Proefschrift ChristineVanVelzenCover+Bladwijzer.indd 1-4 ... · ter verkrijging van de graad Doctor...
150
Transcript of Proefschrift ChristineVanVelzenCover+Bladwijzer.indd 1-4 ... · ter verkrijging van de graad Doctor...

Proefschrift_ChristineVanVelzenCover+Bladwijzer.indd 1-4 15-09-16 17:05


PRENATAL SCREENING FOR CONGENITAL HEART DEFECTS- the results of the standard anomaly scan in the Netherlands -
♥
Christine L. van Velzen
Christine van Velzen.indb 1 20/09/2016 08:26

Title: Prenatal screening for congenital heart defects - the results of the standard anomaly scan in the Netherlands
Author: Christine L. van Velzen
The studies presented in this thesis were performed at the Division of Prenatal Medicine, Department of Obstetrics and Gynecology, VU University Medical Center, Amsterdam, the Netherlands, in cooperation with the Departments of Pediatric Cardiology and the Departments of Obstetrics and Gynecology of the VU University Medical Center, the Leiden University Medical Center and the Academic Medical Center Amsterdam, the Netherlands.
Financial support by the Dutch Heart Foundation for the publication of this thesis is gratefully acknowledged.
Financial support for printing of this thesis was kindly provided byBiomedic | Samsung, Bridea, BMA BV (Mosos), Toshiba Medical Systems Nederland, Chipsoft, Vrije Universiteit
ISBN 978-94-6299-444-7
Cover design: StudioLinLay Out: Jardine MediaPrinting: Ridderprint BV, the Netherlands
Copyright © 2016 Christine van VelzenThesis VU University Medical Center, Amsterdam with summary in Dutch
Christine van Velzen.indb 2 20/09/2016 08:26

V R I J E U N I V E R S I T E I T
PRENATAL SCREENING FOR CONGENITAL HEART DEFECTS- the results of the standard anomaly scan in the Netherlands -
AC A D E M I S C H P R O E F S C H R I F T
ter verkrijging van de graad Doctor aan
de Vrije Universiteit Amsterdam,
op gezag van de rector magnificus
prof.dr. V. Subramaniam,
in het openbaar te verdedigen
ten overstaan van de promotiecommissie
van de Faculteit der Geneeskunde
op donderdag 10 november 2016 om 13.45 uur
in de aula van de universiteit,
De Boelelaan 1105
door
Christine Louise van Velzen
geboren te Utrecht
Christine van Velzen.indb 3 20/09/2016 08:26

Promotoren: prof. dr. C.J.M. de Groot prof. dr. N.A. Blom
Copromotoren: dr. M.C. Haak dr. C.J. Bax
Christine van Velzen.indb 4 20/09/2016 08:26

voor mijn ouders en mijn kinderen
Christine van Velzen.indb 5 20/09/2016 08:26

LEDEN VAN DE BEOORDELINGSCOMMISSIE
prof. dr. C.M. Bilardo University of Groningendr. T.E. Cohen Erasmus University Medical Centerprof. dr. J. Hruda VU University Medical Centerprof. dr. D. Oepkes Leiden University Medical Centerprof. dr. J.I.P. de Vries VU University Medical Center
Christine van Velzen.indb 6 20/09/2016 08:26

TABLE OF CONTENTS
Chapter 1: Introduction 9
Chapter 2: Performance of second trimester screening for prenatal detection of congenital heart defects in unselected populations - systematic review and meta-analysis Submitted
17
Chapter 3: Prenatal detection of congenital heart disease – results of a national screening programBJOG 2016 Feb;123(3):400-7LetterBJOG 2015 Sep; 122(10):1420-1ReplyBJOG 2015 Sep;122(10):1421
49
Chapter 4: Prenatal detection of transposition of the great arteries reduces mortality and morbidityUltrasound Obstet Gynecol 2015 Mar;45(3):320-5
69
Chapter 5: Prenatal diagnosis of congenital heart defects; accuracy and discrepancies in a multi-center cohortUltrasound Obstet Gynecol 2016 May(5);47:616-22
85
Chapter 6: Pregnancy complications in singleton pregnancies with isolated fetal heart defectsAccepted ACTA Obstet Gynecol Scan July 2016
101
Chapter 7: Supraventricular tachycardia in a neonate with the prenatal diagnosis of a single left superior vena cavaUltrasound Obstet Gynecol. 2011 Dec;38(6):731-2
115
Chapter 8: General discussion and perspectives 121
Chapter 9: Summary & Samenvatting 131
Chapter 10: AppendicesContributing authors and affiliationsPublicationsDankwoordOver de auteur
141
Christine van Velzen.indb 7 20/09/2016 08:27

Christine van Velzen.indb 8 20/09/2016 08:27

CHAPTER 1Introduction
Christine van Velzen.indb 9 20/09/2016 08:27

10
Chapter 1
Chapter 1
INTRODUCTION
Ultrasound technology is capable to evaluate many anatomical structures of the fetus in great detail. Targeted ultrasound examination provides the possibility to diagnose a variety of structural malformations. Nowadays, screening for congenital anomalies is off ered as standard obstetric care by ultrasound examination around 20 weeks’ gestation in most Western countries. Screening is the systematic application of a test, to identify individuals at suffi cient risk for a specifi c disorder in order to benefi t from further investigation or preventive action, among persons who have not sought medical attention on account of symptoms of that disorder. 1 A prenatal diagnosis of a congenital heart defect (CHD), may lead to changes in obstetric management and allows for optimal neonatal care which may improve the neonatal outcome. The accuracy and success of detection of anomalies, depends strongly on the skills of the sonographer. 2CHD can be especially diffi cult to detect, and are still amongst the most commonly overlooked lesions in prenatal screening. 3;4
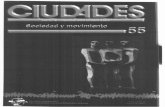
Figure 1 The four standard planes of the cardiac examination in prenatal screening are indicated.
Christine van Velzen.indb 10 20/09/2016 08:27

11
Introduction
Chap
ter 1
The standard anomaly scan (SAS) was introduced in 2007 in the Netherlands. The program was introduced uniformly for all pregnant women. The national organisation makes the Dutch screening program unique, and comprises a scanning protocol and uniform training requisites of the sonographers. The quality of the screening program is continuously monitored biannually by assessment of the images of all ultrasonographers. Furthermore a minimum volume of scans per ultrasonographer per year is required. This is monitored by the 8 regional centers for prenatal screening.
The cardiac examination in a SAS comprises of 4 standard planes (Figure 1). After confirmation of the stomach and heart being situated on the left side of the fetus and the normal left sided arrangement of the aorta in the abdomen, the first plane is a transverse plane through the fetal thorax at the level of the ventricles and atria; the four-chamber view (Figure 2a). In this plane malformations of the ventricles, atria, atrioventricular valves and septa are detectable. Although the four-chamber view is useful for identifying several abnormalities of the fetal heart, defects that involve the outflow tracts may not be demonstrated by an abnormal four-chamber view.
The outflow tracts are assessed in several planes. Just above the level of the four-chamber view the aorta exiting the left ventricle can be visualised by tilting and turning the transducer (Figure 2b). A bit more cranial, but again in a transverse plane, the pulmonary trunk can be visualised, arising from the right ventricle (Figure 2c). And then more cranial, the three-vessel view can been seen (Figure 2d). In this plane the spatial relationship between pulmonary trunk, ascending aorta and vena cava superior can be assessed.
The main two differences between a cardiac examination in a screening setting and a specialised echocardiographic examination are:
• The different expertise and training of the professionals performing the ultrasound (diagnostic fetal echocardiography is performed by a specialised cardiac team, including a pediatric (fetal) cardiologist. These professionals diagnose heart defects frequently and are capable to counsel the parents on the implication of the diagnosis and the treatment options)
• The heart is studied in far more detail. The examination is extended with, for example, evaluation of the valves, cardiac biometry, identification of the pulmonary and systemic veins, Doppler interrogation across the valves, assessment of the aortic and ductal arches, including neck vessels etc.
Christine van Velzen.indb 11 20/09/2016 08:27

12
Chapter 1
Chapter 1
Figure 2a The four chamber view. This plane is indicated in green in Figure 1.*
Figure 2b The aorta arising from the left ventricle. This plane is indicated in red in Figure 1. *
Figure 2c The pulmonary trunk arising from the right ventricle. This plane is indicated in blue in Figure 1. *
Figure 2d The three-vessel view, with from top to bottom the superior vena cava, the cross-section of the ascending aorta and the full length of the pulmonary trunk. This plane is indicated in yellow in Figure 1. *
* Pictures from: Echoscopie in de verloskunde en gynaecologie, M.C. Haak. 2013
Christine van Velzen.indb 12 20/09/2016 08:27

13
Introduction
Chap
ter 1
AIM OF THIS THESIS
The goal of this thesis was to gain insight in the performance of second trimester standard anomaly screening in detecting CHD. Although screening is performed in many countries for several years, reports on screening performance are only sparsely published. A comparison before and after introduction of a program was not possible because SAS was introduced gradually over several decades in most regions. The outcomes can be used to inform future parents about the performance of the SAS, and may provide options to improve the screening performance.
OUTLINE OF THIS THESIS
Chapter 2 is a systematic review of the literature and a meta-analysis on the prenatal detection rates of severe CHD by second trimester screening in unselected populations in Western countries. Severe CHD were defined as being potentially life threatening defects that require surgery or catheterization within the first year of life. Outcomes were evaluated and differentiated per type of heart defect, as well as in cases without additional extra-cardiac anomalies (isolated CHD). Chapter 3 studies the effects of the introduction of the Dutch screening program in 2007 on the prenatal detection, pregnancy outcome and mortality of fetuses and neonates with CHD. Within this cohort we focused on transposition of the great arteries in Chapter 4. Detection rates and the effect of a prenatal diagnosis on mortality and morbidity were studied in infants with a transposition. If a CHD is suspected, the woman is referred to one of the tertiary centres for a fetal echocardiography. In Chapter 5 we studied the diagnostic accuracy of the third level echocardiography. We studied diagnostic errors in detail. The complications in the pregnancies affected by a fetal CHD, in terms of preterm birth and fetal demise, were evaluated in Chapter 6. A rare postnatal complication in an infant with a prenatally detected left superior vena cava, which is usually not associated with complications, is described in Chapter 7. Finally, in the general discussion (Chapter 8) the current status of the SAS in relation to detection of CHD is described and future implications and recommendations are discussed. A summary of the thesis is given in Chapter 9.
Christine van Velzen.indb 13 20/09/2016 08:27

14
Chapter 1
Chapter 1
REFERENCE LIST(1) Antenatal and neonatal screening. In: Wald N, Leck, I, editors. Oxford University press, 2000: xii.
(2) Tegnander E, Eik-Nes SH. The examiner’s ultrasound experience has a significant impact on the detection rate of congenital heart defects at the second-trimester fetal examination. Ultrasound Obstet Gynecol 2006 Jul;28(1):8-14.
(3) Allan L. Screening the fetal heart. Ultrasound Obstet Gynecol 2006 Jul;28(1):5-7.
(4) Garne E, Stoll C, Clementi M. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: experience from 20 European registries. Ultrasound Obstet Gynecol 2001 May;17(5):386-91.
Christine van Velzen.indb 14 20/09/2016 08:27

Christine van Velzen.indb 15 20/09/2016 08:27

Christine van Velzen.indb 16 20/09/2016 08:27

CHAPTER 2Performance of Second Trimester Screening
for Prenatal Detection of Congenital
Heart Defects in Unselected Populations:
Systematic Review and Meta-analysis
C.L. van Velzen, F. Türkeri, J.C.F. Ket, P.M. van de Ven, N.A. Blom, M.C. Haak
Submitted
Christine van Velzen.indb 17 20/09/2016 08:27

18
Chapter 2
Chapter 2
ABSTRACT
This review aims to determine the performance of the second trimester anomaly scan (SAS) to detect congenital heart defects (CHD), differentiated per specific diagnosis. A meta-analysis of studies assessing the detection rate (DR) of population-based prenatal screening for CHD was performed. Cohort studies with unselected or low-risk populations that described prenatal DR per specific diagnosis were eligible for inclusion. A separate analysis was performed for isolated CHD. DRs higher than 90% are found for univentricular defects and heterotaxy cases. Defects like coarctation of the aorta and transposition of the great arteries show lower DRs. Few studies report on isolated CHD.We found that the prenatal DR of a CHD shows a strong correlation with the severity of the heart defect. It remains a challenge to improve the DR of conotruncal anomalies. In order to achieve a higher prenatal detection rate of CHD, a thoroughly organised screening program is essential.
Christine van Velzen.indb 18 20/09/2016 08:27

19
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
INTRODUCTION
Congenital heart disease (CHD) is the most common congenital anomaly. Severe types of CHD affect about 2-3 per 1 000 newborns and are the leading cause of non-infectious neonatal mortality. 1-5 Severe CHD is defined as potentially life threatening heart defects that require surgery or a therapeutic intervention within the first year of life. Increasing evidence shows that a prenatal diagnosis can prevent mortality in several types of severe CHD, due to prompt and appropriate treatment. Furthermore it has been shown that a prenatal diagnosis of CHD results in a more favourable long-term outcome. 6-11 A diagnosis of CHD in the fetus allows for further monitoring, the possibility to test for associated structural or genetic anomalies and counselling of the parents about the management options, including termination of the pregnancy in severe cases. 12
Only 10% of fetal CHD cases occur in pregnancies with known risk factors, such as increased nuchal translucency, family history or fetal extra-cardiac malformations. 13;14 Therefore, population based screening is the only way to detect CHD before birth. The current screening strategy in most western countries is a standard anomaly scan around 20 weeks’ gestational age. 13 National or regional screening protocols mostly require examination of the ‘four chamber view’, accompanied by assessment of the outflow tracts. Depending on the country, region, screening centre or even the individual ultrasonographer, the three vessel view is frequently incorporated in the second trimester anomaly screening (SAS), but often as a non-obligatory item.15 The prenatal detection rate (DR) of CHD has improved in the last decades, but in unselected or low-risk populations the reported DR generally varies between 20% and 50%.3;16-20 The large variation in DR requires a differentiated analysis of the current literature, in order to formulate recommendations to improve prenatal screening. The aim of this study is to determine the current performance of SAS in detecting fetal CHD in unselected populations. As CHD are highly heterogeneous, we evaluate the prenatal DR per type of heart defect, where possible. Cases without additional extra-cardiac anomalies (isolated CHD), were evaluated separately.
MATERIALS AND METHODS
Eligibility criteriaStudies that assessed the prenatal DR for CHD of the SAS in a cohort with an unselected or low-risk population were eligible for inclusion. Isolated CHD was defined as CHD without extracardiac anomalies, chromosomal abnormalities or genetic syndromes. Only a few studies report on isolated CHD and differentiate the data according to the type of CHD. We therefore decided to include studies that report non-isolated cases as well. To have a relevant up-to-date overview on the performance of the anomaly
Christine van Velzen.indb 19 20/09/2016 08:27

20
Chapter 2
Chapter 2
scan, we only included studies in which all scans were performed from 1995 onwards, as ultrasound equipment and guidelines have evolved significantly since the nineties. Studies were included in the meta-analysis if they included cases of pregnancy termination, fetal demise and pre-operative deaths. We excluded studies that reported on less than 200 CHD cases or that presented the results of a single center, as this usually represents a mixed or high-risk population. Studies that did not make any differentiation in CHD diagnoses or did not include all consecutive cases were also excluded. Finally we excluded studies that were not published as a full article.
Sources and searchA review protocol was developed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)-statement (www.prisma-statement.org). PubMed and Embase.com were searched from inception (by CvV and JCFK). PubMed up to the 10th of March 2016 and Embase.com up to the 17th of August 2015. The following terms were used (including synonyms and closely related words) as index terms or free-text words: ‘prenatal diagnosis’ or ‘pregnancy’ and ‘cardiovascular diseases’ or ‘ cardiac defects’ or ‘venes’ or ‘arteries’ and ‘congenital’ and ‘specificity’ or ‘sensitivity’ or ‘cohort study’. The full search strategies can be found in the Supplementary Information. Duplicate articles were removed. All languages were accepted.
Study selectionThe titles were screened by two reviewers (C.V. and F.T.). If the title was not specific enough for decision on inclusion or exclusion, we reviewed the abstract for further selection (flow chart). Two reviewers (C.V. and M.H.) assessed all potentially eligible studies by reading the full-text article. The in- and exclusion criteria as described above were scored (see flow chart). Subsequently, the quality of the articles was assessed. Non-English articles were translated by an native speaker. In some cases the authors were emailed to answer relevant questions. We analyzed the references of the eligible articles for further inclusions.
Data collection and outcomes of interestThe outcomes of interest were the prenatal DR of CHD in total, per type of CHD and per type of CHD in isolated cases. From each study we extracted the reported prevalence of CHD, data concerning the population characteristics, the used definition of severe CHD, the used definition of isolated CHD, the presence of inclusion of data from prenatal, postnatal and pathology databases, the description of the used ultrasound protocol, the description of the type of professionals that perform the SAS and the used time frame for follow-up.
Christine van Velzen.indb 20 20/09/2016 08:27

21
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Studies after removal of duplicates (n=3905)
Studies retrieved for more detailed evaluation (n=70)
Studies excluded on basis of title or abstract (n=3791) No CHD Maternal CHD High risk population Case reports No screening Neonatal screening
Studies included in review (n=14)
Studies excluded (n=56) Expert opinion, review or guideline n=18 Focus on different outcome n=8 Cohort before 1995 n=13 No discrimination for type of CHD n=2 Only abstract published n=8 Not all cases with prenatal diagnosis complete (n=3) Significant part of the cohort without any screening program (n=2) Total number of cases <200 (n=2)
Studies included in meta-analysis 1. reporting on isolated and non-isolated CHD combined (n=7) 2. reporting on isolated CHD separately (n=3)
Studies excluded from meta-analysis (n=4) Not all cases with postnatal diagnosis complete (n=1) Exact diagnosis of CHD not provided (n=3)
Studies identified as potentially relevant through database search (n=6324)
Flow chart. Study inclusion
Christine van Velzen.indb 21 20/09/2016 08:27

22
Chapter 2
Chapter 2
In case of incomplete or unclear data, the authors of the corresponding article were sent an inquiry by email as an attempt to complete or to clarify the data (n= 2). One study covered a timeframe larger than the study period and we excluded the subset of data concerning the period before 1995.16 One study 3 compared DR before and after the introduction of a second trimester screening program. Only the data from the period with the current second trimester screening program were used.
Risk of bias/assessment of methodologyThe quality of the studies was evaluated at study and outcome level by assessing factors we considered important for study validity based on the STARD initiative. 21
Synthesis of results and summary measures The detection rates (percentage of cases with CHD detected by second trimester anomaly screening) found in different studies were pooled separately for each type of CHD using the metaprop command 22 in Stata version 12 (StataCorp 2011). Pooling of the detection rates was done using inverse-variance weights obtained from a random-effects model using the total number of cases and number of cases detected in each study as input. For each type of CHD, forest plots were constructed that give the study-specific sensitivities with 95% exact confidence intervals together with an overall pooled estimate for sensitivity with 95% Wald confidence. For CHDs with a sensitivity reported in at least three different studies, the I2 statistic was calculated. The I2 statistic is interpreted as the percentage of total variation due to heterogeneity between studies.
RESULTS
Study selection and characteristicsThe initial search yielded 6 324 articles (PubMed 3 592, Embase 2 732). After removal of the duplicates, 3 905 studies remained. Screening the titles and abstracts resulted in the selection of 70 articles for more detailed evaluation of the full text of which 14 articles 3;5;16-20;23-29 were included in this review (Flow chart). The studies were published from 2001 to 2015. Study characteristics are shown in Table 1. All studies were designed as cohort studies and reported on unselected geographical cohorts. Only 10 articles reported sufficient details for inclusion in the meta-analyses. Seven reported on the prenatal DR of specific types of CHD, but these studies did not differentiate between isolated heart defects (i-CHD) and non-isolated defects (ni-CHD ). 18-20;23;24;26;27 Three studies reported on the prenatal DR of specific types of CHD in isolated cases. 3;16;17 The quality assessment of the studies that were included in the meta-analysis is shown in Table 2. The populations of the selected studies did not overlap.
Christine van Velzen.indb 22 20/09/2016 08:27

23
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Tabl
e 1
Stu
dy c
hara
cter
istic
s st
udie
s in
clud
ed in
revi
ew
St
udy
coun
try
Recr
uitm
ent
peri
od *
Tota
l nu
mbe
r of
cas
es
Follo
w-u
p pe
riod
Des
crib
ed
asso
ciat
ed
anom
alie
s
Des
crib
ed
mor
talit
ySc
reen
ing
of
feta
l hea
rt †
Crit
eria
in
clud
ed
CHD
Prev
alen
ce
of C
HD
in
popu
lati
on
Diff
eren
tiat
ion
CHD
Excl
uded
CH
D c
ases
Khos
hnoo
d et
al.
2005
Fran
ce19
95-2
000
812
One
wee
kCh
rom
osom
al
and
extr
acar
diac
an
omal
ies
IUFD
, firs
t w
eek
mor
talit
yN
ot g
iven
I5.
4 pe
r 1,0
00Pe
r dia
gnos
is
N=4
Is
olat
ed a
s w
ell
Case
s w
ith
chro
mos
omal
an
omal
ies
Chew
et a
l. 20
07Au
stra
lia19
99-2
002
451
At l
east
on
e ye
arCh
rom
osom
al
anom
alie
sN
ot g
iven
4 CV
+ o
utflo
w
trac
ts13
-26
wee
ks
I7.
8 pe
r 1,0
00Pe
r dia
gnos
is
N=7
Non
-isol
ated
Isol
ated
pat
ent a
rter
ial
duct
or f
oram
en o
vale
Khoo
et a
l. 20
08Au
stra
lia19
99-2
004
467
Five
yea
rsN
ot g
iven
IUFD
, neo
nata
l m
orta
lity
Not
giv
enII
5.2
per 1
,000
Per d
iagn
osis
N
=4N
on-is
olat
ed
Smal
l sep
tal d
efec
ts,
pate
nt a
rter
ial d
uct,
min
or v
alve
lesi
ons
McB
rien
et
al. 2
009
Uni
ted
King
dom
2002
-200
627
2O
ne y
ear
Tris
omie
sIU
FD, n
eona
tal
mor
talit
y4
CV +
out
flow
tr
acts
Se
cond
tr
imes
ter
III3.
0 pe
r 1,0
00D
efec
t vis
ible
in
4 CV
or o
utflo
w
trac
ts
Non
-isol
ated
Isol
ated
pat
ent a
rter
ial
duct
or f
oram
en o
vale
, an
omal
ous
orig
in o
f lef
t co
rona
ry a
rter
yD
uran
d et
al
. 200
9Fr
ance
2003
-200
723
3N
ot g
iven
Chro
mos
omal
, ge
netic
and
ex
trac
ardi
ac
anom
alie
s
IUFD
, pre
-and
po
stop
erat
ive
mor
talit
y
4 CV
+ o
utflo
w
trac
tsSe
cond
tr
imes
ter
IIIN
ot g
iven
Per d
iagn
osis
N
=19
Non
-isol
ated
Isol
ated
atr
ial o
r sm
all
vent
ricle
sep
tal d
efec
t, or
pat
ent a
rter
ial d
uct,
anom
alie
s of
cor
onar
y ar
terie
sG
alin
do e
t al
. 201
0Sp
ain
2004
-200
610
60O
ne y
ear
Extr
acar
diac
an
omal
ies
Not
giv
en4
CV+
outfl
ow
trac
ts18
-22
wee
ks
III4.
1 pe
r 1,0
00Pe
r dia
gnos
is
N=2
0N
on-is
olat
ed
Card
iom
yopa
thie
s or
tu
mou
rs
Bonn
efoy
et
al. 2
011
Fran
ce20
00-2
005
456
Thre
e ye
ars
Chro
mos
omal
an
d ex
trac
ardi
ac
anom
alie
s
IUFD
4 CV
+ o
utflo
w
trac
tsSe
cond
tr
imes
ter
IV11
.3 p
er
1,00
0Pe
r dia
gnos
is
N=7
Non
-isol
ated
min
or v
alve
ano
mal
ies,
Sept
al v
entr
icul
ar
defe
ct <
4 m
m, p
artia
l an
omal
ous
pulm
onar
y ve
nous
retu
rn, a
orto
-pu
lmon
ary
fene
stra
tion,
m
inor
aor
tic
coar
ctat
ion,
ste
nosi
s of
th
e pu
lmon
ary
arte
ries,
pa
tent
art
eria
l duc
t or
fora
men
ova
leM
arek
et a
l. 20
11Cz
ech
Repu
blic
2000
-200
694
6Th
ree
year
sEx
trac
ardi
ac
anom
alie
sIU
FD4
CV +
out
flow
tr
acts
18
-21
wee
ks
IVEs
timat
ed a
t 6.
7 pe
r 1,0
00Pe
r dia
gnos
is,
but n
ot fo
r tim
e fr
ame
2000
-20
06
Isol
ated
dex
troc
ardi
a,
non-
sten
otic
bic
uspi
d ao
rtic
or p
ulm
onar
y va
lve,
asy
mpt
omat
ic
vasc
ular
ano
mal
ies
Christine van Velzen.indb 23 20/09/2016 08:27

24
Chapter 2
Chapter 2
Tabl
e 1
Stu
dy c
hara
cter
istic
s st
udie
s in
clud
ed in
revi
ew (C
ontin
ued)
St
udy
coun
try
Recr
uitm
ent
peri
od *
Tota
l nu
mbe
r of
cas
es
Follo
w-u
p pe
riod
Des
crib
ed
asso
ciat
ed
anom
alie
s
Des
crib
ed
mor
talit
ySc
reen
ing
of
feta
l hea
rt †
Crit
eria
in
clud
ed
CHD
Prev
alen
ce
of C
HD
in
popu
lati
on
Diff
eren
tiat
ion
CHD
Excl
uded
CH
D c
ases
Pint
o et
al.
2012
USA
1997
-200
714
74N
ot g
iven
Addi
tiona
l co
ngen
ital
defe
cts
IUFD
4 CV
+ o
utflo
w
trac
ts 1
6-24
w
eeks
V2.
8 pe
r 1,0
00Pe
r dia
gnos
is
N=3
0 N
on-is
olat
ed
Isol
ated
sep
tal d
efec
ts
(exc
ept i
nlet
VSD
), m
ild
valv
e an
omal
ies
Khos
hnoo
d et
al.
2012
Fran
ce20
05-2
008
2348
At l
east
ei
ght y
ears
Chro
mos
omal
an
d ex
trac
ardi
ac
anom
alie
s
IUFD
, fir
st w
eek
mor
talit
y,
infa
nt
mor
talit
y
Not
repo
rted
IV9.
0 pe
r 1,0
00Cl
assi
ficat
ion
in
grou
ps, n
ot p
er
diag
nosi
s
Isol
ated
pat
ent a
rter
ial
duct
or f
oram
en o
vale
Trin
es e
t al.
2013
Cana
da20
07-2
011
374
One
yea
rEx
clud
edIU
FD, p
re- a
nd
post
oper
ativ
e m
orta
lity
4 CV
18
-24
wee
ksIII
Not
giv
enPe
r dia
gnos
is
N=2
0Is
olat
ed o
nly
Isol
ated
atr
ial o
r sm
all
vent
ricle
sep
tal d
efec
t, or
pat
ent a
rter
ial d
uct
Ross
ier e
t al.
2014
Switz
erla
nd20
03-2
008
535
One
wee
kCh
rom
osom
al
anom
alie
sIU
FD4
CV
seco
nd
trim
este
rIV
12.9
per
1,
000
Clas
sific
atio
n in
gr
oups
, not
per
di
agno
sis
Isol
ated
pat
ent a
rter
ial
duct
or f
oram
en o
vale
Van
Velz
en
et a
l. 20
15
The
Net
herla
nds
2007
-201
289
9O
ne y
ear
Chro
mos
omal
, ge
netic
and
ex
trac
ardi
ac
anom
alie
s
IUFD
, pre
- and
po
stop
erat
ive
mor
talit
y
4 CV
+ o
utflo
w
trac
ts16
-24
wee
ksIII
2.7
per 1
,000
Per d
iagn
osis
N
= 16
Isol
ated
as
wel
l
Isol
ated
pat
ent a
rter
ial
duct
or f
oram
en o
vale
Jørg
ense
n et
al.
2015
Den
mar
k20
08-2
010
408
One
yea
rN
ot g
iven
(c
hrom
osom
al
anom
alie
s ex
clud
ed)
IUFD
4 CV
Seco
nd
trim
este
r
VI4.
5 pe
r 1,0
00Pe
r dia
gnos
is
N=1
0 N
on-is
olat
ed
Mul
tiple
pre
gnan
cies
, ch
rom
osom
al
anom
alie
s, Is
olat
ed
pate
nt a
rter
ial d
uct o
r fo
ram
en o
vale
. CH
D
diag
nose
d af
ter 1
yea
r.
The
stud
ies
shad
ed in
gre
y w
ere
incl
uded
in th
e m
eta-
anal
ysis
. *
In th
e m
eta-
anal
ysis
cas
es w
ere
incl
uded
from
199
5 up
to n
ow.
Onl
y de
tect
ion
rate
s in
the
pres
ence
of s
cree
ning
pro
gram
s w
ere
incl
uded
.†
Min
imum
requ
ired
scre
enin
g pl
anes
in p
roto
col a
nd w
eeks
of g
esta
tiona
l age
incl
uded
as
dete
cted
in s
econ
d tr
imes
ter
IUFD
: int
ra-u
terin
e fe
tal d
emis
e4
CV: f
our c
ham
ber v
iew
Incl
uded
CH
DI:
ICD
-9 c
odes
745
, 746
and
747
, sev
erity
not
defi
ned
II: p
oten
tially
det
ecta
ble
CHD
in
pren
atal
sca
n, d
iagn
osis
mad
e up
to 5
yea
rs o
f age
III: s
ever
e CH
D d
efine
d as
bei
ng p
oten
tially
life
thre
aten
ing
and
requ
iring
sur
gery
or i
nter
vent
ion
with
in th
e fir
st y
ear o
f life
.IV
: all
type
s of
CH
DV:
maj
or C
HD
, not
furt
her s
peci
fied
VI: I
CD-1
0 co
des
DQ
20-D
Q25
Christine van Velzen.indb 24 20/09/2016 08:27

25
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Tabl
e 2
Qua
lity
asse
ssm
ent o
f the
art
icle
s fo
r met
a-an
alys
is
Kh
oshn
ood
2005
Trin
es
2013
Van
Velz
en
2015
Jorg
ense
nPi
nto
Gal
indo
Dur
and
Chew
Khoo
Bonn
efoy
Stud
y de
sign
pro
spec
tive
nopa
rt o
f the
ca
ses
retr
ospe
ctiv
e an
alys
is o
f pr
ospe
ctiv
ely
colle
cted
dat
a
retr
ospe
ctiv
e an
alys
is o
f pr
ospe
ctiv
ely
colle
cted
dat
a
nono
nore
tros
pect
ive
anal
ysis
of
pros
pect
ivel
y co
llect
ed d
ata
nono
Sett
ing
and
recr
uitm
ent p
erio
d de
scrib
edye
sye
sye
sye
sye
sye
sye
sye
sye
sye
s
Elig
ibili
ty c
riter
ia g
iven
yes
yes
yes
yes
yes
yes
yes
yes
yes
yes
Des
crip
tion
of p
opul
atio
n, lo
w
risk
or u
nsel
ecte
dun
sele
cted
unse
lect
edun
sele
cted
unse
lect
edun
sele
cted
unse
lect
edun
sele
cted
unse
lect
edun
sele
cted
unse
lect
ed
Ana
lysi
s pe
rfor
med
per
ty
pe o
f CH
D in
isol
ated
cas
es
sepa
rate
ly
yes
yes
yes
nono
nono
nono
no
Des
crip
tion
of e
xtra
card
iac
anom
alie
s gi
ven
yes
n.a.
yes
noye
sye
sye
slim
ited
limite
dlim
ited
Sear
ched
for a
ll pr
e- a
nd
post
nata
l cas
es, i
nclu
ding
pa
thol
ogy
data
base
s
yes
yes
yes
yes
yes
uncl
ear
yes
yes
yes
yes
Prof
essi
onal
who
per
form
s sc
reen
ing
desc
ribed
not
desc
ribed
not
desc
ribed
yes
not
desc
ribed
yes
yes
yes
yes
yes
yes
Scre
enin
g pr
otoc
ol d
escr
ibed
an
d ge
stat
iona
l age
not
desc
ribed
yes
yes
yes
yes
yes
yes
yes
not
desc
ribed
yes
Prev
alen
ce o
f CH
D in
po
pula
tion
give
nye
sno
yes
yes
noye
sno
yes
yes
yes
Preg
nanc
y ou
tcom
e de
scrib
edye
sye
sye
sye
sye
sye
sye
sno
yes
no
Perin
atal
mor
talit
y de
scrib
edye
sye
sye
sno
nono
yes
noye
sno
Extr
a re
mar
ksre
port
ed
on is
olat
ed
CHD
onl
y
extr
a da
ta fo
r m
eta-
anal
ysis
pr
ovid
ed b
y au
thor
s
excl
uded
ch
rom
osom
al
anom
alie
s
extr
a da
ta
for m
eta-
anal
ysis
pr
ovid
ed b
y au
thor
s
Christine van Velzen.indb 25 20/09/2016 08:27

26
Chapter 2
Chapter 2
Risk of biasContributors to the presence of bias are the variety of the included CHD and their severity, the thoroughness of the description of extracardiac anomalies, the differences in the completeness of inclusion of all CHD cases (not all studies included fetal demises or perinatal deaths), differences in prenatal ultrasound protocols and differences in the follow-up period after birth, all shown in Table 1. Table 2 shows the quality assessment of the articles included in the meta-analysis. The provided data concerning the methods of the study and the outcomes differ between the included articles. By analysing the DR per type of CHD and by excluding non-isolated CHD we tried to acquire the most realistic DR of the SAS in detecting CHD.
Results of meta-analysisThe seven studies that were included in the meta-analysis on prenatal detection of CHD in general (n= 4 992 cases) showed a pooled estimate of prenatal DR of 45.1% [95% CI 33.5-57.0]. 3;18-20;23;24;26 Table 3 shows the results of the meta-analysis on the prenatal detection per type of CHD. (forest plots in Supplemental Information).
Table 3 Prenatal DR per diagnosis of i-CHD and ni-CHD combined.
CHD diagnosisStudies included in meta-analysis (N)
Total cases (N)
Prenatal detection (%)
95% CI
Significant VSD 3 308 36.1 30.7-41.7
AVSD 8 542 60.4 47.0-73.0
Ebstein’s anomaly 4 57 80.1 45.6-99.9
Coarctation of the aorta 6 609 22.3 18.0-27.0
Tetralogy of Fallot 8 503 42.0 30.9-53.6
DORV-Fallot type 4 111 71.5 59.5-82.3
Transposition great arteries 8 361 36.4 21.0-53.3
DORV-Taussig Bing 2 49 61.3 46.9-74.8
Truncus arteriosus 6 133 69.1 43.1-90.6
Pulmonary atresia with VSD 5 58 59.8 45.6-73.2
Congenitally corrected TGA 5 49 72.3 49.8-90.9
HLHS 8 549 87.3 78.3-94.2
Tricuspid valve atresia 3 37 90.8 77.9-99.1
Pulmonary atresia intact IVS 4 59 41.3 25.5-57.9
Complex heterotaxy 3 99 89.1 66.6-100
VSD: ventricular septal defect AVSD: atrioventricular septal defect DORV: double outlet right ventricle TGA: transposition great arteries IVS: interventricular septum
Christine van Velzen.indb 26 20/09/2016 08:27

