10 april, 2018, VSO Voorjaarssymposium, Doorn › resources › ... · Gefuseerde specialisatie met...
87
10 april, 2018, VSO Voorjaarssymposium, Doorn Inleiding Nucleaire Geneeskunde Prof. Dr. L.F. de Geus-Oei Dr. D. Vriens Nucleair geneeskundigen Afdeling Radiologie LUMC, LEIDEN 1
Transcript of 10 april, 2018, VSO Voorjaarssymposium, Doorn › resources › ... · Gefuseerde specialisatie met...
10 april, 2018, VSO Voorjaarssymposium, Doorn
Inleiding Nucleaire Geneeskunde
Prof. Dr. L.F. de Geus-Oei
Dr. D. Vriens
Nucleair geneeskundigen
Afdeling Radiologie
LUMC, LEIDEN
1
Disclosures
2
Research samenwerking met:
•Philips
•Siemens
•GE Healthcare
Wat is nucleaire geneeskunde?
3
4
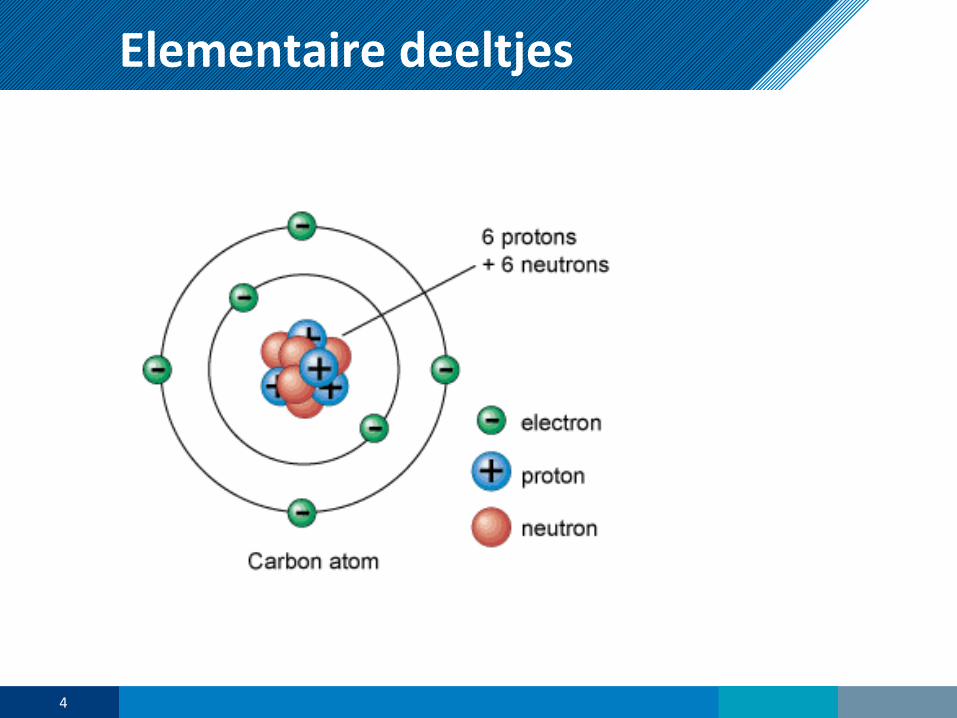
Elementaire deeltjes

farmacon
Radiofarmacon
+
+ isotoop
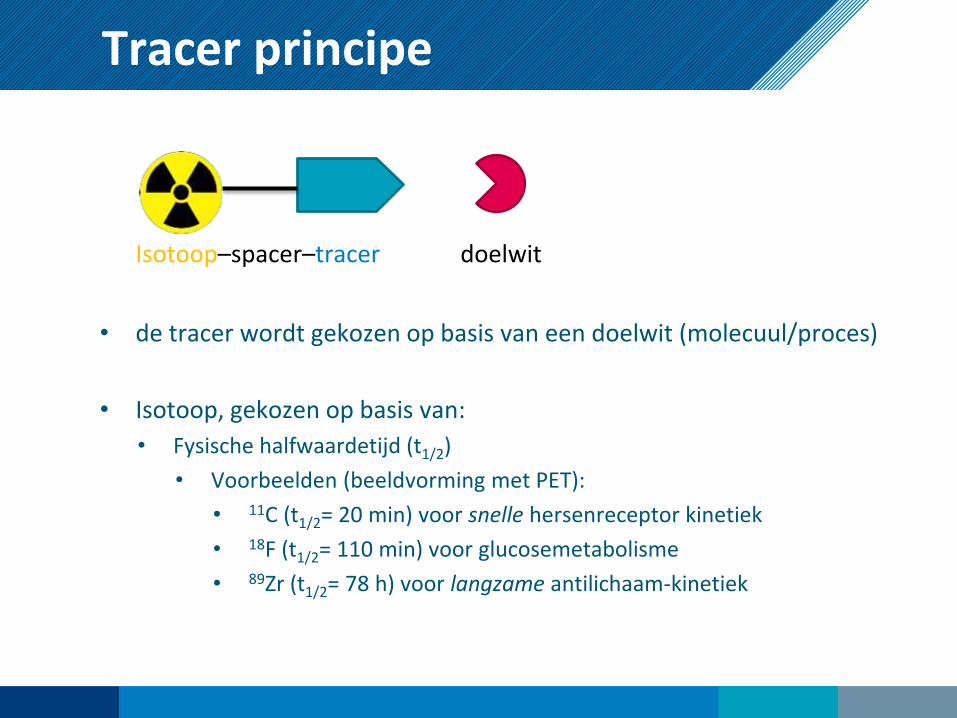
Tracer principe
Isotoop–spacer–tracer doelwit
• de tracer wordt gekozen op basis van een doelwit (molecuul/proces)
• Isotoop, gekozen op basis van:
• Fysische halfwaardetijd (t1/2)
• Voorbeelden (beeldvorming met PET):
• 11C (t1/2= 20 min) voor snelle hersenreceptor kinetiek
• 18F (t1/2= 110 min) voor glucosemetabolisme
• 89Zr (t1/2= 78 h) voor langzame antilichaam-kinetiek

