Gastric Sarcomatoid Carcinoma
3
GI IMAGE Gastric Sarcomatoid Carcinoma Fabio Carboni & Giovanni Battista Levi Sandri & Mario Valle & Renato Covello & Alfredo Garofalo Received: 12 July 2013 /Accepted: 30 July 2013 /Published online: 20 August 2013 # 2013 The Society for Surgery of the Alimentary Tract Abstract Sarcomatoid carcinoma is an uncommon biphasic malignant tumor of the stomach. The histogenesis remains unknown, and a definitive diagnosis is obtained with immunohistochemical staining. Since prognosis is poor after surgery, more effective diagnostic tools are needed in order to select the optimal therapeutic approach. We report the case of an old female patient presenting with an endophytic tumor in the gastric fundus who underwent partial resection of the stomach. Histology revealed a poorly differentiated adenocarcinoma component mixed with sarcomatoid component. Immunohistochemically, the carcinoma components exhibited a positive reaction to pan-cytokeratin, whereas fusiform cells showed positive reactions to vimentin. Keywords Stomach . Carcinosarcoma . Diagnosis . Surgery . Pathology Few cases of resected gastric sarcomatoid carcinoma have been reported in the literature, mostly coming from Eastern countries. 1 – 3 We briefly describe the rare case of an old Caucasian female patient presenting with a symptomatic tumor who underwent partial resection of the stomach. The patient was an 80-year-old woman admitted in our Department with a 4-month complaint of epigastric pain, dys- phagia, asthenia, and weight loss. Past medical history included hypertension, and physical exam was negative. Blood tests revealed severe anemia with hemoglobin concentration of 7.7g/dl, leukocytosis (18.6×10 cp μL), and low protein level (5.7 g/dl). Serum tumor marker (CEA, CA 19–9, CA 72–4) levels were within the normal range. Esophagogastroduo- denoscopy (EGDS) showed a bleeding lobulated polypoid lesion in the gastric fundus (Fig. 1), and biopsies revealed poorly differentiated adenocarcinoma cells with mesenchymal components. Computed tomography (CT) scan confirmed the presence of an endophytic polypoid mass in the gastric fundus with enlarged perigastric nodes (Fig. 2). Considering the his- tology and patient’ s age, a palliative resection of the gastric fundus with omentectomy was performed. Macroscopically, a lobulated polypoid lesion (7.5×5 cm) arising from the gastric fundus was observed. The tumor infiltrated the muscularis propria, and 5 out of 14 metastatic regional lymph nodes from adenocarcinoma were present (pT2N2). Histology revealed a poorly differentiated adenocarcinoma component mixed with sarcomatoid component with necrotic areas (Fig. 3a). Immunohistochemically, the carcinoma components exhibited an intense and diffuse positive reaction to pan-cytokeratin (AE1/AE3) (Fig. 3b), whereas fusiform cells showed intense diffuse positive reactions to vimentin (Fig. 3c) and negative for c-kit and CD34. Postoperative course was uneventful, and the patient was discharged 7 days after the operation. Adjuvant chemotherapy was not administered, and the patient is currently alive without evidence of recurrence at 3 months after the operation. Sarcomatoid carcinoma is an uncommon biphasic malignant tumor of the stomach usually occurring in the sixth decade of life with male gender prevalence, which may arise from all gastric areas. 1 – 3 Patients present with no specific symptoms, including bleeding, obstruction, and pain depending on tumor F. Carboni (*) : G. B. Levi Sandri : M. Valle : R. Covello : A. Garofalo Department of Digestive Surgery, Regina Elena Cancer Institute, Elio Chianesi 53, 00144 Rome, Italy e-mail: [email protected] R. Covello Department of Pathology, Regina Elena Cancer Institute, Rome, Italy J Gastrointest Surg (2013) 17:2025–2027 DOI 10.1007/s11605-013-2310-6
Transcript of Gastric Sarcomatoid Carcinoma

GI IMAGE
Gastric Sarcomatoid Carcinoma
Fabio Carboni & Giovanni Battista Levi Sandri &Mario Valle & Renato Covello & Alfredo Garofalo
Received: 12 July 2013 /Accepted: 30 July 2013 /Published online: 20 August 2013# 2013 The Society for Surgery of the Alimentary Tract
Abstract Sarcomatoid carcinoma is an uncommon biphasic malignant tumor of the stomach. The histogenesis remainsunknown, and a definitive diagnosis is obtained with immunohistochemical staining. Since prognosis is poor after surgery,more effective diagnostic tools are needed in order to select the optimal therapeutic approach. We report the case of an old femalepatient presenting with an endophytic tumor in the gastric fundus who underwent partial resection of the stomach. Histologyrevealed a poorly differentiated adenocarcinoma component mixed with sarcomatoid component. Immunohistochemically, thecarcinoma components exhibited a positive reaction to pan-cytokeratin, whereas fusiform cells showed positive reactions tovimentin.
