Koorts na tropenreis - users.skynet.beusers.skynet.be/fa686441/GAB/GAB-2013/Introductie...
45
Dr.Jan Clerinx Dept. Klinische Wetenschappen Instituut voor Tropische Geneeskunde Antwerpen Koorts na tropenreis
Transcript of Koorts na tropenreis - users.skynet.beusers.skynet.be/fa686441/GAB/GAB-2013/Introductie...

Dr.Jan Clerinx
Dept. Klinische Wetenschappen
Instituut voor Tropische Geneeskunde
Antwerpen
Koorts na tropenreis
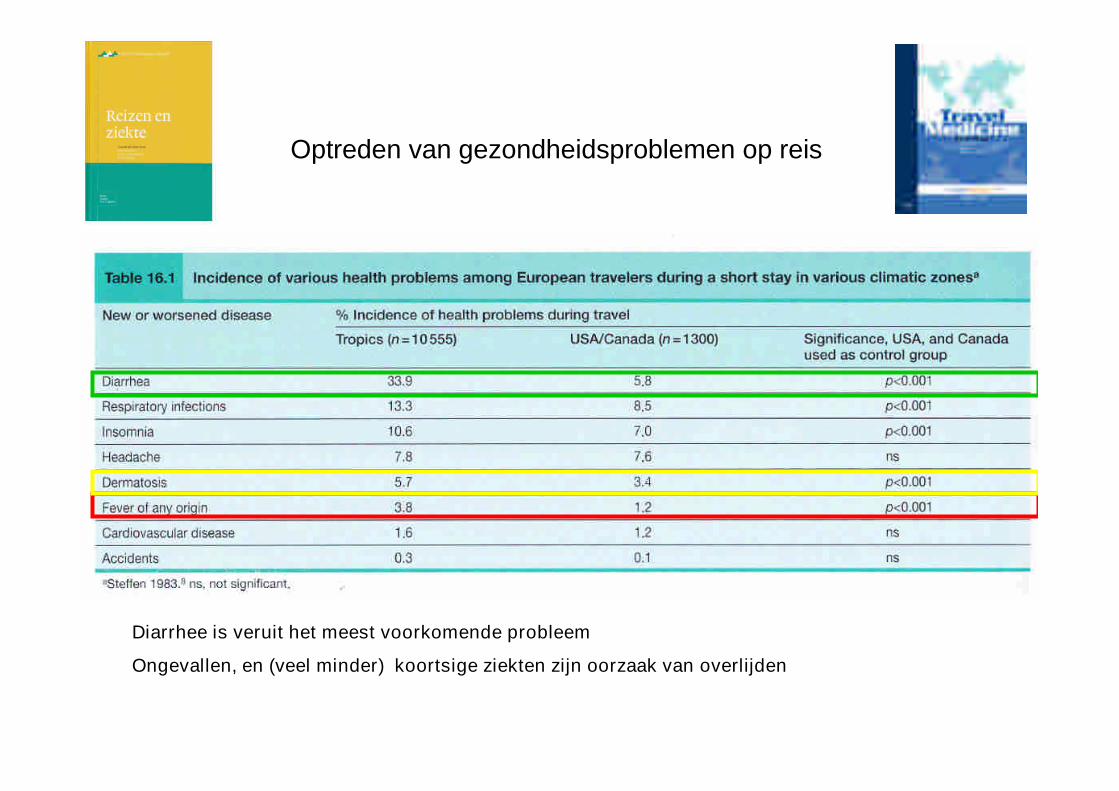
Diarrhee is veruit het meest voorkomende probleem
Ongevallen, en (veel minder) koortsige ziekten zijn oorzaak van overlijden
Optreden van gezondheidsproblemen op reis
Werkonbekwaam na terugkeer
Één of ander gezondheidsprobleem100,000
10,000 Raadpleegde een arts in het buitenland
Voelde zich ziek
1,000
100
10
1
Bleef in bed
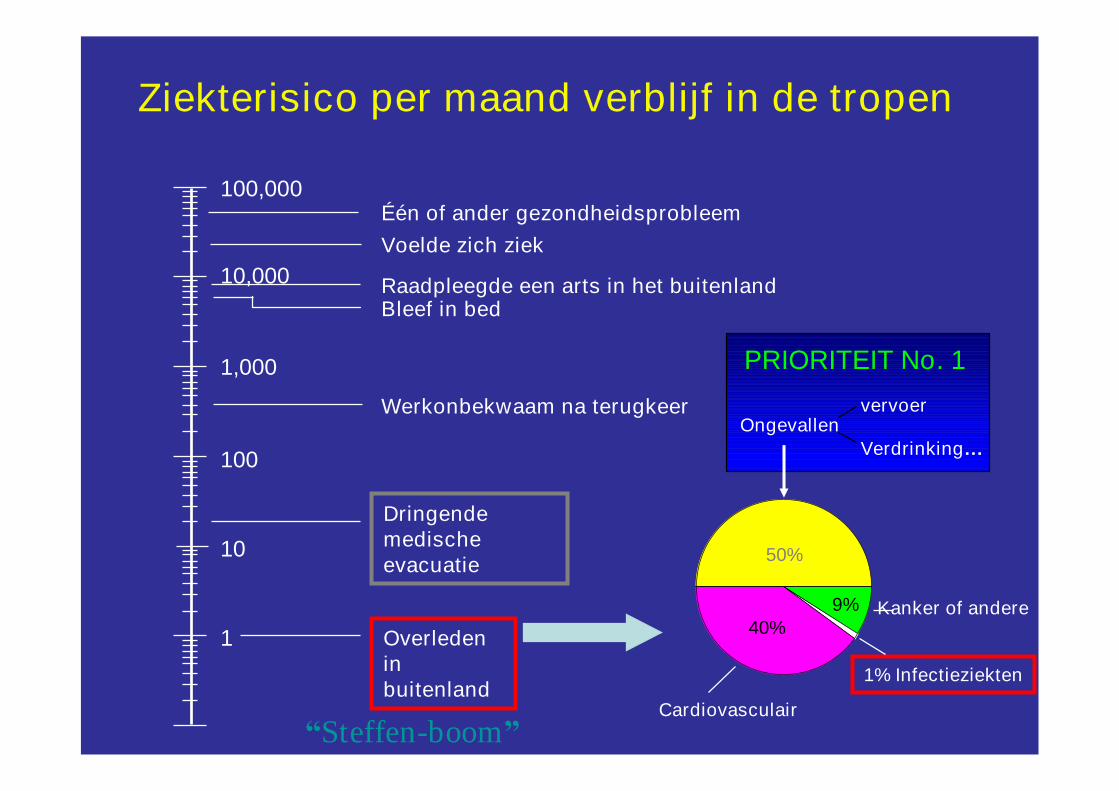
Overledeninbuitenland
Dringendemedischeevacuatie
Ziekterisico per maand verblijf in de tropen
Kanker of andere
Cardiovasculair
Ongevallenvervoer
Verdrinking…
1% Infectieziekten
50%
40%9%
PRIORITEIT No. 1
“Steffen-boom”
100%
10%
1%
0.01%
0.001%
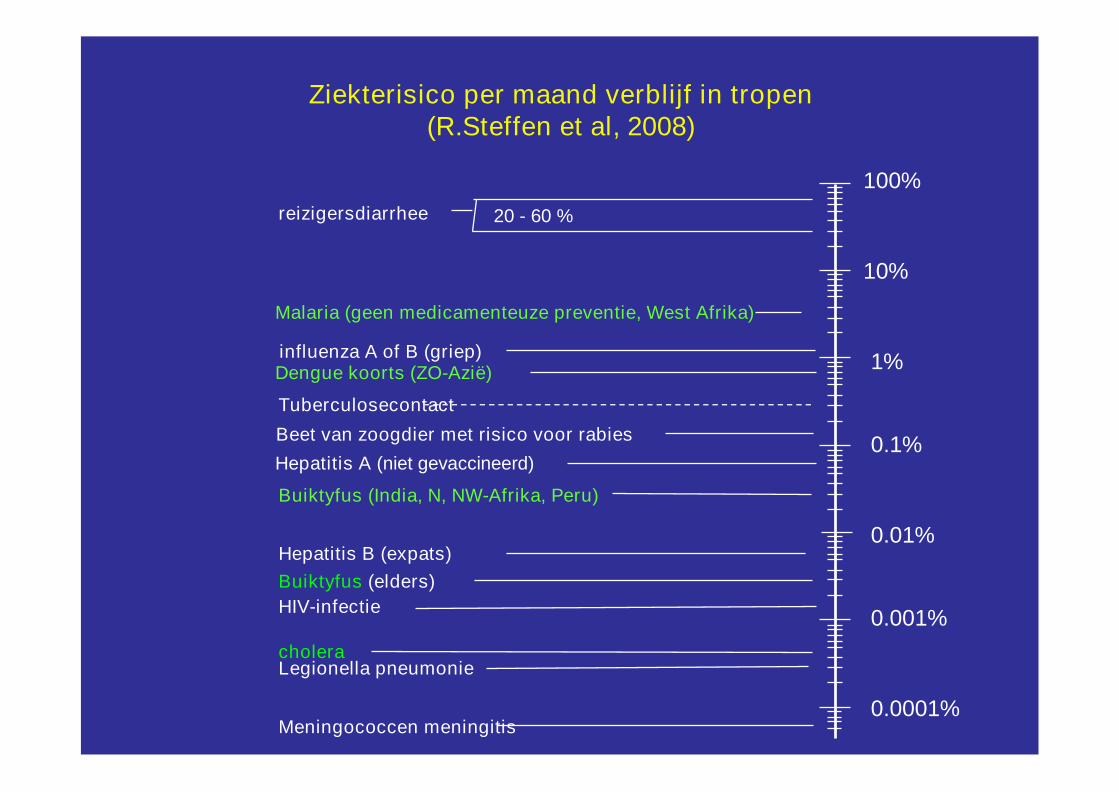
Malaria (geen medicamenteuze preventie, West Afrika)
Buiktyfus (India, N, NW-Afrika, Peru)
Tuberculosecontact
cholera
influenza A of B (griep)
Buiktyfus (elders)
Dengue koorts (ZO-Azië)
Beet van zoogdier met risico voor rabies
Hepatitis B (expats)
HIV-infectie
Legionella pneumonie
Meningococcen meningitis
0.1%
Ziekterisico per maand verblijf in tropen(R.Steffen et al, 2008)
reizigersdiarrhee
0.0001%
20 - 60 %
Hepatitis A (niet gevaccineerd)

…waarschijnlijk, maar stel dat het wat ernstiger is….
Vorige week was ik inGhana, en nu heb ikkoorts en keelpijn…
Griepje,zondertwijfel!
