Esophageal Cancer - EUR · 2016. 5. 20. · Chapter 10 Recurrence pattern in patients with a...
210
Esophageal Cancer preoperative management and postoperative outcome Pieter van Hagen
Transcript of Esophageal Cancer - EUR · 2016. 5. 20. · Chapter 10 Recurrence pattern in patients with a...

Esophageal Cancer preoperative management and postoperative outcome
Pieter van Hagen
Esophageal Cancer preoperative managem
ent and postoperative outcome
Pieter van Hagen
Uitnodiging
Voor het bijwonen van de openbare verdediging
van het proefschrift
Esophageal Cancer;preoperative management and
postoperative outcome
door
Pieter van Hagen
Op woensdag 18 mei 2016 om 13.30 uur.
Professor Queridozaal, Onderwijscentrum Erasmus MC.
Wytemaweg 80, Rotterdam
Receptie aansluitend aan de promotie
ParanimfenZarina Lalmahomed
Karel Klop
Pieter van HagenRolderdiephof 13521 DA Utrecht
13631_Hagen_OM.indd 1 15-04-16 16:43


Esophageal Cancer; Preoperative management and postoperative outcome
Pieter van Hagen

ISBN: 978-94-6299-340-2
Printing: Ridderprint BV - www.ridderprint.nl
Lay-out: Nikki Vermeulen - Ridderprint BV
© Pieter van Hagen, 2016
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or
transmitted, in any form or by any means, electronically, mechanically, by photo-copying, recording,
or otherwise, without the prior permission of the author.

Esophageal Cancer; Preoperative management and postoperative outcome
Slokdarmkanker;
Preoperatieve behandeling en postoperatieve uitkomst
Proefschrift
ter verkrijging van de graad van doctor aan de
Erasmus Universiteit Rotterdam
op gezag van de
rector magnificus
prof.dr. H.A.P. Pols
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
woensdag 18 mei 2016 om 13.30 uur
door
Pieter van Hagengeboren te Leiden

PROMOTIECOMMISSIE
Promotor: Prof.dr. J.J.B. van Lanschot
Overige leden: Prof.dr. A.H.J. Mathijssen
Prof.dr. E.W. Steyerberg
Prof.dr. R. van Hillegersberg
Copromotor: Dr. B.P.L. Wijnhoven

TABLE OF CONTENTS
Chapter 1 General introduction 7
PART 1: Preoperative analysis and treatment 17
Chapter 2 Preoperative chemoradiotherapy for esophageal or junctional cancer. 19
(2012) New England Journal of Medicine, 366(22), pp. 2074-2084.
Chapter 3 Long-term results of a randomized controlled trial comparing neoadjuvant 35
chemoradiotherapy plus surgery with surgery alone for esophageal or
junctional cancer (CROSS trial).
(2015) Lancet Oncology, Sep;16(9):1090-1098.
Chapter 4 Prolonged time to surgery after neoadjuvant chemoradiotherapy increases 53
histopathological response without improving survival in patients with
esophageal or junctional cancer.
(2014) Annals of Surgery, 260(5):807-14.
Chapter 5 Delay in diagnostic workup and treatment of esophageal cancer. 69
(2010) Journal of Gastrointestinal Surgery, 14(3), pp. 476-483.
Chapter 6 Impact of a multidisciplinary tumor board meeting for upper-GI 85
malignancies on clinical decision making: A prospective cohort study.
(2013) International Journal of Clinical Oncology, 18(2), pp. 214-219.
Chapter 7 Human epidermal growth factor receptor 2 overexpression and amplification 97
in endoscopic biopsies and resection specimens in esophageal and junctional
adenocarcinoma.
(2015) Diseases of the Esophagus, 28(4):380-5.
PART 2: Postoperative outcome and prognostication 109
Chapter 8 Prediction of disease-free survival using relative change in FDG-uptake early during 111
neoadjuvant chemoradiotherapy for potentially curable esophageal cancer.
Accepted for publication, Diseases of the Esophagus
Chapter 9 Patterns of recurrence after surgery alone versus preoperative chemoradiotherapy 127
and surgery in the CROSS trials.
(2014) Journal of Clinical Oncology, 32(5):385-391.

Chapter 10 Recurrence pattern in patients with a pathologically complete response after 143
neoadjuvant chemoradiotherapy and surgery for esophageal cancer.
(2013) British Journal of Surgery, 100(2), pp. 267-273.
Chapter 11 Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification 159
for esophageal cancer.
(2012) Annals of Surgical Oncology, 19(7), pp. 2142-2148.
Chapter 12 Vitamin B12
deficiency following esophagectomy for esophageal 173
and esophagogastric cancer.
Submitted
PART 3: Summary and appendices 185
Summary of the thesis 187
Samenvatting in het Nederlands 193
Future perspectives 197
PhD Portfolio 201
Acknowledgements 203
Curriculum Vitae 207

Chapter 1General introduction


General introduction |
9
Cha
pter
1
Esophageal cancer is an aggressive malignancy. With more than 450,000 newly discovered cases
annually, it is the 8th most common cancer worldwide.1,2 Mortality remains high, with an annual
400,000 deaths worldwide and 5-year overall survival rates for patients with potentially curative
disease rarely exceeding 30%.2-4 In general, two types of esophageal cancer can be distinguished,
i.e. esophageal adenocarcinoma and squamous cell carcinoma. Globally, squamous cell carcinoma
is the most common subtype, accounting for more than 80% of cases. However, in many Western
countries, the incidence of esophageal adenocarcinoma exceeds that of squamous cell carcinoma
and is still rising.1 Because advanced tumors can obstruct the esophageal lumen, most patients with
esophageal cancer present with dysphagia and weight loss. Due to the aggressive character of the
tumor, with invasion into adjacent organs and/or hematogenous dissemination, roughly 50% of
patients are incurable at the time of diagnosis.5,6
Esophageal cancer is most often staged using the tumor-node-metastasis (TNM) classification.7 This
classification is developed by the Union Internationale Contre le Cancer (UICC) and the American
Joint Committee on Cancer (AJCC), and comprises the T-stage that classifies the depth of tumor
infiltration, the N-stage that reflects the presence and number of lymph node metastases, and the
M-stage that describes the presence of distant metastases. The TNM classification is widely used for
defining treatment strategies and prognostication.
Surgery remains the cornerstone of potentially curative treatment for resectable tumors. 8,9 Partly due
to centralization, postoperative mortality is now generally below 5% , however, morbidity remains
high.6,10 Despite extensive preoperative staging, a microscopically radical resection (R0) can only be
performed in 75% of patients treated with primary surgery.11,12 An R0 resection is a strong prognostic
factor and should be pursued whenever possible.13,14 Neoadjuvant chemo(radio)therapy may induce
shrinkage of the tumor, and thereby increase the chance on an R0 resection. Over the past decades,
neoadjuvant treatment with chemo(radio)therapy has been extensively investigated.3,11,15-20 There is
growing evidence that neoadjuvant therapy prolongs long-term survival.21-24
The effect of neoadjuvant chemoradiotherapy can be evaluated in the surgical resection specimen
by quantifying the histopathologic response. This pathological response predicts survival, with a
pathologically complete response having the best long term survival. Partial responders also might
benefit from neoadjuvant therapy, in contrast to non-responders, who only risk exposure to the
toxicity that accompanies the treatment.25-29
Fluorodeoxyglucose Positron Emission Tomography (FDG-PET) is a nuclear imaging technique that
quantifies metabolic activity of tumors, which is increased in most cases of malignant disease.30,31
By administering radioactively labeled glucose, increased glucose uptake in malignant tumors and
possible distant metastases can be detected. This technique has a role in the pretreatment staging
of advanced carcinomas and in detecting metastases in the interval between neoadjuvant treatment
and surgery.32 Also, several studies have been published investigating the potential of FDG-PET to
predict pathological response during or after completion of neoadjuvant chemoradiotherapy.33,34
Unfortunately, it was shown not to be possible to accurately predict histopathological response
early during chemoradiotherapy, which would have facilitated to discontinue the therapy in non-
responders and thus to avoid possible unnecessary toxicity.34

| Chapter 1
10
After completion of neoadjuvant therapy, a certain period of time is needed for the patient to recover
from the therapy before undergoing operative therapy. There is no consensus on how long this
interval between neoadjuvant treatment and surgery should be, but in general, a minimum period
of four weeks is abided. In rectal cancer, it was shown that a longer interval to surgery resulted in a
larger proportion of patients with a pathologically complete response.35-41 In esophageal cancer, there
is only limited evidence for accepting a longer interval.42,43
Besides conventional chemotherapeutic agents, more individualized targeted therapy in esophageal
cancer is currently explored.44 In gastric cancer, targeted palliative therapy with anti-epidermal growth
factor receptor (EGFR) agents was investigated in a randomized trial and proved to lengthen overall
survival in metastatic patients.45 In esophageal cancer, many targets for therapy have been identified,
including Human epidermal growth factor receptor 2 (HER2/neu), a receptor in the EGFR family.46-49
These targets might be used for immunotherapy in a (neo)adjuvant setting, however, so far there is no
clear evidence to justify their use in daily practice for patients with esophageal carcinoma.
Esophagectomy with gastric tube reconstruction changes the anatomy of the upper gastrointestinal
tract, often leading to functional problems and reduced quality of life.50 After a total gastrectomy,
patients are at high risk of developing a vitamin B12
deficiency, as a result of a shortage of intrinsic
factor.51 Intrinsic factor is essential for vitamin B12
metabolism and is produced by the parietal cells
in the gastric mucosa.52 In bariatric patients, vitamin B12
deficiency was also found in patients who
underwent gastric sleeve resections, in which only a part of the gastric mucosa is removed, analogue
to a gastric tube reconstruction.53 So far, it is unknown if there is an increase in vitamin B12
deficiency
after esophagectomy with gastric tube reconstruction.
OUTLINE OF THE THESIS
This thesis is composed of studies that focused on preoperative analysis and treatment (part 1) and on
postoperative outcome and prognostication (part 2). In part 1, neoadjuvant multimodality treatment
(including possible biological targets) of esophageal cancer as well as delay in treatment and other
targets for treatment are discussed. In part 2, the focus is on prognostication after treatment, patterns
of recurrence and long-term consequences of esophageal resection such as vitamin B12
deficiency.
PART 1: PREOPERATIVE ANALYSIS AND TREATMENT
Although surgery remains the cornerstone in the potentially curative treatment of esophageal
cancer, the potential additional value of neoadjuvant treatment has been studied extensively during
the recent decades, with varying results. Multiple meta-analyses were published, however, none
were able to provide definitive support for the use of neoadjuvant chemoradiotherapy for treating
esophageal cancer. Therefore, a multicenter randomized controlled trial comparing neoadjuvant
chemoradiotherapy followed by surgery with surgery alone for patients with potentially curable
esophageal or esophagogastric junction cancer was initiated. In Chapter 2 the long-term results

General introduction |
11
Cha
pter
1
of this trial are described. To further investigate the effects of neoadjuvant chemoradiotherapy on
survival, follow-up was performed five years after completion of the trial. The results of this ultra long
term follow-up are described in Chapter 3.
The time-intervals between preoperative staging, neoadjuvant therapy and surgery have been subject
of debate. The length of these intervals might affect post-operative complications, pathological
staging after surgery, and long term survival. Under analogous circumstances, in rectal cancer, a
positive effect of a prolonged interval between neoadjuvant therapy and surgery was found, resulting
in more pathologically complete responders. In Chapter 4, the effects of a prolonged interval
between neoadjuvant chemoradiotherapy and surgery on pathological outcome and survival are
described. In Chapter 5, we evaluated if the length of the intervals between onset of complaints and
diagnosis (the pre-hospital delay) and between pre-operative staging and surgery (the hospital delay)
were of influence on postoperative morbidity and/or long term survival.
The treatment of esophageal cancer is a multidisciplinary effort, and Dutch guidelines require every
new patient to be presented in a multidisciplinary tumor board prior to treatment. In Chapter 6, the
impact of such a tumor board on clinical decision making is evaluated.
Human epidermal growth factor receptor 2 (HER2/neu) is overexpressed in many solid tumors,
creating a potential target for (neo)adjuvant treatment with immunotherapeutic agents. It has been
shown previously that a subset of esophageal adenocarcinomas also express HER2/neu. However,
it is unclear if overexpression can be reliably established in the preoperatively obtained biopsies,
given the intratumoral heterogeneity. In Chapter 7, the results of a multicenter study are described,
investigating the representativeness of preoperative biopsies for the entire primary tumor in terms of
HER2/neu expression.
PART 2: POSTOPERATIVE OUTCOME AND PROGNOSTICATION 18FluoroDeoxyGlucose Positron Emission Tomography (FDG-PET) proved to successfully distinguish
between responders and non-responders in patients treated with neoadjuvant chemotherapy.
Ancillary to the randomized trial that is described in chapter one, the NEOPEC-trial was initiated.54
In this trial, an FDG-PET was performed immediately prior to nCRT and two weeks after the start of
nCRT. By doing this, a change in metabolic activity of the tumor during therapy can be objectified. For
patients treated with nCRT, FDG-PET was not reliable in predicting pathological response when used
early during therapy. However, the correlation between FDG-PET results and long term survival would
provide a more definitive answer to the usefulness of FDG-PET in prognostication. Therefore, patients
who were included in the NEOPEC- trial were subjected to long term follow-up, which was correlated
with FDG-PET results. This study is described in Chapter 8.The mode of action of chemoradiotherapy is mostly ascribed to its radiotherapy component, while
the chemotherapy is thought to have rather radiosensitizing than systemic effects. To fully understand
the action of both components of neoadjuvant chemoradiotherapy in the treatment of esophageal
cancer, it is essential to scrutinize those cases where multimodality treatment failed. In Chapter 9,

| Chapter 1
12
the pattern of recurrence is described that was encountered in patients treated with neoadjuvant
chemoradiotherapy according to the CROSS-regimen. Furthermore, the recurrence pattern was
established in patients who had a pathologically complete response in the resection specimen after
neoadjuvant chemoradiotherapy. These results are shown in Chapter 10.
For prognostication after surgery in esophageal cancer patients, the TNM classification is the most
widely used. In 2007, the UICC published its 7Th edition of the TNM-classification for solid tumors.
This classification differed strongly from the previous edition, especially for esophageal cancer. To
evaluate and validate the predictive value of the latest edition of the classification, its prognostic
power was compared to that of the sixth edition, using a large external cohort. The results of this
study are described in Chapter 11.
It has been suggested that patients who have undergone esophageal resection with gastric tube
reconstruction are more prone to develop a vitamin B12
deficiency postoperatively, due to the
decreased availability of intrinsic factor. However, the incidence and timing of such deficiency
have never been objectified. Therefore, we commenced a prospective multicenter cohort study
investigating the incidence and prevalence of vitamin B12
deficiency amongst patients who underwent
esophagectomy. In Chapter 12, the results of this study are described.

General introduction |
13
Cha
pter
1REFERENCES1. Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological
subtype in 2012. Gut. 2014 Oct 15.
2. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2014 Sep 13.
3. Boonstra JJ, Kok TC, Wijnhoven BP, van Heijl M, van Berge Henegouwen MI, Ten Kate FJ, et al. Chemotherapy followed by surgery versus surgery alone in patients with resectable oesophageal squamous cell carcinoma: long-term results of a randomized controlled trial. BMC Cancer. 2011;11:181.
4. Hulscher JB, van Sandick JW, de Boer AG, Wijnhoven BP, Tijssen JG, Fockens P, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002 Nov 21;347(21):1662-9.
5. Koshy M, Esiashvilli N, Landry JC, Thomas CR, Jr., Matthews RH. Multiple management modalities in esophageal cancer: epidemiology, presentation and progression, work-up, and surgical approaches. Oncologist. 2004;9(2):137-46.
6. Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003 Dec 4;349(23):2241-52.
7. Sobin L.H. GMK, Wittekind C. TNM classification of malignant tumors. 7th edition. Oxford: Wiley-Blackwell; 2010.
8. Graham AJ, Shrive FM, Ghali WA, Manns BJ, Grondin SC, Finley RJ, et al. Defining the optimal treatment of locally advanced esophageal cancer: a systematic review and decision analysis. Ann Thorac Surg. 2007 Apr;83(4):1257-64.
9. Low DE. Update on staging and surgical treatment options for esophageal cancer. J Gastrointest Surg. 2011 May;15(5):719-29.
10. van Lanschot JJ, Hulscher JB, Buskens CJ, Tilanus HW, ten Kate FJ, Obertop H. Hospital volume and hospital mortality for esophagectomy. Cancer. 2001 Apr 15;91(8):1574-8.
11. Kelsen DP, Ginsberg R, Pajak TF, Sheahan DG, Gunderson L, Mortimer J, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med. 1998 Dec 31;339(27):1979-84.
12. van Meerten E, van der Gaast A. Systemic treatment for oesophageal cancer. Eur J Cancer. 2005 Mar;41(5):664-72.
13. Scheepers JJ, van der Peet DL, Veenhof AA, Cuesta MA. Influence of circumferential resection margin on prognosis in distal esophageal and gastroesophageal cancer approached through the transhiatal route. Dis Esophagus. 2009;22(1):42-8.
14. Dexter SP, Sue-Ling H, McMahon MJ, Quirke P, Mapstone N, Martin IG. Circumferential resection margin involvement: an independent predictor of survival following surgery for oesophageal cancer. Gut. 2001 May;48(5):667-70.
15. Bosset JF, Gignoux M, Triboulet JP, Tiret E, Mantion G, Elias D, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med. 1997 Jul 17;337(3):161-7.
16. Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996 Aug 15;335(7):462-7.
17. Lin CC, Hsu CH, Cheng JC, Wang HP, Lee JM, Yeh KH, et al. Concurrent chemoradiotherapy with twice weekly paclitaxel and cisplatin followed by esophagectomy for locally advanced esophageal cancer. Ann Oncol. 2007 Jan;18(1):93-8.

| Chapter 1
14
18. Reynolds JV, Muldoon C, Hollywood D, Ravi N, Rowley S, O’Byrne K, et al. Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer. Ann Surg. 2007 May;245(5):707-16.
19. Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol. 2009 Oct 20;27(30):5062-7.
20. van Meerten E, Muller K, Tilanus HW, Siersema PD, Eijkenboom WM, van Dekken H, et al. Neoadjuvant concurrent chemoradiation with weekly paclitaxel and carboplatin for patients with oesophageal cancer: a phase II study. Br J Cancer. 2006 May 22;94(10):1389-94.
21. Fiorica F, Di Bona D, Schepis F, Licata A, Shahied L, Venturi A, et al. Preoperative chemoradiotherapy for oesophageal cancer: a systematic review and meta-analysis. Gut. 2004 Jul;53(7):925-30.
22. Sjoquist KM, Burmeister BH, Smithers BM, Zalcberg JR, Simes RJ, Barbour A, et al. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011 Jul;12(7):681-92.
23. Gebski V, Burmeister B, Smithers BM, Foo K, Zalcberg J, Simes J, et al. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: a meta-analysis. Lancet Oncol. 2007 Mar;8(3):226-34.
24. Urschel JD, Vasan H. A meta-analysis of randomized controlled trials that compared neoadjuvant chemoradiation and surgery to surgery alone for resectable esophageal cancer. Am J Surg. 2003 Jun;185(6):538-43.
25. Mandard AM, Dalibard F, Mandard JC, Marnay J, Henry-Amar M, Petiot JF, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer. 1994 Jun 1;73(11):2680-6.
26. Donington JS, Miller DL, Allen MS, Deschamps C, Nichols Iii FC, Pairolero PC. Tumor response to induction chemoradiation: Influence on survival after esophagectomy. Eur J Cardio-Thorac Surg. 2003;24(4):631-7.
27. Van Meerten E, Van Der Gaast A, Tilanus HW, Poley JW, Muller K, Van Dekken H. Pathological analysis after neoadjuvant chemoradiotherapy for esophageal carcinoma: The Rotterdam experience. J Surg Oncol. 2009;100(1):32-7.
28. Schneider PM, Baldus SE, Metzger R, Kocher M, Bongartz R, Bollschweiler E, et al. Histomorphologic tumor regression and lymph node metastases determine prognosis following neoadjuvant radiochemotherapy for esophageal cancer: implications for response classification. Ann Surg. 2005 Nov;242(5):684-92.
29. Swisher SG, Hofstetter W, Wu TT, Correa AM, Ajani JA, Komaki RR, et al. Proposed revision of the esophageal cancer staging system to accommodate pathologic response (pP) following preoperative chemoradiation (CRT). Ann Surg. 2005 May;241(5):810-7; discussion 7-20.
30. Czernin J, Phelps ME. Positron emission tomography scanning: current and future applications. Annu Rev Med. 2002;53:89-112.
31. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med. 2001 May;42(5 Suppl):1S-93S.
32. Blom RL, Schreurs WM, Belgers HJ, Oostenbrug LE, Vliegen RF, Sosef MN. The value of post-neoadjuvant therapy PET-CT in the detection of interval metastases in esophageal carcinoma. Eur J Surg Oncol. 2011 Sep;37(9):774-8.
33. Vallbohmer D, Holscher AH, Dietlein M, Bollschweiler E, Baldus SE, Monig SP, et al. [18F]-Fluorodeoxyglucose-positron emission tomography for the assessment of histopathologic response and prognosis after completion of neoadjuvant chemoradiation in esophageal cancer. Ann Surg. 2009 Dec;250(6):888-94.
34. van Heijl M, Omloo JM, van Berge Henegouwen MI, Hoekstra OS, Boellaard R, Bossuyt PM, et al. Fluorodeoxyglucose positron emission tomography for evaluating early response during neoadjuvant chemoradiotherapy in patients with potentially curable esophageal cancer. Ann Surg. 2011 Jan;253(1):56-63.

General introduction |
15
Cha
pter
1
35. Dolinsky CM, Mahmoud NN, Mick R, Sun W, Whittington RW, Solin LJ, et al. Effect of time interval between surgery and preoperative chemoradiotherapy with 5-fluorouracil or 5-fluorouracil and oxaliplatin on outcomes in rectal cancer. J Surg Oncol. 2007 Sep 1;96(3):207-12.
36. Francois Y, Nemoz CJ, Baulieux J, Vignal J, Grandjean JP, Partensky C, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol. 1999 Aug;17(8):2396.
37. Tulchinsky H, Shmueli E, Figer A, Klausner JM, Rabau M. An interval >7 weeks between neoadjuvant therapy and surgery improves pathologic complete response and disease-free survival in patients with locally advanced rectal cancer. Ann Surg Oncol. 2008 Oct;15(10):2661-7.
38. Wolthuis AM, Penninckx F, Haustermans K, De Hertogh G, Fieuws S, Van Cutsem E, et al. Impact of interval between neoadjuvant chemoradiotherapy and TME for locally advanced rectal cancer on pathologic response and oncologic outcome. Ann Surg Oncol. 2012 Sep;19(9):2833-41.
39. de Campos-Lobato LF, Geisler DP, da Luz Moreira A, Stocchi L, Dietz D, Kalady MF. Neoadjuvant therapy for rectal cancer: the impact of longer interval between chemoradiation and surgery. J Gastrointest Surg. 2011 Mar;15(3):444-50.
40. Sloothaak DA, Geijsen DE, van Leersum NJ, Punt CJ, Buskens CJ, Bemelman WA, et al. Optimal time interval between neoadjuvant chemoradiotherapy and surgery for rectal cancer. Br J Surg. 2013 Jun;100(7):933-9.
41. Petrelli F, Sgroi G, Sarti E, Barni S. Increasing the Interval Between Neoadjuvant Chemoradiotherapy and Surgery in Rectal Cancer: A Meta-Analysis of Published Studies. Ann Surg. 2013 Nov 20.
42. Ruol A, Rizzetto C, Castoro C, Cagol M, Alfieri R, Zanchettin G, et al. Interval between neoadjuvant chemoradiotherapy and surgery for squamous cell carcinoma of the thoracic esophagus: does delayed surgery have an impact on outcome? Ann Surg. 2010 Nov;252(5):788-96.
43. Kim JY, Correa AM, Vaporciyan AA, Roth JA, Mehran RJ, Walsh GL, et al. Does the timing of esophagectomy after chemoradiation affect outcome? Ann Thorac Surg. 2012 Jan;93(1):207-12; discussion 12-3.
44. Ku GY, Ilson DH. Emerging mAbs for the treatment of esophagogastric cancer. Expert Opin Emerg Drugs. 2014 Dec 6:1-12.
45. Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010 Aug 28;376(9742):687-97.
46. Jankowski J, Coghill G, Hopwood D, Wormsley KG. Oncogenes and onco-suppressor gene in adenocarcinoma of the oesophagus. Gut. 1992 Aug;33(8):1033-8.
47. al-Kasspooles M, Moore JH, Orringer MB, Beer DG. Amplification and over-expression of the EGFR and erbB-2 genes in human esophageal adenocarcinomas. Int J Cancer. 1993 May 8;54(2):213-9.
48. Hardwick RH, Shepherd NA, Moorghen M, Newcomb PV, Alderson D. c-erbB-2 overexpression in the dysplasia/carcinoma sequence of Barrett’s oesophagus. J Clin Pathol. 1995 Feb;48(2):129-32.
49. Polkowski W, van Sandick JW, Offerhaus GJ, ten Kate FJ, Mulder J, Obertop H, et al. Prognostic value of Lauren classification and c-erbB-2 oncogene overexpression in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol. 1999 Apr-May;6(3):290-7.
50. Sanghera SS, Nurkin SJ, Demmy TL. Quality of life after an esophagectomy. Surg Clin North Am. 2012 Oct;92(5):1315-35.
51. Pitney WR, Beard MF. Vitamin B12
deficiency following total gastrectomy. AMA Arch Intern Med. 1955 Apr;95(4):591-3.

| Chapter 1
16
52. Kapadia CR. Vitamin B12
in health and disease: part I--inherited disorders of function, absorption, and transport. Gastroenterologist. 1995 Dec;3(4):329-44.
53. Majumder S, Soriano J, Louie Cruz A, Dasanu CA. Vitamin B12 deficiency in patients undergoing bariatric surgery: preventive strategies and key recommendations. Surg Obes Relat Dis. 2013 Nov-Dec;9(6):1013-9.
54. van Heijl M, Omloo JM, van Berge Henegouwen MI, Busch OR, Tilanus HW, Bossuyt PM, et al. NEOadjuvant therapy monitoring with PET and CT in Esophageal Cancer (NEOPEC-trial). BMC Med Phys. 2008;8:3.

PART IPreoperative analysis and treatment

P. van Hagen
M.C.C.M. Hulshof
J.J.B. van Lanschot
E.W. Steyerberg
M.I. van Berge Henegouwen
B.P.L. Wijnhoven
D.J. Richel
G.A.P. Nieuwenhuijzen
G.A.P. Hospers
J.J. Bonenkamp
M.A. Cuesta
R.J.B. Blaisse
O.R.C. Busch
F.J.W. ten Kate
G.-J. Creemers
C.J.A. Punt
J.T.M. Plukker
H.M.W. Verheul
E.J. Spillenaar Bilgen
H. van Dekken
M.J.C. van der Sangen
T. Rozema
K. Biermann
J.C. Beukema
A.H.M. Piet
C.M. van Rij
J.G. Reinders
H.W. Tilanus
A. van der Gaast
for the CROSS Group
The New England Journal of Medicine 2012; 366:2074-2084

Chapter 2Preoperative chemoradiotherapy for
esophageal or junctional cancer

| Chapter 2
20
ABSTRACT
BACKGROUNDThe role of neoadjuvant chemoradiotherapy in the treatment of patients with esophageal or
esophagogastric-junction cancer is not well established. We compared chemoradiotherapy followed
by surgery with surgery alone in this patient population.
METHODSWe randomly assigned patients with resectable tumors to receive surgery alone or weekly
administration of carboplatin (doses titrated to achieve an area under the curve of 2 mg per milliliter
per minute) and paclitaxel (50 mg per square meter of body-surface area) for 5 weeks and concurrent
radiotherapy (41.4 Gy in 23 fractions, 5 days per week), followed by surgery.
RESULTSFrom March 2004 through December 2008, we enrolled 368 patients, 366 of whom were included
in the analysis: 275 (75%) had adenocarcinoma, 84 (23%) had squamous-cell carcinoma, and 7
(2%) had large-cell undifferentiated carcinoma. Of the 366 patients, 178 were randomly assigned
to chemoradiotherapy followed by surgery, and 188 to surgery alone. The most common major
hematologic toxic effects in the chemoradiotherapy–surgery group were leukopenia (6%) and
neutropenia (2%); the most common major nonhematologic toxic effects were anorexia (5%) and
fatigue (3%). Complete resection with no tumor within 1 mm of the resection margins (R0) was
achieved in 92% of patients in the chemoradiotherapy–surgery group versus 69% in the surgery
group (P<0.001). A pathological complete response was achieved in 47 of 161 patients (29%) who
underwent resection after chemoradiotherapy. Postoperative complications were similar in the two
treatment groups, and in-hospital mortality was 4% in both. Median overall survival was 49.4 months
in the chemoradiotherapy–surgery group versus 24.0 months in the surgery group. Overall survival
was significantly better in the chemoradiotherapy–surgery group (hazard ratio, 0.657; 95% confidence
interval, 0.495 to 0.871; P = 0.003).
CONCLUSIONSPreoperative chemoradiotherapy improved survival among patients with potentially curable
esophageal or esophagogastric-junction cancer. The regimen was associated with acceptable
adverse-event rates.

Preoperative chemoradiotherapy for esophageal or junctional cancer |
21
Cha
pter
2
INTRODUCTION
With new diagnoses in more than 480,000 patients annually, esophageal cancer is the eighth most
common cancer worldwide.1 It is a highly lethal disease, causing more than 400,000 deaths per
year.2 The incidence of esophageal adenocarcinoma is rapidly rising, whereas that of squamous-cell
carcinoma remains unchanged.3 Despite adequate preoperative staging, 25% of patients treated
with primary surgery have microscopically positive resection margins (R1), and the 5-year survival
rate rarely exceeds 40%.4 The role of neoadjuvant chemoradiotherapy has been debated for several
decades. In most randomized trials, no survival benefit could be shown, and the trials were criticized
for inadequate trial design, samples that were too small, and poor outcomes in the surgery-alone
group.
Meta-analyses suggest a survival benefit from neoadjuvant chemoradiotherapy, albeit frequently at
the cost of increased postoperative morbidity and mortality.5,6 We previously reported a phase 2 trial
of neoadjuvant chemoradiotherapy consisting of weekly administration of carboplatin and paclitaxel
with concurrent radiotherapy.7 This regimen was associated with a low rate of serious toxic effects,
and a complete resection with no tumor within 1 mm of the resection margins (R0) was achieved in all
patients who underwent resection. These results encouraged us to initiate a multicenter, randomized,
controlled, phase 3 study comparing neoadjuvant chemoradiotherapy followed by surgery with
surgery alone in patients with potentially curable esophageal or esophagogastricjunction carcinoma.8
METHODS
Eligibility criteria
Patients with histologically confirmed, potentially curable squamous-cell carcinoma, adenocarcinoma, or large-cell undifferentiated carcinoma of the esophagus or esophagogastric junction (i.e., tumors
involving both the cardia and the esophagus on endoscopy) were eligible for inclusion in the study.
The upper border of the tumor had to be at least 3 cm below the upper esophageal sphincter. Patients
who had proximal gastric tumors with minimal invasion of the esophagus were excluded. The length
and width of the tumor could not exceed 8 cm and 5 cm, respectively. Only patients with tumors
of clinical stage T1N1 or T2-3N0-1and no clinical evidence of metastatic spread (M0), according to
the International Union against Cancer (UICC) tumor–node–metastasis (TNM) classification,9 were
enrolled. Eligible patients were 18 to 75 years of age, had a World Health Organization (WHO)
performance status score of 2 or lower (on a scale of 0 to 5, with 0 indicating fully active, 1 unable
to carry out heavy physical work, and 2 up and about more than half the day but unable to work),
and had lost 10% or less of body weight. Patients also had to have adequate hematologic, renal,
hepatic, and pulmonary function, as well as no history of other cancer or previous radiotherapy or
chemotherapy.
All patients provided written informed consent. The institutional review board at each participating
center approved the study protocol.8 The protocol, including the statistical analysis plan, is available
with the full text of this article at NEJM.org. No commercial support was involved in the study; the

| Chapter 2
22
drugs were purchased. No one who is not an author contributed to the manuscript. The first, fourth,
and last authors vouch for the accuracy and completeness of the reported data and the fidelity of the
study to the protocol.
Staging
All patients underwent pretreatment staging. This included a history taking; physical examination;
pulmonary-function tests, routine hematologic and biochemical tests; upper gastrointestinal
endoscopy with histologic biopsy and endoscopic ultrasonography; computed tomography of
the neck, chest, and upper abdomen; and external ultrasonography of the neck, with fine-needle
aspiration of lymph nodes when cancer was suspected. For the final analysis, the available endoscopic
reports were centrally reviewed.
Treatment
Chemotherapy
On days 1, 8, 15, 22, and 29, carboplatin targeted at an area under the curve of 2 mg per milliliter per
minute and paclitaxel at a dose of 50 mg per square meter of body-surface area were administered
intravenously. All patients were intravenously premedicated with dexamethasone, clemastine, and
ranitidine as well as standard antiemetic agents. The patients were closely monitored for toxic effects
of chemotherapy with the use of the National Cancer Institute’s Common Terminology Criteria for
Adverse Events, version 3.0.10
Radiotherapy
A total radiation dose of 41.4 Gy was given in 23 fractions of 1.8 Gy each, with 5 fractions administered
per week, starting on the first day of the first chemotherapy cycle. All patients were treated by means
of external-beam radiation. A detailed description of the methods of administration of chemotherapy
and radiotherapy can be found in Appendix 1 in the Supplementary Appendix, available at NEJM.org.
Surgery
Patients in the chemoradiotherapy–surgery group underwent surgery as soon as possible after
completion of chemoradiotherapy (preferably, within 4 to 6 weeks), and patients in the surgery
group were treated as soon as possible after randomization. A transthoracic approach with two-field
lymph-node dissection was performed for tumors extending proximally to the tracheal bifurcation.
For tumors involving the esophagogastric junction, a transhiatal resection was preferred. Peritruncal
dissection was carried out with both approaches. For all other tumors, the approach depended on
the characteristics of the patient and on local preferences. Gastric-tube reconstruction with a cervical
anastomosis was the preferred technique for restoring the continuity of the digestive tract.

Preoperative chemoradiotherapy for esophageal or junctional cancer |
23
Cha
pter
2
Pathological analysis
Reports on pathological examination had to describe the tumor type and extension, lymph nodes,
and resection margins. In the absence of macroscopic tumor, any abnormal-appearing tissue was
paraffin-embedded in total in order to make an adequate assessment for the presence of residual
tumor and the effects of therapy.
To grade the response to therapy, we classified the degree of histomorphologic regression into
four categories as follows: grade 1, no evidence of vital residual tumor cells (pathological complete
response); grade 2, less than 10% vital residual tumor cells; grade 3, 10 to 50%; and grade 4, more
than 50%.11,12 If a vital tumor was present at 1 mm or less from the proximal, distal, or circumferential
resection margin, it was considered to be microscopically positive (R1).
Follow-up
During the first year after treatment was completed, patients were seen every 3 months. In the
second year, follow-up took place every 6 months, and then at the end of each year until 5 years
after treatment. Late toxic effects, disease recurrence, and death were documented. Recurrences
were scored at the moment of the first recurrence. During follow-up, diagnostic investigations were
performed only when recurrence was suspected.
Statistical analysis
We calculated that 175 patients were needed in each group in order to detect a difference in median
overall survival of 22 months in the chemoradiotherapy–surgery group versus 16 months in the surgery
group (two-sided test; alpha level, 0.05; beta level, 0.80). Stratification factors included histologic tumor
type, treatment center, lymph-node (N) stage as determined by endoscopic ultrasonography, and
WHO performance score. Block randomization was performed centrally by telephone or at the central
trial office, according to computer-generated randomization lists for each stratum, with random block
sizes of 4 or 6.
Data were analyzed according to the intention-to-treat principle. The primary end point was overall
survival. All other described outcomes were secondary end points. No post hoc analyses were
performed. Survival was calculated from the date of randomization until death. All data collected
through December 2010 were included in the analysis, which guaranteed a potential minimal follow-
up of 2 years.
The Kaplan–Meier method was used to estimate survival, with the log-rank test to determine
significance. A Cox proportional-hazards model was used to estimate the treatment effect with
adjustment for prognostic factors for survival. Moreover, Cox models were used to identify possible
interactions in treatment effect between subgroups, both with and without adjustment for prognostic
factors. Subgroups were predefined according to sex, histologic subtype of tumor, clinical N stage,
and WHO performance score. Statistical analysis was performed with the use of SPSS software, version
17.0 (SPSS).

| Chapter 2
24
837 Assessed and operated
for esophageal / EGJ cancer
469 Not randomized
180 Allocated to CRT+S arm 2 Withdrew their consent
7 Did not receive any CRT
168 Underwent surgery
161 Underwent resecon
188 Allocated to S arm
0 Withdrew their consent
186 Underwent surgery 161 Underwent resecon
178 Analyzed
0 Lost to follow-up 0 Lost to follow-up
188 Analyzed
Enrollment
Allocaon
Analysis
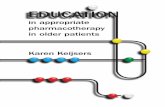
Figure 1. Flow chart
FIGURE 1. Flow chart
RESULTS
Characteristics of the patients
From March 2004 through December 2008, we enrolled 368 patients in the study, of whom 180 were
randomly assigned to the chemoradiotherapy–surgery group, and 188 to the surgery group. Two
patients who were randomly assigned to the chemoradiotherapy–surgery group withdrew consent
and were not included in the analysis (Fig. 1).
Prognostic factors were well balanced between the two treatment groups (Table 1). In both groups,
the median age was 60 years; 134 of 178 patients (75%) in the chemoradiotherapy–surgery group
were men, as compared with 152 of 188 patients (81%) in the surgery group. Most patients (275 of
366 [75%]) had an adenocarcinoma. In both groups, the median tumor length was 4 cm. Most tumors
were located in the distal esophagus (in 211 of 366 patients [58%]) or at the esophagogastric junction
(in 88 [24%]). In the chemoradiotherapy–surgery group, 116 of 178 patients (65%) had positive lymph
nodes as determined by endoscopic ultrasonography, as compared with 120 of 188 (64%) in the
surgery group.

Preoperative chemoradiotherapy for esophageal or junctional cancer |
25
Cha
pter
2
TABLE 1. Characteristics of patients with resectable esophageal or esophagogastric-junction cancer, according to treatment group.*
Characteristic Chemoradiotherapy and Surgery (N = 178)
Surgery Alone (N = 188)
Age — yr
Median 60 60
Range 36-79 36-73
Male sex — no. (%) 134 (75) 152 (81)
Tumor type — no. (%)
Adenocarcinoma 134 (75) 141 (75)
Squamous-cell carcinoma 41 (23) 43 (23)
Other 3 (2) 4 (2)
Tumor length — cm†
Median 4 4
Interquartile range 3–6 3–6
Tumor location — no. (%)†
Esophagus
Proximal third 4 (2) 4 (2)
Middle third 25 (14) 24 (13)
Distal third 104 (58) 107 (57)
Esophagogastric junction 39 (22) 49 (26)
Missing data 6 (3) 4 (2)
Clinical T stage — no. (%)‡
cT1 1 (1) 1 (1)
cT2 26 (15) 35 (19)
cT3 150 (84) 147 (78)
cT4 0 1 (1)
Could not be determined§ 1 (1) 4 (2)
Clinical N stage — no. (%)¶
N0 59 (33) 58 (31)
N1 116 (65) 120 (64)
Could not be determined§ 3 (2) 10 (5)
WHO performance status score — no. (%)ǁ
0 144 (81) 163 (87)
1 34 (19) 25 (13)
* Percentages may not add up to 100 because of rounding. WHO denotes World Health Organization.† Tumor length and location were determined by means of endoscopy.‡ Clinical tumor (cT) stage was assessed by means of endoscopic ultrasonography or computed tomography (CT) and was classified according to the International Union against Cancer (UICC) tumor–node–metastasis (TNM) classification.9
§ This category included patients in whom the tumor could not be fully investigated by means of a transducer for endoscopic ultrasonography owing to a stenosis caused by the tumor.¶ Clinical lymph-node (N) stage was assessed by means of endoscopic ultrasonography, CT, or 18F-fluorodeoxyglucose positron-emission tomography and was classified according to UICC TNM classification.9
|| WHO performance status scores are on a scale of 0 to 5, with lower numbers indicating better performance status; 0 indicates fully active, and 1 unable to carry out heavy physical work.

| Chapter 2
26
Delivery and toxic effects of chemoradiotherapy
Seven patients (4%) in the chemoradiotherapy–surgery group did not receive any chemoradiotherapy:
5 because of disease progression before commencing therapy and 2 because they declined
the therapy. A total of 162 patients (91%) received the full treatment regimen of five cycles of
chemoradiotherapy, and 164 (92%) received the full dose of radiotherapy. Two patients (1%) received
a higher dose of radiotherapy (45.0 and 54.0 Gy, respectively). The most common reason for not
completing all chemotherapy cycles was a low platelet count.
In 12 of 171 patients (7%) who received treatment in the chemoradiotherapy–surgery group, grade
3 hematologic toxic effects were observed; a grade 4 hematologic toxic effect and neutropenic fever
developed in 1 patient. One patient died while awaiting surgery after chemoradiotherapy, probably
owing to a perforation of the esophagus, accompanied by major hemorrhage in the absence of
thrombocytopenia. All other major nonhematologic toxic effects of grade 3 or higher occurred in
less than 13% of patients in this group. All serious adverse events that occurred during treatment are
summarized in Table 2.
Surgery
In the chemoradiotherapy–surgery group, 168 patients (94%) underwent surgery, as compared with
186 (99%) in the surgery group (P = 0.01). Reasons for not undergoing surgery were the patient’s
decision (2 patients in the chemoradiotherapy–surgery group), disease progression during treatment
(7 in the chemoradiotherapy–surgery group and 1 in the surgery group), diagnosis of a second
cancer before surgery (1 in the surgery group), and death before surgery due to toxic effects of
chemoradiotherapy (1). No patients were considered medically unfit for surgery.
The median time between randomization and surgery was 97 days in the chemoradiotherapy–surgery
group and 24 days in the surgery group. The median time between the end of chemoradiotherapy
and surgery was 6.6 weeks (interquartile range, 5.7 to 7.9). In 7 of 168 patients (4%) in the
chemoradiotherapy–surgery group, a resection was not possible because the primary tumor or
lymph nodes were identified during surgery as unresectable, as compared with 25 of 186 patients
(13%) in the surgery group (P = 0.002).
Postoperative complications are summarized in Table 2. No significant differences in the occurrence
of complications were found between the two treatment groups. Six of 168 patients (4%) in the
chemoradiotherapy–surgery group died in the hospital, as did 8 of 186 (4%) in the surgery group (P =
0.70). Four patients (2%) in the chemoradiotherapy– surgery group died within 30 days after surgery,
as compared with 5 (3%) in the surgery group (P = 0.85).

Preoperative chemoradiotherapy for esophageal or junctional cancer |
27
Cha
pter
2
TABLE 2. Adverse events during neoadjuvant chemoradiotherapy and after surgery.*
Event Chemoradio-therapy and Surgery (N = 171)
Surgery Alone
(N = 186)
Postoperative events — no. of patients/total no. (%)†
Pulmonary complications‡ 78/168 (46) 82/186 (44)
Cardiac complications§ 36/168 (21) 31/186 (17)
Chylothorax¶ 17/168 (10) 11/186 (6)
Mediastinitis‖ǁ 5/168 (3) 12/186 (6)
Anastomotic leakage** 36/161 (22) 48/161 (30)
Death
In hospital 6/168 (4) 8/186 (4)
After 30 days 4/168 (2) 5/186 (3)
Events of any grade during chemoradiotherapy — no. of patients (%)
Anorexia 51 (30
Alopecia 25 (15)
Constipation 47 (27)
Diarrhea 30 (18)
Esophageal perforation 1 (1)
Esophagitis 32 (19)
Fatigue 115 (67)
Nausea 91 (53)
Neurotoxic effects 25 (15)
Vomiting 43 (25)
Leukopenia 103 (60)
Neutropenia 16 (9)
Thrombocytopenia 92 (54)
Events of grade ≥3 during chemoradiotherapy — no. of patients (%)
Anorexia 9 (5)
Constipation 1 (1)
Diarrhea 2 (1)
Esophageal perforation 1 (1)
Esophagitis 2 (1)
Fatigue 5 (3)
Nausea 2 (1)
Vomiting 1 (1)
Leukopenia 11 (6)
Neutropenia 4 (2)
Thrombocytopenia 1 (1)
* Adverse events were graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events, version 3.0.10
† Of the 171 patients who received treatment with chemoradiotherapy, 168 underwent surgery.‡ Pulmonary complications were pneumonia (isolation of pathogen from sputum culture and a new or progressive infiltrate on chest radiograph), serious atelectasis (lobar collapse on chest radiograph), pneumothorax (collection of air between the visceral and parietal pleural surfaces, requiring drainage), pleural effusion (collection of fluid between the visceral and parietal pleural surfaces, requiring drainage), pulmonary embolus (embolus detected on spiral CT or a ventilation–perfusion mismatch on a lung scintigram), and acute respiratory failure (partial pressure of arterial oxygen <60 mm Hg while breathing ambient air).

| Chapter 2
28
§ Cardiac complications were arrhythmia (any change in rhythm on the electrocardiogram, requiring treatment), myocardial infarction (two or three of the following: previous myocardial infarction, electrocardiographic changes suggesting myocardial infarction, or enzyme changes suggesting myocardial infarction), and left ventricular failure (marked pulmonary edema on a chest radiograph).¶ Chylothorax was recorded when elevated levels of triglycerides in intrathoracic fluid (>1 mmol per liter [89 mg per deciliter]) were found.|| Mediastinitis was scored when reported by the local investigator.** Anastomotic leakages were recorded when they were diagnosed on physical or radiologic examination in the patients who underwent resection. Leakage was classified as subclinical if it was diagnosed on radiologic examination or endoscopy and as clinical if a salivary fistula was present.
Pathological assessment
An R0 resection was achieved in 148 of 161 patients (92%) in the chemoradiotherapy–surgery group,
as compared with 111 of 161 (69%) in the surgery group (P<0.001). A pathological complete response
(ypT0N0; y denotes underwent neoadjuvant chemoradiotherapy, and p denotes by pathological
assessment) was seen in the resection specimens from 47 patients (29%) in the chemoradiotherapy–
surgery group. A pathological complete response was observed in 28 of 121 patients with
adenocarcinoma (23%) versus 18 of 37 with squamous-cell carcinoma (49%) (P = 0.008). A median
of 15 lymph nodes were resected in patients in the chemoradiotherapy–surgery group, as compared
with 18 in patients in the surgery group (P = 0.77). One or more positive lymph nodes in the resection
specimen were found in 50 patients (31%) in the chemoradiotherapy–surgery group, as compared
with 120 patients (75%) in the surgery group (P<0.001). The pathological findings in all resection
specimens are summarized in Appendix 2 in the Supplementary Appendix.
Survival
For surviving patients, the median follow-up was 45.4 months (range, 25.5 to 80.9). Of the 61 patients
in the chemoradiotherapy–surgery group who underwent resection and died after having been
discharged, 52 (85%) died from recurrent cancer and 9 (15%) from other causes (2 from sepsis, 2
from cardiac failure, 2 from respiratory insufficiency, 1 from kidney failure, 1 from a second primary
tumor, and 1 after reconstructive surgery for a persistent postoperative neo-esophagotracheal
fistula). Of the 83 patients in the surgery group who underwent resection and died after having been
discharged, 78 (94%) died from recurrent cancer, 4 (5%) from other causes (2 from cardiac failure, 1
from respiratory failure, and 1 from a thromboembolic event), and 1 from an unknown cause (P =
0.14). The median disease-free survival for patients who underwent resection was not reached in the
chemoradiotherapy–surgery group and was 24.2 months in the surgery group (hazard ratio, 0.498;
95% confidence interval [CI], 0.357 to 0.693; P<0.001).
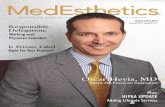
An intention-to-treat analysis that included all patients showed a median overall survival of 49.4
months in the chemoradiotherapy–surgery group versus 24.0 months in the surgery group (P = 0.003
by the log-rank test; hazard ratio, 0.657; 95% CI, 0.495 to 0.871) (Fig. 2A). The respective overall survival
rates at 1, 2, 3, and 5 years were 82%, 67%, 58%, and 47% in the chemoradiotherapy–surgery group,
as compared with 70%, 50%, 44%, and 34% in the surgery group. Adjustment for baseline prognostic
factors led to a similar effect estimate (hazard ratio, 0.665; 95% CI, 0.500 to 0.884).

