Proefschrift van Zoonen
170
-
Upload
nicole-nijhuis -
Category
Documents
-
view
222 -
download
0
description
Â
Transcript of Proefschrift van Zoonen



An Ounce of Prevention is worth a Pound of Cure
Help-seeking and the onset of depression in people with subclinical depression
Kim van Zoonen

This thesis was prepared at the Department of Clinical Psychology, Faculty of Psychology and Education, VU University Amsterdam, within the EMGO Institute for Heath and Care Research. The project was funded by the Netherlands Organisation for Health Research and Development (ZonMw grant: 50-51510-98-009)Financial support for printing of this thesis was kindly provided by:
• Department of Clinical Psychology VU University Amsterdam• NETQ Healthcare. This project used NETQ online surveys• GGZinGeest, Amsterdam• PuntP Preventie, onderdeel van Arkin• Minddistrict. e-health solutions in mental health care
ISBN: 978-94-6108-988-5
© 2015 by K. van Zoonen, Amsterdam.All rights reserved. No part of this thesis may be produced, stored in a retrieval center of any nature, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the permission of the author.
Design cover: Joeri Mastop & Kim van Zoonen, basic picture of libra by Oksana Alekseeva/shutterstock.comDesign layout: Nicole Nijhuis & Kim van Zoonen

VRIJE UNIVERSITEIT
An Ounce of Prevention is worth a Pound of Cure
Help-seeking and the onset of depression in people with subclinical depression
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aande Vrije Universiteit Amsterdam,
op gezag van de rector magnificusprof.dr. F.A. van der Duyn Schouten,
in het openbaar te verdedigenten overstaan van de promotiecommissie
van de Faculteit der Psychologie en Pedagogiekop donderdag 18 juni 2015 om 13.45 uur
in de aula van de universiteit,De Boelelaan 1105
door
Kim van Zoonen
geboren te Amsterdam

promotoren: prof.dr. P. Cuijpers prof.dr. A.T.F. Beekmancopromotoren: prof.dr. J.H. Smit dr. A.M. Kleiboer

leescommissie: prof.dr. A. van Straten prof.dr. H. de Vries prof.dr. T. Brugha prof.dr. C. Hosman prof.dr. R. Schoevers dr. E. Dozeman


Contents
Part I Introduction Chapter 1 General Introduction 11 Part II Preventive care for depression Chapter 2 Are preventive interventions for depression effective? A meta-analysis 27
Part III Reasons for (not) seeking help Chapter 3 Reasons and determinants of (not) seeking help 55Chapter 4 How well do people identify their symptoms? 75Chapter 5 How do people view the available care (professional care, informal help, and self-reliance) 91 Part IV Who will benefit from preventive care? Chapter 6 Conversion of subclinical depressive symptoms into depressive disorders 113 Part V Discussion and summary Chapter 7 General Discussion 131 Summary 145 Samenvatting (summary in Dutch) 149 Part VI Dankwoord/Acknowledgments Dankwoord 155 Part VII About the author About the author 161 Part VIII List of Publications Publications 165


Part I: Introduction


Chapter 1
General Introduction

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
12 | Chapter 1

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 13
An ounce of prevention is worth a pound of cure – Benjamin Franklin -
These famous words are also known as the more common saying; “Prevention is better than cure”, meaning it is better to stop something bad from happening before it occurs than it is to deal with it after it has happened. But is this true? Natural instincts and many diverse situations might incline you to say yes. However, there is a certain complexity to prevention and, therefore, this saying when you look at mental health prevention. In mental health it is difficult to predict if a certain disorder will develop or not, what happens when you try to prevent something of which you cannot predict it will happen? Is prevention better or feasible when it is uncertain what can be done to prevent an illness from developing? For example, there are several mental health disorders in which the outcome (e.g. a full-blown disorder) is unpredictable, even for people who are diagnosed as ‘at risk’.
One of the most prevalent and disabling mental health disorders is depression. Unfortunately, it is unknown which people will develop a depressive disorder and which people will not. However, we do know that certain people are at high(er) risk of developing depression, such as people with a subclinical depression. People with subclinical depression report depressive symptoms, but fail to meet the criteria of major depression according to the Diagnostic and Statistical Manual of Mental Disorders V (DSM-V) (1). Although it is known that preventive interventions for depression can prevent or, at the very least, delay the onset of depression, it is unknown which people with subclinical depression will develop a depressive disorder and which people will not (2). In other words, it is unknown which people might benefit from preventive interventions. Another important shortcoming in the literature is that we do not know if the people that might benefit from preventive care receive or seek this care or how people view their symptoms and how they feel about (preventive) care. This leads to the following research questions;
(1) Can people benefit from preventive interventions?(2) Which people with subclinical depression (are willing to) participate in
preventive interventions for depression?(3) How do people view their symptoms?(4) What are their attitudes towards care?(5) Which people with subclinical depression develop depressive disorders?
This thesis aims to answer these questions and provide more insight into the onset of depression and reasons for (not) seeking help in people with subclinical depression. This chapter will introduce the general background and provide an overview of the chapters.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
14 | Chapter 1
Prevention of depression
Depression is a worldwide health concern and affects one in every eight men and one in every five women (3, 4). It is associated with considerable morbidity and mortality (5-7). Moreover, depression impacts the ability to function at home, affecting marital and parenting behaviour, as well as the ability to function at work, resulting in absenteeism and reduced productivity (8). Depression can be best viewed on a continuum ranging from no symptoms to many symptoms (9-11). Prevalence rates of major depression range from 14.6% in high-income countries to 5.9% in low- to middle-income countries (12). The incidence rates are around 2% in the general population (13).
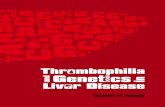
As the saying suggests, treatment and prevention are two different things (Figure 1). Treatment, even under optimal conditions, cannot reduce the burden of disease associated with depression sufficiently (14, 15). A way to further reduce the burden is to reduce the incidence. This is the focus of prevention rather than treatment. However, it is more difficult to convince people, health care professionals and government agencies of the advantages of prevention compared to treatment, as people are not sure a bad event will happen and there is no direct benefit for taking action. Therefore, the urgency to deal with symptoms is less pronounced. This is the area of prevention and there are three levels of prevention; 1) Universal preventive strategies or interventions targeting the entire population. 2) Selective preventive interventions focusing on specific subgroups within the
population who are considered at high risk due to common characteristics (e.g. traumatic events, poverty, etc).
3) Indicated prevention targeting people who suffer from early stages or symptoms of depression (e.g. people with subclinical depression).
The model in Figure 1 also describes “promotion” and “recovery”. Promotion is not necessarily focused on preventing depression. However, due to the focus of promotion on producing healthy and resilient mood states, it is likely to also prevent depression. Recovery focuses more on curing during treatment or after treatment has ended and as such is not part of prevention.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 15
13
Figure 1. Promotion, prevention, treatment and recovery (8)
From a clinical perspective early detection of a mental illness is important (16) and
focusing on people who are at risk of developing depression (e.g. people with subclinical
depression) is an effective way of doing this. In the past 2 decades more and more research
has demonstrated that preventive interventions can be effective in delaying and preventing
the onset of major depression by 22% (17, 18). Therefore, the current thesis will focus on
people with subclinical depression and indicated prevention, since these people are at high
risk of developing depression and subclinical depression has been consistently found to be
one of the best predictors of major depression (2, 19, 20).
In the Netherlands, an infrastructure that structurally embeds prevention in mental
health care has been implemented in the past 30 years, which makes the Dutch health care
system unique. Depression prevention is freely available to the general public, including
people with subclinical depression, in about forty specialized mental health facilities at
little to no costs. However, despite the wide availability of depression prevention in the
Figure 1. Promotion, prevention, treatment and recovery (8)
From a clinical perspective early detection of a mental illness is important (16) and focusing on people who are at risk of developing depression (e.g. people with subclinical depression) is an effective way of doing this. In the past 2 decades more and more research has demonstrated that preventive interventions can be effective in delaying and preventing the onset of major depression by 22% (17, 18). Therefore, the current thesis will focus on people with subclinical depression and indicated prevention, since these people are at high risk of developing depression and subclinical depression has been consistently found to be one of the best predictors of major depression (2, 19, 20).
In the Netherlands, an infrastructure that structurally embeds prevention in mental health care has been implemented in the past 30 years, which makes the Dutch health care system unique. Depression prevention is freely available to the general public, including people with subclinical depression, in about forty specialized mental health facilities at little to no costs. However, despite the wide availability of depression prevention in the Netherlands, participation rates in preventive interventions for depression are low, which is similar to participation rates in other countries (21-23).
Subclinical depression
Subclinical depression is part of the depression continuum and is considered a prodromal phase. It is well known that subclinical depression is one of the best predictors of major depression, but there is also an increased risk of developing other mood and anxiety

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
16 | Chapter 1
disorders as well as an increased risk of suicidal ideation and attempts (2, 19, 20, 24). Subclinical depression has a significant impact on daily functioning and is associated with great economic costs (19, 25).
There are several ways of operationalizing subclinical depression, such as (1) a score above a threshold on a screening instrument, but failing to meet the criteria for major depression according to the Diagnostic and Statistical manual of Mental Disorders (DSM-V) or (2) having a depressed mood accompanied with additional symptoms, but not as severe or as many as the DSM-V criteria for major depression (1, 2, 20). In the current thesis we mostly used the first definition; depressive symptoms that do not yet meet the diagnostic criteria of a full-blown depression (26).
Incidence and prevalence rates vary widely due to differences in population, definition and instruments that are used, with incidence rates ranging from 2% to 13% and prevalence rates varying from 2% to 32% (27-30). These prevalence rates are equal or higher than those for full-blown depressive disorders (29). The prevalence in a population-based study in the US was 12% (24), in the Netherlands approximately 7.5% of the general population suffers from subclinical depression (19).
As stated before, it is well known that people who suffer from subclinical depression have an increased risk of developing major depression and research has shown that between 20% to 34% of people with subclinical depression will develop a major depression (31, 32). Other research has indicated that a considerable proportion of adults and older people with subclinical depression experience recurrent episodes or develop a chronic form of subclinical depression (33). However, little is known about which people with subclinical depression will develop a depressive disorder, which people will not, and which people will recover or, in other words, the individual course of subclinical depression (2, 24).
The few studies that have examined the onset of depressive disorders in people with subclinical depression have identified several factors that influence the onset of depressive disorders (20, 31, 34, 35). Some of these factors can be categorized as characteristics of depression, such as feelings of worthlessness and severity of depressive symptoms, other factors can be categorized as individual characteristics, such as family history of depression, suffering from a chronic illness, and mastery.
Help-seeking
Since we know that not everyone with subclinical depression will develop a depressive disorder, it is imperative to know who will need (professional) care in order to prevent the onset of major depression (e.g. which people do not naturally recover from subclinical depression). A good and necessary first step is to examine help-seeking behaviour and

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 17
identify reasons for (not) seeking help in people with subclinical depression, regardless of the onset of depression.
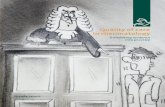
Literature on help-seeking in (mental) health care is often guided by the Behavioural Model of Health Service Use by Andersen and Newman (36). This model, as presented in Figure 2, explains the use of health care by looking at three interrelating factors: need, predisposing, and enabling factors (37). Need factors can be described as both perceived (e.g. how people view and experience their own health and illness symptoms) and actual need (e.g. defined by professional assessment and objective measurement of the symptoms a person experiences or their health status) for health care (38-41). Help-seeking in depression has shown that need factors, such as recognizing symptoms and severity of symptoms, determine whether someone is more likely to seek help (42, 43).
Predisposing factors consist of demographic factors, social structure and belief factors (e.g. attitudes, values, and health beliefs) (37). Some research has shown that young people, people with more positive experiences in mental health care and people who acknowledge their mental problems were more likely to receive mental health treatment (44, 45). However, other research indicates that increasing age is related to greater need for mental health care (46-48). Also, research has shown that people with higher scores on neuroticism, higher education, female gender, and who are in a relationship with a significant other tend to seek more care for their mental health problems (48-52). Furthermore, research indicates that stigma and embarrassment are related to help-seeking in young people (53).
17
Figure 2. Andersen’s model of health care utilization (36)
Enabling factors relate to organisational factors which affect the availability and
affordability of mental health care. These can be individual factors, such as a person’s
financial situation (54), organizational factors, such as location and distribution of health
care facilities, or contextual factors, such as resources that are available to a person (23).
Due to the infrastructure in the Netherlands, mental health care is available and mostly free
to everyone who needs it, however not everyone might know of this type of care or feel it is
applicable to them.
The Behavioural Model of Health Service Use, however, fails to explain what
happens with these three factors and their influence on help-seeking when need factors are
less important or pronounced (e.g. lower severity of symptoms), which is the case in people
ENVIRONMENT POPULATION CHARACTERICTS HEALTH BEHAVIOUR
OUTCOME
Health Care System External Environment
Predisposing Enabling Need Characteristic Resources
Personal Health Practices Use of Health services
Perceived Health Status Evaluated Health Status Consumer Satisfaction
Figure 2. Andersen’s model of health care utilization (36)

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
18 | Chapter 1
Enabling factors relate to organisational factors which affect the availability and affordability of mental health care. These can be individual factors, such as a person’s financial situation (54), organizational factors, such as location and distribution of health care facilities, or contextual factors, such as resources that are available to a person (23). Due to the infrastructure in the Netherlands, mental health care is available and mostly free to everyone who needs it, however not everyone might know of this type of care or feel it is applicable to them.
The Behavioural Model of Health Service Use, however, fails to explain what happens with these three factors and their influence on help-seeking when need factors are less important or pronounced (e.g. lower severity of symptoms), which is the case in people with subclinical depression. Research has indicated that many people with mental health problems do not perceive a need for help, because they do not perceive they have mental health problems, they feel symptoms are temporary or not serious enough (55, 56). This, combined with the natural recovery rate in people with subclinical depression, indicates that people might be correct not to seek help for their symptoms.
Summary
Preventive interventions for depression can help prevent or delay the onset of depression in people who are at high risk of developing depression, such as people with subclinical depression. Although there is no consensus on the definition of subclinical depression, researchers have agreed that depression exists on a continuum and subclinical depression is considered a prodromal phase of depression (2). Furthermore, it is considered the best predictor of major depression. However, the individual course of subclinical depression is unknown which makes it impossible to tell who will benefit from preventive interventions and who will not or, in other words, who should seek-help in order to prevent depressive symptoms converting into a depressive disorder (2).
Research on help-seeking in people with subclinical depression is scarce, however existing research indicates that people’s (poor) self-identification of their symptoms and the judgment of their ability to deal with the symptoms on their own are reported most often as reasons for not seeking help. On the other hand, practical reasons (e.g. lack of time or money) are reported less often as barriers to seeking care (56). These barriers could be categorized, according to the Andersen and Newman model of health care utilization, into need, predisposing and enabling factors, which interrelate to one another.
Although people could benefit from preventive care, participation rates across the world are low. This is also the case in the Netherlands, despite its unique infrastructure which makes mental health care available to everyone at little to no costs. It is not yet clear which of the discussed factors might explain the low participation rates in preventive

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 19
interventions for depression or what people with subclinical depression report as reasons for not seeking preventive care. A possible explanation might be the severity of symptoms or the natural recovery rate of subclinical depression. It is imperative to gain better insight into help-seeking and the onset of depression in people with subclinical depression and this thesis provides a first step by examining if preventive interventions are (still) effective, what reasons people with subclinical depression have for (not) seeking help and what predicts the onset of a depressive disorder in people with subclinical depression.
Overview of the chapters
This thesis will examine the reasons of people with subclinical depression to (not) seek help and the onset of depression in this high risk group. Chapter 2 will focus on answering the first research question and includes a meta-analysis examining the effectiveness of preventive interventions for depression. Chapters 3 to 5 examine the second research question by investigating reasons and determinants for (not) seeking help in people with subclinical depression, whether the patient perspective corresponds to the professional perspective (Chapter 4), and how people with subclinical depression view professional mental health care, informal care (e.g. help from friends and/or family) or being self-reliant (Chapter 5). Finally, this thesis will examine the third research question by providing insight into the onset of a depressive disorder within a one year period in people with subclinical depression and examine characteristics that predict the onset of depression (Chapter 6). Chapter 7 will provide a general discussion on the findings discussed in the previous chapters. As a final note to the reader I would like to draw attention to the fact that chapters 2, 3, 4, 5, and 6 are separate journal articles and can be read independently.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
20 | Chapter 1
References
1. APA. DSM 5: American Psychiatric Association; 2013.2. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder:
a systematic review of prospective studies. Acta Psychiatrica Scandinavica. 2004;109(5):325-31.
3. Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. The Lancet. 2007;370(9590):841-50.
4. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of general psychiatry. 1994;51(1):8-9.
5. Celano CM, Huffman JC. Depression and cardiac disease: a review. Cardiology in review. 2011;19(3):130-42.
6. Pan A, Lucas M, Sun Q, van Dam RM, Franco OH, Willett WC, et al. Increased mortality risk in women with depression and diabetes mellitus. Archives of general psychiatry. 2011;68(1):42-50.
7. Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder: results from the National Epidemiologic Survey on Alcoholism and Related Conditions. Archives of general psychiatry. 2005;62(10):1097-106.
8. Muñoz RF, Cuijpers P, Smit F, Barrera AZ, Leykin Y. Prevention of major depression. Annual Review of Clinical Psychology. 2010;6:181-212.
9. Geiselman B, Bauer M. Subthreshold depression in the elderly: Qualitative or quantitative distinction? Comprehensive Psychiatry. 2000;41(2, Supplement 1):32-8.
10. Goldberg D. Plato versus Aristotle: Categorical and dimensional models for common mental disorders. Comprehensive Psychiatry. 2000;41(2, Supplement 1):8-13.
11. Rodríguez MR, Nuevo R, Chatterji S, Ayuso-Mateos JL. Definitions and factors associated with subthreshold depressive conditions: a systematic review. BMC psychiatry. 2012;12(1):181.
12. Bromet E, Andrade LH, Hwang I, Sampson NA, Alonso J, de Girolamo G, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC medicine. 2011;9(1):90.
13. De Graaf R, Bijl R, Ravelli A, Smit F, Vollebergh W. Predictors of first incidence of DSM-III-R psychiatric disorders in the general population: findings from the Netherlands Mental Health Survey and Incidence Study. Acta Psychiatrica Scandinavica. 2002;106(4):303-13.
14. Andrews G, Wilkinson DD. The prevention of mental disorders in young people. Medical Journal of Australia. 2002;177(7):S97.
15. Chisholm D, Sanderson K, Ayuso-Mateos JL, Saxena S. Reducing the global burden of depression Population-level analysis of intervention cost-effectiveness in 14 world regions. The British Journal of Psychiatry. 2004;184(5):393-403.
16. Insel TR. Translating scientific opportunity into public health impact: a strategic plan for research on mental illness. Archives of General Psychiatry. 2009;66(2):128-33.
17. Cuijpers P, Van Straten A, Smit F, Mihalopoulos C, Beekman A. Preventing the Onset of Depressive Disorders: A Meta-Analytic Review of Psychological Interventions. American Journal of Psychiatry. 2008;165(10):1272-80.
18. Cuijpers P, Koole SL, van Dijke A, Roca M, Li J, Reynolds CF. Psychotherapy for subclinical depression: meta-analysis. The British Journal of Psychiatry. 2014;205(4):268-74.
19. Cuijpers P, de Graaf R, van Dorsselaer S. Minor depression: risk profiles, functional disability, health care use and risk of developing major depression. Journal of Affective Disorders. 2004;79(1–3):71-9.
20. Eaton W, Badawi M, Melton B. Prodromes and precursors: epidemiological data for primary prevention of disorders with slow onset. American Journal of Psychiatry. 1995;152:967-72.
21. de Jonge M, Ruiter M. Aard- en omvangstudie GGZ- en verslavingspreventie 2007. Utrecht: Trimbos Instituut, 2008.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 21
22. Dijkstra M, Ruiter M. Aard en omvang GGZ- en verslavingspreventie 2010; ontwikkelingen in de inhoud, organisatie en omvang van de GGZ- en Verslavingspreventie. Utrecht: Trimbos Instituut, 2010.
23. Cuijpers P, Warmerdam L, Van Straten A, Rooy MJ. Het bereik van preventieve interventies voor depressie. TVGW. 2010;88(5):278-84.
24. Pietrzak R, Kinley J, Afifi T, Enns M, Fawcett J, Sareen J. Subsyndromal depression in the United States: prevalence, course, and risk for incident psychiatric outcomes. Psychological medicine. 2013;43(07):1401-14.
25. Rapaport MH, Judd LL. Minor depressive disorder and subsyndromal depressive symptoms: functional impairment and response to treatment. Journal of Affective Disorders. 1998;48(2–3):227-32.
26. Smit F. Factsheet Prevention: Preventing Depression2007 29-12-2014:[4 p.]. Available from: http://www.trimbos.nl/webwinkel/productoverzicht-webwinkel/preventie/af/~/media/files/gratis%20downloads/af0426%20lsp%20factsheet%20preventing%20depression.ashx.
27. Rivas M, Nuevo R, Ayuso-Mateos JL. Subclinical depression in Spain: Prevalence and health impact. Revista de Psiquiatría y Salud Mental (English Edition). 2011;4(3):144-9.
28. Goldney RD, Fisher LJ, Dal Grande E, Taylor AW. Subsyndromal depression: prevalence, use of health services and quality of life in an Australian population. Social psychiatry and psychiatric epidemiology. 2004;39(4):293-8.
29. Rucci P, Gherardi S, Tansella M, Piccinelli M, Berardi D, Bisoffi G, et al. Subthreshold psychiatric disorders in primary care: prevalence and associated characteristics. Journal of Affective Disorders. 2003;76(1–3):171-81.
30. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. Journal of Affective Disorders. 1997;45(1–2):19-30.
31. Cuijpers P, Beekman ATF, Smit F, Deeg D. Predicting the onset of major depressive disorder and dysthymia in older adults with subthreshold depression: a community based study. International journal of geriatric psychiatry. 2006;21(9):811-8.
32. Hill RM, Pettit JW, Lewinsohn PM, Seeley JR, Klein DN. Escalation to Major Depressive Disorder among adolescents with subthreshold depressive symptoms: Evidence of distinct subgroups at risk. Journal of Affective Disorders. 2014;158(0):133-8.
33. Hermens MLM, van Hout HPJ, Terluin B, van der Windt DAWM, Beekman ATF, van Dyck R, et al. The prognosis of minor depression in the general population: a systematic review. General Hospital Psychiatry. 2004;26(6):453-62.
34. Cuijpers P, Smit F, Willemse G. Predicting the onset of major depression in subjects with subthreshold depression in primary care: a prospective study. Acta Psychiatrica Scandinavica. 2005;111(2):133-8.
35. Crum RM, Cooper-Patrick L, Ford DE. Depressive symptoms among general medical patients: prevalence and one-year outcome. Psychosomatic medicine. 1994;56(2):109-17.
36. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? Journal of health and social behavior. 1995;36(1):1-10.
37. Andersen RM, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Quarterly. 2005;83(4):Online-only.
38. Anderson JG. Demographic Factors Affecting Health Services Utilization: A Causal Model. Medical Care. 1973;11(2):104-20.
39. Babitsch B, Gohl D, von Lengerke T. Re-revisiting Andersen’s Behavioral Model of Health Services Use: a systematic review of studies from 1998–2011. GMS Psycho-Social-Medicine. 2012;9.
40. Andersen RM, Davidson PL, Baumeister SE. Improving access to care. Changing the US health care system: key issues in health services policy and management. 2013:33.
41. Parslow RA, Jorm AF. Who uses mental health services in Australia? An analysis of data from the National Survey of Mental Health and Wellbeing. Australian & New Zealand Journal of Psychiatry. 2000;34(6):997-1008.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
22 | Chapter 1
42. Verhaak PF, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJ, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
43. Nease D, Volk RJ, Cass AR. Does the severity of mood and anxiety symptoms predict health care utilization? Journal of Family Practice. 1999;48(10):769-77.
44. Andrews G, Issakidis C, Carter G. Shortfall in mental health service utilisation. Br J Psychiatry. 2001;179:417-25.
45. Verhaak PFM, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJLM, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
46. Areán PA, Alvidrez J, Barrera A, Robinson GS, Hicks S. Would Older Medical Patients Use Psychological Services? The Gerontologist. 2002;42(3):392-8.
47. Mackenzie CS, Gekoski WL, Knox VJ. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging & Mental Health. 2006;10(6):574-82.
48. Berger JM, Levant R, McMillan KK, Kelleher W, Sellers A. Impact of Gender Role Conflict, Traditional Masculinity Ideology, Alexithymia, and Age on Men’s Attitudes Toward Psychological Help Seeking. Psychology of Men & Masculinity. 2005;6(1):73-8.
49. Oliver MI, Pearson N, Coe N, Gunnell D. Help-seeking behaviour in men and women with common mental health problems: cross-sectional study. Br J Psychiatry. 2005;186:297-301.
50. Koydemir-Özden S. Self-Aspects, Perceived Social Support, Gender, and Willingness to Seek Psychological Help. International Journal of Mental Health. 2010;39(3):44-60.
51. Seekles WM, Cuijpers P, Van de Ven P, Penninx BWJH, Verhaak PFM, Beekman ATF. Perceived need for Mental Health Care and personality among Primary Care patients. Journal of Affective Disorders. 2012;136(3):666-74.
52. Ten Have M, Oldehinkel A, Vollebergh W, Ormel J. Does neuroticism explain variations in care service use for mental health problems in the general population? Social Psychiatry & Psychiatric Epidemiology. 2005;40(6):425-31.
53. Gulliver A, Griffiths K, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. 2010;10(1):113.
54. Bartels SJ. Improving the United States’ System of Care for Older Adults With Mental Illness: Findings and Recommendations for The President’s New Freedom Commission on Mental Health. The American Journal of Geriatric Psychiatry. 2003;11(5):486-97.
55. Mojtabai R, Olfson M, Mechanic D. Perceived need and help-seeking in adults with mood, anxiety, or substance use disorders. Archives of General Psychiatry. 2002;59(1):77-84.
56. van Beljouw I, Verhaak P, Prins M, Cuijpers P, Penninx B, Bensing J. Reasons and determinants for not receiving treatment for common mental disorders. Psychiatric Services. 2010;61(3):250-7.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
1
General Introduction | 23


Part II: Preventive care for depression


Chapter 2
Are preventive interventions for depression effective?
A meta-analysis
This chapter is published as:Van Zoonen, K., Buntrock, C., Ebert, D. D., Smit, F., Reynolds III,
C. F., Beekman, A. T. F., Cuijpers, P. (2014).
Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions.
International Journal of Epidemiology, 43, 318 – 329.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
28 | Chapter 2
Abstract
Background: Depressive disorders are highly prevalent, have a detrimental impact on the quality of life of patients and their relatives, are associated with increased mortality rates, high levels of service use and substantial economic costs. Current treatments are estimated to only reduce about one third of the disease burden of depressive disorders. Prevention may be an alternative strategy to further reduce the disease burden of depression.
Method: We conducted a meta-analysis of randomized controlled trials examining the effects of preventive interventions in participants with no diagnosed depression at baseline on the incidence of diagnosed depressive disorders at follow-up. We identified 32 studies that met our inclusion criteria.
Results: We found that the relative risk of developing a depressive disorder was IRR = 0.79 (95% CI: 0.69-0.91), indicating a 21% decrease in incidence in prevention groups in comparison to control groups. Heterogeneity was low (I2=24%). The number needed to treat (NNT) to prevent one new case of depressive disorder was 20. Sensitivity analyses revealed no differences between type of prevention (e.g. selective, indicated or universal) nor between type of intervention (e.g. CBT, IPT or other). However, data on NNT did show differences.
Conclusions: Prevention of depression seems feasible and may, in addition to treatment, be an effective way to delay or prevent the onset of depressive disorders. By preventing or delaying these disorders it may contribute to the further reduction of the disease burden and economic costs associated with depressive disorders.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 29
Introduction
About 150 million people worldwide are affected with depression at any moment in time, and one in every 5 women and 1 in every 8 men experience an episode of major depression over the course of their life (1-3).
Depression is a major factor in quality of life decrements and is also associated with premature death (4). People suffering from depressive disorders experience substantial loss in quality of life (5). Between 1990 and 2010, major depression has increased from the 15th to11th in terms of global disease burden measured in DALYs (6) and it is projected to become the single leading cause of disease burden by 2030 (7). Depressive disorders are associated with high levels of service use and economic costs stemming from productivity losses (8). Although effective treatments are available, it has been estimated that, even under optimal conditions, contemporary treatments can reduce only about one-third of the disease burden associated with major depressive disorder (MDD) (9, 10).
A way to further reduce the disease burden of major depression could be to reduce the influx of new cases that is, to reduce the incidence. This is done by prevention rather than treatment. Strengthening protective factors (e.g. social, cognitive or problem-solving skills) or alleviating prodromal disease stages (e.g. reducing severity of depressive symptoms) have been investigated in a considerable number of preventive studies (11-13). Several studies examining the effects of preventive interventions have found favourable effects on the incidence of new cases (14-20), but several others did not (21-24). Whether the effect of the currently available preventive interventions decays over time, indicating effectiveness only when a person is participating in the preventive intervention, is being investigated.
There are different types of prevention. Universal prevention focuses on the general public or a whole population group regardless of risk status. Selective prevention targets individuals or subgroups that are at higher risk of developing mental disorders than average individuals or subgroups. Indicated prevention focuses on individuals who are identified as having prodromal symptoms or biological markers to mental disorders, but who not yet meet the diagnostic criteria for a full-blown diagnosis (25, 26). In a previous meta-analysis of studies examining the effects of preventive interventions on the incidence of new cases, we found an overall effect of universal, selective and indicated prevention on the incidence of depressive disorders (13). Universal prevention was only examined in two studies and it was therefore impossible to investigate effectiveness (21, 27). The studies included in that meta-analysis were conducted among various populations and the interventions differed considerably, which might have influenced the results.
One way to examine whether preventive interventions are effective is to look at the numbers needed to treat (NNT). The NNT indicates the number of people who would

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
30 | Chapter 2
have to receive a preventive intervention in order to prevent one new case of depression. This leads to the expectation that NNT is inversely related to the a priori risk of the disorder (i.e. lower NNTs in indicated prevention).
In our earlier meta-analysis we could include 19 trials examining the effects of preventive interventions, whereas we identified 32 studies for the current meta-analysis, using even more stringent criteria for inclusion. It was therefore deemed opportune to update the earlier meta-analysis, thus allowing us to not only estimate the overall effects of preventive interventions with greater precision, but also to examine characteristics of the interventions and participants as moderators of outcome. In addition, the large number of included studies allows us to examine subfields of prevention in more detail and with greater statistical power, such as prevention of postpartum depression, prevention at schools and prevention of depression in people with somatic illnesses. Also, we focus on whether the effect of type of intervention decays over time, thereby investigating if type of intervention works as a protection or inoculation against new onsets of MDD.
Methods
Search strategies and selection of studiesWe conducted a comprehensive search of the literature in bibliographical databases. All relevant articles published between 1966 and March 2012 were included.
The searches of these databases were done by combining terms indicative of prevention and depression. We specified the search for both MeSH terms and free-text words, but limiting the search to effectiveness studies (e.g. randomized trials, controlled trials, clinical trials). Furthermore, we examined the references of relevant previous meta-analyses and reviews (these are marked with an asterisk in the reference list) and we reviewed the reference lists of retrieved articles.
Studies were included when they used a pretest-posttest randomized controlled design and examined the effects of a preventive, psychological intervention on the incidence of new cases of depressive disorders compared with a control group.
Prevention was defined as reducing the incidence of new cases of MDD. Therefore, we selected studies where participants did not meet the diagnostic criteria (according to the DSM-III-R or DSM-IV) at baseline and were “at risk” of becoming depressed at follow-up – as assessed with a diagnostic instrument. We also included studies examining universal, selective and indicated prevention (28). Studies focusing on preventing depressive disorders after a specific live event (e.g. postnatal depression) were also included.
A study was excluded when the participants were receiving a treatment for another mental disorder. Also, studies on maintenance treatment or relapse prevention were excluded.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 31
Quality AssessmentWe used four basic criteria of the ‘Risk of bias’ tool to assess possible sources of bias (29): sequence generation (the method used to generate the allocation sequence is described in sufficient detail to allow an assessment of whether it should produce comparable groups); allocation concealment (the method used to conceal allocation is described in sufficient detail to see whether intervention allocations were foreseeable in advance of, or during enrolment); blinding of outcome assessors (all measures used to blind personnel as well as study participants to knowledge of which intervention participants were allocated); and incomplete outcome data (methods described whether all randomized participants were used in the analyses). The quality assessment was conducted independently by two reviewers (P.C. and K.v.Z.). Disagreements were solved by consensus.
AnalysesWe used the Comprehensive Meta-Analysis Software package, version 2.2.021 (Biostat, Englewood, N.J.) for all analyses. First we calculated the incidence rate ratio (IRR) for developing a depressive disorder in the intervention compared with the control group for each study. Then we calculated the pooled mean of the IRRs. We investigated both the fixed and the random-effects model (29). The random-effects model assumes that the included studies are drawn from “populations” of studies that may differ from each other and we feel this is more appropriate to use in the current study. The effect sizes resulting from included studies are allowed to differ under this model, not only because of the sample error of each study, but also due to true (systematic) variation across studies.
We also calculated the numbers NNT. This indicates how many people would have to receive a preventive intervention in order to prevent one new case of depression. The NNT was calculated as the inverse of the pooled absolute risk difference.
As a test of homogeneity of effect sizes, we calculated the I2-statistic, which is an indicator of heterogeneity. The I2-statistic can be expressed as a percentage, where a value of 0% indicates no heterogeneity, and 25%, 50% and 75% can be interpreted as low, moderate, and high levels of heterogeneity (30, 31). We calculated 95% confidence intervals (Cis) around I2, using the non-central chi-squared-based approach within the heterogeneity command in Stata (32). We also calculated the Q-statistic and tested the level of significance.
Subgroup and meta-regression analyses were conducted according to the procedures implemented in the Comprehensive-Meta-Analysis software. We used mixed-effects analyses, which pooled studies within subgroups with the random-effects model but tested for differences between subgroup with the fixed-effects model.
Publication bias was tested by inspecting the funnel plot on the primary outcome measure and by Duval and Tweedie’s trim-and-fill procedure which yields an estimate

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
32 | Chapter 2
of the effect size after the publication bias has been taken into account (again, as implemented in the Comprehensive Meta-Analysis program) (33). Also, we performed Egger’s test.
Results
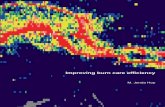
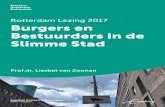
Searches and inclusion of studiesThe literature search resulted in a total of 7447 articles found in PubMed (n = 2006), Cochrane Central Register of Controlled Trials (n = 2707), PsychInfo (n = 932), and EMBASE (n = 1802). We removed duplicates, leaving 4591 articles to be examined. We retrieved a total of 235 full-text articles that potentially met our inclusion criteria. Of these, 203 were excluded. Most (n = 135) were excluded because they lacked a diagnosis at the baseline and/or the follow up. Another reason for not including studies was the lack of randomization (n = 18). All reasons for exclusion are noted in Figure 1. Control groups primarily consisted of care as usual, with some exceptions such as: placebo pill, booklet or no intervention (Table 1).
Characteristics of included studiesA total of 32 studies with 6214 participants (3312 in the prevention groups and 2902 in the control groups) met all inclusion criteria (14-21, 23, 24, 27, 34-56). In one study three different intervention groups were examined (27), so we were able to include 34 comparisons between preventive interventions and control groups. Table 1 shows selected characteristics of the included studies. Sheffield et al. (2006) investigated an universal preventive intervention and two indicated preventive interventions. One other study examined universal prevention, whereas both indicated prevention and selected prevention were each investigated by 15 other studies.
The majority of studies (21) focused on preventing MDD, 9 studies aimed at postpartum depression (PMDD), and 4 dealt with mood mixed disorder (e.g. a combination of MDD, dysthymia and/or minor depression). These were diagnosed by diagnostic instruments, like the SCID (Table 1), which use DSM-III-R or DSM-IV criteria. Most studies did not inform whether they excluded or included participants with a history of depressive disorders (n = 20). Four studies reported using participants with first episode of depression. Eight studies reported including participants with a history of depression, however participants did not experience a depressive disorder at the time of the baseline measure. Eight studies focused on adults in general, 1 study focused on adults with diabetes, 6 studies on pregnant women and 3 studies on (new) mothers, but most studies focused on adolescents or students (n = 14). Fifteen interventions were based on the principle of cognitive behavioural therapy. Some studies based their

