8358289 Acute Gastroenteritis
54
I. INTRODUCTI ON Gastroenteritis is a catchall term for infection or irritation of the digestive tract, particularly the stomach and intestine. It is frequently referred to as the stomach or intestinal flu, although the influenza virus is not associated with this illness. Major symptoms include nausea and vomiting, diarrhea, and abdominal cramps. These symptoms are sometimes also accompanied by fever and overall weakness. Gastroenteri tis typically last s about three days. Adu lts usually recover wit hout problem, but children, the elderly, and anyone with an underlying disease are more vulnerable to complications such as dehydration. (www.wikipedia.com ) Bacterial gastroenteritis is frequently a result of poor sanitation, the lack of safe drinking water, or contaminated food—conditions common in developing nations. Natural or man-made disasters can make underlying problems in sanitation and food safety worse. In developed nations, the modern food production system potentially exposes millions of people to disease-causing bact er ia through its intensive production and distribution methods. Common types of bacterial gastroenteritis can be linked to Salmonella and Campylobacter bacteria; however, Escherichia coli 0157 and Listeria monocytogenes are creating increased concern in developed nations. Cholera and Shigella remain two diseases of great concern in developing countries, and research to de ve lop long-term vaccines against them is underway. ( www.emedicines.com) Gastroenteritis is an uncomfortable and inconvenient ailment, but it is rarely life-threa ten ing in the Uni ted States and other develo ped nations. How ever , an estimated 220,000 children yo unger th an age five are hospitali ze d with gastroenteritis symptoms in the United States annually. Of these children, 300 die as a result of severe diarrhea and dehydration. In developing nations, diarrheal illnesses are a major source of mortality. In 1990, approximately three million deaths occurred worldwide as a result of diarrheal illness.(www.emedicines.com) Loc all y, In Jul y 22, 200 4, the De par tme nt of Hea lth (DOH), Philip pine s dec lare d an epidemic (outbreak) of a water/food-borne disease called acute gastroenteritis in 45 towns in Centr al Pangasinan. Acute gastr oenterit is is a human enteric (inte stinal) dise ase primarily caused by inge stion of s poiled o r bacte rial conta minate d water or food. According to the DOH Secretary, Dr. Manuel Dayrit, a total of 2,778 cases of the said intestinal infection were recorded in just 45 days (from May 31 to July16, 2004). From the studies on the medical diagnoses of 81 cases, Dayrit concluded that infectious (transmittable) cholera disease was the main cause of the epidemic.( www.doh.gov.ph)
-
Upload
earl-montaner-samula -
Category
Documents
-
view
232 -
download
0
Transcript of 8358289 Acute Gastroenteritis
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 1/54
I. INTRODUCTION
Gastroenteritis is a catchall term for infection or irritation of the digestive tract,particularly the stomach and intestine. It is frequently referred to as the stomach orintestinal flu, although the influenza virus is not associated with this illness. Majorsymptoms include nausea and vomiting, diarrhea, and abdominal cramps. Thesesymptoms are sometimes also accompanied by fever and overall weakness.Gastroenteritis typically lasts about three days. Adults usually recover withoutproblem, but children, the elderly, and anyone with an underlying disease are morevulnerable to complications such as dehydration. (www.wikipedia.com)
Bacterial gastroenteritis is frequently a result of poor sanitation, the lack of safe drinking water, or contaminated food—conditions common in developing nations.Natural or man-made disasters can make underlying problems in sanitation and foodsafety worse. In developed nations, the modern food production system potentiallyexposes millions of people to disease-causing bacteria through its intensiveproduction and distribution methods. Common types of bacterial gastroenteritis canbe linked to Salmonella and Campylobacter bacteria; however, Escherichia coli 0157and Listeria monocytogenes are creating increased concern in developed nations.Cholera and Shigella remain two diseases of great concern in developing countries,and research to develop long-term vaccines against them is underway.( www.emedicines.com)
Gastroenteritis is an uncomfortable and inconvenient ailment, but it is rarelylife-threatening in the United States and other developed nations. However, anestimated 220,000 children younger than age five are hospitalized withgastroenteritis symptoms in the United States annually. Of these children, 300 die asa result of severe diarrhea and dehydration. In developing nations, diarrheal illnessesare a major source of mortality. In 1990, approximately three million deaths occurredworldwide as a result of diarrheal illness.(www.emedicines.com)
Locally, In July 22, 2004, the Department of Health (DOH), Philippines declared an
epidemic (outbreak) of a water/food-borne disease called acute gastroenteritis in 45 towns inCentral Pangasinan. Acute gastroenteritis is a human enteric (intestinal) disease primarily caused
by ingestion of spoiled or bacterial contaminated water or food.
According to the DOH Secretary, Dr. Manuel Dayrit, a total of 2,778 cases of the saidintestinal infection were recorded in just 45 days (from May 31 to July16, 2004). From the studies
on the medical diagnoses of 81 cases, Dayrit concluded that infectious (transmittable) cholera
disease was the main cause of the epidemic.(www.doh.gov.ph)

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 2/54
Locally, here in Tagum City, at Davao Regional Hospital pediatric department acute
gastroenteritis was considered number 3 among the most common pediatric cases. It is common in
this area because some of the people are not aware regarding the proper handling and preparationof food.
Gastroenteritis is a general term referring to inflammation or infection of thegastrointestinal tract, primarily the stomach and intestines.[1] It can be caused by infection with
bacteria, viruses, or other parasites, or less commonly reactions to new foods or medications. Itoften involves stomach pain (sometimes to the point of crippling), diarrhea and/or vomiting, with
noninflammatory infection of the upper small bowel, or inflammatory infections of the colon. It
usually is of acute onset, normally lasting fewer than 10 days and self-limiting. Sometimes it isreferred to simply as 'gastro'. It is often called the stomach flu or gastric flu even though it is not
related to influenza. If inflammation is limited to the stomach, the term gastritis is used, and if the
small bowel alone is affected it is enteritis. As such, this has a relationship on the concept fluidsand electrolyte. Because dehydration the most common complication of gastroenteritis if not
treated or no immediate intervention done it could lead to shock and eventually can lead to death.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 3/54
OBJECTIVES
General:
1. To fully understand the underlying disease process of aplastic anemia.
Specific:
1. To identify the epidemiological data of aplastic anemia globally,
nationally and locally.
2. To learn about the major etiologies of aplastic anemia.
3. To determine the previous and present clinical history of the patient.
4. To perform physical assessment with special attention on the systems
focus.
5. To show the laboratory examination results with the corresponding
normal values, actual result from the patient, and it interpretation.
6. To understand the anatomy and physiology of the blood and blood
formation and its pathology during aplastic anemia.
7. To trace and understand the pathophysiology of aplastic anemia.
8. To learn the basic principle of medical management of aplastic
anemia.
9. To use the nursing process to identify nursing problems from the client
and provide the appropriate nursing care plan.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 4/54
10. To understand the pharmacological management set on the client and
provide nursing interventions.
11. To identify the discharge plan for the patient’s rehabilitation to conduct
an evaluation of the client’s condition from admission to present.
II. ASSESSMENT
A. BIOGRAPHIC DATA
Name : Bb. Zoo Sy
Case Number : 185098
Age : 3 months old
Sex : Male
Weight (upon admission) : 43 kgs.
Civil Status : Single
Birthdate : January 8, 2007
Address : Prk. 1 #96 Linoan Montevista, ComVal
Nationality : Filipino
Attending Physician : Dr. Dagooc
B. CHIEF COMPLAINT
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 5/54
Based on the patient’s chart, it appears that seizure, dyspnea,weakness, poor suckling, LBM with watery stool were the chief complaints experience by Bb. Zoo Sy which eventually made her familysought for admission.
C. HISTORY OF PRESENT ILLNESS
One week prior to admission, patient experienced on and off fever,no consultation and medicines given to the patient at home. Until 3 daysprior to admission patient was positive of several episodes of LBM,yellowish to greenish in color, mucoid, non blood streaked and positivefever again no consultation done. Upon admission, the patientexperienced 2 episodes of upward rolling of eyeballs with cycling motionof extremities at the ER. With admitting vital signs of BP- 70/50 mmHg,CR- 140bpm, RR- 58cpm, Temp- 36.4˚C, with pulse oxymeter reading of 96% O2 saturation.
D. PAST MEDICAL HISTORY
E. PERSONAL, FAMILY AND SOCIO-ECONOMIC
Bb. Zoo Sy was born January 8, 2007. He was the youngest of the4 children in the family. Two weeks prior to admission Bb. Zoo Sytogether with his siblings were left by their mother. While his father wasa hardworking businessman who was then at GenSan. The income of hisfather is just enough to support their basic needs.
III. REVIEW OF SYSTEMS (PHYSICAL ASSESSMENT)
A. GENERAL SURVEY
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 6/54
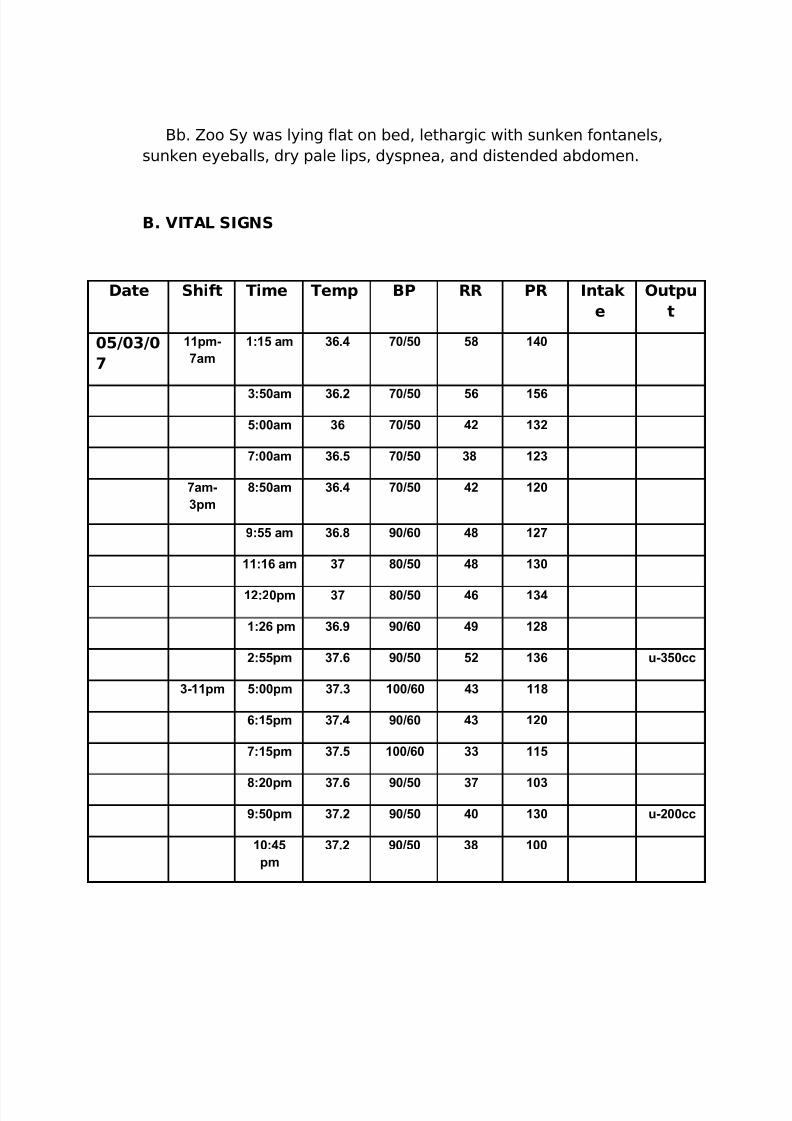
Bb. Zoo Sy was lying flat on bed, lethargic with sunken fontanels,sunken eyeballs, dry pale lips, dyspnea, and distended abdomen.
