
La ligue cardiologique belge ASBL créée en 1968 · 2018-05-24 · Statins are among the most...
106
Transcript of La ligue cardiologique belge ASBL créée en 1968 · 2018-05-24 · Statins are among the most...

Slide 5
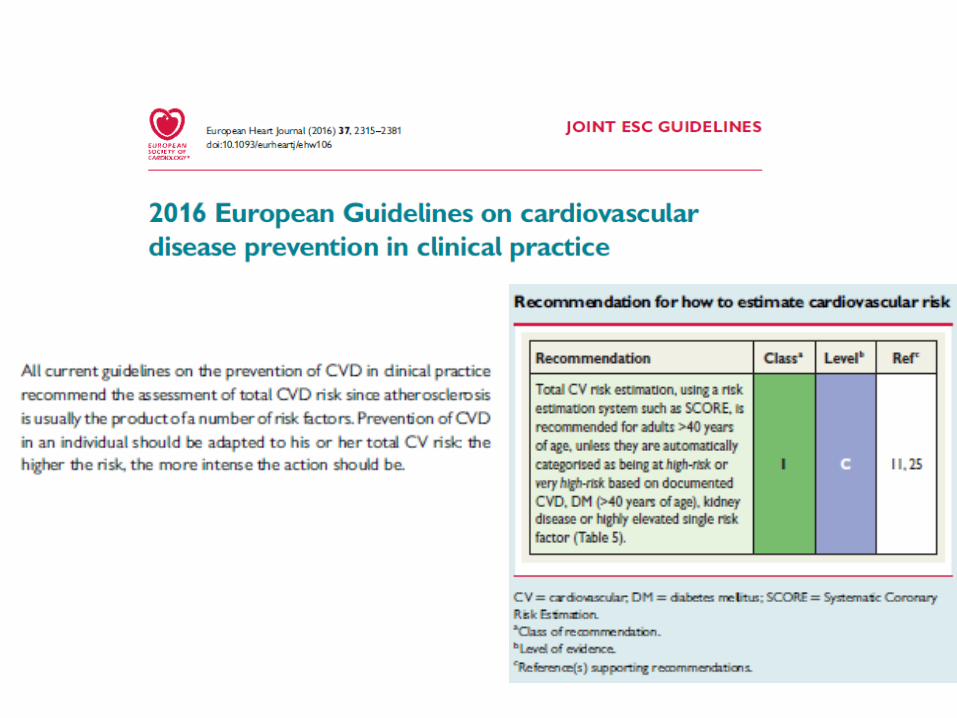
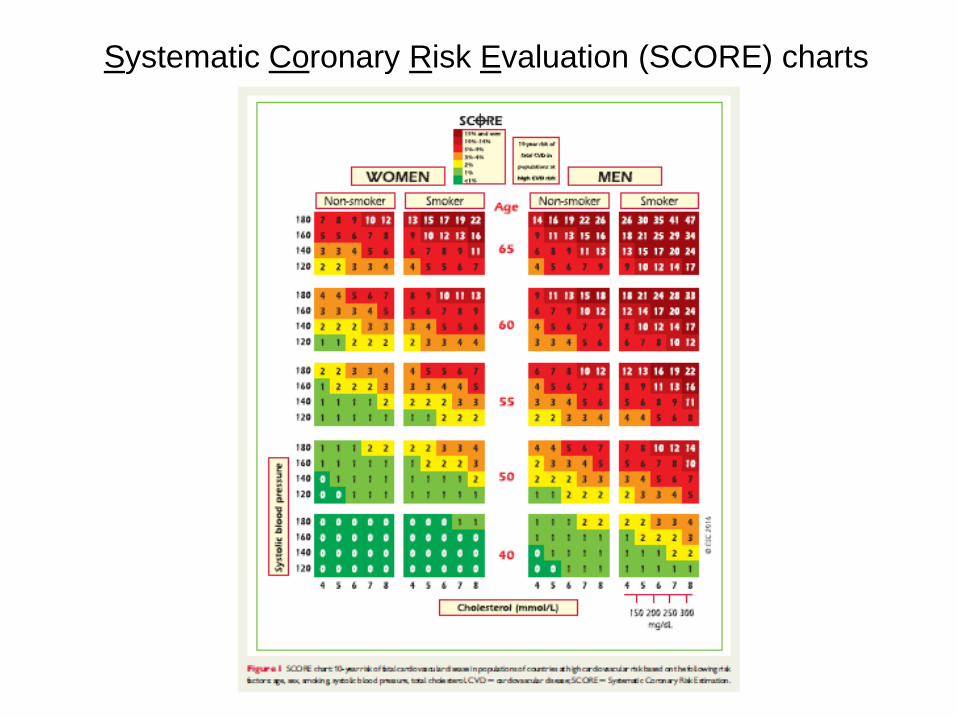
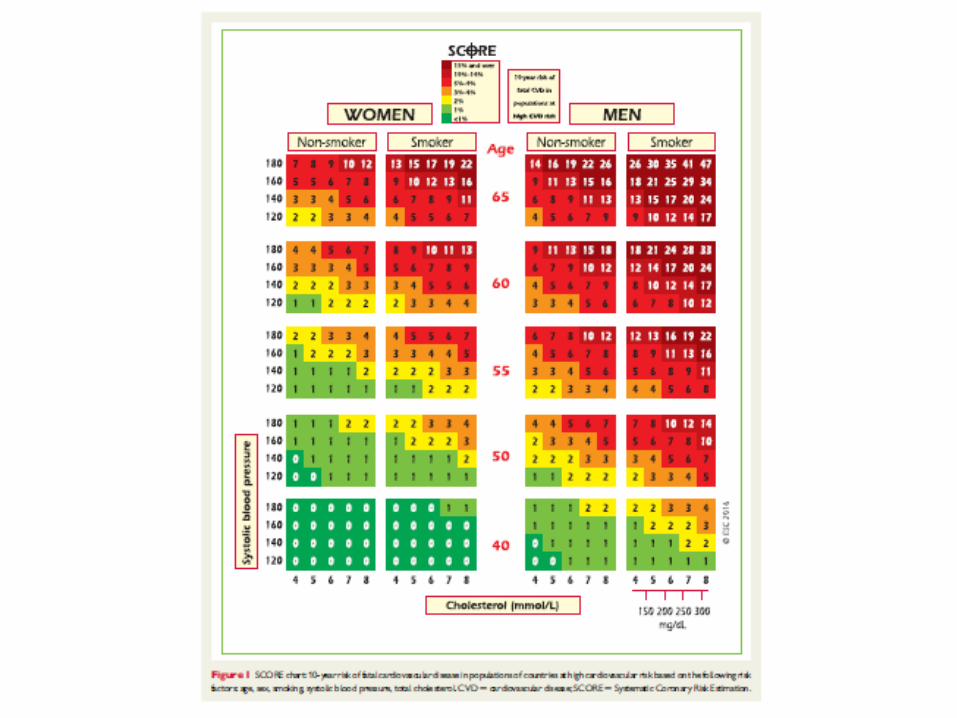
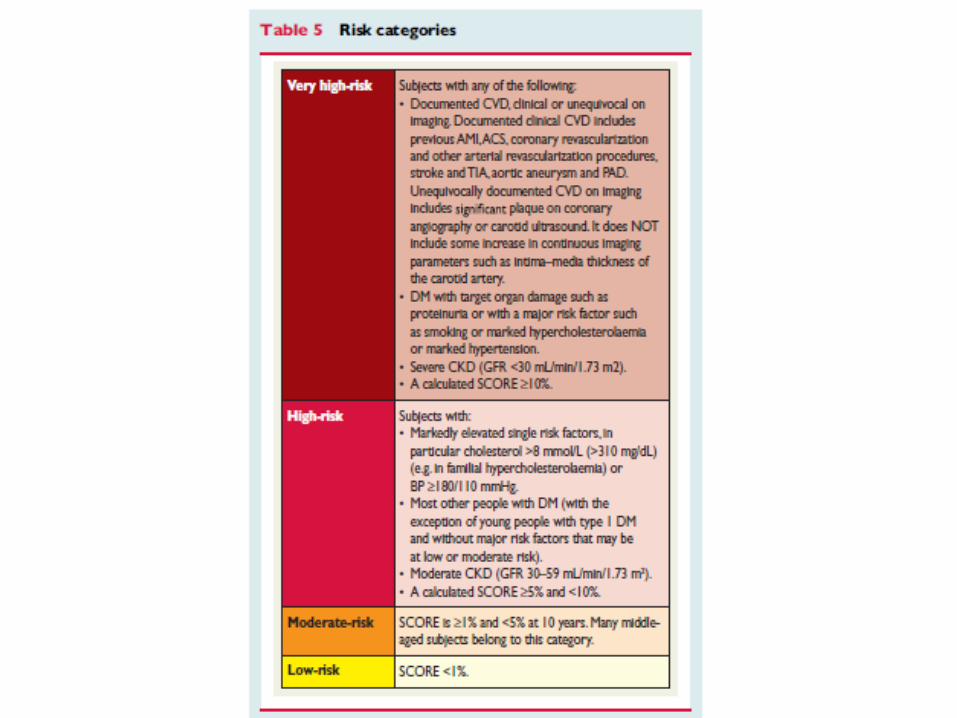
Systematic Coronary Risk Evaluation (SCORE) charts
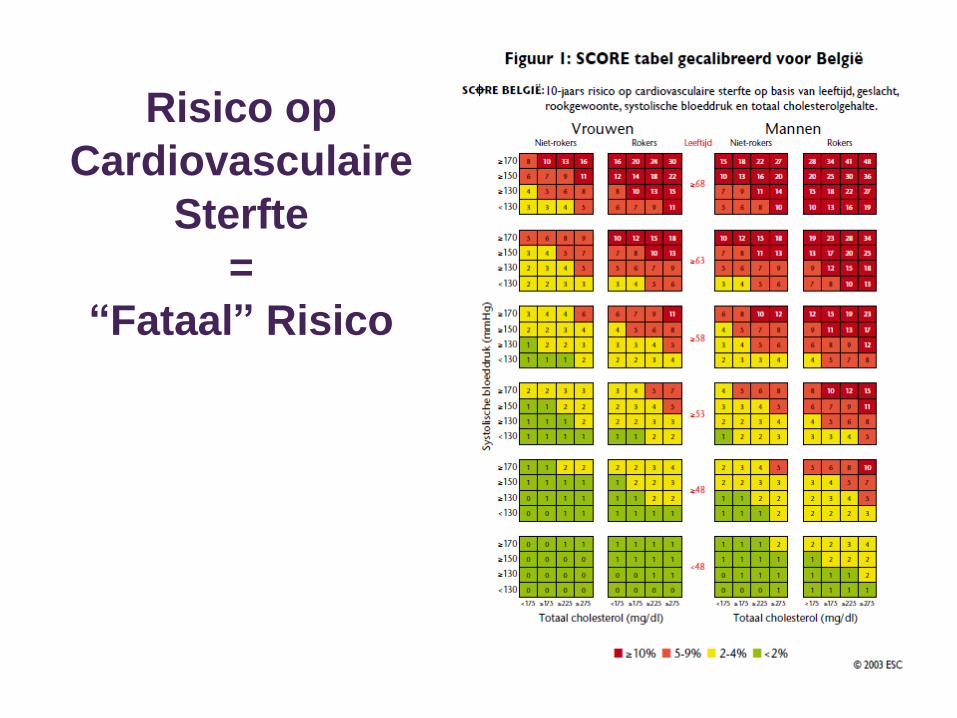
Risico op
Cardiovasculaire
Sterfte
=
“Fataal” Risico
Risiconiveaus
Om het risico op een fataal CV voorval te
converteren naar fataal én niet fataal CV voorval:
– X 3 voor ♂
– X 4 voor ♀
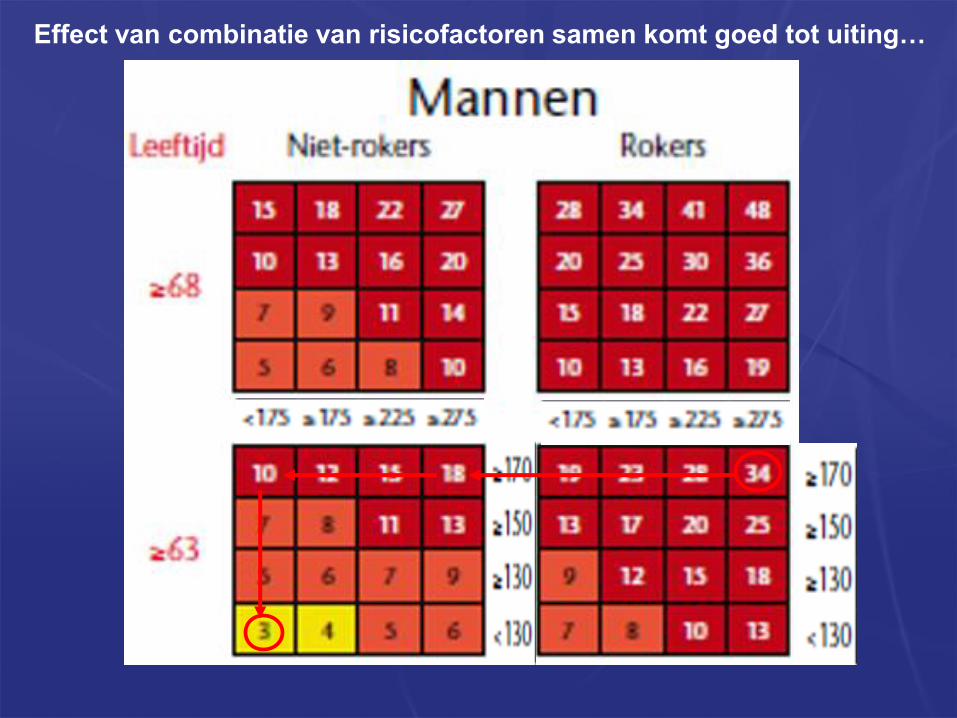
Effect van combinatie van risicofactoren samen komt goed tot uiting…
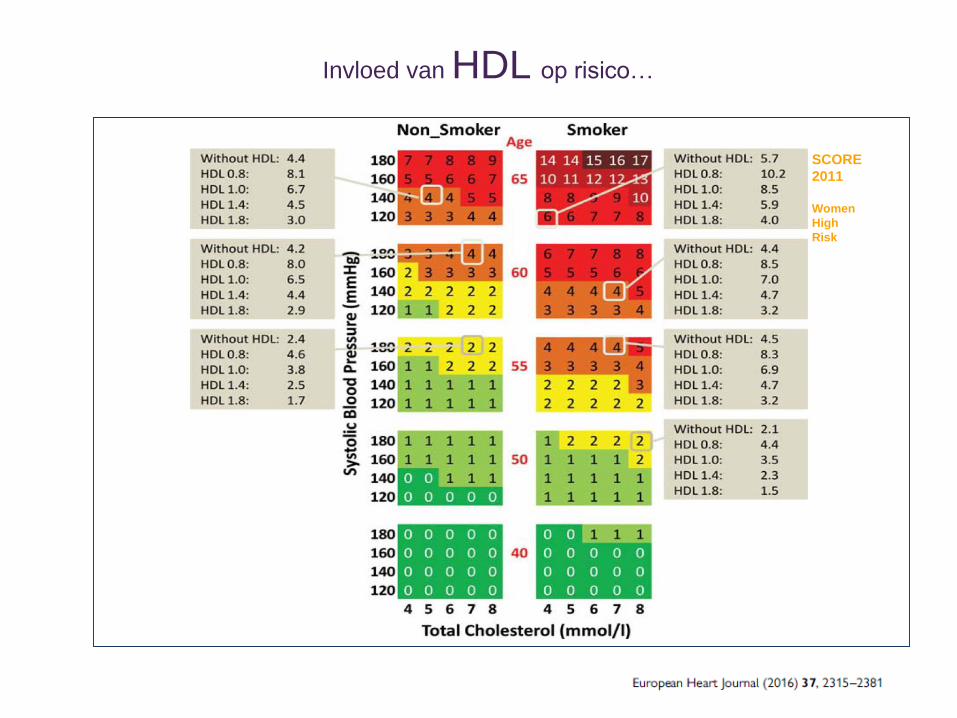
SCORE
2011
Women
High
Risk
Invloed van HDL op risico…
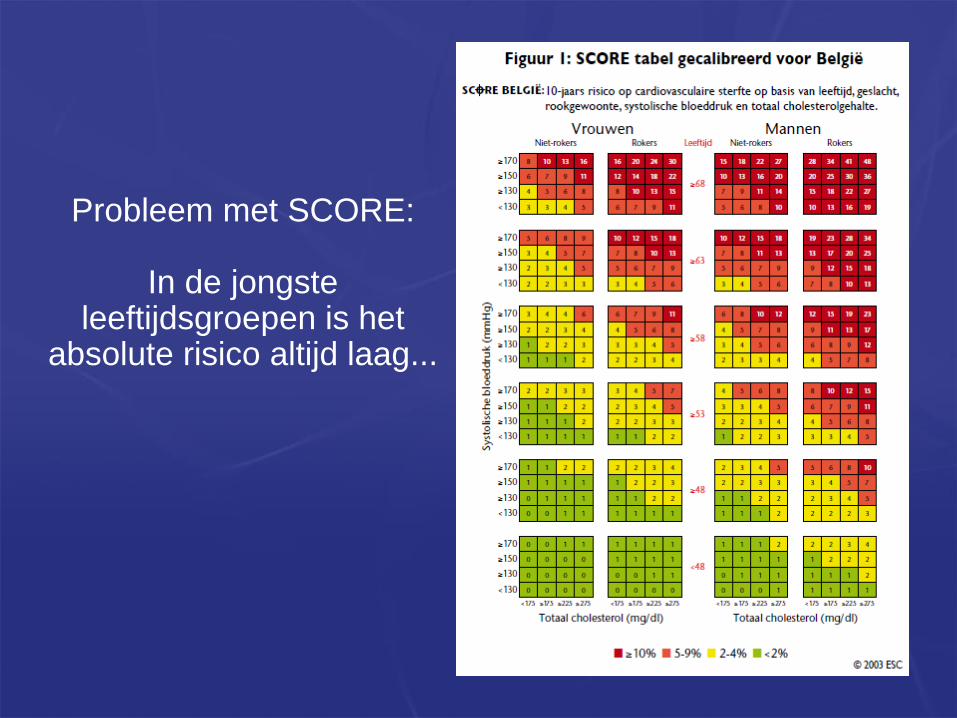
Probleem met SCORE:
In de jongsteleeftijdsgroepen is het
absolute risico altijd laag...
