jaundice - gmch.gov.ingmch.gov.in/sites/default/files/documents/jaundice.pdf · Ask when jaundice...
27
Neonatal Jaundice
Transcript of jaundice - gmch.gov.ingmch.gov.in/sites/default/files/documents/jaundice.pdf · Ask when jaundice...

Neonatal Jaundice

Neonatal Jaundice
Visible form of bilirubinemia – Adult sclera >2mg / dl – Newborn skin >5 mg / dl
Occurs in 60% of term and 80% of preterm neonates However, significant jaundice occurs in 6 % of term babies
Teaching Aids: NNF NJ - 2

Bilirubin metabolism
Hb → globin + haem 1g Hb = 34mg bilirubin
Non – heme source 1 mg / kg
Bilirubin glucuronidase
Bilirubin
Bilirubin Ligandin (Y - acceptor)
Bil glucuronide
Teaching Aids: NNF NJ - 3
β glucuronidase
Intestine
Bil glucuronide
Stercobilin
bacteria

Clinical assessment of jaundice
Area of body Bilirubin levels mg/dl
Face 4-8 Upper trunk 5-12 Lower trunk & thighs 8-16 Arms and lower legs 11-18 Palms & soles > 15
Teaching Aids: NNF NJ - 4

Physiological jaundice
Characteristics Appears after 24 hours Maximum intensity by 4th-5th day in term & 7th day in preterm Serum level less than 15 mg / dl Clinically not detectable after 14 days Disappears without any treatment
Note: Baby should, however, be watched for worsening jaundice
Teaching Aids: NNF NJ - 5

Why does physiological jaundice develop?
Increased bilirubin load Defective uptake from plasma Defective conjugation Decreased excretion Increased entero-hepatic circulation
Teaching Aids: NNF NJ - 6

Bili
rubi
n le
vel
mg/
dl
Course of physiological jaundice
15
10
5
Term Preterm
1 2 3 4 5 6 10 11 13 1412
Age in Days
Teaching Aids: NNF NJ- 7

Pathological jaundice
Appears within 24 hours of age Increase of bilirubin > 5 mg / dl / day Serum bilirubin > 15 mg / dl Jaundice persisting after 14 days Stool clay / white colored and urine staining clothes yellow Direct bilirubin> 2 mg / dl
Teaching Aids: NNF NJ - 8

Causes of jaundice
Appearing within 24 hours of age Hemolytic disease of NB : Rh, ABO Infections: TORCH, malaria, bacterial G6PD deficiency
Appearing between 24-72 hours of life Physiological Sepsis Polycythemia Concealed hemorrhage Intraventricular hemorrhage Increased entero-hepatic circulation
Teaching Aids: NNF NJ - 9

Causes of jaundice After 72 hours of age
Sepsis Cephalhaematoma Neonatal hepatitis Extra-hepatic biliary atresia Breast milk jaundice Metabolic disorders
Teaching Aids: NNF NJ - 10

Risk factors for jaundice
JAUNDICE J - jaundice within first 24 hrs of life A - a sibling who was jaundiced as neonate U - unrecognized hemolysis N – non-optimal sucking/nursing D - deficiency of G6PD I - infection C – cephalhematoma /bruising E - East Asian/North Indian
Teaching Aids: NNF NJ - 11

Common causes in India
Exaggerated physiological Blood group incompatibility – ABO,Rh G6PD deficiency Bruising and cephalhaematoma Intrauterine and postnatal infections Breast milk jaundice
Teaching Aids: NNF NJ - 12

Approach to jaundiced baby
Ascertain birth weight, gestation and postnatal age Ask when jaundice was first noticed Assess clinical condition (well or ill) Decide whether jaundice is physiological or pathological Look for evidence of kernicterus* in deeply jaundiced NB
*Lethargy and poor feeding, poor or absent Moro's, opisthotonus or convulsions
Teaching Aids: NNF NJ - 13

Workup
Maternal & perinatal history Physical examination Laboratory tests (must in all)* – Total & direct bilirubin* – Blood group and Rh for mother and baby* – Hematocrit, retic count and peripheral smear* – Sepsis screen – Liver and thyroid function – TORCH titers, liver scan when conjugated
hyperbilirubinemia
Teaching Aids: NNF NJ - 14

Management
Rationale: reduce level of serum bilirubin and prevent bilirubin toxicity Prevention of hyperbilirubinemia: early feeds, adequate hydration Reduction of bilirubin levels: phototherapy, exchange transfusion, drugs
Teaching Aids: NNF NJ - 15

Principle of phototherapy
450-460nmNative bilirubin Photo isomers of bilirubin of light
Insoluble Soluble
Teaching Aids: NNF NJ - 16

Phototherapy equipment
White light tubes 6-8*/ 4 blue light tubes Cradle or incubator Eye shades
*May use 150 W halogen bulb
Teaching Aids: NNF NJ - 17

Babies under phototherapy
Baby under conventional phototherapy
Baby under triple unit intense phototherapy

Phototherapy
Technique Perform hand wash Place baby naked in cradle or incubator Fix eye shades Keep baby at least 45 cm from lights, if using closer monitor temperature of baby Start phototherapy
Teaching Aids: NNF NJ - 19

Phototherapy
Frequent extra breast feeding every 2 hourly Turn baby after each feed Temperature record 2 to 4 hourly Weight record- daily Monitor urine frequency Monitor bilirubin level
Teaching Aids: NNF NJ - 20