Preoperative chemoradiotherapy for esophageal or junctional cancer |
29
Cha
pter
2
Follow up in months
a.
Prop
ortio
nal s
urvi
val
No. at riskCRT+surgery 178 145 119 75 49 28Surgery alone 188 131 94 62 33 17Total 366 276 213 137 82 45
p=0.003
CRT+S
Surgery alone
.
.
.
.
.
.
.
.
.
.
.
Follow up in months
b.
Prop
ortio
nal s
urvi
val
No. at risk AC CRT+S 134 107 87 53 34 18AC S 141 99 73 50 25 10SCC CRT+S 41 35 30 21 15 8SCC S 43 29 19 11 8 4Total 359 270 209 135 82 40
AC p=0.049SCC p=0.011
SCC CRT+S
SCC S
AC CRT+S
AC S
.
.
.
.
.
.
.
.
.
.
.
FIGURE 2. a. Kaplan-Meier plot of the estimated overall 5-year survival of patients with esophageal or esophagogastric junction cancer treated with neoadjuvant chemoradiotherapy (CRT) followed by surgery (solid line, n=178) or with surgery alone (interrupted line, n=188), according to an intention-to-treat analysis. b. Kaplan-Meier plot of the estimated overall 5-year survival of patients with adenocarcinoma treated with neoadjuvant chemoradiotherapy followed by surgery (AC CRT+S, solid grey line, n=134) or with surgery alone (AC S, interrupted grey line, n=141), or squamous cell carcinoma treated with CRT followed by surgery (SCC CRT+S, solid black line, n=41) or with surgery alone (SCC S, interrupted black line, n=43), according to an intention-to-treat analysis. Other tumor types were excluded from this analysis.
Figure 3. Forest plot with Hazard Raos (HR) for death (square) and 95% confidence intervals (CI, error bars) for 366 paents with esophageal or esophagogastric juncon cancer, according to baseline characteriscs. Univariate Hazard raos [95% CI] per subgroup category are shown in the le column. Hazard raos [95% CI] for subgroup effect, adjusted for baseline covariates and p-values are shown in the middle and right column respecvely.
Univariate HR [95% CI] Adjusted HR [95%CI] p-value for adjusted HRAll paents 0.66 [0.495-0.871] 0.67 [0.500-0.884] 0.005All paents by subpopulaon
Sex Female 0.91 [0.482-1.729] 0.93 [0.487-1.766] 0.819 Male 0.61 [0.446-0.841] 0.61 [0.447-0.845] 0.003 Histology Other 0.62 [0.056-6.970] Adenocarcinoma 0.73 [0.524-0.998] 0.74 [0.536-1.024] 0.069 SSC 0.45 [0.243-0.844] 0.42 [0.226-0.788] 0.007 Clinical N-stage cN0 0.41 [0.2340.732] 0.42 [0.239-0.747] 0.003 cN1 0.79 [0.567-1.108] 0.80 [0.576-1.130] 0.212 cNx 0.55 [0.066-4.602] WHO performance score WHO 0 0.62 [0.452-0.844] 0.63 [0.456-0.857] 0.004 WHO 1 0.86 [0.433-1.726] 0.90 [0.753-1.631] 0.765
0.0 1.0 2.0 3.0
Favors CRT+S Favors S
FIGURE 3. Forest plot with Hazard Ratios (HR) for death (square) and 95% confidence intervals (CI, error bars) for 366 patients with esophageal or esophagogastric junction cancer, according to baseline characteristics. Univariate Hazard ratios [95% CI] per subgroup category are shown in the left column. Hazard ratios [95% CI] for subgroup effect, adjusted for baseline covariates and p-values are shown in the middle and right column respectively.

| Chapter 2
30
Separate curves for overall survival according to histologic subtype (i.e., adenocarcinoma or squamous-
cell carcinoma) are shown in Figure 2B. The benefit of neoadjuvant chemoradiotherapy on survival
was consistent across subgroups, without any significant interaction identified. Hazard ratios for the
subgroup effects, with and without adjustment for baseline covariates, are shown in Figure 3.
DISCUSSION
This large, randomized trial of neoadjuvant chemoradiotherapy in patients with esophageal or
esophagogastric-junction cancer showed significantly better overall and disease-free survival among
patients who received a chemoradiotherapy regimen based on carboplatin and paclitaxel, followed by
surgery, as compared with those treated with surgery alone. The chemoradiotherapy was associated
with a low frequency of high-grade toxic effects and could be given as an outpatient treatment.
The preoperative treatment did not result in higher postoperative morbidity or early mortality in this
group, as compared with the surgery group. Patients treated with neoadjuvant chemoradiotherapy
followed by surgery had a 34% lower risk of death during follow-up (hazard ratio, 0.657).
The chemoradiotherapy regimen was designed on the basis of our experience in a previous phase 2
study,7 which used the same dosages of radiotherapy and chemotherapy. In that study, it was possible
to administer this regimen on an outpatient basis, and all the patients had resection margins that
were microscopically negative. On the basis of these results, an alteration of the chemoradiotherapy
regimen was not thought to be necessary.
The present study was designed to detect a difference in median survival of 6 months in favor of the
combined regimen of chemoradiotherapy and surgery, as compared with surgery alone (22 months
vs. 16 months). The observed survival in both groups was superior to the anticipated survival and to
that reported in earlier randomized trials.6,13-17 In line with the results of other studies, the survival of
patients treated with surgery alone has improved,18,19 probably owing to ongoing improvements in
surgical techniques, patient selection, and staging methods over the years. The difference in overall
survival in the present study is not due to poor survival in the surgery group but can clearly be
attributed to improved survival in the chemoradiotherapy–surgery group.
In the chemoradiotherapy–surgery group, 94% of patients underwent surgery, and 90% of tumors
could be resected. In the surgery group, 99% of patients underwent surgery, and 86% underwent
resection. These percentages indicate that the preoperative chemoradiotherapy did not significantly
change the individual chance of undergoing a resection.14,15,17 Postoperative complication rates,
although similar between groups, were higher than expected and higher than reported in other
studies.20 We could not find a plausible explanation for this finding, other than the fact that all
postoperative events were meticulously recorded. This relatively high incidence of postoperative
events in both treatment groups did not result in an increased postoperative mortality, which was
low and similar in the two groups.
Complete remission in both the primary tumor and the lymph nodes (ypT0N0) was the best
possible pathological outcome of chemoradiotherapy. The observed percentage of patients with a

Preoperative chemoradiotherapy for esophageal or junctional cancer |
31
Cha
pter
2
pathological complete response (29%) is in line with the reported percentages in other phase 2 and
phase 3 studies.7,13,14,18,21 The substantial downstaging as a result of chemoradiotherapy is also reflected
in the significantly higher percentage of R0 resections in the chemoradiotherapy–surgery group.
Despite the higher rate of pathological complete response among patients with squamous-cell
carcinoma, as compared with those with adenocarcinoma, histologic tumor type was not a prognostic
factor for survival. That is, patients with adenocarcinoma and patients with squamous- cell carcinoma
both benefited from neoadjuvant chemoradiotherapy.
Whether esophageal and esophagogastricjunction tumors should be treated with preoperative
chemoradiotherapy or with perioperative chemotherapy, as suggested by the Medical Research
Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial22 and the Actions Concertées dans
les Cancer Colorectaux et Digestifs (ACCORD) 07 trial,23 is unclear. Both trials included gastric tumors as
well as esophagogastric-junction tumors, whereas in the current trial only patients with esophageal or
esophagogastric-junction tumors were treated. In the POET trial, only patients with esophagogastric-
junction tumors were included and randomly assigned to preoperative chemotherapy or
chemoradiotherapy.24 In that study, there was a nonsignificant trend in favor of preoperative
chemoradiotherapy. Because a substantial percentage of patients in the chemoradiotherapy–surgery
group in the present study (22%) had an esophagogastric-junction tumor, we favor preoperative
chemoradiotherapy for such patients, as was also suggested by the POET study, especially because of
the limited toxic effects that were observed with this treatment regimen.
In conclusion, preoperative chemoradiotherapy (five courses of carboplatin and paclitaxel, with 41.4
Gy of concurrent radiotherapy) is safe and leads to a significant increase in overall survival among
patients with adenocarcinoma or squamous-cell carcinoma of the esophagus or esophagogastric
junction.

| Chapter 2
32
REFERENCES1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008:
GLOBOCAN 2008. Int J Cancer 2010;127:2893-917.
2. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000: the global picture. Eur J Cancer 2001;37:Suppl 8:S4-S66.
3. Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in theUnited States. Cancer 1998;83:2049-53.
4. Kelsen DP, Ginsberg R, Pajak TF, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998; 339:1979-84.
5. Malthaner R, Fenlon D. Preoperative chemotherapy for resectable thoracic esophageal cancer. Cochrane Database Syst Rev 2001;1:CD001556.
6. Urba SG, Orringer MB, Turrisi A, Iannettoni M, Forastiere A, Strawderman M. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol 2001;19:305-13.
7. van Meerten E, Muller K, Tilanus HW, et al. Neoadjuvant concurrent chemoradiation with weekly paclitaxel and carboplatin for patients with oesophageal cancer: a phase II study. Br J Cancer 2006; 94:1389-94.
8. van Heijl M, van Lanschot JJ, Koppert LB, et al. Neoadjuvant chemoradiation followed by surgery versus surgery alone for patients with adenocarcinoma or squamous cell carcinoma of the esophagus (CROSS). BMC Surg 2008;8:21.
9. International Union against Cancer. TNM classification of malignant tumours. 6th ed. New York: Wiley-Liss, 2002.
10. Trotti A, Colevas AD, Setser A, et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003;13:176-81..
11. Mandard AM, Dalibard F, Mandard JC, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma: clinicopathologic correlations. Cancer 1994;73:2680-6.
12. Chirieac LR, Swisher SG, Ajani JA, et al. Posttherapy pathologic stage predicts survival in patients with esophageal carcinoma receiving preoperative chemoradiation. Cancer 2005;103:1347-55.
13. Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med 1996;335:462-7. [Erratum, N Engl J Med 1999;341:384.]
14. Bosset JF, Gignoux M, Triboulet JP, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med 1997;337:161-7.
15. Burmeister BH, Smithers BM, Gebski V, et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomized controlled phase III trial. Lancet Oncol 2005;6:659-68.
16. Lin CC, Hsu CH, Cheng JC, et al. Concurrent chemoradiotherapy with twice weekly paclitaxel and cisplatin followed by esophagectomy for locally advanced esophageal cancer. Ann Oncol 2007;18:93-8.
17. Tepper J, Krasna MJ, Niedzwiecki D, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol 2008;26:1086-92.
18. Lee JL, Park SI, Kim SB, et al. A single institutional phase III trial of preoperative chemotherapy with hyperfractionation radiotherapy plus surgery versus surgery alone for resectable esophageal squamous cell carcinoma. Ann Oncol 2004;15:947-54.

Preoperative chemoradiotherapy for esophageal or junctional cancer |
33
Cha
pter
2
19. Portale G, Hagen JA, Peters JH, et al. Modern 5-year survival of resectable esophageal adenocarcinoma: single institution experience with 263 patients. J Am Coll Surg 2006;202:588-96.
20. Fiorica F, Di Bona D, Schepis F, et al. Preoperative chemoradiotherapy for oesophageal cancer: a systematic review andmeta-analysis. Gut 2004;53:925-30.
21. Gannett DE, Wolf RF, Takahashi GW, et al. Neoadjuvant chemoradiotherapy for esophageal cancer using weekly paclitaxel and carboplatin plus infusional 5-fluorouracil. Gastrointest Cancer Res 2007;1:132-8.
22. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 2006; 355:11-20.
23. Ychou M, Boige V, Pignon JP, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol 2011;29:1715-21.
24. Stahl M, Walz MK, Stuschke M, et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol 2009;27:851-6.

J. Shapiro
J.J.B. van Lanschot
M.C.C.M. Hulshof
P. van Hagen
M.I. van Berge Henegouwen
B.P.L. Wijnhoven
H.W.M. van Laarhoven
G.A.P. Nieuwenhuijzen
G.A.P. Hospers
J.J. Bonenkamp
M.A. Cuesta
R.J.B. Blaisse
O.R.C. Busch
F.J.W. ten Kate
G.-J. Creemers
C.J.A. Punt
J.T.M. Plukker
H.M.W. Verheul
E.J. Spillenaar Bilgen
H. van Dekken
M.J.C. van der Sangen
T. Rozema
K. Biermann
J.C. Beukema
A.H.M. Piet
C.M. van Rij
J.G. Reinders
H.W. Tilanus
E.W. Steyerberg
A. van der Gaast
For the CROSS study group
Lancet Oncology 2015 Sep;16(9):1090-1098

Chapter 3Neoadjuvant chemoradiotherapy plus surgery versus
surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial

| Chapter 3
36
ABSTRACT
BACKGROUND
Initial results of the ChemoRadiotherapy for Oesophageal cancer followed by Surgery Study (CROSS)
comparing neoadjuvant chemoradiotherapy plus surgery versus surgery alone in patients with
squamous cell carcinoma and adenocarcinoma of the oesophagus or oesophagogastric junction
showed a significant increase in 5-year overall survival in favour of the neoadjuvant chemoradiotherapy
plus surgery group after a median of 45 months’ follow-up. In this Article, we report the long-term
results after a minimum follow-up of 5 years.
METHODS
Patients with clinically resectable, locally advanced cancer of the oesophagus or oesophagogastric
junction (clinical stage T1N1M0 or T2–3N0–1M0, according to the TNM cancer staging system, sixth
edition) were randomly assigned in a 1:1 ratio with permuted blocks of four or six to receive either
weekly administration of five cycles of neoadjuvant chemoradiotherapy (intravenous carboplatin
[AUC 2 mg/mL per min] and intravenous paclitaxel [50 mg/m2 of body-surface area] for 23 days) with
concurrent radiotherapy (41·4 Gy, given in 23 fractions of 1·8 Gy on 5 days per week) followed by
surgery, or surgery alone. The primary endpoint was overall survival, analysed by intention-to-treat.
No adverse event data were collected beyond those noted in the initial report of the trial. This trial is
registered with the Netherlands Trial Register, number NTR487, and has been completed.
FINDINGS
Between March 30, 2004, and Dec 2, 2008, 368 patients from eight participating centres (five
academic centres and three large non-academic teaching hospitals) in the Netherlands were enrolled
into this study and randomly assigned to the two treatment groups: 180 to surgery plus neoadjuvant
chemoradiotherapy and 188 to surgery alone. Two patients in the neoadjuvant chemoradiotherapy
group withdrew consent, so a total of 366 patients were analysed (178 in the neoadjuvant
chemoradiotherapy plus surgery group and 188 in the surgery alone group). Of 171 patients who
received any neoadjuvant chemoradiotherapy in this group, 162 (95%) were able to complete the
entire neoadjuvant chemoradiotherapy regimen. After a median follow-up for surviving patients
of 84·1 months (range 61·1–116·8, IQR 70·7–96·6), median overall survival was 48·6 months (95% CI
32·1–65·1) in the neoadjuvant chemoradiotherapy plus surgery group and 24·0 months (14·2–33·7)
in the surgery alone group (HR 0·68 [95% CI 0·53–0·88]; log-rank p=0·003). Median overall survival for
patients with squamous cell carcinomas was 81·6 months (95% CI 47·2–116·0) in the neoadjuvant
chemoradiotherapy plus surgery group and 21·1 months (15·4–26·7) in the surgery alone group (HR
0·48 [95% CI 0·28–0·83]; log-rank p=0·008); for patients with adenocarcinomas, it was 43·2 months
(24·9–61·4) in the neoadjuvant chemoradiotherapy plus surgery group and 27·1 months (13·0–41·2) in
the surgery alone group (HR 0·73 [95% CI 0·55–0·98]; log-rank p=0·038).

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
37
Cha
pter
3
INTERPRETATION
Long-term follow-up confirms the overall survival benefits for neoadjuvant chemoradiotherapy when
added to surgery in patients with resectable oesophageal or oesophagogastric junctional cancer. This
improvement is clinically relevant for both squamous cell carcinoma and adenocarcinoma subtypes.
Therefore, neoadjuvant chemoradiotherapy according to the CROSS trial followed by surgical resection
should be regarded as a standard of care for patients with resectable locally advanced oesophageal or
oesophagogastric junctional cancer.
INTRODUCTION
Oesophageal cancer is an aggressive disease, characterised by a high degree of locoregional and
distant recurrence after primary surgical resection and poor 5-year overall survival that rarely exceeds
40%.1, 2 and 3 Much effort has been put into improving tumour resectability, long-term locoregional
control, and overall survival, through the addition of chemotherapy, radiotherapy, or both, to surgery,
in a neoadjuvant or adjuvant setting.2, 3, 4 and 5 However, many studies have not shown a significant
long-term survival benefit of such approaches.6 and 7
The randomised controlled ChemoRadiotherapy for Oesophageal cancer followed by Surgery Study
(CROSS) trial8 compared neoadjuvant chemoradiotherapy plus surgery versus surgery alone. The
trial enrolled 368 patients between March 30, 2004, and Dec 2, 2008, from eight Dutch participating
centres (five academic centres and three large non-academic teaching hospitals). Initial results were
published in 2012 after a minimum follow-up of 24 months (median follow-up 45 months [range
25·2-80·9, IQR 32·6-60·6]). We recorded an absolute benefit in 5-year overall survival in favour of the
multimodality group. The neoadjuvant chemoradiotherapy regimen was completed by 162 (95%)
of 171 patients who received any neoadjuvant chemoradiotherapy, with a low occurrence of grade
3 or adverse events for this setting (29 [17%] of 171 patients). Furthermore, a microscopically radical
resection (ie, no vital tumour present at <1 mm from the proximal, distal, or circumferential resection
margins) was achieved in 148 (92%) of 161 patients in the multimodality group, compared with 112
(69%) of 162 in the surgery alone group (p<0·001).
In this Article, we investigate the consistency of longer-term results with our previous findings and
analyse secondary endpoints, such as progression-free survival and disease recurrence patterns.
METHODS
Study design and participants
Full details of patients’ eligibility criteria and the procedures of this open-label, multicentre,
randomised controlled trial have been reported previously.8 and 9 In brief, eligible patients were aged
75 years or younger; had adequate haematological, renal, hepatic, and pulmonary function; and a
WHO performance score of 2 or better, without a past or present history of other malignancy. Only

| Chapter 3
38
patients with locally advanced (clinical stage T1N1M0 or clinical stage T2–3N0–1M0, according to
the Union for International Cancer Control [UICC] TNM cancer staging, 6th edition10), histologically
proven, and potentially curable squamous cell carcinoma or adenocarcinoma of the oesophagus or
oesophagogastric junction (i.e., tumours involving both the cardia and the oesophagus on endoscopy)
were eligible for inclusion. The main exclusion criteria were past or current history of malignancy other
than the oesophageal malignancy, previous chemotherapy and/or radiotherapy, and weight loss of
more than 10% of the original bodyweight. The institutional review board at each participating centre
approved the study protocol. All patients provided written informed consent.
Randomisation and masking
Patients were randomly assigned 1:1 to each treatment group, and were stratified according to
histological tumour type (adenocarcinoma vs squamous cell carcinoma), treatment centre, clinical
nodal status (cN0 vs cN1), and WHO performance score (WHO-0 vs WHO-1 vs WHO-2). Randomisation
was done centrally at the Clinical Trial Center at Erasmus MC (Rotterdam, the Netherlands), by computer-
generated randomisation lists for each stratum, with random permuted block sizes of four or six.
Procedures
All patients underwent pretreatment staging, including upper gastrointestinal endoscopy with
histological biopsy and endoscopic ultrasonography; CT scan of the neck, chest, and upper abdomen;
and external ultrasonography of the neck, with fine-needle aspiration of suspected lymph nodes on
indication.
For patients assigned to receive neoadjuvant chemoradiotherapy, carboplatin (AUC 2 mg/mL per
min) and paclitaxel (50 mg/m2 of body-surface area) were administered intravenously for five cycles,
starting on days 1, 8, 15, 22, and 29. A total concurrent radiation dose of 41·4 Gy was given in 23 fractions
of 1·8 Gy, on 5 days per week (excluding weekends), starting on the first day of the first chemotherapy
cycle. The total duration of neoadjuvant treatment was 23 days (5 days per week in weeks 1, 2, 3,
and 4, then 3 days in week 5). If on days 8, 15, 22, or 29 the white blood cell count was lower than
1·0 × 109 cells per L or the platelet count was lower than 50 × 109 per L, administration of neoadjuvant
chemoradiotherapy was delayed by 1 week until recovery above these thresholds. Furthermore, in case
of mucositis with oral ulcers or protracted vomiting despite antiemetic premedication, neoadjuvant
chemoradiotherapy was delayed by 1 week. Further chemotherapy was withheld in case of febrile
neutropenia (defined as a neutrophil count <0·5 × 109 cells per L and a body temperature >38·5°C),
persistent creatinine clearance of less than 50% of the pretreatment level, symptomatic cardiac
arrhythmia or atrioventricular block (with the exception of first-degree atrioventricular block), or other
major organ toxicity at grade 3 or worse (with the exception of oesophagitis). During neoadjuvant
chemoradiotherapy, laboratory tests (including complete blood cell counts and serum creatinine
measurement) were done on a weekly basis, whereas radiological assessments were done only on
indication. All patients in the neoadjuvant chemoradiotherapy plus surgery group were included into

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
39
Cha
pter
3
the intention-to-treat analysis, irrespective of total dose of neoadjuvant chemoradiotherapy received.
Patients in the surgery alone group were operated on as soon as possible, whereas those in the
neoadjuvant chemoradiotherapy plus surgery group were preferably operated on within 4–6
weeks after completion of chemoradiotherapy. For carcinomas at or above the level of the carina, a
transthoracic oesophageal resection with two-field lymph node dissection was done. For carcinomas
located well below the level of the carina, either a transthoracic approach with two-field lymph node
dissection or a transhiatal approach was used, depending on both patient characteristics and local
preferences. For carcinomas involving the oesophagogastric junction, a transhiatal oesophageal
resection was preferred. In both approaches, an upper abdominal lymphadenectomy, including
resection of nodes along the hepatic artery, splenic artery, and left gastric artery, was done.
For TNM classification, tumour grading, and stage grouping, the sixth edition of the UICC TNM
cancer staging was used.10 Proximal, distal, and circumferential resection margins were assessed.
Microscopically radical resection (R0) was defined as a tumour-free resection margin of at least 1 mm.
During the first year after treatment completion, patients were seen every 3 months. In the second
year, follow-up took place every 6 months, and annually thereafter until 5 years after treatment.
Additional interim visits were scheduled if complaints such as renewed dysphagia and unexplained
weight loss or pain arose before the next scheduled visit. Diagnostic investigations were only
undertaken as necessary during follow-up. No data for adverse events were collected beyond the
initial report of this trial.8
Outcomes
The primary endpoint was overall survival, which was calculated from the date of randomisation to
the date of all-cause death or to the last day of follow-up. Secondary endpoints included progression-
free survival and progression-free interval. Progression-free survival was defined as the interval
between randomisation and the earliest occurrence of disease progression resulting in primary (or
peroperative) irresectability of disease, locoregional recurrence (after completion of therapy), distant
dissemination (during or after completion of treatment), or death from any cause. This definition
for progression-free survival was taken from the modified STEEP criteria for neoadjuvant treatment
trials.11 and 12 The last day of follow-up for progression-free survival varied, depending on the most
recent (scheduled) contact with the patient. Progression-free interval was similar to progression-
free survival, with the difference that treatment-related deaths and non-oesophageal cancer-related
deaths were not counted as events. Locoregional progression was defined as either progression of
locoregional disease during treatment (resulting in irresectability) or as locoregional recurrence after
completion of treatment. Locoregional sites included the mediastinum, the supraclavicular region,
and the coeliac trunk region. Distant progression was defined as occurrence of disseminated disease,
either during or after completion of treatment. Distant disease included cervical and (para-aortic)
lymph node dissemination below the level of the pancreas, malignant pleural effusions, peritoneal
carcinomatosis, and further haematogenous (organ) dissemination.

| Chapter 3
40
Statistical analysis
Data were analysed according to an intention-to-treat principle. To detect a difference of 6 months in
median overall survival (22 months in the neoadjuvant chemoradiotherapy plus surgery group vs 16
months in the surgery alone group, according to a two-sided test with αlevel 0·05 and β level 0·80),
we calculated that we needed to enrol at least 175 patients in each treatment group. The statistical
significance level was set to 0·05.
We used the Kaplan-Meier method to estimate overall and progression-free survival, with the log-rank
test to ascertain significance. We used univariable and multivariable Cox proportional hazards models
to establish the effect of neoadjuvant chemoradiotherapy in subgroups, adjusting for baseline
covariates.8 Univariable Cox regression modelling was used to analyse differences in progression-free
interval between treatment groups, expressed as hazard ratios (HRs). Follow-up time was divided to
study the temporal distribution of disease progression. Three separate analyses were done, including
follow-up until 6 months, 12 months, and 24 months after randomisation. Progression was defined
as locoregional or distant. Patients in whom both types of disease progression occurred had events
scored in both categories. In the scoring of disease progression in one category, disease progression in
the other category and death without progression were censored. For each timepoint, we compared
the number of events between treatment groups, before the cutoff timepoint and afterwards.
Statistical analysis was done by JS and EWS, using SPSS version 21.0. This trial is registered with the
Netherlands Trial Register, number NTR487.
Role of the funding source
The funder of the study had no role in the study design, data collection, data analysis, data
interpretation, or writing of the report. The corresponding author had full access to all the data in the
study and had final responsibility for the decision to submit for publication.
RESULTS
368 patients from eight participating centres (five academic centres and three large non-academic
teaching hospitals) in the Netherlands were enrolled in the study. 180 patients were randomly
assigned to the neoadjuvant chemoradiotherapy plus surgery group (of whom two later withdrew
consent and were not included in the analysis), and 188 were randomly assigned to the surgery alone
group (figure 1).
Baseline characteristics were well balanced between the two treatment groups (table 1). One
patient in the surgery alone group was originally misclassified as not having received a resection.
However, in the present update, we discovered that this patient had undergone a resection abroad.
This misclassification had no effect on current or previous analyses because of the intention-to-
treat principle. Furthermore, a patient in the neoadjuvant chemoradiotherapy plus surgery group

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
41
Cha
pter
3
moved abroad and was therefore lost to follow-up 73 months after randomisation. Of 171 patients
who received any neoadjuvant chemoradiotherapy in this group, 162 (95%) were able to complete
the entire neoadjuvant chemoradiotherapy regimen. 13 (8%) of 171 patients had grade 3 or worse
haematological toxicity and 18 (11%) had grade 3 or worse non-haematological toxicity. The most
common grade 3 or worse toxicities were leucopenia in 11 (6%) of 171 patients, anorexia in nine (5%),
and fatigue in five (3%).8 In the neoadjuvant chemoradiotherapy plus surgery group, 161 (90%) of
178 patients underwent resection, compared with 162 (86%) of 188 in the surgery alone group. The
proportion of patients with transhiatal resections was similar between both treatment groups (72
[45%] of 161 in the neoadjuvant chemoradiotherapy plus surgery group and 72 [44%] of 162 in the
surgery alone group; χ2=0·01, p=0·96).
837 patients assessed and operated for esophageal or esophagogastric junction cancer
469 excluded
368 patients enrolled and randomly assigned
188 assigned to surgery alone 187 underwent surgery* 161 underwent resection
180 assigned to neoadjuvant chemoradiotherapy and surgery 2 withdrew their consent 5 received CRT only 5 underwent surgery only 5 received neither CRT nor surgery 161 underwent resection
178 were included in the analysis
188 were included in the analysis
FIGURE 1. Trial profile. * One patient had disease progression in waiting period to surgery.

| Chapter 3
42
TABLE 1. Baseline characteristics.
Neoadjuvant chemoradio-therapy plus surgery (n=178) Surgery alone (n=188)
Age, years 60 (55–67) 60 (53–66)
Sex
Women 44 (25%) 36 (19%)
Men 134 (75%) 152 (81%)
Tumour histology
Squamous cell carcinoma 41 (23%) 43 (23%)
Adenocarcinoma 134 (75%) 141 (75%)
Could not be established 3 (2%) 4 (2%)
Tumour length, cm 4 (3–6) 4 (3–6)
Tumour location
Proximal third oesophagus 4 (2%) 4 (2%)
Middle third oesophagus 25 (14%) 24 (13%)
Distal third oesophagus 104 (58%) 107 (57%)
Oesophagogastric junction 39 (22%) 49 (26%)
Missing data 6 (3%) 4 (2%)
Clinical tumour (cT) stage
cT1 1 (1%) 1 (1%)
cT2 26 (15%) 35 (19%)
cT3 150 (84%) 147 (78%)
cT4 0 1 (1%)
Could not be established 1 (1%) 4 (2%)
Clinical nodal (cN) stage
cN0 59 (33%) 58 (31%)
cN1 116 (65%) 120 (64%)
Could not be established 3 (2%) 10 (5%)
WHO performance score
0 144 (81%) 163 (87%)
1 34 (19%) 25 (13%)
Data are median (IQR) or n (%).
The final day of follow-up was Dec 31, 2013, guaranteeing a minimum potential follow-up of 60
months for all included patients. At the time of this analysis, median follow-up for surviving patients
was 84·1 months (range 61·1-116·8; IQR 70·7-96·6). Of the 366 analysed patients, 126 were still alive at
the final analysis (73 [41%] of 178 patients in the neoadjuvant chemoradiotherapy plus surgery group
and 53 [28%] of 188 in the surgery alone group). These results correspond with 19 and 21 additional

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
43
Cha
pter
3
deaths, respectively, since the last follow-up of the original publication.8 Median overall survival was
48·6 months (95% CI 32·1-65·1) in the neoadjuvant chemoradiotherapy plus surgery group and 24·0
months (14·2-33·7) in the surgery alone group (HR 0·68 [95% CI 0·53-0·88]; figure 2A). Median overall
survival for patients with squamous cell carcinomas was 81·6 months (95% CI 47·2-116·0) in the
neoadjuvant chemoradiotherapy plus surgery group and 21·1 months (15·4-26·7) in the surgery alone
group (HR 0·48 [95% CI 0·28-0·83]), and median overall survival for patients with adenocarcinomas was
43·2 months (24·9-61·4) in the neoadjuvant chemoradiotherapy plus surgery group and 27·1 months
(13·0-41·2) in the surgery alone group (HR 0·73 [95% CI 0·55-0·98]; figure 2B). Overall survival was 81%
(95% CI 76-86) at 1 year, 67% (60-74) at 2 years, 58% (51-65) at 3 years, and 47% (39-54) at 5 years in the
neoadjuvant chemoradiotherapy plus surgery group, compared with 70% (63-76), 50% (43-57), 44%
(37-51), and 33% (26-40), respectively, in the surgery alone group (HR 0·57 [95% CI 0·37-0·88] at 1 year,
0·59 [0·43-0·82] at 2 years, 0·65 [0·49-0·88] at 3 years, and 0·67 [0·51-0·87] at 5 years). During follow-up,
16 patients died from treatment-related causes (ie, during neoadjuvant chemoradiotherapy or during
postoperative hospital stay), of whom nine were in the neoadjuvant chemoradiotherapy plus surgery
group and seven in the surgery alone group. 23 patients died from non-disease-related causes beyond
the first 90 days postoperatively (13 in the neoadjuvant chemoradiotherapy plus surgery group and
ten in the surgery alone group).
The estimated number of patients who need to be treated to prevent one additional death at 5
years was 7·1 (95% CI 4·6-13·2).13 The overall survival benefit of neoadjuvant chemoradiotherapy plus
surgery was generally confirmed across subgroups (table 2). The concordance of the multivariable
model for overall survival in all patients was 0·584.15 The proportionality of hazards assumption for the
main analysis was not violated (χ2=0·77, p=0·38).16
Of the 366 analysed patients, 116 were alive and disease free (eventually without evidence of
recurrent disease) at final analysis: 69 (39%) of 178 patients in the neoadjuvant chemoradiotherapy
plus surgery group and 47 (25%) of 188 patients in the surgery alone group. Median progression-
free survival was 37·7 months (95% CI 23·7-51·8) in the neoadjuvant chemoradiotherapy plus surgery
group and 16·2 months (10·7-21·7) in the surgery alone group (HR 0·64 [95% CI 0·49-0·82]; figure
3A). Median progression-free survival for patients with squamous cell carcinomas was 74·7 months
(95% CI 55·1-94·4) in the neoadjuvant chemoradiotherapy plus surgery group and 11·6 months (4·4-
18·8) in the surgery alone group (HR 0·48 [95% CI 0·28-0·82]; figure 3B). Median progression-free
survival for patients with adenocarcinomas was 29·9 months (95% CI 15·9-43·9) in the neoadjuvant
chemoradiotherapy plus surgery group and 17·7 months (11·9-23·5) in the surgery alone group (HR
0·69 [95% CI 0·52-0·92]; figure 3B). Progression-free survival in the neoadjuvant chemoradiotherapy
plus surgery group was 71% (95% CI 65-78) at 1 year, 60% (52-67) at 2 years, 51% (43-58) at 3 years,
and 44% (37-52) at 5 years, compared with 54% (47-61), 41% (34-48), 35% (28-42), and 27% (21-33),
respectively, in the surgery alone group (HR 0·55 [95% CI 0·39-0·77] at 1 year, 0·57 [0·42-0·77] at 2 years,
0·62 [0·47-0·82] at 3 years, and 0·61 [0·47-0·78] at 5 years).

| Chapter 3
44
TABL
E 2.
Uni
varia
ble
and
mul
tivar
iabl
e H
Rs fo
r all-
caus
e m
orta
lity,
acc
ordi
ng to
sub
grou
p ch
arac
teris
tics.
Uni
vari
able
ana
lysi
sM
ultiv
aria
ble
anal
ysis
Neo
adju
vant
ch
emor
adio
ther
apy
plus
sur
gery
(n=1
78)
Surg
ery
alon
e (n
=188
)In
tera
ctio
n p
valu
eH
R (9
5% C
I)p
valu
eaH
R (9
5% C
I)p
valu
e
All
patie
nts
105
(59%
)13
5 (7
2%)
0·07
80·
68 (0
·53-
0·88
)0·
003
0·69
(0·5
3-0·
89)
0·00
4
Sex
0·45
1
Wom
en25
(14%
)24
(13%
)0·
83 (0
·47-
1·45
)0·
502
0·85
(0·4
8-1·
50)
0·57
0
Men
80 (4
5%)
111
(59%
)0·
65 (0
·49-
0·86
)0·
003
0·66
(0·4
9-0·
88)
0·00
4
Tum
our h
isto
logy
0·20
7
Squa
mou
s ce
ll ca
rcin
oma
21 (1
2%)
32 (1
7%)
0·48
(0·2
8-0·
83)
0·00
90·
46 (0
·26-
0·79
)0·
005
Ade
noca
rcin
oma
81 (4
6%)
101
(54%
)0·
73 (0
·55-
0·98
)0·
037
0·75
(0·5
6-1·
01)
0·05
9
Clin
ical
nod
al (c
N) s
tage
0·17
0
cN0
27 (1
5%)
42 (2
2%)
0·50
(0·3
1-0·
80)
0·00
40·
49 (0
·30-
0·80
)0·
004
cN1
77 (4
3%)
85 (4
5%)
0·81
(0·5
9-1·
10)
0·17
60·
83 (0
·61-
1·13
)0·
237
WH
O p
erfo
rman
ce s
core
0·72
9
084
(47%
)11
7 (6
2%)
0·66
(0·5
0-0·
88)
0·00
40·
67 (0
·51-
0·90
)0·
006
121
(12%
)18
(10%
)0·
75 (0
·40-
1·41
)0·
367
0·79
(0·4
1-1·
51)
0·47
3
Dat
a ar
e n
(%),
unle
ss o
ther
wis
e in
dica
ted.
Mul
tivar
iabl
e an
alys
is in
clud
ed th
e fo
llow
ing
base
line
char
acte
ristic
s: se
x, tu
mou
r his
tolo
gy, c
linic
al ly
mph
nod
e (N
) sta
ge, a
nd
WH
O p
erfo
rman
ce s
core
. Clin
ical
N s
tage
was
bas
ed o
n en
dosc
opic
ultr
ason
ogra
phy,
CT,
or 18
F-flu
orod
eoxy
gluc
ose
PET
(in w
hich
cN
0=no
nod
es s
uspe
cted
or p
ositi
ve,
and
cN1=
at le
ast
one
node
sus
pect
ed o
r po
sitiv
e). W
HO
per
form
ance
sta
tus:14
gra
de 0
=ab
le t
o ca
rry
out
all n
orm
al a
ctiv
ity w
ithou
t re
stric
tions
, gra
de 1
=re
stric
ted
in
phys
ical
ly s
tren
uous
act
ivity
but
am
bula
tory
and
abl
e to
do
light
wor
k. H
R=ha
zard
ratio
(nC
RT p
lus
surg
ery
vs s
urge
ry a
lone
). aH
R=ad
just
ed h
azar
d ra
tio.

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
45
Cha
pter
3
The estimated number of patients who need to be treated to prevent one additional disease
progression at 5 years was 6·1 (95% CI 4·2–10·0).13 The progression-free survival benefit of neoadjuvant
chemoradiotherapy plus surgery was generally confirmed across subgroups (appendix p 3).
TABLE 3. Patients with locoregional or distant progression in the two treatment groups.
Neoadjuvant chemoradiotherapy plus surgery (n=178)
Surgery alone (n=188)
HR (95% CI) p value
Locoregional progression 39 (22%) 72 (38%) 0·45 (0·30–0·66) <0·0001
Distant progression 70 (39%) 90 (48%) 0·63 (0·46–0·87) 0·0040
Overall progression 87 (49%) 124 (66%) 0·58 (0·44–0·76) <0. 0001
Data are n (%), unless otherwise indicated. Comparison between treatment groups was based on univariable cause-specific Cox regression modelling of progression-free intervals. Deaths from non-disease-related causes were censored. Overall progression was defined as either locoregional progression or distant progression. Patients with both locoregional disease progression and distant disease progression (22 patients in the neoadjuvant chemoradiotherapy plus surgery group and 38 in the surgery alone group) were counted in both locoregional progression and distant progression categories. HR=hazard ratio.
We studied the progression-free intervals, in addition to progression-free survival, to focus in more
detail on recurrence patterns in both treatment groups. From randomisation, 211 patients showed
disease progression (table 3). In the neoadjuvant chemoradiotherapy plus surgery group, 87 patients
had disease progression, of whom 39 had locoregional progression and 70 had distant progression
(22 patients had both locoregional and distant progression). In the surgery alone group, 124 patients
had disease progression, of whom 72 had locoregional progression and 90 had distant progression
(38 patients had both). Disease progression during treatment (causing adjustment from curative
to palliative treatment intent) occurred in 17 patients in the neoadjuvant chemoradiotherapy plus
surgery group and in 26 patients in the surgery alone group.
Compared with patients in the surgery alone group, those in the neoadjuvant chemoradiotherapy
plus surgery group had significantly less locoregional progression and significantly less distant
progression (table 3). The reduction in locoregional progression was already apparent during the first
6 months of follow-up and remained significant after the first 24 months of follow-up (appendix p
5). This finding indicates that the effect of reduction in locoregional progression continued for an
extended period after randomisation. The reduction in distant progression was also already recorded
during the first 6 months of follow-up and remained significant during the first 24 months of follow-
up but not thereafter, which suggests that the reduction in distant progression mainly occurred
within the first 24 months after randomisation.

| Chapter 3
46
FIG
URE
2. O
vera
ll su
rviv
al.
(A) B
y tr
eatm
ent g
roup
. (B)
By
trea
tmen
t gro
up a
nd h
isto
logi
cal t
umou
r typ
e; fo
ur p
atie
nts i
n th
e su
rger
y al
one
grou
p an
d th
ree
in th
e ne
oadj
uvan
t che
mor
adio
ther
apy
plus
su
rger
y gr
oup
wer
e ex
clud
ed fr
om th
is a
naly
sis
beca
use
thei
r his
tolo
gica
l tum
our t
ype
coul
d no
t be
asce
rtai
ned.
SCC
=sq
uam
ous
cell
carc
inom
a. A
C=
aden
ocar
cino
ma.

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
47
Cha
pter
3
FIG
URE
3. P
rogr
essi
on-fr
ee s
urvi
val
(A)B
y tr
eatm
ent g
roup
. (B)
By
trea
tmen
t gro
up a
nd h
isto
logi
cal t
umou
r typ
e; fo
ur p
atie
nts
in th
e su
rger
y al
one
grou
p an
d th
ree
in th
e ne
oadj
uvan
t che
mor
adio
ther
apy
plus
sur
gery
gro
up w
ere
excl
uded
from
this
ana
lysi
s be
caus
e hi
stol
ogic
al tu
mou
r typ
e co
uld
not b
e as
cert
aine
d. S
CC=
squa
mou
s ce
ll ca
rcin
oma.
AC
=ad
enoc
arci
nom
a

| Chapter 3
48
DISCUSSION
These long-term results, after a median follow-up for surviving patients of 84 months, confirm the
initially reported survival benefit for neoadjuvant chemoradiotherapy plus surgery compared with
surgery alone. The improvement in distant disease control occurred within the first 2 years after
initiation of treatment, whereas the improvement in locoregional control continued for a longer
period. These findings further support the clinical value of this multimodality treatment strategy.
The overall survival benefit and the progression-free survival benefit were confirmed for both
histological subtypes of oesophageal or oesophagogastric junctional cancer and for other clinically
relevant subgroups. Although univariable and multivariable hazard ratios for individual subgroups
were reported for informative purposes, no significant interactions in treatment effect were identified
for any of the subgroups, which means that differences in treatment effect between subgroups
could well have arisen by chance, and the overall treatment effect should be regarded as valid for all
considered subgroups. In other words, no clear evidence exists to support the assumption that the
adjusted overall treatment effect of neoadjuvant chemoradiotherapy does not also apply to patients
with adenocarcinoma. We therefore conclude that both patients with squamous cell carcinoma and
those with adenocarcinoma benefit significantly from the CROSS multimodality treatment regimen.
The addition of neoadjuvant chemoradiotherapy to primary surgery significantly improved
locoregional disease control. Notably, the largest reported trials with neoadjuvant chemotherapy
only showed limited improvement in rates of R0 resection, pathologically complete response, and
locoregional recurrence. Furthermore, two small randomised trials17 and 18 comparing neoadjuvant
chemotherapy plus surgery to neoadjuvant chemoradiotherapy plus surgery both reported similar R0
resection rates between treatment groups, but significantly higher pathologically complete response
rates and lower locoregional recurrence rates in the neoadjuvant chemoradiotherapy plus surgery
groups. Therefore, the results from these trials point towards neoadjuvant radiotherapy combined
with sensitising chemotherapy rather than neoadjuvant chemotherapy alone as the likely cause of
improved locoregional control, as achieved in the CROSS trial.
In the CROSS trial, not only locoregional control, but also distant disease control improved significantly
in the neoadjuvant chemoradiotherapy plus surgery group. Theoretically, several potential
explanations exist for this improved distant disease control. First, if fewer locoregional recurrences
occur, then possibly less distant dissemination develops from these locoregional recurrences.
Second, effective treatment of the primary tumour in the presence of disseminated disease has been
reported to prolong survival in some cancer types.19 and 20 Therefore, a mechanism by which improved
locoregional control might improve distant disease control could be merely control of the primary
tumour itself, thereby removing a presently unknown stimulus for disseminated tumour outgrowth.
A third explanation is that improved distant disease control could be caused by a direct systemic
effect of chemotherapy. In the present study, we recorded a significant reduction in distant disease
progression already within the first 6 months after randomisation (appendix p 5). Such an early
reduction in distant disease progression, without evidence of a reduction beyond the first 24 months,

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
49
Cha
pter
3
supports a direct systemic effect of this neoadjuvant chemotherapy regimen. The reduction in distant
disease progression achieved by this neoadjuvant chemoradiotherapy regimen is similar to reductions
achieved with more protracted (and more toxic) perioperative chemotherapy regimens.4 and 5
Results from this trial might not be readily extrapolated to patients with poorer performance status,
older patients, or those with tumours located in the proximal or middle oesophagus, because of the
relative scarcity of patients in these categories. The value of this treatment regimen will need to be
confirmed for these patients in future follow-up studies.
Despite recent advances in curative treatment of oesophageal or junctional cancers, the benefit
of (neo)adjuvant treatment is generally quite limited and a definitive statement on the optimum
perioperative treatment in terms of survival is still absent. A recent meta-analysis suggested a
(non-significant) advantage of neoadjuvant chemoradiotherapy over neoadjuvant chemotherapy
alone in both a direct comparison (HR 0·77 [95% CI 0·53–1·12]) and in an indirect comparison (0·88
[0·76–1·01]).7 The ongoing Japanese randomised NExT trial (JCOG1109)21 and the Irish randomised
Neo-AEGIS trial (ICORG 10-14)22 will hopefully provide more definitive evidence on the best possible
perioperative treatment for squamous cell carcinoma and adenocarcinoma, respectively. Unless
convincing results to the contrary become available, strong evidence from the CROSS trial continues
to support neoadjuvant chemoradiotherapy as a standard of care for both squamous cell carcinoma
and adenocarcinoma of the oesophagus or oesophagogastric junction.
In conclusion, chemoradiotherapy according to the CROSS regimen improves long-term overall and
progression-free survival in patients with oesophageal and junctional cancer. This improvement is
statistically significant and clinically relevant for both squamous cell carcinoma and adenocarcinoma
subtypes. Neoadjuvant chemoradiotherapy according to CROSS followed by surgical resection
should be viewed as a standard of care for patients with resectable locally advanced oesophageal or
junctional cancer.

| Chapter 3
50
REFERENCES1. JBF Hulscher, JW van Sandick, AGEM de Boer, et al. Extended transthoracic resection compared with limited
transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med, 347 (2002), pp. 1662–1669
2. DP Kelsen, KA Winter, LL Gunderson, et al. Long-term results of RTOG trial 8911 (USA Intergroup 113): a random assignment trial comparison of chemotherapy followed by surgery compared with surgery alone for esophageal cancer. J Clin Oncol, 25 (2007), pp. 3719–3725
3. WH Allum, SP Stenning, J Bancewicz, PI Clark, RE Langley. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol, 27 (2009), pp. 5062–5067
4. D Cunningham, WH Allum, SP Stenning, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer N Engl J Med, 355 (2006), pp. 11–20
5. M Ychou, V Boige, JP Pignon, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol, 29 (2011), pp. 1715–1721
6. V Gebski, B Burmeister, BM Smithers, et al. Survival benefits from neoadjuvant chemoradiotherapy or chemotherapy in oesophageal carcinoma: a meta-analysis. Lancet Oncol, 8 (2007), pp. 226–234
7. KM Sjoquist, BH Burmeister, BM Smithers, et al. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol, 12 (2011), pp. 681–692
8. P van Hagen, MC Hulshof, JJ van Lanschot, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med, 366 (2012), pp. 2074–2084
9. M van Heijl, JJB van Lanschot, LB Koppert, et al.Neoadjuvant chemoradiation followed by surgery versus surgery alone for patients with adenocarcinoma or squamous cell carcinoma of the esophagus (CROSS). BMC Surg, 8 (2008), p. 21
10. LH Sobin, C Wittekind, et al. TNM classification of malignant tumors (6th edn), Wiley-Liss, New York (2002)
11. CA Hudis, WE Barlow, JP Costantino, et al. Proposal for standardized definitions for efficacy end points in adjuvant breast cancer trials: the STEEP system. J Clin Oncol, 25 (2007), pp. 2127–2132
12. D Fumagalli, PL Bedard, Z Nahleh, et al. A common language in neoadjuvant breast cancer clinical trials: proposals for standard definitions and endpoints. Lancet Oncol, 13 (2012), pp. e240–e248
13. DG Altman, PK Andersen. Calculating the number needed to treat for trials where the outcome is time to an event. BMJ, 319 (1999), pp. 1492–1495
14. MM Oken, RH Creech, DC Tormey, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol, 5 (1982), pp. 649–655
15. FE Harrell Jr, RM Califf, DB Pryor, KL Lee, RA Rosati. Evaluating the yield of medical tests. JAMA, 247 (1982), pp. 2543–2546
16. PM Grambsch, TM Therneau. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika, 81 (1994), pp. 515–526
17. M Stahl, MK Walz, M Stuschke, et al. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol, 27 (2009), pp. 851–856
18. BH Burmeister, JM Thomas, EA Burmeister, et al. Is concurrent radiation therapy required in patients receiving preoperative chemotherapy for adenocarcinoma of the oesophagus? A randomised phase II trial. Eur J Cancer, 47 (2011), pp. 354–360

Neoadjuvant chemoradiotherapy for oesophageal or junctional cancer (CROSS): long-term results |
51
Cha
pter
3
19. RC Flanigan, SE Salmon, BA Blumenstein, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med, 345 (2001), pp. 1655–1659
20. E Rapiti, HM Verkooijen, G Vlastos, et al. Complete excision of primary breast tumor improves survival of patients with metastatic breast cancer at diagnosis. J Clin Oncol, 24 (2006), pp. 2743–2749
21. K Nakamura, K Kato, H Igaki, et al . Three-arm phase III trial comparing cisplatin plus 5-FU (CF) versus docetaxel, cisplatin plus 5-FU (DCF) versus radiotherapy with CF (CF-RT) as preoperative therapy for locally advanced esophageal cancer (JCOG1109, NExT study). Jpn J Clin Oncol, 43 (2013), pp. 752–755
22. N Keegan, F Keane, S Cuffe, M Cunningham, N Ravi, G Lee. ICORG 10-14: Neo-AEGIS: a randomized clinical trial of neoadjuvant and adjuvant chemotherapy (modified MAGIC regimen) versus neoadjuvant chemoradiation (CROSS protocol) in adenocarcinoma of the esophagus and esophagogastric junction. Proc Am Soc Clin Oncol, 32 (5 suppl) (2014) abstr TPS4145.