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 33
intervention on other psychological approaches, such as problem solving therapy (n = 2) or interpersonal group therapy (n = 5). The number of sessions ranged from 4 to 15. Most studies used interventions which consisted of 12 sessions (n = 7), 2 studies used preventive interventions which consisted of 4 sessions and 2 studies used preventive interventions consisting of 15 sessions.
Eleven studies were conducted in Europe, 14 in the United States and 9 elsewhere. The follow-up periods of these studies varied between 2 and 60 months (median = 9 months). Only one study reported a follow-up of 5 years (57) and one study reported a follow-up of 36 months (34). One study (24) reported a follow-up period of 2 months and 8 studies reported a follow-up period of 3 months.
36
Records identified through database searching
(n = 7447)
Scre
enin
g In
clud
ed
Elig
ibili
ty
Iden
tific
atio
n
Additional records identified through other sources
(n = 0)
Records after duplicates removed (n = 4591)
Records screened (n = 4591)
Records excluded (n = 4356)
Full-text articles assessed for eligibility
(n = 235)
Full-text articles excluded, with reasons (n = 203) - Duplicate publication: 19 - No random assignment/No RCT: 18 - No diagnosis at baseline and/or follow up: 135 - Insufficient data: 8 - No data on depression: 1 - PDF unavailable: 8 - Protocol study: 5 - Treatment, not prevention study: 9
Studies included in quantitative synthesis
(meta-analysis) (n = 32)
Figure 1. Flow chart of included studies Figure 1. Flow chart of included studies

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
34 | Chapter 2
Most studies, however, also reported a follow-up period of 6 or 12 months (n = 28). Drop-out rates in the studies varied between 2% and 64%. Intention-to-treat-analyses were done by most studies (n = 19).
Quality of the articles was relatively high. Quality of studies was assessed on four criteria; allocation concealment, incomplete outcome data, blinding of outcome assessors, and sequence generation. Sixteen studies reported that blinding of the allocation of interventions was done adequately. Eight studies met all four criteria, 18 studies met two or three criteria, and 6 studies met no or only one criterion.
Overall incidence rate ratios (IRR)We calculated the mean IRR by combining the IRRs at different follow-up times into a single estimate. When looking at the fixed-effects model the IRR for all 34 comparisons from the 32 studies was 0.82 (95% confidence interval [CI]: 0.73 – 0.91; p = 0.000). Focusing on the random-effects model, the IRR for all 34 comparisons from the 32 studies was 0.79 (95% CI: 0.69- 0.91; p = 0.001). Heterogeneity was low (I2= 24%). Because the differences between the fixed- and the random-effects models were small, we only report the results for the random effects model (Table 2 and Figure 2).
There was one study27 that compared three interventions with one control group. Since these comparisons were not independent from each other, we examined whether removal of these comparisons would increase heterogeneity. The overall analyses of 32 studies resulted in a mean IRR of 0.77 (95% CI: 0.66-0.90, p = 0.005), with low heterogeneity (I2=29%). This was comparable to the mean IRR found in the total sample.
Since the IRR could differ at varying follow-up periods, we conducted several sensitivity analyses. We examined the IRR for each follow-up period separately (<5 months; 6 months, 7-12 months, ≥13 months; Table 2).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 35
41
We also conducted a separate analysis in which we used only the last follow-up period reported in each
study (0.78; 95% CI: 0.68-0.89; p = 0.001; I2=29), and another analysis with only the first follow-up
period of each study (0.79; 95% CI: 0.69-0.92; p = 0.002; I2=29). As can be seen in Table 2, we found
few indications that the outcomes differed very much from the IRR in which all follow-up periods were
pooled.
IRR Lower limit
Upper limit
p-value
IRR (95% CI)a
Allart et al. 2007
1.07 0.57 2.01 0.84
Arnarson et al., 2009 0.15 0.03 0.88 0.04 Austin et al. 2008 0.99 0.58 1.67 0.96 Bot et al. 2010 1.15 0.67 1.99 0.61 Brugha et al. 2000 0.85 0.46 1.59 0.61 Clarke et al. 1995 0.57 0.27 1.20 0.14 Clarke et al. 2001 0.82 0.38 1.75 0.60 Compas et al. 2009 0.44 0.18 1.10 0.08 De Jonge et al. 2009 0.58 0.38 0.90 0.01 Elliott et al. 2000 0.83 0.39 1.79 0.63 Garber et al. 2009 0.66 0.45 0.96 0.03 Garcia et al. 2010 0.41 0.11 1.47 0.17 Gillham et al. 2006 1.00 0.60 1.67 1.00 Hagan et al. 2004 1.50 0.60 3.72 0.38 Joling et al. 2012 1.47 0.89 2.54 0.14 Konnert et al. 2009 0.29 0.01 6.18 0.43 Lara et al. 2010 0.43 0.18 1.03 0.06 Martinovic et al. 2006 0.14 0.01 2.55 0.19 Muñoz et al. 1995 0.54 0.10 2.87 0.47 Muñoz et al. 2007 0.80 0.06 10.23 0.88 Robinson et al. 2008 0.63 0.26 1.50 0.29 Rovner et al. 2007 0.62 0.34 1.12 0.11 Seligman et al. 1999 0.83 0.61 1.12 0.22 Sheffield et al., 2006A 0.76 0.43 1.34 0.34 Sheffield et al., 2006B 0.87 0.50 1.49 0.60 Sheffield et al., 2006C 1.05 0.64 1.72 0.85 Spence et al., 2003 1.18 0.83 1.68 0.35 Van ‘t Veer et al., 2009 0.38 0.15 0.97 0.04 Willemse et al., 2004 0.66 0.35 1.26 0.21 Young et al., 2006 0.26 0.02 2.90 0.27 Young et al., 2010 0.18 0.02 1.98 0.16 Zlotnick et al., 2001 0.08 0.01 1.34 0.08 Zlotnick et al., 2006 0.22 0.05 0.97 0.05 Zlotnick et al., 2011 1.11 0.39 3.22 0.84 Overall 0.79 0.69 0.91 0.00 Figure 2. The effects of preventive interventions on the incidence of depressive disorders; incidence rate ratios and numbers needed to treat.
a) Lines represent IRR and 95% CI; the size of the square indicates the weight of each study
Figure 2. The effects of preventive interventions on the incidence of depressive disorders; incidence rate ratios and numbers needed to treat.
a) Lines represent IRR and 95% CI; the size of the square indicates the weight of each study

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
36 | Chapter 2
Tabl
e 1.
Sel
ecte
d ch
arac
teris
tics o
f stu
dies
exa
min
ing
the
effec
ts o
f int
erve
ntio
ns o
n th
e in
cide
nce
of n
ew ca
ses o
f dep
ress
ive
diso
rder
s.St
udy
Type
R
ecru
itmen
tTa
rget
Po
pula
tion
Incl
usio
n C
rite
ria
Prev
ente
d D
isor
der
Con
ditio
nsN
Inte
rven
tion
FU
(mn)
Dro
p-ou
t (%
)
ITT
Alla
rt e
t al.
2007
34In
dC
omm
unity
Adu
lts
BDI ≥
10; n
o cu
rren
t M
DD
MD
D1.
CBT
2.
CA
U61 41
12 C
BT g
rp se
ssio
ns
1225
Y
Arn
arso
n &
C
raig
head
,20
0915
Ind
Scre
enin
g at
sc
hool
sA
dole
scen
tsC
DI,
CA
SQ ≥
; no
curr
ent D
DM
DD
1. E
clec
tic
2. C
AU
81 90
14 e
clec
tic g
rp se
ssio
ns12
34N
Aus
tin e
t al
. 200
824Se
lA
nten
atal
cl
inic
sA
nten
atal
w
omen
EPD
S >
10; A
NRQ
>
23; h
x of
DD
Anx
iety
and
PM
DD
1. C
BT
2. B
ookl
et
191
866
CBT
grp
sess
ions
+ 1
bo
oste
r4
52Y
Bot e
t al.
2010
35In
dou
tpat
ient
cl
inic
sPe
ople
with
di
abet
es≥
55 y
ears
; ≥ 1
6 C
ES-D
MD
D1.
step
ped
care
2.
CA
U
58 5612
wee
ks
2436
N
Brug
ha e
t al
. 200
036Se
lSc
reen
ing
Prim
ipar
ous
wom
enRi
sk fa
ctor
for
depr
essi
onM
DE
1. C
BT
2. C
AU
94 966
CBT
+ P
ST su
ppor
t grp
se
ssio
ns3
9Y
Cla
rke
et
al. 1
99537
Ind
scho
ols
Ado
lesc
ents
(1
5-16
)C
ES-D
>24;
no
curr
ent M
DD
/DYS
MD
D +
D
ysth
ymia
1. C
BT2.
CA
U55 70
15 C
BT g
rp se
ssio
ns
1227
N
Cla
rke
et
al. 2
00114
Ind
HM
OA
dole
scen
ts
(13-
18)
CES
-D >
24;
≥1
DSM
-IV
MD
D +
D
ysth
ymia
1. C
BT
2. C
AU
43 4715
CBT
grp
sess
ions
2417
Y
Com
pas e
t al
. 200
938Se
lM
enta
l hea
lth
clin
ics
Ado
lesc
ents
(9
-15)
CES
D/K
-SA
DS-
PL
MD
E1.
CBT
2. W
ritte
n in
fo
56 5312
sess
ions
, fou
r fam
ilies
ea
ch g
roup
2422
Y
De
Jong
e et
al.
2009
40In
dH
ospi
tal
Patie
nts w
ith
phys
ical
illn
ess
CES
-D, M
INI
MD
D1.
nur
sed-
led
2. C
AU
47 53Su
pp co
uns o
r psy
ch o
r a
mul
ti-di
scip
linar
y ca
se
conf
eren
ce
1233
Y
Ellio
tt et
al
. 200
016Se
lSc
reen
ing
Preg
nant
w
omen
Vuln
erab
le (L
Q)
PMD
D1.
PE
2. C
AU
47 5311
PE
sess
ions
+ m
utua
l su
ppor
t3
15N
Gar
ber e
t al
. 200
917In
dU
nive
rsiti
es
and
heal
th
cent
res
Ado
lesc
ent
(13-
17) o
f pa
rent
s with
de
pres
sion
CES
D >
20
and/
or 2
m
n re
mis
sion
from
M
DD
or b
oth
MD
D1.
CBT
2.
CA
U
159
157
8 C
BT g
rp se
ssio
ns +
6
cont
inua
tion
sess
ions
99
Y

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 37
Tabl
e 1.
Sel
ecte
d ch
arac
teris
tics o
f stu
dies
exa
min
ing
the
effec
ts o
f int
erve
ntio
ns o
n th
e in
cide
nce
of n
ew ca
ses o
f dep
ress
ive
diso
rder
s.St
udy
Type
R
ecru
itmen
tTa
rget
Po
pula
tion
Incl
usio
n C
rite
ria
Prev
ente
d D
isor
der
Con
ditio
nsN
Inte
rven
tion
FU
(mn)
Dro
p-ou
t (%
)
ITT
Alla
rt e
t al.
2007
34In
dC
omm
unity
Adu
lts
BDI ≥
10; n
o cu
rren
t M
DD
MD
D1.
CBT
2.
CA
U61 41
12 C
BT g
rp se
ssio
ns
1225
Y
Arn
arso
n &
C
raig
head
,20
0915
Ind
Scre
enin
g at
sc
hool
sA
dole
scen
tsC
DI,
CA
SQ ≥
; no
curr
ent D
DM
DD
1. E
clec
tic
2. C
AU
81 90
14 e
clec
tic g
rp se
ssio
ns12
34N
Aus
tin e
t al
. 200
824Se
lA
nten
atal
cl
inic
sA
nten
atal
w
omen
EPD
S >
10; A
NRQ
>
23; h
x of
DD
Anx
iety
and
PM
DD
1. C
BT
2. B
ookl
et
191
866
CBT
grp
sess
ions
+ 1
bo
oste
r4
52Y
Bot e
t al.
2010
35In
dou
tpat
ient
cl
inic
sPe
ople
with
di
abet
es≥
55 y
ears
; ≥ 1
6 C
ES-D
MD
D1.
step
ped
care
2.
CA
U
58 5612
wee
ks
2436
N
Brug
ha e
t al
. 200
036Se
lSc
reen
ing
Prim
ipar
ous
wom
enRi
sk fa
ctor
for
depr
essi
onM
DE
1. C
BT
2. C
AU
94 966
CBT
+ P
ST su
ppor
t grp
se
ssio
ns3
9Y
Cla
rke
et
al. 1
99537
Ind
scho
ols
Ado
lesc
ents
(1
5-16
)C
ES-D
>24;
no
curr
ent M
DD
/DYS
MD
D +
D
ysth
ymia
1. C
BT2.
CA
U55 70
15 C
BT g
rp se
ssio
ns
1227
N
Cla
rke
et
al. 2
00114
Ind
HM
OA
dole
scen
ts
(13-
18)
CES
-D >
24;
≥1
DSM
-IV
MD
D +
D
ysth
ymia
1. C
BT
2. C
AU
43 4715
CBT
grp
sess
ions
2417
Y
Com
pas e
t al
. 200
938Se
lM
enta
l hea
lth
clin
ics
Ado
lesc
ents
(9
-15)
CES
D/K
-SA
DS-
PL
MD
E1.
CBT
2. W
ritte
n in
fo
56 5312
sess
ions
, fou
r fam
ilies
ea
ch g
roup
2422
Y
De
Jong
e et
al.
2009
40In
dH
ospi
tal
Patie
nts w
ith
phys
ical
illn
ess
CES
-D, M
INI
MD
D1.
nur
sed-
led
2. C
AU
47 53Su
pp co
uns o
r psy
ch o
r a
mul
ti-di
scip
linar
y ca
se
conf
eren
ce
1233
Y
Ellio
tt et
al
. 200
016Se
lSc
reen
ing
Preg
nant
w
omen
Vuln
erab
le (L
Q)
PMD
D1.
PE
2. C
AU
47 5311
PE
sess
ions
+ m
utua
l su
ppor
t3
15N
Gar
ber e
t al
. 200
917In
dU
nive
rsiti
es
and
heal
th
cent
res
Ado
lesc
ent
(13-
17) o
f pa
rent
s with
de
pres
sion
CES
D >
20
and/
or 2
m
n re
mis
sion
from
M
DD
or b
oth
MD
D1.
CBT
2.
CA
U
159
157
8 C
BT g
rp se
ssio
ns +
6
cont
inua
tion
sess
ions
99
Y
Gar
cia
et
al. 2
01041
Sel
prim
ary
care
Prim
ary
care
pa
tient
s18
-65
yrs;
SPPI
no
DSM
-IV A
xis
Som
atof
orm
di
sord
ers
1. p
sych
o-ed
ucat
iona
l 2.
no
inte
rv.
52 52
Five
120
-min
gro
up
sess
ions
by
fam
ily d
octo
r60
21N
Gill
ham
et
al. 2
00618
Ind
Thro
ugh
HM
OEa
rly
adol
esce
nts
(11-
12)
CD
I ≥ 7
/9; n
o cu
rren
t MD
D D
YSM
DD
, DYS
1. C
BT
2. C
AU
14
712
412
CBT
grp
sess
ions
2441
Y
Hag
an e
t al
. 200
423Se
lne
onat
al u
nit
Mot
hers
ver
y pr
eter
m b
abie
sN
o cu
rren
t DD
Post
part
um
depr
essi
on1.
CBT
2.
CA
U10
198
6 C
BT g
rp se
ssio
ns +
PE
1212
Y
Jolin
g et
al
., 20
1242
Sel
Mem
ory
clin
ics,
gene
ral
prac
tices
, hom
e ca
re se
tting
s
Car
egiv
ers
dem
entia
pa
tient
s
MIN
Ide
pres
sive
or
anx
iety
di
sord
er
1. fa
mily
m
eetin
gs
2. C
AU
96 96
6 in
-per
son
coun
selli
ng
mee
tings
onc
e ev
ery
2 to
3
mon
ths
1226
Y
Kon
nert
et
al. 2
00943
Ind
Resi
dent
s of
nurs
ing
hom
esN
ursi
ng h
ome
resi
dent
s (ov
er
60)
No
MD
E, G
DS
≥ 9
MD
D1.
CBT
2. C
AU
20 23
13 C
BT se
ssio
ns6
33N
Lara
et a
l. 20
0944
Ind
Hos
pita
l, cl
inic
an
d co
mm
unity
he
alth
care
ce
ntre
Preg
nant
w
omen
in
Mex
ico
CES
-D ≥
16
and/
or se
lf-re
port
hx
of
MD
D
MD
D1.
CBT
2.
CA
U
250
127
8 PE
grp
sess
ions
4-9
64Y
Mar
tinov
ic
et a
l. 20
0645
Sel
Com
mun
ity +
cl
inic
Ado
lesc
ents
(1
3-19
) with
ep
ileps
y
sD; n
o cu
rren
t DD
MD
D1.
CBT
2. C
AU
15 15
12 C
BT g
rp se
ssio
ns9
6Y
Muñ
oz e
t al
. 199
546Se
lG
ener
al
prac
tice
reco
rds
GP
patie
nts
No
MD
D in
pas
t 6
mn
MD
D,
dyst
hym
ia1.
CBT
2. C
AU
72 78
8 C
BT g
rp se
ssio
ns
(CW
D)
128
N
Muñ
oz e
t al
. 200
747
Ind
Scre
enin
g Pr
egna
nt
Latin
a w
omen
CES
-D ≥
16;
hx
of
MD
DPM
DD
1. C
BT
2. C
AU
21 2012
CBT
grp
sess
ions
(C
WD
)12
9N
Robi
nson
et
al.
2008
48Se
lC
omm
unity
, un
iver
sitie
s &
hosp
itals
Post
-str
oke
patie
nts
No
curr
ent D
D,
HA
M-D
< 11
; SC
IDPo
stst
roke
de
pres
sion
1.
PST
2. P
lace
bo
59 586
PST
sess
ion
+ 6
boos
ter
sess
ions
129
Y
Rovn
er e
t al
. 200
749Se
lSc
reen
ing
in
outp
atie
nt
cent
ers
Old
er p
atie
nts
No
curr
ent D
D;
SAD
SM
DD
or
min
or d
epr.
1. P
ST2.
CA
U95 99
6 in
dv P
ST se
ssio
ns6
13N

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
38 | Chapter 2
Selig
man
et
al.
1999
50Se
lA
ll ne
w
stud
ents
Und
ergr
adua
te
stud
ents
ASQ
= b
otto
m
quar
tile,
no
curr
ent
MD
D
MD
D1.
CBT
2. C
AU
10
611
98
CBT
grp
sess
ions
364
N
Sheffi
eld
et
al. 2
00627
Uni
/In
dSc
hool
All
stud
ents
of
36 sc
hool
sH
igh-
sym
ptom
st
uden
ts, n
o M
DD
/D
YS
MD
D,
dyst
hym
ia1.
CBT
-Uni
2.
CBT
-Ind
3.C
BT-In
d 4.
CA
U
107
100
110
125
8 C
BT +
1 P
ST g
rp
less
ons
1815
N
Spen
ce e
t al
. 200
321U
niSc
hool
Stud
ents
of 1
8 hi
gh sc
hool
sA
DIS
-CM
ajor
de
pres
sion
1. C
BT2.
CA
U75
174
98
grp
less
ons o
f CBT
+
PST
1215
N
Van
‘t Ve
er-
Taze
laar
et
al. 2
00951
Ind
PIK
Opr
ojec
tO
lder
adu
lts in
pr
imar
y ca
reN
o M
DE;
CES
-D ≥
16M
DD
/ an
xiet
y1.
CBT
+
PST
2. C
AU
86 843
mon
ths C
BT +
nur
se
calls
/vis
its, t
hen
7 PS
T se
ssio
ns
2424
Y
Will
emse
et
al.
2004
53In
dge
nera
l pra
ctic
eA
dults
(18-
65)
One
MD
D co
re
sym
ptom
, no
MD
D
in p
ast 6
mn
(CID
I)
MD
D,
dyst
hym
ia
1. C
BT
2. C
AU
10
710
91
ftf co
ntac
t + se
lf-he
lp
book
+ 6
shor
t tel
epho
ne
cons
ulta
tions
(CW
D)
1237
Y
Youn
g et
al
. 200
619In
dsc
hool
Ado
lesc
ents
(1
5-16
)C
ES-D
≥ 1
6; 2
sy
mpt
oms;
no
MD
D/D
YS
MD
D,
dyst
hym
ia
(K-S
AD
S)
1. IP
T 2.
CA
U
27 142
indv
+ 8
IPT
grp
sess
ions
62
Y
Youn
g et
al
. 201
055In
dTw
o-st
age
scre
enin
g A
dole
scen
ts
(13-
17)
CES
-D 1
6 –
39;
K-S
AD
S-PI
M
DD
1. IP
T-A
ST2.
SC
36 211.
2 p
re-g
rp se
ssio
ns +
8
90-m
in g
rp se
ssio
ns2.
30-
45 m
in in
dv co
uns.
1823
Y
Zlot
nick
et
al. 2
00156
Sel
hosp
itals
Preg
nant
w
omen
≥1 ri
sk in
dica
tors
PD
D, n
o M
DD
PMD
D1.
IPT
2. C
AU
17 184
IPT
grp
sess
ions
35
Y
Zlot
nick
et
al. 2
00620
Sel
hosp
itals
Preg
nant
w
omen
Hig
h sc
ore
risk
surv
ey, n
o cu
rren
t M
DD
PMD
D
(LIF
E)1.
IPT
2. C
AU
17 46
4 IP
T gr
p se
ssio
ns3
13N