20 Januari
2013
Casus:‘first things first’
• Jonge vrouw 21 j
• 3 weken in Kinshasa, familiebezoek
• 14 dagen na terugkeer: hoge koorts 39°C, rillingen en wat hoest
• Raadpleegt huisarts die akute bronchopneumonie vermoedt :
R/ amoxycilline
• Koorts blijft aanhouden
• 4 dagen later: doodziek, dyspnee, snelle pols, bleek, hypotensief…
• Dringend gehospitaliseerd: ernstige anemie, verminderde nierfunctie,
icterisch, hypotensie, longinfiltraten…
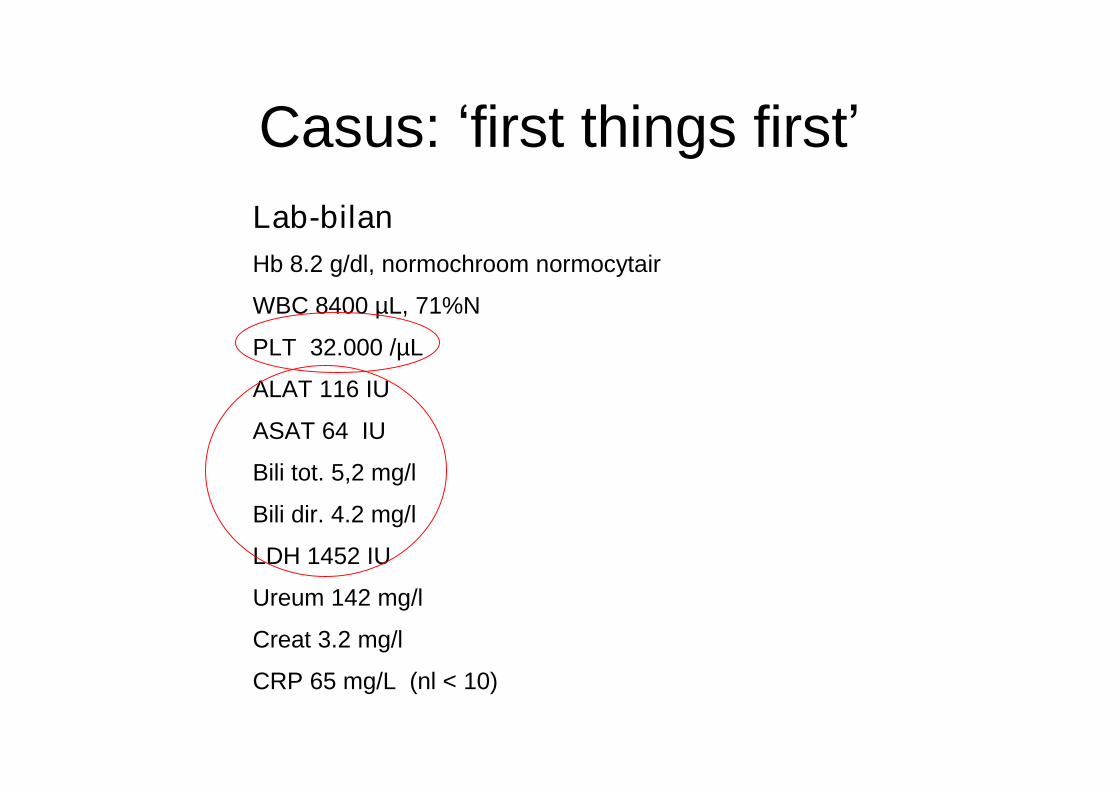
Casus:‘first things first’Lab-bilanHb 8.2 g/dl, normochroom normocytair
WBC 8400 µL, 71%N
PLT 32.000 /µL
ALAT 116 IU
ASAT 64 IU
Bili tot. 5,2 mg/l
Bili dir. 4.2 mg/l
LDH 1452 IU
Ureum 142 mg/l
Creat 3.2 mg/l
CRP 65 mg/L (nl < 10)
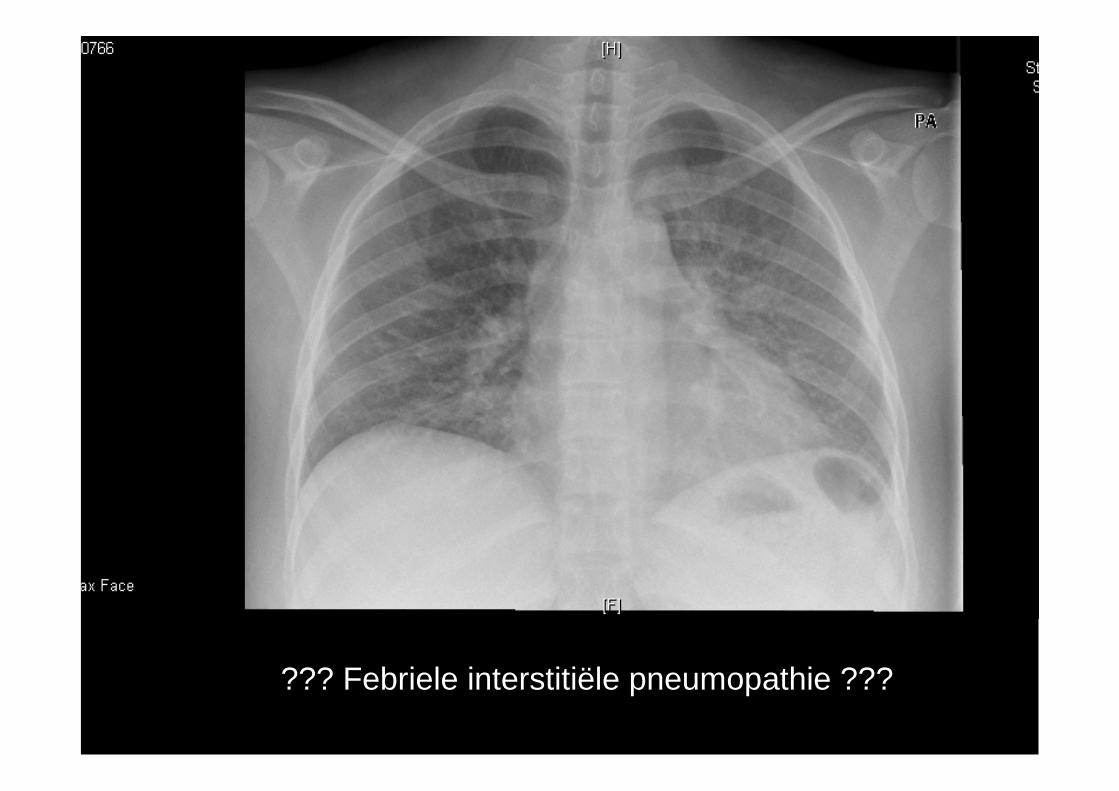
??? Febriele interstitiële pneumopathie ???
Casus:‘first things first’
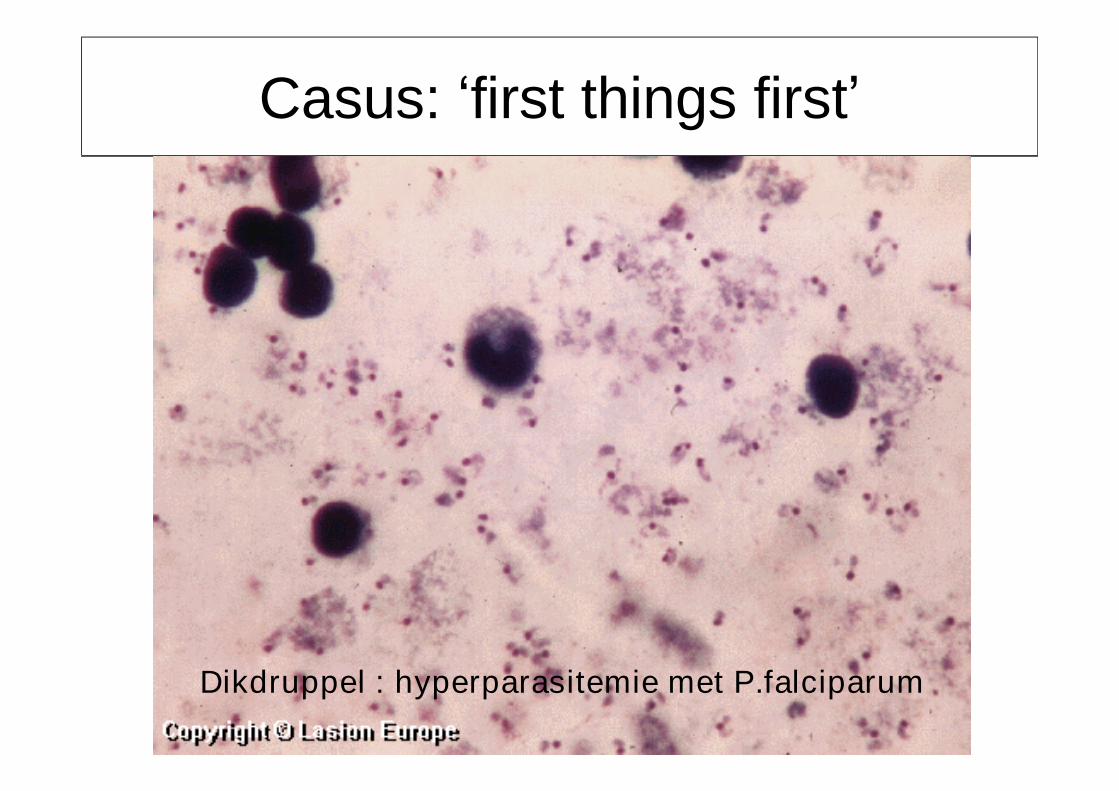
Dikdruppel : hyperparasitemie met P.falciparum
Dikdruppel bij hospitalisatie:Plasmodium falciparum, 54% RBC geinfecteerd!
R/ Hospitalizatie Intensive Care Unit
-- StartStart IVIV KinineKinine** ladingsdosis 20 mg/kg, verder 10 mg/kg /8 uladingsdosis 20 mg/kg, verder 10 mg/kg /8 u
-- WisseltransfusieWisseltransfusie** 4 + 2 u4 + 2 u PCPC
-- HemodialysisHemodialysis
