kreis RW, Middelkoop E. Long-term results of a clinical trial on dermal substitution. A light microscopy and Fourier analysis based evaluation. Burns 2002; 28(2):151-160.
(17) de Vries HJ, Enomoto DN, van Marle J, van Zuijlen PP, Mekkes JR, Bos JD. Dermal organization in scleroderma: the fast Fourier transform and the laser scatter method objectify fibrosis in nonlesional as well as lesional skin. Lab Invest 2000; 80(8):1281-1289.
(18) Alonso M, Segura RJ, Prada C, Caeiro S, Cachaldora JA, Diaz E et al. Cryopreserved arterial homografts: preliminary results in infrageniculate arterial reconstructions. Ann Vasc Surg 1999; 13(3):261-267.
(19) Dardik H, Wengerter K, Qin F, Pangilinan A, Silvestri F, Wolodiger F et al. Comparative decades of experience with glutaraldehyde-tanned human umbilical cord vein graft for lower limb revascularization: an analysis of 1275 cases. J Vasc Surg 2002; 35(1):64-71.
(20) Timaran CH, Stevens SL, Freeman MB, Goldman MH. Infrainguinal bypass grafting using lyophilized saphenous vein allografts for limb salvage. Cardiovasc Surg 2002; 10(4):315-319.
Fahner.indd 54 5-5-2014 14:35:10

Morphological and functional alterations in glycerol preserved rat aortic allografts | 55
3
(21) Crowe D, O’Loughlin K, Knox L, Mitchell G, Hurley J, Romeo R et al. Morphologic change in rabbit femoral arteries induced by storage at four degrees Celsius and by subsequent reperfusion. J Vasc Surg 1995; 22(6):769-779.
(22) Wolff KD, Dienemann D. Vessel preservation with glycerol: an experimental study in rats. J Oral Maxillofac Surg 1990; 48(9):914-918.
(23) Bruel A, Ortoft G, Oxlund H. Inhibition of cross-links in collagen is associated with reduced stiffness of the aorta in young rats. Atherosclerosis 1998; 140(1):135-145.
(24) Pitt TT, Humphries NL. Microarterial anastomoses in the rat: the influence of different suture materials on the patency, strength and the electron microscopic appearance of the vessels. Br J Plast Surg 1982; 35(2):150-155.
(25) von Smitten K, Jiborn H, Ahonen J. Bursting strength of syngeneic aortic vein grafts in the rat. Acta Chir Scand 1981; 147(2):115-119.
(26) Ruiz-Razura A, Lan M, Hita CE, Khan Z, Hwang NH, Cohen BE. Bursting strength in CO2 laser-assisted microvascular anastomoses. J Reconstr Microsurg 1988; 4(4):291-296.
(27) Lauritzen C, Bagge U. A technical and biomechanical comparison between two types of microvascular anastomoses. An experimental study in rats. Scand J Plast Reconstr Surg 1979; 13(3):417-421.
(28) Kolb S, Wray RC, Weeks PM. Bursting strength of microarterial repairs. Surg Forum 1979; 30:531-533.
(29) Noel AA, Gloviczki P, Cherry KJ, Jr., Safi H, Goldstone J, Morasch MD et al. Abdominal aortic reconstruction in infected fields: early results of the United States cryopreserved aortic allograft registry. J Vasc Surg 2002; 35(5):847-852.
(30) Moriyama S, Utoh J, Murai Y, Hagiwara S, Kunitomo R, Nishi K et al. Functional, metabolic, and histological changes of vascular tissues after warm ischemia. Ann Thorac Cardiovasc Surg 2001; 7(3):143-149.
(31) Vischjager M, Van Gulik TM, Kromhout JG, Van Marle J, Pfaffendorf M, Klopper PJ et al. Morphology and function of preserved microvascular arterial grafts: an experimental study in rats. Ann Vasc Surg 1997; 11(3):284-291.
(32) Vischjager M, Van Gulik TM, Van Marle J, Pfaffendorf M, Jacobs MJ. Function of cryopreserved arterial allografts under immunosuppressive protection with cyclosporine A. J Vasc Surg 1996; 24(5):876-882.
(33) Muller-Schweinitzer E, Mihatsch MJ, Schilling M, Haefeli WE. Functional recovery of human mesenteric and coronary arteries after cryopreservation at -196 degrees C in a serum-free medium. J Vasc Surg 1997; 25(4):743-750.
(34) Christy JP, Lupinetti FM, Mardan AH, Thompson SA. Endothelial cell viability in the rat aortic wall. Ann Thorac Surg 1991; 51(2):204-207.
(35) Pober JS, Collins T, Gimbrone MA, Jr., Libby P, Reiss CS. Inducible expression of class II major histocompatibility complex antigens and the immunogenicity of vascular endothelium. Transplantation 1986; 41(2):141-146.
(36) Salomon RN, Hughes CC, Schoen FJ, Payne DD, Pober JS, Libby P. Human coronary transplantation-associated arteriosclerosis. Evidence for a chronic immune reaction to activated graft endothelial cells. Am J Pathol 1991; 138(4):791-798.
(37) Hayry P, von Willebrand E, Parthenais E, Nemlander A, Soots A, Lautenschlager I et al. The inflammatory mechanisms of allograft rejection. Immunol Rev 1984; 77:85-142.
(38) Ellingsworth LR, DeLustro F, Brennan JE, Sawamura S, McPherson J. The human immune response to reconstituted bovine collagen. J Immunol 1986; 136(3):877-882.
(39) Walles T, Herden T, Haverich A, Mertsching H. Influence of scaffold thickness and scaffold composition on bioartificial graft survival. Biomaterials 2003; 24(7):1233-1239.
Fahner.indd 55 5-5-2014 14:35:10

56 | Chapter 3
(40) Berry CL, Sosa-Melgarejo JA, Greenwald SE. The relationship between wall tension, lamellar thickness, and intercellular junctions in the fetal and adult aorta: its relevance to the pathology of dissecting aneurysm. J Pathol 1993; 169(1):15-20.
(41) Russ JC, editor. Processing images in frequency space. The image processing handbook. Boca Raton: CRC Press, 1995: 283-346.
(42) van Zuijlen PP, de Vries HJ, Lamme EN, Coppens JE, van Marle J, Kreis RW et al. Morphometry of dermal collagen orientation by Fourier analysis is superior to multi-observer assessment. J Pathol 2002; 198(3):284-291.
Fahner.indd 56 5-5-2014 14:35:10

4Glycerol preserved arterial allografts
evaluated in the infrarenal rat aorta
P.J. Fahner1, M.M. Idu1, T.M. van Gulik1, B. van Wijk1, A.C. van der Wal2, D.A. Legemate1
1Department of Surgery and 2Department of PathologyAcademic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
Eur Surg Res 2009;42:78-86
Fahner.indd 57 5-5-2014 14:35:10

58 | Chapter 4
Abstract
Background. Vascular transplantation has become an alternative for prosthetic grafts. Suitable
storage methods for vascular allografts are therefore necessary. For small calibre arterial
allografts, cryopreservation and cold storage showed discouraging results. Since glycerol
preservation proved effective for the storage of skin allografts, this preservation method was
investigated for vascular allografts using a rat aortic transplantation model.
Methods. Glycerol preserved allografts (GA) were transplanted to the infrarenal aorta (n=18) in
Wistar rats. A control group (n=18) underwent immediate auto transplantation (AU) of an equal
length of aorta.
Results. Cumulative graft patency at 90 days follow-up was 93% for AU and 78% for GA (ns).
No aneurysm formation was detected in both groups. Intraluminal endothelial cell coverage,
integrity of the media and smooth muscle cell repopulation were comparable in both groups.
Intimal thickness was less in GA compared to AU and inflammatory reaction in the adventitia
was diminished in GA.
Conclusion. Glycerol preserved allografts were successfully grafted with an acceptable patency
rates if compared with autografts, while intima hyperplasia and adventitial inflammatory reaction
were less.
Fahner.indd 58 5-5-2014 14:35:10

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 59
4
Introduction
Transplantation of small diameter allografts is an alternative for patients who need an infrainguinal
arterial bypass graft, especially if autologous veins cannot be used. Vascular allografts require
proper storage techniques to ensure instantaneous availability. Owing to lower or absent
antigenic potential, preserved vascular allografts are by far superior to fresh allografts. Fresh
Brown Norway rat aorta segments induced a higher inflammatory reaction when subcutaneously
implanted in Lewis recipients compared to cryopreserved and glutaraldehyde preserved segments.
Cryopreserved aorta segments were stored for two weeks and glutaraldehyde segments for
three days before implantation (1). Different preservation methods such as cryopreservation,
glutaraldehyde tanning and cold storage have been the focus of extensive research for several
decades (2). Allograft function is hampered by antigenicity and graft rejection which can lead to
graft dilatation, intimal cell proliferation and graft rupture. Studies on cold-stored allografts have
been unsuccessful, due to disintegration and rapid rejection of the graft material. In the study
of van Reedt Dortland et al (3), cold-stored venous homografts, denatured for at least 6 weeks,
were used in femorodistal arterial reconstructions in patients when a suitable autologous vein was
not available. These grafts developed aneurysms in 58% after 5 years. Rebane et al performed
infrainguinal reconstructions for limb salvage in 107 patients. The venous allografts were cold
stored up to 10 days. Early thrombosis, indicating acute rejection, occurred in 16% and 5 year
graft patency rate was only 20% (3;4). Cryopreservation on the other hand has been extensively
used as a preservation method in the clinical setting, but mainly for large calibre arterial vessels
such as aortic allografts. Long-term patency of small calibre cryopreserved vascular grafts is poor
with reported patency rates of less than 50% at one year (5-7). Therefore, better preservation
techniques are necessary to improve the patency rate of small diameter vascular allografts.
Research on preservation techniques of skin allografts (8-10) showed that glycerol preservation
is superior to cryopreservation in regard to graft acceptance and immunogenicity. Glycerol skin
allografts, with a storage life of at least 2 years, were evaluated in 39 patients with extensive
third-degree burns. Cryopreserved allografts failed before epithelialisation was established
and glycerol allografts results in a complete graft take in 73% at one week postoperative. If
glycerol allografts were applied, wound epithelialisation by autologous epithelium was enhanced
compared to fresh-frozen allografts (11). Glycerol preservation of skin allografts attenuates
allograft reaction and has antiviral and antibacterial properties (12-17). The fact that glycerol
preservation results in a tissue matrix without living cells diminishes immunogenicity of the graft.
Previous experiments in our laboratory demonstrated that glycerol preservation of the rat aorta
preserves the biomechanical characteristics and architecture of the vessel wall (18).
The aim of this study was to evaluate in an aortic transplantation model in the rat i) long-term
patency of glycerol preserved arterial allografts in the infrarenal aortic position ii) aneurysmal
Fahner.indd 59 5-5-2014 14:35:11

60 | Chapter 4
degeneration of glycerol preserved arterial allografts, iii) histological features of the glycerol
preserved vessel wall after implantation, with emphasis on restoration of endothelial cell lining,
inflammatory response, degenerative changes of the vessel wall and intimal hyperplasia.
Materials and methods
Preparation of glycerol preserved allografts
The glycerolization protocol consists of three stages;
1. Incubation in a glycerol 50% solution for 4 hours at room temperature
2. Incubation in a glycerol 70% solution for 3 hours at 33°C
3. Incubation in a glycerol 85% solution for 3 hours at 33°C
After completion of the protocol, the grafts were stored in glycerol 85% for 12 hours at 4°C.
Previous in-vitro experiments in our laboratory showed that this protocol resulted in optimal
glycerol preservation of arterial allografts (18).
Experimental design
The experimental protocol was approved by the Animal Ethics Committee of the Academic
Medical Centre, University of Amsterdam, The Netherlands. Male outbred Wistar rats (Unilever
and Harlan), 300-370 g, were used as donors and recipients of aortic grafts (Charles Rivers,
Maastricht, The Netherlands). The animals were housed one week prior to the experiments,
had free access to water and chow and maintained on a 12-hour light-dark cycle. All operative
procedures were performed under clean but not sterile conditions. In the experimental (allograft)
group a 10 mm long segment of the infrarenal abdominal aorta was excised and a donor glycerol
preserved abdominal aortic allograft of similar length was implanted as an interposition graft. In
the control (autograft) group a segment of 10 mm of the infrarenal abdominal aorta was excised
and immediately reanastomosed to restore aortic continuity. Before implantation the glycerol
preserved aortic allograft was immerged in saline to diminish the tissue content of glycerol in the
graft at 33°C for at least 20 minutes. Both control and experimental groups consisted of eighteen
rats. Scheduled sacrifice was on post-operative day 1, 3, 7, 14, 30 and 90 respectively. On these
days three animals were sacrificed in both experimental and control group.
Aortic allograft implantation and harvesting
All animals were anesthetized by inhalation of a mixture of O2/N2O 1:1 and isoflurane 0.8 - 2.0%.
After endotracheal intubation the rats were ventilated and anaesthesia was maintained with
the same mixture. The rats were placed on a heating pad and positioned under a heating lamp
Fahner.indd 60 5-5-2014 14:35:11

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 61
4
to maintain a rectally measured core temperature between 36°C and 37°C. After a midline
laparotomy, the infrarenal abdominal aorta was exposed, clamped and a 10 mm segment was
excised using an operation microscope (Zeiss™, Germany). The grafts and the aortic stumps were
flushed with saline. No heparin or anticoagulant medication was used in the study. The end-
to-end anastomoses were performed with interrupted 9.0 sutures (Ethylon™). After restoring
the blood flow intra-operative patency was determined by visualization of a pulse distally to
the graft. Operation time and aortic clamping time averaged 90 and 45 minutes, respectively.
After sacrifice of the rat the graft was harvested en-bloc, flushed with saline and fixed in 10%
formaldehyde.
Duplex scanning and angiography
To assess graft patency and aneurysm formation, defined as a consistent 50% increase in graft
diameter, colour duplex scanning (19) and angiography were performed. Duplex scanning
(Hewlett Packard Sonos 5000) was performed under general anaesthesia using a miniature
15 MHz probe at post-operative day 1, 3, 7, 14, 30 and 90 respectively. The abdominal aorta was
examined from the renal arteries to the aortic bifurcation. Diameters of the aorta were measured
in B-mode on the following five locations; proximal native vessel, proximal anastomosis, mid-
graft, distal anastomosis and distal native vessel. To investigate the presence of flow-limiting
lesions peak systolic velocity (PSV) was measured. The PSV-max was defined as the maximum
peak systolic velocity in a stenosis, and the PSV-ratio as the PSV in the stenosis divided by the PSV
in the pre- or poststenotic region. A significant stenosis was defined as a PSV-ratio of ≥ 2.5 or a
PSV-max of ≥ 250 cm/sec. Before excision of the aortic allograft a digital subtraction angiography
(DSA) was performed (Philips™) by injection of three ml radio contrast solution (Visipaque™
320 mg I/ml, Nycomed, The Netherlands) through a catheter introduced into the carotid artery.
Preparation and histological staining of specimens
All explanted graft segments were flushed with 10% buffered formaldehyde, dehydrated and
embedded in paraffin for light microscopic examination. Grafts were divided into three equal
segments of 3-4 mm length: one proximal segment including the proximal anastomosis, one
midgraft segment and one distal segment including the distal anastomosis. Of each segment,
5 µm sagittal sections were cut and stained with haematoxylin-eosin (H&E), picosirius red (PSR)
and Elastica van Gieson (EvG) respectively. PSR stains all types of collagen bright red and EvG
stains elastic fibres deep black. Two additional sections were mounted for immunohistochemistry.
We used Anti-vWF (von Willebrand factor) antibody (DAKO, dilation 1: 100, visualizes all
endothelial cells) and anti-alpha-actin-antibody (DAKO, dilution 1: 400, visualizes vascular smooth
muscle cells at all stages of maturation) as primary antibodies. For detection of immunoreactivity
Fahner.indd 61 5-5-2014 14:35:11

