
Een abnormale eiwitelectroforese: wat nu? · MGUS • Aanwezigheid van stabiel paraproteïne in...
35
& Een abnormale eiwitelectroforese: wat nu? J. Lemmens 21/5/2019 1
Transcript of Een abnormale eiwitelectroforese: wat nu? · MGUS • Aanwezigheid van stabiel paraproteïne in...

&
Een abnormale
eiwitelectroforese: wat nu?J. Lemmens
21/5/2019
1

Abnormale piek in het eiwitprofiel
Albumine, A1: antitrypsine/orosmucoid, A2: macroglobuline, haptoglobine, ceruloplasmB: transferrine, hemopexine C3, Gammaglobulines
Is elke Ig-stijging kwaadaardig?
• Infecties!• “Goedaardige” Ig ziekten:
– Ig monoclonale piek (MGUS), bij jonge ptn steeds laten investigeren
– Koude agglutinine ziekte
– Hepatitis C- cryoglobuline
• Niet- goedaardige Ig ziekten:
– Monoclonale gammopathie met renale significantie (MGRS)
– AL-amyloïdose
– Heavy-chain disease
– Extraskeletaal plasmocytoom
– Solitair plasmocytoom
– Smoldering myeloma / Multipel myeloom of Kahler
– Andere Non-Hodgkin lymfomen
– Waldenström

MGUS
• Aanwezigheid van stabiel paraproteïne in serum (of urine) zonder Kahler, Waldenström, amyloïdose, NHL
• Mediane leeftijd is 66 jaar, incidentie 1% op 50 j, 5% boven 80 j
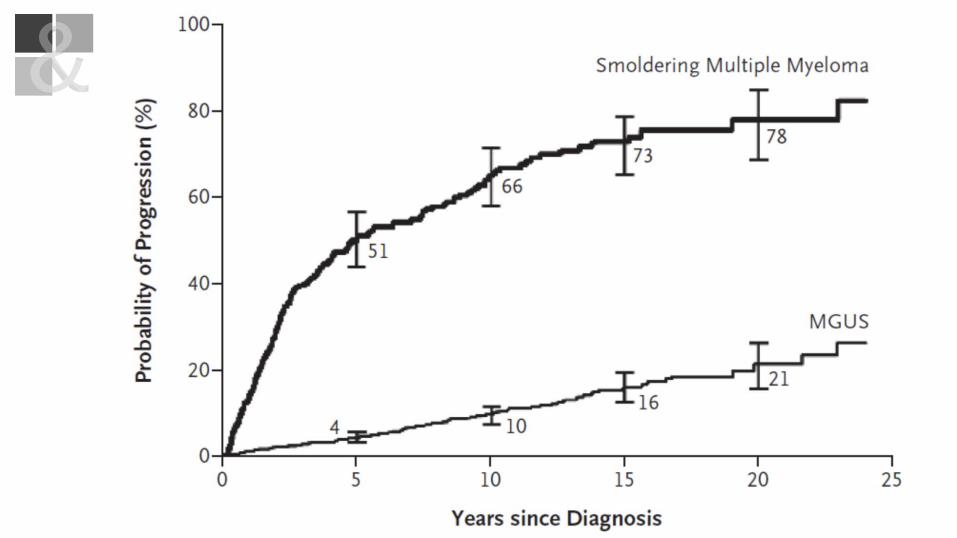
• Risico op transformatie naar maligniteit groeit met de tijd: 1,5% per jaar, 15% per 10 jaar, 30% per 20-30 j.
• 1/10 evolueert binnen de 8 jaar, ¼ pas na 25 jaar
• Iets verhoogd risico op infecties en thrombosen

< 3 g/dL serum
AND
< 10%
AND
Absent
Monoclonal
Gammopathy of
uncertain significance
(MGUS)
Present(serum/urine)
AND
> 10%
AND
Present
Multiple
Myeloma
3 g/dL serum
AND/OR
10-60%
AND
Absent
Smoldering
Multiple
Myeloma
(SMM)
Monoclonal
component
Bone Marrow
Plasma Cells (%)
Myeloma defining-event
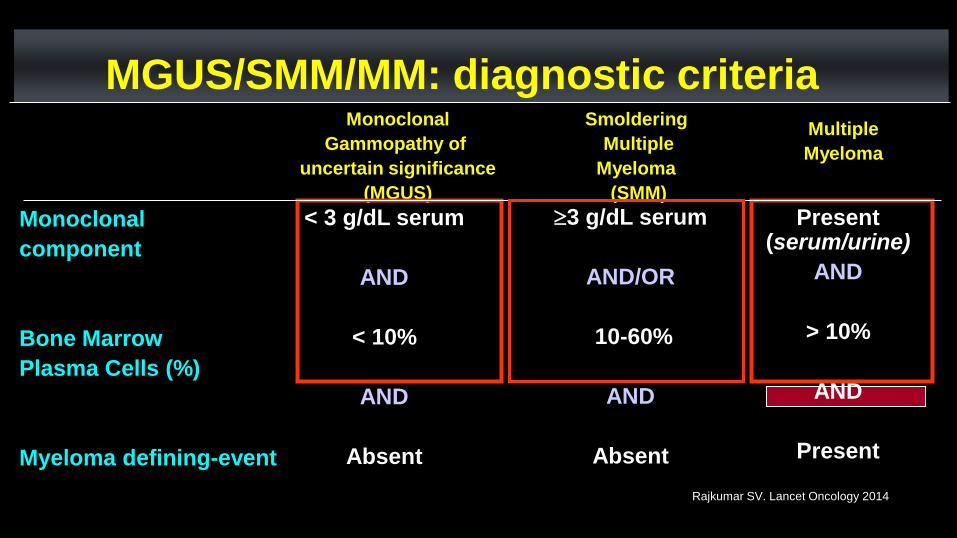
MGUS/SMM/MM: diagnostic criteria
Rajkumar SV. Lancet Oncology 2014
MGUS: diagnostische criteria
• Monoclonale piek < 3 g/dl
• Urinair paraproteïne: minimaal of afwezig
• BM plasmacellen: < 10%
• “No CRAB”
– hyperCalcemie
– Renal damage
– Anemia
– Bone disease
MGUS: risico op evolutie
• Risico factor:
– Normale kappa/lambda verhouding (0,26-1,65)
– IgG paraproteïne
– Paraproteïne <1,5 g/dl
• Risico score: 20 j progressie risico:
– 0 abnl 5 %
– 1 abnl 21 %
– 2 abnl 37 %
– 3 abnl 58 %
Rajkumar et al., Lancet Oncology 2014
MGUS: therapie
• Geen! (evt infectie- en thrombosepreventie?)