27
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Only three studies reported on prenatal DR in isolated CHD (i-CHD). 3;16;17 Two studies presented the total number of isolated CHD in their cohort; in total 901 cases. 3;17 The pooled estimate of the prenatal DR for isolated CHD in general was 46.7% [95% CI 43.5-50.0]. Table 4 shows the results of the meta-analysis on the prenatal detection per diagnosis in isolated CHD. (forest plots in Supplemental Information).
Table 4 Prenatal DR per diagnosis in isolated CHD
CHD diagnosis Studies N Total cases NPrenatal detection %
95% CI
Coarctation of the aorta 3 151 30.6 19.1-43.5
Tetralogy of Fallot 2 67 49.2 37.1-61.3
Transposition great arteries 3 116 48.5 24.2-73.1
Pulmonary atresia with VSD 2 81 37.8 27.2-49.1
HRHS 2 30 63.7 45.1-80.1
HLHS 3 131 90.7 82.1-96.9
Complex heterotaxy 2 44 86.5 74.2-95.6
HRHS: hypoplastic right heart syndromeHLHS: hypoplastic left heart syndrome
Studies not included in the meta-analysisFour studies relevant for this review could not be included in the meta-analysis. Marek et al. described a large cohort of prenatally diagnosed fetuses with CHD in a setting of a nationwide screening program. 5 The number of postnatally diagnosed CHD cases was, however, not reported, which led to exclusion for the meta-analysis. The estimated detection rates of 96% for HLHS, 26% for TGA, 37% for Tetralogy of Fallot and 20% for coarctation of the aorta are comparable to the found DR in the meta-analysis. Three other studies were excluded due to the absence of detection rates per specific diagnosis.25;28;29 Overall DRs were 26, 27 and 52% for severe CHD. Khoshnood et al. published a large cohort, but the CHD cases were categorized in an unconventional classification system, which makes their results incomparable to the other studies.
DISCUSSION
Screening for CHD by SAS in unselected populations yields a prenatal detection rate of approximately 45%. This meta-analysis shows that the prenatal DR differs per type of heart defect. DRs higher than 90% are found for univentricular defects and heterotaxy cases. Defects like coarctation of the aorta, TGA and VSDs show lower DRs, with the lowest rate of 22% for coarctation.
Christine van Velzen.indb 27 20/09/2016 08:27

28
Chapter 2
Chapter 2
Depending on type of CHD, the DR shows a large variation. Therefore it is not very informative to report on prenatal detection of CHD in general, which is common in current literature. This meta-analysis shows a strong relation between the prenatal DR and the severity of the heart defect. The prenatal detection of CHD at the severe end of the spectrum (univentricular CHD) is above 90%, which is a relevant figure to incorporate in counselling about prenatal screening. For conotruncal defects (Tetralogy of Fallot, TGA and coarctation) we believe that there is room for improvement. It has been shown that the addition of the three vessel view, together with training of ultrasonographers, increases the DRs of the SAS. 30 On the other hand, cardiac defects like coarctation may present with completely normal cardiac images at 20 weeks’ gestational age.31;32 As a consequence the prenatal DR will never be very high for these defects. Total abnormal pulmonary venous return is another example of a defect that is very difficult to diagnose prenatally, partly because the pulmonary veins are not routinely assessed in the screening setting.33 For several heart defects we found wide confidence intervals, which can be explained by the relatively small total number of cases (Ebstein’s anomaly, DORV-Fallot, DORV-Taussig Bing and congenitally corrected TGA). For some defects, however, the detection rates vary substantially amongst the included studies despite an adequate number of cases (TGA, truncus arteriosus and pulmonary atresia with intact VS). For example, the prenatal DR of TGA ranged from 11 to 69%. 18;24;26;27 The given explanations for the low DR are: a relatively low uptake of the SAS, socio-economic influences 18 and a lack of standardised referral criteria with a high threshold for referral. 24 The two studies with the relatively high DR for TGA are both French.26;27 France is known for high prenatal detection rates in general, a high uptake of screening and the use of the three vessel view in the SAS. 34;35 It is remarkable that the majority of the included studies in this meta-analysis did not incorporate the three vessel view as an obligatory item in the SAS protocol, since the inclusion of this ultrasonographic plane is proven beneficial and recommended in international guidelines.30 Only very few studies report on isolated CHD. Data on i-CHD are important, since the outcome for the infant depends solely on the cardiac defect. In this meta-analysis the DR of i-CHD is comparable to the DR of i-CDH and ni-CHD combined. This is a remarkable finding, since isolated congenital defects in general, are known to be detected less frequently.28;36 Unfortunately almost all studies included either exclusively i-CHD or ni-CHD, which makes a comparison between these two groups difficult. Nevertheless, one study did report on DR in both i-CHD and ni-CHD 3 and showed that, as expected, the DR of i-CHD was significantly lower compared to ni-CHD. If we compare the screening performance for CHD of SAS to other methods of screening (nuchal translucency (NT) measurement and postnatal pulse-oximetry 37;38),
Christine van Velzen.indb 28 20/09/2016 08:27

29
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
the sensitivity in relation to the number of false positives is best for SAS. In the era of NIPT, it is advocated by many to sustain NT screening programs to identify fetuses that are at increased risk for CHD. 39 The costs of such a program, if NIPT becomes a first-tier test, do not outweigh the fact that only 6-7% of the cases of CHD are detected through NT screening. 40;41 Moreover, in NT screening for CHD a relation with the severity of the CHD is absent. The disadvantage of postnatal pulse-oximetry screening is the timing. A prenatal diagnosis of a CHD allows for further prenatal (genetic) testing and for counselling the parents about the treatment strategies. In severe cases a prenatal diagnosis provides the parents a choice to discontinue the pregnancy. On the other hand, since prenatal detection of CHD will never be 100%, the postnatal pulse-oximetry screening could be complementary to optimize diagnosing infants with CHD. A limitation of our study is that not all the studies included in the meta-analyses used the same inclusion criteria. The inclusion criterium ‘severe CHD’ differed from “potentially detectable CHD in prenatal scan, diagnosis made up to 5 years of age” to “severe CHD defined as being potentially life threatening and requiring surgery or intervention within first year of life”(Table 1). Another potential source of bias is that the follow-up period varied from one week to eight years, influencing the completeness of the included cases. Both differences are also reflected by the varying prevalence of CHD amongst the studies.All included studies were population based studies describing prenatal DR in unselected populations and rates were given per type of CHD. Moreover, in all included studies an effort was made to include all possible CHD cases in the defined region. The study selection was carried out without language restrictions, and attention was paid to quality assessment by using scoring lists and evaluation by multiple investigators, limiting selection and publication bias.
In conclusion, the DR of CHD of the SAS in unselected populations is around 45%. DRs show a strong correlation with the severity of the heart defect. It remains an important challenge to improve the DR of conotruncal anomalies. We expect better results with a global incorporation of the 3VV in the SAS. Essential conditions to optimize screening results are the accessibility to and thorough organization of the prenatal screening, as the highest DRs are found in such programs. Investing in training ultrasonographers, establishing quality monitoring systems and lowering thresholds for referral to fetal cardiology units should help to achieve a higher prenatal detection rate of CHD.
Christine van Velzen.indb 29 20/09/2016 08:27

30
Chapter 2
Chapter 2
REFERENCE LIST(1) Hoffman JI, Kaplan S, Liberthson RR. Prevalence of congenital heart disease. Am Heart J 2004; 147(3):
425-439.
(2) van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011; 58(21): 2241-2247.
(3) van Velzen C, Clur S, Rijlaarsdam M, Bax C, Pajkrt E, Heymans M et al.Prenatal detection of congenital heart disease-results of a national screening programme. BJOG 2016; 123(3): 400-407.
(4) Dolk H, Loane M, Garne E. Congenital heart defects in Europe: prevalence and perinatal mortality, 2000 to 2005. Circulation 2011; 123(8): 841-849.
(5) Marek J, Tomek V, Skovranek J, Povysilova V, Samanek M. Prenatal ultrasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart 2011; 97(2): 124-130.
(6) Jaeggi ET, Sholler GF, Jones OD, Cooper SG. Comparative analysis of pattern, management and outcome of pre- versus postnatally diagnosed major congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2001; 17(5): 380-385.
(7) Kumar RK, Newburger JW, Gauvreau K, Kamenir SA, Hornberger LK. Comparison of outcome when hypoplastic left heart syndrome and transposition of the great arteries are diagnosed prenatally versus when diagnosis of these two conditions is made only postnatally. Am J Cardiol 1999; 83(12): 1649-1653.
(8) Allan LD, Apfel HD, Printz BF. Outcome after prenatal diagnosis of the hypoplastic left heart syndrome. Heart 1998; 79(4): 371-373.
(9) Bonnet D, Coltri A, Butera G, Fermont L, Le Bidois J, Kachaner J et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999; 99(7):916-918.
(10) Fuchs IB, Muller H, Abdul-Khaliq H, Harder T, Dudenhausen JW, Henrich W. Immediate and long-term outcomes in children with prenatal diagnosis of selected isolated congenital heart defects. Ultrasound Obstet Gynecol 2007; 29(1): 38-43.
(11) van Velzen CL, Haak MC, Reijnders G, Rijlaarsdam ME, Bax CJ, Pajkrt E et al. Prenatal detection of transposition of the great arteries reduces mortality and morbidity. Ultrasound Obstet Gynecol 2015; 45(3): 320-325.
(12) Yates RS. The influence of prenatal diagnosis on postnatal outcome in patients with structural congenital heart disease. Prenat Diagn 2004; 24(13): 1143-1149.
(13) Sharland G. Fetal cardiac screening and variation in prenatal detection rates of congenital heart disease: why bother with screening at all? Future Cardiol 2012; 8(2): 189-202.
(14) Allan L. Antenatal diagnosis of heart disease. Heart 2000; 83(3): 367.
(15) Cardiac screening examination of the fetus: guidelines for performing the ‘basic’ and ‘extended basic’ cardiac scan. Ultrasound Obstet Gynecol 2006; 27(1): 107-113.
(16) Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D et al. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983-2000: a population-based evaluation. Pediatrics 2005; 115(1): 95-101.
(17) Trines J, Fruitman D, Zuo KJ, Smallhorn JF, Hornberger LK, Mackie AS. Effectiveness of prenatal screening for congenital heart disease: assessment in a jurisdiction with universal access to health care. Can J Cardiol 2013; 29(7): 879-885.
(18) Pinto NM, Keenan HT, Minich LL, Puchalski MD, Heywood M, Botto LD. Barriers to prenatal detection of congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2012; 40(4): 418-425.
(19) Galindo A, Herraiz I, Escribano D, Lora D, Melchor JC, de la Cruz J. Prenatal detection of congenital heart defects: a survey on clinical practice in Spain. Fetal Diagn Ther 2011; 29(4): 287-295.
(20) Jorgensen DE, Vejlstrup N, Jorgensen C, Maroun LL, Steensberg J, Hessellund A, et al. Prenatal detection of congenital heart disease in a low risk population undergoing first and second trimester screening. Prenat Diagn 2015; 35(4): 325-330.
(21) Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig LM, et al.The STARD statement for reporting studies of diagnostic accuracy: explanation and elaboration. Clin Chem 2003; 49(1): 7-18.
Christine van Velzen.indb 30 20/09/2016 08:27

31
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
(22) Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health 2014; 72(1):39.
(23) Chew C, Halliday JL, Riley MM, Penny DJ. Population-based study of antenatal detection of congenital heart disease by ultrasound examination. Ultrasound Obstet Gynecol 2007; 29(6): 619-624.
(24) Khoo NS, Van Essen P, Richardson M, Robertson T. Effectiveness of prenatal diagnosis of congenital heart defects in South Australia: a population analysis 1999-2003. Aust N Z J Obstet Gynaecol 2008; 48(6): 559-563.
(25) McBrien A, Sands A, Craig B, Dornan J, Casey F. Major congenital heart disease: antenatal detection, patient characteristics and outcomes. J Matern Fetal Neonatal Med 2009; 22(2):101-105.
(26) Durand I, David N, Blaysat G, Marguet C. Diagnosis of congenital heart disease in a nonselected population in Upper Normandy: retrospective study between 2003 and 2007. Arch Pediatr 2009; 16(5): 409-416.
(27) Bonnefoy R, Poinsot J, Vaillant MC, Chantepie A. Evolution of prenatal diagnosis of congenital heart diseases in Indre-et-Loire (France) over a period of 15years. Arch Pediatr 2011; 18(5): 512-517.
(28) Khoshnood B, Lelong N, Houyel L, Thieulin AC, Jouannic JM, Magnier S et al. Prevalence, timing of diagnosis and mortality of newborns with congenital heart defects: a population-based study. Heart 2012; 98(22): 1667-1673.
(29) Rossier M-C, Mivelaz Y, Addor M-C, Sekarski N, Meijboom EJ, Vial Y. Evaluation of prenatal diagnosis of congenital heart disease in a regional controlled case study. Swiss Med Wkly 2014; 144:w14068.
(30) International Society of Ultrasound in Obstetrics and Gynecology, Carvalho JS, Allan LD, Chaoui R, Copel JA, DeVore GR, Hecher K et al. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol 2013; 41(3): 348-359.
(31) Durand I, Deverriere G, Thill C, Lety AS, Parrod C, David N, et al.
Prenatal Detection of Coarctation of the Aorta in a Non-selected Population: A Prospective Analysis of 10 Years of Experience. Pediatr Cardiol 2015; 36(6): 1248-1254.
(32) Liberman RF, Getz KD, Lin AE, Higgins CA, Sekhavat S, Markenson GR, Anderka M. Delayed diagnosis of critical congenital heart defects: trends and associated factors. Pediatrics 2014; 134(2): e373-e381.
(33) Seale AN, Carvalho JS, Gardiner HM, Mellander M, Roughton M, Simpson J, et al.
Total anomalous pulmonary venous connection: impact of prenatal diagnosis. Ultrasound Obstet Gynecol 2012; 40(3): 310-318.
(34) Garne E. Prenatal diagnosis of six major cardiac malformations in Europe--a population based study. Acta Obstet Gynecol Scand 2001; 80(3):224-228.
(35) Grandjean H, Larroque D, Levi S. The performance of routine ultrasonographic screening of pregnancies in the Eurofetus Study. Am J Obstet Gynecol 1999; 181(2): 446-454.
(36) Garne E, Stoll C, Clementi M. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: experience from 20 European registries. Ultrasound Obstet Gynecol 2001; 17(5): 386-391.
(37) Ewer AK, Middleton LJ, Furmston AT, Bhoyar A, Daniels JP, Thangaratinam S, et al.
Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx): a test accuracy study. Lancet 2011; 378(9793): 785-794.
(38) Thangaratinam S, Daniels J, Ewer AK, Zamora J, Khan KS. Accuracy of pulse oximetry in screening for congenital heart disease in asymptomatic newborns: a systematic review. Arch Dis Child Fetal Neonatal Ed 2007; 92(3): F176-F180.
(39) Wilson RD, Poon LC, Ghidini A. Current controversies in prenatal diagnosis 3: is there still a value in a nuchal translucency screening ultrasound in conjunction with maternal plasma non-invasive cell-free DNA testing? Prenat Diagn 2016; 36(1): 20-24.
(40) Hyett J, Perdu M, Sharland G, Snijders R, Nicolaides KH. Using fetal nuchal translucency to screen for major congenital cardiac defects at 10-14 weeks of gestation: population based cohort study. BMJ 1999; 318(7176): 81-85.
(41) Ghi T, Huggon IC, Zosmer N, Nicolaides KH. Incidence of major structural cardiac defects associated with increased nuchal translucency but normal karyotype. Ultrasound Obstet Gynecol 2001; 18(6): 610-614.
Christine van Velzen.indb 31 20/09/2016 08:27

32
Chapter 2
Chapter 2
SUPPLEMENTARY INFORMATION
Search strategy for PubMed (8 September 2015)[Mesh] = Medical subject headings[Mesh:noexp] = MeSH without explosion[tiab] = words in title OR abstract[ot] = words as other terms, especially author keywords
Search Query Items found
#15 (“Prenatal Diagnosis”[Mesh:noexp] OR “Ultrasonography, Prenatal”[Mesh] OR ((“Echocardiography”[Mesh] OR “Ultrasonography”[Mesh:noexp] OR “ultrasonography”[Subheading] OR echocardiograph*[tiab] OR ultraso*[tiab] OR sonograph*[tiab] OR diagnos*[tiab] OR echograph*[tiab] OR echocardiograph*[ot] OR ultraso*[ot] OR sonograph*[ot] OR echograph*[ot] OR diagnos*[ot]) AND (prenatal*[tiab] OR fetal*[tiab] OR fetus*[tiab] OR foetal*[tiab] OR foetus*[tiab] OR intrauterine[tiab] OR antenatal*[tiab] OR prenatal*[ot] OR fetal*[ot] OR fetus*[ot] OR foetal*[ot] OR foetus*[ot] OR intrauterine[ot] OR antenatal*[ot]))) AND (cardiovasc*[tiab] OR cardiolog*[tiab] OR heart[tiab] OR septum[tiab] OR septal[tiab] OR valve[tiab] OR valves[tiab] OR valvular*[tiab] OR tricuspid*[tiab] OR mitral*[tiab] OR atrium[tiab] OR atrial[tiab] OR ventric*[tiab] OR aorta[tiab] OR aortic[tiab] OR (pulmona*[tiab] AND (trunc*[tiab] OR artery[tiab] OR arteries[tiab] OR arterial[tiab] OR atresia*[tiab])) OR “vena cava superior”[tiab] OR caval vein*[tiab] OR “vena cava inferior”[tiab] OR ((pulmona*[tiab] OR systemic*[tiab]) AND (vene[tiab] OR venes[tiab] OR venous[tiab] OR vein[tiab] OR veins[tiab])) OR ebstein*[tiab] OR inlet*[tiab] OR foramen oval*[tiab] OR polyvalv*[tiab] OR cardiovasc*[ot] OR cardiolog*[ot] OR heart[ot] OR septum[ot] OR septal[ot] OR valve[ot] OR valves[ot] OR valvular*[ot] OR tricuspid*[ot] OR mitral*[ot] OR atrium[ot] OR atrial[ot] OR ventric*[ot] OR aorta[ot] OR aortic[ot] OR (pulmona*[ot] AND (trunc*[ot] OR artery[ot] OR arteries[ot] OR arterial[ot] OR atresia*[ot])) OR “vena cava superior”[ot] OR caval vein*[ot] OR “vena cava inferior”[ot] OR ((pulmona*[ot] OR systemic*[ot]) AND (vene[ot] OR venes[ot] OR venous[ot] OR vein[ot] OR veins[ot])) OR ebstein*[ot] OR inlet*[ot] OR foramen oval*[ot] OR polyvalv*[ot]) AND (diseas*[tiab] OR defect*[tiab] OR abnormal*[tiab] OR anomal*[tiab] OR stenos*[tiab] OR dysplas*[tiab] OR insufficien*[tiab] OR coarctati*[tiab] OR hypoplas*[tiab] OR interrupt*[tiab] OR isolat*[tiab] OR obstruct*[tiab] OR double*[tiab] OR atresi*[tiab] OR absent*[tiab] OR window*[tiab] OR closure*[tiab] OR diseas*[ot] OR defect*[ot] OR abnormal*[ot] OR anomal*[ot] OR stenos*[ot] OR dysplas*[ot] OR insufficien*[ot] OR coarctati*[ot] OR hypoplas*[ot] OR interrupt*[ot] OR isolat*[ot] OR obstruct*[ot] OR double*[ot] OR atresi*[ot] OR absent*[ot] OR window*[ot] OR closure*[ot] OR vsd[tiab] OR asd[tiab] OR avsd[tiab] OR fallot*[tiab] OR Taussig Bing*[tiab] OR truncus arterios*[tiab] OR transposition*[tiab] OR hemitrunc*[tiab] OR criss cross*[tiab] OR Isomeris*[tiab] OR heterotax*[tiab] OR dextrocardia*[tiab] OR rhabdomyoma*[tiab] OR discrepan*[tiab] OR vsd[ot] OR asd[ot] OR avsd[ot] OR fallot*[ot] OR Taussig Bing*[ot] OR truncus arterios*[ot] OR transposition*[ot] OR hemitrunc*[ot] OR criss cross*[ot] OR Isomeris*[ot] OR heterotax*[ot] OR dextrocardia*[ot] OR rhabdomyoma*[ot] OR discrepan*[ot] OR “Cardiovascular Abnormalities”[Mesh]) AND ((cohort[ot] OR (case[ot] AND (control[ot] OR controll*[ot] OR comparison[ot] OR referent[ot])) OR risk[ot] OR causation[ot] OR causal[ot] OR “odds ratio”[ot] OR etiol*[ot] OR aetiol*[ot] OR “natural history”[ot] OR predict*[ot] OR prognos*[ot] OR outcome[ot] OR course[ot] OR cohort[tiab] OR (case[tiab] AND (control[tiab] OR controll*[tiab] OR comparison[tiab] OR referent[tiab])) OR risk[tiab] OR causation[tiab] OR causal[tiab] OR “odds ratio”[tiab] OR etiol*[tiab] OR aetiol*[tiab] OR “natural history”[tiab] OR predict*[tiab] OR prognos*[tiab] OR outcome[tiab] OR course[tiab] OR “Epidemiologic Studies”[Mesh]) OR (((“Sensitivity and Specificity”[Mesh] OR specific*[tiab] OR sensitiv*[tiab] OR detection*[tiab] OR specific*[ot] OR sensitiv*[ot] OR detection*[ot])))) AND (congenital*[tiab] OR congenital*[ot])
2,361
Christine van Velzen.indb 32 20/09/2016 08:27

33
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Search Query Items found
#14 ((((“Echocardiography”[Mesh] OR “Ultrasonography”[Mesh:noexp] OR “ultrasonography”[Subheading] OR echocardiograph*[tiab] OR ultraso*[tiab] OR sonograph*[tiab] OR echograph*[tiab] OR echotomograph*[tiab] OR echocardiograph*[ot] OR ultraso*[ot] OR sonograph*[ot] OR echograph*[ot] OR echotomograph*[ot]) AND (“Prenatal Diagnosis”[Mesh:noexp] OR “Ultrasonography, Prenatal”[Mesh] OR prenatal*[tiab] OR fetal*[tiab] OR fetus*[tiab] OR foetal*[tiab] OR foetus*[tiab] OR intrauterine[tiab] OR antenatal*[tiab] OR prenatal*[ot] OR fetal*[ot] OR fetus*[ot] OR foetal*[ot] OR foetus*[ot] OR intrauterine[ot] OR antenatal*[ot]) AND (((cardiovasc*[tiab] OR cardiolog*[tiab] OR heart[tiab] OR septum[tiab] OR septal[tiab] OR valve[tiab] OR valves[tiab] OR valvular*[tiab] OR tricuspid*[tiab] OR mitral*[tiab] OR atrium[tiab] OR atrial[tiab] OR ventric*[tiab] OR aorta[tiab] OR aortic[tiab] OR (pulmona*[tiab] AND (trunc*[tiab] OR artery[tiab] OR arteries[tiab] OR arterial[tiab] OR atresia*[tiab])) OR “vena cava superior”[tiab] OR caval vein*[tiab] OR “vena cava inferior”[tiab] OR ((pulmona*[tiab] OR systemic*[tiab]) AND (vene[tiab] OR venes[tiab] OR venous[tiab])) OR ebstein*[tiab] OR eustachia*[tiab] OR triatriat*[tiab] OR inlet*[tiab] OR foramen oval*[tiab] OR polyvalv*[tiab] OR cardiovasc*[ot] OR cardiolog*[ot] OR heart[ot] OR septum[ot] OR septal[ot] OR valve[ot] OR valves[ot] OR valvular*[ot] OR tricuspid*[ot] OR mitral*[ot] OR atrium[ot] OR atrial[ot] OR ventric*[ot] OR aorta[ot] OR aortic[ot] OR (pulmona*[ot] AND (trunc*[ot] OR artery[ot] OR arteries[ot] OR arterial[ot] OR atresia*[ot])) OR “vena cava superior”[ot] OR caval vein*[ot] OR “vena cava inferior”[ot] OR ((pulmona*[ot] OR systemic*[ot]) AND (vene[ot] OR venes[ot] OR venous[ot])) OR ebstein*[ot] OR eustachia*[ot] OR triatriat*[ot] OR inlet*[ot] OR foramen oval*[ot] OR polyvalv*[ot]) AND (diseas*[tiab] OR defect*[tiab] OR abnormal*[tiab] OR anomal*[tiab] OR stenos*[tiab] OR dysplas*[tiab] OR insufficien*[tiab] OR coarctati*[tiab] OR hypoplas*[tiab] OR interrupt*[tiab] OR isolat*[tiab] OR obstruct*[tiab] OR double*[tiab] OR atresi*[tiab] OR absent*[tiab] OR window*[tiab] OR straddl*[tiab] OR closure*[tiab] OR diseas*[ot] OR defect*[ot] OR abnormal*[ot] OR anomal*[ot] OR stenos*[ot] OR dysplas*[ot] OR insufficien*[ot] OR coarctati*[ot] OR hypoplas*[ot] OR interrupt*[ot] OR isolat*[ot] OR obstruct*[ot] OR double*[ot] OR atresi*[ot] OR absent*[ot] OR window*[ot] OR straddl*[ot] OR closure*[ot])) OR alcapa[tiab] OR vsd[tiab] OR asd[tiab] OR avsd[tiab] OR fallot*[tiab] OR Taussig Bing*[tiab] OR truncus arterios*[tiab] OR transposition*[tiab] OR hemitrunc*[tiab] OR criss cross*[tiab] OR Isomeris*[tiab] OR heterotax*[tiab] OR williams*[tiab] OR dextrocardia*[tiab] OR rhabdomyoma*[tiab] OR discrepan*[tiab] OR alcapa[ot] OR vsd[ot] OR asd[ot] OR avsd[ot] OR fallot*[ot] OR Taussig Bing*[ot] OR truncus arterios*[ot] OR transposition*[ot] OR hemitrunc*[ot] OR criss cross*[ot] OR Isomeris*[ot] OR heterotax*[ot] OR williams*[ot] OR dextrocardia*[ot] OR rhabdomyoma*[ot] OR discrepan*[ot] OR “Cardiovascular Abnormalities”[Mesh]) AND (cohort[ot] OR (case[ot] AND (control[ot] OR controll*[ot] OR comparison[ot] OR referent[ot])) OR risk[ot] OR causation[ot] OR causal[ot] OR “odds ratio”[ot] OR etiol*[ot] OR aetiol*[ot] OR “natural history”[ot] OR predict*[ot] OR prognos*[ot] OR outcome[ot] OR course[ot] OR cohort[tiab] OR (case[tiab] AND (control[tiab] OR controll*[tiab] OR comparison[tiab] OR referent[tiab])) OR risk[tiab] OR causation[tiab] OR causal[tiab] OR “odds ratio”[tiab] OR etiol*[tiab] OR aetiol*[tiab] OR “natural history”[tiab] OR predict*[tiab] OR prognos*[tiab] OR outcome[tiab] OR course[tiab] OR “Epidemiologic Studies”[Mesh]))) AND (diagno*[tiab] OR screen*[tiab] OR diagno*[ot] OR screen*[ot])) AND (congenital[tiab] OR congenital[ot])
1,187
Christine van Velzen.indb 33 20/09/2016 08:27

34
Chapter 2
Chapter 2
Search strategy for Embase.com (17 August 2015)/exp = EMtree keyword with explosion/de = EMtree keyword without explosion:ab,ti = words in title OR abstractNEXT/x = words in that order next to each other, x places apart
Search Query Items found
#11 #8 OR #10 2,732
#10 #1 AND #7 AND #9 2,528
#9 ‘congenital heart disease’/de OR ‘congenital heart malformation’/de 58,127
#8 #1 AND #3 AND #4 AND #5 AND #7 504
#7 #2 OR #6 8,330,015
#6 ‘sensitivity and specificity’/exp OR specific*:ab,ti OR sensitiv*:ab,ti OR detection*:ab,ti 4,161,583
#5 diseas*:ab,ti OR defect*:ab,ti OR abnormal*:ab,ti OR anomal*:ab,ti OR stenos*:ab,ti OR dysplas*:ab,ti OR insufficien*:ab,ti OR coarctati*:ab,ti OR hypoplas*:ab,ti OR interrupt*:ab,ti OR isolat*:ab,ti OR obstruct*:ab,ti OR double*:ab,ti OR atresi*:ab,ti OR absent*:ab,ti OR window*:ab,ti OR closure*:ab,ti OR vsd:ab,ti OR asd:ab,ti OR avsd:ab,ti OR fallot*:ab,ti OR (taussig NEXT/1 bing*):ab,ti OR truncus AND arterios*:ab,ti OR transposition*:ab,ti OR hemitrunc*:ab,ti OR (criss NEXT/1 cross*):ab,ti OR isomeris*:ab,ti OR heterotax*:ab,ti OR dextrocardia*:ab,ti OR rhabdomyoma*:ab,ti OR discrepan*:ab,ti OR ‘cardiovascular malformation’/de
130,927
#4 cardiovasc*:ab,ti OR cardiolog*:ab,ti OR heart:ab,ti OR septum:ab,ti OR septal:ab,ti OR valve:ab,ti OR valves:ab,ti OR valvular*:ab,ti OR tricuspid*:ab,ti OR mitral*:ab,ti OR atrium:ab,ti OR atrial:ab,ti OR ventric*:ab,ti OR aorta:ab,ti OR aortic:ab,ti OR (pulmona*:ab,ti AND (trunc*:ab,ti OR artery:ab,ti OR arteries:ab,ti OR arterial:ab,ti OR atresia*:ab,ti)) OR ‘vena cava superior’:ab,ti OR (caval NEXT/1 vein*):ab,ti OR ‘vena cava inferior’:ab,ti OR (pulmona*:ab,ti OR systemic*:ab,ti AND (vene:ab,ti OR venes:ab,ti OR venous:ab,ti OR vein:ab,ti OR veins:ab,ti)) OR ebstein*:ab,ti OR inlet*:ab,ti OR (foramen NEXT/1 oval*):ab,ti OR polyvalv*:ab,ti
1,894,719
#3 congenital*:ab,ti 241,691
#2 ‘cohort analysis’/exp OR ‘case control study’/exp OR ‘prospective study’/exp OR ‘retrospective study’/exp OR ‘longitudinal study’/exp OR cohort:ab,ti OR (case:ab,ti AND (control:ab,ti OR controll*:ab,ti OR comparison:ab,ti OR referent:ab,ti)) OR risk:ab,ti OR causation:ab,ti OR causal:ab,ti OR ‘odds ratio’:ab,ti OR etiol*:ab,ti OR aetiol*:ab,ti OR ‘natural history’:ab,ti OR predict*:ab,ti OR prognos*:ab,ti OR outcome:ab,ti OR course:ab,ti
5,237,341
#1 ‘prenatal diagnosis’/de OR ‘fetus echography’/de OR (‘echocardiography’/exp OR ‘echography’/de OR echocardiograph*:ab,ti OR ultraso*:ab,ti OR sonograph*:ab,ti OR diagnos*:ab,ti OR echograph*:ab,ti AND (prenatal*:ab,ti OR fetal*:ab,ti OR fetus*:ab,ti OR foetal*:ab,ti OR foetus*:ab,ti OR intrauterine:ab,ti OR antenatal*:ab,ti))
126,588
Christine van Velzen.indb 34 20/09/2016 08:27

35
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Forest plots meta-analysis prenatal detection per type of CHD (non-isolated: indicating no differentiation made between isolated or associated CHD, isolated: indicating CHD without any other congenital anomalies)
Overall (I^2 = 98.56%, p = 0.00)
Galindo
Chew
Pinto
Jørgensen
Durand
Study
Khoo
Van Velzen
45.08 (33.46, 56.98)
52.64 (49.58, 55.68)
52.77 (48.05, 57.46)
38.94 (36.44, 41.48)
21.32 (17.45, 25.62)
70.82 (64.52, 76.57)
ES (95% CI)
22.48 (18.77, 26.55)
59.73 (56.44, 62.96)
100.00
14.43
14.25
14.47
14.22
13.97
%
Weight
14.26
14.40
45.08 (33.46, 56.98)
52.64 (49.58, 55.68)
52.77 (48.05, 57.46)
38.94 (36.44, 41.48)
21.32 (17.45, 25.62)
70.82 (64.52, 76.57)
ES (95% CI)
22.48 (18.77, 26.55)
59.73 (56.44, 62.96)
100.00
14.43
14.25
14.47
14.22
13.97
%
Weight
14.26
14.40
0 20 40 60 80 100Percentage detected
Non-isolated CHD: Total CHD
Overall (I^2 = 0.00%, p = 0.66)
Galindo
Bonnefoy
Study
Van Velzen
36.10 (30.69, 41.69)
34.81 (27.42, 42.79)
28.57 (8.39, 58.10)
ES (95% CI)
38.97 (30.73, 47.70)
100.00
51.21
4.68
Weight
44.10
%
36.10 (30.69, 41.69)
34.81 (27.42, 42.79)
28.57 (8.39, 58.10)
ES (95% CI)
38.97 (30.73, 47.70)
100.00
51.21
4.68
Weight
44.10
%
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: VSD
Christine van Velzen.indb 35 20/09/2016 08:27

