
Atriumfibrilleren: van eerste presentatie naar chronische ... · Atriumfibrilleren: van eerste...
57
Atriumfibrilleren: van eerste presentatie naar chronische behandeling. Dr. D.P. Muijs-Kolditz Cardioloog, MC Zuiderzee, Lelystad
Transcript of Atriumfibrilleren: van eerste presentatie naar chronische ... · Atriumfibrilleren: van eerste...
Atriumfibrilleren: van eerste presentatie
naar chronische behandeling.
Dr. D.P. Muijs-Kolditz Cardioloog, MC Zuiderzee, Lelystad
(potentiële) belangenverstrengeling Geen / Zie hieronder
Voor bijeenkomst mogelijk relevante relaties met bedrijven
Bedrijfsnamen
Sponsoring of onderzoeksgeld Honorarium of andere (financiële)
vergoeding Aandeelhouder Andere relatie, namelijk …
Disclosure belangen spreker
Program
• 17:00 uur - part 1:
- Atriumfibrilleren van eerste behandeling naar chronische behandeling
• 19:00 uur - part 2:
– Huisartsen: cardioloog - D.P. Muijs-Kolditz
– POH: hartfalenverpleegkundige - T. Hermans
Outline – part I
Huisarts and POH:
• What is atrial fibrillation ?
• Pathofysiology
• Incidence/prevalence
• Morbidity/mortality
• Classification of AF
• Concomittant diseases
• Complications in AF
• In practise:
- Diagnosis
- Therapy in AF (NHG standaard)
- Samenwerkingsafspraken regio
Outline- part II
Huisartsen:
• Verwijsbeleid huisarts- cardioloog en terug
• Casuïstiek
- CHADS-VASC / HASBLED
- VKA versus NOAC
- Rate versus rhythm control
- RF-ablation
• Follow-up chronisch AF in huisartsen praktijk
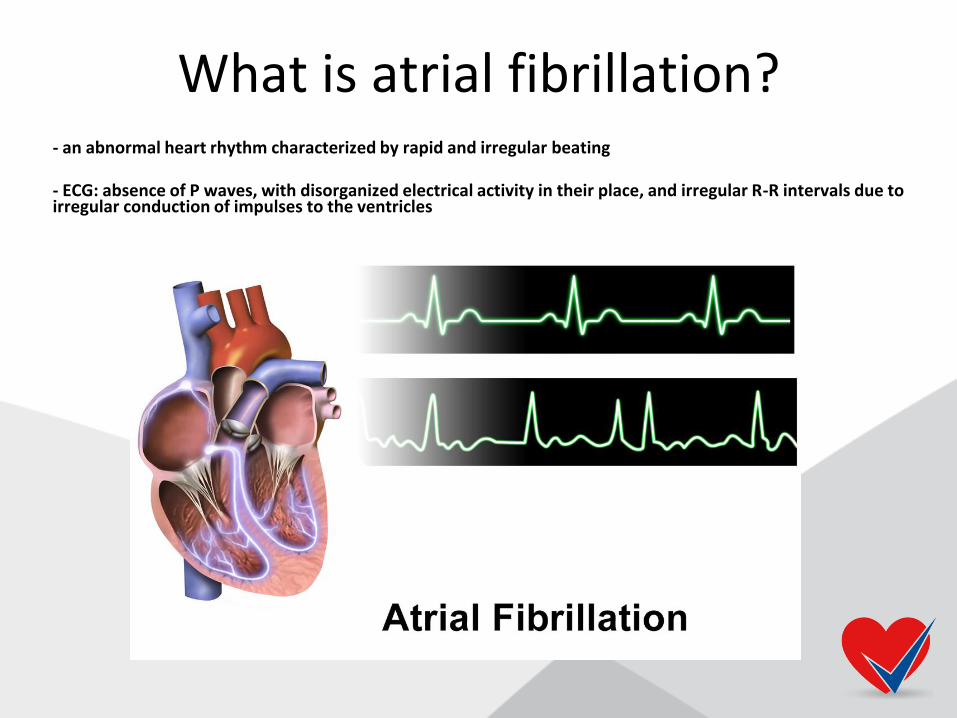
What is atrial fibrillation? - an abnormal heart rhythm characterized by rapid and irregular beating - ECG: absence of P waves, with disorganized electrical activity in their place, and irregular R-R intervals due to irregular conduction of impulses to the ventricles
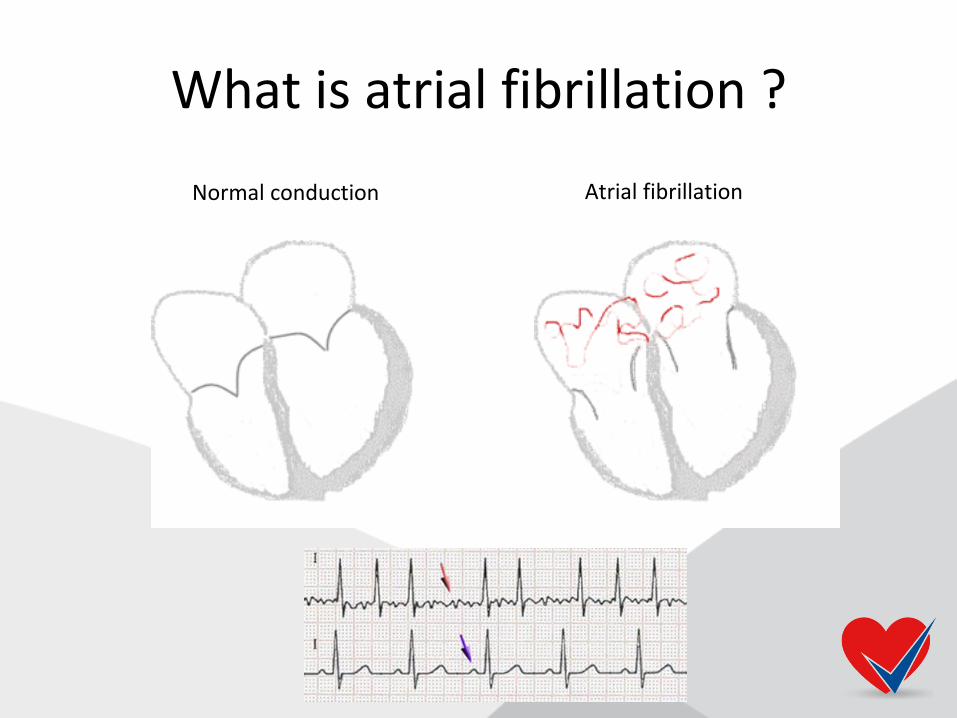
What is atrial fibrillation ?
Normal conduction Atrial fibrillation
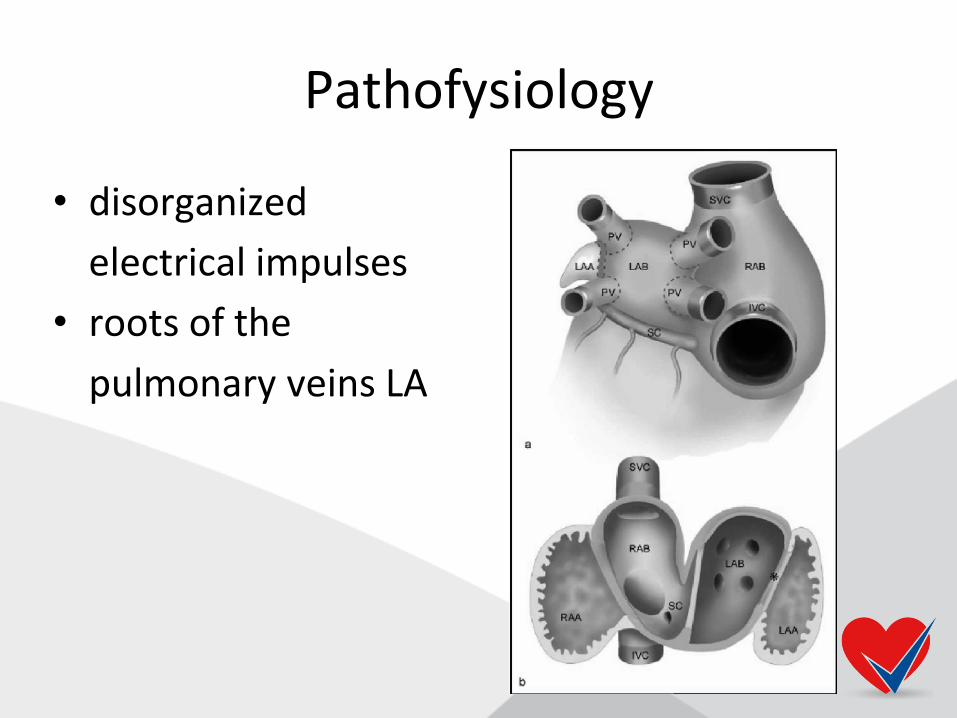