• Wel 6-maandelijks opvolgen
– Bloed
– Urine
• Ook 12-24 maandelijks RX skelet
• Nieuw beenmergonderzoek bij vaststelling evolutie naarKahler
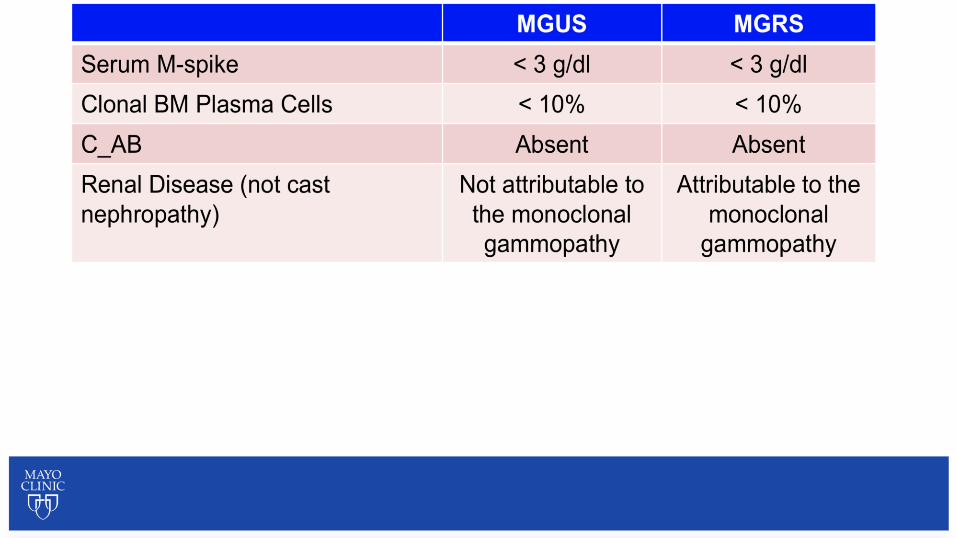
&MGRS
• Renale schade zonder criteria myeloma
• Therapie noodzakelijk om nierftie te beschermen
• Snellere progressie naar myeloma (x 5 ivm MGUS)
• Risico op progressie/1j 10%, (1% bij MGUS)
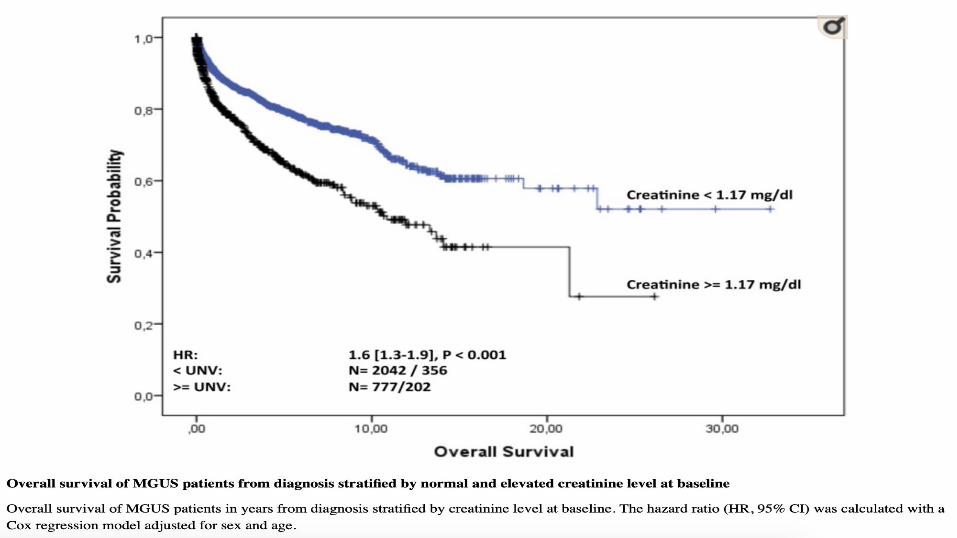
• Impact op overleving vnl bij aantasting nierftie (gestegen
creatinine)
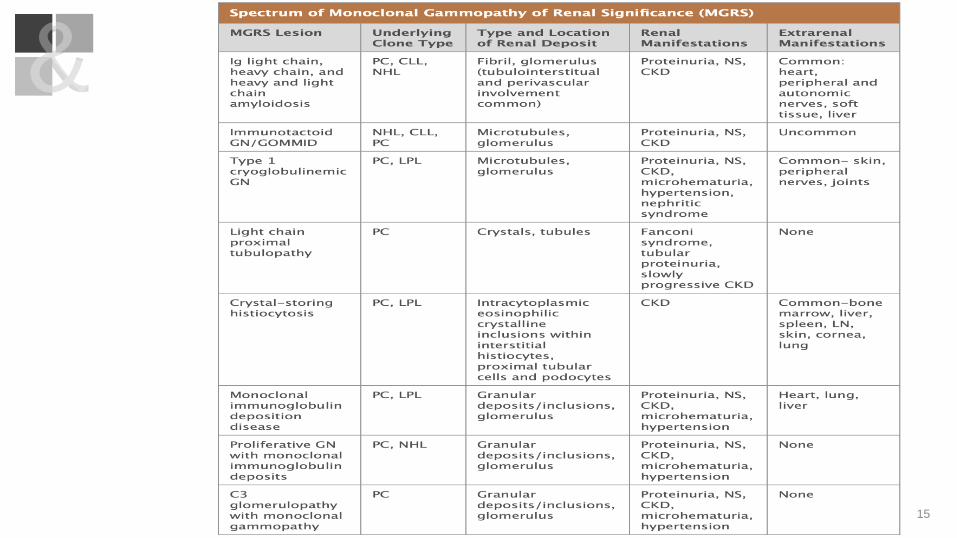
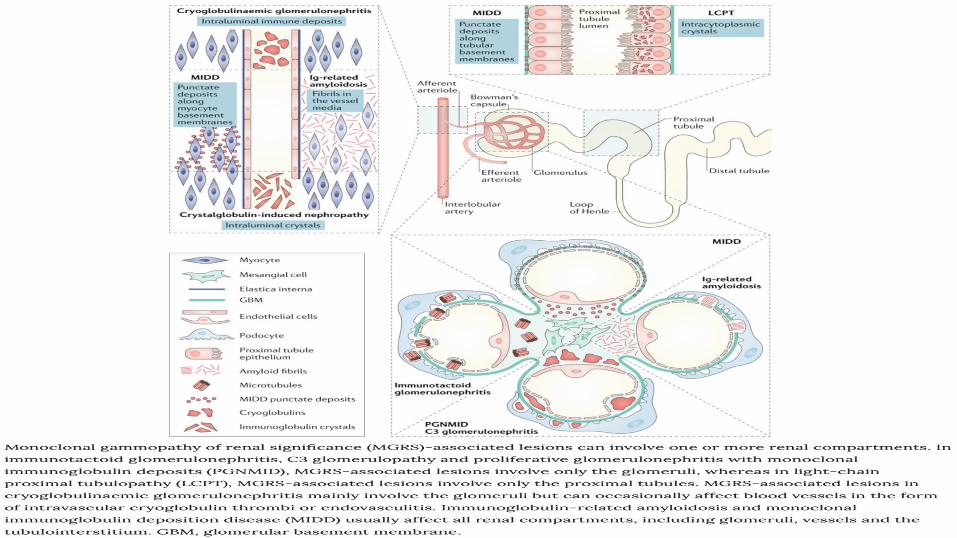
&MGRS
• Bij 1,5% van de MGUS ptn
• M/V 60/40
• IgG 46%, IgM 25%, IgA 7%, light chain 21%
• Bij 27% is amyloïdose geassocieerd, bij 21% light chain
depositie, 18% membranoproliferatieve GP, 9%
membraneuze GP
&
15
16
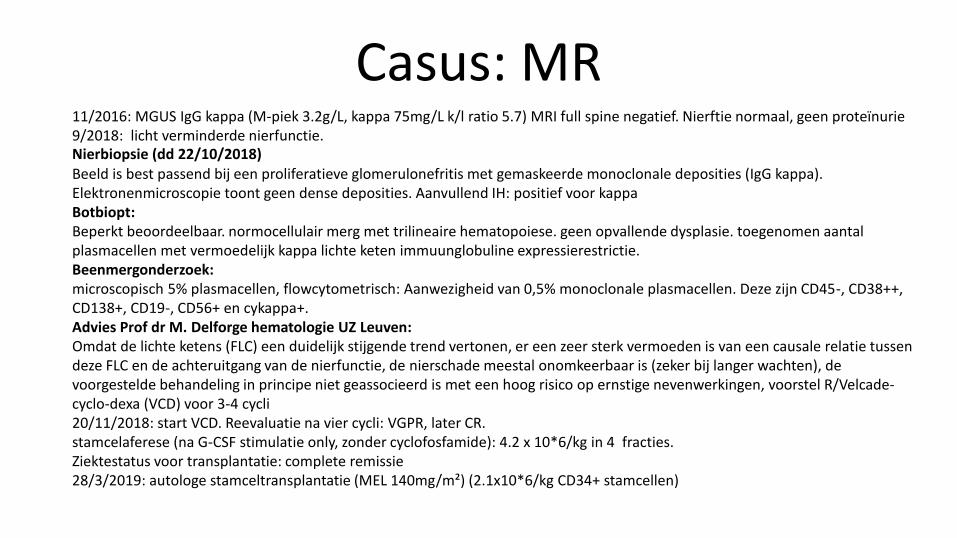
Casus: MR11/2016: MGUS IgG kappa (M-piek 3.2g/L, kappa 75mg/L k/l ratio 5.7) MRI full spine negatief. Nierftie normaal, geen proteïnurie9/2018: licht verminderde nierfunctie. Nierbiopsie (dd 22/10/2018)Beeld is best passend bij een proliferatieve glomerulonefritis met gemaskeerde monoclonale deposities (IgG kappa). Elektronenmicroscopie toont geen dense deposities. Aanvullend IH: positief voor kappaBotbiopt:Beperkt beoordeelbaar. normocellulair merg met trilineaire hematopoiese. geen opvallende dysplasie. toegenomen aantal plasmacellen met vermoedelijk kappa lichte keten immuunglobuline expressierestrictie. Beenmergonderzoek: microscopisch 5% plasmacellen, flowcytometrisch: Aanwezigheid van 0,5% monoclonale plasmacellen. Deze zijn CD45-, CD38++, CD138+, CD19-, CD56+ en cykappa+.Advies Prof dr M. Delforge hematologie UZ Leuven:Omdat de lichte ketens (FLC) een duidelijk stijgende trend vertonen, er een zeer sterk vermoeden is van een causale relatie tussen deze FLC en de achteruitgang van de nierfunctie, de nierschade meestal onomkeerbaar is (zeker bij langer wachten), de voorgestelde behandeling in principe niet geassocieerd is met een hoog risico op ernstige nevenwerkingen, voorstel R/Velcade-cyclo-dexa (VCD) voor 3-4 cycli 20/11/2018: start VCD. Reevaluatie na vier cycli: VGPR, later CR.stamcelaferese (na G-CSF stimulatie only, zonder cyclofosfamide): 4.2 x 10*6/kg in 4 fracties.Ziektestatus voor transplantatie: complete remissie28/3/2019: autologe stamceltransplantatie (MEL 140mg/m²) (2.1x10*6/kg CD34+ stamcellen)
