LLL ICU algemene principes van nutritioneel management · 1/05/2011 1 Dr. J. Nollet Intensieve...
19
1/05/2011 1 Dr. J. Nollet Intensieve Zorg, MICU UZ Gent 30 april 2011 Algemene principes van nutritioneel management Algemene principes van nutritioneel management • Bepalen voedingsstatus: biochemische parameters/anthropometrie • Enteraal en/of parenteraal? • Timing? (laat vsvroeg) • Keuze enteraal of parenteraal: welk voedingspreparaat? • Zo enteraal: maag vsdarm Voorgeschiedenis Antropometrie Biochemie musculaire/immunologische tests -biochemische parameters Bepalen voedingsstatus
Transcript of LLL ICU algemene principes van nutritioneel management · 1/05/2011 1 Dr. J. Nollet Intensieve...
1/05/2011
1
Dr. J. Nollet
Intensieve Zorg, MICU
UZ Gent
30 april 2011
Algemene principes
van nutritioneel management
Algemene principes van nutritioneelmanagement
• Bepalen voedingsstatus: biochemische parameters/anthropometrie
• Enteraal en/of parenteraal?
• Timing? (laat vs vroeg)
• Keuze enteraal of parenteraal: welk voedingspreparaat?
• Zo enteraal: maag vs darm
�Voorgeschiedenis
�Antropometrie
�Biochemie
�musculaire/immunologische tests
- biochemische parameters
Bepalen voedingsstatus
1/05/2011
2
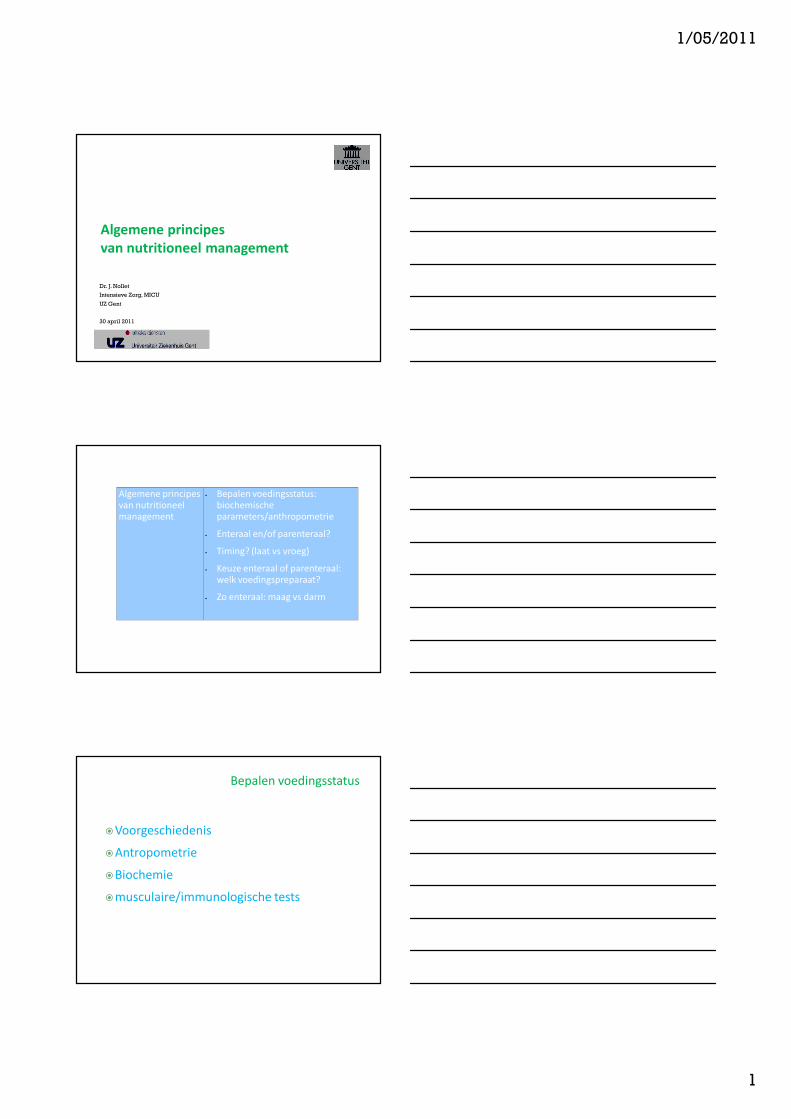
Bepalen voedingsstatus :
(Voedings-)anamnese
�
Excretie nutrienten
�
metabolisme�
Vertering&
absorptie
�
Voedsel inname
(Radiatie-)enteritis ?
Uitgebreide resectiediarree ?
…
Eetlust ?
Kauwen ?Slikken ?