Pathofysiology
• disorganized
electrical impulses
• roots of the
pulmonary veins LA
Pathofysiology
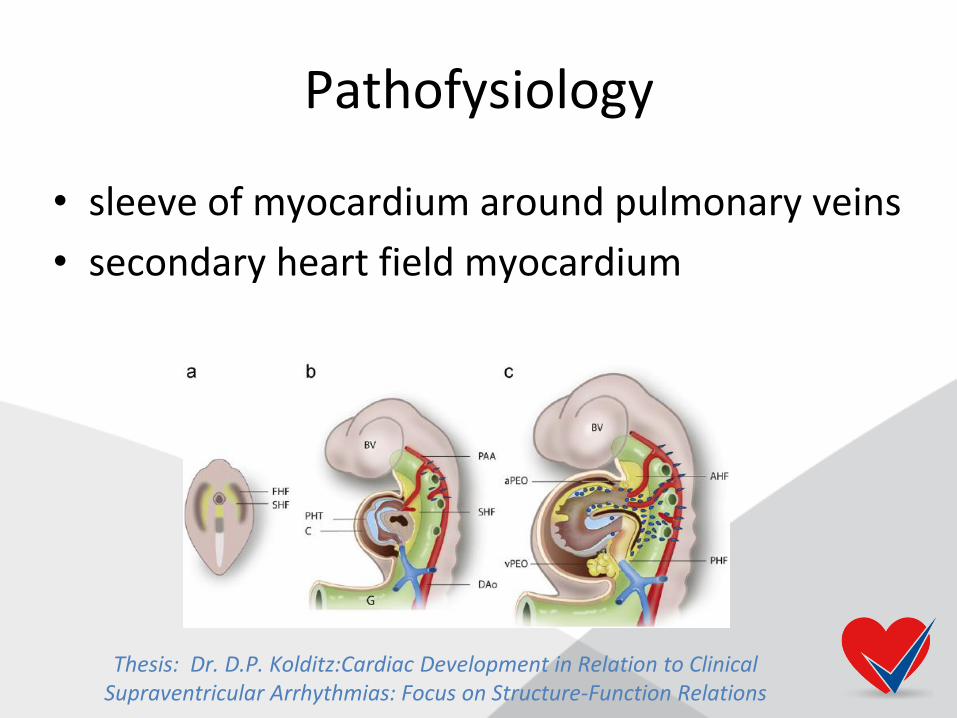
• sleeve of myocardium around pulmonary veins
• secondary heart field myocardium
Thesis: Dr. D.P. Kolditz:Cardiac Development in Relation to Clinical Supraventricular Arrhythmias: Focus on Structure-Function Relations
Pathofysiology
• Disturbance around pulmonary veins:
- automatic foci, often localized at one of the pulmonary veins,
- or a small number of localized sources in the form of either reentrant electrical spiral waves (rotors) or repetitive focal beats;
- mostly in the left atrium near the pulmonary veins or in a variety of other locations through both the left or right atrium.
Pathofysiology
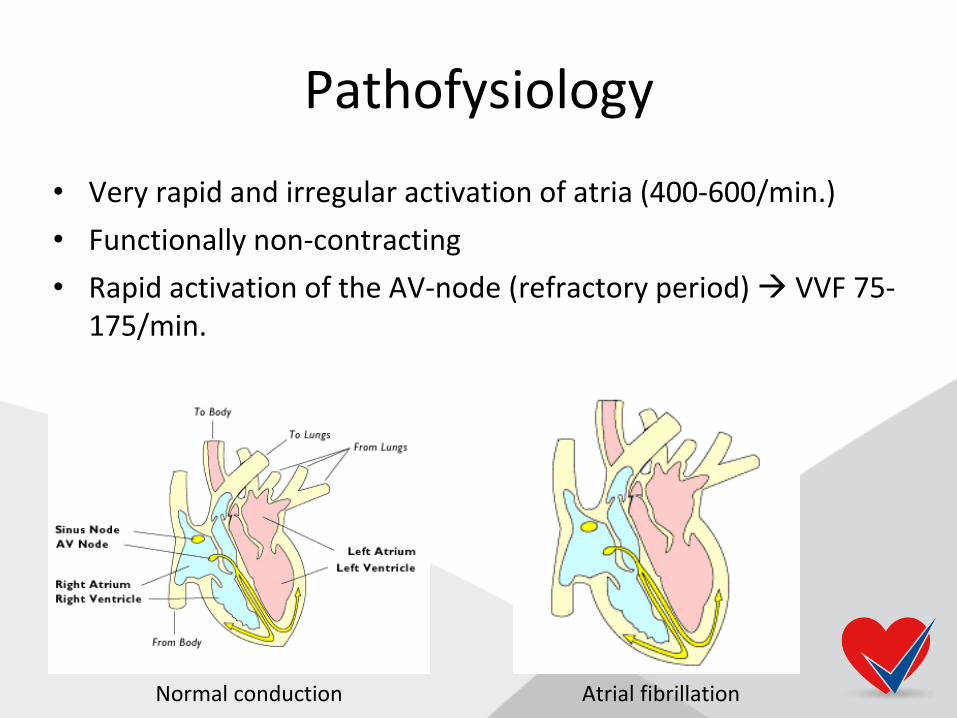
• Very rapid and irregular activation of atria (400-600/min.)
• Functionally non-contracting
• Rapid activation of the AV-node (refractory period) VVF 75-175/min.