7
Toediening Radiofarmacon
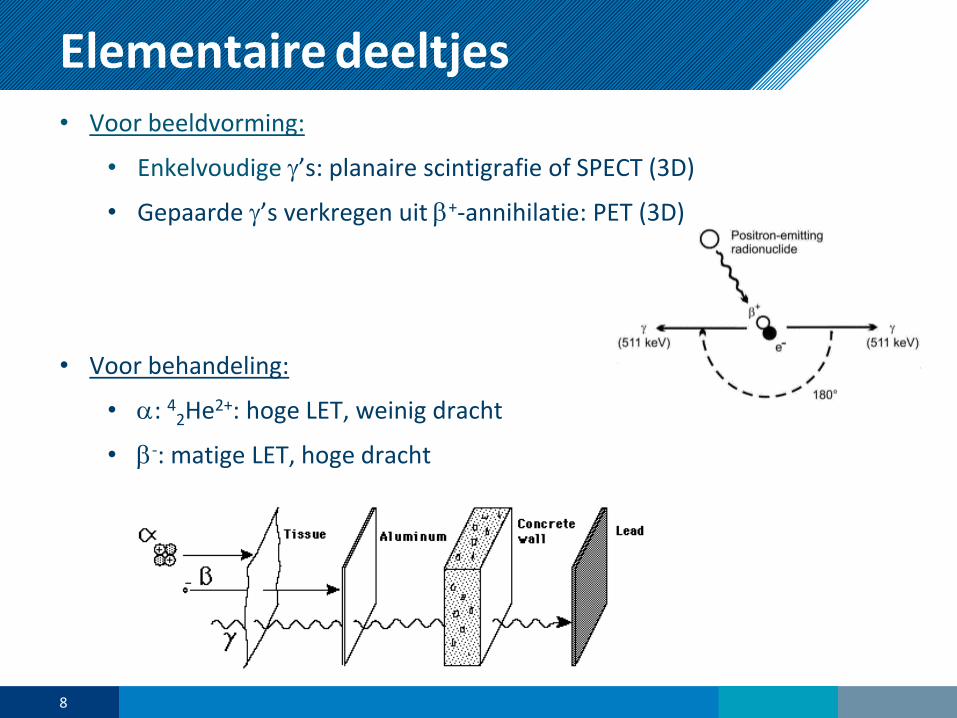
Elementaire deeltjes• Voor beeldvorming:
• Enkelvoudige g’s: planaire scintigrafie of SPECT (3D)
• Gepaarde g’s verkregen uit b+-annihilatie: PET (3D)
• Voor behandeling:
• a: 42He2+: hoge LET, weinig dracht
• b-: matige LET, hoge drachtHollandPTC
8
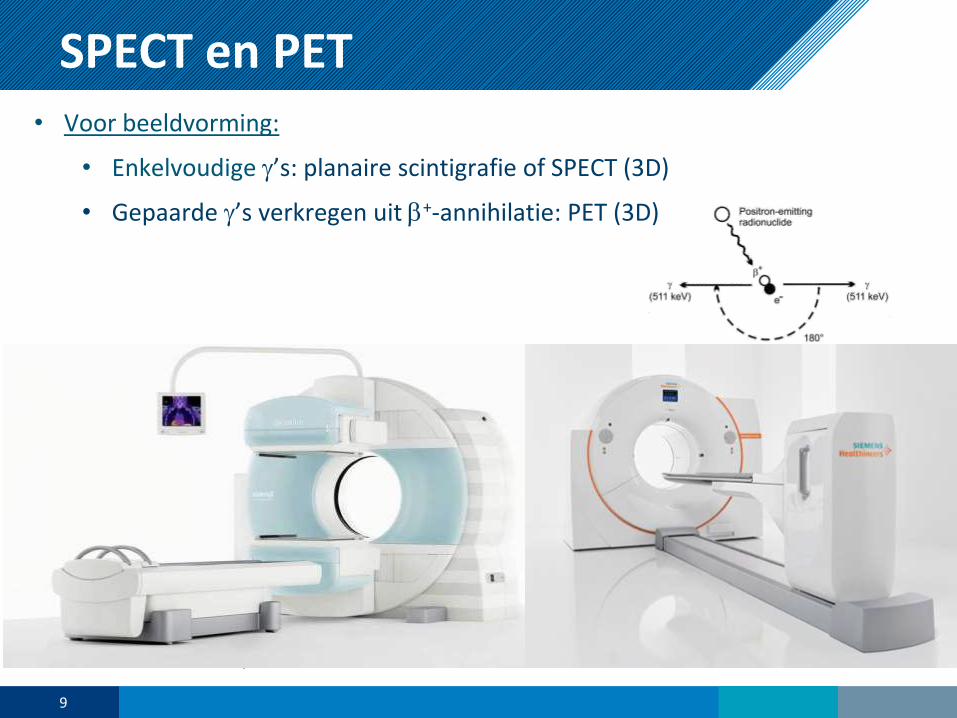
SPECT en PET• Voor beeldvorming:
• Enkelvoudige g’s: planaire scintigrafie of SPECT (3D)
• Gepaarde g’s verkregen uit b+-annihilatie: PET (3D)
• Voor behandeling:
• a: 42He2+: hoge LET, weinig dracht
• b-: matige LET, hoge drachtHollandPTC
9
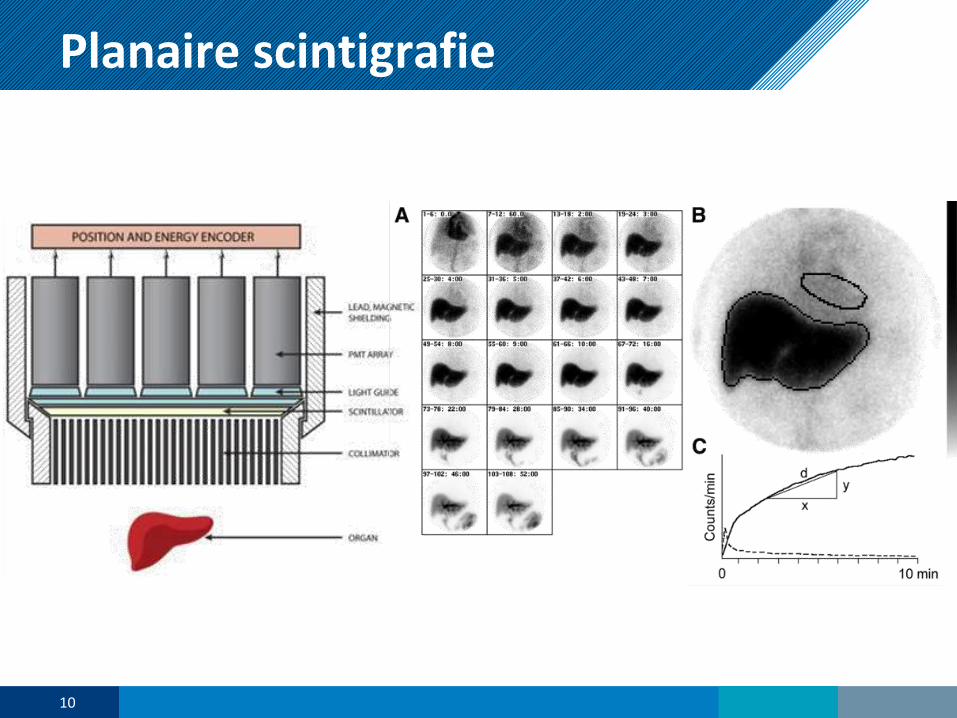
Planaire scintigrafie
HollandPTC
10
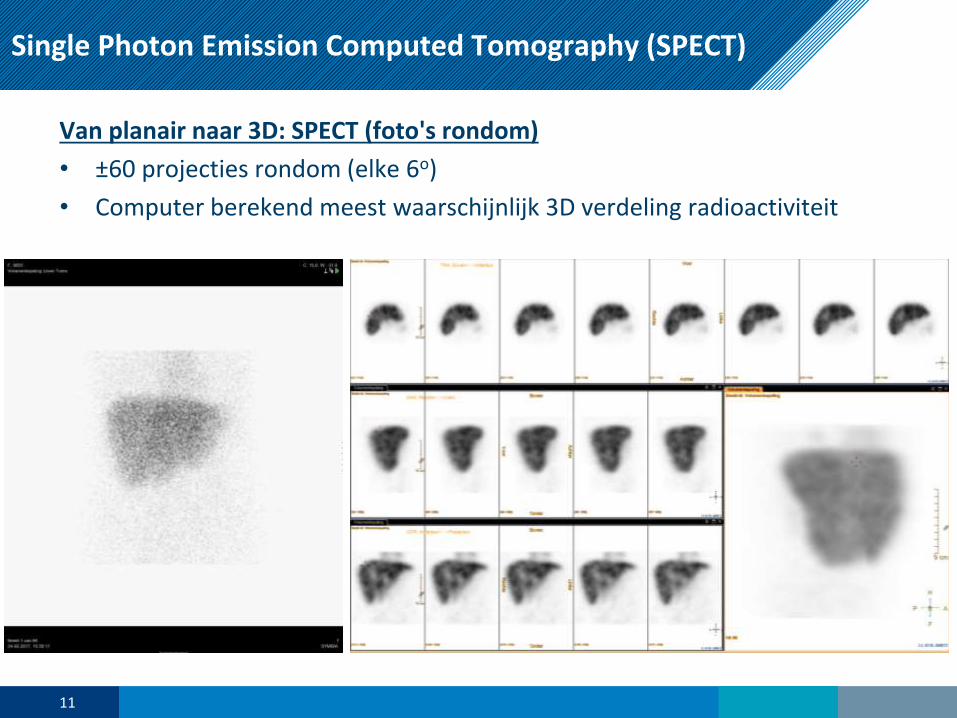
Single Photon Emission Computed Tomography (SPECT)
Van planair naar 3D: SPECT (foto's rondom)
• ±60 projecties rondom (elke 6o)
• Computer berekend meest waarschijnlijk 3D verdeling radioactiviteit
11
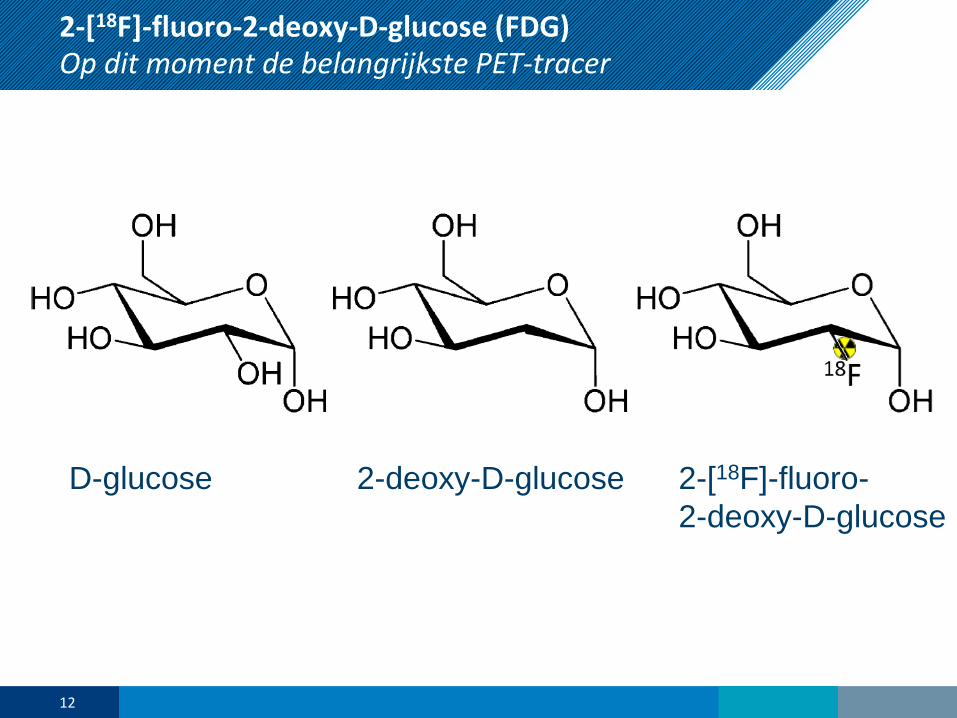
D-glucose 2-deoxy-D-glucose 2-[18F]-fluoro-
2-deoxy-D-glucose
12
2-[18F]-fluoro-2-deoxy-D-glucose (FDG) Op dit moment de belangrijkste PET-tracer
13
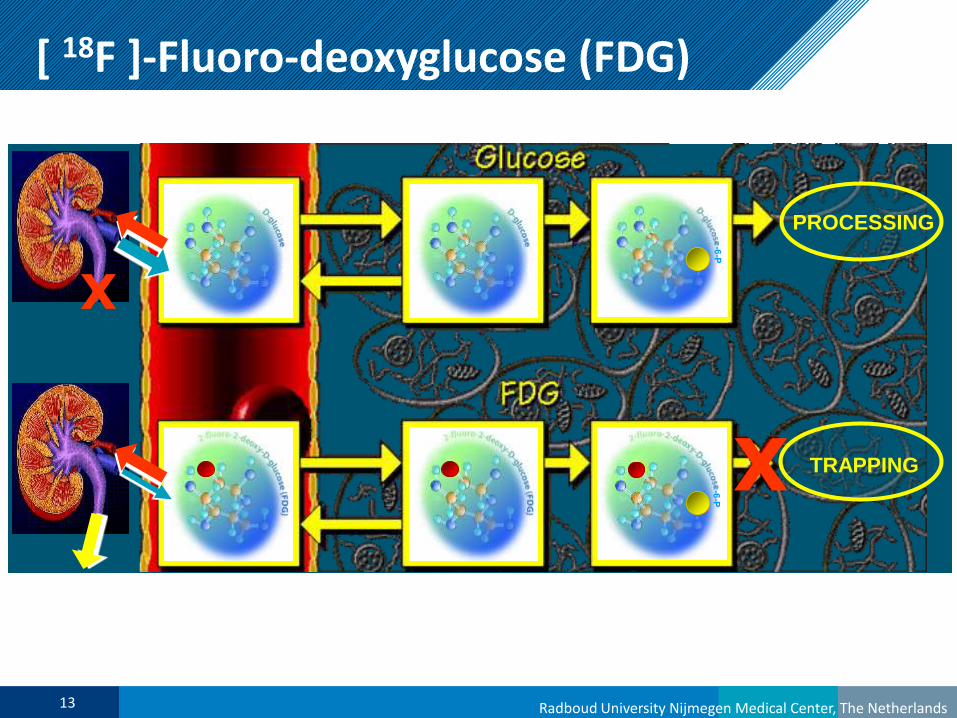
[ 18F ]-Fluoro-deoxyglucose (FDG)
Radboud University Nijmegen Medical Center, The Netherlands
[ 18F ]-Fluoro-deoxyglucose (FDG)
het meest belangrijke PET-radiopharmaconPROCESSING
TRAPPINGX
X
14 Radboud University Nijmegen Medical Center, The NetherlandsRadboud University Nijmegen Medical Center, The Netherlands
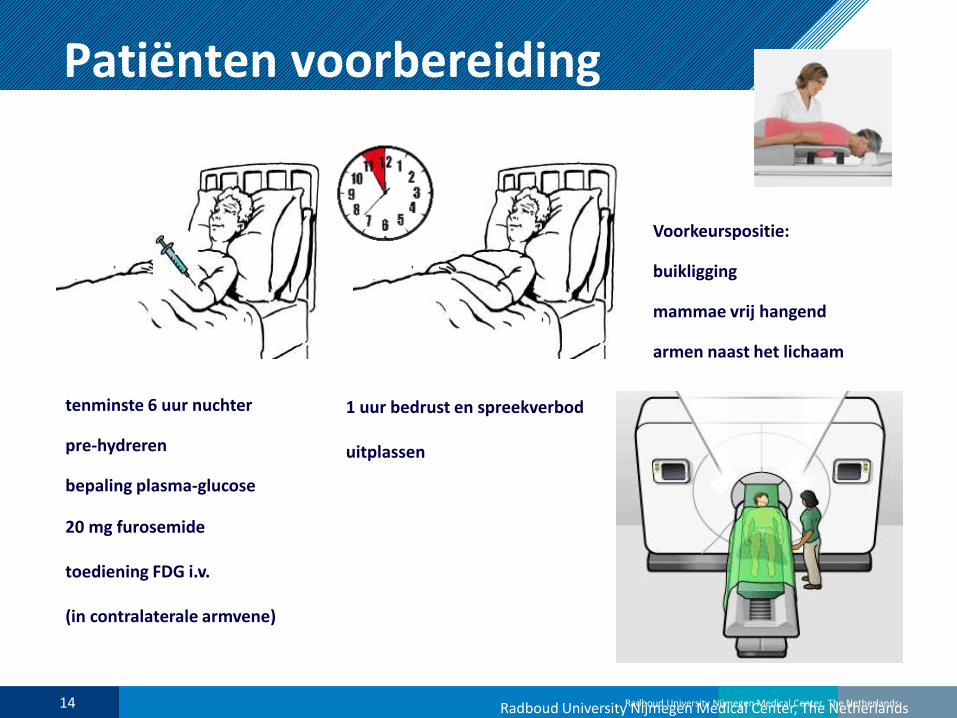
Patiënten voorbereiding
FDG
tenminste 6 uur nuchter
pre-hydreren
bepaling plasma-glucose
20 mg furosemide
toediening FDG i.v.
(in contralaterale armvene)
1 uur bedrust en spreekverbod
uitplassen
Voorkeurspositie:
buikligging
mammae vrij hangend
armen naast het lichaam
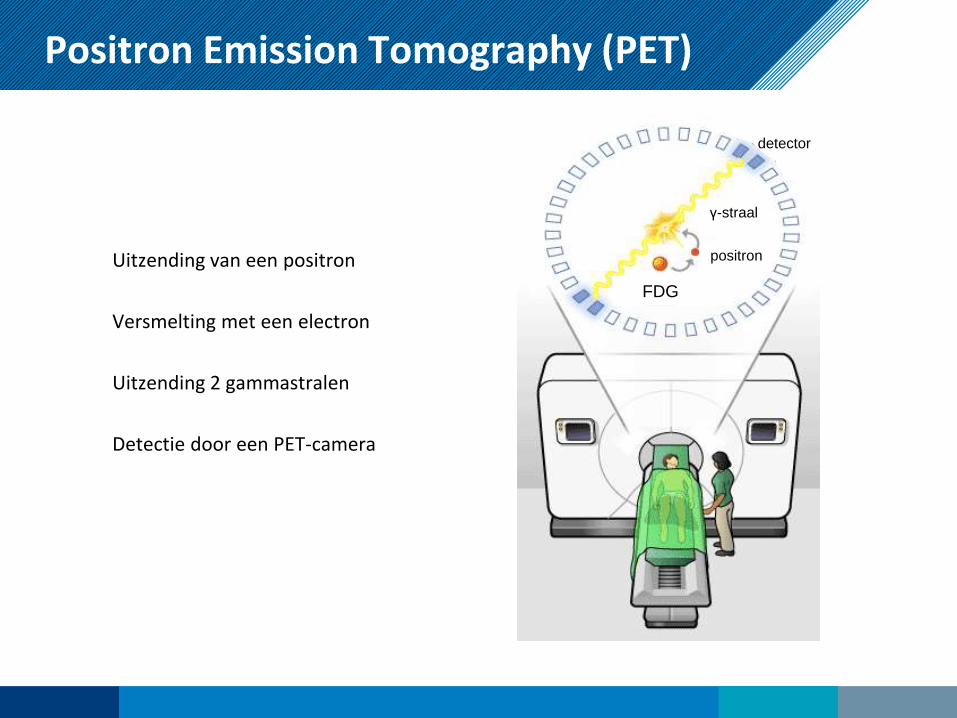
Positron Emission Tomography (PET)
Uitzending van een positron
Versmelting met een electron
Uitzending 2 gammastralen
Detectie door een PET-camera
FDG
positron
γ-straal
detector
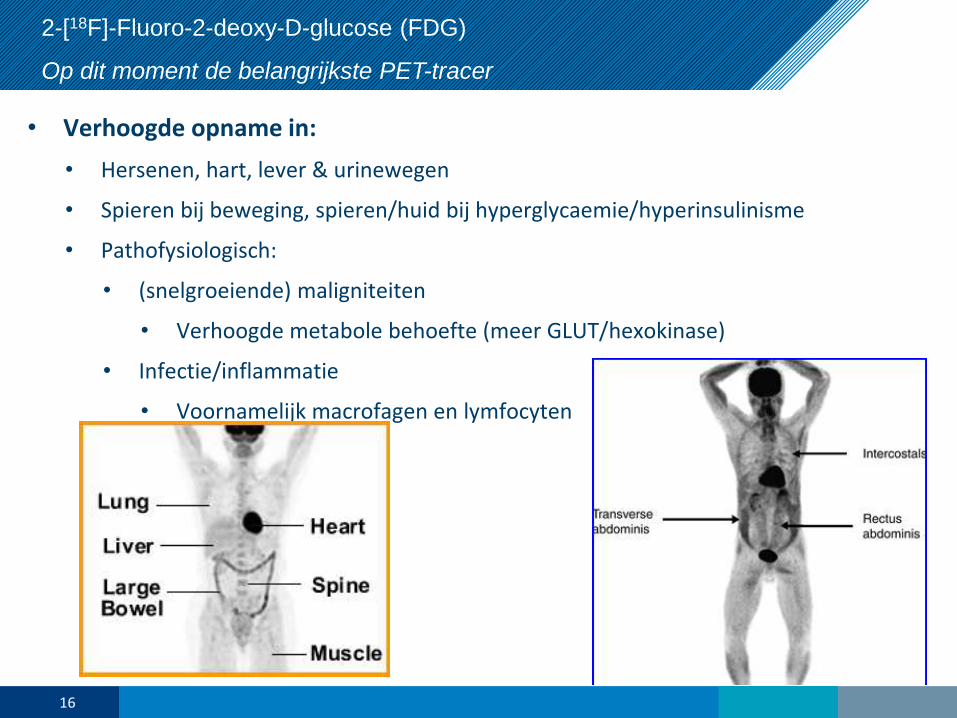
2-[18F]-Fluoro-2-deoxy-D-glucose (FDG)
Op dit moment de belangrijkste PET-tracer
• Verhoogde opname in:
• Hersenen, hart, lever & urinewegen
• Spieren bij beweging, spieren/huid bij hyperglycaemie/hyperinsulinisme
• Pathofysiologisch:
• (snelgroeiende) maligniteiten
• Verhoogde metabole behoefte (meer GLUT/hexokinase)
• Infectie/inflammatie
• Voornamelijk macrofagen en lymfocyten
16
Wat is nucleaire geneeskunde?
Nucleaire geneeskunde en moleculaire beeldvorming is het klinisch en ondersteunend
specialisme dat zich bezig houdt met het
• kwantificeren,
• afbeelden
• behandelen
van biologische processen door gebruik te maken van ioniserende straling welke aan de
patiënt wordt toegediend.
Gefuseerde specialisatie met radiologie (sinds 2015)
Dus NIET:
• Beeldvorming met CT/MRI/US/X-ray: klassieke radiologie
• Therapie met uitwendige bestraling/brachytherapie: radiotherapie
17
18
Welke indicaties?
•bij het stellen van de diagnose
•om beeldgeleide puncties te verrichten
•bij het bepalen van het tumorstadium
•om het operatiegebied te bepalen
•om het bestralingsvolume vast te stellen
•om het effect van de therapie te evalueren
•om de radicaliteit van de behandeling te bepalen
•bij verdenking op terugkeer van de ziekte

