
DR. Mouli Edward, dr. Mkes. SpOT(K) Teddy Heri Wardhana,dr ...

VOL 1 • NO 1
PANGEA PROJECT
THE FREE NUCLEAR MEDICINE & MOLECULAR IMAGING EDUCATIONAL MAGAZINE AVAILABLE WORLDWIDE
NUCLEAR MEDICINEMADE SIMPLE
LA MÉDECINENUCLÉAIRESIMPLIFIÉE
MEDICINA NUCLEAREN PALABRAS
SENCILLAS
核醫學
簡單

4 EDITORIAL BOARD
5 ePATIENT PUBLICATION
6 PANGEA PROJECT : LE PATIENT MAGAZINE
7 THE 7.4 BILLION CITIZEN EDUCATIONAL PANGEA
10 STRESS TESTING: QUESTIONS AND ANSWERS
12 USO DA MEDICINA NUCLEAR NA AVALIAÇÃO DA FUNÇÃO VENTRICULAR
16 PERFUSION MYOCARDIQUE AU RUBIDIUM-82
18 THE UNIVERSITY OF COLORADO DOSE-RISK SMARTCARD
20 INTERVIEW WITH : DR. AKRAM AL IBRAHEEM
22 THE CANADIAN ASSOCIATION OF NUCLEAR MEDICINEASSOCIATION CANADIENNE DE MÉDECINE NUCLÉAIRE
24 新型SPECT肺通气灌注三维定量分析在预测肺癌患者肺叶切除术后残余肺功能的临床价值
25 INTERVIEW WITH : DR. BENNETT S. GREENSPAN
26 VENTILATION/PERFUSION SCINTIGRAPHY IN THE FOLLOW-UP OF PULMONARY EMBOLISM
28 INTERVIEW WITH : DR. RODRIGO JAIMOVICH
29 LE DIAGNOSTIC DE L’EMBOLIE PULMONAIRE
32 INTERVIEW WITH : DR. ANDREW SCOTT
34 INTERVIEW WITH : DR. GERALD DODD
36 MEDICINA NUCLEAR EN TROMBOEMBOLISMO PULMONAR
40 INTERVIEW WITH : DR. RAYMOND RUSSELL
42 INTERVIEW WITH : DR. JUN HATAZAWA
Content
Editors: Dr. Jean-Luc Urbain & Francois Lamoureux
Editorial Board:Dr. Francois Lamoureux - Dr. Jean-Luc UrbainDr. Zvi Bar-Sever - Dr. Paige Bennett - Dr. Salah-Eddine Bouyoucef - Dr. Sanjay Gambhir -Dr. Bennett Greenspan - Dr. Juan Hatazawa - Dr. Wei He - Dr. Fernando Mutt - Dr. Raymond Russel - Dr. Einat Sapir - Dr. Mike Sathekge - Dr. Jean-Philippe Vuillez - Dr. Nadia Whithofs
Featured in this issue:Dr. Akram Al-Ibraheem - Dr. Gerald Dodd & his team -Dr. Bennett S. Greenspan - Dr. Jean Grégoire -Dr. Jun Hatazawa - Dr. Wei He - Dr. Roland Hustinx -Dr. Rodrigo Jaimovich - Dr. Francois Lamoureux - Dr. Normand Laurin - Dr. Juan Luis Londono Blair - Dr. Claudio T Mesquita - Dr. Andrew Ross - Dr. Raymond Russel - Dr. Andrew Scott - Dr. Jean Luc Urbain - Dr. Wei He
Director of the publication: Nicolas Rondeau Lapierre
Publisher:Les Éditions Multi-Concept inc.
Artistic direction and printing: Le Groupe Communimédia inc.communimedia.ca
Correction and proofreading: Anik Messier
Advertisement information: Nicolas Rondeau Lapierre 514-331-0661 #[email protected]
Disclaimer: Authors are selected according to theextent of their expertise in a given specialty. TheePatient/Pangea project publication does not vouchfor the expertise of its collaborators and may notbe held liable for their statements. The textspublished in the ePatient/Pangea project are onlybinding to the authors.
The ePatient magazine is published quarterly by thepublishing company, Les Éditions Multi-ConceptInc. 1600 Henri-Bourassa Blvd West, Suite 405,Montreal, Quebec, H3M 3E2
Secretarial office:Tel.: (514) 331-0661Fax: (514) 331-8821Email : [email protected]
All ads for pharmaceuticals products have beenapproved by the Council by the PharmaceuticalAdvertising Advisory Board.
Legal Deposit:Library and Archives CanadaLibrary and Archives Canada
Post-Publication AgreementNo. 40011180
Subscription information: Quarterly publication, nmpangea.com
3
SUBSCRIBE HERE ! INSCRIVEZ-VOUS ICI ! SUSCRÍBETE AQUÍ ! 在这里签名!
Don’t miss our next issue: Oncology/Theranostics and Neuro-imaging

4
EDITORIAL BOARD
Dr. Lamoureux and I are thrilled to introduce our outstanding editorial boardmembers. Through our travel and NM lecturing around the globe, we havemet terrific scientists and colleagues. Most, if not all of them, are reallypassionate about and true advocates for the field of nuclear medicine. Theystrongly believe in the power, usefulness and safe use of NM diagnostic andtherapeutic procedures for the betterment of public healthcare worldwide.We are delighted that the following leaders have embraced the concept ofthe Pangea-ePatient magazine and accepted to share their invaluableexpertise and experience with patients, referring colleagues, health careadministrators, government agencies and insurance companies.
Dr. Jean-Luc UrbainDr. Francois Lamoureux, M.D.,M.Sc., FRCP(C), President-elect CANM, Canada
Dr. Jean-Luc Urbain, M.D., Ph.D., CPE, Past President CANM, Canada
Dr. Zvi Bar-Sever, M.D.,Chair Pediatric Nuclear MedicineCouncil, EANM; Director, InstituteSchneider Children’s Hospital, Israel
Dr. Paige Bennett, M.D., Nuclear Medicine/Medical ImagingSpecialist , Wake Forest University, USA
Dr. Salah-Eddine Bouyoucef, M.D.,Ph.D., Chief Nuclear Medicine , CHU Bab El Oued, Alger, Algeria
Dr. Jun Hatazawa, M.D., Ph.D., President of the AOFNMB, Japan
Dr. Wei He, M.D., Ph. D., Director of Nuclear Medicine andPET/CT, Center Fu Dan University,China
Dr. Sanjay Gambhir, M.D., Ph.D.,Chief/Chair, Nuclear Medicine, University of Lucknow, India
Dr. Bennett Greenspan, M.D., President of the SNMMI, USA
Dr. Fernando Mutt, M.D., Past President ALASBIMN, Uruguay
Dr. Raymond Russel, M.D., Ph.D., Associate Professor of Medicine Warren Alpert Medical School ofBrown University, Director, NuclearCardiology, Rhode Island Hospital & President, American Society of Nuclear Cardiology, USA
Dr. Einat Sapir, M.D., Ph.D., Professor, Sackler School of Medicine, Tel Aviv University & Head, Department of Nuclear Medicine Tel Aviv Sourasky Medical Center, Israel
Dr. Mike Sathekge, M.D., Prof., University of Pretoria, Head of Nuclear Medicine Steve Biko Acade-mic Hospital & President, Colleges of Medicine of South Africa, South Africa
Dr. Jean-Philippe Vuillez, M.D.,Ph.D., Prof., Vice-Doyen Formation Directeur desétudes PU-PH – Médecine Nucléaire,France
Dr. Nadia Whithofs, M.D., Ph.D, Division of Nuclear Medicine and Oncological Imaging, CHU of Liege, Belgium
The Canadian Association of Nuclear Medicinewelcomes you to our inaugural ePatient
publication aimed at providing doctors and patientsinformation to help them understand how thisvibrant area of medicine can help in diagnosing andtreating often difficult medical conditions. At onetime, nuclear medicine was sometimes called“unclear medicine” because the pattern of dotsproduced by the Polaroid cameras which made theimages appeared more as Rorschach psychologicaltesting cards than medical images to untrained eyes.
Today, Nuclear Medicine provides high detail twoand three-dimensional images looking at how thebody functions and what may be wrong in disease.Additionally, the new generation of cameras haveCTs or even MRs, which give anatomic informationproviding precise location and information. Theseimages are from the radioactive molecules, calledmedical isotopes, injected which demonstratespecific functions in the body. There are numerousmedical isotopes in use and more underdevelopment demonstrating more detailed ability totarget precisely certain functions and diseases.
Some had predicted the death of nuclear medicineseveral decades ago, however far from this, the field
continues to expand andprovide even more infor-mation and diagnosisand, as well, vitaltreatment options forpatients with seriousdiseases. With themove to what is calledper-sonalized medicinewhere diagnosis andtreatments are tailoredto the individual patient,nuclear medicine, morethan any other specialty, hasthe tools to be able to furtherthis exciting reality.
The Canadian Association of Nuclear Medicinestrongly believes the future is bright and in thesedays of electronic communication and informationsystems, we provide you with information and toolsto understand and be able to use it for better health.Enjoy your time looking at this emagazine. Feedbackis always welcome at the contact information for theAssociation.
5
ePATIENT PUBLICATION
Andrew RossM.D., FRCP
Head of Nuclear MedicineQE11 Health Sciences CentreHalifax Nova ScotiaCanadaPresident CanadianAssociation of NuclearMedicine (CANM)

Over the past fewdecades, the medical
imaging communities andassociations have made anextensive effort to educatetheir members aboutradiopharma-ceuticals andnuclear medicine scanners.
As an end user, the nuclear medicine professional isentirely dependent upon patient referrals from itscolleagues. Unfortunately and unlike radiology andcardiology, the nuclear medicine community andnuclear medicine associations/societies have notoutreached proactively and consistently to theirstakeholders (patients, referring physicians,government agencies, hospital administrators….). Asa result, the nuclear medicine field has largelyremained a self-contained and limited environmentthat is always struggling to thrive.
About 10 years ago, Dr. François Lamoureux, Presidentof the Quebec Association of Nuclear Medicine,decided to embark into a provincial outreach effortoutside the Quebec nuclear medicine community. Hestarted an educational magazine in French called “LePatient” (htpp://www.lepatient.ca). The basic principleof “Le Patient” is based on the writing of short articles(2-3 pages max) by nuclear medicine professionals thatare easily readable/understandable by referringpractitioners, health care executives and governmentagencies personnel.
The success of Dr. Lamoureux’s magazine in Quebecis reflected by the clinical strength of nuclearmedicine and the number and quality of the nuclearmedicine procedures performed in Quebec. Forexample, the Province of Quebec performs annuallymore V/Q scan than most Europeans countries. Afew additional factors have also played a significantrole in the strength of nuclear medicine in Quebec.One of them is the fact that nuclear medicinephysicians practice as true consultant to theircolleagues and patients.
The idea behind the Pangea Project is to export to theworldwide NM community the concept of themagazine “Le Patient” and to make current andfuture nuclear medicine diagnostic tests andtherapies known and understandable to prescribingphysicians, patients, health authorities and hospitaladministrators on a global scale.
Two years ago, at the start of our bidding campaignto host the 2022 WFNMB congress, we started to talkabout this idea to our colleagues in Asia, Europe, andthe Americas and to the Nuclear Medicine Industry.Not only did we receive praises and encouragements,we were also told by the nuclear medicine industrythat this “niche” endeavor would fill a badly neededtool for the field and the industry.
With the endorsement of the large regional and mostof the national associations of nuclear medicine, wehave moved forward with our international version ofthe magazine. We are really pleased to introduce toyou our first issue. For this October publication, wehave articles in English, French, Spanish and Chineseas main languages and an article in Portuguese. In theupcoming issues the four main languages will bemaintained; in addition and based on request, we willalso have articles in a specific language, e.g. polish, fortargeting/consumption of a specific country. While theformat of the publication of the magazine Le Patienthas largely been based on a hard copy in the past, wehave moved gradually towards an electronic platformwith easy access and download of the issues onsmartphone, tablets, laptops and desktop computers.
We are very excited about this globalinitiative and hope that youwill enjoy sharing the issuesof Pangea with yourcolleagues and friendsinterested to knowmore about the benefitof the use of medicalisotopes to diagnoseand treat diseases.
PANGEA PROJECT: THE NEW PATIENT MAGAZINE
6
Jean-Luc Urbain
M.D., Ph.D., CPEPast President, CANM
François Lamoureux
M.D.,M.Sc., FRCP(C)President-elect CANM
Derived etymologically from the Latin “educo”,the word education is defined by two major
components: the action or process of teaching andthe knowledge, skills and understanding acquired.The purpose, content and tools of education haveevolved dramatically through the history of humankind.
In prehistoric and primitive culture, the purpose ofeducation was to teach survival tools and culturalvalues and to guide individuals and children tobecome good members of the tribes or bands. Atthe time, it was carried through symboliccommunication systems during initiation, rituals andprobably through stone carving and paintings incaves. It was more relevant to what scientists nowcall socialization or enculturation.
As cultures began to extend their knowledge beyondindividuals and survival skills, new forms of educationemerged. The origin of classes and schools that westill know today parallels the start of civilization inEgypt and Mesopotamia about 3500 BCE withpriests, scribes and government officials dispensingknowledge as teachers.
For millennia, education was reserved to the elite andthe privileged. Bringing new ideas and challengingthe dogma and authority of the Aristocracy andCatholic Church, the Age of enlightenment of the15th and 16th centuries in Europe enabled togradually provide education, literacy and learning torich and poor alike. Today, in most countries, full-time education, whether at school or otherwise, iscompulsory for all children up to a certain age.
Jean-Luc Urbain
M.D., Ph.D., CPEPast President, CANM
THE 7.4 BILLION CITIZEN EDUCATIONAL PANGEA
7