62 | Chapter 4
we applied a streptavidin biotin complex method with DAB as substrate. Fresh full thickness
arterial wall was used as positive control tissue.
Histopathologic evaluation of grafts
Endothelial cell lining, integrity of elastin meshwork of the media, presence of medial smooth
muscle cells and adventitial inflammation were assessed on a semi quantitative basis. Two
observers (PJF and BvW) independently scored all sections which were blinded for study group
and follow-up period.
Morphometry
For morphometric analyses we used Image Pro-4 software (Image Pro-plus 4.5) (20). The
specimens were evaluated with a 10 times magnification objective of the light microscope
(Olympus, BX60). Intima thickness (distance between inner surface and internal elastica lamina)
and media thickness (distance between inner and outer elastica lamina) were automatically
measured at 6 places in each specimen and mean values were calculated.
Collagen content of the media and adventitia were quantified planimetrically on Picosirius
red stains for which we used grey scale detection with fixed threshold.
Statistical analysis
All statistical analyses were performed with GraphPad Prism 4.00 programme (GraphPad
Software, San Diego, USA). For comparison of cumulative graft patency data the log rank test
was used. Differences between groups in the morphological and morphometric analyses were
tested with Student-t test for continuous data and with the Mann-Whitney U test for comparison
of the semi-quantitative scores. The Kruskal-Wallis test was used to compare more than two
unpaired groups. A p-value of less than 0.05 was considered statistical significant.
RESULTS
Animal survival and graft patency
All animals survived the postoperative period until scheduled sacrifice, except one in the glycerol
group which was sacrificed at day 6 postoperatively because of severe weight loss. Macroscopic
examination of the harvested aorta revealed occlusion of the allograft. Of all other animals,
4 grafts occluded, one in the control group and three in the glycerol group. All occlusions
occurred within the first 3 postoperative days as was determined by duplex scanning. Cumulative
graft patency at 3 months follow-up for the autografts and the glycerol preserved allografts was
93% and 78% respectively (p = 0.14).
Fahner.indd 62 5-5-2014 14:35:11

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 63
4
PNal PNau PAal PAau MGal MGau DAal DAau DNal DNau0
25
50
75
100
125
150
175
localization of measurement in native vessel and graft
mea
n PS
V a
t da
y 7(
cm/s
ec)
Figure 1. Mean peak systolic velocities (cm/sec) of glycerol allografts and autografts after 7 days follow-up. Error bars depict SEM. PN = proximal native vessel, PA = proximal anastomosis, MG = midgraft, DA = distal anastomosis, DN = distal native vessel, al = glycerol allograft, au = autograft. (MGal and MGau; p< 0.01).
= autograft = glycerol allograft
PNal PNau PAal PAau MGal MGau DAal DAau DNal DNau0
102030405060708090
100110120130
localization of measurement in native vessel and graft
mea
n PS
V a
t da
y 9
0 (c
m/s
ec)
Figure 2. Mean peak systolic velocities (cm/sec) of glycerol allografts and autografts after 90 days follow-up. Error bars depict SEM. PN = proximal native vessel, PA = proximal anastomosis, MG = midgraft, DA = distal anastomosis, DN = distal native vessel, al = glycerol allograft, au = autograft. (PNal and PNau; p< 0.01).
= autograft = glycerol allograft
Fahner.indd 63 5-5-2014 14:35:11

64 | Chapter 4
Duplex sonography and angiographic parameters
The mean PSV at the different sites of the graft in both groups are represented in figure 1 and
2. Two autografts and one allograft showed a significant stenosis. In the midgraft part of the
transplanted allografts the mean PSV after 7 days follow-up was significantly lower compared
to the autografts (p< 0.01). No significant difference was detected after one months and after
3 months follow-up the mean PSV was consistently lower in the allografts at all locations although
only significantly different in the proximal native vessel in the transplanted allografts (p< 0.01).
No aneurysm formation or graft-disintegration was found during follow-up. After 7 and
90 days follow-up no significant difference in graft diameter was measured between both
graft types. After one month the mean diameter of the allografts was significantly higher at
the proximal anastomosis (p< 0.01) and midgraft (p= 0.02) as shown in figure 3. Percentage
graft stenosis on angiograms was not encountered in the midgraft segments, neither in the
allografts or autografts. In 4 autografts a stenosis was measured at the proximal anastomosis
and in 6 autografts at the distal anastomosis. Three glycerol allografts developed a stenosis at
the proximal anastomosis and one at the distal anastomosis. No significant difference existed
between autografts and allografts (p= 0.17).
Morphological and morphometric results
Intima
Endothelial cell (EC) coverage was assessed with anti-Vwf immunostaining. When pooling
the scores of the endothelial cell coverage at all time points for both graft types, intraluminal
endothelial cell coverage was more abundant in the proximal and distal segments compared to
the midgraft segments (p= 0.26). Endothelial cell coverage is presented in figure 4 in relation
with implantation time. There are no consistent differences in endothelial cell coverage between
autografts and glycerol grafts during the implantation period.
Intimal thickness was evaluated in the same segments using H&E stained sections. Increase in
intimal thickness, interpreted as intimal hyperplasia, was first observed in the glycerol allografts
at day 3 and in the autografts at day 14. When pooling the neo-intimal thickness of all graft
segments, intimal thickness was significantly greater in the autografts compared to the glycerol
preserved allografts after 1 and 3 months follow- up (figure 5, p< 0.01).
Media
The integrity of the elastic meshwork of the media, evaluated in Elastica van Gieson stained
sections, did not differ significantly between both types of grafts (p = 0.64). The length of
implantation period did not affect elastin network integrity which was comparable in all graft
segments.
Fahner.indd 64 5-5-2014 14:35:11

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 65
4PAal PAau MGal MGau DAal DAau
0
1
2
3
localization in graft
graf
t d
iam
eter
at
day
30
(mm
)
Figure 3. Mean graft diameter measurements (mm) of allografts and autografts after 30 days follow-up. Error bars depict SEM. PA = proximal anastomosis, MG = midgraft, DA = distal anastomosis, al = glycerol allograft, au = autograft. (PAal and PAau; p> 0.01, MGal and MGau; p= 0.02).
= autograft = glycerol allograft
gl1 a1 gl3 a3 gl7 a7 gl14 a14 gl30 a30 gl90 a90
0
1
2
3
4
follow up (days)
mea
n to
tal s
core
Figure 4. Mean score of intraluminal endothelial cells (Factor VIII staining) after pooling of results for proximal, midgraft and distal segments. Error bars depict SEM. Score 0 = complete coverage, 1 = some endothelial lining, 2 = no endothelial cells. gl = glycerol allograft, a = autograft.
= autograft = glycerol allograft
Fahner.indd 65 5-5-2014 14:35:11

66 | Chapter 4
0
10
20
30
40
50
60
follow up (days)
intim
al t
hick
ness
(μm
)
1 3 7 14 30 90
Figure 5. Pooled results of proximal, midgraft and distal mean intimal thickness of allografts and autografts. Error bars depicts SEM.
= autograft = glycerol allograft
Medial width in proximal, mid and distal graft segments was significantly less in the glycerol
allografts compared to the autografts (p<0.01). Figure 6a shows a mid segment of a glycerol
allograft and figure 6b shows a mid segment of an autograft. Differences were most prominent
after day-1 and day-3 postoperatively and diminished during further follow-up. The pooled mean
thickness (SD) was 52.2 (12.9) μm for glycerol allografts and 71.1 (27.3) μm for autografts.
In all segments, apart from scant mononuclear infiltration around the sutures, no inflammatory
reaction was observed in both graft types.
The pooled mean collagen content of the media was lower in autografts compared to
allografts at all time points. In the autografts a decrease of the mean collagen content was
measured in the first three days postoperatively which however recovered, and after 14 days
exceeded the amount at day-1. For the glycerol allografts collagen content remained almost
similar at all time points (figure 7).
Fahner.indd 66 5-5-2014 14:35:11

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 67
4
Figure 6A. Haematoxylin-eosin staining of a glycerol allograft midgraft segment (10x).
Figure 6B. Haematoxylin-eosin staining of an autograft midgraft segment (10x). Arrows point to the media in both fi gures.
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
follow-up (days)
perc
enta
ge c
olla
gen
in m
edia
(%)
1 3 7 14 30 90
Figure 7. Results of pooled data of percentage collagen in media of glycerol allografts and autografts, referring to proximal, midgraft and distal graft segments.
= autograft = glycerol allograft
Fahner.indd 67 5-5-2014 14:35:12

68 | Chapter 4
gl1 a1 gl3 a3 gl7 a7 gl14 a14 gl30 a30 gl90 a900
1
2
3
4
5
6
7
*
follow up (days)
mea
n to
tal s
core
Figure 8. Mean score of α-smooth muscle cell (smc) staining of medial cells after pooling of results for proximal, midgraft and distal segments. Scores of all three segments were added and the mean calculated (score for single segment; 0 = > 50% smc ingrowth, 1 = < 50% smc ingrowth, 2 = some smc, n=3 for each follow-up). Mean maximal score is 3x2, mean minimal score is 3x0. * p= 0.01. Error bars depict SEM.
= autograft = glycerol allograft
Presence of smooth muscle cells in the extra cellular tissue matrix was evaluated with anti
α- smooth muscle actin immunostaining. Both graft types showed slightly lower numbers of
smooth muscle cells in the distal segments compared to the proximal and medial segments. As
expected, the highest amount of positively stained cells was found in the autograft segments
at day-1 postoperatively. In the glycerol allografts this amount diminished in the first week
postoperatively and recovered to almost the level of day three after three months follow-up
(figure 8). No consistent differences in smooth muscle cell repopulation between autografts and
glycerol allografts exist during follow-up.
Adventitial parameters
Quantification of collagen in the adventitia of both graft types and in the different graft segments
showed equal results.
Both graft types showed a higher score of inflammatory reaction at the sites of anastomosis.
The pooled score at the proximal and distal segments was lower for the glycerol allografts
Fahner.indd 68 5-5-2014 14:35:12

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 69
40 10 20 30 40 50 60 70 80 90 100
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
follow up (days)
tota
l sco
re f
or in
flam
mat
ion
Figure 9. Results of adventitial inflammation scoring in haematoxylin-eosin stained sections. Data shown are the result of pooling of the proximal, medial and distal segments ( = allografts, ----- = autografts). Score 0 = some lymphocytes, 1 = clusters of lymphocytes, 2 = diffuse infiltration.
compared to the autografts. This indicates a less extensive inflammatory reaction in the
glycerol allografts after implantation. The pooled score of the midgraft segments was slightly
lower in the allografts. The calculated total inflammatory score for proximal, medial and distal
segments reached its maximum earlier in glycerol grafts compared to autografts (day 14 and day
30 respectively). During follow-up a decrease in inflammation was measured in both groups,
inflammation being less in the allografts (figure 9).
Fahner.indd 69 5-5-2014 14:35:12

70 | Chapter 4
DISCUSSION
The infrarenal rat aortic replacement model is well established in the investigation of alternatives
for the venous or arterial autograft (21-24). It is clear that for the reconstruction of large arteries
synthetic vascular grafts (e.g. ePTFE or Dacron) are the conduits of choice. However, for small
diameter reconstructions such prosthetic grafts have low cumulative patencies, ranging from
24% to 58% after three years (25;26). These results have stimulated research in alternatives to
prosthetic grafts such as preserved vascular allografts and xenografts, and the use of biomaterials
to serve as a vascular tissue matrix (27;28). Extra cellular matrix scaffolds can serve as templates
for cellular attachment and ingrowth of recipient cells (29;30). Main efforts in this field have been
directed to minimizing immunogenicity and inflammation of the graft, while preserving extra
cellular matrix integrity and mechanical properties (31).
More details of the glycerol preservation process in skin allografts were clarified by Huang
et al and Ross et al. In the permeation of glycerol in skin a process of diffusion and binding is
involved. Both histological and ultra structural analysis showed that the integrity of skin structure
was maintained and degradation of the skin avoided due to effective sequestration of water
(32;33). The preservation of connective tissue after glycerolization was confirmed by glycerol
preservation of ovine cardiac valve allografts and mechanical properties maintained for 6 months
after implantation in the ovine descending aorta (34;35).
In the present study, glycerol preserved aortic allografts were examined as an alternative
biomaterial for arterial grafting. Patency rate after 3 months was 78% for glycerol preserved
allografts. These results are in accordance with the high patency rates after 100 days reported
by Wolff et al who transplanted rat aortic allografts and femoral veins preserved in 98% glycerol
(36). In the study of Wolff, however, no angiography or sonography was performed rendering
reliability of patency detection uncertain. Also possible aneurysm formation could have easily
been missed in this report. In our study aneurysm formation could be ruled out and owing to
the histological examinations new insight was provided into the performance of the glycerol
preserved allografts after implantation. The results of the present study and that of the study of
Wolff are different from the total graft occlusions after two weeks reported by Bishop et al (37).
In this study glycerol preserved DA strain rat femoral vein was transplanted into the common iliac
artery of Lewis rats. In the same study hind leg and foreleg veins were preserved in glycerol 98%
and transplanted to the common carotid artery. After six month of follow up a patency rate of
64% was reached. They reported a very strong allograft reaction as a result of the two rat strains
which obviously influenced patency rates.
Two pathways are involved in the immune response against allografts in transplant
vasculopathy. At first, donor endothelial cells and antigen presenting cells (APC) of the allograft
induces proliferation of recipient T- cells. Donor MHC I molecules on the surface of transplanted
Fahner.indd 70 5-5-2014 14:35:12