Normal conduction Atrial fibrillation
Pathofysiology
• Chain of events
• Atrial fibrosis
• Due to atrial dilatation: valvular heart disease, hypertension, heart failure, inflammation

Incidence, prevalence
• Worldwide (7 miljard):
– males: prevalence 20.9 million
– females: prevalence 12,6 million
• Incidence higher in developed countries
• 1:4 middle-aged adults develops AF
• Incidence in EU: 120.000-215.000 AF de novo/year

Incidence, prevalence
• Netherlands (NHG-standaard):
- prevalence: 0,5%
- 25-45 years: 0,04%
- >75 years: 6%
- 50% of patient with AF is > 75 years
- males > females
- 25-35% of patients with AF = silent AF
Incidence, prevalence
• Increase in AF prevalence due to:
- better detection
- increasing mean age
- conditions predisposing to AF
High risk groups
• Hogere prevalentie van AF bij: - hogere leeftijd - hypertensie - coronarialijden - klepvitia - obesitas - OSAS - diabetes mellitus - chronische nierinsufficientie

Morbidity, mortality
• AF is independently associated with:
- a 2-fold increased risk of all-cause mortality in women
- a 1.5-fold increased risk of all-cause mortality in men
• 10-40% of AF patients is hospitalized each year
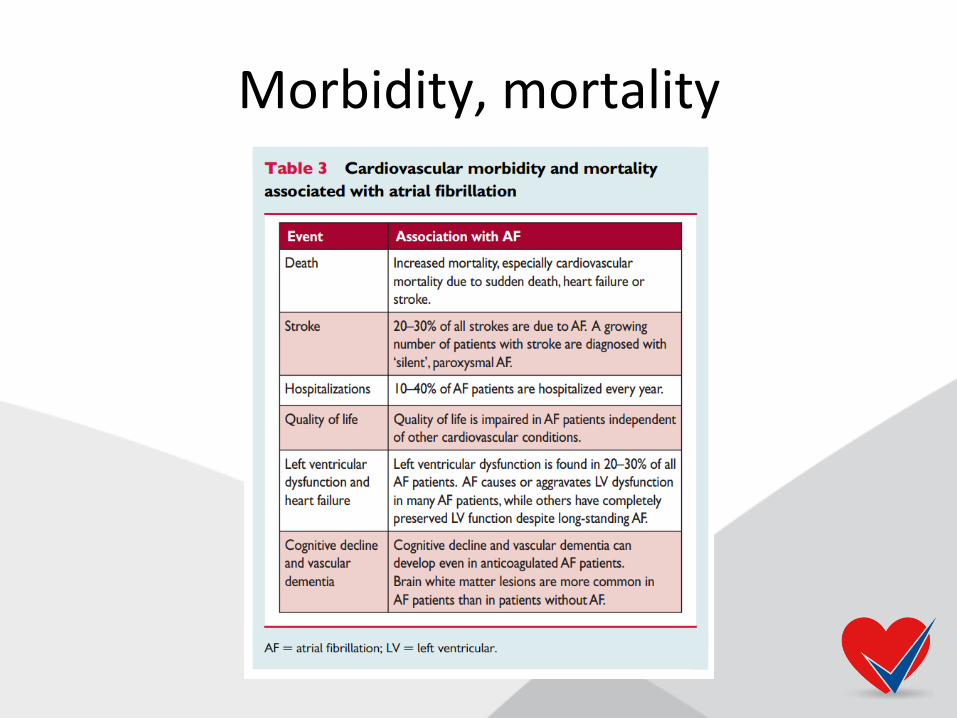
Morbidity, mortality

Overt versus silent AF
• Screening for silent AF:
- cost-effective in patient > 65 years of age
- prevalence of chronic AF 2.3%
- screening by pulse palpation or short-term ECG
- paroxysmal AF often missed
- innovation: smartphones with ECG electrodes, smart watches and
BB machines, MyDiagnostick
AF and cryptogenic stroke
• Cryptogenic stroke: a stroke in which the cause could not be identified after extensive investigation
• ECG monitoring detects AF in 24% of stroke survivors
• Prolonged ECG monitoring is advised, at least 72 hours

Classification of atrial fibrillation
5 types of AF
Concomitant CV-diseases
• AF en heart failure:
– Coincide in many patients
– Cause and exacerbate each
other:
• Structural cardiac
remodelling
• Activation of neurohumoral mechanisms
• Rate related impairment of LV function

Concomitant CV-diseases
• AF and hypertension:
– both stroke risk factor
– RAAS inhibition gives rise to structural remodeling and recurrence of AF
– ACE and ARBs beneficial effect on occurence of AF upstream therapy
Concomitant CV-diseases
• AF and valvular heart disease:
– 30% of patient with AF have
valvular heart disease
– In severe valveular disease, AF is a marker for progressive disease valve repair
– Valvular AF: only in patient with rheumatic valvular disease of mechanical valves
Concomitant CV-diseases
• AF and diabetes mellitus:
– Both risk factor for stroke
– Frequently co-exsist
– Intensive glucose control had no effect of AF occurence
Concomitant CV-diseases
• AF and obesity :
– Obesity increases risk for AF:
• More LV diastolic dysfunction
• Increased sympathetic activation & fatty infiltration
– 10-15 kg weight loss, fewer symptoms
– Higher recurrence rate after AF-ablation in obesity
Concomitant CV-diseases
• AF and OSAS:
– CPAP reduces AF recurrence
– OSAS screening in AF patients ?