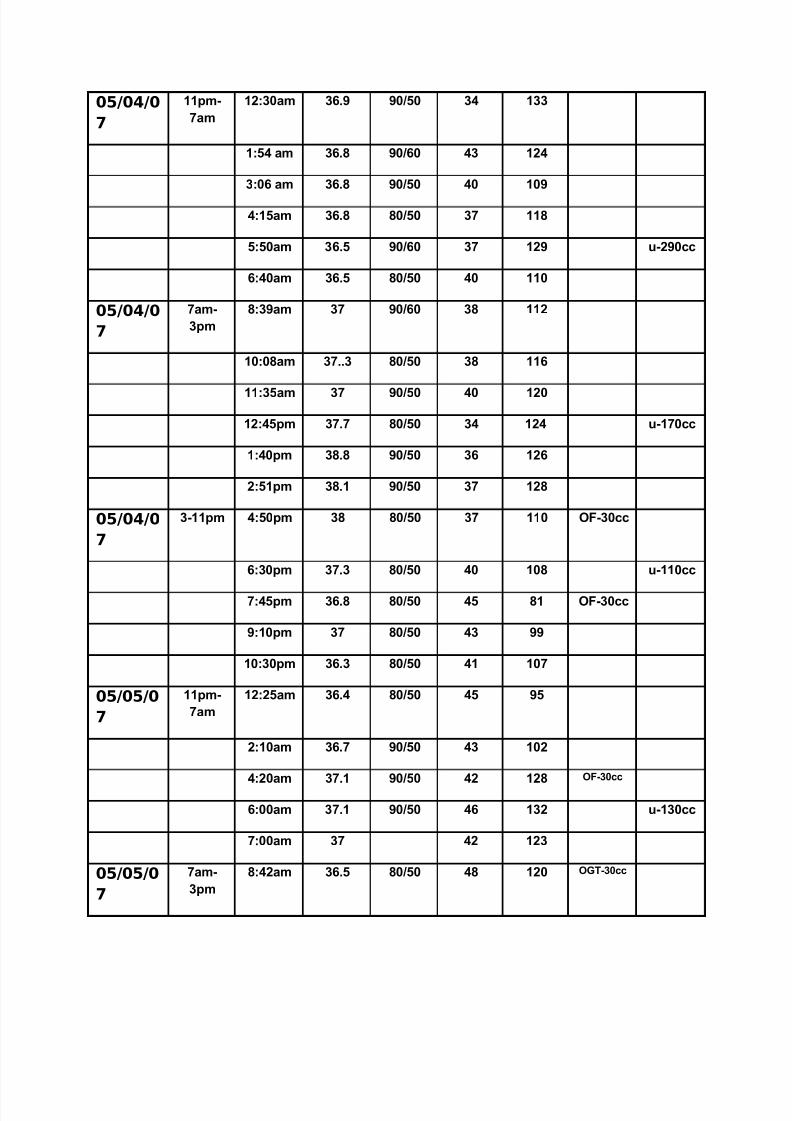
B. VITAL SIGNS
Date Shift Time Temp BP RR PR Intak
e
Outpu
t
05/03/0
7
11pm-
7am
1:15 am 36.4 70/50 58 140
3:50am 36.2 70/50 56 156
5:00am 36 70/50 42 132
7:00am 36.5 70/50 38 123
7am-
3pm
8:50am 36.4 70/50 42 120
9:55 am 36.8 90/60 48 127
11:16 am 37 80/50 48 130
12:20pm 37 80/50 46 134
1:26 pm 36.9 90/60 49 128
2:55pm 37.6 90/50 52 136 u-350cc
3-11pm 5:00pm 37.3 100/60 43 118
6:15pm 37.4 90/60 43 120
7:15pm 37.5 100/60 33 115
8:20pm 37.6 90/50 37 103
9:50pm 37.2 90/50 40 130 u-200cc
10:45
pm
37.2 90/50 38 100
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 7/54
05/04/0
7
11pm-
7am
12:30am 36.9 90/50 34 133
1:54 am 36.8 90/60 43 124
3:06 am 36.8 90/50 40 109
4:15am 36.8 80/50 37 118
5:50am 36.5 90/60 37 129 u-290cc
6:40am 36.5 80/50 40 110
05/04/0
7
7am-
3pm
8:39am 37 90/60 38 112
10:08am 37..3 80/50 38 116
11:35am 37 90/50 40 120
12:45pm 37.7 80/50 34 124 u-170cc
1:40pm 38.8 90/50 36 126
2:51pm 38.1 90/50 37 128
05/04/0
7
3-11pm 4:50pm 38 80/50 37 110 OF-30cc
6:30pm 37.3 80/50 40 108 u-110cc
7:45pm 36.8 80/50 45 81 OF-30cc
9:10pm 37 80/50 43 99
10:30pm 36.3 80/50 41 107
05/05/0
7
11pm-
7am
12:25am 36.4 80/50 45 95
2:10am 36.7 90/50 43 102
4:20am 37.1 90/50 42 128 OF-30cc
6:00am 37.1 90/50 46 132 u-130cc
7:00am 37 42 123
05/05/0
7
7am-
3pm
8:42am 36.5 80/50 48 120 OGT-30cc
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 8/54
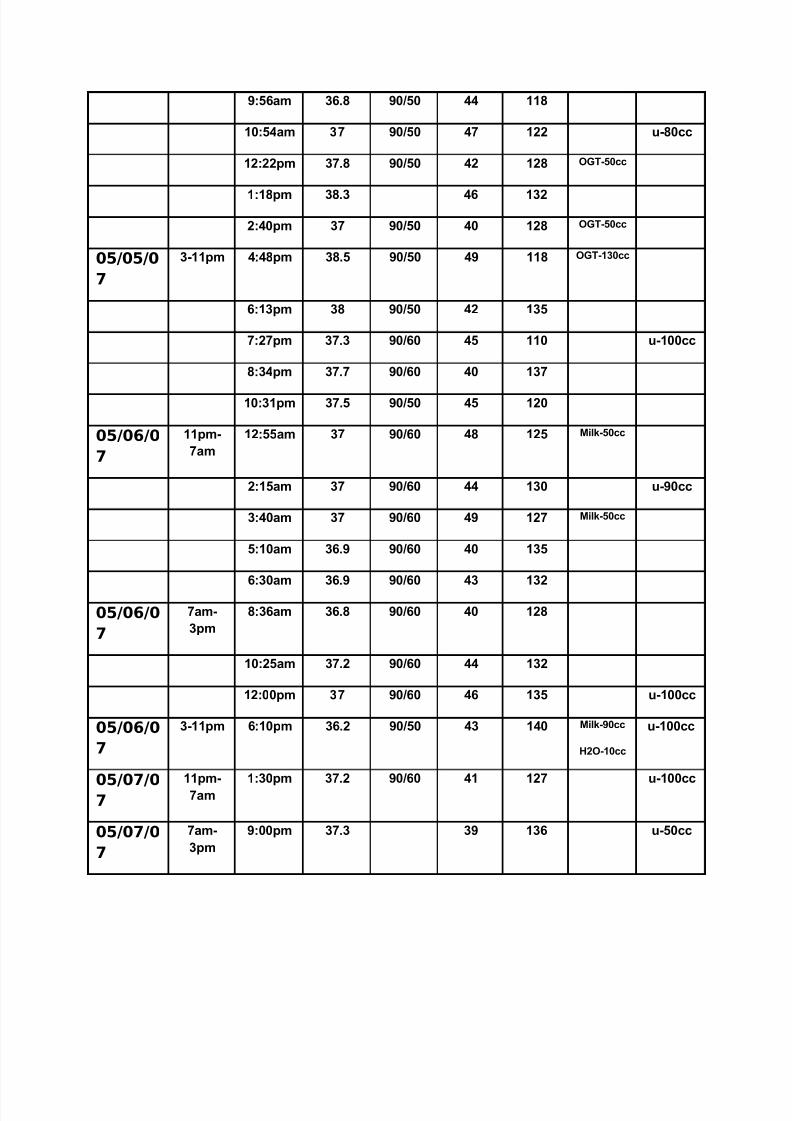
9:56am 36.8 90/50 44 118
10:54am 37 90/50 47 122 u-80cc
12:22pm 37.8 90/50 42 128 OGT-50cc
1:18pm 38.3 46 132
2:40pm 37 90/50 40 128 OGT-50cc
05/05/0
7
3-11pm 4:48pm 38.5 90/50 49 118 OGT-130cc
6:13pm 38 90/50 42 135
7:27pm 37.3 90/60 45 110 u-100cc
8:34pm 37.7 90/60 40 137
10:31pm 37.5 90/50 45 120
05/06/0
7
11pm-
7am
12:55am 37 90/60 48 125 Milk-50cc
2:15am 37 90/60 44 130 u-90cc
3:40am 37 90/60 49 127 Milk-50cc
5:10am 36.9 90/60 40 135
6:30am 36.9 90/60 43 132
05/06/0
7
7am-
3pm
8:36am 36.8 90/60 40 128
10:25am 37.2 90/60 44 132
12:00pm 37 90/60 46 135 u-100cc
05/06/0
7
3-11pm 6:10pm 36.2 90/50 43 140 Milk-90cc
H2O-10cc
u-100cc
05/07/07
11pm-
7am
1:30pm 37.2 90/60 41 127 u-100cc
05/07/0
7
7am-
3pm
9:00pm 37.3 39 136 u-50cc
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 9/54
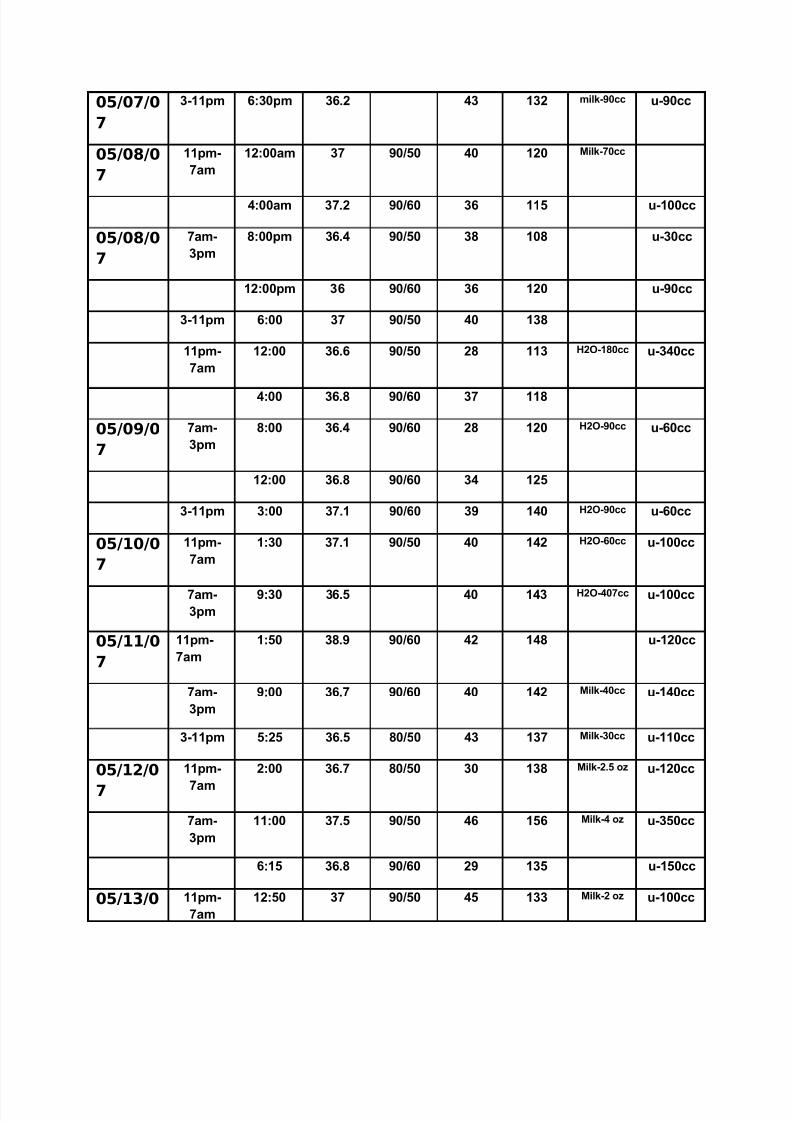
05/07/0
7
3-11pm 6:30pm 36.2 43 132 milk-90cc u-90cc
05/08/0
7
11pm-
7am
12:00am 37 90/50 40 120 Milk-70cc
4:00am 37.2 90/60 36 115 u-100cc
05/08/0
7
7am-
3pm
8:00pm 36.4 90/50 38 108 u-30cc
12:00pm 36 90/60 36 120 u-90cc
3-11pm 6:00 37 90/50 40 138
11pm-
7am
12:00 36.6 90/50 28 113 H2O-180cc u-340cc
4:00 36.8 90/60 37 118
05/09/0
7
7am-
3pm
8:00 36.4 90/60 28 120 H2O-90cc u-60cc
12:00 36.8 90/60 34 125
3-11pm 3:00 37.1 90/60 39 140 H2O-90cc u-60cc
05/10/0
7
11pm-
7am
1:30 37.1 90/50 40 142 H2O-60cc u-100cc
7am-
3pm
9:30 36.5 40 143 H2O-407cc u-100cc
05/11/0
7
11pm-
7am
1:50 38.9 90/60 42 148 u-120cc
7am-
3pm
9:00 36.7 90/60 40 142 Milk-40cc u-140cc
3-11pm 5:25 36.5 80/50 43 137 Milk-30cc u-110cc
05/12/0
7
11pm-
7am
2:00 36.7 80/50 30 138 Milk-2.5 oz u-120cc
7am-
3pm
11:00 37.5 90/50 46 156 Milk-4 oz u-350cc
6:15 36.8 90/60 29 135 u-150cc
05/13/0 11pm-
7am
12:50 37 90/50 45 133 Milk-2 oz u-100cc
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 10/54
7
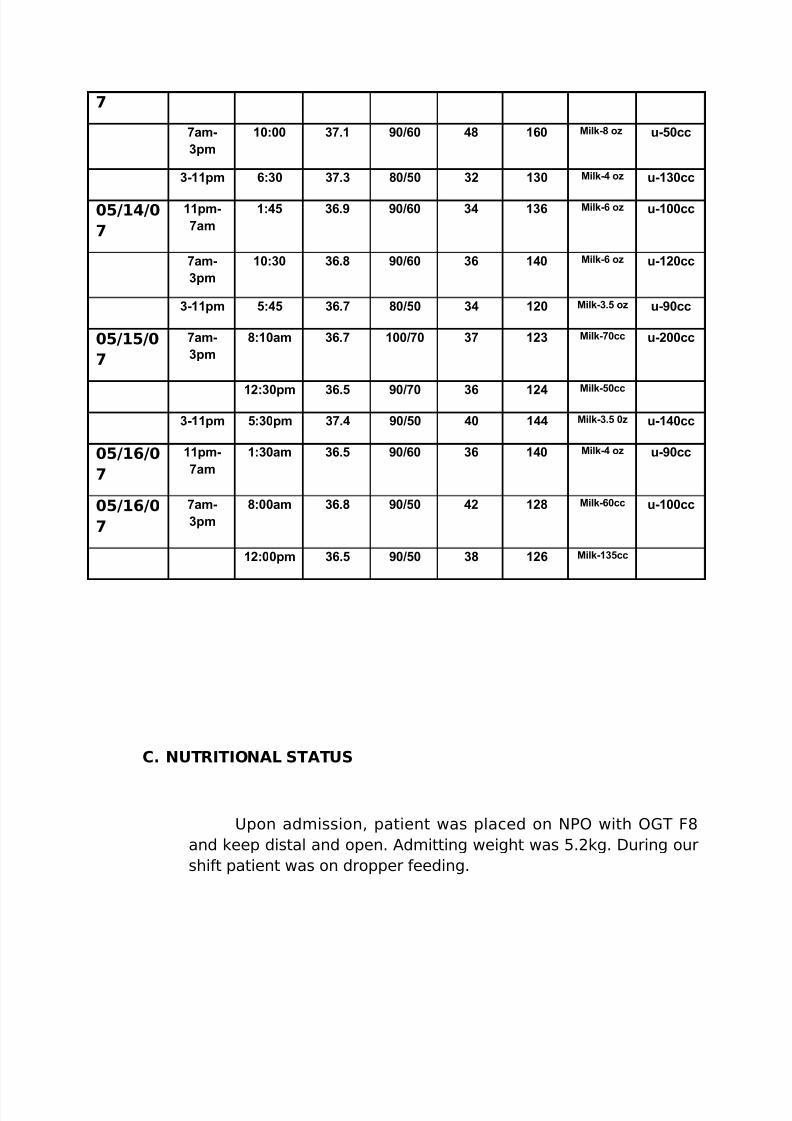
7am-
3pm
10:00 37.1 90/60 48 160 Milk-8 oz u-50cc
3-11pm 6:30 37.3 80/50 32 130 Milk-4 oz u-130cc
05/14/0
7
11pm-
7am
1:45 36.9 90/60 34 136 Milk-6 oz u-100cc
7am-
3pm
10:30 36.8 90/60 36 140 Milk-6 oz u-120cc
3-11pm 5:45 36.7 80/50 34 120 Milk-3.5 oz u-90cc
05/15/0
7
7am-
3pm
8:10am 36.7 100/70 37 123 Milk-70cc u-200cc
12:30pm 36.5 90/70 36 124 Milk-50cc
3-11pm 5:30pm 37.4 90/50 40 144 Milk-3.5 0z u-140cc
05/16/0
7
11pm-
7am
1:30am 36.5 90/60 36 140 Milk-4 oz u-90cc
05/16/0
7
7am-
3pm
8:00am 36.8 90/50 42 128 Milk-60cc u-100cc
12:00pm 36.5 90/50 38 126 Milk-135cc
C. NUTRITIONAL STATUS
Upon admission, patient was placed on NPO with OGT F8and keep distal and open. Admitting weight was 5.2kg. During ourshift patient was on dropper feeding.

