Congenitalhemiparesis, unilateralpolymicrogyriaand ...2Fepd.2013.0612.pdf · María Celeste...
11
doi:10.1684/epd.2013.0612 Epileptic Disord, Vol. 15, No. 4, December 2013 417 Correspondence: Roberto Caraballo, Department of Neurology, Hospital de ni ˜ nos “Prof Juan P Garrahan”, Combate de los Pozos 1881, Buenos Aires, CP 1245, Argentina <[email protected]> Original article Epileptic Disord 2013; 15 (4): 417-27 Congenital hemiparesis, unilateral polymicrogyria and epilepsy with or without status epilepticus during sleep: a study of 66 patients with long-term follow-up Roberto Horacio Caraballo, Ricardo Oscar Cersósimo, Pablo Sebastián Fortini, Lorena Ornella, María Celeste Buompadre, Carolina Vilte, Juan Pablo Princich, Natalio Fejerman Department of Neurology, Hospital Nacional de Pediatría Juan P Garrahan, Buenos Aires, Argentina Received April 08, 2013; Accepted August 28, 2013 ABSTRACT – Aim. We retrospectively analysed the electroclinical features, treatment, and outcome in patients with unilateral polymicrogyria (PMG), focussing on epileptic syndrome with or without encephalopathy, with sta- tus epilepticus during sleep (ESES) or continuous spikes and waves during slow sleep (CSWS) syndrome. Methods. From June 1990 to December 2012, 39 males and 27 females, aged 5-26 years, were studied. We did not include patients with bilateral PMG or cases with unilateral PMG associated with other cerebral lesions. The mean follow-up period was 12 years (range: 3-22 years). Results. Mean age at epilepsy onset was 6.5 years. Focal motor seizures occurred in all cases and 25 had secondary generalised seizures. Six patients also had complex focal seizures. Interictal EEG recordings showed focal spikes in all cases. For 43 of 53 patients with epilepsy, aged 2-9.5 years, the electroclinical features changed. An increase in frequency of focal motor seizures was reported in 20 patients, negative myoclonus occurred in 32 patients, atypical absences in 25 patients, and positive myoclonus in 19 patients. All patients had a continuous symmetric or asymmetric pattern of spike-wave activity during slow-wave sleep. Conclusion. For patients pre- senting with congenital hemiparesis, negative or positive myoclonus, and absences and focal motor seizures with ESES/CSWS, unilateral PMG should be considered. Brain MRI is mandatory to confirm this cortical malforma- tion. The most commonly used treatments were clobazam, ethosuximide, and sulthiame, alone or in combination. For refractory cases, high-dose steroids were administered and surgery was performed in two patients. Outcome was relatively benign. Key words: congenital hemiparesis, epilepsy, negative myoclonus, continuous spikes and waves, sleep, unilateral polymicrogyria
Transcript of Congenitalhemiparesis, unilateralpolymicrogyriaand ...2Fepd.2013.0612.pdf · María Celeste...
-
do
i:10.
1684
/ep
d.2
013.
0612
Epileptic Disord, Vol. 15, No. 4, December 2013
Correspondence:Roberto Caraballo,Department of Neurology,Hospital de niños “Prof Juan P Garrahan”,Combate de los Pozos 1881,Buenos Aires, CP 1245, Argentina
Original articleEpileptic Disord 2013; 15 (4): 417-27
Congenital hemiparesis,unilateral polymicrogyria andepilepsy with or without statusepilepticus during sleep:a study of 66 patientswith long-term follow-upRoberto Horacio Caraballo, Ricardo Oscar Cersósimo,Pablo Sebastián Fortini, Lorena Ornella,María Celeste Buompadre, Carolina Vilte, Juan Pablo Princich,Natalio FejermanDepartment of Neurology, Hospital Nacional de Pediatría Juan P Garrahan,Buenos Aires, Argentina
Received April 08, 2013; Accepted August 28, 2013
ABSTRACT – Aim. We retrospectively analysed the electroclinical features,treatment, and outcome in patients with unilateral polymicrogyria (PMG),focussing on epileptic syndrome with or without encephalopathy, with sta-tus epilepticus during sleep (ESES) or continuous spikes and waves duringslow sleep (CSWS) syndrome. Methods. From June 1990 to December 2012,39 males and 27 females, aged 5-26 years, were studied. We did not includepatients with bilateral PMG or cases with unilateral PMG associated withother cerebral lesions. The mean follow-up period was 12 years (range:3-22 years). Results. Mean age at epilepsy onset was 6.5 years. Focal motorseizures occurred in all cases and 25 had secondary generalised seizures. Sixpatients also had complex focal seizures. Interictal EEG recordings showedfocal spikes in all cases. For 43 of 53 patients with epilepsy, aged 2-9.5years, the electroclinical features changed. An increase in frequency of focalmotor seizures was reported in 20 patients, negative myoclonus occurredin 32 patients, atypical absences in 25 patients, and positive myoclonus in 19patients. All patients had a continuous symmetric or asymmetric pattern ofspike-wave activity during slow-wave sleep. Conclusion. For patients pre-senting with congenital hemiparesis, negative or positive myoclonus, andabsences and focal motor seizures with ESES/CSWS, unilateral PMG shouldbe considered. Brain MRI is mandatory to confirm this cortical malforma-tion. The most commonly used treatments were clobazam, ethosuximide,and sulthiame, alone or in combination. For refractory cases, high-dosesteroids were adminOutcome was relativ
Key words: congencontinuous spikes an
417
istered and surgery was performed in two patients.ely benign.