Egyptian hieroglyphs, Chineseoracle bones, wax coveredwriting boards, clay tablets,strips of bark from trees, tickleaves, parchment andvellum made of goat skinand calf skin have been useduntil the Middles Ages to
teach humanities and subjectssuch as science, medicine,
mathematics and geometry. Inthe Middles Ages, Gutenberg’s
printing press invention played a keyrole in the development of the scientific
revolution and laid the material basis for thespread of learning to and by the masses. Theinvention of the blackboard, in the 18th century, thatreplaced individual writing slates was also pivotal tothe teaching of classrooms. By the middle of the 19th
century, almost every classroom in America had ablackboard. Invented at the end of the 19th century,the overhead projector was only introduced inclassrooms in the 1950’s and early 1960’s. From the60’s to the 90’s slide projectors were commonly usedfor presentations.
Before the advent of microcomputers in the 1980’s,mainframe computers were used to deliver printeddrill and practice and simple tutorials for teachingstudents lessons. When microcomputers beganpopulating classrooms in the late 80’s and 90’s, theyrapidly transformed the multi-millennial era ofanalog education into our digital epoch. Thedevelopment of inexpensive multimedia computersand the eruption of the Internet in the mid-1990’sand social media tools in the mid-2000’s havedramatically transformed the nature of education.
Nowadays digital communications tools (e.g., e-mail,social media…) and multimedia (e.g. videoconference, webinars…) dominate our world andlife. Besides the traditional elementary, primary,secondary, higher and adult forms of education,people across the world have, could or should begiven access to alternative, indigenous, informal,open and self-directed education.
Your reading of this article in this magazine or via theweb portal (www.lepatient.ca) illustrates nicely theeducational evolution in our field. Dedicated toeducation of patients and physicians outside theirscope of practice and field of expertize, themagazine “Le Patient” is among the first and rareexamples of dissemination of simple, practical anduseful medical and nuclear medicine information tothe masses.
Less than a century old and largely an outcome ofthe WWII Manhattan Project, the field nuclearmedicine has evolved into a vast, multidisciplinaryand complex body of knowledge. In parallel to itsenormous impact on human health through unique
diagnostic and therapeutic approaches, nuclearmedicine has also become a multi-billion dollarsindustry that is part of the economic fiber ofcontinents.
Technologists, scientists and physicians involved innuclear medicine have always been eager to sharetheir findings, discoveries and developments in thefield through communications and publications. Overthe past 50 years and in partnership with theindustry, national, regional and international nuclearmedicine organizations (SNMMI, EANM, AANM,ALASBIMN, AOCNMB, IAEA, WFNMB, WHO) havefostered a vast and collaborative environment for thedissemination of knowledge and the education ofour community.
Unfortunately, mostly preoccupied to develop thefield and to improve patients’ services, nuclearmedicine professionals have neglected to focus onand to develop initiatives for the teaching of patientsand non-nuclear medicine professionals that remainconcerned about the use of radioactive material.
The recent involvement of patient advocacy groupsin government agencies and the availability oftargeted radiopharmaceuticals for the treatment ofcancers have created a new paradigm and challengefor our community: the need to educate governmentbureaucrats, patients and non-nuclear medicineprofessionals about the safe use of medical isotopesfor the diagnosis and treatment of diseases.
In partnership with the industry and in collaborationwith our sister organizations, some members of theCanadian Association of Nuclear Medicine areembarking into a major educational initiative acrossthe globe.
Taking advantage of 21st century cognitiveintelligence, Internet, social media andcommunication tools, we aim to create a unique,useful, multilingual educational reference nuclearmedicine library understandable by patients,colleagues and public servants.
8

When I recommend that a patient undergostress testing, I try to anticipate the questions
they may have about the test and how theinformation gained from the test will change theircare. By answering these questions, I hope to helpmy patient make the most informed decisionsconcerning the stress test itself and the managementdecisions that arise from the stress test. Making surethat our patients are well-informed concerning theirtesting and treatment options is an importantresponsibility of any physician.
Why do I need a stress test?
Far and away, the most common reason thatsomeone needs a stress test is because they haveexperienced some sort of symptom that isconcerning for the presence of significant coronary
artery disease (CAD), or blockages of the arteries thatfeed the heart. The symptom may be angina, that is,chest pressure that occurs with exertion. However,someone may have other symptoms that increase mysuspicion for the presence of CAD. These mayinclude atypical pain or pressure symptoms insomeone who is at risk for CAD, or new orworsening shortness of breath with exertion.
In addition, stress testing may be performed inpatients who have developed congestive heart failureand I am concerned that CAD may be causing theirheart failure. Similarly, some patients who developdangerous rhythm disturbances of the heart mayundergo stress testing to help determine the causeof that rhythm. In addition, some patients mayundergo stress testing because of another study,such as an echocardiogram or a coronary calciumscoring test, that was abnormal.
What is involved in a stress test?
Stress tests come in a variety of forms and everyeffort is made to focus the test on the patient, theircapabilities with respect to exercising, and theinformation that is needed. The first step in thedecision process is to determine what type of“stress” will be used for the study. In general, thebest type of stress test is one in which the patientexercises, either on a treadmill or on a stationarybicycle. This is because there is very usefulinformation that comes from observing howsomeone responds to exercise. However, physiciansrecognize that not all patients are able to exercise,either safely or to an adequate level, to providediagnostic information on the stress test. For thoseindividuals, a drug (adenosine, dipyridamole,regadenoson, or dobutamine) is given that dilatesthe coronary arteries that feed the heart to mimicwhat occurs during exercise. If a patient undergoessuch a pharmacologic stress test, it is very importantto follow the instructions provided to them inpreparation for the stress test.
Raymond Russell, III, MD, PhD, FASNC, FACCAssociate Professor of Medicine
Warren Alpert Medical School of Brown UniversityDirector, Nuclear Cardiology, Rhode Island HospitalPresident, American Society of Nuclear Cardiology
Disclosures: Spouse employed by Novartis Institutes for Biomedical Research
Stress testing: Questions and Answers
10
Figure 1. A normalstress test imaging
study. The stress imagesare shown in the rowsmarked A and the rest
images are shown inthe rows marked B. The
uptake of theradioactive dye is similar
throughout the heartmuscle shown in threedifferent orientations:
short axis (top), verticallong axis (middle), and
horizontal long axis(bottom).
The second step in the decision process is todetermine whether some type of imaging of theheart is required to increase the ability to detectdecreased blood flow (ischemia) in the heart. Thereare several types of imaging that can be performed,nuclear perfusion imaging, echocardiographicfunctional imaging, or cardiac magnetic resonanceperfusion imaging. In this article, I will focus onnuclear perfusion imaging. If a patient is at low riskof having CAD, and they can exercise, and they havea normal electrocardiogram, then an exercise stresstest without any form of imaging is generallyappropriate. If the patient has risk factors for CADor has an established diagnosis of CAD, thenimaging is likely to be an important adjunct to detectCAD. If the patient cannot exercise adequately, thenthey will require a pharmacologic stress test withimaging to detect CAD.
On the day of the stress test, the patient will be“prepped” for the procedure. This includes have anintravenous (i.v.) catheter inserted for theadministration of a pharmacologic stress agent (ifneeded) and the radioactive dye to image the heart(if needed). In general, both exercise andpharmacologic stress tests are safe, but the insertionof an i.v. catheter also allows for the ability to giveother medications if needed. In addition,electrocardiographic electrodes are attached to thebody to record the ECG during the study.
For an exercise stress test, the patient will exercise atincreasing levels of exertion up to the point that theycannot exercise any further. At this point, aradioactive dye is injected by vein and is taken up bythe heart. For the pharmacologic stress test, one ofthe vasodilating agents is injection to increase bloodflow to the heart and then the radioactive dye isinjected to once again evaluate blood flow to theheart. It is not uncommon for someone to experiencesymptoms such as shortness of breath or chest painduring the injection of the pharmacologic agents.The patient’s blood pressure and electrocardiogramare monitored continuously during the stress test bya nurse or physician and they will ask about anysymptoms that the patient may have.
After the radioactive dye is injected, the patient willrest for 10-45 minutes before being placed in aspecial camera that detects the radioactivity taken upby the heart. Depending on the type of camera, apatient may lay under/inside the camera for 5-30minutes. In addition to the images obtained afterstress testing, a patient may need to have restingimages taken for comparison. This involves all of thesteps described above, except for the stress testing.
What information comes from the stress test?
The stress test and imaging that are performedprovide very valuable information for the referringphysician. An example of a normal stress test, inwhich the blood flow is normal throughout theheart, is shown in figure 1. An example of an
abnormal stress test, with significant decreases inblood flow, is shown in figure 2.
The information from the stress test, in addition tothe imaging study provides a “yes/no” answer to thequestion of whether someone had blockages in thecoronary arteries. But more importantly, the dataprovides an assessment of risk of having a heartattack (myocardial infarction) or experiencing cardiacdeath over the next year. In other words, someonewho has a small decrease in blood flow to their hearton the stress test is at low risk of having a heartattack or cardiac death over the ensuing year andmay be best served by starting with a treatment planthat focuses on medical therapy and risk factormanagement. In contrast, someone who has severe,diffuse decreases in blood flow would be consideredat high risk of cardiac events and may be betterserved by undergoing a treatment plan that includescardiac catheterization and revascularization toimprove blood flow to the heart, either byangioplasty and stenting or by bypass surgery.
These are just some of the questions that I get askedwhen someone is undergoing a stress test, and everyindividual has different questions and concerns asthey face testing. In addition, based on variety offactors, your stress test may not follow the exactcourse I have described above and the treatmentdecisions similarly may be different. Be sure that youunderstand what sort of testing your physician hasrecommended and that your questions areanswered.
11
Figure 2. An abnormal stress test image. The stress and restimages are once again shown as described in Figure 1. There isdecreased blood flow in the stress images, as indicated by thewhite arrows, that improves in the resting images. These findingsare consistent with the presence of significant blockages in thecoronary arteries.

Introdução: A avaliação quantitativa da função contrátil dascâmaras cardíacas é ponto de grande interesse clínicopois têm elevada importância diagnóstica eprognóstica. Como principal ponto de utilidadeclínica, a insuficiência cardíaca (IC) tem como alicercediagnóstico central a avaliação da presença dedisfunção sistólica do ventrículo esquerda que agrupaos pacientes em Insuficiência Cardíaca com Fração deEjeção Reduzida (ICFER) que tem como baseterapêutica a detecção de etiologias potencialmentereversíveis da disfunção sistólica e o tratamento combetabloqueadores e inibidores da enzima deconversão da angiotensina II. Em contrapartida apresença de uma fração de ejeção preservada aliadaa outros dados clínicos e laboratoriais configura odiagnóstico de Insuficiência Cardíaca com Fração deEjeção Preservada (ICFER) que corresponde a até 50%dos casos de IC e que muda radicalmente aabordagem terapêutica da condição (1).
A avaliação da função ventricular também éum poderosa ferramenta prognóstica e servepara guiar a terapêutica. Os pacientes comdisfunção sistólica do ventrículo esquerdo têmmaior morbidade e mortalidade em diversascondições como na cardiopatia isquêmica,miocardiopatia dilatada, valvopatias, afecçõesinflamatórias do miocárdio como miocardite ena cardiotoxidade decorrente do uso dedrogas antineoplásicas. A presença dedisfunção ventricular serve como critérioprincipal para indicação de implante dedispositivos de alta complexidade como ocardioversor desfibrilador implantável (DCI),que é fortemente indicado em pacientes comcardiopatia isquêmica ou não isquêmica eFEVE < 30% persistente após 3 meses detratamento clínico otimizado, sendo que omesmo pode ser considerado quando a FEVEestiver entre 31%e 35% (2).
A cardio-oncologia representa a interseção entre acâncer e as doenças cardiovasculares. Diversostratamentos do câncer estão associados com odesenvolvimento de cardiotoxicidade, sendo as maisgraves o espasmo coronariano, angina, infarto domiocárdio, arritmias, hipertensão arterial, disfunçãoventricular esquerda e insuficiência cardíaca (4). Amonitoração seriada da fração de ejeção do ventrículoesquerdo durante quimioterapia tem sido a base paramodificação ou interrupção do uso de drogasantineoplásicas por muitos anos. A avaliação precisada função ventricular esquerda é fundamental paraque as decisões referentes ao tratamento do câncerpossam ser feitas com segurança, evitando expor opaciente ao risco de um tratamento potencialmentefatal enquanto levando em consideração o uso deuma droga com capacidade de atuar de modopositivo no tratamento do câncer (4).
O objetivo desta revisão é abordar as principaistécnicas de avaliação da função ventricular pelamedicina nuclear: (1) ventriculografia radionuclídicade primeira passagem; (2) ventriculografiaradionuclídica de equilíbrio e (3) GATED SPECT.
1. Ventriculografia radionuclídica de primeirapassagem: é a técnica cintilográfica que avalia apassagem de um bôlus do radiotraçador que passapelas câmaras cardíacas permitindo o cálculo dafração de ejeção de ambos ventrículos, e nos casosde shunts intracardíacos, estimar o volume do débitocardíaco que é desviado do seu trajeto normal.Normalmente este exame é realizado em repousocom o paciente deitado em posição supina em frenteao detector da gama câmara. As imagens sãorealizadas em intervalos de 20-30 mseg (24-48/ciclo)durante 45-60 segundos e são obtidasimediatamente após injeção do bolo doradiofármaco. A qualidade da injeção do bolusradioativo e da sincronização eletrocardiográfica écrucial para bons resultados. São geradas curvas
Claudio T Mesquita MD, FACC, PhD
Chief of section of nuclear medicine of Hospital Universitário Antonio Pedro Immediate Past-President of Brazilian S
ociety of Nuclear Medicine (2015-2016)Editor-in-Chief of International Journal of Cardiovascular Sciences
Professor of Medicine, Universidade Federal Fluminense, Rio de Janeiro, Brazil.
USO DA MEDICINA NUCLEAR NA AVALIAÇÃODA FUNÇÃO VENTRICULAR
12
tempo-atividade para cálculo da fração de ejeção decada um dos ventrículos (figura 1). Como há umamelhor separação temporal entre as câmarascardíacas a fração de ejeção do ventrículo direito émelhor avaliada por esta técnica em comparaçãocom a ventriculografia de equilíbrio. Atualmente aventriculografia de primeira passagem é maisempregada na avaliação da função ventriculardireita, especialmente em pacientes com janelaecocardiográfica comprometida, pacientes comdispositivos cardíacos implantáveis (que limitam ouso da ressonância magnética) e noacompanhamento de pacientes com hipertensãoarterial pulmonar. Uma fração de ejeção doventrículo direito inferior a 40% é consideradadefinitivamente anormal (5).
A fração de ejeção do ventrículo direito (FEVD)calculada pela ventriculografia de primeira passagemé um reconhecido preditor de maior mortalidade empacientes com insuficiência cardíaca congestiva (6).Outra aplicação importante é na avaliação doprognóstico de pacientes hipertensão arterialpulmonar, sendo que aqueles que demonstramqueda na fração de ejeção do ventrículo direito pós-exercício ou maior tempo de trânsito pulmonar doradiotraçador têm pior prognóstico (7).
2. Ventriculografia de equilíbrio: nesta técnica oradiotraçador é administrado por via venosa e apósum período de equilíbrio do mesmo na circulaçãosão tomadas imagens sincronizadas do coração como intuito de avaliar a fração de ejeção das câmarasventriculares. Em geral é utilizado o pirofosfatoestanhoso com o objetivo de reduzir a hemoglobinadas hemácias e permitir a marcação das hemáciascom o 99mTcO4- (pertecnetato) que é administradopor via venosa após 15 minutos da administração dopirofosfato. Após o período de 10 a 15 minutos deequilíbrio são tomadas imagens planaressincronizadas com o eletrocardiograma em pelomenos três projeções : anterior, obliqua anterioresquerda (com melhor separação dos ventrículos quefor possível) e lateral esquerda. A avaliação da funçãodiastólica também é possível com um mínino de 32
frames/ciclo. Para o exame ter adequada taxa decontagens (500 mil a 1 milhão de contagens porprojeção) são necessários 10 a 15 minutos deaquisição (8).
A ventriculografia de equilíbrio permite a análise dotamanho das câmaras cardíacas, avaliação da funçãosistólica global e regional, avaliação da funçãodiastólica e do sincronismo intraventricular pelaanálise de fase. A quantificação da função ventricularesquerda sistólica e diastólica é obtida pela curvatempo-atividade da projeção obliqua anterioresquerda, em que o ventrículo direito não superpõeo ventrículo esquerdo. A análise paramétrica dafunção ventricular permite a avaliação da motilidaderegional de modo quantitativo (amplitude) e da
sincronia contrátil das paredes(fase). Uma fração de ejeçãoabaixo de 50% já éconsiderada como anormal namaioria das instituições (figura2). Além da avaliação da funçãosistólica a ventriculografia deequilíbrio permite a avaliaçãoda função diastólica, sendoos índices mais frequentementeavaliados a taxa máxima deenchimento ventricularesquerdo (valor normal > 2,5Volumes diastólicosfinais/segundo) e o tempo taxamáxima de enchimentoventricular esquerdo (valornormal < 180 ms).
A aquisição tomográfica pode ser realizada e geraimagens tridimensionais que adicionalmentepermitem a avaliação dos volumes das câmarascardíacas.
A grande vantagem da ventriculografiaradionuclídica é a sua alta reprodutibilidade eacurácia, o que a torna superior à ventriculografia deprimeira passagem para avaliar a função doventrículo esquerdo e uma ferramenta útil paramonitoramento da função contrátil de modo
13
Figura 1:Ventriculografia deprimeira passagemdemonstrandodisfunção ventriculardireita (fração deejeção do VD = 28%)em um paciente com50 anos, enfisemapulmonar e sintomasde insuficiênciacardíaca direita.
Figura 2:Ventriculografia deequilíbrio demonstrandodisfunção ventricularesquerda (FEVE = 37%) em um paciente commiocardite viral.Observar que ohistograma de fasedemonstra significativoretardo contrátil naregião apical doventrículo esquerdo (cor amarela).