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 39
Zlot
nick
et
al. 2
01157
Sel
Prim
ary
care
cl
inic
s + p
rivat
e O
BGYN
clin
ic
Preg
nant
w
omen
(18-
40yr
s)
EPD
S/SC
IDM
DD
/PM
DD
1. IP
T 2.
CA
U
28 264
IPT
+ bo
oste
r ses
sion
315
Y
Abb
revi
atio
ns: A
DIS
-C =
Anx
iety
dis
orde
rs i
nter
view
sch
edul
e ch
ildre
n, A
NQ
R =
Ant
enat
al R
isk
Que
stio
nnai
re, B
DI
= Be
ck
Dep
ress
ion
Inve
ntor
y, (C
) ASQ
=( C
hild
ren’
s) A
ttrib
utio
nal S
tyle
Que
stio
nnai
re, C
AU
= ca
re a
s usu
al, C
BT =
cogn
itive
beh
avio
ural
th
erap
y, C
DI =
Chi
ldre
n’s
Dep
ress
ion
Inve
ntor
y, C
ES-D
= C
ente
r fo
r Ep
idem
iolo
gica
l Stu
dies
-Dep
ress
ion
Scal
e, C
WD
= C
opin
g w
ith d
epre
ssio
n, D
AS
= D
ysfu
nctio
nal A
ttitu
de S
cale
, DD
= d
epre
ssiv
e di
sord
er, D
YS =
Dys
thym
ia, E
PDS
= Ed
inbu
rgh
Post
nata
l D
epre
ssio
n Sc
ale,
GD
S =
Ger
iatr
ic D
epre
ssio
n Sc
ale,
HA
M-D
= H
amilt
on r
atin
g sc
ale
Dep
ress
ion,
IN
D =
Ind
icat
ed,
IPT
= In
terp
erso
nal t
hera
py, K
/SA
DS/
PL =
Kid
die-
Sads
-Pre
sent
and
Life
time
Vers
ion,
LQ
= L
ever
ton
Que
stio
nnai
re, M
DD
= m
ajor
de
pres
sive
dis
orde
r, M
DE
= m
ajor
dep
ress
ive e
piso
de, M
INI =
Min
i-Int
erna
tiona
l Neu
rops
ychi
atric
Inte
rvie
w, P
MD
D =
pos
tpar
tum
de
pres
sion
, PST
= p
robl
em so
lvin
g th
erap
y, S
AD
S =
Sche
dule
for A
ffect
ive D
isor
ders
and
Sch
izop
hren
ia, S
CID
= S
truc
ture
d C
linic
al
Inte
rvie
w fo
r DSM
-IV, S
EL =
sele
ctiv
e, S
PPI =
Sta
ndar
dize
d Po
lyva
lent
Psy
chia
tric
Inte
rvie
w, V
AS
= Vi
sual
Ana
logu
e Sc
ale,
Uni
=
univ
ersa
l.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
40 | Chapter 2
We also conducted a separate analysis in which we used only the last follow-up period reported in each study (0.78; 95% CI: 0.68-0.89; p = 0.001; I2=29), and another analysis with only the first follow-up period of each study (0.79; 95% CI: 0.69-0.92; p = 0.002; I2=29). As can be seen in Table 2, we found few indications that the outcomes differed very much from the IRR in which all follow-up periods were pooled.
We also conducted meta-regression analyses to see whether there was any effect decay over time. First, we examined the association between IRR and the first follow-up period reported in the study. We did not find an association between IRR and first follow-up period (the point estimate of the slope was 0.003; 95% CI: -0.007 to 0.013), although there was a trend (p = 0.06) suggesting that the effects of the interventions are lower at longer follow-up periods (median = 7.5 months; range = 2 months to 60 months). In the second meta-regression analysis we used the last follow-up period reported in the studies. Again, these results did not show an association between IRR and last follow-up moment (p = 0.06; the point estimate of the slope was -0.000; 95% CI: -0.01 to 0.01), suggesting that the longer it takes before the last follow-up period, the lower the incidence of depression is (median = 12; range = 3 months to 60 months).
Inspection of the funnel plot (Figure 3) and Duval and Tweedie’s trim-and-fill procedure attested to the possible presence of publication bias. After adjustment for publication bias, the effect size was increased from 0.82 to 0.86 (95% CI: 0.74-1.00; number of trimmed studies: 10). The Egger’s Test also indicated an asymmetric funnel plot (intercept: -1.24, 95% CI: -1.95 to -0.53, degree of freedom (df) 32, p = 0.001). The fail-safe n was 175, indicating that 175 studies with an effect size of 0 would have to be included to not find a publication bias.
Subgroup analyses We conducted a series of subgroup analyses (Table 2). We examined whether the IRR differed according to type of prevention (indicated, universal or selective), type of intervention (CBT, IPT or other), age group (adolescent, adults or elderly), number of sessions (1-7, 8-11, ≥12; one study did not report the number of intervention sessions), country of publication (USA, EU or other), and target group (school-based, general medical, perinatal or other).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 41
43
The IRR did not differ in any of the subgroups (Table 2). The difference between CBT and IPT
interventions, found by Cuijpers et al. in 2008, could not be replicated in the current meta-analyses.
This null finding might be caused by the low number of studies using IPT as an intervention (n = 5).
However, when looking at NNT, as indicated in Table 2, there was a difference between
number needed to treat of CBT (NNT = 71), IPT (NNT = 7) and other (NNT = 12) interventions (p =
0.003), suggesting that preventive interventions using IPT are more effective than preventive
interventions using CBT.
In most subgroup analyses the heterogeneity was low to moderate. No heterogeneity was found
in several subgroups of studies; subgroups using CBT, focusing on elderly, using a target population of
general medical patients (41). Also, no heterogeneity was found in subgroups having 8-11 sessions,
having a publication score of 3 or 4, or studies not published in Europe.
-3-3-3-3 -2-2-2-2 -1-1-1-1 0000 1111 2222 3333
0,00,00,00,0
0,50,50,50,5
1,01,01,01,0
1,51,51,51,5
2,02,02,02,0
Sta
ndar
d Err
orS
tand
ard E
rror
Sta
ndar
d Err
orS
tand
ard E
rror
Log risk
ratioLog
risk
ratioLog
risk
ratioLog
risk
ratio
Funnel Plot
of
Standard
Error
by
Log
risk
ratioFunnel
Plot
of
Standard
Error
by
Log
risk
ratioFunnel
Plot
of
Standard
Error
by
Log
risk
ratioFunnel
Plot
of
Standard
Error
by
Log
risk
ratio
Figure 3. Funnel Plot
The IRR did not differ in any of the subgroups (Table 2). The difference between CBT and IPT interventions, found by Cuijpers et al. in 2008, could not be replicated in the current meta-analyses. This null finding might be caused by the low number of studies using IPT as an intervention (n = 5).
However, when looking at NNT, as indicated in Table 2, there was a difference between number needed to treat of CBT (NNT = 71), IPT (NNT = 7) and other (NNT = 12) interventions (p = 0.003), suggesting that preventive interventions using IPT are more effective than preventive interventions using CBT.
In most subgroup analyses the heterogeneity was low to moderate. No heterogeneity was found in several subgroups of studies; subgroups using CBT, focusing on elderly, using a target population of general medical patients (41). Also, no heterogeneity was found in subgroups having 8-11 sessions, having a publication score of 3 or 4, or studies not published in Europe.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
42 | Chapter 2Ta
ble
2. M
eta-
Ana
lyse
s of
stu
dies
exa
min
ing
the
effec
ts o
f pre
vent
ive
inte
rven
tions
on
the
inci
denc
e of
dep
ress
ive
diso
rder
s: In
cide
nce
rate
ra
tios,
hete
roge
neity
and
num
bers
nee
ded
to tr
eat (
NN
T). N
IRR
95%
CI
I2 95
% C
IP
NN
T95
% C
IP
Dep
ress
ive
diso
rder
s34
0.79
0.69
~0.9
124
0~50
2013
.33~
37.0
4Sh
effiel
d ex
clud
ed31
0.77
0.66
~0.9
029
0~54
1611
.11~
30.3
0O
nly
last
follo
w u
p m
omen
t34
0.78
0.68
~0.8
929
0~53
1711
.90~
30.3
0O
nly
first
follo
w u
p m
omen
t34
0.79
0.69
~0.9
229
0~54
2113
.89~
45.4
5
Follo
w u
p Pe
riod
<5 m
onth
s11
0.81
0.55
~1.1
829
0~65
158.
40~7
6.92
66
0.51
0.30
~0.8
641
0~76
154.
81~1
3.89
7-12
120.
820.
66~1
.01
370~
6825
14.2
9~10
0>1
35
0.89
0.66
~1.2
10
2.75
5 4
249.
00~3
4.48
Subg
roup
ana
lyse
s
Type
of t
hera
pyC
BT19
0.86
0.76
-0.9
80
0~49
0.10
671
33.3
3-50
00.
003
IPT
50.
360.
13-0
.96
320~
747
4.27
-20.
41O
ther
100.
680.
49-0
.95
521~
7712
7.14
-37.
04
Age
Stud
ents
140.
810.
67-0
.97
250~
600.
231
2212
.66-
71.4
30.
419
Adu
lts16
0.84
0.66
-1.0
130
0~62
2211
.11-
333.
33El
derly
40.
550.
36-0
.85
00~
8511
6.80
-32.
26
Targ
et g
roup
a)
Scho
ol-b
ased
140.
810.
68-0
.97
2517
.221
130
0.58
621
12.3
5-71
.43
0.75
9Pe
rinat
al d
epre
ssio
n9
0.81
0.59
-1.1
122
10.2
75 8
209.
80-7
1.43
Gen
eral
Med
ical
100.
690.
54-0
.89
08.
585
915
8.85
-41.
67O
ther
1
Prev
entio
n ty
pea)
IND
170.
740.
61-0
.90
1418
.594
16
0.50
713
9.09
-25.
640.
284
SEL
150.
810.
65-1
.01
2619
.034
14
2112
.05-
90.9
1U
NI
2
Num
ber o
f ses
sion
sa)1-
710
0.81
0.61
-1.0
751
18.2
07 9
0.77
520
10.9
9-12
50.
159
8-11
110.
850.
68-1
.07
09.
268
1042
18.1
8-14
2.86
≥12
120.
750.
58-0
.97
912
.101
11
148.
62-3
1.25
nr1
Publ
icat
ion
coun
try
USA
140.
670.
54-0
.82
00~
550.
051
138.
93-2
50.
002
Euro
pe11
0.77
0.57
-1.0
447
0~73
168.
62-9
0.91
Oth
er
90.
940.
79-1
.10
00~
6514
335
.71-
71.4
3
Qua
lity
scor
e<3
120.
790.
59-1
.06
5310
~76
0.89
414
7.87
-71.
430.
234
3 or
422
0.77
0.67
-0.9
00
0~46
2918
.52-
71.4
3
Abb
revi
atio
ns:
CBT
, co
gniti
ve b
ehav
iour
al t
hera
py;
IND
, in
dica
ted
prev
entio
n; I
PT,
Inte
rper
sona
l th
erap
y; I
RR,
inci
denc
e ra
te r
atio
; I2 ,
hete
roge
neity
; MD
D, m
ajor
dep
ress
ive
diso
rder
; N, n
umbe
r of
stu
dies
; NN
T, n
umbe
rs n
eede
d to
trea
t; N
R, n
ot re
port
ed; P
MD
D, p
ostp
artu
m
maj
or d
epre
ssiv
e di
sord
er; S
EL, s
elec
tive
prev
entio
n; U
NI,
univ
ersa
l pre
vent
ion.
b) W
hen
subg
roup
incl
udin
g le
ss th
an 3
stu
dies
ana
lysi
s w
as
done
with
out t
hat s
ubgr
oup.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 43
Tabl
e 2.
Met
a-A
naly
ses
of s
tudi
es e
xam
inin
g th
e eff
ects
of p
reve
ntiv
e in
terv
entio
ns o
n th
e in
cide
nce
of d
epre
ssiv
e di
sord
ers:
Inci
denc
e ra
te
ratio
s, he
tero
gene
ity a
nd n
umbe
rs n
eede
d to
trea
t (N
NT)
. NIR
R95
% C
II2
95%
CI
PN
NT
95%
CI
PD
epre
ssiv
e di
sord
ers
340.
790.
69~0
.91
240~
5020
13.3
3~37
.04
Sheffi
eld
excl
uded
310.
770.
66~0
.90
290~
5416
11.1
1~30
.30
Onl
y la
st fo
llow
up
mom
ent
340.
780.
68~0
.89
290~
5317
11.9
0~30
.30
Onl
y fir
st fo
llow
up
mom
ent
340.
790.
69~0
.92
290~
5421
13.8
9~45
.45
Follo
w u
p Pe
riod
<5 m
onth
s11
0.81
0.55
~1.1
829
0~65
158.
40~7
6.92
66
0.51
0.30
~0.8
641
0~76
154.
81~1
3.89
7-12
120.
820.
66~1
.01
370~
6825
14.2
9~10
0>1
35
0.89
0.66
~1.2
10
2.75
5 4
249.
00~3
4.48
Subg
roup
ana
lyse
s
Type
of t
hera
pyC
BT19
0.86
0.76
-0.9
80
0~49
0.10
671
33.3
3-50
00.
003
IPT
50.
360.
13-0
.96
320~
747
4.27
-20.
41O
ther
100.
680.
49-0
.95
521~
7712
7.14
-37.
04
Age
Stud
ents
140.
810.
67-0
.97
250~
600.
231
2212
.66-
71.4
30.
419
Adu
lts16
0.84
0.66
-1.0
130
0~62
2211
.11-
333.
33El
derly
40.
550.
36-0
.85
00~
8511
6.80
-32.
26
Targ
et g
roup
a)
Scho
ol-b
ased
140.
810.
68-0
.97
2517
.221
130
0.58
621
12.3
5-71
.43
0.75
9Pe
rinat
al d
epre
ssio
n9
0.81
0.59
-1.1
122
10.2
75 8
209.
80-7
1.43
Gen
eral
Med
ical
100.
690.
54-0
.89
08.
585
915
8.85
-41.
67O
ther
1
Prev
entio
n ty
pea)
IND
170.
740.
61-0
.90
1418
.594
16
0.50
713
9.09
-25.
640.
284
SEL
150.
810.
65-1
.01
2619
.034
14
2112
.05-
90.9
1U
NI
2
Num
ber o
f ses
sion
sa)1-
710
0.81
0.61
-1.0
751
18.2
07 9
0.77
520
10.9
9-12
50.
159
8-11
110.
850.
68-1
.07
09.
268
1042
18.1
8-14
2.86
≥12
120.
750.
58-0
.97
912
.101
11
148.
62-3
1.25
nr1
Publ
icat
ion
coun
try
USA
140.
670.
54-0
.82
00~
550.
051
138.
93-2
50.
002
Euro
pe11
0.77
0.57
-1.0
447
0~73
168.
62-9
0.91
Oth
er
90.
940.
79-1
.10
00~
6514
335
.71-
71.4
3
Qua
lity
scor
e<3
120.
790.
59-1
.06
5310
~76
0.89
414
7.87
-71.
430.
234
3 or
422
0.77
0.67
-0.9
00
0~46
2918
.52-
71.4
3
Abb
revi
atio
ns:
CBT
, co
gniti
ve b
ehav
iour
al t
hera
py;
IND
, in
dica
ted
prev
entio
n; I
PT,
Inte
rper
sona
l th
erap
y; I
RR,
inci
denc
e ra
te r
atio
; I2 ,
hete
roge
neity
; MD
D, m
ajor
dep
ress
ive
diso
rder
; N, n
umbe
r of
stu
dies
; NN
T, n
umbe
rs n
eede
d to
trea
t; N
R, n
ot re
port
ed; P
MD
D, p
ostp
artu
m
maj
or d
epre
ssiv
e di
sord
er; S
EL, s
elec
tive
prev
entio
n; U
NI,
univ
ersa
l pre
vent
ion.
b) W
hen
subg
roup
incl
udin
g le
ss th
an 3
stu
dies
ana
lysi
s w
as
done
with
out t
hat s
ubgr
oup.
Discussion
We examined whether preventive interventions are effective in reducing the incidence of MDD. Results showed that preventive interventions lowered the incidence of depression by 21%, compared to controls. This is in agreement with the results of the previous meta-analyses (13). A reduction in incidence of 21% can be considered clinically relevant. In the current meta-analysis we only included studies that used diagnostic criteria at baseline and follow-up, to exclude cases of depression at baseline and assess diagnostic status at follow-up. Using these rigorous criteria and the relatively large number of trials, this meta-analysis offers the most robust evidence on the impact of preventive interventions on the incidence of new depressions than any previous meta-analysis.
The current meta-analyses did not show IPT to be more effective than CBT. This is in contrast to the findings of our earlier meta-analyses. Examining the NNT, however, shows that IPT (NNT = 7) is more effective than CBT (NNT = 71). Furthermore, there is no overlap in the 95% confidence intervals, reinforcing our suggestion that IPT might have a greater prophylactic effect than CBT. This result is consisted with our results from the previous meta-analysis conducted in 2008. It should, however, be interpreted with caution, since the number of studies using IPT (5) was considerably lower than the studies using CBT (20). If IPT is indeed more effective, this might be related to the fact that this type of intervention focuses more directly on the current problems and high-risk situations. This might be exactly what people in high-risk situations or with subthreshold symptoms need. Also, results did not suggest that indicated prevention (IRR = 0.74) was more effective than selective prevention (IRR=0.81). However, only two studies investigated universal prevention and those were therefore excluded from analysis.
This does not necessarily imply that universal intervention might not be effective in high-risk subgroups. Rose (58) discussed that there are two strategies to prevention; a population strategy of prevention, which targets a whole population regardless of individual differences in risk status and an individual strategy of prevention, which targets individuals at high risk for an adverse health outcome (59). Our meta-analysis is mainly focused on individual prevention. When we would use less rigorous inclusion criteria (e.g. no diagnostic instrument to determine whether participants have a diagnosis) we might find results similar to similar to another meta-analysis conducted in 2012 (60). This analysis found a beneficial effect in the prevention of postpartum depression in a range of interventions, both individually based as well as multiple contacts. This shows that population-based strategies for prevention are interesting from a public health point of view and have the potential of reducing the incidence of depression considerably. However, our study also makes clear that there are no studies yet that show that population-based strategies actually reduce the incidence of depressive disorders.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
44 | Chapter 2
Although prevention of depression seems to be effective, the NNT appears high (20 in the overall analysis), which is comparable to the NNT in the earlier analyses by Cuijpers (NNT = 22). There are, however, no normative thresholds for lower or higher NNT (13). Considering the impact depressive disorders have on social, economic and physical life and the clinical relevance, it seems an acceptable number. As discussed earlier, universal prevention might have a very different approach and yield very different results compared to selective and indicated prevention. Also, there were only two studies using universal prevention in this analysis. Therefore, it might be a consideration to not include universal prevention in other reviews like the current review. Other research did not show that the implemented intervention reduced the depressive symptoms in adolescents at high risk. The intervention was implemented under everyday life situations. The sample consisted of non-referred adolescents from the community. This study was, however, not included in the current meta-analysis because the researchers did not use a diagnostic instrument to diagnose depressive disorders at follow up (61). However, the study shows that it is important to investigate the risk factors for depression, this could be due to premorbid vulnerability or due to the experience of previous episodes of depression. Future research should take history of depression into account.
Furthermore, the control/comparison groups in the included studies consisted mostly of treatments like care-as-usual or waitlist. These are passive rather than active forms of ‘treatments”. There is, therefore, no control for face to face time and attention. These are, however, nonspecific aspects of structured interventions like IPT or CBT. If future research included more active comparators, it would greatly improve the strength with which conclusions can be drawn about the specific prophylactic value of learning based psychotherapies.
Most follow-up periods were between 6 and 12 months (28), only 2 studies had follow-up periods beyond 2 years. Therefore, it is not clear whether preventive interventions actually prevented the incidence of depression or simply delayed the onset of depressive episodes. We performed analyses per follow-up (<5, 6, 7-12, ≥13 months). Comparing the effects of preventive interventions and first follow-up months showed a small positive association, indicating that the more months pass, the more effective the preventive intervention is. However, comparing the effects of preventive interventions and last follow-up period, this had a very small negative association. This might indicate that the effects of the preventive intervention became smaller over longer follow-up periods, suggesting that the preventive interventions delay the onset of disorders rather than preventing them altogether. However, only few studies had longer follow-up periods than 2 years. From a clinical point of view preventing new onsets of depression would obviously be preferable since it would completely avoid the burden of disease in all prevented cases. However, delaying the onset is also important. Every year a disorder is delayed, is a year without suffering.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 45
We acknowledge several limitations of this study. First, several studies examined different populations and used different types of interventions. That said, according to I2 statistic, heterogeneity was low to moderate, indicating that it may be a fairly homogenous set of studies. Second, the follow-up periods differed between studies. We, therefore, examined the various follow-up periods. However, we also conducted regression analysis with only the first follow-up moment and regression analysis with only the last follow-up moment to see whether there was any effect decay over time. Third, the number of studies in some of the subgroup-analyses were rather small and show only correlations. Therefore results should be interpreted with caution.
In conclusion, it is encouraging that we found positive effects of preventive interventions on the incidence of major depression, which are clinically relevant. Prevention of depressive disorders is possible, and may, in addition to treatment, be an important way to further reduce the burden of disease due to a very prevalent and disabling condition: depression.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
46 | Chapter 2
References
1. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of general psychiatry. 1994;51(1):8-9.
2. Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. The Lancet. 2007;370(9590):841-50.
3. O’Kearney R, Kang K, Christensen H, Griffiths K. A controlled trial of a school-based Internet program for reducing depressive symptoms in adolescent girls. Depression and Anxiety. 2009;26(1):65-72.
4. Cuijpers P, Smit F. Excess mortality in depression: a meta-analysis of community studies. Journal of affective disorders. 2002;72(3):227-36.
5. De Graaf R, Bijl R, Ravelli A, Smit F, Vollebergh W. Predictors of first incidence of DSM-III-R psychiatric disorders in the general population: findings from the Netherlands Mental Health Survey and Incidence Study. Acta Psychiatrica Scandinavica. 2002;106(4):303-13.
6. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet. 2012;380(9859):2197-223.
7. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS medicine. 2006;3(11):e442.
8. Smit F, Cuijpers P, Oostenbrink J, Batelaan N, De Graaf R, Beekman A. Excess costs of common mental disorders: population-based cohort study. J Ment Health Policy Econ. 2006;9(4):193-200.
9. Andrews G, Wilkinson DD. The prevention of mental disorders in young people. Medical Journal of Australia. 2002;177(7):S97.
10. Chisholm D, Sanderson K, Ayuso-Mateos JL, Saxena S. Reducing the global burden of depression Population-level analysis of intervention cost-effectiveness in 14 world regions. The British Journal of Psychiatry. 2004;184(5):393-403.
11. Petersen I, Bhana A, Swartz L. Mental health promotion and the prevention of mental disorders in South Africa: review. African journal of psychiatry. 2012;15(6):411-6.
*12. Cuijpers P, Van Straten A, Smit F. Preventing the incidence of new cases of mental disorders: a meta-analytic review. The Journal of nervous and mental disease. 2005;193(2):119-25.
*13. Cuijpers P, Van Straten A, Smit F, Mihalopoulos C, Beekman A. Preventing the Onset of Depressive Disorders: A Meta-Analytic Review of Psychological Interventions. American Journal of Psychiatry. 2008;165(10):1272-80.
14. Clarke GN, Hornbrook M, Lynch F, Polen M, Gale J, Beardslee W, et al. A randomized trial of a group cognitive intervention for preventing depression in adolescent offspring of depressed parents. Archives of general psychiatry. 2001;58(12):1127-34.
15. Arnarson EÖ, Craighead WE. Prevention of depression among Icelandic adolescents. Behaviour research and therapy. 2009;47(7):577-85.
16. Elliott SA, Leverton TJ, Sanjack M, Turner H, Cowmeadow P, Hopkins J, et al. Promoting mental health after childbirth: a controlled trial of primary prevention of postnatal depression. British Journal of Clinical Psychology. 2000;39(3):223-41.
17. Garber J, Clarke GN, Weersing VR, Beardslee WR, Brent DA, Gladstone TR, et al. Prevention of depression in at-risk adolescents: a randomized controlled trial. jama. 2009;301(21):2215-24.
18. Gillham JE, Hamilton J, Freres DR, Patton K, Gallop R. Preventing depression among early adolescents in the primary care setting: A randomized controlled study of the Penn Resiliency Program. Journal of abnormal child psychology. 2006;34(2):195-211.
19. Young JF, Mufson L, Davies M. Efficacy of Interpersonal Psychotherapy-Adolescent Skills Training: an indicated preventive intervention for depression. Journal of Child Psychology and Psychiatry. 2006;47(12):1254-62.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 47
20. Zlotnick C, Miller I, Pearlstein T, Howard M, Sweeney P. A preventive intervention for pregnant women on public assistance at risk for postpartum depression. American Journal of Psychiatry. 2006;163(8):1443-5.
21. Spence SH, Sheffield JK, Donovan CL. Preventing adolescent depression: an evaluation of the problem solving for life program. Journal of consulting and clinical psychology. 2003;71(1):3.
22. Priest SR, Henderson J, Evans SF, Hagan R. Stress debriefing after childbirth: a randomised controlled trial. The Medical Journal of Australia. 2003;178(11):542-5.
23. Hagan R, Evans SF, Pope S. Preventing postnatal depression in mothers of very preterm infants: a randomised controlled trial. BJOG: An International Journal of Obstetrics & Gynaecology. 2004;111(7):641-7.
24. Austin M-P, Frilingos M, Lumley J, Hadzi-Pavlovic D, Roncolato W, Acland S, et al. Brief antenatal cognitive behaviour therapy group intervention for the prevention of postnatal depression and anxiety: a randomised controlled trial. Journal of affective disorders. 2008;105(1):35-44.
25. Muñoz RF, Cuijpers P, Smit F, Barrera AZ, Leykin Y. Prevention of major depression. Annual Review of Clinical Psychology. 2010;6:181-212.
26. Greenberg MT, Domitrovich C, Bumbarger B. Preventing mental disorders in school-age children: A review of the effectiveness of prevention programs. Prevention Research Center for the Promotion of Human Development, College of Health and Human Development, Pennsylvania State University. 2000.
27. Sheffield JK, Spence SH, Rapee RM, Kowalenko N, Wignall A, Davis A, et al. Evaluation of universal, indicated, and combined cognitive-behavioral approaches to the prevention of depression among adolescents. Journal of consulting and clinical psychology. 2006;74(1):66.
28. Mrazek PJ, Haggerty RJ. Reducing Risks for Mental Disorders:: Frontiers for Preventive Intervention Research: National Academies Press; 1994.
29. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions Version 5.1. 0 [updated March 2011]. The Cochrane Collaboration, 2011. www cochrane-handbook org. 2012.
30. Ioannidis J, Patsopoulos NA, Evangelou E. Uncertainty in heterogeneity estimates in meta-analyses. Bmj. 2007;335(7626):914-6.
31. Higgins J, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Bmj. 2003;327(7414):557-60.
32. Orsini N, Bottai M, Higgins J, Buchan I. Heterogi: Stata module to quantify heterogeneity in a meta-analysis. Statistical Software Components. 2006.
33. Duval S, Tweedie R. Trim and fill: a simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455-63.
34. Bot M, Pouwer F, Ormel J, Slaets JP, De Jonge P. Predictors of incident major depression in diabetic outpatients with subthreshold depression. Diabetic Medicine. 2010;27(11):1295-301.
35. Brugha TS, Wheatley S, Taub NA, Culverwell A, Friedman T, Kirwan P, et al. Pragmatic randomized trial of antenatal intervention to prevent post-natal depression by reducing psychosocial risk factors. Psychological medicine. 2000;30(06):1273-81.
36. Clarke GN, Hawkins W, Murphy M, Sheeber LB, Lewinsohn PM, Seeley JR. Targeted prevention of unipolar depressive disorder in an at-risk sample of high school adolescents: A randomized trial of a group cognitive intervention. Journal of the American Academy of Child & Adolescent Psychiatry. 1995;34(3):312-21.
37. Compas BE, Forehand R, Keller G, Champion JE, Rakow A, Reeslund KL, et al. Randomized controlled trial of a family cognitive-behavioral preventive intervention for children of depressed parents. Journal of consulting and clinical psychology. 2009;77(6):1007.
38. Compas BE, Forehand R, Thigpen JC, Keller G, Hardcastle EJ, Cole DA, et al. Family group cognitive–behavioral preventive intervention for families of depressed parents: 18-and 24-month outcomes. Journal of consulting and clinical psychology. 2011;79(4):488.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
48 | Chapter 2
39. de Jonge P, Bel Hadj F, Boffa D, Zdrojewski C, Dorogi Y, So A, et al. Prevention of major depression in complex medically ill patients: preliminary results from a randomized, controlled trial. Psychosomatics. 2009;50(3):227-33.
40. García-Campayo J, Arevalo E, Claraco LM, Alda M, Lopez del Hoyo Y. A prevention programme for somatoform disorders is effective for affective disorders. Journal of affective disorders. 2010;122(1):124-32.
41. Joling KJ, van Marwijk HW, Smit F, van der Horst HE, Scheltens P, van de Ven PM, et al. Does a family meetings intervention prevent depression and anxiety in family caregivers of dementia patients? A randomized trial. PloS one. 2012;7(1):e30936.
42. Konnert C, Dobson K, Stelmach L. The prevention of depression in nursing home residents: A randomized clinical trial of cognitive–behavioral therapy. Aging and Mental Health. 2009;13(2):288-99.
43. Lara MA, Navarro C, Navarrete L. Outcome results of a psycho-educational intervention in pregnancy to prevent PPD: A randomized control trial. Journal of Affective Disorders. 2009;122(1):109-17.
44. Martinović Ž, Simonović P, Djokić R. Preventing depression in adolescents with epilepsy. Epilepsy & Behavior. 2006;9(4):619-24.
45. Muñoz RF, Ying Y-W, Bernal G, Pérez-Stable EJ, Sorensen JL, Hargreaves WA, et al. Prevention of depression with primary care patients: A randomized controlled trial. American Journal of Community Psychology. 1995;23(2):199-222.
46. Muñoz RF, Le H-N, Ippen CG, Diaz MA, Urizar Jr GG, Soto J, et al. Prevention of Postpartum Depression in Low-Income Women: Development of the Mamás y Bebés/Mothers and Babies Course. Cognitive and Behavioral Practice. 2007;14(1):70-83.
47. Robinson RG, Jorge RE, Moser DJ, Acion L, Solodkin A, Small SL, et al. Escitalopram and problem-solving therapy for prevention of poststroke depression: a randomized controlled trial. Jama. 2008;299(20):2391-400.
48. Rovner BW, Casten RJ, Hegel MT, Leiby BE, Tasman WS. Preventing depression in age-related macular degeneration. Archives of General Psychiatry. 2007;64(8):886-92.
49. Seligman ME, Schulman P, DeRubeis RJ, Hollon SD. The prevention of depression and anxiety. Prevention & Treatment. 1999;2(1):8a.
50. van’t Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, van Hout HP, van der Horst HE, Cuijpers P, et al. Stepped-care prevention of anxiety and depression in late life: a randomized controlled trial. Archives of General Psychiatry. 2009;66(3):297-304.
51. van’t Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, van der Horst HE, Smit F, Cuijpers P, et al. Prevention of late-life anxiety and depression has sustained effects over 24 months: a pragmatic randomized trial. The American Journal of Geriatric Psychiatry. 2011;19(3):230-9.
52. Willemse GR, Smit F, Cuijpers P, Tiemens BG. Minimal-contact psychotherapy for sub-threshold depression in primary care Randomised trial. The British Journal of Psychiatry. 2004;185(5):416-21.
53. Young JF, Gallop R, Mufson L. Mother–child conflict and its moderating effects on depression outcomes in a preventive intervention for adolescent depression. Journal of Clinical Child & Adolescent Psychology. 2009;38(5):696-704.
54. Young JF, Mufson L, Gallop R. Preventing depression: a randomized trial of interpersonal psychotherapy-adolescent skills training. Depression and anxiety. 2010;27(5):426-33.
55. Zlotnick C, Johnson SL, Miller IW, Pearlstein T, Howard M. Postpartum depression in women receiving public assistance: pilot study of an interpersonal-therapy-oriented group intervention. American Journal of Psychiatry. 2001;158(4):638-40.
56. Zlotnick C, Capezza NM, Parker D. An interpersonally based intervention for low-income pregnant women with intimate partner violence: a pilot study. Archives of women’s mental health. 2011;14(1):55-65.
57. Allart-van Dam E, Hosman C, Hoogduin C, Schaap C. Prevention of depression in subclinically depressed adults: follow-up effects on the ‘Coping with Depression’course. Journal of affective disorders. 2007;97(1):219-28.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 49
58. Rose G. Sick individuals and sick populations. International journal of epidemiology. 2001;30(3):427-32.
59. McLaren L, McIntyre L, Kirkpatrick S. Rose’s population strategy of prevention need not increase social inequalities in health. International journal of epidemiology. 2010;39(2):372-7.
*60. Dennis CL, Dowsell T. Psychosocial and psychological interventions for preventing portpartum depression. Cochrane Database Syst Rev. 2013: 2: CD001134. Doi: 10.1002/14651858.CD001134.pub3.
61. Stallard P, Sayal K, Phillips R, Taylor JA, Spears M, Anderson R, et al. Classroom based cognitive behavioural therapy in reducing symptoms of depression in high risk adolescents: pragmatic cluster randomised controlled trial. BMJ: British Medical Journal. 2012;345.
*62. Boath E, Bradley E, Henshaw C. The prevention of postnatal depression: a narrative systematic review. J Psychosom Obstet Gynaecol. 2005 Sep;26(3):185-92.
*63. Brunwasser SM, Gillham JE, Kim ES. A meta-analytic review of the Penn Resiliency Program’s effect on depressive symptoms. J Consult Clin Psychol. 2009 Dec;77(6):1042-54.
*64. Boath E, Bradley E, Henshaw C. The prevention of postnatal depression: a narrative systematic review. J Psychosom Obstet Gynaecol. 2005 Sep;26(3):185-92.
*65. Brunwasser SM, Gillham JE, Kim ES. A meta-analytic review of the Penn Resiliency Program’s effect on depressive symptoms. J Consult Clin Psychol. 2009 Dec;77(6):1042-54.
*66. Calear, A. L. and H. Christensen (2010). “Systematic review of school-based prevention and early intervention programs for depression.” Journal of Adolescence 33(3): 429-438.
*67. Cole MG, Dendukuri N. The feasibility and effectiveness of brief interventions to prevent depression in older subjects: a systematic review. Int J Geriatr Psychiatry. 2004 Nov;19(11):1019-25.
*68. Cuijpers P, Muñoz RF, Clarke GN, Lewinsohn PM.Psychoeducational treatment and prevention of depression: the “Coping with Depression” course thirty years later. Clin Psychol Rev. 2009 Jul;29(5):449-58. Epub 2009 Apr 18.
*69. Cuijpers P, Smit F, van Straten A. Psychological treatments of subthreshold depression: a meta-analytic review. Acta Psychiatr Scand. 2007 Jun;115(6):434-41.
*70. Dennis CL, Creedy D. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst Rev. 2004 Oct 18;(4):CD001134.
*71. Dennis CL. Psychosocial and psychological interventions for prevention of postnatal depression: systematic review. BMJ. 2005 Jul 2;331(7507):15.
*72. Forsman AK, Schierenbeck I, Wahlbeck K. Psychosocial interventions for the prevention of depression in older adults: systematic review and meta-analysis. J Aging Health. 2011 Apr;23(3):387-416. Epub 2010 Oct 8.
*73. Garber, Judy; Downs, Lindsay E. Prevention of depression in youth: Sex differences in effects. In: Depression in adolescent girls: Science and prevention. Strauman, Timothy J. (Ed.); Costanzo, Philip R. (Ed.); Garger, Judy (Ed.); New York, NY, US: Guilford Press, 2011. pp. 193-234.
*74. Hackett ML, Anderson CS, House A, Halteh C. Interventions for preventing depression after stroke. Cochrane Database Syst Rev. 2008 Jul 16;(3):CD003689.
*75. Horowitz JL, Garber J. The prevention of depressive symptoms in children and adolescents: A meta-analytic review. J Consult Clin Psychol. 2006 Jun;74(3):401-15.
*76. Jané-Llopis E, Hosman C, Jenkins R, Anderson P. Predictors of efficacy in depression prevention programmes. Meta-analysis. Br J Psychiatry. 2003 Nov;183:384-97.
*77. Martin A, Sanderson K, Cocker F. Meta-analysis of the effects of health promotion intervention in the workplace on depression and anxiety symptoms. Scand J Work Environ Health. 2009 Jan;35(1):7-18. Epub 2008 Dec 9.
*78. Mead N, Lester H, Chew-Graham C, Gask L, Bower P. Effects of befriending on depressive symptoms and distress: Systematic review and meta-analysis. British Journal of Psychiatry, Vol 196(2), Feb, 2010. pp. 96-101.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
50 | Chapter 2
*79. Merry S, McDowell H, Hetrick S, Bir J, Muller N. Psychological and/or educational interventions for the prevention of depression in children and adolescents. Cochrane Database Syst Rev. 2004;(1):CD003380.
*80. Merry SN, Hetrick SE, Cox GR, Brudevold-Iversen T, Bir JJ, McDowell H. Psychological and educational interventions for preventing depression in children and adolescents. Cochrane Database Syst Rev. 2011 Dec 7;12:CD003380.
*81. Mihalopoulos C., Vos T., Pirkis J., Smit F., Carter R. Do indicated preventive interventions for depression represent good value for money? Australian and New Zealand Journal of Psychiatry 2011 45:1 (36-44)
*82. Siegenthaler E, Munder T, Egger M. Effect of preventive interventions in mentally ill parents on the mental health of the offspring: systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. 2012 Jan;51(1):8-17.e8. Epub 2011 Dec 3.
*83. Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analytic review of depression prevention programs for children and adolescents: factors that predict magnitude of intervention effects. J Consult Clin Psychol. 2009 Jun;77(3):486-503.
*84. Stuart S, O’Hara MW, Gorman LL. The prevention and psychotherapeutic treatment of postpartum depression. Arch Womens Ment Health. 2003 Aug;6 Suppl 2:S57-69. Epub 2003 Aug 9.
*85. van der Waerden JE, Hoefnagels C, Hosman CM. Psychosocial preventive interventions to reduce depressive symptoms in low-SES women at risk: a meta-analysis. J Affect Disord. 2011 Jan;128(1-2):10-23. Epub 2010 Mar 25.
*86. Waddell C, Hua JM, Garland OM, Peters RD, McEwan K. Preventing mental disorders in children: a systematic review to inform policy-making. Can J Public Health. 2007 May-Jun;98(3):166-73.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
2
Are preventive interventions for depression effective? A meta-analysis | 51


Part III: Reasons for (not) seeking help


Chapter 3
Reasons and determinants of (not) seeking help
This chapter is published as:Van Zoonen, K., Kleiboer, A. M., Beekman, A. T. F., Smit, J. H.,
Boerema, A. M., Cuijpers, P. (2014). Reasons and determinants of help-seeking in people with a subclinical depression.
Journal of Affective Disorders, 173, 105 – 112.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
56 | Chapter 3
Abstract
Background: Subclinical depression is common. Although interventions have proven to be effective, participation rates are low. This study first aimed to get more insight in help-seeking and reasons for (not) seeking care. The second aim was to identify characteristics that distinguish people who receive help, those with an unmet need, or no perceived need for care.
Methods: Respondents with a subclinical depression (n = 162) were recruited from the general population. They were eligible for participation if they were aged 18 years or older, scored 20 or higher on the K10 screening instrument for depression, and did not meet the criteria for major depression.
Results: Of all participants, 27% received help, 33% had an unmet need, and 40% had no perceived need for care. Participants with no perceived need reported not to experience symptoms, were able to solve problems on their own, and could mobilize their own support. They were characterized by lower scores on neuroticism and an older age than those who received care.
Limitations: The response rate in this study was relatively low which may have caused a selection bias.
Conclusion: Not all people with subclinical depression may need help for their symptoms, some are able to deal with problems on their own. However, others experience a need for care but do not receive any. Gaining insight into potential barriers for help seeking and receiving in people with an unmet need is important so appropriate measures can be taken to ensure that those who need care get the help they want.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 57
Introduction
Subclinical depression is common and has a significant impact on daily functioning (1, 2) while at the same time creating a large burden for the society (3). Subclinical depression can be defined in different ways such as (1) a score above a threshold on a screening instrument without meeting the full criteria for major depression according to the DSM-V or (2) having a depressed mood accompanied with additional symptoms, but not as severe or as many as the DSM-V criteria for major depression (4-6). The definitions proposed in the DSM-V of clinical and subclinical depression suggest a qualitative difference between the two, however, research indicates that depression is best viewed on a continuum from no symptoms to many symptoms (7-9). Subclinical depression is considered part of the prodromal phase of depression and is one of the best predictors of major depression (1, 5).
The incidence and prevalence rates of subclinical depression vary widely depending on the definition, population, and instruments that are used. Estimates of the incidence rates range from 2.3% to 12.9% and prevalence rates vary from 2.2% to 24% in community samples (10, 11). Compared to the prevalence of full blown depressive disorders these prevalence rates are equal or higher. It is estimated that, in the Netherlands, approximately 7.5% of the general population meets the criteria for a subclinical depression (1). Although research has shown that effective interventions are available to ameliorate symptoms in individuals with a subclinical depression and to prevent the onset of major depression (12), only few people who could benefit from these treatments actually participate in these interventions. Help-receiving rates in individuals with a subclinical depression range between 1% and 32% (13). Since preventive treatments have shown to be effective, it is important to know what the reasons are for people with subclinical depression not to seek help, and what kind of people do or do not seek help for their symptoms.
Research on help seeking behaviour is often guided by Andersen and Newman’s model for health services utilization that distinguishes three interrelated factors; need factors, predisposing factors, and enabling factors (14). According to this model need factors include both the individual’s own judgment of their health and symptoms (perceived need) and the professional assessment of the individual’s symptoms and health based on a clinical instrument (actual need) (14-16).
Predisposing factors consist of personal, social, and cultural characteristics of individuals such as demographic factors (e.g. gender), social structure (e.g. education, relationship status), and belief factors towards the health care system and symptoms (e.g. expectations of treatment outcome and/or their health) (17). Enabling factors relate to organisational factors which affect the availability and affordability of mental health care (e.g. individual’s financial situation, location and distribution of health care facilities) (18).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
58 | Chapter 3
The model of Andersen and Newman contains feedback loops between the various factors, illustrating the interrelations between those factors. For example, the ability to recognize symptoms (a need factor) is closely related to age and the level of education (both predisposing factors), health related quality of life (e.g. when people do not experience a burden of disease they might not seek help) and the severity of symptoms (actual need) (17, 19).
Furthermore, looking at (actual) need factors, research in the general population has shown that depressive disorders are often accompanied by alcohol use disorders, with depressed individuals having a 2-to-3-fold increased risk of alcohol use disorders (20-22). Research on help-seeking in people with and without an alcohol disorder is contradictory with some studies showing no difference in help-receiving (23) and others showing a reduced tendency to seek care in people with an alcohol disorder (24, 25). Also, previous episodes of depression tend to make people with recent depressive episodes seek help more quickly (26).
Research on age is not clear cut with some research indicating that increasing age is related to a greater need for and receiving of professional help (27-29) and other studies showing that young people, people with more positive experiences of their mental health care, and people who acknowledge their mental problems receive more mental health treatment (13, 19, 30, 31). Research on gender and help-seeking showed that men are less likely than women to seek help, which might be due to gender-role differences and what is viewed as masculine (28, 32). Furthermore, research on stigma and help-seeking in depression is contradictory, with some research showing a relation between stigma and help-seeking (33-35) and others not finding a relation (36). Further research has shown that people with higher scores on neuroticism, a higher education, and those who are in a relationship with a significant other tend to seek more help for their mental health problems (13, 16, 29, 32, 37). However, research in people with affective symptoms has shown that people who have a partner are less likely to seek professional help (38). Above literature shows that there is a lot of information on help-seeking in mental health care and full-blown depressive disorders. However, not many studies have focused on help-seeking in populations with subclinical depression. In the Netherlands preventive care is easily accessible and mostly free of charge to everyone which will minimize the influence of enabling factors.
In the current study we recruited a sample with subclinical depression from the general population in order to get more insight in help-seeking and the reasons for (not) seeking help. In order to do so, we distinguished between people who had: (1) no perceived need for professional help, (2) an unmet need (i.e. they did not receive professional help, but perceived a need for help), and (3) received professional help (people who received care for their symptoms). Furthermore, we examined what type of professional help was used by people who received care.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 59
The second aim was to examine if we could identify characteristics that distinguished people with an unmet need, no perceived need, and those who received professional help. We examined differences in predisposing factors such as, sex, age, education, marital status, mastery, neuroticism, and need factors such as, health related quality of life (HRQoL), alcohol use, duration of symptoms, severity of depression and anxiety symptoms, and comorbid anxiety disorder.
Methods
Participants and procedure Subjects with subclinical depression were recruited from the general population between September 2012 and February 2013 in collaboration with Municipal Public Health Services (GGD) in three different areas in the Netherlands: Amsterdam, Zuid-Holland West, and Zuid-Holland Zuid. In collaboration with several mental health institutions, the availability of preventive interventions in these areas was optimized and widely advertised (i.e. extensive advertisement through local newspapers, flyers and leaflets with information on the preventive interventions and mental health institutions prevention these were delivered to GPs and individual’s homes to make health care professionals as well as the general population aware of the preventive interventions). In each area the preventive interventions were well distributed, however with the optimisation the emphasize was on five preventive interventions; two web-based interventions and three group interventions: mindfulness training, a coping with depression course, and exercise therapy. Advertisement were focused on people with symptoms of depression such as low mood or feelings of sadness and who wanted to do something about them. We specifically asked about these five interventions, because they form a good representation of the broad range in available preventive interventions throughout the Netherlands and provide enough diversity for people to choose from. Since the focus of these interventions is to prevent (or at least delay) the onset of depressive disorders they are considered preventive interventions. Subjects were also able to indicate if they preferred other interventions.
GGD in the Netherlands are obliged by law to gain insight into the health situation of their citizens and a health survey among a random sample of the population is one way of doing so. The current study joined this survey in 2012. This survey is usually conducted every four years by the GGD and contains questions about physical, mental, and social health and lifestyle. A screening instrument for depression, the Kessler-10 (K10) was included in the 2012 survey (39). Subjects who scored 20 or higher on the K10 screening instrument for depression (40), who were 18 years or older, and who had given permission to be contacted for further research at the health survey were invited

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
60 | Chapter 3
to take part in the current study. They received a letter containing more information about the study and an informed consent form that could be returned to the research team in a prepaid envelope. Subjects with insufficient comprehension of the Dutch language (spoken or written) were excluded. Subjects who were willing to take part and who had signed and returned the informed consent form were contacted by telephone for a diagnostic interview, the Composite International Diagnostic Interview (CIDI) (41), to determine depression status. Respondents who scored negative for a diagnosed depressive disorder in the past 6 months (no major depression or dysthymia according to DSM-IV criteria) were identified as having subclinical depression and were included in the current study. Respondents who met criteria for major depression and/or dysthymia remained in the study, but were not included in this paper. Respondents with subclinical depression received an online questionnaire covering several domains including health care use, personality and perceived need for care, followed by questions concerning their knowledge of preventive interventions and mental health care. As these questions needed more elaboration and explanation by the researchers they were assessed during a short telephone call. Some respondents preferred to answer the questions of the online questionnaire by telephone (n=40), by paper-and-pencil (n=3) or during a home visit (n=3).
InstrumentsDiagnostic interviewThe Composite International Diagnostic Interview (CIDI) is developed by the WHO for use by lay interviewers and for research purposes. The instrument has shown adequate validity and excellent reliability for depressive and anxiety disorders (42). In the current study the 6 month version of the CIDI was administered to establish a diagnosis of anxiety (section D) and/or depression (section E) and the lifetime version to identify past episodes of anxiety or depression disorder. The lifetime version was used to establish whether participants had ever had a diagnosis of major depression and/or dysthymia or not. The interview was carried out by Master level students in Clinical Psychology that received 8 hours of training and worked under supervision. It took about 60 minutes to complete, depending on the answers given by respondents.
Help-seekingTo distinguish people who had received professional help from those with an unmet need, and those with no perceived need we used questions from the Trimbos/iMTA questionnaire that measures health care uptake associated with Psychiatric Illness (TiC-P) (43) and answers to questions at the short telephone questionnaire.
To establish whether respondents had received (professional) help for depressive

