Fertiliteitspreservatie aan vrouwelijke, oncologische ... · 9 juli 2015 Gastheren: ... •...
93
Fertiliteitspreservatie aan vrouwelijke, oncologische patiënten 9 juli 2015 Gastheren: - Prof. dr. Joop Laven, Erasmus MC - Dr. Marcel van Hooff, Sint Franciscus Vlietland Groep
Transcript of Fertiliteitspreservatie aan vrouwelijke, oncologische ... · 9 juli 2015 Gastheren: ... •...

Fertiliteitspreservatie aan vrouwelijke, oncologische
patiënten
9 juli 2015 Gastheren: - Prof. dr. Joop Laven, Erasmus MC - Dr. Marcel van Hooff, Sint Franciscus Vlietland Groep
Van ‘ik & mijn patiënt’ naar ‘wij & gedeelde zorg’
Doelstelling: kwaliteit van de zorg in de regio op een nóg hoger niveau tillen door middel van concrete, zinvolle en
kansrijke samenwerkingsinitiatieven.
Welkom! De start van dit initiatief

Van 4 naar 11 ziekenhuizen
Welkom! Toelichting op de bijeenkomst
Van Gynaecologie naar alle betrokken professionals
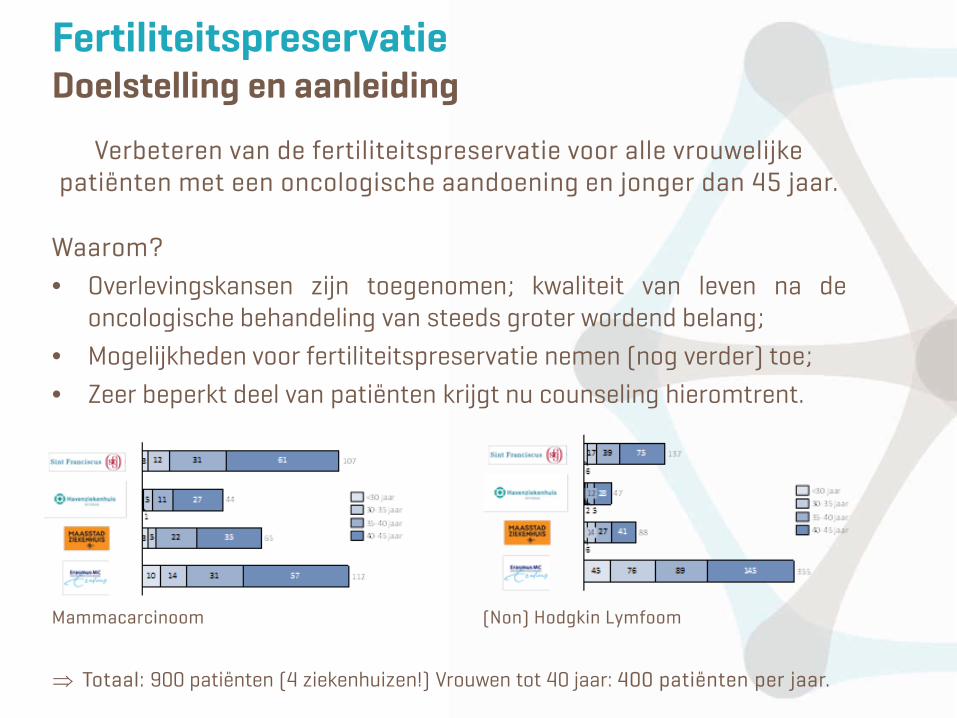
Verbeteren van de fertiliteitspreservatie voor alle vrouwelijke patiënten met een oncologische aandoening en jonger dan 45 jaar.
Waarom? • Overlevingskansen zijn toegenomen; kwaliteit van leven na de
oncologische behandeling van steeds groter wordend belang; • Mogelijkheden voor fertiliteitspreservatie nemen (nog verder) toe; • Zeer beperkt deel van patiënten krijgt nu counseling hieromtrent.
Mammacarcinoom (Non) Hodgkin Lymfoom
⇒ Totaal: 900 patiënten (4 ziekenhuizen!) Vrouwen tot 40 jaar: 400 patiënten per jaar.
Fertiliteitspreservatie Doelstelling en aanleiding
Elke vrouw <40 jaar met oncologische aandoening heeft recht op uitstekende counseling en, indien mogelijk en gewenst, het behouden van haar vruchtbaarheid.
Hoe • Met een zeer goed programma fertiliteitspreservatie dat betrekking
heeft op zowel counseling en behandeling en waarin patiënt en verwijzer optimaal bediend worden.
• Koppeling van patiëntenzorg aan wetenschappelijk onderzoek waardoor zorginnovatie mogelijk wordt.
Fertiliteitspreservatie De visie

Bijdrage prof. Joop Laven
9 juli 2015 – Fertiliteitspreservatie aan oncologische patiënten
• Past President of the Dutch Society for Reproductive Medicine
• Past Chairman of the Task force Reproductive Endocrinology of the RDCOG.
• Board member of Genovum, company for valorisation of genetic findings.
• Received unrestricted research grants from (in alphabetical order) – Ferring®, – Merck Serono®, – MSD®, – Organon®, – Serono® – Shering-Plough®.
• Received grants from the Erasmus Trust Fund and from Erasmus MC Holding.
• Received grants from the Dutch Genomics Initiative
Disclosures