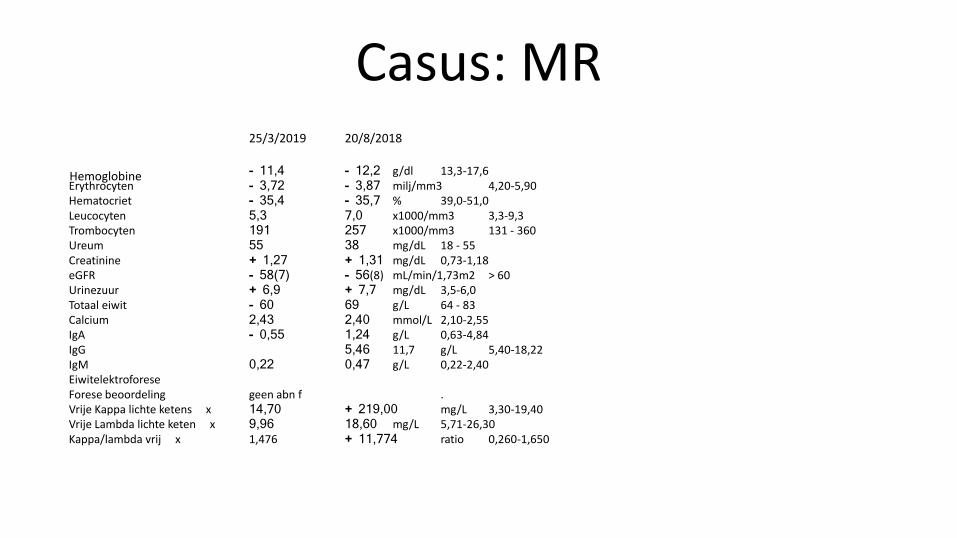
Casus: MR25/3/2019 20/8/2018
Hemoglobine - 11,4 - 12,2 g/dl 13,3-17,6Erythrocyten - 3,72 - 3,87 milj/mm3 4,20-5,90Hematocriet - 35,4 - 35,7 % 39,0-51,0Leucocyten 5,3 7,0 x1000/mm3 3,3-9,3Trombocyten 191 257 x1000/mm3 131 - 360Ureum 55 38 mg/dL 18 - 55Creatinine + 1,27 + 1,31 mg/dL 0,73-1,18eGFR - 58(7) - 56(8) mL/min/1,73m2 > 60Urinezuur + 6,9 + 7,7 mg/dL 3,5-6,0Totaal eiwit - 60 69 g/L 64 - 83Calcium 2,43 2,40 mmol/L 2,10-2,55IgA - 0,55 1,24 g/L 0,63-4,84IgG 5,46 11,7 g/L 5,40-18,22IgM 0,22 0,47 g/L 0,22-2,40EiwitelektroforeseForese beoordeling geen abn f . Vrije Kappa lichte ketens x 14,70 + 219,00 mg/L 3,30-19,40Vrije Lambda lichte keten x 9,96 18,60 mg/L 5,71-26,30Kappa/lambda vrij x 1,476 + 11,774 ratio 0,260-1,650
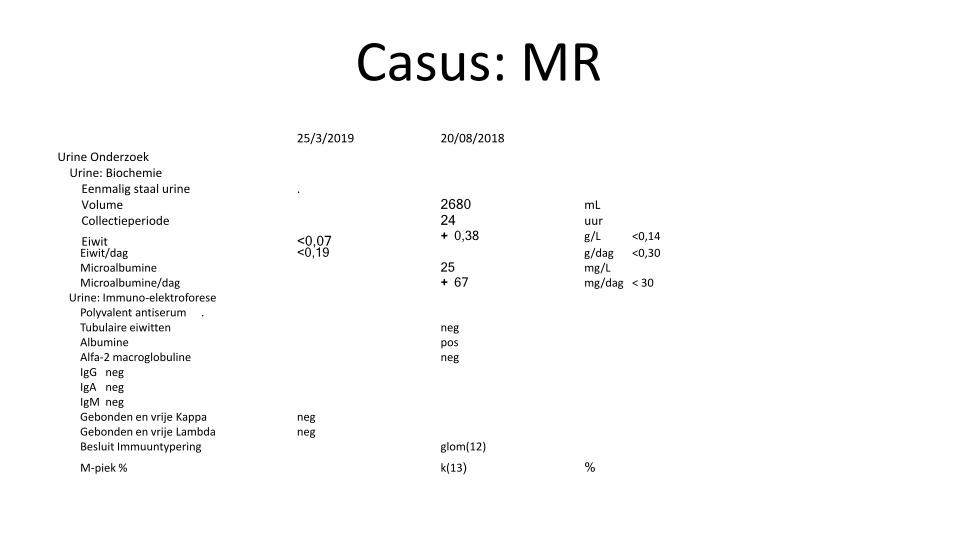
Casus: MR25/3/2019 20/08/2018
Urine OnderzoekUrine: Biochemie
Eenmalig staal urine .Volume 2680 mLCollectieperiode 24 uur
Eiwit <0,07 + 0,38 g/L <0,14
Eiwit/dag <0,19 g/dag <0,30Microalbumine 25 mg/LMicroalbumine/dag + 67 mg/dag < 30