�speeksel ?…
� E behoefte ? GI (Faecaal
verlies, braken, stoma)
brandwonden
malnutritie
ICU
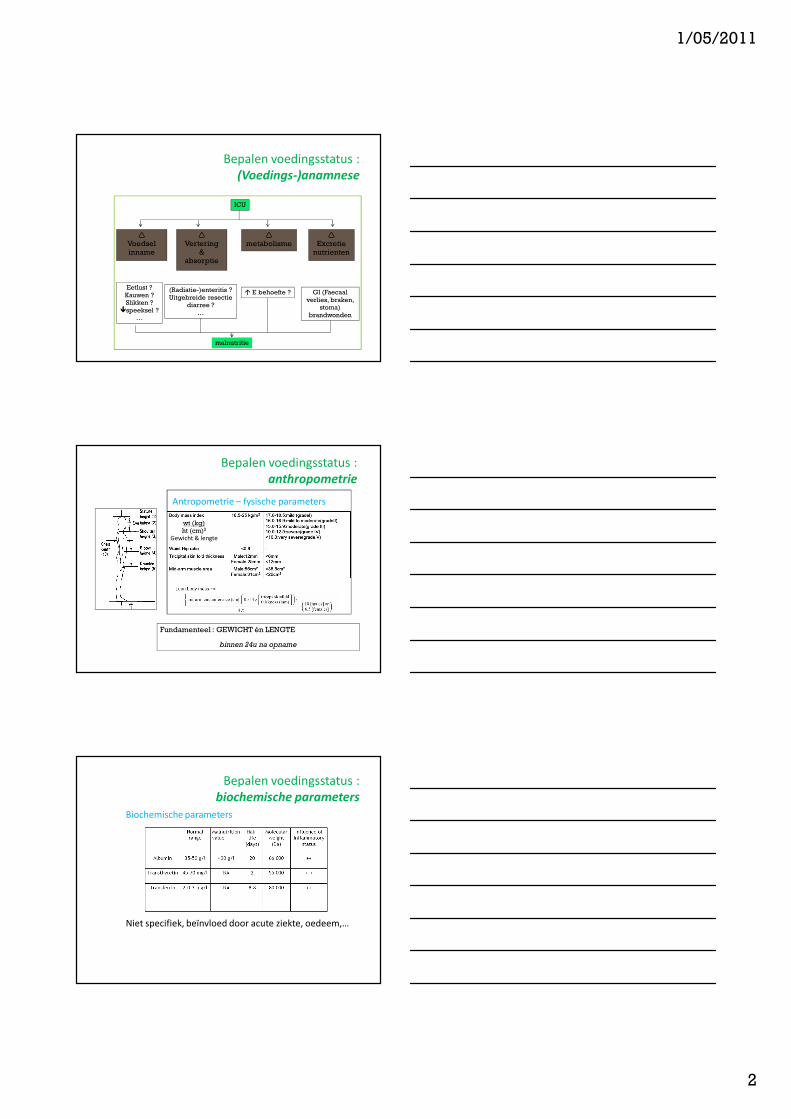
Bepalen voedingsstatus :
anthropometrie
Antropometrie – fysische parameters
wt (kg)
ht (cm)2
Gewicht & lengte
Fundamenteel : GEWICHT én LENGTE
binnen 24u na opname
Bepalen voedingsstatus :
biochemische parameters
Biochemische parameters
Niet specifiek, beïnvloed door acute ziekte, oedeem,…
1/05/2011
3
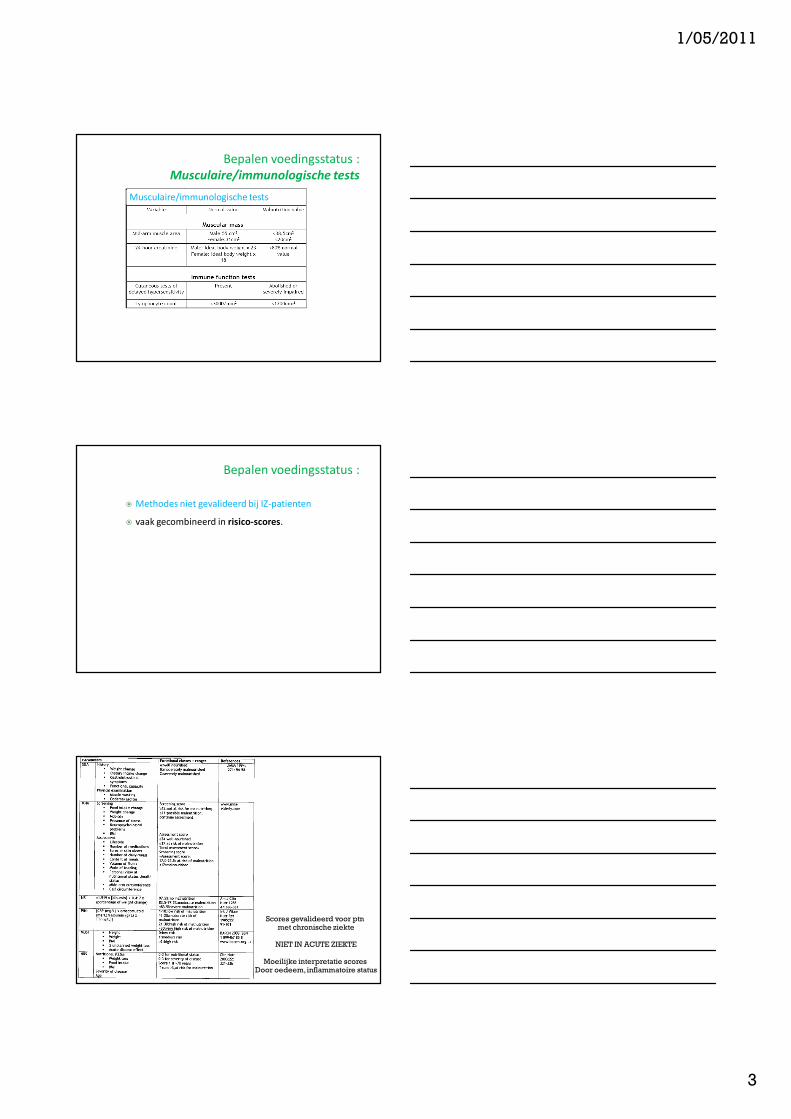
Bepalen voedingsstatus :
Musculaire/immunologische tests
� musculaire/immunologische testsMusculaire/immunologische tests
Bepalen voedingsstatus :
� Methodes niet gevalideerd bij IZ-patienten
� vaak gecombineerd in risico-scores.