Learning Objectives
• Provide some basic understanding about survival after Childhood Cancer
• Discuss some issues concerning Long term Health Sequelae especially Ovarian dysfunction in Childhood Cancer patients
• Briefly review some basic aspects of Ovarian Function throughout a women’s life
• Summarize the data on ovarian function after Childhood Cancer treatment
• Provide some guidance for assessing ovarian function after childhood cancer treatment
• Review the different treatment options for fertility preservation in children and young adults with cancer
• Summarize the data on pregnancy in childhood cancer survivors
• Finish with some concluding remarks
SURVIVAL AFTER CHILDHOOD CANCER
Ovarian function in Long-term Survivors of Childhood Cancer
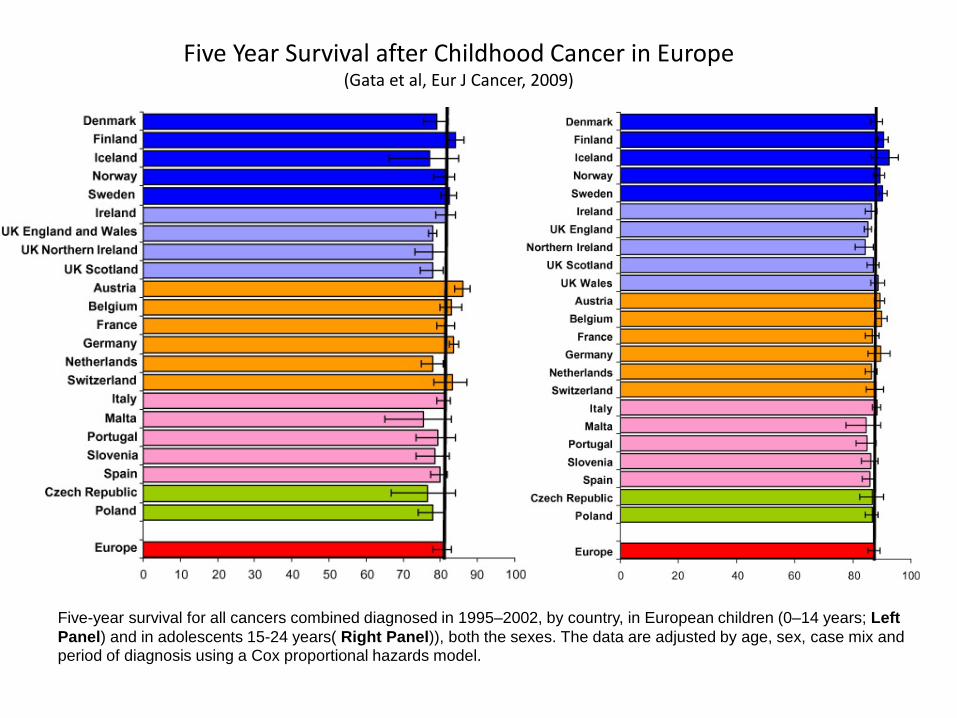
Five Year Survival after Childhood Cancer in Europe (Gata et al, Eur J Cancer, 2009)
Five-year survival for all cancers combined diagnosed in 1995–2002, by country, in European children (0–14 years; Left Panel) and in adolescents 15-24 years( Right Panel)), both the sexes. The data are adjusted by age, sex, case mix and period of diagnosis using a Cox proportional hazards model.
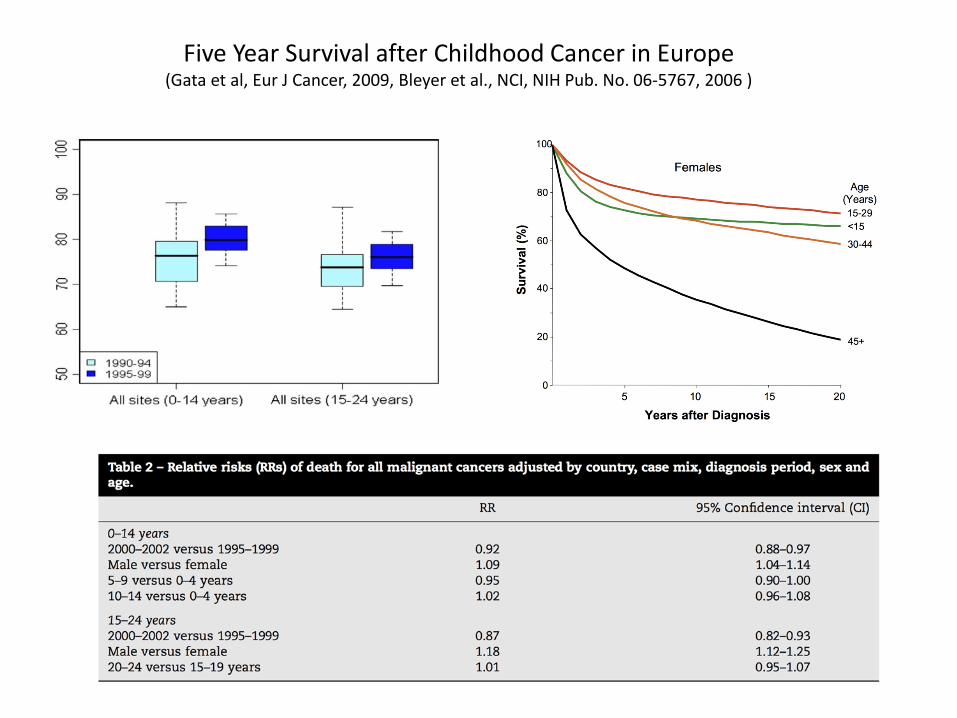
Five Year Survival after Childhood Cancer in Europe (Gata et al, Eur J Cancer, 2009, Bleyer et al., NCI, NIH Pub. No. 06-5767, 2006 )
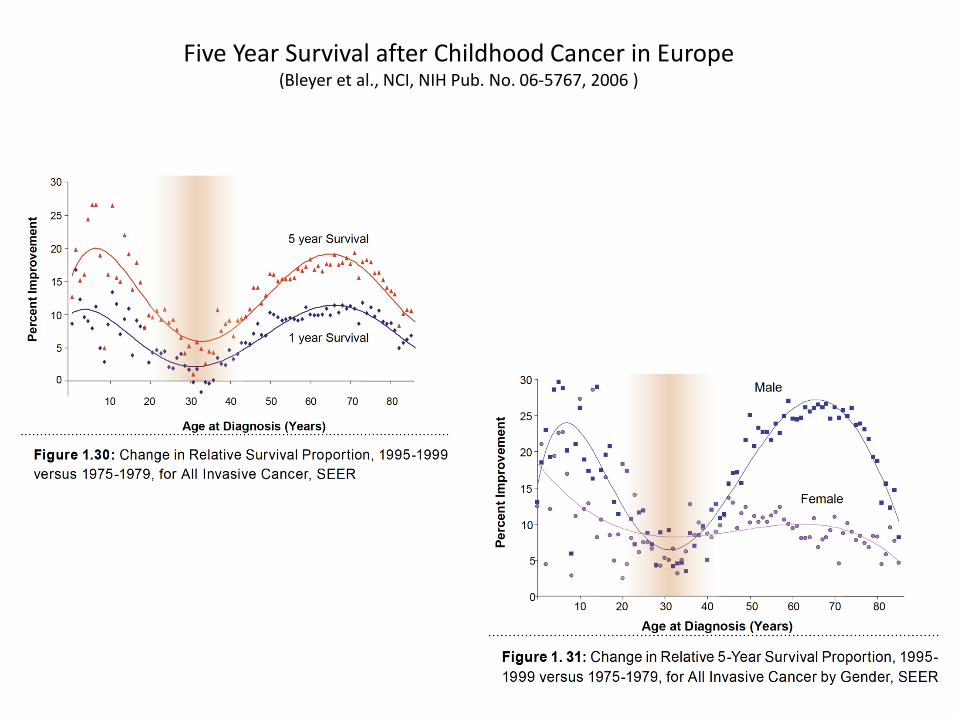
Five Year Survival after Childhood Cancer in Europe (Bleyer et al., NCI, NIH Pub. No. 06-5767, 2006 )
HEALTH ISSUES AFTER CHILDHOOD CANCER
Ovarian function in Long-term Survivors of Childhood Cancer
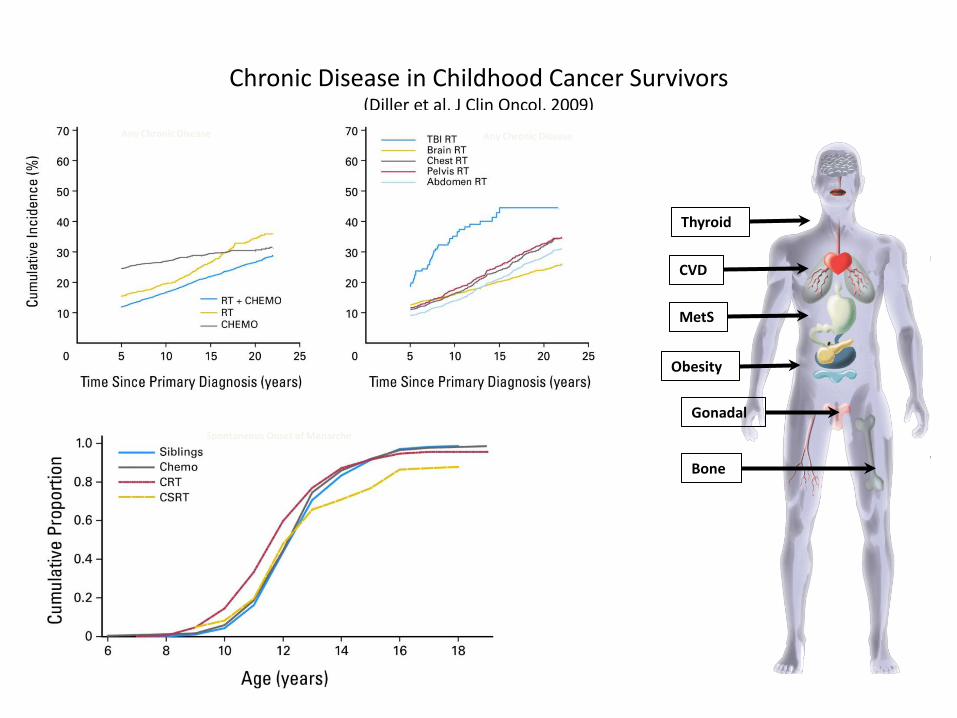
Chronic Disease in Childhood Cancer Survivors (Diller et al, J Clin Oncol, 2009)
Spontaneous Onset of Menarche
Any Chronic Disease Any Chronic Disease
CVD
Gonadal
MetS
Bone
Obesity
Thyroid
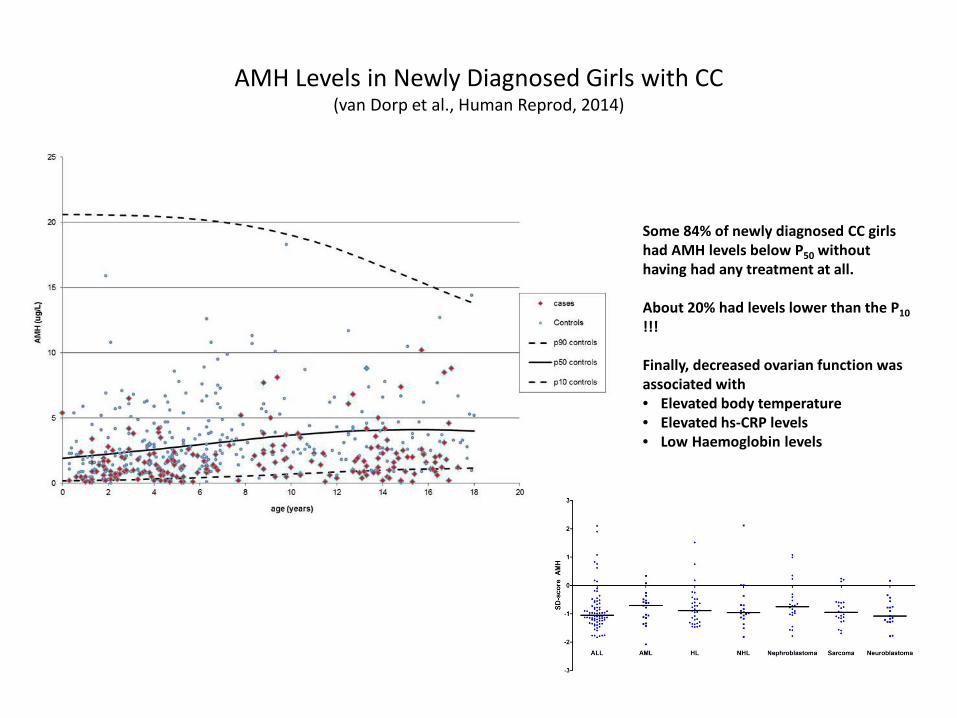
AMH Levels in Newly Diagnosed Girls with CC (van Dorp et al., Human Reprod, 2014)
Some 84% of newly diagnosed CC girls had AMH levels below P50 without having had any treatment at all. About 20% had levels lower than the P10 !!! Finally, decreased ovarian function was associated with • Elevated body temperature • Elevated hs-CRP levels • Low Haemoglobin levels
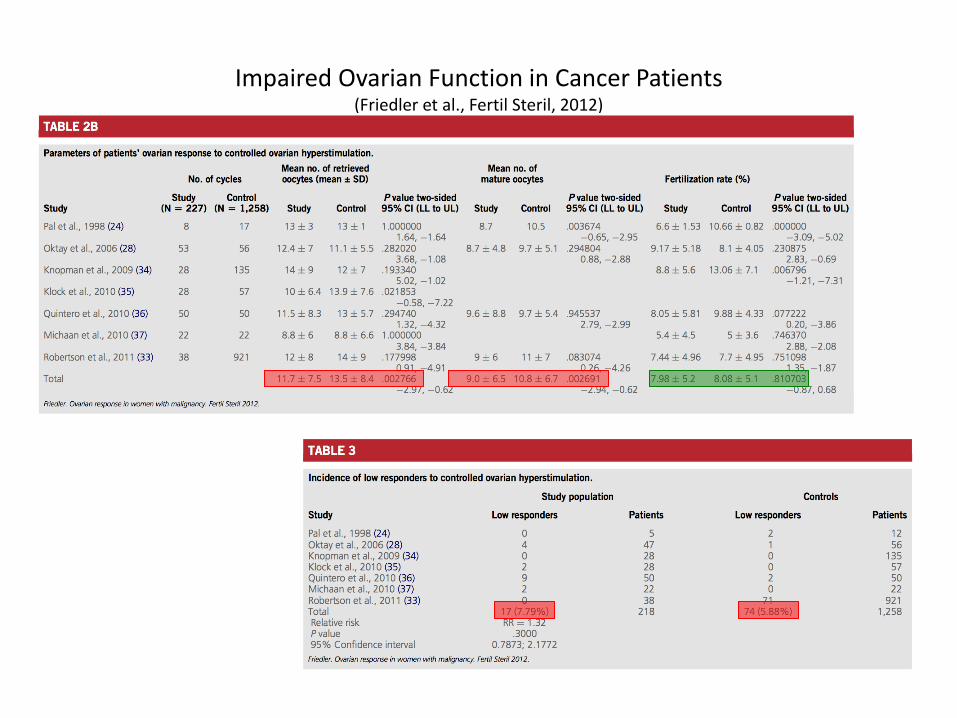
Impaired Ovarian Function in Cancer Patients (Friedler et al., Fertil Steril, 2012)
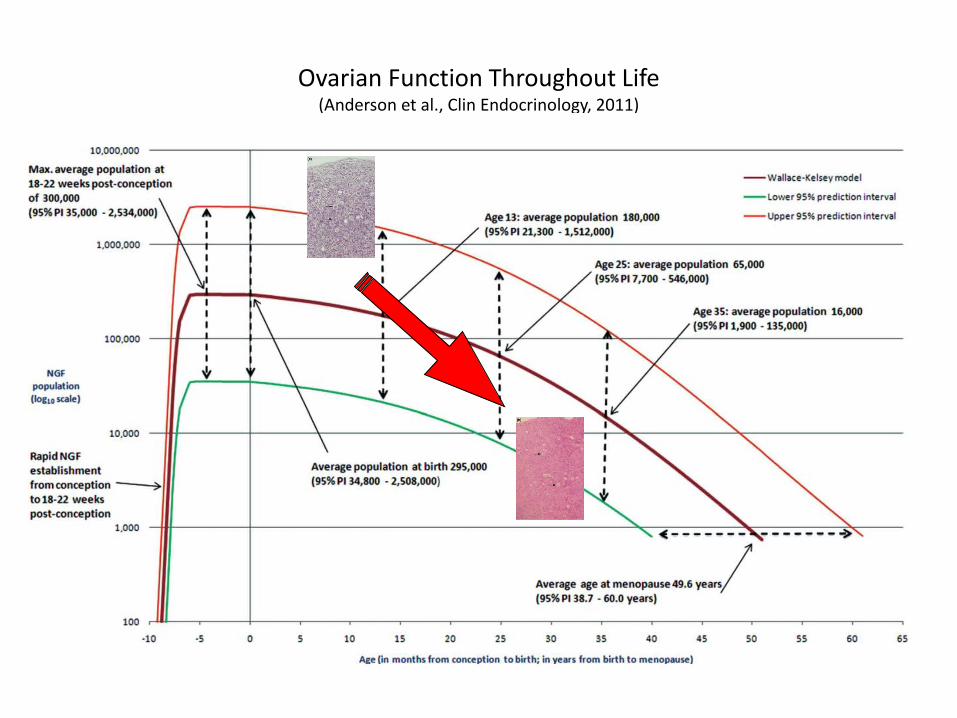
Ovarian Function Throughout Life (Anderson et al., Clin Endocrinology, 2011)