Urine: Immuno-elektroforesePolyvalent antiserum .Tubulaire eiwitten negAlbumine posAlfa-2 macroglobuline negIgG negIgA negIgM negGebonden en vrije Kappa negGebonden en vrije Lambda negBesluit Immuuntypering glom(12)
M-piek % k(13) %
&Smoldering Myeloma
• Asymptomatische staat tussen MGUS en myeloma.
• Risico op evolutie naar myeloma: 10%/jaar.
• Biologisch heterogeen: low risk <> ultra high risk.
• Effect van type Ig, hoogte Ig, aanwezigheid light chains in
urine of K/L, # beenmergplasmacellen, focaal botletsel
(MRI), cytogenetica
&Smoldering Myeloma
< 3 g/dL serum
AND
< 10%
AND
Absent
Monoclonal
Gammopathy of
uncertain significance
(MGUS)
Present(serum/urine)
AND
> 10%
AND
Present
Multiple
Myeloma
3 g/dL serum
AND/OR
10-60%
AND
Absent
Smoldering
Multiple
Myeloma
(SMM)
Monoclonal
component
Bone Marrow
Plasma Cells (%)
Myeloma defining-event
MGUS/SMM/MM: diagnostic criteria
Rajkumar SV. Lancet Oncology 2014
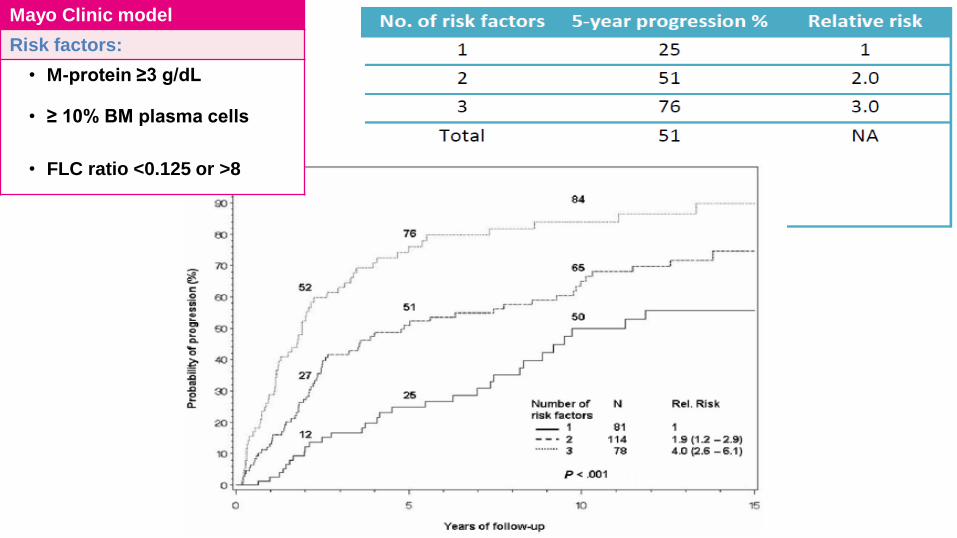
Mayo Clinic model
Risk factors:
• M-protein ≥3 g/dL
• ≥ 10% BM plasma cells
• FLC ratio <0.125 or >8
1. Rajkumar SV et al. N Engl J Med 2011; 365:474-475