� risico-scores
Scores gevalideerd voor ptnmet chronische ziekte
NIET IN ACUTE ZIEKTE
Moeilijke interpretatie scores Door oedeem, inflammatoire status
1/05/2011
4
anthropometrie
Bepalen voedingsstatus :
biochemische parameters/anthropometrie
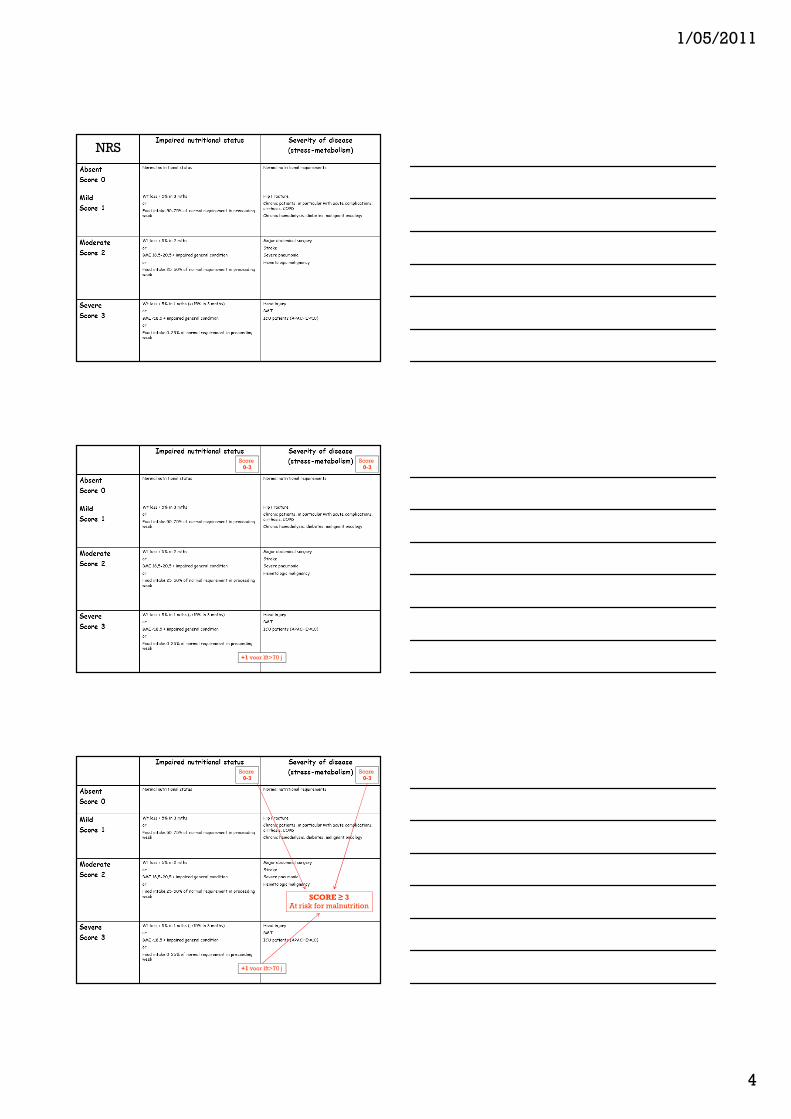
NRS
anthropometrie
Bepalen voedingsstatus :
biochemische parameters/anthropometrie
Score 0-3
Score 0-3
+1 voor lft>70 j
anthropometrie
Bepalen voedingsstatus :
biochemische parameters/anthropometrie
Score 0-3
Score 0-3
+1 voor lft>70 j
SCORE ≥ 3At risk for malnutrition
1/05/2011
5
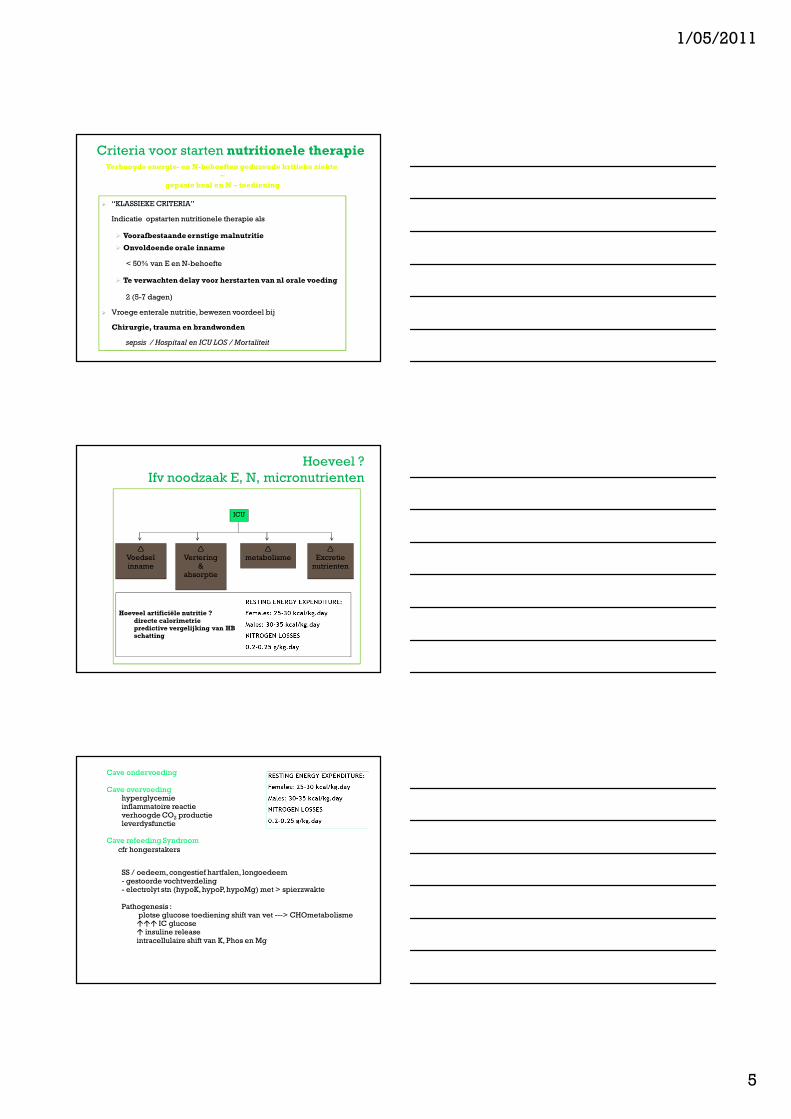
Criteria voor starten nutritionele therapie
� “KLASSIEKE CRITERIA”
Indicatie opstarten nutritionele therapie als
� Voorafbestaande ernstige malnutritie
� Onvoldoende orale inname
< 50% van E en N-behoefte
� Te verwachten delay voor herstarten van nl orale voeding
2 (5-7 dagen)
� Vroege enterale nutritie, bewezen voordeel bij
Chirurgie, trauma en brandwonden
sepsis / Hospitaal en ICU LOS / Mortaliteit
Verhoogde energie- en N-behoeften gedurende kritieke ziekte
~
gepaste kcal en N – toediening
Hoeveel ?