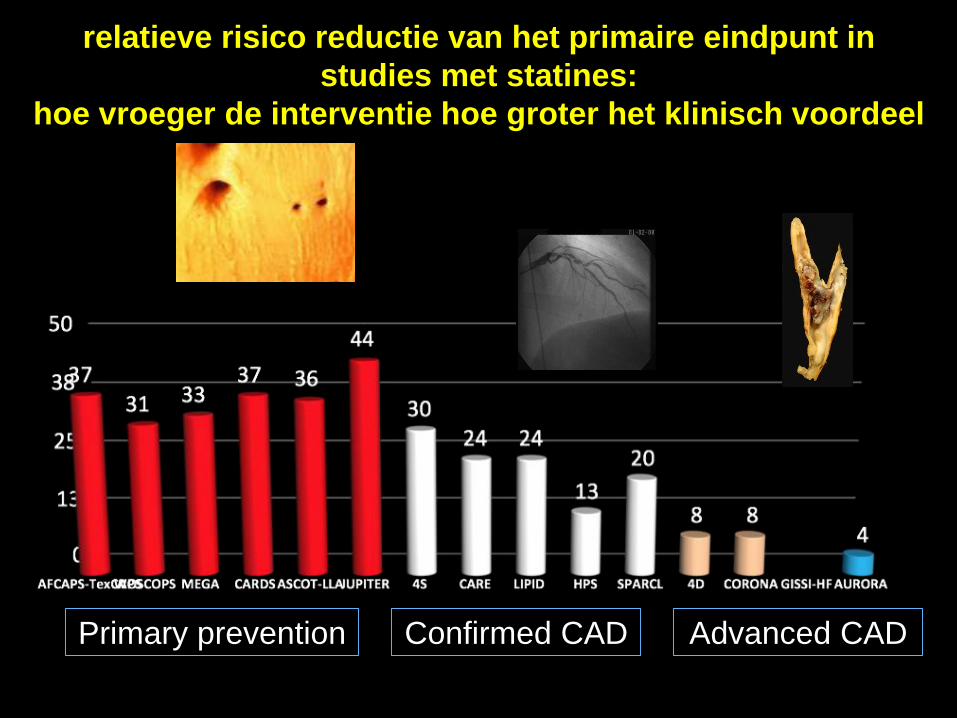
relatieve risico reductie van het primaire eindpunt in
studies met statines:
hoe vroeger de interventie hoe groter het klinisch voordeel
Primary prevention Confirmed CAD Advanced CAD
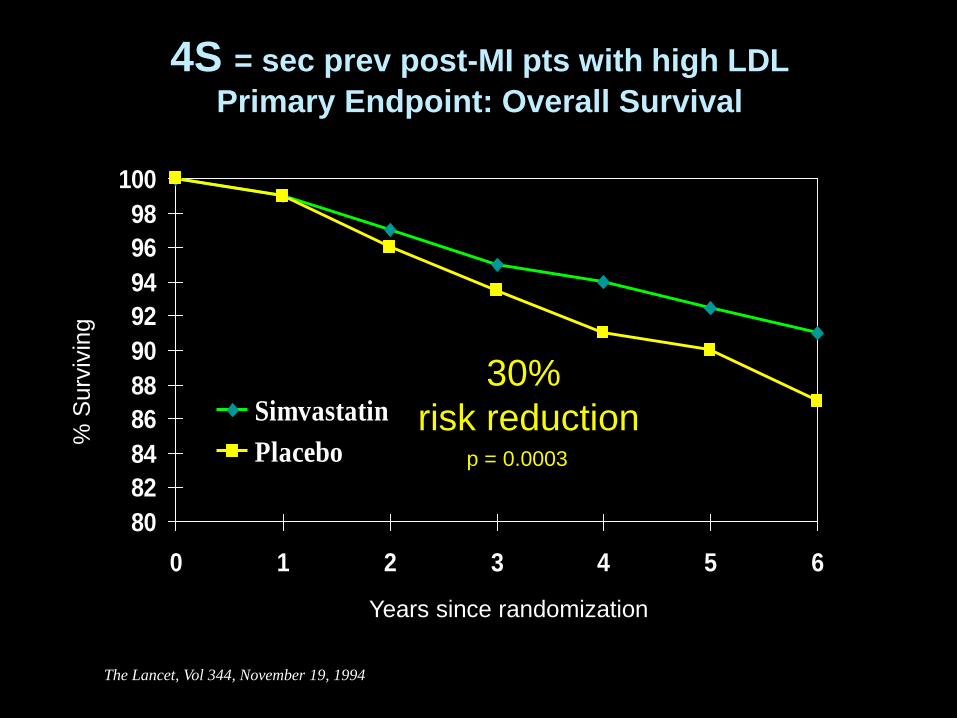
4S = sec prev post-MI pts with high LDL
Primary Endpoint: Overall Survival
80
82
84
86
88
90
92
94
96
98
100
0 1 2 3 4 5 6
Simvastatin
Placebo
Years since randomization
% S
urv
ivin
g
30%
risk reductionp = 0.0003
The Lancet, Vol 344, November 19, 1994
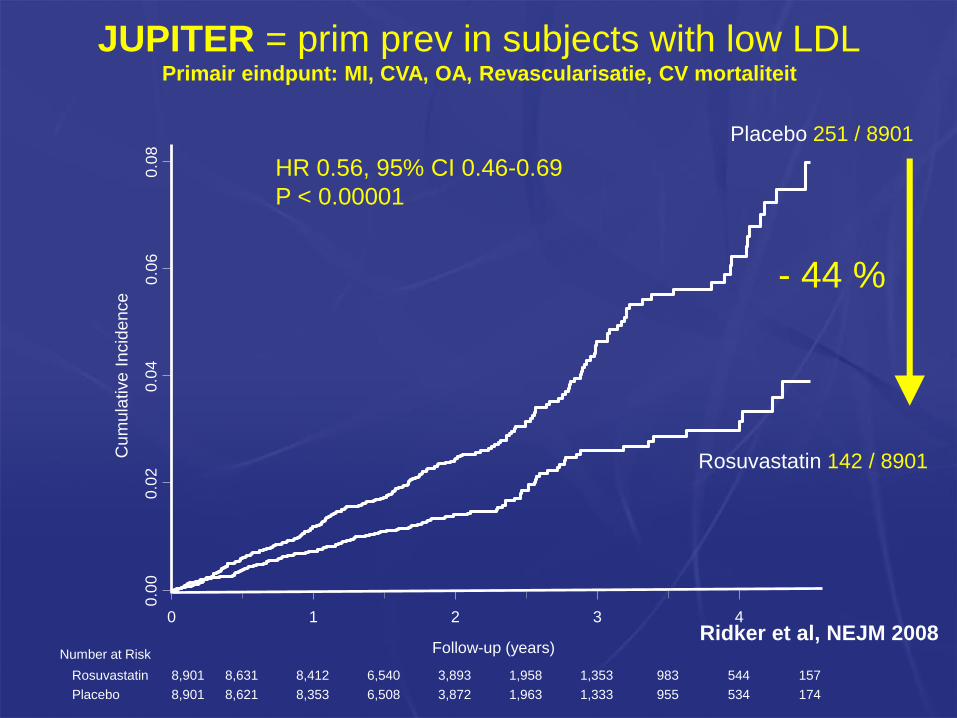
Placebo 251 / 8901
Rosuvastatin 142 / 8901
HR 0.56, 95% CI 0.46-0.69
P < 0.00001
- 44 %
0 1 2 3 4
0.0
00
.02
0.0
40
.06
0.0
8
Cu
mu
lative
In
cid
en
ce
Number at Risk Follow-up (years)
Rosuvastatin
Placebo
8,901 8,631 8,412 6,540 3,893 1,958 1,353 983 544 157
8,901 8,621 8,353 6,508 3,872 1,963 1,333 955 534 174
JUPITER = prim prev in subjects with low LDLPrimair eindpunt: MI, CVA, OA, Revascularisatie, CV mortaliteit
Ridker et al, NEJM 2008
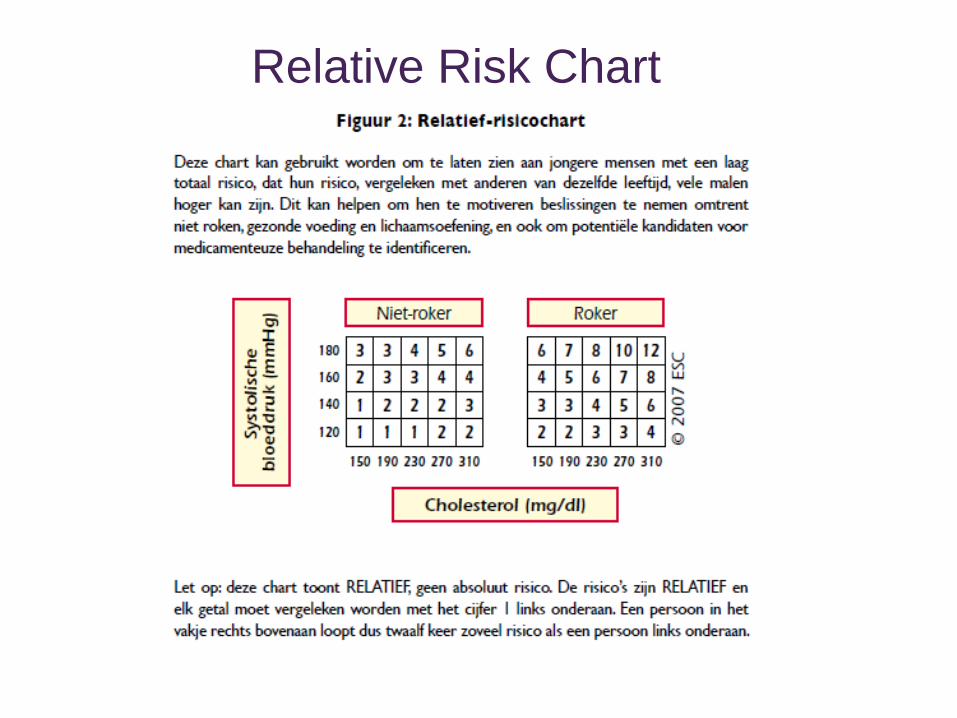
Relative Risk Chart
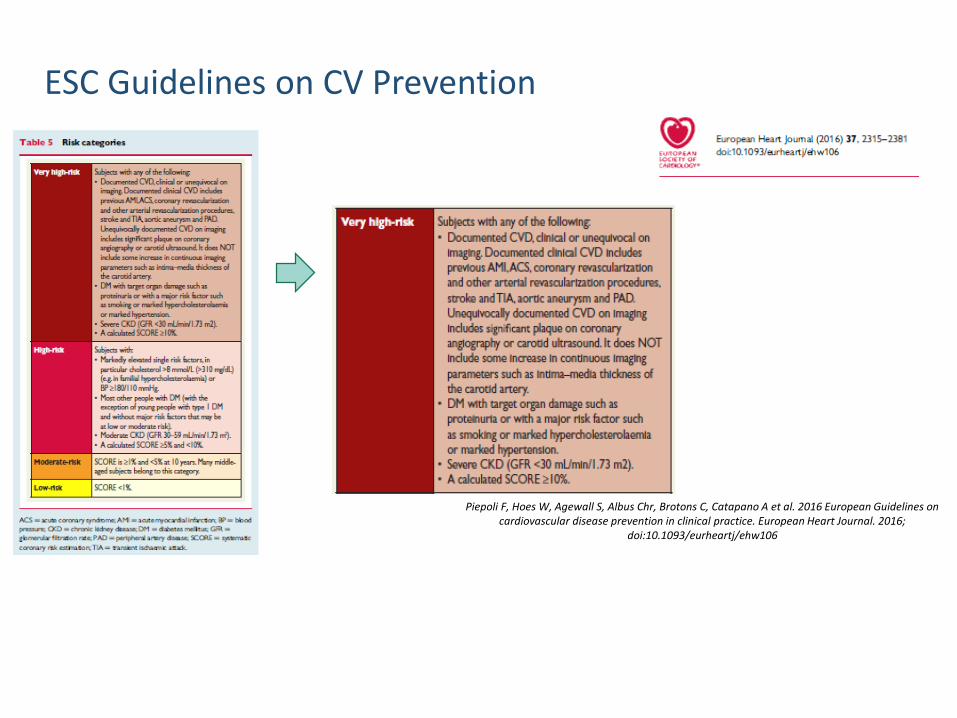
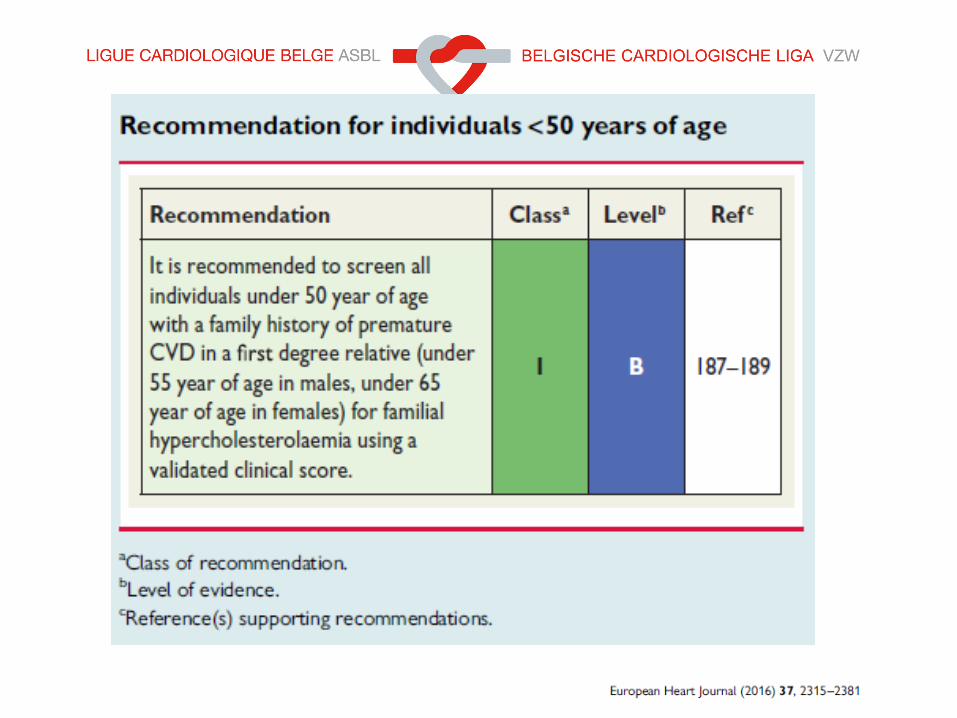
Piepoli F, Hoes W, Agewall S, Albus Chr, Brotons C, Catapano A et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal. 2016;
doi:10.1093/eurheartj/ehw106
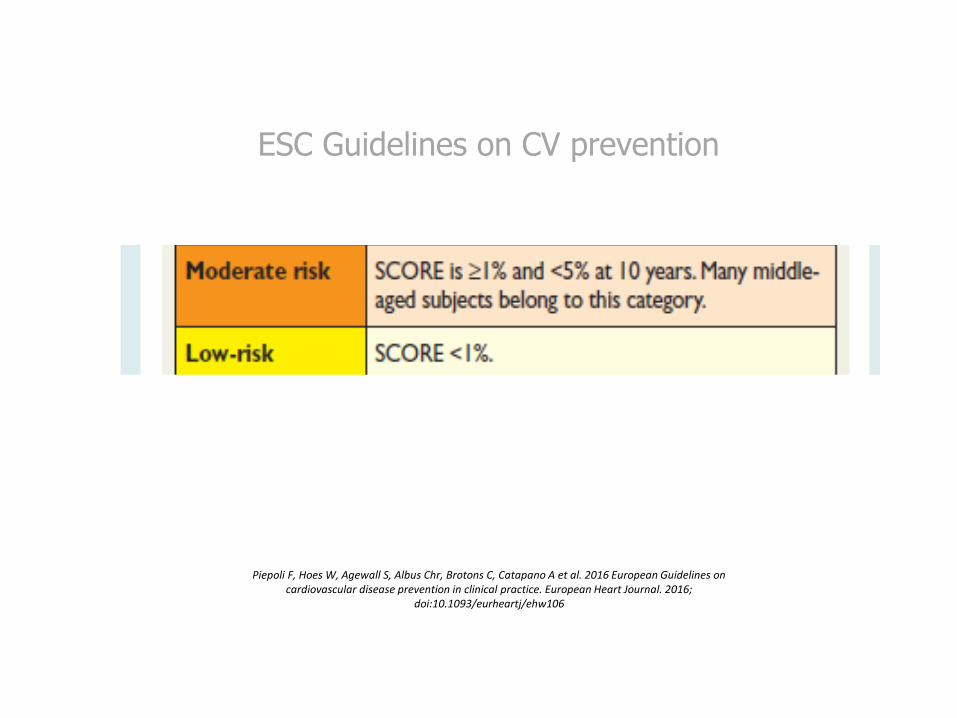
ESC Guidelines on CV Prevention
Piepoli F, Hoes W, Agewall S, Albus Chr, Brotons C, Catapano A et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal. 2016;
doi:10.1093/eurheartj/ehw106
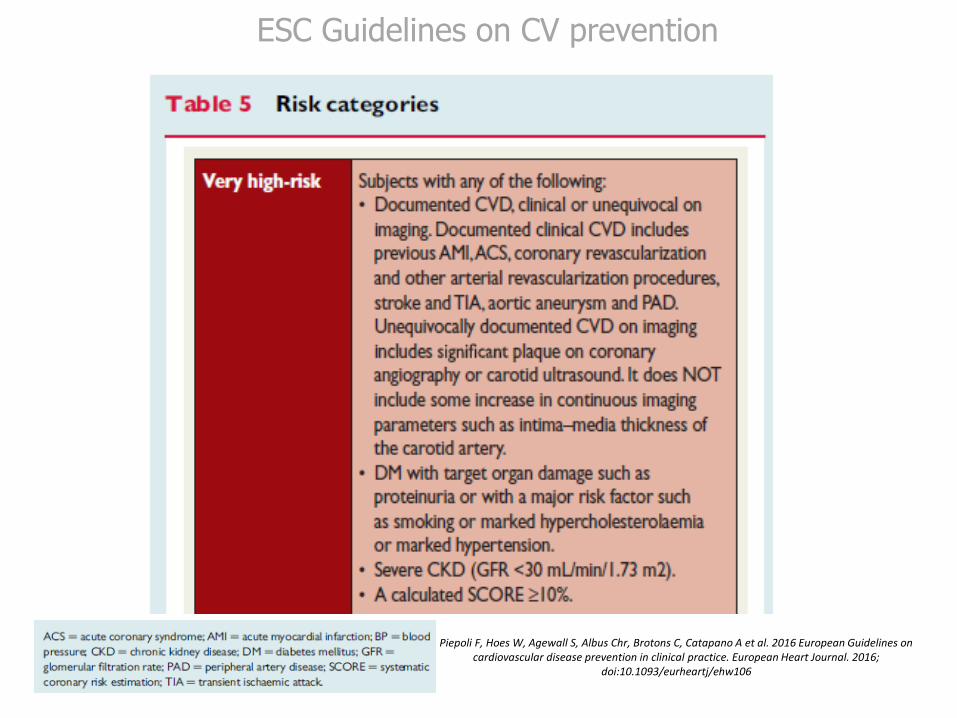
ESC Guidelines on CV prevention
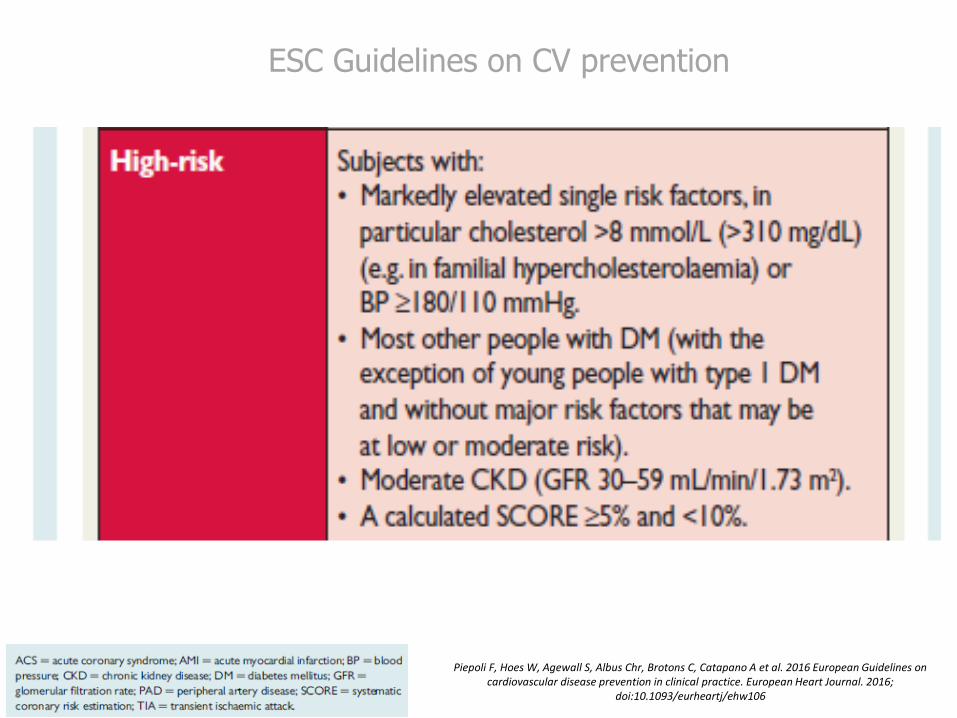
Piepoli F, Hoes W, Agewall S, Albus Chr, Brotons C, Catapano A et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal. 2016;
doi:10.1093/eurheartj/ehw106
ESC Guidelines on CV prevention
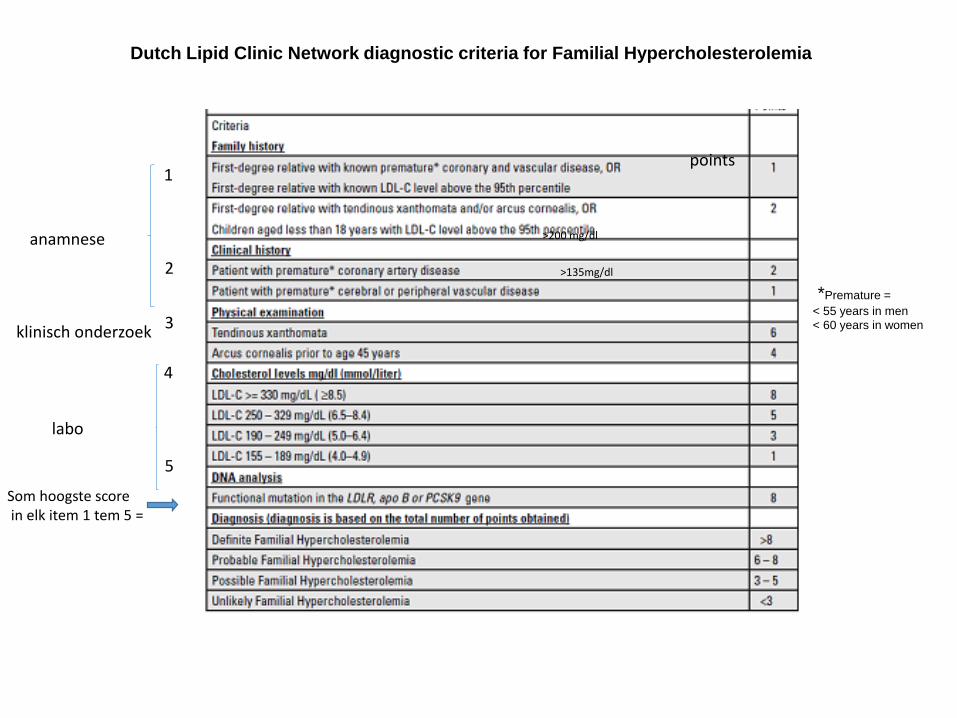
Dutch Lipid Clinic Network diagnostic criteria for Familial Hypercholesterolemia
*Premature =
< 55 years in men
< 60 years in women
points1
2
3
4
5
Som hoogste scorein elk item 1 tem 5 =
anamnese
klinisch onderzoek
labo
>200 mg/dl
>135mg/dl
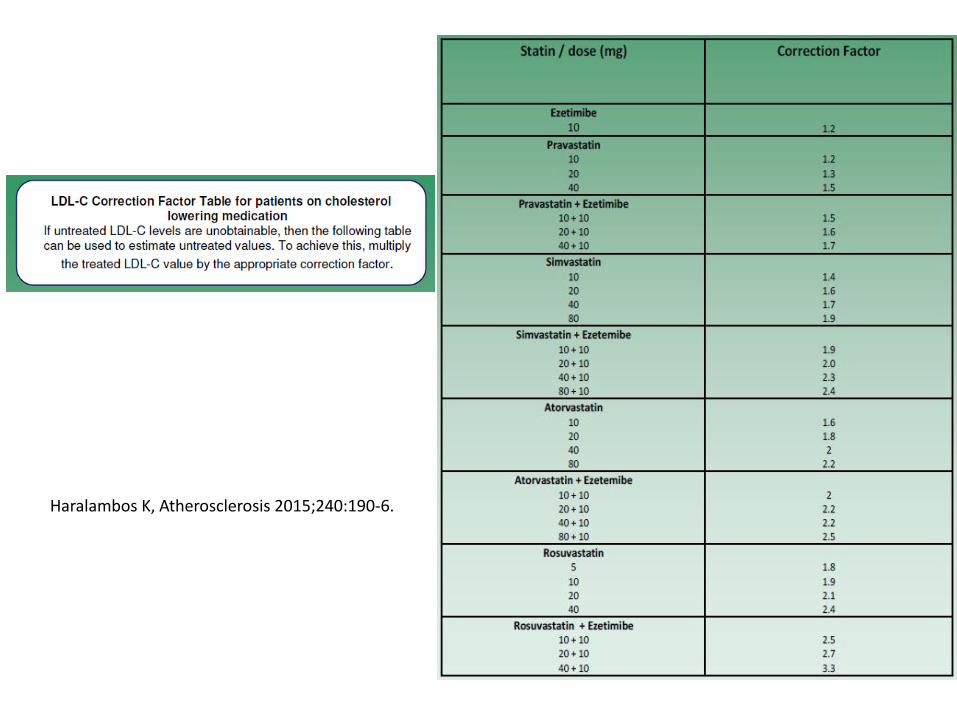
Haralambos K, Atherosclerosis 2015;240:190-6.