OVARIAN FUNCTION AFTER TREATMENT IN CCS
Ovarian function in Long-term Survivors of Childhood Cancer
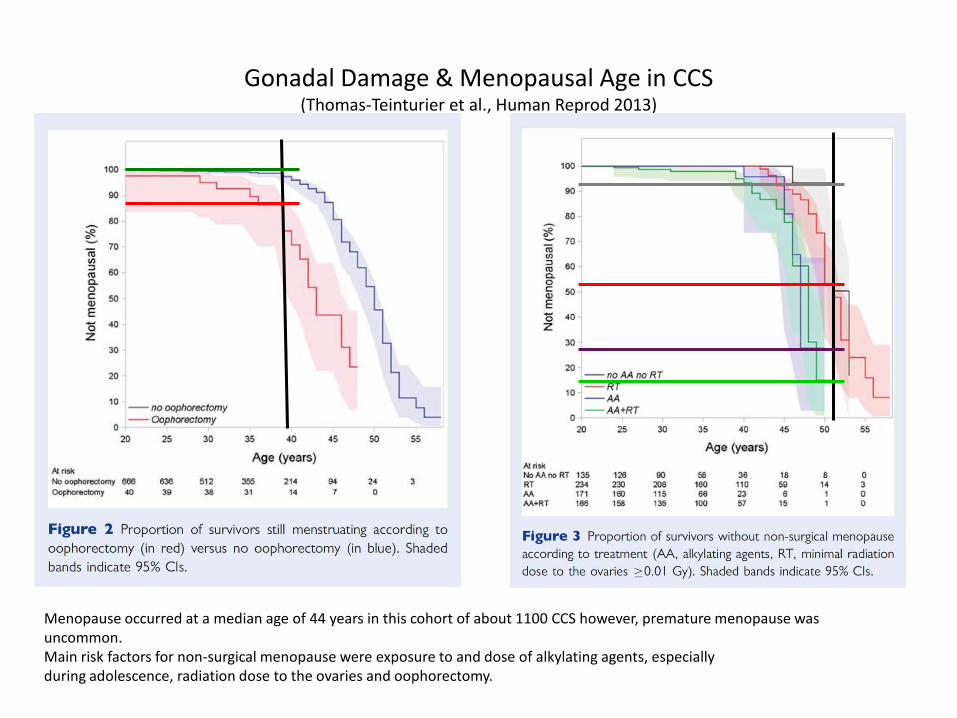
Gonadal Damage & Menopausal Age in CCS (Thomas-Teinturier et al., Human Reprod 2013)
Menopause occurred at a median age of 44 years in this cohort of about 1100 CCS however, premature menopause was uncommon. Main risk factors for non-surgical menopause were exposure to and dose of alkylating agents, especially during adolescence, radiation dose to the ovaries and oophorectomy.
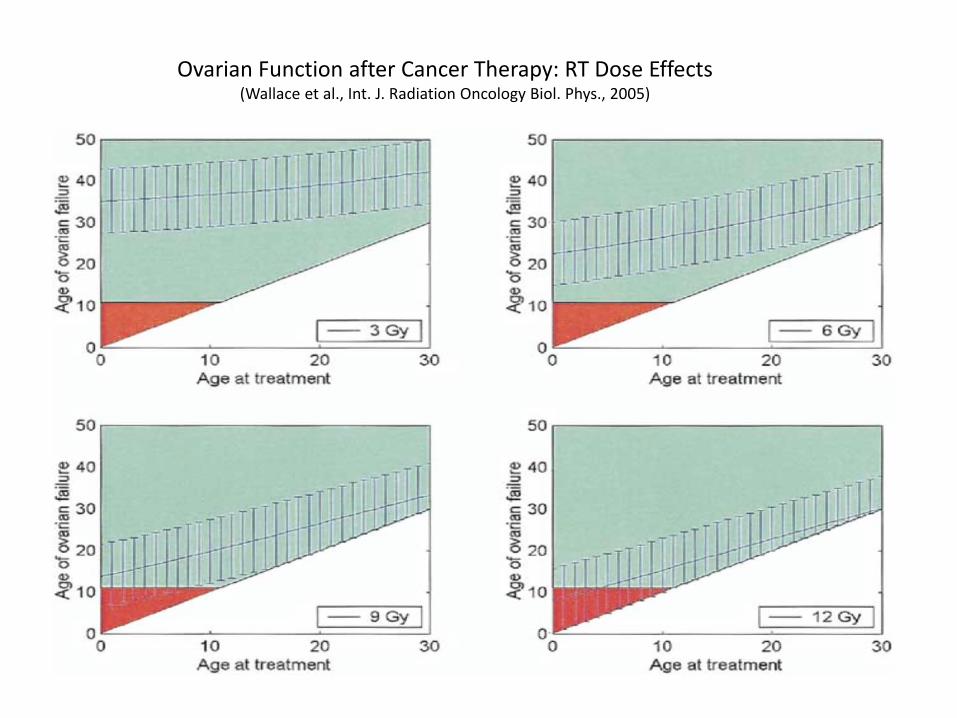
Ovarian Function after Cancer Therapy: RT Dose Effects
(Wallace et al., Int. J. Radiation Oncology Biol. Phys., 2005)
05
10AM
H n
g/m
l
0 2 4 6 8 10Alkylating agent dose scores (AAD)
AMH ng/ml predicted AMH95% confidence Interval
020
4060
8010
0FS
H M
iu/m
l
0 2 4 6 8 10Alkylating agent dose scores (AAD)
FSH Miu/ml predicted FSH95% confidence interval
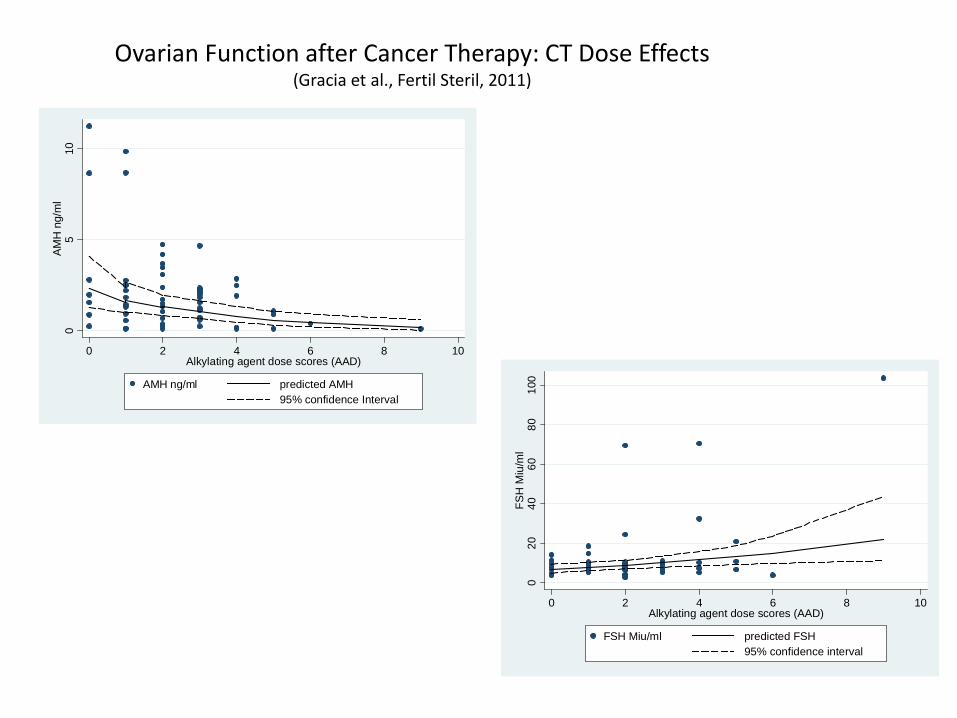
Ovarian Function after Cancer Therapy: CT Dose Effects (Gracia et al., Fertil Steril, 2011)
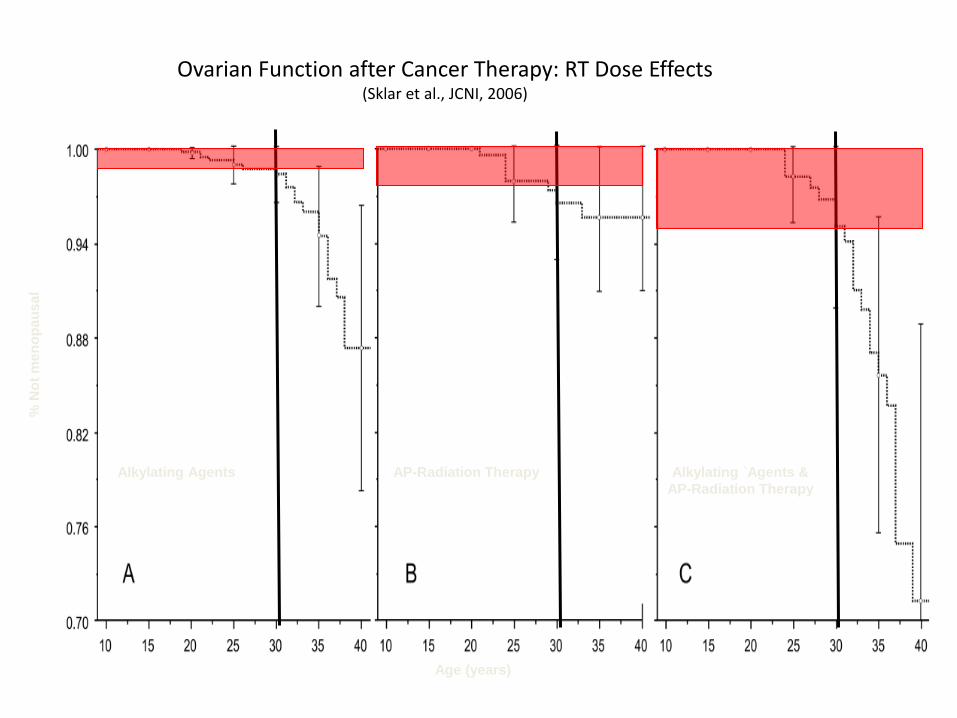
Ovarian Function after Cancer Therapy: RT Dose Effects
(Sklar et al., JCNI, 2006)
% N
ot m
enop
ausa
l
Age (years)
Alkylating Agents AP-Radiation Therapy Alkylating `Agents & AP-Radiation Therapy
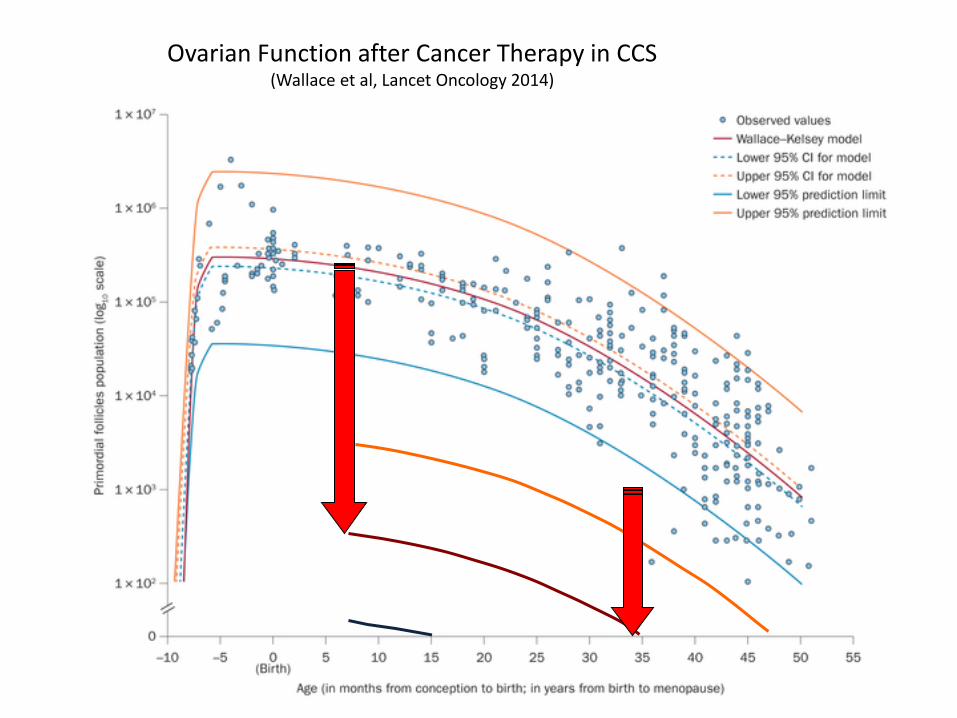
Ovarian Function after Cancer Therapy in CCS (Wallace et al, Lancet Oncology 2014)
Summary: Ovarian Function after Treatment CCS
• CCS treated with alkylating agents or those who had radiotherapy on one or both ovaries are at risk of premature ovarian insufficiency and its implications for future fertility.
• Counselling regarding the risk of POI and its impact on fertility (DOR) is recommended for these survivors
• Combination therapy of alkylating agents along with abdominal or pelvic radiotherapy is especially gonadotoxic
• Menopause occurred earlier in CCS
• Premature menopause however, was uncommon
• Main risk factors for non-surgical menopause were – Exposure to and dose of alkylating agents – Adolescence – Radiation dose to the ovaries and oophorectomy
SURVEILLANCE AFTER CHILDHOOD CANCER
Ovarian function in Long-term Survivors of Childhood Cancer
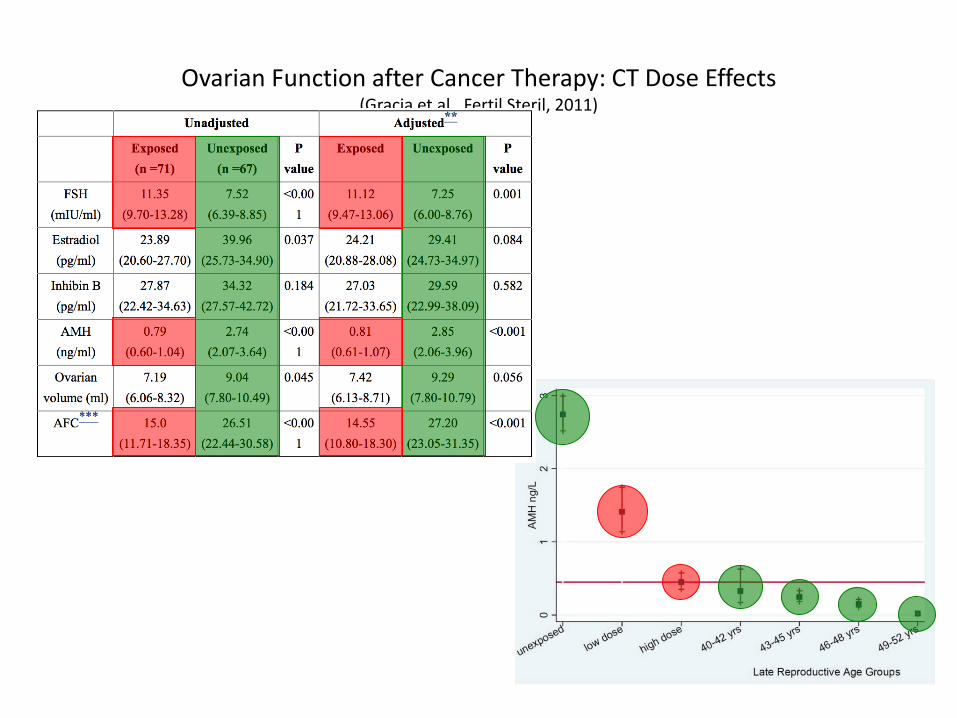
Ovarian Function after Cancer Therapy: CT Dose Effects (Gracia et al., Fertil Steril, 2011)
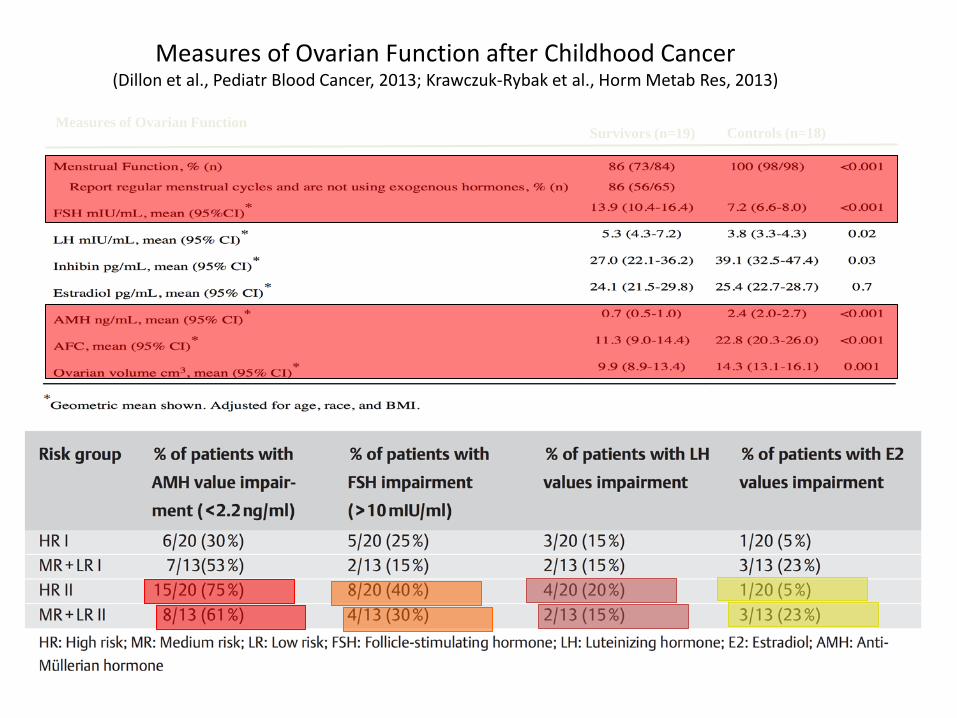