Ifv noodzaak E, N, micronutrienten
�
Excretie nutrienten
�
metabolisme�
Vertering&
absorptie
�
Voedsel inname
Hoeveel artificiële nutritie ?directe calorimetriepredictive vergelijking van HBschatting
ICU
Cave ondervoeding
Cave overvoedinghyperglycemieinflammatoire reactieverhoogde CO2 productieleverdysfunctie
Cave refeeding Syndroom
cfr hongerstakers
SS / oedeem, congestief hartfalen, longoedeem- gestoorde vochtverdeling- electrolyt stn (hypoK, hypoP, hypoMg) met > spierzwakte
Pathogenesis : plotse glucose toediening shift van vet ---> CHOmetabolisme��� IC glucose� insuline releaseintracellulaire shift van K, Phos en Mg
1/05/2011
6
Malnutritie op IZ
XXXXX
IZ-patiënten- normo- of hypermetabool (verhoogd rustmetabolisme)- hypercatabool (verhoogde N2 uitscheiding)- voorafbestaande malnutritie
+ kcal en EW deficiet
+ « vasten » op IZ- > % normale GIT � ??
Malnutritie op IZ ???
Darm barrière (epitheliale cel
junctie )
Verhoogde permeabiliteit voor
macro-molecules en micro-
organismen ( bacteriën, fungi)
Enterocyten Verhoogde adhesie van bacteriën
Intestinale flora Overgroei van pathogenen
Submucosaal immuunsysteem Atrofie van de Peyerse platen
Verminderde productie van IgA
Belangrijke trigger voor systemische infecties
tgv typische gastro-intestinale micro-organismen
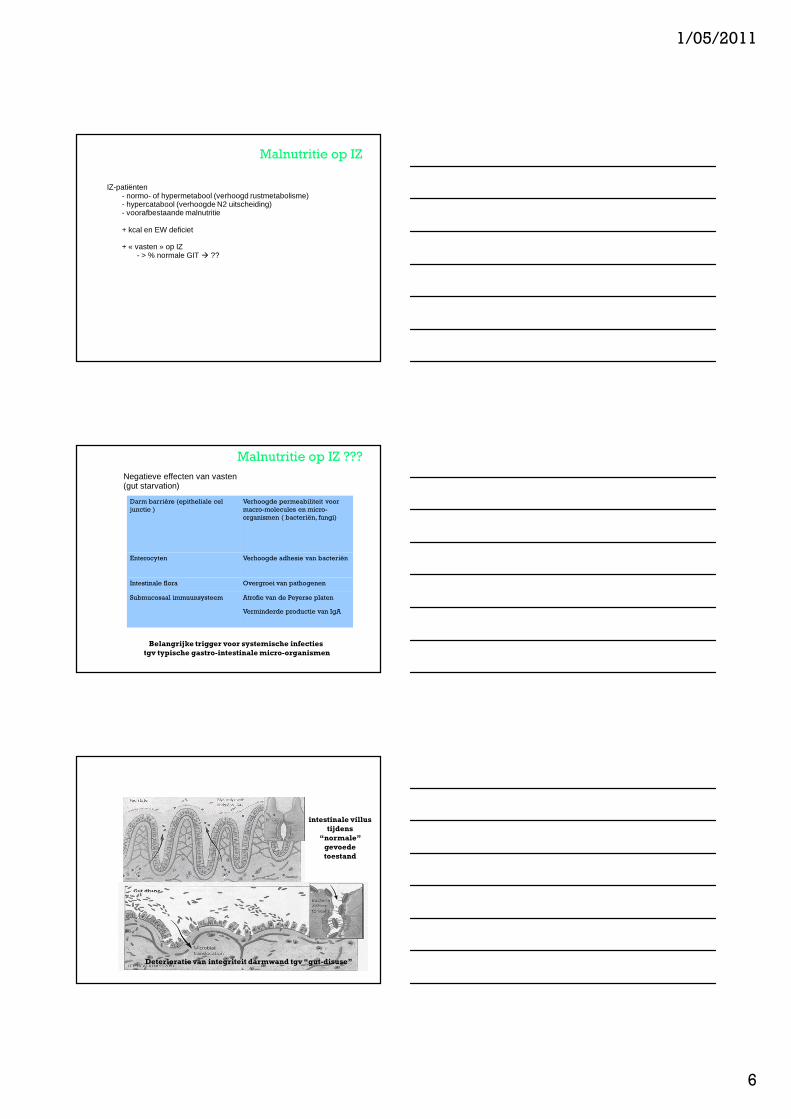
Negatieve effecten van vasten (gut starvation)
intestinale villus
tijdens
“normale”
gevoede
toestand
Deterioratie van integriteit darmwand tgv “gut-disuse”
McClave. J of critical illness. 2001:16:198-202;
1/05/2011
7
intestinale villus
tijdens
“normale”
gevoede
toestand
Deterioratie van integriteit darmwand tgv “gut-disuse”
McClave. J of critical illness. 2001:16:198-202;
Belang« trickle feeding »
« gut trophic »
Malnutritie op IZ
XXXXX
Vasten op IZ ??