seriado. Desta forma as principais indicações parauso da ventriculografia radionuclídica envolvem adeterminação com precisão da fração de ejeção doventrículo esquerdo, como em pacientes pós-infartoem se requer a definição para implante decardioversor desfibrilador, pacientes com valvopatiasem que a queda da fração de ejeção constitui-seindicação cirúrgica, pacientes em uso de drogascardiotóxicas como antraciclínicos e trastuzumab. Aventriculografia radionuclídica é um método maisreprodutível e acurado que as medidasbidimensionais obtidas pelo ecocardiografia, sendo
muito útil em pacientes acompanhados em uso dedrogas cardiotóxicas (9). Uma limitação ao uso daventriculografia é a exposição à radiação decorrentedos múltiplos exames, entretanto a técnica é usadacom frequência pela confiabilidade dos seusresultados. Estudo recente demonstrou que no MDAnderson Cancer Center 28% dos pacientes em usode trastuzumab eram monitorados com aventriculografia radionuclídica (10).
3. Gated SPECT: a cintilografia de perfusãomiocárdica com 99mTc-sestamibi, com contagensestatísticas superiores às observadas no exames com201Tálio, permitiu que a sincronização da aquisiçãodas imagens com eletrocardiográfica trouxesse obenefício da avaliação da função ventricularesquerda. A técnica não aumenta a exposição àradiação ou o tempo de aquisição do exame eagrega avaliação de importantes parâmetros daanálise da função ventricular esquerda global eregional, além da fração de ejeção do ventrículoesquerdo pós-estresse e os volumes ventriculares aofinal da sístole e da diástole. Mais recentemente foiagregado ao Gated SPECT a avaliação da funçãodiastólica e a avaliação da análise de fase econsequentemente do sincronismo intraventricular(11).
14
Figura 3: Ventriculografiatomográfica de equilíbrio(blood pool gated SPECT)demonstrando disfunção
sistólica avançadabiventricular e aumento de
ambas câmaras ventricularesem um pacientes com
miocardiopatia chagásica.
Uma das vantagens em relação à ventriculografiaradionuclídica, em que se observa a motilidade dascamaras, no GATED Spect podemos avaliar oespessamento parietal, que é extremamenteimportante, pois a presença de espessamento domiocárdio é um indicativo direto de viabilidademiocárdica. Áreas de infarto contida entresegmentos com contratilidade normal podemapresentar motilidade normal, entretanto oespessamento será alterado. Em decorrência destainformação o GATED Spect se tornou também umaferramenta para diferenciar áreas de artefatos deatenuação (em que há hipoperfusão comespessamento preservado) de áreas de infarto prévio(hipoperfusão concomitante com redução doespessamento). Outra informação relevante obtida apartir do Gated SPECT é a redução da funçãoregional transitória que pode ser observada naaquisição pós-estresse, que está associada à isquemiasignificativa na região, um fenômeno denominadode atordoamento miocárdico.
Por fim, o Gated SPECT também oferece aoportunidade da analise da fase ventricular esquerda,ou seja do momento do início da contração parietal,de modo preciso e reprodutível. Esta avaliação estásendo testada como parâmetro de dissincronismoventricular nos casos de pacientes com bloqueio deramo esquerdo e insuficiência cardíaca avançada queestão sendo considerados para Terapia deRessincronização Cardíaca (TRC). Além de avaliar apresença de dissincronismo mecânico, o GATED Spectpermite avaliar se o último segmento a se contrair éviável (tem perfusão adequada do traçador), pois istoé um ponto crucial para o implante do eletrodo doventrículo esquerdo na TRC.
Conclusão: A medicina nuclear tem ferramentas validadas,acuradas, reprodutíveis e de fácil acesso paraavaliação da função ventricular. A sua utilizaçãopermite beneficiar pacientes em diversos cenários,sendo que o reconhecimento da sua aplicabilidade éimportante para clínicos, cirurgiões e cardiologistas.
Referências: __________________________
1. Redfield MM. Heart Failure with Preserved EjectionFraction. N Engl J Med. 2017 Mar 2;376(9):897
2. Bennett M, Parkash R, Nery P, Sénéchal M, Mondesert B,Birnie D, Sterns LD, Rinne C, Exner D, Philippon F, CampbellD, Cox J, Dorian P, Essebag V, Krahn A, Manlucu J, Molin F,Slawnych M, Talajic M. Canadian CardiovascularSociety/Canadian Heart Rhythm Society 2016 ImplantableCardioverter-Defibrillator Guidelines. Can J Cardiol. 2017Feb;33(2):174-188.
3. Russell RR, Alexander J, Jain D, Poornima IG, SrivastavaAV, Storozynsky E, Schwartz RG. The role and clinicaleffectiveness of multimodality imaging in the managementof cardiac complications of cancer and cancer therapy. J NuclCardiol. 2016 Aug;23(4):856-84
4. Russell RR, Alexander J, Jain D, Poornima IG, SrivastavaAV, Storozynsky E, Schwartz RG. The role and clinicaleffectiveness of multimodality imaging in the managementof cardiac complications of cancer and cancer therapy. J NuclCardiol. 2016 Aug;23(4):856-84.
5. Friedman JD, Berman DS, Borges-Neto S, Hayes SW,Johnson LL, Nichols KJ, Pagnanelli RA, Port SC; QualityAssurance Committee of the American Society of NuclearCardiology. First-pass radionuclide angiography. J NuclCardiol. 2006 Nov;13(6):e42-55.
6. Murninkas, Daniel et al. Right Ventricular Function andPrognosis in Stable Heart Failure Patients. Journal of CardiacFailure , Volume 20 , Issue 5 , 343 - 349
7. Wu YW, Hsu PY, Lin YH, Cheng MF, Ko CL, Huang YH,Yen RF, Chen JS, Lin JW, Hsu HH. Diagnostic and PrognosticImplications of Exercise Treadmill and Rest First-PassRadionuclide Angiography in Patients With PulmonaryHypertension. Clin Nucl Med. 2017 Sep;42(9):e392-e399.
8. Nicol A, Avison M, Harbinson M, Jeans S, Waddington W,Woldman S; BNCS; BNMS; IPEM. Procedure guideline forplanar radionuclide cardiac ventriculogram for theassessment of left ventricular systolic function. Nucl MedCommun. 2009 Mar;30(3):245-52.
9. Virani SA, Dent S, Brezden-Masley C, Clarke B, Davis MK,Jassal DS, Johnson C, Lemieux J, Paterson I, Sebag IA,Simmons C, Sulpher J, Thain K, Thavendiranathan P,Wentzell JR, Wurtele N, Côté MA, Fine NM, Haddad H,Hayley BD, Hopkins S, Joy AA, Rayson D, Stadnick E,Straatman L. Canadian Cardiovascular Society Guidelines forEvaluation and Management of CardiovascularComplications of Cancer Therapy. Can J Cardiol. 2016Jul;32(7):831-41.
10. Chavez-MacGregor M, Niu J, Zhang N, Elting LS, SmithBD, Banchs J, Hortobagyi GN, Giordano SH. CardiacMonitoring During Adjuvant Trastuzumab-BasedChemotherapy Among Older Patients With Breast Cancer. JClin Oncol. 2015 Jul 1;33(19):2176-83.
11. Abidov A, Germano G, Hachamovitch R, Slomka P,Berman DS. Gated SPECT in assessment of regional andglobal left ventricular function: an update. J Nucl Cardiol.2013 Dec;20(6):1118-43;
__________________________
15
Figura 4: Gated Spect em repouso e após estressedemonstrando redução da motilidade e do espessamentoapós o estresse na parede anterior, achado consistentecom isquemia miocárdica estresse induzida na região :atordoamento miocárdico (stunning myocardium).

IntroductionDepuis près d’un demi-siècle, la scintigraphie de laperfusion myocardique s’est développée progres-sivement pour devenir une modalité de choix dans lediagnostic et le pronostic de la maladie coronarienne.Des percées technologiques importantes ont étéréalisées en médecine nucléaire conventionnelle, autantdu côté des radiotraceurs (Potassium-43, Thallium-201,Sestamibi-99mTc, Tétrofosmine-99mTc) que des appareilsscintigraphiques (planaires, tomographiques (SPECT),tomographiques dédiées à la cardiologie, couplés à untomodensitomètre (TDM)). En parallèle à cetteprogression permettant à la médecine nucléairecardiaque de prendre une place importante dansl’évaluation des patients porteurs ou potentiellementporteurs d’une maladie coronarienne athérosclérotique,les études utilisant la tomographie par émission depositrons (TEP) offraient des avancées majeures dans lacompréhension de la physiopathologie des maladiescardiaques. Dans certains milieux ultraspécialisés, latechnologie TEP s’implante progressivement, devenantune modalité de choix pour évaluer la maladiecoronarienne en clinique.
Perfusion myocardiqueLes radiotraceurs de perfusion myocardique injectés parvoie intraveineuse ont la propriété de se distribuer dansle muscle cardiaque en proportion avec la quantité desang nourrissant celui-ci. L’examen est fait en deuxparties : une injection du traceur avec imagerie au repos
et une injection avec imagerie lors de l'augmentationde la perfusion myocardique suite à un effort ou unestimulation pharmacologique. La comparaison des deuxséries d’images permet de différencier les zonesnormalement perfusées de celles qui sont en souffrance,mais que l’on pourrait traiter ainsi que de celles qui sontirrémédiablement atteintes suite à un infarctus.
Présentement, la très grande majorité des centreseffectuant de la médecine nucléaire cardiaque utilise latechnologie SPECT (avec ou sans TDM) et des agentstechnétiés (Sestamibi-99mTc, Tétrofosmine-99mTc). Unemultitude d’études a démontré l’utilité de cettetechnique pour diagnostiquer la maladie coronariennesténosante et, le cas échéant, déterminer le risqueassocié à la sévérité de la maladie afin d’orienter lathérapie (traitement médical versus revascularisation).
Tomographie par émission de positronsLa technologie TEP est utilisée en clinique depuisplusieurs années, principalement en oncologie. Alorsque la capacité d’effectuer des études TEP en cardiologien’était réservée qu’aux rares centres académiquespossédant un cyclotron, l’arrivée du rubidium-82 (Rb-82) a permis d’augmenter progressivement la capacitéd’offrir des études de perfusion myocardique en TEP.Étant produit par un générateur, le Rb-82 ne nécessitepas d’être fabriqué sur place par un cyclotron. Les deuxphases de l’examen, au repos et sous stimulationpharmacologique, sont effectuées séquentiellement
Jean Grégoire, MD, FRCPC
Département de radiologie et de médecine nucléaireInstitut de cardiologie de Montréal
Professeur adjoint de cliniqueDépartement de radiologie, radio-oncologie et médecine nucléaire
Université de Montréal
PERFUSION MYOCARDIQUEAU RUBIDIUM-82
16
sous la caméra TEP, alors que le patient reçoit le Rb-82via un générateur à son chevet. Cette configuration faitque la stimulation doit être effectuée via unvasodilatateur pharmaceutique, habituellement ledipyridamole, et qu’un test à l’effort n’est pas possible.
Les appareils TEP récents sont couplés à untomodensitomètre (TDM), ce qui permet de corriger lesscintigraphies pour l’atténuation causée par les tissusadjacents au cœur (seins, diaphragme, etc.) etd’accroitre la qualité des images. Chez l’humain, lesappareils TEP ont une résolution spatiale supérieure auxcaméras SPECT. L’efficacité de la TEP pour le diagnosticde la maladie coronarienne obstructive est légèrementsupérieure à la technologie conventionnelle. Cettecaractéristique est particulièrement avantageuse chezles patients obèses. La demi-vie du Rb-82 étant trèscourte, ceci permet d’acquérir rapidement des imagesde qualité tout en diminuant de façon importante ladose de radiation reçue par le patient. Un examencomplet peut être complété plus rapidement qu’un testconventionnel, soit en environ 45 minutes.
Un des avantages marqués de la perfusion myo-cardique du Rb-82 découle de sa capacité à obtenir desmesures quantitatives de perfusion myocardique.Contrairement aux études conventionnelles où l’ondétermine la perfusion myocardique relative d’uneparoi cardiaque par rapport à une autre, les études auRb-82 permettent de mesurer la perfusion myocardiquede façon absolue. Il est possible de calculer la réservemyocardique, c’est-à-dire la capacité du système artérielcoronarien d’augmenter son flot lors d’unevasodilatation coronarienne. Ceci est optimal pourévaluer les patients atteints d’une maladie coronarienneimpliquant plusieurs vaisseaux causant de l’ischémiebalancée ainsi que chez les individus porteurs d’uneatteinte des petits vaisseaux coronariens (atteintemicrovasculaire).
Considérations financières et logistiquesActuellement au Québec, on assiste à une mise en placede la technologie TEP-Rb-82 limitée à quelques centresultraspécialisés en cardiologie. Pour que les coûts de cetexamen soient acceptables, l’implantation de cettetechnique doit se faire dans des centres effectuant unnombre important d'études de perfusion myocardique.
Bien que la différence se soit atténuée au fil des ans,une caméra TEP est plus couteuse qu’une caméraconventionnelle SPECT. De plus, l’achat d’un générateurde Rb-82 comporte un coût fixe important sur une baseannuelle. Par contre, les coûts variables sont faibles. Plusun générateur de rubidium sera utilisé, plus le coût parpatient sera moindre. Avec un appareil TEP dédié etpour une journée habituelle de travail, il est possibled’effectuer 10 à 12 études complètes par jour sur unappareil TEP, soit environ 2500 à 3000 examens parannée. Si la demande le justifie, la capacité d’étendreles heures de travail en soirée et les weekendsdiminuerait d’autant le coût de revient de l’étude.
On ne doit pas négliger les avantages importantsassociés à la capacité d’effectuer une étude de perfusionmyocardique plus rapidement, en particulier pour lespatients observés à l’urgence ou une réponse rapidepermet d’accélérer la prise en charge.
ConclusionLa technologie TEP-Rubidium constitue une progressionmajeure dans l’étude de la perfusion myocardique.Actuellement, les coûts associés à cette technique nepermettent que de justifier son implantation dans descentres ultraspécialisés en cardiologie. Comme pour lesautres progressions dans le passé, il est à prévoir quecette technique deviendra progressivement plusaccessible et que davantage de nos patients pourronten bénéficier.
17
Avantages de la TEP-Rubidium :• Radiation moindre : de l’ordre de cinq à 10 fois • Plus rapide : examen complet en 45 minutes• Quantitatif : permet de quantifier la réserve myocardique et de
détecter la maladie microvasculaire et l’ischémie balancée• Efficacité diagnostique légèrement supérieure au SPECT• Meilleure qualité d’images, en particulier chez les patients obèses• Coûts variables faibles : radiotraceur toujours disponible• Évaluation de la fonction ventriculaire gauche au repos et per-stimulation
Désavantages du rubidium-82 :• Coûts fixes élevés : appareil TEP, générateur de rubidium• Uniquement sous stimulation pharmacologique
Perfusion myocardique au rubidium sous dypridamole(Str) et au repos (Rst) – Examen normal
L’analyse des coupes scintigraphiques ainsi que descartes polaires montre une distribution uniforme du
radiotraceur. Les mesures de flot absolu montrent qu’ily a une réserve myocardique supérieure à 3 pour
l’ensemble du ventricule gauche ainsi que pour chacundes principaux territoires vasculaires.
Perfusion myocardique au rubidium sous dypridamole(Str) et au repos (Rst) – Examen anormalL’analyse des coupes scintigraphiques ainsi que descartes polaires montre un déficit de perfusiond’étendue sévère et dont le gradient est modéré auniveau de la paroi latérale et plus léger au niveau de laparoi antéro-latérale. Les mesures de flot absolumontrent qu’il y a une réserve myocardique de 1,8dans le territoire de l’artère circonflexe alors que lesvaleurs sont supérieures à 2,5 pour les autresterritoires vasculaires.