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 11/54
D. NEUROLOGIC STATUS
Patient was lethargic as observed by NOD.
E. INTEGUMENTARY SYSTEM
Fine and evenly distributed, thin and dry hair was noted. Hisnails were in convex shape, smooth in texture , capillary refill of five seconds an untrimmed finger nails with poor skin turgor. Hisskin was pale, dry, with fine and fare complexion
F. HEENT
The size of head was in proportion with the body. The eyeswere symmetrical with the ears; with sunken fontanels and eyes.When the eyes were tested papillary reaction to light, the pupilconstricted to 2mm. Ear had no discharges noted. Nasal septum
were intact and in the midline. Patient had cleft lip. The throat wasfunctioning well and in normal condition.
G. PULMONARY SYSTEM
Respiratory rate was 58 cpm and dyspnic. Upon
auscultation, crackles were heard and with symmetrical chestexpansion. With history of Pneumonia.
H. CARDIOVASCULAR SYSTEM
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 12/54
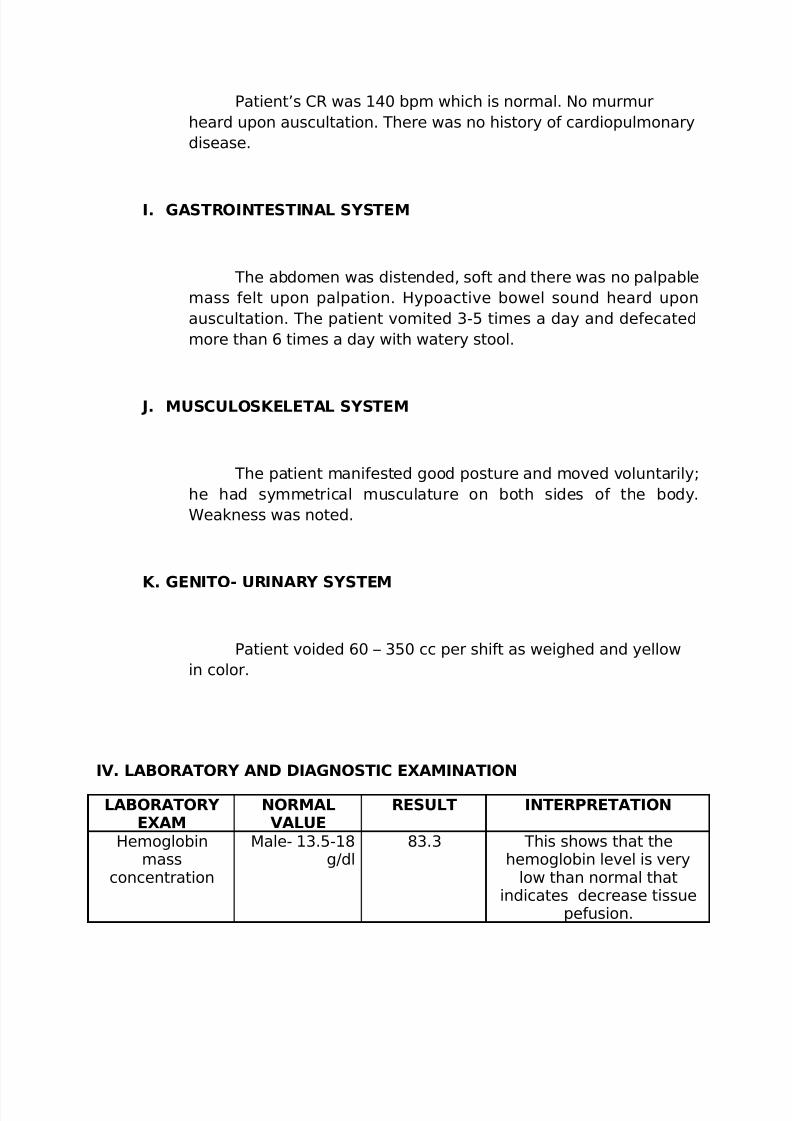
Patient’s CR was 140 bpm which is normal. No murmurheard upon auscultation. There was no history of cardiopulmonarydisease.
I. GASTROINTESTINAL SYSTEM
The abdomen was distended, soft and there was no palpablemass felt upon palpation. Hypoactive bowel sound heard uponauscultation. The patient vomited 3-5 times a day and defecatedmore than 6 times a day with watery stool.
J. MUSCULOSKELETAL SYSTEM
The patient manifested good posture and moved voluntarily;he had symmetrical musculature on both sides of the body.Weakness was noted.
K. GENITO- URINARY SYSTEM
Patient voided 60 – 350 cc per shift as weighed and yellowin color.
IV. LABORATORY AND DIAGNOSTIC EXAMINATION
LABORATORY EXAM
NORMALVALUE
RESULT INTERPRETATION
Hemoglobinmass
concentration
Male- 13.5-18g/dl
83.3 This shows that thehemoglobin level is very
low than normal thatindicates decrease tissue
pefusion.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 13/54
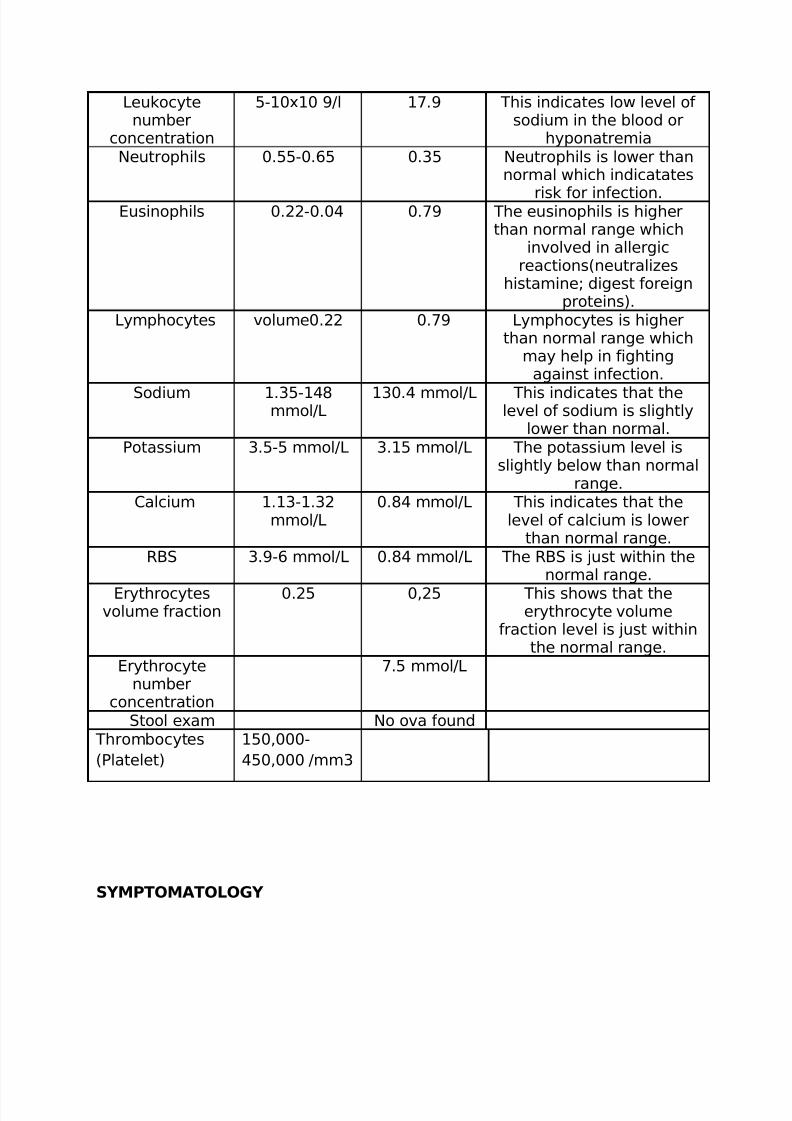
Leukocytenumber
concentration
5-10x10 9/l 17.9 This indicates low level of sodium in the blood or
hyponatremiaNeutrophils 0.55-0.65 0.35 Neutrophils is lower than
normal which indicatates
risk for infection.Eusinophils 0.22-0.04 0.79 The eusinophils is higherthan normal range which
involved in allergicreactions(neutralizes
histamine; digest foreignproteins).
Lymphocytes volume0.22 0.79 Lymphocytes is higherthan normal range which
may help in fightingagainst infection.
Sodium 1.35-148mmol/L
130.4 mmol/L This indicates that thelevel of sodium is slightly
lower than normal.Potassium 3.5-5 mmol/L 3.15 mmol/L The potassium level is
slightly below than normalrange.
Calcium 1.13-1.32mmol/L
0.84 mmol/L This indicates that thelevel of calcium is lower
than normal range.RBS 3.9-6 mmol/L 0.84 mmol/L The RBS is just within the
normal range.
Erythrocytesvolume fraction
0.25 0,25 This shows that theerythrocyte volume
fraction level is just withinthe normal range.
Erythrocytenumber
concentration
7.5 mmol/L
Stool exam No ova found Thrombocytes(Platelet)
150,000-450,000 /mm3
SYMPTOMATOLOGY
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 14/54
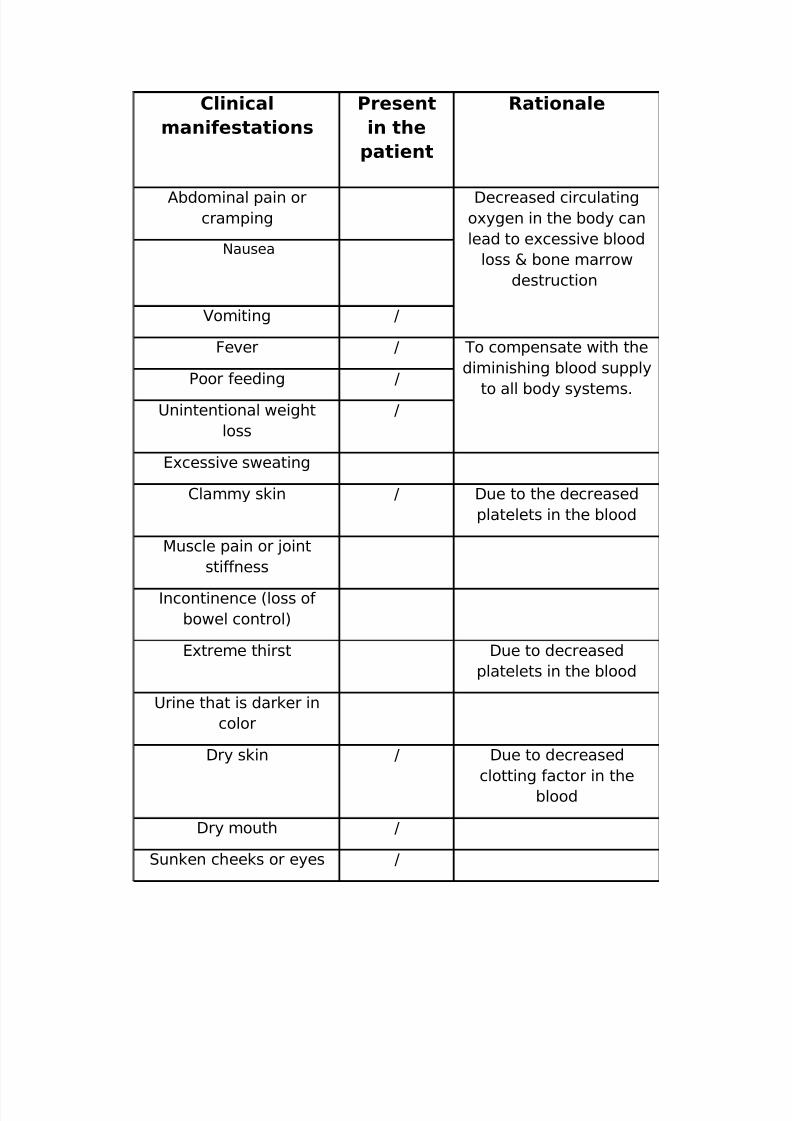
Clinical
manifestations
Present
in the
patient
Rationale
Abdominal pain orcramping
Decreased circulatingoxygen in the body canlead to excessive blood
loss & bone marrowdestruction
Nausea
Vomiting /
Fever / To compensate with thediminishing blood supply
to all body systems.
Poor feeding /
Unintentional weightloss
/
Excessive sweating
Clammy skin / Due to the decreasedplatelets in the blood
Muscle pain or jointstiffness
Incontinence (loss of bowel control)
Extreme thirst Due to decreasedplatelets in the blood
Urine that is darker incolor
Dry skin / Due to decreasedclotting factor in the
blood
Dry mouth /
Sunken cheeks or eyes /

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 15/54
In infants, dry diapers(for more than 4-6 hrs)
V. ANATOMY AND PHYSIOLOGY
Anatomy of the Digestive System
If a human adult’s digestive tract were stretched out, it would be 6 to 9 m (20
to 30 ft) long. In humans, digestion begins in the mouth, where both mechanical and
chemical digestion occur. The mouth quickly converts food into a soft, moist mass.

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 16/54
The muscular tongue pushes the food against the teeth, which cut, chop, and grind
the food. Glands in the cheek linings secrete mucus, which lubricates the food,
making it easier to chew and swallow. Three pairs of glands empty saliva into the
mouth through ducts to moisten the food. Saliva contains the enzyme ptyalin, which
begins to hydrolyze (break down) starch—a carbohydrate manufactured by green
plants.
Once food has been reduced to a soft mass, it is ready to be swallowed. The
tongue pushes this mass—called a bolus—to the back of the mouth and into the
pharynx. This cavity between the mouth and windpipe serves as a passageway both
for food on its way down the alimentary canal and for air passing into the windpipe.
The epiglottis, a flap of cartilage, covers the trachea (windpipe) when a person
swallows. This action of the epiglottis prevents choking by directing food from thewindpipe and toward the stomach.
Mouth
The mouth plays a role in digestion, speech, and breathing. Digestion begins
when food enters the mouth. Teeth break down food and the muscular tongue pushes
food back toward the pharynx, or throat. Three salivary glands—the sublingual gland,
the submandibular gland, and the parotid gland—secrete enzymes that partially
digest food into a soft, moist, round lump. Muscles in the pharynx swallow the food,
pushing it into the esophagus, a muscular tube that passes food into the stomach.
The epiglottis prevents food from entering the trachea, or windpipe, during
swallowing.
Esophagus
The presence of food in the pharynx stimulates swallowing, which squeezes the
food into the esophagus. The esophagus, a muscular tube about 25 cm (10 in) long,
passes behind the trachea and heart and penetrates the diaphragm (muscular wall
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 17/54
between the chest and abdomen) before reaching the stomach. Food advances
through the alimentary canal by means of rhythmic muscle contractions (tightenings)
known as peristalsis. The process begins when circular muscles in the esophagus wall
contract and relax (widen) one after the other, squeezing food downward toward the
stomach. Food travels the length of the esophagus in two to three seconds.