� uitstellen van start EN
(geen maagsonde, meerdere pogingen voor plaatsen post-pylore sonde)
� « morgen herevalueren »
� MS eruit getrokken of verstopt
� onderbrekingen voor OK / tests / procedures
� Stoppen SV in anticipatie van extubatie
�….
XXXXX
1/05/2011
8
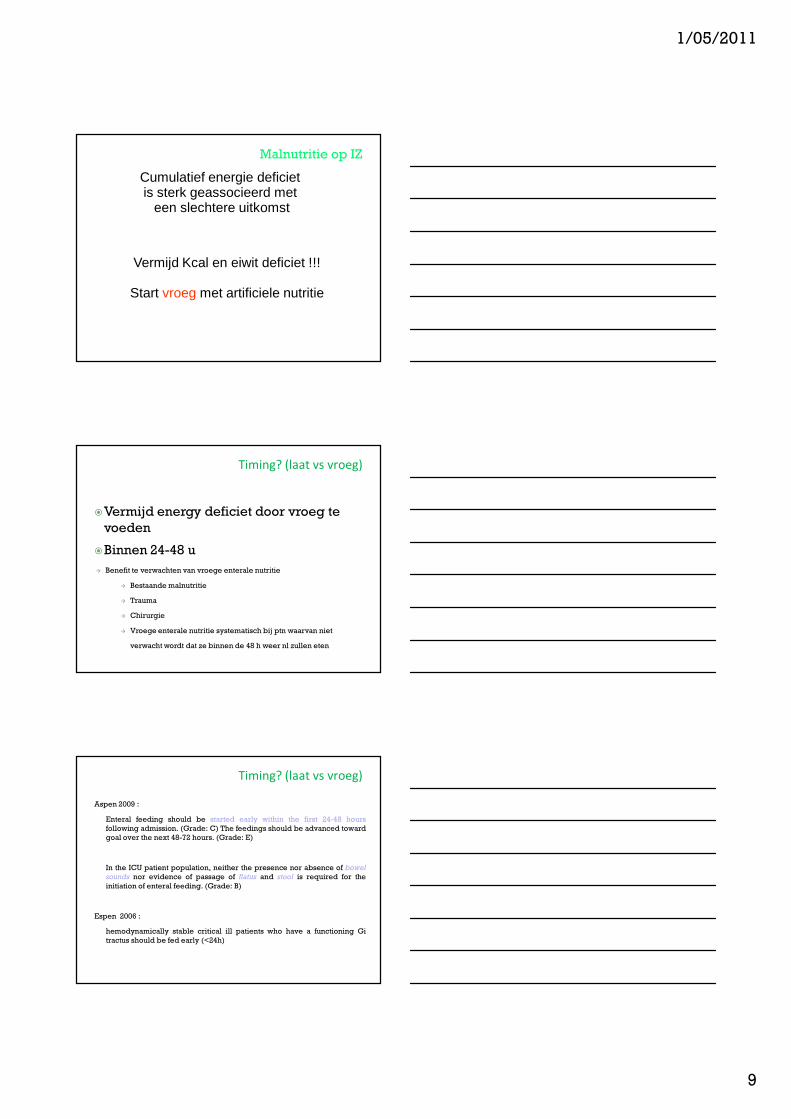
XXXXX
et al.
Cumulatieve negatieve energie-balans ~
aantal infectieuse complicaties
Villet et al, Clin Nutr 24:502 (2005)
1/05/2011
9
Malnutritie op IZ
XXXXX
Vermijd Kcal en eiwit deficiet !!!
Start vroeg met artificiele nutritie
Cumulatief energie deficiet is sterk geassocieerd met
een slechtere uitkomst
Timing? (laat vs vroeg)
�Vermijd energy deficiet door vroeg te
voeden
�Binnen 24-48 u
� Benefit te verwachten van vroege enterale nutritie
� Bestaande malnutritie
� Trauma
� Chirurgie
� Vroege enterale nutritie systematisch bij ptn waarvan niet
verwacht wordt dat ze binnen de 48 h weer nl zullen eten
Aspen 2009 :
Enteral feeding should be started early within the first 24-48 hours
following admission. (Grade: C) The feedings should be advanced toward
goal over the next 48-72 hours. (Grade: E)
In the ICU patient population, neither the presence nor absence of bowel
sounds nor evidence of passage of flatus and stool is required for the
initiation of enteral feeding. (Grade: B)
Espen 2006 :
hemodynamically stable critical ill patients who have a functioning Gi
tractus should be fed early (<24h)
Timing? (laat vs vroeg)
1/05/2011
10
Enteraal en/of parenteraal?
EN
ORAAL
Enteraal
(oraal niet vergeten !!!)
