
UITNODIGING lifestyle · e m s-J o n g s m a L i f e s t y l e c h a n g e i n a d u l t s w i t h...
178
in adults intellectual disabilities lifestyle with M a r i ë l W i l l e m s - J o n g s m a J U s e a n d e f f e c t i v e n e s s o f b e h a v i o u r c h a n g e t e c h n i q u e s
Transcript of UITNODIGING lifestyle · e m s-J o n g s m a L i f e s t y l e c h a n g e i n a d u l t s w i t h...
in adults intellectual disabilities
lifestylewith
Mariël Willems-Jongsma
in adults intellectual disabilities
Mariël Willems-J-J-JJongsma
Use and effectiveness of behaviour change techniques
Ma
riëlWillem
s-Jong
sma
Lifestylecha
nge
ina
dults
with
intellectuald
isab
ilitiesJ
g
UITNODIGING
Voor het bijwonen van de openbare verdediging
van het proefschrift
Lifestyle change in adults withintellectual disabilities
Use and effectiveness ofbehaviour change techniques
door
Mariël Willems-Jongsma
Op maandag 9 december 2019om 14.30 uur
in het academiegebouw vande Rijksuniversiteit Groningen,
Broerstraat 5 te Groningen
Paranimfen:
Gerjan Willems 0610394409Ilse Mol-Jongsma 0641422911
Mariël Willems-Jongsma
Goudsbloemstraat 508012XN Zwolle

Lifestyle change in adults with intellectual disabilities
Use and effectiveness of behaviour change techniques
Mariël Willems-Jongsma
138541-Willems_BNW.indd 1 31-10-19 10:07
The work presented in this thesis was performed at the Research Group Healthy Ageing, Allied Health Care and
Nursing, Hanze University of Applied Sciences, Groningen, the Netherlands, at the Research Institute SHARE of
the Groningen Graduate School of Medical Sciences of the University Medical Center Groningen, University of
Groningen, the Netherlands.
Printing Ridderprint BV, www.ridderprint.nl
ISBN 978-94-034-2140-7
ISBN 978-94-034-2139-1 (E-book)
© 2019 Mariël Willems-Jongsma
All rights reserved. No parts of this publication may be reproduced, stored in a retrieval system or transmitted in
any form or by any means, without the prior written permission of the copyright owner.
Lifestyle change in adults with intellectual disabilities
Use and effectiveness of BCTs
Proefschrift
ter verkrijging van de graad van doctor aan de Rijksuniversiteit Groningen
op gezag van de rector magnificus prof. dr. C. Wijmenga
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 9 december 2019 om 14.30 uur
door
Mariël Jongsma
geboren op 19 januari 1991 te Almelo
138541-Willems_BNW.indd 2 31-10-19 10:07
The work presented in this thesis was performed at the Research Group Healthy Ageing, Allied Health Care and
Nursing, Hanze University of Applied Sciences, Groningen, the Netherlands, at the Research Institute SHARE of
the Groningen Graduate School of Medical Sciences of the University Medical Center Groningen, University of
Groningen, the Netherlands.
Printing Ridderprint BV, www.ridderprint.nl
ISBN 978-94-034-2140-7
ISBN 978-94-034-2139-1 (E-book)
© 2019 Mariël Willems-Jongsma
All rights reserved. No parts of this publication may be reproduced, stored in a retrieval system or transmitted in
any form or by any means, without the prior written permission of the copyright owner.
Lifestyle change in adults with intellectual disabilities
Use and effectiveness of BCTs
Proefschrift
ter verkrijging van de graad van doctor aan de Rijksuniversiteit Groningen
op gezag van de rector magnificus prof. dr. C. Wijmenga
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
maandag 9 december 2019 om 14.30 uur
door
Mariël Jongsma
geboren op 19 januari 1991 te Almelo
138541-Willems_BNW.indd 3 31-10-19 10:07
Promotor Prof. dr. C.P. van der Schans
Copromotores
Dr. A. Waninge
Dr. J. de Jong
Dr. T.I.M. Hilgenkamp
Beoordelingscommissie
Prof. dr. M. Hagedoorn
Prof. dr. A.A.J. van der Putten
Prof. dr. G. Leusink
Contents
Chapter 1 General introduction 14
Chapter 2 Effects of lifestyle change interventions for people with intellectual 25
disabilities: Systematic review and meta-analysis of randomized
controlled trials
Journal of Applied Research in Intellectual Disabilities, 31(6), 949-961
Chapter 3 Use of behaviour change techniques in lifestyle change interventions 55
for people with intellectual disabilities: A systematic review
Research in Developmental Disabilities, 60, 256-268
Chapter 4 Exploration of suitable behaviour change techniques for lifestyle change in 95
individuals with mild intellectual disabilities: A Delphi study
Journal of Applied Research in Intellectual Disabilities, 32(3), 543-557
Chapter 5 Behaviour change techniques used in lifestyle support of adults with mild 119
intellectual disabilities
Manuscript submitted
Chapter 6 Training professional caregivers in changing lifestyle behaviour of adults 135
with mild intellectual disabilities: a pilot-study
Manuscript submitted
Chapter 7 General discussion 153
Nederlandse samenvatting 162
Dankwoord 168
Research Institute for Health Research SHARE 173
138541-Willems_BNW.indd 4 31-10-19 10:07
Promotor Prof. dr. C.P. van der Schans
Copromotores
Dr. A. Waninge
Dr. J. de Jong
Dr. T.I.M. Hilgenkamp
Beoordelingscommissie
Prof. dr. M. Hagedoorn
Prof. dr. A.A.J. van der Putten
Prof. dr. G. Leusink
Contents
Chapter 1 General introduction 14
Chapter 2 Effects of lifestyle change interventions for people with intellectual 25
disabilities: Systematic review and meta-analysis of randomized
controlled trials
Journal of Applied Research in Intellectual Disabilities, 31(6), 949-961
Chapter 3 Use of behaviour change techniques in lifestyle change interventions 55
for people with intellectual disabilities: A systematic review
Research in Developmental Disabilities, 60, 256-268
Chapter 4 Exploration of suitable behaviour change techniques for lifestyle change in 95
individuals with mild intellectual disabilities: A Delphi study
Journal of Applied Research in Intellectual Disabilities, 32(3), 543-557
Chapter 5 Behaviour change techniques used in lifestyle support of adults with mild 119
intellectual disabilities
Manuscript submitted
Chapter 6 Training professional caregivers in changing lifestyle behaviour of adults 135
with mild intellectual disabilities: a pilot-study
Manuscript submitted
Chapter 7 General discussion 153
Nederlandse samenvatting 162
Dankwoord 168
Research Institute for Health Research SHARE 173
138541-Willems_BNW.indd 5 31-10-19 10:07

Chapter 1
General introduction
138541-Willems_BNW.indd 6 31-10-19 10:07
Chapter 1
General introduction
138541-Willems_BNW.indd 7 31-10-19 10:07
1 | ADULTS WITH INTELLECTUAL DISABILITIES
An intellectual disability (ID) can be defined as a “disorder with onset during the developmental period that
includes both intellectual and adaptive functioning deficits in conceptual, social and practical domains”
(American Psychiatric Association, 2013, p. 33). Adults with ID experience: a) limitations in intellectual
functioning (for example: reasoning, problem solving, planning, abstract thinking), b) deficits in adaptive
functions and c) onset of deficits during the developmental period (American Psychiatric Association, 2013).
Specifically, adults with mild ID (IQ 50-69) need support with abstract thinking, executive functioning, academic
skills and additional support in daily living (American Psychiatric Association, 2013). According to the
International Statistical Classification of Diseases and Related Health Problems (ICD-10), it is important to notice
the emotional and social development because of its influence on daily functioning (Schalock et al., 2002; WHO,
1992).
2 | HEALTHY LIFESTYLE OF ADULTS WITH INTELLECTUAL DISABILITIES
In the Netherlands, 47.7% of the adults are overweight or obese (Gezondheidsraad, 2017). Only 44% of adults in
the Netherlands achieve the latest Dutch physical activity guidelines in 2017 (Gezondheidsraad, 2017). These
guidelines state that adults should include 150 minutes exercise of moderate to severe intensity on multiple days
per week. Additionally, bone and muscle strengthening exercises should be conducted and one should prevent
too much time sitting (Gezondheidsraad, 2017). Adults with ID experience much more health problems and
health inequalities in comparison to adults from the general population (Van Schrojenstein Lantman-De Valk &
Walsh, 2008). Specifically, with regard to physical activity and nutrition, they experience physical inactivity
(Hilgenkamp, Reis, Van Wijck & Evenhuis, 2012; Peterson, Janz & Lowe, 2008), have high levels of sedentary
behaviour (Melville et al., 2017) as well as unhealthy eating habits (Haveman et al., 2010; Hsieh, Rimmer, &
Heller, 2014). Also, their level of health needs are higher (Cooper & Bailey, 2001; Wilson & Haire, 1990) and these
needs are often unmet (Lennox & Kerr, 1997; Wilson & Haire, 1990).
Using the International Classification of Functioning, Disability and Health (ICF), health consists of five underlying
constructs, namely “functions,” “activities,” “participation,” “personal factors” and “environmental factors”
(World Health Organisation, 2001). Moreover, a healthy lifestyle is related to improved quality of life, more
participation in society (Heller, McCubbin, Drum, & Peterson, 2011) and more independency in activities of daily
living (Hilgenkamp, Van Wijck & Evenhuis, 2011; Van Schijndel-Speet, Evenhuis, Van Wijck & Echteld, 2014). It is
thus of main importance to improve the health of adults with ID from an individual as well as a societal
perspective.
3 | DUTCH ID CARE ORGANISATIONS AND LIFESTYLE CHANGE
To improve the lifestyle behaviour of their caretakers, a Dutch consort of 9 ID care organisations was formed, an
innovative collaboration for practice. These organisations (De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo
Zorggroep, Talant, Cosis, Koninklijke Visio Noord Nederland, Philadelphia and Vanboeijen) aim to improve and
maintain a healthy lifestyle for their caretakers. They want to know if their current interventions and lifestyle
9
approaches are effective and how their employees can improve the lifestyle behaviour of their caretakers.
Together they formulated research questions and supported research to promote a healthy life for people with
intellectual disabilities. For all research performed within this consortium, the central theme is lifestyle change
of individuals with ID. This thesis is part of this research programme, which aims to target adults with ID as well
as their social and physical environment and ID care organisation policies.
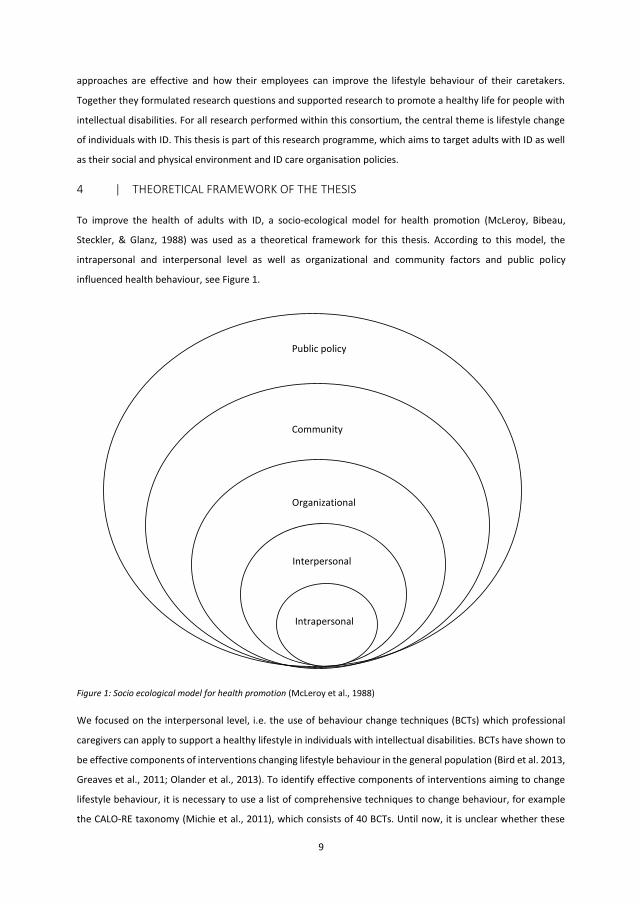
4 | THEORETICAL FRAMEWORK OF THE THESIS
To improve the health of adults with ID, a socio-ecological model for health promotion (McLeroy, Bibeau,
Steckler, & Glanz, 1988) was used as a theoretical framework for this thesis. According to this model, the
intrapersonal and interpersonal level as well as organizational and community factors and public policy
influenced health behaviour, see Figure 1.
Figure 1: Socio ecological model for health promotion (McLeroy et al., 1988)
We focused on the interpersonal level, i.e. the use of behaviour change techniques (BCTs) which professional
caregivers can apply to support a healthy lifestyle in individuals with intellectual disabilities. BCTs have shown to
be effective components of interventions changing lifestyle behaviour in the general population (Bird et al. 2013,
Greaves et al., 2011; Olander et al., 2013). To identify effective components of interventions aiming to change
lifestyle behaviour, it is necessary to use a list of comprehensive techniques to change behaviour, for example
the CALO-RE taxonomy (Michie et al., 2011), which consists of 40 BCTs. Until now, it is unclear whether these
Public policy
Interpersonal
Organizational
Intrapersonal
Community
138541-Willems_BNW.indd 8 31-10-19 10:07
1 | ADULTS WITH INTELLECTUAL DISABILITIES
An intellectual disability (ID) can be defined as a “disorder with onset during the developmental period that
includes both intellectual and adaptive functioning deficits in conceptual, social and practical domains”
(American Psychiatric Association, 2013, p. 33). Adults with ID experience: a) limitations in intellectual
functioning (for example: reasoning, problem solving, planning, abstract thinking), b) deficits in adaptive
functions and c) onset of deficits during the developmental period (American Psychiatric Association, 2013).
Specifically, adults with mild ID (IQ 50-69) need support with abstract thinking, executive functioning, academic
skills and additional support in daily living (American Psychiatric Association, 2013). According to the
International Statistical Classification of Diseases and Related Health Problems (ICD-10), it is important to notice
the emotional and social development because of its influence on daily functioning (Schalock et al., 2002; WHO,
1992).
2 | HEALTHY LIFESTYLE OF ADULTS WITH INTELLECTUAL DISABILITIES
In the Netherlands, 47.7% of the adults are overweight or obese (Gezondheidsraad, 2017). Only 44% of adults in
the Netherlands achieve the latest Dutch physical activity guidelines in 2017 (Gezondheidsraad, 2017). These
guidelines state that adults should include 150 minutes exercise of moderate to severe intensity on multiple days
per week. Additionally, bone and muscle strengthening exercises should be conducted and one should prevent
too much time sitting (Gezondheidsraad, 2017). Adults with ID experience much more health problems and
health inequalities in comparison to adults from the general population (Van Schrojenstein Lantman-De Valk &
Walsh, 2008). Specifically, with regard to physical activity and nutrition, they experience physical inactivity
(Hilgenkamp, Reis, Van Wijck & Evenhuis, 2012; Peterson, Janz & Lowe, 2008), have high levels of sedentary
behaviour (Melville et al., 2017) as well as unhealthy eating habits (Haveman et al., 2010; Hsieh, Rimmer, &
Heller, 2014). Also, their level of health needs are higher (Cooper & Bailey, 2001; Wilson & Haire, 1990) and these
needs are often unmet (Lennox & Kerr, 1997; Wilson & Haire, 1990).
Using the International Classification of Functioning, Disability and Health (ICF), health consists of five underlying
constructs, namely “functions,” “activities,” “participation,” “personal factors” and “environmental factors”
(World Health Organisation, 2001). Moreover, a healthy lifestyle is related to improved quality of life, more
participation in society (Heller, McCubbin, Drum, & Peterson, 2011) and more independency in activities of daily
living (Hilgenkamp, Van Wijck & Evenhuis, 2011; Van Schijndel-Speet, Evenhuis, Van Wijck & Echteld, 2014). It is
thus of main importance to improve the health of adults with ID from an individual as well as a societal
perspective.
3 | DUTCH ID CARE ORGANISATIONS AND LIFESTYLE CHANGE
To improve the lifestyle behaviour of their caretakers, a Dutch consort of 9 ID care organisations was formed, an
innovative collaboration for practice. These organisations (De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo
Zorggroep, Talant, Cosis, Koninklijke Visio Noord Nederland, Philadelphia and Vanboeijen) aim to improve and
maintain a healthy lifestyle for their caretakers. They want to know if their current interventions and lifestyle
9
approaches are effective and how their employees can improve the lifestyle behaviour of their caretakers.
Together they formulated research questions and supported research to promote a healthy life for people with
intellectual disabilities. For all research performed within this consortium, the central theme is lifestyle change
of individuals with ID. This thesis is part of this research programme, which aims to target adults with ID as well
as their social and physical environment and ID care organisation policies.
4 | THEORETICAL FRAMEWORK OF THE THESIS
To improve the health of adults with ID, a socio-ecological model for health promotion (McLeroy, Bibeau,
Steckler, & Glanz, 1988) was used as a theoretical framework for this thesis. According to this model, the
intrapersonal and interpersonal level as well as organizational and community factors and public policy
influenced health behaviour, see Figure 1.
Figure 1: Socio ecological model for health promotion (McLeroy et al., 1988)
We focused on the interpersonal level, i.e. the use of behaviour change techniques (BCTs) which professional
caregivers can apply to support a healthy lifestyle in individuals with intellectual disabilities. BCTs have shown to
be effective components of interventions changing lifestyle behaviour in the general population (Bird et al. 2013,
Greaves et al., 2011; Olander et al., 2013). To identify effective components of interventions aiming to change
lifestyle behaviour, it is necessary to use a list of comprehensive techniques to change behaviour, for example
the CALO-RE taxonomy (Michie et al., 2011), which consists of 40 BCTs. Until now, it is unclear whether these
Public policy
Interpersonal
Organizational
Intrapersonal
Community
138541-Willems_BNW.indd 9 31-10-19 10:07
10
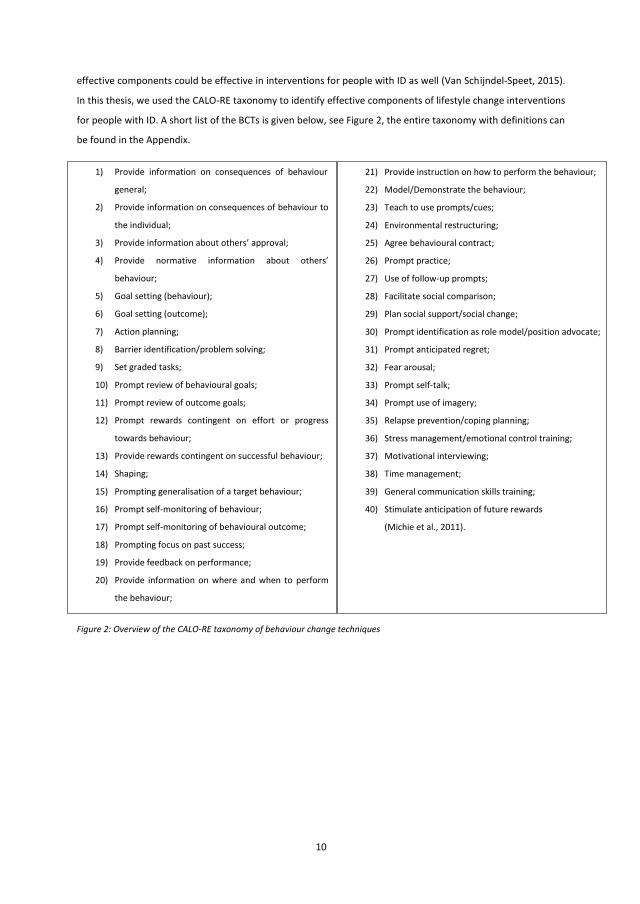
effective components could be effective in interventions for people with ID as well (Van Schijndel-Speet, 2015).
In this thesis, we used the CALO-RE taxonomy to identify effective components of lifestyle change interventions
for people with ID. A short list of the BCTs is given below, see Figure 2, the entire taxonomy with definitions can
be found in the Appendix.
Figure 2: Overview of the CALO-RE taxonomy of behaviour change techniques
21) Provide instruction on how to perform the behaviour;
22) Model/Demonstrate the behaviour;
23) Teach to use prompts/cues;
24) Environmental restructuring;
25) Agree behavioural contract;
26) Prompt practice;
27) Use of follow-up prompts;
28) Facilitate social comparison;
29) Plan social support/social change;
30) Prompt identification as role model/position advocate;
31) Prompt anticipated regret;
32) Fear arousal;
33) Prompt self-talk;
34) Prompt use of imagery;
35) Relapse prevention/coping planning;
36) Stress management/emotional control training;
37) Motivational interviewing;
38) Time management;
39) General communication skills training;
40) Stimulate anticipation of future rewards
(Michie et al., 2011).
1) Provide information on consequences of behaviour in
general;
2) Provide information on consequences of behaviour to
the individual;
3) Provide information about others’ approval;
4) Provide normative information about others’
behaviour;
5) Goal setting (behaviour);
6) Goal setting (outcome);
7) Action planning;
8) Barrier identification/problem solving;
9) Set graded tasks;
10) Prompt review of behavioural goals;
11) Prompt review of outcome goals;
12) Prompt rewards contingent on effort or progress
towards behaviour;
13) Provide rewards contingent on successful behaviour;
14) Shaping;
15) Prompting generalisation of a target behaviour;
16) Prompt self-monitoring of behaviour;
17) Prompt self-monitoring of behavioural outcome;
18) Prompting focus on past success;
19) Provide feedback on performance;
20) Provide information on where and when to perform
the behaviour;
11
5 | LIFESTYLE CHANGE IN ADULTS WITH MILD INTELLECTUAL DISABILITIES
It is necessary to improve the lifestyle of adults with ID, to reduce health risks and health inequalities (Alesi &
Pepi, 2015). However, evidence for the effectiveness of lifestyle change interventions in adults with ID is limited
(Brooker et al., 2015; Scott & Havercamp, 2016; Spanos, Melville, & Hankey, 2013). Some studies found small
significant changes on health outcomes (Curtin et al., 2013, Marks, Sisirak, & Chang, 2013, Van Schijndel-Speet,
Evenhuis, Van Wijck, Montfort, & Echteld, 2017), whereas other studies lacked significant effects (Bergström,
Hagströmer, Hagberg, & Elinder, 2013, Melville et al., 2015, Shields & Taylor, 2015). Since health needs are
different in adults with different levels of ID (Kinnear et al., 2018), lifestyle change interventions need to be
tailored to level of ID. Until now, an overview of lifestyle change interventions and their effectiveness is missing,
as well as knowledge about effective behaviour change techniques for people with mild ID.
Also, the role of professional caregivers is of great importance in changing health behaviour of adults with ID
(Alesi & Pepi, 2015; Grondhuis & Aman, 2014; Heller et al., 2011; Melville, Hamilton, Hankey, Miller & Boyle,
2007; Naaldenberg, Kuijken, van Dooren & De Valk, 2013) and might be the key to a successful behavioural
intervention (Felce, Lowe, Beecham, & Hallam, 2000). However, until now, no knowledge is available if and how
BCT’s are used by caregivers in daily support of persons with mild ID. Also, it is important to improve training for
caregivers (Ptomey et al., 2018), as they have significant training needs promoting healthy behaviour (Melville
et al., 2009). Which specific wishes and needs they have, is still unclear.
So far, training and development focussed on knowledge and competences was still ineffective (O’Connor-
Fleming, Parker, Higgins, & Gould, 2006). If professional caregivers would be able support adults with mild ID
effectively to change their lifestyle behaviour, adults with mild ID may live healthier, longer and experience a
higher quality of life. Therefore, the main aim of this thesis is to investigate the usage and effectiveness of lifestyle
change interventions by professional caregivers to support adults with ID.
6 | CONTENT OF THE THESIS
The first question of this thesis is whether there are already effective lifestyle change interventions for adults
with ID, which will be answered in Chapter 2. The International Classification of Functioning, Disability and Health
(ICF) (World Health Organisation, 2001) will be introduced to categorize the outcome measures in underlying
constructs, including “functions,” “activities,” “participation,” “personal factors” and “environmental factors”.
Afterwards, the main aim of Chapter 3 is to provide an overview of current lifestyle change interventions for
people with ID. It aims to introduce the identification of BCTs in lifestyle change interventions and determines
the quality of studies investigating lifestyle change interventions. The question whether BCTs are suitable for use
in lifestyle change in people with mild ID will be answered in Chapter 4, whereas the main aim of Chapter 5 is to
investigate the use of BCTs by professional caregivers in daily support of people with mild ID. Also, this chapter
aims to provide a comparison between the suitable BCTs and the BCTs used in daily support. The results of an
intervention to train professional caregivers in one of the most suitable BCTs, called “Action planning”, will be
138541-Willems_BNW.indd 10 31-10-19 10:07
10
effective components could be effective in interventions for people with ID as well (Van Schijndel-Speet, 2015).
In this thesis, we used the CALO-RE taxonomy to identify effective components of lifestyle change interventions
for people with ID. A short list of the BCTs is given below, see Figure 2, the entire taxonomy with definitions can
be found in the Appendix.
Figure 2: Overview of the CALO-RE taxonomy of behaviour change techniques
21) Provide instruction on how to perform the behaviour;
22) Model/Demonstrate the behaviour;
23) Teach to use prompts/cues;
24) Environmental restructuring;
25) Agree behavioural contract;
26) Prompt practice;
27) Use of follow-up prompts;
28) Facilitate social comparison;
29) Plan social support/social change;
30) Prompt identification as role model/position advocate;
31) Prompt anticipated regret;
32) Fear arousal;
33) Prompt self-talk;
34) Prompt use of imagery;
35) Relapse prevention/coping planning;
36) Stress management/emotional control training;
37) Motivational interviewing;
38) Time management;
39) General communication skills training;
40) Stimulate anticipation of future rewards
(Michie et al., 2011).
1) Provide information on consequences of behaviour in
general;
2) Provide information on consequences of behaviour to
the individual;
3) Provide information about others’ approval;
4) Provide normative information about others’
behaviour;
5) Goal setting (behaviour);
6) Goal setting (outcome);
7) Action planning;
8) Barrier identification/problem solving;
9) Set graded tasks;
10) Prompt review of behavioural goals;
11) Prompt review of outcome goals;
12) Prompt rewards contingent on effort or progress
towards behaviour;
13) Provide rewards contingent on successful behaviour;
14) Shaping;
15) Prompting generalisation of a target behaviour;
16) Prompt self-monitoring of behaviour;
17) Prompt self-monitoring of behavioural outcome;
18) Prompting focus on past success;
19) Provide feedback on performance;
20) Provide information on where and when to perform
the behaviour;
11
5 | LIFESTYLE CHANGE IN ADULTS WITH MILD INTELLECTUAL DISABILITIES
It is necessary to improve the lifestyle of adults with ID, to reduce health risks and health inequalities (Alesi &
Pepi, 2015). However, evidence for the effectiveness of lifestyle change interventions in adults with ID is limited
(Brooker et al., 2015; Scott & Havercamp, 2016; Spanos, Melville, & Hankey, 2013). Some studies found small
significant changes on health outcomes (Curtin et al., 2013, Marks, Sisirak, & Chang, 2013, Van Schijndel-Speet,
Evenhuis, Van Wijck, Montfort, & Echteld, 2017), whereas other studies lacked significant effects (Bergström,
Hagströmer, Hagberg, & Elinder, 2013, Melville et al., 2015, Shields & Taylor, 2015). Since health needs are
different in adults with different levels of ID (Kinnear et al., 2018), lifestyle change interventions need to be
tailored to level of ID. Until now, an overview of lifestyle change interventions and their effectiveness is missing,
as well as knowledge about effective behaviour change techniques for people with mild ID.
Also, the role of professional caregivers is of great importance in changing health behaviour of adults with ID
(Alesi & Pepi, 2015; Grondhuis & Aman, 2014; Heller et al., 2011; Melville, Hamilton, Hankey, Miller & Boyle,
2007; Naaldenberg, Kuijken, van Dooren & De Valk, 2013) and might be the key to a successful behavioural
intervention (Felce, Lowe, Beecham, & Hallam, 2000). However, until now, no knowledge is available if and how
BCT’s are used by caregivers in daily support of persons with mild ID. Also, it is important to improve training for
caregivers (Ptomey et al., 2018), as they have significant training needs promoting healthy behaviour (Melville
et al., 2009). Which specific wishes and needs they have, is still unclear.
So far, training and development focussed on knowledge and competences was still ineffective (O’Connor-
Fleming, Parker, Higgins, & Gould, 2006). If professional caregivers would be able support adults with mild ID
effectively to change their lifestyle behaviour, adults with mild ID may live healthier, longer and experience a
higher quality of life. Therefore, the main aim of this thesis is to investigate the usage and effectiveness of lifestyle
change interventions by professional caregivers to support adults with ID.
6 | CONTENT OF THE THESIS
The first question of this thesis is whether there are already effective lifestyle change interventions for adults
with ID, which will be answered in Chapter 2. The International Classification of Functioning, Disability and Health
(ICF) (World Health Organisation, 2001) will be introduced to categorize the outcome measures in underlying
constructs, including “functions,” “activities,” “participation,” “personal factors” and “environmental factors”.
Afterwards, the main aim of Chapter 3 is to provide an overview of current lifestyle change interventions for
people with ID. It aims to introduce the identification of BCTs in lifestyle change interventions and determines
the quality of studies investigating lifestyle change interventions. The question whether BCTs are suitable for use
in lifestyle change in people with mild ID will be answered in Chapter 4, whereas the main aim of Chapter 5 is to
investigate the use of BCTs by professional caregivers in daily support of people with mild ID. Also, this chapter
aims to provide a comparison between the suitable BCTs and the BCTs used in daily support. The results of an
intervention to train professional caregivers in one of the most suitable BCTs, called “Action planning”, will be
138541-Willems_BNW.indd 11 31-10-19 10:07

12
described in Chapter 6. The main findings of this thesis and implications for clinical practice and future research
will be discussed in Chapter 7.
13
REFERENCES
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome:
Investigating Parental Beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61-80.
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5
(5th Ed.). Washington, DC: Author.
Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention to
improve diet and physical activity among adults with intellectual disabilities in community residences:
a cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847-3857.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used to
promote walking and cycling: A systematic review. Health psychology, 32(8), 829.
Brooker, K., Van Dooren, K., McPherson, L., Lennox, N., & Ware, R. (2015). Systematic review of interventions
aiming to improve involvement in physical activity among adults with intellectual disability. Journal of
Physical Activity and Health, 12(3), 434-444.
Cooper, S. A., & Bailey, N. M. (2001). Psychiatric disorders amongst adults with learning disabilities
prevalence and relationship to ability level. Irish Journal of Psychological Medicine, 18(2), 45-53.
Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., Eliasziw, M., Maslin, M., & Fleming, R. K.
(2013). Parent support improves weight loss in adolescents and young adults with Down syndrome. The
Journal of Pediatrics, 163(5), 1402-1408.
Felce, D., Lowe, K., Beecham, J., & Hallam A. (2000). Exploring the relationships between costs and quality of
services for adults with severe intellectual disabilities and the most sever challenging behaviours in
Wales: A multivariate regression analysis. Journal of Intellectual & Developmental Disability, 25(4), 307-
26.
Gezondheidsraad (2017). Beweegrichtlijnen 2017 [physical activity guidelines 2017]. The Hague, the
Netherlands: Gezondheidsraad. Retrieved from
https://www.gezondheidsraad.nl/organisatie/leefstijl/documenten/adviezen/2017/08/22/
beweegrichtlijnen-2017
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P.
(2011). Systematic review of reviews of intervention components associated with increased
effectiveness in dietary and physical activity interventions. BMC public health, 11(1), 119.
Grondhuis, S. N., & Aman, M. G. (2014). Overweight and obesity in youth with developmental disabilities: a
call to action. Journal of Intellectual Disability Research, 58(9), 787-799.
138541-Willems_BNW.indd 12 31-10-19 10:07
12
described in Chapter 6. The main findings of this thesis and implications for clinical practice and future research
will be discussed in Chapter 7.
13
REFERENCES
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome:
Investigating Parental Beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61-80.
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5
(5th Ed.). Washington, DC: Author.
Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention to
improve diet and physical activity among adults with intellectual disabilities in community residences:
a cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847-3857.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used to
promote walking and cycling: A systematic review. Health psychology, 32(8), 829.
Brooker, K., Van Dooren, K., McPherson, L., Lennox, N., & Ware, R. (2015). Systematic review of interventions
aiming to improve involvement in physical activity among adults with intellectual disability. Journal of
Physical Activity and Health, 12(3), 434-444.
Cooper, S. A., & Bailey, N. M. (2001). Psychiatric disorders amongst adults with learning disabilities
prevalence and relationship to ability level. Irish Journal of Psychological Medicine, 18(2), 45-53.
Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., Eliasziw, M., Maslin, M., & Fleming, R. K.
(2013). Parent support improves weight loss in adolescents and young adults with Down syndrome. The
Journal of Pediatrics, 163(5), 1402-1408.
Felce, D., Lowe, K., Beecham, J., & Hallam A. (2000). Exploring the relationships between costs and quality of
services for adults with severe intellectual disabilities and the most sever challenging behaviours in
Wales: A multivariate regression analysis. Journal of Intellectual & Developmental Disability, 25(4), 307-
26.
Gezondheidsraad (2017). Beweegrichtlijnen 2017 [physical activity guidelines 2017]. The Hague, the
Netherlands: Gezondheidsraad. Retrieved from
https://www.gezondheidsraad.nl/organisatie/leefstijl/documenten/adviezen/2017/08/22/
beweegrichtlijnen-2017
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P.
(2011). Systematic review of reviews of intervention components associated with increased
effectiveness in dietary and physical activity interventions. BMC public health, 11(1), 119.
Grondhuis, S. N., & Aman, M. G. (2014). Overweight and obesity in youth with developmental disabilities: a
call to action. Journal of Intellectual Disability Research, 58(9), 787-799.
138541-Willems_BNW.indd 13 31-10-19 10:07
14
Haveman, M., Heller, T., Lee, L., Maaskant, M., Shooshtari, S., & Strydom, A. (2010). Major health risks in aging
persons with intellectual disabilities: an overview of recent studies. Journal of Policy and Practice in
Intellectual Disabilities, 7(1), 59-69.
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: what is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477-483.
Hilgenkamp, T. I., Van Wijck, R., & Evenhuis, H. M. (2011). (Instrumental) activities of daily living in older adults
with intellectual disabilities. Research in Developmental Disabilities, 32(5), 1977-1987.
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851-863.
Kinnear, D., Morrison, J., Allan, L., Henderson, A., Smiley, E., & Cooper, S. A. (2018). Prevalence of
physical conditions and multimorbidity in a cohort of adults with intellectual disabilities with and
without Down syndrome: cross-sectional study. BMJ open, 8(2), e018292.
Lennox, N. G., & Kerr, M. P. (1997). Primary health care and people with an intellectual disability: the
evidence base. Journal of Intellectual Disability Research, 41(5), 365-372.
Marks, B., Sisirak, J., & Chang, Y. C. (2013). Efficacy of the HealthMatters Program Train‐the Trainer Model.
Journal of Applied Research in Intellectual Disabilities, 26(4), 319-334.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion
programs. Health education quarterly, 15(4), 351-377.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Melville, C. A., Hamilton, S., Miller, S., Boyle, S., Robinson, N., Pert, C., & Hankey, C. R. (2009). Carer
knowledge and perceptions of healthy lifestyles for adults with intellectual disabilities. Journal of
Applied Research in Intellectual Disabilities, 22(3), 298-306.
Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., Melling, C., & Mutrie, N.
(2015). Effectiveness of a walking programme to support adults with intellectual disabilities to increase
physical activity: walk well cluster-randomised controlled trial. International Journal of Behavioral
Nutrition and Physical Activity, 12(1), 1-11.
Melville, C. A., Oppewal, A., Elinder, L. S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T. I. M., (…) & Giné-
Garriga, M. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with
intellectual disabilities—A systematic review. Preventive Medicine, 97, 62-71.
15
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: a structured review of literature. Research in
Developmental Disabilities, 34(12), 4534-4545.
O’Connor-Fleming, M. L., Parker, E., Higgins, H., & Gould, T. (2006). A framework for evaluating health
promotion programs. Health Promotion Journal of Australia: Official Journal of Australian Association of
Health Promotion Professionals, 17(1), 61–66.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity,
10(29), 1-15.
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., (…) & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
Ras, M., Verbeek-Oudijk, D., & Eggink, E. (2013). Lasten onder de loep. De kostengroei van de zorg voor
verstandelijk gehandicapten ontrafeld [Charges Unravelled: The Cost Growth of the Care for People with
an Intellectual Disability]. The Hague, The Netherlands: Sociaal en Cultureel Planbureau.
Scott, H. M., & Havercamp, S. M. (2016). Systematic Review of Health Promotion Programs Focused on Behavioral
Changes for People With Intellectual Disability. Intellectual and developmental disabilities, 54(1), 63-76.
Schalock, R., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., . . . Parmenter, T. (2002).
Conceptualization, Measurement, and Application of Quality of Life for Persons with Intellectual
Disabilities: Report of an International Panel of Experts. Mental Retardation 40(6):457-470.
Shields, N., & Taylor, N. F. (2015). The feasibility of a physical activity program for young adults with Down
syndrome: A phase II randomised controlled trial. Journal of Intellectual and Developmental Disability,
40(2), 115-125.
Snell, M. E., Luckasson, R., Borthwick-Duffy, W. S., Bradley, V., Buntinx, W. H., Coulter, D. L., (...) &
Yeager, M. H. (2009). Characteristics and needs of people with intellectual disability who have higher
IQs. Intellectual and Developmental Disabilities, 47(3), 220-233.
138541-Willems_BNW.indd 14 31-10-19 10:07
14
Haveman, M., Heller, T., Lee, L., Maaskant, M., Shooshtari, S., & Strydom, A. (2010). Major health risks in aging
persons with intellectual disabilities: an overview of recent studies. Journal of Policy and Practice in
Intellectual Disabilities, 7(1), 59-69.
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: what is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477-483.
Hilgenkamp, T. I., Van Wijck, R., & Evenhuis, H. M. (2011). (Instrumental) activities of daily living in older adults
with intellectual disabilities. Research in Developmental Disabilities, 32(5), 1977-1987.
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851-863.
Kinnear, D., Morrison, J., Allan, L., Henderson, A., Smiley, E., & Cooper, S. A. (2018). Prevalence of
physical conditions and multimorbidity in a cohort of adults with intellectual disabilities with and
without Down syndrome: cross-sectional study. BMJ open, 8(2), e018292.
Lennox, N. G., & Kerr, M. P. (1997). Primary health care and people with an intellectual disability: the
evidence base. Journal of Intellectual Disability Research, 41(5), 365-372.
Marks, B., Sisirak, J., & Chang, Y. C. (2013). Efficacy of the HealthMatters Program Train‐the Trainer Model.
Journal of Applied Research in Intellectual Disabilities, 26(4), 319-334.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion
programs. Health education quarterly, 15(4), 351-377.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Melville, C. A., Hamilton, S., Miller, S., Boyle, S., Robinson, N., Pert, C., & Hankey, C. R. (2009). Carer
knowledge and perceptions of healthy lifestyles for adults with intellectual disabilities. Journal of
Applied Research in Intellectual Disabilities, 22(3), 298-306.
Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., Melling, C., & Mutrie, N.
(2015). Effectiveness of a walking programme to support adults with intellectual disabilities to increase
physical activity: walk well cluster-randomised controlled trial. International Journal of Behavioral
Nutrition and Physical Activity, 12(1), 1-11.
Melville, C. A., Oppewal, A., Elinder, L. S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T. I. M., (…) & Giné-
Garriga, M. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with
intellectual disabilities—A systematic review. Preventive Medicine, 97, 62-71.
15
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: a structured review of literature. Research in
Developmental Disabilities, 34(12), 4534-4545.
O’Connor-Fleming, M. L., Parker, E., Higgins, H., & Gould, T. (2006). A framework for evaluating health
promotion programs. Health Promotion Journal of Australia: Official Journal of Australian Association of
Health Promotion Professionals, 17(1), 61–66.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity,
10(29), 1-15.
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., (…) & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
Ras, M., Verbeek-Oudijk, D., & Eggink, E. (2013). Lasten onder de loep. De kostengroei van de zorg voor
verstandelijk gehandicapten ontrafeld [Charges Unravelled: The Cost Growth of the Care for People with
an Intellectual Disability]. The Hague, The Netherlands: Sociaal en Cultureel Planbureau.
Scott, H. M., & Havercamp, S. M. (2016). Systematic Review of Health Promotion Programs Focused on Behavioral
Changes for People With Intellectual Disability. Intellectual and developmental disabilities, 54(1), 63-76.
Schalock, R., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., . . . Parmenter, T. (2002).
Conceptualization, Measurement, and Application of Quality of Life for Persons with Intellectual
Disabilities: Report of an International Panel of Experts. Mental Retardation 40(6):457-470.
Shields, N., & Taylor, N. F. (2015). The feasibility of a physical activity program for young adults with Down
syndrome: A phase II randomised controlled trial. Journal of Intellectual and Developmental Disability,
40(2), 115-125.
Snell, M. E., Luckasson, R., Borthwick-Duffy, W. S., Bradley, V., Buntinx, W. H., Coulter, D. L., (...) &
Yeager, M. H. (2009). Characteristics and needs of people with intellectual disability who have higher
IQs. Intellectual and Developmental Disabilities, 47(3), 220-233.
138541-Willems_BNW.indd 15 31-10-19 10:07
16
Soresi, S., Nota, L., & Wehmeyer, M. L. (2011). Community involvement in promoting inclusion, participation
and self‐determination. International Journal of Inclusive Education, 15(1), 15- 28.
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with
intellectual disabilities and obesity: a systematic review of the evidence. Nutrition Journal, 12, 1-16.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., (…) Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
United Nations (2006). Convention on the rights of persons with disabilities. Retrieved from
http://www.un.org/disabilities/documents/convention/convoptprot-e.pdf.
Van Schijndel-Speet, M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544
Van Schijndel‐Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Van Schijndel‐Speet, M., Evenhuis, H. M., van Wijck, R., van Montfort, K. C. A. G. M., & Echteld, M. A.
(2017). A structured physical activity and fitness programme for older adults with intellectual
disabilities: results of a cluster‐randomised clinical trial. Journal of Intellectual Disability
Research, 61(1), 16-29.
Van Schrojenstein Lantman-De Valk, H. M. J., & Walsh, P. N. (2008). Managing health problems in people with
intellectual disabilities. British Medical Journal: BMJ, 8(1), A2507.
Wilson, D. N., & Haire, A. (1990). Health care screening for people with mental handicap living in the
community. BMJ, 301(6765), 1379-1381.
Woittiez, I., Eggink, E., Putman, L., & Ras, M. (2018). An international comparison of care for people with
intellectual disabilities: an exploration. The Hague, the Netherlands: The Netherlands Institute for
Social Research.
Woittiez, I., Putman, L., Eggink E., & Ras, M. (2014). Zorg beter begrepen. Verklaringen voor de groeiende
vraag naar zorg voor mensen met een verstandelijke beperking. [Care Better Understood: Explanations
for the Growing Demand to Care for People with an Intellectual Disability]. The Hague, The Netherlands:
Sociaal en Cultureel Planbureau.
World Health Organization (WHO) (2001). International classification of functioning, disability and health: ICF.
Geneva, Switzerland: World Health Organisation.
17
APPENDIX | CALO-RE Taxonomy (Michie et al., 2011)
1. Provide information on consequences of behaviour in general
Information about the relationship between the behaviour and its possible or likely consequences in the general case, usually
based on epidemiological data, and not personalised for the individual (contrast with technique 2).
2. Provide information on consequences of behaviour to the individual
Information about the benefits and costs of action or inaction to the individual or tailored to a relevant group based on that
individual’s characteristics (i.e. demographics, clinical, behavioural or psychological information). This can include any
costs/benefits and not necessarily those related to health, e.g. feelings.
3. Provide information about others’ approval
Involves information about what other people think about the target person’s behaviour. It clarifies whether others will like,
approve or disapprove of what the person is doing or will do.
NB: Check that any instance does not also involve techniques 1 (Provide information on consequences of behaviour in
general) or 2 (Provide information on consequences of behaviour to the individual) or 4 (Provide normative information about
others’ behaviour).
4. Provide normative information about others’ behaviour
Involves providing information about what other people are doing i.e. indicates that a particular behaviour or sequence of
behaviours is common or uncommon amongst the population or amongst a specified group – presentation of case studies of
a few others is not normative information.
NB: this concerns other people’s actions and is distinct from the provision of information about others’ approval (technique
3 (Provide information about others’ approval)).
5. Goal setting (behaviour)
The person is encouraged to make a behavioural resolution (e.g. take more exercise next week). This is directed towards
encouraging people to decide to change or maintain change.
NB: This is distinguished from technique 6 (goal setting – outcome) and 7 (action planning) as it does not involve planning
exactly how the behaviour will be done and either when or where the behaviour or action sequence will be performed. Where
the text only states that goal setting was used without specifying the detail of action planning involved then this would be an
example of this technique (not technique 7 (action planning)). If the text states that ‘goal setting’ was used if it is not clear
from the report, if the goal setting was related to behaviour or to other outcomes, technique 6 should be coded. This includes
sub-goals or preparatory behaviours and/or specific contexts in which the behaviour will be performed. The behaviour in this
technique will be directly related to or be a necessary condition for the target behaviour (e.g. shopping for healthy eating;
buying equipment for physical activity).
NB: check if techniques applied to preparatory behaviours should also be coded as instances of technique 9 (Set graded tasks).
6. Goal setting (outcome)
The person is encouraged to set a general goal that can be achieved by behavioural means but is not defined in terms of
behaviour (e.g. to reduce blood pressure or lose/maintain weight), as opposed to a goal based on changing behaviour as
such. The goal may be an expected consequence of one or more behaviours, but is not a behaviour per se (see also techniques
5 (Goal setting – behaviour) and 7 (Action planning)). This technique may co-occur with technique 5 if goals for both behaviour
and other outcomes are set.
7. Action planning
Involves detailed planning of what the person will do including, as a minimum, when, in which situation and/or where to act.
‘When’ may describe frequency (such as how many times a day/week or duration (e.g. for how long). The exact content of
138541-Willems_BNW.indd 16 31-10-19 10:07

16
Soresi, S., Nota, L., & Wehmeyer, M. L. (2011). Community involvement in promoting inclusion, participation
and self‐determination. International Journal of Inclusive Education, 15(1), 15- 28.
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with
intellectual disabilities and obesity: a systematic review of the evidence. Nutrition Journal, 12, 1-16.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., (…) Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
United Nations (2006). Convention on the rights of persons with disabilities. Retrieved from
http://www.un.org/disabilities/documents/convention/convoptprot-e.pdf.
Van Schijndel-Speet, M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544
Van Schijndel‐Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Van Schijndel‐Speet, M., Evenhuis, H. M., van Wijck, R., van Montfort, K. C. A. G. M., & Echteld, M. A.
(2017). A structured physical activity and fitness programme for older adults with intellectual
disabilities: results of a cluster‐randomised clinical trial. Journal of Intellectual Disability
Research, 61(1), 16-29.
Van Schrojenstein Lantman-De Valk, H. M. J., & Walsh, P. N. (2008). Managing health problems in people with
intellectual disabilities. British Medical Journal: BMJ, 8(1), A2507.
Wilson, D. N., & Haire, A. (1990). Health care screening for people with mental handicap living in the
community. BMJ, 301(6765), 1379-1381.
Woittiez, I., Eggink, E., Putman, L., & Ras, M. (2018). An international comparison of care for people with
intellectual disabilities: an exploration. The Hague, the Netherlands: The Netherlands Institute for
Social Research.
Woittiez, I., Putman, L., Eggink E., & Ras, M. (2014). Zorg beter begrepen. Verklaringen voor de groeiende
vraag naar zorg voor mensen met een verstandelijke beperking. [Care Better Understood: Explanations
for the Growing Demand to Care for People with an Intellectual Disability]. The Hague, The Netherlands:
Sociaal en Cultureel Planbureau.
World Health Organization (WHO) (2001). International classification of functioning, disability and health: ICF.
Geneva, Switzerland: World Health Organisation.
17
APPENDIX | CALO-RE Taxonomy (Michie et al., 2011)
1. Provide information on consequences of behaviour in general
Information about the relationship between the behaviour and its possible or likely consequences in the general case, usually
based on epidemiological data, and not personalised for the individual (contrast with technique 2).
2. Provide information on consequences of behaviour to the individual
Information about the benefits and costs of action or inaction to the individual or tailored to a relevant group based on that
individual’s characteristics (i.e. demographics, clinical, behavioural or psychological information). This can include any
costs/benefits and not necessarily those related to health, e.g. feelings.
3. Provide information about others’ approval
Involves information about what other people think about the target person’s behaviour. It clarifies whether others will like,
approve or disapprove of what the person is doing or will do.
NB: Check that any instance does not also involve techniques 1 (Provide information on consequences of behaviour in
general) or 2 (Provide information on consequences of behaviour to the individual) or 4 (Provide normative information about
others’ behaviour).
4. Provide normative information about others’ behaviour
Involves providing information about what other people are doing i.e. indicates that a particular behaviour or sequence of
behaviours is common or uncommon amongst the population or amongst a specified group – presentation of case studies of
a few others is not normative information.
NB: this concerns other people’s actions and is distinct from the provision of information about others’ approval (technique
3 (Provide information about others’ approval)).
5. Goal setting (behaviour)
The person is encouraged to make a behavioural resolution (e.g. take more exercise next week). This is directed towards
encouraging people to decide to change or maintain change.
NB: This is distinguished from technique 6 (goal setting – outcome) and 7 (action planning) as it does not involve planning
exactly how the behaviour will be done and either when or where the behaviour or action sequence will be performed. Where
the text only states that goal setting was used without specifying the detail of action planning involved then this would be an
example of this technique (not technique 7 (action planning)). If the text states that ‘goal setting’ was used if it is not clear
from the report, if the goal setting was related to behaviour or to other outcomes, technique 6 should be coded. This includes
sub-goals or preparatory behaviours and/or specific contexts in which the behaviour will be performed. The behaviour in this
technique will be directly related to or be a necessary condition for the target behaviour (e.g. shopping for healthy eating;
buying equipment for physical activity).
NB: check if techniques applied to preparatory behaviours should also be coded as instances of technique 9 (Set graded tasks).
6. Goal setting (outcome)
The person is encouraged to set a general goal that can be achieved by behavioural means but is not defined in terms of
behaviour (e.g. to reduce blood pressure or lose/maintain weight), as opposed to a goal based on changing behaviour as
such. The goal may be an expected consequence of one or more behaviours, but is not a behaviour per se (see also techniques
5 (Goal setting – behaviour) and 7 (Action planning)). This technique may co-occur with technique 5 if goals for both behaviour
and other outcomes are set.
7. Action planning
Involves detailed planning of what the person will do including, as a minimum, when, in which situation and/or where to act.
‘When’ may describe frequency (such as how many times a day/week or duration (e.g. for how long). The exact content of
138541-Willems_BNW.indd 17 31-10-19 10:07

18
action plans may or may not be described, in this case code as this technique if it is stated that the behaviour is planned
contingent to a specific situation or set of situations even if exact details are not present.
NB: The terms ‘goal setting’ or ‘action plan’ are not enough to ensure inclusion of this technique unless it is clear that plans
involve linking behavioural responses to specific situational cues, when only described as ‘goal setting’ or ‘action plan’ without
the above detail it should be regarded as applications of techniques 5 and 6.
8. Barrier identification/problem solving
This presumes having formed an initial plan to change behaviour. The person is prompted to think about potential barriers
and identify the ways of overcoming them. Barriers may include competing goals in specified situations. This may be described
as ‘problem solving’. If it is problem solving in relation to the performance of a behaviour, then it counts as an instance of this
technique. Examples of barriers may include behavioural, cognitive, emotional, environmental, social and/or physical
barriers.
NB: Closely related to techniques 7 (action planning) and 9 (set graded task), but involves a focus on specific obstacles to
performance. It contrasts with technique 35 (relapse prevention/coping planning), which is about maintaining behaviour that
has already been changed.
9. Set graded tasks
Breaking down the target behaviour into smaller easier to achieve tasks and enabling the person to build on small successes
to achieve target behaviour. This may include increments towards target behaviour or incremental increases from baseline
behaviour.
NB: The key difference to technique 7 (Action planning) lies in planning to perform a sequence of preparatory actions (e.g.
remembering to take gym kit to work), task components or target behaviours which are in a logical sequence or increase in
difficulty over time – as opposed to planning ‘if-then’ contingencies when/where to perform behaviours. General references
to increasing physical activity as intervention goal are not instances of this technique.
10. Prompt review of behavioural goals
Involves a review or analysis of the extent to which previously set behavioural goals (e.g. take more exercise next week) were
achieved. In most cases, this will follow previous goal setting (see technique 5, ‘goal setting-behaviour’) and an attempt to
act on those goals, followed by a revision or readjustment of goals, and/or means to attain them.
NB: Check if any instance also involves techniques 6 (goal setting – behaviour), 8 (barrier identification/problem solving), 9
(set graded tasks) or 11 (prompt review of outcome goals).
11. Prompt review of outcome goals
Involves a review or analysis of the extent to which previously set outcome goals (e.g. to reduce blood pressure or
lose/maintain weight) were achieved. In most cases, this will follow previous goal setting (see technique 6, goal setting-
outcome’) and an attempt to act on those goals, followed by a revision of goals, and/or means to attain them. NB: Check that
any instance does not also involve techniques 5 (goal setting – outcome), 8 (barrier identification/problem solving), 9 (set
graded tasks) or 10 (prompt review of behavioural goals).
12. Prompt rewards contingent on effort or progress towards behaviour
Involves the person using praise or rewards for attempts at achieving a behavioural goal. This might include efforts made
towards achieving the behaviour or progress made in preparatory steps towards the behaviour, but not merely participation
in intervention. This can include self-reward.
NB: This technique is not reinforcement for performing the target behaviour itself, which is an instance of technique 13
(provide rewards contingent on successful behaviour).
13. Provide rewards contingent on successful behaviour
19
Reinforcing successful performance of the specific target behaviour. This can include praise and encouragement as well as
material rewards but the reward/incentive must be explicitly linked to the achievement of the specific target behaviour i.e.
the person receives the reward if they perform the specified behaviour but not if they do not perform the behaviour. This
can include self-reward. Provisions of rewards for completing intervention components or materials are not instances of this
technique. References to provision of incentives for being more physically active are not instances of this technique unless
information about contingency to the performance of the target behaviour is provided. NB: Check the distinction between
this and techniques 7 (action planning) and 17 (prompt self-monitoring of behavioural outcome) and 19 (provide feedback
on performance).
14. Shaping
Contingent rewards are first provided for any approximation to the target behaviour e.g. for any increase in physical activity.
Then, later, only a more demanding performance, e.g. brisk walking for 10 min on 3 days a week would be rewarded. Thus,
this is graded use of contingent rewards over time.
15. Prompting generalisation of a target behaviour
Once behaviour is performed in a particular situation, the person is encouraged or helped to try it in another situation. The
idea is to ensure that the behaviour is not tied to one situation but becomes a more integrated part of the person’s life that
can be performed at a variety of different times and in a variety of contexts.
16. Prompt self-monitoring of behaviour
The person is asked to keep a record of specified behaviour(s) as a method for changing behaviour. This should be an explicitly
stated intervention component, as opposed to occurring as part of completing measures for research purposes. This could
e.g. take the form of a diary or completing a questionnaire about their behaviour, in terms of type, frequency, duration and/or
intensity. Check the distinction between this and techniques 17 (prompt self-monitoring of behavioural outcome).
17. Prompt self-monitoring of behavioural outcome
The person is asked to keep a record of specified measures expected to be influenced by the behaviour change, e.g. blood
pressure, blood glucose, weight loss, physical fitness. NB: It must be reported as part of the intervention, rather than only as
an outcome measure. Check the distinction between this and techniques 16 (Prompt self-monitoring of behaviour).
18. Prompting focus on past success
Involves instructing the person to think about or list previous successes in performing the behaviour (or parts of it). NB: This
is not just encouragement but a clear focus on the person’s past behaviour. It is also not feedback because it refers to
behaviour preceded the intervention.
19. Provide feedback on performance
This involves providing the participant with data about their own recorded behaviour (e.g. following technique 16 (prompt
self-monitoring of behaviour)) or commenting on a person’s behavioural performance (e.g. identifying a discrepancy with
between behavioural performance and a set goal – see techniques 5 (Goal setting – behaviour) and 7 (action planning) – or a
discrepancy between one’s own performance in relation to others’ – note this could also involve technique 28 (Facilitate
social comparison).
20. Provide information on where and when to perform the behaviour
Involves telling the person about when and where they might be able to perform the behaviour this e.g. tips on places and
times participants can access local exercise classes. This can be in either verbal or written form. NB: Check whether there are
also instances of technique 21 (Provide instruction on how to perform the behaviour).
21. Provide instruction on how to perform the behaviour
Involves telling the person how to perform behaviour or preparatory behaviours, either verbally or in written form. Examples
of instructions include; how to use gym equipment (without getting on and showing the participant), instruction on suitable
138541-Willems_BNW.indd 18 31-10-19 10:07

18
action plans may or may not be described, in this case code as this technique if it is stated that the behaviour is planned
contingent to a specific situation or set of situations even if exact details are not present.
NB: The terms ‘goal setting’ or ‘action plan’ are not enough to ensure inclusion of this technique unless it is clear that plans
involve linking behavioural responses to specific situational cues, when only described as ‘goal setting’ or ‘action plan’ without
the above detail it should be regarded as applications of techniques 5 and 6.
8. Barrier identification/problem solving
This presumes having formed an initial plan to change behaviour. The person is prompted to think about potential barriers
and identify the ways of overcoming them. Barriers may include competing goals in specified situations. This may be described
as ‘problem solving’. If it is problem solving in relation to the performance of a behaviour, then it counts as an instance of this
technique. Examples of barriers may include behavioural, cognitive, emotional, environmental, social and/or physical
barriers.
NB: Closely related to techniques 7 (action planning) and 9 (set graded task), but involves a focus on specific obstacles to
performance. It contrasts with technique 35 (relapse prevention/coping planning), which is about maintaining behaviour that
has already been changed.
9. Set graded tasks
Breaking down the target behaviour into smaller easier to achieve tasks and enabling the person to build on small successes
to achieve target behaviour. This may include increments towards target behaviour or incremental increases from baseline
behaviour.
NB: The key difference to technique 7 (Action planning) lies in planning to perform a sequence of preparatory actions (e.g.
remembering to take gym kit to work), task components or target behaviours which are in a logical sequence or increase in
difficulty over time – as opposed to planning ‘if-then’ contingencies when/where to perform behaviours. General references
to increasing physical activity as intervention goal are not instances of this technique.
10. Prompt review of behavioural goals
Involves a review or analysis of the extent to which previously set behavioural goals (e.g. take more exercise next week) were
achieved. In most cases, this will follow previous goal setting (see technique 5, ‘goal setting-behaviour’) and an attempt to
act on those goals, followed by a revision or readjustment of goals, and/or means to attain them.
NB: Check if any instance also involves techniques 6 (goal setting – behaviour), 8 (barrier identification/problem solving), 9
(set graded tasks) or 11 (prompt review of outcome goals).
11. Prompt review of outcome goals
Involves a review or analysis of the extent to which previously set outcome goals (e.g. to reduce blood pressure or
lose/maintain weight) were achieved. In most cases, this will follow previous goal setting (see technique 6, goal setting-
outcome’) and an attempt to act on those goals, followed by a revision of goals, and/or means to attain them. NB: Check that
any instance does not also involve techniques 5 (goal setting – outcome), 8 (barrier identification/problem solving), 9 (set
graded tasks) or 10 (prompt review of behavioural goals).
12. Prompt rewards contingent on effort or progress towards behaviour
Involves the person using praise or rewards for attempts at achieving a behavioural goal. This might include efforts made
towards achieving the behaviour or progress made in preparatory steps towards the behaviour, but not merely participation
in intervention. This can include self-reward.
NB: This technique is not reinforcement for performing the target behaviour itself, which is an instance of technique 13
(provide rewards contingent on successful behaviour).
13. Provide rewards contingent on successful behaviour
19
Reinforcing successful performance of the specific target behaviour. This can include praise and encouragement as well as
material rewards but the reward/incentive must be explicitly linked to the achievement of the specific target behaviour i.e.
the person receives the reward if they perform the specified behaviour but not if they do not perform the behaviour. This
can include self-reward. Provisions of rewards for completing intervention components or materials are not instances of this
technique. References to provision of incentives for being more physically active are not instances of this technique unless
information about contingency to the performance of the target behaviour is provided. NB: Check the distinction between
this and techniques 7 (action planning) and 17 (prompt self-monitoring of behavioural outcome) and 19 (provide feedback
on performance).
14. Shaping
Contingent rewards are first provided for any approximation to the target behaviour e.g. for any increase in physical activity.
Then, later, only a more demanding performance, e.g. brisk walking for 10 min on 3 days a week would be rewarded. Thus,
this is graded use of contingent rewards over time.
15. Prompting generalisation of a target behaviour
Once behaviour is performed in a particular situation, the person is encouraged or helped to try it in another situation. The
idea is to ensure that the behaviour is not tied to one situation but becomes a more integrated part of the person’s life that
can be performed at a variety of different times and in a variety of contexts.
16. Prompt self-monitoring of behaviour
The person is asked to keep a record of specified behaviour(s) as a method for changing behaviour. This should be an explicitly
stated intervention component, as opposed to occurring as part of completing measures for research purposes. This could
e.g. take the form of a diary or completing a questionnaire about their behaviour, in terms of type, frequency, duration and/or
intensity. Check the distinction between this and techniques 17 (prompt self-monitoring of behavioural outcome).
17. Prompt self-monitoring of behavioural outcome
The person is asked to keep a record of specified measures expected to be influenced by the behaviour change, e.g. blood
pressure, blood glucose, weight loss, physical fitness. NB: It must be reported as part of the intervention, rather than only as
an outcome measure. Check the distinction between this and techniques 16 (Prompt self-monitoring of behaviour).
18. Prompting focus on past success
Involves instructing the person to think about or list previous successes in performing the behaviour (or parts of it). NB: This
is not just encouragement but a clear focus on the person’s past behaviour. It is also not feedback because it refers to
behaviour preceded the intervention.
19. Provide feedback on performance
This involves providing the participant with data about their own recorded behaviour (e.g. following technique 16 (prompt
self-monitoring of behaviour)) or commenting on a person’s behavioural performance (e.g. identifying a discrepancy with
between behavioural performance and a set goal – see techniques 5 (Goal setting – behaviour) and 7 (action planning) – or a
discrepancy between one’s own performance in relation to others’ – note this could also involve technique 28 (Facilitate
social comparison).
20. Provide information on where and when to perform the behaviour
Involves telling the person about when and where they might be able to perform the behaviour this e.g. tips on places and
times participants can access local exercise classes. This can be in either verbal or written form. NB: Check whether there are
also instances of technique 21 (Provide instruction on how to perform the behaviour).
21. Provide instruction on how to perform the behaviour
Involves telling the person how to perform behaviour or preparatory behaviours, either verbally or in written form. Examples
of instructions include; how to use gym equipment (without getting on and showing the participant), instruction on suitable
138541-Willems_BNW.indd 19 31-10-19 10:07
20
clothing, and tips on how to take action Showing a person how to perform a behaviour without verbal instruction would be
an instance of technique 22 only. NB: Check whether there are also instances of techniques 5, 7, 8, 9 and 22. Instructions to
follow a specific diet or programme of exercise without instructions how to perform the behaviours are not included in this
definition. Cooking and exercise classes as well as personal trainers and recipes should always be coded as this technique,
but may also be coded as 22 (model/demonstrate the behaviour).
22. Model/Demonstrate the behaviour
Involves showing the person how to perform a behaviour e.g. through physical or visual demonstrations of behavioural
performance, in person or remotely. NB: This is distinct from just providing instruction (technique 21) because in
‘demonstration’ the person is able to observe the behaviour being enacted. This technique and techniques 21 (Provide
instruction on how to perform the behaviour) and may be used separately or together. Instructing parents or peers to perform
the target behaviour is not an instance of this technique as fidelity would be uncertain.
23. Teach to use prompts/cues
The person is taught to identify environmental prompts which can be used to remind them to perform the behaviour (or to
perform an alternative, incompatible behaviour in the case of behaviours to be reduced). Cues could include times of day,
particular contexts or technologies such as mobile phone alerts which prompt them to perform the target behaviour. NB:
This technique could be used independently or in conjunction with techniques 5 (goal setting - behaviour) and 7 (action
planning; see also 24 (environmental restructuring)).
24. Environmental restructuring
The person is prompted to alter the environment in ways so that it is more supportive of the target behaviour e.g. altering
cues or reinforcers. For example, they might be asked to lock up or throw away or their high calorie snacks or take their
running shoes to work. Interventions in which the interveners directly modify environmental variables (e.g. the way food is
displayed in shops, provision of sports facilities) are not covered by this taxonomy and should be coded independently.
25. Agree behavioural contract
Must involve written agreement on the performance of an explicitly specified behaviour so that there is a written record of
the person’s resolution witnessed by another.
26. Prompt practice
Prompt the person to rehearse and repeat the behaviour or preparatory behaviours numerous times. Note this will also
include parts of the behaviour e.g. refusal skills in relation to unhealthy snacks. This could be described as ‘building habits or
routines’ but is still practice so long as the person is prompted to try the behaviour (or parts of it) during the intervention or
practice between intervention sessions, e.g. as ‘homework’.
27. Use of follow-up prompts
Intervention components are gradually reduced in intensity, duration and frequency over time, e.g. letters or telephone calls
instead of face to face and/or provided at longer time intervals.
28. Facilitate social comparison
Involves explicitly drawing attention to others’ performance to elicit comparisons. NB: The fact the intervention takes place
in a group setting, or have been placed in groups on the basis of shared characteristics, does not necessarily mean social
comparison is actually taking place. Social support may also be encouraged in such settings and this would then involve
technique 29 (plan social support/social change). Group classes may also involve instruction (technique 21 (provide
instruction on how to perform the behaviour)) demonstration (technique 22 (model/demonstrate the behaviour)) and
practice (technique 26 (prompt practice)).
29. Plan social support/social change
21
Involves prompting the person to plan how to elicit social support from other people to help him/her achieve their target
behaviour/outcome. This will include support during interventions e.g. setting up a ‘buddy’ system or other forms of support
and following the intervention including support provided by the individuals delivering the intervention, partner, friends and
family.
30. Prompt identification as role model/position advocate
Involves focusing on how the person may be an example to others and affect their behaviour, e.g. being a good example to
children. Also includes providing opportunities for participants to persuade others of the importance of adopting/changing
the behaviour, for example, giving a talk or running a peer-led session.
31. Prompt anticipated regret
Involves inducing expectations of future regret about the performance or non-performance of a behaviour. This includes
focusing on how the person will feel in the future and specifically whether they will feel regret or feel sorry that they did or
did not take a different course of action. Do not also code instances of this technique as the more generic providing
information on consequences (techniques 1 (provide information on consequences of behaviour in general and 2 (provide
information on consequences of behaviour to the individual)).
32. Fear arousal
Involves presentation of risk and/or mortality information relevant to the behaviour as emotive images designed to evoke a
fearful response (e.g. ‘smoking kills!’ or images of the grim reaper). Do not also code instances of this technique as the more
generic providing information on consequences (techniques 1 (provide information on consequences of behaviour in general)
and 2 (provide information on consequences of behaviour to the individual)).
33. Prompt self-talk
Encourage the person to use talk to themselves (aloud or silently) before and during planned behaviours to encourage,
support and maintain action.
34. Prompt use of imagery
Teach the person to imagine successfully performing the behaviour or to imagine finding it easy to perform the behaviour,
including component or easy versions of the behaviour. Distinct from recalling instances of previous success without imagery
(technique 18 (prompting focus on past success)).
35. Relapse prevention/coping planning
This relates to planning how to maintain behaviour that has been changed. The person is prompted to identify in advance
situations in which the changed behaviour may not be maintained and develop strategies to avoid or manage those situations.
Contrast with techniques 7 (action planning) and 8 (barrier identification/problem solving) which are about initiating
behaviour change.
36. Stress management/emotional control training
This is a set of specific techniques (e.g. progressive relaxation) which do not target the behaviour directly but seek to reduce
anxiety and stress to facilitate the performance of the behaviour. It might also include techniques designed to reduce negative
emotions or control mood or feelings that may interfere with performance of the behaviour, and/or to increase positive
emotions that might help with the performance of the behaviour. NB: Check whether there are any instances of technique 8
(barrier identification/ problem solving), which includes identifying emotional barriers to performance, in contrast to the
current technique, which addresses stress and emotions, whether they have been identified as barriers or not.
37. Motivational interviewing
This is a clinical method including a specific set of techniques involving prompting the person to engage in change talk in
order to minimise resistance and resolve ambivalence to change (includes motivational counselling). NB: Only rate this
138541-Willems_BNW.indd 20 31-10-19 10:07

20
clothing, and tips on how to take action Showing a person how to perform a behaviour without verbal instruction would be
an instance of technique 22 only. NB: Check whether there are also instances of techniques 5, 7, 8, 9 and 22. Instructions to
follow a specific diet or programme of exercise without instructions how to perform the behaviours are not included in this
definition. Cooking and exercise classes as well as personal trainers and recipes should always be coded as this technique,
but may also be coded as 22 (model/demonstrate the behaviour).
22. Model/Demonstrate the behaviour
Involves showing the person how to perform a behaviour e.g. through physical or visual demonstrations of behavioural
performance, in person or remotely. NB: This is distinct from just providing instruction (technique 21) because in
‘demonstration’ the person is able to observe the behaviour being enacted. This technique and techniques 21 (Provide
instruction on how to perform the behaviour) and may be used separately or together. Instructing parents or peers to perform
the target behaviour is not an instance of this technique as fidelity would be uncertain.
23. Teach to use prompts/cues
The person is taught to identify environmental prompts which can be used to remind them to perform the behaviour (or to
perform an alternative, incompatible behaviour in the case of behaviours to be reduced). Cues could include times of day,
particular contexts or technologies such as mobile phone alerts which prompt them to perform the target behaviour. NB:
This technique could be used independently or in conjunction with techniques 5 (goal setting - behaviour) and 7 (action
planning; see also 24 (environmental restructuring)).
24. Environmental restructuring
The person is prompted to alter the environment in ways so that it is more supportive of the target behaviour e.g. altering
cues or reinforcers. For example, they might be asked to lock up or throw away or their high calorie snacks or take their
running shoes to work. Interventions in which the interveners directly modify environmental variables (e.g. the way food is
displayed in shops, provision of sports facilities) are not covered by this taxonomy and should be coded independently.
25. Agree behavioural contract
Must involve written agreement on the performance of an explicitly specified behaviour so that there is a written record of
the person’s resolution witnessed by another.
26. Prompt practice
Prompt the person to rehearse and repeat the behaviour or preparatory behaviours numerous times. Note this will also
include parts of the behaviour e.g. refusal skills in relation to unhealthy snacks. This could be described as ‘building habits or
routines’ but is still practice so long as the person is prompted to try the behaviour (or parts of it) during the intervention or
practice between intervention sessions, e.g. as ‘homework’.
27. Use of follow-up prompts
Intervention components are gradually reduced in intensity, duration and frequency over time, e.g. letters or telephone calls
instead of face to face and/or provided at longer time intervals.
28. Facilitate social comparison
Involves explicitly drawing attention to others’ performance to elicit comparisons. NB: The fact the intervention takes place
in a group setting, or have been placed in groups on the basis of shared characteristics, does not necessarily mean social
comparison is actually taking place. Social support may also be encouraged in such settings and this would then involve
technique 29 (plan social support/social change). Group classes may also involve instruction (technique 21 (provide
instruction on how to perform the behaviour)) demonstration (technique 22 (model/demonstrate the behaviour)) and
practice (technique 26 (prompt practice)).
29. Plan social support/social change
21
Involves prompting the person to plan how to elicit social support from other people to help him/her achieve their target
behaviour/outcome. This will include support during interventions e.g. setting up a ‘buddy’ system or other forms of support
and following the intervention including support provided by the individuals delivering the intervention, partner, friends and
family.
30. Prompt identification as role model/position advocate
Involves focusing on how the person may be an example to others and affect their behaviour, e.g. being a good example to
children. Also includes providing opportunities for participants to persuade others of the importance of adopting/changing
the behaviour, for example, giving a talk or running a peer-led session.
31. Prompt anticipated regret
Involves inducing expectations of future regret about the performance or non-performance of a behaviour. This includes
focusing on how the person will feel in the future and specifically whether they will feel regret or feel sorry that they did or
did not take a different course of action. Do not also code instances of this technique as the more generic providing
information on consequences (techniques 1 (provide information on consequences of behaviour in general and 2 (provide
information on consequences of behaviour to the individual)).
32. Fear arousal
Involves presentation of risk and/or mortality information relevant to the behaviour as emotive images designed to evoke a
fearful response (e.g. ‘smoking kills!’ or images of the grim reaper). Do not also code instances of this technique as the more
generic providing information on consequences (techniques 1 (provide information on consequences of behaviour in general)
and 2 (provide information on consequences of behaviour to the individual)).
33. Prompt self-talk
Encourage the person to use talk to themselves (aloud or silently) before and during planned behaviours to encourage,
support and maintain action.
34. Prompt use of imagery
Teach the person to imagine successfully performing the behaviour or to imagine finding it easy to perform the behaviour,
including component or easy versions of the behaviour. Distinct from recalling instances of previous success without imagery
(technique 18 (prompting focus on past success)).
35. Relapse prevention/coping planning
This relates to planning how to maintain behaviour that has been changed. The person is prompted to identify in advance
situations in which the changed behaviour may not be maintained and develop strategies to avoid or manage those situations.
Contrast with techniques 7 (action planning) and 8 (barrier identification/problem solving) which are about initiating
behaviour change.
36. Stress management/emotional control training
This is a set of specific techniques (e.g. progressive relaxation) which do not target the behaviour directly but seek to reduce
anxiety and stress to facilitate the performance of the behaviour. It might also include techniques designed to reduce negative
emotions or control mood or feelings that may interfere with performance of the behaviour, and/or to increase positive
emotions that might help with the performance of the behaviour. NB: Check whether there are any instances of technique 8
(barrier identification/ problem solving), which includes identifying emotional barriers to performance, in contrast to the
current technique, which addresses stress and emotions, whether they have been identified as barriers or not.
37. Motivational interviewing
This is a clinical method including a specific set of techniques involving prompting the person to engage in change talk in
order to minimise resistance and resolve ambivalence to change (includes motivational counselling). NB: Only rate this
138541-Willems_BNW.indd 21 31-10-19 10:07

22
technique if explicitly referred to by name, not if one identifies specific elements of it, this may happen if you have prior
experience with this technique.
38. Time management
This includes any technique designed to teach a person how to manage their time in order to make time for the behaviour.
These techniques are not directed towards performance of target behaviour but rather seek to facilitate it by freeing up times
when it could be performed. NB: Only rate this technique if explicitly referred to by name, not if one identifies specific
elements of it, this may happen if you have prior experience with this technique.
39. General communication skills training
This includes any technique directed at general communication skills but not directed towards a particular behaviour change.
Often this may include role play and group work focusing on listening skills or assertive skills. NB: Practicing a particular
behaviour-specific interpersonal negotiation e.g. refusal skills in relation to cigarettes or alcohol would not be an instance of
this technique.
40. Stimulate anticipation of future rewards
Create anticipation of future rewards without necessarily reinforcing behaviour throughout the active period of the
intervention. Code this technique when participants are told at the onset that they will be rewarded based on behavioural
achievement.
138541-Willems_BNW.indd 22 31-10-19 10:07
22
technique if explicitly referred to by name, not if one identifies specific elements of it, this may happen if you have prior
experience with this technique.
38. Time management
This includes any technique designed to teach a person how to manage their time in order to make time for the behaviour.
These techniques are not directed towards performance of target behaviour but rather seek to facilitate it by freeing up times
when it could be performed. NB: Only rate this technique if explicitly referred to by name, not if one identifies specific
elements of it, this may happen if you have prior experience with this technique.
39. General communication skills training
This includes any technique directed at general communication skills but not directed towards a particular behaviour change.
Often this may include role play and group work focusing on listening skills or assertive skills. NB: Practicing a particular
behaviour-specific interpersonal negotiation e.g. refusal skills in relation to cigarettes or alcohol would not be an instance of
this technique.
40. Stimulate anticipation of future rewards
Create anticipation of future rewards without necessarily reinforcing behaviour throughout the active period of the
intervention. Code this technique when participants are told at the onset that they will be rewarded based on behavioural
achievement.
138541-Willems_BNW.indd 23 31-10-19 10:07

Chapter 2
Effects of lifestyle change interventions for people with intellectual
disabilities: Systematic review and meta-analysis of randomized controlled
trials
Mariël Willems
Aly Waninge
Thessa I.M. Hilgenkamp
Pepijn van Empelen
Wim P. Krijnen
Cees P. Van der Schans
Craig A. Melville
Journal of Applied Research in Intellectual Disabilities, 2018, 31(6), 949-961
138541-Willems_BNW.indd 24 31-10-19 10:07
Chapter 2
Effects of lifestyle change interventions for people with intellectual
disabilities: Systematic review and meta-analysis of randomized controlled
trials
Mariël Willems
Aly Waninge
Thessa I.M. Hilgenkamp
Pepijn van Empelen
Wim P. Krijnen
Cees P. Van der Schans
Craig A. Melville
Journal of Applied Research in Intellectual Disabilities, 2018, 31(6), 949-961
138541-Willems_BNW.indd 25 31-10-19 10:07

26
ABSTRACT
Background: Promotion of a healthy lifestyle for people with intellectual disabilities is important; however, the
effectiveness of lifestyle change interventions is unclear. Aims: This research will examine the effectiveness of
lifestyle change interventions for people with intellectual disabilities.
Methods and Procedures: Randomized controlled trials (RCTs) of lifestyle change interventions for people with
intellectual disabilities were included in a systematic review and meta- analysis. Data on study and intervention
characteristics were extracted, as well as data on outcome measures and results. Internal validity of the selected
papers was assessed using the Cochrane Collaboration’s risk bias tool.
Outcomes and Results: Eight RCTs were included. Multiple outcome measures were used, whereby outcome
measures targeting environmental factors and participation were lacking and personal outcome measures were
mostly used by a single study. Risks of bias were found for all studies. Meta- analysis showed some effectiveness
for lifestyle change interventions, and a statistically significant decrease was found for waist circumference.
Conclusion and Implications: Some effectiveness was found for lifestyle change interventions for people with
intellectual disabilities. However, the effects were only statistically significant for waist circumference, so current
lifestyle change interventions may not be optimally tailored to meet the needs of people with intellectual
disabilities.
27
1 | INTRODUCTION
Adults with intellectual disabilities experience greater health risks compared to the general population, including
overweight and obesity (Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Waninge et al., 2013; Yamaki, 2005),
physical inactivity (Hilgenkamp, Reis, van Wijck, & Evenhuis, 2012; Peterson, Janz, & Lowe, 2008) and high levels
of sedentary behaviour (Melville et al., 2017). An unhealthy lifestyle is a risk factor for a shorter life expectancy
(Bittles et al., 2002; Melville et al., 2007; Patja, Iivanainen, Vesala, Oksanen, & Ruoppila, 2000), diminished quality
of life (Pett et al., 2013) and higher dependence in performing activities in daily living (Hilgenkamp, Van Wijck, &
Evenhuis, 2011; Van Schijndel-Speet, Evenhuis, Van Wijck, & Echteld, 2014; Van Schijndel-Speet, Evenhuis, Van
Wijck, Van Empelen, & Echteld, 2014). To reduce health inequalities and improve the health of people with
intellectual disabilities, promotion of healthier lifestyles is important (Alesi & Pepi, 2015).
In the general population, lifestyle change interventions are effective in improving health outcomes (Avery et al.,
2015; Dusseldorp, Van Genugten, Van Buuren, Verheijden, & Van Empelen, 2014; Fjeldsjoe, Nuehaus, Winkler,
& Eakin, 2011). For people with intellectual disabilities, there have been many studies of interventions that aim
to improve health by targeting nutrition, physical activity or both (Willems, Hilgenkamp, Havik, Waninge, &
Melville, 2017). However, a number of methodological issues complicate general conclusions about the
effectiveness on lifestyle change, like the inappropriate definition of important concepts, for example “follow-
up,” level of intellectual disability and use of outcome measures (Willems et al., 2017). Other methodological
issues reported previously include inadequate reporting of intervention content, small sample sizes and
unsustainable implementation (Bartlo & Klein, 2011; Heller, McCubbin, Drum, & Peterson, 2011; Hithersay,
Strydom, Moulster, & Buszewicz, 2014; Maïano, Normand, Aimé, & Bégarie, 2014; Ogg-Groenendaal, Hermans,
& Claessens, 2014; Öhman, Savikko, Strandberg, & Pitkälä, 2014; Willems et al., 2017). In addition, a previous
review found that only a limited number of effect studies described the use of an underlying theory to design
the intervention (Willems et al., 2017), which is necessary to understand why effects take place or not. Missing
information about demographics, outcome measures, dropout rates and follow-up measurements further limits
interpretation of the results (Willems et al., 2017). Due to these limitations, robust evidence on the influence
and effectiveness of lifestyle change interventions for people with intellectual disabilities is scarce (Casey &
Rasmussen, 2013; Hithersay et al., 2014; Jinks, Cotton, & Rylance, 2011; Maïano et al., 2014; Spanos, Melville, &
Hankey, 2013).
Reviews for the general population found heterogeneous evidence for the effectiveness of lifestyle change
interventions in changing health outcomes (Dombrowski et al., 2012; Foster, Hillsdon, Thorogood, Kaur, &
Wedatilake, 2005; Greaves et al., 2011; Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Ogilvie et al.,
2007) as some interventions were very effective in changing health behaviour whereas other interventions lack
effectiveness. Despite these differences, based on outcomes of various meta-analyses on behavioural change
interventions targeting physical activity and dietary intake of the general population, an average effect size (g)
of 0.31 is achieved on physical activity and behaviour, as well as weight loss (Dombrowski et al., 2012; Michie et
al., 2009). Some studies of lifestyle change interventions for people with intellectual disabilities have reported
small significant effects on health outcomes (Curtin et al., 2013; Marks, Sisirak, & Chang, 2013; Van Schijndel-
138541-Willems_BNW.indd 26 31-10-19 10:07

26
ABSTRACT
Background: Promotion of a healthy lifestyle for people with intellectual disabilities is important; however, the
effectiveness of lifestyle change interventions is unclear. Aims: This research will examine the effectiveness of
lifestyle change interventions for people with intellectual disabilities.
Methods and Procedures: Randomized controlled trials (RCTs) of lifestyle change interventions for people with
intellectual disabilities were included in a systematic review and meta- analysis. Data on study and intervention
characteristics were extracted, as well as data on outcome measures and results. Internal validity of the selected
papers was assessed using the Cochrane Collaboration’s risk bias tool.
Outcomes and Results: Eight RCTs were included. Multiple outcome measures were used, whereby outcome
measures targeting environmental factors and participation were lacking and personal outcome measures were
mostly used by a single study. Risks of bias were found for all studies. Meta- analysis showed some effectiveness
for lifestyle change interventions, and a statistically significant decrease was found for waist circumference.
Conclusion and Implications: Some effectiveness was found for lifestyle change interventions for people with
intellectual disabilities. However, the effects were only statistically significant for waist circumference, so current
lifestyle change interventions may not be optimally tailored to meet the needs of people with intellectual
disabilities.
27
1 | INTRODUCTION
Adults with intellectual disabilities experience greater health risks compared to the general population, including
overweight and obesity (Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Waninge et al., 2013; Yamaki, 2005),
physical inactivity (Hilgenkamp, Reis, van Wijck, & Evenhuis, 2012; Peterson, Janz, & Lowe, 2008) and high levels
of sedentary behaviour (Melville et al., 2017). An unhealthy lifestyle is a risk factor for a shorter life expectancy
(Bittles et al., 2002; Melville et al., 2007; Patja, Iivanainen, Vesala, Oksanen, & Ruoppila, 2000), diminished quality
of life (Pett et al., 2013) and higher dependence in performing activities in daily living (Hilgenkamp, Van Wijck, &
Evenhuis, 2011; Van Schijndel-Speet, Evenhuis, Van Wijck, & Echteld, 2014; Van Schijndel-Speet, Evenhuis, Van
Wijck, Van Empelen, & Echteld, 2014). To reduce health inequalities and improve the health of people with
intellectual disabilities, promotion of healthier lifestyles is important (Alesi & Pepi, 2015).
In the general population, lifestyle change interventions are effective in improving health outcomes (Avery et al.,
2015; Dusseldorp, Van Genugten, Van Buuren, Verheijden, & Van Empelen, 2014; Fjeldsjoe, Nuehaus, Winkler,
& Eakin, 2011). For people with intellectual disabilities, there have been many studies of interventions that aim
to improve health by targeting nutrition, physical activity or both (Willems, Hilgenkamp, Havik, Waninge, &
Melville, 2017). However, a number of methodological issues complicate general conclusions about the
effectiveness on lifestyle change, like the inappropriate definition of important concepts, for example “follow-
up,” level of intellectual disability and use of outcome measures (Willems et al., 2017). Other methodological
issues reported previously include inadequate reporting of intervention content, small sample sizes and
unsustainable implementation (Bartlo & Klein, 2011; Heller, McCubbin, Drum, & Peterson, 2011; Hithersay,
Strydom, Moulster, & Buszewicz, 2014; Maïano, Normand, Aimé, & Bégarie, 2014; Ogg-Groenendaal, Hermans,
& Claessens, 2014; Öhman, Savikko, Strandberg, & Pitkälä, 2014; Willems et al., 2017). In addition, a previous
review found that only a limited number of effect studies described the use of an underlying theory to design
the intervention (Willems et al., 2017), which is necessary to understand why effects take place or not. Missing
information about demographics, outcome measures, dropout rates and follow-up measurements further limits
interpretation of the results (Willems et al., 2017). Due to these limitations, robust evidence on the influence
and effectiveness of lifestyle change interventions for people with intellectual disabilities is scarce (Casey &
Rasmussen, 2013; Hithersay et al., 2014; Jinks, Cotton, & Rylance, 2011; Maïano et al., 2014; Spanos, Melville, &
Hankey, 2013).
Reviews for the general population found heterogeneous evidence for the effectiveness of lifestyle change
interventions in changing health outcomes (Dombrowski et al., 2012; Foster, Hillsdon, Thorogood, Kaur, &
Wedatilake, 2005; Greaves et al., 2011; Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Ogilvie et al.,
2007) as some interventions were very effective in changing health behaviour whereas other interventions lack
effectiveness. Despite these differences, based on outcomes of various meta-analyses on behavioural change
interventions targeting physical activity and dietary intake of the general population, an average effect size (g)
of 0.31 is achieved on physical activity and behaviour, as well as weight loss (Dombrowski et al., 2012; Michie et
al., 2009). Some studies of lifestyle change interventions for people with intellectual disabilities have reported
small significant effects on health outcomes (Curtin et al., 2013; Marks, Sisirak, & Chang, 2013; Van Schijndel-
138541-Willems_BNW.indd 27 31-10-19 10:07
28
Speet, Evenhuis, Van Wijck, Montfort, & Echteld, 2016), other studies did not find significant effects (Bergström,
Hagströmer, Hagberg, & Elinder, 2013; Melville et al., 2015; Shields & Taylor, 2015). Previous systematic reviews
of lifestyle change interventions for adults with intellectual disabilities have described and compared the content
of published lifestyle interventions or health promotion programmes. However, to date, the effectiveness of
these interventions and programmes has not been systematically analysed. Meta-analyses of the effects of
lifestyle change interventions could reveal topics for future research and could give more insight if the current
lifestyle change interventions really change the lifestyle of people with intellectual disabilities. Therefore, the
current systematic review and meta-analysis aim to determine the effects of lifestyle change interventions,
aimed at physical activity, nutrition or both physical activity and nutrition for people with intellectual disabilities.
2 | METHODS
The Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) (Moher, Liberati, Tetzlaff,
& Altman, 2009) and the Cochrane Handbook for systematic review of interventions (Higgins et al., 2011) were
used to guide this systematic review and meta- analysis.
2.1 | Search strategy
A search strategy (see Appendix 1) was developed with a research librarian and used to retrieve papers from
seven electronic databases: Embase.com, Medline (OvidSP), Web of Science, PsycINFO (OvidSP) Cochrane,
PubMed publisher and Google Scholar. This search was conducted in April 2016. Only peer- reviewed journal
papers, published between 2000 and 2016 and written in English, were eligible for inclusion. The full search
strategy is available from the corresponding author.
2.2 | Selection criteria for studies
2.2.1 | Inclusion criteria
Papers were eligible if they reported outcomes for lifestyle change interventions for adults with intellectual
disabilities, aged over 18 years, with all levels of intellectual disabilities. Only studies using a randomized
controlled trial (RCT) design and explicitly aimed at supporting change in dietary and/or physical activity
behaviour were included. The intervention had to target changes in physical activity (PA) or nutrition (e.g.,
improving nutrition habits, increasing level of physical activity or fitness or reducing weight). Study outcomes
had to include at least one aspect of participants’ PA levels, cardiorespiratory fitness, body composition (e.g.,
weight, body mass index, waist circumference), dietary intake or adherence to PA programmes.
2.2.2 | Exclusion criteria
The present authors excluded studies using interventions focusing only on staff or caregivers of people with
intellectual disabilities and studies discussing interventions for people with autism, schizophrenia or other
psychiatric disorders without explicitly mentioning intellectual disabilities. Studies with study outcomes solely on
improving motor performance or skills, inflammation, oxidative stress, blood composition, muscle mass, solely
improving fitness components other than cardiorespiratory fitness (such as strength, balance, flexibility, reaction
29
time, speed, agility) or on cognitive outcomes, were excluded. Furthermore, interventions using laboratory-
based, as opposed to community- based, training or exercise programmes and interventions with hormone
therapy or other medical treatment for weight control, or interventions focusing on smoking cessation, alcohol
or drug use, were excluded. Studies with less than six participants, review papers, conference abstracts and
editorials were also excluded.
2.2.3 | Screening and selection process
The selection process was conducted independently by two investigators (MW and AW), including title screening,
abstract screening and reading full- text papers to identify studies that met the inclusion criteria. Disagreements
were resolved by consensus discussion. During full- text screening, all full- text papers were available. When
relevant outcome data were missing, the present authors emailed the corresponding author.
2.3 | Data extraction
A data extraction form was developed and tested by two authors (MW and CM). Two reviewers (MW and CM)
independently performed both data extraction. Results were compared, and disagreements were resolved by
consensus discussion. In the case of any remaining uncertainty, a third author (TH) was consulted. Published
protocol papers about the included interventions were also used for data extraction on study design,
intervention characteristics and outcome measures (Bergström et al., 2013; Melville et al., 2015; Van Schijndel-
Speet et al., 2016).
Data extracted from the studies were as follows:
1) General study characteristics (aim of intervention, study design, sample characteristics);
2) Intervention characteristics (short description, theoretical framework, setting, duration, frequency,
intensity, deliverer and mode of delivery of intervention);
3) Outcome measures and results for the outcome measures (mean and standard deviation). The outcome
measures and results are categorized in “functions,” “activities,” “participation,” “personal factors” and
“environmental factors” using the International Classification of Functioning, Disability and Health (ICF)
(World Health Organisation, 2001), with the following underlying constructs:
- Activity: daily physical activity and food intake/nutrition
- Participation: activities of daily living (ADL)
- Functions: body composition, cardiovascular risk factors, physical capacity, flexibility
- Personal factors: quality of life, psychological functioning, perceived health, health literacy
- Environmental factors: social/environmental supports (SESE), work routine.
2.4 | Risk of bias assessment
The internal validity of the selected papers was assessed by two authors (MW & CM), using the Cochrane
Collaboration’s tool for assessing risk of bias (Higgins et al., 2011). This risk of bias tool includes six domains of
bias, namely selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias (Higgins
138541-Willems_BNW.indd 28 31-10-19 10:07
28
Speet, Evenhuis, Van Wijck, Montfort, & Echteld, 2016), other studies did not find significant effects (Bergström,
Hagströmer, Hagberg, & Elinder, 2013; Melville et al., 2015; Shields & Taylor, 2015). Previous systematic reviews
of lifestyle change interventions for adults with intellectual disabilities have described and compared the content
of published lifestyle interventions or health promotion programmes. However, to date, the effectiveness of
these interventions and programmes has not been systematically analysed. Meta-analyses of the effects of
lifestyle change interventions could reveal topics for future research and could give more insight if the current
lifestyle change interventions really change the lifestyle of people with intellectual disabilities. Therefore, the
current systematic review and meta-analysis aim to determine the effects of lifestyle change interventions,
aimed at physical activity, nutrition or both physical activity and nutrition for people with intellectual disabilities.
2 | METHODS
The Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) (Moher, Liberati, Tetzlaff,
& Altman, 2009) and the Cochrane Handbook for systematic review of interventions (Higgins et al., 2011) were
used to guide this systematic review and meta- analysis.
2.1 | Search strategy
A search strategy (see Appendix 1) was developed with a research librarian and used to retrieve papers from
seven electronic databases: Embase.com, Medline (OvidSP), Web of Science, PsycINFO (OvidSP) Cochrane,
PubMed publisher and Google Scholar. This search was conducted in April 2016. Only peer- reviewed journal
papers, published between 2000 and 2016 and written in English, were eligible for inclusion. The full search
strategy is available from the corresponding author.
2.2 | Selection criteria for studies
2.2.1 | Inclusion criteria
Papers were eligible if they reported outcomes for lifestyle change interventions for adults with intellectual
disabilities, aged over 18 years, with all levels of intellectual disabilities. Only studies using a randomized
controlled trial (RCT) design and explicitly aimed at supporting change in dietary and/or physical activity
behaviour were included. The intervention had to target changes in physical activity (PA) or nutrition (e.g.,
improving nutrition habits, increasing level of physical activity or fitness or reducing weight). Study outcomes
had to include at least one aspect of participants’ PA levels, cardiorespiratory fitness, body composition (e.g.,
weight, body mass index, waist circumference), dietary intake or adherence to PA programmes.
2.2.2 | Exclusion criteria
The present authors excluded studies using interventions focusing only on staff or caregivers of people with
intellectual disabilities and studies discussing interventions for people with autism, schizophrenia or other
psychiatric disorders without explicitly mentioning intellectual disabilities. Studies with study outcomes solely on
improving motor performance or skills, inflammation, oxidative stress, blood composition, muscle mass, solely
improving fitness components other than cardiorespiratory fitness (such as strength, balance, flexibility, reaction
29
time, speed, agility) or on cognitive outcomes, were excluded. Furthermore, interventions using laboratory-
based, as opposed to community- based, training or exercise programmes and interventions with hormone
therapy or other medical treatment for weight control, or interventions focusing on smoking cessation, alcohol
or drug use, were excluded. Studies with less than six participants, review papers, conference abstracts and
editorials were also excluded.
2.2.3 | Screening and selection process
The selection process was conducted independently by two investigators (MW and AW), including title screening,
abstract screening and reading full- text papers to identify studies that met the inclusion criteria. Disagreements
were resolved by consensus discussion. During full- text screening, all full- text papers were available. When
relevant outcome data were missing, the present authors emailed the corresponding author.
2.3 | Data extraction
A data extraction form was developed and tested by two authors (MW and CM). Two reviewers (MW and CM)
independently performed both data extraction. Results were compared, and disagreements were resolved by
consensus discussion. In the case of any remaining uncertainty, a third author (TH) was consulted. Published
protocol papers about the included interventions were also used for data extraction on study design,
intervention characteristics and outcome measures (Bergström et al., 2013; Melville et al., 2015; Van Schijndel-
Speet et al., 2016).
Data extracted from the studies were as follows:
1) General study characteristics (aim of intervention, study design, sample characteristics);
2) Intervention characteristics (short description, theoretical framework, setting, duration, frequency,
intensity, deliverer and mode of delivery of intervention);
3) Outcome measures and results for the outcome measures (mean and standard deviation). The outcome
measures and results are categorized in “functions,” “activities,” “participation,” “personal factors” and
“environmental factors” using the International Classification of Functioning, Disability and Health (ICF)
(World Health Organisation, 2001), with the following underlying constructs:
- Activity: daily physical activity and food intake/nutrition
- Participation: activities of daily living (ADL)
- Functions: body composition, cardiovascular risk factors, physical capacity, flexibility
- Personal factors: quality of life, psychological functioning, perceived health, health literacy
- Environmental factors: social/environmental supports (SESE), work routine.
2.4 | Risk of bias assessment
The internal validity of the selected papers was assessed by two authors (MW & CM), using the Cochrane
Collaboration’s tool for assessing risk of bias (Higgins et al., 2011). This risk of bias tool includes six domains of
bias, namely selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias (Higgins
138541-Willems_BNW.indd 29 31-10-19 10:07