A circular muscle called the esophageal sphincter separates the esophagus
and the stomach. As food is swallowed, this muscle relaxes, forming an opening
through which the food can pass into the stomach. Then the muscle contracts, closing
the opening to prevent food from moving back into the esophagus. The esophageal
sphincter is the first of several such muscles along the alimentary canal. These
muscles act as valves to regulate the passage of food and keep it from moving
backward.
Stomach
The stomach, located in the upper abdomen just below the diaphragm, is a
saclike structure with strong, muscular walls. The stomach can expand significantly to
store all the food from a meal for both mechanical and chemical processing. The
stomach contracts about three times per minute, churning the food and mixing it with
gastric juice. This fluid, secreted by thousands of gastric glands in the lining of the
stomach, consists of water, hydrochloric acid, an enzyme called pepsin, and mucin
(the main component of mucus). Hydrochloric acid creates the acidic environment
that pepsin needs to begin breaking down proteins. It also kills microorganisms that
may have been ingested in the food. Mucin coats the stomach, protecting it from the
effects of the acid and pepsin. About four hours or less after a meal, food processed
by the stomach, called chyme, begins passing a little at a time through the pyloric
sphincter into the duodenum, the first portion of the small intestine.
Liver
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 18/54
The liver is the largest internal organ in the human body, located at the top of
the abdomen on the right side of the body. A dark red organ with a spongy texture,
the liver is divided into right and left lobes by the falciform ligament. The liver
performs more than 500 functions, including the production of a digestive liquid
called bile that plays a role in the breakdown of fats in food. Bile from the liver passes
through the hepatic duct into the gallbladder, where it is stored. During digestion bile
passes from the gallbladder through bile ducts to the small intestine, where it breaks
down fatty food so that it can be absorbed into the body. Nutrient-rich blood passes
from the small intestine to the liver, where nutrients are further processed and
stored. Deoxygenated blood leaves the liver via the hepatic vein to return to the
heart.
Small Intestine
Most digestion, as well as absorption of digested food, occurs in the small
intestine. This narrow, twisting tube, about 2.5 cm (1 in) in diameter, fills most of the
lower abdomen, extending about 6 m (20 ft) in length. Over a period of three to six
hours, peristalsis moves chyme through the duodenum into the next portion of the
small intestine, the jejunum, and finally into the ileum, the last section of the smallintestine. During this time, the liver secretes bile into the small intestine through the
bile duct. Bile breaks large fat globules into small droplets, which enzymes in the
small intestine can act upon. Pancreatic juice, secreted by the pancreas, enters the
small intestine through the pancreatic duct. Pancreatic juice contains enzymes that
break down sugars and starches into simple sugars, fats into fatty acids and glycerol,
and proteins into amino acids. Glands in the intestinal walls secrete additional
enzymes that break down starches and complex sugars into nutrients that the
intestine absorbs. Structures called Brunner’s glands secrete mucus to protect theintestinal walls from the acid effects of digestive juices.
The small intestine’s capacity for absorption is increased by millions of
fingerlike projections called villi, which line the inner walls of the small intestine. Each
villus is about 0.5 to 1.5 mm (0.02 to 0.06 in) long and covered with a single layer of
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 19/54
cells. Even tinier fingerlike projections called microvilli cover the cell surfaces. This
combination of villi and microvilli increases the surface area of the small intestine’s
lining by about 150 times, multiplying its capacity for absorption. Beneath the villi’s
single layer of cells are capillaries (tiny vessels) of the bloodstream and the lymphatic
system. These capillaries allow nutrients produced by digestion to travel to the cells
of the body. Simple sugars and amino acids pass through the capillaries to enter the
bloodstream. Fatty acids and glycerol pass through to the lymphatic system.
Large Intestine
A watery residue of indigestible food and digestive juices remains unabsorbed.
This residue leaves the ileum of the small intestine and moves by peristalsis into thelarge intestine, where it spends 12 to 24 hours. The large intestine forms an inverted
U over the coils of the small intestine. It starts on the lower right-hand side of the
body and ends on the lower left-hand side. The large intestine is 1.5 to 1.8 m (5 to 6
ft) long and about 6 cm (2.5 in) in diameter.
The large intestine serves several important functions. It absorbs water—about
6 liters (1.6 gallons) daily—as well as dissolved salts from the residue passed on by
the small intestine. In addition, bacteria in the large intestine promote the breakdown
of undigested materials and make several vitamins, notably vitamin K, which the
body needs for blood clotting. The large intestine moves its remaining contents
toward the rectum, which makes up the final 15 to 20 cm (6 to 8 in) of the alimentary
canal. The rectum stores the feces—waste material that consists largely of
undigested food, digestive juices, bacteria, and mucus—until elimination. Then,
muscle contractions in the walls of the rectum push the feces toward the anus. When
sphincters between the rectum and anus relax, the feces pass out of the bod

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 20/54
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 21/54
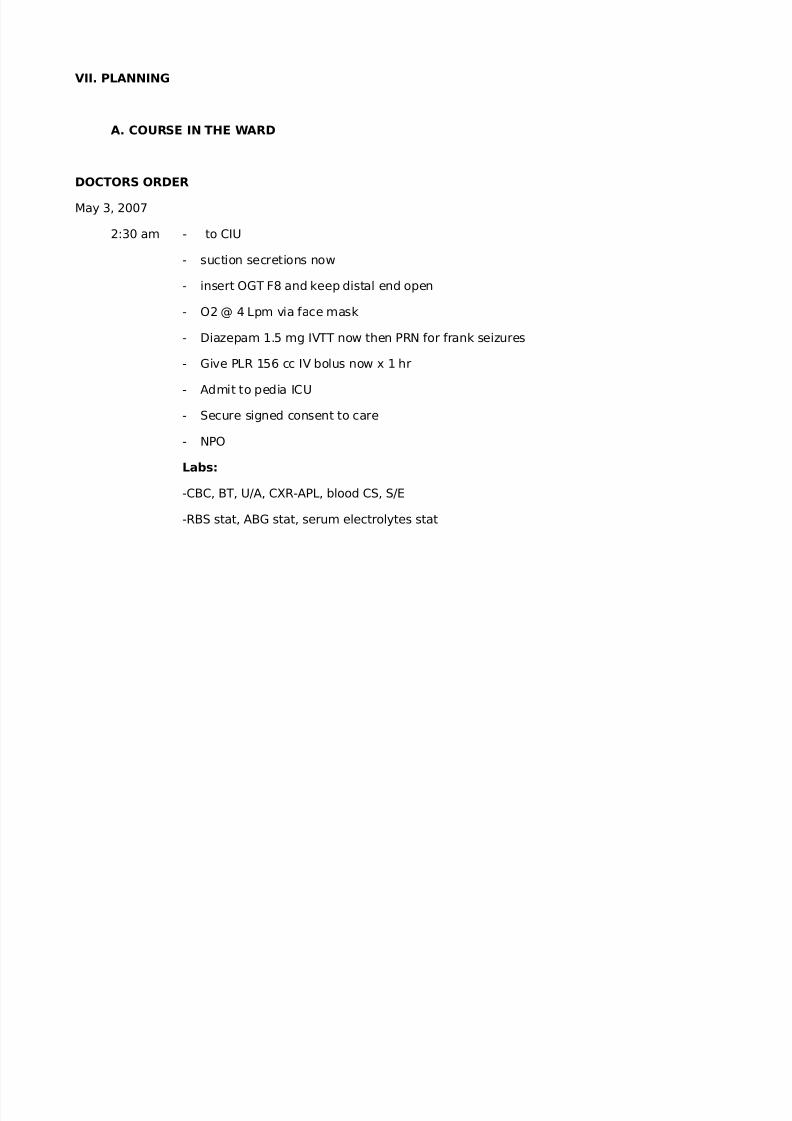
VII. PLANNING
A. COURSE IN THE WARD
DOCTORS ORDER
May 3, 2007
2:30 am - to CIU
- suction secretions now
- insert OGT F8 and keep distal end open
- O2 @ 4 Lpm via face mask
- Diazepam 1.5 mg IVTT now then PRN for frank seizures
- Give PLR 156 cc IV bolus now x 1 hr
- Admit to pedia ICU
- Secure signed consent to care
- NPO
Labs:
-CBC, BT, U/A, CXR-APL, blood CS, S/E
-RBS stat, ABG stat, serum electrolytes stat
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 22/54
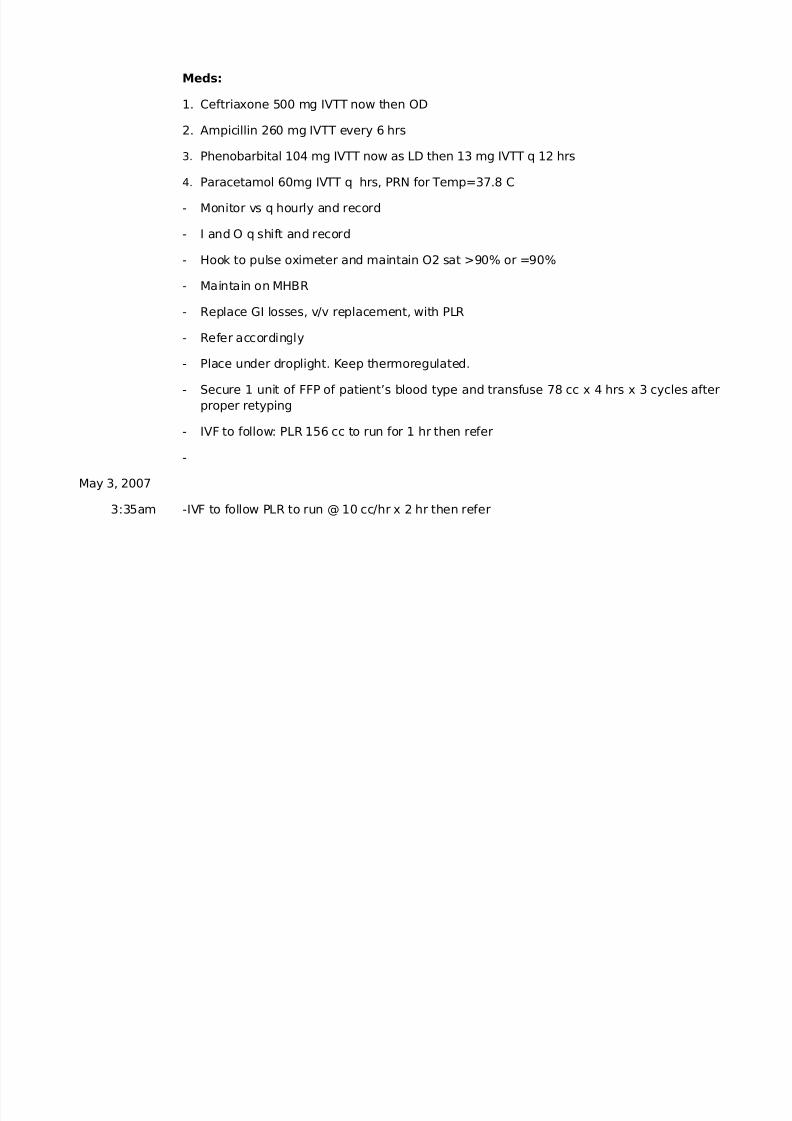
Meds:
1. Ceftriaxone 500 mg IVTT now then OD
2. Ampicillin 260 mg IVTT every 6 hrs
3. Phenobarbital 104 mg IVTT now as LD then 13 mg IVTT q 12 hrs
4. Paracetamol 60mg IVTT q hrs, PRN for Temp=37.8 C
- Monitor vs q hourly and record
- I and O q shift and record
- Hook to pulse oximeter and maintain O2 sat >90% or =90%
- Maintain on MHBR
- Replace GI losses, v/v replacement, with PLR
- Refer accordingly
- Place under droplight. Keep thermoregulated.