ital hemiparesis, epilepsy, negative myoclonus,d waves, sleep, unilateral polymicrogyria
mailto:[email protected]
-
4
PcbnfclilwtBgUoh1RtftBothwhCcTcE(cleewepicdtdeecfpsBPdb
mJbS(Aa(Hfuoddf
M
FgwtPsg(a1flssvrgCaeSccaefEiEo
olymicrogyria (PMG) is secondary to abnormal corti-al organisation. In PMG, the neurons reach the cortexut do not form normal cortical or intracortical con-ections and result in multiple small gyri. The classic
orm is represented by four-layered polymicrogyricortex with a molecular layer, an organised intercellu-ar layer, a cell-sparse layer, and a slightly unorganisednner cellular layer. However, a broad range of histo-ogical abnormalities has been found including casesith an unlayered and completely unorganised cor-
ex (Barkovich et al., 1996; Palmini, 2000; Kuzniecky andarkovich, 2001; Barkovich et al., 2001). PMG may beeneralised, focal, or multifocal (Barkovich et al., 1996).nilateral PMG may affect the whole hemisphere ornly part of it. Large malformations are associated withypoplasia of the affected hemisphere (Guerrini et al.,993).ecently, in a new classification proposal of malforma-
ions of cortical development, PMG was divided intoour groups: A) with schizencephalic clefts or calcifica-ions, presumably due to infection or vascular causes;) without clefts or calcifications, which may be geneticr disruptive; C) as part of genetically-defined mul-
iple congenital anomaly syndromes (some of whichave an atypical histology); and D) in conjunctionith inborn errors of metabolism (also with atypicalistology) (Barkovich et al., 2012).olamaria and co-workers (1989) reported a boy withongenital hemiparesis, unilateral PMG, and epilepsy.he authors described an ictal asterixis, an electroclini-al phenomenon that, according to the polygraphicEG recording, corresponded to a negative myoclonusColamaria et al., 1989). Subsequently, patients withongenital hemiparesis, unilateral PMG, and a particu-ar type of epilepsy have been published (Colamariat al., 1991; Caraballo et al., 1992, 1997, 1999; Guerrinit al., 1993, 1996, 1998a). These patients startedith focal motor seizures evolving into particularlectroclinical features, characterised by myoclonias,seudoataxia, atonic seizures, and absences. The inter-
ctal EEG showed bilateral, symmetric and asymmetric,ontinuous or subcontinuous spikes and spike-wavesuring slow sleep, with a more benign course than
hat in patients with epilepsy associated with corticalysplasias (Caraballo et al., 1992, 1997, 1999; Guerrinit al., 1993, 1996, 1998a; Aicardi, 1994; Dalla Bernardinat al., 1996). Subsequently, more detailed electro-linical descriptions have been reported, confirmingavourable evolution (Caraballo et al., 2007). Bilateral
18
erisylvian polymicrogyria or congenital bilateral peri-ylvian syndrome has been described (Barkovich, 2010,arkovich et al., 2012; Guerrini and Barba, 2011).MG may occur as an isolated lesion or associate withifferent entities (Guerrini and Barba, 2011). PMG haseen associated with different chromosomal abnor-
siM3ws
alities (Leventer et al., 2008; Dobyns et al., 2008aglin et al., 2009; Barkovich, 2010). PMG has alsoeen related to mutations of several genes, such asRPX2, PAX6, TBR2, KIAA1279, RAB3GAP1, and COLI8A1Glaser et al., 1994; Sertié et al., 2000; Brooks et al., 2005;ligianis et al., 2005; Roll et al., 2006; Baala et al., 2007). Inddition, copy number variations have been describedGuerrini and Parrini, 2010).ere, we retrospectively analysed the electroclinical
eatures, treatment, and outcome in 66 patients withnilateral PMG, focussing on epileptic syndrome withr without encephalopathy, with status epilepticusuring sleep (ESES) or continuous spikes and wavesuring slow sleep (CSWSS) syndrome, with long-term
ollow-up.
aterial and methods
rom June 1990 to December 2012, 66 patients with con-enital hemiparesis associated with unilateral PMG,ith or without epilepsy, were included for inves-
igation. We did not include patients with bilateralMG or cases with unilateral PMG associated withchizencephaly, porencephaly, heterotopias, or ule-yria. The mean period of follow-up was 12 yearsrange: 3-22 years) with repeat clinical examinationsnd EEGs. Video-EEG recordings were carried out in5 patients. Polygraphic EEG recordings were not per-ormed. The lack of polygraphic EEG recordings is aimitation of this study. However, all the myocloniceizures were observed by the first author, and inome patients, the seizures were also registered byideo-EEG recording. Based on clinical phenomenonather than EEG abnormalities, we were able to distin-uish whether the myoclonus was negative or positive.omputed tomography (CT) and MRI was obtained inll cases. All patients were psychometrically evaluat-d with the Wechsler Intelligence or Terman Merrillcales. Antiepileptic drugs (AEDs) were given in allases with epilepsy, and modified according to clini-al and EEG evolution. Therapeutic alternatives, suchs the ketogenic diet and surgery, were also consider-d. Karyotypes and metabolic investigations were per-ormed in 61 and 6 patients, respectively.EG recordings were performed with the 10-20nternational system using 22 electrodes. SerialEG recordings during wakefulness and sleep werebtained for all patients. We analysed seizure onset,emiology, distribution, and frequency, as well as inter-
Epileptic Disord, Vol. 15, No. 4, December 2013
ctal and ictal EEG findings.RI was performed on a 0.5-T and 1.5-T scanner for
5 and 36 patients, respectively. Intermediate- and T2-eighted axial and coronal images and T1-weighted
agittal images were obtained for all patients.