Piepoli F, Hoes W, Agewall S, Albus Chr, Brotons C, Catapano A et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. European Heart Journal. 2016;
doi:10.1093/eurheartj/ehw106
ESC Guidelines on CV prevention
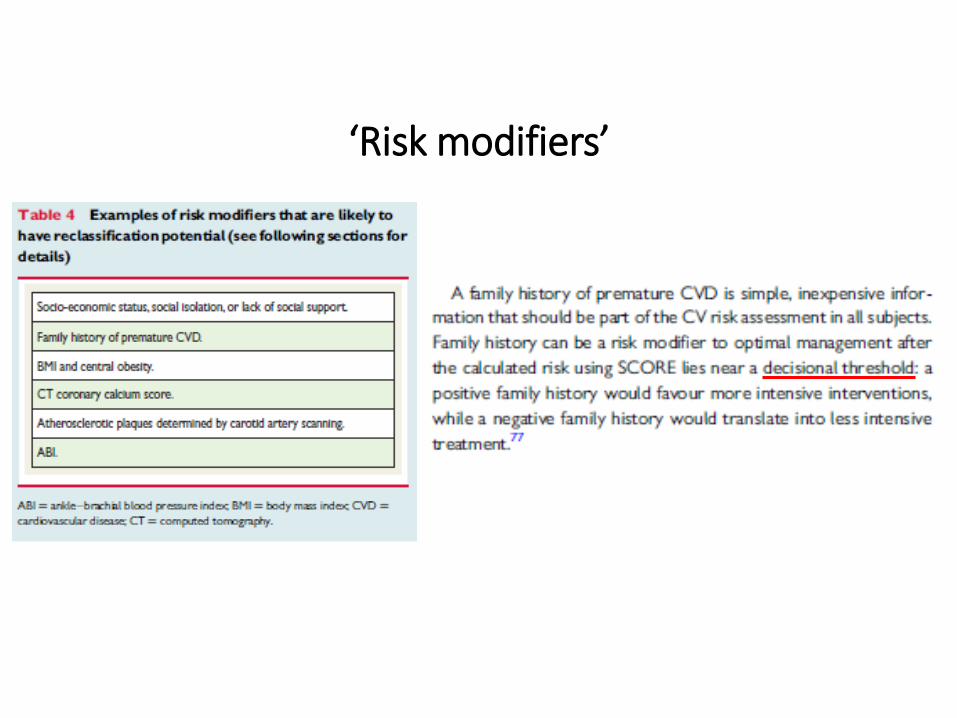
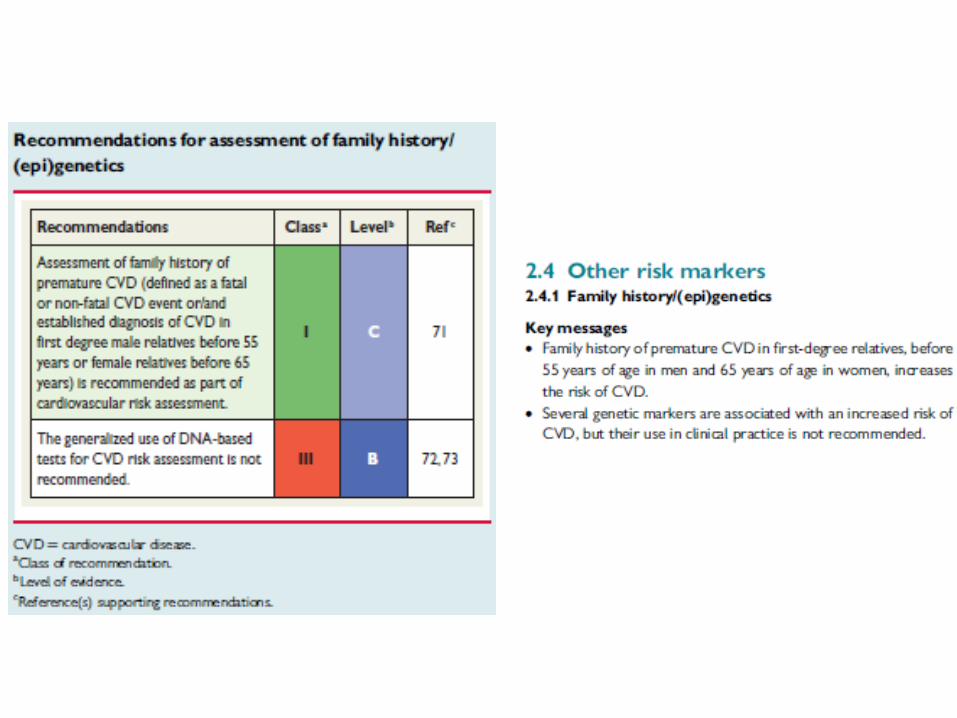
‘Risk modifiers’
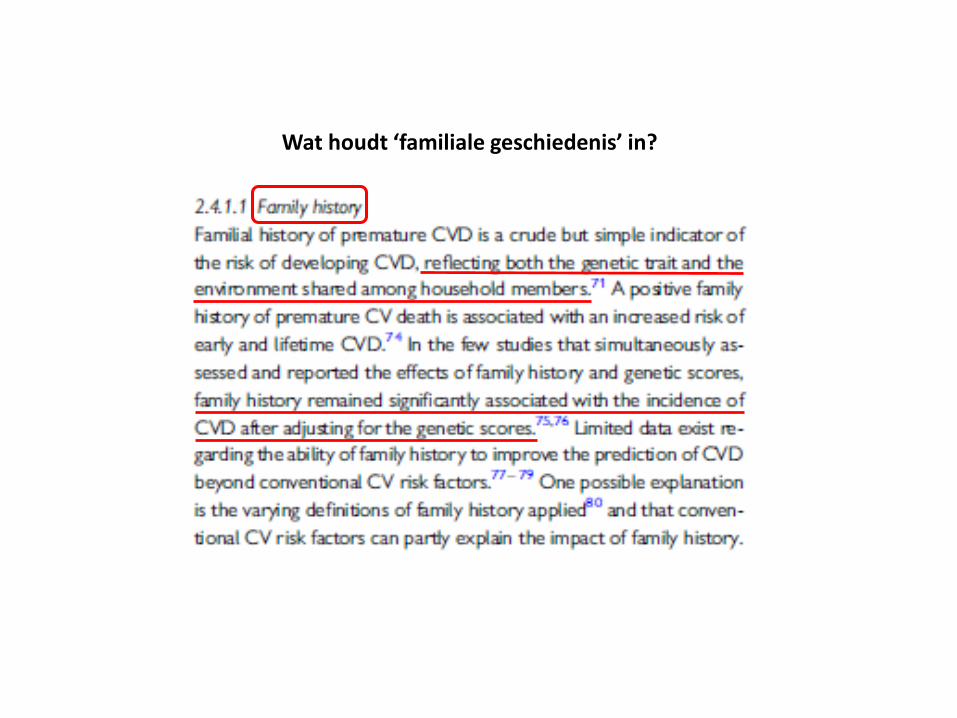
Wat houdt ‘familiale geschiedenis’ in?
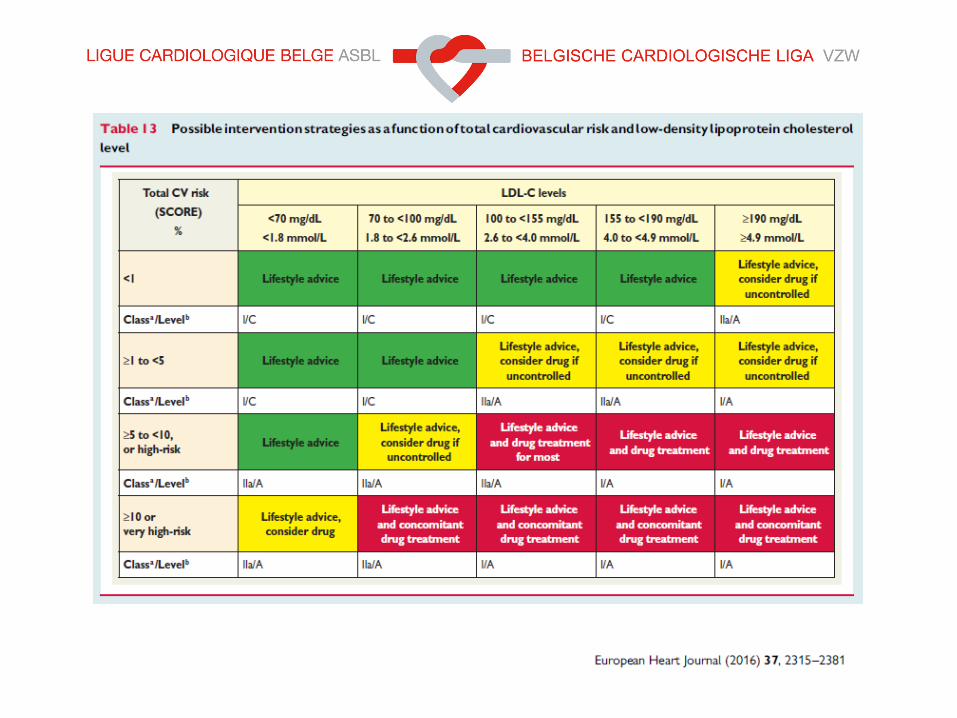
General principle of prevention:
The higher the risk, the more intense the action should be.
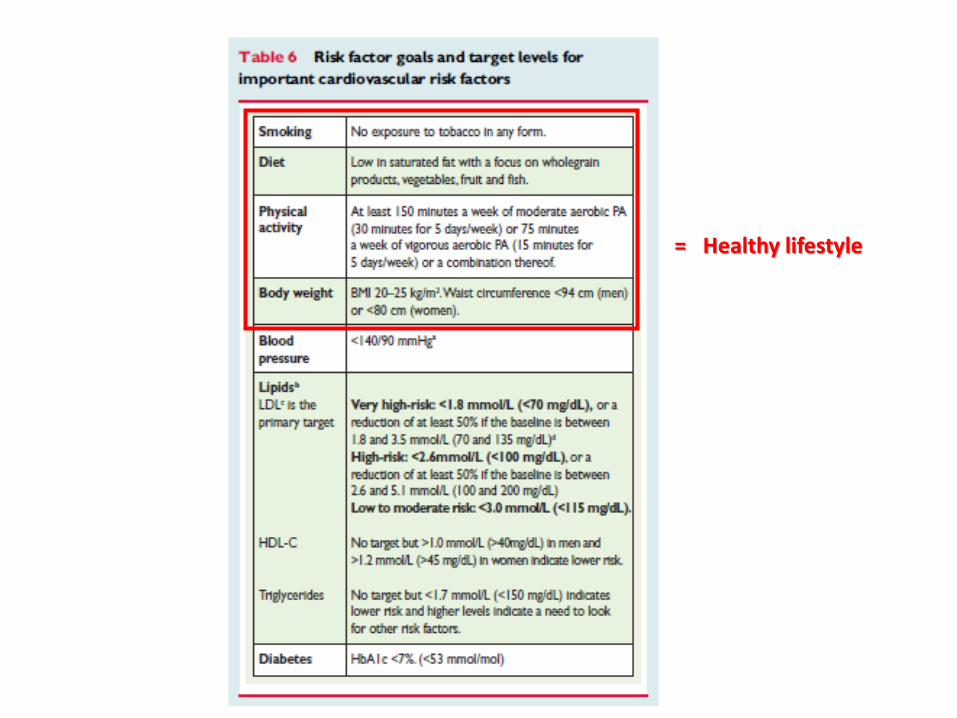
= Healthy lifestyle
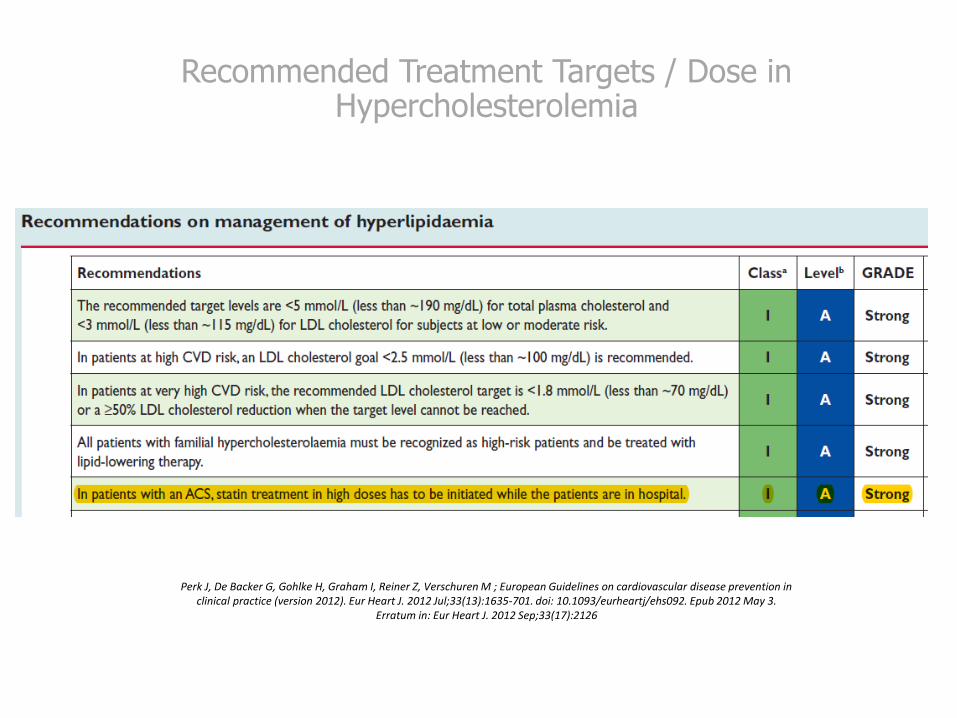
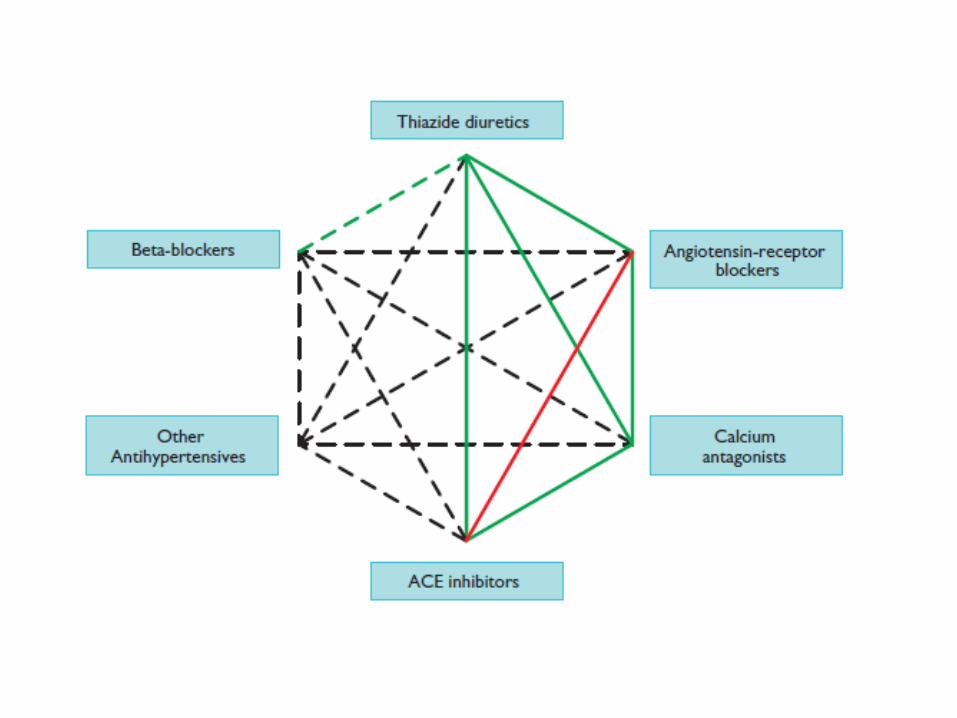
Recommended Treatment Targets / Dose in Hypercholesterolemia
Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M ; European Guidelines on cardiovascular disease prevention inclinical practice (version 2012). Eur Heart J. 2012 Jul;33(13):1635-701. doi: 10.1093/eurheartj/ehs092. Epub 2012 May 3.
