Visual Performance in Homonymous Hemianopia: Assessment ...
203
Transcript of Visual Performance in Homonymous Hemianopia: Assessment ...


9LVXDO�3HUIRUPDQFH�LQ�+RPRQ\PRXV�+HPLDQRSLD�$VVHVVPHQW��7UDLQLQJ�DQG�'ULYLQJ

Stellingenbehorende bij het proefschrift
Visual Performance in Homonymous Hemianopia: Assessment, Training and Driving.Mark L.M. Tant
1. Alles kan beter.
2. Een sensorische visuele stoornis wordt dikwijls met een cognitieve visuele stoornisverward.
3. Een testprestatie op zich verklapt niets over de onderliggende mechanismen.
4. “Gezichtsveld” is een even (on)duidelijke term als “geheugen” en “aandacht”.
5. Compenseren betekent niet problemen oplossen, maar ze verstoppen.
6. Een patiënt met homonieme hemianopsie, die er optimaal voor compenseert, is moeilijk teonderscheiden van zijn of haar doorsnee leeftijdsgenoot.
7. Het kijkgedrag bij patiënten met een homonieme hemianopsie is meestal te verbeteren.
8. De werkelijkheid is soms een stuk eenvoudiger dan de manier waarop we ze proberen uitte leggen.
9. Neglectgedrag wijst niet altijd op een neglectstoornis.
10. De visuele prestatie tijdens het autorijden is sterk gerelateerd aan visuo-spatieelneuropsychologisch functioneren.
11. Mensen met een linker en een rechter homonieme hemianopsie zijn even gelimiteerd.
12. De helft van onze kennissenkring presteert onder het gemiddelde.
13. Homonieme hemianopsie leidt niet noodzakelijk tot praktische rijongeschiktheid.
14. Wanneer men de term “contralateraal” gebruikt, moet men erbij vermelden aan wat.
15. Sublimatie is in de psychoanalyse het verdedigingsmechanisme waarbij energie afkomstigvan niet toelaatbare angsten en vrezen omgezet wordt in sociaal meer aanvaardbarevormen. Belgenmoppen zijn daar voorbeelden van.
16. Het afstemmen van de testen op het doel en op de patiënten verhoogt de bruikbaarheidvan de testen, maar dikwijls ook het frustratieniveau van de patiënten.
17. Voor optimaal succes en voldoening in de revalidatie moet het revalidatiedoel afgestemdworden op het functioneringsniveau van de patiënt.
18. Statistisch onafhankelijke maten hoeven in de praktijk niet onafhankelijk te zijn.
19. Er zijn in de wereld drie soorten mensen: zij die kunnen tellen en zij die niet kunnentellen.

Paranimfen: Marleen J.J. GerritsenFlorian A. Salomons
This projectwas carried out at
Department of Psychology, Division Biopsychology and NeuropsychologyHeymans Institute for Basic Psychological Research
collaborated withLaboratory of Experimental Ophthalmology (LEO), Faculty of Medical SciencesCentraal Bureau Rijvaardigheidsbewijzen (CBR), Rijswijk
was funded byHeymans Institute for Basic Psychological ResearchSchool of Behavioral and Cognitive Neurosciences (BCN)
University of Groningen (RUG)

RIJKSUNIVERSITEIT GRONINGEN
9LVXDO�3HUIRUPDQFH�LQ�+RPRQ\PRXV�+HPLDQRSLD�$VVHVVPHQW��7UDLQLQJ�DQG�'ULYLQJProefschrift
ter verkrijging van het doctoraat in dePsychologische, Pedagogische en Sociologische Wetenschappen
aan de Rijksuniversiteit Groningenop gezag van de
Rector Magnificus, dr. D.F.J. Bosscher,in het openbaar te verdedigen op
donderdag 3 januari 2002om 14.15 uur
door
Mark Lieven Marcel Tantgeboren op 8 januari 1972
te Brugge (België)

Promotores Prof. dr. W.H. BrouwerProf. dr. A.C. Kooijman
Referent Dr. F.W. Cornelissen
Beoordelingscommissie Prof. dr. J. ZihlProf. dr. B.G. DeelmanProf. dr. K. Postema
ISBN-nummer: 90-367-1544-X

1,/�1(48,7�$025(liefde kan alles)

Dankwoord'DQNZRRUGDe aandachtige lezer zal het merken. Die andere wijs ik er op: deze tekst werd niet verbeterd.Het is te zeggen: mijn promotoren, begeleiders en andere welwillenden keken deze tekst nietna. Het gevolg laat zich duidelijk merken: minder begrijpelijke en gebruikelijke taal wellicht,geen helder gestructureerde en rechtlijnige redeneringen, geen censuur, geen politiekecorrectheid, geen nuances of verzachtende omstandigheden; maar wel de waarheid en nietsdan de waarheid. …. Waarmee ik niet wil impliceren dat laatstgenoemden het laatstgenoemdeniet zouden genegen zijn. Een deel van waarvoor ik u waarschuwde, is hierbij reedsgeïllustreerd.
U wist het al langer: De wereld is niet eerlijk. 9HOHQ hebben bijgedragen, maar er is er maarppQ die met de hoofdprijs gaat lopen. Gelukkig ben ik die “ppQ”. Het daarnet gestelde euvelbeschouw ik daarmee als deels gecompenseerd. De “YHOHQ” rest een eervolle vermelding.Daarom had ik nog graag, zoals dat in het Schoon Vlaams dan heet, een “woordje geplaceerd”(U merkt dat er dan ook een stukje Frans aan te pas komt).
Vasthouden is loslaten.Mijn ouders zagen Tanja en ik het land uit trekken, eerst naar Engeland. Maar dat zeons naar Nederland (naar Holland!) lieten gaan, bewijst hun onvoorwaardelijke steunen vertrouwen. Zonder hen stond ik nu niet waar ik nu sta. Merci.
Weggaan is terugkomen.Residentie Braeckevelt was altijd een oord van uitbundige blijdschap en mateloosplezier bij repatriëring. Mia, Steven, lieve Sara en kleine Robbe, bedankt voor julliegastvrijheid in de voorbije jaren. Dat we nog veel mogen komen (spelen).
Verdedigen is aanvallen.Martien en Jan wisselden de landsverdediging ook meermaals af met grens-overschrijdende diepe penetraties op Nederlandse grondgebied; steevast metverkennende en vredelievende objectieven. Ik salueer.
En dan ben je in het hoge Noorden. “Ja, maar wij zeggen dat zo niet, Komt U uit het Zuiden?,Ik had het niet gemerkt dat u uit België kwam”. Men is altijd beleefd gebleven.
Nemen is geven.De voltallige afdeling Neuropsychologie (huidig en verleden) wil ik bedanken “ommij op te nemen in hun midden”. Samen met de afdeling Oogheelkunde, met in hetbijzonder het Laboratorium voor Experimentele Oogheelkunde, zorgden zij voor eenvruchtbare, stimulerende en uitdagende werkomgeving. De faculteit PPSW, samenmet het BCN, lagen aan de basis van deze mooie multidisciplinaire samenwerking.Ik dank alle studenten die zich door mij lieten begeleiden. Hun opleiding was voor eenstuk de mijne. Ik denk in het bijzonder aan Else, Ursula, Erik, John en Jorrit. Ik dankook “mijn” patiënten. Zonder hun medewerking en inspanning bleven mijn ideeënideeën. Ik hoop dat iedereen iets bijgeleerd heeft en dat het uiteindelijk resulteerde ineen verhoging van hun kwaliteit van leven.De mensen op de polikliniek Oogheelkunde, en Albert, dank ik voor hunondersteuning bij en tijdens mijn oogheelkundige bezigheden. Voor statistische enandere culinaire vragen kon ik terecht bij Ivo Molenaar. Voor de neurologischeaspecten werd ik bijgestaan door Jan Kuks.

Dankwoord
Ik dank ook het Centraal Bureau Rijvaardigheidsbewijzen (CBR) voor hun weten-schappelijke interesse, openheid en medewerking voor en aan dit onderzoek. Ik dankin het bijzonder Ruud Bredewoud, Sander Bison en Rinus Kempeneers. In dezelfdeadem zeg ik dankjewel aan Rijschool Bosman, met in het bijzonder %ert %osman. “Werijden onder het alziende oog van %%” zal nooit meer dezelfde betekenis hebben. Ookhet Verkeerskundig Studiecentrum bedank ik, want niet iedereen mocht de echte wegop. Ik bedank verder alle doorverwijzende instanties. Het waren er veel, over heelNederland verspreid. De kans is dus reëel dat ik iemand vergeet en daarom omzeil ikhet probleem: Ik dank alle interne en perifere oogartsen, neurologen en neuro-psychologen alsook de vele (visuele) revalidatiecentra die patiënten doorverwezenen/of expertise uitwisselden.
Schrijven is schrappen.Na het verzamelen van de gegevens, volgde een periode van (poging tot) rapportage.Sommigen hebben van deze periode genoten, wat hun goed recht is. Het corrigerenvan teksten wordt tot op heden niet beschouwd als een volwaardige sport. Maar als ikJacques Rogge (huidig voorzitter van het Internationaal Olympisch Comité) nog eensspreek, zal ik dit zeker aan de orde stellen. Wiebo, Aart, Frans en Tanja: bedankt ommij op het taalkundig rechte pad te houden.
Spreken is luisteren.Ik heb “de stiel” zo goed mogelijk geleerd. Ik dank dus in het bijzonder mijn directebegeleiders; Wiebo in de eerste plaats. Ik kon hem meteen volgen, zoals wij datzeggen, en hij mij. Behalve die keer dat hij, bij zeer geringe temperatuur, matig tot vrijsterke wind en uiterst schaars gekleed, de Waddenzee indook. Toen heb ik, in eenmoment van zwakte, getwijfeld. Aan Aart heb je een uitstekende discussiepartner bijwie de rooster een veel “gebezigd” voorwerp is. Met een passie voor detail belichaamtAart de te-weing-begrepen idee dat “een gelijkspel een overwinning kan zijn”. Determ “stimulering” wijs ik toe aan Frans. Hoe zou je anders zeilinitiatie, eerste(poster)presentaties, eerste fietstochtorganisatie, computerprogrammering,experimentuitvoering, Eyelinks en MACdoctrine samenvatten? U mag altijd ietsbeters suggereren.
Werken is ontspannen.Groene Uilen Heren-3. Vrienden, kameraden en ander basketballend gespuis, nogeven voor de duidelijkheid: Een korf is niet enkel om fruit in te dragen, een plein isniet enkel een marktplaats, een dakgoot is niet enkel een regenafvoerpijp en een oude-mannen-move is eigenlijk een beredeneerde en op ervaring berustende efficiëntehandeling, waar “jonkies” altijd in trappen. Iedereen heeft van mij nog eenvriendelijke elleboogstoot te goed.
Gedeeld is dubbel.Het meest dank ik Tanja. Jaja «ZRRUGHQ�GRHQ�KLHU�RQUHFKW��,N�]ZLMJ�GXV�PDDU�EHWHU�
Aan alles komt een eind. Behalve aan een worstje. Maar dit is een begin.

Contents&RQWHQWV$OJHPHQH�VDPHQYDWWLQJ ������������������������������������������������������������������������������������������������������������
1. Homonieme Hemianopsie ..................................................................................................12. Deel I: Algemene vraagstelling en methode.......................................................................13. Deel II: Het project .............................................................................................................34. Deel III: Enkele bevindingen bij homonieme hemianopsie en gerelateerde stoornissen ...55. Appendix: Een analytische oefening ..................................................................................7
*HQHUDO�VXPPDU\ ����������������������������������������������������������������������������������������������������������������������1. Part I: Introduction and methods ........................................................................................92. Part II: The project............................................................................................................113. Part III: Additional findings in patients with HH and related impairments .....................124. Appendix: An analytic exercise........................................................................................14
3DUW�,��,QWURGXFWLRQ�DQG�0HWKRGV,QWURGXFWLRQ�DQG�$LP�RI�WKH�SURMHFW ���������������������������������������������������������������������������������������
1. General: Fitness to drive and Homonymous Hemianopia ................................................162. Fitness to drive: requirements and characteristics ............................................................163. Homonymous Hemianopia ............................................................................................... 164. Goals .................................................................................................................................17
7HUPV�DQG�&RQFHSWV �����������������������������������������������������������������������������������������������������������������1. General..............................................................................................................................182. ICF applied to the current research...................................................................................18
2.1. General structure and terms .......................................................................................182.2. Interactions and further examples..............................................................................222.3. Neuropsychological tests ...........................................................................................242.4. Fitness to Drive..........................................................................................................25
'ULYLQJ�UHODWHG�5HVHDUFK ���������������������������������������������������������������������������������������������������������1. The importance of Vision in Driving................................................................................26
1.1. General.......................................................................................................................261.2. Lower and Higher-order Visual Function .................................................................261.3. Impairment and Limitation ........................................................................................271.4. Consequences ............................................................................................................271.5. Conclusion .................................................................................................................27
2. Visual Function.................................................................................................................282.1. General.......................................................................................................................282.2. Need and goal of assessment .....................................................................................282.3. Lower-order (sensory) Visual Function ....................................................................282.4. Higher-order Cognitive Function ..............................................................................342.5. Visuo-spatial impairment and driving(-related) performance ...................................39
3. Conclusion and Implications ............................................................................................474. Reference List ...................................................................................................................48

Contents
$�9LVXR�VSDWLDO�WHVW�EDWWHU\ �����������������������������������������������������������������������������������������������������1. General..............................................................................................................................52
1.1. Introduction ...............................................................................................................521.2. Evaluating Visuo-spatial performance ......................................................................521.3. Pre-driver and Driver assessment ..............................................................................531.4. Summary....................................................................................................................53
2. The Visuo-Spatial Factors and Tests ................................................................................542.1. Factor 1: Basic Visual Scanning and Search (BVSS) ...............................................542.2. Factor 2: Visuo-Constructive and Organisational tasks (VCO) ................................ 602.3. Factor 3: Visuo-Integrative tasks (VI) .......................................................................612.4. Factor 4: Dynamic Tracking task (Dy) ......................................................................63
3. Driver Assessment ............................................................................................................643.1. The Practical Driving Test.........................................................................................643.2. Evaluating Practical Fitness to Drive ........................................................................64
4. Conclusion ........................................................................................................................655. Reference List ...................................................................................................................65
3DUW�,,��7KH�3URMHFW'ULYLQJ�DQG�9LVXR�VSDWLDO�7HVW�SHUIRUPDQFH�LQ�+RPRQ\PRXV�+HPLDQRSLD ����������������������
1. Abstract.............................................................................................................................692. Introduction ......................................................................................................................693. Method..............................................................................................................................72
3.1. Patients ......................................................................................................................723.2. Test procedures..........................................................................................................74
4. Results ..............................................................................................................................774.1. Practical Driving Test ................................................................................................ 774.2. CVD Questionnaire ...................................................................................................794.3. Visuo-spatial Tests ....................................................................................................794.4. Associations with visual performance during driving ...............................................83
5. Discussion.........................................................................................................................865.1. Practical Driving Test ................................................................................................ 865.2. CVD questionnaire ....................................................................................................885.3. Visuo-spatial factors and their components............................................................... 895.4. Predicting visual performance during driving ...........................................................90
6. Conclusion ........................................................................................................................927. Reference List ...................................................................................................................93
9LVXDO�UHKDELOLWDWLRQ�LQ�+RPRQ\PRXV�+HPLDQRSLD�DQG�UHODWHG�GLVRUGHUV �������������������������1. Introduction ......................................................................................................................962. Visual Field Defects and related disorders: forms, frequency of occurrence and diagnosis..............................................................................................................................................96
2.1. Homonymous hemianopia and related disorders.......................................................962.2. Homonymous Hemianopia and visual Neglect: differential diagnosis .....................972.3. Visual fields: assessment and properties .................................................................100
3. Rehabilitation..................................................................................................................1013.1. Visual disorders related to Homonymous Hemianopia ...........................................101

Contents
3.2. Homonymous Hemianopia ......................................................................................1024. The Integrated Saccadic Compensation Training Program ............................................111
4.1. Establishing global understanding of visual problem and general aim ofrehabilitation program ....................................................................................................1114.2. First phase: Saccadic eye movement training..........................................................1124.3. Second phase: Application and integration of eye movements into the scanningpattern .............................................................................................................................1144.4. Third phase: Application and integration of scanning pattern into ADL: driving a car........................................................................................................................................1174.5. Results .....................................................................................................................1174.6. Conclusion ...............................................................................................................118
5. General conclusion .........................................................................................................1186. References.......................................................................................................................118
3UHGLFWLRQ�DQG�(YDOXDWLRQ�RI�'ULYLQJ�DQG�9LVXR�6SDWLDO�3HUIRUPDQFH�LQ�+RPRQ\PRXV+HPLDQRSLD�DIWHU�&RPSHQVDWLRQDO�7UDLQLQJ ������������������������������������������������������������������������1. Abstract...........................................................................................................................1212. Introduction ....................................................................................................................1213. Methods ..........................................................................................................................123
3.1. Patients ....................................................................................................................1233.2. Visual Assessment ...................................................................................................1243.3. Procedure .................................................................................................................126
4. Results ............................................................................................................................1274.1. Practical Driving Test ..............................................................................................1274.2. Neuropsychological Test Battery ............................................................................1274.3. Visual performance during driving (VIS) ............................................................... 128
5. Discussion.......................................................................................................................1295.1. Reduction of visuo-spatial limitations .....................................................................1295.2. Interrelations and predictability...............................................................................1325.3. Prediction of improvement ......................................................................................1335.4. Implications and conclusions...................................................................................133
6. Reference List .................................................................................................................134
3DUW�,,,��$GGLWLRQDO�ILQGLQJV�LQ�SDWLHQWV�ZLWK�++�DQG�UHODWHG�LPSDLUPHQWV*UH\�6FDOHV�XQFRYHU�VLPLODU�DWWHQWLRQDO�HIIHFWV�LQ�KRPRQ\PRXV�KHPLDQRSLD�DQG�YLVXDOKHPL�QHJOHFW �����������������������������������������������������������������������������������������������������������������������������
1. Abstract...........................................................................................................................1382. Introduction ....................................................................................................................1383. Method............................................................................................................................140
3.1. Participants ..............................................................................................................1403.2. Stimuli .....................................................................................................................1433.3. Procedure .................................................................................................................1433.4. Scoring.....................................................................................................................143
4. Results ............................................................................................................................1445. Discussion.......................................................................................................................1446. References.......................................................................................................................148

Contents
+HPLDQRSLF�9LVXDO�)LHOG�'HIHFWV�HOLFLW�+HPLDQRSLF�6FDQQLQJ ��������������������������������������������1. Abstract...........................................................................................................................1522. Introduction ....................................................................................................................1523. Methods ..........................................................................................................................154
3.1. Subjects....................................................................................................................1543.2. Dot counting Task and Apparatus ...........................................................................1543.3. Procedure .................................................................................................................1553.4. Statistical analysis....................................................................................................155
4. Results ............................................................................................................................1564.1. General analysis: Multivariate .................................................................................1564.2. General analysis: Univariate....................................................................................1574.3. Directional analysis .................................................................................................1584.4. Hemispace analysis..................................................................................................1594.5. Trend analysis..........................................................................................................160
5. Discussion.......................................................................................................................1616. Reference List .................................................................................................................164
(YDOXDWLRQ�RI�WKH�HIIHFWLYHQHVV�RI�D�KHPL�QHJOHFW�UHKDELOLWDWLRQ�SURJUDP�DQGJHQHUDOLVDWLRQ�WR�GULYLQJ��D�FDVH�VWXG\�����������������������������������������������������������������������������������1. Introduction ....................................................................................................................1662. Methods ..........................................................................................................................166
2.1. Case .........................................................................................................................1662.2. Evaluation methods .................................................................................................1672.3. The Tracking task ....................................................................................................1672.4. The Driving Simulator.............................................................................................1682.5. Training methods .....................................................................................................168
3. Results and Discussion ...................................................................................................1683.1. Part one: Visual Scanning training ..........................................................................1683.2. Part two: Reading training .......................................................................................1693.3. Part three: Matrix training .......................................................................................1693.4. Part four: Picture description ...................................................................................1693.5. Assessments of non-trained tasks ............................................................................1703.6. The Driving Simulator.............................................................................................1713.7. Head Movements .....................................................................................................1713.8. Lateral Position........................................................................................................1713.9. Speed .......................................................................................................................172
4. Conclusions ....................................................................................................................1725. References.......................................................................................................................173
4XDGUDQRSLD�FDQ�VKLIW�WR�+HPLDQRSLD�ZLWK�VKLIW�RI�WDVN�GHPDQGV ������������������������������������1. Introduction ....................................................................................................................1742. Method: Perimetric tests .................................................................................................174
2.1. The Goldmann perimetric test .................................................................................1742.2. The Humphrey Field Analyzer ................................................................................174
3. Case report, Results and Discussion ...............................................................................1743.1. Case .........................................................................................................................174

Contents
3.2. Perimetry .................................................................................................................1753.3. The Attention task ...................................................................................................175
4. References.......................................................................................................................177
$SSHQGL[��$Q�DQDO\WLF�H[HUFLVH$VVHVVLQJ�YLVXDO�VHDUFK�LQ�WKH�$)29�WHVW ������������������������������������������������������������������������������
1. Aim .................................................................................................................................1792. Methods ..........................................................................................................................1793. Requirements of the measure of distribution ..................................................................180
3.1. Different measures for efficiency of distribution ....................................................1803.2. A limited range and easy to interpret.......................................................................1803.3. Unaffected by constant differences across individuals............................................1813.4. Measures of variability ............................................................................................181
4. PDM: a measure of distribution......................................................................................1824.1. PDM, percentage deviation from the median ..........................................................1824.2. Features of the PDM................................................................................................ 183
5. Hemi-spatial lateralisation ..............................................................................................1855.1. Required features .....................................................................................................1865.2. The Asymmetry Index .............................................................................................1865.3. Examples .................................................................................................................187

Algemene samenvatting1
Algemene samenvatting
We kijken met onze ogen, maar zien met onze hersenen. Beschadigingen van het breinkunnen dus leiden tot visuele problemen. De visuele problematiek kan van een “hogere orde”zijn, bijvoorbeeld het niet meer kunnen herkennen van bekende gezichten. Echter,hersenbeschadiging kan ook resulteren in stoornissen van een “lagere orde” zoalsbijvoorbeeld stoornissen in het gezichtsveld. Het gezichtsveld is het blikveld dat we in éénoogopslag kunnen waarnemen.
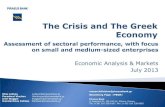
1. Homonieme HemianopsieDe visuele informatie, gestuurd door het oog, wordt in eerste instantie langs een specifiekeweg naar de achterkant van onze hersenen getransporteerd. Deze weg noemen we de visuelebanen (zie Fig. 1). Beschadigingen van die visuele banen leiden tot gezichtsveld uitvallen. Devisuele banen zijn op zo’n maniergeorganiseerd dat, na het chiasmaopticum, het linker gezichtsveld inde rechter hersenhelft terecht komten het rechter gezichtsveld in delinker hersenhelft. Dit noemt men“contralaterale representatie”.Verder is het zo dat het bovenstegedeelte van het gezichtsveld doorde onderste visuele banen gestuurdwordt en het onderste gedeelte doorde bovenste banen. Een volledigebeschadiging van de visuele banenna het chiasma opticum in de rechterhersenhelft leidt bijgevolg tot eenhalfzijdige linker gezichtsvelduitvalen een volledige beschadiging in delinker hersenhelft leidt tot een rechter gezichtsvelduitval. Dit noemt men “homoniemehemianopsie” of halfzijdige blindheid. Gedeeltelijke beschadigingen leiden tot gedeeltelijkeuitvallen. Bijvoorbeeld, beschadiging van enkel de bovenste visuele banen leidt tot eenhomonieme onder-quadranopsie, waarbij de patiënt slechts in een kwart van het gezichtsveldblind is (in dit geval het onderste kwart). Verdere informatie omtrent mogelijke oorzaken,frequentie van voorkomen van homonieme hemianopsie en eraan gerelateerde stoornissenwordt besproken in 3DUW� ,,��9LVXDO� UHKDELOLWDWLRQ� LQ�+RPRQ\PRXV�+HPLDQRSLD� DQG� UHODWHGGLVRUGHUV.2. Deel I: Algemene vraagstelling en methodePatiënten met een homonieme hemianopsie hebben specifieke visuele klachten zoalsbijvoorbeeld het opbotsen tegen mensen of dingen en problemen met lezen. Verder mogen zijniet als bestuurder aan het autoverkeer deelnemen. De Europese richtlijnen eisen eengezichtsveld van minstens 120° ononderbroken horizontale diameter, terwijl patiënten meteen homonieme hemianopsie slechts ongeveer 90° ter beschikking hebben. Het niet (meer)mogen autorijden kan ernstige sociale ongemakken met zich mee brengen. Deze en andereklachten en gevolgen vragen enerzijds om een behandeling en anderzijds om een nader
Fig. 1. Schematische voorstelling van de visuele banen in dehersenen. De linker figuur toont een horizontale doorsnede. Inde figuur zijn de visuele banen na het chiamsa opticum roodgekleurd. De rechter figuur toont een overlangse doorsnedevan de visuele banen vanaf de nucleus geniculate lateralis(LNG).
Chiasma Opticum
LNG

Algemene samenvatting2
onderzoek naar de relatie van de visuele problematiek met het autorijden. Deze achterliggendegedachten die aan de basis liggen van het huidige proefschrift worden geformuleerd in 3DUW�,�,QWURGXFWLRQ�DQG�DLP�RI�WKH�SURMHFW .Om de visuele problematiek en hun gevolgen te duiden wordt terminologie aangewend dieniet voor iedereen meteen inzichtelijk is. In 3DUW�,��7HUPV�DQG�FRQFHSWV worden veel gebruiktetermen geïntroduceerd en gesitueerd in een omvattend kader, namelijk de InternationalClassification of Functioning, Disability and Health. We beargumenteren dat het algemeenfunctioneren het best in kaart kan gebracht worden met een combinatie van gedragsmaten(activiteiten) en tests die iets vertellen over de toestand en integriteit van het lichaam. Wemaakten daarbij het onderscheid tussen tests op het niveau van de activiteit en tests op hetniveau van de stoornis. Het cruciale onderscheid tussen beide niveaus is dat ze aanverschillende invloeden onderhevig zijn. Namelijk, voor activiteiten (en hun limitaties) wordtgesteld dat deze het gevolg zijn van een complexe bio-psycho-sociale interactie. Hoe depatiënt zelf omgaat met een stoornis (in zeer algemene bewoording “de algemene context”)bepaalt gedeeltelijk zijn of haar testprestatie. Dus of een patiënt al dan niet een behandelingachter de rug heeft, kan bepalend zijn voor het functioneren op het activiteitsniveau. Echter,de uitkomst van een test op het stoornisniveau wordt enkel bepaald door de stoornis zelf en isderhalve niet onderhevig aan invloeden van bijvoorbeeld een behandeling. We stelden verderdat de meeste neuropsychologische tests en de praktische rijtest, uitgevoerd door patiëntenmet een homonieme hemianopsie, te situeren zijn op het niveau van de activiteit. Dit heeftverschillende implicaties. Bijvoorbeeld, (visueel) neuropsychologische tests meten bij dezemensen misschien wel niet (meer) wat ze bij andere mensen meten, waardoor hun belang eninterpretatie anders wordt. We introduceren tenslotte het onderscheid tussen (medische)rijgeschiktheid en de (praktische) rijvaardigheid en besluiten dat een praktische testrit, diespeciaal rekening houdt met de visuele problematiek, het gewenste criterium is omrijgeschiktheid te beoordelen. Een testrit in het echte verkeer, waarbij specifiek situatiesopgezocht worden waarin de visuele problematiek zich kan uiten en waarbij door eenaanpassingsdeskundige gelet wordt op hoe de patiënt al dan niet compenseert voor deaandoening, geeft een goed beeld van de praktische rijgeschiktheid.
Het onderzoek gerelateerd aan het autorijden wordt samengevat in 3DUW� ,�� 'ULYLQJ�UHODWHG5HVHDUFK. Visuele functies maken een belangrijk deel uit van de rijtaak. Een goede evaluatievan deze functies is dus noodzakelijk om rijgeschiktheid te evalueren. Echter, de evaluatievan de visuele functies hoeft niet enkel een beoordelende functie te hebben, maar kan ookindicaties bieden omtrent mogelijke behandeling en revalidatie. Uit de voorgaande literatuurblijkt dat evaluatie van sensorische visuele functies (zoals gezichtsscherpte) slechts een matigverband vertonen met verkeersveiligheid. Ook wanneer er gezichtsvelduitvallen zijn, is derelatie met verkeersveiligheid niet altijd duidelijk. Daarom is het belangrijk om ook de relatiemet hogere-orde visuele stoornissen te bestuderen. Algemeen gesteld ontstaan dezestoornissen door een hersenletsel en worden ze gemeten met visueel neuropsychologischetests. Na een studie van de relatie tussen neuropsychologische prestaties en het autorijden,besluiten we dat we tests moeten gebruiken die het best passen bij “onze” patiëntengroep. Hetniet afstemmen van de gebruikte tests op de groep van patiënten die men onderzoekt, leidtvolgens ons immers tot het vinden van slechts relatief zwakke verbanden met het autorijden.De discussie wordt verder toegespitst op (patiënten met) specifiek visuo-spatiële stoornissen.Een visuo-spatiële stoornis uit zich bijvoorbeeld in het niet meer kunnen herkennen van

Algemene samenvatting3
bekende voorwerpen, het niet meer kunnen kopiëren van een ingewikkelde figuur, het steedsverloren lopen in een toch bekende omgeving, of in het steeds opbotsen tegen mensen ofdingen. We benadrukken dat niet alle dergelijke stoornissen even belemmerend zijn voor hetautorijden, maar dat vooral de zogenaamde hemi-spatiële visuele stoornissen een zeerverstorende rol kunnen spelen. Bij deze laatste stoornissen doen de problemen zich steeds aandezelfde kant voor, bijvoorbeeld men stoot zich steeds aan dingen die zich aan de linker kantbevinden. De “aangedane kant” is dus meestal de kant van de homonieme hemianopsie (dusde kant waar de patiënt blind is), maar ook andere (hogere-orde) oorzaken kunnen in het spelzijn. De literatuur die we vonden omtrent de relatie tussen hemi-spatieel functioneren en hetautorijden laat eveneens geen duidelijke conclusies toe. Sommige studies geven aan dat eenhemi-spatiële problematiek zonder enige uitzondering leidt tot onaanvaardbaar rijgedrag. Uitdeze studies zou dus volgen dat geen enkele patiënt met een homonieme hemianopsie eenrijbewijs zou mogen hebben. Uit andere studies blijkt dan weer het tegendeel of moet menbesluiten dat sommige patiënten er wel en andere er niet in slagen adequaat auto te rijden.Daarmee rijst de vraag “welke patiënten wel slagen en welke niet”. Dit bracht er ons toe omhet hemi-spatieel functioneren van homonieme hemianopsie patiënten gedetailleerd in kaart tebrengen met behulp van een visuo-spatiële testbatterij.
Onze uitgebreide visuo-spatiële testbatterij wordt voorgesteld in 3DUW� ,��$�9LVXR�VSDWLDO� WHVWEDWWHU\. We gebruikten naast bestaande neuropsychologische, ook zelf ontwikkelde ofaangepaste taken. De tests werden op voorhand ingedeeld in vier factoren. Met deze factorenworden verschillende (maar niet van elkaar onafhankelijke) visuo-spatiële functies gemeten,zoals eenvoudig scannen en zoeken (BVSS), visuo-constructieve functies (VCO), visuo-integratieve functies (VI) en functies waar dynamiek en beweging een belangrijke rol spelen(Dy). Naast snelheid en accuraatheid creëerden we ook een asymmetrie index (AI). Dit is eenmaat voor een verschil in prestatie aan de linker kant ten opzichte van de rechter kant,waarmee we een onderscheid willen maken tussen een algemeen visuo-spatieel (weinigverschil tussen links en rechts) en een hemi-visuo-spatieel probleem (veel verschil tussenlinks en rechts).Tenslotte beschrijven we de praktische rijtest en de scoringsmethode met behulp van hetTRIPprotocol. Gelijkaardig aan de visuo-spatiële neuropsychologische factoren werden ookop voorhand TRIPfactoren samengesteld. Een TRIPfactor bundelt gelijkaardige (enbelangrijke) aspecten van het autorijden. Gezien onze speciale interesse voor de visueleprestaties, hechten we vooral belang aan de visuele factor.
3. Deel II: Het projectDe logisch volgende stap is het in de praktijk brengen en toepassen van de geschetstemethodieken. Dit wordt naar voren gebracht in Part II van het proefschrift. In 'ULYLQJ� DQG9LVXR�VSDWLDO� 7HVW� SHUIRUPDQFH� LQ� +RPRQ\PRXV� +HPLDQRSLD bestudeerden we de relatietussen visuo-spatiële neuropsychologische testprestatie en visuele prestaties tijdens hetautorijden bij 28 patiënten met een homonieme hemianopsie. Conform aan de verwachtingen,scoorden de patiënten minder goed op de visuele factor van het autorijden dan op de anderefactoren. Gemiddeld genomen was de rijprestatie eerder laag tot matig. De meestterugkomende opmerking was onacceptabel slingergedrag. Maar gezien toch vier patiëntenvolgens de aanpassingsdeskundige zouden geslaagd zijn, kunnen we niet besluiten dathomonieme hemianopsie altijd vlot en veilig autorijden uitsluit. Bij het voorspellen van devisuele prestatie tijdens het autorijden aan de hand van de visuo-spatiële neuropsychologische

Algemene samenvatting4
testprestatie hanteerden we een specifiek functioneel kijkmodel. In ons model gaan we ervanuit dat homonieme hemianopsie kan leiden tot een verschil in testprestatie in de “aangedanekant” ten opzichte van de “niet aangedane” kant (differentiële lateralisatie gemeten door eenAsymmetrie Index) en we beschouwen dit ook als een typisch en primair gevolg van degezichtsveldaandoening. Hiervoor compenseren kost aandacht en energie en daardoor zal detestprestatie minder snel en/of minder accuraatheid worden. Dit model pasten we toe bij destatistische voorspellingsprocedures, waarbij we dus eerst en vooral rekening hielden metmate van differentiële lateralisatie, daarna met de tijd en tenslotte met de accuraatheid. Visuo-spatieel neuropsychologisch functioneren, gedefinieerd met behulp van het voornoemdekijkmodel aan de hand van de gemaakte visuo-spatiële factoren, verklaarde een groot deel(77%) van de variantie in kijkgedrag tijdens het autorijden. Dit betekent dat we aan de handvan de neuropsychologie goed konden voorspellen hoe patiënten zouden presteren tijdens hetautorijden.
We vonden, niet geheel onverwacht, een laag tot matige prestatie op de visuo-spatiële taken,zowel bij de neuropsychologische tests als tijdens het autorijden. Mede gesterkt door desubjectieve klachten van de patiënten en de sociale gevolgen van de visuele problematiek,suggereert dit de noodzaak en het belang van (onderzoek naar) een specifieke behandeling,temeer omdat tot op heden er in de reguliere zorgsector weinig of geen gestructureerde entheoretisch onderbouwde hulp aangeboden wordt aan patiënten met een homoniemehemianopsie. In 3DUW� ,,�� 9LVXDO� UHKDELOLWDWLRQ� LQ� +RPRQ\PRXV� +HPLDQRSLD� DQG� UHODWHGGLVRUGHUV wordt onder meer een overzicht geboden van de bestaande revalidatietechnieken en-methodes. Naast het spontaan herstel, wat slechts bij de minderheid van de patiëntenvoorkomt, onderscheiden we drie types technieken, te weten restoratie, adaptatie encompensatie. Met restoratie wordt bedoeld het herstel van (een deel van) het verlorengezichtsveld door visuele training. Uit de literatuur blijkt dat deze methode zeerarbeidsintensief is, mogelijk slechts op een zeer beperkt deel van de patiënten van toepassingkan zijn en het herstel meestal vrij klein is. De tweede techniek is adaptatie en veronderstelteen vorm van aanpassing. We bespreken het gebruik van optische hulpmiddelen, bijvoorbeeldprisma’s, lenzen en spiegels. Het toepassen van prisma’s wordt uitgebreid toegelicht, omdatdeze techniek (vooralsnog vooral in Amerika) in opmars is en omdat op basis van debeschikbare literatuur blijkt dat deze revalidatietechniek aanzienlijke en positieve effecten kanhebben. De derde, en door ons gebruikte methode, is de techniek van de compensatie. Decompensatoire technieken zijn ontstaan uit de aanname dat de meeste homoniemehemianopsie klachten het gevolg zijn van het ontbreken van een snel en volledig (visueel)overzicht van de beschikbare ruimte. Dit gebrek is enerzijds het gevolg van hetgezichtsveldverlies en anderzijds van een onaangepast kijkgedrag. Dit kijkgedrag uit zichbijvoorbeeld in kleine stapsgewijze oogsprongen (saccades) naar de blinde kant toe. Het doelvan de compensatoire technieken is het leren en toepassen van een aangepaste kijktechniekom het verlies aan het gezichtsveld goed te maken of op te vangen. De technieken, in hetverleden reeds toegepast, zijn gebaseerd op het gebruiken van grote oogsprongen om op diemanier een globaal overzicht te creëren, zodat men (snel) weet wat er allemaal te zien is enmen daarna kan beslissen wat bijvoorbeeld eerst bekeken moet worden. Onze techniek, een“geïntegreerde saccadische compensatie training”, is gestoeld op deze principes. We lichtenonze interventie uitgebreid toe. We beschrijven het doel van onze training als het verminderenvan de gevolgen van het gezichtsveldverlies, met name tijdens het autorijden. Ons programmabestaat uit drie fasen. In de eerste fase wordt de beoogde kijktechniek geïntroduceerd en

Algemene samenvatting5
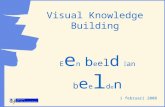
aangeleerd in een laboratoriumsituatie. De basis van de (nieuwe) kijktechniek is het aanlerenvan (te) grote, frequente, en snelle oogbewegingen naar de blinde kant toe. Deze wordenstapsgewijs aangeleerd. In de tweede fase moeten deze oogbewegingen worden toegepast.Daarvoor ontwikkelden wij taken dieeen aangepast kijkgedrag veronder-stellen, zoals bijvoorbeeld het kopiërenvan ingewikkelde lijntekeningen, het be-schrijven van plaatjes en het besturenvan een virtuele auto. Deze twee laatstetaken werden aangeboden, zoals ook deoefeningen tijdens de eerste fase, op eengroot projectiescherm (zie Fig. 2). In delaatste fase werd de aangeleerde kijk-techniek toegepast tijdens het autorijden.De patiënten kregen rijlessen in eenwagen met dubbele bediening en onderbegeleiding van een ervaren rij-instructeur.
In 3DUW� ,,�� 3UHGLFWLRQ� DQG� (YDOXDWLRQ� RI� 'ULYLQJ� DQG� 9LVXR�6SDWLDO� 3HUIRUPDQFH� LQ+RPRQ\PRXV�+HPLDQRSLD�DIWHU�&RPSHQVDWLRQDO�7UDLQLQJ wordt de behandeling geëvalueerd.Echter, we zijn niet enkel geïnteresseerd in de evaluatie, maar ook (en opnieuw) gaan we naof we de visuele prestatie tijdens het autorijden kunnen voorspellen aan de hand van hetvisuo-spatieel neuropsychologisch functioneren. Zoals we hoopten, vonden we eenverbetering in visuele prestatie tijdens het autorijden. Deze verbetering was echter over hetalgemeen onvoldoende om de norm te bereiken die gesteld wordt door het Centraal Bureauvoor Rijvaardigheidbewijzen (CBR). Toch slaagden, na onze vrij korte behandeling, twee vande 17 patiënten op de testrit. Niemand van deze groep was geslaagd vóór de behandeling.Omdat we na de behandeling specifieke verbetering vonden, met name enkel op visueel vlak,concluderen we dat verdere investering van energie en faciliteiten in cognitieve visuelerevalidatieprogramma’s gerechtvaardigd is. Met betrekking tot het voorspellen van (deverbetering van) het rijgedrag concludeerden we enerzijds (opnieuw) dat visuo-spatieelneuropsychologisch functioneren (zoals door ons gemeten en voorgesteld) samenhangt met devisuele prestaties tijdens het autorijden. Anderzijds bleek dat de mate van verbetering niet konvoorspeld worden op basis van het neuropsychologisch functioneren. Daarom moet in hetvervolg het revalidatiedoel afgestemd worden op het niveau van functioneren van de patiënt.Naast autorijden voor licht visueel dysfunctionerende patiënten, kunnen lagere doelen alszelfstandig lopen, of het gebruik van fiets of scootmobiel, gesteld worden aan ernstig totmatig visueel dysfunctionerende patiënten.
4. Deel III: Enkele bevindingen bij homonieme hemianopsie en gerelateerde stoornissenTwee tests uit de visuo-spatiële testbatterij, namelijk de Grey Scales taak en de stippenteltaak, bespreken we uitgebreid in Part III. Bij de bespreking van het visuo-spatieelfunctioneren en het veronderstelde functioneel kijkmodel introduceerden we de AsymmetrieIndex (AI). Het idee van de AI, ook wel perceptuele asymmetrie genoemd, werd in hetverleden vooral gebruikt bij het hemi-neglectsyndroom. Visueel hemi-neglect is een hogere-orde hemi-spatiële (aandachts)stoornis, waarbij de patiënt nalaat te reageren op visuele
Fig. 2. Opstelling van de kijktraining door middel vande virtuele auto. Een virtuele weg wordt geprojecteerdover de breedte van het projectiescherm (lijn).

Algemene samenvatting6
stimuli, meestal aan de linker zijde. Homonieme hemianopsie en visueel hemi-neglect zijnaan elkaar gerelateerde stoornissen (zie 3DUW� ,,�� 9LVXDO� UHKDELOLWDWLRQ� LQ� +RPRQ\PRXV+HPLDQRSLD� DQG� UHODWHG� GLVRUGHUV). In 3DUW� ,,,�� *UH\� 6FDOHV� XQFRYHU� VLPLODU� DWWHQWLRQDOHIIHFWV�LQ�KRPRQ\PRXV�KHPLDQRSLD�DQG�YLVXDO�KHPL�QHJOHFW onderzochten we wat de oorzaakkan zijn van een perceptuele asymmetrie. Wanneer men de keuze heeft tussen tweegelijkwaarde opties, waarvan één links en één rechts, en men kiest systematisch voor ofwel delinker ofwel de rechter optie, dan vertoont men een perceptuele asymmetrie. We vonden,zoals verwacht, dat “gezonde” personen een lichte voorkeur hebben voor “links” en dat hemi-neglectpatiënten een sterke voorkeur hebben voor “rechts”. Maar verder toonden we aan datpatiënten met een linker hemianopsie zonder hemi-neglect ook een voorkeur hadden voor“rechts” (maar minder sterk) en dat patiënten met een rechter hemianopsie een voorkeurhadden voor “links”. Deze bevinding suggereert dat de perceptuele asymmetrie niet enkelveroorzaakt kan worden door een letsel in de rechter hersenhelft of door een (hogere-orde)aandachtsstoornis, zoals voorheen aangenomen werd. Ook een lagere-orde perceptuelestoornis (met name een homonieme hemianopsie) kan een perceptuele asymmetrieveroorzaken, zij het in een lichtere mate. We concluderen hieruit dat op gedragsniveau er eencontinuüm bestaat gaande van “gezond” (zonder of met een kleine linker voorkeur), overlinker hemianopsie patiënten (met een matige rechter voorkeur) tot aan visueel hemi-neglect(met een extreem rechter voorkeur). Deze bevindingen bevestigen dat homoniemehemianopsie en hemi-neglect gerelateerde stoornissen zijn en dat ze op gedragsniveau somsmoeilijk van elkaar te onderscheiden zijn. Echter, de oorzaak van hun visuele problematiekkan duidelijk verschillen. Dit bevestigt (en voor een stuk rechtvaardigt) de in de klinischepraktijk dikwijls ondervonden problemen bij de differentiële diagnose.
De relatie tussen de effecten van hogere- en lagere-orde stoornissen wordt ook behandeld in3DUW�,,,��+HPLDQRSLF�9LVXDO�)LHOG�'HIHFWV�HOLFLW�+HPLDQRSLF�6FDQQLQJ . In de literatuur werdgesteld dat de visuele problematiek bijhomonieme hemianopsie, met het nameafwijkend zoek- en oogbewegingsgedragtijdens een stippentel taak, gerelateerd was aande grootte van het opgelopen hersenletsel. Wijgingen na of het hebben van een hersenletselwel noodzakelijk was of dat de aanwezigheidvan een homonieme hemianopsie, zonder eenhersenletsel, ook het typische (afwijkende)oogbewegingsgedrag zou kunnen veroorzaken.Daarvoor creëerden we een homoniemehemianopsie bij gezonde mensen. Wegebruikten hiervoor geavanceerde apparatuur(zie Fig. 3), waardoor we op gedetailleerdewijze alle oogbewegingen konden registrerenen tegelijkertijd een homonieme hemianopsiekonden simuleren. Onze gesimuleerdepatiënten (dus gezonde personen met eenhomonieme hemianopsie maar zonderhersenletsel) vertoonden een kijkgedrag vergelijkbaar aan echte patiënten. We concludeerdendaaruit dat het hemianopische kijkgedrag, tijdens de stippentel taak, voor een belangrijk deel
Fig 3. Opstelling bij de oogbewegingsregistratie:twee met elkaar verbonden computers. Ditsysteem is verbonden met een helm. Aan de helmzijn twee kleine camera’s bevestigd, elk gerichtop een oog. Met behulp van speciaal ontwikkeldeprogrammatuur kan bijna elk type gezichts-velduitval gesimuleerd worden. Homoniemehemianopsie wordt gesimuleerd door op hetscherm alles links of rechts van het fixatiepunt tewissen.

Algemene samenvatting7
veroorzaakt wordt door de gezichtsvelduitval en niet door het hersenletsel. We toonden dus(nogmaals) aan dat lagere-orde (perceptuele) stoornissen, in dit geval een homoniemehemianopsie zonder hersenletsel, aanleiding kan geven tot het ontstaan van een afwijkendekijkprestatie, die als een hogere-orde stoornis kan (mis)geïnterpreteerd worden. Dit benadrukthet belang van een gulden regel in de neuropsychologie, namelijk nooit tot een hogere-ordestoornis te besluiten als de invloed van een lagere-orde stoornis niet uitgesloten is. Verdervonden wij, dat ouderen met een gesimuleerde hemianopsie meer belemmerd worden danjongeren en, op het eerste zicht paradoxaal, dat een hemianopsie het meest belemmerend kanzijn in ogenschijnlijk de meest eenvoudige situaties.
Omdat het visueel hemi-neglectsyndroom gerelateerd is aan homonieme hemianopsie,evalueerden we, bij één persoon, in de aanloop van het onderzoek een revalidatiemethode dieontwikkeld werd in Italië. Later zouden we delen van deze methode gebruiken en combinerenmet andere methodes, wat uiteindelijk leidde tot onze “geïntegreerde saccadische compensatietraining” die we toepasten bij de hemianopsie patiënten (zie 3DUW�,,��9LVXDO�UHKDELOLWDWLRQ�LQ+RPRQ\PRXV� +HPLDQRSLD� DQG� UHODWHG� GLVRUGHUV ). De aanpassingen aan de origineleneglectmethode en de evaluatie van de effectiviteit ervan staat beschreven in 3DUW� ,,,�(YDOXDWLRQ�RI�WKH�HIIHFWLYHQHVV�RI�D�KHPL�QHJOHFW�UHKDELOLWDWLRQ�SURJUDP�DQG�JHQHUDOL]DWLRQ�WRGULYLQJ��D�FDVH�VWXG\. Onze evaluatiemethodes bestonden niet enkel uit traditionele klinischeneglecttests. We evalueerden ook door middel van een dynamische tracking taak (een zeereenvoudige rijsimulator) en door middel van een geavanceerde rijsimulator. Na debehandeling vonden we een sterke verbetering in de klinische (niet-getrainde) neglecttests,waardoor we klinisch gesproken, de neglectdiagnose niet meer zouden mogen stellen. Zowelin de dynamische trackingtaak als in de meer realistische rijsimulator observeerden we na detraining enerzijds nog onaanvaardbaar veel slingergedrag, maar anderzijds nog weinigkenmerken typisch voor hemi-neglect. We concludeerden hieruit dat de behandeling wel leidttot het beter oplossen van de klinische tests, maar niet noodzakelijk leidt tot een verbeteringbij het uitvoeren van complexe taken of alledaagse activiteiten.
Tenslotte signaleren we een probleem bij het meten en beoordelen van gezichtsvelden(perimetrie) in 3DUW�,,,��4XDGUDQRSLD�FDQ�VKLIW�WR�+HPLDQRSLD�ZLWK�VKLIW�RI�WDVN�GHPDQGV . Wevonden dat de vorm en uitgebreidheid van het gezichtsveld afhankelijk kan zijn van degebruikte perimetrische techniek. Wanneer de perimetrie bepalend is voor het wel of nietbehouden van het rijbewijs dient de officieel te gebruiken techniek dus eenduidiggespecificeerd te zijn omdat de resultaten, en dus ook de daarmee verbonden conclusies,drastisch kunnen verschillen naargelang de methode die men gebruikt.
5. Appendix: Een analytische oefeningIn de appendix bespreken we hoe een zoektaak, met name de AFOV, kan gebruikt worden omde efficiëntie van het visueel zoekgedrag uit te drukken. In $VVHVVLQJ� YLVXDO� VHDUFK� LQ� WKH$)29�WHVW�stellen we dat efficiënt zoeken gekenmerkt wordt door snelheid enerzijds en eengelijkmatige verdeling van de capaciteiten over het zoekveld anderzijds. We introduceerdenen vergeleken verschillende maten en besloten dat twee statistisch onafhankelijke parameters,namelijk een combinatie van de aanbiedingstijd en een genormeerde variantie (PDM) het(AFOV)zoekgedrag kwalitatief en kwantitatief kunnen beschrijven. Dit laat toe om metdezelfde test en dezelfde maten verschillend zoekgedrag te onderscheiden dat kenmerkendkan zijn voor verschillende types slechtziendheid. Met één of met een zeer algemene maat is

Algemene samenvatting8
dit niet mogelijk. Deze twee maten kunnen nog aangevuld worden met een Asymmetrie Index(AI), om de (linker-rechter) asymmetrie van de verdeling aan te geven. Deze laatste is eenmaat voor hemi-spatieel dysfunctioneren, zodat de test ook specifiek bij patiënten met eenhomonieme hemianopsie en met het visueel hemi-neglectsyndroom kan gebruikt worden.

General summary9
General summary
This dissertation concentrates on visual performance in patients with homonymoushemianopia (HH). Homonymous hemianopia indicates blindness for half the field of vision, inboth eyes to approximately the same extent and for the same hemifield (either left or right).This visual field defect is caused by post-chiasmal brain damage. We studied visuo-spatialperformance in neuropsychological tests and during driving in HH.
1. Part I: Introduction and methodsIn 3DUW�,��,QWURGXFWLRQ�DQG�DLP�RI�WKH�SURMHFW we introduce the general questions and aims ofthe dissertation. We indicate that both practical and theoretical objectives can be formulated.On the one hand, valuable clinical application of the findings can be in the form of givingpatients and caretakers realistic advice, and formulating and improving rehabilitationmethods. On the other hand, theoretical interest is in testing predictions of (opportunities for)visual compensation in the driving task by visuo-spatial neuropsychological test performance.Several aspects of driving can be studied, for example accident rates. We focussed on fitnessto drive. Fitness to drive is a medico-legal term indicating a prerequisite for holding a drivers’license. In Europe, the requirement with regard to horizontal field size is 120° or more. Bythis standard, patients with HH, in whom the visual field size is approximately 90°, areexcluded from driving. As we live in a motorised society, the social and economic restrictionsfollowing being declared unfit to drive, are not to be underestimated. In the Netherlands,however, the regulations allow an assessment procedure on the road in the case of visual fieldextent (somewhat) below the norm. During this procedure the opportunity is offered to theclients to actually demonstrate their ability to drive fluently and safely in spite of visualimpairment. The aspects of driving assessed as such, are referred to as practical fitness todrive.
The aforementioned and other crucial concepts, at the basis of this dissertation, are introducedin 3DUW� ,�� 7HUPV� DQG� FRQFHSWV. The description of visual and cognitive functions, theirdetermining factors, the classification of the various tests which we use, and the qualifyingterms, can be approached from various points of view. We adopt the new conceptualframework offered by the World Health Organisation (WHO), namely the InternationalClassification of Functioning, Disability and Health (ICF). In ICF, human functioning isviewed as the outcome of an interaction of a person’s physical or mental condition and thesocial and physical environment. We introduce this conceptual framework and explain how itassociates to our research. We suggest that the outcomes of the visuo-spatialneuropsychological tests used are at the activity level rather than the impairment level and areto be qualified as performance rather than capacity. We discuss the consequences of these andother suggestions. We suggest for example that, in our patient population, neuropsychologicaltests with substantial visual components, no longer exclusively assess the functions they wereoriginally devised for. We therefore question whether standard norms and interpretation canbe maintained. To conclude we situate the concept of practical fitness to drive in thisframework. The fitness or unfitness to drive is, in our study, a decision based on the results ona practical test-ride which attributes special emphasis on visual function and related visuallimitations and compensations. The test-ride is hence situated on the activity level, as it is anassessment of actual driving ability presented by the client. Unfitness to drive is thereforeconceptually an activity limitation. In contrast, medical fitness to drive is a decision based on

General summary10
medical information (for example visual acuity or visual field extent), not on actual drivingperformance. Both practical and medical fitness to drive (can) lead to a participationrestriction, i.c. not being allowed to drive. We point out that the restriction based on medicalunfitness to drive bypasses the activity level in the framework. We suggest that fitness-to-drive decisions should (and can be in the Netherlands) be based on the outcome of a practicaltest-ride (activity level), because the resulting restrictions (if any) are then evidence based,namely on driving limitations. This is ethically and socially more acceptable.
Factors which can cause restrictions and limitations related to driving are discussed in 3DUW�,�'ULYLQJ�UHODWHG� 5HVHDUFK. Here it is explained why and how it can be expected thatneuropsychological test performance can be related to driving(-related) performance. Asvisual information processing takes up a large part in the driving task, a detailed assessmentof this processing is essential to understand and predict practical fitness to drive. In visualinformation processing, both lower- (i.e. sensory) and higher-order (i.e. cognitive) aspects areto be considered. Although sensory visual functions are appropriate for clinical assessment of(loss of) visual function, they clearly do not reflect the visual complexity of the driving task.From the reviewed literature it appears that HH by itself, does not necessarily lead to (hemi-spatial) limitation, or to practical unfitness to drive. Therefore, in addition to detailed andspecific ophthalmological assessment, also higher-order visual functions, measured byneuropsychological tests, should receive considerable attention as to meaningfully andsuccessfully relate visual functioning to practical fitness to drive. We explain why and, morespecifically, which (class of) tests should be included in our test battery. We suggest thatselectivity in test choice and selectivity in patient population are of considerable importanceand consequently further restrict our focus to visual hemi-spatial impairment in patients withexpected visuo-spatial limitation. The observed interrelationships can be used for predictionand evaluation, but could additionally guide the therapist as to which components, skills orfunctions need specific attention in rehabilitation and assist in understanding why a client is(currently) unfit to drive, and perhaps what is the prognosis for future evaluation andimprovement.
A test battery which could serve our purpose is presented in 3DUW� ,�� $� 9LVXR�VSDWLDO� WHVWEDWWHU\. In our aim to specifically and fully assess visuo-spatial functioning, we chose for anumber of different assessments. We classified our range of tests, on an a priori basis, intofour factors, namely basic visual scanning and search (BVSS), visuo-constructive andorganisational tasks (VCO), visuo-integrative tasks (VI) and a task with a dynamiccomponent (Dy). These tasks were evaluated in terms of speed and accuracy. Additionally,since we are more specifically interested in visual hemi-spatial impairment and limitation, wedetermined (when possible) a lateralisation score computed as an asymmetry index (AI). TheAI expresses a lateralised perceptual bias, measured by the degree of differential lateralisedperformance, independently from general performance. This AI, combined with generalperformance, can help to distinguish between a hemi-spatial (and thus lateralised) impairmentand a more general spatial, attentional or scanning deficit. We adopted a similar approach inscoring driving performance during the test-ride. A structured protocol was used withpredetermined observational items. Those items were on a priori basis assigned to factorsrepresenting different aspects of the driving task. Given our specific interest, we specificallyfocussed upon visual performance during driving, reflected in the visual factor.

General summary11
2. Part II: The projectIn part I, we presented the general aim and questions of the project and the tools toaccommodate them. The second part of the manuscript reflects the general structure of theproject, starting with a pre-assessment, followed by an intervention which is subsequently re-assessed (post-assessment).
In 3DUW� ,,�� 'ULYLQJ� DQG� 9LVXR�VSDWLDO� 7HVW� SHUIRUPDQFH� LQ� +RPRQ\PRXV� +HPLDQRSLD , weposed two general questions namely one concerning the practical fitness to drive in HHpatients and the other whether the visual performance during driving could be related tovisuo-spatial neuropsychological test performance. With respect to the first issue, we foundthat driving performance during our practical driving test was generally modest in our HHpatient group. The most frequent remark by the driving expert was a lack of stability insteering. Four of the 28 patients passed the driving test. We concluded that this confirms thatHH cannot be an absolute contra-indication for practical fitness to drive and justifies ourcurrent investment of effort in studying and hopefully future investment of improving fitnessto drive in HH. With respect to the second issue, we found that visual performance duringdriving was significantly related to visuo-spatial neuropsychological test performance, whichwas operationally defined as a function of typical visual HH disability. A specificcombination of the lateralisation, speed and accuracy components derived from the visuo-spatial neuropsychological factors explained a considerable part of the variance (77%) invisual performance during driving.
The observed modest visual performance, and the subjective complaints and restrictionsreported and experienced by the patients suggest the need for (research on) specificrehabilitation. In 3DUW� ,,�� 9LVXDO� UHKDELOLWDWLRQ� LQ� +RPRQ\PRXV� +HPLDQRSLD� DQG� UHODWHGGLVRUGHUV we focussed on the rehabilitation of visual field defects in general and of HH inparticular. We also briefly referred to visual rehabilitation in hemi-neglect and other relateddisorders. After briefly discussing spontaneous recovery, only apparent to some extent and inthe vast minority of patients, we introduced three types of rehabilitation techniques, namelyrestitution, adaptation and compensation. Restoration means (partially) restoring or enlargingthe lost visual field. We concluded that this approach is very time consuming and onlyapplicable in the minority of patients. The small size and location of the restored visualfunction questions its practical relevance. The second technique we discussed was adaptationusing auxiliary optical devices. We specifically focussed on the use of prisms because thisapproach is currently popular in the US and preliminary evaluations are promising. The third,and by us adopted approach is the compensatory technique. The compensatory techniquesoriginate from the plausible assumption that most complaints, limitations and restrictions arethe result of a lack of a quick and full overview of the available visual space. This lack is aconsequence of viewing behaviour which is not adapted to the visual field defect. Inhemianopic patients it is characterised by small-amplitude ‘staircase’ saccades towards theblind hemifield and frequent repetitions of the scan paths during visual search and inspection.With our “Integrated Saccadic Compensation Training Program” we aimed at combiningpositive aspects from several approaches as to facilitate the learning of an optimalcompensatory viewing strategy, which is integrated in a personal scanning style, andapplicable in all daily life situations. Our training consists of three consecutive phases. In afirst phase, large amplitude saccades towards the blind hemifield are trained usingcomputerised programs. This type of eye movement makes it possible to glance over visual

General summary12
space quickly. To enhance transfer, in the second phase, the eye movement principles areapplied in several tasks requiring efficient scanning behaviour. In the third and final phase,the newly learned visual style is practised during car driving, again to promote transfer.
In SDUW� ,,�� 3UHGLFWLRQ� DQG� (YDOXDWLRQ� RI� 'ULYLQJ� DQG� 9LVXR�6SDWLDO� 3HUIRUPDQFH� LQ+RPRQ\PRXV� +HPLDQRSLD� DIWHU� &RPSHQVDWLRQDO� 7UDLQLQJ our intervention is evaluated.Seventeen HH patients, taking part in our training program, were again subjected to ourvisuo-spatial neuropsychological test battery and the driving test. We compared andinterrelated visuo-spatial performance in driving and in neuropsychological tests, before andafter the training. The results were in concordance with previously made claims. Firstly,visual performance during driving, an important aspect of the driving task, was related tovisuo-spatial neuropsychological test performance. Secondly, patients with HH can be fit todrive, since not all of our patients failed the driving test. Although visual performance duringdriving significantly improved, driving performance did not meet the standard for passing thedriving test for each patient, nor did we find any clear evidence of substantial improvement inneuropsychological test performance. The specificity of the improvement argues against anon-specific placebo effect. As indicated by our patients, more rehabilitation time and perhapsalso more attention to aspects other than pure visuo-spatial function, should be incorporated inthe rehabilitation program, as to reduce even more visual limitations and restrictions.Alternatively, in contrast to a collective rehabilitation aim, the rehabilitation goal could betuned to the degree of limitation of the patient. We concluded that visuo-spatial disability,common and apparent in HH patients and consequential for practical fitness to drive, can bepositively influenced by our visual rehabilitation program, and that continuation of(improvement of) rehabilitation efforts for HH is justified and highly desired. However, tovalidate the exact therapeutic effects, a randomised controlled trial with HH patients who arenot trained is needed, but we questioned the ethical aspect of this option.
3. Part III: Additional findings in patients with HH and related impairmentsWe employ two tests from the visuo-spatial battery to draw some more fundamentalconclusions, namely on the relationship of lower- and higher-order visual impairment and theeffects the former can have on the latter.
In 3DUW�,,,��*UH\�6FDOHV�XQFRYHU�VLPLODU�DWWHQWLRQDO�HIIHFWV� LQ�KRPRQ\PRXV�KHPLDQRSLD�DQGYLVXDO�KHPL�QHJOHFW we discuss the Grey Scales task. This task has been developed to quantifythe early, automatic, (perhaps obligatory) ipsilesional orienting of visual attention, frequentlyassumed as the first component of the attentional deficits in visual hemi-neglect. This lateralattentional bias has been demonstrated in controls, in whom it is expressed as a leftwardperceptual asymmetry and in neglect patients, expressed as an extreme rightward bias.Explanations for this attentional imbalance were up until now mainly formulated in terms ofright hemisphere activation. We reproduced previous literature findings, considering controlsand neglect patients. Additionally, we presented this Grey Scale task to 32 patients with left-and right-sided HH who had no clinical signs of impaired lateralised attention. Resultsrevealed that HH patients showed an ipsilesional bias, albeit to a lesser degree than in neglect.Left-sided HH patients presented a quantitatively similar, but qualitatively opposite bias thanthe right-sided HH patients. We concluded that sensory effects can be an alternative source ofattentional imbalance, which can interact with the previously proposed (right) hemisphericeffects. This suggests that the perceptual asymmetry is not necessarily an indicator of

General summary13
impaired right hemisphere attention. It rather suggests a pattern of functional cerebralasymmetry, which can also be caused by asymmetric sensory input and hence illustrates ourpoint that a lower-order visual impairment can give rise to an apparently higher-order effect.
A similar conclusion was drawn in 3DUW� ,,,�� +HPLDQRSLF� 9LVXDO� )LHOG� 'HIHFWV� HOLFLW+HPLDQRSLF� 6FDQQLQJ. Previous explanations for the defective hemianopic scanningbehaviour and for the variability in success of compensating for HH had been in terms ofextent of the brain injury. We investigated whether brain injury is necessary to elicit theselimitations or whether merely a visual field defect would be sufficient. We thereforesimulated HH in 16 healthy subjects without brain damage by using on-line eye movementregistrations and compared their scanning performance, on a dot counting task, to their own“normal” condition and to real HH patients’ performance. We evidenced clear parallelsbetween simulated and real HH, suggesting that hemianopic scanning behaviour largely isvisually elicited, namely by the visual field defect, and not by the brain damage. Weconcluded that most typical HH oculomotor dysfunctions, as for example ipsilateralhypometric saccades, do not result from the brain damage but are visually elicited and thatcomplaints as for example slowness of vision and prolongation of scanpaths, can no longer bemerely associated to brain damage. We further observed age-related processes incompensating for the HH, namely worse compensation to the created visual impairment withhigher age and, at first sight paradoxically, that the visually elicited limitations can be mostpronounced during (seemingly) the simpler situations. We further concluded that at least forsome HH patients, more emphasis can be devoted to visual than to cognitive components inrehabilitation and that diagnosing higher-order visuo-spatial impairment can only occur in thelight of concomitant lower-order visual impairment.
In preparing the HH project and devising the “Integrated Saccadic Compensation TrainingProgram”, we evaluated by means of a case study, an Italian neglect rehabilitation program.The modifications to the original program and its evaluation is described in 3DUW� ,,,�(YDOXDWLRQ�RI�WKH�HIIHFWLYHQHVV�RI�D�KHPL�QHJOHFW�UHKDELOLWDWLRQ�SURJUDP�DQG�JHQHUDOL]DWLRQ�WRGULYLQJ�� D� FDVH� VWXG\. We evaluated by means of traditional and clinical neglect tasks,complemented by a dynamic tracking task (a basic driving simulator) and by a test-ride in anadvanced driving simulator. After the program, we observed strong improvements on theclinical (non-trained) neglect tasks. By that performance, the patient would no longer bediagnosed with the neglect-syndrome. However, in the tracking task and the moreecologically valid driving simulator, we still observed unacceptable lateral positions on theroad and unsteadiness in steering in spite of acceptable visual exploration. We concluded thatthis training can help to compensate for the scanning deficit, most pronounced in clinicaltasks. But since some aspects of real life tasks do not change even after this intensive training,we have no evidence of functional improvement of neglect. We concluded that not everyvisually related aspect of activities of daily life can easily be compensated for.
Finally, we notify a problem in measuring and evaluating visual field defects (perimetry) in3DUW�,,,��4XDGUDQRSLD�FDQ�VKLIW�WR�+HPLDQRSLD�ZLWK�VKLIW�RI�WDVN�GHPDQGV . We found that theform and extent of the visual field defect in a patient who had suffered brain damage, wasstrongly dependent on the perimetric procedure used. When perimetry is determinative forholding or withdrawing drivers’ licences, this suggests that the procedure needs to be

General summary14
explicitly and unambiguously specified as the outcome and therefore the conclusions cansubstantially differ.
4. Appendix: An analytic exerciseIn $VVHVVLQJ�YLVXDO�VHDUFK�LQ�WKH�$)29�WHVW��DSSHQGL[� we discuss how the AFOV (AttendedField Of View) test can be used to assess and express the efficiency of visual search. Wedefine an efficient search strategy as a strategy which allows the subject to respond to targetsin a fast and evenly distributed manner. Hence, the test should provide a measure of generalsearch time as well as a measure of distribution. The mean threshold presentation time iscalculated as an estimate of general search time. We further present a measure expressing the‘flatness’ and a measure expressing the ‘asymmetry’ of the distribution across the searchfield. We suggest that both measures in combination with the mean threshold presentationtime give an adequate description of the efficiency of visual search in the AFOV test. Byconsidering these three parameters, typical visual search patterns associated with specificvisual field impairments can be differentiated.