P. van Hagen
J. Shapiro
H.F. Lingsma
B.P.L. Wijnhoven
K. Biermann
F.J.W. ten Kate
E.W. Steyerberg
A. van der Gaast
J.J.B. van Lanschot
on behalf of the CROSS Study Group
Annals of Surgery 2014 Nov;260(5):807-13

Chapter 4Prolonged time to surgery after neoadjuvant
chemoradiotherapy increases histopathological response without affecting survival in patients
with esophageal or junctional cancer

| Chapter 4
54
ABSTRACT
OBJECTIVE
To determine the relation between time to surgery (TTS) after neoadjuvant chemoradiotherapy
(nCRT) and pathologically complete response (pCR), surgical outcome, and survival in patients with
esophageal cancer.
BACKGROUND
Standard treatment for potentially curable esophageal cancer is nCRT plus surgery after 4 to 6 weeks.
In rectal cancer patients, evidence suggests that prolonged TTS is associated with a higher pCR rate
and possibly with better survival.
METHODS
We identified patients treated with nCRT plus surgery for esophageal cancer between 2001 and 2011.
TTS (last day of radiotherapy to day of surgery) varied mainly for logistical reasons. Minimal follow-
up was 24 months. The effect of TTS on pCR rate, postoperative complications, and survival was
determined with (ordinal) logistic, linear, and Cox regression, respectively.
RESULTS
In total, 325 patients were included. Median TTS was 48 days (p25-p75 = 40-60). After 45 days, TTS was
associated with an increased probability of pCR [odds ratio (OR) = 1.35 per additional week of TTS,
P = 0.0004] and a small increased risk of postoperative complications (OR = 1.20, P = 0.976 and
P = 0.139, respectively).
CONCLUSIONS
Prolonged TTS after nCRT increases the probability of pCR and is associated with a slightly increased
probability of postoperative complications, without affecting disease-free and overall survivals. We
conclude that TTS can be safely prolonged from the usual 4 to 6 weeks up to at least 12 weeks,
which facilitates a more conservative wait-and-see strategy after neoadjuvant chemoradiotherapy to
be tested.

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
55
Cha
pter
4
INTRODUCTION
Recent studies show that, in patients with potentially curable esophageal or esophagogastric junction
cancer, the addition of neoadjuvant chemoradiotherapy (nCRT) to surgery improves locoregional
control and long-term survival.1,2 Therefore, nCRT plus surgery has become the standard of care for
patients with potentially curable esophageal or junctional cancer in many countries.
Reasons for prolonged time to surgery (TTS) after nCRT include patients’ malnutrition or poor physical
status, comorbidities such as infections and cardiopulmonary problems, and logistical problems such
as hospital bed and operating room availability.
Tumor response to neoadjuvant therapy is classified in several tumor regression grading (TRG)
systems.3-6 A pathologically complete response (pCR; ie, no viable tumor cells found in the resection
specimen) has been recognized as a valuable prognostic factor for long-term survival.3,7-10 It remains
unclear, however, whether prolonged TTS has an impact on pCR rate, on short-term surgical outcome
and on long-term survival.
Theoretically, prolonged TTS might increase pCR rate and possibly improve disease-free survival
(DFS) because of a prolonged effect of nCRT. Conversely, prolonged TTS might lead to residual tumor
outgrowth, increased difficulty of surgical resection with a higher postoperative complication rate,
and possibly a worse overall survival (OS).
In rectal cancer patients, several studies have shown that prolonged TTS probably increases the
percentage of pathologically complete responders.11-18 Perioperative morbidity and mortality, DFS
and OS, seem less clearly correlated with TTS.12,13,15-22 Comparable studies in esophageal cancer
patients have shown no effect of TTS on pCR rate and no (or little) effect on DFS.23,24
We aimed to investigate the impact of TTS after nCRT on pCR rate, short-term surgical outcome, and
DFS and OS in a cohort of patients with potentially curable esophageal or junctional cancer, who
underwent neoadjuvant chemoradiotherapy according to CROSS 2 followed by surgical resection.
PATIENTS AND METHODS
Patients
We included patients treated with nCRT according to CROSS 2 followed by surgical resection within
a previously published single-center phase II trial (February 2001-January 2004),25 a multicenter
randomized controlled phase III trial (March 2004-November 2008)2 and as standard therapy in the
period after completion of the 2 trials (March 2009-December 2011) at the Erasmus MC-University
Medical Center Rotterdam (a tertiary referral hospital in Rotterdam, The Netherlands).
Patients who did not receive at least 80% of planned nCRT or who received a different nCRT regimen
were excluded. Also, patients with irresectable tumors (cT4b) and/or disseminated disease (M1) were
excluded.

| Chapter 4
56
Treatment and pathological assessment
The neoadjuvant treatment regimen has been described before in detail.2 Esophagectomy was
planned 4 to 6 weeks after completion of nCRT. The resection specimens (primary tumor and all
resected lymph nodes) were processed according to a standardized protocol.26 The TRG was scored
with the modified Mandard scoring system as reported by Chirieac et al.3,4 A microscopically radical
resection (R0) was defined as a tumor-free resection margin of 1 mm or more.
Follow-up and data collection
Clinical, surgical, and histopathological characteristics were retrieved from prospectively maintained
institutional databases. TTS was determined as the interval between the last day of radiotherapy and
the day of surgery. After surgery, patients were routinely followed; every 3 months during the first
postoperative year, every 6 months during the second postoperative year, and yearly until the fifth
postoperative year. During follow-up, diagnostic investigations were performed only when recurrence
was suspected clinically. Recurrences were scored at the time of first failure. Survival was determined
using hospital records and municipal registers.
Surgical outcome
Surgical outcome was described by duration of operation in minutes, intraoperative blood loss in
milliliters, and length of hospital stay in days. Postoperative complications were categorized according
to the Clavien-Dindo classification,27,28 a postoperative complication ranking system: grade 0-no
complications; grade I-complications requiring no or minimal (nonpharmacological) treatment; grade
II-complications requiring pharmacological treatment; grade III-complications requiring surgical,
endoscopic, or radiological intervention; grade-IV-life-threatening complications requiring intensive
care unit-level care; and grade V-postoperative death.
Potential delay-related confounders
To correct for the possibility that variations in TTS were not only caused by random logistical
difficulties but also by patient-related characteristics (i.e. intentionally longer TTS in more vulnerable
patients), effects of TTS on pCR and on surgical outcome were adjusted for 3 potential delay-related
confounders.
First, this was the Charlson comorbidity index 29 at diagnosis, an indicator of comorbidity. For this
index, each condition present at diagnosis is assigned a standard score of 1, 2, 3, or 6 (determined by
the estimated risk of dying from this condition). The total sum per patient is predictive for mortality.
Second, the Karnofsky performance status 30,31 at the end of nCRT, an indicator of general well-
being. The scale ranges from 100 (normal health) to 0 (death). A score of 90 indicates minor signs and/
or symptoms of disease, 80 indicates mild signs and/or symptoms of disease, etc. Third, weight loss
during nCRT, defined as the difference in body weight (in kilograms) between the start of the first cycle
of chemotherapy and the start of the fifth cycle of chemotherapy. Weight gains were set to zero loss.

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
57
Cha
pter
4
Statistical analysis
Baseline data were described as medians with the interquartile range in case of continuous variables
and as frequencies with percentages in case of categorical variables. Missing baseline data were
imputed with a single imputation technique based on correlations with relevant baseline variables
and outcome. TTS was truncated at 5% and 95% to reduce leverage effects of outliers. The effect of
TTS on pCR and on surgical outcome was determined using univariable and multivariable logistic
regression. Nonlinearity of the effect of TTS was assessed with restricted cubic splines (3 knots).32 To
correct for the possibility that TTS was intentionally longer in more vulnerable patients, the effects of
TTS on surgical outcome was adjusted in multivariable regression analysis for the 3 potential delay-
related confounders together with surgical approach (adjusted odds ratio, aOR). Subsequently, the
effects of pCR and TTS on DFS and OS were assessed using Cox regression with adjustment for the
3 potential delay-related confounders alone and in combination with postoperative complications
(adjusted hazard ratio, aHR).
RESULTS
Patient and treatment-related characteristics
In total, 325 patients with potentially curable esophageal or junctional cancer were included who
underwent nCRT according to CROSS 2 followed by resection between February 2001 and December
2011. Fifty-one included patients participated in the phase II trial,25 157 patients participated in
the multimodality arm of the randomized phase III trial,2 and 117 patients were treated with nCRT
followed by resection as standard therapy in the period after completion of the phase III trial. In total,
344 patients completed nCRT within the 3 cohorts. Of these, 4 patients did not undergo surgery
(primarily due to patient preferences) and 15 additional patients did not undergo resection (due to
disease progression).
Clinical, surgical, and histopathological characteristics of included patients are summarized in
Table 1. Median age at diagnosis was 60 years. The majority of patients were male (78%), had an
adenocarcinoma (76%), and were clinically staged as cT3 (77%), cN1 (63%). Before truncation, TTS
ranged from 18 to 291 days, with a median of 48 days (interquartile range: 40-60 days), as also shown
in Figure 1. Median TTS in irresectable patients was 46 days (interquartile range: 40-61 days), which
was similar to TTS in resected patients (P = 0.99). Surgical resection was performed regularly via both
transhiatal approach (48%) and transthoracic approach (50%). Median duration of operation was 368
minutes, median volume of intraoperative blood loss was 900 mL, and median length of hospital
stay was 14 days. Postoperative complications requiring pharmacological, interventional, or surgical
treatment (>= grade-II) were reported in 55% of patients. Postoperative in-hospital mortality was
4%. Histopathological staging showed frequent ypT0 and ypT3 stages (34% and 32%, respectively),
whereas ypN0 was the most frequent nodal stage (68%). A pCR (TRG1) was found in 28% of patients.
The microscopically radical resection rate (R0) was 93%.

| Chapter 4
58
TABLE 1 . Clinical, surgical, and histopathological characteristics of 325 included patients with potentially curable esophageal or junctional cancer, treated with neoadjuvant chemoradiotherapy according to CROSS2 followed by surgical resection.
Characteristic N (total) N %*
Age [years] 325
median (p25-p75) 60 (55 – 67)
Sex 325
Male 253 78%
Female 72 22%
Tumor type 325
Squamous cell carcinoma 73 23%
Adenocarcinoma 247 76%
Other 5 2%
cT-stage§ 323
cT1 9 3%
cT2 60 19%
cT3 250 77%
cT4 4 1%
cN-stage‡ 324
cN0 120 37%
cN1 204 63%
Time to surgery [days] ₪ 325
median (p25-p75) 48 (40 – 60)
Surgical approach 325
Transhiatal approach 156 48%
Transthoracic approach 164 50%
Thoraco-phreno-laparotomy 5 2%
Length of operation [min] 308
median (p25-p75) 368 (262 – 388)
Intraoperative blood loss [ml] 281
median (p25-p75) 900 (550 – 1350)
Length of hospital stay [days] 319
median (p25-p75) 14 (12 – 23)
Clavien–Dindo classification (26, 27) ∆ 324
Grade 0 72 22%
Grade I 73 23%
Grade II 82 25%
Grade III 43 13%

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
59
Cha
pter
4
TABLE 1 . Continued
Characteristic N (total) N %*
Grade IV 40 12%
Grade V 14 4%
ypT-stage• 324
ypT0 110 34%
ypT1 49 15%
ypT2 59 18%
ypT3 103 32%
ypT4 3 1%
ypN-stage• 325
ypN0 222 68%
ypN1 74 23%
ypN2 21 7%
ypN3 8 3%
Tumor regression grade (TRG) ¥ 325
1 90 28%
2 102 31%
3 77 24%
4 56 17%
Radicality◊ 325
R0303 93%
R122 7%
* Percentages may not add up to 100 due to rounding§ cT-stage: clinical T-stage as defined by endo-ultrasonography and/or CT-scanning according to the Union
Internationale Contre le Cancer (UICC) TNM Cancer Staging, 7th edition. ‡ cN-stage: clinical N-stage as defined by endo-ultrasonography and/or CT-scanning and/or FDG-PET-scanning
according to UICC TNM Cancer Staging, 7th edition.₪ Time to surgery was determined as the interval between the last day of radiotherapy and the day of surgery. ∆ Clavien-Dindo classification, a postoperative complication ranking system. Grade 0: no complications,
grade I: complications requiring none or minimal (non-pharmacological) treatment, grade II: complications requiring pharmacological treatment, grade III: complications requiring surgical, endoscopic or radiological intervention, grade IV: life-threatening complications requiring ICU-level care, grade V: postoperative death.
• ypT and ypN-stage: pathological T-stage and pathological N-stage in the resection specimen following neoadjuvant chemoradiotherapy, according to UICC TNM Cancer Staging, 7th edition.
¥ Tumor regression grade was defined as: TRG1: no residual tumor cells found (pathologically complete response= pCR); TRG2: 1-10% residual tumor cells; TRG3: 11-50% residual tumor cells; TRG4: > 50% residual tumor cells.
◊ R0 was defined as a tumor-free resection margin ≥ 1 mm. R
1 was defined as a macroscopically radical resection,
with a microscopically tumor-free resection margin < 1 mm.

| Chapter 4
60
FIGURE 1 . Distribution of TTS (before truncation) in 340 patients who completed neoadjuvant chemoradiotherapy according to CROSS 2 and underwent surgery for potentially curable esophageal or junctional cancer, 15 of these patients were irresectable due to disease progression, whereas 325 patients underwent resection.
Effect of TTS on pCR
Median TTS was 48 days (p25-p75: 40-60 days, p5-p95: 18-83 days). The association of TTS with pCR
was nonlinear (P = 0.025). After approximately 45 days (Supplementary Fig. 1, available at http://links.
lww.com/SLA/A672), additional TTS was associated with an increased probability of pCR (OR = 1.35
per additional week after 45 days, P = 0.0004).
In itself a pathologically complete response was associated with a significantly better DFS and OS
HR = 0.29, P < 0.0001 and 0.44, P < 0.0001, respectively). The effect of pCR on OS was sustained after
correction for the 3 potential delay-related confounders (aHR = 0.44, P < 0.0001).
Effect of TTS on short-term surgical outcome
The effect of TTS on short-term surgical outcome was reasonably linear (nonlinearity, P = 0.920).
Increased TTS was associated with prolonged duration of operation (12 minutes per additional week
of TTS, P < 0.001), prolonged length of hospital stay (1.55 day per additional week of TTS, P = 0.006),
and more severe postoperative complications (OR 1.20 per additional week of TTS, P < 0.001). No
association was found with intraoperative blood loss (-3 mL per additional week of TTS, P = 0.898).
However, these associations were partly explained by the 3 potential delay-related confounders
together with surgical approach. After adjustment, the effects were reduced for duration of operation
(6 minutes per additional week of TTS, P = 0.031), length of hospital stay (1.03 days per additional
week of TTS, P = 0.071), and for postoperative complications (aOR 1.10 per additional week of TTS, P
= 0.132, Table 3.)

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
61
Cha
pter
4
TABLE 2. Three potential delay-related confounders in 325 included patients with potentially curable esophageal or junctional cancer, treated with neoadjuvant chemoradiotherapy according to CROSS2 followed by surgical resection.
Characteristic N (total) N %*
Charlson comorbidity index28 §at initial diagnosis
324
0
243 75%
1
63 19%
2
15 5%
3
2 1%
4
1 0%
Karnofsky performance status 29,30 ‡ at the end of nCRT 269
100 80 30%
90 171 64%
≤80 18 7%
Weight loss [kg] •
during nCRT297
median (p25-p75) 1 (0 – 3)
* Percentages may not add up to 100 due to rounding§ Charlson comorbidity index, an indicator of comorbidity. Each condition present at diagnosis is assigned a
standard score of 1, 2, 3 or 6 (determined by the estimated risk of dying from this condition). The total sum per patient is predictive for mortality.
‡ Karnofsky performance status, an indicator of general well-being. The scale ranges from 100 (normal health) to 0 (death). A score of 90 indicates minor signs and/or symptoms of disease, 80 indicates mild signs and/or symptoms of disease, etc.
• Weight loss during nCRT was defined as the difference in body weight (in kilograms) between the start of the first cycle of chemotherapy and the start of the fifth cycle of chemotherapy. Weight gains were set to zero loss.

| Chapter 4
62
TABLE 3. Effect of time to surgery on short-term surgical outcome and postoperative complications in 325 included patients treated with CROSS 2 followed by surgical resection, adjusted for the three potential delay-related confounders together with surgical approach.
Outcomebeta(per additional week)
Padjusted beta (per additional week)
P
Length of operation (minutes) 12 <0.001 6 0.031
Intraoperative blood loss (ml) -3 0.898 -3 0.898
Length of hospital stay (days) 1.55 0.006 1.03 0.071
Postoperative complications (according to the Clavien-Dindo
classification 26, 27))1.20* <0.001 1.10* 0.132
*Odds ratioAdjustment for the 3 delay-related confounders (Charlson comorbidity index29 at diagnosis, Karnofsky performance status 30,31 during the last week of nCRT, and weight loss during nCRT) together with surgical approach.
The potential delay-related confounders are summarized in Table 2. The majority of patients had a
pretreatment Charlson comorbidity index of 0 (75%) and a Karnofsky performance score at the end of
nCRT of 90 (64%). Median weight loss during nCRT was 1 kg (p25-p75: 0-3).
Effects of TTS on survival
The effect of TTS on DFS and OS was reasonably linear (nonlinearity, P = 0.566). Increased TTS was not
associated with DFS (HR = 1.00, P = 0.976; aHR = 0.98, P = 0.620), nor with OS (HR = 1.06, P = 0.139;
aHR = 1.03, P = 0.465, Table 4).
TABLE 4. Effect of time to surgery on OS in 325 included patients with potentially curable esophageal or junctional cancer, treated with neoadjuvant chemoradiotherapy according to CROSS followed by surgical resection
TTS HR for OS(Per Additional Week) P
Univariate 1.06 0.139
Adjusted for 3 potential delay-related confounders 1.04 0.387
Adjusted for 3 potential delay-relatedconfounders + postoperativecomplications (shows effect ofTTS on OS via increased pCR)
1.030.465
Delay-related confounders: Charlson comorbidity index29 at diagnosis, Karnofsky performance status30,31 during the last week of nCRT, and weight loss during nCRT.

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
63
Cha
pter
4
DISCUSSION
Results show that prolonged TTS, beyond 45 days after completion of nCRT, significantly increased
the probability of pCR. Longer TTS was also associated with a small increased risk of postoperative
complications. Furthermore, pCR in the resection specimen was associated with significantly
improved DFS. However, prolonged TTS (with increased probability of pCR) was not associated with
improved DFS.
Although prolonged TTS was associated with an increased pCR rate, DFS was not accordingly
improved. The comparable DFS between patients with shorter and longer TTS implies that their
disease is biologically similar, despite differences in pCR rate. The increase in pCR after prolonged TTS
is attributed to patients who presumably would have been noncomplete responders at shorter TTS.
Interestingly, these patients, who become pathologically complete responders relatively late after
completion of nCRT, do not contribute to an improved DFS after prolonged TTS. This can be explained
if “late complete responders” would already behave as biologically complete responders at shorter
TTS, despite a pathologically noncomplete response in their resection specimens. Therefore, the
(minimal) residual disease found at histological examination after shorter TTS in these late complete
responders is presumed to be biologically nonrelevant. We hypothesize that prolonged TTS does
not truly improve the biological pCR rate, but that prolonged TTS simply allows for a more precise
histopathological distinction between viable residual tumor cells and biologically nonrelevant tumor
cell debris by the pathologist.
In this cohort, prolonged TTS was significantly associated with a prolonged duration of operation,
a prolonged length of hospital stay, and increased postoperative complications. However, these
associations were partly explained by the 3 potential delay-related confounders, that is, Charlson
comorbidity index 29 at diagnosis, Karnofsky performance status 30,31 at the end of nCRT, and weight loss
during nCRT (besides surgical approach; Table 3). These potential confounding factors were chosen to
reflect the overall condition of patients at the end of nCRT, which might have influenced the surgeons’
decision to delay surgical resection after nCRT, independent of logistical planning. Therefore, these
results indicate that the association of prolonged TTS with negative short-term surgical outcome
and increased postoperative complications is partly the result of an intentionally prolonged TTS in
patients with a worse overall condition at the end of nCRT and that prolonged TTS has at most a small
association with short-term surgical outcome and postoperative complications.
Two previous studIes investigated the association between TTS and surgical and oncological outcome
in patients with esophageal cancer. Both studies did not find a correlation with pCR rate.23,24 This
discrepancy with the present study might be related to the heterogeneity of nCRT protocols used
in both previous studies. In our cohort, all patients completed the same nCRT protocol, and in all
patients there was a similar initial intention to undergo surgery after 4 to 6 weeks, possibly allowing
for a clearer delineation of the effect of TTS on pCR rate. Also, the present study investigated the
association between TTS and pCR in all patients using logistic regression, resulting in more power to
detect subtle effects as compared to subgroup analyses. Last, this study focused on the association

| Chapter 4
64
between TTS and DFS, which was lacking in the study by Kim and colleagues.24
Currently, controversy exists concerning the management of cancer patients with a clinically
complete response after neoadjuvant therapy. For rectal cancer patients, more conservative strategies
have already been proposed and tested in clinically complete responders.33-36 The goal of these wait-
and-see approaches is organ preservation and overall reduction in treatment-related morbidity and
mortality. However, it has remained difficult to clinically distinguish truly complete responders from
nearly complete responders. Patients belonging to the latter group might be incorrectly identified as
clinically complete responders and could thus be exposed to potentially harmful disease progression
during the wait-and-see period. For esophageal cancer, the challenge to distinguish complete from
nearly complete responders seems even more difficult.37-40
However, if surgery can be safely postponed beyond the usual 4 to 6 weeks, without negatively
affecting oncological outcome as suggested in the present study, more time is allowed to identify
noncomplete responders. Such a strategy would not focus on distinguishing complete from
noncomplete responders at a single instance, but would rather use intense surveillance, with targeting
of the mucosa and submucosa41 during repeated instances, for the detection of residual or recurrent
disease. Thereby, possibly allowing more time to differentiate between truly complete responders and
noncomplete responders.
Limitations of the study
The first limitation is that this study was a retrospective analysis. However, all parameters in this study
were collected prospectively. Furthermore, all 3 cohorts used the same neoadjuvant CROSS regimen
and all 3 cohorts had a similar intention to perform surgery at 4 to 6 weeks after completion of nCRT.
The second limitation of this study is that the number of patients with a TTS beyond 10 weeks was
relatively small. Therefore, a subtle effect of TTS on DFS and OS cannot be excluded in patients with a
TTS beyond 10 weeks.
Conclusions
In patients with potentially curable esophageal or junctional cancer, prolonged TTS (beyond 45
days) after neoadjuvant chemoradiotherapy increases the probability of a pathologically complete
response, without improving DFS and OS. It might also slightly increase the probability of postoperative
complications, which can be partly explained by intentional postponement of surgery in some
high-risk patients with worse overall condition. We hypothesize that prolonged TTS allows for more
accurate determination of histopathological response due to continued disintegration of nonviable
cells in some patients, without affecting actual prognosis after neoadjuvant chemoradiotherapy. We
conclude that TTS can be safely prolonged from the usual 4 to 6 weeks up to at least 12 weeks,
which facilitates a more conservative wait-and-see strategy after neoadjuvant chemoradiotherapy to
be tested.

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
65
Cha
pter
4
REFERENCES1. Sjoquist KM, Burmeister BH, Smithers BM, et al. Survival after neoadjuvant chemotherapy or chemoradiotherapy
for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12:681-692.
2. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074-2084.
3. Mandard AM, Dalibard F, Mandard JC, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma: clinicopathologic correlations. Cancer. 1994;73:2680-2686.
4. Chirieac LR, Swisher SG, Ajani JA, et al. Posttherapy pathologic stage predicts survival in patients with esophageal carcinoma receiving preoperativeBNchemoradiation. Cancer. 2005;103:1347-1355.
5. Schneider PM, Baldus SE, Metzger R, et al. Histomorphologic tumor regression and lymph node metastases determine prognosis following neoadjuvant radiochemotherapy for esophageal cancer: implications for response classification. Ann Surg.2005;242:684-692.
6. Donohoe CL, O’Farrell NJ, Grant T, et al. Classification of pathologic response to neoadjuvant therapy in esophageal and junctional cancer: assessment of existing measures and proposal of a novel 3-point standard. Ann Surg. 2013;258:784-792.
7. Ancona E, Ruol A, Santi S, et al. Only pathologic complete response to neoadjuvant chemotherapy improves significantly the long-term survival of patients with resectable esophageal squamous cell carcinoma: final report of a randomized, controlled trial of preoperative chemotherapy versus surgery alone. Cancer. 2001;91:2165-7214.
8. Reynolds JV, Muldoon C, Hollywood D, et al. Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer. Ann Surg. 2007;245:707-716.
9. Verlato G, Zanoni A, Tomezzoli A, et al. Response to induction therapy in oesophageal and cardia carcinoma using Mandard tumour regression grade or size of residual foci. Br J Surg. 2010;97:719-725.
10. Vallbohmer D, Holscher AH, DeMeester S, et al. A multicenter study of survival after neoadjuvant radiotherapy/chemotherapy and esophagectomy for ypT0N0M0R0 esophageal cancer. Ann Surg. 2010;252:744-749.
11. Francois Y, Nemoz CJ, Baulieux J, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol. 1999;17:2396-2402.
12. Dolinsky CM, Mahmoud NN, Mick R, et al. Effect of time interval between surgery and preoperative chemoradiotherapy with 5-fluorouracil or 5-fluorouracil and oxaliplatin on outcomes in rectal cancer. J Surg Oncol. 2007;96:207-212.
13. Tulchinsky H, Shmueli E, Figer A, et al. An interval >7 weeks between neoadjuvant therapy and surgery improves pathologic complete response and disease-free survival in patients with locally advanced rectal cancer. Ann Surg Oncol. 2008;15:2661-2667.
14. Kalady MF, de Campos-Lobato LF, Stocchi L, et al. Predictive factors of pathologic complete response after neoadjuvant chemoradiation for rectal cancer. Ann Surg. 2009;250:582-589.
15. de Campos-Lobato LF, Geisler DP, da Luz Moreira A, et al. Neoadjuvant therapy for rectal cancer: the impact of longer interval between chemoradiation and surgery. J Gastrointest Surg. 2010;15:444-450.
16. Wolthuis AM, Penninckx F, Haustermans K, et al. Impact of interval between neoadjuvant chemoradiotherapy and TME for locally advanced rectal cancer on pathologic response and oncologic outcome. Ann Surg Oncol. 2012;19:2833-2841.
17. Sloothaak DA, Geijsen DE, van Leersum NJ, et al. Optimal time interval between neoadjuvant chemoradiotherapy and surgery for rectal cancer. Br J Surg. 2013;100:933-939.

| Chapter 4
66
18. Petrelli F, Sgroi G, Sarti E, et al. Increasing the interval between neoadjuvant chemoradiotherapy and surgery in rectal cancer: a meta-analysis of published studies. Ann Surg. November 20, 2013 [Epub ahead of print].
19. Moore HG, Gittleman AE, Minsky BD, et al. Rate of pathologic complete response with increased interval between preoperative combined modality therapy and rectal cancer resection. Dis Colon Rectum. 2004;47:279-286.
20. Habr-Gama A, Perez RO, Proscurshim I, et al. Interval between surgery and neoadjuvant chemoradiation therapy for distal rectal cancer: does delayed surgery have an impact on outcome? Int J Radiat Oncol Biol Phys. 2008;71:1181-1188.
21. Kerr SF, Norton S, Glynne-Jones R. Delaying surgery after neoadjuvant chemoradiotherapy for rectal cancer may reduce postoperative morbidity without compromising prognosis. Br J Surg. 2008;95:1534-1540.
22. Lim SB, Choi HS, Jeong SY, et al. Optimal surgery time after preoperative chemoradiotherapy for locally advanced rectal cancers. Ann Surg. 2008;248:243-251.
23. Ruol A, Rizzetto C, Castoro C, et al. Interval between neoadjuvant chemoradiotherapy and surgery for squamous cell carcinoma of the thoracic esophagus: does delayed surgery have an impact on outcome? Ann SUrg. 2010;252:788-796.
24. Kim JY, Correa AM, Vaporciyan AA, et al. Does the timing of esophagectomy after chemoradiation affect outcome? Ann Thorac Surg. 2012;93:207-213.
25. van Meerten E, Muller K, Tilanus HW, et al. Neoadjuvant concurrent chemoradiation with weekly paclitaxel and carboplatin for patients with oesophageal cancer: a phase II study. Br J Cancer. 2006;94:1389-1394.
26. van Meerten E, van der Gaast A, Tilanus HW, et al. Pathological analysis after neoadjuvant chemoradiotherapy for esophageal carcinoma: the Rotterdam experience. J Surg Oncol. 2009;100:32-37.
27. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205-213.
28. Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250:187-196.
29. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383.
30. Karnofsky DA, Burchenal JH. The clinical evaluation of chemotherapeutic agents in cancer. In: MacLeod CM, ed. Evaluation of Chemotherapeutic Agents. New York, NY: Columbia University Press; 1949:191-205.
31. Mor V, Laliberte L, Morris JN, et al. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer. 1984;53:2002-2007.
32. Harrell FE Jr, Lee KL, Pollock BG. Regression models in clinical studies: determining relationships between predictors and response. J Natl Cancer Inst. 1988;80:1198-1202.
33. Habr-Gama A, Perez RO, Nadalin W, et al. Operative versus nonoperative treatment for stage 0 distal rectal cancer following chemoradiation therapy: long-term results. Ann Surg. 2004;240:711-718.
34. Habr-Gama A, Perez RO. Non-operative management of rectal cancer after neoadjuvant chemoradiation. Br J Surg. 2009;96:125-127.
35. Maas M, Beets-Tan RG, Lambregts DM, et al. Wait-and-see policy for clinical complete responders after chemoradiation for rectal cancer. J Clin Oncol. 2011;29:4633-4640.
36. Bokkerink GM, de Graaf EJ, Punt CJ, et al. The CARTS study: Chemoradiation therapy for rectal cancer in the distal rectum followed by organ-sparing transanal endoscopic microsurgery. BMC Surg. 2011;11:34.

Prolonged time to surgery after neoadjuvant chemoradiotherapy for esophageal or junctional cancer |
67
Cha
pter
4
37. Lordick F, Ott K, Krause BJ, et al. PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: the MUNICON phase II trial. Lancet Oncol. 2007;8:797-805.
38. Schneider PM, Metzger R, Schaefer H, et al. Response evaluation by endoscopy, rebiopsy, and endoscopic ultrasound does not accurately predict histopathologic regression after neoadjuvant chemoradiation for esophageal cancer. Ann Surg. 2008;248:902-908.
39. Vallbohmer D, Holscher AH, Dietlein M, et al. [18F]-Fluorodeoxyglucose-positron emission tomography for the assessment of histopathologic response and prognosis after completion of neoadjuvant chemoradiation in esophageal cancer. Ann Surg. 2009;250:888-894.
40. van Heijl M, Omloo JM, van Berge Henegouwen MI, et al. Fluorodeoxyglucose positron emission tomography for evaluating early response during neoadjuvant chemoradiotherapy in patients with potentially curable esophageal cancer. Ann Surg. 2011;253:56-63.
41. Shapiro J, ten Kate FJ, van Hagen P, et al. Residual esophageal cancer after neoadjuvant chemoradiotherapy frequently involves the mucosa and submucosa. Ann Surg. 2013;258:678-688.

B.A. Grotenhuis
P. van Hagen
B.P.L. Wijnhoven
M.C.W. Spaander
H.W. Tilanus
J.J.B. van Lanschot
Journal of Gastrointestinal Surgery 2010;14(3):476-83

Chapter 5Delay in diagnostic workup and treatment of esophageal cancer

| Chapter 5
70
ABSTRACT
INTRODUCTION
Esophageal cancer should preferably be detected and treated at an early stage, but this may be
prohibited by late onset of symptoms and delays in referral, diagnostic workup, and treatment.
The aim of this study was to investigate the impact of these delays on outcome in patients with
esophageal cancer.
METHODS
For 491 patients undergoing esophagectomy for cancer between 1991 and 2007, patients’ short- and
long-term outcome were analyzed according to different time intervals between onset of symptoms,
diagnosis, and surgical treatment.
RESULTS
Length of prehospital delay (from onset of symptoms until endoscopic diagnosis) did not affect
patient’s short- or long-term outcome. A shorter hospital delay between establishing the diagnosis
of esophageal cancer on endoscopy and surgery was associated with lower overall morbidity and in-
hospital mortality. Patients of ASA classes I and II experienced a shorter hospital delay than patients
of ASA classes III and IV. Length of hospital delay between endoscopic diagnosis and surgery did not
affect pathological tumor–node–metastasis stage or R0-resection rate. Longer hospital delay did not
result in worse survival: Overall survival after esophagectomy for cancer was not significantly different
between patients with hospital delay <5, 5–8, or >8 weeks (24.7%, 21.7%, and 32.3%, respectively;
p = 0.12).
CONCLUSION
A longer hospital delay (between endoscopic diagnosis and surgery) resulted in worse patient’s short-
term outcome (higher overall morbidity and mortality rates) but not in a worse long-term outcome
(overall survival). This may be explained by a more time-consuming diagnostic workup in patients
with a poorer physical status and not by tumor progression.

Delay in diagnostic workup and treatment of esophageal cancer |
71
Cha
pter
5
INTRODUCTION
The 5-year survival rate for esophageal cancer patients after esophagectomy with curative intent has
improved up to 40%.1-3 As further improvement in survival from a single modality approach, such as
surgery, is unlikely, considerable interest has grown in other strategies that may improve patients’
survival (neoadjuvant chemo- and/or radiotherapy in particular). In many types of cancer, the prognosis
of patients with small, localized tumors is better than with locally advanced or metastatic disease.
Similar to other malignancies such as colorectal and breast cancer, the outcome of esophageal cancer
is related to the pathological tumor–node–metastasis (pTNM) stage of the disease.2,4,5 Therefore,
detection and treatment of esophageal cancer at an early stage could also improve long-term survival.
Early detection of esophageal cancer may be prohibited not only by the late onset of symptoms but
also by delays in referral to an appropriate specialist, establishment of the diagnosis, further diagnostic
workup, and start of treatment. However, the impact of these delays on both short- and long-term
outcome for patients undergoing esophagectomy for cancer is unclear.
In patients with breast cancer, delays of 3–6 months between the onset of symptoms and start
of treatment are associated with lower survival, caused by a more advanced tumor stage.6 In two
systematic reviews, no association was found between diagnostic and therapeutic delay and survival
in colorectal cancer patients7 nor between these delays and disease stage.8 A few studies have
investigated the impact of delays in diagnosis and treatment of esophageal cancer. Drawbacks of
these studies are small numbers of patients included,9 analyses that do not cover the complete track
between onset of symptoms and surgical treatment,10,11 combined patient groups with gastric and
esophageal carcinoma,12,13 and studies lacking survival analyses.9, 11-13
We hypothesized that longer delays between onset of symptoms, endoscopic diagnosis, and surgical
treatment are associated with a worse short-term outcome (morbidity, reoperation rate, and in-
hospital mortality), worse tumor stage, and hence, worse long-term outcome (overall survival)
following potentially curative esophagectomy in patients with esophageal cancer.
PATIENTS AND METHODS
The Erasmus Medical Center in Rotterdam is a tertiary referral center for patients with esophageal
cancer in The Netherlands. Most patients are referred to the Erasmus MC outpatient clinic for (surgical)
treatment after the diagnosis of esophageal cancer has been established in a referring hospital (group
A). The minority of patients is directly referred by the general practitioner (GP) to the Erasmus MC for
clinical investigations of symptoms suggestive of cancer (group B). In all patients (groups A and B)
upper gastrointestinal endoscopy with biopsy is (re)done in the Erasmus MC to confirm the diagnosis
of esophageal cancer and to determine the exact location of the tumor. Staging is performed routinely
with endoscopic ultrasonography, CT scanning of thorax and abdomen, and external ultrasound of the
neck. Every patient is discussed in a weekly multidisciplinary oncology meeting in which a definitive
treatment plan is designed. If eligible for surgery, patients are put on the waiting list for surgery. On the

| Chapter 5
72
same day, the patient is referred to the Department of Anesthesiology for preoperative counseling. If
needed, additional cardiac and/or pulmonary function tests are scheduled.
Between January 1991 and December 2007, 791 patients underwent esophagectomy for cancer of
the esophagus or gastroesophageal junction in the Erasmus MC. To obtain a homogeneous cohort
of patients in terms of treatment and to circumvent possible stage migration following chemo-
and/or radiotherapy, patients receiving (neo)adjuvant therapy were excluded from this analysis.
In our hospital, patients received neoadjuvant chemo(radio)therapy in the context of randomized
controlled trials.14,15 Induction chemo- and/or radiotherapy was given in patients with either a cT4
tumor without distant metastases or in patients with gross involvement of celiac trunk lymph nodes
(M1a), who were not considered eligible for primary surgical therapy. There were 214 patients who
were excluded because of chemo- and/or radiotherapy prior to surgery. In 44 patients, the hospital
delay from endoscopic diagnosis to surgery could not be calculated, as the date of their first upper
gastrointestinal endoscopy performed in the referring hospital was unknown. Another 42 patients
were excluded, as they participated in a Barrett’s esophagus surveillance program. Over recent years,
multiple attempts for endoscopic treatment of early lesions delayed referral to the Department of
Surgery in such way that this group was not representative for patients treated for (more advanced)
esophageal cancer. Finally, data of 491 patients were analyzed in the present study. The vast majority
of these patients underwent a transhiatal esophagectomy with locoregional lymphadenectomy only
(N = 477). In 14 patients, a transthoracic resection with extended lymphadenectomy was performed.
The applied surgical techniques have been described previously.3, 16 Tumors were assigned pTNM
stages according to the Union Internationale Contre le Cancer 2002 system.17
Data on patients’ demographics, diagnostic tests, surgery, postoperative morbidity, in-hospital
mortality, and survival have been collected prospectively and stored in a database by a data manager.
From this database, the following time points were defined:
- Date of upper gastrointestinal endoscopy in the referring hospital, on which the diagnosis of
esophageal cancer had been established by histology from biopsies (only applicable for group A)
- Date of first visit at the Erasmus MC outpatient clinic: Department of Surgery, Gastroenterology,
or Medical Oncology
- Date of upper gastrointestinal endoscopy in the Erasmus MC, on which the diagnosis of
esophageal cancer had been established by histology from biopsies
- Date of the multidisciplinary oncology meeting, after which the patient had been put on the
operative waiting list if eligible for surgery
- Date of surgery.
To summarize all different time points that have been marked in the process between onset of
symptoms and surgery, we divided this time span into two major time intervals that have been
analyzed separately: pre-hospital and hospital delay (see Fig. 1). Subsequently, data were analyzed in
three different ways:

Delay in diagnostic workup and treatment of esophageal cancer |
73
Cha
pter
5
- Impact of prehospital delay: time from onset of symptoms until diagnosis on first endoscopy
(either in the referring hospital for group A or in Erasmus MC for group B)
- Impact of hospital-delay: time from diagnosis on patient’s first endoscopy undertaken until
surgery
- Impact of specific time intervals between diagnosis on first endoscopy and surgery. In order to
examine the hospital-delay in more detail, the effect of specific time intervals between diagnosis
in the referring hospital, first visit at the outpatient clinic in Erasmus MC, diagnosis on endoscopy in
Erasmus MC, multidisciplinary oncology meeting, and surgery on short- and long-term outcome
were analyzed. For this purpose, only data from patients in group A were used.
Onset of symptoms Diagnosis on endoscopy -Referring hospital (group A)
-Erasmus MC (group B)
Multidisciplinary oncology meeting
Surgery
FIGURE 1. Analysis of prehospital and hospital delays encountered by patients who underwent surgical resection for esophageal cancer in Erasmus MC.
Statistics
Follow-up was recorded until December 2008 or until death if earlier and was complete for all patients.
Statistical analysis for non-parametric data was used. Grouped data were compared using the chi-
square, Mann–Whitney U, or Kruskall–Wallis H test. Patients who died due to complications following
esophagectomy (in-hospital mortality) were not excluded from survival analysis. Overall survival
was calculated from the date of operation until the date of last follow-up or death according to the
Kaplan–Meier method. Disease-free survival was assessed from the date of operation until the date of
disease recurrence in case of locoregional recurrence or distant metastases. Univariate analyses were
performed with the log-rank test to identify prognostic variables associated with overall survival after
esophagectomy. Data analyses were carried out with SPSS version 15.0 (SPSS, Chicago, IL, USA).
RESULTS
Patients’ characteristics are shown in Table 1. Three hundred sixty-five patients (74.3%), in whom the
diagnosis esophageal cancer was established in another hospital, were referred to the Erasmus MC
for further staging and treatment (group A). One hundred twenty-six patients (25.7%) were referred
directly to the Erasmus MC by the general practitioner for investigation of symptoms suggestive

| Chapter 5
74
of esophageal cancer (group B). Patients’ first visit to the Erasmus MC was at the Department of
Surgery (N = 338, 68.8%), Department of Gastroenterology (N = 147, 29.9%), or Department of Medical
Oncology (N = 6, 1.3%).
TABLE 1. Clinicopathological characteristics of 491 patients who underwent surgical resection for esophageal cancer and who were included in the present study.
Characteristic N (range)
Age (in years)a 65 (28–89)
N (%)
Gender
Male 399 (81.3%)
Female 92 (18.7%)
ASA classification
I 77 (15.7%)
II 316 (64.4%)
III 96 (19.6%)
IV 2 (0.4%)
Tumor location
Proximal esophagus 8 (1.6%)
Mid esophagus 27 (5.5%)
Distal esophagus 196 (39.9%)
Gastroesophageal junction 260 (53.0%)
Histology
Squamous cell carcinoma 73 (14.9%)
Adenocarcinoma 418 (85.1%)
ASA classification American Society of Anesthesiologists classification.aAge is given as median (range).
Impact of prehospital delay: time from onset of symptoms until first endoscopy
The majority of patients underwent endoscopy for investigation of obstructive symptoms suggestive
of cancer like dysphagia, odynophagia, and weight loss (N = 462, 94.1%). Other indications for
endoscopy encompassed investigation of hematemesis (N = 12, 2.4%), anemia (N = 9, 1.8%), or melena
(N = 8, 1.6%). Prehospital delay (from onset of symptoms until first endoscopy) lasted a median time
period of 3.0 months (range, 0–36 months). Patient’s short-term (morbidity, reoperation rate, and
in-hospital mortality) and long-term outcome (overall 5-year survival) after esophagectomy were
comparable for patients who experienced symptoms for a period of 3 months or less versus more
than 3 months until endoscopy was performed (Table 2).

Delay in diagnostic workup and treatment of esophageal cancer |
75
Cha
pter
5
TABLE 2. Impact of prehospital delay from onset of symptoms to first endoscopy on short- and long-term outcome after esophagectomy; comparison of prehospital delay ≤3 months (N = 308) versus >3 months (N = 183).
Prehospital delay ≤3 months, N = 308
Prehospital delay >3 months, N = 183 p value
Morbidity 199 (64.6%) 104 (56.8%) 0.09
Reoperation 34 (11.0%) 16 (8.7%) 0.42
In-hospital mortality 18 (5.8%) 9 (4.9%) 0.66
Overall 5-year survival 24.0% 29.3% 0.10
Impact of hospital delay: time from endoscopic diagnosis until surgery
The hospital delay from establishing the diagnosis of esophageal cancer on endoscopy (either in the
referring hospital for group A or in Erasmus MC for group B) until surgery was 49 days (given as median,
range of 5–175 days). This delay encompassed a median time period of 28 days (range, 0–147 days)
from diagnosis on patient’s first endoscopy until the multidisciplinary oncology meeting (staging
delay), and a median time period of 15 days from this meeting until surgery (operative waiting list,
range of 1–67 days). Median hospital delay between diagnosis and surgery increased during the study
period (1991–2007): 3.9 weeks in 1991 toward 10.9 weeks in 2007 (Fig. 2). This increase in hospital
delay should rather be ascribed to the 3.4 times increase in length of the operative waiting list (1.6
weeks in 1991 towards 5.6 weeks in 2007) than to the 1.5 times increase in staging delay (3.3 weeks in
1991 towards 4.9 weeks in 2007).
3,9
4,7
6,6 6,6 7
7,9
6,9
10,6 10,9
0
2
4
6
8
10
12
1991-1992 1993-1994 1995-1996 1997-1998 1999-2000 2001-2002 2003-2004 2005-2006 2007
FIGURE 2. Median hospital delay (in weeks) between endoscopic diagnosis and surgery increased during the study period (1991–2007): 3.9 weeks in 1991 toward 10.9 weeks in 2007.

| Chapter 5
76
A shorter hospital delay between establishing the diagnosis of esophageal cancer on patient’s first
endoscopy and surgery was associated with significantly lower overall morbidity and mortality (Table
3). These associations appeared to be linear: morbidity (p = 0.001) and in-hospital mortality (p = 0.01)
increased with longer hospital delay. Patients of ASA classes I and II experienced a shorter hospital
delay than patients of ASA classes III and IV (hospital delay <5 weeks, 28.8%; 5–8 weeks, 36.9%; and >8
weeks, 34.4% versus <5 weeks, 15.3%; 5–8 weeks, 41.8%; and > 8 weeks, 42.9%, respectively; p = 0.02).
Length of hospital delay did not affect pTNM stage or R0-resection rate (Table 3).
TABLE 3. Impact of the hospital delay from diagnosis on patient’s first endoscopy until surgery: hospital delay <5 weeks (N = 128), 5–8 weeks (N = 186), and >8 weeks (N = 177).
Delay <5 weeks, N = 128
Delay 5–8 weeks, N = 186
Delay >8 weeks, N = 177 p value
Morbidity 62 (48.4%) 122 (65.6%) 119 (67.2%) <0.01
In-hospital mortality 2 (1.6%) 10 (5.4%) 15 (8.5%) 0.03
Reoperation 7 (5.5%) 20 (10.8%) 23 (13.0%) 0.10
pT stage
pT1–pT2 30 (23.4%) 57 (30.6%) 54 (30.5%) 0.31
pT3–pT4 98 (76.6%) 129 (69.4%) 123 (69.5%)
pN stage
pN0 42 (32.8%) 66 (35.5%) 62 (35.0%) 0.88
pN1 86 (67.2%) 120 (64.5%) 115 (65.0%)
pM stage
pM0 103 (80.5%) 150 (80.6%) 131 (74.0%) 0.24
pM1a–M1b 25 (19.5%) 36 (19.4%) 46 (26.0%)
Radicality of resection
R0 86 (67.2%) 124 (66.7%) 130 (73.4%) 0.32
R1–R2 42 (32.8%) 62 (33.3%) 47 (26.6%)
Longer hospital delay did not result in worse survival (Fig. 3): Overall 5-year survival was 24.7% in
patients with a hospital delay less than 5 weeks, 21.7% in patients with a hospital delay between 5
and 8 weeks and 32.3% in patients in whom the hospital delay was more than 8 weeks. Although
overall survival appeared to be longer in patients with a longer hospital delay, this difference was not
statistically significant (p = 0.12).