We developed the University of Colorado Dose-Risk Smartcard shown on the following
page(s) to summarize the effective doses andradiation risks of common radiological examinations(1). We have found it useful to radiologists, medicalphysicists, radiology and nuclear medicinepersonnel, referring physicians, and other medicalpersonnel interested in understanding radiationrisks and in communicating those risks to patients.Understanding radiation risks, along with otherrisks and benefits of an exam or procedure,empowers patients to make informed medicaldecisions.
Effective doses estimates for many exams andprocedures come from a 2008 article by Mettler,et.al. (2). Effective doses and risk estimates formammography exams come from recent articles byHendrick, et.al. (3-5). Most estimates of cancer riskfrom radiation exposures in the Smartcard arebased on the International Commission onRadiological Protection Report #103 (ICRP-103) (6).ICRP-103 estimates of radiation risk are age-averaged for adults ages 18-65 years and gender-averaged, resulting in a fatal cancer induction riskof 4.1% per Sievert (Sv) of effective dose or aprobability factor of 0.041 per Sv. Risks estimatesspecific to females undergoing mammography arebased on the National Academy of Sciences’Biological Effects of Ionizing Radiation (BEIR-VII)report (7,4,5).
Both ICRP-103 and BEIR-VII assume alinear, no-threshold (LNT) relationship
between radiation dose and cancerrisk for solid tumors to
extrapolate from the high-dose,high linear energy transfer(LET) exposures, such as thoseto atomic bomb survivorswhere subsequent radiation-induced cancers have beendocumented, to the low-dose,
low-LET exposures fromdiagnostic radiology exams,
where no direct cancer-causingeffect has been found in humans.
Evidence from the study of atomic bomb survivorsindicates that organ doses above 100 milliSieverts(mSv) result in a small, but statistically significant,increase in cancer risk. The risks shown on theSmartcard use the LNT model to extrapolate thedose-risk relationship down to the low dose levelsused in diagnostic exams. These risk estimates areconservative in terms of protecting patients andmay overestimate rather than underestimateradiation risk from medical exams. We understandthat there are those who challenge the validity ofthe LNT model (8).
The Smartcard puts doses and risks in perspectiveby comparing effective doses from variousradiological exams to natural background radiationlevels, and includes a scale corresponding to theACR Appropriateness Criteria relative radiation leveldesignation (9, 10). The Smartcard also provides acolor-coded scale categorizing the level of risk of afatal radiation-induced cancer and compares thosecategories to risks of death from other causes.
In many cases, there are significant age-dependentand gender-dependent variations in both radiationdose and risk estimates (7, 11-13). We have notattempted to incorporate all of those variations inthe Smartcard, but instead to provide arepresentative estimate of effective doses andradiation risks to adults.
We recognize that major efforts have taken placeto reduce patient doses from radiological examssince the effective dose estimates appearing inMettler et al (2), particularly for CT and nuclearmedicine exams (14-18). As a result, some patientdoses and estimated radiation risks may be lowerthan those shown because of those dose-reductionefforts.
Like other radiology departments, the University ofColorado Department of Radiology is dedicated tothe goal of ensuring that only necessary exams areperformed and that patients undergoing diagnosticexams receive the lowest radiation dose necessaryto convey medical benefit.
R. Edward Hendrick, Ph.D. Gary D. Fullerton, Ph.D.
William R. Hendee, Ph.D.James P. Borgstede, M.D.
Fred Larke, M.S.
THE UNIVERSITY OF COLORADODOSE-RISK SMARTCARD
18
1. Hendrick RE, Dodd GD, Fullerton GD, Hendee WR, Borgstede JP, Larke F. TheUniversity of Colorado radiology adult dose-risk Smartcard. JACR 2012; 9 (4): 290-292.
2. Mettler FA, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology andnuclear medicine: a catalog. Radiology 2008; 248:254-263.
3. Hendrick RE, Pisano ED, Averbukh A, et.al. Comparison of acquisition parameters andbreast dose in digital mammography and screen-film mammography in the AmericanCollege of Radiology Imaging Network Digital Mammographic Screening Trial. Am. J.Roentgenology 2010; 194: 362-369.
4. Hendrick RE. Radiation doses and cancer risks from breast imaging studies.Radiology 2010; 257: 246-253.
5. Hendrick RE, Tredennick T. Benefit to radiation risk of breast-specific gammaimaging compared with mammography in screening asymptomatic women withdense breasts. Radiology 2016: 281: 583-588.
6. ICRP 2007: International Commission on Radiological Protection.“Recommendations of the International Commission on Radiological Protection”,ICRP Publication No. 103. Ann ICRP. 1(3), 2007.
7. Health risks from exposure to low levels of ionizing radiation –BEIR VII, Phase 2.Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation,National Research Council of the National Academies, Washington, DC: NationalAcademies Press, 2006.
8. Siegel JA, Pennington CW, Sacks B. Subjecting radiologic imaging to the linearno-threshold hypothesis: A non-sequitur of non-trivial proportion. J Nucl. Med. 2017;58: 1–6.
9. ACR Appropriateness Criteria® Radiation Dose Assessment Introduction, available athttps://www.acr.org/~/media/ACR/Documents/AppCriteria/RadiationDoseAssessmentIntro.pdf?la=en , last accessed on 3/24/17.
10. Amis ES, Jr., Butler PF, Applegate KE, et al. American College of Radiology whitepaper on radiation dose in medicine. J Am Coll Radiol 2007; 4(5):272-284.
11. Brenner DJ, Hall EJ. Computed tomography: an increasing source of radiationexposure. N. Engl. J. Med. 2007; 357: 2277-2284.
12. Shuryak I, Sachs RK, Brenner DJ. Cancer risks after radiation exposure in middleage. J. Natl. Cancer Inst. 2010; 102: 1628-1636.
13. Brenner DJ, Shuryak I, Einstein, AJ. Impact of reduced patient life expectancy onpotential cancer risks from radiologic imaging. Radiology 2011; 261: 193-198.
14. Amis ES. CT radiation dose: trending in the right direction. Radiology 2011; 261:5-8.
15. White Paper: Initiative to Reduce Unnecessary Radiation Exposure fromMedical Imaging, available at: https://www.fda.gov/Radiation-EmittingProducts/RadiationSafety/RadiationDoseReduction/ucm199994.htm (last accessed on 3/24/17).
16. Image GentlySM , at http://www.imagegently.org/ (last accessed on 3/24/17).
17.Image WiselyTM, Radiation safety in adult medical imaging, athttp://imagewisely.org/ (last accessed on 3/24/17).
18. Singh S, Kalra MK, Thrall JH, Mahesh M. Pointers for optimizing radiation dosein chest CT protocols. JACR 2011; 8: 663-665.
19
References:___________________________________________________________________________________________________________________
Gerald D. Dodd III, M.D.
Figures:The following
figures comprise thefront and back of atrifold University ofColorado Dose-Risk
Smartcard. They canbe cutout, taped
together and foldedinto a pocketsizetrifold for use in
clinics.

The Arab Society of Nuclear Medicine is arelatively young society. For those who arenot familiar with the ARSNM, can you describesuccinctly its role in the field of nuclearmedicine?
Until recently, nuclear medicine in our region was notrepresented by any organizing body. As nuclearmedicine physicians, we have perceived that thisdisadvantaged situation undermined our scientificand medical community and resulted in loss of manyopportunities, whether at national or internationalslevels. This unprivileged condition has triggered ourinitiative to establish and promote the Arab Societyof Nuclear Medicine (ARSNM).
Promoting and advocating nuclear medicine specialtyin the region is a vigorous objective for ARSNM. Oneof our principal goals is to support education effortsfor nuclear physicians, physicists, technologists, radiopharmacists and radio chemists from the Arab world.
In achieving its programmatic goals, the ARSNM willwork with its members, national societies andleaders in the fields, as well as with internationalhealth and scientific bodies like the InternationalAtomic Energy Agency (IAEA) and the WorldFederation of Nuclear Medicine and Biology(WFNMB). This will empower us to enhance nuclearmedicine education and improve access to thehighest quality nuclear medicine and molecularimaging care in the medical community resulting inmany benefits for our patients.
What are the most dramatic changes that youhave seen in the field of nuclear medicine overthe past 10 years?
In the past decade, hybrid imaging, namely, thepositron imaging tomography combined withcomputed tomography (PET/CT) has reshaped thepractice of medicine particularly in the field ofoncology. Chairing the nuclear medicine departmentin one of the pioneer comprehensive cancer centerin the Middle East region, King Hussein CancerCenter, has enabled me to live and contribute tothese dramatic changes. It has been a gradualprocess with some resistance in the beginning, butnow we are sure that nuclear medicine physicianbecomes an essential part of the multidisciplinaryteam of most common cancers and PET/CT results isindispensable for the proper management plan ofmany cancer patients. This growing role has beenendorsed in the clinical practice guidelines atinstitutional and regional levels. Reimbursement forthis powerful modality has also been approved andbroadened. Now, we can clearly see the status ofnuclear medicine is perceptively on the rise over thelast 10 years, thanks to the PET/CT and the robustevidence based medicine for this new nuclearmedicine technique contributed by the dedicatedprofessionals in the nuclear medicine field.
How do you see the field of nuclear medicineevolving during the next decade in yourregion?
In my opinion, theranostics is the key word for theevolving nuclear medicine in the next decade. Iconsider this advancement as the new milestone innuclear medicine that has just been recognized in theclinical practice and will be empowered andexpanded in the next decade. Peptide receptorsradionuclide therapy (PPRT) for neuroendocrinetumors is the best example to be inspired. I perceivenuclear medicine as the non-invasive approach tointegrate the molecular diagnostic and targetedtherapeutic capabilities into a single platformresulting in an effective method for detecting andcharacterizing disease at cellular and molecularlevels. This will eventually tailor a precisepersonalized medicine. Ga-68 PSMA and Lu-177PSMA for diagnosis and treatment of prostatecancer, respectively, are another example of thistargeted approach. As a nuclear medicinecommunity, we are brightly expecting new and morespecific tracers to make in-road from the bench intothe bedside in the coming few years that woulddefine the particular biological processes taking placein cancer. PET/CT has the potential to non-invasivelydepict these processes and project the biologicalsignatures of different malignancies.
To your opinion, what role do you see thePangea-ePatient magazine play for nuclearmedicine?
The huge advancements in the nuclear medicine fieldthat have been already achieved and expected to beaccomplished in the next years, unquestionably needa robust approach to ensure it is will deliverable andutilized in the medical community. Equal inimportance is to promote the public awareness forsuch advances in molecular and personalizedmedicine. I see the Pangea-ePatient magazine as apowerful asset that can significantly contribute tothis robust approach.
Successfully passing the establishment phase,availability of fund and the dedicated team ofPangea-ePatient magazine are among the importantfactors that would ensure influential outreach tocolleagues in other disciplines and patients.
Nuclear medicine physicians should practice as trueconsultant to their colleagues and patients to makesuch advancements sufficiently visible in the medicalcommunity and public awareness. Pangea-ePatientmagazine is perceived as important niche in thisjourney.
Interview with: Dr. Akram Al IbraheemMD, FEBNM, DCBNC, FANMBPRESIDENT, ARAB SOCIETY OF NUCLEAR MEDECINECHAIRMAN, DEPARTMENT OF NUCLEAR MEDECINE, KHCC
20 21