15
Part I: Introduction and Methods

Part I: Introduction and Aim16
Introduction and Aim of the project
1. General: Fitness to drive and Homonymous HemianopiaThis dissertation concentrates on fitness to drive in persons with a homonymous hemianopicvisual field defect. Homonymous hemianopia (HH) denotes the loss of one hemi-field and iscaused by post-chiasmal brain damage, usually following stroke. Fitness to drive is a medico-legal term indicating a prerequisite for holding a drivers license. It is defined in terms ofminimal functional requirements described in legal regulations. In almost any country, therequirements for visual function are defined in terms of static visual acuity and horizontalvisual field size. The standard in Europe with regard to horizontal field size is 120 degrees ormore. By this requirement, patients with HH, in whom the visual field size is approximately90 degrees, are excluded from driving. As we live in a motorised society, the social andeconomic restrictions following being declared unfit to drive, should not be underestimated.
2. Fitness to drive: requirements and characteristicsThe origin of the requirements is historic and has never been put to empirical test. In fact, theevidence supporting their validity is rather weak. The question is whether these standardsshould not be subjected to rigorous investigation and perhaps revision. Because of the legalcharacter of the requirements, such research is often precluded. In the Netherlands, however,the regulations allow an assessment procedure on the road in the case of (mild) cognitiveimpairment. Similar opportunities are created in the case of visual field extent (somewhat)below the norm. During this procedure the opportunity is offered to actually demonstrate thatthe subject is able to drive fluently and safely in spite of visual impairment. The aspects ofdriving assessed as such, are referred to as practical fitness to drive. This original approach isbased on theoretical and pragmatic evidence that driving allows for a great deal ofcompensation for limitations. This may involve compensatory strategies on the tactical andstrategical level. Tactical adaptations could be anticipatory adjustments of speed and of theaverage following distance, providing time for compensatory eye-movements. Strategicaladaptation could be choosing route and time for trips in which driving is not very time-pressured. In terms of the World Health Organisation’s (WHO) International Classification ofFunctioning, Disability and Health (ICF), formerly International Classification ofImpairments, Disabilities and Handicaps (ICIDH), practical fitness to drive is defined on theactivity (formerly disability) level, and is evaluated accordingly1. It is thus recognised thatfitness to drive is as closely related to learned driving skills and compensatory behaviours asto medical status. This is in contrast to the traditional medical concept of fitness to drive,which is only related to impairments.
3. Homonymous HemianopiaHomonymous hemianopia (HH) is a frequent consequence of post-chiasmal stroke, estimatedto strike some 48% of survivors. In comparison to this relatively high prevalence, only fewHH patients have made use of the opportunity to have their practical fitness to drive assessed.As is shown in the files of the licensing authorities, of those HH patients who were actuallyassessed, a substantial percentage was declared fit to drive. However, this may have been a-typical sample. At present, it is not at all clear what are the characteristics of those who doand those who do not pass the assessment of practical fitness to drive. Further, it is not clear
1 In the course of realisation of this dissertation, WHO terminology changed from ICIDH to ICF.

Part I: Introduction and Aim17
which features determine, if and to what extent a HH patient could profit from drivingoriented rehabilitation or visual aids, if a patient initially fails the driving assessment.
4. GoalsAn important aim of this study is to provide more insight into these questions about individualcharacteristics, making use of standardised assessments and rehabilitation applied in arepresentative sample of HH patients. Based both on literature and on clinical experience,these characteristics are primarily sought in terms of neuropsychological test performance inthe cognitive and visuo-perceptual and visuo-spatial domain. Having a better knowledgeabout the role of these individual characteristics is important both clinically and theoretically.Valuable clinical application can be in the form of giving patients and caretakers realisticadvice, and improving rehabilitation methods. The theoretical interest lies in testingpredictions of opportunities for compensation in the driving task as derived from cognitivepsychological driver models. Besides its direct clinical and theoretical importance, the projectmay have policy implications for regulations with regard to fitness to drive, as implied above.

Part I: Terms and Concepts18
Terms and Concepts
1. GeneralThroughout this dissertation a variety of terminology is used. Especially, as in thisdissertation, when research is done interdisciplinary, a priori clarification and definition of thekey-terms is highly recommendable. We will use the terms consistently as we are about todescribe them. The description of visual and cognitive functions, their determining factors,the classification of tests which assess them, and the qualifying terms, can be approachedfrom various points of view. We adopt the new conceptual framework offered by the WorldHealth Organisation (WHO), namely the International Classification of Functioning,Disability and Health (ICF1), formerly International Classification of Impairments,Disabilities and Handicaps (ICIDH). The ICF classification provides a unified and standardlanguage and framework for understanding, studying, and describing health and health-relatedstates in a bio-psycho-social model that emphasis the universal nature of disablement. ICFclassifies functioning and is essentially an aetiology neutral classification. In this respect, itsupplements the International Classification of Diseases, Tenth Edition (ICD-10) whichprovides an etiological framework. In ICF, human functioning is viewed as the outcome of aninteraction between a person’s physical or mental condition and the social and physicalenvironment. We will use this conceptual framework for it’s terminology and will alsoclassify and situate our procedures in it, although ICF is not primarily intended for this atpresent. The framework, and how it in our view associates to our research, is summarised inTable 1.
2. ICF applied to the current research2.1. General structure and terms2.1.1. Functioning and DisabilityICF organises information in two parts, namely in )XQFWLRQLQJ�DQG�'LVDELOLW\, and &RQWH[WXDO)DFWRUV. Functioning and Disability has two components, namely one component concerningthe ERG\ (in a broad sense) and one component concerning aspects of action, termed DFWLYLWLHVDQG�SDUWLFLSDWLRQ. The body component comprises two domains, namely for IXQFWLRQV of bodysystems and for the body VWUXFWXUHV. It is important to note that the “body” refers to the humanorganism as a whole and hence also includes the brain and its psychological or cognitivefunctions in addition to, for example, sensory functions. Cognitive (neuro)psychologists havethe inclination to stress the conceptual differentiation of “body” and “mind” and parallel thedistinction with “hardware” and “software”. Inapparently for them, in ICF both terms are atthe body-level, the former referring to “structure”, the latter to “mental function”. ICF lists atotal of 873 body items. We will use the term “cognitive” or “higher-order” function for whatin the classification is referred to as mental function. The cognitive functions, most relevant toour research are orientation in place (b1141), attention (b140), and perception (b156). Fromthe latter (perceptual functions), we will specifically address visual perception (b1561) andvisuo-spatial perception (b1565). In addition to mental function, also sensory function isincluded in ICF, for which we will use the terms “sensory” or “lower-order” function. In thisdissertation, visual sensory or lower-order functions (b210) will be focussed upon, morespecifically functions of the visual field (b2101), which include scotomas and (hemi-)anopias.
1 The version we used is the ICIDH-2 Final Draft but has been approved by the WHO’s governing bodies andwill be referred to as ICF. This document and further information can be found on the Internet at:http://www3.who.int/icf/icftemplate.cfm

Part I: Terms and Concepts19
Also qualitative functions involving light sensitivity, colour vision, contrast sensitivity andoverall picture quality (b2102) can be relevant. Other functions of the body, addressed in thisdissertation, are reflexive (b750) and voluntary (b760) control of movements. Applied tovisual-compensational topics, we will discuss movements of the eye and head.
In addition to the functional aspects of the body, the ICF also addresses structural aspects.Body structures are anatomical parts of the body and include i.a. different structures of thebrain (s110).In ICF, changes in body function and body structure are considered to have physiological andanatomical causation respectively. In both domains, a negative change is termed anLPSDLUPHQW, which can either be an anomaly, defect, lack, loss or reduction, addition orexcess, or a significant deviation in body structure or in (lower- or higher-order) function.Hence, visual field defects, defective attentional and visuo-spatial function, and brain damageare referred to as impairments.
The second component in the Function and Disability-part, concerns action and is captured bythe Activities and Participation-label. In a sense, all behaviour displayed by the subject inquestion resorts under this label. ICF defines DFWLYLW\ as the execution of a task or action by anindividual, for example an experimental test or reading and writing, or driving a car.3DUWLFLSDWLRQ entails involvement in a life situation, for example social contact by beingmobile, participation in community activities, obtaining a driving license. ICF provides aclassification of 617 activities and 106 participations, unified as OLIH� DUHDV. The listedcategories of life areas, most applicable for our research, are purposeful visual sensoryexperience (namely watching, d115), basic learning (namely acquiring skills, d155), applyingknowledge (namely focussing attention, d160), communicating with -receiving- visual stimuli(namely comprehending the meaning represented by signs, symbols, drawings, photographsetc., d315), and moving around using transportation (namely driving, d475). Conceptually,whether a category is considered an activity or a participation depends on the adoptedtheoretical framework.
$FWLYLW\ OLPLWDWLRQV (henceforth limitations) are difficulties an individual may have inexecuting tasks (formerly disabilities in ICIDH). Activities can be limited in nature, duration,and quality. 3DUWLFLSDWLRQ UHVWULFWLRQV (henceforth restrictions) are problems an individualmay experience in involvement in life situations (formerly handicaps in ICIDH). Participationmay be restricted in nature, duration and quality. In ICF, IXQFWLRQLQJ is an umbrella term forthe positive aspects referring to body functions and structures, activities and participations.Similarly, GLVDELOLW\ refers to impairments, limitations and restrictions. In this dissertation,lower-order functioning, refers to sensory (body) functioning. Lower-order impairment refersto sensory impairment. Homonymous hemianopia (HH), a key-concept in this dissertation, isa lower-order sensory impairment. Higher-order functioning, in this dissertation, refers tocognitive or brain-related (in ICF termed “mental”) functioning. Higher-order impairment isformulated likewise. Agnosia and dyslexia are (neuropsychological) examples of higher-orderimpairment. Hemi-spatial neglect and visuo-spatial impairment are other examples and key-concepts in this dissertation.
Although ICF is basically not a classification of procedures, different types of tests can besituated in the framework. For example, it can be argued that a driving test is an assessment of

Table 1. ICF terminology related to the current projectParts Functioning and Disability Contextual FactorsComponents Body Activities and Participation Environmental Personal� Body FunctionsDomains/Constructs v Body Structures
Qualifiers:
Capacity&
Performance
External influences offeatures of the
physical, social, andattitudinal world
Internal influences ofattributes of the
person
Outcome
� visuo-spatial perceptionvisual field
eye movement
“ideal” neuro-psychological tests
fMRI scanperimetric testExamples
v optic tractoccipital lobe CT scan
“actual” neuropsychological testspractical driving test
glasses, lenses,prejudices,
rehabilitationprograms, laws and
regulations
age, gender,education, driving
experience, scanningstyle
Positive Aspect Functional and structural integrity
Life areas:
Activities&
Participation
Facilitator (Facilitator)
Functioning
Negative Aspect ImpairmentActivity limitation
Participation restrictionBarriers (Barrier)
Disability

Part I: Terms and Concepts21
an activity, whereas measuring intensity of social contact is at the participation level. In thepresent dissertation, most tests used are at the activity level. Activity is defined as the natureand extent of functioning at the level of the person and intrinsically implies human behaviour.However, we are in the opinion that a full description of human functioning should not onlybe composed of functioning at the level of the person, but also at the level of the body. Thelatter tests typically have a minimal (or non-)behavioural dependence and are at present notincorporated in ICF. These tests which reveal direct information about body function andstructure are measures of impairments (in contrast to activities). CT-scans, for example, areapplicable in ICF classification, as they can reveal structural changes in body aspects.Similarly, measurement of visual evoked potentials have (ideally) a minimal behaviouralcomponent, but can reveal brain-related impairment. Ideally, the same can be argued forperimetric tests, which reveal functional body aspects (i.c. visual field function).Consideration of this type of test outcome complements, in our opinion, significantly to thecompleteness of describing human functioning and disability.We would like to stress that, by definition, tests at the impairment level are not prone to thesame influences as tests at the activity level. The latter are considered to be the product of acomplex bio-psycho-social interaction, whereas the former are mere registrations ofimpairments, and are hence (ideally) not influenced by such interactions.
As a consequence and for the benefit of the completeness of describing functioning anddisability, we performed some additions to the existing ICF framework (see grey areas inTable 1). We added a new column in the “Body” component hosting the non-behaviourally-dependent type of tests i.e. tests at the impairment level. We combined this cell with the“Activity and Participation” component. The combination is termed “outcome” which is aneutral term indicating test result but not implying active behaviour. The position of the newcell expresses the close relationship with (only) the body and the (relative) unproneness tocontextual influences (distinct from activities and participation).
The above mentioned life areas (i.e. both activities and participations) are qualified by the twoqualifiers of SHUIRUPDQFH and FDSDFLW\�(note the linkage and orthogonal orientation in Fig. 1).The performance describes an individual executing a task or an action in his or her currentcontext or situation, which includes all personal and environmental factors (to be discussedfurther). The capacity qualifier describes an individual’s ability to execute a task or an actionand indicates the highest probable level of functioning that a person may reach in a givendomain at a given moment. Hence, capacity reflects the environmentally adjusted ability ofthe individual, as a full ability is to be assessed in a uniform and standard context.Performance and capacity will appear to provide a crucial conceptual difference in thisdissertation. Namely, we will (later) argue, based on cognitive-neuropsychologicaltheorisation, that, in the HH population, neuropsychological tests are measures ofperformance, in spite of that they frequently are considered to be capacity assessments andeven ideally assessments at the impairment level.
2.1.2. Contextual factorsAs previously mentioned, ICF organises information into two parts (left and right parts inTable 1). We discussed the first part above, namely functioning and disability. The secondpart comprises the &RQWH[WXDO� )DFWRUV, including two components, namely (QYLURQPHQWDO)DFWRUV and 3HUVRQDO� )DFWRUV. The contextual factors interact with (i.e. influence) theconstructs from functioning and disability, as for example “light” (environment) interacts with

Part I: Terms and Concepts22
“seeing” (body function), or the law on (obtaining and denying) drivers’ licences interactswith social contact.The personal factors are not currently classified in ICF, but comprise internal influences andcharacteristics of the subject like age, gender, race, coping style, fitness, lifestyle, habits,character style, social status and background, education, individual psychological assets,overall behaviour pattern etc. They comprise the particular background of an individual’s lifeand living. Another example of a personal factor, and key-concept in this dissertation, is thepersonal scanning style or viewing method and strategy. An adapted scanning styledetermines if and how a patient with HH visually compensates for the visual impairment, andhence influences how the effects of the visual field defect translate to limitations andrestrictions. Positive and negative aspects are not discussed in ICF, but we introduce the sameterms as for the environmental factors (namely facilitators and barriers respectively).Examples of the former are driving experience for driving performance, and for the latter,misconception of the visual impairment resulting in non-effective or deleterious head-movements hindering effective compensation by eye-movements.The environmental factors make up the physical, social and attitudinal environment in whichpeople live and conduct their lives and can be IDFLOLWDWRUV (positive aspect) or a EDUULHUV(negative aspect). ICF provides classifications of which the following are most relevant forour research. Firstly, there are the assistive products and technologies, defined as any product,instrument, equipment or technical system, especially produced or generally available,preventing, compensating, monitoring, relieving or neutralising disability. Specificapplications are the adaptations to indoor and outdoor mobility transportation means (e1201),but also specifically designed products, such as specialised vision devices (glasses, lenses,prisms, e1551) are important environmental factors. Another class of environmental factorsare attitudes, namely observable consequences of customs, practices, ideologies, values,norms, factual beliefs and religious beliefs. These attitudes influence individual behaviour andsocial life at all levels. The attitudes classified are those of people external to the personwhose situation is being described, and are hence not those of the person themselves.Relevant to our research are the individual attitudes of people in positions of authority (e430).Also part of the environment are the services, systems and policies. Services are the provisionof benefits, structured programmes and operations, in order to meet the needs of individuals.Systems are administrative control and monitoring mechanisms. Policies are the establishedrules, regulations and standards, which govern or regulate the systems that control services,programmes and other infrastructural activities. Relevant to our research are the healthservices, system and policies (e580). These are services and programmes aimed at deliveringinterventions to individuals for their physical, psychological and social well-being, such asprimary care services, acute care, rehabilitation and long-term care services. In addition,specifically in relation to driving, the legal services, systems and policies (e545) will bementioned, since in most countries HH precludes legal driving.
2.2. Interactions and further examplesA person's functioning and disability is conceived as a dynamic interaction between healthconditions (diseases, disorders, injuries, traumas, etc.) and contextual factors. Contextualfactors include both personal and environmental factors. There is a dynamic interactionamong all entities: interventions in one entity have the potential to modify one or more of theother entities. The interactions are specific, complex and can be bi-directional. We summarisethe most obvious relationships applied to the current research (see Fig. 1).

Part I: Terms and Concepts23
Impairments in body functions are usually linked to impairments in body structures, as forexample a homonymous visual field defect is caused by unilateral post-chiasmal braindamage. The impairment can have consequences for activities and hence may lead tolimitations. For example a visual field defect may result in a scanning deficit (assessed by avisual scanning task) or problems with reading (assessed with a reading test). Impairmentdoes not necessarily lead to limitation, as for example specially designed lenses, or asuccessful rehabilitation program (i.e. contextual factors) may help to compensate sufficientlyfor the impairment and limitation imposed by it. Limitation may lead to restriction, i.e. whenthe consequences are also discernible in life situations, as for example a reading limitationmay result in not reading the newspaper any more and hence being deprived from some typeof information leading to ignorance. However, also restrictions can be apparent withoutaccompanying (or eliciting) limitations. They can directly result from impairments incombination with contextual factors (i.c. barriers). For example, patients with HH may bedeclared unfit to drive by law (and hence do not drive any more and are thereby deprivedfrom some types of social events), despite sufficient capacity to drive fluently and safely.
Performance
Capacity
Performance
Capacity
Environmental
Personal
Body Function
Body Structure
Body Action Context
Activity
Participation
Fig. 1. Interrelations in ICF.

Part I: Terms and Concepts24
Similarly, a limitation does not necessarily lead to a restriction, as contextual factors (i.c.facilitators) can reduce the influence of an impairment on real-life situations. For example,specific adaptations to entrances of public buildings can make it perfectly possible for ahemiplegic patient not to be deprived from cultural and social happenings.
Whether an activity or participation is qualified as capacity (environmentally adjusted) orperformance (executing tasks under influence of current personal context), depends on itsdetermination by contextual factors. Conceptually, if test result is dependent onenvironmental and/or personal factors, then by definition performance is observed, in contrastto capacity, which is context-free.Further, as previously argued, if outcome is at the impairment level and hence minimallybehaviourally-related (as e.g. CT scans, perimetric tests), it is also considered to be context-free, defining impairment assessments as measures of capacity. In ICF, it is stated that bothcapacity and performance qualifiers can be used with and without assistive devices andpersonal assistance. This seems paradoxical, as assistive devices, in ICF, are environmentalfactors, and as such are by definition incompatible with the notion of capacity. But whenassistive devices (and personal assistance) do not act upon the function at hand or areconsidered to be part of the uniform and standard environment, then the paradox is resolved.For example, when dyslexia (reading function) is assessed, subjects can wear their correctivelenses or spectacles, such that reading is not complicated by blurry letters. Obviously,corrective lenses or spectacles do not fundamentally distort the reading function. Optimaloptical correction is considered to be part of the uniform and standard environment. On theother hand, whispering the words to-be-read to the (dyslexic) subject, would fundamentallyact upon the reading function at hand. Consequently the reading outcome would obviously notbe considered to reflect reading capacity.
2.3. Neuropsychological testsFundamental to this dissertation are the higher-order visual functions which are assessed. Themajority of the neuropsychological tests used, aim at assessing visual attention and visuo-spatial function and hence pretend to be measures at the impairment level. In table 1 they arereferred to as “ideal” neuropsychological tests. However, we would like to argue that in ourpatient group their outcome should be conceptualised at the level of activity (“actual”neuropsychological tests). For this it is crucial to (re)appreciate a fundamental issue ininterpreting neuropsychological test results, namely never to conclude to a higher-orderimpairment, if influences at another or lower level have not been excluded. Applied to ourHH patient population, it could be argued that for any test, in which visual information is ofsubstantial importance, its outcome is determined by the lower-order impairment (i.c. thevisual field defect) and by contextual factors (e.g. non-adapted scanning style). Hence, theoutcome which is observed is at the activity level and is further to be qualified as performancerather than capacity. These considerations are not without consequences.Firstly, it could be questioned whether the standard norms for visually based tests can validlybe used in our patient group, as we argue that the tests could be considered assessments atdifferent levels (ideal versus actual neuropsychological tests; impairment versus activity).Secondly, interpretation of neuropsychological test at the performance level is not a standardenterprise. The effects of a visual impairment on performance will be negative, whereas thecontextual effects can go either way. Contextual factors can facilitate, for example havingparticipated in a visual rehabilitation program which allows patients to effectively compensatefor the visual impairment. On the other hand, absence of (immediate) care could result in

Part I: Terms and Concepts25
depressive states or improper and ineffective compensational efforts, hence forming a barrier.Since the performance is effected by several factors which each can be positive or negative,conclusions about the function (which was the primary reason for applying theneuropsychological test) become extremely complicated and opaque.Thirdly and on the basis of the above, it can be questioned whether indications of truecapacity can still be obtained in our patients using visually based tests. Even if so, it can beargued that this is not “normal” capacity but rather “hemianopic” capacity. Namely, maximalperformance (i.e. capacity) can only be obtained when fully and perfectly compensating forthe visual impairment. Hence behaviour displayed by non-or suboptimally compensating HHpatients are always indications of performance. Performance can be improved for exampleafter visual cognitive rehabilitation and at this stage would approximate (more) the level ofcapacity (shift in status). As a consequence of this shift in status, comparison of visualneuropsychological test results by HH patients before and after a (successful) visualrehabilitation program might be considered conceptually problematic.
2.4. Fitness to DriveTraditionally fitness to drive is defined in medico-legal terms. The visual (body) functions,which are used to decide on whether someone is fit to drive, are of a lower-order nature,namely visual acuity and horizontal visual field extent. Not acquiring the norm resultsautomatically in being declared (legally) unfit to drive. Note that we use, in this respect, theterm “declaration”, which suggests the involvement of authority rather than outcome of testresults in the decision process. Using ICF terminology and conceptualisation, an interaction oflower-order impairment (medico) and environmental factors (legal) results in a participationrestriction, namely being refused to drive a car or obtaining a driving license and hence beingdeprived from this popular and socially important type of mobility. Further note that this is anexample of the presence of a participation restriction, without touching upon the activityconstruct. Typically a restrictions (e.g. not driving a car anymore) is jointly caused by alimitation (e.g. not being able to drive a car). Medico-legal unfitness to drive restricts drivingwithout personal evidence-based limitation information. It is uniquely associated with (lower-order) impairment and is hence likewise conceptualised in ICF terminology.
In the Netherlands, a different conceptualisation of fitness to drive is used, namely practicalfitness to drive, as opposed to medical fitness to drive. Practical fitness to drive is situated atthe activity-performance level, and is hence assessed accordingly, namely by a practicaldriving test. We would like to stress that we consider fitness to drive to be related to activityand to be contextually influenced, qualifying it as performance.Practical fitness to drive is assessed by an on-the-road driving test (activity). Drivingperformance is thereby evaluated, attributing special emphasis on visual function, and relatedor to-be expected (visual) limitations. When fitness to drive is evaluated, it is recognised thatboth lower- and higher-order impairments (e.g. visual field defects and visuo-spatialimpairment respectively) and contextual factors (e.g. driving experience, visualcompensation, personality characteristics, etc.) can be crucial determining elements. Patientswith HH, considered medico-legally unfit to drive, may prove to be practically fit to drive byadequately performing the test-ride. They can do so by effectively compensating for the visualimpairment for example after visual rehabilitation, spontaneous adaptation, or using assistivedevices. We suggest that the outcome of such a test-ride should (and can be in theNetherlands) be the basis for fitness-to-drive decisions because the resulting restrictions (ifany) are then evidence based, which is ethically and socially more acceptable.

Part I: Driving-related Research26
Driving-related Research
In this chapter it is explained why it can be expected that neuropsychological test performancein the domain of higher-order visual functions is related to practical fitness to drive. It will beargued that visual information-processing takes up a large part in the driving task. This visualinformation processing can be influenced by both lower- and higher-order visual impairment(dysfunction) and should be assessed accordingly. It will be explained why and, morespecifically, which class of tests of visual function should be included in a battery used tounderstand and predict practical fitness to drive. We will plead that selectivity in test choiceand selectivity in patient population are of considerable importance in this line of research.Since our particular interest in visual hemi-spatial impairment, we will therefore focus onpatients with homonymous hemianopia (HH) and related hemi-spatial disability. We willargue that only detailed and specific ophthalmological and neuropsychological tests canmeaningfully and successfully be related to practical fitness to drive. This conduct is imposedby the conclusion that HH by itself, does not necessarily lead to hemi-spatial limitation, or topractical unfitness to drive. In addition to the need for specificity and selectivity, the testsneed to be sensitive, as to be able to observe different levels of hemi-spatial disability. By ourown research, to be reported further, we aim to enhance insights into the relationship betweenhemi-spatial (dys)function and practical fitness to drive.
1. The importance of Vision in Driving1.1. GeneralDriving is a complex skill requiring many sub-skills on the strategical, tactical and operationallevel. These skills require adequate perceptual, cognitive and motor processes. Theseprocesses are linked by a mental schema in a co-ordinated manner, presumably stored inprocedural memory (Van Winsum & Brouwer, 1997; Brouwer, in press). It is assumed thatthe application of the schemata is triggered by the visual context of the driving situation andhence is very much dependent on visual information-processing. Thus, although auditory,kinaesthetic, and vestibular senses are of importance, the most substantial information beingprocessed while driving is of a visual nature. Rockwell (1972) is referred to, in nearly alldriving-related texts, stating that vision constitutes over 90% of information-input to thedriver.
1.2. Lower and Higher-order Visual FunctionAlthough sensory visual functions are appropriate for clinical assessment of (loss of) visualfunction, they clearly do not reflect the visual complexity of the driving task (nor of any otheractivity of daily living for that matter). In visual sensory tests, perceptual influences which areimportant and inherent to driving, such as searching and finding targets in a cluttered array,stimulus uncertainty, simultaneous processing of information etcetera, are minimised. Higher-order impairment can also be a limiting factor, as alternative or in addition to obviousphysical and sensory impairment (e.g. Sivak, Olson, Kewman, Won, & Henson, 1981). Shinarand Schieber (1991) argue that higher-order perceptual functions are conceptually morerelevant to the driving demands and manifest a much faster rate of age-related deterioration.In this respect, concepts of visual search, visual speed, visual and divided attention, andvisuo-spatial impairments are frequently put forward as alternative determinants of practicalfitness to drive (e.g. Shinar & Schieber, 1991; Brouwer, in press). In the following discussion,a clear distinction will thus be made between lower- and higher-order visual function.

Part I: Driving-related Research27
1.3. Impairment and LimitationThe confusing status of the term “fitness to drive” has been elucidated in previous discussion.It has been argued that practical fitness to drive is situated at the activity-performance leveland is assessed accordingly. This is in contrast to medical fitness to drive, which is arestriction resulting from impairment. Assessments of primary visual functions and higher-order cognitive functions are ideally evaluations on the impairment level and can thus (only)possibly be related to medical fitness to drive. This is not to say that these impairments areirrelevant, as obviously they can elicit limitation and thus influence practical fitness to drive.However, and in addition, also other 'individual' factors (such as e.g. driving experience,compensatory behaviour etc.) and non-specific cognitive factors (such as e.g. fluidintelligence) can have as much influence on test performance at the activity level ( Brouwer,in press). Hence, it is imperative to keep in mind that performance on a practical driving test(or on most tests for that matter) can be influenced by a variety of different factors frompossibly different levels and their interactions.
1.4. ConsequencesAssessments paying attention to only one (e.g. lower-order visual function) or a few factors,result necessarily in poverty of explaining variability in or in low correlations with practicalfitness to drive (Van Zomeren, Brouwer, Rothengatter, & Snoek, 1988; Brouwer, in press).From the point of view of accurately predicting practical fitness to drive, this has at least twoconsequences. Firstly, only when very specific sub-tasks of the general driving task areconsidered (e.g. reading signs), the correlations with assessments on the impairment level areincreased (Van Zomeren et al., 1988). It is intuitive that for example reading signs or readinglicence plates could well be highly related to visual acuity. But then only one aspect of thedriving task is considered, and thus practical fitness to drive is only partly addressed.Secondly, when the total driving task is considered (which is actually our aim), the mostpredictive (neuropsychological) task will have to be equally influenced by the same lower-and higher-order, specific and non-specific factors as the real driving task itself. This testcould prove to be difficult to construct and only be approximated (perhaps by e.g. a tracking-task).
1.5. ConclusionIn conclusion, visual function is an important and predominant aspect of the driving task.Visual impairment can thus have clear negative effects on driving performance. It is howeverof theoretical and practical importance to distinguish and study both lower- and higher-ordervisual function. Successfully performing the driving task (i.e. being practically fit to drive)entails more than adequate visual function as driving entails a multitude of sub-tasks andappeals to a multitude of functions, all possibly interacting. This is to say that practical fitnessto drive is situated at the activity-performance level an can thus possibly be influenced by (amultitude of) impairments, and by individual and non-specific cognitive factors. This hasclear consequences for choosing (neuropsychological) tasks when trying to accurately predictpractical fitness to drive.Keeping in mind these general limitations in studying practical fitness to drive, and for theremainder of this discussion, I will focus on visual (dys)function, later narrowing toparticularly visual hemi-spatial impairment resulting from brain damage.

Part I: Driving-related Research28
2. Visual Function2.1. GeneralChanges in visual (and other sensory) structures and lower-order functions may result in adecline of performance on the routine tasks essential to the individual’s daily living includingdriving. An evenly serious effect can arise from higher-order visual impairment or from acombination of both lower- and higher-order impairments. Visual function was previouslyconceptualised as incorporating two aspects namely lower-order (sensory) visual function andhigher-order (cognitive) visual function, both possibly resulting in limitations. Not being ableto quickly overview a visual scene, recognise common objects, faces, words, or signs orfailing to notice events on one side of (visual) space, can be further be very restricting. For theremainder, visual field defects (VFDs) and associated higher-order visual impairment will befocussed upon. The associated higher-order visual impairments of our particular interest, arehemi-spatial in nature. The resulting visual limitations may arise as a by-effect or knock-oneffect of homonymous visual field loss or may be the direct resultant of brain damage (orboth). Behaviourally, the disabilities may appear the same but the causation and perhaps alsothe rehabilitation might be different. Assessment of visual functioning will thus include testsfor both lower and higher-order aspects and, will specifically involve perimetry (i.e. visualfield assessment) and visuo-spatial neuropsychological tests. For the remainder, I will try toindicate why and, more specifically, which tests of visual function should be included in abattery used to understand and predict the safety and fluency of driving performance.
2.2. Need and goal of assessmentStudies indicate that general practitioners and occupational therapists as well as clients andtheir families express the need for standardised and theoretically validated methods forevaluating driver performance (Korner-Bitensky, Sofer, Gelinas, & Mazer, 1998) and thusassessing fitness to drive. As standard procedures do not exist and on-the-road testing issometimes considered dangerous, often have unknown reliability and objectivity, and arecostly in terms of time, money and energy (Galski, Bruno, & Ehle, 1992), it can be desirableto have a set of valid alternative tests closely related to and wishfully capable of predictingpractical fitness to drive. Additionally, test results could not only serve the purpose ofevaluation but could also guide the therapist as to which components, skills or functions needspecific attention in rehabilitation (Brouwer & Withaar, 1997). As such, these results couldalso help practitioners, researchers, clients and families, to understand why a client is(currently) unfit to drive, perhaps what is the prognosis for further evaluation anddevelopment and what are the learning or adaptive potentials. Finally, the accumulated resultscould yield valuable information about goals and means for improving road and carinfrastructure (e.g. additional mirrors) and possible other “personal” adaptations as forexample prisms in spectacles.
2.3. Lower-order (sensory) Visual Function2.3.1. GeneralLower-order visual function was previously conceptualised as what is often referred to asvisual function in medical and ophthalmic terms. The most well-known of those functions arevisual acuity, contrast sensitivity and visual fields. They are usually assessed by a medicalexpert and measured for each eye separately. Impairments are very often caused by retinal,eye or optic nerve disease but also cortical malfunctioning can be at its basis.

Part I: Driving-related Research29
Visual acuity refers to the ability to perceive details presented with good contrasts and isusually assessed by a letter recognition task (e.g. Snellen chart). Usually visual acuity is notimpaired after unilateral post-chiasmatic brain damage, except in cases where also the optictract is involved (Zihl, 2000). Whether or not reduction in visual acuity leads to limitations,frequently depends on whether further visual impairments (e.g. contrast sensitivity) arepresent.Spatial contrast sensitivity is usually assessed by measuring contrast detection thresholds forblack-white grating stimuli (e.g. Vistech chart). Patients with impairments in contrastsensitivity, usually complain of “blurred” or “foggy” vision in the presence of normal visualacuity and other visual functions.However, the present focus is on visual field defects (VFDs). The monocular visual field canbe defined as the perceptual space available to the fixating eye. The binocular visual field isthe sum of the perceptual spaces available to both fixating eyes. In general, the extent of anormal visual field totals approximately 200 degrees horizontally but is usually measured upuntil 180 degrees. This extent tends to decrease with age. This age-related decrease is due to aloss of visual sensitivity, which is more pronounced with increasing eccentricity (e.g. Ball,Owsley, & Beard, 1990). Pathological visual field loss can result from ocular and optic nervedisease like macular degeneration, glaucoma and neuritis optica. It can also result from braindamage. Different perimetric techniques and devices can be used to assess the visual fields.They can be automated or manually operated, using static or dynamic, white or colouredtargets of different sizes and intensities. Clinically frequently used are the Goldmann and theHumphrey Field Analyzer. Zihl (1994, 1999, 2000) estimates that about 80% of subjects withposterior brain damage suffer from visual field loss. In 89% of cases this loss is unilateral (i.e.affecting only one hemi-field). The most common type of unilateral VFD is HH (65%),followed by quadranopia (16%), hemiamblyopia (11%) and paracentral scotoma (8%). In HH,also termed hemi-field blindness, only (left or right) half of the perceptual space as definedabove is available and can therefore be defined as a lower-order visual hemi-spatialimpairment. In quadranopia only one quarter of the perceptual space is available, either upperor lower. Hemiamblyopia indicates that light vision is spared but depressed, while colour andform vision are lost. Paracentral scotoma indicate islands of blindness in the parafoveal fieldregion. Following these percentages, approximately 46% of subjects acquiring and survivingposterior brain damage suffer unilateral HH, further referred to as HH.
2.3.2. Lower-order Visual Function and driving(-related) performanceIn a recent review article by Owsley and McGwin (Owsley & McGwin, 1999), therelationship between various eye conditions and driving habits, performance and safety isdiscussed. They conclude that visual acuity, although the most commonly used visualscreening test for driving licensure, is only very mildly associated with driving safety. Visualfield assessment, another commonly used screening procedure, does not provide forconsistent and conclusive findings either. However, it seems quite intuitive that theimportance of intact visual fields or rather the impediments imposed by VFDs should not beunderestimated. They can bring about limitations even in the absence of brain damage as isshown by for example Kuyk and co-workers (Kuyk, Elliott, & Fuhr, 1998). These authorsstudied the relationship between vision and mobility as a function of the subject’s type ofvision loss. They assessed 165 visually impaired subjects on many different aspects ofsensory and higher-order visual function. Sensory tests included, amongst others, assessmentsof visual acuity, contrast sensitivity, motion sensitivity, colour confusion and visual fields.The visual fields were measured binocularly using the Goldmann perimeter and associated

Part I: Driving-related Research30
procedures. Higher-order visual functions were assessed by tests of figure-grounddiscrimination, embedded figures discrimination and scanning reaction time. Also mobilityperformance was measured on a high-density indoor obstacle course. This route consisted ofan indoor track, being 1-1.5m wide and approximately 100m long, passing through severalrooms. In addition to the common and usual obstacles in the rooms, 60 objects of differentsizes were placed in the travel path. Subjects were instructed to walk through the course atwhatever pace they felt comfortable with, to stay within the boundaries, and to avoid collidingwith or touching objects. Mobility performance was measured in terms of the coursecompletion time and the total number of contacts made with boundaries and objects. Threetypes of vision loss were defined: either an acuity loss, a visual field restriction, or acombination of both. All impairments had been caused by ocular or optic nerve disease.Interestingly, it was found that the group with visual field restriction displayed the highest(i.e. better) scores on the higher-order visual perception tests. However, the authors note thatthe results may have been contaminated by sensory function. The acuity group might havebeen placed at a disadvantage because the items might not have been equally well visible.More importantly for this discussion, visual field extent and scanning efficiency were foundto be the variables most closely related to the mobility results. More specifically, as visualfield extent and scanning efficiency decreased, the mobility performance degraded both interms of completion time and collisions. Further analysis of the mobility task revealed that theacuity-loss group spent less time and made fewer errors than both other groups with VFDs.These results indicate that the size of the visual field can be an important sensory determinantof mobility performance. However, also another aspect of vision, namely visuo-spatialfunction as measured by the scanning score, appears to be an important factor related tomobility performance.
This has led researchers (e.g. Owsley et al., 1999) to conclude that visual perception duringdriving, or any other complex task for that matter, is dependent not exclusively on visualsensory function and physiologic optics, but also on higher-order functions, which they referto as “central processing skills”. Higher-order visual functions can be argued to have perhapsmore face validity to safe driving than visual sensory thresholds (e.g. Shinar et al., 1991). Onesuch higher-order function which appears to be relevant to safe driving appears to be visualspeed, sometimes referred to as visual attention. As Owsley and McGwin discuss,assessments of visual processing speed and visual attention as for example assessed with theuseful field of view test (UFOV; Visual Resources, Inc., Chicago, IL) appear to be betterscreening tests than assessments of sensory functions. They further briefly mention that alsoother higher-order visual processing functions like visual search, sequencing, selectiveattention, spatial memory and perception of three-dimensional structure from motion are alsofound to be associated with safe driving. In addition, from the previous discussion on ICFterminology, it should be clear that a combination of visual impairment, and personal andnon-specific characteristics and their interactions influence practical fitness to drive. Owsleyand McGwin further justly note that these and many other (higher-order) impairments havenot been fully explored. The role of eye-movement disorders, motion perception and opticflow phenomena such as heading have indeed a great deal of face validity but have receivedrelatively little research attention. Thus another aspect of “vision” is largely left unexplorednamely the higher-order visuo-perceptual, visuo-spatial and visuo-motor processing functions(Owsley et al., 1999). Neuropsychological tests of higher-order visual function could thusalso and perhaps more successfully serve the purpose of screening, evaluating andunderstanding practical fitness to drive and guiding possible rehabilitation and adaptation.

Part I: Driving-related Research31
From the previous discussion of lower-order visual function, it emerged that extent of thevisual field or presence of VFDs can be an important factor determining practical fitness todrive. Additional evidence for this statement was provided by Hartje and colleagues (Hartje,Willmes, & Pach, 1991) and by Hannen, Hartje and Skreczek (1998), who also addressed theissue of VFDs. The cause of the VFDs in their patient groups differs from the previousreported studies as both studies include brain damaged patients suffering cognitiveimpairment. A small number of these patients additionally suffered from lower-order visualimpairment, namely homonymous narrowing of the visual fields, not caused by ocular oroptic nerve disease, but due to post-chiasmal brain damage. Of the patients with the VFDs,hardly any of them passed a practical driving test. As this was not the primary topic in thesestudies, the authors do not indicate the exact reasons or specific problems associated with theVFDs.
Hartje and colleagues (Hartje et al., 1991) compared performance of 36 aphasic and 29 non-aphasic patients on neuropsychological tests and on a on-the-road driving test. Theneuropsychological test battery consisted of visuo-spatial tests, reaction time measures, andan intelligence test. Visuo-spatial functioning is operationally defined as rapid visualorientation, speed of visual perception, visual search, and visual simple and complex reactiontimes. The practical driving test was a nearly 50 km on-the-road assessment with arepresentative mixture of varying day-time traffic conditions and levels of driving difficulty.Performance was scored by an experienced licensed driving instructor using a protocol with280 observational items. Their sample consisted of 45, 7 and 13 subjects with respectivelyleft, right and bilateral brain damage. The sample was unselected in terms of perceptual,motor, and cognitive impairment. Fifty five percent of the patients passed the practical drivingexamination with the aphasic patients (42%) being less successful than the non-aphasicpatients (72%). Only a minority of neuropsychological test scores were significantly related tothe outcome of the practical driving test. Those tests that showed a relationship, had visuo-spatial components. In the non-aphasic group only a complex (partly visual) reaction timetask proved to be significant. In the aphasic group this test was complemented by atachistoscopic perception test and a cancellation task. Important in this respect is theobservation that hemiparesis nor any other neurological deficit was related to the outcome ofthe driving test. However, all (eight) patients with VFDs failed the practical driving test.These VFDs were due to a “homonymous narrowing of the visual fields” (as indicated by anot specified perimetric examination) but were not HH, since this was an exclusion criterion.
A comparable negative effect of homonymous VFDs in a brain damaged population ondriving performance was found by Hannen, Hartje and Skreczek (1998). They subjected 116brain damaged patients to a neuropsychological test battery and to an on-the-road driving test.The testing protocol is identical to Hartje et al. (1991), as previously discussed, comprising ofvisuo-spatial tests, reaction time measures, and a global intelligence test. The on-the-roadassessment was a nearly 50 km test-ride with real and representative traffic conditions.Performance was scored using a detailed and extensive protocol. Sixty two percent of thepatients had left-sided, 14% right-sided and 24% had bilateral brain damage. Similar to theprevious study, 58% of the patients passed the driving test. Also in this study, the sameneuropsychological tasks were significantly related to the driving results. These tasks assessedcomplex information processing (under dual-task conditions) and had strong visuo-spatialcomponents. There were no significant effects of the laterality of the brain damage, nor of

Part I: Driving-related Research32
presence of aphasia or hemiplegia. However, 11 of the 13 patients with VFDs failed the test-ride. The type or rather severity of the VFDs is described by the authors as “mild”, and thusare supposedly also due to a homonymous narrowing of the visual fields, but not HHs. In 10of these 11 patients, the driving instructor was forced to actively intervene during the test-rideto prevent hazardous situations. Again, the presence of VFDs caused by brain damage appearsto be a strong indicator of unfitness to drive.
2.3.3. Lower-order visual Hemi-spatial impairment and driving(-related) performanceIn the studies by Hartje et al. (1991) and Hannen et al. (1998) it could be observed thathomonymous VFDs due to brain damage resulted in nearly all cases in failure on an on-the-road driving test, suggesting clear negative effects of homonymous VFDs on fitness to drive.However, not all literature points inexorably at the devastating effects of such visualimpairments on driving or driving-related performance. An early demonstration that HH notnecessarily results in unfitness to drive was provided by Vos and Riemersma (1976). This hasbeen confirmed several times by more recent research findings. A similar conclusion was forexample drawn in an abstract by Warmink et al. (Warmink, de Jong, & Kempeneers, 1998).In their research, they assessed the driving performance of more than 100 patients with HH. Astudy by Szlyk et al. (Szlyk, Brigell, & Seiple, 1993) shows clearly that different levels ofperformance can be observed within the hemianopic patient group and that perhaps age is anevenly important factor for practical driving performance in a brain damaged population. Thisstudy will be reported further on in more detail. Racette and Casson (1999) comparedretrospectively visual field assessments with an evaluation of an on-the-road driving test in aCanadian sample. They report data from 13 patients with HH and seven patients withhomonymous quadranopia. It was found that only 23% of the hemianopic patients weredeemed as unsafe drivers. Twenty-three percent were judged to be safe and the remainingpatients were referred to be re-assessed. From the quadranopic group, no one was judged tobe unsafe and 57% was found to be safe. The remaining patients had to be re-assessed.Clearly, the evidence provided by these reports indicate that homonymous VFDs and HH byitself can not be an absolute and inevitable contra-indication for practical fitness to drive.
A similar positive conclusion was reached by Schulte and co-workers (Schulte, Strasburger,Muller-Oehring, Kasten, & Sabel, 1999). Their subject sample consisted of nine patients withvisual field defects, whom were judged to be otherwise neuropsychologically andophthalmologically intact. They investigated whether driving performance in a drivingsimulator would be impaired. All patients were found to be without neuropsychologicaldeficits measured by tests of attention, perceptual speed and dyslexia, and had intact fovealvision (macular sparing). Patients had lesions of either primary visual cortex or optic nerve.Visual field assessment was performed with a standard static luminance threshold perimeter,complemented by a qualitative high-resolution campimetry. Three patients presented withHH, two with quadranopia, two with homonymous scotoma, one patient had paracentraldefects and one had only monocular (but otherwise intact) vision. The driving simulationconsisted of driving a car with automatic transmission. The field of view was 21°(horizontally) by 16° (vertically). Assessments included driving speed, reaction time to asuddenly appearing deer and traffic violations. The test was preceded by familiarisation over adistance of 2.6 km. For the test, the subject was instructed to drive a 5.2 km roadway at 100km/hr, and to pass slower cars while obeying all traffic rules.Several interesting results emerged from this study. No differences were found between thevisually impaired and the age-matched control subjects on any simulator parameter. Larger

Part I: Driving-related Research33
field losses tended to be associated with slower driving but the correlation did not reachstatistical significance (possibly because of the small number of subjects). Time since onset ofthe visual impairment did not correlate with any of the simulator performances. Reactiontimes in moments of danger (a deer suddenly crossing the road) were also found to beidentical in both groups. Thus, in this study, no negative effects of VFDs are found withrespect to measures of driving performance in this simulator task, suggesting thathomonymous VFDs do not necessarily and by definition lead to decline in drivingperformance. However, by using automatic transmission and simulating a roadway (nointersections), performance-influencing factors other that those caused by the visual field loss(e.g. interference from divided attention) are minimised. Hence, it is important to observe thatby the nature of the simulation, the driving task is rather simplified. It could for example beargued that by the rather small used field of view, control subjects could not profit from theiravailable wider field of view.
It is further important to note that these hemianopic patients were reported to be“neuropsychologically intact” and thus this sample is (perhaps) not representative for thewider population of HH patients. A similar critical comment can be made on the study byWarmink et al. (1998). In co-operation with the Dutch Licensing Authority, they officiallyassessed more than 100 hemianopic patients on an practical driving test. For the vast majorityof subjects, the decision by an official driving instructor was positive. Several reasons can beformulated as to why this sample is most likely not representative for the hemianopicpopulation. One of them is that only subjects whom are confident of their performance arelikely to volunteer for this official test ride. Since the subjects do not find themselves visuallydisabled, they are probably also “neuropsychologically intact”.As presented, this study also warrants against the absolute negative influence of HH onpractical fitness to drive. It seems that the sample of hemianopic patients covers severalsubgroups of patients with different levels of hemi-spatial limitations.
2.3.4. ConclusionIn summary, lower-order (sensory) impairment (e.g. a VFD) as a standard, does not lead tounequivocal decisions about practical fitness to drive. Driving performance -apart frompersonal characteristics- can also be influenced by impairments at a higher-order level.Perceptual and cognitive disorders are well recognised to accompany brain damage. It isestimated that of persons who suffered a stroke, 75% have residual perceptual-cognitiveimpairment (Korner-Bitensky et al., 1998) and only 25% are free of these kind ofimpairments. For most brain damaged patients, cars can be adapted to their new physicalrequirements, for example automatic transmission and steering knobs for hemiplegia. Butthese adaptations are of little use for the possible accompanying cognitive higher level,perceptual and spatial impairments. These will be focussed upon subsequently. In thefollowing, I will try to shed some light on the possible role of higher-order cognitiveimpairment, later specifying to visuo-spatial and hemi-spatial visual impairments, alone or incombination with lower-order hemi-spatial impairment. This will eventually lead to thegeneral aim of the current project, namely to investigate which HH subjects are fit or unfit todrive and what is the cause of this. We will be particularly interested in the limitationstypically associated with hemi-spatial impairment.

Part I: Driving-related Research34
2.4. Higher-order Cognitive Function2.4.1. General: Brain damage and Cognitive FunctionIt seems very intuitive that brain damage can negatively effect a wide variety of activities andperformances, including driving. Several studies indicate (e.g. Haselkorn, Mueller, & Rivara,1998) that not the brain damage in itself is the limiting factor. Only when the brain damageresults in higher-order impairment, practical driving performance is negatively affected. Forcomprehensive and recent reviews on brain damage and driving, I refer to Brouwer andWithaar (1997), Brouwer (in press) and Withaar et al. (2000). They conclude firstly that in thebrain damaged population, cognitively impaired subjects perform worse on bothneuropsychological tasks and on driving tasks. Secondly, neuropsychological test results canbe shown to correlate moderately high with measures of driving performance. Specificallyvisual speed and measures of divided (visual) attention prove to be more informative thanglobal indicators of severity of illness. However thirdly, the large range in test scores makes itdifficult to discriminate between cognitively impaired subjects who are or are not practicallyfit to drive, purely on the basis of neuropsychological test performance.
2.4.2. Neuropsychological FunctioningAs neuropsychological tests are assumed to measure higher-order cognitive functioning andwith economic, therapeutic and conceptual reasons in mind, neuropsychological tests havebeen incorporated into procedures to evaluate and assess (residual) impairment related todriving. In reviewing the relevant literature, it will be noticed that numerousneuropsychological tests have been used in relation to different kinds of performances relatedto driving. As a result, reports on the validity and reliability of these kinds of tests in relationto any kind of driving performance have been inconsistent and sometimes incomparable.Another possible reason for this is offered by Galski et al. (1992). They question thetheoretical basis for the selection of neuropsychological tests. They specifically argue thatmostly the tests are not meaningfully related to the behind-the-wheel performance. It can benoticed however that not only a-theoretical selection but also different theories with respect todriving performance have been used.
2.4.2.1. Neuropsychological test scores and driving(-related) performance2.4.2.1.1. Correlation with driving(-related) performanceA more elaborate discussion for the low to moderate correlations between test scores anddriving performance can be found in Withaar et al. (2000). They discuss, amongst othertopics, the selection of participants, choice of tests and method of driving assessment. It issuggested that participants are usually too small in numbers and not representative for ageneral population. The direct relationship between many neuropsychological measures andactual driving performance is questioned. The authors point at the multiple determination ofthe quality of the driving performance and it is noted that in many studies this has not beentaken into account. They further accentuate that the importance of task-specific experience(specifically with respect to driving) may blur the (direct) relationship betweenneuropsychological function and driving. In addition, it is rightfully commented that thedriving task itself can, theoretically as well as practically, be conceptualised in different waysand there has been no consistency in theories used so far. One theoretical approach which hasproven to be fruitful, defines the driving task using a hierarchical cognitive structure (Michon,1971; Van Zomeren, Brouwer, & Minderhoud, 1987) in terms of strategic, tactical, andoperational subtasks. However, this and many other theoretical accounts have been used,leading to relative incomparability in studies. Practically, driving, as a dependent variable, can

Part I: Driving-related Research35
and has also been evaluated in many different ways. Assessment can thus take differentformats: Subjective and objective reports on accidents (and near accidents), drivingfrequency, licence renewal, etcetera. can and have been used as an indication of drivingperformance. The quality of actual and real driving performance can instantly and moredirectly be assessed on open and closed circuits, with real (and adapted) cars or using drivingsimulators with different reality similarities. The performance can be evaluated using differentprotocols and rating scales by different criteria. This variability results in modestcomparability between studies and low insights into the subcomponents of the driving task,again moderating possible correlations with other (neuropsychological) tests.
2.4.2.1.2. SpecificityIn our opinion a further point can be raised approaching the research from the side of thesubject, in this case the patient, rather than exclusively from the side of the (driving) task.Namely, it can be argued that in previous studies, most tests are not specifically assessing themost likely and prominent impairments of the patients under study. This idea originates forexample from reports by Galski et al. (Galski, Bruno, & Ehle, 1993). They showed that onlycarefully selected tests can be used to evaluate fitness to drive. Not all cognitive testsadversely affected or were equally related to driving performance. Additionally, confusionabout the relative importance of tests can be created considering the well establishedobservation that tests which successfully discriminate between brain damaged and non-braindamaged patients are not necessarily highly correlated to driving performance (e.g. VanZomeren et al., 1988). Thus, tests serving one purpose (e.g. patient-group classification), donot necessarily serve another (relationship to driving). This leads to the conclusion, not onlythat merely very specific tests are useful in neuropsychological assessments, but also that therelatedness of the tests to driving can very well be determined by the specific patient-population (which and) because they exhibit specific limitations. It is not inconceivable that ina population with left-hemisphere brain damage, visuo-spatial tasks will be less revealing andfunctional than in a right-hemisphere group or that “frontal tests” will be more predictive in a“frontal brain damaged group” than in any other group of patients. Support for this idea isprovided by Mazer et al. (Mazer, Korner-Bitensky, & Sofer, 1998) conducting a study with 84brain damaged subjects tested on a neuropsychological battery consisting of various mainlyvisual perceptual tests, and on an on-the-road driving test. The driving test was based on thestandard test procedure used by the provincial licensing board in Quebec (Canada) and wasevaluated using a 43-item assessment form covering use of controls, manoeuvring, andspecific and general driving skills. The score resulted in a pass/fail decision. Logisticregression models were created and it was found that for left and right brain damagedsubjects, different perceptual tests were the best predictors of the on-the-road assessment. Forright brain damaged subjects, a joint measure of visual discrimination, spatial relations andfigure-ground discrimination yielded the best prediction. These tests hold strong spatialcomponents, usually associated with right-sided brain damage. For the left brain damagedgroup, the Trailmaking Test part B was the best predictor. The Trailmaking Test part B tapsmultiple conceptual tracking, sequencing, and alternating divided attention. Furthermore, itholds an additional “language component”, typically associated with the left hemisphere.Summarising this point, we argue that the tests directed towards the typical problemsexhibited by the patient population will be most predictive for driving performance. This is inline with a previous general point we made, namely that only when very specific sub-tasks ofthe driving task are considered, correlations with (specific) neuropsychological tests can beincreased. When patients suffer a specific and well isolated impairment, assumed that these

Part I: Driving-related Research36
impairments can be neuropsychologically tapped, and these impairments are related toimportant aspects of fitness to drive, this specific neuropsychological test performance can behighly related to practical fitness to drive.
From previous points, it follows that selectivity in test choice and selectivity in patientpopulation are logically linked. The need for selectivity follows from the conceptualisation ofthe driving task (what components of the driving task can be adequately measured byneuropsychological tests) and from the specific impairments of a specific patient population.The brain damaged population in general might well be a too broadly defined category to beeffective in pinpointing a specific and limited range of impairments relevant to practicalfitness to drive. Therefore, specific subgroups of patients should be considered (e.g. welldocumented HH patients), assessed with specific tests (e.g. visuo-spatial tests).
2.4.2.2. Other (inter-)related general topics: hemispheric differences, selection criteria,and range in outcomes2.4.2.2.1. Hemispheric differencesAs it is not unreasonable to assert that driving has a high visuo-spatial component, it can beexpected that right hemisphere brain damaged patients perform worse on both practicaldriving and visuo-spatial tests than patients suffering from left hemisphere brain damagebecause of the traditionally assumed hemispheric specialisation of the right hemisphere forspatial function. Brouwer (in press) remarks that most studies indeed show this expectedtendency. However, he points at the possible selection bias inherent in many studies. Quigleyand DeLisa (1983) notice that although left CVA patients performed better on their visuo-spatial test battery, needed less training sessions (class-room driving instruction and in-cartraining) and were more successful on a driving test, fewer are in practice referred to driver-training programs. Thus, although some research suggests higher levels of performance of leftrelative to right CVA patients, fewer actually enrol in (clinical) driver-training programs. It issuggested that left CVA patients have less tendency of actually expressing the desire tocontinue driving, possibly as a consequence of language impairment to some degree. This isin contrast to right-sided brain damaged patients, who frequently have low insight into theirown pathology. These patients do not see at all, why they should not drive or participate indriving-programs. Other reasons for skewness are the possible more prominent limitations fordriving caused by right hemiparesis, associated with left-sided brain damage. However,despite of that these limitations can quite easily be diminished with the appropriate technicalcar-adaptations, frequently right hemiparesic patients decline from driving. These tendenciesare likely to skew the proportion of actual left versus right CVA drivers on the road, temptingto inaccurate and biased interpretations when using measures of driving performance as, forexample, return-to-driving-after-stroke.This skewness is also suspected to influence subject selection and inclusion in driving relatedstudies, especially when stringent inclusion criteria are used, as for example minimum ofdriving experience since the brain damage, and when patients are studied who voluntarilyapply for participation. This also might result in exclusion of left CVA patients with relativelyhigh potential and overinclusion of right CVA patients, skewing and biasing overall test-outcomes and hence interpretation. Brouwer (in press) therefore rightfully concludes thatprecise numbers and conclusions with respect to hemispheric differences should then also betreated with caution. To stress this point, Hannen and colleagues (1998), assessing 116patients with acquired brain damage, found no significant effects of the laterality of braindamage on an on-the-road driving test. This emphasises the point that hemispheric differences

Part I: Driving-related Research37
with respect to the quality of driving performance, although plausible, are not as yetaccounted for by strong evidence. This suggests the need for studies where this kind of patientselection is brought to a minimum.In the light of topics to be discussed further on, this has important implications, sincelaterality of brain damage is typically associated with (contra-)laterality of potential HH. Theabsence of established differences due to laterality of brain damage indicates the potentialabsence of differences in limitations between left- and right-sided HH patients. This suggeststhe need for studies including both kinds of patients, with a minimum of additional in- andexclusion criteria. If in such studies differences are to be found, these are not a prioriattributable to laterality of brain damage per se, but could be due to specific (visual)problems, typically associated with either left- or right sided HH.
2.4.2.2.2. Selection biases and range in outcomesFrom the previous remarks, it should be clear that selection biases can cause caveats withrespect to data interpretation. It was shown that possible selection (or exclusion) of patientsmight influence research outcomes with respect to laterality of brain damage and its relationto driving-related outcomes. In addition, selection biases can also influence the range of testscores. Highly restricting selection can decrease the range in neuropsychological and drivingoutcomes. In general, narrow ranges are likely to result in low correlational measures andpoor predictive powers. To put it extremely simple: if all test performance is at ceiling orfloor level, no association between them can be observed. This was for example witnessed ina study by Lundqvist and colleagues (Lundqvist et al., 1997). Several neuropsychological anddriving tests (simulator and on-the-road) were subjected to 29 patients. Neuropsychologicaltests assessed perceptual, cognitive, and executive functioning. The driving simulatorconsisted of an advanced moving-base system, providing the driver a realistic dynamicimpression of a 80-km two-lane road with realistic traffic conditions. During simulatordriving, speed, lateral position, complex reaction time, time to collision and distance tocollision were recorded. The on-the-road driving was performed over 25-km in actual trafficin the participant’s own car. Speed, manoeuvring, lateral position, attention and trafficbehaviour were evaluated. All patients had good recovery from brain damage, no VFDs, nohemiplegia, no deficits as non-fluency and other intellectual impairments. Patients withoutdrivers license or who were not driving at that moment were also excluded. These stringentcriteria are very likely to produce skewed outcome ranges to the positive end. In other words,these criteria produce a patient population without (expected) limitations, which is non-representative for a brain damaged population. This is confirmed by the observation that onlytwo of the five simulator driving parameters (speed and lateral position) and three of the fiveon-the-road driving parameters (speed, manoeuvring and lateral position) showed significantdifferences between the patient and control group.The important and striking observation in this study is that the neuropsychological test resultswere found not to be significantly related to the simulator driving outcomes and thatadditionally the simulator driving outcomes were not related to the on-the-road drivingoutcomes. This seems very odd and counter-intuitive, but, as we have argued, it might be as aconsequence of very limited ranges in all outcome measures.
The significance of the range of outcome measures is also confirmed in a study by Nouri andLincoln (1992). It further demonstrates that, if any constriction in driving outcome, it ispreferably to the negative end; not to the positive end as in the previously reported Lundqvistet al. (1997) study. The test battery of Nouri and Lincoln (1992) consisted of measures of,

Part I: Driving-related Research38
amongst others, spatial function, visual inattention and concentration, reasoning function, andvisual memory. These were complemented with typical driving related tests as road sign andhazard recognition. Also, an representative on-the-road driving test was administered. Thesubjects were first graded into either a pass or fail group by an instructor on the basis of anoverall subjective impression of the quality of driving performance. Discriminant equationswere then derived from the results of a subgroup of randomly selected patients. Suchequations incorporate a profile of neuropsychological test results and produce a predictivevalue. Two values are obtained per subject, namely a predictive value for whether the subjectwould pass the driving test and a value whether the subjects would fail. The higher value istaken to indicate the likely outcome. This resulted in 82% correct classifications.These equations were then applied to the remainder of the subjects to examine their predictivevalue in another but similar group of patients. These new classification results demonstratedthat the predictive equations were approximately equally effective in overall classification(79% correct classifications). But more important for this discussion is the observation thatthe equations were more effective at identifying those subjects that were to fail the drivingtest than those who were to pass. Thus, in the light of effectiveness of predicting drivingperformance, when driving outcomes are biased, this study suggests it preferably to be to thenegative end, since it is suggested that failure is more predictable than passing the drivingtest.This might explain why in the Lundqvist et al.-study non-significant predictive equationswere observed: driving outcomes were strongly biased to the positive end. The preferred biasof driving performance to the negative end does not necessarily have to be problematic sincehigh effectiveness for predicting failure is for screening purposes perhaps a more desiredproperty.
2.4.3. Visuo-spatial FunctionIt was previously argued that the driving task is comprised of many different aspects ondifferent levels and that the quality of driving performance can thus be influenced by manydifferent factors. In previous discussion we indicated that neuropsychological test choice hasto depend firstly on preferably consistent and unified task analysis and model building of thedriving task and secondly on the specific population the tests will be applied to, in order to beable to significantly relate outcomes of both types of assessments.Given that a great deal of information-processing in the driving task is of a visual and spatialnature and that later action is highly dependent on this visuo-spatial information, the specificinterest in visuo-spatial functioning is a logical consequence. Additionally, since wespecifically limit our focus on patients suffering homonymous VFDs due to post-chiasmalbrain damage (and HH in particular) and since this condition is known frequently toaccompany, intensify and/or provoke visual-spatial limitation, it follows that the tests of ourinterest should have prominent visuo-perceptual and visuo-spatial components.
Visuo-spatial perception is one component of cognitive functioning which globally refers toour ability to process and interpret visual information about where (parts of) objects are inspace. It is a vital aspect of cognitive functioning as it is a necessary element for successfullyperforming a wide range of activities of daily living. For instance, it underlies our ability tomove around in an environment and orient ourselves appropriately. Visuo-spatial perceptionis also involved in our ability to accurately reach for objects in visual space and our ability toshift our gaze to different points in space in order to effectively scan and search for objects.Some visuo-spatial impairments are commonly associated with right hemisphere brain

Part I: Driving-related Research39
damage. Such impairments could be for example impaired discrimination of complex stimuli,recognition, figure-ground differentiation and visual integration. Other visuo-spatialimpairments are defective localisation of points in space, judgement of direction and distance,and topographic disorientation. Subjective complaints as having a limited overview, bumpinginto obstacles or persons, getting lost while going for a walk, finding reading very exhausting,missing or misreading words, getting dizzy in busy streets etcetera, are frequently reported byHH patients. These complaints are (at least partly) due to visuo-spatial impairment, resultingin defective visual scanning.
The most severe disabling spatial impairment is the neglect syndrome, usually caused by righthemisphere brain damage. Hemi-spatial visual neglect can be described as a failure to report,respond, or orient to novel or meaningful stimuli, usually on the side of space or objectsopposite the side of lesion (e.g. Robertson & Halligan, 1999). This failure is not primarily dueto hemi-field blindness although it often co-occurs. It has been estimated that approximately70% of the neglect patients also suffer from a homonymous VFD (Kerkhoff & Schindler,1997). However, these percentages have to be treated with caution, since the differentialdiagnosis can prove to be complex. Due to the severity of the limitations frequently imposedby this condition, it is usually presupposed that this condition in incompatible with safedriving.
Our aim is to study patients suffering HH and patients suffering related impairments whichwill be inherently visuo-spatial (and specifically hemi-spatial) in nature. We will denote thisgroup of patients as suffering from hemi-spatial visual limitation. Hemi-spatial limitation canbe thus caused by lower-order hemi-spatial impairment (i.e. HH), and by higher-order hemi-spatial impairment (i.e. hemi-spatial neglect), or by both. Both types of impairments arisefrom unilateral (post-chiasmal) brain damage and can be expressed in lateralised visuallimitation and restriction, implying more visual problems on one particular side (left or right)of visual space, usually contralateral to the side of brain damage (i.e. contra-lesionally). In thefollowing paragraphs, we will try to highlight studies specifically discussing hemi-spatialimpairment and its influence on the quality of driving performance or driving relatedperformance.
2.5. Visuo-spatial impairment and driving(-related) performance2.5.1. Observational and anecdotal informationWe previously alluded to limitations related to visuo-spatial impairment. Examples of suchimpairments, likely to influence fitness to drive, are visual dysorientation and environmentalagnosia. One particular class of visuo-perceptional, visuo-spatial and visuo-cognitiveimpairment are visual (object)agnosias. Though generally visuo-spatial in nature, theseimpairments are usually not hemi-spatial in nature and imply difficulty in identifying objectsusing visual information. This higher-order impairment is not to be explained (fully) on thebasis of lower visual impairment. Frequently, these agnosias are category-specific. For a shortbut comprehensive description of several types of agnosias, we refer to Zihl (2000). In thecourse of our own research we encountered several types of agnosic patients. Although mostof these subjects are quite disabled in some respects, not all of them present a reduction in thequality of driving performance. A prosopagnosic patient (difficulty in visually recognisingfamiliar faces and learning new faces) from our own hemianopic patient sample, had nodifficulty at all adequately performing an on-the-road practical driving test. This is notunsuspected, since driving has no relation to recognising faces. Not exactly similar is the case