36
Chapter 2
Chapter 2
Overall (I^2 = 87.38%, p = 0.00)
Bonnefoy
Study
Pinto
Van Velzen
Galindo
Chew
Jørgensen
Durand
Khoo
60.36 (47.01, 73.02)
80.00 (44.39, 97.48)
ES (95% CI)
48.50 (40.71, 56.35)
67.02 (56.56, 76.38)
76.12 (67.99, 83.06)
46.48 (34.55, 58.71)
50.00 (27.20, 72.80)
88.00 (68.78, 97.45)
23.81 (8.22, 47.17)
100.00
8.48
Weight
14.89
14.33
%
14.71
13.95
10.93
11.62
11.08
60.36 (47.01, 73.02)
80.00 (44.39, 97.48)
ES (95% CI)
48.50 (40.71, 56.35)
67.02 (56.56, 76.38)
76.12 (67.99, 83.06)
46.48 (34.55, 58.71)
50.00 (27.20, 72.80)
88.00 (68.78, 97.45)
23.81 (8.22, 47.17)
100.00
8.48
Weight
14.89
14.33
%
14.71
13.95
10.93
11.62
11.08
0 20 40 60 80 100Percentage detected
Non-isolated CHD: AVSD
Overall (I^2 = 80.16%, p = 0.00)
Galindo
Study
Pinto
Van Velzen
Durand
80.14 (45.58, 99.98)
100.00 (54.07, 100.00)
ES (95% CI)
42.86 (26.32, 60.65)
87.50 (47.35, 99.68)
87.50 (47.35, 99.68)
100.00
%
22.30
Weight
29.67
24.02
24.02
80.14 (45.58, 99.98)
100.00 (54.07, 100.00)
ES (95% CI)
42.86 (26.32, 60.65)
87.50 (47.35, 99.68)
87.50 (47.35, 99.68)
100.00
%
22.30
Weight
29.67
24.02
24.02
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Ebstein's Anomaly
Christine van Velzen.indb 36 20/09/2016 08:27

37
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Overall (I^2 = 22.12%, p = 0.27)
Pinto
Van Velzen
Bonnefoy
Jørgensen
Chew
Study
Galindo
22.34 (17.96, 27.01)
18.49 (14.60, 22.91)
25.71 (16.01, 37.56)
25.00 (3.19, 65.09)
23.53 (10.75, 41.17)
26.09 (14.27, 41.13)
ES (95% CI)
28.72 (19.86, 38.98)
100.00
42.73
15.66
2.32
%
8.59
11.13
Weight
19.58
22.34 (17.96, 27.01)
18.49 (14.60, 22.91)
25.71 (16.01, 37.56)
25.00 (3.19, 65.09)
23.53 (10.75, 41.17)
26.09 (14.27, 41.13)
ES (95% CI)
28.72 (19.86, 38.98)
100.00
42.73
15.66
2.32
%
8.59
11.13
Weight
19.58
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Coarctation of the aorta
Overall (I^2 = 81.93%, p = 0.00)
Bonnefoy
Durand
Study
Chew
Pinto
Van Velzen
Galindo
Khoo
Jørgensen
42.03 (30.89, 53.56)
75.00 (42.81, 94.51)
66.67 (46.04, 83.48)
ES (95% CI)
43.12 (33.67, 52.95)
26.25 (19.62, 33.78)
41.67 (27.61, 56.79)
51.52 (41.25, 61.68)
21.43 (8.30, 40.95)
25.00 (8.66, 49.10)
100.00
8.27
%
11.41
Weight
14.96
15.47
13.23
14.81
11.54
10.30
42.03 (30.89, 53.56)
75.00 (42.81, 94.51)
66.67 (46.04, 83.48)
ES (95% CI)
43.12 (33.67, 52.95)
26.25 (19.62, 33.78)
41.67 (27.61, 56.79)
51.52 (41.25, 61.68)
21.43 (8.30, 40.95)
25.00 (8.66, 49.10)
100.00
8.27
%
11.41
Weight
14.96
15.47
13.23
14.81
11.54
10.30
0 20 40 60 80 100Percentage detected
Non-isolated CHD: Tetralogy of Fallot
Christine van Velzen.indb 37 20/09/2016 08:27

38
Chapter 2
Chapter 2
Overall (I^2 = 40.79%, p = 0.17)
Jørgensen
Galindo
Study
Van Velzen
Pinto
71.50 (59.46, 82.25)
55.56 (30.76, 78.47)
67.86 (47.65, 84.12)
ES (95% CI)
82.93 (67.94, 92.85)
70.83 (48.91, 87.38)
100.00
19.52
25.66
Weight
%
31.39
23.43
71.50 (59.46, 82.25)
55.56 (30.76, 78.47)
67.86 (47.65, 84.12)
ES (95% CI)
82.93 (67.94, 92.85)
70.83 (48.91, 87.38)
100.00
19.52
25.66
Weight
%
31.39
23.43
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: DORV-Fallot type
Overall (I^2 = 89.54%, p = 0.00)
Durand
Pinto
Bonnefoy
Jørgensen
Study
Van Velzen
Chew
Galindo
Khoo
36.38 (20.95, 53.30)
68.75 (49.99, 83.88)
13.04 (6.14, 23.32)
60.00 (26.24, 87.84)
41.94 (24.55, 60.92)
ES (95% CI)
44.19 (29.08, 60.12)
17.02 (7.65, 30.81)
52.94 (42.80, 62.90)
11.11 (2.35, 29.16)
100.00
12.48
13.45
9.73
12.43
Weight
12.93
13.04
13.75
12.19
%
36.38 (20.95, 53.30)
68.75 (49.99, 83.88)
13.04 (6.14, 23.32)
60.00 (26.24, 87.84)
41.94 (24.55, 60.92)
ES (95% CI)
44.19 (29.08, 60.12)
17.02 (7.65, 30.81)
52.94 (42.80, 62.90)
11.11 (2.35, 29.16)
100.00
12.48
13.45
9.73
12.43
Weight
12.93
13.04
13.75
12.19
%
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: TGA
Christine van Velzen.indb 38 20/09/2016 08:27

39
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Overall
Study
Van Velzen
Pinto
61.28 (46.91, 74.77)
ES (95% CI)
66.67 (40.99, 86.66)
58.06 (39.08, 75.45)
100.00
%
Weight
37.00
63.00
61.28 (46.91, 74.77)
ES (95% CI)
66.67 (40.99, 86.66)
58.06 (39.08, 75.45)
100.00
%
Weight
37.00
63.00
0 20 40 60 80 100Percentage detected
Non-isolated CHD: DORV-Taussig Bing
Overall (I^2 = 85.65%, p = 0.00)
Durand
Pinto
Jørgensen
Study
Van Velzen
Chew
Galindo
69.08 (43.10, 90.54)
75.00 (19.41, 99.37)
23.68 (11.44, 40.24)
100.00 (39.76, 100.00)
ES (95% CI)
85.19 (66.27, 95.81)
66.67 (46.04, 83.48)
69.70 (51.29, 84.41)
100.00
%
11.88
19.43
11.88
Weight
18.80
18.80
19.19
69.08 (43.10, 90.54)
75.00 (19.41, 99.37)
23.68 (11.44, 40.24)
100.00 (39.76, 100.00)
ES (95% CI)
85.19 (66.27, 95.81)
66.67 (46.04, 83.48)
69.70 (51.29, 84.41)
100.00
%
11.88
19.43
11.88
Weight
18.80
18.80
19.19
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Truncus arteriosus
Christine van Velzen.indb 39 20/09/2016 08:27

40
Chapter 2
Chapter 2
Overall (I^2 = 0.00%, p = 0.43)
Study
Bonnefoy
Durand
Galindo
Pinto
Van Velzen
59.75 (45.66, 73.20)
ES (95% CI)
100.00 (29.24, 100.00)
61.54 (31.58, 86.14)
44.44 (13.70, 78.80)
50.00 (21.09, 78.91)
61.90 (38.44, 81.89)
100.00
%
Weight
5.79
22.31
15.70
20.66
35.54
59.75 (45.66, 73.20)
ES (95% CI)
100.00 (29.24, 100.00)
61.54 (31.58, 86.14)
44.44 (13.70, 78.80)
50.00 (21.09, 78.91)
61.90 (38.44, 81.89)
100.00
%
Weight
5.79
22.31
15.70
20.66
35.54
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Pulmonary atresia with VSD
Overall (I^2 = 40.35%, p = 0.15)
Pinto
Jørgensen
Study
Durand
Van Velzen
Galindo
72.26 (49.82, 90.88)
54.17 (32.82, 74.45)
50.00 (1.26, 98.74)
ES (95% CI)
100.00 (39.76, 100.00)
88.89 (51.75, 99.72)
60.00 (26.24, 87.84)
100.00
33.71
8.29
Weight
13.23
21.75
23.02
%
72.26 (49.82, 90.88)
54.17 (32.82, 74.45)
50.00 (1.26, 98.74)
ES (95% CI)
100.00 (39.76, 100.00)
88.89 (51.75, 99.72)
60.00 (26.24, 87.84)
100.00
33.71
8.29
Weight
13.23
21.75
23.02
%
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Congenitally corrected TGA
Christine van Velzen.indb 40 20/09/2016 08:27

41
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Overall (I^2 = 0.00%, p = 0.43)
Durand
Study
Van Velzen
Galindo
90.82 (77.90, 99.06)
100.00 (63.06, 100.00)
ES (95% CI)
88.24 (63.56, 98.54)
83.33 (51.59, 97.91)
100.00
22.08
Weight
%
45.45
32.47
90.82 (77.90, 99.06)
100.00 (63.06, 100.00)
ES (95% CI)
88.24 (63.56, 98.54)
83.33 (51.59, 97.91)
100.00
22.08
Weight
%
45.45
32.47
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Tricuspid valve atresia
Overall (I^2 = 84.70%, p = 0.00)
Bonnefoy
Jørgensen
Khoo
Chew
Van Velzen
Galindo
Durand
Pinto
Study
87.24 (78.28, 94.23)
94.12 (71.31, 99.85)
92.59 (75.71, 99.09)
60.61 (42.14, 77.09)
84.62 (74.67, 91.79)
97.56 (91.47, 99.70)
86.41 (78.25, 92.37)
96.55 (82.24, 99.91)
74.44 (67.42, 80.64)
ES (95% CI)
100.00
9.48
11.08
11.70
13.71
13.79
14.15
11.31
14.78
Weight
%
87.24 (78.28, 94.23)
94.12 (71.31, 99.85)
92.59 (75.71, 99.09)
60.61 (42.14, 77.09)
84.62 (74.67, 91.79)
97.56 (91.47, 99.70)
86.41 (78.25, 92.37)
96.55 (82.24, 99.91)
74.44 (67.42, 80.64)
ES (95% CI)
100.00
9.48
11.08
11.70
13.71
13.79
14.15
11.31
14.78
Weight
%
0 20 40 60 80 100Percentage detected
Non-isolated CHD: HLHS
Christine van Velzen.indb 41 20/09/2016 08:27

42
Chapter 2
Chapter 2
Overall (I^2 = 33.01%, p = 0.21)
Van Velzen
Study
Durand
Galindo
Pinto
41.26 (25.45, 57.93)
61.54 (31.58, 86.14)
ES (95% CI)
50.00 (15.70, 84.30)
38.89 (17.30, 64.25)
25.00 (8.66, 49.10)
100.00
23.54
%
Weight
16.75
28.93
30.79
41.26 (25.45, 57.93)
61.54 (31.58, 86.14)
ES (95% CI)
50.00 (15.70, 84.30)
38.89 (17.30, 64.25)
25.00 (8.66, 49.10)
100.00
23.54
%
Weight
16.75
28.93
30.79
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: PA, intact IVS
Overall (I^2 = 69.41%, p = 0.04)
Pinto
Van Velzen
Jørgensen
Study
89.09 (66.61, 100.00)
72.73 (60.36, 82.97)
93.55 (78.58, 99.21)
100.00 (15.81, 100.00)
ES (95% CI)
100.00
47.69
%
41.52
10.78
Weight
89.09 (66.61, 100.00)
72.73 (60.36, 82.97)
93.55 (78.58, 99.21)
100.00 (15.81, 100.00)
ES (95% CI)
100.00
47.69
%
41.52
10.78
Weight
0 20 40 60 80 100
Percentage detected
Non-isolated CHD: Complex heterotaxy
Christine van Velzen.indb 42 20/09/2016 08:27

43
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Overall
Trines (2013)
Van Velzen (2015)
Study
46.72 (43.47, 49.99)
50.27 (45.08, 55.45)
44.21 (39.92, 48.57)
ES (95% CI)
100.00
41.52
58.48
Weight
%
46.72 (43.47, 49.99)
50.27 (45.08, 55.45)
44.21 (39.92, 48.57)
ES (95% CI)
100.00
41.52
58.48
Weight
%
0 20 40 60 80 100
Percentage detected
Isolated CHD: Total CHD
Overall (I^2 = 61.81%, p = 0.07)
Khoshnood (2005)
Study
Van Velzen (2015)
Trines (2013)
30.64 (19.09, 43.51)
42.42 (25.48, 60.78)
ES (95% CI)
20.63 (11.47, 32.70)
32.73 (20.68, 46.71)
100.00
28.39
Weight
36.62
34.99
%
30.64 (19.09, 43.51)
42.42 (25.48, 60.78)
ES (95% CI)
20.63 (11.47, 32.70)
32.73 (20.68, 46.71)
100.00
28.39
Weight
36.62
34.99
%
0 20 40 60 80 100
Percentage detected
Isolated CHD: Coarctation of the aorta
Christine van Velzen.indb 43 20/09/2016 08:27

44
Chapter 2
Chapter 2
Overall
Van Velzen (2015)
Study
Khoshnood (2005)
49.20 (37.11, 61.34)
29.41 (15.10, 47.48)
ES (95% CI)
69.70 (51.29, 84.41)
100.00
50.74
%
Weight
49.26
49.20 (37.11, 61.34)
29.41 (15.10, 47.48)
ES (95% CI)
69.70 (51.29, 84.41)
100.00
50.74
%
Weight
49.26
0 20 40 60 80 100
Percentage detected
Isolated CHD: Tetralogy of Fallot
Overall (I^2 = 86.69%, p = 0.00)
Trines (2013)
Study
Van Velzen (2015)
Khoshnood (2005)
48.47 (24.23, 73.08)
29.41 (15.10, 47.48)
ES (95% CI)
42.86 (27.72, 59.04)
72.50 (56.11, 85.40)
100.00
%
32.78
Weight
33.71
33.51
48.47 (24.23, 73.08)
29.41 (15.10, 47.48)
ES (95% CI)
42.86 (27.72, 59.04)
72.50 (56.11, 85.40)
100.00
%
32.78
Weight
33.71
33.51
0 20 40 60 80 100
Percentage detected
Isolated CHD: Transposition of great arteries
Christine van Velzen.indb 44 20/09/2016 08:27

45
Performance of second trimester screening for prenatal detection of congenital heart defects
Chap
ter 2
Overall
Study
Trines (2013)
Van Velzen (2015)
37.82 (27.17, 49.05)
ES (95% CI)
34.78 (23.71, 47.21)
58.33 (27.67, 84.83)
100.00
%
Weight
84.76
15.24
37.82 (27.17, 49.05)
ES (95% CI)
34.78 (23.71, 47.21)
58.33 (27.67, 84.83)
100.00
%
Weight
84.76
15.24
0 20 40 60 80 100
Percentage detected
Isolated CHD: Pulmonary atresia with VSD
Overall
Trines (2013)
Van Velzen (2015)
Study
63.71 (45.09, 80.62)
72.22 (46.52, 90.31)
50.00 (21.09, 78.91)
ES (95% CI)
100.00
59.68
%
40.32
Weight
63.71 (45.09, 80.62)
72.22 (46.52, 90.31)
50.00 (21.09, 78.91)
ES (95% CI)
100.00
59.68
%
40.32
Weight
0 20 40 60 80 100
Percentage detected
Isolated CHD: HRHS
Christine van Velzen.indb 45 20/09/2016 08:27

46
Chapter 2
Chapter 2
Overall (I^2 = 48.44%, p = 0.14)
Khoshnood (2005)
Trines (2013)
Van Velzen (2015)
Study
90.67 (82.05, 96.89)
88.89 (70.84, 97.65)
84.91 (72.41, 93.25)
96.08 (86.54, 99.52)
ES (95% CI)
100.00
26.03
37.31
%
36.66
Weight
90.67 (82.05, 96.89)
88.89 (70.84, 97.65)
84.91 (72.41, 93.25)
96.08 (86.54, 99.52)
ES (95% CI)
100.00
26.03
37.31
%
36.66
Weight
0 20 40 60 80 100
Percentage detected
Isolated CHD: HLHS
Overall
Van Velzen (2015)
Trines (2013)
Study
86.46 (74.15, 95.59)
88.89 (65.29, 98.62)
84.62 (65.13, 95.64)
ES (95% CI)
100.00
41.11
58.89
Weight
%
86.46 (74.15, 95.59)
88.89 (65.29, 98.62)
84.62 (65.13, 95.64)
ES (95% CI)
100.00
41.11
58.89
Weight
%
0 20 40 60 80 100
Percentage detected
Isolated CHD: Complex heterotaxy
Christine van Velzen.indb 46 20/09/2016 08:27

Christine van Velzen.indb 47 20/09/2016 08:27

Christine van Velzen.indb 48 20/09/2016 08:27

CHAPTER 3Prenatal Detection of
Congenital Heart Disease:
Results of a National Screening Programme
CL van Velzen, SA Clur, MEB Rijlaarsdam, CJ Bax, E Pajkrt, MW Heymans, MN Bekker,J Hruda, CJM de Groot, NA Blom, MC Haak.
BJOG 2016 Feb;123(3):400-7
LetterP Ramaekers, D Mannaerts, Y Jacquemyn
BJOG 2015 Sep; 122:1420-1
ReplyCL van Velzen, E Pajkrt, MC Haak
BJOG 2015 Sep; 122:1421
Christine van Velzen.indb 49 20/09/2016 08:27

50
Chapter 3
Chapter 3
ABSTRACT
Objective Congenital heart disease (CHD) is the most common congenital malformation and causes major morbidity and mortality. Prenatal detection improves the neonatal condition before surgery, resulting in less morbidity and mortality. In the Netherlands a national prenatal screening programme was introduced in 2007. This study evaluates the effects of this screening programme.
Design Geographical cohort study.
Setting Large referral region of three tertiary care centres.
Population Fetuses and infants diagnosed with severe CHD born between 1 January 2002 and 1 January 2012.
Methods Cases were divided into two groups: before and after the introduction of screening.
Main outcome measures Detection rates were calculated.
Results The prenatal detection rate (n = 1912) increased with 23.9% (95% confidence interval [95% CI] 19.5–28.3) from 35.8 to 59.7% after the introduction of screening and of isolated CHD with 21.4% (95% CI 16.0–26.8) from 22.8 to 44.2%. The highest detection rates were found in the hypoplastic left heart syndrome, other univentricular defects and complex defects with atrial isomerism (>93%). Since the introduction of screening, the ‘late’ referrals (after24 weeks of gestation) decreased by 24.3% (95% CI 19.3–29.3).
Conclusions This is the largest cohort study to investigate the prenatal detection rate of severe CHD in an unselected population. A nationally organised screening has resulted in a remarkably high detection rate of CHD (59.7%) compared with earlier literature.
Christine van Velzen.indb 50 20/09/2016 08:27

51
Prenatal detection of CHD - national screening
Chap
ter 3
INTRODUCTION
Congenital heart disease (CHD) is the most common congenital malformation and affects approximately 6–11 per 1000 newborns. 1–4 About 20–30% of these heart defects are severe, defined as being potentially life threatening and requiring surgery within the first year of life. 2,5–7 Only 10% of CHD cases occur in pregnancies with identifiable risk factors, such as fetal extracardiac malformations. 8,9 The current screening strategy in most western countries is a standard anomaly scan at 20 weeks of gestation. 8Although the prenatal detection rate of CHD has improved in the last decades, 5,10 the reported detection rate in low-risk populations does not exceed 35–40%. 7,10–14 Prenataldetection of specific types of CHD may reduce neonatal mortality and morbidity. 15–19 It allows for planning the delivery at a tertiary-care centre ensuring optimal neonataland perisurgical care. Furthermore, parents can consider termination of pregnancy (TOP) in severe cases. 20–22 In the Netherlands in January 2007 a nationwide screeningprogramme, with the aim to detect congenital anomalies, was introduced. Before 2007 fetal ultrasound was exclusively performed for the evaluation of obstetric complications during pregnancy or in pregnancies with an increased risk of fetal abnormalities (first- or second-degree family member with CHD or other congenital anomalies). The defined and uniform introduction of the national standard anomaly scan for all pregnant women provided the unique opportunity to study the effect of such a programme. The primary aim of this study was to evaluate the effectiveness of the national screening programme on the prenatal detection of severe CHD in an unselected population in the Netherlands. The secondary aims were to assess the gestational age at prenatal diagnosis and to study the effect of the screening programme on the mortality rates.
METHODS
Region and referral systemThis was a geographical cohort study, conducted in the northwest region of the Netherlands. In this area 72 000 infants are born per year, which is approximately 40% of all live births in the Netherlands. Three tertiary referral centres, Academic Medical Centre Amsterdam, VU Medical Centre Amsterdam and Leiden University Medical Centre Leiden, are responsible for the care of children with CHD in this region. All infant cardiothoracic surgery is performed in the Leiden University Medical Centre. This collaboration is called the CAHAL (Centre for congenital heart defects Amsterdam and Leiden—in Dutch Centrum voor Aangeboren Hartafwijkingen Amsterdam-Leiden). Prenatal screening in the Netherlands is mostly performed in primary and secondary healthcare centers by ultrasonographers and obstetricians (performing respectively 96% and 4% of the standard anomaly scans). Only the women with an increased risk
Christine van Velzen.indb 51 20/09/2016 08:27

52
Chapter 3
Chapter 3
of having offspring with a congenital anomaly are screened in tertiary centres. All ultrasonographers are educated and are required to take a practical and a theoretical examination according to the Fetal Medicine Foundation criteria. Furthermore, they are required to conduct at least 150 structural anomaly scans per year. Every 2 years the quality of their scans is assessed by regional surveillance committees. The standard anomaly scan is performed between 18 and 22 weeks gestational age according to a national protocol. The assessment of the fetal heart in the Dutch anomaly scan entailed the assessment of the four-chamber view (size of the heart and position in thorax, symmetry of the atria and ventricles, identification of atrioventricular valves and crux) and the right and left outflow tract views. 23 The assessment of the three-vessel view (a transverse section of the fetal thorax, just above the level of the four-chamber view) 23 was only made compulsory from January 2012, once the ultrasonographers’ cardiac scanning experience had increased. The three-vessel view depicts the spatial relationship of the aorta and pulmonary artery and is beneficial in the detection of outflow tract anomalies. In case a congenital (heart) defect is suspected, the woman is referred to one of the tertiary centres. In the tertiary centres fetal echocardiography is performed by a specialised perinatologist in collaboration with a paediatric cardiologist. After a prenatal diagnosis of CHD, karyotyping was routinely recommended.
CasesWe included all cases with a prenatal or postnatal diagnosis of severe CHD born between 1 January 2002 and 1 January 2012, irrespective of presence or absence of additional congenital anomalies. For inclusion the mother of the fetus or the infant had to be resident within the study region at the time of birth. Severe CHD was defined as being potentially life threatening and requiring surgery or intervention within the first year of life. All cases with severe abnormal cardiac findings in the pregnancy (including pregnancies with fetal demise or TOP) were identified in the prenatal ultrasound databases of the tertiary centres. Fetal cases were prospectively entered in these databases. The case list was complemented with all postnatally diagnosed infants with a CHD who needed surgery or therapeutic cardiac catheterisation or who died within the first year of life. They were selected from the paediatric cardiology departmental databases and cross-checked with catheterisation schedules, operating schedules and emergency admissions. The postnatal cases were prospectively entered in the paediatric departmental databases. The postmortem databases of the departments of pathology were studied for cardiac anomalies, to identify cases in which death had occurred outside a hospital or in which the child was dead on arrival at an emergency room. Finally, the database of the Dutch sudden infant death syndrome registry was searched for all cardiac causes that may not have been recorded in the hospital databases. All the cases were reviewed and the
Christine van Velzen.indb 52 20/09/2016 08:27

53
Prenatal detection of CHD - national screening
Chap
ter 3
prenatal and postnatal data were matched. To assess the effectiveness of the national screening programme on the prenatal detection of CHD, data from the period 2002–2006 were compared with data from 2007 to 2011. Cases of isolated fetal or neonatal arrhythmia were not included. We excluded isolated secundum atrial septal defects and/or isolated persistent arterial ducts as these conditions are normal in fetal life. In the Netherlands, by participating in prenatal screening, pregnant women automatically give consent to use the anonymised data of the pregnancy and the outcome for research. Approval from the Medical Ethical Committee of the VU University Medical Centre was obtained for this study. This study complies with the Declaration of Helsinki.
Data collectionData concerning the mother, pregnancy, birth and infant were collected from medical files. The gestational ages at both referral and diagnosis were retrieved. The final prenatalcardiac diagnosis was recorded. In cases in which data about prenatal screening were missing, infants born after 1 May 2007 were considered screened prenatally (since the national screening programme was introduced on 1 January 2007). The postnatal echocardiography, surgical report, autopsy or magnetic resonance imaging determined the definitive diagnosis in the analysis of the data. The postnatal diagnoses were coded and categorised as depicted in Table 1. In cases with more than one cardiac diagnosis the most important heart anomaly (in terms of determining the prognosis) of the fetus or infant was stated (for example a coarctation of the aorta combined with a ventricular septal defect [VSD] was coded as a coarctation). We defined heart defects as univentricular, when in postnatal life the heart could only be surgically managed as a single ventricle. In cases in which a postnatal diagnosis was not available (e.g. in some cases with TOP or intrauterine fetal death without a postmortem), the prenatal diagnosis was used to categorise the heart defect. The presence of extracardiac congenital anomalies, either as a prenatal or a postnatal finding, was recorded. Prenatally detected extracardiac anomalies were categorised as: single or multiple extracardiac structural anomaly/ies, intrauterine growth restriction, oligohydramnios or polyhydramnios, fetal hydrops and nuchal translucency >3.5 mm. Prenatally detected aneuploidy and genetic syndromes were also recorded. Postnatally diagnosed congenital anomalies were categorised as: aneuploidy, confirmed genetic syndrome, multiple or single extracardiac anomaly/ies. Isolated CHD was defined as CHD without any other congenital anomalies (except single umbilical artery).
Statistical analysisThe prenatal detection rate of CHD in the years before introduction of the screening programme was estimated at 20%, a little higher than the last Dutch data published in
Christine van Velzen.indb 53 20/09/2016 08:27

54
Chapter 3
Chapter 3
1996 (16.7%). 11 After the introduction we anticipated a detection rate of around 40% according to earlier published international studies with comparable programmes. A sample size of 300 cases was necessary to show a significant difference in detection rate (power 90% and α = 0.01). Comparisons were made between the group before and after introduction of the national screening programme. A chi-square test was used to test associations between categorical variables, the Student’s t test was used to test differences between numeric variables. For dichotomous outcomes, differences between the groups were tested using the two-sample z-test for proportions. Confidence intervals were also calculated. We considered P values <0.05 as statistically significant; all tests were two-sided. We corrected for multiple testing by using Bonferroni correction, in other words for each subgroup of outcome measures the P value was adjusted by dividing the P value of 0.05 by the number of tests. Data analysis was generated using SPSS software (version 20; SPSS Inc., Chicago, IL, USA).
RESULTS
Inclusions and follow upIn total, 1965 cases were eligible for inclusion in the study. Fifty-three cases were excluded from further analysis for the following reasons; date of birth in 2012 or postnatal cases with the first cardiac surgery after the age of 12 months. This resulted in 1912 inclusions. In the study period 1413 infants were liveborn with a severe CHD in this region. The total live birth rate in this period in the same region was 720 138 (data supplied by Statistics Netherlands, CBS), resulting in a live birth prevalence for severe CHD of 2.0 per 1000 in this region. Overall, the total birth (including stillbirth and termination of pregnancy) prevalence of severe CHD was 2.7 per 1000 births. A flow chart of the inclusions and follow up is shown in Figure 1. Follow up of all cases was at least 1 year after birth. Only 0.3% of the cases was lost to follow-up (two cases without information on pregnancy outcome and four cases lacking information on first-year mortality). The lost-to-follow-up cases were all included in the analysis.
Prenatal detection of CHDAn overview of the prenatal detection rate of categorised groups of CHD in our cohort is shown in Table 1. The detection rate of all CHD increased significantly from 35.8% before to 59.7% after the introduction of the national screening programme (P < 0.001). The detection rate of isolated CHD increased from 22.8 to 44.2% (P < 0.001). The highest prenatal detection rates after introduction of screening were found in hypoplastic left heart syndrome, other univentricular defects and the complex heart defects with atrial isomerism (>93%).
Christine van Velzen.indb 54 20/09/2016 08:27

55
Prenatal detection of CHD - national screening
Chap
ter 3
An overview of the prenatal detection of specifi c diagnosis of CHD—with a number large enough to present results—are shown in Table 2. Signifi cant improvements were made in the prenatal detection of hypoplastic left heart syndrome, coarctation of the aorta, double outlet right ventricle with VSD and pulmonary stenosis (DORV-Fallot), transposition of the great arteries with intact ventricular septum (TGA), truncus arteriosus and pulmonary atresia with VSD.
Figure 1 Flow chart showing inclusions and pregnancy outcomes
Exclusion criteria 53
Examined for eligibility 1,965
Inclusions 1,912
Stillbirths 94 (4.9%)
Live-births 1,413 (73.9%)
Termination of pregnancy 403 (21.1%)
Lost to follow-up 2 (0.1%)
Lost to follow-up 4 (0.3%)
Figure 1 Flow chart showing inclusions and pregnancy outcomes
Christine van Velzen.indb 55 20/09/2016 08:27

56
Chapter 3
Chapter 3
Table 1 Prenatal detection per category of congenital heart disease before and after introduction of the screening program
Before introductionof screening
After introductionof screening
Heart defect category Total (n)
Prenatal detection(%)
Total (n)
Prenatal detection(%)
Difference in prenatal detection(95% CI)
p
1.Septal defects 272 37.1 230 50.4 13.3 (4.7-21.9) 0.003
2.Valvular anomalies, biventricular heart
65 20.0 65 32.3 12.3 (-2.7-27.3) 0.110
3.Venous return anomalies 23 4.3 27 11.1 6.8 (-7.7-21.3) 0.380
4.Aortic arch anomalies 117 12.0 91 29.7 17.7 (6.6-28.8) 0.001
5.Conotruncal anomalies 267 26.6 229 59.8 33.2 (24.9-41.5) <0.001
6.Hypoplastic Right Heart syndrome
22 50.0 18 66.7 16.7 (-13.5-46.9) 0.289
7.Hypoplastic Left Heart syndrome
85 54.1 82 97.6 43.5 (32.3-54.7) <0.001
8.Other univentricular heart defects
83 57.8 78 94.9 37.1 (25.3-48.9) <0.001
9.Complex defects with atrial isomerism
31 64.5 31 93.5 29.0 (10.1-47.9) 0.005
10.Miscellaneous 48 20.8 48 20.8 0 0.100
Total 1013 35.8 899 59.7 23.9 (19.5-28.3) <0.001
Isolated CHD 619 22.8 527 44.2 21.4 (16.0-26.8) <0.001
Legend: p value (Bonferroni corrected) is considered significant if <0.005.Categories consist of:1. Ventricular septal defect(s), balanced atrioventricular septal defect2. Pulmonary or aortic valve stenosis, mitral stenosis, Ebstein’s anomaly, tricuspid dysplasia, tricuspid or mitral
regurgitation3. Total or partial abnormal pulmonary venous return, giant eustachian valve/cor triatriatum dexter or sinister4. Aortic coarctation, hypoplastic or interrupted aortic arch, multiple level left heart obstruction, double aortic arch 5. Tetralogy of Fallot, double outlet right ventricle-fallot type or DORV and VSD and/or pulmonary stenosis, simple
transposition of great arteries (without signficant VSD), complex TGA (with significant VSD and/or PS), DORV Taussig Bing (= TGA type), truncus arteriosus, pulmonary atresia with VSD, congenitally corrected TGA, absent pulmonary valve syndrome, aortopulmonary window, hemitruncus
6. Pulmonary atresia with intact ventricular septum, critical pulmonary valve stenosis with right ventricular hypoplasia 7. Aortic valve atresia or critical aortic valve stenosis with left ventricular hypoplasia8. Double inlet left ventricle, tricuspid valve atresia, absent left A-V connection, unbalanced AVSD, TGA with RV hypoplasia
and straddling tricuspid valve, criss-cross, DORV with mitral valve and LV hypoplasia, congenitally corrected TGA with RV hypoplasia, isolated AV discordance with hypoplastic RV and VSD
9. Left or right atrial isomerism, heterotaxy syndromes10. Cardiomyopathy, generalized arteriopathy, complex severe heart defect in aneuploidy other than trisomy 21,
polyvalvular disease, isolated double chambered right ventricle, right atrial aneurysm, aortic root dilatation (Marfan)
Christine van Velzen.indb 56 20/09/2016 08:27

57
Prenatal detection of CHD - national screening
Chap
ter 3
Table 2 Prenatal detection per type of severe CHD before and after introduction of the screening program
Before introductionof screening
After introductionof screening
Heart defect Total(n)
Prenatal detection (%)
Total(n)
Prenatal detection (%)
Difference in prenatal detection(95% CI)
p
Ventricular septal defect 167 28.7 136 39.0 10.3 (-0.4-21.0) 0.060
Atrioventricular septal defect, balanced
105 50.5 94 67.0 16.5 (3.0-30.0) 0.018
Pulmonary valve stenosis 25 8.0 26 19.2 11.2 (-7.3-29.7) 0.244
Aortic valve stenosis 23 8.7 26 26.9 18.2 (-2.4-38.8) 0.100
Atrioventricular valve dysplasia/stenosis/regurgitation*
17 47.1 13 69.2 17.6 (-12.4-56.6) 0.367
Totally/partially abnormal pulmonary venous return
22 9.1 20 10.0 0.9 (-16.9-18.7) 0.639
Coarctation of aorta 86 8.1 70 25.7 17.6 (5.9-29.3) 0.003
Tetralogy of Fallot 63 22.2 48 41.7 19.5 (2.2-36.8) 0.028
Double outlet right ventricle (Fallot-type)
35 48.6 41 82.9 34.3 (14.1-54.5) 0.001
Transposition of great arteries, simple
63 14.3 43 44.2 29.9 (12.5-47.3) 0.001
TGA complex (with significant VSD and/or DORV or pulmonary stenosis)
34 26.5 32 53.1 26.6 (3.8-49.4) 0.027
Truncus arteriosus 19 31.6 27 85.2 53.6 (28.5-78.7) <0.001
Pulmonary atresia with VSD (± main aortico-pulmonary collateral arteries)
33 24.2 21 61.9 37.7 (12.3-63.1) 0.006
Tricuspid valve atresia 20 55.0 17 88.2 33.2 (6.0-60.4) 0.028
Unbalanced AVSD 18 77.8 28 92.9 15.1 (-6.3-36.5) 0.138
Legend: All heart defects in this table required surgery or caused deatha p value (Bonferroni corrected) of <0.0033 was considered statistically significant* Ebstein’s anomaly included
Christine van Velzen.indb 57 20/09/2016 08:27

