Hepatocellulair Carcinoma: behandeling
41
11de Antwerpse Oncologiedag - 28 maart 2014 “Viraal geïnduceerde kankers” Hepatocellulair Carcinoma: behandeling D. Ysebaert, T. Chapelle, G. Roeyen, K. De Greef, B. Bracke Dienst Hepatobiliaire, Transplantatie en Endocriene Heelkunde UZ Antwerpen
Transcript of Hepatocellulair Carcinoma: behandeling

11de Antwerpse Oncologiedag - 28 maart 2014
“Viraal geïnduceerde kankers”
Hepatocellulair Carcinoma:
behandeling D. Ysebaert, T. Chapelle, G. Roeyen, K. De Greef, B. Bracke
Dienst Hepatobiliaire, Transplantatie en Endocriene Heelkunde
UZ Antwerpen

HCC : therapie
Uitgangsvragen
• Plaats en mogelijkheden van chirurgie ?
• Levertransplantatie ?
• Locoregionale therapie ?
• Welke systemische therapie wordt aanbevolen bij HCC patiënten?

BCLC schema

BCLC staging system (Barcelona Clinic Liver Cancer)
stage Tumor size Cirrhosis therapy prognosis
A “early”
1 tumor <5cm or 3 tumors <3cm
compensated Curative intend : Resection Transplantation RFA
5 year survival: 50 – 75%
B “intermediate”
multinodularity no vascular invasion no extrahepatic spread
compensated TACE (Resection) ? (Transplantation) ? (RFA) ?
3 year survival 50%
C “advanced”
vascular invasion and/or extrahepatic spread
compensated or decompensated
no Resection no Transplantation no RFA (TACE) ? Antitumoral agents
3 year survival < 10%
D “terminal”
Major symptoms related to cancer invasion
decompensated symptomatic 1 year survival < 10%

Surgery for HCC
= only treatment with curative intent
3 techniques:
– Liver resection
– Liver transplantation
– (Ablation techniques)
but: Cirrhosis = “the Achilles heel” of surgery for HCC

Resection for HCC: liver factors
Tumor factors
• Single tumor (Ercolani, 2003)
also: multiple tumors?
• Diameter ≤ 5cm Poon, 2005)
also ≥ 5cm ?
• no vascular invasion • no extrahepatic spread
Liver factors
• Child-Pugh A (compensated)
• Normal liver function – bilirubin – albumin – PT
• no portal hypertension
– hepatic vein gradient < 10 mmHg
(Bruix Gastroenterol, 1996)
• Remnant liver volume

Resection for HCC: tumor-factors

Resection for HCC: safe?
Compare: < 1% mortality after resection in non-cirrhotic

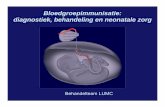
Resection for HCC: impact of portal hypertension and bilirubin
(Llovet, Lancet 2003)

Hepatic venous pressure gradient in the assessment of portal hypertension before liver resection in patients with cirrhosis
Measurement portal pressure by:
– Direct: HVPG (hepatic venous pressure gradient)
– Indirect: oesaphageal varices; splenomegaly; thrombocytopenia
(E.Boleslawski, F.R.Pruvot, BJS 2012;99:855-863)
40 pts
atypical resection
up to
major hepatectomy

Hepatic resection for HCC in patients with Child A cirrhosis: is clinical evidence of portal hypertension a contraindication?
• 223 pts with cirrhosis BCLC stage A
• PTHN: oesaphageal varices; splenomegaly; thrombocytopenia
• 2 groups: N/Y
• Limited liver resections: 31%/17% (<2 segments)
• Morbidity: 14%/29%
(R Santombrogio, D Cherqui, HPB 2013,15,78-84)

Resection for HCC: 3y and 5y survival
(Emond, 2005)
3y survival : ± 65% 5y survival : ± 45%

Resection for HCC: disease-free survival
(Emond, 2005)
± 2/3 patients: recurrence 3 y after resection of HCC !!