Specifieke indicatiesiKNL / HOVON
19
20
Specifieke indicatiesMammacarcinoom
• (Her)stadiëring:
• Schildwachtklierprocedure:
T1-2(-3)N0, evt. DCIS. >95% succesvol. Indien SWK+ gevolgd door OKD.
Bij pN0: veilig alternatief OKD, minder morbiditeit.
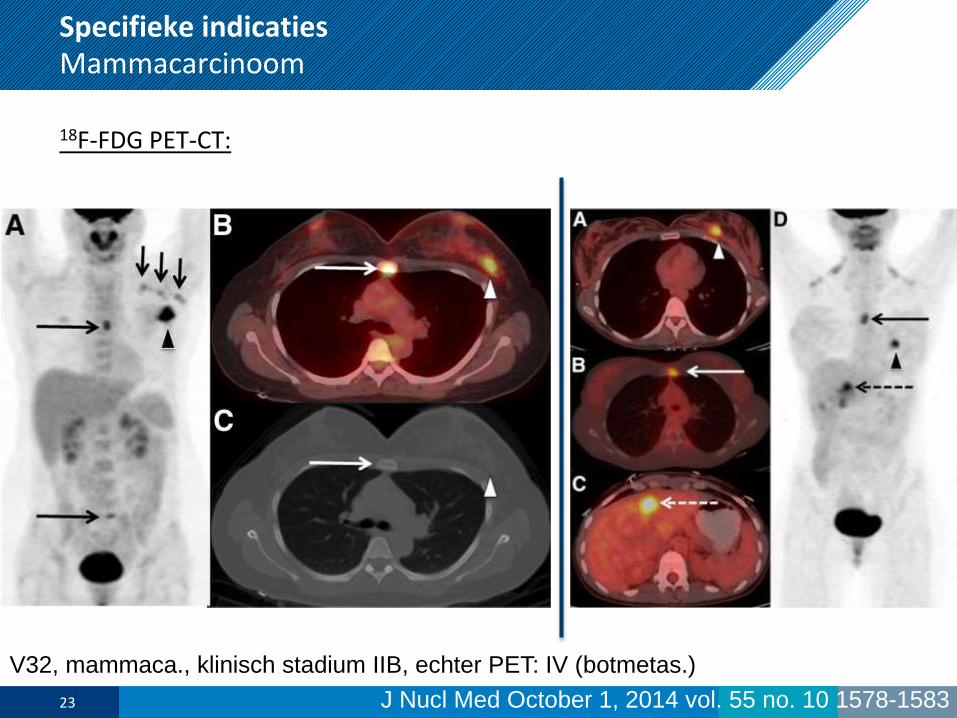
• 18F-FDG PET-CT:
Ter vervanging van het conventionele stadiëringsonderzoek.
Geadviseerd bij stadium III. Overweeg bij stadium II ikv neoadjuvante
behandeling of bij klachten wijzend op recidief/M+.
- T: Se 80% (T1 68%, T2 92%)
- N: Se 63%; Sp 94%
- Recidiefdetectie/M+: Se 93%
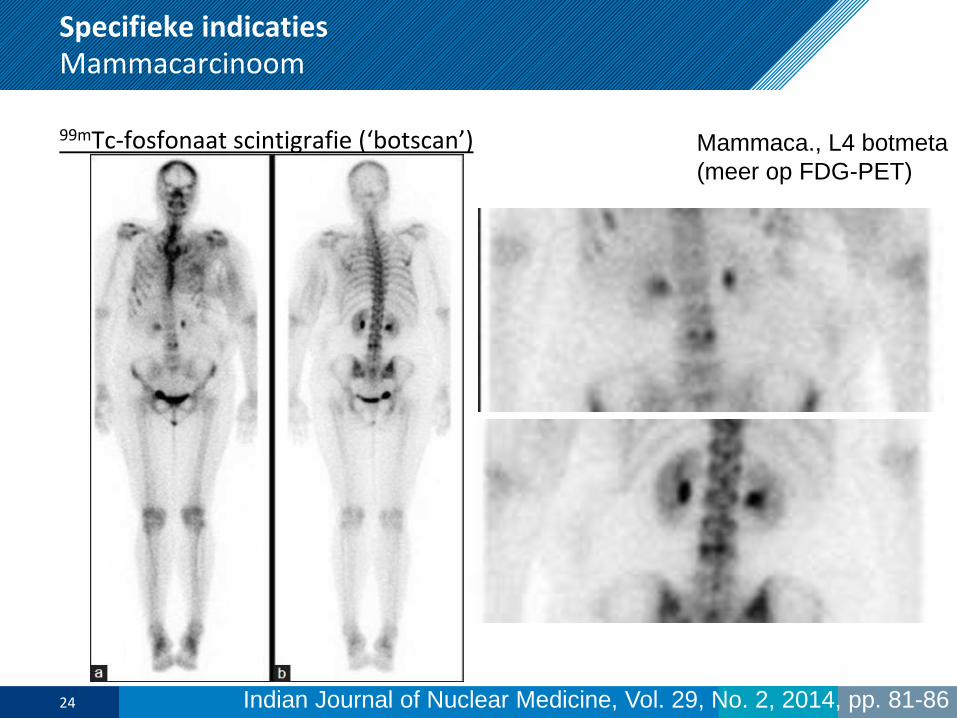
• Botscintigrafie:
Als onderdeel bij stadiering van stadium III. Specifiek bij klachten.21
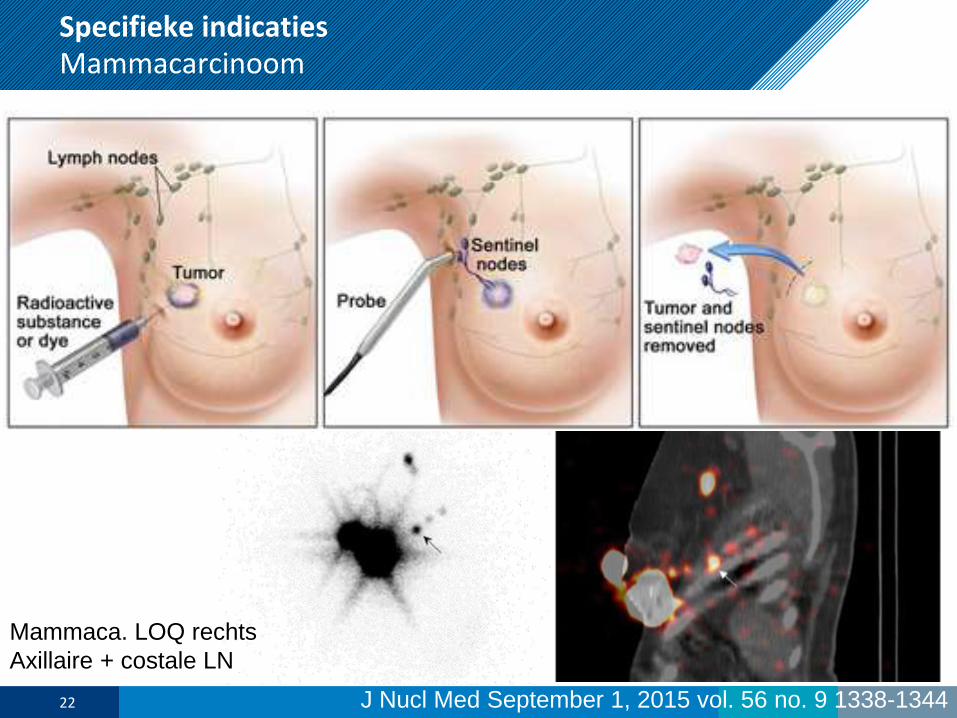
Specifieke indicatiesMammacarcinoom
J Nucl Med September 1, 2015 vol. 56 no. 9 1338-134422
Mammaca. LOQ rechts
Axillaire + costale LN
Specifieke indicatiesMammacarcinoom
18F-FDG PET-CT:
23 J Nucl Med October 1, 2014 vol. 55 no. 10 1578-1583
V32, mammaca., klinisch stadium IIB, echter PET: IV (botmetas.)
Specifieke indicatiesMammacarcinoom
99mTc-fosfonaat scintigrafie (‘botscan’)
24 Indian Journal of Nuclear Medicine, Vol. 29, No. 2, 2014, pp. 81-86
Mammaca., L4 botmeta
(meer op FDG-PET)
Specifieke indicatiesMammacarcinoom
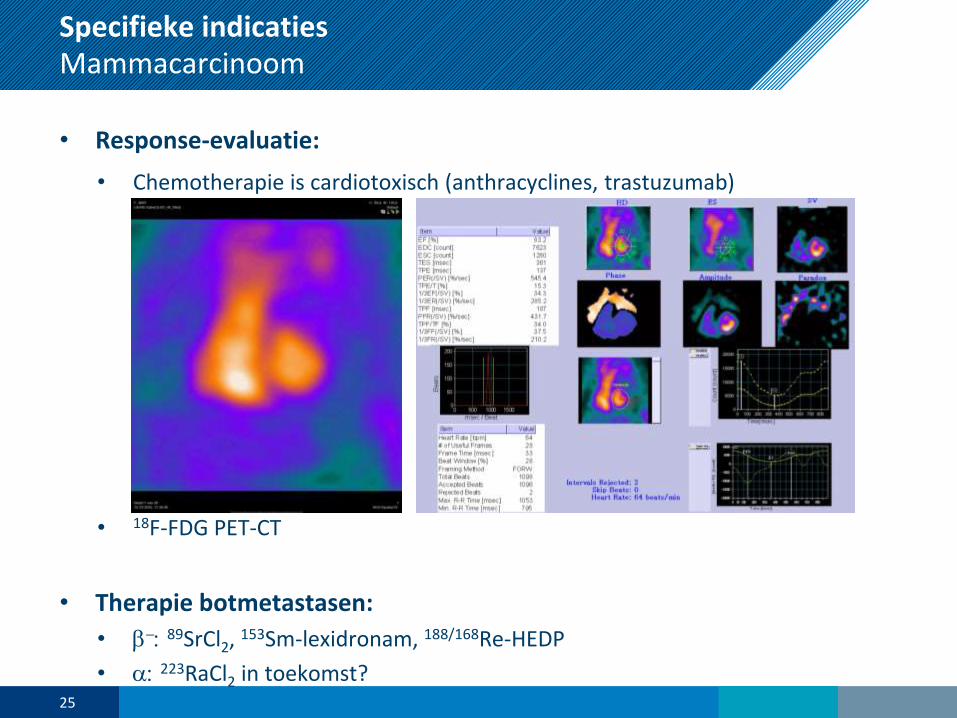
• Response-evaluatie:
• Chemotherapie is cardiotoxisch (anthracyclines, trastuzumab)
• 18F-FDG PET-CT
• Therapie botmetastasen:
• b-: 89SrCl2, 153Sm-lexidronam, 188/168Re-HEDP
• a: 223RaCl2 in toekomst?25