Keywords Stomach .Carcinosarcoma .Diagnosis .Surgery .
Pathology
Few cases of resected gastric sarcomatoid carcinoma havebeen reported in the literature, mostly coming from Easterncountries.1
–3 We briefly describe the rare case of an oldCaucasian female patient presenting with a symptomatictumor who underwent partial resection of the stomach.
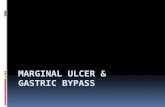
The patient was an 80-year-old woman admitted in ourDepartment with a 4-month complaint of epigastric pain, dys-phagia, asthenia, and weight loss. Past medical history includedhypertension, and physical exam was negative. Blood testsrevealed severe anemia with hemoglobin concentrationof 7.7g/dl, leukocytosis (18.6×10cpμL), and low protein level(5.7 g/dl). Serum tumor marker (CEA, CA 19–9, CA 72–4)levels were within the normal range. Esophagogastroduo-denoscopy (EGDS) showed a bleeding lobulated polypoid
lesion in the gastric fundus (Fig. 1), and biopsies revealedpoorly differentiated adenocarcinoma cells with mesenchymalcomponents. Computed tomography (CT) scan confirmed thepresence of an endophytic polypoid mass in the gastric funduswith enlarged perigastric nodes (Fig. 2). Considering the his-tology and patient’s age, a palliative resection of the gastricfundus with omentectomy was performed. Macroscopically, alobulated polypoid lesion (7.5×5 cm) arising from the gastricfundus was observed. The tumor infiltrated the muscularispropria, and 5 out of 14 metastatic regional lymph nodes fromadenocarcinoma were present (pT2N2). Histology revealed apoorly differentiated adenocarcinoma component mixed withsarcomatoid component with necrotic areas (Fig. 3a).Immunohistochemically, the carcinoma components exhibitedan intense and diffuse positive reaction to pan-cytokeratin(AE1/AE3) (Fig. 3b), whereas fusiform cells showed intensediffuse positive reactions to vimentin (Fig. 3c) and negative forc-kit and CD34. Postoperative course was uneventful, and thepatient was discharged 7 days after the operation. Adjuvantchemotherapywas not administered, and the patient is currentlyalive without evidence of recurrence at 3 months after theoperation.
