Proefschrift Martin
223
Counseling for prenatal anomaly screening
-
Upload
nicole-nijhuis -
Category
Documents
-
view
220 -
download
0
description
Â
Transcript of Proefschrift Martin

Counseling for prenatal anomaly screening
Counseling for prenatal anomaly screening
Uitnodiging
Counseling for prenatal anomaly screening
door
Amsterdam
Paranimfen



The study presented in this thesis has been performed within the department of Midwifery Science of the EMGO+ Institute for Health and Care Research, the VU Medical Center, and the AVAG Midwifery Academy Amsterdam Groningen in collaboration with NIVEL (Netherlands institute for health services research), Utrecht.
Financial funding by the AVAG is gratefully acknowledged.
Thesis, Free University, Amsterdam, the NetherlandsISBN/EAN: 978-94-6108-984-7
©Copyright 2015 Linda Martin, the Netherlands All rights reserved. No part of this book may be reproduced, stored in a retrieval system or transmitted in any form or by any means, without prior permission of the author.
Design cover: Ruben Timman, www.nowords.nlLayout: Gildeprint EnschedePrinted by: Gildeprint Enschede

VRIJE UNIVERSITEIT
Counseling for prenatal anomaly screeningParents’ perspectives,
midwives’ perspectives, andclient-midwife communication
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad Doctor aande Vrije Universiteit Amsterdam,
op gezag van de rector magnificusprof.dr. F.A. van der Duyn Schouten,
in het openbaar te verdedigenten overstaan van de promotiecommissie
van de Faculteit der Geneeskundeop maandag 15 juni 2015 om 13.45 uur
in de aula van de universiteit,De Boelelaan 1105
door
Linda Martin
geboren te Hoorn

promotoren: prof.dr. E.K. Hutton prof.dr. A.M. van Dulmencopromotor: dr. E.R. Spelten

Beoordelingscommissie:
prof.dr. M.C. Cornelprof.dr. H. Eideprof.dr. J.M.M. van Lithprof.dr. J. van der Veldenprof.dr. T. van der Weijdendr. M.P. Amelink-Verburg
Paranimfen:
Drs. F. MartinL. Martin
Voor mijn kinderen Aniek, Teun en Koen en voor alle aanstaande ouders


TABLE OF CONTENTS
Chapter 1 General introduction 9
Chapter 2 Prenatal counseling for congenital anomaly tests: 29 parental preferences and perceptions of midwife performance
Chapter 3 Midwives’ views on appropriate antenatal counseling for congenital 53 anomaly tests: do they match clients’ preferences?
Chapter 4 Introducing video recording in primary care midwifery for research 75 purposes: procedure, dataset, and use
Chapter 5 Antenatal counseling for congenital anomaly tests: an exploratory 95 video-observational study about client-midwife communication
Chapter 6 Midwives’ perceptions of communication during videotaped 119 counseling for prenatal anomaly tests: how do they relate to clients’ perceptions and independent observations?
Chapter 7 Exploring non-verbal communication of counselors during prenatal 145 counseling for congenital anomaly tests
Chapter 8 General discussion 163
Chapter 9 Summary & Samenvatting 191
List of publications 207Curriculum Vitae 211Dankwoord 215


Chapter 1General introduction
‘Om te zijn moet met eerst en vooral verantwoordelijkheid aanvaarden. Men moet een taak op zich nemen.’
A. de Saint-Exupéry

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
10

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
11
1“Yes, yes, [counseling should be] really a conversation. Not like hm ... it was a bit uh, too little attention was paid to it. I got that impression a little bit [because the midwife said:] Yes, you can do that, but yes, I do not really know what to tell you about this, we have a leaflet … and, well read that one.” (A client about her counseling needs).
This thesis is about the conversation between clients and midwives concerning prenatal anomaly screening in early pregnancy. In order to gain knowledge about counseling for prenatal anomaly screening in the Dutch, midwifery-led care context, we focused on two different aspects: 1) the perspectives on counseling of clients and of midwives, and 2) the actual communication between midwives and clients during prenatal counseling. Both aspects are brought together in chapter 6. Before introducing the relevance of investigating midwife prenatal counseling, we first explain the approach to prenatal screening in the Netherlands.
Prenatal anomaly screening
From a positive pregnancy test to considering prenatal anomaly screeningMost expectant parents are happy to discover that they are expecting a baby and probably search the internet for the next step [1]. The client website of the Royal Dutch Association of Midwives (KNOV) recommends that women make an appointment with a midwife for primary, prenatal midwifery led care as soon as they know they are pregnant. The website also recommends women to attend their first appointment together with their partner [2]. Coming together to this intake visit is important for several reasons, including the fact that during the appointment midwives take both clients’ and partners’ family history regarding inherited birth defects, and provide counseling for prenatal anomaly tests, with the aim to facilitate clients’ decision-making regarding whether or not to opt for prenatal anomaly screening [2-6]. For most couples, the decision whether to opt for anomaly screening or not is a decision couples want to make together, which underlines the importance to provide counseling to both of them, to make sure they both have the relevant information and support in making their decision [7,8]. As a result, when it comes to counseling for prenatal anomaly screening, partners are also midwives’ clients. In this thesis we consider both pregnant women and their partners as clients; their perspectives regarding counseling for prenatal anomaly screening is our first focus. Most women and their partners feel excited about their pregnancy but also a bit nervous about the first visit at their midwife [3,9]. At the end of this intake visit, or sometimes in a separate consultation, the midwife introduces the Dutch prenatal anomaly screening program, which aims to detect congenital anomalies in order to provide expectant parents with, if they choose to participate, reproductive choices [4]. Even the offering of the program is cause for parents to confront the fact that although most children are born with no diagnosed anomaly, in

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
12
every pregnancy there is a risk that the unborn child has a congenital anomaly [4]. As a result, some expectant parents may struggle to shift from their context of happily expecting a baby to talking about prenatal anomaly screening. The prenatal anomaly screening offer is timed in early pregnancy, because the first test can be completed around 12 weeks of gestation [10]. Because they have a ‘right not to know’ anything about prenatal anomaly tests, by about 10 weeks gestational age, clients need to make the first decision about prenatal screening: that is to decide whether they want any information about prenatal anomaly tests [11-13].
Dutch prenatal screening offerIf expectant parents accept the information offer about prenatal anomaly screening, the information process starts [14,15]. According to Van Agt et al. [16] expectant parents should get information about the available prenatal anomaly tests, the aim of these tests, medical information about the target anomalies and the prevalence of these anomalies. So, at the time of this study (data collection between 2010-2011), clients should have been informed that the Dutch prenatal screening program comprised two tests: 1) the Combined Test (CT) undertaken around 12 weeks gestational age to calculate a pregnancy related risk for Down Syndrome (trisomy 21) [4,10]; and 2) the Fetal Anomaly ultrasound Scan (FAS) done at around 20 weeks gestational age, to detect structural anomalies [4,10]. In January 2011, risk assessments for Edwards- (trisomy 18) and Patau syndrome (trisomy 13) were added to the CT. Since April 2014, the Non-Invasive Prenatal Test (NIPT) is also offered to clients who are identified to be at increased risk on the CT, defined as ≥1:200, or family history [4,17,18]. The NIPT is a blood-screening test for Down-, Edwards- and Patau syndrome [17].Regarding the target anomalies of the CT and NIPT, clients should be informed that children with Down syndrome have a decreased cognitive function, but that cognition can vary from normal or low intelligence to profoundly impaired. In addition certain complications and risks, such as congenital cardiac defects and ear, nose and throat defects, are higher among individuals with Down syndrome compared to the average population [19]. Clients should hear that children diagnosed with Edwards- and Patau syndrome show much more severe clinical manifestations than trisomy 21; only rarely do affected infants survive to one year of life [10]. Prevalence of Down-, Edwards- and Patau are respectively 1:500, 1:3000, and 1:6000 yearly [10,20].Further, clients should be informed about test procedures, the meaning of test results (screening versus diagnostic), including detection percentages, options after a positive screening outcome and the costs [16]. Thus, clients will be told that the CT comprises a blood test and ultrasound and is, like the FAS, considered harmless for both mother and unborn child [10]. For the client, the CT results indicate personal risk of a trisomy, which will indicate if follow-up prenatal diagnostic is indicated based on a cutoff value ≥ 1:200 [4]. The test result of the FAS can be divided into three main categories to make clients clear what they can

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
13
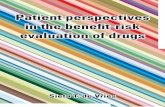
1expect; outcome 1, no anomaly is detected, but clients have to know that, for instance, 25-50% of heart defects are missed; outcome 2, a sole marker is seen that is of no known clinical significance; or outcome 3, a structural anomaly is seen or suspected [10]. When clients receive a positive screening outcome of the CT and/or FAS, and/or NIPT, clients can choose to follow up prenatal anomaly screening by a diagnostic test. Diagnostic, invasive tests are only offered on indication. In addition to positive screens, at the time of this study, maternal age ≥ 36 years of age and family history of birth defects were indications for direct access to diagnostic anomaly tests [12,21]. The FAS and, if indicated, diagnostic tests were free of charge, whereas the CT had to be paid for by women younger than 36 years of age [12,22].Diagnostic, prenatal anomaly tests comprise an advanced ultrasound, chorion vilus sampling or amniocentesis, aiming to confirm the outcome of screening by providing a diagnosis. Parents should be informed that chorion vilus sampling and amniocentesis are associated with a miscarriage risk of about 0.5%, because the procedures involve the insertion of a needle into the uterus [10,23-25]. Finally, parents ought to be informed about the possibilities for action after diagnostic tests. Such information should comprise the two options continuing or terminating the pregnancy if an unborn child is diagnosed with an anomaly, treatment options and legal terms for termination of the pregnancy [16] (see flowchart Dutch prenatal anomaly test offer). The right (not) to knowThe above information is, in a nutshell, what expectant parents might hear during one of the first visits with their midwife. It is up to the pregnant women and her partner to decide whether to opt for anomaly screening or not and subsequently, whether or not to take a further diagnostic path. In other words: prenatal anomaly screening and diagnosis is offered using an opt-in approach; expectant parents have the right (not) to know and are thus encouraged to make their own reproductive choices based on reliable information [3,11,12,14]. To make a personal, reproductive choice is not always perceived as easy by clients [26,27]. The offer of prenatal anomaly screening seems to be an answer to one of clients’ main concerns, that is, the wellbeing of their unborn child. At the same time the prenatal screening offer forces clients also to answer moral questions such as ‘how welcome are children with an anomaly in my world, my life, my family?’ or ‘what does this pregnancy mean to me?’ or ‘how do I feel about the risk of a miscarriage in relation to my wish to know that my child does not suffer from a congenital anomaly?’ [27-33]. Ultimately, clients can be confronted with the question whether to continue the pregnancy or to terminate the pregnancy in case of a confirmed, congenital anomaly [4,27,33]. Furthermore, prenatal anomaly screening is becoming better known to the general public. Both to take or decline the offer can be challenging in the resulting context of societal expectations and reactions of family and friends [34,35,36]. Consequently, regardless of whether clients opt for anomaly test or not, the offer of prenatal

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
14
Rig
ht (
not)
to k
now
any
thin
g ab
out
pren
atal
ano
mal
y te
sts
Clie
nts
do n
ot w
ant t
o ge
t in
form
atio
n ab
out p
rena
tal
anom
aly
test
s. N
o co
unse
ling
Clie
nts
wan
t to
get i
nfor
mat
ion:
st
art p
rena
tal c
ouns
elin
g
Preg
nant
wom
en <
36
year
s of
age
:C
ombi
ned
Test
(C
T): a
bout
150
eur
o’s
Feta
l Ano
mal
y ul
tras
ound
Sca
n (F
AS)
: fre
ePr
enat
al d
iagn
ostic
s: o
nly
acce
ssib
le a
fter
a p
ositi
ve C
T (r
isk ≥1
:20
0)
Preg
nant
wom
en ≥
36
year
s of
age
:C
ombi
ned
Test
(C
T): f
ree
Feta
l Ano
mal
y ul
tras
ound
Sca
n (F
AS)
: fre
ePr
enat
al d
iagn
ostic
s: fr
ee
Rig
ht (
not)
to k
now
any
thin
g ab
out
even
tual
ano
mal
ies
with
in th
eir
unbo
rn c
hild
Clie
nts
decl
ine
the
CT
and/
or F
AS
and/
or p
rena
tal d
iagn
ostic
s. E
nd o
f co
unse
ling
for t
he d
eclin
ed te
st(s
)
No
cong
enita
l ano
mal
y:C
ontin
uatio
n of
the
preg
nanc
y
Dia
gnos
is o
f a c
onge
nita
l ano
mal
y:C
ontin
uatio
n of
the
preg
nanc
y O
R
term
inat
ion
of th
e pr
egna
ncy
Clie
nts
opt f
or C
T
Posi
tive
CT (
risk ≥1
:20
0):
No
furt
her i
nves
tigat
ions
Pren
atal
Dia
gnos
tic
Neg
ativ
e CT
(ris
k <1
:20
0):
Wom
en o
f all
ages
: No
furt
her i
nves
tigat
ions
W
omen
≥ 3
6 ye
ars
of a
ge: P
rena
tal D
iagn
ostic
Clie
nts
opt f
or p
rena
tal d
iagn
ostic
sC
lient
s op
t for
the
FAS
Neg
ativ
e FA
SN
o fu
rthe
r inv
estig
atio
ns
FAS
show
s a
sole
mar
ker:
No
furt
her i
nves
tigat
ions
FAS
show
s st
ruct
ural
ano
mal
y O
R
susp
icio
n of
the
pres
ence
of a
n an
omal
y:N
o fu
rthe
r inv
estig
atio
nPr
enat
al D
iagn
ostic
sO
nly
dire
ct a
cces
s fo
r wom
en ≥
36
year
s of
age
Acc
ess
for a
ll w
omen
END
STA
RT
END

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
15
1anomaly screening alone forces parents to make a difficult choice [26]. Such a difficult choice takes time. Clients might want to (re)read information leaflets, talk to important others, visit advised websites, use a web-based decision-clarification aid, or ask for a second visit to their midwife [4,37].If expectant parents choose to opt for prenatal screening, the midwife refers them to a provider of prenatal tests. Clients will receive the test result either by the provider of the test or by their midwife; in both cases midwives talk about the test results with the clients [4]. If prenatal anomaly diagnostic tests are to be considered, clients will receive counseling from professionals of one of the eight prenatal screening centers in the Netherlands [4].
Midwives as counselors
A new roleMidwives’ perspective on counseling for prenatal anomaly screening is another important focus of this thesis. Midwives provide primary maternity care to approximately 80% of the Dutch pregnant women and are consequently the designated counselors in these pregnancies [4,11,38]. In 2006, midwives provided 202,000 counseling consultations (pre- and post-test counseling) to about 160,000 pregnant women who started prenatal midwifery-led care [38,39]. It is unclear what these figures indicate in terms of the number of counseling sessions per client. The Dutch midwifery profession has evolved through, among other things, the continuous addition of tasks being added to midwives’ responsibilities [39,40]. This was probably especially challenging for midwives between circa 2000 and 2005, when there was a huge shortage of midwives in the Netherlands [41]. At the end of this period, in 2005, the KNOV published a new Professional profile of midwives, with a strong emphasis on client-centered care: “Within daily care, the midwife should find a balance between the expectations, needs, desires and the identity of the individual client and her own professional standards as a midwife” [42]. In order to give midwives more practical guidance, client-centered care was further specified in professional roles and tasks. One of these roles was the role of counselor, which is client-centered by nature [43]: “The midwife as a counselor guides the woman to be her best self (empowerment). She offers the client guidance in gaining insight into her own feelings and behavior and will equip and assist her in making (emotional) decisions. The midwife as a counselor is characterized by her openness, sincerity, respect, listening skills, conversation skills, empathy, and especially her non-directivity” [42].Although the role of counselor is relevant during conversations about preference sensitive decisions in general, Dutch midwives most often associate counseling with prenatal anomaly tests. This is understandable, since soon after the introduction of the new professional profile, in 2007, the task to provide prenatal counseling for anomaly screening and the role of being

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
16
a counselor became part of primary, prenatal midwifery-led care [12]. At the time of this study, the role of counselor was relatively new to midwives. Being a counselor requires the addition of other professional attitudes, associated knowledge and skills than midwives used to have. Midwives were familiar with the provision of information to clients, but not so much with empowering clients to make their own decision. To be oriented to the counselor role, all midwives were required to take a course in prenatal counseling for anomaly screening. This course is a prerequisite for offering prenatal counseling, for all midwives who graduated prior to 2007, at which time counseling became part of the educational requirements [4]. During a course about counseling for prenatal anomaly screening, information about relevant genetics, congenital anomalies, test characteristics and interpretation of test-results was offered as well as information and training regarding risk-communication and the competencies needed to facilitate decision-making in a non-directive, client-centered way while addressing moral and psychosocial issues [4,10]. The course for midwives about prenatal counseling for anomaly tests seem to be constructed in line with the international consensus about how counseling for preference sensitive choices, including prenatal anomaly screening, should be done.
Counseling for prenatal anomaly screening
A counseling modelIn a review, Meiser et al., [5] describe two models of genetic counseling, which are used in practice; the ‘teaching model’ and the ‘counseling model’. Within the ‘teaching model’, counselors focus on information-giving and education, because the information that is transmitted is often seen as very complex, extensive and difficult to understand. For instance, explaining the value of a medical risk assessment, the differences between screening and diagnosis, the variety of the abilities of children with Down syndrome, the huge diversity of anomalies that could be detected with the FAS, the eligibility to screening in the Dutch health care context and recently the introduction of the NIPT, make the information complex and difficult to understand. In the ‘teaching model’, counselors’ main goal is as a medical expert providing information in order to accurately educate their clients.Within the ‘counseling model’, the main goal is to promote informed-decisions and to facilitate psychosocial understanding of the personal risks and conditions that could be tested for. Within the ‘counseling model’, increasing the emotional well-being of clients is also seen as a crucial part of genetic counseling. The ‘counseling model’ has been described as a psychotherapeutic process in which the counselor listens carefully to the client’s story while asking client-centered questions; questions which follow and facilitate the clients’ lines of reasoning in giving personal sense to the prenatal screening offer [4,5,6,36,43-48]. In a critical review of empirical studies regarding genetic counseling, Meiser et al. [5] suggested a two function counseling model. This model comprises both ‘teaching’ and ‘counseling’ in order

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
17
1to enhance the key goal of genetic counseling; that is the facilitation of clients’ autonomous, informed decision-making [4].
A non-directive attitude and client-centered approachCounselors’ guidelines and policy statements have advised counselors to use a non-directive counseling attitude, which means a non-persuasive communication style while facilitating clients’ decision-making about prenatal anomaly screening [3,12,22,49,50] The rationale for the emphasis on a non-directive attitude was to remove the counselors’ personal views regarding a particular course of action, because the decision whether to opt for prenatal anomaly screening, or not, is preference sensitive: one course of action is not seen as better than another course of action [14,49,51,52]. Another core concept of genetic counseling is the use of a client-centered approach. Client-centered communication regarding the provision of information, that is the teaching component, focusses on tailoring the information to individuals’ preferences, knowledge, interests and concerns [3,53-55]. When client-centered communication is used to facilitate a client’s decision-making process, in the counseling function, counselors should follow the client’s lead, encourage the client to share their deliberations and help them to make a ‘decision-balance’, a personal list of pros and cons of prenatal anomaly tests [48,56]. As clients are, in the end, the expert regarding their concerns, values and preferences concerning the decisions at hand, counselors should take the role of an engaged professional guide [37,48].Recently, more and more authors point to the problems arising in practice from the use of a non-directive counseling approach; provision of information is always framed one way or the other and at least some clients seem interested to hear the opinion of the professional regarding whether they should opt for an anomaly test or not [8,50-52].
Perspectives of clients and midwives
Research on the development of guidelines about counseling for anomaly testing has shown that clients’ preferences and counselors’ views on appropriate counseling are relevant to incorporate in the ongoing development process of counseling guidelines [57,58]. At the time of this study research into clients’ preferences regarding counseling for prenatal anomaly screening and counselors’ views on appropriate prenatal counseling was minimal, although the two function counseling model seems to have been adapted within prenatal counseling for anomaly screening.
Clients: pregnant women and their partnersWith regard to the ‘teaching’ function of prenatal counseling for anomaly screening, most clients indicated that some balance between details and brevity was optimal, since the wide

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
18
range of options could led to confusion [59]. However, clients also feel a need for detailed, accurate information about the day-today symptoms that result from the anomalies that the unborn child could potentially be tested for, including information on potential suffering, and the potential quality of life for the child and his or her family [60,61]. Additional important aspects are the logistics of testing, follow-up if the test is positive, and options and resources if the child is affected with a disorder [59]. Clients seem to have mixed feelings about information stated with uncertainty and risks assessments, because the usefulness of risk assessments is not always clear to them [62,63]. Regarding the ‘teaching’ function, research shows that clients prefer information that is adapted to their social, ethnic and cultural background and provided in simple and accessible language, supported by written documents and photos [58,64,65]. During counseling, the client wants to be seen as an equal member of the team; a team in which care-providers know the limits of their knowledge and are willing to refer [58,61].Research has focused almost exclusively on the ‘teaching’ function of counseling. Limited attention has been given to clients’ preferences regarding the ‘counseling’ function, despite the fact that most clients do not want to be given ‘information only’, without guidance. The resulting lack of detailed and systematic insight into clients’ ‘counseling’ preferences is problematic, because within health care, optimizing client empowerment, health decisions, and health behavior requires tailored communication; that is, communication that is adapted to the preferences, interests, and concerns of the individual [3,43,53-66,67]. Furthermore, whereas pregnant women have been included in counseling research, their partners have rarely been. Because of the important role of partners in decisions around prenatal screening for anomalies, we viewed partners to also be midwives’ clients. Therefore, both pregnant women’s and their partners’ preferences regarding prenatal counseling for anomaly screening are investigated within this study.
Midwives’ perspectivesCounselors’ views on appropriate counseling are important to understand, because these views will reflect the way counseling is carried out in daily practice [6]. From the relatively little available literature it is known that genetic counselors in general, perceive the ‘teaching’ function as part of their role, but only a minority of counselors view also the ‘counseling’ function as part of their role [6]. With regard to the ‘teaching’ function, counselors primarily stressed the importance of informed consent while balancing the information that is given compared to the information that is withheld. Regarding the ‘counseling’ function, counselors struggle with directiveness versus non-directiveness. Some counselors admitted to provide ‘teaching’ and ‘counseling’ based on their own (predictably limited) experience, and gave advice based on the choices they themselves would make. This may led to a huge variety in counselors’ views about appropriate counseling and in daily practice of counseling [61,68,69].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
19
1Moreover, several researchers concluded that clients and counselors do have very different perspectives on appropriate counseling and value information and professional behavior, such as non-directiveness, differently [61,70]. These findings and the fact that they were found in a relative small sample of obstetric-, midwife-, nurse- and general genetic counselors underline the relevance to investigate midwives’ views on appropriate counseling and clients’ preferences in relation to each other.
Communication during counseling
Actual communication during counseling has been investigated in several studies among health care providers with diverse backgrounds, e.g. genetic counselors and cancer genetic counselors [6,71,72]. Studies focus on the provision of the two genetic and/or prenatal counseling functions, ‘teaching’ and ‘counseling’ in practice. Counseling has been shown to focus on ‘teaching’ and that more attention is needed for providing ‘counseling’ [6,71,73-77]. However, little research has been done to investigate real life communication during prenatal counseling for anomaly screening. Such information is relevant, since it is known that prenatal counseling does not always lead to informed decisions [75,78,79]. As a result, in practice, clients sometimes have to be counseled again once they are already in the room to have the ultrasound of the CT. This is problematic in some cases, when following the receipt of additional information, the clients appreciate the purpose of anomaly screening that they did not grasp earlier and determine just prior to the test being done, that they actually do not want to take the test. It might also indicate that more than one pre-test counseling consultation is needed. For instance, one session to exchange information and another to talk about clients’ questions and the decision whether to opt for screening, may be the best approach for some clients. For parents involved in prenatal testing, the today offer of pre- and post-test counseling might be too limited [37].
Study design
This study is embedded in the DELIVER study, a nationwide, multicenter cross-sectional study investigating the organization, accessibility and quality of primary midwifery led care in the Netherlands [80]. Seventeen of the 20 midwifery practices across the country that participated in the DELIVER study, participated in the present study. We studied client and midwife perspectives regarding appropriate prenatal counseling for anomaly screening. Furthermore, we made video recordings of midwife-client interactions during the prenatal intake visit to study prenatal counseling for anomaly screening by midwives in daily practice. The communication process was investigated by means of clients’ experiences, midwives’ self-evaluations and observations of the video recorded counseling consultations. We used a

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
20
mixed methods approach in order to gain knowledge about prenatal counseling by midwives based on multiple perspectives, positions, and standpoints, e.g. the standpoints of qualitative and quantitative research [81].
Perspectives of clients and midwivesAt the time of this study there was no measurement tool available to investigate clients’ preferences and experiences regarding prenatal counseling for anomaly screening. However, a commonly used measurement tool to measure the perspectives of clients, e.g. their preferences and experiences with care, is the QUOTE (QUality Of care Through the patient’s Eyes); a series of questionnaires adapted to a diverse range of healthcare contexts [67,82,83,84]. Each QUOTE-questionnaire consists of two parts. In part one, the pre-counseling questionnaire, clients are asked to what extent they consider aspects, related to the care they are about to receive, as important. In part two, the post-counseling questionnaire, clients are asked to evaluate the consultation regarding the same aspects of care as mentioned in the pre-counseling questionnaire. So, the QUOTE-questionnaires can be used to both investigate clients’ perspectives on preferable care and their perspectives on the extent to which these aspects are addressed [83,84]. This focus on clients’ perspectives is extremely useful for getting information about clients’ preferences, needs, opinions and ideas regarding counseling which can be used to optimize client-centered counseling in practice. We adapted the original QUOTE questionnaire to measure client preferences and experiences regarding prenatal counseling for anomaly screening.To measure midwives’ views on appropriate counseling and their self-evaluation we wanted to use a similar measurement tool that could be compared with clients. We developed a pre-counseling questionnaire to measure midwives’ views on appropriate counseling and a post-counseling questionnaire, to measure midwives’ self-evaluation of the prenatal counseling they just offered. Both midwifery questionnaires mirrored those of the clients.
Communication during prenatal counselingIn communication research, observational studies are designed to investigate the communication process [5]. In this type of research, recordings of actual health care consultations using audio or video taping are typically used for analyses. Within the Dutch midwifery research context at the time we started our study making audio or video tapes of consultations had never been done. Despite this possible barrier, we felt videotaping was the most effective means to gain a better understanding about what exactly happens during midwives’ prenatal counseling. To be able to open the ‘black box’ and to know more about the coherence between the counseling practice, the prenatal counseling theory, and the perspectives of Dutch clients and midwives on appropriate counseling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
21
1A widely used and valid scheme for coding audio or video taped healthcare encounters is the Roter Interaction Analysis System (RIAS) [6,77,85]. The RIAS focuses on the smallest unit of expression or statement (utterance) to which a meaningful code can be assigned [6,86]. The main focus of the RIAS is verbal behavior. A distinction is made between affective utterances and instrumental utterances, thereby complying clients’ most urgent needs: the need to feel known and understood (to be fulfilled by using affective communication) and the need to know and understand (for which instrumental communication is needed) [87,88]. The affective categories include social conversation, such as emotional statements, e.g. empathy. The instrumental categories refer to the communication aspects that primarily focus on solving problems, such as giving information, asking questions and providing counseling [6, 86]. Several studies have adapted the RIAS, to make the coding scheme more suitable and reliable for their coding context [82,89-91]. We adapted the RIAS for coding videotapes of prenatal counseling for anomaly screening by midwives to the items of the QUOTE. We added coding of client-directed gaze to the coding protocol in order to have information about one of the most important forms of nonverbal communication [92-97]. Our adaptation of the RIAS also allowed us to integrate the results of the video recordings with the results of client and midwife questionnaires.
Aims of the thesis
The overall aim of this thesis was to investigate clients’ preferences and midwives’ views regarding appropriate prenatal counseling for anomaly screening. Furthermore, this study aims to provide knowledge about how prenatal counseling for anomaly screening by midwives is performed in daily practice, from the perspectives of clients, midwives and observers.
Outline of this thesisThe first study of this thesis is about the development and validation of a QUOTE-questionnaire that assesses clients’ and their partners’ preferences and experiences regarding prenatal counseling for congenital anomaly tests. The resulting questionnaire was used in a cross-sectional study design in primary midwifery care in the Netherlands. Data were used to assess clients’ pre-counseling preferences regarding prenatal counseling and clients’ experiences. Data of socio-demographic background characteristics of clients were used to determine possible differences between different groups of clients in pre-counseling preferences and post-counseling experiences (chapter 2). The final client questionnaire was mirrored for midwives so that it could be used as a pre-counseling instrument for measuring midwives’ views on appropriate counseling. All Dutch midwives who were a member of the KNOV were asked to complete this questionnaire. Midwives’ views on appropriate prenatal counseling for anomaly tests were compared to clients’ preferences and the functions described in the

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
22
theoretical prenatal counseling model (chapter 3). To examine actual prenatal counseling for anomaly screening in daily practice, we introduced video recording in primary midwifery care. Chapter 4 describes the introduction procedure, resulting dataset, and use of data for research purposes. In chapter 5 we used the video recorded prenatal counseling consultations to describe how the functions of prenatal counseling were expressed in daily, midwifery practice. We described the conversational contribution of both clients and midwives during counseling and explored characteristics, which were associated with the performance of midwives’ prenatal counseling. After each video recorded counseling consultation midwives completed a post-counseling questionnaire, to evaluate their own counseling. Data of post-counseling client questionnaires, video-observations and midwives’ self-evaluations were compared to each other (chapter 6). Nonverbal behavior was the topic of the last study within this thesis. In this study we examined if and how the nonverbal behavior ‘client-directed gaze’ was related to clients’ psychosocial communication, which is an important part of the decision-making support function of counseling. In addition to midwives’ psychosocial questioning, we also examined the relation between verbal affective communication, and clients’ psychosocial communication (chapter 7).The thesis ends with a general discussion of the findings including suggestions for further research and practical implications.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
23
1REFERENCES
[1] http://www.medicinfo.nl.[2] http://www.deverloskundige.nl.[3] De Boer J, Zeeman K. KNOV-guideline prenatal midwifery led care: recommendation for coaching,
interaction and information giving. Utrecht: KNOV, 2008; p.17–46 [In Dutch].[4] RIVM. Scenario Prenatal Screening. Down syndrome and fetal anomaly ultrasound scan. Dutch
Translation: Draaiboek Prenatale Screening. Downsyndroom en Structureel Echoscopisch Onderzoek. Versie 4.0; 2014. www.rivm.nl [In Dutch].
[5] Meiser B, Irle J, Lobb E, Barlow-Stewart K. Assessment of the Content and Process of Genetic Counselling: A Critical Review of Emperical Studies. JOGC 2008; 17:434-451.
[6] Roter D, Ellington L, Hamby Erby L, Larson S, Dudley W. The genetic counselling Video project (GCVP). Am J Med Genet 2006; 142C:209-20.
[7] Martin L, Van Dulmen S, Spelten E, Hutton E. Prenatal genetic counseling: Future parents prefer to make decisions together, using professional advice. Prenat Diagn 2012; 32(1): 1–128.
[8] Hillman SC, Skelton J, Quinlan-Jones E, Wilson A, Kilby MD. “If it helps . . .” The Use of Microarray Technology in Prenatal Testing: Patient and Partners Reflections. Am J Med Genetics 2013; 161A(7):1619-27.
[9] Barry CA, Bradley CP, Britten N, Stevenson FA, Barber N. “Patients’ unvoiced agendas in general practice consultations: qualitative study”. BMJ 2000; 320(7244): 1246-50.
[10] www.prenatalescreening.nl including: Teachers Manuel Skills training Prenatal Screening. Developed by: KNOV, SSOV, VAA, VAG, AVM, SROV, NHG, NVOG, VSOP, erfocentrum en VKGN, 2007 [In Dutch].
[11] Health Council of the Netherlands: Prenatal Screening: Down’s Syndrome, Neural Tube Defects, Routine-Ultrasonography. Dutch Translation: Prenatale Screening op Downsyndroom, Neuralebuisdefecten, Routine-Echoscopie; 2001.2001/11 [In Dutch].
[12] Health Council of the Netherlands: Population Screening Act: Prenatal Screening: Down’s Syndrome and Neural Tube Defects. Dutch Translation: Wet Bevolkingsonderzoek: Prenatale Screening op Downsyndroom en Neuralebuisdefecten; 2007. 2007/05WBO [In Dutch].
[13] Ministry of Dutch Civil Code Book 7: Article 449. Medical Treatment Agreements Act. Dutch Translation: Burgerlijk Wetboek 7: Artikel 449. Wet op de Geneeskundige Behandelingsovereenkomst (WGBO) [In Dutch].
[14] Crombag NM, Vellinga YE, Kluijfhout SA, Bryant LD, Ward PA, Iedema-Kuiper R, Schielen PC, Bensing JM, Visser GH, Tabor A, Hirst J. Explaining variation in Down’s syndrome screening uptake: comparing the Netherlands with England and Denmark using documentary analysis and expert stakeholder interviews. BMC Health Serv Res 2014; 25(14):437-8.
[15] Engels MAJ. Prenatal Down Syndrome Screening; Screening policies revised. Doctoral thesis. Amsterdam; Vrije Universiteit Amsterdam; 2014.
[16] Van Agt HME, Schoonen HMHJD, Wildschut HIJ, De Koning HJ, Elsink-Bot ML. Education about prenatal and neonatal screening programs: Questionnaires for national evaluation of the test-offer procedure. Erasmus MC, Eindrapportage 2007 [In Dutch].
[17] www.niptconsortium.nl.[18] www.meerovernipt.nl.[19] https://pedclerk.bsd.uchicago.edu/page/trisomy-21-down.[20] www.rivm.nl including: Quality requirements Counselor prenatal screening (version 5,
set by the Central Organization Prenatal Screening; 03 June 2014). http://www.rivm.nl/dsresource?objectid=rivmp:50878&type=org&disposition=inline&ns_nc=1 [In Dutch].
[21] Fracheboud J, Van Agt HME, De Koning HJ. Monitoring of reported uptake of the screening program Down syndrome / Fetal Anomaly Scan 2010. Bilthoven, RIVM, Eindrapport Juli 2012 [In Dutch].
[22] Oepkes P, Wieringa J. The right to know; the 20-weeks ultrasound investigation facilitates a conscious choice. Medisch Contact 2008; 31/32:1296-1297 [In Dutch].
[23] Feenstra I, Van der Burht I, Voskuilen D. Prenatal diagnostics anno 2011. Bijblijven 2011; 27 (9):34-41 [In Dutch].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
24
[24] Ekelund CK, Petersen OB, Skibsted L, Kjaergaard S, Vogel I, Tabor A. First-trimester screening for trisomy 21 in Denmark: implications for detection and birth rates of trisomy 18 and trisomy 13. Ultrasound Obstet Gynecol 2011; 38:140–4.
[25] Tabor A, Alfirevic Z. Update on procedure-related risks for prenatal diagnosis techniques. Fetal Diagn Ther 2010; 27:1-7.
[26] Bosk CL. All God’s Mistakes. Genetic counseling in a pedriatic hospital. Chicago and London, The university of Chicago Press, 1995; p. 1-19.
[27] Gitsels-van der Wal JT, Martin L, Manniën J, Verhoeven P, Hutton EK, Reinders HS. A qualitative study on how Muslim women of Moroccan descent approach antenatal anomaly screening. Midwifery 2015. doi: 10.1016/j.midw.2014.12.007.
[28] Garcia Gonzalez ME. In search of good motherhood. How prenatal screening shapes women’s views on their moral duties to their family. Doctoral thesis. Nijmegen, Radboud University; 2011.
[29] Van Zwieten M. Communication about ethical issues in medical practice. In: Medical psychology, Kaptein AA, Prins JB, Collette EH, Hulsman RL (red). 2e herziene druk. Houten: Bohn Stafleu Van Loghum, 2010; p. 213-224 [In Dutch].
[30] Williams C, Sandalla J, Lewando-Hundt G, Heymand B, Spencerb K, Grellier R. Women as moral pioneers? Experiences of first trimester antenatal screening. Soc Sci Med 2005; 61(9):1983–1992.
[31] Hunt LM, De Voogd KB, Castañeda H. The routine and the traumatic in prenatal genetic diagnosis: does clinical information inform patient decision-making? Patient Educ Couns 2005; 56(3):302–312.
[32] Van den Berg M. Decision making in prenatal screening. Doctoral thesis, VU medical centre Amsterdam, 2006.
[33] De Jong A, Dondorp WJ, De Die-Smulders CEM, De Wert GMWR. The dynamics of prenatal screening. Medisch Contact 2010; 39:2007-2009 [In Dutch].
[34] Horstman K. Should we do everything that is possible? Bijblijven 2008; 24(6):65-72 [In Dutch].[35] Geelen EGM, Horstman K, Widdershoven GAM. Needless worry. Experiences of pregnant women
with risk assessments. Medisch Contact 2004; 59(45):1770-3 [In Dutch].[36] Garcia E, Timmermans DRM, Van Leeuwen E. Rethinking autonomy in the context of prenatal
screening decision-making. Prenat diagn 2008; 28(2):115-120.[37] Van Zwieten M, Willems D, Knegt L, Leschot N. Communication with patients during the prenatal
testing procedure: An explorative qualitative study. Patient Educ Couns 2006; 63:161–168.[38] Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands.
BMC Pregnancy and Childbirth 2009; 9:18.[39] Wiegers TA, Hingstman l. The changing responsibilities of midwives: new figures about time spent
on specific tasks. Tijdschrift voor Verloskundigen 2008; 33(3):19-24 [In Dutch].[40] Verburg MP. The role of primary care midwives in the Netherlands. Evaluation of midwifery care
in the Dutch maternity care system: a descriptive study. Doctoral thesis. Amsterdam, AMC-UvA, 2011: H1.
[41] Wiegers TA, van der Velden LFJ, Hingstman L. Estimated need for midwives 2004 – 2015; Utrecht, NIVEL 2005 [In Dutch].
[42] Liefhebber S, Van Dam C, Waelput A. Dutch professional profile midwives. Utrecht: Royal Dutch organization of Midwives (KNOV), 2005 [In Dutch].
[43] Mearns D, Thorne B. Person-Centered Counselling in Action. London: Sage Publications, (2nd ed), 1999; p. 5–21.
[44] Health Council of the Netherlands: Committee Genetic screening. Genetic Screening. The Hague: Health Council, 1994; publication no. 1994/22 [In Dutch].
[45] Resta RG. Defining and redefining the scope and goals of genetic counseling. Am J Med Genetics 2006; 142C:269–75.
[46] Flessel MC, Lorey FW. The California Prenatal Screening Program: “options and choices” not “coercion and eugenics”. Genetic Medicine 2011; 13(8):711–3.
[47] Jakobsen TR, Sogaard K, Tabor A. Implications of a first trimester Down’s syndrome screening program on timing of malformation detection. Acta Obstetrica et Gynecologica Scandinavica. Nord Fed Society Obstet Gyn 2011; 90:728–36.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
25
1[48] Smith RC, Hoppe RB. The patient’s story: integrating the patient- and physician-centered
approaches to interviewing. Ann Intern Med 1991; 115:470–7.[49] O’Connor AM, France Légaré, Dawn Stacey. Risk communication in practice: the contribution of
decision aids. BMJ 2003; 327:736-740.[50] Chieng WS, Chan N, Lee SC. Non-directive genetic counselling-respect for autonomy or
unprofessional practice? Ann Acad Med Singapore 2011; 40(1):36-42.[51] Pennacchini M, Pensieri C. Is non-directive communication in genetic counseling possible? Clin
Ter 2011; 162:141-144.[52] Vanstone M, Kinsella EA, Nisker J. Information-sharing to promote informed choice in prenatal
screening in the spirit of the SOGC clinical practice guideline: a proposal for an alternative model. J Obstet Gynaecol Can 2012; 34:269-675.
[53] Durand MA, Stiel M, Boivin J, Elwyn G. Information and decision support needs of parents considering amniocentesis: interviews with pregnant women and health professionals. Health Expect 2010; 13(2):125–38.
[54] Kreuter MW, Strecker VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Ann Behav Medicine 1999; 21(4):276–83.
[55] Todd J, Bohart AC. Foundations of Clinical and Counseling Psychology. New York: HarperCollins College Publishers, (3rd ed), 2005; p. 209–39.
[56] Van Staveren R. Patient centered communication; a guide for medical practice. Utrecht, DeTijdstroom, september 2010 [In Dutch].
[57] Bernhardt BA, Geller G, Doksum T, Larson SM, Roter D, Holtzman NA. Prenatal Genetic Testing: Content of Discussions Between Obstetric Providers and Pregnant Women. Obstet Gynecol 1998; 91:0029-7844.
[58] Bernhardt BA, Barbara B. Biesecker, Carrie L. Mastromarino. Goals, Benefits, and Outcomes of Genetic Counseling: Client and Genetic Counselor Assessment. Am J Med Genet 2000; 94:189–197.
[59] Ormond KEM, Banuvar I, Minogue SJ, Annas GJ, Elias S. What do Patients Prefer: Informed Consent Models for Genetic Carrier Testing. J Genet Counsel 2007; 16:539–550.
[60] Ahmed S, Hewison J, Green JM, Cuckle HS, Hirst J, Thornton JG. Decisions About Testing and Termination of Pregnancy for Different Fetal Conditions: A Qualitative Study of European White and Pakistani Mothers of Affected Children. J Genet Counsel 2008; 17:560–572.
[61] Wertz D, Gregg R. Genetics services in a social, ethical and policy context: a collaboration between consumers and providers. J Med Ethics 2000; 26(4):261–265.
[62] Shiloh S, Gerad L, Goldman B. Patients’ Information Needs and Decision-Making Processes: What Can Be Learned From Genetic Counselees? Health Psychology 2006; 25(2):211–219.
[63] Hsieh Y, Flatley Brennan P. What Are Pregnant Women’s Information Needs and Information Seeking Behaviors Prior to Their Prenatal Genetic Counseling? AMIA 2005 Symposium Proceedings Page: 355-359.
[64] Alouini S, Moutel G, Venslauskaite G, Gaillard M, Truc JB, Herve C. Information for patients undergoing a prenatal diagnosis. Eur J Obstet Gynaecol Reprod Biol 2007; 134:9–14.
[65] Browner CH, Preloran HM, Casado MC, Bass HN, Walker AP. Genetic counseling gone awry: miscommunication between prenatal genetic service providers and Mexican-origin clients. Soc Sci Med 2003; 56(9):1933-46.
[66] Petty R, Cacioppo J. The elaboration likelihood model of persuasion. Advances Experimental Social Psychology 1986; 19:123–205.
[67] Weert van JCM, Jansen J, Bruijn de GJ, Noordman J, van Dulmen S, Bensing JM.QUOTE chemo: a patient-centered instrument to measure quality of care preceding chemotherapy treatment through the patient’s eyes. Europ J Cancer 2009; 45(17):2967–76.
[68] Bramwell R, Carter D. An exploration of midwives’ and obstetricians’ knowledge of genetic screening in pregnancy and their perception of appropriate counselling. Midwifery 2001; 17(2):133-41.
[69] Veach PM, Bartels DM, LeRoy BS. Ethical and professional challenges posed by patients with genetic concerns: a report of focus group discussions with genetic counselors, physicians, and nurses. J Genet Couns 2001; 10(2):97-119.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 1
26
[70] Sheets KB, Best RG, Brasington CK, Will MC. Balanced information about Down syndrome: what is essential? Am J Med Genet A 2011; 155A(6):1246-57.
[71] Pieterse A, Van Dulmen S, Ausems M, Schoemaker A, Beemer F, Bensing J. QUOTE-GENEca: development of a counselee-centered instrument to measure needs and preferences in genetic counselling for hereditary cancer. Psycho Oncology 2005; 14:361–75.
[72] Pieterse AH, Van Dulmen AM, Beemer FA, Ausems MGEM, Bensing JM. Tailoring communication in cancer genetic counselling through individual video-supported feedback: a controlled pretest-posttest design. Patient Educ Couns 2006; 60(3):326-335.
[73] Michie S, Dormandy E, Marteau TM. Informed choice: understanding knowledge in the context of screening uptake. Patient Educ Couns 2003; 3:247-53.
[74] Barr O, Skirton H. Informed decision making regarding antenatal screening for fetal abnormality in the United Kingdom: A qualitative study of parents and professionals. Nurs Health Sci 2013; 15:318-25.
[75] Van den Berg M, Timmermans DRM, Ten Kate LP, Van Vugt JMG, Van der Wal G. Are pregnant women making informed choices about prenatal screening? Genet Med 2005; 7:767–76.
[76] Farrelly E, Cho MK, Erby L, Roter D, Stenzel A, Ormond K. Genetic counseling for prenatal testing: where is the discussion about disability? J Genet Couns 2012; 21(6):814-24.
[77] Ellington L, Kelly KM, Reblin M, Latimer S, Roter D. Communicationin genetic counseling: cognitive and emotional processing. Health Commun 2011; 26:667–675.
[78] Fransen MP, Essink-Bot ML, Vogel I, Mackenbach JP, Steegers EA, Wildschut HI. Ethnic differences in informed decision-making about prenatal screening for Down ‘s syndrome. J. Epidemiol. Community Health 2010; 64:262–268.
[79] Schoonen HM, Essink-Bot ML, Van Agt HM, Wildschut HI, Steegers EA, De Koning HJ. Informed decision-making about the fetal anomaly scan: what knowledge is relevant?. Ultrasound Obstet. Gynecol 2011; 37:649–657.
[80] Manniën J, Klomp T, Wiegers T, Pereboom M, Brug J, De Jonge A, Van der Meijde M, Hutton EK, Schellevis F, Spelten ER. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Serv Res 2012; 12:69-78.
[81] Johnson RB, Onwuegbuzie AJ, Turner LA. Toward a definition of mixed methods research. J Mix Methods Res 2007; 1(2):112-133.
[82] Pieterse AH, Van Dulmen AM, Beemer FA, Bensing JM, Ausems MG. Cancer genetic counseling: communication and counselees’ post-visit satisfaction, cognitions, anxiety, and needs fulfillment. J Genet Couns 2007; 16(1):85-96.
[83] Sixma HJ, Van Campen C, Kerssens JJ, Peters L. Quality of care from the patients’ perspectives: from theoretical concept to a new measuring instrument. Health Expect 1998; 1:82–95.
[84] Nijkamp MD, Sixma HJ, Afman H, Hiddema F, Koopmans SA, van den Borne B, Hendrikse F, Nuijts RM. Quality of care from the perspective of the cataract patient: the reliability and validity of the QUOTE-cataract. British J Ophthalmol 2002; 86:840–2.
[85] Roter DL, Hall JA, Blanch-Hartigan D, Larson D, Frankel RM. Slicing it thin: New methods for brief sampling analysis using RIAS-coded medical dialogue. Patient Educ Couns 2011; 82:410–419.
[86] Roter DL, Larson SM, Beach MC, Cooper LA. Interactive and evaluative correlates of dialogue sequence: a simulation study applying the RIAS to turn taking structures. Patient Educ Couns 2008; 71(1):26-33.
[87] Engel GL. (1988) How much longer must medicine’s science be bound by a seventeenth century world view. In The Task of Medicine: Dialogue at Wickenburg (ed. K.White), pp. 113–116. Menlo Park: The Henry Kaiser Foundation.
[88] Bensing JM. Bridging the gap: the separate worlds of evidence-based medicine and patient-centred medicine. Patient Educ Couns 2000; 39(1):17-251.
[89] Weert JCM, Van Dulmen AM, Spreeuwenberg PMM, Ribbe MW, Bensing JM. Effects of snoezelen, integrated in 24-h dementia care, on nurse-patient communication during morning care. Patient Educ Couns 2005; 58(3):312-26.
[90] Albada A, Ausems MG, Van Dulmen S. Counselee participation in follow-up breast cancer genetic counselling visits and associations with achievement of the preferred role, cognitive outcomes, risk perception alignment and perceived personal control. Soc Sci Med 2014; 116:178-86.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General introduction
27
1[91] Noordman J, Verhaak P, Van Dulmen S. Web-enabled video-feedback: a method to reflect on the
communication skills of experienced physicians. Patient Educ Couns 2011; 82:335-340.[92] Henry SG, Fuhrel-Forbis A, Rogers MA, Eggly S. Association between nonverbal communication
during clinical interactions and outcomes: a systematic review and meta-analysis. Patient Educ Couns 2012; 86:297-315.
[93] Gorawara-Bhat R, Cook MA. Eye contact in patient-centered communication. Patient Educ Couns 2011; 82:442–447.
[94] Zimmermann C, Del Piccolo L, Finset A. Cues and concerns by patients in medical consultations: A literature review. Psychological Bulletin 2007; 133:438-463.
[95] Marcinowicz L, Konstantynowicz J, Godlewski C. Patients’ perceptions of GP non-verbal communication: a qualitative study. Br J Gen Pract 2010; 60(571):83-7.
[96] Stepanikova Q, Zhang D, Wieland GP, Eleazer T, Stewart. Non-Verbal Communication Between Primary Care Physicians and Older Patients: How Does Race Matter? J Gen Intern Med 2011; 27:576–81.
[97] Bensing JM, Kerssens JJ, Van der Pasch M. Patient-directed gaze as a tool for discovering and handling psychosocial problems in general practice. J Nonverbal Behav 1995; 19(4):223-242.