Part I: Driving-related Research40
in (pure) alexia. This impairment implies difficulties identifying individual letters and/orconstructing words out of the string of letters (“letter-by-letter reading”). Our hemianopic andpure alexic patient expectedly complained of difficulties in following instructions during thetest-ride as “on the next crossing, follow the direction to <<placename>>” or followinstructions on information boards due to unexpected deviations. This impairment isobviously more disabling with respect to driving performance, since reading is a small but canbe an important aspect for fluent driving. We found visual object agnosia the far mostdisabling type. Our hemianopic and visual agnosic patient displayed a complete disability invisually identifying and recognising any type of object. Painted markings on the road-surfaceand crossings with multiple-lane roads, totally confused our subject. During the test-ride, thesubject was able to describe most road-signs in terms of colour and shape but was totallyunable to identify their meaning, although the symbols (e.g. crossing pedestrians) are verystraight-forward to “gnosic” viewers. When a short distance further, a previously and recentlyexplained road-sign was encountered, once again, it was not recognised. When passingthrough a road-construction area the following happened. Traffic from two opposing laneswas reduced into one lane. This process was supervised by two typically dressed road-construction officials. These visually conspicuous officials (both male, orange uniforms,helmets, and flags) took standard positions at the beginning and end of the one-way lane. Atthe end of this lane, just before the second official, our subject abruptly stopped the car,making a ‘gentleman-like’ gesture to “let this lady cross the road”. Being “a gentleman intraffic”, he did not have a clue who this person was, what the specific traffic situation was andwhat all the symbols meant. The test-ride was never considered dangerous by our experienceddriving instructor, was sometimes humorous but clearly the impairment is as limiting thatquality of driving becomes unacceptable.By these anecdotes, we indicate that different types of visuo-spatial impairment can result indifferent levels of limitation. For the remainder, we will specifically focus on hemi-spatialimpairment and limitation.
2.5.2. Hemi-spatial visual impairment and driving(-related) performance2.5.2.1. Legal, ethical and empirical groundsWe previously argued that hemi-spatial impairment can be considered to be a negativeindicator for adequate driving performance. This conclusion has not always been basedexclusively on objective research findings. Subjective, ethical and legal motives can also bethe basis for, for example, withdrawal of drivers licenses. In some studies, such a mixture ofmatters can be observed as for example in Sundet et al. (Sundet, Goffeng, & Hofft, 1995).Sundet and co-workers investigated whether the judgement concerning fitness to drive (thusnot an actual test) by a professional team was related to performance on a neuropsychologicalscreening battery. They investigated 29 left-sided and 43 right-sided brain damaged subjectsand decided that respectively 41% and 58% did not meet the fitness criteria for a driver’slicense. Results indicated that neither sex, laterality of the lesion nor hemiplegia were ofinfluence on the decision of whether or not the patient was allowed to drive. In predicting thefitness decision, it proved that neuropsychological test results provided a major part of theinformation used by the team in the decision process. Trailmaking Test part B showed to bethe single most potent predicting variable. However, a possible judgement bias might haveinfluenced the observed relationships. When HH and/or hemi-spatial neglect was diagnosed,the conclusion was negative without any exception. The expectation can however be raisedthat this conclusion was based on legal and ethical grounds rather that on empirical evidenceas one can read: “Brain damaged subjects with impairments such as loss of visual field or

Part I: Driving-related Research41
significant visuo-spatial inattention, are not allowed to drive. A controlled study designed tocompare driving skills between patients with and without hemianopia/neglect is thus neitherlegally nor ethically advisable”. We would like to notify that decisions whether or not asubject is considered fit to drive has serious social consequences for the subject and safetyconsequences for the public. Hence these decisions are not to be made on the basis ofsupposedly common sense, subjective impressions, “clinical feeling”, or historically grownhabits. They should be underpinned by clear empirical evidence.
2.5.2.2. Empirical evidenceOther studies do present empirical evidence and from this literature, it is not evident thathemi-spatial impairment necessarily results in negative driving outcomes, suggesting thateither lower- or higher-order hemi-spatial impairment not necessarily results in hemi-spatiallimitation. As is the case for general higher-order visual impairment (e.g. the agnosias),apparently some forms of hemi-spatial impairment result in a higher degree of limitation. Itwill for example be argued that hemi-spatial neglect is be much more impeding than HHwithout other cognitive dysfunction.
To illustrate our points, a (rather limited) number of literature reports can be quoted. In all thefollowing papers, hemi-spatial limitation is apparent. And since hemi-spatial limitationindicates either lower- or higher-order hemi-spatial impairment, or both, these reports arerelevant for this discussion. However, not all papers are conclusive about the specific natureand cause of the hemi-spatial limitation. Only a few studies discuss explicitly HH. In thesestudies, the status of the visual fields has objectively been established. Additionally isreported whether the lower-order impairment are accompanied by higher-order hemi-spatialimpairment. Using the impairment as a point of departure, the relationship with limitation isfocussed upon. These studies will be highlighted in the next paragraph. Further we willdiscuss in extent a study using, not the impairment, but the hemi-spatial limitation as the pointof departure. In this study, the presence of hemi-spatial impairment can be inferred from theobvious hemi-spatial limitation. Whether it’s nature is of a lower- or higher-order can notsimply be resolved. The profoundness of the observed limitations and other information as forexample aetiology, leads us to suspect that most patients suffer hemi-spatial neglect.However, the presence of HH, or the combination of both can not be ruled out. In the finalparagraph, we mention some studies, not specifically focussing on either hemi-spatialimpairment nor hemi-spatial limitation. In these papers, neither constructs were amongst theinclusion criteria and were thus accounted for. The studies rather include brain damagedpatients in general. However, some of these studies mention in their discussion section, somepresence (in some patients) of hemi-spatial limitation. It is therefore apparent that the patientpopulation under study consist of a "mixed" group. Therefore, although clearly limited, theytoo can be of some importance for this discussion.
2.5.2.2.1. Homonymous hemianopia and driving(-related) performanceEvidently, not all literature reports are unclear with respect to the presence and classificationof visual and/or hemi-spatial impairment. Pitifully, the evidence provided by those papersdoes not provide simple and clear conclusions about the degree of limitation imposed by theseimpairments. In a previous paragraph discussing lower-order visual hemi-spatial impairmentin relation to driving performance, we already mentioned the studies by Hannen et al. (1998)and Hartje et al. (1991). In these studies, nearly all patients with a homonymous VFD, failedan on-the-road driving test. By these studies, a clear negative relationship with the quality of

Part I: Driving-related Research42
driving performance is suggested. In the same paragraph, and in contrast to this suggestednegative relationship, we also mentioned the reports by Vos and Riemersma (1976), Warminket al. (1998) and by Schulte et al. (1999). These reports warrant against an absolute negativeinfluence of HH on practical fitness to drive. Thus with the reports discussed so far, weindicated that, with respect to HH, some authors provide clear negative relationships, whereasothers do not find significant differences with controls on practical driving performance ordriving-related parameters.
More moderate conclusions are drawn by Szlyk and co-workers (Szlyk et al., 1993). Theyassessed the driving performance of six older patients in an interactive driving simulator andcompared it to performance of seven normally sighted age-matched controls and to a youngercontrol group (31 youngsters). The patients had extended occipital lobe damage resultingfrom CVAs. Visual field assessment was done by means of a Goldmann perimeter (V4etarget) and showed that three and four patients respectively had left and right sidedhomonymous VFDs (either hemianopia or quadranopia). The authors also report threepatients neglecting their missing hemi-field of whom one with left and two with right sidedhemi-spatial impairment. Driving was simulated by means of car with automatic transmission(consisting of a seat, steering wheel, acceleration and pedal brakes) in a world provided bythree large colour monitors simulating a dynamic and realistic visual environment of 160°horizontally by 35° vertically. Subjects were allowed a 15 min training session followed by a5 min test course where they were instructed to operate the simulated vehicle as they wouldnormally drive and to obey all traffic regulations. Several challenges were encountered duringthe test-ride including intersections with crossing traffic, cars passing on the left, a cowapproaching and crossing from the right, and cars merging on the roadway. Several simulatorindexes were analysed including lateral position, speed, slowing and stopping, and accidents.Results showed worse driving performance by patients relative to the age-matched groupsuggesting a negative influence of the brain damage and VFDs. This was evidenced on forexample lane boundary crossing and variability in lane position. But on other indices asabsolute lane position, steering and vehicle angle, average slowing and stopping, speed,acceleration and brake pedal pressure, accidents and eye-movements, no differences werefound. Thus on most of the indices, most of the patients performed at levels (nearly)equivalent to age-matched controls. These patients showed greater head-movements thancontrols, enabling them to compensate for the visual field loss. Thus, as a group, thesepatients showed relatively little abnormalities, but clearly some specific patients showedmarked limitations. One patient with reported left hemi-field neglect, failed to stop at any ofthe traffic signals. Another patient, with reported right hemi-field neglect had outlierperformance on nearly all indices. Hence within the hemianopic patient group, cleardifferential performance can be observed ranging from normal to highly deficient. Comparingpatient and age-matched groups to the younger group revealed strong effects of age. This is,all older individuals (both controls and patients) performed worse than the younger ones. Thisreveals that not exclusively the brain damage and VFDs negatively effect driving performancebut that age is also a significant factor in this simulator task. Szlyk and colleagues (Szlyk etal., 1993) conclude that age-related losses when compounded by brain damage-associatedimpairments, may further increase the on-the-road risk of the older hemianopic patients whiledriving. This suggests that with increasing age, impairment might lead to higher levels oflimitation. This is in line with a previous point we made namely that limitation is notexclusively determined by impairment, but that also 'personal characteristics' exert a possibleimportant influence.

Part I: Driving-related Research43
2.5.2.2.2. Hemi-spatial Neglect and driving(-related) performanceAn interesting study, not starting from the impairment level but from the limitation level, is astudy by Webster et al. (Webster et al., 1995). However, although these authors report(severe) hemi-spatial limitation (also in driving-related performance) in their patient group,they do not provide clear indication about its specific cause. In addition to the discussion ofhemi-spatial limitation, this paper is also for other reasons relevant for our purposes. Namely,the study specifically addresses the issue of hemi-spatial neglect and the caveats concerningresearch on fitness to drive with this group of patients. We will therefore first discuss thispaper by Webster and colleagues and subsequently complement it with more general findingson hemi-spatial neglect and driving.
Before discussing their results in more detail, we will first describe the included subjects as tojustify our interest. Patients were classified in three subgroups on the basis of the severity ofhemi-spatial limitation (which is indicative for hemi-spatial impairment) as evidenced inneuropsychological tests (to be specified further on). Lesion analysis of the patients' (CT orMRI) brain scans (when available) were performed to investigate the possible relationshipbetween lesion location and hemi-spatial limitation. This revealed for nine of the ten subjectsin the most hemi-spatially limited subgroup (L-Omit, see further) right inferior parietal lobeand right thalamic damage. The other subject had right thalamic damage. These sites arecommonly associated with hemi-spatial neglect (e.g. Vallar, 1993). In a second, modestlyhemi-spatially limited, group (R-bias, see further), lesions involved the right parietal lobe(two subjects) and the right frontal lobe and/or right basal ganglia (six subjects). These sitesare also suggestive for hemi-spatial neglect (e.g. Vallar, 1993). A third group (non-Neglect,see further) suffered more anterior brain damage, not involving the right parietal lobe (foursubjects). On the basis of both hemi-spatial limitation and anatomy, only the latter group canbe 'free of suspicions' of suffering hemi-spatial impairment, either lower-, higher-order orboth. On the same grounds, the information concerning both former groups is highlyindicative for hemi-spatial impairment. It is very plausible to interpret the hemi-spatiallimitations as a result of hemi-spatial neglect to a severe or mild degree respectively. Inaddition, on the basis of frequency of co-occurrence (previously discussed), and on the basisof lesion location and presented hemi-spatial limitation, these patients can also validly besuspected of suffering from left-sided HH.Hence, this is a relevant study, firstly on the basis of the (severe) hemi-spatial limitationspresented by two subgroups of this right hemisphere brain damaged patient group. Secondly,Both lower- and higher-order visual hemi-spatial impairment can be expected in at least twoof the three patient groups.Having justified our interest concerning the patients, we further need to account for the reasonwhy, in this study, there is no driving assessment in the format of an on-the-road test. Asalready mentioned, hemi-spatial neglect might be considered as an extreme case of hemi-spatial impairment resulting in severe hemi-spatial limitation. Therefore, severe neglect isoften considered as highly indicative for unfitness to drive. Hence, on-the-road drivingassessment is usually considered as very hazardous and alternative testing imposes itself. Inthis study, a wheelchair mobility task was favoured. This task has clear similarities to a realdriving task as equivalent variables as lateral position, speed, (near) accidents etcetera can beobserved and evaluated. As a consequence, in spite of severe visuo-spatial limitation, similarvisuo-spatial functions, as used in real driving, can be assessed under less dangerousconditions.

Part I: Driving-related Research44
Having clarified the reasons for presentation, we can now in more detail discuss the paper andits implications. In this study 55 patients with right sided brain damage were classified intothree groups on the basis of performance on two neuropsychological tests. These tests werethe Rey-Osterrieth Complex Figure Drawing and a Letter Cancellation Test from which twodependent variables were derived. The first variable considers the number of omitted items.Expressed as left-sided relative to right-sided omissions, this measure indicates differentiallateral performance and thus hemi-spatial limitation. For the second measure, task initiationlocations (starting points) were recorded. Deviation from the mean starting point displayed bycontrols, is expressed as a left/right orienting bias. Controls almost always start on the left.Applying these two “lateralisation” parameters, one group was termed the L-Omit group.These 32 patients omitted left-sided stimuli on both tasks and tended to start the tasks more tothe right side than controls. The authors note that they preferred to label this group in terms ofomissions (limitations) rather than refer to it as the “severe neglect” group (higher-orderimpairment) because “QRW� DOO� VXEMHFWV� SUHVHQWHG� DOO� WKH� FDUGLQDO� IHDWXUHV� RI� WKH� WUDGLWLRQDOQHJOHFW�V\QGURPH”. This confirms our suspicion that this group indeed not only consisted ofwhat are traditionally called “neglect patients”, but also included patients with lower-orderhemi-spatial impairment (i.c. left-sided HH). The same remark holds for the second group (R-bias) which consisted of 11 subjects who showed a rightward orienting bias, namely theyexceeded criteria for starting to the right on at least one task, but did not meet the criteria forthe left-sided omissions. The third group (Non-Neglect) consisted of 12 patients who showedneither the left-sided omissions nor the rightward orienting bias. The control group comprisedof 20 chronic pain patients with no history of brain damage.Standard hospital incident reports (when available) on all types of falls were reviewed andevaluated. Results show that both L-Omit and R-bias groups fell more than both other groups.Within one week of completing both neuropsychological tests, a 122 m wheelchair obstaclecourse was traversed and evaluated. The route consisted of six left and six right turns, and 12obstacles occurring at each side. The path-width was demarcated by a rope and was 81 cmwide (standard door width). Each subject was instructed to propel the wheelchair through thepath without striking anything, in a manner that they would usually do, and as safe aspossible. They were told they had unlimited time. The control subjects were asked to use onlythe right arm and leg to propel the wheelchair as to approximate the motor disadvantageexperienced by the majority of patients. For evaluation, direct frontal hits and sideswipes(contacts made with the side of the wheelchair) were counted.
In general, the results from the wheelchair obstacle course were in line with the pattern ofresults of the falls. Both L-Omit and R-bias groups made more left-sided sideswipes than theother groups. However, only the L-Omit group made right-sided direct frontal hits and madealso significantly more left-sided direct frontal hits (most severe error) than any other group.Several notable conclusions can be drawn from this study. Firstly, severity of hemi-spatiallimitation as measured by neuropsychological tests, by reports of fall-data, and by this visuo-spatial wheelchair mobility and navigation task, are in concordance. Secondly, the fall-datadid not differentiate L-Omit and R-bias groups and showed a clear difference with the Non-Neglect group and controls. In concordance with this are the results of the side-swipes in thewheelchair course. It is thus suggested that, not only “obvious neglect patients” but alsopatients with similar but less pronounced and “more subtle hemi-spatial tendencies” (R-biasgroup) are at a greater risk for falls and wheelchair collisions (i.c. side-swipes ) than patientswithout any such symptoms. It could hence be concluded that neuropsychological visuo-

Part I: Driving-related Research45
spatial test performance (which was the basis for group assignment), and in particular left-sided omissions and spatial location of the patient’s initial approach to these paper and penciltests, has clinical significance in that they could be associated with increased accident risk. Asalready argued, this wheelchair mobility course can be defended to have equivalentcomponents to a real driving task. Though, it would still be interesting to study theserelationships with real driving performance. Thirdly, in contrast, the wheelchair coursediffered from the fall-data in that the L-Omit group (alleged severe neglect group) was theonly group that showed right-sided direct hits and had more left-sided direct hits than anyother group, including the R-bias group (alleged mild neglect group). This suggests that in thegroup of patients with hemi-spatial impairment, different levels of limitation can be observedusing this 'ecological' wheelchair obstacle course.These points taken together indicate that, when using sensitive neuropsychological visuo-spatial tasks, a continuum can be demonstrated ranging from “severe hemi-spatially limited”to “normal”, with the patients evidencing more subtle hemi-spatial impairment in between.These tasks can still have clinical significance. This suggests that considerable effort shouldbe invested in any (pre-driver) neuropsychological test battery, in prevention of using notsensitive enough measures for quantifying hemi-spatial impairment.
Having described this group-study on relating hemi-spatial neglect to driving-relatedperformance, we would like to complement the discussion with more general remarks onhemi-spatial neglect and driving. Systematic investigations relating hemi-spatial neglect toactual practical driving performance are very scarce, presumably because of safety reasons orbecause nothing more than a disastrous driving outcome is expected. Occasional case reportshave been described which show that visual field defects in association with neglectbehaviour can be potentially dangerous for driver and pedestrian (Robertson et al., 1999).Denial of impairment (anosognosia) is a characteristic feature of the neglect syndrome andcases have been described where only after fatal accidents and prolonged court casescessation of active driving by the patient could be accomplished. Other case reports on hemi-spatial neglect explicitly mention driving problems during everyday driving and are mostlyindicated by the partner. In a cognitive rehabilitation study by Rao and Bieliauskas (Rao &Bieliauskas, 1983), the partner of the patient reports “accidents caused by misperception ofcars approaching from the left side”. In a case study by Barrett and colleagues (Barrett,Schwartz, Crucian, Kim, & Heilman, 2000) showing differential neglect symptomatology inperi- and extrapersonal space, the patient was reported to have a “disturbing tendency to veerto the right towards people or objects present on that side of the road”. In our own work (Tant,Brouwer, Kooijman, & Cornelissen, in press), we observed suboptimal scanning behaviourbut also extreme (left) deviant lateral positions, on assessment in a realistic interactive drivingsimulator in a neglect patient after an otherwise successful rehabilitation program. We too, incase of indication of severe neglect, opted for assessment using a 'realistic interactive drivingsimulation', instead of a the usual practical driving test, because of safety reasons. Our criteriafor the diagnosis of severe hemi-spatial neglect are described elsewhere.
In conclusion, although severe hemi-spatial neglect is frequently considered to be a definitecontra-indication for practical fitness to drive, overgeneralizations have to be avoided sincethe relationship has only scarcely objectively been investigated. The study by Webster et al.(1995) shows and confirms that hemi-spatial neglect can be confused with left-sided HH.However, the impairments should be clearly differentiated, both with respect to differentialrehabilitation methods and -outcomes, but also on the basis of severity of limitation and hence

Part I: Driving-related Research46
its differential implications on practical fitness to drive. Further, since it can be argued thatthe severity of hemi-spatial limitation can cover a broad range, a (hemi-spatial) neuro-psychological battery should be able to differentiate between these different levels. Thus, anadequate screening battery for severe hemi-spatial neglect in addition to a range of sensitivetests for hemi-spatial functioning is in order as to subtlety indicate the severity of hemi-spatiallimitation.
2.5.2.2.3. Mixed groups and driving(-related) performanceIn our introduction, we argued that not all studies relevant for our points, specificallyinvestigated hemi-spatial impairment, but did touch upon this topic indirectly. Since suchstudies are merely “suspectedly” relevant, they will be dealt with rather briefly.As previously discussed, not all studies are unequivocal with respect to patient selection.Hence, some studies including brain damaged patients are not unambiguous with respect toeither presence or measurement of the VFDs in their patient sample. On some occasions theactual perimetric technique is not mentioned or the diagnosis is based on a confrontationaltechnique, for which unquestionably more accurate alternatives can be chosen. In otherreports, VFDs are not explicitly mentioned as an exclusion criterion, suggesting that they maybe included in the sample. The same caveat holds with respect to higher-order hemi-spatialimpairment. The type, severity, and localisation of brain damage and some typical observedbehaviours (i.c. hemi-spatial limitations) make it highly likely that some samples did in factcontain (at least some) patients with homonymous VFDs or higher-order hemi-spatialimpairment (or both). These samples can thus be suspected to be “mixed” groups as is forexample possibly the case in a study by Sivak (Sivak et al., 1981).
In this study, twenty-three persons with brain damage were compared to 10 controls and toeight patients with spinal-cord damage. The brain damaged group consisted of 10 patientswith left-sided, six patients with right-sided and seven with bilateral brain damage. Eachsubject’s performance was evaluated using three sets of tests: a set of 12 perceptual-cognitiveneuropsychological tests, a closed-course driving test and an open-road driving test, eachassessed on several parameters. The neuropsychological tests were chosen on the basis ofexpected relatedness to driving performance, involving minimal motor requirements andexpected deficiency in a brain damaged population. The closed-course driving test consistedof performing several basic driving tasks on a private parking lot. For the open-road drivingtest, the subjects drove a 17 km course under different (common) traffic conditions.In general, brain damaged subjects performed worse than controls and than patients withspinal cord damage. In accordance with the dominance of both hemispheres, the authorsreport worse performance of left brain damaged subjects on tasks with a high verbalcomponent versus worse performance of right brain damage subjects on tasks with high non-verbal and perceptual components. This general pattern of performance was observed in allthree sets of tests. Interestingly and making these results relevant for this discussion, in theclosed-course driving test, the brain damaged subjects exhibited problems on tracking of theroad contralateral to their brain damage: left-sided and right-sided brain damaged subjects hitmore cones on the right and left side of the road respectively. Thus, although indicated byhemi-spatial visual limitations, the authors do not provide information whether or not andwhich of the patients suffered any kind of hemi-spatial impairment.Having observed hemi-spatial visual limitation and inferred suspected hemi-spatialimpairment, we can briefly discuss their further findings. Not all subjects were judged orproved to be competent enough to allow for safe testing conditions in the open-road driving

Part I: Driving-related Research47
test. It was completed by thirty-seven subjects. Correlational analyses indicated that, amongother indices, age, sex, education, driving experience and time since lesion were notsignificantly related to the composite driving index (i.e. a measure reflecting overall drivingperformance). The only difference found was that patients who had driving experience sincethe acquisition of the brain damage, performed better than those who had not been drivingsince. When analysed for all subjects simultaneously, most of the neuropsychological testsand closed-course driving measures correlated significantly with the composite driving index.However, the tests which proved to correlate significantly with this overall measure of thequality of driving performance were different for patients with and without brain damage. Itwas further observed that, for the brain damaged group, none of the closed-course measurescorrelated with the composite driving index. This is in contrast to the control group, whereseveral of the measures correlated significantly. Both patterns of results might indicate thatthe nature of the driving task is different in both groups.
Thus, although no conclusive evidence is provided on the presence of homonymous VFDs orother hemi-spatial impairment in this sample, the results could still be relevant, indicated bythe specific observation of lateralised visual limitations. Generally, the results confirm ourprevious point that different patterns of results can be observed for different (patient-)groupsindicating different (specific) impairments. It could thus be concluded that the nature of thedriving task for patient and control groups might be different and that the closed-coursedriving manoeuvres might not tap the on-the-road driving-related skills of brain damagedpatients. But more to the point for this discussion, is the indication that visuo-spatialfunctioning, as measured by these neuropsychological tests, is related to driving performancealso in this non-specific brain damaged sample (mixed group). This is firstly suggested by theobservation that a higher-order visual test of field (in)dependence (Oltman's Rod-and-Frametest) was the best indicator for whether or not patients would perform and complete the open-road driving test. Secondly, the tests which were significantly correlated with the compositedriving index, proved to have strong visuo-spatial components. A final note to be made is thatthe most potent patient characteristic related to the composite driving index was found to bedriving experience since the brain damage.The presentation of this paper, not only has theoretical value (although limited), but is alsoclinically of importance. It clearly suggests that studying visuo-spatial tasks (i.c. driving) in anon-specified brain damaged population almost inherently yields indefinite conclusions.Especially, since the relatively high occurrence of homonymous VFDs following post-chiasmal brain damage, and the frequent co-occurrence of higher-order hemi-spatialimpairment (see previous discussion), this dictates detailed and specific quantification ofthese deficits. Finally, more positively, it could be inferred that gaining experience with theacquired impairment, can be an important aspect of rehabilitation- or training programs, sincesubjects who had driving experience since their brain damage performed better. It could beargued that these patients gained more experience in this specific situation, and could thusadapt better to the impairment.
3. Conclusion and ImplicationsWe conceptualised visual function as consisting of two aspects, namely lower-order andhigher-order visual function, both possibly resulting in limitations (and restrictions). Thelower-order visual impairments of our interest are VFDs, more specifically HH which is ahemi-field loss. Due to it's cause, namely post-chiasmal brain damage, it can be accompaniedby higher-order visual impairment, often of a (hemi-)spatial nature. This possible co-

Part I: Driving-related Research48
occurrence might explain the variability in research outcomes concerning practical fitness todrive in this patient population. Hence our interest in hemi-spatial impairment. This interest isalso fed by the nature of the driving task. The driving task is composed of many differentaspects on different levels. It was argued that visual and spatial information-processing areclearly essential. A battery aimed at relating test performance to the quality of drivingperformance, should include ophthalmological and neuropsychological tests with strongvisual hemi-spatial components.Thus, in our own research, we aim at selectivity in test choice and in patient population. Wechoose to focus on patients suffering from HH and related hemi-spatial impairment. Thereforewe will apply a predominantly visual hemi-spatial test battery to relate ophthalmological andneuropsychological test performance to practical driving performance. Fitness to drive will beevaluated on the basis of practical driving test. An on-the-road test is, in our opinion the bestchoice for evaluating practical fitness to drive and is the golden standard in the Netherlands.In constructing and selecting our ophthalmological and neuropsychological tests, it has beenour aim to be accurate, specific, and detailed with regard to the quantification of the visual(hemi-)spatial impairment, both in terms of lower- and higher-order visual impairment.Standardised perimetric assessments will evaluate the type and extent of the VFD. A visuo-spatial screening should demarcate patients with the most severe hemi-spatial limitations (i.c.severe hemi-neglect patients), since this extreme condition is almost always found to beincompatible with standard and safe on-the-road driving-assessment. The remaining visuo-spatial tasks should be sensitive enough to show the also more subtle hemi-spatial limitations,as to be able to observe a continuum in severity of hemi-spatial limitation and impairment,and relate this to practical fitness to drive.
4. Reference ListBall,K., Owsley,C., & Beard,B. (1990). Clinical visual perimetry underestimates
peripheral field problems in older adults. Clinical Vision Science, 5, 113-125.
Barrett,A.M., Schwartz,R.L., Crucian,G.P., Kim,M., & Heilman,K.M. (2000).Attentional grasp in far extrapersonal pace after thalamic infarction. Neuropsychologia, 38,778-784.
Brouwer,W.H. (in press). Attention and driving: a cognitive neuropsychologicalapproach. In P. Zimmerman & M. Leclercq (Eds.), Applied Neuropsychology of Attention.Hove: Psychology Press.
Brouwer,W.H., & Withaar,F.K. (1997). Fitness to Drive After Traumatic BrainInjury. Neuropsychological Rehabilitation, 7, 177-193.
Galski,M., Bruno,R.L., & Ehle,H.T. (1992). Driving after cerebral damage: amodel with implications for evaluation. American Journal of Occupational Therapy, 46, 324-323.
Galski,M., Bruno,R.L., & Ehle,H.T. (1993). Prediction of behind-the-wheelDriving Performance in patients with Cerebral Brain Damage: a Discriminant FunctionAnalysis. American Journal of Occupational Therapy, 47, 391-396.

Part I: Driving-related Research49
Hannen,P., Hartje,W., & Skreczek,W. (1998). [Evaluating driving ability afterbrain damage. Neuropsychological diagnosis and driving test]. Nervenarzt, 69, 864-872.
Hartje,W., Willmes,K., & Pach,R. (1991). Driving Ability of Aphasic and Non-aphasic Brain-damaged Patients. Neuropsychological Rehabilitation, 1, 161-174.
Haselkorn,J.K., Mueller,B.A., & Rivara,F.A. (1998). Characteristics of drivers anddriving record after traumatic and nontraumatic brain injury. Archives of Physical Medicineand Rehabilitation, 79, 738-742.
Kerkhoff,G., & Schindler,I. (1997). [Hemi-neglect versus hemianopia. Differentialdiagnosis]. Fortschritte der Neurologie-Psychiatrie, 65, 278-289.
Korner-Bitensky,N.A., Sofer,S., Gelinas,I., & Mazer,B.L. (1998). EvaluatingDriving Potential in Persons With Stroke: A Survey of Occupational Therapy Practices.American Journal of Occupational Therapy, 52, 916-919.
Kuyk,T., Elliott,J.L., & Fuhr,P.S. (1998). Visual correlates of obstacle avoidancein adults with low vision. Optometry and Vision Science, 75, 174-182.
Lundqvist,A., Alinder,J., Alm,H., Gerdle,B., Levander,S., & Ronnberg,J. (1997).Neuropsychological Aspects of Driving After Brain Lesion: Simulator Study and On-RoadDriving. Applied Neuropsychology, 4, 220-230.
Mazer,B.L., Korner-Bitensky,N.A., & Sofer,S. (1998). Predicting ability to driveafter a stroke. Archives of Physical Medicine and Rehabilitation, 79, 743-750.
Michon,J.A. (1971). Psychonomie Onderweg (inaugural lecture). Groningen:Wolters Noordhoff.
Nouri,F.M., & Lincoln,N.B. (1992). Validation of a cognitive assessment:predicting driving performance after a stroke. Clinical Rehabilitation, 6, 275-281.
Owsley,C., & McGwin,G., Jr. (1999). Vision impairment and driving. Survey ofOphthalmology, 43, 535-550.
Quigley,F.L., & DeLisa,J.A. (1983). Assessing the driving potential of cerebralvascular accident patients. American Journal of Occupational Therapy, 37, 474-478.
Racette,L., & Casson,E. (1999). Visual field loss and driving performance: aretrospective study [Abstract]. Abstracts of the Eighth International Conference Vision inVehicles,
Rao,S.M., & Bieliauskas,L.A. (1983). Cognitive rehabilitation two and one-halfyears post right temporal lobectomy. Journal of Clinical Neuropsychology, 5, 313-320.
Robertson,I.H., & Halligan,P.W. (1999). Spatial Neglect: a clinical handbook fordiagnosis and treatment. Hove, UK: Psychology Press.

Part I: Driving-related Research50
Rockwell,T.H. (1972). Skills, judgement and information acquisition in driving. InT. W. Forbes (Ed.), Human Factors in Highway Traffic Safety Research. (pp. 133-164). NewYork: Wiley-Interscience.
Schulte,T., Strasburger,H., Muller-Oehring,E.M., Kasten,E., & Sabel,B.A. (1999).Automobile driving performance of brain-injured patients with visual field defects. AmericanJournal of Physical Medicine and Rehabilitation, 78, 136-142.
Shinar,D., & Schieber,F. (1991). Visual requirements for safety and mobility ofolder drivers. Human Factors, 33, 507-519.
Sivak,M., Olson,P.L., Kewman,D.G., Won,H., & Henson,D.L. (1981). Drivingand perceptual/cognitive skills: behavioral consequences of brain damage. Archives ofPhysical Medicine and Rehabilitation, 62, 476-483.
Sundet,K., Goffeng,L., & Hofft,E. (1995). To drive or not to drive:Neuropsychological assessment for driver's license among stroke patients. ScandinavianJournal of Psychology, 36, 47-58.
Szlyk,J.P., Brigell,M., & Seiple,W. (1993). Effects of age and hemianopic visualfield loss on driving. Optometry and Visual Science, 70, 1031-1037.
Tant,M.L.M., Brouwer,W.H., Kooijman,A.C., & Cornelissen,F.W. (in press).Evaluation of the effectiveness of a hemi-neglect rehabilitation program and generalization todriving: a case study. In A. G. Gale, I. D. D. Brown, C. M. Haslegrave, & S. P. Taylor (Eds.),Vision in Vehicles VIII. Amsterdam: Elsevier.
Vallar,G. (1993). The Anatomical Basis of Spatial Hemineglect in Humans. In I.H. Robertson & J. C. Marchall (Eds.), Unilateral Neglect: Clinical and Experimental Studies.(pp. 27-59). Hove (UK): Lawrence Erlbaum Associates, Publishers.
Van Winsum,W., & Brouwer,W.H. (1997). Time-headway in car-following andoperational performance during unexpected braking. Perceptual and Motor Skills, 84, 1247-1257.
Van Zomeren,A.H., Brouwer,W.H., & Minderhoud,J.M. (1987). Acquired braindamage and car driving: a review. Archives of Physical Medicine and Rehabilitation, 68,697-705.
Van Zomeren,A.H., Brouwer,W.H., Rothengatter,J.A., & Snoek,J.W. (1988).Fitness to drive a car after recovery from severe head injury. Archives of Physical Medicineand Rehabilitation, 69, 90-96.
Vos,J.J., & Riemersma,J.B.J. (1976). On the behavior in traffic of a homonymoushemianope. Ophthalmologia, 173, 427-428.
Warmink,H.H., de Jong,P.T.V.M., & Kempeneers,M.A. (1998). Hemianopsia isno absolute contra-indication for driving. [Abstract]. Book of Abstracts of the XXVIIIthInternational Congress of Ophthalmology,

Part I: Driving-related Research51
Webster,J.S., Roades,L.A., Rapport,L.J., Abadee,P.S., Sowa,M.V., Dutra,R., &Godlewski,M.C. (1995). Rightward Orienting Bias, Wheelchair Maneuvering, and Fall Risk.Archives of Physical Medicine and Rehabilitation, 76, 924-928.
Withaar,F.K., Brouwer,W.H., & Van Zomeren,A.H. (2000). Fitness to drive inolder drivers with cognitive impairment. Journal of the International NeuropsychologicalSociety, 6, 480-490.
Zihl,J. (1994). Rehabilitation of visual impairments in patients with brain damage.In A. C. Kooijman, P. L. Looijestijn, J. A. Welling, & G. J. van der Wildt (Eds.), Low VisionResearch and New Developments in Rehabilitation. (pp. 287-295). Amsterdam and Oxford:IOS Press.
Zihl,J. (1999). Oculomotor scanning performance in subjects with homonymousvisual field disorders. Visual Impairment Research, 1, 23-31.
Zihl,J. (2000). Rehabilitation of Visual Disorders After Brain Injury. Hove, EastSussex: Psychology Press Ltd.

Part I: A Visuo-spatial test battery52
A Visuo-spatial test battery
1. General1.1. IntroductionIn the previous chapter, it was argued that the use of cognitive and perceptual tasks canprovide significant information about multiple aspects related to driving performance. It wasargued that specifically both lower-order and higher-order aspects of visual functioning arerelevant in this respect. This focussing is in line with the nature of the driving task and theplausible hemi-spatial visual impairments and limitations displayed by the specific subjectgroup of interest, namely patients suffering homonymous hemianopia (HH) and relateddisorders. Therefore, our neuropsychological test battery is aimed at assessing visuo-spatialfunctioning. Visuo-spatial functioning can be expressed in many tasks.
In the previously reviewed studies, many different tests have been subjected to the patients.Additionally, different types of assessment of driving performance have been applied todifferent and sometimes unclearly defined patient groups. In these studies, only a limitedrange of visuo-spatial tests were used, which renders it impossible to compare their relativeefficiency. Therefore, selection of testing methods, purely on empirical grounds is lessobvious. Hence, a broad range of visuo-spatial tests were selected, which have beensuccessfully related to driving performance in previous studies. The selectivity in test choice,for which we argued, is applicable on the class of function assessed, namely visuo-spatialfunction. The range of visuo-spatial assessments has the further advantage of assessingdifferent aspects of visuo-spatial functioning. Additionally, their interrelatedness can bestudied, and by combining their outcomes, a detailed indication can be provided concerningthe nature and severity of visuo-(hemi-)spatial impairment.
1.2. Evaluating Visuo-spatial performance1.2.1. Basic performance: Speed and AccuracyThe selected tests can be evaluated on different aspects, as to increase their efficiency andsensitivity. Speed and accuracy are evident and frequently used dependants to quantify thequality of test performance. Both on theoretical and empirical grounds, it was concluded byBrouwer (in press) that tests of visual speed are moderately correlated to driving performanceas assessed in test-rides. In general, this concerns speed of detecting and identifying simplediscrete stimuli (e.g. Ball, Owsley, & Beard, 1990) and visual search speed (Withaar, 2000).Thus, to get a reliable indication of this speed component, reaction times (RTs) andcompletion times on several tests from different visuo-spatial domains are recorded.
Accuracy is also an indicator of efficiency of performance. However, speed and accuracy canbe highly interdependent. It is important to appreciate this interrelatedness to fully andadequately interpret the test-results. The interrelatedness of speed and accuracy often resultsfrom the nature of the task, the instructions and the preference of the subject. For example,when stimuli are presented for a very limited time, accuracy is actually an indication of speed.This is for example the case in a test where the minimum presentation time (speedcomponent) is determined to identify (accuracy component) simple stimuli. In contrast, whenstimuli are presented in a very inconspicuous manner, speed reflects accuracy. A difficultrecognition task (accuracy component) might better be analysed in terms of speed, becauseeventually all subjects would recognise the picture, when given ample time. Also the subject

Part I: A Visuo-spatial test battery53
may voluntarily choose to perform fast and less accurate or vice versa. Our instructions were,unless otherwise specified by formal and official test-instructions, to perform as adequate andfast as possible, in order to approximate an optimal balance of speed and accuracy. Furtheron, the visuo-spatial tasks and respective methods of analysis will be explained, accountingfor this interdependence.
1.2.2. Lateralised performance: the Asymmetry IndexThus, most tests will be evaluated on one or both of the basic parameters of speed andaccuracy. These dependent variables give an indication of visuo-spatial performance ingeneral. But since we are more specifically interested in visual hemi-spatial impairment andlimitation, we additionally compute (when possible) a lateralisation score or asymmetry index(AI). This index can be computed from for example differential accuracy or speed measuresin the left and right hemi-space, from the location of task initiation, from the (side of)deviation from an expected location, from a preference for either left or right hemi-spaceetcetera. This AI expresses a lateralised perceptual bias, measured by the degree ofdifferential lateralised performance, independently from general performance. Combined withgeneral performance, the AI distinguishes between a hemi-spatial (and thus lateralised)impairment and a more general spatial, attentional or scanning deficit. In the former there willbe a bias in performance on one particular side, resulting in an apparent and high AI. In thelatter, the performance level will be more equally distributed across both hemi-spaces,resulting in a low AI. Unless otherwise stated, the AI is calculated as
+−
eperformancleft eperformancright eperformancleft eperformancright . In terms of RTs this would be
This formula results in a statistic ranging from -1 to +1. A score of 0 indicates no differentialperformance. Scores tending to -1 and +1 indicate a relative preponderance of performance onthe left and right respectively. Additional information and theoretical considerations on the AIcan be found in the chapter “Grey scales uncover similar attentional effects in homonymoushemianopia and visual hemi-neglect” in this dissertation.
1.3. Pre-driver and Driver assessmentIn a previous chapter, we discussed the notion of fitness to drive. As it is our aim to study thequality of driving performance, we administer an on-the-road driving test. As such, thedriving outcome can be considered an independent variable, as are the neuropsychologicaloutcomes. But since it is our aim to relate performance on the neuropsychological tests to thequality of performance on the driving test, the driving outcome can be considered a criterion.The outcome on the neuropsychological test battery and the ophthalmological screening arethen the predictors. As such, neuropsychological and ophthalmological outcomes can bereferred to as "pre-driver" assessments.
1.4. SummaryIn a previous chapter, we argued for selectivity and specificity in test choice. On the basis ofprevious research, no specific or limited number of tests emerges which can successfullypredict practical fitness to drive. However, the specific patient population of interest, namelyHH patients, suffering specific impairment, and the nature of the driving task, both stronglysuggest to focus on visuo-spatial functioning.
left RT+right RTleft RT-right RT

Part I: A Visuo-spatial test battery54
Visuo-spatial perception is one component of cognitive functioning which globally refers toour ability to process and interpret visual information about where (parts of) objects are inspace. It underlies our ability to move around in an environment and orient ourselvesappropriately. Visuo-spatial perception is further involved in our ability to accurately reachfor objects in visual space and our ability to shift our gaze to different points in space in orderto effectively scan and search for objects. Impairments in visuo-spatial functioning could befor example impaired discrimination of complex stimuli, recognition, figure-grounddifferentiation and visual integration. Other visuo-spatial dysfunctions are defectivelocalisation of points in space, judgement of direction and distance, and topographicdisorientation. These impairments can result in subjective complaints as having a limitedoverview, bumping into obstacles or persons, getting lost while going for a walk, findingreading very exhausting, missing or misreading words, getting dizzy in busy streets etcetera.
In our aim to assess as many relevant aspects, finding a balance between quality and quantity,we chose for a number of assessments. We classified our range of tests, on an a priori basis,into four “factors”, namely basic visual scanning and search (BVSS), visuo-constructive andorganisational tasks (VCO), visuo-integrative tasks (VI) and the tracking task (Dy). Fromthese tasks (or factors) multiple aspects can be evaluated, namely basic performance in termsof speed and accuracy, and differential lateralised performance in terms of left-rightasymmetry. In the following paragraphs, the construction of the visuo-spatial factors will bepresented, the tests are described and the associated dependent variables will be indicated.This is visualised and summarised in Table 1.
2. The Visuo-Spatial Factors and Tests2.1. Factor 1: Basic Visual Scanning and Search (BVSS)As previously argued, visuo-spatial perception is involved in ability to shift our gaze todifferent points in space in order to effectively scan and search for objects. This is consideredto be a very basic ability as it is frequently described by the patients as "not effectively orforgetting looking around, not simply finding things, failing to notice (visual) events on time,always looking and searching in the same direction, etcetera". Tests from this factor all hold apredominantly simple scanning and/or search component. This component is minimallyinfluenced by other cognitive factors as visual integration, segmentation etcetera. The varietyof tests include different types of stimuli (symbols, letters, numbers), under differentpresentation modes (paper, computer screen, projection screen), requiring different responsemodes (key-press, pencil, oral), under different conditions (limited or unlimited presentationtimes). Also, tests which are usually considered as 'visual-attentional' tasks are a part of thisfactor because of the close relationship of visual-attention and scanning. Thus, clinical visualneglect tests (delineated in the table), such as line bisection and cancellation tasks, are a partof this factor. Also reading is included, since our primary interest in reading is the substantialscanning component.

Part I: A Visuo-spatial test battery55
Table 1. Summary of visuo-spatial factor construction.Visuo-spatial Dependent Variables
Factor Test Basic performance LateralisationSpeed Accuracy AI
Trail Making Test üCounting Dots üPosition Discrimination üTAP Eye movements ü üTAP Visual Scanning ü ü üThe Attended Field of View Test ü üDetection Task ü üReading words ü ü üReading strings ü ü üZihl Dotcounting test ü üLine bisection ü üAlbert’s line cancellation Test ü üMesulam Structured Shape cancellation ü ü üSearch for O's ü ü üThe Bells Test ü ü ü
%DVLF�9LVXDO6FDQQLQJ�DQG6HDUFK��%966�
Grey scales üWAIS-R Block Design Test üMatrix copy test üRepresentational Drawing test ü ü
9LVXR�&RQVWUXFWLYHDQG�2UJDQLVDWLRQDO�9&2�Complex Figure Test ü ü üPosition Determination üBlocks üHidden Figures Test ü
9LVXR�,QWHJUDWLYH�9,�Overlapping Figures Task ü ü ü'\QDPLF��'\� Tracking task ü ü
2.1.1. Trail Making TestTrail Making Test part A (TMTa) (Reitan, 1992) is a test for speed of visual search, attentionand motor function. It requires the connection, by making pencil lines, in ascending orderbetween 25 encircled numbers randomly arranged on a page. Trail Making Test part B(TMTb) (Reitan, 1992) is similar to part A, except that the B-version consists of 25 encirclednumbers and letters which have to be connected in alternating order. As such, it is also a testfor speed of mental flexibility (Spreen & Strauss, 1991). For both parts, basic performance isexpressed in terms of the time (in seconds) required to connect all circles.
2.1.2. Counting DotsThis test is subtask 5 from the Visual Object and Space Perception Battery (VOSP)(Warrington & James, 1991). It consists of 10 white cards (150x210 mm2) containing 5-9black dots (5 mm) randomly scattered. It entails localising and simple scanning as the task isto count the dots (no time limit). Performance is indicated by the number of correctly countedcards.

Part I: A Visuo-spatial test battery56
2.1.3. Position DiscriminationThis test is subtask 6 from the VOSP (Warrington and James, 1991). One item consists of twohorizontally aligned black squares (80x80 mm2). Each square contains one black dot (5 mm).Only one of the dots is positioned exactly in the centre of its square. The task is to find andindicate the centre-dot (no time limit). Performance is scored as the total number of correctlyanswered items (max 20).
2.1.4. TAP Eye movementsThis task is a subtask of the Testbattery for Attentional Performance (TAP) (Zimmerman &Fimm, 1994). It measures the speed of an overt orienting response, namely a saccadic eye-movement. Stimuli consist of small white squares (15x15 mm2) on a black background. In thetarget stimulus, the square has an opening on top. Stimuli are randomly presented on threepossible positions (horizontally aligned): centre of the screen, left and right. The peripheralstimuli were 135 mm separated from the centre position. Viewing distance was approximately450 mm. The subject pressed a button when the target stimulus appeared. Basic performanceis the overall RT. The difference in RT between central and (left or right) peripheral targetsgives an indication of lateralised performance (and is indicated by an AI).
2.1.5. TAP Visual ScanningThis task is a subtask of the Testbattery for Attentional Performance (TAP) (Zimmerman andFimm, 1994). It gives an indication of speed and strategy of visual search. One item consistsof a 110x110 mm2 matrix of (5x5) white squares. The squares measure 15x15 mm2 and allhave one discontinuous (i.e. open) side. The target stimulus holds the open side on top. Ineach matrix, there is only one target, if any. The task of the subject is to indicate whether ornot the target stimulus was present by pressing one of two buttons (present vs not present).Basic performance is scored in terms of the overall reaction time (RT) and the number ofcorrect decisions. Correlational analysis (RT by position) results in row- and column-correlations, indicating the method and direction of search (top to bottom or vice versa, andleft to right or vice versa). The column correlation gives an indication of lateralisedperformance.
2.1.6. The Attended Field Of View TestThis visual search task (AFOV) is extensively described by Coeckelbergh (Coeckelbergh,Cornelissen, Brouwer, & Kooijman, submitted). After central fixation, a display of 31 circlesis presented. The positions of the circles are organised in three elliptical rings subtending 60°by 24°. One circle (target) has a gap. The task of the subject is to indicate the direction of thegap (left, right, up or down). The presentation time of the display is adjusted by a staircaseprocedure determining 75% correct identifications of the gap-direction at that particularlocation. Performance is scored in terms of speed and efficiency of distribution. In theappendix of this dissertation, a detailed description of the method of scoring of the AFOV isdescribed in “Assessing visual search in the AFOV test”.
2.1.7. Detection TaskIn this scanning task, digits (1-9) or symbols (X or O) are singly and randomly presented inone of 48 different positions (4 rows x 12 columns) on a large projection screen(approximately 100° horizontally and 60° vertically). The stimulus software is developed anddescribed by Pizzamiglio and colleagues (e.g. Pizzamiglio et al., 1992). We adapted theoriginal procedure by using a voice-key which registers the naming/detection latency. The

Part I: A Visuo-spatial test battery57
mean RT is taken as a measure of speed. The standard deviation is a measure of consistencyof search. An AI is calculated based on the differential RTs and STDs on left and right side ofthe projection screen.
2.1.8. Reading2.1.8.1. Word versionIn the reading test, 90 unrelated Dutch words are presented over 16 lines on a A4 sheet ofpaper in landscape orientation. Words are printed in bold Arial 20 point font. Mean wordlength is 8.2 letters and varies from 2 to 18 letters. Longer words usually are compositions(e.g. sunflower). The mean number of words per line is 5.6 and varies from 3 to 8 words. Theleft and right margins are varied, as is the spacing between the words, resulting in a irregulartype page.We started with two different reading tests and constructed parallel versions of each one,changing the words but keeping their positions and approximate lengths. Not all words werechanged completely: in some words only the first or last composite part was replaced (e.g.sunflower into cauliflower).
We record reading time and accuracy. We calculate the mean reading speed per word bydividing the total reading time by the number of words actually read. For accuracy, weconsider the number and type of errors. Errors are scored on two dimensions: the word leveland the line level. A word-error is committed when part of a word is not read. Not reading acomplete word is scored as a word-omission. We also note the number and location of wordsread more than once (word-repetitions). A line-error is committed when the subject does notstart or end reading respectively at the first or last letter on that line, and is scored as a left- orright-sided line error, respectively. The location of the error within the word (left or right part)is noted as is the location of omissions and repetitions on the line. Reading accuracy isoperationally defined as the sum of the proportion of all errors. From the accuracy measures,an AI is deduced.
2.1.8.2. Letter-string versionTo investigate the influence of the direction of gaze during reading and to minimise the effectof word recognition, we devised also an alternative ‘reading’ test, based on the previousword-reading test. This alternative test was constructed by again replacing all the words whilekeeping the positions. All words were replaced by strings of random letters and numbers ofequal length as the words they replaced. The subjects were asked to read all the stringscharacter by character, first as they would read a normal page (i.e. from left to right in theword and starting from the leftmost string on the page, proceeding rightwards). Subsequentlythey were asked to do the same but in reversed order on the word level thus ‘reading’ thestrings backwards but again starting with the leftmost word on the line (i.e. from right to leftin the string, but left to right on the line). Performance is scored in the same manner as theword-reading tests.
2.1.9. Zihl Dotcounting testZihl (e.g. 1995) presented a task to assess the presence (if any) and quality of a compensatoryscanning strategy displayed by HH patients. This test consists of one trial in which 20 dots arepresented on a computer screen and have to be counted. We adapted the work of Zihl by usingmore dot patterns and varying the distribution and the total number of dots. We presented intotal 29 trials. The total number of dots in a particular trial was 5, 7, 9 ,11 ,13 ,15,17, 19, 20 or

Part I: A Visuo-spatial test battery58
21 dots. The screen dimensions were 36° and 27° horizontally and vertically respectively. Thedot size was 1°. Dots were white on a grey background. Subject are instructed to count and toreport verbally the number of dots presented as quickly and accurately as possible. Wecompute the mean response time as speed measurement and the mean absolute error asaccuracy measurement. The response time is the time between presentation of the trial andverbal response. The absolute error is the unsigned value of the difference between the actualnumber of dots and the reported number. For a more elaborate discussion of the dotcountingtask, we refer to the relevant chapter in this dissertation (part III: Hemianopic Visual FieldDefects elicit Hemianopic Scanning).
2.1.10. Clinical Neglect tasksThe neglect battery (marked in the table) is the collection of the following tests, which areclinically frequently used to diagnose (visual) hemi-spatial neglect. The battery is used notonly to quantify (parts of) visual scanning and search, but also to diagnose severe neglect asthis was an exclusion criterion for the actual HH-project. Hence, these tests are part of boththe pre-driver and the screening assessment. The rationale for exclusion is described in thescreening section of the chapter addressing “Driving and Visuo-spatial Test performance inHomonymous Hemianopia” in this dissertation. Used as screening tests, the performance isscored with reference to cut-off scores. As pre-driver assessment tests, performance is scoredin more detail, as will be described. At this point, only five of the six clinical neglect tests arepresented. The representational drawing test will be described when addressing the VCO-factor.
2.1.10.1. Line bisectionThe line bisection task (Schenkenberg, Bradford, & Ajax, 1980) consists of an A4 sheet ofpaper (landscape orientation) with 20 horizontal lines. Eighteen of the lines are organised inthree sets of six lines, so that one set is situated primarily on the left, one set on the right andone in the middle of the page. Each set contains lines of 100-200 mm, with 20 mmincrements. The order of the lines is random with respect to line length and position, and arevertically distributed across the page. Two 150 mm centre lines are added at top and bottomof the page for instruction purposes and are not included in the analysis.Scoring is achieved as described in Schenkenberg and colleagues (1980) and entails thecomputation of an average percent deviation score. The absolute value of this deviation scoregives an indication of basic performance. The average percent deviation score is comparableto an AI.
2.1.10.2. Cancellation tasksWe will first specify the four cancellation tasks we selected, after which the scoring procedurewill be described as the rationale is identical for all four of them. We chose to selectcancellation tasks of different difficulty levels and different stimuli.Both the Albert's line test and the Mesulam's test are of a moderately difficulty level as thereare respectively few and unambiguous targets or he position of the stimuli is structured,promoting structured search. Both other tests are unstructured, have many targets, havedifferent types of stimuli (symbols or letters), and have different page orientations (landscapeor portrait).In each cancellation task basic performance is scored in terms of completion time andaccuracy. The completion time is the time from presentation of the sheet until indication bythe subject of being finished. The completion time was not measured in the modified Albert’s

Part I: A Visuo-spatial test battery59
Lines test. Accuracy is expressed by the number of omissions. Using left- and right-sidedomissions, an AI is calculated.
2.1.10.2.1. Modified Albert’s line cancellation TestThis line-cancellation task (Albert, 1973; Halligan & Marshall, 1989) is a test frequentlyemployed for diagnosing severe visual neglect. The task consists of an A4 sheet of paper inlandscape orientation, with an array of 40 variously orientated black lines. These lines, eachof 25 mm, are pseudorandomly distributed in six columns of six lines each, and one centralcolumn of four lines. The purpose of the test is demonstrated by the examiner by crossing outthe four central lines, leaving 36 lines to cancel for the subject (18 on the left and 18 on theright).
2.1.10.2.2. Mesulam Structured Shape cancellationThis cancellation task was introduced by Weintraub and Mesulam (1988). In their study theyexamined the effect of stimulus material on the severity of neglect. They varied severalstimulus dimensions as for example the type of material (letters vs geometric shapes) andstimulus array (random vs structured). We opted only for the structured–shapes version. Thestimuli are displayed on an A4 sheet of paper in landscape orientation. There are 60 blacktargets to be found and circled. These targets can be described as "an open circle withradiations and a single slanted line". They are equally divided over the four quadrants of thepage and are interspersed with 300 distracters in total. The stimuli are linearly organised inrows and columns (structured) and the targets are in symmetrical locations with respect to thehorizontal and vertical axes of the page.
2.1.10.2.3. The Bells TestThe Bells Test (Gauthier, Dehaut, & Joannette, 1989; Vanier et al., 1990) consists of 315figures pseudorandomly distributed on an A4 sheet op paper (landscape orientation). Allfigures are black silhouettes of familiar objects and are about 0.7 cm2 in size. Of these 315figures, 35 are bells (targets) and 280 are distracters (guitar, house, key etc.). The positions ofthe bells are organised into seven columns (five bells per column). The purpose of this test isto find and circle all the bells.
2.1.10.2.4. Search for O'sIn this cancellation task (OZO) the subject is presented with an A4 sheet of paper in portraitorientation. This sheet contains black letters pseudorandomly distributed. There are 40 targetletters (“o”), ten in each quadrant and 430 distracter letters (all the other letters of thealphabet). The purpose of this cancellation task is to find and circle all the o's. To ourknowledge this test is not publicly available, but is however widely used for diagnosticpurposes in the Netherlands.
2.1.11. Grey scalesThe Grey Scales task was originally described by Mattingley and colleagues (Mattingley,Bradshaw, Bradshaw, & Nettleton, 1994). Initially, it was designed to assess the early,automatic orienting of attention towards the ipsilesional side of space, frequently supposed inneglect patients. This test proved to assess this chronic attentional bias in neglect byexpressing it as a lateral preference (or lateral bias).Our version contains 26 items. An item consists of an A4 (landscape orientation) white sheetof paper with two vertically aligned rectangular grey scales of equal length. A grey scale is a

Part I: A Visuo-spatial test battery60
rectangular strip with a thin black border. Its dimensions are 20 mm in height and 20 to 260mm in width with 20 mm increments. This rectangular is filled-in by a semi-continuous scaleof different grey shades varying between black and white. This filling-in is achieved bydefining 33 strips of different grey shades. The width of these band is adjusted according tothe length of the rectangular. Grey scales are thus presented in pairs (and vertically aligned)so that one grey scale is the mirror reverse of the other. Hence, one of the grey scales is blackon the left and white on the right. The other is exactly the opposite. Each item is presentedonce with top/bottom position counterbalanced resulting in 26 items.The subject is asked to judge which of the two grey scales (top or bottom) appears overalldarker. The subject is encouraged to make a judgement based upon spontaneous and ratherimmediate apprehension rather than on prolonged and detailed inspection but is told that thereis no time limit. This test results only in an AI based on the number of items judged with arightward and leftward bias. For a more elaborate discussion we refer to the chapter “Greyscales uncover similar attentional effects in homonymous hemianopia and visual hemi-neglect” in this dissertation.
2.2. Factor 2: Visuo-Constructive and Organisational tasks (VCO)The nature of this type of visuo-spatial functioning is (partly) different from the previousfactor, in that in the present tests "spatial insight" is predominant. This function is mainlyexpressed in spatial constructions and spatial organisations. To acquire, use and maintain thisspatial cognition, basic visual scanning and search are a prerequisite though not sufficient. Weopted for tests with and without time limits, always minimising the memory component sincethis is not our primary interest.
2.2.1. WAIS-R Block Design TestThis test is a subtest of the Wechsler Adult Intelligence Scale Revised (Wechsler, 1981) andinvolves having the subject duplicate specific designs using blocks with different colouredsides. The designs are presented (two dimensional) on a small booklet. The subject uses aprespecified number of blocks in order to duplicate the design in a limited amount of time.Standard procedures for instruction and scoring are used. The raw score is used as themeasure of basic performance.
2.2.2. Matrix Copy testThis test is based on a part of a training method for neglect as mentioned in for examplePizzamiglio et al. (Pizzamiglio et al., 1992). An item consists of a A4 sheet of paper inlandscape orientation, containing two matrices separated by a thick black line in the middle ofthe page. A matrix is a set of structurally ordered black dots. In one of both matrices, the dotsare connected by lines (i.e. the stimulus), forming a pattern. The successive items (and thuspatterns) are of increasing difficulty. The first dimension used to increase difficulty is the sizeof the matrix. The first set of matrices is composed of 2x2 dots, followed by 2x3, 3x3, 4x4,4x5 and 5x5. Within each set, the difficulty level is increased by increasing the number ofconnected dots, the length of the lines and the number of line crossings. The first three setsconsist of three items each, the latter three sets contain each four items, adding up to 21 itemsin total. The task for the subject is to copy the line pattern onto the empty matrix, as quicklyand accurately as possible. No instructions or limitations are imposed except for the startingpoint (dot marked by a small square). Items are presented one at a time with the stimulusmatrix on the same side as the visual field defect. The test is ceased when at least one error ismade on three consecutive items. Performance is expressed by the total number of errors (i.e.

Part I: A Visuo-spatial test battery61
faulty line segments) divided by the maximum number of faulty line segments, given thenumber of items attempted. This error-proportion takes into account both number of errorsand number of items attempted.
2.2.3. Representational Drawing testThis drawing task is part of the Behavioral Inattention Test (BIT) (Wilson, Cockburn, &Halligan, 1987) and belongs to both screening and pre-driver evaluation, as it is a clinicalmethod for diagnosing (visual) hemi-spatial neglect (described earlier). For each drawing thesubject is presented with a blank A4 sheet of paper in landscape orientation with the centre ofthe page positioned directly in front of the sagital midline of the body of the subject. Thesubject is first asked to draw a clock face with numbers. They are also invited to set a time atown preference. Next they are urged to draw a simple man or woman and finally to produce asimple sketch of a butterfly. For each drawing, a new sheet of paper is used.The scoring system provided by the manual of the BIT was applied for screening purposes,but was found to be too basic for our assessment purpose. Therefore, the basic quality of thedrawings is scored using a self-constructed system taking both global form and details intoaccount. The reported scores are the average of two independent raters. Scoring also results inan AI based on the absence/presence of (a)symmetry in the drawings.
2.2.4. Rey-Osterrieth Complex Figure TestIn this test the subject is presented with the Rey-Osterrieth figure (Osterrieth, 1944) and isasked to copy it on a sheet of paper, as accurately and quickly as possible. We did not includereproductions from memory. For scoring basic performance, we use the Boston QualitativeScoring System (BQSS),which provides a global score for accuracy and organisation (Stern etal., 1999). We additionally recorded the completion time. For evaluating asymmetry, we useaccuracy scores for left- and right-sided items as suggested by Rapport, Dutra, Webster,Charter, and Morrill (1995).
2.3. Factor 3: Visuo-Integrative tasks (VI)In contrast to the previous factor, tasks from this factor do not mainly hold constructional andmore active spatial components. In the previous (VI-)factor, the more passive, receptive andapperceptive spatial functions are envisaged as visuo-spatial comprehension andunderstanding, figure-ground separation, field-(in)dependence etcetera. For adequateperformance, many different high and low level visuo-spatial information has to be integratedand fused. Basic visual scanning and search can again be considered a prerequisite, but notsufficient for successful visuo-spatial integration. We opted for minimal involvement ofmemory and motor components.
2.3.1. Position DeterminationThis test is subtask 7 from the VOSP (Warrington and James, 1991) and consists of 10 items.One item contains two vertically aligned black squares (62x62 mm2). The top square containsnumbers (1-9) at randomly placed positions. The bottom square contains one black dot. Itsposition matches the position of one of the numbers of the top square. The task is to find thematching number. Standard procedure for administration is used and as such there is no timelimit. The total number of correctly answered items is taken as indication of basicperformance.

Part I: A Visuo-spatial test battery62
2.3.2. BlocksThis test of interpreting two dimensional depictions of a three dimensional object, is subtask 8from the VOSP (Warrington and James, 1991). It enquires the perception of complex spatialrelations. The tests consists of 10 in-perspective drawings of a spatial construction of blocks.The difficulty level is systematically increased as the total number of blocks increases (5-10)and the number of 'hidden blocks' increases (0-3). The task is to count the number of blocksthe construction consists of. Standard procedure for administration is used and as such there isno time limit. Basic performance is scored as the total number of correctly answered items.
2.3.3. Hidden Figures TestThis hidden figures test consists of 51 Gottschaldt-like figures partitioned over four parts andis based on Thurstone's Hidden Figures Test (Thurstone, 1944). For each part, the task is tofind and trace a stimulus figure which is embedded in a more complex figure. A coloured felt-tip is used for the tracings. The first part consists of 37 pairs of items. Each pair consists of asimple stimulus figure (on the left) which is embedded and has to be marked in the complexfigure on the right. The second part consists of seven complex figures in which a (one andthus always the same) given stimulus figure is embedded. The third part is similar to thesecond part in that again seven (different) complex figures are presented. But instead of one,two stimulus figures are offered. Thus one of both stimulus figures is embedded in eachcomplex design. The fourth part is identical to the third part (two different stimulus figures),only it offers 10 complex stimuli which are also more complicated. Instructions were to markthe hidden figures as quickly and accurately as possible. For each part a maximum time wasset at 10 minutes. As a measure of basic performance, we divide the total number of correctlymarked items by the total completion time.
2.3.4. Overlapping Figures TaskThe Overlapping Figures task (OFT) was constructed using the principles mentioned byGainotti and colleagues (Gainotti, D'Erme, Monteleone, & Silveri, 1986). Our version haseight stimulus and response cards. Each stimulus card (A4 sheet, landscape orientation) hasfive black line drawings of common objects all belonging to the same category. We use fiveclearly nameable themes: both small and large elements from both the categories of utensilsand animals, and transportation means. The three other categories are less nameable: upper,and lower case Greek letters, and symbols from flow charts. The stimulus cards are composedof two figures transparently overlapping on the left, two transparently overlapping on theright, and a fifth larger figure in the centre of the card transparently overlapping both left andright pairs. Each composition is approximately 100x130 mm2 in size. Each response card (A4sheet, portrait orientation) contains eight drawings vertically aligned across the page in acounterbalanced order. Four of them (targets) are identical to the four lateralised figures onthe corresponding stimulus card. Each target is matched with a visually similar distracterbelonging to the same category.To explain the test to the subject, an instruction item is used. This stimulus card contains onlythree drawings. This card is not used in the analysis. Cards are placed in front of the subject,with the centre of the pages aligned with the sagital midline of the body. The response card isplaced below the stimulus card. Subjects are asked to point, on the response card, to theidentical figures they could recognise on the stimulus card. There is no time limitation. Whensubjects indicate being finished, the examiner asks if they pointed to all the figures they couldrecognise.