Tumour recurrence after liver resection for HCC
liver recurrence: 70 -85 % at 5 y
– 2/3 intrahepatic satellite tumors, undetected at
resection
often < 2y after resection
– 1/3 de novo tumors
often > 2y after resection

Why liver transplantation for HCC ?
PRO
• Replacement of cirrhotic liver
• Prevention de novo HCC
• Treatment unrecognised
satellite tumors
• Treatment of decompensated
cirrhosis (Child B / C)
• Perspective of cure from
hepatitis B/C
CONTRA
• Risks of transplantation
– Immunosuppressive therapy
– Opportunistic infections
– Agressive tumor recurrence ?
• Waiting time & tumour
progression
• Competition on waiting list
between HCC and non-HCC
candidates for OLTx

Liver transplantation offers the perspective of cure from Hepatitis B/C
Hepatitis B
• Patients without active replication before LTX : HBIG (Hepacaf®, 5000 IE/flacon) – 10 000 IU IV in 1 hour during anhepatic phase
– then daily 10 000 IU for 1 week
– then every 4-8 weeks in order to keep anti-HBs titers > 100-150 IU/L
• Patients with active replication: start antiviral therapy before LTX + – HBIG 10 000 IU IV in 1 hour during anhepatic phase
– then daily 10 000 IU for 1 week
– then every 4-8 weeks in order to keep anti-HBs titers > 500 IU/L for the first month, > 250 IU/L until 3 months and > 100-150 IU/L thereafter
Duration of treatment : - 1 year for acute hepatitis B - lifelong for chronic hep B or until proven reinfection
Failure : 5-10 %

Liver transplantation offers the perspective of cure from Hepatitis B/C
Hepatitis C
• 100 % recurrence within 1-6 months
• Until recently : no profylaxis possible
• Perspective : Pre-transplant treatment with sofosbuvir (Sovaldi ®) + ribavirin until liver transplantation (awaiting reimbursement)

Liver Tx for HCC: organ allocation
• MELD (Model for End-stage Liver Disease) – INR
– Bilirubine
– Creatinine
predicts 3-month mortality in chronic liver disease
• Laboratory MELD does not reflect mortality risk of HCC/ChildA
• Standard exception: extra points for HCC (early stage), reflecting 10% increased mortality risk/ 3 months on waiting list
• UNOS = Eurotransplant

Recommendations for liver transplantation for HCC: an international consensus conference report
Tumour criteria for OLTx?
Level of evidence
Strength of recommendation
Preoperative assessment of the size of the largest tumour or total diameter of tumours should be the main consideration in selecting patients with HCC for OLTx
2a Strong
The Milan Criteria are currently the benchmark for the selection of HCC pts for OLTx and the basis for comparison with other suggested criteria
2a Strong
P.A Clavien et al, Lancet Oncol 2012;13:e11-22 Based on International Consensus conference, Zürich, Dec 2-4 2010

Liver Tx for HCC: indications
General Tumor - related
• Milan-criteria – 1 tumor < 5 cm – 3 tumors < 3 cm
(Mazzaferro, Liver transpl 2011)
• no macrovascular invasion • no extrahepatic disease
Mijn dokter zegt: “Eén glas alcohol per
dag.”
Ik kan daar mee leven !

Vascular involvement in HCC: impact on LTx
Macrovascular involvement
• On imaging
• Portal and/ or hepatic vein
• = major contra-indication for OLTx
Microvascular involvement
– On microscopy
– Poorer outcome & more recurrences after OLTx
– Often associated with larger nodules , multiple nodules, moderate or poor differentiation, confluent multinodular pattern
– No reliable detection pre-OLTX possible
– Currently not useful as contra-indication in OLTx
(J.P.Llovet, V. Mazzaferro, Sem in liver dis. 2006; 25:181-200)