2. Kastritis E, et al. Leukemia. 2013 Apr;27(4):947-53
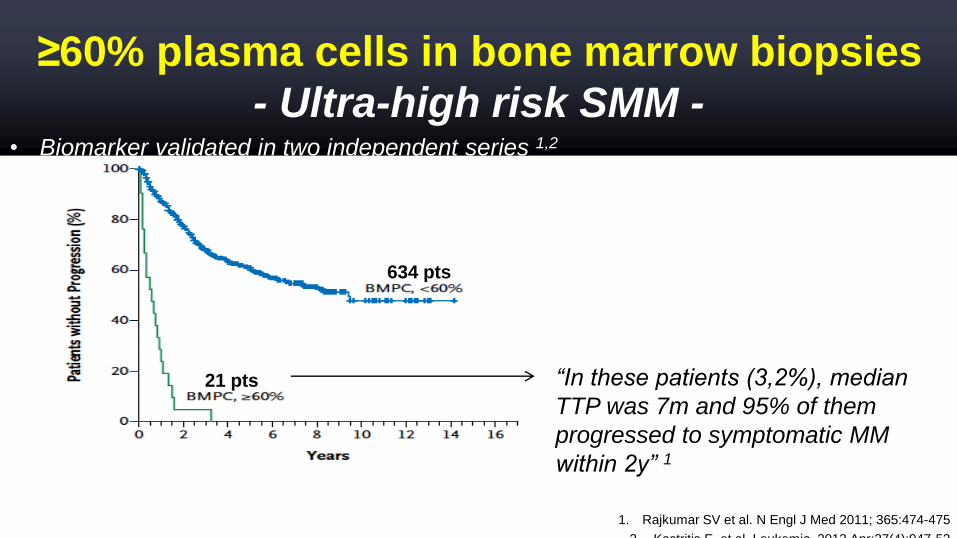
≥60% plasma cells in bone marrow biopsies
- Ultra-high risk SMM -
21 pts
634 pts
“In these patients (3,2%), median
TTP was 7m and 95% of them
progressed to symptomatic MM
within 2y” 1
• Biomarker validated in two independent series 1,2
1. Rajkumar SV et al. N Engl J Med 2011; 365:474-475
2. Kastritis E, et al. Leukemia. 2013 Apr;27(4):947-53
3. Waxman AJ, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 8607)
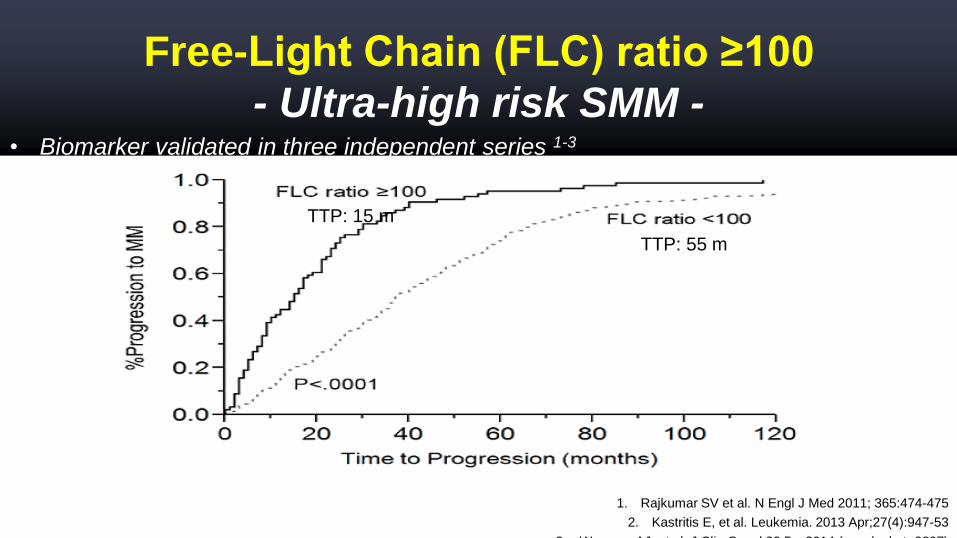
Free-Light Chain (FLC) ratio ≥100
- Ultra-high risk SMM -
TTP: 55 m
TTP: 15 m
• Biomarker validated in three independent series 1-3
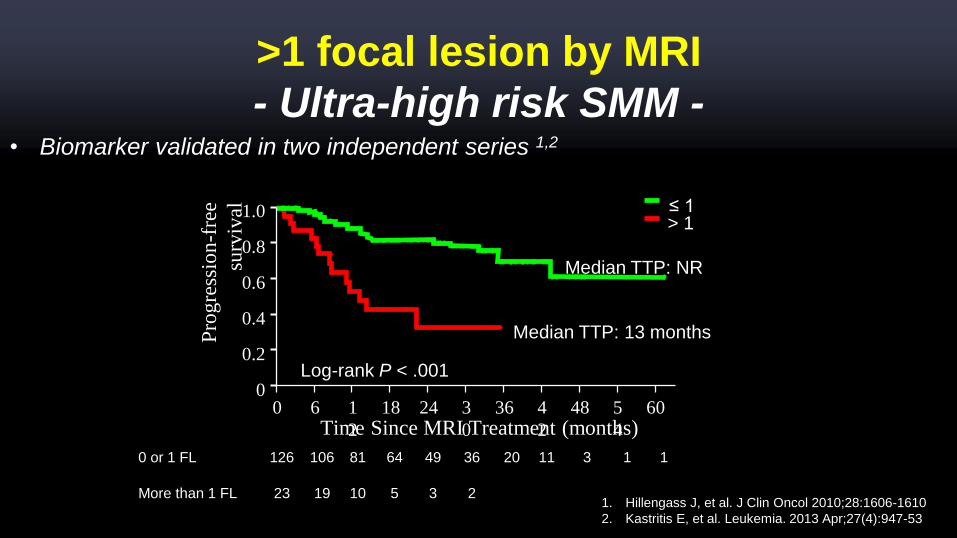
Median TTP: 13 m
Median TTP: NR
1. Hillengass J, et al. J Clin Oncol 2010;28:1606-1610
2. Kastritis E, et al. Leukemia. 2013 Apr;27(4):947-53
Median TTP: 13 months
Median TTP: NR
Pro
gre
ssio
n-f
ree
surv
ival
Time Since MRI Treatment (months)
1.0
60 181
2
3
0
24 4
2
36 5
4
48 60
0.8
0.6
0.4
0.2
0
> 1
Log-rank P < .001
0 or 1 FL 126 106 81 64 49 36 20 11 3 1 1
More than 1 FL 23 19 10 5 3 2