Measures of Ovarian Function after Childhood Cancer (Dillon et al., Pediatr Blood Cancer, 2013; Krawczuk-Rybak et al., Horm Metab Res, 2013)
Measures of Ovarian Function Survivors (n=19) Controls (n=18)
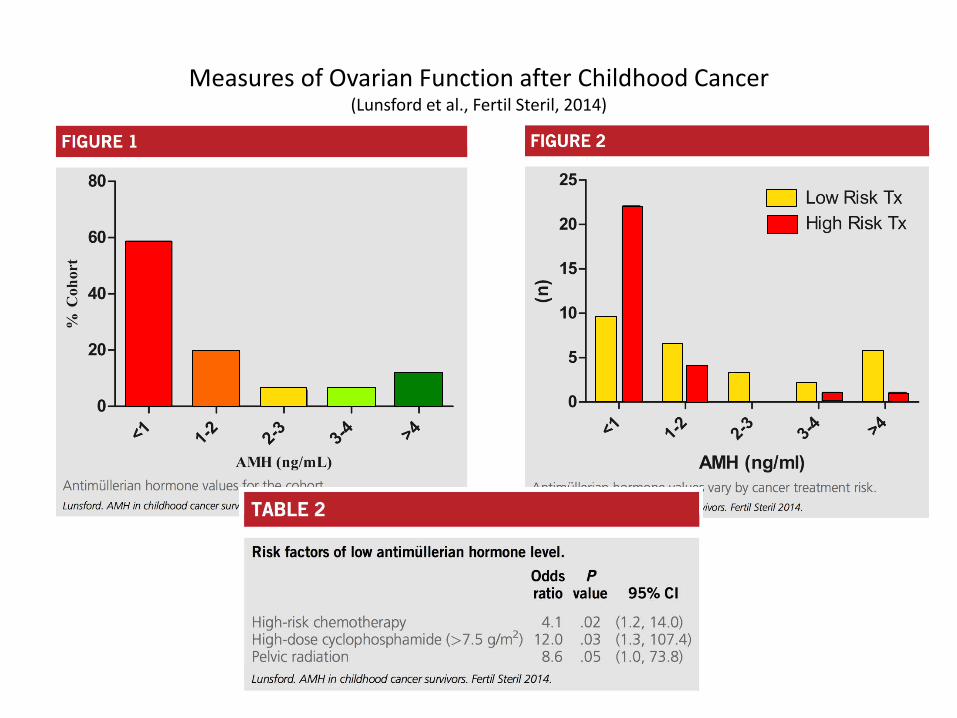
Measures of Ovarian Function after Childhood Cancer (Lunsford et al., Fertil Steril, 2014)
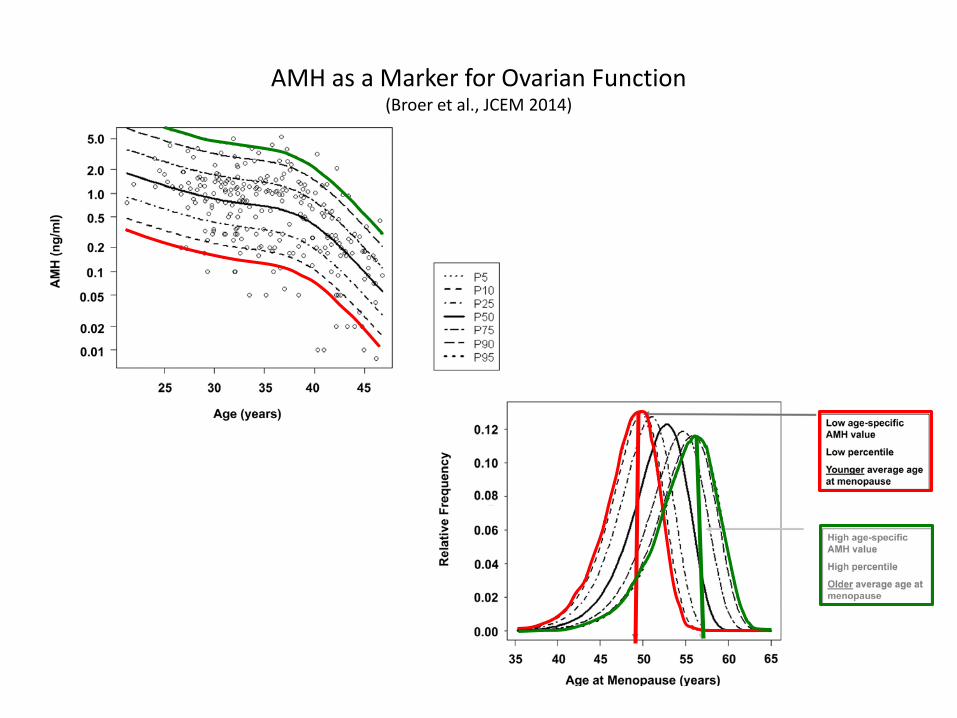
AMH as a Marker for Ovarian Function (Broer et al., JCEM 2014)
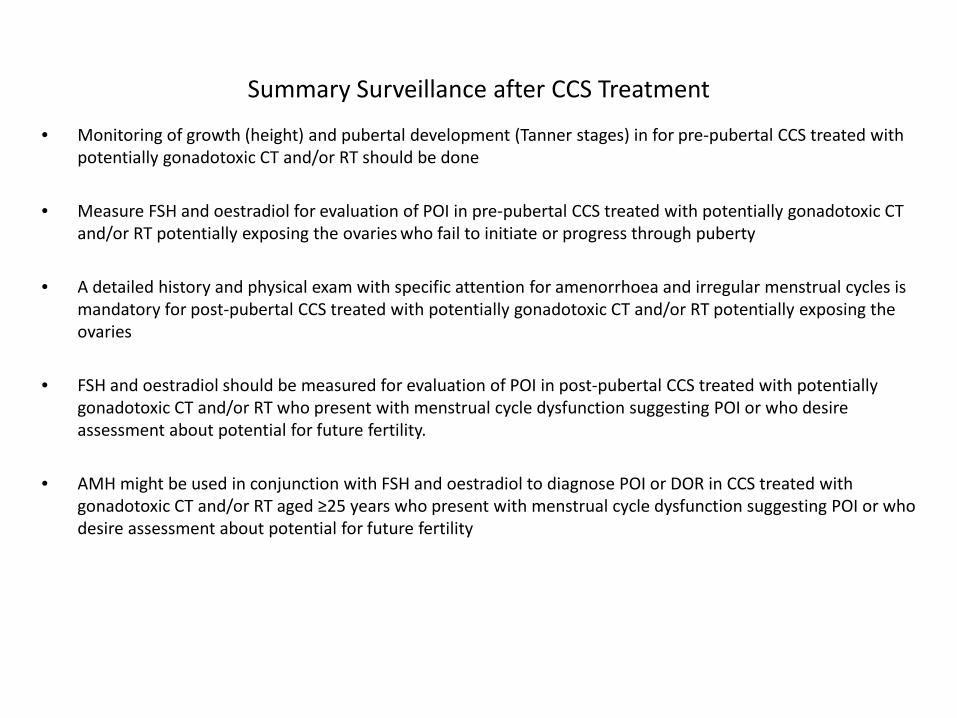
Summary Surveillance after CCS Treatment
• Monitoring of growth (height) and pubertal development (Tanner stages) in for pre-pubertal CCS treated with potentially gonadotoxic CT and/or RT should be done
• Measure FSH and oestradiol for evaluation of POI in pre-pubertal CCS treated with potentially gonadotoxic CT
and/or RT potentially exposing the ovaries who fail to initiate or progress through puberty
• A detailed history and physical exam with specific attention for amenorrhoea and irregular menstrual cycles is mandatory for post-pubertal CCS treated with potentially gonadotoxic CT and/or RT potentially exposing the ovaries
• FSH and oestradiol should be measured for evaluation of POI in post-pubertal CCS treated with potentially gonadotoxic CT and/or RT who present with menstrual cycle dysfunction suggesting POI or who desire assessment about potential for future fertility.
• AMH might be used in conjunction with FSH and oestradiol to diagnose POI or DOR in CCS treated with gonadotoxic CT and/or RT aged ≥25 years who present with menstrual cycle dysfunction suggesting POI or who desire assessment about potential for future fertility
TREATMENT OPTIONS AFTER CHILDHOOD CANCER
Ovarian function in Long-term Survivors of Childhood Cancer
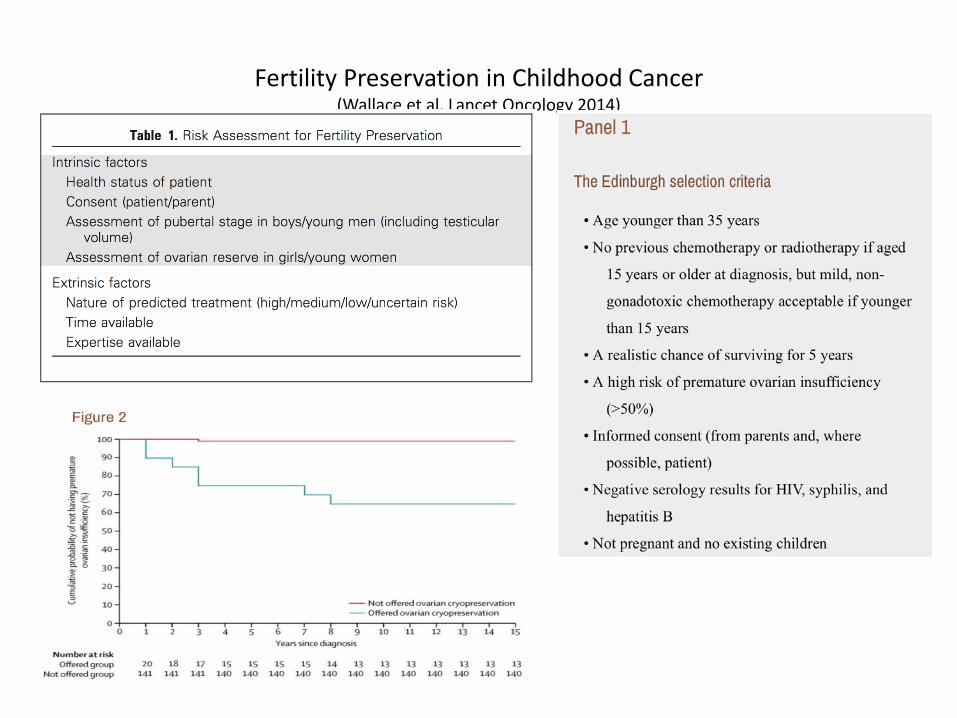
Fertility Preservation in Childhood Cancer (Wallace et al, Lancet Oncology 2014)
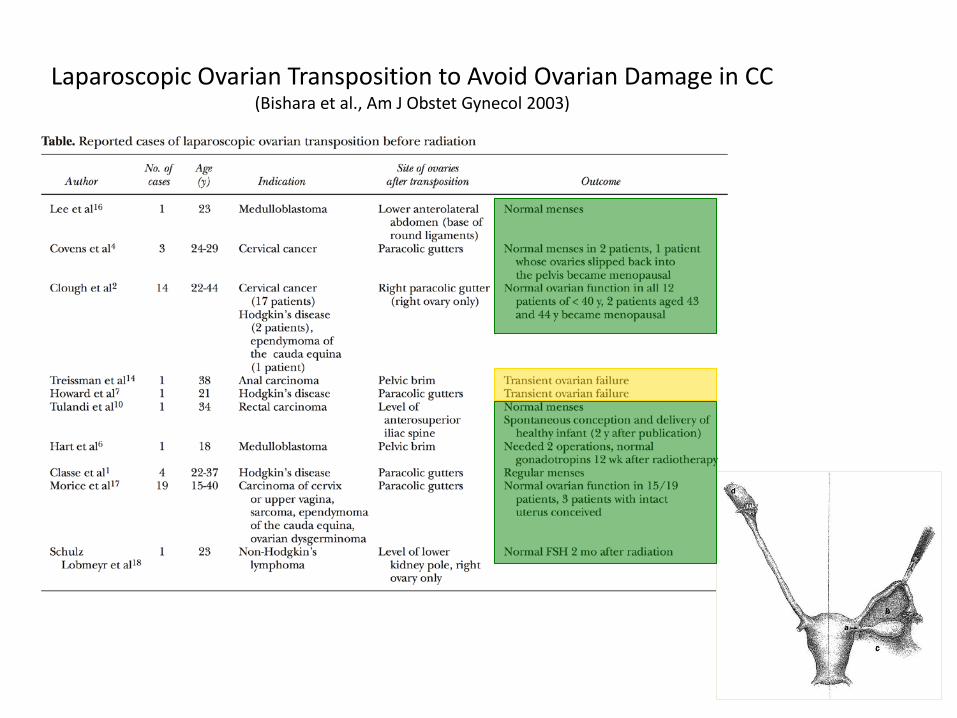
Laparoscopic Ovarian Transposition to Avoid Ovarian Damage in CC (Bishara et al., Am J Obstet Gynecol 2003)
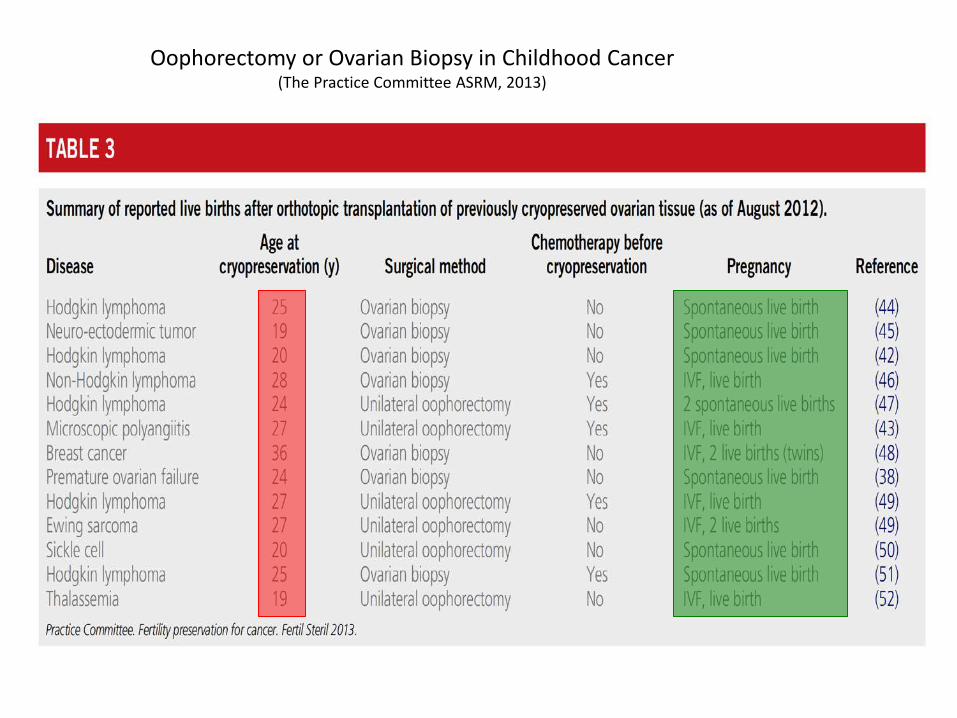
Oophorectomy or Ovarian Biopsy in Childhood Cancer (The Practice Committee ASRM, 2013)
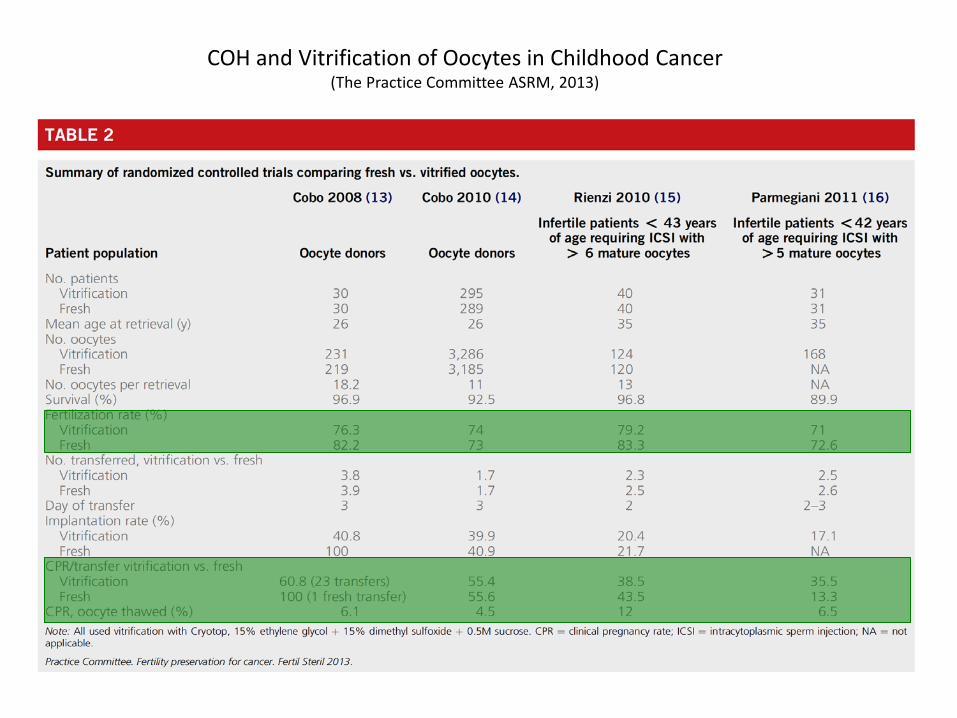
COH and Vitrification of Oocytes in Childhood Cancer (The Practice Committee ASRM, 2013)
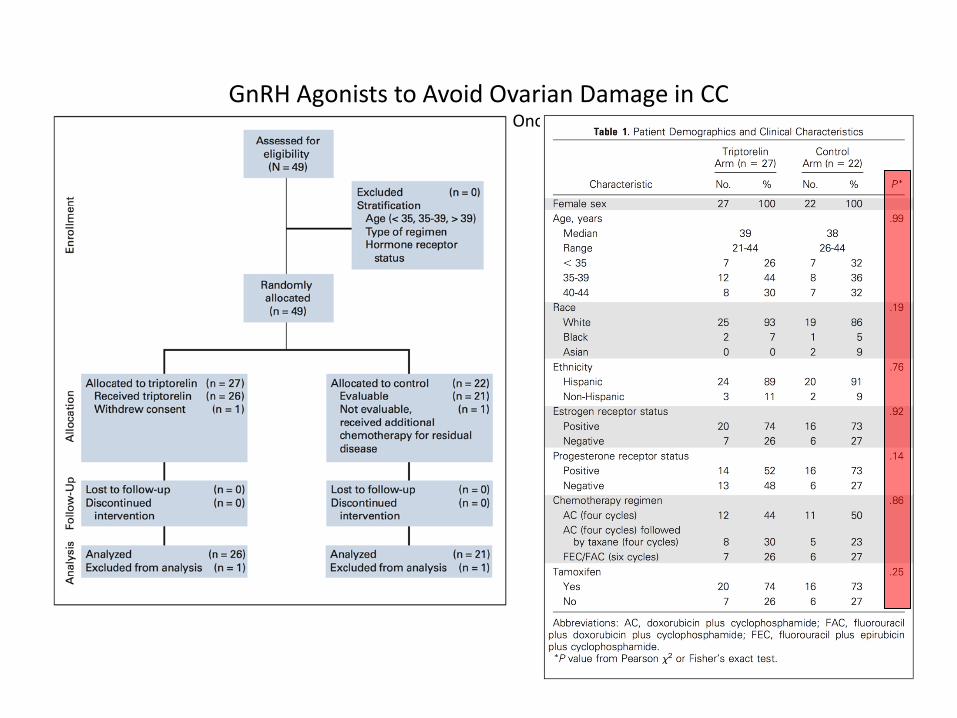
GnRH Agonists to Avoid Ovarian Damage in CC
(Munster et al., J.Clin Oncol, 2012)
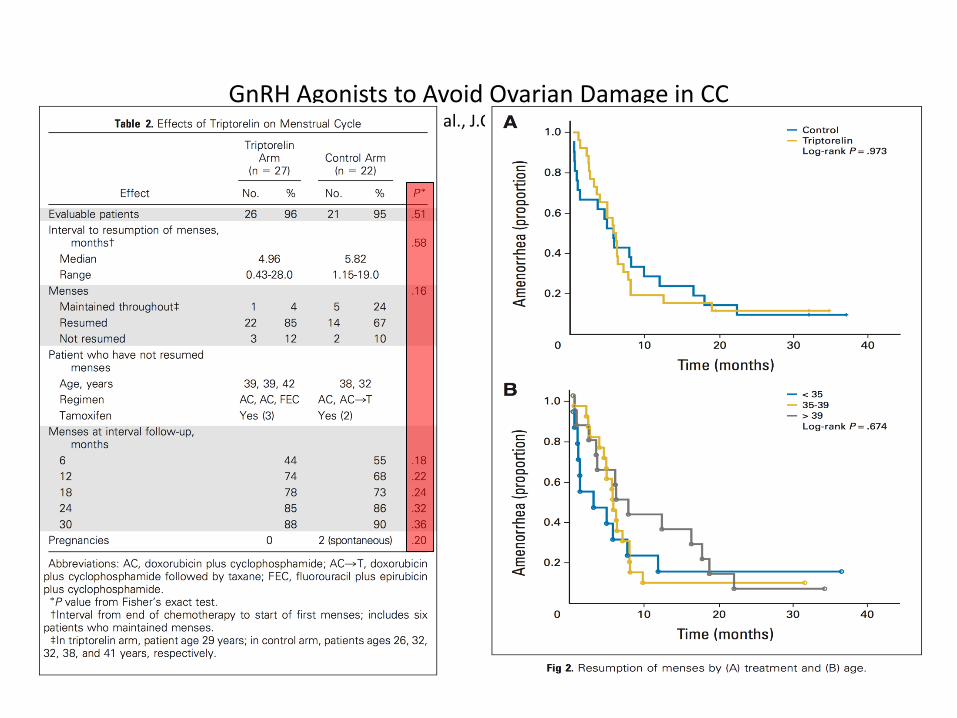
GnRH Agonists to Avoid Ovarian Damage in CC
(Munster et al., J.Clin Oncol, 2012)