President, Dr. Andrew Ross, président
Past-President, Dr. Norman Laurin,président sortant
Vice-President, Dr. Francois Lamoureux,President Elect
Secretary-Treasurer, Dr.Glenn Ollenberger, se-crétaire- trésorier
Member-at-Large, Dr. Jean-Luc Urbain,membre à titre personnel
Member-at-Large, Dr. Christopher O’Brien,membre à titre personnel
Member-at-Large, Dr. Daniel Levin,membre à titre personnel
Member-at-Large, Dr. Philip Cohen,membre à titre personnel
Member-at-Large, Dr. Antoine Leblond,membre à titre personnel
Member-at-Large, Dr. Anna Danilenko,membre à titre personnel
Member-at-Large, Dr. Salem Yuoness,membre à titre personnel
Member-at-Large, Dr. Denise Chan,membre à titre personnel
THE CANM
3 Its dedication to promote the transfer of scientific bench discoveries into molecular & personalized medical diagnostics and therapies.
3 Its ability to promote, develop and support the use of medical isotopes in the emerging countries.
3 Its proven commitment to educate and provide high level training to nuclear medicine professionnals from across the world, particularly from emerging countriesin collaboration with the Royal College of Canada.
3 The Pangea project
BOARD OF DIRECTOR / CONSEIL D’ADMINISTRATION
THE PANGEA PROJECT • Promoting nuclear medicine• Education / teaching around the world
• Continuous training
INFO CONTACTExecutive Director / Directrice ExécutiveCanadian Association of Nuclear Medicine / Association Canadienne de Médecine Nucléaire
[email protected] www.canm-acmn.ca
1.613.882.5097
Hélène Samson
nmpangea.com
SISTER ORGANIZATIONS
CANM 2017-2018 SPONSORS
Picture taken during the signature of thedocument formalizing the educational strategicalliance between Cyclopharm and the Canadian
Association of Nuclear Medicine for the safe,sound and appropriate performance of lung
ventilation/perfusion studies and theadvancement of nuclear medicine across
the globe.
From left to right:
Pr. Claudio Tinoco Mesquita, Past President, Brazilian Society of Nuclear MedicineMs. Lynn McLauchlinn, General Manager, Cyclomedica Canada Limited
Pr. Francois Lamoureux, President Elect, Canadian Association of Nuclear MedicinePr. Sanjay Gambhir, Past President, Society of Nuclear Medicine India
Pr. Andrew Ross, President, Canadian Association of Nuclear MedicinePr. Jean-Luc Urbain, Past President, Canadian Association of Nuclear Medicine
Mr.James McBrayer, CEO & Managing Director, Cyclopharm. Ltd
[email protected] www.canm-acmn.ca
1.613.882.5097

新型SPECT肺通气灌注三维定量分析在预测肺癌患者肺叶切除术后残余肺功能的临床价值
【摘要】 目的 探讨新型SPECT肺通气灌注三维(3D)定量分析预测肺癌患者肺叶切除术后残余肺功能的能力。方法 对拟在我院行肺叶切除术的80名肺癌患者,术前1个月内行常规肺功能,高分辨率CT和SPECT肺通气灌注扫描检查。肺功能以第1秒用力呼气容积(FEV1L)表示。对SPECT肺通气灌注扫描资料分别进行2D和3D定量分析,根据获得的数值,相应计算术后肺功能的公式,得出FEV1L预测值,配对进行t检验,并与手术后2-3个月患者常规肺功能复查的实测值进行配对t检验、Pearson相关性检验和Bland-Altman一致性分析。结果 2D灌注预测值与3D灌注预测值,2D通气预测值与3D通气预测值比较差别均有统计学意义(P<0.05)。2D灌注预测值与2D通气预测值,3D灌注预测值与3D通气预测值比较差别均无统计学意义。FEV1L预测值与术后实测值比较差别均有统计学意义(P<0.05)。2D灌注预测值、2D通气预测值、3D灌注预测值、3D通气预测值与术后实测值相关系数 r 值分别为:0.711、0.695、0.884、0.862(P<0.05)。Bland-Altman—致分析结果:2D灌注预测值、2D通气预测值、3D灌注预测值、3D通气预测值与术后实测值差值的平均值和一致性界限分别为-0.346L(-0.899L,0.313L)、-0.323L(-1.075L,0.469L)、 -0.293L(-0.801L, 0.109L)、 -0.303L(-0.811L, 0.165L)。结论 新型SPECT肺通气灌注三维(3D)定量分析创新新型混合式3D肺叶定量SPECT肺通气预测肺癌患者肺叶切除术后残余肺功能的结果与手术后肺功能实测值之间有较强的相关性和一致性,较传统2D定量分析预测值更准确,可能作为预测肺叶切除术后呼吸功能的手段。
【关键词】 肺癌;肺叶切除术;体层摄影术;单
光子发射型计算机断层扫描;呼吸功能预测
Wei He,M.D., PH. D.,
Director of nuclear medicinedepartement and PET/CTCenter Fu Dan University,
affiliated with ShanghaiHua Dong Hospital
China
新型SPECT肺通气灌注三维定量分析在预测肺癌患者肺叶切除术后残余肺功能的临床价值
24 25
You have been a member of the Society of NuclearMedicine and Molecular Imaging for a long timeand just became its President. For those who arenot familiar with the SNMMI, can you describesuccinctly its role in the field of nuclear medicine?
The Society of Nuclear Medicine and MolecularImaging (SNMMI) was founded in 1954 (as theSociety of Nuclear Medicine [SNM]). The mission ofSNMMI is “To improve human health by advancingnuclear medicine, molecular imaging, andradionuclide therapy.” The SNNMI does this bysupporting 5 Domains: 1. Quality of Practice,2. Innovation/Research and Development,3. Workforce pipeline and lifelong learning,4. Advocacy, and 5. Outreach. SNMMI provideseducational materials and an annual meeting thatincludes many scientific sessions and continuingeducation sessions. SNMMI provides guidancedocuments, which include procedure standards thatprovide guidance of best practice for NuclearMedicine physicians, and appropriate use criteria,which will guide clinicians in optimal use of imagingin managing their patients. SNMMI also supportsquality assurance programs in nuclear medicine toconstantly improve the quality of practice. SNMMIpublishes the Journal of Nuclear Medicine, whichcontains the latest research in the field andcontinuing education in basic science. SNMMIpromotes research in the field of Nuclear Medicineby advancing the development and approval of newtracers and radionuclide therapies and otherimaging technologies. SNMMI supports attractingbright young physicians and scientists to work innuclear medicine/molecular imaging, supports highquality training, and supports lifelong learning. InAdvocacy, SNMMI works with governmentregulators, policy makers, and other federalagencies, as well as Congress, to support andimprove the integrity of the isotope supply chain,and promote adequate and appropriatereimbursement for nuclear medicine procedures. InOutreach, SNMMI promotes the value of NuclearMedicine in the care of patients, to referringphysicians, hospital regulators, other medicalsocieties and the public.
What are the most dramatic changes that you haveseen in the field of nuclear medicine over the past10 years?
We have seen dramatic advances in the science ofNuclear Medicine over the past 10 years. These
advances build on the scientific advances in basicsciences, especially biochemistry and immunology.In the past few years, we have seen approval by theUS Food and Drug Administration (FDA) of severaldiagnostic imaging agents, including amyloidimaging tracers, and most recently, Fluorine-18Fluciclovine for imaging prostate cancer andGallium-68 DOTATATE for imaging neuroendocrinetumors. We have also recently obtained FDAapproval for Radium-223 dichloride for radionuclidetherapy of castrate-resistant metastatic prostatecancer.
How do you see the field of nuclear medicineevolving during the next decade?
I believe we will see FDA approvals of a number ofdiagnostic tracers and therapeutic radionuclides forimaging and radionuclide therapy of variouscancers. I think within 10 years, if not sooner, wewill see major advances in radionuclide therapy ofmany cancers, with much better outcomes and farless morbidity. This really will be precision medicine.We may see improvement in diagnosis andevaluation of infectious and inflammatory diseaseswith nuclear medicine techniques. In cardiology, wewill see advances in imaging of heart disease, indiagnosis and risk assessment, especially of cardiacischemia. In neurology, I expect we will see greateruse of imaging for the various types of dementia,for diagnosis and prognosis, and also response totherapy, if we can develop useful therapies.
To your opinion, what role do you see the Pangea-ePatient magazine play for nuclear medicinepractice?
I think this magazine has a wonderful potential toraise awareness in patients, referring physicians andthe public of the value that Nuclear Medicinestudies and Nuclear Medicine therapies can providein patient care. The magazine describes in relativelyshort articles how Nuclear Medicine studies andtherapies can improve patient outcomes, manytimes with much less morbidity, in terms that canbe easily understood by the public, and especiallyby health care administrators, governmentregulators, as well as referring physicians. I see thismagazine as an important adjunct to the growth ofthe practice of Nuclear Medicine.
Interview with: Dr. Bennett S. Greenspan
T P T
2D VS 2D 0.605 >0.05
3D VS 3D 0.860 >0.05
2D VS 3D 2.145 <0.05
2D VS 3D 2.038 <0.05

KEY MESSAGES
• Ventilation/Perfusion scintigraphy (V/Por lung scan) is a powerful tool forpulmonary embolism diagnosis.
• Its performance (accuracy) is comparableto CT pulmonary angiography (CTPA) butwith only a fraction of the radiation dose(3 to 5 times less to the whole-body, 20 to50 times less to the breast in women).
• Follow-up imaging of pulmonary embolismis essential to differentiate incompletelyreperfused old emboli from new embolicevents. It should be done 3 months afterthe initial emboli.
Pulmonary embolism imaging in Nuclear Medicinehas undergone a revolution over the last decade.The replacement of old ventilation agents (Xenonand large aerosols) by ultrafine heated carbon
particles (Technegas) and the use of tomographicimaging (three-dimensional imaging analogous toCT imaging) have greatly improved the quality of ourimages. More importantly, the replacement of oldprobabilistic interpretations (low, intermediate, orhigh probability of embolism) by a binary mode ofinterpretation (embolism absent, embolism present)has proven to be much more acceptable to theclinicians and at the same time very accurate andsafe. In comparison with CTPA, V/P scintigraphy isprobably slightly more sensitive, slightly less specific,with an overall accuracy that is quite similar in theclinical setting of acute embolism. In chronicembolism, the accuracy of V/P scintigraphy is higher.
After an acute pulmonary embolism, a cascade istriggered to remove the embolic material from thepulmonary arteries. This endogenous thrombolyticprocess can be very rapid (a few days) or can takeup to 3-6 months. Younger patients with a smallerembolic load will remove their emboli more rapidlythan older patients with larger loads. Thisreperfusion process can be easily imaged with V/Pscintigraphy, with a minimal radiation dose. It is welldocumented that emboli tend to reperfuse faster onCTPA than on V/P scintigraphy. This may be due to
Norman Laurin MD, CMQ, FRCPC
Nuclear Medicine Specialist, CIUSSS-MCQ Clinical Assistant Professor, Université de Sherbrooke and Université de Montréal
VENTILATION/PERFUSION SCINTIGRAPHY INTHE FOLLOW-UP OF PULMONARY EMBOLISM
26
the inability of CTPA to image small residual anddistal cloths. Therefore, residual cloth may be seenon V/P scintigraphy but not on CTPA. The timing ofthe follow-up V/P scintigraphy must consider thenatural history of pulmonary embolism, the durationand cessation of anticoagulants therapy, and theprobability of a recurrence during and after cessationof therapy. Traditionally, oral anticoagulants areprescribed for a period of 3 months. The reperfusionprocess, partial or complete, progresses very littleafter 3 months and is almost inexistent after 6months. It is recommended that a control study beperformed 3 months after the initial embolic episode(it also coincides with cessation of therapy in mostpatients) to establish a baseline in case of futurerecurrence. This simple measure will prove invaluablein case of recurrence, allowing the distinction of newfrom old emboli with incomplete reperfusion.
27