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 71
4
cells induces T- cell activation (38). Secondly, recipient APC’s present donor MHC and minor
antigens from the allograft to recipient T- cells. This requires recognition of the allogens as
peptides bound to recipient MHC II molecules (39;40).
Direct sensitization of the recipient by Langerhans cells, which have a strong expression
of MHC II molecules and are the APC’s of the skin, will be blocked in glycerol preserved skin
allografts since active migration of Langerhans cells from the allograft is no longer possible due
to cell death after glycerolization.
In the current experiments we used outbred Wistar rats. It could be debated if intimal
hyperplasia would have been more distinct when immunologically more different animal strains
had been used for our aortic transplantation experiments. Osako et al (41) demonstrated more
intimal hyperplasia in fresh and cryopreserved allografts compared to fresh and cryopreserved
isografts in their Lewis rat aortic transplantation model. However, Takeishi et al (42), who
performed cryopreserved femoral artery transplantation in Lewis and Brown Norway rats, found
quite similar patency rates for isografts (100% and 87%) and allografts (100% and 78%) after 1
and 3 months follow up.
Although it is difficult to assess the effect of genetically incompatibility between different
rat strains in relation to patency rates, one should be aware of the genetically relation when
comparing results of vascular implantation studies in which different rat strains were used. The
difference in above mentioned patencies is in agreement with the lower genetically uniformity
between DA and Lewis rats compared to BN and Lewis rat strains. This is confirmed by the higher
amount of cellular damage in DA donor livers compared to BN donor livers in an orthotopic rat
liver transplantation model (43).
The role of intraluminal endothelial cells is crucial in vascular graft patency. Several studies
have been performed to examine preservation methods for maintaining endothelial cell viability.
Preservation of luminal endothelial cell lining in University of Wisconsin (UW) solution appears
more successful compared to phosphate buffered saline (PBS) for up to seven days of cold storage
of rat carotid arteries (44). Longer periods of cold storage however led to endothelial cell death
and incomplete luminal coverage, which resulted in intimal hyperplasia and graft occlusion in
transplanted rabbit femoral arteries (45). Although on the one hand, the best thromboresistant
graft surface is luminal lining with host endothelial cells, transplanted donor endothelial cells on
the other hand, evoke an immunogenic response that will induce pathologic changes in graft
wall architecture (46;47). Furthermore, initial absence of allograft endothelium did not seem to
influence graft patency in the experiments of Komorowska et al (48) in which cryopreserved
femoral arteries were transplanted in a rat model. The absence of endothelium is probably
an advantage of glycerol preservation since no viable endothelial cells are transplanted while
the extracellular tissue matrix is used as template for recipient cell attachment and ingrowth
(49;50). Our study reveals endothelial cells in glycerol preserved allografts after transplantation
Fahner.indd 71 5-5-2014 14:35:12

72 | Chapter 4
which obviously originate from repopulating cells of the recipient. Theoretically this has the
advantage of the development of an antithrombotic luminal surface without the disadvantage
of immunologic reactions after transplantation of viable donor cells (51). Another important
finding is the lesser intimal hyperplasia as measured after one and three months and the lower
inflammatory response after one month follow-up in glycerol preserved allografts. Since intimal
hyperplasia is the common healing response to arterial wall injury and occurs subsequent to
immunoinflammatory endothelial injury, glycerol preservation has potential advantages (52).
The absence of living endothelial cells in the glycerol allografts unable those to induce the
cascade of cellular damage after transplantation which results in proliferation of smooth muscle
cells and fibroblasts involved in intimal hyperplasia. This will be valuable in the application of
glycerol allografts in humans since endothelialization is prolonged in humans (53;54). Although
the endothelialization of prosthetic grafts is at least 7.5 times more pronounced in any animal
model compared to human (including rat, dog and baboon models), interpretation of graft
endothelialization in rat models to humans is complicated by graft dimension difference (55).
In conclusion, in our aortic transplantation model in the rat, glycerol preserved allografts
were successfully grafted and had acceptable graft patencies if compared with autografts in
conjunction with diminished intimal hyperplasia and in the absence of aneurysmatic matrix
degeneration. These results warrant further investigation of this preservation method in a
clinically relevant, large animal model.
Fahner.indd 72 5-5-2014 14:35:12

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 73
4
Reference List
(1) Moriyama S, Utoh J, Sun LB, Tagami H, Okamoto K, Kunitomo R, et al. Antigenicity of cryopreserved arterial allografts: comparison with fresh and glutaraldehyde treated grafts. ASAIO J 2001 May;47(3):202-5.
(2) Dardik H, Wengerter K, Qin F, Pangilinan A, Silvestri F, Wolodiger F, et al. Comparative decades of experience with glutaraldehyde-tanned human umbilical cord vein graft for lower limb revascularization: an analysis of 1275 cases. J Vasc Surg 2002 Jan;35(1):64-71.
(3) van Reedt Dortland RW, van Leeuwen MS, Steijling JJ, Theodorides T, van Vroonhoven TJ. Long-term results with vein homograft in femoro-distal arterial reconstructions. Eur J Vasc Surg 1991 Oct;5(5):557-64.
(4) Rebane E, Tikko H, Tunder E, Lepner U, Helberg A, Pulges A, et al. Venous allografts for infrainguinal vascular bypass. Cardiovasc Surg 1997 Feb;5(1):21-5.
(5) Albertini JN, Barral X, Branchereau A, Favre JP, Guidicelli H, Magne JL, et al. Long-term results of arterial allograft below-knee bypass grafts for limb salvage: a retrospective multicenter study. J Vasc Surg 2000 Mar;31(3):426-35.
(6) Farber A, Major K, Wagner WH, Cohen JL, Cossman DV, Lauterbach SR, et al. Cryopreserved saphenous vein allografts in infrainguinal revascularization: analysis of 240 grafts. J Vasc Surg 2003 Jul;38(1):15-21.
(7) Martin RS, III, Edwards WH, Mulherin JL, Jr., Edwards WH, Jr., Jenkins JM, Hoff SJ. Cryopreserved saphenous vein allografts for below-knee lower extremity revascularization. Ann Surg 1994 Jun;219(6):664-70.
(8) Brown JB, Fryer MP, Randall P, Lu M. Postmortem homografts as biological dressings for extensive burns and denuded areas; immediate and preserved homografts as life-saving procedures. Ann Surg 1953 Oct;138(4):618-30.
(9) Robson MC, Krizek TJ. Predicting skin graft survival. J Trauma 1973 Mar;13(3):213-7.
(10) Schechter I, Belldegrin A, Ben Basat M, Kaplan I. Prolonged retention of glutaraldehyde-treated skin homografts in humans. Br J Plast Surg 1975 Jul;28(3):198-202.
(11) Kreis RW, Vloemans AF, Hoekstra MJ, Mackie DP, Hermans RP. The use of non-viable glycerol-preserved cadaver skin combined with widely expanded autografts in the treatment of extensive third-degree burns. J Trauma 1989 Jan;29(1):51-4.
(12) Basil A. A comparative study of glycerinized and lyophilized porcine skin in dressings for third-degree burns. Plast Reconstr Surg 1982;69:969-74.
(13) de Backere AC. Euro Skin Bank: large scale skin-banking in Europe based on glycerol-preservation of donor skin. Burns 1994;20 Suppl 1:S4-S9.
(14) Richters CD, Hoekstra MJ, van Baare J, du Pont JS, Kamperdijk EW. Morphology of glycerol-preserved human cadaver skin. Burns 1996 Mar;22(2):113-6.
(15) van Baare J, Buitenwerf J, Hoekstra MJ, du Pont JS. Virucidal effect of glycerol as used in donor skin preservation. Burns 1994;20 Suppl 1:S77-S80.
(16) van Baare J, Ligtvoet EE, Middelkoop E. Microbiological evaluation of glycerolized cadaveric donor skin. Transplantation 1998 Apr 15;65(7):966-70.
(17) van Baare J, Cameron PU, Vardaxis N, Pagnon J, Reece J, Middelkoop E, et al. The 1998 Lindberg Award. Comparison of glycerol preservation with cryopreservation methods on HIV-1 inactivation. J Burn Care Rehabil 1998 Nov;19(6):494-500.
(18) Fahner PJ, Idu MM, Legemate DA, Vanbavel E, Borstlap J, Pfaffendorf M, et al. Morphological and functional alterations in glycerol preserved rat aortic allografts. Int J Artif Organs 2004 Nov;27(11):979-89.
Fahner.indd 73 5-5-2014 14:35:12

74 | Chapter 4
(19) Wessely R, Paschalidis M, Wagenpfeil S, Wegener F, Neumann FJ, Theiss W. A comprehensive approach to visual and functional assessment of experimental vascular lesions in vivo. Am J Physiol Heart Circ Physiol 2004 Jun;286(6):H2461-H2467.
(20) Blatt RJ, Clark AN, Courtney J, Tully C, Tucker AL. Automated quantitative analysis of angiogenesis in the rat aorta model using Image-Pro Plus 4.1. Comput Methods Programs Biomed 2004 Jul;75(1): 75-9.
(21) Qin F, Dardik H, Pangilinan A, Robinson J, Chuy J, Wengerter K. Remodeling and suppression of intimal hyperplasia of vascular grafts with a distal arteriovenous fistula in a rat model. J Vasc Surg 2001 Oct;34(4):701-6.
(22) Ribbe EB, Holmin T, Lowenhielm PC. Microvascular polytetrafluoroethylene (Gore-Tex) grafts in the infrarenal rat aorta. Microsurgery 1987;8(2):48-53.
(23) Tizian C, Glass KD, Demuth R. Using expanded polytetrafluoroethylene for bridging arterial microvascular defects: an experimental study with evaluation in the scanning electron microscopy. Thorac Cardiovasc Surg 1980 Aug;28(4):273-6.
(24) Zelder O, Werner HH, Jerusalem CR. The use of microvascular graft as an arterial substitute in the abdominal aorta of the rat. Microsurgery 1983;4(3):157-63.
(25) Eickhoff JH, Broome A, Ericsson BF, Buchardt Hansen HJ, Kordt KF, Mouritzen C, et al. Four years’ results of a prospective, randomized clinical trial comparing polytetrafluoroethylene and modified human umbilical vein for below-knee femoropopliteal bypass. J Vasc Surg 1987 Nov;6(5):506-11.
(26) Johnson WC, Lee KK. A comparative evaluation of polytetrafluoroethylene, umbilical vein, and saphenous vein bypass grafts for femoral-popliteal above-knee revascularization: a prospective randomized Department of Veterans Affairs cooperative study. J Vasc Surg 2000 Aug;32(2):268-77.
(27) Hilbert SL, Ferrans VJ, Jones M. Tissue-derived biomaterials and their use in cardiovascular prosthetic devices. Med Prog Technol 1988;14(3-4):115-63.
(28) Zdrahala RJ. Small caliber vascular grafts. Part I: state of the art. J Biomater Appl 1996 Apr;10(4):309-29.
(29) Stansby G, Berwanger C, Shukla N, Hamilton G. Endothelial cell seeding of vascular grafts: status and prospects. Cardiovasc Surg 1994 Oct;2(5):543-8.
(30) Williams SK, Schneider T, Kapelan B, Jarrell BE. Formation of a functional endothelium on vascular grafts. J Electron Microsc Tech 1991 Dec;19(4):439-51.
(31) Schmidt CE, Baier JM. Acellular vascular tissues: natural biomaterials for tissue repair and tissue engineering. Biomaterials 2000 Nov;21(22):2215-31.
(32) Huang Q, Pegg DE, Kearney JN. Banking of non-viable skin allografts using high concentrations of glycerol or propylene glycol. Cell Tissue Bank 2004;5(1):3-21.
(33) Ross A, Kearney JN. The measurement of water activity in allogeneic skin grafts preserved using high concentration glycerol or propylene glycol. Cell Tissue Bank 2004;5(1):37-44.
(34) Aidulis D, Pegg DE, Hunt CJ, Goffin YA, Vanderkelen A, Van HB, et al. Processing of ovine cardiac valve allografts. Effects of preservation method on structure and mechanical properties. Cell Tissue Bank 2002;3(2):79-89.
(35) Neves J, Abecassis M, Santiago T, Ramos T, Melo J, Gruys E, et al. Processing of ovine cardiac valve allografts. Implantation following antimicrobial treatment and preservation. Cell Tissue Bank 2002;3(2):105-19.
(36) Wolff KD, Dienemann D. Vessel preservation with glycerol: an experimental study in rats. J Oral Maxillofac Surg 1990 Sep;48(9):914-8.
(37) Bishop AJ, Glasby MA, Houlton JE. A morphological assessment of vein allografts preserved in glycerol and used for arterial replacement. J Cardiovasc Surg (Torino) 1987 Sep;28(5):491-7.
Fahner.indd 74 5-5-2014 14:35:12

Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta | 75
4
(38) Denton MD, Davis SF, Baum MA, Melter M, Reinders ME, Exeni A, et al. The role of the graft endothelium in transplant rejection: evidence that endothelial activation may serve as a clinical marker for the development of chronic rejection. Pediatr Transplant 2000 Nov;4(4):252-60.
(39) Watschinger B, Gallon L, Carpenter CB, Sayegh MH. Mechanisms of allo-recognition. Recognition by in vivo-primed T cells of specific major histocompatibility complex polymorphisms presented as peptides by responder antigen-presenting cells. Transplantation 1994 Feb 27;57(4):572-6.
(40) Zdoroveac A, Doebis C, Laube H, Brosel S, Schmitt-Knosalla I, Volk HD, et al. Modulation of Graft Arteriosclerosis in a Rat Carotid Transplantation Model. J Surg Res 2007 Sep 29.
(41) Osako M, Otani H, Yamamura T, Nakao Y, Hattori R, Omiya H, et al. Alloimmune response may be involved in neointimal hyperplasia in cryopreserved aortic allografts. Transplant Proc 2001 Jun;33(4):2566-70.
(42) Takeishi M, Hirase Y, Kojima T. Experimental study of cryopreserved allogeneic transfer of vessel: preliminary report 4. Microsurgery 1994;15(1):55-62.
(43) Mollevi DG, Ginesta MM, Domenech P, Serrano T, Figueras J, Jaurrieta E. Hemostatic status in long-term surviving xenografts. Surgery 2006 Jun;139(6):775-81.
(44) Vischjager M, van Gulik TM, Kromhout JG, van MJ, Pfaffendorf M, Klopper PJ, et al. Morphology and function of preserved microvascular arterial grafts: an experimental study in rats. Ann Vasc Surg 1997 May;11(3):284-91.
(45) Crowe DM, Hurley JV, Mitchell GM, Niazi Z, Morrison WA. Long-term studies of cold-stored rabbit femoral artery and vein autografts. Br J Plast Surg 1998 Jun;51(4):291-9.
(46) Marois Y, Wagner E, Paris E, Roy R, Douville Y, Guidoin R. Comparison of healing in fresh and preserved arterial allografts in the dog. Ann Vasc Surg 1999 Mar;13(2):130-40.
(47) Zhao XM, Green M, Frazer IH, Hogan P, O’Brien MF. Donor-specific immune response after aortic valve allografting in the rat. Ann Thorac Surg 1994 May;57(5):1158-63.
(48) Komorowska-Timek E, Zhang F, Shi DY, Lineaweaver WC, Buncke HJ. Effect of cryopreservation on patency and histological changes of arterial isogeneic and allogeneic grafts in the rat model. Ann Plast Surg 2002 Oct;49(4):404-9.
(49) Wang X, Lin P, Yao Q, Chen C. Development of small-diameter vascular grafts. World J Surg 2007 Apr;31(4):682-9.
(50) Yow KH, Ingram J, Korossis SA, Ingham E, Homer-Vanniasinkam S. Tissue engineering of vascular conduits. Br J Surg 2006 Jun;93(6):652-61.
(51) Borschel GH, Huang YC, Calve S, Arruda EM, Lynch JB, Dow DE, et al. Tissue engineering of recellularized small-diameter vascular grafts. Tissue Eng 2005 May;11(5-6):778-86.
(52) Gomes D, Louedec L, Plissonnier D, Dauge MC, Henin D, Osborne-Pellegrin M, et al. Endoluminal smooth muscle cell seeding limits intimal hyperplasia. J Vasc Surg 2001 Oct;34(4):707-15.
(53) Dixit P, Hern-Anderson D, Ranieri J, Schmidt CE. Vascular graft endothelialization: comparative analysis of canine and human endothelial cell migration on natural biomaterials. J Biomed Mater Res 2001 Sep 15;56(4):545-55.
(54) Rezvan A, Allen FD, Lelkes PI. Steady unidirectional laminar flow inhibits monolayer formation by human and rat microvascular endothelial cells. Endothelium 2004 Jan;11(1):11-6.
(55) Davids L, Dower T, Zilla P. The lack of healing in conventional vascular grafts. In: Zilla PP, Greisler HP, editors. Tissue engineering of vascular prosthetic grafts. Austin, Texas: R.G. Landes; 1999, p. 3-44.
Fahner.indd 75 5-5-2014 14:35:12

Fahner.indd 76 5-5-2014 14:35:12

5Comparison of preserved vascular allografts using
glycerol and University of Wisconsin solution in
a goat carotid artery transplantation model
P.J. Fahner1, D.A. Legemate1, A.C. van der Wal2, J. van Marle3, S.L.M. Peters4, C.F. van Eck1, T.M. van Gulik1, M.M. Idu1
1Department of Surgery and 2Department of PathologyAcademic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
2 Department of Pathology, AMC3 Department of Microscopic Research, AMC
4 Department of Pharmacology & Pharmacotherapy, AMC
Eur Surg Res 2012;48:64-72
Fahner.indd 77 5-5-2014 14:35:12

78 | Chapter 5
Abstract
Background. Prosthetic grafts have poor patency rates in peripheral arterial reconstructions.
Glycerol (GL)-preserved grafts are an alternative. The aim of this study was to examine patency,
graft morphology and function of GL-preserved allografts in a goat carotid artery animal
model.
Methods. The first group (n=7) underwent bilateral replacement of the carotid artery by a carotid
allograft that was preserved in GL for 1 week. In the second group (n=5), a carotid artery allograft
that was preserved in University of Wisconsin solution (UW) for 48 h was used. In the third group
(n=5), the jugular vein (autologous vein, AU) was used. The follow-up was 3 months.
Results. One UW graft and 1 GL graft occluded in the first 24 h postoperatively. Three-month
primary patency rates for GL, UW and AU grafts were 93%, 100% and 80% respectively (p =
0.39). Graft diameter was increased in UW allografts (p < 0.005), whereas GL allografts remained
unchanged. After explantation, GL allografts demonstrated contraction and relaxation capacity
and lower intimal thickness (p < 0.001).
Conclusion. GL preservation has proven to be a feasible method for arterial allograft transplantation
in a large animal model with decreased intimal hyperplasia and renewed functional capacity.
Fahner.indd 78 5-5-2014 14:35:12

solution in a goat carotid artery transplantation model | 79
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
Introduction
Prosthetic vascular grafts have proven less successful when used as small caliber grafts (< 6mm)
in peripheral arterial reconstructions compared to great diameters in aortic repair. Therefore
research in small-diameter, biological or tissue-engineered vascular constructs has continued.
To minimize the immunological response to allogeneic vascular grafts, current research has
focused on the use of decellularized tissue matrices which are potentially repopulated by host
derived endothelial and smooth muscle cells after implantation (1-4). Biological tissues provide an
extracellular matrix scaffold for migrating host cells using host specific adhesion receptors. This
results in diminished or absent immunological response to the grafts and enhanced ingrowth of
host endothelial and smooth muscle cells (5).
The use of biological vascular grafts requires appropriate techniques for graft preservation
and storage. Various preservation methods for vascular allografts have been examined in the
past two decades, of which cryopreservation, glutaraldehyde tanning and cold storage have
found clinical application. Early thrombosis, intimal hyperplasia and aneurysmal degeneration,
however, have hampered optimal performance. Glycerol (GL) preservation of skin allografts is
successfully in the management of burn injuries (6-9). Glycerol, a non-toxic intermediate of the
fatty acids metabolism, leaves the structural integrity of the skin unaffected and after application
on wounds, generates an unspecific host inflammatory reaction rather than an immune response
leading to rejection (10;11). An additional advantage of the use of glycerol is its potency to
eliminate micro-organisms (12). In vitro experiments using infected cadaveric split skin grafts
showed inactivation of herpes simplex virus, polio virus, HIV-1 and elimination of bacterial
growth after prolonged storage (13-15).
The efficacy of glycerol for preservation of skin allografts has encouraged examination of
glycerol for preservation of vascular allografts. Previous in vitro experiments in our laboratory
on glycerol preservation of rat aortic allografts confirmed maintenance of mechanical integrity
and extracellular matrix characteristics after three months preservation (16). In an in vivo rat
aortic transplantation model, glycerol preserved allografts showed a three months patency
rate comparable to autografts, with decreased intima hyperplasia and adventitial inflammatory
reaction (17).
The primary aim of the current study was to assess the use of glycerol preserved arterial
allografts in a preclinical, large animal model, with special emphasis on patency rate, vessel
wall function and graft morphology after implantation. Our secondary aim was to compare
glycerolization of vascular allografts with cold storage preservation using the University of
Wisconsin (UW), as widely used in most types of solid organ transplantation (18).
Because UW preservation is applicable for relatively short preservation times in contrast to
glycerol preservation we hypothozised that glycerol preservation was a feasible preservation
Fahner.indd 79 5-5-2014 14:35:13

80 | Chapter 5
method for vascular allografts with patency rates comparable to UW preserved allografts and
venous autografts.
Materials and methods
Animals and experimental groups
Dutch female milk goats (65kg - 104kg) were used, obtained from an official breeder. The
animals were housed five days prior to the experiments and maintained on a 12-hour light-dark
cycle. The animals had free access to water, bix and hay. The experimental protocol was approved
by the Animal Ethics Committee of the Academic Medical Center, University of Amsterdam,
The Netherlands. This protocol was in accordance with EU regulation on the care and use of
laboratory animals. In addition, the investigation conforms with the Guide for the Care and Use
of Laboratory Animals published by the US National Institutes of Health (NIH Publication No. 84-
23, revised 1996).
The study consisted of three experimental groups. One group (n = 7) underwent bilateral
replacement of the common carotid artery by a glycerol preserved carotid allograft (glycerol
group, GL). In the second group (n = 5) carotid allografts cold preserved in UW solution, were
used for bilateral replacement of the common carotid artery (University of Wisconsin group,
UW). In animals of the third group (n = 5) unilateral autotransplantation of the jugular vein to the
carotid artery was performed (autologous vein group, AU). This group served as golden standard
since autologous venous allografts reached highest patency rates in peripheral arterial bypass
surgery. At the beginning of the study one animal was sacrificed to serve as allograft donor.
In subsequent experiments, the segments of carotid artery which were excised in order to be
replaced by preserved allografts, were preserved and stored until implantation in the following
animal. All grafts were harvested after 3 months follow-up.
Surgical protocol and graft preservation
The animals were premedicated with 20 mg/kg Ketamine and 0.5 mg/kg Midazolam i.m. and
were ventilated using a mixture of O2 / N 2O, 1:1 L and Isoflurane 1-1.5% after endotracheal
intubation and placement of a nasogastric tube. Postoperatively, buprenorfine 5.0 µg/ kg and
finadyne 1.0 mg/kg was administered i.m. for control of pain. Finadyne 1.0 mg/kg injection was
repeated on a weekly basis. Ampicilline (1 g) was given 24 hours preoperatively and on day 1
and 3 postoperatively. All operations were performed under sterile conditions. Using a midline
neck incision, the carotid artery and jugular vein were identified and dissected over a length of
10 cm. Three minutes before clamping of the carotid artery, heparin (100 IU/ kg) was infused
Fahner.indd 80 5-5-2014 14:35:13

solution in a goat carotid artery transplantation model | 81
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
intravenously. A vascular allograft or autograft of 6.0 cm length was implanted as interposition
graft with end-to-end anastomosis using a 6.0 Prolene running suture.
The preservation protocol for the glycerol allografts was in accordance with the protocol
routinely used at the Euro Skin Bank (Beverwijk, The Netherlands) and was optimized for
preservation of arterial allografts (16). Briefly, the grafts were incubated in glycerol solution
(Glycerolum, Genfarma BV, Maarssen, The Netherlands) of increasing concentration as follows:
1. Incubation in a glycerol 50% solution for 4 hr at room temperature
2. Incubation in a glycerol 70% solution for 3 hr at 330C
3. Incubation in a glycerol 85% solution for 3 hr at 330C
After completion of the protocol, the grafts were stored in glycerol 85% for one week at 40C.
Cold storage was performed using University of Wisconsin preservation solution (ViaSpanR,
Barr Laboratories, Inc., NY) in which the grafts were immersed for 48 hr at 40C. Before
implantation all grafts were rinsed in saline for 20 min.
Graft surveillance
Routine color duplex scanning (Hewlett Packerd Sonos 5000) of the grafts was performed at
post-operative day 1, 3, 7 and week 2, 3, 4, 8 and 12. Peak systolic velocity (PSV), end diastolic
velocity (EDV) and vessel diameter were measured. Significant stenosis was arbitrarily defined as a
PSVmax which was 2.5 times increased. Just before explantation, a digital subtraction angiography
(DSA) was performed by puncture of the femoral artery and placement of a 5 Fr angiographic
catheter (Imager IITM, Boston Scientific Corporation, Watertown) in the aortic arch. A PTFE coated
steerable guide wire (2.7 Fr, Back-up Meier, Boston Scientific Corparation, Natick, USA) was
manipulated into the proximal carotid artery. Five ml of radio contrast solution (VisipaqueTM
320mg I/ml, Amersham Cygne BV, Eindhoven, The Netherlands) was manually injected.
Contraction and relaxation experiments
Segments of glycerol allografts (n=10) were tested for functional responses immediately following
explantation. In these experiments, the nonpreserved carotid artery proximal and distal to the
graft (n=12) served as fresh controls. After explantation, contraction and relaxation responses
were studied in 4 mm segments in an organ bath set-up as described previously (16). The initial
resting tension was set at 20 mN and was adjusted throughout the experiment. After one hour
of equilibration, the segments were exposed three times to a 50 mM depolarizing potassium
chloride solution for 5- 10 min intervals. After a rinsing procedure a concentration-response
curve was constructed for L-phenylephrine (1.10-8 – 1.10-4 M) to study receptor-dependent
contractile responses.
Fahner.indd 81 5-5-2014 14:35:13