58
Chapter 3
Chapter 3
Aneuploidy and syndromesThe rates of aneuploidy, genetic syndromes, extracardiac anomalies and pregnancy outcome in prenatally detected CHD with and without extracardiac structural anomalies on prenatal scan are depicted in Table 3. Of the CHD cases identified on prenatal scan without any extracardiac structural anomalies (n = 384) 10.9% had an aneuploidy (of which 45.2% trisomy 21 [T21] presenting with atrioventricular septal defect, 31.0% T21 with another CHD, 4.8% T18 and 7.1% Turner syndrome). Of the CHD cases without a prenatal diagnosis (n = 1012) 11.3% (95% confidence interval [95% CI] 9.4–13.2) had an aneuploidy and 4.9% (95% CI 3.6–6.2) a genetic syndrome. In the total cohort (n = 1912) 2.0% (95% CI 1.4–2.6) had a 22q11 deletion (n = 39). Other genetic syndromes (e.g. CHARGE, Williams, Holt–Oram syndrome) were diagnosed in 3.9% (n = 75) of the total cohort.
Gestational age at referralThe mean gestational age at prenatal referral to a tertiary centre was 22+3 weeks before and 19+3 weeks after the introduction of the screening programme (difference 21 days, 95% CI 16–26, P < 0.001). Since the introduction of screening the ‘late’ referrals (after 24 weeks of gestation, the legal limit for termination of pregnancy in the Netherlands) decreased from 31.0% to 6.7% (difference 24.3%, 95% CI 19.3–29.3, P < 0.001). Seventy-three percent of the cases detected after 24 weeks of gestation since 2007 (n = 34), are CHD that are known to develop later in gestation or that are difficult to detect around 20 weeks of gestation (e.g. coarctation, pulmonary stenosis, VSD).
MortalityThe TOP rate in all severe CHD cases (including cases with chromosomal or other extracardiac anomalies), prenatally diagnosed before 24 weeks of gestation remained similar; 50.0% (124/248) before the introduction versus 52.7% (263/499) after the introduction of screening (difference 2.7%, 95% CI -4.9 to 10.3, P = 0.486). The TOP rate in isolated CHD, diagnosed before 24 weeks of gestation remained similar; 28.6% (28/98)before versus 34.7% (74/213) after the introduction of screening (difference 6.1%, 95%CI-4.9 to 17.1, P = 0.282). The first-year mortality in liveborn infants with isolated CHD decreased from 13.2% to 12.2% (difference 1.0%, 95% CI -2.7 to 3.7, P = 0.612). The presurgical mortality of liveborn infants with isolated CHD was 7.0% before versus 6.3% after the introduction of screening (difference 0.7%, 95% CI _2.0 to 3.6, P = 0.640). The first year postsurgical mortality in isolated CHD went from 6.7 to 6.3% (difference 0.4%, 95% CI -2.4 to 3.2, P = 0.801).
Christine van Velzen.indb 58 20/09/2016 08:27

59
Prenatal detection of CHD - national screening
Chap
ter 3
DISCUSSION
Main findingsThis study presents more than 1900 fetuses and infants with severe CHD. The study assessed the effect of a national screening programme on the prenatal detection rate. A total birth prevalence of severe CHD of 2.7 per 1000 births was found. The prenatal detection rates of severe CHD increased significantly after the introduction of the programme to 59.7% and 44.2% for isolated severe CHD. The highest prenatal detection rates were found in hypoplastic left heart syndrome, other univentricular defects and the complex heart defects with atrial isomerism, all >93%. The groups of CHD in which the prenatal detection has remained relatively low are valve abnormalities in biventricular hearts and pulmonary or systemic venous return anomalies.
Table 3 Aneuploidy, genetic syndromes and pregnancy outcome in prenatally detected severe CHD with and without extracardiac structural anomalies identified on prenatal scan*
Identified on prenatal scan
CHD without extra structural anomalies n (%)
CHD with extra structural anomalies* n (%)
CHD with SUA, IUGR, poly-, or oligohydramniosn (%)
Total n (%)
Outcome
Isolated 303 (78.9) 49 (10.4) † 29 (65.9) 381 (42.3)
Aneuploidy 42 (10.9) 255 (54.0) 7 (15.9) 304 (33.8)
Genetic syndrome ‡ 21 (5.5) 40 (8.5) 2 (4.5) 63 (7.0)
Extracardiac anomaly § 18 (4.7) 125 (26.5) 7 (15.9) 150 (16.7)
Missing ‖ 0 (0) 2 (0.4) 0 (0) 2 (0.2)
Live birth 261 (68.0) 116 (24.6) 28 (63.6) 405 (45.0)
TOP 109 (28.4) 283 (60.0) 11 (25.0) 403 (44.8)
IUFD 14 (3.6) 73 (15.4) 5 (11.4) 92 (10.2)
Total 384 (42.7) 472 (52.4) 44 (4.9) 900 (100)
Legend: SUA; single umbilical arteryIUGR; intra-uterine growth restriction* Extracardiac structural anomaly on prenatal scan includes single or multiple structural anomaly/ies, fetal hydrops and nuchal translucency >3.5mm. † In these cases on prenatal scan an extracardiac structural anomaly was identified, but after birth the infant developed normal (e.g. suspicion esophageal atresia, pyelectasis, hydrops).‡ Genetic syndrome includes microdeletions, duplications and monogenic disorders.§ Extracardiac anomaly after birth without chromosomal anomaly (includes single extracardiac anomaly significantly affecting postnatal outcome or multiple extracardiac anomalies).‖ Data missing on presence of extracardiac anomalies after birth
Christine van Velzen.indb 59 20/09/2016 08:27

60
Chapter 3
Chapter 3
Strengths and limitationsDue to the gradual and heterogeneous introduction of prenatal screening worldwide and continuous technical developments, it has always been challenging to study the actual effects of screening programmes in pregnancy. Therefore, the relatively late, but uniform introduction of a national screening programme in the Netherlands offered a unique possibility to study the effect of such an instrument. This study represents the largest cohort of severe CHD in an unselected population with such a detailed analysis per cardiac diagnosis since the 1990s. 24 The total birth prevalence that was found in this study is consistent with a worldwide accepted birth prevalence of severe CHD. 2,7,10,25 Pathology databases, sudden infant death records and emergency ward admissions were studied for potential cases and we assume that we did not miss a significant number of them. The lost-to-follow-up rate in our cohort is very low. Maximum efforts were made to identify possible risk factors, but maternal data were not available in all postnatally diagnosed cases. However, it is well known that 90% of CHD occur in populations without any identifiable risk factor, 26 so we assume that the effect of potential confounders will be very limited. We could not obtain data of cases that were screened as negative in the study region, but that were born and diagnosed with CHD outside the study region. Those data, however, would not influence the detection rates of our screening programme. Furthermore, we conclude from the data before 2007 that in a small number of pregnancies, an ultrasound was already performed around 20 weeks of gestation in the absence of a screening programme. This implies that the true effect of prenatal screening is even more significant than we can demonstrate here.
InterpretationThe detection rate after the introduction of the programme was 59.7%, which is remarkably high in an unselected population, compared with similar programmes that never exceeded 25–45%. 10,24,27–29 The detection rate of isolated CHD with the screening programme is especially noteworthy (44.2%), compared with 16–23% published in other studies. 28,30
The highest prenatal detection rates (>93%) were found in CHD with abnormal four-chamber view (hypoplastic left heart syndrome, other univentricular defects and the complex heart defects with atrial isomerism) and exceed previously published series. 5,14,29,30 Hypoplastic right heart syndrome is more frequently overlooked (prenatal detection rate 66.7%), as it may present with a relatively good right ventricular cavity around 20 weeks of gestation. 31 Significant improvements were made in the prenatal detection of several (ductal dependent) outflow tract and aortic arch anomalies that require examination of the outlet views in addition to the four-chamber view. The prenatal detection of valve abnormalities in biventricular hearts and pulmonary or
Christine van Velzen.indb 60 20/09/2016 08:27

61
Prenatal detection of CHD - national screening
Chap
ter 3
systemic venous return anomalies has remained relatively low. Valve abnormalities can be very subtle in the first half of pregnancy and usually need the use of colour Doppler. Doppler was not compulsory in the Dutch screening programme. Furthermore, obstructive lesions can develop or progress as pregnancy advances and may not be recognisable around 20 weeks of gestation. 32,33 We believe that another factor that adds to the persistent low detection rates is the fact that training programmes do not sufficiently teach how to diagnose those anomalies in four-chamber and sagittal views. The difficulty in the diagnosis of anomalies of the aortic arch has been widely acknowledged, 34 yet this study showed a significant increase in the detection rate of coarctation of the aorta. The high detection rates in this study are in our opinion, explained by the thoroughly organised national screening programme with well-defined ultrasound protocols. Uniform training, 35 and quality assessments of the ultrasonographers, warrant a quality level that is not restricted to urban areas only, as this cohort contains large rural areas as well. 29,36 A standardised educational programme for ultrasonographers, comparable to the one in the Netherlands, was described by Levy et al. 7 They reached a prenatal detection rate of 74.1% within an integrated managed care consortium. Their study cohort was, however, rather small.
Several studies have shown that the prenatal identification of specific types of CHD reduces mortality. 15–19,37 In this study, the first-year mortality, as well as the presurgical mortality in liveborn infants with isolated severe CHD, remained similar. Mortality in the first year is influenced by multiple factors and perioperative care improves, so it is difficult to show a significant effect of prenatal screening. The detection rate of (ductal dependent) outflow tract anomalies hopefully will improve because of the increased awareness of the importance of the three-vessel view and its inclusion in the Dutch screening protocol as a compulsory item from 2012. 26,38 It is plausible that mortality will consequently decrease.
ConclusionWe have shown that a thoroughly organised national screening programme has resulted in a significant increase in prenatal detection of severe CHD up to 59.7% in an unselected population. More than 90% of the prenatal diagnoses were made before 24 weeks of gestation. Prenatal detection of CHD remains challenging, especially for ultrasonographers who are minimally exposed to these anomalies. We are convinced that continued improvement of training programmes can contribute to even higher prenatal detection.
Christine van Velzen.indb 61 20/09/2016 08:27

62
Chapter 3
Chapter 3
REFERENCES(1) Ferencz C, Rubin JD, McCarter RJ, Brenner JI, Neill CA, Perry LW, et al. Congenital heart disease:
prevalence at livebirth. The Baltimore-Washington Infant Study. Am J Epidemiol 1985;121:31–6.
(2) Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002;39:1890–900.
(3) van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011;58:2241–7.
(4) Schwedler G, Lindinger A, Lange PE, Sax U, Olchvary J, Peters B, et al. Frequency and spectrum of congenital heart defects among live births in Germany: a study of the Competence Network for Congenital Heart Defects. Clin Res Cardiol 2011;100:1111–7.
(5) Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D, et al. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983–2000: a population-based evaluation. Pediatrics 2005;115:95–101.
(6) Germanakis I, Sifakis S. The impact of fetal echocardiography on the prevalence of liveborn congenital heart disease. Pediatr Cardiol 2006;27:465–72.
(7) Levy DJ, Pretorius DH, Rothman A, Gonzales M, Rao C, Nunes ME, et al. Improved prenatal detection of congenital heart disease in an integrated health care system. Pediatr Cardiol 2013;34:670–9.
(8) Sharland G. Fetal cardiac screening and variation in prenatal detection rates of congenital heart disease: why bother with screening at all? Future Cardiol 2012;8:189–202.
(9) Allan L. Antenatal diagnosis of heart disease. Heart 2000;83:367.
(10) Marek J, Tomek V, Skovranek J, Povysilova V, Samanek M. Prenatal ultrasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart 2011;97:124–30.
(11) Buskens E, Grobbee DE, Frohn-Mulder IM, Stewart PA, Juttmann RE, Wladimiroff JW, et al. Efficacy of routine fetal ultrasound screening for congenital heart disease in normal pregnancy. Circulation 1996;94:67–72.
(12) Sharland GK, Allan LD. Screening for congenital heart disease prenatally. Results of a 2 1/2-year study in the South East Thames Region. Br J Obstet Gynaecol 1992;99:220–5.
(13) Stumpflen I, Stumpflen A, Wimmer M, Bernaschek G. Effect of detailed fetal echocardiography as part of routine prenatal ultrasonographic screening on detection of congenital heart disease. Lancet 1996;348:854–7.
(14) Galindo A, Herraiz I, Escribano D, Lora D, Melchor JC, de la Cruz J. Prenatal detection of congenital heart defects: a survey on clinical practice in Spain. Fetal Diagn Ther 2011;29:287–95.
(15) Bonnet D, Coltri A, Butera G, Fermont L, Le Bidios J, Kachaner J, et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999;99:916–8.
(16) Mahle WT, Clancy RR, McGaurn SP, Goin JE, Clark BJ. Impact of prenatal diagnosis on survival and early neurologic morbidity in neonates with the hypoplastic left heart syndrome. Pediatrics 2001;107: 1277–82.
(17) Franklin O, Burch M, Manning N, Sleeman K, Gould S, Archer N. Prenatal diagnosis of coarctation of the aorta improves survival and reduces morbidity. Heart 2002;87:67–9.
(18) Makikallio K, McElhinney DB, Levine JC, Marx GR, Colan SD, Marshall AC, et al. Fetal aortic valve stenosis and the evolution of hypoplastic left heart syndrome: patient selection for fetal intervention. Circulation 2006;113:1401–5.
(19) Kaguelidou F, Fermont L, Boudjemline Y, Le Bidois J, Batisse A, Bonnet D. Foetal echocardiographic assessment of tetralogy of Fallot and post-natal outcome. Eur Heart J 2008;29:1432–8.
(20) Yates RS. The influence of prenatal diagnosis on postnatal outcome in patients with structural congenital heart disease. Prenat Diagn 2004;24:1143–9.
(21) Berkley EM, Goens MB, Karr S, Rappaport V. Utility of fetal echocardiography in postnatal
Christine van Velzen.indb 62 20/09/2016 08:27

63
Prenatal detection of CHD - national screening
Chap
ter 3
management of infants with prenatally diagnosed congenital heart disease. Prenat Diagn2009;29: 654–8.
(22) Jaeggi ET, Sholler GF, Jones OD, Cooper SG. Comparative analysis of pattern, management and outcome of pre- versus postnatally diagnosed major congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2001;17:380–5.
(23) Eik-Nes S, Lee W, Carvalho JS, Chaoui R, Copel J, Hecher K, et al. Cardiac screening examination of the fetus: guidelines for performing the ‘basic’ and ‘extended basic’ cardiac scan. Ultrasound Obstet Gynecol 2006;27:107–13.
(24) Bull C. Current and potential impact of fetal diagnosis on prevalence and spectrum of serious congenital heart disease at term in the UK. British Paediatric Cardiac Association. Lancet 1999;354:1242–7.
(25) Dolk H, Loane M, Garne E. Congenital heart defects in Europe: prevalence and perinatal mortality, 2000 to 2005. Circulation 2011;123:841–9.
(26) Sharland G. Routine fetal cardiac screening: what are we doing and what should we do? Prenat Diagn 2004;24:1123–9.
(27) Tegnander E, Eik-Nes SH. The examiner’s ultrasound experience has a significant impact on the detection rate of congenital heart defects at the second-trimester fetal examination. Ultrasound Obstet Gynecol 2006;28:8–14.
(28) Khoshnood B, Lelong N, Houyel L, Thieulin AC, Jouannic JM, Magnier S, et al. Prevalence, timing of diagnosis and mortality of newborns with congenital heart defects: a population-based study. Heart 2012;98:1667–73.
(29) Pinto NM, Keenan HT, Minich LL, Puchalski MD, Heywood M, Botto LD. Barriers to prenatal detection of congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2012;40:418–25.
(30) Garne E, Stoll C, Clementi M. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: experience from 20 European registries. Ultrasound Obstet Gynecol 2001;17:386–91.
(31) Shinebourne EA, Rigby ML, Carvalho JS. Pulmonary atresia with intact ventricular septum: from fetus to adult: congenital heart disease. Heart 2008;94:1350–7.
(32) Hornberger LK, Sanders SP, Rein AJ, Spevak PJ, Parness IA, Colan SD. Left heart obstructive lesions and left ventricular growth in the midtrimester fetus. A longitudinal study. Circulation 1995;92:1531–8.
(33) Gardiner HM, Belmar C, Tulzer G, Barlow A, Pasquini L, Carvalho JS, et al. Morphologic and functional predictors of eventual circulation in the fetus with pulmonary atresia or critical pulmonary stenosis with intact septum. J Am Coll Cardiol 2008;51:1299–308.
(34) Matsui H, Mellander M, Roughton M, Jicinska H, Gardiner HM. Morphological and physiological predictors of fetal aortic coarctation. Circulation 2008;118:1793–801.
(35) McBrien A, Sands A, Craig B, Dornan J, Casey F. Impact of a regional training program in fetal echocardiography for sonographers on the antenatal detection of major congenital heart disease. Ultrasound Obstet Gynecol 2010;36:279–84.
(36) Gardiner HM. Access to perinatal cardiology in the United Kingdom. Postgrad Med J 2001;77:1–3.
(37) Brown KL, Ridout DA, Hoskote A, Verhulst L, Ricci M, Bull C. Delayed diagnosis of congenital heart disease worsens preoperative condition and outcome of surgery in neonates. Heart 2006;92: 1298–302.
(38) Tongsong T, Tongprasert F, Srisupundit K, Luewan S. The complete three-vessel view in prenatal detection of congenital heart defects. Prenat Diagn 2010;30:23–9.
Christine van Velzen.indb 63 20/09/2016 08:27

64
Chapter 3
Chapter 3
LETTER TO THE EDITOR
Dear Sir,
We have read with interest the article by van Velzen and co-workers that reports asignificant increase in prenatal detection rate of congenital heart disease (CHD) after the introduction of a national screening programme in the Netherlands. 1
Recently we analysed the prenatal detection rate of 1865 fetuses with a morphologicalCHD, diagnosed in pregnancy till their 1st year of age, in the province of Antwerp,Belgium, using data from the European Surveillance of Congenital Anomalies-Antwerp(EUROCAT) over 16 years. Antwerp represents almost 30% of all births in Flanders (thenorthern part of Belgium).In contrast to van Velzen et al. our data revealed a disappointingly low prenataldetection rate of 29.3% for all morphological CHD and 40.2% for severe CHD. Only48.0% of these were diagnosed before the end of the 24th week of pregnancy. This was51.0% for severe CHD. Therefore the detection rate of morphological CHD before theend of the 24th week is 14.1% and 20.5% for severe CHD. The increasing trend of thedetection rate over this 16-year period is significant (p< 0.0001) (table 1). Probably thisis the effect of the mandatory ultrasound course during the training for obstetrics.Both our group and the one from van Velzen have similar demographic characteristics;Flanders and the Netherlands constitute geographic neighbours.In Flanders, standard midtrimester anomaly scans are being performed for over 18years already. Local guidelines are based on the guidelines of the International Society of Ultrasound. 2 The last 10 years, the Flemish Association of Gynaecology and Obstetrics(VVOG) in collaboration with the Flemish Society of Ultrasound (VVVE) have mademajor efforts, to offer training to all sonographers. In contrast to the Netherlands, nolicence is required to perform the anomaly scan and reimbursement by national healthinsurance is independent from training and qualification.The improving detection rate in the group of van Velzen is clearly the result of betterultrasound screening. 1 The study shows that training followed by certification andpermanent quality control are mandatory to maintain the level, which may be expectedby women. 1
Our numbers confirm that constant training can significantly improve detection percentage of CDH in a general population.
Sincerely,
Dr. Paul Ramaekers, Dr. Dominique Mannaerts, Prof. Dr. Yves Jacquemyn
Christine van Velzen.indb 64 20/09/2016 08:27

65
Prenatal detection of CHD - national screening
Chap
ter 3
REFERENCES(1) van Velzen CL, Clur SA, Rijlaarsdam MEB, Bax CJ, Pajkrt E, Heymans MW, Bekker, MN, Hruda J, de Groot
CJM, Blom NA, Haak MC. Prenatal detection of congenital heart disease—results of a national screening programme. BJOG 2015; doi: 10.1111/1471-0528.13274.
(2) International Society of Ultrasound in Obstetrics and Gynecology, Carvalho JS, Allan LD, Chaoui R, Copel JA, DeVore GR, Hecher K, Lee W, Munoz H, Paladini D, Tutschek B, Yagel S. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol. 2013 Mar;41(3):348-59. doi: 10.1002/uog.12403.
Christine van Velzen.indb 65 20/09/2016 08:27

66
Chapter 3
Chapter 3
REPLY
Sir,
We thank colleagues Ramaekers, Mannaerts, and Jacquemyn for their positive comments on our article. They report a markedly lower detection rate for severe congenital heart disease (CHD) in a comparable population, despite efforts to adequately train all ultrasonographers.
They state that certification and permanent quality control may be an important determinant in our detection rates. Although the aim of the study was not to compare the monitoring system in the Netherlands with other systems, we do agree that quality control may contribute to our good results. In the Netherlands, prenatal screening is centrally organised, with a uniform protocol and regulations. The quality control is divided in eight prenatal screening regions, affiliated with the eight academic fetal medicine units and clinical genetics departments. These eight regions are responsible for and carry out quality monitoring of prenatal screening. In this system, licensing is compulsory. In order to perform anomaly scans, an ultrasonographer requires a license from one of the acknowledged training institutes, as well as a contract with one of the eight prenatal screening regions. Without these prerequisites, insurance companies will not reimburse. National regulations on quality management of the anomaly scan comprise a minimal number of anomaly scans per year (250 per year for starters, and 150 per year for experienced ultrasonographers) and a biannual review of their anomaly scans: the regional quality manager checks images of five randomly selected anomaly scans and scores these scans according to a nationally developed scoring system. We believe that these measures help to maintain the high quality of the anomaly scans. The cost-effectiveness of this quality monitoring system has not been investigated. The cost of a routine anomaly scan in the Netherlands is €160, of which €17 is used to run the regional centres. The overhead costs of the National Health Service (RIVM) must also be taken into account. On the other hand, missed congenital defects would also introduce costs to society. These types of costs are extremely difficult to compare. We agree with Ramaekers et al. that if prenatal screening is offered to women, then quality monitoring should be mandatory, and we strongly believe that the Dutch quality monitoring system contributed to our CHD detection rates. We did not, however, elaborate on these details extensively in our article, as the system itself was not our topic of study. The comment from Ramaekers et al. provides us with a welcome opportunity to explain more about this important underlying aspect of our study.
Christine van Velzen.indb 66 20/09/2016 08:27

Christine van Velzen.indb 67 20/09/2016 08:27

Christine van Velzen.indb 68 20/09/2016 08:27

CHAPTER 4Prenatal Detection of Transposition
of the Great Arteries reduces
Mortality and Morbidity
C.L. van Velzen, M.C. Haak, G. Reijnders, M.E.B. Rijlaarsdam, C.J. Bax, E. Pajkrt, J. Hruda, F. Galindo-Garre, C.M. Bilardo, C.J.M. de Groot, N.A. Blom, S.A. Clur.
Ultrasound in O&G 2015 Mar 45;320-5
Christine van Velzen.indb 69 20/09/2016 08:27

70
Chapter 4
Chapter 4
ABSTRACT
Objectives To evaluate the prenatal detection of transposition of the great arteries (TGA), after the introduction of a Dutch screening program in 2007, as well as the effect of prenatal detection on pre- and postsurgical mortality and morbidity.
Methods In a geographical cohort study, all infants with TGA who were born between 1 January 2002 and 1 January 2012 were included. The cases were divided into two groups: those with and those without a prenatal diagnosis. Pre- and postsurgical mortality was assessed, with a follow-up of 1 year. Pre-surgical morbidity was assessed in terms of cardiovascular compromise, metabolic acidosis, renal and/or hepatic dysfunction and closure of the duct before initiation of therapy.
Results Of all cases (n=144), 26.4% were diagnosed prenatally, with detection rates of 15.7% and 41.0% in the first and last 5 years of the study period, respectively. First-year mortality was significantly lower in cases with a prenatal diagnosis of TGA than in those without (0.0% vs 11.4%, respectively). Pre-surgical mortality (4.9%) only occurred in undetected simple TGA cases. Closure of the duct before treatment, renal dysfunction and hypoxia occurred significantly more often in the group without a prenatal diagnosis.
Conclusions The prenatal detection rate of TGA has increased significantly since the introduction of the screening program in 2007. Prenatal diagnosis is an important factor that contributes to survival of the infant in the first postnatal year. Furthermore, some morbidity indicators were significantly higher in the group without a prenatal diagnosis. These results justify efforts to improve prenatal screening programs.
Christine van Velzen.indb 70 20/09/2016 08:27

71
Prenatal detection of transposition of the great arteries
Chap
ter 4
INTRODUCTION
Transposition of the great arteries (TGA) is one of the most common cyanotic congenital heart defects (CHD), with an incidence of 0.2–0.3 per 1000 live births. 1,2 TGA with an intact ventricular septum or a non-significant ventricular septal defect (VSD), also defined as simple TGA, is rarely associated with chromosomal or extracardiac anomalies. 2 The condition is generally well tolerated by the fetus, but life-threatening cyanotic complications occur shortly after birth. Without treatment, 50% of these infants die within the first month and 90% within the first year of postnatal life. 3 Directly after birth, prostaglandin-E1 is administered to keep the ductus arteriosus open to allow for the mixing of oxygen-rich and oxygen-poor blood. If necessary, a Rashkind procedure (atrial septostomy) is an additional measure that can be performed for short-term survival. The arterial switch operation (ASO) restores a normal pulmonary and systemic circulation, with a 20-year survival rate of 97% and a low surgical mortality rate of 2–5%. 4–6 The preoperative mortality rate is, however, around 4–6%. 6,7 The prenatal detection rate of simple TGA is low (3–27%). 8–12 Gardiner et al. 13 recently published data on an improved detection rate of 37% in a geographically discrete region with local training programs. It is essential that the outflow-tract and three-vessel views are included in screening protocols, as simple TGA shows a normal four-chamber view. 14,15 When the standard anomaly scan was introduced into practice in The Netherlands in January 2007, the four-chamber and outflow-tract views were obligatory items in the protocol. The three-vessel view was a recommended item, but was not compulsory until January 2012. 16
Without a prenatal diagnosis, most infants with TGA are born outside of tertiary-care centers, which delays appropriate care. This may result in unnecessary death or multi-organ or neurocognitive damage. The prenatal diagnosis of TGA reduces neonatal mortality. 7,8,17,18 It is difficult to ascertain whether a prenatal diagnosis influences morbidity, as only a few cohort studies on this subject have been published. Although a positive effect has been observed in some studies 7,17,19, this has not been replicated in others. 5,20
The aim of this study was to determine the prenatal detection rate of TGA in a national screening program and to evaluate the effect of prenatal detection on pre- and post-surgical mortality and pre-surgical morbidity.
METHODS
This was a cohort study in an unselected population, conducted in the north-west region of The Netherlands. Three tertiary referral centers – Academic Medical Center (Amsterdam), VU Medical Center (Amsterdam) and Leiden University Medical Center (Leiden) – are responsible for the care of children with CHD in this region. Cases with TGA
Christine van Velzen.indb 71 20/09/2016 08:27

72
Chapter 4
Chapter 4
diagnosed both pre- and postnatally between 1 January 2002 and 1 January 2012 in the referral region of the centers were identified. Prenatal screening in The Netherlands is mostly performed in primary and secondary healthcare centers; when an anomaly is suspected, patients are referred to tertiary centers. In the obstetric departments of the tertiary centers, fetal echocardiography is performed by a perinatologist in collaboration with a pediatric cardiologist. All cases of suspected fetal TGA were identified from the prenatal ultrasound databases of the tertiary centers. The case list was complemented with all infants with TGA that was diagnosed after birth, selected from the pediatric cardiology departmental databases and cross-checked with catheterization schedules, operating schedules and emergency admissions. To identify infants who had died outside a hospital or who were dead on arrival at an emergency room, postmortem reports from pathology departments were studied. Finally, the database of the Dutch sudden infant death syndrome registry was searched for all cardiac cases that may not have been recorded in the hospital databases. All the cases were reviewed and the pre- and postnatal data were matched. To define a uniform cohort, we included cases of TGA with intact ventricular septum or TGA with VSD with or without coarctation of the aorta (CoA) and/or Taussig–Bing syndrome. Early management of these groups of patients is similar and an arterial switch is the major surgical repair required, with the addition of VSD closure or coarctectomy if needed. We excluded cases with double discordance, atrial isomerism, significant pulmonary stenosis, double outlet right ventricle with the pulmonary artery arising more than 50% from the right ventricle and univentricular heart defects, because all these defects require a different surgical approach.We compared cases with a prenatal diagnosis to those without. All analyses were performed separately in the group of simple TGA (TGA with intact ventricular septum or TGA with non-significant VSD), since this is a homogeneous group, the pathophysiology of which requires urgent treatment in the first week after birth.
Data collection and treatmentData concerning the mother, pregnancy, birth and infant were collected from medical files and included: prenatal ultrasound anomalies and diagnosis, pregnancy outcome, gestational age at delivery, birth weight, sex, location of delivery, age at postnatal diagnosis, presence or absence of extracardiac anomalies, aneuploidy or a genetic syndrome and postpartum diagnosis by echocardiography or, when applicable, results of postmortem examination.All prenatally diagnosed patients were born in one of the three tertiary centers and admitted to the neonatal intensive care unit for prostaglandin infusion immediately after birth. Additional medication or ventilation was started when indicated. The pediatric cardiologist examined the patient after birth, performed an echocardiogram to make a
Christine van Velzen.indb 72 20/09/2016 08:27

73
Prenatal detection of transposition of the great arteries
Chap
ter 4
definitive diagnosis and evaluated the need for a Rashkind procedure. In cases without a prenatal diagnosis, the infants were treated similarly, depending on their condition at the time of admission. We retrieved the following data from their medical files: necessity for resuscitation with inotropes presurgery, oxygen saturation at admission, lowest pH and lactate presurgery (after first pH and lactate directly after birth), levels of creatinine, urea, aspartate aminotransferase and alanine aminotransferase measured no later than day 3 after birth or at admission, closure of the arterial duct before initiation of prostaglandin therapy and performance of a Rashkind procedure. Renal dysfunction was defined as a creatinine level >100 μmol/L (or >60 μmol/L if >7 days old) or urea level >7.0 mmol/L. Furthermore, the number of surgical interventions the infant underwent in the first year following birth and their pre- or postoperative mortality were recorded. Follow-up of all cases was for at least 1 year.
Statistical analysisMeans and SD were calculated to describe numeric variables and Student’s t-test was used to study the differences between the prenatal- and the postnatal-diagnosis groups. Frequencies and percentages were used to describecategorical variables and the chi-square test was used to test associations between categorical variables. For the rates of first-year mortality and closure of the arterial duct before initiation of prostaglandin therapy a likelihood ratio test was used, providing a robust test when frequencies were less than five. We considered P <0.05 to be statistically significant; all tests were two-sided. Data analysis was performed with the SPSS software package version 20 (SPSS Inc., Chicago, IL, USA).
RESULTS
Inclusions, prenatal detection and pregnancy outcomeWe identified 144 cases with TGA. The total birth rate (including stillbirth and termination of pregnancy) in this 10-year study period in the same region was 724 089 births (data supplied by Statistics Netherlands, CBS, Geboorte, kerncijfers, StatLine, Central Bureau of Statistics (accessed 10 December 2012)), resulting in a total birth prevalence for TGA of 2.0 per 10 000 births. Simple TGA occurred in 105 cases, TGA with VSD with or without CoA and/or Taussig–Bing syndrome in 39 cases. There was a significant increase in the proportion of cases diagnosed prenatally as the study progressed. In the period between 2002 and 2006, 13 (15.7%) of the 83 cases with TGA were detected prenatally compared with 25 (41.0%) of the 61 cases in the period between 2007 and 2011, a difference of 25.3% (95% CI, 10.7–39.9%) (P=0.001) in the prenatal detection rate of TGA between these periods. The prenatal detection rate for simple TGA increased from 12.9% (8/62)
Christine van Velzen.indb 73 20/09/2016 08:27

74
Chapter 4
Chapter 4
between 2002 and 2006 to 44.2% (19/43) between 2007 and 2011, a difference of 31.3% (95% CI, 14.4–48.3%) (P <0.001). This increase in prenatal detection corresponded with the initiation of the nationwide prenatal screening program in 2007. Figure 1 shows the percentage of TGA cases that were diagnosed prenatally between 2002 and 2011, according to year. Gestational age at delivery and birth weight were similar for the groups with and without a prenatal diagnosis: mean 275 vs 278 days (P=0.186) and 3323 g vs 3446 g (P=0.207), respectively.
Figure 1 Percentage of neonatal cases of transposition of the great arteries that were diagnosed prenatally in 2002–2011 in the north-west region of The Netherlands, according to year (n=144).
Christine van Velzen.indb 74 20/09/2016 08:27

75
Prenatal detection of transposition of the great arteries
Chap
ter 4
Severe extracardiac anomalies in combination with chromosomal or genetic defects were found in four cases (2.8%), of which three were cases of TGA with signifi cant VSD or Taussig–Bing syndrome (pulmonary artery arising <50% from the right ventricle). In two of these cases, the pregnancy was terminated before 24 weeks’ gestation, and one was liveborn. In one case with simple TGA, 18p-syndrome was diagnosed after birth. All four cases were excluded from further analysis because of the severe extracardiac congenital anomalies and subsequent complications that aff ected postnatal outcome. One intra-uterine fetal death occurred in a case with simple TGA owing to an intrauterine infection diagnosed postmortem. A summary of the included cases, pregnancy outcomes and mortality is given in Figure 2. The distribution of cases within the cohort of 139 liveborn infants (without severe extracardiac anomalies) according to the subcategory of TGA and prenatal or postnatal detection is shown in Table 1. The mean age at diagnosis in the group without a prenatal diagnosis was 7.7 days, 61% were diagnosed within 5 days, 20% were diagnosed more than 10 days and 13% were diagnosed more than 20 days after birth. One case with a prenatal diagnosis was lost to follow-up, since the parents and infant moved out of the study region.
Figure 2 Flowchart summarizing inclusions, pregnancy outcomes and deaths of 144 cases of transposition of the great arteries (TGA) diagnosed in the north-west region of The Netherlands in 2002–2011.
CoA: coarctation of the aorta IUFD: intrauterine fetal demise MCA: multiple congenital anomaliesTOP: termination of pregnancy VSD: ventricular septal defect
TotalTGAcases144
IUFD1(postmortem:intra-uterineinfection)TOP2(trisomy18;geneticdefectwithMCA)
Livebirths141
Exclusions:Aneuploidy1(trisomy18)
Geneticsyndrome1(18p-syndrome)
TGA(+/-VSDorCoAo)139
Pre-operativedeaths5Losttofollow-up1
Underwentsurgery133
Post-operativedeathinfirstyearaftersurgery7
Christine van Velzen.indb 75 20/09/2016 08:27