-
E
Congenital hemiparesis, unilateral polymicrogyria, and epilepsy
R
G
T(slptw(MtaoppAceFta
S
Fays
Fpb
esults
eneral features
hirty-nine males and 27 females, aged 5-26 yearsmean: 15 years), were studied. Congenital hemipare-is was present in 64 patients, affecting limbs on theeft side in 36 and on the right side in 28 cases. Sixtyatients with hemiparesis had a mild degree of spas-
icity and four a moderate degree. Mental impairmentas mild in 35 cases (IQ: 60-69) and moderate in 25
IQ: 50-59). Six patients had a normal IQ. Brain CT andRI showed unilateral PMG, localised in the fronto-
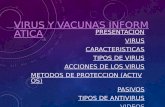
emporal region in 39 cases, in the fronto-temporalnd parietal regions in 5 cases, and in the parieto-ccipital regions in 22 (figures 1 and 2). The CT showederiventricular calcifications associated with PMG in 5atients.personal history of febrile seizures was found in 10
ases (19%) and a family history of febrile seizures andpilepsy was found in 3 and 2 cases, respectively.ifty-nine cases were sporadic, 5 patients had congeni-al cytomegalovirus, 1 patient had Stickler syndrome,nd another was a familial case.
pileptic Disord, Vol. 15, No. 4, December 2013
eizure manifestations and EEG findings
ifty-three of 66 patients (80%) had epilepsy. The meannd median age at onset of epilepsy was 6.5 and 4ears, respectively (range: 0.5-13 years). Focal motoreizures occurred in all cases and 25 had secondary
igure 1. Axial T1-weighted MRI sequence showing left fronto-arietal PMG with ipsilateral hemisphere atrophy in a 10-year-oldoy.
Fao
gfnwsmlpItsswmwipecqi
E
Ba
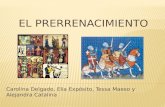
igure 2. T1-weighted MRI sequence showing right hemispheretrophy with PMG in the left parieto-occipital cortex in a 9-year-ld boy.
eneralised seizures. Six patients also had complexocal seizures. Seizures occurred only during wakeful-ess in 30 patients, during sleep in 8, and both duringakefulness and sleep in 15 cases. The duration of the
eizures was brief (less than 5 minutes) in 19 patients,oderate (between 5 and 10 minutes) in 28, and pro-
onged (more than 15 minutes) in 6. During this initialeriod, no other types of seizure were documented.
nterictal EEG recordings showed unilateral fronto-emporal spikes in 25 cases, unilateral fronto-centralpikes in 7, and parieto-occipital spikes in 10. Bilateralpikes, predominantly in the dysplastic hemisphere,ere observed in 11. In 10 patients, the EEG abnor-alities occurred only during sleep. In all but 19 casesith spikes during wakefulness, the EEG abnormalities
ncreased during sleep. In addition to the spikes, 45atients also had focal fast polyspikes and slow waves,specially during sleep, consistent with a structuralause. Hyperventilation did not increase seizure fre-
419
uency. Intermittent photic stimulation was negativen all cases (table 1).
lectroclinical changes
etween ages 2 and 9.5 years (mean: 6; median: 5),n evident change in terms of seizures and EEG
-
4
R.H. Caraballo, et al.
Table 1. Neuroradiological findings,initial electroclinical features, and treatment
in 66 patients with unilateral PMG.
Gender 39 Male; 27 Female
Congenital hemiparesisNo hemiparesis
642
Localisation of PMG Fronto-temporal: 39Fronto-temporo-parietal: 5Parieto-occipital: 22
Mental impairment Normal IQ: 6Mild: 35Moderate: 25
Epilepsy 53/66 (80%)
Median age at onsetof epilepsy
4 years(R: 0.5-7 years)
Type of seizure at onset Motor focal seizureswith or without secondarygeneralisationRare complex focalseizures
Interictal EEG Focal abnormalities: 55Bilateral abnormalities: 11
AEDs used before PHB, PHT, CBZ, OXC, VPA,
POl
oiisiido2(Itamdhbotbc
(dnwrwtTddda((at(
T
Fcd9awrDro3miittetfsscAiocsssethosuximide, clobazam, and sulthiame in 3; corticos-
worsening of seizures TPM, LTG, CLB
HB: phenobarbital; PHT: phenytoin; CBZ: carbamazepine;XC: oxcarbazepine; VPA: valproic acid; TPM: topiramate; LTG:
amotrigine; CLB: clobazam.
ccurred. This electroclinical change was observedn 43 of 53 patients (81%) with epilepsy. An increasen frequency of focal motor seizures with or withoutecondary generalised tonic-clonic seizures occurredn 20 patients (46.5%), negative myoclonus occurredn 32 patients (74.4%), associated gait instability in 20,rop-attacks in 7, and diminished motor initiative inne hemibody in 5. Atypical absences occurred in5 patients (58%) and positive myoclonus in 19 cases44.4%).n the period of three months before the onset ofhe electroclinical change, the EEG recordings showedn increase in interictal abnormalities. During sleep,ore frequent and bilateral spikes were recorded pre-
ominantly in the anterior region and in the dysplastic
20
emisphere (figure 3). Asymmetric and symmetricilateral spikes and spikes and waves were observedn EEG during wakefulness in all cases during
his period of electroclinical change. Some of theseilateral discharges, especially those that were sub-ontinuous, were associated with negative myoclonus
tiigsI
figure 4). The discharges became more frequenturing sleep in all patients and featured the conti-uous symmetric and asymmetric pattern of spike-ave activity during slow-wave sleep in 15 and 28 cases,
espectively (figures 5 and 6). The bilateral dischargesere observed in less than 80% of slow sleep in 14 of
hese children.he following cognitive disturbances were observeduring the period of electroclinical change: attentioneficit hyperactivity disorder in 22 (51%), languageeterioration (non-verbal agnosia) in 12 (27.8%),ggressiveness in 12 (27.8%), memory deficit in 1023.2%), impaired temporo-spatial orientation in 920.9%), non-verbal communication deficit in 9 (20.9%),nd loss of bladder control in 3 patients (6.9%). Intellec-ual deterioration was observed in 28 patients (65.1%)table 2).