30
et al., 2011). Risk of bias assessment involves assigning a judgement to risk of material bias, concerning high, low
or unclear risk. Material bias means “bias of sufficient magnitude to have a notable effect on the results or
conclusions of the trial, recognising the subjectivity of any such judgment” (Higgins et al., 2011). Unclear risk was
scored when information was missing or unclear, or if there was uncertainty. Risk of bias was assessed at study
level. Papers were not rejected based on the internal validity assessment; this assessment gave an overview of
the internal validity of RCT studies in the field of lifestyle interventions in people with intellectual disabilities.
2.5 | Data analyses
Included papers were categorized in the result tables by the aim of the intervention change in physical activity
or physical activity and nutrition. The extracted data were organized by general study and intervention
characteristics, risk of bias, outcome measures and analyses of the effects of the intervention.
Outcome measures were categorized by their aim and underlying construct, and transformed into uniform units
of measurement, for example transforming measurements in pounds (lbs) into kilograms (kg). When studies
reported measurements from different time points, the present authors extracted data from the first time point
following the post- intervention assessment of the outcome measure. The present authors tested heterogeneity
across studies quantitatively using I2 statistic (values of 25%, 50% and 75% respectively, indicate low, moderate
and high heterogeneity). Publication bias was assessed by examining funnel plots for asymmetry.
To determine the effects of lifestyle change interventions, outcomes were analysed on two levels using R v3.3.0
(R Core Team, 2017):
1. Inverse variance weighted random-effects meta-analyses (Borenstein, Hedges, Higgins, & Rothstein,
2009) on standardized change in outcomes measures were performed, only if an outcome measure was used in
three or more studies;
2. The present authors also conducted meta-analyses on underlying constructs of outcome measures using
standardized mean change within groups.
For analysis of change in outcome measures, as well as for analysis on underlying constructs of outcome
measures, only studies using an intervention group and a control group were included to enable comparison on
effectiveness. When a study had more than one relevant intervention group, each group was separately included
in the analysis, according to the guidelines from the Cochrane Handbook for Systematic Reviews of Interventions
(Higgins et al., 2011). In those cases, the control group was split into two groups with equal sample sizes, retaining
mean and standard deviations.
When the mean change or within- group standard deviation was missing for an outcome measure, meta- analysis
was performed with a relatively large within- group correlation of r = .8 between pre- and post- measurement of
the outcome to determine whether there was any effect. When within- group correlation between pre- and post-
measurement of the outcome from other included studies could be calculated for that outcome measure, the
31
present authors compared the used correlation coefficient (r = .8) with the calculated correlation coefficient from
included studies.
For meta- analysis at the construct level, standardized results on multiple outcome measures were included.
When a study used more than one outcome measure related to a construct, the most frequently used outcome
measure was included in the construct meta- analysis. For all meta- analysed outcome measures, leave- one- out
sensitivity analyses were conducted to sustain the validity of the conclusions. Only results of the sensitivity
analyses leading to different conclusions were reported.
3 | RESULTS
3.1 | Literature search
The systematic literature search firstly identified 3,352 papers, resulting in 2,370 papers after removing
duplicates. After the screening and selection process, eight articles passed the inclusion criteria and entered the
systematic review and meta- analysis. One study (Boer & Moss, 2016), described two interventions, which were
used separately in the meta- analysis. Detailed information of the selection process is provided by the flow
diagram in Figure 1.
3.2 | General and intervention characteristics of the studies included
The majority of studies (Table 1) included adults with mild to moderate level of intellectual disabilities as
participants (6/8). There was considerable variation in the number of participants per study, ranging from 16 to
443 participants (Mean 121.5) (Table 1). The setting of the interventions varied between the studies. All the
included studies were recently completed, published between 2012 and 2016 (Table 1).
No interventions focussed on change in nutrition only. Five of eight studies used some theoretical framework
(Table 1), which was social cognitive theory in all five studies. Studies within both study categories (aiming
physical activity or physical activity and nutrition) delivered the intervention face- to- face (8/8), most of them
within a group- wise manner (5/8). Intervention duration ranged from eight weeks to 16 months. Intervention
frequency varied between all studies, ranging from three times in 12 weeks to five times per week. Follow- up
period was used in two studies aiming to improve physical activity (Melville et al., 2015; Van Schijndel- Speet et
al., 2016) and two studies aiming to improve physical activity and nutrition (Curtin et al., 2013; McDermott et al.,
2012). Further intervention characteristics are shown in Table 2.
138541-Willems_BNW.indd 30 31-10-19 10:07
30
et al., 2011). Risk of bias assessment involves assigning a judgement to risk of material bias, concerning high, low
or unclear risk. Material bias means “bias of sufficient magnitude to have a notable effect on the results or
conclusions of the trial, recognising the subjectivity of any such judgment” (Higgins et al., 2011). Unclear risk was
scored when information was missing or unclear, or if there was uncertainty. Risk of bias was assessed at study
level. Papers were not rejected based on the internal validity assessment; this assessment gave an overview of
the internal validity of RCT studies in the field of lifestyle interventions in people with intellectual disabilities.
2.5 | Data analyses
Included papers were categorized in the result tables by the aim of the intervention change in physical activity
or physical activity and nutrition. The extracted data were organized by general study and intervention
characteristics, risk of bias, outcome measures and analyses of the effects of the intervention.
Outcome measures were categorized by their aim and underlying construct, and transformed into uniform units
of measurement, for example transforming measurements in pounds (lbs) into kilograms (kg). When studies
reported measurements from different time points, the present authors extracted data from the first time point
following the post- intervention assessment of the outcome measure. The present authors tested heterogeneity
across studies quantitatively using I2 statistic (values of 25%, 50% and 75% respectively, indicate low, moderate
and high heterogeneity). Publication bias was assessed by examining funnel plots for asymmetry.
To determine the effects of lifestyle change interventions, outcomes were analysed on two levels using R v3.3.0
(R Core Team, 2017):
1. Inverse variance weighted random-effects meta-analyses (Borenstein, Hedges, Higgins, & Rothstein,
2009) on standardized change in outcomes measures were performed, only if an outcome measure was used in
three or more studies;
2. The present authors also conducted meta-analyses on underlying constructs of outcome measures using
standardized mean change within groups.
For analysis of change in outcome measures, as well as for analysis on underlying constructs of outcome
measures, only studies using an intervention group and a control group were included to enable comparison on
effectiveness. When a study had more than one relevant intervention group, each group was separately included
in the analysis, according to the guidelines from the Cochrane Handbook for Systematic Reviews of Interventions
(Higgins et al., 2011). In those cases, the control group was split into two groups with equal sample sizes, retaining
mean and standard deviations.
When the mean change or within- group standard deviation was missing for an outcome measure, meta- analysis
was performed with a relatively large within- group correlation of r = .8 between pre- and post- measurement of
the outcome to determine whether there was any effect. When within- group correlation between pre- and post-
measurement of the outcome from other included studies could be calculated for that outcome measure, the
31
present authors compared the used correlation coefficient (r = .8) with the calculated correlation coefficient from
included studies.
For meta- analysis at the construct level, standardized results on multiple outcome measures were included.
When a study used more than one outcome measure related to a construct, the most frequently used outcome
measure was included in the construct meta- analysis. For all meta- analysed outcome measures, leave- one- out
sensitivity analyses were conducted to sustain the validity of the conclusions. Only results of the sensitivity
analyses leading to different conclusions were reported.
3 | RESULTS
3.1 | Literature search
The systematic literature search firstly identified 3,352 papers, resulting in 2,370 papers after removing
duplicates. After the screening and selection process, eight articles passed the inclusion criteria and entered the
systematic review and meta- analysis. One study (Boer & Moss, 2016), described two interventions, which were
used separately in the meta- analysis. Detailed information of the selection process is provided by the flow
diagram in Figure 1.
3.2 | General and intervention characteristics of the studies included
The majority of studies (Table 1) included adults with mild to moderate level of intellectual disabilities as
participants (6/8). There was considerable variation in the number of participants per study, ranging from 16 to
443 participants (Mean 121.5) (Table 1). The setting of the interventions varied between the studies. All the
included studies were recently completed, published between 2012 and 2016 (Table 1).
No interventions focussed on change in nutrition only. Five of eight studies used some theoretical framework
(Table 1), which was social cognitive theory in all five studies. Studies within both study categories (aiming
physical activity or physical activity and nutrition) delivered the intervention face- to- face (8/8), most of them
within a group- wise manner (5/8). Intervention duration ranged from eight weeks to 16 months. Intervention
frequency varied between all studies, ranging from three times in 12 weeks to five times per week. Follow- up
period was used in two studies aiming to improve physical activity (Melville et al., 2015; Van Schijndel- Speet et
al., 2016) and two studies aiming to improve physical activity and nutrition (Curtin et al., 2013; McDermott et al.,
2012). Further intervention characteristics are shown in Table 2.
138541-Willems_BNW.indd 31 31-10-19 10:07
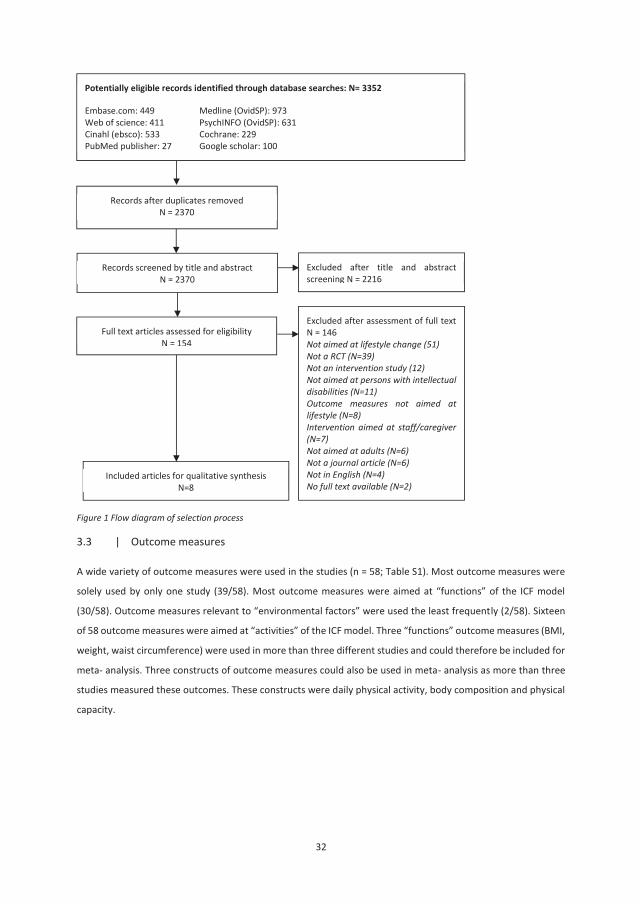
32
Figure 1 Flow diagram of selection process
3.3 | Outcome measures
A wide variety of outcome measures were used in the studies (n = 58; Table S1). Most outcome measures were
solely used by only one study (39/58). Most outcome measures were aimed at “functions” of the ICF model
(30/58). Outcome measures relevant to “environmental factors” were used the least frequently (2/58). Sixteen
of 58 outcome measures were aimed at “activities” of the ICF model. Three “functions” outcome measures (BMI,
weight, waist circumference) were used in more than three different studies and could therefore be included for
meta- analysis. Three constructs of outcome measures could also be used in meta- analysis as more than three
studies measured these outcomes. These constructs were daily physical activity, body composition and physical
capacity.
Potentially eligible records identified through database searches: N= 3352
Embase.com: 449 Medline (OvidSP): 973Web of science: 411 PsychINFO (OvidSP): 631Cinahl (ebsco): 533 Cochrane: 229PubMed publisher: 27 Google scholar: 100
Excluded after title and abstract screening N = 2216
Records screened by title and abstractN = 2370
Full text articles assessed for eligibility N = 154
Excluded after assessment of full text N = 146Not aimed at lifestyle change (51)Not a RCT (N=39)Not an intervention study (12)Not aimed at persons with intellectual disabilities (N=11)Outcome measures not aimed at lifestyle (N=8)Intervention aimed at staff/caregiver (N=7)Not aimed at adults (N=6)Not a journal article (N=6)Not in English (N=4)No full text available (N=2)
Records after duplicates removedN = 2370
Included articles for qualitative synthesis N=8
33
Tabl
e 1:
Gen
eral
char
acte
ristic
s of t
he st
udie
s
Stud
y Ye
ar
Setti
ng
Popu
latio
n N
Mea
n Ag
e (S
D)
Leve
l of
ID
Sex
(%F)
‘F
unct
ion’
out
com
e m
easu
res,
with
sign
ifica
nt
effe
cts r
epor
ted
‘Act
iviti
es’
outc
ome
m
easu
res,
w
ith
signi
fican
t ef
fect
s re
port
ed
‘Par
ticip
atio
n’
outc
ome
m
easu
res,
w
ith
signi
fican
t ef
fect
s re
port
ed
‘Per
sona
l fa
ctor
s’ ou
tcom
e
mea
sure
s, w
ith
signi
fican
t ef
fect
s re
port
ed
‘Env
ironm
enta
l fa
ctor
s’ ou
tcom
e
mea
sure
s, w
ith
signi
fican
t effe
cts
repo
rted
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(4)
Mel
ville
20
15
Part
icipa
nts
hom
e Ad
ults
w
ith ID
10
2 46
.2
All l
evel
s 44
.1
- -
Not
used
-
Not u
sed
Boer
– IT
gr
oup
2016
Un
know
n Ad
ults
w
ith D
S*
21
33.8
(8
.6)
Unkn
own
40.5
Pe
ak o
xyge
n co
nsum
ptio
n (V
O2, L
/min
), re
lativ
e pe
ak
oxyg
en co
nsum
ptio
n (V
O2,
L/m
in),
vent
ilato
r thr
esho
ld
(VT)
, tim
e to
exh
aust
ion,
pea
k he
art r
ate,
wei
ght,
BMI
Not u
sed
Not
used
No
t use
d No
t use
d
Boer
– C
AT
grou
p 20
16
Unkn
own
Adul
ts
with
DS*
21
33
.8
(8.6
) Un
know
n 40
.5
Peak
oxy
gen
cons
umpt
ion
(VO2
, L/m
in),
rela
tive
peak
ox
ygen
cons
umpt
ion
(VO2
, L/
min
), tim
e to
exh
aust
ion,
pe
ak h
eart
rate
, 8-ft
up
and
go,
6-m
inut
e w
alki
ng d
istan
ce
(m),
sit-to
-sta
nd
(am
ount
/30s
), w
eigh
t
Not u
sed
Not
used
No
t use
d No
t use
d
Shie
lds
2015
Un
know
n Yo
ung
adul
ts w
ith
DS*
16
21.4
(3
.2)
Mild
-M
oder
ate
50
- -
Not
used
-
Not u
sed
138541-Willems_BNW.indd 32 31-10-19 10:07

3332
Figure 1 Flow diagram of selection process
3.3 | Outcome measures
A wide variety of outcome measures were used in the studies (n = 58; Table S1). Most outcome measures were
solely used by only one study (39/58). Most outcome measures were aimed at “functions” of the ICF model
(30/58). Outcome measures relevant to “environmental factors” were used the least frequently (2/58). Sixteen
of 58 outcome measures were aimed at “activities” of the ICF model. Three “functions” outcome measures (BMI,
weight, waist circumference) were used in more than three different studies and could therefore be included for
meta- analysis. Three constructs of outcome measures could also be used in meta- analysis as more than three
studies measured these outcomes. These constructs were daily physical activity, body composition and physical
capacity.
Potentially eligible records identified through database searches: N= 3352
Embase.com: 449 Medline (OvidSP): 973Web of science: 411 PsychINFO (OvidSP): 631Cinahl (ebsco): 533 Cochrane: 229PubMed publisher: 27 Google scholar: 100
Excluded after title and abstract screening N = 2216
Records screened by title and abstractN = 2370
Full text articles assessed for eligibility N = 154
Excluded after assessment of full text N = 146Not aimed at lifestyle change (51)Not a RCT (N=39)Not an intervention study (12)Not aimed at persons with intellectual disabilities (N=11)Outcome measures not aimed at lifestyle (N=8)Intervention aimed at staff/caregiver (N=7)Not aimed at adults (N=6)Not a journal article (N=6)Not in English (N=4)No full text available (N=2)
Records after duplicates removedN = 2370
Included articles for qualitative synthesis N=8
33
Tabl
e 1:
Gen
eral
char
acte
ristic
s of t
he st
udie
s
Stud
y Ye
ar
Setti
ng
Popu
latio
n N
Mea
n Ag
e (S
D)
Leve
l of
ID
Sex
(%F)
‘F
unct
ion’
out
com
e m
easu
res,
with
sign
ifica
nt
effe
cts r
epor
ted
‘Act
iviti
es’
outc
ome
m
easu
res,
w
ith
signi
fican
t ef
fect
s re
port
ed
‘Par
ticip
atio
n’
outc
ome
m
easu
res,
w
ith
signi
fican
t ef
fect
s re
port
ed
‘Per
sona
l fa
ctor
s’ ou
tcom
e
mea
sure
s, w
ith
signi
fican
t ef
fect
s re
port
ed
‘Env
ironm
enta
l fa
ctor
s’ ou
tcom
e
mea
sure
s, w
ith
signi
fican
t effe
cts
repo
rted
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(4)
Mel
ville
20
15
Part
icipa
nts
hom
e Ad
ults
w
ith ID
10
2 46
.2
All l
evel
s 44
.1
- -
Not
used
-
Not u
sed
Boer
– IT
gr
oup
2016
Un
know
n Ad
ults
w
ith D
S*
21
33.8
(8
.6)
Unkn
own
40.5
Pe
ak o
xyge
n co
nsum
ptio
n (V
O2, L
/min
), re
lativ
e pe
ak
oxyg
en co
nsum
ptio
n (V
O2,
L/m
in),
vent
ilato
r thr
esho
ld
(VT)
, tim
e to
exh
aust
ion,
pea
k he
art r
ate,
wei
ght,
BMI
Not u
sed
Not
used
No
t use
d No
t use
d
Boer
– C
AT
grou
p 20
16
Unkn
own
Adul
ts
with
DS*
21
33
.8
(8.6
) Un
know
n 40
.5
Peak
oxy
gen
cons
umpt
ion
(VO2
, L/m
in),
rela
tive
peak
ox
ygen
cons
umpt
ion
(VO2
, L/
min
), tim
e to
exh
aust
ion,
pe
ak h
eart
rate
, 8-ft
up
and
go,
6-m
inut
e w
alki
ng d
istan
ce
(m),
sit-to
-sta
nd
(am
ount
/30s
), w
eigh
t
Not u
sed
Not
used
No
t use
d No
t use
d
Shie
lds
2015
Un
know
n Yo
ung
adul
ts w
ith
DS*
16
21.4
(3
.2)
Mild
-M
oder
ate
50
- -
Not
used
-
Not u
sed
138541-Willems_BNW.indd 33 31-10-19 10:07
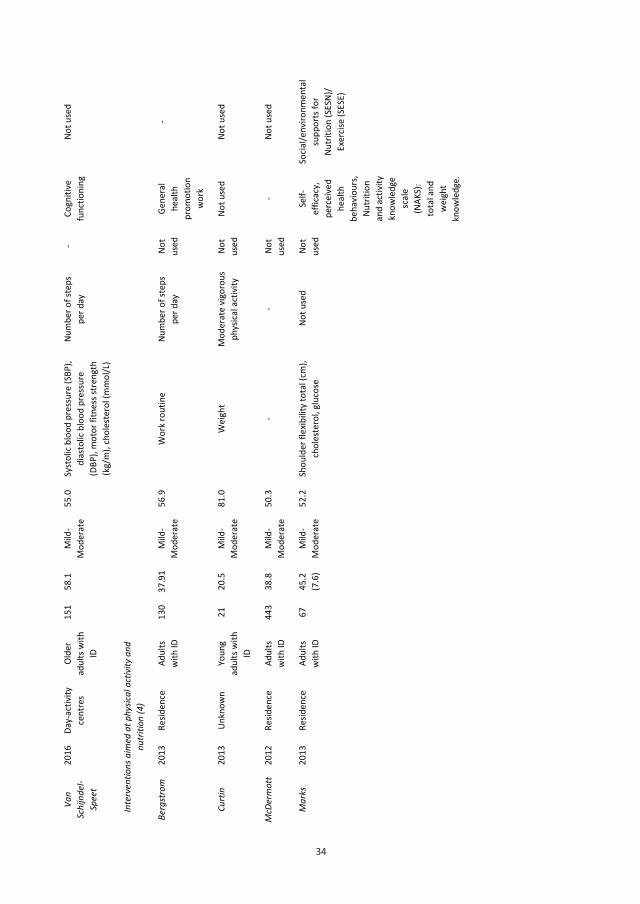
34
34
Van
Schi
jnde
l-Sp
eet
2016
Da
y-ac
tivity
ce
ntre
s Ol
der
adul
ts w
ith
ID
151
58.1
M
ild-
Mod
erat
e 55
.0
Syst
olic
bloo
d pr
essu
re (S
BP),
dias
tolic
blo
od p
ress
ure
(DBP
), m
otor
fitn
ess s
tren
gth
(kg/
m),
chol
este
rol (
mm
ol/L
)
Num
ber o
f ste
ps
per d
ay
- Co
gniti
ve
func
tioni
ng
Not u
sed
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
and
nu
triti
on (4
)
Berg
stro
m
2013
Re
siden
ce
Adul
ts
with
ID
130
37.9
1 M
ild-
Mod
erat
e 56
.9
Wor
k ro
utin
e Nu
mbe
r of s
teps
pe
r day
No
t us
ed
Gene
ral
heal
th
prom
otio
n w
ork
-
Curt
in
2013
Un
know
n Yo
ung
adul
ts w
ith
ID
21
20.5
M
ild-
Mod
erat
e 81
.0
Wei
ght
Mod
erat
e vi
goro
us
phys
ical a
ctiv
ity
Not
used
No
t use
d No
t use
d
McD
erm
ott
2012
Re
siden
ce
Adul
ts
with
ID
443
38.8
M
ild-
Mod
erat
e 50
.3
- -
Not
used
-
Not u
sed
Mar
ks
2013
Re
siden
ce
Adul
ts
with
ID
67
45.2
(7
.6)
Mild
-M
oder
ate
52.2
Sh
ould
er fl
exib
ility
tota
l (cm
), ch
oles
tero
l, gl
ucos
e N
ot u
sed
Not
used
Se
lf-ef
ficac
y,
perc
eive
d he
alth
be
havi
ours
, Nu
triti
on
and
activ
ity
know
ledg
e sc
ale
(NAK
S):
tota
l and
w
eigh
t kn
owle
dge.
Socia
l/env
ironm
enta
l su
ppor
ts fo
r Nu
triti
on (S
ESN)
/ Ex
ercis
e (S
ESE)
35
Tabl
e 2:
Inte
rven
tion
char
acte
ristic
s
St
udy
Year
De
sign
Theo
retic
al fr
amew
ork
Deliv
ery
Num
ber/
fre
quen
cy p
er
wee
k
Inte
rven
tion
dura
tion
(wee
ks)
Follo
w-u
p (w
eeks
)
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(4)
Mel
ville
20
15
RCT
Socia
l Cog
nitiv
e Th
eory
, Tr
anst
heor
etica
l Mod
el
Face
-to-fa
ce,
indi
vidu
ally
3
times
in tw
elve
w
eeks
12
12
Boer
20
16
RCT
None
Fa
ce-to
-face
, in
grou
ps
3 12
Un
know
n
Shie
lds
2015
RC
T No
ne
Face
-to-fa
ce
3-5
8 Un
know
n
Van
Schi
jnde
l-Spe
et
2016
RC
T Th
eory
of P
lann
ed B
ehav
iour
, So
cial C
ogni
tive
Theo
ry, B
ehav
iour
Ch
ange
Tec
hniq
ues
Face
-to-fa
ce, i
n gr
oups
3
8 m
onth
s 6
mon
ths
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
nut
ritio
n (4
)
Berg
stro
m
2013
RC
T So
cial C
ogni
tive
Theo
ry
Face
-to-fa
ce, i
n gr
oups
10
sess
ions
12
-16
mon
ths
Unkn
own
Curt
in
2013
RC
T No
ne
Face
-to-fa
ce, i
n gr
oups
16
sess
ions
6
mon
ths
6 m
onth
s
McD
erm
ott
2012
RC
T So
cial C
ogni
tive
Theo
ry
Face
-to-fa
ce, i
n gr
oups
1
8 10
mon
ths
Mar
ks
2013
RC
T So
cial C
ogni
tive
Theo
ry.
Tran
sthe
oret
ical M
odel
Fa
ce-to
-face
3
12
Unkn
own
138541-Willems_BNW.indd 34 31-10-19 10:07
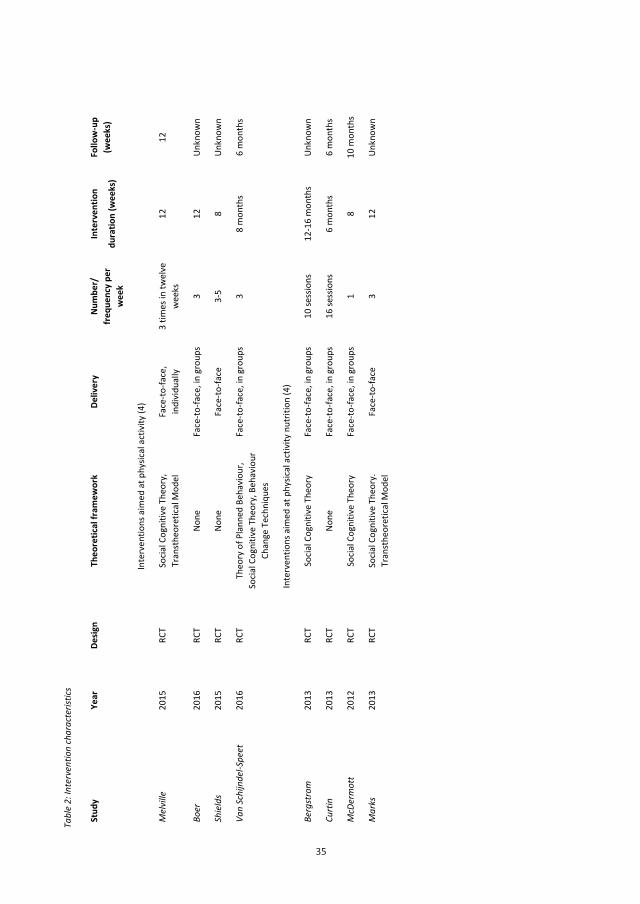
35
35
Tabl
e 2:
Inte
rven
tion
char
acte
ristic
s
St
udy
Year
De
sign
Theo
retic
al fr
amew
ork
Deliv
ery
Num
ber/
fre
quen
cy p
er
wee
k
Inte
rven
tion
dura
tion
(wee
ks)
Follo
w-u
p (w
eeks
)
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(4)
Mel
ville
20
15
RCT
Socia
l Cog
nitiv
e Th
eory
, Tr
anst
heor
etica
l Mod
el
Face
-to-fa
ce,
indi
vidu
ally
3
times
in tw
elve
w
eeks
12
12
Boer
20
16
RCT
None
Fa
ce-to
-face
, in
grou
ps
3 12
Un
know
n
Shie
lds
2015
RC
T No
ne
Face
-to-fa
ce
3-5
8 Un
know
n
Van
Schi
jnde
l-Spe
et
2016
RC
T Th
eory
of P
lann
ed B
ehav
iour
, So
cial C
ogni
tive
Theo
ry, B
ehav
iour
Ch
ange
Tec
hniq
ues
Face
-to-fa
ce, i
n gr
oups
3
8 m
onth
s 6
mon
ths
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
nut
ritio
n (4
)
Berg
stro
m
2013
RC
T So
cial C
ogni
tive
Theo
ry
Face
-to-fa
ce, i
n gr
oups
10
sess
ions
12
-16
mon
ths
Unkn
own
Curt
in
2013
RC
T No
ne
Face
-to-fa
ce, i
n gr
oups
16
sess
ions
6
mon
ths
6 m
onth
s
McD
erm
ott
2012
RC
T So
cial C
ogni
tive
Theo
ry
Face
-to-fa
ce, i
n gr
oups
1
8 10
mon
ths
Mar
ks
2013
RC
T So
cial C
ogni
tive
Theo
ry.
Tran
sthe
oret
ical M
odel
Fa
ce-to
-face
3
12
Unkn
own
138541-Willems_BNW.indd 35 31-10-19 10:07
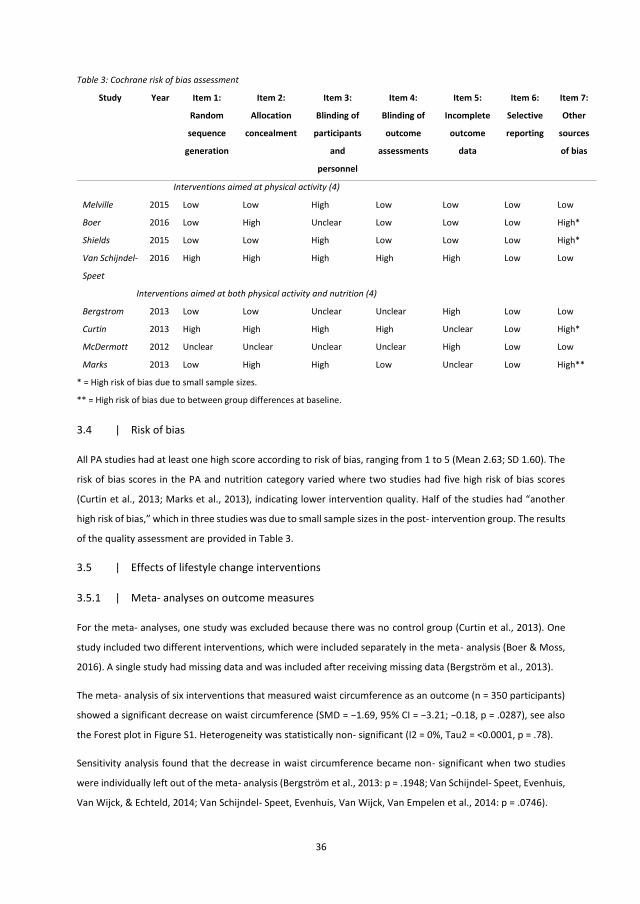
36
Table 3: Cochrane risk of bias assessment
* = High risk of bias due to small sample sizes.
** = High risk of bias due to between group differences at baseline.
3.4 | Risk of bias
All PA studies had at least one high score according to risk of bias, ranging from 1 to 5 (Mean 2.63; SD 1.60). The
risk of bias scores in the PA and nutrition category varied where two studies had five high risk of bias scores
(Curtin et al., 2013; Marks et al., 2013), indicating lower intervention quality. Half of the studies had “another
high risk of bias,” which in three studies was due to small sample sizes in the post- intervention group. The results
of the quality assessment are provided in Table 3.
3.5 | Effects of lifestyle change interventions
3.5.1 | Meta- analyses on outcome measures
For the meta- analyses, one study was excluded because there was no control group (Curtin et al., 2013). One
study included two different interventions, which were included separately in the meta- analysis (Boer & Moss,
2016). A single study had missing data and was included after receiving missing data (Bergström et al., 2013).
The meta- analysis of six interventions that measured waist circumference as an outcome (n = 350 participants)
showed a significant decrease on waist circumference (SMD = −1.69, 95% CI = −3.21; −0.18, p = .0287), see also
the Forest plot in Figure S1. Heterogeneity was statistically non- significant (I2 = 0%, Tau2 = <0.0001, p = .78).
Sensitivity analysis found that the decrease in waist circumference became non- significant when two studies
were individually left out of the meta- analysis (Bergström et al., 2013: p = .1948; Van Schijndel- Speet, Evenhuis,
Van Wijck, & Echteld, 2014; Van Schijndel- Speet, Evenhuis, Van Wijck, Van Empelen et al., 2014: p = .0746).
Study Year Item 1:
Random
sequence
generation
Item 2:
Allocation
concealment
Item 3:
Blinding of
participants
and
personnel
Item 4:
Blinding of
outcome
assessments
Item 5:
Incomplete
outcome
data
Item 6:
Selective
reporting
Item 7:
Other
sources
of bias
Interventions aimed at physical activity (4)
Melville 2015 Low Low High Low Low Low Low
Boer 2016 Low High Unclear Low Low Low High*
Shields 2015 Low Low High Low Low Low High*
Van Schijndel-
Speet
2016 High High High High High Low Low
Interventions aimed at both physical activity and nutrition (4)
Bergstrom 2013 Low Low Unclear Unclear High Low Low
Curtin 2013 High High High High Unclear Low High*
McDermott 2012 Unclear Unclear Unclear Unclear High Low Low
Marks 2013 Low High High Low Unclear Low High**
37
Results of the meta- analysis of the five interventions that measured BMI (n = 433 participants) showed no
significant effect on BMI (SMD = 0.15, 95% CI = −0.13; 0.43, p = .2859), see also the Forest plot in Figure S2. There
was no evidence of heterogeneity (I2 = 0%, Tau2 = 0, p = .8911). Sensitivity analyses did not alter these findings.
Five interventions were included in the meta- analysis for weight change (n = 226 participants). Results of the
meta- analysis found no significant effect on weight (SMD = −0.98, 95% CI = −2.20; 0.25, p = .1191), see also the
Forest plot in Figure S3. No evidence of heterogeneity was found (I2 = 0%, Tau2 = 0, p = .93). Sensitivity analyses
did not alter the findings.
3.5.2 | Meta- analysis at the construct level
Meta- analysis at the construct level of change in outcomes was conducted for physical activity (N = 5), body
composition (N = 7) and physical capacity (N = 5), respectively.
Meta- analysis on physical activity included five studies using three different outcome measures (n = 343
participants). The outcomes showed a borderline significant increase in physical activity (SMD = 0.21, 95% CI
= −0.01; 0.42, p = .0581), see also the Forest plot in Figure S4. There was no evidence of heterogeneity (I2 = 0%,
Tau2 = 0, p = .54). Sensitivity analysis showed a significant increase for physical activity (p = .0297) after leaving
out a single study (McDermott et al., 2012).
Seven included studies (n = 612 participants) for body composition used three included outcome measures,
including waist circumference (N = 5), weight (N = 1) and BMI (N = 1). Based on correlation coefficient r = .8,
meta- analysis showed borderline significant effects on body composition (SMD = −0.15, 95% CI = −0.31; 0.01, p
= .0584), see also the Forest plot in Figure S5. There was no evidence of heterogeneity (I2 = 0%, Tau2 = 0, p =
.80). One study included two different interventions, which were separately included in the meta- analysis (Boer
& Moss, 2016). Sensitivity analysis found a significant decrease for body composition after leaving out either of
two studies (Boer & Mossa, IT group, 2016: p = .0297, McDermott et al., 2012: p = .0265).
Based on correlation coefficient r = .8, the four included studies (n = 125 participants) showed no significant
effect on physical capacity (SMD = 0.38, 95% CI = −0.10; 0.86, p = .1227), see also the Forest plot in Figure S6.
There was no evidence of heterogeneity (I2 = 26.2%, Tau2 = 0.0832, p = .2545). One study included two different
interventions, which were separately included in the meta- analysis (Boer & Moss, 2016). Sensitivity analysis
showed significant increase for physical capacity after leaving out a single study (Marks et al., 2013) of the meta-
analysis (p = .0206).
138541-Willems_BNW.indd 36 31-10-19 10:07
36
Table 3: Cochrane risk of bias assessment
* = High risk of bias due to small sample sizes.
** = High risk of bias due to between group differences at baseline.
3.4 | Risk of bias
All PA studies had at least one high score according to risk of bias, ranging from 1 to 5 (Mean 2.63; SD 1.60). The
risk of bias scores in the PA and nutrition category varied where two studies had five high risk of bias scores
(Curtin et al., 2013; Marks et al., 2013), indicating lower intervention quality. Half of the studies had “another
high risk of bias,” which in three studies was due to small sample sizes in the post- intervention group. The results
of the quality assessment are provided in Table 3.
3.5 | Effects of lifestyle change interventions
3.5.1 | Meta- analyses on outcome measures
For the meta- analyses, one study was excluded because there was no control group (Curtin et al., 2013). One
study included two different interventions, which were included separately in the meta- analysis (Boer & Moss,
2016). A single study had missing data and was included after receiving missing data (Bergström et al., 2013).
The meta- analysis of six interventions that measured waist circumference as an outcome (n = 350 participants)
showed a significant decrease on waist circumference (SMD = −1.69, 95% CI = −3.21; −0.18, p = .0287), see also
the Forest plot in Figure S1. Heterogeneity was statistically non- significant (I2 = 0%, Tau2 = <0.0001, p = .78).
Sensitivity analysis found that the decrease in waist circumference became non- significant when two studies
were individually left out of the meta- analysis (Bergström et al., 2013: p = .1948; Van Schijndel- Speet, Evenhuis,
Van Wijck, & Echteld, 2014; Van Schijndel- Speet, Evenhuis, Van Wijck, Van Empelen et al., 2014: p = .0746).
Study Year Item 1:
Random
sequence
generation
Item 2:
Allocation
concealment
Item 3:
Blinding of
participants
and
personnel
Item 4:
Blinding of
outcome
assessments
Item 5:
Incomplete
outcome
data
Item 6:
Selective
reporting
Item 7:
Other
sources
of bias
Interventions aimed at physical activity (4)
Melville 2015 Low Low High Low Low Low Low
Boer 2016 Low High Unclear Low Low Low High*
Shields 2015 Low Low High Low Low Low High*
Van Schijndel-
Speet
2016 High High High High High Low Low
Interventions aimed at both physical activity and nutrition (4)
Bergstrom 2013 Low Low Unclear Unclear High Low Low
Curtin 2013 High High High High Unclear Low High*
McDermott 2012 Unclear Unclear Unclear Unclear High Low Low
Marks 2013 Low High High Low Unclear Low High**
37
Results of the meta- analysis of the five interventions that measured BMI (n = 433 participants) showed no
significant effect on BMI (SMD = 0.15, 95% CI = −0.13; 0.43, p = .2859), see also the Forest plot in Figure S2. There
was no evidence of heterogeneity (I2 = 0%, Tau2 = 0, p = .8911). Sensitivity analyses did not alter these findings.
Five interventions were included in the meta- analysis for weight change (n = 226 participants). Results of the
meta- analysis found no significant effect on weight (SMD = −0.98, 95% CI = −2.20; 0.25, p = .1191), see also the
Forest plot in Figure S3. No evidence of heterogeneity was found (I2 = 0%, Tau2 = 0, p = .93). Sensitivity analyses
did not alter the findings.
3.5.2 | Meta- analysis at the construct level
Meta- analysis at the construct level of change in outcomes was conducted for physical activity (N = 5), body
composition (N = 7) and physical capacity (N = 5), respectively.
Meta- analysis on physical activity included five studies using three different outcome measures (n = 343
participants). The outcomes showed a borderline significant increase in physical activity (SMD = 0.21, 95% CI
= −0.01; 0.42, p = .0581), see also the Forest plot in Figure S4. There was no evidence of heterogeneity (I2 = 0%,
Tau2 = 0, p = .54). Sensitivity analysis showed a significant increase for physical activity (p = .0297) after leaving
out a single study (McDermott et al., 2012).
Seven included studies (n = 612 participants) for body composition used three included outcome measures,
including waist circumference (N = 5), weight (N = 1) and BMI (N = 1). Based on correlation coefficient r = .8,
meta- analysis showed borderline significant effects on body composition (SMD = −0.15, 95% CI = −0.31; 0.01, p
= .0584), see also the Forest plot in Figure S5. There was no evidence of heterogeneity (I2 = 0%, Tau2 = 0, p =
.80). One study included two different interventions, which were separately included in the meta- analysis (Boer
& Moss, 2016). Sensitivity analysis found a significant decrease for body composition after leaving out either of
two studies (Boer & Mossa, IT group, 2016: p = .0297, McDermott et al., 2012: p = .0265).
Based on correlation coefficient r = .8, the four included studies (n = 125 participants) showed no significant
effect on physical capacity (SMD = 0.38, 95% CI = −0.10; 0.86, p = .1227), see also the Forest plot in Figure S6.
There was no evidence of heterogeneity (I2 = 26.2%, Tau2 = 0.0832, p = .2545). One study included two different
interventions, which were separately included in the meta- analysis (Boer & Moss, 2016). Sensitivity analysis
showed significant increase for physical capacity after leaving out a single study (Marks et al., 2013) of the meta-
analysis (p = .0206).
138541-Willems_BNW.indd 37 31-10-19 10:07

38
4 | DISCUSSION
4.1 | Principal findings
This systematic review aimed to examine the effectiveness of lifestyle change interventions for people with
intellectual disabilities. A small number of RCTs were identified and met the criteria for inclusion in the study. A
large number of outcome measures across all ICF categories were used but meta- analyses could only be
performed for a limited number of outcome measures. Lifestyle change interventions were found to lead to a
statistically significant decrease in waist circumference.
Studies mostly used well quantifiable outcome measures including “function” outcome measures such as weight
or 6- min walking distance. However, outcome measures from the ICF categories “environmental factors” and
“participation” were often neglected and personal outcome measures were mostly used by a single study. This
is surprising, because previous research found that environmental barriers, support from others and personal
motivation are relevant to healthy lifestyles for people with intellectual disabilities (Kuijken, Naaldenberg,
Nijhuis- van der Sanden, & Schrojenstein- Lantman de Valk, 2016; Van Schijndel- Speet, Evenhuis, Van Wijck, &
Echteld, 2014; Van Schijndel- Speet, Evenhuis, Van Wijck, Van Empelen et al., 2014). In addition, persons with
intellectual disabilities experience a healthy lifestyle as more than just functional and do relate more personal,
environmental and participation factors to a healthy lifestyle (Kuijken et al., 2016). For future research,
researchers may consider the use of suitable lifestyle outcome measures, which also target environmental and
personal factors as well as participation. Also, the research field could benefit from consensus about important
outcome measures on all ICF categories of healthy living.
Data on change in mean and standard deviations were missing for some studies, which made it necessary to use
a correlation coefficient for the within- group standard deviations for the constructs body composition and
physical capacity. However, we only found borderline significant effects on the construct of body composition
and no significant effects on the construct of physical capacity. Using this seemingly large correlation coefficient
indicates that further research is necessary to determine whether and how lifestyle change interventions can be
effective in improving body composition and physical capacity. For future research, it is important to report all
relevant data in papers to enable comparison.
Our meta- analysis found some evidence supporting the effectiveness of lifestyle change interventions for people
with intellectual disabilities. A significant decrease was found for waist circumference and borderline significant
effects were found at the construct level for physical activity and body composition. The analysis suggests that
the findings from the included studies may have been influenced by several methodological problems, such as
small sample size, short intervention duration, lack of follow- up and loss of participants during the intervention
resulting in incomplete outcome data. No moderators could be detected that could provide insight into
differences in effects across studies. These tentative results may indicate that the current lifestyle change
interventions are not optimally adapted for people with intellectual disabilities. This is in line with a previous
review which found that carer led health promotion interventions for people with intellectual disabilities were
either ineffective or insufficiently tailored to the needs of people with intellectual disabilities (Hithersay et al.,
39
2014). An explanation for the effectiveness of the interventions on waist circumference might be that this
outcome measure is more sensitive than the other outcome measures used. Previous research in the general
population recommends the use of more specific measures of adiposity than BMI, such as waist circumference,
as the former does not distinguish body composition (Burkhauser & Cawley, 2008). For future research, it is
important to use outcome measures appropriate for people with intellectual disabilities. Also, future research
could benefit from tailoring lifestyle change interventions specifically to people with intellectual disabilities.
4.2 | Strengths and weaknesses of the review
This review and meta- analysis aimed to give more insight into the effects of lifestyle change interventions for
people with intellectual disabilities. A strength of this review was the systematic way in which the search and the
data extraction were performed, as well as the inclusion of RCTs. This rigorous method increased the reliability
of our findings and led to new insights in the effectiveness of lifestyle change interventions for people with
intellectual disabilities. Another strength was the use of meta- analysis, which has not been conducted previously
in the field of lifestyle change interventions for people with intellectual disabilities. As only RCTs were included,
the number of investigated lifestyle change interventions for people with intellectual disabilities was somewhat
limited. However, this inclusion criterion was necessary to conduct a reliable meta- analysis. Because of the small
number of RCTs for lifestyle change interventions, some caution is necessary with respect to the interpretation
of the current findings.
4.3 | Implications for future research
As the field of lifestyle change for people with intellectual disabilities is still young, our findings provide some
guidance for future research to improve the lifestyle of people with intellectual disabilities. The field of lifestyle
change for people with intellectual disabilities could benefit from interventions with a stronger methodological
design as mentioned earlier, for example using a tailored behaviour change theory- based design and the use of
suitable, sensitive outcome measures. Furthermore, it is important to determine in which way lifestyle change
interventions can be adapted for people with intellectual disabilities to avoid dropout and further improve
effectiveness. Further research is necessary to understand the key components of lifestyle change interventions
for people with intellectual disabilities as well as their effect on lifestyle changes.
4.4 | Conclusion
Lifestyle change interventions for people with intellectual disabilities have a small, though, positive effect on
lifestyle, as demonstrated by meta- analyses on BMI, weight, and waist circumference, as well as by meta-
analyses on the constructs physical activity, body composition and physical capacity. However, the effects were
only statistically significant for waist circumference. Therefore, current lifestyle change interventions may not be
optimally tailored to meet the needs of people with intellectual disabilities. This review indicates that there are
still improvements to make in lifestyle change interventions to facilitate a healthier lifestyle of people with
intellectual disabilities.
138541-Willems_BNW.indd 38 31-10-19 10:07

38
4 | DISCUSSION
4.1 | Principal findings
This systematic review aimed to examine the effectiveness of lifestyle change interventions for people with
intellectual disabilities. A small number of RCTs were identified and met the criteria for inclusion in the study. A
large number of outcome measures across all ICF categories were used but meta- analyses could only be
performed for a limited number of outcome measures. Lifestyle change interventions were found to lead to a
statistically significant decrease in waist circumference.
Studies mostly used well quantifiable outcome measures including “function” outcome measures such as weight
or 6- min walking distance. However, outcome measures from the ICF categories “environmental factors” and
“participation” were often neglected and personal outcome measures were mostly used by a single study. This
is surprising, because previous research found that environmental barriers, support from others and personal
motivation are relevant to healthy lifestyles for people with intellectual disabilities (Kuijken, Naaldenberg,
Nijhuis- van der Sanden, & Schrojenstein- Lantman de Valk, 2016; Van Schijndel- Speet, Evenhuis, Van Wijck, &
Echteld, 2014; Van Schijndel- Speet, Evenhuis, Van Wijck, Van Empelen et al., 2014). In addition, persons with
intellectual disabilities experience a healthy lifestyle as more than just functional and do relate more personal,
environmental and participation factors to a healthy lifestyle (Kuijken et al., 2016). For future research,
researchers may consider the use of suitable lifestyle outcome measures, which also target environmental and
personal factors as well as participation. Also, the research field could benefit from consensus about important
outcome measures on all ICF categories of healthy living.
Data on change in mean and standard deviations were missing for some studies, which made it necessary to use
a correlation coefficient for the within- group standard deviations for the constructs body composition and
physical capacity. However, we only found borderline significant effects on the construct of body composition
and no significant effects on the construct of physical capacity. Using this seemingly large correlation coefficient
indicates that further research is necessary to determine whether and how lifestyle change interventions can be
effective in improving body composition and physical capacity. For future research, it is important to report all
relevant data in papers to enable comparison.
Our meta- analysis found some evidence supporting the effectiveness of lifestyle change interventions for people
with intellectual disabilities. A significant decrease was found for waist circumference and borderline significant
effects were found at the construct level for physical activity and body composition. The analysis suggests that
the findings from the included studies may have been influenced by several methodological problems, such as
small sample size, short intervention duration, lack of follow- up and loss of participants during the intervention
resulting in incomplete outcome data. No moderators could be detected that could provide insight into
differences in effects across studies. These tentative results may indicate that the current lifestyle change
interventions are not optimally adapted for people with intellectual disabilities. This is in line with a previous
review which found that carer led health promotion interventions for people with intellectual disabilities were
either ineffective or insufficiently tailored to the needs of people with intellectual disabilities (Hithersay et al.,
39
2014). An explanation for the effectiveness of the interventions on waist circumference might be that this
outcome measure is more sensitive than the other outcome measures used. Previous research in the general
population recommends the use of more specific measures of adiposity than BMI, such as waist circumference,
as the former does not distinguish body composition (Burkhauser & Cawley, 2008). For future research, it is
important to use outcome measures appropriate for people with intellectual disabilities. Also, future research
could benefit from tailoring lifestyle change interventions specifically to people with intellectual disabilities.
4.2 | Strengths and weaknesses of the review
This review and meta- analysis aimed to give more insight into the effects of lifestyle change interventions for
people with intellectual disabilities. A strength of this review was the systematic way in which the search and the
data extraction were performed, as well as the inclusion of RCTs. This rigorous method increased the reliability
of our findings and led to new insights in the effectiveness of lifestyle change interventions for people with
intellectual disabilities. Another strength was the use of meta- analysis, which has not been conducted previously
in the field of lifestyle change interventions for people with intellectual disabilities. As only RCTs were included,
the number of investigated lifestyle change interventions for people with intellectual disabilities was somewhat
limited. However, this inclusion criterion was necessary to conduct a reliable meta- analysis. Because of the small
number of RCTs for lifestyle change interventions, some caution is necessary with respect to the interpretation
of the current findings.
4.3 | Implications for future research
As the field of lifestyle change for people with intellectual disabilities is still young, our findings provide some
guidance for future research to improve the lifestyle of people with intellectual disabilities. The field of lifestyle
change for people with intellectual disabilities could benefit from interventions with a stronger methodological
design as mentioned earlier, for example using a tailored behaviour change theory- based design and the use of
suitable, sensitive outcome measures. Furthermore, it is important to determine in which way lifestyle change
interventions can be adapted for people with intellectual disabilities to avoid dropout and further improve
effectiveness. Further research is necessary to understand the key components of lifestyle change interventions
for people with intellectual disabilities as well as their effect on lifestyle changes.
4.4 | Conclusion
Lifestyle change interventions for people with intellectual disabilities have a small, though, positive effect on
lifestyle, as demonstrated by meta- analyses on BMI, weight, and waist circumference, as well as by meta-
analyses on the constructs physical activity, body composition and physical capacity. However, the effects were
only statistically significant for waist circumference. Therefore, current lifestyle change interventions may not be
optimally tailored to meet the needs of people with intellectual disabilities. This review indicates that there are
still improvements to make in lifestyle change interventions to facilitate a healthier lifestyle of people with
intellectual disabilities.
138541-Willems_BNW.indd 39 31-10-19 10:07
40
ACKNOWLEDGMENTS
The authors thank Wichor Bramer, the information specialist of the Erasmus MC University Medical Center
Rotterdam, for his support with the design and execution of the literature search.
COMPETING INTERESTS
The authors declare that they have no competing interests.
41
REFERENCES
References marked with an * were included in the review
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome: Investigating
parental beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61–80.
Avery, L., Flynn, D., Dombrowski, S. U., Wersch, A., Sniehotta, F. F., & Trenell, M. I. (2015). Successful behavioural
strategies to increase physical activity and improve glucose control in adults with type 2 diabetes.
Diabetic Medicine, 32(8), 1058–1062. https://doi. org/10.1111/dme.12738
Bartlo, P., & Klein, P. J. (2011). Physical activity benefits and needs in adults with intellectual disabilities:
Systematic review of the literature. American Journal on Intellectual and Developmental Disabilities,
116(3), 220–232. https://doi.org/10.1352/1944-7558-116.3.220
* Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention
to improve diet and physical activity among adults with intellectual disabilities in community residences:
A cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847–3857.
https://doi. org/10.1016/j.ridd.2013.07.019
Bittles, A. H., Petterson, B. A., Sullivan, S. G., Hussain, R., Glasson, E. J., & Montgomery, P. D. (2002). The influence
of intellectual disability on life expectancy. The Journals of Gerontology Series A: Biological Sciences and
Medical Sciences, 57(7), M470–M472. https://doi. org/10.1093/gerona/57.7.M470
* Boer, P. H., & Moss, S. J. (2016). Effect of continuous aerobic vs. interval training on selected anthropometrical,
physiological and functional parameters of adults with Down syndrome. Journal of Intellectual Disability
Research, 60(4), 322–334. https://doi.org/10.1111/ jir.12251
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta- analysis. Chichester,
UK: John Wiley. https:// doi.org/10.1002/9780470743386
Burkhauser, R. V., & Cawley, J. (2008). Beyond BMI: The value of more accurate measures of fatness and obesity
in social science research. Journal of Health Economics, 27(2), 519–529.
https://doi.org/10.1016/j.jhealeco.2007.05.005
Casey, A. F., & Rasmussen, R. (2013). Reduction measures and percent body fat in individuals with intellectual
disabilities: A scoping review. Disability and Health Journal, 6(1), 2–7.
https://doi.org/10.1016/j. dhjo.2012.09.002
* Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., … Fleming, R. K. (2013). Parent support
improves weight loss in adolescents and young adults with Down syndrome. The Journal of Pediatrics,
163(5), 1402–1408. https://doi.org/10.1016/j.jpeds.2013.06.081
Dombrowski, S. U., Sniehotta, F. F., Avenell, A., Johnston, M., MacLennan, G., & Araújo-Soares, V. (2012).
Identifying active ingredients in complex behavioural interventions for obese adults with obesity-
138541-Willems_BNW.indd 40 31-10-19 10:07
40
ACKNOWLEDGMENTS
The authors thank Wichor Bramer, the information specialist of the Erasmus MC University Medical Center
Rotterdam, for his support with the design and execution of the literature search.
COMPETING INTERESTS
The authors declare that they have no competing interests.
41
REFERENCES
References marked with an * were included in the review
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome: Investigating
parental beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61–80.
Avery, L., Flynn, D., Dombrowski, S. U., Wersch, A., Sniehotta, F. F., & Trenell, M. I. (2015). Successful behavioural
strategies to increase physical activity and improve glucose control in adults with type 2 diabetes.
Diabetic Medicine, 32(8), 1058–1062. https://doi. org/10.1111/dme.12738
Bartlo, P., & Klein, P. J. (2011). Physical activity benefits and needs in adults with intellectual disabilities:
Systematic review of the literature. American Journal on Intellectual and Developmental Disabilities,
116(3), 220–232. https://doi.org/10.1352/1944-7558-116.3.220
* Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention
to improve diet and physical activity among adults with intellectual disabilities in community residences:
A cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847–3857.
https://doi. org/10.1016/j.ridd.2013.07.019
Bittles, A. H., Petterson, B. A., Sullivan, S. G., Hussain, R., Glasson, E. J., & Montgomery, P. D. (2002). The influence
of intellectual disability on life expectancy. The Journals of Gerontology Series A: Biological Sciences and
Medical Sciences, 57(7), M470–M472. https://doi. org/10.1093/gerona/57.7.M470
* Boer, P. H., & Moss, S. J. (2016). Effect of continuous aerobic vs. interval training on selected anthropometrical,
physiological and functional parameters of adults with Down syndrome. Journal of Intellectual Disability
Research, 60(4), 322–334. https://doi.org/10.1111/ jir.12251
Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta- analysis. Chichester,
UK: John Wiley. https:// doi.org/10.1002/9780470743386
Burkhauser, R. V., & Cawley, J. (2008). Beyond BMI: The value of more accurate measures of fatness and obesity
in social science research. Journal of Health Economics, 27(2), 519–529.
https://doi.org/10.1016/j.jhealeco.2007.05.005
Casey, A. F., & Rasmussen, R. (2013). Reduction measures and percent body fat in individuals with intellectual
disabilities: A scoping review. Disability and Health Journal, 6(1), 2–7.
https://doi.org/10.1016/j. dhjo.2012.09.002
* Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., … Fleming, R. K. (2013). Parent support
improves weight loss in adolescents and young adults with Down syndrome. The Journal of Pediatrics,
163(5), 1402–1408. https://doi.org/10.1016/j.jpeds.2013.06.081
Dombrowski, S. U., Sniehotta, F. F., Avenell, A., Johnston, M., MacLennan, G., & Araújo-Soares, V. (2012).
Identifying active ingredients in complex behavioural interventions for obese adults with obesity-
138541-Willems_BNW.indd 41 31-10-19 10:07
42
related co-morbidities or additional risk factors for co- morbidities: A systematic review. Health
Psychology Review, 6(1), 7–32. https://doi.org/10.1080/17437199.2010.513298
Dusseldorp, E., Van Genugten, L., Van Buuren, S., Verheijden, M. W., & Van Empelen, P. (2014). Combinations of
techniques that effectively change health behavior: Evidence from Meta CART analysis. Health
Psychology, 33(12), 1530. https://doi.org/10.1037/hea0000018
Fjeldsoe, B., Neuhaus, M., Winkler, E., & Eakin, E. (2011). Systematic review of maintenance of behavior change
following physical activity and dietary interventions. Health Psychology, 30(1), 99.
Foster, C., Hillsdon, M., Thorogood, M., Kaur, A., & Wedatilake, T. (2005). Interventions for promoting physical
activity. Cochrane Database of Systematic Reviews, https://doi.org/10.1002/14651858.CD003180. pub2
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P. (2011).
Systematic review of reviews of intervention components associated with increased effectiveness in
dietary and physical activity interventions. BMC Public Health, 11(1), 119.
https://doi.org/10.1186/1471-2458-11-119
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: What is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36. https://doi.org/10.1352/1934-9556-49.1.26
Higgins, J. P. T., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., … Sterne, J. A. C. (2011). The
Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ: British Medical Journal,
343, d5928. https://doi.org/10.1136/bmj.d5928
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
https://doi.org/10.1016/j.ridd.2011.10.011
Hilgenkamp, T. I., Van Wijck, R., & Evenhuis, H. M. (2011). (Instrumental) activities of daily living in older adults
with intellectual disabilities. Research in Developmental Disabilities, 32(5), 1977–1987.
https://doi.org/10.1016/j.ridd.2011.04.003
Hithersay, R., Strydom, A., Moulster, G., & Buszewicz, M. (2014). Carer- led health interventions to monitor,
promote and improve the health of adults with intellectual disabilities in the community: A systematic
review. Research in Developmental Disabilities, 35(4), 887–907.
https://doi.org/10.1016/j.ridd.2014.01.010
Jinks, A., Cotton, A., & Rylance, R. (2011). Obesity interventions for people with a learning disability: An
integrative literature review. Journal of Advanced Nursing, 67(3), 460–471.
https://doi. org/10.1111/j.1365-2648.2010.05508.x
43
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
https://doi.org/10.1111/jir.12243
Maïano, C., Normand, C. L., Aimé, A., & Bégarie, J. (2014). Lifestyle interventions targeting changes in body weight
and composition among youth with an intellectual disability: A systematic review. Research in
Developmental Disabilities, 35(8), 1914–1926. https://doi. org/10.1016/j.ridd.2014.04.014
* Marks, B., Sisirak, J., & Chang, Y. C. (2013). Efficacy of the health matters program train- the trainer model.
Journal of Applied Research in Intellectual Disabilities, 26(4), 319–334.
https://doi.org/10.1111/jar.12045
* McDermott, S., Whitner, W., Thomas-Koger, M., Mann, J. R., Clarkson, J., Barnes, T. L., . . . Meriwether, R. A.
(2012). An efficacy trial of ‘steps to your health’, a health promotion programme for adults with
intellectual disability. Health Education Journal, 71(3), 278–290.
https://doi.org/10.1177/0017896912441240
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223–230.
https://doi. org/10.1111/j.1467-789X.2006.00296.x
* Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., . . . Mutrie, N. (2015).
Effectiveness of a walking programme to support adults with intellectual disabilities to increase physical
activity: Walk well cluster- randomised controlled trial. International Journal of Behavioral Nutrition and
Physical Activity, 12(1), 1–11.
Melville, C. A., Oppewal, A., Elinder, L. S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T. I. M., . . . Giné-Garriga,
M. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual
disabilities—A systematic review. Preventive Medicine, 97, 62–71.
https://doi.org/10.1016/j.ypmed.2016.12.052
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta- regression. Health Psychology, 28(6), 690.
https://doi.org/10.1037/a0016136
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and
meta- analyses: The PRISMA statement. Annals of Internal Medicine, 151(264–269), W64.
Ogg-Groenendaal, M., Hermans, H., & Claessens, B. (2014). A systematic review on the effect of exercise
interventions on challenging behavior for people with intellectual disabilities. Research in
Developmental Disabilities, 35(7), 1507–1517. https://doi.org/10.1016/j.ridd.2014.04.003
138541-Willems_BNW.indd 42 31-10-19 10:07
42
related co-morbidities or additional risk factors for co- morbidities: A systematic review. Health
Psychology Review, 6(1), 7–32. https://doi.org/10.1080/17437199.2010.513298
Dusseldorp, E., Van Genugten, L., Van Buuren, S., Verheijden, M. W., & Van Empelen, P. (2014). Combinations of
techniques that effectively change health behavior: Evidence from Meta CART analysis. Health
Psychology, 33(12), 1530. https://doi.org/10.1037/hea0000018
Fjeldsoe, B., Neuhaus, M., Winkler, E., & Eakin, E. (2011). Systematic review of maintenance of behavior change
following physical activity and dietary interventions. Health Psychology, 30(1), 99.
Foster, C., Hillsdon, M., Thorogood, M., Kaur, A., & Wedatilake, T. (2005). Interventions for promoting physical
activity. Cochrane Database of Systematic Reviews, https://doi.org/10.1002/14651858.CD003180. pub2
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P. (2011).
Systematic review of reviews of intervention components associated with increased effectiveness in
dietary and physical activity interventions. BMC Public Health, 11(1), 119.
https://doi.org/10.1186/1471-2458-11-119
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: What is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36. https://doi.org/10.1352/1934-9556-49.1.26
Higgins, J. P. T., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., … Sterne, J. A. C. (2011). The
Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ: British Medical Journal,
343, d5928. https://doi.org/10.1136/bmj.d5928
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
https://doi.org/10.1016/j.ridd.2011.10.011
Hilgenkamp, T. I., Van Wijck, R., & Evenhuis, H. M. (2011). (Instrumental) activities of daily living in older adults
with intellectual disabilities. Research in Developmental Disabilities, 32(5), 1977–1987.
https://doi.org/10.1016/j.ridd.2011.04.003
Hithersay, R., Strydom, A., Moulster, G., & Buszewicz, M. (2014). Carer- led health interventions to monitor,
promote and improve the health of adults with intellectual disabilities in the community: A systematic
review. Research in Developmental Disabilities, 35(4), 887–907.
https://doi.org/10.1016/j.ridd.2014.01.010
Jinks, A., Cotton, A., & Rylance, R. (2011). Obesity interventions for people with a learning disability: An
integrative literature review. Journal of Advanced Nursing, 67(3), 460–471.
https://doi. org/10.1111/j.1365-2648.2010.05508.x
43
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
https://doi.org/10.1111/jir.12243
Maïano, C., Normand, C. L., Aimé, A., & Bégarie, J. (2014). Lifestyle interventions targeting changes in body weight
and composition among youth with an intellectual disability: A systematic review. Research in
Developmental Disabilities, 35(8), 1914–1926. https://doi. org/10.1016/j.ridd.2014.04.014
* Marks, B., Sisirak, J., & Chang, Y. C. (2013). Efficacy of the health matters program train- the trainer model.
Journal of Applied Research in Intellectual Disabilities, 26(4), 319–334.
https://doi.org/10.1111/jar.12045
* McDermott, S., Whitner, W., Thomas-Koger, M., Mann, J. R., Clarkson, J., Barnes, T. L., . . . Meriwether, R. A.
(2012). An efficacy trial of ‘steps to your health’, a health promotion programme for adults with
intellectual disability. Health Education Journal, 71(3), 278–290.
https://doi.org/10.1177/0017896912441240
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223–230.
https://doi. org/10.1111/j.1467-789X.2006.00296.x
* Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., . . . Mutrie, N. (2015).
Effectiveness of a walking programme to support adults with intellectual disabilities to increase physical
activity: Walk well cluster- randomised controlled trial. International Journal of Behavioral Nutrition and
Physical Activity, 12(1), 1–11.
Melville, C. A., Oppewal, A., Elinder, L. S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T. I. M., . . . Giné-Garriga,
M. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual
disabilities—A systematic review. Preventive Medicine, 97, 62–71.
https://doi.org/10.1016/j.ypmed.2016.12.052
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta- regression. Health Psychology, 28(6), 690.
https://doi.org/10.1037/a0016136
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and
meta- analyses: The PRISMA statement. Annals of Internal Medicine, 151(264–269), W64.
Ogg-Groenendaal, M., Hermans, H., & Claessens, B. (2014). A systematic review on the effect of exercise
interventions on challenging behavior for people with intellectual disabilities. Research in
Developmental Disabilities, 35(7), 1507–1517. https://doi.org/10.1016/j.ridd.2014.04.003
138541-Willems_BNW.indd 43 31-10-19 10:07
44
Ogilvie, D., Foster, C. E., Rothnie, H., Cavill, N., Hamilton, V., Fitzsimons, C. F., & Mutrie, N. (2007). Interventions
to promote walking: Systematic review. British Medical Journal, 334(7605), 1204.
https:// doi.org/10.1136/bmj.39198.722720.BE
Öhman, H., Savikko, N., Strandberg, T. E., & Pitkälä, K. H. (2014). Effect of physical exercise on cognitive
performance in older adults with mild cognitive impairment or dementia: A systematic review. Dementia
and Geriatric Cognitive Disorders, 38(5–6), 347–365.
Patja, K., Iivanainen, M., Vesala, H., Oksanen, H., & Ruoppila, I. (2000). Life expectancy of people with intellectual
disability: A 35- year follow- up study. Journal of Intellectual Disability Research, 44(5), 591–599.
https://doi.org/10.1046/j.1365-2788.2000.00280.x
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
https://doi.org/10.1016/j. ypmed.2008.01.007
Pett, M., Clark, L., Eldredge, A., Cardell, B., Jordan, K., Chambless, C., & Burley, J. (2013). Effecting healthy lifestyle
changes in overweight and obese young adults with intellectual disability. American Journal on
Intellectual and Developmental Disabilities, 118(3), 224–243.
https://doi.org/10.1352/1944-7558-118.3.224
R Core Team (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for
Statistical Computing. https://www.R-project.org/
* Shields, N., & Taylor, N. F. (2015). The feasibility of a physical activity program for young adults with Down
syndrome: A phase II randomised controlled trial. Journal of Intellectual and Developmental Disability,
40(2), 115–125. https://doi.org/10.3109/13668250.2015.1014027
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with intellectual
disabilities and obesity: A systematic review of the evidence. Nutrition Journal, 12(1), 132.
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: A process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401–407. https://doi. org/10.1111/jep.12145
* Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Montfort, K. C. A. G. M., & Echteld, M. A. (2016). A
structured physical activity and fitness programme for older adults with intellectual disabilities: Results
of a cluster- randomised clinical trial. Journal of Intellectual Disability Research, 61(1), 16-29.
https://doi.org/10.1111/jir.12267
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Van Empelen, P., & Echteld, M. A. (2014). Facilitators and
barriers to physical activity as perceived by older adults with intellectual disability. Mental Retardation,
52(3), 175–186.
45
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
https://doi.org/10.1519/JSC.0b013e31828bf1aa
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic review.
Research in Developmental Disabilities, 60, 256–268. https://doi. org/10.1016/j.ridd.2016.10.008
World Health Organization (WHO) (2001). International classification of functioning, disability and health: ICF.
Geneva, Switzerland: World Health Organisation.
Yamaki, K. (2005). Body weight status among adults with intellectual disability in the community. Mental
Retardation, 43(1), 1–10. https://doi. org/10.1352/0047-6765(2005)43<1:BWSAAW>2.0.CO;2
138541-Willems_BNW.indd 44 31-10-19 10:07
44
Ogilvie, D., Foster, C. E., Rothnie, H., Cavill, N., Hamilton, V., Fitzsimons, C. F., & Mutrie, N. (2007). Interventions
to promote walking: Systematic review. British Medical Journal, 334(7605), 1204.
https:// doi.org/10.1136/bmj.39198.722720.BE
Öhman, H., Savikko, N., Strandberg, T. E., & Pitkälä, K. H. (2014). Effect of physical exercise on cognitive
performance in older adults with mild cognitive impairment or dementia: A systematic review. Dementia
and Geriatric Cognitive Disorders, 38(5–6), 347–365.
Patja, K., Iivanainen, M., Vesala, H., Oksanen, H., & Ruoppila, I. (2000). Life expectancy of people with intellectual
disability: A 35- year follow- up study. Journal of Intellectual Disability Research, 44(5), 591–599.
https://doi.org/10.1046/j.1365-2788.2000.00280.x
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
https://doi.org/10.1016/j. ypmed.2008.01.007
Pett, M., Clark, L., Eldredge, A., Cardell, B., Jordan, K., Chambless, C., & Burley, J. (2013). Effecting healthy lifestyle
changes in overweight and obese young adults with intellectual disability. American Journal on
Intellectual and Developmental Disabilities, 118(3), 224–243.
https://doi.org/10.1352/1944-7558-118.3.224
R Core Team (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for
Statistical Computing. https://www.R-project.org/
* Shields, N., & Taylor, N. F. (2015). The feasibility of a physical activity program for young adults with Down
syndrome: A phase II randomised controlled trial. Journal of Intellectual and Developmental Disability,
40(2), 115–125. https://doi.org/10.3109/13668250.2015.1014027
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with intellectual
disabilities and obesity: A systematic review of the evidence. Nutrition Journal, 12(1), 132.
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: A process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401–407. https://doi. org/10.1111/jep.12145
* Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Montfort, K. C. A. G. M., & Echteld, M. A. (2016). A
structured physical activity and fitness programme for older adults with intellectual disabilities: Results
of a cluster- randomised clinical trial. Journal of Intellectual Disability Research, 61(1), 16-29.
https://doi.org/10.1111/jir.12267
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Van Empelen, P., & Echteld, M. A. (2014). Facilitators and
barriers to physical activity as perceived by older adults with intellectual disability. Mental Retardation,
52(3), 175–186.
45
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
https://doi.org/10.1519/JSC.0b013e31828bf1aa
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic review.
Research in Developmental Disabilities, 60, 256–268. https://doi. org/10.1016/j.ridd.2016.10.008
World Health Organization (WHO) (2001). International classification of functioning, disability and health: ICF.
Geneva, Switzerland: World Health Organisation.
Yamaki, K. (2005). Body weight status among adults with intellectual disability in the community. Mental
Retardation, 43(1), 1–10. https://doi. org/10.1352/0047-6765(2005)43<1:BWSAAW>2.0.CO;2
138541-Willems_BNW.indd 45 31-10-19 10:07

46
APPENDICES
APPENDIX 1 – Search string for database searches
Embase.com 449 438
Medline (OvidSP) 973 772
Web of science 411 208
Cochrane 229 43
PubMed publisher 27 21
PsycINFO (OvidSP) 631 431
Cinahl (ebsco) 533 375
Google scholar 100 82
Total 3352 2370
Embase.com
('mental deficiency'/exp OR 'intellectual impairment'/de OR (((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down*
NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND ('lifestyle modification'/exp OR 'diet therapy'/de OR 'diet restriction'/exp OR
'low calory diet'/exp OR 'low carbohydrate diet'/exp OR 'low fat diet'/exp OR 'weight control'/exp OR 'weight reduction'/exp
OR 'dietary intake'/de OR lifestyle/exp OR 'sedentary lifestyle'/exp OR 'body mass'/exp OR 'physical activity'/exp OR
exercise/exp OR kinesiotherapy/exp OR 'treadmill exercise'/exp OR obesity/exp OR (((lifestyle* OR life-style OR calor* OR
nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low NEXT/1 (calor*
OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)) OR 'body mass' OR bmi OR lifestyle OR life-
style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming
OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) NEAR/3 intake*)):ab,ti) AND ((random*
OR factorial* OR crossover* OR (cross NEXT/1 over*) OR placebo* OR ((doubl* OR singl*) NEXT/1 blind*) OR assign* OR
allocat* OR volunteer*):ab,ti OR 'crossover procedure'/de OR 'double-blind procedure'/de OR 'randomized controlled
trial'/de OR 'single-blind procedure'/de) NOT ([Conference Abstract]/lim OR [Letter]/lim OR [Note]/lim OR [Conference
Paper]/lim OR [Editorial]/lim) AND [english]/lim NOT ([animals]/lim NOT [humans]/lim)
Medline (OvidSP)
(exp Intellectual Disability/ OR Mentally Disabled Persons/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR "prader willi").ab,ti.) AND (diet therapy/ OR diet therapy.xs. OR Caloric Restriction/ OR "Diet, Reducing"/
OR "Diet, Carbohydrate-Restricted"/ OR "Diet, Fat-Restricted"/ OR Weight Loss/ OR Weight Reduction Programs/ OR
(((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR
treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*)) OR "body mass"
OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR
kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3
intake*)).ab,ti.) AND (Clinical Trial.pt. OR randomized.ab,ti. OR placebo.ab,ti. OR dt.fs. OR randomly.ab,ti. OR trial.ab,ti. OR
groups.ab,ti.) NOT (letter OR news OR comment OR editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp
animals/ NOT humans/)
47
Cochrane
((((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND
((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)) OR 'body
mass' OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*)):ab,ti)
Web of science
TS=(((((mental* OR intellect*) NEAR/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEAR/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEAR/1 syndrome*) OR "prader willi")) AND
((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/2 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEAR/1 (calor* OR carb* OR fat)) OR (weight NEAR/2 (loss OR losing OR reduction OR control*)) OR "body
mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/2 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/2 intake*))) AND ((random* OR factorial* OR crossover* OR (cross NEAR/1 over*) OR placebo* OR ((doubl*
OR singl*) NEAR/1 blind*) OR assign* OR allocat* ORvolunteer*)) NOT ((animal* OR rat OR rats OR mouse OR mice OR murine
OR pig OR swine OR porcine) NOT (human* OR patient* OR person*))) AND DT=(article)
PubMed publisher
("Intellectual Disability"[mh] OR "Mentally Disabled Persons"[mh] OR (mental deficien*[tiab] OR mental handicap*[tiab] OR
mental disab*[tiab] OR mental retard*[tiab] OR mental impair*[tiab] OR mental challeng*[tiab] OR mentally deficien*[tiab]
OR mentally handicap*[tiab] OR mentally disab*[tiab] OR mentally retard*[tiab] OR mentally impair*[tiab] OR mentally
challeng*[tiab] OR intellectual deficien*[tiab] OR intellectual handicap*[tiab] OR intellectual disab*[tiab] OR intellectual
retard*[tiab] OR intellectual impair*[tiab] OR intellectual challeng*[tiab] OR intellectually deficien*[tiab] OR intellectually
handicap*[tiab] OR intellectually disab*[tiab] OR intellectually retard*[tiab] OR intellectually impair*[tiab] OR intellectually
challeng*[tiab] OR developmental disabilit*[tiab] OR developmental handicap*[tiab] OR developmental deficien*[tiab] OR
Down syndrome*[tiab] OR "prader willi")) AND (diet therapy[mh] OR diet therapy[sh] OR Caloric Restriction[mh] OR "Diet,
Reducing"[mh] OR "Diet, Carbohydrate-Restricted"[mh] OR "Diet, Fat-Restricted"[mh] OR Weight Loss[mh] OR Weight
Reduction Programs[mh] OR (((lifestyle*[tiab] OR life-style OR calor*[tiab] OR nutrition*[tiab] OR diet*[tiab]) AND
(rehab*[tiab] OR modif*[tiab] OR program*[tiab] OR restrict*[tiab] OR therap*[tiab] OR treat*[tiab])) OR (low ADJ
(calor*[tiab] OR carb*[tiab] OR fat)) OR (weight AND (loss OR losing OR reduction OR control*[tiab])) OR "body mass" OR bmi
OR lifestyle OR life-style OR obes*[tiab] OR overweight*[tiab] OR (physical*[tiab] AND activ*[tiab]) OR exercise OR
kinesiotherap*[tiab] OR kinesitherap*[tiab] OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR
((diet*[tiab] OR nutrient*[tiab]) AND intake*[tiab]))) AND (Clinical Trial[pt] OR randomized OR placebo OR drug therapy[sh]
OR randomly OR trial OR groups) NOT (letter[pt] OR news[pt] OR comment[pt] OR editorial[pt] OR congresses[pt] OR
abstracts[pt]) AND english[la] NOT (animals[mh] NOT humans[mh]) AND publisher[sb]
PsycINFO (OvidSP)
(exp Intellectual Development Disorder/ OR Cognitive Impairment/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR "prader willi").ab,ti.) AND (Weight Control/ OR Dietary Restraint/ OR Weight Loss/ OR Lifestyle Changes/
138541-Willems_BNW.indd 46 31-10-19 10:07