Delay in diagnostic workup and treatment of esophageal cancer |
77
Cha
pter
5
TABLE 4. Univariable analyses of potential prognostic variables associated with overall survival after esophagectomy for cancer (N = 491).
Variable Five-year survival (%) p value
Age≤65 years 30.2 0.001
>65 years 21.4
SexMale 25.4 0.84
Female 28.5
ASA classificationI–II 27.0 0.12
III–IV 22.2
pT stagepT1–T2 53.3 <0.001
pT3–T4 15.0
pN stagepN0 50.3 <0.001
pN1 12.2
pM stagepM0 39.8 <0.001
pM1a–M1b 9.5
HistologySquamous cell carcinoma 27.1 0.98
Adenocarcinoma 25.8
Differentiation grade of tumorGood 69.1
Moderate 29.5 <0.001
Poor 16.0
Radicality of resectionR0 35.5 <0.001
R1–R2 5.5
Lymph node ratio≤0.24 36.0 <0.001
>0.24 12.0
ReferralBy another hospital (group A) 25.9 0.65
By GP (group B) 26.2
Prehospital delay≤3 months 24.0 0.10
>3 months 29.3
Hospital delay<5 weeks 24.7
5–8 weeks 21.7 0.12
>8 weeks 32.3
ASA classification American Society of Anesthesiologists classification, GP general practitioner.

| Chapter 5
78
Parameters found to be associated with overall survival in univariate analyses are shown in Table 4:
age younger than 65 years, early pT stage (pT1 or pT2), no lymph node involvement (pN0), absence
of distant metastatic disease (pM0), good differentiation grade of the tumor, R0 resection, and lymph
node ratio smaller than 0.24 were favorable of improved overall survival. Survival analysis with regard
to 5-year disease-free survival paralleled the overall 5-year survival curves (27.0%, 27.7%, and 38.3%,
respectively; p = 0.09).
No at risk 0 months 12 months 24 months 36 months 48 months 60 months >8 weeks 177 107 68 48 38 24 5-8 weeks 186 122 78 54 39 34 <5 weeks 128 80 53 42 32 30
FIGURE 3. Overall 5-year survival for esophageal cancer patients appeared longer for patients with a hospital delay between diagnosis on first endoscopy and surgery >8 weeks (N = 177) versus patients with a hospital delay <5 weeks (N = 128) or 5–8 weeks (N = 186), although this difference did not reach statistical significance (p = 0.12).
Impact of specific time intervals between endoscopic diagnosis and surgery (Group A)
The median hospital delay was 53 days (range, 5–175 days) for patients in group A in whom the
diagnosis esophageal cancer had been established in another hospital and who were referred to
the Erasmus MC for surgical treatment (N = 365). The breakdown of this delay is shown in Table 5,
according to the different time intervals between diagnosis in the referring hospital, first visit to the
outpatient clinic in Erasmus MC, diagnosis on endoscopy in Erasmus MC, multidisciplinary oncology
meeting, and surgery.
When analyzing the impact of the separate time intervals, it appeared that the delay between the
multidisciplinary oncology meeting and surgery (median, 15 days; reflecting the length of the operative
waiting list) was the only time interval that influenced short-term outcome post-esophagectomy.

Delay in diagnostic workup and treatment of esophageal cancer |
79
Cha
pter
5
Although in-hospital mortality was comparable between patients who had been on the waiting list
for 15 days or shorter versus patients who were waiting for more than 15 days (p = 0.14), length of
the operative waiting list did influence morbidity (55.7% versus 67.1%, p = 0.03), and a trend towards
an increased reoperation rate could be noted (7.8% versus 13.9%, p = 0.06). However, in contrast with
the hospital delay between endoscopic diagnosis and surgery, none of the separate time intervals
affected long-term survival.
TABLE 5. Delays encountered by esophageal cancer patients who have been referred from an other hospital to the Erasmus MC for surgical treatment (group A, N = 365).
Diagnosis on endoscopy elsewhere → first visit outpatient clinic Erasmus MC 17 days (1–138)
First visit outpatient clinic Erasmus MC → diagnosis on endoscopy Erasmus MC 6 days (0–36)
Diagnosis on endoscopy Erasmus MC → multidisciplinary oncology meeting 7 days (0–95)
Multidisciplinary oncology meeting → surgery 15 days (1–67)
Total hospital delay
Diagnosis on endoscopy elsewhere → surgery 53 days (5–175
Lengths of delays are given as a median values with the corresponding range in brackets.
DISCUSSION
When initiating the current study, we hypothesized that longer delays between onset of symptoms,
diagnosis, and surgical treatment are associated with worse short-term outcome (in terms of
morbidity, reoperation rate, and mortality) and worse long-term outcome (overall survival) following
esophagectomy for cancer. In the present series, it appeared that length of prehospital delay (from
onset of symptoms until endoscopic diagnosis) did not influence patient’s short-term outcome or
overall 5-year survival. Onset of symptoms is a subjective measurement, and it may be that patients
are not able to recall the exact moment that they first experienced discomfort. Furthermore, although
little information is known about the tumor doubling time of esophageal cancer, the period of time in
which a patient is symptomatic may be relatively short when compared to the total period between
the first presence of malignant cells in the esophagus and the diagnosis of esophageal cancer.
Unfortunately, we did not have information on delays caused by the GP (i.e., time between onset of
symptoms and referral for endoscopy). Nevertheless, we do want to emphasize the importance of
both patient and primary care education that will result in earlier notification of alarming symptoms
such as dysphagia and weight loss.
A longer hospital delay from endoscopic diagnosis until surgery was associated with higher overall
morbidity and mortality. This could be explained by a more thorough and time-consuming diagnostic
workup in patients with a poorer physical status. Indeed, in the present study, patients of ASA classes I
and II experienced a shorter hospital delay than patients of ASA classes III and IV. Alternatively, a longer
delay prior to surgery may also have caused a worse physical status in esophageal cancer patients by

| Chapter 5
80
means of malnutrition. However, this remains speculative, as our database did not provide detailed
information with regard to patients’ preoperative nutritional status (e.g., nutritional risk indices). When
analyzing the impact of the separate time intervals between patient’s first endoscopy and surgery, it
appeared that the length of the operative waiting list was the time interval that influenced short-term
outcome following esophagectomy the most. From the literature, it is also known that the quality of
life in newly diagnosed esophageal cancer patients who are waiting for surgery is seriously impaired.18
Hence, it should be aimed for to keep this time interval to a minimum.
Our second hypothesis was that patients with longer delays would generally present with more
advanced disease and that this relation between delay and stage would result in a poorer survival.
However, pTNM stages were comparable in patients with a hospital delay <5, 5-8, or >8 weeks
between endoscopy and surgery. Surprisingly, it appeared that overall survival was improved in
patients with a longer hospital delay, although this difference was not statistically significant. This is
in line with the results of Kötz et al.10 who showed that a longer delay between diagnosis and surgical
resection was associated with improved survival in esophageal cancer patients. However, the delay
between diagnosis and surgery was not an independent prognostic variable on multivariate analysis
in their study. Kötz et al.10 noted that patients with a longer delay had a higher rate of complete tumor
resection, suggesting that they were more appropriately selected for surgical treatment. In our series,
we could not find evidence that patients were selected more appropriately, as both pTNM stage and
R0-resection rate did not differ between patients with a shorter or longer hospital delay. However,
hospital delay substantially increased especially over the last few years in our hospital (Fig. 2). This
can probably explain the counter-intuitive correlation between longer hospital delay and improved
long-term survival, which is rather reflecting state-of-the-art staging modalities, refined surgical
techniques, and improved intensive care that have been introduced over the past years. Theoretically,
it could also be possible that, in our hospital, patients did not undergo surgery anymore after a longer
hospital delay in case the tumor progressed to a stage that was considered irresectable. However, in
our patient group, the increased hospital delay can rather be ascribed to an increase in length of the
operative waiting list than to an increased staging delay. As the decision on whether to operate or
not has been made during the multidisciplinary oncology meeting, it is unlikely that a longer hospital
delay led to a dropout of patients with irresectable tumors and, hence, a more selected patient group
that underwent esophagectomy.
It is evident that efforts are taken to minimize delays experienced by patients with esophageal cancer
between onset of symptoms, diagnosis, and surgical treatment. The National Health Service cancer
plan was implemented in 2000 in the UK, indicating that all patients with relevant symptoms and
suspected cancer should be able to see a specialist within 2 weeks of their GP referral. The introduction
of these guidelines was associated with reductions in times to first outpatient visit, endoscopy,
and diagnosis in patients with upper gastrointestinal cancer (esophageal or gastric).19,20 However,
the effectiveness of the NHS cancer plan is uncertain, as it can be questioned whether the slightly
improved survival rates after 2000 can be ascribed to this plan.21

Delay in diagnostic workup and treatment of esophageal cancer |
81
Cha
pter
5
In our hospital, we recently introduced a new schedule of diagnostic services for patients with
suspected esophageal cancer. It is attempted to see patients at the outpatient clinic of the Department
of Surgery or Department of Gastroenterology within 1 week after referral. Furthermore, patients are
offered all imaging modalities in 1 week, including upper gastrointestinal endoscopy, endoscopic
ultrasonography, CT scanning of thorax and abdomen, and external ultrasound of the neck. The aim
of this schedule is to minimize the delay between referral to our hospital and establishment of a
definitive treatment plan for each individual patient.
In conclusion, length of prehospital delay (from onset of symptoms until diagnosis) did not affect
patient’s short- or long-term outcome. A longer hospital delay (between endoscopic diagnosis and
surgery) resulted in worse patient’s short-term outcome (higher overall morbidity and mortality
rates) but not in worse long-term outcome (overall survival). This may be explained by a more time-
consuming diagnostic workup in patients with a poorer physical status and not by tumor progression.

| Chapter 5
82
REFERENCES1. Lerut T, De Leyn P, Coosemans W et al. Surgical strategies in esophageal carcinoma with emphasis on radical
lymphadenectomy. Ann Surg 1992;216(5):583–590
2. Siewert JR, Stein HJ, Feith M et al. Histologic tumor type is an independent prognostic parameter in esophageal cancer: lessons from more than 1,000 consecutive resections at a single center in the Western world. Ann Surg 2001;234(3):360–367. (discussion 368–369).
3. Hulscher JB, van Sandick JW, de Boer AG et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med 2002;347(21):1662–1669.
4. Eloubeidi MA, Desmond R, Arguedas MR et al. Prognostic factors for the survival of patients with esophageal carcinoma in the U.S.: the importance of tumor length and lymph node status. Cancer 2002;95(7):1434–1443.
5. Wijnhoven BP, Tran KT, Esterman A et al. An evaluation of prognostic factors and tumor staging of resected carcinoma of the esophagus. Ann Surg 2007;245(5):717–725.
6. Richards MA, Westcombe AM, Love SB et al. Influence of delay on survival in patients with breast cancer: a systematic review. Lancet 1999;353(9159):1119–1126.
7. Ramos M, Esteva M, Cabeza E et al. Relationship of diagnostic and therapeutic delay with survival in colorectal cancer: a review. Eur J Cancer 2007;43(17):2467–2478.
8. Ramos M, Esteva M, Cabeza E et al. Lack of association between diagnostic and therapeutic delay and stage of colorectal cancer. Eur J Cancer 2008;44(4):510–521.
9. Wang J, Liu F, Gao H et al. The symptom-to-treatment delay and stage at the time of treatment in cancer of esophagus. Jpn J Clin Oncol 2008;38(2):87–91.
10. Kotz BS, Croft S, Ferry DR. Do delays between diagnosis and surgery in resectable oesophageal cancer affect survival? A study based on West Midlands cancer registration data. Br J Cancer 2006;95(7):835–840.
11. Rothwell JF, Feehan E, Reid I et al. Delay in treatment for oesophageal cancer. Br J Surg 1997;84(5):690–693.
12. Martin IG, Young S, Sue-Ling H, Johnston D. Delays in the diagnosis of oesophagogastric cancer: a consecutive case series. BMJ 1997;314(7079):467–470.
13. Witzig R, Schonberger B, Fink U et al. Delays in diagnosis and therapy of gastric cancer and esophageal adenocarcinoma. Endoscopy 2006;38(11):1122–1126.
14. Kok TC, Van Lanschot JJB, Siersema PD et al. Neoadjuvant chemotherapy in operable esophageal squamous cell cancer: final report of a phase III multicenter randomized controlled trial. Proc Am Soc Clin Oncol 1997;17:984.
15. van Heijl M, van Lanschot JJ, Koppert LB et al. Neoadjuvant chemoradiation followed by surgery versus surgery alone for patients with adenocarcinoma or squamous cell carcinoma of the esophagus (CROSS). BMC Surg 2008;8:21.
16. Omloo JM, Lagarde SM, Hulscher JB et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg 2007;246(6):992–1000. (discussion 1000–1001).
17. Sobin L. TNM classification of malignant tumors, 6th edn. Wiley: New York, 2002.
18. Visser MR, van Lanschot JJ, van der Velden J et al. Quality of life in newly diagnosed cancer patients waiting for surgery is seriously impaired. J Surg Oncol 2006;93(7):571–577.
19. Logan RF, Behan MW, Campion G, Keating NA. Impact of the two-week referral guideline on time to diagnosis and treatment in oesophago-gastric cancer. Clin Med 2003;3(4):386–387.

Delay in diagnostic workup and treatment of esophageal cancer |
83
Cha
pter
5
20. Spahos T, Hindmarsh A, Cameron E et al. Endoscopy waiting times and impact of the two week wait scheme on diagnosis and outcome of upper gastrointestinal cancer. Postgrad Med J 2005;81(961):728–730.
21. Rachet B, Maringe C, Nur U et al. Population-based cancer survival trends in England and Wales up to 2007: an assessment of the NHS cancer plan for England. Lancet Oncol 2009;10(4):351–369.

P. van Hagen
M.C.W. Spaander
A. van der Gaast
C.M. van Rij
H.W. Tilanus
J.J.B. van Lanschot
B.P.L. Wijnhoven
International Journal of Clinical Oncology 2013;18(2):214-9.

Chapter 6Impact of a multidisciplinary tumor board meeting for
upper-GI malignancies on clinical decision making: a prospective cohort study

| Chapter 6
86
ABSTRACT
BACKGROUND
The Dutch guidelines for diagnosis and treatment of upper-GI malignancies recommend review of
patients by a multidisciplinary tumor board (MDT). The purpose of this study was to determine the
effect on clinical decision making of an MDT for patients with upper-GI malignancies.
METHODS
All physicians participating in the MDT completed an electronic standardized case form to delineate
their proposed treatment plan for the patients they presented, including the intent of treatment and
the modality of treatment. This therapeutic or diagnostic proposal was then compared with the plan
on which consensus was reached by the MDT.
RESULTS
A total of 252/280 (90.0%) forms were completed and suitable for analysis. In 87/252 (34.5%) of the
case presentations, the MDT altered the proposed plan of management. In 29/87 (33.3%) cases, a
more extensive diagnostic work-up was decided upon. In 8/87 (9.2%) cases the curative intent of the
proposed treatment was altered to palliation only. In 2/75 (2.7%) cases, however, it was decided that a
patient could be treated with curative intent instead of the proposed palliative intent.
CONCLUSION
In over 1/3 of cases, the diagnostic work-up or treatment plan is altered after evaluation by a
multidisciplinary tumor board. This study supports Dutch guidelines recommending discussion of
patients with upper-GI malignancies by a multidisciplinary tumor board.

Impact of a multidisciplinary tumor board meeting for upper-GI malignancies on clinical decision making |
87
Cha
pter
6
INTRODUCTION
Diagnosis and treatment of upper-GI malignancies can be challenging, and most cases require a
multidisciplinary approach. The wide variety of diagnostic tools, (neo)adjuvant treatment regimens,
surgical techniques, and palliative treatment options makes it almost impossible for an individual
specialist to stage and treat a patient with esophageal or gastric cancer1. Many Dutch University
and community hospitals have multidisciplinary tumor board (MDT) meetings in which patients are
discussed by a team of dedicated specialists. The need for multidisciplinary treatment of patients is
also acknowledged in the Dutch guidelines for treating esophageal and gastric malignancies2.
In many other fields of oncologic practice, it has been shown that discussing patients in an MDT can
improve survival3 and resection rates4 and alter treatment plans for many patients. These alterations
of treatment plans have been reported for 24% of patients with head and neck malignancies5 and for
up to 52% of breast cancer patients6 discussed in an MDT. Overall, the variety of decisions made by
individual practitioners can be greatly reduced by the process of multidisciplinary decision making7.
Especially nowadays, when most patients with upper-GI malignancies are offered multimodal
treatment and the number of treatment options is increasing, communication between the treating
specialists should be optimum, to decide on the best possible care. MDTs can substantially contribute
to efficient and clear communication between specialists8.
The exact clinical effect of decisions made by an MDT is hard to determine. In several studies, alteration
of treatment plans after discussion by an MDT is taken as a measure of clinical effect5,6,9. In contrast
with, for instance, breast, lung, and gynecologic malignancies, little is known about the value of MDTs
for patients with upper-GI malignancies. The purpose of this study was to determine the effect of the
MDT for upper-GI malignancies on clinical decision making in a tertiary referral center.
METHODS
In our tertiary referral center, a weekly MDT meeting for upper-GI malignancies is held in which an
upper-GI surgeon, medical oncologist, gastroenterologist, radiation oncologist, and pathologist
participate. For newly diagnosed GI malignancies, patients were discussed by the MDT after
standardized pretreatment work-up had been performed. Patients with endoscopically resectable
tumors (T1N0) were discussed only after failure of endoscopic treatment. The participating specialist
to whom the patient was initially referred presents the case to the MDT. After discussion by the MDT,
consensus is reached on a treatment plan or further diagnostic workup. The decision made by the
MDT is binding and is digitally recorded in the patients’ electronic medical records.
Over an 8-month period, participating physicians were asked to complete the first part of a
standardized digital case form. Detailed description of patient demographics, results of diagnostic
tests, and proposed treatment are obligatory before a patient is discussed by an MDT. After this
discussion, the second part of the case form is completed by the chairman of the MDT; this contains

| Chapter 6
88
a summary of the decision of the panel, and the definitive plan of management. Possible treatment
plans that could be proposed by the presenting specialist and then decided upon by the MDT are
shown in Fig. 1.
new diagnosis recurrence second opinion pathology results other
curative palliative not applicable
primary surgery transhiatal resection transthoracic resection (neo)adjuvant/induction therapy followed by transthoracic resection transhiatal resection definitive chemoradiotherapy other
chemotherapy radiotherapy external beam radiotherapy brachytherapy chemoradiotherapy endoluminal stenting other
follow-up further diagnostic work-up - radiologic - gastroduodenoscopy/ endo-ultrasonography - histologic investigation no therapeutic options
definitive treatment plan
definitive treatment plan
definitive treatment plan
Reason for presentation
Intent of treatment
Treatment modality
Other options
Definitive treatment plan
FIGURE 1. Options for filling out the standardised digital multidisciplinary tumour (MDT) board meeting case form. All options are valid for both proposed and definitive treatment plan.
For this analysis, the initially proposed treatment plans were compared with the definitive treatment
plans. If after discussion by the MDT the treatment plan was altered, the level at which this alteration
occurred was determined and scored. Alterations could occur at the level of intent of treatment (e.g.
curative intent was altered to “not applicable” because further diagnostic work-up had to take place),
at the level of treatment modality (e.g. primary surgery was altered to definitive chemoradiotherapy),
and within the level of treatment modality (e.g. transthoracic resection was altered to transhiatal

Impact of a multidisciplinary tumor board meeting for upper-GI malignancies on clinical decision making |
89
Cha
pter
6
resection). Alterations in treatment plans that were made after discussion by the MDT were not
assessed by a third party.
Because all data were anonymized, obtaining patients’ informed consent for this study was not
obligatory according to the medical ethics committee in our center. Alterations in treatment plan
were expressed as percentage of discussed cases, or as percentage of cases in which alteration of
a treatment plan occurred. Statistical analysis was performed by use of Statistical Package for Social
Sciences version 17.0 (SPSS, Chicago, IL, USA).
RESULTS
Over an 8-month period, 34 MDT meetings were held, in which 171 patients were discussed. A total
of 280 case forms were completed, one for each time a patient was discussed. Of these case forms,
252 were complete and suitable for analysis. For most patients the case was presented to the panel by
the upper-GI surgeon (54.0%), followed by the medical oncologist, gastroenterologist, and radiation
oncologist (23.8, 18.3 and 3.2%, respectively).
One hundred-and-eight (42.9%) case forms were completed for patients with newly diagnosed
esophagogastric malignancies whereas for 33 (13.1%) the reason for presentation was recurrent
disease. Fifteen (6.0%) patients were discussed as a second opinion and in 39 (15.5%) cases the
pathology results after resection were discussed. In 57 (22.6%) patients, there was another reason for
presentation, for example re-evaluation after chemo(radio)therapy or new diagnostic findings. The
clinical characteristics of patients, the number of patients per presenting specialty, and the reasons for
presentation are summarized in Table 1.
One hundred-and-eighteen (46.8%) of the 252 proposed treatment plans were initially curative, and
75/252 (29.8%) palliative. In 59/252 (23.4%) of the cases presented, a curative or palliative intent could
not be scored, for example when pathologic findings after resection were evaluated.
For 87/252 (34.5%) of the proposed treatment plans, the MDT altered the proposed treatment. In
8/118 (6.8%) cases for which a curative treatment plan was proposed, the treatment plan was altered
to palliative treatment. Only 2/75 (2.7%) cases with a proposed palliative treatment plan were altered
to curative treatment. Of the proposed treatment plans for which no intent of treatment could be
applied, because further diagnostic work up was proposed, 6/59 (10.2%) were altered to curative or
palliative treatment after discussion.
For 31/87 (35.6%) cases in which an alteration occurred, another treatment modality was decided
upon, without altering the intent of treatment. In 29/87 (33.3%) cases, a more extensive diagnostic
work-up was decided upon. In 2/87 (2.3%) cases, another treatment within the same modality
(another form of radiotherapy) was decided on. All proposed and definitive management plans are
summarized in Table 2.

| Chapter 6
90
TABLE 1. Characteristics of 171 patients presented to the multidisciplinary tumor board (MDT)
Characteristic n (%)
Age (n = 171)
Median 63
Range 39–86
Sex (n = 171)
Male 129 (75.4%)
Female 42 (24.6%)
Tumor histology (n = 171)
Squamous cell carcinoma 46 (26.9%)
Adenocarcinoma 113 (66.1%)
Other 12 (7.0%)
Tumor location (n = 171)
Esophagus 94 (55.0%)
EGJ 34 (19.9%)
Stomach 41 (24.0%)
Not applicable 2 (1.2%)
cT-stagea (n = 171)
0 1 (0.6%)
1 9 (5.3%)
2 21 (12.3%)
3 87 (50.9%)
4 17 (9.9%)
Unknown 36 (21.1%)
cN-stagea (n = 171)
0 29 (17.0%)
1 117 (68.4%)
Unknown 25 (14.6%)
cM-stageb (n = 171)
0 107 (62.6%)
1a 24 (14.0%)
1b 21 (12.3%)
Unknown 19 (11.1%)
Presenting specialty (n = 252)
Surgery 136 (54.0%)
Medical oncology 60 (23.8%)
Gastroenterology 46 (18.3%)

Impact of a multidisciplinary tumor board meeting for upper-GI malignancies on clinical decision making |
91
Cha
pter
6
TABLE 1. Continued
Characteristic n (%)
Radiotherapy 8 (3.2%)
Other 2 (0.8%)
Reason for presentation (n = 252)
Newly diagnosed 108 (42.9%)
Recurrent disease 33 (13.1%)
Second opinion 15 (6.0%)
Pathology results 39 (15.5%)
Other 57 (22.6%)
EGJ, esophago-gastric junctionaClinical T-stage and N-stage according to the 6th edition of the TNM classification of the Union International Contre le Cancer (UICC), determined by use of endo-ultrasonography (and/or computed tomography for T4 tumors)bClinical M-stage according to the 6th edition of the TNM classification of the Union International Contre le Cancer (UICC), determined by use of computed tomography and/or external ultrasonography of the neck.

| Chapter 6
92
TABL
E 2.
Pro
pose
d an
d de
finiti
ve m
anag
emen
t pl
ans
for
252
cons
ecut
ive
case
s di
scus
sed
by t
he m
ultid
isci
plin
ary
tum
or b
oard
(M
DT)
for
upp
er g
astr
oint
estin
al
mal
igna
ncie
s
Defi
nitiv
e m
anag
emen
t pla
n
Prop
osed
trea
tmen
t pla
nCu
rativ
e in
tent
prim
ary
surg
ery
tran
shia
tal
rese
ctio
ntr
anst
hora
cic
rese
ctio
not
her
(neo
)adj
uvan
t/in
duct
ion
chem
othe
rapy
defin
itive
ch
emo-
radi
othe
rapy
othe
r
Palli
ativ
e tr
eatm
ent
optio
nsC
hem
o-th
erap
yRa
dio-
ther
apy
Exte
rnal
be
am
radi
atio
nBr
achy
-th
erap
yC
hem
o-ra
diot
hera
pyEn
dolu
min
al
sten
ting
othe
r
no o
ptio
ns/
best
su
ppor
tive
care
Not
ap
plic
able
Follo
w-
up
Furt
her
diag
nost
ic
wor
k-up
118
Cura
tive
inte
nt92
818
35 p
rimar
y su
rger
y23
97
74
12
14
14 tr
ansh
iata
l res
ectio
n9
21
11
8 tr
anst
hora
cic
rese
ctio
n7
1
14 o
ther
72
14
64(n
eo)a
djuv
ant/
indu
ctio
n ch
emot
hera
py1
145
11
32
11
11
9de
finiti
ve
chem
orad
ioth
erap
y7
11
1
10ot
her
73
75Pa
lliat
ive
trea
tmen
t op
tions
262
11
32ch
emot
hera
py 1
192
11
42
4
16ra
diot
hera
py2
87
11
14
11 e
xter
nal b
eam
ra
diat
ion
16
61
3
5 b
rach
ythe
rapy
21
11
11
7ch
emor
adio
ther
apy
15
1
7en
dolu
min
al s
tent
ing
24
1
11ot
her
11
21
14
21
2no
opt
ions
/bes
t su
ppor
tive
care
2
59N
ot a
pplic
able
42
53
32fo
llow
-up
11
31
27fu
rthe
r dia
gnos
tic
wor
k-up
31
11
11
22
252
TOTA
L98
2811
89
509
1172
3015
610
47
8233
4

Impact of a multidisciplinary tumor board meeting for upper-GI malignancies on clinical decision making |
93
Cha
pter
6
DISCUSSION
The purpose of this study was to determine the clinical effect of discussing patients with upper-GI
malignancies in an MDT meeting. These data show that in 87/252 (34.5%) of cases, the initially proposed
management plan was altered after discussion by the MDT. In most cases, alterations concerned
specific details of the initially proposed treatment modality, although in 16/252 (6.4%) cases the intent
of treatment (curative or palliative) was modified.
Diagnosis and treatment of esophageal and gastric malignancies has long been a process in which
the different individual specialists were responsible for sequential steps in the process. Staging
was performed by the gastroenterologist; surgery was then performed by the surgeon and the
radiotherapeutic and medical oncologist were involved when palliation was the only option.
Much has changed, however, over recent decades, resulting in multi-modal treatment for upper-GI
malignancies1, 10, 11. Neoadjuvant and adjuvant therapies are now important in the treatment of upper-
GI malignancies. Moreover, diagnostic tools have evolved, necessitating the input of several specialists
for more accurate staging12. Communication and cooperation between these specialists are of great
importance8, justifying the need for multi-disciplinary discussion by MDTs.
For patients with gynecologic malignancies, Greer et al.9 showed that evaluation by an MDT altered
clinical management in 20.0% of cases that were presented for a review of pathology and in 10.0%
of cases presented for a review of radiology. Another retrospective study performed by Chang et al.13
for 75 patients with breast malignancies showed that the multidisciplinary panel disagreed with the
external presenting physician in 43% of cases. However, both studies were retrospective in nature, and
involved tumors for which pathology has a much greater effect on clinical decision making than for
upper-GI tumors (e.g. hormone receptor status in breast malignancies).
Wheless et al.5 published a prospective study of patients with head and neck tumors for which the
clinical effect of discussion by an MDT was described. Malignancies of the head and neck are similar to
upper-GI malignancies in that they are often diagnosed and treated by a multidisciplinary team. In that
study, in 27.0% of the cases discussed there was an alteration in primary tumor diagnosis, tumor stage,
or treatment plan. This percentage is comparable with the percentage found in our study.
A study performed by Bumm et al.14 involving the effect of an MDT for upper-GI malignancies showed
that the proposed treatment plan was altered in 36.0% of the cases discussed. In another 6% of cases,
further diagnostic work-up was decided upon. That is, as far as we are aware, the only study performed
so far for patients with an upper-GI malignancy. Unfortunately, that study does not describe the actual
alterations in treatment, so the effect on clinical decision making is hard to determine. One can imagine
that alterations within the same treatment modality have less effect than changing a curative intent to
a palliative intent of treatment (or vice versa).
The data for this study were collected prospectively in a high-volume center with special interest in
this type of patient. The clinical characteristics of the study population are sufficiently heterogeneous
to ensure a wide variety of possible treatments. Devitt et al.15 have already shown that health-care
professionals regard the MDT as a useful tool in the treatment of patients with malignancies and value
the opportunity for peer review that is provided by MDT meetings.

| Chapter 6
94
Case discussion by an MDT may cause a delay between diagnosis and start of treatment. Leo et al.16
found the median delay was 20 days for patients treated for lung malignancies. However, in a study
performed in our center by Grotenhuis et al.17 it was shown that a treatment delay longer than 5
weeks (including discussing patients in the MDT) resulted in more post-operative morbidity, but did
not affect long-term survival. However, as Grotenhuis et al. also stated, higher postoperative morbidity
and mortality for patients with a longer delay is also very likely to be caused by case selection.
Patients with severe co-morbidity usually have a longer preoperative work-up before undergoing
esophagectomy, and are more prone to suffer from post-operative morbidity and even mortality.
CONCLUSION
Discussing patients with upper-GI malignancies in a multidisciplinary tumor board meeting results in
an altered clinical decision in more than one third of cases. This study supports the recommendations
of the Dutch “Guidelines for the diagnosis and treatment of upper-GI malignancies” that all patients
should be discussed in the setting of an MDT before initiation of therapy.

Impact of a multidisciplinary tumor board meeting for upper-GI malignancies on clinical decision making |
95
Cha
pter
6
REFERENCES1. Kaifi JT, Gusani NJ, Jiang Y et al (2011) Multidisciplinary management of early and locally advanced esophageal
cancer. J Clin Gastroenterol 45:391–399
2. Siersema PD, Rosenbrand CJ, Bergman JJ et al (2006) Richtlijn ‘diagnostiek en behandeling oesofaguscarcinoom’ [guideline ‘diagnosis and treatment of oesophageal carcinoma’]. Ned Tijdschr Geneeskd 150:1877–1882
3. Junor EJ, Hole DJ, Gillis CR (1994) Management of ovarian cancer: referral to a multidisciplinary team matters. Br J Cancer 70:363–370
4. Davison AG, Eraut CD, Haque AS et al (2004) Telemedicine for multidisciplinary lung cancer meetings. J Telemed Telecare 10:140–143
5. Wheless SA, McKinney KA, Zanation AM (2010) A prospective study of the clinical impact of a multidisciplinary head and neck tumor board. Otolaryngol Head Neck Surg 143:650–654
6. Newman EA, Guest AB, Helvie MA et al (2006) Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer 107:2346–2351
7. Pfeiffer SI, Naglieri JA (1983) An investigation of multidisciplinary team decision-making. J Learn Disabil 16:588–590
8. Ruhstaller T, Roe H, Thurlimann B et al (2006) The multidisciplinary meeting: an indispensable aid to communication between different specialities. Eur J Cancer 42:2459–2462
9. Greer HO, Frederick PJ, Falls NM et al (2010) Impact of a weekly multidisciplinary tumor board conference on the management of women with gynecologic malignancies. Int J Gynecol Cancer 20:1321–1325
10. Menges M (2011) Gastric cancer: where is the place for the surgeon, the oncologist and the endoscopist today? World J Gastrointest Oncol 3:10–13
11. Quiros RM, Bui CL(2009) Multidisciplinary approach to esophageal and gastric cancer. Surg Clin North Am 89:79–96, viii
12. Low DE (2011) Update on staging and surgical treatment options for esophageal cancer. J Gastrointest Surg 15:719–729
13. Chang JH, Vines E, Bertsch H et al (2001) The impact of a multidisciplinary breast cancer center on recommendations for patient management: the University of Pennsylvania experience. Cancer 91:1231–1237
14. Bumm R, Feith M, Lordick F et al (2009) Impact of multidisciplinary tumor boards on diagnosis and treatment of esophageal cancer. Eur Surg 39:136–140
15. Devitt B, Philip J, McLachlan SA (2010) Team dynamics, decision making, and attitudes toward multidisciplinary cancer meetings: health professionals’ perspectives. J Oncol Pract 6:e17–e20
16. Leo F, Venissac N, Poudenx M et al (2007) Multidisciplinary management of lung cancer: how to test its efficacy? J Thorac Oncol 2:69–72
17. Grotenhuis BA, van Hagen P, Wijnhoven BP et al (2010) Delay in diagnostic workup and treatment of esophageal cancer. J Gastrointest Surg 14:476–483

P. van Hagen
K. Biermann
J.E. Boers
O. Stoss
H.F. Sleddens
J.J.B. van Lanschot
W.N.M. Dinjens
J. Rueschoff
B.P.L. Wijnhoven
Diseases of the Esophagus 2015, 28(4):380-5
This study was financially supported by an unrestricted grant from Roche b.v., Woerden, the Netherlands

Chapter 7Human epidermal growth factor receptor 2
overexpression and amplification in endoscopic biopsies and resection specimens in esophageal
and junctional adenocarcinoma

| Chapter 7
98
ABSTRACT
AIMS
Human Epidermal growth factor Receptor 2 (HER2) is overexpressed in a subset of esophageal
adenocarcinomas. Frequently, biopsy material is used for evaluation of HER2 status. The aim of the
study was to determine if HER2 expression in preoperative endoscopic biopsies is representative for
the entire tumor.
METHODS
Preoperative endoscopic biopsies and matched resection specimens were collected from 75 patients
who underwent esophagectomy for esophageal adenocarcinoma. Immunohistochemical staining
(IHC) on HER2 and dual-color in-situ hybridization (ISH) were performed. HER2 status was determined
by following a clinical algorithm, first determining HER2 overexpression on IHC, and when equivocal
(2+), determining HER2 amplification on ISH.
RESULTS
71/75 (95%) biopsies and 69/75 (92%) resection specimens could be analyzed, due to technical failure.
HER2 positivity was seen in 18/71 (25%) biopsies and in 15/69 (22%) resection specimens. Overall,
HER2 status in the biopsy was concordant with HER2 status in the resection specimen in 94% of
cases. Interobserver agreement on IHC-scoring for all three observers was 83% in biopsies and 85%
in resection specimens.
CONCLUSION
HER2 positivity was detected in 22% of esophageal adenocarcinomas. Although inter-observer
agreement was moderate, HER2 status of a primary tumor can be reliably determined based on the
endoscopically obtained pretreatment biopsy.

HER2/neu overexpression in biopsies and resection specimens of esophageal adenocarcinoma |
99
Cha
pter
7
INTRODUCTION
Cancer of the esophagus is the sixth cause of cancer death worldwide. It is a highly lethal disease in
which only one third of patients have a resectable tumor at the time of presentation. Surgery with
neoadjuvant chemo(radio)therapy offers the best chances for long-term survival.1 However, still half
of patients suffer from recurrence of disease after multimodality therapy.2-4 Clearly, new treatments are
needed to improve the outcome of patients with esophageal cancer.
The Human Epidermal growth factor Receptor 2 (HER2) regulates cell growth and proliferation.
Overexpression of HER2 has been identified in a wide variety of carcinomas, including esophageal
cancer. HER2 overexpression correlates with advanced tumor stage and poor survival.5-9 Trastuzumab,
a monoclonal antibody against the HER2 receptor, inhibits the receptor activity and oncogenic
downstream targets. 10 In HER2-positive breast cancer, trastuzumab improves overall and disease-free
survival in early and metastatic disease. 11 Overexpression of HER2 is not uncommon in esophageal
cancer with up to 43% of the cancers being HER2 positive.10, 12-17 Hence, trastuzumab could well be an
effective drug in the multimodal treatment of esophageal cancer.18 In metastatic gastric cancer, the
addition of Trastuzumab to standard palliative chemotherapy has proved to be of benefit. 19
Trastuzumab is only effective in cancer cells overexpressing HER2 and/or cells that show HER2 gene
amplification 6 The HER2 status is evaluated by immunohistochemical staining (IHC) and HER2 gene
amplification by In Situ Hybridization (ISH).20 Abundant tumor tissue is available for analysis from
the resection specimen. However, preoperative biopsies from esophageal cancer are limited in size.
Moreover, expression of oncogenes and tumor suppressor genes in adenocarcinomas of the upper
gastrointestinal tract are well known to be heterogeneous which questions the representativeness of
a small tissue fragment taken at endoscopy.21 This might lead to under-treatment of patients in whom
HER2 overexpression/amplification was falsely scored negative. On the other hand, false positive
biopsies may lead to an increase of toxicity and costs, and moreover, inadequate prognostication with
a potential negative impact on clinical decision making.
The aims of the present study were to determine if the HER2 status of an esophageal adenocarcinoma
can be reliably determined based on endoscopic biopsies, and to assess the inter-observer agreement
in determining HER status.
MATERIALS AND METHODS
Patients and samples
Patients who had undergone an esophagectomy for adenocarcinoma of the esophagus or OGJ
between January 2000 to January 2010 in the Erasmus MC, Rotterdam, the Netherlands were
identified from the institutional database. Seventy-five patients with a cT2-cT3 tumor were selected.
Excluded were cT1 and cT4 tumors and patients who underwent any form of neoadjuvant or adjuvant
chemo(radio)therapy. cT1 tumors were excluded because of the limited additional effect of neo-

| Chapter 7
100
adjuvant therapy targeted at HER2 that can be expected after resection in this group of tumors which
already has a relatively high survival rate after resection. cT4 tumors were excluded because in our
center, cT4 tumors are not resected but are treated with definitive chemoradiotherapy, after which no
resection specimen is available to compare to the pre-treatment biopsies.
Also patients with incomplete or inadequate archived tumor tissue (either in biopsies or the surgical
resection specimen) were excluded. Patients were selected consecutively whenever possible.
Tissue blocks of the endoscopic biopsies, routinely taken from multiple areas of the tumor, as well as
the resection specimen for each patient were retrieved. All tissue samples had been fixed using 4%
buffered formalin and embedded in paraffin after dehydration. All biopsies and a representative area
of invasive tumor of the resection specimen that was identified using a Haematoxylin and Eosin (H&E)
stain. Subsequently, 4-μm sections were cut from the tissue blocks and were used for IHC and ISH.
Several patient and tumor characteristics were identified including patients’ age (at the time of
diagnosis), sex and tumor stage according to the AICC TNM 6th edition (as determined by endo-
ultrasonography and CT-scanning of the chest and abdomen, or from pathology report when clinical
investigations were not conclusive).22 The study was reviewed and approved by the local medical
ethics committee and the requirement of obtaining patients’ informed consent was waived.
HER2 immunohistochemistry (IHC) and dual-colour In-situ Hybridization (ISH)
The 4-μm sections were mounted on starfrost slides (Knittel Gläser, Braunschweig, Germany) and
dried. The immunohistochemical staining was performed using a BenchMark ULTRA automated
slide staining instrument (Ventana Medical Systems, Tuscon, AZ, USA) and using the PATHWAY HER2
4B5 antibody, according to the manufacturer’s instructions. ISH staining was also performed fully
automated with the BenchMark ULTRA, with the INFORM HER2 DNA probe and the Red ISH V probe
(both Ventana Medical Systems).
Evaluation of HER2 status
HER2 expression and amplification was independently assessed by three experienced pathologists
(KB, JEB and JR) from three institutions (Erasmus MC, University Medical Centre Rotterdam, Rotterdam,
The Netherlands; Isala Clinics Zwolle, The Netherlands, and TARGOS Molecular Pathology, Kassel,
Germany). The pathologists were blinded for the patients. Biopsies and resection specimens were
rotating amongst the centers in three batches making sure that matching biopsies and resection
specimens were never present at the same location simultaneously. The H&E staining, IHC and ISH
results of the tissues from a single patient’s biopsy or resection specimens were at the disposal of the
pathologist.