reatment
rom the onset of epilepsy until the appearance ofhanges in electroclinical features, patients receivedifferent AEDs: phenobarbital in 10, carbamazepine in, phenytoin in 3, oxcarbazepine in 9, valproic acid in 8,nd 3 patients each with valproic acid in combinationith carbamazepine, oxcarbazepine, and clobazam,
espectively.uring the phase of electroclinical change, no
esponse or worsening of electroclinical features wasbserved using the following AEDs: valproic acid in2 patients, lamotrigine in 14, topiramate in 14, carba-azepine in 13, oxcarbazepine in 12, phenobarbital
n 12, primidone in 8, clonazepam in 6, levetiracetamn 5, ethosuximide in 3, and sulthiame in 2. Some ofhese AEDs were prescribed prior to consultation inhe centres participating in this study and all of them,xcept ethosuximide, clobazam, sulthiame, levetirace-am, and clonazepam, exacerbated the electroclinicaleatures of ESES/CSWS in the majority of patients. Awitch of these AEDs to ethosuximide, clobazam, orulthiame may be the first treatment step to signifi-antly improve the electroclinical pattern.
positive response was observed using the follow-ng AEDs, alone or in combination, as well as withther treatment options: ethosuximide in 2 patients;lobazam in 2; sulthiame in 3; clobazam and etho-uximide in 8; clobazam and sulthiame in 8; etho-uximide and valproic acid in 5; ethosuximide andulthiame in 5; levetiracetam and ethosuximide in 2;
Epileptic Disord, Vol. 15, No. 4, December 2013
eroids and valproic acid in 2; corticosteroids and sulth-ame in 2; corticosteroids, ethosuximide, and clobazamn 1; the ketogenic diet and sulthiame in 1; and the keto-enic diet, clobazam, and ethosuximide in 1. Epilepsyurgery was performed with good results in 2 patients.n one of these patients, a partial lesionectomy
-
E
Congenital hemiparesis, unilateral polymicrogyria, and epilepsy
Fp2-Fp1
F8-Fp2
O1-O2
O1-O4
T4-T8
Fp1-F7
F7-T3
T3-O1
300 µV
F kefua
wiwsAtasc
O
Ac2aorsss
h3sbIhmtrTes
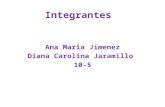
igure 3. The same patient as in Figure 2. EEG recording during wactivity, clearly dominant in posterior regions.
as performed to avoid further motor deficit andn the other, who had unilateral PMG affecting the
hole hemisphere associated with severe hemipare-is, a hemispherectomy was performed.
partial response was observed in 15 patients usinghe following AEDs: sulthiame in 2 patients, valproiccid and ethosuximide in 2, clobazam and etho-uximide in 1, levetiracetam in 2, and diazepam inombination with sulthiame in 1.
utcome
verage follow-up after the period of electroclinicalhange or onset of ESES/CSWS was 13.5 years (range: 3-
pileptic Disord, Vol. 15, No. 4, December 2013
0 years) for 43 children. ESES/CSWS disappeared aftertime, ranging from 2 to 9 months. Seven patients hadne or more relapses. At the last control, 3 patientsemained seizure-free. One of them had undergoneurgery. The EEG recordings showed isolated focalpikes in these 3 patients. Twenty-four patients hadporadic seizures, 5 had seizures every six months, 5
D
Tebid
1 sec
lness shows occipital spikes and bilateral continuous spike-wave
ad two seizures a month, 3 had monthly seizures, andhad weekly seizures. The EEG in these 40 patients
howed focal spikes in 25, multifocal spikes in 3, andilateral asymmetric spikes in 12 patients.
n patients who became seizure-free and those whoad a more than 75% seizure reduction, school perfor-ance and IQ improved significantly. They returned
o baseline cognitive development. Cognitive deterio-ation remained unchanged in 5 patients (11%).he remaining 10 patients with epilepsy withoutlectroclinical changes or ESES/CSWS had sporadiceizures except one, who is currently seizure-free.
421
iscussion
he patients in this series had non-progressivencephalopathy or cerebral palsy, characterisedy congenital hemiparesis associated with mental
mpairment and epilepsy. These patients frequentlyeveloped focal seizures with or without secondary
-
4
R.H. Caraballo, et al.
Fp2-Fp1
F8-Fp2
O1-O2
O1-O4
T4-T8
Fp1-F7
F7-T3
T3-O1
1 sec
300 µV
FT ic bilc limbp
gtmswcnpWEwitsocioAswPpIo
ihemauimu(Bcosrme1
igure 4. A 6-year-old boy with right fronto-parietal PMG.he EEG recording during wakefulness shows asymmetric rhythmharacterised by a sudden loss of muscle tone in the left upperosition.
eneralised tonic-clonic seizures, followed by a par-icular electroclinical pattern of negative and positive
yoclonias, atypical absences, and an increase of focaleizures and ESES/CSWS, secondary to unilateral PMG,ith relatively good outcome. The majority of these
ases had mild, and less frequently, moderate, butever severe, spastic hemiparesis. The majority of theatients also had mild or moderate mental impairment.ith regards to EEG findings, 43/53 of the patients had
SES/CSWS with more or less than 80% of the spike-ave index. If we consider more wide-reaching EEG
nclusion criteria, all the cases with this particular elec-roclinical pattern may correspond to the ESES/CSWSyndrome. PMG is the most frequent structural causef ESES/CSWS syndrome (Caraballo et al., 2013). Inhildren with PMG, early recognition of this entity ismportant to adequately manage this particular typef epilepsy.