82 | Chapter 5
To examine endothelium-dependent relaxation of the smooth muscle cells, a concentration-
response curve was constructed for methacholine (1.10-7 – 1.10-4 M) after rinsing with Tyrode’s
solution and precontraction with L-phenylephrine (1.10-5 M). Subsequently, the segments were
exposed to the NO-donor sodium nitroprusside (1.10-5 – 1.10-4 M) to determine endothelium-
independent relaxation.
Histological and electronmicroscopical examination
Histology
Five-mm ring samples were used for histological examination. Of each graft two samples
were examined in the proximal, mid and distal part of the graft, respectively. Sections of the
native vessel proximal to the implanted graft served as controls. Immediately after harvesting,
the segments were rinsed in saline, fixed in 10% formaldehyde solution (Mallinckrodt Baker,
Deventer, The Netherlands), dehydrated and embedded in paraffin. Transverse sections (5µm)
were stained with hematoxylin-eosin (HE) and Elastin van Gieson (EvG) and were mounted on
slides for microscopic evaluation. Of each slide three measurements of intima and media were
performed at 3, 6, 9 and 12 hour on a clockwise grid. A Leica LB 30 S light microscope (Leica,
Wetzlar, Germany) was used in combination with the Qwin Image pro analysis software (version
2.6, Leica Imaging Systems Ltd., Cambridge).
Scanning electron microscopy
Luminal coverage of the graft with endothelial cells was examined using scanning electron
microscopy. Ring segments were rinsed in saline and fixed for 24 hours in McDowell fixative
(4% paraformaldehyde and 1% glutaraldehyde in 0.1M phosphate buffer). The samples were
dehydrated in graded ethanol’s, immersed in 1,1,1,3,3,3 hexamethyl disilazan (Merck- Schuchardt)
and dried at room temperature for 12 hours. Finally, the tissue segments were mounted on stubs
with conductive carbon cement, sputter-coated with 20 nm gold-palladium and scanned with an
electron microscope (Philips SEM 525 equipped with an Orion frame grabber) operated at 10 kV
and a spot size of 50 nm.
Angiographies, functional and morphological examinations were evaluated by blinded
investigators.
Fahner.indd 82 5-5-2014 14:35:13

solution in a goat carotid artery transplantation model | 83
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
Statistical analysis
One way analysis of variance analysis was performed when means of three or more groups were
compared. If only means of two groups were analyzed the t-test was used. To test if time of
follow-up and graft location had effects on PSVmax values, a two way ANOVA analysis was used.
The log-rank test was used to compare patency rates. All statistical analysis was performed using
the GraphPad Prism 4.0 program (GraphPad Software, San Diego).
RESULTS
Animal follow-up and graft patency
Thirteen out of seventeen animals underwent surgery without any complication. Two animals
developed a graft occlusion within the first 24 hours postoperatively. Both suffered from
postoperative complications. One in the autologous vein autograft group had a postoperative
hemorrhage and thrombosis at the anastomosis requiring thrombectomy and reanastomosis.
The other animal with occlusion of a glycerol allograft developed a postoperative cardiac arrest,
was resuscitated and survived. No graft occlusions were observed after postoperative day
one. Two animals of the UW allograft group were euthanized on postoperative day 14 and 16
respectively, due to severe respiratory distress. The grafts were harvested and autopsy revealed
bilateral pneumonia with abcess formation in both animals. The 90-days primary patency rate
for UW, glycerol and autologous vein grafts was 100%, 93% and 80% respectively (p = 0.39).
Peak systolic velocity and graft diameter
When all measurements at the different locations in the grafts were pooled, the maximal mean
peak systolic velocity (PSVmax) could be depicted for all time-points during follow-up (Fig 1). No
significant stenosis, was detected in any of the experimental groups. As expected, the mean
PSVmax pooled for all time-points at follow-up was lowest in the midgraft segments for all the
three groups (Fig 2). Both graft location and time of follow-up did affect PSV max (p = 0.03 and
p = < 0.001). Flow velocity was significantly lower in the midgraft segments of the autologous
vein grafts whereas flow velocity was higher at the proximal anastomosis of the venous allografts
(p < 0.001). No differences in flow velocity were found between the UW and glycerol allografts.
Results of pooled diameter measurements of each graft during follow-up are shown in
figure 3. The diameter of autologous vein grafts placed as interposition graft in the carotid artery
was increased compared to native, non-operated jugular vein. A significant increase in diameter
was shown during follow-up (p < 0.005) only for the UW preserved allografts. The diameter of
glycerol allografts remained unchanged during 3 months follow-up.
Fahner.indd 83 5-5-2014 14:35:13

84 | Chapter 5
1d 3d 1w 2w 3w 1m 2m 3m60
65
70
75
80
85
90
95
100UW
GL
AU
follow up
mea
n PS
V (c
m/s
ec)
Figure 1. Maximal mean peak systolic velocity (PSVmax) in cm/sec for carotid artery allografts preserved in University of Wisconsin solution (UW, n = 10), in glycerol (GL, n = 14) and jugular vein autografts (AU, n = 5). 1d = 1 day, 1w = 1 week, 1m = 1 month.
pv pa mg da dv pv pa mg da dv pv pa mg da dv0
10
20
30
40
50
60
70
80
90
100
110
120
AU vein UW GLYCgraft locations in research groups
mea
n PS
V (c
m/s
ec)
Figure 2. Mean peak systolic velocity (PSVmax) in cm/sec for jugular vein autografts (AU vein, n = 5), carotid artery allografts preserved in University of Wisconsin solution (UW, n = 10) and glycerol preserved allografts (Glyc, n = 14). Error bars depict SEM. pv = proximal native vessel, pa = proximal anastomosis, mg = mid graft, da = distal anastomosis, dv = distal native vessel.
Fahner.indd 84 5-5-2014 14:35:13

solution in a goat carotid artery transplantation model | 85
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
Angiography
Angiography performed after three months follow-up showed a midgraft stenosis of
approximately 50% in one glycerol allograft. In none of the other glycerol or UW allografts a
stenosis could be detected. The diameter of the venous allografts was 2.3 times the diameter
of the native carotid artery. No aneurysmatic dilatation could be demonstrated in any of the
preserved allografts.
1d 3d 7d 2w 3w 1m 2m 3m 1d 3d 7d 2w 3w 1m 2m 3m 1d 3d 7d 2w 3w 1m 2m 3m0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
1.1
1.2
AU vein UW GLYC
follow up for different research groups
mea
n di
amet
er (c
m)
Figure 3. Mean diameter (cm) of jugular vein autografts (AU vein, n = 5), carotid artery allografts preserved in University of Wisconsin solution (UW, n = 10) and glycerol preserved allografts (GLYC, n = 14) during follow-up. Error bars depict SEM. 1d = 1 day, 1w = 1 week, 1m = 1 month.
Contraction and relaxation response
All grafts showed a modest contractile response to KCL and after stimulation with KCL and
phenylephrine. A dilatory response was measured after administration of both Na+ - nitroprusside
and methacholine. The response to methacholine was limited in both carotid allografts and
control grafts probably explained by damage to the endothelial cells during explantation.
The contractile and dilatory responses were more substantial in the control carotid grafts
(Fig 4).
Morphological and morphometrical analysis
Mean intimal thickness was less in the glycerol allografts in both proximal and midgraft segments
compared to the UW preserved grafts albeit that this difference was statistically significant only
Fahner.indd 85 5-5-2014 14:35:13

86 | Chapter 5
-20
-10
0
10
20
30
carotid graft
carotid control
KCl
SNPMET
50
60
70
80
PHE
∆ c
ontr
actil
e fo
rce
(mN
)
Figure 4. Differences in isometric contractile and relaxation force responses (mN) assessed in ring segments of fresh carotid arteries (carotid control, n = 12) and glycerol preserved allografts (carotid graft, n = 10). Error bars depict SEM. KCl = after stimulation with 50mM potassiumchlorite, SNP = after addition of Na+ - nitroprusside (1.10-5 – 1.10-4M) to determine endothelium-independent relaxation, MET = after addition of methacholine (1.10-7 – 1.10-4M) to examine endothelium-dependent relaxation and PHE = after addition of the α1-adrenoceptor agonist L-phenylephrine (1.10-7.5 – 1.10-4 M)
in the midgraft position (p < 0.001). At the distal anastomosis, the intima was thicker in the
glycerol allografts (Fig 5, p = 0.02). As expected, the autologous vein grafts and control carotid
artery segments showed only thin intimal layers. The results of media thickness are presented in
figure 6. At all locations the glycerol allografts had the smallest thickness of media which was
significantly different compared to the UW allografts (Fig 6, p < 0.01). Pooling of the results at all
locations showed no significant difference in mean intimal thickness between glycerol allografts
and UW allografts (34µm (SD = 5) and 37µm (SD = 4)). For the pooled results of media thickness,
a significant difference (p < 0.001) was found between mean thickness of glycerol and UW
segments (124µm (SD = 56) vs 161µm (SD = 4)).
Scanning electron microscopy
The scanning electron micrographs of the UW allografts showed a confluent layer of endothelial
cells somewhat higher compared to the control carotid artery endothelial cells (Fig 7A and B).
The endothelial cells were partly shriveled up and became less strongly attached to the sub-
endothelial medial layer (Fig 7B insert). Confluent intraluminal coverage was also determined
in the glycerol preserved allografts. A neo-intima was formed (Fig 7C) and the intraluminal
surface of the autologous vein grafts demonstrated a diminished profile compared to the arterial
allografts as seen in Fig 7D. Some damage to the confluent layer of endothelial cells was seen as
small cracks in the intima of the transplanted venous autografts (Fig 7D insert).
Fahner.indd 86 5-5-2014 14:35:14

solution in a goat carotid artery transplantation model | 87
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
gl uw au gl uw au gl uw au ca 0
50
100
150
200
250
prox distmid
med
ia t
hick
ness
(µm
)
Figure 6. Results of mean media thickness (µm) of glycerol preserved carotid allografts (gl, n = 14), carotid allografts preserved in University of Wisconsin solution (uw, n = 10), jugular venous autografts (au, n = 5) and fresh carotid arteries (ca, n = 5). Error bars depict SEM. prox = proximal part of graft, mid = middle part of graft and dist = distal part of graft.
gl uw au gl uw au gl uw au ca 0
10
20
30
40
50
60
prox distmid
intim
al t
hick
ness
(µm
)
Figure 5. Results of mean intimal thickness (µm) of glycerol preserved carotid allografts (gl, n = 14), carotid allografts preserved in University of Wisconsin solution (uw, n = 10), jugular venous autografts (au, n = 5) and fresh carotid arteries (ca, n = 5). Error bars depict SEM. prox = proximal part of graft, mid = middle part of graft and dist = distal part of graft.
Fahner.indd 87 5-5-2014 14:35:14

88 | Chapter 5
Figure 7. Scanning electon micrographs with high-power inserts of luminal coverage with endothelial cells in fresh carotid arteries (a), carotid allografts preserved in UW (b), GL-preserved carotid allografts (c) and AU autografts (d).
A B
C D
DISCUSSION
This study demonstrates the feasibility of glycerol preservation of vascular allografts with
diameters comparable to human peripheral arteries. No signifi cant stenosis was observed in the
glycerol allografts. When compared to UW preserved allografts, glycerol allografts demonstrate
less intimal hyperplasia in midgraft segments and repopulation of the glycerolized tissue matrix
by recipient cells resulting in renewed contraction and relaxation capability of the vessel wall
after transplantation.
The bilateral carotid artery transplantation model used in the current study, is successfully used
for the assessment of pseudo-intima proliferation, for examination of the effect of antiplatelet
drugs, and for assessment of arterial conduits and intravascular thrombectomy devices (19-22).
An important advantage of our model is the similarity of vessel diameter and hemodynamic
properties of the carotid artery in the goat when compared to human peripheral arteries (23).
Fahner.indd 88 5-5-2014 14:35:15

solution in a goat carotid artery transplantation model | 89
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
Limitations of the study include the time of follow up. A prolonged follow up period for up to
6 or 12 months would have facilitate the extrapolation to the clinical setting with patency rates
after 1 or 2 years follow up. Although this had lead to high costs.
Another limitation is that we did not transplantate the upper or lower limb arteries. These are
mainly involved in human peripheral arterial disease. Transplantation of leg arteries in an animal
model is not favourable due to higher risk of infection and traumatic events which hampers
wound healing.
During three months follow up, the mean diameter of the glycerol preserved allografts
stayed close to the initial value of almost 6.0 millimeter. A significant increase in arterial diameter
however, was shown in the UW preserved allografts which consistently increased after one
month of implantation. The increase in diameter potentially leads to aneurysm formation and
ultimately, vessel wall disintegration (24). In a review of explanted synthetic and biological
grafts in clinical peripheral arterial reconstructions, aneurysmal degeneration was the reason
for graft explantation in 72% of allografts used as a blood access for hemodialysis (25). In
general, aneurysmatic dilatation develops in the long term, therefore we are cautious with final
conclusions from our experiments because of the relatively short follow-up. Future research is
necessary to study the long-term risk of aneurysmal degeneration.
Endothelial dysfunction followed by endothelial cell-leucocyte interaction, endothelial
destruction and smooth muscle cell (SMC) loss are processes which play a central role in vascular
allograft rejection and graft dysfunction (26;27). To overcome this cascade, re-endothelialization
and neo-intimal formation, most likely the result of the proliferation of SMCs of recipient origin,
is generated in transplanted vascular allografts (28). Functional endothelial cells and SMCs are
necessary in maintaining a good vasomotor function as alterations in the nitric oxide-endothelin
homeostasis play an important role in the development of allograft transplant vasculopathy (29).
In a rat aorta interposition model transplanted cold stored allografts remain as nonfunctional
conduits after one and two months when they no longer respond to acetylcholine and
phenylephrine (30).
In a previous study glycerol preserved allografts were transplanted in a rat aorta transplantation
model. Anti-von Willebrand factor antibody immunostaining was used to assess endothelial graft
coverage and anti-α-actin antibody to visualize vascular SMC. No differences were found in
endothelial cell coverage and SMC repopulation between GL allografts and autografts after 3
months of follow-up. Given the available techniques in goats, it is not feasible to differentiate
between persisting cells of the donor in the vascular graft after transplantation or ingrowing
cells from the recipient. A mononuclear infiltration was observed only around the sutures of a
GL preservated vascular graft (17). Therefore, we assessed repoplulation of the non-viable tissue
matrix after GL preservation in our study, using the contraction and relaxation experiments.
Fahner.indd 89 5-5-2014 14:35:15

90 | Chapter 5
GL allografts did respond to vasodilating and vasconstricting agents demonstrating neo-
endothelial cell and SMC interactions resulting again in some of the original functionality. This
means ingrowth of recipient endothelial and SMCs in the donor extracellular tissue matrix. GL
preservation results in pyknotic nuclear cells and complete loss of contraction and relaxation
capacity (16).
Bishop et al (31) reported ten days glycerol 98% preservation of venous allografts used as
interposition graft in the common carotid artery in a goat model. Six months patency was 64%
compared to 88% for autografts. Handling and suturing qualities were as good as untreated
fresh vein and aneurysm formation in the vessel wall or at the anastomosis was not detected
suggesting adequate strength and durability of the allografts. Although scanning electron
microscopy and histology revealed endothelial disruption after preservation it apparently did not
result in a sufficiently thrombogenic graft surface to compromise long-term graft function (31).
Differences in patency rates between this experiment and the current study can, apart from the
longer observation time (i.e. 6 months), be explained by a better compliance match between
native artery and glycerol preserved artery compared to glycerol preserved vein.
Neo-intimal thickness was comparable at both proximal and distal anastomoses in both UW
and glycerol preservation groups and was very limited in autologous venous grafts.
In contrast, glycerol allografts showed a significantly thinner intima in the midgraft segments
compared to the UW allografts after three months follow-up. Although a short period of UW
preservation preserves vasomotor activity after cold storage which means that endothelial
cells and SMCs will survive the storage period to some extent, these cells will have sustained
damage due to the 48 hours of cold ischemia (26). These injured cells induce cellular proliferation
probably from surviving native graft SMCs, recipient endothelial cells from both anastomoses
and circulating endothelial progenitor cells (32;33). Extensive neo-intimal formation in UW grafts
can occur secondary to the immunological reaction to graft endothelial cells which results in
chronic intimal injury and enhanced neo-intimal proliferation (34). The diminished neo-intimal
formation in the glycerol preserved allografts in the current study is probably explained by the
fact that glycerol preservation results in a non-viable extracellular tissue from which all living
endothelial cells have been eliminated (16).
An intact intraluminal coverage by an endothelial monolayer in the transplanted vascular
grafts is important in prevention of intravascular coagulation (35). In the current study this
monolayer was present in the control carotid arteries and could also be demonstrated in the
autologous vein grafts. Flat endothelial cells with a smooth surface and without pores and
microvilli are criteria for cells in normal condition (36). Endothelial cells were flattened in the
glycerol allografts too, comparable with the endothelial cells in the autologous veins. However,
the endothelial cells preserved in UW seemed to have decreased in size and have lost cellular
attachment. Endothelial cell remnants seen on top of the neo-endothelial cells in the glycerol
Fahner.indd 90 5-5-2014 14:35:15

solution in a goat carotid artery transplantation model | 91
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
allografts suggest temporary luminal coverage by donor endothelial cells to enable recipient neo-
endothelial cells to proliferate and constitute a new bond with the graft internal elastic lamina.
GL-preserved arterial allografts can probably be used for small caliber vascular bypasses when
AU specimens are not available. UW preserved allografts could only be preserved for a short
period of time (1-2 weeks), whereas GL-preserved allografts could be stored for at least 3 months
with maintenance of structural properties. In view of these prolonged storage opportunities, iliac
and femoral arteries could be procured in multi-organ harvest procedures, preserved in GL and
stored in a vascular tissue bank. The absence of aneurysmal degeneration and the lesser degree
of intimal hyperplasia and inflammatory reaction in GL allografts, as compared to UW allografts,
render GL allografts a feasible alternative to cold-stored vascular grafts.
In conclusion, glycerol preservation of arterial allografts in this large animal model of carotid
artery transplantation, showed a promising patency rate after 3 months. Vessel wall diameter
of the preserved allografts was maintained as well as several functional characteristics owing to
repopulation of the vascular tissue matrix by host cells.
These results encourage us to devise a pilot study using glycerol preserved arterial allografts
in a clinical setting.
Fahner.indd 91 5-5-2014 14:35:15