Chapter 2Prenatal counseling for congenital anomaly tests: parental
preferences and perceptions of midwife performance
Martin L, Van Dulmen S, Spelten ER, De Jonge A, De Cock P, Hutton EK.
Prenatal Diagnosis 2013; 33: 1–12.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
30
ABSTRACT
Objective Evidence-based instruments to evaluate the preferences and experiences of future parents regarding prenatal counseling for congenital anomaly tests are currently lacking. We developed the QUality Of care Through clients’ Eyes prenatal (QUOTE prenatal) questionnaire, a client-centered instrument, and assessed its components. Furthermore, the QUOTE prenatal
was used to provide insight into (1) clients’ pre-counseling preferences and (2) clients’ post-counseling experiences, that is, perceived care provider performance regarding the counseling they received.
Method In the questionnaire survey, a principal component analysis was used to gain insight into the underlying components of the questionnaire. Regression analysis was performed to examine differences between groups.
Results In 17 Dutch midwifery practices, 941 pregnant women and their partners (response rate 79%) completed the 59-item QUOTE prenatal pre-counseling and post-counseling, measuring preferences and perceived performances, respectively. A principal component analysis revealed three counseling components: client–midwife relation, health education and decision-making support. Reponses showed that, pre-counseling, most clients consider the client–midwife relationship and health education to be (very) important. More than one third of the clients consider decision-making support to be (very) important. Nulliparae had higher preferences for health education and decision-making support than multiparous women.
Conclusion Clients perceive that their midwives perform well in building the client–midwife relation and in giving health education. Improvement is needed in decision-making support.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
31
2
What’s already known about this topic?- Optimizing client health decisions requires tailored communication.- In prenatal counseling, such communication should comprise health education and
decision-making support.
What does this study add?- A valid research instrument to evaluate the preferences and experiences of parents
regarding prenatal counseling.- Clients perceive that their midwives perform well in giving health education, an
aspect of care considered important by most clients.- Although fewer clients valued decision-making support, we identified a need for
improvement in this aspect of care.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
32
INTRODUCTION
Over the last decades, prenatal testing for congenital anomalies has developed substantially [1–3]. In the Western world, prenatal tests, such as first and second trimester ultrasounds, are increasingly offered as routine prenatal care, although in fact they are not; clients have the right to refuse such tests [4–7]. Consequently, to help future parents decide whether or not to accept these tests, midwives, gynecologists, and genetic counselors have to offer prenatal counseling including decision-making support. This counseling should be nonbiased, i.e. the counselor does not make the decision or give advice about whether or not to have prenatal tests, and informative, encompassing health educational aspects as well as decision-making support [7–11]. Many process and outcome studies have been carried out to assess the quality of prenatal counseling from the perspective of what care providers think clients should know to make informed choices. Quality measures typically include risk perception accuracy, recall of information provided, decision related outcomes, psychological adjustment and communication style of the counselor [9,12]. Considerably less research has focused on the perspective of the clients, such as their preferences regarding counseling for prenatal congenital anomaly tests and the extent to which these preferences are met. The resulting lack of insight into client preferences is striking, because within health care, optimizing client empowerment, health decisions and health behavior requires tailored communication, that is, communication that focuses on individuals’ preferences, interests and concerns [13–19]. Awareness of client preferences is a prerequisite for tailored communication. Insight into clients’ preferences regarding decision-making support, which are of utmost importance given the gravity of the decision parents may be facing, is particularly lacking [20]. As far as we know, no validated instrument exists to evaluate the preferences and experiences of future parents regarding prenatal counseling. For the present study, we developed the QUality Of care Through clients’ Eyes prenatal (QUOTE prenatal) questionnaire to assess parental preferences and experiences regarding prenatal counseling for congenital anomaly tests, with a focus on both the counseling process and content. In the literature, there is consensus about the health education and decision-making support functions of prenatal counseling [9,21]. However, it is unclear to what extent clients value these functions as important and to what extent these values differ between clients. We therefore compared preferences and experiences within pregnant women and their partners and nulliparous and multiparous women, and finally, we considered the influence of age. Older women have an increased risk of giving birth to a child with a chromosomal abnormality, and therefore, in the Netherlands, women 36 years and older are offered free prenatal testing [22].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
33
2
In summary, there are no instruments available that assess clients’ and their partners’ preferences and experiences regarding prenatal counseling for congenital anomaly tests. The first aim of this study was to develop such an instrument on the basis of their input, that is, following the QUality Of care Through clients’ Eyes procedure [19]. Secondly, using this instrument, we explored preferences and experiences within a large group of clients and their partners. More specifically, we assessed (1) clients’ pre-counseling preferences regarding prenatal counseling, (2) clients’ experiences [the level of perceived performance regarding issues clients value as (very) important], (3) consistency of pre-counseling preferences between women and partners, nulliparae and multiparae, and women younger than and at or older than 36 years of age, and (4) differences in post-counseling experiences between the same groups.
METHODS
The study was conducted in the Dutch healthcare context in which midwives offer prenatal counseling to almost 80% of the pregnant women [43]. Dutch midwives have to pass a training course in genetic knowledge and counseling skills to provide prenatal counseling for congenital anomaly tests to low-risk couples. Couples at increased risk for having a child with a congenital anomaly are referred to clinical geneticists.
ParticipantsSeventeen midwifery practices in the Netherlands were purposefully selected so as to include different-sized practices from all over the country [23]. Participants were recruited from all consecutive new clients (women and their partners), between June 2010 and May 2011. Eligible clients were clients (1) new to counseling about prenatal tests for the current pregnancy, (2) 18 years or older, and (3) able to read Dutch or English. Partners were included only if the pregnant women agreed to participate. Participants were not paid for participating in this study.
InstrumentsThe self-administered questionnaire contained items on socio-demographic variables and medical background. These questions were completed before the visit. Background characteristics of non-responders were recorded by the practice assistant.
QUOTE prenatal: measurement of preferences and experienceWe developed an instrument based on QUOTE questionnaires. These are a group of standardized and validated survey questionnaires aimed at investigating preferences and actual experiences of clients pre-counseling and post-counseling, respectively [19,24,25].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
34
The degree to which (perceived) performances of health and societal care services meet the preferences of persons is defined as quality of care. Attention is paid to quality of generic communication items and target-group-related or specific items [24]. The QUOTE prenatal was based on semi-structured interviews with couples (N= 12) and future mothers (N= 5), existing QUOTE questionnaires [24,26] and guidelines for prenatal counseling [13]. The resulting QUOTE prenatal consists of 59 items. This includes generic items, such as ‘It is important to me that the midwife takes my concerns seriously’; prenatal-specific items, such as ‘It is important to me that the midwife explains which abnormality can be identified using prenatal screening’; and three organizational items. The importance part of the questionnaire asks parents to rate the extent to which specific aspects of information and communication are considered important prior to counseling about prenatal tests (‘preferences’), measured by a 4-point Likert scale (‘It is important to me that the midwife . . .’: ‘1 = not important’, ‘2 = fairly important’, ‘3 = important’, and ‘4 = very important’). In the post-counseling questionnaire, parents are asked to report whether they perceive that these aspects were attended to during the actual counseling, measured by a 4-point Likert scale (‘During the visit, the midwife. . .’: ‘1=no’, ‘2 = a little’, ‘3 = yes’, and ‘4 = very much’) [19,24].The QUOTE prenatal was translated into English by a professional translator and double-checked by a second one. Validation was limited to the Dutch version because of the expected small sample size of English-speaking participants.
Data analysisQUOTE prenatal questionnaire A principal component analysis (PCA) with varimax rotation was performed on the importance scores [24,27]. The three organizational items were left out of the PCA; results were analyzed separately. The appropriateness of the factor analytic model for the remaining 56 items was tested using the Kaiser– Meyer–Olkin measure of sampling adequacy and Barlett’s test of sphericity. Items failing to load at least 0.32 [28] on any component were left out. Cronbach’s a was rated to assess the internal consistency of the QUOTE categories [19,29]. Item– total correlations (ITCs) were calculated for each of the subscales, using 0.30 as criterion [30]. If the percentage of missing values was acceptably low (<15%) and considered to be missing at random, we used the listwise deletion approach. Otherwise, missing values were substituted according to the ‘mean value of valid subtests principle’.
Clients’ preferencesImportance scores on the components and the individual items of the QUOTE prenatal were calculated as the proportion of clients who rated these components and individual items as important or very important [19,31]. We considered pre-counseling scores of 3 or 4 on individual-item level to indicate importance or high importance. Because of the fact that we used mean values of scores on individual items to compute the scores on the components,

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
35
2
we used 2.50 rather than 3 as a threshold to indicate importance or high importance on component-level. The components or individual items of the QUOTE prenatal were classified as important for all clients if components and/or items were identified as important or very important by more than 75% of the participants [19].
Clients’ experiences: perceived performancesPost-counseling measures of experiences were only calculated for clients who had considered certain items as important or very important pre-counseling. Post-counseling scores of 3 or 4 on individual items were considered as indicating that preferences were met well or very well. Post-counseling scores higher than 2.50 on the components were considered as indicating that preferences were well or very well met, an approach similar to that used in earlier studies [24]. The criterion for well-met preferences was defined as having at least 75% of the respondents reporting a performance score of 3 or 4 on item level and higher than 2.50 on components [19].
Analyses of subgroupsImportance scores and perceived performance scores on each component were subsequently rated for the following groups separately: women versus partners, nulliparae versus multiparae (women and partners) and women younger than and at or older than 36 years of age. Groups were compared to examine differences between these groups using regression analysis (method ENTER). Analyses were carried out using SPSS 17.0.2.
Ethical considerationsThe design of the study was approved by the Institutional Review Board of the VU University Medical Centre and the Medical Ethical Committee of the VU Medical Centre, Amsterdam, the Netherlands. Local declarations of intent were provided by all participating midwives.
RESULTS
ParticipantsOf the 680 eligible pregnant women, 538/680 (79%) and 403/538 (75%) of their partners agreed to participate. Pre-counseling data were available for all respondents; the percentage of missing values for items ranged from 0.7% to 2.4% and was considered to be random. The mean age of the pregnant women was 29.4 years (SD=4.2) and of the partners 31.8 years (SD=4.9). About fifty percent of clients had completed education up to high school level, and the other half had completed higher vocational or university education. Of the pregnant women, 219 were nulliparae (41%) and 307 were multiparae (57%). For 205 (51%) of the partners, it was the first time their partner was pregnant, whereas 185 (46%) had prior experience (Table 1). Nine hundred thirty-four (99%) participants completed the Dutch questionnaire and seven (0.7%) the English questionnaire.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
36
A comparison between women who agreed and women who declined to participate in the study showed no significant difference with regard to age (mean 29.4 vs 30.1 years, p=0.11), whereas rates of multiparity (77% vs 58%, p<0.001) and non-Dutch participants (25% vs 15%, p<0.001) were higher in the nonresponse group than in the response group.
Table 1 Demographic characteristics of the test sample.
Characteristics Pregnant women N=538 (%)Mean (SD); missing (%)
Partners N=403 (%)Mean (SD); missing (%)
Age 29.4 years (4.2); 7 (1.3) 31.8 years (4.9); 7 (1.7)Age first pregnancy 27.9 years (4.0); 0 30.4 years (4.5); 0Weeks pregnant 8.6 weeks (2.1); 39 (7.2) 8.6 weeks (SD); 39 (7.2)
ParityNulliparaeMultiparaeMissing
219 (40.7)307 (57.0)12 (2.3)
205 (50.8)185 (45.9)13 (3.3)
EducationLowMiddleHighMissing
7 (1.3)250 (46.5) 278 (51.7)3 (0.5)
6 (1.4)208 (51.6)186 (46.3)3 (0.7)
Ethnic origina
DutchNon-DutchMissing
454 (84.4)79 (14.7)5 (0.9)
346 (85.9)49 (12.1)8 (2)
Marital statusPartnerSingleMissing
515 (95.7)20 (3.7)3 (0.6)
387 (96.0) 12 (3.0) 4 (1.0)
ReligionBelieversNon-believersMissing
262 (48.7)267 (49.6)9 (1.7)
187 (46.4)207 (51.4)9 (2.2)
GenderMaleFemaleMissing
396 (98.2)6 (1.4) 1 (0.4)
a In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one or both of the parents of a person are born outside the Netherlands, this person is considered non-Dutch (Dutch National Office of Statistics; Statistics Netherlands).
QUOTE prenatal questionnaireThe PCAs were conducted for the importance scores on the set of 56 items. The Kaiser–Meyer–Olkinmeasure (0.95) and Barlett test (X2 = 21 607.8; p=0.000) demonstrated the legitimacy of the PCA. A three-component solution that explained 43% of the variance

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
37
2
was chosen (Table 2). The three distinguishable components appeared to represent client–midwife relation, health education and decision-making support. The 15-item component client–midwife relation reflects affective communication such as showing empathy, putting clients at ease, taking time and being professional; the 24-item component health education covers medical test information, (test) procedural information, risk information and societal information (e.g. costs of prenatal tests and eligibility for tests); and the 16-item component decision-making support includes items enquiring about values, social support and pressure on decision-making and discussion about the different options and outcomes of scenarios (Tables 3 and 4). One item, namely ‘it is important that the midwife mentions the costs of prenatal testing’ (Q34), loaded highest on decision-making support but loaded also >0.32 on health education. It was therefore placed in the health education component because we considered it to be a health education topic rather than a decision-making support topic. Table 3 shows the Cronbach’s α found for each of the three components of the QUOTE prenatal – important, 0.85, 0.94 and 0.90, respectively. Most corrected ITCs were higher than the threshold of 0.30 (ranging up to 0.73), except for Q2 (ITC=0.27), which we excluded from further analyses. After PCA, we considered the 15 remaining items of the client–midwife relation component to be generic for counseling and the 40 items of the components health education and decision-making support to be specific to the prenatal counseling setting.
Clients’ preferencesTable 3 shows that two components of the QUOTE prenatal can be considered as important for all clients: client–midwife relation (98%) and health education (89%). More than one third of the clients (39%) considered the component decision-making support as either important or very important. Looking at item level, we can see in Table 4 the percentages of clients who rated the individual items of the three components as important or very important, ranging from high to low. Scores on individual client–midwife relation items ranged from 60% to 100%. Of these fifteen items, 13 can be considered as important for all clients because these items were listed as important or very important by more than 75% of the respondents, with highest scores for the item ‘Listens to what I am trying to ask’ (Q6). Scores on health education items ranged from 54% to 95%. Of the 24 items, 17 were listed as important or very important by more than 75% of the participants and thus can be considered as important to all clients, with highest scores for the item ‘Discusses the possible negative implications of prenatal screening for the unborn child’ (Q29). None of the scores on decision-making support reached the threshold of 75%. The highest score (70%) was found for the item ‘Advises me about whether or not to take the prenatal tests’ (Q9).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
38
Table 2 Varimax rotated component matrix with three-factor solution on the 56 QUOTE prenatal items pre-counseling, capturing 42.6% of the variance, and variance explained by each component (N=941).
Items Component1 2 3
Health educationQ26 explains which anomalies can be identified using prenatal tests .760Q31 explains usefulness of prenatal screening (what can client do with it after obtaining results)
.756
Q32 tells me about all different types of prenatal tests available .752Q41 explains why the client is or is not eligible for certain prenatal tests .720Q43 explains which prenatal tests will be done first and which will be done later, if required and/or necessary
.717
Q48 discuss all my options with regard to prenatal screening and the implications .705Q42 explains what will happen during prenatal tests .691Q39 tells me about MY chances of having a child with a congenital abnormality during the pregnancy
.689
Q27 explains which anomalies can NOT be identified using prenatal tests .688Q45 explains how long I may take to decide whether or not to have the prenatal tests
.657
Q29 discusses possible negative implications of prenatal screening for the unborn child
.642
Q46 explains how long I may take to decide whether or not to terminate the pregnancy, should the test results show an abnormality
.635
Q38 explains how the changes of a birth defect are calculated for our unborn child .604 .334Q28 provides medical information about the anomalies that are being tested for .597Q40 talks to me about how MY risk of having a child with a birth defect will affect me
.584 .423
Q44 explains who will give me the results of the prenatal tests and how (verbally, in writing or by telephone)
.554 .354
Q37 explains how often congenital anomalies occur in pregnant women of my age .546 .353Q35 tells me about the incidence of birth defects in the Netherlands .524 .396Q36 asks about my family’s history of birth defects .513Q13 provides information on prenatal tests .510Q33 tells me how prenatal screening can effect my emotions and mental wellbeing .437 .397Q58 makes sure that the topics I consider to be important are discussed at length .413Q56 only discusses specific information about follow-up tests and possible defects with me if it becomes clear that I will need them
.401
Decision-making supportQ51 asks whether my family, friends or other people close to me would support my decision about prenatal screening
.751
Q54 asks whether my family, friends or other people close to me would support my decision to terminate the pregnancy if the child were to have a congenital abnormality
.745
Q53 asks whether test results indicating that my unborn child has a birth defect would cause problems with my conscience
.304 .696
Q52 asks me what I think constitute a healthy child .693Q55 asks how I think I will react to the results of the prenatal tests .688

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
39
2
Items Component1 2 3
Q49 talks to me about how my family and I would react to a child with a birth defect
.360 .644
Q25 encourages me and my partner to talk together about prenatal screening .597Q14 enquires about my standards, values and views on prenatal tests .540 .300Q21 is interested in who I am .534 .423Q30 tells me what the Dutch government aims to achieve by providing prenatal tests
.313 .515
Q20 asks me questions that make me think .413Q22 responds to what I already know about prenatal screening .402Q34 tells me how much prenatal tests cost .324 .396Q11 is understanding about my ideological background or my religion .394 .327Q3 tells me which internet sites I can use to find information about prenatal testing
.375
Q9 advises me about whether or not to take the prenatal tests .327 .352Client-midwife relationQ6 listens to what I am trying to ask .702Q8 gives me enough time to explain myself properly .683Q5 takes my concerns seriously .683Q15 makes clear that I can ask anything I want to know .604Q4 puts me at ease .563Q1 takes plenty of time to answer my questions .563Q16 uses clear and comprehensible language .520Q12 knows what I am talking about .517Q7 is open and honest about every aspect of my pregnancy .505Q10 shows empathy .430 .489Q18 tells me that I can always contact her/him with any question I may have (including when the practice is closed)
.318 .486
Q24 gives me the feeling that she is tuning in to me as a person .347 .482Q2 is professional .389Q19 accepts my decision on whether or not to agree to prenatal testing .365Q17 gives me (additional) written information .301 .351Q23 paints a realistic picture (not just through ‘rose tinted spectacles’) .333
Extraction Method: Principal Component Analysis; Rotation Method: Varimax with Kaiser Normalization. Rotation converged in 7 iterations. Loadings below 0.30 are not shown.
Table 2 Continued

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
40
Tabl
e 3
Com
pone
nts,
num
ber o
f ite
ms
of th
e Q
UO
TE pr
enat
al an
d co
nten
t.
Com
pone
nts
Num
ber
of it
ems
Cont
ent
Pre-
coun
selin
g im
port
ance
sc
ores
Na (%
)b
Post
-co
unse
ling
posi
tive
pe
rfor
man
ceN
a (%)b
Post
-co
unse
ling
nega
tive
pe
rfor
man
ceN
a (%)b
Croh
nbac
h’s
α
Gen
eric
com
pone
ntCl
ient
-mid
wife
rela
tion
15Ite
ms
refle
ct th
e cl
ient
-cen
tred
atti
tude
of t
he
mid
wife
dur
ing
the
prof
essio
nal c
onsu
ltatio
n or
ite
ms
that
des
crib
e co
nditi
ons
for h
avin
g a
clie
nt-
cent
ered
con
vers
ation
.
865
(97.
9)79
9(9
9.9)
1 (0.1
)0.
85
Pren
atal
-spe
cific
com
pone
nts
Hea
lth e
duca
tion
26M
edic
al te
st in
form
ation
, (te
st) p
roce
dura
l in
form
ation
, risk
info
rmati
on, s
ocie
tal i
nfor
mati
on
(e.g
. cos
ts o
f pre
nata
l tes
ts, e
ligib
ility
for t
ests
)
775
(89.
4)50
6(8
3.4)
101
(16.
6)0.
94
(Mor
al) d
ecisi
on-m
akin
g su
ppor
t16
Expl
orati
on o
f val
ues,
soc
ial s
uppo
rt a
nd p
ress
ure
on d
ecisi
on-m
akin
g, d
iscus
sion
abou
t the
diff
eren
t op
tions
and
out
com
es o
f sce
nario
s
328
(38.
5)24
2(6
5.6)
127
(34.
4)0.
90
Colu
mn
thre
e, f
our
and
five:
pre
-cou
nsel
ing
impo
rtan
ce r
ating
s (s
core
3-4
), po
st-c
ouns
elin
g po
sitive
per
form
ance
(sc
ore
3-4)
and
pos
t-cou
nsel
ing
nega
tive
perf
orm
ance
(sco
re 1
-2).
Colu
mn
six: C
rohn
bach
’s Al
pha
for e
ach
com
pone
nt.
a Sa
mpl
e siz
e va
ries
due
to m
issin
g da
ta a
nd p
re-c
ouns
elin
g pr
efer
ence
sco
res
(onl
y po
st-c
ouns
elin
g ex
perie
nce
scor
es o
f clie
nts
with
pre
-cou
nsel
ing
impo
rtan
ce s
core
s 3
or 4
are
men
tione
d).
b Va
lid p
erce
ntag
es.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
41
2
Post-counseling perceived performancesTable 3 shows that most clients who rate client–midwife relation, health education and decision-making support pre-counseling as important or very important report positive experiences post-counseling regarding the first two components, but these clients report less positive experience regarding decision-making support. At an item level, Table 4 shows that more than 25% of the clients who attached high importance (score 3 or 4) to items of health education experienced a lack of performance (score 1 or 2) on 13 items of this 24-item component. A gap between preferences and perceived performances on the item perceived as most important, ‘Discusses the possible negative implications of prenatal screening for the unborn child’ (Q29), was perceived by 25% of the clients. Moreover, Table 4 shows that more than 25% of the clients rated perceived performance of their midwives as 1 or 2 on 12 items of the 16-item decision-making support component. A gap between preferences and perceived performances on the item perceived as most important of this component, ‘Advises me about whether or not to take the prenatal tests’ (Q9), was perceived by 37% of the clients.
SubgroupsRegression analyses on pre-counseling outcome variables showed that, pre-counseling, significantly less partners rate the client–midwife relation as important than did pregnant women (b=-1.745; p=0.000) and that less multiparae rate both health education and decision making support as important than did nulliparae (b=-0.924, p=0.000, and b=-0.476, p=0.001, respectively; Table 5). Regression analyses on post-counseling outcome variables showed that compared with nulliparae, less multiparae perceived the performance of their midwives in terms of health education to be well performed (b=-1.125, p=0.000; Table 6).
OrganizationTable 4 shows that 76% of the clients wanted to be invited to the counseling consultation together with their partner; less than half of them actually perceived they were.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
42
Tabl
e 4
Clie
nt ra
ting
item
s as (
very
) im
port
ant p
re-c
ouns
elin
g (s
core
s 3 o
r 4);
clie
nts r
epor
ting
post
-cou
nsel
ing
positi
ve p
erfo
rman
ce (s
core
s 3 o
r 4) o
r neg
ative
per
form
ance
(s
core
s 1
or 2
).
Num
ber
Item
des
crip
tion
Pre-
coun
selin
g Im
port
ance
sco
res
N=9
41a (%
)
Post
-cou
nsel
ing
Posi
tive
Per
form
ance
N
b (%)
Post
-cou
nsel
ing
Neg
ative
Perf
orm
ance
Nb (%
)
Gen
eric
com
pone
nt a
nd it
ems
Clie
nt-m
idw
ife re
latio
nQ
2 c
Is p
rofe
ssio
nal
923
(99.
8)84
8 (9
9.7)
3 (0
.3)
Q6
List
ens
to w
hat I
am
tryi
ng to
ask
924
(99.
7)84
8 (9
9.8)
2 (0
.2)
Q5
Take
s m
y co
ncer
ns s
erio
usly
922
(98.
9)83
2 (9
9.2)
7 (0
.8)
Q1
Take
s pl
enty
of ti
me
to a
nsw
er m
y qu
estio
ns
913
(98.
3)84
1 (9
9.6)
3 (0
.4)
Q7
Is o
pen
and
hone
st a
bout
eve
ry a
spec
t of m
y pr
egna
ncy
916
(98.
3)76
8 (9
9.4)
5 (0
.6)
Q4
Puts
me
at e
ase
899
(96.
8)82
7 (9
9.2)
7 (0
.8)
Q16
U
ses
clea
r and
com
preh
ensib
le la
ngua
ge88
5 (9
5.1)
821
(99.
8)2
(0.2
)Q
23Pa
ints
a re
alisti
c pi
ctur
e (n
ot ju
st th
roug
h ‘ro
se-ti
nted
spe
ctac
les’
)87
2 (9
3.8)
731
(96.
8)24
(3.2
)Q
8G
ives
me
enou
gh ti
me
to e
xpla
in m
ysel
f pro
perly
866
(92.
9)74
8 (9
9.6)
3 (0
.4)
Q15
Mak
es c
lear
that
I ca
n as
k an
ythi
ng I
wan
t to
know
858
(92.
5)79
8 (9
8.8)
10 (1
.2)
Q19
Acce
pts
my
deci
sion
on w
heth
er o
r not
to a
gree
to p
rena
tal s
cree
ning
81
3 (8
7.9)
705
(97.
5)18
(2.5
)Q
24G
ives
me
the
feel
ing
that
she
is tu
ning
in to
me
as a
per
son
768
(82.
8)66
3 (9
6.1)
27 (3
.9)
Q12
Know
s w
hat I
am
talk
ing
abou
t75
0 (8
0.9)
580
(83.
2)11
7 (1
6.8)
Q18
Tells
me
that
I ca
n al
way
s co
ntac
t her
/him
with
any
que
stion
s I m
ay h
ave
(incl
udin
g w
hen
the
prac
tice
is cl
osed
)74
2 (7
9.7)
621
(93.
4)44
(6.6
)Q
10Sh
ows
empa
thy
570
(61.
8)53
1 (9
7.2)
15 (2
.8)
Q17
Giv
es m
e (a
dditi
onal
) writt
en in
form
ation
557
(60.
0)42
2 (9
7.2)
12 (2
.8)
Pren
atal
-spe
cific
com
pone
nts
and
item
sH
ealth
edu
catio
nQ
29Di
scus
ses
poss
ible
neg
ative
impl
icati
ons
of p
rena
tal s
cree
ning
for t
he u
nbor
n ch
ild88
6 (9
5.2)
467
(75.
5)18
1 (2
4.5)
Q26
Expl
ains
whi
ch a
nom
alie
s ca
n be
iden
tified
usin
g pr
enat
al s
cree
ning
844
(90.
8)65
5 (8
9.0)
81 (1
1.0)
Q31
Expl
ains
the
usef
ulne
ss o
f pre
nata
l scr
eeni
ng (w
hat I
can
dec
ide
to d
o ev
entu
ally
)83
8 (9
0.0)
651
(89.
3)78
(10.
7)Q
58M
akes
sur
e th
at th
e to
pics
I co
nsid
er to
be
impo
rtan
t are
disc
usse
d at
leng
th82
1 (8
8.8)
665
(92.
4)54
(7.6
)Q
13Pr
ovid
es in
form
ation
on
pren
atal
scr
eeni
ng81
7 (8
8.2)
314
(59.
1)21
7 (4
0.9)
Q42
Expl
ains
wha
t will
hap
pen
DURI
NG
the
pren
atal
test
s81
0 (8
7.0)
485
(69.
4)21
4 (3
0.6)
Q32
Tells
me
abou
t all
the
diffe
rent
type
s of
pre
nata
l tes
ts80
6 (8
6.8)
650
(91.
3)62
(8.7
)Q
27Ex
plai
ns w
hich
ano
mal
ies c
anno
t be
iden
tified
usin
g pr
enat
al te
sts
796
(85.
4)44
9 (6
4.0)
253
(36.
0)Q
39Te
lls m
e ab
out M
Y ch
ance
s of
hav
ing
a ch
ild w
ith a
con
geni
tal a
bnor
mal
ity d
urin
g th
is pr
egna
ncy
773
(83.
6)36
0 (5
8.4)
256
(41.
6)Q
43Ex
plai
ns w
hich
pre
nata
l tes
ts w
ill b
e do
ne fi
rst a
nd w
hich
will
be
done
late
r, if
requ
ired
and/
or n
eces
sary
772
(82.
7)58
3 (8
5.6)
98 (1
4.4)
Q41
Tells
me
why
I am
or a
m n
ot e
ligib
le fo
r cer
tain
pre
nata
l tes
ts76
4 (8
2.4)
497
(68.
6)21
1 (3
1.4)
Q48
Disc
usse
s al
l my
optio
ns w
ith re
gard
to p
rena
tal s
cree
ning
and
the
impl
icati
ons
761
(82.
3)34
4 (8
3.9)
62 (1
6.1)
Q46
Expl
ains
how
long
I m
ay ta
ke to
dec
ide
whe
ther
or n
ot to
term
inat
e th
e pr
egna
ncy,
shou
ld th
e te
st re
sults
sho
w a
n ab
norm
ality
758
(81.
8)38
0 (5
8.8)
289
(43.
2)
Q45
Expl
ains
how
long
I m
ay ta
ke to
dec
ide
whe
ther
or n
ot to
hav
e th
e pr
enat
al te
sts
757
(81.
0)51
8 (7
7.9)
147
(22.
1)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
43
2
Q40
Talk
s to
me
abou
t how
MY
risk
of h
avin
g a
child
with
a b
irth
defe
ct w
ill a
ffect
me
707
(76.
3)23
6 (6
2.3)
143
(37.
7)Q
28Pr
ovid
es m
edic
al in
form
ation
abo
ut th
e an
omal
ies
that
are
bei
ng te
sted
for
708
(76.
0)48
6 (7
7.3)
143
(22.
7)Q
36As
ks a
bout
my
fam
ily´s
hist
ory
of b
irth
defe
cts
719
(77.
1)54
4 (9
4.1)
34 (5
.9)
Q56
Onl
y di
scus
ses
spec
ific
info
rmati
on a
bout
follo
w-u
p te
sts
and
poss
ible
def
ects
with
me
if it
beco
mes
cle
ar th
at I
will
ne
ed th
em69
7 (7
5.1)
351
(59.
7)23
7 (4
0.3)
Q33
Tells
me
how
pre
nata
l scr
eeni
ng c
an a
ffect
my
emoti
ons
and
men
tal w
ellb
eing
696
(74.
9)25
5 (6
8.7)
116
(31.
3)Q
38Ex
plai
ns h
ow th
e ch
ance
s of
a b
irth
defe
ct a
re c
alcu
late
d fo
r our
unb
orn
child
675
(72.
5)44
2 (7
6.7)
134
(23.
3)Q
44Ex
plai
ns w
ho w
ill g
ive
me
the
resu
lts o
f the
pre
nata
l tes
ts a
nd h
ow (v
erba
lly, i
n w
riting
or b
y te
leph
one)
638
(68.
3)32
6 (5
6.3)
253
(43.
7)Q
37Ex
plai
ns h
ow o
ften
cong
enita
l ano
mal
ies
occu
r in
preg
nant
wom
en o
f my
age
638
(68.
4)39
6 (6
9.6)
173
(30.
4)Q
34Te
lls m
e ho
w m
uch
pren
atal
test
s co
st52
1 (5
6.0)
285
(61.
0)18
2 (3
9.0)
Q35
Tells
me
abou
t the
inci
denc
e of
birt
h de
fect
s in
the
Net
herla
nds
508
(54.
4)27
4 (5
9.6)
186
(40.
4)De
cisio
n-m
akin
g su
ppor
tQ
9Ad
vise
s m
e ab
out w
heth
er o
r not
to ta
ke th
e pr
enat
al te
sts
648
(69.
8)30
1 (6
2.7)
179
(37.
3)Q
22Re
spon
ds to
wha
t I a
lread
y kn
ow a
bout
pre
nata
l scr
eeni
ng61
0 (6
5.9)
533
(93.
2)33
(6.8
)Q
20As
ks m
e qu
estio
ns th
at m
ake
me
thin
k60
2 (6
4.9)
396
(61.
7)16
4 (2
9.3)
Q49
Talk
s to
me
abou
t how
my
fam
ily a
nd I
wou
ld re
act t
o a
child
with
a b
irth
defe
ct56
9 (6
1.3)
205
(55.
7)16
3 (4
4.3)
Q50
Asks
me
to e
xpla
in m
y de
cisio
n to
take
/ no
t to
take
the
pren
atal
test
s47
4 (5
1.6)
488
(66.
1)11
2 (3
3.9)
Q21
Is in
tere
sted
in w
ho I
am48
9 (5
0.6)
428
(96.
0)18
(4.0
)Q
55As
ks h
ow I
thin
k I w
ill re
act t
o th
e re
sults
of t
he p
rena
tal t
ests
456
(49.
5)16
6 (4
8.7)
175
(51.
3)Q
53As
ks w
heth
er te
st re
sults
indi
catin
g th
at m
y un
born
chi
ld h
as a
birt
h de
fect
wou
ld c
ause
pro
blem
s w
ith m
y co
nsci
ence
446
(48.
2)15
6 (4
6.0)
183
(54.
0)Q
25En
cour
ages
me
and
my
part
ner t
o ta
lk to
geth
er a
bout
pre
nata
l scr
eeni
ng43
6 (4
7.0)
306
(82.
5)65
(17.
5)Q
14En
quire
s ab
out m
y st
anda
rds,
val
ues
and
view
s on
pre
nata
l tes
ts42
4 (4
5.7)
299
(74.
4)13
0 (2
5.6)
Q52
Asks
me
wha
t I th
ink
cons
titut
es a
hea
lthy
child
415
(45.
1)12
1 (3
8.7)
192
(61.
3)Q
30Te
lls m
e w
hat t
he D
utch
gov
ernm
ent a
ims
to a
chie
ve b
y pr
ovid
ing
pren
atal
test
s39
2 (4
2.3)
186
(52.
2)17
0 (4
7.7)
Q3
Tells
me
whi
ch in
tern
et s
ites
I can
use
to fi
nd in
form
ation
abo
ut p
rena
tal s
cree
ning
343
(37.
0)18
0 (6
2.5)
108
(37.
5)Q
11Is
und
erst
andi
ng a
bout
my
ideo
logi
cal b
ackg
roun
d or
my
relig
ion
298
(32.
3)23
9 (8
7.9)
33 (1
2.1)
Q54
Asks
whe
ther
my
fam
ily, f
riend
s or
oth
er p
eopl
e cl
ose
to m
e w
ould
sup
port
my
deci
sion
to te
rmin
ate
the
preg
nanc
y if
the
child
wer
e to
hav
e a
cong
enita
l ano
mal
y20
4 (2
2.0)
239
(31.
8)10
9 (5
9.2)
Q51
Asks
whe
ther
my
fam
ily, f
riend
s or
oth
er p
eopl
e cl
ose
to m
e w
ould
sup
port
my
deci
sion
abou
t pre
nata
l scr
eeni
ng14
9 (1
6.1)
64 (5
6.4)
74 (5
3.6)
Org
aniz
ation
al it
ems
Q47
Asks
my
part
ner a
nd m
e to
com
e to
the
coun
selin
g se
ssio
n on
pre
nata
l scr
eeni
ng T
OG
ETH
ER70
2 (7
5.6)
295
(49.
2)30
5 (5
0.8)
Q59
Mak
es a
sep
arat
e ap
poin
tmen
t for
me
to d
iscus
s pr
enat
al te
sts
(rat
her t
han
broa
chin
g th
e su
bjec
t dur
ing
my
first
ap
poin
tmen
t)30
7 (3
3.4)
94 (3
1.6)
203
(68.
4)
Q57
Plan
s tw
o ap
poin
tmen
ts to
disc
uss
pren
atal
test
s (1
to p
rovi
de th
e re
leva
nt in
form
ation
and
1 to
disc
uss
the
deci
sion)
20
1 (2
1.8)
67 (3
4.2)
129
(65.
8)
a Sam
ple
size
varie
s du
e to
miss
ing
data
. Val
id p
erce
ntag
es a
re s
how
n.b Fi
gure
s co
ncer
n cl
ient
s co
nsid
erin
g th
e ite
ms
as e
ither
impo
rtan
t or v
ery
impo
rtan
t pre
-cou
nsel
ing
only.
Sam
ple
size
varie
s. V
alid
per
cent
ages
are
sho
wn.
c Th
is qu
estio
n w
as o
mitt
ed fr
om fu
rthe
r ana
lyse
s, b
ecau
se o
f the
ver
y lo
w IT
C.Bo
ld fi
gure
s in
the
first
col
umn
refle
ct it
ems
that
are
impo
rtan
t to
all c
lient
s ac
cord
ing
to th
e th
resh
old
of 7
5% w
e us
ed in
this
stud
y.Bo
ld fi
gure
s in
the
third
col
umn
refle
ct it
ems
that
wer
e pe
rcei
ved
to b
e no
t or s
light
ly m
et d
urin
g pr
enat
al c
ouns
elin
g by
mid
wiv
es in
this
stud
y.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
44
Tabl
e 5
Pre-
coun
selin
g Q
UO
TE pr
enat
al sc
ores
of c
lient
s ra
ting
item
s as
(ver
y) im
port
ant (
scor
e 3
or 4
).
Com
pone
ntA
ll cl
ient
sb
N=9
41a
(%)
Preg
nant
W
omen
N=5
38a
(%)
Part
ners
N=4
03a
(%)
Nul
lipar
aeb
N=4
24a
(%)
Mul
tipa
raeb
N=4
92a
(%)
Wom
en <
36
year
s
N=4
95a
(%)
Wom
en ≥
36
year
s
N=4
3a
(%)
Clie
nt-m
idw
ife re
latio
n86
5(9
7.9)
512
(99.
2)35
3(9
5.9)
394
(97.
3)46
1(9
8.3)
472
(99.
2)40 (1
00)
Hea
lth e
duca
tion
775
(89.
4)45
3(8
4.2)
310
(86.
4)36
8(9
2.9)
386
(83.
9)41
4(8
8.7)
39 (95.
1)De
cisio
n-m
akin
g su
ppor
t32
8(3
8.5)
177
(32.
9)11
3(3
1.5)
156
(39.
8)13
1(2
9.1)
166
(36.
6)11 (2
8.2)
a Sa
mpl
e siz
e va
ries
due
to m
issin
g da
ta. V
alid
per
cent
ages
are
sho
wn.
b W
omen
and
par
tner
s to
geth
er.
Bold
: Sig
nific
ant d
iffer
ence
s be
twee
n gr
oups
(p<.
05).
Tabl
e 6
Post
-cou
nsel
ing
QU
OTE
pren
atal
scor
es o
f clie
nts
ratin
g m
idw
ives
’ per
form
ance
as
(wel
l) do
ne (s
core
3 o
r 4).
Com
pone
ntA
ll cl
ient
sb
N=7
39a
(%)
Preg
nant
W
omen
N
=450
a (%
)
Part
ners
N=2
89a
(%)
Nul
lipar
aeb
N=3
39a
(%)
Mul
tipa
raeb
N=3
92a
(%)
Wom
en <
36
year
s
N=4
17a
(%)
Wom
en ≥
36
year
s
N=
33a
(%)
Clie
nt-m
idw
ife re
latio
n73
9(1
00)
450
(100
)28
9(1
00)
339
(100
)39
2(1
00)
417
(100
)33 (1
00)
Hea
lth e
duca
tion
506
(83.
4)30
0(8
2.0)
206
(85.
5)27
2(9
0.7)
227
(75.
9)28
3(8
3.0)
24 (75.
0)De
cisio
n-m
akin
g su
ppor
t24
2(6
5.6)
135
(63.
4)10
7(6
8.6)
128
(63.
1)11
0(6
8.3)
90 (69.
2)5 (6
2.5)
a Sa
mpl
e siz
e va
ries
due
to m
issin
g da
ta a
nd p
re-c
ouns
elin
g pr
efer
ence
sco
res
(onl
y po
st-c
ouns
elin
g ex
perie
nce
scor
es o
f clie
nts
with
pre
-cou
nsel
ing
impo
rtan
ce s
core
s 3
or 4
are
men
tione
d). V
alid
per
cent
ages
are
sho
wn.
b Pr
egna
nt w
omen
and
par
tner
s to
geth
er.
Bold
: Sig
nific
ant d
iffer
ence
s be
twee
n gr
oups
(p<.
05).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
45
2
DISCUSSION
The current study presents a new research questionnaire to assess parental preferences regarding prenatal counseling for congenital anomaly tests and parental perceptions of midwives’ performance. The QUOTE prenatal consists of three components, which show sufficient reliability: client–midwife relation, health education and decision–making support. In addition, the QUOTE prenatal was used to evaluate current parental preferences concerning prenatal counseling. Results indicate that all clients perceive the client–midwife relation as either important or very important, most clients see health education as important or very important and more than one third of the clients value decision-making support as either important or very important. Furthermore, the present study found that clients perceive that midwives largely act according to their pre-counseling preferences to build a client–midwife relation and receive health education but that they fail to fully oblige clients’ preferences regarding decision-making support.Genetic counseling should ideally consist of health education and decision-making support [9,12,32]. In line with this theoretical model of counseling, our findings showed that most clients have indeed strong preferences for health education. However, only about one third of our population expressed strong preferences for decision-making support, nulliparae more so than multiparae. An explanation for the contradiction of the counseling model and the preferences of clients prior to counseling might be that clients are more familiar with the midwife’s role as a health educator than as a counselor who gives decision-making support. The decision to accept or decline prenatal screening is in some respects a moral decision, and therefore, clients cannot expect professionals to make these decisions for them. However, they can expect support in making these decisions as empowerment to make their own decision, which is part of the nondirective attitude approach during counseling that has been the norm [32–35]. This study suggests that empowerment in making a decision may not be enough; more than two third of the participants prefer getting advice on whether or not to test. This may be a call for a more directive approach of counseling. Our findings reflect the perception of clients whether they got their preferred advice or not. Thus, although our questionnaire was not developed to measure directiveness, the preference of clients that midwives provide advice seems to be in line with more recent research into decision-making support in counseling that stresses the need to use the shared decision-making model during counseling [35–37]. Health professionals using this model can tailor the extent of decision-making support to their clients’ individual preferences. However, Dutch society decided that ultimately the choice for prenatal screening should be well informed but made by couples themselves.The QUOTE prenatal appeared to be able to detect issues that need improvement to ensure that prenatal counseling is in line with client preferences. Despite the relative positive

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
46
experience of clients with the offered health education, midwives in our population only appear to inform clients adequately on about two thirds of the necessary health education aspects; from the clients’ perceptions, one third of the procedural, societal and risk-related aspects of health education was not adequately discussed during counseling. This was more true in perceptions of multiparae compared with those of nulliparae; midwives might have anticipated prior knowledge among multiparae and therefore omitted parts of the health education. The high number of health education issues that need improvement may reflect the results of Houwink et al.[45] that Dutch midwives, at least in the perception of clinical genetic professionals, have a lack of genetic knowledge.Our study indicated that improvement is warranted in decision-making support as well, for those clients who did rate decision-making support as important, which occurred more frequently among nulliparae than multiparae. Prior to initiating, counseling midwives or other prenatal genetic counselors might be advised to consider first whether a client wants support with decision making. The QUOTE prenatal and the shared decision-making model can be used to assess preferences regarding prenatal counseling.To our knowledge, this is the largest nationally representative study of pregnant women’s and their partners’ pre-counseling preferences and post-counseling experiences regarding prenatal counseling for congenital anomaly tests. The proportion of participating clients compared with those eligible was relatively high (79%). Because our sample was heterogeneous in terms of age, parity and religious background, it appears that the findings can be generalized to the wider population of clients of primary midwifery practices, keeping in mind the relatively small proportion of lower-educated participants and participants of non-Dutch origin. The mean age of our pregnant population was similar to the mean age of Dutch pregnant women (29.4 vs 31 years), and the proportions of nulliparae and multiparae (41% and 57%, respectively) differed slightly from the Dutch population (45% and 55%, respectively)[38]. The proportion of non-Dutch participants in our study was 15% versus 20% pregnant residents of non-Dutch origin in the whole country [38]. However, no differentiation between Western origin and non-Western origin of non-Dutch participants was made. Additional research would be useful to assess whether the pre-counseling preferences found in this study also represent the preferences of clients from non-Dutch, non-Western origin.
CONCLUSION
The results of this study indicate that Dutch midwives- largely act according to clients’ preferences with respect to building a client–
midwife relation and receiving health education,- may have to improve some aspects of their health education by discussing
procedural, societal and risk aspects to facilitate an informed choice,

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
47
2
- adjust their counseling for the smaller group of clients who rate decision-making support as important,
- should invite clients together with their partner for prenatal counseling and- can use the QUOTE prenatal to assess their clients preferences pre-counseling to
tailor their counseling to these preferences.
AcknowledgementsWe owe our special thanks to the participating pregnant women and their partners and to the midwives and assistants of the participating midwifery practices, who made this study possible.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
48
REFERENCES
[1] Jakobsen TR, Sogaard K, Tabor A. Implications of a first trimester Down’s syndrome screening program on timing of malformation detection. Acta Obstetrica et Gynecologica Scandinavica. Nord Fed Society Obstet Gyn 2011;90:728–36.
[2] Korenromp M. Prenatal adaptation to termination of pregnancy for fetal anomalies. Utrecht: Dissertation UMC Utrecht, 2006:11–3.
[3] Tischler R, Hudgins L, Blumenfeld YJ, et al. Noninvasive prenatal diagnosis: pregnant women’s interest and expected uptake. Prenat Diagn 2011;31(13):1292–9.
[4] Flessel MC, Lorey FW. The California Prenatal Screening Program: “options and choices” not “coercion and eugenics”. Genetic Medicine 2011;13(8):711–3.
[5] Garcia ME, Timmermans DRM, Van Leeuwen E. Rethinking autonomy in the context of prenatal screening decision-making. Prenat Diagn 2008;28:115–20.
[6] Health Counsel of the Netherlands. Population screening Act: first start with a nationwide program for prenatal screening: Down’s syndrome and neural tube defects. The Hague: Health Counsel of the Netherlands, 2006 publication no. 2006–03.
[7] Resta RG. Defining and redefining the scope and goals of genetic counseling. Am J Med Genetics Part C 2006;142C:269–75.
[8] Liefhebber S, VanDamC,Waelput A. Dutch professional profilemidwives.Utrecht: Royal Dutch organization of Midwives (KNOV), 2005.
[9] Meiser B, Irle J, Lobb E, et al. Assessment of the content and process of genetic counseling: a critical review of empirical. Studies. J Genetic Couns 2008;17:434–51.
[10] Resta R, Bowles - Biesecker B, Bennett RL, et al. A new definition of genetic counseling: National Society of Genetic Counselors’ Task Force report. J Genet Counsel 2006;15(2):77–83.
[11] Van Zwieten MCB. The importance of an informed choice, but what concerns the choice? The complex decision-making in prenatal screening. De Psycholoog 2008;43:20–5.
[12] Roter D, Ellington L, Hamby Erby L, et al. The genetic counseling video project (GCVP). Am J Med Genetics Part C 2006; (142C): 209–20.
[13] De Boer J, Zeeman K. KNOV-guideline prenatal midwifery led care: recommendation for coaching, interaction and information giving. Utrecht: KNOV, 2008:17–46.
[14] Durand MA, Stiel M, Boivin J, et al. Information and decision support needs of parents considering amniocentesis: interviews with pregnant women and health professionals. Health Expect 2010;13(2):125–38.
[15] Kreuter MW, Strecker VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Annals Behav Medicine 1999;21(4):276–83.
[16] Mearns D, Thorne B. Person-Centered Counselling in Action. London: Sage Publications, (2nd edn), 1999;5–21.
[17] Petty R, Cacioppo J. The elaboration likelihood model of persuasion. Advances Experimental Social Psychology 1986;19:123–205.
[18] Todd J, Bohart AC. Foundations of Clinical and Counseling Psychology. New York: HarperCollins College Publishers, (3rd edn), 2005;209–39.
[19] Van Weert JCM, Jansen J, Bruijn de GJ, et al. QUOTE chemo : a patientcentered instrument to measure quality of care preceding chemotherapy treatment through the patient’s eyes. Europ J Cancer 2009;45(17):2967–76.
[20] Shiloh S, Gerad L, Goldman B. Patients’ information needs and decision-making processes: what can be learned from genetic counselees? Health Psychol 2006;25(2):211–9.
[21] Kessler S Psychological aspects of genetic counseling: XI. Teaching and counseling. J Genetic Counsel 1999a;6:287–95.
[22] RIVM. [WWW document]. URL http://www.rivm.nl/Onderwerpen/ Onderwerpen/D/Downscreening.html [accessed on 19 July 2012].
[23] Manniën J, Klomp T, Wiegers T, et al. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Serv Res 2012;12(69), DOI: 10.1186/1472- 6963-12-69.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
49
2
[24] Pieterse A, Van Dulmen S, Ausems M, et al. QUOTE-GENEca: development of a counselee-centered instrument to measure needs and preferences in genetic counselling for hereditary cancer. Psycho-Oncology 2005;14:361–75.
[25] Sixma HJ, Van Campen C, Kerssens JJ, et al. Quality of care from the patients’ perspectives: from theoretical concept to a new measuring instrument. Health Expect 1998;1:82–95.
[26] Van den Brink-Muinen A, Van Dulmen AM, Jung HP, et al. Do our talks with patient meet their expectations? Yes, for the most part. J Fam Pract 2007;56:559–68.
[27] Nijkamp MD, Sixma HJ, Afman H, et al.. Quality of care from the perspective of the cataract patient: the reliability and validity of the QUOTE-cataract. British J Ophthalmol 2002;86:840–2.
[28] Costello AB, Osborne JW. Exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval 2005;10(7):1–9.
[29] Cook DA, Beckman TJ. Current concepts in validity and reliability for psychometric instruments: theory and application. Am J Med 2006;119:166.e7–16.
[30] Field A. Discovering Statistics Using SPSS. London: Sage Publishers, (3rd edn), 2009;627–85. 31. [31] Gutteling JJ, De Man RA, Busschbach JJ, et al. Quality of health care and patient satisfaction in
liver disease: the development and preliminary results of the QUOTE-Liver questionnaire. BMC Gastroenterol 2008;8:25–32.
[32] Ellington L, Roter DL, Dudley W, et al. Communication analysis of BRCA1 genetic counseling. J Genet Couns 2005;14:377–86.
[33] Beckendorf JL, Prince MB, Rose MA, et al. Does indirect speech promote non-directive genetic counseling? Results of a sociolinguistic investigation. Am J Med Genetics 2001;106:199–207.
[34] Van den Berg M, Timmermans DR, Ten Kate LP, et al. Are counsellors’ attitude influencing pregnant women’s attitudes and decisions on prenatal screening? Prenat Diagn 2007;27:518–24.
[35] Smets E, Van Zwieten M, Michie S. Comparing genetic counseling with non-genetic health care interactions: two of a kind? Patient Educ Couns 2007;68:225–34.
[36] Van Zwieten MCB. Non-directivity: a controversial concept. TvG 2003;13(1):20–2.[37] Van Zwieten MCB, Willems D, Knegt L, et al. Communication with patients during the prenatal
testing procedure : an explorative qualitative study. Patient Educ Couns 2006;63:161–8.[38] The Netherlands Perinatal Registry. 10 Years Perinatal Registration in the Netherlands; an
Overview. Utrecht: Stichting Perinatale Registratie Nederland, 2011;26–39.[39] Van den Berg M, Timmermans DR, Ten Kate LP, et al. Informed decision making in the context of
prenatal screening. Patient Educ Couns 2006;63(1–2):110–7.[40] Kleinveld JH. Psychological Consequences of Prenatal Screening. Amsterdam: Dissertation VU
Medical Centre, 2008;18.[41] de Grient- Dreux A, Kooijman H, Korenromp M. Prenatal tests. About Choices and Dilemmas.
Houten: Het Spectrum 2008:46–62.[42] National Public Health Compass. [WWW document]. URL http://www. nationaalkompas.nl/
gezondheid-en-ziekte/ziekte-en-aandoeningen/aangeboren-afwijkingen/centrale-zenuwstelsel/diagnose-behandeling.html [accessed on 19 July 2012].
[43] Wiegers TA, Hingstman L. Het veranderende takenpakket van verloskundigen. Nieuwe cijfers over tijdsbesteding aan specifieke taken. TvV 2008;3:19–24.
[44] Hoogendoorn M, Hamberg-van Reenen HH, van Genugten MLL, et al. Comparison of costs and effects of prenatal screening methods for Down’s syndrome and neural tube defects. Bilthoven: RIVM rapport, 2004; publication no. 230041001/2004: 7–12.
[45] Houwink EJF, van Luijk SJ, Henneman L, et al. Genetic educational needs and role of genetics in primary care: a focus group study with multiple perspectives. BMC Fam Pract 2011;12:5.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 2
50
APPENDIX 1 Prenatal testing in the Netherlands
In the Netherlands, prenatal testing procedures are available to the public. However, Dutch law prohibits the routine introduction of prenatal tests for congenital anomalies in an attempt to protect the population against prenatal testing programs that could be a threat to the psychological and physical health of the person being screened or diagnosed [39]. In other words, this law states that prenatal tests to detect severe anomalies that cannot be cured or prevented should not be offered routinely, but only after thorough informed consent. If pregnant women and their partners in the Netherlands indicate that they want information, the midwife will inform them about the following prenatal tests: Firstly, pregnant women and their partners are offered the opportunity of having the combined test (also known as first trimester screening) early in pregnancy (9–14 weeks).This test provides information on the chance of having a child with Down syndrome (DS), trisomy 13 or 18 based on the combination of nuchal translucency measurement, first trimester maternal serum screening, and maternal age in relation to gestational age. Women older than 36 years have this screening for free, younger women have to pay (people are informed about screening). Secondly, all pregnant women and their partners are offered a Fetal ultrasound Anomaly Scan (FAS) between 18 and 22 weeks gestation. The FAS is made either in hospitals or by certified midwives or sonographers in primary healthcare. Only women at higher risk of carrying a fetus with chromosomal anomalies due to their family history, age 36 years or older, or elevated risk based on the combined test can have amniocentesis or chorionic villus sampling for free [39,40]. Advanced ultrasound is only offered to women if anomalies are seen on the FAS or if they have an increased risk of a child with a structural abnormality which cannot be diagnosed with other prenatal diagnostic tests [41]. Besides these prenatal tests, which are offered in the context of the described law, early in pregnancy (8 to 10 weeks) and in contrast with prenatal tests for congenital abnormality, a routine ultrasound, used to confirm pregnancy, a possible twin pregnancy and the expected date of birth, is offered to all parents. Due to the advanced quality of the ultrasound technology, unexpected findings, such as an increased nuchal translucency, may be found as well [42].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Parental preferences and perceptions regarding prenatal counseling
51
2
APPENDIX 2 Prenatal test uptake in the Netherlands
In the Netherlands, around 160,000 pregnant couples start their prenatal care in primary midwifery care. About 40,000 couples receive obstetrician-led prenatal care in hospitals [40,43]. Seventy-five percent of the low risk couples have the FAS, about 27% of them have the combined test and about one third of all pregnant women older than 36 years have the amniocentesis or chorionic villus sampling [43,44]. Due to governmental policies, the uptake of FAS has increased recently; many women experience FAS as a routine ultrasound and not as a matter in which they have a choice [39,42]. As a result of medical developments and greater focus on the combined test rather than the triple test, the uptake of the combined test has increased, that of prenatal diagnostic tests has decreased [44].