– Theophyllines and beta-adrenergic agonists used for bronchospasme can precipitate AF
– Non-selective beta-blokkers, sotalol and adenosine: not in patients with bronchospasme, safely used in COPD
– Beta-1-selective blockers (bisoprolol, metoprolol, nebivolol): safely used in all astma/COPD patients
Concomitant CV-diseases
• AF and chronic kidney disaese:
– AF in 15-20% of patients with CKD
– CKD: eGFR < 50 ml/min.
– Alle patient with AF, yearly renal function evaluation
– OAS dosage, digoxine dosage
Complications of AF
• STROKE !
• Tachycardiomyopathy
• Heart failure
In practise
Van eerste presentatie naar chronische behandeling
NHG-standaard
Diagnostics
• Active palpitation of heart rhythm in:
• dyspnea
• decrease in toleration for exercise
• dizziness
• (pre) syncope
• heart failure
• TIA/CVA
• Thyroid dysfunction
Diagnostics
• Symptoms:
– palpitations
– Dizziness, collaps
– Chest pain
– Congestion
– Stres
– Sleeping disorders
– Intoxications: alcohol, coffee, drugs

Symptom scale for AF
Diagnostics
• Lichamelijk onderzoek:
– Measure RR
– Auscutation of heart
– Signs of heart failure ?
– Signs of valvular disease ?
Diagnostics
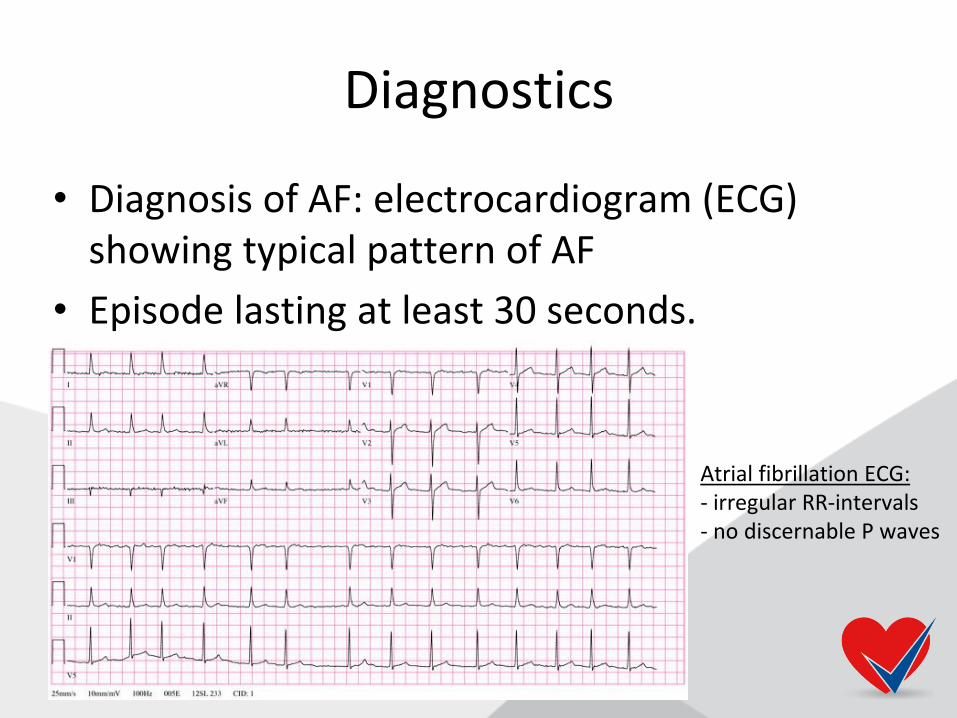
• Diagnosis of AF: electrocardiogram (ECG) showing typical pattern of AF
• Episode lasting at least 30 seconds.