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 61
symptoms in the past 6 months, we used some questions of the TiC-P (43). The TiC-P asks for the number of appointments someone had for psychological problems with the GP, a company doctor, a medical specialist or within specialised mental health care in the past 6 months. We further categorised people into those who had received help in primary care (GP, company doctor, and social worker), those who had received help in specialised mental health care (mental health institution, psychologist or psychiatrist, medical specialist, consultation agency for alcohol and drugs), those with another form of help (e.g. alternative healer), those who received primary care as well as specialized mental health care, those who received primary care as well as other forms of help, those who received specialized mental health care as well as other forms of help, and those who received primary care, specialized mental health care.
In order to establish whether respondents who had not received care, had no perceived need or an unmet need for preventive interventions, we asked whether they would have taken part in one or more of the five preventive interventions (e.g. group cognitive behaviour therapy, group exercise intervention, mindfulness, one of two online interventions, either a problem-solving intervention or an intervention with the focus on cognitive behaviour therapy) if they had known about them in a short telephone questionnaire. If they responded positive, respondents were asked to indicate which intervention(s) they would choose. Also, respondents were able to choose another intervention if they felt none of the preventive interventions were suitable. Respondents that answered negative were asked for the reason as to why they were not willing to take part in these interventions. They were able to choose one or more out of 12 reasons, one answer was an open alternative stating “other”. We recoded all 11 options as well as the open ended option into 7 main categories for not wanting to participate; inability to recognize own symptoms, feeling one can solve his or her own problems, interventions are difficult to reach (for example due to travel distance), people seem unaware of the different aspects of an intervention, people received care in another way (for example from lay people), other external factors, and other reasons.
DemographicsThe demographic characteristics used in this study were marital status, education, gender and age.
Health related Quality of LifeThe European Quality of Life 5-Dimensions 3-Level (EQ-5D-3L) questionnaire was used to determine people’s health related quality of life (HRQoL). This short self-report questionnaire includes 5 domains; mobility, self-care, usual activities, pain/discomfort, anxiety/depression. Each domain has 3 levels of functioning; no problems,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
62 | Chapter 3
some problems, and extreme problems. People indicate which level is applicable to their perceived health. The EQ5D distinguishes 486 unique health states that are related to a utility score which ranges from “poor health” (0) to “perfect health” (1). There is extensive literature on the validity and reliability of the EQ-5D in many populations and conditions (44, 45).
Depressive symptomsThe severity of depressive symptoms was assessed with the screening instrument K-10 (39). This questionnaire consists of 10 questions answered on a 5-point rating scale from “never” to “always”. The Dutch version of the K10 has good internal consistency (α=0.94.). The reliability in the current study was fair α=0.75, which might be caused by the inclusion of people who only score 20 or higher instead of using the whole spectrum (40). This data was derived from the survey of the GGD.
AnxietyTo establish a co-morbid anxiety disorder we used section D of the CIDI 2.1 (42). To assess the severity of anxiety symptoms we used the anxiety subscale of the Hospital Anxiety and Depression Scale (HADS). Respondents were able to answer questions on a 4-point rating scale ranging from “not at all” to “very often”. The HADS has shown good validity in different populations. The concurrent validity of the HADS is good to very good. The reliability of the HADS-A in the current study was good (α=0.81) (46).
Duration of depressive symptoms To establish the duration of the depressive symptoms, respondents were asked to give an estimation in months.
Alcohol useTo establish co-morbid alcohol use we have used data from the survey of the GGD stating if someone was a heavy drinker or not. Someone was considered a heavy drinker when they consumed more than 21 glasses of alcohol per week (men) or more than 14 glasses of alcohol per week (women) on average in the past 6 months.
NeuroticismNeuroticism was assessed with the neuroticism subscale of the NEO-Five Factor Inventory (NEO-FFI) (47). Respondents were asked to answer 12 questions on a 5-point rating scale ranging from “strongly disagree” to “strongly agree”. The reliability in previous research has shown to be fair to good (α=0.64 – α=0.88) and test-retest reliability was good (α=0.75 – α=0.87) (47). The reliability in the current study was good (α=0.84).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 63
MasteryTo assess to what extent respondents felt in control of their life and life-events, we used the short form of the Pearlin Mastery Scale (48). Respondents were able to answer questions on a 5-point rating scale ranging from “strongly agree” to “strongly disagree”. Total scores could range from 5 to 25. Lower scores indicate a more external locus of control, while higher scores indicate a more internal locus of control. The internal consistency was good (α=0.83).
StigmaTo establish levels of personal and perceived stigma the Depression Stigma Scale (DSS) was used (49). This instrument consists of 18 questions answered on a 4-point rating scale ranging from “strongly disagree” to “strongly agree”. There are 2 subscales, each consisting of 9 items, leading to a range of 0 to 36 on both scales. Lower scores indicating less stigma. Both personal and perceived stigma showed good internal consistency (respectively, α=0.72 and α=0.84).
Statistical AnalysisDescriptive statistics were used to determine how many respondents were identified as having received professional care, or experiencing an unmet need or no perceived need, to describe the type of help respondents preferred, and the reasons respondents gave for not perceiving the need to make use of any of the mentioned preventive interventions. To examine whether the predictors (e.g. gender, age, marital status, education level, neuroticism, comorbid anxiety, comorbid alcohol use, mastery, duration of depressive symptoms, severity of depressive symptoms, severity of anxiety symptoms, health related quality of life (HRQoL), previous lifetime diagnosis of depressive disorder, and perceived and personal stigma had an association with help-seeking we first conducted univariate analyses (one way ANOVA, Levene’s test when appropriate, and Chi-square tests). We also conducted post hoc tests for significant Chi-square tests and ANOVAs. We reported the Bonferroni post hoc test, except when Levene’s test was significant we then reported Games Howell post hoc test. Additionally, we performed a multinomial stepwise regression analysis to investigate which of the 12 predictors (gender, education, marital status, alcohol use, comorbid anxiety disorder, duration of symptoms, age, severity of depressive and anxiety symptoms, neuroticism, mastery, HRQoL, previous lifetime diagnosis of depressive disorder, and perceived and personal stigma) influenced receiving care, perceiving an unmet need, or perceiving no need for help the most. The reference category was the group who received help, since this was the only group who had received help, they perceived as needed. Multicollinearity was tested and we also tested the usefulness of the model by looking at the by chance accuracy. This states

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
64 | Chapter 3
the difference between the percentages explained by the tested model compared to a model without predictors. When the percentage explained by the tested model is higher than the percentage explained by the model without any predictors, the tested model is considered useful.
Results
SampleA total of 1191 people were invited to take part in the study, this included people with depressive disorders as well as people with subclinical depression. Of these, 331 people (28%) returned their informed consent form and 291 participants (24%) completed the diagnostic interview. Reasons for not completing the diagnostic interview were no response (n = 9), insufficient knowledge of the Dutch language (n=15), physical or mental inabilities (e.g. stroke, psychological stress) (n=4), and/or not in the mood to participate (n=4), one respondent had moved abroad, one respondent did not have time to participate, and 6 respondents did not provide a reason. One hundred and eighty-five people met criteria for subclinical depression and 162 respondents completed the information on help-seeking.
Table 1 shows the descriptive characteristics of the respondents. Age varied widely, the average age was 57 (SD=18), with a range of 19-94 years. Fifty-six per cent of the respondents were female, most had finished middle education and were involved in a close relationship. Table 1. Descriptives
All Met Need (n=44)
Unmet Need(n=54)
No perceived Need(n=64)
Gender, n (%) Female Male
91 (56.2)71 (43.8)
23 (52.3)21 (47.7)
35 (64.8)19 (35.2)
33 (51.6)31 (48.4)
Age, M (sd) 57.2 (17.8) 51.6 (18.4) 53.6 (14.3) 64.1 (17.7)
Marital Status, n (%) In relationship Single
93 (57.4)69 (42.6)
29 (65.9)15 (34.1)
30 (55.6)24 (44.4)
34 (53.1)30 (46.9)
Education, n (%) Low Middle High
24 (14.8)81 (50.0)57 (35.2)
6 (13.6)22 (50.0)16 (36.4)
5 (9.3)28 (51.9)21 (38.9)
13 (20.3)31 (48.4)20 (31.3)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 65
Received (professional) helpForty-four respondents (27%) with a subclinical depression had received help for their symptoms. Of the respondent who received help, 30% had received help in primary care, 14% in specialized mental health care, 41% in both primary and specialized mental health care, 9% in primary and other care (e.g. alternative healer), and 7% had received primary care, specialized mental health care, and other care. No respondent had received other care only or a combination of specialized mental health care and other care.
Unmet needFifty-four respondents (33%) would have taken part in preventive interventions if they had known about them (unmet need). When asked which preventive intervention (two web-based interventions, mindfulness training, a coping with depression course, and/or exercise therapy) respondents would choose if given the choice, 43% answered they would choose mindfulness, 37% choose group exercise treatment, 33% choose cognitive behavioral treatment, 20% was not able to choose one of the preventive interventions mentioned above, 15% choose the online problem solving treatment “Alles onder controle”, and 13% choose the other online cognitive behavioral treatment “Beter Gestemd Online”. Respondents were able to choose more than one of the preventive interventions.
No perceived needSixty-four respondents (40%) did not perceive a need for (psychological) care (no perceived need). Respondents were asked what their reasons were for not willing to participate in a preventive intervention. They were able to choose more than one reason. Half of the respondents explained that they felt they were able to solve their own problems, 44% of the respondents experienced a lack of knowledge about the courses, 38% did not recognize their symptoms and felt that they were not subclinically depressed. Thirty-four per cent indicated they received another kind of help or treatment, 23% indicated they were too old, had no time, or not enough money to participate, 11% explained the interventions were not accessible to them.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
66 | Chapter 3
Tabl
e 2.
Ass
ocia
tions
of p
redi
ctor
s with
rece
ived
or p
erce
ived
nee
d fo
r hel
pPr
edic
tor
All
Rec
eive
d H
elp
Unm
et N
eed
No
perc
eive
d ne
ed
Test
G
ende
r, n
(%)
Fe
mal
e
Mal
e91
(56.
2)71
(43.
8)23
(52.
3)21
(47.
7)35
(64.
8)19
(35.
2)33
(51.
6)31
(48.
4)χ2 =
(2, n
= 1
62) =
2.4
6, p
= .3
0
Educ
atio
n, n
(%)
Lo
w
Mid
dle
H
igh
24 (1
4.8)
81 (5
0.0)
57
(35.
2)
6 (1
3.6)
22 (5
0.0)
16 (3
6.4)
5 (9
.3)
28 (5
1.9)
21 (3
8.9)
13 (2
0.3)
31 (4
8.4)
20 (3
1.2)
χ2 = (4
, n =
162
) = 3
.05,
p =
.56
Mar
ital s
tatu
s, n
(%)
Si
ngle
In
a R
elat
ions
hip
69 (4
2.6)
93 (5
7.4)
15 (3
4.1)
29 (6
5.9)
24 (4
4.4)
30 (5
5.6)
30 (4
6.9)
34 (5
3.1)
χ2 = (2
, n =
162
) = 1
.86,
p =
.41
Alc
ohol
use
, n (%
)
No
Ye
s13
8 (9
0.2)
15 (9
.8)
37 (9
0.2)
4 (9
.8)
45 (8
6.5)
7 (1
3.5)
56 (9
3.3)
4 (6
.7)
χ2 = (2
, n =
153
) = 1
.46,
p =
.52
Life
time
diag
nosi
s, n
(%)
D
epre
ssiv
e di
sord
er
No
depr
essi
ve d
isor
der
70 (4
3.2)
92 (5
6.8)
23 (5
2.3)
21 (4
7.7)
28 (5
1.9)
26 (4
8.1)
19 (2
9.7)
45 (7
0.3)
χ2 = (2
, n =
162
) = 7
.89,
p <
.05*
Com
orbi
d an
xiet
y, n
(%)
N
o
Yes
127
(78.
4)35
(21.
6)28
(63.
6)16
(36.
4)a
43 (7
9.6)
11 (2
0.4)
56 (8
7.5)
8 (1
2.5)
a
χ2 = (2
, n =
162
) = 8
.84,
p <
.05*
Dur
atio
n sy
mpt
oms,
n (%
)
0 m
onth
s
1-12
mon
ths
>1
2 m
onth
s
mis
sing
52 (3
2.1)
38 (2
3.5)
65 (4
0.1)
7 (4
.3)
9 (2
0.5)
a
10 (2
2.7)
24 (5
4.5)
1 (2
.3)
13 (2
4.1)
16 (2
9.6)
23 (4
2.6)
2 (3
.7)
30 (4
6.9)
a
12 (1
8.8)
18 (2
8.1)
4 (6
.3)
χ2 = (4
, n =
155
) = 1
3.45
, p <
.01*
*
Pers
onal
Stig
ma,
m (S
D)
14.8
6 (4
.18)
14.3
3 (3
.91)
15.0
4 (4
.35)
15.0
6 (4
.24)
F(2,
157
) = 0
.47,
p =
.63
Perc
eive
d St
igm
a, m
(SD
)20
.79
(4.9
7)21
.53
(4.4
8)21
.09
(5.3
5)20
.03
(4.9
1)F(
2, 1
57) =
1.3
2, p
= .2
7Se
verit
y de
pres
sive
sym
ptom
s, m
(SD
)25
.04
(4.9
0)26
.30
( 5.2
8)a
25.7
4 ( 5
.10)
23.6
1 (4
.12)
aF(
2, 1
57) =
4.9
3, p
< .0
1** †
Neu
rotic
ism
, m (S
D)
22.0
4 (7
.84)
24.7
0 (7
.65)
a23
.15
(7.3
4) b
19.2
7 (7
.61)
a,b
F(2,
159
) = 7
.68,
p <
.001
**M
aste
ry, m
(SD
)10
.41
(4.2
3)9.
77 (4
.13)
10.3
1 (4
.01)
10.9
4 (4
.48)
F(2,
159
) = 1
.00,
p =
.37
Age
, m (S
D)
57.2
2 (1
7.68
)51
.61
(18.
40)a
53.5
7 (1
4.27
)b64
.16
(17.
73) a
,bF(
2, 1
59) =
9.1
2, p
< .0
01**
*Se
verit
y an
xiet
y sy
mpt
oms,
m (S
D)
6.52
(3.5
0)7.
68 (3
.36)
a6.
63 (3
.22)
5.63
(3.6
3) a
F(2,
159
) = 4
.749
, p <
.05*
HRQ
oL, m
(SD
)0.
74 (0
.22)
0.74
(0.1
6)0.
73 (0
.25)
0.75
(0.2
2)F(
2, 1
59) =
0.1
1, p
= .9
0
*sig
nific
ant a
t lev
el p
< 0.
05.**
sig
nific
ant a
t lev
el p
< 0.
01 *
** s
igni
fican
t at l
evel
p< 0
.001
. Pos
t hoc
test
s si
gnifi
cant
com
paris
ons;
a =
rece
ived
hel
p co
mpa
red
to n
o pe
rcei
ved
need
, b =
unm
et n
eed
com
pare
d to
no
perc
eive
d ne
ed, † L
even
e’s
test
was
sig
nific
ant,
ther
efor
e th
e W
elch
test
was
re
port
ed

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 67
Univariate associations between dispositional and need factors and help-seekingResults of the univariate analyses showed a significant relation between group and comorbid anxiety disorder (χ2(2)=8.84, p<.05), duration of symptoms (χ2(4)=13.45, p<.01), lifetime depression diagnosis (χ2(2)=7.89, p<.05), severity of depressive symptoms (F(2, 157)=4.93, p<.01) and anxiety symptoms (F(2, 159)=4.45, p<.05), age (F(2, 159)=9.12, p<.001), and neuroticism (F(2, 159)=7.68, p<.001) (see Table 2).
Post hoc analyses showed that people without a comorbid anxiety disorder, who experienced a no symptoms or a short duration of symptoms, those with less severe symptoms of depression and anxiety, who were older and who had lower scores on neuroticism were more likely to not perceive a need compared to the people who received help. Post hoc analysis of lifetime diagnosis did not show significant differences between the individual groups. Respondents who were older and had lower scores on neuroticism were also more likely to not perceive a need for help compared to people with an unmet need. There were no significant associations between the no perceived need, unmet need or received help groups and gender, education, personal and perceived stigma, alcohol use, being in a relationship, health related quality of life (HRQoL) or mastery (Table 2).
Multivariate associations between dispositional and need factors and help-seekingStepwise regression includes variables until there is no significant improvement to the model. Results, as reported in Table 3, showed that age and neuroticism were the best predictors for received or perceived need for help (χ2(4)=23.15, p<.001). The step summary results show that age and neuroticism are significant predictors, with neuroticism showing the strongest effect. Overall the model with both age and neuroticism explains 47.6%, this is 5% more than the model without predictors and so our model is considered useful. The results show that people who are older are more likely to not perceive a need for care, OR=1.04; 95% CI=1.01-1.07; p<.01. More specifically, for every year people get older they are 1.04 times more likely to not experience a need for care. Also, people who scored higher on neuroticism were more likely to have received help. Specifically, the results showed that for every unit increase in neuroticism, their chance of not experiencing a need for care decreases with 0.92.
Neuroticism showed some correlation with other predictors like severity of anxiety and depressive symptoms, mastery and age. Although multicollinearity is not a problem in the current study, we conducted the analyses again without neuroticism. The results showed that age and severity of anxiety symptoms were predictors, with severity of anxiety symptoms showing the strongest effect.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
68 | Chapter 3
Table 3. Multinomial stepwise regression analyses dispositional and need factors on help-seeking95 % CI for Odds Ratio
B (SE) Lower Odds UpperUnmet Need vs Met NeedIntercept 0.42 (1.02)Age 0.01 (0.01) 0.98 1.01 1.03Neuroticism -0.02 (0.03) 0.92 0.98 1.03No perceived Need vs Met NeedIntercept -0.02 (1.09)Age 0.04 (0.01)* 1.01 1.04 1.07Neuroticism -0.08 (0.03)* 0.87 0.92 0.98
Note. R2 = .15 (Cox & Snell), .17 (Nagelkerke). Model χ2 (4) = 23.15, p = 0.00. *p < 0.01.
Discussion
Participation rates in preventive interventions for depression are low despite the availability of effective interventions to reduce symptoms and to prevent the onset of depression (1, 12, 13). In the current study, we examined help-seeking in people with a subclinical depression. Participants with a subclinical depression were divided into three groups that either: (1) received help for their symptoms, (2) did not receive help, but perceived a need for help, (3) did not perceive a need for help. Guided by Anderson and Newman’s model for health care utilization (15, 17, 50) we further examined characteristics of respondents in those groups.
Results showed that 40% of the respondents did not perceive a need for care, 33% had an unmet need and 27% received professional help. People who had received help mostly found help in a combination of primary care and specialized mental health care. Most people who experienced an unmet need preferred group interventions (mindfulness, exercise, or cognitive behavioural therapy) over web-based interventions (problem solving treatment or cognitive behavioural therapy). Mindfulness and exercise interventions are known to be popular treatments for anxiety and depression (51) which may have to do with the interventions being less stigmatizing and having high accessibility compared to more depression-focused interventions (52). Furthermore, web-based interventions are relatively new. This and the relative old age of our sample make it less surprising that they are, as yet, a less popular option as most people are still unfamiliar with these interventions. An important finding was that many people indicated they lacked knowledge to make a well-informed decision to choose a preventive intervention. Apparently, optimizing advertisement for preventive interventions is not sufficient to provide people with the knowledge they need to choose a suitable intervention. This emphasizes a need to reach the people who perceive a need for care and provide them with the information necessary to make a decision on participation in interventions.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 69
Respondents without a perceived need for professional help frequently mentioned that they believed that their symptoms were not severe enough to seek help or that they were able solve their problems on their own. This is in line with previous research showing that people’s perceptions of their symptoms and their ability to deal with them is more often mentioned as a reason not to seek help (24, 53, 54) than practical considerations such as lack of money or time (24, 54). Respondents who did not perceive a need for care also frequently stated that they already received help from family or friends, which indicates that they are able to mobilize their own support. Most people in our sample were in a relationship (e.g. easy access to social support) which may be considered a protective factor for need for professional help (38). Also, most respondents who did not perceive a need for help were more likely to not have had a previous episode of depression. This might make it more difficult to recognize the symptoms. Finally, a large number of respondents without a perceived need for help mentioned that they were not familiar with preventive interventions. This may make it less likely for them to see this as an option when they experience problems and they may seek for other options to deal with their problems first.
Respondents without a perceived need for help were older and had lower scores on neuroticism than people who received help, with age being the strongest determinant of help-seeking. Previous research regarding the relation between age and help-seeking in people with a major depression was inconclusive. Our results are in line with the study of Verhaak and colleagues (31) who showed that younger people are more inclined to seek psychological help. Older people might be more familiar with subclinical depressive symptoms in the past and are willing to see if it passes without professional help or wait until symptoms get more severe. Also, people might be less mobile making professional care less accessible. It is well-known that people with a higher score on neuroticism are more likely to seek help for mental health problems in general and this study confirmed that this was also the case in people with a subclinical depression (16, 31, 37). Unlike other research we did not find a relation between gender and help-seeking (30, 32). The existing literature mostly focuses on full-blown depressive disorders and less is known about subclinical populations and help-seeking behaviour. In the current study, there were more women than men in the unmet need group, but the difference was not significant which may be due to the relatively small group sizes. This might also explain why we did not to find an effect of stigma on perceived need for help. Another explanation might be the differences in the definition of stigma (55). Furthermore, we found that lifetime diagnosis of depression was associated with help-seeking, but there were no differences between the individual groups. Other research has indicated that people with previous depressive disorders tend to seek professional help sooner than people without life time diagnosis (26).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
70 | Chapter 3
The results of our study suggests that dispositional factors (age and neuroticism) were more important determinants of help-seeking than need factors such as the severity of symptoms, comorbidity, lifetime diagnosis of depressive disorder, and the duration of symptoms. However, respondents with no perceived need for help had less severe symptoms, a shorter duration of symptoms (or they did not experience symptoms at all), and less comorbid anxiety. When we looked at all factors together, these need factors were no longer significant. Need factors were strongly related with neuroticism and this could have explained our findings. However, when we removed neuroticism from the analyses, the severity of anxiety symptoms became a significant determinant for help-seeking, but this did not apply to other need factors. More research is needed to examine if dispositional factors are indeed more important for help-seeking in people with a subclinical depression and to what extent (actual) need factors play a role.
We did not identify systematic differences between respondents who received care and those who perceived a need for help but did not actually receive that help. This study did not examine why people with an unmet need did not receive help. They may have been unfamiliar with the health care system or there may have been other reasons to explain why they did not receive or seek help. Future research should provide more insight into this issue so we can take measures to overcome potential barriers and ensure that those people who perceive a need for help, but do not receive help get the help they want.
This study has several strengths and limitations. A strength is that participants were selected from the general population through a Health Survey in a random sample. Identification occurred in a two stage process by selecting people with a high score on a screening instrument and excluding people with a major depressive disorder or dysthymia according to a diagnostic interview in the past 6 months (e.g. CIDI). However, the response rate on the Health survey was relatively low and men, people between 18 and 49 years of age, and immigrants were underrepresented in the Health Survey which has automatically caused underrepresentation of these groups in the current study (56). Not all respondents that participated in the Health Survey gave permission to be contacted for further research which may have further increased bias. Unfortunately, response rates are often low in Health studies in the Netherlands, like NEMESIS (57), which may be a result of people being more often contacted to participate in (commercial) research. We excluded people with insufficient understanding of the Dutch language which also limits the generalizability of our findings. Another limitation of this study was that the K10 is not designed to measure symptoms of depression specifically but is a measure of psychological distress. Therefore, symptoms of the K10 and the anxiety subscale of the HADS may overlap. However, the correlation between these measures was only moderately high and we felt that it was justified to include both measures

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 71
in the analyses. Nevertheless, it would have been better to have a pure measure of depressive symptoms. Finally, although the respondents were equally divided over the three groups with no perceived need for care, an unmet need, and those that received help, the number of people in each group was relatively small which may have limited the statistical power to find an effect.
Despite these limitations we believe that this study provides valuable insight in help-seeking in people with a subclinical depression. A large number of respondents did not perceive a need for care and these people were characterized by lower scores on neuroticism and older age. They felt that they were able to solve their problems on their own, did not recognize their symptoms and were able to mobilize their own support. Research has indicated that recognition of symptoms and impact on daily life are essential in (professional) help-seeking (31, 58). However, it may well be that this group of patients does not need professional care due to the natural recovery in subclinical depression as well as the mobilisation of their own support. However, some people experienced a need for care but did not receive any care. Gaining insight into potential barriers for help seeking and receiving in people with an unmet need is important so that appropriate measures can be taken to ensure that those who perceive a need for care get the help they want.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
72 | Chapter 3
References
1. Cuijpers P, de Graaf R, van Dorsselaer S. Minor depression: risk profiles, functional disability, health care use and risk of developing major depression. Journal of Affective Disorders. 2004;79(1–3):71-9.
2. Rapaport MH, Judd LL. Minor depressive disorder and subsyndromal depressive symptoms: functional impairment and response to treatment. Journal of Affective Disorders. 1998;48(2–3):227-32.
3. Broadhead W, Blazer DG, George LK, Tse C. Depression, disability days, and days lost from work in a prospective epidemiologic survey. JAMA. 1990;264(19):2524-8.
4. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta Psychiatrica Scandinavica. 2004;109(5):325-31.
5. Eaton W, Badawi M, Melton B. Prodromes and precursors: epidemiological data for primary prevention of disorders with slow onset. American Journal of Psychiatry. 1995;152:967-72.
6. APA. DSM 5: American Psychiatric Association; 2013.7. Geiselman B, Bauer M. Subthreshold depression in the elderly: Qualitative or quantitative
distinction? Comprehensive Psychiatry. 2000;41(2, Supplement 1):32-8.8. Goldberg D. Plato versus Aristotle: Categorical and dimensional models for common
mental disorders. Comprehensive Psychiatry. 2000;41(2, Supplement 1):8-13.9. Rodríguez MR, Nuevo R, Chatterji S, Ayuso-Mateos JL. Definitions and factors associated
with subthreshold depressive conditions: a systematic review. BMC psychiatry. 2012;12(1):181.
10. Rucci P, Gherardi S, Tansella M, Piccinelli M, Berardi D, Bisoffi G, et al. Subthreshold psychiatric disorders in primary care: prevalence and associated characteristics. Journal of Affective Disorders. 2003;76(1–3):171-81.
11. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. Journal of Affective Disorders. 1997;45(1–2):19-30.
12. van Zoonen K, Buntrock C, Ebert DD, Smit F, Reynolds CFr, Beekman AT, et al. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. International journal of epidemiology. 2014;43(2):318-29.
13. Andrews G, Issakidis C, Carter G. Shortfall in mental health service utilisation. Br J Psychiatry. 2001;179:417-25.
14. Anderson JG. Demographic Factors Affecting Health Services Utilization: A Causal Model. Medical Care. 1973;11(2):104-20.
15. Babitsch B, Gohl D, von Lengerke T. Re-revisiting Andersen’s Behavioral Model of Health Services Use: a systematic review of studies from 1998–2011. GMS Psycho-Social-Medicine. 2012;9.
16. Parslow RA, Jorm AF. Who uses mental health services in Australia? An analysis of data from the National Survey of Mental Health and Wellbeing. Australian & New Zealand Journal of Psychiatry. 2000;34(6):997-1008.
17. Andersen RM, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Quarterly. 2005;83(4):Online-only.
18. Bartels SJ. Improving the United States’ System of Care for Older Adults With Mental Illness: Findings and Recommendations for The President’s New Freedom Commission on Mental Health. The American Journal of Geriatric Psychiatry. 2003;11(5):486-97.
19. Sherwood C, Salkovskis PM, Rimes KA. Help-Seeking for Depression: The Role of Beliefs, Attitudes and Mood. Behavioural and Cognitive Psychotherapy. 2007;35(05):541-54.
20. Hasin DS, Stinson FS, Ogburn E, Grant BF. Prevalence, correlates, disability, and comorbidity of dsm-iv alcohol abuse and dependence in the united states: Results from the national epidemiologic survey on alcohol and related conditions. Archives of General Psychiatry. 2007;64(7):830-42.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
3
Reasons and determinants of (not) seeking help | 73
21. Pirkola S, Isometsä E, Suvisaari J, Aro H, Joukamaa M, Poikolainen K, et al. DSM-IV mood-, anxiety- and alcohol use disorders and their comorbidity in the Finnish general population. Social Psychiatry and Psychiatric Epidemiology. 2005;40(1):1-10.
22. Burns L, Teesson M. Alcohol use disorders comorbid with anxiety, depression and drug use disorders: Findings from the Australian National Survey of Mental Health and Well Being. Drug and Alcohol Dependence. 2002;68(3):299-307.
23. Ten Have M, de Graaf R, Vollebergh W, Beekman A. What depressive symptoms are associated with the use of care services?: Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Journal of Affective Disorders. 2004;80(2):239-48.
24. Ten Have M, De Graaf R, Ormel J, Vilagut G, Kovess V, Alonso J. Are attitudes towards mental health help-seeking associated with service use? Results from the European Study of Epidemiology of Mental Disorders. Social psychiatry and psychiatric epidemiology. 2010;45(2):153-63.
25. Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha T, Bryson H, et al. Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatrica Scandinavica. 2004;109(s420):47-54.
26. Farmer C, Farrand P, O’Mahen H. ‘I am not a depressed person’: How identity conflict affects help-seeking rates for major depressive disorder. BMC psychiatry. 2012;12(1):164.
27. Gallo JJ, Marino S, Ford D, Anthony JC. Filters on the pathway to mental health care, II. Sociodemographic factors. Psychological medicine. 1995;25(6):1149-60.
28. Mackenzie CS, Gekoski WL, Knox VJ. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging & Mental Health. 2006;10(6):574-82.
29. Bristow K, Patten S. Treatment-seeking rates and associated mediating factors among individuals with depression. Can J Psychiatry. 2002;47:660-5.
30. Bland RC, Newman SC, Orn H. Help-seeking for psychiatric disorders. Can J Psychiatry. 1997;42:935-42.
31. Verhaak PF, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJ, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
32. Oliver MI, Pearson N, Coe N, Gunnell D. Help-seeking behaviour in men and women with common mental health problems: cross-sectional study. Br J Psychiatry. 2005;186:297-301.
33. Barney LJ, Griffiths KM, Jorm AF, Christensen H. Stigma about depression and its impact on help-seeking intentions. Australian and New Zealand Journal of Psychiatry. 2006;40(1):51-4.
34. Schomerus G, Matschinger H, Angermeyer MC. The stigma of psychiatric treatment and help-seeking intentions for depression. European archives of psychiatry and clinical neuroscience. 2009;259(5):298-306.
35. Gulliver A, Griffiths K, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. 2010;10(1):113.
36. Endicott J. Barriers to seeking treatment for major depression. Depression and Anxiety. 1996;4(6):273-8.
37. Ten Have M, Oldehinkel A, Vollebergh W, Ormel J. Does neuroticism explain variations in care service use for mental health problems in the general population? Social Psychiatry & Psychiatric Epidemiology. 2005;40(6):425-31.
38. Burns T, Eichenberger A, Eich D, Ajdacic-Gross V, Angst J, Rössler W. Which individuals with affective symptoms seek help? Results from the Zurich epidemiological study. Acta Psychiatrica Scandinavica. 2003;108(6):419-26.
39. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normands SLT, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine. 2002;32(06):959-76.
40. Donker T, Comijs H, Cuijpers P, Terluin B, Nolen W, Zitman F, et al. The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research. 2010;176(1):45-50.
41. Robins LN, Wing J, Wittchen H, Helzer JE, Babor TF, Burke J, et al. The composite international diagnostic interview: An epidemiologic instrument suitable for use in

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
74 | Chapter 3
conjunction with different diagnostic systems and in different cultures. Archives of General Psychiatry. 1988;45(12):1069-77.
42. Andrews G, Peters L. The psychometric properties of the Composite International Diagnostic Interview. Social Psychiatry & Psychiatric Epidemiology. 1998;33(2):80.
43. Hakkaart-van Roijen L, Straten Av, Tiemens B, Donker MCH. Handleiding Trimbos/iMTA questionnaire for costs associated with psychiatric illness (Tic-P). 2002 January. Report No.
44. van Agt HM, Essink-Bot M-L, Krabbe PF, Bonsel GJ. Test-retest reliability of health state valuations collected with the EuroQol questionnaire. Social science & medicine. 1994;39(11):1537-44.
45. Dyer MT, Goldsmith KA, Sharples LS, Buxton MJ. A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health Qual Life Outcomes. 2010;8(13):1-12.
46. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. Journal of Psychosomatic Research. 2002;52(2):69-77.
47. Costa Jr PT, McCrae RR. Revised NEO Personality Inventory (NEO-PI-R) and the Five Factor Inventory (NEO-FFI): Professional manual. Odessa: Psychological Assessment resources Inc.; 1992.
48. Pearlin LI, Schooler C. The Structure of Coping. Journal of Health and Social Behavior. 1978;19(1):2-21.
49. Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC psychiatry. 2008;8(1):25.
50. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? Journal of health and social behavior. 1995;36(1):1-10.
51. Kessler RC, Soukup J, Davis RB, Foster DF, Wilkey SA, Van Rompay MI, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. American Journal of Psychiatry. 2001;158(2):289-94.
52. Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO. Exercise treatment for depression: Efficacy and dose response. American Journal of Preventive Medicine. 2005;28(1):1-8.
53. Mojtabai R. Unmet need for treatment of major depression in the united states. Psychiatric services. 2001;60(3):297-305.
54. Sareen J, Jagdeo A, Cox B, Clara I, ten Have M, Belik S-L, et al. Perceived barriers to mental health service utilization in the United States, Ontario, and the Netherlands. Psychiatric Services. 2007;58(3):357-64.
55. Aromaa E, Tolvanen A, Tuulari J, Wahlbeck K. Personal stigma and use of mental health services among people with depression in a general population in Finland. BMC psychiatry. 2011;11(1):52.
56. GGD. Gezondheid en welzijn van volwassenen en senioren in Zuid-Holland West - resultaten van het Gezondheidsonderzoek 2012. GGD Zuid-Holland West, 2012.
57. De Graaf R, Ten Have M, van Dorsselaer S. De psychische gezondheid van de Nederlandse bevolking. Nemesis-2: Opzet en eerste resultaten, Trimbos-Instituut, Utrecht. 2010.
58. Andrade L, Alonso J, Mneimneh Z, Wells J, Al-Hamzawi A, Borges G, et al. Barriers to mental health treatment: results from the WHO World Mental Health surveys. Psychological medicine. 2013:1-15.