46
APPENDICES
APPENDIX 1 – Search string for database searches
Embase.com 449 438
Medline (OvidSP) 973 772
Web of science 411 208
Cochrane 229 43
PubMed publisher 27 21
PsycINFO (OvidSP) 631 431
Cinahl (ebsco) 533 375
Google scholar 100 82
Total 3352 2370
Embase.com
('mental deficiency'/exp OR 'intellectual impairment'/de OR (((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down*
NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND ('lifestyle modification'/exp OR 'diet therapy'/de OR 'diet restriction'/exp OR
'low calory diet'/exp OR 'low carbohydrate diet'/exp OR 'low fat diet'/exp OR 'weight control'/exp OR 'weight reduction'/exp
OR 'dietary intake'/de OR lifestyle/exp OR 'sedentary lifestyle'/exp OR 'body mass'/exp OR 'physical activity'/exp OR
exercise/exp OR kinesiotherapy/exp OR 'treadmill exercise'/exp OR obesity/exp OR (((lifestyle* OR life-style OR calor* OR
nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low NEXT/1 (calor*
OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)) OR 'body mass' OR bmi OR lifestyle OR life-
style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming
OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) NEAR/3 intake*)):ab,ti) AND ((random*
OR factorial* OR crossover* OR (cross NEXT/1 over*) OR placebo* OR ((doubl* OR singl*) NEXT/1 blind*) OR assign* OR
allocat* OR volunteer*):ab,ti OR 'crossover procedure'/de OR 'double-blind procedure'/de OR 'randomized controlled
trial'/de OR 'single-blind procedure'/de) NOT ([Conference Abstract]/lim OR [Letter]/lim OR [Note]/lim OR [Conference
Paper]/lim OR [Editorial]/lim) AND [english]/lim NOT ([animals]/lim NOT [humans]/lim)
Medline (OvidSP)
(exp Intellectual Disability/ OR Mentally Disabled Persons/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR "prader willi").ab,ti.) AND (diet therapy/ OR diet therapy.xs. OR Caloric Restriction/ OR "Diet, Reducing"/
OR "Diet, Carbohydrate-Restricted"/ OR "Diet, Fat-Restricted"/ OR Weight Loss/ OR Weight Reduction Programs/ OR
(((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR
treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*)) OR "body mass"
OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR
kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3
intake*)).ab,ti.) AND (Clinical Trial.pt. OR randomized.ab,ti. OR placebo.ab,ti. OR dt.fs. OR randomly.ab,ti. OR trial.ab,ti. OR
groups.ab,ti.) NOT (letter OR news OR comment OR editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp
animals/ NOT humans/)
47
Cochrane
((((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND
((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)) OR 'body
mass' OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*)):ab,ti)
Web of science
TS=(((((mental* OR intellect*) NEAR/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEAR/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEAR/1 syndrome*) OR "prader willi")) AND
((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/2 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEAR/1 (calor* OR carb* OR fat)) OR (weight NEAR/2 (loss OR losing OR reduction OR control*)) OR "body
mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/2 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/2 intake*))) AND ((random* OR factorial* OR crossover* OR (cross NEAR/1 over*) OR placebo* OR ((doubl*
OR singl*) NEAR/1 blind*) OR assign* OR allocat* ORvolunteer*)) NOT ((animal* OR rat OR rats OR mouse OR mice OR murine
OR pig OR swine OR porcine) NOT (human* OR patient* OR person*))) AND DT=(article)
PubMed publisher
("Intellectual Disability"[mh] OR "Mentally Disabled Persons"[mh] OR (mental deficien*[tiab] OR mental handicap*[tiab] OR
mental disab*[tiab] OR mental retard*[tiab] OR mental impair*[tiab] OR mental challeng*[tiab] OR mentally deficien*[tiab]
OR mentally handicap*[tiab] OR mentally disab*[tiab] OR mentally retard*[tiab] OR mentally impair*[tiab] OR mentally
challeng*[tiab] OR intellectual deficien*[tiab] OR intellectual handicap*[tiab] OR intellectual disab*[tiab] OR intellectual
retard*[tiab] OR intellectual impair*[tiab] OR intellectual challeng*[tiab] OR intellectually deficien*[tiab] OR intellectually
handicap*[tiab] OR intellectually disab*[tiab] OR intellectually retard*[tiab] OR intellectually impair*[tiab] OR intellectually
challeng*[tiab] OR developmental disabilit*[tiab] OR developmental handicap*[tiab] OR developmental deficien*[tiab] OR
Down syndrome*[tiab] OR "prader willi")) AND (diet therapy[mh] OR diet therapy[sh] OR Caloric Restriction[mh] OR "Diet,
Reducing"[mh] OR "Diet, Carbohydrate-Restricted"[mh] OR "Diet, Fat-Restricted"[mh] OR Weight Loss[mh] OR Weight
Reduction Programs[mh] OR (((lifestyle*[tiab] OR life-style OR calor*[tiab] OR nutrition*[tiab] OR diet*[tiab]) AND
(rehab*[tiab] OR modif*[tiab] OR program*[tiab] OR restrict*[tiab] OR therap*[tiab] OR treat*[tiab])) OR (low ADJ
(calor*[tiab] OR carb*[tiab] OR fat)) OR (weight AND (loss OR losing OR reduction OR control*[tiab])) OR "body mass" OR bmi
OR lifestyle OR life-style OR obes*[tiab] OR overweight*[tiab] OR (physical*[tiab] AND activ*[tiab]) OR exercise OR
kinesiotherap*[tiab] OR kinesitherap*[tiab] OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR
((diet*[tiab] OR nutrient*[tiab]) AND intake*[tiab]))) AND (Clinical Trial[pt] OR randomized OR placebo OR drug therapy[sh]
OR randomly OR trial OR groups) NOT (letter[pt] OR news[pt] OR comment[pt] OR editorial[pt] OR congresses[pt] OR
abstracts[pt]) AND english[la] NOT (animals[mh] NOT humans[mh]) AND publisher[sb]
PsycINFO (OvidSP)
(exp Intellectual Development Disorder/ OR Cognitive Impairment/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR "prader willi").ab,ti.) AND (Weight Control/ OR Dietary Restraint/ OR Weight Loss/ OR Lifestyle Changes/
138541-Willems_BNW.indd 47 31-10-19 10:07
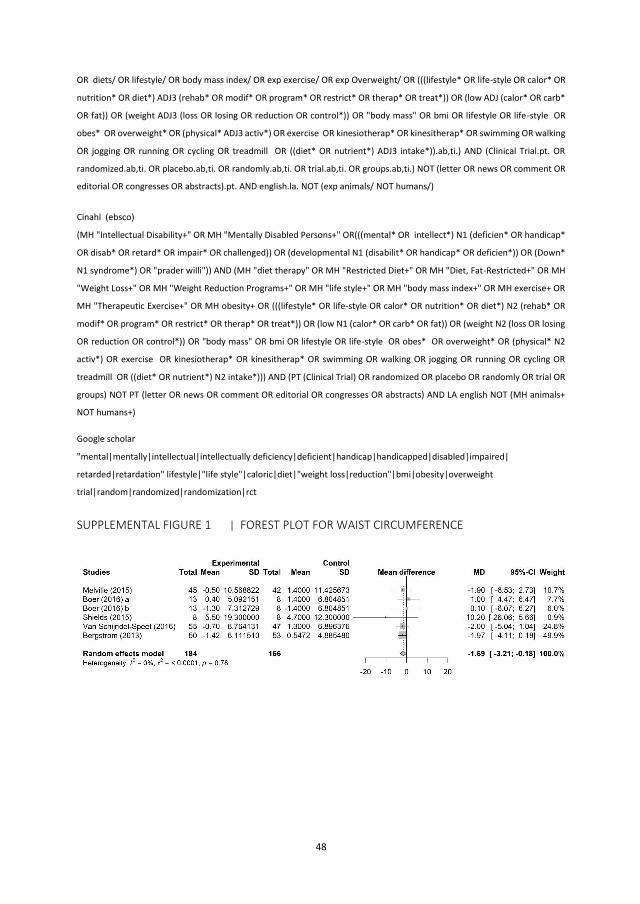
48
OR diets/ OR lifestyle/ OR body mass index/ OR exp exercise/ OR exp Overweight/ OR (((lifestyle* OR life-style OR calor* OR
nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low ADJ (calor* OR carb*
OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*)) OR "body mass" OR bmi OR lifestyle OR life-style OR
obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking
OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3 intake*)).ab,ti.) AND (Clinical Trial.pt. OR
randomized.ab,ti. OR placebo.ab,ti. OR randomly.ab,ti. OR trial.ab,ti. OR groups.ab,ti.) NOT (letter OR news OR comment OR
editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cinahl (ebsco)
(MH "Intellectual Disability+" OR MH "Mentally Disabled Persons+" OR(((mental* OR intellect*) N1 (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental N1 (disabilit* OR handicap* OR deficien*)) OR (Down*
N1 syndrome*) OR "prader willi")) AND (MH "diet therapy" OR MH "Restricted Diet+" OR MH "Diet, Fat-Restricted+" OR MH
"Weight Loss+" OR MH "Weight Reduction Programs+" OR MH "life style+" OR MH "body mass index+" OR MH exercise+ OR
MH "Therapeutic Exercise+" OR MH obesity+ OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) N2 (rehab* OR
modif* OR program* OR restrict* OR therap* OR treat*)) OR (low N1 (calor* OR carb* OR fat)) OR (weight N2 (loss OR losing
OR reduction OR control*)) OR "body mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* N2
activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR
treadmill OR ((diet* OR nutrient*) N2 intake*))) AND (PT (Clinical Trial) OR randomized OR placebo OR randomly OR trial OR
groups) NOT PT (letter OR news OR comment OR editorial OR congresses OR abstracts) AND LA english NOT (MH animals+
NOT humans+)
Google scholar
"mental|mentally|intellectual|intellectually deficiency|deficient|handicap|handicapped|disabled|impaired|
retarded|retardation" lifestyle|"life style"|caloric|diet|"weight loss|reduction"|bmi|obesity|overweight
trial|random|randomized|randomization|rct
SUPPLEMENTAL FIGURE 1 | FOREST PLOT FOR WAIST CIRCUMFERENCE
49
SUPPLEMENTAL FIGURE 2 | FOREST PLOT FOR BMI
SUPPLEMENTAL FIGURE 3 | FOREST PLOT FOR WEIGHT
SUPPLEMENTAL FIGURE 4 | FOREST PLOT FOR PHYSICAL ACTIVITY
SUPPLEMENTAL FIGURE 5 | FOREST PLOT FOR BODY COMPOSITION
138541-Willems_BNW.indd 48 31-10-19 10:07
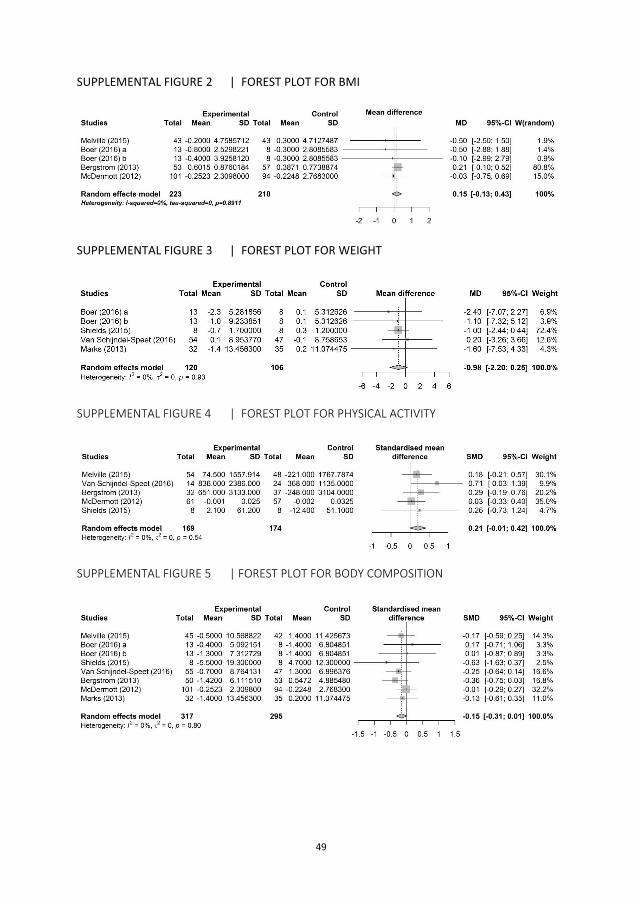
48
OR diets/ OR lifestyle/ OR body mass index/ OR exp exercise/ OR exp Overweight/ OR (((lifestyle* OR life-style OR calor* OR
nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low ADJ (calor* OR carb*
OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*)) OR "body mass" OR bmi OR lifestyle OR life-style OR
obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking
OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3 intake*)).ab,ti.) AND (Clinical Trial.pt. OR
randomized.ab,ti. OR placebo.ab,ti. OR randomly.ab,ti. OR trial.ab,ti. OR groups.ab,ti.) NOT (letter OR news OR comment OR
editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cinahl (ebsco)
(MH "Intellectual Disability+" OR MH "Mentally Disabled Persons+" OR(((mental* OR intellect*) N1 (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental N1 (disabilit* OR handicap* OR deficien*)) OR (Down*
N1 syndrome*) OR "prader willi")) AND (MH "diet therapy" OR MH "Restricted Diet+" OR MH "Diet, Fat-Restricted+" OR MH
"Weight Loss+" OR MH "Weight Reduction Programs+" OR MH "life style+" OR MH "body mass index+" OR MH exercise+ OR
MH "Therapeutic Exercise+" OR MH obesity+ OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) N2 (rehab* OR
modif* OR program* OR restrict* OR therap* OR treat*)) OR (low N1 (calor* OR carb* OR fat)) OR (weight N2 (loss OR losing
OR reduction OR control*)) OR "body mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* N2
activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR
treadmill OR ((diet* OR nutrient*) N2 intake*))) AND (PT (Clinical Trial) OR randomized OR placebo OR randomly OR trial OR
groups) NOT PT (letter OR news OR comment OR editorial OR congresses OR abstracts) AND LA english NOT (MH animals+
NOT humans+)
Google scholar
"mental|mentally|intellectual|intellectually deficiency|deficient|handicap|handicapped|disabled|impaired|
retarded|retardation" lifestyle|"life style"|caloric|diet|"weight loss|reduction"|bmi|obesity|overweight
trial|random|randomized|randomization|rct
SUPPLEMENTAL FIGURE 1 | FOREST PLOT FOR WAIST CIRCUMFERENCE
49
SUPPLEMENTAL FIGURE 2 | FOREST PLOT FOR BMI
SUPPLEMENTAL FIGURE 3 | FOREST PLOT FOR WEIGHT
SUPPLEMENTAL FIGURE 4 | FOREST PLOT FOR PHYSICAL ACTIVITY
SUPPLEMENTAL FIGURE 5 | FOREST PLOT FOR BODY COMPOSITION
138541-Willems_BNW.indd 49 31-10-19 10:07
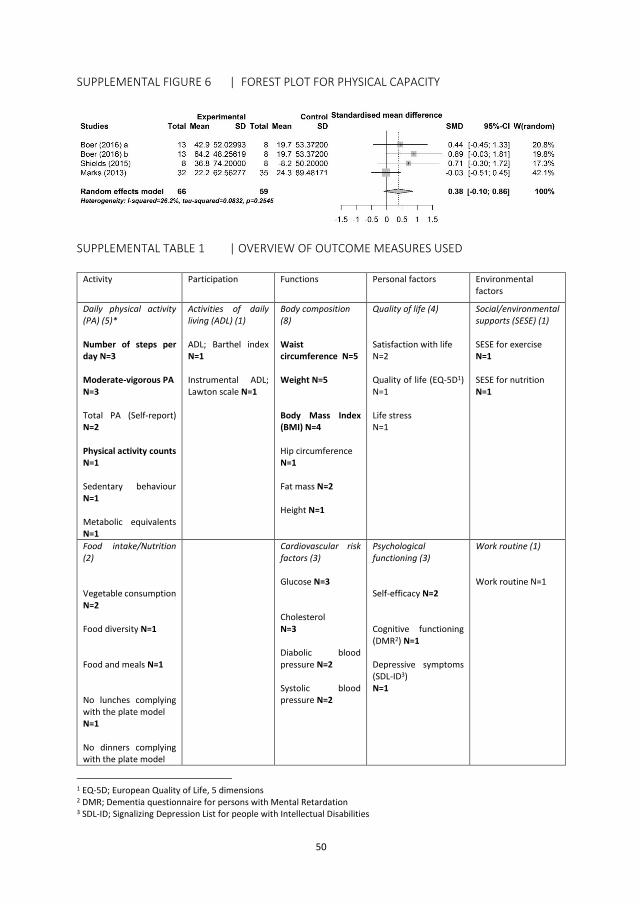
50
SUPPLEMENTAL FIGURE 6 | FOREST PLOT FOR PHYSICAL CAPACITY
SUPPLEMENTAL TABLE 1 | OVERVIEW OF OUTCOME MEASURES USED
Activity Participation Functions Personal factors Environmental factors
Daily physical activity (PA) (5)* Number of steps per day N=3 Moderate-vigorous PA N=3 Total PA (Self-report) N=2 Physical activity counts N=1 Sedentary behaviour N=1 Metabolic equivalents N=1
Activities of daily living (ADL) (1) ADL; Barthel index N=1 Instrumental ADL; Lawton scale N=1
Body composition (8) Waist circumference N=5 Weight N=5 Body Mass Index (BMI) N=4 Hip circumference N=1 Fat mass N=2 Height N=1
Quality of life (4) Satisfaction with life N=2 Quality of life (EQ-5D1) N=1 Life stress N=1
Social/environmental supports (SESE) (1) SESE for exercise N=1 SESE for nutrition N=1
Food intake/Nutrition (2) Vegetable consumption N=2 Food diversity N=1 Food and meals N=1 No lunches complying with the plate model N=1 No dinners complying with the plate model
Cardiovascular risk factors (3) Glucose N=3 Cholesterol N=3 Diabolic blood pressure N=2 Systolic blood pressure N=2
Psychological functioning (3) Self-efficacy N=2 Cognitive functioning (DMR2) N=1 Depressive symptoms (SDL-ID3) N=1
Work routine (1) Work routine N=1
1 EQ-5D; European Quality of Life, 5 dimensions 2 DMR; Dementia questionnaire for persons with Mental Retardation 3 SDL-ID; Signalizing Depression List for people with Intellectual Disabilities
51
N=1 Fruit servings N=1 Treats, kcal/day N=1
Physical capacity (5) 6-Minute walking distance N=3 Time get-up-and-go N=2 Sit-to-stand N=2 Self-selected walking speed N=2 Fast walking speed N=2 Hand Grip Strength N=1 Time to exhaustion N=1 Exercise outcomes N=1 Motor fitness strength N=1 Balance (BBS4) N=1 Aerobic Performance (ISWT5) N=1 Ventilatory Threshold N=1 Relative peak oxygen consumption N=1 Peak oxygen consumption N=1 Peak heart rate N=1
Perceived health (3) Perceived general health N=2 Perceived health behaviour N=1 Subjective vitality N=1
Flexibility Shoulder flexibility N=1 Sit-and-reach N=1
Health literacy (1)
4 BBS; Berg Balance Test 5 ISWT; Incremental Shuttle Walking Test
138541-Willems_BNW.indd 50 31-10-19 10:07
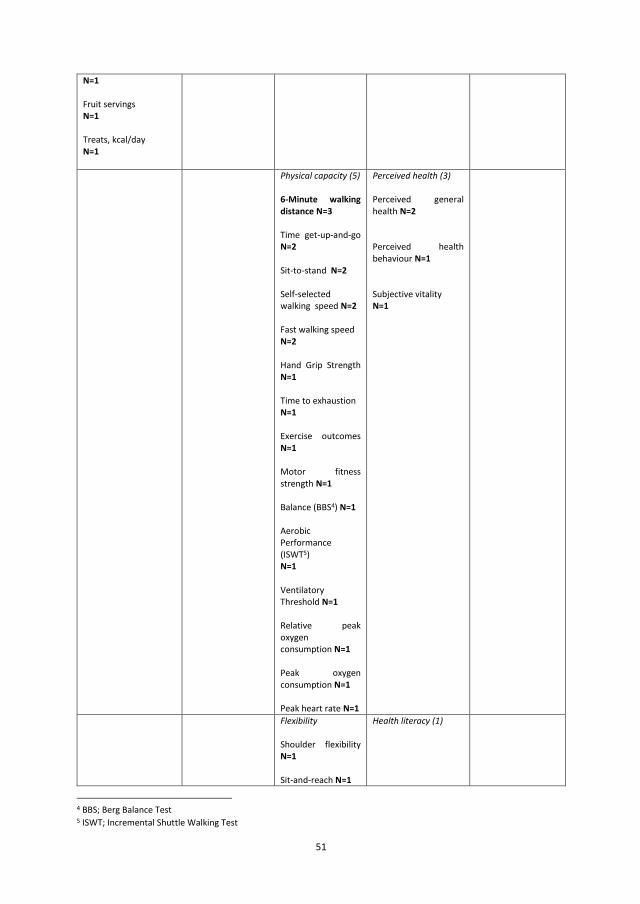
50
SUPPLEMENTAL FIGURE 6 | FOREST PLOT FOR PHYSICAL CAPACITY
SUPPLEMENTAL TABLE 1 | OVERVIEW OF OUTCOME MEASURES USED
Activity Participation Functions Personal factors Environmental factors
Daily physical activity (PA) (5)* Number of steps per day N=3 Moderate-vigorous PA N=3 Total PA (Self-report) N=2 Physical activity counts N=1 Sedentary behaviour N=1 Metabolic equivalents N=1
Activities of daily living (ADL) (1) ADL; Barthel index N=1 Instrumental ADL; Lawton scale N=1
Body composition (8) Waist circumference N=5 Weight N=5 Body Mass Index (BMI) N=4 Hip circumference N=1 Fat mass N=2 Height N=1
Quality of life (4) Satisfaction with life N=2 Quality of life (EQ-5D1) N=1 Life stress N=1
Social/environmental supports (SESE) (1) SESE for exercise N=1 SESE for nutrition N=1
Food intake/Nutrition (2) Vegetable consumption N=2 Food diversity N=1 Food and meals N=1 No lunches complying with the plate model N=1 No dinners complying with the plate model
Cardiovascular risk factors (3) Glucose N=3 Cholesterol N=3 Diabolic blood pressure N=2 Systolic blood pressure N=2
Psychological functioning (3) Self-efficacy N=2 Cognitive functioning (DMR2) N=1 Depressive symptoms (SDL-ID3) N=1
Work routine (1) Work routine N=1
1 EQ-5D; European Quality of Life, 5 dimensions 2 DMR; Dementia questionnaire for persons with Mental Retardation 3 SDL-ID; Signalizing Depression List for people with Intellectual Disabilities
51
N=1 Fruit servings N=1 Treats, kcal/day N=1
Physical capacity (5) 6-Minute walking distance N=3 Time get-up-and-go N=2 Sit-to-stand N=2 Self-selected walking speed N=2 Fast walking speed N=2 Hand Grip Strength N=1 Time to exhaustion N=1 Exercise outcomes N=1 Motor fitness strength N=1 Balance (BBS4) N=1 Aerobic Performance (ISWT5) N=1 Ventilatory Threshold N=1 Relative peak oxygen consumption N=1 Peak oxygen consumption N=1 Peak heart rate N=1
Perceived health (3) Perceived general health N=2 Perceived health behaviour N=1 Subjective vitality N=1
Flexibility Shoulder flexibility N=1 Sit-and-reach N=1
Health literacy (1)
4 BBS; Berg Balance Test 5 ISWT; Incremental Shuttle Walking Test
138541-Willems_BNW.indd 51 31-10-19 10:07
52
Mobility N=1 Nutrition (NAKS6) N=1 Weight (NAKS6) N=1 Total (NAKS6) N=1
* Bolded outcome measures are used in meta-analysis on construct level.
6 NAKS; Nutrition and Activity Knowledge Scale
138541-Willems_BNW.indd 52 31-10-19 10:07

52
Mobility N=1 Nutrition (NAKS6) N=1 Weight (NAKS6) N=1 Total (NAKS6) N=1
* Bolded outcome measures are used in meta-analysis on construct level.
6 NAKS; Nutrition and Activity Knowledge Scale
138541-Willems_BNW.indd 53 31-10-19 10:07

Chapter 3
Use of behaviour change techniques in lifestyle change interventions for
people with intellectual disabilities: A systematic review
Mariël Willems
Thessa I.M. Hilgenkamp
Else Havik
Aly Waninge
Craig A. Melville
Research in Developmental Disabilities, 2017, 60, 256-268
138541-Willems_BNW.indd 54 31-10-19 10:07
Chapter 3
Use of behaviour change techniques in lifestyle change interventions for
people with intellectual disabilities: A systematic review
Mariël Willems
Thessa I.M. Hilgenkamp
Else Havik
Aly Waninge
Craig A. Melville
Research in Developmental Disabilities, 2017, 60, 256-268
138541-Willems_BNW.indd 55 31-10-19 10:07

56
ABSTRACT
Background: People with intellectual disabilities (ID) experience more health problems and have different
lifestyle change needs, compared with the general population.
Aim: To improve lifestyle change interventions for people with ID, this review examined how behaviour change
techniques (BCTs) were applied in interventions aimed at physical activity, nutrition or physical activity and
nutrition, and described their quality.
Methods: After a broad search and detailed selection process, 45 studies were included in the review. For coding
BCTs, the CALO-RE taxonomy was used. To assess the quality of the interventions, the Physiotherapy Evidence
Database (PEDro) scale was used. Extracted data included general study characteristics and intervention
characteristics.
Results: All interventions used BCTs, although theory-driven BCTs were rarely used. The most frequently used
BCTs were ‘provide information on consequences of behaviour in general’ and ‘plan social support/social
change’. Most studies were of low quality and a theoretical framework was often missing.
Conclusion: This review shows that BCTs are frequently applied in lifestyle change interventions. To further
improve effectiveness, these lifestyle change interventions could benefit from using a theoretical framework, a
detailed intervention description and an appropriate and reliable intervention design which is tailored to people
with ID.
57
1 | INTRODUCTION
People with intellectual disabilities (ID) experience up to twice as many health problems as the general
population (Van Schrojenstein Lantman-De Valk & Walsh, 2008). They have very low physical activity levels
(Temple, Frey, & Stanish, 2006; Hilgenkamp, Reis, Van Wijck, & Evenhuis, 2012) and both obesity and overweight
are highly prevalent in this population (Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Waninge et al., 2013).
Factors like low activity levels, use of medication causing weight gain and having Down syndrome (Hsieh, Rimmer,
& Heller, 2014) are associated with higher rates of obesity in people with ID (Peterson, Janz, & Lowe, 2008).
Physical inactivity, obesity and overweight cause serious health problems (WHO, 2009). Due to the health risks
associated with physical inactivity and obesity, research on the promotion of physical activity and healthy eating
habits for people with ID is necessary (Robertson et al., 2000).
Lifestyle change interventions, aimed at weight management in the general population, have found to be
effective in managing weight (Loveman et al., 2011). However, minimal evidence is available for the effectiveness
of lifestyle change interventions in ID populations (Brooker et al., 2015; Scott & Havercamp, 2016; Spanos et al.,
2013). People with ID have different health promotion needs, compared to the general population (Robertson
et al., 2000). They experience intrinsic barriers to a healthy lifestyle and lifestyle change as multimorbidity
(Hermans & Evenhuis, 2014) and barriers related to cognitive, behavioural and mobility impairments. In addition,
persons with ID face many external barriers such as financial barriers, physical limitations and policy guidelines
that limit health choices (Caton et al., 2012; Kuijken, Naaldenberg, Nijhuis-Van der Sande, & Van Schrojenstein-
Lantman de Valk, 2016; Messent, Cooke, & Long, 1999). As a contrast, the general population mostly experiences
barriers as intrinsic to the individual, according to theoretical models of the determinants of physical activity
(Robertson et al., 2000). Considering the cognitive impairments of people with ID and the barriers described
above, programme materials have to be changed to be accessible for people with ID (Elinder, Bergström,
Hagberg, Wihlman, & Hagströmer, 2010). Additionally, people with ID experience barriers to access lifestyle
change services (Van Schrojenstein Lantman-De Valk & Walsh, 2008).
To improve the effectiveness of lifestyle change interventions for people with ID, it is necessary to identify the
effective ingredients within interventions (Michie et al., 2011). However, reporting of intervention content in
published articles is heterogeneous with regards to the used descriptions (Naaldenberg, Kuijken, Van Dooren, &
Van Schrojenstein Lantman-De Valk, 2013) and is often undetailed (Michie, Fixen, Grimshaw, & Eccles, 2009). For
the general population, behaviour change techniques (BCTs) have been found to be an effective component of
interventions changing health behaviours (Bird et al., 2013; Greaves et al., 2011; Olander et al., 2013). Abraham
and Michie (2008) developed a 26-item taxonomy to categorize the BCTs. This taxonomy was later refined by
Michie et al. (2011). Multiple reviews have used these taxonomies to review the BCTs in lifestyle change
interventions for the general population (Dombrowski et al., 2012; Malik, Blake & Suggs, 2014; Olander et al.,
2013; Williams & French, 2011) and have informed the development of new interventions.
Although BCTs have been shown to be effective components of lifestyle change interventions for the general
population, it is unclear whether these BCTs can be used in the same way in interventions for people with ID (Van
138541-Willems_BNW.indd 56 31-10-19 10:07

56
ABSTRACT
Background: People with intellectual disabilities (ID) experience more health problems and have different
lifestyle change needs, compared with the general population.
Aim: To improve lifestyle change interventions for people with ID, this review examined how behaviour change
techniques (BCTs) were applied in interventions aimed at physical activity, nutrition or physical activity and
nutrition, and described their quality.
Methods: After a broad search and detailed selection process, 45 studies were included in the review. For coding
BCTs, the CALO-RE taxonomy was used. To assess the quality of the interventions, the Physiotherapy Evidence
Database (PEDro) scale was used. Extracted data included general study characteristics and intervention
characteristics.
Results: All interventions used BCTs, although theory-driven BCTs were rarely used. The most frequently used
BCTs were ‘provide information on consequences of behaviour in general’ and ‘plan social support/social
change’. Most studies were of low quality and a theoretical framework was often missing.
Conclusion: This review shows that BCTs are frequently applied in lifestyle change interventions. To further
improve effectiveness, these lifestyle change interventions could benefit from using a theoretical framework, a
detailed intervention description and an appropriate and reliable intervention design which is tailored to people
with ID.
57
1 | INTRODUCTION
People with intellectual disabilities (ID) experience up to twice as many health problems as the general
population (Van Schrojenstein Lantman-De Valk & Walsh, 2008). They have very low physical activity levels
(Temple, Frey, & Stanish, 2006; Hilgenkamp, Reis, Van Wijck, & Evenhuis, 2012) and both obesity and overweight
are highly prevalent in this population (Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Waninge et al., 2013).
Factors like low activity levels, use of medication causing weight gain and having Down syndrome (Hsieh, Rimmer,
& Heller, 2014) are associated with higher rates of obesity in people with ID (Peterson, Janz, & Lowe, 2008).
Physical inactivity, obesity and overweight cause serious health problems (WHO, 2009). Due to the health risks
associated with physical inactivity and obesity, research on the promotion of physical activity and healthy eating
habits for people with ID is necessary (Robertson et al., 2000).
Lifestyle change interventions, aimed at weight management in the general population, have found to be
effective in managing weight (Loveman et al., 2011). However, minimal evidence is available for the effectiveness
of lifestyle change interventions in ID populations (Brooker et al., 2015; Scott & Havercamp, 2016; Spanos et al.,
2013). People with ID have different health promotion needs, compared to the general population (Robertson
et al., 2000). They experience intrinsic barriers to a healthy lifestyle and lifestyle change as multimorbidity
(Hermans & Evenhuis, 2014) and barriers related to cognitive, behavioural and mobility impairments. In addition,
persons with ID face many external barriers such as financial barriers, physical limitations and policy guidelines
that limit health choices (Caton et al., 2012; Kuijken, Naaldenberg, Nijhuis-Van der Sande, & Van Schrojenstein-
Lantman de Valk, 2016; Messent, Cooke, & Long, 1999). As a contrast, the general population mostly experiences
barriers as intrinsic to the individual, according to theoretical models of the determinants of physical activity
(Robertson et al., 2000). Considering the cognitive impairments of people with ID and the barriers described
above, programme materials have to be changed to be accessible for people with ID (Elinder, Bergström,
Hagberg, Wihlman, & Hagströmer, 2010). Additionally, people with ID experience barriers to access lifestyle
change services (Van Schrojenstein Lantman-De Valk & Walsh, 2008).
To improve the effectiveness of lifestyle change interventions for people with ID, it is necessary to identify the
effective ingredients within interventions (Michie et al., 2011). However, reporting of intervention content in
published articles is heterogeneous with regards to the used descriptions (Naaldenberg, Kuijken, Van Dooren, &
Van Schrojenstein Lantman-De Valk, 2013) and is often undetailed (Michie, Fixen, Grimshaw, & Eccles, 2009). For
the general population, behaviour change techniques (BCTs) have been found to be an effective component of
interventions changing health behaviours (Bird et al., 2013; Greaves et al., 2011; Olander et al., 2013). Abraham
and Michie (2008) developed a 26-item taxonomy to categorize the BCTs. This taxonomy was later refined by
Michie et al. (2011). Multiple reviews have used these taxonomies to review the BCTs in lifestyle change
interventions for the general population (Dombrowski et al., 2012; Malik, Blake & Suggs, 2014; Olander et al.,
2013; Williams & French, 2011) and have informed the development of new interventions.
Although BCTs have been shown to be effective components of lifestyle change interventions for the general
population, it is unclear whether these BCTs can be used in the same way in interventions for people with ID (Van
138541-Willems_BNW.indd 57 31-10-19 10:07

58
Schijndel-Speet, 2015). The level of complexity and abstraction of some BCTs may complicate their use for this
population, given the intellectual disabilities and special needs of people with ID (Kuijken et al., 2016; Robertson
et al., 2000). Scott and Havercamp (2016) reviewed lifestyle change interventions for people with ID and
described the content and structure of the interventions. However, they did not examine the BCTs used within
the interventions. As a consequence, there is no research on BCTs as a possible effective ingredient used in
lifestyle change interventions for people with ID. Therefore, this review will examine how BCTs are applied in
lifestyle change interventions for people with ID and describes the quality of these studies.
2 | METHODS
2.1 | Search strategy
An extensive search strategy (see Appendix 1) was used to retrieve papers from the electronic databases Embase,
Medline (OvidSP), Web of Science, Psychinfo (OvidSP), Cochrane, PubMed publisher and from Google Scholar.
This search was conducted in March 2015 with an information specialist of the Erasmus MC University Medical
Center Rotterdam. Reference lists from included papers (N = 55) as well as from relevant review papers (n = 51)
retrieved in the original dataset were hand searched for missed papers fulfilling the inclusion criteria.
2.2 | Selection criteria for studies
2.2.1 | Inclusion criteria
Papers were eligible if they discussed lifestyle change interventions for people with ID, in all age ranges, with all
levels of ID. To be included in the review, the intervention had to target changes in physical activity (PA), nutrition
(e.g. increasing levels of physical activity or fitness, improving nutrition habits, or reducing weight) or both
physical activity and nutrition. In the paper, the authors had to state that the intervention program aimed to
achieve a change in daily lifestyle. Only peer-reviewed journal articles, published between 2000 and 2015 and
written in English were eligible for inclusion. Study outcomes had to include at least one aspect of participants’
PA levels, cardiorespiratory fitness, body composition or dietary intake. Adherence to PA or nutrition programs
was also considered a relevant outcome measure.
2.2.2 | Exclusion criteria
Excluded were interventions focusing only on staff or caregivers of people with ID, and papers discussing
interventions for people with autism, schizophrenia or other psychiatric disorders without explicitly mentioning
ID. Papers with study outcomes on improving motor performance or skills, improving inflammation, oxidative
stress, blood composition, or muscle mass, or solely improving other fitness components than cardiorespiratory
fitness (such as strength, balance, flexibility, reaction time, speed, agility) or on cognitive outcomes, were
excluded. Furthermore, interventions using lab-based training or exercise programs (as opposed to community-
based) and interventions with hormone therapy or other medical treatment for weight control, or interventions
focusing on smoking cessation, alcohol or drug use, were excluded. Studies with less than six participants were
59
excluded because the results of small case studies are hard to interpret or generalise for the entire ID population.
Review papers, conference abstracts and editorials were also excluded.
2.2.3 | Screening process
In the first stage of the selection process, 10% of the title screening was conducted by two authors (EH and TH),
resulting in 97.7% agreement; the remaining 90% of titles were screened by one author (EH). Screening all
abstracts and, subsequently, completing inclusion checklists for the full-text papers were done by two authors
(EH and TH) and disagreements were resolved by a consensus discussion. For two records the full-text article was
unavailable, after the authors were contacted. Therefore, these articles were excluded. See Figure 1 for a flow
diagram of the search process.
2.3 | Data extraction
A data extraction form was developed, partly based on Olander et al. (2013), and refined after testing on two
randomly selected studies, by two authors (MW and CM), see Appendix 2. Two reviewers (MW and CM)
independently performed both data extraction and the quality assessment. Results were compared and
disagreements were resolved by consensus discussion. In the case of remaining uncertainty, a third author (TH)
was consulted. Multiple reports of the same intervention study were counted as two papers during the data
extraction, but counted as one in the analysis, e.g. Bodde, Seo, Frey, Lohrmann, and Van Puymbroeck (2012) and
Bodde, Seo, Frey, Van Puymbroeck, and Lohrmann (2012) concerned a study protocol and an outcome paper for
the same study.
Data extracted from the papers were categorized as (1) General study characteristics (aim of intervention, study
design, sample characteristics); (2) Intervention characteristics (short description, theoretical framework,
setting, duration, frequency, intensity, deliverer and mode of delivery of intervention); and (3) Use of BCTs in the
intervention.
For coding of the BCTs the Coventry Aberdeen London Refined (CALORE) taxonomy was used (Michie, Ashford,
Sniehotta et al., 2011). This taxonomy consists of a 40-item list of theory-based definitions of behaviour change
techniques that may be used in interventions aiming to improve physical activity or nutrition. General study
characteristics and intervention characteristics were extracted by one author (MW) and BCTs were coded by two
authors (MW and CM).
138541-Willems_BNW.indd 58 31-10-19 10:07

58
Schijndel-Speet, 2015). The level of complexity and abstraction of some BCTs may complicate their use for this
population, given the intellectual disabilities and special needs of people with ID (Kuijken et al., 2016; Robertson
et al., 2000). Scott and Havercamp (2016) reviewed lifestyle change interventions for people with ID and
described the content and structure of the interventions. However, they did not examine the BCTs used within
the interventions. As a consequence, there is no research on BCTs as a possible effective ingredient used in
lifestyle change interventions for people with ID. Therefore, this review will examine how BCTs are applied in
lifestyle change interventions for people with ID and describes the quality of these studies.
2 | METHODS
2.1 | Search strategy
An extensive search strategy (see Appendix 1) was used to retrieve papers from the electronic databases Embase,
Medline (OvidSP), Web of Science, Psychinfo (OvidSP), Cochrane, PubMed publisher and from Google Scholar.
This search was conducted in March 2015 with an information specialist of the Erasmus MC University Medical
Center Rotterdam. Reference lists from included papers (N = 55) as well as from relevant review papers (n = 51)
retrieved in the original dataset were hand searched for missed papers fulfilling the inclusion criteria.
2.2 | Selection criteria for studies
2.2.1 | Inclusion criteria
Papers were eligible if they discussed lifestyle change interventions for people with ID, in all age ranges, with all
levels of ID. To be included in the review, the intervention had to target changes in physical activity (PA), nutrition
(e.g. increasing levels of physical activity or fitness, improving nutrition habits, or reducing weight) or both
physical activity and nutrition. In the paper, the authors had to state that the intervention program aimed to
achieve a change in daily lifestyle. Only peer-reviewed journal articles, published between 2000 and 2015 and
written in English were eligible for inclusion. Study outcomes had to include at least one aspect of participants’
PA levels, cardiorespiratory fitness, body composition or dietary intake. Adherence to PA or nutrition programs
was also considered a relevant outcome measure.
2.2.2 | Exclusion criteria
Excluded were interventions focusing only on staff or caregivers of people with ID, and papers discussing
interventions for people with autism, schizophrenia or other psychiatric disorders without explicitly mentioning
ID. Papers with study outcomes on improving motor performance or skills, improving inflammation, oxidative
stress, blood composition, or muscle mass, or solely improving other fitness components than cardiorespiratory
fitness (such as strength, balance, flexibility, reaction time, speed, agility) or on cognitive outcomes, were
excluded. Furthermore, interventions using lab-based training or exercise programs (as opposed to community-
based) and interventions with hormone therapy or other medical treatment for weight control, or interventions
focusing on smoking cessation, alcohol or drug use, were excluded. Studies with less than six participants were
59
excluded because the results of small case studies are hard to interpret or generalise for the entire ID population.
Review papers, conference abstracts and editorials were also excluded.
2.2.3 | Screening process
In the first stage of the selection process, 10% of the title screening was conducted by two authors (EH and TH),
resulting in 97.7% agreement; the remaining 90% of titles were screened by one author (EH). Screening all
abstracts and, subsequently, completing inclusion checklists for the full-text papers were done by two authors
(EH and TH) and disagreements were resolved by a consensus discussion. For two records the full-text article was
unavailable, after the authors were contacted. Therefore, these articles were excluded. See Figure 1 for a flow
diagram of the search process.
2.3 | Data extraction
A data extraction form was developed, partly based on Olander et al. (2013), and refined after testing on two
randomly selected studies, by two authors (MW and CM), see Appendix 2. Two reviewers (MW and CM)
independently performed both data extraction and the quality assessment. Results were compared and
disagreements were resolved by consensus discussion. In the case of remaining uncertainty, a third author (TH)
was consulted. Multiple reports of the same intervention study were counted as two papers during the data
extraction, but counted as one in the analysis, e.g. Bodde, Seo, Frey, Lohrmann, and Van Puymbroeck (2012) and
Bodde, Seo, Frey, Van Puymbroeck, and Lohrmann (2012) concerned a study protocol and an outcome paper for
the same study.
Data extracted from the papers were categorized as (1) General study characteristics (aim of intervention, study
design, sample characteristics); (2) Intervention characteristics (short description, theoretical framework,
setting, duration, frequency, intensity, deliverer and mode of delivery of intervention); and (3) Use of BCTs in the
intervention.
For coding of the BCTs the Coventry Aberdeen London Refined (CALORE) taxonomy was used (Michie, Ashford,
Sniehotta et al., 2011). This taxonomy consists of a 40-item list of theory-based definitions of behaviour change
techniques that may be used in interventions aiming to improve physical activity or nutrition. General study
characteristics and intervention characteristics were extracted by one author (MW) and BCTs were coded by two
authors (MW and CM).
138541-Willems_BNW.indd 59 31-10-19 10:07
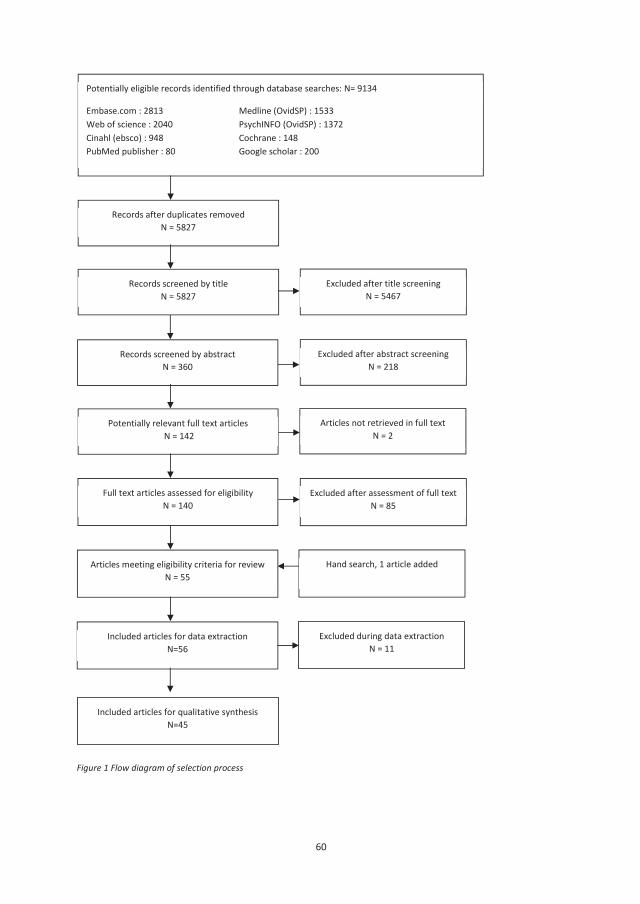
60
Figure 1 Flow diagram of selection process
Potentially eligible records identified through database searches: N= 9134
Embase.com : 2813 Medline (OvidSP) : 1533Web of science : 2040 PsychINFO (OvidSP) : 1372Cinahl (ebsco) : 948 Cochrane : 148PubMed publisher : 80 Google scholar : 200
Records screened by abstractN = 360
Excluded after title screening N = 5467
Excluded after abstract screening N = 218
Potentially relevant full text articlesN = 142
Articles not retrieved in full text N = 2
Articles meeting eligibility criteria for review N = 55
Records screened by title N = 5827
Full text articles assessed for eligibility N = 140
Excluded after assessment of full text N = 85
Records after duplicates removedN = 5827
Included articles for data extraction N=56
Hand search, 1 article added
Included articles for qualitative synthesis N=45
Excluded during data extraction N = 11
61
2.4 | Quality assessment
The quality of the selected articles was assessed using the 10-point Physiotherapy Evidence Database (PEDro)
scale (Maher, Sherrington, Herbert, Moseley, & Elkins, 2003; PEDro, 2015). The purpose of the PEDro scale is to
support users to determine the internal and external validity of studies (PEDro, 2015; Sherrington, Herbert,
Maher, & Moseley, 2000). The first criterion of the scale describes the study’s external validity, but is not used
calculating the final PEDro score. Criteria 2–9 describe the study’s internal validity, while criteria 10 and 11
describe the interpretability of the results (Sherrington et al., 2000). The PEDro scale includes the following
criteria: (1) eligibility criteria were specified (2) random allocation to groups (3) concealed allocation (4) similar
groups at baseline regarding the most important prognostic indicators (5) blinding of all subjects (6) blinding of
all therapists who administered the therapy (7) blinding of all assessors who measured at least one key outcome
(8) measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated
to groups (9) all subjects for whom outcome measures were available received the treatment or control condition
as allocated or, where this was not the case, data for at least one key outcome was analysed by ‘intention to
treat’ (10) reported results of between-group statistical comparisons for at least one key outcome (11) both point
measures and measures of variability are provided for at least one key outcome. The criteria are rated on a yes-
no score and the total of yes-scores gives the PEDro scale score of the article (Sherrington et al., 2000).
2.5 | Synthesis of results
Included articles were categorized together by their aim (e.g. physical activity, nutrition, or both physical activity
and nutrition) in the result tables and the result section in the paper. The extracted data were organized in
general characteristics, intervention characteristics, BCTs and PEDro quality scores.
3 | RESULTS
Table 1 provides an overview of the most important results, categorized by the aim of the studies to change
physical activity, nutrition or both physical activity and nutrition. Table 2 shows the used BCTs in all of the
interventions. Details of the results can be found in four supplemental tables. Table S1 provides an overview of
the study characteristics. Table S2 gives detailed information of the intervention characteristics. Table S3 shows
the ratings for all BCTs. Table S4 shows the results of the PEDro quality assessment.
3.1 | General characteristics
The three categories of studies (aiming to promote physical activity, nutrition or both physical activity and
nutrition) all showed considerable variation in the number of participants, ranging from six to 443 participants
(Table 1). The population of the studies differed between the three study categories: most physical activity
interventions (53%) and physical activity and nutrition interventions (87%) were designed for adults with ID,
while a small majority of the nutrition interventions was designed for children or adolescents with ID (67%). The
level of ID varied in all three study categories. Further details of the study characteristics are provided in
supplementary Table S1.
138541-Willems_BNW.indd 60 31-10-19 10:07
60
Figure 1 Flow diagram of selection process
Potentially eligible records identified through database searches: N= 9134
Embase.com : 2813 Medline (OvidSP) : 1533Web of science : 2040 PsychINFO (OvidSP) : 1372Cinahl (ebsco) : 948 Cochrane : 148PubMed publisher : 80 Google scholar : 200
Records screened by abstractN = 360
Excluded after title screening N = 5467
Excluded after abstract screening N = 218
Potentially relevant full text articlesN = 142
Articles not retrieved in full text N = 2
Articles meeting eligibility criteria for review N = 55
Records screened by title N = 5827
Full text articles assessed for eligibility N = 140
Excluded after assessment of full text N = 85
Records after duplicates removedN = 5827
Included articles for data extraction N=56
Hand search, 1 article added
Included articles for qualitative synthesis N=45
Excluded during data extraction N = 11
61
2.4 | Quality assessment
The quality of the selected articles was assessed using the 10-point Physiotherapy Evidence Database (PEDro)
scale (Maher, Sherrington, Herbert, Moseley, & Elkins, 2003; PEDro, 2015). The purpose of the PEDro scale is to
support users to determine the internal and external validity of studies (PEDro, 2015; Sherrington, Herbert,
Maher, & Moseley, 2000). The first criterion of the scale describes the study’s external validity, but is not used
calculating the final PEDro score. Criteria 2–9 describe the study’s internal validity, while criteria 10 and 11
describe the interpretability of the results (Sherrington et al., 2000). The PEDro scale includes the following
criteria: (1) eligibility criteria were specified (2) random allocation to groups (3) concealed allocation (4) similar
groups at baseline regarding the most important prognostic indicators (5) blinding of all subjects (6) blinding of
all therapists who administered the therapy (7) blinding of all assessors who measured at least one key outcome
(8) measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated
to groups (9) all subjects for whom outcome measures were available received the treatment or control condition
as allocated or, where this was not the case, data for at least one key outcome was analysed by ‘intention to
treat’ (10) reported results of between-group statistical comparisons for at least one key outcome (11) both point
measures and measures of variability are provided for at least one key outcome. The criteria are rated on a yes-
no score and the total of yes-scores gives the PEDro scale score of the article (Sherrington et al., 2000).
2.5 | Synthesis of results
Included articles were categorized together by their aim (e.g. physical activity, nutrition, or both physical activity
and nutrition) in the result tables and the result section in the paper. The extracted data were organized in
general characteristics, intervention characteristics, BCTs and PEDro quality scores.
3 | RESULTS
Table 1 provides an overview of the most important results, categorized by the aim of the studies to change
physical activity, nutrition or both physical activity and nutrition. Table 2 shows the used BCTs in all of the
interventions. Details of the results can be found in four supplemental tables. Table S1 provides an overview of
the study characteristics. Table S2 gives detailed information of the intervention characteristics. Table S3 shows
the ratings for all BCTs. Table S4 shows the results of the PEDro quality assessment.
3.1 | General characteristics
The three categories of studies (aiming to promote physical activity, nutrition or both physical activity and
nutrition) all showed considerable variation in the number of participants, ranging from six to 443 participants
(Table 1). The population of the studies differed between the three study categories: most physical activity
interventions (53%) and physical activity and nutrition interventions (87%) were designed for adults with ID,
while a small majority of the nutrition interventions was designed for children or adolescents with ID (67%). The
level of ID varied in all three study categories. Further details of the study characteristics are provided in
supplementary Table S1.
138541-Willems_BNW.indd 61 31-10-19 10:07
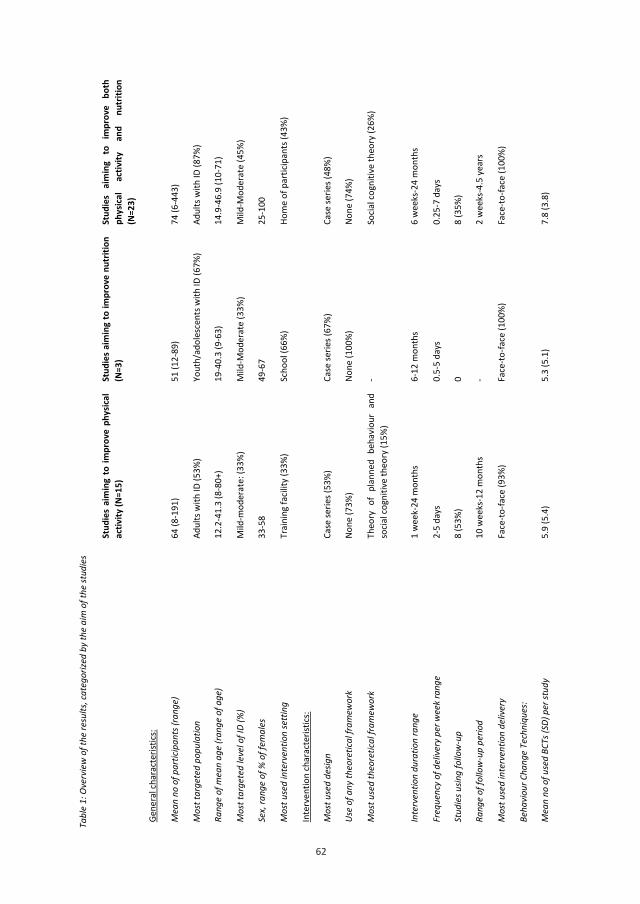
62
62
Tabl
e 1:
Ove
rvie
w o
f the
resu
lts, c
ateg
orize
d by
the
aim
of t
he st
udie
s
St
udie
s ai
min
g to
impr
ove
phys
ical
activ
ity (N
=15)
St
udie
s aim
ing
to im
prov
e nu
triti
on
(N=3
) St
udie
s ai
min
g to
im
prov
e bo
th
phys
ical
activ
ity
and
nutr
ition
(N
=23)
Gene
ral c
hara
cter
istics
:
Mea
n no
of p
artic
ipan
ts (r
ange
) 64
(8-1
91)
51 (1
2-89
) 74
(6-4
43)
Mos
t tar
gete
d po
pula
tion
Adul
ts w
ith ID
(53%
) Yo
uth/
adol
esce
nts w
ith ID
(67%
) Ad
ults
with
ID (8
7%)
Rang
e of
mea
n ag
e (r
ange
of a
ge)
12.2
-41.
3 (8
-80+
) 19
-40.
3 (9
-63)
14
.9-4
6.9
(10-
71)
Mos
t tar
gete
d le
vel o
f ID
(%)
Mild
-mod
erat
e: (3
3%)
Mild
-Mod
erat
e (3
3%)
Mild
-Mod
erat
e (4
5%)
Sex,
rang
e of
% o
f fem
ales
33
-58
49-6
7 25
-100
Mos
t use
d in
terv
entio
n se
ttin
g Tr
aini
ng fa
cility
(33%
) Sc
hool
(66%
) Ho
me
of p
artic
ipan
ts (4
3%)
Inte
rven
tion
char
acte
ristic
s:
Mos
t use
d de
sign
Case
serie
s (53
%)
Case
serie
s (67
%)
Case
serie
s (48
%)
Use
of a
ny th
eore
tical
fram
ewor
k No
ne (7
3%)
None
(100
%)
None
(74%
)
Mos
t use
d th
eore
tical
fram
ewor
k Th
eory
of
plan
ned
beha
viou
r an
d so
cial c
ogni
tive
theo
ry (1
5%)
- So
cial c
ogni
tive
theo
ry (2
6%)
Inte
rven
tion
dura
tion
rang
e 1
wee
k-24
mon
ths
6-12
mon
ths
6 w
eeks
-24
mon
ths
Freq
uenc
y of
del
iver
y pe
r wee
k ra
nge
2-5
days
0.
5-5
days
0.
25-7
day
s
Stud
ies u
sing
follo
w-u
p 8
(53%
) 0
8 (3
5%)
Rang
e of
follo
w-u
p pe
riod
10 w
eeks
-12
mon
ths
- 2
wee
ks-4
.5 y
ears
Mos
t use
d in
terv
entio
n de
liver
y Fa
ce-to
-face
(93%
) Fa
ce-to
-face
(100
%)
Face
-to-fa
ce (1
00%
)
Beha
viou
r Cha
nge
Tech
niqu
es:
Mea
n no
of u
sed
BCTs
(SD)
per
stud
y
5.9
(5.4
) 5.
3 (5
.1)
7.8
(3.8
)
63
Rang
e of
no
of u
sed
BCTs
per
stud
y 1-
14
1-11
2-
15
No o
f BCT
s use
d pe
r cat
egor
y of
stud
ies (
PA, n
utrit
ion
or b
oth
of th
em)
22
12
31
PEDr
o qu
ality
ass
essm
ent:
Mea
n PE
Dro
scor
e (S
D), r
ange
3
(2.0
), 1-
8 1.
7 (1
.5),
0-3
2.8
(1.9
3), 0
-6
Mea
n qu
ality
of i
nter
vent
ions
(PED
ro)
Low
qua
lity
Low
qua
lity
Low
qua
lity
Tabl
e 2:
Ove
rvie
w o
f fre
quen
cies f
or u
sed
BCT
BCT
Freq
uenc
y
BCT
Freq
uenc
y
BCT
Freq
uenc
y
Prov
ide
info
rmat
ion
on c
onse
quen
ces
of b
ehav
iour
in g
ener
al
27
Prom
pt re
war
ds co
ntin
gent
on
effo
rt o
r pro
gres
s
tow
ards
beh
avio
ur
7 Pr
ompt
ing
gene
ralis
atio
n of
a ta
rget
beh
avio
ur
2
Plan
socia
l sup
port
/soc
ial c
hang
e 26
Pr
ompt
self-
mon
itorin
g of
beh
avio
ural
out
com
e 7
Prov
ide
info
rmat
ion
abou
t oth
ers'
appr
oval
1
Prov
ide
inst
ruct
ion
on h
ow to
per
form
the
beha
viou
r
23
Rela
pse
prev
entio
n/co
ping
pla
nnin
g 8
Shap
ing
1
Goal
sett
ing
(beh
avio
ur)
19
Prom
pt re
view
of b
ehav
iour
al g
oals
6 St
imul
ate
antic
ipat
ion
of fu
ture
rew
ards
1
Prom
pt p
ract
ice
17
Goal
setti
ng (o
utco
me)
5
Prov
ide
info
rmat
ion
on c
onse
quen
ces
of b
ehav
iour
to
the
indi
vidu
al
0
Barr
ier i
dent
ifica
tion/
prob
lem
solv
ing
15
Prom
ptin
g fo
cus o
n pa
st su
cces
s 5
Prov
ide
norm
ativ
e in
form
atio
n ab
out
othe
rs'
beha
viou
r
0
Prom
pt se
lf-m
onito
ring
of b
ehav
iour
14
Ge
nera
l com
mun
icatio
n sk
ills t
rain
ing
5 Ag
ree
beha
viou
ral c
ontr
act
0
Actio
n pl
anni
ng
13
Prom
pt re
view
of o
utco
me
goal
s 4
Prom
pt a
ntici
pate
d re
gret
0
Mod
el/d
emon
stra
te th
e be
havi
our
13
Teac
h to
use
pro
mpt
s/cu
es
4 Fe
ar a
rous
al
0
138541-Willems_BNW.indd 62 31-10-19 10:07
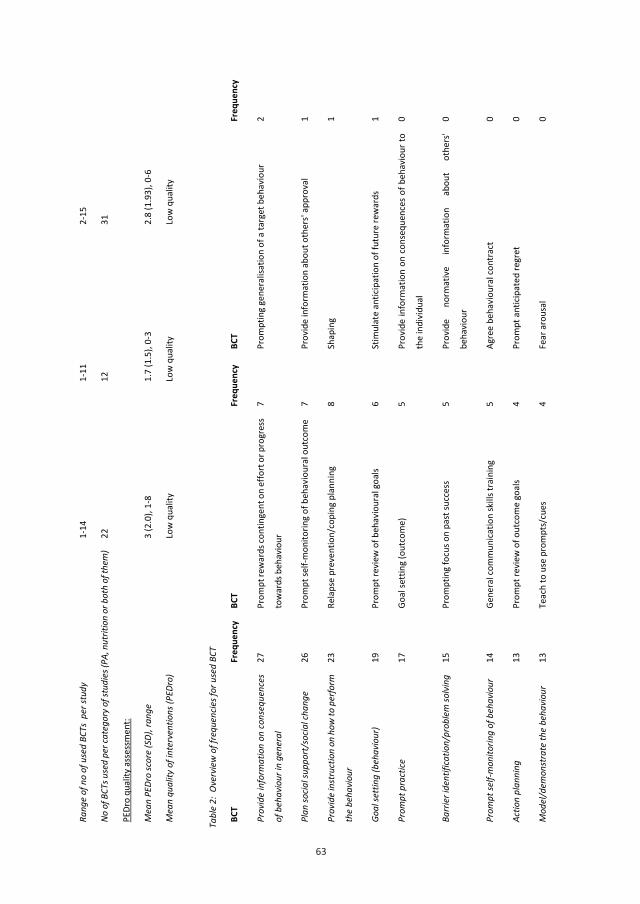
63
63
Rang
e of
no
of u
sed
BCTs
per
stud
y 1-
14
1-11
2-
15
No o
f BCT
s use
d pe
r cat
egor
y of
stud
ies (
PA, n
utrit
ion
or b
oth
of th
em)
22
12
31
PEDr
o qu
ality
ass
essm
ent:
Mea
n PE
Dro
scor
e (S
D), r
ange
3
(2.0
), 1-
8 1.
7 (1
.5),
0-3
2.8
(1.9
3), 0
-6
Mea
n qu
ality
of i
nter
vent
ions
(PED
ro)
Low
qua
lity
Low
qua
lity
Low
qua
lity
Tabl
e 2:
Ove
rvie
w o
f fre
quen
cies f
or u
sed
BCT
BCT
Freq
uenc
y
BCT
Freq
uenc
y
BCT
Freq
uenc
y
Prov
ide
info
rmat
ion
on c
onse
quen
ces
of b
ehav
iour
in g
ener
al
27
Prom
pt re
war
ds co
ntin
gent
on
effo
rt o
r pro
gres
s
tow
ards
beh
avio
ur
7 Pr
ompt
ing
gene
ralis
atio
n of
a ta
rget
beh
avio
ur
2
Plan
socia
l sup
port
/soc
ial c
hang
e 26
Pr
ompt
self-
mon
itorin
g of
beh
avio
ural
out
com
e 7
Prov
ide
info
rmat
ion
abou
t oth
ers'
appr
oval
1
Prov
ide
inst
ruct
ion
on h
ow to
per
form
the
beha
viou
r
23
Rela
pse
prev
entio
n/co
ping
pla
nnin
g 8
Shap
ing
1
Goal
sett
ing
(beh
avio
ur)
19
Prom
pt re
view
of b
ehav
iour
al g
oals
6 St
imul
ate
antic
ipat
ion
of fu
ture
rew
ards
1
Prom
pt p
ract
ice
17
Goal
setti
ng (o
utco
me)
5
Prov
ide
info
rmat
ion
on c
onse
quen
ces
of b
ehav
iour
to
the
indi
vidu
al
0
Barr
ier i
dent
ifica
tion/
prob
lem
solv
ing
15
Prom
ptin
g fo
cus o
n pa
st su
cces
s 5
Prov
ide
norm
ativ
e in
form
atio
n ab
out
othe
rs'
beha
viou
r
0
Prom
pt se
lf-m
onito
ring
of b
ehav
iour
14
Ge
nera
l com
mun
icatio
n sk
ills t
rain
ing
5 Ag
ree
beha
viou
ral c
ontr
act
0
Actio
n pl
anni
ng
13
Prom
pt re
view
of o
utco
me
goal
s 4
Prom
pt a
ntici
pate
d re
gret
0
Mod
el/d
emon
stra
te th
e be
havi
our
13
Teac
h to
use
pro
mpt
s/cu
es
4 Fe
ar a
rous
al
0
138541-Willems_BNW.indd 63 31-10-19 10:07
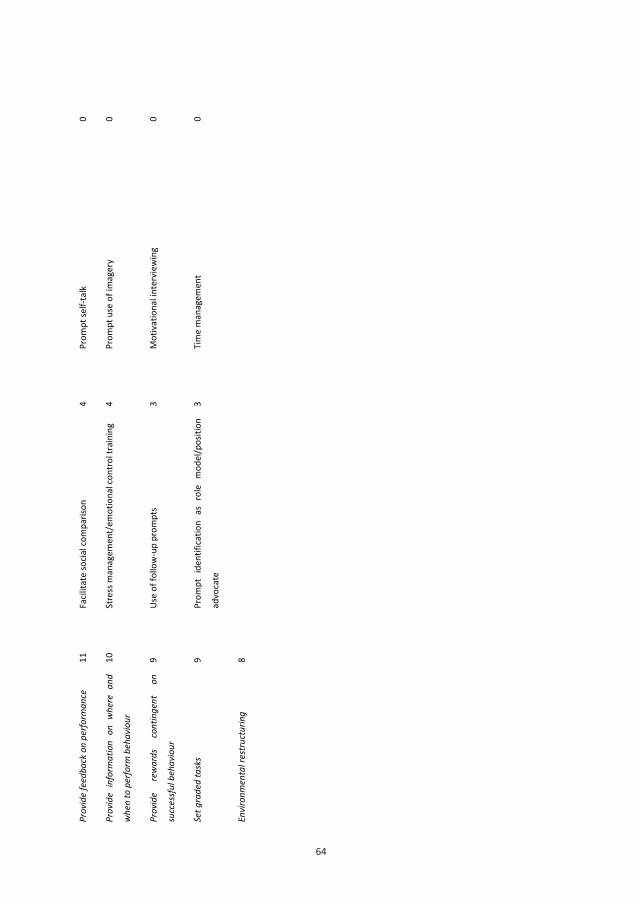
64
64
Prov
ide
feed
back
on
perfo
rman
ce
11
Facil
itate
socia
l com
paris
on
4 Pr
ompt
self-
talk
0
Prov
ide
info
rmat
ion
on w
here
and
whe
n to
per
form
beh
avio
ur
10
Stre
ss m
anag
emen
t/em
otio
nal c
ontr
ol tr
aini
ng
4 Pr
ompt
use
of i
mag
ery
0
Prov
ide
rew
ards
co
ntin
gent
on
succ
essf
ul b
ehav
iour
9 Us
e of
follo
w-u
p pr
ompt
s 3
Mot
ivat
iona
l int
ervi
ewin
g 0
Set g
rade
d ta
sks
9 Pr
ompt
ide
ntifi
catio
n as
rol
e m
odel
/pos
ition
advo
cate
3 Ti
me
man
agem
ent
0
Envi
ronm
enta
l res
truc
turin
g 8
65
3.2 | Intervention characteristics
A case series was the most commonly used design in all three study categories (n = 21) (Table 1). According to
Reeves, Deeks, Higgins, and Wells (2008), a case series is a study that collects observations on a series of
individuals, receiving the same intervention. These observations are made before and after an intervention, with
no control group (Reeves et al., 2008). Another similarity in the three study categories was the lack of a
theoretical framework to inform the design of the intervention (n = 31). Only three studies mentioned the use of
behaviour change techniques in the description of the intervention components (Beeken et al., 2013; Mitchell et
al., 2013; Van Schijndel-Speet, Evenhuis, Van Empelen, Van Wijck, & Echteld, 2013). Two of these studies were
aimed at physical activity (Mitchell et al., 2013; Van Schijndel-Speet et al., 2013) and one aimed both physical
activity and nutrition (Beeken et al., 2013) (Table S2). A few studies (n = 16) included a follow-up period (Tables
1 and S2). All studies used face-to-face delivery, except the physical activity intervention of Thomas and Kerr
(2011), which was delivered by log-books. These log-books contained information about exercise and helped
clients to set personal goals. Details of the intervention characteristics can be found in supplementary Table S2.
3.3 | Behaviour change techniques
All of the interventions used at least one BCT. However, not all of the BCTs were used in the studies (Table 2)
with 9/40 BCTs not used in any of the included studies. The studies in the both physical activity and nutrition
intervention category (n = 23) used the largest proportion of the BCTs, using 31 out of the 40 BCTs, while the
physical activity interventions (n = 15) used 22 different BCTs and the nutrition studies (n = 3) used 12 different
BCTs (Table 1). The mean number of BCTs used in the different categories of interventions was 5.9 (SD 4.0; Range
1–14) for the physical activity interventions, 5.3 (SD 5.10; Range 1–11) for the nutrition interventions and 7.8 (SD
3.8; Range 2–15) for the both physical activity and nutrition interventions. An overview of the ratings for BCTs
used is provided in supplementary Table S3.
The three categories of studies all frequently used “Provide information on consequences of behaviour in
general” (n = 27) and the “Social support” BCT (n = 26) but there was a wide variation in which BCTs were
commonly used (Tables 2 and Table S3). “Social support” means the help of others to achieve a target
behaviour/outcome. This will include support during interventions e.g., setting up a ‘buddy’ system or other
forms of support and following the intervention including support provided by the individuals delivering the
intervention, partner, friends, family (Michie et al., 2011). Physical activity interventions, and nutrition
interventions both frequently used the BCT ‘Instruction on how to perform the behaviour’, but only 50% of the
interventions to improve both physical activity and nutrition used this BCT (Table S3). The nutrition interventions
and the both physical activity and nutrition interventions frequently used the BCT ‘Provide information on
consequences in general’, but this BCT was used in less than half of the physical activity interventions.
3.4 | PEDro quality scores
While most of the interventions in all three categories of studies were of low quality, the RCT studies (10/13)
were of medium or even high quality, in the category of physical activity studies and the category of both physical
138541-Willems_BNW.indd 64 31-10-19 10:07
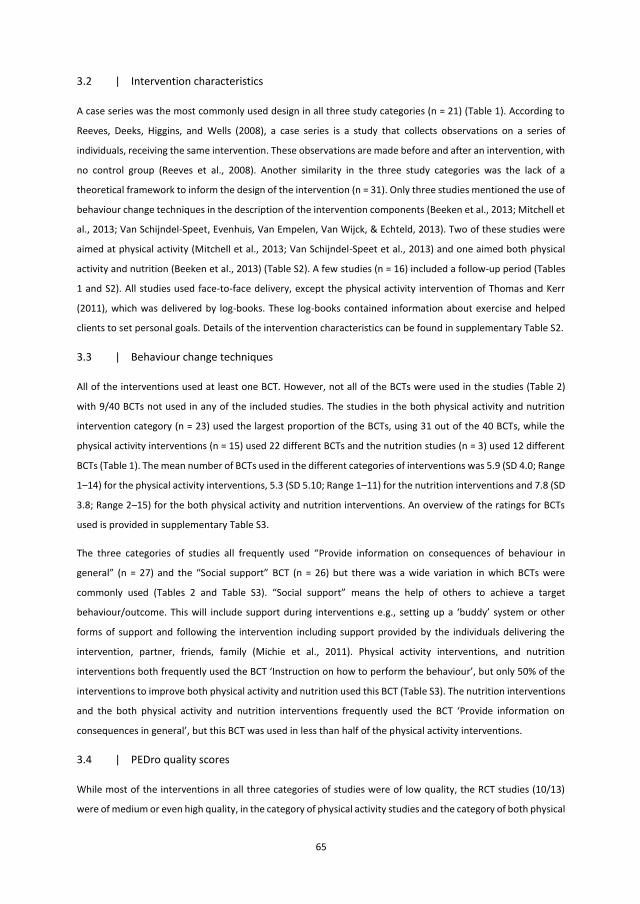
65
3.2 | Intervention characteristics
A case series was the most commonly used design in all three study categories (n = 21) (Table 1). According to
Reeves, Deeks, Higgins, and Wells (2008), a case series is a study that collects observations on a series of
individuals, receiving the same intervention. These observations are made before and after an intervention, with
no control group (Reeves et al., 2008). Another similarity in the three study categories was the lack of a
theoretical framework to inform the design of the intervention (n = 31). Only three studies mentioned the use of
behaviour change techniques in the description of the intervention components (Beeken et al., 2013; Mitchell et
al., 2013; Van Schijndel-Speet, Evenhuis, Van Empelen, Van Wijck, & Echteld, 2013). Two of these studies were
aimed at physical activity (Mitchell et al., 2013; Van Schijndel-Speet et al., 2013) and one aimed both physical
activity and nutrition (Beeken et al., 2013) (Table S2). A few studies (n = 16) included a follow-up period (Tables
1 and S2). All studies used face-to-face delivery, except the physical activity intervention of Thomas and Kerr
(2011), which was delivered by log-books. These log-books contained information about exercise and helped
clients to set personal goals. Details of the intervention characteristics can be found in supplementary Table S2.
3.3 | Behaviour change techniques
All of the interventions used at least one BCT. However, not all of the BCTs were used in the studies (Table 2)
with 9/40 BCTs not used in any of the included studies. The studies in the both physical activity and nutrition
intervention category (n = 23) used the largest proportion of the BCTs, using 31 out of the 40 BCTs, while the
physical activity interventions (n = 15) used 22 different BCTs and the nutrition studies (n = 3) used 12 different
BCTs (Table 1). The mean number of BCTs used in the different categories of interventions was 5.9 (SD 4.0; Range
1–14) for the physical activity interventions, 5.3 (SD 5.10; Range 1–11) for the nutrition interventions and 7.8 (SD
3.8; Range 2–15) for the both physical activity and nutrition interventions. An overview of the ratings for BCTs
used is provided in supplementary Table S3.
The three categories of studies all frequently used “Provide information on consequences of behaviour in
general” (n = 27) and the “Social support” BCT (n = 26) but there was a wide variation in which BCTs were
commonly used (Tables 2 and Table S3). “Social support” means the help of others to achieve a target
behaviour/outcome. This will include support during interventions e.g., setting up a ‘buddy’ system or other
forms of support and following the intervention including support provided by the individuals delivering the
intervention, partner, friends, family (Michie et al., 2011). Physical activity interventions, and nutrition
interventions both frequently used the BCT ‘Instruction on how to perform the behaviour’, but only 50% of the
interventions to improve both physical activity and nutrition used this BCT (Table S3). The nutrition interventions
and the both physical activity and nutrition interventions frequently used the BCT ‘Provide information on
consequences in general’, but this BCT was used in less than half of the physical activity interventions.
3.4 | PEDro quality scores
While most of the interventions in all three categories of studies were of low quality, the RCT studies (10/13)
were of medium or even high quality, in the category of physical activity studies and the category of both physical
138541-Willems_BNW.indd 65 31-10-19 10:07
66
activity and nutrition studies. None of the nutrition studies used an RCT design. All case series were of low quality,
except for one physical activity study (Bodde, Seo, Frey, Lohrmann et al., 2012) and one both physical activity
and nutrition study (Pett et al., 2013), which were of medium quality. The most common limitation was the same
for all three categories of studies, namely insufficient blinding of patients/therapists/assessors. The results of the
PEDro quality assessment are provided in Table S4.
4 | DISCUSSION
4.1 | Principal findings
This systematic review aimed to identify the BCTs used in interventions targeting physical activity, nutrition or
both physical activity and nutrition for people with ID, and to describe the quality of these interventions. All
interventions used at least one BCT, but BCTs were rarely used within the context of a theoretical framework for
intervention design. Given their complexity, it is still unclear to what extent BCTs are accessible for people with
ID.
4.2 | Behaviour change techniques
BCTs were used in all interventions, which may indicate that the importance of BCTs is recognized by researchers
developing interventions. Several of the most commonly used BCTs are similar to facilitators of health behaviour
for people with ID as reported by adults with ID (Kuijken et al., 2016). For example, adults with ID reported that
support from others, motivational support and environmental resources can facilitate health behaviour which
reflects two of the most commonly used BCTs found in this review (Kuijken et al., 2016). In fact, most BCTs in this
review are consistent with these facilitators, as they are aimed at providing social support or maintaining the
motivation of participants. This suggests that the BCTs used in the studies included here meet the needs for
health behaviour of people with ID.
However, many of the BCTs included in the CALORE taxonomy are complex and involve a significant amount of
abstraction. This raises a question about the extent to which BCTs are accessible for people with ID. People with
ID may experience challenges to interpret knowledge and may not be able to live healthy although they have the
required knowledge (Kuijken et al., 2016). This might indicate that complex BCTs will not fit into the capabilities
of people with ID, which may make these BCTs ineffective when included in lifestyle change interventions. For
example, a trial of a walking intervention reported that, even with support from carers, most participants with
ID were unable to use pedometers to self-monitor daily step count (Melville et al., 2015). This is particularly
relevant because self-monitoring has been shown to be important to the effectiveness of lifestyle change
interventions (Michie, Fixsen et al., 2009; Michie, Jochelson et al., 2009). It is recommended that researchers
minimize and simplify the BCTs included in lifestyle change interventions for disadvantaged groups (Michie,
Jochelson, Markham, & Bridle, 2009). However, many of the interventions used ten or more BCTs. To tailor
lifestyle change interventions to the needs of people with ID, researchers should consider testing whether
individual BCTs can be made accessible, for example via support from carers, or using assistive technology, and
67
during the design phase of interventions give careful consideration to which, and how many, BCTs should be
included.
4.3 | Quality of the included studies
Low quality scores were found for a majority of the included lifestyle change interventions, as was also found in
a previous review of Scott and Havercamp (2016). In line with another review, the most common limitation was
blinding of participants, therapists and assessors (Ogg-Groenendaal et al., 2014). Additionally, data presentation
was often incomplete and studies mostly failed to report accurate about recruitment of participants, drop-out
rates and baseline similarities. This may result in different interpretations of the intervention content and issues
with representativeness and generalisation of the findings. This is in line with a review of Scott and Havercamp
(2016), which found that most lifestyle change interventions use weak designs. Weak designs made findings
about effectiveness of the included studies less reliable since the design of the study is used to quantitatively
test the study (Scott & Havercamp, 2016). Our findings correspond with the commentary that there is
heterogeneity in reporting intervention content in lifestyle change research (Michie et al., 2011; Naaldenberg et
al., 2013; Ogg-Groenendaal et al., 2014). Heterogeneity is also found for multiple study characteristics, like levels
of disability, setting of the interventions, the targeted populations and the aimed lifestyle change (nutrition or
PA, or both PA and nutrition). Only three studies were aimed at changing nutrition, which makes it hard to
generalise the findings from this category of studies. This might indicate that lifestyle change is dependent on
the specific social and cultural context, and therefore research in this field might need to be tailored to the
specific situation and context of the people with ID. However, the majority of included studies do not properly
describe context related characteristics, as mentioned above. Also, the varying level of disability could affect the
efficacy of the studies, because the level of ID determines the understanding of participants. Therefore,
intervention content needs to be tailored to the capabilities of the participants.
Although a theoretical base is important for interventions in order to be effective and for understanding of the
results, a majority of the included studies did not use any kind of theoretical framework. In addition, the BCTs
were mostly used in an implicit way, not referring to any theoretical base nor describing the BCT explicitly. In the
field of lifestyle change for the general population, the same lack of theoretical base has been found (Golley,
Hendrie, Slater & Corsini, 2011). Furthermore, the RCT is the gold standard to evaluate lifestyle change
interventions (Tones, 2000), but an RCT design was not often used in the included interventions. This could partly
be explained by perceptions about the ethical issues surrounding the inclusion of people with ID in lifestyle
change research. For example, the conflict between one’s own autonomy to participate and the dependence on
family and staff for participation (Maïano et al., 2014; Naaldenberg et al., 2013; Spanos, Melville, & Hankey,
2013). Also, previous research shows high drop-out rates and large amount of incomplete data in lifestyle change
RCTs for people with ID (Bergström, Hagströmer, Hagberg, & Elinder, 2013; McDermott et al., 2012; Van
Schijndel-Speet, Evenhuis, Van Wijck, Van Montfort, & Echteld, 2016), which may limit the generalizability of the
results. Naaldenberg et al. (2013) called for greater use of other design studies, that can be implemented more
easily, are less expensive and fit the ethical issues experienced in research for people with ID. However, people
with ID are entitled to the same level of evidence based healthcare as all citizens and the RCTs included in this
138541-Willems_BNW.indd 66 31-10-19 10:07
66
activity and nutrition studies. None of the nutrition studies used an RCT design. All case series were of low quality,
except for one physical activity study (Bodde, Seo, Frey, Lohrmann et al., 2012) and one both physical activity
and nutrition study (Pett et al., 2013), which were of medium quality. The most common limitation was the same
for all three categories of studies, namely insufficient blinding of patients/therapists/assessors. The results of the
PEDro quality assessment are provided in Table S4.
4 | DISCUSSION
4.1 | Principal findings
This systematic review aimed to identify the BCTs used in interventions targeting physical activity, nutrition or
both physical activity and nutrition for people with ID, and to describe the quality of these interventions. All
interventions used at least one BCT, but BCTs were rarely used within the context of a theoretical framework for
intervention design. Given their complexity, it is still unclear to what extent BCTs are accessible for people with
ID.
4.2 | Behaviour change techniques
BCTs were used in all interventions, which may indicate that the importance of BCTs is recognized by researchers
developing interventions. Several of the most commonly used BCTs are similar to facilitators of health behaviour
for people with ID as reported by adults with ID (Kuijken et al., 2016). For example, adults with ID reported that
support from others, motivational support and environmental resources can facilitate health behaviour which
reflects two of the most commonly used BCTs found in this review (Kuijken et al., 2016). In fact, most BCTs in this
review are consistent with these facilitators, as they are aimed at providing social support or maintaining the
motivation of participants. This suggests that the BCTs used in the studies included here meet the needs for
health behaviour of people with ID.
However, many of the BCTs included in the CALORE taxonomy are complex and involve a significant amount of
abstraction. This raises a question about the extent to which BCTs are accessible for people with ID. People with
ID may experience challenges to interpret knowledge and may not be able to live healthy although they have the
required knowledge (Kuijken et al., 2016). This might indicate that complex BCTs will not fit into the capabilities
of people with ID, which may make these BCTs ineffective when included in lifestyle change interventions. For
example, a trial of a walking intervention reported that, even with support from carers, most participants with
ID were unable to use pedometers to self-monitor daily step count (Melville et al., 2015). This is particularly
relevant because self-monitoring has been shown to be important to the effectiveness of lifestyle change
interventions (Michie, Fixsen et al., 2009; Michie, Jochelson et al., 2009). It is recommended that researchers
minimize and simplify the BCTs included in lifestyle change interventions for disadvantaged groups (Michie,
Jochelson, Markham, & Bridle, 2009). However, many of the interventions used ten or more BCTs. To tailor
lifestyle change interventions to the needs of people with ID, researchers should consider testing whether
individual BCTs can be made accessible, for example via support from carers, or using assistive technology, and
67
during the design phase of interventions give careful consideration to which, and how many, BCTs should be
included.
4.3 | Quality of the included studies
Low quality scores were found for a majority of the included lifestyle change interventions, as was also found in
a previous review of Scott and Havercamp (2016). In line with another review, the most common limitation was
blinding of participants, therapists and assessors (Ogg-Groenendaal et al., 2014). Additionally, data presentation
was often incomplete and studies mostly failed to report accurate about recruitment of participants, drop-out
rates and baseline similarities. This may result in different interpretations of the intervention content and issues
with representativeness and generalisation of the findings. This is in line with a review of Scott and Havercamp
(2016), which found that most lifestyle change interventions use weak designs. Weak designs made findings
about effectiveness of the included studies less reliable since the design of the study is used to quantitatively
test the study (Scott & Havercamp, 2016). Our findings correspond with the commentary that there is
heterogeneity in reporting intervention content in lifestyle change research (Michie et al., 2011; Naaldenberg et
al., 2013; Ogg-Groenendaal et al., 2014). Heterogeneity is also found for multiple study characteristics, like levels
of disability, setting of the interventions, the targeted populations and the aimed lifestyle change (nutrition or
PA, or both PA and nutrition). Only three studies were aimed at changing nutrition, which makes it hard to
generalise the findings from this category of studies. This might indicate that lifestyle change is dependent on
the specific social and cultural context, and therefore research in this field might need to be tailored to the
specific situation and context of the people with ID. However, the majority of included studies do not properly
describe context related characteristics, as mentioned above. Also, the varying level of disability could affect the
efficacy of the studies, because the level of ID determines the understanding of participants. Therefore,
intervention content needs to be tailored to the capabilities of the participants.
Although a theoretical base is important for interventions in order to be effective and for understanding of the
results, a majority of the included studies did not use any kind of theoretical framework. In addition, the BCTs
were mostly used in an implicit way, not referring to any theoretical base nor describing the BCT explicitly. In the
field of lifestyle change for the general population, the same lack of theoretical base has been found (Golley,
Hendrie, Slater & Corsini, 2011). Furthermore, the RCT is the gold standard to evaluate lifestyle change
interventions (Tones, 2000), but an RCT design was not often used in the included interventions. This could partly
be explained by perceptions about the ethical issues surrounding the inclusion of people with ID in lifestyle
change research. For example, the conflict between one’s own autonomy to participate and the dependence on
family and staff for participation (Maïano et al., 2014; Naaldenberg et al., 2013; Spanos, Melville, & Hankey,
2013). Also, previous research shows high drop-out rates and large amount of incomplete data in lifestyle change
RCTs for people with ID (Bergström, Hagströmer, Hagberg, & Elinder, 2013; McDermott et al., 2012; Van
Schijndel-Speet, Evenhuis, Van Wijck, Van Montfort, & Echteld, 2016), which may limit the generalizability of the
results. Naaldenberg et al. (2013) called for greater use of other design studies, that can be implemented more
easily, are less expensive and fit the ethical issues experienced in research for people with ID. However, people
with ID are entitled to the same level of evidence based healthcare as all citizens and the RCTs included in this
138541-Willems_BNW.indd 67 31-10-19 10:07
68
review suggest that it is feasible to use this design to test the effectiveness of interventions, considering the
mentioned difficulties.
4.4 | Strengths and weaknesses of the review
A strength of this review is the systematic use of the CALO-RE taxonomy to research BCT intervention
components. This systematic way of describing BCTs has been used in the general population (Bird et al., 2013)
but not for people with ID. Another strength is the comprehensive search strategy, which gives a thorough
overview of the field of lifestyle change for people with ID. Finally, the coding of the interventions was conducted
independently by two authors, and then checked for any differences, which increased the reliability and
therefore the quality of this review.
To examine the quality of the interventions, the Physiotherapy Evidence Database (PEDro) Scale was used
whereby the quality coding was checked by two authors. This method increased the reliability of the coding and
therefore the results of this review. The use of PEDro for various intervention designs caused a more general
quality assessment, which may limit the possibility to assess the depth of the studies. However, a general quality
assessment was most appropriate for this review, because we aimed to target the differences in quality between
studies. Additionally, the use of various designs enables a more suitable overview of the actual situation in recent
literature. An even more complete overview would have been provided if not only English articles would have
been included in this review.
4.5 | Implications for future research
A review of the evaluation of effectiveness of interventions is the logical next step to explore possible
relationships between the use of certain BCTs in interventions and the effectiveness of these interventions.
Furthermore, this field could benefit from interventions that are based on an explicitly mentioned theoretical
framework, and a detailed description of intervention content would make a contribution to the existing
knowledge. Since most studies included in this research were of poor quality researchers should aim to use
rigorous designs to minimize the risk of bias.
4.6 | Conclusion
Our findings suggest that the field of lifestyle change for people with ID lacks theory-driven interventions.
Although the inclusion of BCTs can contribute to the quality and effectiveness of lifestyle change interventions,
researchers should strive to include a detailed intervention description and use rigorous research methodologies.
COMPETING INTERESTS
The authors declare that they have no competing interests.
ACKNOWLEDGEMENT
The authors thank Wichor Bramer, the information specialist of the Erasmus MC University Medical Center
Rotterdam, for his support with the design and execution of the literature search.
69
REFERENCES
References marked with an * were included in the review
Abraham, C., & Michie, S. (2008). A taxonomy of behaviour change techniques used in interventions. Health
Psychology, 27(3), 379–387.
* Bartley, J. (2011). Promoting healthy eating and weight loss. Learning Disability Practice, 14(3).
* Bazzano, A. T., Zeldin, A. S., Diab, I. R. S., Garro, N. M., Allevato, N. A., Lehrer, D., & Team, W. P. O. (2009). The
Healthy Lifestyle Change Program: a pilot of a community-based health promotion intervention for
adults with developmental disabilities. American Journal of Preventive Medicine, 37(6), S201-S208.
* Beeken, R. J., Spanos, D., Fovargue, S., Hunter, R., Omar, R., Hassiotis, A., et al. (2013). Piloting a manualised
weight management programme (Shape Up-LD) for overweight and obese persons with mild-moderate
learning disabilities: Study protocol for a pilot randomised controlled trial. Trials, 14(1), 1–9.
* Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention
to improve diet and physical activity among adults with intellectual disabilities in community residences:
A cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847–3857.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used to
promote walking and cycling: A systematic review. Health Psychology, 32(8), 829.
* Bodde, A. E., Seo, D. C., Frey, G. C., Lohrmann, D. K., & Van Puymbroeck, M. (2012). Developing a physical
activity education curriculum for adults with intellectual disabilities. Health Promotion Practice, 13(1),
116–123.
* Bodde, A. E., Seo, D. C., Frey, G. C., Van Puymbroeck, M., & Lohrmann, D. K. (2012). The effect of a designed
health education intervention on physical activity knowledge and participation of adults with intellectual
disabilities. American Journal of Health Promotion, 26(5), 313–316.
* Bradley, S. (2005). Tackling obesity in people with learning disability. Learning Disability Practice, 8(7), 10-14.
Brooker, K., Van Dooren, K., McPherson, L., Lennox, N., & Ware, R. (2015). Systematic review of interventions
aiming to improve involvement in physical activity among adults with intellectual disability. Journal of
Physical Activity and Health, 12(3), 434–444.
* Casey, A., Boyd, C., MacKenzie, S., & Rasmussen, R. (2012). Dual-energy x-ray absorptiometry to measure the
effects of a thirteen-week moderate to vigorous aquatic exercise and nutritional education intervention
on percent body fat in adults with intellectual disabilities from group home settings. Journal of Human
Kinetics, 32, 221-229.
138541-Willems_BNW.indd 68 31-10-19 10:07
68
review suggest that it is feasible to use this design to test the effectiveness of interventions, considering the
mentioned difficulties.
4.4 | Strengths and weaknesses of the review
A strength of this review is the systematic use of the CALO-RE taxonomy to research BCT intervention
components. This systematic way of describing BCTs has been used in the general population (Bird et al., 2013)
but not for people with ID. Another strength is the comprehensive search strategy, which gives a thorough
overview of the field of lifestyle change for people with ID. Finally, the coding of the interventions was conducted
independently by two authors, and then checked for any differences, which increased the reliability and
therefore the quality of this review.
To examine the quality of the interventions, the Physiotherapy Evidence Database (PEDro) Scale was used
whereby the quality coding was checked by two authors. This method increased the reliability of the coding and
therefore the results of this review. The use of PEDro for various intervention designs caused a more general
quality assessment, which may limit the possibility to assess the depth of the studies. However, a general quality
assessment was most appropriate for this review, because we aimed to target the differences in quality between
studies. Additionally, the use of various designs enables a more suitable overview of the actual situation in recent
literature. An even more complete overview would have been provided if not only English articles would have
been included in this review.
4.5 | Implications for future research
A review of the evaluation of effectiveness of interventions is the logical next step to explore possible
relationships between the use of certain BCTs in interventions and the effectiveness of these interventions.
Furthermore, this field could benefit from interventions that are based on an explicitly mentioned theoretical
framework, and a detailed description of intervention content would make a contribution to the existing
knowledge. Since most studies included in this research were of poor quality researchers should aim to use
rigorous designs to minimize the risk of bias.
4.6 | Conclusion
Our findings suggest that the field of lifestyle change for people with ID lacks theory-driven interventions.
Although the inclusion of BCTs can contribute to the quality and effectiveness of lifestyle change interventions,
researchers should strive to include a detailed intervention description and use rigorous research methodologies.
COMPETING INTERESTS
The authors declare that they have no competing interests.
ACKNOWLEDGEMENT
The authors thank Wichor Bramer, the information specialist of the Erasmus MC University Medical Center
Rotterdam, for his support with the design and execution of the literature search.
69
REFERENCES
References marked with an * were included in the review
Abraham, C., & Michie, S. (2008). A taxonomy of behaviour change techniques used in interventions. Health
Psychology, 27(3), 379–387.
* Bartley, J. (2011). Promoting healthy eating and weight loss. Learning Disability Practice, 14(3).
* Bazzano, A. T., Zeldin, A. S., Diab, I. R. S., Garro, N. M., Allevato, N. A., Lehrer, D., & Team, W. P. O. (2009). The
Healthy Lifestyle Change Program: a pilot of a community-based health promotion intervention for
adults with developmental disabilities. American Journal of Preventive Medicine, 37(6), S201-S208.
* Beeken, R. J., Spanos, D., Fovargue, S., Hunter, R., Omar, R., Hassiotis, A., et al. (2013). Piloting a manualised
weight management programme (Shape Up-LD) for overweight and obese persons with mild-moderate
learning disabilities: Study protocol for a pilot randomised controlled trial. Trials, 14(1), 1–9.
* Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L. S. (2013). A multi-component universal intervention
to improve diet and physical activity among adults with intellectual disabilities in community residences:
A cluster randomised controlled trial. Research in Developmental Disabilities, 34(11), 3847–3857.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used to
promote walking and cycling: A systematic review. Health Psychology, 32(8), 829.
* Bodde, A. E., Seo, D. C., Frey, G. C., Lohrmann, D. K., & Van Puymbroeck, M. (2012). Developing a physical
activity education curriculum for adults with intellectual disabilities. Health Promotion Practice, 13(1),
116–123.
* Bodde, A. E., Seo, D. C., Frey, G. C., Van Puymbroeck, M., & Lohrmann, D. K. (2012). The effect of a designed
health education intervention on physical activity knowledge and participation of adults with intellectual
disabilities. American Journal of Health Promotion, 26(5), 313–316.
* Bradley, S. (2005). Tackling obesity in people with learning disability. Learning Disability Practice, 8(7), 10-14.
Brooker, K., Van Dooren, K., McPherson, L., Lennox, N., & Ware, R. (2015). Systematic review of interventions
aiming to improve involvement in physical activity among adults with intellectual disability. Journal of
Physical Activity and Health, 12(3), 434–444.
* Casey, A., Boyd, C., MacKenzie, S., & Rasmussen, R. (2012). Dual-energy x-ray absorptiometry to measure the
effects of a thirteen-week moderate to vigorous aquatic exercise and nutritional education intervention
on percent body fat in adults with intellectual disabilities from group home settings. Journal of Human
Kinetics, 32, 221-229.
138541-Willems_BNW.indd 69 31-10-19 10:07
70
Caton, S., Chadwick, D., Chapman, M., Turnbull, S., Mitchell, D., & Stansfield, J. (2012). Healthy lifestyles for adults
with intellectual disability: Knowledge, barriers and facilitators. Journal of Intellectual & Developmental
Disability, 37(3), 248–259.
* Chapman, M. J., Craven, M. J., & Chadwick, D. D. (2005). Fighting fit? An evaluation of health practitioner input
to improve healthy living and reduce obesity for adults with learning disabilities. Journal of Intellectual
Disabilities, 9(2), 131-144.
* Chapman, M. J., Craven, M. J., & Chadwick, D. D. (2008). Following up fighting fit: the long-term impact of health
practitioner input on obesity and BMI amongst adults with intellectual disabilities. Journal of Intellectual
Disabilities, 12(4), 309-323.
* Cluphf, D., O’Connor, J., & Vanin, S. (2001). Effects of aerobic dance on the cardiovascular endurance of adults
with intellectual disabilities. Adapted Physical Activity Quarterly, 18(1), 60-71.
* Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., ... & Fleming, R. K. (2013). Parent support
improves weight loss in adolescents and young adults with Down syndrome. The Journal of Pediatrics,
163(5), 1402-1408.
Dombrowski, S. U., Sniehotta, F. F., Avenell, A., Johnston, M., MacLennan, G., & Araújo-Soares, V. (2012).
Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related
co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychology
Review, 6(1), 7–32.
* Donnelly, J. E., Saunders, R. R., Saunders, M., Washburn, R. A., Sullivan, D. K., Gibson, C. A., . . . & Rondon, M.
R. (2013). Weight management for individuals with intellectual and developmental disabilities: rationale
and design for an 18 month randomized trial. Contemporary Clinical Trials, 36(1), 116-124.
* Elinder, L. S., Bergström, H., Hagberg, J., Wihlman, U., & Hagströmer, M. (2010). Promoting a healthy diet and
physical activity in adults with intellectual disabilities living in community residences: Design and
evaluation of a cluster-randomized intervention. BMC Public Health, 10(1), 761.
* Ewing, G., McDermott, S., Thomas-Koger, M., Whitner, W., & Pierce, K. (2004). Evaluation of a cardiovascular
health program for participants with mental retardation and normal learners. Health Education &
Behavior, 31(1), 77-87.
* Geller, J. S., & Crowley, M. (2009). An empowerment group visit model as treatment for obesity in
developmentally delayed adults. Journal of Developmental and Physical Disabilities, 21(5), 345-353.
Golley, R. K., Hendrie, G. A., Slater, A., & Corsini, N. (2011). Interventions that involve parents to improve
children’s weight-related nutrition intake and activity patterns—what nutrition and activity targets and
behaviour change techniques are associated with intervention effectiveness? Obesity Reviews, 12(2),
114–130.
71
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., et al. (2011). Systematic
review of reviews of intervention components associated with increased effectiveness in dietary and
physical activity interventions. BMC Public Health, 11(1), 119.
Hermans, H., & Evenhuis, H. M. (2014). Multimorbidity in older adults with intellectual disabilities. Research in
Developmental Disabilities, 35(4), 776–783.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual disability.
Journal of Intellectual Disability Research: JIDR, 58(9), 851–863.
* Hubbard, K. L., Bandini, L. G., Folta, S. C., Wansink, B., & Must, A. (2014). The Adaptation of a School‐based
Health Promotion Programme for Youth with Intellectual and Developmental Disabilities: A Community
Engaged Research Process. Journal of Applied Research in Intellectual Disabilities, 27(6), 576-590.
* Jones, M. C., Walley, R. M., Leech, A., Paterson, M., Common, S., & Metcalf, C. (2007). Behavioral and
Psychosocial Outcomes of a 16‐Week Rebound Therapy‐Based Exercise Program for People with
Profound Intellectual Disabilities. Journal of Policy and Practice in Intellectual Disabilities, 4(2), 111-119.
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-Van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
* Lante, K., Stancliffe, R. J., Bauman, A., van der Ploeg, H. P., Jan, S., & Davis, G. M. (2014). Embedding sustainable
physical activities into the everyday lives of adults with intellectual disabilities: a randomised controlled
trial. BMC Public Health, 14(1), 1038.
Loveman, E., Frampton, G. K., Shepherd, J., Picot, J., Cooper, K., Bryant, J., et al. (2011). The clinical effectiveness
and cost-effectiveness of long-term weight management schemes for adults: A systematic review.
Health Technology Assessment-Southampton, 15(2), 1–182.
Maïano, C., Normand, C. L., Aimé, A., & Bégarie, J. (2014). Lifestyle interventions targeting changes in body weight
and composition among youth with an intellectual disability: A systematic review. Research in
Developmental Disabilities, 35(8), 1914–1926.
Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., & Elkins, M. (2003). Reliability of the PEDro scale for
rating quality of randomized controlled trials. Physical Therapy, 83(8), 713–721.
Malik, S. H., Blake, H., & Suggs, L. S. (2014). A systematic review of workplace health promotion interventions for
increasing physical activity. British Journal of Health Psychology, 19(1), 149–180.
138541-Willems_BNW.indd 70 31-10-19 10:07
70
Caton, S., Chadwick, D., Chapman, M., Turnbull, S., Mitchell, D., & Stansfield, J. (2012). Healthy lifestyles for adults
with intellectual disability: Knowledge, barriers and facilitators. Journal of Intellectual & Developmental
Disability, 37(3), 248–259.
* Chapman, M. J., Craven, M. J., & Chadwick, D. D. (2005). Fighting fit? An evaluation of health practitioner input
to improve healthy living and reduce obesity for adults with learning disabilities. Journal of Intellectual
Disabilities, 9(2), 131-144.
* Chapman, M. J., Craven, M. J., & Chadwick, D. D. (2008). Following up fighting fit: the long-term impact of health
practitioner input on obesity and BMI amongst adults with intellectual disabilities. Journal of Intellectual
Disabilities, 12(4), 309-323.
* Cluphf, D., O’Connor, J., & Vanin, S. (2001). Effects of aerobic dance on the cardiovascular endurance of adults
with intellectual disabilities. Adapted Physical Activity Quarterly, 18(1), 60-71.
* Curtin, C., Bandini, L. G., Must, A., Gleason, J., Lividini, K., Phillips, S., ... & Fleming, R. K. (2013). Parent support
improves weight loss in adolescents and young adults with Down syndrome. The Journal of Pediatrics,
163(5), 1402-1408.
Dombrowski, S. U., Sniehotta, F. F., Avenell, A., Johnston, M., MacLennan, G., & Araújo-Soares, V. (2012).
Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related
co-morbidities or additional risk factors for co-morbidities: A systematic review. Health Psychology
Review, 6(1), 7–32.
* Donnelly, J. E., Saunders, R. R., Saunders, M., Washburn, R. A., Sullivan, D. K., Gibson, C. A., . . . & Rondon, M.
R. (2013). Weight management for individuals with intellectual and developmental disabilities: rationale
and design for an 18 month randomized trial. Contemporary Clinical Trials, 36(1), 116-124.
* Elinder, L. S., Bergström, H., Hagberg, J., Wihlman, U., & Hagströmer, M. (2010). Promoting a healthy diet and
physical activity in adults with intellectual disabilities living in community residences: Design and
evaluation of a cluster-randomized intervention. BMC Public Health, 10(1), 761.
* Ewing, G., McDermott, S., Thomas-Koger, M., Whitner, W., & Pierce, K. (2004). Evaluation of a cardiovascular
health program for participants with mental retardation and normal learners. Health Education &
Behavior, 31(1), 77-87.
* Geller, J. S., & Crowley, M. (2009). An empowerment group visit model as treatment for obesity in
developmentally delayed adults. Journal of Developmental and Physical Disabilities, 21(5), 345-353.
Golley, R. K., Hendrie, G. A., Slater, A., & Corsini, N. (2011). Interventions that involve parents to improve
children’s weight-related nutrition intake and activity patterns—what nutrition and activity targets and
behaviour change techniques are associated with intervention effectiveness? Obesity Reviews, 12(2),
114–130.
71
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., et al. (2011). Systematic
review of reviews of intervention components associated with increased effectiveness in dietary and
physical activity interventions. BMC Public Health, 11(1), 119.
Hermans, H., & Evenhuis, H. M. (2014). Multimorbidity in older adults with intellectual disabilities. Research in
Developmental Disabilities, 35(4), 776–783.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual disability.
Journal of Intellectual Disability Research: JIDR, 58(9), 851–863.
* Hubbard, K. L., Bandini, L. G., Folta, S. C., Wansink, B., & Must, A. (2014). The Adaptation of a School‐based
Health Promotion Programme for Youth with Intellectual and Developmental Disabilities: A Community
Engaged Research Process. Journal of Applied Research in Intellectual Disabilities, 27(6), 576-590.
* Jones, M. C., Walley, R. M., Leech, A., Paterson, M., Common, S., & Metcalf, C. (2007). Behavioral and
Psychosocial Outcomes of a 16‐Week Rebound Therapy‐Based Exercise Program for People with
Profound Intellectual Disabilities. Journal of Policy and Practice in Intellectual Disabilities, 4(2), 111-119.
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-Van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
* Lante, K., Stancliffe, R. J., Bauman, A., van der Ploeg, H. P., Jan, S., & Davis, G. M. (2014). Embedding sustainable
physical activities into the everyday lives of adults with intellectual disabilities: a randomised controlled
trial. BMC Public Health, 14(1), 1038.
Loveman, E., Frampton, G. K., Shepherd, J., Picot, J., Cooper, K., Bryant, J., et al. (2011). The clinical effectiveness
and cost-effectiveness of long-term weight management schemes for adults: A systematic review.
Health Technology Assessment-Southampton, 15(2), 1–182.
Maïano, C., Normand, C. L., Aimé, A., & Bégarie, J. (2014). Lifestyle interventions targeting changes in body weight
and composition among youth with an intellectual disability: A systematic review. Research in
Developmental Disabilities, 35(8), 1914–1926.
Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., & Elkins, M. (2003). Reliability of the PEDro scale for
rating quality of randomized controlled trials. Physical Therapy, 83(8), 713–721.
Malik, S. H., Blake, H., & Suggs, L. S. (2014). A systematic review of workplace health promotion interventions for
increasing physical activity. British Journal of Health Psychology, 19(1), 149–180.
138541-Willems_BNW.indd 71 31-10-19 10:07
72
* Mann, J., Zhou, H., McDermott, S., & Poston, M. B. (2006). Healthy behavior change of adults with mental
retardation: attendance in a health promotion program. American Journal on Mental Retardation,
111(1), 62-73.
* Marks, B., Sisirak, J., Heller, T., & Wagner, M. (2010). Evaluation of community‐based health promotion
programs for Special Olympics athletes. Journal of Policy and Practice in Intellectual Disabilities, 7(2),
119-129.
* Marshall, D., McConkey, R., & Moore, G. (2003). Obesity in people with intellectual disabilities: the impact of
nurse‐led health screenings and health promotion activities. Journal of Advanced Nursing, 41(2), 147
153.
* McDermott, S., Whitner, W., Thomas-Koger, M., Mann, J. R., Clarkson, J., Barnes, T. L., et al. (2012). An efficacy
trial of ‘Steps to Your Health’, a health promotion programme for adults with intellectual disability.
Health Education Journal, 71(3), 278–290.
* Melville, C. A., Boyle, S., Miller, S., Macmillan, S., Penpraze, V., Pert, C., . . . & Hankey, C. R. (2011). An open
study of the effectiveness of a multi-component weight-loss intervention for adults with intellectual
disabilities and obesity. British Journal of Nutrition, 105(10), 1553-1562.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223–230.
Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., et al. (2015). Effectiveness
of a walking programme to support adults with intellectual disabilities to increase physical activity: Walk
well cluster-randomised controlled trial. International Journal of Behavioral Nutrition and Physical
Activity, 12(1), 1–11.
Messent, P. R., Cooke, C., & Long, J. (1999). What choice: A consideration of the level of opportunity for people
with mild and moderate learning disabilities to lead a physically active lifestyle. British Journal of
Learning Disabilities, 27(2), 73–77.
Michie, S., Ashford, S., Sniehotta, F. F., Dombrowski, S. U., Bishop, A., & French, D. P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479–1498.
Michie, S., Fixsen, D., Grimshaw, J. M., & Eccles, M. P. (2009). Specifying and reporting complex behaviour change
interventions: The need for a scientific method. Implementation Science, 4(40), 1–6.
Michie, S., Jochelson, K., Markham, W. A., & Bridle, C. (2009). Low-income groups and behaviour change
interventions: A review of intervention content, effectiveness and theoretical frameworks. Journal of
Epidemiology & Community Health, 63(8), 610–622.
73
* Mitchell, F., Melville, C., Stalker, K., Matthews, L., McConnachie, A., Murray, H., et al. (2013). Walk well: A
randomised controlled trial of a walking intervention for adults with intellectual disabilities: Study
protocol. BMC Public Health, 13(1), 1–13.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: A structured review of literature. Research in
Developmental Disabilities, 34(12), 4534–4545.
Ogg-Groenendaal, M., Hermans, H., & Claessens, B. (2014). A systematic review on the effect of exercise
interventions on challenging behavior for people with intellectual disabilities. Research in
Developmental Disabilities, 35(7), 1507–1517.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: A
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity,
10(29), 1–15.
* Pérez-Cruzado, D., & Cuesta-Vargas, A. I. (2013). Improving adherence physical activity with a smartphone
application based on adults with intellectual disabilities (APPCOID). BMC public health, 13(1), 1173.
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
* Pett, M., Clark, L., Eldredge, A., Cardell, B., Jordan, K., Chambless, C., et al. (2013). Effecting healthy lifestyle
changes in overweight and obese young adults with intellectual disability. American Journal on
Intellectual and Developmental Disabilities, 118(3), 224–243.
Physiotherapy Evidence Database PEDro Scale. Retrieved 10.07.15, from www.pedro.org.au.
* Pitetti, K. H., Rendoff, A. D., Grover, T., & Beets, M. W. (2007). The efficacy of a 9-month treadmill walking
program on the exercise capacity and weight reduction for adolescents with severe autism. Journal of
Autism and Developmental Disorders, 37(6), 997-1006.
* Podgorski, C. A., Kessler, K., Cacia, B., Peterson, D. R., & Henderson, C. M. (2004). Physical activity intervention
for older adults with intellectual disability: report on a pilot project. Mental retardation, 42(4), 272-283.
* Ptomey, L. T., Sullivan, D. K., Lee, J., Goetz, J. R., Gibson, C., & Donnelly, J. E. (2015). The use of technology for
delivering a weight loss program for adolescents with intellectual and developmental disabilities.
Journal of the Academy of Nutrition and Dietetics, 115(1), 112-118.
Reeves, B. C., Deeks, J. J., Higgins, J. P. T., & Wells, G. A. (2008). Chapter 13: Including non- randomized studies.
In: Higgins, J. P. T., & Green, S. (Eds), Cochrane Handbook for Systematic Reviews of Interventions.
Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from
www.cochrane-handbook.org.
138541-Willems_BNW.indd 72 31-10-19 10:07
72
* Mann, J., Zhou, H., McDermott, S., & Poston, M. B. (2006). Healthy behavior change of adults with mental
retardation: attendance in a health promotion program. American Journal on Mental Retardation,
111(1), 62-73.
* Marks, B., Sisirak, J., Heller, T., & Wagner, M. (2010). Evaluation of community‐based health promotion
programs for Special Olympics athletes. Journal of Policy and Practice in Intellectual Disabilities, 7(2),
119-129.
* Marshall, D., McConkey, R., & Moore, G. (2003). Obesity in people with intellectual disabilities: the impact of
nurse‐led health screenings and health promotion activities. Journal of Advanced Nursing, 41(2), 147
153.
* McDermott, S., Whitner, W., Thomas-Koger, M., Mann, J. R., Clarkson, J., Barnes, T. L., et al. (2012). An efficacy
trial of ‘Steps to Your Health’, a health promotion programme for adults with intellectual disability.
Health Education Journal, 71(3), 278–290.
* Melville, C. A., Boyle, S., Miller, S., Macmillan, S., Penpraze, V., Pert, C., . . . & Hankey, C. R. (2011). An open
study of the effectiveness of a multi-component weight-loss intervention for adults with intellectual
disabilities and obesity. British Journal of Nutrition, 105(10), 1553-1562.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223–230.
Melville, C. A., Mitchell, F., Stalker, K., Matthews, L., McConnachie, A., Murray, H. M., et al. (2015). Effectiveness
of a walking programme to support adults with intellectual disabilities to increase physical activity: Walk
well cluster-randomised controlled trial. International Journal of Behavioral Nutrition and Physical
Activity, 12(1), 1–11.
Messent, P. R., Cooke, C., & Long, J. (1999). What choice: A consideration of the level of opportunity for people
with mild and moderate learning disabilities to lead a physically active lifestyle. British Journal of
Learning Disabilities, 27(2), 73–77.
Michie, S., Ashford, S., Sniehotta, F. F., Dombrowski, S. U., Bishop, A., & French, D. P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479–1498.
Michie, S., Fixsen, D., Grimshaw, J. M., & Eccles, M. P. (2009). Specifying and reporting complex behaviour change
interventions: The need for a scientific method. Implementation Science, 4(40), 1–6.
Michie, S., Jochelson, K., Markham, W. A., & Bridle, C. (2009). Low-income groups and behaviour change
interventions: A review of intervention content, effectiveness and theoretical frameworks. Journal of
Epidemiology & Community Health, 63(8), 610–622.
73
* Mitchell, F., Melville, C., Stalker, K., Matthews, L., McConnachie, A., Murray, H., et al. (2013). Walk well: A
randomised controlled trial of a walking intervention for adults with intellectual disabilities: Study
protocol. BMC Public Health, 13(1), 1–13.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: A structured review of literature. Research in
Developmental Disabilities, 34(12), 4534–4545.
Ogg-Groenendaal, M., Hermans, H., & Claessens, B. (2014). A systematic review on the effect of exercise
interventions on challenging behavior for people with intellectual disabilities. Research in
Developmental Disabilities, 35(7), 1507–1517.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: A
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity,
10(29), 1–15.
* Pérez-Cruzado, D., & Cuesta-Vargas, A. I. (2013). Improving adherence physical activity with a smartphone
application based on adults with intellectual disabilities (APPCOID). BMC public health, 13(1), 1173.
Peterson, J. J., Janz, K. F., & Lowe, J. B. (2008). Physical activity among adults with intellectual disabilities living in
community settings. Preventive Medicine, 47(1), 101–106.
* Pett, M., Clark, L., Eldredge, A., Cardell, B., Jordan, K., Chambless, C., et al. (2013). Effecting healthy lifestyle
changes in overweight and obese young adults with intellectual disability. American Journal on
Intellectual and Developmental Disabilities, 118(3), 224–243.
Physiotherapy Evidence Database PEDro Scale. Retrieved 10.07.15, from www.pedro.org.au.
* Pitetti, K. H., Rendoff, A. D., Grover, T., & Beets, M. W. (2007). The efficacy of a 9-month treadmill walking
program on the exercise capacity and weight reduction for adolescents with severe autism. Journal of
Autism and Developmental Disorders, 37(6), 997-1006.
* Podgorski, C. A., Kessler, K., Cacia, B., Peterson, D. R., & Henderson, C. M. (2004). Physical activity intervention
for older adults with intellectual disability: report on a pilot project. Mental retardation, 42(4), 272-283.
* Ptomey, L. T., Sullivan, D. K., Lee, J., Goetz, J. R., Gibson, C., & Donnelly, J. E. (2015). The use of technology for
delivering a weight loss program for adolescents with intellectual and developmental disabilities.
Journal of the Academy of Nutrition and Dietetics, 115(1), 112-118.
Reeves, B. C., Deeks, J. J., Higgins, J. P. T., & Wells, G. A. (2008). Chapter 13: Including non- randomized studies.
In: Higgins, J. P. T., & Green, S. (Eds), Cochrane Handbook for Systematic Reviews of Interventions.
Version 5.0.1 [updated September 2008]. The Cochrane Collaboration, 2008. Available from
www.cochrane-handbook.org.
138541-Willems_BNW.indd 73 31-10-19 10:07
74
Robertson, J., Emerson, E., Gregory, N., Hatto, C., Turner, S., Kessissoglou, S., et al. (2000). Lifestyle related risk
factors for poor health in residential settings for people with intellectual disabilities. Research in
Developmental Disabilities, 21(6), 469–486.
* Sailer, A. B., Miltenberger, R. G., Johnson, B., Zetocha, K., Egemo-Helm, K., & Hegstad, H. (2006). Evaluation of
a weight loss treatment program for individuals with mild mental retardation. Child & Family Behaviour
Therapy, 28(2), 15-28.
* Saunders, R. R., Saunders, M. D., Donnelly, J. E., Smith, B. K., Sullivan, D. K., Guilford, B., & Rondon, M. F. (2011).
Evaluation of an approach to weight loss in adults with intellectual or developmental disabilities.
Intellectual and Developmental Disabilities, 49(2), 103-112.
Scott, H. M., & Havercamp, S. M. (2016). Systematic review of health promotion programs focused on behavioral
changes for people with intellectual disability. Intellectual and Developmental Disabilities, 54(1), 63–76.
Sherrington, C., Herbert, R. D., Maher, C. G., & Moseley, A. M. (2000). PEDro. A database of randomized trials
and systematic reviews in physiotherapy. Manual Therapy, 5(4), 223–226.
* Shields, N., Taylor, N. F., & Fernhall, B. (2010). A study protocol of a randomised controlled trial to investigate
if a community based strength training programme improves work task performance in young adults
with Down syndrome. BMC Pediatrics, 10(1), 17.
* Shields, N., Taylor, N. F., Wee, E., Wollersheim, D., O'Shea, S. D., & Fernhall, B. (2013). A community-based
strength training programme increases muscle strength and physical activity in young people with Down
syndrome: A randomised controlled trial. Research in Developmental Disabilities, 34(12), 4385-4394.
* Spanos, D., Hankey, C., Boyle, S., & Melville, C. (2014). Comparing the effectiveness of a multi‐component
weight loss intervention in adults with and without intellectual disabilities. Journal of Human Nutrition
and Dietetics, 27(1), 22-29.
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with intellectual
disabilities and obesity: A systematic review of the evidence. Nutrition Journal, 12, 1–16.
* Stanish, H. I., & Temple, V. A. (2012). Efficacy of a peer‐guided exercise programme for adolescents with
intellectual disability. Journal of Applied Research in Intellectual Disabilities, 25(4), 319-328.
Temple, V. A., Frey, G. C., & Stanish, H. I. (2006). Physical activity of adults with mental retardation: Review and
research needs. American Journal of Health Promotion, 21(1), 2–12.
* Temple, V. A., & Stanish, H. I. (2011). The feasibility of using a peer-guided model to enhance participation in
community-based physical activity for youth with intellectual disability. Journal of Intellectual
Disabilities, 15(3), 209-217.
75
* Thomas, G. R., & Kerr, M. P. (2011). Longitudinal follow-up of weight change in the context of a community
based health promotion programme for adults with an intellectual disability. Journal of Applied Research
in Intellectual Disabilities, 24(4), 381–387.
Tones, K. (2000). Evaluating health promotion: A tale of three errors. Patient Education and Counseling, 39(2),
227–236.
* Ulrich, D. A., Burghardt, A. R., Lloyd, M., Tiernan, C., & Hornyak, J. E. (2011). Physical activity benefits of learning
to ride a two-wheel bicycle for children with Down syndrome: a randomized trial. Physical Therapy,
91(10), 1463-1477.
* Van Schijndel-Speet, M., Evenhuis, H. M., Van Empelen, P., Van Wijck, R., & Echteld, M. A. (2013). Development
and evaluation of a structured programme for promoting physical activity among seniors with
intellectual disabilities: A study protocol for a cluster randomized trial. BMC Public Health, 13(1), 1–11.
* Van Schijndel‐Speet, M., Evenhuis, H. M., van Wijck, R., & Echteld, M. A. (2014). Implementation of a group
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Montfort, K. C. A. G. M., & Echteld, M. A. (2016). A
structured physical activity and fitness programme for older adults with intellectual disabilities: Results
of a cluster- randomised clinical trial. Journal of Intellectual Disability Research, 61(1), 16-29.
https://doi.org/10.1111/jir.12267
Van Schijndel-Speet M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544.
Van Schrojenstein Lantman-De Valk, H. M. J., & Walsh, P. N. (2008). Managing health problems in people with
intellectual disabilities. British Medical Journal: BMJ, 8(1), A2507.
* Wallén, E. F., Müllerdorf, M., Christensson, K., & Marcus, C. (2013). Eating Patterns among Students with
Intellectual Disabilities after a Multifactorial School Intervention Using the Plate Model. Journal of Policy
and Practice in Intellectual Disabilities, 10(1), 45-53.
* Wallén, E. F., Müllersdorf, M., Christensson, K., & Marcus, C. (2013). A school-based intervention associated
with improvements in cardiometabolic risk profiles in young people with intellectual disabilities. Journal
of Intellectual Disabilities, 17(1), 38-50.
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
138541-Willems_BNW.indd 74 31-10-19 10:07
74
Robertson, J., Emerson, E., Gregory, N., Hatto, C., Turner, S., Kessissoglou, S., et al. (2000). Lifestyle related risk
factors for poor health in residential settings for people with intellectual disabilities. Research in
Developmental Disabilities, 21(6), 469–486.
* Sailer, A. B., Miltenberger, R. G., Johnson, B., Zetocha, K., Egemo-Helm, K., & Hegstad, H. (2006). Evaluation of
a weight loss treatment program for individuals with mild mental retardation. Child & Family Behaviour
Therapy, 28(2), 15-28.
* Saunders, R. R., Saunders, M. D., Donnelly, J. E., Smith, B. K., Sullivan, D. K., Guilford, B., & Rondon, M. F. (2011).
Evaluation of an approach to weight loss in adults with intellectual or developmental disabilities.
Intellectual and Developmental Disabilities, 49(2), 103-112.
Scott, H. M., & Havercamp, S. M. (2016). Systematic review of health promotion programs focused on behavioral
changes for people with intellectual disability. Intellectual and Developmental Disabilities, 54(1), 63–76.
Sherrington, C., Herbert, R. D., Maher, C. G., & Moseley, A. M. (2000). PEDro. A database of randomized trials
and systematic reviews in physiotherapy. Manual Therapy, 5(4), 223–226.
* Shields, N., Taylor, N. F., & Fernhall, B. (2010). A study protocol of a randomised controlled trial to investigate
if a community based strength training programme improves work task performance in young adults
with Down syndrome. BMC Pediatrics, 10(1), 17.
* Shields, N., Taylor, N. F., Wee, E., Wollersheim, D., O'Shea, S. D., & Fernhall, B. (2013). A community-based
strength training programme increases muscle strength and physical activity in young people with Down
syndrome: A randomised controlled trial. Research in Developmental Disabilities, 34(12), 4385-4394.
* Spanos, D., Hankey, C., Boyle, S., & Melville, C. (2014). Comparing the effectiveness of a multi‐component
weight loss intervention in adults with and without intellectual disabilities. Journal of Human Nutrition
and Dietetics, 27(1), 22-29.
Spanos, D., Melville, C. A., & Hankey, C. R. (2013). Weight management interventions in adults with intellectual
disabilities and obesity: A systematic review of the evidence. Nutrition Journal, 12, 1–16.
* Stanish, H. I., & Temple, V. A. (2012). Efficacy of a peer‐guided exercise programme for adolescents with
intellectual disability. Journal of Applied Research in Intellectual Disabilities, 25(4), 319-328.
Temple, V. A., Frey, G. C., & Stanish, H. I. (2006). Physical activity of adults with mental retardation: Review and
research needs. American Journal of Health Promotion, 21(1), 2–12.
* Temple, V. A., & Stanish, H. I. (2011). The feasibility of using a peer-guided model to enhance participation in
community-based physical activity for youth with intellectual disability. Journal of Intellectual
Disabilities, 15(3), 209-217.
75
* Thomas, G. R., & Kerr, M. P. (2011). Longitudinal follow-up of weight change in the context of a community
based health promotion programme for adults with an intellectual disability. Journal of Applied Research
in Intellectual Disabilities, 24(4), 381–387.
Tones, K. (2000). Evaluating health promotion: A tale of three errors. Patient Education and Counseling, 39(2),
227–236.
* Ulrich, D. A., Burghardt, A. R., Lloyd, M., Tiernan, C., & Hornyak, J. E. (2011). Physical activity benefits of learning
to ride a two-wheel bicycle for children with Down syndrome: a randomized trial. Physical Therapy,
91(10), 1463-1477.
* Van Schijndel-Speet, M., Evenhuis, H. M., Van Empelen, P., Van Wijck, R., & Echteld, M. A. (2013). Development
and evaluation of a structured programme for promoting physical activity among seniors with
intellectual disabilities: A study protocol for a cluster randomized trial. BMC Public Health, 13(1), 1–11.
* Van Schijndel‐Speet, M., Evenhuis, H. M., van Wijck, R., & Echteld, M. A. (2014). Implementation of a group
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., Montfort, K. C. A. G. M., & Echteld, M. A. (2016). A
structured physical activity and fitness programme for older adults with intellectual disabilities: Results
of a cluster- randomised clinical trial. Journal of Intellectual Disability Research, 61(1), 16-29.
https://doi.org/10.1111/jir.12267
Van Schijndel-Speet M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544.
Van Schrojenstein Lantman-De Valk, H. M. J., & Walsh, P. N. (2008). Managing health problems in people with
intellectual disabilities. British Medical Journal: BMJ, 8(1), A2507.
* Wallén, E. F., Müllerdorf, M., Christensson, K., & Marcus, C. (2013). Eating Patterns among Students with
Intellectual Disabilities after a Multifactorial School Intervention Using the Plate Model. Journal of Policy
and Practice in Intellectual Disabilities, 10(1), 45-53.
* Wallén, E. F., Müllersdorf, M., Christensson, K., & Marcus, C. (2013). A school-based intervention associated
with improvements in cardiometabolic risk profiles in young people with intellectual disabilities. Journal
of Intellectual Disabilities, 17(1), 38-50.
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
138541-Willems_BNW.indd 75 31-10-19 10:07
76
WHO. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. Geneva,
Switzerland: World Health Organization.
* Wilhite, B., Biren, G., & Spencer, L. (2012). Fitness intervention for adults with developmental disabilities and
their caregivers. Therapeutic Recreation Journal, 46(4), 245.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308–322.
* Yen, C. F., Lin, J. D., Wu, C. L., & Hu, J. (2012). Promotion of physical exercise in institutionalized people with
intellectual disabilities: age and gender effects. International Journal of Developmental Disabilities,
58(2), 85-94.
77
APPENDICES
APPENDIX 1 – Search string for database searches
Embase.com
('mental deficiency'/exp OR 'intellectual impairment'/de OR (((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down*
NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND (('lifestyle modification'/exp OR 'diet therapy'/de OR 'diet restriction'/exp
OR 'low calory diet'/exp OR 'low carbohydrate diet'/exp OR 'low fat diet'/exp OR 'weight control'/exp OR 'weight
reduction'/exp OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR
restrict* OR therap* OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction
OR control*))):ab,ti) OR (('dietary intake'/de OR lifestyle/exp OR 'sedentary lifestyle'/exp OR 'body mass'/exp OR 'physical
activity'/exp OR exercise/exp OR kinesiotherapy/exp OR 'treadmill exercise'/exp OR obesity/exp OR ('body mass' OR bmi OR
lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR kinesiotherap* OR
kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) NEAR/3
intake*)):ab,ti) AND ('education program'/exp OR 'health education'/de OR 'health promotion'/de OR 'nutrition
education'/de OR 'program development'/exp OR 'program evaluation'/exp OR 'health program'/exp OR 'intervention
study'/exp OR 'randomized controlled trial'/exp OR (program* OR promoti* OR educat* OR interven* OR randomi* OR
trial*):ab,ti))) NOT ([Conference Abstract]/lim OR [Letter]/lim OR [Note]/lim OR [Conference Paper]/lim OR [Editorial]/lim)
AND [english]/lim NOT ([animals]/lim NOT [humans]/lim)
Medline (OvidSP)
(exp Intellectual Disability/ OR Mentally Disabled Persons/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR prader willi).ab,ti.) AND ((diet therapy/ OR diet therapy.xs. OR Caloric Restriction/ OR "Diet, Reducing"/
OR "Diet, Carbohydrate-Restricted"/ OR "Diet, Fat-Restricted"/ OR Weight Loss/ OR Weight Reduction Programs/ OR
(((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR
treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*))).ab,ti.) OR ((life
style/ OR sedentary lifestyle/ OR body mass index/ OR exp exercise/ OR exp exercise therapy/ OR exp Overweight/ OR (body
mass OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap*
OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3
intake*)).ab,ti.) AND (health education/ OR "Patient Education as Topic"/ OR exp health promotion/ OR program
development/ OR program evaluation/ OR intervention studies/ OR randomized controlled trial.pt. OR (program* OR
promoti* OR educat* OR interven* OR randomi* OR trial*).ab,ti.))) NOT (letter OR news OR comment OR editorial OR
congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cochrane
((((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND
(((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*))):ab,ti)
OR ((('body mass' OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*)):ab,ti) AND ((program* OR promoti* OR educat* OR interven* OR randomi* OR trial*):ab,ti)) )
138541-Willems_BNW.indd 76 31-10-19 10:07