Chapter 3Midwives’ views on appropriate antenatal counseling for congenital
anomaly tests: do they match clients’ preferences?
Martin L, Hutton EK, Spelten ER, Gitsels-van der Wal JT, Van Dulmen S.
Midwifery 2014; 30(6): 600–609.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
54
ABSTRACT
Objective This study aims to provide insight into: a) midwives´ views on appropriate prenatal counseling for congenital anomaly tests, and b) whether these views match clients´ preferences regarding prenatal counseling.
Design A comparative (midwives versus clients) questionnaire survey. Cognitive interviews (N=8) were used to validate the internal validity of the midwifery questionnaire results.
Participants and setting 1416 Dutch midwives (response 62%) completed a questionnaire measuring their views on appropriate prenatal counseling for congenital anomaly tests.
Measurements We used the 58-item midwives’ version of the QUOTE prenatal, an instrument to assess clients’ counseling preferences. Descriptive statistics were used to explore midwives’ views on appropriate counseling and how these relate to client preferences as measured previously with the clients’ version of the QUOTE prenatal.
Findings Almost all midwives consider the client-midwife relation (100%) and health education (95%) to be (very) important for appropriate prenatal counseling for congenital anomaly tests. Almost half of the midwives consider decision-making support (47%) to be (very) important. These findings are practically congruent with client preferences. Still, clinically relevant differences were found regarding 13 individual items, e.g. more clients than midwives value ‘medical information about congenital anomalies’ and ‘getting advice whether to take prenatal tests or not’.
Key conclusion Like clients, most midwives value a good client-midwife relation and health education as (very) important for prenatal counseling for congenital anomaly tests. Less than half of them value decision-making support. These findings are in contrast with the literature in which decision-making support is seen as the most important part of prenatal counseling for congenital anomaly tests.
Implication for practice Preferably, prenatal counseling for congenital anomaly tests should be consistent with the three-function model of prenatal counseling i.e. maintaining a client-midwife relation, providing health education as well as decision-making support, and tailored to clients’ individual preferences. Since not all midwives subscribe to these functions, reflection on their views is important. Furthermore, midwives need to bridge their views on appropriate prenatal counseling and client preferences. To do so, midwives may benefit from the Shared Decision Making approach.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
55
3
INTRODUCTION
Medical and policy developments in prenatal screening and diagnostic testing have led to a rapid increase in the number of congenital anomalies for which testing is available [1,2]. The amount of information about testing that is communicated to clients has increased and seems difficult to manage for both counselors and clients [3,4]. In the Netherlands, prenatal screening for congenital anomalies has been available since 2007. Primary care midwives are the designated counselor in about 80% of the pregnancies [5,6]. They are trained to offer prenatal counseling to help clients understand information about congenital anomaly tests and to help clients in making autonomous, informed decisions [7,8].Appropriate counseling usually serves the two functions teaching and counseling, embedded within a non-directive approach [9-11]. In the context of prenatal counseling, these counseling functions are referred to as health education and decision-making support [12]. An important third function, i.e. maintaining a patient-provider relationship, is considered to be a prerequisite for enabling these two counseling functions [13,14].While providing health education, midwives enhance clients’ knowledge by giving medical information about topics such as the prenatal tests available and the anomalies that can be diagnosed, but no golden standard exists for the information needed to make an informed decision about participation in prenatal screening [15-18]. During decision-making support counselors help clients in making autonomous, informed decisions by for instance discussing diverse scenario’s and putting moral issues on the agenda [8,19]. A good client-counselor relation can be established by showing empathy and unconditional support regardless of the decision a client makes about taking or refusing a prenatal test or by terminating or continuing a pregnancy [14,20].Clients differ in the value they attach to the three functions of the prenatal counseling model, including the non-directive approach. Most Dutch clients do value the client-midwife relation and health education as important functions of prenatal counseling. A relatively smaller group values decision-making support as an important function, although more than two third of the clients value one specific aspect of decision-making support, i.e. ‘getting advice on whether to have prenatal tests or not’ [12]. So, for the majority of clients, the three function prenatal counseling model fits well with their preferences, and a significant number of clients indicate that they value a directive approach during decision-making support expressed in the need for advice. This suggests that a personalized approach to counseling that takes clients’ individual preferences regarding the topics discussed as well as their need for decision-making support (e.g. non-directive versus more directive or Shared Decision Making) into account will be most likely to meet client needs [12]. These findings are consistent with client preferences for personalized health care in general and prenatal care in particular [21-24].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
56
There has been little investigation of the views of counselors regarding the three-function model of prenatal counseling, including the non-directive approach. Roter et al. [9] describes some scepticism regarding the desire of genetic counselors to fully address the decision-making support function of counseling. The study of Sheets et al. [25] illustrates that genetic counselors and parents differ in the importance they attach to different aspects of information (or health education) about having a child with Down syndrome. In the context of end of life counseling health care providers seem to be reluctant to offer advice about treatment options even when patients specifically asked for it [26]. Understanding counselors’ views on appropriate counseling is important. If counselors do not endorse all three functions of the prenatal counseling model, the provision of appropriate, personalized prenatal counseling may be at risk. This paper aims to describe midwives’ views on appropriate prenatal counseling for congenital anomaly tests focussing on the three functions of the prenatal counseling model, health education, decision-making support and the client-midwife relation and to compare midwives’ views to previous findings on clients´ preferences [12]. The following research questions are addressed: a) what are midwives´ views on appropriate prenatal counseling for congenital anomaly tests, and b) do these views match clients´ preferences regarding prenatal counseling? It was hypothesized that midwives attach more importance to health education than to decision-making support as a result of the extensive amount of information they are obliged to give according to Dutch educational programs and research [15-18]. Midwives are also most familiar with the role of health educator since the role of counselor has been relatively recently (2005) introduced in the midwifery profession as well as in the prenatal screening program in the Netherlands (2007) [6,27] (See for more information about the Dutch prenatal counseling setting Appendix A).
METHODS
This study is part of the DELIVER study, a multi-center national research program to evaluate the quality and provision of primary midwifery care in the Netherlands [28].The design of the current nation-wide cross-sectional study was approved by the Institutional Review Board and the Medical Ethical Committee of the VU University Medical Centre, Amsterdam, The Netherlands.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
57
3
Participants
MidwivesAll midwives who were members of the Royal Dutch Associations of Midwives (KNOV) were invited to participate in our cross-sectional survey questionnaire in November 2010. 87% of the Dutch, working midwifery population and 98% of the midwives working in primary midwifery care are members of the KNOV [29].
ClientsIn the current study we used data from our cross-sectional study about parental preferences and experiences regarding prenatal counseling for congenital anomaly tests by midwives [12] and compared those findings with the results of the midwife questionnaire. In the study of clients, 941 parents from 17 Dutch midwifery practices, including 538 women and 403 partners, participated. The sample of participating women was representative for the Dutch pregnant population except for level of education (the sample was higher educated compared to the pregnant Dutch population) and ethnicity (the sample contained lower percentages of non-Dutch compared to the pregnant Dutch population). Significantly more pregnant women valued the client-midwife relation as important or very important compared to partners, 99% versus 96% respectively. Women and their partners placed the same value on the health education function; 85% valued this prenatal counseling function as important or very important. Decision-making support was valued important or very important by more than one third of the women and their partners [12]. Since the differences between women and partners regarding their valuation of the client-midwife relation seem to have no practical relevance, we use the overall results of women and partners in this study.
MeasuresBackground characteristics The self-administered questionnaire for midwives contained socio-demographic items such as age, gender, work experience, country of origin and religion.
Midwives’-version QUOTE prenatal questionnaireThe questionnaire used to measure midwives’ views on appropriate prenatal counseling for congenital anomaly tests mirrored the 58-item QUOTE prenatal questionnaire (Quality of care through the patients’ eyes), that we developed to assess clients’ preferences and experiences regarding this type of prenatal counseling. Used among parents, the QUOTE prenatal questionnaire showed high levels of internal consistency measured with Cronbach’s alpha [12]. We used the same items of the QUOTE prenatal in this study, but rephrased them in order to change the focus to midwives’ views on appropriate prenatal counseling (see tables 3a,3b,3c for the resulting midwives’-version QUOTE prenatal questionnaire).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
58
The questionnaire contains generic communication items and specific items about prenatal counseling for congenital anomaly tests [12]. The three functions of prenatal counseling were addressed in the three components of the QUOTE prenatal questionnaire: 15 items covered the client-midwife relation (i.e. generic items), 24 items covered health education (i.e. specific items) and 16 items concerned decision-making support (i.e. specific items) (Table 2 and Tables 3a, 3b, 3c). The remaining 3 items covered statements about organizational aspects of prenatal counseling, such as number of consultations used for pre-test counseling. The items of the questionnaire were formulated as importance statements (‘As a midwife I perceive as important for prenatal counseling, that…’) to be answered on a 4-point scale. Response options were 1, ‘not important’; 2, ‘fairly important’; 3, ‘important’; and 4, ‘very important’. When used in the midwife population, we found good Cronbach’s alpha estimates of internal consistencies for the three components of the questionnaire: client-midwife relation 0.86, health education 0.86 and decision-making support 0.82. Item-total correlations (ITCs) were higher than the threshold of 0.30 we used (ranging up to 0.65), except for Q56, Q3 and Q9 [30]. These three items with low ITC scores were not removed when we adapted the questionnaire for use with care providers so that the measurement tool would mirror the results from the client QUOTE prenatal as much as possible. We undertook internal validation of the findings of the questionnaire using Cognitive Interviews (CI) (N=8) [31]. During the Cognitive Interviews midwives, who had not yet completed the questionnaire, were asked to complete the questionnaire while thinking aloud, including the indication of their rating for each questionnaire item. Participants were instructed to complete the questionnaire from the perspective of their view on appropriate prenatal counseling for congenital anomaly tests as if there were no practical limitations such as time and rewarding system. The interviews were audio-taped and transcribed verbatim. Results of the CI show that midwives indeed interpreted and rated most items of the questionnaire focusing on their views of appropriate counseling without letting practical limitations disturb their ratings. Still, 15 items were partially interpreted and answered while taking into account the limitations of daily practice (Tables 3a,b,c items marked with #).
ProceduresQuestionnaires were sent to the home address of midwife participants in order to minimize bias due to influences of colleagues. A prepaid and preaddressed return envelope could be used to return the questionnaires. After two weeks, non-responders received a reminder including a new questionnaire and return envelope.
Analyses If 15% or less of the values were missing on item level of the questionnaire, the missing values were replaced by the mean on the sub-scale. Analyses were carried out using SPSS 17.0.2.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
59
3
Participants Descriptive statistics were used to describe the demographic characteristics of participants who completed the questionnaire. We compared characteristics of respondents with characteristics of the National midwifery population to examine the representativeness of our research sample concerning the variables: age, gender and location of vocational education.
Midwives’ views on appropriate counselingIn line with our earlier study using the QUOTE prenatal methodology [12] importance scores on the three components of the questionnaire were used to rate views on aspects of appropriate counseling. Importance scores were calculated as the percentage of midwives who rated individual items as important (score 3) or very important (score 4) or components as important or very important (scores ≥2.50).
Midwives´ views on appropriate prenatal counseling and clients’ preferences Midwives’ views on aspects of appropriate prenatal counseling for congenital anomaly tests were compared to clients’ preferences regarding prenatal counseling as reported in our previous paper [12]. If both midwives and clients value the same components or items of the components as important or very important, this was considered as congruence between midwives’ views and client preferences. If more than 75% of the midwives listed components and/or items as important or very important for appropriate counseling, but less than 75% of the clients or vice versa, with a difference of at least 10%, we considered this as a clinically relevant difference in midwives’ views on appropriate counseling and client preferences.
FINDINGS
Participants Of the 2300 eligible midwives, 1416 (62%) completed and returned the questionnaire. Table 1 shows that 1354 (98%) of the participating midwives were female, 24 (2%) were male. Mean age was 37.9 years, (SD=10.4). Mean years of work experience was 11.9 years (SD=9.3). A comparison with the characteristics of the study population and the Dutch midwifery population showed no differences in percentages of >5%, except for the category ‘other’ regarding ‘place of education’. Five hundred and forty seven (39%) of the respondents were religious and 737 (52%) were non-religious. As missing data per item were ≤5% for each of the items of the questionnaire, missing values were not replaced.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
60
Table 1 Demographic Characteristics of the test Sample Midwives (N=1416) and of the Dutch midwifery population.
Characteristics Sample of Midwives Dutch midwifery population a
Membership KNOV N=1416 (100%) N=2264 (86.7%)AgeMean; SD; missing 37.9 years; 10.4; 41 (2.9%)N (%) < 40 years 835 (60.1) 1644 (63) N (%) > 55 years 95 (6.8) 198 (7.6)GenderMaleFemaleMissing
N (%)24 (1.7)1354 (95.6)38 (2.7)
N (%)43 (1.6)2569 (98.4)
Place of graduationAmsterdamGroningenMaastrichtRotterdamOther / AbroadMissing
383 (27.0)74 (5.2)373 (26.3)356 (25.1) 174 (12.3)56 (4.1)
641 (25)147 (6)660 (25)638 (24) 523 (20)3 (0.1)
Religious backgroundReligiousNon-religiousMissing
547 (38.6)737 (52.0)132 (9.4)
Not available
Work experienceMean; SD; Missing (%) 11.9 years; 9.3; 44 (3.1) Not available
a Hingstman and Kenens, 2011.
Midwives’ views on appropriate counseling Table 2 shows that two of the three functions of prenatal counseling as measured with the components of the questionnaire, client-midwife relation (100%) and health education (95%), are perceived as important for appropriate prenatal counseling for congenital anomaly tests by almost all midwives. Forty seven percent of the midwives considered the component decision-making support as either important or very important for appropriate counseling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
61
3
Table 2 Components of the questionnaire and the content. Column three and four: Midwives and clients rating the three components (very) important for prenatal counseling (scores 3-4).
Component Content Midwives N=1416a
(%)*
Clientsb N=941 (%)*
Client-midwife relation
Items reflect the client-centered attitude of the midwife during the professional consultation or items that describe conditions for having a client-centered conversation
1293(99.9)
865(97.9)
Health education Medical test information, (test) procedural information, risk information, societal information (e.g. costs of prenatal tests, eligibility for tests)
1154(95.4)
775(89.4)
Decision-making support
Exploration of values, social support and pressure on decision-making, discussion about the different options and outcomes of scenarios
581(47.0)
328(38.5)
* Valid percentages.a Sample size varies due to missing data. Missing value analyses showed 91% (N = 1283) complete cases for the component client-midwife relation, 85% (N = 1198) complete cases for Health education and 87% (N = 1226) completed cases for Decision-making support. b Clients: pregnant women and partners.
Looking at item level, tables 3a, 3b and 3c show the percentages of midwives who rated the individual items of the three components as important or very important, ranked from high to low. Scores on the 15 individual items, concerning the client-midwife relation, ranged from 100% to 76%, with highest scores for the items ‘Listen to what the client is trying to ask’ (Q6); ‘Use clear and comprehensible language’ (Q16). The two items with lowest percentages were ‘Show empathy (Q10)’ and ‘Tell the client that she can always contact me about questions she may have (including when the practice is closed)’(Q18). Percentages of scores on the 24 items concerning health education ranged from 98% to 41%. Thirteen of these 24 items were listed as important or very important for appropriate counseling by more than 75% of the participating midwives, with highest percentages for the items ‘Explain the usefulness of prenatal screening to the client’ (Q31) and ‘Tell the client about all the different types of prenatal tests’ (Q32) (Table 3b). The two items with lowest percentages were: ‘only discuss specific information about follow-up test and possible anomalies with the client if it becomes clear that the client will need them’ (Q56) and ‘Tell the client about the incidence of birth defects in the Netherlands’ (35) (Table 3b).Furthermore, table 3c shows that percentages of scores on five of the 16 items concerning decision-making support reached the 75%, with highest percentages for the two items concerning tailored communication: ‘Respond to what the client already knows about prenatal screening’ (Q22) and ‘Am interested in who the client is’ (Q21). The two items with lowest percentages were: ‘Ask whether client’s family, friends or other people close to her would support her decision about prenatal screening’ (Q51) and ‘Ask whether client’s family,

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
62
friends or other people close to her would support her decision to terminate the pregnancy if the child were to have a congenital abnormality’ (Q54) (Table 3c).Regarding organizational items of prenatal counseling none of the items were interpreted as important for appropriate counseling by more than 75% of the participants. Most midwives value asking the client to come together with their partner to the prenatal counseling as important or very important (67%) and scheduling a separate appointment for counseling was least valued (19%).
Table 3a Items of the QUOTE prenatal regarding the client-midwife relation. Figures show the number and percentage of midwives and clients who rated these items as (very) important (scores 3 or 4).
Number Item description:For me it is important that I as a midwife…
Midwives N=1416a (%)*
Clientsb
N=941 (%)* Client – midwife relation
Q6 Listen to what my client is trying to ask 1347 (100) (99.7)Q16 Use clear and comprehensible language 1348 (99.9) (95.1)Q1#& Take plenty of time to answer clients questions 1342 (99.6) (98.3)Q5& Take clients concerns seriously 1343 (99.5) (98.9)Q19 Accept clients’ decisions on whether or not to opt for
prenatal screening1321 (98.1) (87.9)
Q15& Make clear that my client can ask anything she wants to know
1320 (97.8) (92.5)
Q23# Paint a realistic picture (not just through ‘rose-tinted spec-tacles’)
1314 (97.3) (93.8)
Q4 Put my client at ease 1307 (97.1) (96.8)Q7 Am open and honest about every aspect of the pregnancy 1293 (96.1) (98.3)Q12 Know what the client is talking about 1291 (96.1) (80.9)Q8#& Give the client enough time to explain herself properly 1270 (94.7) (92.9)Q17 Give the client (additional) written information 1260 (93.5) (60.0)Q24& Give my client the feeling that I am tuning in to her as a
person1254 (92.8) (82.8)
Q18# Tell the client that she can always contact me with any questions she may have (including when the practice is closed)
1229 (91.2) (79.8)
Q10 Show empathy 1015 (75.5) (61.7) *Valid percentages. a Sample size varies due to missing data. Missing data were found for 25 items of the questionnaire ranging from 5% to 10%.b Clients: pregnant women and partners.Bold figures contain items which are either important for ≥ 75% of the midwives, but not for ≥ 75% of the clients or vice versa. # Items that were at least partially interpreted and answered in the context of the limitations of daily practice. & Items that were answered in the context of required prenatal counseling, although limitations of daily practice prevented participant from acting accordingly.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
63
3
Table 3b Items of the QUOTE prenatal regarding the health education. Figures show the number and percentage of midwives and clients who rated these items as (very) important (scores 3 or 4).Number Item description:
For me it is important that I as a midwife…Midwives N=1416a (%)*
Clientsb
N=941 (%)*
Health educationQ31& Explain the usefulness of prenatal screening (what the client can decide to do
eventually)1320 (98.1) (90.0)
Q32# Tell the client about all the different types of prenatal tests 1318 (98.0) (86.8)Q13 Impart information on prenatal testing 1310 (97.8) (88.2)Q26& Explain which anomalies can be identified using prenatal screening 1300 (96.7) (90.7)Q58 Make sure that the topics the client consider to be important are discussed at
length1286 (95.9) (88.8)
Q43 Explain which prenatal tests will be done first and which will be done later, if required and/or necessary
1278 (94.9) (82.7)
Q45 Explain how long the client may take to decide whether or not to have the prenatal tests
1271 (94.5%) (81.0)
Q48# Discuss all clients options with regard to prenatal screening and the implications 1206 (90.1) (82.3)Q29& Discuss possible negative implications of prenatal screening for the unborn child 1201 (89.8) (95.2)Q36 Ask about clients family´s history of birth defects 1206 (89.7) (77.1)Q33& Tell the client how prenatal screening can affect her emotions and mental
wellbeing1181 (87.9) (74.9)
Q41 Tell the client why she is or is not eligible for certain prenatal tests 1164 (86.7) (82.4)Q42 Explain what will happen DURING the prenatal tests 1120 (83.5) (87.0)Q27# Explain which anomalies cannot be identified using prenatal tests 985 (73.3) (85.4)Q39 Tell the client about HER chances of having a child with a congenital
abnormality during this pregnancy984 (73.3) (83.6)
Q40 Talk to the client about how HER risk of having a child with a birth defect will affect her
982 (73.2) (76.3)
Q44 Explain who will give the client the results of the prenatal tests and how (verbally, in writing or by telephone)
982 (73.0) (68.3)
Q37 Explain how often congenital anomalies occur in pregnant women of clients age 937 (69.6) (68.4)Q46 Explain how long the client may take to decide whether or not to terminate
the pregnancy, should the test results show an anomaly933 (69.5) (81.8)
Q34& Tell the client how much prenatal tests cost 890 (66.1) (55.9)Q38# Explain how the chances of a birth defect are calculated for the clients unborn
child843 (62.7) (72.5)
Q28 Provide medical information about the anomalies that are being tested for 681 (50.6) (76.0)Q56@ Only discuss specific information about follow-up tests and possible
anomalies with the client if it becomes clear that the client will need this information
640 (50.4) (75.1)
Q35 Tell the client about the incidence of birth defects in the Netherlands 550 (41.0) (54.4)
*Valid percentages. a Sample size varies due to missing data. Missing data were found for 25 items of the questionnaire ranging from 5% to 10%. b Clients: pregnant women and partners.Bold figures contain items which are either important for ≥ 75% of the midwives, but not for ≥ 75% of the clients or vice versa. # Items which are at least partially interpreted and answered in the context of the limitations of daily practice.& Items that were answered in the context of required prenatal counseling, although limitations of daily practice prevented participant from acting accordingly.@ Items with low Item Total Correlation (≤ .30).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
64
Table 3c Items of the QUOTE prenatal regarding the decision-making support. Figures show the number and percentage of midwives and clients who rated these items as (very) important (scores 3 or 4).Number Item description:
For me it is important that I as a midwife…Midwives N=1416a (%)*
Clientsb N=941 (%)*
Decision making supportQ22& Respond to what the client already knows about prenatal screening 1232 (91.3) (65.9)Q21 Am interested in who the client is 1186 (88.4) (50.6)Q11 Am understanding about clients ideological background or religion 1183 (87.6) (32.3)Q20 Ask the client questions that makes her think 1168 (86.6) (65.0)Q25 Encourage the client and her partner to talk together about prenatal
screening1151 (85.3) (47.0)
Q55 Ask how the client thinks she will react to the results of the prenatal tests 821 (61.2) (49.5)Q14# Enquire clients’ standards, values and views on prenatal screening and
diagnostic738 (54.9) (45.7)
Q49# Talk to the client about how her family and she would react to a child with a birth defect
727 (54.2) (61.3)
Q50# Ask the client to explain her decision to take / not to take the prenatal tests 624 (46.5) (51.7)Q3@ Tell which websites the client can use to find information about prenatal
screening and diagnostic617 (45.9) (37.0)
Q53 Ask whether test results indicating that clients unborn child has a birth defect would cause problems with her conscience
578 (43.2) (48.2)
Q30# Tell the client what the Dutch government aims to achieve by providing prenatal tests
434 (32.4) (42.4)
Q52# Ask the client what for her constitutes a healthy child 294 (21.9) (45.1)Q9@& Advise the client about whether or not to take the prenatal tests 214 (16.5) (69.8)Q54 Ask whether clients family, friends or other people close to her would
support her decision to terminate the pregnancy if the child were to have a congenital abnormality
185 (13.8) (22.0)
Q51 Asks whether clients family, friends or other people close to her would support her decision about prenatal screening
100 (7.5) (16.2)
Organizational itemsQ47# Ask the client and her partner to come to the counseling session on
prenatal screening TOGETHER898 (67.0) (75.5)
Q59 Plan two appointments to discuss prenatal tests (1 to provide the relevant information and 1 to discuss the decision)
328 (24.7) (33.4)
Q57# Make a separate appointment for the client to discuss prenatal tests (rather than broaching the subject during the first appointment)
258 (19.3) (21.8)
*Valid percentages. a Sample size varies due to missing data. Missing data were found for 25 items of the PAC questionnaire ranging from 5% to 10%. b Clients: pregnant women and partners.Bold figures contain items which are either important for ≥ 75% of the midwives, but not for ≥ 75% of the clients or vice versa. # Items which are at least partially interpreted and answered in the context of the limitations of daily practice.& Items that were answered in the context of required prenatal counseling, although limitations of daily practice prevented participant from acting accordingly.@ Items with low Item Total Correlation (≤ 0.30).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
65
3
Midwives´ views on appropriate prenatal counseling and clients’ preferences Table 2 shows that two of the three components of appropriate counseling can be considered as important for most midwives and clients; the client-midwife relation (100%midwives and 98%clients) and health education (95%midwives and 89%clients). Decision-making support is considered important or very important for appropriate counseling by fewer midwives and fewer clients (47%midwives and 39%clients).At item level, focussing only on items valued as important or very important by ≥75% of the midwives or clients, Tables 3a, 3b and 3c show incongruence of ≥10% between midwives and clients on 13 of the 58 items of the questionnaire in the valuation of aspects of prenatal counseling. Concerning the client-midwife relation items Q10 and Q17 were considered important or very important by most midwives but not by most clients with the biggest divergence found for ‘Give the client (additional) written information’ (Q17: 94%midwives and 60%clients).Regarding health education five items were considered important by most clients but not by most midwives (Q27, Q28, Q33, Q39, Q46, Q56). The biggest divergence was found for ‘only discuss specific information about follow-up tests and possible anomalies with the clients if it becomes clear that the client will need them’ (Q56: 50%midwives and 75%clients) and ‘provide medical information about the anomalies that are being tested for’ (Q28: 51%midwives and
76%clients). As for decision-making support five items (Q11, Q20, Q21, Q22, Q25) were considered (very) important by most midwives but not by most clients. The biggest divergence was found for ‘Am understanding about clients ideological background or religion’ (Q11: 88%midwives and 32%clients) and ‘encourage the client and her partner to talk together about prenatal screening’ (Q25: 85%midwives and 47%clients). Furthermore, Table 3c shows that, in particular, most midwives value item Q22 ‘respond to what the client already knows about prenatal screening’ (91%midwives and 66%clients) important, whereas most clients value item Q9 ‘advise the client about whether or not to take the prenatal tests’ (17%midwives and 70%clients) important of this component.
DISCUSSION
The first aim of the study was to explore midwives’ views on appropriate prenatal counseling for congenital anomaly tests. The second aim was to evaluate whether these views of midwives match clients’ preferences regarding prenatal counseling.The current questionnaire survey suggests that of the participating midwives, although most consider that appropriate counseling includes building a good client-midwife relation and giving health education, less than half perceived decision-making support as an important or very important function of appropriate counseling. Therefore, our findings suggest that more than half of the midwives do not fully subscribe the three function model of prenatal counseling for congenital anomalies as described in the literature.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
66
Comparisons between midwives’ views on appropriate prenatal counseling and client preferences show congruence in the importance they assign to the three counseling functions client-midwife relation, health education and decision-making support. However, results on item-level suggest clinically relevant differences between midwives’ views and clients’ preferences regarding prenatal counseling for congenital anomaly tests.
Midwives’ views on appropriate prenatal counselingAmongst the health education items regarding prenatal counseling for congenital anomaly tests midwives value as most important items about the content and chronology of the Dutch prenatal screening program. The least valued health education items could be characterized as either items with the potential to negatively impact on the experience of pregnancy or as risk communication and procedural aspects of prenatal screening tests. An explanation might be that midwives do not want to disturb the feelings of happiness their clients may have about the pregnancy by addressing – during the first contact they have with their clients – the possible unfortunate outcomes of the pregnancy. In addition, midwives, like other prenatal counselors [4], may have problems addressing all health education topics that have to be discussed and therefore prefer not to talk about procedural aspects of prenatal congenital anomaly tests; clients can learn about this after they choose to take a prenatal test. Therefore, it may be that this information is seen as less important for achieving informed decision making in clients and thus consistent with appropriate prenatal counseling for congenital anomaly tests.Concerning decision-making support, midwives in this study perceived ‘being interested in who the client is’ and ‘tailoring their counseling to the individual client’ as (very) important, but most of them did not perceive questions about social support or pressure as such. In addition, according to almost all participating midwives ‘giving advice’ seemed inappropriate in the process of prenatal counseling. This may be due their interpretation of non-directive counseling; an approach that is associated with forbearance of giving advice and anything that comes close to that [8]. Dutch midwives are educated according to this non-directive approach and this study shows that they seem to agree with it [7]. An explanation for the apparent contradiction between the relatively high importance midwives assign to ‘asking questions that make the client think’ and the relatively low importance they assign to the examples of such questions in our questionnaire, could be found in the results of the Cognitive Interviews (CI). The results of the CI show that at least four of the items that could be used to make clients think more deeply about their decision were answered in the context of the limitations of daily practice; i.e. midwives might find these items important but do not use them in practice due to a lack of time and therefore mark them as not important or fairly important completing the questionnaire. In other words, the results regarding decision-making support could be an underestimation of the importance midwives attach

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
67
3
to these items in order to reach appropriate prenatal counseling for congenital anomaly tests. Therefore, midwives might benefit from developing communication skills so that they can better explore their clients’ wishes and are subsequently better prepared to help clients make decisions even in the context of the limitations of daily practice.
Midwives’ views and clients’ preferencesPersonalized, appropriate prenatal counseling for congenital anomaly tests is only possible if professionals provide counseling which is consistent with the principles of the gold standard of prenatal counseling and also meets the needs of each individual client. Within the perspective of the three function model of prenatal counseling as reflected in the three components of the questionnaire, this study shows high congruence between midwives’ views on appropriate counseling and client preferences, but low congruence to the golden standard which includes decision-making support as an important aspect of prenatal counseling. Furthermore, there are some important differences on item level between midwives’ views and client preferences. Regarding the client-midwife relation, relatively more midwives than clients value ‘giving the client (additional) written information’. Knowing the relatively small amount of information people can recall after a health consultation [33] and the need for clients to make an informed decision, to give written information seems reasonable. However, the most important part is that clients actually read this information. If clients do not value written information, it seems unlikely they will read it unless, during the counseling, they are motivated to do so. It might be useful to test whether more clients would highly value written material that was directly referred to during the counseling visit or material that was provided as ‘homework’ before the actual counseling, especially if during the counseling this information was tailored to the individual client.A comparison on item-level of midwives’ views on prenatal counseling and client preferences regarding the health education component items, shows that more clients prefer to get medical, risk and procedural information than midwives in this study seem to perceive to be important for appropriate prenatal counseling. In literature there is no consensus about what information should be given [15] although some guidelines exist [15-18]. These guidelines, however, only partially account for the perspective and preferences of clients; they are based on expert group opinions [15,18]. Midwives in our study did not fully subscribe to the importance of the items that should be addressed during health education according to the current guidelines. This study also detected a discrepancy between what midwives think is relevant information to guarantee informed decision-making and what the bigger group of clients perceive as important to make their personal choice to take or refuse congenital anomaly tests. It seems reasonable that client preferences should be addressed, while midwives have also to make clear why the information they share with clients is important

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
68
for them to know in the context of the decision about prenatal congenital anomaly tests. The Shared Decision Making model could facilitate this communication, because it structures the discussion about relevant information exchange and makes clear that the role of expert can shift from professional to client and vice versa [13].Concerning decision-making support items, reflecting a genuine interest in the client and stimulating the client to make an informed, autonomous, personal decision about whether to take the prenatal tests or not, seems to be relevant for almost all midwives. None of these topics seems to be relevant to many clients. Furthermore, the important topic for most clients, ‘getting advice whether to take prenatal tests or not’ is not seen as important by most midwives. These results seem to reflect that midwives are willing to help their clients in making their decision, using counseling techniques such as asking exploring questions that make clients really think about the decision they face. Clients, conversely, appear to want at least a more clearly focused discussion about what to do. The Shared Decision Making model could serve as a bridge between both midwife and client expectations for decision-making support, including the notion that it is the client that has to make the ultimate decision about whether to take or refuse prenatal congenital anomaly tests; at least in Dutch society. Therefore, like other researchers, we emphasize the importance of flexibility in the way prenatal counselors structure the decision-making process so that individual differences in client preferences can be respected while incorporating the goals of prenatal counseling, prenatal testing and who the expert is in the area at hand [8,32,34,35]. As many parents prefer to make their informed choices about prenatal tests together, it is easy to understand why clients value the opportunity for joint counseling. So, although, one third of the midwives do not value having partners invited to attend the prenatal counseling for congenital anomaly tests, we suggest that they should invite them explicitly.The counseling role is a recent one for Dutch midwives. Counseling for prenatal congenital anomaly tests is one example of the counseling topics midwives have to address in the context of the increasing medicalization of pregnancy and childbearing and the resulting preference sensitive decisions that have to be made [27,36]. From the perspective of the unique history of Dutch midwifery, characterized by a minimal use of medical interventions, the client’s views on specific medical advice on these prenatal tests are highly relevant, and might signal a historical shift in expectations of the role of midwives in the more and more medicalised pregnancy and birth process. The shared decision making (SDM) approach could be seen as an answer to this shift towards more clients involvement in decision-making. This approach is recently found to be worthwhile in view of other obstetric decisions such as the decision about birth position [37]. The SDM model would move midwives from a health care provider-centered approach in which the midwife sets the agenda and makes the decisions to a model wherein midwives and clients work together towards personalised care and decision-making. Although the SDM model is being advocated as the solution for strengthening the patient’s

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
69
3
role, it remains challenging to accomplish this in every day practice, because of the many other demands good practice make on the provider-patient interaction [38,39]. Nevertheless seems the SDM model promising in addressing clients’ expectations for the role of midwives.
Strengths and limitations To our knowledge, this is the largest nationally representative study of midwives’ views on appropriate prenatal counseling for congenital anomaly tests. The response rate of participating midwives was relatively high (62%). Since our sample was heterogeneous in terms of age, years of experience and religious background, the findings can be generalized to the wider population of Dutch midwives. The proportion of midwives younger than 40 years in our population (60%) was similar to this proportion in Dutch midwifery population (63%) and the proportion of male midwives was the same in our population compared to the general midwifery population (1.7% versus 1.6% respectively).The internal consistency of the midwives’-version QUOTE prenatal questionnaire was good, based on the Cronbach’s alphas we found in this study. ITC of three items were too low (Q3, Q9 and Q56). If we had removed these items from analyses on component level, the overall importance midwives attach to the corresponding prenatal counseling functions (i.e. health education and decision-making support) would be higher, because midwives address relatively low importance to these aspects of the counseling functions. Consequently, the congruence between midwives’ views and the three function model of prenatal counseling as described in literature would have been better than is reflected in the results of this study. Midwives were asked to rate the items of the questionnaire as if working in an ideal world without problems such as a lack of time or knowledge. However, the results of the Cognitive Interviews suggested that although midwives were asked to refer to their ideal practice, daily practice have also been influencing their answers. Therefore, the findings of this study have to be seen in the light of the possibly undesirable impact of clinical midwifery practice on the reported views on appropriate prenatal counseling. The midwives’ version of the QUOTE prenatal questionnaire could be used in future research, keeping in mind the limitations we mentioned. Further research of our research group will be done to investigate to what extent views on appropriate prenatal counseling for congenital anomaly tests actually influence this counseling in daily practice. Such data will potentially provide insight into aspects that contribute to the performance of counselors in clinical practice.
Key Conclusion Midwives in our study do not all subscribe fully to the three function model of prenatal counseling for congenital anomaly test. Like clients, almost every midwife looks upon counseling as consisting of building a good client-midwife relation and providing health

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
70
education. Almost half of the participating midwives perceive decision-making support as a (very) important function of appropriate prenatal counseling. This focus on giving information may inhibit midwives in daily practice from establishing a real dialogue during prenatal counseling. Consequently, it may cause difficulties in adapting prenatal counseling to individual client preferences - which midwives consider to be important - because engaging in dialogue is required to get to appreciate individual preferences. It may also cause problems in reaching the prenatal counseling goal (informed, autonomous decision making by clients) for which the three functions of prenatal counseling are required.
Implication for practice Midwives and other professionals who provide prenatal counseling should discuss their attitude towards their role as prenatal counselor with clients in order to ensure that client preferences may be met in conformity with professional standards. Literature based guidelines, professional expertise and client preferences all together determine appropriate, client specific prenatal counseling. The Shared Decision Making model may be useful in establishing a dialogue with clients (women and partners) in order to cope with incongruences between midwives’ views on appropriate counseling and client preferences, especially regarding the health education and decision-making support functions of counseling.
AcknowledgementsWe gratefully acknowledge the AVAG for funding this study. We also thankfully admit the contribution of the midwives in the Netherlands, who provided data for this study. We also thank M. Piksen, B. Meijer, W. Stavenuiter and C. van Schoor, students of the Midwifery Academy Amsterdam in June 2011, for their work on the Cognitive Interviews. Last but not least we gratefully acknowledge the contribution of Lisanne Gitsels and Lotte Smits for data entry in SPSS.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
71
3
REFERENCES
[1] Jakobsen TR, Sogaard K, Tabor A. Implications of a first trimester Down’s syndrome screening program on timing of malformation detection. Acta Obstetrica et Gynecologica Scandinavica 2011; 90: 728-736.
[2] Tischler R, Hudgins L, Blumenfeld YJ, Greely HT, Ormond KE. Noninvasive prenatal diagnosis: pregnant women’s interest and expected uptake. Prenatal Diagnosis 2011; 31(13): 1292-1299.
[3] Shiloh S, Gerad L, Goldman B. Patients’ information needs and decision-making processes: what can be learned from genetic counselees? Health Psychology 2006; 25(2): 211-9.
[4] Yu J. A systematic review of issues around antenatal screening and prenatal diagnostic testing for genetic disorders: women of Asian origin in western countries. Health and Social Care in the Community 2012; 4: 329-346.
[5] Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands. BMC Pregnancy Birth 2009; 9: 18.
[6] National Institute for Public Health & Environment (RIVM). Scenario Prenatal Screening. Down Syndrome and Structural Ultrasound Investigation version 2.0. National Institute for Public Health & Environment, Bilthoven 2011; [in Dutch].
[7] Stichting Samenwerkende Opleidingen Verloskunde (SSOV); KNOV, NHG, NVOG, VKGN, VSOP & Erfocentrum, 2007. Teachers guideline for training communication skills regarding prenatal screening SSOV, Bilthoven [in Dutch].
[8] van Zwieten MCB. The importance of a conscious choice but what is the choice about? The set of possibilities during decision-making about prenatal congenital anomaly tests. De Psycholoog 2008; 43: 20-25 [in Dutch].
[9] Roter D, Ellington L, Hamby Erby L, Larson S, Dudley W. The genetic counselling Video project (GCVP). American Journal of Medical Genetics Part C 2006; 142C: 209-220.
[10] Pirzadeh SM, McCarthy Veach P, Bartels DM, Kao J, Leroy BS. A national survey of genetic counselors’ personal values. Journal of Genetic Counseling 2007; 16(6): 763-73.
[11] Meiser B, Irle J, Lobb E, Barlow-Stewart K. Assessment of the Content and Process of Genetic Counselling: A Critical Review of Emperical Studies. Journal of Genetic Counseling 2008; 17: 434-451.
[12] Martin L, van Dulmen S, Spelten E, de Jonge A, de Cock P, Hutton E. Prenatal counseling for congenital anomaly tests: Parental preferences and perceptions of midwife performance. Prenatal Diagnosis 2013; 33: 1–12.
[13] Elwyn G. Arriving at the postmodern medical consultation. European Journal of General Practice 2004; 10(3): 93-7.
[14] Smets E, van Zwieten M, Michie S. Comparing genetic counselling with non-genetic health care interactions: Two of a kind? Review article. Patient Education and Counselling 2007; 68: 225-234.
[15] Schoonen HM, van Agt HME, Essink-Bot ML, Wildschut HI, Steegers EAP, de Koning HJ. Informed decision-making in prenatal screening for Down’s syndrome: What knowledge is relevant? Patient Education and Counseling 2011; 84(2): 265-270.
[16] van Agt HME, Schoonen HMHJD, Wildschut HIJ, De Koning HJ, Essink-Bot ML. Health education for the pre- and neonatal screening program: Questionnaires regarding the national evaluation of the providing procedures. Erasmus MC, Rotterdam 2007 [in Dutch].
[17] KNOV. Digital Individual post-graduate Course (DIN), 2010. KNOV, Utrecht [in Dutch]. Checked on: 06-02-2012. URL: http://leden.knov.nl/leden/30werken_aan_kwaliteit/19bij_en_nascholing/Digitale_individuele_nascholing_DIN.
[18] Schoonen HM, Essink-Bot ML, van Agt HM, Wildschut HI, Steegers EA, de Koning HJ. Informed decision-making about the fetal anomaly scan: what knowledge is relevant? Utrasound in Obstetrics and Gynecology 2011; 37(6): 649-57.
[19] O’Connor AM, Légaré F, Stacey D. Risk communication in practice: the contribution of decision aids. British Medical Journal 2003; 327: 736-740.
[20] Mearns D, Thorne B. Person-centered counselling in Action. London: Sage Publications,1999; 2nd ed.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 3
72
[21] de Boer J, Zeeman K. KNOV-guideline Prenatal midwifery led care: recommendation for coaching, interaction and information giving. KNOV, Utrecht 2008 [in Dutch].
[22] Rademakers J, Delnoij D, de Boer D. Structure, process or outcome: which contributes most to patients’ overall assessment of healthcare quality? British Medical Journal Quality Safety 2011; 20: 326-331.
[23] Kramer P. The general practitioner-patient relation anno 2011. TNS NIPO, Amsterdam 2011.[24] Mazzi MA, Bensing J, Rimondini M, Flicher I, van Vliet L, Zimmerman C, Deveugele M. How do
lay people assess the quality of physicians’ communicative responses to patients’ emotional cues and concerns? An international multicentre study based on videotaped medical consultations. Patient Education and Counseling 2012; 90(3): 347-53.
[25] Sheets KB, Best RG, Brastington CK, Will MC. Balanced information about Down syndrome: what is essential? American Journal of Medical Genetics Part A 2011; 155(6): 1246-57.
[26] Corke CF, Stow PJ, Green DT, Agar JW, Henry MJ, 2004. Learning in practice. How doctors discuss major interventions with high risk patients: an observational study. Britisch Medical Journal 2005; 330: 182.
[27] Liefhebber S, van Dam C, Waelput A. Professional profile of midwives. KNOV, Bilthoven. 2005 [in Dutch].
[28] Manniën J, Klomp T, Wiegers T, Pereboom M, Brug J, de Jonge AM, van der Meijde M, Hutton EK, Schellevis F, Spelten ER. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). Bio Medical Central Health Services Research 2012; 12: 69-79.
[29] Hingstman L, Kenens RJ. Numbers from the midwifery registrations. Nivel, Utrecht 2011 [in Dutch].
[30] Field A. Discovering Statistics Using SPSS. London: Sage Publishers, 2009 3rd ed.[31] Willis GB. Cognitive interviewing. A tool for improving questionnaire design. Sage Publications,
London, 2005.[32] Charles C, Gafnia A, Whelan T. Decision-making in the physician-patient encounter: revisiting the
shared treatment decision-making model. Social Science and Medicine 1999; 49: 651-661.[33] Jansen J, Butow PN, van Weert JC, van Dulmen S, Devine RJ, Heeren TJ, Bensing, JM, Tattersall
MH. Does age really matter? Recall of information presented to newly referred patients with cancer. Journal of Clinical Oncology 2008; 26(33): 5450-5457.
[34] Durand MA, Stiel M, Boivin J, Elwyn G. Information and decision support needs of parents considering amniocentesis: interviews with pregnant women and health professionals. Health Expectations 2010; 13(2): 125-38.
[35] van Zwieten M, Willems D, Knegt L, Leschot N. Communication with patients during the prenatal testing procedure: An explorative qualitative study. Patient Education and Counseling 2006; 63: 161-168.
[36] Christiaens W, Nieuwenhuijze MJ, De Vries R. Trends in the medicalisation of childbirth in Flanders and the Netherlands, Midwifery 2013; 29(1): e1-8.
[37] Nieuwenhuijze MJ, de Jonge A, Korstjens I. Influence of birthing positions affects women’s sense of control in second stage of labour. Midwifery 2013; 29(11): e107-14.
[38] van den Brink-Muinen A, van Dulmen AM, de Haes CJM, Visser HCJM, Schellevis FG, Bensing JM. Has patients’ involvement in the decision-making process changed over time? Health Expectations 2006; 9: 333–342.
[39] Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, Cording E, Tomson D, Dodd C, Rollnick S, Edwards A, Barry M. Shared Decision Making: A Model for Clinical Practice. Journal of General Internal Medicine 2012; 27(10): 1361-1367.
[40] Health Council. Act population screening on Down syndrome and nuraltube defects. Gezondheidsraad, Den Haag publication no. 2007/05WBO [in Dutch].
[41] Oepkes P, Wieringa J. The right to know; the 20-weeks ultrasound investigation facilitates a conscious choice. Medisch Contact 2008; 31/32: 1296-1297 [in Dutch].
[42] Fracheboud J, Van Agt HME, De Koning HJ. Monitoring 2010 van gerapporteerde verrichtingen van het screeningsprogramma Down syndroom /Structureel Echoscopisch Onderzoek Eindrapport Juli 2012. Rotterdam, RIVM. http://www.rijksoverheid.nl/onderwerpen/zwangerschap-en-geboorte/

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ views on appropriate antenatal counseling for anomaly screening
73
3
APPENDIX A Dutch setting
Since 2007 prenatal screening is offered to all Dutch pregnant women using an opt-in approach [16,40,41]. The screening program includes two non-invasive tests: the combined test (CT) a risk assessment for Down-, Patau- and Edwards syndrome (around 12th weeks gestational age), and the Fetal Anomaly ultrasound Scan (FAS) for detecting physical anomalies (around 20th weeks gestational age). The FAS is free for all women, the CT has to be paid for by women younger than 36 years of age [40,41]. Mean uptake of the FAS in the Netherlands in 2011 was around 92% and the uptake for the CT is about 30% for women younger than 30 years of age and 59% for women older than 36 years of age. Invasive tests are offered on indication (e.g. maternal age ≥ 36 years of age, family history) [42].


Chapter 4Introducing video recording in primary care midwifery for research
purposes: procedure, dataset, and use
Spelten ER, Martin L, Gitsels-van der Wal JT, Pereboom MTR, Hutton EK, Van Dulmen S.
Midwifery 2015; 31(1):95-102.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
76
ABSTRACT
Background Video recording studies have been found to be complex, however very few studies describe the actual introduction and enrolment of the study, the resulting dataset and its interpretation. In this paper we describe the introduction and the use of video recordings of health care provider (HCP)-client interactions in primary care midwifery for research purposes. We also report on the process of data management, data coding and the resulting data set.
Methods We describe our experience in undertaking a study using video recording to assess the interaction of the midwife and her client in the first prenatal consultation, in a real life clinical practice setting in the Netherlands. Midwives from six practices across the Netherlands were recruited to videotape 15-20 intakes. The introduction, complexity of the study and intrusiveness of the study were discussed within the research group. The number of valid recordings and missing recordings were measured; reasons not to participate, non-response analyses, and the inter-rater reliability of the coded videotapes were assessed. Video recordings were supplemented by questionnaires for midwives and clients. The Roter Interaction Analysis System (RIAS) was used for coding as well as an obstetric topics scale.
Results At the introduction of the study, more initial hesitation in cooperation was found among the midwives than among their clients. The intrusive nature of the recording on the interaction was perceived to be minimal. The complex nature of the study affected recruitment and data collection. Combining the dataset with the questionnaires and medical records proved to be a challenge. The final dataset included videotapes of 20 midwives (7-23 recordings per midwife). Of the 460 eligible clients, 324 gave informed consent. The study resulted in a significant dataset of first prenatal consultations involving recording 269 clients and 194 partners.
Conclusion Video recording of midwife-client interaction was both feasible and challenging and resulted in a unique dataset of recordings of midwife-client interaction. Video recording studies will benefit from a tight design, and vigilant monitoring during the data collection to ensure effective data collection. We provide suggestions to promote successful introduction of video recording for research purposes.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
77
4
BACKGROUND
Video recording of health care-provider (HCP)-client communication has become an accepted part of health care education and research. In education, video recording provides feedback on work habits by assessing communication during clinical performance. In research, video recording enables the assessment of communication performance or intervention fidelity as well as the confirmation of best practices in health care provider-client communication by observing daily practice, often in combination with other research measures such as questionnaires [1,2,3].In the Netherlands, nearly 80% of all pregnant women start obstetric care in a midwifery practice [4]. In the first prenatal consultation, the midwife provides health education on a large number of important topics, e.g. on health life style such as smoking, drinking, weight gain, and on infectious diseases. In 2007, midwives became the primary counselors for prenatal screening for congenital anomalies [4]. To date, no research has considered how midwives counsel clients in practice, how they provide health care education during a consultation, or what topics are addressed during the first consultation. We felt video recorded HCP-client interaction in midwifery practices would be an ideal approach to studying these complex interactions. We anticipated that the use of video recordings for research purposes in health care practice would be complex; however, very few studies describe the actual introduction and enrolment of the study, the resulting dataset and its interpretation. From a number of studies on video recording we extracted three elements that seem to shape the feasibility of a video recording study: introduction of the study, complexity of the data collection and intrusion of the video camera. A good introduction is crucial to the feasibility of the study. Both client and health care worker need to be briefed adequately in order to enhance participation [2]. Complexity of the data collection refers to additional questionnaires that need to be completed, filling in of forms such as non-participant forms, and managing the actual recording. It has been found that a more complex research protocol results in reduced participation [2].A third element to consider is the potential intrusive nature of the camera for both the health care worker and the patient. The actual recording could act as an intervention. However, there is little evidence that care providers behave differently when on camera [5] and in practice, the majority of patients do not object to being video recorded, as long as there are careful privacy and safety procedures [2,6,7]. We found little information in the literature on the construction of a meaningful data set in terms of quantity: e.g. about how many recordings should be made in total and per health professional, how many health professionals should be included to allow for generalizability of the observations. It is our impression that the challenges encountered with the complex and time-consuming nature of video recording may in the end determine the amount of data collected rather than realising a predefined number of recordings.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
78
In this report, we use a framework made of the elements extracted from the literature: introduction, complexity and intrusion, to which we have added quantity as a fourth important element to consider in planning and implementing video recording studies. This is the first study in which midwife-client interactions in primary care midwifery practices in the Netherlands were video recorded. The purpose of the study was to gain insight into the midwife-client interaction in relation to the quality of care provided by midwives. There are very few papers recounting the complex recording process. This paper describes the introduction of video recording in midwifery practices for research purposes, the coding process, and the resulting dataset. Analyses of observational data are described in separate papers [8,9].
METHODS
The video study focused on the interaction of the midwife and her client in the first prenatal consultation. The study was embedded in the DELIVER study, a large scale multi-centre multidisciplinary prospective national survey into the quality and provision of primary midwife led care in the Netherlands in which twenty midwifery practices and their clients participated [10-12]. The design of the DELIVER study, including the video recordings of first prenatal consultations, was approved by the Institutional Review Board of the VU University Medical Centre as well as by the Medical Ethical Committee of the VU Medical Centre, Amsterdam, the Netherlands, supplemented by consent from all participating midwives.
Data collection: quantity of video recordingsIn order to have an adequate sample to perform quantitative analysis and to develop consistency around our observations of communication for each midwife and across the group, we aimed to obtain at least 15-20 recordings per midwife and to include at least 6 practices across the country. The number of recordings was also based on the fact the sometimes the first recording needs to be discarded due to getting acquainted with video recording [13] and sometimes technical problems are encountered rendering the recording unusable. At recruitment for the DELIVER study, all twenty DELIVER practices, which were purposively sampled from the north, east, west, and south region of the Netherlands were automatically asked to participate in the video recording study, even though we anticipated that would be more than sufficient for our video data collection. All midwives in a practice were requested to participate; however in larger practices the number was set at a maximum of 6 midwives, to limit the relative influence of one practice on the entire dataset. In all participating practices, midwives decided which of them participated.Midwives were eligible to participate if they: (1) had a work contract at the midwifery practice; (2) were fully qualified midwives (e.g. not student-midwives); and (3) if prenatal counseling consultations were part of their usual work.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
79
4
Clients were eligible if they: (1) were new to counseling about prenatal congenital anomaly tests for the current pregnancy; (2) waived their right not to know about prenatal anomalies tests; (3) were aged 18 years or older; and (4) were able to read Dutch or English. Data collection was carried out between June 2010 and May 2011.
Data managementAll video recordings were digitalized, analyzed in The Observer XT version 7.0 [14]. Coded data were transported to the statistical software package SPSS 20.0 (SPSS inc., Chicago, IL). Data from the analysis of the video recordings were entered in SPSS 20.0 together with the questionnaire data. Through anonymous patient numbers, data from the video recordings were connected to the questionnaire data and the medical record files of the DELIVER study.
Introduction of video recording researchPractices were first approached by phone, followed by written information to those who agreed to consider participation, and finally a visit was made to explain the study procedure. For the recording, participating midwives received a camera, empty tapes, and a recording protocol. They were made familiar with the actual recording of the consultation: setting up of the camera, starting and stopping recording, camera angle, changing of tapes, completion of the study forms, etc. Researchers were not present at the actual recordings but could be reached by phone.Midwives also received questionnaires, information leaflets for clients and informed consent forms. Practice assistants who did the initial recruitment, received protocol instructions from the midwives.
Enrolment of clientsThe enrolment procedure for this study is described as a flow chart in Figure 1. Pregnant women and their partners were recruited from all consecutive new clients at the six midwifery practices involved. Eligible clients received information about the study and were invited to participate. Interested clients signed an informed consent form prior to the consultation, which stated that they could withdraw at any time during or after the consultation without consequences.If clients declined to participate in the study, the practice assistant recorded reasons for refusal of participation as well as the clients’ age, parity, level of education and ethnicity.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
80
Figure 1. Flowchart for video recording study.
Client calls practice to make an appointment for first prenatal consultation.
Practice assistant (1) checks eligibility of client, (2) uses scripted dialogue to inform client of the study and their right not to know, (3) asks for participation, (4) and sends consenting client and their partner a packet containing the pre-visit questionnaires, an METC-client-information-letter, a flyer, and an informed consent form, (5) non-consenting women were asked to reasons and baseline characteristics recorded.
Client arrives at practice for first prenatal consultation.
Client hands in completed pre-visit questionnaire or completes questionnaire at the practice, together with her partner.
Both midwife and client / partner complete a post-visit questionnaire.
All midwives complete a questionnaire at the start of the study.
The consultation is video recorded.
This is either a consultation including counseling on prenatal screening or a separate consultation on counseling for prenatal screening or only the counseling section of a first prenatal consultation.
Figure 1 Flowchart for video recording study.
QuestionnairesTo supplement the recordings, we collected demographic information and background characteristics from midwives, clients, and their partners. We asked participants to complete the QUOTE prenatal questionnaire twice, once before and once after the recorded consultation. This questionnaire focuses on clients’ preferences and experiences regarding prenatal counseling for congenital anomaly tests [15]. On request, an English version of the questionnaire was available.The midwives completed the midwives’ version of the QUOTE prenatal including items on the midwife-client relationship once, at the start of the study to assess their views on appropriate