Chapter 4
How well do people identify their symptoms?
This chapter is submitted as:Van Zoonen, K., Crisp, D., Griffiths, K. M. (2015).
Concurrence between self-assessment of anxiety and depression and actual scores on a screening instrument for anxiety and depression.
Manuscript submitted for publication to the Journal of Affective Disorders.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
76 | Chapter 4
Abstract
Background: Recognizing the symptoms of a mental illness such as anxiety or depression in oneself (e.g. insight) is one of the most important precursors for people to seek professional help. However, how accurate people are in identifying anxiety or depression in themselves compared to screening or diagnostic instruments is unknown. This study aimed to: 1) examine the concordance between an individual’s self-diagnosis and their status on a validated screening instrument; and 2) investigate what factors predicted an individual’s lack of insight into (underestimation of) their current depression and anxiety status.
Methods: Respondents (n=11940) from the general population completed a postal survey assessing perceptions and experiences of mental illness. All participants were aged between 18 and 65 years, with a mean of 46 years (SD=12.6).
Results: Most participants were accurate in their self-diagnosis of anxiety or depression; However, 20.9% of those who scored above the cut-off point for caseness on the K10 failed to self-report current depression or anxiety (95% CI: 0.78 - 0.81). Higher personal stigma, being separated or divorced and younger age were predictors of underestimating depression/anxiety symptoms.
Limitations: The response rate was low which may have caused a selection bias and the results might therefore not be representative of the general population.
Conclusions: This study suggest that members of the community are mostly capable of accurately identifying their current mental health status. However, a clinically relevant number of people underestimate their symptoms. Lowering stigma might improve an individual’s insight and subsequently increase help-seeking.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 77
Introduction
Depression and anxiety are among the most common mental disorders worldwide (1-3) and frequently co-occur (4-6). Both disorders result in significant loss of quality of life, and high economic costs and public health burden (7-9). Furthermore, depression is a highly recurrent and chronic disorder (8, 10) and associated with a high mortality risk due to suicide (11).
Although there are effective evidence-based treatments for both conditions, only around one-third of people experiencing anxiety problems or depression make use of health services (4, 9, 12). Many different barriers to seeking help have been suggested in the literature, such as stigma, lack of access to professionals and treatments, and a belief in self-reliance (13-16). Moreover, there is evidence to support that recognizing and acknowledging the experience of symptoms (e.g. self-identification), and the severity of depressive symptoms experienced, are crucial to seeking mental health care for depression or anxiety (17-19).
Many studies have focused on comparing self- and other-knowledge and predictions in several settings (e.g. 20, 21) or the capacity to recognise depression in ‘others’ in the form of vignettes depicting depression (e.g. 22, 23), showing that there are certain asymmetries between people’s self-identification and the identification by others about them. However, there is limited research comparing people’s self-identification of depression and/or anxiety to that of an objective measure or the factors underlying the accuracy of self-identification. One study has indicated that stigma influences a person’s willingness to accept that they have a mental illness (24). However, the possibility that stigma may affect the individual’s ability to self-identify their own symptoms correctly has not yet been investigated in the literature. Another study showed that people who did not perceive a mental health problem were characterised by less severe symptoms of anxiety and depression; they may therefore have been less in need of care and better placed to solve their problems without professional help (25). However, the study used the Perceived Need for Care Questionnaire (PNCQ; (26) which does not specifically assess whether people believe they suffer from anxiety or depression and the study did not specify what question or questions were used to identify if a person perceived that they had a mental problem. Furthermore, this paper did not focus on the accuracy of participant’s self-identification or factors that might have influenced accuracy.
It is critical to understand not only the capacity of individuals to accurately evaluate whether they suffer from anxiety or depression, but also to understand the characteristics that underlie self-identification in order to inform intervention strategies to promote help-seeking. Accordingly, the current study sought to investigate in a sample of members of the community: (i) the correspondence between an individual’s self-assessment of

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
78 | Chapter 4
anxiety or depression and their status on a validated screening instrument; and, since no research to date has examined the accuracy of self-identification, (ii) the demographic and attitudinal factors, such as gender, age, marital status, stigma and education, which predict self-identification into an individual’s personal current depression and anxiety status.
Methods
Participants and procedureThe present study comprised 11940 adults aged 18 to 65 years who responded to the “Wellbeing Survey”, a large survey of the emotional health of residents in several regions of Australia (27, 28). A total of 70,000 Australians randomly selected from the electoral rolls of eight Australian electoral divisions (4 rural, 4 metropolitan) were invited to complete the survey. Registration on the electoral roll is compulsory in Australia. Response rate of the survey was 18.1%. The study was approved by The Australian National University Human Research Ethics Committee (protocol 2007/2259). MeasuresThe Well-Being survey comprised a range of measures to assess perceptions and experiences of mental illness, including symptoms of anxiety and depression, attitudes toward mental illness and information needs. Details of this survey have been reported previously (27). The focus of the present study was on measures of psychological distress, self-reported diagnosis, stigma and demographic characteristics such as: age, gender, level of education, and marital status.
Psychological Distress The Kessler Psychological Distress (K10) scale was used to assess individual’s level of anxiety and depression. This scale has been shown to be a good indicator of depression and anxiety in the Australian community (29). The K10 consists of 10 items responded to on a 5-point Likert scale ranging from 1 (never) to 5 (always). Total scores range from 10 to 50, with higher scores indicating greater psychological distress. Scores of 20 or more have been shown to indicate anxiety or depressive disorders (29). The sensitivity and specificity of the scale using a cut-off score of 20 is .80 and .81 for any depressive or anxiety disorder (30).
Self-reported Diagnosis Self- reported diagnosis - whether respondents believed they suffered from anxiety, depression or both - was assessed using two individual items: “Do you currently suffer

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 79
from depression?” and “Do you currently suffer from anxiety?” Response options were 0 (No) or 1 (Yes). Respondents were categorised as self-reporting no diagnosis or as self-reporting that they suffered from anxiety/depression.
Stigma Stigma was assessed using the personal sub-scale of the Depression Stigma Scale (DSS) (31). Personal stigma refers to an individual’s own attitude toward people with depression (31). The scale consists of 9 items responded to on a 5-point scale from 1 (strongly agree) to 5 (strongly disagree). Total scores for the subscale range from 9 to 45; higher scores indicate greater stigma. The scale has demonstrated good reliability and validity (32). Internal consistency in the current study was good (α=0.83).
Current treatment status To examine treatment status, two questions were used asking whether respondents were receiving treatment for their anxiety or depression. Response options were 0 (No) or 1 (Yes). In addition, another question examined whether participants were currently receiving treatment from a psychologist, psychiatrist or mental health support group. Again, response options were 0 (No) or 1 (Yes).
Demographic variables The following demographic characteristics were collected: gender (0=male; 1=female), age (mean centred at 45.7 years), marital status (coded 0=married/de-facto, 1=separated/divorced, 2=widowed, 3=never married), with ‘married’ being the reference category, and level of education of participants (mean centred at 14.08 years).
Analysis Data analysis was conducted using SPSS Statistics Version 22. Respondents with missing data for ‘self-reported diagnosis’ or key demographic characteristics (i.e. gender, marital status, years of education) were removed from the dataset (2.6%). Other missing data (<3%) on continuous variables was imputed using maximum likelihood estimation via the EM algorithm (33). Age and years of education were mean centred and stigma total scores were converted to standardized z-scores to assist in the interpretation of the magnitude of effects found.
To examine the accuracy of a self-reported diagnosis we compared the respondent’s self-reported diagnosis with their score on the K10. This allowed us to construct four possible categories of accuracy: 1) accurate with no self-reported diagnosis and a score below the cut-off on the K10; 2) underestimation (no self-reported diagnosis of anxiety/depression and a score above the cut-off on the K10); 3) overestimation (a self-reported

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
80 | Chapter 4
diagnosis of anxiety/depression and scoring below the cur-off score on the K10); 4) accurate with a self-reported diagnosis of anxiety/depression and a score above the cut-off on the K10).
Initial descriptive statistics were examined to determine the concordance of respondent self-reported disorder with their indicated level of psychological distress on the K-10. This allowed us to identify the four categories of individuals in terms of accuracy of self-reported diagnosis (i.e. accurate without symptoms, overestimators, underestimatators, and accurate with anxiety/depression). In addition, we examined the sensitivity and specificity of self-reported diagnosis of anxiety/depression against the K10. Univariate analyses (one-way ANOVA and Chi-square tests) were then conducted to examine the association between demographic characteristics (e.g. gender, age, marital status, level of education), personal stigma, and accuracy of self-reported diagnosis. Post-hoc comparisons were based on the standardized residual for each cell in the Chi-square tests. Values greater than (+/-) 1.96 indicated a significant difference at a p-value of .05. The post hoc comparisons of the ANOVA tests were undertaken using the Tukey HSD. Finally, a logistic regression analysis using generalized linear models was conducted to further examine predictors of underestimators (those with a lack of insight) as compared to people who accurately identified their symptoms (accurate with anxiety/depression). Interquartile odds ratios were calculated for continuous variables (personal stigma, age, and years of education) (34). These ratios represent the odds of respondents at the 25th compared to the 75th percentile on the DSS sub-scale underestimating their symptoms.
Results
Sample characteristicsTable 1 shows the descriptive characteristics of the analyzed sample. The study comprised 11940 individuals of whom over 60% were female. Respondents were aged 18 to 65 years (M=46 years, SD=12.6). The majority of participants were married or in a de-facto relationship (71.4%). Twenty-two percent of respondents scored above the cut-off score of 20 on the K10 while 30% of the respondents had reported that they currently suffered from anxiety/depression.
Using the K10, over 80% of respondents accurately self-reported their mental health status with 65% falling below the cut-off on the K10 and self-reporting no symptoms and 18% with K10 scores above the cut-off and self-reporting anxiety/depression. Of the total sample (n=11940), 13% were identified as overestimating a condition (e.g. self-reporting diagnosis of anxiety/depression, but scoring below the K10 cut-off) and 5% underestimated their mental health problems self-reporting no diagnosis of anxiety/depression, but having a K10 score above the cut-off (Table 2).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 81
Table 1. Demographic characteristics as a function of accuracy of self-identificationPredictor All
(n=11940)
Accurate without anxiety/depression(n=7742)
Under-estimators
(n=551)
Over-estimators
(n=1560)
Accurate with anxiety/depression(n=2087)
p
Gender, n (%) Female Male
7366 (61.7)4574 (38.3)
4617 (59.6)3125 (40.4)
345 (62.6)206 (37.4)
1032 (66.2)528 (33.8)
1372 (65.7)715 (34.3)
0.00
Marital status, n (%) Married/de-facto Separated/Divorced Widowed Never married
8523 (71.4)1149 (9.6)181 (1.5)2087 (17.5)
5898 (76.2)587 (7.6)102 (1.3)1155 (14.9)
337 (61.2)49 (8.9)10 (1.8)155 (28.1)
1111 (71.2)143 (9.2)33 (2.1)273 (17.5)
1177 (56.4)370 (17.7)36 (1.7)504 (24.1)
0.00
Age, m (SD) 45.6 (12.6) 46.4 (12.5) 41.0 (13.5) 45.8 (12.0) 43.3 (12.5) 0.00Stigma, m (SD) 20.1 (5.6) 20.0 (5.5) 21.7 (5.6) 18.8 (5.5) 20.9 (6.0) 0.00Years of education, m (SD)
14.1 (2.4) 14.2 (2.4) 13.8 (2.5) 14.3 (2.4) 13.6 (2.5) 0.00
Note: Gender and marital status were examined using Chi-square analyses. Age, stigma and education were examined using ANOVAs.
In investigating the accuracy of self-report diagnosis as compared to K10 scores we acknowledge that some participants (specifically those self-reporting a diagnosis of depression) may have already been receiving treatment. All participants responding that they were currently experiencing anxiety or depression were asked if they were currently receiving treatment for the condition. In addition, all participants were asked if they were currently receiving treatment from a psychologist, psychiatrist or mental health support group (e.g. specialized care). Table 3 summarizes the results of help-seeking for anxiety/depression. Less than 1% of the respondents who were categorized as accurate without current symptoms had sought help for depression or for anxiety. In contrast, 57% and 45% of the group who were accurate with anxiety/depression reported they had sought help for depression and anxiety respectively.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
82 | Chapter 4
Table 2. Accuracy, self-report and self-identificationTotal n=11940 n (%)Self-identification No diagnosis anxiety/depression
8293 (69.5)3647 (30.5)
Self-report score (K-10) Below 20 20 or higher
9302 (77.9)2638 (22.1)
Accuracy Accurate without anxiety/depression Accurate with anxiety/depression Underestimators Overestimators
7742 (64.8)2087 (17.5)551 (4.6)1560 (13.1)
Note: anxiety/depression refers to anxiety, depression or both
Approximately one-third of the respondents who overestimated their symptoms indicated they had sought help for depression or anxiety symptoms. However, only approximately 2% of respondents who underestimated their symptoms reported they sought help. Finally, only 2% of the respondents who were categorized as accurate without anxiety/depression and 4% of the underestimators reported currently seeing a mental health professional. Of the respondents who were accurate with anxiety/depression 26% had sought help from a psychologist, psychiatrist or mental health support group, compared to 10% of the overestimators.
Table 3. Professional help-seeking for depression and anxietyAccurate without anxiety or depressionn=7742
Accurate with anxiety or depressionn=2087
Underestimators
n=551
Overestimators
n=1560
Seeking help, n (%)Depression Yes No Missing
57 (0.7)308 (4.0)7377 (95.3)
1186 (56.8)520 (24.9)381 (18.3)
13 (2.4)52 (9.4)486 (88.2)
525 (33.7)324 (20.8)711 (45.6)
Anxiety Yes No Missing
58 (0.7)432 (5.6)7252 (93.7)
928 (44.5)680 (32.6)479 (23.0)
9 (1.6)71 (12.9)471 (85.5)
505 (32.4)650 (41.7)405 (26.0)
Currently seeing a mental health professional, n (%) Yes No Missing
114 (1.5) 7571 (97.8)57 (0.7)
536 (25.7)1536 (73.6)15 (0.7)
24 (4.4) 520 (94.4)7 (1.3)
157 (10.1) 1392 (89.2)11 (0.7)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 83
Specificity and sensitivitySpecificity and sensitivity for the self-reported diagnosis of anxiety/depression was calculated using a spreadsheet developed by Mackinnon (35). Results indicated that overall respondents were good at identifying if they were experiencing anxiety or depression in concordance with the K10 screening. Specificity for people who were accurate with anxiety/depression was 0.83 (95% CI: 0.82 – 0.84) and the sensitivity was 0.79 (95% CI: 0.78 – 0.81). Table 4 shows the number of respondents categorized by their score on the K10.
Table 4. Number of respondents categorized by score on K10. n (%)
Below cut-off K10: 9302 (100) Overestimators 1560 (16.8) Accurate without Anxiety/depression 7742 (83.2)
Above cut-off K10: 2638 (100) Underestimators 551 (20.9) Accurate with anxiety/depression 2087 (79.1)
Univariate associations between demographics, stigma and accuracy of self-reported diagnosisUnivariate analyses were conducted to examine differences between the groups on all predictors (Table 1). Significant differences were found across all predictors. Post hoc comparisons indicated that for gender, males were more likely to be accurate without symptoms, and less likely to be overestimators or accurate with anxiety/depression. In contrast, females were more likely to either overestimate or be accurate with anxiety/depression, but less likely to be classified as accurate without anxiety/depression.
There was also an effect for marital status. Respondents who were married or in a de-facto relationship were more likely to be accurate without symptoms, and less likely to be underestimators or accurate with anxiety/depression. In contrast, individuals never married or separated/divorced were more likely to be accurate with anxiety/depression and less likely to be accurate without symptoms. Those who had never married were also more likely to be underestimators.
Education was significantly associated with accuracy, F(3, 11936)=35.23, p<.001. Post hoc analysis indicated that underestimators reported lower levels of education compared to respondents who were classified as accurate without symptoms (p<.001), and overestimators (p<.001). Respondents classified as accurate with anxiety/depression reported significantly lower levels of education compared to people who were classified as accurate without symptoms (p<.001) and overestimators (p<.001).
A significant association was also found between age and accuracy, F(3, 11936)=59.41, p<.001. Respondents who underestimated their self-reported diagnosis were significantly

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
84 | Chapter 4
younger compared to overestimators (p<.001), respondents classified as accurate without symptoms (p<.001), and respondents who were accurate with anxiety/depression (p=.001). Respondents classified accurate with anxiety/depression were also significantly younger than those classified as accurate without symptoms and overestimators (p<001).
Personal stigma was also significantly associated with accuracy, F(3, 11936)=57.01, p<.001. Respondents who underestimated their self-reported diagnosis reported higher levels of stigma compared to overestimators (p<.001), respondents classified as accurate without symptoms (p<.001), and respondents who were accurate with anxiety/depression (p=.03). Furthermore, respondents who were accurate with anxiety/depression reported higher stigma than both individuals who were accurate without symptoms (p<.001) and people who overestimated their self-reported disorder (p<.001). Respondents who were classified as accurate without symptoms reported higher levels of stigma than those who were classified as overestimators (p<.001).
Predictors of underestimationA multivariate logistic regression was then conducted to examine specifically the predictors of underestimating symptoms anxiety and depression when providing self-report, as compared to those accurately self-reporting depression and/or anxiety. The results showed that stigma was associated with the underestimation of symptoms (e.g. self-reported no depression or anxiety, but scored above cut-off) (Table 5). In addition, marital status independently predicted the underestimation of anxiety/depression as did age, albeit with a small effect. Specifically, underestimators reported higher stigma, were more likely to be married or in a de-facto relationship, and were younger compared to those who were accurate in reporting depression or anxiety.
Table 5. Predictors of underestimating symptomsB(SE) OR (95% C.I.)
Model 1 Constant -1.18 (.09)*** .31 (.26-.37)Age -.01 (.01)** 0.77b (.98-1.00)Education .00 (.02) 1.00b (.96-1.04)Gender (Female) -.13 (.10) .88 (.72-1.08)Marital Statusa
Separated/divorcedWidowedNever Married
.72 (.17)***
.12 (.36)-.12 (.13)
.49 (.69-1.15)1.13 (.55-2.32)-.89 (.35-0.67)
Personal Stigma .12 (.05)* 1.17b (1.02-1.24)
*p<.05;**p<.01;***p<.001; a reference category is ‘married’; b Odds ratios represent the 25th compared to the 75th percentile on the DSS sub-scale.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 85
Discussion
Accuracy of self-identification This study investigated the accuracy with which members of the community are able to identify their current mental health status. We found a high level of accuracy in self-reported mental health. Nevertheless, of respondents categorised as scoring below the cut-off on the screening measure 16.8% inaccurately self-reported themselves as currently anxious or depressed or both (specificity = 83.2%). Conversely, 20.9% of those who scored above the cut-off score failed to self-report current depression or anxiety (sensitivity = 79.11%).
Help-seeking of respondentsMany respondents who were considered overestimators indicated they had sought help, with 34% seeking help for anxiety, 32% for anxiety and 14% for both depression and anxiety. In such cases successful treatment may have lowered K10 scores leading to the categorisation of such individuals as overestimators. Research indicates that females seek help more often than males so one explanation for the higher help-seeking rates in overestimators might be that they were more often female than male (36, 37). Furthermore, it is possible that some respondents reported the presence of anxiety and/or depression based on residual symptoms or on a view that it is diagnosis and treatment of depression or anxiety rather than current level of symptoms which defines their mental health status.
The current study demonstrated that lack of insight is associated with substantially reduced levels of help seeking. Very few respondents who were underestimators sought help for depression or anxiety (2%). This might be due to a failure to recognize their symptoms or to an unwillingness to disclose and seek help due to their higher stigma levels (14, 24). Furthermore, this reluctance might have led to an unwillingness to report their anxiety and/or depression as such.
At the same time the findings indicate that insight may not be sufficient to prompt help seeking, In particular, we found that respondents who accurately self-reported anxiety and/or depression showed low help-seeking rates with 45% seeking help for their anxiety and 57% seeking help for depression. This failure to seek help by a substantial percentage of those suffering from high prevalence disorders even in the context of correct self-identification is significant. It implies that self-identification into one’s symptoms or disorder (e.g. accurately identifying the symptoms or disorder) alone is insufficient to prompt professional help-seeking suggesting that although the recognition of symptoms may be important, it is only one factor in promoting help seeking. This is in line with results from a previous study in perceived need and help-seeking (19).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
86 | Chapter 4
Predicting poor self-identificationThe finding that those who lack insight demonstrate substantially lower levels of help seeking is of clinical relevance. We investigated the demographic and attitudinal factors, such as gender, age, marital status, stigma and education, which predicted lack of insight into an individual’s personal current depression and anxiety status. Significantly, we found that underestimators reported higher levels of personal stigma when compared to those who were accurate with anxiety/depression. These results are consistent with previous research indicating that higher levels of stigma are associated with a reluctance to acknowledge or agree one has a mental health problem (e.g. insight) and/or that there is a need to seek professional care (19, 24). This might have caused respondents to be reluctant in admitting they suffer from anxiety and/or depression. It is therefore imperative to continue efforts directed to reducing the stigma associated with mental illness. However, lowering stigma might not be sufficient to improve help-seeking. Therefore a better understanding of other interrelated barriers, such as stigma and sociodemographic factors, to help-seeking is imperative.
We also found that underestimators were more likely to be younger and more likely to be separated or divorced compared to respondents who were accurate with anxiety/depression. The finding that younger people are less accurate in their self-reported diagnosis (e.g. have less insight) is consistent with results from other research showing that recognizing one’s symptoms is closely related to age (19, 25). This suggests that awareness raising programs on anxiety and depression should target the younger population and people who are divorced.
Limitations Results of this study should be considered in the context of several limitations. First, sensitivity and specificity were assessed with reference to a screening instrument rather than a diagnostic interview. Both measures are based on self-report, which might have led to higher agreement between the outcomes. However, the ability to self-identify symptoms could be influenced by stigma and social desirability which are known to influence self-report measures. Therefore, the data provide a good first step in exploring the accuracy of self-report relative to a validated measure of depressive and anxiety disorders (30). Second, the response rate to the survey was low and not representative of the general population; this is common in large population-based studies (6, 38). As this might have caused a selection bias the results should be considered with caution. However, the study constitutes one of the first steps in examining whether people can accurately self-assess if they suffer from depression/anxiety and what factors predict lack of insight into one’s own depression or anxiety. Future research should be undertaken using a diagnostic interview as the ‘gold standard’.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 87
Implications and ConclusionsOur results suggest that a significant minority of people with depression and/or anxiety fail to recognize their condition. Although our research indicates that recognising symptoms is insufficient by itself to prompt help seeking, help-seeking was higher among those who were aware of their depression and/or anxiety status in the current study. Significantly, people who do not seek care, but are at risk for developing depression/anxiety (e.g. showing subclinical symptoms) have a significantly higher chance of developing a disorder (39, 40). It is therefore important to continue to deliver educational programs on anxiety and depressive disorders to the community. In addition, given that underestimators were characterised by higher personal stigma, there is a need to implement evidence-based programs to lower stigma. Such programs should target the entire community, but also particularly young people who, according to the current findings, are at most risk of failing to recognise that they are suffering from depression or anxiety. Finally, future research should further examine the relation between insight and help-seeking.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
88 | Chapter 4
References
1. Fletcher JR, Bassilios B, Kohn F, Naccarella L, Blashki GA, Burgess PM, et al. Meeting demand for psychological services for people with depression and anxiety: recent developments in primary mental health care. Medical Journal of Australia. 2008;188(12):S107.
2. Kessler RC, Merikangas KR, Wang PS. Prevalence, comorbidity, and service utilization for mood disorders in the United States at the beginning of the twenty-first century. Annu Rev Clin Psychol. 2007;3:137-58.
3. Baxter A, Scott K, Vos T, Whiteford H. Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med. 2012;10:1-14.
4. Johansson R, Carlbring P, Heedman Å, Paxling B, Andersson G. Depression, anxiety and their comorbidity in the Swedish general population: point prevalence and the effect on health-related quality of life. PeerJ. 2013;1:e98.
5. Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980–2013. International journal of epidemiology. 2014:dyu038.
6. Slade T, Johnston A, Oakley Browne MA, Andrews G, Whiteford H. 2007 National Survey of Mental Health and Wellbeing: methods and key findings. Australasian Psychiatry. 2009;43(7):594-605.
7. ten Doesschate MC, Koeter MWJ, Bockting CLH, Schene AH. Health related quality of life in recurrent depression: A comparison with a general population sample. Journal of Affective Disorders. 2010;120(1–3):126-32.
8. Kessler RC. The costs of depression. The psychiatric Clinics of north America. 2012;35(1):1.9. Kessler RC, Ruscio AM, Shear K, Wittchen HU. Epidemiology of Anxiety Disorders. In:
Stein MB, Steckler T, editors. Behavioral Neurobiology of Anxiety and Its Treatment. Current Topics in Behavioral Neurosciences. 2: Springer Berlin Heidelberg; 2010. p. 21-35.
10. Burcusa SL, Iacono WG. Risk for recurrence in depression. Clinical Psychology Review. 2007;27(8):959-85.
11. Lépine J-P, Briley M. The increasing burden of depression. Neuropsychiatric disease and treatment. 2011;7(Suppl 1):3.
12. Andrews G, Sanderson K, Slade T, Issakidis C. Why does the burden of disease persist? Relating the burden of anxiety and depression to effectiveness of treatment. Bulletin of the world Health Organization. 2000;78(4):446-54.
13. Goldman LS, Nielsen NH, Champion HC. Awareness, diagnosis, and treatment of depression. Journal of General Internal Medicine. 1999;14(9):569-80.
14. Gulliver A, Griffiths K, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry. 2010;10(1):113.
15. Zell E, Krizan Z. Do People Have Insight Into Their Abilities? A Metasynthesis. Perspectives on Psychological Science. 2014;9(2):111-25.
16. Dunning D, Heath C, Suls JM. Flawed self-assessment implications for health, education, and the workplace. Psychological science in the public interest. 2004;5(3):69-106.
17. Coles ME, Coleman SL. Barriers to treatment seeking for anxiety disorders: initial data on the role of mental health literacy. Depression and Anxiety. 2010;27(1):63-71.
18. Nease D, Volk RJ, Cass AR. Does the severity of mood and anxiety symptoms predict health care utilization? Journal of Family Practice. 1999;48(10):769-77.
19. Verhaak PF, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJ, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
20. Carlson EN, Vazire S, Oltmanns TF. Self-Other Knowledge Asymmetries in Personality Pathology. Journal of personality. 2013;81(2):155-70.
21. Epley N, Dunning D. The mixed blessings of self-knowledge in behavioral prediction: Enhanced discrimination but exacerbated bias. Personality and Social Psychology Bulletin. 2006;32(5):641-55.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
4
How well do people identify their symptoms? | 89
22. Jorm AF, Christensen H, Griffiths KM. The impact of beyondblue: the national depression initiative on the Australian public’s recognition of depression and beliefs about treatments. Australian and New Zealand Journal of Psychiatry. 2005;39(4):248-54.
23. Christensen H, Batterham PJ, Grant JB, Griffiths KM, Mackinnon AJ. A population study comparing screening performance of prototypes for depression and anxiety with standard scales. BMC medical research methodology. 2011;11(1):154.
24. Van Voorhees BW, Fogel J, Houston TK, Cooper LA, Wang N-Y, Ford DE. Beliefs and attitudes associated with the intention to not accept the diagnosis of depression among young adults. The Annals of Family Medicine. 2005;3(1):38-46.
25. van Beljouw I, Verhaak P, Prins M, Cuijpers P, Penninx B, Bensing J. Reasons and determinants for not receiving treatment for common mental disorders. Psychiatric Services. 2010;61(3):250-7.
26. Meadows G, Harvey C, Fossey E, Burgess P. Assessing perceived need for mental health care in a community survey: development of the Perceived Need for Care Questionnaire (PNCQ). Social Psychiatry & Psychiatric Epidemiology. 2000;35(9):427.
27. Griffiths KM, Crisp D, Christensen H, Mackinnon AJ, Bennett K. The ANU WellBeing study: a protocol for a quasi-factorial randomised controlled trial of the effectiveness of an Internet support group and an automated Internet intervention for depression. BMC psychiatry. 2010;10(1):20.
28. Griffiths KM, Crisp DA. Unmet depression information needs in the community. Journal of Affective Disorders. 2013;146(3):348-54.
29. Andrews G, Slade T. Interpreting scores on the Kessler psychological distress scale (K10). Australian and New Zealand journal of public health. 2001;25(6):494-7.
30. Donker T, Comijs H, Cuijpers P, Terluin B, Nolen W, Zitman F, et al. The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research. 2010;176(1):45-50.
31. Griffiths KM, Christensen H, Jorm AF, Evans K, Groves C. Effect of web-based depression literacy and cognitive–behavioural therapy interventions on stigmatising attitudes to depression Randomised controlled trial. The British Journal of Psychiatry. 2004;185(4):342-9.
32. Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC psychiatry. 2008;8(1):25.
33. Schafer JL, Graham JW. Missing data: our view of the state of the art. Psychological methods. 2002;7(2):147.
34. Mackinnon A. The interquartile odds ratio: a suggestion for the presentation of results from continuous predictors in logistic regression. International Journal of Methods in Psychiatric Research. 1992;2:233-5.
35. Mackinnon A. A spreadsheet for the calculation of comprehensive statistics for the assessment of diagnostic tests and inter-rater agreement. Computers in biology and medicine. 2000;30(3):127-34.
36. Mackenzie CS, Gekoski WL, Knox VJ. Age, gender, and the underutilization of mental health services: The influence of help-seeking attitudes. Aging & Mental Health. 2006;10(6):574-82.
37. Oliver MI, Pearson N, Coe N, Gunnell D. Help-seeking behaviour in men and women with common mental health problems: cross-sectional study. Br J Psychiatry. 2005;186:297-301.
38. Galea S, Tracy M. Participation rates in epidemiologic studies. Annals of epidemiology. 2007;17(9):643-53.
39. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. Journal of Affective Disorders. 1997;45(1–2):19-30.
40. Georgiades K, Lewinsohn PM, Monroe SM, Seeley JR. Major depressive disorder in adolescence: the role of subthreshold symptoms. Journal of the American Academy of Child & Adolescent Psychiatry. 2006;45(8):936-44.


Chapter 5
How do people view the available care
(i.e. professional care, informal help, self-reliance)
This chapter is submitted as:Van Zoonen, K., Kleiboer A. M., Cuijpers, P., Smit, J. H., Penninx, B., Verhaak,
P., Beekman, A. T. F. (2015). Determinants of attitudes towards professional mental health care, informal help,
and self-reliance in people with subclinical depressionManuscript submitted for publication to Social Psychiatry & Psychiatric Epidemiology.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
92 | Chapter 5
Abstract
Purpose: Although little is known about which people with subclinical depression should receive care to prevent the onset of depression, it is clear that remediating symptoms of depression is important. However, depending on the beliefs people hold about help, some people will seek professional help, while others seek informal help or solve problems on their own. The current study examined associations between these attitudes about help and sociodemographic variables, mastery, severity of depressive symptoms, accessibility to care, and health care utilization at baseline and 4 year follow-up.
Methods: Data were derived from a large cohort study, the Netherlands Study of Depression and Anxiety (NESDA). A total of 235 respondents with subclinical depression completed questionnaires at baseline and follow-up. Attitude was assessed using a short version of the “Trust in mental health care” questionnaire.
Results: Positive attitude towards professional care was associated with being male, younger age, higher mastery, and easy accessibility to care. Positive attitude towards informal help was associated with higher mastery and unemployment. Older age, less accessibility to care, and lower mastery were associated with positive attitude in self-reliance. Furthermore, a change in care utilization was associated with a more positive attitude towards informal help at follow-up.
Conclusion: Attitude towards professional care is influenced by a change in care utilization. Furthermore, older people have a more positive attitude towards being self-reliant. It is imperative to improve attitude in order to lower the reluctance to seek care, but also establish if being self-reliant is sufficient in coping with subclinical depressive symptoms.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 93
Introduction
Subclinical depression is common (1, 2), impairs health-related quality of life of individuals substantially (3), and is associated with a large societal burden (4). It can be defined as a score above a threshold for depressive symptoms, but failing to meet the diagnostic criteria of major depression (5) or as a depressed mood accompanied with less severe symptoms than those required for DSM-V diagnosis. Estimates of the prevalence rates of subclinical depression in samples range from 2 to 24% (6, 7) depending on the definition, population, and instrument used.
Subclinical depression is an important risk factor for developing a major depression. Depending on the sample, 20% to 34% of people with a subclinical depression develop major depression (8, 9). Randomized trials have shown that the onset of depression can be prevented by preventive interventions (10). However, few people with subclinical depression seek help for their symptoms, with numbers of patients that seek help at 1%. Three categories of determinants of help-seeking behaviour are often distinguished: need factors such as severity and duration of symptoms, enabling factors such as organizational factors, and predisposing factors such as personality and attitudinal factors (11, 12). In people with subclinical depression, need factors are often less pronounced compared to people with for example a full-blown depression, therefore other factors may become more important.
Attitudinal factors have been identified as one of the most important barriers of intentions to seek help and utilization of health services. These attitudes include stigma related concerns, fears or embarrassment about revealing personal details, beliefs that one should handle problems by oneself, and beliefs about the probability that a service will help resolve a problem (13). To get a better understanding of how people view mental health care and what might influence people’s beliefs it is important to know more about who has these attitudes and if these attitudes change over time.
Consequently, the current study has examined determinants of the attitude towards
mental health care (e.g. professional mental health care, informal help and self-reliance) in people with subclinical depression. The relationship between various factors (e.g. age, gender, education level, marital status, employment status, severity of symptoms, mastery, accessibility to professional care, whether or not people had used professional care in the past) and attitudes towards mental health care were examined first. Secondly, we examined if a change in factors (mastery, severity of depressive symptoms, and use of care at baseline and follow-up) was associated with a change in attitudes between baseline and follow-up.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
94 | Chapter 5
Methods
Design, participants and procedureData from the Netherlands Study of Depression and Anxiety (NESDA) were used. Details can be found in another paper by Penninx et al. (14). NESDA was designed to examine the long-term course of anxiety and depression in a longitudinal cohort study. In the current study we used data from wave 1 (baseline) and wave 3 (4 year follow-up). Respondents were recruited from the general population, general practices, and mental health care centers in Amsterdam, Groningen, and Leiden. Recruitment took place between September 2004 and February 2007. Recruitment procedures were the same across regions and recruitment setting. Exclusion criteria included insufficient understanding of the Dutch language and a primary clinical diagnosis of a psychiatric condition that was not the subject of NESDA (e.g. psychotic disorders). Written consent was obtained from all respondents. The NESDA protocol has been approved by the Ethical Review Committee of the VU University Medical Center and local boards of every participating center.
We included people with a score above 19 on the Kessler 10 (K10) screening instrument (15) who did not meet the diagnostic criteria for depression or anxiety in the past 6 months according to the Composite International Diagnostic Interview (CIDI) (15, 16). Those participants with incomplete data at one or both assessments were excluded. A total of 1289 respondents scored 20 or higher on the K10, 561 of these respondents (51.5%) met the criteria for clinical depression in the six months prior to recruitment. This resulted in 528 respondents with subclinical depression. However, 115 respondents had missing data at baseline and/or follow-up, leading to a total of 413 respondents. Of these 413 respondents, 178 respondents (43%) met criteria for current anxiety disorders, leaving a total of 235 respondents with subclinical depression.
InstrumentsDepression screening instrumentThe K10 was used as a screening instrument for depressive symptoms (15). This self-report questionnaire has shown to have good sensitivity and specificity for detecting people with major depressive disorder (17). The questionnaire consists of 10 questions which are answered on a 5 point Likert scale ranging from “never” to “always”. The Dutch version of the K10 has good psychometric properties (α=0.94) (17).
Diagnostic instrument The CIDI version 2.0 was used to establish depression status (16). This diagnostic instrument was developed by the World Health Organization (WHO) for research