76
WHO. (2009). Global health risks: Mortality and burden of disease attributable to selected major risks. Geneva,
Switzerland: World Health Organization.
* Wilhite, B., Biren, G., & Spencer, L. (2012). Fitness intervention for adults with developmental disabilities and
their caregivers. Therapeutic Recreation Journal, 46(4), 245.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308–322.
* Yen, C. F., Lin, J. D., Wu, C. L., & Hu, J. (2012). Promotion of physical exercise in institutionalized people with
intellectual disabilities: age and gender effects. International Journal of Developmental Disabilities,
58(2), 85-94.
77
APPENDICES
APPENDIX 1 – Search string for database searches
Embase.com
('mental deficiency'/exp OR 'intellectual impairment'/de OR (((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down*
NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND (('lifestyle modification'/exp OR 'diet therapy'/de OR 'diet restriction'/exp
OR 'low calory diet'/exp OR 'low carbohydrate diet'/exp OR 'low fat diet'/exp OR 'weight control'/exp OR 'weight
reduction'/exp OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR
restrict* OR therap* OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction
OR control*))):ab,ti) OR (('dietary intake'/de OR lifestyle/exp OR 'sedentary lifestyle'/exp OR 'body mass'/exp OR 'physical
activity'/exp OR exercise/exp OR kinesiotherapy/exp OR 'treadmill exercise'/exp OR obesity/exp OR ('body mass' OR bmi OR
lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR kinesiotherap* OR
kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) NEAR/3
intake*)):ab,ti) AND ('education program'/exp OR 'health education'/de OR 'health promotion'/de OR 'nutrition
education'/de OR 'program development'/exp OR 'program evaluation'/exp OR 'health program'/exp OR 'intervention
study'/exp OR 'randomized controlled trial'/exp OR (program* OR promoti* OR educat* OR interven* OR randomi* OR
trial*):ab,ti))) NOT ([Conference Abstract]/lim OR [Letter]/lim OR [Note]/lim OR [Conference Paper]/lim OR [Editorial]/lim)
AND [english]/lim NOT ([animals]/lim NOT [humans]/lim)
Medline (OvidSP)
(exp Intellectual Disability/ OR Mentally Disabled Persons/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap* OR
disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR prader willi).ab,ti.) AND ((diet therapy/ OR diet therapy.xs. OR Caloric Restriction/ OR "Diet, Reducing"/
OR "Diet, Carbohydrate-Restricted"/ OR "Diet, Fat-Restricted"/ OR Weight Loss/ OR Weight Reduction Programs/ OR
(((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap* OR
treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*))).ab,ti.) OR ((life
style/ OR sedentary lifestyle/ OR body mass index/ OR exp exercise/ OR exp exercise therapy/ OR exp Overweight/ OR (body
mass OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap*
OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3
intake*)).ab,ti.) AND (health education/ OR "Patient Education as Topic"/ OR exp health promotion/ OR program
development/ OR program evaluation/ OR intervention studies/ OR randomized controlled trial.pt. OR (program* OR
promoti* OR educat* OR interven* OR randomi* OR trial*).ab,ti.))) NOT (letter OR news OR comment OR editorial OR
congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cochrane
((((mental* OR intellect*) NEXT/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEXT/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEXT/1 syndrome*) OR 'prader willi'):ab,ti) AND
(((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEXT/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*))):ab,ti)
OR ((('body mass' OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*)):ab,ti) AND ((program* OR promoti* OR educat* OR interven* OR randomi* OR trial*):ab,ti)) )
138541-Willems_BNW.indd 77 31-10-19 10:07

78
Web of science
TS=(((((mental* OR intellect*) NEAR/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEAR/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEAR/1 syndrome*) OR "prader willi")) AND
(((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEAR/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)))) OR
((("body mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*))) AND ((program* OR promoti* OR educat* OR interven* OR randomi* OR trial*)))) NOT
((animal* OR rat OR rats OR mouse OR mice OR murine OR pig OR swine OR porcine) NOT (human* OR patient* OR person*)))
PubMed publisher
(Intellectual Disability[mh] OR Mentally Disabled Persons[mh] OR (mental deficien*[tiab] OR mental handicap*[tiab] OR
mental disab*[tiab] OR mental retard*[tiab] OR mental impair*[tiab] OR mental challenged*[tiab] OR mentally deficien*[tiab]
OR mentally handicap*[tiab] OR mentally disab*[tiab] OR mentally retard*[tiab] OR mentally impair*[tiab] OR mentally
challenged*[tiab] OR intellectual deficien*[tiab] OR intellectual handicap*[tiab] OR intellectual disab*[tiab] OR intellectual
retard*[tiab] OR intellectual impair*[tiab] OR intellectual challenged*[tiab] OR intellectually deficien*[tiab] OR intellectually
handicap*[tiab] OR intellectually disab*[tiab] OR intellectually retard*[tiab] OR intellectually impair*[tiab] OR intellectually
challenged*[tiab] OR developmental disabilit*[tiab] OR developmental handicap*[tiab] OR developmental deficien*[tiab] OR
Down syndrome*[tiab] OR prader willi*[tiab])) AND ((diet therapy[mh] OR diet therapy[sh] OR Caloric Restriction[mh] OR
"Diet, Reducing"[mh] OR "Diet, Carbohydrate-Restricted"[mh] OR "Diet, Fat-Restricted"[mh] OR Weight Loss[mh] OR Weight
Reduction Programs[mh] OR (((lifestyle*[tiab] OR life-style OR calor*[tiab] OR nutrition*[tiab] OR diet*[tiab]) AND
(rehab*[tiab] OR modif*[tiab] OR program*[tiab] OR restrict*[tiab] OR therap*[tiab] OR treat*[tiab])) OR low calor*[tiab] OR
low carb*[tiab] OR low fat*[tiab] OR weight loss*[tiab] OR losing weight*[tiab] OR weight reduction*[tiab] OR weight
control*[tiab])) OR ((life style[mh] OR sedentary lifestyle[mh] OR body mass index[mh] OR exercise[mh] OR exercise
therapy[mh] OR Overweight[mh] OR (body mass OR bmi OR lifestyle OR life-style OR obes*[tiab] OR overweight*[tiab] OR
(physical*[tiab] AND activ*[tiab]) OR exercise OR kinesiotherap*[tiab] OR kinesitherap*[tiab] OR swimming OR walking OR
jogging OR running OR cycling OR treadmill OR ((diet*[tiab] OR nutrient*[tiab]) AND intake*[tiab]))) AND (health
education[mh] OR "Patient Education as Topic"[mh] OR health promotion[mh] OR program development[mh] OR program
evaluation[mh] OR intervention studies[mh] OR randomized controlled trial.pt. OR (program*[tiab] OR promoti*[tiab] OR
educat*[tiab] OR interven*[tiab] OR randomi*[tiab] OR trial*[tiab])))) NOT (letter[pt] OR news[pt] OR comment[pt] OR
editorial[pt] OR congresses[pt] OR abstracts[pt]) AND english[la] NOT (animals[mh] NOT humans[mh]) AND publisher[sb]
PsycINFO (OvidSP)
(exp Intellectual Development Disorder/ OR Cognitive Impairment/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR prader willi).ab,ti.) AND ((Weight Control/ OR Dietary Restraint/ OR Weight Loss/ OR Lifestyle Changes/
OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*))).ab,ti.) OR
((diets/ OR lifestyle/ OR body mass index/ OR exp exercise/ OR exp Overweight/ OR (body mass OR bmi OR lifestyle OR life-
style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming
OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3 intake*)).ab,ti.) AND (health
education/ OR "client Education"/ OR exp health promotion/ OR program development/ OR program evaluation/ OR
79
intervention/ OR (program* OR promoti* OR educat* OR interven* OR randomi* OR trial*).ab,ti.))) NOT (letter OR news OR
comment OR editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cinahl (ebsco)
(MH "Intellectual Disability+" OR MH "Mentally Disabled Persons+" OR (((mental* OR intellect*) n1 (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental n1 (disabilit* OR handicap* OR deficien*)) OR (Down*
n1 syndrome*) OR prader willi)) AND ((MH "diet therapy" OR MH "Restricted Diet+" OR MH "Diet, Fat-Restricted+" OR MH
"Weight Loss+" OR MH "Weight Reduction Programs+" OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) N3
(rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low n1 (calor* OR carb* OR fat)) OR (weight N3
(loss OR losing OR reduction OR control*)))) OR ((MH "life style+" OR MH "body mass index+" OR MH exercise+ OR MH
"Therapeutic Exercise+" OR MH obesity+ OR (body mass OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR
(physical* N3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR
cycling OR treadmill OR ((diet* OR nutrient*) N3 intake*))) AND (MH "health education+" OR MH "Patient Education+" OR
MH "health promotion+" OR MH "program development+" OR MH "program evaluation+" OR MH "Experimental Studies+"
OR MH "Randomized Controlled Trials+" OR (program* OR promoti* OR educat* OR interven* OR randomi* OR trial*))))
NOT PT (letter OR news OR comment OR editorial OR congresses OR abstracts) AND LA english NOT (MH animals+ NOT
humans+)
Google scholar
"mental|mentally|intellectual|intellectually
deficiency|deficient|handicap|handicapped|disabled|impaired|retarded|retardation"lifestyle|"life style"|
caloric|diet|"weight loss|reduction"|bmi|obesity|overweight program|promotion|education|intervention
APPENDIX 2 – Data Extraction Form
Author & record info
Data extraction author name
Date of data extraction
Article record nor in Endnote
Title
Authors
Year of publication
GENERAL CHARACTERISTICS
Intervention aimed at behavioural / lifestyle changes in
Physical activity, nutrition, both
Sample characteristics:
Sample Size Number of subjects, (if more groups, nor of subjects for each group)
Age Mean age (if more groups, mean age for each group)
Age group Children (<12), adolescents (12-18), adults (18-45), seniors (45+)
Sex Percentage of females in sample (if more groups, % for each group)
138541-Willems_BNW.indd 78 31-10-19 10:07

78
Web of science
TS=(((((mental* OR intellect*) NEAR/1 (deficien* OR handicap* OR disab* OR retard* OR impair* OR challenged)) OR
(developmental NEAR/1 (disabilit* OR handicap* OR deficien*)) OR (Down* NEAR/1 syndrome*) OR "prader willi")) AND
(((((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) NEAR/3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low NEAR/1 (calor* OR carb* OR fat)) OR (weight NEAR/3 (loss OR losing OR reduction OR control*)))) OR
((("body mass" OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR (physical* NEAR/3 activ*) OR exercise OR
kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR
nutrient*) NEAR/3 intake*))) AND ((program* OR promoti* OR educat* OR interven* OR randomi* OR trial*)))) NOT
((animal* OR rat OR rats OR mouse OR mice OR murine OR pig OR swine OR porcine) NOT (human* OR patient* OR person*)))
PubMed publisher
(Intellectual Disability[mh] OR Mentally Disabled Persons[mh] OR (mental deficien*[tiab] OR mental handicap*[tiab] OR
mental disab*[tiab] OR mental retard*[tiab] OR mental impair*[tiab] OR mental challenged*[tiab] OR mentally deficien*[tiab]
OR mentally handicap*[tiab] OR mentally disab*[tiab] OR mentally retard*[tiab] OR mentally impair*[tiab] OR mentally
challenged*[tiab] OR intellectual deficien*[tiab] OR intellectual handicap*[tiab] OR intellectual disab*[tiab] OR intellectual
retard*[tiab] OR intellectual impair*[tiab] OR intellectual challenged*[tiab] OR intellectually deficien*[tiab] OR intellectually
handicap*[tiab] OR intellectually disab*[tiab] OR intellectually retard*[tiab] OR intellectually impair*[tiab] OR intellectually
challenged*[tiab] OR developmental disabilit*[tiab] OR developmental handicap*[tiab] OR developmental deficien*[tiab] OR
Down syndrome*[tiab] OR prader willi*[tiab])) AND ((diet therapy[mh] OR diet therapy[sh] OR Caloric Restriction[mh] OR
"Diet, Reducing"[mh] OR "Diet, Carbohydrate-Restricted"[mh] OR "Diet, Fat-Restricted"[mh] OR Weight Loss[mh] OR Weight
Reduction Programs[mh] OR (((lifestyle*[tiab] OR life-style OR calor*[tiab] OR nutrition*[tiab] OR diet*[tiab]) AND
(rehab*[tiab] OR modif*[tiab] OR program*[tiab] OR restrict*[tiab] OR therap*[tiab] OR treat*[tiab])) OR low calor*[tiab] OR
low carb*[tiab] OR low fat*[tiab] OR weight loss*[tiab] OR losing weight*[tiab] OR weight reduction*[tiab] OR weight
control*[tiab])) OR ((life style[mh] OR sedentary lifestyle[mh] OR body mass index[mh] OR exercise[mh] OR exercise
therapy[mh] OR Overweight[mh] OR (body mass OR bmi OR lifestyle OR life-style OR obes*[tiab] OR overweight*[tiab] OR
(physical*[tiab] AND activ*[tiab]) OR exercise OR kinesiotherap*[tiab] OR kinesitherap*[tiab] OR swimming OR walking OR
jogging OR running OR cycling OR treadmill OR ((diet*[tiab] OR nutrient*[tiab]) AND intake*[tiab]))) AND (health
education[mh] OR "Patient Education as Topic"[mh] OR health promotion[mh] OR program development[mh] OR program
evaluation[mh] OR intervention studies[mh] OR randomized controlled trial.pt. OR (program*[tiab] OR promoti*[tiab] OR
educat*[tiab] OR interven*[tiab] OR randomi*[tiab] OR trial*[tiab])))) NOT (letter[pt] OR news[pt] OR comment[pt] OR
editorial[pt] OR congresses[pt] OR abstracts[pt]) AND english[la] NOT (animals[mh] NOT humans[mh]) AND publisher[sb]
PsycINFO (OvidSP)
(exp Intellectual Development Disorder/ OR Cognitive Impairment/ OR (((mental* OR intellect*) ADJ (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental ADJ (disabilit* OR handicap* OR deficien*)) OR (Down*
ADJ syndrome*) OR prader willi).ab,ti.) AND ((Weight Control/ OR Dietary Restraint/ OR Weight Loss/ OR Lifestyle Changes/
OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) ADJ3 (rehab* OR modif* OR program* OR restrict* OR therap*
OR treat*)) OR (low ADJ (calor* OR carb* OR fat)) OR (weight ADJ3 (loss OR losing OR reduction OR control*))).ab,ti.) OR
((diets/ OR lifestyle/ OR body mass index/ OR exp exercise/ OR exp Overweight/ OR (body mass OR bmi OR lifestyle OR life-
style OR obes* OR overweight* OR (physical* ADJ3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming
OR walking OR jogging OR running OR cycling OR treadmill OR ((diet* OR nutrient*) ADJ3 intake*)).ab,ti.) AND (health
education/ OR "client Education"/ OR exp health promotion/ OR program development/ OR program evaluation/ OR
79
intervention/ OR (program* OR promoti* OR educat* OR interven* OR randomi* OR trial*).ab,ti.))) NOT (letter OR news OR
comment OR editorial OR congresses OR abstracts).pt. AND english.la. NOT (exp animals/ NOT humans/)
Cinahl (ebsco)
(MH "Intellectual Disability+" OR MH "Mentally Disabled Persons+" OR (((mental* OR intellect*) n1 (deficien* OR handicap*
OR disab* OR retard* OR impair* OR challenged)) OR (developmental n1 (disabilit* OR handicap* OR deficien*)) OR (Down*
n1 syndrome*) OR prader willi)) AND ((MH "diet therapy" OR MH "Restricted Diet+" OR MH "Diet, Fat-Restricted+" OR MH
"Weight Loss+" OR MH "Weight Reduction Programs+" OR (((lifestyle* OR life-style OR calor* OR nutrition* OR diet*) N3
(rehab* OR modif* OR program* OR restrict* OR therap* OR treat*)) OR (low n1 (calor* OR carb* OR fat)) OR (weight N3
(loss OR losing OR reduction OR control*)))) OR ((MH "life style+" OR MH "body mass index+" OR MH exercise+ OR MH
"Therapeutic Exercise+" OR MH obesity+ OR (body mass OR bmi OR lifestyle OR life-style OR obes* OR overweight* OR
(physical* N3 activ*) OR exercise OR kinesiotherap* OR kinesitherap* OR swimming OR walking OR jogging OR running OR
cycling OR treadmill OR ((diet* OR nutrient*) N3 intake*))) AND (MH "health education+" OR MH "Patient Education+" OR
MH "health promotion+" OR MH "program development+" OR MH "program evaluation+" OR MH "Experimental Studies+"
OR MH "Randomized Controlled Trials+" OR (program* OR promoti* OR educat* OR interven* OR randomi* OR trial*))))
NOT PT (letter OR news OR comment OR editorial OR congresses OR abstracts) AND LA english NOT (MH animals+ NOT
humans+)
Google scholar
"mental|mentally|intellectual|intellectually
deficiency|deficient|handicap|handicapped|disabled|impaired|retarded|retardation"lifestyle|"life style"|
caloric|diet|"weight loss|reduction"|bmi|obesity|overweight program|promotion|education|intervention
APPENDIX 2 – Data Extraction Form
Author & record info
Data extraction author name
Date of data extraction
Article record nor in Endnote
Title
Authors
Year of publication
GENERAL CHARACTERISTICS
Intervention aimed at behavioural / lifestyle changes in
Physical activity, nutrition, both
Sample characteristics:
Sample Size Number of subjects, (if more groups, nor of subjects for each group)
Age Mean age (if more groups, mean age for each group)
Age group Children (<12), adolescents (12-18), adults (18-45), seniors (45+)
Sex Percentage of females in sample (if more groups, % for each group)
138541-Willems_BNW.indd 79 31-10-19 10:07
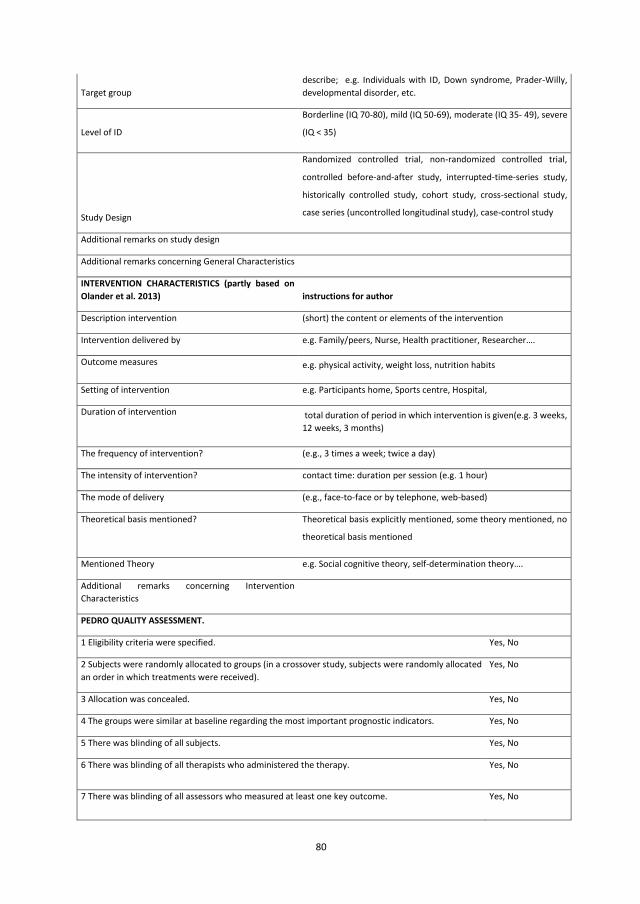
80
Target group describe; e.g. Individuals with ID, Down syndrome, Prader-Willy, developmental disorder, etc.
Level of ID
Borderline (IQ 70-80), mild (IQ 50-69), moderate (IQ 35- 49), severe
(IQ < 35)
Study Design
Randomized controlled trial, non-randomized controlled trial,
controlled before-and-after study, interrupted-time-series study,
historically controlled study, cohort study, cross-sectional study,
case series (uncontrolled longitudinal study), case-control study
Additional remarks on study design
Additional remarks concerning General Characteristics
INTERVENTION CHARACTERISTICS (partly based on Olander et al. 2013) instructions for author
Description intervention (short) the content or elements of the intervention
Intervention delivered by e.g. Family/peers, Nurse, Health practitioner, Researcher….
Outcome measures e.g. physical activity, weight loss, nutrition habits
Setting of intervention e.g. Participants home, Sports centre, Hospital,
Duration of intervention total duration of period in which intervention is given(e.g. 3 weeks, 12 weeks, 3 months)
The frequency of intervention? (e.g., 3 times a week; twice a day)
The intensity of intervention? contact time: duration per session (e.g. 1 hour)
The mode of delivery (e.g., face-to-face or by telephone, web-based)
Theoretical basis mentioned? Theoretical basis explicitly mentioned, some theory mentioned, no
theoretical basis mentioned
Mentioned Theory e.g. Social cognitive theory, self-determination theory….
Additional remarks concerning Intervention Characteristics
PEDRO QUALITY ASSESSMENT.
1 Eligibility criteria were specified. Yes, No
2 Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received).
Yes, No
3 Allocation was concealed. Yes, No
4 The groups were similar at baseline regarding the most important prognostic indicators. Yes, No
5 There was blinding of all subjects. Yes, No
6 There was blinding of all therapists who administered the therapy. Yes, No
7 There was blinding of all assessors who measured at least one key outcome. Yes, No
81
8 Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups.
Yes, No
9 All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”.
Yes, No
10 The results of between-group statistical comparisons are reported for at least one key outcome. Yes, No
11 The study provides both point measures and measures of variability for at least one key outcome. Yes, No
BEHAVIOR CHANGE TECHNIQUES
(based on CALORE Taxonomy for behavioural change Techniques (Michie et al. 2011))
1 Provide information on consequences of behaviour in general
2 Provide information on consequences of behaviour to the individual
3 Provide information about others' approval
4 Provide normative information about others' behaviour
5 Goal setting (behaviour)
6 Goal setting (outcome)
7 Action planning
8 Barrier identification/problem solving
9 Set graded tasks
10 Prompt review of behavioural goals
11 Prompt review of outcome goals
12 Prompt rewards contingent on effort or progress towards behaviour
13 Provide rewards contingent on successful behaviour
14 Shaping
15 Prompting generalization of a target behaviour
16 Prompt self-monitoring of behaviour
17 Prompt self-monitoring of behavioural outcome
18 Prompting focus on past success
19 Provide feedback on performance
20 Provide information on where and when to perform behaviour
21 Provide instruction on how to perform the behaviour
22 Model/demonstrate the behaviour
23 Teach to use prompts/cues
24 Environmental restructuring
25 Agree behavioural contract
26 Prompt practice
138541-Willems_BNW.indd 80 31-10-19 10:07
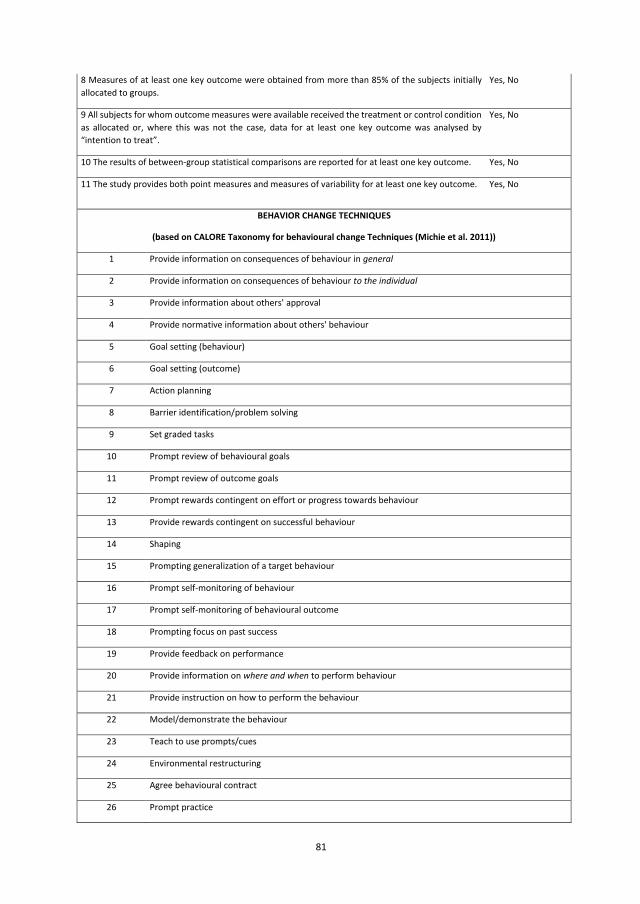
80
Target group describe; e.g. Individuals with ID, Down syndrome, Prader-Willy, developmental disorder, etc.
Level of ID
Borderline (IQ 70-80), mild (IQ 50-69), moderate (IQ 35- 49), severe
(IQ < 35)
Study Design
Randomized controlled trial, non-randomized controlled trial,
controlled before-and-after study, interrupted-time-series study,
historically controlled study, cohort study, cross-sectional study,
case series (uncontrolled longitudinal study), case-control study
Additional remarks on study design
Additional remarks concerning General Characteristics
INTERVENTION CHARACTERISTICS (partly based on Olander et al. 2013) instructions for author
Description intervention (short) the content or elements of the intervention
Intervention delivered by e.g. Family/peers, Nurse, Health practitioner, Researcher….
Outcome measures e.g. physical activity, weight loss, nutrition habits
Setting of intervention e.g. Participants home, Sports centre, Hospital,
Duration of intervention total duration of period in which intervention is given(e.g. 3 weeks, 12 weeks, 3 months)
The frequency of intervention? (e.g., 3 times a week; twice a day)
The intensity of intervention? contact time: duration per session (e.g. 1 hour)
The mode of delivery (e.g., face-to-face or by telephone, web-based)
Theoretical basis mentioned? Theoretical basis explicitly mentioned, some theory mentioned, no
theoretical basis mentioned
Mentioned Theory e.g. Social cognitive theory, self-determination theory….
Additional remarks concerning Intervention Characteristics
PEDRO QUALITY ASSESSMENT.
1 Eligibility criteria were specified. Yes, No
2 Subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received).
Yes, No
3 Allocation was concealed. Yes, No
4 The groups were similar at baseline regarding the most important prognostic indicators. Yes, No
5 There was blinding of all subjects. Yes, No
6 There was blinding of all therapists who administered the therapy. Yes, No
7 There was blinding of all assessors who measured at least one key outcome. Yes, No
81
8 Measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups.
Yes, No
9 All subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome was analysed by “intention to treat”.
Yes, No
10 The results of between-group statistical comparisons are reported for at least one key outcome. Yes, No
11 The study provides both point measures and measures of variability for at least one key outcome. Yes, No
BEHAVIOR CHANGE TECHNIQUES
(based on CALORE Taxonomy for behavioural change Techniques (Michie et al. 2011))
1 Provide information on consequences of behaviour in general
2 Provide information on consequences of behaviour to the individual
3 Provide information about others' approval
4 Provide normative information about others' behaviour
5 Goal setting (behaviour)
6 Goal setting (outcome)
7 Action planning
8 Barrier identification/problem solving
9 Set graded tasks
10 Prompt review of behavioural goals
11 Prompt review of outcome goals
12 Prompt rewards contingent on effort or progress towards behaviour
13 Provide rewards contingent on successful behaviour
14 Shaping
15 Prompting generalization of a target behaviour
16 Prompt self-monitoring of behaviour
17 Prompt self-monitoring of behavioural outcome
18 Prompting focus on past success
19 Provide feedback on performance
20 Provide information on where and when to perform behaviour
21 Provide instruction on how to perform the behaviour
22 Model/demonstrate the behaviour
23 Teach to use prompts/cues
24 Environmental restructuring
25 Agree behavioural contract
26 Prompt practice
138541-Willems_BNW.indd 81 31-10-19 10:07
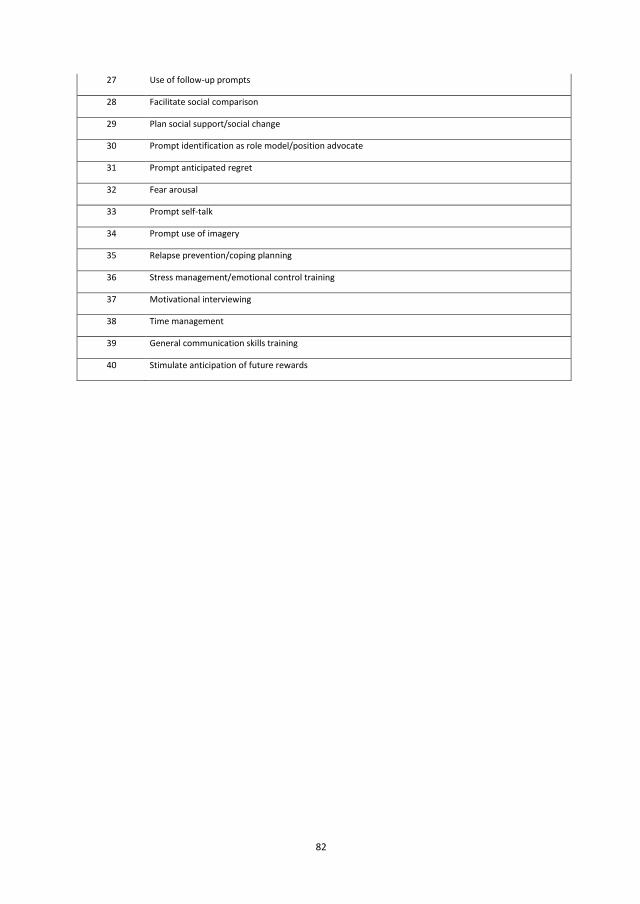
82
27 Use of follow-up prompts
28 Facilitate social comparison
29 Plan social support/social change
30 Prompt identification as role model/position advocate
31 Prompt anticipated regret
32 Fear arousal
33 Prompt self-talk
34 Prompt use of imagery
35 Relapse prevention/coping planning
36 Stress management/emotional control training
37 Motivational interviewing
38 Time management
39 General communication skills training
40 Stimulate anticipation of future rewards
83
SUPP
LEM
ENTA
L TA
BLE
1 –
Gen
eral
cha
ract
erist
ics
7 The
se re
sults
are
com
bine
d w
ith th
e pr
oces
s eva
luat
ion
pape
r fro
m B
odde
et a
l. (2
012)
des
crib
ing
the
sam
e st
udy.
8 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om S
hiel
ds e
t al.
(201
0) d
escr
ibin
g th
e sa
me
stud
y.
9 The
se re
sults
are
com
bine
d w
ith th
e pr
otoc
ol p
aper
from
Van
Sch
ijnde
l-Spe
et e
t al.
(201
3) d
escr
ibin
g th
e sa
me
stud
y.
Stud
y Ye
ar
Setti
ng
Popu
latio
n N
Age
(M)
Leve
l of I
D Se
x (%
F)
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(15)
Podg
orsk
i 20
04
Day
habi
litat
ion
sett
ing
Olde
r adu
lts w
ith ID
12
40
-80+
Al
l lev
els.
Mild
= 40
%; M
oder
ate=
13.3
%;
Seve
re=
20.0
%; P
rofo
und=
26.7
%
46.7
Jone
s 20
07
Resid
entia
l fac
ility
Pe
ople
with
ID
8 41
.3 (S
D= 6
.5)
Seve
re (1
00%
) Un
know
n
Pite
tti
2007
Gy
mna
sium
Ad
oles
cent
s/yo
uth
with
se
vere
dev
elop
men
tal
disa
bilit
ies
10
17 (1
4-19
yea
rs,
SD=
1.9)
M
oder
ate-
seve
re. M
ild I=
10%
; Sev
ere=
60%
; ID
unc
lass
ified
= 20
%; A
sper
ger
synd
rom
e=10
%
40
Gelle
r 20
09
Com
mun
ity h
ealth
cent
re
Over
wei
ght a
dults
with
de
velo
pmen
tal d
elay
43
42
.6
All l
evel
s 58
.1
Tem
ple
2011
YM
CA fi
tnes
s cen
tre
Yout
h w
ith ID
in th
e co
mm
unity
20
17
.8
(15-
21
year
s, SD
= 1.
6)
Mild
(100
%)
50
Thom
as
2011
Un
know
n Ad
ults
with
ID
191
42 (1
9-72
year
s)
Unkn
own
38.2
Ulric
h 20
11
Trai
ning
facil
ity
Child
ren
(8-1
5 ye
ars)
w
ith D
own
Synd
rom
e 46
12
.2 (8
-15)
Un
know
n 56
.5
Bodd
e7 20
12
Agen
cies t
hat s
erve
adu
lts
with
ID
Ambu
lato
ry a
dults
with
ID
42
38
.8
(19-
62
year
s)
Mild
-mod
erat
e 50
Stan
ish
2012
YM
CA B
ranc
hes
Adol
esce
nts w
ith ID
20
17
.8
(15-
21
year
s, SD
= 1.
6)
Mild
-mod
erat
e 50
Yen
2012
In
stitu
tion
Adul
ts w
ith ID
, liv
ing
in
inst
itutio
n 13
5 33
.7
(19-
67
year
s, SD
= 10
.0)
All l
evel
s. M
ild=
3.6%
; Mod
erat
e= 3
0.4%
; Se
vere
=31
.9%
; Pro
foun
d= 3
4.15
33
.3
Mitc
hell
2013
Pa
rtici
pant
’s ho
me
Adul
ts w
ith ID
Pr
otoc
ol
Prot
ocol
Al
l lev
els
Prot
ocol
Pere
z-Cr
uzad
o 20
13
Occu
patio
nal c
entr
e Pe
ople
with
ID
Prot
ocol
Pr
otoc
ol
Mild
-mod
erat
e Pr
otoc
ol
Shie
lds8
2013
Gy
mna
sium
Ad
oles
cent
s with
Dow
n Sy
ndro
me
68
17.9
(1
4-22
ye
ars,
SD=
2.6)
M
ild-m
oder
ate.
Mild
=50%
; Mod
erat
e=50
%
44
Lant
e 20
14
Loca
l com
mun
ity se
tting
s Ad
ults
with
ID
90
18-5
5 ye
ars
Unkn
own
Unkn
own
Van
Schi
jnde
l-Sp
eet9
2014
Da
y ac
tivity
cent
re
Olde
r ind
ivid
uals
with
ID
14
6 44
+ ye
ars
Mild
-mod
erat
e Un
know
n
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
138541-Willems_BNW.indd 82 31-10-19 10:07
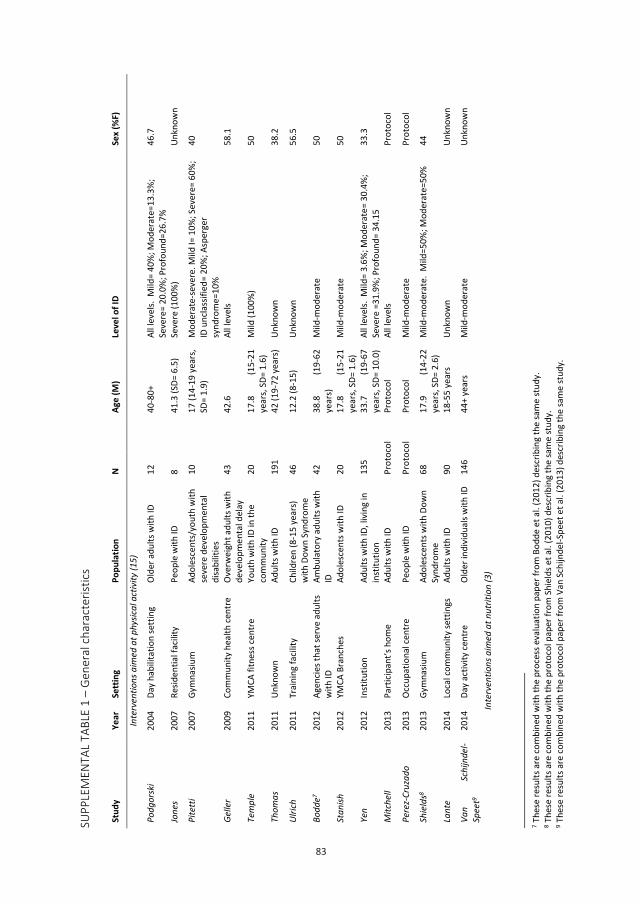
83
82
27 Use of follow-up prompts
28 Facilitate social comparison
29 Plan social support/social change
30 Prompt identification as role model/position advocate
31 Prompt anticipated regret
32 Fear arousal
33 Prompt self-talk
34 Prompt use of imagery
35 Relapse prevention/coping planning
36 Stress management/emotional control training
37 Motivational interviewing
38 Time management
39 General communication skills training
40 Stimulate anticipation of future rewards
83
SUPP
LEM
ENTA
L TA
BLE
1 –
Gen
eral
cha
ract
erist
ics
7 The
se re
sults
are
com
bine
d w
ith th
e pr
oces
s eva
luat
ion
pape
r fro
m B
odde
et a
l. (2
012)
des
crib
ing
the
sam
e st
udy.
8 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om S
hiel
ds e
t al.
(201
0) d
escr
ibin
g th
e sa
me
stud
y.
9 The
se re
sults
are
com
bine
d w
ith th
e pr
otoc
ol p
aper
from
Van
Sch
ijnde
l-Spe
et e
t al.
(201
3) d
escr
ibin
g th
e sa
me
stud
y.
Stud
y Ye
ar
Setti
ng
Popu
latio
n N
Age
(M)
Leve
l of I
D Se
x (%
F)
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(15)
Podg
orsk
i 20
04
Day
habi
litat
ion
sett
ing
Olde
r adu
lts w
ith ID
12
40
-80+
Al
l lev
els.
Mild
= 40
%; M
oder
ate=
13.3
%;
Seve
re=
20.0
%; P
rofo
und=
26.7
%
46.7
Jone
s 20
07
Resid
entia
l fac
ility
Pe
ople
with
ID
8 41
.3 (S
D= 6
.5)
Seve
re (1
00%
) Un
know
n
Pite
tti
2007
Gy
mna
sium
Ad
oles
cent
s/yo
uth
with
se
vere
dev
elop
men
tal
disa
bilit
ies
10
17 (1
4-19
yea
rs,
SD=
1.9)
M
oder
ate-
seve
re. M
ild I=
10%
; Sev
ere=
60%
; ID
unc
lass
ified
= 20
%; A
sper
ger
synd
rom
e=10
%
40
Gelle
r 20
09
Com
mun
ity h
ealth
cent
re
Over
wei
ght a
dults
with
de
velo
pmen
tal d
elay
43
42
.6
All l
evel
s 58
.1
Tem
ple
2011
YM
CA fi
tnes
s cen
tre
Yout
h w
ith ID
in th
e co
mm
unity
20
17
.8
(15-
21
year
s, SD
= 1.
6)
Mild
(100
%)
50
Thom
as
2011
Un
know
n Ad
ults
with
ID
191
42 (1
9-72
year
s)
Unkn
own
38.2
Ulric
h 20
11
Trai
ning
facil
ity
Child
ren
(8-1
5 ye
ars)
w
ith D
own
Synd
rom
e 46
12
.2 (8
-15)
Un
know
n 56
.5
Bodd
e7 20
12
Agen
cies t
hat s
erve
adu
lts
with
ID
Ambu
lato
ry a
dults
with
ID
42
38
.8
(19-
62
year
s)
Mild
-mod
erat
e 50
Stan
ish
2012
YM
CA B
ranc
hes
Adol
esce
nts w
ith ID
20
17
.8
(15-
21
year
s, SD
= 1.
6)
Mild
-mod
erat
e 50
Yen
2012
In
stitu
tion
Adul
ts w
ith ID
, liv
ing
in
inst
itutio
n 13
5 33
.7
(19-
67
year
s, SD
= 10
.0)
All l
evel
s. M
ild=
3.6%
; Mod
erat
e= 3
0.4%
; Se
vere
=31
.9%
; Pro
foun
d= 3
4.15
33
.3
Mitc
hell
2013
Pa
rtici
pant
’s ho
me
Adul
ts w
ith ID
Pr
otoc
ol
Prot
ocol
Al
l lev
els
Prot
ocol
Pere
z-Cr
uzad
o 20
13
Occu
patio
nal c
entr
e Pe
ople
with
ID
Prot
ocol
Pr
otoc
ol
Mild
-mod
erat
e Pr
otoc
ol
Shie
lds8
2013
Gy
mna
sium
Ad
oles
cent
s with
Dow
n Sy
ndro
me
68
17.9
(1
4-22
ye
ars,
SD=
2.6)
M
ild-m
oder
ate.
Mild
=50%
; Mod
erat
e=50
%
44
Lant
e 20
14
Loca
l com
mun
ity se
tting
s Ad
ults
with
ID
90
18-5
5 ye
ars
Unkn
own
Unkn
own
Van
Schi
jnde
l-Sp
eet9
2014
Da
y ac
tivity
cent
re
Olde
r ind
ivid
uals
with
ID
14
6 44
+ ye
ars
Mild
-mod
erat
e Un
know
n
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
138541-Willems_BNW.indd 83 31-10-19 10:07
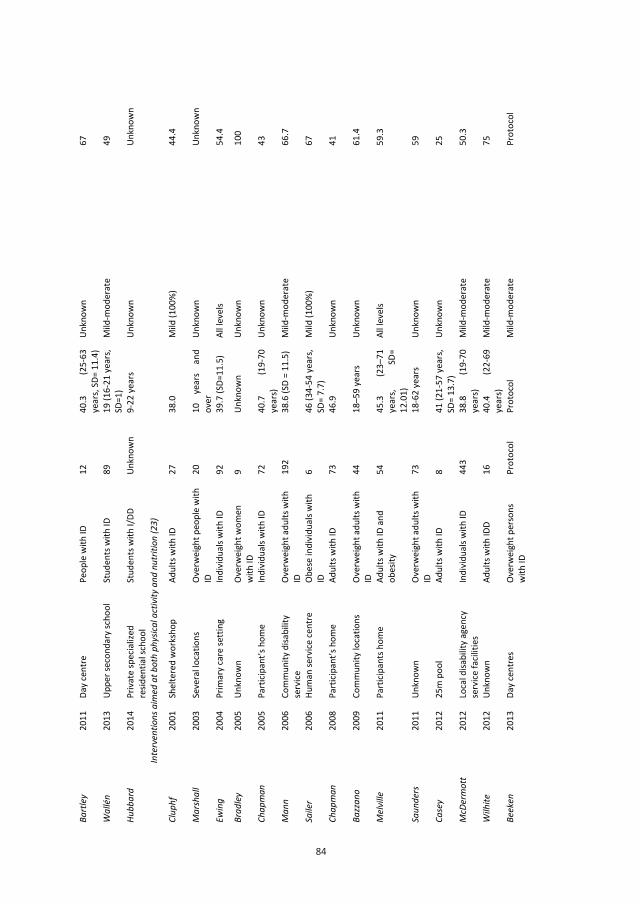
84
84
Bart
ley
2011
Da
y ce
ntre
Pe
ople
with
ID
12
40.3
(2
5-63
ye
ars,
SD=
11.4
) Un
know
n 67
Wal
lén
2013
Up
per s
econ
dary
scho
ol
Stud
ents
with
ID
89
19 (1
6-21
yea
rs,
SD=1
) M
ild-m
oder
ate
49
Hubb
ard
2014
Pr
ivat
e sp
ecia
lized
re
siden
tial s
choo
l St
uden
ts w
ith I/
DD
Unkn
own
9-22
yea
rs
Unkn
own
Unkn
own
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Clup
hf
2001
Sh
elte
red
wor
ksho
p Ad
ults
with
ID
27
38.0
M
ild (1
00%
) 44
.4
M
arsh
all
2003
Se
vera
l loc
atio
ns
Over
wei
ght p
eopl
e w
ith
ID
20
10
ye
ars
and
over
Un
know
n Un
know
n
Ewin
g 20
04
Prim
ary
care
setti
ng
Indi
vidu
als w
ith ID
92
39
.7 (S
D=11
.5)
All l
evel
s 54
.4
Brad
ley
2005
Un
know
n Ov
erw
eigh
t wom
en
with
ID
9 Un
know
n Un
know
n 10
0
Chap
man
20
05
Part
icipa
nt’s
hom
e In
divi
dual
s with
ID
72
40.7
(1
9-70
ye
ars)
Un
know
n 43
Man
n 20
06
Com
mun
ity d
isabi
lity
serv
ice
Over
wei
ght a
dults
with
ID
19
2 38
.6 (S
D =
11.5
) M
ild-m
oder
ate
66.7
Saile
r 20
06
Hum
an se
rvice
cent
re
Obes
e in
divi
dual
s with
ID
6
46 (3
4-54
yea
rs,
SD=
7.7)
M
ild (1
00%
) 67
Chap
man
2008
Pa
rtici
pant
’s ho
me
Adul
ts w
ith ID
73
46
.9
Unkn
own
41
Bazz
ano
2009
Co
mm
unity
loca
tions
Ov
erw
eigh
t adu
lts w
ith
ID
44
18–5
9 ye
ars
Unkn
own
61.4
Mel
ville
20
11
Part
icipa
nts h
ome
Adul
ts w
ith ID
and
ob
esity
54
45
.3
(23–
71
year
s, SD
= 12
.01)
All l
evel
s 59
.3
Saun
ders
20
11
Unkn
own
Over
wei
ght a
dults
with
ID
73
18
-62
year
s Un
know
n 59
Case
y 20
12
25m
poo
l Ad
ults
with
ID
8 41
(21-
57 y
ears
, SD
= 13
.7)
Unkn
own
25
McD
erm
ott
2012
Lo
cal d
isabi
lity
agen
cy
serv
ice fa
ciliti
es
Indi
vidu
als w
ith ID
44
3 38
.8
(19-
70
year
s)
Mild
-mod
erat
e 50
.3
Wilh
ite
2012
Un
know
n Ad
ults
with
IDD
16
40.4
(2
2-69
ye
ars)
M
ild-m
oder
ate
75
Beek
en
2013
Da
y ce
ntre
s Ov
erw
eigh
t per
sons
w
ith ID
Pr
otoc
ol
Prot
ocol
M
ild-m
oder
ate
Prot
ocol
85
SUPP
LEM
ENTA
L TA
BLE
2 –
Inte
rven
tion
char
acte
ristic
s
10 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
11
The
se re
sults
are
com
bine
d w
ith th
e pr
oces
s eva
luat
ion
pape
r fro
m B
odde
et a
l. (2
012)
des
crib
ing
the
sam
e st
udy.
Berg
stro
m10
20
13
Resid
ence
Ad
ults
with
ID li
ving
in
resid
ence
s 12
9 37
.8
(20-
66
year
s)
Mild
-mod
erat
e 56
.9
Cu
rtin
20
13
Unkn
own
Adol
esce
nts a
nd y
oung
ad
ults
with
dow
n sy
ndro
me
21
20.5
(1
3-26
ye
ars,
SD=
3.2)
M
ild-m
oder
ate
81.0
Donn
elly
20
13
Part
icipa
nt’s
hom
e Ov
erw
eigh
t adu
lts w
ith
ID a
nd D
D 15
0 18
ye
ars
and
over
M
ild-m
oder
ate
Desig
n/ra
tiona
le
Mar
ks
2013
Co
mm
unity
-bas
ed
orga
nisa
tions
Ad
ults
with
ID
67
45.2
(3
1-64
ye
ars,
SD=7
.6)
Mild
-mod
erat
e 52
Pett
20
13
Recr
eatio
n ce
ntre
Ob
ese
hom
e dw
ellin
g yo
ung
adul
ts w
ith ID
30
24
.2
(18-
33
year
s, SD
= 4.
2)
Mild
-mod
erat
e 60
Wal
lén
2013
Up
per s
econ
dary
scho
ol
Stud
ents
with
ID
27
20.7
(19
.2-2
1.8
year
s)
Mild
-mod
erat
e 33
.3
Span
os
2014
Pa
rtici
pant
’s ho
me
Adul
ts w
ith ID
52
51
(26-
73 ye
ars)
M
ild, m
oder
ate,
seve
re
60.9
Ptom
ey
2015
Pa
rtici
pant
s hom
e Ad
oles
cent
s with
IDD
with
ove
rwei
ght
22
14.9
(1
1-18
ye
ars,
SD=
2.2)
M
ild-m
oder
ate.
Mild
= 60
%; M
oder
ate=
40%
45
Stud
y Ye
ar
Desig
n Th
eore
tical
fram
ewor
k De
liver
y Nu
mbe
r/
freq
uenc
y pe
r w
eek
Inte
rven
tion
dura
tion
(wee
ks)
Follo
w-u
p
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(15)
Podg
orsk
i 20
04
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
4
12
9 m
onth
s
Jone
s 20
07
Case
serie
s No
ne
Face
-to-fa
ce
3-5
16
3 m
onth
s
Pite
tti
2007
No
n-RC
T No
ne
face
-to-fa
ce, g
roup
3
9 m
onth
s No
ne
Gelle
r 20
09
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
and
in
divi
dual
ly
2 13
,5 m
onth
s No
ne
Tem
ple
2011
Ca
se se
ries
None
Fa
ce-to
-face
, gro
up
2
15
None
Thom
as
2011
Ca
se se
ries
None
lo
gboo
ks
Unkn
own
24 m
onth
s No
ne
Ulric
h 20
11
RCT
Dyna
mic
syst
ems t
heor
y Fa
ce-to
-face
5
cons
ecut
ive
days
5
cons
ecut
ive
days
12
mon
ths
Bodd
e11
2012
Ca
se se
ries
Theo
ry o
f pla
nned
beh
avio
ur
Face
-to-fa
ce, g
roup
8
sess
ions
in to
tal
Unkn
own
None
138541-Willems_BNW.indd 84 31-10-19 10:07
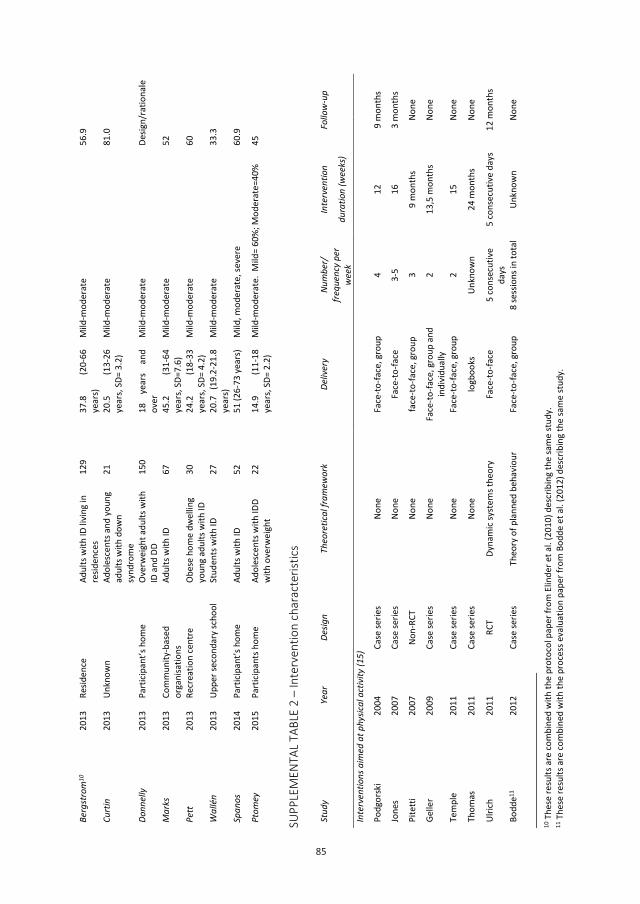
85
85
SUPP
LEM
ENTA
L TA
BLE
2 –
Inte
rven
tion
char
acte
ristic
s
10 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
11
The
se re
sults
are
com
bine
d w
ith th
e pr
oces
s eva
luat
ion
pape
r fro
m B
odde
et a
l. (2
012)
des
crib
ing
the
sam
e st
udy.
Berg
stro
m10
20
13
Resid
ence
Ad
ults
with
ID li
ving
in
resid
ence
s 12
9 37
.8
(20-
66
year
s)
Mild
-mod
erat
e 56
.9
Cu
rtin
20
13
Unkn
own
Adol
esce
nts a
nd y
oung
ad
ults
with
dow
n sy
ndro
me
21
20.5
(1
3-26
ye
ars,
SD=
3.2)
M
ild-m
oder
ate
81.0
Donn
elly
20
13
Part
icipa
nt’s
hom
e Ov
erw
eigh
t adu
lts w
ith
ID a
nd D
D 15
0 18
ye
ars
and
over
M
ild-m
oder
ate
Desig
n/ra
tiona
le
Mar
ks
2013
Co
mm
unity
-bas
ed
orga
nisa
tions
Ad
ults
with
ID
67
45.2
(3
1-64
ye
ars,
SD=7
.6)
Mild
-mod
erat
e 52
Pett
20
13
Recr
eatio
n ce
ntre
Ob
ese
hom
e dw
ellin
g yo
ung
adul
ts w
ith ID
30
24
.2
(18-
33
year
s, SD
= 4.
2)
Mild
-mod
erat
e 60
Wal
lén
2013
Up
per s
econ
dary
scho
ol
Stud
ents
with
ID
27
20.7
(19
.2-2
1.8
year
s)
Mild
-mod
erat
e 33
.3
Span
os
2014
Pa
rtici
pant
’s ho
me
Adul
ts w
ith ID
52
51
(26-
73 ye
ars)
M
ild, m
oder
ate,
seve
re
60.9
Ptom
ey
2015
Pa
rtici
pant
s hom
e Ad
oles
cent
s with
IDD
with
ove
rwei
ght
22
14.9
(1
1-18
ye
ars,
SD=
2.2)
M
ild-m
oder
ate.
Mild
= 60
%; M
oder
ate=
40%
45
Stud
y Ye
ar
Desig
n Th
eore
tical
fram
ewor
k De
liver
y Nu
mbe
r/
freq
uenc
y pe
r w
eek
Inte
rven
tion
dura
tion
(wee
ks)
Follo
w-u
p
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(15)
Podg
orsk
i 20
04
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
4
12
9 m
onth
s
Jone
s 20
07
Case
serie
s No
ne
Face
-to-fa
ce
3-5
16
3 m
onth
s
Pite
tti
2007
No
n-RC
T No
ne
face
-to-fa
ce, g
roup
3
9 m
onth
s No
ne
Gelle
r 20
09
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
and
in
divi
dual
ly
2 13
,5 m
onth
s No
ne
Tem
ple
2011
Ca
se se
ries
None
Fa
ce-to
-face
, gro
up
2
15
None
Thom
as
2011
Ca
se se
ries
None
lo
gboo
ks
Unkn
own
24 m
onth
s No
ne
Ulric
h 20
11
RCT
Dyna
mic
syst
ems t
heor
y Fa
ce-to
-face
5
cons
ecut
ive
days
5
cons
ecut
ive
days
12
mon
ths
Bodd
e11
2012
Ca
se se
ries
Theo
ry o
f pla
nned
beh
avio
ur
Face
-to-fa
ce, g
roup
8
sess
ions
in to
tal
Unkn
own
None
138541-Willems_BNW.indd 85 31-10-19 10:07
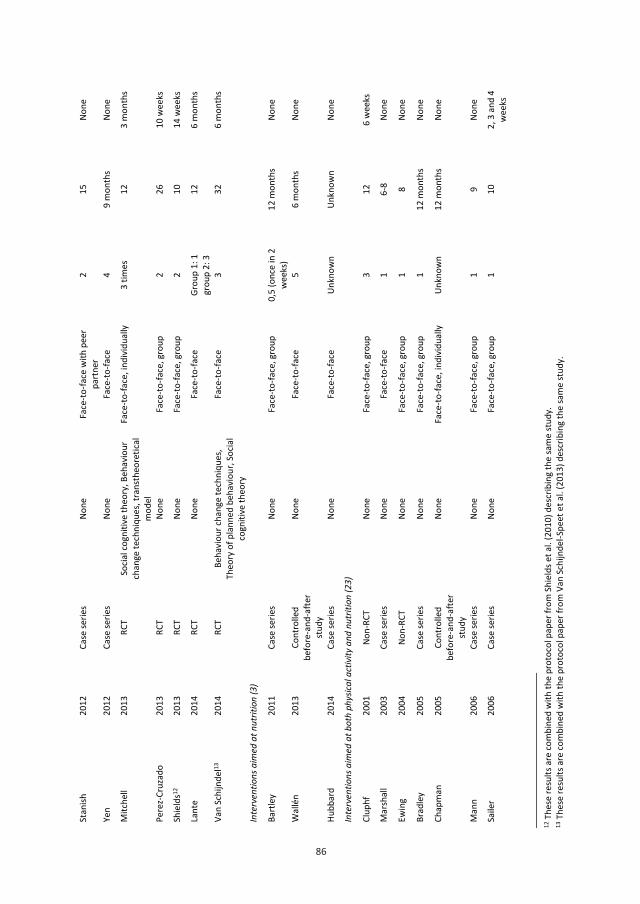
86
86
12 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om S
hiel
ds e
t al.
(201
0) d
escr
ibin
g th
e sa
me
stud
y.
13 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om V
an S
chijn
del-S
peet
et a
l. (2
013)
des
crib
ing
the
sam
e st
udy.
Stan
ish
2012
Ca
se se
ries
None
Fa
ce-to
-face
with
pee
r pa
rtne
r 2
15
None
Yen
2012
Ca
se se
ries
None
Fa
ce-to
-face
4
9 m
onth
s No
ne
Mitc
hell
2013
RC
T So
cial c
ogni
tive
theo
ry, B
ehav
iour
ch
ange
tech
niqu
es, t
rans
theo
retic
al
mod
el
Face
-to-fa
ce, i
ndiv
idua
lly
3 tim
es
12
3 m
onth
s
Pere
z-Cr
uzad
o 20
13
RCT
None
Fa
ce-to
-face
, gro
up
2 26
10
wee
ks
Shie
lds12
20
13
RCT
None
Fa
ce-to
-face
, gro
up
2 10
14
wee
ks
Lant
e 20
14
RCT
None
Fa
ce-to
-face
Gr
oup
1: 1
gr
oup
2: 3
12
6
mon
ths
Van
Schi
jnde
l13
2014
RC
T Be
havi
our c
hang
e te
chni
ques
, Th
eory
of p
lann
ed b
ehav
iour
, Soc
ial
cogn
itive
theo
ry
Face
-to-fa
ce
3
32
6 m
onth
s
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
Bart
ley
2011
Ca
se se
ries
None
Fa
ce-to
-face
, gro
up
0,5
(onc
e in
2
wee
ks)
12 m
onth
s No
ne
Wal
lén
2013
Co
ntro
lled
befo
re-a
nd-a
fter
stud
y
None
Fa
ce-to
-face
5
6 m
onth
s No
ne
Hubb
ard
2014
Ca
se se
ries
None
Fa
ce-to
-face
Un
know
n Un
know
n No
ne
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Clup
hf
2001
No
n-RC
T No
ne
Face
-to-fa
ce, g
roup
3
12
6 w
eeks
Mar
shal
l 20
03
Case
serie
s No
ne
Face
-to-fa
ce
1 6-
8 No
ne
Ewin
g 20
04
Non-
RCT
None
Fa
ce-to
-face
, gro
up
1 8
None
Brad
ley
2005
Ca
se se
ries
None
Fa
ce-to
-face
, gro
up
1 12
mon
ths
None
Chap
man
20
05
Cont
rolle
d be
fore
-and
-afte
r st
udy
None
Fa
ce-to
-face
, ind
ivid
ually
Un
know
n 12
mon
ths
None
Man
n 20
06
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
1
9 No
ne
Saile
r 20
06
Case
serie
s No
ne
Face
-to-fa
ce, g
roup
1
10
2, 3
and
4
wee
ks
87
14 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
Chap
man
2008
Co
ntro
lled
befo
re-a
nd-a
fter
stud
y
None
Fa
ce-to
-face
4-
5 pe
r yea
r 18
mon
ths
4,5
year
s
Bazz
ano
2009
Ca
se se
ries
Socia
l cog
nitiv
e th
eory
Fa
ce-to
-face
2
7 m
onth
s No
ne
Mel
ville
20
11
Case
serie
s No
ne
Face
-to-fa
ce, i
ndiv
idua
lly
1 in
2-3
wee
ks
24
None
Saun
ders
20
11
Case
serie
s No
ne
Face
-to-fa
ce, i
ndiv
idua
lly
Mon
thly
6
mon
ths
6 m
onth
s
Case
y 20
12
Case
serie
s No
ne
Face
-to-fa
ce
4 13
No
ne
McD
erm
ott
2012
RC
T So
cial c
ogni
tive
theo
ry
Face
-to-fa
ce, g
roup
1
8 10
mon
ths
Wilh
ite
2012
Ca
se se
ries
None
Fa
ce-to
-face
, ind
ivid
ually
3
12
None
Beek
en
2013
RC
T So
cial c
ogni
tive
theo
ry, c
ontr
ol
theo
ry, B
ehav
iour
chan
ge
tech
niqu
es
Face
-to-fa
ce, g
roup
1
12
3 m
onth
s
Berg
stro
m14
20
13
RCT
Socia
l cog
nitiv
e th
eory
Fa
ce-to
-face
, gro
up
10 se
ssio
ns
12-1
6 m
onth
s No
ne
Curt
in
2013
RC
T No
ne
Face
-to-fa
ce, g
roup
1
6 m
onth
s 6
mon
ths
Donn
elly
20
13
RCT
None
Fa
ce-to
-face
5-
7 18
No
ne
Mar
ks
2013
RC
T Tr
anst
heor
etica
l mod
el, s
ocia
l co
gniti
ve th
eory
Fa
ce-to
-face
3
12
None
Pett
2013
Ca
se se
ries
Tran
sthe
oret
ical m
odel
, soc
ial
cogn
itive
theo
ry, B
ronf
enbr
enne
r ec
olog
ical t
heor
y of
hum
an
deve
lopm
ent
Face
-to-fa
ce
2 12
3
mon
ths
Wal
lén
2013
Hi
stor
ically
co
ntro
lled
stud
y No
ne
Face
-to-fa
ce
2-3
24 m
onth
s No
ne
Span
os
2014
Ca
se se
ries
None
Fa
ce-to
-face
, ind
ivid
ually
9
sess
ions
16
No
ne
Ptom
ey
2015
RC
T No
ne
Face
-to-fa
ce
1 8
None
138541-Willems_BNW.indd 86 31-10-19 10:07
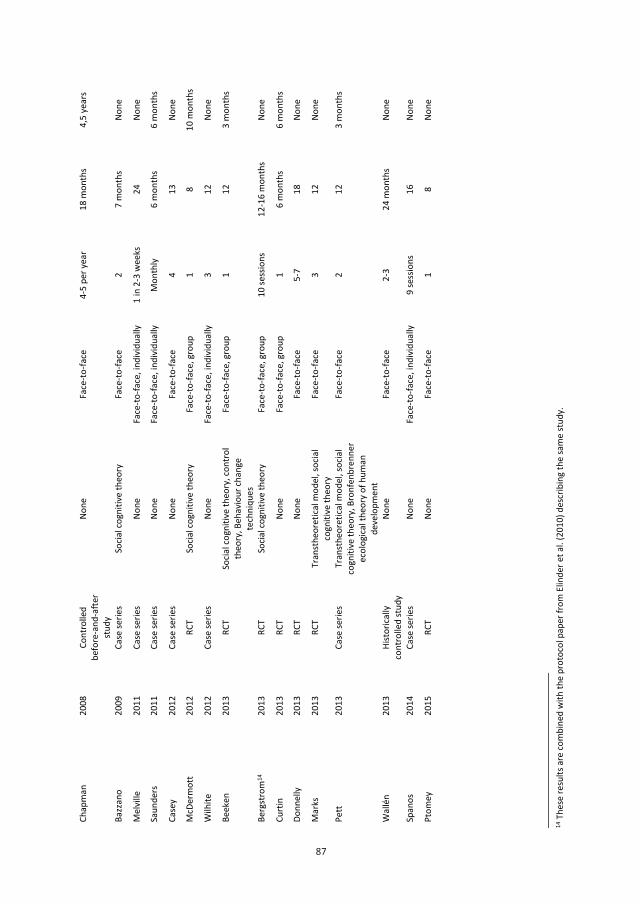
87
87
14 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
Chap
man
2008
Co
ntro
lled
befo
re-a
nd-a
fter
stud
y
None
Fa
ce-to
-face
4-
5 pe
r yea
r 18
mon
ths
4,5
year
s
Bazz
ano
2009
Ca
se se
ries
Socia
l cog
nitiv
e th
eory
Fa
ce-to
-face
2
7 m
onth
s No
ne
Mel
ville
20
11
Case
serie
s No
ne
Face
-to-fa
ce, i
ndiv
idua
lly
1 in
2-3
wee
ks
24
None
Saun
ders
20
11
Case
serie
s No
ne
Face
-to-fa
ce, i
ndiv
idua
lly
Mon
thly
6
mon
ths
6 m
onth
s
Case
y 20
12
Case
serie
s No
ne
Face
-to-fa
ce
4 13
No
ne
McD
erm
ott
2012
RC
T So
cial c
ogni
tive
theo
ry
Face
-to-fa
ce, g
roup
1
8 10
mon
ths
Wilh
ite
2012
Ca
se se
ries
None
Fa
ce-to
-face
, ind
ivid
ually
3
12
None
Beek
en
2013
RC
T So
cial c
ogni
tive
theo
ry, c
ontr
ol
theo
ry, B
ehav
iour
chan
ge
tech
niqu
es
Face
-to-fa
ce, g
roup
1
12
3 m
onth
s
Berg
stro
m14
20
13
RCT
Socia
l cog
nitiv
e th
eory
Fa
ce-to
-face
, gro
up
10 se
ssio
ns
12-1
6 m
onth
s No
ne
Curt
in
2013
RC
T No
ne
Face
-to-fa
ce, g
roup
1
6 m
onth
s 6
mon
ths
Donn
elly
20
13
RCT
None
Fa
ce-to
-face
5-
7 18
No
ne
Mar
ks
2013
RC
T Tr
anst
heor
etica
l mod
el, s
ocia
l co
gniti
ve th
eory
Fa
ce-to
-face
3
12
None
Pett
2013
Ca
se se
ries
Tran
sthe
oret
ical m
odel
, soc
ial
cogn
itive
theo
ry, B
ronf
enbr
enne
r ec
olog
ical t
heor
y of
hum
an
deve
lopm
ent
Face
-to-fa
ce
2 12
3
mon
ths
Wal
lén
2013
Hi
stor
ically
co
ntro
lled
stud
y No
ne
Face
-to-fa
ce
2-3
24 m
onth
s No
ne
Span
os
2014
Ca
se se
ries
None
Fa
ce-to
-face
, ind
ivid
ually
9
sess
ions
16
No
ne
Ptom
ey
2015
RC
T No
ne
Face
-to-fa
ce
1 8
None
138541-Willems_BNW.indd 87 31-10-19 10:07
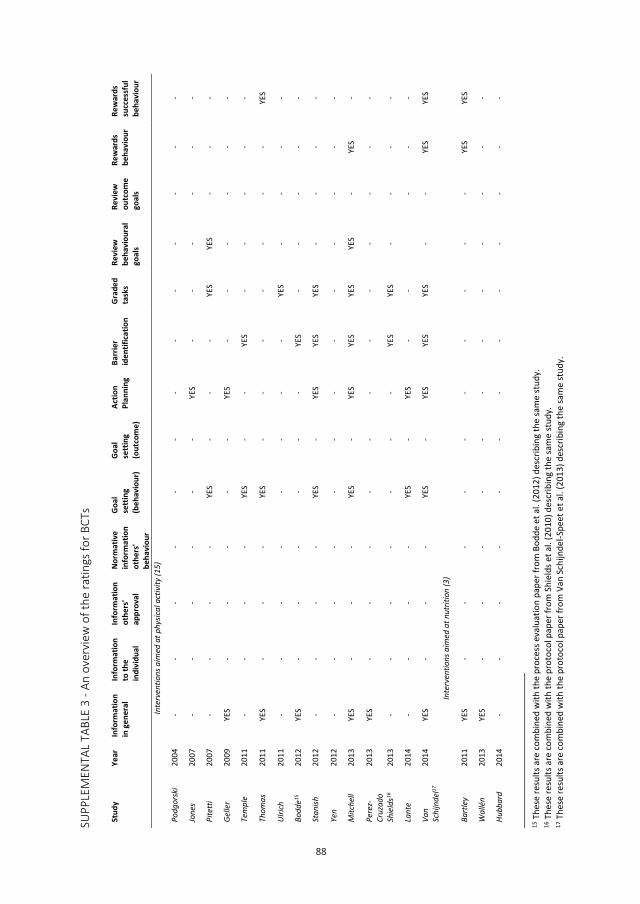
88
88
SUPP
LEM
ENTA
L TA
BLE
3 - A
n ov
ervi
ew o
f the
ratin
gs fo
r BCT
s
15 T
hese
resu
lts a
re co
mbi
ned
with
the
proc
ess e
valu
atio
n pa
per f
rom
Bod
de e
t al.
(201
2) d
escr
ibin
g th
e sa
me
stud
y.
16 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om S
hiel
ds e
t al.
(201
0) d
escr
ibin
g th
e sa
me
stud
y.
17 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om V
an S
chijn
del-S
peet
et a
l. (2
013)
des
crib
ing
the
sam
e st
udy.
Stud
y Ye
ar
Info
rmat
ion
in g
ener
al
Info
rmat
ion
to th
e in
divi
dual
Info
rmat
ion
othe
rs'
appr
oval
Norm
ativ
e in
form
atio
n ot
hers
' be
havi
our
Goal
se
tting
(b
ehav
iour
)
Goal
se
tting
(o
utco
me)
Actio
n Pl
anni
ng
Barr
ier
iden
tifica
tion
Grad
ed
task
s Re
view
be
havi
oura
l go
als
Revi
ew
outc
ome
goal
s
Rew
ards
be
havi
our
Rew
ards
su
cces
sful
be
havi
our
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(15)
Podg
orsk
i 20
04
- -
- -
- -
- -
- -
- -
-
Jone
s 20
07
- -
- -
- -
YES
- -
- -
- -
Pite
tti
2007
-
- -
- YE
S -
- -
YES
YES
- -
-
Gelle
r 20
09
YES
- -
- -
- YE
S -
- -
- -
-
Tem
ple
2011
-
- -
- YE
S -
- YE
S -
- -
- -
Thom
as
2011
YE
S -
- -
YES
- -
- -
- -
- YE
S
Ulric
h 20
11
- -
- -
- -
- -
YES
- -
- -
Bodd
e15
2012
YE
S -
- -
- -
- YE
S -
- -
- -
Stan
ish
2012
-
- -
- YE
S -
YES
YES
YES
- -
- -
Yen
2012
-
- -
- -
- -
- -
- -
- -
Mitc
hell
2013
YE
S -
- -
YES
- YE
S YE
S YE
S YE
S -
YES
-
Pere
z-Cr
uzad
o 20
13
YES
- -
- -
- -
- -
- -
- -
Shie
lds16
20
13
- -
- -
- -
- YE
S YE
S -
- -
-
Lant
e 20
14
- -
- -
YES
- YE
S -
-
- -
-
Van
Schi
jnde
l17
2014
YE
S -
- -
YES
- YE
S YE
S YE
S -
- YE
S YE
S
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
Bart
ley
2011
YE
S -
- -
- -
- -
- -
- YE
S YE
S
Wal
lén
2013
YE
S -
- -
- -
- -
- -
- -
-
Hubb
ard
2014
-
- -
- -
- -
- -
- -
- -
89
18 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Clup
hf
2001
-
- -
- -
- -
- -
- -
YES
YES
Mar
shal
l 20
03
YES
- -
- -
- -
- -
- -
- -
Ewin
g 20
04
YES
- -
- -
- YE
S YE
S -
- -
- -
Brad
ley
2005
YE
S -
- -
- -
- -
- -
- -
-
Chap
man
20
05
YES
- -
- -
- YE
S YE
S -
- -
- -
Man
n 20
06
YES
- -
- -
- -
- -
- -
- -
Saile
r 20
06
YES
- -
- -
YES
- -
- -
YES
YES
YES
Chap
man
2008
YE
S -
- -
- -
YES
- -
- -
- -
Bazz
ano
2009
YE
S -
- -
- -
- -
- -
- -
YES
Mel
ville
20
11
YES
- -
- YE
S YE
S -
YES
YES
YES
YES
- -
Saun
ders
20
11
- -
- -
YES
- -
YES
- -
- -
YES
Case
y 20
12
YES
- -
- YE
S YE
S -
- YE
S -
- YE
S -
McD
erm
ott
2012
YE
S -
- -
- -
- YE
S -
- -
- -
Wilh
ite
2012
YE
S -
- -
YES
- YE
S -
- YE
S -
- YE
S
Beek
en
2013
YE
S -
- -
YES
- -
- -
- -
- -
Berg
stro
m18
20
13
YES
- YE
S -
YES
- YE
S -
- -
- -
-
Curt
in
2013
YE
S -
- -
YES
- YE
S -
- -
- YE
S -
Donn
elly
20
13
YES
- -
- YE
S YE
S -
YES
- YE
S YE
S -
YES
Mar
ks
2013
YE
S -
- -
YES
- -
YES
- -
- -
-
Pett
20
13
YES
- -
- YE
S -
- YE
S -
- -
- -
Wal
lén
2013
YE
S -
- -
- -
- -
- -
- -
-
Span
os
2014
-
- -
- YE
S -
YES
- -
- -
- -
Ptom
ey
2015
-
- -
- YE
S YE
S -
YES
YES
YES
YES
- -
Tota
l -
27
0 1
0 19
5
13
15
9 6
4 7
9
138541-Willems_BNW.indd 88 31-10-19 10:07
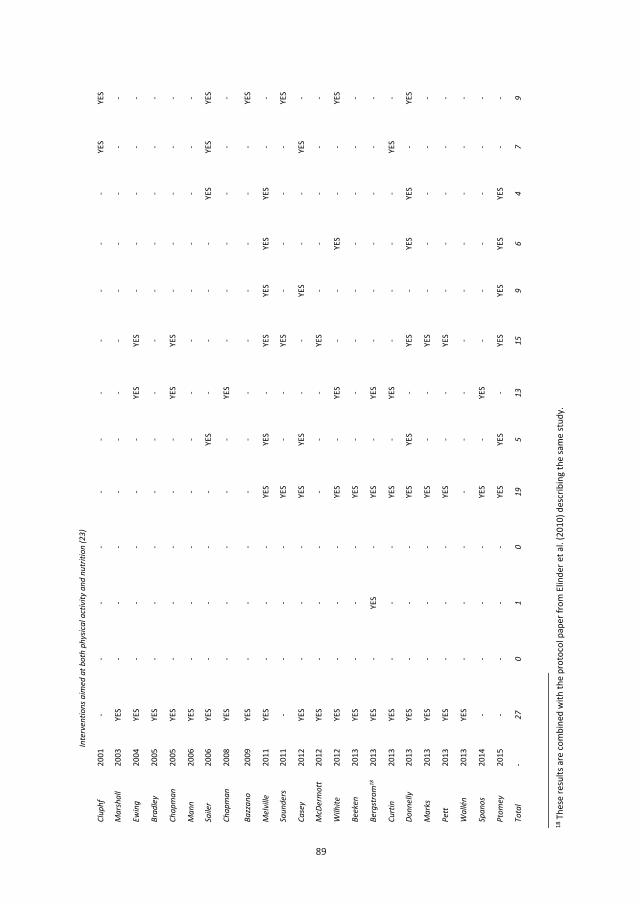
89
89
18 T
hese
resu
lts a
re co
mbi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Clup
hf
2001
-
- -
- -
- -
- -
- -
YES
YES
Mar
shal
l 20
03
YES
- -
- -
- -
- -
- -
- -
Ewin
g 20
04
YES
- -
- -
- YE
S YE
S -
- -
- -
Brad
ley
2005
YE
S -
- -
- -
- -
- -
- -
-
Chap
man
20
05
YES
- -
- -
- YE
S YE
S -
- -
- -
Man
n 20
06
YES
- -
- -
- -
- -
- -
- -
Saile
r 20
06
YES
- -
- -
YES
- -
- -
YES
YES
YES
Chap
man
2008
YE
S -
- -
- -
YES
- -
- -
- -
Bazz
ano
2009
YE
S -
- -
- -
- -
- -
- -
YES
Mel
ville
20
11
YES
- -
- YE
S YE
S -
YES
YES
YES
YES
- -
Saun
ders
20
11
- -
- -
YES
- -
YES
- -
- -
YES
Case
y 20
12
YES
- -
- YE
S YE
S -
- YE
S -
- YE
S -
McD
erm
ott
2012
YE
S -
- -
- -
- YE
S -
- -
- -
Wilh
ite
2012
YE
S -
- -
YES
- YE
S -
- YE
S -
- YE
S
Beek
en
2013
YE
S -
- -
YES
- -
- -
- -
- -
Berg
stro
m18
20
13
YES
- YE
S -
YES
- YE
S -
- -
- -
-
Curt
in
2013
YE
S -
- -
YES
- YE
S -
- -
- YE
S -
Donn
elly
20
13
YES
- -
- YE
S YE
S -
YES
- YE
S YE
S -
YES
Mar
ks
2013
YE
S -
- -
YES
- -
YES
- -
- -
-
Pett
20
13
YES
- -
- YE
S -
- YE
S -
- -
- -
Wal
lén
2013
YE
S -
- -
- -
- -
- -
- -
-
Span
os
2014
-
- -
- YE
S -
YES
- -
- -
- -
Ptom
ey
2015
-
- -
- YE
S YE
S -
YES
YES
YES
YES
- -
Tota
l -
27
0 1
0 19
5
13
15
9 6
4 7
9
138541-Willems_BNW.indd 89 31-10-19 10:07
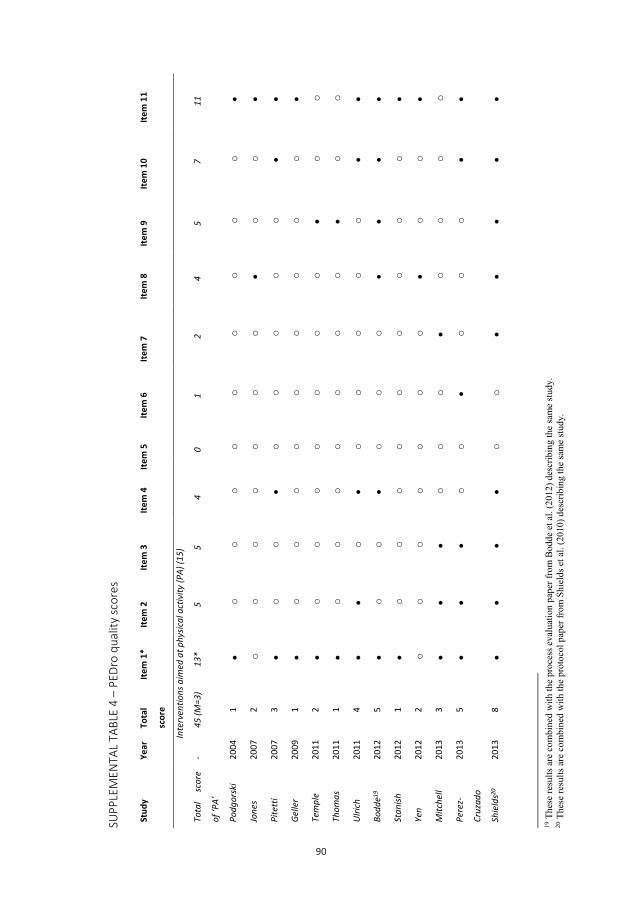
90
90
SUPP
LEM
ENTA
L TA
BLE
4 –
PEDr
o qu
ality
scor
es
19 T
hese
resu
lts a
re c
ombi
ned
with
the
proc
ess e
valu
atio
n pa
per f
rom
Bod
de e
t al.
(201
2) d
escr
ibin
g th
e sa
me
stud
y.
20 T
hese
resu
lts a
re c
ombi
ned
with
the
prot
ocol
pap
er fr
om S
hiel
ds e
t al.
(201
0) d
escr
ibin
g th
e sa
me
stud
y.
Stud
y Ye
ar
Tota
l
scor
e
Item
1*
Item
2
Item
3
Item
4
Item
5
Item
6
Item
7
Item
8
Item
9
Item
10
Item
11
Inte
rven
tions
aim
ed a
t phy
sical
act
ivity
(PA)
(15)
Tota
l sc
ore
of ‘P
A’
- 45
(M=3
) 13
* 5
5 4
0 1
2 4
5 7
11
Podg
orsk
i 20
04
1
o
o
o
o
o
o
o
o
o
Jone
s 20
07
2 o
o
o
o
o
o
o
o
o
Pite
tti
2007
3
o
o
o
o
o
o
o
Gelle
r 20
09
1
o
o
o
o
o
o
o
o
o
Tem
ple
2011
2
o
o
o
o
o
o
o
o
o
Thom
as
2011
1
o
o
o
o
o
o
o
o
o
Ulric
h 20
11
4
o
o
o
o
o
o
Bodd
e19
2012
5
o
o
o
o
o
Stan
ish
2012
1
o
o
o
o
o
o
o
o
o
Yen
2012
2
o
o
o
o
o
o
o
o
o
Mitc
hell
2013
3
o
o
o
o
o
o
o
Pere
z-
Cruz
ado
2013
5
o
o
o
o
o
Shie
lds20
20
13
8
o
o
91
21 T
hese
resu
lts a
re c
ombi
ned
with
the
prot
ocol
pap
er fr
om V
an S
chijn
del-S
peet
et a
l. (2
014)
des
crib
ing
the
sam
e st
udy.
Lant
e 20
14
5
o
o
o
o
o
van
Schi
jnde
l21
2013
2
o
o
o
o
o
o
o
o
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
Tota
l sco
re
of ‘n
utrit
ion’
- 5
(M=1
.7)
1*
0 0
1 0
0 0
1 0
1 1
Bart
ley
2011
2
o
o
o
o
o
o
o
o
o
Wal
lén
2013
3
o
o
o
o
o
o
o
o
Hubb
ard
2014
0
o
o
o
o
o
o
o
o
o
o
o
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Tota
l sc
ore
of ‘b
oth’
- 69
(M=3
)
15*
8 5
6 0
0 3
12
6 13
16
Clup
hf
2001
3
o
o
o
o
o
o
o
o
Mar
shal
l 20
03
2 o
o
o
o
o
o
o
o
o
Ewin
g 20
04
1 o
o
o
o
o
o
o
o
o
o
Brad
ley
2005
1
o
o
o
o
o
o
o
o
o
o
Chap
man
20
05
3 o
o
o
o
o
o
o
o
Man
n 20
06
1
o
o
o
o
o
o
o
o
o
Saile
r 20
06
1 o
o
o
o
o
o
o
o
o
o
Chap
man
2008
3
o
o
o
o
o
o
o
o
Bazz
ano
2009
0
o
o
o
o
o
o
o
o
o
o
Mel
ville
20
11
2
o
o
o
o
o
o
o
o
138541-Willems_BNW.indd 90 31-10-19 10:07
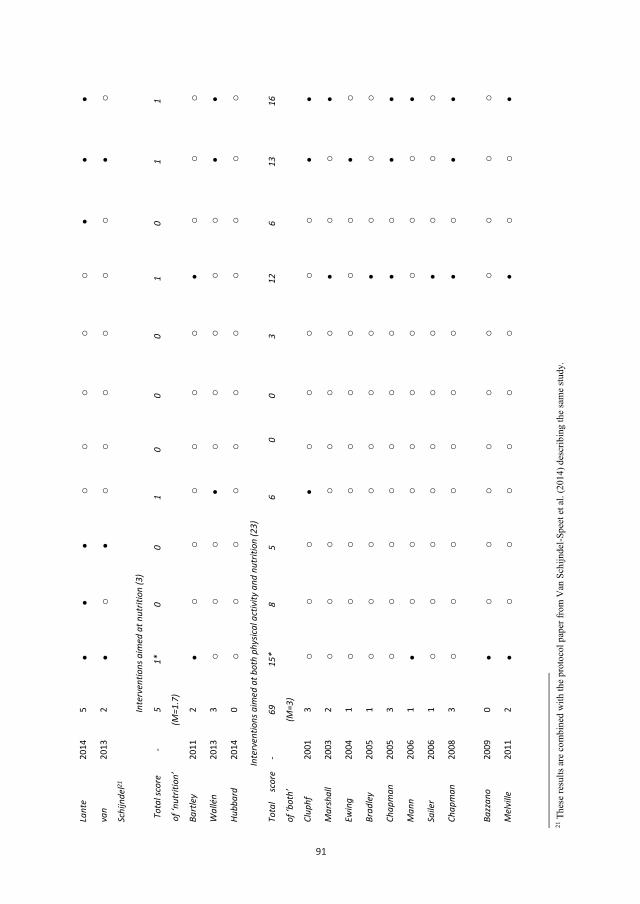
91
91
21 T
hese
resu
lts a
re c
ombi
ned
with
the
prot
ocol
pap
er fr
om V
an S
chijn
del-S
peet
et a
l. (2
014)
des
crib
ing
the
sam
e st
udy.
Lant
e 20
14
5
o
o
o
o
o
van
Schi
jnde
l21
2013
2
o
o
o
o
o
o
o
o
Inte
rven
tions
aim
ed a
t nut
ritio
n (3
)
Tota
l sco
re
of ‘n
utrit
ion’
- 5
(M=1
.7)
1*
0 0
1 0
0 0
1 0
1 1
Bart
ley
2011
2
o
o
o
o
o
o
o
o
o
Wal
lén
2013
3
o
o
o
o
o
o
o
o
Hubb
ard
2014
0
o
o
o
o
o
o
o
o
o
o
o
Inte
rven
tions
aim
ed a
t bot
h ph
ysica
l act
ivity
and
nut
ritio
n (2
3)
Tota
l sc
ore
of ‘b
oth’
- 69
(M=3
)
15*
8 5
6 0
0 3
12
6 13
16
Clup
hf
2001
3
o
o
o
o
o
o
o
o
Mar
shal
l 20
03
2 o
o
o
o
o
o
o
o
o
Ewin
g 20
04
1 o
o
o
o
o
o
o
o
o
o
Brad
ley
2005
1
o
o
o
o
o
o
o
o
o
o
Chap
man
20
05
3 o
o
o
o
o
o
o
o
Man
n 20
06
1
o
o
o
o
o
o
o
o
o
Saile
r 20
06
1 o
o
o
o
o
o
o
o
o
o
Chap
man
2008
3
o
o
o
o
o
o
o
o
Bazz
ano
2009
0
o
o
o
o
o
o
o
o
o
o
Mel
ville
20
11
2
o
o
o
o
o
o
o
o
138541-Willems_BNW.indd 91 31-10-19 10:07
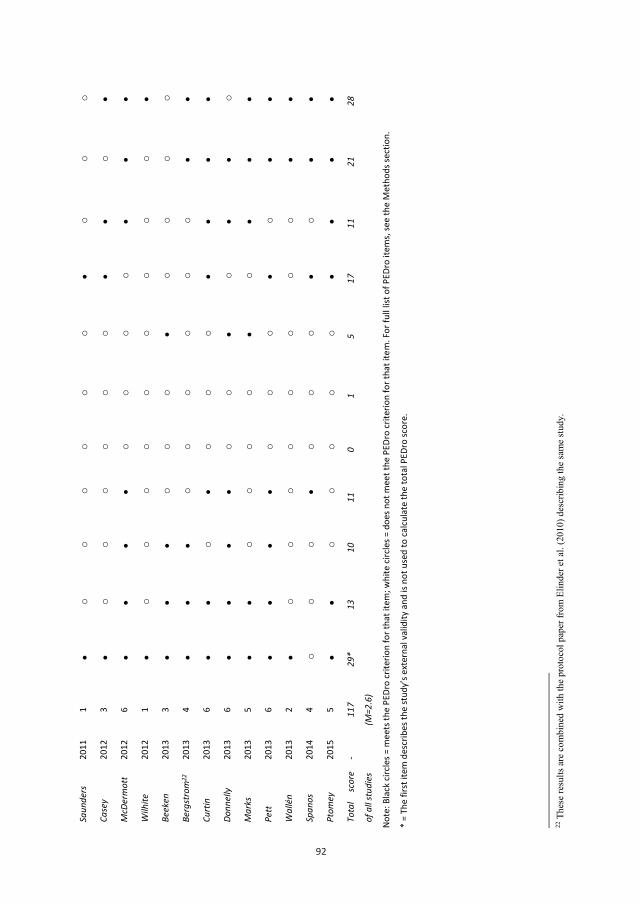
92
92
Note
: Bla
ck ci
rcle
s = m
eets
the
PEDr
o cr
iterio
n fo
r tha
t ite
m; w
hite
circ
les =
doe
s not
mee
t the
PED
ro cr
iterio
n fo
r tha
t ite
m. F
or fu
ll lis
t of P
EDro
item
s, se
e th
e M
etho
ds se
ctio
n.
* =
The
first
item
des
crib
es th
e st
udy’
s ext
erna
l val
idity
and
is n
ot u
sed
to ca
lcula
te th
e to
tal P
EDro
scor
e.
22 T
hese
resu
lts a
re c
ombi
ned
with
the
prot
ocol
pap
er fr
om E
linde
r et a
l. (2
010)
des
crib
ing
the
sam
e st
udy.
Saun
ders
20
11
1
o
o
o
o
o
o
o
o
o
Case
y 20
12
3
o
o
o
o
o
o
o
McD
erm
ott
2012
6
o
o
o
o
Wilh
ite
2012
1
o
o
o
o
o
o
o
o
o
Beek
en
2013
3
o
o
o
o
o
o
o
Berg
stro
m22
20
13
4
o
o
o
o
o
o
Curt
in
2013
6
o
o
o
o
Donn
elly
20
13
6
o
o
o
o
Mar
ks
2013
5
o
o
o
o
o
Pett
20
13
6
o
o
o
o
Wal
lén
2013
2
o
o
o
o
o
o
o
o
Span
os
2014
4
o
o
o
o
o
o
o
Ptom
ey
2015
5
o
o
o
o
o
Tota
l sc
ore
of a
ll st
udie
s
- 11
7
(M=2
.6)
29*
13
10
11
0 1
5 17
11
21
28
138541-Willems_BNW.indd 92 31-10-19 10:07