Part I: A Visuo-spatial test battery63
Completion time and number of correct identifications are measures of basic performance. AnAI is derived from the number of lateralised omissions. A second AI is based on the strategy.This AI indicates the tendency to preferentially first explore one side of the composition. Forthis we record in each composition the side (left or right) of the first object identified.
2.4. Factor 4: Dynamic Tracking task (Dy)As it has previously been suggested, more dynamic aspects of visuo-spatial processing, inrelation to driving performance, have received relatively little research attention. Yet, motionand optic flow perception do have a great deal of face validity in this respect, since drivingessentially implies also movement. We therefore chose not to include exclusively static butalso a dynamic visuo-spatial task. The task in question calls for multiple visuo-spatialfunctions as scanning, construction and integration, in a moving environment. Hence, by itsunderlying components, but also by its implementation, it simulates in some aspects (visuo-spatially) the real driving event.
The tracking task aspires to assess two basic skills closely related to driving, namely lanekeeping and detection of peripheral events. The experimental set-up is partly described inBrouwer, Rothengather and van Wolffelaar (1992). It consists of a central (20 inch) screen,flanked by two peripheral screens. A steering wheel, in which press-buttons are incorporated,is placed in front of the central screen. The central screen represents a (straight) road-scene asseen through the windshield of a car. Both peripheral screens present (peripheral) targets, i.c.triangular traffic signs in which black arrows can appear. This set-up covers approximately75� of visual angle.In the first phase of this task, using only the central screen, the subject tries to keep the car oncourse, in the middle of the right lane, while a distortion signal is imposed on the steeringsignal. This distortion signal is referred to as an "unpredictable sidewind" and causesunpredictably being pushed out of course. By compensatory steering, the lateral displacementis to be corrected for. For each subject, a computer routine adapted the signal-amplitude, in15s intervals, until a stable course of 90% of the time is reached. The individually attainedsidewind-factor provides an indication of the ability of psycho-motor tracking (Brouwer,Rothengather, & Wolffelaar, 1992) and is the first measure of basic performance. In thesecond phase, the average lateral position on the road (LP) and the average standard deviationof the lateral position (STDLP) of the car are determined, while keeping lane with theindividually achieved sidewind factor. The LP provides a second basic measure ofperformance. The LP, expressed as a deviation from its ideal (middle of the right lane),provides an indication of lateralisation, comparable to an AI. The STDLP is a measure ofvariability and can be interpreted as a measure of swing i.e. how well subjects can keepcourse. This measure should be similar at this stage for each subject as all subjects drive withtheir individually attained sidewind factor. In the third phase, only using the peripheralscreens and the press-buttons in the steering wheel, stimuli are presented randomly on left andright peripheral screens. The subject does not have to keep lane, but only reacts on detection(pushes buttons on the steering wheel). The overall reaction time (RT) is taken as a basicmeasure of detection. The RTs on left and right sided stimuli provide an AI. During the finalphase, both tasks (lane keeping and peripheral detection) are performed at the same time(dual-task condition). The same dependent variables as in both single task conditions, arecomputed in this dual task condition.

Part I: A Visuo-spatial test battery64
3. Driver Assessment3.1. The Practical Driving TestWe previously discussed driving performance with reference to fitness to drive. Traditionally,fitness to drive is defined in medico-legal terms. We however use a differentconceptualisation, namely practical fitness to drive, which is to be located at the activity-performance level and is hence assessed accordingly. Also from previous discussion, itappeared that numerous kinds and formats of driving tests have been applied (e.g. open andclosed circuits, on-the-road and in realistic simulated environments etc.) and we argued formore universal and comparable formats. Therefore, driving will be evaluated on-the-road aswe consider this to be the primary and most direct method for determining practical fitness todrive. Our practical driving test is as close to real-life as possible. It is identical (except for thescoring system) to the "practical test-ride" as conducted by the Dutch Licensing Authority,Department of Adaptations, as this is considered to be the golden standard for determiningfitness to drive in the Netherlands. In the test-ride, it is examined whether the subject candrive adequately, given the visual impairment. Hence, the test-ride is not a regular on-the-roaddriving examination, as applied for obtaining a drivers' licence. Such a conventional test-rideis meant to get an overall impression of driving skill. The practical test-ride we apply, is usedto assess driving competence on the level of activity-performance. Its aim is therefore toevaluate how an impairment is manifested and compensated for during driving. Thus, duringthe test-ride, specific and potentially problematic situations are focussed upon.
The on-the-road test took place in and near the city of Groningen, and was conducted by acertified and official driving examiner of the Dutch Licensing Authority, using the standardtest-routes, and protocols. The cars used for the on-the-road test had dual operation and weremaximally adapted to the needs, imposed by motor impairment, of the individual patient.Possible adaptations were for example automatic gears, reverse pedal control, steering knobs,etcetera. The examiner, who conducted the behind-the-wheel assessment, was not blind to theperceptual status of the subjects. Because of safety reasons, it was found to be unreasonable tolet the examiner ignorant of the subject's perceptual deficits. Hence, the examiner could anddid seek circumstances which taxed the subjects potential weaknesses in order to observe if,and how well, these could be compensated for by the subject. During the driving test,difficulty levels (in terms of speed, busyness and complexity) were systematically increasedwhen judged to be safe. When fully administered, the driving test took approximately onehour and was representative for real and average day-time traffic.
3.2. Evaluating Practical Fitness to DriveThe prognostic validity of even a practical driving test cannot be taken for granted. Inprinciple, a practical driving examination does not necessarily yield an objective measurementof driving competence. The judgment given by a driving instructor or traffic expert issubjective in nature. Therefore, to judge the performance while driving and in an attempt totry to reduce effects of rater bias, a structured protocol, with predetermined observationalitems, was used.The structured protocol (Test Ride for Investigating Practical fitness to drive, i.e. TRIP) is achecklist of different aspects of the driving task. Previous versions were used by for exampleWithaar (2000) and De Raedt (2000). We added some items which specifically asked forvisual and visually related performance. Our version contains 55 items asking for specificqualities and behaviours during driving scored on a 4-point scale (1-4). In case of suboptimalperformance, the examiner is asked to provide a clarification of the problem or situation. At

Part I: A Visuo-spatial test battery65
the end of the protocol, both a global impression and end-verdict are provided, based on all(subjective) observations.From the 55 items, separate subscales or factors were constructed, based on a prioriconsiderations. The visual factor (VIS) joins all items in which predominantly visuo-perceptual behaviour is reflected. This includes visual scanning, visuo-spatial, and visuo-integrative aspects like assessment of eye- and head-movements in different situations,perception of traffic signals, visual communication with other traffic participants etcetera.This factor holds 25 different items. The operational factor (OPER) joins 8 items and reflectsfluency of instrumental and psycho-motor aspects of driving like handling the brakes andshifting gears. The tactical factor (TACT) reflects all aspects in which (tactical) choices,anticipation, and adaptation are represented. This factor is comprised of 15 items. Some itemsare represented in more than one factor. The global impression (GLOB) is the combination ofthree items, each scored on the same 4-point scale, namely a global impression of practicalfitness to drive, technical execution, and traffic insight. These factors are expressedproportional to the maximum factor-score for ease of intercomparison. The end-verdictindicates whether or not the subject would be declared fit to drive (pass or fail).
4. ConclusionUsing the proposed visuo-spatial neuropsychological test battery, and applied and analysed inthe proposed way, we hope to be able to qualify and quantify in detail the visuo-spatiallimitations in our patient group. It is our intention to relate these measures to (aspects of)driving performance. We are aware that, especially for the new and adapted tests, detailedinformation about their psychometric properties is lacking.
5. Reference List
Albert,M.L. (1973). A simple test of visual neglect. Neurology, 23, 658-664.
Ball,K., Owsley,C., & Beard,B. (1990). Clinical visual perimetry underestimatesperipheral field problems in older adults. Clinical Vision Science, 5, 113-125.
Brouwer,W.H. (in press). Attention and driving: a cognitive neuropsychologicalapproach. In P. Zimmerman & M. Leclercq (Eds.), Applied Neuropsychology of Attention.Hove: Psychology Press.
Brouwer,W.H., Rothengather,T., & Wolffelaar,P.C. (1992). Older drivers and roadinformatics. In H. Bouma & J. A. M. Graafmans (Eds.), Gerontechnology. (pp. 317-338).Amsterdam: IOS Press.
Coeckelbergh,T.R.M., Cornelissen,F.W., Brouwer,W.H., & Kooijman,A.C.(submitted). Age-related changes in the functional visual field: Further evidence for aninverse age by eccentricity effect. Journal of Gerontology: Psychological Sciences,
De Raedt,R. (2000). Cognitive/Neuropsychological functioning and compensationrelated to car driving performance in older adults. Free University Brussels.
Gainotti,G., D'Erme,P., Monteleone,D., & Silveri,M.C. (1986). Mechanisms ofunilateral spatial neglect in relation to laterality of cerebral lesions. Brain, 109, 599-612.

Part I: A Visuo-spatial test battery66
Gauthier,L., Dehaut,F., & Joannette,Y. (1989). The Bells Test: A quantitative andqualitative test for visual neglect. International Journal of Clinical Neuropsychology, 49-54.
Halligan,P.W., & Marshall,J.C. (1989). Is neglect (only) lateral? A quadrantanalysis of line cancellation. Journal of Clinical and Experimental Neuropsychology, 11,793-798.
Mattingley,J.B., Bradshaw,J.L., Bradshaw,J.A., & Nettleton,N.C. (1994). Residualrightward attentional bias after apparent recovery from right hemisphere damage: implicationsfor a multicomponent model of neglect. Journal of Neurology, Neurosurgery, and Psychiatry,57, 597-604.
Osterrieth,P.A. (1944). Le test de copie d'une figure complexe. Archives dePsychologie, 30, 206-356.
Pizzamiglio,L., Antonucci,G., Judica,A., Montenero,P., Razzano,C., &Zoccolotti,P. (1992). Cognitive rehabilitation of the hemineglect disorder in chronic patientswith unilateral right brain damage. Journal of Clinical and Experimental Neuropsychology,14, 901-923.
Rapport,L.J., Dutra,R.L., Webster,J.S., Charter,R., & Morrill,B. (1995).Hemispatial Deficits on the Rey-Osterrieth Complex Figure Drawing. The ClinicalPsychologist, 9 , 169-179.
Reitan,R.M. (1992). Trail Making Test: Manual for Administration and Scoring.South Tucson, Arizona: Reitan Neuropsychology Laboratoy.
Schenkenberg,T., Bradford,D.C., & Ajax,E.T. (1980). Line bisection andunilateral visual neglect in patients with neurologic impairment. Neurology, 30, 509-517.
Spreen,O., & Strauss,E. (1991). A Compendium of Neuropsychological Tests:administration, norms, and commentary. New York: Oxford University Press.
Stern,R.A., Javorsky,D.J., Singer,E.A., Singer-Harris,N.G., Somerville,J.A.,Duke,L.M., Thompson,J.A., & Kaplan,E. (1999). The Boston Qualitative Scoring System forthe Rey-Osterrieth Complex Figure. Odessa, FL: Psychological Assessment Resources, Inc.
Thurstone,L.L. (1944). A factorial study of perception. Chicago, IL: UniversityChicago Press.
Vanier,M., Gauthier,L., Lambert,J., Pepin,E.P., Robillard,A., Dubouloz,C.J.,Gagnon,R., & Joannette,Y. (1990). Evaluation of left visuospatial neglect: Norms anddiscrimination power of two tests. Neuropsychology, 4, 87-96.
Warrington,E.K., & James,M. (1991). The Visual Object and Space battery. BurySt. Edmunds, England.
Wechsler,D. (1981). WAIS-R manual. New York: The PsychologicalCorporation.

Part I: A Visuo-spatial test battery67
Weintraub,S., & Mesulam,M.M. (1988). Visual hemispatial inattention: stimulusparameters and exploratory strategies. Journal of Neurology, Neurosurgery, and Psychiatry,51, 1481-1488.
Wilson,B., Cockburn,J., & Halligan,P. (1987). Development of a behavioral test ofvisuospatial neglect. Archives of Physical Medicine and Rehabilitation, 68, 98-102.
Withaar,F.K. (2000). Divided Attention and driving: The effects of aging andbrain injury. University of Groningen.
Zihl,J. (1995). Visual scanning behavior in patients with homonymoushemianopia. Neuropsychologia, 33, 287-303.
Zimmerman,P., & Fimm,B. (1994). Testbatterie zur Aufmerksamkeitsprüfung.Freiburg-Würselen: Psychologische Testsysteme.

68
Part II: The Project

Part II: Driving and Visuo-spatial Test performance69
Driving and Visuo-spatial Test performance in Homonymous Hemianopia*
1. AbstractWe studied practical fitness to drive in 28 patients with homonymous hemianopia (HH). Wefocussed upon visual performance during driving and related this to neuropsychologicalvisuo-spatial test performance. Visuo-spatial tests were classified a priorily in four visuo-spatial factors, and were evaluated on three components, namely lateralisation, speed andaccuracy. Driving safety and fluency was assessed by means of a practical test-ride and scoredusing a structured protocol. We conclude that HH can not be considered a definite contra-indication for holding a drivers licence since not all patients failed the test-ride. The mostfrequent remark made by the driving expert was a lack of stability in steering. We found thatvisual performance during driving was significantly related to visuo-spatial test performance,which was operationally defined as a function of typical visual HH disability. A specificcombination of the lateralisation, speed and accuracy components derived from the visuo-spatial factors explained 77% of the variance in visual performance during driving.For deciding which type of mobility-rehabilitation goal is feasible in HH, our results suggestto administer the Grey Scales task, the Trailmaking test, the Bells test and a Hidden FiguresTest.
2. IntroductionAlthough auditory, kinaesthetic, and vestibular senses are of importance, the most substantialinformation being processed while driving is of a visual nature. Visual function can, at theimpairment level, be conceptualised as incorporating two aspects namely lower-order(sensory) visual function and higher-order (cognitive) visual function, both possibly resultingin disabilities, including impaired driving performance.
Although sensory visual functions are appropriate for clinical assessment of (loss of) visualfunction, they clearly do not reflect the visual complexity of the driving task. Higher-orderdeficits can be an alternative limiting factor, in addition to obvious physical and sensorylimitations (e.g. Sivak, Olson, Kewman, Won, & Henson, 1981). In a recent review article byOwsley and McGwin (1999), the relationship between various eye conditions and drivinghabits, performance and safety is discussed. They conclude that visual acuity, although themost commonly used visual screening test for driving licensure, is only very mildly associatedwith driving safety. Visual field assessment, another commonly used screening procedure,does not provide for consistent and conclusive findings either. These lower-order visualfunctions do show some relationship with driving in some patients, but clearly do not providea full account. This has led researchers (e.g. Owsley & McGwin, 1999) to conclude thatvisual perception during driving, or any other complex task for that matter, is dependent notexclusively on visual sensory function and physiologic optics, but also on higher-order visualfunctions. Neuropsychological tests, assessing these of higher-order visual functions, couldthus also and perhaps more successfully serve the purpose of screening, evaluating andunderstanding practical fitness to drive and guiding possible rehabilitation and adaptation.
Traditionally, fitness to drive is defined in medico-legal terms, and is related to impairments,as defined by the WHO classification. We however use a different conceptualisation, namely
* This manuscript was submitted to Neuropsychological Rehabilitation (Tant, Brouwer, Kooijman &Cornelissen).

Part II: Driving and Visuo-spatial Test performance70
“practical fitness to drive”, which is to be located at the disability level and is hence assessedaccordingly. Fluency and safety of driving was therefore evaluated on-the-road, as weconsider this to be the primary and most direct method for determining practical fitness todrive. This practical driving test is (except for the scoring system) similar to the "test-ride" asconducted by the Dutch Licensing Authority (Department of Adaptations), as this isconsidered to be the golden standard for determining fitness to drive in the Netherlands. In thetest-ride, it is examined whether the subject can drive adequately, given the visualimpairment.
Neuropsychological test performance has previously been used in relation to studyingpractical fitness to drive. In this respect, concepts of visual search, visual speed, visual anddivided attention, and visuo-spatial impairments are frequently put forward as alternativedeterminants (e.g. Shinar & Schieber, 1991; Brouwer, in press). However, not all cognitiveimpairments are expected to adversely affect practical fitness to drive. Specific cognitiveimpairments, like visuo-spatial dysfunctioning, are more likely to be related to safe and fluentdriving. Visuo-spatial perception is one component of cognitive functioning which globallyrefers to our ability to process and interpret visual information about where (parts of) objectsare in space. It underlies our ability to move around in an environment and orient ourselvesappropriately. It is not unreasonable to assert that driving has a high visuo-spatial component,and that ongoing and related action is highly dependent on this visuo-spatial information.
A specific interest in visuo-spatial functioning can hence be considered to be a logicalconsequence of the nature of the driving task. Additionally, since we specifically limit ourfocus on patients suffering homonymous visual field defects due to post-chiasmal braindamage (and homonymous hemianopia in particular) and since this condition is knownfrequently to accompany, intensify and/or provoke visual-spatial disability, it validates oureffort of studying visuo-spatial test performance in this patient group in relation to driverperformance.
From discussions on lower-order visual function (e.g. Owsley & McGwin, 1999), it emergedthat extent of the visual field or presence of visual field defects can be an important factordetermining practical fitness to drive. Further evidence for this statement is for exampleprovided by Hartje and colleagues (Hartje, Willmes, & Pach, 1991) and by Hannen andcolleagues (Hannen, Hartje, & Skreczek, 1998). In these studies, it was reported thathomonymous visual field defects due to brain damage resulted, in nearly all cases, in failureon an on-the-road driving test, suggesting clear negative effects of homonymous visual fielddefects on practical fitness to drive. However, not all literature points inexorably at thedevastating effects of homonymous visual field defects on the safety and fluency of driving ordriving-related performance. There is evidence which indicates that homonymous visual fielddefects and homonymous hemianopia by itself can not be an absolute and inevitable contra-indication for holding a drivers licence.An early demonstration that homonymous hemianopia not necessarily results in unfitness todrive was provided by Vos & Riemersma (1976) and was confirmed by Warmink andcolleagues (Warmink, de Jong, & Kempeneers, 1998). Further, a study by Szlyk et al. (Szlyk,Brigell, & Seiple, 1993) shows clearly that different levels of driving performance can beobserved within the hemianopic patient group. A similar conclusion was drawn by Racetteand Casson (1999). An even more optimistic conclusion was reached by Schulte and co-

Part II: Driving and Visuo-spatial Test performance71
workers (Schulte, Strasburger, Muller-Oehring, Kasten, & Sabel, 1999). In their study, nonegative effects of visual field defects were found with respect to measures of drivingperformance in a driver simulator task, suggesting that homonymous visual field defects donot necessarily and by definition lead to decline in (simulator)driving performance.
The current research hence focuses on two main questions. The first concerns practical fitnessto drive in patients with homonymous hemianopia (HH). The second questions concerns therelationship between visual performance during driving and other visually relatedcharacteristic, with a special emphasis on neuropsychological visuo-spatial test performance.We will study driver performance by means of a practical test-ride. The study population willbe patient suffering HH. Our interest is in studying the effects of a visual field defect andassociated disorders. We will therefore invest effort in differentiating HH from hemi-spatialneglect, which is considered to be primarily a hemi-spatial attentional problem, rather thanprimarily a hemi-spatial visual problem.Patients with hemi-spatial neglect frequently suffer right sided brain damage, in combinationwith left HH. Hemi-spatial neglect might be considered as an extreme case of hemi-spatialdysfunction resulting in severe hemi-spatial disability. Therefore, severe neglect is oftenconsidered as highly indicative for unfitness to drive. Occasional case reports have beendescribed which show that visual field defects in association with neglect behaviour arepotentially dangerous for driver and pedestrian (Robertson & Halligan, 1999; Barrett,Schwartz, Crucian, Kim, & Heilman, 2000; Tant, Brouwer, Kooijman, & Cornelissen, inpress). As a consequence, on-the-road driving assessment is usually considered as veryhazardous and alternative testing (if at all) is usually suggested. Hence, homonymoushemianopia and hemi-spatial neglect need to be clearly differentiated, both on the basis ofrehabilitation methods and -outcomes, but also on the basis of severity of disability and henceits differential implications for practical fitness to drive.By excluding patient with hemi-spatial neglect, we aim at studying the population of patientssuffering visual and visually related impairments, rather than primarily attentionalimpairments. As a consequence, we do not expect any differences in disabilities between leftand right HH patients, since they suffer equal (but inverse) visual impairment.
The second question concerns relating visual performance during driving to other visualfactors. As already mentioned, lower-order visual dysfunctions (like acuity or the presence ofa visual field defect) can not be the sole cause of practical unfitness to drive. In our research,these factors will be held constant, namely our patients will have optimal acuity and HH. Wewill investigate if other personal characteristics like age, time since lesion, driving experienceetc. are perhaps also important factors in relation to visual performance during driving.Macular sparing is in this respect an interesting characteristic. It is well recognised (e.g.Kerkhoff, 1999) that field sparing and reading speed are nearly linearly related. We areinterested in its relationship to driving performance. As we conceptualise driving as aprimarily visuo-spatial task, in which orientation and global overview are more importantthan e.g. reading directions, we do not expect macular sparing to be a crucial factor in drivingperformance. The presence of homonymous visual field defects can lead to subjective visualcomplaints. We will examine whether these subjective visual complaints (as measured by aquestionnaire) can also be related to practical fitness to drive.
Our primary interest is however in relating higher-order visual function to practical drivingperformance. As already argued, we will focus on visuo-spatial functioning, both in

Part II: Driving and Visuo-spatial Test performance72
neuropsychological tests and during driving. From previous research, no specific or limitednumber of tests emerged which showed a consistently high correlation with practical fitnessto drive. Therefore, a small selection of testing methods, purely on empirical grounds, is notobvious. Hence, a broad range of visuo-spatial tests were selected, which had beenmoderately correlated to practical driving performance in previous studies. These tests areclassified a priorily in different visuo-spatial factors, and are evaluated on differentcomponents, namely lateralisation, speed and accuracy.
Our envisaged model predicting visual performance during driving by these factors andcomponents is strongly bound by a priori considerations. Firstly, we assume that a (structural)lateralised visual field defect can result in (functional) differential lateralised performance.Homonymous hemianopia is a lateralised visual dysfunction that, if not properly compensatedfor, will lead to relatively poor visual performance with regard to the side of the blind hemi-field. As we assume that good compensation for the HH is a prerequisite for practical fitnessto drive and other visuo-spatial tasks, we presume that the extent of differential lateralisedperformance is a basic component in a model predicting practical fitness to drive. Thislateralisation is considered to be a measure of typical hemianopic disability, possibly andmost likely affecting all other components. We find it intuitive that highly differentiallateralised performance leads in general to more difficulties in constructing an accuratemental spatial representation which is essential in these visuo-spatial tasks. This will lead tomore time consumption and less accurate performance. Forcing lateralisation firstly in theprediction model expresses our assumed basic and primary status of this component.Secondly, HH is caused by brain damage. It is commonly observed that brain damage resultsin mental slowness. In addition, it can safely be argued that the mere visual effects of thelateralised visual field defect will primarily result in more time consumption during visualtasks (Zihl, 1999). We will therefore force speed as the second component in the model.Thirdly and finally, we will force accuracy in the model. We expect that visual performanceduring driving can be related to this specific visuo-spatial information. To support ourconceptualisation of the status of our components, we expect to observe the traditional speedand accuracy trade-off. More importantly, we hope to observe that worse performance interms of speed and accuracy is related to higher (i.e. worse) lateralisation scores.Additionally, we are interested in which visuo-spatial factors are of most importance inrelation to driving and by which specific tests they are represented.To conclude, we will try to shed more light on the relationship of visuo-spatial impairmentand visual performance during driving. We hypothesise that not all HH patients are practicallyunfit to drive and that visual performance during driving is related to visuo-spatial testperformance, operationally defined as a function of components of typical visual HHdisability.
3. Method3.1. Patients3.1.1. GeneralThirty-two brain damaged patients were referred to us by either ophthalmologists,neurologists or neuropsychologists because either the caretakers or the patient had expressedthe desire for the patient to be assessed on fitness to drive. All patients had a binocularoptimally corrected acuity of 0.8 or better and contrast sensitivity within normal ranges. Allhad complete or incomplete homonymous hemianopia (HH) as confirmed by automatedperimetry using the Humphrey Field Analyzer (Full Field 246 screening program, age

Part II: Driving and Visuo-spatial Test performance73
corrected, 3-zone strategy). One patient, with left HH, only had (right) monocular vision.Three patients were excluded on the basis of severe hemi-spatial neglect (see further). Onepatient with left HH suffered severe object-agnosia. As several tests proved not to beapplicable and/or resulted in extremely deviant performances, inclusion of this patient wouldhave highly distorted group analyses. As a consequence and as severe object-agnosia is notconsidered to be typical for HH, this patient was also excluded from the analyses. Hence,twenty-eight patients participated in this study. Table 1 provides some relevant characteristicsof these patients.
A number of chi square tests were performed to analyse the patient characteristics. Thereproved to be no significant difference in the number of left and right HH patients in thissample (χ2 (1, N=28) = .143, ns). There are significantly more males than females, (χ2 (1,N=28) = 9.143, P <.005), equally distributed across both left and right HH groups (χ2 (1,N=28) = 1.257, ns). Also the aetiologies are equally distributed across both groups (χ2 (2,N=28) = 2.45, ns). T-tests reveal no differences in age (t (26) = -.059, P <.954), macularsparing (t (26) = -.122, ns), time since injury (t (26) = -.644, ns) or driving experience beforeinjury (t (26) = 4.27, ns) between both HH-groups. Chi square test show that more patientsdiscontinued driving since injury (χ2 (1, N=28) = 7.001, P <.01) but the distribution ofpatients who (dis)continued driving since injury is equal across both HH groups (χ2 (1, N=28)= .048, ns).
3.1.2. Neuropsychological ScreeningPrior to the visuo-spatial assessment and driver assessments, all subjects were subjected to ageneral neuropsychological screening battery. Standardised tests were administered toexclude dementia, aphasia and apraxia. For each individual patient, there was no indication ofglobal cognitive decline as assessed by the Cognitive Screening Test (CST) (De Graaf &Deelman, 1991) and the Mini Mental Status Examination (MMSE). For assessing aphasia,
Table 1. Summary of patient characteristics
Hemianopia TotalCharacteristic value Left RightPatients (number) 15 13 28Age (years) mean 53 53 53
range 29-76 24-68 24-76Gender (number) male 13 9 22
female 2 4 6Time since injury (months) mean 34.4 45.1 39.3
range 6.4-157 3.2-142 3.2-157Aetiology (number) CVA 12 11 23
TBI 1 2 3Tumour 2 0 2
Macular sparing (°) mean 2.8 2.9 2.85range 0-10 0-8 0-10
Driving experience before injury (years) mean 27 25 26range 5-47 0-44 0-47
Continued driving since injury (number) yes 4 3 7no 11 10 21

Part II: Driving and Visuo-spatial Test performance74
two subtests from the SAN test (Deelman, Liebrand, Koning-Haanstra, & van der Burg, 1987)were administered evaluating receptive verbal abilities. There was no indication of receptiveaphasia in this sample. Ideational and ideomotor apraxia was assessed using a modifiedversion of a method by De Renzi (De Renzi, Faglioni, & Sorgato, 1982). No impairmentswere found. Further, all patients performed within the normal limits on a form discriminationscreening test (VPOR), confirming adequate general lower-order aspects of visual function,apart from the HH.
In order to exclude patients with severe hemi-spatial visual neglect, we used a battery of fourclinical cancellation tasks, a line bisection task and a drawing tests. We used the cut-offcriteria reported and found in literature reports or manuals of the tests in question (see table2). For each cancellation task, we imposed an additional “lateralisation-requirement". Thiswas done in order to make a distinction between a general inattention deficit resulting in ageneral scanning deficit, and hemi-inattention resulting in a lateralised scanning deficit. Thisrequirement holds that for a "neglect-score" (as opposed to a "general attention deficit-score")the difference between left-sided and right-sided omissions should also be equal to or exceedthe cut-off score (i.e. there should be a clear lateralisation). When applicable, the laterality islabelled as either "left" or "right" depending on the side of the anomalies. We decided that,using this battery and cut-off criteria, a patient is considered to suffer severe hemi-spatialvisual neglect, if at least four (of maximally six) neglect-scores are obtained and if thesescores are identical in laterality. As previously mentioned, three patients were excluded on thebasis of these neglect-criteria.
33AtaaaTp
Table 2: Hemi-neglect battery consisting of four cancellation tasks (1-4), a line bisection test (5) and adrawing test (6). For each test the cut-off score in terms of omissions is indicated as are relevant references.Clinical Hemi-neglect tests Cut-off
(omissions)Reference
1. Albert’s line cancellation Test 2 Halligan & Marshal (1989); Vanier, Gauthier,Lambert, Pepin, Robbillard, Dubouloz, Gagnon, &Joanette (1990)
2. Mesulam Structured Shapecancellation
3 Weintraub and Mesulam (1988)
3. Search for O's 3 clinical practice4. The Bells Test 4 Gauthier, Dehaut, & Joanette (1989); Vanier,
Gauthier, Lambert, Pepin, Robbillard, Dubouloz,Gagnon, & Joanette (1990)
5. Line bisection 2 Schenkenberg, Bradford, & Ajax, 1980; VanDeusen (1984); Soukup, Harrell, & Clark, T.(1994)
6. Representational Drawing test 2 Wilson, Cockburn and Halligan (1987)
.2. Test procedures
.2.1. Driving Assessment practical test-ride is used to assess driving competence on the level of disability. The on-
he-road test took place in and near the city of Groningen, and was conducted by a certifiednd official driving examiner of the Dutch Licensing Authority, using the standard test-routesnd protocols. The cars used for the on-the-road test had dual operation and were maximallydapted to the needs imposed by motor impairments of the individual patient.o assess performance while driving in a detailed manner, a structured protocol, withredetermined observational items was added to the procedure. This structured protocol (Test-

Part II: Driving and Visuo-spatial Test performance75
ride for Investigating Practical fitness to drive, i.e. TRIP) is a checklist of different aspects ofthe driving task and had to be filled in by the expert after the test-ride. It contains 55 itemsjudging specific qualities and behaviours during driving. These items are scored on a 4-pointscale, where a score of “1” indicates insufficient and inadequate performance, a score of “2”indicates dubious performance, “3” indicates sufficient and “4” indicates good performance.Based on a priori considerations, we constructed separate subscales or factors with these 55items. The visual factor (VIS) was constructed by joining all items in which, in our opinion,predominantly visuo-perceptual behaviour was reflected. This included visual scanning,visuo-spatial, and visuo-integrative aspects like assessment of eye- and head-movements indifferent situations, perception of traffic signals, visual communication with other trafficparticipants etc. This factor held 25 different items. The operational factor (OPER) joined 8items and reflected fluency of instrumental and psycho-motor aspects of driving like handlingthe brakes and shifting gears. The tactical factor (TACT) reflected all aspects in which(tactical) choices, anticipation, and adaptation were represented. This factor was comprised of15 items. Some items were represented in more than one factor. The sum of all TRIP items isindicated by the TOT factor. These four factors (VIS, OPER, TACT and TOT) are hence alldirectly derived from (combinations of) specific TRIP items.At the end of the TRIP, both a global impression and end-verdict were provided, based on aglobal and subjective impression of the expert. The global impression was provided byevaluating three global aspects, namely practical fitness to drive, technical handling andexecution, and traffic insight, each scored on the 4-point scale. Similarly to the other factors, aGLOB factor was constructed, combining these three items. All these factors were expressedproportional to their respective maximum factor score for ease of inter-comparison and willsubsequently be referred to as factor scores. A factor score of .25 indicates performance at the“insufficient and inadequate” level. Factor scores of .50, .75 and 1 indicate performance atrespectively “dubious”, “sufficient” and “good” level. The minimum level for passing wouldbe the “sufficient” (i.e. .75) level. The end-verdict provided by the expert indicates whether ornot the subject would be declared fit to drive (pass or fail).Whenever the driving expert scored an item as “insufficient and inadequate”, he was given theopportunity to also qualitatively express his opinion on the cause and reason for the specificinadequacy. This provides some qualitative indications of the practical driving performance.
3.2.2. Visuo-spatial Assessment3.2.2.1. Cerebral Visual Disorders (CVD) QuestionnaireThe quality of the subjective reports of the visual (field) impairment can be considerablyimproved by using a structured protocol with specific items assessing specific disabilities(Zihl, 2000). Providing likely examples from everyday life enhances recognisability, accuracyand reliability of the subjective reports by the patients. We use a (translated) Cerebral VisualDisorder questionnaire, originally developed and described by Kerkhoff et al. (Kerkhoff,Schaub, & Zihl, 1990) and modified by Dittrich (1996, version E1.1, personalcommunication). This questionnaire quantitatively and qualitatively assesses visualdisabilities by way of specific descriptions as bumping into or avoiding people or obstacles,judging the height of the next step when climbing stairs, getting dazzled by bright lights etc.Kerkhoff et al. (1990) significantly correlated the subjective complaints as measured by theirquestionnaire with objective measurements of visual dysfunction. The concordance of visualimpairment expressed by the subjective complaints and verified by objective measurements,

Part II: Driving and Visuo-spatial Test performance76
proved to be correct in 80% to 98% of the 269 brain damaged people tested. The complaintsmost characteristic for HH were bumping into obstacles and slow vision (Zihl, 2000).We scored eight visual disabilities as absent or present (0-1) (Kerkhoff et al.-part) and 12specific situations on a 5-point scale, ranging from “no problem” (0) to “mostly a problem”(4) (Dittrich-part). For each part, the scores are summed and divided by the maximum score,resulting in a proportion disability score. The reported subjective disability score is theaverage of the proportion of both parts.
3.2.2.2. Visuo-spatial Tests: factor (component) scoresPreviously we argued for selectivity and specificity in test choice, namely for testing visuo-spatial functioning. In our aim to assess as many relevant aspects, finding a balance betweenquality and quantity, we chose for a battery of visuo-spatial test, which we classified, on an apriori basis, into four factors, namely basic visual scanning and search (BVSS), a visuo-constructive and organisational factor (VCO), a visuo-integrative factor (VI) and a dynamicfactor (Dy). From these factors, multiple components can be evaluated, namely performancein terms of lateralisation, speed, and accuracy. The speed and accuracy components aretraditional aspects for evaluating general test performance. Lateralisation, expressed as anasymmetry index (AI), qualifies and quantifies a lateral perceptual bias. It expresses thenature and degree of differential lateral performance, independently of general performance.The details on the construction of the factors are discussed elsewhere but are summarised intable 3. We can confine ourselves here in summarising the rationale. The BVSS factor isconstructed of 16 different visuo-spatial tasks. The speed, accuracy and lateralisationcomponents of this factor are combinations of respectively 12, 11 and 13 differentmeasurements. The VCO factor is constructed by combining four tests. One test results in aspeed component, all four tests lead to an accuracy measurement, and two tests result in alateralisation measure. Also four tests are part of the VI factor. One test leads to a speedevaluation, all four tests lead to an accuracy evaluation and one test results in a lateralisationscore. The Dy factor is the evaluation of different aspects of the tracking task. The speedcomponent is a combination of RTs and sidewind factor. The lateralisation index is acombination of differential RTs and an evaluation of the lateral position. There is no accuracycomponent in this factor.When necessary and possible, transformations were inforced on the raw data, followingsuggestions by Stevens (Stevens, 1996), to approximate normal distributions of the scores.The data were then normalised for intercomparison. The respective component scores of eachfactor were then averaged, providing a factor component score.Visuo-spatial test performance is hereby operationally defined a comprising four differentvisuo-spatial factors, with are evaluated in terms of lateralisation, speed, and accuracy. Theserespective factor component scores can hence be entered into a model, according to our apriori considerations, to predict visual performance during driving.

Part II: Driving and Visuo-spatial Test performance77
Table 3. Summary of construction of the Visuo-Spatial factors. The components used for each test aremarked.
Visuo-spatial Dependent VariablesFactor Test Basic performance Lateralisation
Speed Accuracy AI
Trail Making Test üCounting Dots üPosition Discrimination üTAP Eye movements ü üTAP Visual Scanning ü ü üThe Attended Field of View Test ü üDetection Task ü üReading words ü ü üReading strings ü ü üZihl Dotcounting test ü üLine bisection ü üAlbert’s line cancellation Test ü üMesulam Structured Shape cancellation ü ü üSearch for O's ü ü üThe Bells Test ü ü ü
%DVLF�9LVXDO6FDQQLQJ�DQG6HDUFK��%966�
Grey scales üWAIS-R Block Design Test üMatrix copy test üRepresentational Drawing test ü ü
9LVXR�&RQVWUXFWLYHDQG�2UJDQLVDWLRQDO�9&2�Complex Figure Test ü ü üPosition Determination üBlocks üHidden Figures Test ü
9LVXR�,QWHJUDWLYH�9,�Overlapping Figures Task ü ü ü'\QDPLF��'\� Tracking task ü ü
4. Results4.1TwcomtheiteminvThThtrafunsespthesid
. Practical Driving Testenty eight HH patients performed the practical test-ride, after which the TRIP protocol waspleted by the driving expert. After quantitatively scoring the items, the driving expert had
opportunity to comment on salient and unacceptable aspects during the driving test for thes which he had rated as insufficient or doubtful. The comments of the 28 protocols were
entoried. Then we tagged per protocol whether the comment was either present or not.is showed that lack of stability in steering is the most reoccurring comment (11 protocols).is deficiency is especially evident in complex situations. Complex situations could be busyfic, difficult road design, distraction by conversation or an upcoming manoeuvre. Theteadiness tended to be more apparent in the left HH group but the higher occurrence wasecially evident in simple situations. Unacceptable lateral deviations, either to the left or to right, were reported in eight protocols. Surprisingly, there was no relationship between thee of the lateral deviation and the side of the HH. These large lateral deviations (and their

Part II: Driving and Visuo-spatial Test performance78
corrections) led to unacceptable “swinging over the road”. It was remarked that in some cases,this was most apparent on broad roads, with minimal markings and low traffic. Moreobstacles and narrow roads led to better performance. In five protocols the driving instructorcommented that the patient could not adequately overview a complex traffic scene (e.g. largeintersection) and as a consequence chose a wrong lane. Viewing performance was labelled asunstable, variable or inconsequent in seven protocols. Five of them pertained to right HHpatients. Although the viewing behaviour was described as adequate, it was only apparent insome situations, hence the viewing style not being a routine. Some of the patients performedbest in uncomplicated situations and while not being distracted. However, in others theopposite was observed. Their scanning behaviour improved when complicated situations wereat hand or expected. The speed was commented upon as too high in eight protocols, equallydistributed across both HH groups. Too low speeds were also frequently observed (10protocols), as well in city as in rural areas. In seven protocols, driving behaviour was labelledas too uncertain, sometimes despite adequate viewing behaviour. These patients tended todecrease their speed. This frequently intensified the impression (by others) of this uncertaintyand as a result led these patients in being an obstacle for other traffic participants. Driving tooclosely to the right side of the road and taking rightwards turns too widely was commentedupon in four and five protocols respectively, all pertaining to right HH patients.
MANOVA analysis was performed entering all factor scores derived from the practicaldriving test, as dependants and the side of hemianopia as between-subjects factor. Thisrevealed no significant effect of hemianopia (F(5, 22) = .737, ns). Chi square analysis on thedata of the end-verdict revealed that significantly more patients failed than passed (χ2 (1,N=28) = 14.286, P <.001), but the distribution was equal in both HH groups (χ2 (1, N=28) =.862, ns). The factor scores are summarised in table 4.
Finding ngroups anfrom "sufsignificantyielded sig
Table 4. Summary of mean TRIP factor scores for both HH groups and pooled data.Standard deviations in brackets. For the End verdict frequencies are reported.
TRIP Factors LHH RHH Pooled dataVIS .53 (.21) .57 (.14) .55 (.18)OPER .63 (.16) .66 (.11) .65 (.14)TACT .62 (.15) .68 (.10) .65 (.13)TOT .58 (.18) .61 (.12) .60 (.15)GLOB .53 (.17) .54 (.15) .53 (.16)End verdict pass 3 1 4
fail 12 12 24
o interactions with the side of the hemianopia, we pooled the data from both HHd performed one-sample T-tests to evaluate whether the factor scores were differentficient"-level (i.e. .75) and from "dubious"-level (i.e. .50). All factor scores werely different from "sufficient"-level. All factors, except the VIS and GLOB factornificant differences from "dubious" level (see table 5).
Table 5. Summary of T-test evaluation of TRIP factor scores.Test value TRIP factor score Test value
Dubious (.50) (mean) Sufficient (.75)t (27) = 1.501, ns = VIS (.55) < t (27) = -5.946, P <.001t (27) = 5.576, P <.001 < OPER (.65) < t (27) = -3.971, P <.001t (27) = 5.748, P <.001 < TACT (.65) < t (27) = -4.198, P <.001t (27) = 3.325, P <.005 < TOT (.60) < t (27) = -5.369, P <.001t (27) = 1.142, ns = GLOB (.53) < t (27) = -7.253, P <.001

Part II: Driving and Visuo-spatial Test performance79
For the remainder of the analyses, we will only consider the VIS factor as our specific interestis in visual performance during driving. For prediction, we do not consider the other factors.The Pearson correlations of the different factors were all highly significant and ranged from.71 to .98 (all P < .001). We do not use the end-verdict as the to-be predicted score, since weobserved far more failures than passes and logistic regression results in 86% correctclassifications without any factors in the model.
4.2. CVD QuestionnaireSince the CVD questionnaire comprises two parts, we firstly checked if both partsconsiderably agreed in both HH groups. We therefore performed an MANOVA entering the"Kerkhoff et al. part", the "Dittrich part" and the subjective disability score with side of thehemianopia as between-subjects factor. This analysis yielded no significant result (F(2, 25) =.832, ns). Since also the correlations between the parts proved to be significantly high (seetable 6), we will henceforth only use the subjective disability score, which is a combination ofboth constituent parts.
4.3. Vi4.3.1. F4.3.1.14.3.1.1The spPearsoBVSSstests wand letwith th.75). Fletter-r
4.3.1.1The acand is worse factorsperformscannincorrelaobservDotcou
Table 6. Correlations of the CVD questionnaire parts.Kerkhoff et al Dittrich Subjective Disability score
Kerkhoff et al. .557** .926**
Dittrich .517*/.613* .829**
Subjective Disability score .910**/.943** .825**/.841**
above the diagonal: correlations for the pooled patient population (N=28)below the diagonal: correlations for LHH (N=15) and RHH (N=13) respectively* correlation is significant at .05 level (2-tailed)** correlation is significant at .01 level (2-tailed)
suo-spatial Testsactors and factor components
. BVSS factor components
.1. speedeed component of the BVSS factor (BVSSsp) consists of 12 speed assessments. Alln correlations, except of the TAP eye movement test (r(28) = .333, ns), with thep factor were significant and ranged from .48 (P < .01) to .82 (P < .001). The threeith the highest correlations were the Bells test (r = .82), Trailmaking part B (r = .80)ter-reading speed (r = .75). The three highest correlations for the left HH group weree Trailmaking part A and B (r = .86 and r = .79) and the Mesulam cancellation (r =or the right HH group, the three highest correlations were with the Bells test (r = .91),eading speed (r = .88) and Search of O’s (r = .87).
.2. accuracycuracy component of the BVSS factor (BVSSac) consists of 11 accuracy assessmentsexpressed in terms of omissions, errors and deviations. A higher score hence indicatesperformance. For the remainder and for comparing accuracy components scores across, we will use the inverted factor components score so that higher scores indicate better
ance. Only the accuracy of the Line bisection test (r = .07) and the TAP visualg (r = .16) did not correlate significantly with the BVSSac factor. All other Pearson
tions ranged from .38 (P < .05) to .78 (P < .001). The three highest correlations wereed with the Bells test (r = .78), Position Discrimination (r = .70) and the Zihlnting test (r = .69). The Bells test (r = .78), the Search of O’s (r = .76) and the Position

Part II: Driving and Visuo-spatial Test performance80
Discrimination (r = .68) showed the highest correlations in the left HH group. The Mesulamcancellation ( r = .76), the Bells test (r = .62) and the Zihl Dotcounting test (r = .58) showedthe highest correlations for the right HH group.
4.3.1.1.3. lateralisationThe lateralisation component of the BVSS factor (BVSSai) consists of 13 lateralisationindices. The AIs resulting from the Line bisection (r = .30), Search of O’s (r = .14), AlbertsLine Test (r = .02), the Bells test (r = .06) and the TAP visual scanning (r = .34), did notcorrelate significantly with the BVSSai. All other Pearson correlations were significant andranged from .40 (P < .05) to .82 (P < .001). The Grey Scales (r = .81), the lateralisation basedon the standard deviations of the Detection Task (r = .75), the AFOV and the TAP eyemovements (both r = .65) showed the highest correlations. For the left HH group, the threehighest correlations were observed with the word reading test (r = .65), the AFOV (r = .62)and the Detection Task (standard deviations) (r = .61). For the right HH group, these were theSearch of O’s (r = .66), the Bells test (r = .45, ns) and the letter reading test (r = .41, ns).
4.3.1.1.4. intercorrelationsWe intercorrelated the BVSS factor components. We used the unsigned values of thelateralisation scores to correlate with. The factor components were not significantlyinterrelated. The results are summarised in table 7.
4.3.1.2. VCO factor4.3.1.2.1. speedThe speed componethe normalised Comp
4.3.1.2.2. accuracyThe accuracy compoand is expressed as better performance. correlations ranged fobserved with the Btest (r = .40). For tComplex Figure Tesright HH group, onlComplex Figure Tesignificantly correlat
Table 7. Pearson intercorrelations of the BVSS components.Speed Accuracy lateralisation
Speed -.17 .35Accuracy -.30 / -.12 -.24Lateralisation .32 / .39 -.29 / -.21above the diagonal: correlations for the pooled patientpopulation (N=28)below the diagonal: correlations for LHH (N=15) and RHH(N=13) respectivelyno significant correlations were found at .05 level (2-tailed)
nt of the VCO factor (VCOsp) only consists of the speed assessment oflex Figure test score.
nent of the VCO factor (VCOac) consists of 4 accuracy measurementsnumber of items or elements completed. Hence, a higher score indicatesAll test scores correlated significantly with the VCOac factor. Pearsonrom .38 (P < .05) to .79 (P < .001). The three highest correlations werelock Design (r = .53), the Complex Figure Test (r = .42) and the Matrixhe left HH group, the highest correlations were respectively with thet (r = .90), the Matrix test (r = .72) and the Block Design (r = .70). For they the correlation with the Block Design was significant (r = .40). Thest and the Representational Drawing test (both r = .44) were noted with VCOac in the right HH group.

Part II: Driving and Visuo-spatial Test performance81
4.3.1.2.3. lateralisationThe lateralisation component of the VCO factor (VCOai) consists of two AIs. The observedPearson correlations were .87 for the Representational Drawing test (P < .001) and .38 (P <.05) for the Complex Figure Test. For the left HH group, we observed correlations ofrespectively .76 (P < .001) and .42 (ns) for these tests. For the right HH group, the samepattern was observed, namely r = .95 and .05 respectively.
4.3.1.2.4. intercorrelationsWe intercorrelated the VCO factor components. They were significantly correlated. Theresults are summarised in table 8. We used the unsigned values of the lateralisation scores tocorrelate with. The significant correlations in the RHH group disappeared for the Speedcomponent.
4.3.1.3. VI factor4.3.1.3.1. speedThe speed componFigures test.
4.3.1.3.2. accuracyThe accuracy compexpressed as numbbetter performance(r = .34, ns). The oBlocks and .52 fcorrelations were Overlapping Figursignificantly (r = ..33) did not reach s
4.3.1.3.3. lateralisThe lateralisation measurements of omissions. They respectively). For and r = .66. For the
4.3.1.3.4. intercorWe intercorrelatedboth in the poole
Table 8. Intercorrelations of the VCO componentsSpeed Accuracy lateralisation
Speed -.33* .45*
Accuracy -.62* / .01 -.65*
Lateralisation .64* / .31 -.62*. / -.68*
above the diagonal: correlations for the pooled patientpopulation (N=28)below the diagonal: correlations for LHH (N=15) and RHH(N=13) respectively* correlation is significant at .05 level (2-tailed)
ent of the VI factor (VIsp) consists of the assessment of the Overlapping
onent of the VI factor (VIac) consists of four assessments. Performance iser of items successfully completed. Hence, a higher VIac score indicates. The Position Discrimination test did not correlate significantly with VIacther Pearson correlations were .72 for the Hidden Figures test, .67 for the
or the Overlapping Figures test. For the left HH group the observed.81 for the Blocks, .73 for the Hidden Figures test and .52 for thees test. In the right HH group, only the Hidden Figures test correlated79, P < .001). The Overlapping Figures test (r = .52) and the Blocks (r =ignificance.
ationcomponent of the VCO factor (VCOai) consists of two different
the Overlapping Figures test, namely AIs based on strategy and onboth correlated significantly with the VCOai (r = .77 and r = .73the left HH group, the Pearson correlations were respectively r = .48 (ns) right HH group, the correlations were r = .82 and r = .80 respectively.
relations the VI factor components. Speed and accuracy correlated significantly,d sample as for each HH group. The significant pooled correlation of

Part II: Driving and Visuo-spatial Test performance82
accuracy and lateralisation disappeared in the respective HH groups. The results aresummarised in table 9. We used the unsigned values of the lateralisation scores to correlatewith.
4.3.1.4. Dy factor4.3.1.4.1. speedThe speed componcorrelated significa.85, P < .001). The and the sidewind fain the left HH groudouble task RT (r =
4.3.1.4.2. accuracyThere is no accurac
4.3.1.4.3. lateralisaThe lateralisation cboth in single and dAIs based on the Rpositions in single and r = .91; P < .00.81 and r = .82 for t
4.3.1.4.4. intercorrWe intercorrelated results are summaricorrelate with.
Table 9. Intercorrelations of the VI componentsSpeed Accuracy lateralisation
Speed .-.56** .33Accuracy -.53* / -.62* .-40*
Lateralisation .25 / .48 -.31 / -.54above the diagonal: correlations for the pooled patientpopulation (N=28)below the diagonal: correlations for LHH (N=15) and RHH(N=13) respectively* correlation is significant at .05 level (2-tailed)** correlation is significant at .01 level (2-tailed)
ent of the Dy factor (Dysp) consists of three measurements which allntly. The RT in the single task correlated significantly with the Dysp (r =Pearson correlation of RT in the double task condition was .73 (P < .001)ctor correlated .52 with Dysp (P < .005). The same pattern was observedp (respectively .88, .66 and .52). For the right HH group, the pattern was .89), single task RT (r= .87) and sidewind (r = .57).
y component in this factor
tionomponent of the Dy factor (Dyai) is derived of RTs and lateral positionsouble task conditions and hence consists of four measurements. Neither ofTs, correlated significantly with the Dyai. The AIs based on the lateraland double task conditions correlated significantly (respectively r = .75,1). For the left and right HH group, the pattern was identical, namely r =
he left HH and r = .87 and r = .97 for the right HH group.
elationsthe Dy factor components. They were not significantly correlated. Thesed in table 10. We used the unsigned values of the lateralisation scores to
Table 10. Intercorrelations of the Dy componentsSpeed Lateralisation
Speed -.13
Lateralisation .-.45 / .23above the diagonal: correlations for the pooled patientpopulation (N=28)below the diagonal: correlations for LHH (N=15) andRHH (N=13) respectivelyno significant correlations were found at .05 level (2-tailed)

Part II: Driving and Visuo-spatial Test performance83
4.3.2. Factor components: IntracorrelationsWe intracorrelated the respective factor components. All speed factor componentsintracorrelated significantly (and positively) in the pooled patient population, and ranged from.41 (P < .05) to .74 (P <.01). The pattern of intracorrelations generally corresponded well inboth HH groups.All accuracy factors correlated positively. The correlations between the BVSS and VI factordid not reach significance (r = .37, ns).The other Pearsons correlations were .69 (BVSS xVCO, P < .01) and .57 (VI x VCO, P < .01). This pattern of intracorrelations correspondedwell in both HH groups.
Using raw lateralisation scores and pooling data from both patient populations with mainlyquantitatively similar but qualitatively opposite results (see also Tant, Brouwer, Kooijman, &Cornelissen, submitted) can obscure underlying associations. We therefore used the absolutevalues of the respective AIs for intercomparisons. None of the Pearson correlations reachedstatistical significance.
We finally averaged the respective speed, accuracy and lateralisation components of the fourdifferent factors into global component scores. Their intracorrelations are displayed in table11. For the lateralisation indices, unsigned values were used. We observe a negativecorrelation between speed and accuracy. Lateralisation is not significantly correlated neitherwith speed or accuracy. The nature of the trend is indicative however: positively for speed andnegatively for accuracy.
4.4. Associations4.4.1. Patient chaPatient characteriwere computed continuation) poicomputed for exptable 12.
Table 11. Intracorrelations of the Global factor component scoresSpeed Accuracy Lateralisation
Speed -.46** .32Accuracy -.61** / -.20 -.34Lateralisation .24 / .39 -.44 / -.33above the diagonal: correlations for the pooled patient population(N=28)below the diagonal: correlations for LHH (N=15) and RHH(N=13) respectively* correlation is significant at .05 level (2-tailed)** correlation is significant at .01 level (2-tailed)
with visual performance during drivingracteristics and visual performance during driving
stics were correlated with the visual factor score (VIS). Pearson correlationsfor the continuous data. For dichotomous data (gender and drivingnt-biserial correlations were used (Howel, 1992). The Eta statistic wasressing the association with the aetiology. The results are summarised in

Part II: Driving and Visuo-spatial Test performance84
We obssurprisicorrelafor agecharactexperiepatternproved
EnterinanalysiexperieTime sanalysi
Table 12. Association of patient characteristics with VISual factor scorePooled HHgroup (N=28)
LHH (N=15) RHH (N=13)
Age -.70**a -.75**a -.60*a
Time since injury (months) -.13a -.23a -.01a
Macular sparing .41*a .47a .29a
Driving experience before injury(years)
-.50**a -.61*a -.35a
Gender .02b .15b .19b
Driving continuation .50**b .53*b .50b
Aetiology .26c .35c .01c
* correlation is significant at .05 level (2-tailed), ** correlation is significant at .01 level (2-tailed)a Pearson correlation, b point-biserial correlation, c Eta statistic
erved high negative correlations of visual performance during driving with age, andngly also with driving experience. Since age and driving experience are highlyted (r = .90, P <.001), we recomputed the correlations with the VIS factor, controlling. These partial correlations are displayed in table 13. For the pooled group, alleristics measured, except gender, correlated significantly with the VIS factor. Drivingnce and macular sparing correlated positively, time since injury negatively. This of results is confirmed in both HH groups. None of the respective Pearson correlations to be different in both HH groups.
s
is
Table 13. Association of patient characteristics with VISual factor score when controlledfor age
Pooled HHgroup (N=28)
LHH (N=15) RHH (N=13)
Time since injury (months) -.41*a -.54*a -.26a
Macular sparing .47*a .40a .54a
Driving experience before injury(years)
.41*a .63*a .37a
Gender .14b .42b .08b
Driving continuation .45*b .43b .50b
* correlation is significant at .05 level (2-tailed), ** correlation is significant at .01 level (2-tailed)a Pearson correlation, b point-biserial correlation
g the four continuous data sources of patient characteristics in a stepwise regression with the VIS factor as dependent, yielded a model with age, sparing and driving
nce as significant predictors explaining 66.7% of the variance (F(3,24) = 16, P <.001).nce lesion was not included in the model. More detailed statistics resulting from this can be seen in table 14.
Table 14. Statistics from stepwise Regression Analysis entering continuous datasources from the patient characteristics with VIS factor as dependent.Variables Entered R2 (Adj. R2) R2 Change Change StatisticsAge .49 (.47) .49 F(1,26) = 24, P < .001Sparing .60 (.57) .11 F(1,25) = 7, P < .012Driving Experience .67 (.62) .06 F(1,24) = 4, P < .045

Part II: Driving and Visuo-spatial Test performance85
4.4.2. Visuo-spatial assessment and visual performance during driving4.4.2.1. CVD and VISual factorThe Pearson correlation between the subjective disability score and the VIS factor scoreproved not to be significant (r(28) = -.12, ns), neither for the pooled population, nor for theleft (r(15) = .01, ns) and right HH groups (r(13) = -.36, ns).
4.4.2.2. Factor components and VISual factorAs argumented, our envisaged model predicting visual performance during driving by visuo-spatial factor component scores, is strongly bound by our a priori considerations. Wehypothesised that lateralisation should be the first component of our model, due to its status ofprimary disability and its expected knock-on effect on subsequent processes. We also justifiedthe argumentation for forcing speed secondly and accuracy thirdly.
A preliminary regression analysis predicting the VIS factor and using the three globalcomponent scores as predictors and forced into the model in the suggested sequence, resultedin an R2 of .58 (F(3,24) = 11, P < .001; R2 adj. = .52). This analysis indicates that visuo-spatial performance during driving can be predicted by global visuo-spatialneuropsychological test performance. Each component added significantly to the increase ofvariance explained. Interestingly, when age was forced into the model (before these threecomponents), the total R2 increased to .61 (F(4, 24) = 9, P < .001; R2 adj. = .54), butlateralisation and speed did no longer add significantly to the R2 increase. When age wasentered lastly, it did not add significantly to the R2 increase (F(1, 23) = 2, ns).
Our primary aim was however to relate specific (rather than global) neuropsychological testperformance to visual performance during driving. As suggested by our a priori framework,we performed a regression analysis predicting the VIS factor score, using the 11 factorcomponents scores . As argued, we entered the respective component scores in a blockwisemanner. We forced lateralisation as the first block, speed the second, followed by accuracy.Within the respective (component)blocks, the method was stepwise for factor determination.Hence, we firstly forced into the model all four lateralisation factor components in a stepwisemanner, secondly, all four speed factor components were forced, also in a stepwise manner,and finally, the accuracy factor components. This procedure produced four models. The finalmodel explained 76.8% of the variance (F(4, 23) = 19, P < .001; R2 adj = .73). From thelateralisation components, only the BVSS factor was retained. This was also the case for thespeed component, given the previous retention of lateralisation components. Finally, theaccuracy components from the BVSS and VI factor (in this sequence) were retained, givenprevious retained components (see table 15).
Table 15. Statistics from Regression Analysis predicting the VIS factor and entering therespective factor components blockwise, with a stepwise procedure within the blocks.
Variables EnteredComponents Factors R2 (Adj. R2) R2 Change Change StatisticsLateralisation BVSS .22 (.19) .22 F(1,26) = 7, P < .012Speed BVSSS .51 (.47) .29 F(1,25) = 15, P < .001Accuracy BVSS .71 (.68) .20 F(1,24) = 17, P < .001
VI .77 (.73) .05 F(1,23) = 5, P < .029

Part II: Driving and Visuo-spatial Test performance86
5. Discussion5.1. Practical Driving TestIn the practical driving test, it is examined whether the subject can drive safely, fluently, andadequately, given the visual impairment. This test-ride differs form a regular drivingexamination in the sense that specific situations and occurrences are sought and observed inwhich the impairment in question is thought to be a hampering factor. Since we are studyingpatients with expected visuo-spatial disabilities, we focussed upon the visuo-spatialperformance during driving.
Although the left HH group tended to perform slightly worse, we found no significantdifference in driving performance between left and right HH groups. Although left and rightHH results from right and left sided brain damage respectively, our result does not imply thatoverall left and right sided brain damaged patients perform equally well on the practicaldriving test. As mentioned in the patient section, we took effort to exclude the patients withsevere hemi-neglect, both on theoretical and practical reasons. These patients frequentlysuffer right sided brain damage, in combination with left HH, and are thus an integral part ofunselected right sided brain damaged groups. As hemi-spatial neglect is considered to be anextreme case of hemi-spatial dysfunction resulting in severe hemi-spatial disability, inclusionof these hemi-neglect patients hence degrades overall performance in (unselected) right sidedbrain damaged groups. Hence, not finding differences between left and right HH groupsindicates that we were successful in selecting HH patients with quantitatively comparableimpairment and disability. In this sense, our left and right HH groups are not representativefor unselected right and left sided brain damaged groups.
In the HH group in general, typical problems are expected, namely in the visual and visuo-spatial domain. Indeed with respect to practical driving performance, we observed the VISfactor to be worse than the other factors. This is based on the observation that the VIS factorscore is not statistically different from “dubious” level, while the other factors (OPER, TACTand TOT) are significantly better (table 5).However, although some factors are significantly better than “dubious” level, we canconclude that the overall quality of the practical driving performance is generally low (table4-5). This is firstly suggested by the global appreciation of the driving expert (GLOB score),which is not statistically different from the “dubious” level (table 5). This indicates that thedriving expert, based on his global and subjective impression, scored the driving performancejust as “dubious”. Secondly, none of the TRIP factor scores reached the “sufficient” level(table 5). This indicates that, whatever aspect measured during the driving test, it was neverrated as “sufficient”, which is the minimum level for passing. Finally, only four patients inour group actually passed the practical driving test, as indicated by the end-verdict (table 4).This number is too low to be used in any prediction attempt, since a negative prediction for allcases would result in 86% correct classifications. This overall negative conclusion is in clearcontradiction with some reports (Vos and Riemersma, 1976; Warmink et al., 1998; Schulte etal., 1999). This contradiction can at least partly be explained by our selection methods andcriteria. We believe that our HH population is less positively selected, and hence morerepresentative for the “HH population”. Our population can be described as patients, withoutsevere hemi-neglect, suffering HH and having a question related to their fitness to drive. Thisquery often was formulated in terms of the possibility of re-evaluation of their fitness to drive,or evaluation of the safety of their driving participation. The outcome was in most cases

Part II: Driving and Visuo-spatial Test performance87
expected or feared to be negative, since this was, in most cases, the reason for referral. In theWarmink et al. (1998) study (personal communication) most of the patients volunteered for anofficial (and hence decisive) driving evaluation. These patients were possibly encouraged byothers or by their own experience of a likely positive outcome. This would suggest that, intheir population, a clear self-selection bias (to the positive end) could be present, in that onlythe very best performing HH patients are included. This would account for the high number ofpatients passing the driving test in their (selected) sample. The study by Schulte et al. (1999)also suggested absence of driving-related disabilities in HH patients. However, they used adriver-simulator task, which was inherently a simplification of a real world driving situation(i.a. automatic transmission, no intersections etc.). Further, it is important to note that theirnine patients were reported to be “neuropsychologically intact” and thus their sample is(perhaps) not representative for the wider population of HH patients. We neither had thispositive bias (rather the opposite if any), nor this simplification of the driving test (againrather the opposite if any) and hence our results are more indicative of the performance levelin a less self-selected HH (without hemi-neglect) patient population.
It was our aim, by constructing the different factors from the TRIP items, to differentiatedifferent aspects of the driving task, namely visually related performance (VIS), andbehaviours related to more operational (OPER) and tactical (TACT) skills . These werecomplemented by a total sumscore of the TRIP items (TOT) and a more global and subjectiveimpression (GLOB). It could be hypothesised that (at least some of) these factors could beindependent of each other. However, in our sample, clearly they were all highly related, withcorrelations ranging from .71 to .98. As a consequence, one could question the validity of thedifferent skills or aspects. However, this interrelationship can have several reasons. Firstly, itcould be that problems in one domain are also expressed in other domains. Brain damage, forexample, is causing the visual impairment and can thus result in visual disability. Butadditionally, it can also result in forms of motor impairment, possibly affecting the OPERfactor. The brain damage can further lead to diminished insight, empathy and anticipation andincreased impulsivety, resulting in a depressed TACT score. Hence, brain damage caninfluence the VIS, OPER and TACT score and hereby (at least partly) account for theinterrelatedness of these factors. A similar argument can be made for the possible “knock-on”effects of the visual field defect. It is highly likely that compensational efforts for the visualimpairment absorb attentional resources, leaving less to allocate to other tasks as for exampleanticipation, or simultaneously handling brakes and gears. The visual compensationalbehaviour also consumes time. So, when visually exploring the environment in order to obtainan overview, there is less time to devote to other aspects as for example visual communicationwith other traffic participants. The combination of brain damage and visual impairment couldalso have its effects on visuo-spatial memory and space representation. For example, it couldtake more effort and time to find and handle the gear-stick, where one used to find it blindlyusing visual space representation and memory. These are all possible reasons whytheoretically unrelated factors could now be related, i.e. because one disorder (e.g. braindamage) or one impairment (e.g. a HH) can be expressed in different types of disability.A second reason for the high intercorrelations between the factor scores is a possible raterbias by the driving expert. The TRIP protocol is completed after the practical driving test.During the test, the expert observes the performance of the patient and hence forms an overallquality opinion. This opinion (expressed by the end-verdict and the GLOB factor) is