≤ 1
• Biomarker validated in two independent series 1,2
>1 focal lesion by MRI
- Ultra-high risk SMM -
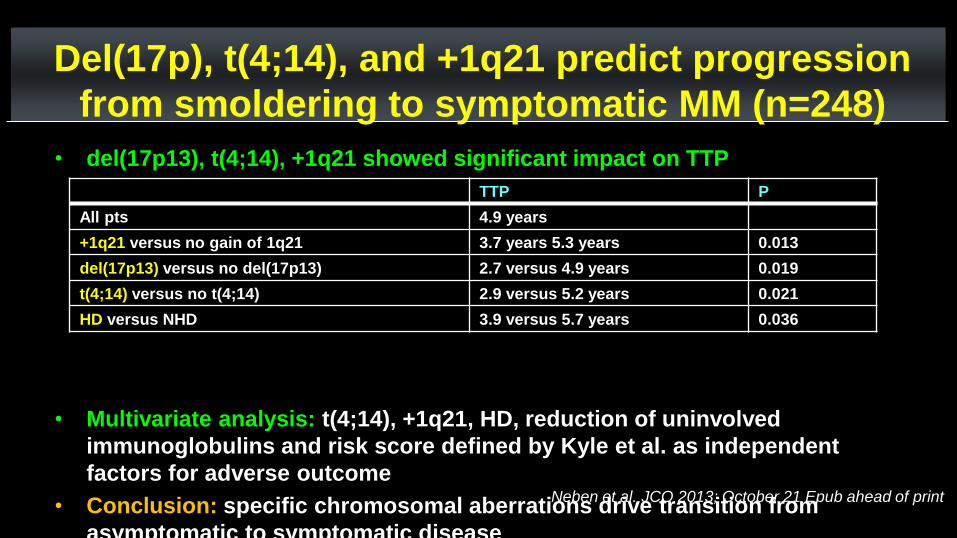
• del(17p13), t(4;14), +1q21 showed significant impact on TTP
• Multivariate analysis: t(4;14), +1q21, HD, reduction of uninvolved
immunoglobulins and risk score defined by Kyle et al. as independent
factors for adverse outcome
• Conclusion: specific chromosomal aberrations drive transition from
asymptomatic to symptomatic disease
TTP P
All pts 4.9 years
+1q21 versus no gain of 1q21 3.7 years 5.3 years 0.013
del(17p13) versus no del(17p13) 2.7 versus 4.9 years 0.019
t(4;14) versus no t(4;14) 2.9 versus 5.2 years 0.021
HD versus NHD 3.9 versus 5.7 years 0.036
Del(17p), t(4;14), and +1q21 predict progression
from smoldering to symptomatic MM (n=248)
Neben et al. JCO 2013; October 21 Epub ahead of print

Gene Expression Profiling of purified CD138+
tumor cells in SMM (n: 105)
Dhodapkar MV et al. Blood 2013
Khan RC et al. Haematologica 2015
The validated 70-gene model (GEP-70) identified SMM patients with GEP70>-0.26 with a 51% of
progression risk at 2 yrs.