Side effects of phototherapy
Increased insensible water loss Loose stools Skin rash Bronze baby syndrome Hyperthermia Upsets maternal baby interaction May result in hypocalcemia
Teaching Aids: NNF NJ - 21

Choice of blood for exchange blood transfusion
ABO incompatibility – Use O blood of same Rh type, ideal O cells
suspended in AB plasma Rh isoimmunization – Emergency 0 -ve blood
Ideal 0 -ve suspended in AB plasmaor baby's blood group but Rh -ve
Other situations – Baby's blood group
Teaching Aids: NNF NJ - 22

.....I u O> E -· C :.c :, .... i:D E :::, ,_ (.1)
(f)
ai ;§
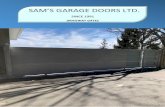
25 ----------------------------------428
20 --~11 __ ..... _---11--+--1--+--1---+---..... ~---•~·-·-·--..... '---_-_--+-______ ....,. ______ ..... ___ _..,-I _ .. - 342
-·· -15 ,.• .... 257
10 l-~1--+••---1 .... -~---1.-...r~-+---lf--+--l--+--l---l----ll--+---lf--+--t . .... ... 171
5 15-4.,,~--~;.a__...i. __ ..... _...._ _ __. __ ...,._ ..... _____ ...., ___ ~_ ...... _ ..... _____ ...., ..... -' • • • • Infants at lower risk (~ 38 wk and well)
: ., - - Infants at medium risk (2: 38 wk + risk factors or 35-37 6/7 wk. and well ·------
85
1 .... 1 --+--- _ Infants at higher risk (35-37 6/7 wk. + risk factors)
O 1 , , , , i , , , 1 1 1 1 , -- 0
Birth 24 h 48h 72 h 96 h 5 Days 6 Days 7 Days
Age
• Use total bilirubin. Do not subtract direct reacting or conjugated bilirubin. • Risk factors == isoimmune hemolytic disease, G6PO deficiency, asphyxia, significant lethargy, temperature instability;
sepsis, acidosis, or albumin < 3.0g/dL (if measured) • For well infants 35-37 6(7 wk can adjust TSB levels for intervention around the medium risk line. It is a.n option to
lntervene at lower TSB levels for infants closer to 35 wks and at higher TSB levels for those closer to 37 6/7 wk. • It is an option to provid'e conventional phototherapy in hospital or at home at TSB levels 2-3 mg/dL (35-S0mmol/L)
below those shown but home phototherapy should not be used in any infant with risk factors.
....J ::::. 0 E :1
Phototherapy
Teaching Aids: NNF NJ - 23

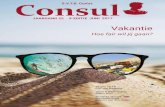
...J 25 -0 0)
s !;:
:0 ~ I..
ai 20 E ::} ,_ Ql
(/}
"tij
i2 15
10
I I I I I I I I I I I I I •••• I nfan1s at lower risk (~ 38 wk and well)
- - Infants at medium risk (~ 38 wk + risk factors or 35-37 en wk. and well - Infants at higher risk {35-37 6n wk. + risk factors)
_ ... ···•-•• •• -· ... - - - I -- - ■ . - - - - ■ . •• ... -
• --. ., ; .,,. ~
... V , ~ ~ -[_; ~~
_,_ .,,. ~ .,,,. .,,.
1....-
-J
Birth 24 h 48 h 72h 96 h 5 Days 6 Days 7 Days
Age
•The dashed lines fo r the first 24 hours indicate uncertainty due to a wide range of clinical ctrcumstances and a range of responses to phototherapy_
• Immediate exchange transfusion is recommended if infant shows signs of acute bilirubin encephalopathy (hypertonia, arching, retrocollis, opisthotonos, fever, high pitched cry) or ii TSB is 2:5 mgldl (85 µmol/L) above these lines.
• Risk factors - isoimmune hemolytic disease, G6PD deficiency, asphyxia, significant lethargy, temperature instability, sepsis, acidosis.
• Measure serum albumin and calculate BIA raUo (See legend) • Use total bilirubin. Do not subtract direct reacting or conjugated bilirubin • If infant is well and 35-37 sn wk (median risk} can individualize TSB levels for exchange based on actual
gestational age.
428
342
257
171
Exchange Transfusion
Teaching Aids: NNF NJ - 24

Prolonged indirect jaundice
Causes
Crigler Najjar syndrome
Breast milk jaundice
Hypothyroidism
Pyloric stenosis
Ongoing hemolysis, malaria
Teaching Aids: NNF NJ - 25

Conjugated hyperbilirubinemia
Suspect High colored urine White or clay colored stool
Caution Always refer to hospital for investigations so that
biliary atresia or metabolic disorders can be diagnosed and managed early
Teaching Aids: NNF NJ - 26

Conjugated hyperbilirubinemia
Causes Idiopathic neonatal hepatitis Infections -Hepatitis B, TORCH, sepsis Biliary atresia, choledochal cyst Metabolic -Galactosemia, tyrosinemia, hypothyroidism Total parenteral nutrition
Teaching Aids: NNF NJ - 27













![quality assess R4 2211 toklara[1] - European Social Survey · 2013. 11. 22. · brina.malnar@fdv.uni‐lj.si The Central Coordinating Team of the ESS requests that the following form](https://static.fdocuments.nl/doc/165x107/613776640ad5d2067648a2a0/quality-assess-r4-2211-toklara1-european-social-survey-2013-11-22-brinamalnarfdvunialjsi.jpg)