HER2/neu overexpression in biopsies and resection specimens of esophageal adenocarcinoma |
101
Cha
pter
7
Positive
2+ 1+ 3+
Negative
Dc-SISH
HER2:CEP17 <2.2 HER2:CEP17 >2.2
IHC staining
FIGURE 1. Algorithm for the assessment of HER2 status IHC: ImmunohistochemistryIntensity of reactivity: 0-1+ = absent - faint, 2+ = moderate, 3+ = strongISH: dual color-silver in situ hybridizationHER2:CEP17 : HER2 and centromeric probe 17 ratio
For determining the HER2 status an algorithm was used (Fig 1.). In case of no or weak HER2 expression
(1+) the tumor is scored as HER2 negative, and in case of strong expression (3+), the tumor is scored
as HER2 positive. In case of moderate expression (2+), the results of ISH are evaluated, and the HER2
status is determined based on the absence (negative) or presence (positive) of HER2 amplification
(Fig 2.).
Evaluation of the IHC for HER2 was done according to the scoring system for gastric and OGJ cancer.23 In
brief: HER2 expression in the resection specimen was scored as 2+ when ≥10% of tumor cells showed
a weak to moderate complete or basolateral membranous reactivity. For preoperative biopsies, the
presence of cohesive IHC 3+ and/or ISH+ clones resulted in a positive HER2 status irrespective of
size.23 For ISH evaluation, the HER2: CEP17 (centromeric probe 17) ratio was determined. A sample was
considered positive for HER2 amplification when this ratio was >2.2.
Statistical analysis
HER2 status was defined as positive or negative.23 The statistical analysis was performed using
Statistical Package for Social Sciences version 17.0 (SPSS Inc., Chicago, IL, USA).

| Chapter 7
102
RESULTS
Patients
A total of 75 patients were selected who met the inclusion criteria. The male: female ratio was 3:1 and
the mean age was 63 years. Forty-eight patients (64%) had a cT3 tumor and 45 (60%) patients were
staged as node positive. (Table 1)
TABLE 1. Patient and tumor characteristics of 75 patients with esophageal or esophagogastric junction adenocarcinoma
Characteristics
Gender (n, %)malefemale
5619
(75%)(25%)
Age [years] mean (SD) 63 (11%)
Tumor differentiation (n, %)goodmoderatepoormissing
32942 1
( 4%)(39%)(56%)( 1%)
Clinical T-stage (n, %)†cT2cT3no endoscopic pass
2048 7
(27%)(64%)( 9%)
Clinical N-stage (n, %)‡N0N1missing
2345 7
(31%)(60%)( 9%)
SD: Standard deviation† Clinical T-stage: T-stage as defined by endo-ultrasonography and/or CT-scanning according to UICC TNM Cancer Staging, 6th edition. ‡Clinical N-stage: clinical N-stage as defined by endo-ultrasonography and/or CT-scanning and/or FDG-PET according to UICC TNM Cancer Staging, 6th edition.
Biopsies
A mean of 5 biopsies (standard deviation ± 2) per patient were collected. The biopsies of four (5%)
patients could not be evaluated for HER2 expression by IHC. One biopsy was identified as squamous
cell carcinoma and in the three remaining biopsies the IHC failed. In 16/71 (23%) patients, expression
of HER2 by IHC was 3+, in 3/71 (4%) patients this was 2+. Two of these biopsies showed HER
amplification. Hence, 18/71 (25%) biopsies were HER2 positive. (Table 2)

HER2/neu overexpression in biopsies and resection specimens of esophageal adenocarcinoma |
103
Cha
pter
7
Resection specimens
Six (8%) patients were excluded: there was one squamous cell carcinoma, two samples contained no
representative tumor cells and in three IHC staining failed. Thirteen patients (19%) were 3+, whilst 3/69
(4%) were 2+. Two of these showed HER2 gene amplification, resulting in a total of 15/69 (22%) HER2
positive resection specimens. In the third 2+ specimen the ISH failed, resulting in one specimen which
could not be classified as positive or negative after using the clinical algorithm. (Table 2)
TABLE 2. Conventional immunohistochemistry scoring and results with the application of a clinical algorithm† of 71 evaluable biopsies and 69 evaluable resection specimens of esophageal adenocarcinoma
IHC After following algorithm
0-1+ 2+ 3+ Neg Pos NE
Biopsies (n=71) 52 (73%) 3 (4%) 16 (23%) 53 (75%) 18 (25%) 0 (0%)
Resection specimens (n=69) 53 (78%) 3 (4%) 13 (19%) 53 (77%) 15 (22%) 1 (1%)
IHC: ImmunohistochemistryNeg: negativePos: positiveNE: not evaluableIntensity of reactivity: 0-1+: absent - faint, 2+: moderate, 3+: strong† Clinical algorithm:IHC 0-1+: HER2 negative; IHC 2+ à HER2/centromere17 ratio on ISH <2.2: HER2 negative; >2.2: HER2 positive IHC3+: HER2 positive
Concordance, sensitivity and specificity
Concordance of HER2 positivity between the biopsies and matching resection specimens was found
in 14/18 (78%) patients. In 3 (16%) patients the matching resection specimens were HER2 negative,
and in one patient the resection specimen could not be evaluated due to technical failure.
For the positive resection specimens, 14/15 (93%) biopsies were concordant with the positive
status. One of the 53 (2%) HER2 negative biopsies was collected from a tumor that showed HER2
overexpression in the resection specimen. (Table 3) Sensitivity for determining HER2 status of a tumor
in an endoscopic biopsy was 93%, specificity was 94%. The positive predictive value of HER2 testing in
biopsies was 82%, the negative predictive value was 98%.
Inter-observer agreement
There was agreement amongst the pathologists for the assessment of HER2 expression in 83% of
biopsies and in 85% of the resection specimens. Agreement on HER2 gene amplification was found in
55% of the biopsies and 47% of the resection specimens.

| Chapter 7
104
TABLE 3. Concordance in HER2 status (based on clinical algorithm† for HER2 status) in 75 matched pairs of biopsies and resection specimen of esophageal adenocarcinoma
Resection specimen
negative positive NE total
Biop
sy
negative 47 1 5 53
positive 3 14 1 18
NE 3 0 1 4
total 53 15 7 75
NE: not evaluable
† Clinical algorithm:IHC 0-1+: HER2 negative; IHC 2+ à HER2/centromeric probe 17 ratio by ISH <2.2: HER2 negative; >2.2: HER2 positive IHC3+: HER2 positive
FIGURE 2. HE (a1, b1), IHC (a2, b2) and ISH (a3, b3) in two different invasive esophageal adenocarcinomas. In (a), the adenocarcinoma is HER2 negative in IHC, and correspondingly there is no amplification of HER2 gene in ISH. In contrast, adenocarcinoma in example two shows moderate HER2 expression (2+) and the corresponding ISH revealsHER2 amplification in some, but not all tumor cells. Magnification a1, b1, a2: 1:200. b2: 1:400, a3 and b3: 1:600

HER2/neu overexpression in biopsies and resection specimens of esophageal adenocarcinoma |
105
Cha
pter
7
DISCUSSION
The treatment of esophageal cancer with monoclonal antibodies targeted against the HER2 receptor
is only indicated when HER2 is overexpressed.6 Hence, careful selection of HER2-positive tumors is
essential to prevent unnecessary (neo-) adjuvant treatment of patients with HER2-negative tumors,
who are not likely to benefit. This study found that 22% of the esophageal adenocarcinomas are HER2
positive. Most importantly, we showed that HER2 expression can be evaluated in small diagnostic
tissue fragments taken at the time of upper GI endoscopy and HER2 status in these biopsies matches
the HER2 status of the resection specimen available after surgery in 94% of the cases.
The findings of this study are of importance for clinical practice. In many patients only a formalin-
fixed, paraffin-embedded endoscopic biopsy is available in which this HER2 status can be determined.
Hence, the indication for cancer treatment with Trastuzumab relies on accurate determination of HER
2 expression in these small tissue fragments. Nowadays, neoadjuvant therapy is given to most patients
with esophageal cancer which induces complete tumor regression in 25% of patients and no vital
tumor cells are present for HER2 evaluation. Also genetic modifications may take place during chemo-
and radiotherapy which can make determination of the HER2 status unreliable or impossible. 24
It has been questioned that small pretreatment biopsies are not representative for the genetic profile
of the primary tumor. Great heterogeneity was observed in HER2 expression throughout esophageal
adenocarcinomas.25 Several other studies were performed using tissue arrays for determining
HER2 status, risking false-positive or false-negative results due to sampling error in heterogeneous
tumors.26,27 By evaluating all biopsies taken during the first endoscopy from multiple areas of the
tumor and representative sections of the resection specimens, we feel that this possible sampling
error was reduced to a minimum in the present study. However, since we still encountered three false
positive biopsies, sampling error might still be an issue, even when using multiple biopsies.
Problems were encountered with the quality of the ISH. Because IHC already provided sufficient
information to determine HER2 status according to the algorithm, it was only necessary to repeat ISH
in two patients that had been scored as HER 2+ by IHC. Also the use of archival material has not led to
a deviating proportion of HER positive tumors. In fact, 22% positivity for HER2 is well within the range
of other studies.12,13,16,17
A concordance rate of 89-98% for HER2 expression between core biopsies and excision specimens
has been demonstrated for breast cancer.28-30 This is comparable to the 94% concordance rate in the
present study. However, it is also known that after neoadjuvant treatment the HER2-status of a tumor
can differ from the pretreatment status, which might make it more difficult to show concordance in
patients who were neoadjuvantly treated.12
When considering both neoadjuvant and adjuvant treatment, the concordance in HER2-status
between the primary tumor and metastases (both regional and distant) is of importance. A study by
Reichelt et al. reported 100% concordance in HER2 status between the primary tumor and lymph-
node metastases as well as distant metastatic deposits of esophageal cancer when analysed using
a FISH technique.26 A more recent study by Bozetti et al. also found high levels of concordance

| Chapter 7
106
between primary gastric tumors and metastasis.31 Fassan et al found a concordance between primary
esophagogastric junction tumors and lymph-node metastases of more than 98%, using a CISH
technique.32 These results suggest that both neoadjuvant and adjuvant treatment targeted at HER2
in patients with tumors of the upper gastro-intestinal tract will affect the primary tumor as well as
possible metastases in the majority of cases.
The IHC scoring algorithm complicates a comparison in HER2 expression between biopsies and
resection specimens. Discrepant HER2 expression between biopsies and resection specimens could
be explained by different cut-off criteria for HER2 positivity or be true differences based on biology.
However, the different cut-off criteria would only lead to a false positive result in biopsies (due to the
10% rule in resection specimens) and this also only holds true for IHC 1+ or IHC 0 resection specimens
with a focus of less than 10% of strong membrane staining. These cases are rare.
In the present study, the interobserver agreement was moderate with respect to the assessment of
ISH. There are several possible explanations for this finding. First, experience in evaluating ISH results
differed between the observers. Secondly, the equipment used for the analyses was likely not the
same in the three centers influencing the quality of the staining. However, the disagreement amongst
the pathologists is likely reduced to a minimum when using the algorithm, not affecting the finally
determined HER2 status of a specimen.
The developments in HER2 targeted therapy for cancers of the upper gastro-intestinal tract raise
questions about the accuracy of determining the HER2 status of the tumor in small tissue fragments.
The present study shows that this can be reliably performed by following an algorithm, when using
multiple endoscopically obtained pretreatment biopsies.

HER2/neu overexpression in biopsies and resection specimens of esophageal adenocarcinoma |
107
Cha
pter
7
REFERENCES1. van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, et al.
Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012 May 31;366(22):2074-84.
2. Burmeister BH, Smithers BM, Gebski V, Fitzgerald L, Simes RJ, Devitt P, et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomised controlled phase III trial. Lancet Oncol. 2005 Sep;6(9):659-68.
3. Tepper J, Krasna MJ, Niedzwiecki D, Hollis D, Reed CE, Goldberg R, et al. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol. 2008 Mar 1;26(7):1086-92.
4. Urba SG, Orringer MB, Turrisi A, Iannettoni M, Forastiere A, Strawderman M. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol. 2001 Jan 15;19(2):305-13.
5. Dreilich M, Wanders A, Brattstrom D, Bergstrom S, Hesselius P, Wagenius G, et al. HER-2 overexpression (3+) in patients with squamous cell esophageal carcinoma correlates with poorer survival. Dis Esophagus. 2006;19(4):224-31.
6. Hudis CA. Trastuzumab--mechanism of action and use in clinical practice. N Engl J Med. 2007 Jul 5;357(1):39-51.
7. Polkowski W, van Sandick JW, Offerhaus GJ, ten Kate FJ, Mulder J, Obertop H, et al. Prognostic value of Lauren classification and c-erbB-2 oncogene overexpression in adenocarcinoma of the esophagus and gastroesophageal junction. Ann Surg Oncol. 1999 Apr-May;6(3):290-7.
8. Sato-Kuwabara Y, Neves JI, Fregnani JH, Sallum RA, Soares FA. Evaluation of gene amplification and protein expression of HER-2/neu in esophageal squamous cell carcinoma using Fluorescence in situ Hybridization (FISH) and immunohistochemistry. BMC Cancer. 2009;9:6.
9. Tanner M, Hollmen M, Junttila TT, Kapanen AI, Tommola S, Soini Y, et al. Amplification of HER-2 in gastric carcinoma: association with Topoisomerase IIalpha gene amplification, intestinal type, poor prognosis and sensitivity to trastuzumab. Ann Oncol. 2005 Feb;16(2):273-8.
10. al-Kasspooles M, Moore JH, Orringer MB, Beer DG. Amplification and over-expression of the EGFR and erbB-2 genes in human esophageal adenocarcinomas. Int J Cancer. 1993 May 8;54(2):213-9.
11. Slamon DJ, Godolphin W, Jones LA, Holt JA, Wong SG, Keith DE, et al. Studies of the HER-2/neu proto-oncogene in human breast and ovarian cancer. Science. 1989 May 12;244(4905):707-12.
12. Schoppmann SF, Jesch B, Zacherl J, Wrba F, Hejna M, Maresch J, et al. HER-2 status in primary oesophageal cancer, lymph nodes and distant metastases. Br J Surg. 2011 May 25.
13. Radu OM, Foxwell T, Cieply K, Navina S, Dacic S, Nason KS, et al. HER2 amplification in gastroesophageal adenocarcinoma: correlation of two antibodies using gastric cancer scoring criteria, H score, and digital image analysis with fluorescence in situ hybridization. Am J Clin Pathol. 2012 Apr;137(4):583-94.
14. Jankowski J, Coghill G, Hopwood D, Wormsley KG. Oncogenes and onco-suppressor gene in adenocarcinoma of the oesophagus. Gut. 1992 Aug;33(8):1033-8.
15. Hardwick RH, Shepherd NA, Moorghen M, Newcomb PV, Alderson D. c-erbB-2 overexpression in the dysplasia/carcinoma sequence of Barrett’s oesophagus. J Clin Pathol. 1995 Feb;48(2):129-32.
16. Schoppmann SF, Jesch B, Friedrich J, Wrba F, Schultheis A, Pluschnig U, et al. Expression of Her-2 in carcinomas of the esophagus. Am J Surg Pathol. 2010 Dec;34(12):1868-73.
17. Yoon HH, Shi Q, Sukov WR, Wiktor AE, Khan M, Sattler CA, et al. Association of HER2/ErbB2 expression and gene amplification with pathologic features and prognosis in esophageal adenocarcinomas. Clin Cancer Res. 2012 Jan 15;18(2):546-54.

| Chapter 7
108
18. Safran H, Dipetrillo T, Akerman P, Ng T, Evans D, Steinhoff M, et al. Phase I/II study of trastuzumab, paclitaxel, cisplatin and radiation for locally advanced, HER2 overexpressing, esophageal adenocarcinoma. Int J Radiat Oncol Biol Phys. 2007 Feb 1;67(2):405-9.
19. Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010 Aug 28;376(9742):687-97.
20. Schneider S, Uchida K, Brabender J, Baldus SE, Yochim J, Danenberg KD, et al. Downregulation of TS, DPD, ERCC1, GST-Pi, EGFR, and HER2 gene expression after neoadjuvant three-modality treatment in patients with esophageal cancer. J Am Coll Surg. 2005 Mar;200(3):336-44.
21. Grabsch H, Sivakumar S, Gray S, Gabbert HE, Muller W. HER2 expression in gastric cancer: Rare, heterogeneous and of no prognostic value - conclusions from 924 cases of two independent series. Cell Oncol. 2010;32(1-2):57-65.
22. Sobin LH, Wittekind C, International Union against Cancer. TNM : classification of malignant tumours. 6th ed. New York: Wiley-Liss; 2002.
23. Hofmann M, Stoss O, Shi D, Buttner R, van de Vijver M, Kim W, et al. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology. 2008 Jun;52(7):797-805.
24. Adams AL, Eltoum I, Krontiras H, Wang W, Chhieng DC. The effect of neoadjuvant chemotherapy on histologic grade, hormone receptor status, and HER2/neu status in breast carcinoma. Breast J. 2008 Mar-Apr;14(2):141-6.
25. Boers JE, Meeuwissen H, Methorst N. HER2 status in gastro-oesophageal adenocarcinomas assessed by two rabbit monoclonal antibodies (SP3 and 4B5) and two in situ hybridization methods (FISH and SISH). Histopathology. 2011 Feb;58(3):383-94.
26. Reichelt U, Duesedau P, Tsourlakis M, Quaas A, Link BC, Schurr PG, et al. Frequent homogeneous HER-2 amplification in primary and metastatic adenocarcinoma of the esophagus. Mod Pathol. 2007 Jan;20(1):120-9.
27. Thompson SK, Sullivan TR, Davies R, Ruszkiewicz AR. HER-2/neu Gene Amplification in Esophageal Adenocarcinoma and Its Influence on Survival. Ann Surg Oncol. 2011 Jan 26.
28. Shousha S, Peston D, Amo-Takyi B, Morgan M, Jasani B. Evaluation of automated silver-enhanced in situ hybridization (SISH) for detection of HER2 gene amplification in breast carcinoma excision and core biopsy specimens. Histopathology. 2009 Jan;54(2):248-53.
29. Sutela A, Vanninen R, Sudah M, Berg M, Kiviniemi V, Rummukainen J, et al. Surgical specimen can be replaced by core samples in assessment of ER, PR and HER-2 for invasive breast cancer. Acta Oncol. 2008;47(1):38-46.
30. Apple SK, Lowe AC, Rao PN, Shintaku IP, Moatamed NA. Comparison of fluorescent in situ hybridization HER-2/neu results on core needle biopsy and excisional biopsy in primary breast cancer. Mod Pathol. 2009 Sep;22(9):1151-9.
31. Bozzetti C, Negri FV, Lagrasta CA, Crafa P, Bassano C, Tamagnini I, et al. Comparison of HER2 status in primary and paired metastatic sites of gastric carcinoma. Br J Cancer. 2011 Apr 26;104(9):1372-6.
32. Fassan M, Ludwig K, Pizzi M, Castoro C, Guzzardo V, Balistreri M, et al. Human epithelial growth factor receptor 2 (HER2) status in primary and metastatic esophagogastric junction adenocarcinomas. Hum Pathol. 2012 Aug;43(8):1206-12.

PART IIPostoperative outcome and prognostication

P. van Hagen
M. van Heijl
M.I. van Berge Henegouwen
R. Boellaard
P.M.M. Bossuyt
F.J.W. ten Kate
H. van Dekken
O.S. Hoekstra
G.W. Sloof
J.J.B. van Lanschot
Diseases of the Esophagus (accepted for publication)

Chapter 8Prediction of disease-free survival using
relative change in FDG-uptake early during neoadjuvant chemoradiotherapy for potentially
curable esophageal cancer: A prospective cohort study

| Chapter 8
112
ABSTRACT
BACKGROUND18F-Fluorodeoxyglucose positron emission tomography (FDG-PET) has been investigated as a tool for
monitoring response to neoadjuvant chemo- and chemoradiotherapy (CT and CRT respectively) and
as a predictor for survival in patients with esophageal cancer. In contrast to patients who undergo
neoadjuvant CT, it is not known whether patients who are clinically identified as responders after
neoadjuvant CRT show better disease-free survival (DFS) than patients identified as nonresponders.
The aim of the study was to determine the predictive value of FDG-uptake measured prior to and early
during neoadjuvant CRT.
METHODS
Patients treated with neoadjuvant CRT between 2004 and 2009 within a randomized trial were
included. FDG-uptake was measured at baseline and after 14 days of CRT. According to the PERCIST-
criteria, patients were allocated to have metabolic response, stable disease or progression. Patients
were followed until recurrence of disease or death. The predictive value of FDG-PET was determined
with uni- and multivariable analysis in patients who underwent potentially curative surgery.
RESULTS
One-hundred and six patients were included in the analysis. Minimal follow-up for surviving patients
was 60 months. No significant differences in DFS were found between patients with metabolic
response, stable disease or progression, with five-year DFS rates of 66%, 53% and 67% respectively
(p=0.39).
CONCLUSION
Relative change in FDG uptake after 14 days of CRT is not associated with disease-free survival in
patients with esophageal cancer undergoing neoadjuvant chemoradiotherapy followed by surgery.
These measurements should not be used for prognostication in this specific group of patients.

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
113
Cha
pter
8
INTRODUCTION
In the Western world, the overall incidence of esophageal cancer is rising.1 Despite many improvements
in diagnosis and treatment, five-year survival rates rarely exceed 40% even after careful preoperative
selection.2,3
Evidence in favor of neoadjuvant chemoradiotherapy (CRT) followed by surgery versus surgery alone
is growing steadily, in terms of improved long-term survival.4,5 It is however well established that only a
proportion of patients treated with neoadjuvant CRT shows a (substantial) histopathological response
in the resection specimen.5-9 The non-responding patients do not benefit from neoadjuvant CRT, but
are still exposed to its toxicity.
If it would be possible to identify non-responders early during neoadjuvant CRT, these patients
would discontinue this therapy and undergo surgery directly. This strategy was designed and already
successfully executed by the Munich group, in patients undergoing FDG-PET monitoring during
neoadjuvant chemotherapy for esophagogastric cancer in the MUNICON-1 and -2 trial.13-14
18F-Fluorodeoxyglucose positron emission tomography (FDG-PET) is a non-invasive imaging
technique which enables quantification of tumor activity based on tissue glucose uptake, which is
generally increased in malignant tissue.10-12 FDG-PET has been investigated as a tool to monitor (early)
response to neoadjuvant therapy and as a predictor for survival.13-16
Definitive evidence for the usefulness of FDG-PET in distinguishing between responding and non-
responding patients would be a difference in (disease-free) long-term survival between patients
identified by FDG-PET as responders compared to non-responders.
The aim of the present study was, therefore, to evaluate the predictive value of pretreatment FDG-
uptake and relative change in FDG-uptake measured early during neoadjuvant chemoradiotherapy.
PATIENTS AND METHODS
Study design
In September 2004, a multicenter randomized phase-III trial was initiated in the Netherlands,
comparing neoadjuvant CRT followed by surgery with surgery alone in patients with potentially
curable esophageal cancer.5 Details of the study design and the final results have been reported
previously.4,5,17,18
The present report concerns an ancillary study within that randomized trial, evaluating the value of
FDG-PET scanning before and two weeks after the start of neoadjuvant CRT in the multimodality
treatment arm.19
Patients
Inclusion criteria for patients were previously described.5 Patients with histologically proven carcinoma
of the esophagus or esophago-gastric junction underwent extensive preoperative staging. Only

| Chapter 8
114
patients with cT1N1 and cT2-3N0-1 tumors were eligible. Eligible patients who had provided written
informed consent were randomly allocated to neoadjuvant CRT followed by surgery or to surgery
alone. Patients allocated to the neoadjuvant arm were subsequently invited to undergo the ancillary
FDG-PET protocol.
Neoadjuvant concurrent chemoradiotherapy
Over a five week period, concurrent chemoradiotherapy was applied on an outpatient basis. Paclitaxel
(50 mg/m2) and Carboplatin (area-under-curve=2) were administered by i.v. infusion once weekly
during the radiation period. External beam radiation with a total dose of 41.4 Gy was given in 23
fractions of 1.8 Gy, five fractions a week.
Surgery
Either transhiatal or transthoracic esophagectomy was performed, preferably within 6 weeks after
completion of the CRT. Only centers performing at least ten esophagectomies per year were allowed
to participate in this trial.20
Evaluation of tumor response by FDG-PET
A tumor-focused static FDG-PET scan was performed after injection of 5 MBq/kg 18F-FDG at baseline
and at day 14 after the start of CRT. Acquisition was started 90 minutes after injection. FDG-PET
scans were performed in five centers, using standardized acquisition and image reconstruction, with
centralized data-analysis (VUmc PET data-analysis center) and after interinstitutional calibration of
scanners.21,22 For every patient, the two scans were performed in the same institution on the same
scanner.
For quantitative analysis of FDG uptake, the maximum standardized uptake value (SUV) was used
according to previously validated methodology and corrected for body weight and serum glucose
(SUV-bw-g).22-27
Histopathological response
The disease stage after CRT was evaluated based on the histology in the surgical resection specimen.
Tumor regression grade (TRG) was classified according to the modified Mandard-score which is
based on the percentage of viable residual tumor cells in relation to the area of fibrosis/necrosis.28
The classification was performed by one of two experienced gastrointestinal pathologists (FJWtK and
HvD).

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
115
Cha
pter
8
Follow-up
After completion of the treatment protocol, patients were seen every three months for the first year,
every six months for the second year, and then each year until five years after treatment, to document
recurrent disease.
Analysis
Disease-free survival was used as primary outcome, counted from the start of CRT up to the time of a
first relapse or death, when no relapse occurred. Only patients who completed the PET protocol and
underwent an operation were analyzed. Follow-up was performed to the time of first relapse, the last
hospital visit or until death. For patients with tumors found to be irresectable during surgery, the date
of operation was used as cut-off for disease-free survival. For patients who showed progression of
disease prior to surgery, censoring was performed on the date on which progression was discovered.
Disease-free and overall survival curves were constructed by the Kaplan–Meier method, and the
log-rank test was used to determine significance (P<0.05 [two-sided] was considered statistically
significant). For the relative change in SUV, patients were allocated to three groups: patients with
metabolic response, those with metabolically stable disease, and those with metabolic progression of
disease. Metabolic response was defined as a relative decrease of SUV of 30% or more, or a reduction
of absolute SUV of >1 unit. Metabolic progression was defined as a relative increase of SUV of 30%
or more, or an increase of absolute SUV with >1 unit. All other patients were defined as having
metabolically stable disease.29
Univariable Cox regression analysis for disease-free survival was used to determine the predictive
significance of pretreatment SUV measurements and of relative change in SUV as continuous
variables. Relative change in SUV (%) was defined as: (100 * (SUV 14 days – SUV baseline)/SUV baseline).
Multivariable Cox regression analyses were used to determine the predictive significance of FDG-PET,
corrected for possible confounding factors.
Furthermore, a time dependent receiver operating characteristic (ROCt) analysis was performed to
estimate the discriminating value of the relative SUV change for cumulative disease free survival
at 5 years. The ROCt-curve and the area under the curve (AUC) were computed according to the
method by Heagerthy and colleagues, and the accompanying R package (The R-project for statistical
computing, http://www.r-project.org/ 10 October 2014, date last accessed).30, 31
RESULTS
Of the 180 patients that were included in the multimodality arm of the randomized trial (parent
study), 145 patients could be included in the current study. One hundred and forty patients
underwent the first FDG-PET, due to withdrawal of two patients and disease progression in 3 patients.
After the first FDG-PET, another patient withdrew from the study. Of the remaining 139 patients, 33

| Chapter 8
116
had to be excluded from further analysis for the following reasons: no FDG uptake on the first PET
(n=6), progression during chemoradiotherapy (n=4), no fasting before FDG-PET (n=3), second FDG-
PET was performed on a different scanner (n=5), nausea during PET (n=1), no FDG available (n=1),
PET technically not analyzable (n=3), no second FDG-PET performed due to logistic reasons (n=10).
Baseline characteristics of the 106 analyzed patients were comparable to the characteristics of all
patients included in the CRT-arm of the randomized CROSS trial (data not shown).
TABLE 1. Patient, PET and tumor characteristics for 106 included patients.
All patientsn = 106
Female / male (%) 26 / 80 (25% / 76%)
Age (y) median [range] 59 [37 to 76]
Tumor type: Adenocarcinoma / Squamous cell carcinoma (%) 87 / 19 (82% / 18%)
Pretreatment SUV (median) [IQR] 10.8 [7.2 to 17.2]
SUV 14 days after start of chemoradiotherapy (median) [IQR] 8.2 [5.4 to 11.0]
%SUV change 14 days after start of chemoradiotherapy (median) [IQR] -26.9 [-47.3 to 0.73]
ypT-stage (n, %)
T0 (complete regression) 34 (34%)
T1 16 (15%)
T2 17 (16%)
T3 33 (31%)
Tx (not resected) 6 ( 6%)
pN-stage (n, %)
N0 72 (68%)
N1 27 (26%)
Nx (not resected or no LN in resection specimen) 7 ( 7%)
Histopathological response* 64 (60%)
Resectability (n, %)
R0 94 (89%)
R1 6 ( 6%)
Irresectable 6 ( 6%)
Median follow-up time in months [IQR]# 76.6 [68.56 to 91.31]
Patients with recurrent / residual disease (n, %) 62 (58%)
SUV: standardized uptake value, IQR: interquartile rangepT stage: pathological T-stage (UICC TNM Cancer Staging, 6th edition)pN stage: pathological N-stage (UICC TNM Cancer Staging, 6th edition)R0: no viable tumor cells within 1mm of all resection marginsR1: viable tumor cells within 1 mm of one of the resection margins *Histopathological response: grade of 1 or 2 on the modified Mandard score # after exclusion of deceased patients

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
117
Cha
pter
8
Eighty men and 26 women with a median age of 59 years (range 37 to 76) completed the PET
protocol and were available for further analysis. Eighty-two percent had an adenocarcinoma and 18%
a squamous cell carcinoma. (Table 1) Disease progression occurred in 5 patients, detected either
during neoadjuvant CRT or during surgery, and one patient died before surgical resection due to a
bleeding from the tumor. Pathological assessment of the resection specimens revealed complete
regression due to CRT in 34 patients, a ypT1 tumor in 16 patients, ypT2 in 17 patients and ypT3 in
33 patients. A microscopically radical resection (no viable tumor cells within 1mm of the resection
margins, R0) was achieved in 94/100 (94%) patients.
One patient was lost to follow-up before the minimal time to follow-up was reached. For all other
patients, the minimal time of follow-up for surviving patients was 60 months, median follow-up for
surviving patients was 76.6 months (interquartile range 68.56-91.31 months). During follow-up, 62
patients deceased, of whom 5 did not have recurrence of disease and died from other causes. In 62
patients (58%), recurrent disease (locoregional, metastatic or both) was found during follow-up.
The log-rank test showed no significant difference in the five year disease-free survival between
patients with a pretreatment SUV above the median of 10.8 and those with a SUV below the median:
51% versus 62% respectively (p=0.32). (Figure 1)
No. at risk
SUV > median 53 40 32 27 25 22
SUV < median 53 40 35 31 28 28
FIGURE 1. Kaplan-Meier curves for estimated five year disease-free survival in 106 patients. (According to pretreatment SUV-uptake above (green line) or below (blue line) the median uptake. Error bars represent 95% confidence intervals)
Metabolic response was found in 49 patients. In 48 patients, metabolically stable disease was found,
while nine patients showed metabolic progression.
The estimated disease-free survival after five years was comparable between patients with
metabolically progressive disease and patients with metabolic response (67% vs. 53% respectively),

| Chapter 8
118
who both showed better survival than patients with metabolically stable disease (40%). These
differences in five year DFS between the groups were not statistically significant (P=0.39 by log rank
test).(Figure 2)
Metabolic response 49 38 34 30 27 26Metabolically stable disease 48 34 27 22 20 18Metabolic progression 9 8 6 6 6 6
FIGURE 2. Kaplan-Meier curves for estimated five year disease-free survival in 106 patients.Metabolic response: a relative SUV decrease of 30% of more (and an absolute reduction of SUV of >1 unit). Metabolically stable disease: SUV decrease of less than 30%, or SUV increase of less than 30%. Metabolic progression was defined as more than 30% increase in SUV, (and an absolute increase of SUV with >1 unit). Dotted lines represent the 95% confidence intervals.
FIGURE 3. Time dependent receiver operating characteristic curve for the prediction of five year disease free survival using relative change in SUV 14 days after the start of chemoradiotherapy in 106 patients. [AUC = 0.58 (95% CI: 0.44 to 0.67)]

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
119
Cha
pter
8
When compared with patients with metabolic progression, 5-year DFS in univariate analysis was
lower in patients with metabolic response and those with metabolically stable disease (HRs 2.02
and 2.72 respectively), however these differences were not statistically significant (p-values 0.25 and
0.10 respectively). When corrected for possible confounding baseline covariates, HRs for metabolic
response and metabolically stable disease were 3.89 and 3.70 respectively, both not statistically
significant (p-values 0.07 and 0.09 respectively).
Subgroup analysis for patients having adenocarcinoma or squamous cell carcinoma, and for patients
who underwent a microscopically radical resection showed no significant correlations between SUV-
max and DFS (data not shown).
When using a cut off of 0% (increased or decreased SUV after 14 days), no significant differences were
found in five year DFS between patients with an increase in SUV and patients with a decrease in SUV
(data not shown).
The time dependent ROC-curve that was computed is shown in Figure 3. The corresponding
estimated AUC at 5 years was 0.57 (95% CI: 0.444 to 0.671).
DISCUSSION
The data analyzed in this prospective trial show that the relative change in FDG-uptake 14 days after
start of neoadjuvant chemoradiotherapy or pretreatment PET measurements is not a significant
predictor of disease-free survival in patients with esophageal cancer undergoing potentially curative
esophagectomy.
Most studies describing FDG-PET as a tool for assessment of response to neoadjuvant therapy use
histopathological response as primary outcome. This is probably because, compared to survival, this
is a (dichotomous) outcome for which one can more easily determine optimal cut-off values. A more
relevant and convincing demonstration for the usefulness of FDG-PET in distinguishing responding
from non-responding patients is whether the patients identified by PET as responders also show
better disease-free survival compared to patients identified by PET as non-responders.
In a previous paper from our group, it was found that FDG-PET response had a positive predictive
value of 76% for histopathological response, while the negative predictive value was found to be
too low (75%) to justify the use of FDG-PET response for early discontinuation of neoadjuvant CRT. 17 As histopathological response determined after neoadjuvant CRT has an association with survival
in several studies,2,24,28,29 it might be expected that there is a (significant) difference in disease-free
survival between patients with a metabolic response on FDG-PET compared to patients in whom
metabolically stable disease or metabolic progression was observed.
FDG-PET has proven to be relatively successful in differentiating between histopathologic responders
and non-responders early during neoadjuvant chemotherapy without radiation.13,34,35 According to
these studies, patients identified by FDG-PET as responder had a significantly better survival compared
to patients identified as non-responder. Previous studies show limited evidence for a similar potential

| Chapter 8
120
in patients treated with concurrent neoadjuvant chemoradiotherapy, but specific data on the relation
between response according to early FDG PET monitoring and long-term survival after combination
therapy are scarcely available.15,36,37 Two of these studies suggested that FDG-PET could actually be
used for early response assessment.15,37
In accordance with our previously presented data, Gillham et al. also concluded that FDG-PET was
not able to predict histopathological response, based on an analysis of 32 patients with esophageal
cancer treated with neoadjuvant chemoradiotherapy.21,36
The most plausible explanation for the limited value of FDG-PET for early response assessment in
patients treated with neoadjuvant chemoradiotherapy is probably the local (inflammatory) response
to radiation, which will cause increased glucose uptake and hence interfere with the FDG-uptake
measurement associated with the treatment effect.38 The fact that nearly all studies investigating early
response to chemotherapy (without concurrent radiotherapy) show more promising results supports
this hypothesis. 13,34,35
Also, the observed metabolic progression in patients in the current study might be caused by an
increase in SUV due to inflammation rather than by tumor progression, which would explain why
this group had survival comparable with the responders, and why time-dependent ROC analysis only
showed a moderate AUC of 0.58.
A recent systematic review by Schollaert et al. shows that metabolic response on FDG-PET after
chemoradiotherapy is significantly associated with better disease-free survival (HR 0.47, 95%CI 0.38-
0.57).39 However, the heterogeneity in timing of the second PET-scan is great, with several studies
performing the second FDG-PET scan even 5 or 6 weeks after the completion of chemoradiotherapy.
Unfortunately, no subgroup analysis was performed for the studies in which the second FDG-PET scan
was performed during CRT.
The sample-size for this ancillary study was based on the sensitivity and specificity of FDG-PET in
predicting histopathologic response on CRT. Disease-free survival was a secondary endpoint, which
leaves room for a type-I error. This could be an explanation for the fairly wide confidence intervals
that accompany the HR’s for DFS according to the PERCIST criteria. This problem might have been
overcome with a larger sample-size.
Whereas measuring relative change in FDG-uptake early during neoadjuvant therapy might have
direct therapeutic consequences, the role of using pretreatment FDG-PET measurements is limited
to the purpose of prognostication which has been described extensively in previous papers.40 Most
of these studies show pretreatment FDG-uptake to be a significant predictor of survival in univariable
analysis. Most impressive are the results of the relatively large but retrospective study by Cerfolio
et al.(N = 89), in which a high four year survival rate was described (89%) for patients with a low
pretreatment SUV value.41 This was significantly higher compared to the survival rate in patients with
a high pretreatment SUV value (31%). In the present analysis the 5-year disease-free survival rate for
patients with a low versus a high pretreatment SUV value was 40% and 56% respectively. The reason
why the results of Cerfolio et al. could not be duplicated in the present study remains unclear.

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
121
Cha
pter
8
In conclusion, the change in FDG-uptake as measured by FDG-PET before and 14 days after the start of
neoadjuvant chemoradiotherapy was found not to be associated with disease-free survival in patients
with potentially curable esophageal cancer. Therefore, the present study indicates, in accordance with
our previous findings, that FDG-PET should not be applied for early response assessment in patients
with potentially curable esophageal cancer who undergo neoadjuvant chemoradiotherapy followed
by surgery.

| Chapter 8
122
REFERENCES1. Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five
continents: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol. 2006 May 10;24(14):2137-50.
2. Berger AC, Farma J, Scott WJ, et al. Complete response to neoadjuvant chemoradiotherapy in esophageal carcinoma is associated with significantly improved survival. J Clin Oncol. 2005 Jul 1;23(19):4330-7.
3. Omloo JM, Lagarde SM, Hulscher JB, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg. 2007 Dec;246(6):992-1000; discussion -1.
4. Shapiro J, van Lanschot JJ, Hulshof MC et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015 Sep, 16(9):1090-1098
5. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012 May 31;366(22):2074-84.
6. Bosset JF, Gignoux M, Triboulet JP, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med. 1997 Jul 17;337(3):161-7.
7. Burmeister BH, Smithers BM, Gebski V, et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomised controlled phase III trial. Lancet Oncol. 2005 Sep;6(9):659-68.
8. Urba SG, Orringer MB, Turrisi A, Iannettoni M, Forastiere A, Strawderman M. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol. 2001 Jan 15;19(2):305-13.
9. Walsh TN, Noonan N, Hollywood D, Kelly A, Keeling N, Hennessy TP. A comparison of multimodal therapy and surgery for esophageal adenocarcinoma. N Engl J Med. 1996 Aug 15;335(7):462-7.
10. Czernin J, Phelps ME. Positron emission tomography scanning: current and future applications. Annu Rev Med. 2002;53:89-112.
11. Gambhir SS, Czernin J, Schwimmer J, Silverman DH, Coleman RE, Phelps ME. A tabulated summary of the FDG PET literature. J Nucl Med. 2001 May;42(5 Suppl):1S-93S.
12. Rohren EM, Turkington TG, Coleman RE. Clinical applications of PET in oncology. Radiology. 2004 May;231(2):305-32.
13. Lordick F, Ott K, Krause BJ, et al. PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: the MUNICON phase II trial. Lancet Oncol. 2007 Sep;8(9):797-805.
14. zum Büschenfelde CM, Herrmann K, Schuster T, et al. (18)F-FDG PET-guided salvage neoadjuvant radiochemotherapy of adenocarcinoma of the esophagogastric junction: the MUNICON II trial. J Nucl Med. 2011;52(8):1189-96
15. Westerterp M, Omloo JM, Sloof GW, et al. Monitoring of response to pre-operative chemoradiation in combination with hyperthermia in oesophageal cancer by FDG-PET. Int J Hyperthermia. 2006 Mar;22(2):149-60.
16. Westerterp M, van Westreenen HL, Reitsma JB, et al. Esophageal cancer: CT, endoscopic US, and FDG PET for assessment of response to neoadjuvant therapy--systematic review. Radiology. 2005 Sep;236(3):841-51.
17. van Heijl M, Omloo JM, van Berge Henegouwen MI, et al. Fluorodeoxyglucose positron emission tomography for evaluating early response during neoadjuvant chemoradiotherapy in patients with potentially curable esophageal cancer. Ann Surg. 2011 Jan;253(1):56-63.

Prediction of disease-free survival using relative change in FDG-uptake early during neoadjuvant chemoradiotherapy |
123
Cha
pter
8
18. van Heijl M, van Lanschot JJ, Koppert LB, et al. Neoadjuvant chemoradiation followed by surgery versus surgery alone for patients with adenocarcinoma or squamous cell carcinoma of the esophagus (CROSS). BMC Surg. 2008;8:21.
19. van Heijl M, Omloo JM, van Berge Henegouwen MI, et al. NEOadjuvant therapy monitoring with PET and CT in Esophageal Cancer (NEOPEC-trial). BMC Med Phys. 2008;8:3.
20. van Lanschot JJ, Hulscher JB, Buskens CJ, Tilanus HW, ten Kate FJ, Obertop H. Hospital volume and hospital mortality for esophagectomy. Cancer. 2001 Apr 15;91(8):1574-8.
21. Boellaard R, Oyen WJ, Hoekstra CJ, et al. The Netherlands protocol for standardisation and quantification of FDG whole body PET studies in multi-centre trials. Eur J Nucl Med Mol Imaging. 2008 Dec;35(12):2320-33.
22. Young H, Baum R, Cremerius U, et al. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: review and 1999 EORTC recommendations. European Organization for Research and Treatment of Cancer (EORTC) PET Study Group. Eur J Cancer. 1999 Dec;35(13):1773-82.
23. Hoekstra CJ, Hoekstra OS, Stroobants SG, et al. Methods to monitor response to chemotherapy in non-small cell lung cancer with 18F-FDG PET. J Nucl Med. 2002 Oct;43(10):1304-9.
24. Hoekstra CJ, Paglianiti I, Hoekstra OS, et al. Monitoring response to therapy in cancer using [18F]-2-fluoro-2-deoxy-D-glucose and positron emission tomography: an overview of different analytical methods. Eur J Nucl Med. 2000 Jun;27(6):731-43.
25. Krak NC, Hoekstra OS, Lammertsma AA. Measuring response to chemotherapy in locally advanced breast cancer: methodological considerations. Eur J Nucl Med Mol Imaging. 2004 Jun;31 Suppl 1:S103-11.
26. Kroep JR, Van Groeningen CJ, Cuesta MA, et al. Positron emission tomography using 2-deoxy-2-[18F]-fluoro-D-glucose for response monitoring in locally advanced gastroesophageal cancer; a comparison of different analytical methods. Mol Imaging Biol. 2003 Sep-Oct;5(5):337-46.
27. Westerterp M, Pruim J, Oyen W, et al. Quantification of FDG PET studies using standardised uptake values in multi-centre trials: effects of image reconstruction, resolution and ROI definition parameters. Eur J Nucl Med Mol Imaging. 2007 Mar;34(3):392-404.
28. Mandard AM, Dalibard F, Mandard JC, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer. 1994 Jun 1;73(11):2680-6.
29. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J Nucl Med. 2009 May;50 Suppl 1:122S-50S.
30. Heagerty PJ, Lumley T, Pepe MS. Time-dependent ROC curves for censored survival data and a diagnostic marker. Biometrics. 2000 Jun;56(2):337-44.
31. Heagerty PJ, Zheng Y. Survival model predictive accuracy and ROC curves. Biometrics. 2005 Mar;61(1):92-105.
32. Brucher BL, Becker K, Lordick F, et al. The clinical impact of histopathologic response assessment by residual tumor cell quantification in esophageal squamous cell carcinomas. Cancer. 2006 May 15;106(10):2119-27.
33. Schneider PM, Baldus SE, Metzger R, et al. Histomorphologic tumor regression and lymph node metastases determine prognosis following neoadjuvant radiochemotherapy for esophageal cancer: implications for response classification. Ann Surg. 2005 Nov;242(5):684-92.
34. Ott K, Weber WA, Lordick F, et al. Metabolic imaging predicts response, survival, and recurrence in adenocarcinomas of the esophagogastric junction. J Clin Oncol. 2006 Oct 10;24(29):4692-8.

| Chapter 8
124
35. Weber WA, Ott K, Becker K, et al. Prediction of response to preoperative chemotherapy in adenocarcinomas of the esophagogastric junction by metabolic imaging. J Clin Oncol. 2001 Jun 15;19(12):3058-65.
36. Gillham CM, Lucey JA, Keogan M, et al. (18)FDG uptake during induction chemoradiation for oesophageal cancer fails to predict histomorphological tumour response. Br J Cancer. 2006 Nov 6;95(9):1174-9.
37. Wieder HA, Brucher BL, Zimmermann F, et al. Time course of tumor metabolic activity during chemoradiotherapy of esophageal squamous cell carcinoma and response to treatment. J Clin Oncol. 2004 Mar 1;22(5):900-8.
38. Hautzel H, Muller-Gartner HW. Early changes in fluorine-18-FDG uptake during radiotherapy. J Nucl Med. 1997 Sep;38(9):1384-6.
39. Schollaert P, Crott R, Bertrand C, D’Hondt L,Borght TV, Krug B. A systematic review of the predictive value of (18)FDG-PET in esophageal and esophagogastric junction cancer after neoadjuvant chemoradiation on the survival outcome stratification. J Gastrointest Surg 2014 May;18(5):894-905.
40. Omloo JM, van Heijl M, Hoekstra OS, van Berge Henegouwen MI, van Lanschot JJ, Sloof GW. FDG-PET parameters as prognostic factor in esophageal cancer patients: a review. Ann Surg Oncol. 2011 Nov;18(12):3338-52.
41. Cerfolio RJ, Bryant AS. Maximum standardized uptake values on positron emission tomography of esophageal cancer predicts stage, tumor biology, and survival. Ann Thorac Surg. 2006 Aug;82(2):391-4; discussion 4-5.


V. Oppedijk
A. van der Gaast
J.J.B. van Lanschot
P. van Hagen
R. van Os
C.M. van Rij
M.J. van der Sangen
J.C. Beukema
H. Rütten
P.H. Spruit
J.G. Reinders
D.J. Richel
M.I. van Berge Henegouwen
M.C.C.M. Hulshof
Journal of Clinical Oncology 2014 Feb 10;32(5):385-91.

Chapter 9Patterns of recurrence after surgery alone
versus preoperative chemoradiotherapy and surgery in the CROSS trials

| Chapter 9
128
ABSTRACT
PURPOSE
To analyze recurrence patterns in patients with cancer of the esophagus or gastroesophageal junction
treated with either preoperative chemoradiotherapy (CRT) plus surgery or surgery alone.
PATIENTS AND METHODS
Recurrence pattern was analyzed in patients from the previously published CROSS I and II trials in
relation to radiation target volumes. CRT consisted of five weekly courses of paclitaxel and carboplatin
combined with a concurrent radiation dose of 41.4 Gy in 1.8-Gy fractions to the tumor and pathologic
lymph nodes with margin.
RESULTS
Of the 422 patients included from 2001 to 2008, 418 were available for analysis. Histology was mostly
adenocarcinoma (75%). Of the 374 patients who underwent resection, 86% were allocated to surgery
and 92% to CRT plus surgery. On January 1, 2011, after a minimum follow-up of 24 months (median,
45 months), the overall recurrence rate in the surgery arm was 58% versus 35% in the CRT plus
surgery arm. Preoperative CRT reduced locoregional recurrence (LRR) from 34% to 14% (P < .001)
and peritoneal carcinomatosis from 14% to 4% (P < .001). There was a small but significant effect on
hematogenous dissemination in favor of the CRT group (35% v 29%; P = .025). LRR occurred in 5%
within the target volume, in 2% in the margins, and in 6% outside the radiation target volume. In 1%,
the exact site in relation to the target volume was unclear. Only 1% had an isolated infield recurrence
after CRT plus surgery.
CONCLUSION
Preoperative CRT in patients with esophageal cancer reduced LRR and peritoneal carcinomatosis.
Recurrence within the radiation target volume occurred in only 5%, mostly combined with outfield
failures.

Patterns of recurrence in the CROSS trials |
129
Cha
pter
9
INTRODUCTION
Patients with esophageal cancer have poor prognosis; at the time of diagnosis; ≥ 50% present with
distant metastasis or irresectable disease.1 For potentially curable patients, for decades, surgical
resection had been the main treatment. However, incomplete resections occurred in up to 25%2
and locoregional recurrence (LRR) in 30% to 40%, with 5-year survival rarely exceeding 25%.3 Most
randomized controlled trials (RCTs) investigating the role of preoperative chemoradiotherapy versus
surgery alone failed to show a significant survival benefit, mostly because of a lack of statistical power.
However, a recent meta-analysis showed a survival benefit for patients treated with preoperative
chemoradiotherapy (CRT) or chemotherapy compared with surgery alone.4
The results of the CROSS (Chemoradiotherapy for Oesophageal Cancer Followed by Surgery Study)
trial have recently been published. This was an RCT comparing preoperative CRT followed by surgery
with surgery alone.5 CRT consisted of 41.4 Gy in 1.8-Gy fractions combined with weekly concurrent
carboplatin and paclitaxel. After a minimum follow-up of 24 months, there was a significant estimated
5-year overall survival benefit of 13% in favor of the CRT plus surgery arm. The CRT regimen was well
tolerated, with little added toxicity.5
Patterns of recurrence of esophageal cancer after surgery compared with CRT plus surgery are
infrequently reported in the literature. Meguid et al6 and Denham et al7 describe relapse patterns after
CRT plus surgery, and CRT plus surgery and definitive CRT, respectively; however, those patient groups
were not compared with surgery alone. Understanding relapse patterns provides insight into the
effectiveness of the combined treatment and may lead to improvements. Therefore, we analyzed the
recurrence pattern of patients treated in the CROSS trial and the preceding phase II trial investigating
the same preoperative regimen.8 In particular, we related the site of recurrence to the radiation fields
employed.
PATIENTS AND METHODS
Patient Population
The patient population consisted of patients enrolled onto the CROSS trial, an RCT in which eligible
patients were randomly assigned between CRT plus surgery and surgery alone,5 and patients included
in the preceding phase II trial8 investigating the same preoperative regimen followed by surgery.
All patients had histologically proven and resectable squamous cell carcinoma (SCC) or
adenocarcinoma (AC) of the esophagus, stage cT1N1M0 or cT2-3N0-1M0 according to the Union
International Contre Cancer (sixth edition, 2002). The upper border of the tumor had to be ≥ 3 cm
below the upper esophageal sphincter. Those with tumors of the gastroesophageal junction were
also eligible, provided that the primary tumor did not extend ≥ 4 cm into the stomach.
Patients had to be age 18 to 75 years with a WHO performance score ≤ 2. Weight loss had to be ≤
10%. No past or current history of malignancy other than the entry diagnosis was allowed, except for
nonmelanomatous skin cancer, curatively treated carcinoma in situ of the cervix, or a nonrecurred

| Chapter 9
130
malignancy treated ≥ 5 years before enrollment. No previous radiotherapy or chemotherapy was
allowed. Written informed consent was required from all patients before random assignment. The
medical ethics committees of all eight participating centers approved the study protocol.
Staging
Pretreatment staging included elaborate history taking, physical examination, routine blood workup
and pulmonary function tests, an upper GI endoscopy, endoultrasonography, and computed
tomography (CT) of neck, chest, and upper abdomen. On indication, ultrasound of the neck was
performed with fine-needle aspiration.
Chemotherapy
Chemotherapy consisted of five cycles of concurrent paclitaxel 50 mg/m2 and carboplatin targeted at
area under the curve of 2, starting on days 1, 8, 15, 22, and 29. Toxicity of CRT was closely monitored
using the National Cancer Institute Common Terminology Criteria for Adverse Events (version 3.0).9
Radiotherapy
A total radiation dose of 41.4 Gy was administered in 23 fractions of 1.8 Gy, five fractions per week,
starting on the first day of chemotherapy. All patients were treated with external-beam radiation
using a three-dimensional conformal radiation technique. Gross tumor volume was drawn on each
relevant slice of the planning CT and was defined by the primary tumor and any enlarged regional
lymph nodes. The planning target volume (PTV) provided a proximal and distal margin of 4 cm and
a radial margin of 1.5 cm around the gross tumor volume. A distal margin of 3 cm was chosen in
case the tumor extended into the gastric cardia. Individually shaped beams were used in each field
by either cerrobend blocks or multileaf collimators to ensure optimal sparing of normal tissue. The
daily prescription dose of 1.8 Gy was specified at the International Commission on Radiation Units
and Measurement 50/62 reference point, and the 95% isodose had to encompass the entire PTV.
The maximum dose to the PTV was not to exceed the prescription dose by > 7%. Tissue density
inhomogeneity correction was used.
Surgery
Patients randomly assigned to the surgery arm were treated as soon as possible after random
assignment. Patients in the CRT plus surgery arm preferably underwent surgery at 6 weeks after
completion of CRT; surgery consisted of a transthoracic approach with a two-field lymph node
dissection or transhiatal approach, depending on tumor localization, patient characteristics, and
local expertise. A wide local excision of the N1 lymph nodes, including standard excision of the celiac
nodes, was carried out in both techniques. Continuity of the digestive tract was restored by gastric
tube reconstruction or colonic interposition procedure with cervical anastomosis.