- Secure 1 unit of FFP of patient’s blood type and transfuse 78 cc x 4 hrs x 3 cycles afterproper retyping
- IVF to follow: PLR 156 cc to run for 1 hr then refer
-
May 3, 2007
3:35am -IVF to follow PLR to run @ 10 cc/hr x 2 hr then refer
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 23/54
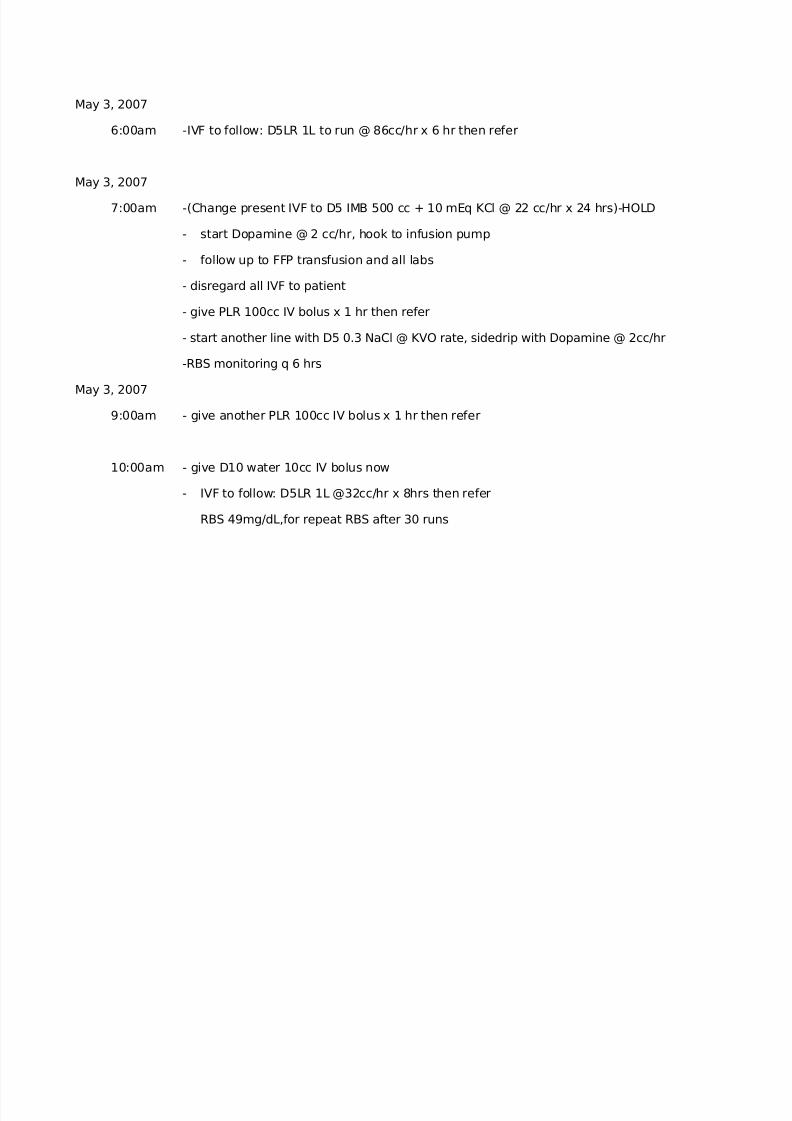
May 3, 2007
6:00am -IVF to follow: D5LR 1L to run @ 86cc/hr x 6 hr then refer
May 3, 2007
7:00am -(Change present IVF to D5 IMB 500 cc + 10 mEq KCl @ 22 cc/hr x 24 hrs)-HOLD
- start Dopamine @ 2 cc/hr, hook to infusion pump
- follow up to FFP transfusion and all labs
- disregard all IVF to patient
- give PLR 100cc IV bolus x 1 hr then refer
- start another line with D5 0.3 NaCl @ KVO rate, sidedrip with Dopamine @ 2cc/hr
-RBS monitoring q 6 hrs
May 3, 2007
9:00am - give another PLR 100cc IV bolus x 1 hr then refer
10:00am - give D10 water 10cc IV bolus now
- IVF to follow: D5LR 1L @32cc/hr x 8hrs then refer
RBS 49mg/dL,for repeat RBS after 30 runs
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 24/54
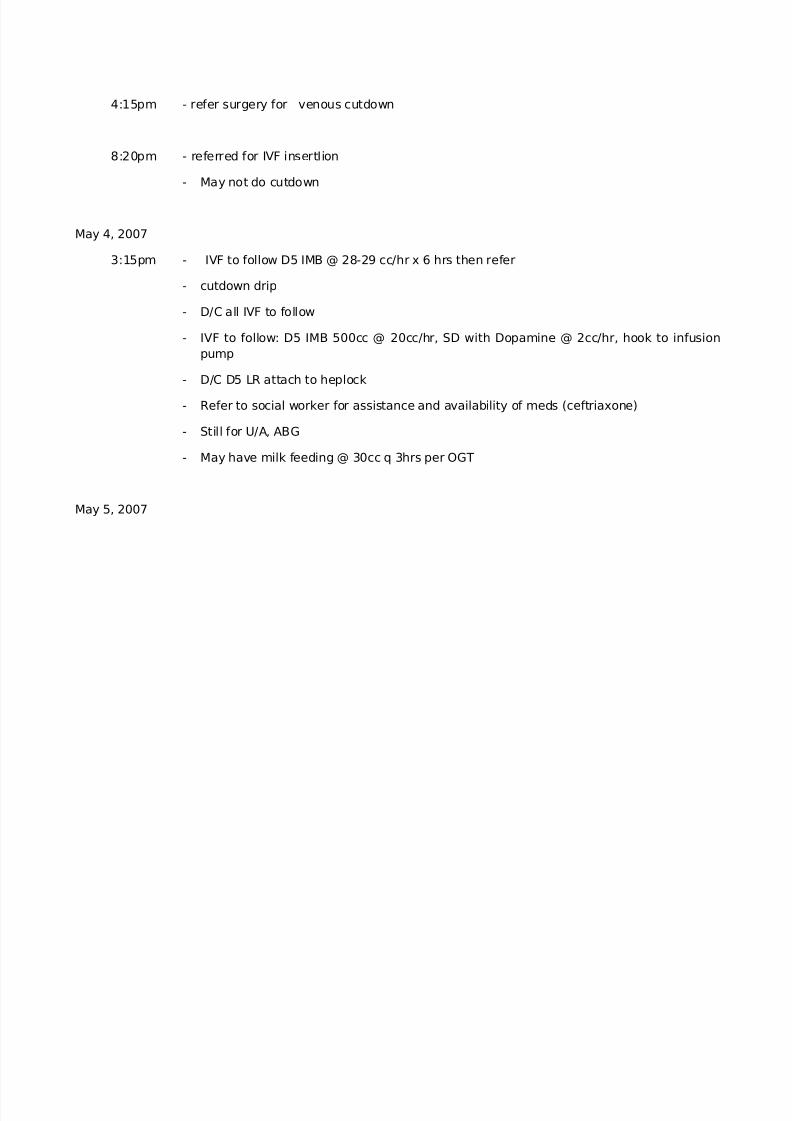
4:15pm - refer surgery for venous cutdown
8:20pm - referred for IVF insertIion
- May not do cutdown
May 4, 2007
3:15pm - IVF to follow D5 IMB @ 28-29 cc/hr x 6 hrs then refer
- cutdown drip
- D/C all IVF to follow
- IVF to follow: D5 IMB 500cc @ 20cc/hr, SD with Dopamine @ 2cc/hr, hook to infusionpump
- D/C D5 LR attach to heplock
- Refer to social worker for assistance and availability of meds (ceftriaxone)
- Still for U/A, ABG
- May have milk feeding @ 30cc q 3hrs per OGT
May 5, 2007

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 25/54
11:30 am - IVF to ff : D5 IMB 500 cc @ 3 cc/hr x 24 hours (50 kcal)
- increase milk feeding @ 50 cc @ 3 hours
- continue meds
- decrease 02 to 2 LPM via nasal cannula
9:40 pm - may have dropper feeding @ 50 cc every 3 hrs with SAP
May 6, 2007
7:45 am - Transferred patient to GW-Gastro
- VS monitoring q 4 hours and meds
- D/C 02 inhalation
- IVF to ff D5IMB 500 cc to run @ 5 cc/hr x 24
- Still for U/A and fecalysis
- D/C dopamine drip
May 7, 2007
8:30 am - C/D IVF and attach to heplock
- continue meds

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 26/54
May 8, 2007
9:30 am - continue meds
- increase dropper feeding + 70 cc/hr with SAP (71 kcal)
- Pls. ff up cranial CT scan, U/A, blood CS, fecalysis., serum electrolyte
- For repeat CBC plt. Today
May 9, 2007
10:40 am - for LP today
- Pls. secure consent for LP
- Ff up cranial CT scan
- Continue meds
- Shift Phenobarbital IV to PO Phenobarbital 6 g/tab. Dissolve 1 Tab into 5 cc give it toBID
May 10, 2007
9:30 am - Silver sulfadiazine cream apply to affected area TID
- Still for LP

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 27/54
- Continue meds
May 11, 2007
9:55 am - for LP today
- NPO x 4 hrs starting 12 pm
- Pls. give Diazepam 1.5 g IVTT prior to LP
- Continue meds
May 12, 2007
6:45 am - Post LP order
- NPO x 4 hrs
- Feed on bed x 4 hrs
- For RBS stat
- Refer for cyanosis, apnea, dyspnea and other S/S
- Refer accordingly
May 13, 2007
9:30 am - Transfer to neuroservice under Dr. Gazmen/Golingay
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 28/54
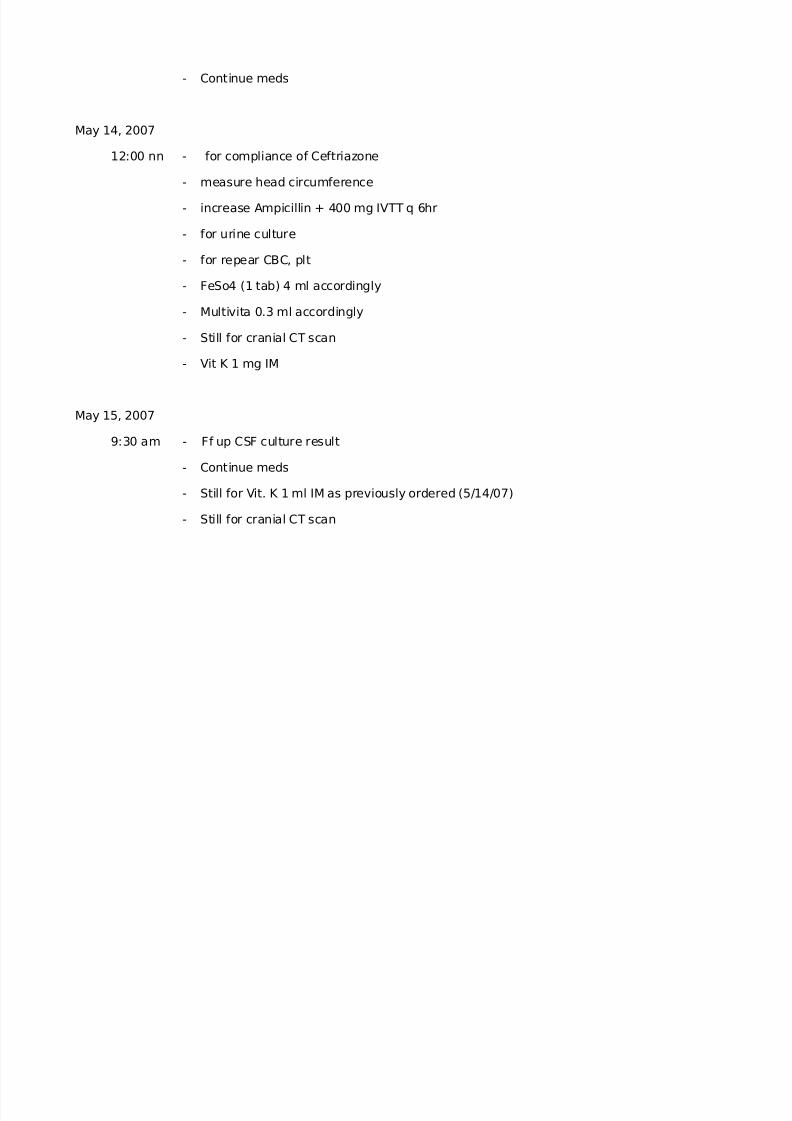
- Continue meds
May 14, 2007
12:00 nn - for compliance of Ceftriazone
- measure head circumference
- increase Ampicillin + 400 mg IVTT q 6hr
- for urine culture
- for repear CBC, plt
- FeSo4 (1 tab) 4 ml accordingly
- Multivita 0.3 ml accordingly
- Still for cranial CT scan
- Vit K 1 mg IM
May 15, 2007
9:30 am - Ff up CSF culture result
- Continue meds
- Still for Vit. K 1 ml IM as previously ordered (5/14/07)
- Still for cranial CT scan

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 29/54
- Measure head circumference pls and chart
- Still for repeat CBC, plt, pls facilitate
May 16, 2007
7:00 am - Continue meds
- for cranial ultrasound pls give request
- facilitate repeat CBC plt
- Transfer to MR
NURSES’ NOTES
May 3,2007
11pm-7am 1:15am>Admitted this 3 months old, male child, lethargic, afebrile, dyspneic in due todifficulty in breathing. Vital signs checked. Seen and examined by Dr. Dagooc with ordersmade. Lab exams requested. IVF of PLR IL @ 156 cc as IV bolus. OGT inserted. O2
inhalation @ 4 Lpm per face mask. Suctioning of secretions done. For CXR-ADL. Ushered toward per wheelchair. Endorsed to NOD.
2:50am>In from ER per wheelchair, stupurous. On NPO with Ogt distal end to bedsidebottle. With an IVF of PLR, with ongoing infusion of 156ccx1hr. with O2 inhalation on @4Lpm via face mask. Ushered to room. Placed on bed comfortably. O2 inhalationcontinued. vs checked and recorded. Lab exams and medicines prescribed followed up.Watched for.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 30/54
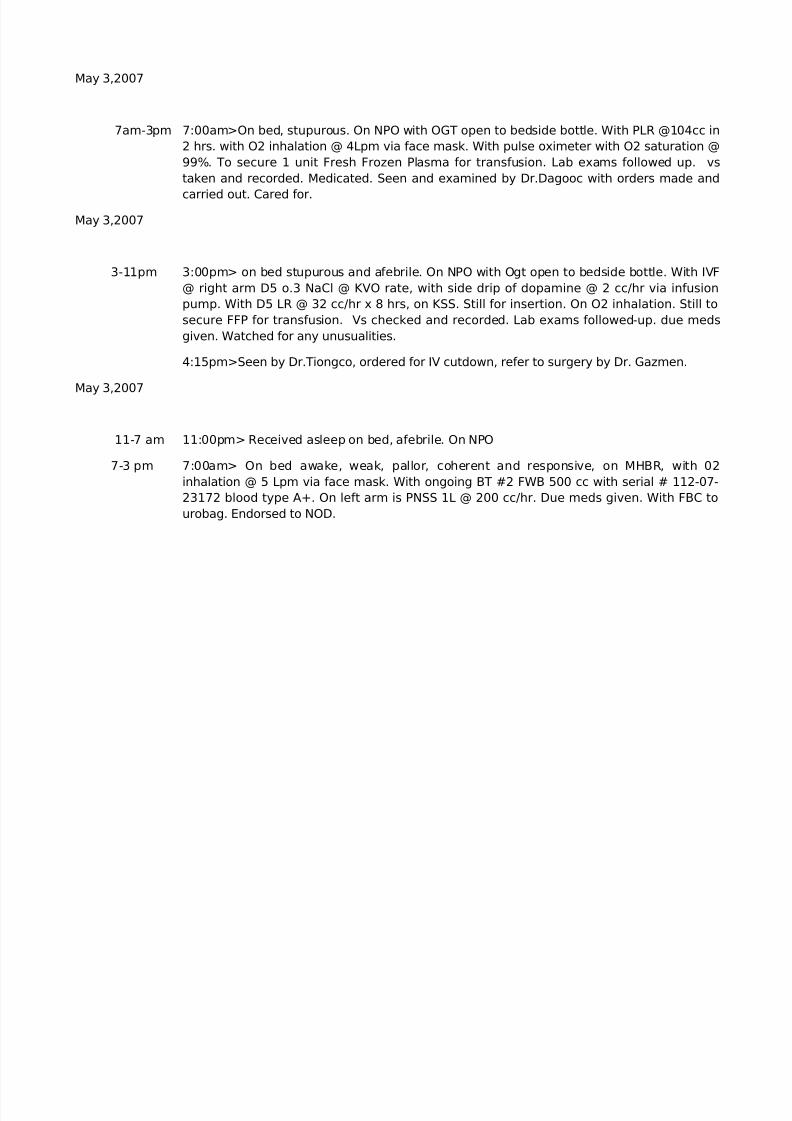
May 3,2007
7am-3pm 7:00am>On bed, stupurous. On NPO with OGT open to bedside bottle. With PLR @104cc in2 hrs. with O2 inhalation @ 4Lpm via face mask. With pulse oximeter with O2 saturation @99%. To secure 1 unit Fresh Frozen Plasma for transfusion. Lab exams followed up. vstaken and recorded. Medicated. Seen and examined by Dr.Dagooc with orders made and
carried out. Cared for.
May 3,2007
3-11pm 3:00pm> on bed stupurous and afebrile. On NPO with Ogt open to bedside bottle. With IVF@ right arm D5 o.3 NaCl @ KVO rate, with side drip of dopamine @ 2 cc/hr via infusionpump. With D5 LR @ 32 cc/hr x 8 hrs, on KSS. Still for insertion. On O2 inhalation. Still tosecure FFP for transfusion. Vs checked and recorded. Lab exams followed-up. due medsgiven. Watched for any unusualities.