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
81
4
counseling for prenatal congenital anomaly tests [16]. To assess their reflections on daily practice, midwives completed the same questionnaire again at the end of each recorded consultation.
The video recordingThe midwife positioned the unmanned camera to show her full face, in line with protocol instruction; the client and her partner were usually seen from behind or from the side. The recording was started before the client entered the consultation room. The midwife recorded the identification numbers of the practice, national registration of herself and the number of the client on video before the client entered. The midwife notified the client and her partner that the video had started recording. The tape was turned off at the end of the (counseling part of the) consultation.
Approach to analysesCodingCoding of the recordingsFor the purpose of analysing the collected data, a valid and reliable coding scheme was used to quantify the data. The best known and most frequently used coding scheme for HCP-patient interaction during the patient visit is the Roter Interaction Analysis System (RIAS). RIAS is also the most extensive coding scheme available [17-19]. Coding was done in two separate runs for verbal and nonverbal behaviour, respectively. In the coding for communication a distinction was made between point events and state events. Point events refer to a straightforward count of occurrences, e.g. does a midwife inform the client of her risk of having a child suffering from a congenital abnormality and if so, how often is the theme discussed. The occurrence is noted and therefore the frequencies can be counted. No time indication is given. State events refer to elements in the communication that are linked to a time indication, e.g. client-directed gaze or the duration of the prenatal counseling.
Coding of the recordings for verbal behaviourThe main focus of the coding was on verbal behaviour related to prenatal counseling for congenital anomaly tests. The RIAS is applied to the smallest unit of expression or statement to which a meaningful code can be assigned. These units are assigned to mutually exclusive and exhaustive categories that reflect the content and form of the dialogue. RIAS has demonstrated levels of reliability and concurrent validity [17,19].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
82
Furthermore, for the purpose of the study, we developed an obstetric topics scale to code each topic addressed during the intake to allow for all relevant components of a first prenatal consultation to be addressed in the analyses, inclusive aspects of prenatal counseling for congenital anomaly tests. The main categories of this obstetric topic scale were: family history (including family genetics, consanguinity), obstetric history, pregnancy-related health and well-being, life style (smoking, alcohol, drugs, weight, nutrition), infectious diseases, use of medication, counseling and philosophy of life and physical examination. An open category was used to note remarkable occurrences such as “the video-recording could not be used because another consultation was recorded on top of it”.
Coding of the recordings for nonverbal behaviourFor nonverbal behaviour, the affect or emotional context of the dialogue, the Global Affect Measure (GAM), which is part of RIAS, and client-directed gaze were rated. The GAM ratings are based on overall affective impressions of the health care provider on such dimensions as dominance, friendliness, attentiveness, and hurrying or rushing. Impressions of the clients are based on dimensions such as emotional distress, assertiveness, and friendliness. Ratings of the GAM were assigned for both the midwife and client (and her partner) on scales from low to high (scale 1-6). Ratings of “3” or “4” are considered “average” affect (www.riasworks.com).Client-directed gaze is the time the midwife looked directly into the pregnant woman or her partner’s face. Client-directed gaze has previously been found to facilitate a discussion about psychosocial issues [20] and is thus an important factor of communication.
Approach to establishing coding reliabilityBefore observing and coding the videotapes, three researchers and three research assistants participated in a RIAS course. These coders were split in two teams: one team with two researchers (JG, MP) and one research assistant (KvA) coded the content of the first prenatal consultation, GAM and client-directed gaze. The second team with one researcher (LM) and two research assistants (LG and VS) coded the communication of the prenatal counseling only, with a distinction between verbal and nonverbal behavior using the RIAS. At the start of the coding process, coders of each team compared three coded tapes, adjusted unclear items and made a final coding model. The team coding the content started the coding process, the other team followed. To establish inter-rater reliability, within each team, the coders compared in total approximately 10% of the tapes with each other, and continued to do so, on a regular basis using also a coding memo to exchange coding experiences, to check and maintain consensus. Coders used direct entry software, The Observer XT version 7.0-computer system, which is especially designed for coding behavioural interactions from video recordings [14], and coded directly from the digitized videotaped sessions.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
83
4
DatasetDescriptive statistics were used to report characteristics of the participating practice, the midwives, clients (and partner) and the first prenatal consultation recordings. The participating and non-responding clients were compared using t-tests to examine differences in age and chi square tests to examine differences in parity, level of education and ethnicity. Proportions were used to identify the relative contribution of the practices and midwives to the total dataset.
RESULTS
Introduction: feasibility of the studySix of the twenty practices that participated in the DELIVER-study were asked to participate. They were selected on the basis of regional coverage, size of the practice and the client characteristics within the different areas. When two declined, two other DELIVER practices in the same region were approached, and they agreed to participate. Per practice two to six midwives agreed to be recorded, in two practices one or more midwives refused to participate. In the six practices, recordings were made of 22 midwives and unintentionally of two non-midwife ultrasound specialists who provided prenatal counseling. The recordings from the ultra sound specialists were excluded from the data because the focus was on midwives. Correctly recorded videotapes per midwife ranged from 2 to 24. If less than seven complete recordings were made of an individual midwife, the recordings of this midwife were excluded. In the research team it was decided that this number was considered too low to give a valid impression of the midwife’s client communication skills.The increased awareness of being recorded may have prompted a tendency towards ‘best behaviour’ for midwives or may have increased self-consciousness. This could have affected the first recording when adjustment takes place. However, we found no discernible learning curve with regards to the content and the amount of information given in the first recorded video consultation were compared to all other recorded video consultations. First recordings were therefore not discarded [9].
DatasetQuantityAn overview of the data collection is given in Table 1. The table shows that video recordings from 20 midwives were taken into the analyses. The number of midwives per practice ranged from one to five midwives, and recordings ranged from 7 to 23 per midwife.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
84
Table 1 Data collection: practices, midwives and recordings.
Practice code
Midwife code
Recordings/clients per midwife
% Recordings per practice
% Recordings per midwife
1 1 20 7.42 19 7.13 19 7.14 15 5.6
Subtotal 73 27.12 5 14 5.2
6 12 4.5Subtotal 26 9.73 7 14 5.2
8 16 6.09 12 4.510 11 4.1
Subtotal 50 18.64 11 12 4.5
12 11 4.113 16 6.014 23 8.6
Subtotal 62 23.15 15 9 3.3
16 11 4.117 8 3.018 11 4.119 12 4.5
Subtotal 51 19.06 20 7 2.6 2.6N=6 N=20 N=269
Of the 460 eligible clients (pregnant women approached to participate), 324 (70.4%) agreed, resulting in the same number of video recordings, since each client was recorded once. Of 269 (58.5% of all approached clients), the video recording could be used for analyses and were included in the resulting dataset. A flow chart summarizing the number of clients approached, down to the final number of recordings included in the dataset, including description of the reduction of numbers can be found in Table 2. Three types of recordings were made: a whole routine first prenatal consultation including counseling (N=191), a recording limited to the counseling part of the consultation (N=71), and a separate counseling consultation (N=7).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
85
4
Table 2 Inclusion and exclusion of clients and recordings.460 Eligible clients- 136 Did not agree to participate for various reasons324 Agreed to participate, total number of recordings made
Exclusion grounds for recordings:- 19 Failed recordings- 7 Recording stopped /halted- 1 Partner withdrew from study for privacy reasons- 2 No unique code- 2 Unmatched second recording- 1 Consultation of 38 weeks gestation- 18 Recordings from ultrasound specialists- 4 Too few recordings per midwife269 Total number of recordings in final dataset
Adequacy and representativeness of sample The sample characteristics are described on three levels: for the midwives, for the clients and for the recordings, respectively in Table 3, 4 and 5.The mean age of the 20 participating midwives was 32.8 years (range 23 to 54 years), with a mean of years of work experience of 8.3 years (range: just started to 33 years). Demographic and professional characteristics of the midwives are shown in Table 3.Data on background characteristics of clients are shown in Table 4. Data on background characteristics of clients were available for 89.6% (N=241/269) and data on background characteristics for partners were available for 88.1% (N=171/194). The mean age of the pregnant women was 29.2 years, (range 20 to 40 years) and the mean age of partners was 31.8 years (range 18 to 47 years). Recordings were combined with questionnaires and with medical records. The latter was complicated and resulted in a large reduction in numbers of matched data; a match of 54 of 269 (20%).Data on the recordings of the consultations are summarised in Table 5, which contains information on the number of recordings and on the duration of the different recordings.Twelve tapes could not be coded on client-directed gaze because of the angle of the recording and for one tape only RIAS coding was done, due to administrative error of the coders, no other coding was undertaken. The intake consultations, including prenatal counseling (N=191), lasted on average 39.55 minutes and ranged from 11.08 minutes to 95.58 minutes. The counseling part of these consultations lasted on average 9.48 minutes and ranged from 1.92 minutes to 25.12 minutes.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
86
Table 3 Demographic and professional characteristics of midwives and of the Dutch midwifery populationa.
Characteristics Midwives N=20 (%)
The Dutch midwifery population N=2612(%)
Age (years)≤ 29 years≥ 30 years
10 (50)10 (50)
< 40 years = 1644 (63)> 55 years = 198 (7.6)
GenderMaleFemale
-20 (100)
43 (1.6)2569 (98.4)
Ethnicityb
DutchNon Dutch – Non Western ethnicityNon Dutch – Western ethnicity
14 (70)2 (10)4 (20)
Not available
Place of graduationAmsterdamGroningenMaastrichtRotterdamAbroadMissing
8 (40)1 (5)3 (15)3 (15)4 (20)1 (5)
641 (25)147 (6)660 (25)638 (24) 523 (20)3 (0.1)
Year of graduation≤ 2003≥ 2004
9 (45)11 (55)
Not available
Work experience (years)≤ 2 years3 – 11 years≥ 12 years
4 (20)12 (60)4 (20)
Not available
Religious backgroundNone believersBelievers
11 (55)9 (45)
Not available
a [25].b In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one of the parents (or both of them) of a person is born outside the Netherlands, this person is non-Dutch [26].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
87
4
Table 4 Characteristics of pregnant women and (if available) their partners.
Characteristics Pregnant women N=241* (%)
Partner N=170* (%)
GenderMaleFemale
-241 (100.0)
168 (99.4)1 (0.6)
Age (years)
≤ 25 years26 – 30 years31 – 35 years≥ 36 years
44 (18.5)108 (45.4)73 (30.7)13 (5.5)
21 (12.6)45 (26.9)69 (41.3)32 (19.2)
Highest level of educationUp to high schoolHigher vocational education / university
115 (47.9)125 (52.1)
88 (52.1)81 (47.9)
OccupationSchoolPaid jobUnemployedDisabledHousewife / Husband
12 (5.1)198 (84.6)12 (5.1)1 (0.4)11 (4.7)
4 (2.4)158 (94.0)2 (1.2)3 (1.8)1 (0.6)
Marital statusSingleDivorcedMarried / Partner
11 (4.6)0 (0.0)227 (95.4)
4 (2.4)0 (0.0)164 (97.6)
Ethnicitya
DutchNon-Dutch
184 (77.0)55 (23.0)
135 (80.8)32 (19.2)
Religious background
NoneChristianMuslimOther
112 (47.1)102 (42.9)22 (9.2)2 (0.8)
80 (47.9)78 (46.7)7 (4.2)2 (1.2)
Pregnancy duration≤ 11 weeks≥ 12 weeks
204 (92.3)17 (7.7)
147 (94.2)9 (5.8)
ParityNulliparaMultipara
98 (41.2)140 (58.8)
92 (55.1)75 (44.9)
*Due to missing and inapplicable answers the N can vary from variable to variable.a In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one of the parents (of both of them) of a person is born outside the Netherlands, this person is non-Dutch [26].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
88
Table 5 Characteristics of the video-taped consultations.
N (%) Minutes (SD in minutes)
Number of videos analysednumber of content analyses 268 (99.6)number of RIAS analyses 269 (100.0)number of integrated consultations 191 (71.0)number of separate counseling consultationsnumber of integrated consultations only counseling on tape
7 (2.6)71 (26.4)
analysis of client-directed gaze 253 (94.1)analysis of GAM 245 (91.1)Durationoverall duration of video-tapes 269 (100.0) 31.33 (16.68)duration of first consultation including counselingoverall duration of counseling
191 (71.0)269 (100.0)
39.55 (11.11)9.21 (4.26)
duration of counseling part the first consultation 191 (71.0) 9.49 (4.37)duration of counseling if only counseling was video-taped 71 (26.4) 8.49 (3.91)duration of separate counseling consultations 7 (2.6) 8.89 (4.40)
Information on clients declining participationNon-response information was available from five of the six participating practices, from 136 pregnant women, not from their partners. These five practices provided 97.5% data. We only found a significant difference for parity: the percentage of multiparas in the non-participant group (75.6%) was higher compared to the percentage multiparas among participants (59.9%), Chi-square test for independence (with Yates Continuity Correction) was p=0.003. No significant differences were found for age or ethnic origin. Education level was only noted in 15.4% of the cases, thus a statistical comparison could not be made. The main reasons noted to refuse participation were: client just does not want to participate; partner refuses to participate, client has a difficult (medical) history.
Reliability of the recordingsInter-rater reliability of content and non-verbal communicationInter-rater reliability between the observers was tested for each scoring item in the protocol for 26 out of 268 video consultations (9.7%); the Kappa coefficient per item ranged from 0.31 to 0.78 (mean 0.56) indicating moderate to very good agreement [21]. Regarding client-directed gaze the inter-rater reliability was calculated on a random sample of 10.3% (N=26) of the video-tapes for which this coding was possible (N=253); the Intraclass Correlation Coefficient (ICC, single measures) ranged from 0.64 to 0.92 indicating moderate to very good agreement.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
89
4
Inter-rater reliability of RIASInter-rater reliability was calculated on a random sample of 9.7 % (N=26) of the study videotapes (N=269). Intraclass correlation (ICC) was used to measure the inter-rater reliability for midwife, client and partner categories with a mean occurrence greater than 2% (i.e. any occurrence had to be at least 2% of the total), which proved to be adequate [22,23]. The ICC was rated as Kappa. Coding categories for midwives had a substantial mean ICC (ICC single measures) of 0.62 (Range = 0.58 – 0.65). The average ICC of client coding categories (ICC single measures) was moderate with 0.53 (Range = 0.30 – 0.56) and the mean ICC of partner categories (ICC single measures) was good with 0.71 (Range = 0.59 – 0.82). The partner category consisted of only one category, namely backchannels. The mean ICC of the counseling topic was also almost perfect with 0.99 (Range = 0.99 – 1.00).
DISCUSSION
In this paper, we describe the introduction and resulting dataset of video recordings in a naïve population: primary care midwifery. Midwives in the Netherlands, unlike many other health professionals, had not yet been exposed to video recording as a tool for research. Also, in the recorded first prenatal visit, there is no established relation between the midwife and her client, which may require more effort to gain trust needed to consent to the recording. Because of the new situation for both midwives and their clients and because there are very few papers recounting the complex recording process, in this paper, we describe the Introduction process. In addition, we report on the data coding procedure and the resulting dataset in terms of quantity and quality.The use of recordings for research purposes posed a number of challenges. These challenges are described in terms of the framework introduced earlier: the introduction in the practice setting, the complexity of the associated data collection including data-linking, the possible intrusiveness of the camera, and determining the needed quantity of the recordings. For the introduction, we identified the need to ensure commitment of health care providers to the research prior to enrolling the practice group as part of the study. Despite initial consent, some practices and midwives did not agree to participate. Voiced reasons for non-participation at practice level were not video-related (i.e. not convenient for the practice at the moment, on grounds of a pregnant colleague and, not convenient for fear that clients would decide to change to a different practice). Because we wanted to limit the relative contribution of a larger practice on the dataset, this provided midwives in larger practices with an opting out option. In the end, the practices that agreed to participate turned all out to be larger practices (≥ 4 midwives) and in these practices, not all midwives agreed to participate. This was left at the discretion of the practice; it could be that individual midwives

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
90
did not participate because recording was unfamiliar to them or for practice management reasons.Second, an introductory period provided opportunity to adjust to the recording process, allowing for necessary changes to be made to the initial protocol. In our study, the provision of a word-by-word script to invite clients to participate in the study proved to be crucial for commitment of midwives to the study and for recruitment of clients. A subsequent change to the protocol related to the recording. Depending on the preference of the practice, three different recordings could be made: a complete first prenatal consultation; only the counseling part within the first prenatal consultation; or for practices that provided a complete, separate session for prenatal counseling, recording of that session only. This change resulted in a recording of the entire first prenatal consultation for most practices, even though the initial focus of the study was on counseling for congenital anomalies. And since all first consultations are likely to be similar in content, this avoided cross-practices comparison issues, which allowed for an extension of our research focus to include all the health education aspects that are included in the first consultation.Finally, we feel that an introductory period may also increase feelings of control for the midwives and their assistants and enhance cooperation. With regards to complexity of the data set, a meticulous description of the recording process, and close monitoring of the data collection by researchers is necessary to prevent loss of data. For example in our study, the 19 failed recordings (table 2) may have been prevented if early check-ins and additional assistance with technical aspects of taping were addressed; 18 sessions taped by non-midwife counselors may have been avoided if we included the credential of who was recording on the clinician data collection form. In studies such as ours, where the video data are to be linked to other data sets, careful attention must be paid to the unique identifiers that will allow the linkages. In our study matching the data with medical records resulted in a considerably reduced sample. The coding system used seemed appropriate, although the complexity of the data coding could negatively influence the results through low ICC’s especially for rare coding categories. The intrusive nature of video recording did not appear to be a problem and may reflect the fact that participating midwives were less concerned about being recorded. Midwives who agreed to participate quickly got used to being recorded and even reported on the fact that being taped itself was already an insightful experience [24]. Even though we were working in a situation where clients would be meeting their midwife for the first time in this pregnancy, client participation was high with nulliparous women being more inclined to participate, suggesting that lack of an established HCP-client relationship was not a barrier to participation in our study. In terms of quantity, the video study has resulted in a dataset consisting of 269 video recordings of first prenatal consultations, involving 269 clients, 194 partners and 20 midwives

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
91
4
from 6 practices, providing unique insight into the communication skills of midwives, with no evidence of it acting as an intervention [9]. The relative contribution of a single midwife and of a practice on the total varied a lot in our sample, which may hamper subsequent analyses. We were not able to record the initially set goal of 15-20 recordings per midwife; instead we required midwives to have recorded a minimum of seven interactions in order to be included in the study. Closer monitoring may have assisted in meeting our original goal and resulted in a more balanced data set in terms of recordings per midwife and participating midwives per practice.
LimitationsOverall, our results indicate that our sampling efforts were adequate. Our purposeful sampling appears to have been adequate. Our sample of midwives compares well to the national sample (table 3). For the client sample, on-going monitoring may have better balanced the number of multiparous women.Video recording as a method may exclude some clients or lead to refusal from others (e.g. clients with personal issues or for example a medical history of miscarriages) and this may lead to bias and reduced generalisability of the results. This may however depend on the research question, e.g. if the focus of the study was on women with personal issues or with a history of miscarriages.Since there was no clear-cut information on cut off points for inclusion for the number of practices, midwives (per practice) and recordings per midwife, we made arbitrary choices. Future research may provide better underpinning for these decisions.
ConclusionsVideo recording in midwifery practice has resulted in a unique database of 269 recording, involving 269 clients, 194 partners and 20 midwives from 6 midwifery practices on midwife-client interaction of primary care midwives in the Netherlands, supplemented with additional data gathered through questionnaires and linked medical records. The implementation of a video recording study requires a tight design, careful attention and vigilant monitoring during the data collection in order to ensure a satisfactory end result.
Author contributions LM, JG and MP conducted the data collection and analysis. ES initiated and coordinated the DELIVER study. EH supervised the DELIVER study. SvD designed and supervised the video observation study. All authors participated in discussing the design of the study and developing the research protocols and questionnaires. ES drafted the manuscript, and all authors read and corrected draft versions of the manuscript and approved the final manuscript.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
92
Acknowledgement We are grateful to all pregnant women, their partners, midwives, and the research assistants: Veerle Steenhuis, Kelly van Almkerk en Lydia Gitsels, who were involved in the study. The study was funded by the Academy of Midwifery Amsterdam-Groningen (AVAG), the Netherlands.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Introducing video recording in primary care midwifery for research purposes
93
4
REFERENCES
[1]. Noordman J, Verhaak P, Van Dulmen S. Web-enabled video-feedback: a method to reflect on the communication skills of experienced physicians. Patient Education and Counselling 2011; 82(3):335-340.
[2]. Van Dulmen S, Humphris G, Eide H. Towards a guideline for person-centered research in clinical communication; lessons learned from three countries. IJPCM 2012; 2:58-63.
[3]. Rushmer R, Themessel-Huber M, Coyle J, Humphris G, Dowell J, Williams B. Is the routine recording of primary care consultations possible... and desirable? Lessons for researchers from a consultation with multiple stakeholders. Patient Education and Counselling 2011; 82:247-253.
[4]. Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands. BMC Pregnancy Birth 2009; 9:18.
[5]. Wolraich ML, Albanese M, Stone G, et al. Medical communication behavior system. An interactional analysis system for medical interactions. Med Care 1986; 24:891–903.
[6]. Pringle M, Stewart-Evans C. Does awareness of being video recorded affect doctors’ consultation behaviour? British Journal of General Practice 1990; 40:455-458.
[7]. Van der Stouwe, R. Voortgang Deliver [Progress of Deliver Study]. Tijdschrift voor Verloskundigen 2010; 35(maart):21-22.
[8]. Martin L, Hutton EK, Gitsels-van der Wal JT, Spelten ER, Kuiper F, Pereboom MTR, Dulmen S van. Prenatal counselling for congenital anomaly tests: an exploratory video-observational study about client-midwife communication. Midwifery 2015; 31(1):37-46.
[9]. Pereboom MTR, Mannien J, Almkerk K van, Spelten ER, Gitsels J, Martin L, Hutton EK, Schellevis FG. What information do Dutch midwives give clients about toxoplasmosis, listeriosis and cytomegalovirus prevention? An exploratory study of videotaped consultations. Patient Education and Counseling 2014; 96(1):29-35.
[10]. Klomp T, Spelten E, Meijde M van der. DELIVER, een studie naar de eerstelijns verloskundige zorg in Nederland [DELIVER, a study into primary care midwifery in the Netherlands]. Tijdschrift voor Verloskunde 2008; juli/augustus: 42-43.
[11]. Manniën, J, Klomp, G, Wiegers, T, Pereboom, M, Brug, J, Jonge, A de, Meijde, M van der, Hutton, E, Schellevis, F, Spelten, E. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Services Research 2012; 12:69-79.
[12]. Spelten E and Nieuwenhuijze M. Midwifery in the Netherlands: research gaining momentum. International Journal of Childbirth 2013; 3(4):195-202.
[13]. Van den Brink-Muinen, A v, Dulmen AM van, Schellevis FG, Bensing JM (eds). Tweede Nationale Studie naar ziekten en verrichtingen in de huisartspraktijk. Oog voor communicatie: huisarts-patiënt communicatie in Nederland[Second National Study into illness and performance in General Pratice. Focus on communication: GP-patient communication in the Netherlands] Utrecht: NIVEL, 2004.
[14]. Noldus LP, Trienes RJ, Henderiksen AH, Jansen H & Jansen RG. The observer video-pro: new software for the collection, management, and presentation of time-structured data from videotapes and digital media files. Behavior Research Methods, Instruments and Computers 2000; 32(1):197-206.
[15]. Martin L, Dulmen, S van, Spelten E, Jonge, A de, Cock P de, Hutton, E. Prenatal counselling for congenital anomaly tests: Parental preferences and perceptions of midwife performance. Prenatal Diagnosis 2013; 33:1–12.
[16]. Martin L., Hutton E.K., Spelten E.R., Gitsels-van der Wal JT., van Dulmen S. Midwives’ views on appropriate antenatal counselling for congenital anomaly tests; do they match clients’ preferences? Midwifery 2014; 30:600-609.
[17]. Ellington L, Kelly KM, Reblin M, Latimer S & Roter D. Communication in genetic counselling: cognitive and emotional processing. Health Communication 2011; 26:667-675.
[18]. Roter DL, Ellington L, Hamby Erby L, Larson S & Dudley W. The genetic counselling video project (GCVP): Models of practice. American Journal of Medical Genetics Part C 2006; 142C:209-220.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 4
94
[19]. Roter DL, Hall JA, Blanch-Hartigan D, Larson D & Frankel RM. Slicing it thin: New methods for brief sampling analysis using RIAS-coded medical dialogue. Patient Education and Counselling 2011; 82 (3):410-419.
[20]. Bensing JM, Kerssens JJ & Pasch M van der. Patient-directed gaze as a tool for discovering and handling psychosocial problems in general practice. Journal of Non-Verbal Behavior 1995; 19(4):223-242.
[21]. Landis JR and Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977; 33:159-174.
[22]. Pieterse AH, Dulmen AM van, Ausems MGEM, Beemer FA & Bensing JM. Communication in cancer genetic counselling: does it reflect counselees’ pre-visit needs and preferences? British Journal of Cancer 2005; 92:1671-1678.
[23]. Pieterse AH, Dulmen AM van, Beemer FA, Ausems MGEM, Bensing JM. Tailoring communication in cancer genetic counselling through individual video-supported feedback: A controlled pretest-posttest design. Patient Education and Counselling 2006; 60(3):326-335.
[24]. Spelten E, Gitsels J, Pereboom M, Martin L, Hutton E, Van Dulmen S. Video recording to improve the quality of prenatal genetic counselling. Prenatal Diagnosis 2012; 32(1):1-128.
[25]. Hingstman, L, Kenens, RJ. Numbers from the midwifery registrations. Nivel, Utrecht, 2011 [In Dutch].
[26]. Dutch National Office of Statistics; Statistics Netherlands. Available from: URL: http://www.cbs.nl/nl-NL/menu/themas/dossiers/allochtonen/methoden/begrippen/default.htm?conceptid=37 [In Dutch].

Chapter 5Antenatal counseling for congenital anomaly tests: an exploratory
video-observational study about client-midwife communication
Martin L, Hutton EK, Gitsels-van der Wal JT, Spelten ER, Kuiper F, Pereboom MTR, Van Dulmen S.
Midwifery 2015; 31(1):37–46.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
96
ABSTRACT
Objective Prenatal counseling for congenital anomaly tests is conceptualized as having both Health Education (HE) and Decision-Making Support (DMS) functions. Building and maintaining a Client-Midwife Relation (CMR) is seen as a necessary condition for enabling these two counseling functions. However, little is known about how these functions are fulfilled in daily practice. This study aims to describe the relative articulation of the prenatal counseling functions; to describe the ratio of client versus midwife conversational contribution and to get insight into clients’ characteristics, which are associated with midwives’ expressions of the functions of prenatal counseling.
Design Exploratory video-observational study.
Participants and setting 269 videotaped prenatal counseling sessions for congenital anomaly tests provided by 20 midwives within 6 Dutch practices.
Measurements We used an adapted version of the Roter Interaction Analysis System to code the client-midwife communication. Multilevel linear regression analyses were used to analyze associations between clients’ characteristics and midwifes’ expressions of prenatal counseling in practice.
Findings Most utterances made during counseling were coded as HE (41%); a quarter as DMS (23%) and 36% as CMR. Midwives contributed the most to the HE compared to clients and their partners (91% versus 9%) and less to the DMS function of counseling (61% versus 39%). Multilevel analyses showed an independent association between parity and shorter duration of prenatal counseling; (β=-3.01; p<.001). The amount of utterances concerning HE and DMS during counseling of multipara was less compared to nulliparous.
Key conclusions Prenatal counseling for congenital anomaly tests by midwives is focused on giving HE compared to DMS. The relatively low contribution of clients during DMS might indicate poor DMS given by midwives. Counseling of multiparae was significantly shorter than counseling of nulliparous women; multiparae received less HE as well as DMS compared to nulliparous women.
Implications for practice Our findings should encourage midwives to reflect on the process of prenatal counseling they offer with regards to the way they address the three prenatal counseling functions during counseling of nulliparous women compared to multiparae.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
97
5
Highlights- We report an exploratory video-observational study about antenatal counseling.- Midwives focused primarily on health education during counseling for antenatal anomaly
tests.- During decision-making support clients contributed most to the conversation.- Parity appears to be independently associated with the way clients are counseled.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
98
INTRODUCTION
Prenatal screening for Down syndrome, other chromosomal and structural congenital anomalies has become common obstetrical practice in many countries [1,2]. Prenatal screening aims to provide timely information to women and their partners about the health of their fetus in order to enhance their reproductive choice [3]. If the fetus is diagnosed with a chromosomal disorder or structural congenital anomaly, prospective parents have the opportunity to either prepare for the birth of a child with a congenital anomaly, or to opt for termination of the pregnancy [4,5]. Screening tests and these options are typically discussed during prenatal counseling. In the Netherlands, since 2007, midwives have provided routine prenatal counseling for congenital anomaly tests to nearly 80% of pregnant population [6]. The purpose of this counseling has been to facilitate autonomous, informed decision-making by prospective parents regarding the uptake of prenatal congenital anomaly tests using an opting in approach [5,7-9]. High quality counseling consists of health education (HE), decision-making support (DMS) and relationship-building [10-12]. The latter function is seen as a necessary condition for enabling the first two counseling functions and could be accomplished by showing empathy and understanding and using partnership statements and social conversation [10,13-15]. Health education topics include providing information about the prenatal tests that are available and the anomalies that can and cannot be detected [9,10,16]. Key elements of decision-making support include empowering clients to find personal meaning in the information given and making psychological sense of the implications for the future. This support is intended to minimize psychological distress and increase personal feelings of control as well as to facilitate autonomous decision-making [11-13,17-19].The extent to which this three-function prenatal counseling model is reflected in daily practice is, so far, unknown. However, because of the extensive amount of information counselors are obliged to give it has been established by Dutch educational and research programs that the health education function requires a lot of time and attention to a variety of information [9,16,20-23]. Furthermore, the role of health educator is more familiar to most counselors in the medical setting compared to the role of providing decision-making support and therefore more counseling activity seems to focus on providing health education [12]. Moreover, clients’ characteristics seem to influence counseling in practice. Counseling with better educated clients seem to contain both more health education and decision-making support, since better educated clients ask probably more questions. The presence of a partner seems also related to both more health education and decision-making support, as it will take more effort to inform two persons and to engage them both into the discussion about the decisions at hand [10,12,24-26].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
99
5
The current study was designed to provide a detailed description of routine prenatal counseling for congenital anomaly tests by midwives in the Netherlands, during videotaped, every day practice (see Appendix A for more information about the Dutch prenatal screening context). This study aims to 1) describe the relative expression of the three functions of the prenatal counseling model (HE, DMS and client-midwife relation: CMR) during counseling by midwives; 2) describe the ratio client versus midwife conversational contribution within the three prenatal counseling functions; 3) explore characteristics which are associated with midwives’ expressions of the three function prenatal counseling model. It was expected that the health education function would be expressed most by midwives compared to decision-making support and that midwives would contribute more to the conversation during counseling compared to clients. With regards to clients’ characteristics it was expected that parity was negatively associated with the amount of health education given during counseling, because midwives might expect multiparae to have former knowledge. Furthermore, it was expected that consultations with better educated clients and / or with partners present would contain both more health education and decision-making support.
METHODS
We used a video observational design to study prenatal counseling. The present study is part of DELIVER, a multi-center national research program investigating the quality and provision of primary midwifery care in the Netherlands [27]. Our study was approved by the Institutional Review Board and the Medical Ethical Committee of the VU University Medical Centre, Amsterdam, the Netherlands, supplemented by local agreements to participate from all participating midwifery practices.
ParticipantsMidwivesFrom the twenty primary care midwifery practices participating in the DELIVER study [27], six practices were purposively sampled based on their practice size and location in the Netherlands (urban versus semi-rural and percentages of clients from non-Dutch origin), and participated between August 2010 and April 2011. Every participating midwife was asked to video-tape 10-20 consultations in order to assure the reliability of the test sample [28] and to complete a pre- and post-counseling questionnaire. As an incentive for participation, each participating midwife was offered an one time amount 80 euro credit note after they finished the video-recordings for this study.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
100
Clients Clients were recruited from all consecutive new clients (pregnant women and their partners) of the six midwifery practices. We used a video observational design to study prenatal counseling between June 2010 and May 2011. Clients (nulliparous or multiparous women) were eligible if they were: (1) new to prenatal counseling for the current pregnancy; (2) aged 18 years or older; (3) able to read Dutch or English.
ProcedureClients were invited to participate in the study by the practice assistant and if they agreed received additional, written information about the study. Participating clients and partners were asked to sign an informed consent form as well as to complete a pre-counseling questionnaire.
MeasurementsMidwifery and client questionnairesMidwives’ characteristics such as age, gender and religion were derived from a questionnaire completed as part of our study regarding midwives’ views on appropriate prenatal counseling [10]. Clients’ background characteristics such as age, parity and ethnicity, were derived from the pre-counseling questionnaire [10].
Measurement to code HE, DMS and CMR on videotapes: RIASThe most well-known and frequently used coding scheme for provider – patient communication with good reliability and concurrent validity is the Roter Interaction Analysis System (RIAS) [12,29,30] (Appendix B). RIAS is also the most exhaustive coding scheme available [29,30]. During the coding procedure meaningful utterances (e.g. a sentence or a thought) of midwives and clients were counted, e.g. the client asking the midwife which anomalies can be found using prenatal screening; or the midwife informing the client of her risk of having a child suffering from a congenital abnormality. The occurrence of utterances with similar themes are categorized and the frequencies are then counted. Three trained observers used an adjusted version of the RIAS to code the video recordings. Health Education was coded using the content areas ‘medical condition’ and ‘medical testing’ concerning topics such as information exchange about the medical conditions which can be detected by prenatal congenital anomaly tests, and ‘societal information exchange’ concerning topics like costs and eligibility of these tests. All codes within these main categories were computed into the categories HE Information, HE Questions and Total HE (Table 5a). Decision-making support was coded using the content area ‘counseling behavior’ (midwives only category) or ‘psychosocial topics’ containing topics that address exploration of clients’ moral dilemma’s concerning the decision about whether to take prenatal congenital anomaly

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
101
5
tests. The main coding area DMS was also divided into two sub-areas DMS Information and DMS Questions. Finally, the client-midwife relation was coded using the ‘affective behavior’ categories of the RIAS; affective behavior facilitates this relation through the development of affinity and responsiveness to the client’s emotions. Examples of this category are: giving verbal attention, agree and backchannel (e.g. “hm, hm” or “ok”) and social behavior.Coding categories per main coding area (HE, DMS and CMR) were derived from the original RIAS and expanded with 32 items of the 58-item QUOTEprenatal questionnaire, a client centered instrument to assess clients’ preferences regarding prenatal counseling for congenital anomaly tests [10]. The 32 items were selected from the possible 58 based on the criterion that they had to be observable as verbal communication during the coding of the video-taped consultations. The 32 items we used of the QUOTEprenatal questionnaire were assigned to the most suitable coding area based on the Principal Component Analysis used in the study of [10] (Table 1).
Coding reliability Inter-rater reliability was calculated on a random sample of 26 (9.3 %) of the 269 study video tapes. Intraclass correlation (ICC) was used to measure the inter-rater reliability for midwife, client and partner categories with a mean occurrence greater than 2% of the total, which proved to be adequate [31,32]. At the start and half way through the coding process levels of agreement were measured; some videos were coded again in order to enhance the coding reliability, which it did. Midwife categories had a substantial mean ICC (ICC single measures) of 0.67 (Range: 0.53 – 0.70). The average ICC of client categories (ICC single measures) was moderate with 0.53 (Range: 0.45 – 0.58) and the mean ICC of partner categories (ICC single measures) was good with 0.82 (Range: 0.72 – 0.91) [33]. Moderate and substantial ICCs such as 0.53 and 0.67 are seen in other video-recording studies using similar approaches [31,34-37].
Data AnalysisDescriptive statistics were used to describe the socio-demographic characteristics of participating midwives, clients and partners. We compared characteristics of midwifery respondents with characteristics of the National midwifery population to examine the representativeness of our research sample with respect to the available information (i.e. age, gender and place of vocational education). Non-response analyses of clients, who declined to participate in this study, were conducted using independent t-tests and X2 tests to compare both groups with regards to background characteristics such as age and parity. Furthermore, descriptive statistics and multilevel regression analyses were used to describe the potentially independent association between clients’ background characteristics and the duration of counseling.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
102
Relative expression of the three prenatal counseling functionsDescriptive statistics (frequencies, percentages) of the coded utterances were used to describe the relative expression of the three counseling functions by clients, partners and midwives together. Throughout the analysis utterances are defined as the smallest unit of expression or statement to which a meaningful code can be assigned, generally a complete thought, expressed by each speaker (client, partner, midwife) throughout the counseling session.
Ratio client versus midwife conversational contributionThe ratio of midwives’ versus clients’ (women and partners separately) contributions to the conversation relative to the total count of utterances were calculated per counseling function using descriptive statistics. For instance HE: midwives’ total HE utterances / total HE utterances; clients’ total HE utterances / total HE utterances and partners’ total HE utterances / total HE utterances.
Characteristics associated with midwives’ expressions of the three prenatal counseling functionsThe data in our dataset came from 20 midwives of 6 practices. Therefore, we assumed dependency of our observations. To control for this clustering, a multivariate multilevel linear regression analysis was used to examine client characteristics that are possibly, independently associated with differences in the expression of the three functions of prenatal counseling by midwives. During multivariate multilevel linear regression analysis the following procedure was used. First, we ran a ‘naïve’ analysis (linear regression analysis) of the relationship between each client characteristic (clients’ age, parity, religion, ethnicity, education and presence of the partner during counseling) and each of the three dependent variables (HE, DMS and client-midwife relation utterances of midwives). Second, we used the likelihood ratio test to determine if a random intercept of ‘midwife’ alone, ‘practice’ alone or ‘midwife and practice’ together would provide the best approach for running the third step. Third we used the likelihood ratio test to evaluate the necessity of a random slope for each independent variable to the model. We built the final association model for each dependent variable separately using a backward selection procedure. For these final analyses we used p≤0.05 to indicate significance, keeping in mind the arbitrary nature of this limit [38]. SPSS 21.0 was used for the analysis.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
103
5
Table 1 Items of the QUOTE prenatal added to the main content areas of the RIAS.
Number Item descriptions per component of the QUOTE prenatal
Client–midwife relationQ17 Give the client (additional) written informationQ18 Tell the client that she can always contact the midwife with any questions she may have (including
when the practice is closed)
Health educationQ26 Explain which anomalies can be identified using prenatal screeningQ27 Explain which anomalies cannot be identified using prenatal testsQ28 Provide medical information about the anomalies that are being tested forQ29 Discuss possible negative implications of prenatal screening for the unborn childQ31 Explain the usefulness of prenatal screening (what the client can decide to do eventually)Q32 Tell the client about all the different types of prenatal testsQ33 Tell the client how prenatal screening can affect her emotions and mental wellbeingQ34 Tell the client how much prenatal tests costQ35 Tell the client about the incidence of birth defects in the NetherlandsQ36 Ask about clients family´s history of birth defectsQ37 Explain how often congenital anomalies occur in pregnant women of clients ageQ38 Explain how the chances of a birth defect are calculated for the unborn childQ39 Tell the client about HER chances of having a child with a congenital abnormality during this
pregnancyQ40 Talk to the client about how HER risk of having a child with a birth defect will affect herQ41 Tell the client why she is or is not eligible for certain prenatal testsQ42 Explain what will happen DURING the prenatal testsQ43 Explain which prenatal tests will be done first and which will be done later, if required and/or
necessaryQ44 Explain who will give the client the results of the prenatal tests and how (verbally, in writing or by
telephone)Q45 Explain how long the client may take to decide whether or not to have the prenatal tests Q46 Explain how long the client may take to decide whether or not to terminate the pregnancy, should
the test results show an abnormalityQ48 Discuss all clients options with regard to prenatal screening and the implications
Decision-making supportQ3 Tell which websites the client can use to find information about prenatal screening and diagnosticQ9 Advise the client about whether or not to take the prenatal testsQ14 Enquire clients’ standards, values and views on prenatal screening and diagnosticQ22 Respond to what the client already knows about prenatal screeningQ30 Tell the client what the Dutch government aims to achieve by providing prenatal testsQ49 Talk to the client about how her family and she would react to a child with a birth defectQ50 Ask the client to explain her decision to take / not to take the prenatal testsQ51 Asks whether clients family, friends or other people close to her would support her decision about
prenatal screeningQ52 Ask the client what for her constitutes a healthy childQ53 Ask whether test results indicating that clients unborn child has a birth defect would cause
problems with her conscienceQ54 Ask whether clients family, friends or other people close to her would support her decision to
terminate the pregnancy if the child were to have a congenital abnormalityQ55 Ask how the client thinks she will react to the results of the prenatal tests

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
104
FINDINGS
ParticipantsMidwives and recorded visits269 video-recordings of 20 midwives working in 6 practices were included in the analyses. Per practice the number of participating midwives ranged from one to five midwives. Recordings per midwife ranged from 7 to 23. The mean age of the participating midwives was 32.8 years of age (range 23 to 54 years of age), and mean years of work experience was 8.3 years (range: just started to 33 years of work experience) (Table 2). One of the midwives offered counseling for prenatal congenital anomaly tests during separate counseling sessions, the other 19 midwives offered this counseling during the routine intake. Within the latter group 191 complete intakes were recorded and in 71 cases the video-recordings were switched on and off to only record the counseling parts of the intake. In cases where the video-recordings contained the whole intake, only the prenatal counseling part was or prenatal counseling parts were analyzed. The coding book for coders provided information about how to decide the counseling was started and ended.
Table 2 Demographic and professional characteristics of midwives.
Characteristics Midwives N=20 (%)
Dutch midwifery population N=2264a (%)
Age (in years)≤ 40 years≥ 41 years
16 (80)4 (20)
1644 (73)620 (27)
GenderMaleFemale
-20 (100)
43 (2)2569 (98)
Ethnicityb
NativeNon-Native - Non Western EthnicityNon Native - Western Ethnicity
14 (70)2 (10)4 (20)
No information available
Work experience (years)≤ 2 years3-11 years≥ 12 years
4 (20)12 (60)4 (20)
No information available
Religious backgroundNon religiousReligious
11 (55)9 (45)
No information available
a [46].b In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one of the parents (of both of them) of a person is born outside the Netherlands, this person is non-Native [56].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
105
5
Table 3 illustrates that the counseling lasted on average 9.13 (SD=4.16) minutes. Only parity was independently and significantly associated with the duration of counseling. Prenatal counseling of multiparae lasted statistical significantly less long compared to nulliparous women (β=-3.01; 95% CI: -3.96 – -2.05; p< .001). The amount of utterances during the counseling was positively related to the duration of counseling and counseling of nulliparae lasted significantly longer compared to multiparae. Therefore, it was decided to measure the ratio client versus midwife conversational contribution overall and for nulliparous (N=98) and multipara (N=141) separately.
Table 3 Characteristics of the video-taped consults.
Duration of consultations and prenatal counseling
N* (%) M (SD in minutes)
Recorded part of the counselingOverall duration of counseling 269 (100.0) 9.13 (4.16)Duration of counseling in integrated consultations 191 (71.0) 9.29 (4.22)Duration of counseling in integrated consultations if video recordings were switched on and of
71 (26.4) 8.32 (3.56)
Duration of separated counseling 7 (2.6) **ParityDuration of counseling nulliparae 98 (41.2) 11.03 (4.09)Duration of counseling multiparae 140 (58.8) 7.91 (3.99)EthnicityDuration of counseling Dutch participants 184 (77.0) 9.46 (4.09)Duration of counseling non-Dutch participants 55 (23.0) 9.01 (4.82)ReligionDuration of counseling religious participants 127 (53.1) 9.08 (4.25)Duration of counseling non-religious participants 112 (46.9) 9.59 (4.22)Level of educationDuration of counseling lower educated women 115 (47.9) 9.28 (4.27)Duration of counseling higher educated women 125 (52.1) 9.40 (4.27)Dyadic / triadic counselingDuration of counseling if partner was present 197 (73.2) 9.85 (4.31)Duration of counseling if partner was absent 72 (28.8) 7.45 (3.59)
* Due to missing data the N can very form variable to variable. Valid percentages are shown.**Number of cases too small for relevant, further analyses.Bold figures indicate independent significantly association between groups (p<0.001).
ClientsOf the 460 eligible clients (pregnant women) invited to take part in the study, 324 (70.4%) agreed to participate, but due to recording and other problems a number 55 video-tapes were lost, leaving 269 clients (269/460=58.5%) to be included in the analysis. Of those

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
106
included, 197 consultations (197/269=73.2%) clients and their partner visited their midwife together. Data on background characteristics were available for 241 clients (241/269=89.6%) and 171 partners (171/197=86.8%). Table 4 shows the background characteristics of clients and partners. The mean age of clients was 29.2 years of age, (range 20 to 40 years) and the mean age of partners was 31.8 years of age (range 18 to 47 years). We analyzed the characteristics of the 136 clients who declined participation. The percentages of multiparae in the non-participant group (75.6%) were higher compared to participants (59.9%) (X2 (1, N=324)=8.58, p=0.003, φ=0.159).
Table 4 Characteristics of pregnant women and (if present) their partners.
Characteristics Pregnant womenN=241* (%)
Partner N=171* (%)
GenderMaleFemale
-241 (100.0)
168 (99.4)1 (0.6)
Age (years)≤ 25 years26 – 30 years31 – 35 years≥ 36 years
44 (18.5)108 (45.4)73 (30.7)13 (5.5)
21 (12.6)45 (26.9)69 (41.3)32 (19.2)
Highest level of educationa
Up to high schoolHigher vocational education / university
115 (47.9)125 (52.1)
88 (52.1)81 (47.9)
Ethnicityb
NativeNon-Native
184 (77.0)55 (23.0)
135 (80.8)32 (19.2)
Religious backgroundNoneChristianMuslimOther
112 (47.1)102 (42.9)22 (9.2)2 (0.8)
80 (47.9)78 (46.7)7 (4.2)2 (1.2)
Pregnancy duration≤ 11 weeks≥ 12 weeks
204 (92.3)17 (7.7)
147 (94.2)9 (5.8)
ParityNulliparaMultipara
98 (41.2)141 (58.8)
92 (55.1)75 (44.9)
*Due to missing and inapplicable answers the N can vary from variable to variable. Valid percentages are shown.a Up to high school includes the Dutch MBO.b In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one of the parents (of both of them) of a person is born outside the Netherlands, this person is non-Native [56].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
107
5
Relative expression of the three prenatal counseling functionsTables 5a and 5b present the total amount of utterances regarding the three functions of counseling for prenatal congenital anomaly tests made by midwives, clients and partners. 41% (20635/50154) of the utterances were coded as HE, 23% (11528/50154) as DMS and 36% (17991/50154) as building a client-midwife relation.
Ratio client versus midwife conversational contributionTables 5a and 5b show that the overall conversational contribution of midwives during prenatal counseling exceeded the contribution of clients and partners (60% versus 32% and 8%, respectively) with no difference for the nulliparous women compared to multiparae ≥ 5%. More specifically, results show that midwives contributed the most to the conversation during HE; they made 91% of the HE utterances, 7% were made by clients and 2% by partners. The majority of the utterances made by midwives were characterized as giving HE Information (90% out of 91%). Also, most utterances of clients and partners were characterized as giving HE Information. With regards to decision-making support tables 5a and 5b show that midwives’ relative contribution to the conversation was 61%, clients 29% and partners made 10% of the utterances regarding the decision-making support function of prenatal counseling. However, these ratios were different for nulliparous women compared to multiparae. Multiparae contributed relatively more to the conversation during decision-making support (34%) compared to nulliparous women (25%). Overall, of the midwifery utterances coded as DMS, the majority (34%) were intended to direct behavior. For example ‘you really have to talk about your decision at home together with your partner’ or utterances stating the ‘opting in’ system used in the Netherlands such as ‘it is important to think about the implications of prenatal testing before you take or refuse them’. The least frequent utterances of midwives were DMS Questions (11%), such as ‘what reasons do you have to take or refuse prenatal tests?’. Both clients and partners made the most utterances regarding giving DMS Information (29% and 10%, respectively), such as ´The combined test is just a risk assessment. I think the results will only upset me´.Regarding the client-midwife relation most utterances of midwives, clients and partners were coded as agree or backchannel.
Characteristics associated with midwives’ expressions of the three prenatal counseling functionsResults of the multivariable multilevel analyses of the whole dataset show that data were clustered within midwives, but not within practices. Regarding the HE function of counseling, the multivariable multilevel analyses shows that of the 5 potential client characteristics that were included in the model (age, religion, level of education, parity and partner being

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
108
Tabl
e 5a
Cou
nsel
ors
(MF)
’, cl
ient
s’ a
nd p
artn
ers’
num
ber
and
perc
enta
ges
of t
otal
cou
nsel
ing
utter
ance
s ac
ross
the
thr
ee f
uncti
ons
of p
rena
tal
coun
selin
g.
MF
(N=2
0)N
(%)
Clie
nts
(N=2
69)
N (%
) Pa
rtne
rs (N
=197
) N
(%)
Tota
lN
(%)
Hea
lth
Educ
ation
Hea
lth e
duca
tion
Que
stion
s24
1 (1
)45
3 (2
)19
2 (0
.9)
886
(4)
Hea
lth e
duca
tion
Info
rmati
on18
520
(90)
936
(5)
293
(1.1
)19
749
(96)
Tota
l Hea
lth E
duca
tion
utter
ance
s18
761
(91)
1389
(7)
485
(2)
2063
5 (1
00)
2063
5/50
154=
41%
Dec
isio
n-m
akin
g su
ppor
tDe
cisio
n-m
akin
g su
ppor
t Que
stion
s11
51 (1
1)35
(0)
34 (0
)De
cisio
n-m
akin
g su
ppor
t Inf
orm
ation
1878
(16)
3359
(29)
1123
(10)
Deci
sion-
mak
ing
supp
ort C
ouns
elin
g39
48 (3
4)-
-To
tal D
ecisi
on-m
akin
g su
ppor
t utt
eran
ces
6977
(61)
3394
(29)
1157
(10)
1152
8 (1
00)
1152
8/50
154=
23%
Clie
nt-m
idw
ife re
lati
onAff
ectiv
e co
mm
unic
ation
: ve
rbal
att
entio
n, s
ocia
l beh
avio
ur, a
gree
and
bac
kcha
nnel
s,
appr
oval
, con
cern
, rea
ssur
ance
, disa
gree
3497
(19)
1109
4 (6
2)26
89 (1
5)
Giv
ing
writt
en in
form
ation
557
(3)
2 (0
)2
(0)
Offe
r the
pos
sibili
ty to
talk
abo
ut p
rena
tal t
ests
aga
in15
0 (1
)-
-To
tal c
lient
-mid
wife
rela
tion
utter
ance
s42
04 (2
3)11
096
(62)
2691
(15)
1799
1 (1
00)
1799
1/50
154=
36%
Tota
l am
ount
of p
rena
tal c
ouns
elin
g utt
eran
ces
2994
2 (6
0)15
879
(32)
43
33 (8
)50
154
(100
)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
109
5
Tabl
e 5b
Cou
nsel
ors
(MF)
’, cl
ient
s’ a
nd p
artn
ers’
num
ber
and
perc
enta
ges
of t
otal
cou
nsel
ing
utter
ance
s ac
ross
the
thr
ee f
uncti
ons
of p
rena
tal
coun
selin
g an
d nu
llipa
rae
and
mul
tipar
ae s
epar
atel
y an
d al
l clie
nts
toge
ther
.
MF
(N=2
0)N
(%)
Clie
nts
(N=2
69)
N (%
) Pa
rtne
rs (N
=197
)N
(%)
Tota
lN
(%)
Hea
lth
Educ
ation
Nul
lipar
a (N
=98)
8849
(92)
553
(6)
236
(2)
9638
(100
)M
ultip
ara
(N=1
41)
8129
(90)
724
(8)
197
(2)
9050
(100
)N
ullip
ara
and
mul
tipar
a to
geth
er (N
=269
)18
761
(91)
1389
(7)
485
(2)
2063
5 (1
00)
Dec
isio
n-m
akin
g su
ppor
tN
ullip
ara
3240
(65)
1252
(25)
494
(10)
4986
(100
)M
ultip
ara
3037
(56)
1854
(34)
514
(10)
5405
(100
)N
ullip
arou
s an
d m
ultip
ara
toge
ther
69
77 (6
1)33
94 (2
9)11
57 (1
0)11
528
(100
) Cl
ient
-mid
wife
rela
tion
Nul
lipar
a 16
37 (2
1)47
08 (6
0)14
80 (1
9)78
25 (1
00)
Mul
tipar
a 21
63 (2
5)54
93 (6
4)91
6 (1
1)85
72 (1
00)
Nul
lipar
ous
and
mul
tipar
a to
geth
er
4204
(23)
1109
6 (6
2)
2691
(15)
1799
1 (1
00)
Tota
l am
ount
of p
rena
tal c
ouns
elin
g utt
eran
ces
Nul
lipar
a13
726
(61)
6513
(29)
2210
(10)
2244
9 (1
00)
Mul
tipar
a 13
329
(58)
8071
(35)
1627
(7)
2302
7 (1
00)
Nul
lipar
a an
d m
ultip
ara
toge
ther
29
942
(60)
1587
9 (3
2)
4333
(8)
5015
4 (1
00)
Bold
figu
res
show
diff
eren
ces
≥ 9%
bet
wee
n th
e re
lativ
e co
ntrib
ution
to th
e co
nver
satio
n be
twee
n co
unse
ling
of n
ullip
ara
vers
us m
ultip
ara.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
110
present or not), only parity was independently and significantly associated with the amount of HE utterances as well as DMS utterances (β=-27,41; CI: -35,20 – -19,63; p< 0.001 and β=-10,62; CI: -14.30 – - 6.95; p< 0.000, respectively); midwives used less health educational and decision-making support utterances during counseling of multiparae compared to counseling of nulliparous women. The expression of building a client-midwife relation was independently and significantly associated with the religious background of clients and the age of the pregnant women. With non-religious clients midwives used less client-midwife relation utterances compared to religious women (β=-2.42; CI: -4.88 – 0.04; p=0.05) and a higher age of pregnant women was associated with more midwives’ utterances regarding the client-midwife relation (β=0.41; CI: 0.11 – 0.70; p=0.01).
DISCUSSION
This study shows that almost half of the utterances made during prenatal counseling for congenital anomaly tests by midwives were coded as related to the health education function of prenatal counseling. About a quarter of the utterances was related to the decision-making support function. Building a client-midwife relation was accomplished by both midwives and clients primarily through active listening techniques such as giving backchannels and agreements. As expected, midwives contributed the most to the conversation coded as health education. Regarding the decision-making support function of counseling, the relative contribution of midwives was less extensive compared to their contribution during health education, while clients and their partners contributed more to the decision-making support conversation compared to their relative contribution during health education. This ‘pattern’ was different for nulliparae compared to multiparae; during decision-making support of multiparae midwives’ relative contribution to the discussion was less compared to their contribution during decision-making support of nulliparous women. Such differences were not found within the other two functions of counseling. Counseling of nulliparous women lasted significantly longer than counseling of multiparous women. Other research on client-counselor communication, also concluded that counseling sessions are largely didactic in nature with relatively little emphasis on the psychological and emotional aspects of the decision-making process of clients and decision-making support [12,31,39]. Most of the counseling took place during the initial intake, although a separate counseling consultation is recommended by national guidelines and the literature [18,24-26,40]. Perceived time pressure may be a reason why most practices choose to counsel within the initial intake, despite recommendations from the national guidelines. Most clients enter midwifery care around 8.6 weeks of pregnancy [10]. Scheduling two appointments (e.g. one intake and one prenatal counseling session) is challenging since the blood test of the CT has