Meestal haalbaar
(WEINIG !!) CI
Voordelen
Enteraal en/of parenteraal?(WEINIG !!) CONTRA-INDICATIES
1. Relatieve contraindicaties – “gut doesn’t work”� Peritonitis
� darmobstructie
� Mesenteriale ischemie
� Belangrijke GI bloeding
� Gecompliceerde enteroenterische fistels
2. Risico voor (niet-occlusieve) darmnecrose
� Patient in resuscitatie-fase (vocht- en/of inotropica-nood en/of
vasoactieve medicatie noodzakelijk voor MAP>60 mmHg)
� EN moet gestart worden eens eindpunten van resuscitatie bereikt zijn.
3. EN niet veilig
� Prone positioning (overweeg jejunal voeding)
� Risico voor aspiratie
� Herhaalde hoge hoeveelheid GVR
� Niet-invasieve ventilatie
� Dreigende intubatie
Enteraal en/of parenteraal?
Enteraal
(WEINIG !!) CI
Voordelen :
- goedkoop : ligdagprijs
- fysiologisch cfr. Darmintegriteit
Nadelen :
aspiratie risico
necrose neusvleugel
diarree
1/05/2011
11
ASPEN 2009 : Enteral nutrition is the preferred route of feeding over
parenteral nutrition (PN) for the critically ill patient who requires nutrition
support therapy. (Grade: B)
Enteraal en/of parenteraal?
EN
ORAAL
Enteraal (oraal niet vergeten !!!)
(WEINIG !!) CI
Voordelen :
- goedkoop : ligdagprijs
- fysiologisch cfr. darmintegriteit
Maar vaak targets niet gehaald
cumulatief deficiet van kcal en EW
Parenteraal = grote schuldige ….
Enteraal en/of parenteraal?
Parenteraal dan ??
1/05/2011
12
Total poisonous nutrition ????
� hetze tegen PN
� Voordeel tov EN tov PN in verschillende prospectieve RCT (trauma, BW, neurotrauma, chirurgie, acute pancreatitis)
� > reductie in infectieuse morbiditeit (pneumonie, catheterinfecties).
� In vele studies voordeel aangetoond
� hospital length of stay
� cost of nutrition therapy
� return of cognitive function (in head injury patients).
1/05/2011
13
Associatie EN + TPN
Enteraal en/of parenteraal?
Nadelen PN- infectie-risico ??? (manipulaties ???)- betere samenstellingen (glutamine, vetten)- metabole complicaties- meeste studies gedaan pre- tight glucose control
- >> kostprijs (in ZH forfait)- vaak « EN of TPN » � gut trophic factor valt weg
Voordelen- adequate Kcal en EW mogelijk bij cachectische ptn
Associatie EN + TPN
Enteraal en/of parenteraal?
Tot op heden geen bewijs voor mortaliteits-verschil
- Vijf meta-analyses : geen verschil in mortaliteit tss EN en PN
- 1 meta-analyse door Simpson en Doig : significantly lower mortality (RR = 0.51; 95% CI 0.27-0.97; P =.04) despite a significantly higher incidence of infectious complications (RR = 1.66; 95% CI 1.09-2.51; P =.02) with use of PN compared to EN.
Feiten :
> % van de IZ patienten = practisch en veilig en goedkoop om enteraal te voeden
Combineren EN +PN : kans om energie en EW deficiet te vermijden
Maar, ptn PN geven als ze enteraal gevoed kunnen worden is geengoed idee
PN zou oa infectieuse morbiditeit kunnen verhogen
Aspen 2009 :
If early EN is not feasible or available the first 7 days following
admission to the ICU, no nutrition support therapy (ie, STD therapy)
should be provided. (Grade: C) In the patient who was previously
healthy prior to critical illness with no evidence of protein-calorie
malnutrition, use of PN should be reserved and initiated only after
the first 7 days of hospitalization (when EN is not available). (Grade:
E)
If there is evidence of protein-caloriemalnutrition on admission and EN
IS NOT FEASIBLE, it is appropriate to initiate PN as soon as possible
following admission and adequate resuscitation. (Grade: C)
Plan : route of feeding
1/05/2011
14
Optimaliseer EN
Vroeg starten = hogere slaagkans
Feeding protocols
ACCEPT trial (Martin et al, CMAJ 2004)
reduced mortality
Positionering 45 °
Motility agents (metoclopramide - erytromycine )
Small bowel feeding tubes
Hyperglycemia and insulin resistance
Overweeg toevoegen van PN
Functionerende GI tract
Onmogelijkheid om adequaat enteraal te voeden
(Ileus , Diarrhea, Abdominal distension, Short bowel,…)
Timing
- afhankelijk van voedingstoestand : bestaande malnutritie ?
- guidelines : als er argumenten zijn dat onvoldoende EN kanvoorzien worden binnen 2 (of 5,7…)
start EN
behoud minstens trickle feed
blijf pogingen ondernemen om EN te optimaliseren
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat?