4:15pm>Seen by Dr.Tiongco, ordered for IV cutdown, refer to surgery by Dr. Gazmen.
May 3,2007
11-7 am 11:00pm> Received asleep on bed, afebrile. On NPO
7-3 pm 7:00am> On bed awake, weak, pallor, coherent and responsive, on MHBR, with 02inhalation @ 5 Lpm via face mask. With ongoing BT #2 FWB 500 cc with serial # 112-07-23172 blood type A+. On left arm is PNSS 1L @ 200 cc/hr. Due meds given. With FBC tourobag. Endorsed to NOD.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 31/54
3-11pm 3:00pm> Received lying on bed, awake, responsive, and coherent to verbalcommunication. On MHBR position. With droopy eyes noted. With pale lips, dry and warmskin noted, capillary refill less than 2 seconds. Established rapport. On NPO exceptmedications. With 02 inhalaltion @ 5 lpm via nasal cannula. With double line IVF- #7 PNSS1L @ 200 cc/hr infusing well @ L brachial vein, #8 PNSS 1L @ 100 cc/hr infusing well @ Rbasilica vein. With FBC attached to urobag draining amber colored urine. On CBR withoutBRP-reinstructed.
4:00pm> VS, I & O checked and recorded every hour.
4:25pm> Above IVF consumed and followed-up with #9 PNSS 1L @ KVO rate @ R basilicvein.
5:20pm> Temp. 37.8 C, NOD aware. TSB done
6:00pm> Above IVF consumed and followed-up with #9 PNSS 1L @ KVO rate @ R basilicvein.
10:00pm> Still to secure 6 units of platelet and 3 units of fresh whole blood. Advise forbone marrow biopsy, still undecided.
11:00pm> Watched and monitored for any unusualities. Endorsed to NOD.
May 4, 2007
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 32/54
11.7 11 pm> Received asleep on bed, afebrile, on milk feeding 30cc every 3 hours per OGT, With IVFof D5IMB @ 20 cc/hr with side of 2 cc/hr, with heplock @ left and right foot, with O2 @4 Lpm, tosecure another unit of fresh frozen plasma followed-up, V/S checked, due meds given, cared andwatched for.
May 5, 2007
7.3 7 am> On bed, on milk feeding/OGT 30cc every 1hr, # 4 D5IMB @ 20cc/hr, with side drip to run@ 2cc/hr, O2 @ 4cc/mask. To secure 1 unit Fresh Frozen Blood for transfusion. Watched andcared for.
3.11 3 pm> Received patient on bed awake, febrile. On milk feeding 30cc every 3hr per OGT,checked patency, with Ivf ofD5IMB 500cc @3cc/hr infusing well, withside drip dopamine @ 2cc/hrper infusion pump, with O2 inhalation @ 5Lpm via face mask, still to secre fresh frozen plasmafollowed-up. V/S checked once recorded. Watched and cared for.
11.7 11pm> On bed asleep, on dropperfeeding 50cc every 3hr, with IVF of D5IMB @ 3cc/hr x 24hr,infusing well @ the level of 400cc/hr, with side drip of dopamine @ 2cc/hr infusing via infusion
pump. O2 @5 Lpm via face mask. Still to secure fresh frozen plasma for transfusion. V/S checkedand recorded. Lab exams followed-up,due meds given. Watched for any unusualities.
May 6, 2007
7.3 7am> On bed asleep, on dropper feeding 50cc every 3hr, with IVF D5IMB @ 3cc/hr x 24hr, withattached O2 @ 5Lpm via face mask, to secure kit fresh frozen plasma for transfusion. Lab examsfollowed-up. V/S taken and checked. Endorsed to NOD.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 33/54
7:45> seen and examined by Dr. Garingalao with orders made and carried out. Transferred toCardio Ward as ordered.
3-11 3pm> On bed, asleep, dropper feeding, with IVF of D5IMB @ 5cc/hr.
Still for blood CS. still to secure urine and stool exam. Followed up availability of fresh frozenplasma. V/S checked. Meds given. Endorsed to NOD.
11.7 11pm. Received on bed asleep, on dropper feeding 50cc every 3hr, with IVF of D5IMB @ 5cc/hron KSS. V/S checked and recorded. Meds followed up. Cared for.
May 7, 2007
7.3 7am> on bed awake, dropper feeding, with IVF regulated infusing well. V/S checked andrecorded. Meds cut off. Watched and cared for.
3-11 3pm> Received on bed awake, on dropper feeding, helock KSS, labs followed up. still to secureblood followed up. V/S checked and recorded, medicated, watched and cared for,
11-7 11pm> received lying on bed, awake, patient not in respiratory distress, minimal wheezes heardupon auscultation, with cleft lip, with good capillary refill, with good skin turgor, warm to touch,with heplock on right metatarsal vein. On dropper feeding, for blood CS, U/A, S/E, ABG.
12am> VS checked and recorded, afebrile. Bedside care done; linens stretched and tucked well.Health teachings rendered to mother such as increasing OFI, encouraged to promote goodhygiene. Instructed to keep child away from allergens such as dust, smoke, ect...instructed torefer any unusualities and to comply medical regimens. Infant was able to defecate 180cc- softin characteristics and yellowish in color.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 34/54
4am> V/S checked and recorded; afebrile; watched and cared for.
5am> morning care done. Intake and output summed up and recorded.
7am> Left on bed with watcher. Endorsed to NOD.
May 8, 2007
7.3 7:30am> received on bed awake with mother on side, with cleft lip palate, with heplock on rightmetatarsal vein; on on respiratory distress. On syringe feeding, able to consume milk feeding50cc, able to defecate with semisolid character of stool and yellowish in color about 30cc. VSchecked and recorded, afebrile T: 36.4, PR:109, RR:39, BP:90/50. Bedside care done. Instructedmother to increase OFI and to report for vomiting and type of stool and its consistency. V/Srechecked and documented. Give ample time for sleeping.
3pm> Health teaching given regarding proper hygiene, milk preparation, proper feedingtechniques and burping of the baby after each feeding. Observed closely for sign of intolerancelike vomiting and nausea.
3.11 3pm> Received on bed, awake on dropper feeding 70cc every 3hr, with heplock attached; stillpatent. V/S checked and recorded, afebrile; lab exams followed up. due meds given, watchedand cared for.
11-7 11pm> Received on bed asleep ,with watcher on side, not in distress, with cleft lip, with goodskin turgor and warm to touch, with heplock in right metatarsal; V/S checked and recordedafebrile; bedside care done. Linens stretched and properly tucked; left on bed comfortably.Health teachings rendered to watcher such as increasing OFI of patient, promote goodventilation and relaxation, encouraged mother to breastfed.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 35/54
May 9, 2007
7.3 7am> Received patient on bed, sleeping with mother on side, with heplock @ right metatarsal
vein, on bottle feeding, able to consumed 90cc. V/S checked and recorded, afebrile, T:36.4,PR:120, RR:28,BP:90/60. instructed mother to feed baby every 3-4 hours and should preparemilk formula using sterile or distilled water and to report any sign of dehydration such as crackedlips and sunken fontanels.
3pm> Endorsed to NOD.
3-11 3pm> received patient on bed awake, on dropper feeding, with heplock attached on; V/S takenand recorded, afebrile. Followed up availability of meds. Watched and cared for.
11-7 11pm> Received asleep on bed, afebrile; on dropper feeding with aspiration precaution, withheplock attached, still for lumbar puncture, with consent, lab exams followed up, meds followedup, V/S checked an recorded. Watched and cared for.
May 10, 2007
7-3 7am> On bed awake, on breast feeding with heplock, patent and intact. V/S checked andrecorded, labs followed up, medicated, watched and cared for.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 36/54
3-11 3pm> Received on bed, awake, on dropper feeding 70cc every 3hrs; with heplock attached. Stillpatent. V/S checked and recorded, afebrile. Lab exams followed up. Due meds given. Cared for.
11-7 11pm> Received on bed, asleep, on dropper feeding; with heplock attached; V/S checked andrecorded; meds given, cared for.
May 11, 2007
7-3 7am> On bed, awake, on dropper feeding, with attached on. V/S checked and recorded, medsgiven. Cared for.
3-11 3pm> Lying on bed asleep, on NPO temporarily; for lumbar puncture any time today withconsent. Still for cranial CT scan. V/S checked and recorded. Medicines provided, followed up
intervention.
11-7 11pm> Received asleep on bed, afebrile, on dropper feeding, with heplock attached, still for LPwith consent. Lab exams and medicines followed up. V/S checked, cared for.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 37/54
May 12, 2007
7-3 7am> On bed awake, NPO for 4 hours reminded, flat on bed x 4 hours, instructed, with heplock,patent and intact, watched and cared for.
3-11 3pm> On bed asleep, on dropper feeding 79cc every 3 hours, with heplock attached on. V/Schecked and recorded. Lab exams followed up. Due meds given; watched for.
11-7 11pm> received asleep on bed, afebrile; on dropper feeding, with strict aspiration precaution,with heplock attached, cranial ultrasound and lab exams followed up, V/S checked, medsfollowed up, cared for.
May 13, 2007
7-3 7am> On bed, awake, with heplock patent and intact, V/S checked and recorded, labs followedup, meds prescribed, watched and cared for.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 38/54
3-11 3pm> Received on bed, awake; on dropper feeding every 3 hours. With heplock attached, stillpatent. V/S cheched and recorded; afebrile. Lab exams followed up. Due meds given. Cared for.
11-7 11pm> Received asleep on bed; afebrile, on dropper feeding, with heplock attached. Urinalysisand cranial ultrasound followed up, V/S checked, due meds given, cared for.
May 14, 2007
7-3 7am> Received patient cuddled by mother, awake. On breastfeeding, with heplock attached on.V/S taken and recorded. Afebrile. Medicated. Watched and cared for.
3.11 3pm> On bed, afebrile, dropper feeding, with heplock attached; followed up cranial ultrasound;urine CS followed up, fresh frozen plasma was available.
11-7 11pm> Received on bed, asleep, on dropper feeding, with heplock; V/S taken and recorded,meds given; cared for.

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 39/54
May 15, 2007
7.3 7am> Received lying flat on bed, asleep with watcher at bedside. With heplock attached to rightmetatarsal vein; still patent and intact. With cleft lip and dry skin warm to touched. With normalcapillary refill less than 2 seconds, with good skin turgor. Instructed on dropper feeding every 3-4 hours.
8am> V/S checked and recorded; within normal ranges. Intake and output monitored closely asordered. Instructed watcher to report any signs of dehydration such as dry lips and skin, sunkeneyes and fontanels, vomiting, LBM, and weakness.
9am> Bed linen stretched and tucked well. Arranged things properly. Provided with restfulenvironment conducive for sleep. Changed soiled diaper into clean one, with semi-solid stool,yellow in color weighing 70gs.
10am> Vitamin K given 1mg IM as ordered. Watched out for any signs of adverse reactions, notnoted. Able to consumed 70cc of milk via bottle feeding.
10:40am> Changed soiled diaper into clean one, with semi- solid formed stool, yellow in colorweighing 80gs. Measured head circumference as ordered: 40cm. health teaching imparted on
proper hygiene, importance of proper feeding and burping after each feeding, and to observe forvomiting and LBM. IVTT meds given by NOD; watched out for any signs of adverse reaction, notnoted.
12nn> V/S rechecked and recorded. Intake and output monitored closely as ordered. Watchedout for any unusualities, not noted. Provided with restful environment conducive for sleep. Needsattended to and cared for.
3pm> Endorsed to NOD.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 40/54
3-11 3pm> On bed asleep. On dropper feeding 70cc every 3 hours, with heplock attached. V/Schecked and recorded. Watched and cared for.
11-7 11pm> Received on bed, asleep. On dropper feeding 70cc every 3 hours. With heplockattached. V/S checked and recorded. Meds given, cared for.
May 16, 2007
7-3 7am> Received carried by watcher per arm, awake andconscious. With no heplockattached. With cleft lip and dry skin warm to touch. With normal capillary refill less than 2seconds, with good skin turgor. Instructed on dropper feeding every 3-4 hours. Still forcranial ultrasound; repeat CBC, platelet; for transfer to miscellaneous room.
8am> V/S checked and recorded; within normal ranges. Intake and output monitoredclosely as ordered. Bed linens stretched and tucked well. Provided with restfulenvironment conducive for sleep. Able to consume 60cc of milk via bottle feeding with
good appetite. Instructed watcher to report any signs of dehydration such as dry lips andskin, sunken fontanels, vomiting and diarrhea.
9am> Asleep; provided with restful and safe environment.
10am> Transferred to miscellaneous room as ordered. Bed linens stretched and tuckedwell. Arranged things in proper place.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 41/54
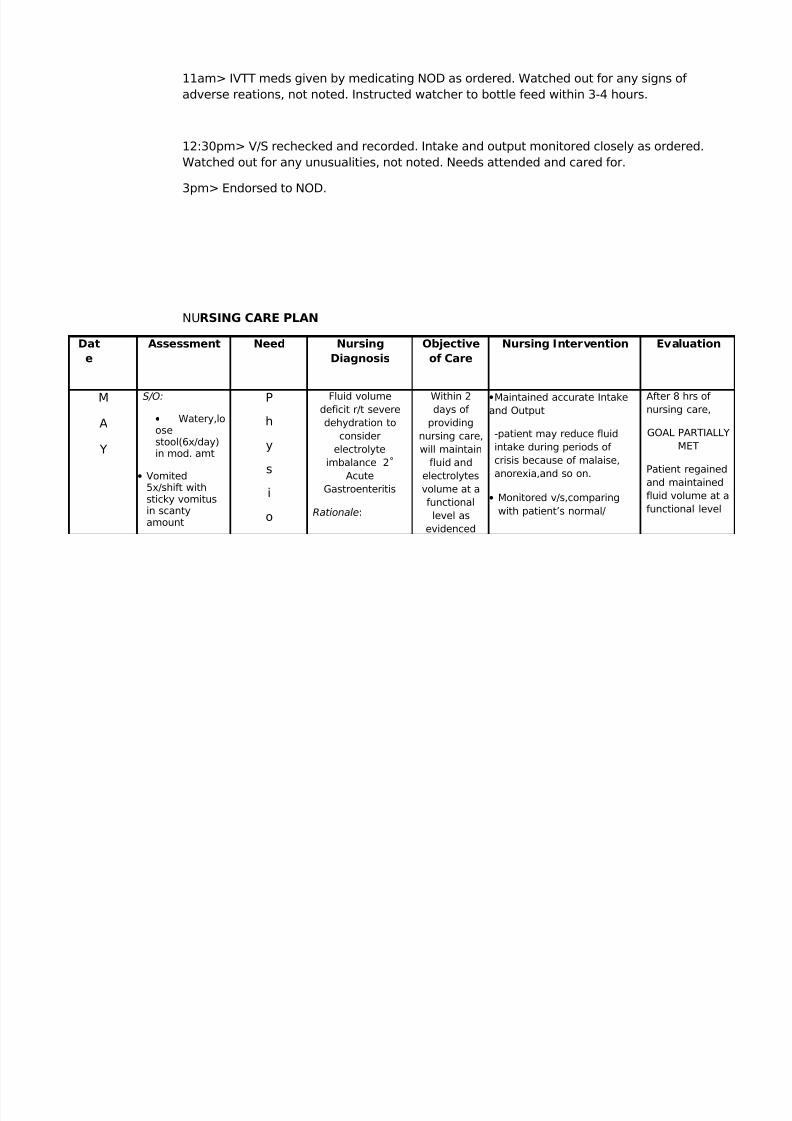
11am> IVTT meds given by medicating NOD as ordered. Watched out for any signs of adverse reations, not noted. Instructed watcher to bottle feed within 3-4 hours.