138541-Willems_BNW.indd 93 31-10-19 10:07
Chapter 4
Exploration of suitable behaviour change techniques for lifestyle change in
individuals with mild intellectual disabilities: A Delphi study
Mariël Willems
Aly Waninge
Johan de Jong
Thessa I.M. Hilgenkamp
Cees P. Van der Schans
Journal of Applied Research in Intellectual Disabilities, 2019, 32(3), 543-557.
138541-Willems_BNW.indd 94 31-10-19 10:07
Chapter 4
Exploration of suitable behaviour change techniques for lifestyle change in
individuals with mild intellectual disabilities: A Delphi study
Mariël Willems
Aly Waninge
Johan de Jong
Thessa I.M. Hilgenkamp
Cees P. Van der Schans
Journal of Applied Research in Intellectual Disabilities, 2019, 32(3), 543-557.
138541-Willems_BNW.indd 95 31-10-19 10:07

96
ABSTRACT
Background: Promotion of a healthy lifestyle for individuals with mild intellectual disabilities is important.
However, the suitability of behaviour change techniques (BCTs) for these individuals is still unclear.
Methods: A Delphi study was performed using the Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy
of BCTs (n = 40). Health professionals (professional caregivers, behavioural scientists, health professionals,
intellectual disability physicians) participated in an online survey to determine whether BCTs were suitable or
unsuitable. Comments from participants were analysed qualitatively.
Results: Consensus was reached for 25 BCTs out of 40.The most suitable BCTs were barrier identification (97%),
set graded tasks (97%) and reward effort towards behaviour (95%). No significant differences were found for
intergroup effects.
Conclusion: Regardless of their position and education level, health professionals reached consensus about the
suitability of BCTs for individuals with mild intellectual disabilities. Increased use of these BCTs could result in
more effective promotion of a healthy lifestyle.
97
1 | INTRODUCTION
Adults with intellectual disabilities are more at risk of being overweight, obese and inactive compared to adults
without intellectual disabilities (Hilgenkamp, Reis, Van Wijck, & Evenhuis, 2012; Melville, Hamilton, Hankey,
Miller, & Boyle, 2007; Waninge et al., 2013). The promotion of a healthy lifestyle, therefore, is important for
individuals with intellectual disabilities (Alesi & Pepi, 2015). Many interventions are aimed at supporting a healthy
lifestyle for this population by targeting nutrition, physical activity or both (Willems, Hilgenkamp, Havik,
Waninge, & Melville, 2017).
To promote a healthy lifestyle, several reviews confirmed the effectiveness of techniques to change behaviour,
called behaviour change techniques (BCTs), for the general population (Bird et al., 2013, Greaves et al., 2011;
Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Olander et al., 2013; Williams & French, 2011).
Bartholomew and Mullen (2011) recommended improving the effectiveness of health‐related behavioural
change and increasing the possibilities of replicating a positive effect by increasing our understanding of the
underlying action mechanisms. One recommendation was to determine techniques to change lifestyle behaviour
(Abraham & Michie, 2008; Rothman, 2004). To achieve this, a 26‐item taxonomy of behaviour change techniques
was developed by Abraham and Michie (2008) which was later refined by Michie et al. (2011) resulting in the 40‐
item Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy. Another taxonomy was developed later,
named the Behavior Change Technique Taxonomy v1 which consisted of 93 techniques (Michie et al., 2013).
However, there was heterogeneity between results with respect to which particular BCTs were effective for the
general population. Also, associations between the number of used BCTs and the effectiveness of the
intervention as well as the combination of particular BCTs are ambiguous (Bird et al., 2013; Olander et al., 2013).
Some BCTs also do not seem to be interchangeable between specific health behaviours (Michie et al., 2011). In
addition, the suitability of BCTs for specific populations is understudied, and they may need to be adapted or
extended (Michie et al., 2011; Van Schijndel‐Speet, 2015).
A review regarding the use of BCTs in lifestyle interventions for individuals with intellectual disabilities
determined that the BCT’s “Plan social support/social change” and “Provide information on consequences of
behaviour in general” were mostly used (Willems et al., 2017). However, it is unclear whether these BCTs are
effective for individuals with intellectual disabilities and whether the use of these BCTs is sufficient for changing
the lifestyles of these individuals. Also, the BCTs that are used in the previous studies are often not explicitly
labelled as such, which may indicate that these BCTs are used unintentionally. Without intended use of BCTs and
evaluation of this use, effectiveness of the used BCTs could not be determined. BCTs targeting an increase in
knowledge and understanding as well as those primarily using executive functioning may be less suitable for
individuals with mild intellectual disabilities because translation of health knowledge into behaviour might be
difficult for these individuals (Kuijken, Naaldenberg, Nijhuis‐van der Sanden, & Schrojenstein‐Lantman de Valk,
2016). Until now, the suitability of BCTs in lifestyle interventions for individuals with intellectual disabilities
remains unclear.
138541-Willems_BNW.indd 96 31-10-19 10:07

96
ABSTRACT
Background: Promotion of a healthy lifestyle for individuals with mild intellectual disabilities is important.
However, the suitability of behaviour change techniques (BCTs) for these individuals is still unclear.
Methods: A Delphi study was performed using the Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy
of BCTs (n = 40). Health professionals (professional caregivers, behavioural scientists, health professionals,
intellectual disability physicians) participated in an online survey to determine whether BCTs were suitable or
unsuitable. Comments from participants were analysed qualitatively.
Results: Consensus was reached for 25 BCTs out of 40.The most suitable BCTs were barrier identification (97%),
set graded tasks (97%) and reward effort towards behaviour (95%). No significant differences were found for
intergroup effects.
Conclusion: Regardless of their position and education level, health professionals reached consensus about the
suitability of BCTs for individuals with mild intellectual disabilities. Increased use of these BCTs could result in
more effective promotion of a healthy lifestyle.
97
1 | INTRODUCTION
Adults with intellectual disabilities are more at risk of being overweight, obese and inactive compared to adults
without intellectual disabilities (Hilgenkamp, Reis, Van Wijck, & Evenhuis, 2012; Melville, Hamilton, Hankey,
Miller, & Boyle, 2007; Waninge et al., 2013). The promotion of a healthy lifestyle, therefore, is important for
individuals with intellectual disabilities (Alesi & Pepi, 2015). Many interventions are aimed at supporting a healthy
lifestyle for this population by targeting nutrition, physical activity or both (Willems, Hilgenkamp, Havik,
Waninge, & Melville, 2017).
To promote a healthy lifestyle, several reviews confirmed the effectiveness of techniques to change behaviour,
called behaviour change techniques (BCTs), for the general population (Bird et al., 2013, Greaves et al., 2011;
Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Olander et al., 2013; Williams & French, 2011).
Bartholomew and Mullen (2011) recommended improving the effectiveness of health‐related behavioural
change and increasing the possibilities of replicating a positive effect by increasing our understanding of the
underlying action mechanisms. One recommendation was to determine techniques to change lifestyle behaviour
(Abraham & Michie, 2008; Rothman, 2004). To achieve this, a 26‐item taxonomy of behaviour change techniques
was developed by Abraham and Michie (2008) which was later refined by Michie et al. (2011) resulting in the 40‐
item Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy. Another taxonomy was developed later,
named the Behavior Change Technique Taxonomy v1 which consisted of 93 techniques (Michie et al., 2013).
However, there was heterogeneity between results with respect to which particular BCTs were effective for the
general population. Also, associations between the number of used BCTs and the effectiveness of the
intervention as well as the combination of particular BCTs are ambiguous (Bird et al., 2013; Olander et al., 2013).
Some BCTs also do not seem to be interchangeable between specific health behaviours (Michie et al., 2011). In
addition, the suitability of BCTs for specific populations is understudied, and they may need to be adapted or
extended (Michie et al., 2011; Van Schijndel‐Speet, 2015).
A review regarding the use of BCTs in lifestyle interventions for individuals with intellectual disabilities
determined that the BCT’s “Plan social support/social change” and “Provide information on consequences of
behaviour in general” were mostly used (Willems et al., 2017). However, it is unclear whether these BCTs are
effective for individuals with intellectual disabilities and whether the use of these BCTs is sufficient for changing
the lifestyles of these individuals. Also, the BCTs that are used in the previous studies are often not explicitly
labelled as such, which may indicate that these BCTs are used unintentionally. Without intended use of BCTs and
evaluation of this use, effectiveness of the used BCTs could not be determined. BCTs targeting an increase in
knowledge and understanding as well as those primarily using executive functioning may be less suitable for
individuals with mild intellectual disabilities because translation of health knowledge into behaviour might be
difficult for these individuals (Kuijken, Naaldenberg, Nijhuis‐van der Sanden, & Schrojenstein‐Lantman de Valk,
2016). Until now, the suitability of BCTs in lifestyle interventions for individuals with intellectual disabilities
remains unclear.
138541-Willems_BNW.indd 97 31-10-19 10:07

98
Specific subgroups need specific BCTs that are tailored to the subgroup or the individuals’ preferences and living
situation (Van Schijndel‐Speet, 2015). To tailor BCTs to people with mild intellectual disabilities, it is necessary to
have a clear understanding of the characteristics of this subgroup. According to the Diagnostic and statistical
manual of mental disorders (DSM 5), they suffer from (a) deficits in intellectual functions (e.g., reasoning,
problem‐solving, planning, abstract thinking), (b) deficits in adaptive functions and (c) onset of deficits during the
developmental period (American Psychiatric Association, 2013). Specifically, people with mild intellectual
disabilities need support with abstract thinking, executive functioning, academic skills and additional support
within daily living (American Psychiatric Association, 2013). According to the International statistical classification
of diseases and related health problems (ICD‐10), it is also important to consider the emotional and social
development because of the influence on daily functioning (WHO, 1992). In sum, there is only minimal insight
into the suitability of BCTs for individuals with intellectual disabilities, and additional insight is needed to
determine which BCTs could be suitable for supporting a change in their lifestyles (Willems et al., 2017). This
study aimed to query experts from the field with the Delphi method in order to investigate the suitability of BCTs
for supporting a change in the lifestyles of people with mild intellectual disabilities.
2 | METHODS
2.1 | Design
In this Delphi study, the consensus of experts was achieved in several rounds with intermediate feedback
regarding the suitability of BCTs in individuals with mild intellectual disabilities (De Meyrick, 2003). This method
is considered appropriate for health‐promotion research in “new” areas with only a small knowledge‐base (De
Meyrick, 2003; Milat, King, Bauman, & Redman, 2013; Whitehead, 2008). The Delphi study was performed
between April 2017 and July 2017. The CALO‐RE taxonomy of BCTs (Michie et al., 2011) was used instead of the
Behavior Change Technique Taxonomy (Michie et al., 2013) since this last taxonomy was too extensive for the
goal in this Delphi study, exploring the suitability of BCTs specifically for people with mild intellectual disabilities.
The panel was completed when 66.67% consensus was reached for the suitability of all BCTs or after a maximum
of three rounds since the literature stated that three rounds are usually enough and considering the (time)
investment of professionals participating in the panel (Boulkedid, Abdoul, Loustau, Sibony, & Alberti, 2011).
2.2 | Sample
2.2.1 | Criteria for participants
The Delphi panel consisted of three groups of professionals working with individuals in the Netherlands with mild
intellectual disabilities, and the desired number of participants was at least ten per group. These groups were
selected since they primarily work with individuals with mild intellectual disabilities and provide support in their
daily lives. The first group consisted of professional caregivers; the second group consisted of behavioural
scientists; and the third group consisted of allied health professionals including physiotherapists, speech
therapists, dieticians, psychomotor therapists, movement scientists, occupational therapists, family therapists
and nurse practitioners.
99
2.2.2 | Recruitment of participants
Participants were approached through multiple channels for both Delphi rounds in order to achieve the broadest
representation possible:
- Through expert networks in the field of lifestyle promotion research for individuals with mild intellectual
disabilities. These researchers were asked to share the questionnaire with professional caregivers,
behavioural scientists and healthcare professionals in their own network.
- Through a consortium of Dutch intellectual disability care provider organizations. These organizations
invited their employees to participate in the panel. Employees were asked to invite colleagues to join
the research.
- Through a conference about lifestyle and persons with mild intellectual disabilities that was held on 5
April 2017. Visitors to the conference were invited to participate in the panel. They could participate by
emailing the first author.
2.3 | Measurements
The Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy was used for designing the questionnaires
and defining BCTs (Michie et al., 2011). This taxonomy consists of a 40‐item list of theory‐based descriptions of
BCTs that are potentially suitable for improving a lifestyle. The CALO‐RE taxonomy was adapted to the CALO‐RE‐
NL in four steps. First, the BCTs were translated into Dutch using the definitions from the CALO‐RE taxonomy.
Second, the wording of the BCTs was simplified in order to be understandable for all of the participants with
different education levels. Third, examples were drafted for all of the BCTs. Fourth, the CALO‐RE‐NL was
converted into a questionnaire. The CALO‐RE‐NL taxonomy is provided in the Appendix.
The questionnaire was pilot‐tested within three groups of intended participants and a group of research experts.
First, it was submitted digitally to experts in research on lifestyle changes in individuals with mild intellectual
disabilities (n = 5). They provided suggestions for further improvements of the formulations and the examples
that were implemented in the questionnaire. Second, the questionnaire was pilot‐tested in a paper form with
professional caregivers (n = 15) who were working with individuals with mild intellectual disabilities in a Dutch
care provider organization. The caregivers completed the questionnaire and offered feedback regarding the
usability (e.g., duration of the questionnaire, the examples used and advised specification of the degree of
intellectual disabilities) with which the questionnaire was further improved. Third, the adapted questionnaire
was pilot‐tested by the other two groups of participants including behavioural scientists (n = 4) and allied health
professionals (n = 4) working with individuals with mild intellectual disabilities. The questionnaire was delivered
using online survey software (www.qualtrics.com), and questions were offered at random. Their feedback (e.g.,
regarding usability of the online version of the questionnaire and used examples) was used to further improve
the questionnaire and the online procedure, for example, the visibility of the questions.
Delphi Round 1: The final questionnaire including the CALO‐RE‐NL taxonomy was used in the first Delphi round.
The 40 translated BCTs and related examples were presented one‐by‐one in random sequence in order to
138541-Willems_BNW.indd 98 31-10-19 10:07

98
Specific subgroups need specific BCTs that are tailored to the subgroup or the individuals’ preferences and living
situation (Van Schijndel‐Speet, 2015). To tailor BCTs to people with mild intellectual disabilities, it is necessary to
have a clear understanding of the characteristics of this subgroup. According to the Diagnostic and statistical
manual of mental disorders (DSM 5), they suffer from (a) deficits in intellectual functions (e.g., reasoning,
problem‐solving, planning, abstract thinking), (b) deficits in adaptive functions and (c) onset of deficits during the
developmental period (American Psychiatric Association, 2013). Specifically, people with mild intellectual
disabilities need support with abstract thinking, executive functioning, academic skills and additional support
within daily living (American Psychiatric Association, 2013). According to the International statistical classification
of diseases and related health problems (ICD‐10), it is also important to consider the emotional and social
development because of the influence on daily functioning (WHO, 1992). In sum, there is only minimal insight
into the suitability of BCTs for individuals with intellectual disabilities, and additional insight is needed to
determine which BCTs could be suitable for supporting a change in their lifestyles (Willems et al., 2017). This
study aimed to query experts from the field with the Delphi method in order to investigate the suitability of BCTs
for supporting a change in the lifestyles of people with mild intellectual disabilities.
2 | METHODS
2.1 | Design
In this Delphi study, the consensus of experts was achieved in several rounds with intermediate feedback
regarding the suitability of BCTs in individuals with mild intellectual disabilities (De Meyrick, 2003). This method
is considered appropriate for health‐promotion research in “new” areas with only a small knowledge‐base (De
Meyrick, 2003; Milat, King, Bauman, & Redman, 2013; Whitehead, 2008). The Delphi study was performed
between April 2017 and July 2017. The CALO‐RE taxonomy of BCTs (Michie et al., 2011) was used instead of the
Behavior Change Technique Taxonomy (Michie et al., 2013) since this last taxonomy was too extensive for the
goal in this Delphi study, exploring the suitability of BCTs specifically for people with mild intellectual disabilities.
The panel was completed when 66.67% consensus was reached for the suitability of all BCTs or after a maximum
of three rounds since the literature stated that three rounds are usually enough and considering the (time)
investment of professionals participating in the panel (Boulkedid, Abdoul, Loustau, Sibony, & Alberti, 2011).
2.2 | Sample
2.2.1 | Criteria for participants
The Delphi panel consisted of three groups of professionals working with individuals in the Netherlands with mild
intellectual disabilities, and the desired number of participants was at least ten per group. These groups were
selected since they primarily work with individuals with mild intellectual disabilities and provide support in their
daily lives. The first group consisted of professional caregivers; the second group consisted of behavioural
scientists; and the third group consisted of allied health professionals including physiotherapists, speech
therapists, dieticians, psychomotor therapists, movement scientists, occupational therapists, family therapists
and nurse practitioners.
99
2.2.2 | Recruitment of participants
Participants were approached through multiple channels for both Delphi rounds in order to achieve the broadest
representation possible:
- Through expert networks in the field of lifestyle promotion research for individuals with mild intellectual
disabilities. These researchers were asked to share the questionnaire with professional caregivers,
behavioural scientists and healthcare professionals in their own network.
- Through a consortium of Dutch intellectual disability care provider organizations. These organizations
invited their employees to participate in the panel. Employees were asked to invite colleagues to join
the research.
- Through a conference about lifestyle and persons with mild intellectual disabilities that was held on 5
April 2017. Visitors to the conference were invited to participate in the panel. They could participate by
emailing the first author.
2.3 | Measurements
The Coventry, Aberdeen & LOndon – REfined (CALO‐RE) taxonomy was used for designing the questionnaires
and defining BCTs (Michie et al., 2011). This taxonomy consists of a 40‐item list of theory‐based descriptions of
BCTs that are potentially suitable for improving a lifestyle. The CALO‐RE taxonomy was adapted to the CALO‐RE‐
NL in four steps. First, the BCTs were translated into Dutch using the definitions from the CALO‐RE taxonomy.
Second, the wording of the BCTs was simplified in order to be understandable for all of the participants with
different education levels. Third, examples were drafted for all of the BCTs. Fourth, the CALO‐RE‐NL was
converted into a questionnaire. The CALO‐RE‐NL taxonomy is provided in the Appendix.
The questionnaire was pilot‐tested within three groups of intended participants and a group of research experts.
First, it was submitted digitally to experts in research on lifestyle changes in individuals with mild intellectual
disabilities (n = 5). They provided suggestions for further improvements of the formulations and the examples
that were implemented in the questionnaire. Second, the questionnaire was pilot‐tested in a paper form with
professional caregivers (n = 15) who were working with individuals with mild intellectual disabilities in a Dutch
care provider organization. The caregivers completed the questionnaire and offered feedback regarding the
usability (e.g., duration of the questionnaire, the examples used and advised specification of the degree of
intellectual disabilities) with which the questionnaire was further improved. Third, the adapted questionnaire
was pilot‐tested by the other two groups of participants including behavioural scientists (n = 4) and allied health
professionals (n = 4) working with individuals with mild intellectual disabilities. The questionnaire was delivered
using online survey software (www.qualtrics.com), and questions were offered at random. Their feedback (e.g.,
regarding usability of the online version of the questionnaire and used examples) was used to further improve
the questionnaire and the online procedure, for example, the visibility of the questions.
Delphi Round 1: The final questionnaire including the CALO‐RE‐NL taxonomy was used in the first Delphi round.
The 40 translated BCTs and related examples were presented one‐by‐one in random sequence in order to
138541-Willems_BNW.indd 99 31-10-19 10:07

100
prevent question order bias. For every BCT, participants were asked if the BCT was suitable for influencing the
lifestyles of individuals with mild intellectual disabilities. Dichotomous answers included “yes, this technique is
suitable” or “no, this technique is not suitable.” With each dichotomous answer, there was also an open field to
write down comments. The first questionnaire was delivered using the web‐based survey software,
Qualtrics.com, that invited participants by email and which included an anonymous hyperlink to the
questionnaire. Participants were asked to respond within 16 days. Personal information was asked about job
position, years of work experience and email address (not obligatory). Answers were collected and anonymously
analysed. Participants provided informed consent before participating in any of the Delphi rounds.
Delphi Round 2: After the data from the first Delphi round were analysed, a second questionnaire was designed
based on the outcomes from it. The purpose of the second round was to determine consensus about the
suitability of the BCTs in which no consensus was reached in the first round. The BCTs and corresponding
examples were similar to the second questionnaire. The only exception concerned some of the examples that
were not completely clear to the participants; this was expressed in the comments provided by the participants
in the open fields in the first round. Only minor changes were made to the examples (e.g., the time period in
which a behaviour goal had to be completed).
Participants were asked whether or not these BCTs were suitable. Again, there was an open field to write down
comments. The group decisions from Round 1 were shown in percentages per technique using only one decimal
in case the percentage decimal was exactly 0.5. Comments from participants in Round 1 were translated into
statements that were more common and comprehensive by the first author (MW) and checked by the second
author (AW). Disagreements were resolved by a consensus discussion. These resumptive comments (e.g.,
“according to participants of the panel, suitability depends on the client characteristics”) were shown per
technique next to the group decisions from Round 1. The questionnaire was tailored to the groups of participants,
and questions were offered in a random order. The second questionnaire was also delivered using the web‐based
survey software, Qualtrics.com, by which participants were invited through an email containing an anonymous
hyperlink to the questionnaire. Participants were asked to respond within 16 days. Personal information was
asked about job position, years of work experience and email address (not obligatory).
2.4 | Data analyses
Round 1: After collecting the data from the first questionnaire, consensus was determined. There is no generally
accepted cut‐off score for the consensus that was reached (Becker, & Roberts, 2009; Boulkedid et al., 2011). The
present authors used a cut‐off score of 66.67% consensus both for evaluating a BCT as suitable or not (in changing
lifestyle) in the first round. The 66.67% consensus was determined by dividing the number of corresponding
answers of the participants (yes, suitable/no, not suitable) by the number of participants for that group. The
present authors calculated the total consensus (in %) of each group and the total consensus (in %) of all of the
groups together. Since the questions were offered at random, the answers from incomplete questionnaires were
also used in the analyses. The comments of participants were analysed by theme and categorized. These
101
categories or themes were used in the second questionnaire in order to give participants’ feedback on the results
of the first round.
Per profession group, the inter‐rater reliability of the binary suitability scores was estimated by the alpha
coefficient from the ordinal factor analysis performed on the tetrachoric correlation coefficients (Revelle &
Zinbarg, 2009). Reliability was considered poor or moderate (ICC < 0.75), good (ICC 0.75–0.90) or very good (ICC
> 0.90) (Portney & Watkins, 2000). To investigate agreement between profession groups, the present authors
computed the two‐way intraclass correlation coefficient (ICC) (McGraw & Wong, 1996) by using the average BCT
score per profession group. Also for the ICC, reliability was considered poor or moderate (ICC < 0.75), good (ICC
0.75–0.90) or very good (ICC > 0.90) (Portney & Watkins, 2000). To investigate whether there was any systematic
bias of a profession group with respect to any other profession group, a mixed model analysis (Pinheiro, & Bates,
2000) was undertaken on the average BCT scores per profession. In the mixed model, random intercepts were
specified for the BCTs and fixed effects for the profession groups. A pairwise comparison (Hothorn, Bretz, &
Westfall, 2008) was used to analyse the intergroup effects. For all statistical analyses, raters with more than 30%
missing BCT suitability evaluations were discarded from further analysis. R v3.3.0 was used (R Core Team, 2017).
Round 2: After data collection, consensus for the BCTs in Round 2 was determined within each group. The total
number of BCTs with consensus and the number of suitable BCTs for this round was not calculated for the total
group since the BCTs in the second questionnaire differed per group depending on the consensus found in the
first round per group. This made it also impossible to compute the agreement between profession groups and
the systematic bias of a profession group with respect to another profession group.
The present authors calculated the total consensus (in %) for all BCTs of each group and that over all groups.
Suitable BCTs were ranked by mean consensus using the percentages of consensus on suitability for all of the
groups. Comments from participants were analysed regarding theme and then categorized. The answers of
behavioural scientists were compared separately with the other groups since this profession group has the most
extensive education and working experience with BCTs. The present authors compared the consensus of the
behavioural scientists with the consensus of the other groups to identify possible differences in consensus.
3 | RESULTS
3.1 | First Delphi round
A total of 97 professionals responded to the questionnaire in the first round. Ten respondents did not answer
any of the questions. Four participants declared that they did not want to participate in the research and,
therefore, did not respond to further questions. Answers from two participants were excluded from the data
analysis as they did not satisfy the inclusion criteria for participants. Answers of 81 participants were included in
the data analysis of which 58 completed the entire questionnaire. No patterns of missing data were found, and
138541-Willems_BNW.indd 100 31-10-19 10:07
100
prevent question order bias. For every BCT, participants were asked if the BCT was suitable for influencing the
lifestyles of individuals with mild intellectual disabilities. Dichotomous answers included “yes, this technique is
suitable” or “no, this technique is not suitable.” With each dichotomous answer, there was also an open field to
write down comments. The first questionnaire was delivered using the web‐based survey software,
Qualtrics.com, that invited participants by email and which included an anonymous hyperlink to the
questionnaire. Participants were asked to respond within 16 days. Personal information was asked about job
position, years of work experience and email address (not obligatory). Answers were collected and anonymously
analysed. Participants provided informed consent before participating in any of the Delphi rounds.
Delphi Round 2: After the data from the first Delphi round were analysed, a second questionnaire was designed
based on the outcomes from it. The purpose of the second round was to determine consensus about the
suitability of the BCTs in which no consensus was reached in the first round. The BCTs and corresponding
examples were similar to the second questionnaire. The only exception concerned some of the examples that
were not completely clear to the participants; this was expressed in the comments provided by the participants
in the open fields in the first round. Only minor changes were made to the examples (e.g., the time period in
which a behaviour goal had to be completed).
Participants were asked whether or not these BCTs were suitable. Again, there was an open field to write down
comments. The group decisions from Round 1 were shown in percentages per technique using only one decimal
in case the percentage decimal was exactly 0.5. Comments from participants in Round 1 were translated into
statements that were more common and comprehensive by the first author (MW) and checked by the second
author (AW). Disagreements were resolved by a consensus discussion. These resumptive comments (e.g.,
“according to participants of the panel, suitability depends on the client characteristics”) were shown per
technique next to the group decisions from Round 1. The questionnaire was tailored to the groups of participants,
and questions were offered in a random order. The second questionnaire was also delivered using the web‐based
survey software, Qualtrics.com, by which participants were invited through an email containing an anonymous
hyperlink to the questionnaire. Participants were asked to respond within 16 days. Personal information was
asked about job position, years of work experience and email address (not obligatory).
2.4 | Data analyses
Round 1: After collecting the data from the first questionnaire, consensus was determined. There is no generally
accepted cut‐off score for the consensus that was reached (Becker, & Roberts, 2009; Boulkedid et al., 2011). The
present authors used a cut‐off score of 66.67% consensus both for evaluating a BCT as suitable or not (in changing
lifestyle) in the first round. The 66.67% consensus was determined by dividing the number of corresponding
answers of the participants (yes, suitable/no, not suitable) by the number of participants for that group. The
present authors calculated the total consensus (in %) of each group and the total consensus (in %) of all of the
groups together. Since the questions were offered at random, the answers from incomplete questionnaires were
also used in the analyses. The comments of participants were analysed by theme and categorized. These
101
categories or themes were used in the second questionnaire in order to give participants’ feedback on the results
of the first round.
Per profession group, the inter‐rater reliability of the binary suitability scores was estimated by the alpha
coefficient from the ordinal factor analysis performed on the tetrachoric correlation coefficients (Revelle &
Zinbarg, 2009). Reliability was considered poor or moderate (ICC < 0.75), good (ICC 0.75–0.90) or very good (ICC
> 0.90) (Portney & Watkins, 2000). To investigate agreement between profession groups, the present authors
computed the two‐way intraclass correlation coefficient (ICC) (McGraw & Wong, 1996) by using the average BCT
score per profession group. Also for the ICC, reliability was considered poor or moderate (ICC < 0.75), good (ICC
0.75–0.90) or very good (ICC > 0.90) (Portney & Watkins, 2000). To investigate whether there was any systematic
bias of a profession group with respect to any other profession group, a mixed model analysis (Pinheiro, & Bates,
2000) was undertaken on the average BCT scores per profession. In the mixed model, random intercepts were
specified for the BCTs and fixed effects for the profession groups. A pairwise comparison (Hothorn, Bretz, &
Westfall, 2008) was used to analyse the intergroup effects. For all statistical analyses, raters with more than 30%
missing BCT suitability evaluations were discarded from further analysis. R v3.3.0 was used (R Core Team, 2017).
Round 2: After data collection, consensus for the BCTs in Round 2 was determined within each group. The total
number of BCTs with consensus and the number of suitable BCTs for this round was not calculated for the total
group since the BCTs in the second questionnaire differed per group depending on the consensus found in the
first round per group. This made it also impossible to compute the agreement between profession groups and
the systematic bias of a profession group with respect to another profession group.
The present authors calculated the total consensus (in %) for all BCTs of each group and that over all groups.
Suitable BCTs were ranked by mean consensus using the percentages of consensus on suitability for all of the
groups. Comments from participants were analysed regarding theme and then categorized. The answers of
behavioural scientists were compared separately with the other groups since this profession group has the most
extensive education and working experience with BCTs. The present authors compared the consensus of the
behavioural scientists with the consensus of the other groups to identify possible differences in consensus.
3 | RESULTS
3.1 | First Delphi round
A total of 97 professionals responded to the questionnaire in the first round. Ten respondents did not answer
any of the questions. Four participants declared that they did not want to participate in the research and,
therefore, did not respond to further questions. Answers from two participants were excluded from the data
analysis as they did not satisfy the inclusion criteria for participants. Answers of 81 participants were included in
the data analysis of which 58 completed the entire questionnaire. No patterns of missing data were found, and
138541-Willems_BNW.indd 101 31-10-19 10:07
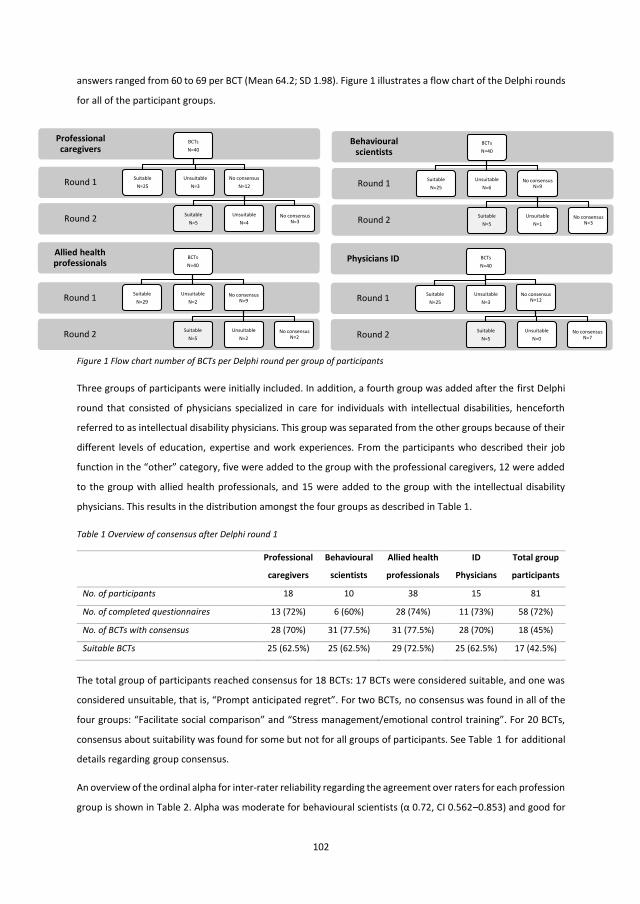
102
answers ranged from 60 to 69 per BCT (Mean 64.2; SD 1.98). Figure 1 illustrates a flow chart of the Delphi rounds
for all of the participant groups.
Figure 1 Flow chart number of BCTs per Delphi round per group of participants
Three groups of participants were initially included. In addition, a fourth group was added after the first Delphi
round that consisted of physicians specialized in care for individuals with intellectual disabilities, henceforth
referred to as intellectual disability physicians. This group was separated from the other groups because of their
different levels of education, expertise and work experiences. From the participants who described their job
function in the “other” category, five were added to the group with the professional caregivers, 12 were added
to the group with allied health professionals, and 15 were added to the group with the intellectual disability
physicians. This results in the distribution amongst the four groups as described in Table 1.
Table 1 Overview of consensus after Delphi round 1
Professional
caregivers
Behavioural
scientists
Allied health
professionals
ID
Physicians
Total group
participants
No. of participants 18 10 38 15 81
No. of completed questionnaires 13 (72%) 6 (60%) 28 (74%) 11 (73%) 58 (72%)
No. of BCTs with consensus 28 (70%) 31 (77.5%) 31 (77.5%) 28 (70%) 18 (45%)
Suitable BCTs 25 (62.5%) 25 (62.5%) 29 (72.5%) 25 (62.5%) 17 (42.5%)
The total group of participants reached consensus for 18 BCTs: 17 BCTs were considered suitable, and one was
considered unsuitable, that is, “Prompt anticipated regret”. For two BCTs, no consensus was found in all of the
four groups: “Facilitate social comparison” and “Stress management/emotional control training”. For 20 BCTs,
consensus about suitability was found for some but not for all groups of participants. See Table 1 for additional
details regarding group consensus.
An overview of the ordinal alpha for inter‐rater reliability regarding the agreement over raters for each profession
group is shown in Table 2. Alpha was moderate for behavioural scientists (α 0.72, CI 0.562–0.853) and good for
Round 2
Round 1
Behavioural scientists
BCTsN=40
SuitableN=25
UnsuitableN=6
No consensus N=9
SuitableN=5
UnsuitableN=1
No consensus N=3Round 2
Round 1
Professional caregivers
BCTsN=40
SuitableN=25
UnsuitableN=3
No consensusN=12
SuitableN=5
UnsuitableN=4
No consensus N=3
Round 2
Round 1
Physicians ID BCTsN=40
SuitableN=25
UnsuitableN=3
No consensus N=12
SuitableN=5
UnsuitableN=0
No consensus N=7Round 2
Round 1
Allied health professionals
BCTsN=40
SuitableN=29
UnsuitableN=2
No consensus N=9
SuitableN=5
UnsuitableN=2
No consensus N=2
103
professional caregivers (α 0.81, CI 0.715– 0.876), allied health professionals (α 0.88, CI 0.820–0.915) and
intellectual disability physicians (α 0.83, CI 0.627–0.915). Among the excluded raters with missing evaluations,
there was one with 38% missing, and the others had more than 50% missing. ICC for agreement between
profession groups was good (ICC 0.876, CI 0.8; 0.929) which indicates a high degree of agreement between the
groups. Analysis of the intergroup effects showed no evidence for significant differences in mean scores between
the four profession groups whereas none of the pairwise comparisons were significant (see also Table 3).
Table 2: Interrater reliability per group of professionals
Profession group Number of raters (total no. of raters) α (ordinal Alpha) 95% CI*
Professional caregivers 13 (18) 0.81 0.715- 0.876
Behavioural scientists 6 (10) 0.72 0.562-0.853
Allied health professionals 28 (38) 0.88 0.820- 0.915
ID Physicians 11 (15) 0.83 0.627-0.915
* CI, Confidence Intervals
Table 3: Group comparisons of mean rating per BCT for each group of professionals
Profession groups Estimate Standard Error p-value
Professional caregivers - Behavioural scientists 0.04872 0.02894 0.3324
Allied health professionals - Behavioural scientists 0.07173 0.02894 0.0632
ID Physicians - Behavioural scientists 0.03333 0.02894 0.6573
Allied health professionals - Professional caregivers 0.02301 0.02894 0.8567
ID Physicians - Professional caregivers -0.01538 0.02894 0.9514
ID Physicians - Allied health professionals -0.03839 0.02894 0.5459
3.2 | Second Delphi round
A total of 123 professionals responded to the questionnaire in the second round. Nine respondents did not
answer any of the questions. Three respondents stated that they did not want to participate further in the
research and, therefore, had not responded to further questions. Two participants stated that they wanted to
participate, however, did not answer any of the further questions. The answers of 112 participants were included
in data analysis, and 87 participants completed the questionnaire. Figure 1 provides a flow chart of the Delphi
rounds.
For the group of professional caregivers, Rounds 1 and 2 resulted in consensus about 30 suitable and seven
unsuitable BCTs; see also Figure 1. For three BCTs, consensus was not reached, that is, “Provide information on
consequences of behaviour to the individual,” “Goal setting (outcome)” and “Agree behavioural contract”. An
overview of consensus after Delphi round 2 is shown in Table 4.
For the group of behavioural scientists, Rounds 1 and 2 resulted in consensus about 30 suitable and seven
unsuitable BCTs (see Figure 1). For three BCTs, consensus was not reached the following: “Prompt review of
outcome goals”, “Environmental restructuring” and “Facilitate social comparison”.
138541-Willems_BNW.indd 102 31-10-19 10:07
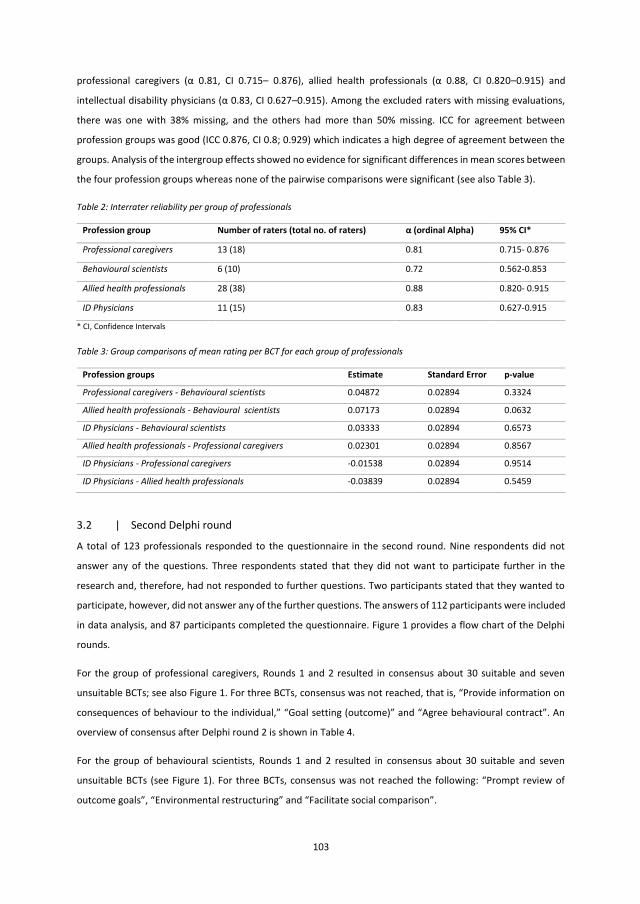
102
answers ranged from 60 to 69 per BCT (Mean 64.2; SD 1.98). Figure 1 illustrates a flow chart of the Delphi rounds
for all of the participant groups.
Figure 1 Flow chart number of BCTs per Delphi round per group of participants
Three groups of participants were initially included. In addition, a fourth group was added after the first Delphi
round that consisted of physicians specialized in care for individuals with intellectual disabilities, henceforth
referred to as intellectual disability physicians. This group was separated from the other groups because of their
different levels of education, expertise and work experiences. From the participants who described their job
function in the “other” category, five were added to the group with the professional caregivers, 12 were added
to the group with allied health professionals, and 15 were added to the group with the intellectual disability
physicians. This results in the distribution amongst the four groups as described in Table 1.
Table 1 Overview of consensus after Delphi round 1
Professional
caregivers
Behavioural
scientists
Allied health
professionals
ID
Physicians
Total group
participants
No. of participants 18 10 38 15 81
No. of completed questionnaires 13 (72%) 6 (60%) 28 (74%) 11 (73%) 58 (72%)
No. of BCTs with consensus 28 (70%) 31 (77.5%) 31 (77.5%) 28 (70%) 18 (45%)
Suitable BCTs 25 (62.5%) 25 (62.5%) 29 (72.5%) 25 (62.5%) 17 (42.5%)
The total group of participants reached consensus for 18 BCTs: 17 BCTs were considered suitable, and one was
considered unsuitable, that is, “Prompt anticipated regret”. For two BCTs, no consensus was found in all of the
four groups: “Facilitate social comparison” and “Stress management/emotional control training”. For 20 BCTs,
consensus about suitability was found for some but not for all groups of participants. See Table 1 for additional
details regarding group consensus.
An overview of the ordinal alpha for inter‐rater reliability regarding the agreement over raters for each profession
group is shown in Table 2. Alpha was moderate for behavioural scientists (α 0.72, CI 0.562–0.853) and good for
Round 2
Round 1
Behavioural scientists
BCTsN=40
SuitableN=25
UnsuitableN=6
No consensus N=9
SuitableN=5
UnsuitableN=1
No consensus N=3Round 2
Round 1
Professional caregivers
BCTsN=40
SuitableN=25
UnsuitableN=3
No consensusN=12
SuitableN=5
UnsuitableN=4
No consensus N=3
Round 2
Round 1
Physicians ID BCTsN=40
SuitableN=25
UnsuitableN=3
No consensus N=12
SuitableN=5
UnsuitableN=0
No consensus N=7Round 2
Round 1
Allied health professionals
BCTsN=40
SuitableN=29
UnsuitableN=2
No consensus N=9
SuitableN=5
UnsuitableN=2
No consensus N=2
103
professional caregivers (α 0.81, CI 0.715– 0.876), allied health professionals (α 0.88, CI 0.820–0.915) and
intellectual disability physicians (α 0.83, CI 0.627–0.915). Among the excluded raters with missing evaluations,
there was one with 38% missing, and the others had more than 50% missing. ICC for agreement between
profession groups was good (ICC 0.876, CI 0.8; 0.929) which indicates a high degree of agreement between the
groups. Analysis of the intergroup effects showed no evidence for significant differences in mean scores between
the four profession groups whereas none of the pairwise comparisons were significant (see also Table 3).
Table 2: Interrater reliability per group of professionals
Profession group Number of raters (total no. of raters) α (ordinal Alpha) 95% CI*
Professional caregivers 13 (18) 0.81 0.715- 0.876
Behavioural scientists 6 (10) 0.72 0.562-0.853
Allied health professionals 28 (38) 0.88 0.820- 0.915
ID Physicians 11 (15) 0.83 0.627-0.915
* CI, Confidence Intervals
Table 3: Group comparisons of mean rating per BCT for each group of professionals
Profession groups Estimate Standard Error p-value
Professional caregivers - Behavioural scientists 0.04872 0.02894 0.3324
Allied health professionals - Behavioural scientists 0.07173 0.02894 0.0632
ID Physicians - Behavioural scientists 0.03333 0.02894 0.6573
Allied health professionals - Professional caregivers 0.02301 0.02894 0.8567
ID Physicians - Professional caregivers -0.01538 0.02894 0.9514
ID Physicians - Allied health professionals -0.03839 0.02894 0.5459
3.2 | Second Delphi round
A total of 123 professionals responded to the questionnaire in the second round. Nine respondents did not
answer any of the questions. Three respondents stated that they did not want to participate further in the
research and, therefore, had not responded to further questions. Two participants stated that they wanted to
participate, however, did not answer any of the further questions. The answers of 112 participants were included
in data analysis, and 87 participants completed the questionnaire. Figure 1 provides a flow chart of the Delphi
rounds.
For the group of professional caregivers, Rounds 1 and 2 resulted in consensus about 30 suitable and seven
unsuitable BCTs; see also Figure 1. For three BCTs, consensus was not reached, that is, “Provide information on
consequences of behaviour to the individual,” “Goal setting (outcome)” and “Agree behavioural contract”. An
overview of consensus after Delphi round 2 is shown in Table 4.
For the group of behavioural scientists, Rounds 1 and 2 resulted in consensus about 30 suitable and seven
unsuitable BCTs (see Figure 1). For three BCTs, consensus was not reached the following: “Prompt review of
outcome goals”, “Environmental restructuring” and “Facilitate social comparison”.
138541-Willems_BNW.indd 103 31-10-19 10:07
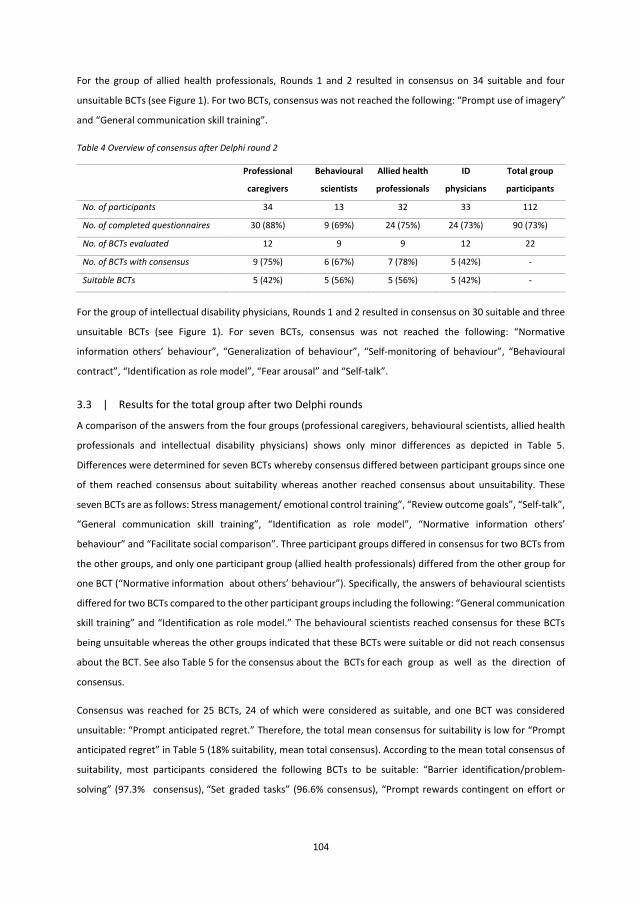
104
For the group of allied health professionals, Rounds 1 and 2 resulted in consensus on 34 suitable and four
unsuitable BCTs (see Figure 1). For two BCTs, consensus was not reached the following: “Prompt use of imagery”
and “General communication skill training”.
Table 4 Overview of consensus after Delphi round 2
Professional
caregivers
Behavioural
scientists
Allied health
professionals
ID
physicians
Total group
participants
No. of participants 34 13 32 33 112
No. of completed questionnaires 30 (88%) 9 (69%) 24 (75%) 24 (73%) 90 (73%)
No. of BCTs evaluated 12 9 9 12 22
No. of BCTs with consensus 9 (75%) 6 (67%) 7 (78%) 5 (42%) -
Suitable BCTs 5 (42%) 5 (56%) 5 (56%) 5 (42%) -
For the group of intellectual disability physicians, Rounds 1 and 2 resulted in consensus on 30 suitable and three
unsuitable BCTs (see Figure 1). For seven BCTs, consensus was not reached the following: “Normative
information others’ behaviour”, “Generalization of behaviour”, “Self‐monitoring of behaviour”, “Behavioural
contract”, “Identification as role model”, “Fear arousal” and “Self‐talk”.
3.3 | Results for the total group after two Delphi rounds
A comparison of the answers from the four groups (professional caregivers, behavioural scientists, allied health
professionals and intellectual disability physicians) shows only minor differences as depicted in Table 5.
Differences were determined for seven BCTs whereby consensus differed between participant groups since one
of them reached consensus about suitability whereas another reached consensus about unsuitability. These
seven BCTs are as follows: Stress management/ emotional control training”, “Review outcome goals”, “Self‐talk”,
“General communication skill training”, “Identification as role model”, “Normative information others’
behaviour” and “Facilitate social comparison”. Three participant groups differed in consensus for two BCTs from
the other groups, and only one participant group (allied health professionals) differed from the other group for
one BCT (“Normative information about others’ behaviour”). Specifically, the answers of behavioural scientists
differed for two BCTs compared to the other participant groups including the following: “General communication
skill training” and “Identification as role model.” The behavioural scientists reached consensus for these BCTs
being unsuitable whereas the other groups indicated that these BCTs were suitable or did not reach consensus
about the BCT. See also Table 5 for the consensus about the BCTs for each group as well as the direction of
consensus.
Consensus was reached for 25 BCTs, 24 of which were considered as suitable, and one BCT was considered
unsuitable: “Prompt anticipated regret.” Therefore, the total mean consensus for suitability is low for “Prompt
anticipated regret” in Table 5 (18% suitability, mean total consensus). According to the mean total consensus of
suitability, most participants considered the following BCTs to be suitable: “Barrier identification/problem‐
solving” (97.3% consensus), “Set graded tasks” (96.6% consensus), “Prompt rewards contingent on effort or
105
progress towards behaviour” (95.3% consensus), “Motivational interviewing” (94.4% consensus) and “Action
planning” (90.8% consensus). For an overview of mean consensus per BCT, see Table 5.
A total number of 613 comments were given in the two Delphi rounds (Mean 15.3; SD 7.9; range 3–38) including
368 comments given with a response that the BCT was suitable and 245 comments with a response that the BCT
was unsuitable. The comments were categorized into five categories, including:
1. Methods/validity: comments about the methods or validity of the study methods or the text in the
questionnaire (e.g., “the example is confusing”);
2. Feasibility: comments about the feasibility of the BCT (e.g., “it depends on what the reward
entails”);
3. Relative techniques: comments about the suitability of the BCT in relationship to other BCTs (e.g.,
“encouraging on itself is rarely enough. Pre‐structuring and shaping is a prerequisite”);
4. Client characteristics: comments about the suitability of the BCT in relationship to client
characteristics (e.g., “depending on the client and his possible fears”);
5. Support from others: comments about the suitability of the BCT in relation to support from others
(e.g., “the BCT is only suitable if the personal caregiver supports the client”).
Consensus seemed to be reached primarily for the BCTs with fewer comments (see, for more details, Table 5).
Most comments were offered for the category “client characteristics” (n = 241), and fewer comments were given
for the category “methods/validity” (n = 31); see also Table 6. The most suitable BCTs (barrier identification,
graded tasks, reward effort towards behaviour, motivational interviewing and action planning) received a lower
number of comments than average (mean 8.4; SD 3.0; range 5–13). Table 7 provides an overview of the number
of comments per category for every BCT ranked by suitability.
138541-Willems_BNW.indd 104 31-10-19 10:08
104
For the group of allied health professionals, Rounds 1 and 2 resulted in consensus on 34 suitable and four
unsuitable BCTs (see Figure 1). For two BCTs, consensus was not reached the following: “Prompt use of imagery”
and “General communication skill training”.
Table 4 Overview of consensus after Delphi round 2
Professional
caregivers
Behavioural
scientists
Allied health
professionals
ID
physicians
Total group
participants
No. of participants 34 13 32 33 112
No. of completed questionnaires 30 (88%) 9 (69%) 24 (75%) 24 (73%) 90 (73%)
No. of BCTs evaluated 12 9 9 12 22
No. of BCTs with consensus 9 (75%) 6 (67%) 7 (78%) 5 (42%) -
Suitable BCTs 5 (42%) 5 (56%) 5 (56%) 5 (42%) -
For the group of intellectual disability physicians, Rounds 1 and 2 resulted in consensus on 30 suitable and three
unsuitable BCTs (see Figure 1). For seven BCTs, consensus was not reached the following: “Normative
information others’ behaviour”, “Generalization of behaviour”, “Self‐monitoring of behaviour”, “Behavioural
contract”, “Identification as role model”, “Fear arousal” and “Self‐talk”.
3.3 | Results for the total group after two Delphi rounds
A comparison of the answers from the four groups (professional caregivers, behavioural scientists, allied health
professionals and intellectual disability physicians) shows only minor differences as depicted in Table 5.
Differences were determined for seven BCTs whereby consensus differed between participant groups since one
of them reached consensus about suitability whereas another reached consensus about unsuitability. These
seven BCTs are as follows: Stress management/ emotional control training”, “Review outcome goals”, “Self‐talk”,
“General communication skill training”, “Identification as role model”, “Normative information others’
behaviour” and “Facilitate social comparison”. Three participant groups differed in consensus for two BCTs from
the other groups, and only one participant group (allied health professionals) differed from the other group for
one BCT (“Normative information about others’ behaviour”). Specifically, the answers of behavioural scientists
differed for two BCTs compared to the other participant groups including the following: “General communication
skill training” and “Identification as role model.” The behavioural scientists reached consensus for these BCTs
being unsuitable whereas the other groups indicated that these BCTs were suitable or did not reach consensus
about the BCT. See also Table 5 for the consensus about the BCTs for each group as well as the direction of
consensus.
Consensus was reached for 25 BCTs, 24 of which were considered as suitable, and one BCT was considered
unsuitable: “Prompt anticipated regret.” Therefore, the total mean consensus for suitability is low for “Prompt
anticipated regret” in Table 5 (18% suitability, mean total consensus). According to the mean total consensus of
suitability, most participants considered the following BCTs to be suitable: “Barrier identification/problem‐
solving” (97.3% consensus), “Set graded tasks” (96.6% consensus), “Prompt rewards contingent on effort or
105
progress towards behaviour” (95.3% consensus), “Motivational interviewing” (94.4% consensus) and “Action
planning” (90.8% consensus). For an overview of mean consensus per BCT, see Table 5.
A total number of 613 comments were given in the two Delphi rounds (Mean 15.3; SD 7.9; range 3–38) including
368 comments given with a response that the BCT was suitable and 245 comments with a response that the BCT
was unsuitable. The comments were categorized into five categories, including:
1. Methods/validity: comments about the methods or validity of the study methods or the text in the
questionnaire (e.g., “the example is confusing”);
2. Feasibility: comments about the feasibility of the BCT (e.g., “it depends on what the reward
entails”);
3. Relative techniques: comments about the suitability of the BCT in relationship to other BCTs (e.g.,
“encouraging on itself is rarely enough. Pre‐structuring and shaping is a prerequisite”);
4. Client characteristics: comments about the suitability of the BCT in relationship to client
characteristics (e.g., “depending on the client and his possible fears”);
5. Support from others: comments about the suitability of the BCT in relation to support from others
(e.g., “the BCT is only suitable if the personal caregiver supports the client”).
Consensus seemed to be reached primarily for the BCTs with fewer comments (see, for more details, Table 5).
Most comments were offered for the category “client characteristics” (n = 241), and fewer comments were given
for the category “methods/validity” (n = 31); see also Table 6. The most suitable BCTs (barrier identification,
graded tasks, reward effort towards behaviour, motivational interviewing and action planning) received a lower
number of comments than average (mean 8.4; SD 3.0; range 5–13). Table 7 provides an overview of the number
of comments per category for every BCT ranked by suitability.
138541-Willems_BNW.indd 105 31-10-19 10:08
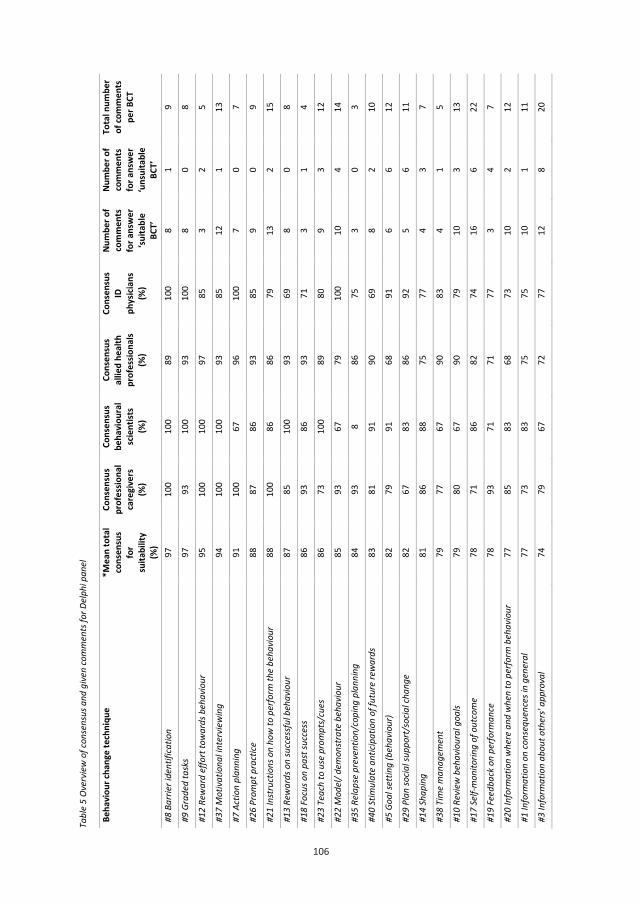
106
106
Tabl
e 5
Ove
rvie
w o
f con
sens
us a
nd g
iven
com
men
ts fo
r Del
phi p
anel
Beha
viou
r cha
nge
tech
niqu
e *M
ean
tota
l co
nsen
sus
for
suita
bilit
y (%
)
Cons
ensu
s pr
ofes
siona
l ca
regi
vers
(%
)
Cons
ensu
s be
havi
oura
l sc
ient
ists
(%)
Cons
ensu
s al
lied
heal
th
prof
essio
nals
(%)
Cons
ensu
s ID
ph
ysici
ans
(%)
Num
ber o
f co
mm
ents
fo
r ans
wer
‘su
itabl
e BC
T’
Num
ber o
f co
mm
ents
fo
r ans
wer
‘u
nsui
tabl
e BC
T’
Tota
l num
ber
of co
mm
ents
pe
r BCT
#8 B
arrie
r ide
ntifi
catio
n 97
10
0 10
0 89
10
0 8
1 9
#9 G
rade
d ta
sks
97
93
100
93
100
8 0
8
#12
Rew
ard
effo
rt to
war
ds b
ehav
iour
95
10
0 10
0 97
85
3
2 5
#37
Mot
ivat
iona
l int
ervi
ewin
g 94
10
0 10
0 93
85
12
1
13
#7 A
ctio
n pl
anni
ng
91
100
67
96
100
7 0
7
#26
Prom
pt p
ract
ice
88
87
86
93
85
9 0
9
#21
Inst
ruct
ions
on
how
to p
erfo
rm th
e be
havi
our
88
100
86
86
79
13
2 15
#13
Rew
ards
on
succ
essf
ul b
ehav
iour
87
85
10
0 93
69
8
0 8
#18
Focu
s on
past
succ
ess
86
93
86
93
71
3 1
4
#23
Teac
h to
use
pro
mpt
s/cu
es
86
73
100
89
80
9 3
12
#22
Mod
el/ d
emon
stra
te b
ehav
iour
85
93
67
79
10
0 10
4
14
#35
Rela
pse
prev
entio
n/co
ping
pla
nnin
g 84
93
8
86
75
3 0
3
#40
Stim
ulat
e an
ticip
atio
n of
futu
re re
war
ds
83
81
91
90
69
8 2
10
#5 G
oal s
ettin
g (b
ehav
iour
) 82
79
91
68
91
6
6 12
#29
Plan
socia
l sup
port
/soc
ial c
hang
e 82
67
83
86
92
5
6 11
#14
Shap
ing
81
86
88
75
77
4 3
7
#38
Tim
e m
anag
emen
t 79
77
67
90
83
4
1 5
#10
Revi
ew b
ehav
iour
al g
oals
79
80
67
90
79
10
3 13
#17
Self-
mon
itorin
g of
out
com
e 78
71
86
82
74
16
6
22
#19
Feed
back
on
perfo
rman
ce
78
93
71
71
77
3 4
7
#20
Info
rmat
ion
whe
re a
nd w
hen
to p
erfo
rm b
ehav
iour
77
85
83
68
73
10
2
12
#1 In
form
atio
n on
cons
eque
nces
in g
ener
al
77
73
83
75
75
10
1 11
#3 In
form
atio
n ab
out o
ther
s' ap
prov
al
74
79
67
72
77
12
8 20
107
#27
Use
of fo
llow
-up
prom
pts
70
71
67
75
67
8 7
15
#31
Prom
pt a
ntici
pate
d re
gret
18
† 29
† 0†
32†
9† 1
12
13
#16
Self-
mon
itorin
g of
beh
avio
ur
- 90
71
87
56
~ 11
7
18
#24
Envi
ronm
enta
l res
truc
turin
g -
81
58~
70
86
10
10
20
#15
Gene
ralis
atio
n of
beh
avio
ur
- 85
71
75
63
~ 10
8
18
#2 In
form
atio
n to
the
indi
vidu
al
- 65
~ 71
68
75
11
9
20
#6 G
oal s
ettin
g (o
utco
me)
-
58~
67
68
75
16
9 25
#36
Stre
ss m
anag
emen
t /em
otio
nal c
ontr
ol tr
aini
ng
- 26
† 91
71
76
18
8
26
#11
Revi
ew o
utco
me
goal
s -
94
42~
76
31†
13
9 22
#33
Self-
talk
-
31†
67
80
54~
13
10
23
#39
Gene
ral c
omm
unica
tion
skill
s tra
inin
g -
67
17†
60~
75
10
9 19
#30
Iden
tifica
tion
as ro
le m
odel
-
73
9† 68
44
~ 10
11
21
#4 N
orm
ativ
e in
form
atio
n ot
hers
' beh
avio
ur
- 16
† 25
† 72
46
~ 14
12
26
#28
Facil
itate
socia
l com
paris
on
- 16
† 40
~ 27
† 70
16
16
32
#25
Beha
viou
ral c
ontr
act
- 55
~ 29
† 20
† 48
~ 13
25
38
#32
Fear
aro
usal
-
29†
33†
31†
35~
6 17
23
#34
Use
of im
ager
y -
13†
33†
48~
0† 7
10
17
Tabl
e 6
Ove
rvie
w o
f giv
en co
mm
ents
in to
tal
M
etho
ds/
valid
ity
Feas
ibili
ty
Rela
tive
tech
niqu
es
Clie
nt
char
acte
ristic
s Su
ppor
t fro
m
othe
rs
Tota
l no.
of
com
men
ts (m
ean)
No. o
f com
men
ts fo
r sui
tabl
e BC
Ts, n
=24
(mea
n*)
8 (0
.33)
75
(3.1
3)
34 (1
.42)
83
(3.4
6)
52 (2
.17)
25
2 (1
0.5)
No
. of c
omm
ents
for u
nsui
tabl
e BC
Ts, n
=1
0 4
1 8
0 13
No
. of c
omm
ents
for B
CTs w
ithou
t con
sens
us, n
=15
(mea
n*)
23 (1
.53)
10
8 (7
.2)
49 (3
.27)
15
0 (1
0)
18 (1
.2)
348
(23.
2)
Tota
l num
ber o
f com
men
ts
31
187
84
241
70
613
* =
mea
n no
. of c
omm
ents
for s
uita
ble
BCTs
or B
CTs f
or w
hich
cons
ensu
s was
not
foun
d
138541-Willems_BNW.indd 106 31-10-19 10:08
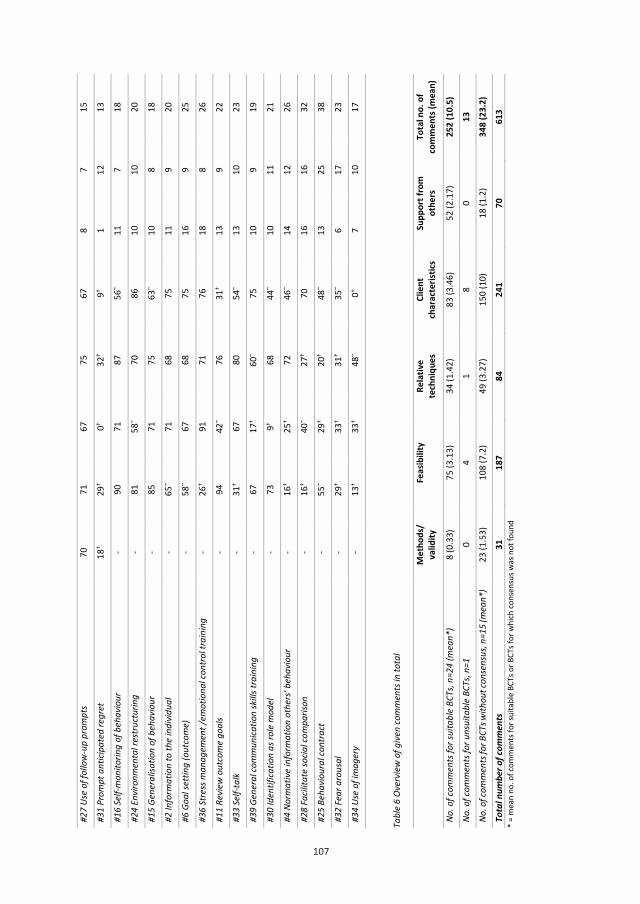
107
107
#27
Use
of fo
llow
-up
prom
pts
70
71
67
75
67
8 7
15
#31
Prom
pt a
ntici
pate
d re
gret
18
† 29
† 0†
32†
9† 1
12
13
#16
Self-
mon
itorin
g of
beh
avio
ur
- 90
71
87
56
~ 11
7
18
#24
Envi
ronm
enta
l res
truc
turin
g -
81
58~
70
86
10
10
20
#15
Gene
ralis
atio
n of
beh
avio
ur
- 85
71
75
63
~ 10
8
18
#2 In
form
atio
n to
the
indi
vidu
al
- 65
~ 71
68
75
11
9
20
#6 G
oal s
ettin
g (o
utco
me)
-
58~
67
68
75
16
9 25
#36
Stre
ss m
anag
emen
t /em
otio
nal c
ontr
ol tr
aini
ng
- 26
† 91
71
76
18
8
26
#11
Revi
ew o
utco
me
goal
s -
94
42~
76
31†
13
9 22
#33
Self-
talk
-
31†
67
80
54~
13
10
23
#39
Gene
ral c
omm
unica
tion
skill
s tra
inin
g -
67
17†
60~
75
10
9 19
#30
Iden
tifica
tion
as ro
le m
odel
-
73
9† 68
44
~ 10
11
21
#4 N
orm
ativ
e in
form
atio
n ot
hers
' beh
avio
ur
- 16
† 25
† 72
46
~ 14
12
26
#28
Facil
itate
socia
l com
paris
on
- 16
† 40
~ 27
† 70
16
16
32
#25
Beha
viou
ral c
ontr
act
- 55
~ 29
† 20
† 48
~ 13
25
38
#32
Fear
aro
usal
-
29†
33†
31†
35~
6 17
23
#34
Use
of im
ager
y -
13†
33†
48~
0† 7
10
17
Tabl
e 6
Ove
rvie
w o
f giv
en co
mm
ents
in to
tal
M
etho
ds/
valid
ity
Feas
ibili
ty
Rela
tive
tech
niqu
es
Clie
nt
char
acte
ristic
s Su
ppor
t fro
m
othe
rs
Tota
l no.
of
com
men
ts (m
ean)
No. o
f com
men
ts fo
r sui
tabl
e BC
Ts, n
=24
(mea
n*)
8 (0
.33)
75
(3.1
3)
34 (1
.42)
83
(3.4
6)
52 (2
.17)
25
2 (1
0.5)
No
. of c
omm
ents
for u
nsui
tabl
e BC
Ts, n
=1
0 4
1 8
0 13
No
. of c
omm
ents
for B
CTs w
ithou
t con
sens
us, n
=15
(mea
n*)
23 (1
.53)
10
8 (7
.2)
49 (3
.27)
15
0 (1
0)
18 (1
.2)
348
(23.
2)
Tota
l num
ber o
f com
men
ts
31
187
84
241
70
613
* =
mea
n no
. of c
omm
ents
for s
uita
ble
BCTs
or B
CTs f
or w
hich
cons
ensu
s was
not
foun
d
138541-Willems_BNW.indd 107 31-10-19 10:08