** heden is IV artesunaat de standaardbehandeling!heden is IV artesunaat de standaardbehandeling!
Casus:‘first things first’
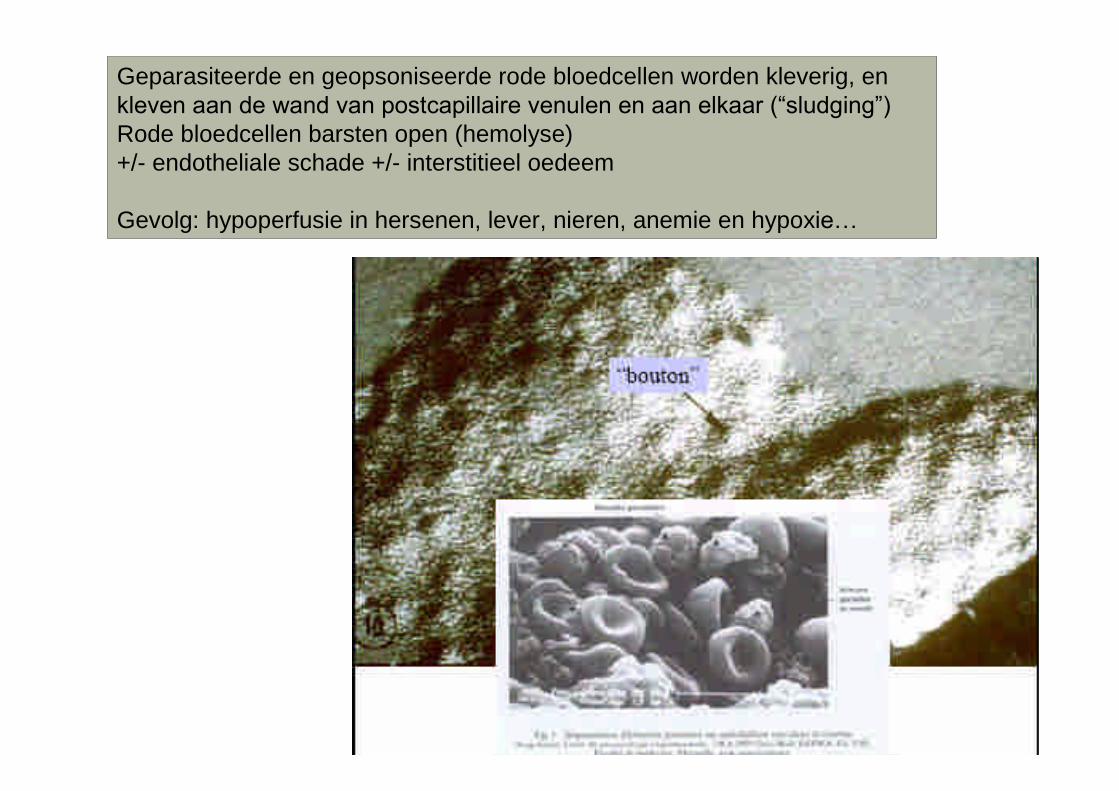
Geparasiteerde en geopsoniseerde rode bloedcellen worden kleverig, enkleven aan de wand van postcapillaire venulen en aan elkaar (“sludging”)Rode bloedcellen barsten open (hemolyse)+/- endotheliale schade +/- interstitieel oedeem
Gevolg: hypoperfusie in hersenen, lever, nieren, anemie en hypoxie…
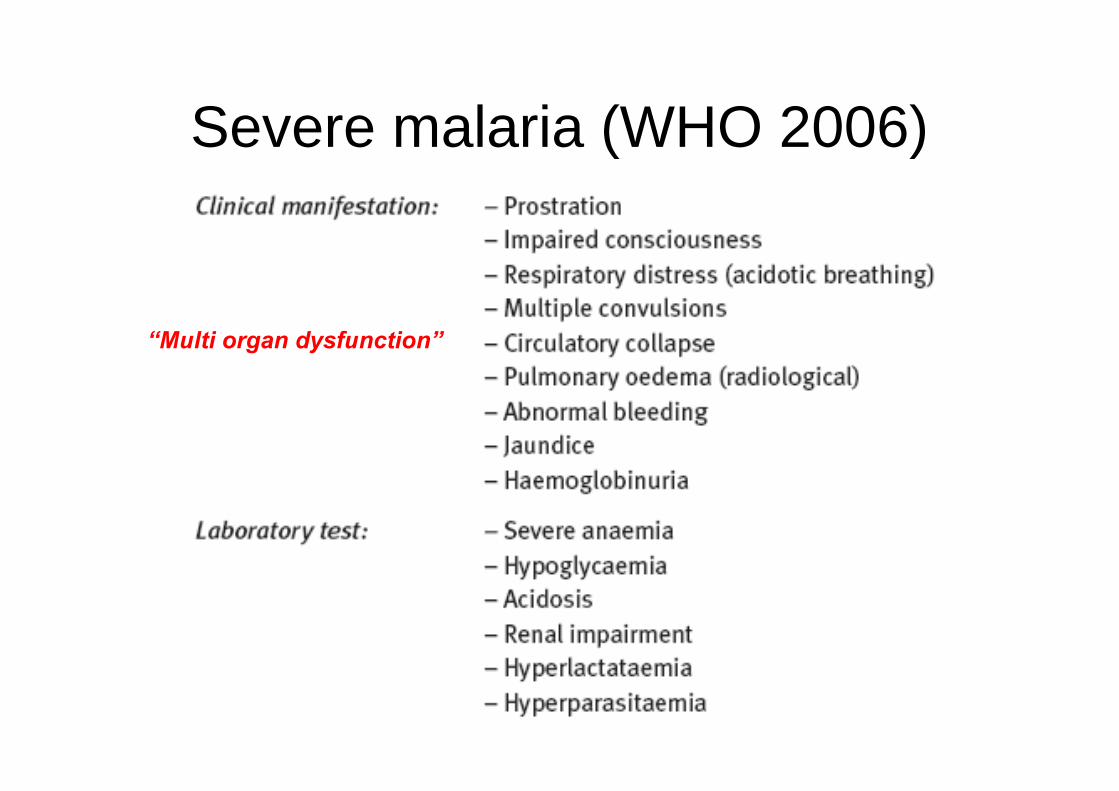
Severe malaria (WHO 2006)
“Multi organ dysfunction”
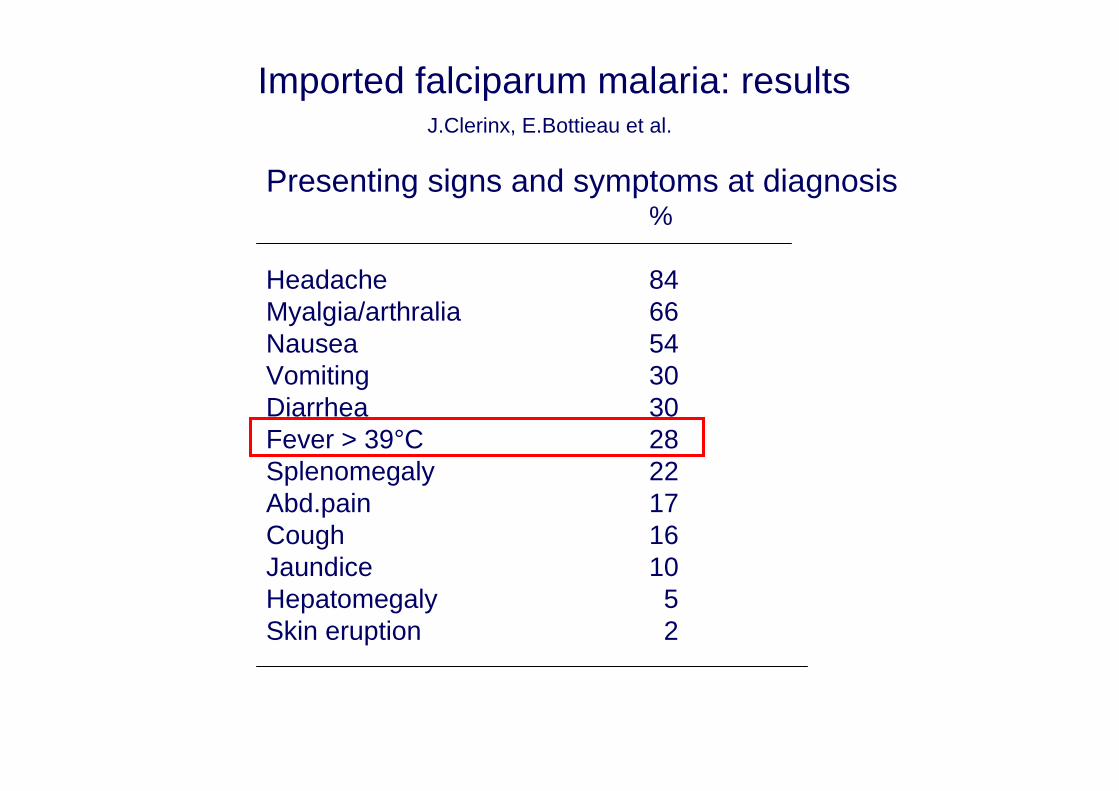
Imported falciparum malaria: resultsJ.Clerinx, E.Bottieau et al.
Presenting signs and symptoms at diagnosis%
Headache 84Myalgia/arthralia 66Nausea 54Vomiting 30Diarrhea 30Fever > 39°C 28Splenomegaly 22Abd.pain 17Cough 16Jaundice 10Hepatomegaly 5Skin eruption 2
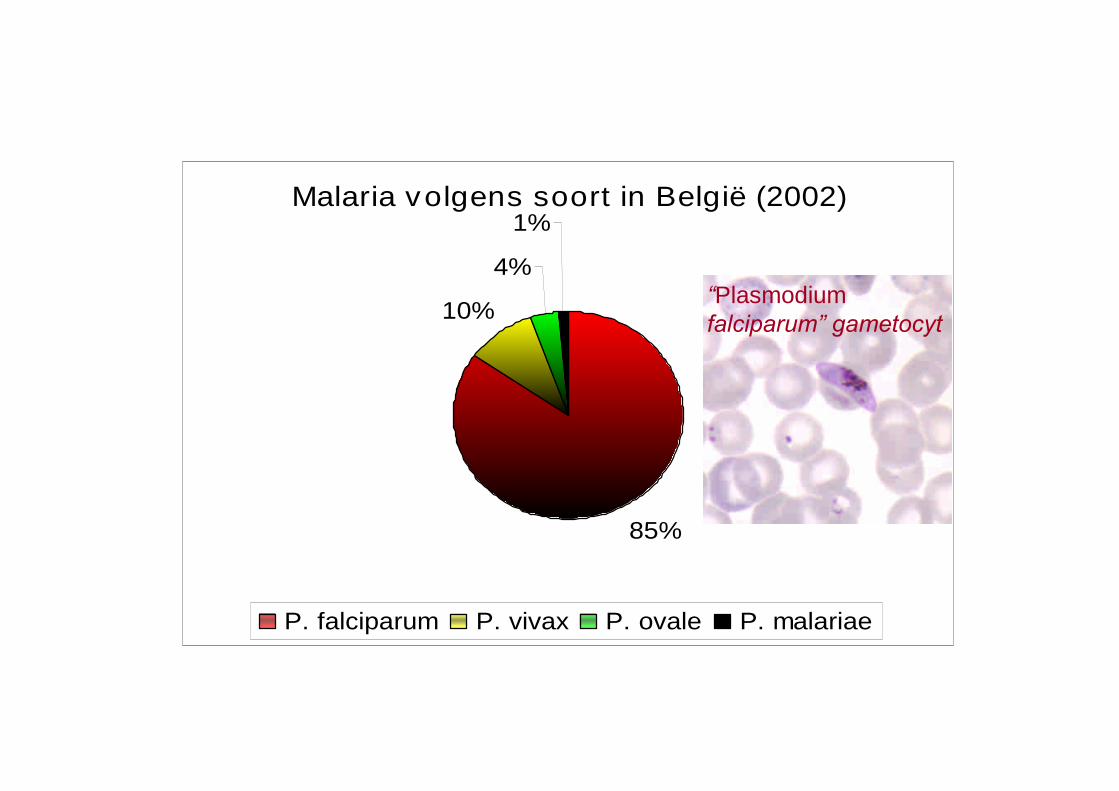
Malaria volgens soort in België (2002)
85%
10%
4%
1%
P. falciparum P. vivax P. ovale P. malariae
“Plasmodiumfalciparum” gametocyt
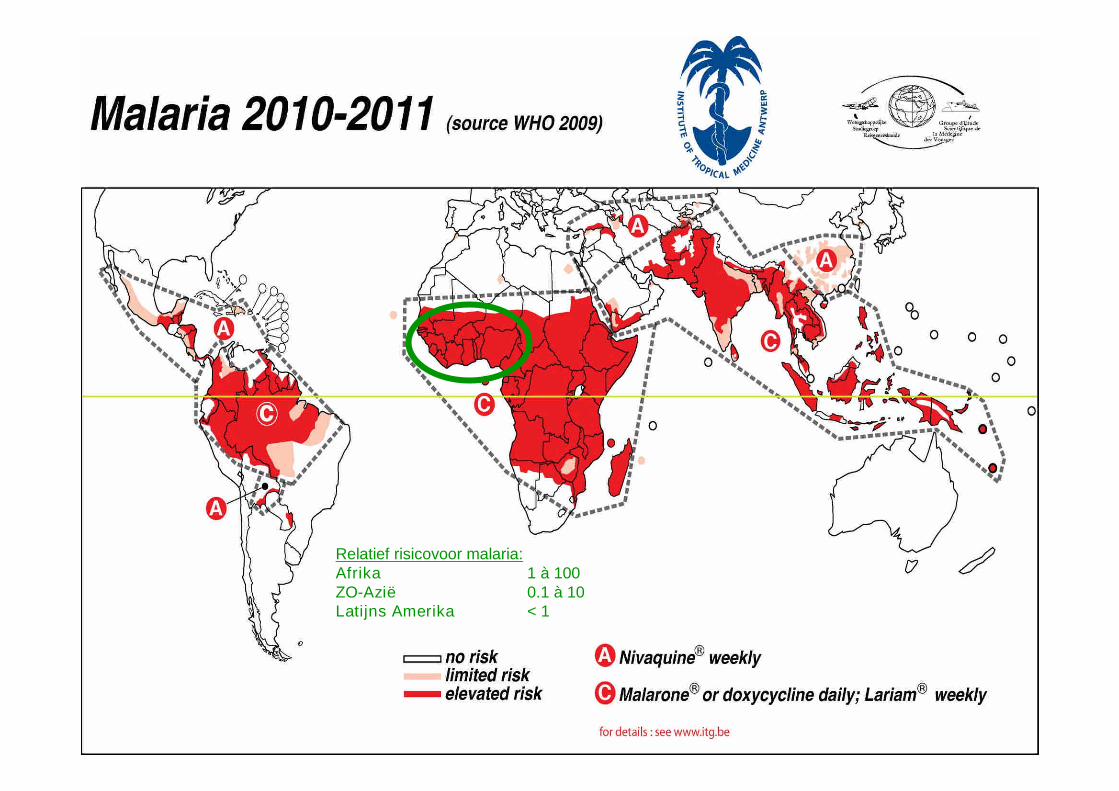
Relatief risicovoor malaria:Afrika 1 à 100ZO-Azië 0.1 à 10Latijns Amerika < 1
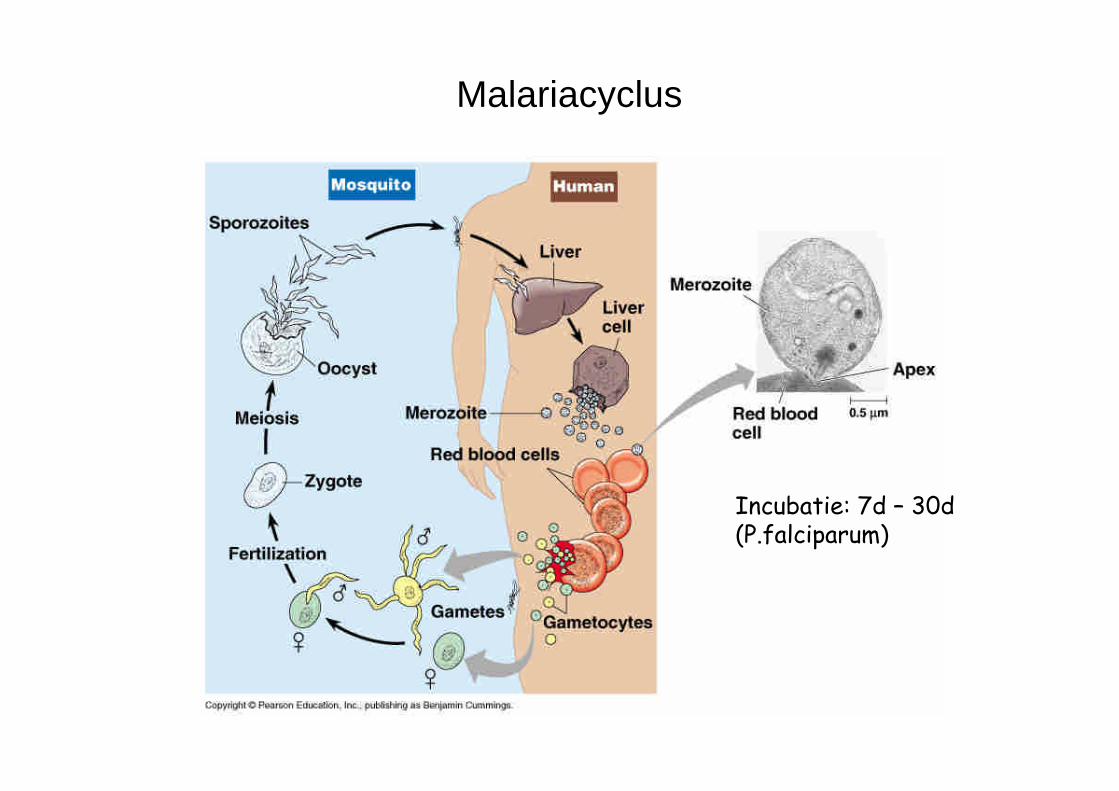
Malariacyclus
Incubatie: 7d –30d(P.falciparum)
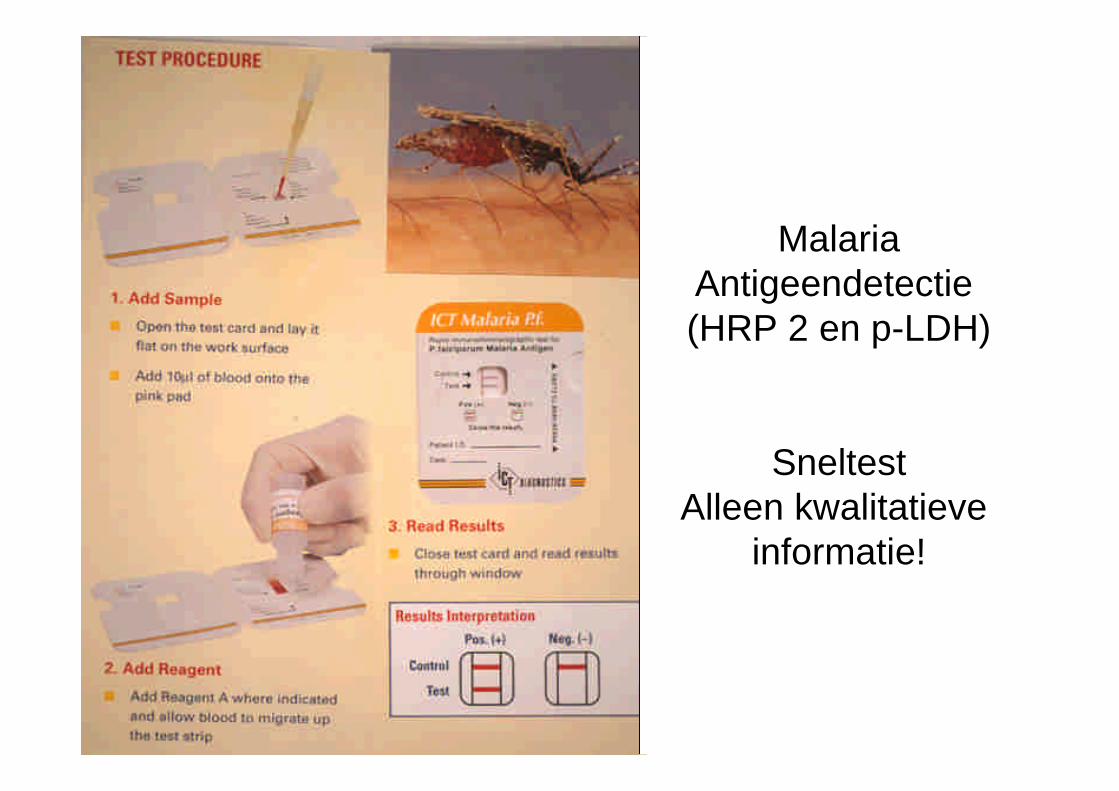