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
111
5
ideally to be done around 10 weeks of the pregnancy. One way to improve this suboptimal situation is to provide clients with more information about choices at hand, prior to the initial consultation. For example by asking clients and partners to complete a decision aid at home and read information. During counseling the counselor can then check knowledge, focus on pros and cons of the options, discuss the outcome of the decision aid and provide client-centered decision-making support [26]. As far as we know, this approach is not commonly used by midwives. Limited time in combination with a client with little or no prior knowledge could have affected the way midwives asked decision-making support questions, i.e. more as rhetorical questions. With regards to the decision-making support function of counseling the results of our study are promising. Midwives seem to understand that during this part of the conversation it is important to step back and listen to the clients’ way of making sense of the information they just received. However, our study shows also that midwives use relatively fewer exploring questions compared to directing behavior. This approach could potentially cause less informed decision-making, because clients are not invited to really answer reflective questions during counseling. As a result, they might not consider them at all and therefore base their decision on uninformed instead of informed preferences. Achieving informed preferences is the optimal goal since decisions will be better understood, based on more accurate expectations about the negative and positive consequences and more consistent with personal preferences [26,41]. Results of the multilevel analyses showed a strong association between parity and the amount of health education and decision-making support provided. Furthermore, as expected, counseling of nulliparous women lasted significantly longer than counseling of multiparae. One explanation could be that multiparae know already more about the available tests and might have experience in making decisions about the test uptake and therefore need less health education and decision-making support and shorter counseling. However, from an earlier study of our research group it is known that significantly fewer multiparae compared to nulliparous women perceive that the health education they received during counseling met their pre-counseling preferences and that a majority of multiparae with strong preferences for decision-making support perceived that these preferences were not fully addressed during counseling [10]. Since we found no random slope for parity and we did find clustering of data within midwives, midwives seem to be the initiator of contributing more to the decision-making support of nulliparous compared to multiparous women. With the current data it remains unclear if this approach together with differences in the duration of counseling is accurate especially within the Dutch context in which the fee midwives receive for counseling of nulliparae and multiparae is the same. The funded pre-test counseling time is 30 minutes [42].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
112
This study indicated that the full funded 30 minutes for counseling was not used, on average. There may be several reasons why midwives do not use the allocated counseling time for pre-test counseling during this first prenatal visit. Perhaps midwives plan to spend additional time later in the pregnancy for example additional counseling for the FAS. Alternatively, they may want to reserve some extra funded time for post-test counseling. Furthermore, maybe there is a difference in perception of time needed between midwives and policy makers. Recent studies demonstrate that a substantial part of the Dutch midwives’ perceptions regarding the content of health education do not entirely match clients’ preferences and that not all midwives fully endorse the counseling function decision-making support, while clients prefer tailored health education as well as decision-making support [10,43]. Using the funded 30 minutes time could improve counseling that meets clients’ individual preferences as well as professional guidelines.The expression of building a client-midwife relation was statistically, independently and significantly associated with the religious background of clients indicating that midwives used more client-midwife relation utterances during counseling of religious women. It is difficult to provide examples of the differences between counseling of religious versus non-religious women, since the client-midwife relation is built during the whole counseling using utterances such as ‘yes, I can imagine it is a difficult decision to make’ or ‘hm, indeed’. However, an explanation for the expression of more client-midwife relation utterances used within counseling of religious women, could be that in general believers indicate obedience to an authority (e.g. God, the bible, doctrines and preacher) as more important than non-believers do [44]. So, from the perspective of a believer, a midwife could be seen as an authoritative person with whom it is important to build a relationship of trust. Furthermore, in general, non-believers are more individualized than believers and one of the characteristics of individualization is the emphasis on interest of the person herself [44,45].
Study limitationsFirst, our study included only 20 midwives of the ca. 2264 midwives in the Netherlands [46]. Therefore, the generalizability of the findings of this explorative study are limited. Some of the midwives video-taped a relatively small amount of their consultations, which might not be representative for their way of counseling. Depending on the medical history of the client and the policy of the midwifery practice, additional counseling sessions could be held. These were not included in the study, because especially during the first consultation, focusing on pre-test counseling, the foundation for a relationship between the midwife and the client (and partner) is laid. However, participating midwives stated that they counseled for both the combined test and the fetal anomaly scan during the recorded counseling sessions and therefore it is likely that most of it was video-taped. Second, although the ratio multiparae versus nulliparae in the current study was the same as the Dutch pregnant population [47]

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
113
5
fewer multiparae participated, and our study sample was more highly educated and of Dutch origin than the Dutch pregnant population although of practices participating in this study were also located in the so called ‘Randstad’ area of the Netherlands, where significantly more people from non-Dutch origin live [47]. This also limits generalizability of our results. Last, using the RIAS for analyses as we did, all utterances get the same count irrespective of whether they refer to words or backchannels such as ‘hm, hm’ or to a whole expression, such as ‘you have to know that the combined test is a risk assessment only’. In general, health education utterances are more likely to be whole expressions and not backchannels. During decision-making support backchannels will more often used reflecting active listening after asking exploring questions. These backchannels are counted as client-midwife relation utterances. As a result, the relative amount of health education utterances compared to decision-making support utterances may have been underestimated.
Key Conclusions- We found that midwives focused primarily on the health education function of
counseling for prenatal anomaly tests. As expected, during health education midwives did most of the talking while clients were listening.
- During decision-making support clients, especially multiparae, contributed more to the conversation compared to their contribution during health education. However, midwives contributed still more to the discussion compared to clients and used relatively few exploring questions.
- Parity appears to be independently associated with the way midwives counsel their clients. Nulliparous women receive more health education as well as decision-making support and contributed less to the conversation during decision-making support compared to multiparae.
Practice Implications Our findings should encourage midwives to reflect on the way they address the three prenatal counseling functions during counseling of nulliparous women compared to multiparous women. Reflections should include the connection to knowledge of clients: ‘what do you know about prenatal screening?’ followed by: ‘can you tell me what additional information you might need from me?’. Regarding decision-making support, in our study a midwife stated ‘The most important thing to do is to think about what you would do if your test informs you that your child has Down syndrome […] I think it is important to talk this through with your boyfriend’. Rather than telling a client what to do, we would encourage midwives to ask open questions such as ‘what would you do in case prenatal tests informs you that your child has Down syndrome?’ and wait for the answer, also when it takes the client some time to formulate it. Another approach to the starting of the counseling could also be considered;

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
114
for example, providing clients with a decision aid to complete prior to starting the counseling session with the midwife. The counseling could start with: ‘What do you want to know about the health of your child during pregnancy?’ or ‘Why would you opt for prenatal screening or / why would you not opt for prenatal screening?’ This directs the counseling more towards DMS compared to HE. The Shared Decision Making model could be used as a practical guideline to optimize both the health education and decision-making support functions of prenatal counseling. The model divides the conversation into three parts: ‘choice talk’: the pros and cons of each choice (e.g. the choices about prenatal screening, the choices about prenatal diagnosis, the eventual choices about termination of pregnancy), ‘option talk’: exploration of preferences and moral values as well as providing further decision support by using decision tools and ‘decision talk’: reflection on the time needed to make the decision.
AcknowledgementsWe gratefully acknowledge the contribution of the clients and midwives in the Netherlands, who provided the data for this study. We also thank Lydia Gitsels and Veerle Steenhuis for their work on the video-coding project. In addition, we thankfully acknowledge AVAG for funding this study.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
115
5
REFERENCES
[1] Leporrier N, Herrou M, Morello R, Leymarie P. Fetuses with Down’s Syndrome detected by prenatal screening are more likely to abort spontaneously than fetuses with Down’s syndrome not detected by prenatal screening. BJOG- An International Journal of Obstetrics and Gynaecology, 2003; 110: 18-21.
[2] Nicolaides KH, Heath V, Cicero S. Increased fetal nuchal translucency measurement at 11-14 weeks. Prenatal Diagnosis, 2002; 22: 308-15.
[3] Economides DL. Early pregnancy screening for fetal abnormalities. Utrasound Obstetrics and Gynecology, 1999; 13: 81-3.
[4] Fransen MP, Wildschut HIJ, Mackenbach JP, Steegers EAP, Essink-Bot ML. Information about prenatal screening for Down syndrome. Ethnic differences in knowledge. Patient Education and Counseling, 2009; 77: 279-288.
[5] Health Council of the Netherlands, 2007. Population screening act. Prenatal screening on down’s syndrome and neural tube defects. Den Haag: Health council of the Netherlands; 2007/05 [In Dutch].
[6] Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands. BMC Pregnancy and Childbirth, 2009; 9:18.
[7] Waelput AJM, Hoekstra J. Midwifery care summarized. In: Public health Forecasts, National Compass Public Health. Bilthoven: RIVM. 2012 [cited 2012 Feb 23]. Available from: URL: http://www.nationaalkompas.nl/zorg/sectoroverstijgend/verloskundige-zorg/verloskundige-zorg-samengevat/ [In Dutch].
[8] Oepkes P, Wieringa J. The right to know; the 20-weeks ultrasound investigation facilitates a conscious choice. Medisch Contact, 2008; 31/32: 1296–1297 [In Dutch].
[9] van Agt HME, Schoonen HMHJD, Wildschut HIJ, de Koning HJ, Essink-Bot ML. Health education for the pre- and neonatal screeningsprogram: Questionnaires regarding the national evaluation of the providing procedures. Erasmus MC, Rotterdam 2007 [In Dutch].
[10] Martin L, van Dulmen S, Spelten E, de Jonge A, de Cock P, Hutton E. Prenatal counseling for congenital anomaly tests: Parental preferences and perceptions of midwife performance. Prenatal Diagnosis, 2013; 33, 1–12.
[11] Meiser B, Irle J, Lobb E, Barlow-Stewart K. Assessment of the content and process of genetic counseling: a critical review of empirical studies. Journal of Genetic Counseling, 2008;17: 434-451.
[12] Roter DL, Ellington L, Hamby Erby L, Larson S, Dudley W. The genetic counseling video project (GCVP): Models of practice. American Journal of Medical Genetics, 2006, Part C; 142C: 209-220.
[13] Smets E, van Zwieten M, Michie S. Comparing genetic counseling with non-genetic health care interactions: Two of a kind? Patient Education and Counseling, 2007; 68: 225-234.
[14] Weil J, Ormond K, Peters J, Peters K, Bowles, Biesecker B, LeRoy B. The relationship of nondirectiveness to genetic counseling: report of a workshop at the 2003 NSGC Annual Education Conference. Journal of Genetic Counseling, 2006; 15(2): 85-93.
[15] www.riasworks.com, last retrieved: March 18th 2013.[16] KNOV, 2010. Digital Individual post-graduate Course (DIN). KNOV, Utrecht (in Dutch). Checked
on: 06-02-2012. URL: http://leden.knov.nl/leden/30werken_aan_kwaliteit/19bij_en_nascholing/Digitale_individuele_nascholing_DIN [In Dutch].
[17] van Zwieten M. Communication on ethical issues in medical practice. In: Kaptein A.A., Prins J.B., Collette E.H., Hulsman R.L., editors. Medical psychology. Houten: Bohn Stafleu van Loghum, 2010; p. 213-223 [In Dutch].
[18] van Zwieten M. The importance of an informed choice - but what concerns the choice? The complex decision-making in prenatal screening. De Psycholoog, 2008; January: 20-25 [In Dutch].
[19] McCarthy Veach P, Bartels DM, LeRoy BS. Coming full circle: A reciprocal-engagement model of genetic counseling practice. Journal of Genetic Counseling, 2007; 16 (6): 713-728.
[20] Schoonen HM, van Agt HME, Essink-Bot ML, Wildschut HI, Steeger EAP, de Koning HJ. Informed decision-making in prenatal screening for Down’s syndrome: What knowledge is relevant? Patient Education and Counseling, 2011; 84 (2), 265-270.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
116
[21] Schoonen HM, Essink-Bot ML, van Agt HM, Wildschut HI, Steegers EA, de Koning HJ. Informed decision-making about the fetal anomaly scan: what knowledge is relevant? Utrasound in Obstetrics and Gynecology, 2011; 37 (6), 649-57.
[22] Schoonen M, van der Zee B, Wildschut H, Beaufort I, de Wert GMWR, de Koning HJ, Essink-Bot ML, Steegers E. Informing on prenatal screening for Down syndrome prior to conception. An empirical and ethical perspective. American Journal of Medical Genetics, 2012a, Part A; 158A (3): 485-497.
[23] Schoonen M, Wildschut H, Essink-Bot ML, Peters I, Steegers E, de Koning H. The provision of information and informed decision-making on prenatal screening for Down syndrome: a questionnaire- and register-based survey in a non-selected population. Patient Education and Counseling, 2012; 7(3):351-9.
[24] Ahmed S, Bryant LD, Tizro Z, Shickle D. Is advice incompatible with autonomous informed choice? Women’s perceptions of advice in the context of antenatal screening: a qualitative study. Health Expectations, 2012; doi:10.111/j.1369-7625.2012.00784.x.
[25] Barr O, Skirton H. Informed decision making regarding antenatal screening for fetal abnormality in the United Kingdom: A qualitative study of parents and professionals. Nursing and Health Sciences, 2013; DOI: 10.1111/nhs.12034
[26] Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, Cording E, et al.. Shared Decision Making: A model for clinical practice. Journal General Internal Medicine, 2012; 27(10): 1361-7.
[27] Manniën J, Klomp T, Wiegers T, Pereboom M, Brug J, de Jonge A, van der Meijde M, Hutton E, Schellevis F, Spelten E. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Services Research, 2012; 12: 69. DOI: 10.1186/1472-6963-12-69.
[28] Fletcher RH, Fletcher SW. Fourth Edition Clinical Epidemiology, The Essentials. Baltimore: Lippincott Williams & Wilkins, 2005; p. 20-21.
[29] Roter DL, Hall JA, Blanch-Hartigan D, Larson D, Frankel RM. Slicing it thin: New methods for brief sampling analysis using RIAS-coded medical dialogue. Patient Education and Counseling, 2011; 82 (3): 410-419.
[30] Ellington L, Kelly KM, Reblin M, Latimer S, Roter D. Communication in genetic counseling: cognitive and emotional processing. Health Communication, 2011; 26: 667-675.
[31] Pieterse AH, van Dulmen AM, Ausems MGEM, Beemer FA, Bensing JM. Communication in cancer genetic counseling: does it reflect counselees’ pre-visit needs and preferences? British Journal of Cancer, 2005; 92: 1671-1678.
[32] Pieterse AH, van Dulmen AM, Beemer FA, Ausems MGEM, Bensing JM. Tailoring communication in cancer genetic counseling through individual video-supported feedback: A controlled pretest-posttest design. Patient Education and Counseling, 2006; 60 (3): 326-335.
[33] Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics, 1977; 33:159-174.
[34] Roter DL, Larson SL. The Roter Interaction Analysis System (RIAS): Utility and flexibility for analysis of medical interactions. Patient Education and Counseling, 2002; 46:243–251.
[35] van Weert JC, Bolle S, van Dulmen S, Jansen J. Older cancer patients’ information and communication needs: what they want is what they get? Patient Education and Counseling, 2013; 92(3):388-97.
[36] Bensing JM, Kerssens JJ, Van der Pasch M. Patient-directed gaze as a tool for discovering and handling psychosocial problems in general practice. Journal of Nonverbal Behavior, 1995; 19 (4): 223-242.
[37] Steinwachs DM, Roter D, Skinner EE, Lehman AF, Fahey M, Cullen B, Smith A, Everett MD, Gallucci G. A Web-Based Program to Empower Patients With Schizophrenia to Discuss Quality of Care With Mental Health Providers. Psychiatric Services, 2011; 62(11): 1296–1302.
[38] Twisk JWR. Applied Multilevel Analysis. Practical guides to biostatistics and epidemiology. Cambridge university press, Cambridge, 2006 UK.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Antenatal counseling for congenital anomaly tests: an exploratory video-observational study
117
5
[39] Pieterse AH, Ausems MGEM, van Dulmen AM, Beemer FA, Bensing JM. Initial cancer genetic counseling consultation: Change in counselees’ cognitions and anxiety, and association with with addressing their needs and preferences. American Journal of Medical Genetics, 2005a; Part A; 137A: 27-35.
[40] de Boer J, Zeeman K. KNOV-guideline “Prenatal midwifery-led care: Recommendations for support, interaction and information.” Utrecht: KNOV, 2008 [In Dutch].
[41] Frosch D, Kaplan R. Shared decision making in clinical medicine: past research and future directions. American Journal of Preventive Medicine, 1999; 17: 285-94.
[42] Scholman HSA. Evaluation prenatal screening performance. Utrecht: Nederlandse Zorgautoriteit, 2009, CV 09-19 [in Dutch].
[43] Martin L. Hutton EK, Spelten ER, Gitsels-van der Wal JT, van Dulmen S, 2014. Midwives’ views on appropriate antenatal counseling for congenital anomaly tests; do they match clients’ preferences? Midwifery, 2014; 30(6):600-9.
[44] Becker J, de Hart J. Religious changes in the Netherlands. Shifts in the binding with the churches and the Christian tradition. Den Haag: Social and Cultural Planning office, 2006.
[45] Beck U, Beck-Gernsheim E. Individualization: Institutionalized Individualism and its Social and Political Consequences, London: Sage Publications, 2002.
[46] Hingstman L, Kenens RJ. Figures from the registration of midwives, poll 2011. NIVEL, dec 2011 [In Dutch].
[47] The Netherlands Perinatal Registry. 10 years perinatal registration in the Netherlands; an overview. Utrecht: Stichting Perinatale Registratie Nederland, 2011: 26-39 [In Dutch].
[48] NVOG, 2007. LZA: Medical practice Late Termination of pregnancy. Version 2.0. 08-06-2007 [In Dutch].
[49] Bosch M, Adriaanse C, ter Maat E, van der Ven J. Results of prenatal screening 2008 in nine primary care ultrasound centers. Tijdschrift voor Verloskundigen, 2010; 6:45-50 [In Dutch].
[50] Fracheboud J, van Agt HME, de Koning HJ. Monitoring 2009 of prenatal screening for Down’s Syndrome and for foetal anomalies in the Netherlands. Final Report RIVM: Bilthoven, 2011.
[51] Schielen PCJI. Quality control parameters of Dutch Down’s syndrome screening laboratories 2010. RIVM Report 230083003: Bilthoven, 2012 [In Dutch].
[52] Bakker M, Birnie E, Pajkrt E, Bilardo CM, Snijders RJM. Low uptake of the combined test in The Netherlands-which factors contribute? Prenatal Diagnosis 2012; 32:1305-1312.
[53] www.prenatalescreening.nl/vruchtwaterpunctie.php, last retrieved: April 8th 2014 [In Dutch].[54] IGZ (Inspectorate for Healthcare). Termination of Pregnancy Act, Annual Report 2011. 11-04-
2013 [In Dutch].[55] Roter DL. The Roter method of interaction process analysis. Bloomberg School of Public Health,
Balitimore, Maryland, 2006.[56] Statistics Netherlands. Terms immigrant. 2012 [cited 2012 March 23]. Available from: URL:
http://www.cbs.nl/nl-NL/menu/themas/dossiers/allochtonen/methoden/begrippen/default.htm?conceptid=37 [In Dutch].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 5
118
APPENDIX A Dutch prenatal screening contextSince 2007 prenatal screening is offered to all Dutch pregnant women using an opting in approach [5,8,9]. The screening program includes two non-invasive tests: the combined test (CT), a blood test and an ultrasound to measure the nuchal translucency, for determining the possibility of Down syndrome, (around 12th weeks gestational age), and the Fetal Anomaly ultrasound Scan (FAS) for detecting physical anomalies (around 20th weeks gestational age). In the case of confirmatory diagnostic testing, two options are available: pregnancy termination before 24 weeks of gestation, or health-oriented prenatal care for the fetus combined with prenatal and postnatal support [48]. Although both tests are part of a population-screening program, they are not offered on the same basis. The FAS is free for all women, while the CT has to be paid for (ca. 150 euro) by women younger than 36 years of age [5,8]. The mean uptake of prenatal anomaly screening tests in the Netherlands has been around 27% for the CT, but varies between different regions (range 12% to 52%) [49-52]; the mean uptake of the FAS has been around 91% (range 80% to 99%) [50,51]. In the Netherlands, an obstetrician, clinic genetic or pediatrician will provide counseling following confirmation of a fetal anomaly and discuss the option of pregnancy termination or health-oriented prenatal care for the fetus [53]. In 2011, 970 of the parents choose to terminate a pregnancy with a confirmed diagnosis of a congenital anomaly (e.g. about 0.5% of the pregnancies) [54].
APPENDIX B RIASThe RIAS distinguishes utterances that are primarily informative (information giving), persuasive (counseling), interrogative (closed and open-ended questions), affective (social, positive, negative and emotional) and process oriented (facilitation, orientation and transitions). Information and question utterances were further specified in: 1) medical condition, symptoms and history; 2) testing and therapeutic intervention; 3) lifestyle, finances, self-care, and preventive behaviors; 4) psychosocial topics related to emotional reactions, coping, family issues, and social relationships; and 5) counseling or directs behavior [12,55].

Chapter 6Midwives’ perceptions of communication during videotaped
counseling for prenatal anomaly tests: how do they relate to
clients’ perceptions and independent observations?
Martin L, Gitsels-van der Wal JT, Pereboom MTR, Spelten ER, Hutton EK, Van Dulmen S.
Patient Education and Counseling 2015; doi: 10.1016/j.pec.2015.02.002

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
120
ABSTRACT
Objective This study aimed to provide insight into Dutch midwives’ self-evaluation of prenatal counseling for anomaly screening in real life practice and, the degree of congruence of midwives’ self-assessments with clients’ perceptions and with observed performance.
Methods Counseling sessions were videotaped. We used the QUOTE prenatal questionnaire to have each midwife (N=20) and her client (N=240) rate the prenatal counseling that they had together. We used an adapted version of the RIAS video-coding system to assess actual counseling during videotaped prenatal counseling (N=240).
Results Midwives perceived the following functions of counseling performed well: 100% of Client-Counselor relation (CCR); 80% of Health Education (HE); and 17% Decision-Making Support (DMS). Congruence on HE of midwives with observers and with clients was ≥75%; congruence on DMS was higher between midwives and observers (80%) compared to midwives and clients (62%).
Conclusion Midwives perceive that during prenatal counseling the CCR and HE functions of counseling were performed well, whereas DMS was not. Furthermore, this study shows incongruence between midwives and clients about the discussion during DMS, indicating DMS is more difficult to assess than HE.
Practice implications The best way to measure prenatal counseling practice might be by using assessments of different sources within one study.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
121
6
INTRODUCTION
The overall aim of prenatal counseling is to support clients in making an informed, autonomous decision about health care issues that are preference sensitive [1]. Often the best strategy for an individual may be unclear and very personal [2,3]. In theory, ‘good’ counseling can be recognized first by the ‘outcome’, i.e. an informed, autonomous decision made by the client (and her partner), and secondly by the ‘process’. In the process, counselors facilitate the informed decision through the provision of Health Education (HE) and Decision-Making Support (DMS) while building a good Client-Counselor Relation (CCR). The latter refers to being conscious about values regarding the subject of choice and its eventual consequences [4-7]. Addressing moral considerations towards testing and the resulting decisions is a recommended part of decision-making support during counseling [8,9,10]. However, counseling has been shown to focus on HE with less attention for providing DMS [6,11-15].The counseling process has been primarily considered from the perspective of clients and the perspective of an independent observer. We identified an inconsistency between the theoretical model of counseling and the experiences of clients, when looking at clients’ perceptions of the prenatal counseling process; clients consider the HE purpose and building a good CCR to be fulfilled in line with their preference, but they felt that preferences regarding DMS were less frequently met [6]. Research on counseling in various settings in which videotaped counseling was observed by independent observers draw similar conclusions [13,15,16]. Furthermore, we know that care providers do not fully comply with all functions of the theoretical counseling model [15,17]. However, we do not know if counselors also experience an inconsistency between theory and daily counseling practice. Insights derived from counselors’ self-assessment of prenatal counseling may inform optimization of the counseling practices, since self-assessment contributes to continuing professional development in daily practice [18-20]. Therefore, such activities are a core component in medical education as part of becoming and being a medical expert [21].Studies that identified a discrepancy between the theoretical prenatal counseling model and daily practice were, to our knowledge, studies in which evaluation of counseling was undertaken from one perspective at the time e.g. the observer OR the client. Comparing assessments of the same counseling sessions from the vantage point of different assessors within one study might lead to additional insights. Comparing counselors’ self-assessments with observed communication will evaluate the accuracy of these self-assessments while comparisons with the client assessments will compare the client experience of counseling with that of the provider. Eventual incongruence between experiences of counselors and counselees potentially provides important eye-openers for health care providers, such as clients struggling with the inclusion of medical information [22-24].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
122
In the Netherlands, midwives are the designated counselors in 80% of pregnancies [3,25]. They are trained to provide non-directive prenatal counseling for anomaly screening. Dutch midwifery led care is the current study context (Appendix A). We aimed to provide insight into: 1) midwives’ self-assessments on three prenatal counseling functions CCR, HE and DMS; 2) the degree of congruence between midwives’ self-assessments with clients’ perceptions and observed performance. We expected high levels of congruence between midwives’ self-assessments and observed communication, since we expected midwives to have at least some experience with self-evaluation as part of their education as medical expert [21].
METHODS
DesignThis study is part of the DELIVER study, a multi-center national research program to evaluate the quality and provision of primary midwifery care in the Netherlands [26].The video-observational design, including additional questionnaires, of the current cross-sectional study was approved by the Institutional Review Board and the Medical Ethical Committee of the VU University Medical Centre, Amsterdam, the Netherlands, supplemented by local feasibility statements from all participating midwifery practices.
SubjectsMidwives of six midwifery practices in the Netherlands were asked to participate in this study. To offset additional costs of participation, each midwife was offered an 80-euro credit note.Clients were recruited from all consecutive new clients of the six midwifery practices between June 2010 and May 2011. Clients (nulliparous and multiparous women) were eligible if they were: 1) new to prenatal screening for the current pregnancy, 2) aged 18 years or older, 3) able to read Dutch or English.
ProcedureFirst, the midwives and practice assistants of the six participating midwifery practices received detailed oral and written information about the video-recording protocol. Each midwife was asked to videotape ten to twenty consultations in order to deliver a reliable research sample [27] and to complete a questionnaire regarding their background. Second, clients were asked to participate in the study by the practice assistant. If they refused to participate, the practice assistant asked for the reason to decline and background information. If clients agreed to participate, clients received additional written information about the study. They were asked to sign for informed consent to videotape the consultation with an unmanned camera and to complete a pre-counseling questionnaire about their background. Third, after each videotaped counseling session both midwives and clients completed a post-counseling

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
123
6
questionnaire to assess the counseling process. More details of the procedure are described elsewhere [13,28].
MeasurementsBackground characteristicsThe self-administered pre-counseling questionnaires for midwives and clients contained background items such as age, gender, country of origin, education, and religion. The questionnaires were used in our earlier studies [6,17].
Assessment of counseling by midwives Midwives’ self-assessments of prenatal counseling were measured by the midwifery version of the QUOTE prenatal – Performance (Quality of care through the patients’ eyes), which mirrored the questionnaire of clients. The QUOTE prenatal aims at investigating preferences (pre-counseling QUOTE prenatal –Importance questionnaire) and actual prenatal counseling experiences (post-counseling QUOTE prenatal –Performance questionnaire) of clients, respectively [6,17]. Fifteen items of the QUOTE prenatal appeared to cover the client-counselor relation, 24 items the health education function, and sixteen items the decision-making support function. The midwifery version of the post-counseling QUOTE prenatal – Performance questionnaire asks midwives to self-assess the extent to which they addressed specific aspects of information and communication directly after each videotaped counseling session, indicating their perceptions of their own counseling performance.
Assessment of counseling by clients and observersClients’ perceptions of counseling were measured using the QUOTE prenatal – Performance. To answer the second research question, we used a selection of the items of the QUOTE prenatal – Performance to observe the counseling performance of midwives. We selected items, that 1) were eligible to be coded objectively during observation of the videotaped counseling and 2) the selected items per function had to reach a substantial internal reliability, e.g. ≥0.70 [29,30]. Thirty-five items met the first eligibility criterion. Based on our previous study, two-items refer to the client-counselor relation (CCR) function (e.g. Q4: Tell the client that she can always contact me with any questions she may have), 21 items refer to providing health education (HE) (e.g. Q28: providing information about the medical condition that the fetus is screened on) and 12 items refer to decision-making support (DMS) (e.g. Q50: discussing personal reasons to opt or decline for prenatal screening) [6]. The reliability of functions HE and DMS was good: Cronbach’s alpha’s were 0.89 and 0.92 respectively. Spearman-Brown test for CCR was 0.41, which was below the threshold of 0.70; therefore, this function was excluded from further analyses. Thirty-three items remained (Appendix B).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
124
Three trained observers rated the extent to which counselors applied the 33 communication aspects of the QUOTE prenatal during the consultation, using an adapted version of the Roter Interaction Analysis System, RIAS [31]. The 33 items of the QUOTE prenatal – Performance were incorporated into the existing RIAS protocol and were rated as point events. Rated point events signify that an item was addressed during counseling and by whom; the midwife or client. Since the direct entry software Observer XT was used for the assessments of independent observers, these assessments were seen as the most objective source of the actual communication during prenatal counseling [32].Inter-rater reliability was already calculated during our earlier study [13] on a random sample of 26 (9.7%) of the 269 study videotapes. Mean Intraclass correlation (ICC) was 0.67, which can be considered as substantial [29,33].
Data analysisWithin this study, we used subsamples of midwives, clients and video-observations from the earlier studies [6,13,17] to reach the research objectives. A non-response analysis between participating clients and non-participants, relevant for the current study, is described in Martin et al. 2014 [13]. The databases of clients’, midwives’ and observers’ assessments were merged to guarantee analyses of full cases only. We assumed this procedure to be non-selective.We dichotomized the independently QUOTE prenatal – Performance Likert scores per item; scores 1-2 were labeled as ‘insufficiently performed’ and scores 3 and 4 were labeled as ‘well performed’ during counseling. Data from the video-observations were also dichotomized. Therefore first, we computed new variables; all utterances of midwives and clients which were coded as the same topic (e.g. midwife: Asked the client to explain her decision to take / not to take the prenatal tests (Q50); client: explained why she decided to opt / decline prenatal screening (G50)) and were computed into one new variable (item 50). Second, we dichotomized the resulting new variables; if an item was coded once or more during counseling, it was recoded as ‘addressed’. All other cases were coded as ‘not addressed’. Third, we computed variables on prenatal counseling function level; e.g. HE and DMS. Since we used dichotomous scores on individual item level to compute the scores on function level, we used 0.50 as a threshold to indicate counseling functions as ‘well performed’ or ‘addressed’.To answer the first research question: midwives’ self-assessment on the three counseling functions, operationalized by the components of the midwife version of the QUOTE prenatal – Performance, we ran the independent frequencies on counseling function level (CCR, HE and DMS) as well as on item level. In line with our earlier research the criterion for ‘well performed’ was defined as having performance scores of 3-4 at least in 75% of the cases [6,17]. Note that the qualifications ‘insufficiently performed’ and visa-versa do not necessarily indicate inappropriate versus appropriate counseling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
125
6
To answer the second research question, we first ran independent frequencies for clients and observers. Again the criterion for ‘well performed’ (clients) or ‘addressed’ items (observation) was defined as having performance scores of 3- 4 at least in 75% of the cases. Second, we ran dependently, descriptive analyses on item level to provide insight into the amount of congruence between midwives’ self-assessments with clients’ perceptions and with observed performance of counseling. We re-ran the analyses for the total score of each counseling function, e.g. HE and DSM. We considered ≥75% congruency between assessors to be adequate and <75% to be inadequate. We did not correct for clustering because of the exploratory nature of the research questions.
RESULTS
ResponseMidwives invited 460 eligible clients to take part in the study; 324 agreed to participate (response rate 70%). In total, 240 videotaped counseling sessions were taken into the analyses, for which we also had the completed QUOTE prenatal – Performance questionnaires of clients and midwives (74%).
Background characteristics midwivesTable 1 shows the background characteristics of the 20 female midwives working in 6 practices and their clients who participated in this study. The number of participating midwives per practice ranged from one to five midwives. Recordings per practice ranged from 5 – 68 and per midwife from 5 to 20.
Midwives’ self-assessmentsOn counseling function level, participating midwives perceived the client-counselor relation (CCR) was ‘performed’ or ‘performed well’ in all, analyzed cases (230; 100%); health education (HE) was perceived as ‘performed’ or ‘performed well’ in 172 cases (81%) and decision-making support (DMS) in 38 cases (17%). Figure 1 shows a summary of counseling performance perceived by midwives and clients and observed counseling performance. On item level, midwives perceived that they addressed all items of the CCR well or very well (range 85%-100%). Furthermore, table 2a shows that 8 items of the 21 HE items of counseling were perceived as ‘performed’ or ‘performed well’ (range of scores: 36%-95%). Scores of ‘performed’ or ‘performed well’ for the DMS function of counseling ranged from 3%-94%; 4 out of 16 items were perceived as ‘performed’ or ‘performed well’ (table 2b). Tables 2a and 2b show also the independent ratings of clients and observers.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
126
Table 1 Characteristics of midwives and participating pregnant women.
Characteristics Pregnant women
N=240* (%)
Midwives
N=20 (%)
Dutch midwifery population N=2264c (%)
GenderMaleFemale
- -20 (100)
43 (2)2569 (98)
Work experience≤ 2 years3-11 years≥ 12 years
- 4 (20)12 (60)4 (20)
No information available
Age (years)Mean (SD)Range ≥ 36 years (N (%)
≤ 40 years≥ 41 years
29.2 (4.07)20 - 4013 (5.5)
16 (80)4 (20)
1644 (73)620 (27)
Ethnicityb
NativeNon Native
187 (77.9)53 (22.1)
14 (70)6 (30)
No information available
Highest level of education a
Up to high schoolHigher vocational education / university
114 (47.7)125 (52.3)
Religious backgroundNone ReligiousReligious
110 (46.4)127 (53.6)
-
Pregnancy duration≤ 11 weeks≥ 12 weeks
202 (91.9)18 (8.1)
-
ParityNulliparaeMultiparae
97 (40.9)140 (59.1)
-
*Due to missing and inapplicable answers the N can vary from variable to variable. Valid percentages are shown.a Up to high school ranges from only primary school up to the Dutch MBO.b In the Netherlands, ethnic origin is defined by country of birth of a person’s parents. If one of the parents (or both of them) of a person is born outside the Netherlands, this person is non-Native (Dutch National Office of Statistics; Statistics Netherlands).c Hingstman, L.; Kenens, RJ., 2011. NIVEL, Figures from the registration of midwives, poll 2011. NIVEL: dec 2011 [In Dutch].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
127
6
0%10%20%30%40%50%60%70%80%90%
Health Education Decision-making support
Figure 1: Frequencies of counseling performance for HE and DMS
Midwives Clients Observers
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Health Education Decision-making support
Figure 2: Congruence on HE and DMS
Midwives vs observers Midwives vs clients
Figure 1 Frequencies of counseling performance for HE and DMS
Congruence between midwives’ assessments versus those of observers and clientsTable 3a and figure 2 show that regarding the HE function of counseling congruence between midwives and observers was ≥75%: 62%HE addressed +19%HE not addressed = 81%. Congruence between midwives’ and clients’ assessments was found in 85% of the cases (75%HE addressed + 10%HE not addressed). Looking at item-level of the 21 HE items, percentages of ≥75% congruence between midwives and observers that an item was ‘addressed’ was found for three items: 26, 31 and 32 and percentages of ≥75% congruence that an item was ‘addressed’ OR ‘not addressed’ was found for seven items: 29, 34, 37, 38, 41, 42 and 46 (‘time to decide on eventual termination pregnancy’). Furthermore, congruence between midwives and clients that an item was ‘addressed’ was found for five items: 26, 31, 32, 36 (‘Asked about clients family´s history of birth defects’) and 43 (‘Explained which prenatal tests will be done first and which will be done later, if required and/or necessary’) and percentages of ≥75% congruence that an item was ‘addressed’ OR ‘not addressed’ was found for six items: 29, 34, 37, 38, 45 and 48 (table 3a).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
128
Table 2a Consultations in which the health education function was addressed according to midwives,
clients and observers (N=240).
QUOTE Item number
Item description:The midwife…
MidwivesN (%)*
ClientsN (%)*
Observers (N%)*
Health education 172 (81.1) 172 (81.1) 172 (81.1)Q26@ Explained which anomalies can be identified using
prenatal screening220 (92.4) 212 (91.0) 208 (86.7)
Q27 Explained which anomalies cannot be identified using prenatal tests
118 (49.6) 146 (63.2) 100 (41.7)
Q28 Provided medical information about the anomalies that are being tested for
129 (55.6) 164 (71.6) 148 (61.7)
Q29@ Discussed possible negative implications of prenatal screening for the unborn child
162 (68.4) 173 (75.5) 156 (65.0)
Q31@ Explained the usefulness of prenatal screening (what the client can decide to do eventually)
206 (86.6) 204 (88.3) 217 (90.4)
Q32@ Told the client about all the different types of prenatal tests
224 (94.9) 214 (92.2) 224 (93.3)
Q33 Told the client how prenatal screening can affect her emotions and mental wellbeing
145 (60.9) 128 (55.9) 112 (46.7)
Q34@ Told the client how much prenatal tests cost 151 (63.4) 144 (62.1) 166 (69.2)Q35 Told the client about the incidence of birth defects in
the Netherlands84 (35.7) 125 (54.1) 66 (27.5)
Q36@ Asked about clients family´s history of birth defects 216 (90.8) 222 (95.3) 20 (8.3)Q37@ Explained how often congenital anomalies occur in
pregnant women of clients age133 (55.6) 160 (69.6) 149 (62.1)
Q38@ Explained how the chances of a birth defect are calculated for our unborn child
174 (72.8) 117 (76.6) 186 (77.5)
Q39 Told the client about HER chances of having a child with a congenital abnormality during this pregnancy
120 (50.4) 134 (58.0) 33 (13.8)
Q40 Talked to the client about how HER risk of having a child with a birth defect will affect her
121 (51.1) 117 (51.3) 9 (3.8)
Q41@ Told the client why she is or is not eligible for certain prenatal tests
161 (67.4) 155 (67.4) 182 (75.8)
Q42@ Explained what will happen DURING the prenatal tests
190 (80.2) 159 (69.4) 181 (75.4)
Q43@ Explained which prenatal tests will be done first and which will be done later, if required and/or necessary
195 (82.6) 199 (86.1) 128 (53.3)
Q44 Explain who will give the client the results of the prenatal tests and how (verbally, in writing or by telephone)
88 (37.0) 115 (50.2) 106 (44.2)
Q45@ Explained how long the client may take to decide whether or not to have the prenatal tests
168 (71.8) 181 (78.0) 130 (54.2)
Q46@ Explained how long the client may take to decide whether or not to terminate the pregnancy, should the test results show an abnormality
101 (42.6) 130 (56.5) 96 (40.0)
Q48@ Discussed all clients options with regard to prenatal screening and the implications
164 (68.4) 199 (86.5) 12 (5.0)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
129
6
QUOTE Item number
Item description:The midwife…
MidwivesN (%)*
- -
Q13** Imparted information on prenatal testing 229 (96.6)Q56** Only discussed specific information about follow-
up tests and possible anomalies with the client if it becomes clear that the client will need them
86 (36.6)
Q58** Made sure that the topics the client consider to be important are discussed at length
228 (96.6)
*Sample size varies due to missing data, valid percentages are shown. **Items that were only taken into the analyses of midwives’ self-assessments.@ Items that are also presented in the table about assessment of congruence (table 3a and 3b).Bold figures indicate that the item was observed or perceived as addressed during ≥ 75% of the counseling.
0%10%20%30%40%50%60%70%80%90%
Health Education Decision-making support
Figure 1: Frequencies of counseling performance for HE and DMS
Midwives Clients Observers
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Health Education Decision-making support
Figure 2: Congruence on HE and DMS
Midwives vs observers Midwives vs clients
Figure 2 Congruence on HE and DMS
Table 2a Continued

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
130
Table 2b Consultations in which the decision-making support function was addressed according to
midwives, clients and observers (N=240).
QUOTE Item Number
Item description:The midwife…
MidwivesN (%)*
ClientN (%)*
Observer (N%)*
Decision-making support 38 (17.3) 83 (39.2) 83 (39.2)Q3@ Tell which websites the client can use to find
information about prenatal screening and diagnostic98 (41.2) 114 (48.7) 83 (34.6)
Q9@ Advised the client about whether or not to take the prenatal tests
17 (7.1) 102 (44.0) 12 (5.0)
Q14 Enquired clients’ standards, values and views on prenatal screening and diagnostic
57 (24.3) 160 (54.8) 11 (4.6)
Q22@ Responded to what the client already knew about prenatal screening
224 (94.1) 225 (96.6) 207 (86.3)
Q30 Told the client what the Dutch government aims to achieve by providing prenatal tests
94 (39.8) 86 (37.6) 179 (74.6)
Q49 Talked to the client about how her family and she would react to a child with a birth defect
94 (39.5) 127 (54.5) 74 (30.8)
Q50 Asked the client to explain her decision to take / not to take the prenatal tests
100 (42.6) 126 (54.8) 109 (45.4)
Q51@ Asked whether clients family, friends or other people close to her would support her decision about prenatal screening
15 (6.3) 40 (17.5) 3 (1.3)
Q52@ Asked the client what for her constitutes a healthy child
21 (8.9) 52 (22.6) 12 (5.0)
Q53@ Asked whether test results indicating that clients unborn child has a birth defect would cause problems with her conscience
35 (14.7) 71 (31.1) 1 (0.4)
Q54@ Asked whether clients family, friends or other people close to her would support her decision to terminate the pregnancy if the child were to have a congenital abnormality
8 (3.3) 36 (15.7) 0 (0.0)
Q55 Asked how the client thinks she will react to the results of the prenatal tests
57 (23.7) 92 (39.8) 82 (34.2)
Q11** Was understanding about clients ideological background or religion
190 (67.3)
Q20** Asked the client questions that makes her think 190 (79.5)Q21** Was interested in who the client is 238 (100)Q25** Encouraged the client and her partner to talk
together about prenatal screening190 (80.2)
*Sample size varies due to missing data, valid percentages are shown. **Items that were only taken into the analyses of midwives’ self-assessments.@ Items that are also presented in the table about assessment of congruence (table 3a and 3b).Bold figures indicate that the item was observed or perceived as addressed during ≥ 75% of the counseling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
131
6
Table 3b and figure 2 show that regarding the DMS function of counseling congruence between midwives and observers was ≥75%: 2%DSM addressed +78%DMS not addressed = 80%. Congruence between midwives’ and clients’ assessments of counseling was found in 62% of the cases (9%DMS addressed + 53%DMS not addressed). Looking at item level, ≥75% of congruence between midwives and observers were found for six items: item 22 (≥75% congruence that the item was ‘performed well’ / ‘addressed’), item 3 (≥75% congruence that the item was ‘addressed’ OR ‘not addressed’) and the items 9 (‘giving advice’), 51, 52, 53 and 54 (≥75% congruence these items were ‘insufficiently performed’ / ‘not addressed’). Additionally, we found levels of congruence of ≥75% between midwives and clients regarding four items: 22 (‘addressed’), items 51 and 54 (‘not addressed’) and item 3 (‘addressed’ OR ‘not addressed’).

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
132
Tabl
e 3a
Ass
essm
ents
of t
he H
ealth
Edu
catio
n fu
nctio
n: c
ongr
uenc
e be
twee
n m
idw
ives
& o
bser
vers
and
mid
wiv
es &
clie
nts
(N=2
40).
Nat
ure
of C
ongr
uenc
e M
idw
ife v
ersu
s
Obs
erve
r N
(%)*
M
idw
ife v
ersu
s Cl
ient
N (%
)*H
ealth
edu
catio
nCo
ngru
ence
func
tion
addr
esse
d13
3 (6
2.1)
140
(74.
9)Co
ngru
ence
func
tion
not a
ddre
ssed
41 (1
9.2)
19 (1
0.2)
QU
OTE
It
em n
umbe
rIt
em d
escr
ipti
on: T
he m
idw
ife…
26Ex
plai
ned
whi
ch a
nom
alie
s ca
n be
iden
tified
usin
g pr
enat
al
scre
enin
g Co
ngru
ence
item
add
ress
ed
194
(81.
5)20
0 (8
6.6)
Cong
ruen
ce it
em n
ot a
ddre
ssed
6 (2
.5)
7 (3
.0)
29Di
scus
sed
poss
ible
neg
ative
impl
icati
ons
of p
rena
tal
scre
enin
g fo
r the
unb
orn
child
Co
ngru
ence
item
add
ress
ed
135
(57.
0)13
5 (5
9.7)
Cong
ruen
ce it
em n
ot a
ddre
ssed
57 (2
4.1)
35 (1
5.5)
31Ex
plai
ned
the
usef
ulne
ss o
f pre
nata
l scr
eeni
ng (w
hat t
he
clie
nt c
an d
ecid
e to
do
even
tual
ly)
Cong
ruen
ce it
em a
ddre
ssed
19
3 (8
1.1)
186
(81.
2)Co
ngru
ence
item
not
add
ress
ed10
(4.2
)13
(5.7
)32
Told
the
clie
nt a
bout
all
the
diffe
rent
type
s of
pre
nata
l tes
ts
Cong
ruen
ce it
em a
ddre
ssed
21
2 (8
9.8)
201
(88.
2)Co
ngru
ence
item
not
add
ress
ed4
(1.7
)2
(0.9
)34
Told
the
clie
nt h
ow m
uch
pren
atal
test
s co
st
Cong
ruen
ce it
em a
ddre
ssed
14
2 (5
9.7)
125
(54.
3)Co
ngru
ence
item
not
add
ress
ed65
(27.
3)66
(28.
7)36
Aske
d ab
out c
lient
s fa
mily
´s h
istor
y of
birt
h de
fect
s Co
ngru
ence
item
add
ress
ed
18 (7
.6)
199
(86.
1)Co
ngru
ence
item
not
add
ress
ed20
(8.4
)-
37Ex
plai
ned
how
ofte
n co
ngen
ital a
nom
alie
s oc
cur i
n pr
egna
nt w
omen
of c
lient
s ag
e Co
ngru
ence
item
add
ress
ed
123
(51.
5)12
2 (5
3.3)
Cong
ruen
ce it
em n
ot a
ddre
ssed
81 (3
3.9)
62 (2
7.1)
38Ex
plai
ned
how
the
chan
ces
of a
birt
h de
fect
are
cal
cula
ted
for o
ur u
nbor
n ch
ild
Cong
ruen
ce it
em a
ddre
ssed
16
8 (7
0.3)
150
(65.
2)Co
ngru
ence
item
not
add
ress
ed48
(20.
1)36
(15.
7)41
Told
the
clie
nt w
hy s
he is
or i
s no
t elig
ible
for c
erta
in
pren
atal
test
s Co
ngru
ence
item
add
ress
ed
142
(59.
4)11
4 (4
9.8)
Cong
ruen
ce it
em n
ot a
ddre
ssed
39 (1
6.3)
32 (1
4.0)
42Ex
plai
ned
wha
t will
hap
pen
DURI
NG
the
pren
atal
test
s Co
ngru
ence
item
add
ress
ed
155
(65.
4)14
1 (6
2.7)
Cong
ruen
ce it
em n
ot a
ddre
ssed
23 (9
.7)
27 (1
2.0)
43Ex
plai
ned
whi
ch p
rena
tal t
ests
will
be
done
firs
t and
whi
ch
will
be
done
late
r, if
requ
ired
and/
or n
eces
sary
Co
ngru
ence
item
add
ress
ed
112
(47.
5)17
7 (7
8.0)
Cong
ruen
ce it
em n
ot a
ddre
ssed
26 (1
1.0)
19 (8
.4)
45Ex
plai
ned
how
long
the
clie
nt m
ay ta
ke to
dec
ide
whe
ther
or
not
to h
ave
the
pren
atal
test
s Co
ngru
ence
item
add
ress
ed
116
(49.
6)14
8 (6
5.5)
Cong
ruen
ce it
em n
ot a
ddre
ssed
55 (2
3.5)
34 (1
5.0)

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
133
6
Nat
ure
of C
ongr
uenc
e M
idw
ife v
ersu
s
Obs
erve
r N
(%)*
M
idw
ife v
ersu
s Cl
ient
N (%
)*46
Expl
aine
d ho
w lo
ng th
e cl
ient
may
take
to d
ecid
e w
heth
er
or n
ot to
term
inat
e th
e pr
egna
ncy,
shou
ld th
e te
st re
sults
sh
ow a
n ab
norm
ality
Cong
ruen
ce it
em a
ddre
ssed
79
(33.
3)78
(34.
2)
Cong
ruen
ce it
em n
ot a
ddre
ssed
121
(51.
1)80
(35.
1)
48Di
scus
sed
all c
lient
s op
tions
with
rega
rd to
pre
nata
l sc
reen
ing
and
the
impl
icati
ons
Cong
ruen
ce it
em a
ddre
ssed
11
(4.6
)16
7 (7
3.2)
Cong
ruen
ce it
em n
ot a
ddre
ssed
47 (1
9.7)
14 (6
.1)
*Sam
ple
size
varie
s du
e to
miss
ing
data
, val
id p
erce
ntag
es a
re s
how
n. F
igur
es d
o no
t add
up
to 1
00%
. Miss
ing
% re
pres
ent i
ncon
grue
nce.
Bold
figu
res
indi
cate
item
s /
func
tions
on
whi
ch t
here
was
a c
ongr
uenc
e th
at t
he it
em /
func
tion
was
add
ress
ed /
not
add
ress
ed o
f ≥75
% b
etw
een
mid
wiv
es a
nd o
bser
vers
or c
lient
s.Ita
lic fi
gure
s in
dica
te it
ems
/ fu
nctio
ns o
n w
hich
ther
e w
as a
con
grue
nce
that
the
item
/ fu
nctio
n w
as a
ddre
ssed
+ n
ot a
ddre
ssed
of ≥
75%
bet
wee
n m
idw
ives
and
obs
erve
rs o
r clie
nts.
Tabl
e 3a
Con
tinue
d

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
134
Tabl
e 3b
Ass
essm
ents
of t
he D
ecisi
on-M
akin
g Su
ppor
t fun
ction
: con
grue
nce
betw
een
mid
wiv
es &
obs
erve
rs a
nd m
idw
ives
& c
lient
s (N
=240
).
Nat
ure
of C
ongr
uenc
eM
idw
ife v
ersu
s
Obs
erve
r N
(%)*
M
idw
ife v
ersu
s Cl
ient
N (%
)*
Deci
sion-
mak
ing
supp
ort
Cong
ruen
ce fu
nctio
n ad
dres
sed
5 (2
.3)
18 (9
.3)
Cong
ruen
ce fu
nctio
n no
t add
ress
ed17
1 (7
7.7)
103
(53.
1)Q
UO
TE
Item
num
ber
Item
des
crip
tion
: The
mid
wife
…
3To
ld w
hich
web
sites
the
clie
nt c
an u
se to
find
info
rmati
on
abou
t pre
nata
l scr
eeni
ng a
nd d
iagn
ostic
Co
ngru
ence
item
add
ress
ed
74 (3
1.1)
78 (3
3.6)
Cong
ruen
ce it
em n
ot a
ddre
ssed
131
(55.
0)10
2 (4
4.0)
9Ad
vise
d th
e cl
ient
abo
ut w
heth
er o
r not
to ta
ke th
e pr
enat
al
test
s Co
ngru
ence
item
add
ress
ed
0 (0
.0)
7 (3
.0)
Cong
ruen
ce it
em n
ot a
ddre
ssed
210
(87.
9)11
9 (5
1.5)
22Re
spon
ded
to w
hat t
he c
lient
alre
ady
knew
abo
ut p
rena
tal
scre
enin
g Co
ngru
ence
item
add
ress
ed
193
(81.
1)21
2 (9
1.8)
Cong
ruen
ce it
em n
ot a
ddre
ssed
2 (0
.8)
1 (0
.4)
51As
ked
whe
ther
clie
nts
fam
ily, f
riend
s or
oth
er p
eopl
e cl
ose
to
her w
ould
sup
port
her
dec
ision
abo
ut p
rena
tal s
cree
ning
Cong
ruen
ce it
em a
ddre
ssed
3
(1.3
)8
(3.5
)Co
ngru
ence
item
not
add
ress
ed22
3 (9
3.7)
181
(79.
7)52
Aske
d th
e cl
ient
wha
t for
her
con
stitu
tes
a he
alth
y ch
ild
Cong
ruen
ce it
em a
ddre
ssed
3
(1.3
)4
(1.8
)Co
ngru
ence
item
not
add
ress
ed20
7 (8
7.3)
159
(70.
0)53
Aske
d w
heth
er te
st re
sults
indi
catin
g th
at c
lient
s un
born
chi
ld
has
a bi
rth
defe
ct w
ould
cau
se p
robl
ems
with
her
con
scie
nce
Cong
ruen
ce it
em a
ddre
ssed
0
(0.0
)14
(6.2
)Co
ngru
ence
item
not
add
ress
ed20
2 (8
4.9)
136
(60.
2)54
Aske
d w
heth
er c
lient
s fa
mily
, frie
nds
or o
ther
peo
ple
clos
e to
he
r wou
ld s
uppo
rt h
er d
ecisi
on to
term
inat
e th
e pr
egna
ncy
if th
e ch
ild w
ere
to h
ave
a co
ngen
ital a
bnor
mal
ity
Cong
ruen
ce it
em a
ddre
ssed
0
(0.0
)3
(1.3
)
Cong
ruen
ce it
em n
ot a
ddre
ssed
231
(96.
7)18
8 (8
2.1)
*Sam
ple
size
varie
s du
e to
miss
ing
data
, val
id p
erce
ntag
es a
re s
how
n. F
igur
es d
o no
t add
up
to 1
00%
. Miss
ing
% re
pres
ent i
ncon
grue
nce.
Bold
figu
res
indi
cate
item
s /
func
tions
on
whi
ch t
here
was
a c
ongr
uenc
e th
at t
he it
em /
func
tion
was
add
ress
ed /
not
add
ress
ed o
f ≥75
% b
etw
een
mid
wiv
es a
nd o
bser
vers
or c
lient
s.Ita
lic fi
gure
s in
dica
te it
ems
/ fu
nctio
ns o
n w
hich
ther
e w
as a
con
grue
nce
that
the
item
/ fu
nctio
n w
as a
ddre
ssed
+ n
ot a
ddre
ssed
of ≥
75%
bet
wee
n m
idw
ives
and
obs
erve
rs o
r clie
nts.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
135
6
DISCUSSION AND CONCLUSION
DiscussionThis study aimed first, to provide insight into midwives’ perceptions of their own prenatal counseling performance in daily practice. Results of midwives’ self-assessments point to the same inconsistency between the theoretical prenatal counseling model and daily practice as was earlier identified [6,13,17]; the CMR and HE functions of counseling were overall assessed as ‘performed’ or ‘performed well’ whereas midwives assessed the DMS function as ‘insufficiently performed’ during most of their counseling sessions. The second study aim was to provide insight into the degree of congruence of midwives’ self-assessments with clients’ perceptions and with observed performance. On the HE counseling function level congruence between midwives and both observers and clients was ≥75%; congruence on DMS was higher between midwives and observers (80%) compared to congruence between midwives and clients (62%), indicating that clients seem to weigh other aspects during their assessment of counseling compared to midwives and observers. On item level congruence between midwives on the one hand and observers and clients on the other hand was relatively poor on about half of the items of both HE and DMS; remarkable differences between the two dyadic assessments of congruence were found, i.e. midwives and clients agreeing that an item was addressed whereas assessments of midwives and observers showed high levels of incongruence. Finally, midwives both overestimated and underestimated their communication compared to observed communication.
The finding that midwives assessed the CCR function of prenatal counseling as ‘performed well’ is in line with clients’ perceptions and observations in our earlier studies [6,13]. It is also known that midwives perceive that CCR is important for appropriate prenatal counseling [17]. Although midwives assessed that they ‘performed well’ the HE function of counseling, results on item level indicate room for improvement especially given the importance clients attach to these items and recommendations of professional guidelines [6,34]. An example is the HE-item ‘offering medical information about the anomalies that are being tested for’. Last, midwives assessed the DMS function as ‘performed well’ in only a few cases. This might indicate that they are aware of room for improvement, since we know that half of the midwives in our earlier study consider the DMS counseling function important for appropriate counseling and thus want to close the gap between theory and daily practice [6].The findings of this study indicate that the nature and size of the gap between prenatal counseling models and counseling in practice may vary with the assessor, which is in line with conclusions of other research [23,24]. Overall, midwives evaluated their counseling with regards to HE more or less equally congruent relative to clients compared to observers (85% versus 81%). However, midwives and observers agreed less that this function was addressed