108
4 | DISCUSSION
In this Delphi study, the present authors found that the mean total consensus amongst professionals who were
working with individuals with mild intellectual disabilities considered 24 out of 40 BCTs suitable for supporting
these individuals for changing their lifestyles. BCTs considered to be most suitable for this were as follows: barrier
identification, set graded tasks, reward effort towards behaviour, motivational interviewing and action planning.
No evidence was found for differences in consensus between groups of professionals.
The present authors ascertained that the BCTs that were considered to be most suitable for changing lifestyle
behaviour were as follows: “Barrier identification”, “Set graded tasks”, “Reward effort towards behaviour”,
“Motivational interviewing” and “Action planning”. According to the literature, suitable BCTs for individuals with
mild intellectual disabilities may need to target monitoring of behaviour (Hutzler & Korsensky, 2010), self‐efficacy
(Bodde & Seo, 2009; Kuijken et al., 2016; Mallet, Guillard, Huillard, Dubertret, & Limosin, 2016; Young, Naji, &
Kroll, 2012) and rewards towards behaviour (Skinner, 1938; Temple, 2009; Van Schijndel‐Speet, Evenhuis, Van
Wijck, & Echteld, 2014); these need to be combined with social support (Bodde & Seo, 2009; Kuijken et al., 2016;
Mallet et al., 2016; Young et al., 2012). Less suitable BCTs may be those targeting an increase in knowledge and
understanding or appealing to executive functioning (Kuijken et al., 2016). Our findings are mostly in accordance
with the literature since the present authors found that BCTs that targeted rewards were considered most
suitable. However, the present authors also found consensus for BCTs that targeted executive functioning (BCTs
targeting planning). An explanation for the suitability of these BCTs or those targeting executive functioning or
cognitive functioning is that these BCTs may be suitable when used in combination with support from others. A
category “support from others” was defined in the results since there were many comments about the need of
social support from others for the suitability of techniques. This finding confirms the current knowledge that a
multidimensional approach is important for lifestyle changes for individuals with mild intellectual disabilities,
including tailoring to client characteristics and support from others (Hutzler & Korsensky, 2010; National Institute
for Health and Clinical Excellence (NICE) 2007; Willems et al., 2018).
A review about the use of BCTs in lifestyle change interventions for people with intellectual disabilities found
that the BCTs “Provide information on consequences of behaviour in general” and “Plan social support/social
change” were most frequently used (Willems et al., 2017). However, according to professionals in this Delphi
study, these BCTs were not the most suitable. For future research and the design of new interventions, it may be
important to investigate step-by‐step what the efficacy is of individual BCTs. The authors recommend to begin
researching the BCTs that were considered as most suitable according to professionals working with people with
mild intellectual disabilities. This may lead to new insights about the use of BCTs in changing lifestyle of people
with mild intellectual disabilities.
The present authors compared the answers of the four groups (professional caregivers, behavioural scientists,
allied health professionals and intellectual disability physicians) and did not find significant differences.
Consensus differed for only seven BCTs. Behavioural scientists were considered as being experts of behavioural
change due to education, working position and experience. Therefore, the answers of behavioural scientists were
109
compared with the answers of the other groups. Two BCTs (“General communication skill training” and
“Identification as a role model”) were considered unsuitable by behavioural scientists while the other
professional groups considered the technique suitable or did not reach consensus. This indicates that,
independent of the working position and education level of professionals, no major difference in rating the
suitability of BCTs was determined for lifestyle changes in individuals with mild intellectual disabilities.
A substantial number of additional comments were provided by the participants that appear to be related to the
suitability of a BCT. The BCTs with the highest mean consensus for all of the groups received fewer comments
than unsuitable BCTs. Apparently, these BCTs needed no further explanation, the feasibility was relatively good,
and the suitability was less dependent on the use of relative techniques, client characteristics and support from
others. This indicates that these BCTs (“Barrier identification,” “Set graded tasks,” “Reward effort towards
behaviour,” “Motivational interviewing” and “Action planning”) are suitable for use in the daily practice of
lifestyle changes in individuals with intellectual disabilities.
4.1 | Strengths and weaknesses
A cut‐off score of 66.7% was used for consensus about the suitability of BCTs. This cut‐off score could not be
supported by literature considering the fact that there is no consensus in the literature regarding the best cut‐
off score (Diamond et al., 2014). Since this is the first study about the suitability of BCTs in lifestyle changes for
individuals with mild intellectual disabilities, the present authors did not want to be too rigorous by excluding
BCTs from being categorized as suitable. The same mild cut‐off score was used for categorizing unsuitable BCTs
which meant that they were categorized as unsuitable if the mild cut‐off score was reached. However, the
present authors found 16 BCTs with a high mean percentage (>80%) of consensus over all of the groups of
participants which may indicate that these BCTs were reliably judged as suitable and relevant for future research.
The BCTs in which most consensus was reached may be used to design new lifestyle change interventions for
individuals with mild intellectual disabilities. However, the level of suitability is not measured in this study. Since
this and the level of consensus of suitability are not the same, our findings are tentative and require further
investigation. Since the field of lifestyle change for individuals with (mild) intellectual disabilities is still in its
infancy, these results can provide guidance for future research.
Questionnaires from both Delphi rounds had a substantial number of participants which indicates a wide reach
of the study. It was not possible to calculate the total number of people who were approached for participation
in this study because the present authors used indirect methods of recruitment. The high consensus rates in the
groups may mean that there was probably data saturation (Guest, Bunce, & Johnson, 2006). Although the study
reach was wide, the questionnaires were not completed by all of the respondents. This may mean that the
awareness and/or knowledge about behaviour change may be small with professionals working with individuals
with mild intellectual disabilities or that the BCTs are still too theoretical. Nevertheless, the present authors used
examples for each BCT from the daily practice of professionals working with individuals with mild intellectual
disabilities to overcome this issue.
138541-Willems_BNW.indd 108 31-10-19 10:08
108
4 | DISCUSSION
In this Delphi study, the present authors found that the mean total consensus amongst professionals who were
working with individuals with mild intellectual disabilities considered 24 out of 40 BCTs suitable for supporting
these individuals for changing their lifestyles. BCTs considered to be most suitable for this were as follows: barrier
identification, set graded tasks, reward effort towards behaviour, motivational interviewing and action planning.
No evidence was found for differences in consensus between groups of professionals.
The present authors ascertained that the BCTs that were considered to be most suitable for changing lifestyle
behaviour were as follows: “Barrier identification”, “Set graded tasks”, “Reward effort towards behaviour”,
“Motivational interviewing” and “Action planning”. According to the literature, suitable BCTs for individuals with
mild intellectual disabilities may need to target monitoring of behaviour (Hutzler & Korsensky, 2010), self‐efficacy
(Bodde & Seo, 2009; Kuijken et al., 2016; Mallet, Guillard, Huillard, Dubertret, & Limosin, 2016; Young, Naji, &
Kroll, 2012) and rewards towards behaviour (Skinner, 1938; Temple, 2009; Van Schijndel‐Speet, Evenhuis, Van
Wijck, & Echteld, 2014); these need to be combined with social support (Bodde & Seo, 2009; Kuijken et al., 2016;
Mallet et al., 2016; Young et al., 2012). Less suitable BCTs may be those targeting an increase in knowledge and
understanding or appealing to executive functioning (Kuijken et al., 2016). Our findings are mostly in accordance
with the literature since the present authors found that BCTs that targeted rewards were considered most
suitable. However, the present authors also found consensus for BCTs that targeted executive functioning (BCTs
targeting planning). An explanation for the suitability of these BCTs or those targeting executive functioning or
cognitive functioning is that these BCTs may be suitable when used in combination with support from others. A
category “support from others” was defined in the results since there were many comments about the need of
social support from others for the suitability of techniques. This finding confirms the current knowledge that a
multidimensional approach is important for lifestyle changes for individuals with mild intellectual disabilities,
including tailoring to client characteristics and support from others (Hutzler & Korsensky, 2010; National Institute
for Health and Clinical Excellence (NICE) 2007; Willems et al., 2018).
A review about the use of BCTs in lifestyle change interventions for people with intellectual disabilities found
that the BCTs “Provide information on consequences of behaviour in general” and “Plan social support/social
change” were most frequently used (Willems et al., 2017). However, according to professionals in this Delphi
study, these BCTs were not the most suitable. For future research and the design of new interventions, it may be
important to investigate step-by‐step what the efficacy is of individual BCTs. The authors recommend to begin
researching the BCTs that were considered as most suitable according to professionals working with people with
mild intellectual disabilities. This may lead to new insights about the use of BCTs in changing lifestyle of people
with mild intellectual disabilities.
The present authors compared the answers of the four groups (professional caregivers, behavioural scientists,
allied health professionals and intellectual disability physicians) and did not find significant differences.
Consensus differed for only seven BCTs. Behavioural scientists were considered as being experts of behavioural
change due to education, working position and experience. Therefore, the answers of behavioural scientists were
109
compared with the answers of the other groups. Two BCTs (“General communication skill training” and
“Identification as a role model”) were considered unsuitable by behavioural scientists while the other
professional groups considered the technique suitable or did not reach consensus. This indicates that,
independent of the working position and education level of professionals, no major difference in rating the
suitability of BCTs was determined for lifestyle changes in individuals with mild intellectual disabilities.
A substantial number of additional comments were provided by the participants that appear to be related to the
suitability of a BCT. The BCTs with the highest mean consensus for all of the groups received fewer comments
than unsuitable BCTs. Apparently, these BCTs needed no further explanation, the feasibility was relatively good,
and the suitability was less dependent on the use of relative techniques, client characteristics and support from
others. This indicates that these BCTs (“Barrier identification,” “Set graded tasks,” “Reward effort towards
behaviour,” “Motivational interviewing” and “Action planning”) are suitable for use in the daily practice of
lifestyle changes in individuals with intellectual disabilities.
4.1 | Strengths and weaknesses
A cut‐off score of 66.7% was used for consensus about the suitability of BCTs. This cut‐off score could not be
supported by literature considering the fact that there is no consensus in the literature regarding the best cut‐
off score (Diamond et al., 2014). Since this is the first study about the suitability of BCTs in lifestyle changes for
individuals with mild intellectual disabilities, the present authors did not want to be too rigorous by excluding
BCTs from being categorized as suitable. The same mild cut‐off score was used for categorizing unsuitable BCTs
which meant that they were categorized as unsuitable if the mild cut‐off score was reached. However, the
present authors found 16 BCTs with a high mean percentage (>80%) of consensus over all of the groups of
participants which may indicate that these BCTs were reliably judged as suitable and relevant for future research.
The BCTs in which most consensus was reached may be used to design new lifestyle change interventions for
individuals with mild intellectual disabilities. However, the level of suitability is not measured in this study. Since
this and the level of consensus of suitability are not the same, our findings are tentative and require further
investigation. Since the field of lifestyle change for individuals with (mild) intellectual disabilities is still in its
infancy, these results can provide guidance for future research.
Questionnaires from both Delphi rounds had a substantial number of participants which indicates a wide reach
of the study. It was not possible to calculate the total number of people who were approached for participation
in this study because the present authors used indirect methods of recruitment. The high consensus rates in the
groups may mean that there was probably data saturation (Guest, Bunce, & Johnson, 2006). Although the study
reach was wide, the questionnaires were not completed by all of the respondents. This may mean that the
awareness and/or knowledge about behaviour change may be small with professionals working with individuals
with mild intellectual disabilities or that the BCTs are still too theoretical. Nevertheless, the present authors used
examples for each BCT from the daily practice of professionals working with individuals with mild intellectual
disabilities to overcome this issue.
138541-Willems_BNW.indd 109 31-10-19 10:08

110
An important strength of the study is the randomized sequence of the questions the present authors used to
avoid question order bias and differences in answer ratings for each BCT. The randomization made it possible to
use the answers of participants who did not complete the questionnaire.
4.2 | Recommendations
To our knowledge, this is the first study exploring the suitability of BCTs for supporting lifestyle changes in
individuals with mild intellectual disabilities. Twenty‐four suitable BCTs were identified and might be applied for
doing so. The present authors did not study the suitability of combinations of BCTs since this was an explorative
study. In practice, BCTs may often not have been used solely. However, the authors recommend step‐by‐step
research to determine the efficacy of individual BCTs using a multidimensional approach for a solid design of an
effective lifestyle change intervention. Increased awareness and knowledge about behaviour change and lifestyle
changes in individuals with mild intellectual disabilities are necessary since this is important for the
implementation of a multidimensional approach. Additional research is necessary on the combination and the
use of BCTs in daily support of these individuals. Since the present authors did not study the effectiveness of
BCTs, more research is also needed to determine this in supporting lifestyle changes in individuals with mild
intellectual disabilities.
4.3 | Conclusion
This explorative Delphi study identified 24 BCTs that are suitable for encouraging lifestyle changes in individuals
with mild intellectual disabilities. The study had a wide reach under professionals (given the number of
participants) working with this population, and the present authors determined that professionals reached
consensus about the suitability of BCTs regardless of their working position. The number of comments offered
for a BCT might indicate the suitability of it inversely; fewer comments indicate higher suitability for that BCTs
and more comments indicate lower suitability. Support from others appears to be important for the suitability
of BCTs.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
111
REFERENCES
Abraham, C., & Michie, S. (2008). A taxonomy of behaviour change techniques used in interventions. Health
Psychology, 27(3), 379–387.
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome: Investigating
parental beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61–80.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders: DSM‐5 (5th
Ed.). Arlington, VA: American Psychiatric Association.
Bartholomew, L. K., & Mullen, P. D. (2011). Five roles for using theory and evidence in the design and testing of
behavior change interventions. Journal of Public Health Dentistry, 71, S20–S33.
https://doi. org/10.1111/j.1752‐7325.2011.00223.x
Becker, G. E., & Roberts, T. (2009). Do we agree? Using a Delphi technique to develop consensus on skills of
hand expression. Journal of Human Lactation, 25(2), 220–225.
https://doi.org/10.1177/0890334409333679
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used
to promote walking and cycling: A systematic review. Health Psychology, 32(8), 829–838.
https://doi.org/10.1037/a0032078
Bodde, A. E., & Seo, D. C. (2009). A review of social and environmental barriers to physical activity for adults
with intellectual disabilities. Disability and Health Journal, 2(2), 57–66.
https://doi.org/10.1016/j. dhjo.2008.11.004
Boulkedid, R., Abdoul, H., Loustau, M., Sibony, O., & Alberti, C. (2011). Using and reporting the Delphi method
for selecting healthcare quality indicators: A systematic review. PLoS ONE, 6(6), e20476.
https:// doi.org/10.1371/journal.pone.0020476
De Meyrick, J. (2003). The Delphi method and health research. Health Education, 103(1), 7–16.
https://doi.org/ 10.1108/09654280310459112
Diamond, I. R., Grant, R. C., Feldman, B. M., Pencharz, P. B., Ling, S. C., Moore, A. M., & Wales, P. W. (2014).
Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi
studies. Journal of Clinical Epidemiology, 67(4), 401–409.
https://doi.org/10.1016/j.jclinepi.2013.12.002
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P. (2011).
Systematic review of reviews of intervention components associated with increased effectiveness in
dietary and physical activity interventions. BMC Public Health, 11(1), 119.
https://doi.org/10.1186/1471-2458-11-119
138541-Willems_BNW.indd 110 31-10-19 10:08

110
An important strength of the study is the randomized sequence of the questions the present authors used to
avoid question order bias and differences in answer ratings for each BCT. The randomization made it possible to
use the answers of participants who did not complete the questionnaire.
4.2 | Recommendations
To our knowledge, this is the first study exploring the suitability of BCTs for supporting lifestyle changes in
individuals with mild intellectual disabilities. Twenty‐four suitable BCTs were identified and might be applied for
doing so. The present authors did not study the suitability of combinations of BCTs since this was an explorative
study. In practice, BCTs may often not have been used solely. However, the authors recommend step‐by‐step
research to determine the efficacy of individual BCTs using a multidimensional approach for a solid design of an
effective lifestyle change intervention. Increased awareness and knowledge about behaviour change and lifestyle
changes in individuals with mild intellectual disabilities are necessary since this is important for the
implementation of a multidimensional approach. Additional research is necessary on the combination and the
use of BCTs in daily support of these individuals. Since the present authors did not study the effectiveness of
BCTs, more research is also needed to determine this in supporting lifestyle changes in individuals with mild
intellectual disabilities.
4.3 | Conclusion
This explorative Delphi study identified 24 BCTs that are suitable for encouraging lifestyle changes in individuals
with mild intellectual disabilities. The study had a wide reach under professionals (given the number of
participants) working with this population, and the present authors determined that professionals reached
consensus about the suitability of BCTs regardless of their working position. The number of comments offered
for a BCT might indicate the suitability of it inversely; fewer comments indicate higher suitability for that BCTs
and more comments indicate lower suitability. Support from others appears to be important for the suitability
of BCTs.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
111
REFERENCES
Abraham, C., & Michie, S. (2008). A taxonomy of behaviour change techniques used in interventions. Health
Psychology, 27(3), 379–387.
Alesi, M., & Pepi, A. (2015). Physical activity engagement in young people with Down syndrome: Investigating
parental beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61–80.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders: DSM‐5 (5th
Ed.). Arlington, VA: American Psychiatric Association.
Bartholomew, L. K., & Mullen, P. D. (2011). Five roles for using theory and evidence in the design and testing of
behavior change interventions. Journal of Public Health Dentistry, 71, S20–S33.
https://doi. org/10.1111/j.1752‐7325.2011.00223.x
Becker, G. E., & Roberts, T. (2009). Do we agree? Using a Delphi technique to develop consensus on skills of
hand expression. Journal of Human Lactation, 25(2), 220–225.
https://doi.org/10.1177/0890334409333679
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behavior change techniques used
to promote walking and cycling: A systematic review. Health Psychology, 32(8), 829–838.
https://doi.org/10.1037/a0032078
Bodde, A. E., & Seo, D. C. (2009). A review of social and environmental barriers to physical activity for adults
with intellectual disabilities. Disability and Health Journal, 2(2), 57–66.
https://doi.org/10.1016/j. dhjo.2008.11.004
Boulkedid, R., Abdoul, H., Loustau, M., Sibony, O., & Alberti, C. (2011). Using and reporting the Delphi method
for selecting healthcare quality indicators: A systematic review. PLoS ONE, 6(6), e20476.
https:// doi.org/10.1371/journal.pone.0020476
De Meyrick, J. (2003). The Delphi method and health research. Health Education, 103(1), 7–16.
https://doi.org/ 10.1108/09654280310459112
Diamond, I. R., Grant, R. C., Feldman, B. M., Pencharz, P. B., Ling, S. C., Moore, A. M., & Wales, P. W. (2014).
Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi
studies. Journal of Clinical Epidemiology, 67(4), 401–409.
https://doi.org/10.1016/j.jclinepi.2013.12.002
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P. (2011).
Systematic review of reviews of intervention components associated with increased effectiveness in
dietary and physical activity interventions. BMC Public Health, 11(1), 119.
https://doi.org/10.1186/1471-2458-11-119
138541-Willems_BNW.indd 111 31-10-19 10:08
112
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data
saturation and variability. Field Methods, 18(1), 59–82. https://doi.org/10.1177/1525822X05279903
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
https://doi.org/10.1016/j.ridd.2011.10.011
Hothorn, T., Bretz, F., & Westfall, P. (2008). Simultaneous inference in general parametric models.
Biometrical journal, 50(3), 346-363. https://doi.org/10.1002/bimj.200810425
Hutzler, Y., & Korsensky, O. (2010). Motivational correlates of physical activity in persons with an intellectual
disability: A systematic literature review. Journal of Intellectual Disability Research, 54(9), 767–786.
https://doi.org/10.1111/j.1365‐2788.2010.01313.x
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
https://doi.org/10.1111/jir.12243
Mallet, J., Guillard, V., Huillard, O., Dubertret, C., & Limosin, F. (2016). Effectiveness of cognitive behavioural
therapy in the treatment of a phobic disorder in a patient with Down syndrome and early Alzheimer's
disease. European Psychiatry, 33, S476. https://doi. org/10.1016/j.eurpsy.2016.01.1739
McGraw, K. O. & Wong, S. P. (1996). Forming Inferences about some intraclass correlation coefficients.
Psychological Methods, 1(1), 30-46. https://doi.org/10.1037/1082‐989X.1.1.30
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
https://doi.org/10.1111/j.1467‐789X.2006.00296.x
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701.
https:// doi.org/10.1037/a0016136
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and healthy
eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
https://doi.org/10.1080/08870446.2010.540664
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J. &
Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered
techniques: building an international consensus for the reporting of behaviour change interventions.
Annals of Behavioral Medicine, 46(1), 81-95.
113
Milat, A. J., King, L., Bauman, A. E., & Redman, S. (January 01, 2013). The concept of scalability: increasing the
scale and potential adoption of health promotion interventions into policy and practice. Health
Promotion International, 28, 3, 285-298.https://doi.org/10.1093/heapro/dar097
National Institute for Health and Clinical Excellence (NICE) (2007). Behaviour change at population, community
and individual levels. London: NICE.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical
Activity, 10(29), 1-15.https://doi. org/10.1186/1479‐5868‐10‐29
Pinheiro, J. C., & Bates, D. M. (2000). Mixed‐effects models in S and SPLUS. New York, NY: Springer‐Verlag.
Portney, L. G., & Watkins, M. P. (2000). Foundations of clinical research (2nd Ed.). Upper Saddle River, NJ:
Prentice Hall.
R Core Team (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation
for Statistical Computing. https:// www.R‐project.org/
Revelle, W., & Zinbarg, R. E. (2009). Coefficients alpha, beta, omega and the glb: Comments on Sijtsma.
Psychometrika, 74(1), 145–154. https://doi.org/10.1007/s11336‐008‐9102‐z
Rothman, A. J. (2004). Is there nothing more practical than a good theory? Why, innovations and advances in
health behavior change will arise if interventions are used to test and refine theory. International
Journal of Behavioral Nutrition and Physical Activity, 1(11), 1–7.
http://www.ijbnpa.org/content/1/1/11.
Skinner, B. F. (1938). The behaviour of organisms. New York, NY: Appleton‐Century‐Crofts.
Temple, V. A. (2009). Factors associated with high levels of physical activity among adults with intellectual
disability. International Journal of Rehabilitation Research, 32, 89–92.
https://doi.org/10.1097/ MRR.0b013e328307f5a0
Van Schijndel-Speet, M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544
Van Schijndel‐Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
138541-Willems_BNW.indd 112 31-10-19 10:08
112
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data
saturation and variability. Field Methods, 18(1), 59–82. https://doi.org/10.1177/1525822X05279903
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477–483.
https://doi.org/10.1016/j.ridd.2011.10.011
Hothorn, T., Bretz, F., & Westfall, P. (2008). Simultaneous inference in general parametric models.
Biometrical journal, 50(3), 346-363. https://doi.org/10.1002/bimj.200810425
Hutzler, Y., & Korsensky, O. (2010). Motivational correlates of physical activity in persons with an intellectual
disability: A systematic literature review. Journal of Intellectual Disability Research, 54(9), 767–786.
https://doi.org/10.1111/j.1365‐2788.2010.01313.x
Kuijken, N. M. J., Naaldenberg, J., Nijhuis-van der Sanden, M. W., & Schrojenstein-Lantman de Valk, H. M. J.
(2016). Healthy living according to adults with intellectual disabilities: Towards tailoring health
promotion initiatives. Journal of Intellectual Disability Research, 60(3), 228–241.
https://doi.org/10.1111/jir.12243
Mallet, J., Guillard, V., Huillard, O., Dubertret, C., & Limosin, F. (2016). Effectiveness of cognitive behavioural
therapy in the treatment of a phobic disorder in a patient with Down syndrome and early Alzheimer's
disease. European Psychiatry, 33, S476. https://doi. org/10.1016/j.eurpsy.2016.01.1739
McGraw, K. O. & Wong, S. P. (1996). Forming Inferences about some intraclass correlation coefficients.
Psychological Methods, 1(1), 30-46. https://doi.org/10.1037/1082‐989X.1.1.30
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
https://doi.org/10.1111/j.1467‐789X.2006.00296.x
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701.
https:// doi.org/10.1037/a0016136
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and healthy
eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
https://doi.org/10.1080/08870446.2010.540664
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J. &
Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered
techniques: building an international consensus for the reporting of behaviour change interventions.
Annals of Behavioral Medicine, 46(1), 81-95.
113
Milat, A. J., King, L., Bauman, A. E., & Redman, S. (January 01, 2013). The concept of scalability: increasing the
scale and potential adoption of health promotion interventions into policy and practice. Health
Promotion International, 28, 3, 285-298.https://doi.org/10.1093/heapro/dar097
National Institute for Health and Clinical Excellence (NICE) (2007). Behaviour change at population, community
and individual levels. London: NICE.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a
systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical
Activity, 10(29), 1-15.https://doi. org/10.1186/1479‐5868‐10‐29
Pinheiro, J. C., & Bates, D. M. (2000). Mixed‐effects models in S and SPLUS. New York, NY: Springer‐Verlag.
Portney, L. G., & Watkins, M. P. (2000). Foundations of clinical research (2nd Ed.). Upper Saddle River, NJ:
Prentice Hall.
R Core Team (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation
for Statistical Computing. https:// www.R‐project.org/
Revelle, W., & Zinbarg, R. E. (2009). Coefficients alpha, beta, omega and the glb: Comments on Sijtsma.
Psychometrika, 74(1), 145–154. https://doi.org/10.1007/s11336‐008‐9102‐z
Rothman, A. J. (2004). Is there nothing more practical than a good theory? Why, innovations and advances in
health behavior change will arise if interventions are used to test and refine theory. International
Journal of Behavioral Nutrition and Physical Activity, 1(11), 1–7.
http://www.ijbnpa.org/content/1/1/11.
Skinner, B. F. (1938). The behaviour of organisms. New York, NY: Appleton‐Century‐Crofts.
Temple, V. A. (2009). Factors associated with high levels of physical activity among adults with intellectual
disability. International Journal of Rehabilitation Research, 32, 89–92.
https://doi.org/10.1097/ MRR.0b013e328307f5a0
Van Schijndel-Speet, M. (2015, February 11). An evidence-based physical activity and fitness programme for
ageing adults with intellectual disabilities (Dissertation). Erasmus University Rotterdam. Retrieved from
http://hdl.handle.net/1765/77544
Van Schijndel‐Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: a process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities.
138541-Willems_BNW.indd 113 31-10-19 10:08
114
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
https://doi.org/10.1519/JSC.0b013e31828bf1aa
Whitehead, D. (2008). An international Delphi study examining health promotion and health education in
nursing practice, education and policy. Journal of Clinical Nursing, 17(7), 891–900.
https://doi. org/10.1111/j.1365‐2702.2007.02079.x
WHO (1992). International statistical classification of diseases and related health problems: ICD‐10, Vol. 1.
Geneva: World Health Organization.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308–322.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256–268
https://doi.org/10.1016/j.ridd.2016.10.008
Willems, M., Waninge, A., Hilgenkamp, T. I., Van Empelen, P., Krijnen, W. P., Van der Schans, C. P., &
Melville, C. A. (2018). Effects of Lifestyle Change Interventions for People with Intellectual
Disabilities: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Applied
Research in Intellectual Disabilities, 31(6), 949-961. https://doi.org/10.1111/jar.12463
Young, A. F., Naji, S., & Kroll, T. (2012). Support for self-management of cardiovascular disease by people with
learning disabilities. Family Practice, 29(4), 467-475. https://doi.org/10.1093/fampra/cmr106
115
APPENDIX – CALO-RE-NL Taxonomy
1) Speak to the client about the consequences of lifestyle behaviour. These may be positive and negative consequences. For
example: you might tell the client that if they switch to a healthier diet they will feel more energetic during the daytime.
2) Speak to the client about the consequences of lifestyle behaviour specifically tailored to them. These may be positive and
negative consequences. For example: you might tell a client with diabetes that if they adopt a healthier diet, their blood sugar
levels will not be as high.
3) Speak to the client about how others feel about the client’s lifestyle behaviour. For example: you might tell the client that
a lot of people approve of their eating healthy food.
4) Speak to the client about other people’s lifestyle behaviour. For example: you might tell the client that a lot of young
people eat healthy meals.
5) Encourage the client to set a behavioural goal for lifestyle behaviour. For example: Encourage the client to set a lifestyle
behaviour goal, such as the goal to cook one healthy meal this week.
6) Encourage the client to set a result-oriented lifestyle behaviour goal. For example: Encourage the client to set a result-
oriented goal, such as the goal to lose 0.5 kg of weight within one week.
7) Encourage the client to plan lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal every week’, you might
encourage the client to plan when they cook that healthy meal.
8) Help the client consider potential lifestyle behaviour barriers and solutions. For example: You might help the client think
about what prevents them from eating healthy food and come with ways of how to change that.
9) Encourage the client to come up with graded (lifestyle behaviour) tasks. For example: If the goal is ‘to cook a healthy meal
every week’, you might encourage the client to come up with graded tasks, such as finding a recipe, making a shopping list,
doing the shopping and cooking the meal.
10) Encourage the client to review their (lifestyle behaviour) goals. For example: If the goal was ‘to cook a healthy meal every
week’, you might encourage the client to reflect on whether they actually did cook a healthy meal every week.
11) Encourage the client to evaluate a result-oriented goal. For example: If the goal was ‘to lose 0.5 kg of weight within one
week’, you might encourage the client to evaluate to what extent they did lose 0.5 kg over the past week.
12) Reward the client for progress they have made to achieve the goal. For example: If the goal is ‘to cook a healthy meal
every week’, the client will receive a reward (which may also simply be a compliment) once they draw up their shopping list.
13) Reward the client for performing the lifestyle behaviour. For example: the client will receive a reward for achieving the
goal ‘to cook a healthy meal every week’.
14) Reward the client so they learn to perform the lifestyle behaviour. The client will first be rewarded for steps made toward
achieving the goal and subsequently they will only be rewarded for performance of the intended lifestyle behaviour. For
example: If the goal is ‘to cook a healthy meal every week’, the client is first rewarded for finding a recipe and subsequently
for doing the shopping for the meal. Eventually, the client is only rewarded for cooking a healthy meal every week.
15) Encourage the client to perform the specified lifestyle behaviour more often. For example: If the goal is ‘to cook a healthy
meal every week’, encourage the client to cook healthy meals more often.
16) Encourage the client to keep a record of how they perform the specified behaviour(s). For example: If the goal is ‘to cook
a healthy meal every week’, encourage the client to keep a record of when they cooked a healthy meal and what they cooked
for themselves.
17) Encourage the client to keep a record of the results of their lifestyle behaviour. For example: If the goal is ‘to lose 0.5 kg
of weight within one week’, then you should encourage the client to monitor their weight and keep a record of their progress.
138541-Willems_BNW.indd 114 31-10-19 10:08

114
The Journal of Strength and Conditioning Research, 27(11), 3150–3158.
https://doi.org/10.1519/JSC.0b013e31828bf1aa
Whitehead, D. (2008). An international Delphi study examining health promotion and health education in
nursing practice, education and policy. Journal of Clinical Nursing, 17(7), 891–900.
https://doi. org/10.1111/j.1365‐2702.2007.02079.x
WHO (1992). International statistical classification of diseases and related health problems: ICD‐10, Vol. 1.
Geneva: World Health Organization.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308–322.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256–268
https://doi.org/10.1016/j.ridd.2016.10.008
Willems, M., Waninge, A., Hilgenkamp, T. I., Van Empelen, P., Krijnen, W. P., Van der Schans, C. P., &
Melville, C. A. (2018). Effects of Lifestyle Change Interventions for People with Intellectual
Disabilities: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Applied
Research in Intellectual Disabilities, 31(6), 949-961. https://doi.org/10.1111/jar.12463
Young, A. F., Naji, S., & Kroll, T. (2012). Support for self-management of cardiovascular disease by people with
learning disabilities. Family Practice, 29(4), 467-475. https://doi.org/10.1093/fampra/cmr106
115
APPENDIX – CALO-RE-NL Taxonomy
1) Speak to the client about the consequences of lifestyle behaviour. These may be positive and negative consequences. For
example: you might tell the client that if they switch to a healthier diet they will feel more energetic during the daytime.
2) Speak to the client about the consequences of lifestyle behaviour specifically tailored to them. These may be positive and
negative consequences. For example: you might tell a client with diabetes that if they adopt a healthier diet, their blood sugar
levels will not be as high.
3) Speak to the client about how others feel about the client’s lifestyle behaviour. For example: you might tell the client that
a lot of people approve of their eating healthy food.
4) Speak to the client about other people’s lifestyle behaviour. For example: you might tell the client that a lot of young
people eat healthy meals.
5) Encourage the client to set a behavioural goal for lifestyle behaviour. For example: Encourage the client to set a lifestyle
behaviour goal, such as the goal to cook one healthy meal this week.
6) Encourage the client to set a result-oriented lifestyle behaviour goal. For example: Encourage the client to set a result-
oriented goal, such as the goal to lose 0.5 kg of weight within one week.
7) Encourage the client to plan lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal every week’, you might
encourage the client to plan when they cook that healthy meal.
8) Help the client consider potential lifestyle behaviour barriers and solutions. For example: You might help the client think
about what prevents them from eating healthy food and come with ways of how to change that.
9) Encourage the client to come up with graded (lifestyle behaviour) tasks. For example: If the goal is ‘to cook a healthy meal
every week’, you might encourage the client to come up with graded tasks, such as finding a recipe, making a shopping list,
doing the shopping and cooking the meal.
10) Encourage the client to review their (lifestyle behaviour) goals. For example: If the goal was ‘to cook a healthy meal every
week’, you might encourage the client to reflect on whether they actually did cook a healthy meal every week.
11) Encourage the client to evaluate a result-oriented goal. For example: If the goal was ‘to lose 0.5 kg of weight within one
week’, you might encourage the client to evaluate to what extent they did lose 0.5 kg over the past week.
12) Reward the client for progress they have made to achieve the goal. For example: If the goal is ‘to cook a healthy meal
every week’, the client will receive a reward (which may also simply be a compliment) once they draw up their shopping list.
13) Reward the client for performing the lifestyle behaviour. For example: the client will receive a reward for achieving the
goal ‘to cook a healthy meal every week’.
14) Reward the client so they learn to perform the lifestyle behaviour. The client will first be rewarded for steps made toward
achieving the goal and subsequently they will only be rewarded for performance of the intended lifestyle behaviour. For
example: If the goal is ‘to cook a healthy meal every week’, the client is first rewarded for finding a recipe and subsequently
for doing the shopping for the meal. Eventually, the client is only rewarded for cooking a healthy meal every week.
15) Encourage the client to perform the specified lifestyle behaviour more often. For example: If the goal is ‘to cook a healthy
meal every week’, encourage the client to cook healthy meals more often.
16) Encourage the client to keep a record of how they perform the specified behaviour(s). For example: If the goal is ‘to cook
a healthy meal every week’, encourage the client to keep a record of when they cooked a healthy meal and what they cooked
for themselves.
17) Encourage the client to keep a record of the results of their lifestyle behaviour. For example: If the goal is ‘to lose 0.5 kg
of weight within one week’, then you should encourage the client to monitor their weight and keep a record of their progress.
138541-Willems_BNW.indd 115 31-10-19 10:08

116
18) Encourage the client to reflect on past lifestyle behaviour successes. For example: If the goal is ‘to cook a healthy meal
every week’, then you should encourage the client to think back to the last time they cooked a healthy meal and how
successful they were.
19) Provide the client with feedback on the performance of their lifestyle behaviour. For example: If the goal is ‘to cook a
healthy meal every week’, then you should tell the client whether they have carried out the cooking task well and whether
they could make improvements.
20) Tell the client where and when they are able to perform the lifestyle behaviour. For example: If the goal is ‘to cook a
healthy meal every week’, you might give the client tips on what day and what time they would be best off cooking.
21) Explain to the client how they should perform the lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal
every week’, explain to the client how they should follow a recipe in order to cook a meal.
22) Demonstrate the lifestyle behaviour to the client. For example: If the goal is ‘to cook a healthy meal every week’,
demonstrate to the client how to follow a recipe and how to cook a healthy meal using that method.
23) Teach the client to use environmental cues/prompts for lifestyle behaviour. For example: If the goal is ‘to cook a healthy
meal every week’, teach the client how to use an app that sends them a reminder to start cooking.
24) Encourage the client to change their environment in such a way as to help them perform the specified behaviour. For
example: If the goal is ‘to lose 0.5 kg of weight within a week’, then encourage the client to throw out any unhealthy snacks.
25) Agree on a behavioural contact with the client. The behavioural contract sets out that the client wishes to achieve a
specific (lifestyle) goal. For example: If the goal is ‘to cook a healthy meal every week’, then the behavioural contract will
state that the client intends to cook a healthy meal at least once a week
26) Encourage the client to practice and rehearse lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal every
week’, then encourage the client to practise cooking healthy meals.
27) Encourage the client to perform the specified lifestyle behaviour. Use follow-up prompts and gradually reduce the
encouragement they receive. For example: If the goal is ‘to cook a healthy meal every week’, then first encourage the client
during daily conversations, gradually only provide encouragement on a weekly basis and finally only occasionally give them
encouragement.
28) Prompt the client to compare themselves with others. For example: If the goal is ‘to cook a healthy meal every week’,
then prompt the client to consider that their friends or family also cook healthy meals.
29) Encourage the client to ask others for social support or encouragement. For example: If the goal is ‘to cook a healthy meal
every week’, then encourage the client to find a friend, or ‘buddy’ that can help them do the cooking.
30) Help the client consider themselves as a role model. For example: If the goal is ‘to cook a healthy meal every week’, then
convince the client that they are a role model to their friends by cooking healthy food.
31) Prompt the client to consider how they would feel if they were not to perform the specified lifestyle behaviour and
whether they would regret that. For example: If the goal is ‘to lose 0.5 kg of weight within a week’, then have the client
consider whether they would regret eating unhealthy food and not lose weight as a result.
32) Provide the client with information on the risks of undesirable behavioural lifestyle behaviour to evoke fear in the client.
For example: You might tell the client that eating unhealthy food can lead to heart disease.
33) Encourage the client to use self-instruction and self-talk (aloud or silently) before or during performance of actions. This
can be used to encourage, support and maintain the behaviour. For example: If the goal is ‘to cook a healthy meal every
week’, then prompt the client to encourage themselves (“I can do this” / “I did well”).
34) Encourage the client to imagine that they are performing the lifestyle behaviour really well or that this type of lifestyle
behaviour is very easy. For example: If the goal is ‘to cook a healthy meal every week’, then prompt the client to imagine how
they would feel if they had already succeeded to cook a healthy meal.
117
35) Encourage the client to identify ways of how they could maintain new lifestyle behaviours and help the client identify
ways of avoiding or managing situations likely to result in readopting risk behaviour or failure. For example: If the goal is ‘to
cook a healthy meal every week’, then encourage the client to identify ways in which they can maintain the behaviour of
cooking a healthy meal every week.
36) Teach the client techniques to reduce anxiety or stress. For example: If the goal is ‘to cook a healthy meal every week’,
then teach the client to breathe in and out deeply before tasting an ingredient they do not like.
37) Introduce a coach to help the client using motivational interviewing. This is a specific method that involves the coach
prompting the client about the client’s lifestyle behaviour and helps them identify what they want or what they value.
38) Teach the client to manage their own time. For example: If the goal is ‘to cook a healthy meal every week’, then teach
the client to draw up a detailed plan of their free time, which includes scheduling the cooking of a healthy meal every week.
39) General communication skills training: the client is taught communication skills, for example through the use of role play
exercises or group discussions.
40) Encourage the client to look forward to a reward in the future. For example: If the goal is ‘to cook a healthy meal every
week’, then remind the client once they have cooked 3 healthy meals for themselves they will be allowed to take part in the
special dinner they planned where they cook for their family.
138541-Willems_BNW.indd 116 31-10-19 10:08

116
18) Encourage the client to reflect on past lifestyle behaviour successes. For example: If the goal is ‘to cook a healthy meal
every week’, then you should encourage the client to think back to the last time they cooked a healthy meal and how
successful they were.
19) Provide the client with feedback on the performance of their lifestyle behaviour. For example: If the goal is ‘to cook a
healthy meal every week’, then you should tell the client whether they have carried out the cooking task well and whether
they could make improvements.
20) Tell the client where and when they are able to perform the lifestyle behaviour. For example: If the goal is ‘to cook a
healthy meal every week’, you might give the client tips on what day and what time they would be best off cooking.
21) Explain to the client how they should perform the lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal
every week’, explain to the client how they should follow a recipe in order to cook a meal.
22) Demonstrate the lifestyle behaviour to the client. For example: If the goal is ‘to cook a healthy meal every week’,
demonstrate to the client how to follow a recipe and how to cook a healthy meal using that method.
23) Teach the client to use environmental cues/prompts for lifestyle behaviour. For example: If the goal is ‘to cook a healthy
meal every week’, teach the client how to use an app that sends them a reminder to start cooking.
24) Encourage the client to change their environment in such a way as to help them perform the specified behaviour. For
example: If the goal is ‘to lose 0.5 kg of weight within a week’, then encourage the client to throw out any unhealthy snacks.
25) Agree on a behavioural contact with the client. The behavioural contract sets out that the client wishes to achieve a
specific (lifestyle) goal. For example: If the goal is ‘to cook a healthy meal every week’, then the behavioural contract will
state that the client intends to cook a healthy meal at least once a week
26) Encourage the client to practice and rehearse lifestyle behaviour. For example: If the goal is ‘to cook a healthy meal every
week’, then encourage the client to practise cooking healthy meals.
27) Encourage the client to perform the specified lifestyle behaviour. Use follow-up prompts and gradually reduce the
encouragement they receive. For example: If the goal is ‘to cook a healthy meal every week’, then first encourage the client
during daily conversations, gradually only provide encouragement on a weekly basis and finally only occasionally give them
encouragement.
28) Prompt the client to compare themselves with others. For example: If the goal is ‘to cook a healthy meal every week’,
then prompt the client to consider that their friends or family also cook healthy meals.
29) Encourage the client to ask others for social support or encouragement. For example: If the goal is ‘to cook a healthy meal
every week’, then encourage the client to find a friend, or ‘buddy’ that can help them do the cooking.
30) Help the client consider themselves as a role model. For example: If the goal is ‘to cook a healthy meal every week’, then
convince the client that they are a role model to their friends by cooking healthy food.
31) Prompt the client to consider how they would feel if they were not to perform the specified lifestyle behaviour and
whether they would regret that. For example: If the goal is ‘to lose 0.5 kg of weight within a week’, then have the client
consider whether they would regret eating unhealthy food and not lose weight as a result.
32) Provide the client with information on the risks of undesirable behavioural lifestyle behaviour to evoke fear in the client.
For example: You might tell the client that eating unhealthy food can lead to heart disease.
33) Encourage the client to use self-instruction and self-talk (aloud or silently) before or during performance of actions. This
can be used to encourage, support and maintain the behaviour. For example: If the goal is ‘to cook a healthy meal every
week’, then prompt the client to encourage themselves (“I can do this” / “I did well”).
34) Encourage the client to imagine that they are performing the lifestyle behaviour really well or that this type of lifestyle
behaviour is very easy. For example: If the goal is ‘to cook a healthy meal every week’, then prompt the client to imagine how
they would feel if they had already succeeded to cook a healthy meal.
117
35) Encourage the client to identify ways of how they could maintain new lifestyle behaviours and help the client identify
ways of avoiding or managing situations likely to result in readopting risk behaviour or failure. For example: If the goal is ‘to
cook a healthy meal every week’, then encourage the client to identify ways in which they can maintain the behaviour of
cooking a healthy meal every week.
36) Teach the client techniques to reduce anxiety or stress. For example: If the goal is ‘to cook a healthy meal every week’,
then teach the client to breathe in and out deeply before tasting an ingredient they do not like.
37) Introduce a coach to help the client using motivational interviewing. This is a specific method that involves the coach
prompting the client about the client’s lifestyle behaviour and helps them identify what they want or what they value.
38) Teach the client to manage their own time. For example: If the goal is ‘to cook a healthy meal every week’, then teach
the client to draw up a detailed plan of their free time, which includes scheduling the cooking of a healthy meal every week.
39) General communication skills training: the client is taught communication skills, for example through the use of role play
exercises or group discussions.
40) Encourage the client to look forward to a reward in the future. For example: If the goal is ‘to cook a healthy meal every
week’, then remind the client once they have cooked 3 healthy meals for themselves they will be allowed to take part in the
special dinner they planned where they cook for their family.
138541-Willems_BNW.indd 117 31-10-19 10:08

Chapter 5
Behaviour change techniques used in lifestyle support of adults with mild
intellectual disabilities
Mariël Willems
Johan de Jong
Annelies Overwijk
Thessa I.M. Hilgenkamp
Cees P. Van der Schans
Aly Waninge
Manuscript submitted
138541-Willems_BNW.indd 118 31-10-19 10:08
Chapter 5
Behaviour change techniques used in lifestyle support of adults with mild
intellectual disabilities
Mariël Willems
Johan de Jong
Annelies Overwijk
Thessa I.M. Hilgenkamp
Cees P. Van der Schans
Aly Waninge
Manuscript submitted
138541-Willems_BNW.indd 119 31-10-19 10:08

120
ABSTRACT
Background: Professional caregivers are important in the daily support of lifestyle change in adults with mild
intellectual disabilities (ID). However, little is known about which behaviour change techniques (BCTs) they
actually use in changing their lifestyle behaviour.
Aim: This study aims to get insight in the use of behaviour change techniques (BCTs) in daily support for lifestyle
behaviour of adults with mild ID, using video observations.
Methods: Professional caregivers (N=14) were observed in their daily work, supporting adults with mild ID. Videos
are analysed using the Coventry Aberdeen London Refined (CALO-RE) taxonomy and BCTs used were coded on a
data report form.
Results: 21 out of 40 BCTs were used by professional caregivers. The BCTs “Information about others' approval”,
“Identification as role model”, “Rewards on successful behaviour”, “Review behavioural goals” and “Instructions
on how to perform the behaviour” were mostly used.
Conclusion: Professional caregivers used BCTs to support lifestyle behaviour of adults with mild ID. However, the
most promising BCTs were rarely used by professional caregivers.
121
1 | INTRODUCTION
Adults with intellectual disabilities (ID) often demonstrate an unhealthy lifestyle (McGuire, Daly, & Smyth, 2007).
They are often sedentary (Haveman et al., 2010), not physically active enough to gain substantial health benefits
(Draheim, Williams, & McCubbin, 2002; Frey & Chow, 2006; Lahtinen, Rintala, & Malin, 2007; Temple, Frey, &
Stanish, 2006), and they experience unhealthy dietary habits (Haveman et al., 2010; Hsieh, Rimmer, & Heller,
2014). Supporting lifestyle change for adults with intellectual disabilities is therefore important.
Lifestyle behaviour can be improved using behaviour change techniques (BCTs) in the general population (Bird
et al. 2013, Greaves et al., 2011; Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Olander et al., 2013;
Williams & French, 2011). For adults with ID, we found frequent use of BCTs in lifestyle change interventions
although mostly implicit (Willems, Hilgenkamp, Havik, Waninge, & Melville, 2017).
According to professionals (professional caregivers, behavioural scientists, health professionals, intellectual
disability physicians) BCTs may be suitable to change lifestyle behaviour in adults with mild ID (Willems, Waninge,
De Jong, Hilgenkamp, & Van der Schans, 2019). Professional caregivers and relatives play an important role in
behaviour change for adults with ID (Alesi & Pepi, 2015; Davison, Jurkowski, Li, Kranz & Lawson, 2013; Grondhuis
& Aman, 2014; Heller, McCubbin, Drum, & Peterson, 2011; Hithersay, Strydom, Moulster, & Buszewicz, 2014;
James & Shireman, 2010; Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Naaldenberg, Kuijken, van Dooren
& De Valk, 2013; Stanish, Temple & Frey, 2006; Van Schijndel-Speet, Evenhuis, Van Wijck, & Echteld, 2014). BCTs
that were considered most suitable were: “Barrier identification”, “Set graded tasks”, “Reward effort towards
behaviour”, “Motivational interviewing”, and “Action planning” (Willems et al., 2019). The perceived suitability
of BCTs was related to personal characteristics of adults with mild ID and the social support from others they
receive. However, to date, there is no insight into the actual use or application of BCTs in the daily support that
professional caregivers provide. This is instrumental knowledge for determining what BCT would be most
effective to focus on in a training or education program. In order to investigate the gaps of knowledge and
expertise, and to design meaningful support for professional caregivers, this observational study aims to observe
and determine the use of BCTs by professional caregivers, assisting lifestyle behaviour of adults with mild ID using
video observations. If BCTs are used by professional caregivers, this study will also investigate whether there is
any relation between the BCTs used and characteristics of the users.
2 | METHODS
2.1 | Design
During this observational study, professional caregivers were observed during their daily work, supporting adults
with mild ID. Between October 2018 and March 2019, data were collected in nine community-based living
facilities where adults with all levels of ID were living and receiving support from professional caregivers.
Observations of professional caregivers providing regular daily support to adults with mild ID took place on three
random weekdays, on various moments of the day.
138541-Willems_BNW.indd 120 31-10-19 10:08

120
ABSTRACT
Background: Professional caregivers are important in the daily support of lifestyle change in adults with mild
intellectual disabilities (ID). However, little is known about which behaviour change techniques (BCTs) they
actually use in changing their lifestyle behaviour.
Aim: This study aims to get insight in the use of behaviour change techniques (BCTs) in daily support for lifestyle
behaviour of adults with mild ID, using video observations.
Methods: Professional caregivers (N=14) were observed in their daily work, supporting adults with mild ID. Videos
are analysed using the Coventry Aberdeen London Refined (CALO-RE) taxonomy and BCTs used were coded on a
data report form.
Results: 21 out of 40 BCTs were used by professional caregivers. The BCTs “Information about others' approval”,
“Identification as role model”, “Rewards on successful behaviour”, “Review behavioural goals” and “Instructions
on how to perform the behaviour” were mostly used.
Conclusion: Professional caregivers used BCTs to support lifestyle behaviour of adults with mild ID. However, the
most promising BCTs were rarely used by professional caregivers.
121
1 | INTRODUCTION
Adults with intellectual disabilities (ID) often demonstrate an unhealthy lifestyle (McGuire, Daly, & Smyth, 2007).
They are often sedentary (Haveman et al., 2010), not physically active enough to gain substantial health benefits
(Draheim, Williams, & McCubbin, 2002; Frey & Chow, 2006; Lahtinen, Rintala, & Malin, 2007; Temple, Frey, &
Stanish, 2006), and they experience unhealthy dietary habits (Haveman et al., 2010; Hsieh, Rimmer, & Heller,
2014). Supporting lifestyle change for adults with intellectual disabilities is therefore important.
Lifestyle behaviour can be improved using behaviour change techniques (BCTs) in the general population (Bird
et al. 2013, Greaves et al., 2011; Michie, Abraham, Whittington, McAteer, & Gupta, 2009; Olander et al., 2013;
Williams & French, 2011). For adults with ID, we found frequent use of BCTs in lifestyle change interventions
although mostly implicit (Willems, Hilgenkamp, Havik, Waninge, & Melville, 2017).
According to professionals (professional caregivers, behavioural scientists, health professionals, intellectual
disability physicians) BCTs may be suitable to change lifestyle behaviour in adults with mild ID (Willems, Waninge,
De Jong, Hilgenkamp, & Van der Schans, 2019). Professional caregivers and relatives play an important role in
behaviour change for adults with ID (Alesi & Pepi, 2015; Davison, Jurkowski, Li, Kranz & Lawson, 2013; Grondhuis
& Aman, 2014; Heller, McCubbin, Drum, & Peterson, 2011; Hithersay, Strydom, Moulster, & Buszewicz, 2014;
James & Shireman, 2010; Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Naaldenberg, Kuijken, van Dooren
& De Valk, 2013; Stanish, Temple & Frey, 2006; Van Schijndel-Speet, Evenhuis, Van Wijck, & Echteld, 2014). BCTs
that were considered most suitable were: “Barrier identification”, “Set graded tasks”, “Reward effort towards
behaviour”, “Motivational interviewing”, and “Action planning” (Willems et al., 2019). The perceived suitability
of BCTs was related to personal characteristics of adults with mild ID and the social support from others they
receive. However, to date, there is no insight into the actual use or application of BCTs in the daily support that
professional caregivers provide. This is instrumental knowledge for determining what BCT would be most
effective to focus on in a training or education program. In order to investigate the gaps of knowledge and
expertise, and to design meaningful support for professional caregivers, this observational study aims to observe
and determine the use of BCTs by professional caregivers, assisting lifestyle behaviour of adults with mild ID using
video observations. If BCTs are used by professional caregivers, this study will also investigate whether there is
any relation between the BCTs used and characteristics of the users.
2 | METHODS
2.1 | Design
During this observational study, professional caregivers were observed during their daily work, supporting adults
with mild ID. Between October 2018 and March 2019, data were collected in nine community-based living
facilities where adults with all levels of ID were living and receiving support from professional caregivers.
Observations of professional caregivers providing regular daily support to adults with mild ID took place on three
random weekdays, on various moments of the day.
138541-Willems_BNW.indd 121 31-10-19 10:08
122
2.2 | Participants
Participants were professional caregivers working with adults with mild ID in ID care provider organizations in
the Netherlands.
Inclusion criteria were:
- Professional caregivers;
- Supporting adults with mild ID (>18 years) in daily living;
- Working on community-based living facility for adults with ID of Dutch ID care provider organizations;
- Minimum of 6 months of working experience;
- Age ≥18 years.
Professional caregivers were approached through a consortium consisting of nine Dutch ID care provider
organizations. These organizations support persons within the whole range of ID. Participants were recruited by
contact persons of these organizations. Informed consent was asked for all participants (professional caregivers).
Since adults with mild ID may also be recorded, informed consent was also given by involved adults with mild ID
or their legal representatives.
2.3 | Ethical approval
Dispensation was obtained from the local medical ethical committee of the University Medical Centre Groningen
(number: 201700241, Medical Ethics Committee, University Medical Centre Groningen, the Netherlands, METc
UMCG) because this study did not concern medical scientific research in humans. Privacy of participants and
adults with mild ID was secured, saving the recordings and personal characteristics separately.
2.4 | Data collection
The observations were made in community-based living facilities. They were made on three weekdays on
different moments of the day, including an observation in the morning (e.g. during breakfast) and in the evening
(e.g. during diner or evening activities). Each video recording moment lasted for two hours to reveal a reliable
representation of the daily support of adults with mild ID. Professionals were asked to engage in their normal
activities like there was no observer. Activities regarding personal hygiene (e.g. showering, bathing) were not
recorded because of the privacy of the adults with mild ID.
The observations were of audio-visual nature, which means that the observations included both picture and
sound. The observations were non-participative, since the observer did not or only minimally participate in the
interaction between professional caregivers and the adults with mild ID they supported. The video recordings
were collected by interns working at the included living facility. The deployment of interns reduced the
infringement on the daily living of adults with mild ID, since the interns were already familiar. Interns were
instructed about the methods of the observations by the first author (MW). Instructions included 1) technical
instructions about how to use the camera 2) the observation method with information on how to film without
participating or interpreting 3) registration of the video recording, e.g. notation of characteristics to recognize
participants and adults with mild ID 4) bias registration, about possible forms of bias during filming and how to
123
register this when necessary 5) data storage instructions on how to store the video recordings safely after
recording. Observations were made with high quality cameras. Before starting the observations, interns had to
sign a declaration of confidentiality. The video camera was stored in a saved locker before, between and after
the observations until the camera was collected by the first author (MW).
The protocol for filming and instruction of the filming procedure were optimized using the first pilot type of
recordings. The latter were checked for correct placement of the camera, optimal visibility of the interaction
between professional caregiver and adults with mild ID and whether relevant information about the environment
and eventual special circumstances was provided by the interns making the video observations.
Before the video observations were made, professional caregivers were asked to complete a questionnaire about
demographic characteristics: age, gender, education level, working experience, current position, number of
colleagues, group size of the adults with mild ID and characteristics of the individuals with ID they were
supporting (age, gender, level of ID, mobility, additional problems). Before starting the observations, the first
author (MW) checked the questionnaires (about the general characteristics) for completeness.
After completion of the observations, the video camera with recordings was collected by the first author (MW).
The recordings were saved on two separate external hard disks, secured with different passwords. The passwords
were saved separately, in a file that was accessible by the researchers involved only. Afterwards, the memory
cards in the video cameras were formatted to erase all data. Names and characteristics of adults with mild ID
were extracted from the online questionnaire filled in by participants to determine which persons on the video’s
had given informed consent and to avoid that parts of the recordings were analysed where someone else was
accidentally filmed. Before data analyses, the first author (MW) checked the recordings for quality of the videos.
2.5 | Data analyses
The Coventry Aberdeen London Refined (CALO-RE) taxonomy (Michie et al., 2011) was used for deductive coding
of the BCTs. A data report form was designed and pilot tested by two authors (MW, AO), using the recordings
from the pilot test observations. No changes were made during pilot testing. The BCTs were coded per video
recording moment on use or non-use, frequency of use was not coded in a video recording moment.
Recordings were scored separately by two trained research assistants, which were instructed for scoring by the
first author (MW). After instruction, the two research assistants and the first author (MW) scored a sample of 2
recordings, including approximately 20 minutes of video material. The sample included recordings from different
observation moments and included a physical activity moment and a nutrition moment. Scorings were compared
and disagreements were solved by consensus discussion. Next, the researchers and first author (MW) scored
another sample of recordings of approximately 20 minutes of video material and interrater reliability was
calculated, disagreements were solved by consensus discussion. Interrater reliability after instruction for first
author and two research assistants (RA1 and RA2) was calculated. One research assistant (RA1) scored the videos
of twelve participants of the sample, whereas the other research assistant (RA2) scored the videos of two
participants. When scorings were halfway, research assistant (RA1) and first author (MW) scored a sample of
recordings (approximately 20 minutes of video material) to check interrater reliability again and solve
138541-Willems_BNW.indd 122 31-10-19 10:08

122
2.2 | Participants
Participants were professional caregivers working with adults with mild ID in ID care provider organizations in
the Netherlands.
Inclusion criteria were:
- Professional caregivers;
- Supporting adults with mild ID (>18 years) in daily living;
- Working on community-based living facility for adults with ID of Dutch ID care provider organizations;
- Minimum of 6 months of working experience;
- Age ≥18 years.
Professional caregivers were approached through a consortium consisting of nine Dutch ID care provider
organizations. These organizations support persons within the whole range of ID. Participants were recruited by
contact persons of these organizations. Informed consent was asked for all participants (professional caregivers).
Since adults with mild ID may also be recorded, informed consent was also given by involved adults with mild ID
or their legal representatives.
2.3 | Ethical approval
Dispensation was obtained from the local medical ethical committee of the University Medical Centre Groningen
(number: 201700241, Medical Ethics Committee, University Medical Centre Groningen, the Netherlands, METc
UMCG) because this study did not concern medical scientific research in humans. Privacy of participants and
adults with mild ID was secured, saving the recordings and personal characteristics separately.
2.4 | Data collection
The observations were made in community-based living facilities. They were made on three weekdays on
different moments of the day, including an observation in the morning (e.g. during breakfast) and in the evening
(e.g. during diner or evening activities). Each video recording moment lasted for two hours to reveal a reliable
representation of the daily support of adults with mild ID. Professionals were asked to engage in their normal
activities like there was no observer. Activities regarding personal hygiene (e.g. showering, bathing) were not
recorded because of the privacy of the adults with mild ID.
The observations were of audio-visual nature, which means that the observations included both picture and
sound. The observations were non-participative, since the observer did not or only minimally participate in the
interaction between professional caregivers and the adults with mild ID they supported. The video recordings
were collected by interns working at the included living facility. The deployment of interns reduced the
infringement on the daily living of adults with mild ID, since the interns were already familiar. Interns were
instructed about the methods of the observations by the first author (MW). Instructions included 1) technical
instructions about how to use the camera 2) the observation method with information on how to film without
participating or interpreting 3) registration of the video recording, e.g. notation of characteristics to recognize
participants and adults with mild ID 4) bias registration, about possible forms of bias during filming and how to
123
register this when necessary 5) data storage instructions on how to store the video recordings safely after
recording. Observations were made with high quality cameras. Before starting the observations, interns had to
sign a declaration of confidentiality. The video camera was stored in a saved locker before, between and after
the observations until the camera was collected by the first author (MW).
The protocol for filming and instruction of the filming procedure were optimized using the first pilot type of
recordings. The latter were checked for correct placement of the camera, optimal visibility of the interaction
between professional caregiver and adults with mild ID and whether relevant information about the environment
and eventual special circumstances was provided by the interns making the video observations.
Before the video observations were made, professional caregivers were asked to complete a questionnaire about
demographic characteristics: age, gender, education level, working experience, current position, number of
colleagues, group size of the adults with mild ID and characteristics of the individuals with ID they were
supporting (age, gender, level of ID, mobility, additional problems). Before starting the observations, the first
author (MW) checked the questionnaires (about the general characteristics) for completeness.
After completion of the observations, the video camera with recordings was collected by the first author (MW).
The recordings were saved on two separate external hard disks, secured with different passwords. The passwords
were saved separately, in a file that was accessible by the researchers involved only. Afterwards, the memory
cards in the video cameras were formatted to erase all data. Names and characteristics of adults with mild ID
were extracted from the online questionnaire filled in by participants to determine which persons on the video’s
had given informed consent and to avoid that parts of the recordings were analysed where someone else was
accidentally filmed. Before data analyses, the first author (MW) checked the recordings for quality of the videos.
2.5 | Data analyses
The Coventry Aberdeen London Refined (CALO-RE) taxonomy (Michie et al., 2011) was used for deductive coding
of the BCTs. A data report form was designed and pilot tested by two authors (MW, AO), using the recordings
from the pilot test observations. No changes were made during pilot testing. The BCTs were coded per video
recording moment on use or non-use, frequency of use was not coded in a video recording moment.
Recordings were scored separately by two trained research assistants, which were instructed for scoring by the
first author (MW). After instruction, the two research assistants and the first author (MW) scored a sample of 2
recordings, including approximately 20 minutes of video material. The sample included recordings from different
observation moments and included a physical activity moment and a nutrition moment. Scorings were compared
and disagreements were solved by consensus discussion. Next, the researchers and first author (MW) scored
another sample of recordings of approximately 20 minutes of video material and interrater reliability was
calculated, disagreements were solved by consensus discussion. Interrater reliability after instruction for first
author and two research assistants (RA1 and RA2) was calculated. One research assistant (RA1) scored the videos
of twelve participants of the sample, whereas the other research assistant (RA2) scored the videos of two
participants. When scorings were halfway, research assistant (RA1) and first author (MW) scored a sample of
recordings (approximately 20 minutes of video material) to check interrater reliability again and solve
138541-Willems_BNW.indd 123 31-10-19 10:08

124
disagreements by consensus discussion. A sample of recording (approximately 20 minutes) was scored again for
calculating the intra-rater reliability.
For the characteristics of participants, means and standard deviations were calculated. The outcomes of the
frequency of usage of top 5 of BCTs used out of a total of 3 are binomial distributed. Therefore, a generalized
linear modelling analysis was performed using the logit link for binomial regression with the explanative variables
sex, age, work years, education, additional lifestyle training and policies.
3 | RESULTS
3.1 | General characteristics
Fourteen professional caregivers participated in the study who supported adults with mild ID in a community
based living facility (N=6), and were filmed during daily support work. Participants had a mean age of 41.9 (SD
12.1) years and their mean working experience was 17.4 (SD 10.1, range 3-35) years. Baseline characteristics of
participants were shown in Table 1. Informed consent was given for 30 adults with mild ID, whereas 12 adults
where supported by 2 participants during the observations. Mean age of adults with mild ID was 51.5 years (SD
18.0). Participants (N=4) dropped out for several reasons: they left the organization during observation period
(n=1), ran out of time to perform the video observation (n=2) or the adults with ID involved did not have mild ID
(N=1). In total, 33:15:47 (h:m:s) film material was obtained and total observation time ranged from 00:13:10 to
04:38:59 per participant. Most participants (N=8) were filmed two moments (n=6) or one moment (n=2) or
instead of three moments, due to scheduling issues. For one participant, videos from two measurements had to
be erased as informed consent for an adult with mild ID was withdrawn. Interrater reliability after instruction
was 82.5% (MW-RA1), 85% (MW, RA2) and 87.5% (RA1-RA2) respectively. Interrater reliability halfway data
analysis for 2 measurements was 92.5% and 90% (MW-RA1). Intra-rater reliability was 97.5%, calculated as
percentage of absolute agreement.
Table 1: General characteristics of participants
Professional caregivers (N=14)
Age, mean (SD) 41.9 (12.1)
sex (% Female) 85.7
Working experience mean (SD) years 17.4
Mean years working in organization 15 (SD 7.5)
Mean working hours per week 18.6 (SD 7.2)
Education level Higher=6, Vocational=8
Supplemental lifestyle training No=9, Yes=5
Lifestyle policy in ID care organization Very little: 0, Little: 1, Not much/not little: 4, Much: 8, Very much: 1
Mean no. of clients per group 12.9 (SD 6.1)
Mean no. of professionals for clients 2.3 (SD 1.0)
125
3.2 | Behaviour change techniques in lifestyle support
A total of 21 BCTs was used by professional caregivers, supporting lifestyle behaviour of adults with mild ID. The
BCTs mostly used were: “Information about others' approval” (N=15), “Identification as role model” (N=15),
“Rewards on successful behaviour” (N=11), “Review behavioural goals” (N=9) and “Instructions on how to
perform the behaviour” (N=8). A total of nine BCTs was used by only two (N=1) or one (N=8) participants, and 19
BCTs were not used at all. See Table 2 for an overview of the frequencies for BCTs used.
Univariate binomial regression analysis were performed on frequency of use of the five mostly used BCTs
(“Information about others' approval”, “Identification as role model”, “Rewards on successful behaviour”,
“Review behavioural goals” and “Instructions on how to perform the behaviour”) one for each characteristic of
the 14 professional caregivers, including: sex, age, work years, education, additional lifestyle training and policies.
A significant effect was found for policies on the BCT “Identification as a role model” (odds ratio 0.04906, 95% CI
[0.00241, 0.2920]), whereas an increase in reported organization policies gives an increase in the BCT used. For
“Instructions on how to perform the behaviour”, an increase in reported policies gave a significant decrease as
well (odds ratio 0.2991; 95% CI [0.07762, 0.9102]). No significant effects were found for other participant
characteristics.
138541-Willems_BNW.indd 124 31-10-19 10:08

124
disagreements by consensus discussion. A sample of recording (approximately 20 minutes) was scored again for
calculating the intra-rater reliability.
For the characteristics of participants, means and standard deviations were calculated. The outcomes of the
frequency of usage of top 5 of BCTs used out of a total of 3 are binomial distributed. Therefore, a generalized
linear modelling analysis was performed using the logit link for binomial regression with the explanative variables
sex, age, work years, education, additional lifestyle training and policies.
3 | RESULTS
3.1 | General characteristics
Fourteen professional caregivers participated in the study who supported adults with mild ID in a community
based living facility (N=6), and were filmed during daily support work. Participants had a mean age of 41.9 (SD
12.1) years and their mean working experience was 17.4 (SD 10.1, range 3-35) years. Baseline characteristics of
participants were shown in Table 1. Informed consent was given for 30 adults with mild ID, whereas 12 adults
where supported by 2 participants during the observations. Mean age of adults with mild ID was 51.5 years (SD
18.0). Participants (N=4) dropped out for several reasons: they left the organization during observation period
(n=1), ran out of time to perform the video observation (n=2) or the adults with ID involved did not have mild ID
(N=1). In total, 33:15:47 (h:m:s) film material was obtained and total observation time ranged from 00:13:10 to
04:38:59 per participant. Most participants (N=8) were filmed two moments (n=6) or one moment (n=2) or
instead of three moments, due to scheduling issues. For one participant, videos from two measurements had to
be erased as informed consent for an adult with mild ID was withdrawn. Interrater reliability after instruction
was 82.5% (MW-RA1), 85% (MW, RA2) and 87.5% (RA1-RA2) respectively. Interrater reliability halfway data
analysis for 2 measurements was 92.5% and 90% (MW-RA1). Intra-rater reliability was 97.5%, calculated as
percentage of absolute agreement.
Table 1: General characteristics of participants
Professional caregivers (N=14)
Age, mean (SD) 41.9 (12.1)
sex (% Female) 85.7
Working experience mean (SD) years 17.4
Mean years working in organization 15 (SD 7.5)
Mean working hours per week 18.6 (SD 7.2)
Education level Higher=6, Vocational=8
Supplemental lifestyle training No=9, Yes=5
Lifestyle policy in ID care organization Very little: 0, Little: 1, Not much/not little: 4, Much: 8, Very much: 1
Mean no. of clients per group 12.9 (SD 6.1)
Mean no. of professionals for clients 2.3 (SD 1.0)
125
3.2 | Behaviour change techniques in lifestyle support
A total of 21 BCTs was used by professional caregivers, supporting lifestyle behaviour of adults with mild ID. The
BCTs mostly used were: “Information about others' approval” (N=15), “Identification as role model” (N=15),
“Rewards on successful behaviour” (N=11), “Review behavioural goals” (N=9) and “Instructions on how to
perform the behaviour” (N=8). A total of nine BCTs was used by only two (N=1) or one (N=8) participants, and 19
BCTs were not used at all. See Table 2 for an overview of the frequencies for BCTs used.
Univariate binomial regression analysis were performed on frequency of use of the five mostly used BCTs
(“Information about others' approval”, “Identification as role model”, “Rewards on successful behaviour”,
“Review behavioural goals” and “Instructions on how to perform the behaviour”) one for each characteristic of
the 14 professional caregivers, including: sex, age, work years, education, additional lifestyle training and policies.
A significant effect was found for policies on the BCT “Identification as a role model” (odds ratio 0.04906, 95% CI
[0.00241, 0.2920]), whereas an increase in reported organization policies gives an increase in the BCT used. For
“Instructions on how to perform the behaviour”, an increase in reported policies gave a significant decrease as
well (odds ratio 0.2991; 95% CI [0.07762, 0.9102]). No significant effects were found for other participant
characteristics.
138541-Willems_BNW.indd 125 31-10-19 10:08
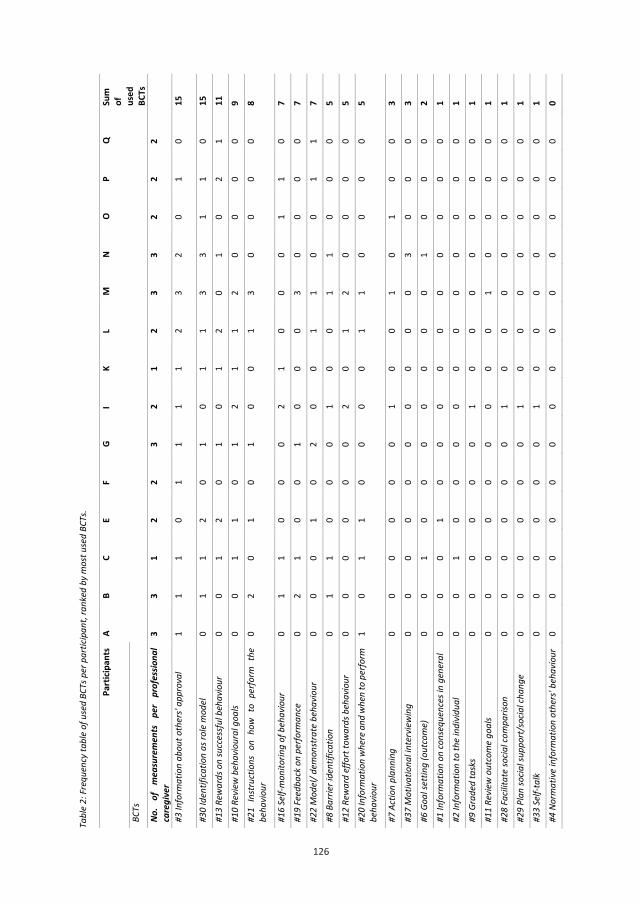
126
126
Tabl
e 2:
Fre
quen
cy ta
ble
of u
sed
BCTs
per
par
ticip
ant,
rank
ed b
y m
ost u
sed
BCTs
.
Part
icipa
nts
A
B C
E F
G I
K L
M
N O
P Q
Sum
of
us
ed
BCTs
BC
Ts
No.
of
mea
sure
men
ts
per
prof
essio
nal
care
give
r 3
3 1
2 2
3 2
1 2
3 3
2 2
2
#3 In
form
atio
n ab
out o
ther
s' ap
prov
al
1 1
1 0
1 1
1 1
2 3
2 0
1 0
15
#30
Iden
tifica
tion
as ro
le m
odel
0
1 1
2 0
1 0
1 1
3 3
1 1
0 15
#1
3 Re
war
ds o
n su
cces
sful
beh
avio
ur
0 0
1 2
0 1
0 1
2 0
1 0
2 1
11
#10
Revi
ew b
ehav
iour
al g
oals
0 0
1 1
0 1
2 1
1 2
0 0
0 0
9 #2
1 In
stru
ctio
ns o
n ho
w t
o pe
rfor
m t
he
beha
viou
r 0
2 0
1 0
1 0
0 1
3 0
0 0
0 8
#16
Self-
mon
itorin
g of
beh
avio
ur
0 1
1 0
0 0
2 1
0 0
0 1
1 0
7 #1
9 Fe
edba
ck o
n pe
rform
ance
0
2 1
0 0
1 0
0 0
3 0
0 0
0 7
#22
Mod
el/ d
emon
stra
te b
ehav
iour
0
0 0
1 0
2 0
0 1
1 0
0 1
1 7
#8 B
arrie
r ide
ntifi
catio
n 0
1 1
0 0
0 1
0 0
1 1
0 0
0 5
#12
Rew
ard
effo
rt to
war
ds b
ehav
iour
0
0 0
0 0
0 2
0 1
2 0
0 0
0 5
#20
Info
rmat
ion
whe
re a
nd w
hen
to p
erfo
rm
beha
viou
r 1
0 1
1 0
0 0
0 1
1 0
0 0
0 5
#7 A
ctio
n pl
anni
ng
0 0
0 0
0 0
1 0
0 1
0 1
0 0
3 #3
7 M
otiv
atio
nal i
nter
view
ing
0 0
0 0
0 0
0 0
0 0
3 0
0 0
3 #6
Goa
l set
ting
(out
com
e)
0 0
1 0
0 0
0 0
0 0
1 0
0 0
2 #1
Info
rmat
ion
on co
nseq
uenc
es in
gen
eral
0
0 0
1 0
0 0
0 0
0 0
0 0
0 1
#2 In
form
atio
n to
the
indi
vidu
al
0 0
1 0
0 0
0 0
0 0
0 0
0 0
1 #9
Gra
ded
task
s 0
0 0
0 0
0 1
0 0
0 0
0 0
0 1
#11
Revi
ew o
utco
me
goal
s 0
0 0
0 0
0 0
0 0
1 0
0 0
0 1
#28
Facil
itate
socia
l com
paris
on
0 0
0 0
0 0
1 0
0 0
0 0
0 0
1 #2
9 Pl
an so
cial s
uppo
rt/s
ocia
l cha
nge
0 0
0 0
0 0
1 0
0 0
0 0
0 0
1 #3
3 Se
lf-ta
lk
0 0
0 0
0 0
1 0
0 0
0 0
0 0
1 #4
Nor
mat
ive
info
rmat
ion
othe
rs' b
ehav
iour
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
127
#5 G
oal s
ettin
g (b
ehav
iour
) 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#14
Shap
ing
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #1
5 Ge
nera
lizat
ion
of b
ehav
iour
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#17
Self-
mon
itorin
g of
out
com
e 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#18
Focu
s on
past
succ
ess
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #2
3 Te
ach
to u
se p
rom
pts/
cues
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#24
Envi
ronm
enta
l res
truc
turin
g 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#25
Beha
viou
ral c
ontr
act
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #2
6 Pr
ompt
pra
ctice
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#27
Use
of fo
llow
-up
prom
pts
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
1 Pr
ompt
ant
icipa
ted
regr
et
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
2 Fe
ar a
rous
al
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
4 Us
e of
imag
ery
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
5 Re
laps
e pr
even
tion/
copi
ng p
lann
ing
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
6 St
ress
man
agem
ent /
emot
iona
l con
trol
tr
aini
ng
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0
#38
Tim
e m
anag
emen
t 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#39
Gene
ral c
omm
unica
tion
skill
s tra
inin
g 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#40
Stim
ulat
e an
ticip
atio
n of
futu
re re
war
ds
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 No
. of (
uniq
uely
) use
d BC
Ts p
er p
rofe
ssio
nal
2 6
10
7 1
7 10
5
8 11
6
3 5
2 21
138541-Willems_BNW.indd 126 31-10-19 10:08
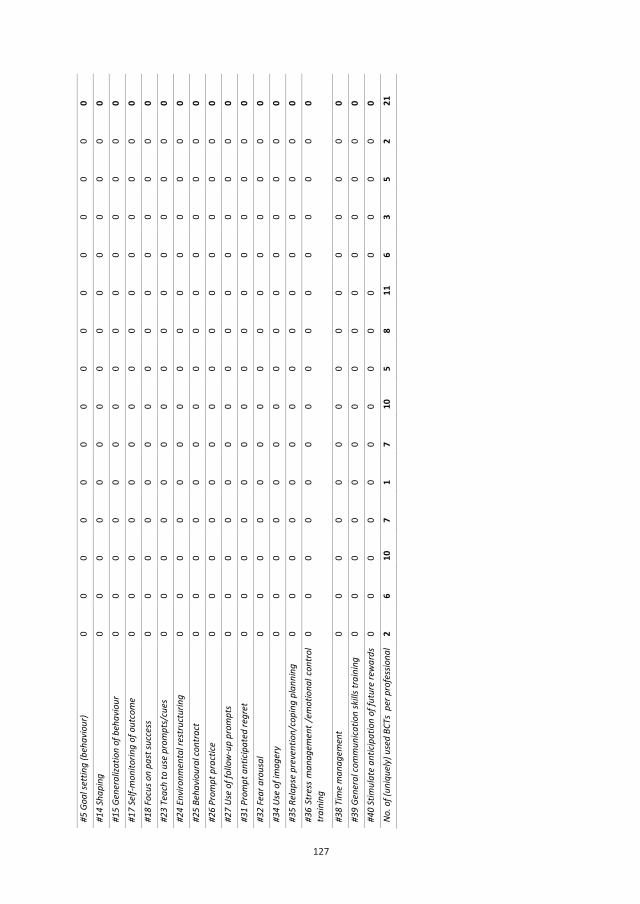
127
127
#5 G
oal s
ettin
g (b
ehav
iour
) 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#14
Shap
ing
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #1
5 Ge
nera
lizat
ion
of b
ehav
iour
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#17
Self-
mon
itorin
g of
out
com
e 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#18
Focu
s on
past
succ
ess
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #2
3 Te
ach
to u
se p
rom
pts/
cues
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#24
Envi
ronm
enta
l res
truc
turin
g 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#25
Beha
viou
ral c
ontr
act
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #2
6 Pr
ompt
pra
ctice
0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#27
Use
of fo
llow
-up
prom
pts
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
1 Pr
ompt
ant
icipa
ted
regr
et
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
2 Fe
ar a
rous
al
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
4 Us
e of
imag
ery
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
5 Re
laps
e pr
even
tion/
copi
ng p
lann
ing
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 #3
6 St
ress
man
agem
ent /
emot
iona
l con
trol
tr
aini
ng
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0
#38
Tim
e m
anag
emen
t 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#39
Gene
ral c
omm
unica
tion
skill
s tra
inin
g 0
0 0
0 0
0 0
0 0
0 0
0 0
0 0
#40
Stim
ulat
e an
ticip
atio
n of
futu
re re
war
ds
0 0
0 0
0 0
0 0
0 0
0 0
0 0
0 No
. of (
uniq
uely
) use
d BC
Ts p
er p
rofe
ssio
nal
2 6
10
7 1
7 10
5
8 11
6
3 5
2 21
138541-Willems_BNW.indd 127 31-10-19 10:08

128
4 | DISCUSSION
4.1 | Main findings
This observation study showed that professional caregivers used BCTs to support lifestyle behaviour of adults
with mild ID. The BCTs “Information about others' approval”, “Identification as role model”, “Rewards on
successful behaviour”, “Review behavioural goals” and “Instructions on how to perform the behaviour” were
mostly used. Only reported organization policies significantly decreased the frequency of use of “Identification
as a role model” and “Instructions on how to perform the behaviour”. No other significant effects were found
for characteristics of professional caregivers on the frequency of use of the five most frequently used BCTs.
The use of BCTs by professional caregivers is important and innovative knowledge, since it was unknown to which
extend professional caregivers used BCTs or whether they used any BCTs at all. However, the effectiveness of
the BCTs used was not researched in this study. Also, it is still unknown whether there is a relation between effect
of BCTs and the characteristics of adults with mild ID (e.g. qualities and disabilities). For example, adults with
mild ID have often issues regarding planning and executive functioning (American Psychiatric Association, 2013),
which implies that BCTs targeting planning like “Action planning”, “Barrier identification/problem solving” and
“Set graded tasks” may support them to change lifestyle behaviour. These BCTs were all used by professional
caregivers, but were not used mostly. Also, social and emotional development of adults with mild ID are
important to take into account (WHO, 1992) and may lead to use BCTs like “Provide information about others’
approval”, “Facilitate social comparison”, “General communication skills training” as well as “Prompt rewards
contingent on effort or progress towards behaviour” or “Provide rewards contingent on successful behaviour”.
Most of these BCTs were used by professional caregivers, with exception of “General communication skills
training”. The BCTs “Provide information about others' approval” and “Provide rewards contingent on successful
behaviour” were applied most frequently, which implicated that professional caregivers might take social and
emotional development of adults with mild ID into account. To further investigate the tailoring of used BCTs in
relation to the social and emotional characteristics of an adult with mild ID, future research could focus on the
effects of BCTs used to improve lifestyle behaviour change in adults with mild ID.
The BCTs “Information about others' approval”, “Rewards on successful behaviour”, “Review behavioural goals”,
“Instructions on how to perform the behaviour” and “Identification as role model” were often used by
professional caregivers. In our previous research, the first four BCTs were considered to be suitable BCTs in
changing lifestyle behaviour of adults with mild ID also (Willems et al., 2019). This means that professional
caregivers already use suitable BCTs, which is good news for clinical practice and professional caregivers.
However, the effects of using BCTs were not measured in this study so it is not clear if the BCTs used indeed
changed the lifestyle of adults with mild ID. The BCT “Identification as role model” was often used by professional
caregivers. However, this BCT was unsuitable according to a panel of behaviour scientists, but suitable according
to a panel of professional caregivers (Willems et al., 2019). This phenomenon is also known as the scientist-
practitioner split (Hoshmand & Polkinghorne, 1992). This finding is important because behavioural scientists are
trained to support professional caregivers about behaviour change, but professional caregivers still use a BCT
129
that is not suitable according to behavioural scientists. An explanation could be that behavioural scientists
interpret this BCT in another way than professional caregivers did. For example: behavioural scientists might
think that role modelling does not fit social and emotional development of adults with mild ID, whereas
professional caregivers did use the BCT in a way that the client is a role model for the professional caregiver on
that specific moment.
Some BCTs that were rarely used by professional caregivers, were considered suitable by health care
professionals. These BCTS were “Barrier identification/problem solving”, “Set graded tasks”, “Prompt rewards
contingent on effort or progress towards behaviour”, “Motivational interviewing” and “Action planning”. This
may imply that clinical practice might take advantage from BCTs that are still unknown by professional caregivers.
Training of professional caregivers in promising BCTs for changing lifestyle behaviour of adults with mild ID was
recommended.
4.2 | Strengths and limitations
Observations were performed using video cameras which increased reliability of the data. Video observation
made it possible to check and recheck the data and coding of the data. This method was independent of self-
report and opinions of participants, as is the case with questionnaires and other self-report methods. An eventual
drawback of video observation was external validity, since participants and adults with mild ID may have behaved
different because of the camera. Observations lasted for two hours, which gave participants the opportunity to
get used to the camera each measurement. However, observations took often less than the scheduled two hours,
which gave participants less time to get used and this might have influenced the study results since less time
could be analysed than was intended. However, this was the first-time clinical practice was observed with video
analysis to investigate the use of BCTs which gives guidance for future lifestyle behaviour change research.
Another strength of this study was the use of a structured taxonomy of BCTs, the CALO-RE taxonomy (Michie et
al., 2011). The systematic coding of BCTs was also used in literature about lifestyle change interventions for adults
with ID (Willems et al., 2017), but never in video observations. Since the taxonomy was not designed for adults
with mild ID, we used an adjusted version used before in a Delphi study about suitable BCTs for adults with mild
ID (Willems et al., 2019). This method gave insight in the use of BCTs in daily support of lifestyle change for adults
with mild ID. However, we did not research whether the use of BCTs was implicit or explicit. Also, the way in
which BCTs were used was not measured, for example whether healthy or even unhealthy behaviour was
supported. The BCTs were only coded as used or not-used instead of the frequency of use per observation
moment, which made differences between participants in time observed of less influence, also known as
selection bias.
Next to the BCTs used according to the CALO-RE taxonomy, we could not code all techniques used to change
behaviour. “Performing lifestyle behaviour together”, “Expressing confidence in one another” and “Checking on
lifestyle behaviour” were some techniques we could not code according to the existing taxonomy. A newer
taxonomy of BCTs, ‘Taxonomy v1’ (Michie et al., 2013), consisting of 93 BCTs was not used in this study because
138541-Willems_BNW.indd 128 31-10-19 10:08
128
4 | DISCUSSION
4.1 | Main findings
This observation study showed that professional caregivers used BCTs to support lifestyle behaviour of adults
with mild ID. The BCTs “Information about others' approval”, “Identification as role model”, “Rewards on
successful behaviour”, “Review behavioural goals” and “Instructions on how to perform the behaviour” were
mostly used. Only reported organization policies significantly decreased the frequency of use of “Identification
as a role model” and “Instructions on how to perform the behaviour”. No other significant effects were found
for characteristics of professional caregivers on the frequency of use of the five most frequently used BCTs.
The use of BCTs by professional caregivers is important and innovative knowledge, since it was unknown to which
extend professional caregivers used BCTs or whether they used any BCTs at all. However, the effectiveness of
the BCTs used was not researched in this study. Also, it is still unknown whether there is a relation between effect
of BCTs and the characteristics of adults with mild ID (e.g. qualities and disabilities). For example, adults with
mild ID have often issues regarding planning and executive functioning (American Psychiatric Association, 2013),
which implies that BCTs targeting planning like “Action planning”, “Barrier identification/problem solving” and
“Set graded tasks” may support them to change lifestyle behaviour. These BCTs were all used by professional
caregivers, but were not used mostly. Also, social and emotional development of adults with mild ID are
important to take into account (WHO, 1992) and may lead to use BCTs like “Provide information about others’
approval”, “Facilitate social comparison”, “General communication skills training” as well as “Prompt rewards
contingent on effort or progress towards behaviour” or “Provide rewards contingent on successful behaviour”.
Most of these BCTs were used by professional caregivers, with exception of “General communication skills
training”. The BCTs “Provide information about others' approval” and “Provide rewards contingent on successful
behaviour” were applied most frequently, which implicated that professional caregivers might take social and
emotional development of adults with mild ID into account. To further investigate the tailoring of used BCTs in
relation to the social and emotional characteristics of an adult with mild ID, future research could focus on the
effects of BCTs used to improve lifestyle behaviour change in adults with mild ID.
The BCTs “Information about others' approval”, “Rewards on successful behaviour”, “Review behavioural goals”,
“Instructions on how to perform the behaviour” and “Identification as role model” were often used by
professional caregivers. In our previous research, the first four BCTs were considered to be suitable BCTs in
changing lifestyle behaviour of adults with mild ID also (Willems et al., 2019). This means that professional
caregivers already use suitable BCTs, which is good news for clinical practice and professional caregivers.
However, the effects of using BCTs were not measured in this study so it is not clear if the BCTs used indeed
changed the lifestyle of adults with mild ID. The BCT “Identification as role model” was often used by professional
caregivers. However, this BCT was unsuitable according to a panel of behaviour scientists, but suitable according
to a panel of professional caregivers (Willems et al., 2019). This phenomenon is also known as the scientist-
practitioner split (Hoshmand & Polkinghorne, 1992). This finding is important because behavioural scientists are
trained to support professional caregivers about behaviour change, but professional caregivers still use a BCT
129
that is not suitable according to behavioural scientists. An explanation could be that behavioural scientists
interpret this BCT in another way than professional caregivers did. For example: behavioural scientists might
think that role modelling does not fit social and emotional development of adults with mild ID, whereas
professional caregivers did use the BCT in a way that the client is a role model for the professional caregiver on
that specific moment.
Some BCTs that were rarely used by professional caregivers, were considered suitable by health care
professionals. These BCTS were “Barrier identification/problem solving”, “Set graded tasks”, “Prompt rewards
contingent on effort or progress towards behaviour”, “Motivational interviewing” and “Action planning”. This
may imply that clinical practice might take advantage from BCTs that are still unknown by professional caregivers.
Training of professional caregivers in promising BCTs for changing lifestyle behaviour of adults with mild ID was
recommended.
4.2 | Strengths and limitations
Observations were performed using video cameras which increased reliability of the data. Video observation
made it possible to check and recheck the data and coding of the data. This method was independent of self-
report and opinions of participants, as is the case with questionnaires and other self-report methods. An eventual
drawback of video observation was external validity, since participants and adults with mild ID may have behaved
different because of the camera. Observations lasted for two hours, which gave participants the opportunity to
get used to the camera each measurement. However, observations took often less than the scheduled two hours,
which gave participants less time to get used and this might have influenced the study results since less time
could be analysed than was intended. However, this was the first-time clinical practice was observed with video
analysis to investigate the use of BCTs which gives guidance for future lifestyle behaviour change research.
Another strength of this study was the use of a structured taxonomy of BCTs, the CALO-RE taxonomy (Michie et
al., 2011). The systematic coding of BCTs was also used in literature about lifestyle change interventions for adults
with ID (Willems et al., 2017), but never in video observations. Since the taxonomy was not designed for adults
with mild ID, we used an adjusted version used before in a Delphi study about suitable BCTs for adults with mild
ID (Willems et al., 2019). This method gave insight in the use of BCTs in daily support of lifestyle change for adults
with mild ID. However, we did not research whether the use of BCTs was implicit or explicit. Also, the way in
which BCTs were used was not measured, for example whether healthy or even unhealthy behaviour was
supported. The BCTs were only coded as used or not-used instead of the frequency of use per observation
moment, which made differences between participants in time observed of less influence, also known as
selection bias.
Next to the BCTs used according to the CALO-RE taxonomy, we could not code all techniques used to change
behaviour. “Performing lifestyle behaviour together”, “Expressing confidence in one another” and “Checking on
lifestyle behaviour” were some techniques we could not code according to the existing taxonomy. A newer
taxonomy of BCTs, ‘Taxonomy v1’ (Michie et al., 2013), consisting of 93 BCTs was not used in this study because
138541-Willems_BNW.indd 129 31-10-19 10:08