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 95
purposes and lay interviewers. The interview has shown good psychometric properties for depressive disorders (16). The current study focused on the 6 month history of depression and was used to establish whether someone met the DSM-IV criteria for major depression or dysthymia.
Attitude towards mental health careTo establish people’s attitude towards mental health care we used a short version of the ‘Trust in mental health care” questionnaire (18). The questionnaire consists of five questions; two measured “confidence in professional help”, two measured “confidence in help from family/friends”, and one single item stating “psychological problems are best kept to one’s self ” (e.g. self-reliance). Items were scored on a 4 point Likert scale with “No” (1) to “Yes” (4), with 2.5 as the neutral “no opinion” option. This resulted in three types of attitudes: Attitude towards professional care, attitude towards in informal help, and attitude towards self-reliance (e.g. psychological problems can be best kept to one’s self).
Demographic variablesDemographic variables (e.g. gender, age, educational level, marital status, employment status) were derived from the baseline measure. Educational level was divided into three groups based on type of education: basic (e.g. elementary education only), intermediate (e.g. lower level vocational education, general middle level education, middle level vocational education, general secondary education), and high (e.g. higher level vocational education, college/university education). Marital status was divided into two categories: “partner/married” (1) and “not married/no partner” (0). Employment status was recoded into two categories; “employed” (currently employed, self-employed, on sickness benefit, pregnancy/maternity leave, other) and “unemployed” (occupationally disabled, early retirement, unemployed, and other). The “other” option was chosen 10 times and referred to variations of employed or unemployed. An example of a typical “other” answer from the sample was; “officially employed, but due to a work related conflict at home and looking for a new job”. These answers were recoded into either employed or unemployed.
Depressive symptoms Severity of depressive symptoms was established by using the Inventory of Depressive Symptoms (IDS) (19). It is a self-report questionnaire containing 30 questions, with 4 answering options to each question (scored from 0 to 3). The psychometric properties of the IDS have shown to be acceptable to good (20, 21).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
96 | Chapter 5
Help-receiving To establish whether people had received help for their mental problems a question from the Quality of care Through the patients’ Eye Questionnaire (QUOTE) was used (22). This questionnaire was specifically designed for the NESDA study to measure the quality of care as it is delivered from the patient’s point of view and consists of 36 items. The first part entails 18 items divided over 6 subscales including: accessibility, GP care, patient centeredness, explanation and advice, self-help, effective care. To establish whether a respondent should fill out the second part of the QUOTE (e.g. questions about experience with previous care) they are asked whether they had ever received care from their GP or other therapist for their mental health problems. They could answer with either “yes” or “no”. The same question was asked at follow-up. To examine a change in help-receiving between baseline and follow-up, a variable with the possible combinations from the answers on baseline and follow-up was created. This leads to 3 possible categories; No help received at baseline, but help was received at follow-up (0), no help received at baseline or follow-up (1), or help was received at both baseline and follow-up (2).
Accessibility to careTo establish perceived accessibility to health care we used questions from the first part of the QUOTE. Items were scored on a 4 point Likert scale from 1 (“no”) to 4 (“yes”), with the score 2.5 as the neutral “does not know” option. The current study used the accessibility subscale that consists of 3 items. Higher scores indicate better accessibility to care.
Locus of controlTo examine locus of control (e.g. Mastery) we used the 5 item Pearlin & Schooler mastery scale (23). Mastery refers to the feeling to which a person perceives him- or herself to be in control of events and ongoing situations. The questionnaire consisted of 5 items which are rated on 5-point scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). This results in a total score between 5 and 25, where higher rates indicate more feelings of mastery. In a non-institutionalized sample it has shown reasonable reliability (α=0.67) (24).
Statistical AnalysisTo examine the association between the determinants and attitude towards care (e.g. professional informal help, and self-reliance) at baseline, we first conducted univariate regression analyses. We created dummy variables for education (reference category was basic education). Next, we carried out multivariate multiple regression analyses to investigate which variable was most strongly associated with attitude at baseline.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 97
Furthermore, we conducted univariate multiple regression analyses to examine if a change in attitude over time was related to a change in other relevant variables (e.g. mastery, severity of depressive symptoms, and use of care). In the regression analyses, attitude at 3 years follow-up was the dependent variable and baseline attitude and other variables were included as the independent variables. We calculated change scores between baseline and follow-up for mastery and severity of depressive symptoms. We created two dummy variables for use of care to indicate the direction of change between baseline and follow-up. The reference category was a received care at follow-up, but not at baseline.
Results
SampleThe average age of respondents was 43 years, with a range of 18 to 65 years. Most respondents were female (n=175, 74%) and 26% were male (n=60). More than half of the respondents had an intermediate level of education (n=122, 52%), 43% of the respondents (n=101) had a high level of education, and only a minority had a basic level of education (n=12, 5%). Most respondents indicated they had used professional care for their mental problems (n=171, 73%) and only 64 respondents (27%) indicated never to have used professional care.
Associations between factors and attitude towards professional care at baselineResults of the univariate linear regression analyses showed that respondents who were younger (b=-.20, p<.01), experienced more control over their lives (b=.21, p<.01), and had a high level of education (b=.37, p<.01) reported a more positive attitude towards mental health care at baseline (Table 2).
Results from the multiple linear regression showed that respondents who were male (b=-.13, p<.05), younger (b=-.02, p<.01), experienced more control over their lives (b=.06, p<.05) and reported better accessibility to care (b=.19, p<.01) reported a more positive attitude towards professional mental health care (Table 2). The model was a good fit to the data, F(10, 224) = 4.34, p<.001, however only 16% of the variance was explained (R2 = .16).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
98 | Chapter 5
Table 1. Descriptive characteristics of respondentsTotal respondents (n = 235)
Baseline Follow-up
Gender, n (%) Male Female
60 (25.5)175 (74.5)
a
Marital Status, n (%) Not married/No partner Married/partner
68 (28.9)167 (71.1)
a
Education, n (%) Basic Intermediate High
12 (5.1)122 (51.9)101 (43.0)
a
Employment status, n (%) Paid job No paid job
163 (69.4)72 (30.6)
a
Accessibility to care, m (SD) 9.4 (1.8) a
Age, m (SD) 43.3 (13.4) a
Use of professional care, n (%) No care used Care used
64 (27.2)171 (72.9)
144 (61.3)91 (38.7)
Severity of symptoms, m (SD) 18.8 (8.5) 15.8 (9.7)
Mastery, m (SD) 17.7 (3.8) 18.2 (4.2)
a= not applicable.
Associations between factors and attitude towards informal help at baselineResults of the univariate linear regression analyses showed that respondents who experienced more control over their lives (b=.17, p<.01) reported a more positive attitude towards informal help at baseline (Table 2).
Multiple linear regression analysis showed that a more positive attitude towards informal help is associated with being unemployed (b=-.39, p<.05) and experiencing more control over one’s life (b=.04, p<.05) (Table 2). However, the model was not a good fit to the data (F(10, 224) = 1.87, p=.05) and explained only 8% of the variance (R2 = .08).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 99
Tabl
e 2.
Uni
varia
te a
nd m
ultiv
aria
te a
ssoc
iatio
ns w
ith a
ttitu
de a
t bas
elin
e(n
= 2
35)
Prof
essi
onal
car
eIn
form
al H
elp
Self
-rel
ianc
eU
niva
riate
Mul
tivar
iate
Uni
varia
teM
ultiv
aria
teU
niva
riate
Mul
tivar
iate
B (S
E)b
B (S
E)b
B (S
E)b
B (S
E)b
B (S
E)b
B (S
E)b
Con
stan
ta
-4.
99 (0
.61)
-***
a
-4.
58 (0
.64)
-***
a-
2.33
(0.3
1)-*
**G
ende
r-0
.24
(0.1
5)-.1
1-0
.31
(0.1
4)-.1
3*-0
.20
(0.1
5)-.0
9-0
.18
(0.1
5)-.0
80.
10 (0
.10)
.06
0.15
(0.1
0).1
0M
arita
l sta
tus
0.04
(0.1
5).0
20.
06 (0
.14)
.03
-0.0
5 (0
.15)
-.02
-0.0
3 (0
.15)
-.01
0.08
(0.1
0).0
50.
04 (0
.10)
.03
Empl
oym
ent s
tatu
s0.
24 (0
.14)
.11-0
.00
(0.1
4)-.0
0-0
.25
(0.1
4)-.1
1-0
.39
(0.1
5)-.1
8*-0
.10
(0.1
0)-.0
70.
05 (0
.10)
.03
Age
-0.0
2 (0
.01)
-.20*
*-0
.02
(0.0
1)-.2
3**
-0.0
0 (0
.01)
-.05
-0.0
1 (0
.01)
-.07
0.01
(0.0
0).2
5***
0.01
(0.0
0).2
7***
Educ
atio
n- I
nter
med
iate
- H
igh
0.33
(0.3
0)0.
75 (0
.30)
.16
.37*
*0.
07 (0
.30)
0.49
(0.3
0).0
3.2
40.
03 (0
.31)
0.26
(0.3
1).0
1.1
3-0
.00
(0.3
1)0.
28 (0
.32)
-.00
.14
-0.1
0 (0
.20)
-0.3
1 (0
.20)
-.0
7-.2
30.
05 (0
.20)
-0.1
5 (0
.20)
.04
-.11
Use
of p
rofe
ssio
nal
care
0.03
(0.1
5).0
10.
08 (0
.14)
.03
-0.1
8 (0
.15)
-.08
-0.1
2 (0
.15)
-.05
-0.1
4 (0
.10)
-.09
-0.1
7 (0
.10)
-.11
Mas
tery
0.
06 (0
.02)
.21*
*0.
04 (.
02)
.16*
0.04
(0.0
2).1
6*0.
04 (0
.02)
.16*
-0.0
4 (0
.01)
-.20*
*-0
.03
(0.0
1)-.1
7*Se
verit
y of
sy
mpt
oms
-0.0
1 (0
.01)
-.12
-0.0
0 (0
.01)
-.01
-0.0
1 (0
.01)
-.09
-0.0
0 (0
.01)
-.01
0.01
(0.0
1).11
0.00
(0.0
1).0
1
Acc
essi
bilit
y 0.
06 (0
.04)
.10
0.10
(0.0
4).1
9**
0.01
(0.0
4).0
10.
03 (0
.04)
.05
-0.0
3 (0
.03)
-.08
-0.0
7 (0
.02)
-.17*
*
a = p
er re
gres
sion
anal
yses
the B
rang
ed fr
om 5
.17
to 6
.62
(pro
fessio
nal c
are)
, 4.2
1 to
5.1
9 (in
form
al h
elp),
1.19
to 2
.25
(self
-reli
ance
). *p
<.05
;**p<
.01;
***p
<.00
1

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
100 | Chapter 5
Associations between factors and attitude towards self-reliance at baselineThe results of the univariate linear regression analyses showed that respondents who were older (b=.01, p<.001) and who experienced less control over their lives (b=-.04, p<.01) reported a more positive attitude towards self-reliance (Table 2).
Multivariate analysis showed that respondents who were older (b=.01, p<.001), experienced less control over their lives (b=-.17, p<.05), and who indicated less accessibility to professional care (b=-.17, p<.01) reported a more positive attitude towards self-reliance (Table 2). The model was a good fit to the data, F(10, 224) = 4.11, p<.001. However, only 16% of the variance was explained by the model (R2 = .16).
Longitudinal descriptive characteristicsWhen examining the possible factors associated with change in attitude (e.g. mastery, severity of symptoms and use of professional care in the past), most people indicated that they had used care at baseline as well as follow-up (73%), 23% indicated to never have used care at baseline or follow-up, whereas the least number of people indicated that they had not used care at baseline, but they had used care at follow-up (4%). Most people reported more control over their lives at follow-up than they did at baseline (52%), 37% reported less control and 11% did not report a change in mastery. Furthermore, most people reported less severe depressive symptoms at follow-up than at baseline (64%), 32% reported an elevation in depressive symptoms and 4% reported an equal severity of depressive symptoms at baseline and follow-up.
Longitudinal analysis of variables on attitude towards professional careResults showed that respondents who have not used professional care (GP or other specialist for mental problems) at baseline or follow-up reported a more negative attitude towards professional care at follow-up compared to respondents who had not used professional care at baseline, but who indicated a use of professional care at 4 year follow-up (p<.05) (Table 3).
Multivariate stepwise analysis showed comparable results (Table 3). Both models showed a significant association between attitude towards professional care at baseline and attitude towards professional care at follow-up. More specifically, positive attitude at baseline is associated with a more positive attitude at follow-up (p<.001, in both models). Furthermore, the second model, with all variables, showed that respondents who reported not to have used professional care at baseline and follow-up reported a less positive attitude towards professional care at baseline. The first model was a good fit to the data, F(1, 233) = 96.13, p<.001. The model explained 29% of the variance (R2=.29). The second model was also a good fit to the data, F(5, 229) = 16.33, p<.001. The model explained 32% of the variance (R2=.32) However, the R2 change was not significant

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 101
(p=.07), indicating the model with all predictors does not explain more of the variance than our first model including attitude at baseline only.
Longitudinal analysis of predictors on attitude towards informal helpTable 3 shows the results for the univariate multiple regression analysis. No significant associations with attitude towards informal help at follow-up were found, except for attitude at baseline (p<.001). Multivariate analysis showed similar results, indicating that attitude towards informal help at baseline was associated with attitude towards informal help at follow-up (Table 3). Both models showed a good fit to the data, model 1 F(1, 233) = 42.71, p<.001; and model 2 F(5, 229) = 10.65, p<.001. The first model explained 16% of the variance (R2=.16), while the second model explained 19% of the variance (R2=.19). The R2 change was not significant (R2 change = .03, p=.05), indicating that the second model, including all predictors, does not explain more of the variance in attitude at follow-up than the first model.
Longitudinal analysis of predictors on attitude towards self-relianceUnivariate regression analysis showed that none of the variables (e.g. mastery, severity of symptoms, and use of professional care) were significantly associated with attitude towards self-reliance at follow-up, except for attitude at baseline (Table 3). Multivariate analysis showed only an association between attitude towards self-reliance at baseline and attitude towards self-reliance at follow-up (p<.001). However, both models seemed a good fit to the data (model 1: F(1, 233) = 45.55, p<.001; model 2: F(5, 229) = 11.31, p<.001). Model 1, including attitude towards self-reliance at baseline only, explained 16% of the variance (R2=.16) and model 2 explained 20% (R2=.20). The change in R2 of 3% (R2 change = .03) was significant (p<.05), indicating the second model was a better fit to the data than model 1.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
102 | Chapter 5
Table 3. Univariate and Multivariate longitudinal analyses of attitude Univariate Multivariate Multivariate
Model 1 Model 2B (SE) b B (SE) b B (SE) b
Professional mental health careAttitude at baseline a a 0.56 (0.06)*** 0.54 0.57 (0.06)*** 0.55Change in mastery 0.01 (0.02) 0.04 0.10 (0.02) 0.07Change in severity of depressive symptoms
0.00 (.01) 0.03 0.00 (0.01) 0.04
Change in use of professional careNo experience at baseline, but experience at follow-upNo experience at baseline and follow-up
0
-0.68 (.31)*
0
-0.27
0
-0.50 (0.23)*
0
-0.28
Experience at baseline and follow-up
-0.39 (0.30) -0.17 -0.34 (0.21) -0.17
Informal helpAttitude at baseline a a 0.41 (0.06)*** 0.39 0.40 (0.06)*** 0.38Change in mastery 0.01 (0.02) 0.05 0.02 (0.02) 0.06Change in severity of depressive symptoms
0.01 (0.01) 0.06 0.01 (0.01) 0.07
Change in use of professional careNo experience at baseline, but experience at follow-upNo experience at baseline and follow-up
0
-0.05 (0.35)
0
-0.02
0
-0.10 (0.24)
0
-0.04
Experience at baseline and follow-up
-0.44 (0.33) -0.19 -0.37 (0.23) -0.15
Self-relianceAttitude at baseline a a 0.41 (0.06)*** 0.40 0.39 (0.06)*** 0.39Change in mastery 0.02 (0.01) 0.40 0.01 (0.01) 0.07Change in severity of depressive symptoms
-0.01 (0.00) -0.08 -.00 (0.01) -0.05
Change in use of professional careNo experience at baseline, but experience at follow-upNo experience at baseline and follow-up
0
0.36 (0.22)
0
0.23
0
0.32 (0.22)
0
0.20
Experience at baseline and follow-up
0.12 (0.21) 0.08 0.09 (0.21) 0.06
a= we controlled for attitude at baseline. Per univariate regression analyses b ranged from: 0.54 to 0.56 (professional care); 0.38 to 0.40 (informal help) and 0.39 to 0.40 (self-reliance). *p<.05;**p<.01;***p<.001.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 103
Discussion
ResultsAlthough not everyone with a subclinical depression will develop a depressive disorder, it is important to gain better insight into their preferences of coping with their symptoms (25). Attitude towards help (i.e. professional help, informal help or self-reliance) is an important factor that will determine how people will cope with their symptoms. However, no research to date has focused on attitudes towards care in people with subclinical depression. Therefore, the current study examined the influences on attitude towards professional mental health care, informal help, and self-reliance in a sample with subclinical depression.
Our results examining attitude at baseline show that being male, younger in age, feeling more control over their lives, and having easy access to professional care were related to a more positive attitude towards professional mental health care at baseline. Being male and having a positive attitude towards professional care, contradicts previous findings that males are less likely to seek professional care (26, 27). This indicates that using care is an interactive process which is influenced by more than attitude. Furthermore, there are some inconsistencies in the literature in regards to age as a predictor of how people cope with problems, however our results seem to support the research that younger adults hold more positive beliefs about professional mental health care (28-31). Positive attitudes towards informal help at baseline were associated with both being unemployed and feelings of more control. Although research in informal help-seeking is scarce, previous research did not find any influence of employment status (32). However, the previous research included more young adults and students among the economically inactive, while people in the current study were mostly employed or economically active.
A more positive attitude towards self-reliance was associated with older age, lower control over one’s lives, and less accessibility to professional care. No studies have examined attitude towards self-reliance, however the results seem to support findings from an earlier study in which older respondents indicated to prefer to solve problems on their own and showing a less positive attitude towards professional care (26, 33). Furthermore, it has been shown that inaccessibility to professional care has a negative influence on attitude towards professional care (34, 35), however it might also make people feel they should solve these problems on their own resulting in a more positive attitude towards being self-reliant.
Attitudes towards mental health care at follow-up were shown to be positively associated to the attitudes towards the same type of mental health care at baseline (e.g. attitude towards professional care at follow-up was positively associated to attitude

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
104 | Chapter 5
towards professional care at baseline). We compared two models, one with attitude at baseline in relation to attitude at follow-up and one model which included a change in mastery, severity of depressive symptoms, and use of care as well as attitude at baseline. Attitude towards informal help at follow-up seems to be strongly associated with attitude towards self-reliance at baseline and the other factors did not influence the variance explained. However, the model with all factors in relation to attitude towards self-reliance did explain more of the variance.
Furthermore, our results showed that people who indicated to have used professional care for their mental health problems at follow-up, but not at baseline reported a more positive attitude towards professional care compared to respondents who had not used professional care at either baseline or follow-up. This experience with care might explain results from other research indicating that people who report using professional care, more readily seek care when they experience problems (34-36). However, these results should be interpreted with caution, since this model did not explain more of the variance than the model with solely attitude towards professional care at baseline.
LimitationsThe current study has some important strengths as well, including the large sample size and the longitudinal design. As far as we know this is the first study that examines the association in change of variables across time on a change in attitude towards different types of care (e.g. professional mental health care, informal help, and self-reliance) across time, within such a large population sample. Therefore, this study provides a good first step in better understanding the attitudes of people with subclinical depression in care (e.g. professionals, friends or family, or themselves). However, there were certain limitations to this study and the results should be interpreted in light of these limitations. The definition of subclinical depression as used in the current study does not distinguish between depression in remission and people who experience depressive symptoms for the first time. However, no clear consensus on the definition of subclinical depression exists. This could influence the results, since people who have experienced a depression might have had more experience with professional care. Nevertheless, it is known that people with subclinical depression are at high risk of developing a depressive disorder and this study provides a good first step in exploring attitudes in people at high risk of developing major depression. Furthermore, the scale on which the different types of attitude were based was derived from a larger questionnaire, this might have caused some information to get lost. More importantly, this study examines only a specific part of attitudes that may be of influence on help-seeking. Finally, even though the study uses longitudinal data, it remains difficult to identify causal relationships. For example, it is not possible to identify whether someone has a positive attitude and this has influenced

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 105
the positive attitude at follow-up or did people seek care because they already had a positive attitude. Nonetheless, the current study enhances our understanding about an important facet of help-seeking that has not been examined before in this high risk group of people with subclinical depression.
Implications and future researchFuture research should focus on identifying which people with subclinical depression will benefit from preventive care and which people will recover on their own. It is clear that not everyone with subclinical depression is in need of care, however we do know that people with subclinical depression are at high risk of developing depression. It is therefore important to increase understanding of how people with subclinical depression will cope with their symptoms. Do they perceive a need for care or not? And if they do not perceive a need for care, will self-reliance suffice to recover from subclinical depression? It is imperative to gain better insight into the course of subclinical depression.
Regardless of its course, however, it is important to increase insight into people’s attitudes and health beliefs. These attitudes determine ways of coping, such as seeking help from family and friends or keeping problems to oneself. An important facet of attitude is people’s confidence in their own abilities and the abilities of others (professionals or family and friends’ abilities). Future research should replicate the results from the current study and expand knowledge by differentiating between people who suffer from first-time subclinical depression and people who report subclinical depression after having suffered a depressive disorder. This history of illness might influence whether or not people have experience with different types of help and this, in turn, might influence people’s attitudes in the different types of help.
Moreover, future research should focus on examining whether or not being self-reliant will suffice in preventing the onset of depression in people with subclinical depression who indicate a more positive attitude towards being self-reliant and who have not sought professional help.
Conclusion
Regardless of the course of subclinical depression and the lack of knowledge on who will benefit from preventive interventions for depression it is important to gain insight into the attitude people report towards professional help, informal help, or being self-reliant. Attitude is an important factor that will influence the way people cope with their symptoms. The current study showed that attitude at baseline is the most important predictor of attitude at follow-up. To improve people’s attitude it is important that professional care is viewed as easily accessible (e.g. no waiting list when trying to make

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
106 | Chapter 5
an appointment) and to increase people’s feeling of control over their lives. Furthermore, older people tend to hold a more positive attitude towards self-reliance. It is important to examine if being self-reliant is sufficient in preventing the depressive symptoms from converting into a depressive disorder.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 107
References
1. Cuijpers P, de Graaf R, van Dorsselaer S. Minor depression: risk profiles, functional disability, health care use and risk of developing major depression. Journal of Affective Disorders. 2004;79(1–3):71-9.
2. Horwath E, Johnson J, Klerman GL, Weissman MM. Depressive symptoms as relative and attributable risk factors for first-onset major depression. Archives of General Psychiatry. 1992;49(10):817-23.
3. Chachamovich E, Fleck M, Laidlaw K, Power M. Impact of major depression and subsyndromal symptoms on quality of life and attitudes toward aging in an international sample of older adults. The Gerontologist. 2008;48(5):593-602.
4. Broadhead W, Blazer DG, George LK, Tse C. Depression, disability days, and days lost from work in a prospective epidemiologic survey. JAMA. 1990;264(19):2524-8.
5. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta Psychiatrica Scandinavica. 2004;109(5):325-31.
6. Rucci P, Gherardi S, Tansella M, Piccinelli M, Berardi D, Bisoffi G, et al. Subthreshold psychiatric disorders in primary care: prevalence and associated characteristics. Journal of Affective Disorders. 2003;76(1–3):171-81.
7. Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. Journal of Affective Disorders. 1997;45(1–2):19-30.
8. Hill RM, Pettit JW, Lewinsohn PM, Seeley JR, Klein DN. Escalation to Major Depressive Disorder among adolescents with subthreshold depressive symptoms: Evidence of distinct subgroups at risk. Journal of Affective Disorders. 2014;158(0):133-8.
9. Cuijpers P, Beekman ATF, Smit F, Deeg D. Predicting the onset of major depressive disorder and dysthymia in older adults with subthreshold depression: a community based study. International journal of geriatric psychiatry. 2006;21(9):811-8.
10. van Zoonen K, Buntrock C, Ebert DD, Smit F, Reynolds CFr, Beekman AT, et al. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. International journal of epidemiology. 2014;43(2):318-29.
11. Andersen RM, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Quarterly. 2005;83(4):Online-only.
12. Anderson JG. Demographic Factors Affecting Health Services Utilization: A Causal Model. Medical Care. 1973;11(2):104-20.
13. Mackenzie CS, Erickson J, Deane FP, Wright M. Changes in Attitudes toward Seeking Mental Health Services: A 40-Year Cross-Temporal Meta-Analysis. Clinical Psychology Review. 2014;34(2):99-106.
14. Penninx BW, Beekman AT, Smit JH, Zitman FG, Nolen WA, Spinhoven P, et al. The Netherlands Study of Depression and Anxiety (NESDA): rationale, objectives and methods. International journal of methods in psychiatric research. 2008;17(3):121-40.
15. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normands SLT, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine. 2002;32(06):959-76.
16. Andrews G, Peters L. The psychometric properties of the Composite International Diagnostic Interview. Social Psychiatry & Psychiatric Epidemiology. 1998;33(2):80.
17. Donker T, Comijs H, Cuijpers P, Terluin B, Nolen W, Zitman F, et al. The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research. 2010;176(1):45-50.
18. Friele R, Verhaak P, Andela M. Vertrouwen in de GGZ: meer duideelijkheid gevraagd. MAANDBLAD VOOR DE GEESTELIJKE VOLKSGEZONDHEID. 2000;55(2):P122-33.
19. Rush AJ, Giles DE, Schlesser MA, Fulton CL, Weissenburger J, Burns C. The inventory for depressive symptomatology (IDS): preliminary findings. Psychiatry Research. 1986;18(1):65-87.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
108 | Chapter 5
20. Gili M, Luciano JV, Bauzá N, Aguado J, Serrano MJ, Armengol S, et al. Psychometric properties of the IDS-SR30 for the assessment of depressive symptoms in spanish population. BMC medical research methodology. 2011;11(1):131.
21. Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The inventory of depressive symptomatology (IDS): psychometric properties. Psychological medicine. 1996;26(03):477-86.
22. Sixma HJ, Kerssens JJ, Campen Cv, Peters L. Quality of care from the patients’ perspective: from theoretical concept to a new measuring instrument. Health expectations. 1998;1(2):82-95.
23. Pearlin LI, Schooler C. The Structure of Coping. Journal of Health and Social Behavior. 1978;19(1):2-21.
24. Penninx BW, Van Tilburg T, Kriegsman DM, Deeg DJ, Boeke AJP, van Eijk JTM. Effects of social support and personal coping resources on mortality in older age: The Longitudinal Aging Study Amsterdam. American journal of epidemiology. 1997;146(6):510-9.
25. Pietrzak R, Kinley J, Afifi T, Enns M, Fawcett J, Sareen J. Subsyndromal depression in the United States: prevalence, course, and risk for incident psychiatric outcomes. Psychological medicine. 2013;43(07):1401-14.
26. Jagdeo A, Cox BJ, Stein MB, Sareen J. Negative attitudes toward help seeking for mental illness in 2 population-based surveys from the United States and Canada. Canadian journal of psychiatry Revue canadienne de psychiatrie. 2009;54(11):757-66.
27. Jorm AF, Wright A. Beliefs of young people and their parents about the effectiveness of interventions for mental disorders. Australasian Psychiatry. 2007;41(8):656-66.
28. Ten Have M, De Graaf R, Ormel J, Vilagut G, Kovess V, Alonso J. Are attitudes towards mental health help-seeking associated with service use? Results from the European Study of Epidemiology of Mental Disorders. Social psychiatry and psychiatric epidemiology. 2010;45(2):153-63.
29. Verhaak PFM, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJLM, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
30. Bland RC, Newman SC, Orn H. Help-seeking for psychiatric disorders. Can J Psychiatry. 1997;42:935-42.
31. Andrews G, Issakidis C, Carter G. Shortfall in mental health service utilisation. Br J Psychiatry. 2001;179:417-25.
32. Brown JS, Evans-Lacko S, Aschan L, Henderson MJ, Hatch SL, Hotopf M. Seeking informal and formal help for mental health problems in the community: a secondary analysis from a psychiatric morbidity survey in South London. BMC psychiatry. 2014;14(1):275.
33. van Zoonen K, Kleiboer AM, Beekman ATF, Smit JH, Boerema AM, Cuijpers P. Reasons and determinants of help-seeking in people with a subclinical depression. Journal of Affective Disorders. 2014;173(0):105-12.
34. Fung K, Wong Y-LR. Factors influencing attitudes towards seeking professional help among East and Southeast Asian immigrant and refugee women. International Journal of Social Psychiatry. 2007;53(3):216-31.
35. Mojtabai R. Americans’ attitudes toward mental health treatment seeking: 1990–2003. Psychiatric Services. 2007;58(5):642-51.
36. Verhaak PF, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJ, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
5
How do people view the available care (i.e. professional care, informal help, self-reliance) | 109


Part IV: Who will benefit from preventive care?


Chapter 6
Conversion of subclinical depressive
symptoms into depressive disorders
This chapter is submitted as:Van Zoonen, K., Kleiboer, A. M., Beekman, A. T. F., Smit, J. H., Boerema,
A. M., Dijkshoorn, H., Cuijpers, P. (2014). Predictors of the conversion of subclinical depressive symptoms to major depressive
and anxiety disorders in the community.Manuscript submitted for publication to Depression & Anxiety.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
114 | Chapter 6
Abstract
Background: Subclinical depression is an important predictor of developing a full-blown depressive disorders. However, it is not known which people with a subclinical depression will develop a full-blown depression and which people will not. The current study examined predictors of the onset of depression (major depression and dysthymia) in people with subclinical depressive symptoms over a one year period. Since anxiety disorders frequently co-occur, we also explored predictors of the onset of anxiety disorders.
Methods: 162 people with subclinical depressive symptoms were recruited from the general population. They were eligible to participate if they were aged 18 years or older, scored 20 or higher on the K10 screening instrument for depression and did not meet criteria for a current depressive disorder (dysthymia or major depression) as established by a diagnostic interview; the Composite International Diagnostic Interview(CIDI). A total of 139 people (86%) completed the CIDI diagnostic interview at one year follow-up.
Results: 31 respondents (22%) developed a depressive disorder within one year and 20 respondents (14%) developed an anxiety disorder. At baseline 35 respondents (22%) met criteria for an anxiety disorder. Lifetime history of depression predicted the onset of a depressive disorder within one year, whereas severity of symptoms predicted the onset of anxiety disorders.
Conclusions: Professionals should be vigilant for people with subclinical depression who report prior depression and/or anxiety disorders, or indicate more severe symptoms on a screening instrument. It is important to further examine possible predictors of depressive disorders in people that are at high risk.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 115
Introduction
Depression affects millions of people worldwide with one in every eight men and one in every 5 women experiencing a depressive disorder once in their lives (1, 2). It is becoming the single leading cause of disease burden and is associated with significant loss in quality of life (3, 4). It is well known that people who suffer from subclinical depression are at high risk of developing a depressive disorder (5, 6). Subclinical depression is seen as a prodromal phase of major depression and can be defined as a score above the cut-off on a screening instrument, but failing to meet the criteria for major depression according to the Diagnostic and Statistical manual of Mental Disorders V (DSM-V) (6-8). The incidence rates of subclinical depression depend on the definition and population used and vary between 2.2% and 24% (9).
Research has shown that preventive interventions are able to prevent the onset of depression (10, 11). Although research on who will develop a major depression is scarce, certain risk factors have been identified in preventing depression (12). These risk factors can be divided into two classes: specific factors, such as severity of symptoms, and nonspecific factors, such as poverty (13). Studies focusing on the onset of depression in people with subclinical depression have shown that specific factors, such as severity of depressive symptoms, family history of depression, feelings of worthlessness or guilt, suffering from chronic illnesses, and mastery are important (8, 14-16). Furthermore, a need for care (e.g. met need, unmet need, or no perceived need) might be important in predicting who will develop a depressive disorder. Most people with mental health problems believe they do not need treatment, because the symptoms are temporary or not serious enough (17).
The first aim of the current study was to identify which people with a subclinical depression had developed a depressive disorder within one year. Since depression and anxiety often co-occur we also examined the onset of anxiety disorders at baseline and one year follow-up. A second aim was to examine what predicts (e.g. severity of symptoms, mastery, lifetime history of depressive and/or anxiety disorders, chronic illness, perceived need for care, loneliness, and demographic factors) the onset of depression or an anxiety.
Materials and Methods
DesignA longitudinal cohort study was conducted in people from the general population where people with subclinical depressive symptoms were followed during a one year period to see if they developed a depressive disorder.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
116 | Chapter 6
Participants, recruitment and procedureParticipants in the general population were recruited in collaboration with Municipal Health Services (GGD) in three different areas in the Netherlands. The current study joined the national Health Survey 2012 of the GGD. In the selected areas preventive interventions were widely advertised and available to everyone. More details can be found elsewhere (18). Recruitment at baseline took place between September 2012 and February 2013. Follow-up measures one year later.
People were eligible to take part when they scored 20 or higher on a screening instrument, Kessler 10 (K10) (19, 20) and were 18 years or older. If permission was granted people received a letter containing information about the current study including the follow-up. Participants with insufficient understanding of the Dutch language, either spoken or written, were excluded.
To establish depression status at baseline and follow-up, participants were contacted by telephone for a diagnostic interview, the Composite International Diagnostic Interview (CIDI, 2.1) (21). When the criteria for major depression and/or dysthymia were met participants remained in the study, but were not included in the current paper. Participants received an online questionnaire covering several domains including health care use and perceived need for care. At baseline this questionnaire was followed by a short questionnaire on people’s knowledge of preventive interventions and mental health care. This questionnaire was conducted by telephone since some questions needed some more elaboration and explanation by the researchers. A total number of 162 respondents with subclinical depression were included at baseline.
InstrumentsDemographicsIn the current study marital status, educational level, employment status, gender and age were used as demographic variables.
Diagnostic interviewThe CIDI was conducted at baseline and follow-up to establish which participant met the criteria for major depression and/or dysthymia. The current study used the lifetime version of the CIDI and two sections were administered; the anxiety (section D) and the depression section (section E). It has shown adequate validity and excellent reliability for depressive disorders (22). The interviews were conducted by trained Master level students in Clinical Psychology who received 8 hours of training and worked under supervision.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 117
Depressive symptomsTo examine the severity of symptoms the K10 was used (19). This screener consists of 10 questions and is mostly focused on depressive symptoms (20). The questions are answered on a 5-point rating scale from “never” (1) to “always” (5). The Dutch version has shown good psychometric properties (20). The baseline scores on the K10 were derived from the Health Survey of the GGD.Perceived need for care
The three categories of need for care at baseline were established using a combination of items from the Trimbos/iMTA questionnaire (TiC-P) and items from a short telephone questionnaire were used. The TiC-P measures health care uptake associated with psychiatric illness (23). A met need, or people who received professional care, in the 6 months prior to baseline were assessed with the TiC-P. Unmet need and no perceived need were established with the short telephone questionnaire, after people reported no experience with professional care on the TiC-P. Respondents who indicated they would have used preventive interventions if they had known about them were considered having an unmet need. Respondents who reported to be unwilling to use preventive interventions were considered having no perceived need.
Chronic illnessTo examine who suffered from a chronic illness in the past 12 months before baseline we used data derived from the GGD-survey. Questions stated if people reported one of the following 19 (chronic) diseases; any form of cancer, diabetes, several types of heart diseases, stroke, severe back problems, COPD and asthma, migraines, involuntary loss of urine, chronic eczema, psoriasis, dizziness with falling, arthrosis, and chronic or severe elbow, wrist or hand problems. When respondents had answered “yes” on 1 or more questions they were considered to suffer from a chronic illness.
Loneliness Loneliness was assessed using the Jong Gierveld Loneliness scale (24). The data were derived from the survey of the GGD. The GGD dichotomized the outcome so respondents either experienced loneliness or they did not. The scale has proved to be a reliable and valid instrument (25).
MasteryMastery (e.g. to what extent respondents felt they had control of their life and life-events) was examined by using the short form of the Pearlin Mastery Scale (26). Questions were answered on a 5-point rating scale from “strongly agree” to “strongly disagree”. The total score has a range of 5 to 25. Lower scores indicate a more external locus of control