MalariaAntigeendetectie(HRP 2 en p-LDH)
SneltestAlleen kwalitatieve
informatie!
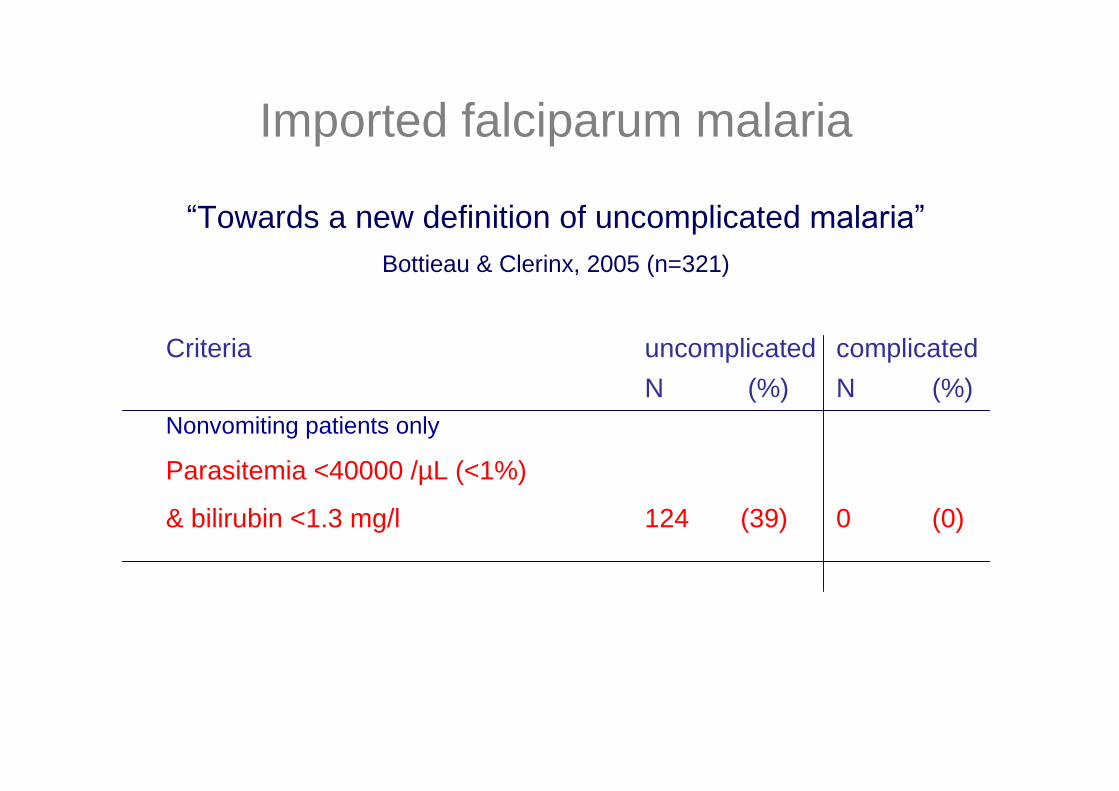
Imported falciparum malaria
“Towards a new definition of uncomplicatedmalaria”Bottieau & Clerinx, 2005 (n=321)
Criteria uncomplicated complicatedN (%) N (%)
Nonvomiting patients only
Parasitemia <40000 /µL (<1%)
& bilirubin <1.3 mg/l 124 (39) 0 (0)

Malaria noodbehandeling
SCHEMA AMalarone® (250 mg atovaquone + 100 mg proguanil),ongeveer 40€ voor12 tablettenPosologie: 4 tabletten éénmaal per dag x 3 dagen, met wat voedsel.
SCHEMA BRiamet® (= Coartem) : (Artemether 20mg en Lumefantrine 120mg)ongeveer 40€ voor 24 tabletten.Posologie: 4 compr.op 0h en na 8h, nadien 4 compr. om de 12 uur.
(In totaal 6 x 4 compr).
Voordeel tov Malarone: snellere parasietenclearance (48h ipv 72h),artemether werkt op jonge malariatrofozoïeten.
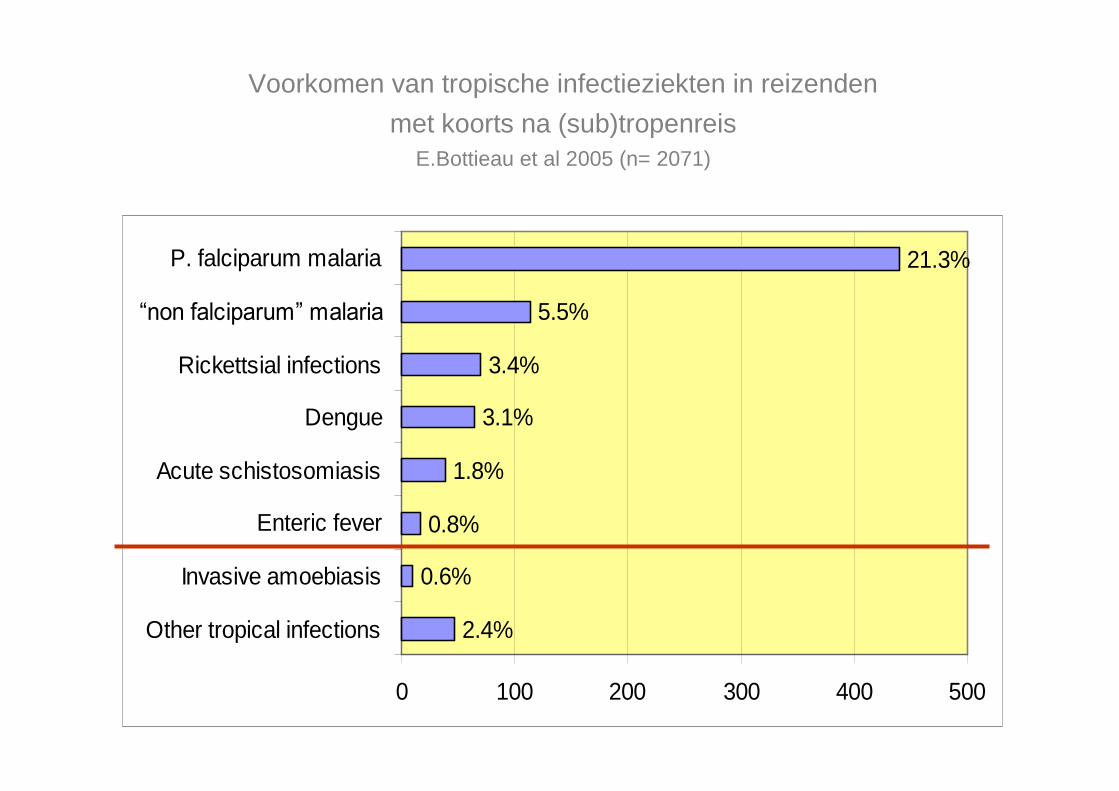
Voorkomen van tropische infectieziekten in reizendenmet koorts na (sub)tropenreis
E.Bottieau et al 2005 (n= 2071)
21.3%
5.5%
3.4%
3.1%
1.8%
0.8%
0.6%
2.4%
0 100 200 300 400 500
Other tropical infections
Invasive amoebiasis
Enteric fever
Acute schistosomiasis
Dengue
Rickettsial infections
“non falciparum” malaria
P. falciparum malaria
The Big Five!