12:30pm> V/S rechecked and recorded. Intake and output monitored closely as ordered.Watched out for any unusualities, not noted. Needs attended and cared for.
3pm> Endorsed to NOD.
NURSING CARE PLAN
Dat
e
Assessment Need Nursing
Diagnosis
Objective
of Care
Nursing Intervention Evaluation
M
A
Y
S/O:
• Watery,loosestool(6x/day)in mod. amt
• Vomited5x/shift withsticky vomitusin scantyamount
P
h
y
s
i
o
Fluid volumedeficit r/t severedehydration to
considerelectrolyte
imbalance 2˚Acute
Gastroenteritis
Rationale:
Within 2days of
providingnursing care,will maintain
fluid andelectrolytesvolume at afunctionallevel as
evidenced
•Maintained accurate Intakeand Output
-patient may reduce fluidintake during periods of crisis because of malaise,anorexia,and so on.
• Monitored v/s,comparingwith patient’s normal/
After 8 hrs of nursing care,
GOAL PARTIALLYMET
Patient regainedand maintainedfluid volume at afunctional level
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 42/54
,
2
0
0
7
7am –
3pm
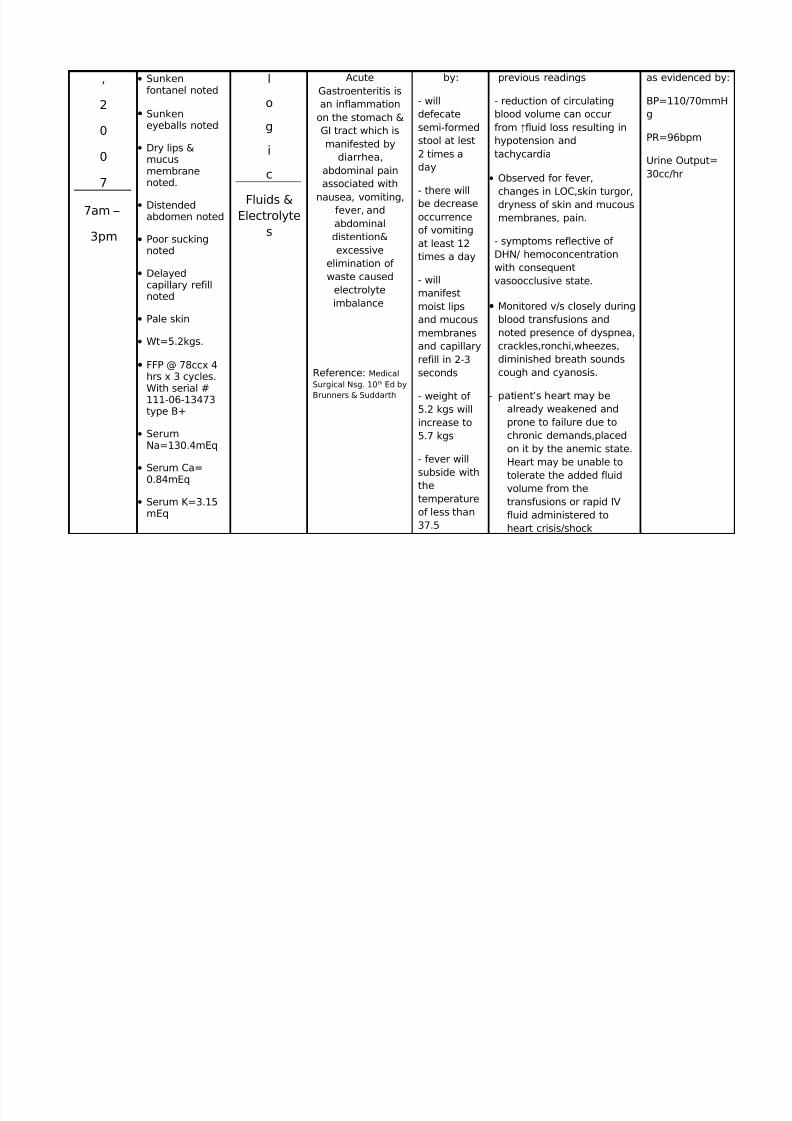
• Sunkenfontanel noted
• Sunkeneyeballs noted
• Dry lips &mucusmembranenoted.
• Distendedabdomen noted
• Poor suckingnoted
• Delayedcapillary refillnoted
• Pale skin
• Wt=5.2kgs.
• FFP @ 78ccx 4hrs x 3 cycles.
With serial #111-06-13473type B+
• SerumNa=130.4mEq
• Serum Ca=0.84mEq
• Serum K=3.15mEq
l
o
g
i
c
Fluids &Electrolyte
s
AcuteGastroenteritis isan inflammation
on the stomach &GI tract which ismanifested by
diarrhea,abdominal painassociated with
nausea, vomiting,fever, andabdominaldistention&excessive
elimination of waste caused
electrolyteimbalance
Reference: MedicalSurgical Nsg. 10th Ed by
Brunners & Suddarth
by:
- willdefecatesemi-formedstool at lest2 times aday
- there willbe decreaseoccurrenceof vomitingat least 12times a day
- willmanifestmoist lipsand mucousmembranesand capillaryrefill in 2-3seconds
- weight of 5.2 kgs willincrease to5.7 kgs
- fever willsubside withthetemperatureof less than37.5
previous readings
- reduction of circulatingblood volume can occurfrom ↑fluid loss resulting inhypotension andtachycardia
• Observed for fever,
changes in LOC,skin turgor,dryness of skin and mucousmembranes, pain.
- symptoms reflective of DHN/ hemoconcentrationwith consequentvasoocclusive state.
• Monitored v/s closely duringblood transfusions andnoted presence of dyspnea,crackles,ronchi,wheezes,diminished breath soundscough and cyanosis.
- patient’s heart may bealready weakened andprone to failure due tochronic demands,placedon it by the anemic state.Heart may be unable totolerate the added fluidvolume from thetransfusions or rapid IVfluid administered toheart crisis/shock
as evidenced by:
BP=110/70mmHg
PR=96bpm
Urine Output=30cc/hr
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 43/54
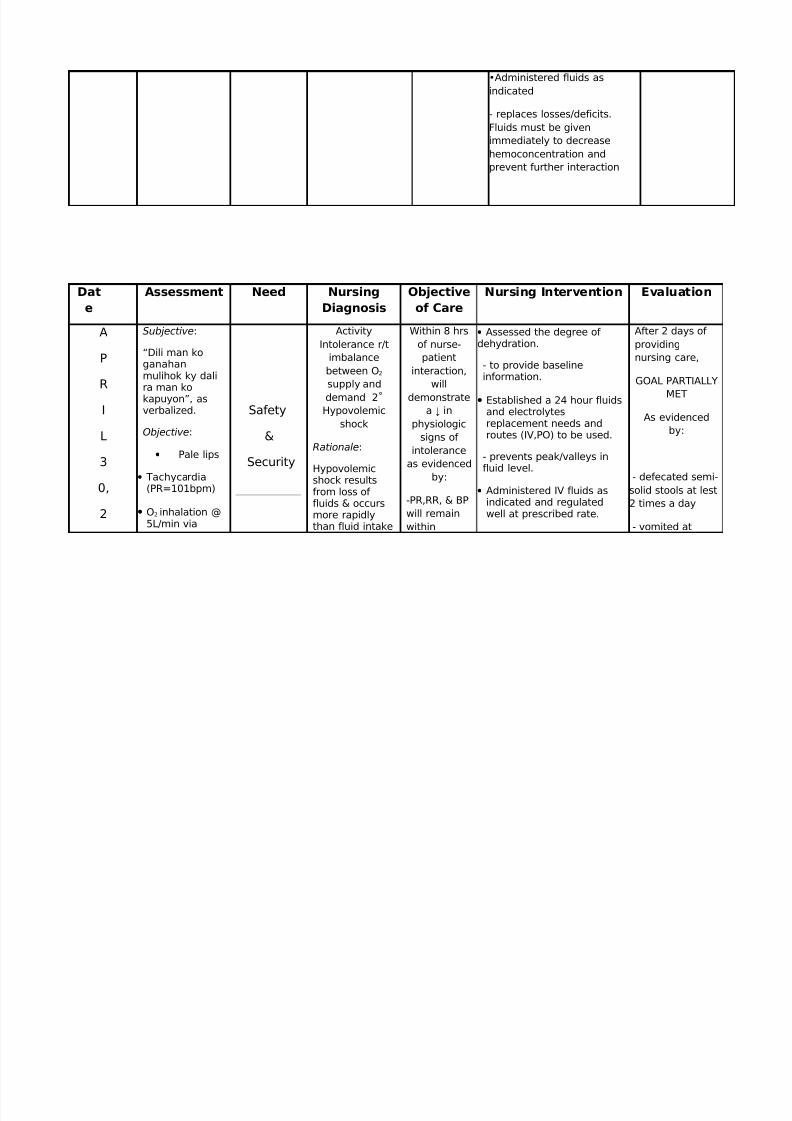
•Administered fluids asindicated
- replaces losses/deficits.Fluids must be givenimmediately to decreasehemoconcentration andprevent further interaction
Dat
e
Assessment Need Nursing
Diagnosis
Objective
of Care
Nursing Intervention Evaluation
A
P
R
I
L
3
0,
2
Subjective:
“Dili man koganahanmulihok ky dali
ra man kokapuyon”, asverbalized.
Objective:
• Pale lips
• Tachycardia(PR=101bpm)
• O2 inhalation @5L/min via
Safety
&
Security
ActivityIntolerance r/t
imbalancebetween O2
supply anddemand 2˚Hypovolemic
shock
Rationale:
Hypovolemicshock resultsfrom loss of fluids & occursmore rapidlythan fluid intake
Within 8 hrsof nurse-patient
interaction,will
demonstratea ↓ in
physiologicsigns of
intoleranceas evidenced
by:
-PR,RR, & BPwill remainwithin
• Assessed the degree of dehydration.
- to provide baselineinformation.
• Established a 24 hour fluidsand electrolytesreplacement needs androutes (IV,PO) to be used.
- prevents peak/valleys influid level.
• Administered IV fluids asindicated and regulatedwell at prescribed rate.
After 2 days of providingnursing care,
GOAL PARTIALLY
MET
As evidencedby:
- defecated semi-solid stools at lest2 times a day
- vomited at
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 44/54
0
0
7
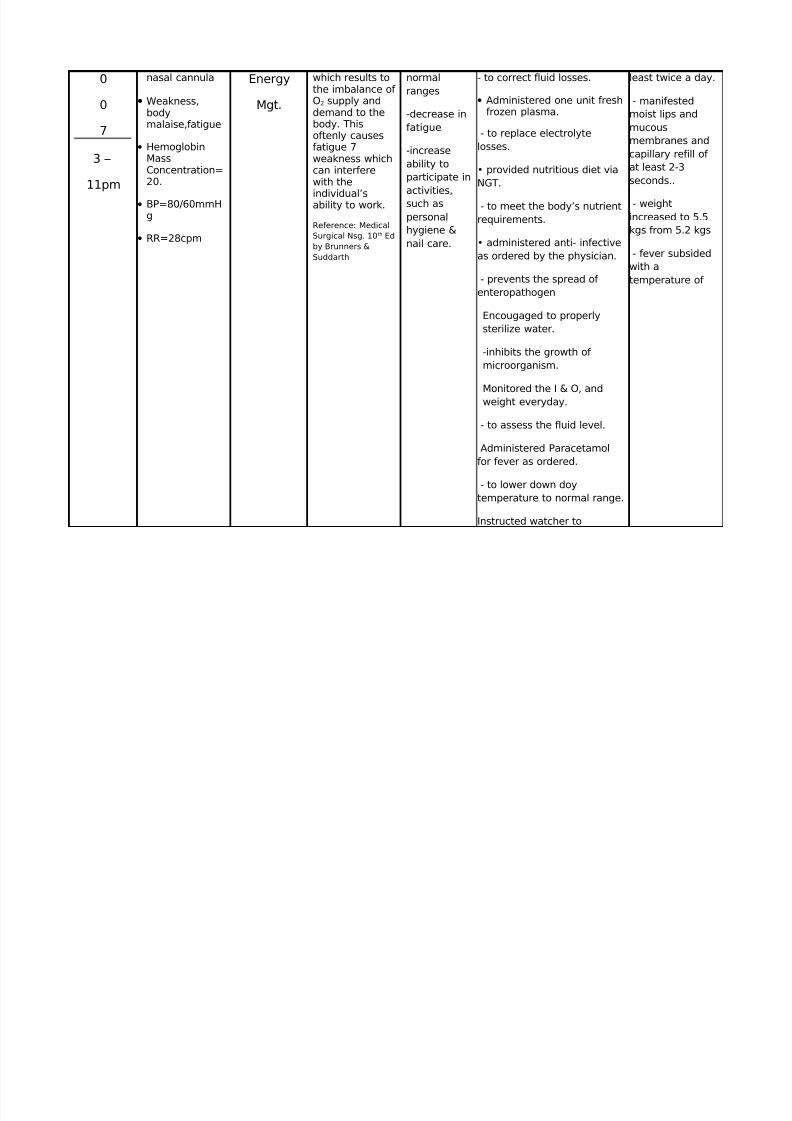
3 –
11pm
nasal cannula
• Weakness,bodymalaise,fatigue
• HemoglobinMassConcentration=20.
• BP=80/60mmHg
• RR=28cpm
Energy
Mgt.
which results tothe imbalance of O2 supply anddemand to thebody. Thisoftenly causesfatigue 7weakness whichcan interferewith the
individual’sability to work.
Reference: MedicalSurgical Nsg. 10th Edby Brunners &Suddarth
normalranges
-decrease infatigue
-increaseability toparticipate in
activities,such aspersonalhygiene &nail care.
- to correct fluid losses.
• Administered one unit freshfrozen plasma.
- to replace electrolytelosses.
• provided nutritious diet viaNGT.
- to meet the body’s nutrientrequirements.
• administered anti- infectiveas ordered by the physician.
- prevents the spread of enteropathogen
Encougaged to properlysterilize water.