Patterns of recurrence in the CROSS trials |
131
Cha
pter
9
Pathologic Analysis
For grading of the therapy response, the degree of histomorphologic regression was classified
into four modified categories, as first described by Mandard et al.10 All resection margins, including
circumferential margins, were evaluated for vital tumor, with a cutoff point of 1 mm. If vital tumor was
present at ≤ 1 mm from a resection margin, that margin was considered to be positive.
Follow-Up
In the first year after completion of the protocol, patients were seen every 3 months. In the second
year, follow-up took place every 6 months and, thereafter, yearly until 5 years after treatment. If
applicable, late toxic effects and recurrence of disease or death were documented. During follow-up,
additional diagnostics were only performed on indication.
Recurrences
Relapses were classified as locoregional or distant. LRRs were defined as recurrences at the site of the
primary tumor or locoregional lymph nodes. Lymph node recurrences at the celiac trunk or in the
supraclavicular region were also considered to be locoregional. Distant recurrences were defined as
nonregional lymph node recurrences, systemic metastases, malignant pleural effusions, or peritoneal
metastases. Most patients suspected of experiencing recurrence underwent a CT scan of thorax and
abdomen or an endoscopy. If necessary, cytology or histology was obtained. If a second recurrence
was detected within 4 weeks after the first occurrence, it was considered to be synchronous.
Localization and date of identification of all locoregional and distant recurrences were scored.
Radiation Target Volumes
In patients with recurrent disease who were treated with CRT plus surgery, radiation target volumes
were analyzed in relation to the site of recurrence. Treatment failures were classified as infield when
relapse occurred within the PTV, outfield when relapse occurred outside the PTV, and borderline
when adjacent to the PTV or field edge. We compared the exact site of recurrence with the treatment
volume on the planning CT scan. When a recurrence was detected endoscopically, the location was
compared with the results of the staging endoscopy. In case of a relapse at the anastomotic site,
endoscopy results, histology reports of the esophageal resection specimen, and planning CT scans
were used to reconstruct the proximal and distal ends of the resection specimen in relation to the
irradiated volume.
Statistical Analysis
Duration of follow-up was defined as the interval between the day of random assignment and death or
the last date of hospital visit or telephone call. The Kaplan-Meier method was used to calculate survival
probabilities. The influence of prognostic factors was analyzed using univariable and multivariable

| Chapter 9
132
Cox regression analyses. The backward-step method was used to optimize the multivariable model.
A univariable Cox regression model was also used to analyze the difference per treatment arm for
each separate location of recurrence. We used one-way analysis of variance test to investigate the
differences between both treatment arms. Analyses were performed using SPSS software (version
18.0; SPSS, Chicago, IL) and the R statistical program (http://www.r-project.org).
CROSS phase II trial: Patients receiving CRT+S
(n=54)
CROSS phase III trial: Patients with esophageal or
GEJ cancer randomly assigned (n=368)
Died after first cycle of CRT (n=1)
Refused surgery (n=1)
Allocated to CRT+S (n=180)
Allocated to S alone (n=188)
Withdrew consent (n=1) Did not receive CRT (n=7)
Underwent resection after completion of CRT
(n=52)
Received CRT (n=171) Underwent surgery (n=168)
Underwent resection (n=161)
Underwent surgery (n=186) Underwent resection
(n=161)
Included in the analysis (n=52)
Included in the analysis (n=161)
Included in the analysis (n=213)
Included in the analysis (n=161)
FIGURE 1. CONSORT diagram. CROSS, Chemoradiotherapy for Oesophageal Cancer Followed by Surgery Study; CRT, chemoradiotherapy; GEJ, gastroesophageal junction; S, surgery.

Patterns of recurrence in the CROSS trials |
133
Cha
pter
9
RESULTS
Patients
A total of 422 patients were included in both trials (Fig 1). Of the 368 patients in the phase III CROSS
trial, two patients were ineligible: one because of withdrawal, and one because of distant metastases
at the time of diagnosis. Of the remaining 366 patients, 188 were randomly assigned to the surgery
arm and 178 to the CRT plus surgery arm. Of the 54 patients included in the phase II trial, 52 completed
the protocol, one patient died after the first course of chemotherapy (probably because of cardiac
arrest), and one patient refused surgery after CRT. The 52 patients who underwent resection were
included in the analysis of the CRT plus surgery arm. Finally, 418 patients were available for analysis.
In the surgery arm, 161 (85.6%) of 188 patients underwent an esophageal resection versus 213 (92.2%)
of 230 in the CRT plus surgery group. A microscopically radical (R0) resection was achieved in 68% of
patients in the surgery arm and in 93% of patients in the CRT plus surgery arm. In the CRT plus surgery
arm, 28% had a pathologic complete response (ypT0N0). One or more pathologically positive lymph
nodes were found in 74% of patients in the surgery arm and in 31% of those in the CRT plus surgery
arm (P < .001).
Patterns of Recurrence
After a minimum follow-up of 24 months and a median survival of 45 months for surviving patients,
57.1% of the resected patients in the surgery group had recurrent disease versus 34.7% in the CRT plus
surgery group. Most patients had distant failure (22%) or combined locoregional and distant failure
(16.5%). Only 9.3% of patients in the surgery arm had an isolated LRR without distant metastasis versus
3.3% in the CRT plus surgery arm. Also, 24.2% versus 10.8% of patients in the surgery and CRT plus
surgery arms, respectively, had concurrent locoregional and distant relapses, and 23.6% versus 20.7%
of patients had distant relapse only in the surgery and CRT plus surgery arms, respectively. The majority
of LRRs occurred within 2 years of follow-up. In the CRT plus surgery arm, no LRRs were observed after
30 months. Figures 2A, 2B, and 2C show the differences between both arms for disease-free survival
(DFS), locoregional DFS, and distant metastasis–free survival, respectively.
Site of Recurrence
Further analysis showed that recurrences at the anastomosis occurred in 8.7% versus 2.8% (P = .008)
of patients in the surgery and CRT plus surgery arms, respectively (Table 2). LRRs at the anastomosis
occurred more often after R1 resections (11%) than after R0 resections (4%) and more often in
patients with pN1 disease (7%) than in those with pN0 disease (3%). Mediastinal relapses occurred
in 20.5% versus 7.0% (P < .001) of patients in the surgery and CRT plus surgery arms, respectively.
Peritoneal carcinomatosis occurred in 13.7% versus 4.2% (P < .001) of patients and hematogenous
metastasis occurred in 35.4% versus 28.6% (P = .025) of patients in the surgery and CRT plus surgery
arms, respectively. There were no significant differences between both arms in recurrence rates at

| Chapter 9
134
the supraclavicular or celiac axis levels (Table 2). Generally, these latter areas were not included in the
radiation target volume.
TABLE 1. Patient demographic and clinical characteristics at diagnosis
Characteristic S Arm (n = 161) CRT + S Arm (n = 213) P*
No. % No. %
Age, years 0.54
Median 60 60
Range 36-73 37-79
Male sex 129 80 169 81 0.85
T stage
T1 1 1 1 0 0.81
T2 35 22 31 15 0.12
T3 122 76 180 85 0.15
Unknown 1 1 1 0 0.40
Nodal stage
N0 50 31 80 38 0.21
N1 106 66 125 61 0.96
Unknown 3 3 3 1 0.96
Nodal status
Positive supraclavicular nodes 0 0 0 0 NA
Positive celiac nodes 6 4 8 4 0.63
Tumor length, cm 0.62
Median 5 5
Range 1-13 1-12
Histology
Adenocarcinoma 122 76 160 75 0.87
SCC 38 24 52 24 0.88
Other 1 1 1 1 0.84
Abbreviations: CRT, chemoradiotherapy; NA, not applicable; S, surgery; SCC, squamous cell carcinoma.* Analysis of variance test.

Patterns of recurrence in the CROSS trials |
135
Cha
pter
9
A B
C
FIGURE 2. (A) Disease-free survival for patients undergoing surgery alone (S) or chemoradiotherapy (CRT) followed by S (CRT + S; hazard ratio [HR], 0.47; 95% CI, 0.35 to 0.64). (B) Locoregional recurrence–free survival; recurrences at anastomotic site, mediastinum, celiac trunk, or supraclavicular lymph nodes (HR, 0.37; 95% CI, 0.23 to 0.59). (C) Distant metastasis–free survival; systemic metastases including nodal metastases other than regional, peritoneal deposits, and malignant pleural effusion (HR, 0.52; 95% CI, 0.38 to 0.73).

| Chapter 9
136
TABLE 2. Results of Univariable Cox Regression Analysis of RFS Time per Treatment Arm in Patients Undergoing Resection (n = 374)
Site of Recurrence S Arm (n = 161) CRT+ S Arm (n=213)HR 95% CI P
No. % No. %
Anastomosis 14 8.7 6 2.8 0.28 0.11 to 0.72 0.008
Mediastinum 33 20.5 15 7.0 0.29 0.16 to 0.53 <0.001
Supraclavicular 7 4.3 9 4.2 0.83 0.31 to 2.2 0.71
Celiac axis 11 6.9 8 3.8 0.42 0.17 to 1.04 0.06
Para-aortic 17 10.6 14 6.6 0.53 0.26 to 1.1 0.08
Peritoneal carcinomatosis
22 13.7 9 4.2 0.27 0.12 to 0.58 0.01
Hematogenous 57 35.4 61 28.6 0.67 0.46 to 0.96 0.03
NOTE. Bold font indicates significance.Abbreviations: CRT, chemoradiotherapy; HR, hazard ratio; RFS, recurrence-free survival; S, surgery.
Site of Recurrence in Relation to the Radiation Target VolumeIn the 74 patients with recurrences after CRT plus surgery, the precise localization of relapse was
determined and correlated to the irradiated field volume (Table 3). Infield recurrences occurred in
11 (5.2%) of 213 patients, of whom only two patients experienced an infield recurrence without
synchronous distant failure. Recurrences at the borders of the treatment volume occurred in five
(2.3%) of 213 patients; three of these occurred at the site of the celiac axis. In two of the borderline
recurrences, the site of relapse was in the anterior-posterior beams but not in the lateral beams.
Regional outfield recurrences occurred in 13 (6.1%) of 213 patients; two of these were solitary LRRs.
Two patients were scored as unknown; one had a relapse at the site of the anastomosis, and for the
other, the diagnostic CT scan of the recurrence could not be retrieved.
TABLE 3. Tumor Recurrences in Relation to Radiation Target Volumes in Patients Undergoing CRT Plus Surgery (n = 213)
Recurrence Infield Outfield Borderline Unknown Total
LRR only 2 2 2 1 7
Distant only 0 43 0 1 44
LRR plus distant 9 11 3 0 23
Total 11 56 5 2 74
Abbreviations: CRT, chemoradiotherapy; LRR, locoregional recurrence.

Patterns of recurrence in the CROSS trials |
137
Cha
pter
9
Potential Prognostic Factors for Developing an LRR
Table 4 lists the results of the analyses per treatment arm. Prognostic factors predicting LRRs in
univariable analysis were surgery alone, pathologically positive lymph nodes (pN1), and R1 resection.
In the multivariable analysis, the backward method showed that surgery alone, pathologic nodal
stage N1, and histology of SCC significantly increased the risk of developing an LRR. After multivariable
analysis, surgery alone, pN1, and SCC remained independent prognostic factors.
In the surgery arm, 47% of patients with SCC developed an LRR compared with 30% of patients with
AC. In the CRT plus surgery arm, there was no significant difference between SCC and AC (15% and
14%, respectively).
Of the 59 patients with a pathologic complete response (pCR) after CRT, 17% developed any recurrent
disease; only one patient (1.7%) had a solitary LRR. Of the 154 patients with no pCR, 42% experienced
a recurrence: LRR ± distant recurrence in 17% and a solitary LRR in 4%. After R1 resection, there was no
significant difference in LRRs between treatment arms, although a trend was present (36% v 29% for
surgery and CRT plus surgery, respectively).
TABLE 4. Univariable and multivariable cox regression analyses for LRRs in patients undergoing resection (n = 374)
Factor LRR Incidence Univariable Multivariable
S Arm CRT + S Arm HR 95% CI HR 95% CI
Method of resection (TTE v THE) 20 v 17 6 v 8 0.83 0.54 to 1.29 NA
Tumor length (≤ 5.0 v > 5.0 cm) 23 v 39 16 v 11 0.89 0.54 to 1.46 NA
Clinical T stage (T1-2 v T3-4) 31 v 35 5 v 17 1.32 0.76 to 2.29 NA
Clinical nodal stage (N0 v N1) 31 v 35 10 v 18 1.50 0.93 to 2.41 NA
Pathologic nodal stage (N0 v N1) 22 v 38 10 v 23 3.66 2.20 to 5.85 2.85 1.59 to 5.11
Involved margins (R0 v R1) 34 v 36 13 v 29 2.29 1.38 to 3.76 NA
Histology (SCC v AC) 47 v 30 15 v 14 0.70 0.44 to 1.12 0.49 0.29 to 0.82
Sex (male v female) 33 v 34 12 v 20 1.12 0.67 to 1.87 NA
Treatment arm (S v CRT + S) 27 14 0.37 0.23 to 0.59 0.50 0.29 to 0.86
pCR after CRT (no v yes)* NA 7 v 17 0.36 0.13 to 1.05 NA
NOTE. Bold font indicates significance.Abbreviations: AC, adenocarcinoma; CRT, chemoradiotherapy; HR, hazard ratio; LRR, locoregional recurrence; NA, not applicable; pCR, pathologic complete response; S, surgery; SCC, squamous cell carcinoma; THE, transhiatal esophagectomy; TTE, transthoracic esophagectomy.* Factor only available in the CRT + S arm and therefore not suitable for multivariable analysis.

| Chapter 9
138
DISCUSSION
In the CROSS phase III trial, preoperative CRT followed by surgery compared with surgery alone
improved DFS, with an absolute difference of 22% at 5 years and an improved overall survival of 13%.
Most patients diagnosed with LRRs also developed synchronous distant metastases. Of the patients
undergoing resection, 24% and 11% had concurrent LRRs and distant relapses and only 9.3% and
3.3% had an isolated LRR in the surgery and CRT plus surgery arms, respectively. Few data are available
on relapse patterns after CRT plus surgery for esophageal and gastroesophageal cancers. In most
RCTs comparing CRT plus surgery with surgery alone, the sites of recurrence are either imprecise
or not reported. LRR rates of 13% to 25% and 12% to 42% after CRT plus surgery and surgery alone,
respectively, have been reported.11–13 Most studies have shown a reduction in LRRs after preoperative
CRT.11,13
In our study, patients with a pCR after CRT had a significantly lower LRR rate compared with patients
with a partial (tumor regression grade 2 to 3) or no response after CRT (tumor regression grade 4 to 5).
Of patients with a pCR, 17% had recurrent disease, of whom only one patient had a solitary LRR. The
only patient experiencing LRR after pCR had no lymph nodes examined in the resection specimen
and should probably be considered as having experienced inadequately staged pCR. These data
compare favorably with those of Meguid et al,6 who in their retrospective series reported five solitary
infield recurrences in 82 patients (6%) achieving pCR after CRT.
A marked difference was seen in the occurrence of peritoneal carcinomatosis in favor of the CRT plus
surgery arm (13.7% v 4.2%; P < .001). This might be explained by a reduction of microscopic residual
disease, because of patients achieving pCR, 1.7% had peritoneal metastasis compared with 5.2% with
no pCR. The reduction in recurrences at the site of anastomosis in the CRT arm might be an effect of
a reduction of microscopically positive surgical margins. Unfortunately, in case of R1 resection, the
site of irradicality was not always reported. This is supposedly more likely at the lateral borders of the
specimen than at the cranial or caudal borders. Irradicality and subsequent tumor spill could also be
considered a cause of recurrence at the anastomosis or in the abdominal cavity.
In both the multivariable and univariable analyses, patients with SCC had a higher probability of
developing LRR; however, this was significant only in the multivariable analysis. Patients with SCC are
known to have a higher risk of LRR after surgery alone,14 which is confirmed by the current data. Of
patients with SCC undergoing resection in the surgery arm, 47% experienced LRRs compared with
30% of those with AC. However, because SCC histology has a higher response rate to CRT, this was not
a prognostic factor in the univariable analysis. After CRT, there was no difference between SCC and
AC regarding LRR. Therefore, in the surgery arm, histology was an independent negative prognostic
factor for LRR, which disappeared after preoperative CRT.
Recurrences of only 5% within the radiation target volumes confirms the hypothesis that preoperative
CRT reduces the LRR rate. Recurrences at the supraclavicular fossae, generally not included in the
radiation target volumes of midesophageal and distal tumors, were similar in both groups (4%), which
further confirms this conclusion. Huang et al15 described supraclavicular lymph node recurrences in

Patterns of recurrence in the CROSS trials |
139
Cha
pter
9
16.7% of 54 patients with SCC of the proximal esophagus after surgery alone, which included removal
of pathologic supraclavicular lymph nodes. In the small group of patients with proximal tumors, no
supraclavicular recurrences were seen, probably because of the proximity of the supraclavicular fossae
to the radiation treatment volume.
Of the 20 patients with a recurrence near the celiac axis, 18 had a primary tumor located in the distal
esophagus, and most of them had synchronous distant metastases. On the basis of these data, elective
inclusion in the radiation target volume of the supraclavicular fossae for mid or distally located tumors
or celiac nodes for mid or proximal tumors would probably not have a large effect on survival. The idea
behind preoperative CRT in the treatment of esophageal cancer and cancer of the gastroesophageal
junction was to improve survival by reducing locoregional failure. However, we also observed a small
but significant effect on the development of hematogenous metastasis. From the current data, it
cannot be concluded whether this was a systemic effect of the chemotherapy or an indirect effect of
reducing LRRs. However, the short interval and frequently occurring synchronous recurrences argue
in favor of the first hypothesis.
In conclusion, preoperative CRT in patients with esopheageal or junctional cancer improves locoregional
control and has an effect on both hematogenous metastasis and peritoneal carcinomatosis. A pCR
after CRT was a favorable prognostic factor for both locoregional and systemic recurrences.

| Chapter 9
140
REFERENCES1. Enzinger PC, Mayer RJ: Esophageal cancer. N Engl J Med 349:2241-2252, 2003
2. Kelsen DP, Ginsberg R, Pajak TF, et al: Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 339:1979-1984, 1998
3. Bosset JF, Gignoux M, Triboulet JP, et al: Chemoradiotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N Engl J Med 337:161-167, 1997
4. Sjoquist KM, Burmeister BH, Smithers BM, et al: Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet Oncol 12: 681-692, 2011
5. van Hagen P, Hulshof MC, van Lanschot JJ, et al: Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 366:2074-2084, 2012
6. Meguid RA, Hooker CM, Taylor JT, et al: Recurrence after neoadjuvant chemoradiation and surgery for esophageal cancer: Does the pattern of recurrence differ for patients with complete response and those with partial or no response? J Thorac Cardiovasc Surg 138:1309-1317, 2009
7. Denham JW, Steigler A, Kilmurray J, et al: Relapse patterns after chemo-radiation for carcinoma of the oesophagus. Clin Oncol (R Coll Radiol) 15:98-108, 2003
8. van Meerten E, van der Gaast A, Tilanus HW, et al: Pathological analysis after neoadjuvant chemoradiotherapy for esophageal carcinoma: The Rotterdam experience. J Surg Oncol 100:32-37, 2009
9. Trotti A, Colevas AD, Setser A, et al: CTCAE v3.0: Development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 13:176-181, 2003
10. Mandard AM, Dalibard F, Mandard JC, et al: Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma: Clinicopathologic correlations. Cancer 73:2680-2686, 1994
11. Burmeister BH, Smithers BM, Gebski V, et al: Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: A randomised controlled phase III trial. Lancet Oncol 6:659-668, 2005
12. Tepper J, Krasna MJ, Niedzwiecki D, et al: Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol 26:1086-1092, 2008
13. Urba SG, Orringer MB, Turrisi A, et al: Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol 19:305-313, 2001
14. Siewert JR, Stein HJ, Feith M, et al: Histologic tumor type is an independent prognostic parameter in esophageal cancer: Lessons from more than 1,000 consecutive resections at a single center in the Western world. Ann Surg 234:360-367, 2001
15. Huang W, Li B, Gong H, et al: Pattern of lymph node metastases and its implication in radiotherapeutic clinical target volume in patients with thoracic esophageal squamous cell carcinoma: A report of 1077 cases. Radiother Oncol 95:229-233, 2010


P. van Hagen
B.P.L. Wijnhoven
P. Nafteux
J. Moons
K. Haustermans
G. DeHertogh
J.J.B. van Lanschot
T. Lerut
British Journal of Surgery 2013;100(2):267-73

Chapter 10Recurrence pattern in patients with a pathologically complete response
after neoadjuvant chemoradiotherapy and surgery for esophageal cancer

| Chapter 10
144
ABSTRACT
BACKGROUND
Little is known about recurrence patterns in patients with a pathologically complete response (pCR)
or an incomplete response after neoadjuvant chemoradiotherapy (CRT) followed by resection for
oesophageal cancer. This study was performed to determine the pattern of recurrence in patients
with a pCR after neoadjuvant CRT followed by surgery.
METHODS
All patients who received neoadjuvant CRT followed by esophagectomy between 1993 and 2009 were
identified from a database, and categorized according to pathological tumor response. Recurrences
were classified as locoregional or distant.
RESULTS
One hundred and eighty-eight patients were included. Median potential follow-up was 71·6 months.
A pCR was achieved in 62 (33·0 per cent) of 188 patients. Recurrence developed in 24 (39 per cent) of
62 patients with a pCR and 70 (55·6 per cent) of 126 without a pCR (P = 0·044). Locoregional recurrence
with or without synchronous distant metastases occurred in eight patients (13 per cent) in the pCR
group and 31 (24·6 per cent) in the non-pCR group (P = 0·095). Locoregional recurrences without
synchronous distant metastases occurred four (6 per cent) and ten (7·9 per cent) patients respectively
(P = 0·945). The overall 5-year survival rate was significantly higher in the pCR group than in the non-
pCR group (52 versus 33·9 per cent respectively; P = 0·019).
CONCLUSION
Of patients with a pCR, 13 per cent still developed a locoregional recurrence. Although pCR is more
favorable for survival, it is not synonymous with cure or complete locoregional disease control.

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
145
Cha
pter
10
INTRODUCTION
Esophageal cancer is the eighth most common cancer worldwide1, causing more than 400 000
deaths per year.2 Esophagectomy is generally considered the treatment of choice for potentially
curable cancers. Neoadjuvant chemoradiotherapy (CRT) is now used widely because it is believed to
facilitate radical resection, improve locoregional control and prolong survival in patients with locally
advanced oesophageal cancer.3–5 Disease recurrence is still seen, however, in approximately half of
patients within 2–3 years of combined modality treatment.6–8
Up to 57 per cent of patients have no tumor left in the resection specimen after preoperative
chemoradiotherapy.3 They are classified as having obtained a pathologically complete response (pCR;
pathological category after neoadjuvant therapy ypT0 N0) and generally have longer survival than
patients with incomplete or poor responses.3, 9, 10
Understanding the pattern and timing of recurrent disease in patients treated with neoadjuvant
CRT followed by surgery is important. If locoregional recurrence in patients who have a pCR is still
frequently encountered, modifying surgery by extended lymphadenectomy or intensifying the
locoregional effects of CRT by widening irradiation fields or increasing radiotherapy doses might be
worthwhile. If distant metastasis is the most common type of recurrence in patients with a pCR, then
new systemic treatments would seem more logical.
The aim of the present study was to define the pattern and timing of disease recurrence in patients
with a pCR compared with those in patients without a pCR after neoadjuvant CRT followed by surgery
for esophageal cancer.
METHODS
Patients were selected from a prospectively assembled database at the Department of Thoracic
Surgery, University Hospital of Leuven, Belgium. All patients who underwent neoadjuvant CRT
followed by esophagectomy for locally advanced cancer (stages T2–4 N0–1 M0) of the esophagus
or esophagogastric junction between January 1993 and January 2009 were eligible for inclusion. All
patients were followed until death or January 2010.
Patients with disease progression during neoadjuvant treatment, unresectable tumors during
exploratory thoracotomy or macroscopically incomplete resection (R2), those who also received
adjuvant chemotherapy, those who died in hospital after surgery, and those lost to follow-up within
12 months after surgery were excluded.
Patients were eligible for neoadjuvant CRT if they were thought to have lymph node metastases (clinical
cN+) on preoperative computed tomography (CT) with or without positron emission tomography
(PET) and/or endoscopic ultrasonography, and/or had tumors of questionable resectability (cT4). CRT
consisted of 80 mg/m2 cisplatin (Platinol®; Bristol-Meyers Squibb, Braine-l’Alleud, Belgium) on days
1 and 21, and 800 mg/m2 5-fluorouracil (5-FU) (Roche, Brussels, Belgium) by continuous infusion
on days 1–4 and 21–24, with concurrent radiotherapy. Patients were treated in the supine position

| Chapter 10
146
with an immobilizing mask. All patients underwent CT in the treatment position with intravenous
contrast. The clinical target volume was delineated based on the results of PET–CT and endoscopic
ultrasound examination. The clinical target volume included the primary tumor with a 5-cm margin
in the craniocaudal direction, the suspected lymph nodes and all regional lymph nodes. A margin of
1 cm was added around the planning target volume. Three-dimensional conformal radiotherapy was
used with at least four beams (anteroposterior–posteroanterior (AP-PA) and 2 oblique beams) and
multileaf collimation. To make the dose distribution more uniform, half beams were used in the AP-PA
direction with wedges and energies varying between 6 and 18 MV in the majority of patients.
Patients underwent surgery within 2 months of completion of CRT, via a left-sided thoracophrenotomy11
for infracarinal tumors or as a two-phase procedure, combining a laparotomy with a thoracotomy12,
when the tumor was located above the carina. In both techniques, a two- or three-field
lymphadenectomy was performed, including resection of the thoracic duct whenever possible.
Gastric tube reconstruction with a cervical anastomosis was the preferred method of reconstruction.
Resection specimens were fixed routinely in formalin. Representative tissue blocks were taken from
macroscopically visible residual tumor, all resection margins, lymph nodes and other lesions if present.
When no tumor was observed macroscopically, the entire tumor bed, identified by the presence of
scar tissue, was submitted for microscopic investigation. Tissue blocks were routinely embedded
in paraffin and a single 5-µm thick section of each block was stained with haematoxylin and eosin.
All slides were examined systematically by dedicated gastro-intestinal pathologists. Lymph nodes
identified macroscopically were halved and a single 5-µm thick section of each node was evaluated.
If there were reasons to assume that any vital tumor could be present in the evaluated lymph
node (such as signs of therapy effects), more sections of that lymph node were cut and evaluated.
Immunohistochemical staining was not performed routinely.
For more rigorous verification of a pCR in patients who subsequently developed locoregional
recurrence, additional immunohistological pankeratin staining was performed on freshly cut 5-µm
thick slides of the tumor bed and lymph node blocks of the archival resection specimens (monoclonal
mouse antihuman cytokeratin antibody, clone AE1/AE3; Dako, Heverlee, Belgium). A skin biopsy was
used as an external positive control, and mesenchymal or lymphoid tissue within the specimen as
an internal negative control. Whenever at least one group (lesions measuring 2·0 mm or less) of
pankeratin-positive, atypical epithelial cells was present within the specimen, immunohistochemical
staining was classified as positive.13 In order to reflect standard clinical practice (where pankeratin
staining is not standard), patients with positive pankeratin staining for isolated primary tumor cells
were still classified as having a pCR.
When no tumor cells were seen within 1 mm of the proximal, distal and circumferential resection
margins, the resection was classified as R0. If tumor cells were present within 1 mm of the surgical
resection margin on microscopic evaluation, the resection was classified as R1.
According to the observed tumour regression in the resection specimen, two groups were identified:
patients who had a pCR and those who did not. A pCR was defined as absence of residual tumor cells

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
147
Cha
pter
10
in the resection specimen, either at the primary tumor site or in any of the resected lymph nodes.
If any vital tumor cells were seen on conventional histopathological examination, the patient was
allocated to the non-pCR group.
Patients were followed for up to 5 years in the outpatient clinic. CT of the neck, chest and abdomen
was carried out routinely every 6 months for at least the first 3 years after surgery. The diagnosis
of recurrence was confirmed by biopsy-positive histopathology or cytopathology. If this was not
possible, clinical deterioration was considered as evidence of recurrence.
In patients with no signs of recurrence, the interval between CT was lengthened to a year in the
fourth and fifth years after operation or until diagnosis of recurrence was established. The last date
of follow-up, date of recurrence (first failure), as well as site of this recurrence (as applicable) were
recorded. Recurrences were defined as locoregional (at the previous site of the primary tumor and/
or in regional lymph nodes within the field of surgical resection and/or the irradiated field), distant
(haematogenous metastases or distant lymph node metastases) or both (synchronous locoregional
and distant recurrence).
Statistical analysis
The χ2 test was used to detect statistical differences between subgroups. Hazard ratios were calculated
using a Cox regression model. Multivariable analysis for prognostic factors was performed using a Cox
proportional hazard model. Only parameters with P < 0·100 in univariable analysis were added to
the multivariable model. Overall and disease-free survival rates were calculated using the Kaplan-
Meier method, and compared by means of the log rank test. P < 0·050 (two-sided) was considered
statistically significant. Statistical analysis was performed using SPSS® version 17.0 (IBM, Armonk, New
York, USA).
RESULTS
Two hundred and sixty-five patients who were scheduled to receive neoadjuvant CRT followed by
surgery between January 1993 and January 2009 were identified. Of these, 77 were excluded, because
of: progressive disease during neoadjuvant CRT (18), unresectability during exploration (3), adjuvant
chemotherapy (10), R2 resection (35), refusal to undergo surgery (4), considered medically unfit for
surgery (2), or they died after surgery before discharge from hospital (5). Of the five patients who died
after operation, three had a pCR in the resection specimen.
Among the 188 included patients (147 men, 41 women), median age was 60 (range 37-80) years. On
clinical staging, the majority of patients (93·6 per cent) had a tumor invading the adventitia (cT3) or
suspicion of invasion of a surrounding structure (cT4). Most (91·5 per cent) had locoregional lymph
node metastases (cN+). Patient and tumor characteristics are summarized in Table 1.

| Chapter 10
148
TABLE 1. Baseline characteristics of 188 patients who underwent neoadjuvant CRT followed by macroscopically radical resection for advanced esophageal cancer.¥
All patients (n=188)
Age [years]medianrange
6037-80
Sex ratio (M:F) 147:41
ASA grade* (n, %)ASA IASA IIASA III
3112928
(17%)(69%)(15%)
Histological type (n, %)SCCACsmall cell carcinoma
107 801
(57%)(43%)( 1%)
cT category^ (n, %)cT2cT3cT4cTx
9112643
( 5%)(60%)(34%)( 2%)
cN grade& (n, %)cN0cN+cNx
15172
1
( 8%)(92%)( 1%)
Tumour location (n, %)proximal thirdmiddle thirddistal thirdGEJ
22638221
(12%)(34%)(44%)(11%)
SCC: Squamous cell carcinomaAC: Adenocarcinoma¥ Percentages may not total 100 because of rounding*ASA grade: American Society of Anesthesiologists Physical Status Classification System^cT grade: clinical T-stage as defined by endo-ultrasonography and/or CT-scanning according to AJCC TNM Cancer Staging, 6th edition.&cN grade: clinical N-stage as defined by endo-ultrasonography and/or CT-scanning and/or FDG-PET-scanning according to AJCC TNM Cancer Staging, 6th edition.
All patients received cisplatin'5-FU-based chemotherapy and concurrent radiotherapy, with a median
dose of 40 (range 36-60) Gy in 20 (range 18-36) fractions. The radiotherapy dose varied during the
study period. In 91 patients (48·4 per cent), a total of 40 Gy was administered in 20 fractions of 2 Gy.
Another 61 patients (32·4 per cent) received a total of 36 Gy in 20 fractions of 1·8 Gy, and 25 (13·3 per
cent) were treated with 45 Gy in 25 fractions of 1·8 Gy. In the remaining 11 patients (5·9 per cent), the
radiotherapy dose varied between 43 and 60 Gy, in fractions of 1·8 Gy.
Ninety-seven patients (51·6 per cent) underwent a left-sided thoracophrenotomy, 89 (47·3 per cent) a
right-sided transthoracic resection and two (1·1 per cent) a left-sided transthoracic resection. A two-

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
149
Cha
pter
10
field lymphadenectomy (chest and upper abdomen) was performed in 100 patients (53·2 per cent)
and a cervical lymph node dissection was also carried out in 75 (39·9 per cent)15. Thirteen patients
(6·9 per cent) had no formal lymphadenectomy.
A pCR was observed in 62 (33·0 per cent) of 188 patients. A further nine patients had a complete
response at the primary tumor site (ypT0), but were allocated to the non-pCR group because of the
presence of lymph node metastases (ypN1). R0 resection was achieved in 183 patients (97·3 per cent).
The results of histopathological examination are summarized in Table 2.
TABLE 2. Results of conventional histopathological examination of resection specimens
All patients (n=188)
ypT-stage (n, %)ypT0ypTis/ypT1ypT2ypT3ypT4
731930624
(39%)(10%)(16%)(33%)( 2%)
ypN-stage (n, %)ypN0ypN+
11969
(63%)(37%)
No. of LNs removed (n)*
medianp25-p75
2414-32
No. of pos LNs (n)*Ω
medianp25-75
20-2
Radicality (n, %)R0R1
1835
(97%)( 3%)
Tumour response (n, %)pCRnon-pCR
62126
(33%)(67%)
Values in parentheses are percentages unless indicated otherwise;*values are median (interquartile range).ΩNumber of positive lymph nodes in patients with positive lymph nodes in the resection specimen. ypT/N, pathological tumor/node category after neoadjuvant therapy in American Joint Committee on Cancer tumor node metastasis staging system (6th edition)14; Tis, tumor in situ; pCR, pathologically complete response.
Median potential follow-up was 71·6 months, 60·0 (range 15·5-190·3) months for the pCR group and
73·0 (13·6-121·7) months for the non-pCR group (P = 0·323). Recurrence was identified in 94 patients
(50·0 per cent). There were 24 recurrences in the pCR group and 70 in the non-pCR group (P = 0·044).
Patterns of recurrence in the two groups are shown in Table 3. There were no significant differences
between the two groups in rates of locoregional recurrence alone (P = 0·945) or locoregional
recurrence with or without synchronous distant spread (P = 0·095). For patients who developed any
locoregional recurrence, the median interval to that recurrence was 8·7 (5·3-100·8) months in the

| Chapter 10
150
pCR group and 12·0 (1·9-69·2) months in the non-pCR group (P = 0·320). For patients who developed
distant metastases, the median interval to their occurrence (with or without synchronous locoregional
recurrence) was 8·7 (2·4-100·8) and 8·5 (0·6-51·9) months in the pCR and non-pCR groups respectively
(P = 0·257).
TABLE 3. Recurrence patterns
nNo recurrence
Locoregional recurrence alone*
Distant metastases alone† Both‡ Site
unknown§
All patients 188 94 (50.0) 14 (7.4) 53 (28.2) 25 (13.3) 2 (1.1)
pCR 62 38 (61) 4 (6) 16 (26) 4 (6) 0 (0)
Non-pCR 126 56 (44.4) 10 (7.9) 37 (29.4) 21 (16.7) 2 (1.6)
Values in parentheses are percentages; percentages may not total 100 because of rounding.*Recurrence of primary tumor and/or tumor in locoregional lymph nodes.†Hematogenous metastases or distant lymph node metastases.‡Synchronous locoregional recurrence and distant metastases.§Insufficient information to determine exact site of recurrence. pCR, pathologically complete response.
Pankeratin staining of the resection specimens of patients who developed recurrent disease after a
pCR revealed small clusters of vital tumour cells (lesions measuring no more than 0·2 mm)13 in the
peri-esophageal lymph nodes in two of eight patients.
Follow up in months3624120
Prop
ortio
nal s
urvi
val
1,0
0,8
0,6
0,4
0,2
0,0
pCR
non-pCR
Page 1
pCR 62 49 41 26non-pCR 126 91 62 47total 188 139 103 73
No. at risk
FIGURE 1. Estimated overall survival among 188 patients who underwent neoadjuvant chemoradiotherapy followed by surgery according to completeness of pathological response in the resection specimen. pCR, pathologically complete response. P=0.019 (log rank test

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
151
Cha
pter
10
Follow up in months3624120
Pro
porti
onal
surv
ival
1,0
0,8
0,6
0,4
0,2
0,0
pCR
non-pCR
Page 1
pCR 62 48 40 25non-pCR 126 91 62 47total 188 139 102 72
No. at risk
FIGURE 2. Estimated disease-specific survival among 188 patients who underwent neoadjuvant chemoradiotherapy followed by surgery according to completeness of pathological response in the resection specimen. pCR, pathologically complete response. P=0.016 (log rank test)
The estimated 5-year overall survival rate for the pCR group was 52 per cent compared with 33·9
per cent for the non-pCR group (P = 0·019) (Fig. 1). Median overall survival was 60·0 and 26·6 months
respectively (hazard ratio 0·59, 95 per cent confidence interval 0·38 to 0·92). The estimated disease-
specific survival rate at 5 years was also significantly better in the pCR group than in the non-pCR
group (70 versus 47·8 per cent respectively; P = 0·016) (Fig. 2). In a multivariable Cox regression analysis,
only ypN category was found to be an independent predictor of survival (Table 4).

| Chapter 10
152
TABLE 4. Univariable and multivariable analysis to identify predictors of survival
Univariable analysis† Multivariable analysis‡
Hazard ratio P Hazard ratio P
Sex 1·05 (0·66, 1·69) 0·828
Age 1·00 (0·99, 1·03) 0·398
ASA grade 0·97 (0·69, 1·36) 0·862
Tumour type 1·08 (0·77, 1·53) 0·655
cT category 0·94 (0·74, 1·12) 0·618
cN category 0·90 (0·62, 1·32) 0·597
ypT category 1·06 (0·99, 1·13) 0·122
Tumour location 1·22 (0·97, 1·53) 0·850
ypN category 2·03 (1·38, 2·98) < 0·001 1·70 (1·02, 2·83) 0·043
Lymph node ratio* 3·98 (1·53, 10·36) 0·005 1·75 (0·52, 5·90) 0·370
pCR 0·59 (0·38, 0·92) 0·021 0·84 (0·50, 1·44) 0·532
Values in parentheses are 95 per cent confidence intervals.*Ratio of positive lymph nodes to total number of lymph nodes in resection specimen. ASA, American Society of Anesthesiologists physical status; cT/N, clinical tumour/node category according to the American Joint Commit-tee on Cancer (AJCC) tumour node metastasis (TNM) staging system (6th edition); ypT/N, pathological tumour/node category after neoadjuvant therapy in AJCC TNM staging system (6th edition); pCR, pathologically com-plete response.† Cox regression;‡ Cox proportional hazards model.
DISCUSSION
A pCR was observed after neoadjuvant chemoradiotherapy in one-third of the patients in this study.
The overall recurrence rate in the pCR group was significantly lower than in the non-pCR group,
although 13 per cent of these patients still developed locoregional recurrence, with or without
synchronous distant metastases. No significant difference was found in the time to locoregional
recurrence or distant dissemination between complete and incomplete responders.
Patterns of recurrence after esophagectomy have been studied in patients undergoing surgery
without neoadjuvant CRT. The locoregional recurrence rate was 13 per cent in 202 patients who
underwent primary, microscopically complete (R0) resection for stage II–IV esophageal carcinoma16,
a similar figure to that in the present pCR group. In a series of 100 consecutive patients with
oesophageal adenocarcinoma who underwent en bloc resection with extended lymphadenectomy
but without neoadjuvant therapy, the local recurrence rate was only 1 per cent, although 32 per
cent of these patients had a pT1 tumour, only 40 per cent a T3 tumour, those who underwent R1–2
resection were excluded and lymph node recurrences outside the surgical field were not scored
as locoregional recurrences.17 Lerut and colleagues15 reported a 5·2 per cent isolated locoregional
recurrence rate and another 9 per cent with synchronous locoregional and distant recurrence after

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
153
Cha
pter
10
three-field lymphadenectomy in a series of 174 patients.15 These data indicate that low locoregional
recurrence rates can also be achieved with appropriate primary surgery alone, raising the question of
how neoadjuvant CRT contributes to locoregional control. The commonly accepted rationale is that
preoperative CRT improves R0 resection rates and decreases the risk of leaving behind both known
and unknown nodal disease.
There have been several reports on recurrence patterns after neoadjuvant CRT and surgery. In a study
of 243 patients treated with cisplatin/5-FU and a radiotherapy dose of 40·0 Gy, 39 (16.0 per cent)
had a pCR. Overall 5-year survival rates in the pCR and non-pCR groups were 50 and 28 per cent
respectively, comparable with rates in the present study.18 In the pCR group, seven patients (18 per
cent) developed locoregional recurrence, with or without distant metastases, compared with 13 per
cent in the present study. In a group of 267 patients, 82 (30.7 per cent) had a pCR, of whom 22 per cent
developed a locoregional and/or distant recurrence, compared with 36 per cent of those without a
pCR19. Within the pCR group, 27 per cent of all these recurrences were located in the mediastinum or
(remnant) esophagus, again similar to the present study. These relatively high in-field recurrence rates
indicate that pCR is not synonymous with complete locoregional control.
It is acknowledged that immunohistochemical staining was not performed on sections from
patients with a pCR who developed distant metastases in the present study. The likelihood of distant
metastases in patients described as having a pCR might be greater if immunohistochemistry were
carried out routinely on all primary tumors and lymph nodes thought not to contain tumor deposits
on conventional histology.
Although significantly fewer patients developed recurrent disease in the pCR group, the time to
recurrence, either locoregional recurrence or distant metastasis, was comparable for patients with and
without a pCR. The disease-free interval in patients who had a pCR was not significantly different from
that in patients without a pCR (for both locoregional recurrences and distant metastases). This is in
contrast to the findings of a study involving 235 patients who underwent CRT followed by surgery, in
which three response types were described: complete (29 per cent), partial (46 per cent) and none (24
per cent); the disease-free interval was significantly longer in complete and partial responders than in
non-responders.20 The significantly longer disease-free interval in that study may be explained by the
different chemoradiation protocols used in the different groups, as well as differences in tumor stage.
One study has specifically examined the impact of surgical radicality (en bloc versus transhiatal
resection) on outcome in the context of preoperative CRT.21 Overall 5-year survival was significantly
better in the en bloc group (51 versus 22 per cent). Better overall 5-year survival in favor of the en bloc
group was also seen both in the presence of a pCR (70 versus 43 per cent) and with no pCR (48 versus
9 per cent). There were no locoregional recurrences in the pCR group suggesting that more radical
surgery, even when allied to neoadjuvant CRT, improved survival as well as decreasing the risk of
locoregional recurrence.
In the present study, after diagnosis of the first recurrence (either locoregional, distant metastases or a
synchronous combination of both), further imaging was driven by clinical need. Further locoregional

| Chapter 10
154
and/or distant failures may well have occurred. This implies that more patients assigned to the pCR
group may have had locoregional failure than were recorded.
Some confounding is inevitable in observational studies of this nature. Patient selection (only patients
with suspicious lymph nodes or questionable resectability were treated with neoadjuvant therapy)
resulted in a less favorable pretreatment tumor stage that might have led to worse outcomes than
reported in series dominated by early-stage tumors. It is acknowledged that the small numbers in
several subgroups of patients invites statistical misinterpretation.
Although it is clear that locoregional control is not always achieved by CRT and surgery, the high
percentage of patients who presented with distant metastases during follow-up was striking. The
radiosensitizing effect of chemotherapy is probably important for the improved locoregional tumor
control, but its systemic impact is clearly far from adequate.22 The lack of systemic chemotherapeutic
efficacy has also been suggested in studies using preoperative chemotherapy without radiotherapy.23
Although locoregional tumor control remains suboptimal after neoadjuvant CRT plus surgery (even in
patients with a pCR), preventing distant dissemination is the major clinical challenge.

Recurrence pattern in patients with pCR after nCRT and surgery for esophageal cancer |
155
Cha
pter
10
REFERENCES1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008:
GLOBOCAN 2008. Int J Cancer 2010;127(12): 2893-2917.
2. Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. Eur J Cancer 2001;37 Suppl 8: S4-66.
3. Gannett DE, Wolf RF, Takahashi GW, Louie J, Wagner RC, Ey FS, Owens MM, Johnson WE, Cook DW, Alberty RE. Neoadjuvant chemoradiotherapy for esophageal cancer using weekly Paclitaxel and Carboplatin plus infusional 5-Fluorouracil. Gastrointest Cancer Res 2007;1(4): 132-138.
4. Lin CC, Hsu CH, Cheng JC, Wang HP, Lee JM, Yeh KH, Yang CH, Lin JT, Cheng AL, Lee YC. Concurrent chemoradiotherapy with twice weekly paclitaxel and cisplatin followed by esophagectomy for locally advanced esophageal cancer. Ann Oncol 2007;18(1): 93-98.
5. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med 2012;366(22): 2074-2084.
6. Burmeister BH, Smithers BM, Gebski V, Fitzgerald L, Simes RJ, Devitt P, Ackland S, Gotley DC, Joseph D, Millar J, North J, Walpole ET, Denham JW, Trans-Tasman Radiation Oncology G, Australasian Gastro-Intestinal Trials G. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: a randomised controlled phase III trial. Lancet Oncol 2005;6(9): 659-668.
7. Tepper J, Krasna MJ, Niedzwiecki D, Hollis D, Reed CE, Goldberg R, Kiel K, Willett C, Sugarbaker D, Mayer R. Phase III trial of trimodality therapy with cisplatin, fluorouracil, radiotherapy, and surgery compared with surgery alone for esophageal cancer: CALGB 9781. J Clin Oncol 2008;26(7): 1086-1092.
8. Urba SG, Orringer MB, Turrisi A, Iannettoni M, Forastiere A, Strawderman M. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol 2001;19(2): 305-313.
9. Schneider PM, Baldus SE, Metzger R, Kocher M, Bongartz R, Bollschweiler E, Schaefer H, Thiele J, Dienes HP, Mueller RP, Hoelscher AH. Histomorphologic tumor regression and lymph node metastases determine prognosis following neoadjuvant radiochemotherapy for esophageal cancer: implications for response classification. Ann Surg 2005;242(5): 684-692.
10. Mandard AM, Dalibard F, Mandard JC, Marnay J, Henry-Amar M, Petiot JF, Roussel A, Jacob JH, Segol P, Samama G, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994;73(11): 2680-2686.
11. Page RD, Khalil JF, Whyte RI, Kaplan DK, Donnelly RJ. Esophagogastrectomy via left thoracophrenotomy. Ann Thorac Surg 1990;49(5): 763-766.
12. Muller JM, Erasmi H, Stelzner M, Zieren U, Pichlmaier H. Surgical therapy of oesophageal carcinoma. Br J Surg 1990;77(8): 845-857.
13. Singletary SE, Greene FL, Sobin LH. Classification of isolated tumor cells: clarification of the 6th edition of the American Joint Committee on Cancer Staging Manual. Cancer 2003;98(12): 2740-2741.
14. Lerut T, Nafteux P, Moons J, Coosemans W, Decker G, De Leyn P, Van Raemdonck D, Ectors N. Three-field lymphadenectomy for carcinoma of the esophagus and gastroesophageal junction in 174 R0 resections: impact on staging, disease-free survival, and outcome: a plea for adaptation of TNM classification in upper-half esophageal carcinoma. Ann Surg 2004;240(6): 962-972; discussion 972-964.
15. Lee PC, Mirza FM, Port JL, Stiles BM, Paul S, Christos P, Altorki NK. Predictors of recurrence and disease-free survival in patients with completely resected esophageal carcinoma. J Thorac Cardiovasc Surg 2011;141(5): 1196-1206.

| Chapter 10
156
16. Hagen JA, DeMeester SR, Peters JH, Chandrasoma P, DeMeester TR. Curative resection for esophageal adenocarcinoma: analysis of 100 en bloc esophagectomies. Ann Surg 2001;234(4): 520-530; discussion 530-521.
17. Reynolds JV, Muldoon C, Hollywood D, Ravi N, Rowley S, O’Byrne K, Kennedy J, Murphy TJ. Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer. Ann Surg 2007;245(5): 707-716.
18. Meguid RA, Hooker CM, Taylor JT, Kleinberg LR, Cattaneo SM, 2nd, Sussman MS, Yang SC, Heitmiller RF, Forastiere AA, Brock MV. Recurrence after neoadjuvant chemoradiation and surgery for esophageal cancer: does the pattern of recurrence differ for patients with complete response and those with partial or no response? J Thorac Cardiovasc Surg 2009;138(6): 1309-1317.
19. Rohatgi PR, Swisher SG, Correa AM, Wu TT, Liao Z, Komaki R, Walsh G, Vaporciyan A, Lynch PM, Rice DC, Roth JA, Ajani JA. Failure patterns correlate with the proportion of residual carcinoma after preoperative chemoradiotherapy for carcinoma of the esophagus. Cancer 2005;104(7): 1349-1355.
20. Rizzetto C, DeMeester SR, Hagen JA, Peyre CG, Lipham JC, DeMeester TR. En bloc esophagectomy reduces local recurrence and improves survival compared with transhiatal resection after neoadjuvant therapy for esophageal adenocarcinoma. J Thorac Cardiovasc Surg 2008;135(6): 1228-1236.
21. Hennequin C, Favaudon V. Biological basis for chemo-radiotherapy interactions. Eur J Cancer 2002;38(2): 223-230.
22. Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol 2009;27(30): 5062-5067.