Results of OLTx for HCC
Within Milan criteria:
• 5y survival 70%
• <10% recurrence rate
Compare with OLTx for non HCC indications:
• 5y survival 65-87%
(European Liver Transplant Registry (ELTR); Organ Procurement an Transplantation Network (OPTN); Australia and New Zealand Liver Transplant Registry (ANZLTR))
(J.Llovet, Liver Transplantation 2011;17:S44-57)

Philosophical approach in OLTx for HCC: “the 5y survival paradox?”
• 5y survival after liver Tx (all indications) should be at least 75- 85% = viewpoint of optimal use of scarce transplant organs
• 5y survival of 35 – 50% in oncology is generally considered as
acceptable/good/excellent often better than palliative treatments eg. liver resection for colorectal liver metastasis = viewpoint of patient

Recommendations for liver transplantation for HCC: an international consensus conference report
Should the survival OLTx for HCC be the same as
for OLTx for non-HCC indications?
Level of evidence
Strength of recommendation
OLTx should be reserved for HCC pts who have a predicted 5y survival comparable to non-HCC pts
NA Weak

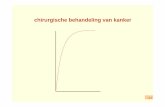
Liver Tx for HCC: 5y survival
(Llovet, Lancet 2003)
UCSF criteria • 1 tumor <6,5cm • 2 or 3 tumors <4,5cm • with total diameter <8cm (Yao, 2001)

UCSF criteria: 5y survival
5y survival based on tumor criteria on pretransplant imaging
Yao, 2008

Expanding tumor criteria in Liver Tx ?

Recommendations for liver transplantation for HCC: an international consensus conference report
LTx outside Milan = should it be done?
Level of evidence
Strength of recommendation
A modest expansion of the number of potential candidates may be considered on the basis of several studies showing comparable survival for patients outside the Milan criteria
3b Weak
Patients with worse prognosis may be considered for OLTx outside the Milan criteria if the dynamics of the waiting list allow it without undue prejudice to other recipients with a better prognosis
NA Weak
P.A Clavien et al, Lancet Oncol 2012;13:e11-22 Based on International Consensus conference, Zürich, Dec 2-4 2010

Adaptation Belgian – Eurotransplant rules (from 2014 on)
• Milan-criteria – 1 tumor < 5 cm – 3 tumors < 3 cm
• no macrovascular invasion • no extrahepatic disease
• Belgian – Eurotransplant criteria – 1 lesion ≥ 2 cm and ≤ 5 cm – 2 or 3 lesions ≥ 1 cm and ≤ 3 cm
• no macrovascular invasion • no extrahepatic disease
Nodules < 1 cm are indeterminate and cannot be considered

Recommendations for liver transplantation for HCC: an international consensus conference report
Role of downstaging for LTx?
Level of evidence
Strength of recommendation
OLTx may be considered after successful downstaging 5 Weak
OLTx after successful downstaging should achieve a 5y survival comparable to that of HCC pts who meet the criteria for OLTx without requiring downstaging
5 Strong
Criteria for successful downstaging should include tumour size and number of viable tumours
4 Strong
Based on existing evidence, no recommendation can be made for preferring a specific locoregional therapy for downstaging over others
NA None
P.A Clavien et al, Lancet Oncol 2012;13:e11-22 Based on International Consensus conference, Zürich, Dec 2-4 2010

Ablative therapies for HCC
• Radiofrequency ablation (RFA )
– less sessions needed
– contra-indications: • subcapsular tumor
• close to hilum or main liver structures
• ascites
• clotting disturbances
• Percutaneous ethanol injection (PEI)
– more sessions needed
• (microwave, cryotherapy, …)

Ablation techniques for HCC: RFA vs PEI
• 4 RCT RFA vs PEI
(Lencioni, 2003; Lin,2004; Shiina, 2005; Lin 2005)
• patient survival and disease free survival
– tumors >2cm: RFA >> PEI (difference 20%)
– tumors <2cm: no difference
• morbidity:
– RFA: 2%
– PEI: 1,3% – 3,2%
(Llovet, Lancet 2003)