76
Chapter 4
Chapter 4
MortalityThe presurgical mortality rate of all liveborn infants with simple TGA was 4.9%. None of the cases with a prenatal diagnosis died before surgery. Moreover, none of the cases with complex TGA died before surgery. Five infants (4.9%) of the 103 with simple TGA, born at home or in local hospitals, died before surgery could be performed; all five were of the 77 cases that did not have a prenatal diagnosis (6.5%). These deaths were distributed equally over the study period (2002–2011). One of them died suddenly at home the day after birth, two of them presented the day after birth at a local hospital requiring immediate resuscitation and died with multi-organ failure; the diagnosis of TGA was made at postmortem examination. The fourth case presented 1 hour after birth in a regional hospital with severe hypoxia, due to a severely restricted foramen ovale. Because the neonate showed severe cerebral damage and a therapy-resistant status epilepticus, ASO was not initiated and the neonate subsequently died several days later. The last neonate that died before surgery presented 13 days after birth requiring resuscitation, and died the same day with multi-organ failure.Of the 133 infants who were operated on, seven (5.3%) died within the first year after surgery (Figure 2). Four of the deaths postsurgery were due to circulatory failure within 30 days after ASO. Another case died after several re-interventions, 4.5 months after ASO, resulting in a first-year mortality rate after ASO of 3.8% (5/131). Two other deaths were related to late presentation with simple TGA (age at diagnosis 21 and 24 days, respectively). A first-stage preparatory operation (pulmonary artery banding with a Blalock–Taussig shunt) was performed. Both infants died before an ASO could be performed. All postoperative deaths occurred in patients without a prenatal diagnosis in the years 2002–2007.Thus, the overall first-year mortality rate of liveborn infants with a prenatal diagnosis was 0/34 (0.0%) vs 12/105 (11.4%) infants with a postnatal diagnosis, a difference of 11.4% (95% CI, 5.3–17.5%), likelihood ratio =0.009.
MorbidityThe frequency of all indicators of presurgical morbidity is shown in Table 2. The group without a prenatal diagnosis had a significantly higher incidence of hypoxia, renal dysfunction and closure of the arterial duct before initiation of prostaglandin treatment than did the group with a prenatal diagnosis. For most variables, the data were >95% complete. However, blood analysis of hepatic function was not performed in a considerable number of infants (40%), especially in the group with a prenatal diagnosis (79% not performed).There was no significant relationship between the age (days) at postnatal diagnosis and the morbidity variables. Fifteen infants required more than one surgical intervention in
Christine van Velzen.indb 76 20/09/2016 08:27

77
Prenatal detection of transposition of the great arteries
Chap
ter 4
Table 1 The distribution of cases within the cohort of 139 live-born infants without severe extracardiac anomalies according to the subcategory of transposition of the great arteries (TGA) and prenatal or postnatal detection
TGA subtype Prenatal diagnosis Postnatal diagnosis Total
Simple TGA 26 (25.2) 77 (74.8) 103 (74.1)
TGA with significant VSD 4 (17.4) 19 (82.6) 23 (16.5)
+CoA 1 (16.7) 5 (83.3) 6 (4.3)
TGA Taussig-Bing 4 (30.8) 9 (69.2) 13 (9.4)
+CoA 2 (33.3) 4 (66.7) 6 (4.3)
Total 34 (24.5) 105 (75.5) 139
Data is given as n (%). CoA, coarctation of the arteries; VSD, ventricular septal defect.
Table 2 Frequency and outcome of indicators of presurgical morbidity in 139 infants with transposition of the great arteries (TGA) between 2002 and 2012
Clinical characteristic Category of TGA With prenatal diagnosis(n=34)
Without prenatal diagnosis (n=105) P
Lowest pH pre-surgery
All 7.20 (0.15) 7.24 (0.12) 0.088
Simple 7.19 (0.16) 7.24 (0.14) 0.113
Highest lactate pre-surgery
All 4.75 (2.45) 4.97 (4.82) 0.807
Simple 4.82 (2.66) 5.44 (5.46) 0.589
Oxygen saturation at admission †
All 73.6 (15.9) 67.0 (15.55) 0.048*
Simple 69.4 (15.6) 63.3 (15.1) 0.099
Renal dysfunction † All 1 (4.3%) 17 (19.1%) 0.039*
Simple 1 (5.6%) 15 (21.7%) 0.021*
AST ‡ All 60.9 (23.9) 204.5 (941.5) 0.633
Simple 59.3 (26.1) 256.0 (1085.0) 0.613
ALT ‡ All 38.7 (29.5) 90.2 (489.6) 0.730
Simple 32.4 (18.3) 112.6 (561.9) 0.673
Closure duct before start PGE †
All - 21 (23.6%) 0.000*
Simple - 13 (19.7%) 0.002*
Inotropes pre-surgery All 7 (21.2%) 27 26.0%) 0.602
Simple 7 (28.0%) 22 (28.6%) 0.712
Rashkind performed All 20 (60.6%) 67 (64.4%) 0.691
Simple 17 (68.0%) 57 (74.0%) 0.557
Data are given as mean plus or minus SD or n/N (%). All TGA (n=139) includes simple TGA (n=103) and TGA with ventricular septal defect or Taussig–Bing syndrome, with or without coarctation of the aorta (n=26). 26 cases of simple TGA had a prenatal diagnosis; 77 had a postnatal diagnosis. Missing data <4% for most variables. *P <0.05. †15% missing data. ‡40% missing data (missing in 79% of cases with prenatal diagnosis; tests were performed only on indication). ALT, alanine aminotransferase; AST, aspartate aminotransferase; PGE, prostaglandin-E.
Christine van Velzen.indb 77 20/09/2016 08:27

78
Chapter 4
Chapter 4
the first year after birth. In five of these cases, a two-stage ASO was performed (three owing to late postnatal diagnosis (>21 days after birth), one owing to premature closure of the foramen ovale and one because of a pulmonary hemorrhage). All other cases (n=10) required re-interventions after ASO owing to postsurgical residual defects. Two or more surgical interventions tended to be needed more frequently in the group without a prenatal diagnosis than in those with a prenatal diagnosis: 12.4% vs 0.6%(P=0.089), respectively. Severe neurological complications in the first year after birth occurred in two cases, of which one died (described previously). The other case was diagnosed 1 day after birth with simple TGA and suffered cerebral infarctions and subdural hemorrhage.
DISCUSSION
This paper describes the largest population-based cohort study of neonates with TGA performed to date, assessing prenatal detection and mortality and morbidity rates in the first year after birth. The total birth prevalence of TGA was 2.0 per 10 000 births, which is in accordance with data in the published literature. 2,8 We found that a prenatal diagnosis of TGA is associated with a first-year mortality rate of 0%. Moreover, this study evaluated multiple objective indicators of the severity of the illness preoperatively and found that several indicators were significantly in favor of the group with a prenatal diagnosis. The prenatal detection rate of TGA and especially simple TGA increased significantly from 15.7% to 41.0% and from 12.9% to 44.2%, respectively, after a national screening program was introduced in 2007. It is known that the prenatal detection rate of TGA and especially simple TGA is generally low (<27%). 8,12 The improvement in prenatal detection in The Netherlands can be attributed to the introduction of a uniform national screening protocol with trained and certified ultrasonographers. In contrast to other CHD, simple TGA has a low prevalence of associated malformations and genetic or chromosomal anomalies likely to influence the outcome. Postnatal survival in newborns with TGA largely depends on the timely initiation of specific treatment after birth. 21 As the surgical results for ASO continue to improve and operative mortality falls below 3% 4, strategies to optimize neonatal presurgical care are essential to reduce the overall mortality rate of TGA and especially simple TGA. Significant decreases in mortality rate have been shown after a prenatal diagnosis. 7,8,17,18 Bonnet et al. 7 described a significant decrease in mortality rate, down to 0% after a prenatal diagnosis. The data they used for their study were from 1988–1997 and were institution-based, which means that only infants referred to their center were included. Since the 1990s, the performance of prenatal screening has improved significantly. 18 More recent population-based studies have also shown a reduced mortality rate in prenatally diagnosed infants, but the
Christine van Velzen.indb 78 20/09/2016 08:27

79
Prenatal detection of transposition of the great arteries
Chap
ter 4
number of cases was rather limited. 8,17,18 Our findings confirm that even in the present era, with modern resuscitation techniques, a prenatal diagnosis is important in order to reduce overall mortality. The first-year mortality rate of liveborn infants with a prenatal diagnosis was 0.0%, compared with 11.4% for infants without a prenatal diagnosis. Presurgical mortality of the simple TGA cases without a prenatal diagnosis was 6.5%. These deaths were equally distributed over the 10-year study period, which rules out a bias due to improved resuscitation and intensive care. The postsurgical deaths all occurred in the first 6 years of the study period. This might be explained by the progress in pediatric diagnostics, pediatric cardiology, cardiac surgery and intensive care in the most recent years. Differences in morbidity within the first year after birth are more complex to evaluate, since morbidity is difficult to capture as a single outcome variable. Bonnet et al. 7 found a significantly higher rate of preoperative mechanical ventilation and metabolic acidosis as well as a significantly longer hospital stay in the group without a prenatal diagnosis. Fuchs et al. 17 found some indicators of morbidity to be significantly in favor of cases with a prenatal diagnosis, however four different cardiac diseases were analyzed as one cohort, without a separate analysis for TGA. Children and adolescents born with TGA have higher rates of neurodevelopmental problems after correction of TGA than do normal populations. 22,23 The main explanation for this is the hypoxic complications that occur before and during surgery. 24 Calderon et al. 19 described better neurocognitive outcomes in children with a prenatal diagnosis. This was attributed to immediate and optimal presurgical care. Since follow-up in our study was for only 1 year after birth, it is not possible to report the long-term neurological follow-up.
We found a significantly higher incidence of preoperative hypoxia, closure of the arterial duct before initiation of prostaglandin treatment and renal dysfunction in those infants without a prenatal diagnosis. Although not statistically significant, two or more surgical interventions were needed more frequently in the group without a prenatal diagnosis. In some cases multiple interventions could have been prevented by a prenatal diagnosis. All these adverse outcomes could contribute to long-term neurodevelopmental problems.All analyses were performed separately in the simple TGA cases. The main argument for performing a separate analysis is the homogeneity of this group, which is not influenced by more complex surgical anatomy, allowing for the most reliable assessment of the effects of prenatal diagnosis. Moreover, this particular group has the most urgent pathophysiology in the first week after birth. We found a significantly higher incidence of closure of the duct before initiation of treatment and of renal dysfunction in the group without a prenatal diagnosis. Although not statistically significant, the rates of hepatic dysfunction and high lactate levels tended to be higher in the group without
Christine van Velzen.indb 79 20/09/2016 08:27

80
Chapter 4
Chapter 4
a prenatal diagnosis. The blood analysis of hepatic function was not performed during admission in a considerable number of infants (40%), especially in the group with a prenatal diagnosis (79% not performed), possibly indicating that the clinical condition of infants with a prenatal diagnosis was more favorable. This was a population-based study in an area where 72 000 infants are born per year, which is approximately 40% of all live births in The Netherlands. All cases in the region were included, from rural as well as urban areas, including deaths outside the hospital.The lost-to-follow-up rate in our cohort was very low. Another strength of this study is that the implementation of the screening program and the training and certification of ultrasonographers have been uniform throughout The Netherlands. Even though this is one of the largest cohorts analyzed, this study is nevertheless limited by the number of cases included and its retrospective character.The detection rate of TGA has improved significantly since 2007, however, over 50% of cases of TGA are still being missed by prenatal screening. The three-vessel view has been included as a compulsory element in the prenatal cardiac screening protocol since January 2012.
With education for ultrasonographers on how to evaluate the three-vessel view plane and the spatial relationship between the aorta and pulmonary trunk, an improved performance of screening for TGA can, we hope, be achieved.In conclusion, first-year and presurgical mortality rates of cases with TGA are significantly decreased by a prenatal diagnosis, from 11.4% to 0% and from 4.9% to 0%, respectively. Moreover, several presurgical morbidity indicators are significantly in favor of the group with a prenatal diagnosis, indicating that these infants are in a better condition presurgery. Still, a substantial number of infants with TGA are diagnosed days to weeks after birth. These results justify all efforts to improve prenatal screening programs.
Christine van Velzen.indb 80 20/09/2016 08:27

81
Prenatal detection of transposition of the great arteries
Chap
ter 4
REFERENCES
(1) Ferencz C, Rubin JD, McCarter RJ, Brenner JI, Neill CA, Perry LW, Hepner SI, Downing JW. Congenital heart disease: prevalence at livebirth. The Baltimore–Washington Infant Study. Am J Epidemiol 1985; 121: 31–36.
(2) Martins P, Castela E. Transposition of the great arteries. Orphanet J Rare Dis 2008; 3: 27.
(3) Liebman J, Cullum L, Belloc NB. Natural history of transpositon of the great arteries. Anatomy and birth and death characteristics. Circulation 1969; 40: 237–262.
(4) Tobler D, Williams WG, Jegatheeswaran A, Van Arsdell GS, McCrindle BW, Greutmann M, Oechslin EN, Silversides CK. Cardiac outcomes in young adult survivors of the arterial switch operation for transposition of the great arteries. J Am Coll Cardiol 2010; 56: 58–64.
(5) Kumar RK, Newburger JW, Gauvreau K, Kamenir SA, Hornberger LK. Comparison of outcome when hypoplastic left heart syndrome and transposition of the great arteries are diagnosed prenatally versus when diagnosis of these two conditions is made only postnatally. Am J Cardiol 1999; 83: 1649–1653.
(6) Soongswang J, Adatia I, Newman C, Smallhorn JF, Williams WG, Freedom RM. Mortality in potential arterial switch candidates with transposition of the great arteries. J Am Coll Cardiol 1998; 32: 753–757.
(7) Bonnet D, Coltri A, Butera G, Fermont L, Le Bidois J, Kachaner J, Sidi D. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999; 99: 916–918.
(8) Blyth M, Howe D, Gnanapragasam J, Wellesley D. The hidden mortality of transposition of the great arteries and survival advantage provided by prenatal diagnosis. BJOG 2008; 115: 1096–1100.
(9) Garne E, Stoll C, Clementi M; Euroscan Group. Evaluation of prenatal diagnosis of congenital heart diseases by ultrasound: experience from 20 European registries. Ultrasound Obstet Gynecol 2001; 17: 386–391.
(10) Jaeggi ET, Sholler GF, Jones OD, Cooper SG. Comparative analysis of pattern, management and outcome of pre- versus postnatally diagnosed major congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2001; 17: 380–385.
(11) Bull C. Current and potential impact of fetal diagnosis on prevalence and spectrum of serious congenital heart disease at term in the UK. British Paediatric Cardiac Association. Lancet 1999; 354: 1242–1247.
(12) Marek J, Tomek V, Skovranek J, Povysilova V, Samanek M. Prenatal ultrasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart 2011; 97: 124–130.
(13) Gardiner HM, Kovasevic A, Van der Heijden LB, Pfeiffer PW, Franklin RC, Gibbs JL, Averiss IE, Larovere JM. Prenatal screening for major congenital heart disease: assessing performance by combining national cardiac audit with maternity data. Heart 2014; 100: 375–382.
(14) Vin˜ als F, Ascenzo R, Poblete P, Comas C, Vargas G, Giuliano A. Simple approach to prenatal diagnosis of transposition of the great arteries. Ultrasound Obstet Gynecol 2006; 28: 22–25.
(15) Yagel S, Cohen SM, Messing B. First and early second trimester fetal heart screening. Curr Opin Obstet Gynecol 2007; 19: 183–190.
(16) International Society of Ultrasound in Obstetrics & Gynecology. Cardiac screening examination of the fetus: guidelines for performing the ‘basic’ and ‘extended basic’ cardiac scan. Ultrasound Obstet Gynecol 2006; 27: 107–113.
(17) Fuchs IB, Mu¨ ller H, Abdul-Khaliq H, Harder T, Dudenhausen JW, HenrichW. Immediate and long-term outcomes in children with prenatal diagnosis of selected isolated congenital heart defects. Ultrasound Obstet Gynecol 2007; 29: 38–43.
(18) Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D, Goffinet F. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983–2000: a population-based evaluation. Pediatrics 2005; 115: 95–101.
Christine van Velzen.indb 81 20/09/2016 08:27

82
Chapter 4
Chapter 4
(19) Calderon J, Angeard N, Moutier S, Plumet MH, Jambaque I, Bonnet D. Impact of prenatal diagnosis on neurocognitive outcomes in children with transposition of the great arteries. J Pediatr 2012; 161: 94-8.
(20) Bartlett JM, Wypij D, Bellinger DC, Rappaport LA, Heffner LJ, Jonas RA, Newburger JW. Effect of prenatal diagnosis on outcomes in D-transposition of the great arteries. Pediatrics 2004; 113: e335–40.
(21) Quaegebeur JM, Rohmer J, Ottenkamp J, Buis T, Kirklin JW, Blackstone EH, Brom AG. The arterial switch operation. An eight-year experience. J Thorac Cardiovasc Surg 1986; 92: 361–384.
(22) Hovels-Gurich HH, Seghaye MC, Schnitker R, Wiesner M, HuberW,Minkenberg R, Kotlarek F, Messmer BJ, Von Bernuth G. Long-term neurodevelopmental outcomes in school-aged children after neonatal arterial switch operation. J Thorac Cardiovasc Surg 2002; 124: 448–458.
(23) Bellinger DC, Wypij D, Rivkin MJ, DeMaso DR, Robertson RL Jr, Dunbar-Masterson C, Rappaport LA, Wernovsky G, Jonas RA, Newburger JW. Adolescents with d-transposition of the great arteries corrected with the arterial switch procedure: neuropsychological assessment and structural brain imaging. Circulation 2011; 124: 1361–1369.
(24) Bellinger DC, Wypij D, Kuban KC, Rappaport LA, Hickey PR, Wernovsky G, Jonas RA, Newburger JW. Developmental and neurological status of children at 4 years of age after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation 1999; 100: 526–532.
Christine van Velzen.indb 82 20/09/2016 08:27

Christine van Velzen.indb 83 20/09/2016 08:27

Christine van Velzen.indb 84 20/09/2016 08:27

CHAPTER 5Prenatal Diagnosis of Congenital Heart
Defects: Accuracy and Discrepancies
in a Multicenter Cohort
C.L. van Velzen, S.A. Clur, M.E.B. Rijlaarsdam, E. Pajkrt, C.J. Bax, J. Hruda, C.J.M. de Groot, N.A. Blom, M.C. Haak
Ultrasound Obstet Gynecol 2016 May(5);47:616-22
Christine van Velzen.indb 85 20/09/2016 08:27

86
Chapter 5
Chapter 5
ABSTRACT
Objective To examine the accuracy of fetal echocardiography in diagnosing congenital heart disease (CHD) at the fetal medicine units of three tertiary care centers.
Methods This was a multicenter cohort study of tertiary echocardiography referrals between 2002 and 2012. Prenatal and postnatal diagnoses were compared and the degree of agreement was classified as ‘correct’ (anatomy correct and the postnatal diagnosis led to a similar outcome as expected), ‘discrepant’ (anatomical discrepancies present but the severity and prognosis of the defect were diagnosed correctly) or ‘no similarity’ (thepre- and postnatal diagnoses differed completely).
Results We included 708 cases with CHD for which both prenatal and postnatal data were available. The prenatal diagnosis was correct in 82.1% of cases and discrepancies were present in 9.9%; however, these did not result in a different outcome. In 8.1% there was no similarity between prenatal and postnatal diagnoses. Disagreement between pre- and postnatal diagnoses occurred significantly more frequently in cases that presented with a normal four-chamber view than in those with an abnormal four-chamber view (5.5% vs 1.9%).Incorrect identification of the outflow tracts and incorrect differentiation between unbalanced atrioventricular septal defect and hypoplastic left heart syndrome were relatively commonly encountered. Inmany cases with disagreement, trisomy 21, extracardiac anomaly or a high maternal body mass index was present.
Conclusions The prenatal diagnosis and estimated prognosis of fetal echocardiography in our tertiary referral centers were appropriate in 92% of cases. Some types of CHD remain difficult to diagnose or rule-out prenatally, therefore awareness and education are of considerableimportance.
Christine van Velzen.indb 86 20/09/2016 08:27

87
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
INTRODUCTION
An accurate prenatal diagnosis of congenital heart defects (CHD) is critical in determining the requirement for immediate postnatal treatment, predicting the course of (surgical) treatment and assessing the prognosis of the defect, including long-term outcome. 1,2
This information is also necessary for determining the location and timing of delivery. A correct diagnosis is essential to enable parents to make an informed decision if they are considering termination of pregnancy (TOP). However, available data on the diagnostic accuracy of fetal echocardiography are limited and mostly based on small cohorts. 3–8
The standard anomaly scan for prenatal screening of congenital defects in The Netherlands is performed in primary and secondary healthcare centers. The anomaly scan is carried out between 18 and 22 weeks’ gestation by well-trained sonographers and obstetricians. This national second-trimester screening program started in 2007 and, since its introduction, the detection rate for CHD has increased from 35.8% in 2007 to 59.7% in 2012. 9 Since 2007, the average number of false-negative second-trimester screening scans, of 72 000 infants born per year in this region, has been 81.If CHD is suspected, fetal echocardiography is performed in a department of prenatal diagnosis in a tertiary center. Women with an increased risk of having offspring with a congenital heart anomaly are screened directly in a tertiary center.This study aimed to explore the diagnostic accuracy of a prenatal diagnosis of cardiac defects at the fetal medicine units of three tertiary care centers in The Netherlands that closely collaborate in the care of children with CHD. The secondary aim was to assess the influence of the type of cardiac anomaly on the accuracy of the diagnosis and to analyze cases with diagnostic errors.
METHODS
This study was performed in the Academic Medical Center, Amsterdam, VU University Medical Center, Amsterdam and Leiden University Medical Center, Leiden. These three tertiary referral centers collaborate in the care of children with CHD in the north-westregion of The Netherlands. Patients with a suspected cardiac anomaly within this geographical area are referred for targeted fetal echocardiography to one of the centers. Here, cases are examined by a fetal medicine specialist. Once a cardiac anomaly is confirmed, the patient is scheduled for a cardiac examination with a pediatric cardiologist. All women are routinely offered karyotyping (more recently quantitative fluorescence polymerase chain reaction with array) if CHD is diagnosed. Over a period of 10 years (2002–2011), all cases diagnosed with CHD by fetal echocardiography in one of the three centers were reviewed to determine the accuracy of the prenatal diagnosis. All prenatal medical records were cross-matched with the postnatal files. 9 The final
Christine van Velzen.indb 87 20/09/2016 08:27

88
Chapter 5
Chapter 5
prenatal cardiac diagnosis was compared with the postnatal anatomy as diagnosed by echocardiography, combined with the findings during catheter intervention or surgery. In cases of neonatal death or TOP (the legal limit for which in The Netherlands is 24 completed weeks’ gestation for non-lethal anomalies), the prenatal diagnosis was compared with the results of a postmortem examination performed by an expert pathologist. When a postnatal diagnosis was not available (e.g. in cases of TOP or intrauterine fetal demise for which the parents declined a postmortem examination) the case was excluded. Cases of trisomy 13 or 18 were also excluded from the analysis, as the aneuploidy itself would have a much greater impact on the outcome than the associated CHD. To locate false-negative cases, we checked whether the mothers of all infants with a postnatal diagnosis of CHD had undergone fetal echocardiography in one of the tertiary centers. 9 All cases were allocated to one of three categories according to the level of agreement between the prenatal and postnatal diagnoses (correct; discrepant; no similarity). The categories were defined as follows:
(1) Correct: postnatal anatomy and diagnosis were in agreement with the prenatal findings and led to a comparable intervention and outcome, as expected prenatally. The detection of small septal defects that were not confirmed postnatally, or the failure to detect ones that were present, along with minor discrepancies in the size of defects found both pre- and postnatally were accepted in this category.
(2) Discrepant: prenatal diagnosis differed from the postnatal diagnosis. If a different surgical intervention was performed from that which was initially predicted, but the severity of the defect and long-term prognosis were the same as expected prenatally, the case was included. Thus cases in which a biventricular repair was predicted but univentricular palliation was needed were not accepted in this category. Examples accepted in this category were cases with a prenatal diagnosis of atrioventricular septal defect (AVSD) with overriding aorta and a postnatal diagnosis of tetralogy of Fallot. Other examples were cases with a prenatal diagnosis of hypoplastic left heart syndrome (HLHS) and a postnatal diagnosis of borderline HLHS (severe coarctation of the aorta, hypoplastic aortic arch and mitral valve stenosis that required univentricular palliation).
(3) No similarity: prenatal and postnatal diagnosis and prognosis were completely different and/or led to a completely different surgical intervention from that which was predicted. The process of categorizing agreement was as follows: The first author (C.L.v.V.) went through all cases and when there was full agreement in prenatal and postnatal diagnoses, they were allocated to the category ‘correct’. All other cases that were not in full agreement were discussed in a committee. All three centers were
Christine van Velzen.indb 88 20/09/2016 08:27

89
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
represented on this committee to ensure an open and critical discussion (C.L.v.V, M.C.H., M.E.B.R. and S.A.C.). Cases that had a significant suspicion of CHD prenatally but had normal anatomy after birth were also included in this category. The data were analyzed with the aim of detecting factors that could influence the diagnostic accuracy of echocardiography.We compared the accuracy of echocardiography in diagnosing cardiac anomalies detectable by examination in the four-chamber view only with the accuracy of diagnosing anomalies that required additional examination of the outflow tracts and presented with a more-or-less normal four-chamber view. 3 We also compared the diagnostic accuracy in cases that presented with prenatally detected extracardiac anomalies (structural anomalies, severe intrauterine growth restriction, fetal hydrops, prenatally detected aneuploidy other than trisomy 13 or 18 or genetic syndromes) with cases that presented prenatally as isolated CHD.
Statistical analysisAbsolute numbers and percentages of accurate diagnoses were calculated. The chi-square test was used to assess for associations between categorical variables, and P < 0.05 was considered as statistically significant; all tests were two-sided. Data analysis was done using SPSS software (version 20; SPSS Inc., Chicago, IL, USA).
RESULTS
Accuracy cohortIn the study period, 1119 fetuses were diagnosed with CHD by prenatal echocardiography. Complete follow-up data were available for all cases. In 348 cases in which fetal demise occurred (n = 73) or TOP (n = 275) was performed, the parents declined postmortem examination. These cases were excluded because comparison between prenatal and postnatal diagnoses could not be carried out. In those with TOP and no postmortem, there were 94 cases of trisomy 13 or 18. Of the remaining 181 cases, 55 (30.4%) had a univentricular heart defect and 119 (65.7%) had another type of CHD combined with anabnormal karyotype, 22q11 deletion or at least one severe extracardiac anomaly. Another 63 cases were excluded because of trisomy 13 or 18, the majority of which did not undergo postmortem examination. Thus a total of 411 cases were excluded, leaving 708 cases in which a prenatal and postnatal diagnosis of CHD was available for inclusion in the analysis. Five hundred and forty-one pregnancies resulted in a live birth, intrauterine fetal demise occurred in 18 and there were 149 cases for which the parents chose TOP and a postmortem examination was performed. In 77.1% of terminated pregnancies, additional anomalies were present, including chromosomal anomalies (e.g. 22q11 deletion or trisomy 21). The mean gestational age at the time
Christine van Velzen.indb 89 20/09/2016 08:27

90
Chapter 5
Chapter 5
of diagnosis was 23+1weeks ± 36 days. A small proportion of these cases (n = 147) have been described previously but were analyzed in a different manner. 7 The prenatal diagnosis was correct in 581/708 (82.1%) cases. In 9.9% (70/708) of cases, a discrepancy between the prenatal and postnatal diagnoses was found. In 8.1% (57/708) of cases, there was no similarity between the prenatal and postnatal diagnoses. In 281 (39.7%) cases, additional congenital anomalies were detected prenatally.There were 13 false-negative cases for which prenatal echocardiography was normal but a postnatal diagnosis of CHD was made among the three tertiary centers duringthe study period (Table 1).
Accuracy according to type of cardiac defectThe size of the cohort enabled us to study the diagnostic accuracy of echocardiography according to the type of CHD diagnosed, as shown in Table 2. Categorization of the CHD was determined by the definitive postnatal diagnosis. The types of CHD that most frequently showed discrepancies or no similarity between the prenatal and postnatal diagnoses were valvular and aortic arch anomalies, abnormal venous return and complex defects with isomerism. Those cases with prenatally suspected heart defects but with normal anatomy after birth are also shown in Table 2. Of the 58 cases with prenatal left/right disproportion, 40 (69.0%) had an aortic arch anomaly after birth and 18 (31.0%) had a normal heart after birth.
Table 1 Postnatal echocardiographic findings in 13 cases of congenital heart defect (CHD) false-negative on prenatal echocardiography
Postnatal diagnosis Number
VSD 4
Partial abnormal pulmonary venous return 1
Truncus arteriosus type I with interruption of aortic arch* 1
Transposition of the great arteries, intact IVS* 2
Coarctation of the aorta, intact IVS* 2
VSD with overriding aorta, no pulmonary artery stenosis 1
Critical aortic valve stenosis* 1
Cardiomyopathy 1
*Ductal-dependent CHD. IVS, interventricular septum.
Christine van Velzen.indb 90 20/09/2016 08:27

91
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
Table 2 Degree of agreement between prenatal and postnatal echocardiographic findings in 708 cases with congenital heart defect, according to type of defect
Heart defect category Total n
Agreement n (%)
Discrepancies n (%)
No similarityn (%)
1.Septal defects 166 155 (93.4) 10 (6.0) 1 (0.6)
2.Valvular anomalies, biventricular heart
31 22 (71.0) 8 (25.8) 1 (3.2)
3.Venous return anomalies 26 18 (69.2) 7 (26.9) 1 (3.8)
4.Aortic arch anomalies 40 30 (75.0) 8 (20.0) 2 (5.0)
5.Conotruncal anomalies 149 130 (87.2) 9 (6.0) 10 (6.7)
6.Hypoplastic Right Heart syndrome 17 15 (88.2) 2 (11.8) -
7.Hypoplastic Left Heart syndrome 71 65 (91.5) 4 (5.6) 2 (2.8)
8.Other univentricular heart defects 87 79 (90.8) 8 (9.2) -
9.Complex defects with atrial isomerism
40 30 (75.0) 9 (22.5) 1 (2.5)
10.Miscellaneous 43 37 (86.0) 5 (11.6) 1 (2.3)
11. Normal heart after birth 38 - - 38 (100)
Total 708 581 (82.1) 70 (9.9) 57 (8.1)
Categories consist of:1. Ventricular septal defect(s) (VSD), balanced atrioventricular septal defect (AVSD)2. Pulmonary or aortic valve stenosis, Ebstein’s anomaly, tricuspid dysplasia or regurgitation3. Partial anomalous pulmonary venous return, isolated persistent left superior caval vein (PLSCV), isolated interrupted
inferior caval vein, isolated pulmonary vein stenosis4. Aortic coarctation (CoAo), hypoplastic or interrupted aortic arch, multiple level left heart obstruction, isolated right
aortic arch 5. Tetralogy of Fallot, double outlet right ventricle (DORV)-Fallot type or DORV and VSD and/or pulmonary stenosis (PS),
simple transposition of great arteries (TGA) (without significant VSD), complex TGA (with significant VSD and/or PS), DORV Taussig Bing (= TGA type), truncus arteriosus, pulmonary atresia with VSD, congenitally corrected TGA (ccTGA), absent pulmonary valve syndrome, aortopulmonary window
6. Pulmonary atresia with intact ventricular septum, critical pulmonary valve stenosis with right ventricular (RV) hypoplasia
7. Aortic valve atresia or critical aortic valve stenosis with left ventricular (LV) hypoplasia8. Double inlet left ventricle, tricuspid valve atresia, absent left A-V connection, unbalanced AVSD, TGA with RV hypoplasia
and straddling tricuspid valve, criss-cross, DORV with mitral valve and LV hypoplasia, congenitally corrected TGA with RV hypoplasia, isolated AV discordance with hypoplastic RV and VSD
9. Left or right atrial isomerism, heterotaxy syndromes10. Myocardial anomalies, rhabdomyoma, non-specific complex heart defect, polyvalvular disease, left/right disproportion,
right atrial aneurysm, aneurysm interventricular septum, aortic root dilatation (Marfan), isolated cardiac malposition
Christine van Velzen.indb 91 20/09/2016 08:27

92
Chapter 5
Chapter 5
Table 3 Degree of agreement between prenatal and postnatal echocardiographic findings in 555 cases with congenital heart defects (CHD) visible only on either four-chamber view or outflow-tract views
CHD visible on Total (n)
Agreement n (%)
Discrepant n (%)
No similarityn (%)
Four chamber view 374 328 (87.7) 39 (10.4) 7 (1.9)
Outflow tract views 181 152 (84.0) 19 (10.5) 10 (5.5)
Table 4 Cardiac anomalies visible mainly on four-chamber view or outflow-tract views
Cardiac anomalies visible in four chamber view Cardiac anomalies predominately visible in the outflow tract views
VSD, balanced AVSD, Ebstein’s anomaly, tricuspid dysplasia or regurgitation, hypoplastic aortic arch, interrupted aortic arch, multiple level left heart obstruction, congenitally corrected TGA, pulmonary atresia with intact ventricular septum, critical pulmonary valve stenosis with RV hypoplasia, aortic valve atresia or critical aortic valve stenosis with LV hypoplasia, double inlet left ventricle, tricuspid valve atresia, absent left AV connection, unbalanced AVSD, TGA with RV hypoplasia and straddling tricuspid valve, criss-cross, DORV with mitral valve and LV hypoplasia, congenitally corrected TGA with RV hypoplasia, isolated AV discordance with hypoplastic RV and VSD, myocardial anomalies, rhabdomyoma, right atrial aneurysm, aneurysm interventricular septum
Tetralogy of Fallot, DORV-fallot type or DORV and VSD and/or pulmonary stenosis, simple TGA (without significant VSD), complex TGA (with significant VSD and/or PS), DORV Taussig Bing (= TGA type), truncus arteriosus, pulmonary atresia with VSD, absent pulmonary valve syndrome, aortopulmonary window, aortic root dilatation (Marfan), isolated pulmonary or aortic valve stenosis, isolated persistent left superior caval vein, isolated right aortic arch
This classification is based on the one published by Sharland (3)List of abbreviations:TGA: transposition of great arteries RV: right ventricularLV: left ventricular AV: atrioventricularDORV: double outlet right ventricle PS: pulmonary stenosis
Table 5 Type of discrepancy in 70 cases with different prenatal and postnatal echocardiographic findings of congenital heart defect
Discrepant n/N
Prenatally diagnosed with trisomy 21 and balanced AVSD, but more extensive heart defects found postnatally
10/49
Prenatally detected severe extracardiac anomaly determining the prognosis more than did the CHD 13/106
Univentricular heart diagnosed prenatally as unbalanced AVSD, determined postnatally to be HLHS (or vice versa)
6/95
Univentricular heart, identification right / left side incorrect 2/175
Mild left/right disproportion, cause of disproportion misinterpreted 11/46
Incorrect identification outflow tract in cases in which the other outflow tract was too small to visualise 4*
Miscellaneous 24*
n=discrepant cases N=cases with this prenatal diagnosis* In these cases the denominator could not be calculated.
Christine van Velzen.indb 92 20/09/2016 08:27