Summary of Treatment Options to Preserve Fertility in CC • Risk assessment for fertility preservation should make use of the Edinburgh selection criteria i.e.
– Age < 35 years – No previous CT or RT if aged >15 years at diagnosis – Mild or non gonadotoxic CT if aged < 15 years – A realistic survival chance – A high risk for POI (>50%) – Informed consent – Negative serology for HIV, syphilis and Hepatitis B – Not pregnant and no existing children
• Treatment options to preserve fertility are:
– GnRH co treatment (investigational) – Ovarian Transposition – Ovariectomy and cryopreservation of ovarian tissue in pre or post-pubertal girls (investigational) – Ovarian hyperstimulation and egg retrieval with subsequent vitrification of oocytes in post pubertal
adolescent girls – IVM of oocytes either after retrieval or from cortical strips (investigational)
• In case of POI HRT should be initiated
PREGNANCY AFTER CHILDHOOD CANCER
Ovarian function in Long-term Survivors of Childhood Cancer
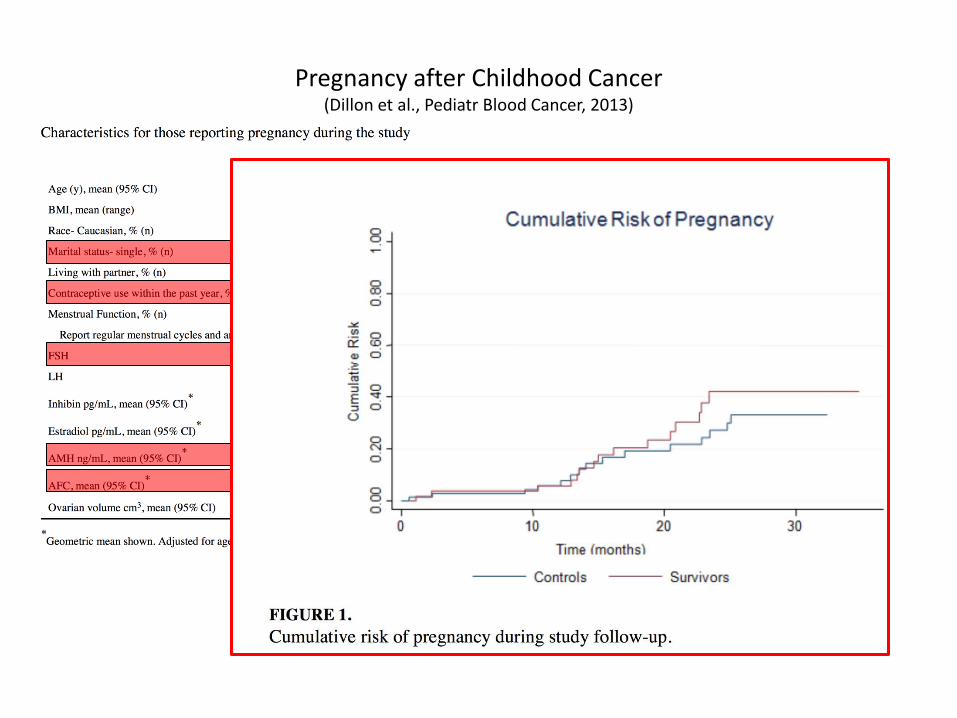
Pregnancy after Childhood Cancer (Dillon et al., Pediatr Blood Cancer, 2013)
Fertility after Cryopreservation of one Ovary (Schmidt et al., Reprod Biomed Online, 2013)
• Fifty-seven women had actively tried to become pregnant after end of treatment
• Of these, • 41 women obtained a total of 68 pregnancies • resulting in 45 live births and five on going pregnancies • 15 spontaneous abortions • 1 ectopic pregnancy • 2 elective abortions.
In the remaining 86 women without a pregnancy wish, there had been
• 5 elective abortions.
• Ninety-three per cent of the pregnancies were after natural conception and only four cases were a result of fertility treatment.
• The overall risk of premature ovarian failure was low (22%).
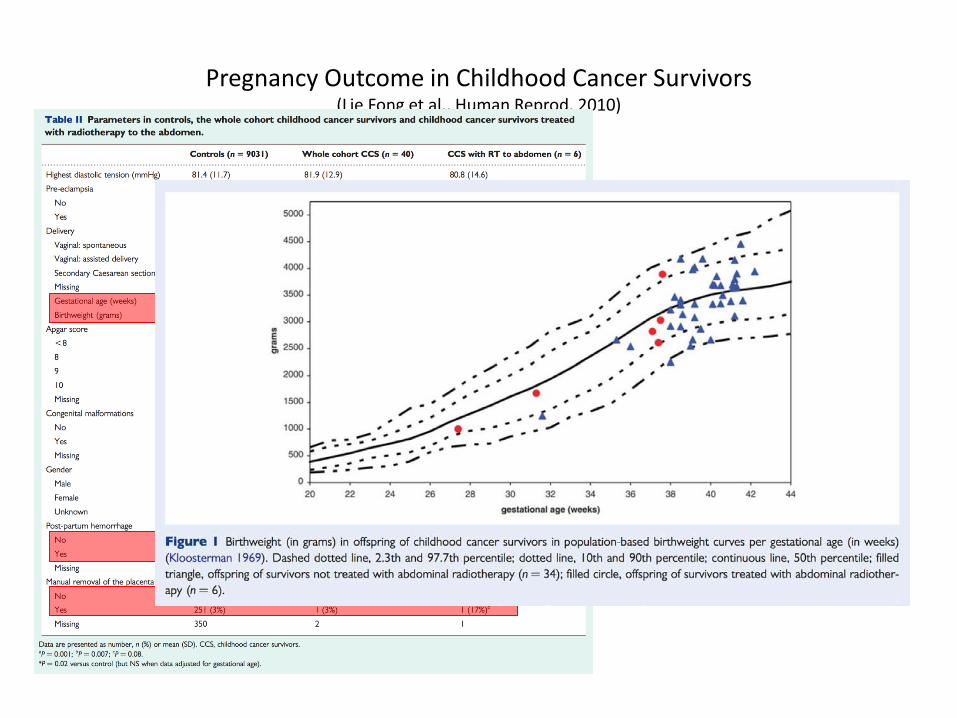
Pregnancy Outcome in Childhood Cancer Survivors (Lie Fong et al., Human Reprod, 2010)
Summary of Fertility after CCS Treatment
• Pregnancy rates after CCS treatment are generally underestimated
• CPR and OPR from long-term follow-up studies of CCS are reassuring
• Pregnancies seem to be complicated by – Preterm-delivery – Post partum Haemorrhage – Disturbances of the third phase of labour – Lower birth weight especially in those CCS who had abdominal or pelvic RT
• Miscarriage rates seem not to be elevated
• Unplanned or unintended pregnancies are also occurring especially in adolescent or young adults
• POI is as common as 20%