92 | Chapter 5
Reference List
(1) Amiel GE, Komura M, Shapira O, Yoo JJ, Yazdani S, Berry J, et al. Engineering of blood vessels from acellular collagen matrices coated with human endothelial cells. Tissue Eng 2006 Aug;12(8):2355-65.
(2) Kaushal S, Amiel GE, Guleserian KJ, Shapira OM, Perry T, Sutherland FW, et al. Functional small-diameter neovessels created using endothelial progenitor cells expanded ex vivo. Nat Med 2001 Sep;7(9):1035-40.
(3) Borschel GH, Huang YC, Calve S, Arruda EM, Lynch JB, Dow DE, et al. Tissue engineering of recellularized small-diameter vascular grafts. Tissue Eng 2005 May;11(5-6):778-86.
(4) Shum-Tim D, Stock U, Hrkach J, Shinoka T, Lien J, Moses MA, et al. Tissue engineering of autologous aorta using a new biodegradable polymer. Ann Thorac Surg 1999 Dec;68(6):2298-304.
(5) Wang X, Lin P, Yao Q, Chen C. Development of small-diameter vascular grafts. World J Surg 2007 Apr;31(4):682-9.
(6) Mackie D. Postal survey on the use of glycerol-preserved allografts in clinical practice. Burns 2002 Oct;28 Suppl 1:S40-S44.
(7) Kreis RW, Vloemans AF, Hoekstra MJ, Mackie DP, Hermans RP. The use of non-viable glycerol-preserved cadaver skin combined with widely expanded autografts in the treatment of extensive third-degree burns. J Trauma 1989 Jan;29(1):51-4.
(8) Vloemans AF, Middelkoop E, Kreis RW. A historical appraisal of the use of cryopreserved and glycerol-preserved allograft skin in the treatment of partial thickness burns. Burns 2002 Oct;28 Suppl 1:S16-S20.
(9) Vloemans AF, Schreinemachers MC, Middelkoop E, Kreis RW. The use of glycerol-preserved allografts in the Beverwijk Burn Centre: a retrospective study. Burns 2002 Oct;28 Suppl 1:S2-S9.
(10) Richters CD, Hoekstra MJ, du Pont JS, Kreis RW, Kamperdijk EW. Immunology of skin transplantation. Clin Dermatol 2005 Jul;23(4):338-42.
(11) Richters CD, Hoekstra MJ, van BJ, du Pont JS, Kamperdijk EW. Immunogenicity of glycerol-preserved human cadaver skin in vitro. J Burn Care Rehabil 1997 May;18(3):228-33.
(12) Ben-Bassat H. Performance and safety of skin allografts. Clin Dermatol 2005 Jul;23(4):365-75.
(13) Cameron PU, Pagnon JC, van BJ, Reece JC, Vardaxis NJ, Crowe SM. Efficacy and kinetics of glycerol inactivation of HIV-1 in split skin grafts. J Med Virol 2000 Feb;60(2):182-8.
(14) van Baare J, Ligtvoet EE, Middelkoop E. Microbiological evaluation of glycerolized cadaveric donor skin. Transplantation 1998 Apr 15;65(7):966-70.
(15) van Baare J, Buitenwerf J, Hoekstra MJ, du Pont JS. Virucidal effect of glycerol as used in donor skin preservation. Burns 1994;20 Suppl 1:S77-S80.
(16) Fahner PJ, Idu MM, Legemate DA, Vanbavel E, Borstlap J, Pfaffendorf M, et al. Morphological and functional alterations in glycerol preserved rat aortic allografts. Int J Artif Organs 2004 Nov;27(11):979-89.
(17) Fahner PJ, Idu MM, van Gulik TM, van Wijk B, van der Wal AC, et al. Glycerol preserved arterial allografts evaluated in the infrarenal rat aorta. Eur Surg Res 2009 Feb;42(2):78-86.
(18) Corner JA, Berwanger CS, Stansby G. Preservation of vascular tissue under hypothermic conditions. J Surg Res 2003 Jul;113(1):21-5.
(19) Hilbert SL, Boerboom LE, Livesey SA, Ferrans VJ. Explant pathology study of decellularized carotid artery vascular grafts. J Biomed Mater Res A 2004 May 1;69(2):197-204.
(20) Pichakron KO, Bui PT, Pickard BJ, Perlstein J, Mathis D, Muir-Padilla J, et al. The application of split-thickness skin graft as an autogenous arterial conduit in a goat (Capra hircus) model. Vasc Endovascular Surg 2006 May;40(3):213-22.
Fahner.indd 92 5-5-2014 14:35:15

solution in a goat carotid artery transplantation model | 93
5
Comparison of preserved vascular allografts using glycerol and University of Wisconsin
(21) Rainwater LM, Plate G, Gloviczki P, Bahn RC, Hollier LH, Kaye MP. Morphologic quantitation of pseudointima and effects of antiplatelet drugs on vascular prostheses in goats. Am J Surg 1984 Aug;148(2):195-202.
(22) van Ommen VG, van der Veen FH, Geskes GG, Daemen M, Habets J, Dassen WR, et al. Comparison of arterial wall reaction after passage of the Hydrolyser device versus a thrombectomy balloon in an animal model. J Vasc Interv Radiol 1996 May;7(3):451-4.
(23) Lemson MS, Daemen MJ, Kitslaar PJ, Tordoir JH. A new animal model to study intimal hyperplasia in arteriovenous fistulas. J Surg Res 1999 Jul;85(1):51-8.
(24) Berry CL, Sosa-Melgarejo JA, Greenwald SE. The relationship between wall tension, lamellar thickness, and intercellular junctions in the fetal and adult aorta: its relevance to the pathology of dissecting aneurysm. J Pathol 1993 Jan;169(1):15-20.
(25) Wagner E, Guidoin R, Marois M, Mantovani D, Roy R, Ricci M, et al. Histopathologic findings in synthetic and biologic explanted grafts used in peripheral arterial reconstruction. ASAIO J 1994 Jul;40(3):M279-M283.
(26) Gohra H, McDonald TO, Verrier ED, Aziz S. Endothelial loss and regeneration in a model of transplant arteriosclerosis. Transplantation 1995 Jul 15;60(1):96-102.
(27) Bigaud M, Schraa EO, Andriambeloson E, Lobstein V, Pally C, Kobel T, et al. Complete loss of functional smooth muscle cells precedes vascular remodeling in rat aorta allografts. Transplantation 1999 Dec 15;68(11):1701-7.
(28) Aziz S, McDonald TO, Gohra H. Transplant arterial vasculopathy: evidence for a dual pattern of endothelial injury and the source of smooth muscle cells in lesions of intimal hyperplasia. J Heart Lung Transplant 1995 Nov;14:S123-S136.
(29) Ramzy D, Rao V, Tumiati LC, Xu N, Miriuka S, Delgado D, et al. Role of endothelin-1 and nitric oxide bioavailability in transplant-related vascular injury: comparative effects of rapamycin and cyclosporine. Circulation 2006 Jul 4;114(1 Suppl):I214-I219.
(30) Andriambeloson E, Bigaud M, Schraa EO, Kobel T, Lobstein V, Pally C, et al. Endothelial dysfunction and denudation in rat aortic allografts. Arterioscler Thromb Vasc Biol 2001 Jan;21(1):67-73.
(31) Bishop AJ, Glasby MA, Houlton JE. A morphological assessment of vein allografts preserved in glycerol and used for arterial replacement. J Cardiovasc Surg (Torino) 1987 Sep;28(5):491-7.
(32) Yokote K, Take A, Nakaseko C, Kobayashi K, Fujimoto M, Kawamura H, et al. Bone marrow-derived vascular cells in response to injury. J Atheroscler Thromb 2003;10(4):205-10.
(33) Xiong W, Gao CJ, Lu XF, Cheng JQ, Li YP. Prolonged cold preservation promotes the recipient’s cell participating in neointima formation but delays the later graft arteriosclerosis in rat model. Transplant Proc 2005 Jan;37(1):312-5.
(34) Lagaaij EL, Cramer-Knijnenburg GF, van Kemenade FJ, van Es LA, Bruijn JA, van Krieken JH. Endothelial cell chimerism after renal transplantation and vascular rejection. Lancet 2001 Jan 6;357(9249):33-7.
(35) Bombeli T, Mueller M, Haeberli A. Anticoagulant properties of the vascular endothelium. Thromb Haemost 1997 Mar;77(3):408-23.
(36) van Leeuwen EB, Molema G, van Luyn MJ, de Jong KP, Dijk F, Slooff MJ, et al. Scanning electron microscopic analysis of endothelial cell coverage and quality in large vessels from multi-organ donors: effects of preservation on endothelial cell integrity. Clin Transplant 2000 Jun;14(3):246-51.
Fahner.indd 93 5-5-2014 14:35:15

Fahner.indd 94 5-5-2014 14:35:15

6Summary and conclusions
Samenvatting en conclusies
Fahner.indd 95 5-5-2014 14:35:15

96 | Chapter 6
SUMMARY AND CONCLUSIONS
In chapter 1, the topic of this thesis is introduced and an outline of the thesis presented.
Chapter 2 provides a systematic review of preservation methods of vascular allografts.
No systematic review of randomized controlled trials concerning the use of preserved vascular
allografts was found in literature. Five randomized controlled trials, 3 prospective cohort or
case series and 15 retrospective case series were identified. Cryopreservation, cold storage and
glutaraldehyde preservation have been methods used for allograft preservation. A wide range
in one-year cumulative primary patency rates and major limb loss was reported for the different
preservation methods used in these studies.
The heterogeneity of studies hampered a formal meta-analysis. The overall graft performance
of glutaraldehyde-preserved human umbilical vein allografts, however, seemed superior to the
other preservation methods. These results underscore the importance of a uniform design in
clinical trials ensuring that patient characteristics, level of anastomosis and anticoagulation
therapy are comparable. No clinical studies on glycerol preservation of vascular grafts were
found. Therefore, a preclinical study measuring the quality of glycerol preservation of arteries in
the ex vivo and in vivo setting, was undertaken in this thesis
In chapter 3, morphological and functional alterations in glycerol preserved allografts were
assessed. Breaking strength, bursting pressure and functional alterations were determined in
glycerol preserved, rat aortic segments. Breaking-strength, bursting pressure and the diameter
of the ruptured vessel wall were not significantly different between glycerol preserved allografts
and control vessels. Although endothelium-dependent or endothelium-independent contraction
or relaxation was abolished, no alterations in elastin-bundle width or mean bundle distance
were detected. The orientation index of the media was, likewise, preserved. Scanning electron
microscopy revealed flattening of the endothelial cells and defragmentation of cellular membranes
in the glycerol preserved allografts. It was concluded that the structural integrity of the aorta was
well preserved after glycerol preservation and that the glycerol preserved aortic wall was strong
enough to withstand normal physiological blood pressure. These results justified further testing
of glycerol preserved arteries in vascular transplantation experiments.
In chapter 4, the outcome of glycerol preserved allografts was studied in a rat aorta transplantation
model. A rat allograft transplantation model was developed in which wdonor rat aortas were
preserved and subsequently transplanted into recipient rats. After three months of follow-up,
the glycerol preserved allografts had a lower peak systolic velocity (PSV) than autografts. No
aneurysms were detected in the allografts implying that glycerol preservation maintained the
Fahner.indd 96 5-5-2014 14:35:15

Summary and conclusions | 97
6
structural integrity of the vessel wall. Furthermore, no significant differences were found in graft
stenosis between the groups. Thickness of the intimal layer was greater in autografts than in
allografts after 1 and 3 months follow-up. Width of the media was less in glycerol allografts and
in both groups, no inflammatory reaction was found in the media. Cumulative graft patency
rates showed no significant differences between both groups. The observation that all viable
cells had died during glycerol preservation implies that the endothelial cells no longer play a role
in the immunological response of the recipient due to the lack of antigen presentation.
Since the results of rat models cannot be directly applied to human vascular transplantation
because of obvious dimensional differences, the next step entailed experiments in a larger animal
model.
Chapter 5 deals with arterial allografts preserved in glycerol or University of Wisconsin (UW)
solution transplanted in a goat model. Donor goat carotid arteries were preserved with glycerol
or with UW solution. The latter is a well established organ preservation solution based on a
colloid component and impermeants. Three months primary patency rates for glycerol allografts,
UW allografts and jugular vein autografts were 93%, 100% and 80%, respectively. Although
graft diameter of UW allografts increased significantly during three months follow-up, the
glycerol allografts showed no aneurysm formation. Glycerol better preserved the matrix of the
vessel wall as compared to UW.
Isometric contraction and relaxation tests in these experiments demonstrated renewed graft
functional capacity after implantation which implicated ingrowth of recipient endothelial and
smooth muscle cells into the preserved vascular tissue matrix. Scanning electron microscopy
showed a confluent layer of endothelial cells in both glycerol and UW allografts.
These results demonstrate the feasibility of a glycerol preserved allograft in a large animal
model.
In Chapter 6 a summary of the studies is presented along with the main concluions.
Chapter 7 provides an overall discussion of the main conclusions of this thesis and ends with a
view on future perspectives concerning the topic.
Fahner.indd 97 5-5-2014 14:35:15