Atrial fibrillation ECG: - irregular RR-intervals - no discernable P waves
Diagnostics
• Laboratory:
– TSH, Hb, glucose, creatinine, kalium
– Pro-BNP (signs of heart failure)
Treatment in AF
1. Rate/rhythm control
2. Anti-thrombotic treatment (VKA/NOAC)
– CHADS-VASC
– HAS-BLED

Therapy in AF (NHG standaard)
• Rate control < 110/min in resting state (lenient rate control)
– beta blocker: metoprolol 50-200 mg
– verapamil/diltiazem 120-360 mg
– digoxine co-medication
• Follow-up after start rate control: weekly
Therapy in AF (NHG standaard)
• Sotalol (rhythm control) only at cardiologist
• Digoxine only with eGFR control:
– < 70 years and normal eGFR: 1dd0.25 mg
– >70 years and eGFR < 50 ml/min: 1dd0.125mg
– > 85 years: 1dd0.625mg

Therapy in AF CHADS2-VASC2 score
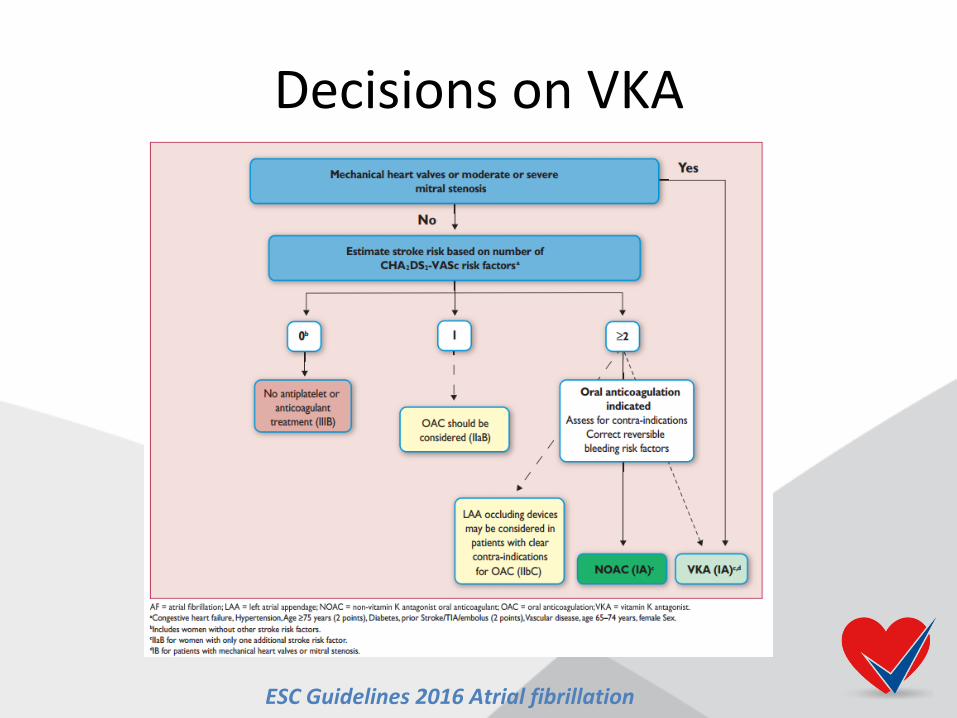
Decisions on VKA
ESC Guidelines 2016 Atrial fibrillation
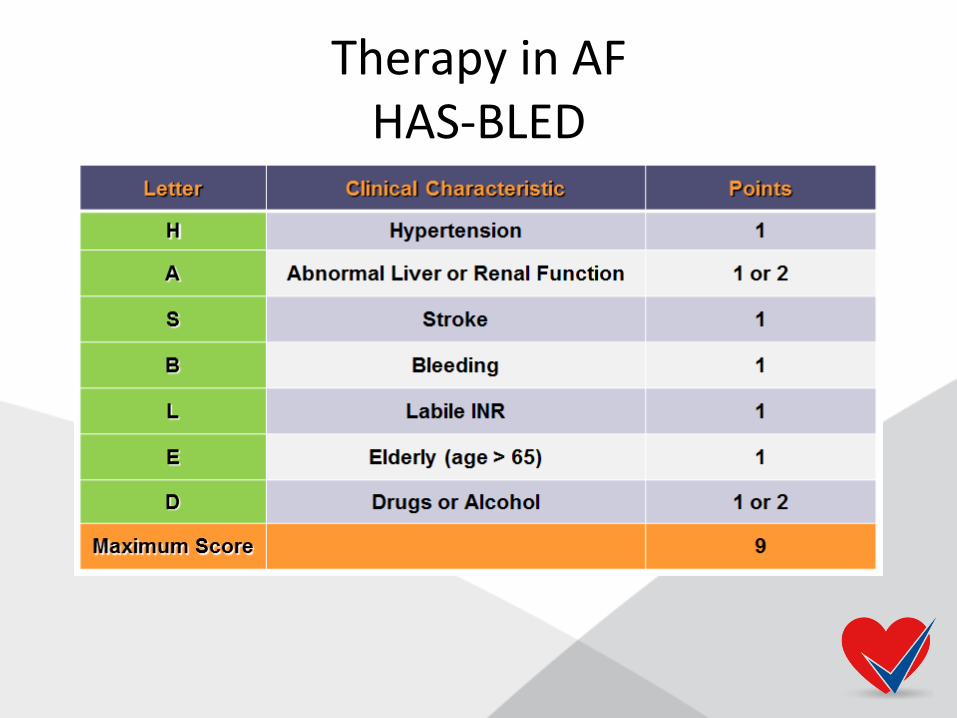
Therapy in AF HAS-BLED
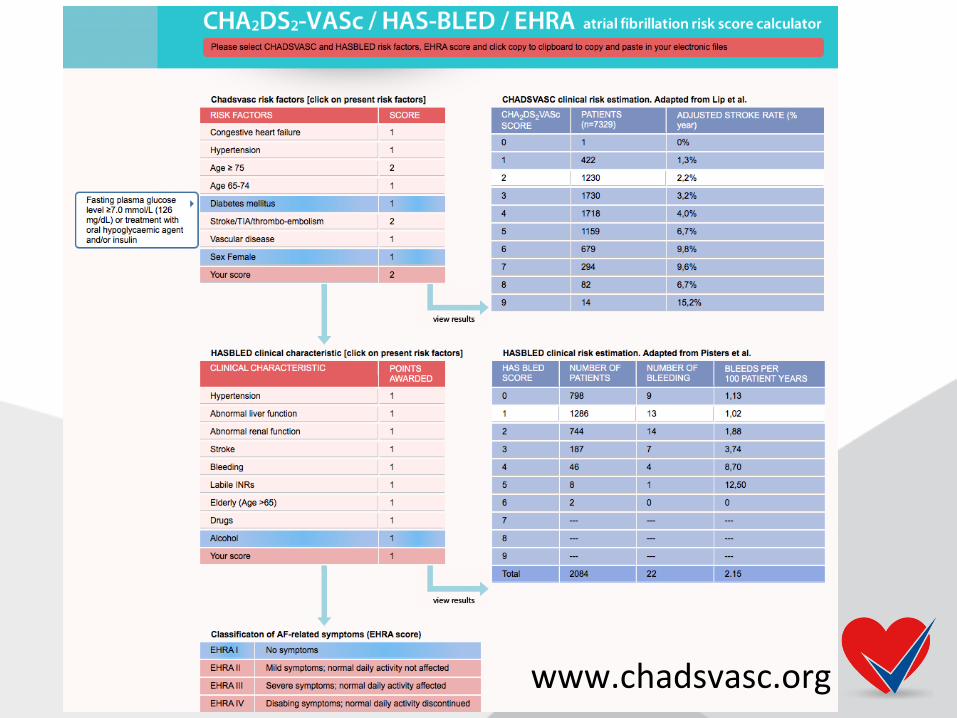
www.chadsvasc.org

Therapy in AF
• CHADS-VASC >> HAS-BLED: start VKA
• HASBLED >> CHADS-VASC:
- consider not starting VKA directly
- however high HAS-BLED – do not withhold VKA completely
- identify bleeding risk factors and treatable risk factors

Therapy in AF
Therapy in AF (NHG standaard)
• AF > 48 hours of PAF VKA
• Only CHADSVASC +2 = VKA not conform ESC guidelines!!!