22
review of patients with hemiparetic cerebral palsyhowed that in 7% of the cases, it was associatedith unilateral cortical dysplasias (Wiklund et al., 1991).MG is the most common cause of congenital hemi-legia (Barkovich, 2010; Caraballo et al., 2007).
n our series, most cases were sporadic andnly one was familial. Inheritance of PMG, includ-
owdamPw
ateral spike-wave discharges with repetitive negative myoclonia,when the patient extended both upper limbs in an antigravity
ng both cases of affected parents and siblings,as been suggested in several reports (Yoshimurat al., 1998; Bartolomei et al., 1999; Caraballo et al., 2000),ost commonly through X-linked transmission. Chang
nd co-workers (2006) identified four families in whichnilateral right-sided PMG, based on MRI, was present
n more than one individual, with pathological confir-ation in one. These findings strongly suggest that
nilateral PMG can have a germline genetic aetiologyChang et al., 2006).ilateral continuous or subcontinuous spike-wave dis-harges during slow-wave sleep with higher voltagever the dysplastic areas indicate a mechanism ofecondary bilateral synchrony (SBS), presumably cor-elating with atypical absences and epileptic negativeyoclonus causing gait instability (Dalla Bernardina
t al., 1989, 1996). Kobayashi and co-workers (1992,994) suggested that SBS implies an initial diffusion
Epileptic Disord, Vol. 15, No. 4, December 2013
f discharges through the corpus callosum, with orithout intervention of centro-encephalic structures,uring generalisation. Spencer and co-workers (1985)lso hypothesized about mesencephalic/diencephalicechanisms for SBS (Spencer et al., 1985).
olymicrogyric abnormalities are often moreidespread than can be shown by MRI and an
-
E
Congenital hemiparesis, unilateral polymicrogyria, and epilepsy
F8-Fp2
O1-O2
O2-T4
T4-T8
Fp1-F7
F7-T3
T3-O1
F us sp
eSccspedpBPtPrrailmvtah
PcHic(cbceatpt2s
Fp2-Fp1
1 sec
300 µV
igure 5. Slow sleep EEG recording shows asymmetric continuo
xtensive area of cortical abnormality may facilitateBS. Enhanced excitation arising from the abnormalortex in PMG and reduced inhibitory activity in theortical surface surrounding PMG can trigger hyper-ynchronous neuronal discharges. For the majority ofatients with unilateral PMG who develop status ofpileptic negative myoclonus, the location of corticalysplasia is fronto-temporal, which may explain thehenomenon of SBS.rain CT and particularly MRI are necessary to identifyMG in detail, and also search for other types of lesionhat may be associated in the same patients. UnilateralMG is most frequently located in the fronto-temporalegions and less frequently in the parieto-occipitalegions. CT may show periventricular calcificationsssociated with PMG. These findings may suggest an
pileptic Disord, Vol. 15, No. 4, December 2013
nfection with cytomegalovirus. An encephalomalacicesion and/or porencephalic cyst associated with PMG
ay occur in the same patient and could represent aascular phenomenon. Brain MRI may also show otherypes of malformation of cortical development, suchs schizencephaly (SCHZ) and nodular periventriculareterotopia.
wbmtpsw
5
ike-wave activity dominant in the left hemisphere.
reviously, we published cases with a unilateral poren-ephalic cyst, with a similar electroclinical picture.owever, in these cases, the cortical region surround-
ng the porencephalic lesion showed a polymicrogyricortex which accounted for the electroclinical findingsCaraballo et al., 2007). This particular electroclini-al pattern associated with unilateral PMG has noteen described for other types of malformation ofortical development. In addition, we compared thelectroclinical features of patients with unilateral PMGnd closed-lip SCHZ. Both conditions are secondaryo abnormal cortical organisation. Nevertheless, theatients with closed-lip SCHZ never developed elec-
roclinical features due to SBS (Caraballo et al.,004). The fact that continuous or subcontinuouspikes and waves during slow sleep due to SBS
423
ere found to be associated with unilateral PMG,ut not with cases with other cortical malformations,ay suggest that a unique anatomo-functional sys-
em is involved. A series of children with prenatal orerinatal unilateral thalamic injuries associated withymptomatic CSWS or sleep slow-wave over-activationere reported (Monteiro et al., 2001; Guzzetta et al.,
-
4
R.H. Caraballo, et al.
F8-Fp2
O1-O2
O2-T4
T4-T8
Fp1-F7
F7-T3
T3-O1
300 µV
F ous
2iie2ImgmfiCAtnccvGdae
tretabadclFatc
Fp2-Fp1
igure 6. EEG recording during slow sleep shows diffuse continu
005; Kelemen et al., 2006). CSWS was also detectedn children with shunted hydrocephalus, suggestingnvolvement of thalamo-cortical circuitries (Veggiottit al., 1998; Ben-Zeev et al., 2004; Caraballo et al.,008).n cases with unilateral PMG without hemiparesis and
ental impairment, the distinction between crypto-enic or idiopathic focal epilepsy with SBS may beore difficult. However, brain MRI findings will con-
rm the diagnosis.are should be taken in the selection of AED treatment.probable association between certain AEDs and
he appearance of continuous spike-wave activity withegative myoclonus has repeatedly been reported in
24
hildren with benign childhood epilepsy exposed toarbamazepine, phenobarbital, phenytoin, and evenalproate (Caraballo et al., 1989; Pratz et al., 1998;uerrini et al., 1998b). This phenomenon has also beenescribed in association with topiramate (Montenegrond Guerreiro, 2002). The majority of these cases werexposed to AEDs, effective against focal seizures, prior
Ilbsees
1 sec.
spike-waves.
o the peculiar evolution of their epilepsy. In our expe-ience, after the onset of continuous or subcontinuouslectroclinical manifestations, the best results are ini-ially obtained with valproic acid, benzodiazepines,nd ethosuximide, either in monotherapy or in com-ination. Oguni and co-workers (1998) and Capovilland co-workers (1999) stated that ethosuximide is therug of choice to treat negative myoclonus. We alsoonsider sulthiame to be a good option, both for non-esional and unilateral PMG (Caraballo et al., 2007;ejerman et al., 2012). Corticosteroid therapy may ben alternative (Caraballo et al., 2007). In cases refrac-ory to these drugs, valproic acid, levetiracetam, and/ororticosteroids should be considered.
Epileptic Disord, Vol. 15, No. 4, December 2013
n refractory cases with hemiparesis and extensive uni-ateral PMG, total or subtotal hemispherectomy coulde useful. In the planning for the surgical strategy, ithould be considered whether the epileptogenic zonextends beyond the polymicrogyric lesion (Chassouxt al., 2008. Any surgical approach to treat epilepsy,econdary to PMG, should be viewed with extreme
-
E
C
Table 2. Electroclinical change in 43 of 53 caseswith epilepsy and unilateral PMG.