A.K. Talsma
P. van Hagen
B.A. Grotenhuis
E.W. Steyerberg
H.W. Tilanus
J.J.B. van Lanschot
B.P.L. Wijnhoven
Annals of Surgical Oncology 2012; 19(7): 2142–2148

Chapter 11Comparison of the 6th and 7th editions
of the UICC-AJCC TNM classification for esophageal cancer

| Chapter 11
160
ABSTRACT
BACKGROUND
The new 7th edition of the Union for International Cancer Control–American Joint Committee on
Cancer (UICC-AJCC) tumor, node, metastasis (TNM) staging system is the ratification of data-driven
recommendations from the Worldwide Esophageal Cancer Collaboration database. Generalizability
remains questionable for single institutions. The present study serves as a validation of the 7th edition
of the TNM system in a prospective cohort of patients with predominantly adenocarcinomas from a
single institution.
METHODS
Included were patients who underwent transhiatal esophagectomy with curative intent between
1991 and 2008 for invasive carcinoma of the esophagus or gastroesophageal junction. Excluded were
patients who had received neoadjuvant chemo(radio)therapy, patients after a noncurative resection
and patients who died in the hospital. Tumors were staged according to both the 6th and the 7th
editions of the UICC-AJCC staging systems. Survival was calculated by the Kaplan–Meier method, and
multivariate analysis was performed with a Cox regression model. The likelihood ratio chi-square test
related to the Cox regression model and the Akaike information criterion were used for measuring
goodness of fit.
RESULTS
A study population of 358 patients was identified. All patients underwent transhiatal esophagectomy
for adenocarcinoma. Overall 5-year survival rate was 38%. Univariate analysis revealed that pT stage,
pN stage, and pM stage significantly predicted overall survival. Prediction was best for the 7th edition,
stratifying for all substages.
CONCLUSIONS
The application of the 7th UICC-AJCC staging system results in a better prognostic stratification
of overall survival compared to the 6th edition. The fact that the 7th edition performs better
predominantly in patients with adenocarcinomas who underwent a transhiatal surgical approach,
in addition to findings from earlier research in other cohorts, supports its generalizability for different
esophageal cancer practices.

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
161
Cha
pter
11
INTRODUCTION
Accurate staging of cancer is important for stage-specific treatment, thus minimizing inappropriate
treatment. Moreover, it allows for interinstitutional comparisons and disclosure of prognosis to patients.1
The staging system for cancer in the esophagus and esophagogastric junction has been revised as
outlined in the 7th edition of the Union for International Cancer Control/Union Internationale Contre
le Cancer (UICC) and the American Joint Committee on Cancer (AJCC), Cancer Staging Manual.2
Retrospective studies suggested that the number of involved lymph nodes is a better predictor of
outcome than classifying lymph node involvement as either present or absent.3,4 Peyre et al. showed
that patients with ≥3 lymph nodes involved have a risk of systemic disease that exceeds 50%. When >8
nodes are involved, the risk of dying is almost 100%.5 Indeed, the latest 7th edition of the UICC-AJCC
esophageal tumor, node, metastasis (TNM) staging system has acknowledged the importance of the
number of involved nodes by revising the N category from site-dependent staging to a numerically
based classification into N0 to N3. Another major change is the definition of regional lymph nodes.
The new UICC-AJCC staging system is the ratification of data-driven recommendations from a database
of >7800 esophageal cancer patients created from a large multi-institutional collaboration involving
13 institutions.6,7 This Worldwide Esophageal Cancer Collaboration (WECC) database overcomes
problems of rarity of this cancer, but generalizability remains questionable for single institutions. WECC
incorporates high-volume centers both from the West (where adenocarcinomas prevail) and from the
East (where most tumors are squamous cell carcinomas). Moreover, the extent of intrathoracic lymph
node dissection can vary greatly between different institutions, leading to potential bias.
The present study serves as a validation of the WECC-based 7th edition of the TNM system in a
cohort of patients with both squamous cell carcinomas and adenocarcinomas from a single Western
high-volume institution. Two studies already showed that the 7th edition criteria resulted in better
prognostic stratification than the 6th edition.8,9 However, both study cohorts consisted of squamous
cell carcinomas or junctional tumors, respectively. Moreover, Gaur et al. included patients who
received (neo)adjuvant therapy.9
The aim of this study was to assess the predictive ability of the 7th edition of the AJCC TNM staging
system for overall survival and to compare this with the 6th edition in a cohort of patients who
underwent transhiatal esophagectomy for adenocarcinomas without (neo)adjuvant therapy.
PATIENTS AND METHODS
Study Population
Included were all patients who underwent a transhiatal esophagectomy with curative intent between
January 1991 and September 2008 at the Erasmus Medical Center (Rotterdam, The Netherlands) for
invasive squamous cell carcinoma and adenocarcinoma of the esophagus or gastroesophageal
junction. Excluded were patients who had received neoadjuvant chemo(radio)therapy, patients

| Chapter 11
162
after a noncurative (R1) resection (tumor-free margin <1 mm) and patients who died in the hospital.
Clinicopathologic data of all patients had been routinely collected in an ongoing prospective registry.
Surgery
Transhiatal esophagectomy with cervical anastomosis was the chosen surgical approach in the
present study. This encompasses the en-bloc dissection of the primary tumor and its adjacent lymph
nodes under direct vision through the widened hiatus of the diaphragm up to the level of the
inferior pulmonary vein. Subsequently, a 3–4-cm-wide gastric tube is created. The left gastric artery is
transected at its origin with resection of celiac trunk lymph nodes. After mobilization and transection
of the cervical esophagus, the intrathoracic middle and upper esophagus is bluntly dissected in an
antegrade fashion with a vein stripper. Esophagogastrostomy is performed in the neck without a
formal cervical lymphadenectomy.
Follow-up
Surviving patients were followed at regular intervals at the outpatient clinic until 5 years after surgery.
Outpatient clinic visits encompassed history taking and physical examination. No routine imaging
was performed. Recurrences were sought afterward, only when clinically indicated, by CT scan or
ultrasound and proven by histology and cytology whenever possible. Overall survival was defined
as the time between date of operation and date of death. Surviving patients were censored on the
day of last follow-up. Patient survival status was calculated after contacting the general practitioners
(performed by a trained data manager). The last follow-up checkpoint was July 2010. If follow-up was
incomplete, survival was verified in the municipal mortality registers.
Statistical Analysis
Tumors were staged according to both the 6th and 7th editions of the UICC-AJCC staging systems.
Survival was calculated by the Kaplan–Meier method, and differences between curves were assessed
by the log rank test.
Two multivariable models were built, one with the 6th edition and one with the 7th edition of the
TNM staging system as categorical variables. The performance was tested for the model in which the
stages were combined into four categories (I–IV) as well as for the model with all substages included
(IA, IB, IIA, IIB, IIIA, IIIB, IIIC, IV). A multivariable model with both 6th and 7th edition criteria included was
used to assess the remaining value of the 6th edition when the 7th edition information was known.
The likelihood ratio chi-square test related to the Cox regression model was used for measuring
goodness of fit. The Akaike information criterion (AIC) was applied to correct for the potential bias
in comparing prognostic systems with different number of stages.10,11 The −2 log likelihood (which is
the parameter in the Cox regression) of the 6th edition was compared to that of the 7th edition; the
smaller the value of this statistic, the better the model.

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
163
Cha
pter
11
AIC was defined as: AIC = −2 log maximum likelihood + 2 × (the number of parameters in the model).
A smaller AIC value indicates a more desirable model for predicting outcome. A value of P < 0.05 was
considered statistically significant. Statistical analysis was performed with SPSS 10 for Windows (SPSS,
Chicago, IL).
RESULTS
Patient Characteristics
A consecutive series of 766 patients underwent esophagectomy with curative intent. In total, 221
patients were excluded because they had received neoadjuvant chemo(radio)therapy in the context
of a randomized, controlled trial.12 Another 165 patients were excluded because of a noncurative (R1)
resection, and 20 patients were excluded because of in-hospital mortality. Two patients had an in situ
carcinoma and were also excluded from the current analysis. This resulted in a final study population
of 358 patients.
Mean follow-up was 51 months (median 37 months). Overall 5-year survival rate was 38%. Most
recurrences of disease occurred within 2 years after surgery. Patient characteristics and overall
survival rates are summarized in Table 1. All patients underwent transhiatal esophagectomy for
adenocarcinoma. Eight patients seemed to have distant metastasis during the operation; their disease
was scored as M1.
Univariate analysis revealed that parameters pT stage, pN stage, and pM stage all significantly
predicted overall survival. Except for histologic grade, no other significant predictors of survival were
detected in this univariate analysis. The median number of dissected nodes per patient was 11. In
patients with negative lymph nodes (pN0), the survival rates did not differ between patients with ≤11
nodes and >11 nodes dissected: 65% vs. 69%, respectively; P = 0.65; data not shown).
Stratification of Prognosis According to 6th and 7th Editions of TNM Staging Systems
The overall survival curves according to the N classifications of the 6th and 7th editions are shown in
Fig. 1a and b, respectively.
Patient stage migration for reclassifying patients from the 6th to the 7th staging system and their
survival rates are listed in Table 2. In 58% of the 358 esophageal cancer patients, stage did not differ in
these two classification systems. Reassignment of disease stage occurred in all other patients, either to
a higher or to a lower tier. According to the 6th edition staging system, 56 (87%) of 64 stage IV patients
were staged as such because of a celiac lymph node metastasis. These patients were reclassified to a
lower tier in the 7th edition: 6 of 64 were staged as stage IIB, 15 as stage IIIA, 19 as IIIB, and 16 as IIIC
(Table 2).

| Chapter 11
164
TABLE 1. Patient demographics and results of univariate analysis for overall survival (N = 358)
Characteristic Value 5-y survival, % P
No. of patients 358
Age, year, mean (range) 62.6 (28–83) 38.8
Gender
Male 293 (82%) 37.2 0.664
Female 65 (18%) 45.9
pT
1 78 (22%) 68.7 <0.001
2 79 (22%) 51.1 <0.001
3 201 (56%) 22.7
pN
0 146 (41%) 65.9 <0.001
1 90 (25%) 28.4 <0.001
2 81 (23%) 17.5 <0.001
3 41 (11%) 3.0
pM
0 350 39.7<0.001
1 8 0.0
Grade
Well differentiated (G1) 31 (9%) 75.3 <0.001
Moderately differentiated (G2) 177 (49%) 39.4 <0.053
Poorly differentiated (G3) 150 (42%) 30.9
Histology
Squamous cell carcinoma 47 (13%) 41.9 0.752
Adenocarcinoma 311 (87%) 38.3
Location
Upper third 6 (2%) 30.4 0.352
Middle third 14 (4%) 42.6 0.325
Lower third (distal + EGJ) 338 (94%) 36.9
Type of surgical approach
Transhiatal esophagectomy 358 (100%)
Transthoracic esophagectomy
T tumor stage (depth of invasion), N lymphatic dissemination stage (according to 7th edition of UICC-AJCC TNM staging system: N0 no positive lymph nodes, N1 1–2 positive lymph nodes, N2 3–6 positive lymph nodes, N3 ≥6 positive lymph nodes), M distant metastasis stage (according to 7th edition of UICC-AJCC TNM staging system: M0 no metastasis, M1 distant metastasis present), EGJ esophagogastric junction.

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
165
Cha
pter
11
FIGURE 1. Kaplan–Meier overall survival curves for 358 patients stratified by N stage according to a 7th edition and b 6th edition UICC-AJCC TNM staging systems (overall log rank P < 0.01)
TABLE 2. Cross table of staging esophageal cancer patients according to the 6th and 7th editions of UICC-AJCC TNM staging
6th editiona5 year-survival according to
7th edition (%)I IIA IIB III IV
7th editionb
IA 43 0 0 0 0 87.7
IB 13 28 0 0 0 73.3
IIA 0 19 0 0 0 55.3
IIB 0 41 24 0 6 40.1
IIIA 0 0 21 50 15 24.3
IIIB 0 0 0 31 19 11.9
IIIC 0 0 4 20 16 3.1
IV 0 0 0 0 8 0.0
5 year-survival according to 6th edition (%) 81.9 56.8 38.3 14.1 12.4
M1a celiac nodes involved in lower esophageal cancer or cervical nodes involved in upper esophageal cancer, M1b beyond locoregional node involvement (i.e., cervical nodes in lower esophageal cancer and celiac nodes in upper esophageal cancer; metastatic involvement of visceral organs, pleura, peritoneum)aThe 6th edition AJCC-UICC TNM staging system: stage I T
1N
0, stage IIA T
2,3N
0, stage IIB T
1,2N
1, stage III T
3N
1 or T
4N
0,
stage IVA Tany
Nany
M1a, stage IVB Tany
Nany
M1b. The 7th edition AJCC-UICC TNM staging system (for adenocarcinoma): stage IA T
1N
0G
1,2, stage IB T
1N
0G
3 or T
2N
0G
1,2, stage IIA T
2N
0, stage IIB T
3N
0 or T
1,2N
1, stage IIIA T
4N
0 or T
3N
1 or T
1,2N
2, stage
IIIB T3N
2, stage IIIC T
anyN
3 or T
4aN
1–3 or T
4bN
any, stage IV T
any,N
any,M
1.

| Chapter 11
166
FIGURE 2. Kaplan–Meier curves of overall survival for 358 patients stratified according to a 6th edition and b 7th edition UICC-AJCC TNM staging systems
FIGURE 3. Kaplan–Meier overall survival curves for 64 UICC-AJCC 6th stage IV patients who were reclassified according to UICC-AJCC 7th edition TNM staging (log rank P = 0.43).
The Kaplan–Meier curves of esophageal cancer patients based on the 6th and 7th editions of the TNM
staging systems are depicted in Fig. 2. Both systems show a relatively ordered monotone distribution
of survival. However, according to the 6th edition staging system, the Kaplan–Meier plot shows

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
167
Cha
pter
11
overlapping curves for stage III and IV. In the 7th edition, no important overlapping occurs among
stages I through IV.
Subgroup analysis among selected patients who had been considered to have stage IV disease
according to the UICC-AJCC 6th edition scoring system showed that patients reclassified from stage
IV disease to a lower tier in the UICC-AJCC 7th edition had a significantly better survival compared to
patients still classified as stage IV according to the UICC-AJCC 7th edition. Moreover, the UICC-AJCC
7th edition was able to make further significant stratification of survival rates of these reclassified
patients (Fig. 3; log rank P = 0.43).
The UICC-AJCC 7th edition staging system defines patients with positive paraesophageal cervical
lymph nodes (n = 10) as having stage IIIA or IIIB disease. These patients, however, had a prognosis as
bad as that of patients with distant metastasis (1-year overall survival rate 30% vs. 33%).
The performance of the 6th and 7th edition staging systems won quantified by the likelihood ratio
chi-square and AIC (Table 3). Predictive ability was best for the full 7th edition criteria stratifying for
all substages (highest likelihood ratio χ2). AIC value was smaller for the 7th edition compared to the
6th edition staging system, indicating that it has a better prognostic stratification. The AIC value was
lowest when patients with cervical lymph node metastasis at a large distance from the primary tumor
(i.e., the lower third of the esophagus) were also classified as having stage IV disease. When the 6th
and 7th edition staging systems are both included in one Cox regression model, the 6th edition no
longer significantly predicted survival, whereas the 7th edition remained a significant stratifier of
prognosis (data not shown).
TABLE 3. Prognostic stratification of the 6th and 7th editions of the UICC-AJCC TNM staging systems
Model Figure Subgroups LR χ2 AIC valuea
6th edition 2a I, II, III, IV 96.9 2607.1
7th edition, full 2b IA, IB, IIA, IIB, IIIA, IIIB, IIIC, IV 128.6 2592.9
7th edition, collapsed I, II, III, IV 99.0 2605.4
AIC Akaike information criteria, LR likelihood ratioaA lower AIC value represents a better discriminatory model
DISCUSSION
This study shows that both the 6th and 7th UICC-AJCC TNM staging systems have a distinctive and
monotone (ordered) relationship of stage group to overall survival for esophageal cancer patients
who have undergone potentially curative surgery without (neo)adjuvant therapy. Distribution of
patients among different stages is in line with that described in the literature. All groups are large
enough for proper statistical analysis, except for stage IIA in the 7th edition.

| Chapter 11
168
Further testing of both systems on the present data shows that the 7th edition has the best
performance because of the lowest AIC (i.e., a better fit) when Cox regression models are used. Survival
curves stratified according to the UICC-AJCC 7th edition TNM staging system did not overlap, which
is in contrast to the curves of the 6th edition. Moreover, further stratification of N stage according to
number of positive lymph nodes in the 7th edition is indeed valuable, as shown in Fig. 1.
A major change in the new TNM staging system is the definition of regional lymph nodes. There
has always been debate regarding the prognostic importance of positive celiac nodes, which were
considered distant metastases in earlier editions.13 In the 6th edition staging system, the Kaplan–Meier
plot showed overlapping curves for stage III and IV. According to the UICC-AJCC 7th edition, only
patients with distant metastasis can be categorized as having stage IV disease. In contrast, according
to the 6th edition, most stage IV disease was due to nonregional celiac lymph node metastasis,
whereas stage IIB and III consisted of regional lymph node metastasis. Hence, 87% (56 of 64) of the
patients with stage IV disease who were assessed according to the 6th edition criteria were reclassified
as having stage IIB, IIIA, IIIB, and IIIC disease according to 7th edition criteria. Because these stages all
had different survivals (Fig. 3), the present results support the new concept that it is unnecessary to
identify nonregional lymph node metastasis and to label these nodes as M1A or M1B.
Two previous studies have compared the performance of 6th with the 7th editions of the TNM staging
system in predicting survival. Hsu et al. evaluated 392 patients who underwent primary surgical
resection through a tri-incisional approach in Taiwan during 1995–2006.8 In the other study, nearly
two-thirds of the patients received neoadjuvant therapy.9
Both Hsu et al. and Gaur et al. concluded that the 7th edition of the staging system was a better model
for predicting outcome.8,9 The most important difference with the present study is tumor histology;
the vast majority of our patients had an adenocarcinoma, and almost all patients underwent a
transhiatal resection.
The WECC-based 7th edition of the TNM staging system was built on data from patients without
neoadjuvant treatment in a squamous cell carcinoma predominant database. Our sample population
from a single institution is of course small compared with the worldwide esophageal cancer
collaboration database, but the surgical procedures were highly uniform throughout the entire
study period. The previous studies of Hsu et al. and Gaur et al., as well as the present study, underline
the generalizability of the 7th edition and make it broadly applicable for daily clinical practice of
esophageal cancer surgery around the world.8,9
The 7th edition of the UICC-AJCC esophageal TNM staging system has acknowledged the importance
of the number of involved nodes by subdividing the N classification into N0 to N3. The transhiatal
approach may profoundly affect the completeness of lymph node dissection and, accordingly, proper
nodal staging. On the basis of data from a Dutch trial, nowadays, tumors proximal of esophagogastric
junction (Siewert type 1) are preferably offered a transthoracic approach in our institution.14,15 The
latter approach will result in the collection of more lymph nodes and might give a more valid node
sampling for staging. To which extent lymph nodes should be sampled for proper staging remains

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
169
Cha
pter
11
an important issue.16 In a study performed by Peyre et al., the number of lymph nodes removed
was an independent predictor of survival and a minimum number of 23 regional lymph nodes was
proposed.17 In the present study, the median number of nodes removed in a transhiatal approach was
11. This relatively scarce lymph node collection result can be seen as a drawback of our study, but it
also gives rise to a remarkable finding. Although all patients underwent a transhiatal esophagectomy,
the survival curves of different N stages (N0–N3; Fig. 1) do not overlap in our data, which probably
indicates that there has been a valid and robust node sampling. On the other hand, there seems
to be a relatively large difference in survival rate between N0 and N1. We know from previous
studies that there is a dichotomy in survival rate between tumors that did and did not lymphatically
disseminate.18 Early tumors (pT1) with lymph node invasion have prognosis comparable to tumors
with more advanced T stage. Lymphatic dissemination is an independent indication of the biological
aggressiveness of the tumor.
However, the large step in survival rate between N0 and N1 might also be due to a stage migrational
effect. This, the so-called Will Rogers effect, means that stage N1 disease might actually include N2
or even N3 disease as a result of invalid node sampling.19 The WECC group has indicated a resection
of a minimum of 10 nodes for T1, 20 for T2, and ≥30 nodes for T3–4 to be resected to obtain optimal
results.20 In N0 patients, such an effect does not occur; we found no significant difference in survival
rates according to the number of resected lymph nodes in lymph node–negative patients. However,
a median of 11 nodes definitely entails the risk of a stage migration effect in the patient group with
positive nodes.
Finally, an important question remains: does a better predictive staging system have consequences
for preoperative decision making? Medical decision making in terms of administering neoadjuvant
chemotherapy and choosing the optimal surgical approach for esophagectomy is often based on
clinical N staging. Lack of accurate preoperative staging is a major problem in allocating treatment
modalities in these patients. It has been recently shown that further stratification according to the
position of the positive node relative to the diaphragm can effectively discriminate between node-
positive patients.21 The overall accuracy for endoscopic ultrasound and CT in predicting the N stage
per station is moderate, however. When the therapeutic approach depends on the status of a specific
lymph node station, a more objective and reliable assessment of lymph nodal involvement (e.g.,
endoscopic ultrasound–fine-needle aspiration) should be considered.22
This study indicates that the application of the 7th UICC-AJCC staging system results in a better
prognostic stratification of overall survival compared to the 6th edition. The fact that the 7th edition
also has a superior prognostic ability in this study population from a single high-volume institution with
predominantly adenocarcinomas and a two-incisional surgical approach supports its generalizability
for different esophageal cancer practices.

| Chapter 11
170
REFERENCES1. Lagarde SM, Franssen SJ, Werven JR, et al. Patient preferences for the disclosure of prognosis after esophagectomy
for cancer with curative intent. Ann Surg Oncol. 2008;15:3289–3298
2. Sobin LH, Gospodarowicz MK, Wittekind C. TNM classification of malignant tumors. 7. Oxford: Wiley-Blackwell; 2010.
3. Thompson SK, Ruszkiewicz AR, Jamieson GG, et al. Improving the accuracy of TNM staging in esophageal cancer: a pathological review of resected specimens. Ann Surg Oncol. 2008;15:3447–3458
4. Kato H, Tachimori Y, Watanabe H, Iizuka T. Evaluation of the new (1987) TNM classification for thoracic esophageal tumors. Int J Cancer. 1993;53:220–223
5. Peyre CG, Hagen JA, DeMeester SR, et al. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on the significance of the number of involved lymph nodes. Ann Surg. 2008;248:979–985
6. Rusch VW, Rice TW, Crowley J, Blackstone EH, Rami-Porta R, Goldstraw P. The seventh edition of the American Joint Committee on Cancer/International Union Against Cancer Staging Manuals: the new era of data-driven revisions. J Thorac Cardiovasc Surg. 2010;139:819–821
7. Rice TW, Rusch VW, Apperson-Hansen C, et al. Worldwide esophageal cancer collaboration. Dis Esophagus. 2009;22:1–8
8. Hsu PK, Wu YC, Chou TY, Huang CS, Hsu WH. Comparison of the 6th and 7th editions of the American Joint Committee on Cancer tumor–node–metastasis staging system in patients with resected esophageal carcinoma. Ann Thorac Surg. 2010;89:1024–1031
9. Gaur P, Hofstetter WL, Bekele BN, et al. Comparison between established and the Worldwide Esophageal Cancer Collaboration staging systems. Ann Thorac Surg. 2010;89:1797–803, 1804 e1791–3
10. Armitage P, Colton T. Encyclopedia of biostatistics. New York: Wiley; 1998. 11. Kee KM, Wang JH, Lee CM, et al. Validation of clinical AJCC/UICC TNM staging system for hepatocellular
carcinoma: analysis of 5,613 cases from a medical center in southern Taiwan. Int J Cancer. 2007;120:2650–2655
12. Heijl M, Lanschot JJ, Koppert LB, et al. Neoadjuvant chemoradiation followed by surgery versus surgery alone for patients with adenocarcinoma or squamous cell carcinoma of the esophagus (CROSS) BMC Surg. 2008;8:21
13. Eloubeidi MA, Wallace MB, Hoffman BJ, et al. Predictors of survival for esophageal cancer patients with and without celiac axis lymphadenopathy: impact of staging endosonography. Ann Thorac Surg. 2001;72:212–219
14. Hulscher JB, Sandick JW, Boer AG, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–1669
15. Siewert JR, Stein HJ. Classification of adenocarcinoma of the esophagogastric junction. Br J Surg. 1998;85:1457–1459
16. Lerut T, Nafteux P, Moons J, et al. Three-field lymphadenectomy for carcinoma of the esophagus and gastresophageal junction in 174 R0 resections: impact on staging, disease-free survival, and outcome: a plea for adaptation of TNM classification in upper-half esophageal carcinoma. Ann Surg. 2004;240:962–972
17. Peyre CG, Hagen JA, DeMeester SR, et al. The number of lymph nodes removed predicts survival in esophageal cancer: an international study on the impact of extent of surgical resection. Ann Surg. 2008;248:549–556
18. Westerterp M, Koppert LB, Buskens CJ, et al. Outcome of surgical treatment for early adenocarcinoma of the esophagus or gastro-esophageal junction. Virchows Arch. 2005;446:497–504
19. Feinstein AR, Sosin DM, Wells CK. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N Engl J Med. 1985;312:1604–1608

Comparison of the 6th and 7th editions of the UICC-AJCC TNM classification for esophageal cancer |
171
Cha
pter
11
20. Rizk NP, Ishwaran H, Rice TW, et al. Optimum lymphadenectomy for esophageal cancer. Ann Surg. 2010;251:46–50
21. Peters CJ, Hardwick RH, Vowler SL, Fitzgerald RC. Generation and validation of a revised classification for esophageal and junctional adenocarcinoma. Br J Surg. 2009;96:724–733
22. Grotenhuis BA, Poley JW, Wijnhoven BPL. Preoperative assessment of tumor location and station-specific lymph nodal status is inaccurate in patients with esophageal adenocarcinoma. World J Surg 2013 Jan;37(1):147-155

P. van Hagen
R. de Jonge
M. I. van Berge Henegouwen
G. J. Hötte
E. P. van der Stok
J. Lindemans
J. J. B. van Lanschot
B. P.L. Wijnhoven
Submitted

Chapter 12Vitamin B12 deficiency after esophagectomy with gastric
tube reconstruction for esophageal cancer

| Chapter 12
174
ABSTRACT
OBJECTIVE
To determine the prevalence and incidence of vitamin B12
deficiency after esophagectomy for cancer.
BACKGROUND
It is unknown if patients after esophagectomy with gastric tube reconstruction are at an increased
risk for vitamin B12
deficiency.
METHODS
A cross sectional cohort (group A) and a prospective cohort (group B) of patients who underwent
esophagectomy for cancer in two tertiary referral centers in the Netherlands were included. Serum
levels of holo-transcobalamin (Holo-TC) and methyl malonic acid (MMA) were determined. Vitamin
B12
deficiency was defined as Holo-TC <21pmol/l and/or MMA >0.45 µmol/l. Vitamin B12
status was
assessed in group A at a single time point between one and three years postoperatively and before
and every three months after resection in group B.
RESULTS
Ninety-nine patients were analyzed in group A. The median time between surgery and analysis
of vitamin B12
deficiency was 19.3 months. In 11 of 99 (11%) patients, vitamin B12
deficiency was
detected. In group B, 5 of 88 (5.6%) patients had vitamin B12
deficiency preoperatively, and another 9
(10.2%) patients developed vitamin B12
deficiency after the operation at a median time of 6 months
postoperatively. The estimated one-year incidence of vitamin B12
deficiency was 18.2%. None of the
patients with vitamin B12
deficiency had a megaloblastic anemia.
CONCLUSION
Vitamin B12
deficiency can be anticipated in 18% of patients after esophagectomy with gastric tube
reconstruction for cancer. During follow-up, Holo-TC and MMA levels should be measured to detect
vitamin B12
deficiency and commence treatment timely.

Vitamin B12
deficiency after esophagectomy with gastric tube reconstruction for esophageal cancer |
175
Cha
pter
12
INTRODUCTION
Vitamin B12
, or cobalamin, is a water-soluble co-enzyme that plays a crucial role in the synthesis of DNA
and the myelinization of neural cells. Vitamin B12
must be obtained through the diet (present mainly
in meat, fish and dairy products), for it cannot be synthesized by the human body.1 After ingestion,
it is bound to intrinsic factor (IF), a glycoprotein which is produced by the parietal cells of the gastric
mucosa. The vitamin B12
-IF complex is then absorbed in the terminal ileum, after which vitamin B12
is
bound to Transcobalamin-II, to form holo-transcobalamin (Holo-TC, active vitamin B12
) and released
into the circulation.2 Methyl malonic acid (MMA) is a precursor of succinyl-CoA, an essential metabolite
in the Krebs cycle. Vitamin B12
is an essential cofactor in the conversion of MMA to succinyl-coA. In case
of vitamin B12 deficiency, MMA will accumulate.
A deficiency of vitamin B12
can lead to a wide variety of signs and symptoms. Megaloblastic anemia
and neurological disorders are the most common and severe complications resulting from vitamin
B12
deficiency.1 When diagnosed early, supplementing vitamin B12
can reverse the deficiency and cure
symptoms.
The incidence of esophageal cancer has risen over the last decades, making it the eighth most
common cancer worldwide.3 About half of the patients are potentially curable at presentation4 The
standard treatment for locally advanced esophageal cancer in the Netherlands is surgical resection,
preceded by neoadjuvant chemoradiotherapy.5 During the operation, the thoracic esophagus is
removed including a substantial part of the proximal stomach. For reconstruction of the digestive
tract, the stomach is tubularized and anastomosed to the cervical esophageal remnant, thereby
performing a so-called gastric tube reconstruction.6 Esophagectomy is accompanied by profound
anatomical and functional changes including a bilateral vagotomy.7-9
In bariatric surgery, there is evidence that partially resecting or functionally bypassing the stomach
can lead to nutritional deficiencies.7 Whether the altered anatomy after gastric tube reconstruction
following esophagectomy induces vitamin B12
deficiency is unknown. The aim of this study was to
determine the prevalence and incidence of vitamin B12
deficiency following esophagectomy with
gastric tube reconstruction in patients treated for potentially curable esophageal cancer.
PATIENTS AND METHODS
Inclusion criteria
Two cohorts of patients were defined: a cross-sectional cohort (group A) and a prospective longitudinal
cohort (group B).
Group A: Patients from group A were recruited from two high volume centers (Erasmus University
Medical Center, Rotterdam and Academic Medical Center, Amsterdam, The Netherlands). Both centers
had an institutional database where all patients were registered who underwent an esophagectomy
in the past 20 years. Patients were eligible to participate if they had undergone esophagectomy with

| Chapter 12
176
gastric tube reconstruction for esophageal cancer between one and three years prior to inclusion
in the study. Excluded were all patients that had clinical signs or symptoms of recurrent disease as
determined by physical examination and/or additional diagnostic examinations.
Group B: All patients who were scheduled for esophagectomy with gastric tube reconstruction for
potentially curable esophageal cancer at the Erasmus University Medical Center Rotterdam were
eligible for inclusion. Patients who were already on enteral or parenteral vitamin B12
were excluded.
All patients had to be eighteen years or older and provide written informed consent before entering
the study. Patients were included one day prior to surgery after informed consent was obtained and
followed for at least one year after the operation. The study protocol was approved by the medical
ethical committees of both participating centers.
Treatment
A transhiatal or transthoracic resection with gastric tube reconstruction was performed as previously
described.4,8 When appropriate, patients were treated with neoadjuvant chemoradiotherapy according
to a previously described regimen of Paclitaxel/Carboplatin with concurrent radiotherapy of 41.4 Gy in
23 fractions.5 The standard treatment protocol for esophageal cancer in both participating centers did
not include routine testing or (prophylactic) substitution of vitamin B12
.
Blood samples
Group A: Blood samples were collected once in the outpatient clinic during a routine visit. If a vitamin
B12
deficiency was diagnosed, substitution treatment was provided.
Group B: Blood samples were collected at baseline (one day before surgery) and during each regular
visit to the outpatient clinic every three months postoperatively. If a patient developed a vitamin B12
deficiency during follow-up, substitution treatment was provided and the patient was excluded from
further follow-up. If progression of disease (i.e. locoregional recurrence or distant dissemination) was
discovered during follow-up, the patient was also excluded from the study.
Laboratory testing
Patients’ blood samples underwent a standard set of laboratory tests. Routine laboratory procedures
(Roche Modular and Cobas 8000; Roche, Almere, the Netherlands) were used to measure serum
creatinin, pre-albumin, c-reactive protein (CRP) and folate (E170/c602). Holo-transcobalamin (Holo-TC,
or active VB12
) (AxSYM analyser; Abbott, Hoofddorp, The Netherlands) and methyl malonic acid (MMA)
(LC-MS/MS) were measured as previously described.9 Hemoglobin (Hb), mean corpuscular volume
(MCV), platelets, and white blood count (WBC) were measured on a Sysmex HST-302 or XN-9000
(Sysmex, Etten-Leur, The Netherlands).

Vitamin B12
deficiency after esophagectomy with gastric tube reconstruction for esophageal cancer |
177
Cha
pter
12
Definition of B12 deficiency
Vitamin B12
deficiency was defined as a level of Holo-TC <21 pmol/l and/or an MMA level of >0.45
µmol/l.9
Statistical analysis
Baseline characteristics, incidence and prevalence of vitamin B12
deficiencies were calculated
using descriptive statistical methods. For group B, the estimated one-year incidence of vitamin B12
deficiency was calculated using the Kaplan-Meier method. Laboratory results that were obtained after
the 12 month limit were excluded from analysis. Post-hoc subgroup analyses were not performed. A
multilevel regression analysis was performed to estimate the mean Holo-TC and MMA levels and to
test for significant increase or decrease of these levels during the follow-up period. A p-value of <0.05
(two-sided) was considered as statistically significant.
RESULTS
Between August 2010 and July 2012, a total of 187 patients were included in the study. Ninety-nine
patients were included in group A (cross-sectional cohort) and 88 patients in group B (longitudinal
cohort). Baseline characteristics of these patients are shown in Table 1.
Group A: The median time after surgery in group A was 19.3 months (IQR 13.5 - 30.0 months). In 11
of 99 (11%) patients, a vitamin B12
deficiency was detected at a median time of 20.8 months (IQR 14.3
- 29.7) after surgery. Five of these 11 patients had a Holo-TC below 21 pmol/l, five of 11 had an MMA
level >0.45 µmol/l and in one patient both Holo-TC and MMA were abnormal (Table 2).
Six of 11 patients in group A with a vitamin B12
deficiency suffered from mild anemia (minimal
measured Hb 8.0 mmol/l). No patients had a megaloblastic anemia (maximum MCV 99 fl).
Group B: Eighteen patients (20%) were followed for the maximum duration of follow-up (12 months),
while 37 (42%) patients could be followed for at least nine months. The median follow-up was 6.4
months for all patients, and 8.9 months for patients who were not excluded from follow-up due to
vitamin B12
deficiency. Other reasons for an incomplete follow-up were progression of disease or death
during the first postoperative year (n=40), incorrect planning of outpatient clinic visits (n=21), patient
withdrawal (n=7) and prescription of vitamin B12
supplements outside the study protocol (n=2).
During the study period, in 14 of 88 (15.9%) patients a vitamin B12
deficiency was detected. Eight of
14 patients had a Holo-TC below 21 pmol/l, five patients had a MMA level >0.45 µmol/l and in one
patient, both Holo-TC and MMA were abnormal (Table 3).
Laboratory results, including the time at which a deficiency was diagnosed, for the 14 patients with
vitamin B12
deficiency in group B are shown in Table 2. Five patients (5.6%) had vitamin B12
deficiency at

| Chapter 12
178
baseline. For the remaining nine patients, the median time to diagnosis of deficiency was 6.0 months
(range 3.5-9.9 months). One patient had severe anemia (Hb 4.8), whilst 6 patients suffered from mild
anemia (Hb from 7 to 8.4). There was no patient with megaloblastic anemia.
The estimated cumulative 1-year incidence of a vitamin B12
deficiency in group B was 22.9% (Figure
1). If patients who were already vitamin B12
deficient at baseline were excluded from analysis, the
estimated 1-year incidence was 18.2%.
TABLE 1. Baseline characteristics of 187 study patients, according to group (cross-sectional analysis (A) or longitudinal analysis (B)).
Group A (n=99) Group B (n=88)
Sex (male, %) 74% 72%
Age (mean, range) 62 (38-79) 63 (19-79)
No of observations12345
99 (100%)N/AN/AN/AN/A
22 (25.0%)18 (20.5%)14 (15.9%)17 (19.3%)17 (19.3%)
Length of follow-up (in days,median, IQR)
589 (412-916) 195 (48-329)
Baseline laboratory results(reference values)
Hemoglobin (mmol/l)(M:8.6-10.5, F: 7.5-9.5)
MCV (fl)(80-100)
Creatinin (umol/l)M: 65-115, F: 55-90)
Folate (nmol/l)(8.0-28.0)
Holo-Transcobalamin* (pmol/l)(>21.0)
MMA (µmol/l)(≤0.45)
Platelets (109/l)(150-370)
WBC (109/l)(3.5-10.0)
(median, range)
8.8 (5.8-10.4)
91 (70-103)
48 (77-148)
19.3 (3.9-45.4)
54 (10-128)
0.21 (0.07-2.87)
228 (123-391)
6.5 (2.8-12.4)
(median, range)
8.1 (5.5-9.8)
92 (70-120)
75 (47-214)
24.4 (9.0-54.4)
61 (20-128)
0.22 (0.02-0.63)
227.5 (16-449)
6.0 (3.8-14.4)
MCV: mean corpuscular volume, WBC: white blood count, MMA: methylmalonic acid N/A: not applicable*maximum possibly measured value of Holo-Transcobalamin was 128 pmol/l (upper linearity limit)

Vitamin B12
deficiency after esophagectomy with gastric tube reconstruction for esophageal cancer |
179
Cha
pter
12
TABLE 2. Laboratory results, timing of vitamin B12
deficiency, hemoglobin and MCV in individual patients who were diagnosed with vitamin B
12 deficiency during follow-up after esophageal resection with gastric tube
reconstruction for potentially curable esophageal carcinoma.
Number, M/FTime from operation to deficiency in months
Holo-TC (pmol/l) MMA (µmol/l) Hemoglobin
(mmol/l) MCV (fl)
Group A
1, M 12.0 24 0.56 8.0 89
2, M 13.9 19 0.31 10.4 95
3, M 14.4 35 0.59 8.2 88
4, M 14.5 39 0.49 9.1 98
5, M 15.6 15 0.2 10.2 91
6, F 19.1 14 0.27 8.2 99
7, M 19.5 20 0.21 10.2 90
8, M 22.5 22 2.87 9.9 99
9, M 29.7 10 2.28 8.4 92
10, M 33.1 13 0.35 8.4 90
11, M 35.1 26 0.67 8.4 88
Group B
1, M 0 33 0.59 7.0 85
2, M 0 66 0.63 8.0 90
3, M 0 55 0.59 9.0 98
4, M 0 20 0.24 8.7 84
5, M 0 20 0.28 7.7 83
6, M 3.5 20 0.25 4.8 87
7, M 3.7 16 0.15 9.2 89
8, M 4.6 25 0.66 8.4 87
9, M 4.9 17 0.34 8.5 92
10, M 6.0 18 0.36 8.3 96
11, F 6.3 34 0.50 7.9 88
12, M 6.5 18 0.19 8.3 86
13, F 8.9 10 0.63 7.5 96
14, M 9.9 16 0.12 9.3 94
M: Male, F: Female, Holo-TC: tolo-transcobalamin, MMA: methyl malonic acid, MCV: mean corpuscular volume

| Chapter 12
180
TABLE 3. Summary of patients in group B, tested at each measuring point during follow-up, including number of vitamin B
12 deficient patients at each point, according to definition of deficiency.
Observation moment 1 (baseline, n=88)
2(n=66)
3(n=49)
4(n=33)
5(n=18)
Total(n=88)
Holo-TC <21 pmol/l 2 3 1 2 0 8
MMA >0.45 µmol/l 3 0 2 0 0 5
Holo-TC <21 pmol/l and MMA >0.45 µmol/l
0 1 0 0 0 1
Total number of vitamin B12
deficiencies
5 4 3 2 0 14
Cumulative number of vitamin B12
deficiencies
5 9 12 14 14
Holo-TC: holo-transcobalamin MMA: methylmalonic acid
Follow-up in months129630
1 - c
umul
ative
dise
ase-
free
surv
ival
1,0
0,8
0,6
0,4
0,2
0,0
Page 1
No at risk 88 60 45 37 17
FIGURE 1. Kaplan Meyer curve (1-year disease-free survival function) for vitamin B12
deficiencies according to clinical algorithm in 88 patients that were followed during one year after esophageal resection with gastric tube reconstruction for potentially curable esophageal cancer.Estimated 1-year incidence: 22.9%
Multilevel regression analysis showed that the predicted mean Holo-TC level significantly decreased
during follow-up at 3, 6, 9 and 12 months after surgery when compared to baseline levels (p<0.001
for all time points) (Figure 2). The predicted lowest mean level of Holo-TC was at 11.4 months (50.0
pmol/l). For MMA levels, no statistically significant increase was seen when comparing the predicted
mean levels with baseline levels during the follow-up period (Figure 2).