Working group Chairs: Hamish Wallace, UK Riccardo Haupt, IT
Advisors: Melissa Hudson, USA Leontien Kremer, NL Renée Mulder, NL
Coordinators: Wendy van Dorp, NL Marry vdn Heuvel-Eibrink, NL
Working Group leaders: Jennifer Levine, USA Marleen vdn Berg, NL Eline van Dulmen, NL Natscia di Iorgi, IT
Members: Andrea Corrias, IT Sebastian Neggers, NL Allison Leiper, UK Hanneke van Santen, NL Clarisa Garcia, USA Uta Dirksen, GER L. Sandy Constine, USA Rebecca Deans, AUS Leah Kroon, USA Alberto Revelli, IT Alessandro Mussa, IT Andy Toogood, USA Lilian Meacham, USA Assunta Albanese, USA Nils Lambalk, NL
www.ighg.org
Conclusions
• Childhood cancer survival rates do increase dramatically and therefore long-term health sequelae of treatment also become more apparent such as ovarian dysfunction and infertility after cancer treatment
• In CCS POI and DOR are more common and generally these women enter menopause early in life
• Assessing ovarian function in pre- as well as in post-pubertal girls and in young adult CS is mandatory. By assessing pubertal development as well as menstrual cycle pattern along with some endocrine measurements like FSH, Oestradiol and AMH seems appropriate
• In case fertility preservation is needed a thorough and prompt assessment of psycho-social factors, survival prospects and limitations of treatment modalities should be done in a multidisciplinary team according to a fixed protocol
• In case a pregnancy is established special attention should be paid antenatal to some known risk factors such as preterm delivery, post partum haemorrhage.