98 | Chapter 6
SAMENVATTING EN CONCLUSIES
In hoofdstuk 1 wordt het onderwerp van dit proefschrift geïntroduceerd en wordt een overzicht
van het proefschrift gepresenteerd.
Hoofdstuk 2 handelt over een systematisch overzicht van preservatie methoden van vasculaire
transplantaten. In de literatuur werd geen systematisch overzicht van gerandomiseerd
gecontroleerde studies gevonden betreffende het gebruik van gepreserveerde vasculaire
transplantaten. Vijf gerandomiseerd gecontroleerde studies, 3 prospectieve cohort of
enkelvoudige studies en 15 retrospectieve enkelvoudige studies werden geïdentificeerd.
Cryopreservatie, koude opslag en glutaaraldehyde preservatie zijn technieken die werden
gebruikt voor transplantaat preservatie. Er bestond een grote spreiding binnen deze studies
waarin verschillende preservatie technieken werden gebruikt voor wat betreft de cumulatieve
primaire patency rate en het verlies van een onderbeen of bovenbeen. De heterogeniteit van
de studies stond het uitvoeren van een formele meta-analyse in de weg. Echter de algehele
prestatie van de glutaaraldehyde gepreserveerde humane navelstreng vene leek superieur ten
opzichte van de andere preservatie technieken. Deze resultaten onderstrepen het belang van
een uniforme studieopzet bij klinische studies waarbij zorg wordt gedragen voor het feit dat
patiënt karakteristieken, het niveau van de anatomose en antistolling therapie met elkaar kunnen
worden vergeleken. Een klinische studie naar het gebruik van een glycerol gepreserveerd vasculair
transplantaat werd niet gevonden. Daarom werd in dit promotie onderzoek een analyse verricht
naar de kwaliteit van glycerol preservatie van arteriën in een ex vivo en in vivo onderzoeksmodel.
In hoofdstuk 3 worden de morfologische en functionele veranderingen in een glycerol
gepreserveerd transplantaat geanalyseerd. Breekkracht, scheurkracht en functionele
veranderingen werden onderzocht in glycerol gepreserveerde aorta segmenten van de
rat. Breekkracht, scheurkracht en de diameter van het vat waarbij de vaatwand scheurde
was niet significant verschillend tussen glycerol gepreserveerde transplantaten en controle
vaatsegmenten. Hoewel endotheel-afhankelijke of endotheel-onafhankelijke contractie en
relaxatie werd uitgeschakeld na glycerolpreservatie werden er geen veranderingen vastgesteld
in breedte van de elastine bundels of gemiddelde onderlinge afstand tussen deze bundels. Ook
de oriëntatie index in de media bleef onaangetast. Scanning elektronen microscopie toonde
een afvlakking van de endotheel cellen en fragmentatie van het celmembraan van het glycerol
gepreserveerde transplantaat. Er werd geconcludeerd dat de structurele integriteit van de aorta
goed bewaard bleef en de vaatwand bestand bleek tegen normale fysiologische bloeddrukken
na glycerol preservatie. Deze resultaten rechtvaardigden vervolg onderzoek naar een glycerol
gepreserveerde arterie in vaat transplantatie experimenten.
Fahner.indd 98 5-5-2014 14:35:15

Samenvatting en conclusies | 99
6
In hoofdstuk 4 worden de resultaten van een glycerol gepreserveerd transplantaat in
een rat aorta transplantatie model beschreven. Een ratten model voor vaattransplantaties
werd ontwikkeld waarbij de aorta van een donor rat werd gepreserveerd en vervolgens
getransplanteerd naar een ontvangende rat. Na een evaluatie periode van drie maanden toonden
de glycerol gepreserveerde transplantaten een lagere piek systolische snelheid (PSV) vergeleken
met de autografts. Er werd geen aneurysma formatie waargenomen in de transplantaten wat
betekende dat na glycerol preservatie de structurele integriteit van de vaatwand bewaard bleef.
Verder bleken er geen significante verschillen te bestaan tussen de groepen voor wat betreft
het optreden van transplantaat stenose. De intima was dikker in de autotransplantaten dan
in de glycerol gepreserveerde transplantaten na een vervolg periode van 1 en 3 maanden. De
media was dunner in de glycerol gepreserveerde transplantaten en in beide groepen werd er
geen ontstekingsreactie gezien in de media. De cumulatieve graad waarin de transplantaten
patent waren, bleek niet verschillend voor beide groepen. De wetenschap dat er geen levende
cellen meer over bleven na de glycerol preservatie betekende dat de endotheel cellen geen
rol meer speelden in de immunologische response van de transplantaat ontvanger vanwege
de afwezigheid van antigeen presentatie. Omdat er natuurlijk duidelijke verschillen zijn in
dimensies tussen rat en mens, kunnen de resultaten vanuit het ratten model niet direct worden
geëxtrapoleerd naar vaat transplantaties bij de mens. Daarom werd als volgende stap een serie
experimenten uitgevoerd in een groter proefdier model.
Hoofdstuk 5 handelt over arteriële transplantaten in een geiten model welke zijn gepreserveerd
in glycerol of in een University of Wisconsin (UW) oplossing. De arteria carotis van donor geiten
werd gepreserveerd in glycerol of UW oplossing. De laatste is een weid geaccepteerd orgaan
preservatie medium gebaseerd op een colloïde en dragerstof. De primaire patency rate na 3
maanden bleek voor glycerol transplantaten, UW transplantaten en autotransplantaten van de
vena jugularis, 93%, 100% en 80% respectievelijk. Hoewel de diameter van de UW transplantaten
na 3 maanden controle significant was toegenomen, werd bij de glycerol transplantaten geen
aneurysma vorming waargenomen. In vergelijk met UW bleef bij glycerolpreservatie de matrix
van de vaatwand beter behouden. De isometrische contractie en relaxatie experimenten
binnen deze studie lieten zien dat er opnieuw functionele contractie en relaxatie mogelijk werd
in de vaatwand na implantatie. Dit impliceerde ingroei van endotheel en gladde spiercellen
van de getransplanteerde dieren in de gepreserveerde vasculaire weefsel matrix. Met behulp
van scanning elektronen microscopie werd aangetoond dat er een aaneengesloten laag van
endotheel cellen was ontstaan in zowel de glycerol als UW transplantaten. De resultaten uit deze
studie toonde aan dat een glycerol gepreserveerd transplantaat kon worden toegepast in een
groot dier model.
Fahner.indd 99 5-5-2014 14:35:15

100 | Chapter 6
In hoofdstuk 6 wordt een overzicht gegeven van de studies aangevuld met de belangrijkste
conclusies.
Hoofdstuk 7 geeft een algemene discussie over de belangrijkste conclusies van dit proefschrift
en sluit af met een visie op mogelijke ontwikkelingen in de toekomst aangaande het onderwerp.
Fahner.indd 100 5-5-2014 14:35:15

7General discussion and future perspectives
Fahner.indd 101 5-5-2014 14:35:15

102 | Chapter 7
Update of systematic review of preservation methods of vascular allografts
The systematic review described in chapter 2, was published in 2006 and included studies
from 1966 until 2004. Therefore, on completion of this thesis in 2014, a renewed systematic
review of clinical studies on peripheral reconstructions using preserved vascular allografts was
performed, covering the last ten years. The same search strategies were followed and the same
in- and exclusion criteria were used to determine key articles in which different types of vascular
allografts were used in arterial reconstructions. A total of twelve clinical studies were retrieved
in the last search. Seven studies were excluded, of which five because of the small number of
patients included. One Czech article was excluded because of translation problems and one
multi-center study evaluated reconstructions with cryopreserved allografts in the aortic position.
Hence, a final set of five additional key articles was obtained (1-5).
Three studies used cryopreserved venous allografts, one retrospective series described
reconstructions using cold stored venous allografts and in one clinical study, the human umbilical
vein (HUV) graft was evaluated. A total of 202 patients were included in the studies using
cryopreserved venous allografts; 43 and 197 patients were enrolled in the cold stored allograft
study and HUV allograft series, respectively.
The weighted mean 1-year cumulative primary graft patency rate was 35% for the
cryopreserved venous allografts, 46% for the cold stored allografts while the 5-year cumulative
primary graft patency rate for the HUV allografts was 54%. The results of the cryopreserved
venous allografts and HUV allografts were comparable to the previous review, showing a
weighted mean 1-year cumulative primary graft patency rate for venous allografts of 41% and
5-year cumulative primary graft patency rate for the HUV allografts of 53%. The patency results
for the cold stored allografts were slightly lower in the recent series since patency rates in the
previous review ranged from 63% to 80%.
This update shows that the conclusion of the former systematic review was confirmed by
the current review. Because studies in which a specific preservation method is compared, are
still lacking, a firm conclusion cannot be made. HUV allografts however, seemed superior to the
other preservation methods showing high 5-year patency-rates.
Transplantation of glycerol preserved allografts.
The implantation studies presented in chapters 4 and 5 demonstrated the feasibility of glycerol
preserved allografts for vascular substitution. It is however important to take caution when
extrapolating patency rates from animal models to humans. The process of endothelialization
Fahner.indd 102 5-5-2014 14:35:15

General discussion and future perspectives | 103
7
for example, is more rapid and complete in animals and different in prosthetic vascular grafts
(6-11) and in animal studies, anticoagulant therapy is usually not used. In clinical application of
glycerol preserved arterial allografts however, anticoagulants are probably needed at least until
intraluminal reendothelialization has been completed. Secondly, in the rat aorta transplantation
model, young animals are used as allograft donors. These animals do not suffer from alterations
in vessel wall constitution such as in atherosclerosis, diabetes mellitus, nicotine abuse or ageing.
These would be all potential factors influencing the results of graft function and patency rates
after application of human glycerol preserved arterial allografts.
Tissue engineering of vascular grafts
While the aforementioned studies concern transplantation of biological vascular tissue, another
area of research is the tissue engineering of synthetic vascular conduits.
As allografts appear to have the advantages of easier placement, lower complication rate
and better resistance to infections, it can be postulated that allografts perform superiorly to
synthetic conduits in revascularization of lower limbs. Future experiments should clarify the
advantages of allografts to synthetic polymers used in combination with biological matrices.
The synthetic polymers include polyglycolic acid, poly-L-lactic acid, poly-DL-lactic-co-glycolic acid
and polyurethanes, the first three being biodegradable (12-15). The degradation process should
follow a timeline that enables the recipient cells to form a functional conduit resistant to the
biomechanical stress and strain imposed on a native vessel. Synthetic scaffolds have the advantage
of reproduction on an industrial scale and the possibilities of quality control at the point of
manufacture (16). A disadvantage of synthetic scaffolds is the lack of biological, cell attachment
factors present in naturally derived scaffolds while their relation with the development of intimal
hyperplasia is uncertain (17;18).
The first tissue-engineered blood vessel was developed by Weinberg and Bell who used
cultured bovine endothelial cells, vascular smooth muscle cells and fibroblasts on a collagen
scaffold (19). Also biodegradable scaffolds seeded with autologous mononuclear cells have been
used in vascular constructs (20). To enable autologous cells to attach to the biological scaffold a
suitable bioreactor system is required. Niklason et al successfully developed the first bioreactor
for vascular tissue engineering (21). Another limitation of this approach is the long culture time of
approximately 8 weeks between the harvest of autologous cells and the culturing of a mature and
durable conduit (22-26). An alternative to endothelialization of the tissue-engineered vascular
graft probably is the utilization of in situ endothelial cells as was reviewed by Melchiorri et al (27).
Fahner.indd 103 5-5-2014 14:35:15

104 | Chapter 7
Future perspectives
Since the applicability of glycerol preservation of arterial allografts has been shown in animal
studies, the next step is the preparation of a glycerol allograft for clinical use.
Although extensive research has been performed in the elimination of bacterial and viral
contamination in glycerol preserved skin allografts, experiments will be needed to examine if
bacterial and/or viral contamination jeopardizes the use of glycerol preserved vascular allografts.
Likewise, contamination studies will be needed looking at human immunodeficiency virus
(HIV), hepatitis B and C, Treponema pallidum, Cytomegalovirus and Toxoplasma. Furthermore,
the duration to safely eliminate these viruses in the process of glycerol preservation must be
established.
Knowing that the attachment of recipient endothelial cells to biological scaffolds is superior
if compared to synthetic constructs, it is interesting to investigate the potential improvements of
complete luminal endothelial cell lining of glycerol preserved arterial allografts via cell seeding.
A potential next step is the development of a vascular tissue bank for glycerol arterial allografts
in collaboration with the established tissue banks using existing infrastructure for cadaveric donor
harvesting protocols. Teams involved in the harvesting of organs and tissues can be trained
to harvest the arteries between the aortic bifurcation and the infragenual popliteal arteries
for glycerol preservation and storage. Ultimately, the efficacy of glycerol preserved allografts
needs to be assessed in properly designed, randomized trials using the venous autograft as gold
standard. Uniform requirements for allograft quality surveillance and anticoagulation therapy
should be established in such protocols.
Fahner.indd 104 5-5-2014 14:35:15