26
Specifieke indicatiesProstaatcarcinoom
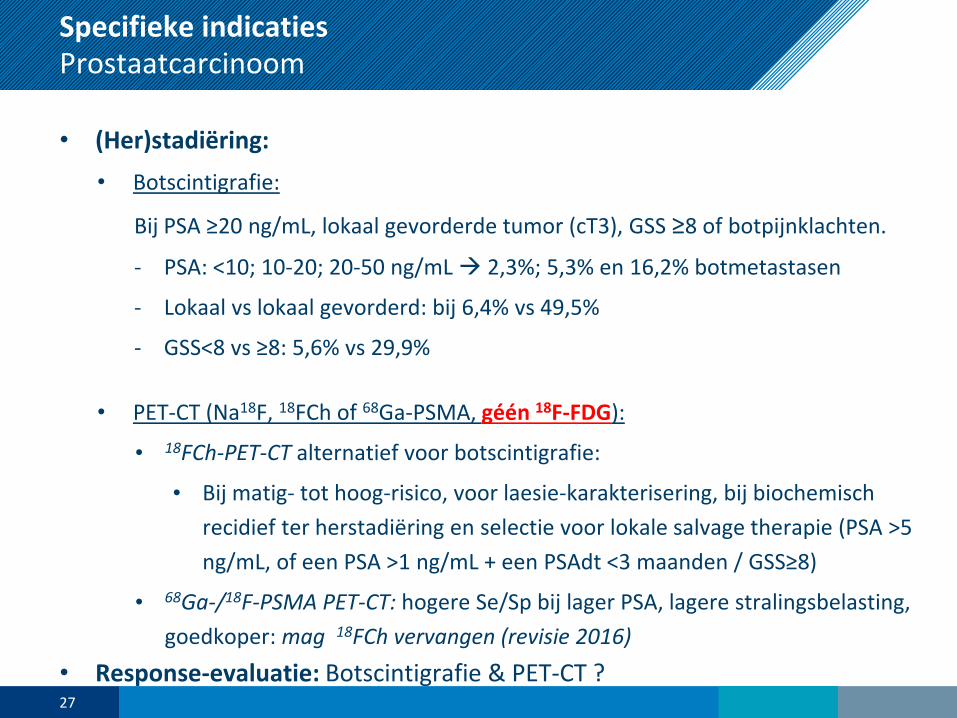
• (Her)stadiëring:
• Botscintigrafie:
Bij PSA ≥20 ng/mL, lokaal gevorderde tumor (cT3), GSS ≥8 of botpijnklachten.
- PSA: <10; 10-20; 20-50 ng/mL 2,3%; 5,3% en 16,2% botmetastasen
- Lokaal vs lokaal gevorderd: bij 6,4% vs 49,5%
- GSS<8 vs ≥8: 5,6% vs 29,9%
• PET-CT (Na18F, 18FCh of 68Ga-PSMA, géén 18F-FDG):
• 18FCh-PET-CT alternatief voor botscintigrafie:
• Bij matig- tot hoog-risico, voor laesie-karakterisering, bij biochemisch
recidief ter herstadiëring en selectie voor lokale salvage therapie (PSA >5
ng/mL, of een PSA >1 ng/mL + een PSAdt <3 maanden / GSS≥8)
• 68Ga-/18F-PSMA PET-CT: hogere Se/Sp bij lager PSA, lagere stralingsbelasting,
goedkoper: mag 18FCh vervangen (revisie 2016)
• Response-evaluatie: Botscintigrafie & PET-CT ?27
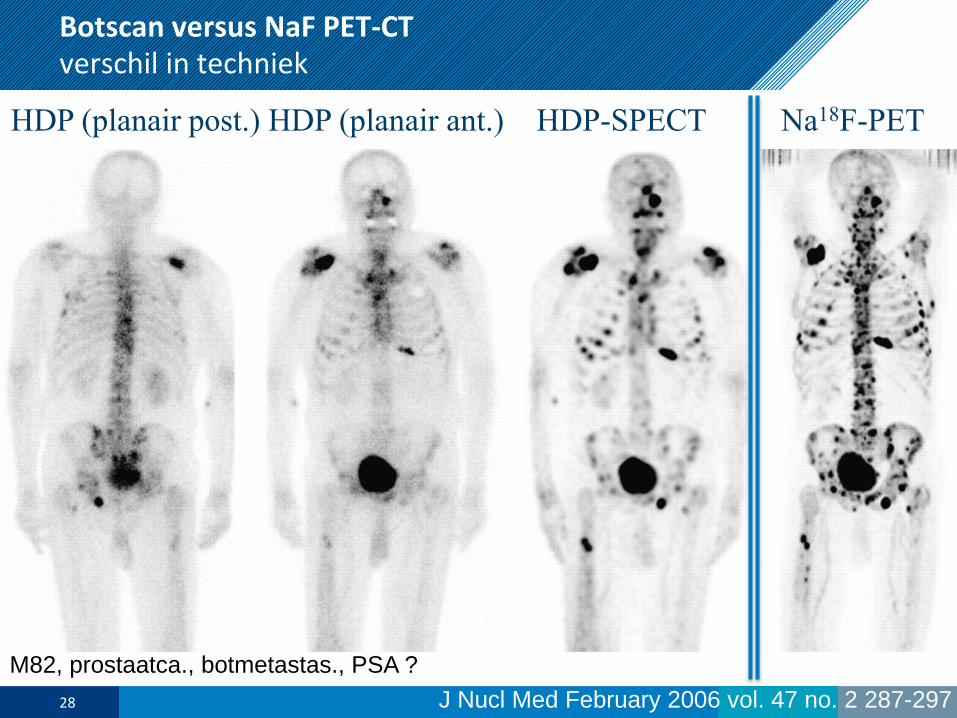
HDP (planair post.) HDP (planair ant.) HDP-SPECT Na18F-PET
J Nucl Med February 2006 vol. 47 no. 2 287-297
Botscan versus NaF PET-CTverschil in techniek
28
M82, prostaatca., botmetastas., PSA ?
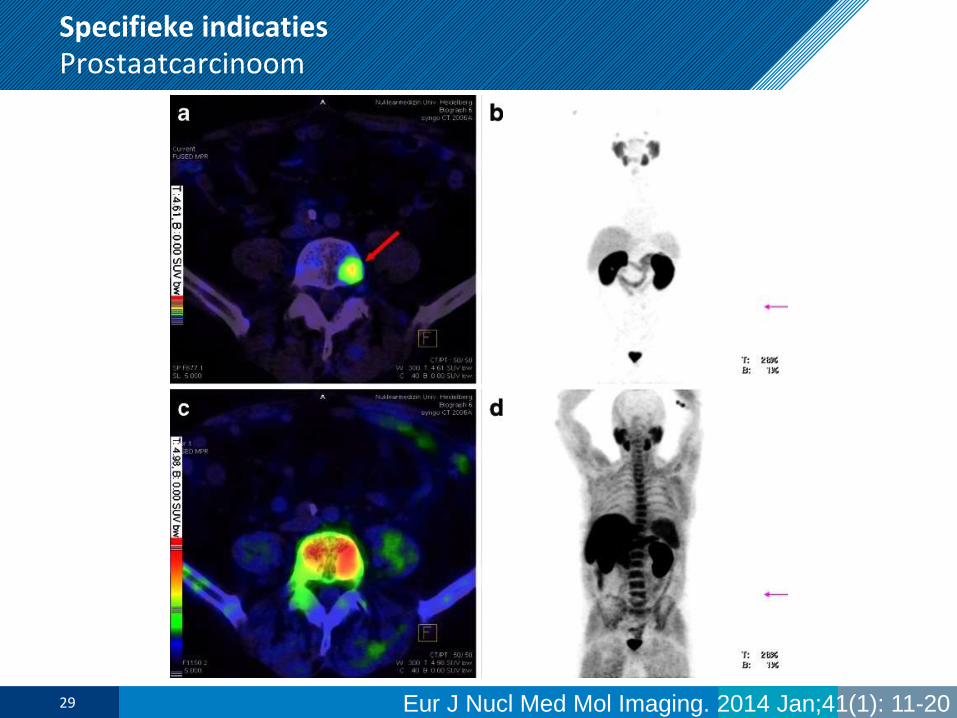
Specifieke indicatiesProstaatcarcinoom
Eur J Nucl Med Mol Imaging. 2014 Jan;41(1): 11-2029
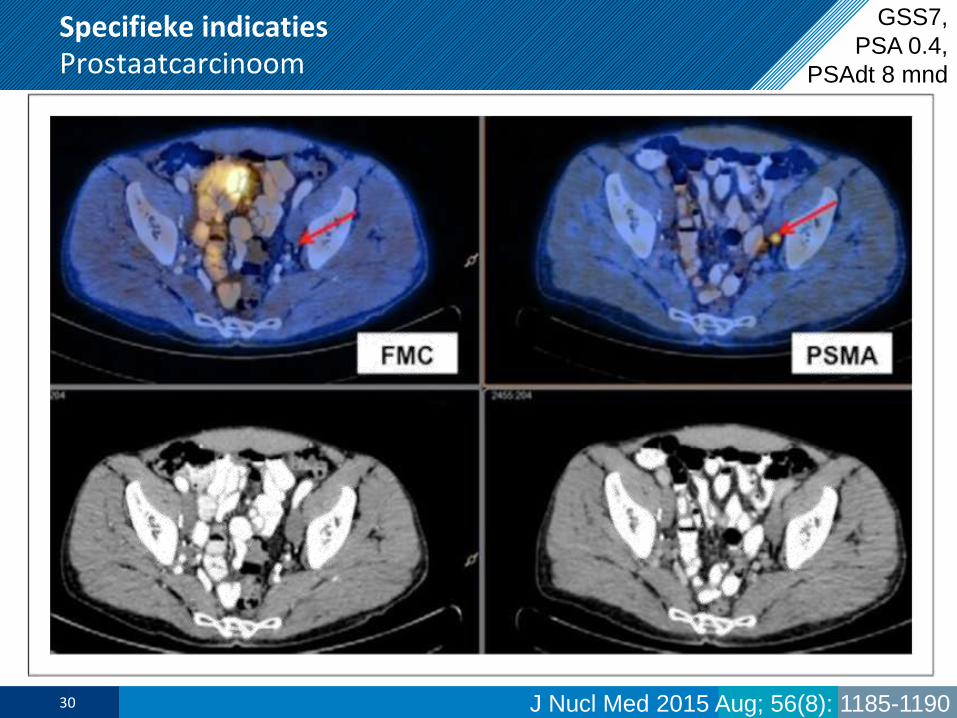
Specifieke indicatiesProstaatcarcinoom
J Nucl Med 2015 Aug; 56(8): 1185-119030
GSS7,
PSA 0.4,
PSAdt 8 mnd
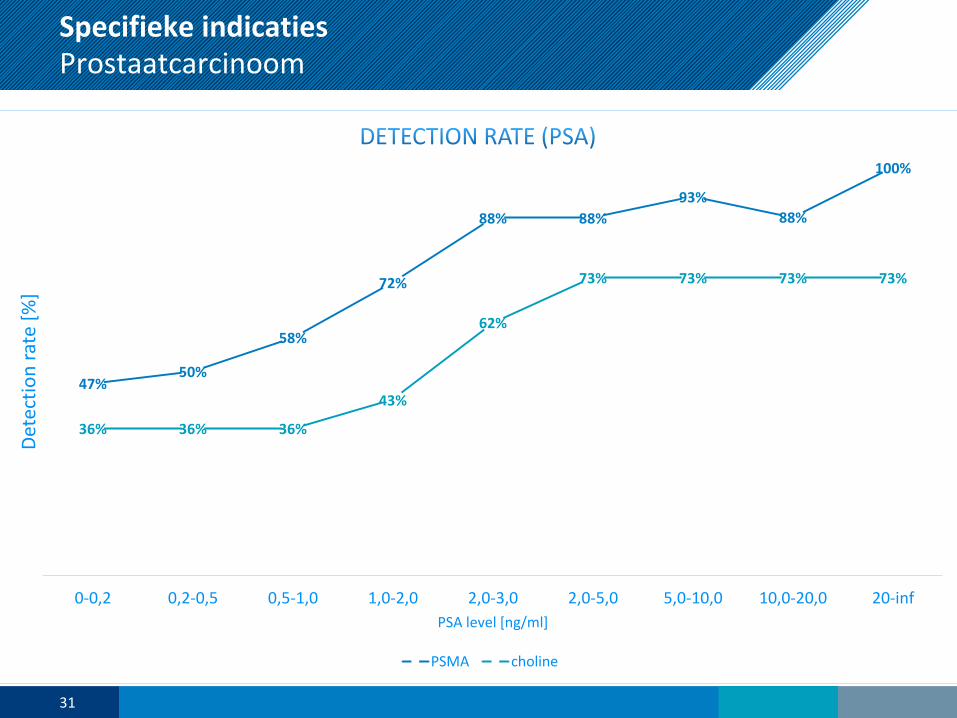
Specifieke indicatiesProstaatcarcinoom
47%50%
58%
72%
88% 88%
93%
88%
100%
36% 36% 36%
43%
62%
73% 73% 73% 73%
0-0,2 0,2-0,5 0,5-1,0 1,0-2,0 2,0-3,0 2,0-5,0 5,0-10,0 10,0-20,0 20-inf
Det
ecti
on
rat
e [%
]
PSA level [ng/ml]
PSMA choline
31
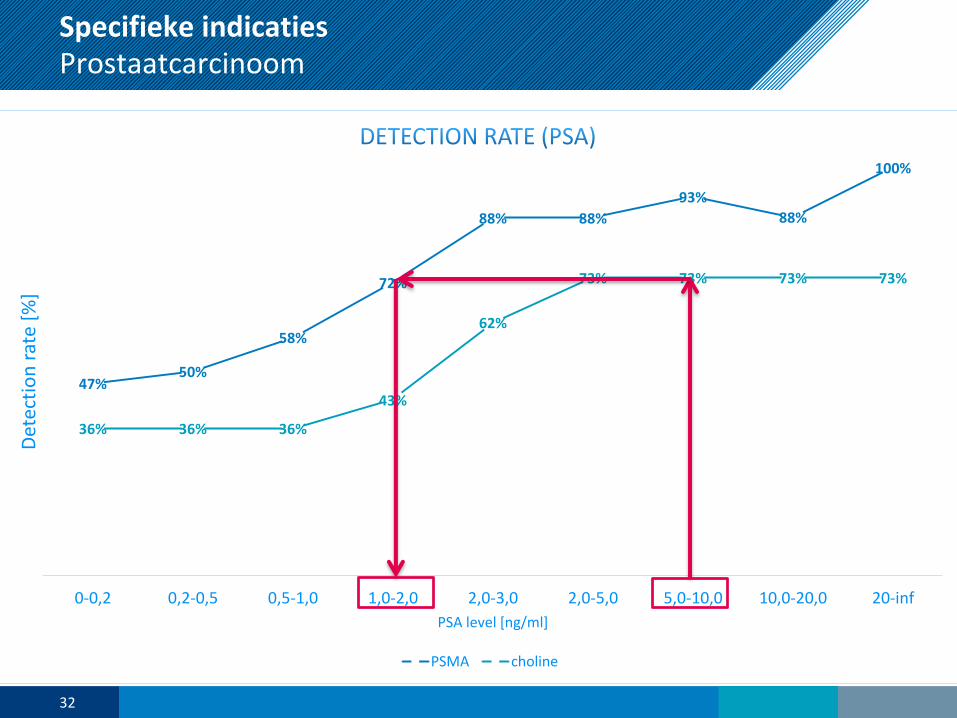
Specifieke indicatiesProstaatcarcinoom
47%50%
58%
72%
88% 88%
93%
88%
100%
36% 36% 36%
43%
62%
73% 73% 73% 73%
0-0,2 0,2-0,5 0,5-1,0 1,0-2,0 2,0-3,0 2,0-5,0 5,0-10,0 10,0-20,0 20-inf
Det
ecti
on
rat
e [%
]
PSA level [ng/ml]
PSMA choline
32
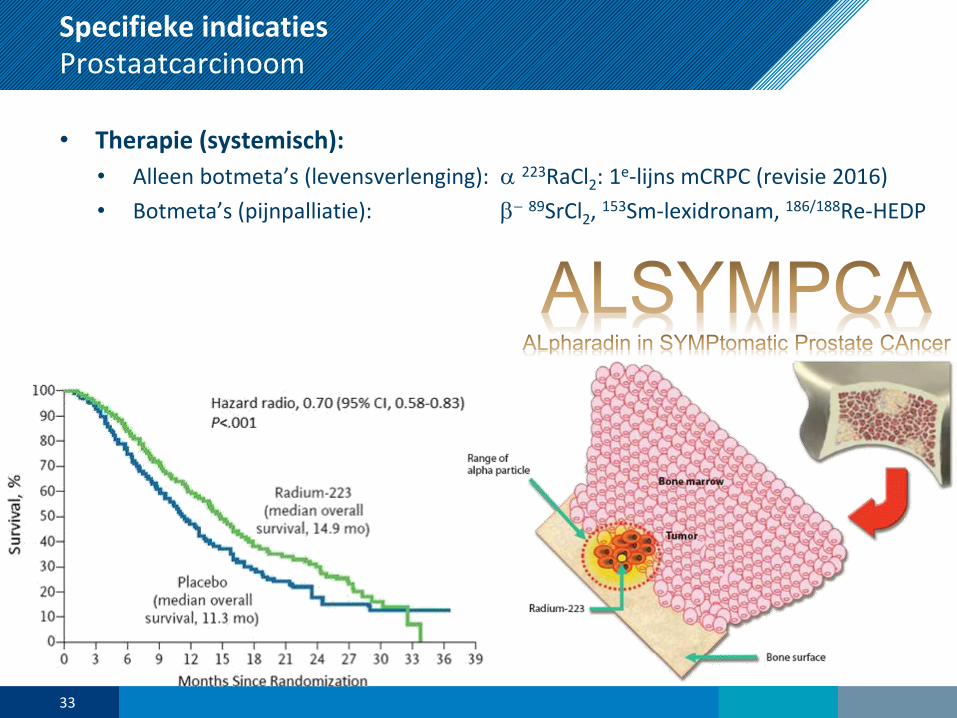
Specifieke indicatiesProstaatcarcinoom
• Therapie (systemisch):
• Alleen botmeta’s (levensverlenging): a 223RaCl2: 1e-lijns mCRPC (revisie 2016)
• Botmeta’s (pijnpalliatie): b- 89SrCl2, 153Sm-lexidronam, 186/188Re-HEDP
33
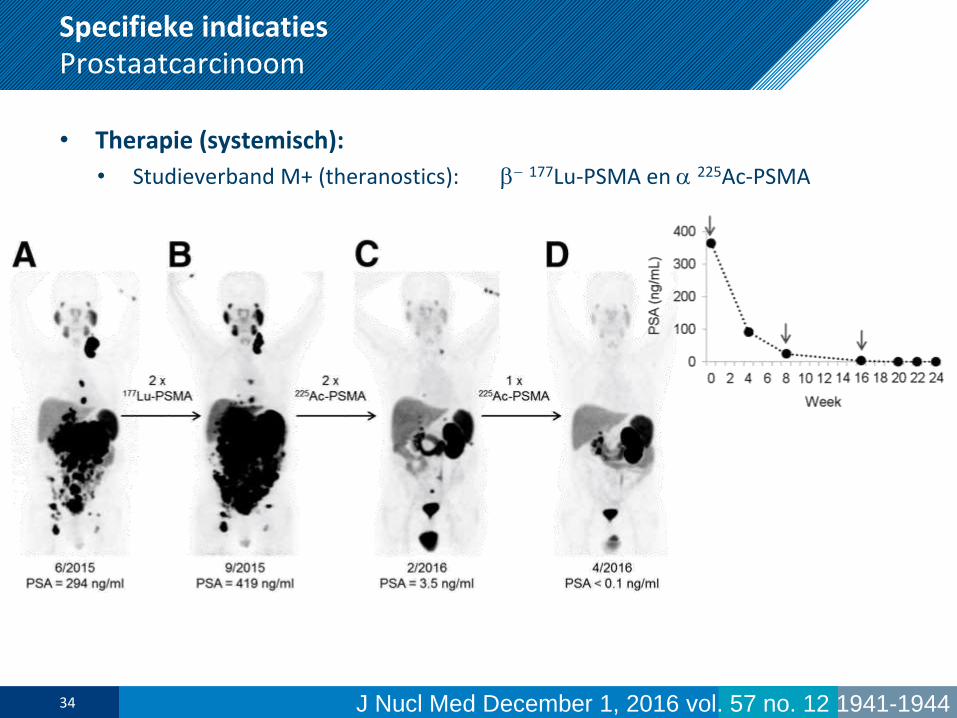
Specifieke indicatiesProstaatcarcinoom
• Therapie (systemisch):
• Studieverband M+ (theranostics): b- 177Lu-PSMA en a 225Ac-PSMA
34 J Nucl Med December 1, 2016 vol. 57 no. 12 1941-1944

35
Specifieke indicatiesMaligne Melanoom
• (Her)stadiëring:
• Schildwachtklierprocedure:
- Bij stadium IB en hoger voor optimale stadiëring en prognose informatie.
- Indien SWK+ (geen m-metastasen), gevolgd door lymfeklierdissectie, echter:
- Overlevingswinst gesuggereerd in MSLT-1 maar niet bevestigd in MSLT-2.
• 18F-FDG PET-ceCT thorax-bekken (revisie 2016):
• Stadiering primaire of recidief: bij stadium IIIB-IV (niet: bij I-IIIA)
• Follow-up: behalve bij in opzet curatief geopereerd stadium III/IV, bij
verdenking op behandelbaar recidief o.b.v. S100B bepalingen (± LDH)
• Response-evaluatie:
• mogelijk met 18F-FDG PET-CT
• nog research-onderwerp voor immunotherapie effect en irAEs
36
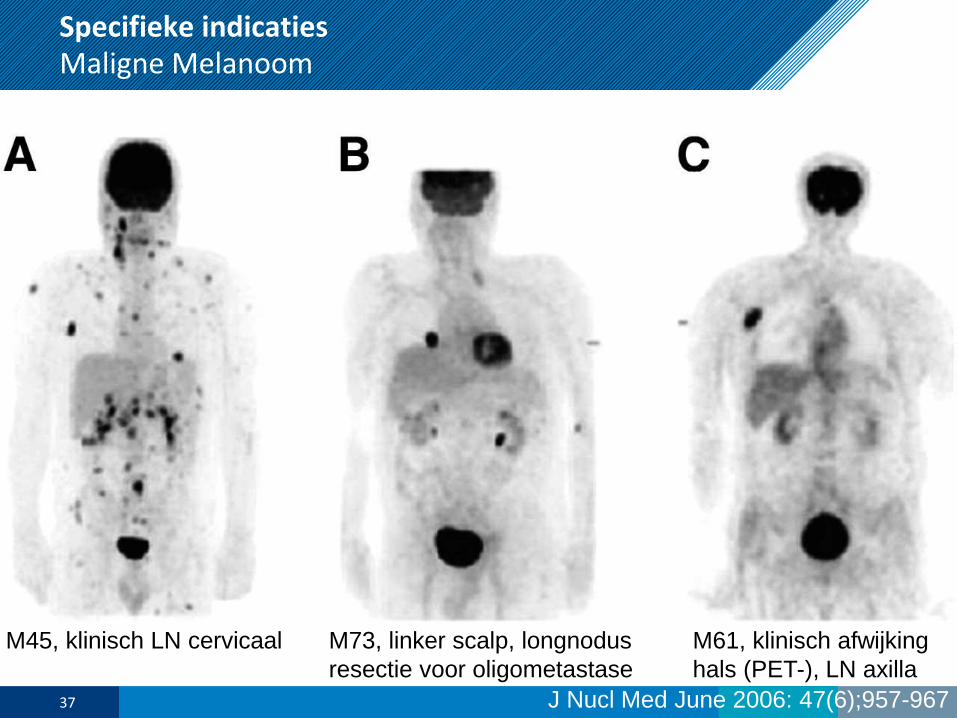
Specifieke indicatiesMaligne Melanoom
J Nucl Med June 2006: 47(6);957-96737
M45, klinisch LN cervicaal M73, linker scalp, longnodus
resectie voor oligometastase
M61, klinisch afwijking
hals (PET-), LN axilla
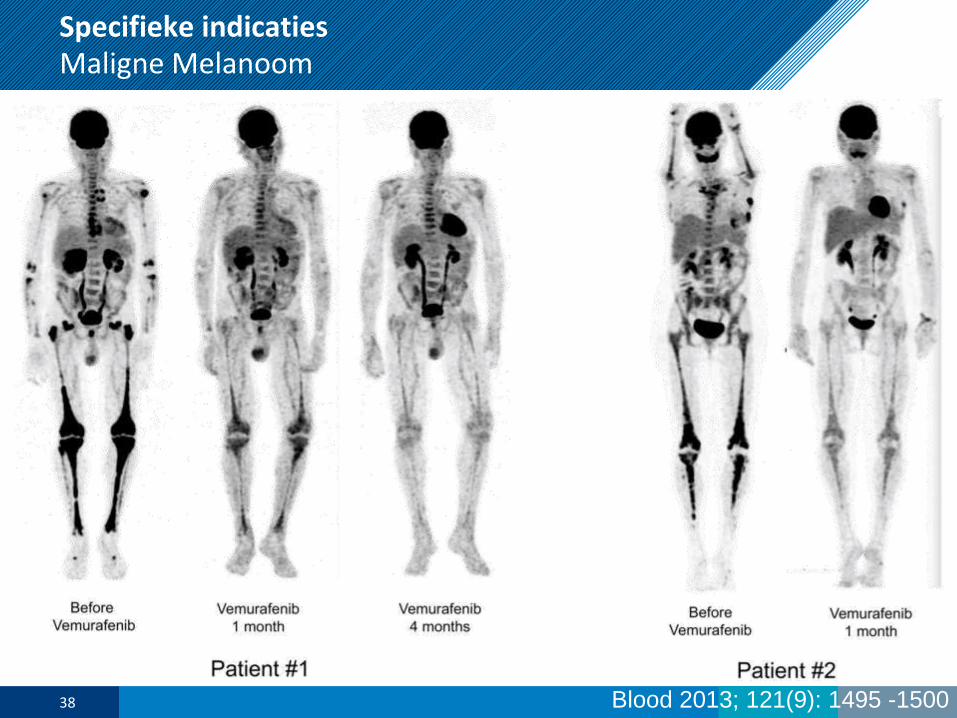
Specifieke indicatiesMaligne Melanoom
Blood 2013; 121(9): 1495 -150038