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
136
compared to midwives and clients (62% versus 75%, respectively). Regarding the DMS function of counseling, levels of congruence between the two dyadic assessments varied substantially (19%). Furthermore, midwives and observers agreed that this function was ‘not addressed’ during counseling in >75% of the cases; midwives and clients agreed that this function was ‘not addressed’ in 53% of the cases.In case of ≥75% congruence between midwives and observers but not between midwives and clients, it seems to mean that in the eyes of both midwives and observers, clients’ were too positive about the topic being addressed. It is possible that clients had problems recalling what was actually discussed during counseling due to information overload, for example [22]. It might also be socially more appropriate for clients to overestimate rather than underestimate midwives counseling, while midwives and clinically removed observers were accurately aware of it. Furthermore, clients might have assessed the counseling from other perspectives than midwives or observers [24]. An explanation for finding high levels of congruence between midwives and observers compared to low levels of congruence between midwives and clients about the topic ‘giving advice’ might be that midwives experience difficulties to recognize and avoid directive elements. For instance, deciding what information to present and how to present it can itself be directive and therefor perceived as giving advice [35]. Observers did not code directive elements, only literally giving advice was coded as such, whereas clients’ experiences might have been actually framed by the directive elements in counseling. We found only ≥75% congruence between midwives and clients but not between midwives and observers regarding items of the HE function of counseling. Although midwives were asked to assess their counseling one by one, their self-assessment might be influenced by their earlier consults whereas clients experienced counseling only once and observers used direct entry software to code the communication and perhaps do not consider the counseling session as a whole. Regarding the topic of ‘asking about clients family’s history of birth defects’, it could be that this issue was addressed at an earlier stage of the intake and not as part the prenatal counseling. Therefore, it was not coded by observers as ‘addressed’, while both midwives and clients experienced it as ‘performed’ during counseling.Within the current study, our findings suggest that both midwives and clients do not perceive as big a gap between theoretical models of appropriate counseling and daily practice as observers do; we found that midwives, clients and observers made a different assessment of the videotaped prenatal counseling. So, the question is ‘who is to say it was a good counseling visit?’ or whose perspective should be preferred in assessing the quality of counseling; the objective, non-involved perspective of the observer or the subjective perspective of the stakeholders, i.e. counselors and clients? Can they all be right? Our results caution against the use of one perspective when assessing the quality of prenatal counseling since this might limit the relevance of research findings [36]. Since, counselors, clients and observers seem to assess different aspects of communication each perspective seems to make its own

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
137
6
contribution to understanding the counseling process. Clients’ experiences seem to reflect what they take home, not necessarily what was most important from a medical perspective or what was said exactly. Counselors self-assessments should be carefully used in research because of the complex, psychological nature of this concept: e.g. did midwives assess themselves relative to what they could have done, to a golden standard, to their personal capacities or to their personal perceptions of appropriate counseling? [18]. Finally, choosing observers as ‘golden’ standard seems reasonable to assess the skills of a counselor, but may also have limitations. Within this study, independent results show that the observers were the most restrained assessors as they were trained to code only verbal communication while a good deal of communication in general is non-verbal [37]. Another challenge regarding video-observation is to reach high levels of inter-rater reliability. In conclusion, if optimization of prenatal counseling is the ultimate goal, this goal should be based on research findings and focused on counselors’ self-improvement through feedback from reliable and valid external sources (experts, clients etc.), and making counselors take the resulting feedback seriously rather than discounting it [18].The study has some limitations. Midwives’ and clients’ assessments of counseling might be influenced by the study procedure. Although both groups were asked to complete the questionnaires directly after counseling, in practice at least some midwives and some clients delayed the completion. It is known that between medical consultation and coming home most clients can only recall 20 to 40% of the topics discussed of which half is incorrectly recalled [22]. These memory changes might also be present in midwives. An additional explanation might be that self-assessment is not a stable skill, but rather a situational bounded cognitive process that is context specific and dependent upon expertise [18]. Another limitation of the study might be the way observers, midwives and clients assessed the prenatal counseling. Point events of the RIAS scores indicate if an item is ‘addressed’ or not, while the results of the QUOTE prenatal – Performance scale do include information about how well an item was perceived as addressed. Therefore, RIAS scores could potentially cause an overestimation of performances compared to results of the QUOTE prenatal – Performance. However, we did not observe such tendency in our study. Finally, although the inter-rater reliability between observers was substantial, there was (an acceptable amount of) variation between the codes that observers gave to a certain statement. Future research could also take the non-verbal communication into account.
ConclusionThis study shows that midwives’ self-assessments indicate the same inconsistency between the prenatal counseling model and daily practice as was identified earlier by clients’ experiences and independent observations; the CCR and HE functions of counseling were overall assessed as ‘performed’ or ‘performed well’ whereas midwives assessed the DMS

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
138
function as ‘insufficiently performed’ during most counseling sessions. Dyadic congruence between midwives and observers was adequate regarding the counseling functions HE and DMS, while congruence between midwives and clients reached only levels of ≥75% for HE. Moreover, on item level congruence for both dyadic analyses was poor in about half of the cases. Therefore, this study shows incongruence about the exact nature of the gap between the theoretical prenatal counseling model and counseling in daily practice.
Practice implicationsMidwives should focus more on DMS to optimize appropriate counseling for prenatal anomaly screening. The best way to measure counselors’ counseling practice might be by using three sources of information: counselors’ self-assessment and assessments from both experts and clients.
AcknowledgementsWe gratefully acknowledge the contribution of the clients and midwives in the Netherlands, who provided the data for this study. We also thank Lydia Gitsels and Veerle Steenhuis for their work on the video-coding project. In addition, we thankfully acknowledge AVAG for funding this study.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
139
6
REFERENCES
[1] Liefhebber S, van Dam C, Waelput A. Professional profile of midwives. Bilthoven: KNOV, 2005 [In Dutch].
[2] O’Connor AM, Légaré F, Stacey D. Risk communication in practice: the contribution of decision aids. BMJ 2003; 327:736-740.
[3] RIVM. Scenario prenatal screening. Down syndrome and structural ultrasound investigation version 2.0. Bilthoven: National Institute for Public Health & Environment (RIVM), 2011 [In Dutch].
[4] O’Connor AM, Mulley AG, Wennberg JE. Standard consultations are not enough to ensure decision quality regarding preference-sensitive options. J Natl Cancer Inst 2003; 95:507 Editorials.
[5] Marteau TM, Dormandy E, Michie S. A measure of informed choice. Health Expect 2001; 4:99-108.
[6] Martin L, van Dulmen S, Spelten ER, de Jonge A, de Cock P, Hutton EK. Prenatal counseling for congenital anomaly tests: Parental preferences and perceptions of midwife performance. Pren Diagn 2013; 33:341-53.
[7] Smets E, van Zwieten M, Michie S. Comparing genetic counselling with non-genetic health care interactions: Two of a kind? Review article. Pat Educ Couns 2007; 68:225-34.
[8] Bhogal AK, Brunger F. Prenatal genetic counseling in cross-cultural medicine. A framework for family physicians. Clinical Review. Can Fam Pfysician 2010; 56:993-99.
[9] van Zwieten MCB. [The importance of a conscious choice but what is the choice about? The set of possibilities during decision-making about prenatal congenital anomaly tests]. De Psycholoog 2008; 43:20-5.
[10] de Jong A, Dondorp WJ, de Die-Smulders CE, Frints SG, de Wert GM. Non-invasive prenatal testing: ethical issues explored. Eur J Hum Genet 2010; 18:272-7.
[11] Barr O, Skirton H. Informed decision making regarding 388 antenatal screening for fetal abnormality in the United Kingdom: A qualitative study of parents and professionals. Nurs Health Sci 2013;15:318-25.
[12] van den Berg M, Timmermans DRM, ten Kate LP, van Vugt JMG, van der Wal G. Are pregnant women making informed choices about prenatal screening? Genet Med 2005; 7:767–76.
[13] Martin L, Hutton EK, Gitsels-van der Wal JT, Spelten ER, Kuiper F, Pereboom MTR, van Dulmen S. Prenatal counselling for congenital anomaly tests: an exploratory video observational study about client-midwife communication. Midwifery 2014;10.1016/j.midw.2014.05.004.
[14] Michie S, Dormandy E, Marteau TM. Informed choice: understanding knowledge in the context of screening uptake. Patient Educ Couns 2003; 50(3):247-253.
[15] Roter D, Ellington L, Hamby Erby L, Larson S, Dudley W. The genetic counselling video project (GCVP). Am J Med Genet 2006; 142C:209-20.
[16] Hack TF, Degner LF, Parker PA. The communication goals and needs of cancer patients: a review. Psycho-Oncology 2005; 14:831-45.
[17] Martin L, Hutton EK, Spelten ER, Gitsels-van der Wal JT, van Dulmen S. Midwives’ views on appropriate antenatal counselling for congenital anomaly tests: Do they match clients’ preferences? Midwifery 2014; 30:600-9.
[18] Eva KW, Regehr G. Self-assessment in the health professions: a reformulation and research agenda. Acad Med 2005; 80: 46-54.
[19] Aukes LC, Geertsma J, Cohen-Schotanus J, Zwierstra RP, Slaets JPJ. The development of a scale to measure personal reflection in medical practice and education. Medical Teacher 2007; 29:177−82.
[20] Epstein RM, Siegel DJ, Silberman J. Self-monitoring in clinical practice: a challenge for medical educators. J contin Educ Health Prof 2008; 28:5-13.
[21] http://www.royalcollege.ca/portal/page/portal/rc/canmeds/framework (last visit April 1st 2014). [22] Kessels RPC. Patients’ memory for medical information. J R Soc Med 2003; 96:219-22.[23] Schinkel S, Schouten BC, van Weert JC. Are GP patients’ needs being met? Unfulfilled information
needs among native-Dutch and Turkish-Dutch patients. Patient Educ Couns 2013; 90:261-7.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
140
[24] Van Weert JCM, Bolle S, van Dulmen S, Jansen J. Older cancer patients’ information and communication needs: what they want is what they get? Patient Educ Couns 2013; 92:388-97.
[25] Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands. BMC Pregnancy Childbirth 2009; 9:18.
[26] Manniën J, Klomp T, Wiegers T, Pereboom M, Brug J, de Jonge A, van der Meijde M, Hutton EK, Schellevis F, Spelten E. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Ser Res 2012; 69-8.
[27] Fletcher RH, Fletcher SW. Clinical Epidemiology: The Essentials. Fourth Ed, 2005, Lippincott Williams & Wilkins; Baltimore, 20-21.
[28] Spelten ER, Martin L, Gitsels JT, Pereboom MTR, Hutton EK, van Dulmen S. Introducing video recording in primary care midwifery for research purposes: procedure, dataset, and use. Midwifery 2014; 10.1016/j.midw.2014.06.007.
[29] Field A. Discovering statistics using SPSS. 3rd ed, 2009, Sage Publishers; London, 50-100.[30] Eisinga R, te Grotenhuis M, Pelzer B. The reliability of a two-item scale: Pearson, Cronbach, or
Spearman-Brown? Int J Public Health 2013; 58:637-42.[31] http://www.riasworks.com/ (last visit June 10th 2014). [32] Noldus LP, Trienes RJ, Henderiksen AH, Jansen H,Jansen RG. The observer video-pro: new software
for the collection, management, and presentation of time-structured data from videotapes and digital media files. Beh Res Methods Instrum Compu 2000; 32:197-206.
[33] Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977; 33:159-74.
[34] RIVM. [National training requirements on counseling; Workgroup version 2. Adopted by the Coordinating Committee prenatal screening, December 7th, 2007]. Bilthoven: RIVM; http://www.rivm.nl/dsresource?objectid=rivmp:50890&type=org&disposition=inline.
[35] Vanstone M, Kinsella EA, Nisker J. Information-sharing to promote informed choice in prenatal screening in the spirit of the SOGC clinical practice guideline: a proposal for an alternative model. J Obstet Gynaecol Can 2012; 34:269-75.
[36] Bensing J. 1991. Doctor-patient communication and the quality of care. Soc Scr Med 1991; 32:1301-10.
[37] van Staveren R. Patiëntgericht communiceren; gids voor de medische praktijk. Houten: De Tijdstroom, 2011; 58-60.
[38] van Agt HME, Schoonen HMHJD, Wildschut HIJ, de Koning HJ, Essink-Bot ML. [Health education for the pre- and neonatal screening program: Questionnaires regarding the national evaluation of the providing procedures]. Roterdam: Erasmus MC, 2007.
[39] Health Council. [Act population screening on Down syndrome and nural tube defects]. Den Haag: Health Council, publication no. 2007/05WBO.
[40] Oepkes P, Wieringa J. [The right to know; the 20-weeks ultrasound investigation facilitates a conscious choice]. Med Contact 2008; 31/32:1296-97.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
141
6
APPENDIX A Dutch Setting Since 2007 prenatal anomaly screening is offered to all Dutch pregnant women using an opting in approach [38, 39, 40]. Primary care midwives are the designated counselor within this prenatal anomaly test program in 80% of the pregnancies [3, 25]. The screening program includes two non-invasive tests: the combined test (CT), a blood test and an ultrasound to measure the nuchal translucency, for determining the possibility of the child having Down syndrome, (around 12th weeks gestational age), and the Fetal Anomaly Scan (FAS) for detecting physical anomalies (around 20th weeks gestational age). In the case of confirmatory diagnostic testing, two options are available: terminating pregnancy before 24 weeks of gestation, or health-oriented prenatal care for the fetus combined with prenatal and postnatal support. Although both tests are part of a population-screening program, they are not offered on the same basis. The FAS is free for all women, the CT has to be paid for (ca. 150 euro) by women younger than 36 years of age [39,40].

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 6
142
APPENDIX B Items of the QUOTE prenatal presented per counseling function: Health Education, Decision-making support and Client-Counselor relation.
Health educationQ26 Explained which anomalies can be identified using prenatal screeningQ27 Explained which anomalies cannot be identified using prenatal testsQ28 Provided medical information about the anomalies that are being tested forQ29 Discussed possible negative implications of prenatal screening for the unborn childQ31 Explained the usefulness of prenatal screening (what the client can decide to do eventually)Q32 Told the client about all the different types of prenatal testsQ33 Told the client how prenatal screening can affect her emotions and mental wellbeingQ34 Told the client how much prenatal tests costQ35 Told the client about the incidence of birth defects in the NetherlandsQ36 Asked about clients family´s history of birth defectsQ37 Explained how often congenital anomalies occur in pregnant women of clients ageQ38 Explained how the chances of a birth defect are calculated for our unborn childQ39 Told the client about HER chances of having a child with a congenital abnormality during
this pregnancyQ40 Talked to the client about how HER risk of having a child with a birth defect will affect herQ41 Told the client why she is or is not eligible for certain prenatal testsQ42 Explained what will happen DURING the prenatal testsQ43 Explained which prenatal tests will be done first and which will be done later, if required
and/or necessaryQ44 Explain who will give the client the results of the prenatal tests and how (verbally, in writing
or by telephone)Q45 Explained how long the client may take to decide whether or not to have the prenatal tests Q46 Explained how long the client may take to decide whether or not to terminate the
pregnancy, should the test results show an abnormalityQ48 Discussed all clients options with regard to prenatal screening and the implicationsQ13** Imparted information on prenatal testingQ56** Only discussed specific information about follow-up tests and possible anomalies with the
client if it becomes clear that the client will need themQ58** Made sure that the topics the client consider to be important are discussed at length
Decision-making supportQ3 Tell which websites the client can use to find information about prenatal screening and
diagnosticQ9 Advised the client about whether or not to take the prenatal testsQ14 Enquired clients’ standards, values and views on prenatal screening and diagnosticQ22 Responded to what the client already knew about prenatal screeningQ30 Told the client what the Dutch government aims to achieve by providing prenatal testsQ49 Talked to the client about how her family and she would react to a child with a birth defectQ50 Asked the client to explain her decision to take / not to take the prenatal testsQ51 Asked whether clients family, friends or other people close to her would support her
decision about prenatal screeningQ52 Asked the client what for her constitutes a healthy child

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests
143
6
Decision-making supportQ53 Asked whether test results indicating that clients unborn child has a birth defect would
cause problems with her conscienceQ54 Asked whether clients family, friends or other people close to her would support her
decision to terminate the pregnancy if the child were to have a congenital abnormalityQ55 Asked how the client thinks she will react to the results of the prenatal testsQ11** Was understanding about clients ideological background or religionQ20** Asked the client questions that makes her thinkQ21** Was interested in who the client isQ25** Encouraged the client and her partner to talk together about prenatal screening
Client-counselor relationQ1* Took plenty of time to answer clients questionsQ4* Putted the client at easeQ5* Took clients concerns seriouslyQ6* Listened to what my client is trying to askQ7* Was open and honest about every aspect of the pregnancyQ8* Gave the client enough time to explain herself properlyQ10* Showed empathyQ12* Knew what the client is talking aboutQ15* Made clear that my client can ask anything she wants to knowQ16* Used clear and comprehensible languageQ17* Gave the client (additional) written informationQ18* Told the client that she can always contact me with any questions she may have (including
when the practice is closed)Q19* Accepted clients’ decisions on whether or not to agree to prenatal screeningQ23* Painted a realistic picture (not just through ‘rose-tinted spectacles’)Q24* Gave the client the feeling that she is tuning in to her as a person
* Items of the QUOTE prenatal we did not use in the current study.**Items that were only taken into the analyses of midwives’ self-assessments.
APPENDIX B Continued


Chapter 7Clients’ psychosocial communication during prenatal counseling
for anomaly screening: how is it related to midwives’
communication and client-directed gaze?
Martin L, Gitsels-van der Wal JT, Pereboom MTR, Spelten ER, Hutton EK, Van Dulmen S.
Under review.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
146
ABSTRACT
Objectives This study focuses on facilitation of clients’ psychosocial communication during prenatal counseling for fetal anomaly screening. We assessed how psychosocial communication by clients is related to midwives’ psychosocial and affective communication, client-directed gaze and counseling duration.
Methods During 184 videotaped prenatal counseling consultations with 20 Dutch midwives, verbal psychosocial and affective behavior was measured by the Roter Interaction Analysis System (RIAS). We rated the duration of client-directed gaze. We performed multilevel analyses to assess the relation between clients’ psychosocial communication and midwives’ psychosocial and affective communication, client-directed gaze and counseling duration.
Results Clients’ psychosocial communication was higher if midwives asked more psychosocial questions and showed more affective behavior (β=0.90; CI: 0.45 – 1.35; p <0.00 and β=1.32; CI: 0.18 – 2.47; p=0.025, respectively). Clients’ psychosocial communication was not related to midwives’ client-directed gaze. Additionally, psychosocial communication by clients was directly, positively related to the counseling duration (β=0.59; CI: 0.20 – 099; p=0.004).
Conclusions In addition to asking psychosocial questions, our study shows that midwives’ affective behavior and counseling duration is likely to encourage client’s psychosocial communication, known to be especially important for facilitating decision-making. In contrast with our expectations, midwives’ client-directed gaze was not related with psychosocial communication of clients.
Highlights- Client’s psychosocial communication is likely to be encouraged by:- midwives’ affective behavior.- Psychosocial communication of clients was not related with:- midwives’ client-directed gaze.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
147
7
INTRODUCTION
As in many other countries, Dutch pregnant women are offered prenatal fetal anomaly screening for chromosomal syndromes, e.g. Down syndrome or structural anomalies, e.g. neural tube defects (Appendix A). An opt-in approach is used, to underline the fundamental right of parents to make an autonomous, informed decision whether to accept or decline prenatal anomaly screening [1,2]. However, expectant parents perceive this decision as difficult [3-5]. During the decision-making phase, parents simultaneously hope to be reassured by test results if they choose to opt for screening, and worry, because they might be confronted with an unfortunate test outcome or need to go on to more definitive diagnostic testing which carries iatrogenic consequences [3-5]. Therefore, pregnant women receive prenatal counseling to support them with the decision to have prenatal anomaly screening or not [2,6]. Such counseling comprises: health education about, for instance, the available anomaly tests and the anomalies that could be detected, and decision-making support by discussing for example clients’ values and views on parenthood and disabled life (psychological issues), and social influences to opt or decline anomaly screening (social issues). In the Netherlands, for about 80% of the pregnancies, primary care midwives are the designated counselors for prenatal anomaly screening [7].Given that preference-sensitive decisions need to be made, historically, genetic counseling has had much in common with Rogers’ client-centered approach to psychotherapy, which is intended to facilitate an autonomous, informed decision using a non-directive counseling attitude and a non-persuasive client-centered communication style [1,8-14]. Within the client-centered approach a good client-counselor relationship is seen as an essential condition for having a dialogue in which the client feels safe enough to express psychosocial issues such as concerns, dilemmas and needs regarding the decision and its eventual consequences. So, a good client-counselor relation is seen as necessary to enable clients to participate in the conversation and therefore to attain autonomous, informed decision-making [14-18].According to the theory of client-centered psychotherapy, building a good client-counselor relation is primarily established by nonverbal behavior, such as client-directed gaze and affective behavior [14]. Research into the role of gaze in healthcare encounters showed that care providers’ client-directed gaze can stimulate the detection of clients’ psychosocial concerns and also encourage clients to express these concerns [19-24]. Since discussing psychosocial concerns is seen as one of the most important prerequisites for decision-making support, nonverbal counseling skills, such as client-directed gaze, are thought to be essential for prenatal counseling for anomaly screening [15,18,25-27]. Affective communication, such as verbal attention, partnership statements and empathy, also enhances the client-counselor relationship and is positively associated with participation of clients for example in negotiations about treatment plans, participation in treatment and moral considerations. Thus affective

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
148
communication can also be seen as a prerequisite for decision-making support [16,17,28,29]. In addition, once a good client-counselor relationship is established, clients’ participation may be facilitated by asking exploring, client-centered questions, which is another key of the client-centered psychotherapeutic process [14]. Within the context of counseling for prenatal anomaly screening, clients want their counselors to set psychosocial issues on the agenda [30-32]. Apparently, talking about psychosocial topics does not come easy; clients need to be invited by for instance psychosocial questions. These questions facilitate clients in giving personal meaning to the pros and cons of screening and are therefore essential during decision-making support [15,25].In daily practice, however, providing decision-making support seems to be challenging for several reasons. A significant number of counselors do not fully subscribe to the decision-making support function of counseling [18,33,34]. Furthermore, because of a perceived lack of communication skills, many counselors feel incapable of providing decision-making support [18]. Midwife counselors in our earlier study, for instance, were more likely to address psychosocial issues by giving psychosocial information and asking rhetorical questions than by using open-ended questions. This might explain the relatively low contribution of clients to the counseling conversation and the largely unmet needs reported by clients regarding decision-support, such as being supported in making a personal decision, and in balancing the pros and cons [15,26,32]. Lastly, appropriate prenatal counseling takes time. This is acknowledged in Dutch healthcare policy by means of a separate fee for prenatal counseling [35]. In daily practice, however, counseling duration appears relatively short, on average 9 minutes, which is shorter than the allotted, billable time of around 30 minutes and may hinder a thorough discussion of clients’ psychosocial issues and questions [26].We hypothesize that talking about psychosocial topics does not come easy for clients but relies on prompting from the midwife. Furthermore, we assume that midwives’ affective communication, the duration of counseling and midwives’ client-directed gaze also help clients to discuss psychosocial topics. As such, gaze can be seen as a nonverbal counseling skill to facilitate decision-making support. The present study aims to examine to what extent psychosocial communication by clients, during prenatal counseling for anomaly screening is related to 1) midwives’ psychosocial questions; 2) midwives’ affective communication; 3) midwives’ client-directed gaze; and 4) the duration of the counseling.
METHODS
This study is part of the DELIVER study, a multi-center, prospective dynamic cohort study investigating the quality and provision of primary midwifery care in the Netherlands [36]. The current study is part of a series of studies about counseling for prenatal anomaly tests, for which the design was approved by the Institutional Review Board and the Medical Ethical

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
149
7
Committee of the VU university Medical Centre, Amsterdam, Netherlands. In this series of studies we used different subsets of data from the same group of clients and midwives. Methods of the prenatal counseling for anomaly screening studies have been described in detail elsewhere [15,26] and - with regards to the current study - are briefly summarized here.
ParticipantsMidwivesFor the DELIVER study, twenty midwifery care practices in the Netherlands were purposefully selected to include different-sized practices from all over the country [36]. Twenty midwives from six of these practices also participated in the video-observation study [37]. One practice offered prenatal counseling within a separate consultation, the others as part of the initial intake visit [26].
ClientsClients of the current study were recruited between June 2010 and May 2011 and asked to participate in the study by the practice assistant or the midwife. Eligible clients were: a) clients new to counseling about prenatal anomaly tests for the current pregnancy; b) aged 18 years or older; and c) able to read Dutch or English. Background characteristics of non-responders were recorded by the practice assistant directly after their refusal. The clients who agreed to participate, were asked to complete a questionnaire booklet before and again just after their visit to the midwife [15]. Since client-directed gaze is interpreted differently among cultures we decided to only include native, Dutch clients in the current study [38,39].
MeasuresThe pre-counseling self-administered questionnaire contained items on background characteristics such as parity, age, ethnicity and familiarity with the midwife.
Psychosocial communication and affective communicationThe prenatal counseling visit was video recorded with an unmanned camera, positioned to show the midwives’ full face and clients from behind or from the side [37]. Verbal communication during counseling was measured using an adapted version [26] of the Roter Interaction Analysis System (RIAS) [40,41]. Clients’ and midwives’ utterances were coded separately. Because of the limited contribution to the conversation, partners were left out the analyses [26]. Utterances were seen as “the smallest unit of expression to which a meaningful code can be assigned, generally a complete thought” [18]. For clients, we computed one psychosocial variable ‘clients’ psychosocial communication’ which comprises both asking psychosocial questions and sharing psychosocial information. For midwives three clusters of coding categories were used: a) affective communication, b) psychosocial (closed and

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
150
open-ended) questions, and c) psychosocial information and counseling. In conformity with previous studies [42,43] we used two clusters of affective communication comprising five codes: 1) Verbal attention: (a) empathy, (b) partnership statements, (c) legitimizes, and 2) Shows: (d) concern or (e) worry (Table 1).
Table 1 Content of the RIAS categories adapted for prenatal counseling for anomaly screening.
Variables current study
RIAS categories Adapted RIAS categories
Examples
ClientsPsychosocial communication
Psychosocial Questions (open- and closed ended)
Psychosocial Questions
‘Why do other clients choose for prenatal screening?
Psychosocial Information giving
Psychosocial Information giving
‘We choose to perform the risk assessment tests, because it is just a bit certainty we both want’
‘We asked ourselves, what should we do with the results of the tests? Nothing! The baby is welcome anyway’
MidwivesAffective communication
Empathy Verbal attention ‘That sounds like a dilemma, it must be difficult’
‘Let me know if I can do something for you to help you with this choice’
Partnership statements,Legitimizes
Shows concern or worry
Shows concern or worry
‘I hope, you’ll feel better when…’
Psychosocial questions
Psychosocial (closed and open ended questions)
Psychosocial Questions
‘What are you struggling with, while thinking about whether to screen or not?’
Psychosocial information
Psychosocial Give Information
Psychosocial Give Information
‘Knowing too much, about the baby, can cause anxiety for some person’
Counsel Psychosocial
Counsel Psychosocial
‘It is important, that you realize in advance what you should do, with the results of the combination test (in case of an increased risk)’
Midwives’ client-directed gazeClient-directed gaze was measured as the time in minutes that the midwife looked directly into the clients’ face for all videotapes in which the face of the midwife was in the picture for the full duration of the video recording. We calculated the percentage of client-directed gaze, by dividing the time a midwife looked at the client by the total duration of the counseling session * 100%. In line with other research, we used percentages of time rather than the absolute length of time spent to client-directed gaze during counseling [20,23,44].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
151
7
Interrator reliabilityThree coders used a computerized observation system that allows direct coding of the videos (OBSERVER:55). The inter-observer reliability for client-directed gaze was measured on a random sample of 10.3% of the included videotapes. The intraclass correlation coefficient (ICC, single measures) ranged from 0.64 to 0.92 [37]. The inter-observer reliability of the RIAS coding was measured on a random subsample of 9.7% of the videotapes [26]. Mean ICC was 0.67, which can be considered as substantial [46,47].
Data analysisThe subsample of videotapes that we used in this study had to meet three inclusion criteria: (1) to show the midwife clearly enough to code client-directed gaze; (2) to match with the data of the pre- and post-visit questionnaire, and (3) to show a recording with a client from Dutch origin. Descriptive statistics were used to describe the background characteristics of the participants.
The outcome variable ‘clients’ psychosocial communication’ was normally distributed, thus we used multivariate multilevel linear regression analysis to examine how midwives’ client-directed gaze, midwives’ psychosocial and affective communication and the duration of the counseling were associated with the manifestation of clients’ psychosocial communication. Using this approach we adjusted the results for clustering of clients within midwives and midwives within practices, due to the hierarchical structure of the data.We used the following procedure: First, we ran a ‘naïve’ linear regression analysis of the relationship between the independent and dependent measures. We did the same for possible confounders, such as familiarity with the midwife, religion, age, level of education, parity and the duration of counseling, which we choose based on findings from our previous study [26]. In that study we found an independent and significant association between parity and the amount of decision-making support utterances (including psychosocial communication) and between age and religion on building a good client-counselor relation (including affective communication) [26]. Second, we used the likelihood ratio test to determine if data were clustered. If so, we examined on what level - ‘midwife’ alone, ‘practice’ alone or ‘midwife and practice’ - the use of a random intercept was the best approach. In this study, we found a random intercept for ‘midwife’ to be the best approach, because the likelihood ratio test significantly declined. Third, we used the likelihood ratio test to evaluate the necessity of a random slope for each variable in the model. In this data, we found the use of random slope not necessary, as the likelihood ratio-test did not significantly decline using this approach. We built the final association model for the outcome variable using a manual backward selection procedure. We present the results of the final model by means of the regression coefficients (β) and 95% confidence intervals (CI) in which p ≤0.05 indicates significance [48]. We used SPSS 21.0 for the analysis.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
152
RESULTS
We started the analysis process with all 269 videotaped counseling consultations. From these, we excluded videotapes that (1) could not be coded for client-directed gaze, because midwives’ faces were not visible enough (N=16); (2) did not match with the data of the pre- and post-visit questionnaire, and/or (3) were of clients from non-Dutch origin (N=69), leaving 184 videotaped prenatal counseling consultations for our analyses. These 184 consultations represent 68% (184/269) of the videotapes coded with the RIAS [26,37]. Twenty midwives from six practices participated in this study; the total of midwives per practice ranged from one to five. Recordings per practice ranged from six to 52 and recordings per midwife ranged from three to sixteen. Prenatal counseling lasted on average 9.5 minutes (SD=3.9 minutes) ranging from 1.9 to 22.7 minutes.
Midwives’ and clients’ characteristicsAs described in more detail elsewhere, midwives were on average 33 years of age, ranging from 23-54 years of age [26]. Participating clients were on average 29 years of age (range 20-40 years of age), 53% of the clients were non-religious. Seventy-four nulliparous women (46%) participated and 86 (54%) multiparae. Ninety clients (56%) completed at least vocational education. Fifty-three (33%) clients were familiar with the midwife who provided the counseling.
Verbal behavior: Midwives’ psychosocial- and affective communicationTable 2 shows how frequently clients expressed utterances containing psychosocial information. Furthermore, this table shows how often affective communication, psychosocial questions and psychosocial information were provided by midwives. When looking more specifically into midwives’ affective and psychosocial communication we found that utterances coded as affective communication were expressed on average one time per consultation and psychosocial questions were expressed on average 6 times per consultation. Utterances were mostly coded as giving psychosocial information, on average 25 utterances per consultation.
Nonverbal behavior: Midwives’ client-directed gazeTime spent on client-directed gaze varied between 29.7% and 96.6% (mean=70.3; median=70.5; SD=13.1). To get more insight into the relation between gaze and duration of counseling we classified the amount of gaze into two groups. The median percentage of client-directed gaze (70.5%) was used as the cut-off point to dichotomize participants into high and low client-directed gaze group. The high client-directed gaze group as well as the low client-directed gaze group comprised 92 participants. In the low client-directed gaze group the average duration of counseling was 9.8 minutes (range 1.9-22.7 minutes) and on average time spent in client-directed gaze was 59.6% (range 29.6-70.4%). In the high client-directed

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
153
7
gaze group counseling lasted on average 9.2 minutes (range 2.0-16.7 minutes) and the mean time spent in client-directed gaze was 80.9% (range 70.6-96.6%) (Table 2). There was no significant difference in mean visit length between visits with high and low gaze.
Table 2 Midwives’ client-directed gaze and observed midwives’ and clients’ verbal behavior.
Behavior All counseling(N=184)
Low gaze counseling(N=92)
High gaze counseling(N=92)
Nonverbal behavior M(range) % M(range) % M(range) %Client-directed gaze 70.3 (29.7 - 96.6%) 59.6 (29.6 - 70.4) 80.9 (70.6 - 96.6)
Verbal behavior M(range); SD M(range); SD M(range); SDClients’ psychosociaal talk 13.4 (1-46); 9.6 13.7 (1-46); 9.9 13.1 (1-45); 9.3
Midwives’Affective communication
0.6 (0-8); 1.1 0.5 (0-5); 1.1 0.7 (0-8); 1.2
Psychosocial questions 5.7 (0-22); 3.8 5.8 (0-22); 3.8 5.6 (0-19); 3.6Psychosocial information 24.6 (0-76); 15.5 24.3 (1-76); 16.2 24.8 (0-62); 14.7
Clients’ psychosocial communicationThe univariate analyses showed no significant association between midwives’ client-directed gaze and ‘clients’ psychosocial communication’ (β=0.02; CI: -0.08 – 0.13; p=0.65). Furthermore, results showed that midwives’ affective communication, psychosocial questions, the duration of counseling and client’s parity were significantly associated with ‘clients’ psychosocial communication’ when adjusted for the percentage of client-directed gaze, midwives’ psychosocial information, clients’ level of education, age, religion and familiarity with the midwife who provided the counseling (Table 3). So, clients communicated more about psychosocial issues the more midwives asked psychosocial questions (β=0.90; CI:0.45 – 1.35; p=0.000); expressed affective behaviour (β=1.32; CI:0.18 – 2.47; p=0.025) and the longer the counseling lasted (β=0.59; CI: 0.20 – 0.99; p=0.004). The clients expressed less ‘psychosocial communication’ when they were nulliparous compared to multiparous (β=-3.83; CI:-6.62 – -1.04; p=0.007).
Table 3 Associations between midwives’ behavior and clients’ psychosocial talk.
Coefficient (β)* 95% CI p-valueIntercept 4.03Psychosocial questions 0.90 0.45 – 1.35 0.000Verbal affective behavior 1.32 0.18 – 2.47 0.025Parity -3.83 -6.62 – -1.04 0.007Duration of counseling 0.59 0.20 – 099 0.004
CI = confidence interval.* Adjusted for midwives’ percentage of client-directed gaze and midwives’ psychosocial information giving, clients’ level of education, age, religion and familiarity with the midwife who provided the counseling.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
154
DISCUSSION AND CONCLUSION
DiscussionThis study aimed to examine the extent to which psychosocial communication by clients during prenatal counseling for anomaly screening was related to midwives’ psychosocial questions, midwives’ affective communication, midwives’ client-directed gaze and the duration of the counseling. We found that the amount of ‘clients’ psychosocial communication’ was positively related to the amount of midwives’ verbal affective communication, midwives’ psychosocial questions and the counseling duration. In addition, multiparous women used psychosocial communication less often than nulliparous women. In contrast to our expectations, client-directed gaze was not significantly associated with clients’ psychosocial communication.The midwives that we observed used a much higher percentage of client-directed gaze (mean 70%) compared to other studies (mean approximately 50%), which decreased the power to show any effect of client-directed gaze [49,20]. It is unclear why midwives in our study had high levels of client-directed gaze. It may be that midwives typically interact differently than other health care providers, or that during counseling they do not usually use computers for registration of medical data; an activity that has been shown to negatively relate to client-directed gaze [44]. Furthermore, in a review, Henry et al. (2012) [19] showed inconsistent associations between client-directed gaze and outcome measures in research of everyday clinical encounters. Within the context of counseling for prenatal anomaly screening, all clients are brought into a situation in which they have to consider psychosocial and moral issues [1,3,5,27]. The content of the counseling prompts psychosocial and moral issues inevitably and these issues are the core of the dialogue during decision-making support, which should be offered by midwives [4,15,50,51]. From other research, we know that clients want their midwives to put psychosocial issues on the agenda, because clients are reluctant to take the initiative and therefore might need more than non-verbal encouragement such as client-directed gaze [30-32]. The finding that midwives’ psychosocial questions were related to clients’ psychosocial communication, might suggest that clients need to be encouraged by questions from the midwife to talk about psychosocial issues. Clients’ needs for encouragement to talk about psychosocial issues could be explained by the prenatal counseling setting. In five of the six practices, prenatal counseling for anomaly screening was provided at the end of the first midwifery visit of the pregnancy; the intake. This intake is primarily focused on taking a medical and obstetric history. Midwives act as medical experts, they set the agenda and consequently midwives’ questions and information guide clients’ contributions to the consultation [52]. However, when it comes to the decision-making support function of counseling, midwives should take into account that clients are the experts regarding their concerns, values and preferences about the decisions at hand. Therefore, the story of the client should guide

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
155
7
the midwife’s additional exploring questions [52,53]. Clients may need to be encouraged to take on this new role of expert through psychosocial questions of their midwife. To prevent midwives from relying too heavily on psychosocial questions only, our results suggest that showing affective behavior, such as reflecting clients’ feelings and deliberation might be a client-centered way of providing decision-making support [14].A number of factors might explain our finding that clients’ psychosocial communication was related to duration of counseling. The simple availability of additional time will provide more opportunity for clients’ psychosocial communication. Alternatively, during longer consultations, midwives may have encouraged their clients more - by asking psychosocial questions and using affective communication- with the result that clients share more psychosocial issues and the consultation time lengthens. However, our results show that the duration of counseling and midwives’ psychosocial questioning are both independently, positively associated with clients’ psychosocial communication. This seems to suggest another mechanism that we were not able to identify, such as the possibility that longer counseling duration is a marker of a client characteristic – better ability to engage in psychosocial interactions - and not so much of midwife’s interventions. Duration of counseling and asking psychosocial questions as well as showing affective behavior might have reinforced each other. Nevertheless, since clients’ psychosocial communication is important to reach the goal of counseling for prenatal anomaly screening, we recommend midwives to take the time for counseling that is reserved for it by healthcare policy; in the Netherlands around 30 minutes per counseling consultation [35].Although nonverbal behavior is considered to be an important clinician or counselor intervention, to our knowledge, this is the first study to investigate midwives’ nonverbal communication in their relatively new role as prenatal screening counselor. Henry and colleagues (2012) [19] stated that until now research failed to consistently and significantly associate, for instance, client-directed gaze with the same set of outcome measures in real life clinician-patient encounters and further, that the use of statistical techniques, which correct for the mutual influences that account for psychosocial communication, would be helpful to build a consistent body of knowledge. In our study we did use multilevel linear regression analyses to correct for the mutual influences on our outcome variables. Furthermore, we conducted our study in a real-life context. Our results confirm the findings of a review conducted by Henry et al. (2012) [19] who concluded that client-directed gaze was not consistently associated with psychosocial communication of clients. Our sample of midwives as counselors was representative for the Dutch midwifery population and we analyzed a relatively large number of videotapes representative for the Dutch, autochthonous, higher educated population of pregnant women [26]. However, the 20 midwives who participated in this study is a small proportion of the overall Dutch midwifery population; this limits the generalizability of our results. Even though our sample

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
156
was large for this type of study, we were limited by the sample in the way we analyzed the data. From our earlier study [26] we know that multi-parity was negatively associated with the number of utterances coded as decision-making support; parity seems to be an effect modifier. Our sample size was underpowered to permit us to analyze the data for nulliparous and multiparous women separately. As partners were in most of the cases present during counseling, they might have influence clients’ psychosocial communication. Further research is needed to investigate the effect of the presence of partners on psychosocial communication of clients. We made no distinction between brief or sustained episodes of client-directed gaze, though the latter is found to be more strongly associated with clients’ psychosocial communication than the first [20]. We also know that timed silences seem to encourage clients to express their concerns [54-56]. The way midwives use or do not use silences might have been a confounder for the relation between client-directed gaze and clients’ psychosocial communication. Further research is needed to know how nonverbal communication together with verbal communication can improve participation of clients during decision-making support, including those from non-Dutch, non-Western origin, since they contributed on average 18% of all live births in the Netherlands up to circa 45% in the major cities [57,58].
ConclusionsIn this quantitative study we analyzed 184 videotapes from 20 midwives of six practices across the Netherlands focused on prenatal counseling for anomaly screening. In addition to the number of psychosocial questions midwives used, clients’ psychosocial communication was positively related to midwives’ affective communication and duration of counseling. We found no relationship between clients’ psychosocial communication and midwives’ client-directed gaze. The positive relations we found might indicate that midwives can improve clients’ psychosocial communication during decision-making support by taking additional time to provide prenatal counseling and showing affective communication in addition to asking psychosocial questions. However, our findings do not indicate causation, so it might be that women who are better at expressing themselves in the psychosocial arena will engage better, thus encouraging midwives to ask them more psychosocial questions resulting in longer sessions.
Practice implications- To improve decision-making support and thus encourage clients to share their
deliberations during prenatal counseling for anomaly screening, midwives might need to consider that for clients it seems to be helpful to take the advised time for counseling.
- Using affective communication in addition to asking psychosocial questions, can be useful to maintain a client-centered approach, which is known to be essential during decision-making support.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
157
7
- Future research on counseling for prenatal anomaly screening should measure more aspects of nonverbal behavior, such as the use of silences and both brief and sustained client-directed gaze episodes. These nonverbal behaviors have to be linked to the content of the conversation at the time they are used. Such approach potentially provides insight into the pathways through which non-verbal communication and clients’ psychosocial communication influence each other. Furthermore, since the use of client-directed gaze was high in our midwife population, future research might learn from studying those cases where gaze was limited.
Acknowledgements We gratefully acknowledge the contribution of the clients and midwives in the Netherlands, who provided the data for this study. We thank Kelly van Almkerk for her contribution to the video-coding. In addition, we thankfully acknowledge AVAG for funding this study.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
158
REFERENCES
[1] Crombag NM, Vellinga YE, Kluijfhout SA, Bryant LD, Ward PA, Iedema-Kuiper R, Schielen PC, Bensing JM, Visser GH, Tabor A, Hirst J. Explaining variation in Down’s syndrome screening uptake: comparing the Netherlands with England and Denmark using documentary analysis and expert stakeholder interviews. BMC Health Serv Res. 14 (2014):437-8.
[2] RIVM, 2014. Roadmap Prenatal Screening for Down’s syndrome and the fetal anomaly scan. (version 4.0, set by the Central Organization Prenatal Screening; March 2014) [In Dutch].
[3] Bosk CL. All God’s Mistakes. Genetic counseling in a pediatric hospital. The university of Chicago Press, Chicago and London, 1995, pp.1-20.
[4] Gitsels-van der Wal J, Martin L, Manniën J, Hutton EK. A qualitative study on how Muslim women of Moroccan descent approach antenatal anomaly screening. Midwifery, DOI 10.1016/j.midw.2014.12.007.
[5] Garcia E, Timmermans DRM, van Leeuwen E. Rethinking autonomy in the context of prenatal screening decision-making. Prenat Diagn. 28 (2010):115-0.
[6] Health Council of the Netherlands: Committee Genetic screening. The Hague: Health Council, 1994; publication no. 1994/22 [In Dutch].
[7] Wiegers TA. The quality of maternity care services as experienced by women in the Netherlands. BMC Pregnancy Childbirth. 9 (2009):18-6.
[8] Chieng WS, Chan N, Lee SC. Non-directive genetic counselling - respect for autonomy or unprofessional practice? Ann Acad Med Singapore. 40 (2011):36-2.
[9] Health Council 2007. [Act population screening on Down syndrome and nural tube defects.] Health Council, The Hague. publication no. 2007/05WBO [In Dutch].
[10] Oepkes P, Wieringa J. Recht op prenatale kennis: 20-weken echo maakt weloverwogen keuze mogelijk. [The right to prenatal knowledge; 20-week untrasound for structural anomalies makes an informed choice possible]. Medisch Contact. 31/32 (2008):1296-7 [In Dutch].
[11] Pennacchini M, Pensieri C. Is non-directive communication in genetic counseling possible? Clin Ter. 162 (2011):141-4.
[12] O’Connor AM, Légaré F, Stacey D. Risk communication in practice: the contribution of decision aids. BMJ. 327 (2003):736-0.
[13] Vanstone M, Kinsella EA, Nisker J. Information-sharing to promote informed choice in prenatal screening in the spirit of the SOGC clinical practice guideline: a proposal for an alternative model. J Obstet Gynaecol Can. 34 (2012):269-5.
[14] Mearns D, Thorne B. Person-centered counselling in Action, second ed, Sage Publications, London, 1999, pp:5-21.
[15] Martin L, van Dulmen S, Spelten ER, de Jonge A, de Cock P, Hutton EK. Prenatal counseling for congenital anomaly tests: parental preferences and perceptions of midwife performance. Prenat Diagn. 33(2013):341-3.
[16] Smets E, van Zwieten M, Michie S. Comparing genetic counseling with non-genetic health care interactions: two of a kind? Patient Educ Couns. 68 (2007):225-4.
[17] Elwyn G. Arriving at the postmodern medical consultation. Eur J Gen Pract. 10 (2004):93-7.[18] Roter D, Ellington L, Hamby-Erby L, Larson S, Dudley W. The genetic counseling video project
(GCVP): Models of practice. Am J Med Genet. 142C(2006):209-0. [19] Henry SG, Fuhrel-Forbis A, Rogers MA, Eggly S. Association between nonverbal communication
during clinical interactions and outcomes: a systematic review and meta-analysis. Patient Educ Couns. 86 (2012):297-5.
[20] Gorawara-Bhat R, Cook MA. Eye contact in patient-centered communication. Patient Educ Couns. 82 (2011):442–7.
[21] Zimmermann C, Del Piccolo L, Finset A. Cues and concerns by patients in medical consultations: A literature review. Psychological Bulletin. 133(2007):438-3.
[22] Marcinowicz L, Konstantynowicz J, Godlewski C. Patients’ perceptions of GP non-verbal communication: a qualitative study. BJGP. (2010):83-7.
[23] Bensing JM, Kerssens JJ, van der Pasch M. Patient-directed gaze as a tool for Discovering and handling psychosocial Problems in general practice. J nonverbal behav. 19 (1995):223-2.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
159
7
[24] Stepanikova I, Zhang Q, Wieland D, Eleazer GP, Stewart T. Non-Verbal Communication Between Primary Care Physicians and Older Patients: How Does Race Matter? J Gen Intern Med. 27(2011): 576–1.
[25] Meiser B, Tucker K, Friedlander M, Barlow-Stewart K, Lobb E, Saunders C, Mitchell G. Genetic counselling and testing for inherited gene mutations in newly diagnosed patients with breast cancer: a review of the existing literature and a proposed research agenda. Breast Cancer Res. 10 (2008):216-0.
[26] Martin L, Hutton EK, Gitsels-van der Wal JT, Spelten ER, Kuiper F, Pereboom MTR, van Dulmen S. Antenatal counselling for congenital anomaly tests: an exploratory video-observational study about client-midwife communication. Midwifery. 31(1) (2015):37-46.
[27] van Zwieten M. Communicatie over ethische issues in de medische praktijk. [Communication about ethical issues in medical practice], in: A.A. Kaptein, J.B. Prins, E.H. Collette, R.L. Hulsman (Eds). Medical psychology, second ed, Bohn Stafleu Van Loghum, Houten, 2010, pp: 213-4 [In Dutch].
[28] Tone EB, Tully EC. Empathy as a “risky strength”: A multilevel examination of empathy and risk for internalizing disorders. Dev Psychopathol. 26 (2014):1547-5.
[29] Jones LM, Huggins TJ. Empathy in the dentist-patient relationship: review and application. N Z Dent J. 110 (2014):98-4.
[30] O’Connor A, O’Brien Pallas LL. Decisional conflict, in Nursing Diagnosis and Intervention, G.K. Mcfarlane, E.A. Mcfarlane (Eds.), Mosby, Toronto, 1998, pp:486–6.
[31] Marteau TM, Dormandy E, Michie S. A measure of informed choice. Health Expect. 2 (2001):99-8.[32] Gitsels-van der Wal JT, Martin L, Verhoeven P, Hutton EK, Reinders HS. Antenatal counselling
for congenital anomaly tests: Muslim Moroccan women’s preferences. Midwifery. 2015, doi: 10.1016/j.midw.2015.01.002.
[33] Martin L, Hutton EK, Spelten ER, Gitsels-van der Wal JT, van Dulmen S. Midwives’ views on appropriate antenatal counselling for congenital anomaly tests: do they match clients’ preferences? Midwifery. 30 (2014):30:600-9.
[34] Gitsels–van der Wal JT, Manniën J, Gitsels L.A, Reinders HS, Verhoeven NS, Ghaly MM, Klomp T, Hutton EK. Prenatal screening for congenital anomalies: exploring midwives’ perceptions of counseling clients with religious backgrounds. BMC pregnancy and childbirth, 14 (2014):237-6.
[35] Scholman HSA. Evaluatie van prenatale screening [Evaluation Prenatal Screening Performance]. Dutch Healthcare authority, Utrecht, CV (2009):09-9 [In Dutch].
[36] Manniën J, Klomp T, Wiegers T, Pereboom M, Brug J, de Jonge A, van der Meijde M, Hutton E, Schellevis F, Spelten E. Evaluation of primary care midwifery in the Netherlands: design and rationale of a dynamic cohort study (DELIVER). BMC Health Services Research. 12 (2012):69-8.
[37] Spelten ER, Martin L, Gitsels JT, Pereboom MTR, Hutton EK, van Dulmen S. Introducing video recording in primary care midwifery for research purposes: procedure, dataset, and use. Midwifery. 31 (2014):95-2.
[38] Shadid W. Culturele diversiteit and interculturele communicatie. [Cultural diversity and intercultural communication], in: H. van Veghel (Eds.): Waarden onder de meetlat: Het Europese waardenonderzoek in discussie. Damon b.v., Budel (2002), pp:1-6.
[39] Fassaert T, Nielen M, Verheij R, Verhoeff A, Dekker J, Beekman A, de Wit M. Quality of care for anxiety and depression in different ethnic groups by family practitioners in urban areas in the Netherlands. Gen Hosp Psychiatry. 32 (2010):368-6.
[40] Roter DL, Larson S. The relationship between residents’ and attending physicians’ communication during primary care visits: an illustrative use of the Roter Interaction Analysis System. Health Commun. 13 (2001):33-8.
[41] Bensing JM, Verheul W, van Dulmen AM. Patient anxiety in the medical encounter: a study of verbal and nonverbal communication in general practice. Health Educ. 108 (2008):373-3.
[42] Pieterse AH, van Dulmen AM, Beemer FA, Ausems MGEM, Bensing JM. Tailoring communication in cancer genetic counselling through individual video-supported feedback: a controlled pretest-posttest design. Patient Educ Couns. 60 (2006):326-5.
[43] Pieterse AH, van Dulmen AM, Beemer FA, Bensing JM, Ausems MGEM. Cancer Genetic Counseling: Communication and Counselees’ Post-Visit Satisfaction, Cognitions, Anxiety, and Needs Fulfillment. J Genet Couns. 16 (2007):85-6.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 7
160
[44] Noordman J, Verhaak P, Beljouw I, van Dulmen S. Consulting room computers and their effect on GP-patient communication: comparing two periods of computer use. Fam Pract. 27 (2010):644-1.
[45] Noldus LP, Trienes RJ, Henderiksen AH, Jansen H, Jansen RG. The observer video-pro: new software for the collection, management, and presentation of time-structured data from videotapes and digital media files. Behav Res Methods, Instrum Comput. 32 (2000):197-6.
[46] Field A. Discovering Statistics Using SPSS. third ed, Sage Publishers, London, 2009, pp:50-100.[47] Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 33
(1977):159-4.[48] Twisk JWR. Applied Multilevel Analysis A Practical Guide for Medical Researchers. (2006) ISNB10:
0521614988, ISBN13: 9780521614986, pp: 1-29.[49] van den Brink-Muinen A, Verhaak PF, Bensing JM, Bahrs O, Deveugele M, Gask L, Mead N, Leiva-
Fernandez F, Perez A, Messerli V, Oppizzi L, Peltenburg M. Communication in general practice: differences between European countries. Fam Pract. 20 (2003):478-5.
[50] van Zwieten M. Het belang van een weloverwogen keuze, maar wat behelst die keuze? De complexe besluitvorming in prenatale screening. [The importance of an informed choice, but what concerns the choice? The complex decision-making in prenatal screening]. De Psycholoog. 43 (2008):20-25 [In Dutch].
[51] Garcia E, Timmermans DRM, van Leeuwen E. The impact of ethical beliefs on decisions about prenatal screening tests: Searching for justification. Soc Sci & Med. (2008):66735-4.
[52] Smith RC, Hoppe RB. The patient’s story: integrating the patient- and physician-centered approaches to interviewing. Ann Intern Med. 115(1991):470–7.
[53] van Zwieten M, Willems D, Knegt L, Leschot N. Communication with patients during the prenatal testing procedure: An explorative qualitative study. Patient Educ Couns. 63 (2006):161–8.
[54] Kreijkamp-Kaspers S, Glasziou P. A is for aphorism - the power of silence. Aust Fam Physician. 41 (2012):909-9.
[55] Shipley SD. Listening: a concept analysis. Nurs Forum. 45 (2010):125-4.[56] Kacperek L. Non-verbal communication: the importance of listening. Br J Nurs. 6 (1997):275-9.[57] Boerleider AW, Francke AL, Manniën J, Wiegers TA, Devillé WLJM. “A mixture of positive and
negative feelings”: a qualitative study of primary care midwives’ experiences with non-western clients living in the Netherlands. Int J Nurs Stud. 50 (2013): 1658-6.
[58] Gitsels-van der Wal JT, Verhoeven PS, Manniën J, Martin L, Reinders HS, Spelten E, Hutton EK. Factors affecting the uptake of prenatal screening tests for congenital anomalies; a multicentre prospective cohort study. BMC Pregnancy Childbirth. 9(2014): 264-8.
[59] Fracheboud J, van Agt HME, de Koning HJ. Monitoring 2009 of prenatal screening for Down’s Syndrome and for Foetal Anomalies in the Netherlands. Final report RIVM, Bilthoven (2011).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Clients’ psychosocial communication during prenatal counseling for anomaly screening
161
7
APPENDIX A Dutch prenatal screening programThe Dutch Screening Program consists of the Combined Test (CT) undertaken at around 12 weeks to detect trisomy 13, 18 or 21 and a Fetal Anomaly ultrasound Scan (FAS) to detect structural anomalies usually done at around 20 weeks. In the Netherlands, the FAS is free for all women, the CT has to be paid for by women younger than 36 years of age [9,10]. Mean uptake of the FAS in the Netherlands is around 92% and the uptake for the CT is on average 23%. Diagnostic, invasive tests are offered on indication (e.g. maternal age ≥ 36 years of age, family history) [58,59]. These tests have important differences in policy and historical context between the Netherlands and other countries including the fee charged for the CT, but also the historically strong emphasis on the implementation of the opt-in approach and ‘right not to know’ about prenatal anomaly screening [1]. As a result, especially regarding the CT, clients intensively deliberate the decision whether to opt for screening or not [4].