A gene signature derived from 4 genes at an optimal binary cut-point of 9.28, identified 14
patients (13%) with a 2-year therapy risk of 85.7%
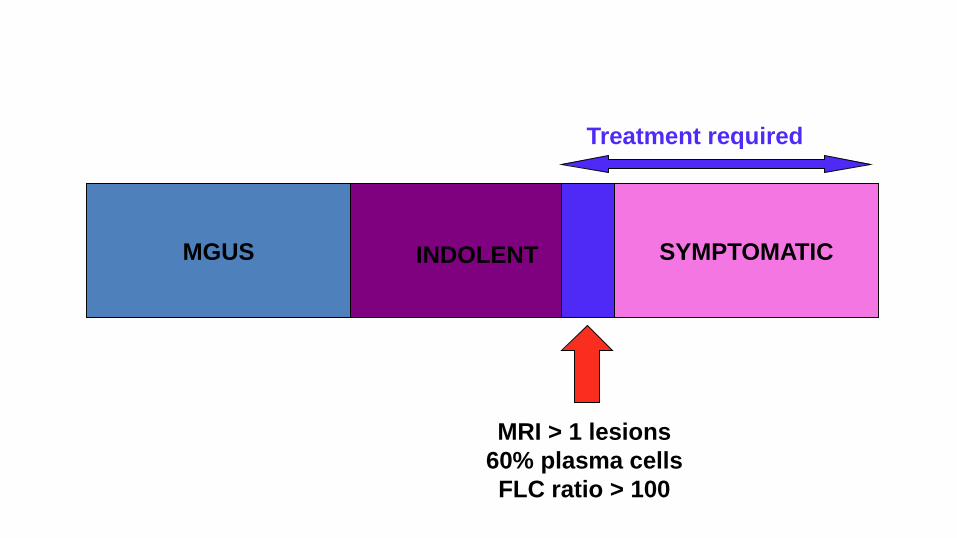
MGUS SYMPTOMATICINDOLENT
MRI > 1 lesions
60% plasma cells
FLC ratio > 100
Treatment required
N Engl J Med 369;5 august 1, 2013
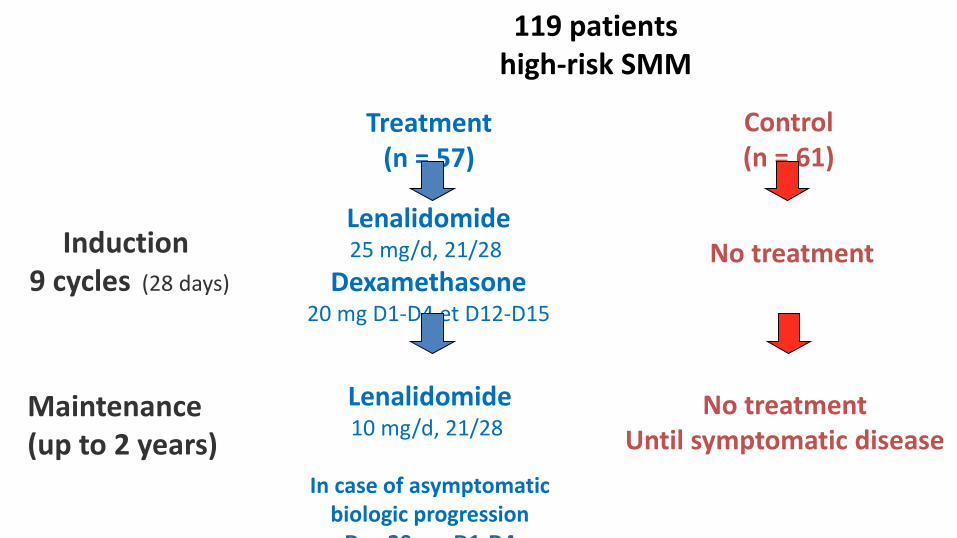
Lenalidomide25 mg/d, 21/28
Dexamethasone20 mg D1-D4 et D12-D15
No treatmentInduction 9 cycles (28 days)
Maintenance(up to 2 years)
Lenalidomide10 mg/d, 21/28
In case of asymptomaticbiologic progression
Dex 20 mg D1-D4
No treatmentUntil symptomatic disease
Treatment(n = 57)
Control(n = 61)
119 patientshigh-risk SMM

Smoldering Multiple MyelomaSmoldering MM
Stratification according tothe risk of progression
Low/Intermediate risk
Follow-up as MGUS
Ultra high risk
Multiple Myeloma
High risk
Close follow-upCandidates to clinical
trials to better know thedisease
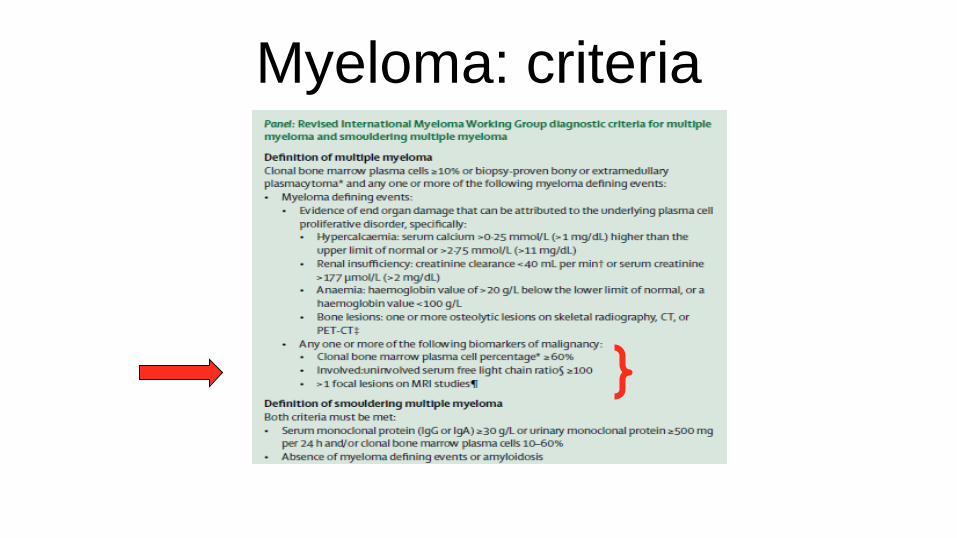
Myeloma: criteria
&Take home message
• Paraproteïne verdient een kritische blik.
• MGUS opvolging: denk aan de urine!
• MGRS vereist een onmiddellijke actie.
• Smoldering myeloma met hoogrisico-kenmerken: te
beschouwen als myeloma en onmiddellijk behandelen!