Erratum in: Eur Heart J. 2012 Sep;33(17):2126
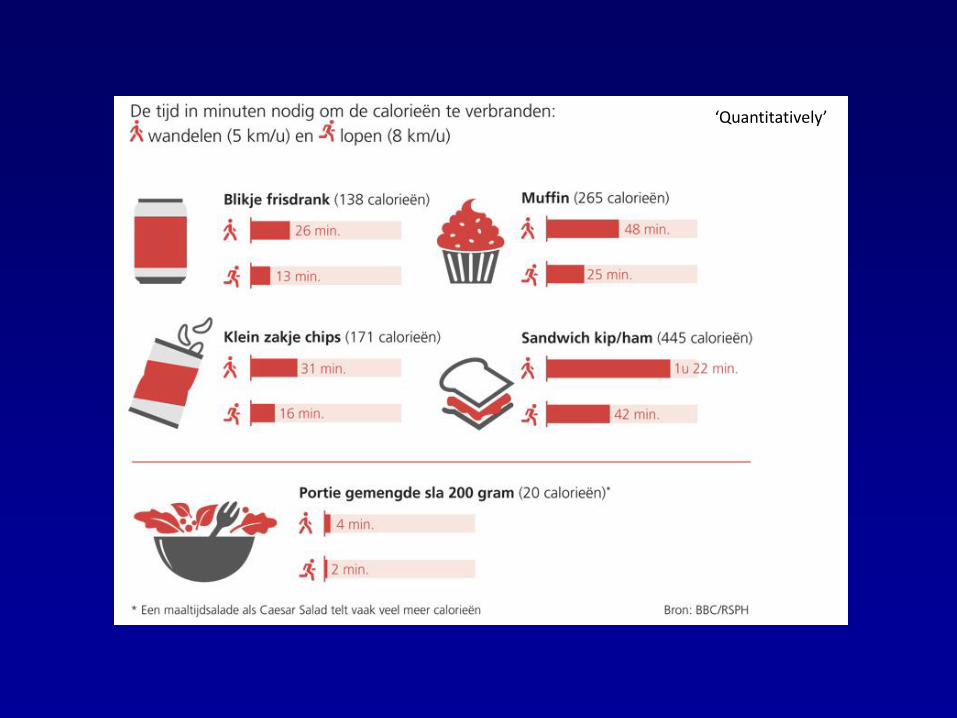
‘Quantitatively’
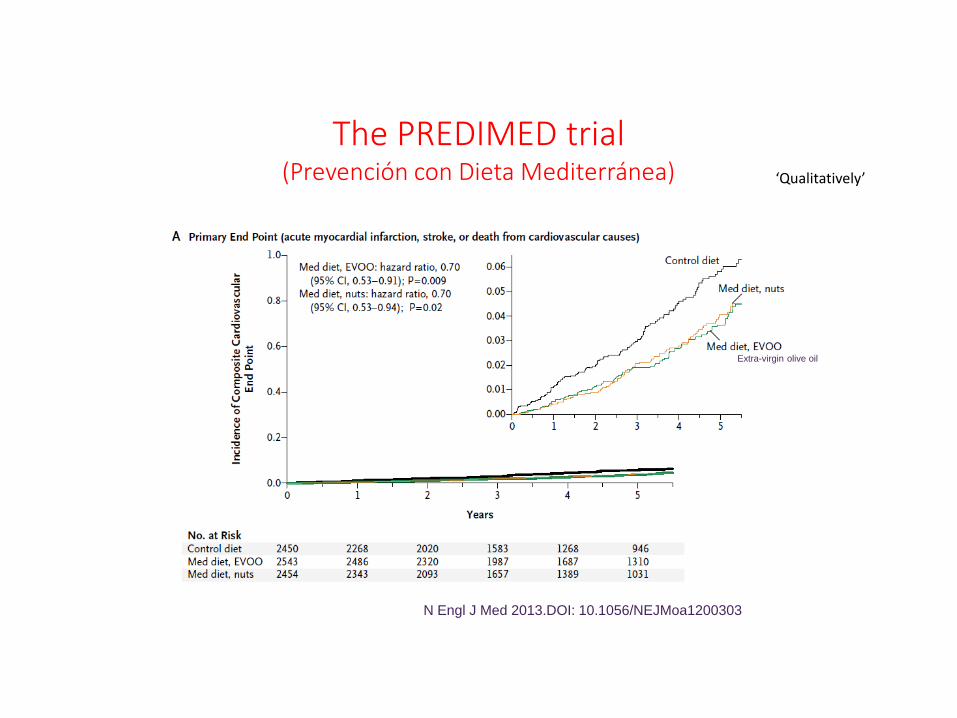
The PREDIMED trial(Prevención con Dieta Mediterránea)
N Engl J Med 2013.DOI: 10.1056/NEJMoa1200303
Extra-virgin olive oil
‘Qualitatively’
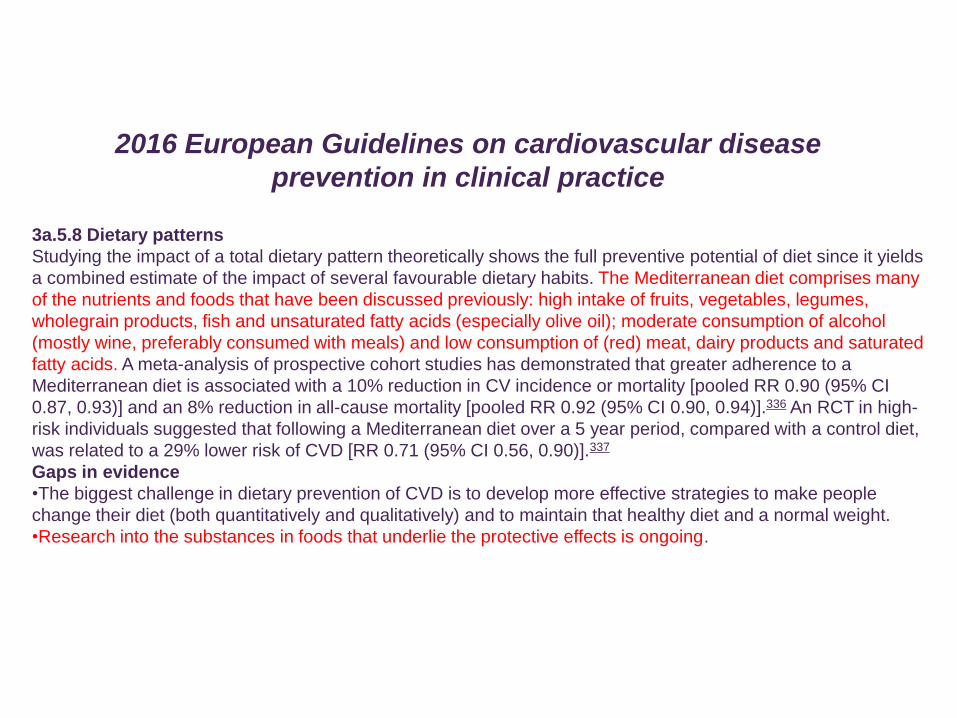
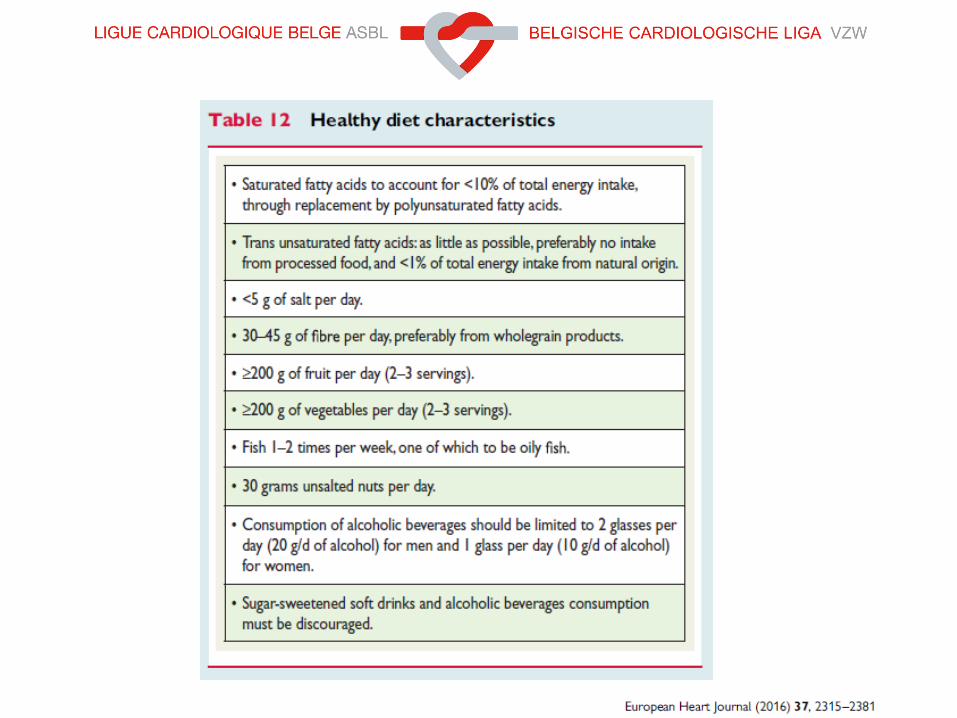
3a.5.8 Dietary patterns
Studying the impact of a total dietary pattern theoretically shows the full preventive potential of diet since it yields
a combined estimate of the impact of several favourable dietary habits. The Mediterranean diet comprises many
of the nutrients and foods that have been discussed previously: high intake of fruits, vegetables, legumes,
wholegrain products, fish and unsaturated fatty acids (especially olive oil); moderate consumption of alcohol
(mostly wine, preferably consumed with meals) and low consumption of (red) meat, dairy products and saturated
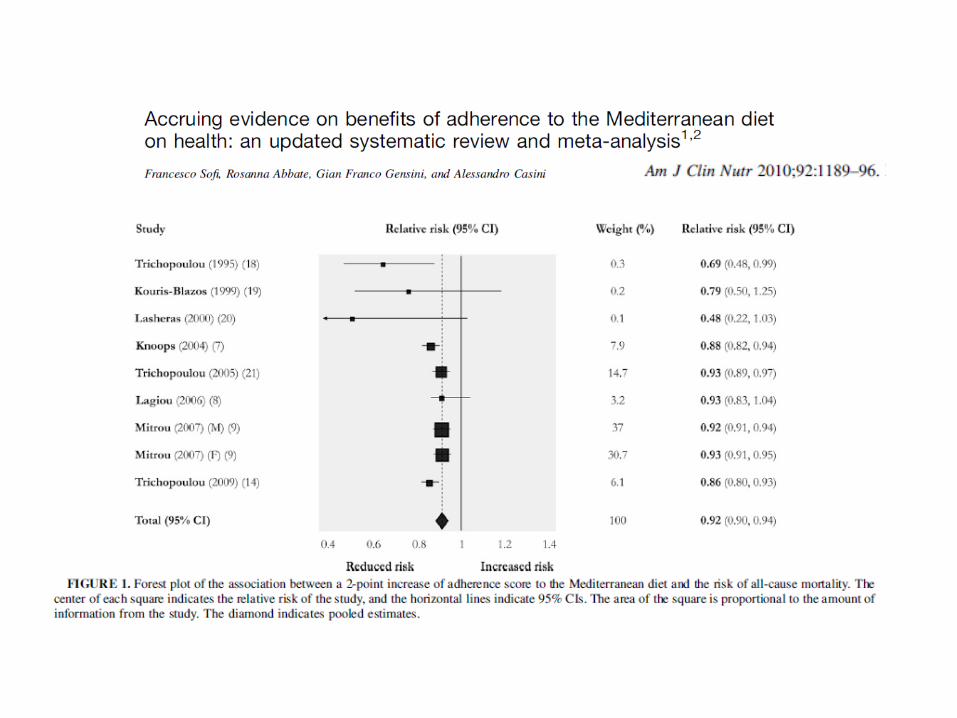
fatty acids. A meta-analysis of prospective cohort studies has demonstrated that greater adherence to a
Mediterranean diet is associated with a 10% reduction in CV incidence or mortality [pooled RR 0.90 (95% CI
0.87, 0.93)] and an 8% reduction in all-cause mortality [pooled RR 0.92 (95% CI 0.90, 0.94)].336 An RCT in high-
risk individuals suggested that following a Mediterranean diet over a 5 year period, compared with a control diet,
was related to a 29% lower risk of CVD [RR 0.71 (95% CI 0.56, 0.90)].337
Gaps in evidence
•The biggest challenge in dietary prevention of CVD is to develop more effective strategies to make people
change their diet (both quantitatively and qualitatively) and to maintain that healthy diet and a normal weight.
•Research into the substances in foods that underlie the protective effects is ongoing.
2016 European Guidelines on cardiovascular disease
prevention in clinical practice
Medicamenteuze Aanpakvan Hypercholesterolemie
Remmen van de cholesterolsynthese
Remmen van de cholesterolopname via de darm
Remmen van de afbraak van de LDL receptor
Statins are among the most studied drugs in CV prevention.
A number of large-scale clinical trials have demonstrated that statins
substantially reduce CV morbidity and mortality in both primary and
secondary prevention.
Statins have also been shown to slow the progression or even promote
regression of coronary atherosclerosis.
Statins
Efficacy in clinical studies
Reiner Z et al., European Heart Journal (2011) 32, 1790
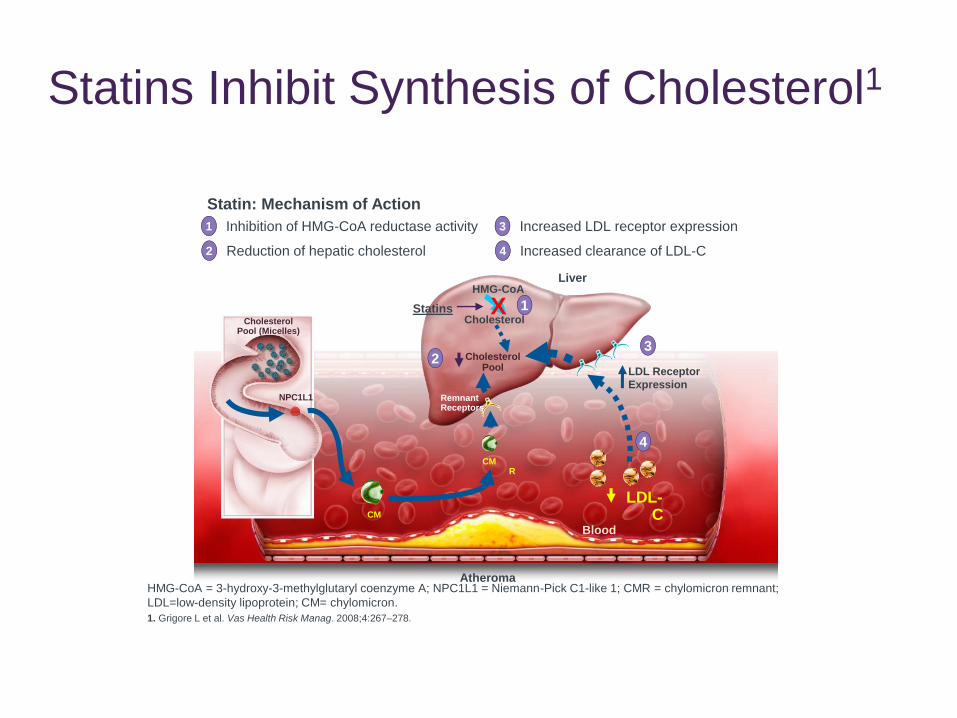
Atheroma
Liver
CholesterolPool (Micelles)
NPC1L1 RemnantReceptors
LDL Receptor
Expression
Cholesterol
HMG-CoA
CMR
CM
Statins X 1
3
1 Inhibition of HMG-CoA reductase activity
2 Reduction of hepatic cholesterol
3 Increased LDL receptor expression
4 Increased clearance of LDL-C
Statin: Mechanism of Action
LDL-C
HMG-CoA = 3-hydroxy-3-methylglutaryl coenzyme A; NPC1L1 = Niemann-Pick C1-like 1; CMR = chylomicron remnant;
LDL=low-density lipoprotein; CM= chylomicron.
1. Grigore L et al. Vas Health Risk Manag. 2008;4:267–278.
Cholesterol Pool
2
4
Statins Inhibit Synthesis of Cholesterol1
Blood
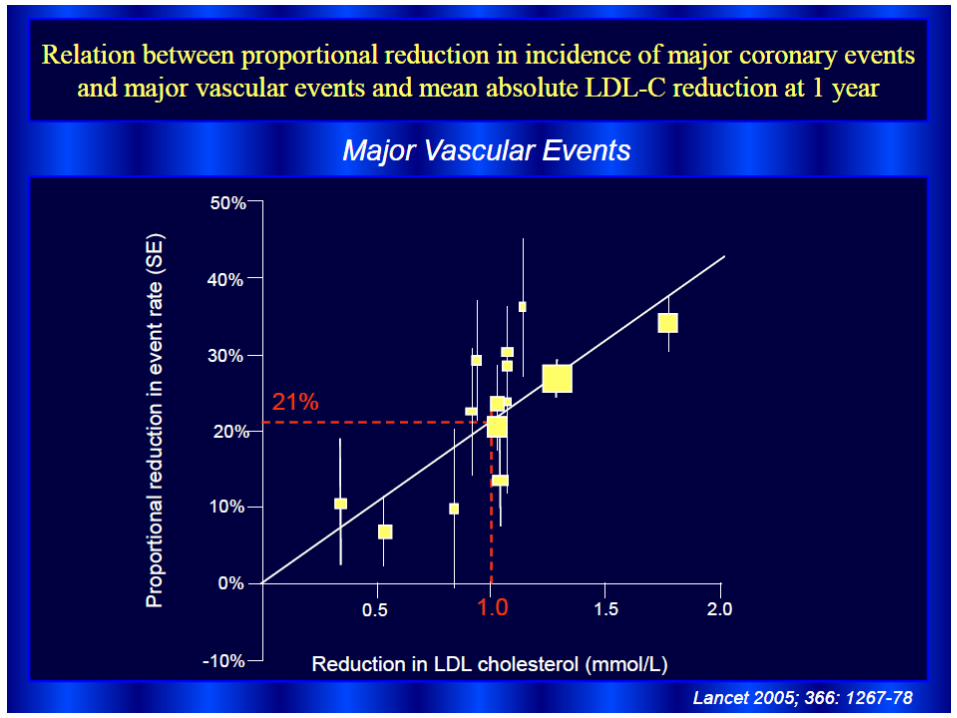
Current available evidence “suggests” that the clinical benefit:
-is largely independent of the type of statin
-but depends on the extent of LDL-C lowering.
Statins
Meta-analyses
Reiner Z et al., European Heart Journal (2011) 32, 1790
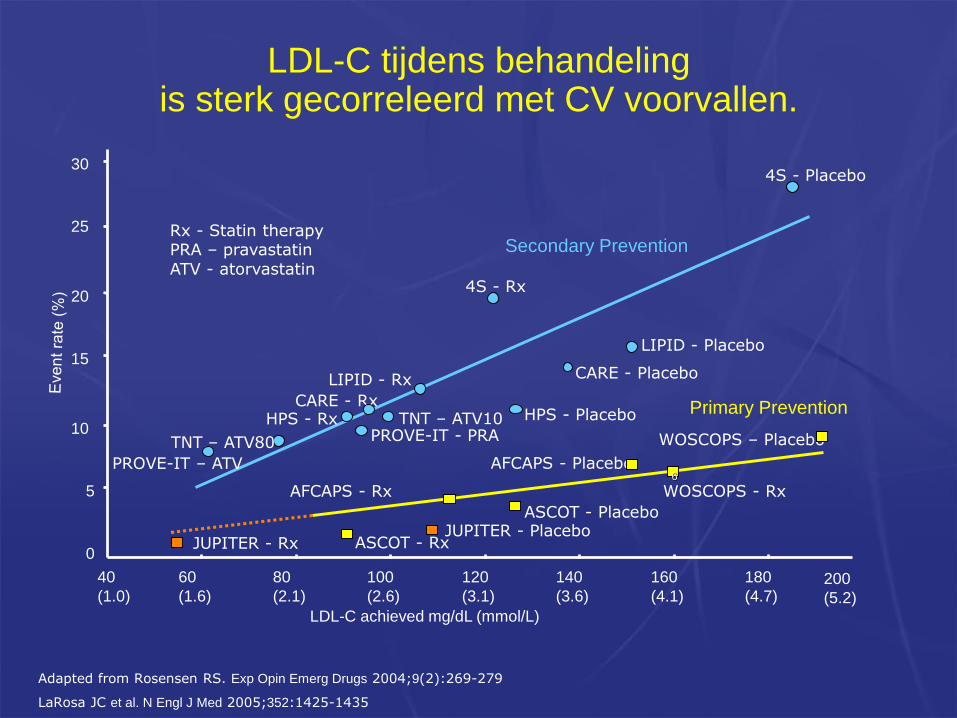
Adapted from Rosensen RS. Exp Opin Emerg Drugs 2004;9(2):269-279
LaRosa JC et al. N Engl J Med 2005;352:1425-1435
LDL-C achieved mg/dL (mmol/L)
WOSCOPS – Placebo
AFCAPS - Placebo
ASCOT - Placebo
AFCAPS - Rx WOSCOPS - Rx
ASCOT - Rx
4S - Rx
HPS - Placebo
LIPID - Rx
4S - Placebo
CARE - Rx
LIPID - Placebo
CARE - Placebo
HPS - Rx
0
5
10
15
20
25
30
40
(1.0)
60
(1.6)
80
(2.1)
100
(2.6)
120
(3.1)
140
(3.6)
160
(4.1)
180
(4.7)
6
Secondary Prevention
Primary Prevention
Rx - Statin therapyPRA – pravastatinATV - atorvastatin
200
(5.2)
PROVE-IT - PRA
PROVE-IT – ATV
TNT – ATV10
TNT – ATV80
LDL-C tijdens behandelingis sterk gecorreleerd met CV voorvallen.
JUPITER - PlaceboJUPITER - Rx

LDL-C ≈ 35 mg/dL
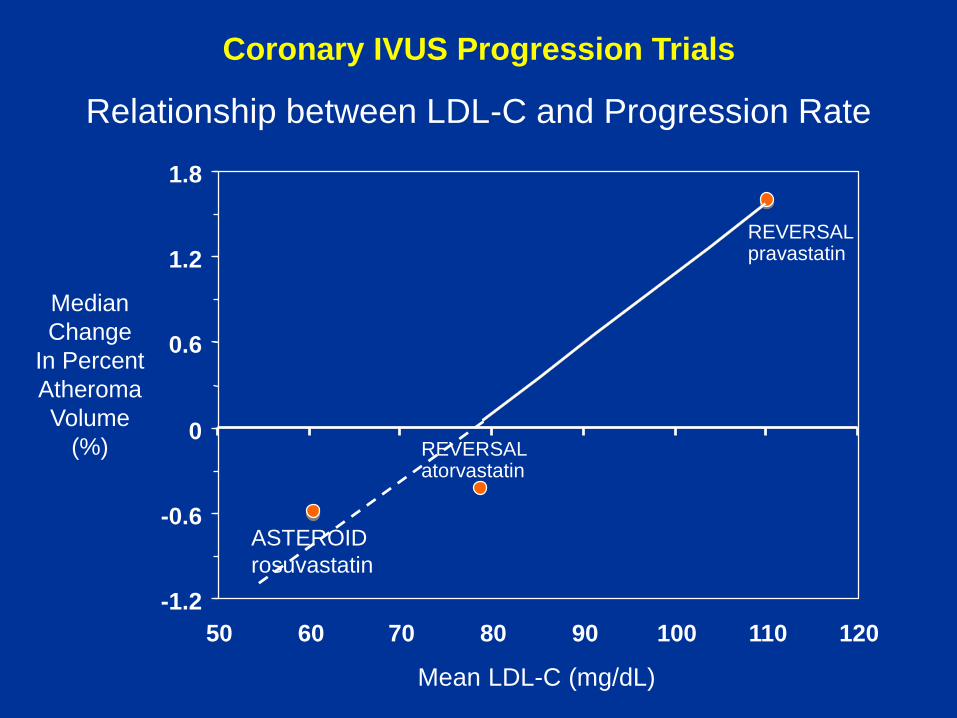
Coronary IVUS Progression Trials
-1.2
-0.6
0
0.6
1.2
1.8
50 60 70 80 90 100 110 120
Median
Change
In Percent
Atheroma
Volume
(%)
Mean LDL-C (mg/dL)
REVERSALpravastatin
REVERSALatorvastatin
Relationship between LDL-C and Progression Rate
ASTEROID
rosuvastatin
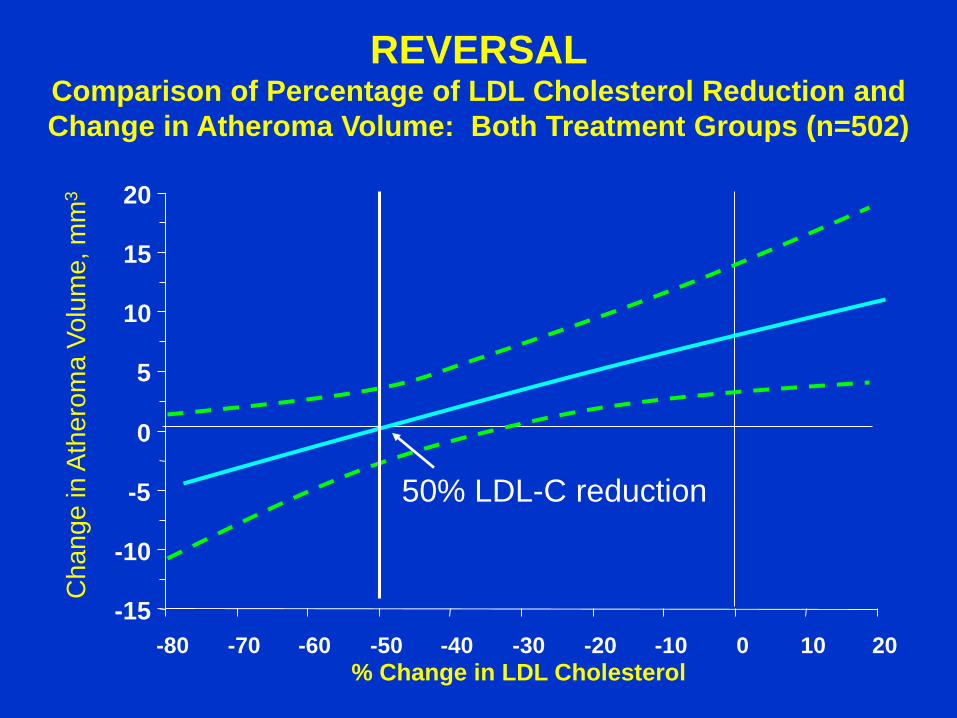
REVERSALComparison of Percentage of LDL Cholesterol Reduction and
Change in Atheroma Volume: Both Treatment Groups (n=502)
% Change in LDL Cholesterol
Ch
an
ge
in
Ath
ero
ma
Vo
lum
e, m
m3
Adapted from Nissen S. et al., JAMA 2004; 291:1071-80.