Vitamin B12
deficiency after esophagectomy with gastric tube reconstruction for esophageal cancer |
181
Cha
pter
12
Follow-up 12 months9 months6 months3 monthsBaseline
Mea
n pr
edic
ted
valu
es o
f Hol
o-TC
70
65
60
55
50
Page 1
Follow-up 12 months9 months6 months3 monthsBaseline
Mea
n pr
edic
ted
valu
es o
f Hol
o-TC
70
65
60
55
50
Page 1
Follow-up12 months9 months6 months3 monthsBaseline
Mea
n pr
edic
ted
valu
es o
f MM
A
,27
,26
,26
,25
,25
,24
p=0.065
p=0.085
p=0.109
p=0.062
P<0.001
P<0.001 P<0.001
P<0.001
FIGURE 2. Mean predicted levels of Holo-TC (upper graph, in pmol/l) and MMA (lower graph, in µmol/l) during 1-year follow-up of 88 patients who underwent esophageal resection with gastric tube reconstruction for potentially curable esophageal cancer. P-values per time point are for change from baseline value.
When combining group A and B, a total of 25 of 187 (13.4%) patients were diagnosed with vitamin B12
deficiency. Fourteen of 88 (15.9%) patients were diagnosed in the first year (group B), 8 of 61 (13.1%)
during the second year (group A), and 3 of 38 (7.9%) during the third year after surgery (group A).

| Chapter 12
182
DISCUSSION
The present study shows that about 18% of patients subjected to esophagectomy for cancer (group
B) develops vitamin B12
deficiency during the first postoperative year. The prevalence of preoperative
vitamin B12
deficiency in this population was 5.6%. The prevalence within the second and third
postoperative year (group A) was 11.1%.
The percentage of patients with a vitamin B12
deficiency preoperatively, i.e. the estimated prevalence
in the non-operated population, is comparable with data from the general population.10-12 Although a
decreased preoperative intake of vitamin B12
might have occurred in these patients with esophageal
cancer (caused by e.g. dysphagia or horror carnis), this does not seem to affect the prevalence of
vitamin B12
deficiencies.
The absorption of vitamin B12
is a multifactorial process.2 After esophagectomy with gastric tube
reconstruction, absorption can be perturbed due to 1) reduced dietary intake of vitamin B12
as a result
of the change in anatomy leading to early satiety, 2) reduced digestion of protein-bound vitamin B12
from food due to reduced acid secretion and reduced length of time that the food is exposed to this
acid in the gastric conduit, and 3) reduced production of intrinsic factor due to a/ reduction of the
gastric mucosal surface, b/ gastritis due to biliary reflux or c/ bilateral truncal vagotomy.8-13 It is unclear
whether all three mechanisms play a role in the development of vitamin B12
deficiencies in patients
following esophagectomy, or if there is a single factor leading to vitamin B12
deficiency.
After bariatric surgery, where the anatomy of the upper gastrointestinal tract is deliberately altered to
reduce both intake and absorption, the prevalence of vitamin B12
deficiency two years after surgery
is between 4 and 36%. This is higher than in the general population.14 Vitamin B12
deficiency is more
frequently seen after a Roux-en-Y gastric bypass compared to a gastric sleeve resection.15 Vitamin
B12
deficiency seems to occur at a later time point than in patients after esophagectomy in the
current study population. In a large Dutch cohort of patients who underwent gastric bypass surgery,
vitamin B12
deficiencies were almost all diagnosed in the second postoperative year (mean time to
deficiency 14.1 months , CI 12.4-15.8 months).16 In the present study, the mean time to deficiency in
the longitudinally observed group was 6 months. This phenomenon is more clearly visible by the
early decrease in mean Holo-TC level during the first postoperative year that was detected in the
multilevel regression and the rise of MMA as an early metabolic marker for vitamin B12
deficiency
(Figure 2). The serum levels of both biochemical markers indicate that there is no stable vitamin B12
turnover after esophagectomy. It remains however unclear why deficiencies develop relatively early
after esophagectomy. Possibly, preoperative consumption of vitamin B12
-containing foods might
be decreased due to an obstructed food passage and/or chemoradiotherapy-induced nausea. This
might result in subnormal levels of vitamin B12
already preoperatively.
There is no worldwide consensus on the definition of vitamin B12
deficiency. Although many clinicians
still use total serum vitamin B12
to detect possible deficiencies, it has become more and more clear
that metabolically relevant deficiencies are better diagnosed by measuring Holo-TC and MMA
levels. Especially an increase in MMA should be considered a consequence of intracellular vitamin

Vitamin B12
deficiency after esophagectomy with gastric tube reconstruction for esophageal cancer |
183
Cha
pter
12
B12
shortage, and is therefore a more specific marker for metabolic deficiency. This is why MMA is
generally considered the golden standard for detecting effective vitamin B12
deficiency.17 Holo-TC is
considered an early marker of a negative vitamin B12 balance. When detected early, decrease in Holo-
TC and increased MMA may precede clinical manifestations of vitamin B12
deficiency, facilitating early
preventive measures. This might also be a reason why in the current study, no megaloblastic anemias
were found.18
In the present study, the focus was on the detection of metabolic vitamin B12
deficiencies using
laboratory testing. Symptoms that patients might have as a result of possible a vitamin B12
deficiency
were not an endpoint. Signs and symptoms of B12
deficiency are rather aspecific and may also develop
following neo-adjuvant and/or surgical treatment. Therefore, postoperative symptoms were not
recorded in this study.5,19
Because patients who underwent esophagectomy might not suffer from malabsorption, but
rather develop deficiencies due to insufficient dietary intake or reduced gastric acid secretion, oral
supplements might also be effective in the prevention and treatment of vitamin B12
deficiency in
this group.20 Studies have shown that high-dosed oral supplements can be as effective as parenteral
hydroxycobalamin in the treatment of vitamin B12
deficiencies.20,21 This may be better tolerated by the
patient and reduce costs.
The Dutch guidelines for the diagnosis and treatment of esophageal cancer do not give specific
recommendations (e.g. frequency and timing) for testing patients for vitamin B12
deficiency after
esophagectomy. The present study indicates that preoperatively and at least once postoperatively,
but not before one year after esophagectomy, assessment of vitamin B12
status is of use. Due to the
design of the study, it cannot be determined at what point in time patients in the cross-sectional
group have developed a deficiency. Therefore, repeated testing of patients with marginal Holo-TC and
MMA levels is recommended.

| Chapter 12
184
REFERENCES1. Stabler SP. Clinical practice. Vitamin B12 deficiency. N Engl J Med. 2013 Jan 10;368(2):149-60.
2. Nielsen MJ, Rasmussen MR, Andersen CB, Nexo E, Moestrup SK. Vitamin B12 transport from food to the body’s cells--a sophisticated, multistep pathway. Nat Rev Gastroenterol Hepatol. 2012 Jun;9(6):345-54.
3. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2014 Sep 13.
4. Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2014 Oct 15.
5. van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012 May 31;366(22):2074-84.
6. Orringer MB, Sloan H. Substernal gastric bypass of the excluded thoracic esophagus for palliation of esophageal carcinoma. J Thorac Cardiovasc Surg. 1975 Nov;70(5):836-51.
7. Majumder S, Soriano J, Louie Cruz A, Dasanu CA. Vitamin B12 deficiency in patients undergoing bariatric surgery: preventive strategies and key recommendations. Surg Obes Relat Dis. 2013 Nov-Dec;9(6):1013-9.
8. Donington JS. Functional conduit disorders after esophagectomy. Thorac Surg Clin. 2006 Feb;16(1):53-62.
9. Heil SG, de Jonge R, de Rotte MC, et al. Screening for metabolic vitamin B12 deficiency by holotranscobalamin in patients suspected of vitamin B12 deficiency: a multicentre study. Ann Clin Biochem. 2012 Mar;49(Pt 2):184-9.
10. Allen LH. How common is vitamin B-12 deficiency? Am J Clin Nutr. 2009 Feb;89(2):693S-6S.
11. Clarke R, Grimley Evans J, Schneede J, et al. Vitamin B12 and folate deficiency in later life. Age Ageing. 2004 Jan;33(1):34-41.
12. Herrmann W, Schorr H, Obeid R, Geisel J. Vitamin B-12 status, particularly holotranscobalamin II and methylmalonic acid concentrations, and hyperhomocysteinemia in vegetarians. Am J Clin Nutr. 2003 Jul;78(1):131-6.
13. Okada N, Nishimura O, Sakurai T, Tsuchihashi S, Juhri M. Gastric functions in patients with the intrathoracic stomach after esophageal surgery. Ann Surg. 1986 Aug;204(2):114-21.
14. Stein J, Stier C, Raab H, Weiner R. Review article: The nutritional and pharmacological consequences of obesity surgery. Aliment Pharmacol Ther. 2014 Sep;40(6):582-609.
15. Kwon Y, Kim HJ, Lo Menzo E, Park S, Szomstein S, Rosenthal RJ. Anemia, iron and vitamin B12 deficiencies after sleeve gastrectomy compared to Roux-en-Y gastric bypass: a meta-analysis. Surg Obes Relat Dis. 2014 Jul-Aug;10(4):589-97.
16. van der Beek ES, Monpellier VM, Eland I, Tromp E, van Ramshorst B. Nutritional deficiencies in gastric bypass patients; incidence, time of occurrence and implications for post-operative surveillance. Obes Surg. 2015 May; 25(5):818-823.
17. Allen RH, Stabler SP, Savage DG, Lindenbaum J. Diagnosis of cobalamin deficiency I: usefulness of serum methylmalonic acid and total homocysteine concentrations. Am J Hematol. 1990 Jun;34(2):90-8.
18. Carmel R. Current concepts in cobalamin deficiency. Annu Rev Med. 2000;51:357-75.
19. Vidal-Alaball J, Butler CC, Cannings-John R, et al. Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency. Cochrane Database Syst Rev. 2005(3):CD004655.
20. Hjelms E, Thirup P, Schou L. Gastric intrinsic factor production and vitamin B12 absorption after oesophageal resection using stomach as substitute. Eur J Cardiothorac Surg. 1999 Sep;16(3):273-5.
21. Kuzminski AM, Del Giacco EJ, Allen RH, Stabler SP, Lindenbaum J. Effective treatment of cobalamin deficiency with oral cobalamin. Blood. 1998 Aug 15;92(4):1191-8.

PART IIISummary and appendices


Summary of the thesis
Samenvatting in het Nederlands
Future perspectives
PhD Portfolio
Acknowledgements
Curriculum Vitae


Summary of the thesis |
189
SUMMARY OF THE THESIS
Esophageal cancer is a highly aggressive disease with a rising incidence, especially in the Western
World. Almost half of the patients who present with esophageal cancer are beyond curative therapy,
and for patients with potentially curable disease, 5-year survival rates rarely exceed 30%. Although
surgical resection is the most important part of the treatment, evidence in favor of neoadjuvant
treatment (i.e. chemo(radio)therapy prior to surgery) is accumulating. These multimodality treatment
regimens can induce shrinkage of the tumor and thereby facilitate a microscopically radical resection,
which is an important prognostic factor for survival. However, this potential benefit should outweigh
the toxicity that neoadjuvant treatment adds to the already high morbidity and mortality that are
associated with the curative resection of esophageal cancer.
This thesis consists of two parts. In part one: “Preoperative analysis and treatment” the benefits of
neoadjuvant chemoradiotherapy (nCRT) are described and the impact of several (pre-)clinical delays
in the treatment are evaluated. Part two: “Postoperative outcome and prognostication” focusses on
(disease-free) survival and prognostication after potentially curative treatment.
Part 1: Preoperative analysis and treatment
Over the past decades, evidence for the positive effect of nCRT in patients with esophageal cancer
has accumulated, especially in meta-analyses. However, due to various reasons, in most randomized
trials no survival benefit could be demonstrated. In chapter 2, the results of a multicenter randomized
trial which compared nCRT followed by surgery with surgery alone in patients with potentially curable
esophageal or esophagogastric junction cancer are described after a minimal follow-up of two years.
This trial, in which 178 patients were allocated to the nCRT arm and 188 to the surgery alone arm,
showed a statistically significant estimated survival benefit at five years of 13%. This might be due to
the high rate of microscopically radical resections, which was 92% in the nCRT arm versus 79% in the
surgery alone arm. The toxicity of the nCRT was acceptable, and postoperative morbidity and mortality
were comparable between groups. The overall rate of pathologically complete response (pCR) was
29%, but with 49% especially high in patients with squamous cell carcinoma. This large randomized
trial confirmed the growing support for incorporating nCRT in the treatment of esophageal cancer.
To affirm the results that were found in chapter 1, a second analysis was performed after a longer
period of follow-up. In chapter 3, these results are shown. After a minimal follow-up of five years for
each patient, the 5-year survival rate differed 14% in favor of nCRT, which was statistically significant.
Also, there was a statistically significant difference in 5-year progression-free survival of 17% in favor
of the nCRT arm. These results show that the effect of nCRT on overall and progression-free survival is
sustained during a longer period of time and nCRT followed by surgery should be accepted as a new
standard of care.
The interval between nCRT and surgery (time to surgery, TTS) can be prolonged by various factors.
One of the reasons of such delay might be, that the nCRT itself can cause a prolonged TTS due

| Summary of the thesis
190
to toxic side-effects, having an effect on patients’ nutritional status or causing hematological or
infectious complications. A prolonged TTS might theoretically cause a more difficult resection with
more complications, or even outgrowth of residual tumor. On the other hand, it might also result in
more pathologically complete responders, as was shown earlier in patients treated witch nCRT for
rectal cancer. In chapter 4, the impact of a prolonged TTS was investigated retrospectively in 325
patients who were treated with nCRT followed by surgery within a ten year period. Prolonged TTS
was associated with an increased probability of pCR. No effect on overall or progression-free survival
could be demonstrated, however, there was a slightly increased risk for postoperative complications
in patients who had a TTS of more than 45 days. Prolonging TTS up to at least twelve weeks could
safely be done. This allows for an active surveillance strategy to be tested in patients who show no
clinical signs of residual tumor after nCRT.
An additional relevant time interval can be recognized between the diagnosis and actual treatment
of esophageal cancer. In chapter 5, the impact of this so called hospital delay was evaluated. It
was found that a prolonged hospital delay had a negative impact on postoperative morbidity and
mortality, resulting in mortality rates up to 8.5% and morbidity rates up to 67.2% in patients with a
delay of more than 8 weeks. However, between all the evaluated time intervals that were tested, no
difference in overall or progression-free survival could be observed. The interval between onset of
complaints and diagnosis (the pre-hospital delay) had no influence on short- or long-term outcome
of patients.
Before the start of any treatment, the patients should be presented and discussed in a multidisciplinary
tumor board (MDT). During this MDT, a personalized definitive treatment plan is established, in which
the appropriate medical, radiotherapeutic and surgical treatment is determined. In chapter 6, the
value of the MDT in a tertiary referral center was evaluated. Over a period of eight months, 171
patients were discussed in 34 MDTs. In more than one third of discussed treatment cases, a substantial
alteration was made in the proposed treatment plan. These results demonstrate the value of a regular
MDT for esophageal cancer and support the Dutch guidelines, in which MDTs are mandatory.
In chapter 7, the HER2/neu status of esophageal adenocarcinoma biopsies of patients who underwent
primary surgery was compared with the HER2/neu status in the primary tumor as determined by three
dedicated pathologists in a multicenter retrospective study. HER2/neu overexpression was found in
22% of the primary tumors. In 93% of these cases, the reported HER2/neu status was concordant with
that in the preoperatively obtained biopsy. Inter-observer agreement amongst all three pathologists
was moderate, especially in the interpretation of the in-situ hybridization results.
Part 2: Postoperative outcome and prognostication 18F-Fluorodeoxyglucose positron emission tomography (FDG-PET) has been investigated as a tool
for monitoring response to neoadjuvant therapy and as a predictor for survival in patients with
esophageal cancer. If non-responders could be identified early during therapy, possible toxicity could
be avoided by proceeding to surgery earlier. In chapter 8, no correlation could be demonstrated

Summary of the thesis |
191
between the change in FDG-PET signal that was measured early during (i.e. two weeks after the
start of ) nCRT and long-term survival. This implies that FDG-PET cannot be used for identifying non-
responders early during nCRT.
Although long-term survival is improving, due to advances in both medical, radiotherapeutic and
surgical treatment, esophageal cancer is still lethal in more than half of the patients initially considered
potentially curable. This implies that multimodality treatment is failing in a large proportion of patients.
To better understand why nCRT followed by surgery is not a guarantee for definitive cure, the pattern
of recurrence in 213 patients who underwent this treatment are described in chapter 9. After nCRT,
significantly less locoregional recurrences were observed when compared to patients treated with
surgery only. A lesser, although still statistically significant, effect was seen for peritoneal metastases
and hematogenous dissemination. Moreover, locoregional recurrences within the radiation field
occurred in only 5% of cases, emphasizing the high locoregional control that is achieved with nCRT.
However, it is known that even in patients who showed pCR (i.e. the best objective pathological result
of nCRT), recurrent disease can develop. In chapter 10, the recurrence pattern of 62 patients with pCR
was compared with that of 126 patients with non-pCR. As expected, significantly more recurrences
occurred in the non-pCR group, however, still 32% of patients with pCR developed a distant metastasis
and 13% suffered from a locoregional recurrence. A reason for this unexpectedly high number
of recurrences might be a sampling error at pathological examination of the resection specimen,
resulting in a falsely negative pathological outcome. This might explain why in multivariable analysis
only lymph node involvement was found to be an independent prognosticator for survival.
In chapter 11, the prognostic power of the 7th edition of the UICC-AJCC TNM classification for solid
tumors was compared to that of the 6th edition in patients with esophageal adenocarcinoma. This
study confirmed that application of the 7th staging system results in a better prognostic stratification
of overall survival compared to the 6th edition. Even though the 7th edition of the TNM classification
was derived from a large cohort of patients with predominantly squamous cell carcinoma who
underwent a transthoracic esophagectomy, it also performs better in patients with adenocarcinoma
who underwent a transhiatal surgical approach, supporting its generalizability for different esophageal
cancer practices.
During esophageal resection, the anatomy of the upper gastrointestinal tract is changed profoundly,
which may lead to problems in the intake and absorption of vitamin B12, a vitamin essential for DNA
synthesis and neural function. In Chapter 12, the incidence, prevalence and timing of vitamin B12
deficiencies was investigated in patients who underwent esophageal resection for potentially curable
esophageal cancer. This analysis showed that during the first postoperative year, the estimated
incidence of vitamin B12
deficiencies is 18.2%. This is remarkably higher than in the general population,
and moreover, these deficiencies developed earlier than expected. Early and routine testing for
vitamin B12
deficiencies is therefore advised during follow-up after esophagectomy.


Samenvatting in het Nederlands |
193
SAMENVATTING
Het slokdarmcarcinoom is een zeer agressieve vorm van kanker waarvan de incidentie nog altijd
toeneemt, met name in de Westerse wereld. Van alle patiënten die zich presenteren met slokdarmkanker
komt ongeveer de helft niet meer in aanmerking voor een in opzet curatieve behandeling, en voor
patiënten met een in potentie curabel carcinoom ligt de 5-jaars overleving zelden boven de 30%.
Hoewel chirurgische resectie de belangrijkste vorm van behandeling betreft, is er groeiend bewijs
voor de effectiviteit van neoadjuvante behandeling, d.w.z. behandeling met chemo(radio)therapie
voorafgaand aan resectie. Deze neoadjuvante behandelingsstrategieën kunnen een reductie
van tumorvolume tot gevolg hebben waardoor microscopisch radicale resectie, een belangrijke
prognostische factor, waarschijnlijker wordt. Echter, om deze neoadjuvante therapieën te kunnen
toepassen moet dit potentiele voordeel opwegen tegen de toxiciteit die zij toevoegen aan de al
hoge morbiditeit en mortaliteit die waarmee de curatieve resectie van slokdarmkanker gepaard gaat.
Dit proefschrift bestaat uit twee delen. In deel één: ‘Preoperatieve analyse en behandeling’ worden
de voordelen van neoadjuvante chemoradiotherapie (nCRT) beschreven, alsmede de invloed die
verschillende (pre)klinische vertragingen in de behandeling hebben op de uitkomst van patiënten.
Deel twee: ‘Postoperatieve uitkomst en prognosticering’ richt zich op de (ziektevrije-) overleving en
de prognose na in opzet curatieve behandeling van slokdarmkanker.
Deel 1: Preoperatieve analyse en behandeling
Gedurende de laatste decennia heeft het bewijs voor de effectiviteit van nCRT zich opgestapeld,
met name door de positieve resultaten die volgden uit meta-analyses. Om verschillende redenen
kon er in de meeste gerandomiseerde trials echter geen overlevingsvoordeel worden bewezen.
In hoofdstuk 2 worden de resultaten van een multicentrisch gerandomiseerd onderzoek
beschreven waarin nCRT gevolgd door chirurgische resectie werd vergeleken met chirurgie alleen
als behandeling voor potentieel curabel slokdarmcarcinoom of carcinoom van de slokdarm-maag
overgang na een minimale follow-up van 2 jaar. In dit onderzoek, waarin 178 patiënten werden
gerandomiseerd voor nCRT + chirurgie en 188 voor chirurgie alleen, werd een statistisch significant
geschat overlevingsvoordeel na vijf jaar van 13% gevonden. Deze winst in overleving zou kunnen
worden veroorzaakt door het grote verschil in microscopisch radicale resecties, dat 92% was in de
nCRT groep tegenover 79% in de chirurgie alleen groep. De toxiciteit van de nCRT bleek acceptabel,
en de postoperatieve morbiditeit en mortaliteit waren vergelijkbaar tussen de groepen. Het
percentage patiënten met een pathologisch complete respons (geen vitale tumorcellen in het gehele
resectiepreparaat, pCR) was 29%, maar was met name hoog (49%) in de groep patiënten met een
plaveiselcelcarcinoom. Dit grote gerandomiseerde onderzoek ondersteunt het gebruik van nCRT bij
de behandeling van slokdarmcarcinoom.
Ter bevestiging van de resultaten die werden gevonden in hoofdstuk 1 werd een tweede analyse
uitgevoerd na een lagere periode van follow-up. De resultaten van deze analyse worden beschreven

| Samenvatting in het Nederlands
194
in hoofdstuk 3. Na een minimale follow-up van 5 jaar van alle geïncludeerde patiënten was het
verschil in 5-jaars overleving 14% ten faveure van de nCRT groep. Ook werd er een significant verschil
gevonden in de ziektevrije 5-jaars overleving van 17% in het voordeel van de nCRT groep. Deze
resultaten laten zien dat het effect op de totale en ziektevrije overleving gedurende een langere
periode aanhoudt en dat nCRT gevolgd door chirurgie als een nieuwe standaardtherapie zou moeten
gelden voor het potentieel curabele slokdarmcarcinoom.
Het tijdsinterval tussen nCRT en chirurgie (tijd tot chirurgie, TTC) kan door verschillende factoren
worden verlengd. Eén van de oorzaken van een dergelijke vertraging zou kunnen zijn, dat de nCRT zelf
hieraan debet is, vanwege het feit dat door de toxiciteit patiënten in een slechte voedingstoestand
komen, of moeten herstellen van hematologische of infectieuze complicaties. Een langere TTC kan
theoretisch een moeilijkere chirurgische resectie tot gevolg hebben met een bijkomende toename
van het aantal complicaties, of zelfs tot progressie van de tumor. Anderzijds kan het ook een hoger
percentage patiënten met pCR tot gevolg hebben, zoals eerder werd aangetoond bij patiënten met
een rectumcarcinoom. In hoofdstuk 4 werd de invloed van een langere TTC retrospectief onderzocht
bij 325 patiënten die werden behandeld met nCRT gevolgd door chirurgie over een periode van
tien jaar. Een langere TTC was geassocieerd met een hogere kans op pCR, er kon echter geen effect
worden aangetoond op de ziektevrije of totale overleving . Wel was er een licht verhoogd risico
op postoperatieve complicaties bij patiënten die een TTC van meer dan 45 dagen hadden. De TTC
kan veilig worden verlengd tot ten minste twaalf weken. Hierdoor kan een strategie van ‘waakzame
surveillance’ worden onderzocht bij patiënten die na nCRT geen aanwijzingen hebben voor residu
van vitale tumor.
Nog een ander tijdsinterval kan kan een rol spelen, namelijk het tijdsinterval tussen de diagnose
en de behandeling van slokdarmkanker. De invloed van dit zogenaamde ‘ziekenhuis-delay’ werd
geëvalueerd in hoofdstuk 5. Hierbij bleek dat een langer ziekenhuis-delay een negatieve invloed
heeft op de postoperatieve uitkomst, resulterend in 8,5% postoperatieve mortaliteit en 67,2%
postoperatieve morbiditeit bij patiënten met een ziekenhuis-delay van meer dan 8 weken. Een
significant verschil in (ziektevrije-)overleving kon niet worden aangetoond. Het tijdsinterval tussen
het begin van symptomen en het stellen van de diagnose slokdarmcarcinoom bleek niet aantoonbaar
van invloed te zijn op de korte- of lange-termijn uitkomst van patiënten.
In de tijd tussen diagnose en behandeling dient iedere patiënt met slokdarmcarcinoom besproken
te worden in een multidisciplinaire tumorbespreking (MDT). Tijdens dit MDT wordt voor de patiënt
een definitief individueel behandelplan vastgesteld met een heldere beschrijving van geschikte
behandeling. De waarde van dit MDT werd onderzocht in hoofdstuk 6. Hiertoe werd de uitkomst
van het MDT bijgehouden gedurende een periode van 8 maanden, waarin 171 patiënten werden
besproken tijdens 34 bijeenkomsten. In meer dan een derde van de besproken ziektegevallen werd
een substantiële wijziging aangebracht in het voorgestelde behandelplan. Dit resultaat bewijst de
waarde van een wekelijks MDT en ondersteunt de Nederlandse richtlijn, waarin een MDT verplicht
wordt gesteld.

Samenvatting in het Nederlands |
195
In hoofdstuk 7 wordt de HER2/neu status van preoperatief afgenomen biopten van het slokdarm
adenocarcinoom van niet voorbehandelde patiënten vergeleken met die van de primaire tumor in
het resectiepreparaat. Dit vond plaats in het kader van een multicentrisch retrospectief onderzoek
waarbij alle preparaten door drie gespecialiseerde pathologen werden beoordeeld. Overexpressie van
HER2/neu was aanwezig in 22% van de tumoren. In 93% van de gevallen kwam de HER2/neu status in
het biopt overeen met die in de primaire tumor. De overeenstemming tussen de drie beoordelende
pathologen was matig, met name waar het de beoordeling van de in-situ-hybridisatie betrof.
Deel 2: Postoperatieve uitkomst en prognosticering.18F-Fluorodeoxyglucose positron emissie tomografie (FDG-PET) werd eerder onderzocht als techniek
om respons op neoadjuvante therapie te monitoren en overleving te voorspellen bij patiënten met
een slokdarmcarcinoom. Als hiermee niet-responderende patiënten vroeg tijdens de therapie zouden
kunnen worden geïdentificeerd, zou de voorbehandeling voortijdig kunnen worden afgebroken,
waardoor eventuele toxiciteit van de therapie zou kunnen worden voorkomen en patiënten eerder
in aanmerking zouden kunnen komen voor chirurgie. In hoofdstuk 8 kon geen correlatie worden
aangetoond tussen de afname in intensiteit van het FDG-PET signaal dat snel na het starten van nCRT
werd gemeten en de lange-termijn overleving. Hieruit kan worden opgemaakt dat FDG-PET niet kan
worden gebruikt voor het identificeren van non-responders kort na het starten van nCRT.
Hoewel de lange-termijn overleving van patienten met een slokdarmcarcinoom verbetert, als
gevolg van ontwikkelingen in de medische, radiotherapeutische en chirurgische behandeling, is de
ziekte toch nog dodelijk in meer dan de helft van de patiënten die initieel als potentieel curabel
werden beoordeeld. De huidige behandelingen falen bij een groot deel van de gevallen. Om beter
te begrijpen waarom de behandeling van patiënten met nCRT gevolgd door chirurgie geen garantie
is voor curatie, werd het patroon van recidivering van de ziekte in kaart gebracht bij 213 patiënten
die een dergelijke behandeling ondergingen. De resultaten van dit onderzoek worden beschreven in
hoofdstuk 9. Na nCRT werden significant minder locoregionale recidieven gevonden dan na chirurgie
alleen. Een minder sterkeffect, hoewel toch statistisch significant, werd gezien voor het optreden
van peritoneale en hematogene metastasering. Bovendien traden slechts 5% van de locoregionale
recidieven op binnen de grenzen van het bestralingsveld, hetgeen de hoge mate van locoregionale
controle benadrukt die wordt bereikt met nCRT gevolgd door chirurgie.
Hoewel een pCR het beste objectieve pathologische resultaat van nCRT is, treden ook bij deze groep
patiënten recidieven op. In hoofdstuk 10 werd het patroon van recidivering van 62 patiënten met
een pCR vergeleken met dat van 126 patiënten zonder pCR die dezelfde nCRT ondergingen. Zoals
verwacht werden er significant minder recidieven gevonden in de pCR groep, echter, bij 32% werd
een metastase op afstand gevonden en bij 13% een locoregionaal recidief. Een verklaring voor dit
hoge aantal recidieven kan wellicht worden gevonden in het feit dat er tijdens de resectie door de
chirurg of tijdens de beoordeling door de patholoog niet-representatief materiaal wordt uitgenomen
respectievelijk beoordeeld hetgeen resulteert in een fout-negatieve pathologische uitkomst. Dit

| Samenvatting in het Nederlands
196
zou verklaren waarom tijdens multivariabele analyse alleen de lymfklierstatus als onafhankelijke
voorspeller voor overleving werd gevonden.
In hoofdstuk 11 werd de prognostische waarde van de zevende editie van de UICC-AJCC TNM
classificatie voor het slokdarmcarcinoom vergeleken met de zesde editie in een cohort patiënten met
slokdarm adenocarcinoom. Dit onderzoek toonde aan dat gebruik van de zevende editie een betere
prognostificatie van totale overleving tot gevolg heeft vergeleken met het gebruik van de zesde editie.
Hoewel de TNM classificatie werd ontwikkeld met gebruikmaking van een groot cohort patiënten
waarin de meeste patiënten een plaveiselcelcarcinoom hadden en werden behandeld met een
transthoracale resectie, presteerde de zevende editie ook beter als het werd toegepast op patiënten
met een adenocarcinoom die een transhiatale resectie ondergingen, wat de bruikbaarheid van het
systeem bewijst wanneer het wordt toegepast bij andere behandelingen van het slokdarmcarcinoom.
Na een oesofagusresectie is de anatomie van het bovenste deel van de tractus digestivus dusdanig
veranderd dat functionele problemen te verwachten zijn. Eén van deze problemen kan zich voordoen
in de inname en absorptie van vitamine B12, een vitamine die essentieel is voor de opbouw van DNA
en het functioneren van neuronen. In hoofdstuk 12 werd de incidentie, prevalentie en timing van
het voorkomen van vitamine B12
deficiënties bij patienten die een oesofagusresectie ondergingen
onderzocht. Uit deze analyse volgde dat de geschatte 1-jaars incidentie van vitamine B12
deficiënties
na oesofagusresectie 18,2% is. Dit is hoger dan in de algemene populatie, en bovendien ontwikkelen
deze deficiënties zich relatief vroeg na de operatie. Het verdient dus aanbeveling om bij patiënten die
een oesofagusresectie hebben ondergaan routinematig en in een vroeg stadium onderzoek te doen
naar een mogelijke vitamine B12
deficiëntie.

Future perspectives |
197
FUTURE PERSPECTIVES
Historically, esophageal cancer has always been a malignancy that is accompanied by high morbidity
and a poor prognosis. Medical research that was performed over the last decades has improved
survival and reduced morbidity significantly by improving patient selection, surgical techniques and
optimizing postoperative care. Despite these improvements, esophageal cancer is still highly lethal,
especially in advanced cases. Recent developments, especially in multimodality modality treatment,
have shown that there is still room for more improvement. This improvement can be expected in
the fields of screening for esophageal cancer, patient selection for more individualized therapy, and
further development of (neo)adjuvant and targeted therapies. In this paragraph, possible options
for diagnosis and treatment are described on which future experimental and clinical research should
focus.
Screening for esophageal cancer
Early stages of esophageal cancer have a better prognosis than advanced stages. It would therefore
be favorable to detect tumors in an early or premalignant (Barrett’s esophagus) stage, also making less
invasive therapies (e.g. endoscopic resection) possible which are accompanied with less morbidity.
Unfortunately, the current modality to detect esophageal cancer (endoscopy with biopsies)
is not sensitive enough, diminishing the diagnostic yield of a screening program. Also, it can be
accompanied by morbidity. This makes a screening program too hazardous and not cost-effective.
However, if other means of detecting esophageal cancer (preferably by using highly sensitive and
specific biomarkers that can be collected non-invasively) could be found, a screening program in
selected groups of patients might be opportune.1
Patient selection for neoadjuvant and targeted therapy
Neoadjuvant chemoradiotherapy has a well-established survival benefit in potentially curable
esophageal cancer patients. Although the toxicity of the treatment is acceptable in large groups of
patients, it is certainly not a therapy that one should be subjected to without an evident indication.
Short term toxicity (e.g. hematologic toxicity of chemotherapy) can delay further treatment and
potentially negatively affect survival, while long term toxicity (e.g. late radiotherapy effects) might
cause serious illness later in life. Therefore, it is of great importance to identify patients who will
potentially benefit from the treatment, but it maybe even more important to identify those who
will suffer harm from the treatment without gaining any profit. Pretreatment pathological findings
can already identify patients who are less likely to benefit from multimodality treatment (e.g. signet
cells, poorly differentiated adenocarcinomas), but these factors are not strong enough predictors to
withhold patients a potentially curative treatment. Genetic profiling (of patient, tumor or both) could
be used to distinguish between responders and non-responders, prior to the start of therapy. In breast
cancer, such a method is already in use, which identifies patients who will benefit from adjuvant
chemotherapy.2

| Future perspectives
198
Response evaluation during neoadjuvant therapy using nuclear imaging techniques have not
been proven to successfully predict response when used early during chemoradiotherapy. The
inflammatory response that is caused by radiotherapy might be interfering with the signal of the
tumor, thereby masking a metabolic response. New nuclear tracers, with more specific affinity for the
tumor might help to overcome this problem, making it possible to stop neoadjuvant therapy and
proceed to surgery in patients who show no response or even progression. However, such tracers are
still under investigation, and more clinical evidence should be gathered before such a strategy can be
confidently followed.3
After neoadjuvant therapy, a substantial number of patients have no detectable vital tumor cells in
the resection specimen, a so called pathologically complete response (pCR). It is questionable if these
patients should have undergone surgical resection, the tumor might well be fully sterilized by the
neoadjuvant therapy and esophagectomy might only induce morbidity and even mortality, without
adding to survival. These patients could therefore potentially benefit from an active surveillance
strategy, in which patients with a clinically complete response are closely monitored and only operated
upon when there is evidence of residual or recurrent disease. Unfortunately, it is not yet clear if a pCR
can be accurately predicted by performing clinical investigations. Ongoing and future studies will
provide the answer to this question, but until then, surgery will remain the cornerstone of treatment
in potentially curable esophageal cancer. (referentie pre-SANO protocol, submitted BMC cancer)
Improving multimodality treatment
Although neoadjuvant chemo(radio)therapy has been proven to improve radicality of resection
and long-term survival, still more than half of the patients with esophageal cancer that are treated
with curative intent develop recurrent disease. To date, there is no cure for these patients. Therefore,
prevention of recurrences seems to be the key in further improving survival in patients with potentially
curable esophageal cancer. To do so, several strategies could be investigated.
First, intensifying neoadjuvant therapy by either expanding radiotherapy fields, increasing radiotherapy
dosage (e.g. adding a so-called booster), or improving neoadjuvant chemotherapy component of
the neoadjuvant treatment might decrease the number of outfield locoregional recurrences, infield
locoregional recurrences, and hematogenous dissemination, respectively. Especially the shift from
locoregional recurrence to hematogenous dissemination that is clinically observed after neoadjuvant
chemoradiotherapy followed by esophagectomy is a target for further improving multimodality
treatment.
Secondly, adjuvant chemotherapy should be considered to be implemented in the treatment of
esophageal cancer, like it already is standard of care in many other malignancies (e.g. breast and colon
cancer). Especially in esophageal adenocarcinoma, which is less responsive to chemoradiotherapy
than squamous cell carcinoma, adjuvant chemotherapy might be a strategy to reduce hematogenous
dissemination. It goes without saying that further investigations on this subject have to be performed
in phase III trials before implementation can be recommended.

Future perspectives |
199
A third option for further investigation is the potential of so called targeted therapies, such as immuno-,
hormonal-, and molecular therapies. Over the past decades, the molecular characteristics of tumors
and their relation with tumor behavior have become more and more clear. Several agents have already
been proven to be effective in other malignancies (e.g. trastuzumab in HER2 positive breast cancer
and cetuximab in colorectal and head-and-neck cancer) , and some have even been investigated
in esophageal cancer.4 However, most of these therapies are only potentially beneficial for (small)
subgroups of patients, which makes further experimental and translational research so important,
hopefully leading to the discovery of more potent targets for therapy in esophageal cancers.
However, perhaps the key to surviving esophageal cancer not only lies in preventing recurrences, but
in treating them as well. For instance, surgical resection or radio frequent ablation of liver metastases
was already found to be a curative therapy in patients with disseminated colorectal cancer, and might
be an option in esophageal cancer as well.5
Although the recent developments in the multimodality treatment of esophageal carcinoma are
substantial, they are only just another step forward, and many more steps have to be taken on the
road ahead to fight this truly malignant disease.
1. Kumar S, Huang J, Abbassi-Ghadi N, Mackenzie HA, Veselkov KA, Hoare JM, et al. Mass Spectrometric Analysis of Exhaled Breath for the Identification of Volatile Organic Compound Biomarkers in Esophageal and Gastric Adenocarcinoma. Ann Surg. 2015 Jan 8.
2. van ‘t Veer LJ, Dai H, van de Vijver MJ, He YD, Hart AA, Mao M, et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature. 2002 Jan 31;415(6871):530-6.
3. Jiang M, Huang Q, Chen P, Ruan X, Luo Z, Zhao L, et al. Monitoring the early biologic response of esophageal carcinoma after irradiation with 18F-FLT: an in-vitro and in-vivo study. Nucl Med Commun. 2014 Dec;35(12):1212-9.
4. Kasper S, Schuler M. Targeted therapies in gastroesophageal cancer. Eur J Cancer. 2014 May;50(7):1247-58.
5. Tomlinson JS, Jarnagin WR, DeMatteo RP, Fong Y, Kornprat P, Gonen M, et al. Actual 10-year survival after resection of colorectal liver metastases defines cure. J Clin Oncol. 2007 Oct 10;25(29):4575-80


PhD Portfolio |
201
PHD PORTFOLIO
Summary of PhD training and teaching
Name PhD student: Pieter van Hagen PhD period: Jan 2009 – Jan 2016
Erasmus MC Department: Surgery Promotor: Prof. dr. J.J.B. van Lanschot
Supervisor: Dr. B.P.L. Wijnhoven
PHD TRAINING Year Workload (ECTS)
General Courses
BROK (Basiscursus Regelgeving Klinisch Onderzoek) 2010 1.0
Introduction to biomedical research 2012 0.9
Biostatistics for clinicians 2012 1.0
Seminars and Workshops
Course Biomedical Research Techniques 2009 0.3
Methodologie van patiëntgebonden onderzoek en 2009 0.3
voorbereiding van subsidieaanvragen.
Systematisch literatuuronderzoek in databases 2012 0.3
Journal Club 2009-2012 2.0
Presentations
National conferences 2009 1.0
National conferences 2010 1.0
International conferences 2010 5.0
National conferences 2011 1.0
International conferences 2011 2.0
National conferences 2012 3.0
International conferences 2012 1.0
National conferences 2013 1.0
2. TEACHING Year Workload (ECTS)
Lecturing for students and nurses at Department of Surgery 2010-2012 1.0
Examination of Basis Life Support of medical students 2009-2012 1.0


Acknowledgements |
203
ACKNOWLEDGEMENTS
Een proefschrift behoeft een dankwoord. Niet zelden is het namelijk het enige hoofdstuk dat écht
wordt gelezen. Dus om er zeker van te zijn dat ook dit proefschrift wordt gelezen spreek ik hieronder
mijn dank uit aan allen die bij naam genoemd zijn en aan allen die ik mogelijk ben vergeten te
noemen. Echter, om te beginnen wil ik mijn dank uitspreken aan alle patiënten die als proefpersoon
hebben meegewerkt aan de verschillende studies die in dit proefschrift beschreven staan. De cijfers
en lijnen in tabellen en grafieken staan voor mensen van wie ik de naam niet ken. Aan hen als eersten
veel dank.
Geachte promotor prof. dr. J.J.B. van Lanschot, beste professor, hartelijk dank voor de kansen die u
mij hebt geboden. Toen ik bij u solliciteerde als promovendus drukte u mij op het hart dat het toch
echt de bedoeling was om in ieder geval drie jaar vol te maken. U zal het met mij eens zijn dat ik
die afspraak ruimschoots ben nagekomen. Het zijn bewogen jaren geweest, met vele hoogte- en
dieptepunten. Ik heb er ongelooflijk veel van geleerd. Uw messcherpe kritieken hebben de artikelen
die dit proefschrift vormen altijd naar een hoger niveau getild. Hartelijk dank voor het vertrouwen en
uw begeleiding!
Geachte co-promotor dr. B.P.L. Wijnhoven, beste Bas, dankjewel voor het enthousiasmeren, corrigeren,
meedenken en sturen, met de VIDEO-studie als kroon op het werk. Maar bovenal dank voor de
gezelligheid. Onze trips naar Leuven zal ik niet gauw vergeten, net zoals de ski-reizen, congressen,
borrels en ‘pauzes’ in de buitenlucht. Ik wens je al het goede!
Geachte prof. dr. E.W. Steyerberg, beste Ewout, veel dank voor je inzet voor verschillende projecten,
bovenal voor de CROSS-studie. Hoewel ik nachtmerries over interactietermen heb gehad wist jij
met een simpele email me toch weer op het rechte statistische pad te krijgen. Dank voor het zitting
nemen in de leescommissie.
Geachte prof. dr. A.H.J. Matthijssen en prof. dr. R. van Hillegersberg, hartelijk dank voor het zitting
nemen in de kleine commissie en het beoordelen van het manuscript.
Dr. A. van der Gaast, beste Ate, jij hebt ‘jouw’ CROSS-studie laten opschrijven door de meest onervaren
arts-onderzoeker die men op dat moment kon vinden. Hoewel we vrijwel alle data cijfer voor cijfer
samen hebben doorgesproken, moet het je toch enigszins benauwd hebben. Gelukkig liepen de
curves gewoon uiteen! Heel veel dank voor al je vertrouwen, nuchterheid en rust.
Geachte prof. dr. F.J. van Kemenade en dr. M.C.C.M. Hulshof, hartelijk dank voor het zitting nemen in
de grote commissie.

| Acknowledgements
204
Lieve Brechtje Grotenhuis, wat een feest om weer met je te mogen werken in het IJsselland!
Chardonnay! Maar wat hebben we ook tijdens onze onderzoekerstijd een lol gehad. Als ik ooit twijfel
over een pathologische q dan weet ik je te vinden! Kip Siam!
Joel Shapiro. Jij in het lab, ik in de Z-flat, en de mentor ergens tussenin. Je bent vervelend slim, maar
dat gaat gelukkig niet ten koste van je karakter. Dank voor je humor , je hulp en je vriendschap. We
maken er op 3 juni een groot feest van! Lieve Eelke Toxopeus, ik had m´n stethoscoop ervoor gegeven,
dat weet je. Gelukkig hoefde dat niet. Dank voor de gezelligheid! Koen Talsma, veel dank voor wat jij
met de ‘777’-database voor elkaar hebt gekregen. Veel geluk!
Mark van Heijl en Rachel Blom, Mrs Guide, wat is het leuk om jullie nog zo regelmatig te zien. Ik
beschouw de klim naar de congreslocatie in Kagoshima nog steeds als mijn grootste prestatie.
Hoewel het wegwerken van 24 dumplings een goede tweede is. Maarten en Vera (om het 020-clubje
compleet te maken), dank voor jullie hulp en samenwerking.
Alle leden van de Slokdarmwerkgroep, hartelijk dank voor jullie hulp. Ik heb in alle uren achter de
computer op vrijdag verschrikkelijk veel geleerd, met name dat oncologie niet in een richtlijn te
vatten is. Katharina Biermann, dankjewel voor het beoordelen, herbeoordelen en nóg eens bekijken
van al die coupes. Beste professor Tilanus, voor sommigen zou het emeritaat wat mij betreft niet
hoeven gelden.
Een speciale vermelding voor Renée Acosta. Lieve Renée, jij bent de beste die een patiënt kan
tegenkomen. Je inzet voor patiënten kent geen grenzen, je durft ruzie voor ze te maken. Heel veel
dank voor al je hulp bij de poliklinische controles van de VIDEO-patiënten, je enthousiasme en alle
gezellige momenten! Je bent een topwijf.
Publiceren doe je niet alleen. Heel veel dank aan alle co-auteurs voor het ontwerpen, includeren,
verzamelen van data, meedenken en meeschrijven.
Zonder het secure werk van alle datamanagers die meewerkten aan de verschillende studies was dit
proefschrift er nooit geweest. Conny Vollebregt spant echter de kroon. Haar werk staat aan de basis
van het grootste deel van de publicaties over slokdarmpathologie uit Rotterdam. Conny, dank voor je
tomeloze inzet. Tonny, Danielle en Aleida, veel dank voor jullie hulp op de poli!
Bewoners van de hunkerbunker!! Bedankt voor het lachen! Als je er zo lang hebt gezeten als ik (vanaf
Tamara Conjo!) zijn er teveel mensen langsgekomen om allemaal persoonlijk te bedanken. Ik beperk
me tot hen die mij letterlijk het meest na waren. Ruggentje, Aaltje Garnaaltje, Marcella Druppel, dank
jullie wel voor de onvergetelijke tijd.

Acknowledgements |
205
Chirurgen en arts-assistenten uit het IJsselland Ziekenhuis, ik had me geen betere plek kunnen
wensen om opgeleid te worden, en dat komt door jullie! Jullie vragen nooit hoe het nou met mijn
promotie gaat. Ook daarvoor veel dank.
Lieve Zarina Lalmahomed, wat hebben we lang naast elkaar gezeten en wat ben ik blij dat je tijdens
mijn verdediging naast mij zal staan. Vanaf het moment dat ik naast je neerplofte achter Martin’s jaren
’70 bureau waren we begonnen! Het nummer van de dag, later uitgebouwd naar thema van de dag,
de satésaus-ontploffing in mijn keuken, de BBQ’s, stafdag-cabarets (inclusief dollemansrit door Delft-
Den Haag-Rijswijk) en als klap op de vuurpijl het chirurgendagen cabaret, we waren er altijd samen
bij. Jouw werklust en doorzettingsvermogen zijn onnavolgbaar. Dankjewel voor de mooie tijd en voor
je vriendschap!
Karel Klop. Goede vrienden zijn goud waard! Samen hebben we onze studententijd nog eens
dunnetjes overgedaan, het was een feest. Als ik alle schitterende avonden zou moeten beschrijven
kwam er geen einde aan dit dankwoord en werd het net zo lang als de bestelling bij de Mac. Gelukkig
gaat het feest door in het IJsselland, ook al mogen we eigenlijk niet meer naast elkaar zitten tijdens de
overdracht. Laten we het erop houden dat ze onze humor gewoon niet zo goed begrijpen. Ik ben blij
dat ik je heb leren kennen en dat jij mijn paranimf wil zijn. Ik hoop dat je tijdens mijn verdediging mijn
huis niet probeert af te branden, dat zou niet zo origineel zijn.
Lieve schoonfamilie, lieve Jeanette, Egge, Irene, Serah, Jasper, Sebastiaan, Joop, Julius, Olivia, Jasmijn
en Rosa. Dank voor de gezelligheid, gastvrijheid, ondersteuning, interesse en warmte. Willen jullie nu
alsjeblieft nooit meer naar mijn onderzoek vragen?
Lieve Monique, Naud, Maxime, Vince, Quint , Isa en Martijn. Familie hoef je niet meteen te zijn, dat kun
je blijkbaar ook worden. Ik zou jullie voor geen goud willen missen!
Lieve Pien, lieve Roos, wij komen uit hetzelfde nest, dat merk je aan alles. Ik had me echt geen betere
zussen kunnen wensen. Dank voor jullie humor en zorgzaamheid. Lieve Bart en Mau, het is ontzettend
fijn als je zussen nieuwe vrienden voor je mee naar huis nemen! Lieve Anna, Gijs en Mies, wat een
verschrikkelijk leuke kinderen zijn jullie! Ik ben er trots op dat ik jullie oom ben.
Lieve mamma, jij weet als geen ander hoe het is om de data voor een grote studie in het gareel te
krijgen. Dank voor je wijze lessen in de GCP en je begrip voor mijn frustraties. Lieve pappa, doctor
zal jij denk ik nooit meer worden, maar ik hoop eigenlijk ooit net zo´n goede dokter als jij te worden.
Lieve mamma, lieve pappa, dank jullie wel voor alles wat jullie mij gegeven hebben, maar bovenal
voor jullie onvoorwaardelijke liefde.

| Acknowledgements
206
Lieve Dee, wat ben ik trots op jou. Jouw gedrevenheid en discipline zijn jaloersmakend. Je zorgt voor
de rustige basis in mijn leven. Wie had kunnen denken dat het liefste meisje ook nog eens de meest
geweldige moeder zou zijn? Samen kunnen we de wereld aan! Ik hou van je.
Lieve, lieve Sara, ik hou zo ongelóóflijk veel van jou. Voor jouw geluk zou ik dit hele proefschrift
inleveren. Ze mogen het houden. Ik kan niet wachten om je in je nieuwe rol als grote zus te zien. Kus!

Curriculum Vitae |
207
CURRICULUM VITAE
Pieter van Hagen werd op 6 juli 1981 geboren te Leiden. Op tweejarige leeftijd verhuisde hij met zijn
ouders naar Rotterdam, waar hij een bijzonder gelukkige jeugd beleefde en in 2000 zijn VWO-diploma
behaalde aan het Rotterdams Montessori Lyceum. In september van dat jaar begon hij aan de studie
geneeskunde aan de Universiteit Utrecht, waar hij in 2007 zijn artsenbul behaalde. In 2008 werkte hij
als ANIOS in het Erasmus Medisch Centrum te Rotterdam (prof. dr. J.N.M. IJzermans), waarna hij in
2009 begon aan een promotietraject onder begeleiding van prof. dr. J.J.B. van Lanschot. In januari
2013 mocht hij beginnen aan de opleiding tot chirurg in de opleidingsregio Rotterdam (dr. B.P.L.
Wijnhoven), waarvan hij het perifere deel van de opleiding mag volgen in het IJsselland Ziekenhuis te
Capelle aan den IJssel (Dr. I. Dawson). Pieter is al jaren gelukkig samen met Deodata. Op 12 maart 2014
werden zij de trotse ouders van Sara.

Esophageal Cancer preoperative management and postoperative outcome
Pieter van Hagen
Esophageal Cancer preoperative managem
ent and postoperative outcome
Pieter van Hagen
Uitnodiging
Voor het bijwonen van de openbare verdediging
van het proefschrift
Esophageal Cancer;preoperative management and
postoperative outcome
door
Pieter van Hagen
Op woensdag 18 mei 2016 om 13.30 uur.
Professor Queridozaal, Onderwijscentrum Erasmus MC.
Wytemaweg 80, Rotterdam
Receptie aansluitend aan de promotie
ParanimfenZarina Lalmahomed
Karel Klop
Pieter van HagenRolderdiephof 13521 DA Utrecht
13631_Hagen_OM.indd 1 15-04-16 16:43