130
of its extensiveness and thus low feasibility. The development of a practical, complete and tailored taxonomy
specific for changing lifestyle behaviour for adults with mild ID is recommended.
4.3 | Implications for future research
This observation study gives insight in BCTs used in lifestyle change for adults with mild ID by professional
caregivers. A logical next step in research would be to determine effective BCTs in changing lifestyle behaviour.
Research into the competencies of professional caregivers in changing lifestyle behaviour as well as training of
professional caregivers in suitable BCTs can give some further insights in changing lifestyle behaviour of adults
with mild ID.
4.4 | Conclusions
Professional caregivers used BCTs to change lifestyle behaviour of adults with mild ID. Most used BCTs were
“Information about others' approval”, “Identification as role model”, “Rewards on successful behaviour”,
“Review behavioural goals” and “Instructions on how to perform the behaviour”. Promising BCTs according to
previous research, were used only a few times. Clinical practice could benefit from the use of these suitable BCTs
to improve lifestyle behaviour of adults with mild ID.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
131
REFERENCES
Alesi, M., & Pepi, A. (2015). Physical Activity Engagement in Young People with Down Syndrome:
Investigating Parental Beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61-80.
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5 (5th
Ed.). Washington, DC: Author.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behaviour change techniques used
to promote walking and cycling: A systematic review. Health Psychology, 32(8), 829.
Davison, K. K., Jurkowski, J. M., Li, K., Kranz, S., & Lawson, H. A. (2013). A childhood obesity intervention
developed by families for families: results from a pilot study. International Journal of Behavioural
Nutrition and Physical Activity, 10(3), 10-1186.
Draheim, C. C., Williams, D. P., & McCubbin, J. A. (2002). Prevalence of physical inactivity and recommended
physical activity in community-based adults with mental retardation. Mental Retardation, 40(6), 436-
444.
Frey, G. C., & Chow, B. (2006). Relationship between BMI, physical fitness, and motor skills in youth with mild
intellectual disabilities. International Journal of Obesity, 30(5), 861.
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P.
(2011). Systematic review of reviews of intervention components associated with increased
effectiveness in dietary and physical activity interventions. BMC Public Health, 11(1), 119.
Grondhuis, S. N., & Aman, M. G. (2014). Overweight and obesity in youth with developmental disabilities: a call
to action. Journal of Intellectual Disability Research, 58(9), 787-799.
Haveman, M., Heller, T., Lee, L., Maaskant, M., Shooshtari, S., & Strydom, A. (2010). Major health risks in aging
persons with intellectual disabilities: an overview of recent studies. Journal of Policy and Practice in
Intellectual Disabilities, 7(1), 59-69.
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: what is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36.
Hithersay, R., Strydom, A., Moulster, G., & Buszewicz, M. (2014). Carer-led health interventions to
monitor, promote and improve the health of adults with intellectual disabilities in the community: A
systematic review. Research in Developmental Disabilities, 35(4), 887-907.
Hoshmand, L. T., & Polkinghorne, D. E. (1992). Redefining the science-practice relationship and professional
training. American Psychologist, 47(1), 55.
138541-Willems_BNW.indd 130 31-10-19 10:08
130
of its extensiveness and thus low feasibility. The development of a practical, complete and tailored taxonomy
specific for changing lifestyle behaviour for adults with mild ID is recommended.
4.3 | Implications for future research
This observation study gives insight in BCTs used in lifestyle change for adults with mild ID by professional
caregivers. A logical next step in research would be to determine effective BCTs in changing lifestyle behaviour.
Research into the competencies of professional caregivers in changing lifestyle behaviour as well as training of
professional caregivers in suitable BCTs can give some further insights in changing lifestyle behaviour of adults
with mild ID.
4.4 | Conclusions
Professional caregivers used BCTs to change lifestyle behaviour of adults with mild ID. Most used BCTs were
“Information about others' approval”, “Identification as role model”, “Rewards on successful behaviour”,
“Review behavioural goals” and “Instructions on how to perform the behaviour”. Promising BCTs according to
previous research, were used only a few times. Clinical practice could benefit from the use of these suitable BCTs
to improve lifestyle behaviour of adults with mild ID.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
131
REFERENCES
Alesi, M., & Pepi, A. (2015). Physical Activity Engagement in Young People with Down Syndrome:
Investigating Parental Beliefs. Journal of Applied Research in Intellectual Disabilities, 28(2), 61-80.
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5 (5th
Ed.). Washington, DC: Author.
Bird, E. L., Baker, G., Mutrie, N., Ogilvie, D., Sahlqvist, S., & Powell, J. (2013). Behaviour change techniques used
to promote walking and cycling: A systematic review. Health Psychology, 32(8), 829.
Davison, K. K., Jurkowski, J. M., Li, K., Kranz, S., & Lawson, H. A. (2013). A childhood obesity intervention
developed by families for families: results from a pilot study. International Journal of Behavioural
Nutrition and Physical Activity, 10(3), 10-1186.
Draheim, C. C., Williams, D. P., & McCubbin, J. A. (2002). Prevalence of physical inactivity and recommended
physical activity in community-based adults with mental retardation. Mental Retardation, 40(6), 436-
444.
Frey, G. C., & Chow, B. (2006). Relationship between BMI, physical fitness, and motor skills in youth with mild
intellectual disabilities. International Journal of Obesity, 30(5), 861.
Greaves, C. J., Sheppard, K. E., Abraham, C., Hardeman, W., Roden, M., Evans, P. H., & Schwarz, P.
(2011). Systematic review of reviews of intervention components associated with increased
effectiveness in dietary and physical activity interventions. BMC Public Health, 11(1), 119.
Grondhuis, S. N., & Aman, M. G. (2014). Overweight and obesity in youth with developmental disabilities: a call
to action. Journal of Intellectual Disability Research, 58(9), 787-799.
Haveman, M., Heller, T., Lee, L., Maaskant, M., Shooshtari, S., & Strydom, A. (2010). Major health risks in aging
persons with intellectual disabilities: an overview of recent studies. Journal of Policy and Practice in
Intellectual Disabilities, 7(1), 59-69.
Heller, T., McCubbin, J. A., Drum, C., & Peterson, J. (2011). Physical activity and nutrition health promotion
interventions: what is working for people with intellectual disabilities? Intellectual and Developmental
Disabilities, 49(1), 26–36.
Hithersay, R., Strydom, A., Moulster, G., & Buszewicz, M. (2014). Carer-led health interventions to
monitor, promote and improve the health of adults with intellectual disabilities in the community: A
systematic review. Research in Developmental Disabilities, 35(4), 887-907.
Hoshmand, L. T., & Polkinghorne, D. E. (1992). Redefining the science-practice relationship and professional
training. American Psychologist, 47(1), 55.
138541-Willems_BNW.indd 131 31-10-19 10:08
132
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851-863.
James, A. S., & Shireman, T. I. (2010). Case Managers' and Independent Living Counselors' Perspectives on Health
Promotion Activities for Adults with Physical and Developmental Disabilities. Journal of Social Work in
Disability & Rehabilitation, 9(4), 274-288.
Lahtinen, U., Rintala, P., & Malin, A. (2007). Physical performance of adults with intellectual disability: A 30-year
follow-up. Adapted Physical Activity Quarterly, 24(2), 125-143.
McGuire, B. E., Daly, P., & Smyth, F. (2007). Lifestyle and health behaviours of adults with an intellectual disability.
Journal of Intellectual Disability Research, 51(7), 497-510.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and
healthy eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J. & Wood,
C. E. (2013). The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques:
building an international consensus for the reporting of behaviour change interventions. Annals of
Behavioural Medicine, 46(1), 81-95.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: a structured review of literature. Research in
Developmental Disabilities, 34(12), 4534-4545.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese adults’ physical activity self-efficacy and behaviour: a systematic
review and meta-analysis. International Journal of Behavioural Nutrition and Physical Activity, 10(29), 1-
15.
Stanish, H. I., Temple, V. A., & Frey, G. C. (2006). Health‐promoting physical activity of adults with mental
retardation. Mental Retardation and Developmental Disabilities Research Reviews, 12(1), 13-21.
Temple, V. A., Frey, G. C., & Stanish, H. I. (2006). Physical activity of adults with mental retardation: review and
research needs. American Journal of Health Promotion, 21(1), 2.
133
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: A process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
WHO (1992). International statistical classification of diseases and related health problems: ICD‐10, Vol. 1.
Geneva: World Health Organization.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256-268.
Willems, M., Waninge, A., De Jong, J., Hilgenkamp, T. I., & Van der Schans, C. P. (2019). Exploration of
suitable behaviour change techniques for lifestyle change of adults with mild ID: A Delphi study. Journal
of Applied Research in Intellectual Disabilities, 32(3), 543–557.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308-322.
138541-Willems_BNW.indd 132 31-10-19 10:08
132
Hsieh, K., Rimmer, J. H., & Heller, T. (2014). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851-863.
James, A. S., & Shireman, T. I. (2010). Case Managers' and Independent Living Counselors' Perspectives on Health
Promotion Activities for Adults with Physical and Developmental Disabilities. Journal of Social Work in
Disability & Rehabilitation, 9(4), 274-288.
Lahtinen, U., Rintala, P., & Malin, A. (2007). Physical performance of adults with intellectual disability: A 30-year
follow-up. Adapted Physical Activity Quarterly, 24(2), 125-143.
McGuire, B. E., Daly, P., & Smyth, F. (2007). Lifestyle and health behaviours of adults with an intellectual disability.
Journal of Intellectual Disability Research, 51(7), 497-510.
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Michie, S., Abraham, C., Whittington, C., McAteer, J., & Gupta, S. (2009). Effective techniques in healthy eating
and physical activity interventions: A meta-regression. Health Psychology, 28(6), 690–701.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and
healthy eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Eccles, M. P., Cane, J. & Wood,
C. E. (2013). The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques:
building an international consensus for the reporting of behaviour change interventions. Annals of
Behavioural Medicine, 46(1), 81-95.
Naaldenberg, J., Kuijken, N., van Dooren, K., & de Valk, H. V. S. L. (2013). Topics, methods and challenges in health
promotion for people with intellectual disabilities: a structured review of literature. Research in
Developmental Disabilities, 34(12), 4534-4545.
Olander, E. K., Fletcher, H., Williams, S., Atkinson, L., Turner, A., & French, D. P. (2013). What are the most
effective techniques in changing obese adults’ physical activity self-efficacy and behaviour: a systematic
review and meta-analysis. International Journal of Behavioural Nutrition and Physical Activity, 10(29), 1-
15.
Stanish, H. I., Temple, V. A., & Frey, G. C. (2006). Health‐promoting physical activity of adults with mental
retardation. Mental Retardation and Developmental Disabilities Research Reviews, 12(1), 13-21.
Temple, V. A., Frey, G. C., & Stanish, H. I. (2006). Physical activity of adults with mental retardation: review and
research needs. American Journal of Health Promotion, 21(1), 2.
133
Van Schijndel-Speet, M., Evenhuis, H. M., Van Wijck, R., & Echteld, M. A. (2014). Implementation of a group-
based physical activity programme for ageing adults with ID: A process evaluation. Journal of Evaluation
in Clinical Practice, 20(4), 401-407.
WHO (1992). International statistical classification of diseases and related health problems: ICD‐10, Vol. 1.
Geneva: World Health Organization.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256-268.
Willems, M., Waninge, A., De Jong, J., Hilgenkamp, T. I., & Van der Schans, C. P. (2019). Exploration of
suitable behaviour change techniques for lifestyle change of adults with mild ID: A Delphi study. Journal
of Applied Research in Intellectual Disabilities, 32(3), 543–557.
Williams, S. L., & French, D. P. (2011). What are the most effective intervention techniques for changing physical
activity self-efficacy and physical activity behaviour—and are they the same? Health Education
Research, 26(2), 308-322.
138541-Willems_BNW.indd 133 31-10-19 10:08

Chapter 6
Training professional caregivers in changing lifestyle behaviour of adults
with mild intellectual disabilities: a pilot-study
Mariël Willems
Cees. P. van der Schans
Johan de Jong
Wim P. Krijnen
Thessa I.M. Hilgenkamp
Aly Waninge
Manuscript submitted
138541-Willems_BNW.indd 134 31-10-19 10:08

Chapter 6
Training professional caregivers in changing lifestyle behaviour of adults
with mild intellectual disabilities: a pilot-study
Mariël Willems
Cees. P. van der Schans
Johan de Jong
Wim P. Krijnen
Thessa I.M. Hilgenkamp
Aly Waninge
Manuscript submitted
138541-Willems_BNW.indd 135 31-10-19 10:08

136
ABSTRACT
Background: Adults with mild ID have low physical activity levels and high levels of overweight and obesity.
Professional caregivers play a significant role supporting these adults with decision making and planning of
healthy behaviour. However, promising BCTs are rarely used by professional caregivers. Training could be an
important step to support professional caregivers to use BCT’s in clinical practice.
Aim: This study aims to develop and pilot-test a theory-driven lifestyle training in the behaviour change technique
(BCT) “Action planning” for professional caregivers supporting adults with mild ID.
Methods: A training including two training sessions for professional caregivers was developed regarding the BCT
“Action planning”, using problem based learning (PBL) theory. The training design was evaluated, whereas
competence, readiness to use “Action planning” and barriers and facilitators to use the BCT were measured
before the start, between the training sessions and after completing the training, using questionnaires. Results
were analysed with descriptive statistics and multilevel analyses. Facilitators and barriers were categorized by
the COM-B model.
Results: Participants were satisfied about the two training sessions and the training in its entirety. Self-reported
competence, and readiness to use “Action planning” were increased significantly (p<0.05) after finishing the
training. Facilitators and barriers in the category ‘Opportunity’ were mentioned the most, compared to the
categories ‘Motivation’ and ‘Capacity’.
Conclusion: Training in the BCT “Action planning” may support professional caregivers in the use of BCT’s and
their readiness to plan lifestyle behaviour actions.
137
1 | INTRODUCTION
In general, adults with intellectual disabilities (ID) have low physical activity levels (Dairo, Collett, Dawes, &
Oskrochi, 2016; Hilgenkamp, Reis, van Wijck, & Evenhuis, 2012; Sundahl, Zetterberg, Wester, Rehn, & Blomqvist,
2016; Waninge et al., 2013) and demonstrate high levels of overweight and obesity (Hsieh, Rimmer, & Heller,
2013; Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Robertson, Emerson, Baines, & Hatton, 2014).
Therefore, it is of utmost importance to support this group in moving towards a positive and healthy lifestyle.
So far, adapted lifestyle change interventions for adults with ID seem to lack evidence for effectiveness (Willems
et al., 2018). This effectiveness may be improved using behaviour change techniques (BCTs). In previous studies,
BCTs used were not explicitly recognized or labelled as such (Willems, Hilgenkamp, Havik, Waninge, & Melville,
2017), and combinations of different BCTs were used, which makes it difficult to study the effectiveness of the
use of individual BCTs (Willems et al., 2018).
Professional caregivers play a significant role supporting adults with mild ID with decision making and planning
of healthy behaviour (Ptomey et al., 2018; Spanos et al., 2013). Therefore, professional caregivers should be able
to use suitable BCTs in their practice. Although professional caregivers have significant training needs for
promoting a healthy lifestyle in adults with ID (Melville et al., 2009), health promotion programs do not promote
their knowledge and competences effectively and the evaluation of health promotion programs is crucial
(O’Connor-Fleming et al., 2006). In addition, improvement of training and support for caregivers to support adults
with ID more effectively has been recommended (Ptomey et al., 2018). Training of professional caregivers in
knowledge and skills about lifestyle behaviour of adults with mild ID could thus be useful to improve the lifestyle
of adults with mild ID.
According to earlier research, professional caregivers considered 24 BCTs to be suitable in supporting lifestyle
change for adults with mild ID (Willems, Waninge, De Jong, Hilgenkamp, & van der Schans, 2019a). The BCTs
considered most suitable were: “Barrier identification/problem solving”, “Set graded tasks”, “Reward effort
towards behaviour” and “Motivational interviewing and action planning” (Willems et al., 2019a). In addition, an
observational study showed that professional caregivers did use BCTs to change lifestyle behaviour of adults with
mild ID (Willems et al., 2019b). However, comparing the most suitable BCTs with the BCTs used in clinical practice,
professional caregivers did not often use BCTs that were considered as most suitable (Willems et al., 2019b).
These findings indicate that although using BCTs might be suitable in changing lifestyle for adults with mild ID,
most promising BCTs were rarely used by professional caregivers.
One of the most potentially suitable BCTs is called “Action planning” and is defined as ‘detailed planning of what
the person will do including, as a minimum, when, in which situation and/or where to act’ (Michie et al., 2011).
Training in this BCT could be an important step to support professional caregivers in clinical practice. This study
aims to develop and pilot-test a theory-driven training in the BCT “Action planning” for professional caregivers
supporting adults with mild ID.
138541-Willems_BNW.indd 136 31-10-19 10:08

136
ABSTRACT
Background: Adults with mild ID have low physical activity levels and high levels of overweight and obesity.
Professional caregivers play a significant role supporting these adults with decision making and planning of
healthy behaviour. However, promising BCTs are rarely used by professional caregivers. Training could be an
important step to support professional caregivers to use BCT’s in clinical practice.
Aim: This study aims to develop and pilot-test a theory-driven lifestyle training in the behaviour change technique
(BCT) “Action planning” for professional caregivers supporting adults with mild ID.
Methods: A training including two training sessions for professional caregivers was developed regarding the BCT
“Action planning”, using problem based learning (PBL) theory. The training design was evaluated, whereas
competence, readiness to use “Action planning” and barriers and facilitators to use the BCT were measured
before the start, between the training sessions and after completing the training, using questionnaires. Results
were analysed with descriptive statistics and multilevel analyses. Facilitators and barriers were categorized by
the COM-B model.
Results: Participants were satisfied about the two training sessions and the training in its entirety. Self-reported
competence, and readiness to use “Action planning” were increased significantly (p<0.05) after finishing the
training. Facilitators and barriers in the category ‘Opportunity’ were mentioned the most, compared to the
categories ‘Motivation’ and ‘Capacity’.
Conclusion: Training in the BCT “Action planning” may support professional caregivers in the use of BCT’s and
their readiness to plan lifestyle behaviour actions.
137
1 | INTRODUCTION
In general, adults with intellectual disabilities (ID) have low physical activity levels (Dairo, Collett, Dawes, &
Oskrochi, 2016; Hilgenkamp, Reis, van Wijck, & Evenhuis, 2012; Sundahl, Zetterberg, Wester, Rehn, & Blomqvist,
2016; Waninge et al., 2013) and demonstrate high levels of overweight and obesity (Hsieh, Rimmer, & Heller,
2013; Melville, Hamilton, Hankey, Miller, & Boyle, 2007; Robertson, Emerson, Baines, & Hatton, 2014).
Therefore, it is of utmost importance to support this group in moving towards a positive and healthy lifestyle.
So far, adapted lifestyle change interventions for adults with ID seem to lack evidence for effectiveness (Willems
et al., 2018). This effectiveness may be improved using behaviour change techniques (BCTs). In previous studies,
BCTs used were not explicitly recognized or labelled as such (Willems, Hilgenkamp, Havik, Waninge, & Melville,
2017), and combinations of different BCTs were used, which makes it difficult to study the effectiveness of the
use of individual BCTs (Willems et al., 2018).
Professional caregivers play a significant role supporting adults with mild ID with decision making and planning
of healthy behaviour (Ptomey et al., 2018; Spanos et al., 2013). Therefore, professional caregivers should be able
to use suitable BCTs in their practice. Although professional caregivers have significant training needs for
promoting a healthy lifestyle in adults with ID (Melville et al., 2009), health promotion programs do not promote
their knowledge and competences effectively and the evaluation of health promotion programs is crucial
(O’Connor-Fleming et al., 2006). In addition, improvement of training and support for caregivers to support adults
with ID more effectively has been recommended (Ptomey et al., 2018). Training of professional caregivers in
knowledge and skills about lifestyle behaviour of adults with mild ID could thus be useful to improve the lifestyle
of adults with mild ID.
According to earlier research, professional caregivers considered 24 BCTs to be suitable in supporting lifestyle
change for adults with mild ID (Willems, Waninge, De Jong, Hilgenkamp, & van der Schans, 2019a). The BCTs
considered most suitable were: “Barrier identification/problem solving”, “Set graded tasks”, “Reward effort
towards behaviour” and “Motivational interviewing and action planning” (Willems et al., 2019a). In addition, an
observational study showed that professional caregivers did use BCTs to change lifestyle behaviour of adults with
mild ID (Willems et al., 2019b). However, comparing the most suitable BCTs with the BCTs used in clinical practice,
professional caregivers did not often use BCTs that were considered as most suitable (Willems et al., 2019b).
These findings indicate that although using BCTs might be suitable in changing lifestyle for adults with mild ID,
most promising BCTs were rarely used by professional caregivers.
One of the most potentially suitable BCTs is called “Action planning” and is defined as ‘detailed planning of what
the person will do including, as a minimum, when, in which situation and/or where to act’ (Michie et al., 2011).
Training in this BCT could be an important step to support professional caregivers in clinical practice. This study
aims to develop and pilot-test a theory-driven training in the BCT “Action planning” for professional caregivers
supporting adults with mild ID.
138541-Willems_BNW.indd 137 31-10-19 10:08

138
2 | METHODS
2.1 | Design
Based on previous research of suitable BCTs in adults with mild ID, a promising BCT called ‘“Action planning” was
selected to be the focus of a training for professional caregivers supporting adults with mild ID. A (multiple) case
study design was used. A training program was developed in cooperation with researchers and education
specialists working in the field of education for professional caregivers. The training program was reviewed by a
professional caregiver working with adults with mild ID.
To evaluate the training program, an online questionnaire was completed three times by participants: at baseline
(one month before the first training session), one month after the first training session and one month after the
second training session). In addition, participants were asked to evaluate 1) the training sessions and 2) training
components.
2.2 | Participants
2.2.1 | Criteria for participants
Participants (N=11) were Dutch professional caregivers working in one team with adults with mild ID. The
professional caregivers were working as a team on one community-based living facility supporting adults with
mild ID.
Inclusion criteria were:
- Professional caregivers;
- Supporting adults with mild ID (>18 years) in daily living;
- Minimum of 6 months of working experience in the field of supporting persons with mild ID;
- ≥18 years;
- Working in a community-based living facility for adults with mild ID;
- Interested in support in promoting a healthy lifestyle in adults with mild ID.
Exclusion criteria were:
- Professional caregivers leaving the organization during training period;
- Professional caregivers becoming long-term ill during training period;
- Students, working as interns.
Participants were approached through a consortium of Dutch ID care provider organisations. One of these
organisations invited professional caregivers of one residential care facility to participate in the training program.
Written informed consent was obtained from the participants.
139
2.3 | Development of the training
The training aimed to support professional caregivers in changing lifestyle behaviour of adults with mild ID. Since
professional caregivers did not often use the BCT “Action planning” in clinical practice, the training focussed on
increasing competences for using the BCT as well as participants’ readiness to use it. To give participants more
insight why they did or did not use the BCT, facilitators and barriers were also part of the training content.
2.3.1 | Theoretical basis
The training was developed using a learning theory, called problem based learning (PBL). Central in PBL is the
focus on specific and concrete problems and have a relationship to prior knowledge of the learner to start the
learning process. It has been applied to various disciplines of postsecondary education (Gijbels, Dochy, Van den
Bossche, & Segers, 2005). However, there is a wide variety in definitions of PBL (Chen, Cowdroy, Kingsland, &
Ostwald, 1995). According to Barrows (1996), there are six core principles:
1) Learning is student-centred;
2) Learning occurs in small student groups;
3) A tutor is present as a facilitator or guide;
4) Authentic problems are presented at the beginning of the learning sequence, before any
preparation or study has occurred;
5) The problems encountered are used as tools to achieve the required knowledge and the problem-
solving skills necessary to eventually solve the problems;
6) New information is acquired through self-directed learning (Gijbels et al., 2005).
Although there is debate about the effectiveness of PBL compared to traditional teaching strategies, PBL was
found to be effective to increase understanding of principles that link concepts to each other (Gijbels et al., 2005),
as well as for long-term retention, skill development and satisfaction (Strobel & van Barneveld, 2009).
2.3.2 | Content and delivery
The training consisted of two training sessions of 2.5 hours and was practically oriented: during the training
professional caregivers practiced their skills, and used knowledge by case discussion and role playing. The training
was offered in a group-wise manner, since PBL assumes that one is dependent from others to achieve new
knowledge using real-life cases. Thereby, co-creation was intended whereas colleagues collaborate to share their
explicit knowledge and reveal their implicit knowledge in a collective process to create knew knowledge (Ehlen,
Van der Klink, Stoffers, & Boshuizen, 2017). Social aspects such as trust and a positive team spirit were important
to stimulate knowledge development in a collective way (Ehlen et al., 2017). The role of the trainer was of
supportive nature, stimulating participants to use each other’s knowledge and skills and helping to deepen the
content of the brain storming and group discussions.
Using PBL, the first training session was designed to start with a brainstorm and a real-life case (problem
description). All participants had to prepare a case on forehand and these cases were merged into one case using
138541-Willems_BNW.indd 138 31-10-19 10:08
138
2 | METHODS
2.1 | Design
Based on previous research of suitable BCTs in adults with mild ID, a promising BCT called ‘“Action planning” was
selected to be the focus of a training for professional caregivers supporting adults with mild ID. A (multiple) case
study design was used. A training program was developed in cooperation with researchers and education
specialists working in the field of education for professional caregivers. The training program was reviewed by a
professional caregiver working with adults with mild ID.
To evaluate the training program, an online questionnaire was completed three times by participants: at baseline
(one month before the first training session), one month after the first training session and one month after the
second training session). In addition, participants were asked to evaluate 1) the training sessions and 2) training
components.
2.2 | Participants
2.2.1 | Criteria for participants
Participants (N=11) were Dutch professional caregivers working in one team with adults with mild ID. The
professional caregivers were working as a team on one community-based living facility supporting adults with
mild ID.
Inclusion criteria were:
- Professional caregivers;
- Supporting adults with mild ID (>18 years) in daily living;
- Minimum of 6 months of working experience in the field of supporting persons with mild ID;
- ≥18 years;
- Working in a community-based living facility for adults with mild ID;
- Interested in support in promoting a healthy lifestyle in adults with mild ID.
Exclusion criteria were:
- Professional caregivers leaving the organization during training period;
- Professional caregivers becoming long-term ill during training period;
- Students, working as interns.
Participants were approached through a consortium of Dutch ID care provider organisations. One of these
organisations invited professional caregivers of one residential care facility to participate in the training program.
Written informed consent was obtained from the participants.
139
2.3 | Development of the training
The training aimed to support professional caregivers in changing lifestyle behaviour of adults with mild ID. Since
professional caregivers did not often use the BCT “Action planning” in clinical practice, the training focussed on
increasing competences for using the BCT as well as participants’ readiness to use it. To give participants more
insight why they did or did not use the BCT, facilitators and barriers were also part of the training content.
2.3.1 | Theoretical basis
The training was developed using a learning theory, called problem based learning (PBL). Central in PBL is the
focus on specific and concrete problems and have a relationship to prior knowledge of the learner to start the
learning process. It has been applied to various disciplines of postsecondary education (Gijbels, Dochy, Van den
Bossche, & Segers, 2005). However, there is a wide variety in definitions of PBL (Chen, Cowdroy, Kingsland, &
Ostwald, 1995). According to Barrows (1996), there are six core principles:
1) Learning is student-centred;
2) Learning occurs in small student groups;
3) A tutor is present as a facilitator or guide;
4) Authentic problems are presented at the beginning of the learning sequence, before any
preparation or study has occurred;
5) The problems encountered are used as tools to achieve the required knowledge and the problem-
solving skills necessary to eventually solve the problems;
6) New information is acquired through self-directed learning (Gijbels et al., 2005).
Although there is debate about the effectiveness of PBL compared to traditional teaching strategies, PBL was
found to be effective to increase understanding of principles that link concepts to each other (Gijbels et al., 2005),
as well as for long-term retention, skill development and satisfaction (Strobel & van Barneveld, 2009).
2.3.2 | Content and delivery
The training consisted of two training sessions of 2.5 hours and was practically oriented: during the training
professional caregivers practiced their skills, and used knowledge by case discussion and role playing. The training
was offered in a group-wise manner, since PBL assumes that one is dependent from others to achieve new
knowledge using real-life cases. Thereby, co-creation was intended whereas colleagues collaborate to share their
explicit knowledge and reveal their implicit knowledge in a collective process to create knew knowledge (Ehlen,
Van der Klink, Stoffers, & Boshuizen, 2017). Social aspects such as trust and a positive team spirit were important
to stimulate knowledge development in a collective way (Ehlen et al., 2017). The role of the trainer was of
supportive nature, stimulating participants to use each other’s knowledge and skills and helping to deepen the
content of the brain storming and group discussions.
Using PBL, the first training session was designed to start with a brainstorm and a real-life case (problem
description). All participants had to prepare a case on forehand and these cases were merged into one case using
138541-Willems_BNW.indd 139 31-10-19 10:08
140
central themes from the participants’ cases. This central case was discussed during the training. Afterwards, a
minimal amount of theory about behaviour change in relation to adults with mild ID was provided, using video
images and brainstorming. According to PBL, self-directed learning was stimulated using role playing to acquire
knowledge and problem-solving skills necessary. The first training session was ended with reflection by
participants on their own learning process.
During the second training session, first an evaluation and reflection took place about the use of the BCT by
participants in the time between the two training sessions. Again, a form of role-playing was used to gain practical
skills, called the fish-bowl technique (Seaman, & Fellenz, 1989). Using this technique, two participants played
roles, two participants stood stand-by to take over a role when necessary and the other participants were
observers giving feedback afterwards. The fish-bowl role playing was used only during the second training
session.
2.3.3 | Review of the training program by professional caregiver
After developing the training program, the design of the training sessions was then discussed with a professional
caregiver working with adults with mild ID. The following topics were discussed:
1) Whether the training was appropriate for the interests, knowledge and learning strategies of the
intended participants;
2) If and in which way the training could be improved to support professional caregivers with the
intended behaviour;
3) Practical issues, such as time span and frequency of the training, potential breaks and location of
the training.
The most important adaptation based on this step in the design process was the integration of more examples
in the training, in particular in the theoretical part of the training. Also, the theory section was divided by breaks
to discuss what participants had learned, to increase opportunities to process the information. Last, observation
was added during the role playing in the first training session; two participants performed role playing and a third
participant observed the role playing.
2.4 | Training evaluation and outcome measures
The information from the baseline measures was used to tailor the training to the needs of the professional
caregivers and as baseline information. The second training session served as a follow-up training as well as an
evaluation moment. The follow-up consisted of repetition of knowledge and collecting knew knowledge of the
BCT as well as any questions from participants. During the evaluation, barriers and facilitators for the use of the
BCT were defined and solved where possible. When participants needed more training, a third training session
was offered.
To evaluate the training design, participants were asked to evaluate 1) the training sessions and 2) training
components:
141
1) Training sessions. Participants had to give the training sessions a report mark. These scores ranged from
1-10 with 1 as the lowest score and 10 as the highest score, using the same range of scores as school report
scores do in the Netherlands. After the second training, participants were also asked to score the training as a
total, using a score range from 1-10. In both questionnaires, participants were also asked whether the time of
training was in proportion with the gaining and the theory in proportion with practice during the training
sessions. Also, the frequency of training sessions as well as the duration of training sessions (score 0 too short,
score 5 too long) and time between training sessions was evaluated (score 0 too little time, score 5 too much
time). Participants could mention whether they would recommend the training to others (score 0 not
recommending the training, score 5 recommending the training).
2) Training components. During the training sessions, several training methods were used, including:
brainstorming, theory, video material, case discussion and roleplaying. These training components were
evaluated in the online questionnaire, whereas participants could score each component on a visual-analogic
scale (VAS), using scores from 0 (does not agree with the statement) to 5 (does agree with the statement).
Next to the evaluation of the training design, the following outcomes were measured:
1) Competence. Since there are a lot of different definitions of competence (Deardorff, 2006), the
definition used in Dutch clinical practice describing competences of professional caregivers of persons with ID
was utilized (Vereniging Gehandicaptenzorg Nederland, 2015), whereas competence included skills, knowledge,
and attitude towards supporting lifestyle behaviour. Competence of professional caregivers was measured
through self-report using (online) questionnaires. A feasible questionnaire was used to measure competence,
called the Attitude of Direct Support Persons- Health Enhancing Physical Activity (ASDP-HEPA) (Steenbergen et
al., 2019). This questionnaire included 6 questions to measure the attitude towards Health Enhancing Physical
Activity (HEPA). The questions were slightly adjusted to the use of the BCT “Action planning”, instead of physical
activity. Two questions were added to measure skills and knowledge towards “Action planning” specifically.
Participants reported on a visual-analogic scale (VAS) their self-experienced knowledge, attitude and skills. See
the Appendix for the questionnaire.
2) Readiness to use the BCT. The readiness of participants to use the BCT was measured using the five
stages of change from the transtheoretical model (Prochaska & Velicer, 1997), including pre-contemplation,
contemplation, preparation, action and maintenance. Participants answered if they already used the BCT for a
longer period (maintenance phase), for only a short period (action phase), or not used the BCT but willing to do
so in the near future (preparation phase) or later on (contemplation phase) or not willing to use the BCT (pre-
contemplation phase). The scores ranged from 0-4, whereas a score 0 meant that the participant did not use the
BCT “Action planning” at all and was not planning to use it in the future. A score 4 meant that the participant
already used the BCT for a longer period (over 6 months).
3) Barriers and facilitators to use the BCT. Participants were asked why they did or did not used the BCT
and what factors would support and withhold them to use the BCT for adults with mild ID. Barriers and facilitators
138541-Willems_BNW.indd 140 31-10-19 10:08
140
central themes from the participants’ cases. This central case was discussed during the training. Afterwards, a
minimal amount of theory about behaviour change in relation to adults with mild ID was provided, using video
images and brainstorming. According to PBL, self-directed learning was stimulated using role playing to acquire
knowledge and problem-solving skills necessary. The first training session was ended with reflection by
participants on their own learning process.
During the second training session, first an evaluation and reflection took place about the use of the BCT by
participants in the time between the two training sessions. Again, a form of role-playing was used to gain practical
skills, called the fish-bowl technique (Seaman, & Fellenz, 1989). Using this technique, two participants played
roles, two participants stood stand-by to take over a role when necessary and the other participants were
observers giving feedback afterwards. The fish-bowl role playing was used only during the second training
session.
2.3.3 | Review of the training program by professional caregiver
After developing the training program, the design of the training sessions was then discussed with a professional
caregiver working with adults with mild ID. The following topics were discussed:
1) Whether the training was appropriate for the interests, knowledge and learning strategies of the
intended participants;
2) If and in which way the training could be improved to support professional caregivers with the
intended behaviour;
3) Practical issues, such as time span and frequency of the training, potential breaks and location of
the training.
The most important adaptation based on this step in the design process was the integration of more examples
in the training, in particular in the theoretical part of the training. Also, the theory section was divided by breaks
to discuss what participants had learned, to increase opportunities to process the information. Last, observation
was added during the role playing in the first training session; two participants performed role playing and a third
participant observed the role playing.
2.4 | Training evaluation and outcome measures
The information from the baseline measures was used to tailor the training to the needs of the professional
caregivers and as baseline information. The second training session served as a follow-up training as well as an
evaluation moment. The follow-up consisted of repetition of knowledge and collecting knew knowledge of the
BCT as well as any questions from participants. During the evaluation, barriers and facilitators for the use of the
BCT were defined and solved where possible. When participants needed more training, a third training session
was offered.
To evaluate the training design, participants were asked to evaluate 1) the training sessions and 2) training
components:
141
1) Training sessions. Participants had to give the training sessions a report mark. These scores ranged from
1-10 with 1 as the lowest score and 10 as the highest score, using the same range of scores as school report
scores do in the Netherlands. After the second training, participants were also asked to score the training as a
total, using a score range from 1-10. In both questionnaires, participants were also asked whether the time of
training was in proportion with the gaining and the theory in proportion with practice during the training
sessions. Also, the frequency of training sessions as well as the duration of training sessions (score 0 too short,
score 5 too long) and time between training sessions was evaluated (score 0 too little time, score 5 too much
time). Participants could mention whether they would recommend the training to others (score 0 not
recommending the training, score 5 recommending the training).
2) Training components. During the training sessions, several training methods were used, including:
brainstorming, theory, video material, case discussion and roleplaying. These training components were
evaluated in the online questionnaire, whereas participants could score each component on a visual-analogic
scale (VAS), using scores from 0 (does not agree with the statement) to 5 (does agree with the statement).
Next to the evaluation of the training design, the following outcomes were measured:
1) Competence. Since there are a lot of different definitions of competence (Deardorff, 2006), the
definition used in Dutch clinical practice describing competences of professional caregivers of persons with ID
was utilized (Vereniging Gehandicaptenzorg Nederland, 2015), whereas competence included skills, knowledge,
and attitude towards supporting lifestyle behaviour. Competence of professional caregivers was measured
through self-report using (online) questionnaires. A feasible questionnaire was used to measure competence,
called the Attitude of Direct Support Persons- Health Enhancing Physical Activity (ASDP-HEPA) (Steenbergen et
al., 2019). This questionnaire included 6 questions to measure the attitude towards Health Enhancing Physical
Activity (HEPA). The questions were slightly adjusted to the use of the BCT “Action planning”, instead of physical
activity. Two questions were added to measure skills and knowledge towards “Action planning” specifically.
Participants reported on a visual-analogic scale (VAS) their self-experienced knowledge, attitude and skills. See
the Appendix for the questionnaire.
2) Readiness to use the BCT. The readiness of participants to use the BCT was measured using the five
stages of change from the transtheoretical model (Prochaska & Velicer, 1997), including pre-contemplation,
contemplation, preparation, action and maintenance. Participants answered if they already used the BCT for a
longer period (maintenance phase), for only a short period (action phase), or not used the BCT but willing to do
so in the near future (preparation phase) or later on (contemplation phase) or not willing to use the BCT (pre-
contemplation phase). The scores ranged from 0-4, whereas a score 0 meant that the participant did not use the
BCT “Action planning” at all and was not planning to use it in the future. A score 4 meant that the participant
already used the BCT for a longer period (over 6 months).
3) Barriers and facilitators to use the BCT. Participants were asked why they did or did not used the BCT
and what factors would support and withhold them to use the BCT for adults with mild ID. Barriers and facilitators
138541-Willems_BNW.indd 141 31-10-19 10:08

142
were measured by self-report. Using open ended questions, participants could mention factors that helped them
to use “Action planning” as well as factors that impedes the use of “Action planning”.
2.5 | Data analysis
To investigate whether the training had any effect on self-reported competence and readiness for BCT usage, a
mixed model analysis (Pinheiro, & Bates, 2000) was undertaken on the sum score of items for self-reported
competence, as well as on readiness for BCT usage. In the mixed model, a random intercept was specified for
each participant and fixed effects for the time effects. The latter corresponds with the differences in means
between time points. The statistical analyses were performed using the Statistical Package for Social Studies
(SPSS) version 22 for Windows with respect to descriptive statistics, and the statistical programming language R
version 3.4.0 (R Core Team, 2017) for the mixed models. Data of the training evaluation were described using
descriptive statistics.
Facilitators and barriers were analysed qualitatively in a deductive way, using the COM-B system (Michie, Van
Stralen, & West, 2011) by the first author (MW). This system is based on the Theoretical Domains Framework
(Cane, O’Connor, & Michie, 2012), and consists of the components Capability (C), Opportunity (O), and
Motivation (M), and Behaviour (B) (see Figure 1). Capability is defined as ‘the individual’s psychological and
physical capacity to engage in the activity concerned. It includes having the necessary knowledge and skills’.
Motivation is defined as ‘all those brain processes that energize and direct behaviour, not just goals and
conscious decision-making. It includes habitual processes, emotional responding, as well as analytical decision-
making’. Opportunity is defined as ‘all the factors that lie outside the individual that make the behaviour possible
or prompt it’ (Michie, Van Stralen, & West, 2011). These components together generate behaviour, and
behaviour influences the three components of the system as well. The sum of all facilitators and barriers was
counted, as well as the sum of all unique answers, using the central theme(s) of each mentioned facilitator and
barrier, whereas comparable answers were counted as one. Coding was checked for agreement by the last author
(AW) and disagreement was solved by consensus discussion.
143
Figure 1 Overview of the relation between the Theoretical Domains Framework and the COM-B system (Bossink, Van der
Putten, & Vlaskamp, 2019).
3. | RESULTS
3.1 | General results
A total of 11 participants was included in the study. Their mean (SD) age was 37 (7.5) years and 73% was female.
All participants (N=11) joined the first training session, two participants did not attend the second training
session, due to illness and holidays. All participants (N=11) completed all three questionnaires.
3.2 | Evaluation of the training
The training had a mean (SD) score of 7.4 (0.5), one participant did not score the training. Participants evaluated
the first training session with a mean (SD) score of 7.7 (0.5). For the scores on the second training session, data
were missing for two participants since they missed the second training session. The second training session was
given a mean (SD) score of 7.4 (0.5). See also Table 1 for evaluation scores of the training sessions.
Table 1 Mean (SD) scores for evaluation of the training sessions
Training session 1 Training session 2 Total training
Theory-practice ratio 3.7 (0.6) 3.4 (0.9) 3.5 (0.5)
Time investment-gaining ratio 3.7 (0.9) 3.6 (0.9) 3.5 (0.8)
Report score 7.7 (0.5) 7.4 (0.5) 7.5 (0.5)
138541-Willems_BNW.indd 142 31-10-19 10:08
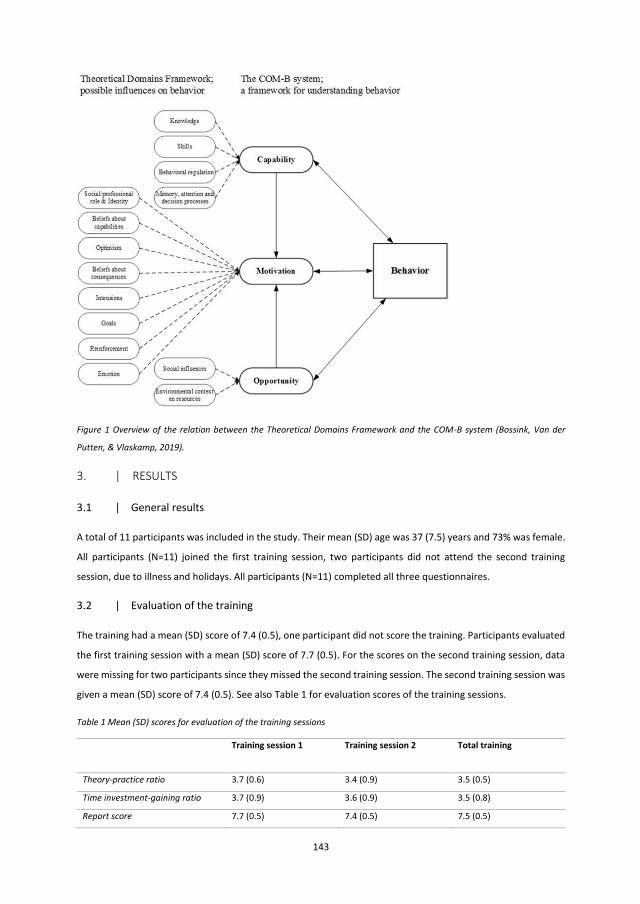
142
were measured by self-report. Using open ended questions, participants could mention factors that helped them
to use “Action planning” as well as factors that impedes the use of “Action planning”.
2.5 | Data analysis
To investigate whether the training had any effect on self-reported competence and readiness for BCT usage, a
mixed model analysis (Pinheiro, & Bates, 2000) was undertaken on the sum score of items for self-reported
competence, as well as on readiness for BCT usage. In the mixed model, a random intercept was specified for
each participant and fixed effects for the time effects. The latter corresponds with the differences in means
between time points. The statistical analyses were performed using the Statistical Package for Social Studies
(SPSS) version 22 for Windows with respect to descriptive statistics, and the statistical programming language R
version 3.4.0 (R Core Team, 2017) for the mixed models. Data of the training evaluation were described using
descriptive statistics.
Facilitators and barriers were analysed qualitatively in a deductive way, using the COM-B system (Michie, Van
Stralen, & West, 2011) by the first author (MW). This system is based on the Theoretical Domains Framework
(Cane, O’Connor, & Michie, 2012), and consists of the components Capability (C), Opportunity (O), and
Motivation (M), and Behaviour (B) (see Figure 1). Capability is defined as ‘the individual’s psychological and
physical capacity to engage in the activity concerned. It includes having the necessary knowledge and skills’.
Motivation is defined as ‘all those brain processes that energize and direct behaviour, not just goals and
conscious decision-making. It includes habitual processes, emotional responding, as well as analytical decision-
making’. Opportunity is defined as ‘all the factors that lie outside the individual that make the behaviour possible
or prompt it’ (Michie, Van Stralen, & West, 2011). These components together generate behaviour, and
behaviour influences the three components of the system as well. The sum of all facilitators and barriers was
counted, as well as the sum of all unique answers, using the central theme(s) of each mentioned facilitator and
barrier, whereas comparable answers were counted as one. Coding was checked for agreement by the last author
(AW) and disagreement was solved by consensus discussion.
143
Figure 1 Overview of the relation between the Theoretical Domains Framework and the COM-B system (Bossink, Van der
Putten, & Vlaskamp, 2019).
3. | RESULTS
3.1 | General results
A total of 11 participants was included in the study. Their mean (SD) age was 37 (7.5) years and 73% was female.
All participants (N=11) joined the first training session, two participants did not attend the second training
session, due to illness and holidays. All participants (N=11) completed all three questionnaires.
3.2 | Evaluation of the training
The training had a mean (SD) score of 7.4 (0.5), one participant did not score the training. Participants evaluated
the first training session with a mean (SD) score of 7.7 (0.5). For the scores on the second training session, data
were missing for two participants since they missed the second training session. The second training session was
given a mean (SD) score of 7.4 (0.5). See also Table 1 for evaluation scores of the training sessions.
Table 1 Mean (SD) scores for evaluation of the training sessions
Training session 1 Training session 2 Total training
Theory-practice ratio 3.7 (0.6) 3.4 (0.9) 3.5 (0.5)
Time investment-gaining ratio 3.7 (0.9) 3.6 (0.9) 3.5 (0.8)
Report score 7.7 (0.5) 7.4 (0.5) 7.5 (0.5)
138541-Willems_BNW.indd 143 31-10-19 10:08
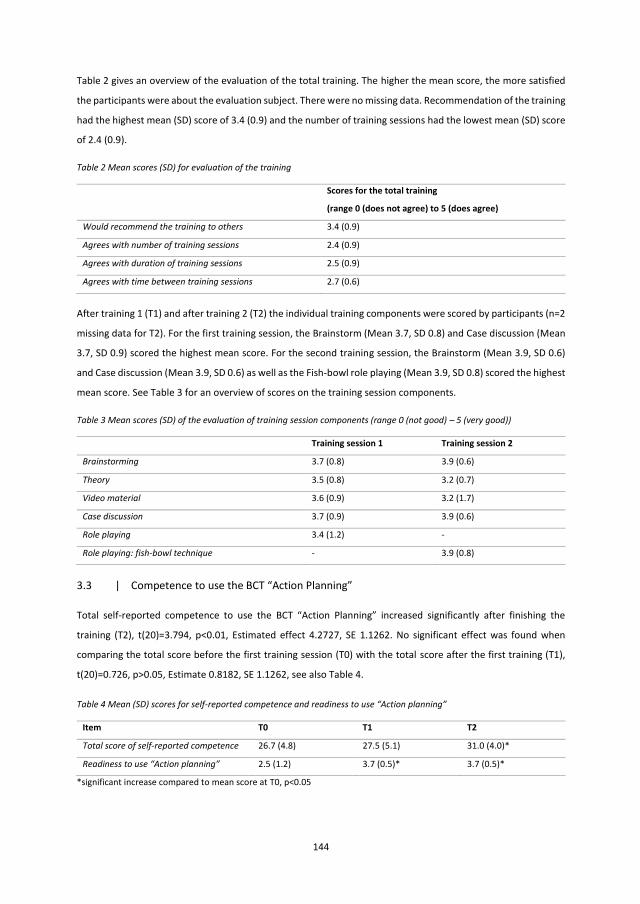
144
Table 2 gives an overview of the evaluation of the total training. The higher the mean score, the more satisfied
the participants were about the evaluation subject. There were no missing data. Recommendation of the training
had the highest mean (SD) score of 3.4 (0.9) and the number of training sessions had the lowest mean (SD) score
of 2.4 (0.9).
Table 2 Mean scores (SD) for evaluation of the training
Scores for the total training
(range 0 (does not agree) to 5 (does agree)
Would recommend the training to others 3.4 (0.9)
Agrees with number of training sessions 2.4 (0.9)
Agrees with duration of training sessions 2.5 (0.9)
Agrees with time between training sessions 2.7 (0.6)
After training 1 (T1) and after training 2 (T2) the individual training components were scored by participants (n=2
missing data for T2). For the first training session, the Brainstorm (Mean 3.7, SD 0.8) and Case discussion (Mean
3.7, SD 0.9) scored the highest mean score. For the second training session, the Brainstorm (Mean 3.9, SD 0.6)
and Case discussion (Mean 3.9, SD 0.6) as well as the Fish-bowl role playing (Mean 3.9, SD 0.8) scored the highest
mean score. See Table 3 for an overview of scores on the training session components.
Table 3 Mean scores (SD) of the evaluation of training session components (range 0 (not good) – 5 (very good))
Training session 1 Training session 2
Brainstorming 3.7 (0.8) 3.9 (0.6)
Theory 3.5 (0.8) 3.2 (0.7)
Video material 3.6 (0.9) 3.2 (1.7)
Case discussion 3.7 (0.9) 3.9 (0.6)
Role playing 3.4 (1.2) -
Role playing: fish-bowl technique - 3.9 (0.8)
3.3 | Competence to use the BCT “Action Planning”
Total self-reported competence to use the BCT “Action Planning” increased significantly after finishing the
training (T2), t(20)=3.794, p<0.01, Estimated effect 4.2727, SE 1.1262. No significant effect was found when
comparing the total score before the first training session (T0) with the total score after the first training (T1),
t(20)=0.726, p>0.05, Estimate 0.8182, SE 1.1262, see also Table 4.
Table 4 Mean (SD) scores for self-reported competence and readiness to use “Action planning”
Item T0 T1 T2
Total score of self-reported competence 26.7 (4.8) 27.5 (5.1) 31.0 (4.0)*
Readiness to use “Action planning” 2.5 (1.2) 3.7 (0.5)* 3.7 (0.5)*
*significant increase compared to mean score at T0, p<0.05
145
3.4 | Readiness to use the BCT “Action planning”
Self-reported readiness to use the BCT “Action planning” increased significantly after finishing the training (T2),
t(20)=3.968 p<0.01, Estimate 1.1818, SE 0.2978. A significant increase was also found after the first training
session (T1), t(20)=3.968 p<0.01, Estimate 1.1818, SE 0.2978, see also Table 4.
3.5 | Facilitators
Facilitators regarding all factors from the COM-B system were mentioned by participants, whereas ‘opportunity
facilitators’ were referred to mostly. Examples of opportunity facilitators were ‘clear and joint agreements’ and
‘time and resources’. ‘Practical tips and tricks’ was an example of a capability facilitator. A motivational facilitator
was about reinforcement of using the BCT “Action planning” for the participant and the adults with mild ID.
Besides the COM-B categories, a category client characteristics was also used to categorize facilitators as well,
for example ‘the attitude of the adults with mild ID about a healthy lifestyle and planning in daily living’. See
Table 5 for an overview of categorized facilitators. For each category of facilitators some answers were
comparable, resulting in differences between the total sum of facilitators and the sum of unique facilitators.
3.6 | Barriers
Barriers from all three COM-B categories were mentioned, opportunity barriers (n=17) were mentioned mostly,
and capability barriers (n=4) were mentioned less. Examples of opportunity barriers were: ‘a lack of consensus
among team members towards “Action planning” and a healthy lifestyle’ and ‘a lack of time’. Examples of
motivational barriers (n=8) were: ‘beliefs about their own professional role’ and ‘believes about their own
responsibility’. An example of a capability barrier was ‘a lack of knowledge and skills to plan action’. Client
characteristics were mentioned in addition to barriers from the categories of the COM-B system, for example
‘the intrinsic motivation of the adults with mild ID’. For each category of barriers some answers were comparable,
resulting in differences between the total sum of barriers and the sum of unique barriers.
Table 5 Facilitators and barriers about usage of the BCT “Action planning” categorized using the COM-B system
* Client characteristics are not a part of the original COM-B system but are added to enable coding of all data.
4. | DISCUSSION
This study showed a significant increase in readiness to use “Action Planning” by professional caregivers after
the lifestyle training provided. Professional caregivers also experienced significantly more competence towards
the usage of “Action planning”. Facilitators and barriers from all three categories of the COM-B model (capability,
Total sum of facilitators Sum of unique facilitators Total sum of barriers Sum of
unique barriers
Capability 8 4 4 2 Opportunity 17 4 17 4 Motivation 2 2 7 2 Client characteristics* 1 1 9 3
138541-Willems_BNW.indd 144 31-10-19 10:08
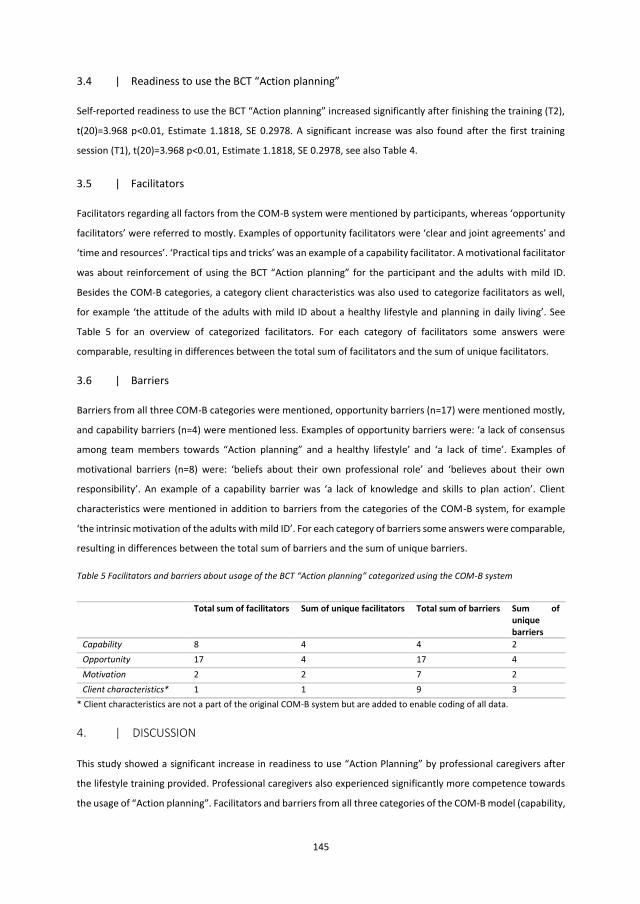
144
Table 2 gives an overview of the evaluation of the total training. The higher the mean score, the more satisfied
the participants were about the evaluation subject. There were no missing data. Recommendation of the training
had the highest mean (SD) score of 3.4 (0.9) and the number of training sessions had the lowest mean (SD) score
of 2.4 (0.9).
Table 2 Mean scores (SD) for evaluation of the training
Scores for the total training
(range 0 (does not agree) to 5 (does agree)
Would recommend the training to others 3.4 (0.9)
Agrees with number of training sessions 2.4 (0.9)
Agrees with duration of training sessions 2.5 (0.9)
Agrees with time between training sessions 2.7 (0.6)
After training 1 (T1) and after training 2 (T2) the individual training components were scored by participants (n=2
missing data for T2). For the first training session, the Brainstorm (Mean 3.7, SD 0.8) and Case discussion (Mean
3.7, SD 0.9) scored the highest mean score. For the second training session, the Brainstorm (Mean 3.9, SD 0.6)
and Case discussion (Mean 3.9, SD 0.6) as well as the Fish-bowl role playing (Mean 3.9, SD 0.8) scored the highest
mean score. See Table 3 for an overview of scores on the training session components.
Table 3 Mean scores (SD) of the evaluation of training session components (range 0 (not good) – 5 (very good))
Training session 1 Training session 2
Brainstorming 3.7 (0.8) 3.9 (0.6)
Theory 3.5 (0.8) 3.2 (0.7)
Video material 3.6 (0.9) 3.2 (1.7)
Case discussion 3.7 (0.9) 3.9 (0.6)
Role playing 3.4 (1.2) -
Role playing: fish-bowl technique - 3.9 (0.8)
3.3 | Competence to use the BCT “Action Planning”
Total self-reported competence to use the BCT “Action Planning” increased significantly after finishing the
training (T2), t(20)=3.794, p<0.01, Estimated effect 4.2727, SE 1.1262. No significant effect was found when
comparing the total score before the first training session (T0) with the total score after the first training (T1),
t(20)=0.726, p>0.05, Estimate 0.8182, SE 1.1262, see also Table 4.
Table 4 Mean (SD) scores for self-reported competence and readiness to use “Action planning”
Item T0 T1 T2
Total score of self-reported competence 26.7 (4.8) 27.5 (5.1) 31.0 (4.0)*
Readiness to use “Action planning” 2.5 (1.2) 3.7 (0.5)* 3.7 (0.5)*
*significant increase compared to mean score at T0, p<0.05
145
3.4 | Readiness to use the BCT “Action planning”
Self-reported readiness to use the BCT “Action planning” increased significantly after finishing the training (T2),
t(20)=3.968 p<0.01, Estimate 1.1818, SE 0.2978. A significant increase was also found after the first training
session (T1), t(20)=3.968 p<0.01, Estimate 1.1818, SE 0.2978, see also Table 4.
3.5 | Facilitators
Facilitators regarding all factors from the COM-B system were mentioned by participants, whereas ‘opportunity
facilitators’ were referred to mostly. Examples of opportunity facilitators were ‘clear and joint agreements’ and
‘time and resources’. ‘Practical tips and tricks’ was an example of a capability facilitator. A motivational facilitator
was about reinforcement of using the BCT “Action planning” for the participant and the adults with mild ID.
Besides the COM-B categories, a category client characteristics was also used to categorize facilitators as well,
for example ‘the attitude of the adults with mild ID about a healthy lifestyle and planning in daily living’. See
Table 5 for an overview of categorized facilitators. For each category of facilitators some answers were
comparable, resulting in differences between the total sum of facilitators and the sum of unique facilitators.
3.6 | Barriers
Barriers from all three COM-B categories were mentioned, opportunity barriers (n=17) were mentioned mostly,
and capability barriers (n=4) were mentioned less. Examples of opportunity barriers were: ‘a lack of consensus
among team members towards “Action planning” and a healthy lifestyle’ and ‘a lack of time’. Examples of
motivational barriers (n=8) were: ‘beliefs about their own professional role’ and ‘believes about their own
responsibility’. An example of a capability barrier was ‘a lack of knowledge and skills to plan action’. Client
characteristics were mentioned in addition to barriers from the categories of the COM-B system, for example
‘the intrinsic motivation of the adults with mild ID’. For each category of barriers some answers were comparable,
resulting in differences between the total sum of barriers and the sum of unique barriers.
Table 5 Facilitators and barriers about usage of the BCT “Action planning” categorized using the COM-B system
* Client characteristics are not a part of the original COM-B system but are added to enable coding of all data.
4. | DISCUSSION
This study showed a significant increase in readiness to use “Action Planning” by professional caregivers after
the lifestyle training provided. Professional caregivers also experienced significantly more competence towards
the usage of “Action planning”. Facilitators and barriers from all three categories of the COM-B model (capability,
Total sum of facilitators Sum of unique facilitators Total sum of barriers Sum of
unique barriers
Capability 8 4 4 2 Opportunity 17 4 17 4 Motivation 2 2 7 2 Client characteristics* 1 1 9 3
138541-Willems_BNW.indd 145 31-10-19 10:08

146
opportunity, and motivation) were mentioned. Opportunity facilitators (e.g. approach shared by the entire team)
and opportunity barriers (e.g. not enough time) were mentioned the most. Participants were satisfied about the
two training sessions and the training in its entirety.
4.1 | Discussion of main findings
This study was, as far as we know, the first one whereby the use of a single BCT was trained and evaluated. This
is an innovative way of training since previous studies did not recognize and labelled BCTs used explicitly and
often lacked a theoretical base for the intervention researched (Willems et al., 2017). It is therefore important
for changing lifestyle behaviour to set small steps towards healthier lifestyle behaviour which can be measured
and evaluated in an unambiguous way. For future research, this training concept could be used also to train
professional caregivers in other promising BCTs to improve lifestyle behaviour of adults with mild ID.
Since “Action planning” was a promising BCT (Willems et al., 2019) but not used much in clinical practice (Willems
et al., 2019b), we chose this BCT as a focus of supporting professional caregivers. However, the use of a single
BCT needs to be reviewed in relation to other BCTs. For example: “Action planning” could be related to the BCT
“goal setting (of behaviour)”, since one has to know which action has to be planned before it can be planned. So
in clinical practice, a single BCT might not always be used separately. For future training of professional
caregivers, this is useful to keep in mind. Thereby, future research could examine which BCTs are (inter)related
to each other, in which ways, and how they can be combined in clinical practice to support lifestyle behaviour of
adults with mild ID.
After finishing the training, professional caregivers felt more competent to plan lifestyle behaviour actions with
the adults with mild ID they supported. This is a promising finding, since competence is an important prerequisite
for performance (Rethans et al., 2002) which implicate that the training studied could influence the usage of the
BCT “Action planning”. This was supported by the significant increase of readiness to use the BCT, as reported by
professional caregivers. Since “Action planning” was rarely used by professional caregivers (Willems et al., 2019b)
but was found to be a promising BCT for changing lifestyle in adults with mild ID (Willems et al., 2019a), this
training could contribute to increased use of this BCT and thus to improved lifestyle behaviour of adults with mild
ID. As this study did not investigate the training effects on the actual use of “Action planning” by professional
caregiver, this is a recommendation for future research.
Professional caregivers described facilitators and barriers from all three categories of the COM-B system
(capability, opportunity and motivation). This is in line with a previous study about physical activity support for
adults with ID (Bossink, Van der Putten, & Vlaskamp, 2019). Most facilitators and barriers could be classified
under opportunity. This might implicate that the usage of the BCT can be increased mostly by enabling
opportunities for professional caregivers to plan lifestyle behaviour actions, such as more time and resources to
plan lifestyle behaviour actions and clear and joint agreements in a team of professional caregivers. A category
called client characteristics was added to the original COM-B system, since professional caregivers mentioned
facilitators and barriers that could not be categorized und the COM-B categories and related to specific
characteristics of the individuals with ID. This new category was used earlier (Bossink et al., 2019) but included
147
mostly barriers. It can be discussed whether resistance and motivation of adults with mild ID was a client
characteristic or that it was also the role of a professional caregiver to influence the motivation of an adult with
ID towards healthy lifestyle behaviour. It might be a combination of client responsibility towards their own
behaviour as well as the role of a professional caregiver to support a client towards healthy lifestyle behaviour.
4.2 | Strengths and limitations
A major strength of this study was that a theory-driven BCT was used to train professional caregivers supporting
lifestyle behaviour of adults with mild ID. This is the first study using a design of training a single BCT for
supporting of professional caregivers. The training format was also based on theory, using the problem-based
learning strategy (PBL), as well as the deductive analysis of the facilitators and barriers influencing the usage of
“Action planning” using the COM-B model. A consideration of this study could be that the training was only
offered to one team of professional caregivers. This might have influenced the results since these participants
have the same working environment and therefore probably experience the same challenges regarding the use
of “Action planning” and might have shared opinions about “Action planning”. Another team of professional
caregivers might experience other challenges and opinions which might have led to other results about
facilitators and barriers towards “Action planning”, as well as towards their readiness to use “Action planning”.
However, since this is a pilot-test of the training, the findings of this study are promising, and can be guiding for
future research in showing the usefulness of a single BCT training for professional caregivers.
4.3 | Recommendations
To our knowledge, this is the first study investigating the effects of a training of a single BCT for professional
caregivers supporting lifestyle behaviour of adults with mild ID. A significant increase in self-experienced
competence and readiness to use the BCT was found after participating in a training in “Action planning”.
Facilitators and barriers mostly fell in the category ‘opportunity’. Since professional caregivers were trainable
and they experienced training needs regarding lifestyle behaviour support of adults with mild ID, research of
training in other suitable, single BCTs is recommended. Since the effects of the training on the use of the BCT and
the lifestyle behaviour of adults with mild ID were not researched in this study, further research is necessary to
determine whether training affects the use of “Action planning” and whether the lifestyle behaviour of adults
becomes healthier.
4.4 | Conclusion
This study researched a training in the BCT “Action planning” supporting professional caregivers, in the use of
BCT’s and their readiness to plan lifestyle behaviour actions of adults with mild ID. Training in the BCT “Action
planning” may support professional caregivers in the use of BCT’s and their readiness to plan lifestyle behaviour
actions.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
138541-Willems_BNW.indd 146 31-10-19 10:08
146
opportunity, and motivation) were mentioned. Opportunity facilitators (e.g. approach shared by the entire team)
and opportunity barriers (e.g. not enough time) were mentioned the most. Participants were satisfied about the
two training sessions and the training in its entirety.
4.1 | Discussion of main findings
This study was, as far as we know, the first one whereby the use of a single BCT was trained and evaluated. This
is an innovative way of training since previous studies did not recognize and labelled BCTs used explicitly and
often lacked a theoretical base for the intervention researched (Willems et al., 2017). It is therefore important
for changing lifestyle behaviour to set small steps towards healthier lifestyle behaviour which can be measured
and evaluated in an unambiguous way. For future research, this training concept could be used also to train
professional caregivers in other promising BCTs to improve lifestyle behaviour of adults with mild ID.
Since “Action planning” was a promising BCT (Willems et al., 2019) but not used much in clinical practice (Willems
et al., 2019b), we chose this BCT as a focus of supporting professional caregivers. However, the use of a single
BCT needs to be reviewed in relation to other BCTs. For example: “Action planning” could be related to the BCT
“goal setting (of behaviour)”, since one has to know which action has to be planned before it can be planned. So
in clinical practice, a single BCT might not always be used separately. For future training of professional
caregivers, this is useful to keep in mind. Thereby, future research could examine which BCTs are (inter)related
to each other, in which ways, and how they can be combined in clinical practice to support lifestyle behaviour of
adults with mild ID.
After finishing the training, professional caregivers felt more competent to plan lifestyle behaviour actions with
the adults with mild ID they supported. This is a promising finding, since competence is an important prerequisite
for performance (Rethans et al., 2002) which implicate that the training studied could influence the usage of the
BCT “Action planning”. This was supported by the significant increase of readiness to use the BCT, as reported by
professional caregivers. Since “Action planning” was rarely used by professional caregivers (Willems et al., 2019b)
but was found to be a promising BCT for changing lifestyle in adults with mild ID (Willems et al., 2019a), this
training could contribute to increased use of this BCT and thus to improved lifestyle behaviour of adults with mild
ID. As this study did not investigate the training effects on the actual use of “Action planning” by professional
caregiver, this is a recommendation for future research.
Professional caregivers described facilitators and barriers from all three categories of the COM-B system
(capability, opportunity and motivation). This is in line with a previous study about physical activity support for
adults with ID (Bossink, Van der Putten, & Vlaskamp, 2019). Most facilitators and barriers could be classified
under opportunity. This might implicate that the usage of the BCT can be increased mostly by enabling
opportunities for professional caregivers to plan lifestyle behaviour actions, such as more time and resources to
plan lifestyle behaviour actions and clear and joint agreements in a team of professional caregivers. A category
called client characteristics was added to the original COM-B system, since professional caregivers mentioned
facilitators and barriers that could not be categorized und the COM-B categories and related to specific
characteristics of the individuals with ID. This new category was used earlier (Bossink et al., 2019) but included
147
mostly barriers. It can be discussed whether resistance and motivation of adults with mild ID was a client
characteristic or that it was also the role of a professional caregiver to influence the motivation of an adult with
ID towards healthy lifestyle behaviour. It might be a combination of client responsibility towards their own
behaviour as well as the role of a professional caregiver to support a client towards healthy lifestyle behaviour.
4.2 | Strengths and limitations
A major strength of this study was that a theory-driven BCT was used to train professional caregivers supporting
lifestyle behaviour of adults with mild ID. This is the first study using a design of training a single BCT for
supporting of professional caregivers. The training format was also based on theory, using the problem-based
learning strategy (PBL), as well as the deductive analysis of the facilitators and barriers influencing the usage of
“Action planning” using the COM-B model. A consideration of this study could be that the training was only
offered to one team of professional caregivers. This might have influenced the results since these participants
have the same working environment and therefore probably experience the same challenges regarding the use
of “Action planning” and might have shared opinions about “Action planning”. Another team of professional
caregivers might experience other challenges and opinions which might have led to other results about
facilitators and barriers towards “Action planning”, as well as towards their readiness to use “Action planning”.
However, since this is a pilot-test of the training, the findings of this study are promising, and can be guiding for
future research in showing the usefulness of a single BCT training for professional caregivers.
4.3 | Recommendations
To our knowledge, this is the first study investigating the effects of a training of a single BCT for professional
caregivers supporting lifestyle behaviour of adults with mild ID. A significant increase in self-experienced
competence and readiness to use the BCT was found after participating in a training in “Action planning”.
Facilitators and barriers mostly fell in the category ‘opportunity’. Since professional caregivers were trainable
and they experienced training needs regarding lifestyle behaviour support of adults with mild ID, research of
training in other suitable, single BCTs is recommended. Since the effects of the training on the use of the BCT and
the lifestyle behaviour of adults with mild ID were not researched in this study, further research is necessary to
determine whether training affects the use of “Action planning” and whether the lifestyle behaviour of adults
becomes healthier.
4.4 | Conclusion
This study researched a training in the BCT “Action planning” supporting professional caregivers, in the use of
BCT’s and their readiness to plan lifestyle behaviour actions of adults with mild ID. Training in the BCT “Action
planning” may support professional caregivers in the use of BCT’s and their readiness to plan lifestyle behaviour
actions.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
138541-Willems_BNW.indd 147 31-10-19 10:08
148
REFERENCES
Barrows, H. S. (1996). Problem-based learning in medicine and beyond. In L. Wilkerson & W. H. Gijselaers
(Eds.), New directions for teaching and learning: Vol. 68. Bringing problem-based learning to higher
education: Theory and practice (pp. 3–13). San Francisco: Jossey-Bass.
Bossink, L. W., Van der Putten, A. A., & Vlaskamp, C. (2019). Physical-activity support for people with
intellectual disabilities: a theory-informed qualitative study exploring the direct support
professionals’ perspective. Disability and Rehabilitation, 1-7.
Cane, J., O’Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in
behaviour change and implementation research. Implementation science, 7(1), 37.
Chen, S. E., Cowdroy, R. M., Kingsland, A. J., & Ostwald, M. J. (Eds.). (1995). Reflections on problem based
learning. Campbelltown, New South Wales, Australia: Australian Problem-based Learning Network.
Dairo, Y. M., Collett, J., Dawes, H., & Oskrochi, G. R. (2016). Physical activity levels in adults with intellectual
disabilities: a systematic review. Preventive Medicine Reports, 4, 209-219.
Deardorff, D. K. (2006). Identification and assessment of intercultural competence as a student outcome of
internationalization. Journal of Studies in International Education, 10(3), 241-266.
Ehlen, C., Van der Klink, D., Stoffers, J., & Boshuizen, H. (2017). The co-creation-wheel: A four dimensional
model of collaborative, interorganisational innovation. European Journal of Training and
Development, 41(7), 628-646
Gijbels, D., Dochy, F., Van den Bossche, P., & Segers, M. (2005). Effects of problem-based learning: A meta-
analysis from the angle of assessment. Review of Educational Research, 75(1), 27-61.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477-483.
Hsieh, K., Rimmer, J. H., & Heller, T. (2013). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851–863. doi:10.1111/jir.12100
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Melville, C. A., Hamilton, S., Miller, S., Boyle, S., Robinson, N., Pert, C., & Hankey, C. R. (2009). Carer
knowledge and perceptions of healthy lifestyles for adults with intellectual disabilities. Journal of
Applied Research in Intellectual Disabilities, 22(3), 298-306.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and healthy
eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
149
Michie, S., Van Stralen, M. M., & West, R. (2011). The behaviour change wheel: a new method for
characterising and designing behaviour change interventions. Implementation Science, 6(1), 42.
O’Connor-Fleming, M. L., Parker, E., Higgins, H., & Gould, T. (2006). A framework for evaluating health
promotion programs. Health Promotion Journal of Australia: Official Journal of Australian
Association of Health Promotion Professionals, 17(1), 61–66.
Pinheiro, J. C., & Bates, D. M. (2000). Mixed‐effects models in S and SPLUS. New York, NY: Springer‐Verlag.
Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American
Journal of Health Promotion, 12(1), 38-48.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., . . . & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical
Computing, Vienna, Austria. URL https://www.R-project.org/.
Rethans, J., Norcini, J., Baron-Maldonado, M., Blackmore, D., Jolly, B., LaDuca, T., . . . & Southgate, L. (2002).
The relationship between competence and performance: Implications for assessing practice
performance. Medical Education, 36(10), 901-909.
Robertson, J., Emerson, E., Baines, S., & Hatton, C. (2014). Obesity and health behaviours of British adults with
self-reported intellectual impairments: cross sectional survey. BMC Public Health, 14(1), 219.
Seaman, D. F., & Fellenz, R. A. (1989). Effective Strategies for Teaching Adults. Columbus, Ohio: Merrill
Publishing Company.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., . . . Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
Steenbergen, H. A., Hilgenkamp, T. I. M., De Jong, J., Bossink, L. W. M., Van der Schans, C. P., Krijnen, W. P., &
Waninge, A. (2019). Evaluating direct support persons’ attitude towards promoting physical activity of
persons with intellectual disabilities: developing a questionnaire. Article in preparation
Strobel, J., & Van Barneveld, A. (2009). When is PBL more effective? A meta-synthesis of meta analyses
comparing PBL to conventional classrooms. Interdisciplinary Journal of Problem based Learning, 3(1),
44-58.
Sundahl, L., Zetterberg, M., Wester, A., Rehn, B., & Blomqvist, S. (2016). Physical activity levels among
adolescent and young adult women and men with and without intellectual disability. Journal of
Applied Research in Intellectual Disabilities, 29(1), 93–98.
138541-Willems_BNW.indd 148 31-10-19 10:08
148
REFERENCES
Barrows, H. S. (1996). Problem-based learning in medicine and beyond. In L. Wilkerson & W. H. Gijselaers
(Eds.), New directions for teaching and learning: Vol. 68. Bringing problem-based learning to higher
education: Theory and practice (pp. 3–13). San Francisco: Jossey-Bass.
Bossink, L. W., Van der Putten, A. A., & Vlaskamp, C. (2019). Physical-activity support for people with
intellectual disabilities: a theory-informed qualitative study exploring the direct support
professionals’ perspective. Disability and Rehabilitation, 1-7.
Cane, J., O’Connor, D., & Michie, S. (2012). Validation of the theoretical domains framework for use in
behaviour change and implementation research. Implementation science, 7(1), 37.
Chen, S. E., Cowdroy, R. M., Kingsland, A. J., & Ostwald, M. J. (Eds.). (1995). Reflections on problem based
learning. Campbelltown, New South Wales, Australia: Australian Problem-based Learning Network.
Dairo, Y. M., Collett, J., Dawes, H., & Oskrochi, G. R. (2016). Physical activity levels in adults with intellectual
disabilities: a systematic review. Preventive Medicine Reports, 4, 209-219.
Deardorff, D. K. (2006). Identification and assessment of intercultural competence as a student outcome of
internationalization. Journal of Studies in International Education, 10(3), 241-266.
Ehlen, C., Van der Klink, D., Stoffers, J., & Boshuizen, H. (2017). The co-creation-wheel: A four dimensional
model of collaborative, interorganisational innovation. European Journal of Training and
Development, 41(7), 628-646
Gijbels, D., Dochy, F., Van den Bossche, P., & Segers, M. (2005). Effects of problem-based learning: A meta-
analysis from the angle of assessment. Review of Educational Research, 75(1), 27-61.
Hilgenkamp, T. I., Reis, D., van Wijck, R., & Evenhuis, H. M. (2012). Physical activity levels in older adults with
intellectual disabilities are extremely low. Research in Developmental Disabilities, 33(2), 477-483.
Hsieh, K., Rimmer, J. H., & Heller, T. (2013). Obesity and associated factors in adults with intellectual
disability. Journal of Intellectual Disability Research, 58(9), 851–863. doi:10.1111/jir.12100
Melville, C. A., Hamilton, S., Hankey, C. R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of
obesity in adults with intellectual disabilities. Obesity Reviews, 8(3), 223-230.
Melville, C. A., Hamilton, S., Miller, S., Boyle, S., Robinson, N., Pert, C., & Hankey, C. R. (2009). Carer
knowledge and perceptions of healthy lifestyles for adults with intellectual disabilities. Journal of
Applied Research in Intellectual Disabilities, 22(3), 298-306.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined
taxonomy of behaviour change techniques to help people change their physical activity and healthy
eating behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
149
Michie, S., Van Stralen, M. M., & West, R. (2011). The behaviour change wheel: a new method for
characterising and designing behaviour change interventions. Implementation Science, 6(1), 42.
O’Connor-Fleming, M. L., Parker, E., Higgins, H., & Gould, T. (2006). A framework for evaluating health
promotion programs. Health Promotion Journal of Australia: Official Journal of Australian
Association of Health Promotion Professionals, 17(1), 61–66.
Pinheiro, J. C., & Bates, D. M. (2000). Mixed‐effects models in S and SPLUS. New York, NY: Springer‐Verlag.
Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior change. American
Journal of Health Promotion, 12(1), 38-48.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., . . . & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
R Core Team (2017). R: A language and environment for statistical computing. R Foundation for Statistical
Computing, Vienna, Austria. URL https://www.R-project.org/.
Rethans, J., Norcini, J., Baron-Maldonado, M., Blackmore, D., Jolly, B., LaDuca, T., . . . & Southgate, L. (2002).
The relationship between competence and performance: Implications for assessing practice
performance. Medical Education, 36(10), 901-909.
Robertson, J., Emerson, E., Baines, S., & Hatton, C. (2014). Obesity and health behaviours of British adults with
self-reported intellectual impairments: cross sectional survey. BMC Public Health, 14(1), 219.
Seaman, D. F., & Fellenz, R. A. (1989). Effective Strategies for Teaching Adults. Columbus, Ohio: Merrill
Publishing Company.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., . . . Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
Steenbergen, H. A., Hilgenkamp, T. I. M., De Jong, J., Bossink, L. W. M., Van der Schans, C. P., Krijnen, W. P., &
Waninge, A. (2019). Evaluating direct support persons’ attitude towards promoting physical activity of
persons with intellectual disabilities: developing a questionnaire. Article in preparation
Strobel, J., & Van Barneveld, A. (2009). When is PBL more effective? A meta-synthesis of meta analyses
comparing PBL to conventional classrooms. Interdisciplinary Journal of Problem based Learning, 3(1),
44-58.
Sundahl, L., Zetterberg, M., Wester, A., Rehn, B., & Blomqvist, S. (2016). Physical activity levels among
adolescent and young adult women and men with and without intellectual disability. Journal of
Applied Research in Intellectual Disabilities, 29(1), 93–98.
138541-Willems_BNW.indd 149 31-10-19 10:08
150
Vereniging Gehandicaptenzorg Nederland (2015). Landelijk competentieprofiel voor beroepskrachten (niveau
ABC) in het primaire proces van de gehandicaptenzorg [National competence profile for professionals
(level ABC) in the primary process of care for persons with intellectual disabilities]. Retrieved from
https://legacy.vgn.nl/media/551d3516b1900/Beroepscompetentieprofiel+ABC+dig.pdf?_ga=2.190538
024.2005256991.1560422018-153282600.1560422018
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple
disabilities. The Journal of Strength and Conditioning Research, 27(11), 3150-3158.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256-268.
Willems, M., Waninge, A., Hilgenkamp, T. I., Van Empelen, P., Krijnen, W. P., Van der Schans, C. P., &
Melville, C. A. (2018). Effects of lifestyle change interventions for people with intellectual
disabilities: systematic review and meta-analysis of randomized controlled trials. Journal of
Applied Research in Intellectual Disabilities, 31(6), 949-961.
Willems, M., Waninge, A., De Jong, J.., Hilgenkamp, T. I. M., & Van der Schans, C. P. (2019a). Exploration of suitable
behaviour change techniques for lifestyle change of individuals with mild intellectual disabilities: A
Delphi study’. Journal of Applied Research in Intellectual Disabilities, 32(3), 543-557.
Willems, M., De Jong, J., Overwijk, A., Hilgenkamp, T. I. M., Van der Schans C. P., Waninge, A., (2019b). Use of
behaviour change techniques in daily support of adults with mild intellectual disabilities. Article in
preparation.
151
APPENDIX – Questionnaire used to measure outcome measures
1) To what extent do you agree with the statements below?
Item 5 point VAS-scale (Not agree – Agree)
I am aware what healthy lifestyle behaviour is for the adults
with mild ID who I support
I have enough practical knowledge and skills to plan healthy
lifestyle behaviour with the adults with mild ID who I
support
I have enough (game) materials to plan healthy lifestyle
behaviour.
I feel supported by my superiors/managers when planning
healthy lifestyle behaviour with the adults with mild ID who
I support
I believe that planning healthy lifestyle behaviour is so
important that I will do anything to plan it in the daily
schedule of the adults with mild ID who I support
I think planning healthy lifestyle behaviour is a fun part of
my work.
I have sufficient skills to plan healthy lifestyle behaviour
with adults with mild ID
I have sufficient knowledge to plan healthy behaviour with
the adults with mild ID who I support
2) I plan healthy lifestyle behaviour with the adults with mild ID who I support:
o Yes, this has been part of my job for at least 6 months
o Yes, I made this part of my job recently (less than 6 months ago)
o No, but I am willing to make this part of my job in the near future
o No, but I want to make this part of my job later on
o No, and I am not willing to make this part of my job
3) What would support you in planning healthy lifestyle behaviour with the adults with mild ID you support?
4) What impedes you to plan healthy lifestyle behaviour with the adults with mild ID you support?
138541-Willems_BNW.indd 150 31-10-19 10:08
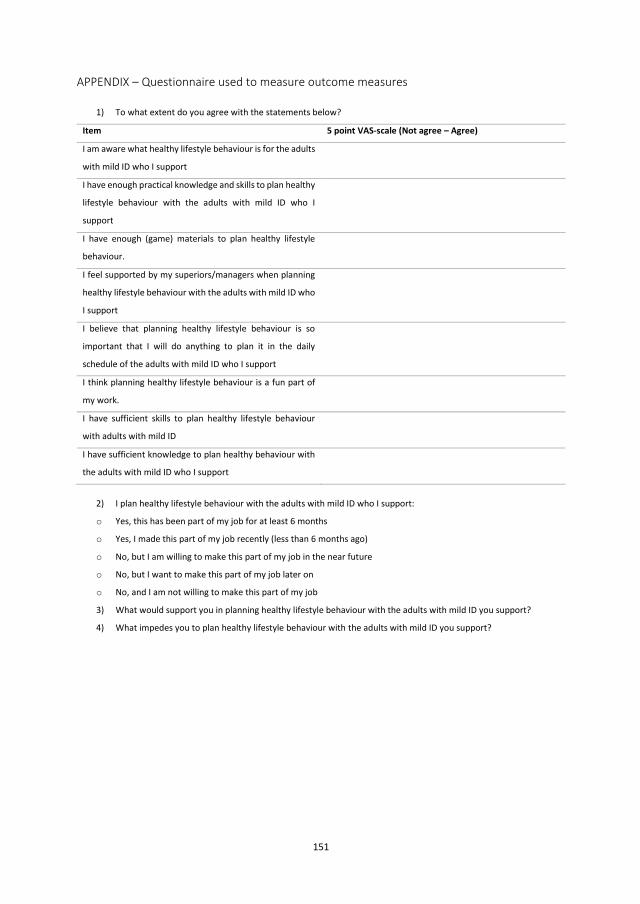
150
Vereniging Gehandicaptenzorg Nederland (2015). Landelijk competentieprofiel voor beroepskrachten (niveau
ABC) in het primaire proces van de gehandicaptenzorg [National competence profile for professionals
(level ABC) in the primary process of care for persons with intellectual disabilities]. Retrieved from
https://legacy.vgn.nl/media/551d3516b1900/Beroepscompetentieprofiel+ABC+dig.pdf?_ga=2.190538
024.2005256991.1560422018-153282600.1560422018
Waninge, A., van der Putten, A. A., Stewart, R. E., Steenbergen, B., van Wijck, R., & van der Schans, C. P. (2013).
Heart rate and physical activity patterns in persons with profound intellectual and multiple
disabilities. The Journal of Strength and Conditioning Research, 27(11), 3150-3158.
Willems, M., Hilgenkamp, T. I., Havik, E., Waninge, A., & Melville, C. A. (2017). Use of behaviour change
techniques in lifestyle change interventions for people with intellectual disabilities: A systematic
review. Research in Developmental Disabilities, 60, 256-268.
Willems, M., Waninge, A., Hilgenkamp, T. I., Van Empelen, P., Krijnen, W. P., Van der Schans, C. P., &
Melville, C. A. (2018). Effects of lifestyle change interventions for people with intellectual
disabilities: systematic review and meta-analysis of randomized controlled trials. Journal of
Applied Research in Intellectual Disabilities, 31(6), 949-961.
Willems, M., Waninge, A., De Jong, J.., Hilgenkamp, T. I. M., & Van der Schans, C. P. (2019a). Exploration of suitable
behaviour change techniques for lifestyle change of individuals with mild intellectual disabilities: A
Delphi study’. Journal of Applied Research in Intellectual Disabilities, 32(3), 543-557.
Willems, M., De Jong, J., Overwijk, A., Hilgenkamp, T. I. M., Van der Schans C. P., Waninge, A., (2019b). Use of
behaviour change techniques in daily support of adults with mild intellectual disabilities. Article in
preparation.
151
APPENDIX – Questionnaire used to measure outcome measures
1) To what extent do you agree with the statements below?
Item 5 point VAS-scale (Not agree – Agree)
I am aware what healthy lifestyle behaviour is for the adults
with mild ID who I support
I have enough practical knowledge and skills to plan healthy
lifestyle behaviour with the adults with mild ID who I
support
I have enough (game) materials to plan healthy lifestyle
behaviour.
I feel supported by my superiors/managers when planning
healthy lifestyle behaviour with the adults with mild ID who
I support
I believe that planning healthy lifestyle behaviour is so
important that I will do anything to plan it in the daily
schedule of the adults with mild ID who I support
I think planning healthy lifestyle behaviour is a fun part of
my work.
I have sufficient skills to plan healthy lifestyle behaviour
with adults with mild ID
I have sufficient knowledge to plan healthy behaviour with
the adults with mild ID who I support
2) I plan healthy lifestyle behaviour with the adults with mild ID who I support:
o Yes, this has been part of my job for at least 6 months
o Yes, I made this part of my job recently (less than 6 months ago)
o No, but I am willing to make this part of my job in the near future
o No, but I want to make this part of my job later on
o No, and I am not willing to make this part of my job
3) What would support you in planning healthy lifestyle behaviour with the adults with mild ID you support?
4) What impedes you to plan healthy lifestyle behaviour with the adults with mild ID you support?
138541-Willems_BNW.indd 151 31-10-19 10:08
Chapter 7
General discussion
138541-Willems_BNW.indd 152 31-10-19 10:08
Chapter 7
General discussion
138541-Willems_BNW.indd 153 31-10-19 10:08

154
1 | SUMMARY OF MAIN FINDINGS
This thesis aimed to investigate the use and effectiveness of current lifestyle change interventions and suitable
behaviour change techniques (BCTs) for professional caregivers to support adults with mild ID to change their
lifestyle behaviour.
First the current level of evidence of lifestyle change interventions for adults with ID was determined. Therefore,
a systematic review and meta-analysis was conducted (Chapter 2) to investigate the effects of lifestyle change
for adults with ID. Outcome measures were categorized using the International Classification of Functioning,
Disability and Health (ICF) (World Health Organisation, 2001). Quantifiable outcome measures from the category
‘Functions’, such as weight, were used most, whereas outcome measures in the categories ‘Environmental
factors’, ‘Participation’, and ‘Personal factors’ were hardly used. Meta-analysis was only possible for three
outcome measures: BMI, weight and waist circumference. A significant decrease was found only for waist
circumference. Consensus about suitable outcome measures to evaluate lifestyle change interventions for adults
with ID is necessary to investigate future interventions. Also, a strong methodological design of studies about
lifestyle change interventions for adults with ID would help to determine potential effects of these interventions.
A systematic review was performed to identify which BCTs have been used in current lifestyle change
interventions for people with ID, aimed at physical activity, nutrition or both (Chapter 3). BCTs were used in all
interventions, but in most cases, they were used implicitly. The most frequently used BCTs were: “Provide
information on consequences of behaviour in general”, “Plan social support/social change”, “Provide instruction
on how to perform the behaviour” and “Goal setting (behaviour)”, as defined in the CALO-RE taxonomy (Michie
et al., 2011). Quality of the studies was often limited, mostly because of insufficient blinding of
patients/therapists/assessors. Thereby, most studies were not based on theory. Interventions often targeted
multiple levels of ID, mostly aiming at individuals with a mild-moderate ID level. For designing future lifestyle
change interventions, it is recommended to determine which BCTs should be included to tailor the interventions
to adults with ID, as well as using theory to substantiate the intervention.
Since there is only little evidence on the effectiveness of lifestyle change interventions in adults with ID, effective
techniques to change lifestyle behaviour could not be identified. Therefore, health care professionals were asked
about the suitability of behaviour change techniques (BCTs) in changing lifestyle behaviour of adults with mild ID
(Chapter 4). Using a Delphi method, consensus was reached for 25 out of 40 BCTs from the CALO-RE taxonomy
(Michie et al., 2011). A total of 24 BCTs was considered to be suitable in changing lifestyle of adults with mild ID.
Health care professionals agreed on the following BCTs as being the most suitable: “Barrier
identification/problem solving” (97%), “Set graded tasks” (97%), “Prompt rewards contingent on effort or
progress towards behaviour” (95%), “Motivational interviewing’ (94%) and “Action planning” (91%). The four
groups of health care professionals, (professional caregivers, behavioural scientists, allied health professionals,
and intellectual disability physicians), did not differ significantly in response regarding suitability of BCTs. For
future research about lifestyle behaviour change in adults with ID, it is advocated to include the BCTs with most
consensus to improve the effectiveness of lifestyle change interventions.
155
No scientific information about the actual use of BCTs in clinical practice supporting adults with mild ID in lifestyle
behaviour change is available, and therefore, an observation study was performed (Chapter 5). The aim of this
study was to identify if and which BCTs are used in clinical practice by professional caregivers supporting adults
with mild ID. A total of 21 out of 40 BCTs was used by professional caregivers (N=14). The BCTs mostly used were:
“Information about others approval”, “Identification as role model”, “Rewards on successful behaviour”, “Review
behavioural goals” and “Instructions on how to perform the behaviour”. However, the most promising BCTs
(including: “Barrier identification/problem solving”, “Set graded tasks”, “Prompt rewards contingent on effort or
progress towards behaviour”, “Motivational interviewing’ and “Action planning”), given high consensus rates of
a panel of health care professionals, were rarely used by professional caregivers.
In order to improve lifestyle behaviour change in adults with mild ID, an intervention was developed to train
professional caregivers supporting adults with mild ID in changing lifestyle behaviour (Chapter 6), using a
promising BCTs entitled “Action planning”. Competence of professional caregivers was significantly increased
after the training, as well as their readiness to plan lifestyle behaviour action. Professional caregivers experienced
several facilitators and barriers, most of them could be classified under the concept ‘opportunity’, and the others
were classified under the categories ‘motivation’, ‘capability’ and ‘client characteristics’. The use of the BCT
“Action planning” could be increased by enabling opportunities to plan lifestyle behaviour actions. In future
research this training could be used as an example for designing lifestyle trainings tailored to professional
caregivers of adults with mild ID.
2 | DISCUSSION OF MAIN FINDINGS AND IMPLICATIONS FOR FUTURE RESEARCH
2.1 | Lifestyle change interventions supporting adults with intellectual disabilities
There are varying levels of intellectual disabilities, ranging from mild to profound ID (Schalock et al., 2002). The
severity of ID is related to the degree of support needs in adaptive functioning and daily life skills (American
Psychiatric Association, 2013). However, current lifestyle change interventions are often aiming at the whole
range of ID levels. This might have influenced the effectiveness of the interventions, because it could be very
hard to meet the specific needs of adults with different levels of ID. Adults with mild ID are more self-sufficient
than adults with more severe levels of ID. They might need more assistance with social interaction in daily living
to do their jobs and to live independently, whereas adults with more severe ID are dependent from others for
their self-care and activities of daily living. It is therefore important to tailor future lifestyle change interventions
to specific level of ID of an individual.
2.2 | Changing lifestyle behaviour in adults with mild intellectual disabilities
BCTs could be suitable in changing lifestyle for adults with mild ID, which is important knowledge for clinical
practice and guiding for future research. However, effectiveness of these BCTs is still unknown. For the general
population, BCTs have been found to positively affect lifestyle behaviour, but it is still complicated to change
behaviour in an effective and sustainable way. For reasons of dependency on others and cognitive limitations,
changing lifestyle change in adults with mild ID is expected to be at least as complicated as it is for the general
population. Personal interests, living situation, social and emotional functioning, as well as the relationship and
138541-Willems_BNW.indd 154 31-10-19 10:08
154
1 | SUMMARY OF MAIN FINDINGS
This thesis aimed to investigate the use and effectiveness of current lifestyle change interventions and suitable
behaviour change techniques (BCTs) for professional caregivers to support adults with mild ID to change their
lifestyle behaviour.
First the current level of evidence of lifestyle change interventions for adults with ID was determined. Therefore,
a systematic review and meta-analysis was conducted (Chapter 2) to investigate the effects of lifestyle change
for adults with ID. Outcome measures were categorized using the International Classification of Functioning,
Disability and Health (ICF) (World Health Organisation, 2001). Quantifiable outcome measures from the category
‘Functions’, such as weight, were used most, whereas outcome measures in the categories ‘Environmental
factors’, ‘Participation’, and ‘Personal factors’ were hardly used. Meta-analysis was only possible for three
outcome measures: BMI, weight and waist circumference. A significant decrease was found only for waist
circumference. Consensus about suitable outcome measures to evaluate lifestyle change interventions for adults
with ID is necessary to investigate future interventions. Also, a strong methodological design of studies about
lifestyle change interventions for adults with ID would help to determine potential effects of these interventions.
A systematic review was performed to identify which BCTs have been used in current lifestyle change
interventions for people with ID, aimed at physical activity, nutrition or both (Chapter 3). BCTs were used in all
interventions, but in most cases, they were used implicitly. The most frequently used BCTs were: “Provide
information on consequences of behaviour in general”, “Plan social support/social change”, “Provide instruction
on how to perform the behaviour” and “Goal setting (behaviour)”, as defined in the CALO-RE taxonomy (Michie
et al., 2011). Quality of the studies was often limited, mostly because of insufficient blinding of
patients/therapists/assessors. Thereby, most studies were not based on theory. Interventions often targeted
multiple levels of ID, mostly aiming at individuals with a mild-moderate ID level. For designing future lifestyle
change interventions, it is recommended to determine which BCTs should be included to tailor the interventions
to adults with ID, as well as using theory to substantiate the intervention.
Since there is only little evidence on the effectiveness of lifestyle change interventions in adults with ID, effective
techniques to change lifestyle behaviour could not be identified. Therefore, health care professionals were asked
about the suitability of behaviour change techniques (BCTs) in changing lifestyle behaviour of adults with mild ID
(Chapter 4). Using a Delphi method, consensus was reached for 25 out of 40 BCTs from the CALO-RE taxonomy
(Michie et al., 2011). A total of 24 BCTs was considered to be suitable in changing lifestyle of adults with mild ID.
Health care professionals agreed on the following BCTs as being the most suitable: “Barrier
identification/problem solving” (97%), “Set graded tasks” (97%), “Prompt rewards contingent on effort or
progress towards behaviour” (95%), “Motivational interviewing’ (94%) and “Action planning” (91%). The four
groups of health care professionals, (professional caregivers, behavioural scientists, allied health professionals,
and intellectual disability physicians), did not differ significantly in response regarding suitability of BCTs. For
future research about lifestyle behaviour change in adults with ID, it is advocated to include the BCTs with most
consensus to improve the effectiveness of lifestyle change interventions.
155
No scientific information about the actual use of BCTs in clinical practice supporting adults with mild ID in lifestyle
behaviour change is available, and therefore, an observation study was performed (Chapter 5). The aim of this
study was to identify if and which BCTs are used in clinical practice by professional caregivers supporting adults
with mild ID. A total of 21 out of 40 BCTs was used by professional caregivers (N=14). The BCTs mostly used were:
“Information about others approval”, “Identification as role model”, “Rewards on successful behaviour”, “Review
behavioural goals” and “Instructions on how to perform the behaviour”. However, the most promising BCTs
(including: “Barrier identification/problem solving”, “Set graded tasks”, “Prompt rewards contingent on effort or
progress towards behaviour”, “Motivational interviewing’ and “Action planning”), given high consensus rates of
a panel of health care professionals, were rarely used by professional caregivers.
In order to improve lifestyle behaviour change in adults with mild ID, an intervention was developed to train
professional caregivers supporting adults with mild ID in changing lifestyle behaviour (Chapter 6), using a
promising BCTs entitled “Action planning”. Competence of professional caregivers was significantly increased
after the training, as well as their readiness to plan lifestyle behaviour action. Professional caregivers experienced
several facilitators and barriers, most of them could be classified under the concept ‘opportunity’, and the others
were classified under the categories ‘motivation’, ‘capability’ and ‘client characteristics’. The use of the BCT
“Action planning” could be increased by enabling opportunities to plan lifestyle behaviour actions. In future
research this training could be used as an example for designing lifestyle trainings tailored to professional
caregivers of adults with mild ID.
2 | DISCUSSION OF MAIN FINDINGS AND IMPLICATIONS FOR FUTURE RESEARCH
2.1 | Lifestyle change interventions supporting adults with intellectual disabilities
There are varying levels of intellectual disabilities, ranging from mild to profound ID (Schalock et al., 2002). The
severity of ID is related to the degree of support needs in adaptive functioning and daily life skills (American
Psychiatric Association, 2013). However, current lifestyle change interventions are often aiming at the whole
range of ID levels. This might have influenced the effectiveness of the interventions, because it could be very
hard to meet the specific needs of adults with different levels of ID. Adults with mild ID are more self-sufficient
than adults with more severe levels of ID. They might need more assistance with social interaction in daily living
to do their jobs and to live independently, whereas adults with more severe ID are dependent from others for
their self-care and activities of daily living. It is therefore important to tailor future lifestyle change interventions
to specific level of ID of an individual.
2.2 | Changing lifestyle behaviour in adults with mild intellectual disabilities
BCTs could be suitable in changing lifestyle for adults with mild ID, which is important knowledge for clinical
practice and guiding for future research. However, effectiveness of these BCTs is still unknown. For the general
population, BCTs have been found to positively affect lifestyle behaviour, but it is still complicated to change
behaviour in an effective and sustainable way. For reasons of dependency on others and cognitive limitations,
changing lifestyle change in adults with mild ID is expected to be at least as complicated as it is for the general
population. Personal interests, living situation, social and emotional functioning, as well as the relationship and
138541-Willems_BNW.indd 155 31-10-19 10:08