Bijdrage dr. Marcel van Hooff
9 juli 2015 – Fertiliteitspreservatie aan oncologische patiënten

Fertiliteitspreservatie Vruchtbaarheid en Kanker
Ervaringen in het SFVG In samenwerking met EMC
Bijdrage dr. Marcel van Hooff
Patienten perspectief Ervaringen in het SFG EMC Beter af met BeterKeten
Patienten perspectief - casus Mw G
• 28 jaar G0P0 • Dec 2011 op SEH – knobbeltje 1-1.5 cm • Mammografie/echografie: echoarme laesie,
beeld fibroadenoom BIRADS 2
• Advies: 6 maanden afwachtend • 22-03-2012 Op verzoek patiënte excisie • 28-03-2012 PA: infiltrerend ductaal carcinoom
– Oestrogeenreceptor negatief – Progesteron receptor negatief – Her2 negatief
• 30-03-2012 lymfklierpunctie • 05-04-2012 gesprek fertiliteitspreservatie

Wat moet ik kiezen ??

FPC – Fertility Preservation Councelling
• Effect behandeling op fertiliteit • Kans op spontane zwangerschap na behandeling • Mogelijke behandelingen fertiliteitspreservatie
met gericht advies • Uitleg behandeling • DNA diagnostiek - genmutatie • Folder NNF
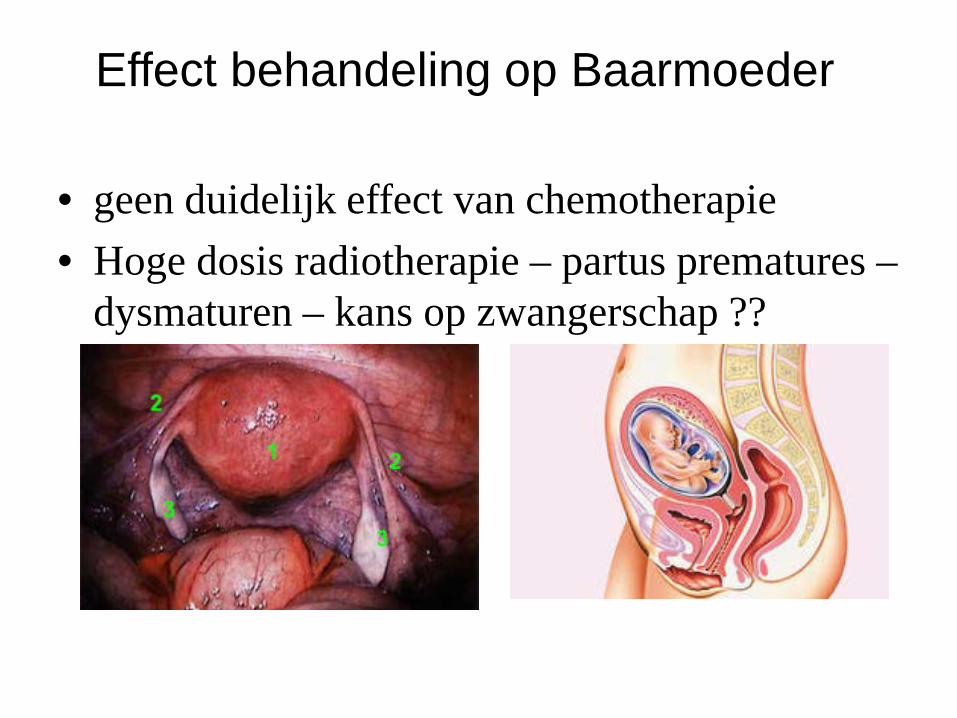
Effect behandeling op Baarmoeder
• geen duidelijk effect van chemotherapie • Hoge dosis radiotherapie – partus prematures –
dysmaturen – kans op zwangerschap ??
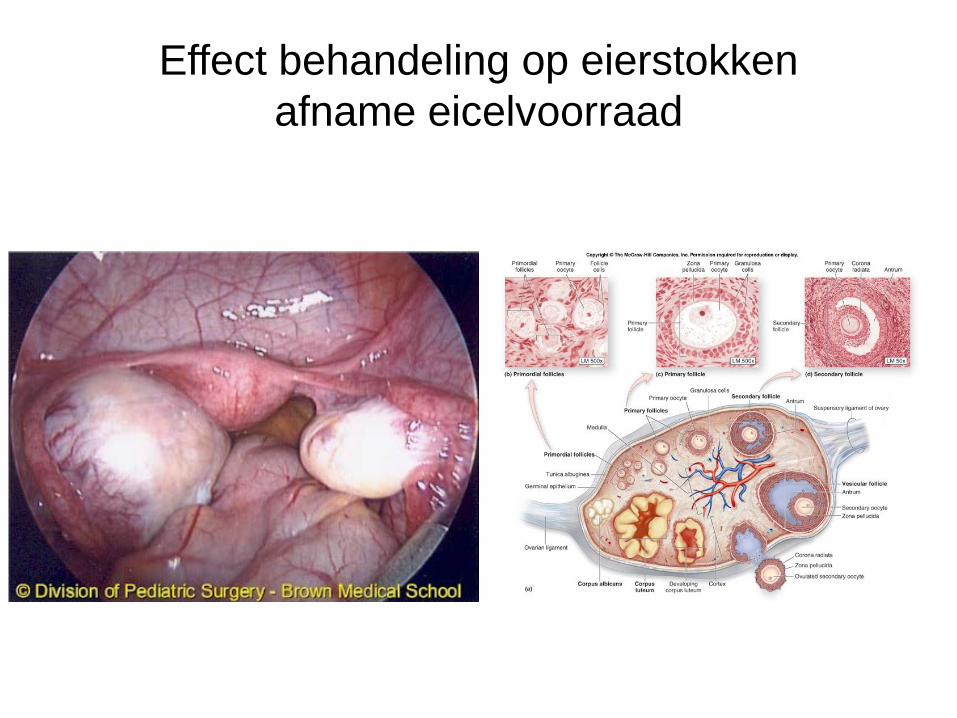
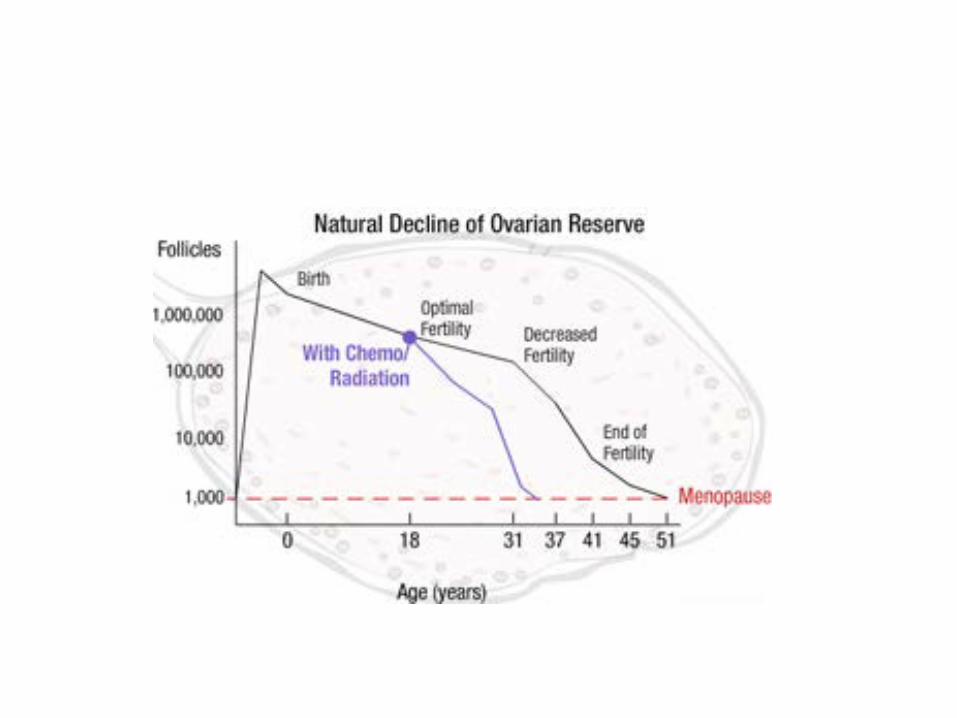
Effect behandeling op eierstokken afname eicelvoorraad

FPC – Fertility Preservation Councelling
• Effect behandeling op fertiliteit • Kans op spontane zwangerschap na behandeling • Mogelijke behandelingen fertiliteitspreservatie
met gericht advies • Uitleg behandeling • DNA diagnostiek - genmutatie • Folder NNF
Ernst schade chemotherapie – Kans op spontane zwangerschap
• Leeftijd • Afname natuurlijke fertiliteit door uitstel
nastreven zwangerschap • Soort en dosis chemotherapie • Vruchtbaarheid voorafgaand aan de
behandeling – Schatten Eicelvoorraad
• Vaginale echoscopie – antrale follikel telling • Bloed: Anti Mullerian Hormoon
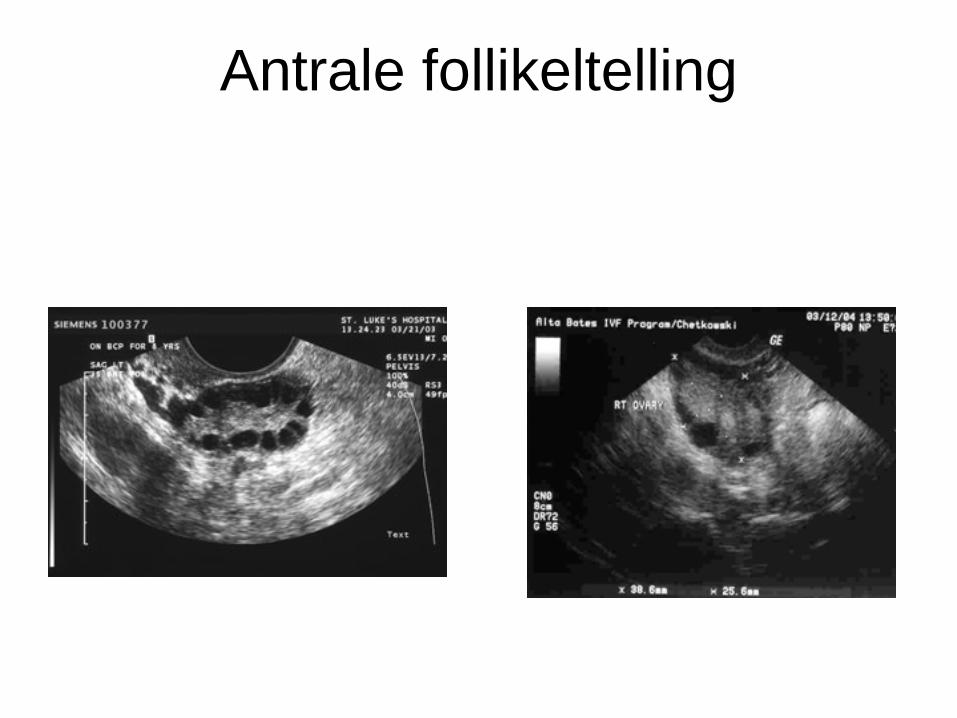
Antrale follikeltelling

FPC – Fertility Preservation Councelling
• Effect behandeling op fertiliteit • Kans op spontane zwangerschap na behandeling • Mogelijke behandelingen fertiliteitspreservatie
met gericht advies • Uitleg behandeling • DNA diagnostiek - genmutatie • Folder NNF
Cryopreservatie ovarium
• Voordeel – Snel mogelijk – 2-3 dagen – geschikt voor vrouwen zonder partner
• Nadeel – Narcose – operatierisico – complicatie – uitstel – Na terugplaatsing duur tot activiteit 85 dagen – Overleving getransplanteerde weefsel 2 maanden tot 4 jaar
geschat – Wereldwijd 17 zwangerschappen (jan 2014) – Herintroductie Tumorcellen???
IVF – Hoe werkt het ?
• Uitsluiten cysten en afwijkingen baarmoeder met vaginale echo
• Hormonale stimulatie – multiple follikelgroei – Dag 2. Start Follikel Stimulerend Hormoon injecties – Dag 6 Start Cetrotide (LHRH antagonist) ter voorkoming
spontane eisprong • Dag 10 eerste echo voor vervolgen groei, vaak meerder
echo’s nodig
• Bij borstkanker - Letrezol


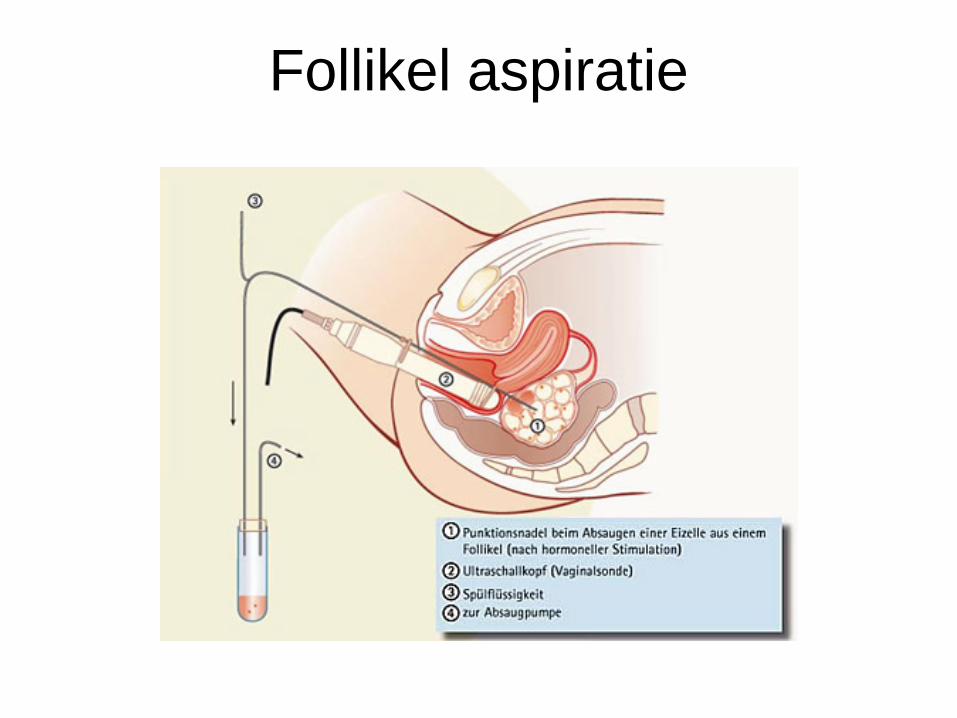
Follikel aspiratie
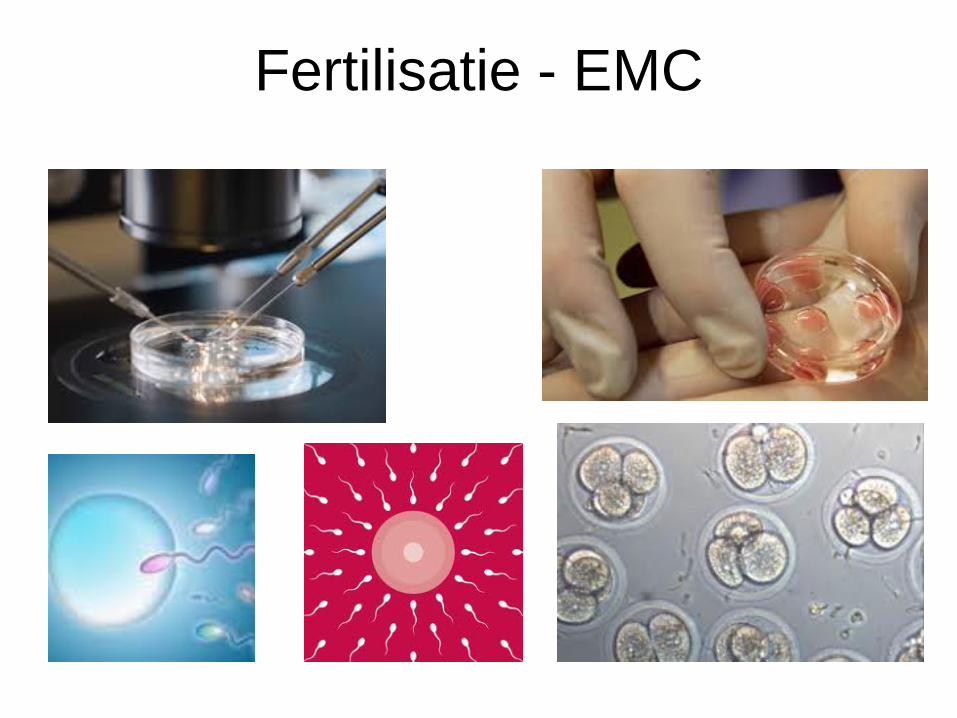
Fertilisatie - EMC
Cryopreservatie - embryo
IVF - afvalrace
• Niet iedere follikel geeft een eicel • Niet iedere eicel wordt bevrucht • Niet iedere bevruchte eicel ontwikkelt zich tot
een embryo • Niet iedere embryo ontwikkelt zich voldoende
om ingevroren te kunnen worden • Niet ieder embryo overleeft het invriezen en
ontdooien
Cryopreservatie eicellen
• Vergelijkbare behandeling met cryopreservatie embryo’s.
• Pas sinds enkele jaren succesvol. • Kans op zwangerschap voorlopig nog kleiner
dan bij invriezen embryo’s. • Geen partner nodig