Roland Hustinx, M.D., Ph.D.Service de Médecine nucléaire,
CHU Liège, Belgique
LE DIAGNOSTIC DE L’EMBOLIE PULMONAIRE
L’embolie pulmonaire est une pathologie fréquente,avec environ 100 000 cas par an en France, et
600 000 aux Etats-Unis. La mortalité en l’absence detraitement peut atteindre 30 %. Les thérapeutiques sonten fait très efficaces, et la majorité des décès sont liés àune absence de diagnostic, donc de traitement, plutôtqu’à un échec du traitement. Il est donc capital d’assurerun diagnostic rapide et fiable. L’embolie pulmonaire sedéfinit comme la migration, totale ou partielle, d’uncaillot dans le réseau artériel pulmonaire, causant ainsiun défaut de perfusion du poumon en aval del’obstruction. Dans la majorité des cas, ce caillot trouveson origine dans le réseau veineux se drainant dans laveine cave inférieure, soit des veines profondes desmembres inférieurs ou du bassin. Dans la moitié des cas,la source de l’embolie n’est pas identifiée. Il existe unecorrélation entre la localisation de la thrombose veineuseprofonde et la fréquence de survenue de l’emboliepulmonaire: plus la veine thrombosée est proximale(proche de la veine cave inférieure), plus les embolies sontfréquentes et sévères. En fait, thrombose veineuseprofonde et embolie pulmonaire relève d’une entitéunique, la maladie thromboembolique veineuse, avec desfacteurs de risques bien identifiés, qu’ils soient génétiquesou acquis.
Lorsqu’on envisage les méthodes diagnostiques del’embolie pulmonaire, il convient de distinguer deuxsituations particulières : La première est l’emboliepulmonaire massive, dans laquelle les répercussionshémodynamiques dominent le tableau clinique (état dechoc) et qui constitue une urgence absolue. La secondeest la maladie thromboembolique chronique, danslaquelle se développent une hypertension artériellepulmonaire et une insuffisance cardiaque. Dans les deuxcas, les stratégies de mise au point sont spécifiques etnous n’envisagerons ici que la stratégie diagnostique del’embolie pulmonaire aiguë, sans répercussionshémodynamique majeures.
La première étape du diagnostic repose avant tout surl’évaluation clinique. Le plus souvent, les signes etsymptômes présentés par le patient sont non spécifiqueset ne permettent pas le diagnostic formel. Néanmoins,lorsque le clinicien, sur base d’une anamnèsesystématique et d’un examen physique complet, associela présence (ou l’absence) de certains signes, symptômeset facteurs de risque, il aboutit à une évaluationquantifiée de la probabilité clinique de présence de lamaladie. Par exemple le score de Genève attribue un
point pour chacun des éléments suivants: antécédentsd’embolie ou de thrombose veineuse profonde,fréquence cardiaque comprise entre 75 et 94 bpm (2points lorsque la fréquence atteint 95 bpm), chirurgie oufracture dans le mois écoulé, hémoptysies (expectorationssanglantes), cancer, douleur dans une jambe, douleur àla palpation du mollet, âge supérieur à 65 ans. Un totalde 0-1 indique une faible probabilité, 2-4 une probabilitéintermédiaire, et au-delà de 4 une probabilité élevée. Onregroupe souvent les scores 0-2 en « embolie peuprobable » et 3 et plus en « embolie probable ». Ce scorede probabilité va guider la stratégie d’exploration, le choixdes examens et l’interprétation de leurs résultats. Lesexamens complémentaires à la disposition du cliniciensont essentiellement au nombre de trois: Le dosage desD-dimères dans le sang, l’angioscanner pulmonaire, et lascintigraphie pulmonaire.
Les D-DimèresIls résultent de la dégradation des produits de la fibrine,et témoignent avec une grande sensibilité de la présenced’un processus thrombotique. Le test est limité par unefaible spécificité: les D-Dimères peuvent en effet êtrefortement accrus dans un grand nombre de pathologiesautres que l’embolie pulmonaire. Citons la thromboseartérielle, le cancer, les traumatismes, les infections etc.Par conséquent, le test est très utile lorsqu’il est négatif,permettant d’exclure l’embolie pulmonaire dans lesscores de probabilité clinique faible ou intermédiaires. Ilest pas recommandé chez les patients hospitalisés, oulorsque la probabilité clinique d’embolie pulmonaire estélevée.
29
You have been a member of the Nuclear Medicinecommunity for a long time and you are now thePresident of ALASBIMN. For those who are notfamiliar with ALASBIMN. Can you describe succinctlyits role in the field of nuclear medicine?
ALASBIMN stands for Association of Latin AmericanSocieties of Nuclear Medicine and Biology. Our mainrole is to promote the development of NuclearMedicine in our region and to provide the means forour different member Societies to interact andcooperate with each other. Currently we arecomposed of 13 different scientific societies orassociations from Central and South America, andalso from Europe (Spain and Portugal). We hold aregional meeting every two years, which is the mostimportant scientific event for Nuclear Medicine inLatin America, that gathers representatives from allour member Societies. As the realities in our differentmember countries is sometimes radically different,the main purpose of this regional meeting is toprovide continuous education to the attendees aswell as to create networks that can improve theirlocal practices. This year we are having our XXVICongress in Santiago, Chile. On 2019 the ALASBIMNcongress will be held in Peru. In addition, theALASBIMN has provided since 1998 an internetbased, free access scientific platform (ALASBIMNJournal) that publishes original research as well asthe abstracts from the different local and regionalmeetings.
What are the most dramatic changes that you haveseen in the field of nuclear cardiology over the past10 years?
As our countries improve their socioeconomic status,we are starting to face the burden of cardiovasculardiseases at a higher rate in our population, but withthe health system infrastructure of under-developedcountries. This has placed the nuclear cardiologystudies, mainly the MPI, as a critical cost-effectiveexam to properly select patients to undergo theexpensive and often unavailable coronaryangiogram. It is true that the coronary CT is solvingmany of these issues worldwide, but in our regionthe Nuclear Medicine units are overtaking this rolewith excellent results. The renewal of the old SPECTgammacameras with the SPECT/CT hybridequipment, as well as the newer reconstructionalgorithms, are allowing our centers to radicallyimprove their throughputs, thus reducing the long
waiting lists. We are still behind in PET perfusionimaging as a region mainly because of the high costinvolved, with the exception of some remarkablecenters that are successfully conducting theseprocedures. Overall, I think that the rising role of theMPI in the decision-making in coronary patients aswell as the cost-effectiveness implied, has been oneof the most dramatic changes in nuclear cardiologyfor our reality.
How do you see the field of nuclear cardiologyevolving during the next decade?
I am very confident that dose and scanning time willcontinue to be reduced with a better image qualityonce the solid state detectors become the standardfor all SPECT/CT cameras, thus globally improving thepatient’s experience in the Nuclear Medicine units.As cardiac PET imaging evolves, we should expect tohave multiple tracers available for different type ofstudies, hopefully with a broader distribution andmore affordable. PET/CT scanners are also expectedto improve in the next decade, with the consequentimpact in cardiological studies. In summary, weshould be able to do shorter, cheaper, lower doseand improved image quality cardiac studies. The roleof absolute flow measurements with PET studieshopefully will be more relevant in the clinical setting,as well as other cardiac PET applications that arebeing developed.
To your opinion, what role do you see the Pangea-ePatient magazine play for nuclear medicine?
The concept of the Pangea-ePatient magazine is veryappealing to our nuclear medicine reality.Traditionally we have focused in disseminatinginformation to our peers, through meetings andtraining courses. However, for some years now, wehave started to change our recipients to referringdoctors and health administrators in order toimprove their knowledge on Nuclear Medicine examsand capabilities. In Chile we stopped organizingregular Nuclear Medicine congresses and instead westarted inviting lecturers to the cardiology meetings,oncology meetings, etc. in order to talk about ourtechniques and results. The Pangea-ePatientmagazine points in that direction, also aiming to ourpatients, and with the prior local success in Quebecwe are very excited to see if this may be replicatedworldwide.
Interview with: Dr. Rodrigo Jaimovich
28

L’angioscannerLa technique tire profit de la très haute résolution spatialede la tomodensitométrie (TDM, CT scan en anglais).Après injection intraveineuse de produit de contraste, desimages sont acquises très rapidement, lors del’opacification de l’arbre artériel pulmonaire. L’examenest très sensible, mais de petites embolies distalespeuvent échapper au diagnostic. L’insuffisance rénale etl’allergie connue au produit de contraste sont des contre-indications.
La scintigraphie pulmonaireL’examen permet d’étudier à la fois la perfusion et laventilation des poumons. Pour l’étude de perfusion, desmacro-agrégats d’albumine (MAA) marqués au 99mTc sontadministrés par voie intraveineuse. Leur taille oscille entre10 et 50 um. Les capillaires pulmonaires ayant unesection de 7 à 10 um, les 99mTc-MAA vont s’emboliserdans les artérioles précapillaires. Injectées au nombre de200 000 à 700 000 ces molécules vont réaliser uneocclusion temporaire de 0,1 à 0,2 % de la circulationpulmonaire. L’image obtenue correspond donc bien, defaçon très physiologique, à l’état de la perfusion artériellepulmonaire, y compris en périphérie. Une emboliepulmonaire apparaît sur l’image scintigraphique commeune zone hypo-active, témoignant d’un défaut deperfusion dans le parenchyme pulmonaire en aval del’occlusion artérielle. De très nombreuses autrespathologies s’accompagnent d’une altération de laperfusion, de telle sorte que l’étude de ventilation estnécessaire pour tirer pleinement parti de la scintigraphie.Plusieurs méthodes sont disponibles, avec pour point
commun l’inhalation par le patient d’un traceur qui va sedéposer au niveau pulmonaire, dans l’arbre broncho-alvéolaire. On peut utiliser des gaz comme le 81mKr, quifournit la meilleure qualité d’image, mais qui souffre deproblèmes de disponibilité et est souvent assez couteux.Une alternative est l’aérosol liquide (nébulisateur), parexemple de 99mTc-DTPA, largement disponible et peucouteux, mais dont la qualité des images est variable, enparticulier si l’état respiratoire du patient ne lui permetpas une pleine collaboration. Enfin, le Technégas est uneoption intermédiaire. Il s’agit d’une dispersion ultrafinede carbone marqué au 99mTc à l’aide d’un dispositif dédié.Il est moins sujet aux dépôts bronchiques observés dansles aérosols liquides, améliorant la qualité des images, etil est plus aisément disponible que le 81mKr. Dans tous lescas, la dosimètre est très favorable, puisque l’examen deperfusion est associé à une dose efficace de 0,017mSv/MBq, soit 0,68 à 2 mSv pour les activitéshabituellement injectées. L’exposition résultant de l’étudede ventilation est encore plus faible, 0,30 à 0,45 mSvpour le Technégas et 0,028 à 0,28 mSv pour le 81mKr.L’exploration est donc très peu irradiante et peut êtreréalisée, si la situation clinique le justifie, chez une femmeenceinte.
Quelle que soit la combinaison des traceurs, l’aspecttypique de l’embolie pulmonaire est celui d’un défaut deperfusion présentant une distribution segmentaire, ousous-segmentaire, avec une ventilation préservée. On estainsi en présence du signe cardinal de l’emboliepulmonaire, le mismatch. Classiquement, les imagesétaient acquises de façon planaire, avec des incidencesantérieures, postérieures et obliques. Depuis les annéesnonante, on connaît parfaitement les performancesdiagnostiques du test et la façon dont il influence la priseen charge du patient. La grande force de la scintigraphiepulmonaire réside dans sa valeur prédictive négative: unaspect normal de la perfusion exclut, de facto, lediagnostic d’embolie pulmonaire. C’est clairementl’examen le plus fiable pour éliminer ce diagnostic, ycompris par rapport à l’angioscan. En revanche, saspécificité est nettement plus limitée, c’est à dire qu’unrésultat positif ne signe pas systématiquement laprésence d’embolie pulmonaire. D’autre part, un nombrenon négligeable d’examens sont interprétés comme noncontributifs, à savoir ni tout à fait normal ni franchementpositif. Cette proportion tend à s’accroitre chez lespatients qui souffrent d’autres maladies cardiaques oupulmonaires, telles que la broncho-pneumopathiechronique obstructive. Chez ces patients, si la fiabilitéd’un test franchement positif ou rigoureusement normal
30
reste haute, de tels résultats, bien tranchés, apparaissentmalheureusement moins fréquents. La figure 1 montreune imagerie plantaire normale, et la figure 2 une imagetypique d’embolies pulmonaires multiples (dans les deuxcas le farceur de ventilation est le 81mKr).
Deux développements récents tendent à améliorersubstantiellement les performances diagnostiques de lascintigraphie: l’acquisition tomographique et le couplageau CT. La notion de tomographie, souvent désignés parl’acronyme anglo-saxon SPECT (Single Photon EmissionComputed Tomography) est pas neuve en médecinenucléaire, mais avec le renouvellement du parc desgamma-caméras, il est devenu plus aisé d’obtenir uneimage des poumons en 3 dimensions, dans un tempsd’acquisition raisonnable. Une étude réalisée récemmentpar Le Roux et al, à Brest, a montré qu’en présence d’unmismatch segmentaire ou de deux mismatches sous-segmentaires, le SPECT réalise le diagnostic l’emboliepulmonaire avec une sensibilité de 92 % et unespécificité de 91 %. Il est désormais également possibled’associer une étude fonctionnelle de la ventilation et dela perfusion (scintigraphie) et une étude anatomique (CTscan), à l’aide des appareils hybrides, appelés SPECT/CT.L’étude scanographique apporte des informationsadditionnelles permettant d’expliquer certaine anomaliesobservées en scintigraphie, en l’absence d’embolie, et deproposer des diagnostics alternatifs. Cette combinaisonpermet non seulement d’améliorer les performancesdiagnostiques du test mais également d’augmenter leniveau de certitude et la confiance avec lequel lediagnostic est posé, réduisant ainsi significativement letaux d’examens dits non ou peu contributifs. Relevonsque lorsque le CT est réalisé avec la scintigraphie, il s’agitd’un examen dont les paramètres d’acquisition sont fixéspour limiter l’exposition (CT « faible dose, < 1mSv) et sansinjection de produit de contraste. Les figures 3 et 4montrent des images typiques d’embolie pulmonaire enSPECT/CT (le traceur de ventilation est le Technégas).
Les recommandations internationales en termes destratégie d’exploration de l’embolie pulmonaire n’ont pasencore intégré ces données les plus récentes. Les
algorithmes sont basés sur les résultats des étudespubliées dans les années nonante et apprécient lascintigraphie essentiellement à la lumière de la très hautevaleur d’un résultat normal pour exclure le diagnostic. Defaçon générale, c’est l’angioscan qui est privilégié commeméthode d’imagerie à réaliser en première ligne. A ladifférence de la scintigraphie, il est disponible 7 jours sur7, 24h sur 24. Si le niveau d’irradiation lié au CT étaitinitialement très élevé, les appareils les plus récentspermettent de considérablement réduire la dose aupatient, pour autant que des protocoles spécifiquessoient appliqués. La dose est dans tous les cas plus faibleen scintigraphie, qui en outre ne fait pas appel au produitde contraste. Par conséquent, la scintigraphie estprivilégiée chez les patients externes avec une faibleprobabilité clinique et une radiographie thoraciquenormale, chez les jeunes patients, en particulier lesfemmes, chez les femmes enceintes, en casd’antécédents d’allergie au produit de contraste ou depoly-allergies et en cas d’insuffisance rénale sévère.
31
Figure 1
Figure 2
Figure 3
Figure 4