50% LDL-C reduction
-15
-10
-5
0
5
10
15
20
-80 -70 -60 -50 -40 -30 -20 -10 0 10 20
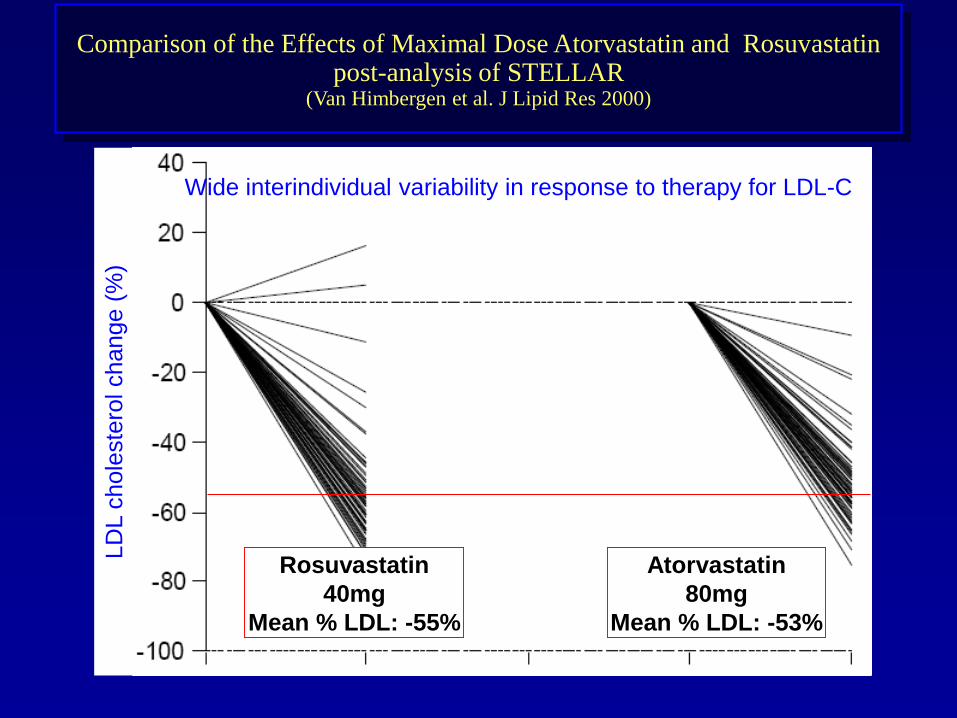
Comparison of the Effects of Maximal Dose Atorvastatin and Rosuvastatinpost-analysis of STELLAR
(Van Himbergen et al. J Lipid Res 2000)
Wide interindividual variability in response to therapy for LDL-C
LD
L c
hole
ste
rol change (
%)
Rosuvastatin
40mg
Mean % LDL: -55%
Atorvastatin
80mg
Mean % LDL: -53%
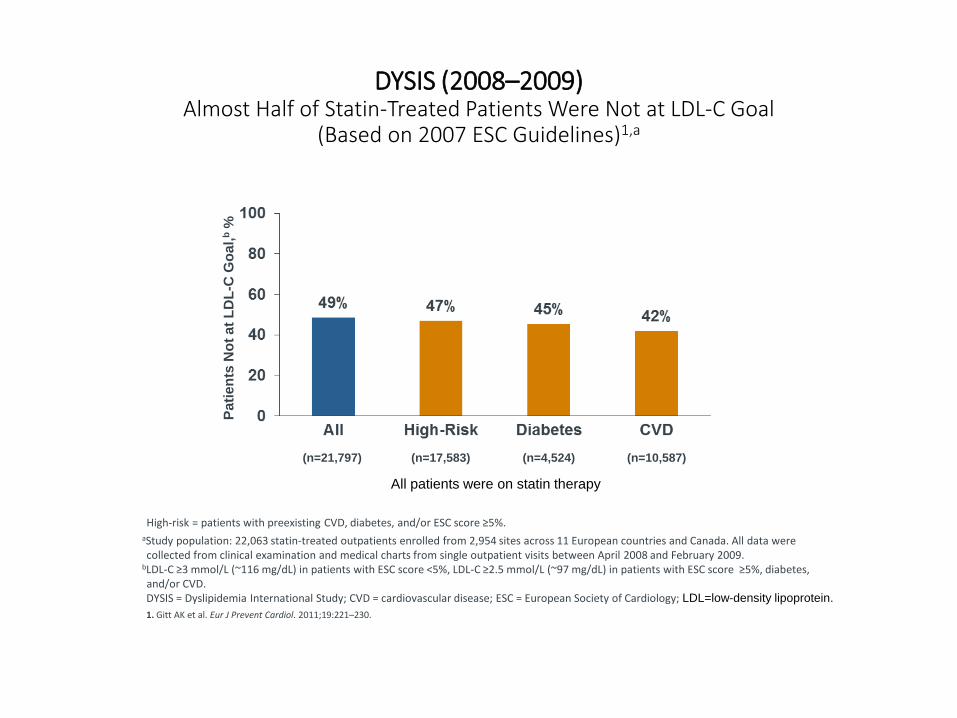
DYSIS (2008–2009)Almost Half of Statin-Treated Patients Were Not at LDL-C Goal
(Based on 2007 ESC Guidelines)1,a
High-risk = patients with preexisting CVD, diabetes, and/or ESC score ≥5%.aStudy population: 22,063 statin-treated outpatients enrolled from 2,954 sites across 11 European countries and Canada. All data were collected from clinical examination and medical charts from single outpatient visits between April 2008 and February 2009.
bLDL-C ≥3 mmol/L (~116 mg/dL) in patients with ESC score <5%, LDL-C ≥2.5 mmol/L (~97 mg/dL) in patients with ESC score ≥5%, diabetes, and/or CVD.DYSIS = Dyslipidemia International Study; CVD = cardiovascular disease; ESC = European Society of Cardiology; LDL=low-density lipoprotein.
1. Gitt AK et al. Eur J Prevent Cardiol. 2011;19:221–230.
All patients were on statin therapy
Pa
tie
nts
No
t a
t L
DL
-C G
oa
l,b
%
(n=21,797) (n=17,583) (n=4,524) (n=10,587)
Medicamenteuze Aanpakvan Hypercholesterolemie
Remmen van de cholesterolsynthese
Remmen van de cholesterolopname via de darm
Remmen van de afbraak van de LDL receptor
Cholesterol Absorption Inhibitors
efficacy in clinical studies
Guidelines ESC
Ezetimibe can be used as second-line therapy in
association with statins when the therapeutic target is not
achieved at maximal tolerated statin dose or in patients
intolerant of statins or with contraindications to these drugs.
Reiner Z et al., European Heart Journal (2011) 32, 1792
54
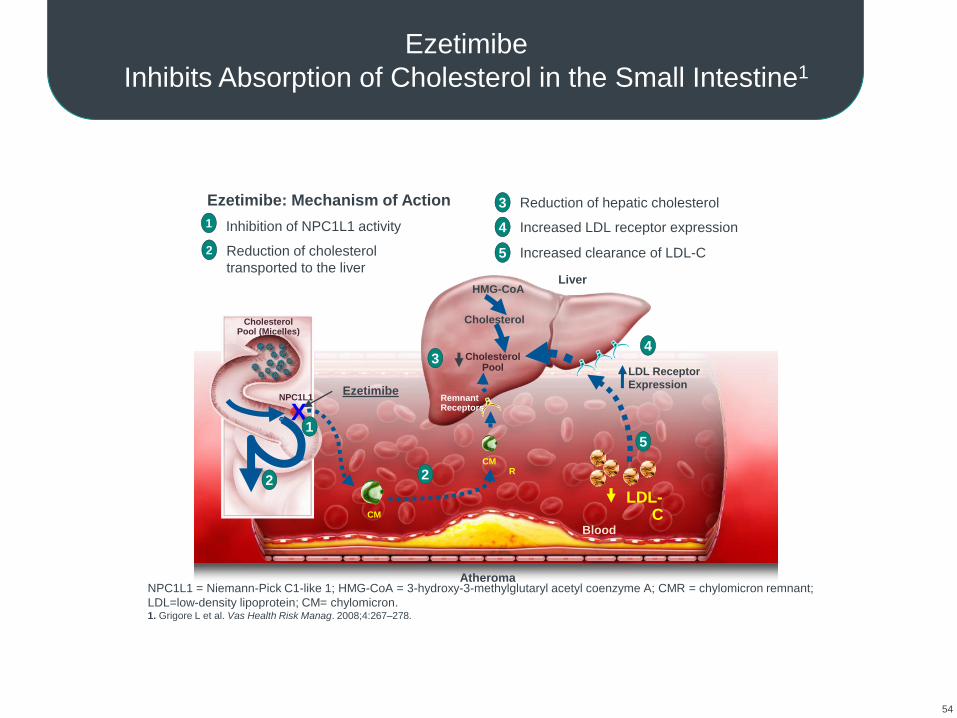
Ezetimibe
Inhibits Absorption of Cholesterol in the Small Intestine1
Atheroma
Liver
Blood
CholesterolPool (Micelles)
NPC1L1 RemnantReceptors
LDL Receptor
Expression
Cholesterol
HMG-CoA
CMR
CM
Ezetimibe
X1
3
5
4
2
1 Inhibition of NPC1L1 activity
2 Reduction of cholesterol
transported to the liver
3 Reduction of hepatic cholesterol
4 Increased LDL receptor expression
5 Increased clearance of LDL-C
2
Ezetimibe: Mechanism of Action
LDL-C
NPC1L1 = Niemann-Pick C1-like 1; HMG-CoA = 3-hydroxy-3-methylglutaryl acetyl coenzyme A; CMR = chylomicron remnant;
LDL=low-density lipoprotein; CM= chylomicron.1. Grigore L et al. Vas Health Risk Manag. 2008;4:267–278.
Cholesterol Pool
55
Atheroma
Liver
CholesterolPool (Micelles)
NPC1L1 RemnantReceptors
LDL Receptor
Expression
Cholesterol
HMG-CoA
CMR
CM
Statins
Ezetimibe
X
2
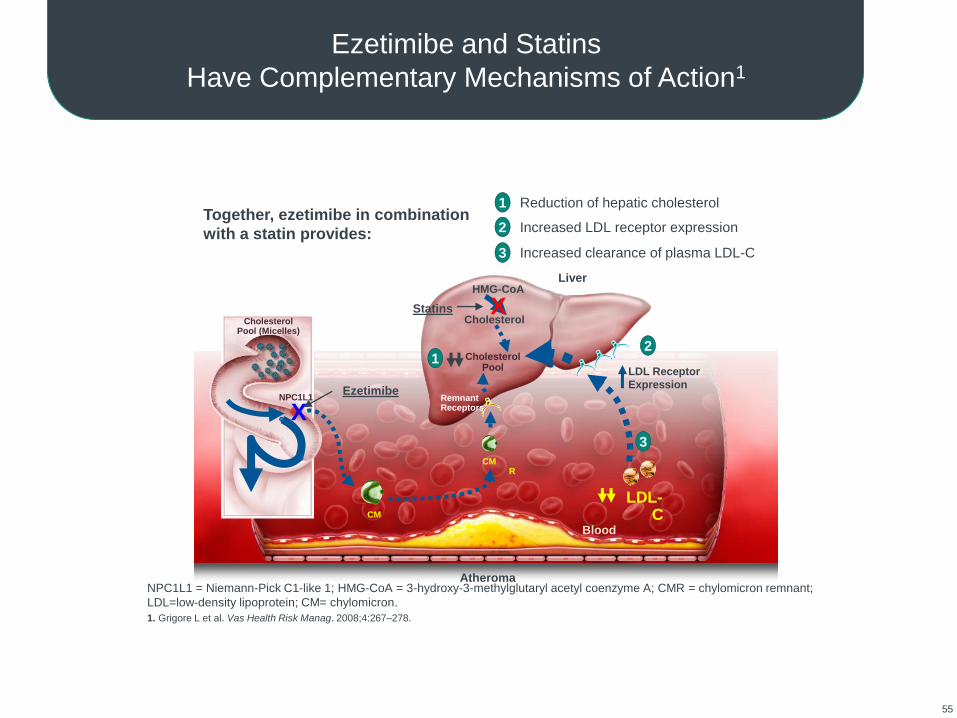
1 Reduction of hepatic cholesterol