Number and genderof cases
27 Male; 16 Female
Localisationof unilateral PMG
Fronto-temporal: 25Fronto-temporo-parietal: 5Parieto-occipital: 13
Affected hemisphere Right: 24Left: 19
Median ageat worsening ofepilepsy
5 years(R: 2-9.5 years)
Type of seizure Negative and positivemyoclonusAtypical absencesFrequent focal seizures withor without SGTCS
EEG findings CSWS > 80% 29 patientsCSWS < 80% 14 patients
AEDs used CLB, ETS, STM, ETS+VPA, LVT
VS
ctctaaWca(eRfvoTcsitspcP
ict
C
IsbssbfiWtcemenIccwTcqa
DN
R
AIY
AaN
BowG
BEdevelopment. Neuropediatrics 1996; 27: 59-63.
Other treatments Corticosteroids, KD, surgery
PA: valproic acid; CLB: clobazam; ETS: ethosuximide;TM: sulthiame; LVT: levetiracetam; KD: ketogenic diet.
aution, and restricted to highly selected cases, givenhat: the outcome of seizures is favourable in mostases; the polymicrogyric cortex may retain its func-ional properties, at least in part; and its removal carrieshigh risk of producing neurological deficits (Guerrinind Barba, 2011).ith a careful selection of AEDs, a relatively benign
ourse of epilepsy in patients with hemiparesis associ-ted with unilateral PMG has repeatedly been reportedCaraballo et al., 1992, 1997, 2004; Aicardi, 1994; Guerrinit al., 1996).esponse to change of treatment is initially good
or the majority of patients, but the evolution canary. A significant number of patients may show oner more relapses of the same electroclinical picture.he seizures usually remit completely before adoles-ence and only a few patients continue with sporadiceizures after this period of age. Even though epilepsy
pileptic Disord, Vol. 15, No. 4, December 2013
n patients with cortical dysplasia is frequently refrac-ory to AEDs, the majority of cases with unilateral PMGhow a favourable outcome. Nevertheless, some of theatients in our series continued with seizures and weonsider that the prognosis of epilepsy in patients withMG is not as benign as that of idiopathic focal epilepsy
BCm
Br
ongenital hemiparesis, unilateral polymicrogyria, and epilepsy
n childhood, however, outcome is more favourableompared to epilepsy secondary to other types of cor-ical dysplasia.
onclusion
n a patient presenting with congenital hemipare-is, particular electroclinical features characterisedy negative myoclonus, absences, and focal motoreizures with continuous or subcontinuous spikes orpike-waves during slow-sleep, unilateral PMG shoulde considered. Brain MRI is mandatory in order to con-rm this cortical malformation.e believe it is important to recognise this par-
icular association between focal PMG conditioningontralateral hemiparesis and the appearance ofpilepsy with peculiar evolution, including one orore periods of frequent inhibitory seizures as an
pileptic negative myoclonus expressing the SBS phe-omenon.
n our study, the most commonly used treatments werelobazam, ethosuximide, and sulthiame, alone or inombination. In refractory cases, high-dose steroidsere administered.he prognosis of these patients with malformation ofortical development is relatively benign and thus ade-uate management may avoid cognitive deteriorationnd surgical intervention. �
isclosures.one of the authors have any conflict of interest to disclose.
eferences
icardi J. Epilepsies characterized by simple partial seizures.n: Aicardi J, ed. Epilepsy in children. 2nd Edition. Nework: Raven Press, 1994, p. 130-64.
ligianis I, Morgan N, Mione M, et al. Mutations of the cat-lytic subunit of RAB3GAP cause Warburg Micro syndrome.at Genet 2005; 37: 221-3.
aala L, Briault S, Etchevers HC, et al. Homozygous silencingf T-box transcription factor EOMES leads to microcephalyith polymicrogyria and corpus callosum agenesis. Natenet 2007; 39: 454-6.
arkovich AJ, Kuzniecky R, Dobyns W, Jackson G, Becker L,vrard P. A classification scheme for malformations of cortical
425
arkovich AJ, Kuzniecky R, Jackson G, Guerrini R, Dobyns W.lassification system for malformations of cortical develop-ent: update 2001. Neurology 2001; 57: 2168-78.
arkovich AJ. Current concepts of polymicrogyria. Neuro-adiology 2010; 52: 479-87.
-
4
R
BWf2
Bet
BKwN
BnmG
CTeJ
Cas
Cpe
Cdd1
Cew
Cc
Csl
Ceeet
CEts2
Cwwf
Cds
Cg1
CoN
CiE
DCtsAp
DEdFe2
Dm1M
FcwtE
Gic
Gar
GteZcP
Gce
Gi1
G
.H. Caraballo, et al.
arkovich AJ, Guerrini R, Kuzniecky RI, Jackson GD, DobynsB. A developmental and genetic classification for mal-
ormations of cortical development: update 2012. Brain012; 135: 1348-69.
artolomei F, Gavaret M, Dravet C, Guerrini R. Familialpilepsy with unilateral and bilateral malformations of cor-ical development. Epilepsia 1999; 40: 47-51.
en-Zeev B, Kivity S, Pshitizki Y, Watemberg N, Brand N,ramer U. Congenital hydrocephalus and continuous spikeave in slow-wave sleep: a common association? J Childeurol 2004; 19: 129-34.
rooks A, Bertoli-Avella A, Burzynski G, et al. Homozygousonsense mutations in KIAA1279 are associated with malfor-ations of the central and enteric nervous systems. Am J Humenet 2005; 77: 120-6.
apovilla G, Beccaria F, Veggliotti P, Rubboli G, Meletti S,assinari CA. Ethosuximide is effective in the treatment ofpileptic negative myoclonus in childhood partial epilepsy.Child Neurol 1999; 14: 395-400.