Sarcomatoid carcinoma is an uncommon biphasic malignanttumor of the stomach usually occurring in the sixth decade oflife with male gender prevalence, which may arise from allgastric areas.1
–3 Patients present with no specific symptoms,including bleeding, obstruction, and pain depending on tumor
F. Carboni (*) :G. B. Levi Sandri :M. Valle :R. Covello :A. GarofaloDepartment of Digestive Surgery, Regina Elena Cancer Institute,Elio Chianesi 53, 00144 Rome, Italye-mail: [email protected]
R. CovelloDepartment of Pathology, Regina Elena Cancer Institute, Rome, Italy
J Gastrointest Surg (2013) 17:2025–2027DOI 10.1007/s11605-013-2310-6

size and location. Most lesions are polypoid and ulcerated inappearance and tend to develop rapidly. According to themacroscopic growth of pattern, they have been classified intothree types: (1) a predominantly intramural infiltration, (2) apredominantly extramural mass, and (3) a predominantly intra-mural mass with exophytic or crater-shaped growth.1
–3
Microscopically, they are classified into two types: truecarcinosarcoma and false carcinosarcoma or so calledsarcomatoid carcinoma.3
, 4 The former shows a relativelysharp demarcation between the two components. The lattershows a sarcomatous part originating from the carcinomawith translational areas. Owing to the low incidence,pathogenesis remains controversial and unclear but twohypotheses have proposed.1
–5 The first is the biclonal originhypothesis that supports the collision tumor theory, accordingto which the carcinosarcoma originates from two differenttumor cell clones. The second is the monoclonal originhypothesis, whereby the carcinosarcoma may originatefrom a common stem cell that is capable of undergoing bothepithelial and mesenchymal differentiation. The mostcommon carcinoma component is tubular or papillaryadenocarcinoma, and the mesenchymal sarcomatouscomponent is variable, and several types of differentiationhave been reported.1
–5
As for other gastric cancers, EGDS is the most frequentlyemployed diagnostic tool while CT scan is useful in thestaging of the disease. However, preoperative biopsies mayshow only an epithelial or sarcomatous component of thetumor, and a definitive diagnosis relies on accurate immuno-histochemical staining.1
–7 CEA, EMA, chromogranin A,CD56, and synaptophysin staining are highly specificmarkers used to identify the carcinoma components, whereasvimentin, desmin, and actin show affinity for the sarcomatouselements.1
, 3, 5
When feasible, radical surgical resection is the standardtreatment of choice but average survival is only about6.5 months, with most recurrences occurring within the firstyear.1
–5, 7 The role of chemotherapy and radiotherapy have notbeen yet defined.3
–5, 7
In conclusion, sarcomatoid carcinoma is a rare gastric neo-plasm that consists of both carcinomatous and sarcomatous
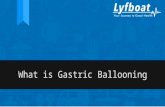
Fig. 3 Histologic findings, sarcomatoid component mixed with adenocarcinoma (HE ×100) (a). Immunohistochemical staining positive for pan-cytokeratin (b) and vimentin (c) (X200)
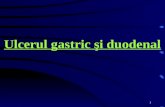
Fig. 2 CT scan showing an endophytic polypoid mass in the gastricfundus
Fig. 1 EGDS showing a lobulated polypoid mass in the gastric fundus
2026 J Gastrointest Surg (2013) 17:2025–2027

components. Usually, a definitive diagnosis is obtainedafter surgical treatment and immunohistochemical stain-ing. Since prognosis is poor, more effective diagnostictools are needed in order to select the optimal therapeuticapproach.
References
1. Cirocchi R, Trastulli S, Desiderio J, et al. Gastric carcinosarcoma: Acase report and review of the literature. Oncol Lett. 2012 Jul;4(1):53–57. Epub 2012 Apr 27
2. Yoshida H, Tanaka N, Tochigi N, et al. Rapidly deforming gastriccarcinosarcoma with osteoblastic component: an autopsy case report.World J Gastroenterol. 2012 Aug 14;18(30):4064–8.
3. Jang SM, Jang SH, Min KW, et al. A Case of Gastric Carcinosarcomawith Neuroendocrine and Smooth Muscle Differentiation. http://dx.doi.org/10.4132/KoreanJPathol.2010.44.1.87.
4. Ikeda Y, Kosugi S, Nishikura K, et al. Gastric carcinosarcoma present-ing as a huge epigastric mass. Gastric Cancer. 2007;10(1):63–8. Epub2007 Feb 23
5. Randjelovic T, Filipovic B, Babic D, et al. Carcinosarcoma of thestomach: a case report and review of the literature. World JGastroenterol. 2007 Nov 7;13(41):5533–6.
6. Kikuyama R, Tanaka K, Tano S, et al. A case of gastric carcinosarco-ma. Endoscopy. 2009;41 Suppl 2:E220-1.
7. Selcukbiricik F, Tural D, Senel ET, et al. Gastric carcinoma withosteoblastic differentiation. Int J Surg Case Rep. 2012;3(11):516–9.
J Gastrointest Surg (2013) 17:2025–2027 2027