2 Increased LDL receptor expression
3 Increased clearance of plasma LDL-C
Together, ezetimibe in combination
with a statin provides:
LDL-C
NPC1L1 = Niemann-Pick C1-like 1; HMG-CoA = 3-hydroxy-3-methylglutaryl acetyl coenzyme A; CMR = chylomicron remnant;
LDL=low-density lipoprotein; CM= chylomicron.
1. Grigore L et al. Vas Health Risk Manag. 2008;4:267–278.
1 Cholesterol Pool
3
Ezetimibe and Statins
Have Complementary Mechanisms of Action1
Blood
X
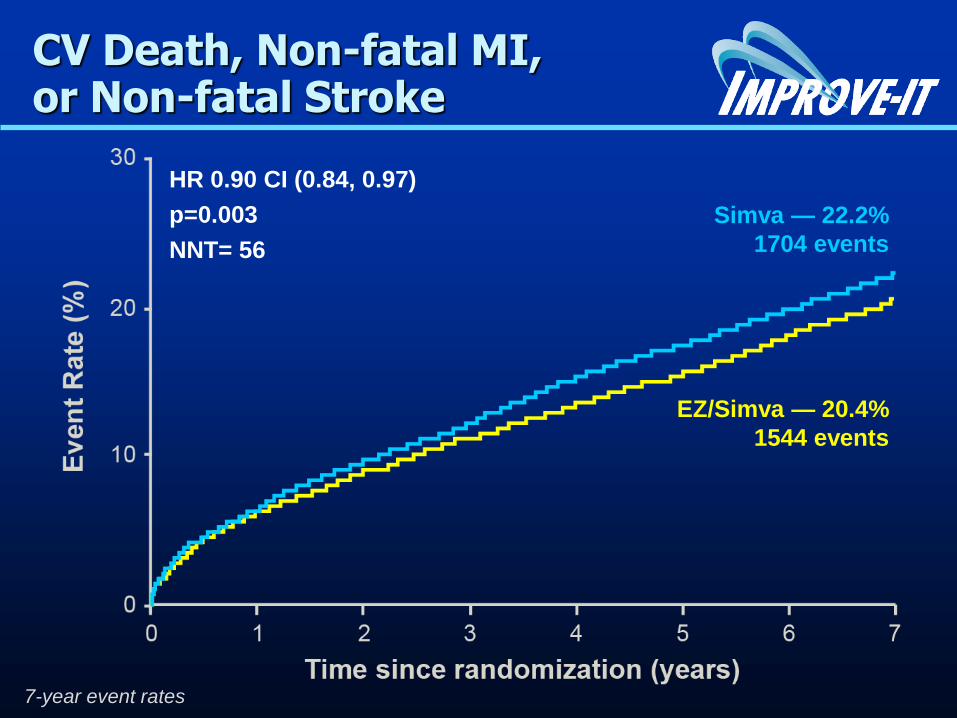
Simva — 22.2%
1704 events
EZ/Simva — 20.4%
1544 events
HR 0.90 CI (0.84, 0.97)
p=0.003
NNT= 56
CV Death, Non-fatal MI, or Non-fatal Stroke
7-year event rates
Medicamenteuze Aanpakvan Hypercholesterolemie
Remmen van de cholesterolsynthese
Remmen van de cholesterolopname via de darm
Remmen van de afbraak van de LDL receptor
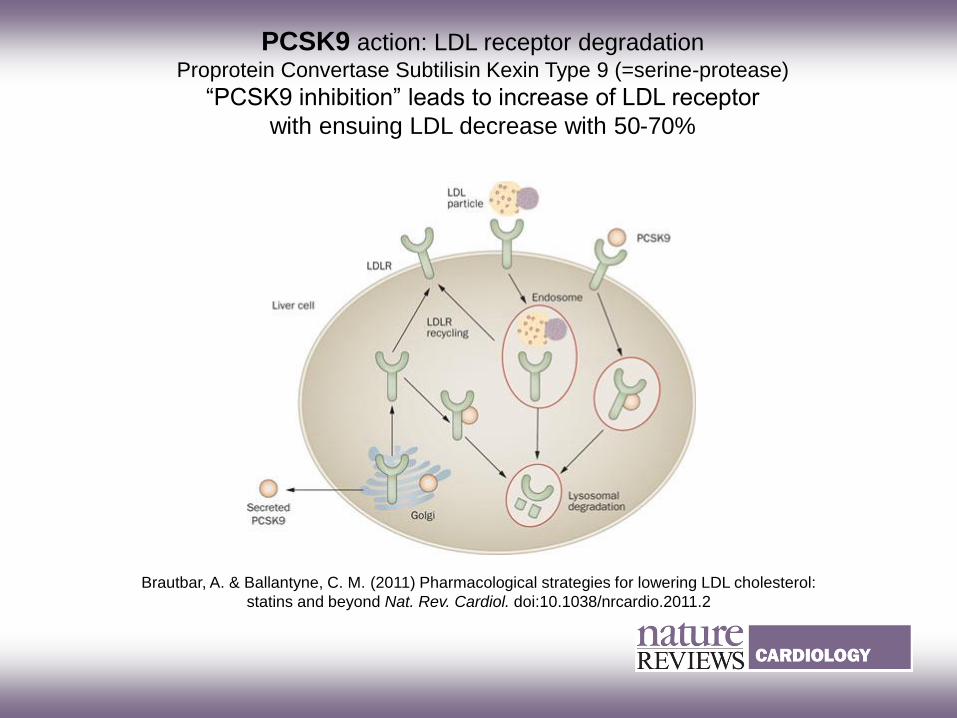
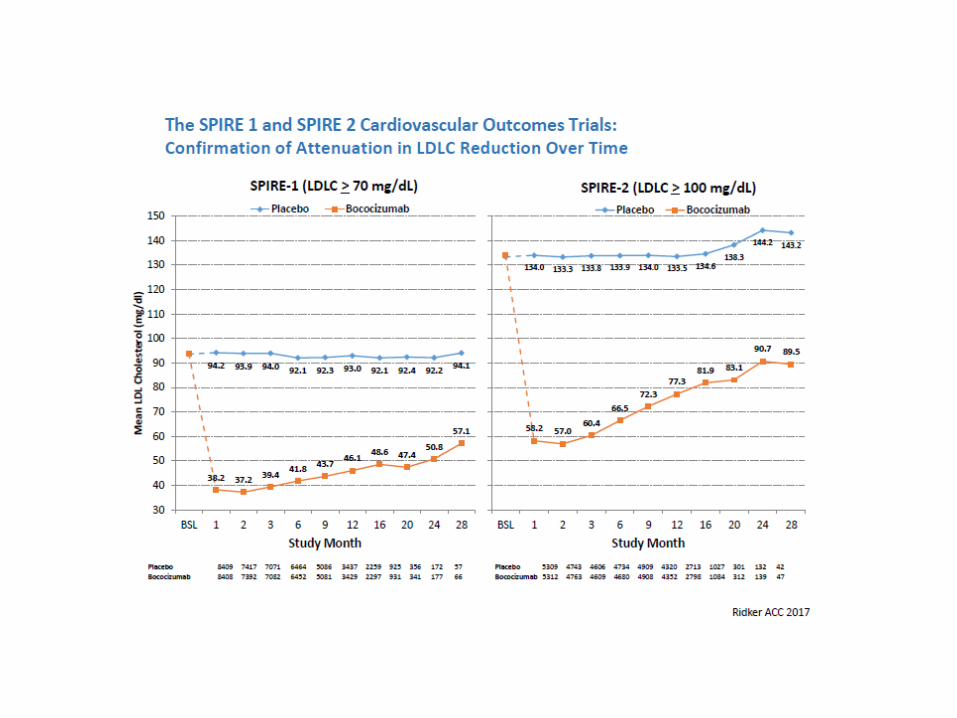
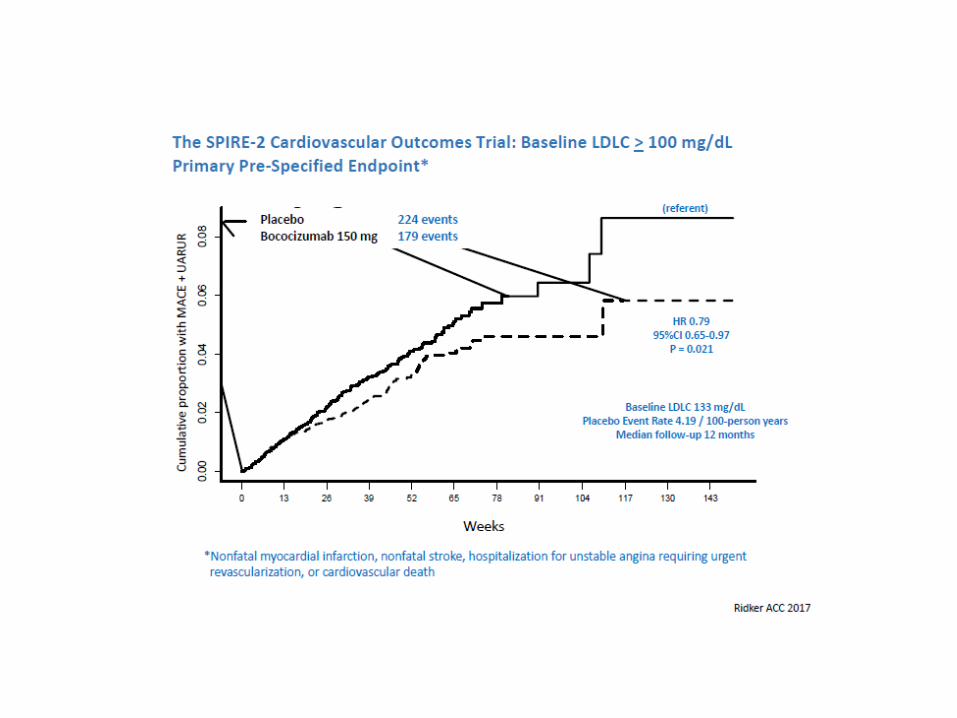
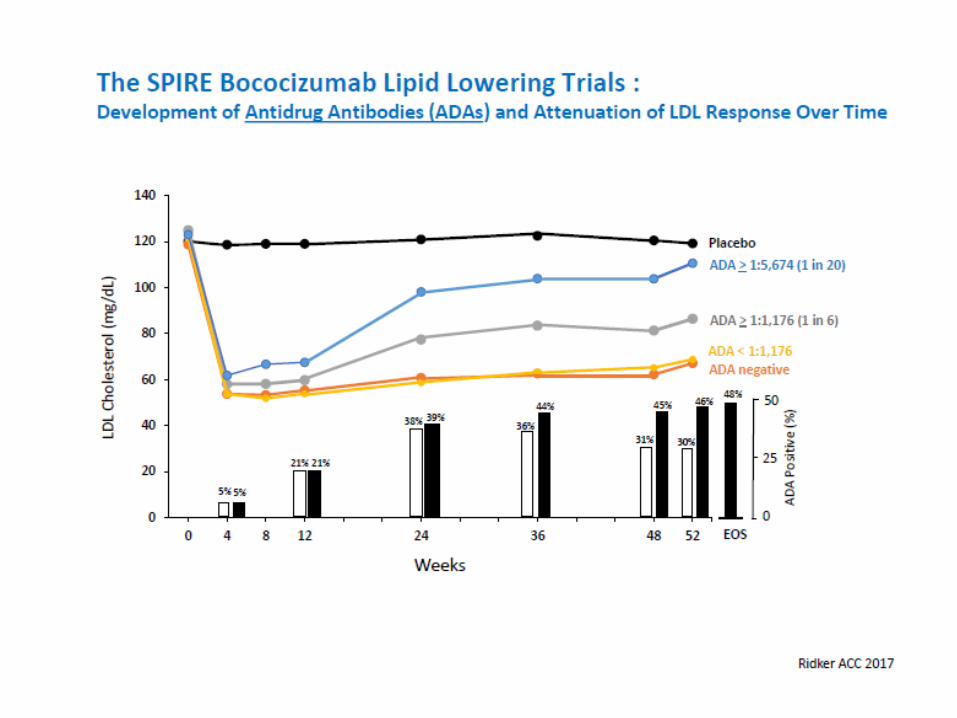
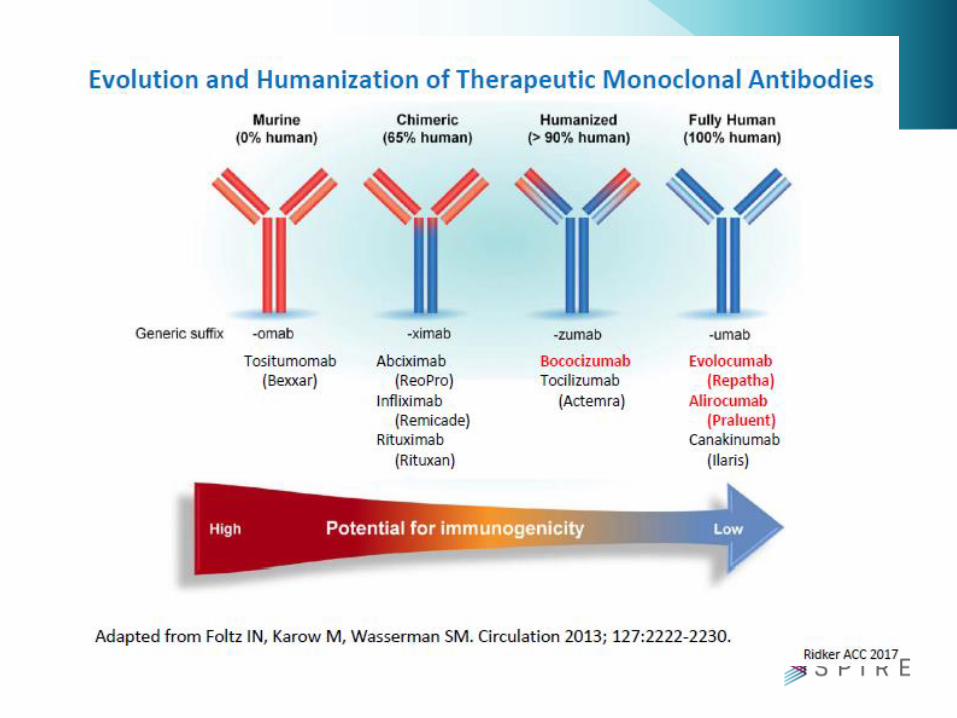
PCSK9 action: LDL receptor degradationProprotein Convertase Subtilisin Kexin Type 9 (=serine-protease)
“PCSK9 inhibition” leads to increase of LDL receptor
with ensuing LDL decrease with 50-70%
Brautbar, A. & Ballantyne, C. M. (2011) Pharmacological strategies for lowering LDL cholesterol:
statins and beyond Nat. Rev. Cardiol. doi:10.1038/nrcardio.2011.2
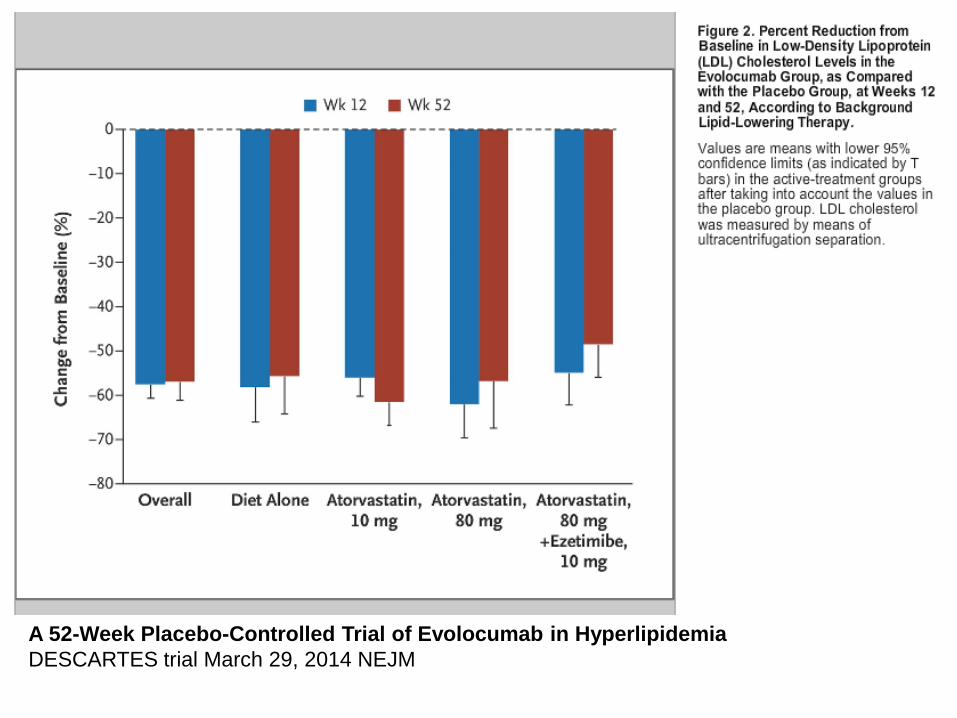
A 52-Week Placebo-Controlled Trial of Evolocumab in Hyperlipidemia
DESCARTES trial March 29, 2014 NEJM
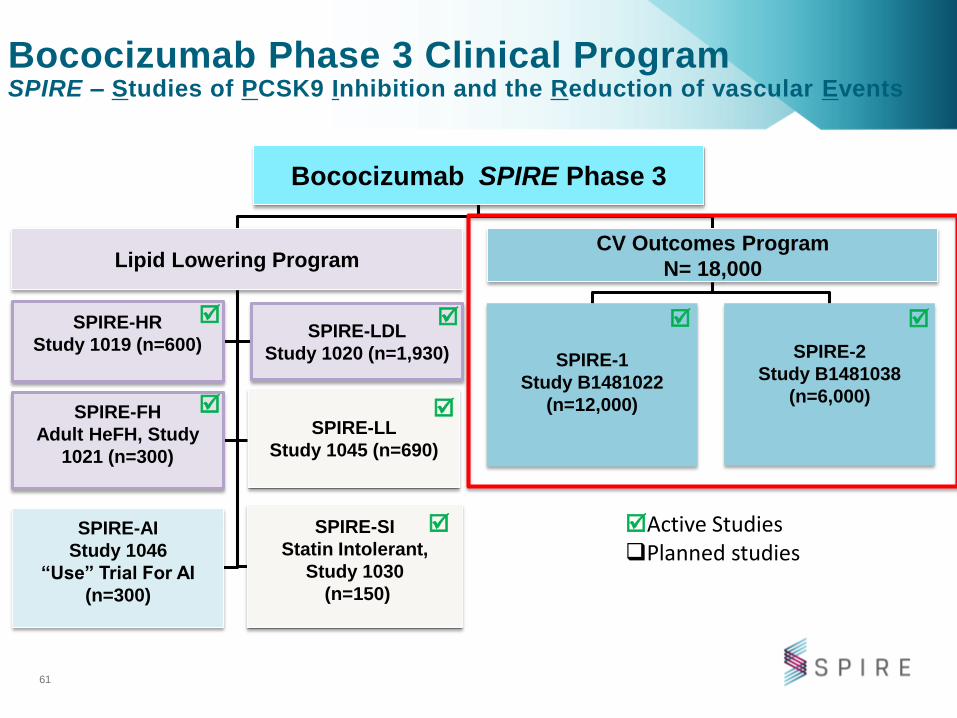
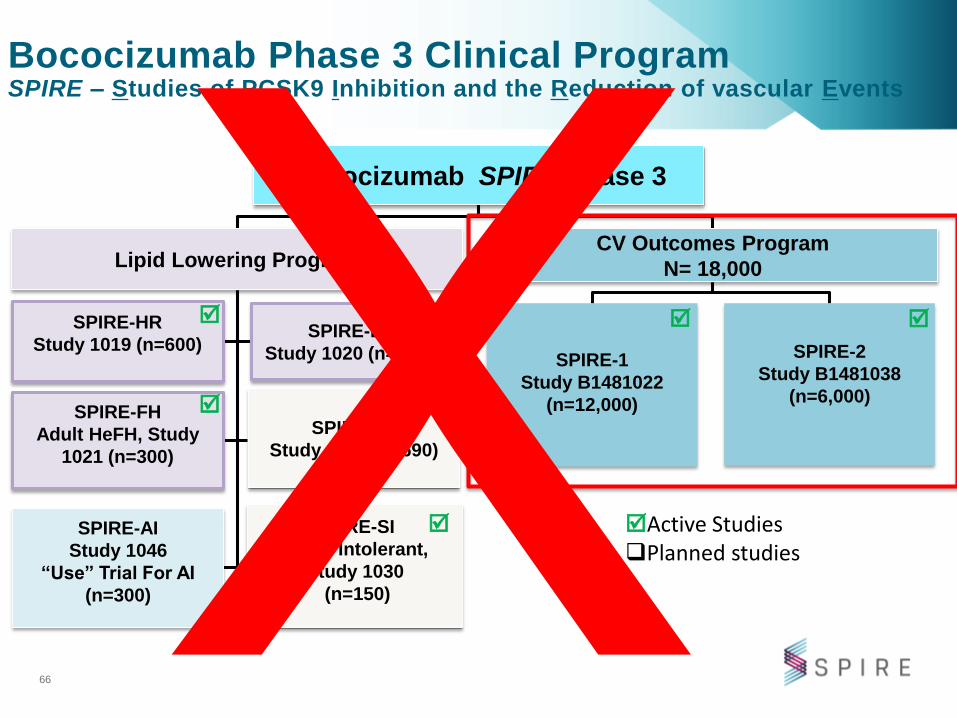
Bococizumab SPIRE Phase 3
CV Outcomes Program
N= 18,000
SPIRE-1
Study B1481022
(n=12,000)
SPIRE-2
Study B1481038
(n=6,000)
SPIRE-HR
Study 1019 (n=600)SPIRE-LDL
Study 1020 (n=1,930)
SPIRE-FH
Adult HeFH, Study
1021 (n=300)
SPIRE-LL
Study 1045 (n=690)
SPIRE-SI
Statin Intolerant,
Study 1030
(n=150)
Lipid Lowering Program
Bococizumab Phase 3 Clinical ProgramSPIRE – Studies of PCSK9 Inhibition and the Reduction of vascular Events
61
Active StudiesPlanned studies
SPIRE-AI
Study 1046
“Use” Trial For AI
(n=300)
Bococizumab SPIRE Phase 3
CV Outcomes Program
N= 18,000
SPIRE-1
Study B1481022
(n=12,000)
SPIRE-2
Study B1481038
(n=6,000)
SPIRE-HR
Study 1019 (n=600)SPIRE-LDL
Study 1020 (n=1,930)
SPIRE-FH
Adult HeFH, Study
1021 (n=300)
SPIRE-LL
Study 1045 (n=690)
SPIRE-SI
Statin Intolerant,
Study 1030
(n=150)
Lipid Lowering Program
Bococizumab Phase 3 Clinical ProgramSPIRE – Studies of PCSK9 Inhibition and the Reduction of vascular Events
66
Active StudiesPlanned studies
SPIRE-AI
Study 1046
“Use” Trial For AI
(n=300)
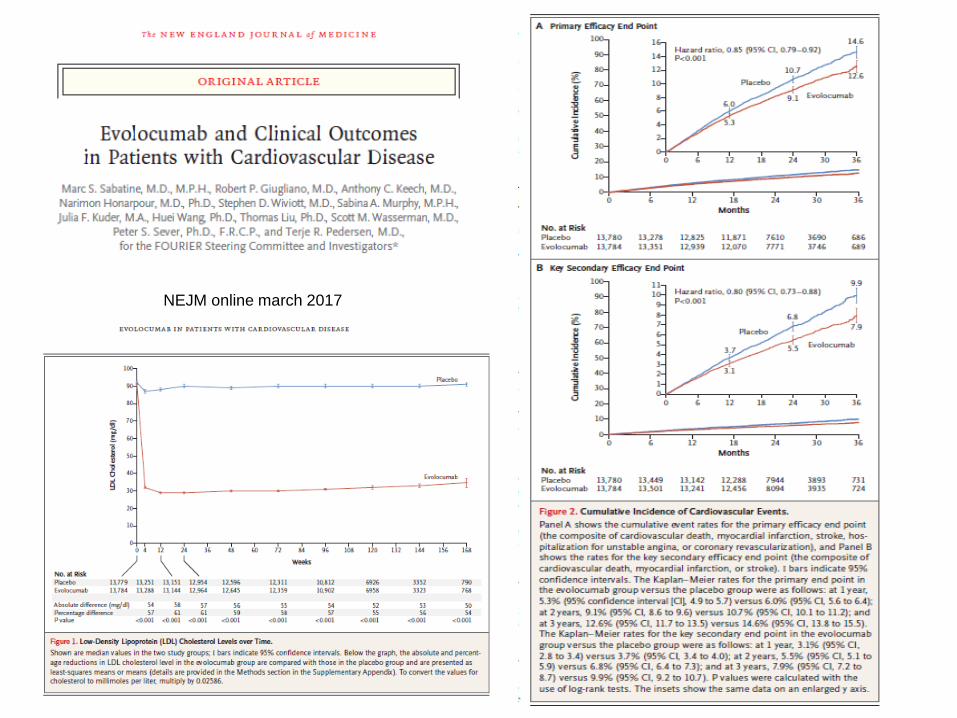
NEJM online march 2017
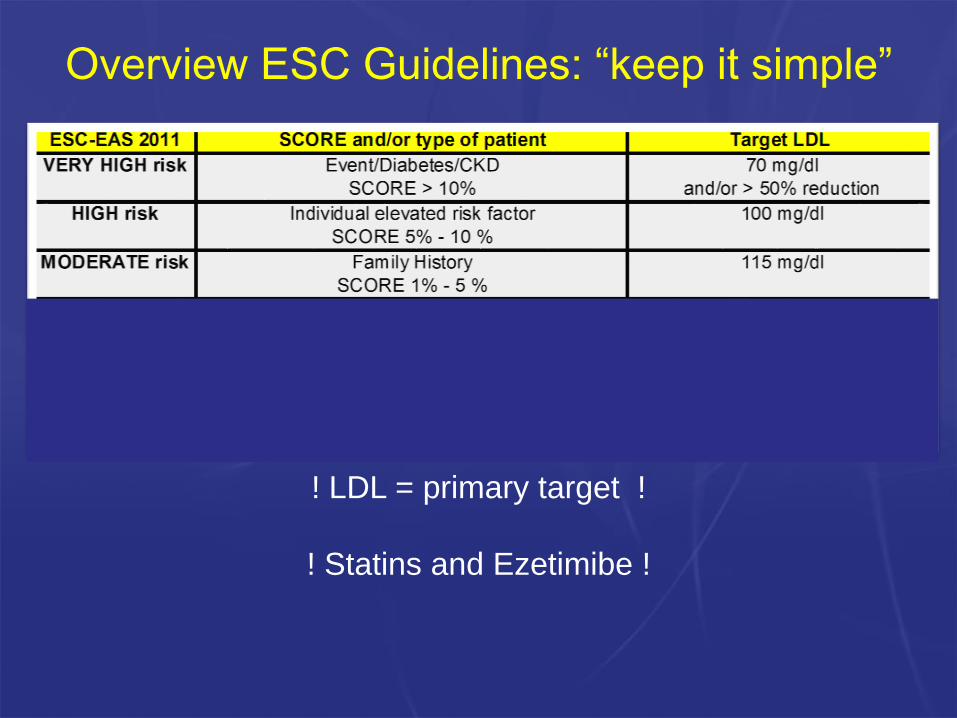
Overview ESC Guidelines: “keep it simple”
! LDL = primary target !
! Statins and Ezetimibe !