Downstaging of HCC prior to OLTx
• Alcohol injection
• RFA
• TACE
• (Liver resection)
• No clear criteria which tumour burden still eligible for downstaging attempt
• Succesful downstaging for large tumour burden + OLTx has same survival as OLTx within Milan
(Ravaioli, Am J Transpl 2012;10:129-137;) (Yao, Hepatology 2008;48:819-827)
• No clear criteria how to evalaute respons to dowstaging:
– Necrosis on imaging ?
– Evolution tumor marker ?

Liver resection/RFA vs OLTx for HCC?
Relationships ?
• Resection/RFA as alternative for OLTx
• Resection/ RFA eventually followed by salvage OLTx for
– Tumour recurrence
– Worsening liver function
• Resection/ RFA as bridge to OLTx consider also TACE (drug eluting beads)
• Resection/RFA as downstaging before OLTx consider also TACE (drug eluting beads)

• TACE drug eluting beads
• stereotactic radiotherapy
• Yttrium-90 radio-embolisation

HCC: systemic therapy
• Child-Pugh A levercirrose stage A, progressive after previous locoregional therapy
• HCC BCLC stadium B en C and impossibility of locoregional therapies

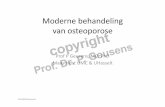
HCC: systemic therapy
“…OS and TRP nearly 3 months longer for sorafenib vs placebo…”
“..diarrhea, weight loss, food-hand syndrome more frequent..”
Llovet JM et al. N Engl J Med 2008;359:378-390
Sharp study Mainly Child A

HCC: systemische therapie
Sorafenib : vergoedingsmodaliteiten (Hfst IV – 2007)
• Voor de behandeling van patiënten met gevorderd HCC en met Child-Pugh A-cirrose die volgens het transplantatie- bilan van een erkend transplantatiecentrum niet in aanmerking komen voor levertransplantatie (MOC attest)
• De diagnose van hepatocellulair carcinoom is vastgesteld aan de hand van een biopsie.
• Max posologie 4 x 200 mg/d
• Alle patiënten moeten na elke periode van 12 weken behandelen of vroeger indien de klinische toestand het vereist geëvalueerd worden. Indien patiënt een radiologische, biochemische en/of klinisch symptomatische progressie vertoont, moet de behandeling stopgezet worden.

HCC: systemische therapie
Sorafenib: herziening vergoedingsmodaliteiten(HfstIV–2010)
• ...voor de behandeling van patiënten met een gevorderd HCC met een Child-Pugh A leverfunctie.
• Indien het gaat om letsel(s) in een cirrotische lever of in geval van Hepatitis B kan de diagnose van HCC gesteld worden aan de hand van medische beeldvorming (dynamische NMR of CT-scan, met contrast en geanalyseerd over verschillende fazen) of een biopsie. In alle andere gevallen of in geval van twijfel, blijft een biopsie noodzakelijk voor de diagnose van HCC.
• Alle patiënten moeten na elke periode van 12 weken behandelen of vroeger indien de klinische toestand het vereist geëvalueerd worden. Indien patiënt een radiologische, biochemische en/of klinisch symptomatische progressie vertoont, moet de behandeling stopgezet worden.

Treatment of HCC: conclusions
• Child A cirrhosis / no PHPN / 1(-3) lesions : - > 3 cm : resection - < 3 cm : RFA (open, laparoscopic, percutaneous)
• Liver transplantion in good candidates : 1 lesion ≥ 2 cm and ≤ 5 cm or 2 or 3 lesions ≥ 1 cm and ≤ 3 cm
• RFA (resection)/ TACE as bridge to LTx
• Consider locoregional therapies if resection/LTX is impossible
• Sorafenib in systematic treatment of intermediate/advanced stage HCC in Child A cirrhosis