93
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
Accuracy in four-chamber-view anomalies vs outflow-tract anomaliesA significant difference (P = 0.019) was found when comparing the degree of accuracy in diagnosing defects visible in the four-chamber view with the accuracy in diagnosing defects that were not visible in the four-chamber view (more-or-less normal four-chamber view) but required additional examination of the outflow tracts (Table 3). The cardiac anomalies visible in each view are classified in Table 4. Some types of CHD, such as coarctation of the aorta, are known to show variation in their presentation, and can show an abnormal four-chamber view, as well as an abnormal outflow-tract view, and therefore these cases were not included in this subset. Fetuses with hearts that were found to be normal after birth were also excluded from this subset.
DiscrepanciesIn cases that showed discrepancy (n = 70), certain groups or patterns could be recognized into which most of the cases could be categorized (Table 5). In 10/49 (20.4%) CHD cases diagnosed with trisomy 21, a discrepancy between the prenatal and postnatal diagnoses was present. Other circumstances in which discrepancies frequently occurred were the presence of other major anomalies or cases with left/right disproportion.
Cases with no similarityThe 57 cases with no similarity between the prenatal and postnatal diagnoses are summarized in Table 6. Factors that could have a negative impact on the quality ofthe ultrasound examination were present in 70.2% of the cases. We evaluated whether at least the ductal dependency of the cardiac defect was prenatally detected. In five cases, ductal dependency was not recognized before birth and, as a consequence, the infant was not treated appropriately with prostaglandin E immediately after birth.
DISCUSSION
This large multicenter cohort study confirms that, in experienced hands, the accuracy of fetal echocardiography is high (82.1% with full agreement between pre- and postnatal diagnosis). If discrepancies that did not lead to a different treatment or prognosis are accepted, the prenatal diagnosis was accurate in 92.0% of cases. These findings are in accordance with those of previous reports in smaller, single-center cohorts. 4–8,10–12
A correct prenatal diagnosis is of great importance, as it determines or influences decisions on postnatal management, delivery location and continuation of the pregnancy. The prenatal diagnosis was not correct in 8.1% of cases, leading to inappropriate treatment immediately after birth in some cases or a different prognosis from that which was expected prenatally. More than one-third of these incorrect diagnoses were left/right disproportion with a normal anatomy after birth. It is known that left/right disproportion can predict coarctation of the aorta, but with low sensitivity and specificity. 13
Christine van Velzen.indb 93 20/09/2016 08:27

94
Chapter 5
Chapter 5
Tabl
e 6
Ove
rvie
w o
f 57
case
s in
whi
ch th
ere
was
no
sim
ilarit
y be
twee
n pr
e- a
nd p
ostn
atal
dia
gnos
is
Pren
atal
dia
gnos
isPo
stna
tal d
iagn
osis
Influ
enci
ng fa
ctor
*D
ucta
l dep
ende
nce
ackn
owle
dged
AV-d
isco
rdan
ce, P
S, V
SD, c
omm
on a
triu
mH
LHS,
aor
tic v
alve
atr
esia
OCA
yes
HLH
SCo
mpl
ete
bala
nced
AVS
D.
Suba
ortic
ste
nosi
s.
Hyp
opla
stic
aor
tic a
rch,
PLS
CV
OCA
, GA
yes
Tric
uspi
d re
gurg
itatio
nCo
Ao
GA
no
(A)V
SD, m
esoc
ardi
a, w
ide
pulm
onar
y tr
unk
HLH
Stw
in, E
-GA
no
AVSD
with
LV<
RV. T
GA
with
nar
row
pul
mon
ary
trun
kH
ypop
last
ic a
ortic
arc
htw
in, O
CA, G
Aye
s
SVT
with
car
diom
egal
y w
ith m
inor
sig
n of
car
diac
failu
reCr
itica
l PS
and
poly
valv
ular
dis
ease
GA
, BM
I, SV
Tno
Card
iom
egal
y an
d tr
icus
pid
regu
rgita
tion
DO
RV+
PSO
CA, G
AN
A
PLSC
V, w
ide
right
SC
VPo
lyva
lvul
ar d
isea
se, n
o PL
SCV
OCA
NA
VSD
Trun
cus
arte
riosu
sBM
IN
A
HLH
SLA
I with
unb
alan
ced
AVSD
(LV<
RV),
TGA
, PS
BMI
yes
DO
RV+
PScc
TGA
GA
NA
VSD
DO
RV+
PSO
CAN
A
DO
RV+
PScc
TGA
twin
, BM
IN
A
DO
RV-T
GA
DO
RV+
PSno
neN
A
Unb
alan
ced
AVSD
PLSC
Vno
neN
A
Fallo
tTG
A c
ompl
ex (T
GA
, VSD
, CoA
o)no
neno
Fallo
t D
ORV
-TG
Ano
neN
A
Asc
endi
ng a
orta
wid
er t
han
norm
al,
mild
aor
tic v
alve
re
gurg
itatio
nTG
A s
impl
eno
neno
VSD
Fallo
tno
neN
A
21 c
ases
with
left
/rig
ht d
ispr
opor
tion,
sus
pect
ed fo
r CoA
oN
orm
al h
eart
aft
er c
losu
re o
f art
eria
l duc
t8
case
s w
ith O
CA, 2
GA
NA
11
case
s w
ith
abno
rmal
4
cham
ber
view
, no
t fu
rthe
r sp
ecifi
ed, w
ith le
thal
ext
raca
rdia
c an
omal
ies
Nor
mal
hea
rt a
t po
st m
orte
m, n
one
of t
hose
11
case
s su
rviv
edA
ll O
CAN
A
6 ca
ses
with
sus
pici
on o
f CH
D i
n ne
ar-t
erm
pre
gnan
cy
(mai
nly
AVSD
s)N
orm
al h
eart
aft
er c
losu
re o
f art
eria
l duc
tA
ll G
AN
A
Lege
nd.
* Fa
ctor
s th
at m
ay h
ave
a po
tent
ial n
egat
ive
influ
ence
on
the
qual
ity o
f the
ultr
asou
nd e
xam
inat
ion
BMI =
BM
I>30
G
A: l
ate
gest
atio
nal a
ge (a
fter
30
wee
ks)
E-
GA
: ear
ly g
esta
tiona
l age
(up
to 1
6 w
eeks
) or t
win
: tw
in p
regn
ancy
SVT:
sup
rave
ntric
ular
tach
ycar
dia
O
CA: o
ther
sev
ere
cong
enita
l ano
mal
ies
N
A: n
ot a
pplic
able
LAI=
left
atr
ial i
som
eris
m
Fa
llot=
Tetr
alog
y of
Fal
lot
Christine van Velzen.indb 94 20/09/2016 08:27

95
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
The size of the cohort allowed a detailed analysis of different types of CHD. For example, outflow tract anomalies like double outlet right ventricle were labeled as ‘discrepancy found’ if the spatial orientation of the outflow tract was not predicted correctly. These cases would be grouped together in the ‘conotruncal’ category in studies that use a broader categorization and, as a consequence, discrepancies would not be detected. Difficulties in identification of the outflow tracts were revealed in this study. This may be explained partly by the more complex multiplanar evaluation of this anatomic area, especially if one outflow tract is small or atretic. This detailed analysis acknowledges the complexity of CHD and fetal echocardiography in general. A simple ‘right’ or ‘wrong’ or a broad categorization does not do justice to the diversity in the anatomy of CHD. Similar to left–right identification of the outflow tracts, identification of the dominant ventricle in univentricular hearts was a challenge, as reported earlier. 14 As the long-term prognosis of univentricular palliative surgery is different for a morphologically right or left ventricle 15, correct identification is important, but could not be achieved in all cases.Several patterns could be recognized in cases with discrepancies (including those with no similarity). If trisomy 21 was diagnosed before birth, a balanced AVSD was frequently diagnosed, however other or accompanying heart defects were also found postnatally.This discrepancy is probably caused by anticipation of an expected diagnosis if trisomy 21 had been detected at the time of the scan. 16 This finding highlights the need to look beyond the obvious, to ensure a complete diagnosis. Differentiation between unbalanced AVSD and a hypoplastic left ventricle (HLV) was a second difficulty. In these cases, the ventricular component of the AVSD was very large, giving the appearance of a univentricular heart. It is possible that errors could be prevented if the position of the crux in the four-chamber view was given more attention. On the other hand, cases like this will remain difficult to diagnose correctly as an unbalanced AVSD with a small LV, and HLV with mitral atresia may produce similar images on ultrasound, even postnatally. In another case a defect presumed to be an unbalanced AVSD was, in fact, a persistent left superior vena cava with a dilated coronary sinus. The false-negative fetal echocardiograms were in accordance with the types of CHD that are known to be missed in the screening setting. Furthermore, some of the undetected defects can develop in the second half of pregnancy. Unfortunately, five cases had ductal-dependent CHD (Table 1).
In cases with no similarity between the prenatal and postnatal diagnoses, 70.2% had factors present that had a negative impact on image quality. This is in line with previous findings. 3,7 In 37.8% of cases with discrepancies (including those with no similarity), severe extracardiac anomalies were present that dominated the overall prognosis for the fetus. It is probable that a less complete echocardiographic examination was
Christine van Velzen.indb 95 20/09/2016 08:27

96
Chapter 5
Chapter 5
performed in these cases (e.g. in a fetus with holoprosencephaly). We believe that this is justifiable, especially if parents request TOP; to perform an additional echocardiographic examination in these circumstances is frequently too emotional and will not influence their decision. It is, however, very important to obtain a karyotype including array comparative genomic hybridization 17, a postmortem examination and a consultation with a clinical geneticist, to rule out inheritable syndromes.Although fetal echocardiography is very accurate in abnormal cases, it may cause unnecessary anxiety. We encountered 21 cases in which the fetus was diagnosed with left/right disproportion but after birth the heart was normal. This particular feature can be the first sign of a life-threatening diagnosis and should always prompt alertness. The difficulty in predicting aortic arch anomalies has been widely acknowledged. 13 Some cases will develop an obstructive lesion when the duct closes, others will not. 18 Often the final diagnosis can only be made after birth. Research to improve the prediction of coarctation of the aorta is ongoing 19, but limited progress is being made. Until better methods to exclude coarctation are devised, the limited diagnostic accuracy has to be accepted, even if it causes anxiety to parents. Prenatal counseling, especially in these cases, should be appropriate for the context.A limitation of this study is the number of cases in which no comparison could be made between the prenatal and postnatal diagnoses owing to the lack of a postmortem examination. In our opinion, postmortem confirmation of a heart anomaly is very important, for both the parents and the diagnostic team. It can reveal additional cardiac anomalies, extracardiac malformations or external dysmorphic features of a fetus that are not visible on ultrasound. These findings may guide the diagnostic genetic work-up and may alter the estimated risk of recurrence. Therefore, even with the reassurance that in 92% of cases no major mistakes are made regarding the diagnosis and treatment plan, we should make every effort to inform parents of the benefits of a postmortem examination.
In conclusion, prenatal diagnosis of CHD is highly accurate in experienced hands. Some types of CHD remain difficult to diagnose or rule out in a fetus. The pitfalls associated with some types of CHD have to be taken into account when making a definitive diagnosis and prognosis. Information on the accuracy and limitations of fetal echocardiography can be used in prenatal counseling.
Christine van Velzen.indb 96 20/09/2016 08:27

97
Prenatal diagnosis of CHD - accuracy and discrepancies
Chap
ter 5
REFERENCES
(1) DonofrioMT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A, Cuneo BF, Huhta JC, Jonas RA, Krishnan A, Lacey S, Lee W, Michelfelder EC Sr, Rempel GR, Silverman NH, Spray TL, Strasburger JF, Tworetzky W, Rychik J; American Heart Association Adults With Congenital Heart Disease Joint Committee of the Council on Cardiovascular Disease in the Young and Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and Council on Cardiovascular and Stroke Nursing. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation 2014; 129: 2183–2242.
(2) Hunter LE, Simpson JM. Prenatal screening for structural congenital heart disease. Nat Rev Cardiol 2014; 11: 323–334.
(3) Sharland G. Fetal cardiac screening and variation in prenatal detection rates of congenital heart disease: why bother with screening at all? Future Cardiol 2012; 8: 189–202.
(4) Galindo A, Mendoza A, Arbues J, Gra ˜ neras A, Escribano D, Nieto O. Conotruncal anomalies in fetal life: accuracy of diagnosis, associated defects and outcome. Eur J Obstet Gynecol Reprod Biol 2009; 146: 55–60.
(5) Forbus GA, Atz AM, Shirali GS. Implications and limitations of an abnormal fetal echocardiogram. Am J Cardiol 2004; 94: 688–689.
(6) Perolo A, Prandstraller D, Ghi T, Gargiulo G, Leone O, Bovicelli L, Pilu G. Diagnosis and management of fetal cardiac anomalies: 10 years of experience at a single institution. Ultrasound Obstet Gynecol 2001; 18: 615–618.
(7) Clur SA, Van Brussel PM, Ottenkamp J, Bilardo CM. Prenatal diagnosis of cardiac defects: accuracy and benefit. Prenat Diagn 2012; 32: 450–455.
(8) Berghella V, Pagotto L, Kaufman M, Huhta JC, Wapner RJ. Accuracy of prenatal diagnosis of congenital heart defects. Fetal Diagn Ther 2001; 16: 407–412.
(9) van Velzen C, Clur S, Rijlaarsdam M, Bax C, Pajkrt E, Heymans M, Bekker M, Hruda J, de Groot C, Blom N, Haak M. Prenatal detection of congenital heart disease – results of a national screening programme. BJOG 2016 Feb;123(3):400-7
(10) Meyer-Wittkopf M, Cooper S, Sholler G. Correlation between fetal cardiac diagnosis by obstetric and pediatric cardiologist sonographers and comparison with postnatal findings. Ultrasound Obstet Gynecol 2001; 17: 392–397.
(11) Berkley EM, Goens MB, Karr S, Rappaport V. Utility of fetal echocardiography in postnatal management of infants with prenatally diagnosed congenital heart disease. Prenat Diagn 2009; 29: 654–658.
(12) Bakiler AR, Ozer EA, Kanik A, Kanit H, Aktas FN. Accuracy of prenatal diagnosis of congenital heart disease with fetal echocardiography. Fetal Diagn Ther 2007; 22: 241–244.
(13) Matsui H, Mellander M, Roughton M, Jicinska H, Gardiner HM. Morphological and physiological predictors of fetal aortic coarctation. Circulation 2008; 118: 1793–1801.
(14) Eik-Nes S, Lee W, Carvalho JS, Chaoui R, Copel J, Hecher K, Paladini D. Cardiac screening examination of the fetus: guidelines for performing the ‘basic’ and ‘extended basic’ cardiac scan. Ultrasound Obstet Gynecol 2006; 27: 107–113.
(15) Khairy P, Fernandes SM, Mayer JE Jr, Triedman JK, Walsh EP, Lock JE, Landzberg MJ. Long-term survival, modes of death, and predictors of mortality in patients with Fontan surgery. Circulation 2008; 117: 85–92.
(16) Mogra R, Alabbad N, Hyett J. Increased nuchal translucency and congenital heart disease. Early Hum Dev 2012; 88: 261–267.
(17) Jansen FA, Blumenfeld YJ, Fisher A, Cobben JM, Odibo AO, Borrell A, Haak MC. Array comparative genomic hybridization and fetal congenital heart defects: a systematic review and meta-analysis. Ultrasound Obstet Gynecol 2015; 45: 27–35.
Christine van Velzen.indb 97 20/09/2016 08:27

98
Chapter 5
Chapter 5
(18) Matsui H, Gardiner H. Coarctation of the aorta: fetal and postnatal diagnosis and outcome. Expert Rev Obstet Gynecol 2009; 4: 191–200.
(19) Gomez-Montes E, Herraiz I, Gomez-Arriaga PI, Escribano D, Mendoza A, Galindo A. Gestational age-specific scoring systems for the prediction of coarctation of the aorta. Prenat Diagn 2014; 34: 1198–1206.
Christine van Velzen.indb 98 20/09/2016 08:27

Christine van Velzen.indb 99 20/09/2016 08:27

Christine van Velzen.indb 100 20/09/2016 08:27

CHAPTER 6Pregnancy Complications in
Singleton Pregnancies
with Isolated Fetal Heart Defects
C.L. van Velzen, F. Türkeri, E. Pajkrt, S.A. Clur, M.E.B. Rijlaarsdam, C.J. Bax, J. Hruda, C.J.M. de Groot, N.A. Blom, M.C. Haak
Accepted ACTA Obstet et Gynecol Scan July 2016
Christine van Velzen.indb 101 20/09/2016 08:27

102
Chapter 6
Chapter 6
ABSTRACT
IntroductionAs the prenatal detection rates of congenital heart defects (CHDs) increase, obstetricians are more frequently faced with pregnancies complicated by a fetal CHD. Congenital anomalies in general are associated with preterm birth and fetal demise. The aim of this study was to gain insight into the prevalence of preterm birth and fetal demise in singleton pregnancies with fetuses with isolated CHDs.
Material and MethodsA geographical cohort study was performed in a large region in the Netherlands. Fetuses and infants from singleton pregnancies diagnosed with severe isolated CHD, born between 1 January 2002 and 1 January 2012, were included. All cases in the CHD cohort were assessed for preterm birth or fetal demise. The proportions of preterm birth and fetal demise were compared to a control group and odds ratios were calculated.
ResultsThe proportion of preterm births in the CHD cohort (n=1013) was 9.1% [95% confidence interval 7.3-10.9] compared to 5.6% [95% CI 5.4-5.8] in the control group, with an odds ratio of 1.7 [95% CI 1.4- 2.1]. The preterm birth started spontaneously in 49.5% and 38.4% were induced. In 15 cases fetal demise occurred(1.5% [95% CI 0.8-2.2]), compared to 0.7% [95% CI 0.6-0.8] in the control group, odds ratio 2.0 [95% CI 1.2-3.4].
ConclusionsHigher rates of preterm birth and fetal demise occur in fetuses with isolated CHD compared to the general population. Prenatal specialists should be vigilant for signs of heart failure, premature closure of the foramen ovale or fetal distress in fetuses with isolated CHDs.
Christine van Velzen.indb 102 20/09/2016 08:27

103
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
INTRODUCTION
Congenital heart defects (CHDs) affect 6 to 11 per 1000 newborns. 20-30% of CHDs are severe. 1-3 Prenatal detection rates are rising and are presently around 50%. 4-9 Thus, obstetricians are increasingly faced with healthy women, pregnant with a fetus with a severe CHD. A prenatal diagnosis of CHDs contributes significantly to an optimal outcome for the affected infant. It allows for the planning of the delivery in a center with pediatric cardiology and neonatology facilities and assures the appropriate management of the neonate after delivery. 5;10;11 In addition, a diagnosis during pregnancy provides the opportunity to detect additional congenital anomalies and to perform chromosomal analysis. Once all essential information is collected, the parents can be counselled appropriately and, when the diagnosis is made timely, they have the opportunity to decide on the continuation of the pregnancy in severe cases. 10;11
Little is known regarding possible associated obstetric morbidity in cases of fetal CHD. These pregnancies generally develop physiologically due to the presence of the fetal shunts (ductus arteriosus and foramen ovale), and obstetric morbidity is assumed to occur with the same prevalence as in pregnancies without fetal heart defects. 12;13 A preterm birth, however, may cause significant problems in the neonatal period, as surgery has to be postponed until the neonate has an acceptable weight. 11;14 Neonates with severe CHDs born prematurely have higher mortality rates than children born at term. 15-17 If a neonate is preterm and, as a consequence, has a lower birthweight, a lethal situation may arise for some heart defects that would have had a good outcome if the child had been born at term. Even an early term birth between 37 to 38 weeks’ gestation is associated with worse outcomes after neonatal cardiac surgery. 18
It is known that in few cases of fetal heart defects (such as Ebstein’s anomaly, premature closure of the foramen ovale in hypoplastic left heart syndrome 12;19;20) fetal cardiac failure and demise can occur. The overall risk for fetal demise related to isolated CHDs in general, is not known. The knowledge of the prevalence of obstetric complications in pregnancies complicated by fetal CHD is important in the obstetric management and counselling of parents. The primary aim of this study is to gain insight into the prevalence of preterm birth and fetal demise in singleton pregnancies with fetuses with isolated CHDs. A secondary aim is to evaluate whether the preterm birth was spontaneous or iatrogenic.
MATERIAL AND METHODS
From a previously described geographical cohort in the North-West Netherlands 9, including 1,912 fetuses and infants born between 2002 and 2012 with severe CHDs, we selected the singleton pregnancies with isolated fetal CHDs. Prenatal detection rates
Christine van Velzen.indb 103 20/09/2016 08:27

104
Chapter 6
Chapter 6
in this cohort were 47% for all CHD combined and 34% for isolated CHD. 9 In 404 cases (51% of the cases with a prenatal diagnosis) the pregnancy was terminated on request of the parents, these cases were excluded. Multiple pregnancies (n=85) were excluded, since in that group a relation to preterm delivery and fetal death is evident. The CHD was isolated in 1,013 of the 1,423 remaining cases. The pregnancy outcome was known in all cases. The cardiac defect was known at the time of birth in 26.4% of the 1,013 cases. All included types of CHD are listed in the legend of Table 1. Data were originally collected from prospectively entered cases in the prenatal ultrasound databases and pediatric cardiology databases. Data concerning the obstetric parameters and, where applicable, post-mortem reports were collected via assessment of the obstetric medical records and pathology databases. We searched all pathology databases in this region for fetal or neonatal cases without a prenatal diagnosis of malformations that turned out to have a CHD. Follow-up of all cases was one year after birth. Approval from the Medical Ethical Committee of the VU University Medical Centre was obtained for this study. (Date of approval: 7 November 2012, reference number 2012/396.)
Severe CHDs were defined as CHDs that required surgery or therapeutic catheterization or caused death within 1 year after birth. As we focused on structural heart defects, we excluded cases with cardiomyopathy or arrhythmia without an underlying structural heart defect. Cases with isolated patent ductus arteriosus or patent foramen ovale were not included in this cohort. All CHD included in this study are listed in the legend of Table 1. Isolated CHDs were defined as CHDs without any additional chromosomal or genetic anomalies or extracardiac malformations (except for single umbilical artery). From this cohort, we assessed all cases with preterm birth or fetal demise. The gestational age was determined by first trimester ultrasound biometry. Preterm birth was defined as a delivery before a gestational age of 37+0 weeks. We subcategorized preterm birth into birth below 28 weeks, between 28 and 32 weeks and between 32 and 37 weeks of gestation. Inclusion of cases started from a gestational age of 19+0 weeks. Term birth was defined as a delivery after 37 completed weeks. In 0.9% of the cases the exact duration of the pregnancy was unknown. These were all postnatally diagnosed cases with a (atrio)ventricular septal defect that underwent surgery several months after birth. In their files there was nothing stated on prematurity or special circumstances around the birth. They were therefore considered as term and included in the analysis.Spontaneous preterm birth was defined as a delivery following spontaneous onset of labor irrespective if labor was subsequently augmented or resulted in a caesarean section in case of failure to progress or fetal distress. Fetal distress was defined as hypoxic changes in the cardiotocogram and/or abnormalities in Doppler velocimetry of the umbilical artery and/or median cerebral artery. Iatrogenic preterm birth was
Christine van Velzen.indb 104 20/09/2016 08:27

105
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
defined as a primary caesarean section in the absence of any signs of spontaneous labor or as medical induction of labor. The reasons for medically induced preterm birth were categorized into fetal, maternal and a combination of fetal and maternal indications. Fetal demise was defined as the intra-uterine death of a fetus and were included after a gestational age of at least 19+0 weeks.The control group consisted of all singleton deliveries (n=68,190) in the year 2010 of women living in the same region (selected by postal code) as the cases. Data on the number of live births at different gestational ages (ranging from 19+0 weeks to 43+0 weeks), fetal demise and neonatal mortality were provided by ’The Netherlands Perinatal Registry’. This is a national medical registry of all deliveries and perinatal mortality in the Netherlands. Comparisons were made between the CHD cohort and the control group and between cases in the CHD cohort with and without a prenatal diagnosis. Information and data were collected and analyzed using SPSS version 20.0. Odds ratios (ORs) and their associated confidence intervals (CIs) were calculated. The chi-square test was used to test for associations between categorical variables. A p-value below 0.05 was considered as statistically significant, all tests were two-sided.
RESULTS
Preterm birth in isolated CHD Of the 1,013 singleton pregnancies with isolated CHD, 9.0% resulted in a preterm birth. If cases with fetal demise were excluded, the proportion of preterm births in isolated CHD was 9.1% [95% CI 7.3-10.9] compared to 5.6% [95% CI 5.4-5.8] in the control group. The odds ratio for preterm birth (<37+0 weeks) in isolated CHD was 1.7 [95% CI 1.4- 2.1]. The odds ratio for birth below 28 weeks, between 28 and 32 weeks and between 32 and 37 weeks of gestation in fetuses with isolated CHD was respectively 2.0, 2.3 and 1.6 compared to the control population (Table 2). The mortality in the first year of life after a preterm birth was 22% (50% in the group born before 32 weeks of gestation), of which 70% was pre-surgery mortality (78% in the group before 32 weeks).The size of the cohort allowed us to assess the prevalence of preterm births per type of CHD (Table 1). Valve abnormalities, septal defects and complex heart defects with atrial isomerism showed the highest rates of live preterm birth. No difference in preterm birth rate was found between the cases in the CHD cohort with a prenatal diagnosis compared to the cases without a prenatal diagnosis (9.7% compared to 9.0% p=0.746).
Christine van Velzen.indb 105 20/09/2016 08:27

106
Chapter 6
Chapter 6
Table 1 Preterm birth per type of CHD
CHD categories N Preterm birth N(%)
Compared to controls OR [95% CI]
1. Septal defects 158 18 (11.4) 2.2 [1.3-3.6]
2. Valve abnormalities in biventricular hearts 101 17 (16.8) 3.4 [2.0-5.8]
3. Pulmonary or systemic venous return abnormalities 40 0 -
4. Aortic arch anomalies 155 13 (8.4) 1.6 [0.9-2.7]
5. Conotruncal anomalies 318 26(8.2) 1.5 [1.0-2.3]
6. Hypoplastic right heart syndrome 20 2 (10.0) 1.9 [0.4-8.1]
7. Hypoplastic left heart syndrome 65 2(3.1) 0.5 [0.1-2.2]
8. Other univentricular heart defects 78 6 (7.7) 1.4 [0.6-3.2]
9. Complex heart defects with atrial isomerism 28 4(14.3) 2.8 [1.0-8.1]
10. Miscellaneous 25 3 (12.0) 2.3 [0.7-7.7]
Total 998 91 (9.1) 1.7 [1.3-2.1]
Categories consist of:1. Ventricular septal defect(s) (VSD), balanced atrioventricular septal defect (AVSD)2. Pulmonary (PS) or aortic valve stenosis, mitral stenosis, Ebstein’s anomaly, tricuspid dysplasia, tricuspid or mitral
regurgitation3. Total or partial abnormal pulmonary venous return, giant eustachian valve/cor triatriatum dexter or sinister4. Aortic coarctation, hypoplastic or interrupted aortic arch, multiple level left heart obstruction, double aortic arch 5. Tetralogy of Fallot, double outlet right ventricle (DORV)-Fallot type with VSD and/or pulmonary stenosis, simple
transposition of great arteries (without signficant VSD), complex TGA (with significant VSD and/or PS), DORV- Taussig Bing (= TGA type), truncus arteriosus, pulmonary atresia with VSD, congenitally corrected TGA, absent pulmonary valve syndrome, aortopulmonary window, hemitruncus
6. Pulmonary atresia with intact ventricular septum, critical pulmonary valve stenosis with right ventricular hypoplasia 7. Aortic valve atresia, critical aortic valve stenosis with left ventricular hypoplasia8. Double inlet left ventricle, tricuspid valve atresia, absent left A-V connection, unbalanced AVSD, TGA with right
ventricular (RV) hypoplasia and straddling tricuspid valve, criss-cross, DORV with mitral valve and left ventricular (LV) hypoplasia, congenitally corrected TGA with RV hypoplasia, isolated atrio-ventricular (AV) discordance with hypoplastic RV and VSD
9. Left or right atrial isomerism, heterotaxy syndromes10. Polyvalvular disease, isolated double chambered right ventricle, right atrial aneurysm
Table 2 Preterm birth in isolated fetal CHD compared to controls Isolated fetal CHD Control cases OR [95% CI]
Birth before 28+0 weeks n (%) 7 (0.7) 231 (0.3) 2.0 [1.0-4.4]
Birth from 28+0 to 31+6 weeks n (%) 11 (1.1) 320 (0.5) 2.3 [1.3-4.3]
Birth from 32+0 to 36+6 weeks n (%) 73 (7.3) 3197 (4.8) 1.6 [1.3-2.0]
Overall preterm birth n (%) 91 (9.1) 3748 (5.6) 1.7 [1.3-2.1]
Total live births n 998 67204
Christine van Velzen.indb 106 20/09/2016 08:27

107
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
Spontaneous versus induced preterm birthWithin the group of preterm born infants (n=91), spontaneous onset of delivery was reported in 49.5% and iatrogenic in 38.4% of the cases. In the remaining 12.1% this information was unavailable because the infant could not be linked to a pregnancy file (cases without a prenatal diagnosis). The indications for preterm induction of the delivery are shown in Figure 1. The most frequent indications were fetal distress and intra-uterine growth restriction (IUGR), either or not in combination with a maternal hypertensive disorder. There was only one pregnancy in which the reason for induction of the delivery was the heart defect itself. The diagnosis was a prematurely closed foramen ovale in a fetus with a small left ventricle leading to heart failure.The proportion of medically induced and total preterm births was comparable between the group with a prenatal diagnosis (3.1% and 9.7% resp.) and the group with a postnatal diagnosis ((3.5% and 9.0% resp.) p=0.746).
Figure 1 Medically induced preterm births (n=35). The numbers in the figure represent percentages.
5,7
17,1
20
14,3
8,6
34,3
Indicationsforinductionofdelivery
fetalhydrops
intra-uterinegrowthrestriction
fetaldistress
hypertensivedisorder
abnormalbloodloss
hypertensivecomplicationcombinedwithfetaldistressorIUGR
Christine van Velzen.indb 107 20/09/2016 08:27

108
Chapter 6
Chapter 6
Fetal demise in isolated CHD There were 15 cases of fetal demise in the CHD cohort (1.5% [95% CI 0.8-2.2]). Compared to the control group (fetal demise rate of 0.7% [95% CI 0.6-0.8]) this resulted in an odds ratio of 2.0 [95% CI 1.2-3.4]. The fifteen cases are described in Table 3.We found a higher percentage of fetal demises in the CHD cases with a prenatal diagnosis compared to the CHD cases without a prenatal diagnosis (5.0% versus 0.3%) (p< 0.001).
DISCUSSION
In an unselected population of over a thousand pregnancies with isolated fetal CHDs an increased risk for preterm birth and fetal demise was found compared to the control population. The odds for a preterm birth were higher in all subcategories. Most preterm births started spontaneously. If induction was performed before 37 completed weeks of gestation, the most common reasons were fetal distress and/or IUGR either or not in combination with a maternal hypertensive disorder.Seven of the 15 cases (47%) with fetal demise could be explained by intra-uterine cardiac failure – due to the CHD. The other eight demise cases (53%) could not be attributed to hemodynamic changes caused by the CHD. The presence of the fetal shunts and the higher pressure in the right ventricle make most CHDs compatible with fetal life. 12;13 There is no evident pattern within this group related to type of defect or gestational age at which the demise occurred, however the cases where cardiac failure was present show common denominators of valvular dysplasia and/or venous obstruction.
Previous reported rates of preterm birth of infants with a CHD vary between 11.5-20.5% with reported corresponding odds ratios of 1.7-2.6. 21-23 The most plausible explanation for the higher rates found, is that previous studies also included cases with non-isolated CHDs 22;23, whereas we excluded non-isolated cases. The proportion of induced preterm birth in those cohorts was not reported. Chromosomal anomalies frequently associated with CHD such as trisomy 13 or 18, are mostly accompanied by severe IUGR and consequently could be a significant cause for the higher rate of preterm deliveries in those studies. The cohort described by Laas et al. did differentiate between isolated and non-isolated CHDs, and the outcomes of that study are the closest to ours. The numbers they presented per type of CHD, however, included cases with multiple extracardiac and/or chromosomal anomalies. 21 Our study is the first study that provides the prevalence of preterm birth per type of CHD in isolated cases and shows that the prevalence is increased, but not to the extent that had been reported previously. This knowledge is useful for counselling parents after genetic analysis has shown no abnormalities.
Christine van Velzen.indb 108 20/09/2016 08:27