39
Specifieke indicatiesColorectaal- en anuscarcinoom
• (Her)stadiëring :
• 18F-FDG PET-CT:
• Colorectaal carcinoom:
T/N: te lage sensitiviteit
M: niet standaard (PET=ceCT), ook niet vóór HIPEC
wel bij ambigue laesies of vóór M-ectomie (20% beleidswijzigingen)
Recidief: onbegrepen verhoogd CEA, vermoeden recidief na RFA/cryo
• Anuscarcinoom:
T: Se 93%; Sp 50% (fysiologische spier-uptake)
N: Se 89% (23% ander stadiëring, >13% beleidswijzigingen)
M: beperkte evidence, gezien beperkte incidentie M1
GTV: bepalen radiotherapie volume
Recidief: te overwegen vóór APR ter exclusie afstandsmetastasen.
• Response-evaluatie: 18F-FDG PET-CT predictief en prognostisch.
• Therapie: Radio-embolisatie met 90Y of 166Ho
40
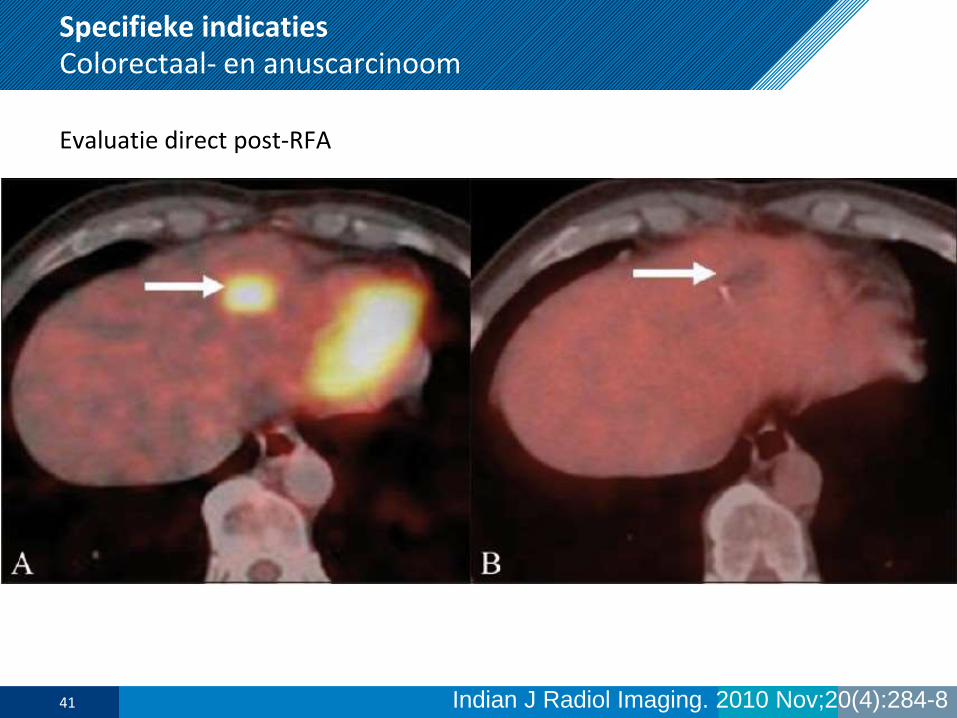
Specifieke indicatiesColorectaal- en anuscarcinoom
Evaluatie direct post-RFA
Indian J Radiol Imaging. 2010 Nov;20(4):284-841
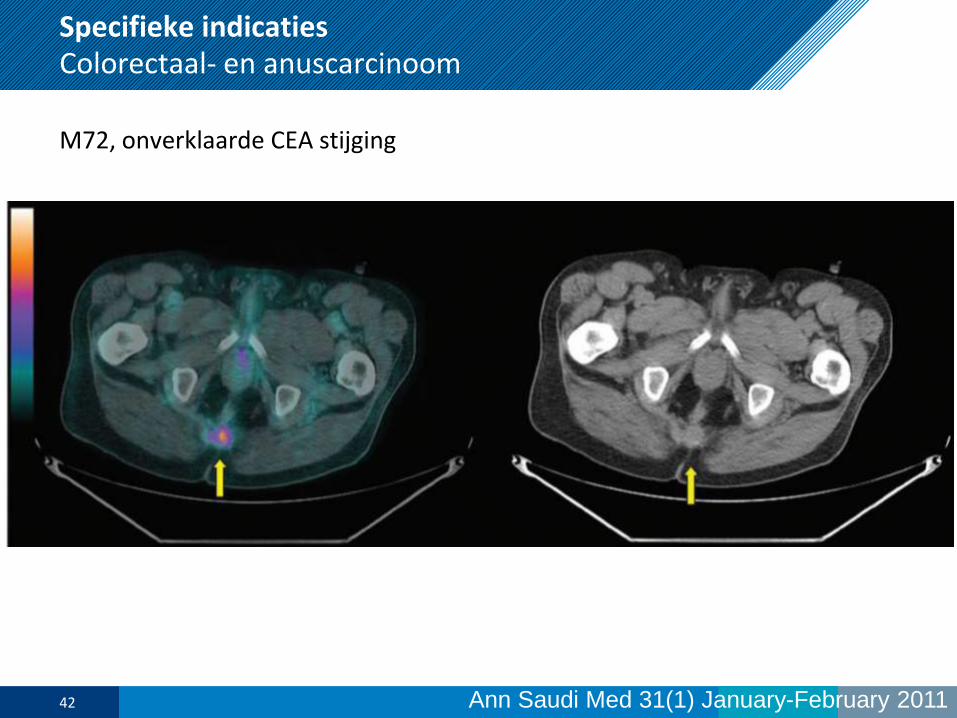
Specifieke indicatiesColorectaal- en anuscarcinoom
M72, onverklaarde CEA stijging
Ann Saudi Med 31(1) January-February 201142
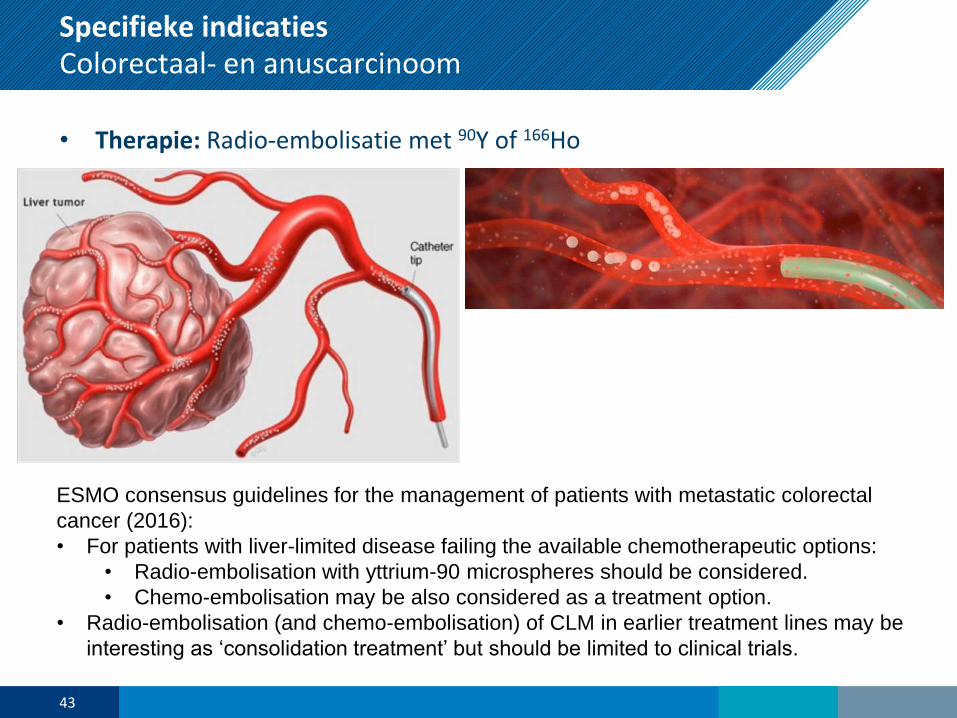
Specifieke indicatiesColorectaal- en anuscarcinoom
• Therapie: Radio-embolisatie met 90Y of 166Ho
43
ESMO consensus guidelines for the management of patients with metastatic colorectal
cancer (2016):
• For patients with liver-limited disease failing the available chemotherapeutic options:
• Radio-embolisation with yttrium-90 microspheres should be considered.
• Chemo-embolisation may be also considered as a treatment option.
• Radio-embolisation (and chemo-embolisation) of CLM in earlier treatment lines may be
interesting as ‘consolidation treatment’ but should be limited to clinical trials.

44
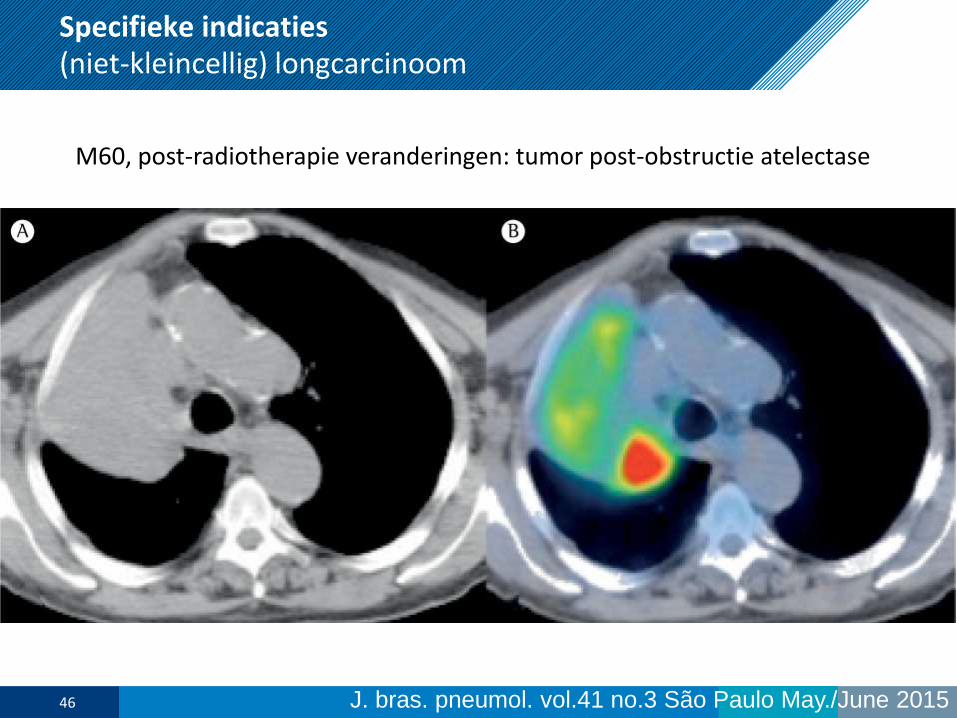
Specifieke indicaties(niet-kleincellig) longcarcinoom
• (Her)stadiëring:
• Botscintigrafie: Obsoleet door 18F-FDG PET-CT
• 18F-FDG PET-CT:
- Vóór iedere in opzet curatieve behandeling (verlaagd futiele thoracotomie,
betere SBRT)
- N: Bij niet-centrale, FDG-avide tumoren zonder vergrote (>1cm) lymfeklieren
kan weefseldiagnostiek achterwegen gelaten worden (Se 92%; Sp 84%).
- M: Se 85%; Sp 56%. Bijnieren: Se 100% als >15mm. NB gevonden bij 10-20%;
- Classificatie solitaire longnodus, zeker indien positief en >1cm
- Groei post-radiotherapeutische veranderingen
• Radiotherapie-planning: 18F-FDG PET-CT
• Response-evaluatie: mogelijk met 18F-FDG PET-CT
45
Specifieke indicaties(niet-kleincellig) longcarcinoom
M60, post-radiotherapie veranderingen: tumor post-obstructie atelectase
J. bras. pneumol. vol.41 no.3 São Paulo May./June 201546

47
Specifieke indicatiesMaligne Lymfoom
• Stadiëring:
• 18F-FDG PET-CT:
- Stadiering baseline voor HL en FDG-avide NHL (10-30% verandering).
- Bepalen bestralingsveld
- Beenmergbetrokkenheid op PET biopsie niet meer nodig (DLBCL)
• Response-evaluatie:
• 18F-FDG PET-CT:
- Beoordeling volgens Deauville 5-puntschaal (interim en end-of-treatment)
- Score 1-2 (FDG-uptake<bloodpool): compleet metabole respons, NPV>90%
- Score 3 (FDG-uptake<lever): compleet metabole respons end-of-treatment
- Maar niet voor studies die de-escalatie overwegen (dan norm: <3)
• Therapie: 90Y-ibtritumomab tiuxetan (anti-CD20)
48
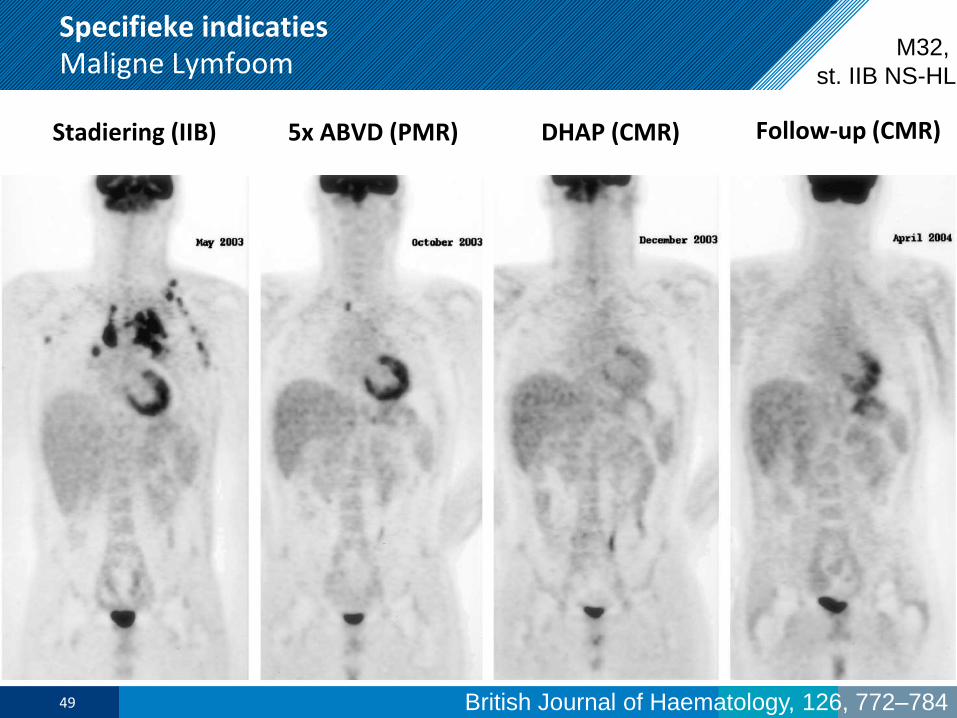
Specifieke indicatiesMaligne Lymfoom
Stadiering (IIB)
British Journal of Haematology, 126, 772–784
5x ABVD (PMR) DHAP (CMR) Follow-up (CMR)
49
M32,
st. IIB NS-HL
50
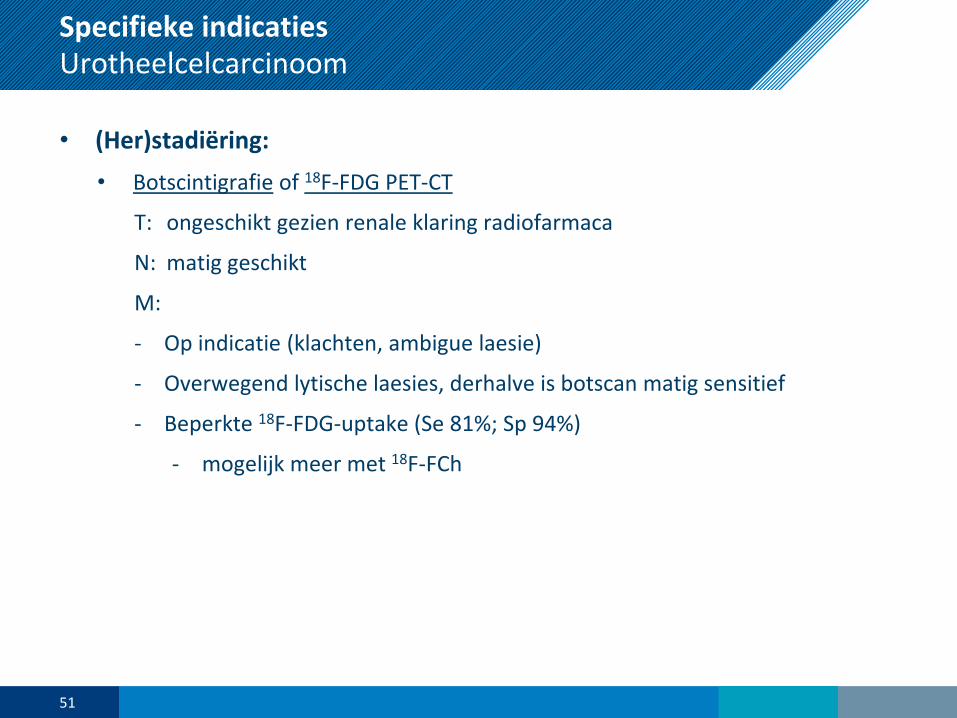
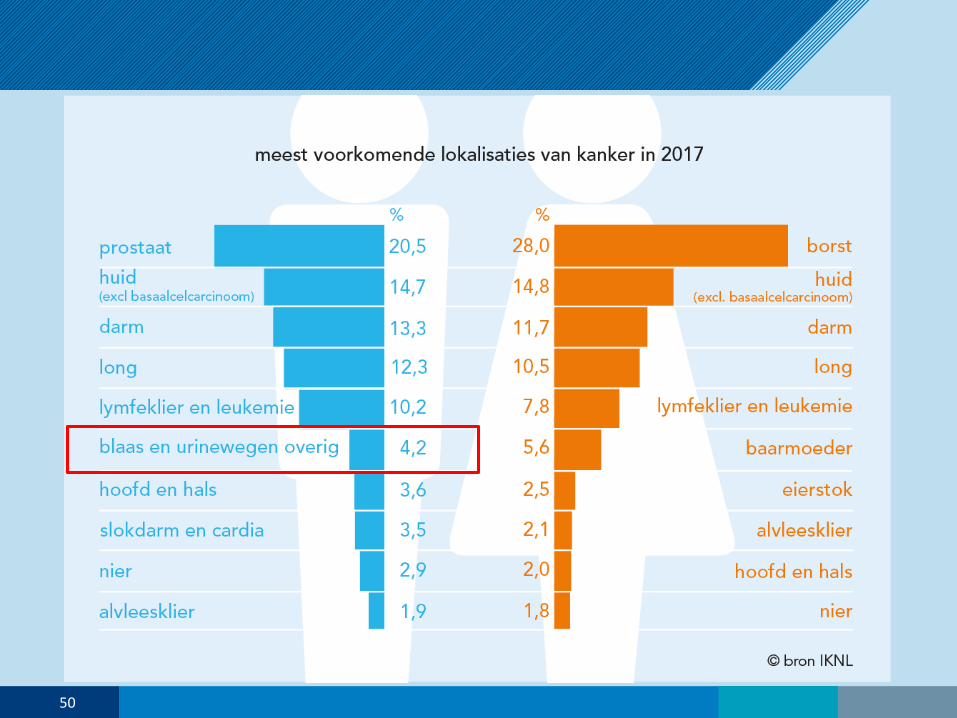
Specifieke indicatiesUrotheelcelcarcinoom
• (Her)stadiëring:
• Botscintigrafie of 18F-FDG PET-CT
T: ongeschikt gezien renale klaring radiofarmaca
N: matig geschikt
M:
- Op indicatie (klachten, ambigue laesie)
- Overwegend lytische laesies, derhalve is botscan matig sensitief
- Beperkte 18F-FDG-uptake (Se 81%; Sp 94%)
- mogelijk meer met 18F-FCh
51