• Male 65-74 years = CHADSVASC +1 consider VKA !!
• Only CHADS-VASC +1 based on female gender is no strict indication for VKA
• NOAC only at cardiologist

Decisions on VKA
CHA2DS2-VASC score = 1
MALE
STRONLY CONSIDER VKA/NOAC
VKA/NOAC
Behandelbeleid atriumfibrilleren
(Terug)verwijs, consultatie-, substitutie- en samenwerkingsafspraken VRM-Atriumfibrilleren (AF) tussen afdeling cardiologie CCG (MC groep) en huisartsen aangesloten bij Medrie regio Flevoland
- Atriumfibrilleren (K78)
Klankbordgroep VRM
Samenwerkingsafspraken
AF-patient verwijzen naar cardioloog:
• leeftijd < 65 jaar en langer dan 48 uur bestaand atriumfibrilleren;
• keuze voor NOAC als antitrombotische medicatie;
• ventrikelfrequentie < 50/min zonder frequentie-verlagende middelen;
• persisterende klachten ondanks adequate ventrikelfrequentie;
• onvoldoende daling van de ventrikelfrequentie door digoxine en betablokker.
• vermoeden van een hartklepafwijking en/of hartfalen;
• aanwezigheid van het Wolff-Parkinson-White-syndroom of plotse hartdood in de familie;
• PAF, wanneer de patiënt therapie wenst ter vermindering van het aantal aanvallen.
• Bij AF: eenmalige echocardiografie ter diagnostiek indien patiënt conform de NHG standaard in de eerstelijn kan worden behandeld (er wordt dan gedeclareerd volgens 1,5 lijns tarief, eerstelijns DBC kan open blijven).