araballo R, Fontana E, Micheliza B, et al. Carbamazepina,ssenze atipiche crisi atoniche e stato di PO continua delonno (POCS). Boll lega It Epil 1989; 66/67: 379-81.
araballo R, Kochen S, Cersósimo R, Fejerman N. Unilateralachygyria with congenital hemiplegia and peculiar type ofpilepsy (Abstract). Pediatr Neurol 1992; 8: 398.
araballo R, Cersósimo R, Fejerman N. Un tipo particulare epilepsia en pacientes con hemiparesia congenita asocia-a a polimicrogiria o paquigiria unilateral. Rev Neurol (Barc)997; 25: 1058-63.
araballo R, Cersósimo R, Fejerman N. A particular type ofpilepsy in children with congenital hemiparesis associatedith unilateral polymicrogyria. Epilepsia 1999; 40: 865-79.
araballo R, Cersósimo R, Mazza E, Fejerman N. Focal polymi-rogyria in mother and son. Brain Dev 2000; 22: 336-9.
araballo R, Cersósimo R, Fejerman N. Unilateral closed-lipchizencephaly and epilepsy: a comparison with cases of uni-ateral polymicrogyria. Brain Dev 2004; 26: 151-7.
araballo R, Cersósimo R, Fejerman N. Symptomatic focalpilepsies imitating atypical evolutions of idiopathic focalpilepsies. In: Fejerman N, Caraballo R, eds. Benign focalpilepsies in infancy, childhood and adolescence. Mon-rouge (France): John Libbey Eurotext, 2007, p. 221-39.
araballo RH, Bongiorni L, Cersosimo R, Semprino M,speche A, Fejerman N. Epileptic encephalopathy with con-inuous spikes and waves during sleep in children withhunted hydrocephalus: a study of nine cases. Epilepsia008; 49: 1520-7.
araballo R, Veggiotti P, Kaltenmeier M, et al. Encephalopathy
26
ith status epilepticus during sleep or continuous spikes andaves during slow sleep syndrome: a multicenter, long-term
ollow-up study of 117 patients. Epilepsy Res 2013; 105: 164-73.
olamaria V, Grimau R, Sgro V, et al. Epilepsia focale con statui punta-onda continua in sonno lento: asterixis critico inoggeto con emipachigiria. Bol Lega It Epil 1989; 66/67: 233-5.
N
GSec3
olamaria V, Franco A, Zamponi N. Emiplegia con-enita, alterazioni corticale ed epilepssia. Bol Lega It Epil991; 74: 169-70.
hang BS, Apse K, Caraballo R, et al. A familial syndromef unilateral polymicrogyria affecting the right hemisphere.eurology 2006; 66: 133-5.
hassoux F, Landre E, Rodrigo S, et al. Intralesional record-ngs and epileptogenic zone in focal polymicrogyria.pilepsia 2008; 49: 51-64.
alla Bernardina B, Fontana E, Michelizza B, Colamaría V,apovilla G, Tassinari C. Partial epilepsies in childhood bila-
eral synchronization, continuous spike-waves during slowleep. In: Manellis J, Bental E, Loeber N, Dreiffus F, eds.dvances in Epileptology: XVllth Epilepsy International Sym-osium. New York: Raven Press, 1989, p. 295-302.
alla Bernardina B, Pérez-Jiménez A, Fontana E, et al.lectroencephalographic findings associated with corticalysplasias. In: Guerrini R, Canapicchi R, Zifkin B, Andermann, Roger J, Pfanner P, eds. Dysplasias of cerebral cortex andpilepsy. Philadelphia: Lippincott-Raven Publishers, 1996, p.35-45.
obyns WB, Mirzaa G, Christian SL, et al. Consistent chro-osome abnormalities identify novel polymicrogyria loci in
p36.3, 2p16.1-p23.1, 4q21.21-q22.1, 6q26-q27, and 21q2. Am Jed Genet A 2008; 146A: 1637-54.
ejerman N, Caraballo R, Cersosimo R, Ferraro SM, Galic-hio S, Amartino H. Sulthiame add-on therapy in childrenith focal epilepsies associated with encephalopathy related
o electrical status epilepticus during slow sleep (ESES).pilepsia 2012; 53: 1156-61.
laser T, Jepeal L, Edwards JG, et al. PAX6 gene dosage effectn a family with congenital cataracts, aniridiaanophtalmia andentral nervous system defects. Nat Genet 1994; 7: 463-71.
uerrini R, Dravet C, Raybaud C, et al. Epilepsy and focal gyralnomalies detected by MRI: electroclinic, morphological cor-elations and follow-up. Dev Med Child Neurol 1993; 34: 706-8.
uerrini R, Pammeggiani M, Bureau M, et al. Localized cor-ical dysplasia: good seizure outcome after sleep-relatedlectrical status epilepticus. In: Guerrini R, Canapicchi R,ifkin B, Andermann F, Roger J, Pfanner P, eds. Dysplasias oferebral cortex and epilepsy. Philadelphia: Lippincott-Ravenublishers, 1996, p. 329-36.
uerrini R, Genton P, Bureau M, et al. Multilobar polymi-rogyria, intractable drop attack seizures, and sleep-relatedlectrical status epilepticus. Neurology 1998a; 51: 504-12.
uerrini R, Belmonte A, Genton P. Antiepileptic drug-nduced worsening of seizures in children. Epilepsia998b; 39: S2-10.
uerrini R, Parrini E. Neuronal migration disorders.
Epileptic Disord, Vol. 15, No. 4, December 2013
eurobiol Dis 2010; 48: 39-48.
uerrini R, Barba C. Polymicrogyria and schizencephaly. In:horvon S, Andermann F, Guerrini R, eds. The causes ofpilepsies: common and uncommon causes in adults andhildren. Cambridge: Cambridge University Press, 2011, p.11-29.