Standaard voedingen
- isocalorisch (1 kcal/cc)
- hypercalorische (1,2-1,5 kcal /cc)
hogere kcal behoefte
volumeload reductie
Mixed fuel
- % KH
- % lipiden
- % EW
RQ Max snelheid van oxydatie
Glucose 4 kcal/g 1.0 3-5 g/kg/d
lipiden 9 kcal/g 0.7 0.5-1.5 g/kg/d
EW 4 kcal/g 0.82 1.2-1.5 g/kg/d
1/05/2011
15
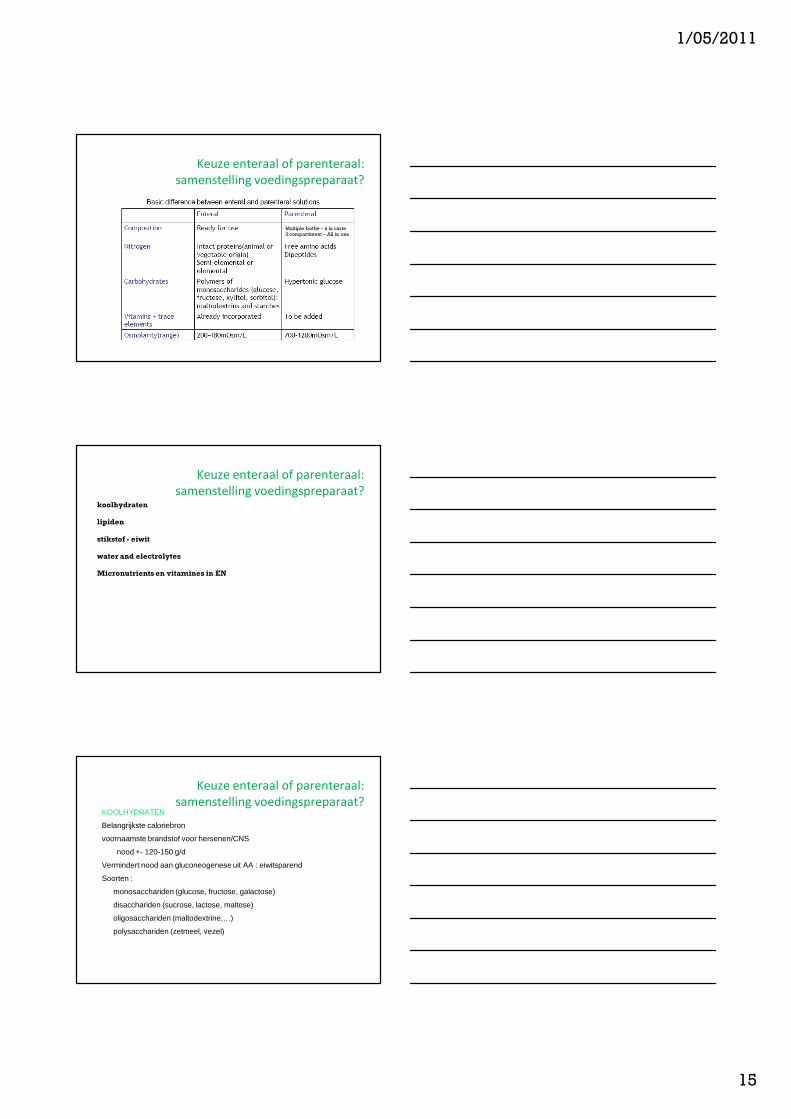
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat?
Multiple bottle – à la carte3 compartiment – All in one
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat? koolhydraten
lipiden
stikstof - eiwit
water and electrolytes
Micronutrients en vitamines in EN
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat? KOOLHYDRATEN
Belangrijkste caloriebron
voornaamste brandstof voor hersenen/CNS
nood +- 120-150 g/d
Vermindert nood aan gluconeogenese uit AA : eiwitsparend
Soorten :
monosacchariden (glucose, fructose, galactose)
disacchariden (sucrose, lactose, maltose)
oligosacchariden (maltodextrine,…)
polysacchariden (zetmeel, vezel)
1/05/2011
16
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat? VETTEN
• Dense energiedrager (9 cal/g)
• Aanbeveling normaal dieet : 30-35 %
• Aanwezig in voeding onder vorm van triglyceriden, fosfolipiden, sterolen
opgebouwd uit vetzuren :
- Verzadigde (vnl dierlijk)
- mono-onverzadigde (oleïnezuur in olijfolie)
- poly-onverzadigde PUFA
ω6 (N6) (> linoleic acid) proinflammatoir
ω3 (N3) antinflammatoir (visolie, koolzaadolie)
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat? EIWITTEN
• Belangrijkste structuurelementen vh lichaam
• SLECHTSTE energieleveranciers
• Aanbeveling normaal dieet 0,8 g/kg/d, 10 E%
• Soorten AA :
- polymere voeding (Intacte EW ) [caseine , soya EW , wei, lactalbumine]
Vereist normale hoeveelheid pancreasenzymes voor vertering
- Semi-elementaire of oligomere voeding (peptiden)
- Elementaire voeding (aminozuren)
Keuze enteraal of parenteraal:
samenstelling voedingspreparaat? MICRONUTRIENTEN
• Essentieel : kleine noden, maar groot belang
• Mineralen : electrisch evenwicht, transport
• Spoorelementen : co-factoren voor enzymatische processen
Vb : Zn, Se
• Vitamines : cofactoren, anti-oxidanten,…
• Vetoplosbare : ADEK
• Wateroplosbare
1/05/2011
17
Keuze enteraal of parenteraal:
compositie voedingspreparaat? Energie-verhoudingen
-Non-proteine kcal
- Koolhydraten (50-70%)
- Vermijd de novo lipogenesis
- Verhoogde CO2 excretie
- Vet (15-30%)
- Leverfunctie ~ samenstelling- [omega]-3 fatty acids
- Parenteraal :
- Monitoring klaring : triglyceride levels <10-20%
boven baseline.
-eiwitten
energieverhoudingen
-Non-proteine kcal
- Koolhydraten (50-70%)
- Vet (15-30%)
-eiwitten (15 - 20% / >20%)
- Optimale EW-toediening !!
- Hoeveelheid :1,2 - 1,5 - 2,0 g/kg/dag- Optimale (non-proteine) CALORIE-STIKSTOF
VERHOUDING
- NPE/N (kcal/gN)
- = maat voor de efficiëntie van de oplossing (EN & TPN)
voldoende NPE geleverd, zodat eiwit maximaal kan
gebruikt worden voor proteïne anabolisme
- 100-150 kcal/gN
>200 kcal/g N : leversteatose<100 kcal/g N : eiwitafbraak � ureum �
energieverhoudingen
-Non-proteine kcal
- Koolhydraten (50-70%)
- Vet (15-30%)
-eiwitten (15 - 20% / >20%)
- Optimale EW-toediening !!