Specifieke indicatiesUrotheelcelcarcinoom
Courtesy prof. Jan Pruim (UMCG)52
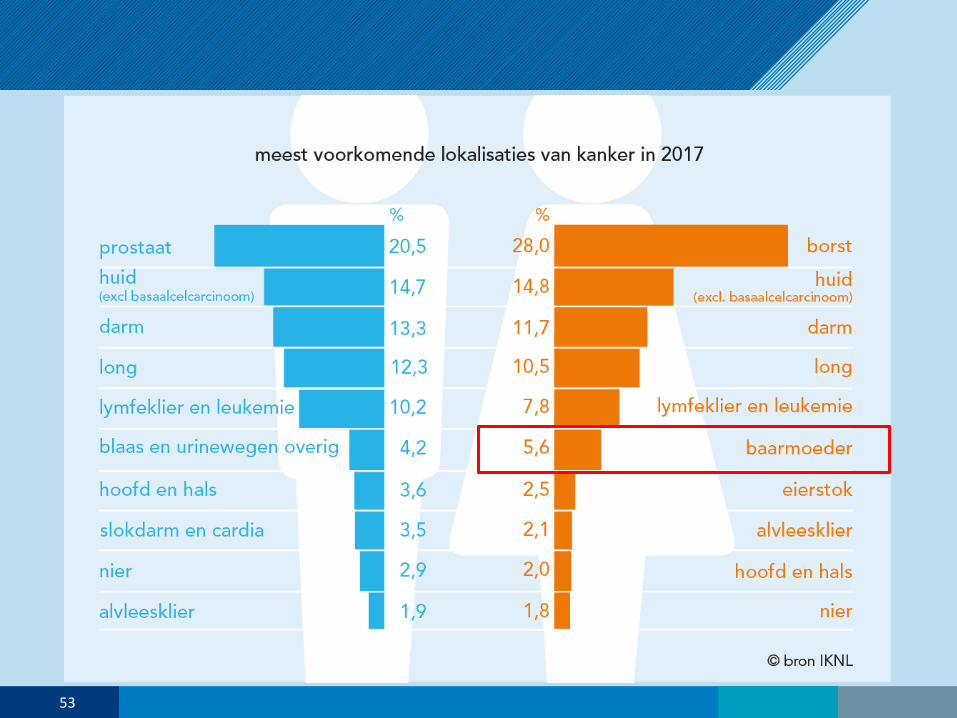
53
Specifieke indicatiesCervix- en Endometriumcarcinoom
• (Her)stadiëring:
• Schildwachtklierprocedure:
- Cervixcarcinoom: in onderzoeksverband (>84% succesvol, Se >77%)
- Endometriumcarcinoom: experimenteel
• 18F-FDG PET-CT:
- Cervixcarcinoom:
- Indien LN/M+ bij beeldvorming of operatie, voor hogere station LN (Se>66%;
Sp >98%) of afstandsmetastasen (Se 100%; Sp >94%)
- Klinische verdenking recidief (Se>87%; Sp >81%)
- Wanneer curatieve radiotherapie / bekken-exenteratie overwogen wordt
- Endometriumcarcinoom:
- geen plaats, MRI vooralsnog beter
- Evt. bij onbegrepen CA-125 stijging
54
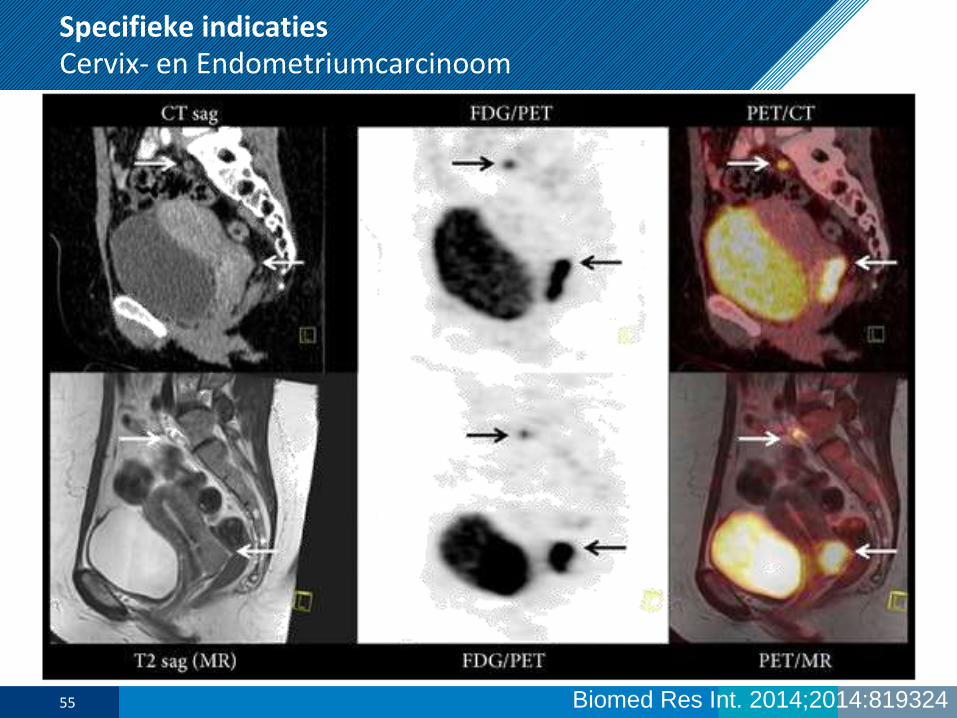
Specifieke indicatiesCervix- en Endometriumcarcinoom
Biomed Res Int. 2014;2014:81932455

56
Specifieke indicatiesHoofd/Hals Plaveiselcelcarcinoom
• (Her)stadiëring:
• 18F-FDG PET-CT:
- Bij een hoog risico op afstandsmetastasen (bv laag jugulaire klieren, bilaterale
halsklieren of N3 klieren).
- Bij carcinoma of unknown primary
- Tijdens follow-up laesie bij CT/MRI of klinische verdenking, zonder PA
- Radiotherapie-planning
- NIET voor uitsluiten 2e primaire
• Schildwachtklierprocedure: experimenteel
• Radiotherapie-planning: 18F-FDG PET-CT
• Response-evaluatie: 18F-FDG PET-CT
57
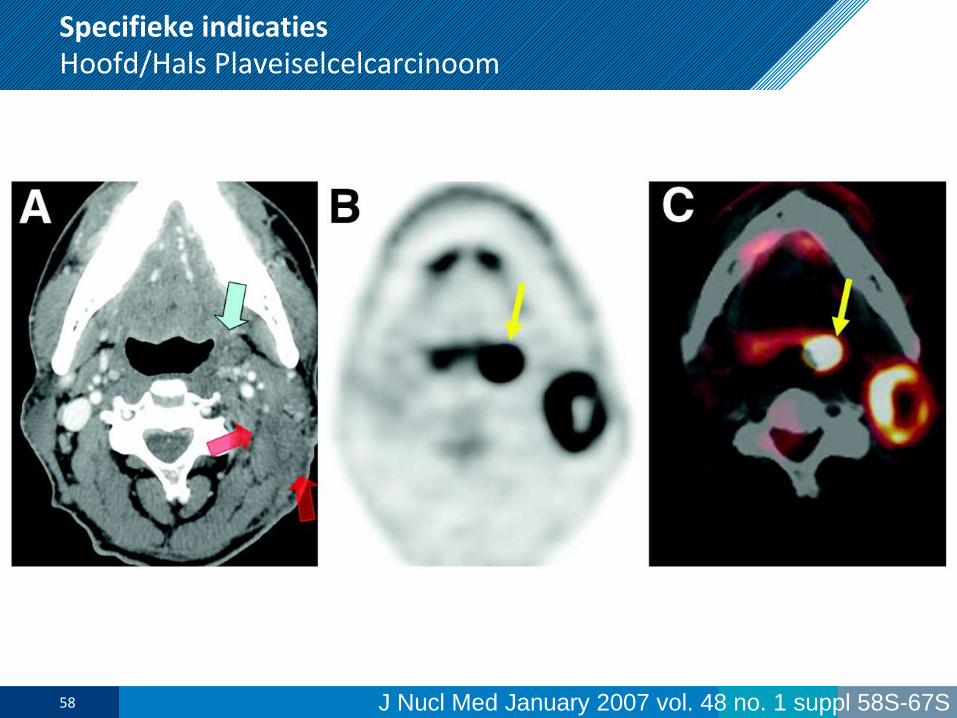
Specifieke indicatiesHoofd/Hals Plaveiselcelcarcinoom
J Nucl Med January 2007 vol. 48 no. 1 suppl 58S-67S58
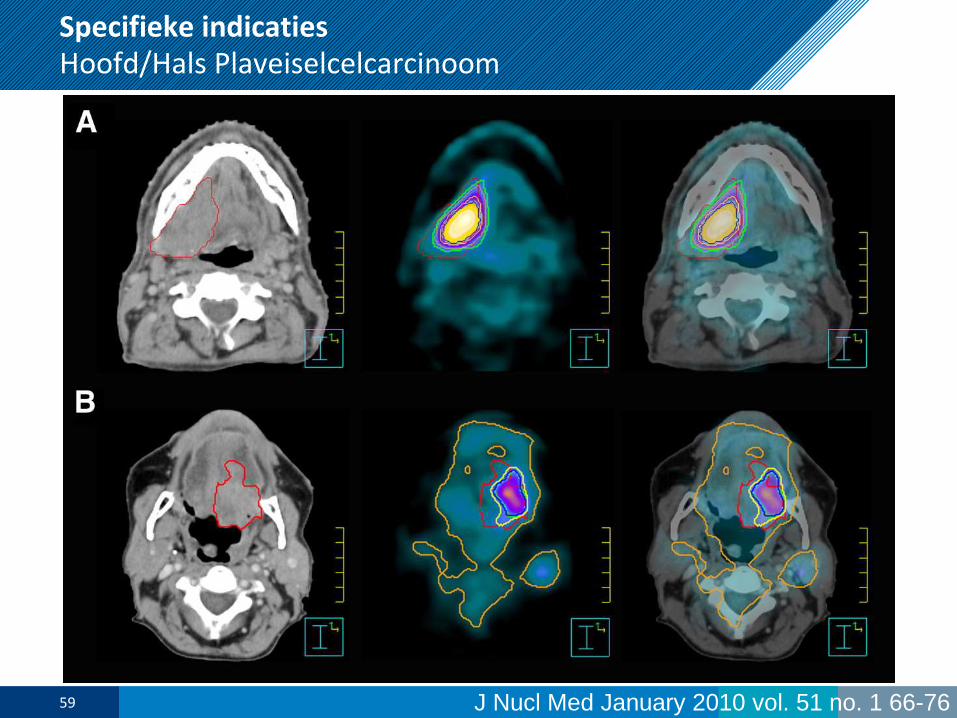
Specifieke indicatiesHoofd/Hals Plaveiselcelcarcinoom
J Nucl Med January 2010 vol. 51 no. 1 66-7659

60
Specifieke indicatiesOvariumcarcinoom
• (Her)stadiëring:
• Geen routine rol voor moleculaire beeldvorming
61

62
Specifieke indicatiesOesophagus(cardia)carcinoom
• (Her)stadiëring:
• 18F-FDG PET-CT:
Bij hoog-risicopatiënten (locally advanced maagcarcinoom T3-4 en/of N+) die in
aanmerking komen voor curatieve chirurgie (na initiële stadiëring), ter aantonen
van eventuele additionele afstandsmetastasen en onnodige chirurgie te
vermijden.
- T: Se 82-100% (behalve T1)
- N:
- Lokaal: matig (Se>35%; Sp>71%), PET+EUS: Se 85%; Sp 100%
- Regionaal: matig (Se 51%; Sp 84%)
- M: Se 67%; Sp 97% (upstaging naar M1 bij ca. 12%)
- Herstadiëring: bij T3 tumoren met curatieve behandelintentie, niet na
adjuvant chemoradiatie.
• Radiotherapie-planning: 18F-FDG PET-CT
• Response-evaluatie: 18F-FDG PET-CT
63
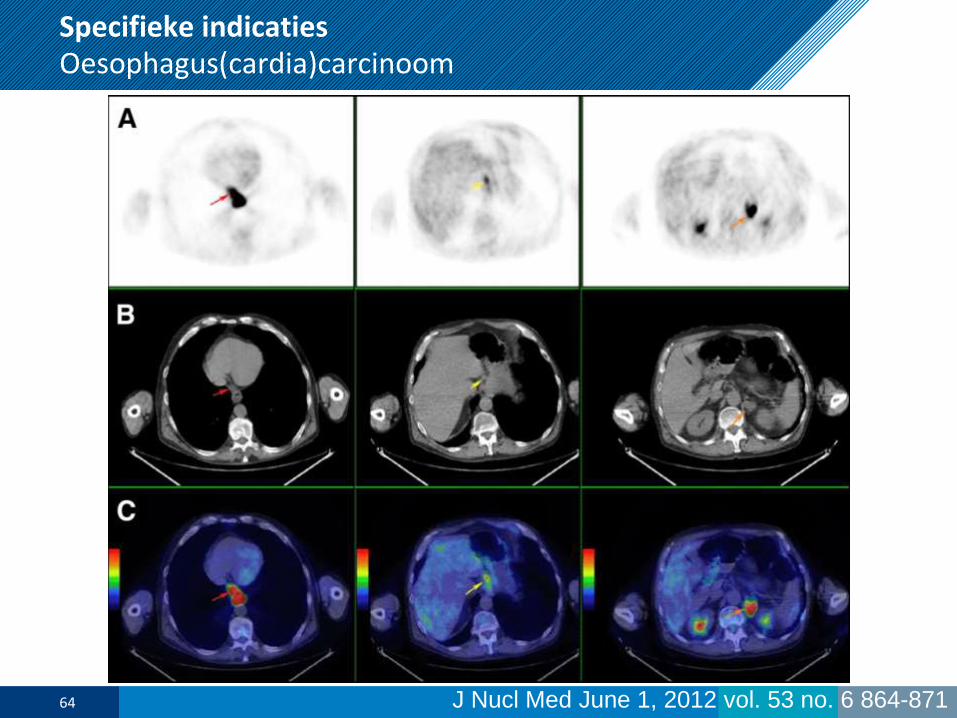
Specifieke indicatiesOesophagus(cardia)carcinoom
J Nucl Med June 1, 2012 vol. 53 no. 6 864-87164