Samenwerkingsafspraken
- De verwijzing vindt plaats via zorgdomein, dus niet via het KIS.
- De huisarts vermeldt minimaal de volgende gegevens: - Ingezette medicamenteuze en niet- medicamenteuze maatregelen en hun resultaat. - Medicatie-historie met reden van staken eerdere relevante medicatie. - Huidige medicatie. - Relevante voorgeschiedenis. - Bereikbaarheid voor overleg (mail via Zorgdomein/telefonisch)

Samenwerkingsafspraken
Direct insturen tweede lijn of direct overleg • Verwijs met spoed per ambulance: - wanneer de patiënt hemodynamisch instabiel is; - bij instabiele angina pectoris. • Overleg direct met de cardioloog wanneer een jonge
patiënt (< 65 jaar) korter dan 48 uur atriumfibrilleren heeft. Cardioversie is dan vaak succesvol en kan zonder antistolling plaatsvinden.
• Overweeg direct overleg met de cardioloog, om dezelfde reden, bij patiënten > 65 jaar, die korter dan 48 uur atriumfibrilleren hebben met veel klachten.
Wat gebeurd er bij de cardioloog?
• Rust-ECG
• Echocardiogram
• Vaak Holter-ECG, evt fietstest
• Zo nodig elektrische cardioversie
• Instellen op rate versus rhythm control
• VKA versus NOAC
• ACE remmer – upstream therapy
• Follow-up van ingezette behandeling
Wat gebeurd er op de AF-poli (T. Hermans)
• Life-style management • Stoppen met roken • Alcohol en drugs beperken • OSAS score !!! • Hypertensie • Heart failure ?? • Follow-up rhythm/rate control • Indication VKA/NOAC • Etc. etc. etc.

Samenwerkingsafspraken
- Terugverwijzing door cardioloog naar 1ste lijn:
- Substitutieafspraak AF: Patiënten met
stabiel AF
- Substitutieafspraak AF: Patiënten met AF zonder onderliggende pathologie met een behandelplan.
Samenwerkingsafspraken
Praktische afspraken bij terugverwijzen:
Cardioloog
• Besluit dat de patiënt overgedragen kan worden naar de huisarts
• Bespreekt dit met de patiënt en geeft informatiebrief mee en geeft de patiënt het advies om een afspraak te maken met zijn eigen huisarts binnen 3 maanden
• Indien de patiënt akkoord gaat stuurt de cardioloog binnen 2 weken na het laatste polibezoek een brief aan de huisarts (zorgmail). In dit bericht staat minimaal:
– Duidelijke vermelding van terugverwijzing en overdracht van zorg aan huisarts.
– Relevante medische gegevens en behandeling
– Resultaten en doelen van de hartrevalidatie (indien nog relevant)
– Resultaten van de cardiovasculaire risico-inventarisatie (linkerventrikelfunctie, beschrijving eventueel verricht (inspannings-)ECG).
– Actuele medicatie: een overzicht van de medicatie met indien ongebruikelijke indicatie of dosering, vermelding van de indicatie en de gebruiksduur. Eventuele gebleken intoleranties voor medicatie en/of stopreden.
– Een advies met betrekking tot anti-stolling (stop plavix etc.).
– Wensen/doelen van de patiënt om mee verder te gaan bij de huisarts (indien bekend)
– Overige betrokken disciplines (indien bekend)
– Contact gegevens: e-mail/telefoonnummer secretariaat.
• De cardioloog licht de patiënt voor over de overdracht van de verdere behandeling door de huisarts en de afspraken die hierover gemaakt zijn, en sluit daarmee de behandeling (en de DOT) af. De patiënt kan daarna met vragen over de medicatie en voor (herhalings)recepten bij de huisarts terecht.
• Cardiologieconsulten voor terugverwezen patiënten worden gedeclareerd conform 1,5 lijns diagnostiek; er wordt geen DOT geopend. Dit betreft:
– AF: eenmalige echocardiografie, ter diagnostiek, indien patiënt conform de NHG standaard in de eerstelijn kan worden behandeld.
Samenwerkingsafspraken
Praktische afspraken bij terugverwijzen:
Huisarts
• De huisarts meldt aan de POH dat patiënt is terugverwezen en draagt er zorg voor dat patiënt actief in het KIS wordt opgenomen. Op deze manier wordt een eerstelijns DBC CVRM geopend en is de huisarts hoofdbehandelaar.
• POH neemt patiënt op in gestructureerde CVRM spreekuur en verwijst naar/onderhoudt z.n. contact met andere disciplines.
Overweeg opnieuw consultatie van een cardioloog:
• Progressief verloop van klachten
• Klachten die mogelijk kunnen worden opgelost met een medicatie-advies



