• 05-04-2014 gesprek fertiliteitspreservatie – Dec 2010 stop anticonceptie – Nastreven zwangerschap sinds 1 jaar – Zeer sterke kinderwens. – LM 18 maart cyclus 26 dagen – In overleg EMC
• Start IVF traject nastreven invriezen embryo’s • Menstruatie afwachten dan start • Schema: Letrezol;, Gonal F, Cetrotide
• 05-04-2012 PA lymfklier - metastase • 11-04-2012 start IVF • 17-04-2012 echo follikelgroei • 21-04-2012 echo follikelgroei • 22-04-2012 lumpectomie met okselklierdissectie • 22-04-2012 avond decapeptyl 2 keer 0,1mg • 24-04-2014 IVF punctie
– 16 eicellen – 12 embryo’s – 10 embryo’s ingevroren

Anticonceptie
• 24-04-2012 PA fibreus mammaweefsel; intramammair gelegen lymfklier met metastase
• 25-04-2012 32 lymfklieren 17 tumorpositief met focaal extranodale doorgroei en veel intravasculaire tumorembolieen
• pT2N3 • Adjuvant chemotherapie en radiotherapie
Chemotherapie : 3 kuren FEC 100 3 kuren - 5FU 500mg/m2 - Epirubicine 100 / m - Cyclofosmadide 500 / m2 - 3 kuren Docetaxel 100 mg/m2
Radiotherapie

FPC – Fertility Preservation Councelling
• Effect behandeling op fertiliteit • Kans op spontane zwangerschap na behandeling • Mogelijke behandelingen fertiliteitspreservatie
met gericht advies • Uitleg behandeling • DNA diagnostiek - genmutatie • Folder NNF

• 5-9-2012: BRCA 1 genmutatie postitief
Erfelijkheid problematiek • Draag ik BRCA1 of 2 gen over naar mijn kind
– Prenatale diagnostiek = testen doormiddel van vruchtwaterpunctie als er een zwangerschap is
– Pre implantatie genetische diagnostiek (PGD) = testen van het embryo op genmutatie voor het wordt geplaatst.
– Niet willen weten

• 5-9-2012: BRCA 1 genmutatie postitief • 6-8-2013: - intake preimplantatie genetische
diagnostiek (PGD) • UMCU – MUMC
En dan ?
• Afwachten beloop behandeling kanker • Hormoontherapie noodzakelijk ? • Akkoord behandelend oncoloog ? – vnl
belangrijk bij hormoongevoelige kanker
• April 2015 verse IVF-ICSI met PGD • 5 eicellen • 1 niet aangedaan embryo – ET – niet zwanger • 2 aangedane embryo’s • 1 niet bevrucht; 1 afwijkend embryo
Mw G “ dit hele traject vind ik zwaarder dan
behandeling van mijn borstkanker”
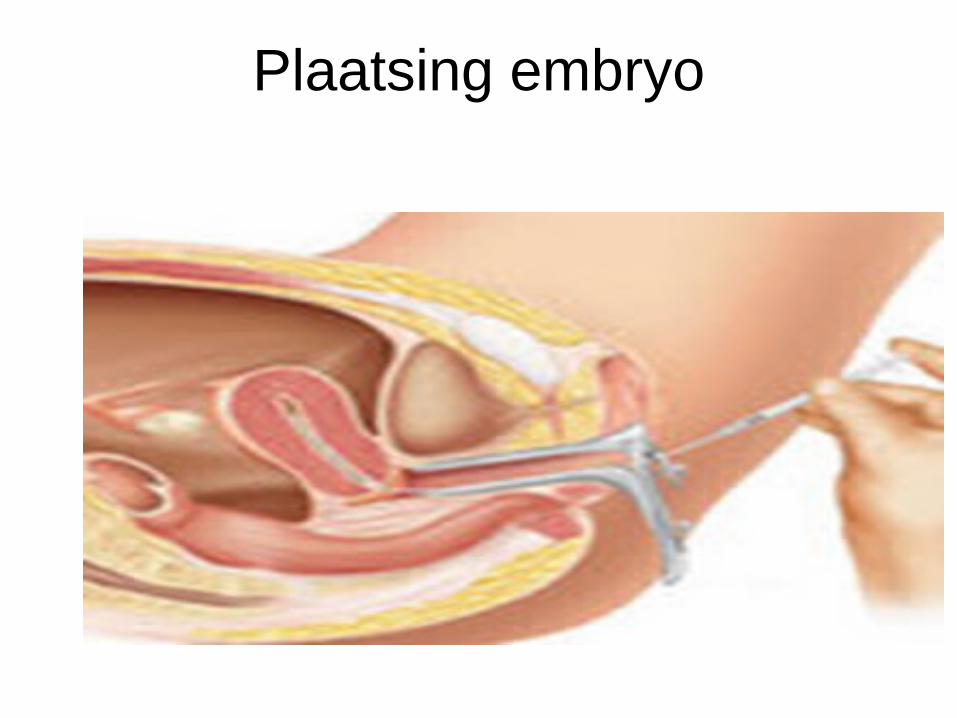
Plaatsing embryo

Wat moet ik kiezen ??
Zwangerschap na kanker
• Vrouwen die zwanger worden na borstkanker hebben vergelijkbare of beter prognose dan vrouwen niet niet zwanger worden – Healthy mother effect
•
Ervaringen samenwerking EMC-SFG • SFVG - 1e vraag vanuit MDO oncologie 2012 • Overleg EMC – councelling / behandeling • 20 patienten jaar
Mammacarcinoom/ M Hodgkin 30-40% kiest voor behandeling 100% tevreden met councelling
Ervaringen samenwerking EMC-SFG - Zorg van onco-haematoloog/ chirurg over uitstel
van behandeling en mogelijk verslechtering prognose.
- Zorg onco-haematoloog/ chirurg over gynaecoloog pushed fertiliteitspreservatie
- Na enige tijd vertrouwen van internist / chirurg op objectieve counselling en snelle behandeling
Ervaringen samenwerking EMC-SFG • Niet iedereen wordt gecouncelled • Aanmelding councelling - soms te laat • Optimaliseren councelling – behandeling binnen
Beter Keten
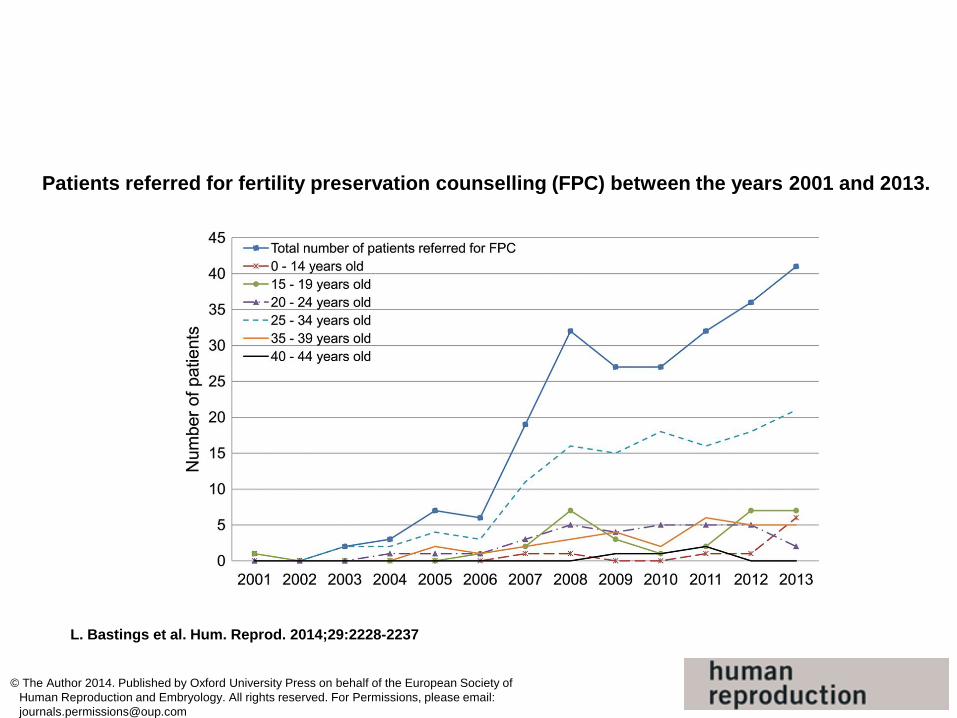
Patients referred for fertility preservation counselling (FPC) between the years 2001 and 2013.
L. Bastings et al. Hum. Reprod. 2014;29:2228-2237
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: [email protected]
Trends in keuze - 1 kind en kinderwens, ja - Geen kinderen en kinderwens, ja - Vaste relatie, ja - Leeftijd 20-27-nee , 28-35- ja, 35-40, wisselt - Kans spontane zwangerschap na behandeling
Ervaringen samenwerking EMC-SFG • Beter af met Beter Keten • Streven naar 100% councelling • Regionaal op alle MDO oncologie
fertiliteitspreservatie voor alle patienten < 45 jaar benoemd.
• Polikliniek counselling EMC • Toegang binnen 48 uur • Aanmelding centraal – tel:010-7033760

FPC – Fertility Preservation Councelling
• Effect behandeling op fertiliteit • Kans op spontane zwangerschap na behandeling • Mogelijke behandelingen fertiliteitspreservatie
met gericht advies • Uitleg behandeling • DNA diagnostiek - genmutatie • Folder NNF
NNF • www.nnf-info.nl • Nederlands netwerk fertiliteitspreservatie
– O.a. Folder fertiliteitspreservatie en borstkanker – www.borstkankerenkinderwens.nl
• App : I save Fertility. (ISF) Keuzehulp wel of niet kiezen voor fertiliteitspreservatie. Wordt vertaald in Nederlands.
Take home message • Fertiliteitspreservatie standaard in MDO oncologie • Counselling fertiliteitspreservatie mogelijk binnen 48
uur (Ma-Wo-Vr) • 010-7033760 • Behandeling altijd in overleg oncoloog/chirurg • Beter af met Beter Keten
– centralisatie informatie – standaard councelling – mogelijkheid wetenschap ter verbetering zorg

Afsluiting en borrel
Bedankt voor uw komst!