You have been a member of the nuclearmedicine community for a long time and youhave been at the helm of the WFNMB forthree years. For those who are not familiarwith the WFNMB, can you succinctly describeits role for the field of nuclear medicine?
The World Federation of Nuclear Medicine andBiology (WFNMB) is the peak nuclear medicineorganisation globally, and has a primary role toprogress and promote nuclear medicine throughoutthe world. It was established in 1970, and itsmembership consists of countries that have nuclearmedicine societies throughout the world, withrepresentatives participating in forums at majornuclear medicine conferences, and contributing toprojects aimed at enhancing nuclear medicinepractice.
In recent years, the WFNMB has undertaken a seriesof projects to enhance nuclear medicine practice,particularly in developing countries, and to engagewith major international organisations (e.g. IAEA,WHO) in advocacy for nuclear medicine in humanhealth. Current projects of the WFNMB include aglobal evaluation of access and availability ofradiopharmaceuticals (in conjunction with SNMMI),aimed at identifying roadblocks to use of diagnosticand therapeutic radiopharmaceuticals and strategiesto improve access; developing guidelines forminimum standards for training of nuclear medicinespecialists (in conjunction with IAEA, and all majorinternational nuclear medicine societies); developinga database of evidence based assessments fornuclear medicine procedures, to assist countries withregulatory and funding approvals of new diagnosticand therapeutic studies; and developing strategies topromote young leaders in Nuclear Medicine fromdeveloped and developing countries.
The WFNMB also runs quadrennial congresses, whichbrings together clinicians and scientists from aroundthe world to engage in educational programs,enhance interactions, and provide a forum forpromotion of nuclear medicine activities. It aims toprovide both informative and cutting-edge lectureson nuclear medicine topics, and provide a vision offuture trends in the field. The next Congress will beheld in Melbourne, Australia from April 20-24, 2018(www.wfnmb.com).
What are the most dramatic changes that youhave seen in the field of nuclear medicine overthe last 10 years?
I believe that over the last 10 years there have beena series of major technological and innovativechanges in diagnostic and therapeutic nuclearmedicine that have dramatically impacted on ourfield. One of the most important changes has beenthe expansion of PET/CT in both developed anddeveloping countries, primarily in oncology, but alsoin other clinical indications (e.g. neurology). This hasbeen largely through the acceptance in the broadermedical community of the evidence for FDG PET incancer patients, and concerted efforts to establishevidence based guidelines that incorporate FDG PETin patient management. In developing countries, the
establishment of PET Centres has been graduallyincreasing, allowing access to FDG PET for cancerpatients. The development and clinicalimplementation of new PET tracers (e.g. 68Ga-DOTATATE, 68Ga-PSMA, 18F-amino acids,18F-β-amyloid) has also provided an excitingopportunity for impact on patient care, and hasgenerated widespread interest in nuclear medicineand broader medical specialists. There is no doubtthat SPECT/CT has enormous potential to enhancethe diagnostic utility of many of our establishednuclear medicine procedures (e.g. bone scans, lungscans), and has increased the accuracy and clinicalrelevance of these studies. Finally, a resurgence intherapeutic nuclear medicine, through 223Radiumdichloride, locoregional therapy (e.g. 90Y-Sirspheres)and more recently the clinical results of multi-centretrials of 177Lu-DOTATATE and 177Lu-PSMA, has shownhow nuclear medicine techniques can make a majorimpact in cancer patients far beyond what ourtraditional areas of therapy (e.g. hyperthyroidism andthyroid cancer) would encompass.
How do you see the field of nuclear medicineevolving during the next decade?
I foresee a bright and exciting future for nuclearmedicine in the next decade. This will be driven bynew diagnostic radiopharmaceuticals, mainly for PETbut also SPECT, that will enhance our ability to
diagnose pathologic processes in oncology,neurology, cardiology, infectious diseases, and othermedical conditions. As the development of newtherapies for dementia emerge, the importance ofaccurate diagnosis of neurodegenerative conditionswill mean an increased need for FDG PET and 18F-β-amyloid, or Tau tracer studies, will occur. A majorparadigm shift in how nuclear medicine can impactin therapeutic treatment of patients, particularlyoncology, will likely emerge, driven by the enormouspotential for 177Lu-based peptide approaches.Prostate cancer treatment alone (with 177Lu-PSMA)will likely provide challenges for nuclear medicinedepartments to meet demands for treatment. Thedevelopment of theranostic approaches for nuclearmedicine therapeutics, as well as for drugdevelopment, will also continue to advance and playan increasingly important role in our clinical andresearch programs.
There are a number of challenges we need to faceto be prepared for these opportunities in diagnosticand therapeutic nuclear medicine. The first is toensure we develop co-ordinated multi-centre trialcapabilities to generate appropriate evidence of theaccuracy and clinical impact of these new diagnosticand therapeutic studies. While pharmaceuticalcompany sponsored trials will occur and lead thefield, we must also develop the ability to conduct co-operative group trials that are of a standard thatprovide relevant evidence suitable for regulatorysubmissions. Co-ordination of trials, and sharing oftechnology assessments, is a key approach we willneed to establish as a nuclear medicine community.Secondly, we will need to ensure our clinicians andscientists have sufficient training in these newtechniques, and ensure this applies in bothdeveloped and developing countries. Workforceissues, and ensuring nuclear medicine as a specialtyis promoted and enhanced, is vital to ensuringongoing innovation and clinical impact of ourspecialty. Lastly, I believe we must develop a strategicapproach to advocacy of nuclear medicine, both forour clinician colleagues, as well as for Governmentand funding bodies, to ensure we can achieveacceptance and approval for these new diagnosticand therapeutic nuclear medicine studies.
In your opinion, what role do you see thePangea-ePatient magazine play for nuclearmedicine?
Communication is the key to achieving improvedawareness of where nuclear medicine is heading inthe future, and to bring our global nuclear medicinecommunity closer together. Pangea-ePatient providesan innovative approach to enhancing nuclearmedicine practice, and ensuring our clinical andscientific colleagues involved in nuclear medicine canbe informed of new trends, major issues facing theprofession, and educational information. I hopePangea-ePatient grows from strength to strength inthe future.
Interview with: Dr. Andrew Scott
32 33

A decade ago you moved from Texas to Coloradoto transform the Radiology Department of theUniversity of Colorado to a Premiere State-of-the-Art Medical Imaging Department. Can you tell usabout your views of what a Medical ImagingDepartment should look in the years to come?
The Imaging Department of the future will changedramatically. The television series “Star Trek” toldus our future. Technology, big data and artificialintelligence will play an ever increasing role inimaging and healthcare. The detection, diagnosisand management decisions of patients will evolveinto an analysis of a bodily fluid and/or a scan ofsome type that will be put into context by big dataand artificial intelligence. Patients will relyincreasingly on personal devices and apps as theinterface to address their healthcare needs. Toensure radiology's future role in healthcare wemust immediately embrace big data and artificialintelligence and the role that they will play in imageanalysis. We must become leaders in the digitalworld of healthcare.
For multiple reasons, the consulting ability ofradiologists and nuclear medicine professionalshas decreased significantly over the past twodecades. In the era of personalized medicine howto we make sure that they are an intimate part ofthe patient care management continuum?
Radiology and Nuclear Medicine must undergo asignificant metamorphosis in the way we providehealthcare. We must adopt the concept of addedvalue in the healthcare delivery system by providinghigh level interactive contemporary care. Renderingreports in an RVU driven model while beinginvisible to our healthcare colleagues and patientsdoes not bode well for our profession. We arebeneficiaries and victims of the digital revolution.PACS has made imaging studies immediatelyaccessible to us and everyone else. This benefit ofaccess has come at a price, our healthcarecolleagues no longer have to come to theDepartment to see imaging studies. While thedecrease in interruptions and ready access toimaging studies has improved our efficiency wehave become silent, faceless providers. This hasdiminished the visibility of our impact on patientcare. We are out of sight and mind. This is a
perilous position because as unknown providers wecan be viewed as unessential and easily replaced.Fortunately, we can change this if we choose to doso. The solution is the same one that hurt us, thedigital world. Digital technology exists that canallow us to provide “just-in-time” virtualconsultations. Through linked PACS, EHRs, andSKYPE-like electronic communication we can beanywhere when needed; we can be "in the room”as healthcare decisions are being formulated andcare delivered. Envision this scenario: a healthcareprovider in an examination room with a patientwho has had an imaging study says to the patient“Let’s ask our imaging physician to review yourstudy results with us.” Using the computerworkstation in the room, he or she requests an
immediate consult with the imaging physician. Theimaging physician at a computer workstation inremote location accepts the electronic request forthe consultation and through SKYPE-like softwareappears immediately on the computer screen in theexamination room and asks, “How may I helpyou?”. Both the healthcare provider and thepatient see a live “in-person” imaging physicianwho through linked computer desktops personally“reads” the imaging study. The value add in thissituation is enormous. It puts us in the middle ofhealthcare delivery as a real and tangible memberof the team.
The University of Colorado Radiology smart dose-risk card is a very innovative way to educatepatients and referring physicians about radiationexposure and to demystify the risks associatiedwith imaging studies. Where did the idea camefrom?
The Dose-Risk Smart Card was a product of theradiation scare about medical imaging that startedto gain traction in the United States about 8-yearsago. At the University of Colorado, we had severalprominent medical physicists and radiologists whowere engaged in the national debate. Throughmultiple discussions we came up with the idea tocreate the card to help healthcare providers speak
with patients about radiation exposure frommedical imaging and the potential increasedlifetime risk that it may cause for dying fromcancer. The card is designed to help place intoperspective the dose and potential risk of radiationexposure from medical imaging versus the averageannual radiation exposure from naturalenvironmental sources and the lifetime risk ofdying from other causes. The card has been verywell received in the medical community. The onerecurring criticism we receive is that the listedradiation exposures from various imaging studiesare higher than the doses at their institutions. Thisis a correct observation as the doses used in thecard predated the development of newer dosereduction techniques. However, the card can stillbe used to place dose and the relative risk intoperspective.
34 35
Interview with: Dr. Gerald Dodd

El tromboembolismo pulmonar (TEP) es unaenfermedad importante, tratable, causada por la
migración de un trombo hacia la circulaciónpulmonar, frecuentemente de la circulación venosade los miembros inferiores. Si esta condición no setrata, puede llevar a la muerte o hacia la hipertensiónpulmonar tromboembólica crónica. Un diagnósticooportuno y certero permite instaurar el tratamientoadecuado y evitar las complicaciones de laenfermedad si ésta no se trata a tiempo.
Se estima que esta enfermedad ocurre en 1 de cada1.000 personas por año. Se encuentra en un 18%de las autopsias. Es raro en personas menores de 15años (menos de 5 por 100.000) e incrementadramáticamente por encima de los 60 años. Ocurrede forma similar en hombres y mujeres.
Factores de riesgo: factores heredados o adquiridos(neoplasias, inmovilización, cirugías, los másimportantes. También puede ocurrir en vuelos delarga distancia, aún en personas sanas.
La mayoría de los trombos se origina en las venas delas pantorrillas, los cuales hasta en un 13% migranhacia venas proximales. Se desarrolla TEP hasta enun 44% de los pacientes que tienen trombosisvenosa profunda (TVP) proximal. Hasta un 40% deestos pacientes pueden tener un TEP de formaasintomática. La TVP y el TEP son manifestacionesdiferentes de una misma enfermedad, llamadatromboembolismo venoso.
La tasa de mortalidad a los 3 meses de ocurrido elevento de TEP es del 15%. Los siguientes factoresse asocian con una mayor mortalidad: pacientes conhipotensiónarterial, falla cardíaca congestiva, cáncer,enfermedad pulmonar obstructiva crónica (EPOC) ypacientes mayores de 70 años.
CUADRO CLÍNICO
Las manifestaciones clínicas son variables, desdepacientes asintomáticos hasta aquellos quepresentan muerte súbita. La mayoría de lospacientes se presentan con disnea inexplicable, dolorprecordial (central o pleurítico), tos, hemoptisis,taquicardia, taquipnea, cianosis, fiebre, hipotensión,
falla cardíaca derecha, hipertensión pulmonar,edema de miembros superiores o síncope. Sinembargo, estos síntomas no son exclusivos de estaenfermedad, ya que también pueden presentarse enpacientes sin TEP.
Los síntomas pueden aparecer de forma abrupta oinsidiosa en varios días o semanas.
No se puede confirmar el TEP solo con lapresentación clínica. Se requiere de otros estudiosde laboratorio y de imágenes para ello.
DIAGNÓSTICO
Si bien el cuadro clínico y los factores predisponentestienen gran utilidad en el diagnóstico, cerca de un50% de los pacientes que se presentan con unprimer episodio de TEP no tienen factores de riesgo.
El dímero D (producto de la descomposición de lasuniones del trombo de fibrina tiene una altasensibilidad (alrededor del 95%) con una bajaespecificidad (del 40%), ya que está presente enotras patologías como infarto agudo del miocardio,inflamación, cáncer activo y embarazo. Suespecificidad desciende con la edad, llegando a serde tan solo un 10% en ancianos.
El electrocardiograma puede orientar con estossignos indirectos de sobrecarga ventricular: el signode S1Q3T3, Bloqueo de rama derecha del Haz deHis, desviación del eje a la derecha y en algunoscasos una P pulmonar.
Los rayos X de tórax pueden mostrar atelectasias,elevación del hemidiafragma, cardiomegalia, infartopulmonar y signo de Westermark (opacidadvascular), que si bien pueden orientar hacia eldiagnóstico, no son patognomónicos de TEP.
Juan Luis Londono, M.D.Médico y Cirujano Universidad Pontificia Bolivariana, Medellín, Colombia
Médico Nuclear Universidad de Buenos Aires, ArgentinaJefe servicio de Medicina Nuclear, San Vicente Fundación,
Hospital Universitario, Medellín, ColombiaPresidente electo, Asociación Colombiana de Medicina Nuclear 2017 - 2019
MEDICINA NUCLEAREN TROMBOEMBOLISMO PULMONAR
36
GAMAGRAFÍA COMBINADA DE VENTILACIÓN YPERFUSIÓN PULMONAR
La gamagrafía de Ventilación y Perfusión Pulmonar(V/Q) se está usando desde la década de 1960.Desde entonces, ha habido avances en la tecnología,el equipamiento y en los radiofármacos utilizados, loque lo ha hecho un estudio rutinario en los serviciosde Medicina Nuclear para el diagnóstico del TEP.
Gamagrafía de VENTILACIÓN PULMONAREsta técnica gamagráfica requiere de laadministración de un gas radioactivo o de unradioaerosol, para luego obtener imágenes de sudistribución en ambos campos pulmonares, lascuales son un reflejo de la ventilación en la vía aérea.
Gases radioactivosEl primer agente de ventilación utilizado fueron losgases inertes como el Kriptón-89 y el Xenón-133,que conservan las propiedades de los gases una vezinhalados, siendo depurados muy rápidamente, porlo que se limita el número de imágenes que sepueden adquirir; además tienen un costo alto y sudisponibilidad es limitada. Su mayor ventaja es suvida media corta, lo cual limita la dosis de exposiciónpara el paciente.
RadioaerosolesSon partículas radiomarcadas, suspendidas en el aire.Pueden ser líquidas, sólidas o una combinación deéstas.
Los radioaerosoles, se obtienen mediante lanebulización del compuesto líquido Ácido DietilenTriamino Pentaacético (DTPA) marcado con Tecnecio-99m. Este aerosol es particulado en su naturaleza;las partículas usualmente tienen un diámetro de 0.5a 5 micras y dado que tiene una tasa de depuraciónmuy lenta, pueden adquirirse imágenes en variasproyecciones, a diferencia de lo que ocurre con losgases. Sin embargo, tienen algunas limitantes:deposición de las partículas en la tráquea y bronquiosprincipales por inercia; deglución de las partículas,con captación en el esófago y el estómago.Enpacientes con enfermedades de las vías aéreas, comoEPOC o enfisema, puede existir acumulación de laspartículas en los grandes bronquios, lo cual puededificultar la interpretación de las imágenes.
El Tecnegas, una partícula ultrafina de carbónmarcado con tecnecio-99m, usada desde la décadade los 80 s produce una dispersión más estructuradadel carbón, que penetra más profundamente en elparénquima pulmonar, con deposición alveolar, porel tamaño y la naturaleza hidrofóbica de laspartículas. Se produce una muy buena penetraciónperiférica con una muy poca fracción retenida en lasvías aéreas, requiriendo solo unas cuantasinhalaciones y con la posibilidad de realizar imágenesen varias proyecciones, con una distribución en elparénquima pulmonar similar a la que se obtienemediante el uso de gases radioactivos.
37
Los estudios imaginológicos son:
1. Angiografía pulmonar2. Angiotomografía3. Gamagrafía de Ventilación y Perfusión Pulmonar4. Angiografía pulmonar con Resonacia Magnética