-inhibits the growth of microorganism.
Monitored the I & O, andweight everyday.
- to assess the fluid level.
Administered Paracetamolfor fever as ordered.
- to lower down doytemperature to normal range.
Instructed watcher to
least twice a day.
- manifestedmoist lips andmucousmembranes andcapillary refill of at least 2-3seconds..
- weightincreased to 5.5kgs from 5.2 kgs
- fever subsidedwith atemperature of
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 45/54
perform TSB.
- provide comfort an loweredbody temperature.
Dat
e
Assessment Need Nursing
Diagnosis
Objective
of Care
Nursing Intervention Evaluation
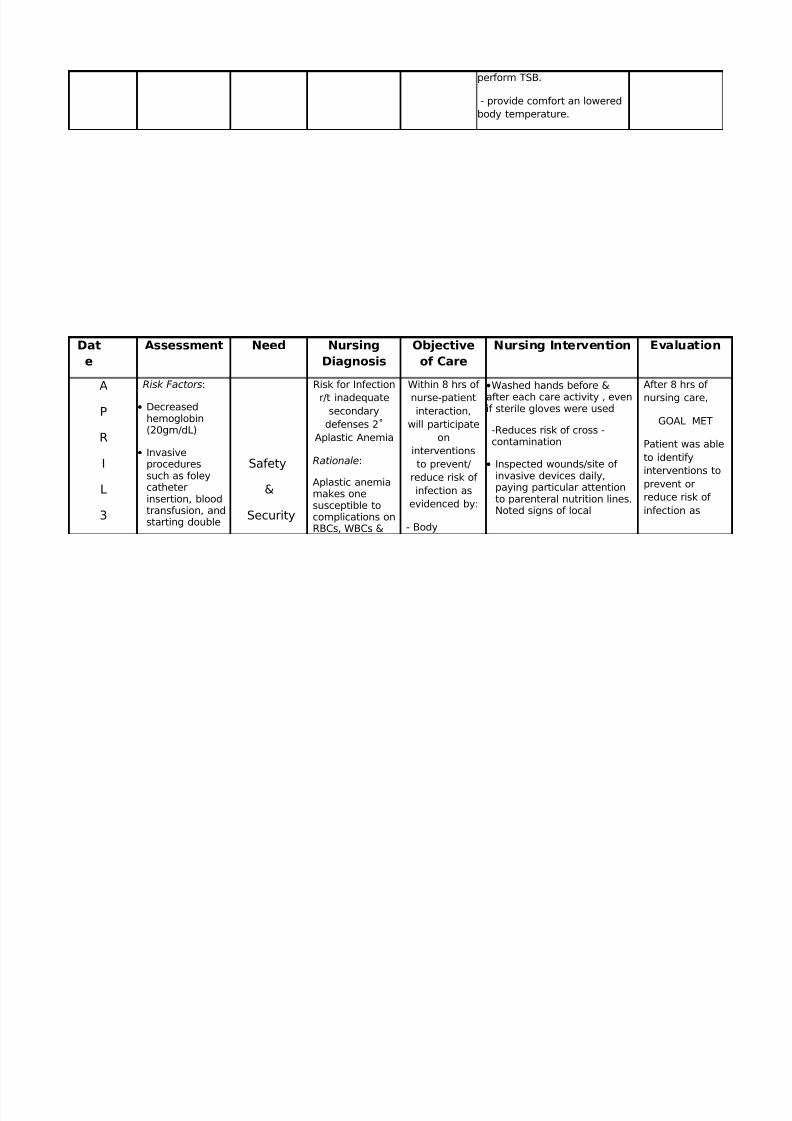
AP
R
I
L
3
Risk Factors:
• Decreasedhemoglobin(20gm/dL)
• Invasiveproceduressuch as foleycatheterinsertion, bloodtransfusion, andstarting double
Safety
&
Security
Risk for Infectionr/t inadequate
secondarydefenses 2˚
Aplastic Anemia
Rationale:
Aplastic anemiamakes onesusceptible tocomplications onRBCs, WBCs &
Within 8 hrs of nurse-patientinteraction,
will participateon
interventionsto prevent/
reduce risk of infection as
evidenced by:
- Body
•Washed hands before &after each care activity , evenif sterile gloves were used
-Reduces risk of cross -contamination
• Inspected wounds/site of invasive devices daily,paying particular attentionto parenteral nutrition lines.Noted signs of local
After 8 hrs of nursing care,
GOAL MET
Patient was ableto identifyinterventions toprevent orreduce risk of infection as
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 46/54
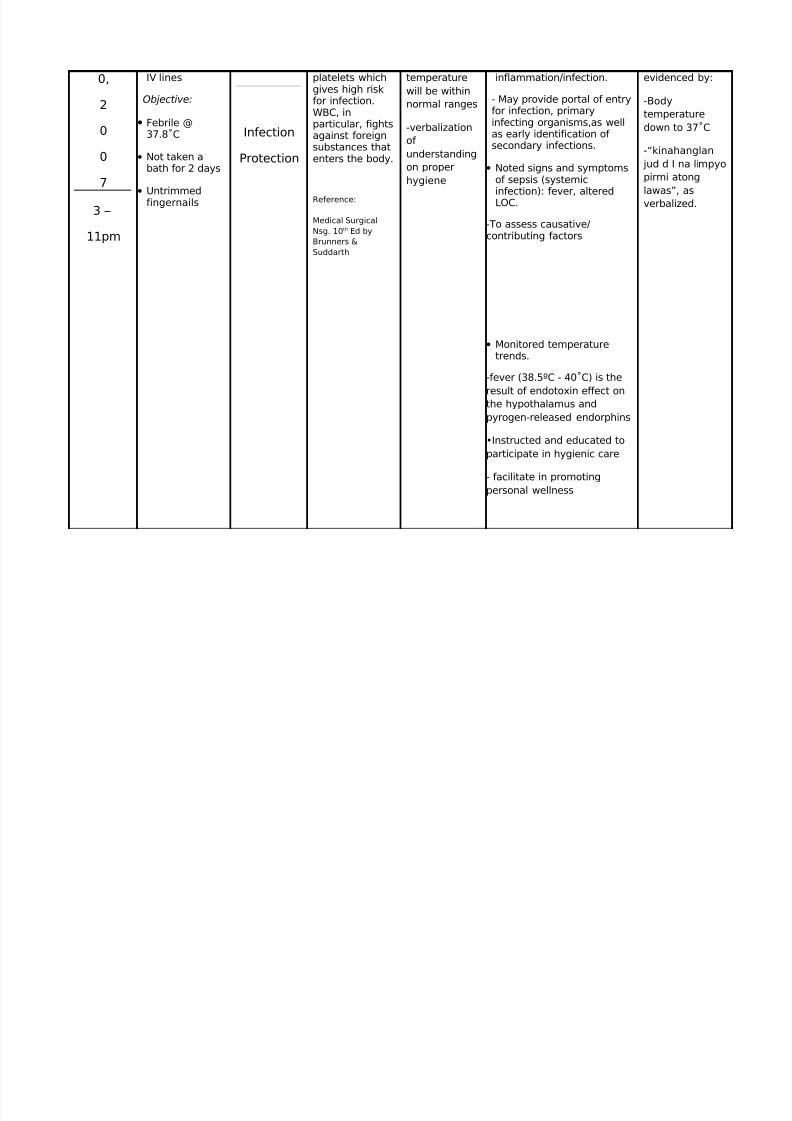
0,
2
0
0
7
3 –
11pm
IV lines
Objective:
• Febrile @37.8˚C
• Not taken abath for 2 days
•
Untrimmedfingernails
Infection
Protection
platelets whichgives high riskfor infection.WBC, inparticular, fightsagainst foreignsubstances thatenters the body.
Reference:
Medical SurgicalNsg. 10th Ed byBrunners &Suddarth
temperaturewill be withinnormal ranges
-verbalizationof understandingon properhygiene
inflammation/infection.
- May provide portal of entryfor infection, primaryinfecting organisms,as wellas early identification of secondary infections.
• Noted signs and symptomsof sepsis (systemic
infection): fever, alteredLOC.
-To assess causative/contributing factors
• Monitored temperaturetrends.
-fever (38.5ºC - 40˚C) is the
result of endotoxin effect onthe hypothalamus andpyrogen-released endorphins
•Instructed and educated toparticipate in hygienic care
- facilitate in promotingpersonal wellness
evidenced by:
-Bodytemperaturedown to 37˚C
-“kinahanglan jud d I na limpyopirmi atong
lawas”, asverbalized.

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 47/54
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 48/54
B. DISCHARGE PLAN
Clients with Acute Gastroenteritis, watchers are instructedto take the following plan for discharge:
M- Medications should be taken regularly as prescribed , onexact dosage, time, & frequency, making sure that thepurpose of medications is fully disclosed by the health careprovider.
E- Exercise should be promoted in a way by stretching hand andfeet every morning and exercise burping every after bottle
feeding.
T- Treatment after discharge is expected for patients andwatcher with Acute Gastroenteritis to fully participate incontinuous treatment.
H- Hygiene must be maintained for patients with AcuteGastroenteritis. Promotion of personal hygiene should beencouraged such as, daily bathing and changing of diaperswhen soiled.
O- OPD such as regular follow-up check-ups should be greatlyencouraged to clients wather with Acute Gastroenteritis asordered by physician to ensure the continuing managementand treatment.
D- Diet should be promoted, since, during admission, the patientwas on NPO. Proper selection of milk that are suitable forbabies will help enhance immunity.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 49/54
VIII. PHARMACOLOGICAL MANAGEMENT
• Diazepam
a. Doctor’s Order: 1.5mg IVTT now then PRN for frank seizures
b. Indication : Management of general anxiety disorder, panicdisorders, and provides pre- operative sedation.
c. Mechanism of Action: Depresses all levels of CNS, including the
limbic and reticular formation, probably through the increasedaction of GABA, which is a major inhibitory neurotransmitter in thebrain.
d. Nursing Responsibilities:
Assess effectiveness of therapy according to diagnosis – seizure.
Monitor RR, HR and BP.
Do not overuse or miss regularly scheduled doses. Administer
drug properly as ordered.
If used or seizures, report immediately lack of seizure control.
• Ceftriaxone
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 50/54
a. Doctor’s Order: 500mg IVTT now then OD
b. Indication: Treatment for lower respiratory tract infection
c. Mechanism of Action : Inhibits bacterial cell wall synthesis by
binding to one or more o the penicillin binding protein.d. Nursing Responsibilities:
Assess for previous history of reaction to other cephalosphorin orpenicillin. Monitor for allergic reactions.
Assess for bowel function (if severe diarrhea occurs, discontinuedrug).
Monitor urine output (if decreased, notify the physician)
• Ampicillin
a. Doctor’s Order: 260mg IVTT q 6hrs
b. Indication : For susceptible bacterial infections
c. Mechanism of Action: Interferes with bacterial cell wall synthesisduring active multiplication, causing cell wall death and resultant
bactericidal against susceptible bacteria.d. Nursing Responsibilities :
Monitor effectiveness of therapy and active reaction, includingdevelopment of opportunistic infections.
• Phenobarbital
a. Doctor’s Order : 104mg IVTT now as LB/13mg IVTT q 12hrs
b. Indication: For generalized tonic clonic (grand mal) and partial
seizures.
c. Mechanism of Action: Interferes with transmission of impulsesfrom the thalamus to the cortex of the brain, resulting in animbalance and facilitatory mechanism.
d. Nursing Responsibilities:

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 51/54
Constant observation and frequent monitoring of BP, RR and HR.
Monitor infusion site for irritating extravasations.
• Paracetamol
a. Doctor’s Order: 60mg IVTT q 4hrs (PRN for temp ≥ 37.8 °C)
b. Indication: For mild to moderate pain and fever.
c. Mechanism of Action: Reduces fever by acting on thehypothalamus to cause vasodilation and sweating.
d. Nursing Responsibilities:
Monitor for effectiveness o therapy.
Recheck Temp 15minutes after administration.
• Dopamine
a. Doctor’s Order: 2cc/°.
b. Indication: Treatment of shock which persist after adequate fluidvolume replacement.
c. Mechanism of Action: Stimulates both adrenergic anddopaminergic receptors, lower doses are mainly dopaminergicstimulating and produce renal and mesenteric vasodilation, higherdoses also are both dopaminergic and Beta1 adrenergicstimulating and produce cardiac stimulation and renalvasodilation.
d. Nursing Responsibilities:
Monitor infusion site for extravasation.
Monitor closely for AR and S/S of overdosage.
• Silver Sulfadiazine
a. Doctor’s Order : Apply to affected area TID.
b. Indication : prevention and treatment of infection and burns.
8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 52/54
c. Mechanism of Action : Acts upon the bacterial cell wall and cellmembrane.
d. Nursing Responsibilities:
Monitor development of granulation.
Observe for hypersensitivity reactions (irritation, redness, burning oritching in unburned areas).
IX. EVALUATION
X. BIBLIOGRAPHY
A. BOOKS
Doenges, Marielyn E., ET. Al. (2002) Nursing Care Plans,Guidelines for Individualizing Patient Care. (6th Edition)

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 53/54
Doenges, Marielyn E., ET. Al. (2004). Nurse’s Pocket Guide. (9th
Edition)
Kozier, Barbara ET. Al. (2004). Fundamentals of Nursing, Concepts,Process and Practice. (7th Edition)
Marieb,Elaine N. (2004). Essential of Human Anatomy andPhysiology. (7th Edition).
MIMS. (105th Edition, 2005)
Smeltzer, Suzanne C. ET. Al. (2000). Textbook of Medical-SurgicalNursing. (9th Edition).
Smeltzer, Suzanne C. ET. Al. (2000). Textbook of Medical-SurgicalNursing. Volume 1 (10th Edition)
Turkoski, Beatrice B., ET. Al. Drug Information Handbook forNursing including Assessment, Administration, MonitoringGuidelines and Patient Education (2000-01).
B. INTERNET
http://en.wikipedia.org/wiki/Aplastic_anemia
http://www.aamds.org
C. OTHERS
Microsoft Encarta Encyclopedia 2007.
A Case Study
On
Aplastic Anemia
-----------------------------------------------------
Presented to:

8/2/2019 8358289 Acute Gastroenteritis
http://slidepdf.com/reader/full/8358289-acute-gastroenteritis 54/54
Ms. Zosi Farah W. Fernandez, RN
--------------------------------------------------------
In Partial Fulfillment of the Requirements
In
Related Learning Experience
Presented by:
Cabibil, Ervin Rol C.
Colita, Arven Troy L.
Abundo, Jissa A.
Albero, Karren Rose A.
Aquino, Sunshine S.
Benilan, Melody E.
Cadiente, Joyce C.
Haguyahay, Faith E.
Hinay, Rodelyn B.
Javier, Kathleen Alyce B.
Legal, Chinki C.
Travilla, Allen Rose Y.
BSN3 A1