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
118 | Chapter 6
and higher scores indicate a more internal locus of control. The internal consistency was good (α = .83).
Statistical AnalysisTo determine how many people had developed a major depression and/or dysthymia or an anxiety disorder between baseline and follow-up descriptive statistics were used. Univariate and multivariate logistic regression analyses were conducted to examine the influence of different baseline characteristics (e.g. severity of symptoms, mastery, lifetime history of depressive and/or anxiety disorders, chronic illness, loneliness, perceived need for care and demographic factors) on depression status and anxiety status within one year after baseline.
Results
SampleAfter filling out the national Health Survey a total of 1191 people with depressive disorders as well as subclinical depressive symptoms were invited to take part in the study. Three hundred and thirty three people (28%) returned their informed consent of whom 291 respondents (24%) completed the diagnostic interview. Reasons for not completing the diagnostic interview were; physical or mental inabilities (e.g. stroke, psychological stress), insufficient knowledge of the Dutch language, no response, lack of motivation to participate, emigration to a foreign country, lack of time, or no given reason.
Another 106 participants were excluded due to meeting the criteria for a depressive disorder, leaving a total of 185 participants with subclinical depressive symptoms of which 162 participants completed all the information at baseline. At follow-up 139 participants (86%) completed the diagnostic interview. Reasons for not completing were; psychological distress (n = 3), no time or not in the mood (n = 3), dissatisfaction with the interview (n = 2), none response (n = 12), or death of the respondent (n = 3).
Table 1 shows the descriptive characteristics of the participants at baseline and follow-up. Age ranged widely from 19 to 94 years, with an average age of 57 (SD = 18) at baseline. Most respondents were female (56%), in a relationship (57%), did not have a paid job (59%), and did not perceive a need for care (40%). Furthermore, most respondents did not suffer from a comorbid anxiety disorder at baseline (78%). Table 2 shows the characteristics of the predictors of the onset of depression or anxiety within a year.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 119
Table 1. Descriptive characteristics of respondents with and without depression or anxiety between baseline and follow-up.
Baseline Between baseline and follow-up
Total Respondents n = 162
Depressive disorder n = 31
No depressive disorder n = 108
Anxiety disorder n = 20
No Anxiety disorder n = 119
Gender, n (%) Female Male
91 (56.2)71 (43.8)
18 (58.1)13 (41.9)
60 (55.6)48 (44.4)
16 (80)4 (20)
62 (52.1)57 (47.9)
Age, M (sd) 57.2 (17.8) 54.0 (13.2) 58.4 (18.1) 54.2 (17.8) 57.9 (17.1)
Marital Status, n (%) In relationship Single
93 (57.4)69 (42.6)
16 (51.6)15 (48.4)
61 (56.5)47 (43.5)
9 (45)11 (55)
68 (57.1)51 (42.9)
Education, n (%) Low Middle High
24 (14.8)81 (50.0)57 (35.2)
3 (9.7)17 (54.8)11 (35.5)
17 (15.7)50 (46.3)41 (38.0)
1 (5)13 (65)6 (30)
19 (16)54 (45.4)46 (38.7)
Employment status, n (%) Paid job No paid job
66 (40.7)96 (59.3)
16 (54.6)15 (48.4)
43 (39.8)65 (60.2)
10 (50)10(50)
49 (41.2)70 (58.8)
Onset of depression between baseline and follow-upAt follow-up 58 respondents (41%) scored below the cut-off score on the K10 and 82 respondents scored (59%) scored above the cut-off score. Between baseline and follow-up, a total of 31 respondents (22%) met the criteria for a depressive disorder and 108 respondents (78%) did not. However, 33 respondents (24%) suffered from a comorbid anxiety disorders at baseline and 9 respondents (27%) developed an anxiety disorder at baseline. On the other hand, most respondents (n=106, 76%) did not suffer from a comorbid anxiety disorder at baseline. Of these 106 respondents, 22 respondents (21%) developed a depressive disorder between baseline and follow-up. Figure 1 shows these results in a flowchart.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
120 | Chapter 6
131
Onset of depression between baseline and follow-up
At follow-up 58 respondents (41%) scored below the cut-off score on the K10 and 82
respondents scored (59%) scored above the cut-off score. Between baseline and follow-up, a
total of 31 respondents (22%) met the criteria for a depressive disorder and 108 respondents
(78%) did not. However, 33 respondents (24%) suffered from a comorbid anxiety disorders at
baseline and 9 respondents (27%) developed an anxiety disorder at baseline. On the other
hand, most respondents (n=106, 76%) did not suffer from a comorbid anxiety disorder at
baseline. Of these 106 respondents, 22 respondents (21%) developed a depressive disorder
between baseline and follow-up. Figure 1 shows these results in a flowchart.
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Sample (n = 139
Subclinical depression (n = 106; 76.3%)
Subclinical depression and anxiety disorder (n = 33; 23.7%)
Depressive disorder (n = 22; 20.8%)
Anxiety disorder (n = 9; 7.1%)
Comorbid depression and anxiety (n = 6; 5.7%)
No depression or anxiety (n = 69; 65.1%)
Depressive disorder (n = 9; 27.3%)
Anxiety disorder (n = 11; 33.3%)
Comorbid depression and anxiety (n = 5; 15.2%)
No depression or anxiety (n = 8; 24.2%)
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Since the only information on depressive symptoms was measured at baseline and follow-up and the diagnostic interview measures the entire year between baseline and follow-up, there is no way to determine the actual recovery of respondents. Interestingly, 7 respondents (16%) who reported a met need, 14 respondents (45%) who reported an unmet need, and 10 respondents (16%) without a perceived need had developed a depressive disorder. However, these differences were not significant. Table 2 presents the characteristics of the predictors of the onset of depression.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 121
Table 2. Characteristics of predictors of the onset of depressive and/or anxiety disorders between baseline and follow-up.
Depressive disorder n = 31
No Depressive disorder n = 108
Anxiety disorder n = 20
No anxiety disorder n = 119
Perceived need, n (%) Met Need Unmet Need No perceived need
7 (22.6)14 (45.2)10 (32.3)
31 (28.7)29 (26.9)48 (44.4)
9 (45)6 (30)5 (25)
29 (24.4)37 (31.1)53 (44.5)
Comorbid anxiety at baseline, n (%) Yes No
9 (29)22 (71)
24 (22.2)84 (77.8)
11 (55)9 (45)
22 (18.5)97 (81.5)
Lifetime depression, n (%) Yes No
20 (64.5)11 (35.5)
43 (39.8)65 (60.2)
13 (65)7 (35)
50 (42)69 (58)
Loneliness, n (%) Yes No
21 (67.7)10 (32.3)
73 (67.6)32 (29.6)
15 (75)5 (25)
79 (66.4)37 (31.1)
Chronic illness, n (%) No illness 1 or more illnesses
4 (12.9)24 (77.4)
19 (17.6)69 (63.9)
3 (15)16 (80)
20 (16.8)77 (64.7)
Mastery, M (sd) 9.5 (4.4) 10.7 (4.3) 6.5 (4.1) 10.6 (4.3)
Severity of symptoms, M (sd) 25.7 (4.6) 24.9 (5.0) 28.0 (5.0) 24.6 (4.7)
a = not applicable
Univariate associations between baseline predictors and depression status within a yearNo significant association were found between perceived need, demographic factors, loneliness, mastery, chronic illness, or severity of depressive symptoms and the development of a depression within a year (Table 3). However, a significant association was found for lifetime history of depression and onset of depression. People with a previous diagnosis of depression were 2.79 times more likely to have developed a depression within a year (OR = 2.79; 95% CI = 1.20-6.31; p<.05).
Multivariate associations between baseline predictors and depression status within a yearA multivariate logistic regression was conducted to examine what factors best predicted the onset of a depressive disorder (Table 3). In line with the univariate analyses, people with a previous episode of depression or anxiety were 3.26 times more likely to develop a major depression than those without a previous episode of depression (OR = 3.26; 95% CI = 1.13-9.40). The model was a good fit to the data, (χ2(8) = 7.71, p = .46). However, the model only explained a modest portion of the variance (Nagelkerke R2 = .19).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
122 | Chapter 6
Onset of anxiety between baseline and follow-upA total of 33 respondents (24%) of the 139 met the criteria for anxiety disorders at baseline and 11 respondents (33%) also met criteria for anxiety disorders at follow-up (See Figure 1). Only 9 respondents (7%) of the respondents who suffered only from subclinical depression (76%) at baseline developed an anxiety disorder within a year. Furthermore, of the 33 respondents with comorbid anxiety at baseline 5 (15%) also reported comorbid depression and anxiety between baseline and follow-up compared to 6% of the respondents who only suffered from subclinical depression.
Univariate associations between baseline predictors and anxiety status within a yearResults of the univariate logistic regression analysis showed significant effects for gender (χ2(1) = 5.84, p<.05), comorbid anxiety disorder at baseline (χ2(1) = 10.91, p<.01), and severity of symptoms (χ2(1) = 7.47, p<.01) on the onset of anxiety (Table 3). Furthermore, lifetime diagnosis of depression showed a trend (χ2(1) = 3.66, p=.06). Females were 3.68 times more likely to develop an anxiety disorder within a year than males (OR = 3.68; 95% CI = 1.16-11.56), people who reported more severe symptoms are 1.13 more likely to develop an anxiety disorder than respondents who reported less severe symptoms (OR = 1.13; 95% CI = 1.04-1.24), and respondents who suffered from comorbid anxiety disorder at baseline were 5.39 times more likely to develop an anxiety disorder within a year compared to respondents who do not suffer from comorbid anxiety disorder (OR = 3.68; 95% CI = 1.16-11.65). Furthermore, respondents who reported a lifetime history of depression were 2.56 more likely to develop an anxiety disorder within one year (OR = 2.56; 95% CI = 0.95-6.89).
Multivariate associations between baseline predictors and anxiety status within a yearA multivariate logistic regression was conducted to investigate what factors best predicted the onset of an anxiety disorder within one year (Table 3). Respondents who reported more severe symptoms on the K10 were 1.15 more likely to develop an anxiety disorder (OR = 1.15; 95% CI = 1.00-1.33). The model was a good fit to the data (χ2(8) = 5.51, p = .70). The model explained 30% of the variance (Nagelkerke R2 = .30).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 123
Tabl
e 3.
Pre
dict
ors o
f the
ons
et o
f dep
ress
ion
and
anxi
ety.
Dep
ress
ion
Anx
iety
Uni
varia
teM
ultiv
aria
teU
niva
riate
Mul
tivar
iate
Pred
icto
rO
R (9
5% C
I)O
R (9
5% C
I)O
R (9
5% C
I)O
R (9
5% C
I)G
ende
r1.
11 (0
.49
– 2.
49)
1.21
(0.4
3 –
3.41
)3.
68 (1
.16
– 11
.56)
*3.
81 (0
.91
– 15
.96)
A
ge0.
99 (0
.96
– 1.
01)
1.01
(0.9
7 –
1.04
)0.
99 (0
.96
– 1.
02)
1.00
(0.9
6 –
1.05
)M
arita
l sta
tus
0.82
(0.3
7 –
1.83
)0.
81 (0
.28
– 2.
34)
0.61
(0.2
4 –
1.59
)0.
88 (0
.25
– 3.
09)
Educ
atio
nal l
evel
a
M
iddl
e
Hig
h1.
93 (0
.50
– 7.
40)
1.52
(0.3
8 –
6.14
)3.
40 (0
.33
– 34
.78)
1.87
(0.1
6 –
22.2
9)4.
57 (0
.56
– 37
.36)
2.48
(0.2
8 –
22.0
0)3.
06 (0
.25
– 37
.89)
2.05
(0.1
4 –
30.6
1)Em
ploy
men
t sta
tus
0.62
(0.2
0 –
1.93
)0.
64 (0
.21
– 2.
02)
0.70
(0.2
7 –
1.81
)0.
52 (0
.13
– 2.
04)
Perc
eive
d ne
ed fo
r car
eb
U
nmet
nee
d
No
perc
eive
d ne
ed2.
14 (0
.76
– 6.
04)
0.92
(0.3
2 –
2.68
)2.
12 (0
.65
– 6.
91)
1.49
(0.4
1 –
5.41
)0.
52 (0
.17
– 1.
64)
0.30
(0.0
9 –
0.99
)0.
35 (0
.08
– 1.
46)
0.71
(0.1
6 –
3.13
)Lo
nelin
ess
0.92
(0.3
9 –
2.18
)0.
54 (0
.16
– 1.
78)
1.41
(0.4
8 –
4.16
)1.
65 (0
.32
– 8.
46)
Chr
onic
illn
ess
1.65
(0.5
1 –
5.35
)1.
66 (0
.41
– 6.
68)
1.39
(0.3
7 –
5.23
)2.
47 (0
.38
– 16
.21)
Life
time
depr
essi
on2.
79 (1
.20
– 6.
31)*
3.26
(1.1
3 –
9.40
)*2.
56 (0
.95
– 6.
89)
1.66
(0.4
7 –
5.85
)C
omor
bid
anxi
ety
diso
rder
at b
asel
ine
1.43
(0.5
8 –
3.52
)0.
64 (0
.19
– 2.
10)
5.39
(1.9
9 –
14.5
8)**
2.36
(0.6
2 –
9.04
)Se
verit
y of
sym
ptom
s1.
04 (0
.96
– 1.
12)
1.02
(0.9
1 –
1.15
)1.
13 (1
.04
– 1.
24)*
*1.
15 (1
.00
– 1.
33)*
Mas
tery
0.93
(0.8
5 –
1.03
)0.
89 (0
.77
– 1.
03)
0.94
(0.8
4 –
1.05
)1.
06 (0
.89
– 1.
29)
a = re
feren
ce ca
tego
ry is
‘low
’; b =
refer
ence
cate
gory
is ‘m
et n
eed’
*p<.
05; *
*p<
.01

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
124 | Chapter 6
Discussion
People with subclinical depression are at high risk of developing a depression (6, 27), but what predicts the onset of depression is unknown. In order to be able to predict who is most in need of preventive care, it is important to examine predictors of the onset of depression in people with subclinical depression. Therefore, the current study has focused on the onset of depressive disorders in a one year period. Since anxiety often co-occurs with depression the current study also explored predictors of anxiety (28).
At follow-up 22% had developed a depressive disorder (dysthymia and/or major depression) within a year after baseline and 12% had developed an anxiety disorder. Incidence rates of major depression in people with subclinical depression varied widely across studies, from 0.15 in general population studies to 0.58 in high-risk studies (6). However, our results show lower incidence rates in a high-risk sample.
People with a lifetime history of depression were more likely to develop a depressive disorder. This is in line with previous studies (6, 27). Furthermore, being female, reporting more severe depressive symptoms, and having a comorbid anxiety disorder at baseline increases the risk of developing an anxiety disorder within one year. However, multivariate analysis only showed higher severity of symptoms predicted the onset of anxiety within a year. The current study emphasizes the importance of lifetime history of depression and severity of symptoms on the onset of depression and anxiety, but could not identify other predictors. It remains difficult to predict the onset of depression (or anxiety) in a high-risk sample. However, the current results support the notion of a depression continuum (29-31).
The results should be interpreted in light of some limitations. The current study had a low response rate. Low response rate, unfortunately, is not uncommon in general population research (32). They propose that the general population is contacted more often for (commercial) research and so people tend to be more reluctant in wanting to participate. However, this has probably led to a selection bias due to the design of the current study. First, the GGD Health Survey reported a selection bias due to underrepresentation of the lower age groups between 18 and 49 years, men, and immigrants (33). Furthermore, not everyone who completed the Health Survey gave permission to be contacted for further research. This might have contributed to selection bias further. Second, the number of respondents in the current study is relatively small and might have limited the power to find an effect. Finally, although the screener K10 is not a “pure measure” for depressive symptoms, it has shown to adequately identify depressive symptoms and disorders (20).
There are some strengths to this study as well. It is one of the very few studies that has examined subclinical depression in the general population and the drop-out rate

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 125
between baseline and follow-up was low (14%). This is encouraging for population-based research that is known to struggle with response and drop-out rates. Another strength is the two-step design. In the first step people with a score above the cut-off on a screener were included and the second step excluded people with a depressive disorder diagnosis according to a diagnostic interview. This makes the current study a unique, first step in identifying predictors of the onset of depression (and anxiety) in a high-risk sample in the general population.
Although the variance explained was relatively small, our results in combination with previous research show that it is important that professionals in mental health care examine and take into account people’s history of depression (and anxiety). They should be vigilant for people who report previous episodes of depression and/or anxiety. Future research should further examine perceived need for care in a larger sample, since the lack of differences between the need categories in this study might be due to the low sample sizes.
Conclusion
Although the current study has shown it might be difficult to predict who will develop a depressive or anxiety disorder in a high risk sample, it is important to continue to identify possible predictors in the onset of depressive and anxiety disorders. Increasing insight will make it possible to tailor and attune preventive care to people who are at risk and will benefit from it. The current study supports the findings from previous research indicating that people that have suffered from a previous depressive disorder are most likely to develop another full-blown depression. Furthermore, severity of symptoms is important in predicting the onset of anxiety. It is important to try and replicate these results in future research.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
126 | Chapter 6
References
1. Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. The Lancet. 2007;370(9590):841-50.
2. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of general psychiatry. 1994;51(1):8-9.
3. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS medicine. 2006;3(11):e442.
4. Cuijpers P, Smit F. Excess mortality in depression: a meta-analysis of community studies. Journal of affective disorders. 2002;72(3):227-36.
5. Cuijpers P, de Graaf R, van Dorsselaer S. Minor depression: risk profiles, functional disability, health care use and risk of developing major depression. Journal of Affective Disorders. 2004;79(1–3):71-9.
6. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta Psychiatrica Scandinavica. 2004;109(5):325-31.
7. APA. DSM 5: American Psychiatric Association; 2013.8. Eaton W, Badawi M, Melton B. Prodromes and precursors: epidemiological data for primary
prevention of disorders with slow onset. American Journal of Psychiatry. 1995;152:967-72.9. Rucci P, Gherardi S, Tansella M, Piccinelli M, Berardi D, Bisoffi G, et al. Subthreshold
psychiatric disorders in primary care: prevalence and associated characteristics. Journal of Affective Disorders. 2003;76(1–3):171-81.
10. van Zoonen K, Buntrock C, Ebert DD, Smit F, Reynolds CFr, Beekman AT, et al. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. International journal of epidemiology. 2014;43(2):318-29.
11. Cuijpers P, Koole SL, van Dijke A, Roca M, Li J, Reynolds CF. Psychotherapy for subclinical depression: meta-analysis. The British Journal of Psychiatry. 2014;205(4):268-74.
12. O’Connell ME, Boat T, Warner KE. Preventing Mental, Emotional, and Behavioral Disorders Among Young People:: Progress and Possibilities: National Academies Press; 2009.
13. Muñoz RF, Beardslee WR, Leykin Y. Major depression can be prevented. American Psychologist. 2012;67(4):285.
14. Crum RM, Cooper-Patrick L, Ford DE. Depressive symptoms among general medical patients: prevalence and one-year outcome. Psychosomatic medicine. 1994;56(2):109-17.
15. Cuijpers P, Smit F, Willemse G. Predicting the onset of major depression in subjects with subthreshold depression in primary care: a prospective study. Acta Psychiatrica Scandinavica. 2005;111(2):133-8.
16. Cuijpers P, Beekman ATF, Smit F, Deeg D. Predicting the onset of major depressive disorder and dysthymia in older adults with subthreshold depression: a community based study. International journal of geriatric psychiatry. 2006;21(9):811-8.
17. Mojtabai R, Olfson M, Mechanic D. Perceived need and help-seeking in adults with mood, anxiety, or substance use disorders. Archives of General Psychiatry. 2002;59(1):77-84.
18. van Zoonen K, Kleiboer AM, Beekman ATF, Smit JH, Boerema AM, Cuijpers P. Reasons and determinants of help-seeking in people with a subclinical depression. Journal of Affective Disorders. 2014;173(0):105-12.
19. Kessler RC, Andrews G, Colpe LJ, Hiripi E, Mroczek DK, Normands SLT, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine. 2002;32(06):959-76.
20. Donker T, Comijs H, Cuijpers P, Terluin B, Nolen W, Zitman F, et al. The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research. 2010;176(1):45-50.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
6
Conversion of subclinical depressive symptoms into depressive disorders | 127
21. Robins LN, Wing J, Wittchen H, Helzer JE, Babor TF, Burke J, et al. The composite international diagnostic interview: An epidemiologic instrument suitable for use in conjunction with different diagnostic systems and in different cultures. Archives of General Psychiatry. 1988;45(12):1069-77.
22. Andrews G, Peters L. The psychometric properties of the Composite International Diagnostic Interview. Social Psychiatry & Psychiatric Epidemiology. 1998;33(2):80.
23. Hakkaart-van Roijen L, Straten Av, Tiemens B, Donker MCH. Handleiding Trimbos/iMTA questionnaire for costs associated with psychiatric illness (Tic-P). 2002 January. Report No.
24. de Jong-Gierveld J, Kamphuls F. The development of a Rasch-type loneliness scale. Applied Psychological Measurement. 1985;9(3):289-99.
25. Gierveld JDJ, Van Tilburg T. A 6-item scale for overall, emotional, and social loneliness confirmatory tests on survey data. Research on Aging. 2006;28(5):582-98.
26. Pearlin LI, Schooler C. The Structure of Coping. Journal of Health and Social Behavior. 1978;19(1):2-21.
27. Muñoz RF, Cuijpers P, Smit F, Barrera AZ, Leykin Y. Prevention of major depression. Annual Review of Clinical Psychology. 2010;6:181-212.
28. Kessler RC, Merikangas KR, Wang PS. Prevalence, comorbidity, and service utilization for mood disorders in the United States at the beginning of the twenty-first century. Annu Rev Clin Psychol. 2007;3:137-58.
29. Goldberg D. Plato versus Aristotle: Categorical and dimensional models for common mental disorders. Comprehensive Psychiatry. 2000;41(2, Supplement 1):8-13.
30. Rodríguez MR, Nuevo R, Chatterji S, Ayuso-Mateos JL. Definitions and factors associated with subthreshold depressive conditions: a systematic review. BMC psychiatry. 2012;12(1):181.
31. Pietrzak R, Kinley J, Afifi T, Enns M, Fawcett J, Sareen J. Subsyndromal depression in the United States: prevalence, course, and risk for incident psychiatric outcomes. Psychological medicine. 2013;43(07):1401-14.
32. De Graaf R, Ten Have M, van Dorsselaer S. De psychische gezondheid van de Nederlandse bevolking. Nemesis-2: Opzet en eerste resultaten, Trimbos-Instituut, Utrecht. 2010.
33. GGD. Gezondheid en welzijn van volwassenen en senioren in Zuid-Holland West - resultaten van het Gezondheidsonderzoek 2012. GGD Zuid-Holland West, 2012.


Part V: Discussion and summary


Chapter 7
General Discussion
Summary
Samenvatting (summary in Dutch)

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
132 | Chapter 7

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 133
Introduction
Depression is a worldwide health concern and it has a big impact on daily life and society. Effective treatments are only able to reduce about one-third of the disease burden. Therefore, preventing the onset of depression is important. However, providing prevention to everyone is expensive and not always necessary. A way to make it more feasible is to prevent depression in people at high risk for depression or indicated prevention. Research has shown that depression exists on a continuum from no symptoms to many symptoms. Subclinical depression is considered a prodromal phase and, as such, is viewed as part of this continuum. Hence, people that suffer from subclinical depression are at high risk of developing depression. Prevention targeting this group is an important first step in lowering the incidence of depression and examining the words of Benjamin Franklin: “An Ounce of Prevention is worth a Pound of Cure”.
This thesis aims to broaden the knowledge on help-seeking and the onset of depression in people with subclinical depression, a group at high risk of developing depression. The following research questions were stated in the introduction:
(1) Can people benefit from preventive interventions?(2) Which people with subclinical depression (are willing to) participate in
preventive interventions for depression?(3) How do people view their symptoms?(4) What are the attitudes towards care?(5) Which people with subclinical depression develop depressive disorders?
In this chapter, the main findings are summarized and the implications of the findings for clinical practice and future research are discussed. Also, the conclusions are stated.
Main findings and previous literature
Effectiveness of preventive interventionsA first important step in examining whether prevention of depression has the potential to lower the incidence of depressive disorders is to examine the effectiveness of preventive interventions for depression. There are three types of prevention: (1) Universal prevention targeting the entire population; (2) Selective prevention targeting individuals or subgroups that are at higher risk of developing mental disorders than average subgroups; (3) Indicated prevention targeting individuals who already show depressive symptoms, but do not yet meet criteria for depressive disorders (1, 2). Previous research has shown an overall effect of universal, selective and indicated prevention of depressive disorders (3). However, universal prevention was only examined in two studies making it impossible to examine its effectiveness. One way to examine whether preventive

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
134 | Chapter 7
interventions are effective is to look at the numbers needed to treat (NNT). The NNT indicates the number of people that would have to receive a preventive intervention in order to prevent one new case of depression.
The findings in chapter 2 of this thesis have shown a relative risk of developing a depressive disorder of 0.79, indicating a 21% reduction in the incidence in depression in the people who received a preventive interventions compared to control groups. The NNT to prevent a new case of a depressive disorder was 20. Although this appears high there are no normative thresholds for lower or higher NNT (3). Considering the impact depressive disorders have on nearly all aspects of daily life, its clinical relevance, and the similar results in other areas of health care, 20 seems an acceptable number.
Help-seeking in people with subclinical depressionAnother way to increase our understanding of prevention and its potential to lower the incidence of depression and its burden of disease is to investigate help-seeking and the onset of depression in people with subclinical depression. Although previous research and the findings in this thesis have shown that preventive interventions for depression are effective in preventing and delaying the onset of depression (3, 4), very few studies have examined help-seeking in people with subclinical depression.
Literature on help-seeking is mostly focused on “general mental conditions” and is often guided by the Behavioural Model of Health Service Use by Andersen and Newman (5). This model identifies three interrelating factors that explain health care use: need, predisposing, and enabling factors (5-7). Need factors include perceived need – how people view and experience their own health and illness symptoms - and actual need – defined by professional assessment and objective measurement of the symptoms a person experiences. Predisposing factors consist of demographic factors, social structure and belief factors, such as attitudes, values and health beliefs. Enabling factors relate to organisational factors that influence availability and affordability of mental health care.
Due to the Dutch health care system, enabling factors were expected not to present a barrier to help-seeking as most preventive care is available to everyone at little to no cost. Furthermore, the need factors were expected to play a less important role compared to help-seeking for full-blown disorders, since the symptoms are less severe. Research has indicated that the ability to recognize symptoms in oneself and attitude are consequently found to influence whether someone will seek help (8, 9).
Our results in chapter 3 showed that many people with subclinical depression (40%) do not perceive a need for care, 33% reported that they felt they needed help, but did not receive any, and 27% received professional help. People who reported no perceived need mostly felt they believed their symptoms were not severe enough to seek help or that they were able to solve problems on their own. Previous research has also shown that

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 135
people’s perception of their symptoms and their ability to deal with them is mentioned more often as a reason not to seek help than more practical reasons, such as lack of money (10-12). Furthermore, people without a perceived need frequently mentioned they were able to mobilize their own support, such as friends or family. They were also more often in a relationship, which is a protective factor for need for professional help (38), had not experienced a previous episode of depression in their life, and reported unfamiliarity with preventive interventions. Therefore, people might not see prevention as an option and seek other options to deal with their problems first. People who did not perceive a need for care were characterized by lower scores on neuroticism and older age compared to those who received care, suggesting that predisposing factors are more important in seeking help than need factors, at least, in people with subclinical depression.
People who received care mostly found this help in a combination of primary and specialized mental health care. People who reported an unmet need preferred group interventions, such as mindfulness, over web-based interventions. This is somewhat contradictory to certain previous studies. However, mindfulness is known to be popular treatment for anxiety and depression and web-based preventive interventions are relatively new (13). This, in combination, with the relatively old age in our study might explain this difference in results.
The ability to recognize one’s own symptoms, or insight, is also an important predictor in help-seeking. The model of Andersen considers this a predisposing factor. However, most research has examined this by using “vignette-studies” (14, 15). The research that has investigated insight has mainly focused on “common mental disorders” and has shown that insight or recognizing one’s symptoms is closely related to level of education and the burden of disease (6, 16). The results in chapter 4 have shown that, although most people are capable in identifying anxiety and depression in themselves, a clinically significant percentage of people underestimate their symptoms. This lack of insight seems to be associated with higher personal stigma, being separated or divorced, and younger age.
Another important factor in help-seeking is how people view the available care, or their attitude towards care. There are multiple types of care, but they can be characterized as: professional care, informal help (e.g. friends or family), or self-reliance (e.g. keep problems to oneself). In order to understand help-seeking it is important to know what influences people’s beliefs about the existing care. Who has these beliefs and are they changeable over time? Chapter 5 focused on this and showed that attitude does not change a lot over time and the attitudes people hold at baseline are consequently related to the attitudes after four years. Furthermore, a more positive attitude towards professional care after four years was associated with a change in mental health acre use. People that had not used care at baseline, but indicated to have used at follow-up

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
136 | Chapter 7
reported a more positive attitude compared to people who had not used mental health care.
The onset of depression in people with subclinical depressionIn order to make prevention of depression useful to people the preventive interventions should be effective in preventing or delaying the onset of depression and people should seek help when they need it. However, not much is known about which people with subclinical depression develop a depressive disorder and which people do not, making it difficult to determine who needs care (17-20). Above I have discussed the effectiveness of preventive interventions for depression and possible important barriers to seeking care in people with subclinical depression, such as neuroticism and age. However, in order to provide care to the people that need it, it is important to determine in which people the subclinical depressive symptoms will convert into a depressive disorder. This will make it possible to tailor the care to the people that need it. Chapter 6 has addressed this question.
Although people with subclinical depression are at higher risk of developing depression, research on which people with subclinical depression develop a depression is scarce. Nevertheless, in other populations certain risk factors have been identified in preventing depression (21). These risk factors include severity of depressive symptoms, suffering from a chronic illness, need for care and mastery (17-19, 22). The findings in chapter 6 showed that 22% had developed a depressive disorder (dysthymia and/or major depression) within a year after baseline and 12% developed an anxiety disorder. However, at baseline certain people already suffered from a comorbid anxiety disorders. Examining people who developed an anxiety disorder without a comorbid anxiety disorder, showed that 7% were new cases of anxiety. The development of depressive and anxiety disorders between people with only subclinical depression and people with subclinical depression and anxiety disorder is shown in Figure 1.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 137
148
6 showed that 22% had developed a depressive disorder (dysthymia and/or major depression)
within a year after baseline and 12% developed an anxiety disorder. However, at baseline
certain people already suffered from a comorbid anxiety disorders. Examining people who
developed an anxiety disorder without a comorbid anxiety disorder, showed that 7% were new
cases of anxiety. The development of depressive and anxiety disorders between people with
only subclinical depression and people with subclinical depression and anxiety disorder is
shown in Figure 1.
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Subclinical depression (n = 106; 76.3%)
Depressive disorder (n = 22; 20.8%)
Anxiety disorder (n = 9; 7.1%)
Comorbid depression and anxiety (n = 6; 5.7%)
No depression or anxiety (n = 69; 65.1%)
Sample (n = 139
Depressive disorder (n = 9; 27.3%)
Anxiety disorder (n = 11; 33.3%)
Subclinical depression and anxiety disorder (n = 33; 23.7%)
Comorbid depression and anxiety (n = 5; 15.2%)
No depression or anxiety (n = 8; 24.2%)
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Lifetime history of depression predicted the onset of depression within a year and severity of symptoms at baseline predicted the onset of anxiety within a year.
Overall discussionThe work in this thesis showed that the difficulty lies not in proving the effectiveness of preventive interventions, but in predicting which people with subclinical depression will develop a depressive disorder and/or an anxiety or, in other words, which people will benefit from preventive interventions. A first step has been taken in this thesis and has shown that lifetime history of depression predicted the onset of depression within a year and severity of symptoms at baseline predicted the onset of anxiety disorders within a year in people with subclinical depression. Taking into account figure 1 of the introduction (p. 9), this indicates that the results of our sample might provide more information on

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
138 | Chapter 7
relapse prevention. This emphasizes the importance of reaching a consensus on what defines prevention. Moreover, it shows that there might be several types of subclinical depression, which could require different (preventive) approaches in dealing with the symptoms. A possible explanation for the difficulty in predicting the onset of depression and anxiety in this high risk group is the heterogeneity of this groups, meaning some people might have remittal symptoms of a previous depressive disorder whereas other people might report depressive symptoms without having suffered from a previous depressive disorder.
Recommendations for Clinical Practice and Policy
The findings in this thesis have implications for clinical practice and lead to the following recommendations. In general, people are difficult to motivate if there is no direct benefit. Therefore, motivating people to seek preventive care is difficult. Prevention focuses on averting a bad event from possibly happening. Furthermore, people are reluctant to seek help for something that is not perceived as an event or illness that has a significant impact on their life. These two things, the uncertainty that something will happen and the lack of impact on daily life, make it difficult to convince people that prevention is useful.
In the Netherlands (and many other countries) we value informing and guiding people in making educated decisions on what is right for them in treating symptoms. This is partly shown in our health care system in which people are free to choose the height of the deductibles. It is important that the government educates people on the risks of developing depression as well as the consequences of suffering from a depression by using campaigns. Moreover, the government should focus on educating health care professionals on prevention and its benefits in seminars and/or campaigns. A good start would be making clinicians aware of the low participation rates in preventive care, but, more importantly, the effectiveness of preventive interventions. This way health care professionals are better able to provide information people can use to make an educated decision on seeking certain care.
Although it is difficult to predict who will develop a depression it is important to be vigilant for people who report lifetime history of depression and/or more severe symptoms according to a screening instrument. Taking into account other factors, such as family history, can make prevention more feasible and tailored in preventing the depressive symptoms from converting into a disorder. Although subclinical depression could have several origins, such as remittal symptoms or prodromal phase, clinicians should be aware of the possibilities of prevention.
Furthermore, care should be easily accessible to everyone (i.e. short waiting lists or travel time). When accessibility to care no longer feels like a barrier people will seek

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 139
help sooner, increasing people’s experience with care. This is important, since experience with care lowers the threshold to seeking (future) care. This is an important finding especially in people who have suffered from previous depression or other disorders. Even though the preventive care in the Netherlands is nearly free of charge this does not seem to be enough to increase awareness or accessibility. A special task might not only lie with GPs and Municipal Health Services, but also with the government. The results in this thesis increase insight into the reasons for not seeking help in people who are at high risk. Most people do not believe their symptoms are severe enough or believe they will be able to handle problems on their own. Since it is known that not everyone will develop a depressive disorder, this might be true in some cases. Furthermore, the predictors of depression identified in chapter 6, lifetime history of depression and severity of depressive symptoms can help clinicians identify people that may benefit from preventive care. However, when people come in with different complaints that might be related to depression or subclinical depression, (mental) health care professionals and Municipal Health services should know where to refer people to. Increasing awareness about prevention in these target groups of professionals is important.
Another important focus for policy makers and professionals should be the people that have indicated their willingness to seek and use help, but have not received any, and people that tend to underestimate their symptoms. Increasing awareness among the general public on what help is available, what the goals are and where this help is available, especially since many people indicated they did not know where to seek care. Also, increasing awareness in the general public might lead to other, more indirect, advantages. Many people report seeking care from friends and family, when awareness about subclinical depression and its consequences is better understood by people, they might be able to provide better care. Furthermore, increasing awareness might lower stigma and this might lower barriers to help-seeking. Moreover, due to people underestimating their symptoms the help they do seek might be for other problems. It is important to educate people on the (preventive) interventions that are available and their goals.
A way of improving this is to consider providing prevention at GP’s and not (only) in specialized mental health institutions or redirecting the focus of preventive interventions to strengthening resilience instead of preventing depression. The focus of the interventions and the location these interventions are provided, might lower stigma in “patients” as well as professionals.
The findings in this thesis, as well as previous research, have shown that prevention of depression is effective in preventing and delaying the onset of depression. Since treatment, even under optimal conditions, can only reduce about one-third of the disease burden of depression, it is essential that prevention of depression is better understood.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
140 | Chapter 7
This research can be two-fold, either focusing on preventing the onset of depression or focus on reducing the symptoms of subclinical depression. Since the consequences of depression as well as other common mental disorders are enormous for both the individual as well as the society, research focused on preventing common mental disorders should be stimulated and financially supported by the government and public health institutions.
Recommendations for future research
In addition to recommendation for clinical practice and policy makers, the results in this thesis also provide recommendations for future research. These can be made to prevention of depression as well as the type of prevention.
Subclinical depression has been defined in several ways; (1) a score above a threshold on a screening instruments without meeting the DSM-V criteria for major depression on a diagnostic instrument or (2) reporting a depressed mood accompanied by additional symptoms, but not as severe as or as many as the DSM-V criteria for major depression (20, 23, 24). In this thesis the first definition was used (25). Future research should determine what constitutes subclinical depression. Are people that report subclinical depressive symptoms as remittal symptoms from a previous depressive episode the same as people who report subclinical depression as prodromal phase to a first onset depressive disorder? It is important to reach some sort of consensus on what constitutes a subclinical depression, since this most likely influences the outcome of results. Lifetime history of depression has shown to predict the onset of depression within a year, however it is likely that these people with subclinical depression most likely suffered from remittal symptoms or were more vulnerable to develop a depression and when they suffer from some addition symptoms these sooner convert into a depressive disorder.
This also shows the importance increasing insight into the course of subclinical depression. Prevention is two-sided, either research can focus on preventing the onset of depression or research can focus on lowering the depressive symptoms. Both sides of depression prevention need more research. The work in this thesis has focused on prevention of depression and future research should examine this in other high-risk groups, such as people with first-degree family members who suffer from depression, and identify people who may benefit from preventive care. Equally important is increasing our understanding of reducing subclinical depressive symptoms. Therefore, research should focus on recovery of subclinical depression as defined in the current thesis. In order to investigate this, researchers will have to measure depressive symptoms more often, which would then have to be cross-examined with the (absence of) diagnosis on a diagnostic instrument. For example, the screener used in the study discussed in