109
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
Table 3 Cases of fetal demise
Cardiac diagnosis Number of cases Remarks
Ebstein’s anomaly with significant tricuspid regurgitation
3 On prenatal scan observed cardiac failure, fetal demise between 25 and 29 weeks of gestational age. Diagnosis confirmed at post-mortem examination in 2 cases, in the third case the post-mortem examination was declined.
Hypoplastic aortic arch 3 1 case with severe maternal preeclampsia with placental abruption at 34 weeks1 case of fetal demise at 35 weeks. Post-mortem examination showed an hypoplastic aortic arch, the size of the LV within normal range, with premature closure of foramen ovale. maternal hyperglycemia, insulin dependent diabetes1 case in combination with persistent left superior caval vein, no extracardiac anomalies found on ultrasound, karyotyping and post-mortem declined, no explanation found for demise *
Aortic coarctation 2 Both cases were not prenatally diagnosed. Post-mortem findings: 1 case demise at 31 weeks with premature closure of foramen ovale, second case* demise at 37 weeks, no other anomalies found
Truncus arteriosus (TA) 2 Same mother in both cases. First case on prenatal scan truncal valve regurgitation and cardiac failure, normal karyotype, fetal demise at 29 weeks. Second case on prenatal scan small truncal valve and interrupted aortic arch, normal karyotype, development of cardiac failure, fetal demise at 29 weeks, post-mortem: TA type 2 ,VSD, quadricuspid dysplastic truncal valve, and patent arterial duct
Tetralogy of Fallot 1 Prenatally detected, normal karyotype. Fetal demise at 39 weeks*, post-mortem diagnosis confirmed, no other abnormalities, except for extremely low placental weight
Complex transposition of great arteries
1 Prenatally detected, fetal demise at 41 weeks*, post-mortem examination confirmed diagnosis: TGA, bicuspid dysplastic pulmonary valve, and dysplastic mitral valve. Hypertrophic right ventricle with a narrow infundibulum. Chorio-amnionitis of the placenta
Tricuspid valve atresia 1 Fetal demise at 19 weeks*. Not prenatally diagnosed. Diagnosis at post-mortem examination: Atresia of the tricuspid valve with hypoplastic right ventricle, hypoplastic pulmonary trunk and dilated right atrium
Left atrial isomerism 1 Fetal demise at 19 weeks, at 13 weeks on prenatal scan: fetal heart block and failure, normal karyotype. Diagnosis at post-mortem examination: left isomerism, situs ambiguous atria, ambiguous AV connection, concordant VA connection, persistent left superior caval vein, AVSD, hypoplastic aortic arch, polyvalvular disease.
Double outlet ventricle 1 Prenatal diagnosis: DORV with aortic and pulmonary valve stenosis, VSD, narrow isthmus of the aortic arch, normal karyotype. Fetal demise at 28 weeks*, post-mortem examination declined
Legend All cases had a prenatal diagnosis of the heart defect, except for the cases with aortic coarctation and the case with tricuspid valve atresia, which were identified in the pathology databases.* no hemodynamic explanation for demise
Christine van Velzen.indb 109 20/09/2016 08:27

110
Chapter 6
Chapter 6
Similar to preterm birth, fetal demise occurs more frequently in fetuses with isolated CHDs compared to the control population. Previous studies report demise rates in fetuses with a CHD from 2.7% to 12%. 2;24-26 Most of the studies, however, report demises in a population including cases with associated extracardiac and chromosomal abnormalities. More importantly, most studies describe cohorts of prenatally diagnosed cases with CHDs, leaving out cases in which the CHD were missed prenatally. This inevitably produces a selection bias towards the more severe heart defects. The reports by Levi et al. 26 and ours are the only studies that focus on isolated CHDs and include fetal demise cases in which the diagnosis was made postnatally by post-mortem examination. The slightly lower proportion of fetal demise found in our study could be explained by the fact that we excluded multiple pregnancies. The higher percentage of demise cases in the group with a prenatal diagnosis can be explained by the fact that more severe CHD usually have higher prenatal detection rates.
Our report is the first that describes the fetal demise cases with the cardiac diagnosis in detail. Only 47% of the cases in our study could be explained by intra-uterine cardiac failure related to the CHD. The cases with a premature closure of the foramen ovale underline the importance of a prenatal diagnosis and prenatal follow-up, especially in CHDs that are known to be at risk. Timely intervention in these cases may prevent fetal demise, with the disadvantage of an induced preterm birth with accompanying risks. Although a part of the pregnancy complications found can be explained by the CHD itself, the reasons for the increased risk for preterm birth and fetal demise in pregnancies with isolated fetal CHD partly remain unclear. A part may be attributed to rhythm disturbances, as it is known that some types of CHD are associated with this complication. Furthermore, genetic and environmental influences may play a role. 27;28 Mutated genes and environmental influences may affect vascular development in the placenta as well. The altered vascular development of the placenta may explain some fetal demise cases. Furthermore a significant association between IUGR and fetal CHDs has been described 29;30, potentially explaining some of the inductions of labor because of fetal distress. It is also known that fetuses with cardiac defects carry a higher risk of genetic syndromes. These syndromes could remain undetected in fetal demise cases were a post-mortem examination was declined by parents or due to the difficulty in detection of mild dysmorphic features in macerated fetuses. It is possible that undiagnosed syndromes could underlie some of the fetal demise cases. These hypotheses do not explain preterm births in neonates with a normal birthweight who had an uneventful long-term outcome. As the cause of spontaneous preterm birth is accepted to be multifactorial 31, it is most likely that preterm birth in fetuses with CHDs has a multifactorial (maybe partly common) cause as well.
Christine van Velzen.indb 110 20/09/2016 08:27

111
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
Our study describes a cohort with a representative number of severe isolated fetal CHDs in singleton pregnancies diagnosed prenatally as well as after birth. We included cases from pathology databases in the study region in which the diagnosis of the CHD was made by post-mortem examination and we could provide a detailed description of the fetal demise cases. We compared fetuses with isolated CHDs to a control group with singleton pregnancies from the same referral area as the affected fetuses. Missing data regarding gestational age at birth was only 0.9%. A limitation in our study is that we were unable to correct for all possible risk factors, except for multiple pregnancies. To minimize the effect of possible confounders we chose a control population from the same region and time period to minimize bias on socio-demographic characteristics. Cases with CHDs or other congenital anomalies could not be excluded from the control group, because The Netherlands Perinatal Registry could not provide full coverage of this type of data. This may account for around 2 % of the births in the control group. If the control group had only contained cases without congenital anomalies, the odds ratio for the outcomes of this study could possibly have been higher.
We were able to produce the prevalence of preterm birth per type of CHD, but the limited sample size still results in wide confidence intervals. Even if a CHD is isolated, higher rates of preterm birth and fetal demise compared to the general population are present. The risks in singleton pregnancies with isolated fetal CHDs are, however, lower than most rates published earlier. For accurate and valid counselling of parents who are expecting a child with a CHD, the prevalence of those complications in singleton pregnancies with isolated CHDs is relevant information. Especially in this modern era, when chromosome analysis including micro-array are offered to parents as standard care, and many significant associated anomalies can be ruled out prenatally, the remaining risk of obstetric complications is essential. Prenatal specialists should be aware of the conditions for a functional fetal circulation: a well-functioning placenta, a patent single ventricular inflow, a patent single ventricular outflow, competent inflow and outflow valves and at least one ventricle that fills normally and can eject sufficiently to sustain the equivalent of the combined cardiac output. When one or more of these is not present, fetal cardiovascular compromise including evolution of heart failure or sudden fetal demise may occur. 32
Christine van Velzen.indb 111 20/09/2016 08:27

112
Chapter 6
Chapter 6
REFERENCE LIST(1) Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002 Jun 19;39(12):1890-
900.
(2) Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D, et al. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983-2000: a population-based evaluation. Pediatrics 2005 Jan;115(1):95-101.
(3) van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011 Nov 15;58(21):2241-7.
(4) Galindo A, Herraiz I, Escribano D, Lora D, Melchor JC, de la Cruz J. Prenatal detection of congenital heart defects: a survey on clinical practice in Spain. Fetal Diagn Ther 2011;29(4):287-95.
(5) Clur SA, Van Brussel PM, Ottenkamp J, Bilardo CM. Prenatal diagnosis of cardiac defects: accuracy and benefit. Prenat Diagn 2012 May;32(5):450-5.
(6) Todros T, Faggiano F, Chiappa E, Gaglioti P, Mitola B, Sciarrone A. Accuracy of routine ultrasonography in screening heart disease prenatally. Gruppo Piemontese for Prenatal Screening of Congenital Heart Disease. Prenat Diagn 1997 Oct;17(10):901-6.
(7) Marek J, Tomek V, Skovranek J, Povysilova V, Samanek M. Prenatal ultrasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart 2011 Jan;97(2):124-30.
(8) Stumpflen I, Stumpflen A, Wimmer M, Bernaschek G. Effect of detailed fetal echocardiography as part of routine prenatal ultrasonographic screening on detection of congenital heart disease. Lancet 1996 Sep 28;348(9031):854-7.
(9) van Velzen C, Clur S, Rijlaarsdam M, Bax C, Pajkrt E, Heymans M, et al. Prenatal detection of congenital heart disease-results of a national screening programme. BJOG 2015 Jan 27.
(10) Landis BJ, Levey A, Levasseur SM, Glickstein JS, Kleinman CS, Simpson LL, et al. Prenatal diagnosis of congenital heart disease and birth outcomes. Pediatr Cardiol 2013 Mar;34(3):597-605.
(11) Andrews RE, Simpson JM, Sharland GK, Sullivan ID, Yates RW. Outcome after preterm delivery of infants antenatally diagnosed with congenital heart disease. J Pediatr 2006 Feb;148(2):213-6.
(12) Friedman AH, Fahey JT. The transition from fetal to neonatal circulation: normal responses and implications for infants with heart disease. Semin Perinatol 1993 Apr;17(2):106-21.
(13) Hunter LE, Simpson JM. Prenatal screening for structural congenital heart disease. Nat Rev Cardiol 2014 Jun;11(6):323-34.
(14) Ades AM, Dominguez TE, Nicolson SC, Gaynor JW, Spray TL, Wernovsky G, et al. Morbidity and mortality after surgery for congenital cardiac disease in the infant born with low weight. Cardiol Young 2010 Feb;20(1):8-17.
(15) Cnota JF, Gupta R, Michelfelder EC, Ittenbach RF. Congenital heart disease infant death rates decrease as gestational age advances from 34 to 40 weeks. J Pediatr 2011 Nov;159(5):761-5.
(16) Costello JM, Polito A, Brown DW, McElrath TF, Graham DA, Thiagarajan RR, et al. Birth before 39 weeks’ gestation is associated with worse outcomes in neonates with heart disease. Pediatrics 2010 Aug;126(2):277-84.
(17) Natarajan G, Anne SR, Aggarwal S. Outcomes of congenital heart disease in late preterm infants: double jeopardy? Acta Paediatr 2011 Aug;100(8):1104-7.
(18) Costello JM, Pasquali SK, Jacobs JP, He X, Hill KD, Cooper DS, et al. Gestational Age at Birth and Outcomes After Neonatal Cardiac Surgery. Circulation. 2014 Jun;129(24):2511-7
(19) Paranon S, Acar P. Ebstein’s anomaly of the tricuspid valve: from fetus to adult: congenital heart disease. Heart 2008 Feb;94(2):237-43.
(20) Donofrio MT. Images in cardiovascular medicine. Premature closure of the foramen ovale and ductus arteriosus in a fetus with transposition of the great arteries. Circulation 2002 Mar 19;105(11):e65-e66.
Christine van Velzen.indb 112 20/09/2016 08:27

113
Pregnancy complications in singleton pregnancies with isolated fetal heart defects
Chap
ter 6
(21) Laas E, Lelong N, Thieulin AC, Houyel L, Bonnet D, Ancel PY, et al. Preterm birth and congenital heart defects: a population-based study.Pediatrics 2012 Oct;130(4):e829-37.
(22) Tanner K, Sabrine N, Wren C. Cardiovascular malformations among preterm infants. Pediatrics 2005 Dec;116(6):e833-8.
(23) Purisch SE, DeFranco EA, Muglia LJ, Odibo AO, Stamilio DM. Preterm birth in pregnancies complicated by major congenital malformations: a population-based study. Am J Obstet Gynecol 2008 Sep;199(3):287-8.
(24) Fesslova’ V, Nava S, Villa L. Evolution and long term outcome in cases with fetal diagnosis of congenital heart disease: Italian multicentre study. Fetal Cardiology Study Group of the Italian Society of Pediatric Cardiology. Heart 1999 Nov;82(5):594-9.
(25) McBrien A, Sands A, Craig B, Dornan J, Casey F. Major congenital heart disease: antenatal detection, patient characteristics and outcomes. J Matern Fetal Neonatal Med 2009 Feb;22(2):101-5.
(26) Levi S, Zhang WH, Alexander S, Viart P, Grandjean H. Short-term outcome of isolated and associated congenital heart defects in relation to antenatal ultrasound screening. Ultrasound Obstet Gynecol 2003 Jun;21(6):532-8.
(27) Nemer M. Genetic insights into normal and abnormal heart development. Cardiovasc Pathol 2008 Jan;17(1):48-54.
(28) Dolk H, Armstrong BF, Lachowycz KF, Vrijheid MF, Rankin JF, Abramsky LF, et al. Ambient air pollution and risk of congenital anomalies in England, 1991-1999. Occup Environ Med 2010 Apr;67(4):223-7.
(29) Wallenstein MB, Harper LM, Odibo AO, Roehl KA, Longman RE, Macones GA, et al. Fetal congenital heart disease and intrauterine growth restriction: a retrospective cohort study. J Matern Fetal Neonatal Med 2012 Jun;25(6):662-5.
(30) Rosenthal GL, Wilson PD, Permutt T, Boughman JA, Ferencz C. Birth weight and cardiovascular malformations: a population-based study. The Baltimore-Washington Infant Study. Am J Epidemiol 1991 Jun 15;133(12):1273-81.
(31) Esplin MS. Overview of spontaneous preterm birth: a complex and multifactorial phenotype. Clin Obstet Gynecol 2014 Sep;57(3):518-30.
(32) Ojala TH, Hornberger LK. Fetal Heart failure. Front Biosci. 2010 Jun;2:891-906.
Christine van Velzen.indb 113 20/09/2016 08:27

Christine van Velzen.indb 114 20/09/2016 08:27

CHAPTER 7Supraventricular Tachycardia in a
Neonate with the Prenatal Diagnosis
of a Single Left Superior Vena Cava
C. L. van Velzen, J. Hruda, L. A. J. Rammeloo and M. C. Haak.
Ultrasound Obstet Gynecol. 2011 Dec;38(6):731-2
Christine van Velzen.indb 115 20/09/2016 08:27

116
Chapter 7
Chapter 7
Persistence of the left superior vena cava (LSVC) in the absence of the right superior vena cava (RSVC) in a fetus with otherwise normal cardiac anatomy is usually not predictive of postnatal complications. A 37-year-old healthy primigravida was referred to our fetalechocardiography unit because of an abnormal three-vessel view (Figure 1) at the 20-week anomaly scan. Echocardiography revealed visceroatrial situs solitus with normal intracardiac anatomy. The innominate vein connected to a single LSVC, entering the dilated coronary sinus (CS) (Figure 2); the RSVC was not visible. The inferior caval vein drained into the right atrium. The ventricles, aortic valve and arch were of adequate size. No additional malformations were found. Amniocentesis was declined by the parents. Follow-up scans confirmed the suspected diagnosis and showed a normal rhythm.
A healthy girl was born at 39 + 1 weeks by normal vaginal delivery. At the age of 3 weeks the neonate presented at the Paediatric Cardiology Department. The prenatal diagnosis was confirmed by echocardiography. Unexpectedly, an atrioventricular re-entry tachycardia of 250 beats per minute was found, with a good peripheral perfusion. The tachycardia could be converted to sinus rhythm with the administration of intravenous adenosine. Electrocardiography demonstrated a normal sinus rhythm, without a pre-excitation pattern. Sotalol was administered for 2 months. No tachycardia occurred afterdiscontinuation.
Persistence of the LSVC in the absence of the RSVC is very rare. An incidence of 0.09% was reported among a postmortem series of children with congenital heart disease. 1 The expectation is that the incidence during fetal life is slightly higher if isolated cases, spontaneous fetal demise and fetuses with multiple malformations are taken into account.A persistent LSVC can be associated with cardiac and extracardiac anomalies 2–4, but in most cases it is an isolated anomaly. 5,6 On prenatal ultrasound an LSVC presents with an abnormal three-vessel view, which is a transverse plane through the fetal thorax at the level of the pulmonary artery leaving the right ventricle. 3,5 Usually the RSVC can be visualized in this plane at the right side of the ascending aorta. An LSVC is present at the left side of the pulmonary artery and generally drains into the CS, causing dilatation. A dilated coronary sinus is visible in the four-chamber view or in an oblique parasagittal plane as a ‘tobacco pipe’. 7 The prognosis for an isolated single LSVC is good. It is an asymptomatic condition without hemodynamic significance. 5,6 Associated arrhythmias have been reported in adulthood, whereas only one study reports on arrhythmias in childhood. 8 The proposed mechanisms for the arrhythmia are stretching of the atrioventricular nodal tissue by the dilated CS, which can cause a re-entry tachycardia 9, or an abnormal development of the sinus node in association with the absence of
Christine van Velzen.indb 116 20/09/2016 08:27

117
Supraventricular tachycardia in a neonate with the prenatal diagnosis of a single left superior vena cava
Chap
ter 7
the RSVC. 10 A prospective study to determine the prevalence of arrhythmias in these children has not been performed and would be unlikely to be feasible considering the low incidence. This case illustrates that it is vital to remain attentive to arrhythmias when associated with single LSVC and that cardiac anomalies that were assumed to be fairly innocuous can have an unexpected outcome.
Figure 1 Three-vessel view at 20 weeks of gestation demonstrating the superior vena cava on the left side of the pulmonary artery.AO, aorta; PA, pulmonary artery; SVC, superior vena cava.
Figure 2 Four-chamber view at 20 weeks of gestation demonstrating a cross-section through the left superior vena cava (arrow)in its course towards the coronary sinus behind the left atrium.
Christine van Velzen.indb 117 20/09/2016 08:27

118
Chapter 7
Chapter 7
REFERENCES(1) Bartram U, Van Praagh S, Levine JC, Hines M, Bensky AS, Van Praagh R. Absent right superior vena cava in
visceroatrial situs solitus. Am J Cardiol 1997; 80: 175–183.
(2) Galindo A, Gutierrez-Larraya F, Escribano D,Arbues J,Velasco JM. Clinical significance of persistent left superior vena cava diagnosed in fetal life. Ultrasound Obstet Gynecol 2007; 30: 152–161.
(3) Barrea C, Ovaert C, Moniotte S, Biard JM, Steenhaut P, Bernard P. Prenatal diagnosis of abnormal cardinal systemic venous return without other heart defects: a case series. Prenat Diagn 2011; 31: 380–388.
(4) Postema PG, Rammeloo LA, van Litsenburg R, Rothuis EG, Hruda J. Left superior vena cava in pediatric cardiology associated with extra-cardiac anomalies. Int J Cardiol 2008; 123: 302–306.
(5) Pasquini L, Belmar C, Seale A, Gardiner HM. Prenatal diagnosis of absent right and persistent left superior vena cava. Prenat Diagn 2006; 26: 700–702.
(6) Guarnieri GF, Romano F, Clerico L, Balducci G. Absent right and persistent left superior vena cava: fetal and neonatal echocardiographic diagnosis. Pediatr Cardiol 2006; 27: 646–648.
(7) Freund M, Stoutenbeek P, ter Heide H, Pistorius L. ‘Tobacco pipe’ sign in the fetus: patent left superior vena cava with absent right superior vena cava. Ultrasound Obstet Gynecol 2008; 32: 593–594.
(8) Ratnasamy C, Idriss SF, Carboni MP, Kanter RJ. Arrhythmias in children having a single left superior vena cava and minimal structural heart disease. J Cardiovasc Electrophysiol 2009; 20: 182–186.
(9) Ucar O, Pasaoglu L, Cicekcioglu H, Vural M, Kocaoglu I, Aydogdu S. Persistent left superior vena cava with absent right superior vena cava: a case report and review of the literature. Cardiovasc J Afr 2010; 21: 164–166.
(10) Lenox CC, Hashida Y, Anderson RH, Hubbard JD. Conduction tissue anomalies in absence of the right superior caval vein. Int J Cardiol 1985; 8: 251–260.
Christine van Velzen.indb 118 20/09/2016 08:27

Christine van Velzen.indb 119 20/09/2016 08:27

Christine van Velzen.indb 120 20/09/2016 08:27

CHAPTER 8General Discussion
Christine van Velzen.indb 121 20/09/2016 08:27

122
Chapter 8
Chapter 8
GENERAL DISCUSSION
The actual effects of ultrasound screening programs in pregnancy have always been challenging to study, due to the gradual and heterogeneous introduction of prenatal screening worldwide, improvements in neonatal care and the continuous technical developments. 1 The standard anomaly scan (SAS) is, however, part of routine prenatal care in almost every developed country. It is known that the SAS is capable to detect a large variety of congenital malformations, ranging from severe malformations like anencephaly to subtle ventricular septal defects.
Congenital heart defects are the most common congenital defects in neonates, occurring in 6-8/1000 live births. One third of these (2-3/1000) are severe CHD, commonly defined as being potentially life threatening and requiring surgery in the first year of life. Severe CHD are the leading cause of non-infectious neonatal mortality in at term born neonates. Only 10% of CHD cases occur in pregnancies with identifiable risk factors, such as fetal extracardiac malformations. Therefore, it is impossible to select all pregnant women that are at ‘high risk’ for having a child with CHD and ultrasonographic screening is required for prenatal detection.Infants with congenital heart defects (CHD) benefit from a prenatal diagnosis. 2-6 Prenatal detection facilitates an accurate diagnosis without the rush and anxiety a life threatening circulatory condition of the newborn would create. Moreover, it provides time for additional prenatal ultrasonographical and genetic testing. In some cardiac diagnosis, the risk for an aneuploidy or genetic syndrome is substantial and these conditions do not only affect the prognosis of the child in general, but can also influence the results of cardiac surgery in a negative manner. Research shows that the long-term prognosis of the physical quality of life is very important for the parents 7 and this should be included in the counselling.
All the information combined, prepares the parents for the time to come and provides a fundament to make a deliberate decision on continuation of the pregnancy. 8;9
This decision is influenced by the kind of congenital defect(s), religion, family circumstances and life experiences. The process of understanding, accepting and decision making should be supported by the medical team and it is essential that parents have a freedom of choice. Increasing evidence shows that a prenatal diagnosis can prevent mortality in several types of severe CHD, due to prompt and appropriate treatment of the neonate in a specialised care centre. This effect is probably most essential in transposition of the great arteries, because this specific heart defect is almost always isolated, and when treated in time, has a very favourable prognosis. Besides a reduction of the mortality, there are
Christine van Velzen.indb 122 20/09/2016 08:27

123
General Discussion
Chap
ter 8
indications that a prenatal diagnosis of severe CHD results in a more favourable long-term outcome in terms of morbidity in the first years of life. 2;10-14 Current screening programs show disappointingly low prenatal detection rates, around 35-50%. 15-20 Detailed data on detection rates stratified per diagnosis were lacking so far. The defined and uniform national introduction of the SAS for all pregnant women in the Netherlands in 2007 provided the unique opportunity to study the effect of the 20 weeks anomaly scan on the detection of heart defects, which was the primary aim of this thesis. Unlike most countries, in which ultrasound screening in not regulated and uniform, the program in the Netherlands was strictly regulated from the beginning onwards, with education and volume requisites for the ultrasonographers and a well-defined uniform scanning protocol. 21
The most important findings of this thesis are that the screening program in the Netherlands resulted in high detection rates for CHD (60% in general) in an unselected population in the Netherlands. 22 A strong relation between the prenatal DR and the severity of the heart defect was present. 22 The prenatal detection of CHD at the severe end of the spectrum (univentricular hearts) is above 90%. Yet, some defects like coarctation of the aorta remain difficult to detect in pregnancy. There is still room for improvement for conotruncal defects in particular (DR around 30-60%). The size of the cohort provided the opportunity to study the pregnancy outcome in sufficient detail. We found that fetal demise (3,6%) and preterm birth occur more frequently in isolated CHD pregnancies compared to the general, unselected population. 23
When a CHD is diagnosed prenatally and appears to be isolated (without any other structural anomalies) on the ultrasound, in 79% of the cases it was confirmed after birth. An aneuploidy was found in 11% and a genetic syndrome in 6% of the cases. 22 Finally, when a CHD is suspected and the woman is referred for a fetal echocardiography in a tertiary care center, the diagnostic accuracy is high. 24
FUTURE PERSPECTIVES
Implications for current screening programThe detection rates for congenital heart defects of the current screening program in the Netherlands are relatively good. Albeit we found that approximately 40% of severe CHD are prenatally missed, and almost all univentricular and other complex heart defects are detected. These results are far better than other studies reporting on regional cohorts, in which detection rates do not exceed 40%. 18;25;26 The studies described in this thesis did not aim to explore the underlying reasons for the screening performance of the SAS, but we hypothesize that the well-organized program
Christine van Velzen.indb 123 20/09/2016 08:27

124
Chapter 8
Chapter 8
can be held responsible for the good results. From the start in 2007 onwards, a national standardized scanning protocol, executed by uniform trained ultrasonographers, was the main principle of the program. Quality is maintained through bi-annual assessments of the scans and volume requirements. The degree of organisation, standardisation and defined prerequisites are substantially different from other countries, and must therefore contribute for a large part to the encountered result.
The results of these studies were collected through the assessment of several sources, like fetal databases, OR and catheterisation registries, emergency ward admission registries and post-mortem examination databases. This was a time consuming process and implicates a risk on missing data because of the partly retrospective approach. The monitoring of the national screening program through assessment of true-positive, false-negative and false positive cases is a very focussed way of reporting on test performance, and thus of the delivered quality of the individual health care workers. Therefore the reported figures in this thesis, which are currently not part of the quality monitoring, are essential, and need to be incorporated in the monitoring program. To achieve this, the database PERIDOS, which registers all prenatal SASs, should be enabled to link the screening results with the results of the subsequent diagnostic scans and the postnatal outcome up to the age of one. Findings after unexpected neonatal death should be incorporated in such registries. Following the example of Scandinavian countries all patients should be registered and traceable by their BSN number and mother and child should be linked to each other. Besides the monitoring of the full program, such a system would allow individual ultrasonographers to get informed about detected or missed anomalies, to directly learn from these cases. Such a registry also provides in the need for a long-term follow-up. The long term outcome, in terms of morbidity, quality of life and reproductive outcomes of infants with congenital malformations is a research subject that is still not elucidated in fetal medicine.
The current prenatal screening program is embedded in the national public health programs of our country. It started with the aim to detect neural tube defects for historical reasons. With the current available results, combined with results of other study groups in our country, 27;28 the objective of the SAS should be changed into the prenatal detection of congenital defects in general. Preferably the screening should be performed around 19 weeks’ gestation, in order to allow reasonable time for additional diagnostics and counselling the parents, since in the Netherlands the law allows to terminate pregnancy up to 24 completed weeks’ gestation. Especially since the possibilities of genetic testing will evolve, which currently takes several weeks to achieve a result.
Christine van Velzen.indb 124 20/09/2016 08:27

125
General Discussion
Chap
ter 8
As the prenatal detection of CHD still caries a vast amount of false negatives, combined with the fact that we encountered a strong relationship between detection rates and the severity of the heart defect, we believe that the detection rates of heart defects would be a very suitable quality indicator of the SAS. The high prevalence of heart defects makes it furthermore a feasible quality indicator, with the opportunity of a relatively fast identification of deviations in quality. In the era of Non-Invasive Prenatal Testing, discussion is raised whether the nuchal translucency screening at 12-13 weeks’ gestation should remain to identify cases at risk for heart defects. The reported incidence of CHD amongst fetuses with an NT >99th percentile is, however, only 6-7% 29, and a relationship between increased nuchal translucency and the severity of the cardiac defect is absent. Considering the screening performance of the SAS, the nuchal translucency measurement as a screening tool to identify cardiac defects cannot be upheld, especially if the costs of such a program are taken into consideration.
Scope for further researchThe detection rate of conotruncal anomalies needs further improvement, especially because these infants may benefit most from a prenatal diagnosis. As a start, the addition of the three vessel view, 30 incorporated as an obligatory item in the Dutch screening protocol since 2012, is expected to increase the detection rates of conotruncal defects further. 31 The effect of training of sonographers is only sparingly studied, but increased detection rates after training were reported. 32 Further research could focus on repetitive training, the effect of on-line availability of image libraries and the use of modern teaching tools like apps or web-based courses and platforms. Furthermore it is unclear if tele-consulting of a fetal medicine specialist, without actual referral of the patient, could help in selecting cases that need expert level real-time echocardiography. Finally, it is unknown what influence personal characteristics and beliefs of the ultrasonographers have on their performance. What makes them doubt and what makes them decide to refer? The importance of these factors seem to play a role, as is proven in breast and lung cancer screening, 33 but it is unknown if these factors can be controlled and guided in obstetric ultrasound.Besides research to study instruments that improve the screening quality, more knowledge is needed about long-term outcome of children with congenital heart defects. Counselling of future parents that are faced with a prenatal diagnosis is hampered by the lack of availability of large series that describe what the outcome is in their specific situation. The available literature on long-term outcome usually starts at the OR table, which is essentially different from cases that are identified at 20 weeks of gestation. The positive effect of a prenatal diagnosis on the morbidity, through the
Christine van Velzen.indb 125 20/09/2016 08:27

126
Chapter 8
Chapter 8
prevention of asphyxia and circulatory collapse by the timely started measures after birth, should be investigated more extensively, including long-term neurological follow up. In several countries, as well as in our study region, the value of postnatal saturation measurement in screening for CHD is currently evaluated. 34 With the current and expected future improvements in prenatal detection of CHD, postnatal screening will probably be superfluous. On the other hand, postnatal saturation measurement can have a value in regions with a lower quality of prenatal screening, and for other indications such as sepsis or persistent pulmonary hypertension.Finally, the possibilities of genetic testing in pregnancy are increasing rapidly. With the developments in non-invasive prenatal testing, a future scenario could be that a test with panels of gene expressions associated with CHD become available for women early in pregnancy or even before pregnancy. Future research will probably demonstrate what the implications will be for the outcome of the pregnancy and the morbidity of the unborn child.
In conclusion, this thesis provides an overview of prenatal screening for fetal heart defect in the current era. The goal should be further improvement of prenatal detection rates of CHD and the reduction of mortality and morbidity of the affected infants.
Christine van Velzen.indb 126 20/09/2016 08:27

127
General Discussion
Chap
ter 8
REFERENCE LIST(1) Eik-Nes SH. The 18-week fetal examination and detection of anomalies. Prenat Diagn 2010 Jul;30(7):624-
30.
(2) Bonnet D, Coltri A, Butera G, Fermont L, Le Bidois J, Kachaner J, et al. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999 Feb 23;99(7):916-8.
(3) Mahle WT, Clancy RR, McGaurn SP, Goin JE, Clark BJ. Impact of prenatal diagnosis on survival and early neurologic morbidity in neonates with the hypoplastic left heart syndrome. Pediatrics 2001 Jun;107(6):1277-82.
(4) Franklin O, Burch M, Manning N, Sleeman K, Gould S, Archer N. Prenatal diagnosis of coarctation of the aorta improves survival and reduces morbidity. Heart 2002 Jan;87(1):67-9.
(5) Kaguelidou F, Fermont L, Boudjemline Y, Le Bidois J, Batisse A, Bonnet D. Foetal echocardiographic assessment of tetralogy of Fallot and post-natal outcome. Eur Heart J 2008 Jun;29(11):1432-8.
(6) Yates RS. The influence of prenatal diagnosis on postnatal outcome in patients with structural congenital heart disease. Prenat Diagn 2004 Dec 30;24(13):1143-9.
(7) Marino BS, Tomlinson RS, Drotar D, Claybon ES, Aguirre A, Ittenbach R, Welkom JS, Helfaer MA, Wernovsky G, Shea JA. Quality-of-life concerns differ among patients, parents, and medical providers in children and adolescents with congenital and acquired heart disease. Pediatrics. 2009Apr;123(4):e708-15
(8) Williams IA, Shaw R, Kleinman CS, Gersony WM, Prakash A, Levasseur SM, et al. Parental understanding of neonatal congenital heart disease. Pediatr Cardiol 2008 Nov;29(6):1059-65.
(9) Hoehn KS, Wernovsky G, Rychik J, Tian ZY, Donaghue D, Alderfer MA, et al. Parental decision-making in congenital heart disease. Cardiol Young 2004 Jun;14(3):309-14.
(10) Jaeggi ET, Sholler GF, Jones OD, Cooper SG. Comparative analysis of pattern, management and outcome of pre- versus postnatally diagnosed major congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2001 May;17(5):380-5.
(11) Kumar RK, Newburger JW, Gauvreau K, Kamenir SA, Hornberger LK. Comparison of outcome when hypoplastic left heart syndrome and transposition of the great arteries are diagnosed prenatally versus when diagnosis of these two conditions is made only postnatally. Am J Cardiol 1999 Jun 15;83(12):1649-53.
(12) Allan LD, Apfel HD, Printz BF. Outcome after prenatal diagnosis of the hypoplastic left heart syndrome. Heart 1998 Apr;79(4):371-3.
(13) Fuchs IB, Muller H, Abdul-Khaliq H, Harder T, Dudenhausen JW, Henrich W. Immediate and long-term outcomes in children with prenatal diagnosis of selected isolated congenital heart defects. Ultrasound Obstet Gynecol 2007 Jan;29(1):38-43.
(14) van Velzen CL, Haak MC, Reijnders G, Rijlaarsdam ME, Bax CJ, Pajkrt E, et al. Prenatal detection of transposition of the great arteries reduces mortality and morbidity. Ultrasound Obstet Gynecol 2015 Mar;45(3):320-5.
(15) Khoshnood B, De Vigan C, Vodovar V, Goujard J, Lhomme A, Bonnet D, et al. Trends in prenatal diagnosis, pregnancy termination, and perinatal mortality of newborns with congenital heart disease in France, 1983-2000: a population-based evaluation. Pediatrics 2005 Jan;115(1):95-101.
(16) Trines J, Fruitman D, Zuo KJ, Smallhorn JF, Hornberger LK, Mackie AS. Effectiveness of prenatal screening for congenital heart disease: assessment in a jurisdiction with universal access to health care. Can J Cardiol 2013 Jul;29(7):879-85.
(17) Pinto NM, Keenan HT, Minich LL, Puchalski MD, Heywood M, Botto LD. Barriers to prenatal detection of congenital heart disease: a population-based study. Ultrasound Obstet Gynecol 2012 Oct;40(4):418-25.
(18) Galindo A, Herraiz I, Escribano D, Lora D, Melchor JC, de la Cruz J. Prenatal detection of congenital heart defects: a survey on clinical practice in Spain. Fetal Diagn Ther 2011;29(4):287-95.
(19) Jorgensen DE, Vejlstrup N, Jorgensen C, Maroun LL, Steensberg J, Hessellund A, et al. Prenatal detection
Christine van Velzen.indb 127 20/09/2016 08:27