Chapter 8General discussion
‘Als je het proces ter harte neemt, dan zorgt het doel wel voor zichzelf’
M.K. Gandhi

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
164

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
165
8
General discussionThis thesis investigates the fairly new field of counseling for prenatal anomaly screening by midwives. The overall aim was to investigate clients’ and midwives’ perspectives about appropriate counseling for prenatal anomaly screening. Additionally, this study aimed to provide knowledge about the client-midwife communication during prenatal counseling in daily practice.For practitioners, this study provides insight into client preferences and experiences. This can be used for enhancing the quality of prenatal counseling. For researchers, this study provides two research tools: the clients’ and midwives’ version of the Quality Of care Through the patients Eyes (QUOTE) prenatal questionnaire, to investigate prenatal counseling from the perspectives of clients, and counselors in a comparable way. In addition, the first time use of video-recordings in midwifery led care, has resulted in information on the introduction of this relatively novel research approach to disciplines unfamiliar with it. Our research, as described by a referee from Patient Education and Counseling: on “the question how the prenatal counseling is perceived by those who practice it, by those who should profit from it […] [and by objective observers] is a rare example of a comparison of three different perceptions on this [counseling for prenatal anomaly screening]”.
Study outlineWe started by adapting the QUOTE questionnaire to the prenatal counseling context. We used the resulting QUOTE prenatal to assess client-centeredness of midwives’ counseling for prenatal anomaly screening by examining the extent to which clients’ pre-counseling preferences were met as reflected in clients’ post-counseling assessments. We assumed prenatal counseling consultations to be triadic rather than dyadic in practice: pregnant women’s partners may play an important role when it comes to the decision whether to opt for prenatal anomaly screening. Therefore, preferences and experiences of partners were also investigated in this study. In our next study we examined midwives’ views on appropriate counseling and to what extent these views reflect the theoretical prenatal counseling functions and match clients’ pre-counseling preferences. We introduced video-recordings as a research tool in midwifery practices to examine counseling for prenatal anomaly screening in practice. We described the process of the introduction and enrolment as well as the resulting dataset. We used video recorded prenatal counseling to explore the client-midwife communication during prenatal counseling for anomaly screening in daily, midwifery practice. We brought the data from midwives, clients and video-observations together, to assess congruence between these three perspectives. Lastly, we assessed midwives’ (non) verbal counseling skills in relation to psychosocial communication of clients. Clients’ psychosocial communication is known to be especially important during the provision of decision-making support, one of the three aspects of prenatal counseling identified in this study.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
166
Summary of the findingsPerspectives of clients and midwivesFifty-five of the 58-item QUOTE prenatal questionnaire appeared to comprise three counseling components which show sufficient reliability: client-midwife relation, health education and decision-making support. The other three items covered organizational aspects of prenatal counseling for anomaly screening. Pre-counseling, most clients considered the client–midwife relation and health education to be important or very important for prenatal counseling. More than one third of the clients valued decision-making support to be important or very important. More nulliparous women had preferences for health education and decision-making support than multiparous women. A comparison between partners and pregnant women showed only statistically significant differences regarding building a good client-midwife relation; more pregnant women compared to partners valued this function to be important or very important. We argued that in practice, when offering triadic counseling, preferences of pregnant women and their partners can be seen as comparable. Pre-counseling, we found that most clients valued being invited together for prenatal counseling. About one third of the clients valued having an appointment that focused primarily on prenatal anomaly testing rather than broaching the subject during the first visit to the midwife. Post-counseling, clients experienced that their needs concerning the client-midwife relation and health education were largely met, although significantly less multiparous women perceived that their health education needs were met compared to nulliparae. Furthermore, about two-third of the clients experienced that their decision-making support needs were addressed [chapter 2].Like clients, most midwives valued a good client–midwife relation and health education as important or very important for prenatal counseling for anomaly screening. Less than half of the midwives valued decision-making support as important. Clients and midwives assessed 13 individual items of the 58-item questionnaire very differently. For instance, more clients than midwives valued ‘receiving medical information about congenital anomalies’ and ‘getting advice whether to take prenatal tests or not’ as important [chapter 3].
Communication during counseling Introducing video-recordings in midwifery practice for research purposes proved to be both feasible and challenging. The result is a set of recommendations for researchers who want to use a video-observational approach and, in addition to our initial aim, a unique dataset of recordings that already have been used for the analyses of the midwife-client interaction regarding other topics than counseling for prenatal anomaly screening [1,2]. In about 65% of the cases partners were present during video-recorded consultations [chapter 4]. In line with clients’ experiences, in our observational study, we found that during prenatal counseling for anomaly screening by midwives most utterances were related to providing health education

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
167
8
compared to decision-making support. The relatively low contribution to the conversation of clients during decision-making support might indicate room for improvement regarding decision-making support given by midwives. Counseling of multiparae was significantly shorter than counseling of nulliparous women; multiparae received less health education as well as less decision-making support compared to nulliparae. Results seem to indicate that partners add verbally less to the triadic conversation compared to pregnant women [chapter 5]. From the perspectives of midwives - midwives’ self-evaluation - prenatal counseling for anomaly screening was performed well with regards to building a good client-midwife relation and providing health education. Midwives perceived that they provided decision-making support in relatively few cases. However, we found incongruence between midwives and clients (only pregnant women) about the discussion during decision-making support. For instance, almost half of the clients reported that they got advice whether to take prenatal screening or not while most midwives perceived they did not give such advice and almost no explicitly expressed advice was observed. Overall, congruence between midwives’ self-evaluation and observed communication was higher compared to midwives’ self-evaluation and clients’ experiences [chapter 6]. In chapter 7 communication concerning decision-making support was further investigated in order to get more insight into midwives’ communication aspects that were related to pregnant women’s’ psychosocial communication. In contrast with our expectations, midwives’ client-directed gaze was not related to the amount of psychosocial communication of clients. Video-observations did show that in addition to asking psychosocial questions, midwives’ affective behavior and the counseling duration were likely to encourage client’s psychosocial communication [chapter 7].
General discussion of the findingsThe findings and conclusions of the six studies together, covering both the perspectives of clients and midwives on prenatal counseling for anomaly screening as well as the communication during prenatal counseling in practice, will be discussed with reference to four subjects: 1) preferences of clients and consequences for prenatal counseling; 2) perceptions of midwives as counselors and the professional context; 3) client-midwife communication; 4) new developments in the field of prenatal anomaly screening and implications for prenatal counseling.
1. Preferences of clients and consequences for counselingIn the literature a two-function genetic counseling model is described containing both ‘teaching’ as well as ‘counseling’ [3-11]. Based on our findings about client preferences, we argued that the model should be extended with a third; building a good client-counselor relationship. Furthermore, we reasoned the necessity of a new terminology instead of using

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
168
the ‘teaching’ and ‘counseling’ terminology. The resulting client-centered prenatal counseling model comprises two, core functions health education and decision-making support and one conditional function, building a good client-counselor relationship [chapter 2]. From the literature it is known that practitioners need practical recommendations in a concrete and easy to understand manner, so that they can use them while preparing and reflecting upon their care in daily practice [12,13]. For prenatal counselors, knowing that clients prefer to get health education and decision-making support while building a good client-counselor relationship, might be too vague. We therefore give some suggestions about how important aspects of counseling in the eyes of clients might be addressed in practice.
Client preferences on health educationOur study on client, (i.e. pregnant women and their partners), preferences adds to the knowledge of the health education function of counseling what clients perceive as important information to talk about during counseling for anomaly screening. In Appendix A, we listed health education items that ≥75% of the clients indicated they would preferred to be discussed. When we compare this topic list to topics found to be important by clients in other research we may conclude that like other clients [14], participants in our study preferred some balance between getting all available test information and getting only information about the prenatal test that is currently relevant (items 6 versus 16, appendix A). Furthermore, clients wanted to know and understand the usefulness of the results of prenatal screening. Also in line with other studies [15,16], participants in our study valued getting information about the anomalies that their unborn child is tested for in case they choose to opt for anomaly screening. Clients indicated, that in case of a positive test result, procedure related aspects of prenatal screening were important in terms of the logistics and procedures of testing and follow-up procedures [chapter 2; 17-19]. Our study adds to the health education literature regarding topics known to be important to address during prenatal counseling. Clients value clarity about the aim of prenatal anomaly tests; about what anomalies (or group of anomalies) prenatal anomaly tests are designed for; and what anomalies are not within the scope of anomaly tests. Clients value information that they can use to know how likely it is that their unborn child has an anomaly. Lastly, in the eyes of clients, it is important to provide insight into the chronological process of prenatal screening and to identify relevant decision timelines in terms of gestational age. For instance, such information might comprise that the Fetal Anomaly Scan (FAS) is performed between 19 -21 weeks of gestational age, so the decision whether to opt for it has to be made around 16 weeks of gestational age in order to have time to make a suitable appointment (appendix A).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
169
8
Client preferences on decision-making supportIn line with other researchers, we found that 70% of the clients did not want to get information only, but also guidance or even advice whether to opt for prenatal anomaly tests or not [chapter 2; 17,20]. It seems important for clients that counselors tailor their counseling activities to clients’ knowledge and preferences [chapter 2; 20-22]. In line with the findings of Gitsels et al [15] we also found that a substantial proportion of clients valued being asked questions that facilitated sharing their deliberations about whether to opt for prenatal anomaly screening or not. Furthermore, it seems to be relevant to explore the scenario of giving birth to a child with a birth defect and to talk about how, for the client important persons, will react to this scenario [23]. Consistent with prior studies, clients participating in our study seem to value a counselor who is really interested in who they are; they want to be seen, known and understood [chapter 2; 24-26].We found no items that were perceived as important or very important by ≥75% of the clients. However, pre-counseling more than one third of the clients did value decision-making support [chapter 2]. In order to provide some insight into relevant items for the smaller group of clients who value decision-making support, we listed the six decision-making support items that were preferred to be discussed by ≥50% of the clients in Appendix B.
Client preferences on client-counselor relationA good client-counselor relation is primarily established by nonverbal behavior, such as eye-contact and showing attention by nodding. (Non)verbal affective behavior, such as showing empathy and asking explicitly if the client has (psychosocial) concerns is another important way to build this relation [27-29]. The clients in our study mentioned the following as the most important aspects of building a good client-midwife relation: ‘listening to what the client is trying to ask’, e.g. listening without interrupting and allowing silences while clients search for words; ‘using clear and comprehensible language’; ‘taking clients’ concerns seriously’, e.g. acknowledging and legitimizing feelings; ‘openness and honesty’, e.g. authenticity; ‘painting a realistic picture’; ‘taking time for the client’; ‘accepting clients’ decision about prenatal anomaly screening’, e.g. unconditional acceptance; and ‘tuning into each individual client’, e.g. person-centeredness [chapter 2; 20-22,27]. Seemingly in contrast with other studies [20-22], less than 75% of the participants valued the two non-related-items ‘empathy’ or ‘getting additional written information’.
Client-centered recommendations for the provision of prenatal counselingThe above paragraph on client preferences indicates that clients prefer a lot of information as well as information tailored to their specific situation. It seems challenging to find a balance between a one size fits all approach in an attempt to provide all information available and tailoring health education to individual preferences of clients. Structuring counseling in line

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
170
with the Shared Decision Making (SDM) model might be helpful to integrate health education and decision-making support, which is one way to deal with the dilemma described. The SDM model is the most widely known and practical communication model in the medical setting to support clients in making preference sensitive choices [13]. The choice of whether to opt for prenatal anomaly screening or not is perceived to be a preference sensitive choice; one course of action is not better compared to another course of action [6]. Furthermore, the SDM model acknowledges that some information is relevant for one client but not for another, and has recently been implemented in midwifery-led care [30,73]. Given this context, and the fact that others have also been advocating the use of the SDM approach in counseling for prenatal anomaly screening [31-33], we recommend using this approach to provide practical, client-centered recommendations about counseling for prenatal anomaly screening. By using the term SDM approach rather than SDM model we try to emphasize the fact that when it comes to decisions about prenatal anomaly tests these decisions remain ‘too personal and too important to be made by anyone other than the woman or the couple involved’ [31]. Incorporating the partner in prenatal counseling and thus the decision-process, might help the couple to make a decision they are both comfortable with. So, in line with our preliminary results on client preferences regarding decision-making, the decision-making journey might be shared, but the ultimate decision should be the women’s or couples only [31,34]. In the Netherlands, from a legal perspective, it is ultimately the woman who decides about whether to opt for prenatal anomaly tests and an eventual termination of the pregnancy [35].To really improve prenatal counseling however, one needs not only a practical communication model, but also an appropriate counseling context. In healthcare, what clients need to know and understand has often been underestimated by care providers [25,26]. Assuming this also applies to clients in the prenatal counseling setting, the question is how to best address these needs if counseling is organized at the end of the first visit with the midwife? This intake already lasts on average 30 minutes [Chapter 4], contains in general a lot of questions and information and is provided to pregnant women in the first trimester of their pregnancy; a period in which women tend to be tired more quickly [36-38]. Barr et al. [37] concluded in their study on informed decision making about prenatal screening for Down syndrome, that clients experienced a negative interference of information on a wide range of topics in the first trimester; information overload distracted clients from their decision about screening. Following the recommendations of Boer et al [36] would involve a separate consultation to provide counseling for prenatal anomaly screening that might minimize the likelihood of information during the intake consultation. Furthermore, a separate prenatal counseling consultation provides clients also an extra opportunity to ask questions that remain, comparable to patients of general practitioners, after the first prenatal visit [39]. For prenatal counselors such scheduling might be helpful to fulfil individual needs to know and understand as well as clients’ need to be known and understood [25,26]. The

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
171
8
latter is seen as essential for facilitating the personal discussion clients need, in order to make the preference sensitive decision about prenatal anomaly screening and thus for counseling for prenatal anomaly screening [23,27,37].
Relevance to practiceHow to provide appropriate counseling for prenatal anomaly screening in practice? It seems relevant to start counseling by setting the choice at hand on the agenda. If we follow a healthcare focused line of reasoning, prenatal anomaly tests can be described as ‘the method’ and detecting congenital anomalies as ‘the objective’. However, from a client perspective ‘the objective’ is more likely to be reassurance that their unborn child does not suffer from an anomaly. Prenatal counselors need to acknowledge this gap [33,40]. Right from the start, one way to do so is by making clear what questions need to be answered in order to make a decision about anomaly screening. Such questions might address: 1) whether clients want to know if their unborn child has an anomaly or not; 2) what anomalies they find important to know about if any at all; and 3) what they might do in case such an anomaly is to be found [41]. Counselors may fear that clients’ answers to question 2 might be beyond the scope of prenatal anomaly screening. Nevertheless these answers place the target of prenatal testing, including what anomalies cannot be detected, directly on the agenda, which is in line with clients’ preferences [chapter 2;15,42]. Furthermore, clients seem to eventually make their decision, whether to opt for prenatal screening or not, based on their moral values regarding for instance disabled life, termination of pregnancy and the procedure related risk of a miscarriage by performing a diagnostic test procedure [33,41,43-45]. These moral topics and considerations will presumably be addressed if counselors start their counseling as suggested and explore the answers of clients to these questions. Note that not only the answers of pregnant women, but also of partners have to be explored in order to know to what extent partners share the values of their pregnant women. Possible consequences of incongruence can be explored. In this way clients’ need to know and understand as well as to be known and understood might be addressed in a more balanced way, compared to a counseling approach that is focused on health education.
2. Perceptions of midwives as counselorsThe role of counselor was relatively new to midwives at the time this study started. Midwives were familiar with building a good client-midwife relation, the role of being a ‘medical expert’ or ‘sender’ who provides information, but not so much with the role of ‘counselor’ or ‘listener’ [36,46,47]. Adapting to the role of counselor, which includes new communication skills, seems to be complex in general medical practice. For instance because of an apparent lack of valuing the new role and skills [4,48]. This might explain the views of midwives on appropriate counseling for prenatal anomaly screening. More than 75% of the

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
172
participating midwives valued all client-midwife relation items as important or very important for appropriate prenatal counseling, but this was only the case for fifty percent of the health education items and one third of the decision-making support items [chapter 3]. Elwyn et al. [13] stress the importance of clinicians who agree with “the need to support autonomy by building good relationships, respecting both individual competence and interdependence on others” as prerequisite to implement the SDM model in practice. Given this context, our finding that most midwives subscribe to all client-midwife relation items seems promising. Reasons to not value all health education items to be important for counseling remain unclear; they are however in line with other studies who found that healthcare providers seem to underestimate their clients’ need to know and understand [49]. Midwives’ views on appropriate counseling do not entirely compare well with client preferences as found in this study. Regarding health education five items were considered important or very important by most clients but not by most midwives. As for decision-making support five items were considered important or very important by most midwives but not by most clients [chapter 2 and 3]. Other studies also found dissimilarity between the value of information and professional behavior between clients and counselors [17,33,50]. This might be problematic for providing client-centered counseling given the knowledge that clients’ preferences regarding decision-making support were not perceived as addressed by one third of the clients [chapter 2].The recently developed Professional midwifery profile [30] and the guideline for prenatal counseling about the NIPT [51] can be considered as an important step in the implementation of client-centered midwifery care and to client-centered prenatal counseling. Professional guidelines tend to be a good starting point for behavioral changes in practice [52]. The Profile is clear about what midwives should do when providing client-centered care, including counseling for prenatal anomaly screening: “Each woman makes her own decisions […]. The midwife assists her clients in making an informed choice on the basis of shared decision-making, thereby guarding her professional boundaries and asking permission of the woman for the care she wants to provide […]. The midwife informs the woman objectively and value-free. Furthermore, the midwife confirms her clients that they are indeed able to make pregnancy related choices themselves. However, not every woman wants or can be fully participating in the decision-making process; the midwife anticipates on this diversity at an individual level.” [30]. As to the role of counselor (coach and communicator) the profile states that the midwife: “Explores the reasons, motivations and barriers for the client and her social environment. [She] builds a professional relationship with her clients based on trust and mutual understanding, and accompanies her clients throughout the care process where continuity of care is pursued. The midwife takes into account ethical, psychological, social, cultural, organizational and economic aspects. The midwife supports the client and her partner / family through education and counseling to come to an informed decision.” [30].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
173
8
We highlighted in bold, parts of the citation to make clear that in essence the description of the role of counselor is compatible with the prenatal counseling functions we focused on in our study. Moreover, the shared decision-making model mentioned as the basis of facilitating informed choice is an explicit shift towards the use of one preferred communication model when it comes to decision-making, even though it is not explicitly linked to counseling for prenatal anomaly screening. The new Professional profile is important for stimulating midwives to provide prenatal counseling that is tailored to clients’ needs, but it might not be enough. In general the implementation of effective clinical communication into everyday practice takes a lot of time and effort [13,48,53,54]. Several interventions have indeed been implemented in order to facilitate midwives in offering appropriate prenatal counseling. Midwives as counselors are trained in the role of prenatal counselor for anomaly screening. Here the topics described in the Professional profile are addressed [55]. For health education, some general guidelines, about what to tell the client and what additional information should be used, exist since 2011 [56] (Appendix C). Furthermore, continuing medical education is provided by the prenatal screening centers on a regular basis [57]. With regard to the decision-making support function, midwives are trained to adopt a non-directive attitude and communication style [5,41,58,59]. Non-directiveness is also the central recommended approach in the counseling guidelines of the National Institute for Public Health and the Environment (RIVM). Nevertheless, the Professional profile of midwives (2014) [30] seems to offer the clearest description of what to do during non-directive counseling. Interestingly, the website of the Prenatal screening foundation southwestern Netherlands only focuses on the health education part of counseling when describing the tasks of the counselor; the topic decision-making support is not described [60]. The aforementioned sources of information and training were published after we finished our data collection. So, at the time of our study, midwives had very little information to rely on while implementing counseling for prenatal anomaly screening in practice. This might have influenced the way midwives viewed appropriate counseling for prenatal anomaly screening. For today’s practice, it seems problematic that no clear guidelines are available about how to offer counseling for prenatal anomaly screening according to standards based on today’s evidence. In contrast to the apparent lack of congruent information on counseling, there are clear guidelines on the organizational aspects of prenatal counseling. Midwives are recommended to organize the counseling for prenatal anomaly screening into a separate consultation during the early pregnancy and to invite partners as well [36,61]. Furthermore, midwives are the designated counselors to offer counseling for anomaly screening. There is a reimbursement for pre-test counseling and ensuing post-test information provision about the test results and

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
174
its consequences [5]. Payment of counseling is based on an average counseling duration of 30 minutes [62]. Since this information was available at the time of our study, one could argue that midwives could have acted accordingly. However, only one of the participating practices offered counseling in a separate consultation. Our results show, that on the one hand only 19% of the midwives value to organize a separate counseling consultation important for appropriate counseling while on the other hand this view might be justifiable since 22% of the clients pre-counseling prefer to have this separate consultation [chapter 3]. However, if midwives intend to use the billable time for counseling, a separate consultation would be most appropriate. When added onto the regular intake, this intake will last 60 to 90 minutes depending on the time reserved for the intake. Information overload and inadequate attention seem unavoidable.
3. Client-midwife communication Our study on introducing video-recordings of midwife-client consultations for research purposes in the Netherlands [chapter 4] is one of the few studies in which the introduction of using videotaped real life consultations is described [63]. Our research on midwife-client communication adds to the wide field of communication research and the smaller field in which video-recordings of daily, medical practice encounters are used [4].We found that midwives, just like counselors in other medical settings, struggle with their role of counselor and that there is room for improvement [chapter 5]. Results indicate that midwives primarily focus on providing health education. These findings are in line with research findings regarding general practitioners. Here also a focus on providing information and advice was found, although clients feel a need for a doctor who listens, supports and shows respect [4,37,64]. Perceived workload and time issues are well known bottlenecks for improving provider-client communication [65]. For midwives, this might especially be true, because their workload was exceptionally high during the early years of the millennium as a result of a shortage of midwives [66]. This problem has been solved, but it probably takes time to change the habit of working as efficient as possible to provide care to all pregnant women. Although, midwives get dedicated pay for this counseling based on a set amount of time, at least in our study, midwives rarely used this allocated time [chapter 4 and 5]. This might inhibit the improvement of midwives’ counseling skills over time. Nevertheless, research results are mixed. We as well as other researchers found that taking more time for a consultation may improve communication in practice [chapter 6 and 7; 67,68]. Other studies do not support these findings [69,70].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
175
8
The non-directive counseling approach, where the counselor refrains from giving direction or advice about the uptake of prenatal tests, seemed difficult to establish in practice [chapter 6], but seventy percent of all clients preferred advice whether or not to take prenatal tests [chapter 2]. Almost 50% of clients perceived that they actually got advice, although both midwives and observers acknowledged that very little explicit advice was given [chapter 2 and 6]. In fact, our results are in line with other research, that addresses on the one hand the difficulties not giving implicit direction when providing information about anomaly screening, and on the other hand proposes the use of a relational approach of autonomy [31,59,71-74]. Relational autonomy is subject of research in the field of family ethics. Studies showed that, in real life, autonomy seems to be ‘relational’, embedded in persons’ social contexts and the relations they have with others [73,74]. As a result, autonomy does not so lead to pure individual choices. With regards to the prenatal anomaly screening context, Garcia et al. (2010) [75] also emphasized the importance of using a new approach of reproductive autonomy. For clients to make choices about prenatal anomaly screening, it is important to freely share their thoughts and feelings about the decision with their partners and other closely related persons [34,75]. The existence of the concept of relational autonomy in prenatal anomaly screening decisions in practice might explain the importance clients attach to the advice of their counselors. Clients seek several opinions of persons relevant to them, for instance to shoulder the decision together with their partner or to get reassured that they made the right decision [75].Therefore, clients’ request for advice should be seen as an opportunity to facilitate clients in clarifying their desires, motives, preferences, values and aims regarding the prenatal anomaly screening offer [34,76,77]. This approach helps clients to a personal understanding of the significance of testing within their own moral framework and to feel confident about their decision [78]. Interestingly, an important website to facilitate decision-making in the Netherlands, provides not only information and tools, but also videos of parents who explain why they opted for anomaly screening or not [55]. This development seems to be in line with the new approach of a relational, reproductive autonomy.
Methodological reflections Three studies reported in this thesis were based on data derived from questionnaire surveys. At the start of this study, it was essential to select the most appropriate questionnaire. We aimed to find an instrument that measured clients’ needs and preferences regarding counseling for prenatal anomaly tests that explicitly involved the input of clients; instead of an instrument based on what experts perceived to be important for prenatal counseling. The QUOTE (Quality Of care Through the patients Eyes) scale seemed to be suitable for measuring our research questions. This scale is based on a concept of quality of care, which is defined as ‘the degree to which (perceived) performances of health and social care services meet the needs of people with respect to aspects that are important to them’ [79]. QUOTE questionnaires

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
176
are described as a group of standardized and validated surveys [79-84], modified for various groups of healthcare consumers, such as patients in need for chemotherapy treatment [80], clients confronted with hereditary cancer [79], patients with a chronic liver disease [85] and cataract patients [86]. We modified existing QUOTE questionnaires following the QUOTE procedure [80], which resulted in the QUOTE prenatal. We undertook certain steps to measure the validity of the QUOTE prenatal questionnaire. We aimed to minimize the burden on respondents. Therefore, we shortened the questionnaire and rephrased difficult questions based on our results of Cognitive Interviews with pregnant women and their partners with low educational level. Dimensionality analyses of the QUOTE prenatal provided a three-factor structure with sufficient reliability of the internal consistency of the factors [chapter 2]. With a threshold for item-total correlations (ITC) set on ≥ 0.30 all but one ITC were acceptable to remain the questions in the QUOTE prenatal. Due to time restraints, we did not investigate the test-retest reliability of the QUOTE prenatal nor the convergent validity; the same sample of data was used for both validation of the questionnaire and for our survey into client preferences and experiences. In contrast with our expectations, we were not able to measure the content validity of the QUOTE prenatal by means of a confirmatory factor analysis. These limitations might have resulted in a questionnaire that does not meet the criteria for a good questionnaire entirely [87]. However, the QUOTE prenatal appeared to be able to detect issues that need improvement to ensure that prenatal counseling is in line with client preferences [chapter 2]. As to the midwives’ version of the QUOTE prenatal we limited validation of the questionnaire to Cognitive Interviews and measurement of the internal consistency, which appeared to be satisfactory [chapter 3].The observational studies reported in this thesis were conducted on a unique dataset of videotaped first consultations including counseling for prenatal anomaly screening by midwives in the Netherlands. To our knowledge, there are no other comparable databases of videotaped material available to study midwife-client communication. This dataset enabled us to answer a wide range of research questions about the first visit of clients to their midwives. However, since we encountered difficulties in recruitment of midwives to participate in our video-observational study, resulting in a lower number of participating midwives and clients, we could not fully avoid selection bias on the part of both the participating midwives and clients. Furthermore, although we introduced the video-recording study to be relevant to answer a variety of research questions, midwives and clients were aware of the focus on counseling for prenatal anomaly screening due to the fact that they completed the complementary QUOTE prenatal questionnaires. Therefore, we can expect a selection bias toward midwives and clients with an interest in prenatal counseling and an effort of midwives to do their very best during videotaped consultations. However, since participating midwives video-taped at least during several months, in most cases whole intake consultations including prenatal counseling, we believe that videotaped material displayed midwives’ usual communication during prenatal counseling [chapter 4].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
177
8
In the observational studies, we used the Roter Interaction Analysis System (RIAS) [88]. An advantage of applying the RIAS coding system is its wide use and proven validity and reliability [89]. During the coding, meaningful utterances, usually a sentence or thought of midwives, pregnant women and their partners, were coded and counted. With the adapted version of the RIAS we were able to identify the focus in communication during prenatal counseling, e.g. health education, decision-making support or building a good client-midwife relation and compare the outcomes of the video-observations with the results of the QUOTE prenatal questionnaire. A possible limitation to our study is that the adapted version of the RIAS was quite extensive, which made coding more difficult and therefore might have negatively influenced inter rater reliability and therefore our results [chapter 5 and 6]. However, this was at least partly compensated by reporting most results on counseling function level and not only on item level.In our studies we used a quantitative approach in which we counted meaningful utterances to study midwife-client communication. The use of state events, which measure the time spent on each utterance, might have given a more realistic and detailed description of the ongoing communication compared to our approach [90]. Due to the extensive amount of variables we used in our study, the mostly triadic nature of counseling and the software we used, we tried but did not manage to use such approach for verbal communication in our study. To measure nonverbal communication, we indeed used state events to code midwives’ client-directed gaze [chapter 7] and silences. Qualitative methods combined with our quantitative approach may have provided broader knowledge about the nature of midwife-client communication during counseling for prenatal anomaly screening. For instance, it would have been interesting to learn, how midwives frame their information in those counseling cases where clients felt they have gotten advice, but where the midwife did not feel she had explicitly provided advice [chapter 6].
To concludeIn the eyes of pregnant women and their partners, prenatal counseling for anomaly screening provided by midwives meets their needs to a large extent, and midwives’ views on appropriate counseling are roughly in line with clients’ preferences. But some important differences exist and midwives’ should take notice of these differences. Especially for multiparous women. Midwives should provide (medical) information about the target anomalies of prenatal screening and endeavor to tailor their counseling to each individual client’s needs. Midwives’ prenatal counseling could presumably be improved by adjusting their counseling to clients who value decision-making support. The increased use of affective communication as well as using all the allocated time available for counselling are relevant for improving decision-making support. Last, introducing video-recording as a research tool in midwifery practice, provided a unique dataset regarding midwives first consultation with their clients and more specifically of prenatal counseling for anomaly screening.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
178
Recommendations As a result of our findings we propose a set of recommendations for prenatal counselors, educators, policy makers and future research.
Recommendations for counselorsBased on our findings we encourage midwives and other professionals who provide prenatal counseling for anomaly screening to reflect on the way they address the three prenatal counseling functions in practice. We recommend that counselors:
- Realise that counseling for prenatal anomaly screening in practice is a triadic instead of dyadic process in which partners should be explicitly invited to join.
- Use the Shared Decision Making approach as a practical guideline to optimize and integrate the health education and decision-making support functions of prenatal counseling.
- Improve some aspects of their health education by discussing the target anomalies, procedural-, societal- and risk- aspects of prenatal screening and thereby to facilitate an informed choice.
- Improve their decision-making support. Counselors need to consider to ask psychosocial questions, use affective communication and take the advised time for counseling.
Recommendations for educators“Without nurturing, the lessons from research and communication training flounder in the face of pressures from inappropriate modelling and apparent lack of valuing” [48]. Therefore, we recommend to:
- Train the trainers / counselors who act as students’ supervisors in practice in the same way students are trained, with the ambition to guarantee appropriate modeling.
- Allocate education time to discuss students’ values on appropriate counseling and to reflect upon these values in the light of professional guidelines and supervisors modeling.
- Provide continuing education, including education credits, on prenatal counseling with the focus on communication skills necessary to integrate health education and decision-making support.
Recommendations for future research- Future research should study clients from non-Dutch, non-Western origin and of
clients with low literacy skills, to assess whether clients’ pre-counseling preferences and post-counseling experiences found in this study also represent theirs.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
179
8
- Nowadays, the Consumer Quality Index (CQ Index), a measurement tool for quality of care, which is based on inter alia the QUOTE-questionnaire, is recommended above the use of QUOTE-questionnaires [91,92]. However, we recommend to use the QUOTE questionnaires, in studies that focus on a particular communication process like prenatal counseling.
- More insight into the decision-making process of pregnant women and their partners/significant others can inform counselors how prenatal counseling could facilitate this process.
- In 10 years, to repeat a video study of the discussion in the consultation room, might provide valuable information about how developments in midwifery care become visible in every day midwifery practice.
Recommendations for policy makers“Progress in the standard of communication in the real world can be disappointingly slow”. Pressures from, for instance, workload and time issues are well known bottlenecks [48]. We, therefore, recommend:
- Monitoring not only the standard of communication of initial and post-initial counseling for prenatal anomaly screening courses [93], but also prenatal counseling in practice.
- Considering an explicit shift from non-directiveness to a Shared Decision Making approach as the leading approach for all preference sensitive choices in pregnancy [30].
- Considering educating some midwives to excel in prenatal counseling so that they can do this task for other midwives, who choose to focus on other midwife responsibilities.
4. Developments in the prenatal anomaly screening offer The offer of tests in the field of prenatal anomaly screening is increasing, so midwives and other stakeholders need to stay attuned. The Non-Invasive Prenatal Test (NIPT) for common aneuploidies was recently added to the prenatal anomaly screening program in a nationwide study setting; the TRIDENT study (Trial by Dutch laboratories for Evaluation of Non-Invasive Prenatal Testing) [94,95]. A license for the TRIDENT study has been granted for two years (starting April 1, 2014) by the Ministry of Health. The NIPT is offered to women with an increased risk for carrying a child with Down-, Patau- and / or Edwards syndrome based on a positive CT (≥ 1:200) or medical indication such as already having a child with trisomy 13, 18 or 21 or carriers of Robertsonian translocations involving chromosome 21 or 13 [5,94,95,96]. Since 2007, the CT was paid by insurance companies for women ≥ 36 years of age. As of January 2015, a change of policy was made. All pregnant women have to pay approximately

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
180
165 euros if they opt for the CT. If women opt for the NIPT, they have to pay the test out of the coinsurance of their health insurance. Depending on the costs of other healthcare consumption, clients may have to pay up to two thirds of the actual costs of the NIPT, ca. 375 euros. Furthermore, women ≥ 36 years of age are no longer directly eligible for invasive prenatal diagnostics, unless they have a family history of birth defects [chapter 6;93,97]. Until now, midwives are the designated professionals to inform their clients about eventual positive test-results of the CT [93]. Inevitably, clients who have an increased risk based on the CT and clients who have a medical indication, might ask questions about available prenatal tests. Midwives may give information about diagnostic tests and the NIPT, based on an information guide for professionals [51]. However, counseling for the NIPT is offered in one of the 8 prenatal screening centers [5], usually by trained obstetricians. These gynaecologists could have completed a post-graduate counselling course together with a range of different care-providers, including midwives [93,97]. However, the current restricted eligibility for NIPT seems to result in a subculture. Pregnant women who are not eligible for NIPT in the Netherlands, can opt to have a NIPT in for instance Belgium or Germany. In those cases NIPT might be used as a first screening test for which pregnant women pay themselves. It is unclear to what extent they are counseled and by whom [98].
Consequences for counselingThe above-described developments have several consequences for midwives as counselors. Obviously, the information they provide about the eligibility for the available prenatal tests and costs has to be updated, as it has been over the past decades. In order to deal with the consequences of the restricted eligibility for the NIPT, in the context of a commercial NIPT-offer abroad, midwives need to excel in sophisticated counseling. The positive characteristics of NIPT - accurate, safe and early testing –could enhance undesirable framing of the NIPT as routine prenatal care. To safeguard voluntary participation, based on informed decision-making will therefore be of utmost importance [99,100,101]. And then again, the choices that are really on the counseling agenda: whether one wants to know about eventual anomalies in the unborn child or not and for what purpose, remain unaltered. The same holds for the information about the target anomalies, in case screening by NIPT stays restricted to aneuploidies of chromosomes 13, 18, and 21 [chapter 7; 100]. If the NIPT is to be offered as the first prenatal anomaly screening in pregnancy, midwives probably will play a crucial role as counselors. The question is how midwives could be trained to both offer counseling to a low-risk population as well as a high-risk population due to for instance ultrasound abnormalities. The clinical eligibility for NIPT might become increasingly challenging to handle because this eligibility happens to be different in both groups. With regards to the health education function of counseling, midwives might need to learn and to discuss with the clients medical indications as well as medical contraindications for the

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
181
8
NIPT. Contraindications for NIPT comprise an increased nuchal translucency, ultrasound abnormalities, vanishing twin, dichorial twins and limited accuracy of the NIPT in over-weighted women [102,103]. So, although clients might view the NIPT to be an attractive test, counselors in some cases have to break the news that NIPT might be not desirable while prenatal diagnostics or an array might be appropriate [94]. Training midwives on the meaning of unexpected findings and for instance the health education topics described above seems reasonable. Furthermore, training on how to provide health education in a personalized way together with the provision of decision-making support seems to be necessary giving the ongoing developments in the field of prenatal anomaly screening and the current prenatal counseling in practice described in this thesis.
With our study, we hope to have contributed to the ongoing discussion and debate in healthcare and policy about what constitutes high quality counseling for prenatal anomaly screening. As a client said: “[To me it was important] to get the feeling that she [the midwife] was talking to ME, and… not just rattle off the information”.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
182
APPENDIX A Topics relevant to address during Health Education according to most clients [chapter 2]
1. Asks about clients’ family’s history of birth defects
2. Explains which anomalies can be identified using prenatal screening
3. Explains which anomalies cannot be identified using prenatal tests
4. Provides medical information about the anomalies that are being tested for
5. Explains the usefulness of prenatal screening (what can the client decide to do eventually)
6. Informs the client about all the different types of prenatal tests
7. Explains what will happen during the prenatal tests
8. Discusses possible negative implications of prenatal screening for the unborn child
9. Informs the client about her chances of having a child with a congenital anomaly during this pregnancy
10. Explains which prenatal tests will be performed first and which will be performed later, if required and/or necessary
11. Tells the client why she is / is not eligible for certain prenatal tests
12. Discusses all clients’ options with regard to prenatal screening and the implications
13. Explains how long the client may take to decide whether or not to terminate the pregnancy, should the test results show an abnormality
14. Explains how long the client may take to decide whether or not to have the prenatal tests
15. Talks with the client about how her risk of having a child with a birth defect will affect her
16. Only discusses specific information about follow-up tests and possible anomalies with the client if it becomes clear that the client will need this information

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
183
8
APPENDIX B Topics relevant to address during Decision-making support according to 50% of the clients [chapter 2]
1. Advise the client about whether or not to take the prenatal tests
2. Respond to what the client already knows about prenatal screening
3. Ask the client questions that make her / him think
4. Talk to the client about how her /his family and the client would react to a child with a birth defect
5. Ask the client to explain her decision to take / not to take the prenatal tests
6. Be interested in who the client is

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
184
APPENDIX C Content of prenatal counseling for anomaly screening
Counseling
Counseling is the provision of information by the obstetric care provider about the combined test and the Fetal Anomaly Scan. The following aspect should be addressed during counseling: The right not to know;
- Information about the anomalies that are the target of screening (down-, edwards- and patau syndrome, neural tube defects, and other physical anomalies);
- Information about the natural course of the disease for which screening is performed and the frequency of occurrence;
- The test characteristics of the CT and FAS. Such as the risk of the anomaly tests, explanation about the test-outcome and the risk of false positive and false negative test results;
- The implications of abnormal test results and possibilities for future research;
- The possible costs of research both tangible and intangible.
In addition, the counselor should give the pregnant women the national information leaflets (of the RIVM). These leaflets contain all important information.
Reference: http://www.prenatale-screening.nl/counseling.html

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
185
8
REFERENCES
[1] Pereboom MT, Manniën J, van Almkerk KD, Spelten ER, Gitsels JT, Martin L, Hutton EK, Schellevis FG. What information do Dutch midwives give clients about toxoplasmosis, listeriosis and cytomegalovirus prevention? An exploratory study of videotaped consultations. Patient Educ Couns 2014; 96(1):29-35.
[2] Baron R, Martin L, Brug J, Hutton EK. Video-observation of lifestyle communication during the first prenatal visit of clients to their midwives. Work in progress.
[3] Meiser B, Irle J, Lobb E, Barlow-Stewart K. Assessment of the Content and Process of Genetic Counselling: A Critical Review of Emperical Studies. JOGC 2008; 17:434-451.
[4] Roter D, Ellington L, Hamby Erby L, Larson S, Dudley W. The genetic counselling Video project (GCVP). Am J Med Genet 2006; 142C:209-20.
[5] RIVM. Draaiboek Prenatale Screening. Downsyndroom en Structureel Echoscopisch Onderzoek. Versie 4.0; 2014. www.rivm.nl [In Dutch].
[6] Health Council of the Netherlands: Committee Genetic screening. Genetic Screening. The Hague: Health Council, 1994; publication no. 1994/22 [In Dutch].
[7] Resta RG. Defining and redefining the scope and goals of genetic counseling. Am J Med Genetics 2006;142C:269–75.
[8] Garcia E, Timmermans DRM, Van Leeuwen E. Rethinking autonomy in the context of prenatal screening decision-making. Prenat diagn 2008; 28(2):115-120.
[9] Flessel MC, Lorey FW. The California Prenatal Screening Program: “options and choices” not “coercion and eugenics”. Genetic Medicine 2011; 13(8):711–3.
[10] Jakobsen TR, Sogaard K, Tabor A. Implications of a first trimester Down’s syndrome screening program on timing of malformation detection. Acta Obstetrica et Gynecologica Scandinavica. Nord Fed Society Obstet Gyn 2011; 90:728–36.
[11] Smith RC, Hoppe RB. The patient’s story: integrating the patient- and physician-centered approaches to interviewing. Ann Intern Med 1991; 115:470–7.
[12] Smits A, Meekes A. Communicatie voor het spreekuur (3). Algemene tips voor een goede communicatie. Huisarts & Wetenschap 2007; 50(2):18-19 [In Dutch].
[13] Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, Cording E, Tomson D, Dodd C, Rollnick S, Edwards A, Barry M. Shared Decision Making: A Model for Clinical Practice. J Genl Intern Med 2012; 27(10):1361-1367.
[14] Ormond KEM, Banuvar I, Minogue SJ, Annas GJ, Elias S. What do Patients Prefer: Informed Consent Models for Genetic Carrier Testing. J Genet Counsel 2007; 16: 539–550.
[15] Gitsels-van der Wal JT, Martin L, Manniën J, Verhoeven P, Hutton EK, Reinders HS. Antenatal counselling for congenital anomaly tests: Pregnant Muslim Moroccan women’s preferences. Midwifery, 2015; doi: 10.1016/j.midw.2015.01.002.
[16] Ahmed S, Hewison J, Green JM, Cuckle HS, Hirst J, Thornton JG. Decisions About Testing and Termination of Pregnancy for Different Fetal Conditions: A Qualitative Study of European White and Pakistani Mothers of Affected Children. J Genet Counsel 2008; 17:560–572.
[17] Wertz D, Gregg R. Genetics services in a social, ethical and policy context: a collaboration between consumers and providers. J Med Ethics 2000; 26(4):261–265.
[18] Shiloh S, Gerad L, Goldman B. Patients’ Information Needs and Decision-Making Processes: What Can Be Learned From Genetic Counselees? Health Psychology 2006; 25(2):211–219.
[19] Hsieh Y, Flatley Brennan P. What Are Pregnant Women’s Information Needs and Information Seeking Behaviors Prior to Their Prenatal Genetic Counseling? AMIA 2005 Symposium Proceedings Page: 355-359.
[20] Bernhardt BA, Biesecker BB, Mastromarino CL. Goals, Benefits, and Outcomes of Genetic Counseling: Client and Genetic Counselor Assessment. Am J Med Genet 2000; 94:189–197.
[21] Alouini S, Moutel G, Venslauskaite G, Gaillard M, Truc JB, Herve C. Information for patients undergoing a prenatal diagnosis. Eur J Obstet Gynaecol Reprod Biol 2007; 134:9–14.
[22] Browner CH, Preloran HM, Casado MC, Bass HN, Walker AP. Genetic counseling gone awry: miscommunication between prenatal genetic service providers and Mexican-origin clients. Soc Sci Med 2003; 56(9):1933-46.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
186
[23] Charles C, Whelan T, Gafni A. What do we mean by partnership in making decisions about treatment? BMJ 1999;319:780–2.
[24] Bensing JM, Kerssens JJ, Van der Pasch M. Patient-directed gaze as a tool for discovering and handling psychosocial problems in general practice. J Nonverbal Behav 1995; 19(4):223-242.
[25] Maassen H. Gezond communiceren: winnaar Spinozapremie laat patiënten panels oordelen over consulten. Medisch Contact, 2006; 61:1924-7 [In Dutch].
[26] Engel GL. How much longer must medicine’s science be bound by a seventeenth century world view. In The Task of Medicine: Dialogue at Wickenburg (ed. K.White), Menlo Park: The Henry Kaiser Foundation, 1988; p. 113–116.
[27] Mearns D, Thorne B. Person-Centered Counselling in Action. London: Sage Publications, (2nd ed), 1999; 5–21.
[28] Ludwig MJ, Burke W. http://depts.washington.edu/bioethx/topics/physpt.html. University of Washington. 2014, Last date modified: October 28, 2014.
[29] www.riasworks.org.[30] Aitink M, Goodarzi B, Martijn L. Beroepsprofiel Verloskundige. Utrecht, KNOV, juni 2014 [In
Dutch].[31] Vanstone M, Kinsella EA, Nisker J. Information-sharing to promote informed choice in prenatal
screening in the spirit of the SOGC clinical practice guideline: a proposal for an alternative model. J Obstet Gynaecol Can 2012; 34: 269-675.
[32] Légaré F, St-Jaques S, Gagnon S, Njoya M, Brisson M, Frémont P, Rousseau F. Prenatal screening for Down syndrome: a survey of willingness in women and family physicians to engage in shared decision-making. Prenat Diagn 2011; 31:319–26.
[33] Hunt LM, De Voogd KB, Castañeda H. The routine and the traumatic in prenatal genetic diagnosis: does clinical information inform patient decision-making? Patient Educ Couns 2005; 56(3):302–312.
[34] Martin L, Van Dulmen S, Spelten E, Hutton E. Prenatal genetic counseling: Future parents prefer to make decisions together, using professional advice. Prenat Diagn 2012; 32(1):1–128.
[35] www.prenatalescreening.nl; http://wetten.overheid.nl/BWBR0003396/geldigheidsdatum_ 16-02-2015.
[36] De Boer J, Zeeman K. KNOV-guideline prenatal midwifery led care: recommendation for coaching, interaction and information giving. Utrecht: KNOV, 2008:17–46 [In Dutch].
[37] Barr O, Skirton H. Informed decision making regarding antenatal screening for fetal abnormality in the United Kingdom: A qualitative study of parents and professionals. Nurs Health Sci 2013; 15:318-25.
[38] Prins M, Van Roosmalen J. Praktische verloskunde. Houten, Bohn Stafleu van Loghum, 2014 [In Dutch].
[39] Barry CA, Bradley CP, Britten N, Stevenson FA, Barber N. “Patients’ unvoiced agendas in general practice consultations: qualitative study”, BMJ 2000; 320(7244):1246-50.
[40] Wildschut HIJ, Van Goudoever JB, Den Hollander NS, Keirse E, De Wert G. Foetale en neonatale screening op aangeboren afwijkingen. Leidraad voor besluitvorming. Amsterdam, Reed Business 2011; p. 385-405 [In Dutch].
[41] Van den Berg M. Decision making in prenatal screening. Doctoral thesis, VU medical centre, Amsterdam, 2006.
[42] Van Zwieten M. Het belang van een weloverwogen keuze – maar wat behelst de keuze. De complexe besluitvorming bij prenataal onderzoek. De Psycholoog 2008; 20-25.
[43] Gitsels-van der Wal JT, Martin L, Manniën J, Verhoeven P, Hutton EK, Reinders HS. A qualitative study on how Muslim women of Moroccan descent approach antenatal anomaly screening. Midwifery 2015. doi: 10.1016/j.midw.2014.12.007.
[44] De Jong A, Dondorp WJ, De Die-Smulders CEM, De Wert GMWR. The dynamics of prenatal screening. 2010; 39:2007-2009 [In Dutch].
[45] Williams C, Sandalla J, Lewando-Hundt G, Heymand B, Spencerb K, Grellier R. Women as moral pioneers? Experiences of first trimester antenatal screening. Soc Sci Med 2005; 61(9):1983–1992.
[46] Liefhebber S, Van Dam C, Waelput A. Dutch professional profile midwives. Utrecht: Royal Dutch organization of Midwives (KNOV), 2005 [In Dutch].