Part II: Driving and Visuo-spatial Test performance88
established by the end of the test-ride. It is not inconceivable that scoring the TRIP itemsafterwards is biased by this overall impression, producing interrelatedness.Assuming that the visual disability is the most characteristic and basic disability in our HHpatient group, we conclude that the evaluation of the practical driving test by means of theTRIP protocol, as currently used in this HH patient group, is highly visually based. Theinterrelatedness of the factors can be caused by one common (i.c. visual) disability orimpairment underlying different aspects of the driving task. But alternatively, theinterrelatedness can also be induced by a (post-hoc) scoring bias. Hence, the validity of thedifferent operationally defined driving aspects or skills does not necessarily have to bequestioned on the basis of the observed intercorrelations.
The most frequent remarks made by the driving expert indicate not that vital information fromthe affected hemi-space was apparently missed or neglected. Most patients showed at leastsome form of (occasional) compensation for their HH and this activity possibly resulted in anunsteadiness in steering, which was the most reported remark. It was however more remarkedin complex situations. This might indicate that the unsteadiness increased with increasingcompensational effort. Further, in situations where creating an overview was rendereddifficult, either by complex road-design, by the large to-be-viewed area, by absence of roadmarkings, or combinations of those, patients tended to show spatial disability, expressed asi.a. deviant lateral positions and misinterpretation of road design and choosing a wrong lane.Another type of compensation adopted was dramatically reducing speed. Although apparentlysafe, this is not always effective, since it frequently resulted in the patients being an(unacceptable) obstacle for other traffic participants. Finally, it appeared that typical lateralanomalies are only observed for the right HH group, as indexed by driving too closely to theright side of the road. This observation is most likely biased and induced by the fact that wedrive on the right side of the road. Quantitatively similar lateral anomalies for the left HHgroup would result in driving to closely to the left side of the lane, approaching or crossingthe midline, dangerously near traffic from the other direction. This upcoming traffic is asource of constant feedback of and correction for the (deviant) lateral position, firstly possiblyresulting in an unsteadiness in steering, which tended to be more apparent in the left HHgroup, but secondly also in a less constant leftward deviation.
5.2. CVD questionnaireWe used the (translated) Kerkhoff et al. (1990) CVD questionnaire, which was adapted byDittrich (1996, version E1.1, personal communication)). Both parts correlated significantly,but not extremely highly (.56) (table 6). Although both parts query visual complaints, theyapparently measure not exactly the same visual disabilities. Therefore a combination of bothparts (i.e. the subjective disability score) provides a better description of the variety of visualcomplaints. However, despite (at least for the Kerkhoff part) of evidence of its high predictivevalue (i.e. subjective complaints verified by objective tests; Kerkhoff et al., 1990), we foundno significant correlation with the VIS factor. Several causes for this absence of correlationcan be formulated. Firstly, the CVD questionnaire does not include any questions related todriving. Secondly, the questions are formulated in terms of simple disabilities, translated from(or due to) primary visual impairments. This accounts of course for the high correspondenceof the questions and the objective measurements. The driving task and also more specifically,the VIS factor however does not stand for a simple disability, because it has more and otherpossibilities for compensation. It is imperative to keep in mind that performance on the

Part II: Driving and Visuo-spatial Test performance89
practical driving test can be influenced by a variety of different factors from possiblydifferent levels and their interactions. For example, driving experience could partlycompensate disabilities caused by reduced visibility due to light-scatter. Hence, a patientcomplaining about light-scatter does not necessarily show a driving disability. We thus wouldsuggest that the CVD questionnaire taps mainly at the impairment level, where drivingperformance and more specifically the VIS factor, is a measure on the disability level. Clearand highly significant relations between impairments and disabilities are not obvious (asevidenced by our data), since compensation can mask the causal relations.
5.3. Visuo-spatial factors and their componentsLower-order (sensory) impairment (e.g. a visual field deficit) as a standard, is notunequivocally related to practical fitness to drive. Practical driving performance -apart frompersonal characteristics- can also be influenced by impairment at a higher-order level. Higher-order cognitive function can be assessed by neuropsychological tests. Neuropsychological testresults are reported to correlate only moderately highly with measures of driving performance(Brouwer, in press). This can have several causes as is discussed by (Withaar, Brouwer, &van Zomeren, 2000). Their arguments can be complemented by the observation that, inprevious studies, most tests are not specifically assessing the most likely and prominentdysfunctions of the patients under study. We argue that selectivity in test choice andselectivity in patient population are logically linked. The necessity for selectivity results fromthe conceptualisation of the driving task (what components of the driving task are importantand can be adequately measured by neuropsychological tests) and from the specificdysfunctions of the patient population. When patients suffer a specific and well definedimpairment, assumed that these impairments can be neuropsychologically tapped, and theseimpairments are related to important aspects of practical fitness to drive, this specificneuropsychological test performance can be strongly related to the safety and fluency ofdriving. We therefore considered a specific group of patients (namely HH patients) assessedwith specific tests (namely visuo-spatial tests). On a priori theoretical considerations, weclassified our neuropsychological visuo-spatial tests from our extensive battery into fourfactors, each representing a visuo-spatial domain. These factors were defined as basic visualscanning and search (BVSS), visuo-constructive and organisational (VCO), visuo-integrative(VI) and dynamic (Dy). These factors were evaluated in terms of lateralisation, speed, andaccuracy (components).
From the significant intercorrelations of the four speed components it can be concluded thatrapidity, with which visuo-spatial tasks are completed, is a prominent and robust variable inall factors. The same conclusion, although to a somewhat lesser degree, can be drawn for theaccuracy component. The importance of the speed component had also been suggested by forexample Brouwer (in press). He argued, both on theoretical and empirical grounds, that visualspeed emerges as a crucial factor of neuropsychological test performance, and that it isassociated with safety and fluency of driving as assessed by test-rides. Contrary to the othercomponents, the lateralisation components are not significantly interrelated. This is inagreement with previous literature on perceptual asymmetries which confirms that, acrosstasks, only low to modest intercorrelations are observed (Nicholls, Bradshaw, & Mattingley,1999). It was suggested that different tasks do not index one single common lateralisationfactor, but tap a set of attentional processes, some of which are overlapping, and others whichare task-specific. This literature refers to tests specifically designed to tap lateralised

Part II: Driving and Visuo-spatial Test performance90
differences (commonly with chimeric stimuli). We however derived the asymmetry indicesmostly from tasks not specifically designed for this purpose. When the intercorrelationsderived from the “specialised” tests are only low to moderately high, our intercorrelations canbe expected to be even less.
We conclude that in general the expected relationships between speed, accuracy andlateralisation were observed. The interrelatedness is expressed as a speed-accuracy trade offas indexed by the negative correlation between the two components. Further, we observe thetrend that worse performance in terms of speed and accuracy is related to a higher (i.e. worse)lateralisation score. Conclusions in terms of causality can not be drawn from this data, but wehypothesise (as also evidenced in our regression analysis) that asymmetry in visualperformance (lateralisation) is the most basic of the components, influencing the others.Hence, we expected that a high asymmetry would result in poorer performance both in termsof speed and accuracy. Although not always statistically significant, the same trend appears inall factors (tables 7-11). It can further be noticed that the significances only arise in the VCO,VI and Dy factor. These factors have higher-order visuo-spatial aspects, either constructive,integrative, or dynamic, whereas tasks from the BVSS factor are more concerned with theelementary process of scanning and search. It appears that the expected relationships betweende different components is only apparent in tasks (factors) where different visuo-spatialaspects are combined.From the absence of interrelatedness of the components in the BVSS factor it can beconcluded that the tests from this factor can adequately convey information about the threeaspects of visuo-spatial performance, assessed relatively independently of each other. Thespeed component of the BVSS factor correlated most highly with performance onunstructured cancellation tasks (e.g. the Bells test) and on the Trailmaking test. The accuracycomponent was most strongly related to unstructured cancellation tasks (e.g. the Bells test) enthe Zihl Dotcounting test. The lateralisation component from the BVSS factor was mosthighly related to the AI derived from the Grey Scales and the AFOV test. In order todramatically reduce the number of tests, still be able to reproduce significant informationabout the three components and taking availability of norms in mind, our results suggest topresent patients the Trailmaking test (part B) for a speed measurement, the Bells test for anaccuracy measurement, and the Grey Scales task for the AI.These three components from the BVSS factor were all retained in our final regressionanalysis (to be discussed further). In this analysis also the accuracy component of the VIfactor was retained. The intercorrelations of the different tests with the VIac componentsuggest that the Hidden Figures test would be the best selection for representation of thisfactor.
5.4. Predicting visual performance during drivingA combination of age, macular sparing and driving experience significantly predicted visualperformance during driving. The combination of the three retained patient characteristicsexplained 67% of the variance in the VIS factor (table 14). When only the objectivelyverifiable/medical characteristics (age and macular sparing) are considered, 60% of thevariance in VIS could be accounted for (table 14). When performing regression analysis onthe basis of neuropsychological information, using the three global component scores(lateralisation, speed and accuracy), 58% of the variance was explained. Hence, prediction onthe basis of global visuo-spatial neuropsychological information is less effective than on the

Part II: Driving and Visuo-spatial Test performance91
information of all retained patient characteristics, but is more effective than on the basis ofage alone (49%). This has practical implications since this suggests that better predictions ofvisual performance during driving can be obtained using global neuropsychological measuresthan using a simple age registration, which would be morally, ethically and politically anincorrect criterion. Further analysis suggested that age did no longer provided additionalinformation after considering the global neuropsychological data. Interestingly, when age wasforced firstly into this model, the lateralisation and speed components no longer addedsignificantly to the prediction model. We take this to indicate that, with respect to visualperformance during driving, lateralisation and speed are highly age dependent and thataccuracy is less influenced by age. This high age-dependedness is not a new finding. A studyby Szlyk et al (1993), observing different levels of driving performance in HH patients,suggests that, besides the effects of visual field loss, age is an evenly important factor in abrain damaged population. These authors conclude that age-related losses, when compoundedby brain damage-associated impairments, may further increase the on-the-road risk of theolder hemianopic patients while driving. This suggests that with increasing age, equaldysfunction might lead to higher levels of disability. This is in line with a previous point wemade namely that disability is not exclusively determined by dysfunctions, but that also'personal characteristics' exert a possible important influence. Another example of such a‘personal characteristic’ is for example driving experience, which can obviously be a sourceof compensation. This is also suggested by our data, since driving experience contributedsignificantly to the prediction model. In the same respect, the importance of macular sparingemerged. Although, it is generally agreed that macular sparing is crucial for e.g. comfortablereading, it is, in our opinion, less obvious how it can be so important for visuo-spatial taskperformance in general, and visual performance while driving in particular. This visualperformance is firstly dependent on using a spatial representation by having and creating anoverview of the (visual) situation. For this stage, we would not expect macular sparing to be acrucial factor. But secondly, using this spatial representation also implies specifying (e.g.identification of objects) and updating it. For this, constant scanning is required. At this stage,macular sparing can be an important factor, since it could reasonably be assumed to bepositively associated with e.g. ease of identification of individual objects and hencenegatively with the amount of compensational effort to be invested. We previously arguedthat compensational effort could be associated with unsteadiness in steering, hence accountingfor the association of macular sparing and practical driving performance in general and visualperformance during driving in particular.
However, as we previously argued for selectivity and specificity, we were most interested inthe regression analysis using the different component scores (lateralisation, speed andaccuracy) from the four visuo-spatial factors (BVSS, VCO, VI and Dy). In this respect, weare using specific neuropsychological information, namely from different domains of visuo-spatial task performance (i.e. different factors) assessed on different aspects (i.e. differentcomponents). As already theoretically argumented, we forced the components by block in aspecific order into the model in accordance with our a priory view on importance and basicstatus of the components. We argued that lateralisation is the most basic component, followedby speed and accuracy. This resulted in a model retaining four factor components explaining77% of the variance in the VIS factor, which is more effective than on the basis of the patientcharacteristics or age alone (67% and 49% respectively). The model included thelateralisation component of the BVSS factor, the speed component of the BVSS factor and

Part II: Driving and Visuo-spatial Test performance92
finally the BVSS and VI accuracy components (table 15). In terms of specific tests, whichproved to be good representatives for the factors, our results suggest the Grey Scales task (forlateralisation), the Trailmaking test (part B) (for speed), the Bells test (for accuracy) and theHidden Figures test (for accuracy). Post-hoc regression analysis, substituting these specifictest performances for their factor components, resulted in 60% of the variance explained (F(4,23) = 9, P < .001; R2 adj. = .53). By administering these four neuropsychological visuo-spatialtests, better prediction of the VIS factor is obtained compared to when only using age, whichhas, as already mentioned, practical implications.
As previously mentioned, logistic regression analysis predicting pass/fail scores is statisticallyfutile, as only four patients passed. In the same respect, detailed analysis producing cut-offscores for the neuropsychological tests is likewise. However, for rehabilitation purposes, it isdesirable to differentiate which patients approximate practical fitness to drive from those whoare dramatically unfit to drive, assuming that specific rehabilitation success in the formergroup is more self-evident. It could be argued that for the former group, rehabilitation specificfor driving could be attempted, whilst for the latter group more modest mobility goals shouldbe formulated. We therefore defined the former group as being represented by the patientswith a visual performance during driving in the upper quartile to present some tentativeindications. This revealed that the AIs from the Grey Scales task ranged from –.69 to +.54 inthe ;upper quartile and from –1 to +1 in the other group. Hence, a Grey Scale lateralisationscore more extreme than [–.69, +.54] could be considered a negative indication. With respectto the Trialmaking test (part B) the longest completion time from the upper quartile was 196 sand the worst performance on the Bells test was five omissions. The lowest score on theHidden Figures test in the lower quartile was .03 (number of correctly marked items persecond). The combination of scores representing worse performances could be considered anegative indication for adaptive visual performance during driving and for success ofrehabilitation related to practical fitness to drive.
6. ConclusionWe posed two general questions namely one concerning the practical fitness to drive in HHpatients and the other whether the visual performance during driving could be related tovisuo-spatial neuropsychological test performance. With respect to the first issue, we wouldlike to give a differentiated answer. Driving performance during our practical driving test wasgenerally modest in our HH patient group. The most frequent remark by the driving expertwas a lack of stability in steering. Only four of the 28 patients passed the driving test. Hence,the majority of the HH patients failed the test-ride, but not all of them. This justifies ourcurrent investment of effort in studying fitness to drive in HH and hopefully future investmentof improving fitness to drive in HH. This further confirms that HH cannot be an absolutecontra-indication for practical fitness to drive. With respect to the second issue, we confirmthat visual performance during driving can be significantly related to visuo-spatial testperformance. A specific combination of the lateralisation, speed and accuracy componentsderived from different visuo-spatial factors explained 77% of the variance. Substitution of theretained factor components by their respective most representative tests, suggests toadminister the Grey Scales task, the Trailmaking test, the Bells test and the Hidden FiguresTest. These are tests which could be administered for deciding whether or not rehabilitationefforts should be invested with respect to driving or, alternatively, that more modestrehabilitation goals should be set with respect to mobility.

Part II: Driving and Visuo-spatial Test performance93
7. Reference List
Barrett,A.M., Schwartz,R.L., Crucian,G.P., Kim,M., & Heilman,K.M. (2000).Attentional grasp in far extrapersonal pace after thalamic infarction. Neuropsychologia, 38,778-784.
Brouwer,W.H. (in press). Attention and driving: a cognitive neuropsychologicalapproach. In P. Zimmerman & M. Leclercq (Eds.), Applied Neuropsychology of Attention.Hove: Psychology Press.
De Graaf,A., & Deelman,B.G. (1991). Cognitieve Screening Test. Lisse: Swets &Zeitlinger.
De Renzi,E., Faglioni,P., & Sorgato,P. (1982). Modality-specific and supramodalmechanisms of apraxia. Brain, 105, 301-312.
Deelman,B.G., Liebrand,W.B.G., Koning-Haanstra,M., & van der Burg,W. (1987).SAN test. Lisse: Swets & Zeitlinger.
Gauthier,L., Dehaut,F., & Joanette,Y. (1989). The Bells Test: A quantitative andqualitative test for visual neglect. International Journal of Clinical Neuropsychology, 11, 49-54.
Halligan,P.W., & Marshall,J.C. (1989). Is neglect (only) lateral? A quadrantanalysis of line cancellation. Journal of Clinical and Experimental Neuropsychology, 11,793-798.
Hannen,P., Hartje,W., & Skreczek,W. (1998). [Evaluating driving ability afterbrain damage. Neuropsychological diagnosis and driving test]. Nervenarzt, 69, 864-872.
Hartje,W., Willmes,K., & Pach,R. (1991). Driving Ability of Aphasic and Non-aphasic Brain-damaged Patients. Neuropsychological Rehabilitation, 1, 161-174.
Howel,D.C. (1992). Statistical methods for psychology. (3rd ed.). Belmont,California: Wadsworth Publishing Company.
Kerkhoff,G. (1999). Restorative and compensatory therapy approaches in cerebralblindness - a review. Restorative Neurology and Neuroscience, 15, 255-271.
Kerkhoff,G., Schaub,J., & Zihl,J. (1990). Die Anamnese zerebral bedingterSehstorungen. Nervenarzt, 61, 711-718.
Nicholls,M.E., Bradshaw,J.L., & Mattingley,J.B. (1999). Free-viewing perceptualasymmetries for the judgement of brightness, numerosity and size. Neuropsychologia, 37,307-314.
Owsley,C., & McGwin,G. (1999). Vision impairment and driving. Survey ofOphthalmology, 43, 535-550.

Part II: Driving and Visuo-spatial Test performance94
Racette,L., & Casson,E. (1999). Visual field loss and driving performance: aretrospective study [Abstract]. Abstracts of the Eighth International Conference Vision inVehicles, p 17.
Robertson,I.H., & Halligan,P.W. (1999). Spatial Neglect: a clinical handbook fordiagnosis and treatment. Hove, UK: Psychology Press.
Schenkenberg,T., Bradford,D.C., & Ajax,E.T. (1980). Line bisection andunilateral visual neglect in patients with neurologic impairment. Neurology, 30, 509-517.
Schulte,T., Strasburger,H., Muller-Oehring,E.M., Kasten,E., & Sabel,B.A. (1999).Automobile driving performance of brain-injured patients with visual field defects. AmericanJournal of Physical Medicine and Rehabilitation, 78, 136-142.
Shinar,D., & Schieber,F. (1991). Visual requirements for safety and mobility ofolder drivers. Human Factors, 33, 507-519.
Sivak,M., Olson,P.L., Kewman,D.G., Won,H., & Henson,D.L. (1981). Drivingand perceptual/cognitive skills: behavioral consequences of brain damage. Archives ofPhysical Medicine and Rehabilitation, 62, 476-483.
Stevens,J. (1996). Applied multivariate statistics for the social sciences. (3rd ed.).Mahwal, New Jersey: Lawrence Erlbaum Associates, Inc.
Szlyk,J.P., Brigell,M., & Seiple,W. (1993). Effects of age and hemianopic visualfield loss on driving. Optometry and Visual Science, 70, 1031-1037.
Tant,M.L.M., Brouwer,W.H., Kooijman,A.C., & Cornelissen,F.W. (in press).Evaluation of the effectiveness of a hemi-neglect rehabilitation program and generalization todriving: a case study. In A. G. Gale, I. D. D. Brown, C. M. Haslegrave, & S. P. Taylor (Eds.),Vision in Vehicles VIII. Amsterdam: Elsevier.
Tant,M.L.M., Brouwer,W.H., Kooijman,A.C., & Cornelissen,F.W. (in press). GreyScales uncover similar attentional effects in homonymous hemianopia and visual hemi-neglect. Neuropsychologia
Van Deusen,J. (1984). Normative Data for Ninety-Three Elderly Persons on theSchenkenberg Line Bisection Test. Physical and Occupational Therapy in Geriatrics, 3, 49-54.
Vanier,M., Gauthier,L., Lambert,J., Pepin,E.P., Robillard,A., Dubouloz,C.J.,Gagnon,R., & Joannette,Y. (1990). Evaluation of left visuospatial neglect: Norms anddiscrimination power of two tests. Neuropsychology, 4, 87-96.
Vos,J.J., & Riemersma,J.B.J. (1976). On the behavior in traffic of a homonymoushemianope. Ophthalmologia, 173, 427-428.

Part II: Driving and Visuo-spatial Test performance95
Warmink,H.H., de Jong,P.T.V.M., & Kempeneers,M.A. (1998). Hemianopsia isno absolute contra-indication for driving. [Abstract]. Book of Abstracts of the XXVIIIthInternational Congress of Ophthalmology
Weintraub,S., & Mesulam,M.M. (1988). Visual hemispatial inattention: stimulusparameters and exploratory strategies. Journal of Neurology, Neurosurgery and Psychiatry,51, 1481-1488.
Wilson,B., Cockburn,J., & Halligan,P. (1987). Development of a behavioral test ofvisuospatial neglect. Archives of Physical Medicine and Rehabilitation, 68, 98-102.
Withaar,F.K., Brouwer,W.H., & van Zomeren,A.H. (2000). Fitness to drive inolder drivers with cognitive impairment. Journal of the International NeuropsychologicalSociety, 6, 480-490.
Zihl,J. (1999). Oculomotor scanning performance in subjects with homonymousvisual field disorders. Visual Impairment Research, 1, 23-31.
Zihl,J. (2000). Rehabilitation of Visual Disorders After Brain Injury. Hove, EastSussex: Psychology Press Ltd.

Part II: Visual rehabilitation96
Visual rehabilitation in Homonymous Hemianopia and related disorders*
1. IntroductionThis chapter focuses on the rehabilitation of visual field defects in general and ofhomonymous hemianopia in particular. Some reference will be made to visual rehabilitationin neglect as a related disorder. Since the differential diagnosis has clear and importantimplications for rehabilitation, it will receive special emphasis. Other related disorders, forexample, the visual agnosias and prosopagnosia, will only be touched upon because of thepresent limitations of specific structured rehabilitation efforts for these particular problems.
2. Visual Field Defects and related disorders: forms, frequency of occurrence anddiagnosis2.1. Homonymous hemianopia and related disordersHomonymous hemianopia or hemianopsia (HH) is a visual field defect (VFD) in which, forboth eyes to the same extent (homonymous), half of the visual field (hemi) is blind (anopia).Like all unilateral VFDs, it is the result of unilateral post-chiasmal brain damage. Nearly 80%of patients with unilateral post-chiasmal brain damage acquire a homonymous VFD (Zihl,1994). Due to the structural organisation of the visual bundles and the crossing of temporalhalf-field information in the optic chiasm, left-sided brain damage results in right-sided VFDsand vice versa. Common causes are cerebrovascular accident (CVA), traumatic brain injury(TBI) and tumours. Forty per cent of HH involve lesions of the occipital lobe, 30% involvethe parietal lobe, 25% involve the temporal lobe and 5% involve the optic tract and lateralgeniculate nucleus (Pambakian & Kennard, 1997). Nearly 66% of the unilateral homonymousVFDs are homonymous hemianopias. The most common other types are quadranopia (about14%) and paracentral scotomas (about 14%) (Zihl, 1994). Quadranopia refers to the loss ofvision in one quadrant of the visual field, either the upper or the lower. Paracentral scotomasare regions of blindness mainly in the central field region but sparing the fovea. It has beenestimated that 20-30% of all patients with CVAs in rehabilitation centres have homonymousVFDs (Kerkhoff, 1999). These percentages indicate the significance of the homonymousVFDs and the importance of structured rehabilitation efforts for this group of patients.
Visual field defects can result in complaints and (visual) dysfunctions. Patients complain, forexample, about having a limited overview, bumping into obstacles or persons, getting lostwhile going for a walk, finding reading very exhausting, missing or misreading words, gettingdizzy in busy streets et cetera. These complaints are partly due to a common underlyingdefective mechanism, namely visual scanning. Visual scanning deficits can be studiedthrough the registration of eye movements. Examples of normal and defective scanningpatterns can be seen in figure 1 A-C. Figure 1A represents normal scanning behaviour whilecounting a number of dots on a computer screen under free viewing conditions. Figures 1Band 1C are illustrations of scanning patterns of hemianopic patients. Figure 1B is a clearillustration of a defective scanning pattern, while figure 1C shows the eye movementsregistered in a neglect patient, clearly ‘neglecting’ the left side of the screen’.
* This chapter is accepted to appear in: Neuropsychological rehabilitation: a cognitive approach. W.H.Brouwer,A.H. van Zomeren, I.J. Berg, J.M. Bouma, & E.H.F. de Haan (Eds.). Amsterdam: Boom(Tant, Bouma, Kooijman, Cornelissen, & Brouwer)

Part II: Visual rehabilitation97
Patients frequently do not understand the nature of their visual deficit (see further notes onhemianopic anosognosia) and cannot explain it to others. This may result in insecurity,depression and social isolation (Zihl & Kennard, 1996). These complaints can be the directresult of the VFD per se, but they can also be caused by other disorders resulting from thepost-chiasmal brain damage. The type and severity of related disorders will depend on thesize and location of the brain damage involved. Impairments in spatial contrast sensitivity,light and dark adaptation and colour vision have been observed in more than 20% of patientswith posterior brain damage (Zihl, 1994). Higher-order visual disorders can also co-occur, forexample visual agnosia, prosopagnosia, disorders in visual space perception, Balint'ssyndrome, visual illusions and hallucinations, and visual neglect. It is very plausible toassume that the presence of a VFD and the resulting scanning deficiency augments thenegative effects of those related disorders. This has indeed been argued in the case of neglect,for example by Webster and colleagues (1984) and by Agrell, Dehlin and Dahlgren (1997).
Perhaps the most common associated disorder is visual neglect. Since neglect is the maintopic of another chapter, it will not be discussed extensively here. Rather we will confineourselves to some general remarks about neglect and discuss the differential diagnosis morethoroughly.Visual neglect can be defined as the tendency not to notice, that is to neglect, contralesional(visual) stimuli. This failure is not due primarily to hemifield blindness, although, asmentioned, the two conditions often co-occur. It has been estimated that approximately 70%of neglect patients also suffer from a homonymous VFD (Kerkhoff & Schindler, 1997).However, these authors suggest interpreting this estimate with caution, since, because bothHH and visual neglect may result in failure to react to visual events in the contralesionalhemifield, the differential diagnosis of HH is difficult. It has further been argued that visualneglect is more severe when it occurs simultaneously with homonymous VFDs (Webster etal., 1984; Agrell et al.,1997).
2.2. Homonymous Hemianopia and visual Neglect: differential diagnosisSince visual neglect occurs more often after right-sided brain lesion, it can co-occur and/or beconfused with left-sided HH. A global guideline for the differential diagnosis in clinicalsettings is that HH patients will try to compensate by turning the head and/or eyes to bring a
Figure 1 A-C. Examples of scanning patterns during a dot counting task. The dots are represented in black.The scanning pattern is visualised by connecting the successive fixations (squares). Figure 1A represents ascanning pattern by a control subject. The scanning pattern is characterised by relatively low number offixations and refixations. There are no repetitions in scanpath. Figure 1B. represents a scanning pattern by asubject with left homonymous hemianopia. The scanning pattern is characterised by a high number offixations and refixations, and repetitions in scanpath. Figure 1C. represents a scanning pattern by a neglectpatient. Although the pattern resembles the pattern from figure 1A. (low number of fixations, refixations,and repetitions), only half of the screen is inspected.
Figure 1A Figure 1CFigure 1B

Part II: Visual rehabilitation98
stimulus into their preserved visual field. In contrast, patients with neglect do not seem to beaware that there is, or could be, anything of interest on their contralesional side. This is trueeven of neglect patients with intact visual fields.Another frequently proposed criterion is the alleged awareness of the visual problem in HH,and its absence in neglect. The lack of awareness of the VFD, due to brain lesion orhemianopic anosognosia (HAN), may range from uncritical underestimation to explicit andintractable denial of the deficit.Two studies, investigating the occurrence of HAN in relation to the presence of neglect(Bisiach, Vallar, Perani, Papagno, & Berti, 1986; Celesia, Brigell, & Vaphiades, 1997),suggested that the relationship is not unequivocal. Forty-eight of the 64 patients described inthe two studies presented with HAN. Of those, 37 were diagnosed with neglect; the remaining11 were found to have no neglect. Thus 24% of the patients with HAN had no neglect.Sixteen patients showed awareness of their VFD (no HAN). Of these, nine were diagnosed ashaving neglect. Thus 56% of the patients with awareness also had neglect.
In conclusion, these results caution against the use of the presence of awareness fordistinguishing visual neglect from HH, as they indicate that most patients with VFDs haveHAN and that neglect patients can also show some form of awareness. Furthermore, very fewof the patients with awareness (no HAN), had complete and full understanding of their deficit.The majority suffered from ‘‘hemianopic misinterpretation’’. They were aware of somedeficit but misinterpreted its cause. Usually the deficit is interpreted as a failure of one eyerather than the blindness of one hemifield. We can ask whether, in terms of rehabilitation ordifferential diagnosis, this difference is important. But apart from this, these findingsdemonstrate that awareness is not the simplest notion and that it is troublesome as adifferential criterion.
Differential diagnosis on the basis of a single criterion proves not to be feasible. Kerkhoff andSchindler (1997) provide ten criteria which can be used to differentiate. They argue that noneof the distinguishing features by themselves can differentiate, but taken as a whole, they cansuccessfully classify almost all patients. We (briefly) summarise the ten criteria.• HH patients can usually describe some of their visual deficits accurately (e.g. specific
reading problems, bumping into obstacles). These deficiencies are usually later confirmedby objective measurements. This contrasts with the subjective reports by neglect patients,which are usually not specific, inaccurate and not relevant.
• Another distinguishing feature is the modality specificity. HH is by definition restricted tothe visual modality. In neglect, the hemispatial deficit is not necessarily restricted to thevisual modality, as forms of tactile, acoustic and motor neglect have been reported.
• Aetiology and location of the lesion can also give informative cues for differentialdiagnosis. HH most often occurs after lesions located at sites supplied by the posteriorarteries. Left and right-sided lesions occur with almost equal frequencies. The mostcommon cause of neglect is reported to be extensive medial cerebral artery territoryinfarctions in the right hemisphere. Most common lesion sites are supplied by the centraland/or parietal branches.
• Extinction is often regarded as a residual symptom of neglect. It is a multimodalphenomenon in which a stimulus which elicits a response when presented singly, nolonger does so under conditions of double simultaneous stimulation (DSS). The neglectedstimulus is usually the stimulus on the left. DSS is usually performed in both hemifields

Part II: Visual rehabilitation99
(with a fixation point in between both stimuli), but can also be presented lateralised (withboth stimuli on the same side as the fixation point). When tested in the intact hemifield,HH patients do not show any form of extinction. Neglect patients either do showextinction or, in contrast to the normal pattern, react more slowly to the more centraltarget (when presented in the right hemifield).
• When drawing inherently symmetrical objects from memory (e.g. a house or the face of aclock), HH patients usually deliver complete and symmetrical drawings, with equal levelof detail on both sides of the drawing. Some neglect patients on the other hand,completely omit one side of the drawing (usually the left), or show a clear discrepancy inaccuracy and level of detail between left and right sides of the figure.
• The presence of visual-spatial dysfunctions renders a neglect diagnosis more likely. Theperception of visual horizonticality and verticality, subjective middle, determination ofposition and orientation are functions associated with the dorsal route. Impairments inthese functions make parietal lesions (and thus neglect) more likely and pure occipitallesions (and thus HH) less likely.
• The size and type of error, made in line bisection tasks, provides another way ofdisentangling neglect and HH. In more than 90% of trials, HH patients mark the midlinewith a contralesional deviation. This means that the deviation is in the direction of theirblind hemifield. Neglect patients, on the other hand, make the opposite bisection error:they deviate ipsilesionally, that is in the direction of their intact hemifield. Further, in ourown work, we very rarely noticed any omissions in the HH group (i.e. not bisecting a linein the case of multiple lines on one page), in contrast to the neglect group.
• If perception (with fixed fixation) in the deficient hemifield can be modulated (e.g. bycueing), the diagnosis of absolute HH is by definition not applicable. Some forms ofcueing can elicit relief (usually transient) of neglect symptomatology. The simplest formof visual cueing would be, for example, to abruptly present a very salient stimulus in theleft hemifield by flashing a white light on a dark background. This stimulus is likely toelicit an orienting response because cueing attracts attention. Once a stimulus has capturedattention, it can be reacted to. This is not the case in HH, because there is, by definition,no possibility of perception in the defective hemifield. However, in HH, there can also besome form of residual perception, for example spared movement perception without lightdetection. This phenomenon is usually referred to as blind-sight and can be understood asthe residual capacity to react to movement, but not to the mere presence of a stationarystimulus. A patient cannot tell whether a stimulus is present or not if it is stationary. Butwhen it starts to move, the direction of the movement can be indicated. In theseexperiments patients make remarks like: µ,�GRQW�NQRZ�LI�DQ\WKLQJ�LV�WKHUH��EXW�LI�WKHUH�LV�P\�IHHOLQJ�WHOOV�PH�LW�PRYHV�XSZDUGV¶. However, these spared functions are not the resultof cueing (attracting attention) but presumably of spared residual capacity, which isalways available, and hence no temporary phenomenon (contrary to cueing). Inconclusion, we would suggest not using moving stimuli as cues but rather simplepresentation of (on/off) stimuli to try to elicit reaction.
• Informative observations can be made during visual field testing. When perimetric testingshows a hemifield deficit, it can be the expression of either neglect symptomatology, HH,or both. However, it was noticed that the HH group performed the perimetric assessmentswithout any problems, with stable fixations and relatively good understanding andconcentration. In contrast, some neglect patients had difficulty maintaining centralfixation. Neglect patients clearly found it difficult to suppress reflexive eye movements to

Part II: Visual rehabilitation100
the light stimuli presented. It was further noticed that repeated measurement and slightmodification of perimetric procedures could affect results significantly in pure neglect butnot in HH. When measured with kinetic perimetry, the VFD in neglect patients appearedlarger and different when targets moved inwards to fixation (standard procedure), thanwhen they moved outwards from fixation. Additionally, a possible influence of thepresence and type of the fixation point suggests visual neglect.
• Finally, measuring visual evoked potentials (VEPs) using hemifield stimulation, canpossibly differentiate. When measuring electrical activity in left and right primary visualcortex, there is a clear discrepancy in response to the stimulation of either hemifield inHH. Usually a (near) normal response is measured when stimulating the intact hemifield,whereas either no signal, or only a negligible signal can be picked up for the blindhemifield. In patients with pure neglect, responses to both hemifields are identical and(near) normal.
2.3. Visual fields: assessment and propertiesTo properly diagnose lost visual field function (e.g. HH) and alternatively residual (e.g.macular sparing) or restored visual field function, very precise assessment is required. Thecontroversy regarding macular sparing is a clear illustration of the importance of precisemeasurement techniques. Macular sparing, or the sparing of a small part of the central visualfield, has been reported in many cases of HH. Some authors report that about 70% of HHpatients show a visual field sparing of (less than) five degrees of visual angle (e.g. Kerkhoff,Munssinger, & Meier, 1994). Yet others have argued that this sparing is a measurementartefact caused by inaccurate fixation during perimetry (e.g. Bischoff, Lang, & Huber, 1995).However, using eye movement measurements and fixation control by scanning laserophthalmoscope (SLO), it was shown that macular sparing and even a small vertical strip ofhemifield overlap does exist (Trauzettel-Klosinski, & Reinhard, 1998). This finding does notdisaffirm that, in past research, the amount of macular sparing could have been overestimated.The most plausible explanations for macular sparing are dual blood supply to the occipitalpole and bilateral cortical representation of the fovea. Controversy exists as to which of thetwo mechanisms is responsible. The second explanation has however been challenged, forexample, by Gray, Geletta, Siegal and Schatz (1997).
Advanced measurement techniques are not always feasible in clinical settings. The mostcrude, but also the fastest method is the confrontational test. It involves the comparison of theVF of the examiner with that of the patient. A major disadvantage of this test is its lack ofstandardisation and the difficulty of reporting the findings objectively. For a more thoroughdiscussion we refer the reader to Elliot, North, and Flanagan (1997). To enhancestandardisation and quality of the output, several perimetric techniques and devices can beused, which can be either automated or manually operated. Depending on the clinical orresearch question, static, dynamic (i.e. moving) or coloured targets can be used. With thesedifferent types of targets, different functional channels or regions of the visual pathway can beprobed.The Goldmann technique is a widely used manual perimetric test with moving (usually white)targets. To quantify the status of visual fields exactly and to ensure the quality of follow-upmeasurements, automated perimetry in combination with continuous fixation control has beensuggested (Schiefer, Skalej, Dietrich and Braun, 1999). Examples of such devices in clinicaluse are the Tübinger Automated Perimeter (TAP) and the Humphrey Field Analyzer (HFA).

Part II: Visual rehabilitation101
Using these techniques, visual field regions can be described as intact or deficient. Inaddition, reference can also be made to ‘grey areas’, as opposed to white (intact) and black(deficient) sectors. A grey area, or relative defect, is an area in the visual field with onlypartial function, for example, residual performance in light detection. It is presumably theresult of spared neuronal fibres in the damaged visual pathway. These areas are usuallysituated between an intact and a deficient area and are therefore also called ‘transition zones’.A transition zone must be distinguished from an island of residual vision in a blind area. Insuch an island of residual vision there is intact visual function. In contrast, a transition zonehosts only inconsistent light detection. Subjectively, stimuli in transition zones are reported asreduced in clarity, brightness or brilliance (Kasten et al., 1999). By assessing and mapping allthese aspects of the functioning of the visual fields, a detailed and precise description ordiagnose concerning the VFD can be provided.
3. RehabilitationWe will extensively discuss rehabilitation efforts for HH patients. As already mentioned, weare not aware of extensive, structured, evaluated specific treatment attempts for relatedhigher-order visual disorders, other than for neglect. We will first briefly mention the fewapproaches to related disorders. Since neglect is the topic of another chapter, we will again bevery brief. We would like to point out that the treatment attempts for HH could also beapplied to the patients with other co-occurring visual disorders. These rehabilitation effortscan have beneficial effects when, for example, a defective scanning strategy, caused by theHH, exacerbates the other disorder. In such cases, partial improvement can be expected. Butsince the treatment approach is specific for the HH, the other co-occurring dysfunction byitself might not improve.
3.1. Visual disorders related to Homonymous HemianopiaSince homonymous VFDs are caused by post-chiasmal brain damage, several other disorderscan co-occur. The type and severity of the related disorders will depend on the size andlocation of the brain damage involved. Higher-order visual disorders include visual agnosia,prosopagnosia, visual neglect, Balint's syndrome, visual illusions and hallucinations. Attemptsto treat visual agnosias are very rare. The main therapeutic approach seems to be to improvevisual recognition by using non-visual cognitive strategies, such as context information. Zihland Kennard (1996) report that no systematic study of the treatment of Balint's syndrome hasbeen attempted. Their own success in treating three patients with Balint's syndrome and threepatients with agnosia was rather limited. The method of treatment of visual illusions andhallucinations depends on the underlying cause. Possible causes are epileptic phenomena,visual deafferentation, delirium, drug intoxication and withdrawal states. When the disorder isdrug related, withdrawal of the drug usually leads to rapid resolution. When it is the result ofabnormal neuronal discharges, anticonvulsants are prescribed. Interestingly, the disorder alsoresponds well to some types of anticonvulsants when caused by reduction of visual input.Zihl and Kennard also note that, so far, no treatment procedure has been reported for other(lower) visual dysfunctions, for example, impairments in spatial contrast sensitivity, light anddark adaptation and colour vision, that have been caused by brain damage.
Almost all therapeutic approaches to neglect are based on some type of cueing. Only a veryfew have been shown to result in lasting improvements. We shall restrict ourselves here to

Part II: Visual rehabilitation102
listing briefly some therapeutic approaches and some references. One group of therapeuticapproaches can be classified as visual-cognitive training programs. This type of approach waspioneered by Diller and Weinberg (1977). Its principles have recently been successfully(re)applied by Pizzamiglio and colleagues (e.g. Pizzamiglio et al., 1992). Other approachesmake fewer demands on cognitive functioning. Robertson uses left limb activation to treatvisual neglect (e.g. Robertson, North, & Geggie, 1992). Caloric stimulation (left ear by coldwater or right ear by warm water) is another example of a non-cognitive treatment method(e.g. Rubens, 1985), as are eye-patching (e.g. Butter and Kirsch, 1992), use of optical aids(e.g. Rossi, Kheyfets, & Reding, 1990) and neck muscle vibration (e.g. Karnath, Christ, &Hartje,1993).
3.2. Homonymous Hemianopia3.2.1. Spontaneous recoveryActive intervention has to be differentiated from (passive) spontaneous recovery andspontaneous adaptation. One might argue that, if spontaneous improvement (either recoveryor adaptation) is expected, therapeutic intervention is not needed. But even if spontaneousimprovement can (still) be expected, therapy should not be denied to the patient. He or shemay develop erroneous compensatory strategies or may become depressed while waiting forintervention (Zihl & Kennard, 1996).Kerkhoff (1999) estimated that in 15% of patients with CVA, spontaneous field recovery ofvariable extent occurred within the first two to three months after brain lesion. Some very rarecases have been reported with longer recovery periods. Due to higher cortical magnificationfactors for peripheral visual fields, field recovery has been reported to be larger in theperiphery (about seven degrees) than in foveal regions (about three degrees) (Kerkhoff, 1999).Higher cortical magnification factors indicate that the visual cortical representation of thefovea is much larger than that of the peripheral retina. As a consequence (to put it simply), aparticular small area of cortex is devoted to a very small area of foveal retina, while an area ofcortex of the same size will respond to a much larger area of peripheral retina. Most fieldrestorations appear to affect peripheral visual fields and are rather small. This raises thepossibility that these limited structural gains will not necessarily lead to significant functionalimprovements other than in performance on perimetric tests. Concerning the quality of vision,Zihl (2000) states that recovery of light sensitivity is typically followed by recovery of colourand form vision. If at all, not all functions are to be restored completely. This is the case inhemiamblyopia, where the recovered region only subserves light detection, and even this mayalso be subnormal.On the basis of eye movement recordings, Zihl (1995) estimated that nearly 60% of HHpatients do not show effective compensatory oculomotor behaviour. It is our opinion thatthere are at least two reasons for this. One reason relates to the lack of awareness of the VFDand the other to the attentional capture phenomenon. As Zihl (2000) correctly points out, it isvery plausible to assume that, if patients are fully aware of missing half of a visual field, theycan spontaneously use adaptive eye movements to compensate for the visual field loss. But asalready mentioned, very few HH patients are aware of their VFD. It seems that patients haveno direct experience and no direct sensation of the absence of vision, so that the visual fieldloss has to be inferred or deduced from visual experience and, in particular, from failures. Itfollows that awareness is never immediate and is more dependent on cognitive abilities suchas memory, and probably also on motivation and personality. This means that compensationwill rarely be automatic and is usually the product of a conscious learning process.

Part II: Visual rehabilitation103
There is a second reason why compensation is not automatic. Attentional capture, and morespecifically the proximity effect, causes eye movements away from the VFD, which isdeleterious for effective compensation. Visual targets can attract attention (attentionalcapture) and consequently elicit eye movements towards them. As a result of the proximityeffect, which refers to the tendency of the eyes to move to the nearest target, targets close tofixation capture attention and elicit eye movements. Since in HH these targets are bydefinition in the preserved hemifield, the eyes have a tendency always to move in thatdirection. Effective compensation, however, requires eye movements in the oppositedirection.
3.2.2. Rehabilitation methodsRehabilitation aims at reducing the degree of the patient’s handicap or participation. This canbe accomplished by restitution, compensation or adaptation. Restorative approaches operateon the level of impairment and aim, in HH, at (partially) restoring or enlarging the lost visualfield. Their success is usually measured by conventional perimetry, indicating structuralimprovement of the visual field in quantitative and/or qualitative terms. Compensationoperates on the level of disability (or activity). It entails replacement of the lost visualfunction (e.g. a hemifield) by another function (e.g. eye movements). Compensation thusimplies behaviour by the patient and is therefore usually assessed by tasks which closelyresemble activities of daily living (ADL). Adaptation can imply adjustment of the patient oradjustment of the environment. Adjustment of the environment is usually not considered to bethe expertise of neuropsychologists but of ergonomists and videologists1. The major emphasisin environmental modification consists of concentrating objects in the seeing hemispace. Forexample, rooms could be organised, so that when the patient sits in his or her ‘comfy chair’,nearly all objects are situated in the seeing hemifield. In the following discussions only theadjustment of the patient will be considered.
3.2.2.1. RestorationAnatomically, the visual system is very strictly organised with very dedicated and specifichard-wired neuronal connections. It therefore seems unlikely for any type of restitution to bepossible. However, there are clear hints at visual system plasticity leading to (partial)restoration of some visual function.
Inducing structural visual field enlargements has been shown to be possible. Some studies atthe beginning of the 1980's and some remarkable cases have been the basis for the optimismconcerning the possibility of inducing some restoration of lost visual function.The earliest studies suggesting induced recovery (e.g. Zihl and von Cramon, 1985) showedsignificant decreases in the extent of the scotoma after repetitive stimulation with light stimuliat the borders of the scotoma. However, most of these early studies suffered from majormethodological problems in the evaluation of the success of the treatments: too little time postlesion, large measurement variability, possible eccentric fixation, changes in detectionstrategies by the subjects and reliance on subjective clinical impressions. Most of theseproblems were later overcome and it was concluded that minor field enlargements (rangingfrom five to twelve degrees) were evident in some of the studies. This hinted at the possibilityof restoring visual fields (Kerkhoff, 1999).
1 Videology regards the research and rehabilitation of visual function due to impairments of the sensory,oculomotor and central nervous system.

Part II: Visual rehabilitation104
Further optimism about the possibility of substantial restoration of lost visual function hasbeen aroused by some remarkable cases which have shown that it is in principle possible toinfluence, at least temporarily, underlying brain structure so as to regain some visualfunctions. Nadeau, Crosson, Swartz, & Heilman (1997) describe a patient with a left-sidedsuperior quadranopia, who showed significant structural enlargement of the visual field whengaze was directed to the far right. Regional blood flow measurements showed a non-specificincrease of nearly 40% in the activity in the damaged hemisphere in this posture. The authorsconclude that these gaze related alterations in visual function and synaptic activity suggestengagement of some form of arousal-like mechanism, since the changes in cerebral bloodflow were broadly distributed rather than restricted to specific areas known to be related tovisual processing. Another remarkable case was reported by Trexler (1998). This patientdemonstrated attentional control over the size of her VFD. More specifically, shedemonstrated the ability voluntarily, or intentionally, to modify/reduce her right homonymoushemianopia to a right upper quadranopia. Her ability to do so, was constrained bymechanisms and manipulations typically related to attention (e.g. fatigue, and stimulusdensity). Perimetric results were complemented by PET imaging techniques suggestingsignificant increases in regional blood flow in several broadly distributed brain areas. Clearlysuch cases are very rare and, in consequence, the mechanisms involved (extreme ipsilesionalgaze and volitional control) are of limited use for application in rehabilitation in general.However, they indicate that restoration of visual function by changing visual processing at thebrain level is a possibility.
3.2.2.1.1. Restoration methodsRecent studies of the induced restoration of visual fields by restorative training have beensummarised by Kasten et al. (1999, see table 2). Several types of studies show inducedrestoration of the VF.Recently, computer based training programs have been developed to stimulate the transitionzones systematically (e.g. Kasten, Strasburger, & Sabel, 1997; Van der Wildt & Bergsma,1997). In a randomised, double-blind, placebo-controlled experiment with nineteen post-chiasmatic patients with VFDs, Kasten and co-workers trained an experimental group forapproximately 175 hours with their computer based Visual Restitution Training (VRT)-program. During VRT, hundreds of light stimuli are presented in succession in the transitionzones. The placebo group performed a fixation training, which required foveal visual search,for a comparable amount of time. The experimental group showed an average increase of 5°in field size. The placebo group showed an average decrease of 1°. Furthermore, the positiveeffects of light detection in the experimental group generalised to colour and formdiscrimination within the crucial areas. The investigators also report some transfer toperformance on paper-and-pencil tests of visual exploration and attention. Further, positiveinfluences on activities of daily living were reported by 72% of the patients from theexperimental group, in contrast to only 17% from the placebo group. These results arepositive and clearly promising, but we would like to caution against too much optimism.Indeed, a 5° increase of VF seems impressive, since as little as 2-3° of foveal vision isgenerally sufficient for reading. However, it is not clear from the report whether therestoration indeed affects foveal vision, and a 5° shift of the visual field border in peripheralfields will have much less functional significance. But then again, it remains unclear to ushow a 5° shift of the visual field border can lead to such impressive subjective improvements.

Part II: Visual rehabilitation105
Not all studies which show evidence of VF restoration had this as their aim. Kerkhoff (1999)reports that saccadic and visual exploration training (a compensatory rather than a restorativerehabilitation approach) also led to a small but significant increase in visual field size (five toseven degrees) in nearly one-third of their patients. This increase is most likely due to theprocedures and techniques used in their compensatory therapy, which are also applied in therestorative training methods, namely repetitive stimulation in transition zones. It thus seemsthat VF restoration can also be attained as a ‘side effect’ of compensatory therapy.
3.2.2.1.2. Mechanisms of restoration of vision and implication for rehabilitationAs is pointed out by Sabel (1999), the plasticity of the human visual system is probably vastlyunderestimated. Sabel argues for a review of the concept of hard-wired visual pathways withstrict, fixed and unchangeable topographical organisation and receptive field properties. Thedominant issue in current discussions of the neural mechanisms, which underlie therestoration of vision, is the role of surviving tissue. Survived fibres within the visual pathwaysmay explain residual and restored vision. There is, however, also the possibility of re-routing.That is, an alternative brain structure takes over the function of the disrupted pathway. Forexample, if the retino-geniculo-striate (‘new’) visual pathway is injured, the retino-tectal(‘old’) pathway might be used to process and mediate some visual information, for example,movement. It is argued that at least some of the rare blindsight phenomena can be ‘explained’this way. Patients have been reported to be able to detect some targets (e.g. moving targets)presented in their blind hemifield. For a comprehensive review on blindsight, see Weiskrantz(1986). Since patients are usually unaware of this residual function and since it can sometimesbe measured only when they are forced to guess, there is little hope that training of ‘theblindsight ability’ in itself can be a useful therapy.
As previously mentioned, the role of surviving tissue dominates the discussion at present.Evidence from animal studies suggests that restoration of vision following brain injury is theresult of the combination of several factors and mechanisms (see Sabel, 1999; Kasten et al.,1999). The most crucial factor, however, seems to be the presence of a minimal number ofresidual neurons which have survived the injury. Sabel and Kasten further point out that brainstructures like the tectum, lateral geniculate and visual cortex probably play the mostprominent role in restoration. Plasticity, in their view, is (partly) due to rewiring in the formof changes in the size and location of receptive fields. We summarise some of their argumentshere.
First, when damage occurs in the receptive fields themselves, that is, following post-chiasmalbrain lesion, less improvement is expected. Indeed, it has been shown that visual fieldenlargement is larger in pre- versus post-chiasmic lesion groups. After pre-chiasmic lesions,there could be a take over of function by the intact neighbouring receptive fields in theprimary visual cortex. A Second argument favouring the involvement of receptive fieldchanges is that improvements in foveal regions occur slowly and are small. The receptivefields for the foveal regions are indeed numerous and small at the V1 level, while receptivefields for peripheral visual field regions are large (cortical magnification factor). Third, theinvolvement of receptive fields allows the possibility of axonal sprouting or the establishmentof new synaptic connections. New lateral connections between neighbouring receptive fieldscan be formed by this mechanism. Alternatively, the disinhibition of silent synapses couldalso be a mechanism influencing receptive field properties. Following disinhibition, pre-

Part II: Visual rehabilitation106
existing but inhibited connections could be activated by the lesion. A final mechanism whichhas been proposed to influence receptive field properties is an increase in synaptic efficiency,for example, by reducing the firing threshold of the few survived neurons so as to increasetheir performance.As a more general remark, but also as a result of the mechanisms proposed to be responsiblefor restoration, the authors caution that there is never complete restoration and that somevisual dysfunction always remains.
Since restoration seems limited and laborious, the obvious question to be answered before theimplementation of training aimed at restoration in rehabilitation settings, is which patients arelikely to benefit? Kerkhoff (1999) suggested that patients with incomplete lesions of thevisual pathways are likely to benefit from restorative training. These patients show someresidual perception of moving targets, the presence of relative scotomata and shallowgradients in the profile of light sensitivity in the scotomata or some striate cortex activity inPET or during fMRI. All these indicators presuppose some spared cortical structure. Thissparing does not need to be massive. Sabel and co-workers argue that as little as 10% of alesioned cortical structure can be sufficient to enable nearly 90% of the normal function ofthis structure.
3.2.2.2. Adaptation: Auxiliary Optical DevicesAnother therapeutic approach is to adjust the patient to theenvironment. This can be achieved using optical aids.Different types of optical devices have been introduced forvisual field rehabilitation purposes. Among these aredevices such as mirrors, partially reflecting mirrors (beamsplitters), reversed telescopes, glass prisms and fresnel(press on) prisms. Such devices can be incorporated intospectacles and have been applied in rehabilitationtechniques, alone or in combination, as monocular (appliedto one eye) or binocular systems (applied to both eyes) (seefigure 2 A-B).
Cohen (1993) provides an overview of techniques used forperipheral field loss. In the following discussion, we willfocus mainly on the prism-approach. Many of the features(both positive and negative) of the prisms are alsoapplicable to the mirrors.The rationale behind the use of prisms is to shiftinformation from the non-seeing side closer to the seeing side. This can be actualised bywedge-shaped prisms with the base positioned towards the blind hemifield. Two effects canbe accomplished with these devices: field relocation and field expansion.
3.2.2.2.1. Field relocationField relocation changes the position of the field loss relative to the environment causing anoptical displacement of (a part of) the visual field. A part of the environment, which was notvisible, now appears. At the same time a different part of the same angular span becomesinvisible and thus disappears, as it is replaced by the previously unseen part of the visual field.
Figure 2 A. A binocular sectorprism.
Figure 2 B. A monocular fullprism system for upper and lowerfields.
From Peli (2000a). © Swets &Zeitlinger. Used with permission.

Part II: Visual rehabilitation107
Binocular full prisms and sector prisms provide only for field relocation. Binocular fullprisms (the entire carrier lens is covered by the prism) induce field loss in the far periphery onthe seeing side. As they are full prisms, they generate this effect independently of eye andhead position.
A binocular sector prism (figure 2 A.) covers only a part of the carrier lens. It is usuallymounted in and near the edge of that portion of the lens corresponding to the non-seeing field.As a consequence, there is natural viewing in primary gaze: one sees an unshifted view whenlooking straight ahead (with the eyes). As gaze moves towards the non-seeing field, itencounters the prism-area and one sees an image which is shifted in the direction of the apexof the prism. This ‘image jump’ or ‘prism jump’, which occurs at the junction of the prismedge, induces an optical scotoma in the centre of the field and is called the jack-in-the-boxphenomenon (Cohen & Waiss, 1996). Objects in that part of the world (angular span equal tothe prism-power in degrees ) will disappear, but may pop into view with head movements.This is where the name ‘jack-in-the-box’ comes from: a toy with a clown’s head (‘Jack’) on aspring, which is put into a box with the spring compressed. When the box is opened, theclown’s head pops all the way out.
3.2.2.2.2. Field expansionThe jack-in-the-box scotoma in a binocular system can be compensated for by headmovements (and partly by eye movements). However it can be overcome by fitting the prismsmonocularly. A monocular sector prism expands the field. Contrary to field relocation, fieldexpansion indicates that the field seen simultaneously is larger with the device than without it(Peli, 1999). Field expansion can be accompanied by central diplopia and confusion. Diplopiameans double vision and should be avoided when possible. It is the most frequently reportednegative side-effect as it is very disturbing. Confusion refers to the perception of two differentobjects in the same perceived direction or at the same spatial location. It thus refers to thesuper-imposition of what is seen with the prism over what is seen without the prism.Importantly, this confusion is the desired effect, because one of these two objects waspreviously unseen.
3.2.2.2.3. ApplicationsThe Visual Field Awareness System (VFAS) approach of Gottlieb, Fuhr, Hatch, & Wright(1998) incorporates a sector prism mounted in and near the edge of the patient’s blindhemifield. It is a monocular system, where the prism is preferably mounted before the eyeipsilateral to the visual field loss. The authors conclude that for most patients, VFAS not onlyimproves visual awareness and increases measured recovery of vision, but also improvesemotional outcomes and increases independence. The main drawbacks are the associatedproblems of central diplopia and confusion. This might explain the negative correlations ofsuccess with age. The initial rejection of the system by the older patients could perhaps be(partly) overcome with time, practice and vision rehabilitation therapy, although the meannumber of treatment sessions for most patients was more than twenty, with each sessionlasting up to three hours. Another disadvantage, in the case of field restoration, is theprogressive repositioning of the prism, which has to be mounted near the edge of the non-seeing field. The vast investment of time and money in the optical adjustments, theaccompanying vision rehabilitation therapy and the problems experienced by older patientsare clearly negative aspects in rehabilitation terms.

Part II: Visual rehabilitation108
As is the case with all sector prisms (monocular or binocular), the effect of this type of systemis limited to instances when the line of sight is directed through the prism sector itself. Thuswhen gaze is at the primary position or directed away from the hemianopic field where theprism is fitted, the sector prism has no effect on the field of view. The obligatory direction ofgaze is a clear drawback because it requires intentional scanning. A slightly larger eyemovement can have the same result in term of field exploration, rendering this prism systemperhaps even superfluous.Peli (1999, 2000a, 2000b) developed an alternative system, with these considerations in mind.His type of hemianopic visual aid expands the field, rather than relocating it. Moreover,intentional scanning is no longer required to benefit from the effects of the prism, as itfunctions in all positions of gaze. And finally, Peli’s system avoids central diplopia. Theseeffects are accomplished by using monocularsector prisms limited to the upper and/or lowerperipheral fields and placed across the wholewidth of the carrier lens (see figure 2 B). Figure 3shows an example of an upper sector prism onthe left carrier lens (the prisms are indicated bythe arrow). As the prisms only shift an upperand/or lower peripheral part of the blindhemifield to the seeing hemifield, they produce confusion only at those locations providingthe field expansion. The combination of these properties results in a system which acts as adetection aid. Stimuli from the non-seeing hemifield can now be detected without activeexploration. To put it simply: some (peripheral) parts of the non-seeing hemifield are shiftedand added to the seeing hemifield. For illustration of the prism-effect, we refer to Peli (2000bfigure 3) and to http://www.eri.harvard.edu/faculty/peli/index.html, where the prism-effectcan be observed in a video simulation.The patient is instructed to fixate only through the carrier lens, not through the prism. Thisway, the desired field expansion is the result of continuous peripheral diplopia (which is verymuch less disturbing than central diplopia) and continuous peripheral confusion. Only objectsfrom the seeing hemifield over the height of the prism segments are seen in diplopia, that is,only objects in the upper and/or lower periphery. Peli (1999, 2000a, 2000b) reports expansionmagnitudes of fifteen to twenty degrees. A further advantage of this type of prisms is that theambiguity that may be associated with the confusion can be reduced. Namely, the objects seenthrough the prisms (shifted) and those seen through the carrier lens (not shifted) can bedistinguished by a spectral cue. The shifted images actually appear slightly distorted in termsof resolution and colour. The ‘peripheral’ side-effects and the reduction in ambiguity canfacilitate adaptation to the system.As previously mentioned, in Peli's approach, the patient is instructed not to look through theprism to avoid central diplopia. Shifting information from the non-seeing side and adding it tothe seeing side, restores the possibility of detecting this visual information. Once an object ofinterest has been detected in the periphery and its location determined (seeing or non-seeingside), it can be inspected and foveated through the carrier lens by making head movements.Since eye movements usually precede the head movements, this requires a new and adaptivetype of gaze and viewing style. Peli (1999, 2000a, 2000b) reports that subjects are instructedonly in the care and use of the prism and therefore assumes this new viewing style will resultfrom an implicit learning process.
Figure 3. Example of a monocular upper prism.
Peli (1999). © Optical Society of America Used withpermission

Part II: Visual rehabilitation109
Of the twelve patients evaluated (Peli, 1999; 2000b), eleven showed the expected fieldexpansion on binocular visual field testing. In contrast to other authors, Peli makes no specialmention of adaptation (or other) problems specific to elderly patients. A crucial factor for thesuccess of the system is, however, intact binocular function. The adaptation period was two tothree weeks per prism and almost all patients reported significant improvement in theavoidance of obstacles after that time. Three patients with a considerable follow-up period ofone year reported large improvements in daily life functioning. Two of them also resumeddriving.
As this type of rehabilitation is relatively new, further improvements and refinements can stillbe expected, as also suggested by Peli (2000b). Further investigation is needed on somecritical points. For example: the effects and necessity of eye and head movements when usingsuch devices need to be considered. Clearly, using this hemianopic visual aid effectivelyrequires a new viewing style. Research on how to teach patients (quickly) to adopt this isneeded. Also the possibilities and limitations of the (cognitive) adaptation process should befurther investigated. The influence of the visuo-spatial distortion that is introduced, and itseffect on the mental representation of space is a question which is not only very interestingbut also crucial for the broader and general use as a rehabilitation method. More specifically,the exact nature of the adaptation (for a suggestion see Peli, 2000b), and the presence of after-effects should be closely investigated.
3.2.2.3. Compensation3.2.2.3.1. Compensatory programsAnother therapeutic approach is the compensation approach. It is fundamentally differentfrom the previous approaches, in that visual input is not altered or changed, but interventionrather focuses on search and scan behaviour. The aim is to enhance the patients’ ability toexplore their blind hemifield. These types of training methods are sometimes called‘awareness enhancement training’ because it is assumed that the patient is trained to be awareof the deficit and to use compensatory eye and head movements for scanning the blind field.It can be a valid alternative and/or complement to the restorative training approaches, sincefield recovery, spontaneous or induced, is rather limited even after extensive training. It canalso be a sound alternative and/or complement to the use of auxiliary optical devices becausesome types of (prism) systems demand intentional scanning (and thus compensation) if theyare to be effective. Other optical systems create new visual problems, like diplopia andconfusion, to which patients must adapt. Adaptation entails implicit learning and could (atleast partly) be accomplished by compensatory behaviour.
The structure and aim of the compensatory therapies reflects the most frequently reportedproblem after visual field loss namely defective visual scanning and exploration (Zihl, 2000).The visual scanning pattern in hemianopic patients can be characterised by small-amplitude‘staircase’ saccades towards the blind hemifield and frequent repetitions of the scan pathsduring search. Increased search times are observed, most pronounced in the blind hemifield,as is a lack of large-scale saccades promoting global spatial orientation (Kerkhoff, 1999).These saccadic or oculomotor problems are at the basis of the saccadic compensation trainingmethods. They have been introduced, explored and used, for example by Zihl and von

Part II: Visual rehabilitation110
Cramon (1985), Zihl (1994, 1995), Kerkhoff, Münssinger, Haaf, Eberle-Strauss, and Stögener(1992) and Kerkhoff et al. (1994). These studies confirm that compensatory strategies can betaught successfully in 10-25 training sessions of about 45 minutes spread over 4-6 weeks. Thegeneral structure of these compensatory treatment approaches can be summarised as follows.Training starts with simple tasks which become progressively more complex. In a first phase,large amplitude saccades towards the blind hemifield are trained using computerisedprograms. This type of eye movement makes it possible to glance over visual space quicklywithout omitting a (portion of the missing) hemispace. Training is usually done in a perimeter(e.g. Zihl, 1995) or on a large computer screen (e.g. Kerkhoff et al, 1992, 1994). The patientis asked to detect and fixate stimuli in the blind hemifield as quickly as possible. Stimulusonset is usually accompanied by an acoustic signal. It is continuously stressed that the patientshould move his/her eyes with one large sweep and not in a step by step manner. Zihl (1994)reports that it takes approximately 400-600 trials for the patient to increase this type of eyemovement. In a second phase, a systematic search pattern, enabling the patient to search blindand intact hemifields without omitting relevant items, is demonstrated and learned. Patientsare encouraged to adopt a systematic row-by-row or column-by-column strategy and starttheir search on the side of the blind hemifield. This has been operationally defined as, forexample, ‘search on projected slides’ (Kerkhoff et al., 1992; Zihl, 1995). In a final step, thecompensatory strategies are trained in everyday life situations. In the study by Kerkhoff andcolleagues (1992), (visual) activities of daily living (ADL) relevant to the patient (e.g. findinga particular spice on a shelf) were listed and subsequently trained, whilst promoting the newlylearned visual strategies.Results show that, with this type of training, a clear improvement can be observed on severalvisual tasks. Zihl (1994) reports that, in a group of 126 patients, the mean extent of the fieldof search increased from 12° to 36° on the side of the blind hemifield, and search timesdecreased by more than 50%. In the study by Kerkhoff et al. (1994), similar improvement inoculomotor function was observed. Transfer to non-trained tasks was also measured:reduction of errors in search tasks, subjective improvements of visual functions as measuredby questionnaires and return to work by 91% of the patients. These results werecomplemented by studies which recorded eye movements, and which reported a normalisationin the number of fixations and refixations and in rates of repetitions of scan paths followingthis type of compensatory training (Zihl, 1995). Since the mean increase in saccadicamplitude was significant but rather small (about 1°), the normalisation is presumablyaccomplished by the acquisition of a systematic, more spatially organised scanning pattern,which has its effect on the entire field of vision.
It is interesting to note that some restitution of the visual field was observed by Kerkhoff et al.(1992) in patients who had followed compensatory therapy. Mean visual field increase aftertherapy was 5° for 37 of 92 patients with visual field defects. The increase for the neglectgroup with VFDs (VFD+) reached 12° for 10 of the 30 patients. Thus in nearly one-third ofthe patients, a partial restitution of the visual field was observed. From the previousdiscussion of measuring visual fields, it should be clear that unless very precise control offixation is guaranteed, the observed improvements can only be regarded as approximations.Further, the authors do not describe exactly where the improvements were located (centralversus peripheral visual field) so that the improvement in functionality cannot be fully beappreciated.