128
Chapter 8
Chapter 8
of congenital heart disease in a low risk population undergoing first and second trimester screening. Prenat Diagn 2015 Apr;35(4):325-30.
(20) Garne E, Loane M, Dolk H, De VC, Scarano G, Tucker D, et al. Prenatal diagnosis of severe structural congenital malformations in Europe. Ultrasound Obstet Gynecol 2005 Jan;25(1):6-11.
(21) van Velzen C, Türkeri F, Ket J, van de Ven P, Blom N, Haak M. Performance of second trimester screening for prenatal detection of congenital heart defects in unselected populations - systematic review and meta-analysis. Submitted work
(22) van Velzen C, Clur S, Rijlaarsdam M, Bax C, Pajkrt E, Heymans M, et al. Prenatal detection of congenital heart disease-results of a national screening programme. BJOG 2015 Jan 27.
(23) van Velzen C, Türkeri F, Pajkrt E, Clur S, Rijlaarsdam M, Bax C, Hruda J, de Groot C, Blom N, Haak M. Pregnancy complications in singleton pregnancies with isolated fetal heart defects. ACTA Obstet Gynec Scan 2016
(24) van Velzen CL, Clur SA, Rijlaarsdam ME, Pajkrt E, Bax CJ, Hruda J, et al. Prenatal diagnosis of congenital heart defects; accuracy and discrepancies in a multi-center cohort. Ultrasound Obstet Gynecol 2015 Sep 9.
(25) Marek J, Tomek V, Skovranek J, Povysilova V, Samanek M. Prenatal ultrasound screening of congenital heart disease in an unselected national population: a 21-year experience. Heart 2011 Jan;97(2):124-30.
(26) Stumpflen I, Stumpflen A, Wimmer M, Bernaschek G. Effect of detailed fetal echocardiography as part of routine prenatal ultrasonographic screening on detection of congenital heart disease. Lancet 1996 Sep 28;348(9031):854-7.
(27) Ensing S, Kleinrouweler CE, Maas SM, Bilardo CM, Van der Horst CM, Pajkrt E. Influence of the 20-week anomaly scan on prenatal diagnosis and management of fetal facial clefts. Ultrasound Obstet Gynecol 2014 Aug;44(2):154-9.
(28) Fleurke-Rozema JH, Vogel TA, Voskamp BJ, Pajkrt E, van den Berg PP, Beekhuis JR, et al. Impact of introduction of mid-trimester scan on pregnancy outcome of open spina bifida in The Netherlands. Ultrasound Obstet Gynecol 2014 May;43(5):553-6.
(29) Ghi T, Huggon IC, Zosmer N, Nicolaides KH. Incidence of major structural cardiac defects associated with increased nuchal translucency but normal karyotype. Ultrasound Obstet Gynecol 2001 Dec;18(6):610-4.
(30) Tongsong T, Tongprasert F, Srisupundit K, Luewan S. The complete three-vessel view in prenatal detection of congenital heart defects. Prenat Diagn 2010 Jan;30(1):23-9.
(31) International Society of Ultrasound in Obstetrics and Gynecology, Carvalho JS, Allan LD, Chaoui R, Copel JA, DeVore GR, et al. ISUOG Practice Guidelines (updated): sonographic screening examination of the fetal heart. Ultrasound Obstet Gynecol 2013 Mar;41(3):348-59.
(32) McBrien A, Sands A, Craig B, Dornan J, Casey F. Impact of a regional training program in fetal echocardiography for sonographers on the antenatal detection of major congenital heart disease. Ultrasound Obstet Gynecol 2010 Sep;36(3):279-84.
(33) Carney PA, Elmore JG, Abraham LA, et al. Radiologist uncertainty and the interpretation of screening. Med Decis Making 2004;24:255-264.
(34) Narayen IC, Blom NA, Bourgonje MS, Haak MC, Smit M, Posthumus F, van den Broek AJ, Havers HM, Te Pas AB. Pulse Oximetry Screening for Critical Congenital Heart Disease after Home Birth and Early Discharge. J Pediatr. 2016 Mar;170:188-192.
Christine van Velzen.indb 128 20/09/2016 08:27

Christine van Velzen.indb 129 20/09/2016 08:27

Christine van Velzen.indb 130 20/09/2016 08:27

CHAPTER 9Summary
Christine van Velzen.indb 131 20/09/2016 08:27

132
Chapter 9
Chapter 9
SUMMARY
Targeted ultrasound examination provides the possibility to diagnose a variety of structural malformations of the fetus. Nowadays, screening for congenital anomalies is offered as standard obstetric care by ultrasound examination around 20 weeks’ gestation in most Western countries. A prenatal diagnosis of a congenital heart defect (CHD), may lead to changes in obstetric management and allows for optimal neonatal care which may improve the neonatal outcome. CHD are still amongst the most commonly overlooked lesions in prenatal screening. CHD are the most common congenital defects in neonates, occurring in 6-8/1000 live births. One third of these (2-3/1000) are severe CHD, commonly defined as being potentially life threatening and requiring surgery in the first year of life. Severe CHD are the leading cause of non-infectious neonatal mortality in at term born neonates. The goal of this thesis was to gain insight in the performance of second trimester standard anomaly screening in detecting CHD and to evaluate the influence of a prenatal diagnosis on the outcome.
First, in Chapter 2, a systematic review was performed, to evaluate the performance of second trimester screening by ultrasound in detecting CHD internationally. A meta-analysis was performed on the detection rates of CHD in low risk or general populations. Analysis were performed differentiated per specific diagnosis, since CHD are very heterogeneous in anatomy, severity and prognosis. A separate analysis was performed for isolated CHD, meaning the CHD being the only congenital defect present, without any genetic or extracardiac structural anomaly. Unfortunately, very few studies report on isolated CHD. Detection rates higher than 90% were found for univentricular defects and heterotaxy cases. Defects like coarctation of the aorta and transposition of the great arteries were detected less frequently. We found that the prenatal detection rate of a CHD generally is correlated with the severity of the heart defect.A large retrospective and partly prospective cohort study was performed in a large region in the Netherlands to evaluate the performance of prenatal screening by ultrasound, including more than 1900 cases of fetuses/neonates with CHD born between 2002 and 2012.
In Chapter 3, we evaluated the effect of the introduction of the national second trimester screening program in the Netherlands in 2007 on the prenatal detection rates of CHD. Cases were divided into two groups: before and after the introduction of screening. The prenatal detection rate increased from 35.8 to 59.7% after the introduction of screening and of isolated CHD from 22.8 to 44.2%. The highest detection rates were found in the hypoplastic left heart syndrome, other univentricular defects and complex defects with atrial isomerism (>93%). Since the introduction of screening, the ‘late’ referrals
Christine van Velzen.indb 132 20/09/2016 08:27

133
Summary
Chap
ter 9
(after 24 weeks of gestation) to a tertiary centre decreased by 24.3%. Of the CHD cases identified on prenatal scan without any extracardiac structural anomalies 10.9% had an aneuploidy. In the total cohort 2.0% had a 22q11 deletion. Other genetic syndromes (e.g. CHARGE, Williams, Holt–Oram syndrome) were diagnosed in 3.9% of the total cohort. Termination of pregnancy is performed in about 50% of all the prenatally diagnosed cases and in about 30% of the prenatally diagnosed cases with isolated CHD. Colleagues from Belgium complemented the Dutch screening program with the high detection rates in a published reply on the study. In a reaction from our side we elaborated on why we think the Dutch screening program has these high detection rates. Essentially the prenatal screening in the Netherlands is centrally organised, with a uniform protocol, training, regulations and close quality monitoring.Transposition of the great arteries (TGA) is one of the most common cyanotic CHDs, with an incidence of 0.2–0.3 per 1000 live births. Simple TGA is rarely associated with chromosomal or extracardiac anomalies. The condition is generally well tolerated by the fetus, but life-threatening cyanotic complications occur shortly after birth. Chapter 4 focuses on the prenatal detection of TGA, as well as the effect of prenatal detection on pre- and postsurgical mortality and morbidity. Of all cases (n=144), 26.4% were diagnosed prenatally, the detection rate was 41.0% after introduction of the second trimester anomaly scan. First-year mortality was significantly lower in cases with a prenatal diagnosis of TGA than in those without (0.0% vs 11.4%, respectively). Pre-surgical mortality (4.9%) only occurred in undetected simple TGA cases. Closure of the duct before treatment, renal dysfunction and hypoxia occurred significantly more often in the group without a prenatal diagnosis.
When a fetal CHD is suspected in a second trimester anomaly scan, the patient is referred to a tertiary center where fetal echocardiography is performed. In Chapter 5 the accuracy of fetal echocardiography in diagnosing CHD is examined. All cases with CHD that were referred prenatally to the three tertiary centers in the study region between 2002 and 2012 were included (n=708). Prenatal and postnatal diagnoses were compared and the degree of agreement was classified as ‘correct’(anatomy correct and the postnatal diagnosis led to a similar outcome as expected), ‘discrepant’ (anatomical discrepancies present but the severity and prognosis of the defect were diagnosed correctly) or ‘no similarity’ (the pre- and postnatal diagnoses differed completely).
The prenatal diagnosis was correct in 82.1% of cases and discrepancies were present in 9.9%; however, these did not result in a different outcome. In 8.1% there was no similarity between prenatal and postnatal diagnoses. Disagreement between pre- and postnatal diagnoses occurred significantly more frequently in cases that presented
Christine van Velzen.indb 133 20/09/2016 08:27

134
Chapter 9
Chapter 9
with a normal four-chamber view than in those with an abnormal four-chamber view (5.5% vs 1.9%). Incorrect identification of the outflow tracts and incorrect differentiation between unbalanced atrioventricular septal defect and hypoplastic left heart syndrome were relatively commonly encountered. In many cases with disagreement, trisomy 21, an extracardiac anomaly or a high maternal body mass index was present.
With the increasing prenatal detection rates of CHD, obstetricians are more frequently faced with pregnancies complicated by a fetal CHD. Congenital anomalies in general are associated with preterm birth and fetal demise. The aim in Chapter 6 was to gain insight into the incidence of preterm birth and fetal demise in singleton pregnancies with fetuses with isolated CHD. In this analysis fetuses and infants from singleton pregnancies diagnosed with severe isolated CHD, born in the study region between 2002 and 2012, were included. All cases in the CHD cohort were assessed for preterm birth or fetal demise. The proportions of preterm birth and fetal demise were compared to a control group (all births in the study region in 2010 (PRN data)) and odds ratios were calculated.
The proportion of preterm births in the CHD cohort (n=1013) was 9.1% compared to 5.6% in the control group, with an odds ratio of 1.7. The preterm birth started spontaneously in 49.5% and 38.4% were induced. In 15 cases fetal demise occurred (1.5%), compared to 0.7% in the control group, odds ratio 2.0.
In Chapter 7 a prenatally diagnosed CHD case is presented with unexpected postnatal complications. Persistence of the left superior vena cava (LSVC) in the absence of the right superior vena cava (RSVC) in a fetus with otherwise normal cardiac anatomy is usually not predictive of postnatal complications. This case report shows that cardiac anomalies that were assumed to be fairly innocuous can have an unexpected outcome.
In Chapter 8 all the findings in this thesis are discussed and suggestions to improve the prenatal screening program and detection rates are postulated in order to achieve a reduction of mortality and morbidity of the affected infants.
Christine van Velzen.indb 134 20/09/2016 08:27

135
Summary
Chap
ter 9
SAMENVATTING
Gericht echoscopisch onderzoek maakt het mogelijk om verschillende typen structurele afwijkingen van de foetus te diagnostiseren. Tegenwoordig wordt het prenatale screenen op congenitale afwijkingen middels echoscopisch onderzoek rond 20 weken amenorroeduur aangeboden als standaard obstetrische zorg in de meeste Westerse landen. Een prenatale diagnose van congenitale hart afwijkingen (CHA), kan leiden tot aanpassingen in het obstetrische beleid en zorgt ervoor dat optimale neonatale zorg kan worden verleend, hetgeen de neonatale uitkomst kan verbeteren. CHA worden nog altijd vrij regelmatig over het hoofd gezien bij de prenatale screening. CHA zijn de meest voorkomende congenitale afwijkingen, 6-8 per 1000 levend geborenen heeft een hartafwijking. Een derde hiervan (2-3/1000) zijn ernstige CHA, gedefinieerd als potentieel levensbedreigende aandoening waarvoor chirurgische behandeling is geïndiceerd in het eerste levensjaar. Ernstige CHA zijn de belangrijkste oorzaak van niet-infectieuze mortaliteit van aterme geboren neonaten. Het doel van dit proefschrift was inzicht te verkrijgen in het functioneren van echoscopische tweede trimester screening en te evalueren of een prenatale diagnose de uitkomst beïnvloedt.
Allereerst, werd in Hoofdstuk 2, een systematische review verricht, teneinde de prenatale detectie van CHA te evalueren van de tweede trimester echoscopische screening internationaal beschouwd. Een meta-analyse werd uitgevoerd naar de detectie ratio van CHA in laag risico danwel algemene populaties. De analyses werden gedifferentieerd per specifieke diagnose uitgevoerd, aangezien CHA zeer heterogeen zijn in de anatomie, ernst en prognose. Een aparte analysis werd uitgevoerd voor geïsoleerde CHA, ofwel foetus/neonaten waarbij de CHA de enige aanwezige congenitale afwijking was, zonder enige andere genetische of extracardiale structurele afwijking. Helaas zijn er maar weinig studies gepubliceerd met getallen over geïsoleerde CHA. Detectie ratio’s van hoger dan 90% werden gevonden voor univentriculaire defecten en heterotaxie afwijkingen. Defecten zoals coarctatio aortae en transpositie van de grote vaten werden minder frequent gedetecteerd prenataal. We zagen dat de prenatale detectie ratio van een CHA over het algemeen een duidelijk verband heeft met de ernst van de hartafwijking.Een grote retrospectieve en deels prospectieve cohort studie werd uitgevoerd in een grote regio in Nederland om het functioneren van de prenatale screening middels echoscopisch onderzoek te evalueren, waarbij meer dan 1900 foetus danwel neonaten met een CHA werden geïncludeerd geboren tussen 2002 en 2012.
In Hoofdstuk 3, evalueerden we het effect van de introductie van het nationale tweede trimester screenings programma (structureel echoscopisch onderzoek) in Nederland in
Christine van Velzen.indb 135 20/09/2016 08:27

136
Chapter 9
Chapter 9
2007 op de prenatale detectie ratio’s of CHA. Cases werden verdeeld in twee groepen: voor en na de introductie van screening. De prenatale detectie ratio verbeterde van 35.8 naar 59.7% na de introductie van screening en voor geïsoleerde CHA van 22.8 naar 44.2%. De hoogste detectie ratio’s werden gevonden bij het hypoplastisch linker hart syndroom, andere univentriculaire defecten en complexe defects met isomerisme van de atria (>93%). Sinds de introductie van de screening, is het percentage van ‘late’ verwijzingen naar een tertiair centrum (na 24 weken amenorroeduur) afgenomen met 24.3%. Van de CHA cases die geïdentificeerd werden bij prenatale echoscopie zonder enige andere extracardiale structurele afwijkingen bleek 10.9% een aneuploidie te hebben. In het totale cohort had 2.0% een 22q11 deletie. Andere genetische syndromen (bijv. CHARGE, Williams, Holt–Oram syndroom) werden gediagnostiseerd in 3.9% van het totale cohort. Er werd gekozen voor een zwangerschapsafbreking voor de 24 weken in ongeveer 50% van alle prenataal gediagnostiseerde cases en in ongeveer 30% van de prenataal gediagnostiseerde cases met geïsoleerde CHA. Collega’s uit België schreven in een reactie op onze studie dat ze het Nederlandse screenings programma prezen om de hoge detectie percentages. In antwoord daarop zetten wij uiteen waarom we denken dat het Nederlands screening programma zo goed functioneert. Samengevat is de prenatale screening in Nederland centraal georganiseerd, met een uniform landelijk protocol, training, regels en nauwgezette kwaliteit monitoring.
Transpositie van de grote vaten (TGV) is een van de meest voorkomende cyanotische hartafwijkingen, met een incidentie van 0.2–0.3 per 1000 levend geborenen. Simpele TGV is zelden geassocieerd met chromosomale of extracardiale afwijkingen. De aandoening wordt in zijn algemeenheid goed verdragen door de foetus, maar levensbedreigende cyanotische complicaties treden op kort na de geboorte. In Hoofdstuk 4 wordt de prenatale detectie van TGV geëvalueerd, en het effect daarvan op pre- en postchirurgische mortaliteit en morbiditeit. Van alle cases (n=144), werd 26.4% prenataal gediagnostiseerd, en de detectie ratio was 41.0% na de introductie van het structureel echoscopisch onderzoek. De mortaliteit in het eerste levensjaar was significant lager in de neonaten met een prenatale diagnose van TGV dan in de neonaten met een diagnose na de geboorte (0.0% vs 11.4%). Pre-chirurgische mortaliteit (4.9%) trad alleen op bij TGV cases zonder prenatale diagnose. Het sluiten van de ductus voor het starten van behandeling, nierfunctie stoornissen en hypoxie traden significant vaker op in de groep zonder prenatale diagnose.
Wanneer een foetale CHA wordt vermoed bij de structurele screenings echo, wordt de patiënt verwezen naar een tertiair centrum waar foetale echocardiografie wordt verricht. In Hoofdstuk 5 wordt de accuratesse van de foetale echocardiografie
Christine van Velzen.indb 136 20/09/2016 08:27

137
Summary
Chap
ter 9
onderzocht. Alle cases met CHA die prenataal verwezen werden naar de drie tertiaire centra in de studie regio tussen 2002 en 2012 werden geïncludeerd (n=708). Prenatale en postnatale diagnoses werden vergeleken en de mate van overeenstemming werd geclassificeerd als ‘correct’(anatomie correct en de postnatale diagnose leidde tot een vergelijkbare uitkomst als voorspeld), ‘discrepantie’ (anatomische discrepantie, maar de ernst en prognose van het defect correct ingeschat) of ‘geen overeenstemming’ (de pre- en postnatale diagnoses verschilden compleet).
De prenatale diagnose was correct in 82.1% van de cases en discrepanties waren aanwezig in 9.9% (niet resulterend in een andere uitkomst). In 8.1% van de cases was er geen overeenstemming tussen de prenatale en postnatale diagnose. Dit trad significant vaker op in cases die zich presenteerden met een normaal 4-kamerbeeld dan in cases met een abnormaal 4-kamerbeeld (5.5% vs 1.9%). Incorrecte identificatie van de outflow tracts en incorrecte differentiatie tussen een ongebalanceerd atrioventriculair septum defect en een hypoplastisch linker hart syndroom kwamen relatief frequent voor. In veel gevallen zonder overeenstemming tussen de pre- en postnatale diagnose was sprake van trisomie 21, een extracardiale anomalie of een hoge maternale BMI.
Met de verbeterende prenatale detectie van CHA, worden obstetrici steeds frequenter geconfronteerd met een zwangerschap die gecompliceerd is door een foetale hartafwijking. Congenitale afwijkingen in het algemeen zijn veelal met partus prematurus en intra-uteriene vruchtdood. Het doel van Hoofdstuk 6 was inzicht te verkrijgen in de incidentie van partus prematurus en intra-uteriene vruchtdood in eenling zwangerschappen van een foetus met een geïsoleerde CHA. Alle foetus en neonaten geboren uit eenling zwangerschappen die gediagnostiseerd waren met een ernstige geïsoleerde CHA, geboren in de studie regio tussen 2002 en 2012, werden geïncludeerd in deze analyse. Van alle cases in het CHA cohort (n=1013) werd nagegaan of er sprake was geweest van een partus prematurus of intra-uteriene vruchtdood. De proportie partus prematurus en intra-uteriene vruchtdood in dit cohort werd vergeleken met een controle groep (bestaande uit alle partus in de studie regio van 2101 (PRN data)) en odds ratio’s werden berekend. De proportie partus prematurus in het CHA cohort was 9.1% tegenover 5.6% in de controle groep, met een odds ratio van 1.7. In 49.5% van de gevallen was de partus prematurus spontaan en in 38.4% van de gevallen werd deze ingeleid. In 15 cases trad intra-uteriene vruchtdood op (1.5%), tegenover 0.7% in de control groep, odds ratio 2.0.
In Hoofdstuk 7 wordt een prenataal gediagnostiseerde CHA case gepresenteerd met een onverwachte postnatale complicatie. Een persisterende linker superior vena cava
Christine van Velzen.indb 137 20/09/2016 08:27

138
Chapter 9
Chapter 9
(LSVC) met afwezige rechter superior vena cava (RSVC) in een foetus met verder een normale cardiale anatomie is meestal niet geassocieerd met postnatale complicaties. Dit case report laat echter een voorbeeld zien van hoe een cardiale afwijking waarvan verwacht wordt dat deze vrij onschuldig is, toch een onverwachte uitkomst kan geven.
In Hoofdstuk 8 worden alle bevindingen beschreven in dit proefschrift bediscussieerd en worden suggesties gedaan teneinde het prenatale screenings programma en de detectie ratios te verbeteren.
Christine van Velzen.indb 138 20/09/2016 08:27

Christine van Velzen.indb 139 20/09/2016 08:27

Christine van Velzen.indb 140 20/09/2016 08:27

CHAPTER 10Appendices
Christine van Velzen.indb 141 20/09/2016 08:27

142
Chapter 10
Chapter 10
CONTRIBUTING AUTHORS AND AFFILIATIONS
Academic Medical Center, Amsterdam, The NetherlandsDepartment of Obstetrics and Gynecology E Pajkrt F. TürkeriDepartment of Pediatric Cardiology N.A. Blom S.A. Clur
Leiden University Medical Center, Leiden, The NetherlandsDepartment of Obstetrics and Gynecology M.C. HaakDepartment of Pediatric Cardiology N.A. Blom M.E.B. Rijlaarsdam
University Medical Center Groningen, Groningen, The NetherlandsDepartment of Obstetrics and Gynecology C.M. Bilardo
VU University Medical Center, Amsterdam, The NetherlandsDepartment of Epidemiology and Biostatistics F. Galindo-Garre M.W. Heymans P.M. van de VenDepartment of Obstetrics and Gynecology C.J. Bax C.J.M. de Groot G. ReijndersDepartment of Pediatric Cardiology J. Hruda L.A.J. RammelooMedical library J.C.F. Ket
Wilhelmina Kinder Ziekenhuis, Utrecht, The NetherlandsDepartment of Obstetrics and Gynecology M.N. Bekker
Christine van Velzen.indb 142 20/09/2016 08:27

143
Appendices
Chap
ter 1
0
PUBLICATIONSC.L. van Velzen, F. Türkeri, E. Pajkrt, S.A. Clur, M.E.B. Rijlaarsdam, C.J. Bax, J. Hruda, C.J.M. de Groot, N.A. Blom, M.C. Haak. Pregnancy complications in singleton pregnancies with isolated fetal heart defects. ACTA Obstet Gynecol Scand July 2016.
Jansen FA, van Zwet EW, Rijlaarsdam ME, Pajkrt E, van Velzen CL, Zuurveen HR, Kragt A, Bax C, Clur S, van Lith JM, Blom NA, Haak MC. Head growth in fetuses with isolated congenital heart defects: lack of influence of aortic arch flow and ascending aorta oxygen saturation. Ultrasound Obstet Gynecol. 2016 Jun.
C.L. van Velzen, S.A. Clur, M.E.B. Rijlaarsdam, E. Pajkrt, C.J. Bax, J. Hruda, C.J.M. de Groot, N.A. Blom, M.C. Haak. Prenatal diagnosis of congenital heart defects; accuracy and discrepancies in a multi-center cohort. Ultrasound Obstet Gynecol 2016 May(5);47:616-22.
Jansen FA, Hoffer MJ, van Velzen CL, Plati SK, Rijlaarsdam ME, Clur SA, Blom NA, Pajkrt E, Bhola SL, Knegt AC, de Boer MA, Haak MC. Chromosomal abnormalities and copy number variations in fetal left-sided congenital heart defects. Prenat Diagn. 2016 Feb;36(2):177-85.
C.L. van Velzen, M.C. Haak, G. Reijnders, M.E.B. Rijlaarsdam, C.J. Bax, E. Pajkrt, J.Hruda, F. Galindo-Garre, C.M. Bilardo, C.J.M. de Groot, N.A. Blom, S.A. Clur. Prenatal detection of transposition of the great arteries affects mortality and morbidity. Ultrasound in Obstetrics and Gynecology 2015 Mar;45(3):320-5.
C.L. van Velzen, S.A. Clur, M.E.B. Rijlaarsdam, C.J. Bax, E. Pajkrt, M.W. Heymans, M.N. Bekker, J. Hruda ,C.J.M. de Groot, N.A. Blom , M.C. Haak. Prenatal detection of congenital heart disease -results of a national screening program. BJOG 2016 Feb;123(3):400-7.
C.L. van Velzen, E. Pajkrt, M.C. Haak. Authors’ reply to Prenatal detection of congenital heart disease -results of a national screening program. BJOG 2015 Sep;122(10):1421.
C.L. van Velzen, B. Adriaanse, L.A.J. Rammeloo, N.A. Blom, J. Hruda. Impact of prenatal diagnosis of ductal origin of the left pulmonary artery. Prenatal Diagnosis 2013 Sep 13:1-3.
E. H.M.N. Westen, P. R. Kolk, C. L. van Velzen, N. S. Mmuni, A.D. Hamisi, R.E. Nakua, A.L.M. Vlek, R. Unkels, H.J. van Beekhuizen. Single-dose versus multiple day antibiotic prophylaxis for caesarean section in low resource setting, a randomised controlled, non-inferiority trial. Acta Obstet Gynecol Scand. 2015 Jan;94(1):43-9.
C.L. van Velzen, J. Hruda, L.A.J. Rammeloo, M.C. Haak. Supraventricular tachycardia in a neonate with the prenatal diagnosis of a single left superior vena cava. Ultrasound in Obstetrics and Gynecology 2011 Dec;38(6):731-2.
Christine van Velzen.indb 143 20/09/2016 08:27

144
Chapter 10
Chapter 10
DANKWOORDGraag wil ik mijn dank uitspreken aan:
Alle patiënten die toestemming hebben gegeven om deel te nemen aan wetenschappelijk onderzoek. Zonder jullie vertrouwen in de wetenschap zou dit proefschrift niet tot stand hebben kunnen komen.
Mijn promotores Prof.Dr. De Groot, Prof.Dr. Blom en copromotores Dr. Haak en Dr. Bax.
Christianne, voor je bereidheid en vertrouwen om mij onder je hoede te nemen, de altijd supersnelle correcties van mijn stukken en ideeën om het onderzoek naar een hoger plan te tillen.
Nico, voor je helicopter view, constructieve meedenken, enthousiasme en zinnige suggesties wanneer ik niet verder leek te komen.
Monique, voor je inspirerende voorbeeld op de werkvloer en daarbuiten, alle wijze professionele en levens-lessen en eindeloze steun.
Caroline, voor je relativeringsvermogen en persoonlijke begeleiding op de werkvloer.
Alle leden van de lees- en promotie commissie, voor jullie tijd, moeite en waardevolle mening.
A special thank you to Professor Gurleen Sharland, from London, for your effort to participate in the opposition committee.
Alle coauteurs voor de hulp en goede samenwerking.
Prof. Dr. Hruda, Jarda voor je enthousiasmerende lessen in de wetenschap en vooral in de kliniek. Het spreekuur op de woensdag ochtend met jou of Lukas was het meest uitdagende en leerzame van de week.
Dr. Clur, Sally-Ann voor alle energie en liefde voor het onderzoek en dat je dat met mij wilde delen.
Drs. Rijlaarsdam, Marry voor de eindeloze tijd en uitleg en je overzichtelijke systematiek. Door jou begreep ik steeds een beetje meer van die verdomd lastige anatomie van cardiale afwijkingen.
Prof. Dr. Pajkrt, Eva voor je ondersteunende ideeën, goede kritieken en directe humor.
Christine van Velzen.indb 144 20/09/2016 08:27

145
Appendices
Chap
ter 1
0
Mijn collega’s op de werkvloer Prenatale Diagnostiek.
Dr. Engels, Melanie voor je betrokkenheid, collegialiteit, je enorme echoscopische ervaring die je met ons deelde en alle gezelligheid.
Collega arts-echoscopisten, Ingeborg, Chantal, Sylvia, Bauke, Nicole, Bloeme wat een fijne tijd heb ik met jullie gehad, we waren een echt team. Ik kijk ernaar uit in de toekomst weer met jullie samen te werken.
Gynaecologen prenatale geneeskunde Dr. Go (Erasmus MC), Drs. Van Hoorn (MC Haaglanden) Dr. Bekker (WKZ Utrecht), Dr. Bakker, Dr. Vandenberghe (UZ Gent), Dr. Sikkel (Radboud UMC Nijmegen) Attie, Marion, Mireille, Petra, Griet, Esther voor de leerzame tijd en fijne samenwerking.
Prof. Dr. Van Vugt, John de samenwerking was helaas kort, maar ik ben eeuwig dankbaar voor de kans die ik heb gekregen.
Prof Dr. De Vries, Hanneke voor de lessen in de foetale neurologie en prettige samenwerking.
Echoscopisten van de VU Marijke, Annemieke, Monique, Sara, Annelieke, Barbara, Helmi, Natasja, Sandra, Sieta, Vicky. Jullie stonden aan de basis en hebben mij de beginselen van de echoscopie geleerd.
Secretariaat prenatale geneeskunde, Ineke, Marijke, Lucia, Brigid, Danielle, Janny, Caroline voor alle ondersteuning en gezelligheid.
Ivan Palmer voor alle keren dat ik ruzie had met de computer.
Alle collega onderzoekers en arts-assistenten in de VU voor de gezellige etentjes, weekenden en koffie.
Prof. Dr. Ottenkamp, voor het monnikenwerk waarop een groot deel van mijn database is gebaseerd.
Fenna Jansen, voor het aanvullen van de database en gezelligheid op congressen.
Alle studenten die ik mocht begeleiden en die bergen werk hebben verzet.
De Landelijke Werkgroep Wiegendood voor het beschikbaar stellen van hun data.
Christine van Velzen.indb 145 20/09/2016 08:27

146
Chapter 10
Chapter 10
Prof. Dr. Scherjon, Sicco, voor je enthousiasmerende begeleiding tijdens mijn studie en het openen van mijn ogen voor de wetenschap.Dr. Verweij en Dr. Holleboom, Robert en Cas, voor de persoonlijke, warme en inspirerende begeleiding tijdens mijn allereerste echte baan.
Alle collega’s in het Zaans Medisch Centrum, voor het warme bad waarin ik mocht starten. Ik vind jullie openheid en eindeloze discussies geweldig.
Dr. Bayram, Neriman, voor je eerlijke, gepassioneerde, persoonlijke en leerzame begeleiding als mijn opleider in Zaandam.
Alle lieve vrienden en vriendinnen, clubgenoten, sletten van H14 voor alle humor, diepgang, interesse, vreugde en verdriet, reizen, skien en al het andere.
Sonja en Jack voor alle interesse, steun en hulp bij de opvang van Julia en Philip.
Sarah, aan een half woord hebben we altijd genoeg, ik weet dat je er altijd zult zijn. Dank voor je vriendschap.
Jeannette, mijn partner in crime tijdens de studie, maar ook vele mooie momenten daarbuiten. Dank voor je interesse en steun en wat fijn dat je op 10 november naast mij zult staan als paranimf. Ik weet zeker dat ik me rot zal blijven lachen met je, totdat we achter de geraniums zitten met tuimelbekers met vla.
Alice, ik voel me bevoorrecht dat ik een zusje heb waar ik echt alles mee kan delen, zelfs onze promoties! Dat jij naast me staat 10 november is een hele geruststellende gedachte. Dank voor al je adviezen en ruggenspraak en voor alles wat we samen hebben meegemaakt.
Papa, voor je goede voorbeeld, motiveringsvermogen, onvoorwaardelijke steun en liefde. En voor je goede wijn- en muzieksmaak.
Mama, voor jouw nooit aflatende hulp, coaching, ondersteuning, er is eigenlijk geen goed woord voor te vinden. Jouw mensenkennis en levenslessen zijn ongeëvenaard en (bijna) altijd zeer bruikbaar. Het is zo fijn zo’n betrokken moeder en de laatste jaren ook oma voor mijn kinderen te hebben.
Bart, mijn grote liefde, you’ve always got my back. Ik hou van je humor, wijsheid, rust en gedrevenheid. Dank voor al je geduld, met jou samen is alles leuker.
Julia en Philip, voor jullie schaterlach en het samen opnieuw ontdekken van de wereld.
Christine van Velzen.indb 146 20/09/2016 08:27

147
Appendices
Chap
ter 1
0
OVER DE AUTEUR
Christine van Velzen werd geboren op 26 september 1980 te Utrecht. Na het behalen van het gymnasium diploma aan het Nieuwe Lyceum te Bilthoven in 1998, studeerde ze een half jaar Spaanse cultuur en taal aan de Academia Mester te Granada, Spanje. Het jaar daarop, toen ze wederom werd uitgeloot voor de studie Geneeskunde, studeerde ze Nederlands Recht aan de Universiteit van Leiden en behaalde de propedeuse.
In het jaar 2000 startte ze met de studie Geneeskunde aan de Universiteit van Leiden. De interesse in de Obstetrie en Gynaecologie ontstond al tijdens het vierde jaar, waarna ze negen maanden een wetenschappelijke stage volgde aan de afdelingen Obstetrie en Immunohematologie onder begeleiding van Prof. Dr. Sicco Scherjon. Tijdens de co-schappen werd de voorkeur voor Obstetrie en Gynaecologie bevestigd. Vervolgens werkte ze zes maanden in het Sokoine Hospital te Lindi, Tanzania, een zeer bijzondere en leerzame ervaring.
Aansluitend kon Christine starten als arts-assistent niet in opleiding op de afdeling Obstetrie en Gynaecologie in het Bronovo Ziekenhuis te Den Haag in 2008. Na een jaar verhuisde ze naar Utrecht en startte in dezelfde functie in het Sint Antonius Ziekenhuis te Nieuwegein. Eind 2009 werd ze aangenomen als arts-echoscopist op de afdeling Prenatale Geneeskunde van het VU Medisch Centrum te Amsterdam. Onder begeleiding van promotores Prof. Dr. Christianne de Groot en Prof. Dr. Nico Blom en co-promotores Dr. Monique Haak en Dr. Caroline Bax werkte ze vanaf begin 2011 aan haar onderzoek op het gebied van foetale echocardiografie, leidend tot deze dissertatie.
Per september 2014 is ze met veel plezier gestart met de opleiding tot gynaecoloog aan het VU Medisch Centrum (opleider Prof. Dr. J.I.P. de Vries). Momenteel volgt zij het eerste deel van haar opleiding in het Zaans Medisch Centrum (opleider Dr. N. Bayram).
Christine is getrouwd met Bart Nieuwkamer en samen hebben zij twee kinderen, Julia (2011) en Philip (2014).
Christine van Velzen.indb 147 20/09/2016 08:27

Proefschrift_ChristineVanVelzenCover+Bladwijzer.indd 1-4 15-09-16 17:05