156
interaction between adults with mild ID and their caregivers may have a great impact on the suitability and
effectiveness of BCTs. Keeping personal characteristics as well as interpersonal relationship in mind is necessary
for future interventions and research. However, it should not be a reason to stop striving to healthy lifestyle
behaviour for this vulnerable group, since improvement of a healthy lifestyle is necessary and seems to be
possible.
Professional caregivers are important for adults with mild ID (Ptomey et al., 2018; Spanos et al., 2013) and were
therefore included as the main focus of this thesis. However, professional caregivers are not the only important
social contacts of adults with mild ID. Family and friends play an important role as well (Miller, Cooper, Cook, &
Petch, 2008). In addition to the social environment, also the physical environment and policies (e.g. policies of
ID care organizations) should be taken in account in future lifestyle change interventions (Steenbergen et al.,
2019). So, all levels that influence health behaviour (including the intrapersonal and interpersonal level as well
as organizational and community factors and public policy) need to be targeted to change lifestyle behaviour, as
emphasized in the ecological model of active living (McLeroy, Bibeau, Steckler, & Glanz, 1988). Acting
unambiguously from a shared vision by all levels, as well as creating opportunities to use suitable BCTs, could be
key factors for successful and sustainable lifestyle behaviour change.
Training professional caregivers in behaviour change is important to improve future lifestyle support for adults
with mild ID. The training in ‘action planning’ is an example of how individual BCTs can be taught to professional
caregivers and how they can be evaluated. This is important, because training in a single BCT allows for
investigation of its individual effectiveness. On the other hand, it is hard to use BCTs independently, since most
BCTs are in some way related to other BCTs. For example: the BCT ‘action planning’ is related to the BCT goal
setting (behaviour)’ as well as ‘goal setting (outcome)’, since you cannot plan any action if you do not know which
action you want to plan. ‘Action planning’ will probably be used together with BCTs like ‘Barrier
identification/Problem solving’, ‘Set graded tasks’ and ‘Provide information on where and when to perform the
behaviour’. Training of single BCTs is necessary for the professional caregivers to understand how to use the BCT
in clinical practice and to investigate suitability and effects of the BCT. At the same time, it is important not to
lose sight on connections between other important BCTs.
Adults with mild ID included in the studies of this thesis were diagnosed as having a mild intellectual disability.
In definitions of mild ID currently used, IQ levels on itself are not enough to diagnose someone having a mild ID.
Also, issues regarding adaptive skills and long term needs for support in daily life need to be identified (American
Psychiatric Association, 2013). In the Netherlands, this shift from the focus on IQ level only to a broader view on
ID was also made to determine support needs and corresponding financial resources for professional support.
This made it possible for persons with borderline cognitive functioning (IQ score 70-85) to get access to ID health
care when necessary (Moonen & Verstegen, 2006). In line with this focus on support needs, a tailored lifestyle
behaviour training was developed (Chapter 6). Since the current situation of lifestyle behaviour support in adults
with mild ID was determined first, the training met training needs of professional caregivers. Thereby, a
theoretical foundation was used since suitable BCTs specifically for adults with mild ID were defined and
compared to BCTs already used by professional caregivers in daily support of adults with mild ID. In future
157
research, a similar approach could be considered to meet lifestyle support for adults with (mild) ID specifically,
since these group could benefit from a tailored lifestyle behaviour approach.
3 | METHODOLOGICAL CONSIDERATIONS/ISSUES
Participating health care professionals included in this thesis were invited by staff management of Dutch ID care
organizations. These organizations participated in a Dutch lifestyle research consortium, aiming to improve and
maintain healthy lifestyle behaviour of their caretakers. As participants were not randomly selected, this
increased the risk of selection bias towards participating health care professionals who were already interested
in lifestyle and lifestyle behaviour change. This might have influenced the results since others who were less
interested in lifestyle might consider a smaller number of BCTs as suitable, may have used less BCTs in changing
lifestyle or might be less positive about the training in ‘action planning’. On the other hand, participants who are
not very interested in lifestyle behaviour could possibly benefit more from training in changing lifestyle behaviour
and that could have increased the effectiveness of the training. For future research, it might be useful to think
about ways to reach professional caregivers who are less motivated to be involved in lifestyle behaviour change.
For example, using the diffusion of innovation theory (Rogers, 1983), professional caregivers who are interested
in lifestyle behaviour change could act as ambassadors and promote the training and use of BCTs to change
lifestyle behaviour. Since a lack of opportunity was mostly mentioned as impeding for lifestyle change support
(Chapter 6), it may help when organisations support less motivated professional caregivers by providing time
and resources as well as encouraging policy and agreements within teams of professionals about lifestyle support
of adults with mild ID.
The methodological quality of lifestyle behaviour change studies so far was usually not high. One of the aims of
this thesis was to contribute to a more thorough way of research by using small steps to gather knew insights
and using these insights to train professionals. However, some methodological considerations remained, such as
small sample sizes and some practical considerations, e.g. the exclusion of adults with mild ID receiving only
ambulatory support. Therefore, future research about lifestyle behaviour change could be optimized using a
thorough design, including a theoretical foundation and outcome measures appropriate for adults with mild ID,
larger sample sizes and small steps towards knew insights.
The used CALO-RE taxonomy was designed for interventions aiming to improve physical activity and nutrition.
This thesis is one of the first using the CALO-RE taxonomy for adults with mild ID, as the taxonomy was designed
for the general population. On the one hand, this taxonomy provided a theoretical framework to this thesis. On
the other hand, it was necessary to adapt some of the definitions of BCTs to make the taxonomy suitable for use
in clinical practice of lifestyle support in adults with mild ID. Despite our best efforts, adapting the taxonomy may
have led to small changes in the interpretation of the BCTs, which makes comparisons slightly more difficult. For
example: BCTs were often formulated as prompting someone to do something (independent), but in clinical
practice professional caregivers often help adults with mild ID to start with a behaviour or even perform the
behaviour together. Recently, a new version of the taxonomy was designed entitled the ‘BCT Taxonomy v1’
(Michie et al., 2013). Since the BCT Taxonomy v1 consisted of many BCTs (93 BCTs), the version with fewer items
138541-Willems_BNW.indd 156 31-10-19 10:08

156
interaction between adults with mild ID and their caregivers may have a great impact on the suitability and
effectiveness of BCTs. Keeping personal characteristics as well as interpersonal relationship in mind is necessary
for future interventions and research. However, it should not be a reason to stop striving to healthy lifestyle
behaviour for this vulnerable group, since improvement of a healthy lifestyle is necessary and seems to be
possible.
Professional caregivers are important for adults with mild ID (Ptomey et al., 2018; Spanos et al., 2013) and were
therefore included as the main focus of this thesis. However, professional caregivers are not the only important
social contacts of adults with mild ID. Family and friends play an important role as well (Miller, Cooper, Cook, &
Petch, 2008). In addition to the social environment, also the physical environment and policies (e.g. policies of
ID care organizations) should be taken in account in future lifestyle change interventions (Steenbergen et al.,
2019). So, all levels that influence health behaviour (including the intrapersonal and interpersonal level as well
as organizational and community factors and public policy) need to be targeted to change lifestyle behaviour, as
emphasized in the ecological model of active living (McLeroy, Bibeau, Steckler, & Glanz, 1988). Acting
unambiguously from a shared vision by all levels, as well as creating opportunities to use suitable BCTs, could be
key factors for successful and sustainable lifestyle behaviour change.
Training professional caregivers in behaviour change is important to improve future lifestyle support for adults
with mild ID. The training in ‘action planning’ is an example of how individual BCTs can be taught to professional
caregivers and how they can be evaluated. This is important, because training in a single BCT allows for
investigation of its individual effectiveness. On the other hand, it is hard to use BCTs independently, since most
BCTs are in some way related to other BCTs. For example: the BCT ‘action planning’ is related to the BCT goal
setting (behaviour)’ as well as ‘goal setting (outcome)’, since you cannot plan any action if you do not know which
action you want to plan. ‘Action planning’ will probably be used together with BCTs like ‘Barrier
identification/Problem solving’, ‘Set graded tasks’ and ‘Provide information on where and when to perform the
behaviour’. Training of single BCTs is necessary for the professional caregivers to understand how to use the BCT
in clinical practice and to investigate suitability and effects of the BCT. At the same time, it is important not to
lose sight on connections between other important BCTs.
Adults with mild ID included in the studies of this thesis were diagnosed as having a mild intellectual disability.
In definitions of mild ID currently used, IQ levels on itself are not enough to diagnose someone having a mild ID.
Also, issues regarding adaptive skills and long term needs for support in daily life need to be identified (American
Psychiatric Association, 2013). In the Netherlands, this shift from the focus on IQ level only to a broader view on
ID was also made to determine support needs and corresponding financial resources for professional support.
This made it possible for persons with borderline cognitive functioning (IQ score 70-85) to get access to ID health
care when necessary (Moonen & Verstegen, 2006). In line with this focus on support needs, a tailored lifestyle
behaviour training was developed (Chapter 6). Since the current situation of lifestyle behaviour support in adults
with mild ID was determined first, the training met training needs of professional caregivers. Thereby, a
theoretical foundation was used since suitable BCTs specifically for adults with mild ID were defined and
compared to BCTs already used by professional caregivers in daily support of adults with mild ID. In future
157
research, a similar approach could be considered to meet lifestyle support for adults with (mild) ID specifically,
since these group could benefit from a tailored lifestyle behaviour approach.
3 | METHODOLOGICAL CONSIDERATIONS/ISSUES
Participating health care professionals included in this thesis were invited by staff management of Dutch ID care
organizations. These organizations participated in a Dutch lifestyle research consortium, aiming to improve and
maintain healthy lifestyle behaviour of their caretakers. As participants were not randomly selected, this
increased the risk of selection bias towards participating health care professionals who were already interested
in lifestyle and lifestyle behaviour change. This might have influenced the results since others who were less
interested in lifestyle might consider a smaller number of BCTs as suitable, may have used less BCTs in changing
lifestyle or might be less positive about the training in ‘action planning’. On the other hand, participants who are
not very interested in lifestyle behaviour could possibly benefit more from training in changing lifestyle behaviour
and that could have increased the effectiveness of the training. For future research, it might be useful to think
about ways to reach professional caregivers who are less motivated to be involved in lifestyle behaviour change.
For example, using the diffusion of innovation theory (Rogers, 1983), professional caregivers who are interested
in lifestyle behaviour change could act as ambassadors and promote the training and use of BCTs to change
lifestyle behaviour. Since a lack of opportunity was mostly mentioned as impeding for lifestyle change support
(Chapter 6), it may help when organisations support less motivated professional caregivers by providing time
and resources as well as encouraging policy and agreements within teams of professionals about lifestyle support
of adults with mild ID.
The methodological quality of lifestyle behaviour change studies so far was usually not high. One of the aims of
this thesis was to contribute to a more thorough way of research by using small steps to gather knew insights
and using these insights to train professionals. However, some methodological considerations remained, such as
small sample sizes and some practical considerations, e.g. the exclusion of adults with mild ID receiving only
ambulatory support. Therefore, future research about lifestyle behaviour change could be optimized using a
thorough design, including a theoretical foundation and outcome measures appropriate for adults with mild ID,
larger sample sizes and small steps towards knew insights.
The used CALO-RE taxonomy was designed for interventions aiming to improve physical activity and nutrition.
This thesis is one of the first using the CALO-RE taxonomy for adults with mild ID, as the taxonomy was designed
for the general population. On the one hand, this taxonomy provided a theoretical framework to this thesis. On
the other hand, it was necessary to adapt some of the definitions of BCTs to make the taxonomy suitable for use
in clinical practice of lifestyle support in adults with mild ID. Despite our best efforts, adapting the taxonomy may
have led to small changes in the interpretation of the BCTs, which makes comparisons slightly more difficult. For
example: BCTs were often formulated as prompting someone to do something (independent), but in clinical
practice professional caregivers often help adults with mild ID to start with a behaviour or even perform the
behaviour together. Recently, a new version of the taxonomy was designed entitled the ‘BCT Taxonomy v1’
(Michie et al., 2013). Since the BCT Taxonomy v1 consisted of many BCTs (93 BCTs), the version with fewer items
138541-Willems_BNW.indd 157 31-10-19 10:08

158
was used in order to explore if this taxonomy would also be suitable for adults with ID. Moreover, for practical
reasons, a smaller number of BCT’s would be more feasible for use in a Delphi panel. It might have been better
to use the newer taxonomy whereas this version would have implemented the newest knowledge and insights.
Since the BCT Taxonomy v1 consists of more BCTs, it might be more complete than the CALO-RE taxonomy. As
both taxonomies were not designed for the ID population, the taxonomy still had to be adapted. Using the CALO-
RE taxonomy gave us the opportunity to suggest some changes and new techniques specifically for adults with
mild ID, without making the list of BCTs more extensive.
4 | IMPLICATIONS FOR CLINICAL PRACTICE, POLICY AND RESEARCH
“Theory without practice is empty; practice without theory is blind” (Immanuel Kant) – Researchers should never
lose the higher goal of supporting practice with their research, whereas health care professionals need the
knowledge gathered by science. Therefore, it is important that health care professionals and researchers co-
operate with the common goal to improve lifestyle behaviour of adults with mild ID. Thereby, clinical practice is
recommended to use the most suitable BCTs founded in the Delphi study (Chapter 4), as well as the training in
‘action planning’ (Chapter 6).
“We do not learn from experience. We learn from reflecting on experience” (John Dewey) – Since much is still
unknown about the use of BCTs to change lifestyle behaviour in adults with mild ID, clinical practice cannot rely
on merely scientific theory. However, instead of becoming passive about healthy lifestyle behaviour, clinical
practice could better use BCTs in an evidence-informed way: using BCTs consciously to change lifestyle behaviour
and reflect on this use until new insights are found, for example by using BCTs which are effective for the general
population.
“If you have knowledge, let others light their candles in it” (Margaret Fuller) – Clinical practice cannot use
knowledge found in research when knowledge is not shared. This implicates that researchers should share their
knowledge not only by scientific articles and presentations, but also through information channels used by
clinical practice. In turn, participation of health care professionals is essential to gather the knowledge necessary
for clinical practice. Also, health care professionals should find ways to share their knowledge with each other,
for example using workshops, conferences, presentations and (online) sharing communities. The Dutch ID care
consort (“Innovatiewerkplaats Active Ageing van mensen met een verstandelijke beperking”) is an example of
sharing information with each other without direct self-interest.
“Never change a winning team” (Alf Ramsey) – Whenever effective strategies are found to changing lifestyle
behaviour of adults with ID, keep using this strategy. This does not imply that reflection and evaluation are not
necessary any more, but constantly switching between strategies does not improve clinical practice nor does it
contributes to knowledge enhancement.
“Disability is the inability to see ability” (Vikas Khanna) – In this thesis, a lifestyle behaviour change approach that
is adapted and therefore suitable for adults with mild ID, given their limitations in social adaptive functioning and
continuing need for support in daily life. It is important to start from and adapt to someone’s abilities and
159
opportunities. A focus on needs is necessary only to help other people in a better way, not to see them as disabled
persons. Keeping this in mind might help to serve the persons for which we performed this thesis, in scientific
research as well as in clinical practice.
“Being a good example is the best form of service” (Sathya Sai Baba) – Using BCTs might help to change lifestyle
behaviour of adults with mild ID, but motivating and stimulating other people to change their behaviour might
work better when the health care professional himself shows healthy lifestyle behaviour. This might be the best
service a health care professional can serve the adult with mild ID.
138541-Willems_BNW.indd 158 31-10-19 10:08

158
was used in order to explore if this taxonomy would also be suitable for adults with ID. Moreover, for practical
reasons, a smaller number of BCT’s would be more feasible for use in a Delphi panel. It might have been better
to use the newer taxonomy whereas this version would have implemented the newest knowledge and insights.
Since the BCT Taxonomy v1 consists of more BCTs, it might be more complete than the CALO-RE taxonomy. As
both taxonomies were not designed for the ID population, the taxonomy still had to be adapted. Using the CALO-
RE taxonomy gave us the opportunity to suggest some changes and new techniques specifically for adults with
mild ID, without making the list of BCTs more extensive.
4 | IMPLICATIONS FOR CLINICAL PRACTICE, POLICY AND RESEARCH
“Theory without practice is empty; practice without theory is blind” (Immanuel Kant) – Researchers should never
lose the higher goal of supporting practice with their research, whereas health care professionals need the
knowledge gathered by science. Therefore, it is important that health care professionals and researchers co-
operate with the common goal to improve lifestyle behaviour of adults with mild ID. Thereby, clinical practice is
recommended to use the most suitable BCTs founded in the Delphi study (Chapter 4), as well as the training in
‘action planning’ (Chapter 6).
“We do not learn from experience. We learn from reflecting on experience” (John Dewey) – Since much is still
unknown about the use of BCTs to change lifestyle behaviour in adults with mild ID, clinical practice cannot rely
on merely scientific theory. However, instead of becoming passive about healthy lifestyle behaviour, clinical
practice could better use BCTs in an evidence-informed way: using BCTs consciously to change lifestyle behaviour
and reflect on this use until new insights are found, for example by using BCTs which are effective for the general
population.
“If you have knowledge, let others light their candles in it” (Margaret Fuller) – Clinical practice cannot use
knowledge found in research when knowledge is not shared. This implicates that researchers should share their
knowledge not only by scientific articles and presentations, but also through information channels used by
clinical practice. In turn, participation of health care professionals is essential to gather the knowledge necessary
for clinical practice. Also, health care professionals should find ways to share their knowledge with each other,
for example using workshops, conferences, presentations and (online) sharing communities. The Dutch ID care
consort (“Innovatiewerkplaats Active Ageing van mensen met een verstandelijke beperking”) is an example of
sharing information with each other without direct self-interest.
“Never change a winning team” (Alf Ramsey) – Whenever effective strategies are found to changing lifestyle
behaviour of adults with ID, keep using this strategy. This does not imply that reflection and evaluation are not
necessary any more, but constantly switching between strategies does not improve clinical practice nor does it
contributes to knowledge enhancement.
“Disability is the inability to see ability” (Vikas Khanna) – In this thesis, a lifestyle behaviour change approach that
is adapted and therefore suitable for adults with mild ID, given their limitations in social adaptive functioning and
continuing need for support in daily life. It is important to start from and adapt to someone’s abilities and
159
opportunities. A focus on needs is necessary only to help other people in a better way, not to see them as disabled
persons. Keeping this in mind might help to serve the persons for which we performed this thesis, in scientific
research as well as in clinical practice.
“Being a good example is the best form of service” (Sathya Sai Baba) – Using BCTs might help to change lifestyle
behaviour of adults with mild ID, but motivating and stimulating other people to change their behaviour might
work better when the health care professional himself shows healthy lifestyle behaviour. This might be the best
service a health care professional can serve the adult with mild ID.
138541-Willems_BNW.indd 159 31-10-19 10:08
160
REFERENCES
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5 (5th
Ed.). Washington, DC: Author.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion
programs. Health education quarterly, 15(4), 351-377.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., . . . Wood, C. E. (2013). The
behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an
international consensus for the reporting of behaviour change interventions. Annals of Behavioral
Medicine, 46(1), 81–95.
Miller, E., Cooper, S. A., Cook, A., & Petch, A. (2008). Outcomes important to people with intellectual
disabilities. Journal of Policy and Practice in Intellectual Disabilities, 5(3), 150-158.
Moonen, X., & Verstegen, D. (2006). LVG-jeugd met ernstige gedragsproblematiek in de verbinding van praktijk
en wetgeving [Youth with mild intellectual disability and severe problem behavior in the connection of
practice and law]. Onderzoek en Praktijk, 4(1), 23–28.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., . . . & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
Rogers, E. M. (1983). Diffusion of innovations. New York: Free Press.
Schalock, R., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., . . . Parmenter, T. (2002).
Conceptualization, Measurement, and Application of Quality of Life for Persons with Intellectual
Disabilities: Report of an International Panel of Experts. Mental Retardation, 40(6), 457-470.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., . . . Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
Steenbergen, H. A., Hilgenkamp, T. I. M., De Jong, J., Bossink, L. W. M., Van der Schans, C. P., Krijnen, W. P., &
Waninge, A. (2019). Evaluating direct support persons’ attitude towards promoting physical activity of
persons with intellectual disabilities: developing a questionnaire. Article in preparation
World Health Organization (WHO) (2001). International classification of functioning, disability and health:
ICF. Geneva, Switzerland: World Health Organisation.
138541-Willems_BNW.indd 160 31-10-19 10:08

160
REFERENCES
American Psychiatric Association (2013). The diagnostic and statistical manual of mental disorders: DSM-5 (5th
Ed.). Washington, DC: Author.
McLeroy, K. R., Bibeau, D., Steckler, A., & Glanz, K. (1988). An ecological perspective on health promotion
programs. Health education quarterly, 15(4), 351-377.
Michie, S., Ashford, S., Sniehotta, F.F., Dombrowski, S.U., Bishop, A., & French, D.P. (2011). A refined taxonomy
of behaviour change techniques to help people change their physical activity and healthy eating
behaviours: The CALO-RE taxonomy. Psychology & Health, 26(11), 1479-1498.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., . . . Wood, C. E. (2013). The
behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an
international consensus for the reporting of behaviour change interventions. Annals of Behavioral
Medicine, 46(1), 81–95.
Miller, E., Cooper, S. A., Cook, A., & Petch, A. (2008). Outcomes important to people with intellectual
disabilities. Journal of Policy and Practice in Intellectual Disabilities, 5(3), 150-158.
Moonen, X., & Verstegen, D. (2006). LVG-jeugd met ernstige gedragsproblematiek in de verbinding van praktijk
en wetgeving [Youth with mild intellectual disability and severe problem behavior in the connection of
practice and law]. Onderzoek en Praktijk, 4(1), 23–28.
Ptomey, L. T., Saunders, R. R., Saunders, M., Washburn, R. A., Mayo, M. S., Sullivan, D. K., . . . & Donnelly, J. E.
(2018). Weight management in adults with intellectual and developmental disabilities: A randomized
controlled trial of two dietary approaches. Journal of Applied Research in Intellectual Disabilities,
31(Suppl. 1), 82-96.
Rogers, E. M. (1983). Diffusion of innovations. New York: Free Press.
Schalock, R., Brown, I., Brown, R., Cummins, R. A., Felce, D., Matikka, L., . . . Parmenter, T. (2002).
Conceptualization, Measurement, and Application of Quality of Life for Persons with Intellectual
Disabilities: Report of an International Panel of Experts. Mental Retardation, 40(6), 457-470.
Spanos, D., Hankey, C. R., Boyle, S., Koshy, P., Macmillan, S., Matthews, L., . . . Melville, C. A. (2013). Carers’
perspectives of a weight loss intervention for adults with intellectual disabilities and obesity: A
qualitative study. Journal of Intellectual Disability Research, 57(1), 90–102.
Steenbergen, H. A., Hilgenkamp, T. I. M., De Jong, J., Bossink, L. W. M., Van der Schans, C. P., Krijnen, W. P., &
Waninge, A. (2019). Evaluating direct support persons’ attitude towards promoting physical activity of
persons with intellectual disabilities: developing a questionnaire. Article in preparation
World Health Organization (WHO) (2001). International classification of functioning, disability and health:
ICF. Geneva, Switzerland: World Health Organisation.
138541-Willems_BNW.indd 161 31-10-19 10:08
162
Nederlandse samenvatting
1 | Inleiding
Mensen met een lichte verstandelijke beperking (LVB) hebben moeite met abstract denken en ingewikkelde
denkprocessen. Ze hebben niet alleen ondersteuning nodig om hun dagelijks leven vorm te geven, maar ook bij
het leggen en onderhouden van sociale contacten en bij het omgaan met hun emoties.
Ook wat betreft gezond leven hebben mensen met een verstandelijke beperking ondersteuning nodig. Ze
ervaren meer gezondheidsproblemen dan mensen uit de algemene bevolking. Van de mensen in Nederland
behaalt slechts 44% de beweegrichtlijnen en heeft 47.7% van de volwassenen overgewicht of obesitas. In
vergelijking met de algemene populatie hebben mensen met een verstandelijke beperking een ongezondere
leefstijl: ze bewegen te weinig, zitten veel en hebben ongezonde eetgewoontes. Het is van belang om de leefstijl
van mensen met een verstandelijke beperking te verbeteren. Dit is van belang omdat een gezonde leefstijl de
kwaliteit van leven verbetert en zorgt dat er betere voorwaarden zijn om mee te doen in de samenleving. Ook
verbetert een gezonde leefstijl de zelfstandigheid in wonen en leven. De dagelijks begeleiders zijn belangrijk bij
de ondersteuning van leefstijlgedrag en gezond leven van mensen met een verstandelijke beperking. Maar het
is nog onduidelijk in hoeverre en op welke manieren de begeleider hun leefstijlgedrag beïnvloedt en of dit ook
verbeterd kan worden. Daarnaast lijken begeleiders behoefte te hebben aan training in het bevorderen van
leefstijlverandering.
Deze vragen rondom het verbeteren van leefstijlgedrag bij mensen met een verstandelijke beperking, vormden
de aanleiding voor negen zorgorganisaties (De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo Zorggroep, Talant,
Cosis, Koninklijke Visio Noord Nederland, Philadelphia en Vanboeijen) om een consortium te vormen om kennis
en praktische handvatten te ontwikkelen, met als doel leefstijlbevordering te stimuleren bij mensen met een
verstandelijke beperking. Naast kennisuitwisseling wordt binnen dit consortium onderzoek uitgevoerd naar het
gebruik en de effectiviteit van leefstijlinterventies en geschikte technieken om leefstijlgedrag te veranderen door
begeleiders van mensen met een verstandelijke beperking.
2 | Leefstijlinterventies voor mensen met een verstandelijke beperking
In hoofdstuk 2 wordt een overzicht gegeven van leefstijlinterventies voor mensen met een verstandelijke
beperking, die in de literatuur zijn beschreven. Daarnaast is de effectiviteit van deze interventies onderzocht. Er
is voor gekozen om alleen artikelen te onderzoeken met een zo sterk mogelijk onderzoeksontwerp: een
Randomized Controlled Trial (RCT) ontwerp. De acht geselecteerde interventies zijn gericht op voeding en/of
fysieke activiteit. Er is gekeken naar algemene kenmerken (zoals de leeftijd van de deelnemers, mate van
verstandelijke beperking) en kenmerken van de interventie (bijv. inhoud, tijdsduur, doel, setting), evenals de
uitkomstmaten en de effecten (resultaten) van de interventie. Het ICF-model (International Classification of
Functioning, Disability and Health) is gebruikt om de uitkomstmaten in te delen naar onderliggend construct,
bijvoorbeeld lichaamssamenstelling of fysieke activiteit (bewegen). De effectiviteit van de leefstijlinterventies is
163
onderzocht door de bevindingen van de acht artikelen te combineren: een meta-analyse op uitkomstmaten, bv.
gewicht, en op onderliggend construct-niveau, bv. lichaamssamenstelling.
De leefstijlinterventies waren voornamelijk bedoeld voor mensen met een lichte tot matige verstandelijke
beperking. Ze richtten zich op fysieke activiteit (bewegen) of op een combinatie van fysieke activiteit en voeding.
Alle interventies werden in direct contact met de deelnemers uitgevoerd, meestal in groepsverband. In alle
studies was wel sprake van onderdelen die kwalitatief gezien niet optimaal waren. Zo was er in de helft van de
onderzoeken sprake van een klein aantal deelnemers aan de interventie. De onderzoeken maakten gebruik van
veel verschillende uitkomstmaten. Daardoor was het ingewikkeld om de effectiviteit van de interventies te
vergelijken. Voor drie uitkomstmaten was dit wel mogelijk, namelijk tailleomtrek, BMI (de verhouding tussen
lengte en gewicht) en gewichtsverandering. Leefstijlinterventies hadden alleen een positief effect op
tailleomtrek. Het was ook mogelijk om de uitkomstmaten op een hoger niveau te bekijken, namelijk op
constructniveau. De onderzochte constructen waren fysieke activiteit, lichaamssamenstelling en fysieke
capaciteit (conditie). Er werden geen aantoonbare effecten gevonden voor deze drie constructen. Er wordt
geconcludeerd dat leefstijlinterventies alleen effect hadden op de tailleomtrek van mensen met een
verstandelijke beperking. Dit betekent dat leefstijlinterventies op dit moment nog niet effectief genoeg zijn om
de leefstijl van mensen met een verstandelijke beperking te verbeteren. De interventies zouden kunnen worden
verbeterd door ze beter theoretisch te onderbouwen en ook door de bewuste inzet van manieren om gedrag te
veranderen bij mensen met verstandelijke beperking.
In hoofdstuk 3 wordt beschreven welke gedragsveranderingstechnieken worden gebruikt in leefstijlinterventies
voor mensen met een verstandelijke beperking, die in de literatuur zijn beschreven. Er is gekeken naar algemene
kenmerken van de mensen waar de interventies zich op richten, zoals de leeftijd van de deelnemers, mate van
verstandelijke beperking en kenmerken van de interventie (bijv. inhoud, tijdsduur, doel, setting). Daarnaast is
onderzocht welke manieren zijn gebruikt om leefstijlgedrag van mensen met een verstandelijke beperking te
veranderen, de gedragsveranderingstechnieken. Om dit te onderzoeken is gebruik gemaakt van de CALO-RE
taxonomie, een lijst van gedragsveranderingstechnieken. De 41 leefstijlinterventies die op basis van de criteria
werden geselecteerd waren gericht op fysieke activiteit, voeding of op beide. Er waren interventies voor alle
maten van verstandelijke beperking, zowel licht-matig als (zeer) ernstig. De interventies werden op veel
verschillende plekken uitgevoerd, bijvoorbeeld op school, op dagbesteding of op de woonlocatie. En ook de duur
en intensiteit van de interventies varieerde, van 1 week tot 24 maanden en qua intensiteit van iedere dag tot
maandelijks. De kwaliteit van de meeste onderzoeken was niet zo sterk en er werd weinig gebruikt gemaakt van
een theoretisch kader.
Gedragsveranderingstechnieken werden in alle interventies gebruikt. Technieken die veel werden gebruikt
waren: ‘geven van informatie over de consequenties van gedrag in het algemeen’ en ‘sociale ondersteuning’.
Echter, de gedragsveranderingstechnieken werden meestal niet specifiek als techniek genoemd in de tekst, maar
werden door de onderzoekers geïdentificeerd in de artikelen. Dat kan betekenen dat de
gedragsveranderingstechnieken niet bewust werden ingezet. Er blijkt dus nog verbetering nodig van
leefstijlinterventies, evenals verder onderzoek naar leefstijlverbetering en het gebruik van
gedragsveranderingstechnieken bij mensen met een verstandelijke beperking. De kwaliteit van veel onderzoeken
138541-Willems_BNW.indd 162 31-10-19 10:08
162
Nederlandse samenvatting
1 | Inleiding
Mensen met een lichte verstandelijke beperking (LVB) hebben moeite met abstract denken en ingewikkelde
denkprocessen. Ze hebben niet alleen ondersteuning nodig om hun dagelijks leven vorm te geven, maar ook bij
het leggen en onderhouden van sociale contacten en bij het omgaan met hun emoties.
Ook wat betreft gezond leven hebben mensen met een verstandelijke beperking ondersteuning nodig. Ze
ervaren meer gezondheidsproblemen dan mensen uit de algemene bevolking. Van de mensen in Nederland
behaalt slechts 44% de beweegrichtlijnen en heeft 47.7% van de volwassenen overgewicht of obesitas. In
vergelijking met de algemene populatie hebben mensen met een verstandelijke beperking een ongezondere
leefstijl: ze bewegen te weinig, zitten veel en hebben ongezonde eetgewoontes. Het is van belang om de leefstijl
van mensen met een verstandelijke beperking te verbeteren. Dit is van belang omdat een gezonde leefstijl de
kwaliteit van leven verbetert en zorgt dat er betere voorwaarden zijn om mee te doen in de samenleving. Ook
verbetert een gezonde leefstijl de zelfstandigheid in wonen en leven. De dagelijks begeleiders zijn belangrijk bij
de ondersteuning van leefstijlgedrag en gezond leven van mensen met een verstandelijke beperking. Maar het
is nog onduidelijk in hoeverre en op welke manieren de begeleider hun leefstijlgedrag beïnvloedt en of dit ook
verbeterd kan worden. Daarnaast lijken begeleiders behoefte te hebben aan training in het bevorderen van
leefstijlverandering.
Deze vragen rondom het verbeteren van leefstijlgedrag bij mensen met een verstandelijke beperking, vormden
de aanleiding voor negen zorgorganisaties (De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo Zorggroep, Talant,
Cosis, Koninklijke Visio Noord Nederland, Philadelphia en Vanboeijen) om een consortium te vormen om kennis
en praktische handvatten te ontwikkelen, met als doel leefstijlbevordering te stimuleren bij mensen met een
verstandelijke beperking. Naast kennisuitwisseling wordt binnen dit consortium onderzoek uitgevoerd naar het
gebruik en de effectiviteit van leefstijlinterventies en geschikte technieken om leefstijlgedrag te veranderen door
begeleiders van mensen met een verstandelijke beperking.
2 | Leefstijlinterventies voor mensen met een verstandelijke beperking
In hoofdstuk 2 wordt een overzicht gegeven van leefstijlinterventies voor mensen met een verstandelijke
beperking, die in de literatuur zijn beschreven. Daarnaast is de effectiviteit van deze interventies onderzocht. Er
is voor gekozen om alleen artikelen te onderzoeken met een zo sterk mogelijk onderzoeksontwerp: een
Randomized Controlled Trial (RCT) ontwerp. De acht geselecteerde interventies zijn gericht op voeding en/of
fysieke activiteit. Er is gekeken naar algemene kenmerken (zoals de leeftijd van de deelnemers, mate van
verstandelijke beperking) en kenmerken van de interventie (bijv. inhoud, tijdsduur, doel, setting), evenals de
uitkomstmaten en de effecten (resultaten) van de interventie. Het ICF-model (International Classification of
Functioning, Disability and Health) is gebruikt om de uitkomstmaten in te delen naar onderliggend construct,
bijvoorbeeld lichaamssamenstelling of fysieke activiteit (bewegen). De effectiviteit van de leefstijlinterventies is
163
onderzocht door de bevindingen van de acht artikelen te combineren: een meta-analyse op uitkomstmaten, bv.
gewicht, en op onderliggend construct-niveau, bv. lichaamssamenstelling.
De leefstijlinterventies waren voornamelijk bedoeld voor mensen met een lichte tot matige verstandelijke
beperking. Ze richtten zich op fysieke activiteit (bewegen) of op een combinatie van fysieke activiteit en voeding.
Alle interventies werden in direct contact met de deelnemers uitgevoerd, meestal in groepsverband. In alle
studies was wel sprake van onderdelen die kwalitatief gezien niet optimaal waren. Zo was er in de helft van de
onderzoeken sprake van een klein aantal deelnemers aan de interventie. De onderzoeken maakten gebruik van
veel verschillende uitkomstmaten. Daardoor was het ingewikkeld om de effectiviteit van de interventies te
vergelijken. Voor drie uitkomstmaten was dit wel mogelijk, namelijk tailleomtrek, BMI (de verhouding tussen
lengte en gewicht) en gewichtsverandering. Leefstijlinterventies hadden alleen een positief effect op
tailleomtrek. Het was ook mogelijk om de uitkomstmaten op een hoger niveau te bekijken, namelijk op
constructniveau. De onderzochte constructen waren fysieke activiteit, lichaamssamenstelling en fysieke
capaciteit (conditie). Er werden geen aantoonbare effecten gevonden voor deze drie constructen. Er wordt
geconcludeerd dat leefstijlinterventies alleen effect hadden op de tailleomtrek van mensen met een
verstandelijke beperking. Dit betekent dat leefstijlinterventies op dit moment nog niet effectief genoeg zijn om
de leefstijl van mensen met een verstandelijke beperking te verbeteren. De interventies zouden kunnen worden
verbeterd door ze beter theoretisch te onderbouwen en ook door de bewuste inzet van manieren om gedrag te
veranderen bij mensen met verstandelijke beperking.
In hoofdstuk 3 wordt beschreven welke gedragsveranderingstechnieken worden gebruikt in leefstijlinterventies
voor mensen met een verstandelijke beperking, die in de literatuur zijn beschreven. Er is gekeken naar algemene
kenmerken van de mensen waar de interventies zich op richten, zoals de leeftijd van de deelnemers, mate van
verstandelijke beperking en kenmerken van de interventie (bijv. inhoud, tijdsduur, doel, setting). Daarnaast is
onderzocht welke manieren zijn gebruikt om leefstijlgedrag van mensen met een verstandelijke beperking te
veranderen, de gedragsveranderingstechnieken. Om dit te onderzoeken is gebruik gemaakt van de CALO-RE
taxonomie, een lijst van gedragsveranderingstechnieken. De 41 leefstijlinterventies die op basis van de criteria
werden geselecteerd waren gericht op fysieke activiteit, voeding of op beide. Er waren interventies voor alle
maten van verstandelijke beperking, zowel licht-matig als (zeer) ernstig. De interventies werden op veel
verschillende plekken uitgevoerd, bijvoorbeeld op school, op dagbesteding of op de woonlocatie. En ook de duur
en intensiteit van de interventies varieerde, van 1 week tot 24 maanden en qua intensiteit van iedere dag tot
maandelijks. De kwaliteit van de meeste onderzoeken was niet zo sterk en er werd weinig gebruikt gemaakt van
een theoretisch kader.
Gedragsveranderingstechnieken werden in alle interventies gebruikt. Technieken die veel werden gebruikt
waren: ‘geven van informatie over de consequenties van gedrag in het algemeen’ en ‘sociale ondersteuning’.
Echter, de gedragsveranderingstechnieken werden meestal niet specifiek als techniek genoemd in de tekst, maar
werden door de onderzoekers geïdentificeerd in de artikelen. Dat kan betekenen dat de
gedragsveranderingstechnieken niet bewust werden ingezet. Er blijkt dus nog verbetering nodig van
leefstijlinterventies, evenals verder onderzoek naar leefstijlverbetering en het gebruik van
gedragsveranderingstechnieken bij mensen met een verstandelijke beperking. De kwaliteit van veel onderzoeken
138541-Willems_BNW.indd 163 31-10-19 10:08

164
kan nog verbeteren door gebruik te maken van een theoretisch kader en informatie duidelijker te beschrijven in
de artikelen.
3 | Gedragsveranderingstechnieken voor mensen met een lichte verstandelijke
beperking
De geschiktheid van gedragsveranderingstechnieken voor leefstijlgedrag van mensen met een lichte
verstandelijke beperking volgens professionals, wordt beschreven in hoofdstuk 4. Er is een Delphi onderzoek
uitgevoerd. Hierbij is in twee rondes aan professionals in de verstandelijk gehandicaptenzorg gevraagd welke
gedragsveranderingstechnieken zij geschikt vinden om leefstijlgedrag bij mensen met een lichte verstandelijke
beperking te veranderen. Deelnemers waren onderverdeeld in vier groepen, namelijk begeleiders,
gedragswetenschappers, paramedici en artsen verstandelijk gehandicapten (AVG). Er werd weer gebruik
gemaakt van de lijst met gedragsveranderingstechnieken die ook in hoofdstuk 3 is gebruikt, de CALO-RE
taxonomie. In de eerste Delphi ronde werden alle technieken van de CALO-RE taxonomie aan de professionals
voorgelegd in een online vragenlijst. Ze konden aangeven of ze iedere techniek geschikt of ongeschikt vonden.
Vervolgens werd de mate van overeenstemming bepaald voor iedere techniek, bij iedere groep van
professionals. In Delphi ronde 2 werden de technieken waarvoor geen consensus was gevonden opnieuw
voorgelegd aan de deelnemers via de online vragenlijst.
Na de twee Delphirondes waren de deelnemers het met elkaar eens over 25 gedragsveranderingstechnieken. Ze
vonden 24 technieken geschikt en 1 techniek ongeschikt, namelijk: ‘je stimuleert de cliënt om na te denken over
hoe hij zich zou voelen als hij het beoogde leefstijlgedrag niet zou doen. En of hij daar spijt van zou krijgen’. De
technieken waarover de meeste consensus was, waren:
- Je denkt met de cliënt na over mogelijke problemen en oplossingen voor leefstijlgedrag;
- Je moedigt de cliënt aan om deeltaken (voor leefstijlgedrag) te bedenken;
- Je beloont de cliënt voor vooruitgang richting het doel;
- Een coach helpt de cliënt met behulp van motiverende gespreksvoering. Hierbij gaat het om een
specifieke methode. De coach gaat met de cliënt in gesprek over het leefstijlgedrag van de cliënt en
helpt hem om na te denken over wat hij wil of belangrijk vindt;
- Je moedigt de cliënt aan om leefstijlgedrag te plannen.
Er wordt geconcludeerd dat de geschikte technieken kunnen worden gebruikt in de ondersteuning van mensen
met een lichte verstandelijke beperking voor het veranderen van hun leefstijlgedrag.
In hoofdstuk 5 worden praktijk observaties beschreven bij begeleiders van mensen met een lichte verstandelijke
beperking om te bepalen of gedragsveranderingstechnieken door hen worden gebruikt als ze hun cliënt
ondersteunen bij gezond leven. Stagiaires filmden begeleiders met videocamera’s tijdens hun werk, samen met
de cliënten die hiervoor toestemming gaven. Begeleiders van verschillende zorgorganisaties in Nederland
hebben meegedaan. Ze werden drie keer gefilmd, op drie verschillende dagen. De videobeelden zijn
geanalyseerd en daarbij is gelet op het gebruik van gedragsveranderingstechnieken. Er werd ook hier weer
165
gebruik gemaakt van de lijst van gedragsveranderingstechnieken, de CALO-RE taxonomie.
Er hebben 14 begeleiders meegedaan aan het onderzoek. Niet alle begeleiders zijn 3 keer gefilmd. Uit de
observaties bleek dat 21 verschillende gedragsveranderingstechnieken werden gebruikt. De meest gebruikte
technieken waren:
- Je vertelt de cliënt wat anderen van het leefstijlgedrag vinden (bijvoorbeeld: wat de begeleider van het
leefstijlgedrag vindt);
- Je helpt de cliënt om zichzelf als rolmodel te zien (bijvoorbeeld doordat de begeleider aan de cliënt
vraagt hoe iets moet: hij/zij is de ‘expert’);
- Je beloont de cliënt voor de uitvoering van het leefstijlgedrag (bijvoorbeeld doordat de begeleider
complimenten geeft);
- Je moedigt de cliënt aan om doelen (over leefstijlgedrag) te evalueren (bijvoorbeeld doordat de
begeleider de cliënt vraagt of het lukt en hoe het gaat met de uitvoering van het gedrag);
- Je legt de cliënt uit hoe hij het leefstijlgedrag moet uitvoeren.
Er wordt geconcludeerd dat begeleiders gebruik maken van gedragsveranderingstechnieken om leefstijlgedrag
bij mensen met een lichte verstandelijke beperking te veranderen. Dit zijn andere technieken dan de meest
geschikte technieken, die uit het eerdere onderzoek (hoofdstuk 4) naar voren kwamen.
Uit hoofdstuk 4 en 5 is gebleken dat begeleiders mogelijk beter andere technieken in kunnen zetten om het
leefstijlgedrag van hun cliënten te ondersteunen. Hoofdstuk 6 bespreekt de ontwikkeling en pilot-test van een
training in het gebruiken van de gedragsveranderingstechniek ‘het plannen van leefstijlgedrag’. Een team van 11
begeleiders heeft deelgenomen aan deze leefstijltraining. De training bestond uit twee bijeenkomsten en richtte
zich op het plannen van leefstijlgedrag. De training is ontwikkeld in samenwerking met leefstijlonderzoekers, een
onderwijsspecialist en een begeleider. Er werd gebruik gemaakt van een casusbespreking, theorie (met behulp
van video’s en brainstorm), rollenspelen en reflectie, volgens de methode van Probleem Gestuurd Onderwijs
(PGO). De begeleiders vulden vragenlijsten in voorafgaand aan het eerste trainingsmoment, tussen de twee
trainingsmomenten en na afronding van de training. Er werd gekeken of begeleiders zich meer competent
voelden om leefstijlgedrag te plannen en of ze bereid waren om dit (vaker) te doen. Daarnaast werd aan
begeleiders gevraagd welke factoren hen hielpen of belemmerden om leefstijlgedrag te plannen met hun
cliënten. Ook werd de training geëvalueerd. De begeleiders waren tevreden over de inhoud en uitvoering van de
training in zijn geheel en ook over de twee trainingsmomenten op zichzelf. Na afloop van de training vonden de
begeleiders dat ze duidelijk meer vaardigheden hadden om leefstijlgedrag te plannen met hun cliënten. Ook
waren ze meer bereid dan voor de training om leefstijlgedrag te gaan plannen. Er werden verschillende factoren
genoemd die hen hielpen of belemmerden om leefstijlgedrag te plannen. Factoren die te maken hadden met het
hebben van gelegenheid zoals voldoende tijd en middelen werden het meest genoemd.
4 | Conclusie
Dit proefschrift laat zien dat de huidige leefstijlinterventies nog niet (voldoende) effectief zijn om het
leefstijlgedrag van mensen met een VB te verbeteren. De gedragsveranderingstechnieken die in deze
138541-Willems_BNW.indd 164 31-10-19 10:08
164
kan nog verbeteren door gebruik te maken van een theoretisch kader en informatie duidelijker te beschrijven in
de artikelen.
3 | Gedragsveranderingstechnieken voor mensen met een lichte verstandelijke
beperking
De geschiktheid van gedragsveranderingstechnieken voor leefstijlgedrag van mensen met een lichte
verstandelijke beperking volgens professionals, wordt beschreven in hoofdstuk 4. Er is een Delphi onderzoek
uitgevoerd. Hierbij is in twee rondes aan professionals in de verstandelijk gehandicaptenzorg gevraagd welke
gedragsveranderingstechnieken zij geschikt vinden om leefstijlgedrag bij mensen met een lichte verstandelijke
beperking te veranderen. Deelnemers waren onderverdeeld in vier groepen, namelijk begeleiders,
gedragswetenschappers, paramedici en artsen verstandelijk gehandicapten (AVG). Er werd weer gebruik
gemaakt van de lijst met gedragsveranderingstechnieken die ook in hoofdstuk 3 is gebruikt, de CALO-RE
taxonomie. In de eerste Delphi ronde werden alle technieken van de CALO-RE taxonomie aan de professionals
voorgelegd in een online vragenlijst. Ze konden aangeven of ze iedere techniek geschikt of ongeschikt vonden.
Vervolgens werd de mate van overeenstemming bepaald voor iedere techniek, bij iedere groep van
professionals. In Delphi ronde 2 werden de technieken waarvoor geen consensus was gevonden opnieuw
voorgelegd aan de deelnemers via de online vragenlijst.
Na de twee Delphirondes waren de deelnemers het met elkaar eens over 25 gedragsveranderingstechnieken. Ze
vonden 24 technieken geschikt en 1 techniek ongeschikt, namelijk: ‘je stimuleert de cliënt om na te denken over
hoe hij zich zou voelen als hij het beoogde leefstijlgedrag niet zou doen. En of hij daar spijt van zou krijgen’. De
technieken waarover de meeste consensus was, waren:
- Je denkt met de cliënt na over mogelijke problemen en oplossingen voor leefstijlgedrag;
- Je moedigt de cliënt aan om deeltaken (voor leefstijlgedrag) te bedenken;
- Je beloont de cliënt voor vooruitgang richting het doel;
- Een coach helpt de cliënt met behulp van motiverende gespreksvoering. Hierbij gaat het om een
specifieke methode. De coach gaat met de cliënt in gesprek over het leefstijlgedrag van de cliënt en
helpt hem om na te denken over wat hij wil of belangrijk vindt;
- Je moedigt de cliënt aan om leefstijlgedrag te plannen.
Er wordt geconcludeerd dat de geschikte technieken kunnen worden gebruikt in de ondersteuning van mensen
met een lichte verstandelijke beperking voor het veranderen van hun leefstijlgedrag.
In hoofdstuk 5 worden praktijk observaties beschreven bij begeleiders van mensen met een lichte verstandelijke
beperking om te bepalen of gedragsveranderingstechnieken door hen worden gebruikt als ze hun cliënt
ondersteunen bij gezond leven. Stagiaires filmden begeleiders met videocamera’s tijdens hun werk, samen met
de cliënten die hiervoor toestemming gaven. Begeleiders van verschillende zorgorganisaties in Nederland
hebben meegedaan. Ze werden drie keer gefilmd, op drie verschillende dagen. De videobeelden zijn
geanalyseerd en daarbij is gelet op het gebruik van gedragsveranderingstechnieken. Er werd ook hier weer
165
gebruik gemaakt van de lijst van gedragsveranderingstechnieken, de CALO-RE taxonomie.
Er hebben 14 begeleiders meegedaan aan het onderzoek. Niet alle begeleiders zijn 3 keer gefilmd. Uit de
observaties bleek dat 21 verschillende gedragsveranderingstechnieken werden gebruikt. De meest gebruikte
technieken waren:
- Je vertelt de cliënt wat anderen van het leefstijlgedrag vinden (bijvoorbeeld: wat de begeleider van het
leefstijlgedrag vindt);
- Je helpt de cliënt om zichzelf als rolmodel te zien (bijvoorbeeld doordat de begeleider aan de cliënt
vraagt hoe iets moet: hij/zij is de ‘expert’);
- Je beloont de cliënt voor de uitvoering van het leefstijlgedrag (bijvoorbeeld doordat de begeleider
complimenten geeft);
- Je moedigt de cliënt aan om doelen (over leefstijlgedrag) te evalueren (bijvoorbeeld doordat de
begeleider de cliënt vraagt of het lukt en hoe het gaat met de uitvoering van het gedrag);
- Je legt de cliënt uit hoe hij het leefstijlgedrag moet uitvoeren.
Er wordt geconcludeerd dat begeleiders gebruik maken van gedragsveranderingstechnieken om leefstijlgedrag
bij mensen met een lichte verstandelijke beperking te veranderen. Dit zijn andere technieken dan de meest
geschikte technieken, die uit het eerdere onderzoek (hoofdstuk 4) naar voren kwamen.
Uit hoofdstuk 4 en 5 is gebleken dat begeleiders mogelijk beter andere technieken in kunnen zetten om het
leefstijlgedrag van hun cliënten te ondersteunen. Hoofdstuk 6 bespreekt de ontwikkeling en pilot-test van een
training in het gebruiken van de gedragsveranderingstechniek ‘het plannen van leefstijlgedrag’. Een team van 11
begeleiders heeft deelgenomen aan deze leefstijltraining. De training bestond uit twee bijeenkomsten en richtte
zich op het plannen van leefstijlgedrag. De training is ontwikkeld in samenwerking met leefstijlonderzoekers, een
onderwijsspecialist en een begeleider. Er werd gebruik gemaakt van een casusbespreking, theorie (met behulp
van video’s en brainstorm), rollenspelen en reflectie, volgens de methode van Probleem Gestuurd Onderwijs
(PGO). De begeleiders vulden vragenlijsten in voorafgaand aan het eerste trainingsmoment, tussen de twee
trainingsmomenten en na afronding van de training. Er werd gekeken of begeleiders zich meer competent
voelden om leefstijlgedrag te plannen en of ze bereid waren om dit (vaker) te doen. Daarnaast werd aan
begeleiders gevraagd welke factoren hen hielpen of belemmerden om leefstijlgedrag te plannen met hun
cliënten. Ook werd de training geëvalueerd. De begeleiders waren tevreden over de inhoud en uitvoering van de
training in zijn geheel en ook over de twee trainingsmomenten op zichzelf. Na afloop van de training vonden de
begeleiders dat ze duidelijk meer vaardigheden hadden om leefstijlgedrag te plannen met hun cliënten. Ook
waren ze meer bereid dan voor de training om leefstijlgedrag te gaan plannen. Er werden verschillende factoren
genoemd die hen hielpen of belemmerden om leefstijlgedrag te plannen. Factoren die te maken hadden met het
hebben van gelegenheid zoals voldoende tijd en middelen werden het meest genoemd.
4 | Conclusie
Dit proefschrift laat zien dat de huidige leefstijlinterventies nog niet (voldoende) effectief zijn om het
leefstijlgedrag van mensen met een VB te verbeteren. De gedragsveranderingstechnieken die in deze
138541-Willems_BNW.indd 165 31-10-19 10:08

166
interventies worden gebruikt, worden veelal niet bewust ingezet. In de praktijk gebruiken begeleiders
gedragsveranderingstechnieken, maar nog lang niet altijd de meest veelbelovende. Training lijkt echter uitkomst
te bieden om begeleiders te ondersteunen bij het inzetten van gedragsveranderingstechnieken. Verdere
ontwikkeling van effectieve en passende trainingen is nodig om begeleiders bekwaam te maken in het
veranderen van leefstijlgedrag van mensen met een lichte verstandelijke beperking.
138541-Willems_BNW.indd 166 31-10-19 10:08

166
interventies worden gebruikt, worden veelal niet bewust ingezet. In de praktijk gebruiken begeleiders
gedragsveranderingstechnieken, maar nog lang niet altijd de meest veelbelovende. Training lijkt echter uitkomst
te bieden om begeleiders te ondersteunen bij het inzetten van gedragsveranderingstechnieken. Verdere
ontwikkeling van effectieve en passende trainingen is nodig om begeleiders bekwaam te maken in het
veranderen van leefstijlgedrag van mensen met een lichte verstandelijke beperking.
138541-Willems_BNW.indd 167 31-10-19 10:08

168
Dankwoord
Promoveren was niet iets wat ik voor mezelf in gedachten had. En toch is er nu dit proefschrift met mijn naam
erop. Een mooie kans, een interessante uitdaging was voor mij het promotie-traject toen ik hier vier jaar geleden
mee startte. En ik had het beslist niet willen missen! Daarom wil ik graag iedereen bedanken die me heeft
geholpen, gesteund en vertrouwd om dit onderzoek te kunnen uitvoeren.
Een groot aantal zorgorganisaties in Noord-Nederland zag het belang van een gezonde leefstijl voor mensen met
een verstandelijke beperking: De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo Zorggroep, Talant, Cosis,
Koninklijke Visio Noord Nederland, Philadelphia en Vanboeijen. Ik wil jullie bedanken voor de mogelijkheid om
dit promotie-traject uit te voeren, het inhoudelijk meedenken met de onderzoeksvragen en de ondersteuning in
de praktische zin, onder andere door medewerkers van de organisaties die deelnamen aan het onderzoek.
De begeleiders en hun cliënten, gedragswetenschappers, paramedici en artsen verstandelijk gehandicapten
(AVG’s) wil ik heel hartelijk bedanken voor hun deelname aan dit onderzoek. Jullie tijdsinvestering, meedenken
en hun openheid waren onmisbaar om inhoud te geven aan dit proefschrift. Ook de wettelijk vertegenwoordigers
van mensen met een verstandelijke beperking wil ik bedanken voor het gestelde vertrouwen en toestemming
zodat de persoon die zij vertegenwoordigen kon deelnemen aan het onderzoek.
Beste Cees, jij was mijn ‘hoofdbegeleider’ en dat deed je op een fijne manier! Door jouw overstijgende kijk, werd
ik telkens teruggeroepen naar de hoofdlijnen en verloor ik me niet in details. Je praktische manier van denken
was geregeld een verademing, evenals je toegankelijke manier van doen: je stimuleerde juist om gebruik te
maken van de expertise van het begeleidingsteam waar ik dat nodig had. Jouw kennis over wetenschappelijk
onderzoek, gezondheid en het promotie-traject op zichzelf hebben me enorm geholpen om dit traject tot een
succes te maken!
Beste Aly, wat heb ik het getroffen met jou als mijn dagelijks begeleider! Je was altijd betrokken, hielp mee bij
het bepalen van de goede richting en wist altijd positieve woorden aan te vinden die me hielpen om weer verder
te gaan. Je maakte vaak direct tijd vrij om mee te denken wanneer dat nodig was en had een luisterend oor. Je
was bereid om met ieder stuk opnieuw mee te kijken en mede door jouw snelle reageren is het gelukt om dit
proefschrift in vier jaar af te ronden. Dankjewel voor je hulp tijdens mijn zwangerschapsverlof en je presentaties
over mijn onderzoek tijdens congressen. Je enthousiasme voor mensen met een verstandelijke beperking en hun
gezondheid werkten aanstekelijk en inspirerend. Dankjewel voor alles!
Beste Johan, je was tijdens mijn promotie traject wat meer vanaf een afstand betrokken en dat maakte dat je
dingen meer vanuit overstijgend perspectief bekeek. Dit hielp me om de grote lijn vast te houden, heel
waardevol! Ook hielpen jouw opmerkingen om soms vanuit een andere invalshoek naar het onderwerp te kijken
en te bezinnen op de gekozen richting. Jouw enthousiasme voor gezondheid en bewegen en hun theoretische
onderbouwing zorgden geregeld voor duidelijke verbeteringen van dit proefschrift, bedankt!
169
Beste Thessa, jij bent wat later een van mijn officiële co-promotores geworden, maar al in het begin van mijn
promotie-traject maakten we kennis vanwege onze samenwerking bij de systematische review. Ik ben heel blij
met jouw betrokkenheid bij mijn promotietraject! Je nuchtere kijk, heldere schrijfstijl en expertise in onderzoek
bij mensen met een verstandelijke beperking hielpen me om koers en focus te houden, inhoudelijk de diepte te
zoeken en uitgevoerde onderzoeken goed op papier te krijgen. Ook voor je fijne manier van communiceren en
omgaan met elkaar wil ik je bedanken!
Beste Ruud, jij was niet officieel betrokken bij mijn promotie-traject, maar had er beslist een belangrijke rol in!
Dankjewel voor je aanwezigheid bij vele overleggen, je expertise op het gebied van onderzoek en mensen met
een verstandelijke beperking en je feedback op geschreven stukken. Je inbreng heeft het proefschrift naar een
hoger niveau getild!
Naast mijn begeleiders hebben ook anderen meegeschreven en meegeholpen met de artikelen uit dit
proefschrift. Craig Melville, thank you for your guidance and patience with me, especially during our
collaboration for the systematic review. I was just starting as a PhD candidate and you approached me like a full
researcher, taking my reasoning’s seriously and answering to simple questions. Thank you for your work on the
meta-analyses as well! Else Havik, dankjewel voor al jouw werk voor de systematische review: het opzetten van
de methode en het screenen van alle artikelen. Zonder jouw inzet en hulp was de review minder snel afgerond
en minder goed geweest! Pepijn van Empelen, dankjewel voor het meeschrijven aan de meta-analyse! Wim
Krijnen, dankjewel voor al je hulp met statische vraagstukken. Je maakte tijd vrij om mee te denken over de opzet
van (statistische) methodes, beantwoordde geduldig allerlei basisvragen over statistiek en gaf waardevolle
feedback op geschreven stukken. Wichor Bramer, dankjewel voor je hulp bij de zoekstring en uitvoeren van de
zoekopdracht in de verschillende databases.
Prof. Dr. Annette van der Putten, Prof. Dr. Mariët Hagedoorn en Prof. Dr. Geraline Leusink, heel hartelijk bedankt
dat jullie wilden deelnemen aan de beoordelingscommissie. Ik hoop dat mijn proefschrift interessant was om te
lezen tijdens de zomervakantie.
Beste Rianne en Annelies, het was fijn om met jullie als collega’s op te trekken. We hebben samen de leuke en
lastige momenten kunnen delen en dat luchtte soms echt even op! Ook hielp het om met elkaar te delen waar
we mee bezig waren en samen na te denken over de volgende stap(pen). Ook de presentaties die we samen
hebben gegeven tijdens de Workshops voor de IWP-VB, de netwerkbijeenkomst Uniek Sporten en de overleggen
vanuit de IWP-VB en ‘De krachten gebundeld’ waren gewoon leuker omdat we ze samen deden! Dank jullie wel
voor de gezellige tijd, samen met Kristel, tijdens het IASSID congres in Belfast. Ik wens jullie veel succes bij de
afronding van jullie promotie-traject, dat gaat helemaal goed komen! Dinette en Annemarie, bedankt voor alle
gezelligheid en het delen van jullie ervaringen en tips met de afronding van het proefschrift en de voorbereiding
van de promotieplechtigheid!
Ook de collega’s van het lectoraat Healthy Ageing, Allied Health Care and Nursing wil ik bedanken. De
onderwerpen van onze onderzoeken verschilden soms behoorlijk, maar het plezier, de dilemma’s en de
138541-Willems_BNW.indd 168 31-10-19 10:08

168
Dankwoord
Promoveren was niet iets wat ik voor mezelf in gedachten had. En toch is er nu dit proefschrift met mijn naam
erop. Een mooie kans, een interessante uitdaging was voor mij het promotie-traject toen ik hier vier jaar geleden
mee startte. En ik had het beslist niet willen missen! Daarom wil ik graag iedereen bedanken die me heeft
geholpen, gesteund en vertrouwd om dit onderzoek te kunnen uitvoeren.
Een groot aantal zorgorganisaties in Noord-Nederland zag het belang van een gezonde leefstijl voor mensen met
een verstandelijke beperking: De Trans, De Zijlen, Stichting Sprank, ’s Heerenloo Zorggroep, Talant, Cosis,
Koninklijke Visio Noord Nederland, Philadelphia en Vanboeijen. Ik wil jullie bedanken voor de mogelijkheid om
dit promotie-traject uit te voeren, het inhoudelijk meedenken met de onderzoeksvragen en de ondersteuning in
de praktische zin, onder andere door medewerkers van de organisaties die deelnamen aan het onderzoek.
De begeleiders en hun cliënten, gedragswetenschappers, paramedici en artsen verstandelijk gehandicapten
(AVG’s) wil ik heel hartelijk bedanken voor hun deelname aan dit onderzoek. Jullie tijdsinvestering, meedenken
en hun openheid waren onmisbaar om inhoud te geven aan dit proefschrift. Ook de wettelijk vertegenwoordigers
van mensen met een verstandelijke beperking wil ik bedanken voor het gestelde vertrouwen en toestemming
zodat de persoon die zij vertegenwoordigen kon deelnemen aan het onderzoek.
Beste Cees, jij was mijn ‘hoofdbegeleider’ en dat deed je op een fijne manier! Door jouw overstijgende kijk, werd
ik telkens teruggeroepen naar de hoofdlijnen en verloor ik me niet in details. Je praktische manier van denken
was geregeld een verademing, evenals je toegankelijke manier van doen: je stimuleerde juist om gebruik te
maken van de expertise van het begeleidingsteam waar ik dat nodig had. Jouw kennis over wetenschappelijk
onderzoek, gezondheid en het promotie-traject op zichzelf hebben me enorm geholpen om dit traject tot een
succes te maken!
Beste Aly, wat heb ik het getroffen met jou als mijn dagelijks begeleider! Je was altijd betrokken, hielp mee bij
het bepalen van de goede richting en wist altijd positieve woorden aan te vinden die me hielpen om weer verder
te gaan. Je maakte vaak direct tijd vrij om mee te denken wanneer dat nodig was en had een luisterend oor. Je
was bereid om met ieder stuk opnieuw mee te kijken en mede door jouw snelle reageren is het gelukt om dit
proefschrift in vier jaar af te ronden. Dankjewel voor je hulp tijdens mijn zwangerschapsverlof en je presentaties
over mijn onderzoek tijdens congressen. Je enthousiasme voor mensen met een verstandelijke beperking en hun
gezondheid werkten aanstekelijk en inspirerend. Dankjewel voor alles!
Beste Johan, je was tijdens mijn promotie traject wat meer vanaf een afstand betrokken en dat maakte dat je
dingen meer vanuit overstijgend perspectief bekeek. Dit hielp me om de grote lijn vast te houden, heel
waardevol! Ook hielpen jouw opmerkingen om soms vanuit een andere invalshoek naar het onderwerp te kijken
en te bezinnen op de gekozen richting. Jouw enthousiasme voor gezondheid en bewegen en hun theoretische
onderbouwing zorgden geregeld voor duidelijke verbeteringen van dit proefschrift, bedankt!
169
Beste Thessa, jij bent wat later een van mijn officiële co-promotores geworden, maar al in het begin van mijn
promotie-traject maakten we kennis vanwege onze samenwerking bij de systematische review. Ik ben heel blij
met jouw betrokkenheid bij mijn promotietraject! Je nuchtere kijk, heldere schrijfstijl en expertise in onderzoek
bij mensen met een verstandelijke beperking hielpen me om koers en focus te houden, inhoudelijk de diepte te
zoeken en uitgevoerde onderzoeken goed op papier te krijgen. Ook voor je fijne manier van communiceren en
omgaan met elkaar wil ik je bedanken!
Beste Ruud, jij was niet officieel betrokken bij mijn promotie-traject, maar had er beslist een belangrijke rol in!
Dankjewel voor je aanwezigheid bij vele overleggen, je expertise op het gebied van onderzoek en mensen met
een verstandelijke beperking en je feedback op geschreven stukken. Je inbreng heeft het proefschrift naar een
hoger niveau getild!
Naast mijn begeleiders hebben ook anderen meegeschreven en meegeholpen met de artikelen uit dit
proefschrift. Craig Melville, thank you for your guidance and patience with me, especially during our
collaboration for the systematic review. I was just starting as a PhD candidate and you approached me like a full
researcher, taking my reasoning’s seriously and answering to simple questions. Thank you for your work on the
meta-analyses as well! Else Havik, dankjewel voor al jouw werk voor de systematische review: het opzetten van
de methode en het screenen van alle artikelen. Zonder jouw inzet en hulp was de review minder snel afgerond
en minder goed geweest! Pepijn van Empelen, dankjewel voor het meeschrijven aan de meta-analyse! Wim
Krijnen, dankjewel voor al je hulp met statische vraagstukken. Je maakte tijd vrij om mee te denken over de opzet
van (statistische) methodes, beantwoordde geduldig allerlei basisvragen over statistiek en gaf waardevolle
feedback op geschreven stukken. Wichor Bramer, dankjewel voor je hulp bij de zoekstring en uitvoeren van de
zoekopdracht in de verschillende databases.
Prof. Dr. Annette van der Putten, Prof. Dr. Mariët Hagedoorn en Prof. Dr. Geraline Leusink, heel hartelijk bedankt
dat jullie wilden deelnemen aan de beoordelingscommissie. Ik hoop dat mijn proefschrift interessant was om te
lezen tijdens de zomervakantie.
Beste Rianne en Annelies, het was fijn om met jullie als collega’s op te trekken. We hebben samen de leuke en
lastige momenten kunnen delen en dat luchtte soms echt even op! Ook hielp het om met elkaar te delen waar
we mee bezig waren en samen na te denken over de volgende stap(pen). Ook de presentaties die we samen
hebben gegeven tijdens de Workshops voor de IWP-VB, de netwerkbijeenkomst Uniek Sporten en de overleggen
vanuit de IWP-VB en ‘De krachten gebundeld’ waren gewoon leuker omdat we ze samen deden! Dank jullie wel
voor de gezellige tijd, samen met Kristel, tijdens het IASSID congres in Belfast. Ik wens jullie veel succes bij de
afronding van jullie promotie-traject, dat gaat helemaal goed komen! Dinette en Annemarie, bedankt voor alle
gezelligheid en het delen van jullie ervaringen en tips met de afronding van het proefschrift en de voorbereiding
van de promotieplechtigheid!
Ook de collega’s van het lectoraat Healthy Ageing, Allied Health Care and Nursing wil ik bedanken. De
onderwerpen van onze onderzoeken verschilden soms behoorlijk, maar het plezier, de dilemma’s en de
138541-Willems_BNW.indd 169 31-10-19 10:08

170
investering zijn vaak een feest van herkenning. Trudy, Ineke en Hillie, het was heel fijn dat ik altijd bij jullie kon
aankloppen voor alle praktische zaken, bedankt!
Onderzoek naar leefstijl bij mensen met een verstandelijke beperking wordt door het hele land gedaan, gelukkig!
De (half)jaarlijkse bijeenkomsten met collega-onderzoekers waren leerzaam, gezellig en fijne momenten om te
sparren over de inhoud van ons onderzoek en gebruikte methodes, evenals het uitwisselingen van ervaringen
met promoveren. Bedankt!
Manouk en Mirjam, bedankt voor jullie hulp bij de uitvoering van dit onderzoek. Manouk, jij hebt me echt
geholpen door tijdens mijn zwangerschapsverlof de coördinatie van de observatiestudie met Aly op je te nemen,
bedankt! Mirjam, jij hebt de codering van alle video-bestanden grotendeels uitgevoerd, een grote klus die je
nauwkeurig en in korte tijd hebt weten uit te voeren, dankjewel!
Naast mijn collega’s bij de Hanzehogeschool had ik het voorrecht dat ik ook collega’s had binnen Stichting Sprank.
Stichting Sprank wil ik bedanken voor de mogelijkheid om dit promotieonderzoek uit te voeren en voor het
gestelde vertrouwen. Lieve (oud)collega-gedragsdeskundigen; Annemarieke, Christien, Lara, Liesbeth, Petra,
Riëtte en Ab, dankjewel voor jullie interesse, steun en fijne samenwerking! Lieve Tineke, jij was een van mijn
begeleiders toen ik net startte bij Stichting Sprank en maakte me wegwijs in de zorg voor mensen met een
verstandelijke beperking. Dankjewel voor het delen van jouw kennis en kunde en je hulp, vertrouwen en
interesse! Lieve Rineke, ook jij hielp me bij mijn start in de VG-sector. Door jouw vertrouwen in mijn kunnen
groeide mijn zelfvertrouwen. Je stimuleerde me om door te zetten, verder te kijken. Ik heb veel geleerd van je
expertise van en zorg voor mensen met een verstandelijke beperking. Ook onze gesprekken over geloof en leven
als christen zijn me heel waardevol. Dankjewel!
Lieve papa en mama, dankjewel voor wie jullie voor me zijn en zijn geweest. Jullie vertrouwen in mij gaf me
zelfvertrouwen en hielp me door te zetten. Het was fijn om met jullie te kunnen praten over dingen waar ik
tegenaan liep of blij van werd, ook al waren jullie zelf niet zo bekend met wetenschappelijk onderzoek. Jullie zijn
een voorbeeld voor me en ik hou heel veel van jullie!
Lieve schoonouders, wat is jullie huis een thuis voor mij geworden. Bedankt voor jullie liefde, interesse en alle
hulp: soms werd er even in huis gepoetst of pasten jullie een keer extra op Jade. Ik heb het enorm getroffen met
jullie en hou veel van jullie!
Lieve Wim, Els, Ilse, Dorienke, lieve zwagers en schoonzussen: familie is familie voor altijd. Jullie
onvoorwaardelijke liefde en steun zijn voor mij een belangrijke basis om te leven en werken. Het is een zegen
om deel uit te maken van zulke liefdevolle en gezellige gezinnen! Lieve Ils, dankjewel dat jij mijn paranimf wilt
zijn, dat betekent veel voor me. Ik hou van jullie, dank jullie wel voor alles!
Lieve vrienden, jullie zijn met velen en wat is dat een zegen! Ontspanning, afleiding, humor en leuke dingen doen
evenals een luisterend oor: ik had er niet zonder gekund. Dank jullie wel voor alle mooie dingen die we samen al
hebben beleefd, ik hoop nog heel lang deel uit te mogen maken van jullie levens! Lieve Elsemiek en Marcia, jullie
171
zijn mijn oudste vriendinnetjes en wat hebben we het goed samen. Het is fijn om elkaar zo goed te kennen,
samen tijd door te brengen en met elkaar mee te leven in mooie en moeilijke momenten. Ik hou van jullie!
Lieve Ger, het mooiste voor het laatst bewaren.. Dat is waarom je pas hier wordt genoemd in het dankwoord. Jij
bent al zo lang mijn maatje en geliefde en nog steeds hebben we het zo goed samen! Je liefde, steun, vertrouwen,
geduld, toewijding en geloof zijn mijn vaste basis. Je was er altijd voor me, had een luisterend oor, gaf me de
ruimte om extra te werken wanneer dat nodig was (Mar, het is geen typemachine..), had geduld als ik even niet
zo gezellig was en wist me op te fleuren met gezelligheid, humor en een kop thee. Het is niet voor niets dat jij
mijn paranimf bent. Je bent zo vertrouwd voor me en ik ben stapelgek op je! Wat is het heerlijk dat we samen
een prachtige dochter mochten krijgen. Jade is ons wondertje en geeft ons zoveel plezier en levensinhoud. En
nu verwachten we nog een (a)pril wondertje, wat een mooi vooruitzicht! Ik bid dat onze levens voor altijd aan
elkaar verbonden blijven en we samen nog heel veel mooie momenten mogen beleven. Dankjewel voor wie je
bent!
‘Laat ieder van u de gaven die hij van God heeft gekregen, gebruiken om anderen daarmee te helpen’ (1 Petrus
4:10a). De vaardigheden die ik nodig had om dit proefschrift te schrijven, heb ik mezelf niet gegeven. Ik dank
Hem die mij heeft gemaakt voor Zijn liefde voor ons allemaal! Prijs de Heer!
138541-Willems_BNW.indd 170 31-10-19 10:08

170
investering zijn vaak een feest van herkenning. Trudy, Ineke en Hillie, het was heel fijn dat ik altijd bij jullie kon
aankloppen voor alle praktische zaken, bedankt!
Onderzoek naar leefstijl bij mensen met een verstandelijke beperking wordt door het hele land gedaan, gelukkig!
De (half)jaarlijkse bijeenkomsten met collega-onderzoekers waren leerzaam, gezellig en fijne momenten om te
sparren over de inhoud van ons onderzoek en gebruikte methodes, evenals het uitwisselingen van ervaringen
met promoveren. Bedankt!
Manouk en Mirjam, bedankt voor jullie hulp bij de uitvoering van dit onderzoek. Manouk, jij hebt me echt
geholpen door tijdens mijn zwangerschapsverlof de coördinatie van de observatiestudie met Aly op je te nemen,
bedankt! Mirjam, jij hebt de codering van alle video-bestanden grotendeels uitgevoerd, een grote klus die je
nauwkeurig en in korte tijd hebt weten uit te voeren, dankjewel!
Naast mijn collega’s bij de Hanzehogeschool had ik het voorrecht dat ik ook collega’s had binnen Stichting Sprank.
Stichting Sprank wil ik bedanken voor de mogelijkheid om dit promotieonderzoek uit te voeren en voor het
gestelde vertrouwen. Lieve (oud)collega-gedragsdeskundigen; Annemarieke, Christien, Lara, Liesbeth, Petra,
Riëtte en Ab, dankjewel voor jullie interesse, steun en fijne samenwerking! Lieve Tineke, jij was een van mijn
begeleiders toen ik net startte bij Stichting Sprank en maakte me wegwijs in de zorg voor mensen met een
verstandelijke beperking. Dankjewel voor het delen van jouw kennis en kunde en je hulp, vertrouwen en
interesse! Lieve Rineke, ook jij hielp me bij mijn start in de VG-sector. Door jouw vertrouwen in mijn kunnen
groeide mijn zelfvertrouwen. Je stimuleerde me om door te zetten, verder te kijken. Ik heb veel geleerd van je
expertise van en zorg voor mensen met een verstandelijke beperking. Ook onze gesprekken over geloof en leven
als christen zijn me heel waardevol. Dankjewel!
Lieve papa en mama, dankjewel voor wie jullie voor me zijn en zijn geweest. Jullie vertrouwen in mij gaf me
zelfvertrouwen en hielp me door te zetten. Het was fijn om met jullie te kunnen praten over dingen waar ik
tegenaan liep of blij van werd, ook al waren jullie zelf niet zo bekend met wetenschappelijk onderzoek. Jullie zijn
een voorbeeld voor me en ik hou heel veel van jullie!
Lieve schoonouders, wat is jullie huis een thuis voor mij geworden. Bedankt voor jullie liefde, interesse en alle
hulp: soms werd er even in huis gepoetst of pasten jullie een keer extra op Jade. Ik heb het enorm getroffen met
jullie en hou veel van jullie!
Lieve Wim, Els, Ilse, Dorienke, lieve zwagers en schoonzussen: familie is familie voor altijd. Jullie
onvoorwaardelijke liefde en steun zijn voor mij een belangrijke basis om te leven en werken. Het is een zegen
om deel uit te maken van zulke liefdevolle en gezellige gezinnen! Lieve Ils, dankjewel dat jij mijn paranimf wilt
zijn, dat betekent veel voor me. Ik hou van jullie, dank jullie wel voor alles!
Lieve vrienden, jullie zijn met velen en wat is dat een zegen! Ontspanning, afleiding, humor en leuke dingen doen
evenals een luisterend oor: ik had er niet zonder gekund. Dank jullie wel voor alle mooie dingen die we samen al
hebben beleefd, ik hoop nog heel lang deel uit te mogen maken van jullie levens! Lieve Elsemiek en Marcia, jullie
171
zijn mijn oudste vriendinnetjes en wat hebben we het goed samen. Het is fijn om elkaar zo goed te kennen,
samen tijd door te brengen en met elkaar mee te leven in mooie en moeilijke momenten. Ik hou van jullie!
Lieve Ger, het mooiste voor het laatst bewaren.. Dat is waarom je pas hier wordt genoemd in het dankwoord. Jij
bent al zo lang mijn maatje en geliefde en nog steeds hebben we het zo goed samen! Je liefde, steun, vertrouwen,
geduld, toewijding en geloof zijn mijn vaste basis. Je was er altijd voor me, had een luisterend oor, gaf me de
ruimte om extra te werken wanneer dat nodig was (Mar, het is geen typemachine..), had geduld als ik even niet
zo gezellig was en wist me op te fleuren met gezelligheid, humor en een kop thee. Het is niet voor niets dat jij
mijn paranimf bent. Je bent zo vertrouwd voor me en ik ben stapelgek op je! Wat is het heerlijk dat we samen
een prachtige dochter mochten krijgen. Jade is ons wondertje en geeft ons zoveel plezier en levensinhoud. En
nu verwachten we nog een (a)pril wondertje, wat een mooi vooruitzicht! Ik bid dat onze levens voor altijd aan
elkaar verbonden blijven en we samen nog heel veel mooie momenten mogen beleven. Dankjewel voor wie je
bent!
‘Laat ieder van u de gaven die hij van God heeft gekregen, gebruiken om anderen daarmee te helpen’ (1 Petrus
4:10a). De vaardigheden die ik nodig had om dit proefschrift te schrijven, heb ik mezelf niet gegeven. Ik dank
Hem die mij heeft gemaakt voor Zijn liefde voor ons allemaal! Prijs de Heer!
138541-Willems_BNW.indd 171 31-10-19 10:08

173
Research Institute for Health Research SHARE
This thesis is published within the Research Institute SHARE (Science in Healthy Ageing and healthcaRE) of the
University Medical Center Groningen / University of Groningen. Further information regarding the institute and
its research can be obtained from our internet site: http://www.share.umcg.nl/.
More recent theses can be found in the list below.
(supervisors are between brackets)
2019
Ong KJ
Economic aspects of public health programmes for infectious disease control; studies on Human
Immunodeficiency Virus & Human Papillomavirus
(prof MJ Postma, prof M Jit, dr K Soldan, dr AJ van Hoek)
Oosterhaven J
Hand eczema; impact, treatment and outcome measures
(dr MLA Schuttelaar, prof PJ Coenraads)
Postma DBW
Affordance-based control in running to catch fly balls
(prof KAPM Lemmink, dr FTJM Zaal)
Nuenen FM van
Screening of distress and referral need in Dutch oncology practice
(prof HBM van de Wiel, dr JEHM Hoekstra-Weebers, dr SM Donofrio)
Olthof SBH
Small-sided games in youth soccer; performance and behavior compared to the official match
(prof KAPM Lemmink, dr WGP Frencken)
Yin H
Epidemiology and treatment of mental disorders in a rapidly developing urban region in China; a study of
prevalence, risk factors and e-applications
(prof RA Schoevers, dr KJ Wardenaar)
Kuipers DA
Design for transfer; figural transfer through metaphorical recontextualization in games for health
(prof JPEN Pierie, dr JT Prins)
138541-Willems_BNW.indd 172 31-10-19 10:08

173
Research Institute for Health Research SHARE
This thesis is published within the Research Institute SHARE (Science in Healthy Ageing and healthcaRE) of the
University Medical Center Groningen / University of Groningen. Further information regarding the institute and
its research can be obtained from our internet site: http://www.share.umcg.nl/.
More recent theses can be found in the list below.
(supervisors are between brackets)
2019
Ong KJ
Economic aspects of public health programmes for infectious disease control; studies on Human
Immunodeficiency Virus & Human Papillomavirus
(prof MJ Postma, prof M Jit, dr K Soldan, dr AJ van Hoek)
Oosterhaven J
Hand eczema; impact, treatment and outcome measures
(dr MLA Schuttelaar, prof PJ Coenraads)
Postma DBW
Affordance-based control in running to catch fly balls
(prof KAPM Lemmink, dr FTJM Zaal)
Nuenen FM van
Screening of distress and referral need in Dutch oncology practice
(prof HBM van de Wiel, dr JEHM Hoekstra-Weebers, dr SM Donofrio)
Olthof SBH
Small-sided games in youth soccer; performance and behavior compared to the official match
(prof KAPM Lemmink, dr WGP Frencken)
Yin H
Epidemiology and treatment of mental disorders in a rapidly developing urban region in China; a study of
prevalence, risk factors and e-applications
(prof RA Schoevers, dr KJ Wardenaar)
Kuipers DA
Design for transfer; figural transfer through metaphorical recontextualization in games for health
(prof JPEN Pierie, dr JT Prins)
138541-Willems_BNW.indd 173 31-10-19 10:08
174
Belak A
The health of segregated Roma: first-line views and practices
(prof SA Reijneveld, prof A Geckova, dr JP van Dijk)
Kieffer TEC
Adaptation and modulation of memory and regulatory T cells in pregnancy
(prof SA Scherjon, dr MM Faas, dr JR Prins)
Kuiper D
Health of offspring of subfertile couples
(prof M Hadders-Algra, prof A Hoek, prof MJ Heineman)
Huang Y
Use of real-world evidence in pharmacoeconomic analysis
(prof FM Haaijer-Ruskamp, prof MJ Postma, dr P Vemer)
Cuijpers LS
Coordination dynamics in crew rowing
(prof KAPM Lemmink, dr FTJM Zaal, dr HJ de Poel)
Dittmar D
Multiple aspects of contact allergy; immunology, patch test methodology and epidemiology
(dr MLA Schuttelaar, prof PJ Coenraads)
Beemster T
Quality improvement of vocational rehabilitation in patients with chronic musculoskeletal pain and reduced work
participation
(prof MF Reneman, prof MHW Frings-Dresen, prof CAM van Bennekom, dr JM van Velzen)
28.08.2019 EXPAND
Geerse O
The impact of lung cancer; towards high-quality and patient-centered supportive care
(prof HAM Kerstjens, prof MY Berger, dr TJN Hiltermann, dr AJ Berendsen)
Dierselhuis EF
Advances of treatment in atypical cartilaginous tumours
(prof SK Bulstra, prof AJH Suurmeijer, dr PC Jutte, dr M Stevens)
175
Gils A van
Developing e-health applications to promote a patient-centered approach to medically unexplained symptoms
(prof JGM Rosmalen, prof RA Schoevers)
Notenbomer A
Frequent sickness absence; a signal to take action
(prof U Bultmann, prof W van Rhenen, dr CAM Roelen)
Bishanga DR
Improving access to quality maternal and newborn care in low-resource settings: the case of Tanzania
(prof J Stekelenburg, dr YM Kim)
Tura AK
Safe motherhood: severe maternal morbidity and mortality in Eastern Ethiopia
(prof SA Scherjon, prof J Stekelenburg, dr TH van den Akker)
Vermeiden CJ
Safe motherhood : maternity waiting homes in Ethiopia to improve women’s access to maternity care
(prof J Stekelenburg, dr TH van den Akker)
Schrier E
Psychological aspects in rehabilitation
(prof PU Dijkstra, prof JHB Geertzen)
For earlier theses visit our website.
138541-Willems_BNW.indd 174 31-10-19 10:08
174
Belak A
The health of segregated Roma: first-line views and practices
(prof SA Reijneveld, prof A Geckova, dr JP van Dijk)
Kieffer TEC
Adaptation and modulation of memory and regulatory T cells in pregnancy
(prof SA Scherjon, dr MM Faas, dr JR Prins)
Kuiper D
Health of offspring of subfertile couples
(prof M Hadders-Algra, prof A Hoek, prof MJ Heineman)
Huang Y
Use of real-world evidence in pharmacoeconomic analysis
(prof FM Haaijer-Ruskamp, prof MJ Postma, dr P Vemer)
Cuijpers LS
Coordination dynamics in crew rowing
(prof KAPM Lemmink, dr FTJM Zaal, dr HJ de Poel)
Dittmar D
Multiple aspects of contact allergy; immunology, patch test methodology and epidemiology
(dr MLA Schuttelaar, prof PJ Coenraads)
Beemster T
Quality improvement of vocational rehabilitation in patients with chronic musculoskeletal pain and reduced work
participation
(prof MF Reneman, prof MHW Frings-Dresen, prof CAM van Bennekom, dr JM van Velzen)
28.08.2019 EXPAND
Geerse O
The impact of lung cancer; towards high-quality and patient-centered supportive care
(prof HAM Kerstjens, prof MY Berger, dr TJN Hiltermann, dr AJ Berendsen)
Dierselhuis EF
Advances of treatment in atypical cartilaginous tumours
(prof SK Bulstra, prof AJH Suurmeijer, dr PC Jutte, dr M Stevens)
175
Gils A van
Developing e-health applications to promote a patient-centered approach to medically unexplained symptoms
(prof JGM Rosmalen, prof RA Schoevers)
Notenbomer A
Frequent sickness absence; a signal to take action
(prof U Bultmann, prof W van Rhenen, dr CAM Roelen)
Bishanga DR
Improving access to quality maternal and newborn care in low-resource settings: the case of Tanzania
(prof J Stekelenburg, dr YM Kim)
Tura AK
Safe motherhood: severe maternal morbidity and mortality in Eastern Ethiopia
(prof SA Scherjon, prof J Stekelenburg, dr TH van den Akker)
Vermeiden CJ
Safe motherhood : maternity waiting homes in Ethiopia to improve women’s access to maternity care
(prof J Stekelenburg, dr TH van den Akker)
Schrier E
Psychological aspects in rehabilitation
(prof PU Dijkstra, prof JHB Geertzen)
For earlier theses visit our website.
138541-Willems_BNW.indd 175 31-10-19 10:08

in adults intellectual disabilities
lifestylewith
Mariël Willems-Jongsma
in adults intellectual disabilities
Mariël Willems-J-J-JJongsma
Use and effectiveness of behaviour change techniques
Ma
riëlWillem
s-Jong
sma
Lifestylecha
nge
ina
dults
with
intellectuald
isab
ilitiesJ
g
UITNODIGING
Voor het bijwonen van de openbare verdediging
van het proefschrift
Lifestyle change in adults withintellectual disabilities
Use and effectiveness ofbehaviour change techniques
door
Mariël Willems-Jongsma
Op maandag 9 december 2019om 14.30 uur
in het academiegebouw vande Rijksuniversiteit Groningen,
Broerstraat 5 te Groningen
Paranimfen:
Gerjan Willems 0610394409Ilse Mol-Jongsma 0641422911
Mariël Willems-Jongsma
Goudsbloemstraat 508012XN Zwolle


