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
187
8
[47] Wouda J. Medische communicatie. Gespreksvaardigheden voor de arts. Utrecht, de Tijdstroom, 2000 [In Dutch].
[48] Silverman J, September 2014, www.each.eu.[49] Bensing JM, Verheul W, Van Dulmen AM. Patient anxiety in the medical encounter: a study of
verbal and nonverbal communication in general practice. Health Education 2008; 108(5):373-383.
[50] Sheets KB, Best RG, Brasington CK, Will MC. Balanced information about Down syndrome: what is essential? Am J Med Genet 2011; 155A(6):1246-57.
[51] Counselors manual for counselors to inform clients about NIPT: http://www.rivm.nl/Documenten_en_publicaties/Professioneel_Praktisch/Stappenplannen/Preventie_Ziekte_Zorg/Down_seo/Gespreksleidraad_voor_counselors_prenatale_screening_Informeren_over_NIPT [In Dutch].
[52] Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. Lancet 2003; 362:1225-30.
[53] Noordman J, Van der Weijden T, Van Dulmen S. Effects of video-feedback on the communication, clinical competence and motivational interviewing skills of practice nurses: a pre-test posttest control group study. J Adv Nurs 2014; 70(10):2272-2283.
[54] Noordman J, Verhaak P, Van Dulmen S. Web-enabled video-feedback: a method to reflect on the communication skills of experienced physicians. Patient Educ Couns 2011; 82(3):335-340.
[55] www.prenatalescreening.nl [In Dutch].[56] Information leaflets prenatal screening RIVM, 2014: http://www.prenatalescreening.nl/folders_
downloaden.php [In Dutch].[57] Continuing medical education of counselors: http://prenatalescreeningzon.mumc.nl/
regiobijeenkomst-2015 [In Dutch].[58] Teaching manual: training counseling for prenatal screening: http://prenatalescreening.nl/
archief/Docentenhandleiding%20vaardigheidstraining%20prenatale%20screening%20(2).pdf [In Dutch].
[59] Smets E, van Zwieten M, Michie S. Comparing genetic counseling with non-genetic health care interactions: Two of a kind? Patient Educ Couns 2007; 68:225–234.
[60] Information for counselors of the Stichting prenatal screening South-West of the Netherlands. www.prenatale-screening.nl. Last accessed: 27-11-2014.
[61] Client information: www.deverloskundige.nl [In Dutch].[62] Scholman HSA. Evaluation prenatal screening performance. Utrecht: Nederlandse Zorgautoriteit,
2009; CV 09-19 [In Dutch].[63] Van Dulmen S, Humphris G, Eide H. Towards a guideline for person-centered research in clinical
communication; lessons learned from three countries. IJPCM 2012; 2:58-63.[64] Butalid L. Changes in doctor-patient communication in general practice. Doctoral thesis, Nivel,
Utrecht, 2015; p. 131-152.[65] Van Dulmen S, Van Bijnen E. What makes them (not) talk about proper medication use with their
patients? An analysis of the determinants of GP communication using reflective practice. IJPCM 2011; 1(1):27-34.
[66] Wiegers TA, Van der Velden LFJ, Hingstman L. Estimated need for midwives 2004 – 2015; Utrecht, NIVEL 2005 [In Dutch].
[67] Van den Brink-Muinen A, Van Dulmen S, Jung HP, Bensing J. Communiceren huisartsen volgens de verwachtingen van hun patiënten? Huisarts & Wetenschap, 2008; 51(3):141-146.
[68] Tarn DM, Paterniti DA, Kravitz RL, Heritage J, Liu H, Kim S, Neil S, Wenger NS. How much time does it take to prescribe a new medication? Patient Educ Couns 2008; 72(2):311–319.
[69] Butalid L, Bensing JM, Verhaak PFM. Talking about psychosocial problems: An observational study on changes in doctor-patient communication in general practice between 1977 and 2008. Patient Educ Couns 2014; 94:314-321.
[70] Bensing JM, Tromp F, Van Dulmen S, Van den Brink-Muinen A, Verheul W, Schellevis F. De zakelijke huisarts en de niet-mondige patiënt: veranderingen in communicatie. Een observatieonderzoek naar consulten met hypertensie patiënten. Huisarts & Wetenschap 2008; 51(1):6-12.
[71] Van Zwieten M, Willems D, Knegt L, Leschot N. Communication with patients during the prenatal testing procedure: An explorative qualitative study. Patient Educ Couns 2006; 63:161–168.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 8
188
[72] Van Zwieten M. Uit de praktijk. Directief counselen: en dan? Psychologisch commentaar. Tijdschrift voor Gezondheidszorg en Ethiek 2003; 13(1):20-22 [In Dutch].
[73] Nieuwenhuijze MJ. On speaking terms. Choice and shared decision-making in maternity care. Doctoral thesis, Radboud University Nijmegen, 2014; p.141-163.
[74] Verkerk M. Care ethics as a feminist perspective on bioethics. In: Gastmans C, Dierickx K, Nys H, Schotmans P, editors. New pathways to European ethics. Antwerp: Intersentia; 2007.
[75] Garcia E, Timmermans DRM, van Leeuwen E. Rethinking autonomy in the context of prenatal screening decision-making. Prenat Diagn 2010; 28:115-0.
[76] Van den Berg M, Timmermans DR, Kleinveld JH, Van Eijk JT, Knol DL, Van der Wal G, Van Vugt JM. Are counsellors’ attitude influencing pregnant women’s attitudes and decisions on prenatal screening? Prenat Diagn 2007; 27:518–24.
[77] Redelmeier DA, Rozin P, Kahneman D. Understanding patients’ decisions. Cognitive and emotional perspectives. JAMA 1993; 270(1):72-6.
[78] Garcia Gonzalez ME. In search of good motherhood. How prenatal screening shapes women’s views on their moral duties to their family. Doctoral thesis. Nijmegen, Radboud University; 2011.
[79] Pieterse A, Van Dulmen S, Ausems M, Schoemaker A, Beemer F, Bensing J. QUOTE-gene ca: development of a counselee-centred instrument to measure needs and preferences in genetic counseling for hereditary cancer. Psycho-Oncology 2005; 14(5):361-375.
[80] Van Weert JCM, Jansen J, De Bruijn GJ, Noordman J, Van Dulmen S, Bensing JM. QUOTEchemo: A patient-centred instrument to measure quality of communication preceding chemotherapy treatment through the patient’s eyes. Eur J Cancer 2009; 45(17):2967-76.
[81] Van den Brink-Muinen, Verhaak PFM, Bensing JM, et al. Doctor-patient communication in different European health care systems: relevance and performance from the patients’ perspective. Patient Educ Couns 2000; 39:115–27.
[82] Brouwer W, Sixma H, Triemstra M, Delnoij D. Kwaliteit van zorg rondom een staaroperatie vanuit het perspectief van patiënten. Meetinstrument ontwikkeling [Quality of care surrounding cataract operation through the eyes of patients. Development of a measurement instrument]. Utrecht: NIVEL; 2005 [In Dutch].
[83] Sixma HJ, Van Campen C, Kerssens JJ, Peters L. Quality of care from the patients’ perspectives: from theoretical concept to a new measuring instrument. Health Expect 1998; 1:82–95.
[84] Stubbe JH, Gelsema T, Delnoij DMJ. The consumer quality index hip knee questionnaire measuring patients’ experiences with quality of care after a total hip of knee arthroplasty. BMC Health Serv Res 2007; 7:60.
[85] Gutteling JJ, de Man RA, Busschbach JJV, Darlington ASE. Quality of health care and patient satisfaction in liver disease: The development and preliminary results of the QUOTE-Liver questionnaire. BMC Gastroenterology 2008; 8:25-35.
[86] Nijkamp MD, Sixma HJ, Afman H, Hiddema F, Koopmans SA, van den Borne B, Hendrikse F, Nuijts RM. Quality of care from the perspective of the cataract patient: the reliability and validity of the QUOTE-cataract. British J Ophthalmol 2002; 86:840–2.
[87] Quality Handbook EMGO+ Institute: www.emgo.nl[88] Roter DL. The Roter Method of Interaction Process Analysis (unpublished manual). Baltimore:
RIASWorks; 1993.[89] Roter D, Larson S. The Roter interaction analysis system (RIAS): utility and flexibility for analysis of
medical interactions. Patient Educ Couns 2002; 46:243-51.[90] Eide H, Graugaard P, Holgersen K, Finset A. Physician communication in different phases of a
consultation at an oncology outpatient clinic related to patient satisfaction. Patient Educ Couns 2003; 51:259–266.
[91] Information on QUOTE questionnaires: www.nivel.nl.[92] Zuidgeest M. Measuring and improving the quality of care from the healthcare user perspective:
the Consumer Quality Index = Het meten en verbeteren van de kwaliteit van zorg vanuit het zorggebruikers perspectief: de Consumer Quality Index. Doctoral Thesis, Tilburg, Tilburg University; 2011.
[93] Monitoring quality of prenatal counseling courses: www.rivm.nl.[94] Trident study: www.meerovernipt.nl.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
General discussion
189
8
[95] Trident study: http://www.emgo.nl/research/quality-of-care/research-projects/1451/trident-study-trial-by-dutch-laboratories-for-evaluation-of-non-invasive-prenatal-testing-nipt/background/.
[96] www.knov.nl.[97] www.niptconsortium.nl.[98] www.niptconsortium.nl/nieuws.[99] van Schendel RV, Kleinveld JH, Dondorp WJ, Pajkrt E, Timmermans DR, Holtkamp KC, Kartsen
M, Vlietstra AL, Lachmeijer AM, Henneman L. Attitudes of pregnant women and male partners towards non-invasive prenatal testing and widening the skope of prenatal screening. Eur J Hum Genet 2014; 22:1345-50.
[100] Van Lith JMM, Faas BHW, Bianchi DW. Current controversies in prenatal diagnosis 1: NIPT for chromosome abnormalities should be offered to women with low a priori risk. Prenat Diagn 2015, 35, 8–14.
[101] Verweij J, Romeijn E, Koelewijn J, Heetkamp K, de Boer M, Oepkes D. Prenatale screening en de non-invasieve prenatale test: hoe denken eerstelijns verloskundigen erover? TvV 2015; (1):16-20.
[102] Benn P, Borell A, Chiu R, Cuckle H, Dugoff L, Faas B, Gross S, Johnson J, Maymon R, Norton M, Odibo A, Schielen P, Spencer K, Huang T, Wright D, Yaron Y. Aneuploidy screening: a position statement from the aneuploidy screening committee on behalf of the Board of the International Society for Prenatal Diagnosis. Prenat Diagn 2013; 33(7):622-9.
[103] Canick JA, Kloza, EM, Lambert-Messerlian GM, Haddow JE, Ehrich M, Boom D van der, Bombard AT, Deciu C, Palomaki GE. DNA sequencing of maternal plasma toidentify Down syndrome and other trisomies in multiple gestations. Prenat Diagn 2012; 32:1-5.


Chapter 9Summary & Samenvatting

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
192

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary
193
9
SUMMARY
Chapter 1 IntroductionIn the Netherlands, the prenatal anomaly test program consists of both screening and diagnostic tests. The prenatal screening program includes the combined test, a first trimester risk assessment for trisomy 21, 18 and 13, and the fetal anomaly scan, a second trimester ultrasound to detect structural anomalies such as neural tube defects. The prenatal diagnosis program includes amniocentesis or chorionic villus sampling to detect chromosomal anomalies and an advanced ultrasound scan. Parents have to decide whether they want to be informed about these tests and once informed whether they want to have the tests. Parents do not always find these choices easy. They might struggle with questions such as ‘what do I feel is a serious anomaly?’; ‘what will I do if an anomaly is found in my unborn child?’; and ‘how will my family and friends judge my choices?’. Counseling is offered to facilitate parents’ decision about prenatal anomaly screening. In about 80% of the Dutch pregnancies, primary care midwives offer this counseling for prenatal anomaly screening to their clients. The aim of prenatal counseling is to inform clients about prenatal anomaly testing, e.g. to provide information about the target anomalies and test characteristics, and to facilitate clients’ informed decision-making whether to opt for prenatal anomaly tests or not e.g. to explore together with clients their values regarding raising a disabled child. Most research on counseling for prenatal anomaly screening has focused on the assessment of the quality of clients’ risk perception accuracy, recall of information provided, decision related outcomes, psychological adjustment and communication style of the counselor. Little is known about parental preferences for counseling or about their experience of being counseled for prenatal anomaly screening. Furthermore, relatively little is known about counselors’ views on appropriate counseling and how they counsel in daily practice.The aim of this thesis was to examine prenatal counseling from the perspectives of clients and midwives and to examine client-midwife communication during counseling in daily, midwifery led-care practice. The research conducted consists of six studies.
Chapter 2 Prenatal counseling for congenital anomaly tests: parental preferences and perceptions of midwife performance.
Counseling for prenatal anomaly tests is largely based on the theoretical concept that counseling should comprise both health education and decision-making support. To our knowledge, little is known about how clients value and experience this theoretical concept in practice. An evidence-based instrument to evaluate the preferences and experiences of future parents regarding prenatal counseling is currently lacking. Therefore, we adapted the existing QUOTE (quality of care through the patients eyes) questionnaire into the QUOTE prenatal, a client centered questionnaire to measure clients’ pre-counseling preferences and post-counseling experiences, and assessed its validity.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
194
In seventeen Dutch midwifery practices, 941 pregnant women and their partners completed the QUOTE prenatal pre- and post-counseling. The QUOTE prenatal appeared to consist of three components, which show sufficient reliability: health education, decision–making support and building a good client–midwife relation. Building a good client-midwife relation (CMR) to enable the two prenatal counseling functions health education (HE) and decision-making support (DMS) in practice appeared to be relevant. We proposed to add this function as an important component of prenatal counseling. The QUOTE prenatal questionnaire is a reliable instrument to measure client preferences and experiences regarding CMR, HE and DMS. Most clients consider the client-midwife relation and health education to be (very) important for prenatal counseling. More than one third of the clients consider decision-making support to be important. More nulliparous women had preferences for health education and decision-making support compared to multiparae. Furthermore, the results of our study suggest that overall pregnant women and their partners have comparable needs regarding prenatal counseling for anomaly screening. As a consequence, our findings suggest that counselees are likely to benefit from paired prenatal counseling. That way each of their individual counseling needs can be met and couples can benefit from both receiving the same information and support in making their decisions towards prenatal anomaly tests. Post-counseling, clients perceived that their midwives performed well in building the client–midwife relation and in giving health education. About one third of the clients indicated that they preferred more decision-making support than they received, indicating that improvement is needed in decision-making support. Chapter 3 Midwives’ views on appropriate prenatal counseling for congenital anomaly tests: do they match clients’ preferences?The data for this study were collected in November 2010. We aimed to provide insight into midwives´ views on appropriate counseling for prenatal anomaly tests, and determine whether these views were concordant with clients´ preferences regarding prenatal counseling. Therefore, we mirrored the QUOTE prenatal so that it could be used to assess midwives’ views on appropriate counseling. 1416 Dutch midwives completed the questionnaire. Data of midwives were compared to the 941 QUOTE prenatal questionnaire-data of clients. Like clients, most midwives value a good client-midwife relation and health education as important or very important for counseling for prenatal anomaly tests. A more detailed look into health education items showed several items that were perceived important by most midwives but not by most clients and vice versa. Preferably, counseling for prenatal anomaly tests should be consistent with the prenatal counseling model that includes health education, decision-making support and building a good client-midwife relation, but should also be tailored to clients’ individual preferences.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary
195
9
Our findings show that only half of the midwives participating in this study seem to subscribe to the decision-making support function of prenatal counseling. This might result in prenatal counseling which does not meet the aims of the counseling or the perceived needs of clients. We therefore recommended that midwives reflect upon their views on prenatal counseling. Furthermore, midwives need to bridge the differences between their views on appropriate prenatal counseling and client preferences in daily practice.
Chapter 4 Introducing video recording in primary care midwifery for research purposes: procedure, dataset, and use.Research to support evidence for the actual introduction and enrolment of video-recording studies has been limited. In this chapter we describe how we introduced and used a nationwide video-recording research project of health care provider (HCP)-client interactions in primary midwifery-led care for research purposes. The video-recording study provided data for three of the other papers included in this thesis: Chapter 5, Chapter 6 and chapter 7. Following an invitation to participate, midwives from six practices across the Netherlands volunteered to videotape 15-20 intake consultations. We measured the number of valid recordings and missing recordings; reasons not to participate, non-response analyses, and the inter-rater reliability of the coded videotapes. Video recordings were supplemented by questionnaires for midwives and clients. We used the Roter Interaction Analysis System (RIAS) for coding as well as a newly developed obstetric topics scale. The introduction, complexity of the study and intrusiveness of the study were discussed within the research group. At the introduction of the study, more initial hesitation in cooperation was found among the midwives than among their clients. The intrusive nature of the recording on the interaction was perceived to be minimal. The complex nature of the study affected recruitment, data collection and combining the dataset with the questionnaires and medical records of clients. Although challenging to obtain, video recording of midwife-client interaction proved to provide a unique dataset. Data could be used to answer a wide range of research questions, for instance about lifestyle communication, pregnancy related health education and prenatal counseling for anomaly screening. Researchers planning to use a video recording research approach will benefit from a tight design, vigilant monitoring during the data collection, and a study-design that is as simple as possible.
Chapter 5 Prenatal counseling for congenital anomaly tests: an exploratory video- observational study about client-midwife communication.This study focusses on how the counseling functions health education, decision-making support and building a good client-counselor relation were performed in daily, midwifery practice. The data for this exploratory video-observational study were collected between June 2010 and May 2011. Pregnant women, and if present their partners, were included if

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
196
they were new to prenatal counseling for the current pregnancy, aged 18 years or older, and able to read Dutch or English. 269 videotapes on counseling for prenatal anomaly screening provided by 20 midwives within 6 Dutch primary midwifery-led care practices were used to code the client-midwife communication with the RIAS. Midwives tended to focus their counseling on HE compared to DMS. The relatively low contribution of clients during the decision-making support conversation might indicate poor DMS given by midwives. Counseling of multiparae was shorter than counseling of nulliparous women; multiparae received less HE as well as DMS compared to nulliparous women. This might be appropriate in the light of their personal experiences during an earlier pregnancy, but might also indicate that multiparous women do not get what they need, given their experiences that their needs seem to be unfulfilled after about a quarter of the prenatal counseling consultations. Since in 28% of the cases partners were not present during prenatal counseling, it remains unclear to what extent they contributed to the counseling conversation. Chapter 6 Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests: how do they relate to clients’ perceptions and independent observations?Chapter 6 describes how Dutch midwives evaluate their own counseling for prenatal anomaly screening in real life practice and how these evaluations relate to clients’ experiences and observed performance. 240 of the videos of 20 midwives could be included in this study. Post-counseling the QUOTE prenatal questionnaire was completed by both midwives and clients. Observers coded a selection of the QUOTE prenatal items using the adapted version of the RIAS video-coding system.We found that in all 240 cases midwives perceived that they performed well on building a good client-midwife relation. During 80% of the prenatal counseling, midwives perceived that they provided appropriate health education. Decision-making support was evaluated as provided by midwives in 17% of the cases. Experiences of clients and observations were highly congruent with those of midwives with regards to the HE functions of counseling. Regarding DMS congruence of assessments was higher between midwives and observers (80%) compared to midwives and clients (62%).Our results indicate that DMS is more difficult to assess compared to HE. An interesting incongruence on item level was found on the item ‘provided advice whether to opt for prenatal anomaly screening’; clients perceived to have gotten advice in 40% of the cases while midwives and observers assessed giving advice in about 6% of the cases.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Summary
197
9
Chapter 7 Clients’ psychosocial communication during prenatal counseling for anomaly screening: how is it related to midwives’ communication and client-directed gaze?Chapter 7 describes an exploratory study of 184 videotaped prenatal counseling consultations by 20 midwives. We aimed to assess the facilitation of clients’ psychosocial communication, known to be especially important for facilitating decision-making, during prenatal counseling for fetal anomaly screening. We assumed that midwives’ psychosocial and affective communication, client-directed gaze and counseling duration were positively related to clients’ psychosocial communication. We rated the duration of client-directed gaze and used the RIAS to code the client-midwife communication.Our results indicate that initiating discussion about psychosocial topics does not come easily; clients need to be invited by, for instance, psychosocial questions. We also found that midwives’ affective behavior and counseling duration is likely to encourage client’s psychosocial communication. Psychosocial communication of clients was, in contrast with our expectations, not related to midwives’ client-directed gaze.
Chapter 8 General DiscussionActive involvement in counseling for prenatal anomaly screening is important for expectant parents as it facilitates their decision-making process. Clients, meaning both pregnant women and their partners, prefer their counselors to build a good client-midwife relation and to provide health education. Decision-making support was considered to be important to a less substantial group of participants in our study. The views of midwives are largely in line with the preferences of clients. It is not entirely in line with the theoretical prenatal counseling model, which indicates that the aim of counseling is only accomplished when both health education as well as decision-making support are provided. Furthermore, several relevant differences between midwives’ views on appropriate counseling and clients’ preferences exist. Therefore, to realize appropriate counseling for prenatal anomaly screening, midwives need to find a way to overcome the differences between their own views about appropriate prenatal counseling, the theoretical functions of counseling and client preferences. The video-recording project provided a unique, multi-useful research dataset of prenatal intake consultations and prenatal counseling by midwives. The complementary use of the QUOTE prenatal questionnaire, for clients and midwives, delivered three different foci to look at counseling for prenatal anomaly screening in practice. This methodological triangulation provided valuable information, such as, how to interpret the findings of each separate focus e.g. observations of the client-midwife communication, experiences of clients and self-evaluations of midwives. The ongoing developments in prenatal anomaly screening, e.g. the Non Invasive Prenatal Test, stress the importance for such developments in counseling practice, since medical

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
198
progress might result in complex choices if an anomaly is indicated in the unborn child. To do so in line with client preferences, further research could be focused on the preferences and needs of clients with low literacy and how they might benefit from the use of value-clarification- or decision aids.Overall, we concluded that counseling for prenatal anomaly screening by midwives, seemed to be in line with communication during counseling of other health care providers since it was focused on the provision of health education. We therefore recommended that prenatal counselors improve the provision of decision-making support and thus encourage clients to share their deliberations whether to opt for anomaly screening or not during prenatal counseling for anomaly screening. Doing so, counselors may benefit from the Shared Decision Making approach as a practical guideline to optimize both the health education and decision-making support functions of prenatal counseling.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting
199
9
SAMENVATTING
Hoofdstuk 1 InleidingIn Nederland bestaat het testaanbod voor het opsporen van aangeboren afwijkingen tijdens de zwangerschap uit zowel screenings- als diagnostische tests. Het prenatale screening programma omvat de combinatietest (CT), een eerste trimester kansberekening voor trisomie 21, 18 en 13 (respectievelijk Down-, Edwards- en Patau sydroom) en het structureel echoscopisch onderzoek (SEO), een tweede trimester echo om structurele afwijkingen, zoals neurale buis defecten, te detecteren. Het prenatale diagnostische aanbod omvat een vlokkentest of vruchtwaterpunctie ten einde eventuele chromosomale afwijkingen te diagnosticeren en een geavanceerd ultrageluidsonderzoek (GUO) om structurele afwijkingen mee te diagnosticeren. Ouders beslissen zelf of ze willen worden geïnformeerd over deze prenatale tests en eenmaal geïnformeerd of ze de test(s) willen laten uitvoeren. Ouders vinden deze keuzes niet altijd eenvoudig. Ze kunnen worstelen met vragen zoals ‘wat vinden wij een ernstige afwijking?’, ‘wat doen we als er een ernstige afwijking wordt gevonden bij ons ongeboren kind?’ en ‘wat zullen onze familie en vrienden van onze keuzes vinden?’.Counseling over prenatale tests op aangeboren afwijkingen wordt aangeboden om ouders te faciliteren bij het nemen van een besluit over prenatale screening en diagnostiek. In ongeveer 80% van de Nederlandse zwangerschappen bieden eerstelijns verloskundigen deze counseling aan hun cliënten aan; de overige 20% van de zwangeren wordt in de tweede lijn begeleid. Het doel van prenatale counseling is om cliënten te informeren over prenatale screening en diagnostiek, bijvoorbeeld door het verstrekken van informatie over het doel van deze testen en de testkarakteristieken. Tevens heeft prenatale counseling tot doel cliënten te faciliteren bij het nemen van een geïnformeerd besluit om wel of niet te kiezen voor prenatale tests op aangeboren afwijkingen, bijvoorbeeld door met cliënten hun waarden met betrekking tot het opvoeden van een eigen gehandicapt kind te verkennen. Het meeste onderzoek naar prenatale counseling heeft zich gericht op de beoordeling van de kwaliteit en de juistheid van de risicoperceptie van cliënten, de hoeveelheid correcte informatie die cliënten zich na de counseling herinneren, de mate van geïnformeerde besluitvorming, psychologische aspecten van prenatale counseling en de communicatiestijl van de counselor. Er is weinig bekend over de ouderlijke voorkeuren voor de wijze van counseling of over hun ervaringen met counseling over prenatale screening en diagnostiek op aangeboren afwijkingen. Bovendien is er relatief weinig bekend over opvattingen van counselors betreffende optimale counseling en hoe zij counselen in de dagelijkse praktijk.Het doel van dit proefschrift was om prenatale counseling vanuit het perspectief van de cliënt en de verloskundige te onderzoeken en tevens te kijken naar de cliënt-verloskundige communicatie tijdens counseling in de dagelijkse, eerstelijns verloskundige praktijk. Het onderzoek bestaat uit zes studies.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
200
Hoofdstuk 2 Counseling over prenatale testen op aangeboren afwijkingen: ouderlijke voorkeuren en hun ervaringen met de verloskundige als counselor.Counseling over prenatale testen op aangeboren afwijkingen is grotendeels gebaseerd op het theoretische concept dat deze begeleiding zowel gezondheidsvoorlichting als begeleiding bij besluitvorming omvat. Voor zover wij weten, is er weinig bekend over de manier waarop cliënten dit theoretische concept waarderen en over hun ervaring hiermee in de praktijk. Een gevalideerd instrument om de voorkeuren van cliënten in kaart te brengen en hun ervaringen met prenatale counseling te meten ontbreekt tot op heden. Daarom pasten wij de bestaande QUOTE (quality of care through the patients eyes) vragenlijst aan resulterend in de QUOTE prenatal, een cliëntgerichte vragenlijst om pre-counseling de voorkeuren van cliënten te meten en post-counseling hun ervaringen met prenatale counseling te meten. Tevens is de validiteit van de vragenlijst beoordeeld.In zeventien, Nederlandse, verloskundige praktijken vulden 941 zwangere vrouwen en hun partners de QUOTE prenatal pre-counseling en post-counseling in. De QUOTE prenatal bleek te bestaan uit drie betrouwbare componenten: gezondheidsvoorlichting, hulp bij besluitvorming en het opbouwen van een goede cliënt-verloskundige relatie. Het opbouwen van een goede cliënt-verloskundige relatie werd gezien als voorwaardelijk om de twee andere functies van prenatale counseling, gezondheidsvoorlichting en hulp bij besluitvorming, mogelijk te maken in de praktijk. We stelden voor om deze functie toe te voegen aan de twee functies van het theoretisch counselingsmodel als een belangrijke component van prenatale counseling.De QUOTE prenatal vragenlijst is een betrouwbaar instrument om de voorkeuren en ervaringen met betrekking tot de cliënt-verloskundige relatie, gezondheidsvoorlichting en hulp bij besluitvorming van cliënten aangaande prenatale counseling te meten. De meeste cliënten beschouwen de cliënt-verloskundige relatie en gezondheidsvoorlichting als (zeer) belangrijk voor prenatale counseling. Ruim een derde van de cliënten vindt hulp bij besluitvorming (zeer) belangrijk. Meer nullipara dan multipara hadden een voorkeur voor gezondheidsvoorlichting en hulp bij besluitvorming. Daarnaast geven de resultaten van onze studie aan dat zwangere vrouwen en hun partners vergelijkbare behoeften hebben op het gebied van counseling over prenatale tests op aangeboren afwijkingen. Deze bevindingen suggereren dat cliënten waarschijnlijk profiteren van counseling waarbij de partner aanwezig is. Op die manier kan tegemoet gekomen worden aan individuele behoeften èn kunnen koppels profiteren van zowel het ontvangen van dezelfde informatie als de begeleiding bij het nemen van besluiten betreffende prenatale anomalie testen.Post-counseling gaven cliënten aan dat zij ervaren dat hun verloskundige goed de cliënt-verloskundige relatie opbouwt en passende gezondheidsvoorlichting geeft. Ruim een derde van de cliënten geeft aan dat zij liever meer hulp bij besluitvorming hadden ontvangen, hetgeen betekent dat verbetering nodig is in het begeleiden van cliënten in hun besluitvormingsproces.

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting
201
9
Hoofdstuk 3 Visies van verloskundigen betreffende adequate counseling over prenatale testen op aangeboren afwijkingen: komen deze visies overeen met de voorkeuren van cliënten?De gegevens voor dit onderzoek werden verzameld in November 2010. Ons doel was om inzicht te bieden in de visies van verloskundigen betreffende counseling over prenatale anomalie testen, en na te gaan of deze visies congruent waren met voorkeuren van cliënten aangaande prenatale counseling. Daarom gebruikten we een gespiegelde versie van de QUOTE prenatal, zodat de visies van verloskundigen en voorkeuren van cliënten met elkaar vergeleken konden worden. 1416 Nederlandse verloskundigen vulden de vragenlijst in. Opvattingen van deze verloskundigen zijn vergeleken met de 941 QUOTE prenatal vragenlijst-gegevens van cliënten. Net als cliënten waarderen de meeste verloskundigen een goede cliënt-verloskundige relatie en gezondheidsvoorlichting als belangrijk of zeer belangrijk voor prenatale counseling. Op item-niveau bleken echter verschillen te bestaan tussen de visies van verloskundigen en voorkeuren van cliënten betreffende gezondheidsvoorlichting; verscheidene items die belangrijk werden ervaren door de meeste cliënten, werden niet van belang gevonden door de meeste verloskundigen en vice versa.Bij voorkeur wordt counseling over prenatale anomalie testen in overeenstemming met het prenatale counseling model uitgevoerd, dat de drie functies gezondheidsvoorlichting, hulp bij besluitvorming en het opbouwen van een goede cliënt-verloskundige relatie omvat, waarbij tevens wordt aansloten bij de individuele voorkeuren van cliënten. Onze bevindingen tonen aan dat slechts de helft van de aan deze studie deelnemende verloskundigen hulp bij besluitvorming als een belangrijke functie van adequate prenatale counseling lijkt te zien. Dit kan resulteren in prenatale counseling die niet voldoet aan de doelstellingen van deze counseling of de behoeften van de cliënten. We raden dan ook aan dat verloskundigen reflecteren op hun visie op adequate prenatale counseling. Bovendien zullen verloskundigen in de praktijk de verschillen tussen hun opvattingen betreffende prenatale counseling en die van cliënten moeten zien te overbruggen.
Hoofdstuk 4 Introductie van video-opnames voor onderzoeksdoeleinden in de eerstelijns verloskundige praktijk: procedure, dataset en gebruik.Onderzoek dat bijdraagt aan wetenschappelijke kennis over de introductie en invoering van video-opnames van gezondheidszorg consulten, voor onderzoeksdoeleinden, is beperkt. In dit hoofdstuk beschrijven we hoe wij een landelijk video-opname onderzoeksproject van in de eerstelijns-verloskundige praktijk hebben geïntroduceerd en gebruikt voor onderzoeksdoeleinden. De video-opnames hebben tevens geresulteerd in een dataset voor de drie andere hoofdstukken in dit proefschrift: Hoofdstuk 5, hoofdstuk 6 en hoofdstuk 7.Naar aanleiding van een uitnodiging voor deelname boden verloskundigen uit zes praktijken verspreid over Nederland aan video-opnamen te maken van 15-20 consulten waarin

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
202
prenatale counseling plaatsvond. We registreerden het aantal bruikbare opnamen en onbruikbare opnamen en redenen van cliënten om niet deel te nemen aan de studie ten behoeve van een non-respons analyse. We gebruikten zowel het Roter Interaction Analysis System (RIAS) voor het coderen van cliënt-verloskundige communicatie gedurende prenatale counseling als een nieuw ontwikkelde obstetrische items schaal om de inhoud van niet counseling gebonden onderwerpen te coderen. De inter-beoordelaar betrouwbaarheid van gecodeerde videobanden werd berekend. Gegevens van video-opnames werden aangevuld met vragenlijsten voor zowel verloskundigen als cliënten. De invoering, complexiteit en de impact van de studie op verloskundigen en cliënten werden binnen de onderzoeksgroep besproken. Bij de invoering van de studie, aarzelden verloskundigen meer om deel te nemen dan hun cliënten. De waargenomen invloed van het maken van video-opnamen op de cliënt-verloskundige interactie bleek minimaal. De complexe studie-opzet van het onderzoek beïnvloedde rekrutering van verloskundigen, het verzamelen van volledige gegevens en het combineren van de resulterende video-dataset met de datasets van vragenlijsten en medische dossiers van cliënten.Hoewel een uitdaging om te verkrijgen, bleken de video-opnames van de cliënt-verloskundige interactie te zorgen voor een unieke dataset. De gegevens kunnen worden gebruikt om een breed scala van onderzoeksvragen te beantwoorden, bijvoorbeeld over de leefstijl van zwangeren, de cliënt-verloskundige communicatie, zwangerschap gerelateerde gezondheidsproblemen en prenatale counseling over screening op aangeboren afwijkingen. Onderzoekers die van plan zijn om gebruik maken van een onderzoeksopzet met video-opnames zullen profiteren van een strak design, alerte monitoring van gegevensverzameling, en een studieontwerp dat zo een eenvoudig mogelijk is.
Hoofdstuk 5 Prenatale counseling over testen op aangeboren afwijkingen: een verkennende video-observatie studie betreffende cliënt-verloskundige communicatie.Dit onderzoek gaat na hoe de counselingsfuncties gezondheidsvoorlichting, hulp bij besluitvorming en het opbouwen van een goede cliënt-verloskundige relatie werden uitgevoerd in de dagelijkse verloskundige praktijk. De gegevens voor deze verkennende video-observatie studie zijn verzameld tussen juni 2010 en mei 2011. Zwangere vrouwen en, indien aanwezig, hun partners konden deelnemen aan de studie als zij nog niet gecounseld waren over prenatale screening in de huidige zwangerschap, 18 jaar of ouder waren, en in staat om Nederlands of Engels te lezen. 269 video-opnamen van counseling over prenatale screening, van 20 verloskundigen uit 6 eerstelijns praktijken verspreid over Nederland, werden gebruikt om de cliënt-verloskundige communicatie te coderen door middel van het RIAS.Verloskundigen hadden de neiging om hun counseling meer te richten op gezondheidsvoorlichting in vergelijking met het bieden van hulp bij besluitvorming. De

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting
203
9
relatief beperkte bijdrage van cliënten aan de conversatie aangaande de counselingsfunctie hulp bij besluitvorming zou kunnen wijzen op matig uitgevoerde hulp bij besluitvorming door verloskundigen. Counseling van multipara was korter dan counseling van nullipara; multipara ontvingen minder gezondheidsvoorlichting evenals minder hulp bij besluitvorming vergeleken met nullipara. Dit zou passend kunnen zijn in het licht van hun persoonlijke ervaringen tijdens een eerdere zwangerschap, maar kan ook aangeven dat multipara niet krijgen wat ze nodig hebben, gezien het gegeven dat ongeveer een kwart van de multipara ervaart dat er niet tegemoet gekomen is aan hun behoeften gedurende prenatale counseling. Aangezien in 28% van de gesprekken partners niet aanwezig waren, blijft onduidelijk in hoeverre zij participeerden in de counseling over prenatale screening en diagnostiek.
Hoofdstuk 6 Verloskundige percepties van de communicatie tijdens op video opgenomen counseling over prenatale anomalie testen: hoe verhouden deze zich tot cliënt percepties en onafhankelijke observaties?In hoofdstuk 6 staat beschreven hoe de Nederlandse verloskundigen in deze studie hun eigen counseling voor prenatale anomalie screening in de praktijk evalueren en in hoeverre deze evaluaties corresponderen met ervaringen van cliënten en waarnemingen van observatoren. 240 video’s van 20 verloskundigen zijn gebruikt in deze studie. De post-counseling QUOTE prenatal vragenlijst werd door zowel verloskundigen als cliënten ingevuld na elk opgenomen counselingsgesprek. Observatoren codeerden een selectie van de QUOTE prenatal items met behulp van de aangepaste versie van het RIAS. We vonden dat in alle 240 gevallen verloskundigen ervaren dat ze een goede cliënt-verloskundige relatie opbouwden. Gedurende 80% van de prenatale counseling evalueerden verloskundigen de door hen zelf gegeven gezondheidsvoorlichting als passend. Verloskundigen vonden dat zij in 17% van de gesprekken het geven van hulp bij besluitvorming adequaat uitvoerden. Ervaringen van cliënten en observaties waren zeer congruent met de zelf-evaluaties van verloskundigen als het gaat om het uitvoeren van de counselingsfunctie gezondheidsvoorlichting. Met betrekking tot de functie hulp bij besluitvorming was de congruentie tussen zelf-evaluaties van verloskundigen en observaties van de cliënt-verloskundige communicatie hoger (80%) dan tussen zelf-evaluaties van verloskundigen en ervaringen van cliënten (62%).Onze resultaten geven aan dat hulp bij besluitvorming moeilijker is te evalueren en te beoordelen vergeleken met gezondheidsvoorlichting. Een interessante incongruentie op itemniveau werd gevonden voor het item ‘de verloskundige verstrekt advies om wel of niet te kiezen voor prenatale screening op aangeboren afwijkingen’; cliënten ervaren advies te hebben gekregen in 40% van de gesprekken, terwijl verloskundigen en observatoren aangeven dat dit advies in ongeveer 6% van de gesprekken daadwerkelijk is gegeven.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Chapter 9
204
Hoofdstuk 7 Psychosociale communicatie van cliënten tijdens prenatale counseling over screening op aangeboren afwijkingen: hoe is deze gerelateerd aan de verloskundige communicatie en de mate waarin de verloskundige naar haar cliënt kijkt?In hoofdstuk 7 staat een verkennende studie beschreven waarvoor 184 video-opnamen van prenatale counseling door 20 verloskundigen gebruikt zijn. Het doel was na te gaan in hoeverre cliënten gefaciliteerd werden om psychosociale onderwerpen te bespreken; psychosociale communicatie wordt gezien als belangrijk gedurende het verlenen van hulp bij besluitvorming. Wij veronderstelden dat psychosociale- en affectieve communicatie doorverloskundigen, het kijken naar de cliënt en de counselingsduur positief waren gerelateerd aan psychosociale communicatie van cliënten. We maten de duur van het kijken naar de cliënt en gebruikten het RIAS om de cliënt-verloskundige communicatie te coderen.Onze resultaten laten zien dat het initiëren van een gesprek over psychosociale onderwerpen niet gemakkelijk is; cliënten moeten hiervoor worden uitgenodigd, bijvoorbeeld door psychosociale vragen. Wij constateerden ook dat affectief gedrag van verloskundigen en een langere counselingsduur cliënten waarschijnlijk aanmoedigt te praten over psychosociale onderwerpen. Psychosociale communicatie van cliënten was, in tegenstelling tot onze verwachtingen, niet gerelateerd aan de tijd die verloskundigen naar hun cliënt keken.
Hoofdstuk 8 Algemene DiscussieActieve betrokkenheid bij prenatale counseling over screening op aangeboren afwijkingen is belangrijk voor aanstaande ouders, omdat dit hun besluitvorming om wel of niet gebruik te maken van prenatale testen faciliteert. Cliënten, zowel zwangere vrouwen als hun partners, stellen het op prijs dat de verloskundige tijdens prenatale counseling aandacht besteed aan het opbouwen van een goede cliënt-verloskundigen relatie en gezondheidsvoorlichting geeft. Hulp bij besluitvorming werd van belang geacht door een minder aanzienlijke groep deelnemers in onze studie. De visie van verloskundigen ten aanzien van adequate counseling komt grotendeels overeen met de voorkeuren van cliënten, maar niet geheel met het theoretische prenatale counselingsmodel. Dit model geeft aan dat het doel van de counseling alleen wordt bereikt wanneer zowel gezondheidsvoorlichting als hulp bij besluitvorming worden aangeboden. Bovendien vonden wij diverse relevante verschillen tussen voorkeuren van cliënten en visies van verloskundigen. Om passende prenatale counseling te kunnen aanbieden dienen verloskundigen een manier te vinden om de verschillen tussen hun eigen opvattingen over adequate counseling, voorkeuren van cliënten en de theoretische functies van prenatale counseling te overbruggen.Het onderzoeksproject met video-opnames voorziet ons van een unieke, breed-bruikbare dataset betreffende prenatale intakes en prenatale counseling door verloskundigen. Het aanvullende gebruik van de QUOTE prenatal vragenlijst, voor cliënten en verloskundigen, maakt

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Samenvatting
205
9
het bovendien mogelijk vanuit drie verschillende foci te kijken naar prenatale counseling over screening op aangeboren afwijkingen in de praktijk. Deze methodologische aanpak heeft waardevolle informatie opgeleverd, zoals hoe de resultaten van elke afzonderlijke focus, bijvoorbeeld observaties van de cliënt-verloskundige communicatie, geïnterpreteerd kunnen worden gezien de ervaringen van cliënten en zelfevaluaties van verloskundigen. De huidige ontwikkelingen in de prenatale anomalie screening, bijvoorbeeld de in studie-verband aangeboden Non-Invasieve Prenatale Test (NIPT), en de bevindingen van dit proefschrift benadrukken het belang van het voortdurende in ontwikkeling blijven van prenatale counseling in de praktijk. Deze counseling dient aangepast te worden aan de medische ontwikkelingen die kunnen leiden tot complexe keuzes als een anomalie in het ongeboren kind wordt aangetroffen. Het ontwikkelen van counseling die in lijn is met de voorkeuren van cliënten vraagt echter ook om nader onderzoek gericht op de wensen en behoeften van laaggeletterde cliënten en hoe deze cliënten bijvoorbeeld kunnen profiteren van het gebruik van keuzehulpen.In grote lijnen concluderen we dat prenatale counseling over screening op aangeboren afwijkingen door verloskundigen overeen lijkt te komen met de communicatie tijdens cliënt-begeleiding door andere zorgverleners, omdat verloskundigen zich, net als zij, met name richtten op het verstrekken van gezondheidsvoorlichting. Daarom bevelen wij aan dat prenatale counselors hun hulp bij besluitvorming verbeteren om daarmee cliënten aan te moedigen om hun overwegingen wel of niet te kiezen voor prenatale screening tijdens de prenatale counseling te delen. Counselors kunnen bij het optimaliseren van hun counseling profiteren van het model voor Gezamenlijke besluitvorming als een praktische leidraad voor het verbeteren van zowel het geven van cliënt-gerichte gezondheidsvoorlichting als het verlenen van hulp bij besluitvorming; de twee centrale functies van prenatale counseling.


Publications

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Publications
208

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Publications
209
P
1. Martin L, Gitsels-van der Wal JT, Pereboom MT, Spelten ER, Hutton EK, van Dulmen S. Midwives’ perceptions of communication during videotaped counseling for prenatal anomaly tests: How do they relate to clients’ perceptions and independent observations? Patient Educ Couns 2015; doi: 10.1016/j.pec.2015.02.002.
2. Gitsels-van der Wal JT, Martin L, Manniën J, Verhoeven P, Hutton EK, Reinders HS. Antenatal counselling for congenital anomaly tests: pregnant Muslim Moroccan women’s preferences. Midwifery 2015; 31(3):e50-7.
3. Gitsels-van der Wal JT, Martin L, Manniën J, Verhoeven P, Hutton EK, Reinders HS. A qualitative study on how Muslim women of Moroccan descent approach antenatal anomaly screening. Midwifery 2015; 31(3):e43-9.
4. Martin L, Hutton EK, Gitsels-van der Wal JT, Spelten ER, Kuiper F, Pereboom MTR, van Dulmen S. Antenatal counselling for congenital anomaly test: An exploratory video-observational study about client-midwife communication. Midwifery 2015; 31(1):37-46.
5. Spelten ER, Martin L, Gitsels JT, Pereboom MT, Hutton EK, van Dulmen S. Introducing video recording in primary care midwifery for research purposes: Procedure, dataset and use. Midwifery 2015; 31(1):95-102.
6. Martin L, Hutton EK, Spelten ER, Gitsels-van der Wal JT, van Dulmen S. Midwives’ views on appropriate antenatal counselling for congenital anomaly tests: Do they match clients’ preferences? Midwifery 2014; 30(6): 600-609.
7. Pereboom MT, Manniën J, van Almkerk KD, Spelten ER, Gitsels JT, Martin L, Hutton EK, Schellevis FG. What information do Dutch midwives give clients about toxoplasmosis, listeriosis and cytomegalovirus prevention? An exploratory study of videotaped consultations. Patient Educ Couns 2014; 96(1):29-35.
8. Gitsels–van der Wal JT, Verhoeven PS, Manniën J, Martin L, Reinders HS, Spelten E, Hutton EK. Factors affecting the uptake of prenatal screening tests for congenital anomalies; a multicentre prospective cohort study. BMC Pregnancy and Childbirth 2014; 14(1):264-273.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Publications
210
9. Martin L, van Dulmen S, Spelten E, de Jonge A, de Cock P, Hutton E. Prenatal counseling for congenital anomaly tests: parental preferences and perceptions of midwife performance. Prenat Diagn 2013; 33(4):341-353.
10. Martin L, van Dulmen S, Spelten E, Hutton E. Prenatal genetic counseling: Future parents prefer to make decisions together, using professional advice. Prenat Diagn 2012; 32(Supl.1): 1–128.
11. Evelien Spelten, Janneke Gitsels, Monique Pereboom, Linda Martin, Eileen Hutton, Sandra van Dulmen. Video recording to improve the quality of prenatal genetic counseling. Prenat Diagn 2012; 32(Supl.1): 1-128.
12. van Knippenberg B, Martin L, Tyler T. Process-orientation versus outcome-orientation during organizational change: The role of organizational identification. J Org Behav 2006; 27: 685–704.

Curriculum Vitae

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Curriculum Vitae
212

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Curriculum Vitae
213
CV
Linda Martin is, na het behalen van haar VWO diploma, in 1995 afgestudeerd als oefentherapeut-Mensendieck. In januari 1997 is zij naast haar werk als zelfstandig oefentherapeut begonnen aan haar studie psychologie aan de Vrije Universiteit te Amsterdam. In 1998 is zij gevraagd docent te worden aan de opleiding voor oefentherapie-Mensendieck, Hogeschool van Amsterdam. In 2000 heeft zij haar laatste patiënten als oefentherapeut-Mensendieck behandeld.
In 2002 behaalde zij haar doctoraal Psychologie. Gedurende haar studiejaren en jaren als docent heeft zij tevens de docentenopleiding FBW afgerond. Daarnaast was zij als staflid werkzaam voor de Nederlandse Vereniging voor Oefentherapeuten Mensendieck, die in dezelfde periode voorbereidingen trof om te fuseren met de beroepsvereniging van Oefentherapeuten Cesar. Hierover heeft zij haar doctoraalscriptie geschreven.
Vanaf 2003 is Linda werkzaam aan de Verloskunde Academie Amsterdam als docent Psychologie en communicatie. Na aanvankelijk een zeer breed takenpakket te hebben uitgevoerd wilde zij zich meer verdiepen in het psychologisch en communicatief vakgebied. Dit heeft in 2010 geleid tot de start van haar promotieonderzoek betreffende prenatale counseling door verloskundigen over screening op congenitale afwijkingen aan de vakgroep Midwifery Science van het EMGO+ Instituut VUmc, Amsterdam. Zij is sinds 2014 lid van het docententeam dat de basis- en vervolgcursussen voor prenatale counseling verzorgd in Noord-Holland en de regio rond het AMC en VUmc.
Linda heeft samen met haar partner Erik Scholte drie kinderen: Aniek (2004), Teun (2006) en Koen (2010).
Maart, 2015


Dankwoord
‘Hij ging op weg [naar de regenboog],’ zei de nar, ‘en hij reisde lange tijd. Hij trok langs steden en dorpen, door velden en woestijnen, over stromende rivieren en door dichte
wouden. […] en hij wist dat het niet om de regenboog zelf ging, maar om het zoeken ernaar.’Uit: De brief voor de koning. Tonke Dragt

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord
216

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord
217
D
‘Promoveren doe je samen’, is mijn ervaring. De hulp en betrokkenheid van velen is onontbeerlijk gebleken. Daarom wil ik iedereen bedanken die heeft bijgedragen aan het tot stand komen van dit proefschrift. Een aantal mensen noem ik hier in het bijzonder.
Dit onderzoek was niet mogelijk geweest zonder de (zwangere) vrouwen, hun partners en verloskundigen die bereid waren mee te doen aan dit onderzoek. Bedankt voor de openhartige gesprekken, wijze woorden, jullie tijd en inzet.
Dan mijn twee promotores, Eileen Hutton en Sandra van Dulmen. Beste Eileen, je hebt van grote afstand in weinig contactmomenten een wezenlijke bijdrage geleverd aan elk onderdeel van dit proefschrift. Ik waardeer de gedegen werkwijze die je voorstaat en naleeft, je kritische vragen, jouw wijze van ‘bedside teaching’ en je flexibiliteit om in de rijdende trein van mijn promotie te stappen. Ik ben blij dat juist jij onze eerste hoogleraar Midwifery Science bent geworden.
Beste Sandra, je hebt mij geholpen de wereld van het communicatieonderzoek te verkennen en eigen te maken. Bij onze besprekingen van de hoofdstukken gaf je heldere feedback, waardoor ik scherper de lijn van het verhaal voor ogen zag en tevens behoed werd voor het volledig decimeren van de resultaten. Met jouw immer overvolle agenda vond je altijd, met de jou zo kenmerkende rust, tijd om mijn vragen te beantwoorden; veel dank daarvoor.
Mijn copromotor, Evelien Spelten. Beste Evelien, zonder jou was ik niet aan promoveren begonnen. Dank dat je in mij een promovenda zag en dat je mij de afgelopen jaren steeds opnieuw weer hebt geholpen mijn blik te scherpen. Jouw focus op de grote lijnen en aandacht voor wat je goed vond aan mijn werk heeft mij gesterkt steeds opnieuw een betere versie van mijn stukken te schrijven. Daarnaast heb ik genoten van onze wetenschappelijke reizen naar het buitenland; voor mij onvergetelijke momenten van de afgelopen jaren.
Beste overige leden van mijn promotiecommissie, prof. dr. M.C. Cornel, prof. dr. H. Eide, prof. dr. J.M.M. van Lith, prof. dr. J. van der Velden, prof. dr. T. van der Weijden en dr. M.P. Amelink-Verburg hartelijk dank voor jullie bereidwilligheid mijn proefschrift op zijn wetenschappelijke waarde te beoordelen.
Beste (oud) directeuren, opleidingsmanagers en fasecoördinatoren van de AVAG, jullie visie op de relevantie om AVAG docenten te laten promoveren heeft mij gebracht waar ik nu sta; dank daarvoor. Voor mij is de rol van docent/onderzoeker een gouden combinatie gebleken, omdat die mij de ruimte gaf de praktische aanbevelingen in mijn artikelen op hun merites te toetsen bij hen die het betreft.

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord
218
Beste collegae van Midwifery Science, jullie collegialiteit was hartverwarmend. Ank, kort maar krachtig is jouw bijdrage aan mijn promotie traject geweest. Jij zat naast mij voor de computer om mijn weggezakte SPSS vaardigheden op te halen. Wat mij enorm heeft geholpen is de volgende uitspraak van jou: ‘bedenk dat alleen jij straks de keuzes in je artikelen moet verdedigen’. Beste promovendi-groep, Ruth, Carien, Catja, Doug en Myrte, dank voor jullie nimmer afnemende belangstelling voor het verloop van mijn promotietraject, voor het kritisch meedenken en delen van jullie ervaringen tijdens de promovendi dagen. Doctores Monique, Agatha, Trudy en Esther, jullie zijn mij voorgegaan! Ook dank voor jullie tips aangaande het regelen van de onvoorstelbare hoeveelheid praktische zaken na de goedkeuring van het manuscript en voor jullie voorbeeld in hoe een verdediging aan te pakken.
Beste collegae van Community Genetics, dank voor jullie gastvrijheid en uitnodiging mijn onderzoek met jullie te delen, mij aan te sluiten bij colloquia en andere leerzame bijeenkomsten. Beste Martina, dank voor de korte tijd dat je mijn promotor was. De cirkel is weer rond nu jij ook bereid bent geweest mijn proefschrift op zijn wetenschappelijke waarde te beoordelen. Beste Lidewij, wat fijn dat wij elkaar hebben leren kennen. Dank dat je de tijd hebt genomen feedback te geven op een deel van mijn proefschrift. Voor mij ben je een onderzoeker die laat zien hoe kennis en netwerken delen leidt tot een bredere verbinding tussen wetenschap en praktijk. In ons project met studenten van de AVAG geniet ik van onze samenwerking. Graag zet ik deze in de toekomst voort.
Beste collegae van de AVAG, ieder op een eigen manier hebben jullie bijgedragen aan het tot stand komen van dit proefschrift. Jullie feedback, het sparren, meelezen, meedenken, meewerken, samen studenten begeleiden en meeleven was hartverwarmend en leerzaam. Dank daarvoor. Beste Joyce, mijn kamer genoot. Dank voor de korte gesprekjes die wij voerden over allerlei zaken betreffende mijn promotie. Vlot, met kennis van zaken en to the point heb je me geholpen een grote verscheidenheid aan hordes die ik de afgelopen jaren ben tegen gekomen te nemen. Mocht je ook willen promoveren, dan weet je mij te vinden. Beste Winnie en Bernadette, dank voor al jullie hulp, advies en interesse in mijn promotie-traject en het ongevraagd doorsturen van artikelen die mogelijk interessant voor mij zouden kunnen zijn.
Beste student-assistenten, wat fijn om met jullie samen te werken aan mijn promotie. Jullie enthousiasme werkte aanstekelijk en jullie bijdragen hebben het afronden van mijn proefschrift aanzienlijk versneld (ik denk aan het coderen van al die videobanden, de enorme stapels vragenlijsten om in te voeren in SPSS, de interviews en al het werk dat daarbij hoorde etc.).

R1R2R3R4R5R6R7R8R9R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord
219
D
Lieve vrienden en familie, zonder de vele wandelingen, jullie interesse, hulp bij oppas- en logistieke problemen, speel- en logeerpartijen van de kinderen, samenzang en etentjes was mijn accu veel te snel op geweest om dit promotie-traject vol te houden. Dank voor jullie vriendschap en begrip als ik niet zoveel van mij liet horen.
Lieve Janneke, het grootste cadeau van deze promotie is mijn vriendschap met jou. Dank voor je gastvrijheid, je begrip, het inzicht in de verloskunde praktijk dat je mij geeft, ‘mijn’ eerste bevalling, de (kleine) attenties, de bijdrage van jouw praktijk aan mijn dataset, het delen van je netwerk, onze onvergetelijke reis naar Miami; kortom dank voor je vriendschap! “Ik ben je dankbaar omdat je me neemt zoals ik ben. Wat moet ik met een vriend(in) die mij beoordeelt?” (A. Saint-Exupéry). Hans, onzeglijk veel dank voor het beschikbaar stellen van je werkkamer; ik heb er met heel veel plezier gewerkt. En dank voor je gastvrijheid ook als ik om 7.00 ’s morgens weer op de stoep stond. Xander, de tijd dat ik met Janneke op jouw boot gewerkt heb is onvergetelijk. Dank dat ik daar mocht komen.
Mijn paranimfen, Freya en Laura, het geeft mij een intens gevoel van blijdschap dat jullie naast mij staan bij de verdediging. Lieve Freya, dank voor je betrokkenheid en bevrijdende opmerkingen als ik de te maken keuzes wat zwaar opnam. Lieve Laura, dank voor de leerzame momenten die je mij gaf tijdens de trainingen over prenatale counseling aan verloskundigen (in opleiding). Ik prijs me gelukkig dat jullie mijn zussen zijn.
Lieve papa en mama, met jullie authentieke visie op dit project en interesse in de tussenresultaten hebben jullie mij mijn motto ‘niet het eindpunt maar de weg daarnaartoe is het doel’ optimaal kunnen laten leven. Ik ben dankbaar voor de basis die jullie gelegd hebben om kritisch na te denken over wat wezenlijk is.
Lieve Aniek, Teun en Koen, jullie verbinden mij intens met het onderwerp van dit proefschrift en tonen mij elke dag opnieuw wat van waarde is in het leven.
En dan. Lieve, lieve Erik, mijn rots in de branding. Zo rustig toen ik geheel in paniek meldde dat ik zwanger was van, zoals we nu weten, onze Koen. Diep in de materie van voorliggend onderzoek gedoken zag ik alléén nog maar vergrote kansen op aangeboren afwijkingen, want … ik was een ‘oude’ zwangere. Jij bracht kalmte, rust en vertrouwen. En zo heb je steeds naast mij gestaan. Wie A zegt moet ook B zeggen, ook als het moeilijk wordt. Moeilijk is het meerdere malen geworden; wat een leerweg om daarmee om te gaan! Mijn promotie is afgerond; het leren gaat door. Op naar de toekomst!

R1R2R3R4R5R6R7R8R9
R10R11R12R13R14R15R16R17R18R19R20R21R22R23R24R25R26R27R28R29R30R31R32R33R34R35R36R37R38R39
Dankwoord
220
‘Er zijn geen geheimen meer’, zei Tiuri.
De Dwaas rimpelde zijn voorhoofd. ‘Geen geheimen meer?’ herhaalde hij. ‘Ze noemen mij de Dwaas, maar dat geloof ik niet, dat er geen geheimen meer zijn.’
Tiuri keek hem aan, plotseling met wat eerbied.
‘Ja,’ zei hij, ‘je hebt gelijk. Mijn geheim mag ik nu vertellen, maar er zijn natuurlijk vele andere. De geheimen van het Wilde Woud bijvoorbeeld en nog een heleboel meer. Ja, van
sommige hebben we misschien nooit gehoord.’
Uit: De brief voor de koning. Tonke Dragt

Counseling for prenatal anomaly screening
Counseling for prenatal anomaly screening
Uitnodiging
Counseling for prenatal anomaly screening
door
Amsterdam
Paranimfen