General discussion and future perspectives | 105
7
Reference List
(1) Zehr BP, Niblick CJ, Downey H, Ladowski JS. Limb salvage with CryoVein cadaver saphenous vein allografts used for peripheral arterial bypass: role of blood compatibility. Ann Vasc Surg 2011 Feb;25(2):177-81.
(2) Randon C, Jacobs B, De RF, Beele H, Vermassen F. Fifteen years of infrapopliteal arterial reconstructions with cryopreserved venous allografts for limb salvage. J Vasc Surg 2010 Apr;51(4):869-77.
(3) Bannazadeh M, Sarac TP, Bena J, Srivastava S, Ouriel K, Clair D. Reoperative lower extremity revascularization with cadaver vein for limb salvage. Ann Vasc Surg 2009 Jan;23(1):24-31.
(4) Matia I, Janousek L, Marada T, Adamec M. Cold-stored venous allografts in the treatment of critical limb ischaemia. Eur J Vasc Endovasc Surg 2007 Oct;34(4):424-31.
(5) Neufang A, Espinola-Klein C, Dorweiler B, Messow CM, Schmiedt W, Vahl CF. Femoropopliteal prosthetic bypass with glutaraldehyde stabilized human umbilical vein (HUV). J Vasc Surg 2007 Aug;46(2):280-8.
(6) Burkel WE, Graham LM, Stanley JC. Endothelial linings in prosthetic vascular grafts 4. Ann N Y Acad Sci 1987;516:131-44.
(7) Clagett GP, Burkel WE, Sharefkin JB, Ford JW, Hufnagel H, Vinter DW, et al. Platelet reactivity in vivo in dogs with arterial prostheses seeded with endothelial cells. Circulation 1984 Mar;69(3):632-9.
(8) Merzkirch C, Davies N, Zilla P. Engineering of vascular ingrowth matrices: are protein domains an alternative to peptides? Anat Rec 2001 Aug 1;263(4):379-87.
(9) Stanley JC, Burkel WE, Graham LM, Lindblad B. Endothelial cell seeding of synthetic vascular prostheses. Acta Chir Scand Suppl 1985;529:17-27.
(10) Wu MH, Shi Q, Wechezak AR, Clowes AW, Gordon IL, Sauvage LR. Definitive proof of endothelialization of a Dacron arterial prosthesis in a human being. J Vasc Surg 1995 May;21(5):862-7. (11)
(11) Burkel WE, Ford JW, Vinter DW, Kahn RH, Graham LM, Stanley JC. Fate of knitted dacron velour vascular grafts seeded with enzymatically derived autologous canine endothelium 4. Trans Am Soc Artif Intern Organs 1982;28:178-84.
(12) Kim BS, Mooney DJ. Development of biocompatible synthetic extracellular matrices for tissue engineering 4. Trends Biotechnol 1998 May;16(5):224-30.
(13) Niklason LE, Abbott W, Gao J, Klagges B, Hirschi KK, Ulubayram K, et al. Morphologic and mechanical characteristics of engineered bovine arteries. J Vasc Surg 2001 Mar;33(3):628-38.
(14) Tiwari A, Salacinski H, Seifalian AM, Hamilton G. New prostheses for use in bypass grafts with special emphasis on polyurethanes. Cardiovasc Surg 2002 Jun;10(3):191-7.
(15) Borschel GH, Huang YC, Calve S, Arruda EM, Lynch JB, Dow DE, et al. Tissue engineering of recellularized small-diameter vascular grafts. Tissue Eng 2005 May;11(5-6):778-86.
(16) Yow KH, Ingram J, Korossis SA, Ingham E, Homer-Vanniasinkam S. Tissue engineering of vascular conduits. Br J Surg 2006 Jun;93(6):652-61.
(17) Kim BS, Mooney DJ. Development of biocompatible synthetic extracellular matrices for tissue engineering. Trends Biotechnol 1998 May;16(5):224-30.
(18) Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 1993 Apr 29;362(6423):801-9.
(19) Weinberg CB, Bell E. A blood vessel model constructed from collagen and cultured vascular cells. Science 1986 Jan 24;231(4736):397-400.
(20) Hibino N, Villalona G, Pietris N, Duncan DR, Schoffner A, Roh JD, et al. Tissue-engineered vascular grafts form neovessels that arise from regeneration of the adjacent blood vessel. FASEB J 2011 Aug;25(8):2731-9.
Fahner.indd 105 5-5-2014 14:35:15

(21) Niklason LE, Gao J, Abbott WM, Hirschi KK, Houser S, Marini R, et al. Functional arteries grown in vitro. Science 1999 Apr 16;284(5413):489-93.
(22) Anders E, Alles JU, Delvos U, Potzsch B, Preissner KT, Muller-Berghaus G. Microvascular endothelial cells from human omental tissue: modified method for long-term cultivation and new aspects of characterization. Microvasc Res 1987 Sep;34(2):239-49.
(23) Pronk A, Leguit P, Hoynck van Papendrecht AA, Hagelen E, van Vroonhoven TJ, Verbrugh HA. A cobblestone cell isolated from the human omentum: the mesothelial cell; isolation, identification, and growth characteristics. In Vitro Cell Dev Biol 1993 Feb;29A(2):127-34.
(24) Sharp WV, Schmidt SP, Meerbaum SO, Pippert TR. Derivation of human microvascular endothelial cells for prosthetic vascular graft seeding. Ann Vasc Surg 1989 Apr;3(2):104-7.
(25) Tiwari A, Salacinski HJ, Hamilton G, Seifalian AM. Tissue engineering of vascular bypass grafts: role of endothelial cell extraction. Eur J Vasc Endovasc Surg 2001 Mar;21(3):193-201.
(26) Williams SK. Human clinical trials of microvascular endothelial cell sodding. In: Zilla P, Greisler HP, editors. Tissue Engineering of Vascular Prosthetic Grafts. Landes: Austin: 1999, p. 143-7.
(27) Melchiorri AJ, Hibino N, Fisher JP. Strategies and techniques to enhance the in situ endothelialization of small-diameter biodegradable polymeric vascular grafts. Tissue Eng Part B Rev 2013 Aug;19(4):292-307.
Fahner.indd 106 5-5-2014 14:35:15

Dankwoord | 107
Dankwoord
In de overtuiging dat elke nieuwe dag een geschenk is uit Gods hand zijn wij Hem dankbaar voor
al die gaven die we in de achterliggende jaren mochten ontvangen.
Prof. dr. T.M. van Gulik, beste Thomas. Zeer dank voor de mogelijkheid die jij gaf om te werken
op het Chirurgisch Laboratorium van het AMC. Een enthousiaste en inspirerende omgeving
wist jij daar te creëren om de experimenten op te zetten en uit te voeren. Je ontwapenende
presentatie gaf altijd het gevoel dat ik bij je welkom was. Dank voor de uitmuntende lezing van
de engelse teksten.
Prof. dr. D.A. Legemate, beste Dink. Dankzij de mede door jou opgezette samenwerking
tussen de experimentele chirurgie en vaatchirurgie werd het onderzoek mogelijk. Dank voor je
begeleiding in de opzet van de verschillende onderzoeken en het bewaken van de voortgang. Je
grote kennis over de opzet en analyse van een systematic review bewonder ik.
Dr. M.M. Idu, beste Mirza. Veel hulp heb je gegeven bij de praktische uitvoering van de
experimenten. We hebben heel wat hechtdraadjes verbruikt voor alle anastomosen. Nederland
zijn we doorgereisd van noord naar zuid ter voorbereiding van de volgende studie. Dank voor je
niet afnemende doorzettingsvermogen.
Prof. dr. E.T. van Bavel, Dr. M. Heger, Prof. dr. B.A.J.M. de Mol, Dr. J.I. Rotmans, Prof. dr. C.J.A.M.
Zeebregts, geachte leden van de promotiecommissie. Dank voor uw bereidheid het manuscript
te willen beoordelen en van commentaar te voorzien. Prof. dr. B.H. Walpoth, dear Beat. Thank
you very much for your valuable discussions we have had in Szeged, Hungary and in Athens,
Greece on the Congress of the European Society for Surgical Research. Thanks a lot for your
introduction in your research laboratory at Hôpitaux Universitaires de Genève and for your
willingness to participate in the doctoral committee.
Beste IWO bewoners, dank voor de plezierige samenwerking. Beste kamergenoten, Ivo
Schoots, Geert Koffeman, Bob Heijnen en Suzanne van Veen. Dank jullie zeer voor de
gezellige tijd samen. Collega onderzoekers, Maud Bessems, Oktay Camlidag, Sander Dinant,
Benedict Doorschot, Maarten Jansen, Maarten-Paul van de Kerkhove, Jeroen Lips, Paul Poyck,
Reeta Vetelainen, Annebeth de Vries. We hebben heel veel teamvergaderingen, retraites,
onderzoekervergaderingen en buitenlandse reizen met elkaar kunnen beleven. Dank voor de
Fahner.indd 107 5-5-2014 14:35:16

108 | Dankwoord
stimulerende ontmoetingen. Beste (bio)technici en analisten, Adri Maas, Goos Huijzer, Henk de
Wit, Marloes Klein, Peter Schneider, Robin Hartman, Maringa Emons, Esther Posno en Albert van
Wijk. Zonder jullie ondersteuning waren de experimenten nooit van de grond gekomen. Dank
voor jullie altijd durende behulpzaamheid. Beste Postdoc´s, Irene Straatsburg, Ruurtje Hoekstra
en Leo Abrahamse. Dank voor jullie wetenschappelijke support.
Beste Wouter Florijn, Henriette Griffioen, Ties van de Berg en Kor Brandsma. Dank voor jullie hulp
bij het toezicht op de naleving en correcte uitvoering van de onderzoeksprotocollen.
Beste onderzoeksstudenten, Jaap Borstlap, Bram van Wijk en Carola van Eck. Dank voor jullie
hulp bij de experimenten, data invoer en analyse. Het was een eer jullie begeleider te mogen
zijn. Dear Dora Bedreaga, it was a great pleasure to me that you have participated as a research
student in our group. Best Kitty Cisse en Andrea de Leeuw. Hartelijk dank voor de vele manieren
waarop jullie secretariële ondersteuning hebben verleend.
Medewerkers van het vaatcentrum en de afdeling radiologie van het AMC, beste Johan van
Gurp, Dianne Hanson, Ineke Zwiers en Theo van de Storm. Hoe vaak zijn jullie niet met je echo
apparaat op pad gegaan door alle gangetjes richting het IWO? Jullie lieten het gewoon nooit
afweten. Hartelijk dank voor de inzet. Theo bedankt voor je hulp bij de angio´s.
Medewerkers van de afdeling Medische fysica, Farmacotherapie, Pathologie en Microscopisch
onderzoek van het AMC. Prof. Dr. Pfaffendorf, MJ Mathy, Stephan Peters, Allard van der Wal
en Jan van Marle. Dank jullie voor de expertise die jullie hebben ingebracht en de enthousiaste
bereidheid tot samenwerking.
Mevrouw G.E.E. van Noppen, beste Wendy. Dank voor je mooie cursus en begeleiding van de
eerste stappen bij het schrijven van engelse teksten.
Medewerkers van het Rode Kruis Ziekenhuis en de Euro Skin Bank te Beverwijk. Prof. Dr. R.W. Kreis,
Dr. R.S. Breederveld, Paul van Zuijlen, Jeroen van Baare, Hans Hoekstra, Esther Middelkoop,
Nelleke Richters en Jos Vloemans. Door jullie bereidheid tot inzicht in het preservatieprotocol
van de glycerol donorhuiden werd het onderzoek op vaten mogelijk gemaakt. Dank voor jullie
discussies en getoonde interesse in het verloop van het onderzoek.
Beste Adelheid Schokker, dank voor je hulp bij de invoer van data en je blijvende interesse
voor het onderzoek. Dank ook voor je grote gastvrijheid en de gezellige ontmoetingen in de
Fahner.indd 108 5-5-2014 14:35:16

Dankwoord | 109
achterliggende jaren. In zeer dierbare herinnering aan je echtgenoot Bob Schokker die ik heb
mogen leren kennen als kundig arts, tactisch bestuurder en bovenal als waardevolle vriend.
Dr C.F. Gattuso van de Kring Oost van de Rijksdienst voor de keuring van vee en vlees voor het
verlenen van toestemming om 1 geitenkop te vervoeren vanuit Slachthuis Midden Nederland
te Twello naar het AMC. Hierdoor werd het mogelijk mij voorafgaand aan de experimenten te
verdiepen in de halsanatomie van de geit.
Beste collegae en medewerkers van ziekenhuis De Sionsberg. Bedankt voor de wijze waarop jullie
me in jullie midden hebben opgenomen. Dank aan het hele team van de afdeling radiologie voor
jullie betrokkenheid. Het is me een groot genoegen met jullie te mogen samenwerken.
Geliefde familie en vrienden. Dank voor jullie getoonde interesse in de onderzoeksjaren. Al moest
ik nog wel eens verstek laten gaan bij feesten en partijen, de onderlinge banden bleven bestaan.
Beste Hanneke van Krimpen en André Janse, dank voor jullie langdurige vriendschap. Het is
prachtig dat jullie paranimf willen zijn.
Lieve kinderen, Anne-Fleur, Joachim, Jean-Luc en Florentijn. We mochten jullie ontvangen in de
achterliggende jaren en genieten elke dag van jullie aanwezigheid. Misschien raken jullie later
ook wel gemotiveerd voor het doen van onderzoek. Lieve Anneke, je bent van onschatbare
waarde gebleken. Niet in het minst in de jaren waarin je heel wat keren de honneurs alleen
moest waarnemen. Ik blijf je voor altijd dankbaar.
Fahner.indd 109 5-5-2014 14:35:16

Fahner.indd 110 5-5-2014 14:35:16

Curriculum Vitae | 111
Curriculum Vitae
The author was born on February 18th, 1972 in Angguruk, Indonesia. He graduated from high
school, Van Lodestein College, in 1991 and obtained his medical degree at Erasmus University
Rotterdam in 1998. He was resident in internal medicine (Ziekenhuis Velp, Velp) urology (Canisius
Wilhelmina Ziekenhuis, Nijmegen) and surgery (Eemland Ziekenhuis, Amersfoort, Rode Kruis
Ziekenhuis, Beverwijk and St Lukas Andreas Ziekenhuis, Amsterdam). From 2001 until 2004 he
was PhD fellow at the Surgical Laboratory of the Academic Medical Center, Amsterdam under
supervision of Prof. dr. D.A. Legemate and Prof. dr. T.M. van Gulik. From 2006 until 2012 he
followed his residency in radiology at the University Medical Center Groningen under supervision
of Prof. dr. M. Oudkerk, Prof. dr. E.J. van der Jagt and Dr. L.M. Kingma. Since 2012 he works as
a radiologist in Ziekenhuis de Sionsberg, Dokkum.
Fahner.indd 111 5-5-2014 14:35:16

Experim
ental Stu
dies o
n G
lycerol Preserved
Vascu
lar Allo
grafts
Peter Fahn
er
Experimental Studies on Glycerol Preserved Vascular Allografts
Peter Fahner
UITNODIGING
voor het bijwonen van
de openbare verdediging
van het proefschrift
Experimental Studieson Glycerol Preserved
Vascular Allografts
op vrijdag 6 juni 2014
om 13.00 uur
in de Aula van de
Universiteit
van Amsterdam
Oude Lutherse Kerk
Singel 411, hoek Spui
1012 WN Amsterdam
Aansluitend receptie in de
naastgelegen
Tetterode Bibliotheek
Paranimfen:
Hanneke van Krimpen
André Janse
Peter [email protected]