Part II: Visual rehabilitation111
Another interesting and important observation by Kerkhoff et al. (1992) is that frequent headmovements had a clear negative effect on the success of the compensation training. Patientswho made no head movements received on average 12 treatment sessions. This numberincreased to 21 and 26 sessions for the mid-frequent and frequent groups respectively. Thereason suggested for this is that these head movements are too slow for rapid orienting. Thisclearly contradicts the assumption that head movements are a helpful compensatorymechanism for VFD patients. This should be taken into account when devising therapeuticmethods.
3.2.2.3.2. An integrated saccadic compensation trainingWith these principles and positive findings in mind, we devised a similar approach. Ourmethod combines previously mentioned principles of saccadic compensation training withprinciples and materials from the neglect rehabilitation training by Pizzamiglio and co-workers (e.g. Pizzamiglio et al., 1992). Our aim is to combine positive aspects from severalapproaches so as to facilitate the learning of an optimal compensatory strategy, which isintegrated in a personal scanning style, and applicable in all daily life situations.
Our program contains three consecutive phases, each of which can last for a maximum of 6hours. In the first phase, compensatory saccadic eye movements are trained. To enhancetransfer, in the second phase the eye movement principles are applied in several tasksrequiring efficient scanning behaviour. Some tasks from phase two had their origins in theneglect rehabilitation program of Pizzamiglio’s group (e.g. Pizzamiglio et al., 1992). In thethird and final phase, the newly learned visual style is practised in daily life, again to enhancetransfer. Unlike the original saccadic compensation training programs, we chose one taskfrom daily life with a high practical and social value, and a large and highly demanding visualscanning component, namely driving a car. Patients have then to apply their scanning stylewhile driving a car, in real traffic, under the close supervision of a driving instructor.
In the following paragraphs, we will try to give the reader a clear impression of how thiscompensatory training is carried out. We will therefore mainly focus on the principles,procedures and methods, minimising reports on results.
4. The Integrated Saccadic Compensation Training Program4.1. Establishing global understanding of visual problem and general aim ofrehabilitation programAll training sessions are on a one therapist–one subject basis. Before the first phase begins,primary visual functions are assessed and discussed extensively with the patient. Our patientgroup had normal or corrected to normal vision, except for the apparent VFDs. The existenceand the cause of the VFD is shown, demonstrated and explained to the patient by means of theperimetric output and by confrontation. When available, scans from imaging techniques werealso shown. Becoming aware of and understanding the nature and cause of the visual problemis believed to be the first step towards compensatory behaviour. Awareness of the deficitrequires its discovery. The patient frequently does not directly sense but rather discovers theabsence of the hemifield. The demonstration of the difference in perception in blind and not-blind hemifields was a very unpleasant surprise for some subjects, which shows that not allhemianopic patients are aware of their visual field defect (as previously discussed). Each ofthe three phases starts with a statement of the aim of the training involved, so as to further

Part II: Visual rehabilitation112
increase understanding and motivation in the patient. A relatively large amount of time isdevoted to explanation, understanding and instruction of the first training phase, as thesuccess of following phases is dependent on its success. In this first phase, the ‘tools’ areprovided which will have to be used in later phases.
4.2. First phase: Saccadic eye movement trainingIn the first phase, saccadic eye movements are trained. Our set-up enables us to projectstimuli on a large screen, covering an area of approximately 100° horizontally by 60°vertically. The software presents a single target (digit or symbol) at a prespecified location fora prespecified maximum presentation time. Presentation time can be individually adjusted,but is kept to a minimum to speed up the response by the subject. The task of the subject is toname the target as quickly as possible. This vocal response was captured by a voice keywhich terminated the presentation of the current stimulus and initiated presentation of the nexttarget. The interstimulus interval (ISI) could also be individually adjusted.The eye movement training is structured into several blocks of increasing difficulty, as will befurther explained. Patients run through the blocks in a fixed order, as each block incorporatespreviously trained principles. A block is offered only after the previous block has beencompleted successfully. Success is defined as running through the sequence without any stopor delay at the prespecified time parameters using the suggested principles (see further).Maximum training time is six hours.
4.2.1. Establishing understanding and aim of first phaseThe first session of the training begins by clarifying why we train eye movements. We explainthat when people without VFDs look straight ahead, they receive visual information fromboth hemi-spaces while our patients receive only half of this information. As a consequencethey need to acquire the missing information actively. One (and in our view a very efficient)way of doing this is by employing the type of eye movements we are about to train. Thus, firstit is stressed that the rehabilitation program aims at making frequent, large and fast saccadiceye movements into the blind hemifield (and back). These eye movements should be largeand fast in order to create an overview of the full (hemi)space quickly. They should befrequent in order to anticipate new events and/or changes in the blind hemispace.Secondly, we explain that priority should always be given to the movements of the eye, andnot to movements of the head. The difference between eye and head movements is explainedby demonstrating both possible ways of compensating. We explain that it is amisunderstanding to think that head movements are the only way of compensating for a visualfield loss and that, sometimes, head movements can lead to the belief that one iscompensating while in fact one is not. This is illustrated by making head movements whilesimultaneously making contralateral eye movements. To demonstrate this, the therapistfixates a point (e.g. the nose of the patient) while making large head movements. With thisdemonstration, it can be shown that the missing hemifield is linked to the position andmovements of the eye, rather than the head. Other advantages of using eye movements arethat they are faster and more accurate than head movements. Furthermore they cannot lead toneck-muscle complaints. For this reason, at the start of the training, the patient is stronglyurged not to make any head movements at all. During the course of the training, as theamplitudes of the required eye movements become larger, it becomes impossible not to movethe head. At that time, it is explained that in this instance the head and eye should collaboratein a sort of ‘rubber band way’. The emphasis remains on the movements of the eye, while the

Part II: Visual rehabilitation113
head only assists at the last stage of the movement. Thus, the eye moves first and the headfollows in a second step.Finally, we emphasise the importance of overshooting the target. An overshoot means(deliberately) making an eye movement which is too large. This is stressed by pointing out thehazards of an undershoot. We explain and demonstrate that when an eye movement into theblind hemifield undershoots a target, this target cannot be detected. In this case, the patientcannot be certain about the presence of a target: either there is no target and he/she can safelyglance somewhere else or the target was missed because it was just a bit further away (in theblind hemifield). The safest action at that point is to check further laterally into the blindhemifield for a possible target. At the next, and all following fixations, this uncertainty willrecur. This leads to an extensive and time consuming, piecemeal scanning pattern with manysmall amplitude saccades. This can be prevented by performing an overshoot as the startingsaccade. ‘Jumping’ to the extreme end of the blind hemispace shifts all possible targets intothe intact hemifield so that they can be detected. Absolute certainty about the presence of atarget can be acquired only with one (large and fast) eye movement.
This part of the training is concluded by emphasising that the principles learned should beintegrated into a new personal scanning style, which is adapted to the patient’s specific VFD.
4.2.2. MethodThe method used to elicit the desired type of eye movements isdifferent from previous reported approaches, where only anacoustic signal indicates the presence of a target. With ourmethod, we provide predictability in time and space for alltargets. We elicit the desired eye movements by a sequence ofthree events (triad) (see figure 4). The triad principle ismaintained throughout the entire eye movement training. The firstevent or target in the triad is the ‘orientation point’. This pointinitiates the sequence and determines the orientation and positionof the head. The subject knows that from this point on, the orientatifixed. The orientation point is followed by a small and easy hmovement (into the seeing hemifield). This second event is alwhorizontal contralateral eye movement (into the blind hemifield). Itaction is the one to be trained and that the previous actions are for pBy explaining and maintaining this triad, the patient can predict the upossible to program and prepare all eye movements. Further, by usiare defined in time and space. The subject is strongly encouraged toplan and program the eye movements. The training starts with oneillustration. This simple sequence is repeated several times, forming following block, the same triad (and repetitions of it) is presented onprojection screen so that eventually the same triad is performed on side of the screen with respectively a left (initial) head orientation,head orientation and a right (initial) head orientation. In this way, texperience that the same eye movements can be performed withposition. In the next set of blocks, the amplitude of the contrasystematically enlarged. When the amplitude becomes too large, heausing the previously described principle (rubber band view). The ini
3 1 2
Figure 4. Event 1-3 of atriad in the case of a leftHH.
on of the head should beorizontal ipsilateral eye
ays followed by a large is stressed that the thirdreparation purposes only.pcoming event making it
ng a fixed ISI, the targets use this predictability to triad as in the previous
a block of practice. In the another part of the largethe left, middle and right a straight ahead (initial)he subject learns through a totally different headlateral eye movement isd movements are allowedtial head position is to be

Part II: Visual rehabilitation114
restored, as soon as the orientation point reoccurs. The different amplitudes are again repeatedon different parts of the screen (‘same eye movements, different main head orientations’-principle). In this set of blocks, the basic features of the program are trained: contralateral eyemovements which are frequent, large and fast.
In the next blocks, four triads occur within the same blockforming a ‘chain’. The chains are repeated several times. Thetriads are identical except for their vertical position (see figure 5).They thus vary by row, starting at the top, moving downwards.As a consequence ,all (four) orientation points are verticallyaligned, as are events two and three. This again results in perfectpredictability of the target positions. Thus, within one chain, alarge part of the screen is systematically covered by four largecontralateral eye movements. The same logic is applied asbefore: the location of the chain on the screen is varied and theamplitude of the contralateral eye movement within the chain issystematically enlarged.The next set of chains is composed of identical but horizontallydisplaced sequences (see figure 6). Here, the initial head positionchanges within a block, but the eye movements remain identical.Again the amplitude of the contralateral eye movements issystematically enlarged. To end this set of blocks, the chains arefinally composed of horizontally and vertically varied identicalsequences. The order of the sequences within a chain remainsfixed. The amplitude of the contralateral eye movement is againsystematically increased. In this set of blocks the basics of theeye movements are incorporated into a systematic scanning pattern.In all previous blocks, the sequences within the chains were identical in terms of theamplitude of the different eye movements. To train the overshoot principle the previous setsare repeated, but the amplitude of the contralateral eye movements now becomesunpredictable (but remains large) (see figure 7). Thus the patient is strongly encouraged toadopt a safe, quick but strenuousscanning pattern.The eye movement training isconcluded with a set of blocksconsisting of sequences with diagonaldirections (see figure 8). Allaforementioned principles andvariations are again applied.
4.3. Second phase: Application and integration of eye movements into the scanningpattern4.3.1. GeneralThe second step in the rehabilitation process is to learn to use this type of eye movementeffectively. In the first phase, all eye movements were elicited by using predictability in timeand space as a cue. In the second phase, the patient is encouraged to plan and generate the eyemovements endogenously. All tasks had to meet the following criteria. Firstly, the task had to
2
5
8
11
1
4
7
10
3
6
9
12
Figure 5. a chain of fourtriads for a left HHcovering a large part of thescreen.
9 6 3 7 4 8 5 1 2
Figure 6. Horizontally variedtriads in the case of a leftHH.
21
3
Figure 8. Triad for diagonaleye movements.
? ? ? 1 2
Figure 7. Triad for trainingthe overshoot.

Part II: Visual rehabilitation115
allow self-initiated eye movements so that most eye movements would be elicitedendogenously (in contrast to exogenously), making the patient an active participant in therehabilitation process. Secondly, the task had to be adaptive in that difficult levels werepreceded by easy levels. This way, performance could be improved gradually. Finally, thetask had to allow (almost) instantaneous feedback, either via evaluation by the therapist or bythe personal experience of the patient. These principles are important for motivation and forcorrective interventions, in the case of suboptimal performance.
For this purpose, we offered four different tasks with a large and difficult visual scanningcomponent. In order to perform these tasks successfully, an overview of the visual space inquestion has to be created and used either for recognition, comparison or action, as will beexplained further. The tasks selected, and the amount of time spent on them, depended on thespecific problems and interests of the patient. In total, a maximum of six hours of training wasgiven. The four possible training tasks were describing a picture, copying a matrix, readingand driving a car in a simple simulator. Care was taken to ensure that at least two differenttasks were attempted, usually finishing with the driving simulation. The reading training wasvery rarely chosen (it was perhaps to easy for this patient group). For this reason, it will not bediscussed here. The driving simulation was developed in our lab for this specific trainingpurpose. The other training tasks were adaptations of the neglect rehabilitation program fromthe Pizzamiglio group, (e.g. Pizzamiglio et al., 1992), for use with our HH patient group.
4.3.2. Picture descriptionA large variety of different pictures was gatheredfrom the internet: photographs, drawings, pictorialart of every day and imaginary objects and scenes,humans and animals. These pictures are presentedusing an LCD projector and a large projectionscreen allowing for picture sizes of up to 100° by90°. The task is to describe the pictures verballywithout omitting relevant items. To do this, thepatients have to scan a considerable size of visualspace effectively. They are expected to organise and plan the scanning strategy themselvesusing the large saccadic eye movements practised in previous sessions. This proved not to bea trivial task: imagine seeing figure 9 at 85cm viewing distance at a size of 220 x 165cm. Ittakes considerable scanning to survey, integrate and finally recognise the picture. Wheneverfull recognition or description fails (e.g. omission of an element in the blind hemifield), thetherapist intervenes and urges the patient to explore the picture more carefully. In the case of afailure of recognition, the therapist can assist in pointing out the important or relevant visualcues. When the patient is verbally less fluent, specific and directed questions can be askedabout the picture, so as to elicit full exploration. The patient could make use of a laser pointerto point at elements he or she was describing. This way, the therapist could evaluate theamount of visual space covered (when in doubt).
4.3.3. Matrix copyingThe original idea and principle was described by the Pizzamiglio group and has again beenadapted for our HH patients. A stimulus consists of two identical matrices of dots separatedby a midline. Each stimulus is presented on an A4 sheet of paper in landscape orientation (see
Figure 9. Example of a picture which had tobe described.

Part II: Visual rehabilitation116
figure 10). In one of these matrices a line pattern is drawnconnecting some dots. To elicit maximum scanning andexploration, the matrix with the pattern to be copied is alwaysipsilateral to the non-seeing hemifield. The level of difficultyvaries with number of dots making up the matrix (4, 6, 9, 16, 20and 25), the number and length of line segments to be copied, andthe number of lines that cross.
The standard task for the patient is to copy this pattern of lines onto the other matrix. Weadapted this task in several ways. First, when the patient makes one or more errors, thesecondary task is to find and correct them as quickly as possible. Second, when the patientmakes no errors at all, the therapist completes some extra matrices, either correctly orincorrectly. The patient has then to evaluate their completeness and correctness and, whennecessary, complete and/or correct the pattern.Patients are encouraged not to perform these tasks using a safe but piecemeal approach, thatis, exploring one dot at a time. Rather, they are asked to adopt a kind of ‘gestalting strategy’,that is, organising the line patterns and working with larger components. This way we elicitthe construction of an overview, using the eye movements learned in previous sessions.Further, we asked the patients, especially when they were finding and correcting errors, tobegin by inspecting the full pattern ‘broadly, widely and quickly’, so as to get a kind of senseabout its correctness and completeness. This was intended to promote global viewing andhence the construction of an overview of the matrices.
4.3.4. Driving simulationThe program developed in our lab presents a moving-roadscene similar to commercial racing games (see figure 11).Using an LCD projector and projecting on a large screen, thetotal scene covers approximately 90° by 75°. The patient facesthe screen and is first asked to keep the car in the middle of theroad using a steering wheel. The difficulty of the task is variedby introducing a weak or strong ‘sidewind’, which ‘pushes’ thecar randomly to the side of the road. In order to compensate forthis, the patient must make corrective steering movementsbased on their evaluation of the current position on the road. Toevaluate their position, they must compare the distance between the left and right sides of theroad. For this, effective and quick scanning of the road is required. The patient is againstrongly encouraged to use the previously practiced scanning principles.As this task becomes familiar, a secondary task is introduced. Targets (traffic signs ofapproximately 3°) are presented just above the horizon, at eccentricities of 10°, 25° and 40°on the left and the right, in random order.Presentation time of these targets is set at three seconds with ISI's ranging from two to fiveseconds. The patient is asked to push any button in the steering wheel on detection of a target.He/she is warned of misses by an acoustic signal. This component in particular relies on thespeed of scanning and the overshoot principle. Thus, to successfully complete bothcomponents of this training, extensive, fast and effective scanning of total space is required.
Figure 10. Example of amatrix.
Figure 11. Illustration of thedriving simulation.

Part II: Visual rehabilitation117
4.4. Third phase: Application and integration of scanning pattern into ADL: driving acarFrom this point on in therapy, we assume that the proposed scanning principles can beemployed autonomously by the patient. In the third phase of the training, we offer drivinglessons, in real traffic, under the close supervision of a qualified driving instructor. Amaximum of six hours of instruction was given. The cars used for the lessons had dualcontrols and were maximally adapted to the needs of the individual patient. The adaptationsincluded automatic gear shifting, reverse pedal control, steering knobs et cetera.Since all patients had driven previously (before their HH-acquisition), the basic technical,theoretical and legal aspects of driving were skipped. The instructions to the instructor wereto guide the patient safely through traffic, advising him/her on all possible aspects of driving.Again, difficulty levels (in terms of speed, traffic congestion and complexity) weresystematically increased, when judged to be safe. The patient was told that the instructor wasnot a qualified (visual) therapist and that his assignment was to point out the important cues,signs and events for driving. The task for the patient was to pick up these cues, signs andevents using the scanning principles trained previously. As such, the scanning goal is set bythe traffic situation; the scanning method has to be developed and displayed by the patient,preferably using the principles trained previously.
4.5. ResultsWe applied this training program with 19 HH patients. After completing the program, allpatients subjectively reported an improvement in their vision. They felt they perceived more,and reported experiencing less disability. This was usually confirmed by their partners.Although some subjects clearly had the impression that their visual field was larger,perimetric assessment indicated that no visual field restoration had occurred. This suggeststhat these patients were compensating for their visual impairment by adopting a betterscanning strategy, which permitted them to perceive more in less time. These subjectivereports were generally confirmed by objective measurements. Details of the assessments andresults will be described elsewhere. In the present discussion, only general and tentativeconclusions are presented.We administered an assessment battery, before and after training, to evaluate scanningperformance. Effective scanning is a prerequisite for, and an integral part of adequate visuo-spatial function and was evaluated using standard neuropsychological, experimental andecological tasks. The mean interval between both assessments was six months. Group analysisrevealed significant improvements on neuropsychological visuo-spatial tasks such as theWAIS Block Design and a Hidden Figures Test. Not all subjects improved, however.Depending on the specific tests, tentative and coarse inspection of the data reveals mostlyimprovement, some status-quo and decreases in performance in a very small number ofpatients. Future inspection of the data should shed some light on the characteristics of thosefew patients whose performance tended to decrease. Possible subclinical manifestations ofhemi-spatial neglect and/or dementia could be important factors. A similar observation wasmade, analysing the results of the experimental visuo-spatial tasks such as the Attended Fieldof View test (AFOV, Coeckelbergh et al, submitted). This experimental assessment ofscanning behaviour generally revealed improvement, but patients who did not improve on theneuropsychological tests tended also not to improve on this test. The final observations arebased on an ecological, practical on-the-road driving test. Performance was measured bymeans of a structured protocol. From this protocol, we derived a ‘visual-factor score’. This

Part II: Visual rehabilitation118
score gives an indication of visual performance during driving. We observed significantimprovement after training. But again the previous remark holds: not all patients improvedand those who did not, also tended not to have improved on the other tests. Additionally,although improvement was generally observed, the performance level was not necessarily atstandard (“sufficient”) level. This finding suggests that, although compensation is possible,complete compensation is very difficult.
4.6. ConclusionThese results are positive, but they raise further questions, which we hope to be able toanswer, at least partly, in the near future. For example, what characterises patients who do anddo not improve objectively after following the program? Is there a relationship with age,aetiology, time since lesion, general cognitive function et cetera.? These issues can be ofconsiderable importance for the development and future implementation of rehabilitationprograms specifically for hemianopic patients.
5. General conclusionTreatment for hemianopic field loss should more often be the focus of systematicrehabilitation efforts than it is at present. The absence of generally accepted and widely usedrehabilitation techniques is perhaps the result of the view that the visual disorder can not betreated or that it poses no apparent problem for the patient. We hope to have shown thecontrary with this chapter. The consequences for visual and cognitive functioning of the lossof a hemifield due to post-chiasmatic brain lesion should not be underestimated.
In this chapter, we briefly reviewed several therapeutic methods that can be applied at present.They all have their pros and cons, and they need more systematic exploration, refinement andevaluation. Future work and experiences will bring new insights in the possibilities ofrehabilitation. In our opinion, compensatory strategies, complemented by the application ofstrategies to enhance transfer, seem to be a good choice for rehabilitation. These methodshave proven to be effective, they do not demand too much of either patient or therapist, andthey have a direct and positive impact on the disabilities. Also the ‘adaptive approach’,devising auxiliary optical aids, is in our view very promising. To make a start for futuredevelopments, we would like to stress that the different approaches need not to be mutuallyexclusive and that different (combinations of) approaches can be chosen on the basis of theneeds, preferences, and abilities of the individual patient. In our view, an interesting approachcould be a combination of optical devices and compensatory training.
6. ReferencesAgrell, B. Dehlin, O. I., & Dahlgren C. J. (1997). Neglect in elderly stroke patients: A
comparison of five tests. Psychiatry and Clinical Neurosciences, 51, 295-300.Bischoff, P., Lang, J., & Huber, A. (1995). Macular sparing as a perimetric artifact. American
journal of ophthalmology, 119, 72-80.Bisiach, E., Vallar, G., Perani, D., Papagno, C., & Berti, A. (1986). Unawareness of disease
following lesions of the right hemisphere: anosognosia for hemiplegia and anosognosiafor hemianopia. Neuropsychologia, 24, 471-482.
Butter, C.M., & Kirsch, N. (1992). Combined and separate effects of eye patching and visualstimulation on unilateral neglect following stroke. Archives of Physical and Medicineand Rehabilitation, 73, 1133-1139.

Part II: Visual rehabilitation119
Celesia, G., G., Brigell, M., G., & Vaphiades, M., S. (1997). Hemianopic anosognosia.Neurology, 49, 88-97.
Cohen, J. M. (1993). An overview of enhancement techniques for peripheral field loss.Journal of the American Optometric Association, 64, 60-70.
Cohen, J. M., & Waiss, B. (1996). Visual field remediation. In R. G. Cole & B. P. Rosenthal(Eds.). Remediation and Management of Low Vision (pp 1-25), Mosby, St. Louis.
Diller, L., & Weinberg, J. (1977). Hemi-inattention in rehabilitation: the evolution of arational remediation program. Advances in Neurology, 18, 63-82.
Elliot, D. B., North, I., & Flanagan, J. (1997). Confrontation visual field tests. Ophthalmicand physiological optics, 17, 17-24.
Gottlieb, D. D., Fuhr, A., Hatch, W. V, & Wright, K. D. (1998). Neuro-optometric facilitationof vision recovery after acquired brain injury. NeuroRehabilition, 11, 175-199.
Gray, L., G., Galetta, S., L., Siegal, T., & Schatz, N., J. (1997). The Central Visual Field inHomonymous Hemianopia. Evidence for Unilateral Representation. Archives ofNeurology, 54, 312-317.
Karnath, H.O., Christ, K., & Hartje, W. (1993). Decrease of contralateral neglect by neckmuscle vibration and spatial orientation of trunk midline. Brain, 116, 383-396.
Kasten, E., Poggel, D. A., Müller-Oehring, E., Gothe, J., Schulte, T., & Sabel, B. A. (1999).Restoration of vision II: Residual functions and training-induced visual fieldenlargement in brain-damaged patients. Restorative Neurology and Neuroscience, 15,273-287.
Kasten, E., Strasburger, H., & Sabel, B. A. (1997). Programs for diagnosis and therapy ofvisual field deficit in vision rehabilitation. Spatial Vision, 10, 499-503.
Kerkhoff, G, & Schindler, I. (1997). Hemineglekt versus Hemianopsie. Hinweise zurDifferentialdiagnose. Fortschritte der Neurologie Psychiatrie, 65, 278-289.
Kerkhoff, G. (1999). Restorative and compensatory therapy approaches in cerebral blindness– a review. Restorative Neurology and Neuroscience, 15, 255-271.
Kerkhoff, G., Münssinger, U., & Meier, E. K (1994). Neurovisual rehabilitation in cerebralblindness. Archives of Neurology, 51, 474-481.
Kerkhoff, G., Münssinger, U., Haaf, E., Eberle-Strauss, & Stögener, E. (1992). Rehabilitationof hemianopic dyslexia in patients with postgeniculate field disorders.Neuropsychological Rehabilitation, 2, 21-42.
Nadeau, S. E., Crosson, B., Swartz, R. L., & Heilman, K. M. (1997). Gaze relatedenhancement of hemispheric blood flow in a stroke patient. Journal of Neurology,Neurosurgery and Psychiatry, 62, 538-540.
Pambakian, A, L., M., & Kennard, C. (1997). Can visual function be restored in patients withhomonymous hemianopia? British Journal of Ophthalmology, 81, 324-328.
Peli, E. (1999). Field Expansion for Homonymous Hemianopia using Prism and PeripheralDiplopia. Technical Digest on Vision Science and it Applications, Technical DigestSeries,1, 74-77.
Peli E. (2000a). Treating Hemianopia Using Prisms to Create Peripheral Diplopia. In C.Stuen, A. Ariditi, A. Horowitz, M. A. Lang, B. Rosenthal, & K. R. Seidman (eds).Vision Rehabilitation: Assessment, Intervention and Outcomes. Selected papers fromVision '99: International Conference on Low Vision., (pp. 104-109) Swets & Zeitlinger,Lisse.
Peli, E. (2000b). Field expansion for Homonymous Hemianopia by Optically InducedPeripheral Exotropia. Optometry and Vision Science, 77, 453-464.

Part II: Visual rehabilitation120
Pizzamiglio, L., Antonucci, G., Judica, A., Montenero, P., Razzano, C. & Zoccolotti, P.(1992). Cognitive rehabilitation of the hemineglect disorder in chronic patients withunilateral right brain damage. Journal of Clinical and Experimental Neuropsychology,14, 901-923.
Robertson, I., H., North, N., T., & Geggie, C. (1992). Spatiomotor cueing in unilateral leftneglect: three case studies of its therapeutic effects. Journal of Neurology, Neurosurgeryand Psychiatry, 55, 799-805.
Rossi, P., W., Kheyfets, S., & Reding, M., J. (1990). Fresnel prisms improve visualperception in stroke patients with homonymous hemianopia or unilateral neglect.Neurology, 40, 1597-1599.
Rubens, A., B. (1985). Caloric stimulation and unilateral visual neglect. Neurology, 35, 1019-1024.
Sabel, B., A. (1999). Restoration of vision I: Neurobiological mechanisms of restoration andplasticity after brain damage – a review. Restorative Neurology and Neuroscience, 15,177-200.
Schiefer, U., Skalej, M., Dietrich, T., J., & Braun, C. (1999). Detection and follow-up ofhomonymous visual field defects – perimetric essentials for evaluation of sponteneousrecovery. Restorative Neurology and Neuroscience, 15, 201-217.
Trauzettel-Klosinski, S. , & Reinhard, J. (1998). The vertical field border in hemianopia andits significance for fixation and reading. Investigative ophthamology and visual science,39, 2177-2186.
Trexler, L. E. (1998). Volitional control of homonymous hemianopsia: a single case study.Neuropsychologia, 36, 573-580.
Van der Wildt, G. J. & Bergsma, D. P. (1997). Visual field enlargement byneuropsychological training of a hemianopsia patient. Documenta Ophthalmologica, 93,277-292.
Webster, J. S., Jones, S., Blanton, P., Gross, R., Beissel, G. F., & Wofford, J. D. (1984).Visual scanning Training with stroke patients. Behaviour Therapy, 15, 129-143.
Weiskrantz, L. (1986). Blindsight: A case study and implications. Oxford: Oxford UniversityPress.
Zihl, J. (1994). Rehabilitation of visual impairments in patients with brain damage. In A. C.Kooijman, P. L. Looijestijn, J. A. Welling and G. J. van der Wildt (Eds.) Low vision.Research and New developments in Rehabilitation (pp 287-295). Amsterdam, IOSPress.
Zihl, J. (1995). Visual scanning behaviour in patients with homonymous hemianopia.Neuropsychologia, 33, 287-303.
Zihl, J. (2000). Rehabilitation of visual disorders after brain injury. Hove, East Sussex:Psychology Press.
Zihl, J, & Kennard, C. (1996). Disorders of Higher Visual Function. In T. Brandt, L. R.Caplan, J. Dichjans, H. C. Diener, & C. Kennard (Eds.) Neurological disorders: Courseand Treatment (pp 201-212). San Diego: Academic Press.
Zihl, J., & von Cramon, D. (1985). Visual field recovery form scotoma in patients withpostgeniculate damage. A review of 55 cases. Brain, 108, 335-365.

Prediction and Evaluation121
Prediction and Evaluation of Driving and Visuo-Spatial Performance inHomonymous Hemianopia after Compensational Training*
1. AbstractIn a previous study we observed that the majority of patients with homonymous hemianopia(HH) showed low to modest visuo-spatial performance on neuropsychological tests andduring a driving test administered by an expert of the Dutch licensing authority, suggestingthe need for specific therapeutic intervention.Seventeen HH patients took part in a saccadic compensation training to reduce visuo-spatiallimitation, with a special focus on compensation during driving. We compared andinterrelated visuo-spatial performance in driving and in neuropsychological tests, before andafter the training.Generally, analysis corroborated results of the previous study, confirming that visualperformance during driving is moderately correlated with visuo-spatial neuropsychologicaltest performance. We found an improvement in visuo-spatial performance during driving afterrehabilitation, but not in other aspects of driving, nor in neuropsychological test performance.This argues against a non-specific placebo-effect.Our results suggest that HH is not necessarily a contra-indication for fitness to drive and thatvisuo-spatial limitation, common and apparent in HH and consequential for fitness to drive,can be reduced by the compensation training. Despite this improvement, driving performancedid not meet the necessary standards in most patients, suggesting either that morerehabilitation is required or lower rehabilitation goals should be set.
2. IntroductionNearly 80% of patients with unilateral post-chiasmal brain damage acquire a homonymousvisual field defect (VFD), and nearly 66% of the unilateral homonymous VFDs arehomonymous hemianopias (HHs) (Zihl, 1994). Patients with HH typically complain aboutbumping into obstacles, difficulties in reading, and having a limited overview, resulting inconsiderable restrictions in every day life1. These limitations and restrictions suggest, inaddition to the structural visual impairment (i.c. HH), also reduced visuo-spatial function(Zihl, 2000; Meienberg, Zangemeister, Rosenberg, Hoyt, & Stark, 1981; Kerkhoff, 1999).Visuo-spatial functioning, is one component of higher-order (cognitive) functioning whichcan be evaluated using specific neuropsychological tests. In addition, this cognitive functionrelates to many activities of daily living, as for example driving.In previous work (Tant, Brouwer, Kooijman, & Cornelissen, submitted), we assessed visuo-spatial performance in HH patients, both by an extensive neuropsychological test battery andby a practical driving test. We found that visuo-spatial neuropsychological test performancecan be significantly related to visual performance during driving, as observed in an on-the-road test-ride. Additionally, it was observed that the majority of the HH patients failed thetest-ride, and showed modest visuo-spatial neuropsychological and driving performance,suggesting the need for specific therapeutic intervention.
* This manuscript was submitted to Neuropsychological Rehabilitation (Tant, Brouwer, Kooijman &Cornelissen)1 We use terminology defined by the World Health Organisation (WHO) in the International Classification ofFunctioning, Disability, and Health (ICF).

Prediction and Evaluation122
Driving-related therapeutic intervention in brain-injured patients has been discussed byBrouwer and Withaar (1997). They suggested to give all brain-injured patients, except thosewho are obviously unfit to drive (e.g. severe neglect patients), driving(-related) rehabilitationand suggested two different approaches. Firstly, to give all patients rehabilitation until acertain criterion of fitness to drive is attained. The associated research question would be topredict the amount of necessary training. Secondly, to give all patients the same amount ofrehabilitation and assess their fitness to drive (before and) after training. The researchquestion would be to predict fitness to drive after training and the progression resulting fromthe training. This last approach, which we adopted for this study, allows more stringentresearch planning and control.
Therapeutic approaches specific for HH have been scarce, despite the high occurrence ofsubstantial visual disabilities (Neetens, 1994; Kerkhoff, Munssinger, Haaf, Eberle-Strauss, &Stogerer, 1992; Nelles et al., 2001). Although limited visual field recovery is definitelypossible in some patients with HH, it is rarely sufficient to eliminate the limitations andrestriction resulting from the VFD (Kerkhoff, 1999) and hence specific (adaptational orcompensational) therapeutic approaches are needed. The use of optical devices has recentlybeen (re)suggested but not fully evaluated (Peli, 2000; 2001). Another therapeutic approach isthe acquisition of oculomotor compensational strategies and has been suggested to be aneffective method for treatment of visual limitations and restrictions resulting from HH(Kerkhoff et al., 1992; Kerkhoff, Munssinger, & Meier, 1994; Nelles et al., 2001; Tant,Bouma, Kooijman, Cornelissen, & Brouwer, in press; Webster et al., 1984; Zihl & Kennard,1996; Zihl, 2000). In addition to the significant improvement in basic oculomotorperformance, as suggested by these authors, also transfer to visually related activities has beenreported (e.g. Kerkhoff et al., 1994; Zihl, 2000). This confirms the potential of this type ofintervention for reducing activity limitations and their consequences for every day life(restrictions).We hence invested considerable effort in (improving) this type of therapeutic intervention asto reduce visuo-spatial disability in our HH group, with a special focus on the application ofthe principles during driving, as we were guided by the low to modest (visuo-spatial) drivingperformance in our previous study (Tant et al., submitted). This modest performance can beexplained by the limited driving experience after acquisition of the HH and/or can result as aconsequence of non-adaptive viewing behaviour. We addressed both aspects in our integratedsaccadic compensation training, which is described in detail in Tant et al. (in press). In brief,the compensational training consisted of three phases, each lasting for six hours maximally. Inthe first phase, saccadic eye-movements into the blind hemifield, which are frequent, fast, and(too) large, were trained. The aim of the second phase was to effectively use this type of eye-movements, during specifically designed visuo-spatial experimental tasks. In the third phaseof the training, we offered driving lessons, in real traffic, under close supervision of aqualified driving instructor, in order to improve the integration of the learned principles into apersonal and general scanning style.
The main issues of the present research concern the relationships of neuropsychological testperformance, driving performance, and the effectivity of our therapeutic intervention. First,can an integrated saccadic compensation training lead to better driving performance and morespecifically to improved visuo-spatial performance during driving. Does this also lead tobetter visuo-spatial neuropsychological test performance. Second, can visuo-spatial

Prediction and Evaluation123
neuropsychological test performance predict visual aspects of driving performance aftertherapeutic intervention and do we observe similar relationships as before the therapeuticintervention. Third, can the effect of the intervention be predicted, from neuropsychologicaltest performance or from other characteristics. To answer these questions, we will use andcompare neuropsychological data and data from an on-the-road test-ride, both before and afterthe rehabilitation program.We expect that visually related activity limitations will be reduced after the rehabilitationprogram and that visuo-spatial neuropsychological performance is related to visualperformance during driving. More specifically, as this was the aim of the therapeuticintervention, we expect an improvement in visual performance during driving. Since wepreviously established a significant relationship between visuo-spatial neuropsychologicalmeasures and visual performance during driving, we do expect to find similar improvementsin visuo-spatial neuropsychological test performance. With respect to the third question, weexpect that patients with more limitations will benefit more from the intervention, as there ismore opportunity for improvement. Personal characteristics, like age and time since lesion,are also expected to be related to the degree of improvement.
3. Methods3.1. PatientsThe seventeen patients reported are part of a larger HH patient population previously reported(Tant et al., submitted). They were referred by specialists who indicated the need forassessment on fitness to drive. All patients failed a practical test ride (see Tant et al.,submitted for details) and expressed the desire for participation in the visual rehabilitationprogram, which we offered (see Tant et al., in press for details).
A summary of the patient characteristics can be seen in Table 1. There is no significantdifference in the number of left- and right-sided HH patients. There are significantly moremales than females ($2 (1, N=17) = 7.2, P <.01), equally distributed across both left- andright-sided HH groups. The higher proportion of males is probably induced by ourrecruitment procedure, in combination with social factors. Namely, we recruited patients withdriving needs. Being refused to drive is probably less restricting in the (elderly) femalepopulation because, a priorily, they drove less (than their husbands) and also are lessdependent on themselves for transportation. We suppose that experiencing less restrictionswould result in less interest in participating in a driving-study. Most of the patients werevictims of stroke, but the different aetiologies are equally distributed across both HH groups.There are no differences in age, macular sparing, time since injury, or driving experiencebefore injury between both HH groups. Most patients discontinued driving since injury ($2 (1,N=17) = 7.2, P <.01), but the distribution of patients who (dis)continued is equal across bothHH groups.Standardised tests were administered to exclude dementia (De Graaf & Deelman, 1991;Folstein, Folstein, & McHugh, 1975), receptive aphasia (Deelman, Liebrand, Koning-Haanstra, & van der Burg, 1987) and apraxia (De Renzi, Faglioni, & Sorgato, 1982).Adequate general lower-order aspects of visual function, apart from the HH, were confirmedby a form discrimination screening test (Warrington & James, 1991). We excluded patientswith severe hemi-spatial visual neglect and severe object agnosia (see Tant et al., submitted).

Prediction and Evaluation124
Table 1. Summary of patient characteristicsHemianopia Total
Characteristic value Left RightPatients (number) 9 8 17
Age (years) mean 57 59 58range 29-76 50-68 29-76
Gender (number) male 8 6 14female 1 2 3
Time since injury (months) mean 33.6 36.8 35.1range 6.4-157 6.4-123 6.4-157
Aetiology (number) CVA 6 7 13CHI 2 1 2Tumour 1 0 1
Macular sparing (number) yes 7 6 13no 2 2 4
Macular sparing (°) mean 2.0 3.0 2.47range 0-3 0-5 0-5
Driving experience before injury (years) mean 30 31 30range 5-47 18-44 5-47
Continued driving since injury (number) yes 2 1 3no 7 7 14
3.2. Visual AssessmentVisuo-spatial assessment consists of both a practical driving test and an extensiveneuropsychological test battery. For detailed procedure and scoring, we refer to Tant et al.(Tant et al., submitted; Tant, in preparation).
3.2.1. Practical Driving TestA practical test-ride is used to assess driving performance on the level of activity. The on-the-road test took place in and near the city of Groningen, and was conducted by a certified andofficial driving examiner of the Dutch Licensing Authority, using the standard test-routes andprotocols. The cars used for the on-the-road test had dual operation and were maximallyadapted to the needs imposed by motor impairments of the individual patient (if any).To assess performance while driving, a structured protocol, was added to the standardprocedure. This structured protocol (Test-ride for Investigating Practical fitness to drive, i.e.TRIP) is a checklist of different aspects of the driving task and was completed by the expertafter the test-ride. Previous versions were used by Withaar (Withaar, 2000) and De Raedt (DeRaedt, 2000). The 55 items, judging specific driving qualities and behaviours, were scored ona 4-point scale, ranging form “1” (indicating insufficient and inadequate performance) to “4”(good performance). Based on a priori considerations, we constructed separate factors (orsubscales) with these 55 items. Four driving factors (namely VIS, OPER, TACT and TOT)are directly derived from (combinations of) specific TRIP items. Some items wererepresented in more than one factor. In the visual factor (VIS, 25 items), predominantly visuo-

Prediction and Evaluation125
perceptual behaviour was reflected. This included visual scanning, visuo-spatial, and visuo-integrative aspects like assessment of eye- and head-movements in different situations,perception of traffic signals, visual communication with other traffic participants etc. Theoperational factor (OPER, 8 items), was to reflect fluency of instrumental and psycho-motoraspects of driving like handling the brakes and shifting gears. The tactical factor (TACT, 15items) reflected all aspects in which (tactical) choices, anticipation, and adaptation wererepresented. The sum of all TRIP items is indicated by the TOT factor (55 items).At the end of the TRIP, both a global impression (GLOB) and end-verdict were provided,based on a global and subjective impression of the expert. The global impression wasprovided by evaluating three global aspects, namely practical fitness to drive, technicalhandling and execution, and traffic insight, each scored on the 4-point scale. The end-verdictindicated whether the expert (officially) would declare the subject fit to drive (pass or fail).The VIS, OPER, TACT, TOT, and GLOB factors are expressed proportional to theirrespective maximum factor score for ease of inter-comparison and will subsequently bereferred to as factor scores (range: .25 – 1). Factor scores of .25, .50, .75 and 1 indicateperformance at respectively “insufficient and inadequate”, “dubious”, “sufficient” (i.e.passing) and “good” level.
3.2.2. Neuropsychological Test BatteryThe neuropsychological battery consisted of 25 clinically available or experimental visuo-spatial tests (see Table 2). These were classified, on an a priori basis, into four factorsrepresenting different aspects of visuo-spatial function, namely basic visual scanning andsearch (BVSS, 16 tests), a visuo-constructive and organisational factor (VCO, 3 tests), avisuo-integrative factor (VI, 4 tests) and a dynamic factor (Dy, 1 test). These four factors wereevaluated on multiple components, namely performance in terms of lateralisation, speed, andaccuracy. The speed and accuracy components are traditionally used for evaluating generaltest performance. As HH is a lateralised visual dysfunction which, if not properlycompensated for, will lead to relatively poor visual performance with regard to the side of theblind hemi-field, we assume that differential lateralised performance is a typical characteristicof HH visual disability. The lateralisation component qualifies and quantifies the nature anddegree of differential lateral performance, independently of general performance. The nature(qualitative aspect) is expressed by the sign the lateralisation index, where a positive indexindicates better right-sided than left-sided performance (as expected in left-sided HH) and theopposite for a negative index (expected in right-sided HH). The degree of the lateraliseddifference (quantitative aspect) varies between 0 an 1, where the former indicates nodifference and the latter indicates maximal difference. Hence the lateralisation index variesbetween –1 and +1. When assessing (only) the quantitative aspect and comparing left- andright-sided HH, the absolute values of the lateralisation scores will be used.
When necessary and possible, transformations were inforced on the raw test data, followingsuggestions by Stevens (1996), to approximate normal distributions of the individual testscores. The speed and accuracy data were then normalised for intercomparison. For eachfactor, the measures of lateralisation, speed, and accuracy of the comprising tests wereaveraged, providing for each factor, a factor (lateralisation, speed, and accuracy) componentscore. Visuo-spatial test performance is hereby operationally defined by four different visuo-spatial factors (namely BVSS, VCO, VI, and Dy), which are evaluated in terms of threecomponents (namely lateralisation, speed, and accuracy). There is no accuracy component in

Prediction and Evaluation126
the Dy factor (see Table 2). Averaging the four lateralisation, four speed, and three accuracycomponents of the respective factors, provides a global lateralisation, global speed, and globalaccuracy component score. For more details, we refer to Tant et al. (Tant et al., submitted;Tant, in preparation).
Table 2. Summary of construction of the Visuo-Spatial factors. The components used for each test aremarked.
Visuo-spatial ComponentsFactor Test Speed Accuracy Lateralisation
Trail Making Test üCounting Dots üPosition Discrimination üTAP Eye movements ü üTAP Visual Scanning ü ü üThe Attended Field of View Test ü üDetection Task ü üReading words ü ü üReading strings ü ü üZihl Dotcounting test ü üLine bisection ü üAlbert’s line cancellation Test ü üMesulam Structured Shape cancellation ü ü üSearch for O's ü ü üThe Bells Test ü ü ü
%DVLF�9LVXDO6FDQQLQJ�DQG6HDUFK��%966�
Grey scales üWAIS-R Block Design Test üMatrix copy test ü
9LVXR�&RQVWUXFWLYHDQG�2UJDQLVDWLRQDO�9&2� Complex Figure Test ü ü üPosition Determination üBlocks üHidden Figures Test ü
9LVXR�,QWHJUDWLYH�9,�Overlapping Figures Task ü ü ü'\QDPLF��'\� Tracking task ü ü
3.3. ProcedureAfter inclusion in the larger study, 28 patients were assessed by both a practical driving testand an extensive visuo-spatial neuropsychological test battery (pre-assessment). Twenty fourpatients failed the test ride, as indicated by the end-verdict of the driving expert. Thesepatients were invited to participate in our saccadic compensation program (see Tant et al., inpress for details). Eighteen patients accepted. One patient did not complete the rehabilitationprogram, due to a new brain insult. The total rehabilitation time for each patient was fixed to18 hours, but the time span of the rehabilitation program was on average 25 weeks, rangingfrom eight to 73 weeks. After completion of the rehabilitation program, the driving test andneuropsychological battery were repeated (post-assessment).

Prediction and Evaluation127
4. ResultsTo address the issues of the effectivity of the rehabilitation program, both in terms of drivingand neuropsychological test performance, the results of the practical driving tests and theneuropsychological test battery will be presented firstly and separately. The issues ofprediction of visual performance during driving and improvement will be reportedsubsequently.
4.1. Practical Driving TestAll 17 patients had failed the practical driving test before the visual rehabilitation program, asindicated by the end-verdict of the driving expert. After the rehabilitation program, twopatients (12%) (one left- and one right-sided HH) achieved a positive end-verdict, and hencepassed the practical driving test. For the remainder of the analyses, in order to evaluatedriving performance, we will use the TRIP factor scores (VIS, OPER, TACT, TOT andGLOB).All TRIP factor scores intracorrelated significantly before the rehabilitation program, as wellas after. Pearson’s R ranged from .68 to .97 and from .69 to .98 respectively (N= 17; all P <.005). Also the respective TRIP factor scores (pre- versus post-assessment) intercorrelatedsignificantly (R-range: .72 - .85, N=17, all P < .001).
A MANOVA on the TRIP factor scores showed no difference in performance between left-and right sided HH, and revealed an effect of the rehabilitation program (F(5,11) = 4.6, P <.05). Univariate analysis showed a significant improvement only of the VIS factor (F(1,15) =8.1, P < .05) (Fig. 1), which evaluates visual performance during driving. On average, none ofthe TRIP factor scores (pre- and post-assessment) reached the “sufficient-level” (all meanscores significantly differed from .75, as indicated by one-sample T-tests). However, for bothpatients who passed, all TRIP factor scores were at sufficient level (range: .75 - .78) after therehabilitation program, while for those who did not pass, mean TRIP factor scores rangedfrom .47 to .59. For comparison, before the rehabilitation program, TRIP factor scores rangedfrom .58 to .77 for the two patients who passed. The mean TRIP factors, for those who did notpass, ranged from .44 to .60.
4.2. Neuropsychological Test BatteryVisuo-spatial neuropsychological testperformance was a priorily classifiedinto four factors (Basic Visual Scanningand Search (BVSS), Visuo-Constructiveand Organisational (VCO), Visuo-Integrative (VI), and Dynamic (Dy)),evaluated on different components(lateralisation, speed, and accuracy).After averaging the respectivecomponent scores of the different factorsinto a global lateralisation, global speed,and global accuracy score, it showed thatall global scores significantly correlatedpre- versus post assessment (r(N=17) =.88, P < .0005 for speed; r(N=17) = .96,
Practical Driving Test
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
VIS OPER TACT TOT GLOBTRIP Factors
Fact
or s
core
s
Pre TrainingPost Training
Figure 1. Results on the practical driving test: TRIPfactor scores before and after rehabilitation. Error barsare standard errors.

Prediction and Evaluation128
P < .0005 for accuracy and r(N=17) = .61, P < .01 for lateralisation). All respective factorcomponent scores, except the lateralisation component of the VCO factor, intercorrelatedsignificantly pre- versus post assessment. Pearson’s R ranged from .49 (N = 17, P < .05) to.94 (N = 17, P < .0005). The global speed x global accuracy correlation was -.42 (ns) and -.59(P < .05) in pre- and post-assessment respectively. Averaged over both assessments, thisspeed-accuracy trade-off was evidenced by a correlation of -.53 (P < .05).
In contrast to the significant improvement in the visual driving factor (VIS, pre- versus post-assessment), we did not observe any multivariate (or univariate) effect of the rehabilitation inthe global (visuo-spatial neuropsychological) component scores. MANOVA showed only asignificant multivariate effect of side of the HH (F(3, 13) = .48, P < .05). Subsequentunivariate analysis revealed this effect to be observed only in the global lateralisation score(F(1, 15) = 11.2, P < .005). This multivariate (and univariate) effect disappeared when usingthe absolute values of the global lateralisation scores, indicating that only the qualitative, notthe quantitative aspect of the lateralisation component differed in both HH groups.
MANOVAs (and ANOVAs), performed separately for the respective (four) lateralisation,(four) speed, and (three) accuracy components of the different visuo-spatial factors, did notreveal any effect of the rehabilitation as indicated by a lack of statistical change, from pre- topost-assessment, in either speed, accuracy or lateralisation component. As was the case for theglobal component scores, for the lateralisation components, we did observe a multivariateeffect of the side of the HH (F(4, 12) = 16.48, P < .0005). Univariate analysis showed that theleft- and right-sided HH patients significantly differed on the BVSS (F(1, 15) = 67.8, P <.0005) and the VI (F(1, 15) = 12.07, P < .005) lateralisation. This multivariate (and univariate)effect disappeared when using the absolute values of the lateralisation scores, indicating thatonly the qualitative, not the quantitative aspect of the lateralisation component differed inboth HH groups.
MANOVAs, performed separately for the four visuo-spatial factors (BVSS, VCO, VI, andDy) using their respective component scores (lateralisation, speed, and accuracy), indicatedno statistical change, from pre- to post-assessment, in either of the four analyses. Multivariateeffects of the side of the HH were observed for the BVSS factor (F(3, 13) = .17, P < .0005),and the VI factor (F(3, 13) = .47, P < .05). This effect disappeared for the VI factor, whenusing the absolute values for the lateralisation score (as previously indicated). However, forthe BVSS factor, in doing similarly, the effect of the side of the HH remained and univariateanalysis revealed that left-sided HH patients showed worse BVSS accuracy scores (Mean = -.202, SD = .50) than right-sided HH patients (Mean = .227, SD = .31) (F(1, 15) = 5.7, P <.05).
4.3. Visual performance during driving (VIS)Due to the nature of the visual impairment, visuo-spatial limitations can be expected in HH.We therefore focussed on the visual performance during driving (VIS factor derived fromTRIP scores), which, as already indicated, significantly improved after the rehabilitationprogram. Bearing the restraints imposed by the low number of subjects in mind, we examinedthe interrelations of the VIS factor with personal characteristics and global(neuropsychological) component scores.

Prediction and Evaluation129
4.3.1. Personal characteristicsAfter correlating the VIS factor with the personal characteristics of the patients, we observedthat age correlated significantly at pre-assessment (r(N=17) = -.60, P < .05), but thiscorrelation disappeared at post-assessment (r(N=17) = -.34, ns), indicating, at pre-assessment,worse visual performance during driving with higher age. Neither macular sparing nor drivingexperience did show any significant relationship with the VIS factors, either at pre- or post-assessment. Driving experience was however highly correlated with age (r(N=17) = .88, P <.0005). When corrected for age, driving experience did correlate significantly with VIS at pre-assessment (r(N=17) = .51, P < .05), but not at post-assessment (r(N=17) = .38, ns),indicating, at pre-assessment, better visual performance during driving with more drivingexperience. In contrast to this pattern, time since injury did not correlate with VIS at pre-assessment (r(N=17) = -.39, ns), but did so at post-assessment (r(N=17) = -.56, P < .05),indicating, at post-assessment, worse visual performance with more time since injury.
4.3.2. Global (neuropsychological) component scoresWe entered the global (lateralisation, speed and accuracy) component scores into a regressionanalysis, predicting visual performance during driving (VIS factor). The VIS factors couldsignificantly be predicted by the global components derived from the same assessmentoccasion, namely at pre-assessment (R2 = .44, F(3, 13) = 3.4, P < .05), and slightly better atpost-assessment (R2 = .50, F(3, 13) = 4.3, P < .05). Interestingly, it appeared that VIS at pre-assessment could also be predicted on the basis of the component scores at post-assessment(R2 = .54, F(3, 13) = 5.1, P < .05). The reverse, however, did not yield a significant model (R2
= .33, F(3, 13) = 2.2, ns).
4.3.3. ImprovementTo assess the predictability of improvement in visual performance during driving, we forcedthe global neuropsychological component scores from either pre- or post-assessment into aregression analysis predicting the difference (from pre- to post-assessment) in VIS factors.Neither analyses resulted in a significant model, suggesting that visuo-spatialneuropsychological test performance cannot predict the visuo-spatial driving improvement.We also used an alternative strategy to investigate the predictability of the rehabilitationeffects and came to the same conclusions. We predicted visual performance during driving atpost-assessment, first by entering the VIS factor at pre-assessment (R2 = .52, F(1, 15) = 16.5,P < .001), after which we entered the global component scores from either pre- or post-assessment and evaluated their addition to the variance explained. We observed no significantaddition in either analyses, indicating that visuo-spatial neuropsychological test performancecannot explain any residual variance in visual performance during driving after rehabilitationwhich has not already been explained by visual performance during driving beforerehabilitation.We further investigated whether any of the personal characteristics showed any relation to theimprovement in visual performance during driving. None of the characteristics correlatedsignificantly with the difference score.
5. Discussion5.1. Reduction of visuo-spatial limitationsIn the on-the-road driving test, it is assessed whether the patient can drive adequately, giventhe visual impairment. This test-ride is not a regular driving examination, as specific concern

Prediction and Evaluation130
and importance is allocated to situations in which the HH can cause difficulties (limitations).To evaluate driving performance, we used a structured protocol (TRIP) from which wederived three factors, each representing an important aspect of driving. Since our visualrehabilitation program (integrated saccadic compensation training, (Tant et al., in press)aimed at reducing visuo-spatial limitations and restrictions, we focussed on visuo-spatialperformance, specifically during driving.Although only two patients (12%) finally passed the driving test (as indicated by the end-verdict of the driving expert) after the rehabilitation program, we did observe an overallimprovement of visual performance during driving (VIS). This conformed to our expectationsand aim, since our rehabilitation program is visuo-spatially in nature. The operational (OPER)and tactical (TACT) aspects of driving, did not improve accordingly. As a result, the totalTRIP score (TOT) and the global impression (GLOB), which incorporate all aspects and arehence global and general measures of driving performance, did not improve significantly (Fig.1). All aspects were still subject to improvement, since none of them reached the “sufficient”level, suggesting the non-improvement not to be due to ceiling-effects. We need to remark inthis respect that it cannot be excluded that the driving expert, in scoring the TRIP items, didnot use the full range of scores (at the higher end), hence hereby lowering the maximum scoreand discrediting our conclusion concerning ceiling-effects.In the current (pre versus post) design, influences other than the treatment effect, cannotsimply be ruled out, but the specificity of improvement, namely only in visual performance,argues against a general and non-specific learning effect. In addition, Coeckelbergh et al.(Coeckelbergh, Kooijman, Brouwer, & Cornelissen, 1999) found no change in general drivingperformance in two post-treatment driving assessments, using similar protocols and drivingtests. Our results hence suggest that we succeeded in improving visual performance duringdriving by the visual rehabilitation program.Since visual information is generally considered to be the most important source ofinformation in driving (Rockwell, 1972), our result is of considerable practical relevance formobility-rehabilitation. Namely, it justifies the efforts in (improving) visual rehabilitation,since visual disability is apparent, consequential, and can be decreased in driving. On theother hand, since the improvement was not sufficient to meet the necessary standards, itsuggests that more rehabilitation is required. This was also confirmed by the comments of thepatients, who urged that they needed more rehabilitation time, especially in the third (driving)phase. Ideally, not only more time, but also other aspects, important for adequate driving,would need to be more addressed, since for passing the driving test, all aspects would need tomeet at least the “sufficient” level.
As in previous work (Tant et al., submitted), in driving performance, we did not observe anydifference between left- and right-sided HH patients. However, we did observe less accurateperformance by left-sided HH patients on the BVSS factor. This result is not surprising, sinceleft-sided HH patients suffered right-sided brain damage, frequently associated with visuo-spatial dysfunction (e.g. Zihl, 2000). That this differential performance was not a robust andgeneral effect is not surprising either, since we excluded patients with hemi-spatial neglect.Such patients are visuo-spatially strongly impaired, and since in general they suffered right-sided brain damage, inclusion typically results in differential performance between left- andright-sided unselected brain damage groups. Since our left- and right-sided brain damagedpatients (respectively with right- and right-sided HH) were “selected” in this respect, we didnot expect to find robust quantitative differences in performance.

Prediction and Evaluation131
Neuropsychological test performance has previously been related to practical fitness to driveand has been reported to correlate only moderately high with measures of drivingperformance (e.g. Withaar, Brouwer, & van Zomeren, 2000; Brouwer, 2001; Engum, Cron,Hulse, Pendergrass, & Lambert, 1988; Engum, Lambert, Womac, & Pendergrass, 1988;Engum, Lambert, & Scott, 1990; Sivak, Olson, Kewman, Won, & Henson, 1981; Galski,Bruno, & Ehle, 1992; Nouri, Tinson, & Lincoln, 1987; Mazer, Korner-Bitensky, & Sofer,1998; Nouri & Lincoln, 1993; Lincoln & Fanthome, 1994). In previous research, weconfirmed a significant interrelatedness of visual performance during driving and visuo-spatial neuropsychological test performance in a larger HH sample (Tant et al., submitted).Since our visual rehabilitation program was aimed at reducing visuo-spatial limitations andrestrictions, and since we observed improvement in visual performance during driving, wewould also expect similar improvements in visuo-spatial neuropsychological testperformance. Despite that we observed the expected intercorrelations of the visuo-spatialneuropsychological factors and their components from pre- to post-assessment, and theexpected speed x accuracy trade-offs, each accrediting the general validity of ourneuropsychological data, we did not observe any statistical improvement inneuropsychological test performance.
Low power due to the modest number of patients, high variability in individualneuropsychological test results, typical in brain damaged populations, and lack of sensitivityof the neuropsychological tests to the (type of) improvements, might account for the absenceof statistical significances. Further, individual neuropsychological tests usually are short intime duration, while the driving tests typically lasted for one hour. It is generally accepted that“true function” can be more validly assessed over a longer period of time, as to minimiseeffects of coincidental fluctuations in performance. As a consequence, although obviouslyrelated, visuo-spatial driving performance and visuo-spatial neuropsychological performancedo not share exactly the same functions and properties, and hence are not necessarily liable tothe same influences.Similarly, Webster and colleagues (Webster et al., 1984) concluded that their visual trainingdid not improve (hemi-spatial) neuropsychological test performance, but did lessen theinfluence of the impairments on functional activities, leading to a similar suggestion, namelythat both types of performances can be prone to different influences or differentiallyinfluenced by the same mechanisms. Conceptually clarifying this point, it can be argued thatthe visual rehabilitation program, due to its compensational nature, is likely to influence thedriving performance and the neuropsychological test performance differently. Practical fitnessto drive, as defined by our assessment and scoring procedure, is situated at the (activity-)performance level, as it is considered to be influenced by a combination of factors at theimpairment level (HH and perhaps cognitive dysfunction) and by contextual (environmentaland personal) factors. As a consequence, driving is relatively highly liable to influences ofcompensation (contextual factor). Neuropsychological tests aim at measuring (pure) cognitivefunctions, which are ideally indications of capacities (i.e. true abilities). In contrast toperformances, capacities are (ideally) not liable to compensation and hence improvement. Wetherefore suggest that, although related, visual performance during driving andneuropsychological test performance are measures at conceptually different levels, and as aconsequence are differently influences by our compensatory training.

Prediction and Evaluation132
5.2. Interrelations and predictabilityThe (patterns of) correlations, observed in this study, of the personal characteristics and thevisual performance during driving (VIS scores) at pre-assessment, correspond well withobserved correlations in a previous (larger) study (Tant et al., submitted). We observed worseVIS scores with increasing age and better VIS scores with increasing driving experience.Surprisingly, these relationships disappeared at post-assessment and a new relationshipappeared, namely better VIS scores with shorter time since injury. Far from being obviouswhat causes this change of pattern from pre- to post-assessment, we suggest it to be related tothe intervention in between, namely the rehabilitation program. The effects of the visualcompensation somehow seem to weaken the influence of age and driving experience andstrengthen the influence of time since injury.As we previously conceptually suggested, we consider visual performance during driving (atpre-assessment) to be influenced by visual (i.c. HH) and probably by cognitive impairments(caused by the brain damage). In addition, in this pre-compensation state, performance isinfluenced by obvious personal characteristics, like age and driving experience. Byparticipating in the visual rehabilitation program, an additional contextual factor isintroduced, possibly blurring other influences (of age and driving experience in this case). Onthe other hand, the effects of visual compensation can also be conceived as a removal of (partof) the visual consequences of the visual impairment (i.c. HH), possibly revealing newinfluences. Both conceptualisations (addition of contextual factor and removal of influence ofimpairment) are directly inspired by ICF theorisation, which also suggests that theinterpretations need not to be mutually exclusive. In the last interpretation and following ICF,visuo-spatial function would be more purely measured at post-assessment, as measurementsare less distorted by negative effects of the visual impairment. We did find some indicationsfor this suggestion in our results. Namely, we observed that the VIS factor could be predicted(as evidenced by the regression models) on the basis of the global (neuropsychological)component scores. This was our expectation, since it can be assumed that visuo-spatialfunction as measured during driving and as measured by neuropsychological tests, should berelated. We observed that the prediction at post-assessment (R2 = .50) seemed better than atpre-assessment (R2 = .44). This confirms our suggestion, as we previously argued that at post-assessment neuropsychologically-assessed visuo-spatial function is more purely measured(less distorted by the visual impairment) than at pre-assessment, and it can be assumed thattwo more pure measures interrelate more strongly than when one is confounded. Additionally,and perhaps at first hand unobviously, as post-assessment neuropsychological performancegives a better indication of (“true”) visuo-spatial function than pre-assessment performance,visuo-spatial performance during driving at pre-assessment should at least equally well, oreven more strongly, be related to neuropsychological performance at post-assessment than atpre-assessment (without the reverse being true). This pattern was observed in our data (VIS atpre-assessment by global factor scores at post-assessment: R2 = .54 versus VIS at post-assessment by global factor scores at pre-assessment: R2 = .33).
Clearly our results are suggestive for a change in visuo-spatial performance between bothassessments. Although it can never be conclusively decided that this change is due to thevisual rehabilitation program, the selective improvement in visuo-spatial performance duringdriving argues against a non-specific placebo-effect. But if the compensational effect is to beconceived as a relief of visual consequences of the visual impairment, it remains puzzlingwhy it was not expressed in better visuo-spatial neuropsychological performance.

Prediction and Evaluation133
5.3. Prediction of improvementAlthough visual performance during driving (VIS), before as well as after the rehabilitationprogram, could be predicted by visuo-spatial neuropsychological test performance, theimprovement in VIS could not. Also, age, driving experience and time since lesion wererelated to, at least one of, the VIS measurements. None of them, however, were related to theimprovement in VIS. Taken the limitations of the low number of patients in mind, these datasuggest that all patients benefited equally from the intervention. This implies that this type ofintervention can be applied for all patients but that the goals of rehabilitation should bedependent on the degree of limitation, so that modest goals are set for moderately limitedpatients and higher goals can be attempted for less limited patients.
5.4. Implications and conclusionsThe transfer of treatment-related gains, as this is one of the major aims of cognitiverehabilitation (Levin, 1990) has been evaluated scarcely (Kerkhoff, 1999). Transfer to non-treatment related (visuo-spatially dependent) activities has previously been reported. Kerkhoff(1999) summarised the improvements of compensational scanning training as betteridentification and location of objects in the blind hemifield, reduction of errors in visualsearch, increase in search speed, and subjective improvements of visual functions as measuredby a questionnaire. Additionally, also transfer of treatment related gains to daily life has beenreported. Kerkhoff et al. (1994) showed significant improvements on a Table Test (findingobjects on a table) and Webster et al. (1984) showed significant improvements on wheelchairobstacle-course performance. The improvements we observed, i.c. in visual performanceduring driving, can be classified as (part of) a socially important daily life activity. However,whether this improvement can be classified as transfer to a non-treatment related activity isdebatable, since driving lessons were a part of the visual rehabilitation program, but the test-ride itself was never exercised. This does not devaluate the suggested positive effects of therehabilitation program, since the ultimate aim of the program was to reduce visuo-spatiallimitations and restrictions, where finally activities of daily living (rather than pureneuropsychological task performance) are the norm.
In conclusion, our results are in concordance with previously made claims. Firstly, visualperformance during driving, an important aspect of the driving task, can be related to visuo-spatial neuropsychological test performance. Secondly, patients with HH can be fit to drive,since not all of our patients failed the driving test. Furthermore, since visuo-spatial disability,common and apparent in these patients and consequential for practical fitness to drive, can bepositively influenced by our visual rehabilitation program, continuation of (improvement of)rehabilitation efforts for HH is justified and highly desired.Although visual performance during driving significantly improved, driving performance didnot meet the standard for passing the driving test for each patient, nor did we find any clearevidence of substantial improvement in neuropsychological test performance. As indicated byour patients, more rehabilitation time and perhaps also more attention to aspects other thanpure visuo-spatial function, should be incorporated, as to reduce even more visual limitationsand restrictions. Alternatively, in contrast to a collective rehabilitation aim, the goal could betuned to the degree of limitation of the patient.

Prediction and Evaluation134
Finally, to validate the exact therapeutic effects of the visual rehabilitation program, arandomised controlled trial with HH patients who are not trained is needed, but whether this isan ethically defendable option, is however debatable.
6. Reference ListBrouwer,W.H. (2001). Attention and driving: a cognitive neuropsychological
approach. In P. Zimmerman & M. Leclercq (Eds.), Applied Neuropsychology of Attention.Hove: Psychology Press.
Brouwer,W.H., & Withaar,F.K. (1997). Fitness to Drive After Traumatic BrainInjury. Neuropsychological Rehabilitation, 7, 177-193.
Coeckelbergh,T.R.M., Kooijman,A.C., Brouwer,W.H., & Cornelissen,F.W. (1999).Improving Driving Performance of Persons with Visual Field Defects: Results of a PilotStudy. In A. G. Gale, I. D. Brown, C. M. Haslegrave, & S. P. Taylor (Eds.), Vision inVehicles-VII. (pp. 119-127). Amsterdam: Elsevier Science.
De Graaf,A., & Deelman,B.G. (1991). Cognitieve Screening Test. Lisse: Swets &Zeitlinger.
De Raedt,R. (2000). Cognitive/Neuropsychological functioning and compensationrelated to car driving performance in older adults. Free University Brussels.
De Renzi,E., Faglioni,P., & Sorgato,P. (1982). Modality-specific and supramodalmechanisms of apraxia. Brain, 105, 301-312.
Deelman,B.G., Liebrand,W.B.G., Koning-Haanstra,M., & van der Burg,W. (1987).SAN test. Lisse: Swets & Zeitlinger.
Engum,E.S., Cron,L., Hulse,C.K., Pendergrass,T.M., & Lambert,W. (1988).Cognitive behavioral driver's inventory. Cognitive Rehabilitation, 6, 34-50.
Engum,E.S., Lambert,W., & Scott,T. (1990). Criterion-related validity of thecognitive behavioral driver's inventory: brain injured patients versus normal controls.Cognitive Rehabilitation, 8, 20-26.
Engum,E.S., Lambert,W., Womac,J., & Pendergrass,T.M. (1988). Norms anddecision making rules for the cognitive behavioral driver's inventory. CognitiveRehabilitation, 6, 12-18.
Folstein,M.F., Folstein,S.E., & McHugh,P.R. (1975). "Mini-mental state". Apractical method for grading the cognitive state of patients for the clinician. Journal ofPsychiatric Research, 12, 189-198.
Galski,M., Bruno,R.L., & Ehle,H.T. (1992). Driving after cerebral damage: amodel with implications for evaluation. American Journal of Occupational Therapy, 46, 324-323.