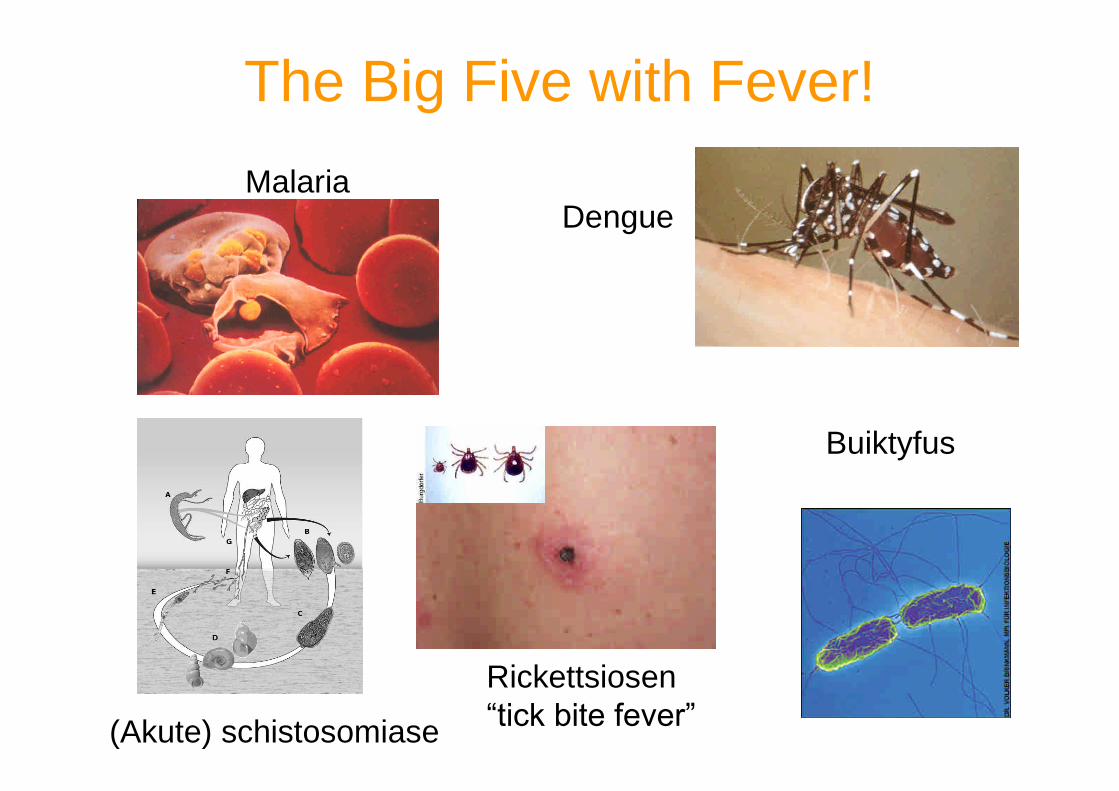
The Big Five with Fever!
MalariaDengue
(Akute) schistosomiase
Rickettsiosen“tick bite fever”
Buiktyfus
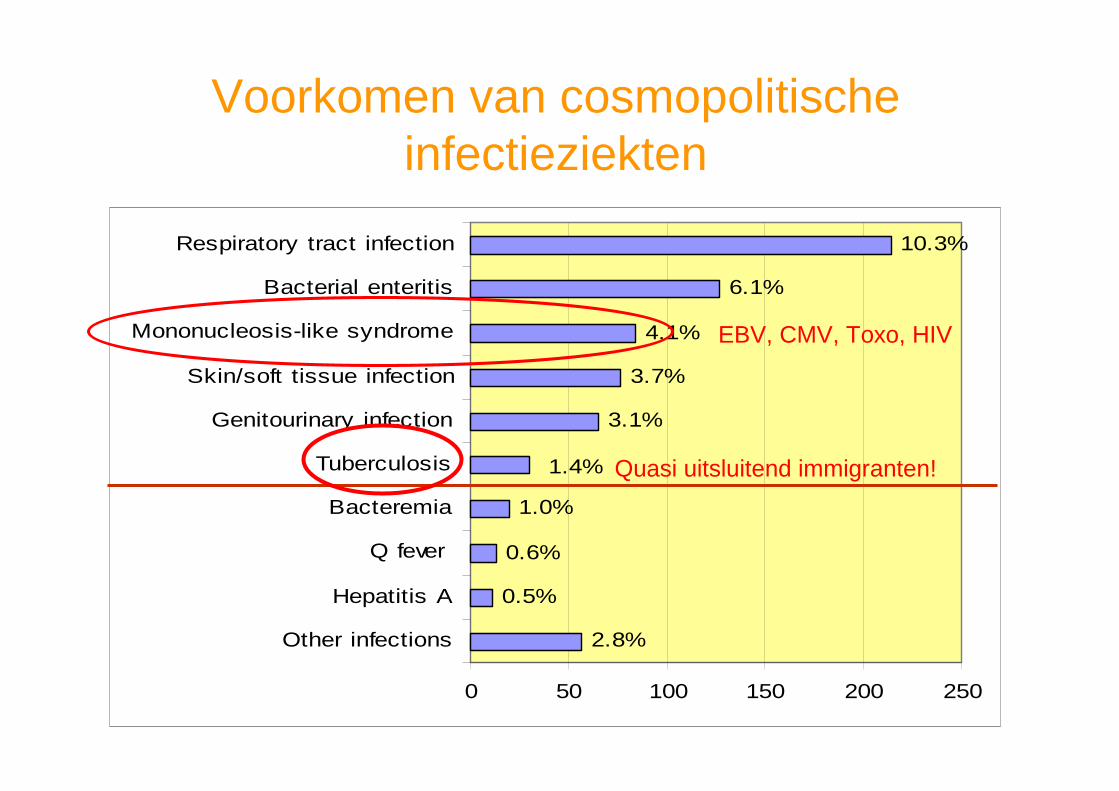
Voorkomen van cosmopolitischeinfectieziekten
10.3%
6.1%
4.1%
3.7%
3.1%
1.4%
1.0%
0.6%
0.5%
2.8%
0 50 100 150 200 250
Other infections
Hepatitis A
Q fever
Bacteremia
Tuberculosis
Genitourinary infection
Skin/soft tissue infection
Mononucleosis-like syndrome
Bacterial enteritis
Respiratory tract infection
Quasi uitsluitend immigranten!
EBV, CMV, Toxo, HIV
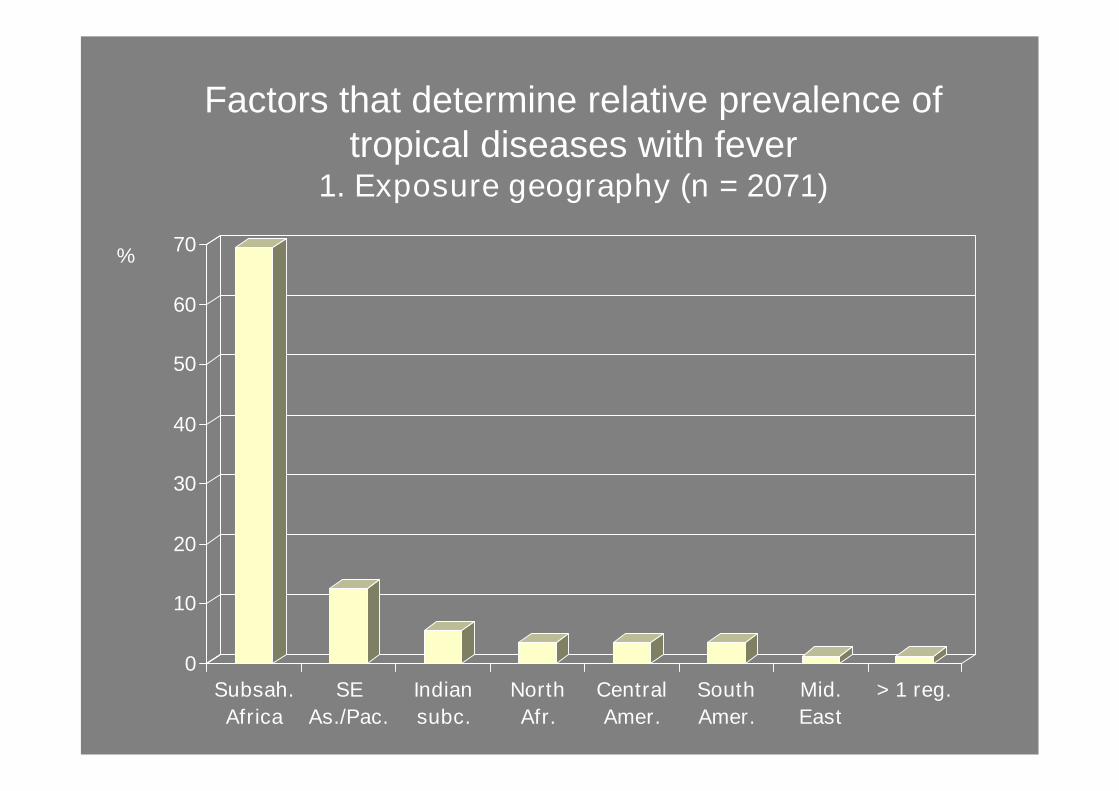
0
10
20
30
40
50
60
70%
Subsah.Africa
SEAs./Pac.
Indiansubc.
NorthAfr.
CentralAmer.
SouthAmer.
Mid.East
> 1 reg.
Factors that determine relative prevalence oftropical diseases with fever
1. Exposure geography (n = 2071)
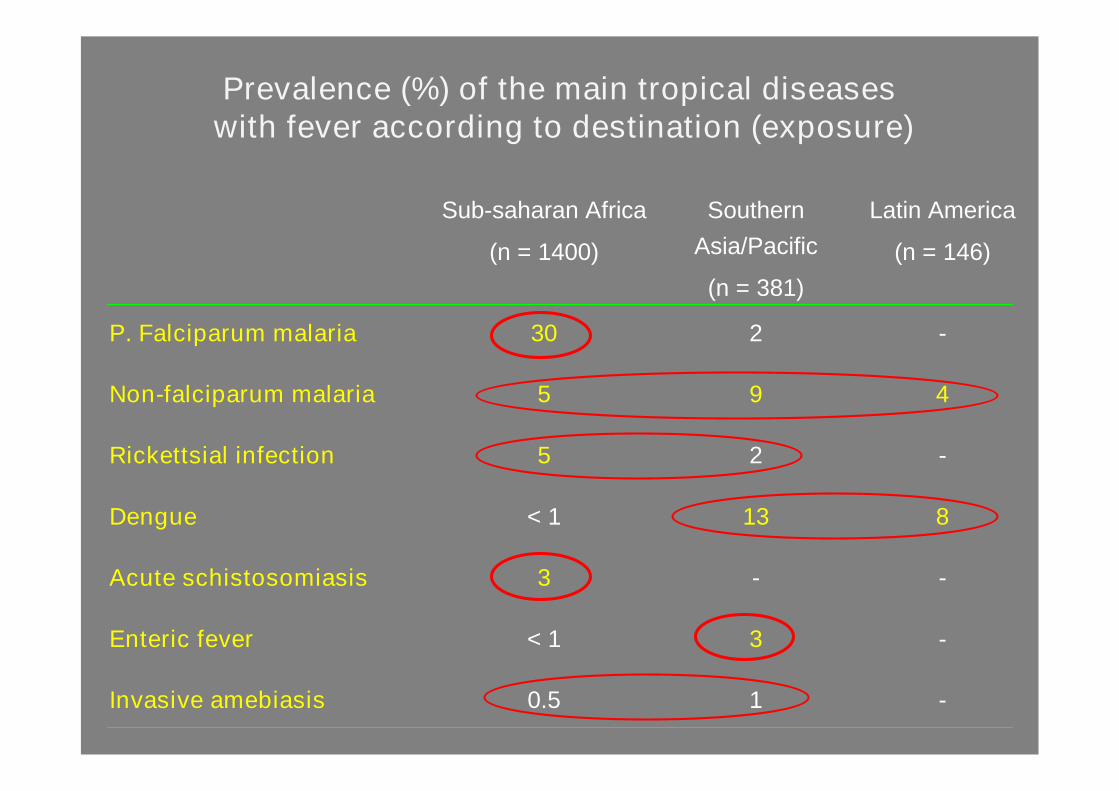
-10.5Invasive amebiasis
-3< 1Enteric fever
--3Acute schistosomiasis
813< 1Dengue
-25Rickettsial infection
495Non-falciparum malaria
-230P. Falciparum malaria
Latin America
(n = 146)
SouthernAsia/Pacific
(n = 381)
Sub-saharan Africa
(n = 1400)
Prevalence (%) of the main tropical diseaseswith fever according to destination (exposure)