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 141
chapters 3 and 6 is reliable in asking four to six weeks prior to the date of completion. It is necessary to synchronize the completion of the screening to the diagnosis on the diagnostic instrument.
It is imperative to identify which factors predict the onset of a disorder even if the target group is fairly heterogeneous. Depression is a very debilitating disease and has immense economic costs at individual as well as societal level. Preventive interventions have shown to be effective, however it is important to make sure the right people receive the care they need. Providing prevention to everyone means wasting valuable resources, since many people do not develop depression and therefore do not need care. Tailoring prevention to people that need it, is important. Tailoring interventions may depend on the target group and setting in which they are provided, for example depending on age, education and setting. Future research should identify predisposing, need and enabling factors that predict the onset of depression in several other people at (high) risk. In order to tailor interventions, more information is needed on target groups. This will lead to adaptations as small as linguistics or as big as implementation. For example, implementing preventive care in high school settings will require a different approach than employment settings.
Furthermore, it is important to know how effective preventive interventions are in the long run. This could be examined by a prospective longitudinal study examining the onset of disorders in people at high risk who have used preventive interventions compared to people at high risk who have not used preventive care.
Conclusion
“An Ounce of Prevention is worth a Pound of Cure” is not as simple as it looks when applied to prevention of depression and certain issues need to be clarified. The work in this thesis allows us to conclude that preventive interventions for depression are effective. Although it remains difficult to determine who will benefit from preventive interventions, in most cases the subclinical depressive symptoms do not convert into a depressive disorder. Although many people can accurately identify their symptoms, a clinically relevant number of people with subclinical depression, who would benefit from care, underestimate their symptoms and do not seek help.
Lifetime history of depression and severity of symptoms seem to predict the onset of depression or anxiety in people with subclinical depression. Professionals should be vigilant of people who report more severe symptoms and who have suffered from a depressive disorder in the past. It is imperative to make (and keep) care easily accessible and tailor prevention to people that need it. It is especially important that care is provided to people who reported an unmet need.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
142 | Chapter 7
References
1. Muñoz RF, Cuijpers P, Smit F, Barrera AZ, Leykin Y. Prevention of major depression. Annual Review of Clinical Psychology. 2010;6:181-212.
2. Greenberg MT, Domitrovich C, Bumbarger B. Preventing mental disorders in school-age children: A review of the effectiveness of prevention programs. Prevention Research Center for the Promotion of Human Development, College of Health and Human Development, Pennsylvania State University. 2000.
3. Cuijpers P, Van Straten A, Smit F, Mihalopoulos C, Beekman A. Preventing the Onset of Depressive Disorders: A Meta-Analytic Review of Psychological Interventions. American Journal of Psychiatry. 2008;165(10):1272-80.
4. van Zoonen K, Buntrock C, Ebert DD, Smit F, Reynolds CFr, Beekman AT, et al. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. International journal of epidemiology. 2014;43(2):318-29.
5. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? Journal of health and social behavior. 1995;36(1):1-10.
6. Andersen RM, Newman JF. Societal and individual determinants of medical care utilization in the United States. Milbank Quarterly. 2005;83(4):Online-only.
7. Anderson JG. Demographic Factors Affecting Health Services Utilization: A Causal Model. Medical Care. 1973;11(2):104-20.
8. Verhaak PF, Prins MA, Spreeuwenberg P, Draisma S, van Balkom TJ, Bensing JM, et al. Receiving treatment for common mental disorders. General Hospital Psychiatry. 2009;31(1):46-55.
9. Mackenzie CS, Erickson J, Deane FP, Wright M. Changes in Attitudes toward Seeking Mental Health Services: A 40-Year Cross-Temporal Meta-Analysis. Clinical Psychology Review. 2014;34(2):99-106.
10. Ten Have M, De Graaf R, Ormel J, Vilagut G, Kovess V, Alonso J. Are attitudes towards mental health help-seeking associated with service use? Results from the European Study of Epidemiology of Mental Disorders. Social psychiatry and psychiatric epidemiology. 2010;45(2):153-63.
11. Mojtabai R. Unmet need for treatment of major depression in the united states. Psychiatric services. 2001;60(3):297-305.
12. Sareen J, Jagdeo A, Cox B, Clara I, ten Have M, Belik S-L, et al. Perceived barriers to mental health service utilization in the United States, Ontario, and the Netherlands. Psychiatric Services. 2007;58(3):357-64.
13. Kessler RC, Soukup J, Davis RB, Foster DF, Wilkey SA, Van Rompay MI, et al. The use of complementary and alternative therapies to treat anxiety and depression in the United States. American Journal of Psychiatry. 2001;158(2):289-94.
14. Jorm AF, Christensen H, Griffiths KM. The impact of beyondblue: the national depression initiative on the Australian public’s recognition of depression and beliefs about treatments. Australian and New Zealand Journal of Psychiatry. 2005;39(4):248-54.
15. Christensen H, Batterham PJ, Grant JB, Griffiths KM, Mackinnon AJ. A population study comparing screening performance of prototypes for depression and anxiety with standard scales. BMC medical research methodology. 2011;11(1):154.
16. van Beljouw I, Verhaak P, Prins M, Cuijpers P, Penninx B, Bensing J. Reasons and determinants for not receiving treatment for common mental disorders. Psychiatric Services. 2010;61(3):250-7.
17. Crum RM, Cooper-Patrick L, Ford DE. Depressive symptoms among general medical patients: prevalence and one-year outcome. Psychosomatic medicine. 1994;56(2):109-17.
18. Cuijpers P, Beekman ATF, Smit F, Deeg D. Predicting the onset of major depressive disorder and dysthymia in older adults with subthreshold depression: a community based study. International journal of geriatric psychiatry. 2006;21(9):811-8.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
7
General Discussion | 143
19. Cuijpers P, Smit F, Willemse G. Predicting the onset of major depression in subjects with subthreshold depression in primary care: a prospective study. Acta Psychiatrica Scandinavica. 2005;111(2):133-8.
20. Eaton W, Badawi M, Melton B. Prodromes and precursors: epidemiological data for primary prevention of disorders with slow onset. American Journal of Psychiatry. 1995;152:967-72.
21. O’Connell ME, Boat T, Warner KE. Preventing Mental, Emotional, and Behavioral Disorders Among Young People:: Progress and Possibilities: National Academies Press; 2009.
22. Mojtabai R, Olfson M, Mechanic D. Perceived need and help-seeking in adults with mood, anxiety, or substance use disorders. Archives of General Psychiatry. 2002;59(1):77-84.
23. Cuijpers P, Smit F. Subthreshold depression as a risk indicator for major depressive disorder: a systematic review of prospective studies. Acta Psychiatrica Scandinavica. 2004;109(5):325-31.
24. APA. DSM 5: American Psychiatric Association; 2013.25. Smit F. Factsheet Prevention: Preventing Depression2007 29-12-2014:[4 p.]. Available
from: http://www.trimbos.nl/webwinkel/productoverzicht-webwinkel/preventie/af/~/media/files/gratis%20downloads/af0426%20lsp%20factsheet%20preventing%20depression.ashx.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
144 | Chapter 7

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
S
Summary | 145
Summary
One of the most common and debilitating disorders is depression. Its impact on daily life and society is enormous, with suicide (attempts) as an extreme outcome. Therefore, preventing or delaying the onset of depression is important. Prevention can be divided into three types; (1) universal prevention, which targets the entire population, (2) selective prevention, which targets specific subgroups within the population who are considered at risk due to common characteristics (e.g. traumatic events, poverty, etc), (3) indicated prevention which targets people who suffer from early stages or symptoms of depression (e.g. people with subclinical depression).
Subclinical depression is seen as a prodromal phase of depression and the best predictor of major depression, hence people who report subclinical depressive symptoms are at high risk of developing depression. There are several ways to define subclinical depression (1) a score above a threshold on a screening instrument without meeting the diagnostic criteria for major depression according to the DSM-V or (2) having a depressed mood accompanied by additional symptoms, but not as severe or as many as the DSM-V criteria for major depression. Subclinical depression is common and causes significant impact on daily functioning while at the same time creating a large burden for the society. In the Netherlands it is estimated that approximately 7.5% of the general population suffers from subclinical depression.
Preventing the onset of depression in people that are at high risk can significantly lower the incidence of depression. As subclinical depression is consistently found as the best predictor of depression, the focus of this thesis was on people who already reported depressive symptoms, but failed to meet criteria of a depressive disorder according to the DSM-IV and was, therefore, focused on indicated prevention. Benjamin Franklin’s famous words: “An Ounce of Prevention is worth a Pound of Cure” might particularly be true in people at high risk. This thesis aimed to provide insight into help-seeking behaviour and onset of depression in people with subclinical depression.
Chapter 1 presents the general introduction. The definition of subclinical depression, help-seeking and onset of depressive disorders are discussed as well as the outline and scope of this thesis.
Chapter 2 shows that preventive interventions are effective in lowering the incidence of depressive disorders with 21%. There were no difference between types of prevention. However, research on universal prevention is scarce. The numbers need to treat (NNT) in order to prevent one new case of depression was 20. Although there is no norm to indicate a high or low NNT, 20 seems to be an acceptable number. Especially, taking into account the impact depressive disorders have on social, economic and physical life.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
146 | Chapter 7
Chapter 3 provides reasons and determinants of (not) seeking help in people with subclinical depression. Three groups of people were identified; (1) people that reported a met need (e.g. had received care), (2) people that reported an unmet need (e.g. people reported having a need for care, but not receiving any care), (3) people who reported no perceived need (e.g. people indicated not to be willing to participate in preventive interventions). Many people (40%) did not perceive a need for care, because they did not experience symptoms, felt they were able to solve problems on their own or were able to mobilize their own support. These people reported lower scores on neuroticism and were older compared to people with a met need. Although not everyone with subclinical depression might be in need of care, a significant number of people (33%) indicated an unmet need for care. Increasing our understanding of barriers to help-seeking in this group is extremely important to be able to ensure that people who perceive a need for care, receive that care.
Chapter 4 describes how well people can identify depression and anxiety symptoms in themselves or, in other words, insight into their symptoms. Most research has focused on how well people are able to identify these disorders in other people using so called ‘vignette studies’. It is important to know whether or not people recognize their own symptoms, since this is one of the primary incentives to seek help. Although most people seemed to be able to correctly identify their symptoms, a significant number of people tends to underestimate their symptoms. This was associated with higher personal stigma, being separated or divorced, and younger age. Lowering stigma might improve people’s help-seeking.
Chapter 5 examined people’s attitude towards the available care. Mental health care can be found in a variety of settings; professional (e.g. professional care), family or friends (e.g. informal help), or within oneself (e.g. self-reliance). Research has shown that not everyone is in need of care, however the help-seeking rates are significantly lower than the number of people that is expected to develop full-blown depression. What people’s beliefs are about care is an important determinant of how they will cope with their symptoms. Positive attitude towards professional care was associated with being male, younger age, higher mastery, and easy accessibility to professional care. Positive attitudes towards informal help was associated with unemployment and higher mastery. Older age, less accessibility to professional care and lower mastery is associated with a more positive attitude towards being self-reliant. Attitudes at baseline were all associated to their corresponding attitude at follow-up. Remarkably, our results show that people who think they should keep problems to themselves report lower control over their lives. This might be due to the problems being too internalized to be able to talk about them or not believing that discussing these problems could be effective.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
S
Summary | 147
Chapter 6 reports on the onset of depressive and anxiety disorders in people with subclinical depression and what factors predicted the onset. Between baseline and follow-up, 22% met the criteria for a depressive disorder. At baseline, 24% suffered from a comorbid anxiety disorders. On the other hand, most respondents (76%) did not suffer from a comorbid anxiety disorder at baseline. Figure 1 shows the development of anxiety and depression in people with and without a comorbid anxiety disorder at baseline.
161
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Although predicting depressive disorders (or anxiety disorders) in people with
subclinical depression remains difficult, the findings in this thesis show that lifetime history of
depression predicts if someone will develop a depressive disorder within a year. The onset of
anxiety disorders is predicted by higher severity of symptoms as reported on our screening
instrument. Increasing insight into predictors of depression and anxiety is important as it gives
professionals the opportunity to make preventive care more feasible, tailored and attuned to
people that need it the most.
Subclinical depression (n = 106; 76.3%)
Depressive disorder (n = 22; 20.8%)
Anxiety disorder (n = 9; 7.1%)
Comorbid depression and anxiety (n = 6; 5.7%)
No depression or anxiety (n = 69; 65.1%)
Sample (n = 139
Depressive disorder (n = 9; 27.3%)
Anxiety disorder (n = 11; 33.3%)
Subclinical depression and anxiety disorder (n = 33; 23.7%)
Comorbid depression and anxiety (n = 5; 15.2%)
No depression or anxiety (n = 8; 24.2%)
Figure 1. Flowchart of diagnosis within a year in respondents with and without anxiety disorders at baseline
Although predicting depressive disorders (or anxiety disorders) in people with subclinical depression remains difficult, the findings in this thesis show that lifetime history of depression predicts if someone will develop a depressive disorder within a year. The onset of anxiety disorders is predicted by higher severity of symptoms as reported on our screening instrument. Increasing insight into predictors of depression

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
148 | Chapter 7
and anxiety is important as it gives professionals the opportunity to make preventive care more feasible, tailored and attuned to people that need it the most.
Chapter 7 summarizes the main findings and discussed suggestions for future research. Furthermore, the importance of these findings for policy as well as clinical practice are discussed.
Participation rates in preventive interventions for depression are low across many countries, even though these interventions have shown to be effective. The Netherlands has a unique mental health care system in which preventive care is widely available to everyone at little to no costs, however the participation rates are still very low. The results of this thesis expand on previous research on predicting the onset of depression by examining need for care, help-seeking, and the onset of depressive disorders in people who are at high risk of developing a depressive disorder.
The results suggest that although it is difficult to predict who will develop a depressive or anxiety disorder, it is important to take severity of symptoms and lifetime history of depression into account. Furthermore, not all cases of depressive symptoms might convert into a depression, but mental health institutions, municipal health services and government officials should focus on providing care to people that report an unmet need. People are capable of correctly identifying their symptoms, however people that are younger, divorced or separated, and report higher stigma are more likely to underestimate their symptoms. This might lead to delayed help-seeking and worsening symptoms. Therefore, lowering stigma, especially in younger people or people that are divorced or separated, is important.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
S
Samenvatting (summary in Dutch) | 149
Samenvatting (summary in Dutch)
Één van de meest voorkomende en slopende ziektes is depressie. De impact op het dagelijks functioneren en op de samenleving is enorm, waarbij de meest extreme consequentie suïcide is. Het voorkomen of verlaten van het ontstaan van een depressie is daarom van groot belang. Dit kan bereikt worden door preventie. Er zijn 3 typen preventie: (1) universele preventie, waarbij op de gehele populatie gemikt wordt, (2) selectieve preventie, waarbij alleen specifieke groepen mensen worden benaderd die bepaalde risicofactoren gemeen hebben (bijvoorbeeld traumatische gebeurtenissen, armoede, enz.), (3) geïndiceerde preventie, waarbij alleen gekeken wordt naar mensen die zich in een vroeg stadium van depressie bevinden of alleen symptomen van depressie vertonen, maar nog niet voldoen aan de criteria voor depressie (ook wel subklinische depressie).
Subklinische depressie wordt gezien als een prodromale fase van depressie en daarmee ook als de beste voorspeller op het ontwikkelen van een depressie. Mensen met een subklinische depressie vormen daarom een hoog-risico groep op het krijgen van een depressie. Er zijn verschillende manieren om subklinische depressie te operationaliseren; (1) een score boven een afkapwaarde op een screeningsinstrument, zonder dat voldaan wordt aan de DSM-V criteria voor depressie of (2) het hebben van een sombere stemming samen met andere symptomen, waarbij dit er minder zijn in aantal en ernst vergeleken met de DSM-V criteria voor een depressie. Subklinische depressie komt vaak voor en heeft, net als depressie, grote impact op het dagelijks leven en de maatschappij. Naar verwachting zijn er in Nederland 7.5% mensen, in de algemene populatie, die lijden aan subklinisch depressieve symptomen.
Het voorkomen van depressie in mensen die een verhoogd risico hebben op het ontwikkelen van een depressie is een goede eerste stap in het verlagen van de incidentie (nieuwe gevallen) van depressie. Subklinische depressie is in de literatuur consistent aangetoond als beste voorspeller voor het ontwikkelen van depressie. Dit proefschrift heeft zich daarom gericht op mensen die al depressie symptomen rapporteerden, maar niet voldeden aan de DSM-IV criteria voor een depressie diagnose en daarmee dus op geïndiceerde preventie. Hiermee komen de bekende woorden van Benjamin Franklin: “An Ounce of Prevention is worth a Pound of Cure” wellicht tot zijn recht. Het doel van dit proefschrift was om meer inzicht te krijgen in het hulp-zoek gedrag en het ontstaan van depressie in mensen met subklinische depressie.
Hoofdstuk 1 bevat een algemene introductie tot het onderwerp. Hierin wordt de definitie van subklinische depressie benoemd en wordt de literatuur omtrent hulp-zoek gedrag en preventie besproken.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
150 | Chapter 7
Hoofdstuk 2 beschrijft de effectiviteit van preventieve cursussen (of interventies). De incidentie blijkt met 21% verlaagt te worden wanneer men preventieve interventies volgt. Er was geen verschil tussen de verschillende typen preventie, maar dit is wellicht beïnvloedt doordat onderzoek naar universele preventie schaars is. Het aantal mensen dat behandeld moet worden om 1 nieuw geval van depressie te voorkomen (NNT) is 20. Er is geen literatuur beschikbaar over wat hoge of lage NNT’s zijn, maar gezien de gevolgen van depressie op het leven, zowel economisch, sociaal, als fysiek lijkt 20 een acceptabel aantal.
Hoofdstuk 3 ligt de redenen en factoren toe om (niet) deel te willen aan preventieve cursussen. Er werden 3 groepen mensen geïdentificeerd; (1) mensen die hulp hebben gekregen (vervulde behoefte), (2) mensen die aangeven wel hulp te willen ontvangen, maar dit niet hebben gekregen (onvervulde behoefte), (3) mensen die aangeven geen behoefte aan hulp te hebben (geen behoefte). Bijna de helft van de mensen (40%) gaf aan geen behoefte aan zorg te ervaren. Zij gaven aan geen symptomen te ervaren, in staat te zijn om de problemen zelf op te lossen, of zelf steun te vinden in de eigen omgeving. Mensen die geen behoefte aan zorg rapporteerden scoorde lager op neuroticisme en waren ouder in vergelijking tot mensen die een vervulde behoefte rapporteerden. Hoewel niet iedereen met subklinische depressie hulp nodig heeft, blijkt een belangrijk deel (33%) van de mensen een onvervulde behoefte te ervaren. Een groter begrip creëren over het hulp-zoek gedrag in deze groep mensen is belangrijk zodat de mensen die aangeven hulp nodig te hebben en te willen ontvangen, dit ook daadwerkelijk ontvangen.
Hoofdstuk 4 beschrijft hoe goed mensen eigenlijk zijn in het identificeren van (symptomen van) depressie en angst bij henzelf. Het overgrote deel van de literatuur heeft zich gericht op hoe goed mensen depressie kunnen herkenning in anderen door middel van zogenaamde “vignette” studies. Dit zijn studies die fictieve personen omschrijven met en zonder depressie en vragen mensen dan om te identificeren welk fictief persoon wel en welke geen depressie hebben. Ook heeft onderzoek zich gericht op de vergelijking tussen het herkennen van symptomen bij mensen zelf in vergelijking tot wat anderen (vrienden, partner, familie) zien bij die persoon. Het is echter belangrijk om te weten hoe goed mensen het bij zichzelf kunnen herkennen, omdat dit één van de sterkste redenen is om hulp te zoeken. Hoewel de meeste mensen goed in staat lijken te zijn om de symptomen te identificeren bij zichzelf, is er een belangrijke minderheid die dit kan. Deze mensen onderschatten de symptomen die zij hebben. Dit was geassocieerd met meer persoonlijk stigma, gescheiden zijn, en een jongere leeftijd. Het verlagen van stigma bij de mensen lijkt dus belangrijk en zou kunnen zorgen voor beter hulp-zoek gedrag.
In hoofdstuk 5 werd onderzocht hoe mensen tegen mentale gezondheidszorg aankeken. Mentale gezondheidszorg kan onderverdeeld worden in verschillende vormen:

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
S
Samenvatting (summary in Dutch) | 151
professionele zorg, informele zorg (bijvoorbeeld vrienden of familie) en de overtuiging dat men psychische problemen voor zichzelf houdt of zelfvoorzienend. Onderzoek heeft aangetoond dat niet iedereen hulp nodig heeft, maar de hoeveelheid mensen die wel hulp zoekt is drastisch lager dan de hoeveelheid die uiteindelijk een depressie ontwikkeld (en die dus baat hadden gehad bij hulp).Hoe men tegen zorg aankijkt (attitude) is bepalend in hoe zij omgaan met problemen. Mannen, jongere leeftijd, hogere controle op het leven, en makkelijke toegankelijkheid tot zorg leiden tot een positieve attitude ten opzichte van professionele zorg. Daarentegen blijken oudere leeftijd, lagere controle op het leven en mindere toegankelijkheid tot zorg samen te hangen met een positievere attitude ten opzichte van zelfvoorzienend zijn. Het niet hebben van werk en hogere controle op het leven hangen samen een positievere attitude ten opzichte van informele hulp. De attitude die men aan het begin van de studie had bepaalde in hoge mate de attitude na 4 jaar. Opvallend was dat uit de resultaten bleek dat mensen die problemen liever voor zich houden een mindere mate van controle op het leven rapporteerden. Een mogelijke verklaring hiervoor is dat de problemen nog te veel geïnternaliseerd zijn en men er nog niet over kan praten of dat men denkt dat er over praten geen zin zal hebben.
Hoofdstuk 6 toont de ontwikkeling van depressie en angststoornissen in mensen met een subklinische depressie. Tussen de basismeting en het follow-up moment blijkt 22% van de mensen te voldoen aan de criteria voor depressie (unipolair en/of dysthymie). Bij de basismeting bleek een minderheid (24%) een comorbide angststoornis te hebben. Figuur 1 laat het ontstaan van depressie en angst zien in mensen met subklinische depressie en mensen met subklinische depressie en een comorbide angststoornis.
Hoewel het voorspellen van depressie en angststoornissen in mensen met subklinische depressie moeilijk blijft, laten de resultaten in dit proefschrift zien dat een levensgeschiedenis van depressie stoornissen een voorspeller is voor het opnieuw ontwikkelen van een depressie. De ernst van symptomen op het screeningsinstrument bleek het ontstaan van angststoornissen te voorspellen. Het vergoten van inzicht in welke factoren voorspellen of een depressie of angststoornis zal ontwikkelen is belangrijk, omdat dit preventie beter mogelijk maakt en kan helpen om de preventieve interventies aan te bieden en aan te passen aan mensen die er baat bij hebben.
Hoofdstuk 7 vat de resultaten samen en bespreekt de suggesties voor verder onderzoek. Daarnaast worden de implicaties voor de klinische praktijk en beleid besproken.
Overal ter wereld is de deelname aan preventieve interventies laag, ook al is aangetoond dat deze interventies effectief zijn. In Nederland is er een uniek gezondheidszorg stelsel waarin preventieve zorg in principe toegankelijk is voor iedereen tegen weinig tot geen kosten, maar ook in Nederland is de deelname bijzonder laag. Dit proefschrift vergroot de bestaande kennis en is een goede eerste stap om de behoefte aan zorg, het hulp-zoek

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
152 | Chapter 7
gedrag en het ontstaan van depressieve stoornissen in mensen die een hoog risico lopen beter te begrijpen.
168
kosten, maar ook in Nederland is de deelname bijzonder laag. Dit proefschrift vergroot de
bestaande kennis en is een goede eerste stap om de behoefte aan zorg, het hulp-zoek gedrag en
het ontstaan van depressieve stoornissen in mensen die een hoog risico lopen beter te
begrijpen.
Figuur 1. Flowchart van diagnoses na 1 jaar in mensen met en zonder comorbide angststoornis. De resultaten uit dit proefschrift tonen aan dat, hoewel het moeilijk blijkt om het ontstaan van
depressie te voorspellen, het belangrijk is om naar de ernst van symptomen en de
levensgeschiedenis van depressie stoornissen te kijken. Daarbij moet men zich bewust zijn van
het feit dat niet in alle gevallen de depressieve symptomen zich ontwikkelen tot een
depressieve stoornis. Het is echter wel belangrijk dat GGZ-instellingen, huisartsen, GGD-en en
Subklinische depressie (n = 106; 76.3%)
Depressieve stoornis (n = 22; 20.8%)
Angst stoornis (n = 9; 7.1%)
Comorbide depressie en angst stoornissen (n = 6; 5.7%)
Geen depressie of angst (n = 69; 65.1%)
Sample (n = 139
Depressieve stoornis (n = 9; 27.3%)
Angst stoornis (n = 11; 33.3%)
Subklinische depressie en angst stoornis (n = 33; 23.7%)
Comorbide depressie en angst stoornissen (n = 5; 15.2%)
Geen depressie of angst (n = 8; 24.2%)
Figuur 1. Flowchart van diagnoses na 1 jaar in mensen met en zonder comorbide angststoornis.
De resultaten uit dit proefschrift tonen aan dat, hoewel het moeilijk blijkt om het ontstaan van depressie te voorspellen, het belangrijk is om naar de ernst van symptomen en de levensgeschiedenis van depressie stoornissen te kijken. Daarbij moet men zich bewust zijn van het feit dat niet in alle gevallen de depressieve symptomen zich ontwikkelen tot een depressieve stoornis. Het is echter wel belangrijk dat GGZ-instellingen, huisartsen, GGD-en en de overheid zich inzetten om zorg te leveren aan mensen die een onvervulde behoefte aan zorg rapporteren. Mensen zijn over het algemeen goed in staat om symptomen in zichzelf te identificeren, maar jonge mensen, gescheiden mensen en mensen die meer stigma ervaren hebben een grotere kans om hun symptomen te

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
S
Samenvatting (summary in Dutch) | 153
onderschatten. Dit kan leiden tot uitstel in het zoeken van hulp. De kans is namelijk groot dat deze mensen pas hulp zoeken wanneer de symptomen ernstiger worden. Het verlagen van stigma, met name in jonge mensen of mensen die gescheiden zijn, is belangrijk.


Part VI: Dankwoord/Acknowledgments

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
156 | Part VI

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
D
Dankwoord - Acknowledgments | 157
Promoveren is altijd een samenwerking. Ik heb tijdens mijn promotie samengewerkt met en hulp gehad van veel verschillende mensen die ik in dit hoofdstuk graag wil bedanken.
Allereerst wil ik de deelnemers aan mijn project bedanken. Zonder jullie was dit proefschrift er niet geweest. Daarnaast wil ik mijn (co)promotoren bedanken. Pim, jij hebt mij de kans geboden om te promoveren op één van de allermooiste projecten (ooit)! Jij hebt mij dan alle ruimte gegeven om te leren en te groeien als onderzoeker, maar ook als persoon. Bedankt daarvoor. Aartjan en Jan, jullie wil ik enorm bedanken voor alle overleggen en sparmomenten. Op de één of andere manier kwam ik altijd met nog meer enthousiasme over mijn project en artikelen bij jullie vandaan. Ik bewonder jullie passie voor onderzoek, maar bovenal jullie kunde om het beste uit onderzoekers te halen. Annet, ik heb zo ontzettend veel van jou geleerd. Jij hebt mij geleerd wat het betekent om een onderzoeker te zijn en extra kritisch te zijn op jezelf en je werk. Bedankt voor jouw geduld en verhelderende feedback! Ik heb daarnaast ontzettend genoten van onze sparmomenten, discussies, en gesprekken over alledaagse dingen. Tevens wil ik de leescommissie; prof. dr. Annemieke van Straaten, prof. dr. Robert Schoevers, prof. dr. Terry Brugha, prof. dr. Hein de Vries, prof. dr. Clemens Hosman en dr. Els Dozeman bedanken voor het lezen en beoordelen van mijn proefschrift.
Mijn project was een logistieke puzzel waarbij ik heb samengewerkt met verschillende GGD-en en GGZ-instellingen in Nederland. Ik wil daarom heel graag een aantal mensen bedanken voor hun (tomeloze) inzet: Henriëtte, Jessie, Johan, Jessica, Roelien, Anne-Marie, Mhamed, Marieke, en Clarien. Daarnaast ben ik dank verschuldigd aan de masterstudenten Klinische Psychologie die hebben geholpen bij de dataverzameling door het afnemen van diagnostische interviews. Ik wil met name Reen en Melany ontzettend bedanken voor de toewijding, energie en tijd die zij hebben gestoken in de logistiek en training omtrent de afname van deze interviews. De database is ontwikkeld in samenwerking met GGZinGeest en daarvoor wil ik Ho Ming, Denise en Jonathan bedanken.
Alle collega’s van de afdeling Klinische Psychologie wil ik bedanken voor de momenten bij ‘het zitje’, de borrels en de hulp bij statistiek, schrijven of het oplossen van andere ‘uitdagingen’. Johan, jou wil ik in het bijzonder bedanken, voor je eindeloze geduld als er weer eens een afspraak met 10 agenda’s gepland moest worden of als ik een formulier verkeerd had ingevuld. Furthermore, I would like to thank my ‘colleagues’ at the NIHMR at ANU. Kathy, thank you for giving me the opportunity to visit. A special thanks to Bregje, John, Fiona and BJ for all the great off-work experiences, there was never a dull moment! Fiona and Jacqui, thank you for putting up with me for 3 months. Ook wil ik

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
158 | Part VI
de beste (oud)roomies ooit bedanken; Anke, Heleen, Jessica, Willemijn en Lisette. Ik kon altijd bij jullie mijn ervaringen en mening ventileren, maar bovenal bedankt voor alle niet werk gerelateerde gesprekken.
Daarnaast ben ik een heleboel andere mensen dank verschuldigd, omdat de afleiding waar jullie voor hebben gezorgd essentieel was om het plezier te behouden en mijn werk goed te kunnen doen. Mijn teamies wil ik bedanken dat ik me het afgelopen jaar ‘asociaal’ heb mogen gedragen en jullie me dit niet kwalijk hebben genomen. Bedankt dat ik mijn hoofd elke maandag en woensdag heb mogen “leeg trainen”. Daphne, Lukas, Kalynda, Eva, Melinde, Hanneke, Frank, en Brian bedankt voor al jullie etentjes, uitjes, high-tea’s, sportmomenten en gesprekken. Ze zijn essentieel geweest om niet aan werk te kunnen en hoeven denken. A special shout-out to Narda, Carlijn en Annemiek. Ladies, what can I say; you rock! Ik hoop dat wij nog heel veel (cocktail)dinners, high-teas, lunches, spelletjesavonden, etc gaan hebben. Jullie geven mijn leven de nodige balans.
Anke en Jessanne. Ik kan me geen betere paranimfen wensen! Anke, jij bent na 1,5 jaar mijn partner in crime geworden en ik wil je danken voor je inzet. Elk project heeft zijn hobbels, maar ik heb het altijd fijn gevonden om deze samen met jou glad te strijken. Jes, mijn awesome BFF, wat hebben wij al veel meegemaakt samen! Ik weet niet waar ik moet beginnen, maar ik ben zo ontzettend vereerd dat jij mijn paranimf wilt zijn. Bedankt dat jij nog steeds mijn tegenpool bent en me hebt geleerd dat dingen ook anders benaderd kunnen worden. Bedankt ook voor alle gekke, hilarische en emotionele momenten. Ik vind het heel bijzonder dat wij dit soort momenten samen kunnen delen.
Pap en mam, bedankt dat jullie mij alle kansen hebben geboden om dit te kunnen en mogen doen. Bovenal heb ik aan jullie de karaktereigenschappen te danken die er voor hebben gezorgd dat ik dit proefschrift binnen 4 jaar heb afgerond, doorzettingsvermogen met een gezonde dosis eigenwijsheid. Het is mijn beste prestatie tot nu toe. Ward, kleine “Grote” broer; zet hem op, dan ben je over 2 jaar ook zo ver. Hopelijk blijven we elkaar motiveren om beter te zijn. Dave, “kleinste” broertje, dank voor je filosofische koffietjes op de VU. Het was heerlijk om met je te kunnen discussiëren en verhalen uit te wisselen over verre reizen en ervaringen. Josta (Jos, Josti-tosti), heerlijk ‘klein’ zusje van me! Blijf wie je bent, ik geniet van al je avonturen en (herkenbare) onhandigheid. Ik had me geen leuker zusje kunnen wensen (en ben nog steeds blij dat je geen broertje bent). Agnes, dank voor jouw frisse blik en je zachte aard. Ik heb veel van je geleerd. Marie-Claire, merci beaucoup for always making me feel welcome, in Paris or at my Dad’s. Wim en Annelies, mijn 2e thuis, bedankt voor jullie warmte, liefde en leuke discussies. Er zijn zoveel momenten die ik nooit zal vergeten, van Canasta tot “chatten” op de zolder. Joeri, dank voor jouw feedback, expertise en creatieve geest bij het ontwikkelen van de omslag.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
D
Dankwoord - Acknowledgments | 159
Mijn ‘schoonfamilie’; bedankt dat ik me altijd welkom voel bij jullie en ik altijd bij jullie terecht kan. Jullie staan altijd voor mij/ons klaar en ik ben jullie daar ontzettend dankbaar voor. Cora, Tobias, Laura, Emma, Michiel, Jet, Tiny, John, Diede, en Nikee bedankt voor de fantastische vakanties. Ze hebben mijn wereld en relativeringsvermogen vergroot. Schoonzusjes en -nichtjes, dank voor jullie humor en wii-dance avonden. Ze hebben voor de broodnodige ontspanning gezorgd. Mette, soms is het heel prettig om weer even kind te kunnen zijn. Bedankt dat jij mijn excuus kunt zijn!
Last, but definitely not least, Ruben. Je bent mijn rots in de branding en jij zorgt voor richting aan en ontspanning in mijn leven. Ik ben en zal nooit een rustig iemand zijn, maar jij geeft mij altijd de tijd en ruimte die ik nodig heb om uit te razen. Jij was er altijd met jouw liefde, geduld en zorgzaamheid. Ook, of juist, op momenten met veel stress en/of weinig tijd voor jou. Bovenal prijs ik mezelf gelukkig dat ik iemand heb gevonden die mij stimuleert om mijn (individuele) dromen na te jagen, zelfs als daarbij jouw wensen/dromen op een tweede plek lijken te komen. Ik zal je nooit duidelijk kunnen maken hoe dankbaar ik je daarvoor ben en hoeveel liefde ik voel voor jou, maar mijn leven is zoveel mooier en leuker met jou samen. Ik kan en wil me geen toekomst voorstellen zonder jou. Ik hou van jou!


Part VII: About the author

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
162 | Part VII

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
A
About the author | 163
Kim van Zoonen was born on February 25, 1984 in Amsterdam, the Netherlands. She grew up in Bilthoven and attended high school there at ‘Het Nieuwe Lyceum’. In 2002 she started her bachelor in psychology at Leiden University. She received her master’s degree Clinical Psychology in 2006. Her hunger and curiosity to learn more on disorders, psychological wellbeing and physical illness made her decide to enroll for the 2-year master Medical Psychology at Tilburg University. She received her degree in 2009. Preferring to gain more experience in logistically challenging work she started as an inter-agent. However, after a short while she realized her passion lies in conducting research which made her pursue a PhD. Her interests lie in public (mental) health, depression and psychological wellbeing. Her PhD-project examined the low participation rates in preventive interventions for depression. This epidemiologic cohort study provided her with the scientific and logistic challenges she was looking for. The project was supervised by Pim Cuijpers (VU), Aartjan Beekman (GGZinGeest), Jan Smit (GGZinGeest), and Annet Kleiboer (VU) and resulted in the current thesis.


Part VIII: List of Publications

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
166 | Part VIII

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
L
List of Publications | 167
Published:Van Zoonen, K., Buntrock, C., Ebert, D. D., Smit, F., Reynold III, C. F., Beekman, A. T. F., Cuijpers, P. Preventing the onset of major depressive disorder: A meta-analytic review of psychological interventions. International journal of Epidemiology. 2014; 1-13.
Van Zoonen, K., Kleiboer, A. M., Beekman, A. T. F., Smit, J. H., Boerema, A. M., Cuijpers, P. Reasons and determinants of help-seeking in people with a subclinical depression. Journal of Affective Disorders. 2014; 173; 105 – 112. Doi: 10.1016/j.jad.2014.10.062.
Under Review:Van Zoonen, K., Crisp, D., Griffiths, K. Concurrence between self-assessment of anxiety and depression and actual scores on a screening instrument for anxiety and depression. Under review of Journal of Affective Disorders.
Van Zoonen, K., Kleiboer, A. M., Cuijpers, P., Beekman, A. T. F., Smit, J. H., Verhaak, P., Penninx, B. Determinants of attitudes towards professional mental health care, informal help, and self-reliance in people with subclinical depression. Under review of Social Psychiatry & Psychiatric Epidemiology.
Van Zoonen, K., Kleiboer, A. M., Beekman, A. T. F., Smit J. H., Boerema A. M., Dijkshoorn H., Cuijpers, P. Predictors of the conversion of subclinical depressive symptoms to major depressive and anxiety disorders in the community. Under review of Depression & Anxiety.
Boerema, A. M., Kleiboer, A. M., Beekman A. T. F., van Zoonen, K., Dijkshoorn, H., Cuijpers, P. Determinants of help-seeking behavior in depression: a cross-sectional study. Under review of BMC Psychiatry.
In Preparation:Van Zoonen, K., Kleiboer, A.M., Boerema, A. M., Smit, F. Health care utilization and costs in people with depression and subclinical depression.
Boerema, A.M., van Zoonen, K., Kleiboer, A.M. Validation of the Dutch version of the Depression Stigma Scale.
Other publications:Van Zoonen, K., Boerema, A. M., Kleiboer, A. M. GGD Rapportage: “Hulpzoeken bij mensen met subklinische en klinische depressie onder de Nederlandse bevolking 2014”.