-
E
C
Gas
JtN
KTa2
KsbdN
KEa1
Km
Lm1M
Mnop
Mt2
OMmn
PN
PdP
Ro2
SBirt2
SEe1
VCs
uzzetta F, Battaglia D, Veredice C, et al. Early thalamic injuryssociated with epilepsy and continuous spike-wave duringlow sleep. Epilepsia 2005; 46: 889-900.
aglin XH, Poirier K, Saillour Y, et al. Mutations in the beta-ubulin gene TUBB2B result in asymmetrical polymicrogyria.at Genet 2009; 41: 746-52.
elemen A, Barsi P, Gyorsok Z, Sarac J, Szucs A, Halász P.halamic lesion and epilepsy with generalized seizures, ESESnd spike-wave paroxysms - Report of three cases. Seizure006; 15: 454-8.
obayashi K, Ohtsuka Y, Oka E, Ohtahara S. Primary andecondary bilateral synchrony in epilepsy: differentiationy stimulation of interhemispheric small time differencesuring short spike-wave activity. Electroencephalogr Clineurophysiol 1992; 83: 93-103.
obayashi K, Nishibayashi N, Ohtsuka Y, Oka E, Ohtahara S.pilepsy with electrical status epilepticus during slow sleepnd secondary bilateral synchrony. Epilepsia 1994; 35: 1097-03.
uzniecky R, Barkovich J. Malformations of cortical develop-ent and epilepsy. Brain Dev 2001; 23: 2-11.
eventer R, Martin C, Gajecka M, Shaffer L. Consistent chro-osome abnormalities identify novel polymicrogyria loci in
p36.3, 2p16.1-p23.1, 4q21.21-q22.1, 6q26-q27, and 21q2. Am Jed Genet A 2008; 146A: 1637-54.
pileptic Disord, Vol. 15, No. 4, December 2013
onteiro JP, Roulet-Perez JP, Davidoff V, Deonna T. Primaryeonatal thalamic haemorrhage and epilepsy with continu-us spike-wave during sleep: a longitudinal follow-up of aossible significant relation. Eur J Paediatr Neurol 2001; 5: 41-7.
ontenegro MA, Guerreiro MM. Electrical status epilep-icus of sleep in association with topiramate. Epilepsia002; 43: 1436-40.
YF1
Wab1
ongenital hemiparesis, unilateral polymicrogyria, and epilepsy
guni H, Uehara T, Tanaka T, Sunahara M, Hara M, Osawa. Dramatic effect of ethosuximide on epileptic negativeyoclonus: implications for the neurophysiological mecha-
ism. Neuropediatrics 1998; 29: 29-34.
almini A. Disorders of cortical development. Curr Opineurol 2000; 13: 183-92.
ratz JM, Garaizar C, García-Nieto ML, Madoz P. Antiepilepticrugs and atypical evolution of idiopathic partial epilepsy.ediatr Neurol 1998; 18: 402-6.
oll P, Rudolf G, Pereira S, et al. SRPX2 mutations in dis-rders of language cortex and cognition. Hum Mol Genet006; 15: 1195-207.
ertié AL, Sossi V, Camargo AA, Zatz M, Brahe C, Passos-ueno MR. Collagen XVIII, containing an endogenous
nhibitor of angiogenesis and tumor growth, plays a criticalole in the maintenance of retinal structure and in neuralube closure (Knobloch syndrome). Hum Mol Genet 2000; 9:051-8.
pencer SS, Spencer DD, Williamson PD, Mattson RH.ffects of corpus callosum sections on secondary bilat-rally synchronous interictal EEG discharges. Neurology985; 35: 1689-94.
eggiotti P, Beccaria F, Papalia G, Termine C, Piazza F, Lanzi G.ontinuous spikes and waves during sleep in children with
hunted hydrocephalus. Childs Nerv Syst 1998; 14: 188-94.
427
oshimura K, Hamada F, Tomoda T, Wakiguchi H, Kurashige T.ocal pachy-polymicrogyria in three siblings. Pediatr Neurol998; 18: 435-8.
iklund L, Uvebrant P, Flodniar K. Computed tomographys an adjunct in etiological analysis of hemiplegic cere-ral palsy: children born at term. Neuropediatrics 1991; 22:21-8.
/ColorImageDict > /JPEG2000ColorACSImageDict > /JPEG2000ColorImageDict > /AntiAliasGrayImages false /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic /GrayImageResolution 300 /GrayImageDepth -1 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict > /GrayImageDict > /JPEG2000GrayACSImageDict > /JPEG2000GrayImageDict > /AntiAliasMonoImages false /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 1200 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict > /AllowPSXObjects false /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (Coated FOGRA27 \050ISO 12647-2:2004\051) /PDFXOutputCondition () /PDFXRegistryName (http://www.color.org) /PDFXTrapped /Unknown
/DetectCurves 0.100000 /EmbedOpenType false /ParseICCProfilesInComments true /PreserveDICMYKValues true /PreserveFlatness false /CropColorImages false /ColorImageMinResolution 150 /ColorImageMinResolutionPolicy /OK /ColorImageMinDownsampleDepth 1 /CropGrayImages false /GrayImageMinResolution 150 /GrayImageMinResolutionPolicy /OK /GrayImageMinDownsampleDepth 2 /CropMonoImages false /MonoImageMinResolution 1200 /MonoImageMinResolutionPolicy /OK /CheckCompliance [ /None ] /PDFXOutputConditionIdentifier (FOGRA27) /Description > /Namespace [ (Adobe) (Common) (1.0) ] /OtherNamespaces [ > > /FormElements true /GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks false /IncludeInteractive false /IncludeLayers false /IncludeProfiles true /MarksOffset 14.173230 /MarksWeight 0.250000 /MultimediaHandling /UseObjectSettings /Namespace [ (Adobe) (CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /UseName /PageMarksFile /RomanDefault /PreserveEditing true /UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling /LeaveUntagged /UseDocumentBleed false >> ]>> setdistillerparams> setpagedevice