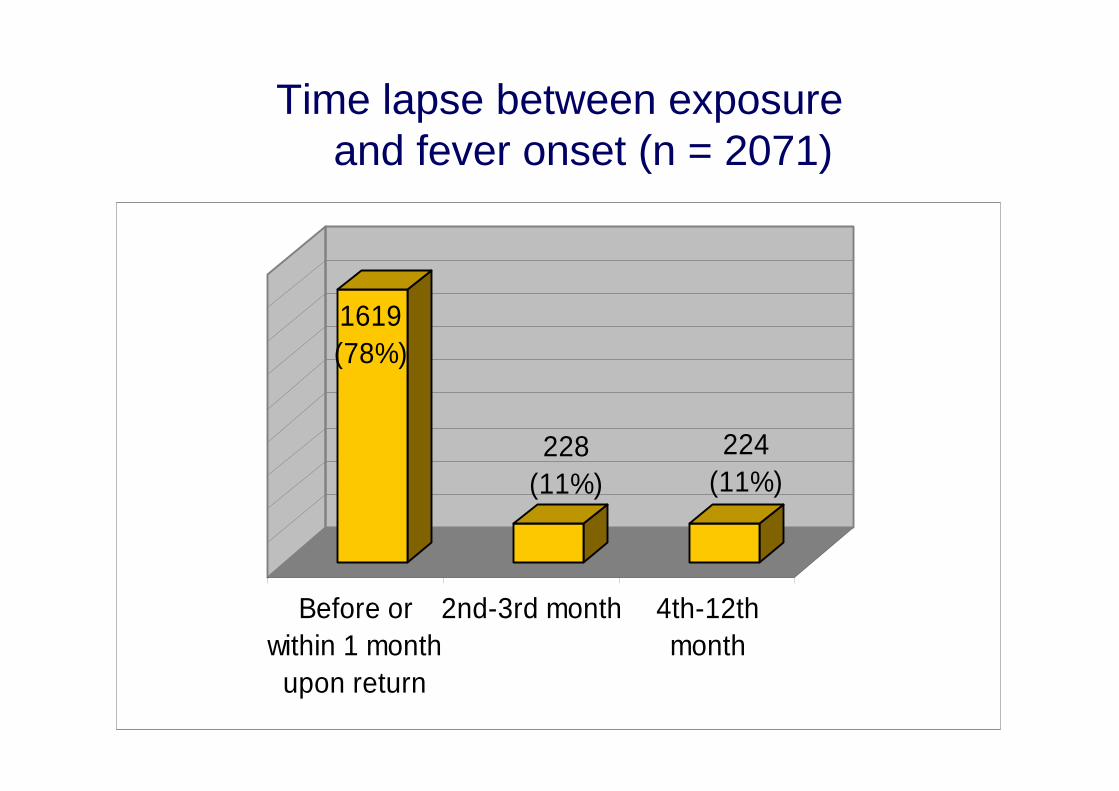
Time lapse between exposureand fever onset (n = 2071)
1619(78%)
228(11%)
224(11%)
Before orwithin 1 month
upon return
2nd-3rd month 4th-12thmonth
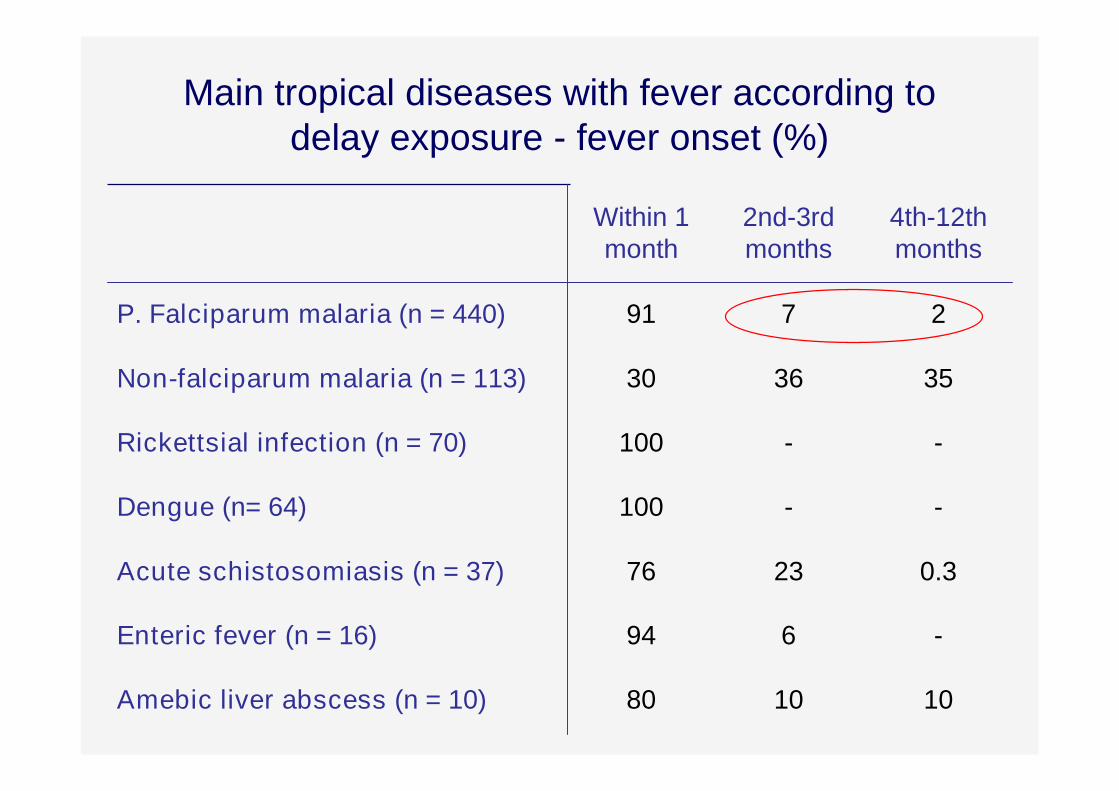
Main tropical diseases with fever according todelay exposure - fever onset (%)
101080Amebic liver abscess (n = 10)
-694Enteric fever (n = 16)
0.32376Acute schistosomiasis (n = 37)
--100Dengue (n= 64)
--100Rickettsial infection (n = 70)
353630Non-falciparum malaria (n = 113)
2791P. Falciparum malaria (n = 440)
4th-12thmonths
2nd-3rdmonths
Within 1month
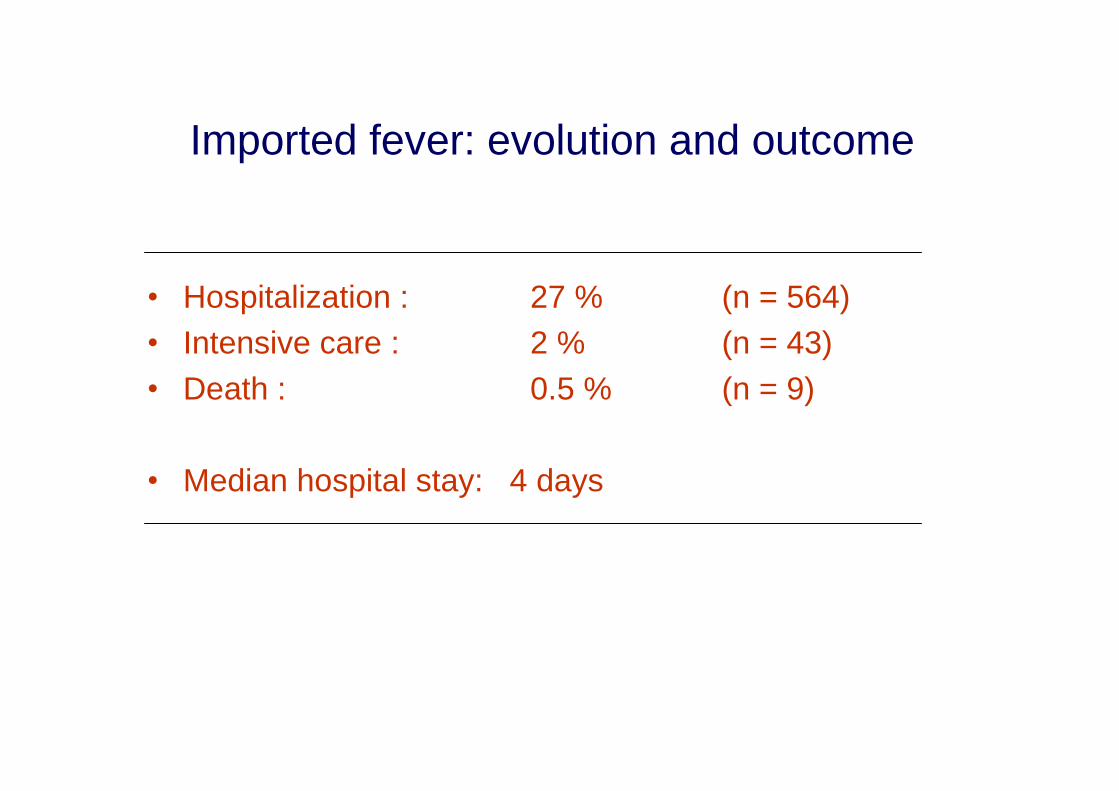
Imported fever: evolution and outcome
•Hospitalization : 27 % (n = 564)• Intensive care : 2 % (n = 43)•Death : 0.5 % (n = 9)
•Median hospital stay: 4 days
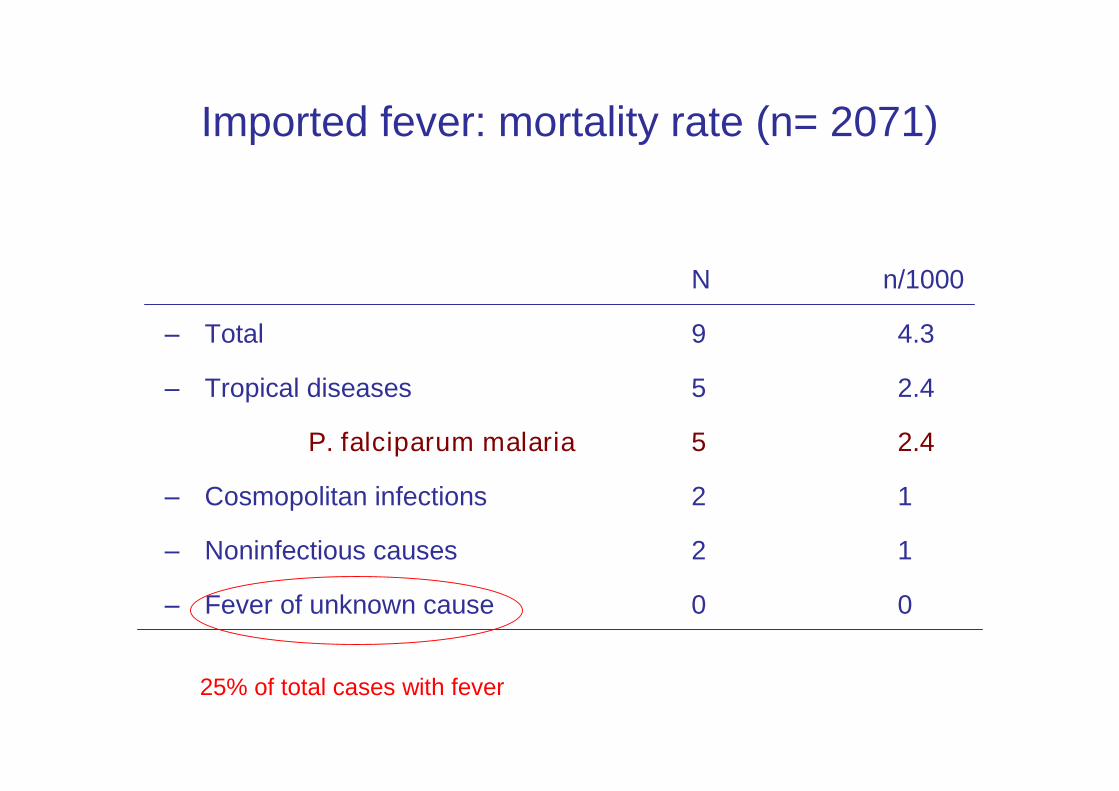
Imported fever: mortality rate (n= 2071)
N n/1000
– Total 9 4.3
– Tropical diseases 5 2.4
P. falciparum malaria 5 2.4
– Cosmopolitan infections 2 1
– Noninfectious causes 2 1
– Fever of unknown cause 0 0
25% of total cases with fever

“We kunnen niets specifieks vinden, dus ik zal umoeten behandelen voor een “akutesymptoom deficiëntie”
DossierITG

Hoe pakHoe pakik datik dataan?aan?