65
Specifieke indicatiesPancreascarcinoom / GEP-NET
• (Her)stadiëring:
• 18F-FDG PET-CT (adenocarcinoom):
- Geen routine plaats, beperkte toegevoegde waarde
- Bij radiologisch verdachte laesies: beperkt specifiek
• Octreotide-imaging (NET):
- Graad I/II: 111In-pentetreotide SPECT-CT of 68Ga-DOTA-octreotide PET-CT
- Graad III: 18F-FDG PET-CT (indien octreotide-negatief)
• Therapie (NET):
• 177Lu-octreotide (PRRT): ErasmusMC, NKI/AvL, MUMC+, Radboudumc
66

Specifieke indicatiesPancreascarcinoom / GEP-NET
Eur J Nucl Med Mol Imaging (2015) 42:1144–115567

68
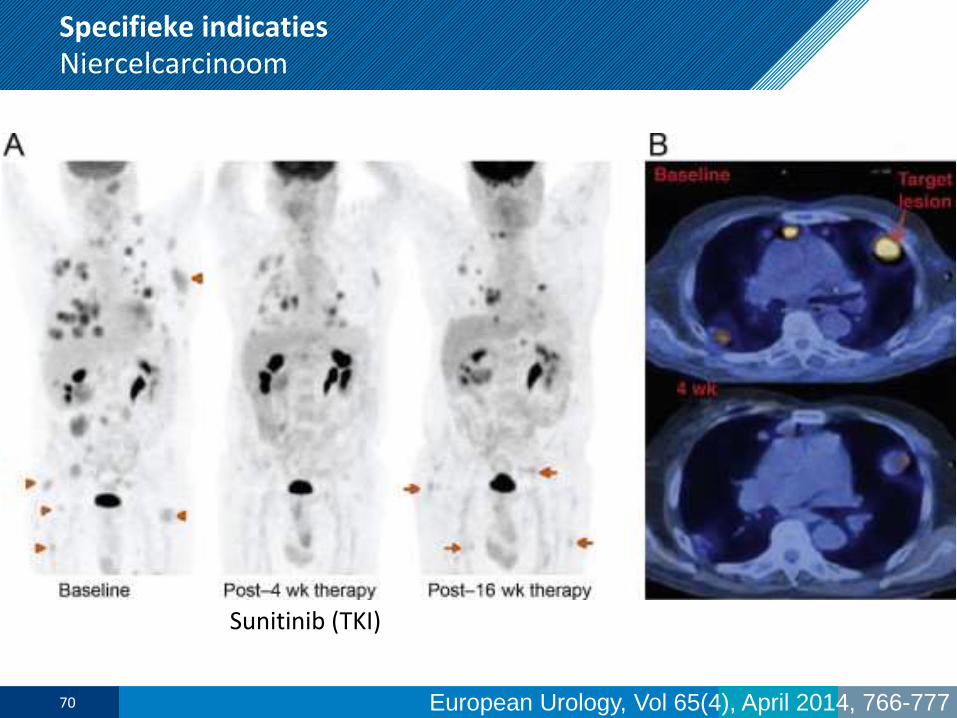
Specifieke indicatiesNiercelcarcinoom
• (Her)stadiëring:
• Botscintigrafie:
Geen plaats: voornamelijk osteolytisch (Se<60%)
• 18F-FDG PET-CT:
Geen routinematig gebruik (Se>32%; Sp>70%)
Evt. bij verdenking recidief op inconclusieve CT
• Response-evaluatie: mogelijk 18F-FDG PET-CT
69
Specifieke indicatiesNiercelcarcinoom
Sunitinib (TKI)
European Urology, Vol 65(4), April 2014, 766-77770
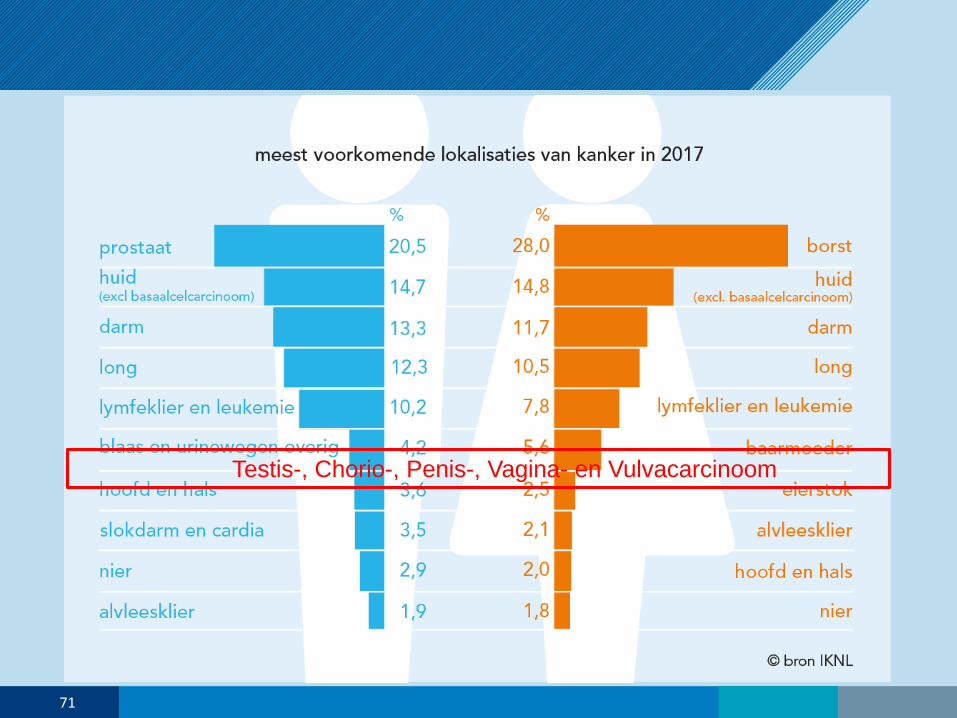
Testis-, Chorio-, Penis-, Vagina- en Vulvacarcinoom
71
Specifieke indicatiesTestis-, Chorio-, Penis-, Vagina- en Vulvacarcinoom
• (Her)stadiëring:
• Schildwachtklierprocedure:
- Vulva: standaard bij unifocaal PCC, Ø<4cm, cN0
- Testis, Penis, Vagina & Endometrium: Experimenteel
• 18F-FDG PET-CT:
- Locoregionale stadiering vagina-carcinoom (als alternatief voor MRI)
- Bepalen vitaal seminoom na therapie (rest op CT)
- Bepalen matuur teratoom vs. rest non-seminoom (rest op CT)
- Onbegrepen verhoogde tumormarkers (AFP) bij kiemceltumoren
72
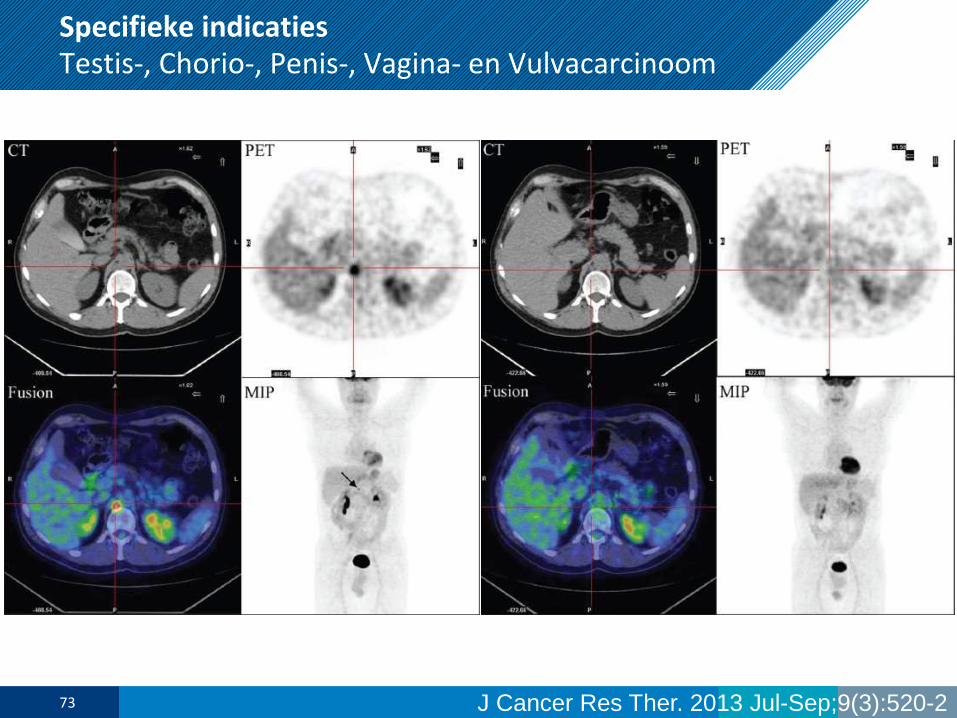
Specifieke indicatiesTestis-, Chorio-, Penis-, Vagina- en Vulvacarcinoom
J Cancer Res Ther. 2013 Jul-Sep;9(3):520-273
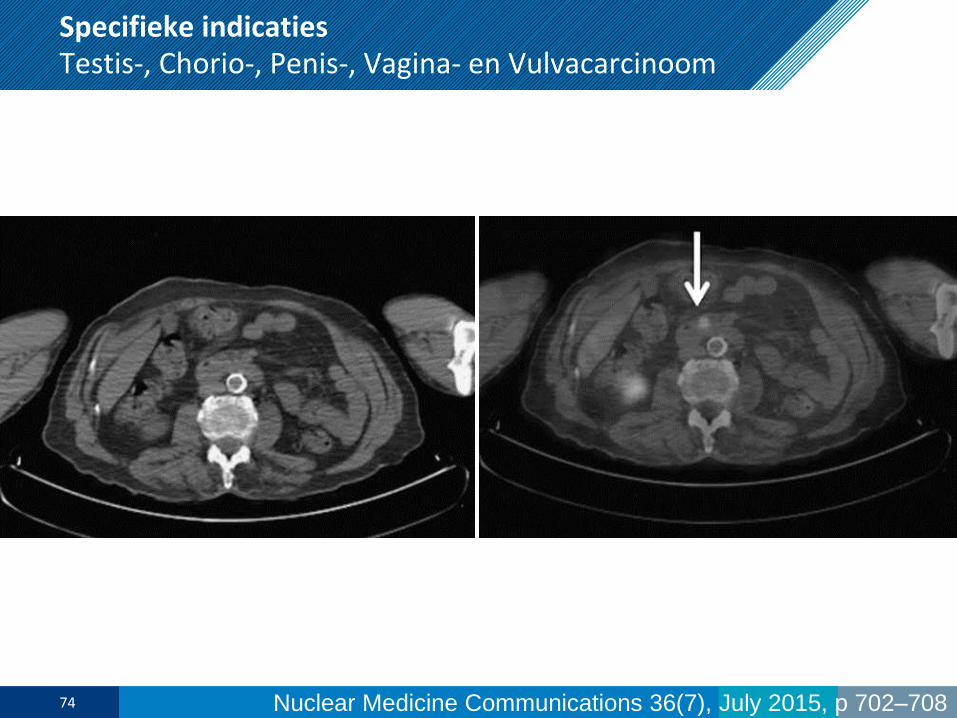
Specifieke indicatiesTestis-, Chorio-, Penis-, Vagina- en Vulvacarcinoom
Nuclear Medicine Communications 36(7), July 2015, p 702–70874
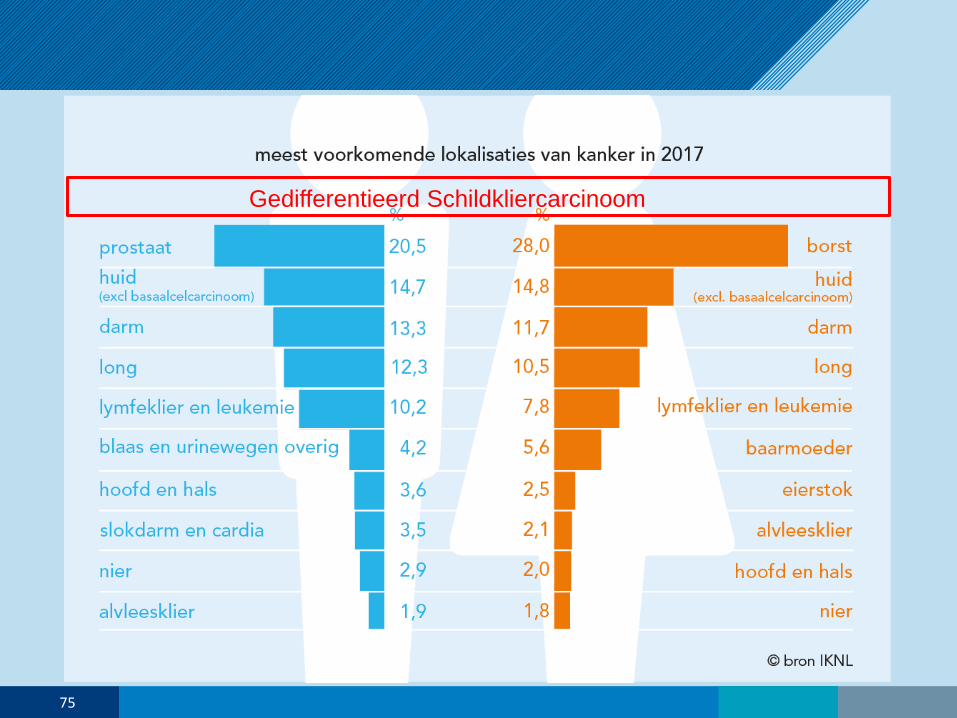
Gedifferentieerd Schildkliercarcinoom
75
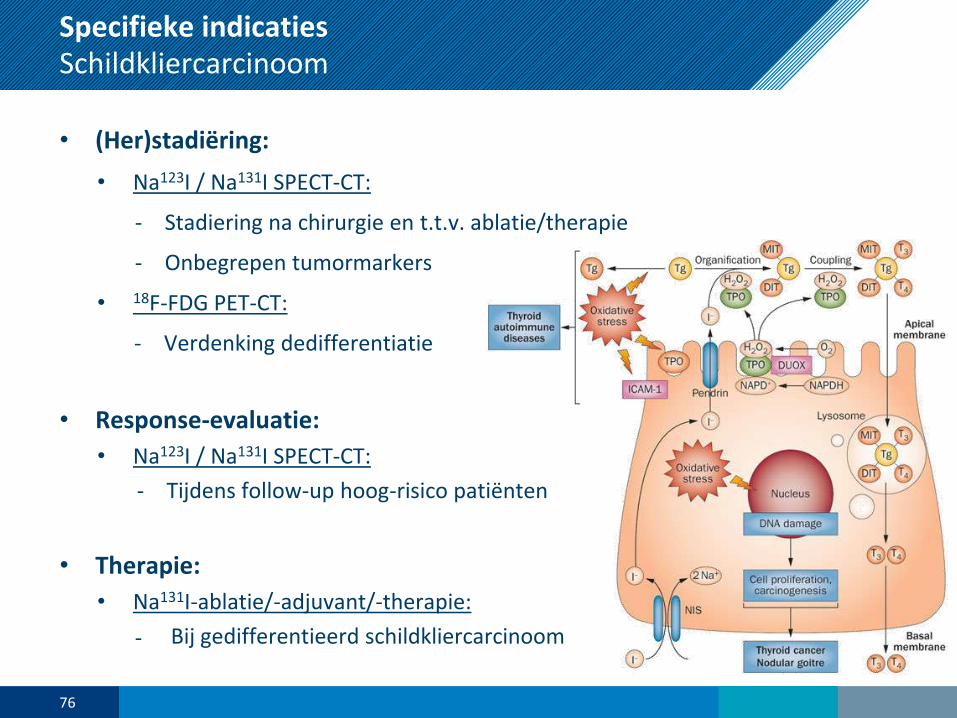
Specifieke indicatiesSchildkliercarcinoom
• (Her)stadiëring:
• Na123I / Na131I SPECT-CT:
- Stadiering na chirurgie en t.t.v. ablatie/therapie
- Onbegrepen tumormarkers
• 18F-FDG PET-CT:
- Verdenking dedifferentiatie
• Response-evaluatie:
• Na123I / Na131I SPECT-CT:
- Tijdens follow-up hoog-risico patiënten
• Therapie:
• Na131I-ablatie/-adjuvant/-therapie:
- Bij gedifferentieerd schildkliercarcinoom
76
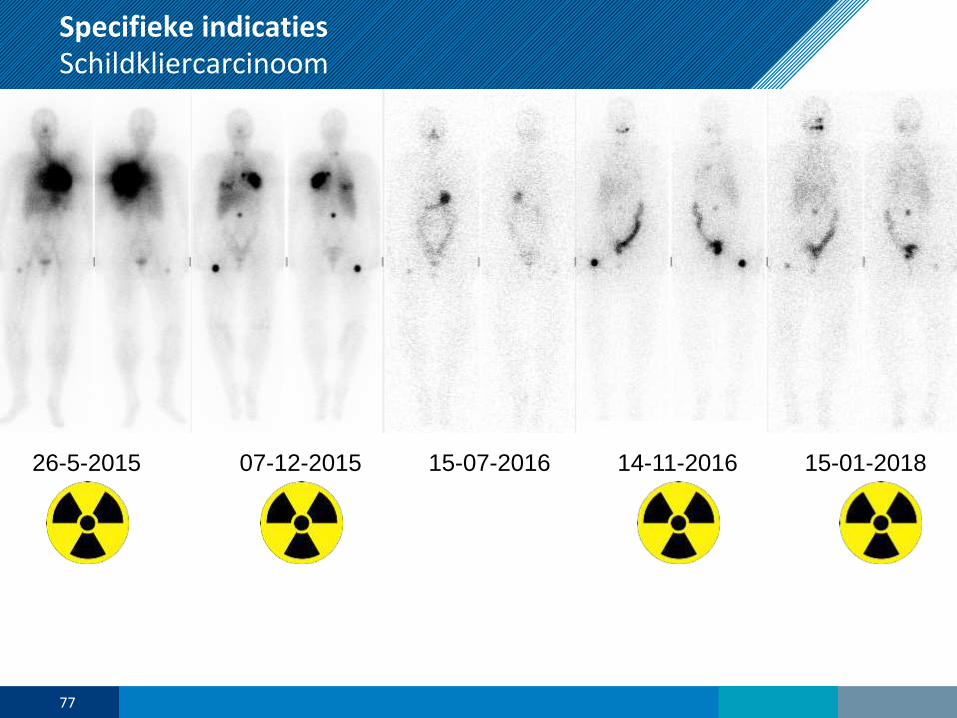
Specifieke indicatiesSchildkliercarcinoom
77
26-5-2015 07-12-2015 15-07-2016 14-11-2016 15-01-2018
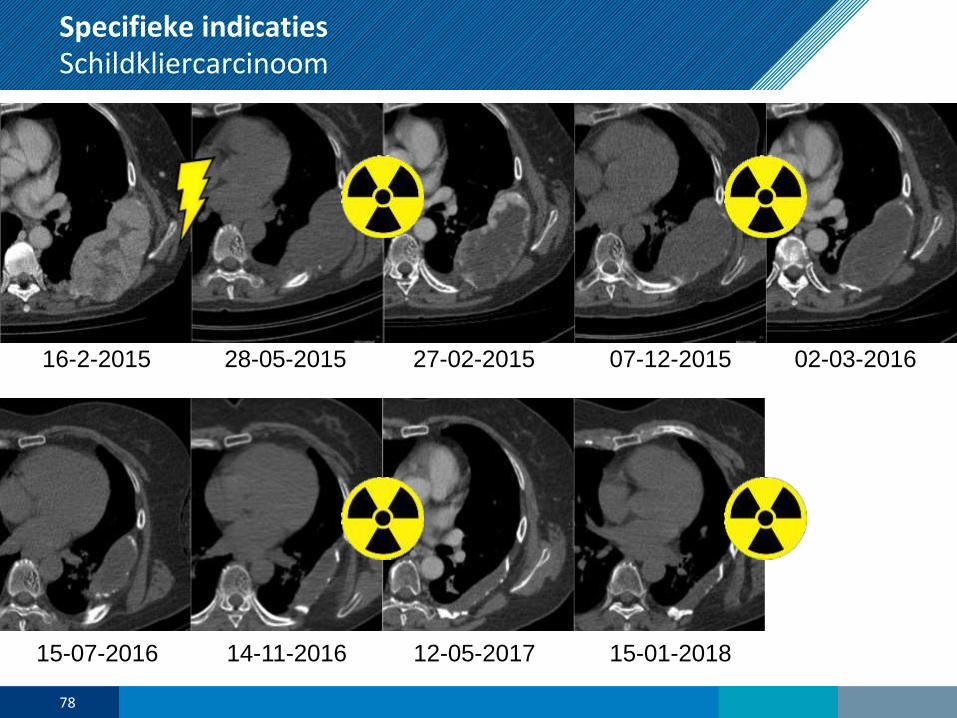
Specifieke indicatiesSchildkliercarcinoom
78
16-2-2015 28-05-2015 27-02-2015 07-12-2015 02-03-2016
15-07-2016 14-11-2016 12-05-2017 15-01-2018
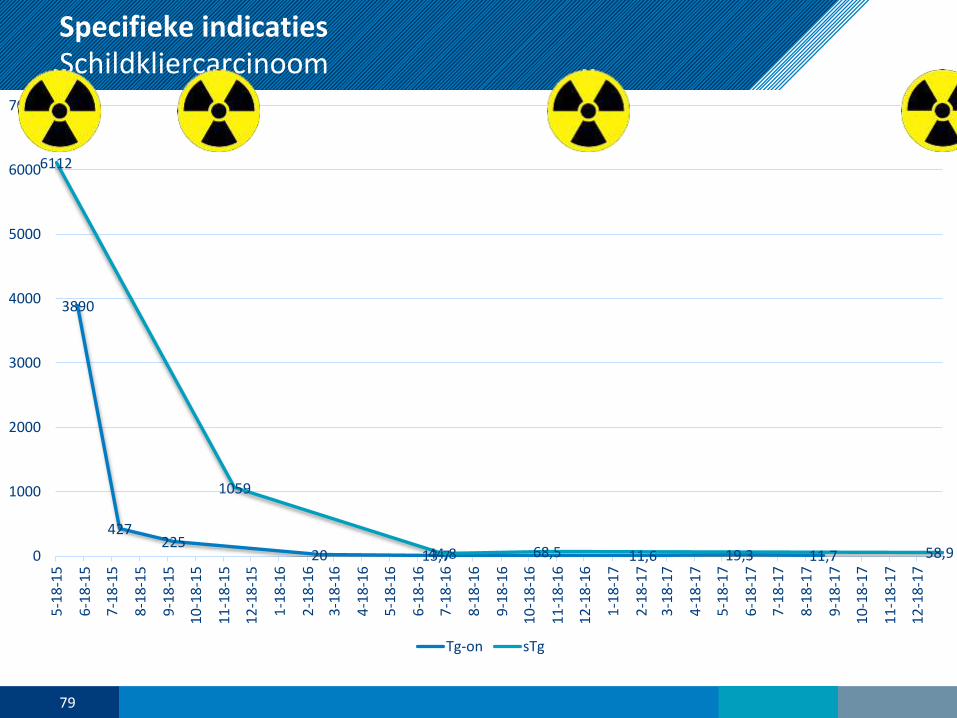
Specifieke indicatiesSchildkliercarcinoom
79
3890
427225
20 13,7 11,6 19,3 11,7
6112
1059
44,8 68,5 58,90
1000
2000
3000
4000
5000
6000
7000
5-1
8-1
5
6-1
8-1
5
7-1
8-1
5
8-1
8-1
5
9-1
8-1
5
10
-18
-15
11
-18
-15
12
-18
-15
1-1
8-1
6
2-1
8-1
6
3-1
8-1
6
4-1
8-1
6
5-1
8-1
6
6-1
8-1
6
7-1
8-1
6
8-1
8-1
6
9-1
8-1
6
10
-18
-16
11
-18
-16
12
-18
-16
1-1
8-1
7
2-1
8-1
7
3-1
8-1
7
4-1
8-1
7
5-1
8-1
7
6-1
8-1
7
7-1
8-1
7
8-1
8-1
7
9-1
8-1
7
10
-18
-17
11
-18
-17
12
-18
-17
Tg-on sTg
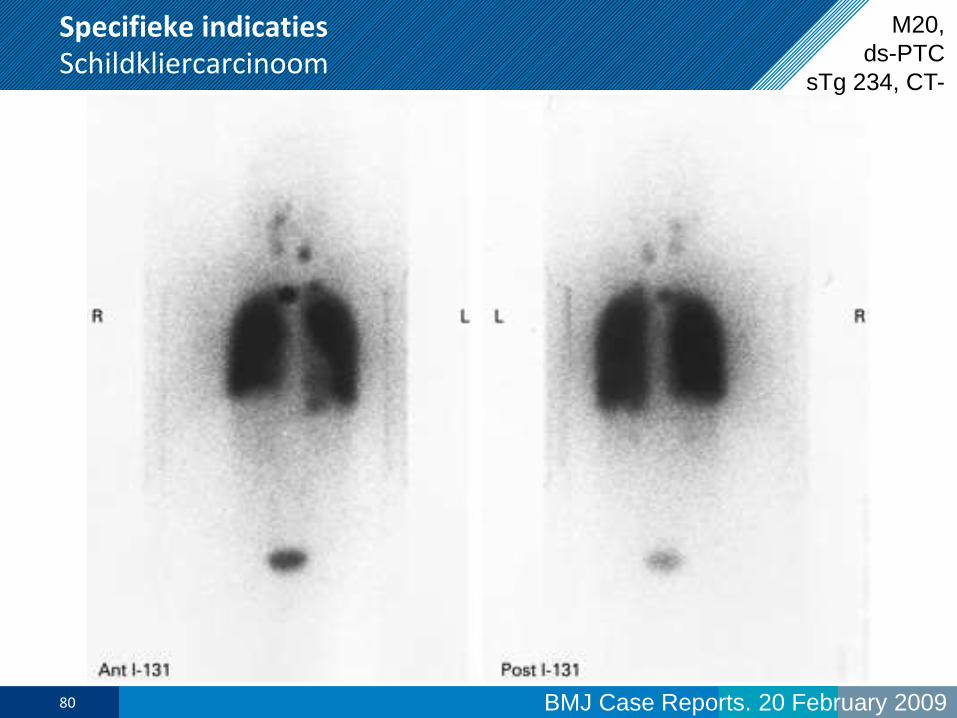
Specifieke indicatiesSchildkliercarcinoom
BMJ Case Reports. 20 February 200980
M20,
ds-PTC
sTg 234, CT-
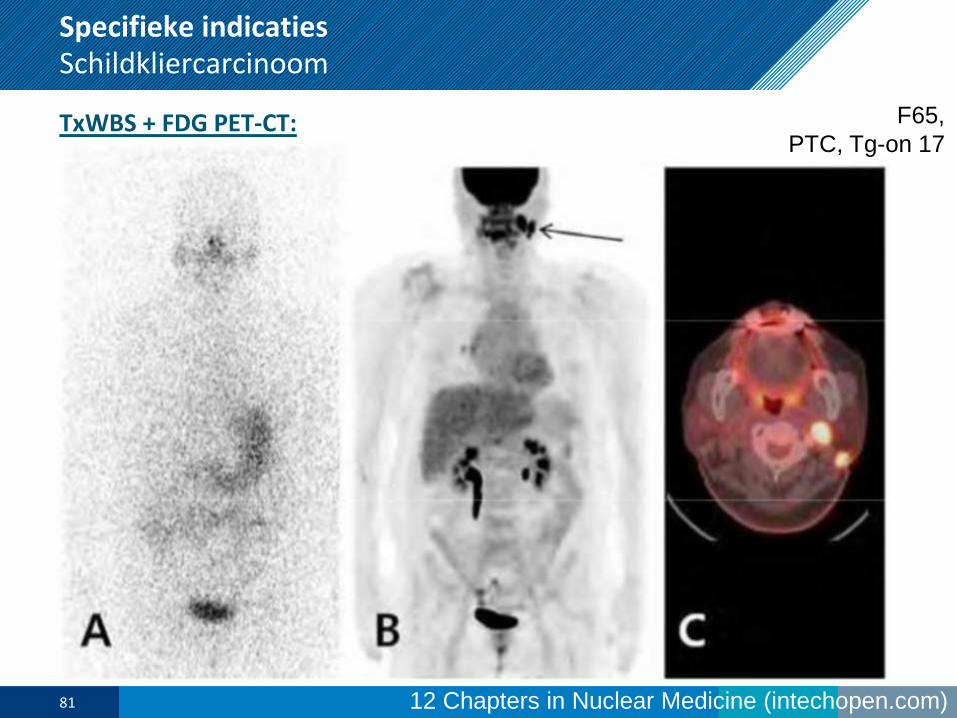
12 Chapters in Nuclear Medicine (intechopen.com)
Specifieke indicatiesSchildkliercarcinoom
TxWBS + FDG PET-CT:
81
F65,
PTC, Tg-on 17
Research
82
Researchoncologie
Volop tracers in ontwikkeling
• metabole tracers als surrogaat uitkomstmaten voor snellere studieresultaten
• markers voor
• hypoxie (gevoeligheid bestraling)
• DNA-metabolisme en eiwitsynthese
• membraan-synthese en vetzuurmetabolisme
• neovascularisatie en matrix
• catecholamine-transporter (o.a. neuroblastoom)
• precursors (F-DOPA, HTP)
• receptoren (bombesine, GLP-1) en hormonale markers (o.a. ER, PR)
• specifieke antigenen (o.a. HER2neu, PSMA, CAIX, CEA, CD20)
• Gelabelde farmaca (bv 11C-erlotinib, 89Zr-CTLA4/-PD1/-PDL1) voor o.a. PK, targetexpressie)
• Combinatie met optische labeling voor interoperatief augmented reality
• In vivo cel-labeling voor host respons op immunotherapie (bv CD4 en CD8)
• etc. etc. etc.
83