Gamagrafía de PERFUSIÓN PULMONARLa gamagrafía de perfusión pulmonar hace uso de laexclusiva anatomía segmentaria pulmonar arterial.Cada segmento broncopulmonar es irrigado por unasola arteria terminal. Por lo tanto, los trombosoclusivos que afectan arterias individuales producendefectos lobares, segmentarios o subsegmentariosperiféricos, en forma de cuña, de base periférica yvértice central.
Las imágenes se obtienen después de realizar unamicroembolización con partículas radiomarcadasinyectadas en una vena periférica. Las partículasson de Macro Agregados de Albúmina (MAA)marcados con Tecnecio-99m. Tienen un tamañode 15-100micras, por lo que se alojan en loscapilares pulmonares y en las arteriolasprecapilares. Su distribución es el reflejo de lacirculación pulmonar.
TIPOS DE IMÁGENES GAMAGRÁFICAS
Se adquieren imágenes con la técnica de SPECT (porlas siglas en inglés de Single Photon EmissionComputed Tomography) en las cuales se hace unaadquisición de imágenes tomográficas, obteniendosensibilidad de 96% con especificidad de 97% yvalor predictivo negativo (la certeza de no tener laenfermedad) de un 98,5% en el diagnóstico del TEP,cifras comparables a las de la angiotomografía.
La técnica de SPECT permite obtener tanto imágenesen 3D como cortes tomográficos, que permitenvisualizar todos los segmentos, incluyendo el medialbasal del lóbulo inferior derecho, que no se ve bienen las imágenes bidimensionales; provee mejordefinición de los segmentos pulmonares y tiene unamejor detección y caracterización de los defectos yuna importante disminución en los reportesindeterminados
INTERPRETACIÓN DE LAS IMÁGENES
Imágenes normales:Las imágenes normales de ventilación reflejan laanatomía broncopulmonar; deben mostrar unadistribución uniforme del radioaerosol, cuyaspartículas son lo suficientemente pequeñas comopara alcanzar el árbol traqueobronquial distal, sinque se observen zonas de defecto de captación enel parénquima pulmonar.
Las imágenes de perfusión muestran la distribuciónde la anatomía arterial pulmonar. Las imágenesdeben mostrar una distribución uniforme delradiotrazador, sin defectos de captación.Un patrónde perfusión normal excluye un TEP.
Las imágenes deben cotejarse con una radiografía detórax reciente, ya que en ésta pueden aparecerlesiones que podrían afectar el diagnósticogamagráfico, como por ejemplo un derrame pleuralo una atelectasia.
Figura 1. Gamagrafía de Ventilación/Perfusiónpulmonar. Estudio normal
Patrón anormal, con discordancia de las imágenes deVentilación y Perfusión:
En los segmentos broncopulmonares afectados porel TEP, la ventilación usualmente está preservada.Este patrón de ventilación preservada, con perfusiónausente en un segmento pulmonar da origen alfundamento diagnóstico del VQ scan: el patrón dediscordancia de Ventilación y Perfusión
38
El TEP es generalmente múltiple ya que el émbolofrecuentemente se fragmenta a su paso por lascavidades derechas y las arterias pulmonaresprincipales. Puede ser un evento único o un procesorecurrente que da lugar a múltiples émbolos enperíodos cortos o largos. El patrón anormal, condiscordancia de las imágenes de Ventilación yPerfusión puede ocurrir también en pacientes que notienen TEP, y que pueden tener alguna de estasenfermedades preexistentes: anomalías pulmonaresvasculares congénitas, vasculitis, cáncer pulmonar oadenopatía tuberculosa mediastinal.
Figura 2. Gamagrafía de Ventilación/Perfusiónpulmonar. Estudio anormal, compatible contromboembolismo pulmonar
Patrón anormal, con concordancia de las imágenesde Ventilación y Perfusión:
La circulación arterial pulmonar puede verse afectadapor otras patologías diferentes al TEP y es el caso enque se afecta tanto las imágenes de ventilación comolas de perfusión, lo que está generalmente causadopor alteraciones de las vías aéreas del parénquima,como en EPOC, fibrosis pulmonar, y otras patologíascrónicas de la vía aérea.
Figura 3. Gamagrafía de Ventilación/Perfusiónpulmonar. Estudio anormal, compatible conenfermedad pulmonar
TEP CRONICO
El TEP crónico es una entidad diferente. Supresentación clínica es usualmente insidiosa. Esprogresiva y si no se trata tiene un mal pronóstico.Ocurre hasta en un 1 – 5% después de un TEPagudo. La mortalidad se debe a la hipertensiónpulmonar, falla cardíaca derecha y arritmias. Lagamagrafía de V/P es uno de los pilaresprincipalespara el diagnóstico de hipertensión pulmonartromboembólica crónica. Los diversos estudios handemostrado que la gamagrafía de V/P es superiorcomparada con la Angiotomografía, que tienemenor sensibilidad y especificidad diagnóstica en elTEP crónico
TEP EN EMBARAZO
El TEP es una causa importante de mortalidadmaterna. Existe un riesgo 4 – 5 veces mayor dedesarrollar TEP en embarazo y en el períodoperiparto; esto por el incremento en la estasisvenosa, incremento en la distensibilidad y capacidadvenosa, aumento en los niveles de coagulación ycambios en el estilo de vida.
El TEP es una enfermedad que pone en riesgo la vidade la madre y del feto. Puede ser difícil dediagnosticar y los beneficios de un diagnósticoadecuado sobrepasan a los riesgos potenciales de losestudios imaginológicos con radiación ionizante,como la gamagrafía o la angiotomografía. La dosisde radiación de ambos métodos es similar; sinembargo, en pacientes en embarazo, se realizaúnicamente la gamagrafía de perfusión pulmonarutilizando un protocolo de dosis reducidas delradiofármaco, con lo cual la dosis al feto se reducehasta en un 60%
SeguridadLa gama VQ es altamente segura. Se han reportadoalgunos efectos secundarios a los radiofármacos engeneral, de un 1-3 por 100.000 pacientes, muchomenor que con otros estudios diagnósticos como laangiografía pulmonar. No existen contraindicacionesabsolutas para su uso.
Dosis de radiaciónCon las dosis utilizadas, según el InternationalComission on Radiological Protection (ICRP), la dosisde radiación es de 1.2 – 2 mSv La dosis absorbidaestimada en la mama femenina se estima en 0.8mGy, mucho menor que con estudios diagnósticostomográficos como la angiografía pulmonar,llegando a ser la dosis de la gamagrafía solo un 35 –40% de la de los estudios tomográficos.
39

You have been a member of the Nuclear Cardiologycommunity for a long time and you are now thePresident of ASNC. For those who are not familiarwith ASNC, can you describe succinctly its role in thefield of nuclear medicine
The American Society of Nuclear Cardiology wasfounded almost 25 years ago to promote educationin nuclear cardiology, to provide nuclear cardiologistswith the tools they need to produce high-qualitystudies that will improve the care of their patients,and to advocate for nuclear cardiologists in thegovernmental and regulatory arenas. Over the years,ASNC has grown to a membership of about 4500members from 63 nations and it is our goal toprovide the support each of those members need toadvance the use of nuclear cardiology.
What are the most dramatic changes that you haveseen in the field of nuclear cardiology over the past10 years?
The past 10 years have seen dramatic advances intechnology that have improved the diagnosticcapabilities of nuclear cardiology. The first innovationis the development of solid-state nuclear medicinecameras that have significantly greater sensitivity andresolution than standard nuclear medicine cameras.This innovation allows us to use smaller doses ofradiotracer to image patients and in shorter amountsof time. Taken together, these characteristicsenhance patient safety and comfort.
Second, we have seen a greater emphasis on the useof positron emission tomography (PET) for cardiacstudies. The greater sensitivity and specificity of PETcompared to single photon emission computedtomography (SPECT), improves the diagnosticaccuracy of our cardiac studies. In addition, PETallows for the quantitative analysis of myocardialperfusion, so that it is possible to evaluate coronarymicrovascular function in addition to blockages inthe major coronary arteries.
Third, we have seen an expansion of the use ofnuclear cardiology outside of perfusion imaging,which is used to detect coronary artery disease.Specifically, PET-based metabolic imaging is being
used to evaluate for inflammatory disorders in theheart, such as cardiac sarcoid or intracardiac deviceinfection. In addition, we are seeing an increase inthe use of nuclear cardiac imaging to diagnosecardiac amyloidosis. These nuclear based techniquesincrease the chances that a patient can avoid a heartbiopsy, which is an invasive procedure.
How do you see the field of nuclear cardiologyevolving during the next decade?
During the next 10 years, I foresee nuclear cardiologyplaying an important role in personalized medicine.As we continue to see innovations in cameratechnology and molecularly-based radiotracers,nuclear cardiac imaging can provide important,patient-specific data to help establish diagnoses andguide therapy. The innovations will also improve theaccessibility to nuclear cardiac imaging studies.
The next 10 years will also see continued andenhanced collaboration between ASNC and othersocieties, such as the Canadian Association ofNuclear Medicine, the Society of Nuclear Medicineand Molecular Imaging, the European Association ofNuclear Medicine, and the International AtomicEnergy Agency. These collaborations are essential inproviding the education and guidelines necessary toensure that physicians world-wide are providingstate-of-the-art nuclear cardiac imaging for theirpatients.
To your opinion, what role do you see the Pangea-ePatient magazine play for nuclear medicine?
Just as the dissemination of information to ourphysicians is important, providing information to ourpatients is essential. I see Pangea-ePatient as avaluable resource for patients to gain a greaterunderstanding of their medical problems and thetests that can be used to help in the diagnosis andmanagement of those disorders. Such informationempowers an individual to navigate complexhealthcare systems and make informed decisions intheir health care.
Interview with: Dr. Raymond Russell
40

You have been a member of the NM community for a longtime and are now the President of the AOFNMB. For thosewho are not familiar with the AOFNMB, can you describesuccinctly its role in the field of nuclear medicine.
AOFNMB was launched in 1992 with the support of 74member states from Oceania, West Asia, Central Asia,South Asia, South East Asia, and North East Asia topromote nuclear medicine practice in these regions. Overthe past 25 years, nuclear medicine practice hasexploded in Asia and there is a constant and everincreasing demand for education and expertise.Competent, well trained and properly qualified humanresources are vital to further develop and continue toprovide quality, efficient and safe nuclear medicineservices to patients. Dedicated, harmonized andsustainable educational tools and training in nuclearmedicine sciences are at the heart of the mission of theAOFNMB is such a platform to promote nuclearmedicine practice in the region. Through a biennalinternational scientific meeting, The Asia Oceania Journalof Nuclear Medicine and Biology, the official Journal ofAOFNMB, The Asia Oceania Research Initiative Networkand a close partnership with the nuclear medicineindustry, the AOFNMB is developing, supporting andpromoting NM research and practice in the region.
What are the most dramatic changes that you have seenin the field of nuclear medicine over the past 10 years?
When I started my PET research fellowship in 1981 atthe Hammersmith Hospital, inLondon, UK, nobody couldhave predicted that 18F-FDG PET would be the dailyimaging work horse of diagnostic oncology. In my mind,over the past decade, hybrid imaging and radionuclidetherapy with radionuclide have revolutionized andchallenged the field of nuclear medicine. By providinganatomic correlates to the metabolic, phenotypic andgenotypic information provided by nuclear medicine
studies we can now offer our colleagues precise andaccurate information about their patients’ ailments. Wealso have the tools to asses the efficacy of theirtreatments. The ability to diagnose, localize and treatearly recurrent prostate cancers in their very early stagewith radiolabeled peptides is a very good example ofprecision medicine that nuclear medicine can offer. Theneed for an in depth knowledge and expertize inmolecular biology, CT, MR and dosimetry constitute thecurrent major challenges that we have embraced andare tackling through our various educational initiatives.
How do you see the field of nuclear medicine evolvingduring the next decade?
In house cyclotrons, refined and automatedradiochemistry along with highly sensitive hybrid PET/CT,SPECT/CT and PET/MR scanners, powerful computingsystems and information technology along with thecontinuous unraveling of the molecular landmarks ofdiseases will will enable us to develop exquisitely specifictargeting diagnostic and therapeutic agents and topinpoint precisely their location in the body. Theavailability of both specific and innovative diagnosticand therapeutic radiopharmaceuticals for the diagnosisand therapy of diseases (Theranostics), particularly inoncology will enable us to deliver on the promises ofmolecular and precision medicine, particularly inoncology.
To your opinion, what role do you see the Pangea-ePatient magazine play for nuclear medicine?
In contrast to medicine, surgery, radiation therapy andthe other main disciplines of medicine, the field ofnuclear medicine is very unique and, in general, not verywell known by patients and referring physicians. Wemust play a major role in educating patients andcolleagues about the usefulness and benefits ofdiagnostic and therapeutic nuclear medicineapproaches and services. In Japan, we recently launchedan annual educational and working conference onTheranostics which gathers patients, nuclear medicinephysicians, referring doctors, industries, the JapanRadioisotope Association, and regulatory authorities.Having an educational magazine that uses all possible21st century digital electronic plateforms likecomputers, tablets, smartphones and that is available24/7 365 days a year at home, at the office and on theroad to educate and share the most recent developmentand innovation in nuclear medicine would be a fantasticasset for the nuclear medicine profession. The Pangea-ePatient magazine promises to deliver on these premisesand I am delighted to contribute to this issue and serveon its medical and scientific advisory board.
Interview with: Dr. Jun Hatazawa
42www.cyclomedica.ca
V/Q imaging using TECHNEGAS is the OPTIMAL choice for SCREENING and FOLLOWING PE
Ventilation / Perfusion Lung Imaging with
TECHNEGASNow expanding BEYOND PE Screening to Functional and Quantitative Lung Imaging
Volumes [%] Perfusion [%] Ventilation [%]
Right Left Right Left Right Left
Upper 24.1 19.1 29 16.2 31.1 9.48
Middle 17.4 N/A 11.5 N/A 23.4 N/A
Lower 15.9 23.4 17.6 25.7 16.1 20
Total 57.4 42.6 58.1 41.9 70.6 29.4
Images and 3D Quantification provided by
THINK FUNCTIONAL IMAGING – CONQUER THE SILENT ZONE
- COPD
- Emphysema
- Pre-Operative Quantification
- Radiation Oncology Planning
- Baseline Imaging
Upper
Middle
olumes [%]V erfusion [%]P
Upper
Middle
entilation [%]V
Lower
otalTTo
Lower

www.hermesmedical.com - [email protected]
End-to-end vendor-neutral connectivity and data integration
Consistency in clinical workflows
ENTERPRISE MOLECULAR IMAGING
ENTERPRISEMOLECUL
ENTERPRISE IMAGINGARMOLECUL
ENTERPRISE IMAGING
connectivit
Consistency in clinical workflows
-end vendorEnd-toy and data integrconnectivit
Consistency in clinical workflows
-neutr-end vendory and data integr
Consistency in clinical workflows
al-neutration y and data integr
Consistency in clinical workflows
.hermesmedical.com - [email protected]
.hermesmedical.com - [email protected]
.hermesmedical.com - [email protected]
.hermesmedical.com - [email protected]
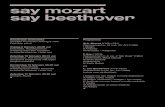
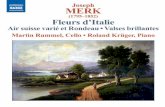





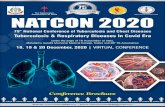




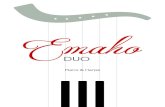





![W ] v [ ' µ€¦ · Dr Jalal Ahmed ( Bangladesh ) Dr Jayant V Iyer ( Singapore ) Dr Kazi Shabbir Anwar ( Bangladesh ) Dr Magdy Khallaf ( Egypt ) Dr Manju Subramaniam ( USA ) Dr Milind](https://static.fdocuments.nl/doc/165x107/5f6754f8b760912f7e5cd7fe/w-v-dr-jalal-ahmed-bangladesh-dr-jayant-v-iyer-singapore-dr-kazi.jpg)