Koorts na verblijf in tropen
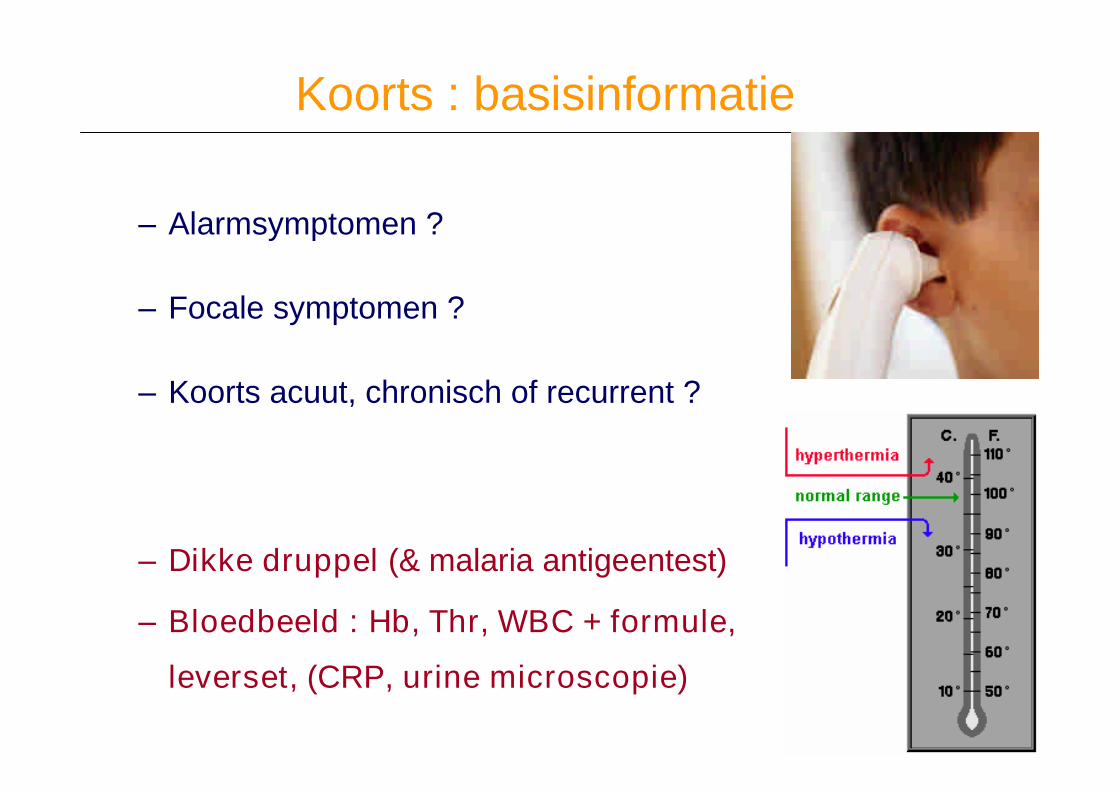
Koorts : basisinformatie
–Alarmsymptomen ?
–Focale symptomen ?
–Koorts acuut, chronisch of recurrent ?
–Dikke druppel (& malaria antigeentest)
–Bloedbeeld : Hb, Thr, WBC + formule,
leverset, (CRP, urine microscopie)
Koorts : onderzoek in 2e instantie
–Rx Thorax
–Echo abdomen-bekken
–Microscopie : urine - faeces - beenmerg - lumbaalvocht -
sputum - wondvocht
–Puncties : abces, gewricht, lymfeklier, pleura, …
–Culturen en Serologie
Nieuwe diagnosemethoden
…in het researchlab…
Ik zorg wel voor de bloedtests……en laat mij met de stront zitten!
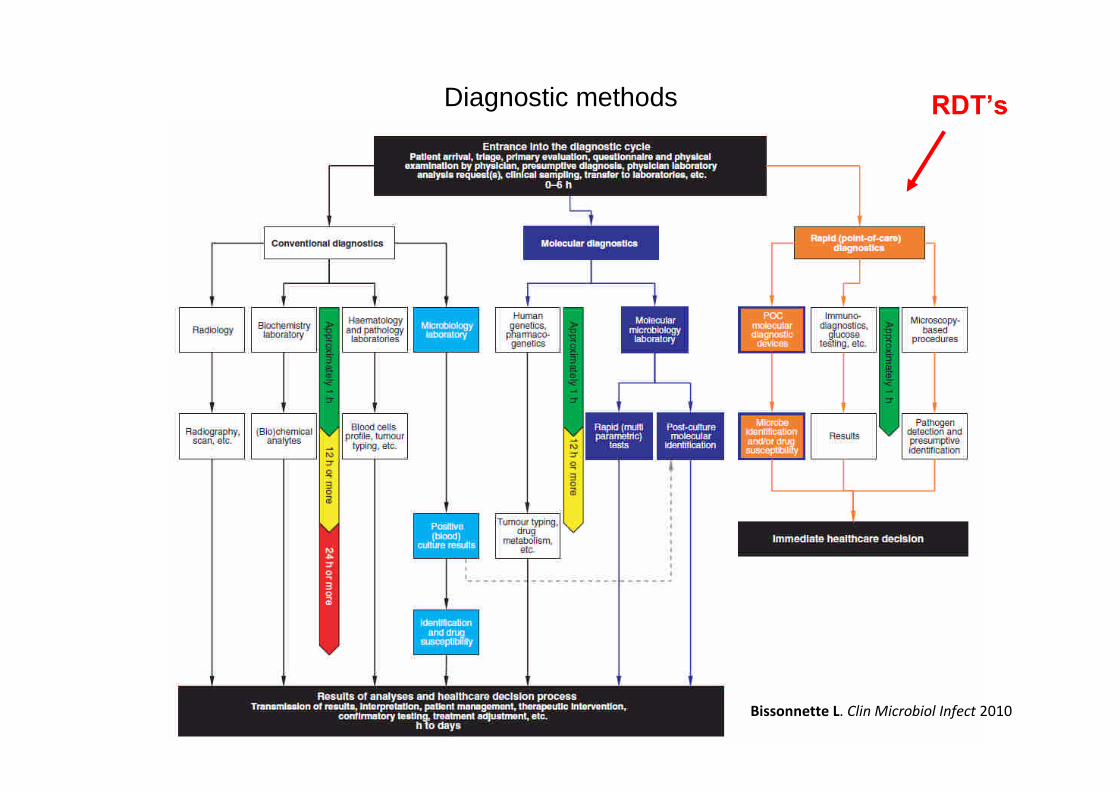
Diagnostic methods
Bissonnette L. Clin Microbiol Infect 2010
RDT’s
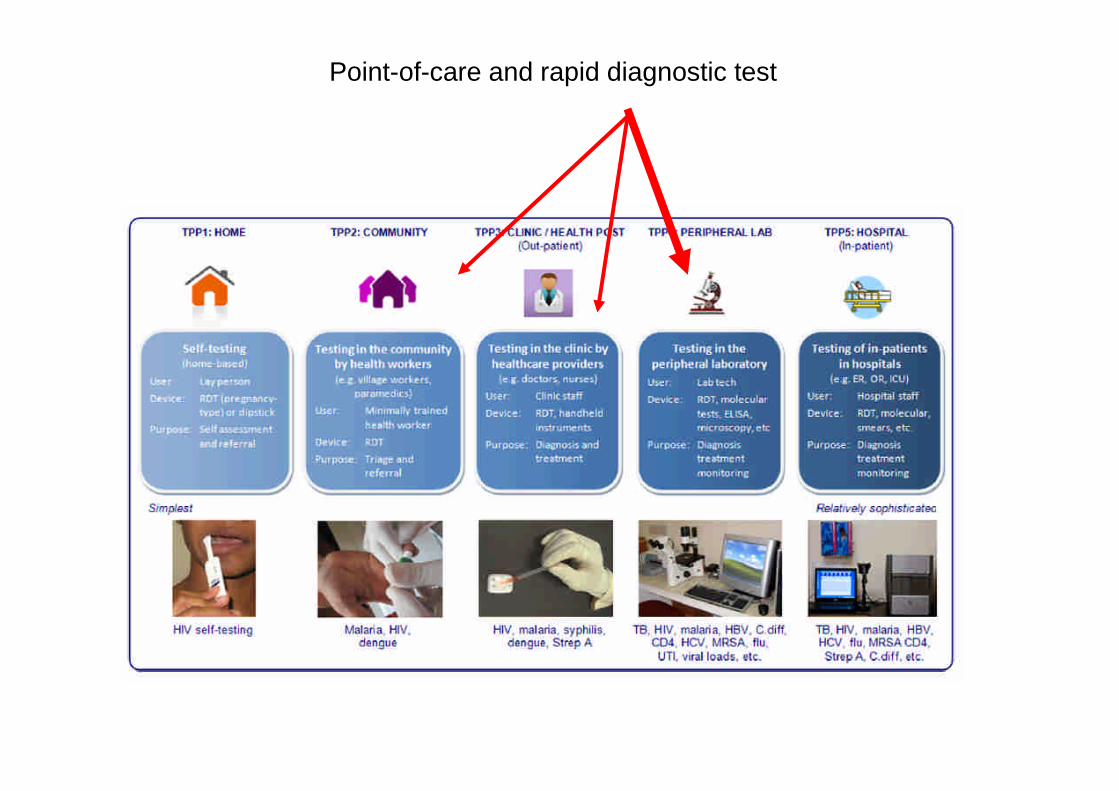
Point-of-care and rapid diagnostic test
Pai NP et al. PLoS Med 2012
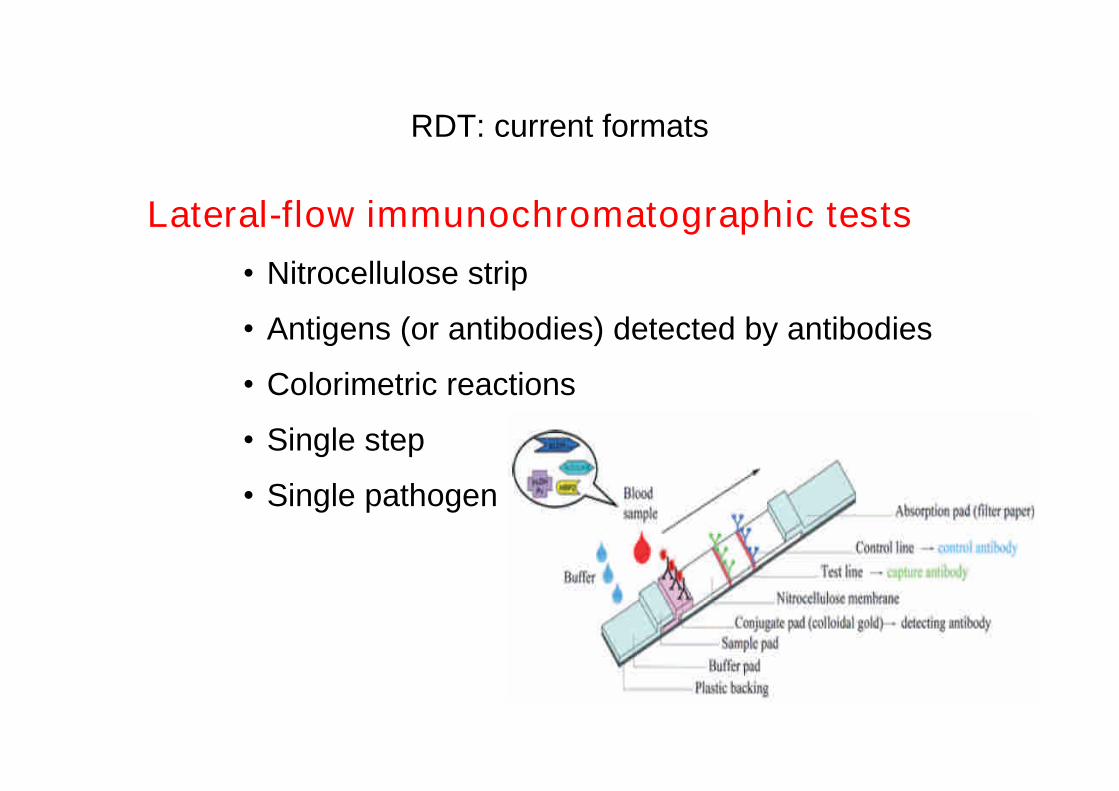
RDT: current formats
Lateral-flow immunochromatographic tests
•Nitrocellulose strip
•Antigens (or antibodies) detected by antibodies
•Colorimetric reactions
•Single step
•Single pathogen
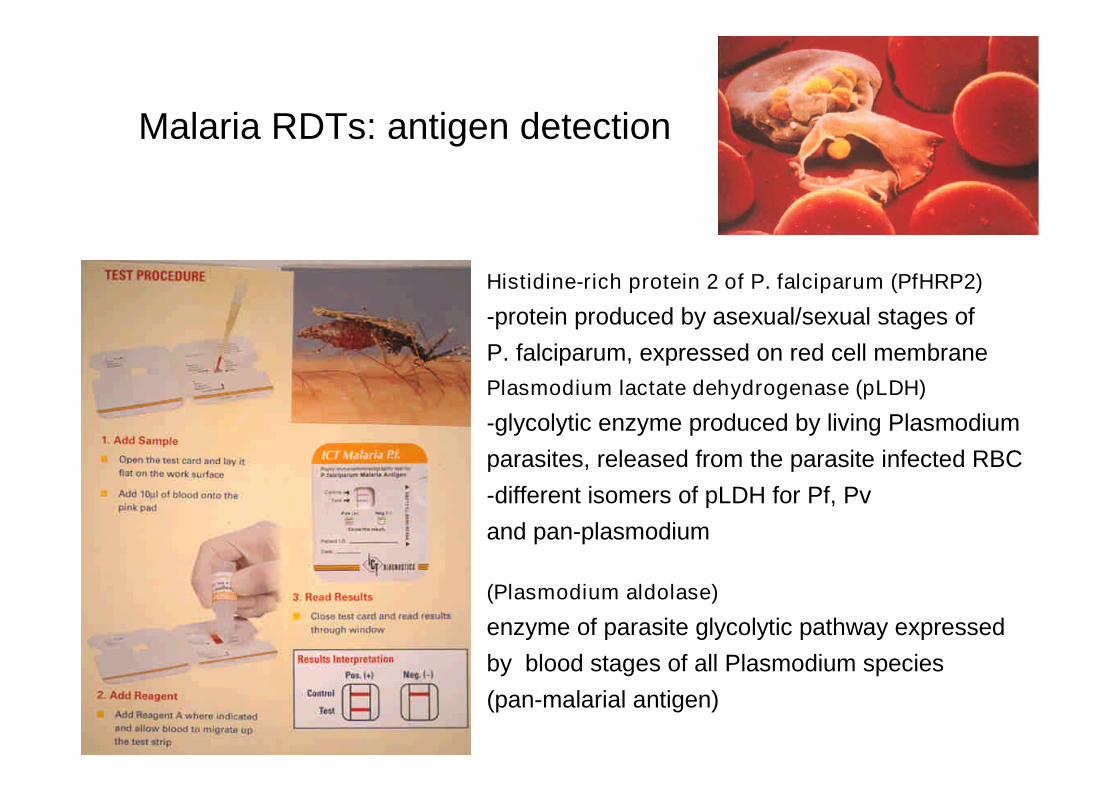
Malaria RDTs: antigen detection
Histidine-rich protein 2 of P. falciparum (PfHRP2)
-protein produced by asexual/sexual stages ofP. falciparum, expressed on red cell membranePlasmodium lactate dehydrogenase (pLDH)
-glycolytic enzyme produced by living Plasmodiumparasites, released from the parasite infected RBC-different isomers of pLDH for Pf, Pvand pan-plasmodium
(Plasmodium aldolase)
enzyme of parasite glycolytic pathway expressedby blood stages of all Plasmodium species(pan-malarial antigen)
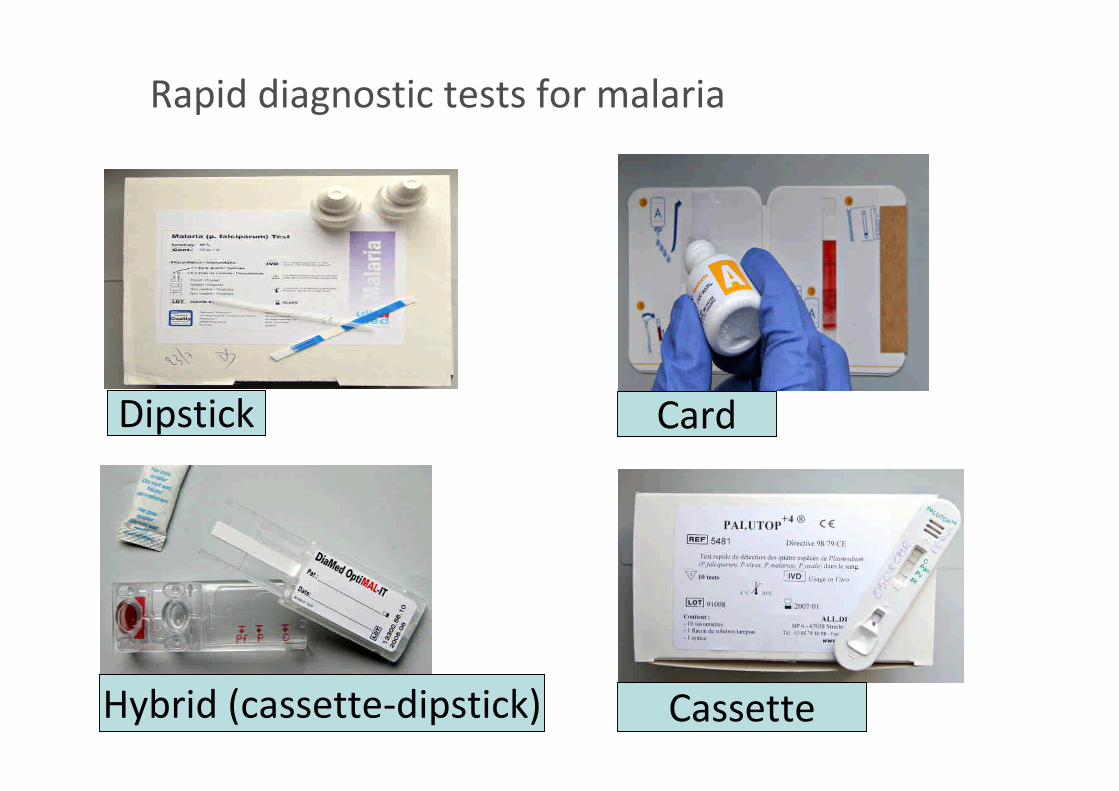
Rapid diagnostic tests for malaria
Dipstick
Hybrid (cassette-dipstick) Cassette
Card
Malaria RDTs: performance