Samenvatting & ‘take-home’ messages
84
Samenvatting en ‘take-home messages’
Nucleaire Geneeskunde:
- diagnostiek met g- of b+-isotopen (<20% van mogelijkheden getoond)
- vaak in combinatie met CT of MRI (daarom fusie opleidingen 2015)
- vaak zeer sensitief, maar beperkt specifiek (FP resultaten)
- soms echter wel erg specifiek (bv octreotide-scan): FN resultaten
- behandelbeslissingen:
- stratificatie (de beste therapie voor iedere patiënt)
- begeleiding (volgen van orgaanfunctie van organen die risico lopen)
- evaluatie behandel-effect
- diagnostische dilemma’s
- Therapie met a- of b--isotopen
- Arsenaal wordt nog altijd uitgebreid
85
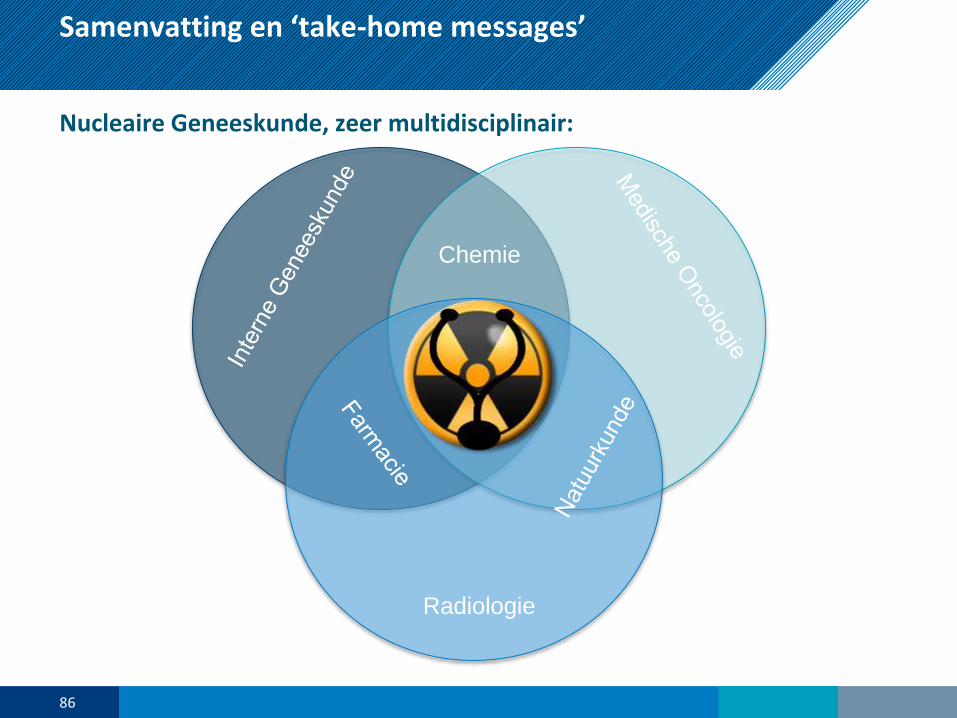
Radiologie
Chemie
Samenvatting en ‘take-home messages’
Nucleaire Geneeskunde, zeer multidisciplinair:
86

Vragen?
Dank voor uw aandacht
87