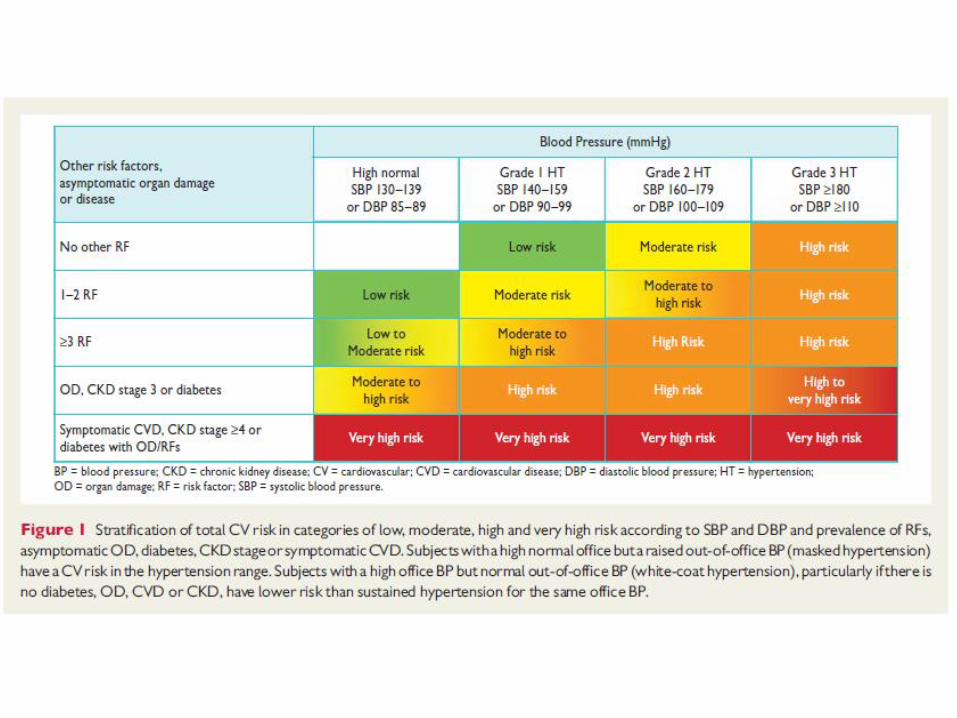
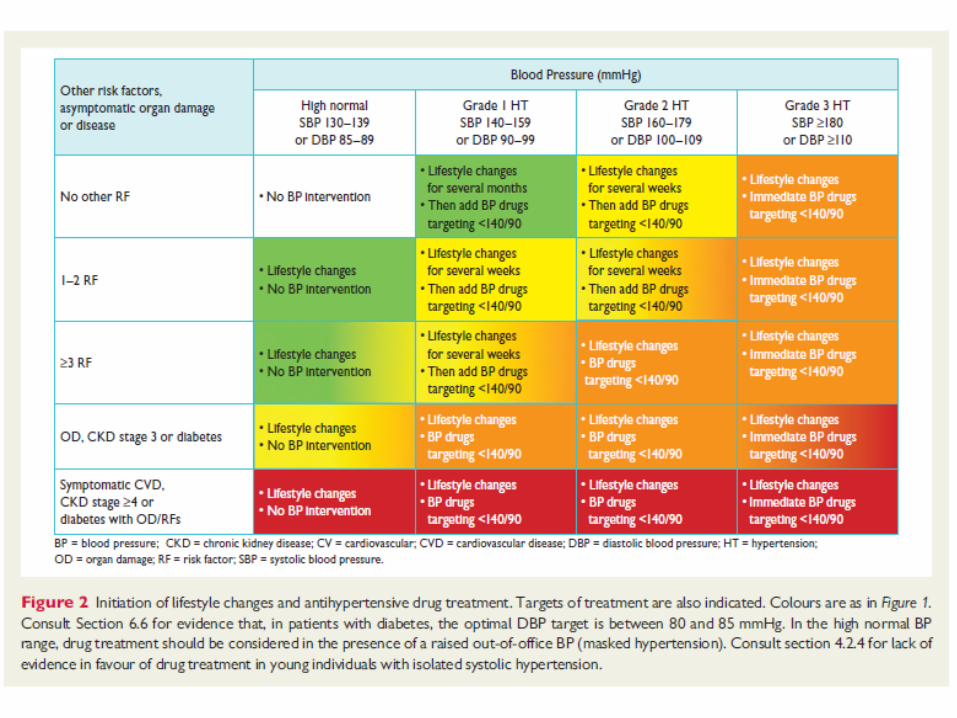
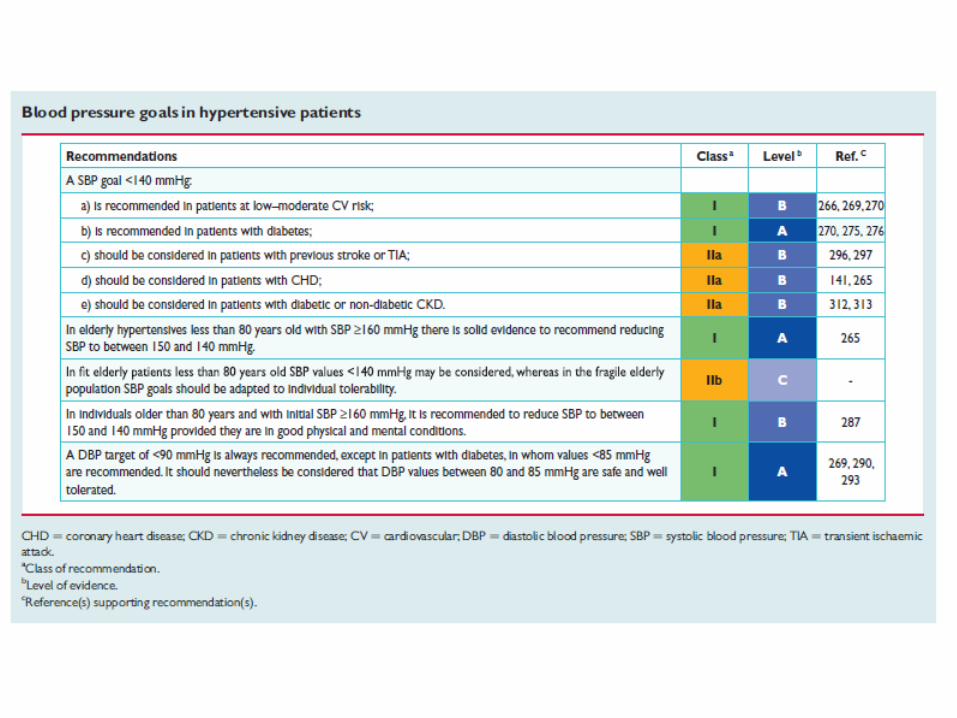
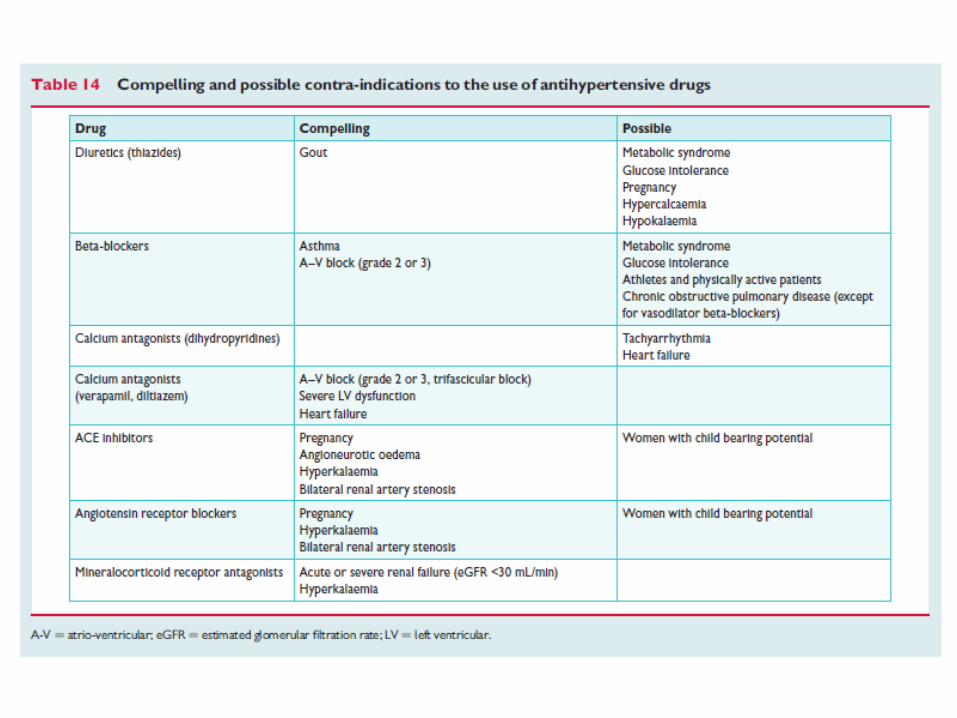
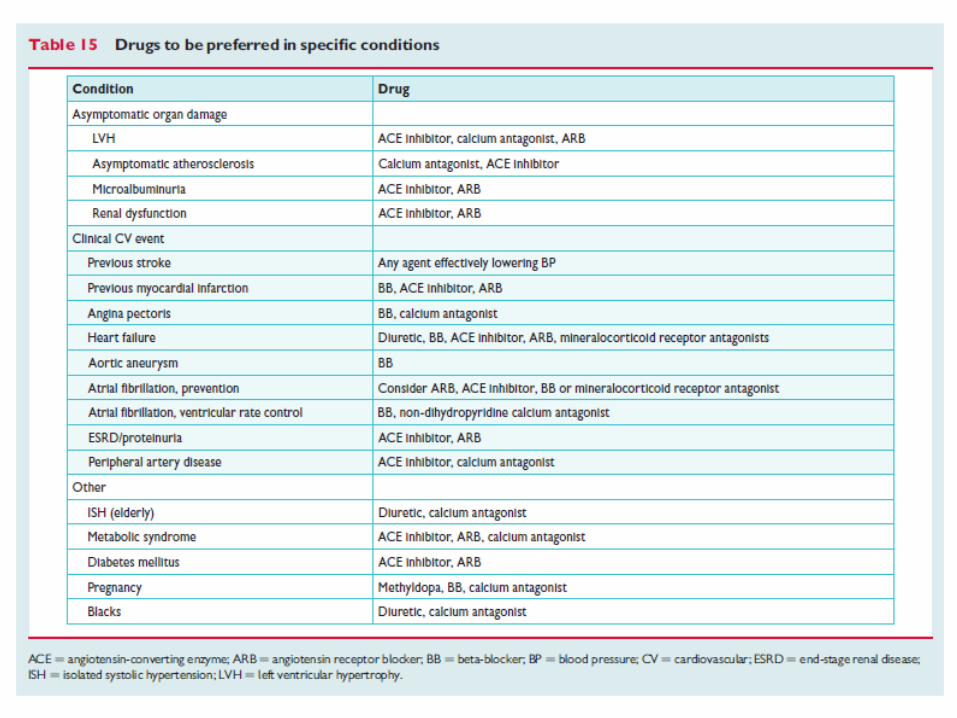
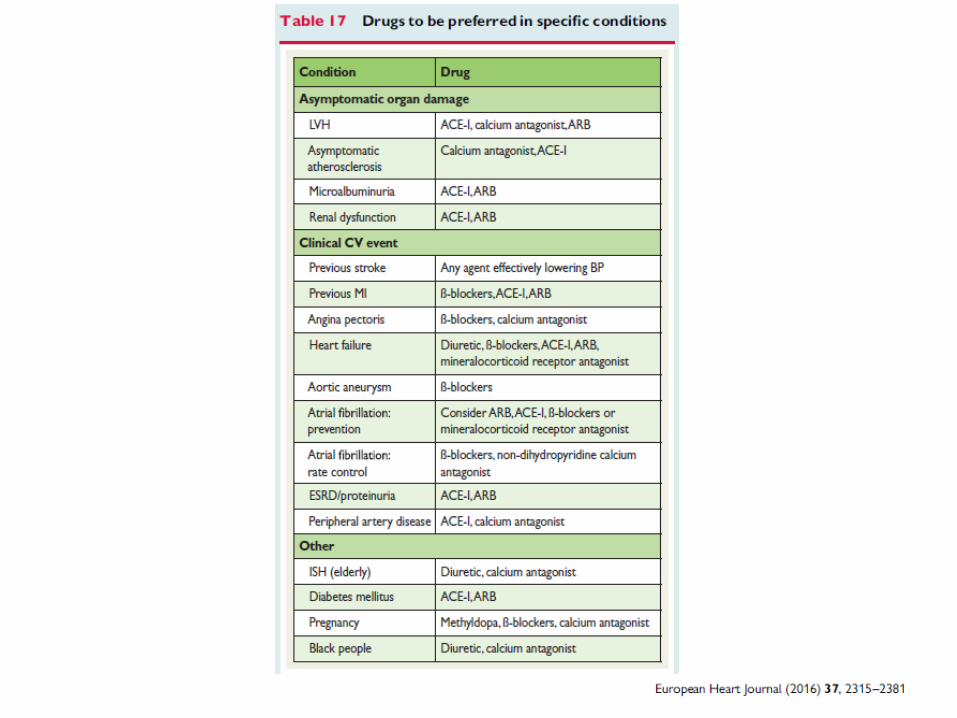
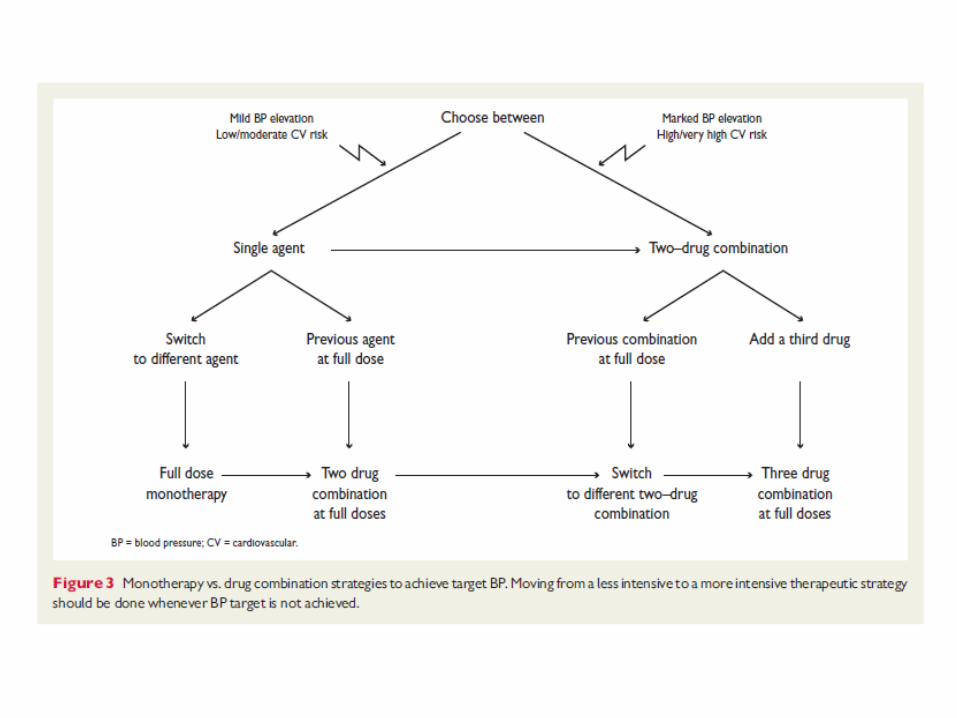
Hypertension
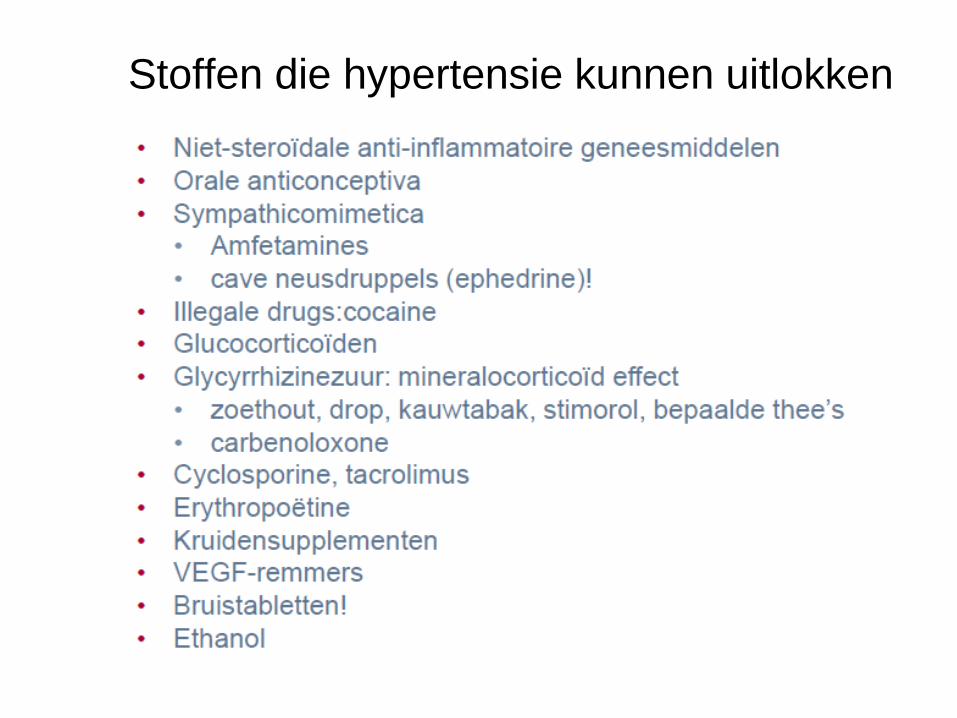
Stoffen die hypertensie kunnen uitlokken

Additional slides on special topics relating toCV risk / prevention / treatment of risk factors
Genetic Risk versus LifestylePCSK9 inhibition

Luc Missault, MD, DSc
Cardiologie St Jan Ziekenhuis Brugge
Genetisch risico vs gezonde
levensstijl en coronair risico
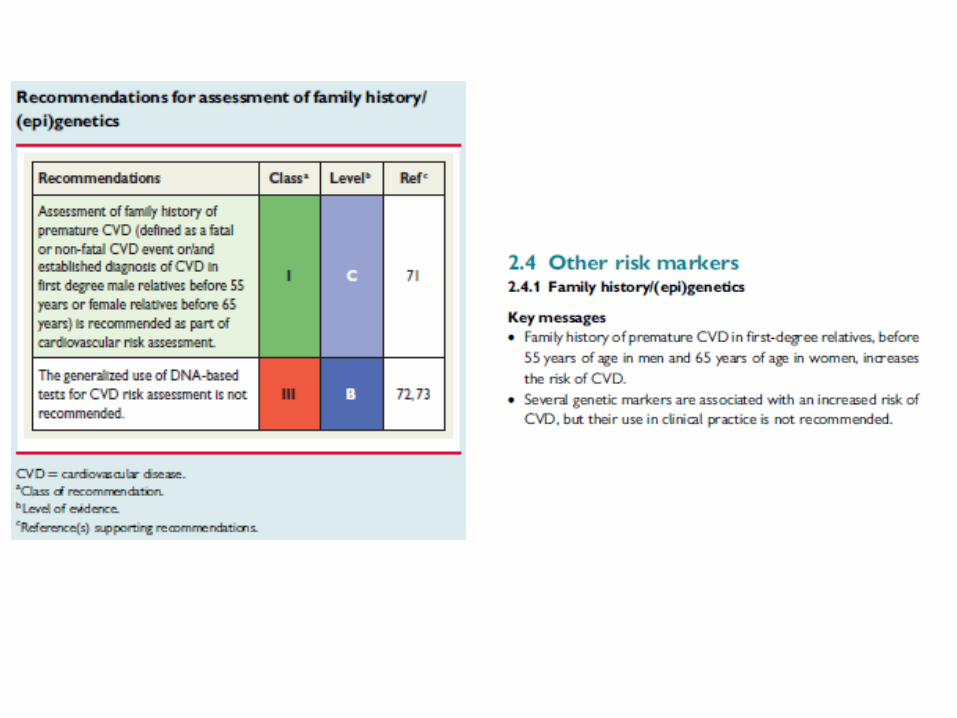
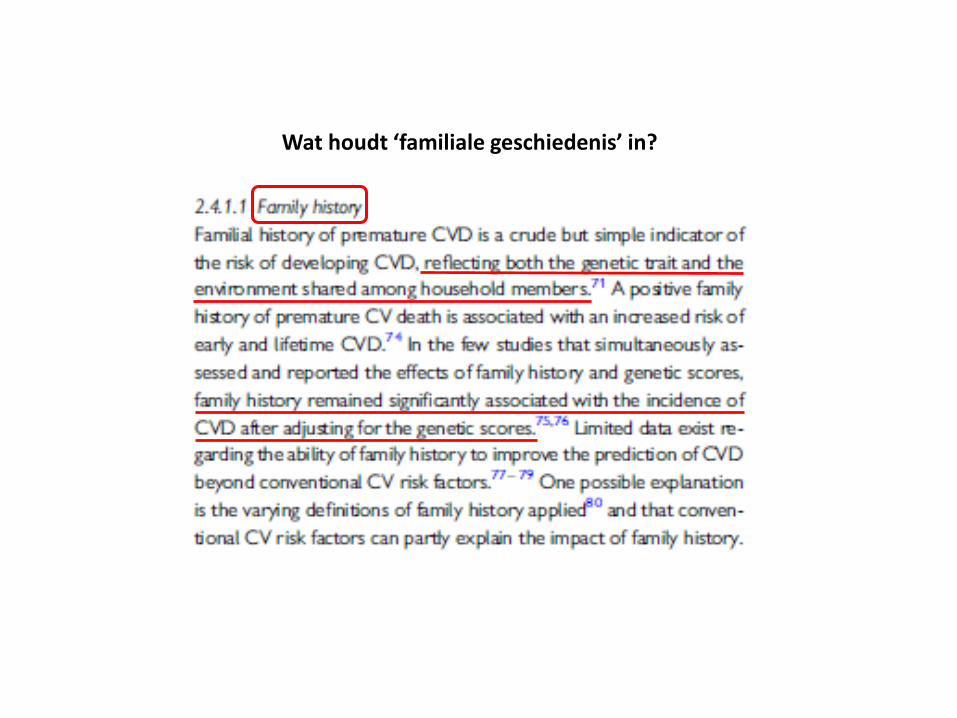
Wat houdt ‘familiale geschiedenis’ in?