• Current RDTs are accurate for P. falciparum diagnosis–Sensitivity > 95%–Specificity > 95%
• Less accurate than expert microscopy–50 parasites/µL
• Equivalent to/better than routine microscopy– In low-resource field settings
• Batwala et al. Malar J 2010• Hendriksen et al. Clin Infect Dis 2011
– In US hospitals• Palmer et al. J Clin Microbiol 2003• Stauffer et al. Clin Infect Dis 2009
WHO: 95% sensitivity atparasitemia of 100/µl

Malaria RDTs: recommendations in travel medicine
• In travel clinics
– ALWAYS perform both RDT AND microscopy
•Quantification of parasite load
•Cross checking
•Microscopy may be delayed if RDT neg (Rossi et al. Malar J 2012)
– Repeat RDT (/microscopy) within 12-24h if first test negative
•Shown to be safe (Bottieau et al. Eur J Clin Microbiol Infect Dis 2006)
• In travelers (peer/lay diagnosis)
– Urgent need to address some RDT shortcomings
– Need for technical training
– Need for clear instructions (If RDT positive AND if negative)
– Value and safety still to investigate in field studies
Dengue RDTs
RDT IgM/IgG
= classic serology = molecular testing
RDT NS1
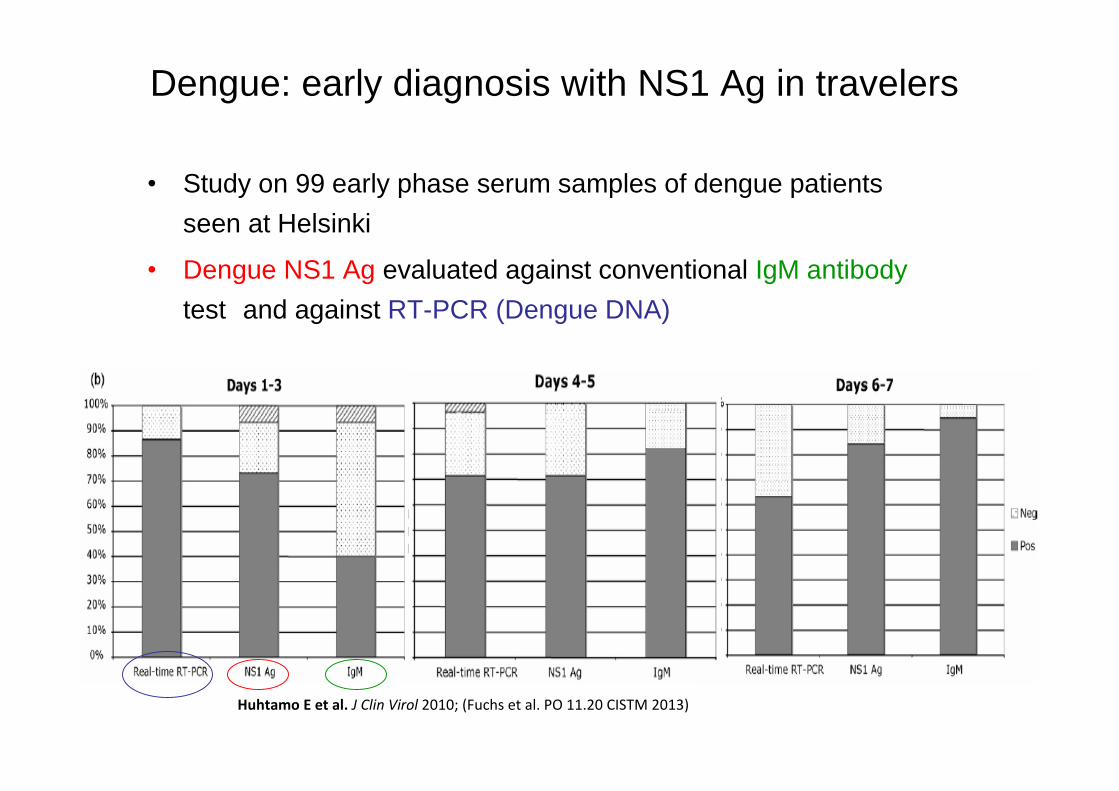
Dengue: early diagnosis with NS1 Ag in travelers
Huhtamo E et al. J Clin Virol 2010; (Fuchs et al. PO 11.20 CISTM 2013)
• Study on 99 early phase serum samples of dengue patientsseen at Helsinki
• Dengue NS1 Ag evaluated against conventional IgM antibodytest and against RT-PCR (Dengue DNA)
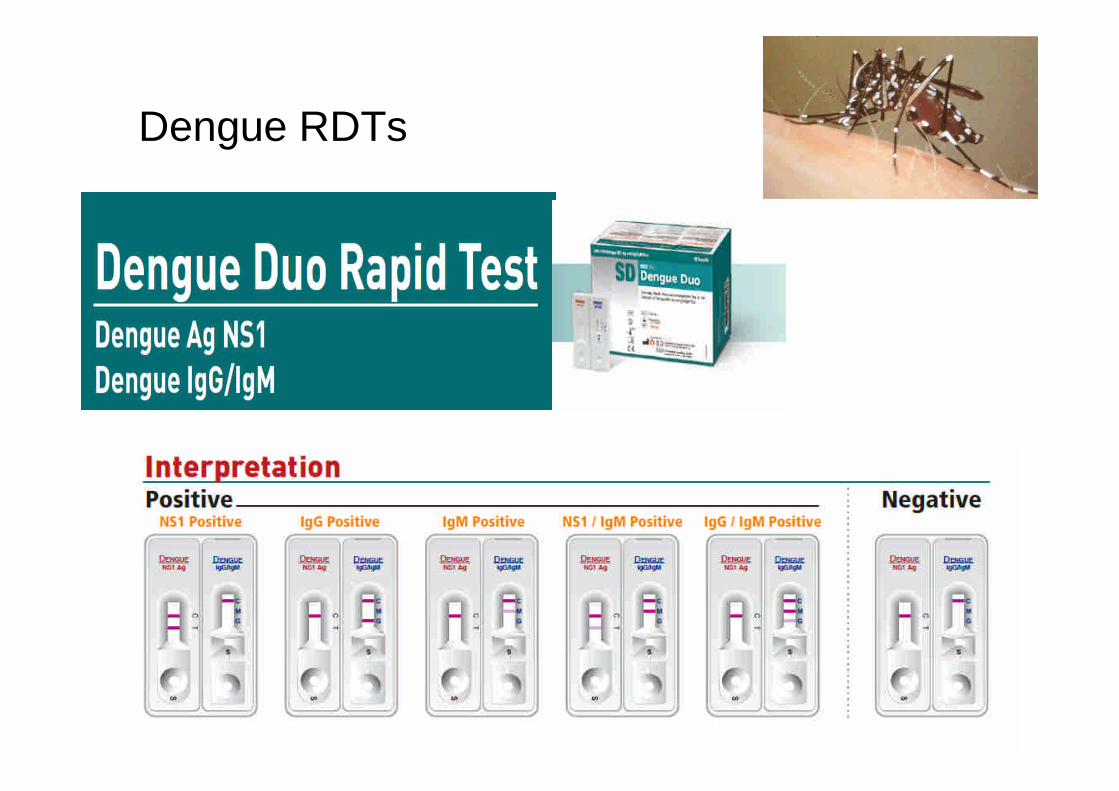
Dengue RDTs
Casuistiek







![Ppt0000020 [Alleen-lezen] - Proximususers.skynet.be/fa686441/GAB/GAB-2013/NIPT_Willems_1311.pdf · Microsoft PowerPoint - Ppt0000020 [Alleen-lezen] Author: gdepourcq Created Date:](https://static.fdocuments.nl/doc/165x107/60560c0c8469cf1b4f17c2c5/ppt0000020-alleen-lezen-microsoft-powerpoint-ppt0000020-alleen-lezen-author.jpg)