- Hoeveelheid :1,2 - 1,5 - 2,0 g/kg/dag- NPE/N 100-150 kcal/gN
Vb. Patiënt - IBW 75 kg
eiwit 1,2-1,5 gr/kg/dag� 75x1,2 = 90 gram eiwit6,25 gr eiwit = 1 gram N
� 90 gr/6 = 14 gram stikstof
N/NPE 1:150 � kalorie aanbreng = 150 x1 4 = 2100 kcal
meer: leversteatoseminder: eiwitafbraak � ureum �
1/05/2011
18
Keuze enteraal of parenteraal:
compositie voedingspreparaat?
Welke keuze van voedingskeuze voor specifieke patiënt
-Meeste patiënten
- Iso-energetisch (1 kCal/cc) of hoog-energetisch (1, 2-1,5 kCal/cc)- Polymere voeding (Whole protein)- PN
- Standaard ternaire parenterale oplossingen- Afwezigheid centrale lijn : producten met lage osmolariteit
- EN - Semi-elementair of elementair : short bowel, malabsorptie,
pancreasinsufficientie- Vochtrestrictie : hoog-energetisch- Diarree : vezelrijk
- Additioneel : vitamines en spore-elementen- Niet aanwezig in TPN : dagelijks toevoegen
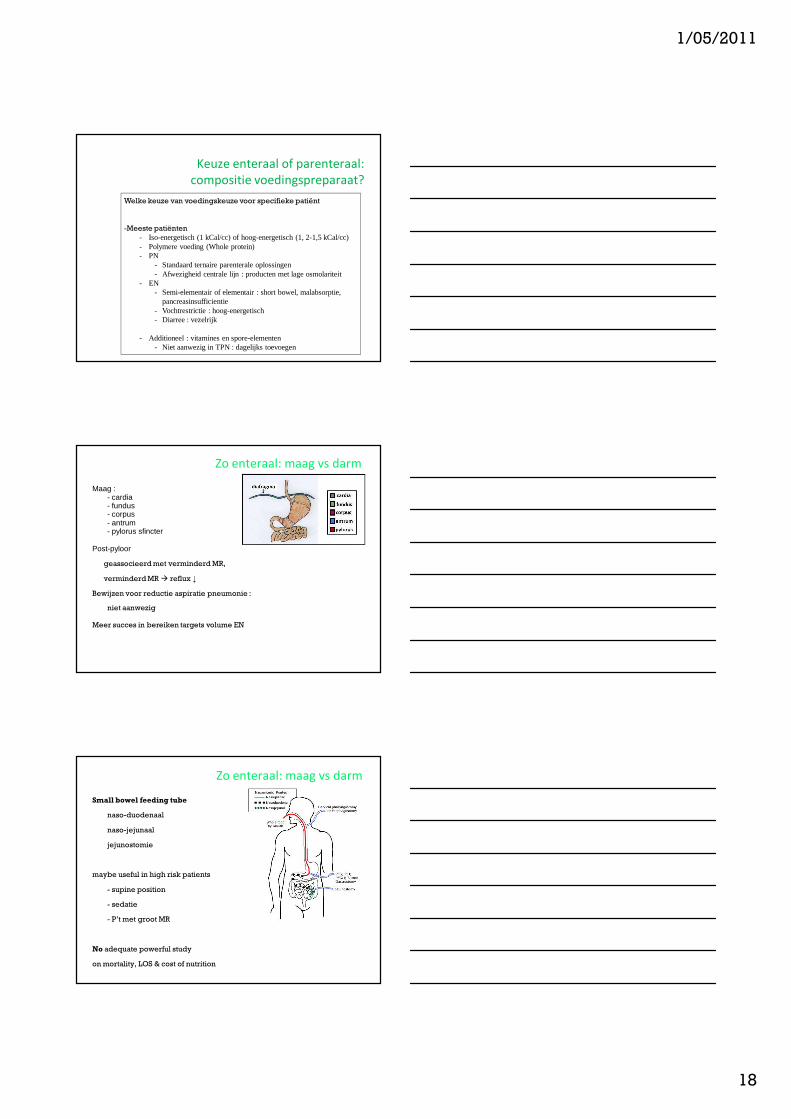
Zo enteraal: maag vs darm
Maag :- cardia- fundus- corpus - antrum- pylorus sfincter
Post-pyloor
geassocieerdmet verminderdMR,
verminderdMR � reflux ↓
Bewijzen voor reductie aspiratie pneumonie :
niet aanwezig
Meer succes in bereiken targets volume EN
Zo enteraal: maag vs darm
Small bowel feeding tube
naso-duodenaal
naso-jejunaal
jejunostomie
maybe useful in high risk patients
- supine position
- sedatie
- P’t met groot MR
No adequate powerful study
on mortality, LOS & cost of nutrition
1/05/2011
19
Zo enteraal: maag vs darm
maybe useful in high risk patients
No adequate powerful study
on mortality, LOS & cost of nutrition
SB feeding improvestime to reach target goalssuccess at achieving target goals
SB feeding may be associated with less pneumonia
Afhankelijk van locale praktijk
Algemene principes van nutritioneel
management
• Bepalen voedingsstatus:
• Identificeer ondervoede patiënten
• Identificeer vermoedelijke langliggers
• Enteraal en/of parenteraal?
• Geef de voorkeur aan EN, maar combineer EN en PN
• Timing? (laat vs vroeg)
• Vermijd energie-deficiet
• Keuze enteraal of parenteraal: welk voedingspreparaat?
• Zo enteraal: maag vs darm