Prediction and Evaluation135
Kerkhoff,G. (1999). Restorative and compensatory therapy approaches in cerebralblindness - a review. Restorative Neurology and Neuroscience, 15, 255-271.
Kerkhoff,G., Munssinger,U., Haaf,E., Eberle-Strauss,G., & Stogerer,E. (1992).Rehabilitation of homonymous scotoma in patients with postgeniculate damage of the visualsystem: saccadic compensation training. Restorative Neurology and Neuroscience, 4, 245-254.
Kerkhoff,G., Munssinger,U., & Meier,E.K. (1994). Neurovisual rehabilitation incerebral blindness. Archives of Neurology, 51, 474-481.
Levin,H.S. (1990). Cognitive rehabilitation. Unproved but promising. Archives ofNeurology, 47, 223-224.
Lincoln,N.B., & Fanthome,Y. (1994). Reliability of the Stroke Drivers ScreeningAssessment. Clinical Rehabilitation, 8, 157-160.
Mazer,B.L., Korner-Bitensky,N.A., & Sofer,S. (1998). Predicting ability to driveafter a stroke. Archives of Physical Medicine and Rehabilitation, 79, 743-750.
Meienberg,O., Zangemeister,W.H., Rosenberg,M., Hoyt,W.F., & Stark,L. (1981).Saccadic eye movement strategies in patients with homonymous hemianopia. Annals ofNeurology, 9, 537-544.
Neetens,A. (1994). Revalidation of homonymous hemianopic patients. In A. C.Kooijman, P. L. Looijestijn, J. A. Welling, & G. J. van der Wildt (Eds.), Low Vision.Research and New Developments in Rehabilitation. (pp. 296-300). Amsterdam and Oxford:IOS Press.
Nelles,G., Esser,J., Eckstein,A., Tiede,A., Gerhard,H., & Diener,H.C. (2001).Compensatory visual field training for patients with hemianopia after stroke. NeuroscienceLetters, 306, 189-192.
Nouri,F.M., & Lincoln,N.B. (1993). Predicting driving performance after stroke.British medical journal, 307, 482-483.
Nouri,F.M., Tinson,D.J., & Lincoln,N.B. (1987). Cognitive ability and drivingafter a stroke. International Disability Studies, 9, 110-115.
Peli,E. (2000). Field Expansion for Homonymous Hemianopia by OpticallyInduced Peripheral Exotropia. Optometry and Vision Science, 77, 453-464.
Peli,E. (2001). Vision multiplexing - an engineering approach to visionrehabilitation device development. Optometry and Vision Science, 78, 304-315.
Rockwell,T.H. (1972). Skills, judgement and information acquisition in driving. InT. W. Forbes (Ed.), Human Factors in Highway Traffic Safety Research. (pp. 133-164). NewYork: Wiley-Interscience.

Prediction and Evaluation136
Sivak,M., Olson,P.L., Kewman,D.G., Won,H., & Henson,D.L. (1981). Drivingand perceptual/cognitive skills: behavioral consequences of brain damage. Archives ofPhysical Medicine and Rehabilitation, 62, 476-483.
Stevens,J. (1996). Applied multivariate statistics for the social sciences. (3rd ed.).Mahwal, New Jersey: Lawrence Erlbaum Associates, Inc.
Tant,M.L.M. (in preparation). Visual Performance in Homonymous Hemianopia:Assessment, Training and Driving. University of Groningen.
Tant,M.L.M., Bouma,J.M., Kooijman,A.C., Cornelissen,F.W., & Brouwer,W.H.(in press). Visual rehabilitation in Homonymous Hemianopia and related disorders. In W. H.Brouwer, A. H. van Zomeren, I. J. Berg, J. M. Bouma, & E. H. F. de Haan (Eds.),Neuropsychological rehabilitation: a cognitive approach. Amsterdam: Boom.
Tant,M.L.M., Brouwer,W.H., Kooijman,A.C., & Cornelissen,F.W. (submitted).Driving and Visuo-Spatial Test performance in Homonymous Hemianopia.Neuropsychological Rehabilitation.
Warrington,E.K., & James,M. (1991). The Visual Object and Space battery. BurySt. Edmunds, England.
Webster,J.S., Jones,S., Blanton,P., Gross,R., Beissel,G.F., & Wofford,J.D. (1984).Visual scanning training with stroke patients. Behaviour Therapy, 15, 129-143.
Withaar,F.K. (2000). Divided Attention and driving: The effects of ageing andbrain injury. University of Groningen.
Withaar,F.K., Brouwer,W.H., & van Zomeren,A.H. (2000). Fitness to drive inolder drivers with cognitive impairment. Journal of the International NeuropsychologicalSociety, 6, 480-490.
Zihl,J. (1994). Rehabilitation of visual impairments in patients with brain damage.In A. C. Kooijman, P. L. Looijestijn, J. A. Welling, & G. J. van der Wildt (Eds.), LowVision. Research and New Developments in Rehabilitation. (pp. 287-295). Amsterdam andOxford: IOS Press.
Zihl,J. (2000). Rehabilitation of Visual Disorders After Brain Injury. Hove, EastSussex: Psychology Press Ltd.
Zihl,J., & Kennard,C. (1996). Disorders of Higher Visual Function. In T. Brandt,L. R. Caplan, J. Dichjons, H. C. Diener, & C. Kennard (Eds.), Neurological Disorders:Course and Treatment. (pp. 201-212). San Diego, California: Academic Press.

137
Part III: Additional findings in patients with HH and related impairments

Grey Scales138
Grey Scales uncover similar attentional effects in homonymous hemianopiaand visual hemi-neglect*
1. AbstractMulti-component models of visual hemi-neglect have postulated that visual hemi-neglect ischaracterised by various attentional deficits. A Grey Scales-task has been developed toquantify the early, automatic, (perhaps obligatory) ipsilesional orienting of visual attention,frequently assumed as the first of these attentional deficits. Explanations for this attentionalimbalance are up until now mainly formulated in terms of right hemisphere activation. Thislateral attentional bias has also been demonstrated in controls, in whom it is expressed as aleftward perceptual asymmetry. We reproduced previous literature findings on a Grey Scales-task, considering controls and neglect patients. Three patients with neglect showed an extremeipsilesional lateral bias. This bias did not change during or after cognitive rehabilitation.Additionally, we presented this Grey Scale-task to 32 patients with left- and right-sidedhomonymous hemianopia (HH). Homonymous hemianopia is the loss of sight in one visualhemi-field. The HH patients had no clinical signs of impaired lateralised attention. Resultsrevealed that HH patients showed a similar ipsilesional bias, albeit to a lesser degree than inneglect. Left-sided HH patients presented a quantitatively similar, but qualitatively oppositebias than the right-sided HH patients. We suggest that sensory effects can be an alternativesource of attentional imbalance, which can interact with the previously proposed (right)hemispheric effects. This suggests that the perceptual asymmetry in the Grey Scales-task isnot necessarily an indicator of impaired right hemisphere attention. It rather suggests a patternof functional cerebral asymmetry, which can also be caused by asymmetric sensory input.
2. IntroductionSeveral authors (e.g. [16, 11, 23]) suggested that the clinical syndrome of unilateral visualspatial neglect (UN) can be described/explained as a series of successive attentional eventsbeginning with (1) an early, automatic, chronic, perhaps obligatory, orienting of attentiontoward the ipsilesional half space, followed by (2) a deficit in disengaging attention from thatside in order to reorient it toward the contralateral half space. In addition to these two deficits,(3) a generalised (i.e. directionally non-specific) reduction in attentional-informationprocessing capacity is assumed. The first component underlies an anomalous lateralpreference. The second component gives rise to the clinical signs of UN (e.g. left-sidedomissions on cancellation tasks) [23]. Karnath [16] proposed that this second component(reorienting) recovers faster than the other two, and this has been confirmed by severalauthors (e.g. [28, 23]). Mattingley and colleagues [23] concluded that the apparent recovery ofUN constituted of the restitution in reorienting of attention, but that the early ipsilesionalorienting remained. They further postulated this (residual) attentional bias to be characteristicof right hemisphere dysfunction, and posed that it could be predictive of persistent neglect-type behaviours.
This attentional bias has been demonstrated in right hemisphere patients, not only using RTparadigms (e.g. [3]), but also under more naturalistic free viewing conditions. It has beendemonstrated using several indexes and tasks. Gainotti et al. [11] operationally defined it as a"position preference", namely as the tendency to identify first (and consistently) those parts ofa composite diagram lying on the right or on the left of its centre. As a result of the early,
* This manuscript was accepted by Neuropsychologia (Tant, Kuks, Kooijman, Cornelissen & Brouwer)

Grey Scales139
automatic orienting of attention, UN patients frequently start scanning on the right side of agiven composite stimulus (i.e. show a rightward bias). A further frequently used indexexpressing this lateral orienting bias is an Asymmetry Index (AI) derived from mainlyparadigms using chimeric stimuli. For example, Mattingley et al. [24, 23] concluded that thislateral preference is expressed (in UN) by a tendency to choose or prefer the right side of acomposite image (rightward bias). In a face-matching task by Mattingley et al. [23], subjectswere required to indicate which of two bisymmetrical composites (one composed of the twoleft halves of an original face, the other composed of the two right halves) more closelyresembled the (inherently asymmetrical) original. Patients with UN tended to judge the facescomposed of the two right halves as more similar to the original one than the face composedof two left halves (rightward bias). In another chimeric faces task, presented by the sameauthors, patients were required to judge which face of a given pair appeared "happier". Thefaces were composed of two half-faces of the same person, one half smiling, the other in aneutral expression. In one pair, the smiling face was on the left, in the other on the right.Again, UN patients tended to judge the face with the "right-smile" as happier. This rightwardbias was also demonstrated using Grey Scales [24]. In this task, the patient was required tocompare two vertically aligned rectangular bars and indicate which one appears overalldarker. The bars consisted of scales of semi-continuous shades of grey, ranging from white onone end to black on the other. Both bars were identical, but mirror-reversed. Patients with UNtended to choose the bar which was black on the right side as the darker one.
Lateral biases have also been demonstrated in healthy subjects using identical or comparableparadigms (e.g. [27, 24, 23, 21]). Contrary to patients with UN, healthy subjects exhibit asignificant leftward bias. Since this bias is displayed by healthy subjects, and hence isconsidered to be "normal", it is often termed as a "perceptual asymmetry" instead of a "bias"(which suggests deviation from normality).This left perceptual asymmetry in healthy subjects has been demonstrated using face-stimuli(judgements of emotions, similarity, and femininity) [24, 23, 21], using Grey Scales (e.g.[24]), and using stimuli asking for comparisons of dot numerosity and roundness (e.g. [21]),and size (e.g. [27]). The leftward bias occurs in all these tasks in more or less comparableintensities. Despite of the similar levels of perceptual asymmetry, only low to modestintercorrelations are observed. Nicholls and colleagues [27] suggest that these tasks do notindex one single common factor, but tap a set of attentional processes, some of which areoverlapping, and others which are task-specific. The communality is suggested to consist inthe common right hemisphere involvement.
Summarising the explanations provided in the literature, in healthy subjects the lateral bias isexplained as the result of more right hemisphere activation due to the visuo-spatial nature ofthe stimuli [21,22, 23,28]. It is argued that the differential activation of the right hemispheregenerates a bias of attention to the left hemispace, creating an attentional imbalance. In UNpatients, the lateral bias results from disturbed right hemisphere function. It is suggested[19,20,24,23] that each hemisphere controls a contralaterally directed attentional vector.Damage to one hemisphere results in dysfunction of the associated vector and gives rise to anipsilesional bias. In all accounts, the perceptual asymmetry is explained in terms of functionalcerebral asymmetry and more specifically in terms of differential attentional right hemisphereactivation. One other alternative account was proposed by Nicholls et al. [27]. They suggestedthe possibility that the asymmetry may be related to effects of directional scanning. In support

Grey Scales140
of this proposal, they report a study by Sakhuja et al. [29] who found that readers of Hindi(left-to-right) showed the expected leftward bias, whereas readers of Urdu (right-to-left)showed the opposite bias. Nicholls and colleagues argue that the preferred directionalscanning habit may lead to an over-representation of one side (i.e. ipsi-directional) of thestimulus and hence can influence the nature of the perceptual asymmetry. Thisconceptualisation, namely as a lateralised over-representation, also can be interpreted as anattentional account. It suggests an alternative nature or cause of attentional imbalance.
In our opinion, further alternative causes of the attentional imbalance can not be ruled out onthe basis of previous experiments. Mattingley et al. [23] demonstrated that patients no longershowing classical signs of UN, continued to show the ipsilesional attentional bias. Theauthors interpreted the persisting ipsilesional attentional bias in terms of a higher-orderattentional right hemisphere dysfunction. However, five of the 13 patients also had visualfield defects (VFDs), i.c. either homonymous hemianopia (HH) or quadranopia. Hence, theobserved residual (group-)effects (in terms of the bias) could be attributable, not to a higher-order right hemisphere attentional problem, but alternatively to effects of the (lower-order)left-sided VFDs.It is well recognised that visuo-spatial perception can be impaired in “pure” hemianopicpatients (i.e. in patients with HH and without UN) [39]. Hemianopic patients have beenreported to show impaired visuo-spatial exploration, especially in the hemianopic hemi-field[40]. Also a deviated subjective midline or subjective straight-ahead in visuo-spatialjudgements has frequently been reported [e.g. 18, 2, 8]. Karnath and Ferber [17] discussreports which show that misperception of horizontal space (hemimicropsia) exists in (some)pure hemianopic patients. It is thus apparent that a homonymous VFD can give rise tolateralised visual impairments. Hence it is not inconceivable that HH, which results inherentlyin a chronic differential lateralised visual input, also gives rise to an imbalance in processingefficiency of the visual space. We thus suggest that an attentional imbalance is not necessarilythe result of a higher-order attentional right hemisphere dysfunction, but also can arise by thepresence of a lower-order VFD.
It is hence our aim to investigate what is or can be the cause of the attentional imbalanceresulting in the observed lateral biases. As argued, hemispheric specialisation for visuo-spatialprocessing, hemispheric specificity with respect to directional attentional vectors and readinghabits or scanning direction have been suggested as underlying mechanisms. We investigate ifhomonymous VFDs (i.c. HH), resulting in asymmetric visual input, can also be added to thelist of mechanisms or factors producing attentional imbalance. If so, it should do so both inleft-sided and right-sided HH, but in opposing directions (i.e. both contralaterally to the sideof the VFD). If this is confirmed, previous explanations of the attentional imbalance stressingexclusively higher-order right hemisphere involvement may have to be revised.
3. Method3.1. Participants3.1.1. ControlsSixty-three control subjects participated in this study (25 females, 38 males). All participantswere naive as to the aims and expected outcomes of the study and reported to be right-handed.They all had normal or corrected-to-normal visual acuity. Their mean age was 47 years,ranging from 17 to 86 years.

Grey Scales141
3.1.2. PatientsPrior to testing, we administered a screening battery to exclude dementia [5, 9], aphasia [7]and apraxia [6]. No impairments were found. All patients performed within the normal limitson the form discrimination screening test [36] confirming perceptual functions to be adequatefor form discrimination. The nature and extent of the VFD was determined using theHumphrey Field Analyzer, which is a clinically widely used automated perimeter. We usedthe Full Field 246, age corrected, 3-zone strategy, screening program.
In order to identify patients with severe UN, we constructed a battery of clinical UN tests,namely, four clinical cancellation tasks, and a line bisection task. For Albert’s linecancellation Test the cut-off score is two omissions [13, 35]. For the Mesulam StructuredShape cancellation this was three omissions [38], for The Bells Test four omissions [12, 35],and three omissions on the Search for O's. This last unstructured cancellation task is notpublically available, but very frequently used for diagnostic purposes in the Netherlands. Alsothe Line bisection task was scored as a function of omitted lines (cut-off = 2) [30, 34,31].For each task, we additionally imposed more stringent criteria. This was done in order tomake a distinction between a general inattention deficit resulting in a general scanning deficit,and hemi-inattention resulting in a lateralised scanning deficit. We therefore imposed anadditional “lateralisation-requirement", namely that for a "UN-score" (as opposed to a"general attention deficit-score") the difference between left-sided and right-sided omissionsshould also be equal to or exceed the cut-off score. For example, if the cut-off score for aparticular test is three omissions, a UN-score is obtained only if also the number of omissionson either side exceeds the other side by at least three. Two left-sided omissions and one right-sided omission hence would not result in a UN-score, although it is indicative of a generalattention and scanning deficit.We decided that using this battery and cut-off criteria, a patient is considered to suffer severeUN if at least three (of maximally five) UN-scores are obtained and if these scores areidentical in laterality (i.e. reach the lateralisation-requirements of the respective tests due toomissions on the same side).
3.1.2.1. UN patientsThree patients were classified as UN patients using our criteria. They were all males andsuffered a right-sided stroke, resulting in UN and left-sided HH. One patient underwentextensive clinical rehabilitation in a clinical setting before participating, but the UN persisted.The other two patients were referred by their ophthalmologists because of “peculiar visualbehaviour”. Their mean time since lesion was 16 months. Their visual acuity and contrastsensitivity were within normal limits. Their mean age was 64 years. Additional clinicalinformation is provided in table 1. On average they omitted 13 items (SD = 9) on the Albert’sline cancellation Test, 23 items (SD = 22) on the Mesulam Structured Shape cancellation, 17items (SD = 9) on The Bells Test, 17 items (SD = 14) on the Search for O's, and three lines(SD = 3) on the Line bisection task.

Grey Scales142
Table 1. Clinical data for the brain-damaged subjectsAge/
GenderTSLa type of HHb and
macular sparingLocationc and caused of
lesionOther remarks
UN group Right-sided brain damage1 50/M 34 C-I, no T-O-P IC, CVA extensive clinical rehabilitation2 74/M 7 C-C, no O dS, CVA left leg hemiparesic3 70/M 7 C-C, no O-P, CVA
Left-sided HH group Right-sided brain damage1 76/M 13 I-I, yes T-O-P, CVA2 69/M 12 I-C, yes O-P, CVA3 53/M 24 I-C, yes O-P, CVA4 56/M 9 I-C, yes O, CVA5 49/M 18 I-I, yes O-T, tumor blindsight6 29/M 9 I- , yes oC, CHI right eye blind7 36/F 107 I-C, yes O, CVA8 56/F 157 C-C, no O-T, CVA left hemiplegic9 73/M 6 I-I, yes O-P, CVA10 31/M 12 C-C, yes O, CVA11 70/M 13 I-C, no O, CVA12 34/M 64 I-C, yes O-P-F, CHI left hemiplegic13 54/M 24 I-C, yes T-O-P Th, CVA left hemiplegic, agnosia14 53/M 11 C-C, no O, CVA letter-by-letter reading15 37/M 12 I-C, yes O-P, tumor16 67/M 47 C-C, no O-T, CVA left hemiparesic
Right-sided HH group Left-sided brain damage1 50/M 390 C-C, yes O, tumor2 51/F 57 C-C, yes O, CVA3 50/M 28 I-I, no T-O-P, CHI word finding difficulties4 39/F 142 I-C, yes O, CVA5 66/M 123 I-I, yes O, CVA6 18/M 225 I-I, yes O-P*, hydrocephalus mild balance problem7 43/F 60 C-C, yes O-T, CVA letter-by-letter reading8 52/M 6 I-I, yes Nd, CVA9 64/F 10 I-C, yes O-T, CVA10 65/M 32 I-C, yes Na, CVA11 48/F 11 I-I, yes O-P, CVA12 53/M 22 C-C, yes O-T, CVA13 56/M 14 I-I, yes O-T Th, CVA left hemiparesic, blindsight14 68/M 25 I-I, no T-O-P, CVA word finding difficulties15 24/M 63 C-C, no Nd, CHI16 57/M 3 C-C, no O, CVA word finding difficulties
a Time Since Lesion in monthsb Complete (C) versus Incomplete (I) – Congruent (C) versus Incongruent (I) Homonymous Hemianopiac O: occipital, T: temporal, P: parietal, F: frontal, Th: thalamus, IC: internal capsula, oC: optic chiasm, dS: diffusesubcortical damage, Nd: no abnormalities detected on CT, Na: no CT available.d CVA: cerebrovascular accident, CHI: closed head injury* Patient refused to give permission for scan inspection. Localisation is based on clinically motivated assumptionand verbal description.
3.1.2.2. HH patientsThirty-two patients with HH participated in this study. Their mean age was 51 years. Themean time since lesion was 55 months (SD = 80). Sixteen patients had left-sided HH (16

Grey Scales143
males, 2 females). Sixteen patients had right-sided HH (11 males, 5 females). All patients hadnormal or corrected-to-normal visual acuity and normal contrast sensitivity. For additionalclinical data, see table 1. None of these patients fulfilled the aforementioned UN criteria.Neither of them had ever been treated for or diagnosed with UN. They omitted no items onthe Albert’s line cancellation Test and on the Line bisection task, on average three items (SD= 9) on the Mesulam Structured Shape cancellation, three items (SD = 4) on The Bells Test,and one item (SD = 3) on the Search for O's.
3.2. StimuliWe used Grey Scales as described in Mattingley etal.[24]. Our version contains 26 items. An itemconsists of an A4 (landscape orientation) white sheetof paper with two vertically aligned rectangular GreyScales of equal lengths. A Grey Scale is a rectangularbar with a thin black border (see fig. 1). Itsdimensions are 20 mm in height and 20 to 260 mm inwidth with 20 mm increments. This rectangular isfilled-in by a semi-continuous scale of different greyshades varying between black and white at theextremes. This filling-in is achieved by defining 33 strips of different grey shades. The widthof these band is adjusted according to the length of the rectangular. Grey Scales are thuspresented in pairs (and vertically aligned) so that one Grey Scale is identical to, but the mirrorreverse of, the other. Each item is presented once with top/bottom position counterbalanced,resulting in 26 items.
3.3. ProcedureA booklet containing the 26 items is placed and remains in front of the subject at readingdistance. The subject is asked to judge which of the two Grey Scales appears overall darker.The choice is indicated by saying "top" or "bottom" after which the page is turned and thenext item is presented. The subject is encouraged to make a judgement based uponspontaneous and immediate apprehension rather than on prolonged and detailed inspectionbut is told that there is no time limit and hence can view freely. Most patients respondedfluently and confidently. Many controls, on the other hand, felt they were making arbitrarychoices. In addition to this standard procedure, on a second occasion, we asked the UNpatients to touch the left side of each bar, prior to judging, to ascertain the perception of thefull length of the bars.
3.4. ScoringScoring is achieved as in Mattingley et al. [24]. For each stimulus, a response is defined asleft-bias or right-bias respectively if the subject chose the Grey Scale with the black side onthe left and right side respectively as the darker one. The Asymmetry Index (AI) wascalculated as the number of items with a rightward bias, minus the number of items with aleftward bias, divided by the total number of items. This AI varies between -1 and +1,representing an extreme leftward and rightward bias respectively. An AI of zero indicates nobias.
Fig. 1. Example of an item in the GreyScales task. Upper and lower bar areidentical but mirror-reversed.

Grey Scales144
4. ResultsWe firstly checked whether we were able to replicate previous findings with control subjects.The mean AI was -0.3370 (SD = .4304) which is significantly different from zero (t(62) = -6.215, p < .0005). This confirms a significant leftward bias in control subjects. Secondly, weconfirmed the extreme lateral bias displayed by our three UN patients. All AIs were equal toone (mean = 1, SD = 0), also on the second occasion, when both left ends of the bars had to betouched.We then performed a one-way ANOVA, with both left-sided and right-sided HH groups andcontrol subjects as a between-subjects (group)factor. This revealed a significant group effect(F(2, 92) = 40.757, p < .0005). The mean AI for left-sided hemianopic patients was .6317 (SD= .3725) and for right-sided hemianopic patients -.5417 (SD = .3967). Post-hoc comparisonswith Bonferroni correction revealed the HH groups to differ from each other (t(30) = 8.6, p <.0005) and the left-sided HH patients to differ from the control group (t(77) = 8.2, p < .0005) .There was no significant difference between the right-sided hemianopic patients and controlsubjects (t(77) = -1.7, ns). The patients with UN were not included in the ANOVA analysisbecause of the low number of patients and the absence of variation in their AIs. To testwhether the AIs by the left-sided HH patients significantly deviated from the AIs by the UNpatients, we performed a one sample T-test on the data by the left-sided hemianopic patientswith the AI from the UN patients (i.e. 1) as test value . This analysis revealed a significantdifference (t(15) = -3.956, p < .001). With the same type of analysis but with the absolutevalue of the AI by the right-sided HH patients as the test value, we confirmed that the strengthof the AI by both HH groups did not differ from each other (t(15) = .966, ns).
In the control group, we found no effects of educational level, nor of age. However, in thepooled HH-group, the effect of age was marginally significant as indicated by a Pearsonscorrelation of age with the absolute value of the AI (r(32) = .338, p < .059). Further, timesince lesion proved to correlate significantly with the absolute value of the AI (r(32) = -.436,p < .05). Time since lesion and age did not correlate in this sample (r(32) = -.283, ns). Noneof the measures of the clinical UN battery correlated significantly with the absolute value ofthe AI.We further had the opportunity to test 15 HH (7 left-sided and 8 right-sided) patients on twodifferent occasions (one week interval, same standard procedure). The AIs on both occasionscorrelated significantly (r(15) = .968, p < .0005), and a paired T-test comparison showed nosignificant difference (t(14) = -1.662, ns) between the means.
5. DiscussionWe replicated previous findings confirming (left) perceptual asymmetries under free viewingconditions in control subjects. Our AI (-.337) clearly is in line with the AI reported byMattingley et al. [24] using similar Grey Scales (-.323). It is also well within the range ofother AIs, using different types of chimeric stimuli ranging from -.208 to -.450 [27, 24, 23,21]. In controls, we found no effect of age, nor of educational level, suggesting the lateral biasto be a fairly robust phenomenon.
We secondly observed an extreme right-sided bias (AI = 1) in patients with UN. At first hand,our AIs might appear to be more extreme than those reported by Mattingley et al. [24] (AI =.849 for the Grey Scales). However, the authors report that four (of the twelve right-sidedbrain damaged) patients did not have UN. Removing those four patients from their results

Grey Scales145
would increase their observed AI, since three of the four lowest scores on the Grey Scales areby a non-UN patient. Not including these non-UN patients would result in all AIs (exceptone) to be above .9.One of our patients with UN participated in a cognitive rehabilitation program based on theprinciples mentioned in Pizzamiglio et al. [28] and was relatively successfully trained [32].His AI, after rehabilitation, remained at its extreme. This confirms claims made by Mattingleyet al. [23] that the AI represents a strong ipsilesional attentional bias which is insensitive torehabilitation. We further confirmed the persistency of the lateral bias by, additionally and ona second occasion, asking our left-sided hemianopic UN patients to touch the left side of eachbar separately before judging which one appeared darker. In order to touch the left side ofeach bar, the patients have to fixate the left side of it (as a consequence of their left-sidedHH). This brings the total bar in the right (and normally perceiving) visual hemi-field,ascertaining us that, at least once, both bars have been fully perceived. Also in this condition,all AIs remained at their extremes. This suggests this bias to be a chronic, very early (low-level) component in the visuo-attentional process, not subjected to effects of behaviouralcompensation. Previously made claims that this ipsilesional bias represents a relatively early,automatic, chronic, perhaps even obligatory orienting of attention [23] are herebystrengthened.
We previously summarised present accounts of the attentional imbalance. Mattingley andcolleagues [23] and Luh [22] suggested that the observed perceptual asymmetry in controls isthe result the selective activation of the right hemisphere, as it is specifically dedicated toprocessing visuo-spatial stimuli. In line with this, Luh et al. [21] previously had argued thatthere is a great deal of evidence that the performance of cognitive tasks for which onehemisphere is specialised, does result in an asymmetric activational pattern. This had alreadybeen recognised very early on by Trevarthen [33]. He further suggested that one hemispherecould be differentially activated by many conditions such as electrical stimulation of onehemisphere and unilateral brain damage.Similarly, Nicholls and colleagues [27] discuss an activation model of perceptual asymmetrypresented by Milner et al. [26]. This model suggests that the asymmetry can be conceptualisedas an attentional imbalance between resources allocated to the left and right hemispaces.Activation of the right hemisphere generates a bias of attention to the left hemispace,increasing the salience of stimuli located there. And since the right hemisphere is specialisedfor judgements of brightness [4], numerosity [25] and shape [10], performing the abovediscussed perceptual asymmetry tasks specifically activates the right hemisphere, resulting ina leftward bias. Nicholls et al. [27] argue that this activation model can account for numerousobservations in controls (e.g. the relatively low intercorrelations between the different, butequal in size, asymmetry scores), but fail to explain how this model could account for therightward bias in right hemisphere brain damaged patients.
As already briefly mentioned, other authors have attempted to explain the rightward biaspresent in UN patients and also stressed the involvement of the right hemisphere. Mattingleyet al. [24] suggest that the lateral bias reflects a gradient in perceptuo-attentional processingefficiency and note that the observed rightward bias is consistent with a model of spatialattention suggested by Kinsbourne [19, 20] which stresses the directional nature of space-related behaviour. It is argued that each hemisphere controls a contralaterally directedattentional vector. The net effect of both vectors gives rise to an attentional gradient (which

Grey Scales146
can be conceptualised as processing efficiency) imposed on the attentional field. Damage toone hemisphere results in dysfunction of the associated vector and hence results in anipsilesional bias. As such the attentional field is characterised by a gradient which allocates"more weight" or processing efficiency to the ipsilesional side. A unilateral lesion would alsorelease the opposing hemisphere from inhibition, and thereby further inducing a pathologicalipsilesional bias. A second critical element in Kinsbourne's vectorial model is that the strengthof the attentional vectors controlled by either hemisphere can be modulated by the activationof that hemisphere.
Hence, Kinsbourne’s vectorial model in combination with the assumed hemisphericspecialisation for visuo-spatial events, accommodates the rightward bias in UN and theleftward bias in controls (attentional/hemispheric account). By this view, the perceptualasymmetries reflect patterns of differential functional cerebral activity and specifically stressthat right hemisphere activity is a key concept. This right hemisphere predominance isconsidered to be exclusively based on its own internal properties i.c. its directional attentionalnature or its specialisation for visuo-spatial stimuli or tasks. We however argue that, inaddition to this hemispheric influence, also differential sensory input can be of influence.Several indications are provided by our results.
Firstly, we found differential performances within the right hemisphere brain damage group.Namely, all our UN patients presented extreme rightward biases, while the patients with left-sided HH were significantly less extreme, though clearly in the same direction andsignificantly different from no bias and from controls. The difference in performance, withinthe right hemisphere damage group, suggests that mere right hemisphere involvement (assuggested by previous accounts) can not be the sole explanation for the observed right-wardbias. However, since we did not have access to detailed neurological information, we cannotrule out the possibility that the size of the right hemisphere lesion can account for theobserved difference. A second confounding factor in our data is the marked difference in timesince lesion between both right hemisphere brain damage groups. This difference could thusalso, at least partly, account for the differential performance within this group. Hence, ourdata show differential performance in the right hemisphere brain damage group, suggestingother factors to be at hand than mere right hemisphere involvement. But alternatively, size of,and time since the right hemisphere lesion can not be ruled out as valid determinants.
However, secondly, we showed that right- and left-sided HH patients present a quantitativelysimilar, but qualitatively opposite pattern of results. Both HH groups are virtually identical,but suffer a mirror-reversed visual dysfunction and present an identical but also reversedlateral bias. The side of the attentional imbalance is clearly linked to side of the HH. Wehypothesise, conceptually in line with the previously mentioned “reading habit” assertion, thatthe VFDs lead to an over-representation of the ipsilesional hemi-space. It is commonlyassumed that visual attention has two aspects, namely exogenous (stimulus-induced) andendogenous (voluntary). Stimulus-induced attention is considered to be very dominant [15,14] and this directing of attention is thought to be guided by the saliency of (visual) objects.In patients with HH, objects from the non-perceiving hemifield cannot attract attention (i.e.have no saliency). All stimulus-driven capturing of attention is exclusively and consistently inthe ipsilesional direction. We conceptualise that this bias leads to an over-representation ofthe ipsi-lesional hemi-space, and hence an attentional imbalance. Our results suggest that

Grey Scales147
these effects in the HH group are conceptually different from attentional/hemispheric effects,as traditionally conceptualised, since none of the clinical UN measures correlated with the AI.
We hence argue that the sensory effects can be another source of attentional imbalance, whichcan interact with the hemispheric effects. In controls, the (normal) leftward bias is due to righthemisphere specialisation for visuo-spatial events. This bias seems enhanced by the sensoryeffect of a right-sided VFD. This enhancement did however not reach statistical significancein our sample. Damage to the right hemisphere removes the (hemispheric) leftward bias, andinduces a rightward bias. Right hemisphere brain damage can disrupt typical visuo-attentionaland directional processes, thought to be typical in UN. But a similar rightward bias can alsobe elicited by left-sided VFDs, for the same (i.e. sensory) reason as with right-sided VFDs.In our study, we cannot dissociate the sensory and attentional/hemispheric components, but itwas shown by Mattingley et al. [24] that UN patients without VFDs, all showed an extremeAI on the Grey Scales task. In our patients with UN (and left-sided HH), both sensory andhemispheric components are combined, leading in all cases to extreme and persistentrightward biases. In our left-sided VFD patients, only the sensory component is present (withpossibly a minor hemispheric component). The bias is qualitatively similar to the UN patients,but less extreme. Warranted, as already argued, by the possible size and time since righthemisphere lesion effects, this suggests the sensory component to be less dominant.
Firstly, this would strengthen the claim that UN is more severe when it occurs simultaneouslywith HH (e.g. [1,37]) since this condition entails both sensory and attentional/hemisphericcomponents. Secondly, this would underpin our claim that one symptom of UN behaviour(namely the lateral bias) can also be displayed by non-UN patients, namely also by HHpatients. This suggests, at least at the behavioural level, a continuum in disability, giving riseto the notion “subclinical neglect”. This term would indicate subtle indications of UN(-behaviour), without objective clinical signs or evidence of UN.
In previous literature, it was not clear whether the attentional imbalance was considered to bethe cause of UN (as suggested by Kinsbourne's model) or whether it resulted as aconsequence of another dysfunction (e.g. a contralesional attentional deficit in UN, or a VFDas in HH). Previous literature had shown that, in pure UN (UN without VFDs), an ipsilesionalbias could be demonstrated (e.g. [23, 24]), suggesting an attentional/hemispheric component.We found that HH also gives rise to a qualitatively similar bias, suggesting a sensorycomponent. We therefore conclude that the attentional imbalance can be multiply influencedand is hence a consequence rather than cause. This has the further implication that anattentional imbalance is not necessarily and unequivocally to be associated with UN.
We feel that the Grey Scales task has strong clinical potential. Firstly, as was suggested inprevious literature, the AI can be considered a sensitive measure of attentional imbalance,with UN as its extreme. Secondly, the AI can give the clinician a clear indication of thepossible presence and side of a homonymous VFD. Namely, in our brain damaged patientgroup with homonymous VFDs, we observed a sensitivity and specificity of .94 and .88 inpredicting the side of the HH, given the direction of the AI. Thirdly, contrary to mostcancellation tasks or other tasks clinically used to diagnose differential lateral performance,almost any patient can perform the Grey Scales task, because it has no identificationcomponent. We hence successfully applied this test to a patient with complete object-agnosia,

Grey Scales148
while all cancellation tasks appeared unachievable. Finally, although not extensivelyinvestigated, we feel that the AI can also have some practical significance. In a larger studyinvestigating practical fitness to drive in patients with HH (to be published), we foundevidence that the AI was significantly related to visual performance during driving (r(29) = -.510, p < .005), while AIs from other tasks were not or significantly less strongly related. Thissuggests the Grey Scales task to have some practical significance to at least this type ofactivity of daily living.
In conclusion, we do not refute that perceptual biases reflect a pattern of functional cerebralasymmetry. But the imbalance can not be uniquely related to specialisation of the righthemisphere for visuo-spatial attentional function, since left- and right-sided hemianopicpatients, with right- and left-sided brain damage respectively, show similar but inverse lateralbiases. Asymmetric activation of one hemisphere can be the result of asymmetric sensoryinput, caused by the HH.
To further understand the nature and cause of the different components which can give rise tothe attentional imbalance, future research could concentrate on patients with left- and right-sided brain damage, without clinical signs of UN and without VFDs. This could elucidate thepossible differential hemispheric involvement. Further, other types of homonymous VFDscould also contribute to the insight into the involvement of the sensory influences. In bilateralsuperior and inferior quadranopia (i.e. missing a lower and upper hemifield respectively) andwith the Grey Scales items 90 degrees rotated, the attentional imbalance should result in aquantitatively similar upper and lower bias respectively. We also envisage experiments wheredifferent types of homonymous VFDs can be simulated on (non-brain damaged) controlsusing sophisticated eye-movement equipment. In these kinds of paradigms, the observedasymmetries (if any) are unconfounded with respect to VFDs and brain damage. Finally, forclinical and practical use, the relationship with performance during activities of everyday lifeshould be further investigated and confirmed.
6. References
[1]Agrell, B M, Dehlin, O I, Dahlgren, C J. Neglect in elderly stroke patients: a comparison offive tests. Psychiatry and Clinical Neuroscience 1997;��:295-300.
[2]Barton, J J, Behrmann, M, Black, S. Ocular search during line bisection. The effects ofhemi-neglect and hemianopia. Brain 1998;���:1117-1131.
[3]D'Erme, P, Robertson, I, Bartolomeo, P, Daniele, A, Gainotti, G. Early rightwardsorienting of attention on simple reaction time performance in patients with left-sidedneglect. Neuropsychologia 1992;��:989-1000.
[4]Davidoff, J B. Hemispheric differences in the perception of lightness. Neuropsychologia1975;��:121-124.
[5]De Graaf, A, Deelman, B G. Cognitieve Screening Test. Lisse: Swets & Zeitlinger, 1991.
[6]De Renzi, E, Faglioni, P, Sorgato, P. Modality-specific and supramodal mechanisms ofapraxia. Brain 1982;���:301-312.

Grey Scales149
[7]Deelman, B G, Liebrand, W B G, Koning-Haanstra, M, van der Burg, W. SAN test. Lisse:Swets & Zeitlinger, 1987.
[8]Ferber, S, Karnath, H O. Parietal and occipital lobe contributions to perception of straightahead orientation. Journal of Neurology, Neurosurgery and Psychiatry 1999;��:572-578.
[9]Folstein, M F, Folstein, S E, McHugh, P R. "Mini-mental state". A practical method forgrading the cognitive state of patients for the clinician. Journal of Psychiatric Research1975;��:189-198.
[10]Fontenot, D J. Visual field differences in the recognition of verbal and nonverbal stimuliin man. Journal of Comparative and Physiological Psychology 1973;��:564-569.
[11]Gainotti, G, D'Erme, P, Bartolomeo, P. Early orientation of attention toward the halfspace ipsilateral to the lesion in patients with unilateral brain damage. Journal ofNeurology, Neurosurgery, and Psychiatry 1991;��:1082-1089.
[12]Gauthier, L, Dehaut, F, Joannette, Y. The Bells Test: A quantitative and qualitative testfor visual neglect. International Journal of Clinical Neuropsychology. 1989;��:49-54.
[13]Halligan, P W, Marshall, J C. Is neglect (only) lateral? A quadrant analysis of linecancellation. Journal of Clinical and Experimental Neuropsychology 1989;��:793-798.
[14]Hikosaka, O, Miyauchi, S, Shimojo, S. Focal visual attention produces illusory temporalorder and motion sensation. Vision Research 1993;��:1219-1240.
[15]Hikosaka, O, Miyauchi, S, Shimojo, S. Voluntary and stimulus-induced attention detectedas motion sensation. Perception 1993;��:517-526.
[16]Karnath, H O. Deficits of attention in acute and recovered visual hemi-neglect.Neuropsychologia 1988;��:27-43.
[17]Karnath, H O, Ferber, S. Is space representation distorted in neglect? Neuropsychologia1999;��:7-15.
[18]Kerkhoff, G. Displacement of the egocentric visual midline in altitudinal postchiasmaticscotomata. Neuropsychologia 1993;��:261-265.
[19]Kinsbourne, M. Mechanisms of unilateral neglect. In: Jeannerod, M, editor.Neurophysiological and Neuropsychological Aspects of Spatial Neglect. Amsterdam,North-Holland,1987:69-86.
[20]Kinsbourne, M. Orientational bias model of unilateral neglect: Evidence from attentionalgradients within a hemispace. In: Robertson, I H, Marchal, J C, editors. UnilateralNeglect: Clinical and Experimental Studies. Hove: Lawrence Erlbaum, 1993;63-86.

Grey Scales150
[21]Luh, K E, Rueckert, L M, Levy, J. Perceptual asymmetries for free viewing of severaltypes of chimeric stimuli. Brain and Cognition 1991;��:83-103.
[22]Luh, K E. Line bisection and perceptual asymmetries in normal individuals: What you seeis not what you get. Neuropsychology. 1995;�:435-448.
[23]Mattingley, J B, Bradshaw, J L, Bradshaw, J A, Nettleton, N C. Residual rightwardattentional bias after apparent recovery from right hemisphere damage: implicationsfor a multicomponent model of neglect. Journal of Neurology, Neurosurgery, andPsychiatry 1994;��:597-604.
[24]Mattingley, J B, Bradshaw, J L, Nettleton, N C, Bradshaw, J A. Can task specificperceptual bias be distinguished from unilateral neglect? Neuropsychologia1994;��:805-817.
[25]McGlone, J, Davidson, W. The relation between cerebral speech laterality and spatialability with special reference to sex and hand preference. Neuropsychologia1973;��:105-113.
[26]Milner, A D, Brechmann, M, Pagliarini, L. To halve and to halve not: an analysis of linebisection judgements in normal subjects. Neuropsychologia 1992;��:515-526.
[27]Nicholls, M E, Bradshaw, J L, Mattingley, J B. Free-viewing perceptual asymmetries forthe judgement of brightness, numerosity and size. Neuropsychologia 1999;��:307-314.
[28]Pizzamiglio, L, Antonucci, G, Judica, A, Montenero, P, Razzano, C, Zoccolotti, P.Cognitive rehabilitation of the hemineglect disorder in chronic patients with unilateralright brain damage. Journal of Clinical and Experimental Neuropsychology1992;��:901-923.
[29]Sakhuja, T, Gupta, G C, Singh, M, Vaid, J. Reading habits affect asymmetries in facialaffect judgements: a replication. Brain and Cognition 1996;��:162-165.
[30]Schenkenberg, T, Bradford, D C, Ajax, E T. Line bisection and unilateral visual neglectin patients with neurologic impairment. Neurology 1980;��:509-517.
[31]Soukup, V M, Harrell, E H, Clark, T. Right hemispace presentation and left cueing onRaven's Coloured Progressive Matrices among right brain-damaged neglect patients.Brain Injury 1994;�:449-455.
[32]Tant, M L M, Brouwer, W H, Kooijman, A C, Cornelissen, F W. Evaluation of theeffectiveness of a hemi-neglect rehabilitation program and generalization to driving: acase study. In: Gale, A G, Brown, I D, Haslegrave, C M, Taylor, S P, editors. Visionin Vehicles VIII. Amsterdam: Elsevier, in press.
[33]Trevarthen, C. Brain bisymmetry and the role of the corpus callosum in the behavior andconscious experience. In: Cernacek, J, Padivinsky, F, editors. Cerebral hemisphericrelations. Bratislava: Slovak Academy of Sciences, 1972.

Grey Scales151
[34]Van Deusen, J. Normative Data for Ninety-Three Elderly Persons on the SchenkenbergLine Bisection Test. Physical and Occupational Therapy in Geriatrics 1984;�:49-54.
[35]Vanier, M, Gauthier, L, Lambert, J, Pepin, E P, Robillard, A, Dubouloz, C J, Gagnon, R,Joannette, Y. Evaluation of left visuospatial neglect: Norms and discrimination powerof two tests. Neuropsychology 1990;�:87-96.
[36]Warrington, E K, James, L. The Visual Object and Space Perception Battery. Bury St.Edmunds: Thames Valley Test Company, 1991.
[37]Webster, J S, Jones, S, Blanton, P, Gross, R, Beissel, G F, Wofford, J D. Visual scanningtraining with stroke patients. Behaviour Therapy 1984;��:129-143.
[38]Weintraub, S, Mesulam, M M. Visual hemispatial inattention: stimulus parameters andexploratory strategies. Journal of Neurology, Neurosurgery, and Psychiatry1988;��:1481-1488.
[39]Zihl, J. Rehabilitation of Visual Disorders After Brain Injury. Hove, East Sussex:Psychology Press Ltd, 2000.
[40]Zihl, J, von Cramon, D. Visual field recovery from scotoma in patients withpostgeniculate damage. A review of 55 cases. Brain 1985;���:335-365.

Hemianopic Visual Field Defects152
Hemianopic Visual Field Defects elicit Hemianopic Scanning*
1. AbstractPrevious explanations for the variability in success of compensating for homonymoushemianopia (HH) has been in terms of extent of the brain injury. In using on-line eyemovement registrations, we simulated HH in 16 healthy subjects and compared their scanningperformance, on a dot counting task, to their own “normal” condition and to real HH patients’performance.We evidenced clear parallels between simulated and real HH, suggesting that hemianopicscanning behaviour largely is visually elicited, namely by the visual field defect, and not bythe brain damage. We further observed age-related processes in compensating for the HH.
2. IntroductionHomonymous hemianopia (HH) is a visual field defect (VFD) in which, for both eyes to thesame extent, half of the visual field is blind. This condition results from unilateral post-chiasmal brain damage. Nearly 80% of patients with unilateral post-chiasmal brain damageacquire a homonymous VFD (Zihl, 1994). Common causes are cerebrovascular accident,traumatic brain injury and tumours (e.g. Kerkhoff, 1999; Zihl, 2000).
Visual field defects often lead to visually related complaints and dysfunctions. Patientscomplain for example about having a limited overview, bumping into obstacles or personsand experience their vision as being too “slow”. These disabilities are related to the degree ofcompensation for the visual field loss. For comprehensive reviews we refer to Kerkhoff(1999) and Zihl (2000). Oculomotor compensation, i.e. adaptive visual scanning behaviour,can be assessed by recording eye movements (e.g. Zihl, 1995, 1999, 2000; Zangemeister,Meienberg, Stark, & Hoyt, 1982; Zangemeister & Oechsner, 1996).
A paradigm to objectively and quantitatively assess oculomotor compensational behaviourwas introduced by Zihl (e.g. 1995, 1999, 2000) and consisted of inspection of a dot pattern.The stimulus display consists of 20 randomly arranged dots projected onto a screen. Subjectsare asked to fixate the centre of the screen, after which the dot pattern is presented and eyemovements are recorded. Subjects subsequently scan the pattern and silently count thenumber of dots. Upon completion they report the number of dots. The relatively simplestimulus display was chosen to restrict visual scanning to the process of visual samplingwithout any further identification component (Zihl, 1999), or the primary involvement ofother complex higher-order visual functions. Using this paradigm, it was found that in HHtypical defective oculomotor scanning behaviour is characterised by longer scanning timesand scan paths, higher number of fixations and re-fixations, and, at least in part, longerfixation durations and shorter saccadic amplitudes (e.g. Zihl, 1995, 1999, 2000). Thesefindings are in concordance with other reports (e.g. Kerkhoff, 1999; Zangemeister &Oechsner, 1996; Meienberg, Zangemeister, Rosenberg, Hoyt, & Stark, 1981; Chedru,Leblanc, & Lhermitte, 1974; Ishiai, Furukawa, & Tsukagoshi, 1987; Neetens, 1994;Zangemeister et al., 1982).
* This manuscript was submitted to Vision Research (Tant, Cornelissen, Kooijman & Brouwer)We thank E.M. Havik for collecting the healthy subjects data.

Hemianopic Visual Field Defects153
In large, it was found that about 40% of the HH patients spontaneously compensateeffectively for their VFD (Zihl, 1995, 1999, 2000) and that the subjective visual complaintsby HH patients were substantiated by eye movement recordings during the dot counting task,confirming its practical relevance. Interestingly, it was concluded (Zihl, 1999, 2000) that thepresence, time since, and severity of the VFDs could not sufficiently explain the observedscanning deficit and that additional factors are crucial for explaining the impaired oculomotorscanning. Zihl suggested that the extent of the brain injury is a crucial factor and that occipito-parietal and posterior thalamic brain injury may be responsible for inefficient compensation.
Nevertheless, there are some peculiar aspects in the results, which cast doubt on the providedexplanation for the individual differences in the efficiency of compensation for HH. Firstly, itwas noted by Zihl (1999) that the scanning (e.g. in terms of scanning time) was found to beimpaired in this very simple visual sampling task. Hence, even in a task, in which complexhigher-order (i.e. brain related) functions are not involved, a disability appears. This calls intoquestion the crucial importance of the integrity of the brain for the visual disability. Zihltherefore cautions against the (mis)interpretation of the results in term of “unspecific”cognitive slowing, suggesting in our view, an interpretation in terms of mere visual slowing.He suggested that the “slowness of vision” may, at least in part, be explained by the use ofhypometric saccades which are provoked by a homonymous VFD.
Secondly, it was found that the side of the VFD (and therefore the side of the brain lesion)was not a crucial factor. Zihl (1999) comments this observation to be surprising, because ofthe assumed specialisation of the right (posterior) hemisphere for visuo-spatial function,including the spatial guidance of eye movements. If predominantly higher-order visual (i.e.brain related) functions were involved, one would have expected left-sided HH patients (withright-sided brain damage) to perform worse, due to hemispheric specialisation and theinherently visuo-spatial nature of the dot counting task.
Both observations suggest that the deficit in visual exploration is perhaps not predominantlyrelated to additional brain damage, but is merely a knock-on effect of the lower-orderdysfunction, i.c. the hemianopic visual field loss. In order to preclude the effects of braindamage, we simulated HH in healthy subjects and compared the visual exploration to theirown ‘normal’ condition. By simulating the hemianopic visual field loss, we ‘create’ subjectswith the lower-order visual dysfunction, but without higher-order dysfunctions caused bybrain damage. The observed disabilities (if any) during simulation result from the visuallimitation only and do not require a further explanation in terms of brain damage. If visualexploration deficits in real HH are predominantly provoked by the VFD, the visualexploration behaviour, displayed in simulated and real HH, should be comparable, includingthe variability in performance between individuals. Our primary research question henceconcerns the influence of the pure visual component on hemianopic visual exploration duringa dot counting task. We also included real HH patients in this study to compare the patterns ofperformance with simulated and real HH.
A secondary question concerns the explanation of individual differences in the efficiency ofcompensating for HH. Apart from differences in extent and site of brain injury in patients, inhealthy subjects there are large individual differences in higher-order visual and cognitiveabilities, for example differences in visual speed and other components of intelligence. Some

Hemianopic Visual Field Defects154
of these abilities are highly dependent on age, for example perceptual speed and spatialorientation (Schaie & Willis, 1993) and fluid intelligence (Rybash, Roodin, & Hoyer, 1995).As was also suggested by Szlyk and colleagues (Szlyk, Brigell, & Seiple, 1993), it is quiteconceivable that such age-related abilities play an important role in the efficient compensationof HH. To investigate the effect of ageing on the efficiency of compensation, we includedboth younger and older adults in the study. It is predicted that the older subjects will havesignificantly more problems in coping with HH.In summary of the research questions, we expect to find typical HH scanning performance inhealthy subjects with a simulated hemianopic VFD, since we hypothesise that HH scanning isprimarily generated by the VFD and not by brain damage. To fully compare and characteriseHH scanning performance, we will perform, in addition to general analysis, also directional,hemispace, and trend analysis (see further). Secondly, we expect to find the disabilities to bemore pronounced in an older age group, since we assume that individual differences inperceptual and intellectual abilities, which tend to decrease with age, are important factorsgoverning the compensation process.
3. Methods3.1. SubjectsSixteen healthy subjects participated in this study (seven males, eight females). Their meanage was 40 years (range 16-71). Two age groups were included: a younger group with a meanage of 21 years (range 16-23) and an older age group with a mean age of 60 years (range 46-71), each consisting of eight subjects. They showed no signs of cognitive decline (CST; DeGraaf & Deelman, 1991), reported to be right-handed, and had normal or corrected-to-normalvisual acuity. They declared to have no visually related complaints.
Twenty-nine patients were included (23 males, 6 females). They showed no evidence ofcognitive decline (CST; De Graaf & Deelman, 1991 and MMSE; Folstein, Folstein, &McHugh, 1975), aphasia (SAN; Deelman, Liebrand, Koning-Haanstra, & van der Burg, 1987)or apraxia (De Renzi, Faglioni, & Sorgato, 1982). Neither of them showed severe unilateralvisual hemi-neglect (UN) or visual agnosia. The selection procedure for UN is describedelsewhere (Tant, Brouwer, Kooijman, & Cornelissen, submitted). All patients had a binocularoptimally corrected acuity of 0.8 or better and contrast sensitivity within normal ranges. Allhad complete or incomplete HH as confirmed by automated perimetry using the HumphreyField Analyzer (Full Field 246 screening program, age corrected, 3-zone strategy). Fourteenpatients had left-sided HH. Their mean age was 54 years (range 29-76), the mean time sincelesion was 32 months (range 6-157), and the mean macular sparing subtended 3 degrees(range 0-10). All were victims of stroke, except two patients, who were surgically operatedfor tumour. One patient, with left-sided HH, only had (right) monocular vision. Fifteenpatients had right-sided HH. Their mean age was 50 years (range 17-68), the mean time sincelesion was 80 months (range 3-390), and the mean macular sparing subtended 3 degrees(range 0-8). One patient was surgically operated for hydrocephalus, and one for tumour. Twopatients suffered closed head injury. The remaining patients were victims of stroke.
3.2. Dot counting Task and ApparatusOur dot counting task is based upon the work of Zihl (e.g. 1995). We presented in total 29patterns of dots. The screen dimensions were 36° and 27° horizontally and verticallyrespectively. The dot size was 1°. Dots were white (luminance 25 cd/m2) on a grey

Hemianopic Visual Field Defects155
background (50% contrast). The viewing distance was 52 cm. We presented five differentpatterns consisting of 19, 20 and 21 dots each (i.e. 15 trials). The spatial distribution of thedots in these patterns was random but fixed over subjects. Additionally we presented patternsconsisting of 5-17 dots (two-dot increment), which each were presented twice (i.e. 14 trials).Their spatial distribution was randomly generated on each presentation. The 29 trials werepresented in a random order. Before each trial, a fixation dot (1.5°) was presented in thecentre of the screen. Upon stable fixation, the trial was initiated. The subject was asked tocount the number of dots. When the subject verbally indicated being finished, the trial wasaborted, and the answer registered.
During the experiment the eye movements were recorded using an EyeLink Gaze tracker(SensoMotoric Instruments GmbH, Teltow, Germany) which registers real-time gaze at 250Hz. When simulating HH, a window, with the same properties as the background,continuously and completely blanked one side of the screen with reference to the current gazeposition. This could either be left or right of fixation in order to simulate left- or right-sidedHH respectively. Prior to the experiment, the equipment was calibrated using a nine-pointgrid. The initial central fixation dot, prior to each trial, was also used for drift correctionwhich may result from slips of the Eyelink’s headset. Small head-movements were allowed(and corrected for) during the experiment. This equipment allows for relatively normal freeviewing conditions.
3.3. ProcedureThe healthy subjects performed the task on two different occasions. On each occasion, theyfirstly performed the task in a non-simulation (i.e. normal) and subsequently in a simulationcondition. During the task in a simulation condition, the side of the simulated homonymoushemianopia (sHH) was fixed. On the second occasion, the side of the sHH was changed foreach subject. During simulation, half of the subjects had a macular sparing of 2.7° on bothoccasions. The patients performed the task once. Obviously, no simulation was imposed.
3.4. Statistical analysisThe oculomotor parameters are number and duration of the fixations, number and amplitudeof the saccades, and the length of the scanpath, which is sum of the saccadic amplitudes.When both number of fixations and number of saccades are used in the same analysis, onlythe number of fixations are reported. As a saccade typically follows a fixation, bothparameters are logically linked and hence the number of one or the other provides noadditional information. We further report the absolute error in counting the dots (henceforthreferred to as error) and the search time. Additionally, we perform directional and hemispaceanalysis. Since the healthy subjects suffered no actual brain damage, directions and side of thehemispace are defined with respect to the side of the VFD. “Ipsilateral” and “contralateral”hence refer to “in or towards” the affected and intact visual hemifield respectively.Directional analysis is performed on the amplitudes and number of saccades. Hemispaceanalysis is applicable for the fixation parameters. The hemispace is defined in terms of thecentre of the screen, which is also the start of exploration in each trial. To further characterisethe scanning performance, we perform a trend analysis using the errors, search time, numberof fixations, and length of the scanpath to investigate how the difficulty of the task(operationally defined by the number of dots in each pattern) influences performance in eachsubject group.

Hemianopic Visual Field Defects156
To analyse the data by the healthy subjects, we performed a MANOVA on a doubly repeatedmeasures design. When significant multivariate effects were observed, the univariate effectswere inspected. When necessary, we additionally performed simple-main-effects analysis, tountangle the interaction-components. For this last type of analysis, only p-values will bereported. The design is graphically depicted in Fig. 1. We included the factors of age(Young/Old), macular sparing (yes/no), and sequence (A/B) as between-subjects factors. Thesequence factor represents whether subjects were first imposed with a left- (A) or right-sidedsHH (B). Within-subject factors were measurement (first or second occasion) and mode(Normal/simulated HH). The measurement-, mode- and age-factors are interpretable as main-effects factors. Since the sparing factor has no relevance in the normal mode and can onlyexert effects during simulation, a main effect of sparing will arise as a mode x sparinginteraction. Effects of the side of the sHH are inferred from simple-main-effect analysis on themeasurement x mode x sequence interactions. Namely, a significant measurement x sequenceinteraction, within the simulation mode, reveals differential performances by left- and right-sided sHH subjects. When observed, further analysis and inspection of the means will thenreveal the nature of the effects of the side of sHH and the consistency of the differencebetween left- and right-sided sHH in both sequences. Absence of this 2-way interactionindicates no difference in left- versus right-sided sHH. Although statistically interactional, theeffects of both sparing and side of the sHH will be reported as main-effects.The patient data conform to a repeated measures design with side of the HH as a between-subjects variable. We analysed the same parameters as for the healthy subjects.
Figure 1. Graphical depiction of the healthy subjects design. Between-subject factorsare Sequence, Age, and Sparing. Within-subject factors are Measurement and Mode.
Measurement First occasion Second occasionMode Normal Simulation Normal Simulation
Sequence Age SparingnoY yesnoA
O yes
N left-sidedsHH N right-sided
sHH
noY yesnoB
O yes
N right-sidedsHH N left-sided
sHH
4. Results4.1. General analysis: MultivariateMANOVA failed to reveal significant multivariate main effects of measurement and age,suggesting that nor repetition of the experiment or age did have any overall influence on thedata. There was a significant mode-effect ()(7,2) = 147, 3� < .007), suggesting an overalleffect of the simulation. We observed no effect of sparing, indicating that macular sparing didnot lead to better performance in sHH. We found no measurement x mode interaction,confirming the absence of learning effects in both modes. Age, however, did interactsignificantly with mode ()(7,2) = 62, 3�< .016). The age effect will be explored further. Weobserved a significant measurement x mode x sequence interaction ()(7,2) = 27, 3�< .036),suggesting a possible influence of the side of the sHH. Simple-main-effect analyses will beperformed to reveal the nature of these effects and interactions.

Hemianopic Visual Field Defects157
4.2. General analysis: UnivariateIn the simulation mode (compared to the normal mode), subjects took more time and mademore errors in counting the dots. They fixated more and the mean fixation duration waslonger. Also the scanpath was prolonged (Fig. 2). All parameters showed significantdifferences, except the saccadic amplitudes ()-range: 11-184, 3-range: .011-.0001).
In comparison to right-sided sHH, subjects with left-sided sHH made more errors ()(1,8) =13, 3�< .007) and presented a longer search time ()(1,8) = 11, 3�< .01) (Table 1). Simple-main-effects analysis had revealed that none of the parameters produced significantdifferences in normal modes. Significantly worse performance by left-sided HH was alsoobserved in the patient group, but only for the errors ()(1,27) = 9, 3�< .005) (Table 1).
Search Time
0
2
4
6
8
10
12
14
Dur
atio
n (s
)
Errors
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Mea
n ab
solu
te e
rror
Fixations
0
5
10
15
20
25
30
35
40
Num
ber
Fixations
0
100
200
300
400
500
600
700
Dur
atio
n (m
s)
Scanpath
0
50
100
150
200
250
Leng
th (d
egre
e)
Saccades
0
2
4
6
8
10
12
Ampl
itude
(deg
ree)
Figure 2. Simulated HH (black) provokes longer search times, more errors, morefixations, longer fixation durations, and longer scanpaths than in normal conditions(white). Patient data (hatched bars) for comparison. Error bars are 1 standard error.

Hemianopic Visual Field Defects158
Table 1. Effects of the side of the VFD in simulated (sHH) and realhemianopia (HH). Left-sided sHH subjects take more time and make moreerrors than right-sided sHH. Left-sided HH patients make more errors thanright-sided HH. The difference between left- and right-sided HH was notstatistically significant for the search time. Standard errors betweenbrackets.
Side of the VFDleft right
Errors sHH .95 (.11) .34 (.11)HH .68 (.10) .25 (.10)
Search Time (s) sHH 13.2 (.83) 10.2 (.83)HH 10.1 (.67) 8.8 (.65)
The effect of age wasapparent in the search time()(1,8) = 19, 3� < .002) andnumber of fixations ()(1,8) =19, 3� < .006). The increasefor both parameters in thesimulation mode was greaterfor the older age group (Fig.3). Exploratory, we plottedthe search time per dot (i.e.relative search time) infunction of the trial order,and observed that, althoughalways present, the ageeffects are especially evidentin the beginning of the task(Fig. 4). We observed similarage effects in the patientpopulation, as evidenced bythe Pearson’s correlation ofage with search time (U(29) = .38, 3� < .05) and number of fixations (U(29) = .42, 3� < .05).
4.3. Directional analysisMultivariate directional analysis on the healthy subjects data, including the number andamplitude of the saccades, was significant ()(2,13) = 4, 3�< .05) for the mode x directioninteraction. The saccadic amplitudes in either direction did not differ in the normal mode, butthere was a significant directional effect in the simulation mode ()(1,14) = 5, 3� < .05).Namely, ipsilateral saccadic amplitudes were smaller than contralateral amplitudes (Table 2).There was no effect of the side of the sHH, indicating that the amplitudes of saccades into theblind hemifield are smaller than into the seeing hemifield, for both left- and right-sided sHH.This pattern of results was paralleled in the patient group. Multivariate analysis failed toreveal any effect of the side of the HH, but presented a significant directionality effect ()(2,26) = 11, 3�< .000). Inspection of the univariate analysis showed the saccadic amplitudes tobe smaller in ipsilateral than in contralateral direction ()(1, 27) = 19, 3�< .000) (Table 2).
Search Time
0
2
4
6
8
10
12
14
16
N sHH
Dur
atio
n (s
)
YoungOld
Fixations
0
5
10
15
20
25
30
35
N sHH
Num
ber
YoungOld
Figure 3. Subjects from the older age group had longer search timesand made more fixations (and saccades) in the simulated conditions.N: Normal condition, sHH: simulated condition. Error bars are 1standard error.

Hemianopic Visual Field Defects159
4.4. Hemispace analysisA multivariate hemispace analysiswas performed on the number anddurations of the fixations by thehealthy subjects. A multivariatemode x field interaction wasfound ()(2,13) = 11, 3�< .002).Univariate analysis showed asignificant effect of fixationduration ()(1,14) = 9, 3�< .010).This effect was however notapparent in the simulationcondition. In the normal mode, thedurations proved to be longerwhen they occurred on the rightside of the screen than on the leftside (352 ms and 411 ms for leftand right hemispace respectively,3� < .004). Tentatively, in thesimulation mode, inspection of themeans would suggest ipsilateral fixation durations (577 ms) to be longer than contralateralones (533 ms), but this difference proved not to be significant.There was also a significant effect of hemispace on the number of fixations ()(1,14) = 8, 3�<.012). In the normal mode, there were as many fixations in either left or right hemispace, butclearly more fixations in the ipsilateral hemispace in the simulation mode (3�< .009) (Table2). There was no interaction with the side of the sHH, indicating that, in both left- and right-sided sHH, subjects fixated more on the same side of the screen as their VFD.This pattern of results was paralleled in the patient group. We observed a multivariate effectof hemispace ()(2,26) = 55, 3�< .000) and no effect of side of the HH. Both left- and right-sided HH patients fixated more in the ipsilateral hemispace ()(1,27) = 93, 3�< .000) (Table 2).
Table 2. Directional and Hemispace analysis. Saccadic amplitudes are smaller inipsilateral than in contralateral direction in simulated (sHH) and real hemianopia (HH).In the normal condition (N), there were no differences in amplitudes between saccadesto the left or to the right (in table termed ipsilateral and contralateral receptively). Inboth HH groups, there are more fixations in ipsilateral than in contralateral hemispace.We observed no such difference in the normal condition. Standard errors betweenbrackets.
Ipsilateral ContralateralSaccadic Amplitude (degree) N 8.4 (.59) 8.7 (.55)
sHH 9.08 (.96) 10.81 (1.2)HH 7.00 (.18) 8.2 (.31)
Number of Fixations N 7.3 (.39) 7.2 (.41)sHH 12.5 (1.2) 8.9 (1.1)HH 15.7 (.94) 9.1 (.48)
Age effects in sHH
0
0.5
1
1.5
2
2.5
3
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29Order of trials
Rel
ativ
e S
earc
h Ti
me
(s)
NYsHHYNOsHHOHH
Figure 4. The age effects in sHH are especially evident in hetbeginning of the experiment. N: Normal condition, sHH:simulated condition, Y: Younger age group, O: Older agegroup, HH: patient group.