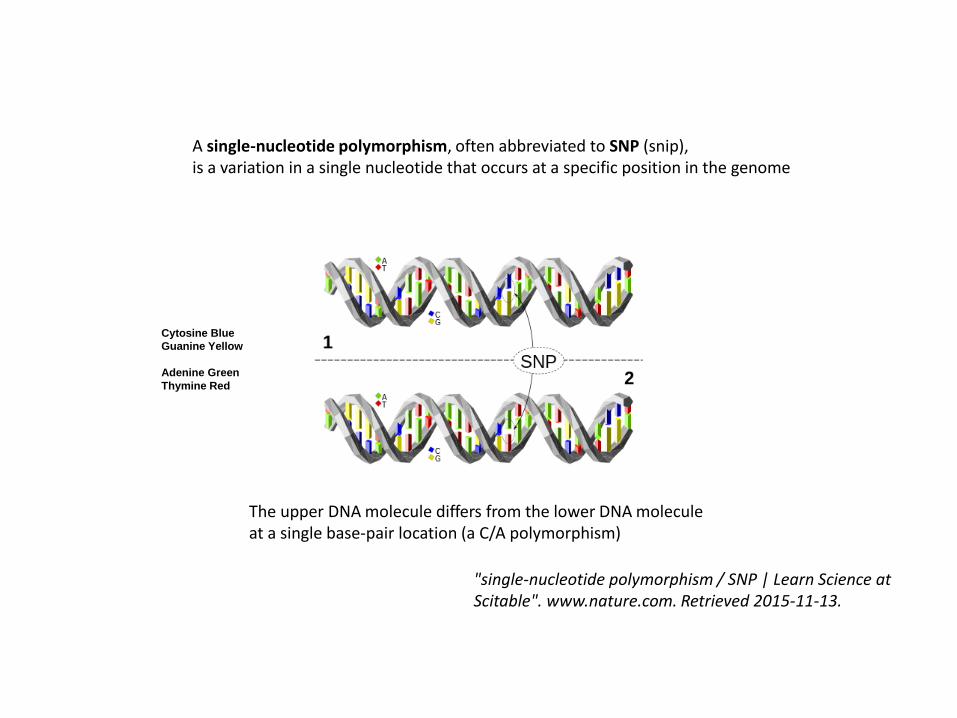
The upper DNA molecule differs from the lower DNA molecule at a single base-pair location (a C/A polymorphism)
Cytosine Blue
Guanine Yellow
Adenine Green
Thymine Red
A single-nucleotide polymorphism, often abbreviated to SNP (snip),is a variation in a single nucleotide that occurs at a specific position in the genome
"single-nucleotide polymorphism / SNP | Learn Science at Scitable". www.nature.com. Retrieved 2015-11-13.
‘Genetic scores’
• Studies van het volledige genoom (GWAS of genome wideassociation studies) hebben aangetoond dat er veel kandidaat SNPsgeassocieerd zijn aan CVD.
• Het effect van een individuele SNP is meestal klein.
• Daarom werden GENETISCHE SCORES ontwikkeld (de som van de SNP’s vermenigvuldigd met hun risicoverhoging).
• Er is nog geen consensus omtrent de te gebruiken SNPs. Er is geen consensus omtrent een ‘standaard’ genetische risicoscore.
• Er is nog evenmin consensus bereikt omtrent een te gebruiken ‘standaard’ methode om het genetisch risico uiteindelijk te berekenen.
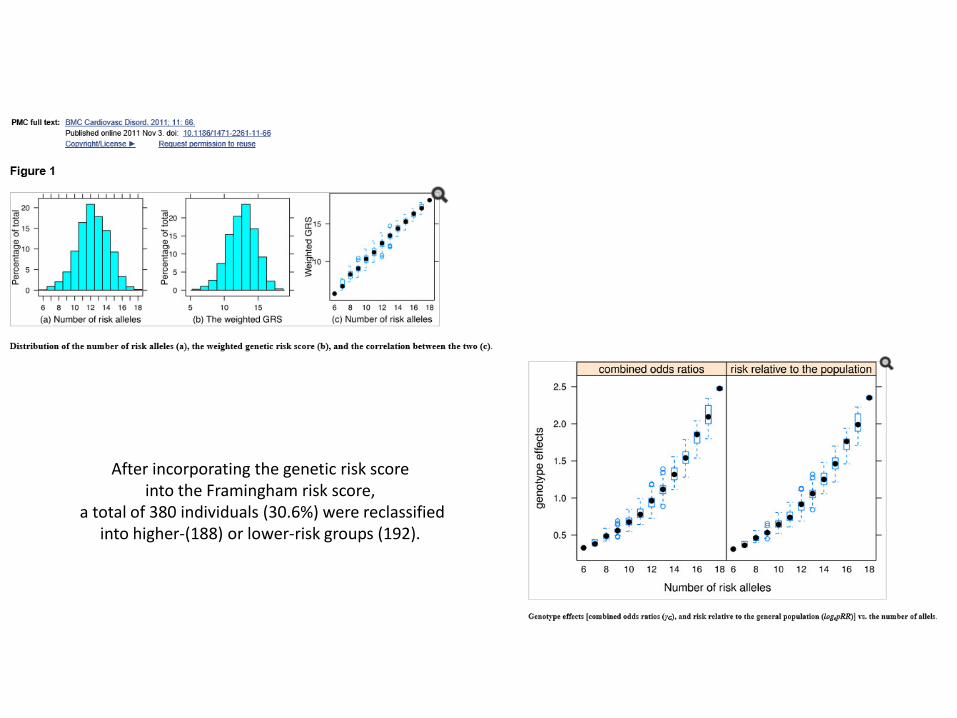
After incorporating the genetic risk score into the Framingham risk score,
a total of 380 individuals (30.6%) were reclassified into higher-(188) or lower-risk groups (192).
‘Genetic scores’
• Studies van het volledige genoom hebben aangetoond dat er veel kandidaat SNPs geassocieerd zijn aan CVD.
• Het effect van een individuele SNP is meestal klein.
• Daarom werden GENETISCHE SCORES ontwikkeld (de som van de SNP’s vermenigvuldigd met hun risicoverhoging).
• Er is nog geen consensus omtrent de te gebruiken SNPs. Er is geen consensus omtrent een ‘standaard’ genetische risicoscore.
• Er is nog evenmin consensus bereikt omtrent een te gebruiken ‘standaard’ methode om het genetisch risico uiteindelijk te berekenen.
Genetische scores en CVD risico (1)
• Ook na correctie voor klassieke RF blijft er een associatie tussen risico en bepaalde genetische scores
• Meerdere scores beschreven (delta risk per score eenheid van 1,02 tot 1,49)
• Vooral bij intermediair risico ~ herklassificatie
• Minder igv ‘hoog risico obv klassieke RF’
• studievb: 1 additioneel event per 318 personen (analogie NNT) zou kunnen voorkomen worden indien men een welbepaalde CHZ specifieke score zou toevoegen aan de klassieke risicofactoren
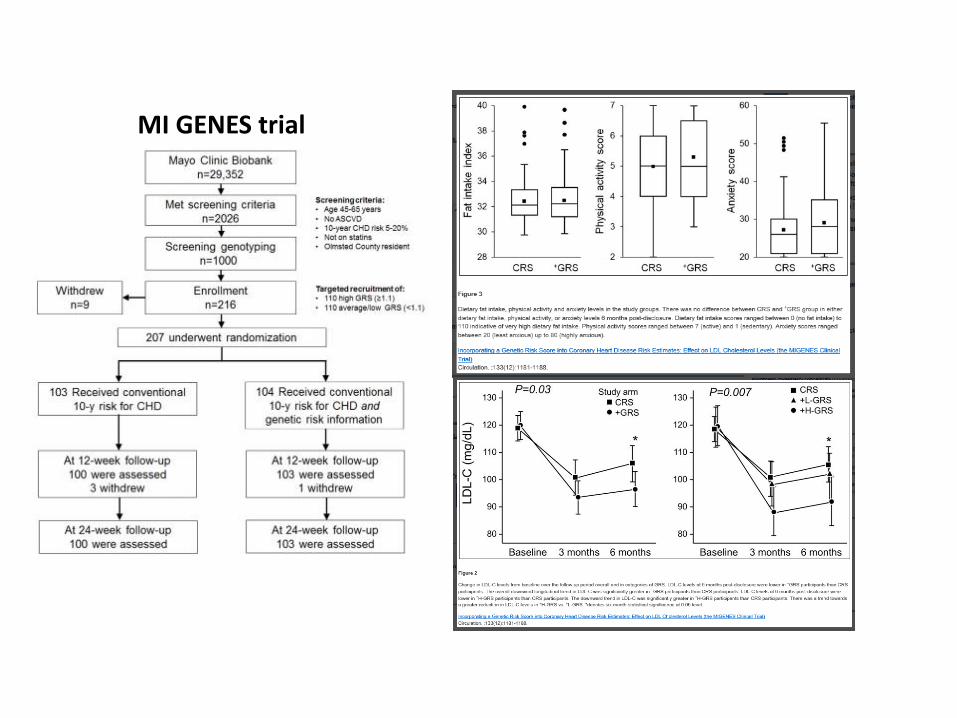
MI GENES trial
Genetische scores en CVD risico (2)
• Bvb een bepaalde genetische score die gebruikt maakt van 27 genetische varianten laat toe om personen te identificeren die het meest baat zouden hebben van een statine in preventie van CVD
• CAVE: klassieke statine studies waren hier niet op gericht en hielden hier geen rekening mee
• Nood aan prospectieve studies in dergelijke groepen (…ethiek)
• Commerciele kits bestaan en het gebruik wordt door sommigen sterk aangeraden (‘strong pressure’; lobbying?)
• Nog geen consensus omtrent: welke genetische merkers te gebruiken? welke genetische score? Voorspellende waarde?
‘Gaps’ in evidence
• Impact van het toevoegen van familiale geschiedenis aan de huidige score risico berekening is nog niet prospectief onderzocht
• Nog geen studies omtrent het bijkomend preventief effect van het incorporeren van een ‘genetische risico score’ aan onze huidige standaard risicoberekening
(hoeveel bijkomende events voorkomen? Kosten effectief?)

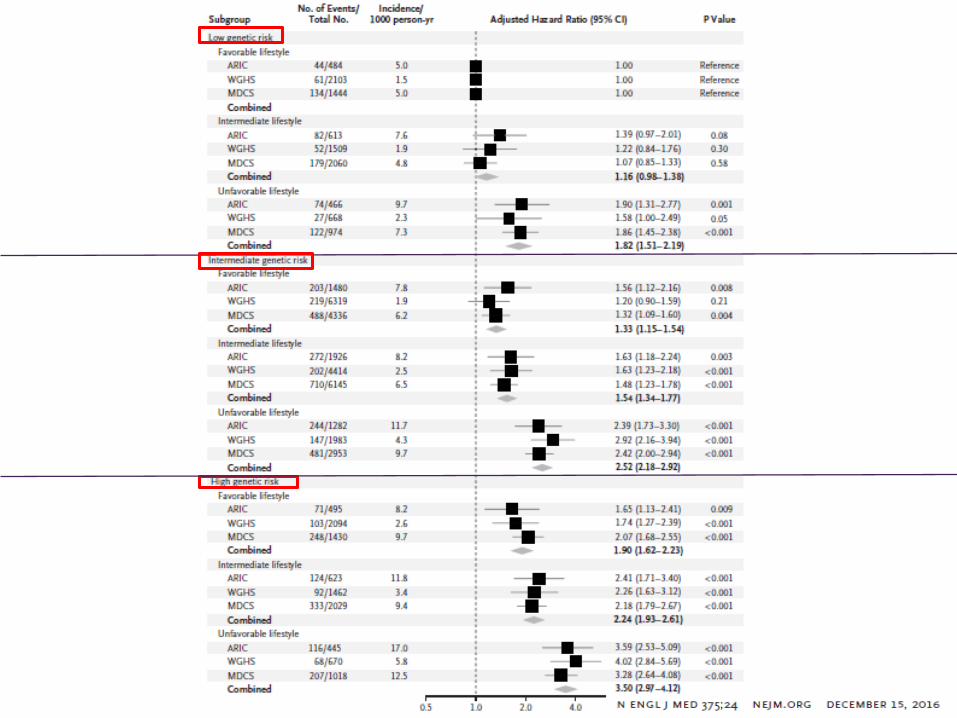
Methods:
-Gebruikte genetische score: gebaseerd op 50 verschillende genetische polymorfismen (SNP’s) geassocieerd aan incidentie van coronair lijden
-Geïncludeerd in een berekende polygenische score
-Aldus indeling in 3 groepen met ‘high’, ‘intermediate’ en ‘low’ genetic risk
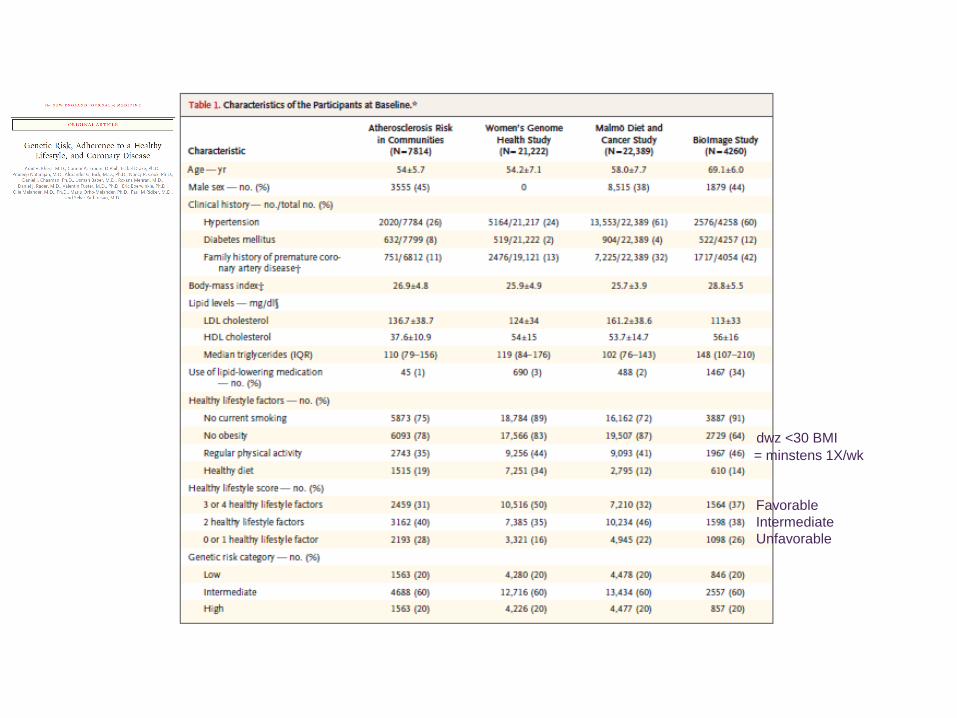
= minstens 1X/wk
dwz <30 BMI
Favorable
Intermediate
Unfavorable
Results:
Elke individuele lifestyle factor beinvloedt (significant) het risico:
• HR voor non-smoking 0,56
• HR voor no-obesity 0,66
• HR voor fysische activiteit 0,88
• HR voor gezonde voeding 0,91
Results: High genetic risk bleek onafhankelijk te zijn van lifestyle.
High genetic risk betekent een HR 1,91 voor CVD.
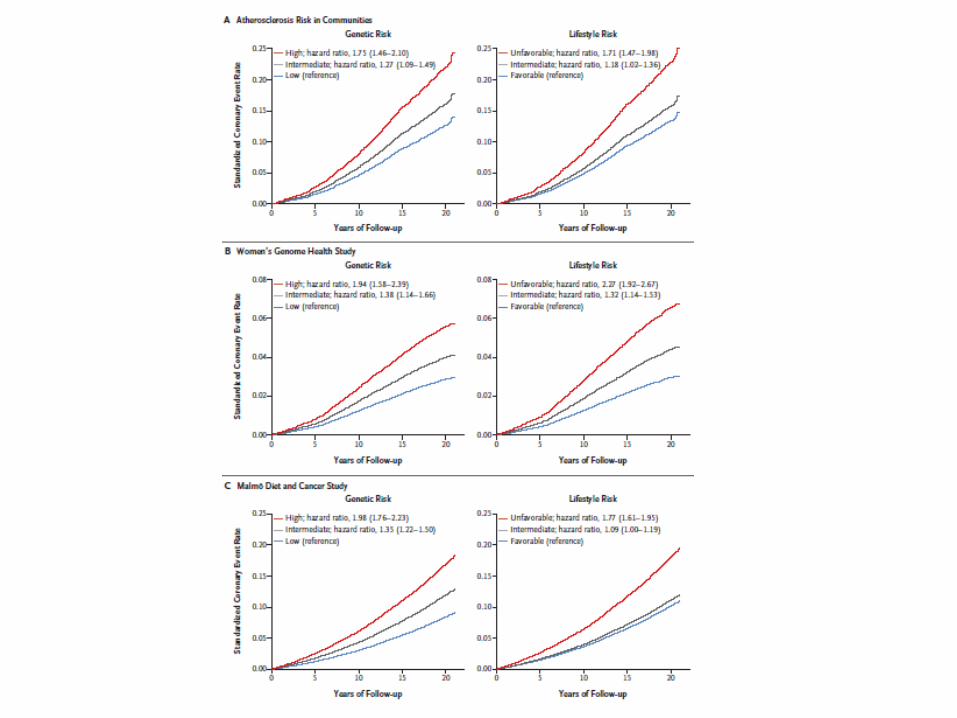
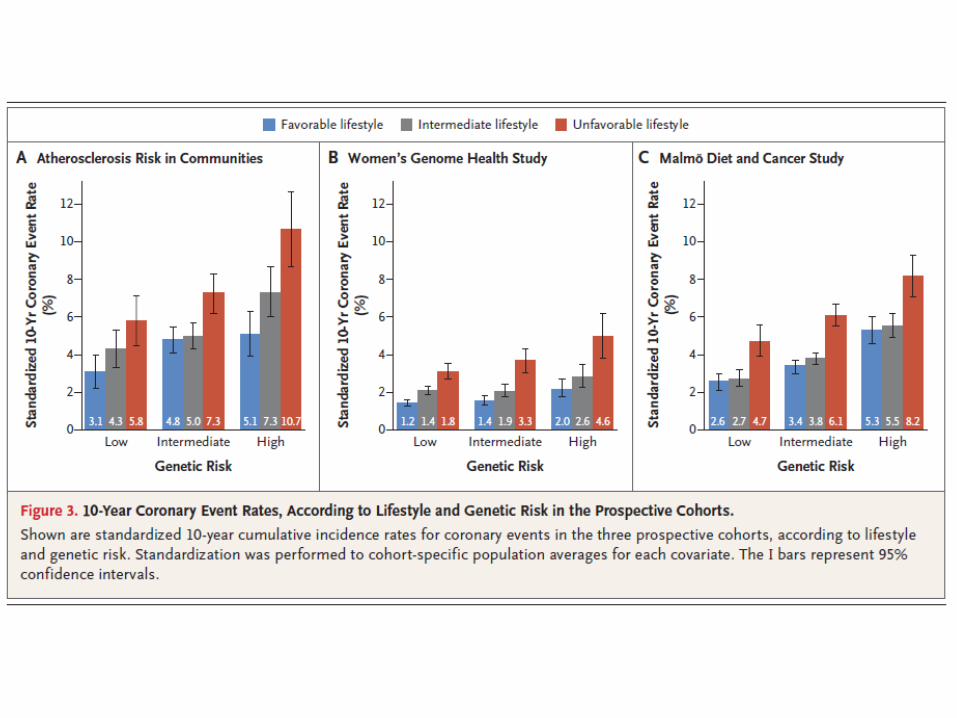
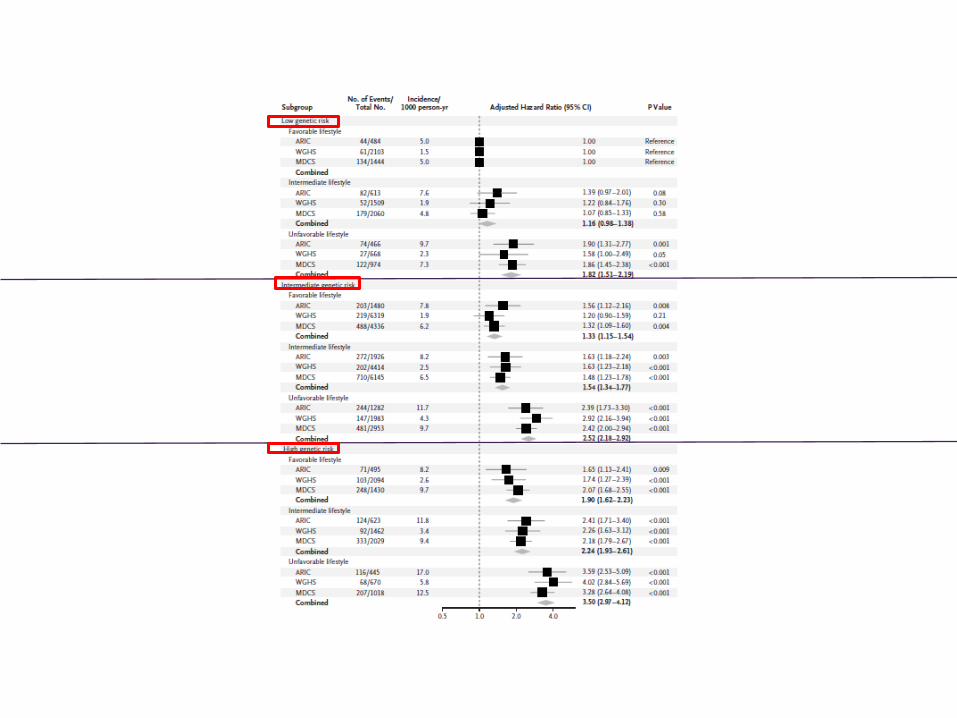

Among participants at high genetic risk, favorable lifestyle was associated with a 46% lower
relative risk of coronary events than unfavorable lifestyle (HR 0.54; 95% CI, 0.47 to 0.63).
This corresponded to a reduction in the standardized 10-year incidence of coronary events
from 10.7% for unfavorable lifestyle to 5.1% for favorable lifestyle in ARIC,
from 4.6% to 2.0% in WGHS,
from 8.2% to 5.3% in MDCS.









![Sodium sulfate heptahydrate in weathering phenomena1. Introduction 10 Sodium sulfate heptahydrate was studied later on by De Coppet [19,20], Hannay [21], and D’Arcy [23]. Their findings](https://static.fdocuments.nl/doc/165x107/60b1d8d26e356d21cd12581c/sodium-sulfate-heptahydrate-in-weathering-1-introduction-10-sodium-sulfate-heptahydrate.jpg)