Hemianopic Visual Field Defects160
Table 3. Trend Analysis assessing the influence of the number of dots for the normal (N) andsimulated condition (sHH) and for the patients (HH). # indicates presence of higher-order trends.ns: not statistically significant.
TrendsLinear Quadratic
Error N F(1,15) = 13, p<.002 nssHH F(1,15) = 19, p<.001 F(1,15) = 5, p<.046HH F(1,27) = 38, p<.000 #
Search Time N ns nssHH F(1,15) = 15, p<.001 nsHH F(1,27) = 5, p<.026 F(1,27) = 15, p<.001
Number of Fixations N F(1,15) = 24, p<.000 nssHH F(1,15) = 42, p<.000 F(1,15) = 8, p<.012HH ns F(1,27) = 7, p<.015 #
Length of Scanpath N F(1,15) = 11, p<.004 nssHH F(1,15) = 50, p<.001 nsHH F(1,27) = 56, p<.000 F(1,27) = 29, p<.000 #
4.5. Trend analysisTo assess the relative difficulty level of the patterns, induced by the number of constituentdots, we expressed the errors, search time, number of fixations, and length of the scanpath asrelative measures in dividing them by the number of dots in the patterns. These parametershence indicate the performance per dot. We then performed a trend analysis by way ofpolynomial contrasts, separately for the normal and simulation mode. If the dot counting taskfunctionally is performed in the same manner in both groups (N and sHH), the same trendsshould appear. If different or additionaltrends appear, the number of dots assert adifferent influence on the performance,suggesting functionally differentsubcomponents or processes. The results aresummarised in Table 3. For all but oneparameter, at least one additional trend waspresent in the simulation mode compared tothe normal mode. For the length of thescanpath, only linear trends were present inboth modes, but in simulation mode being farmore distinct (as evidenced by the )-valuebeing almost five times higher). This overallpattern was observed to be continuated forthe patient data, except that occasionally alsoadditional higher-order trends were present(Table 3). For illustrative purposes, we plotthe search time per dot in function of thenumber of dots (Fig. 5). It can be observedthat in (s)HH, there is relatively more time
Trends
0
0.2
0.4
0.6
0.8
1
1.2
1.4
5 7 9 11 13 15 17 19 20 21Number of Dots
Rel
ativ
e Se
arch
Tim
e (s
)
NsHHHH
Figure 5. Trends for relative search time infunction of number of dots.In the normal condition(N) no trend is present. In the simulated condition(sHH), a linear trend was found. For the patients(HH), both a linear and quadratic trend waspresent. Different trends suggest differentfunctional components.

Hemianopic Visual Field Defects161
consumption for the patterns with less dots, as evidenced by the linear trends. We similarlyobserved relatively increasing number of fixations and the length of the scanpaths withdecreasing number of dots. The reverse pattern was found for the errors (not in Figs).
5. DiscussionWe did observe hemianopic scanning behaviour in healthy subjects without brain damagewith an imposed HH. This suggests that hemianopic scanning behaviour largely is visuallyelicited, namely by the VFD. The parallels between simulated and real HH are evidenced byseveral findings. Firstly we found elevated search times, errors, number and duration offixations and length of scanpath (Fig. 1) in sHH compared to the normal condition. We didnot observe a main effect of saccadic amplitude. These findings are in perfect concordancewith previous findings reported by Zihl (1995, 1999, 2000) for real HH patients andconfirmed by our own patient data (Fig. 1). In sHH, we also found in general longer fixationdurations, which was not observed in our patient data (Fig. 1). Zihl (1999) reported the meanfixation duration to be longer in some (“impaired”) and shorter in other (“unimpaired”) HHpatients. We did not create these subgroups, and hence are likely to have a pooled patientpopulation in this respect. This could account for the total null-effect of fixation duration inour patient group (compared to the normal condition, Fig. 2). The finding that we do observefixation duration increase, fortified by the elevation of the other parameters, suggests that, inmany respects, our sHH subjects resemble the “impaired” HH patients. The observation that,for most parameters, the performance in sHH is more deviant (from the normal condition)than in HH, is agreement with this suggestion. Alternatively, the HH patients did have (more)time to adapt to their VFD, while for the sHH subjects, the acquisition of the VFD was veryrecent.
The second parallel between real and simulated HH concerns the side of the VFD, which waspreviously reported not to affect any oculomotor parameter in real HH patients (Zihl, 1999).This was confirmed by our patient data. We did however find left-sided HH patients to countless accurately than right-sided HH patients (Table 1). Zihl did not observe this difference. Inhis paradigm, only one pattern (one trial) was presented and subjects made no errors. Sincewe presented 29 trials, we were more likely to observe errors, and hence our data are notoptimally comparable in this respect. The absence of effects of the side of the VFD inoculomotor parameters and the worse error performance in left-sided HH was paralleled insHH (Table 1). We did additionally find a longer search time in left-sided sHH. Hence, theresults in sHH parallel the results in HH in that the side of the VFD does not differentiallyinfluence oculomotor performance. Left-sided sHH subjects however tend to make moreerrors and need more time than subjects with right-sided sHH. This was also the case withrespect to the errors for the HH patient group.
Thirdly, directional and hemispace analyses further confirm the same pattern of results insHH and HH (Table 2) and are in concordance with previously reported findings. Differentialhemifield distribution of the fixations has previously been reported (e.g. Zihl, 1995, 1999,2000; Kerkhoff, 1999; Zangemeister & Oechsner, 1996; Meienberg et al., 1981; Chedru et al.,1974; Ishiai et al., 1987). Also in our data, both sHH and HH fixated more in the ipsilateralhemispace. Saccadic dysmetria and more specifically ipsilateral hypometric saccades areconsidered typical for hemianopic scanning (e.g. Zihl, 2000; Neetens, 1994; Zangemeister et

Hemianopic Visual Field Defects162
al., 1982; Chedru et al., 1974; Ishiai et al., 1987; Meienberg et al., 1981, Zangemeister &Oechsner, 1996). Our data, both for sHH and HH, confirm saccadic amplitudes in ipsilateraldirection to be smaller than in contralateral direction. As in previous studies (e.g. Zihl, 1995)no effects of the side of the VFD were found.
Hence, all aspects known to be typical for hemianopic scanning behaviour we were able toreplicate with simulated HH. These healthy subjects did not suffer brain damage, but wereimposed with a simulated homonymous hemianopic VFD. It follows that the typical HHscanning behaviour is largely due to the VFD (i.e. visually elicited) and not to concomitantbrain damage. To further explore underlying components in the scanning behaviour, weperformed the trend analysis in function of the number of dots (Table 3). We assume thatfunctionally different components will result in different trends. In the normal condition, weobserved linear relationships between the number of dots and the errors, number of fixationsand length of the scanpath per dot. The search time per dot did not seem to be influenced bythe number of dots. These same trends appeared in sHH, suggesting the same underlyingmechanisms. However, in nearly all parameters, also other (higher-order) trends wereobserved, suggesting additional components. It is reasonable to assume that these additionaltrends are brought about by the simulated VFD, since this was the only difference with thenormal condition. These additional trends are suggested to be visually elicited. We alreadyargued that the scanning behaviour displayed in sHH is in many respects identical to real HH.This was partly confirmed, by the trend analysis, in that most trends present in sHH, alsoappeared in HH (Table 3).
Upon visual inspection of the trends, a paradox appeared. Fig. 5 shows that relatively, thesearch time increases with decreasing number of dots. A similar pattern was observed for thenumber of fixations and the length of the scanpath. We suggest that this pattern can beexplained as the time cost and effort for (s)HH to check the whole visual field. When healthysubjects, in the normal condition, fixate the centre of the screen, they can parafoveallyperceive the whole screen and spatially represent the dot pattern as to effectively andeconomically organise their scanning pattern. They will cluster neighbouring dots and devotemore attention and time to densely crowded parts of the screen and no attention to emptyparts. This immediately available spatial representation is not available in (s)HH. In additionand as a result, even (eventually apparent) empty parts of the screen require visualexploration. It follows that, as the result of the VFD, apparently easier configurations lead tomore dysfunction in (s)HH. In such a configuration, a priori clustering and identification ofunimportant parts of the screen, leads to gain in effectivity in the normal condition, contraryto (s)HH. We suggest that this is partly at the basis of the visual slowness reported in HH: avisual slowness brought about by the absence of an immediately available spatialrepresentation and the need to standardly fully explore all parts of the screen, also when thisis, as ultimately appears, not necessary.However, the additional trends in HH, compared to sHH (e.g. quadratic in Fig. 5), suggestthat still additional components are into play in real HH scanning. Although different subjectscomprise the sHH and HH groups, and hence are not ideally comparable, this suggests thatalso brain damage functionally influences the scanning behaviour. More dots most likelysummon more visuo-spatial, memory and organisational functions. Brain damage is likely toaffect (some of) these functions, which are likely to interact reciprocally with adequate visualexploration and proper cerebral representation of space, hence resulting in the appearance of

Hemianopic Visual Field Defects163
additional trends. Alternatively, the appearance of the additional trends could be statisticallyinduced by generally better performance by the HH subjects (compared to sHH). As a result,HH subjects sooner perform at their maximal effectivity, inducing flattening of the (relative)performance curve, which will appear as additional trends. With this statistical alternative inmind, we would like to indicate that the additional trends can at least be suggestive for theadditional impact of brain damage on the HH scanning behaviour, but also thatpsychometrically fully comparable data is needed to support our suggestion.In summary, we can conclude that HH scanning behaviour is largely visually elicited, namelyby the VFD. We further suggest that subtle interplay of brain-related functions and the VFDcomplete real HH scanning.
Our interest in the effects of age were aroused by Szlyk et al. (1993) who suggested that age-related losses, when compounded by CVA-associated impairments, significantly influencedvisuo-spatial performance i.c. driving related skills. Such an age-related loss could be fluidintelligence, defined as the ability to new-problem solving. Our healthy subjects were exposedto a new experience (sHH) for which adaptive behaviour was required. We found thiscompensation indeed to be worse for the search time in the older age group. This age effectremained when the log-transformed values were used, as suggested by Cornelissen andKooijman (2000). Clear differences were also observed for the number of fixations, in that theincrease in the sHH condition was far greater in the older age group (Fig. 3). These findingswere paralleled in the patient group. Hence, becoming (simulated) hemianopic seems moredisabling for older subjects. It would follow that on second simulation, these effects wouldweaken, since it then is no longer a new situation. The absence of a learning effect seems tocontradict this, but since on both occasions the side of the sHH was changed, it can not beconsidered a valid test for our hypothesis. We therefore explored the compensation effectswithin the simulation conditions by trial order. The rationale is that the sHH is very new at thefirst trial, but less with increasing trials. If the older age group is less capable of new-problemsolving, it should be most prominent during the first trials. This is exactly what we observed(Fig. 4). This pattern, although still very prominent, was slightly reduced on second occasionfor the older age group (not in Fig.). For the younger age group, patterns on both occasionswere identical (not in Fig.). We therefore conclude with Szlyk and colleagues that age-relatedprocesses are related to hemianopic compensation, but we add this to be the case even if thedisabilities are merely visually elicited and hence are not specific for brain damaged subjects.
In conclusion, HH scanning behaviour, as assessed by eye movement recordings during a dotcounting task, can largely be accounted for by the VFD. It follows that most typical HHoculomotor dysfunctions, as for example ipsilateral hypometric saccades, do not result fromthe brain damage but are visually elicited. Age-related processes, i.c. worse compensation tothese visually elicited disabilities were apparent. The implication of this study is that at leastsome typical HH disabilities and complaints as for example slowness of vision andprolongation of scanpaths, can no longer be merely associated to brain damage, as they alsodo appear in subjects with sHH. A further implication would be that these visually elicitedimpairments can be most pronounced during (seemingly) the simpler situations.This can have also ramifications for both for rehabilitation and diagnosis. Firstly, these resultssuggest that, at least for some HH patients, more emphasis can be devoted to visual than tocognitive components in rehabilitation. Secondly, diagnosing higher-order visuo-spatialimpairment can only occur in the light of concomitant lower-order visual impairment.

Hemianopic Visual Field Defects164
6. Reference List
Chedru, F., Leblanc, M., & Lhermitte, F. (1974). Visual searching in normal and brain-damaged subjects. &RUWH[���� 94-111.
Cornelissen, F. W. & Kooijman, A. C. (2000). Does age change the distribution of visualattention? A comment on McCalley, Bouwhuis, and Juola (1995). -RXUQDOV� RI*HURQWRORJ\�6HULHV�%�3V\FKRORJLFDO�6FLHQFHV�DQG�6RFLDO�6FLHQFHV����� 187-190.
De Graaf, A. & Deelman, B. G. (1991). &RJQLWLHYH�6FUHHQLQJ�7HVW� Lisse: Swets & Zeitlinger.
De Renzi, E., Faglioni, P., & Sorgato, P. (1982). Modality-specific and supramodalmechanisms of apraxia. %UDLQ������ 301-312.
Deelman, B. G., Liebrand, W. B. G., Koning-Haanstra, M., & van der Burg, W. (1987). 6$1WHVW� Lisse: Swets & Zeitlinger.
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state". A practicalmethod for grading the cognitive state of patients for the clinician. -RXUQDO� RI3V\FKLDWULF�5HVHDUFK����� 189-198.
Ishiai, S., Furukawa, T., & Tsukagoshi, H. (1987). Eye-fixation patterns in homonymoushemianopia and unilateral spatial neglect. 1HXURSV\FKRORJLD����� 675-679.
Kerkhoff, G. (1999). Restorative and compensatory therapy approaches in cerebral blindness -a review. 5HVWRUDWLYH�1HXURORJ\�DQG�1HXURVFLHQFH����� 255-271.
Meienberg, O., Zangemeister, W. H., Rosenberg, M., Hoyt, W. F., & Stark, L. (1981).Saccadic eye movement strategies in patients with homonymous hemianopia. $QQDOVRI�1HXURORJ\���� 537-544.
Neetens, A. (1994). Revalidation of homonymous hemianopic patients. In A.C.Kooijman, P.L. Looijestijn, J. A. Welling, & G. J. van der Wildt (Eds.), /RZ�9LVLRQ��5HVHDUFK��DQG1HZ� 'HYHORSPHQWV� LQ� 5HKDELOLWDWLRQ (pp. 296-300). Amsterdam and Oxford: IOSPress.
Rybash, J. M., Roodin, P. A., & Hoyer, W. J. (1995). $GXOW�GHYHORSPHQW�DQG�DJLQJ� (3rd ed.)Boston MA: McGraw-Hill.
Schaie, K. W. & Willis, S. L. (1993). Age difference patterns of psychometric intelligence inadulthood: Generalizability within and across ability domains. 3V\FKRORJ\�DQG�$JLQJ��� 44-55.
Szlyk, J. P., Brigell, M., & Seiple, W. (1993). Effects of age and hemianopic visual field losson driving. 2SWRPHWU\�DQG�9LVXDO�6FLHQFH����� 1031-1037.

Hemianopic Visual Field Defects165
Tant, M. L. M., Brouwer, W. H., Kooijman, A. C., & Cornelissen, F. W. (in press). GreyScales uncover similar attentional effects in homonymous hemianopia and visualhemi-neglect. 1HXURSV\FKRORJLD.
Zangemeister, W. H., Meienberg, O., Stark, L., & Hoyt, W. F. (1982). Eye-head coordinationin homonymous hemianopia. -RXUQDO�RI�1HXURORJ\������ 243-254.
Zangemeister, W. H. & Oechsner, U. (1996). Evidence for scanpaths in hemianopic patientsshown through string editing methods. In W.H. Zangemeister, H. S. Stiehl, & C.Freksa (Eds.), 9LVXDO� $WWHQWLRQ� DQG� &RJQLWLRQ (pp. 197-220). Amsterdam: ElsevierScience.
Zihl, J. (1994). Rehabilitation of visual impairments in patients with brain damage. InA.C.Kooijman, P. L. Looijestijn, J. A. Welling, & G. J. van der Wildt (Eds.), /RZ9LVLRQ��5HVHDUFK��DQG�1HZ�'HYHORSPHQWV�LQ�5HKDELOLWDWLRQ (pp. 287-295). Amsterdamand Oxford: IOS Press.
Zihl, J. (1995). Visual scanning behavior in patients with homonymous hemianopia.1HXURSV\FKRORJLD����� 287-303.
Zihl, J. (1999). Oculomotor scanning performance in subjects with homonymous visual fielddisorders. 9LVXDO�,PSDLUPHQW�5HVHDUFK���� 23-31.
Zihl, J. (2000). 5HKDELOLWDWLRQ� RI� 9LVXDO� 'LVRUGHUV� $IWHU� %UDLQ� ,QMXU\� Hove, East Sussex:Psychology Press Ltd.

Evaluation of a neglect rehabilitation program166
Evaluation of the effectiveness of a hemi-neglect rehabilitation program andgeneralisation to driving: a case study*
1. IntroductionIn the past 30 years various rehabilitation programs and therapeutic interventions have beendesigned to attempt to improve the recovery of patients with unilateral neglect (UN). Just asthere is a multitude of theoretical accounts trying to explain and comprehend the UNsyndrome there are multiple ways of trying to treat or compensate for this functional deficit.Research in rehabilitation of functional impairments in brain-damaged patients in general andin UN in particular is a laborious and difficult enterprise. One of the main problems concernsthe methodology including comparing patients across studies. Another important issue is thediscussion concerning the amount of generalisation of the observed effects. This can beachieved by using testing materials different from training materials, including only patientswith chronic and persistent UN and assessing and comparing non-trained functions likedegree of anosagnosia pre and post treatment, or success of functioning in activities of dailyliving (ADL). Therefore it is of the utmost importance to report well documented case-studieswith regard to the characteristics of the patient as well as with regard to therapeutic andevaluation methods.Recently a promising program has been reported by e.g. Pizzamiglio et al. (1992) andAntonucci et al. (1995). These authors claim that their systematic, comprehensive andintensive program is able to produce significant and long lasting results which also generaliseto non-trained and everyday life situations. This program consists of 4 main procedures:visual scanning training, reading and copying training, copying of line drawings on a dotmatrix and picture description training. The specific characteristics of the entire program canbe summarised as follows: there is a great diversity of stimulus material and responses, thelevel of difficulty can easily be adapted to the patients performance level, and it is quiteintensive in time.
As only multiple and independent replications of both group and single-case studies can leadus with confidence to adopt a particular therapeutic method we took this promising programas a basis for a single-case study. Besides evaluation with clinical tests with static stimuli, wealso assessed the performance post-training on two different driving simulator tasks: a lanetracking task with variable side-wind conditions and conditions of divided attention, and atest-ride in an advanced driving simulator.
2. Methods2.1. CaseKd is a 52-year-old right-handed male who suffered in September 1995 a right sided deepparaventricular heamatoma resulting in damage to the internal capsule sparing the thalamus.At the start of the intervention in 1998, he presented a hemiplegia in his left leg and had aparetic left arm. His primary visual functions (visual acuity and contrast sensitivity) werenormal. Perimetric testing revealed a complete left-sided homonymous hemianopia with nomacular sparing. Visual evoked potentials with half-field stimulation revealed no activityupon left half-field checkerboard pattern reversals. General neuropsychological testing and
* This manuscript is accepted to appear in: Vision in Vehicles VIII. A.G.Gale, I.D.D. Brown, C.M. Haslegrave,& S.P. Taylor (Eds.), Amsterdam: Elsevier. (Tant, Brouwer, Kooijman & Cornelissen)

Evaluation of a neglect rehabilitation program167
observation revealed no signs of dementia, aphasia nor apraxia. At start of the programseveral neglect tests (clinical and experimental) were administered to assess the existence andseverity of neglect. On all the administered tests he showed severe neglect (see result section).
2.2. Evaluation methodsThe clinical evaluation tests were the Albert’s line crossing test (“Albert”) (Albert, 1973), TheBells Test (“Bells”) (Vanier et al., 1990), an unstructured letter cancellation task (“OZO”), theMesulam structured Shapes cancellation (“ShCs”) (Weintraub & Mesulam, 1988), and anoverlapping figures task (“OFT”). These clinical neglect tests were to be assessed severaltimes to follow the progression of the interventions. At no point in time was any feed-backgiven concerning these assessment measures nor were strategies provided to complete thosetasks. The number of omissions on clinical neglect cancellation tasks can be seen in figure 5(pre scan). These results indicate a severe neglect.
2.3. The Tracking taskThe tracking task has two components: a lane tracking task on a 20 inch central screen and aperipheral identification task. In the lane tracking task subjects continuously have to keepcourse while a variable sidewind (i.e. a distortion signal of three superimposed sine waves)which “pushes” the subject off course. The experimental setup is partly described in Brouwer,Rothengather and van Wolffelaar (1992). The subject is seated in front of a 20-inch videoscreen on which the road is projected (i.e. what one sees when looking out of the windshieldof a car; one does not actually see a car). He or she is told to drive as straight as possible inthe middle of the right lane. The car moves at about 50 km/h. Steering was done by means ofa steering wheel that was placed in front of the PC screen. The visual angle covered for thistask is about 25°. On the left and right of this main screen where the road was projected aretwo peripheral screens on which traffic signs could be projected. Arrows appeared in thesesigns and were presented randomly on left and right peripheral screen. The subject was askedto push a button on the steering wheel when an arrow appeared. The visual angle covered bythese two additional screens is about 75° (viewing distance is about 75cm). Our subjectsteered and pressed the button using only his right hand. This tracking task is composed ofeight stages. In stage 1 the subject can get familiar with the central task. He or she isencouraged to “play” with the steering wheel for example to see what happens if they driveinto the roadside. Stage 2-3 are adaptive blocks of 3 minutes each. Here the sidewind factor isindividually adjusted. This is done in a stepwise manner until the subject is able to keepcourse for 90% of the time. A factor is obtained at the end of stage 3 by averaging thesidewind factors of stage 3. The individual sidewind factor is then maintained throughout thewhole task. Stage 4 is an actual testing stage where the subject has to keep course for 2minutes in the middle of the right lane while “the individual sidewind” is blowing. Stage 5 isagain a practice stage where the peripheral task is introduced. The subject has to push a buttonon the steering wheel when an arrow appears on one of the peripheral screens. He does nothave to keep course but is advised to keep his eyes as long as possible on the road.Performance is tested in stage 6. Stages 7-8 are dual-task stages (combination of central andperipheral task) where subjects have to keep course while also pushing the button when anarrow appears on the peripheral screens. Performance is assessed in stage 8. We recordedlateral position (LP), standard deviation of the lateral position (STDLP) for the central taskand reaction times (RTs) for the peripheral task.

Evaluation of a neglect rehabilitation program168
2.4. The Driving SimulatorThe Driving Simulator of the Centre for Environmental and Traffic Psychology (COV)consists of a car installed on a fixed base with a large video projection screen displaying thetraffic scenery viewed through the car’s windscreen. The car is a modified BMW 518containing all its original controls. The screen image has horizontal and vertical viewingangles of 150° and 40° respectively. The outside world is displayed in three-dimensionalperspective. The route consists of built-up area (50 km/h limit), main road (80 km/h limit) andhighway (120 km/h limit). There are a total of 14 intersections with possible traffic comingfrom left, right and front. There are also parts of road with and without oncoming cars. Thetotal distance of the route is 37 km. While driving, we record among other things lateralposition (LP), standard deviation of the lateral position (STDLP), speed (S) and headmovements (HM). The head movements are measured by a potential which is connected by aflexible hinge to a very light helmet.
2.5. Training methodsWe administered the program serially instead of each component in every session as is doneby Pizzamiglio et al. (1992). We first did the visual scanning training, secondly the readingtraining, then the matrix training and with some overlap finally the figure description.For a detailed description of the program itself, we again refer to Pizzamiglio et al. (1992).We used the same principles to construct our own materials (Dutch versions). We additionallyconstructed tests to measure improvements during training.
3. Results and DiscussionWe do not report progression during training parts; only before and after each trainingcomponent (pre and post training respectively).
3.1. Part one: Visual Scanning trainingOur patient trained a total of 18 hours in 12 weekswhich is comparable to the training hours reportedby Pizzamiglio et al. (1992) (20 hours). Figure 1shows the first and the last test sequence. Thetraining effects can clearly be seen: the overall RT islower post-training, as is the standard error. Howeverthe responses on the leftmost targets still seems topoint to some neglect symptomatology. We thereforecompared these RTs to those of a left hemianopicpatient without any signs of neglect. This patient alsoshows the elevation of RTs of the leftmost stimuli(Figure 2). We also checked his performance 8weeks, 9 weeks and 23 weeks after his last session ofvisual scanning training (see Figure 3). It can be seenthat follow-up performance shows the same patternas post-training performance.
0500
10001500200025003000350040004500
123456789101112Position
Rea
ctio
n Ti
me
(ms)
Pre TrainingPost Training
Figure1. Reaction times by Kd on unpredictableTest sequence before and after training. Errorbars are Standard Errors. Position 12 is far left,position 1 is far right. Subject is sitting betweenposition 6 and 7.NB: The utmost left stimulus was never noticedbefore training.

Evaluation of a neglect rehabilitation program169
3.2. Part two: Reading trainingWe trained for 14 hours divided over 7 sessions which is less than reported by Pizzamiglio etal. (1992) who trained for 20 hours. Reading times decreased after training but increasedagain at follow up. Both types of errors decreased after training and remained stable (seeTable 1).
3.3. Part three: Matrix trainingWe trained for 6.5 hours in 10 sessions which again is less than the mean reported byPizzamiglio et al. (1992) (10 hours). During pre training assessment he completed 47% of theitems. This percentage increased to 95% during post training assessment. Additionally, thepercentage of errors per item (erroneous line segments per matrix) decreased form 10% to5%.
3.4. Part four: Picture descriptionWe trained for 2.5 hours over 4 sessions. As we did not have a testing method for this trainingpart, we recorded the number of problems (misidentifications, omissions of important partsetc.) in each category. The results can be seen in table 2.To our surprise Kd disliked this training the most and found it also quite difficult andstressful. Indeed, while hisperformance on previous testswas relatively good, he mademany errors. Even in the easiestcategory, he made relativelymany errors which againdecreased in the medium and hard
Table 2. Misidenof pictures betwCategoryEasyMediumHardExtra hard
0500
10001500200025003000350040004500
123456789101112
Position
Rea
ctio
n Ti
me
(ms)
KdLeft H. HemianopiaControl
Figure 2. Comparison of Reaction times by Kdon unpredictable Test sequence after trainingwith a Left H. Hemianopia patient and a controlsubject. Error bars are Standard Errors.
tifications in picture description (actual numbereen brackets).
Errors on first presentation (%)36.36 (8)20.00 (9)27.27 (9)47.05(16)
Table 1. Results of Reading training.Assessment Reading Time (s) Word Errors (%) Line Errors (%)Pre 285.5 27.5 75.0Post 196.75 3.3 3.16 weeks 280.5 4.4 6.2
0500
10001500200025003000350040004500
123456789101112Position
Rea
ctio
n Ti
me
(ms)
Pre TrainingPost Training8 weeks9 weeks23 weeks
Figure 3. Comparison of Reaction times by Kdon the unpredictable Test sequence before andafter training with performance after 8, 9and 23weeks without training. Error bars are StandardErrors.

Evaluation of a neglect rehabilitation program170
categories. This can be interpreted as again a training effect. The extra hard pictures wereclearly too difficult to comprehend and describe adequately. The high number of problemsencountered suggests that picture description comprises at least some components other thanthe already trained ones. The picture description task clearly needs more attention and shouldbe improved.
3.5. Assessments of non-trained tasksTo assess any generalisation effect ofthe trained components to other tasks orcomponents, the assessments should bedifferent from training materials. Wetherefore assessed with traditionalclinical neglect tests at different pointsin time. The results can be seen infigure 5.It can clearly be noted that theperformance on the non-trained clinicalneglect tests already greatly improvedafter the visual scanning training anddid not further substantially improve.Furthermore on the basis of the combination of tests administered after the visual scanningtraining, one could argue that clinically one could not diagnose neglect any more on the basisof those tests. This does not mean however that all neglect components had improved. Thedata seem to suggest that some compensation strategies have been taught, namely scanningthe environment. But the persistent problems with the picture description and the results onthe OFT suggest that the some deficits remain (under some conditions). This again arguesagainst a complete generalisation of training effects and suggests that the effects are due tocompensatory mechanisms instead of functional improvement.Some results suggest a functional improvement of the neglect syndrome. To further test thishypothesis we should also study more ecologically valid tasks. We chose to assess drivingperformance. Before any training, we tried to administer the Tracking task. This failedcompletely. In spite of extensive explanation and instructions our subject could not grasp theconcept of simulating driving. He could not understand that the graphics on the screendepicted a road. He constantly wanted to see a car he could navigate around. Even afterdemonstration of what brings about the turning of the steering wheel, he could notcomprehend the simulating situation. However, after the first training component, when allbut one of the clinical neglect tests considerably improved (see figure 5), we were successfulin administering this task. His sidewind factor was 0.7 which is extremely low if oneconsiders that the starting value is 1 and that with factors below 1 it is generally better not tosteer at all to keep a straight course. We compared his lateral position (LP) in stage 4 and 8(single and dual task respectively). Figure 6 shows the LP during both stages. When thesubject is driving in the middle of the right lane the LP is 0, the right border corresponds withLP 200, the middle of the road with –200, the left border with –600. The mean LP for stage 4and 8 respectively was –122.75 and –293.75. T-test analysis revealed this difference to besignificant (t=2.404, p<0.05). The STDLP in the two conditions was 107.5 and 79.5respectively (t=1.04, n.s.). These values were twice as high as controls. This means that oursubject was driving too much to the left of the road. This tendency increased in the dual task
02468
1012141618
pre scan post scan post read end
Assessment
Om
issi
ons
(num
ber)
AlbertBellsOZOSh CsOFT
Figure 5. Number of omissions on clinical neglect tests.

Evaluation of a neglect rehabilitation program171
situation. He could not handle any sidewind to keep course. In spite of that, he swayed a lotbut this did not increase in the dual task situation.In the peripheral tasks he saw (and reacted to) a total of 20 arrows during the single task and18 arrows in the dual task. He missed a total of 1 arrow (left screen, dual task). He wasapparently scanning both left and right half fields. We further analysed the RTs of stages 6and 8 (single and dual task situation respectively of peripheral task). We included the stages(6-8) and the side of the screen (left-right) as factors in an ANOVA analysis. Both factors andinteraction effect proved to be significant. As can be seen in figure 7, he reacted generallyfaster in the single task condition (F(1, 33)=11.36, p<.005) and to arrows on the right screen(F(1, 33)=42.49, p<.001). In the dual task condition the difference increased disproportionallyon the left side (F(1,33)=14.45, p<.005).
3.6. The Driving SimulatorAfter completion of the full training program we wanted to use a test still more ecologicallyvalid. We chose again driving. For safety reasons we did not administer a real driving test butused the driving simulator. The experimental test ride takes about 45 minutes (practiceincluded). Again it took a while to fully comprehend the simulated environment. Foranalysing purposes, we make a distinction between A- and B-sections. The part of roadsstarting from an intersection to the moment when the next intersection is perceived (markedby a clear slowing of speed) are A-sections. Near-intersection parts are B-sections.
3.7. Head MovementsWhen considering the head movements wenoticed that he was actually looking around, notneglecting the left side. In figure 8, we show themaximum angle of head movement per part ofroute on B-sections. One can see that most ofthe time he did look to the left although theamplitudes are generally larger to the right. Onparts 9 and 11 he did not look to the left. Thesewere however intersections with right-of-way.
3.8. Lateral PositionIn figures 9 and 10 we plotted the mean LP for sections A and B respectively. Since theSTDLP is again quite high, the means could quite disguise extreme LPs. We therefore
Time
Mea
n La
tera
l Pos
ition
Single TaskDual Task
Figure 6. Lateral Position during tracking task
0
500
1000
1500
2000
2500
3000
3500
Left RightScreen
Rea
ctio
n Ti
me
(mse
c)
S ingle TaskDual Task
Figure 7. Reaction times on signs on left andright screens
01020304050607080
1 2 3 4 5 6 7 8 9 10 11 12 13Part of Route
Hea
d M
ovem
ents
(d
egre
es v
isua
l ang
le)
to Leftto Right
Figure 8. Amplitude of head movements to leftand right on B-sections

Evaluation of a neglect rehabilitation program172
included in the same figures minimal and maximal LPs, giving an impression of the mostextreme LPs of our subject on the road. Positions 0 and 6 are left and right bordersrespectively, 1.5 and 4.5 are middle of the left and right lane (dotted), 3 is middle of the road(full line). We estimated the car being 1.80m in width and depicted those as error bars in thefigures.As can be seen, our subject again showed a clear tendency to drive too far to the left. Thistendency was to its very extreme in B-sections. This may not be very obvious looking only atthe means, but when considering the maximum LPs in combination with the estimated widthof the car this reveals very dangerous positions. On nearly all parts of the route, the front-leftof the car was at least once on the left side of the road, possibly obstructing oncoming cars.When approaching intersections, he even found himself once in the middle of the left lane. Anoncoming car could not possibly have passed.
3.9. SpeedHe generally drove too slowly and refused tospeed up when asked to. Figure 11 shows hisaverage speed on A-sections for each speed limit.The error bars indicate the maximum speed hereached.
4. ConclusionsWe successfully replicated the training paradigmby Pizzamiglio and colleagues (1992). At firsthand we would also have suggested that weobserved generalisation effects because we seeimprovements on most non-trained tasks. Thesetasks were however clinical neglect tests. We alsoasked our patient how he subjectively evaluatedthe training. His remarks were very positiveespecially with regard to the first trainingcomponent. Indeed, we also saw most of the improvements after this type of training. Not allassessment tests improved or were within normal range however. When looking at theTracking task, he was actually looking around although more effectively to the right side. Hisscanning component could be judged relative to standard. Although performance decreased in
0
3
6
1 2 3 4 5 6 7 8 9 10 11 12 13
Part of Route
Mea
n La
tera
l Pos
ition
Minimum LPMaximum LPMean LP
Figure 9. Lateral Postition on A-sections
0
3
6
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Part of Route
Mea
n La
tera
l Pos
ition
Minimum LPMaximum LPMean LP
Figure 10. Lateral Postition on B-sections
0
20
40
60
80
100
120
50 80 120Limit on road (km/h)
Spee
d (k
m/h
)
Figure 11. Speed (km/h) on A-sections.

Evaluation of a neglect rehabilitation program173
dual-task conditions, his LP and course keeping was and remained below standard. A similarpicture emerged from the even closer to real life situation Driving Simulator. Although hewas looking around, his LP was dramatically to the left.These results suggest that training can help to compensate for the scanning deficit in mostsituations. Since some aspects of real life tasks do not change even after this intensivetraining, we have no evidence of functional improvement of neglect.
5. References
Albert, M. L. (1973). A Simple test of visual neglect. Neurology, 23, 658-664.
Antonnuci, G., Guariglia, C., Judica, A., Magnotti, L., Paolucci, L. & Zoccolotti, P.(1995). Effectiveness of neglect rehabilitation in a randomised group study. Journal ofClinical and Experimental Neuropsychology, 17, 383-389.
Brouwer W. H., Rothengather, T. & van Wolffelaar, P.C. (1992). Older drivers and roadinformatics. In H. Bouma and J.A.M. Graafmans (Eds.), Gerontechnology. Amsterdam: IOSPress, pp. 317-238.
Pizzamiglio, L., Antonucci, G., Judica, A., Montenero, P., Razzano, C. & Zoccolotti, P.(1992). Cognitive rehabilitation of the hemineglect disorder in chronic patients with unilateralright brain damage. Journal of Clinical and Experimental Neuropsychology, 14, 901-923.
Vanier, M., Gauthier, L., Lambert, J., Pepin, E.P., Robbillard, A., Dubouloz, C.J.,Gagnon, R., & Joanette, Y. (1990). Evaluation of left visuospatial neglect: Norms anddiscrimination power of two tests. Neuropsychology, 4, 87-96.
Weintraub, S. & Mesulam, M.M. (1988). Visual hemispatial inattention: stimulus parametersand exploratory strategies. Journal of Neurology, Neurosurgery and Psychiatry, 51,1481-1488.

Quandranopia can shift to Hemianopia174
Quadranopia can shift to Hemianopia with shift of task-demands*
1. IntroductionDriving is a complex task that requires good perceptual and cognitive abilities. Restrictions ofthe visual field, confusion between left and right, reduced awareness, inadequate scanning ofthe environment, and distractibility are important functions for safe driving that are oftenimpaired after brain damage. It is estimated that approximately 90% of the informationprocessed while driving is of a visual nature (Wylie, 1978). Therefore there are establishedand strict baseline visual requirements for the issuing of a valid driver’s license. One of thevisual requirements is the extent of the visual field. In the Netherlands the legal standard is:the horizontal visual field, either monocular or binocular, exceeds 140°. Therefore braindamaged subjects with hemianopia are prohibited from driving.Homonymous hemianopia is the most frequent visual field disorder after postchiasmatic braindamage. Hemianopia indicates that half of the visual field had been affected. The term‘homonymous’ means ‘the same side’. A left or right homonymous hemianopia indicates thatthe patient is blind to one half of the entire visual field. About 75% of patients with visualfield impairments resulting from acquired posterior brain injury suffer from (a form of) thiscondition. In about 75% of these cases, field sparing does not exceed 5°. These patientsmainly complain of difficulties with reading, detecting stimuli and hence finding objects inthe visual hemi-space which corresponds to the affected hemi-field (Zihl, 1995).The extent and shape of the visual fields can be measured using different procedures andmethodologies. In clinical practice these measures are used interchangeably and choice isusually depending on time/effort considerations. For a review on comparison of differentconfrontational visual field tests we refer to Elliott, North and Flanagan (1997). In this studywe used two widely used perimetric tests namely the Goldmann and the Humphrey FieldAnalyzer.
2. Method: Perimetric tests2.1. The Goldmann perimetric testIsopters for white stimuli were plotted by a conventional kinetic technique with a targetvelocity of approximately 3° per second. In general, for normal subjects, isopters are plottedalong each of the 15° meridians of the Goldmann chart. In patients with abnormal fields,however, stimulus presentation is performed in succession, perpendicular to the border of thefield defect. Bowl luminosity was 31.5 asb. The stimuli we used were I4 and V4.
2.2. The Humphrey Field AnalyzerThe Humphrey Field Analyzer (HFA) is an automated projection perimeter. It has a bowlluminance of 31.5 asb. and a viewing distance of 33 cm. We presented static white stimuli inthe 246 Full Field Screening Test with a 3-zone strategy. Stimulus size is III4 equivalent. Theintensity is slightly brighter than the subject expected threshold (age corrected).
3. Case report, Results and Discussion3.1. CaseJH is a 75 year old man . CT scans revealed a dilated ventricular system. It shows a righttempero-parietal infarction with slight cortical atrophy. An ophthalmic investigation revealed
* This manuscript is accepted to appear in: Vision in Vehicles VIII. A.G.Gale, I.D.D. Brown, C.M. Haslegrave,& S.P. Taylor (Eds.), Amsterdam: Elsevier. (Tant, Brouwer, Kooijman & Cornelissen)

Quandranopia can shift to Hemianopia175
no abnormalities except for a left sided field defect. Neuropsychological examination showedno signs of dementia, apraxia, aphasia or neglect.
3.2. PerimetryThe Goldmann visual fields reveal a homonymous lower left quadranopia (HQ) (figures 1 and2).
On thperimecompaqualitathe mcompa
3.3. TWe trimodiftask anto idecryingeccenttasks.
Figure
Figure 1. Goldmann visual field, left eye. Figure 2. Goldmann visual field, right eye.
e same day we administered the 246 Full Field Screening Test of the HFA. Thistric test showed an asymmetric partial homonymous hemianopia (HH). For purposes ofrison we overlapped Goldmann and HFA-plots in figures 3 and 4. This shows thetive difference in the appearance of the visual field between both tests. We overlappedean of the isopters of the Goldmann which would be III-4 and is thus directlyrable to the isopters used in the HFA.
he Attention tasked to replicate this qualitative difference using the same paradigm. For this we used aication of the Useful Field of View Test (Ball & Owsley, 1991). This test is an attentiond has a central and a peripheral component. For the central component the subject has
ntify the mouth of a face in the centre of the screen which can either be laughing or. For the peripheral component a circle is presented on 24 possible positions (3ricities along 8 meridians). The field size used is 40° diameter. This test has 4 phases orTask 1 is an adaptive phase with only the peripheral component. In this phase stimulus
3. Goldmann over HFA visual field, left eye. Figure 4. Goldmann over HFA visual field,right eye.

Quandranopia can shift to Hemianopia176
presentation duration is defined where the subject reaches at least 90% correct identifications.For our subject this was 25 ms. This presentation time is maintained throughout the furthertest. In task 2 both components are present: the subject has to report the position of the mouthand the position of the circle. Task 3 has again only the peripheral component but now thecircle is embedded in a field of distracters. Now all possible positions are occupied by stimuli.One of them is the target (circle), the others are squares (distracters). Task 4 is identical totask 2 but now again with the distracters. Thus, the level of difficulty increases with thenumber of the task. Task 1 is a measure of selective attention because there is only theperipheral task to perform. In task 2 there is selective attention and divided attention sinceboth peripheral and central tasks have to be performed. This is thus a more difficult task to do.Tasks 3 and 4 have the same rationale but now the targets are hidden among distracters,rendering the peripheral (divided attention) task more difficult.
In figure 5 the percentage correct identifications (peripheral tasks) are presented for controlsubjects. It can be noted that performance degrades from task 2 to 3, but not from 3 to 4. Infigure 6 we plot the same percentages but by half-field for our subject. It is apparent that thepattern of results of the controls is mirrored is his right half-field. However in the left half-field we see a quadranopic-like performance in task 2 (nearly 50% points seen in this halffield) degrading to a hemianopic-like performance in task 4 (approximately 5% points seen).Thus within the same test using the same stimuli and conditions but varying the attentionaldemands, we shifted a quadranopic to a hemianopic performance. We therefore conclude thattask-load is a crucial factor determining the extent and shape of the visual field of JH.This means however that the choice of the perimetric test could influence the diagnosis of the
visual deficit. The diagnosis, in turn, influences the decision on the drivers permit. Followingthe Goldmann visual fields, a drivers permit in the Netherlands would be granted because thehorizontal axis seems preserved. The conclusion of the ophthalmologist accordingly was ³«EXW�WKH�KRUL]RQWDO�YLVXDO�ILHOG�LV�DERXW�������7KHUH�VHHPV�WR�PH�WR�EH�QR�UHDVRQ�WR�GHFODUH�-+XQILW� WR�GULYH´. But considering the Attention task and looking at the HFA visual fields thehorizontal visual field is not preserved at all, making him unfit to drive. Clearly bothperimetric tests do not measure the same construct namely the visual field. The extent andshape of this presumed constant entity can be dependent on task-load. It is therefore crucial toselect a task-load fitted to the desired goal-task, in this case driving. Since driving can beconsidered a complex task with high load demands and distracters in the environment, it iscloser to the HFA and the fourth task of the Attention Task.
0
20
40
60
80
100
Poin
ts s
een
(%)
Task 2Task 3Task 4
Figure 5. Percentage pointsseen by control subjects on theAttention Task.
0
20
40
60
80
100
LHF RHF
Poin
ts s
een
(%)
Task 2Task 3Task 4
Figure 6. Percentage points seen by JHon the Attention Task. LHF: left halffield. RHF: right half field.

Quandranopia can shift to Hemianopia177
4. ReferencesBall, K. & Owsley, C. (1991). Identifying correlates of accident involvement for the older
driver. Human Factors, 33, 583-595.
Elliot, D. B, North, I. & Flanagan, J. (1997). Confrontation visual field tests. Ophthalmicand Physiological Optics, 17, 17-24.
Wylie, E. J. (1978). Vision and driving. Canadian Journal of Optometry, 40, 70-74.Zihl, J. (1995). Visual Scanning behavior in patients with Homonymous Hemianopia.
Neuropsychologia, 33, 287-303.

178
Appendix: An analytic exercise

AFOV179
Assessing visual search in the AFOV test1
1. AimThe AFOV (Attended Field Of View) test aims at assessing the efficiency of visual search(Coeckelbergh et al., submitted). An efficient search strategy is here defined as a strategy thatallows the subject to respond to targets in a fast and evenly distributed manner. Hence, the testshould provide a measure of general search time as well as a measure of distribution. Themean threshold presentation time (see Methods) is calculated as an estimate of general searchtime. Two scores to assess the distribution of threshold presentation times across the field ofview will be discussed. We will present a measure expressing the ‘flatness’ and a measureexpressing the ‘asymmetry’ of the distribution. In our opinion, both measures in combinationwith the mean threshold presentation time give an adequate description of the efficiency ofvisual search in the AFOV test. By considering these three parameters, typical visual searchpatterns associated with specific visual field impairments can be differentiated.
2. MethodsThe AFOV test makes use of a visual search paradigm. Thirty-one stimuli are presented on a20-inch screen (stimulus luminance = 40 cd/m2, background luminance = 16 cd/m2, roomluminance = 500 lux). The stimuli are arranged in three elliptical rings around a centralstimulus. The visual angle of this stimulus array is 60 degrees horizontally and approximately24 degrees vertically. No stimuli are presented on the vertical axis. The subject is sitting infront of the screen at a viewing distance of 30 cm and is instructed to locate an open circle(e.g., C) among 30 closed circles (O) and subsequently indicate the direction of the gap (left,right, top or bottom of the circle). The target can appear at any of 31 positions (Figure 1a).Some positions were pooled and analysed as one position. Figure 1b identifies the pooled datapoints. All 7 positions on the horizontal axis are analysed as individual data points. Perquadrant three more positions are analysed. Data of the three stimulus elements on the outerring are pooled, as are the two elements in the middle ring. In this way, six positions aretested per ellipse (Figure 1b).
1 In collaboration with Tanja R.M. Coeckelbergh. This paper is also presented in Coeckelbergh, T.R.M. (2002).Effect of compensatory viewing strategies on practical fitness to drive in subjects with visual field defects causedby ocular pathology. Unpublished doctoral dissertation, University of Groningen, The Netherlands.
-15-10-505
1015
-25 -20 -15 -10 -5 0 5 10 15 20 25verti
cal d
ista
nce
(deg
rees
)
horizontal distance (degrees)
a b
horizontal distance (degrees)-25 -20 -15 -10 -5 0 5 10 15 20 25
Figure 1a depicts an example of the actual AFOV stimulus as presented to the subject. Figure 1b representsthe 19 positions which are analysed. Pooled positions are connected.

AFOV180
The size of the stimulus elements is determined by eccentricity and can be adjusted in relationto visual acuity. Eye and head movements are allowed after the central fixation marker hasdisappeared (a diamond consisting of four red dots, luminance = 14 cd/m2). The stimuli arepresented with varying presentation times (range: 8ms - 10s). By means of a staircaseprocedure the presentation time at which the subject can correctly identify the target in 67 percent of the trials is determined foreach of the 19 positions and this isdefined as the thresholdpresentation time. Figure 2represents the graphical output ofthe threshold presentation times bya subject with a central fielddefect. The mean of the 19threshold presentation times perposition is termed the meanthreshold presentation time and isconsidered as an estimate ofgeneral search time.
3. Requirements of the measure of distributionIn a next step, we wanted to describe the search pattern in terms of its distribution. An even orflat distribution is here defined as a distribution with equal threshold presentation times for allpositions. In our view, a distribution score should describe different kinds of distributions andshould allow us to compare the distributions directly. It should be easy to interpret and have alimited range. Finally, it should be independent of general search time.
3.1. Different measures for efficiency of distributionThe visual search paradigm of the AFOV test provides a tool to assess scanning behaviourindirectly. Inefficient scanning techniques will cause high threshold presentation times and/ora poor distribution. Scanning behaviour is frequently impaired in patients with visual fielddefects and can be very diversified. A hemianopic patient, for example, may have an efficientscanning pattern in his intact visual field but a chaotic scanning pattern (if any) in his blindvisual field. A patient with tunnel vision may have a slow but structured scanning pattern or afast but chaotic scanning pattern. These different scanning patterns will lead to differentsearch times and different distributions. In our opinion, a measure of distribution should beapplicable for all kinds of visual field defects such as central scotoma, peripheral constriction,quadranopia or hemianopia.
3.2. A limited range and easy to interpretThe measure of distribution should be easy to interpret and its range should be limited, forinstance on a scale from 0 to 100. A score of 0 would indicate a flat distribution in which thethreshold presentation times are equal for all positions in the field. A score of 100 would beindicative of a search pattern in which the subject performs at the worst level (i.e. responds atthe highest presentation times) at half of the positions and at the best level (i.e. responds at thelowest presentation times) at the other half of the positions.
-15
-10
-5
0
5
10
15
-25 -20 -15 -10 -5 0 5 10 15 20 25
verti
cal d
ista
nce
(deg
ree)
horizontal distance (degree)
0
500
1000
1500
Figure 2. Graphical depiction of AFOV performance by a subjectwith a central field defect.

AFOV181
3.3. Unaffected by constant differences across individualsThe measure of distribution should be independent of the absolute value of search time i.e. themean threshold presentation time and the measure of distribution should be statisticallyindependent. It should be statistically possible to observe a high mean threshold presentationtime in combination with a low distribution score and a low threshold presentation time incombination with a high distribution score. This statistical independence between thedistribution score and the mean threshold presentation time would result in the samedistribution score in case of a subject with high threshold presentation times and a subjectwith low threshold presentation times but otherwise equal search patterns. Equal searchpatterns are represented by parallel lines when threshold presentation times are graphicallyplotted by subject as a function of stimulus position (see figure 3). If the mean thresholdpresentation time and the distribution score were statistically dependent (i.e. a prioricorrelated), a slow search strategy (i.e. high mean threshold presentation times) would nearlyalways result in a high distribution score. As we want to assess and evaluate search time anddistribution independently (for example, before and after training), an intertwining of thesevariables has to be avoided.
3.4. Measures of variabilityThe distribution of threshold presentation times across all positions in the field of view can beexpressed by a measure of variability. A flat distribution characterises low variabilityindicating that the time needed by the subject to detect the target is approximately the samefor every position in the field. Common measures of variability are the range, the standarddeviation or the mean absolute deviation. We will briefly discuss these measures,demonstrating their properties and explaining whether or not these properties are desirable forour purposes. To do so, we will use simplified and extreme examples in which data pointsrepresent threshold presentation times for several positions in the field. The number ofpositions and the values are arbitrarily chosen for the purpose of illustration. Plotting thethreshold presentation times as a function of their position contributes to the insight of theintuitive notion of distribution (e.g. see figure 3).
Range, the difference between the lowest and the highest score is, for our purpose, not anadequate measure as it does not discriminate between short presentation times on all but oneposition (subject 1) and e.g. short presentation times on all but three positions (subject 2).
subject 1: 2 2 2 2 2 2 2 2 8 range = 6subject 2: 8 2 2 2 8 2 2 2 8 range = 6
We consider the distribution of subject 1 as more efficient than the distribution of subject 2because subject 1 shows only one "peak", whereas subject 2 shows three peaks. Thisdifference should be represented in the distribution measure.
More sophisticated measures, like the mean absolute deviation and the standard deviation, canaccommodate this difference in some way and seem thus more appropriate. However, neitherthe mean absolute deviation, nor standard deviation and derivatives such as the coefficient ofvariation are suitable for our purpose, as they calculate deviation with respect to the mean.The mean is highly influenced by outliers. As we are particularly interested in the number andvalue of these extreme scores, we need to avoid a distribution score in which the reference

AFOV182
(i.c. the mean) is contaminated by these extremes. We therefore prefer the use of the PHGLDQas a reference to calculate a deviation. The mean absolute deviation with the median as areference fits our requirements and is represented in the following formula:
An example might illustrate this point. Imagine a subject with a right peripheral visual fielddefect, resulting in the following threshold presentation times:
subject 3: 2 2 2 2 2 2 2 2 80
In our view, the peak of 80 is due to the visual field defect whereas the value of 2 is thebaseline value. We presume that if subject 3 would not have had a visual field defect, thedistribution would have been completely flat. We therefore prefer to use the median (2) as areference and not the mean (10.67), because the median more closely reflects the ‘real’performance level of this subject. A value of 10.67 seconds would indicate that subject 3 isquite slow in detecting the target, whereas we believe that the subject is actually quite fast (2seconds) with the exception of one position where the subject cannot perceive the target dueto an uncompensated visual field defect.
4. PDM: a measure of distribution4.1. PDM, percentage deviation from the medianA measure with reference to the median, which is easy to interpret and has a limited range isthe PDM, the percentage deviation from the median:
The deviation from the median of each position ([L) is calculated, summed and divided by thenumber of positions (Q). This score is further divided by the maximum deviation. Themaximum deviation is the distribution at which a subject responds at a maximum presentationtime at half of the positions and at a minimum presentation time at the other half and istherefore based on a fixed number of positions and a fixed range of presentation times.Finally, the score is multiplied by 100 to fit a range from 0 to 100. A score of 100 indicatesthat a subject responds at a maximum presentation time at half of the positions and at aminimum presentation time at the other half. This is the worst possible form of distribution. A0 score is the resultant of equal presentation times across all positions, representing the bestpossible (i.e. flat) distribution.
In case of the AFOV test with 19 positions and presentation times ranging from 8milliseconds to 10 seconds, the formula becomes:
100max
×
−
=
∑
GHYLDWLRQQPHGLDQ[3'0 L
100733.419
×
−
=
∑ PHGLDQ[3'0 L
QPHGLDQ[PHGLDQIURPGHYLDWLRQDEVROXWH L∑ −=

AFOV183
The maximum deviation is 4.733 and is, as already mentioned, based on a distribution atwhich a subject responds at a maximum presentation time at half of the positions and at aminimum presentation time at the other half. In case of 19 positions, two situations render themaximum deviation: 10 positions at maximum presentation time and 9 positions at minimumpresentation time or vice versa. One of these situations is illustrated below:
GDWD�SRLQWV��UHSUHVHQWLQJ�PD[LPXP�GHYLDWLRQ�10
10
10
10
10
10
10
10
10
10
0.008
0.008
0.008
0.008
0.008
0.008
0.008
0.008
0.008PHGLDQ: 10DYHUDJH�PHDQ�GHYLDWLRQ�IURP�PHGLDQ:
The formula can easily be adapted for different minimum and maximum presentation timesand for different number of positions. For example, in case of 5 data points and presentationtimes ranging from 8 ms to 10 s, two points are set at 10 seconds and three points at 0.008seconds (or vice versa). In a next step, the average absolute deviation from the median iscalculated, as described above. In case of analysing 5 positions of the AFOV test, themaximum deviation would be 3.9968.
4.2. Features of the PDM4.2.1. Unaffected by constant differences between subjectsThe PDM is not affected byconstant differences between thethreshold presentation times ofsubjects. Subjects 5 and 6 showthe same pattern of distributionbut are consistently one resp.three seconds slower than subject4 (figure 3). As a consequence,their mean threshold presentationtime will be different. The PDMs,in contrast, are the same.
As a consequence, a non-compensating subject withmacular degeneration (MD),performing very fast in all areasof the field except the central areawill have the same PDM as a non-compensating subject with tunnel vision (RP) who can onlyperceive the central stimuli (figure 4). The mean threshold presentation times, as an indicationof search speed, are different. The PDMs are equal as in both cases only three datapointsdeviate from the rest. In the example below, mean presentation time is 2.421 seconds for theMD patient and 8.579 for the RP patient. Median presentation times are 1 second and 10seconds respectively. PDM is in both cases 30.
733.419
=
−∑ PHGLDQ[L
0
1
2
3
4
5
6
1 3 5 7 9 11 13 15 17 19position
thre
shol
d pr
esen
tatio
n tim
e (s
)
subject 4subject 5subject 6
Figure 3. Threshold presentation times of three subjects. Constantdifferences at every position (represented as parallel lines) betweensubjects yield different mean threshold presentation times butidentical PDMs.

AFOV184
Similarly, the PDM of a hemianopic patient with macular sparing will be equal to the PDM ofa hemianopic patient without macular sparing although their mean threshold presentationtimes will be different. In the example below, mean threshold presentation times are 5.263seconds (with sparing) and 5.737 (without sparing). Median values are 1 second and 10seconds respectively. PDM equals 90.07 in both cases.
4.2.2. Linear relationship between disability and PDMThe PDM scores can easily be compared to each other. A hemianopic patient, missing half ofthe visual field and not making compensatory eye movements, will not be able to find thetarget when presented in his blind field. Thus, when not compensating, threshold presentationtimes will be very high in the affected hemi-field (e.g. 10s). If the patient is very fast in theunaffected field (e.g. performing at minimum presentation times), the PDM equals 100. Aquadranopic patient, missing a quarter of the visual field, with the same features (notperceiving targets in the blind field and responding at minimum presentation times in theunaffected field) will have a PDM of 50 which is half of the PDM of the hemianopic patient.This is illustrated in the following example (in case of 8 data points, maximum variabilityequals 4.996):
positions
thre
shol
d pr
esen
tatio
n tim
e (s
)
Hemianopic patientwith macularsparing
0
24
6
8
10
1 3 5 7 9 11 13 15 17 19
Hemianopic patientwithout macularsparing
0
2
4
68
10
positions1 3 5 7 9 11 13 15 17 19
Figure 5. Graphical depiction of the threshold presentation times of a non-compensating subject with right-sided homonymous hemianopia with (left) and without (right) macular sparing. In both cases the PDM isidentical, whereas the mean threshold presentation times are different.
thre
shol
d pr
esen
tatio
n tim
e (s
)
MD
0
24
68
10
1 3 5 7 9 11 13 15 17 19positions
RP
positions
24
68
10
1 3 5 7 9 11 13 15 17 190
Figure 4. Graphical depiction of the threshold presentation times of a non-compensating subject with MD(left) and RP (right). In both cases the PDM is identical, whereas the mean threshold presentation times aredifferent.

AFOV185
hemianopia: 0.008 0.008 0.008 0.008 10 10 10 10PHDQ������� PHGLDQ������� 3'0�����quadranopia: 0.008 0.008 0.008 0.008 0.008 0.008 10 10PHDQ������� PHGLDQ������� 3'0����
The relationship between performance in uncompensated hemianopia, missing half of thevisual field, and uncompensated quadranopia, missing a quarter of the visual field is thusreflected in the PDM. In the AFOV test with 19 positions, a hemianopic patient would miss 9or 10 points, resulting in a (averaged) PDM of 100. A quadranopic patient would miss 4 or 5targets, resulting in an averaged PDM of 50. The ratio equals 2 (100:50=2). This ratioperfectly reflects the degree of impairment since the visual field defect in case of hemianopiais twice as large as the visual field defect in case of quadranopia. In contrast, the standarddeviation of this hemianopic patient equals 5.13 and the (averaged) standard deviation of thisquadranopic patient equals 4.35, resulting in a ratio of 1.18. This outcome does not correctlyreflect the difference in degree of impairment between a (non-compensating) subject withhemianopia and a (non-compensating) subject with quadranopia. Similarly, measurementsrelated to the mean (such as the percentage deviation from mean) result in ratios unequal to 2.As a consequence of the properties of these distribution scores, only the PDM is linearlyrelated to the degree ofdisability. This isdepicted in Figure 6. A(linear) increase innumber of deviatingpoints, results in alinear increase in PDMor, in other words,equal steps in degree ofuncompensatedimpairment yield equalsteps in PDM. Neitherthe standard deviation,nor any other measurerepresenting deviationfrom the mean, holdthis linear relationshipto the degree ofdisability.
5. Hemi-spatial lateralisationIn the previous sections, a measure of distribution, which is statistically independent ofthreshold presentation time was presented. It was argued that the PDM provides an adequatemeasure for expressing ‘flatness’ of the distribution. However, the properties of a searchpattern can still be further characterised. This interest in further specification emanates fromthe desire to specifically describe lateralised performance. Since homonymous visual fielddefects are a common type of visual field disorder and often result in hemi-spatial disability,lateralised performance can be expected. It is our aim to express this lateralisation,statistically independent of the mean threshold presentation time and the PDM.
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19number of positions at max. threshold presentation
time
PD m
edia
n/m
ean
0
1
2
3
4
5
stan
dard
dev
.
PDM% deviation from meanst.dev.
Figure 6. Relationships between degree of disability and measurement ofvariability. Disability is schematically expressed as the number of positions notseen (i.e. at the maximum presentation time) while the remaining positions arerecorded at the minimum presentation times. Only the PDM is linearly relatedto the degree of disability.

AFOV186
A distribution with a high PDM can be the result of both a general scanning deficit (chaoticand ineffective scanning all over the field) and a lateralised scanning deficit (e.g. neglecting ahemi-field). In the first case, the positions of worse performance will be randomly distributedacross the search field whereas in the second case, they will be grouped and lateralised. ThePDM can not account for this difference, since it is derived from the number of deviatingpoints, irrespective of their location. The measure to be proposed, expresses this lateralisation.
5.1. Required featuresSimilarly as for the ‘flatness’ of distribution (i.e. the PDM), we seek an index which expresseslateralised performance, irrespective of the mean threshold presentation time and PDM, with aclearly defined and easy-to-interpret range. It should give an indication of both GHJUHH�andVLGH of lateralisation. We will refer to this measure as the Asymmetry Index (AI).
With equal and high PDMs, the AI should differentiate between a totally chaotic distribution(AI=low) and a distribution which is systematic in that worse performance is perfectlylateralised to either left or right hemi-space (AI=high). Equal PDMs and equal AIs shouldresult from completely identically distributed performances or from inverse search patternssuch as shown in Figure 4. A non-compensating subject with a central field defect and a non-compensating subject with tunnel vision should produce equal PDMs and equal AIs. Bothvalues should be low in these examples; the mean threshold presentation times willdifferentiate both cases. It was previously shown that the PDM differentiates uncompensatedhemianopic performance from e.g. quadranopic (but otherwise equivalent) performance.However, in spite of different PDMs, both types of search behaviour are similar in that theyare perfectly lateralised. Hence, the asymmetry index should give identical and high values.Not only the GHJUHH�of lateralisation but also the VLGH�of lateralisation should be representedby the asymmetry index. The degree of lateralisation will be expressed by the absolute valuewhereas of the AI the side of lateralisation will be indicated by its sign. Hence, the range ofthe AI will vary from -1 to +1, indicating respectively extreme lateralisation to left and righthemi-space. No lateralisation (AI=0) results from e.g. only central impairment. Additionally,when the threshold presentation times at homologous stimulus positions are identical or incase of a completely unsystematic distribution, AI will equal 0. Hence, in the previousdiscussion, a ORZ AI should be paraphrased as WHQGLQJ�WR�� and a KLJK AI would be WHQGLQJ�WRHLWKHU����RU���.
5.2. The Asymmetry IndexIt was previously described that in this version of the AFOV test, 19 different locations can beanalysed (see Methods section). Except for the centre location, all other 18 points are situatedeither in the left or right hemi-space (nine points each) (see Figure 1). To expresslateralisation, we will calculate the asymmetry index as:
( )( )
+−
= KHPLVSDFHOHIWKHPLVSDFHULJKW KHPLVSDFHOHIWKHPLVSDFHULJKW ;; ;;$,where KHPLVSDFH; indicates the mean presentation time of the nine locations in the respectivehemispace. This index varies from -1 to +1, and is statistically independent from absolutesearch time and PDM. It further produces identical values for all types of complementarysearch patterns (e.g. MD vs. RP) and uncompensated hemi-spatial disability (e.g. hemianopiavs. quadranopia).

AFOV187
5.3. ExamplesThe examples below are AFOV performances by patients with left-sided homonymoushemianopia (subjects 1-2, 4) and right-sided homonymous hemianopia (subject 3). Althoughthese subjects have similar visual field defects, their scanning behaviour, as measured by theAFOV test, clearly differs.
We illustrate the four different combinations of high (grey) and low PDMs and AIs.
Subject 1 Subject 2 Subject 3 Subject 4Mean Threshold Presentation Time (s) 1.87 3.00 0.75 1.21PDM 29 36 10 8AI -0.71 -0.08 0.56 -0.12
In the AFOV test as presented, performance can thus be evaluated using three different andstatistically independent measures. The mean threshold presentation time indicates generalsearch time. The PDM provides an indication of the ‘flatness’ of distribution across the searchfield. The AI provides a measure of hemi-spatial lateralisation.
-15-10-505
1015
-30-25-20 -15-10 -5 0 5 10 15 20 25 30
01234
thresholdpresentation
time (s)
Subject 1: Graphical depiction of AFOV performance by aleft-sided hemianopic patient. This performance results in ahigh PDM and a high AI.
-15-10-505
1015
-30-25-20-15-10 -5 0 5 10 15 20 25 30
01234
thresholdpresentation
time (s)
Subject 2: Graphical depiction of AFOV performance by aleft-sided hemianopic patient. This performance results in ahigh PDM and a low AI.
-15-10-505
1015
-30-25-20 -15-10 -5 0 5 10 15 20 25 30
01234
thresholdpresentation
time (s)
Subject 3: Graphical depiction of AFOV performance by aleft-sided hemianopic patient. This performance results in alow PDM and a high AI.
-15-10-505
1015
-30-25-20 -15-10 -5 0 5 10 15 20 25 30
01234
thresholdpresentation
time (s)
Subject 4: Graphical depiction of AFOV performance by aleft-sided hemianopic patient. This performance results in alow PDM and a low AI.

Notes188






![Visual storytelling [storytelling matters]](https://static.fdocuments.nl/doc/165x107/54b865614a795970478b4802/visual-storytelling-storytelling-matters.jpg)