dr#A.P.A#Beers,#oogarts# … · M#retina:# #astrocytoom,#CHRPE ... Symptoms such as blurred vision,...
59
dr A.P.A Beers, oogarts Ziekenhuis St Jansdal Harderwijk
Transcript of dr#A.P.A#Beers,#oogarts# … · M#retina:# #astrocytoom,#CHRPE ... Symptoms such as blurred vision,...
dr#A.P.A#Beers,#oogarts#Ziekenhuis#St#Jansdal#Harderwijk##
! MSc#Module#Posterior#Segment#and#Eye#Disease#
! 3#dagen#13#onderwerpen#1#examen#
Anatomy#&#Embryology#Investigative#Techniques#
Neoplasia#VitreoMretinal#Disease#
Inherited#Retinal#Dystrophies#Vitreous#&#Choroid#
Infections#Vascular#Disorders#I#and#II#
Maculopathy#Uveitis#and#Systemic#disease#
#Clinical#Management#of#ARMD#Grand#Rounds#Gene#Therapy#
#
Anatomy#&#Embryology#Investigative#Techniques#
Neoplasia)Vitreo-retinal)Disease)
Inherited#Retinal#Dystrophies#Vitreous#&#Choroid#
Infections#Vascular#Disorders#I#and#II#
Maculopathy#Uveitis#and#Systemic#disease#
#Clinical#Management#of#ARMD#Grand#Rounds#Gene#Therapy#
#

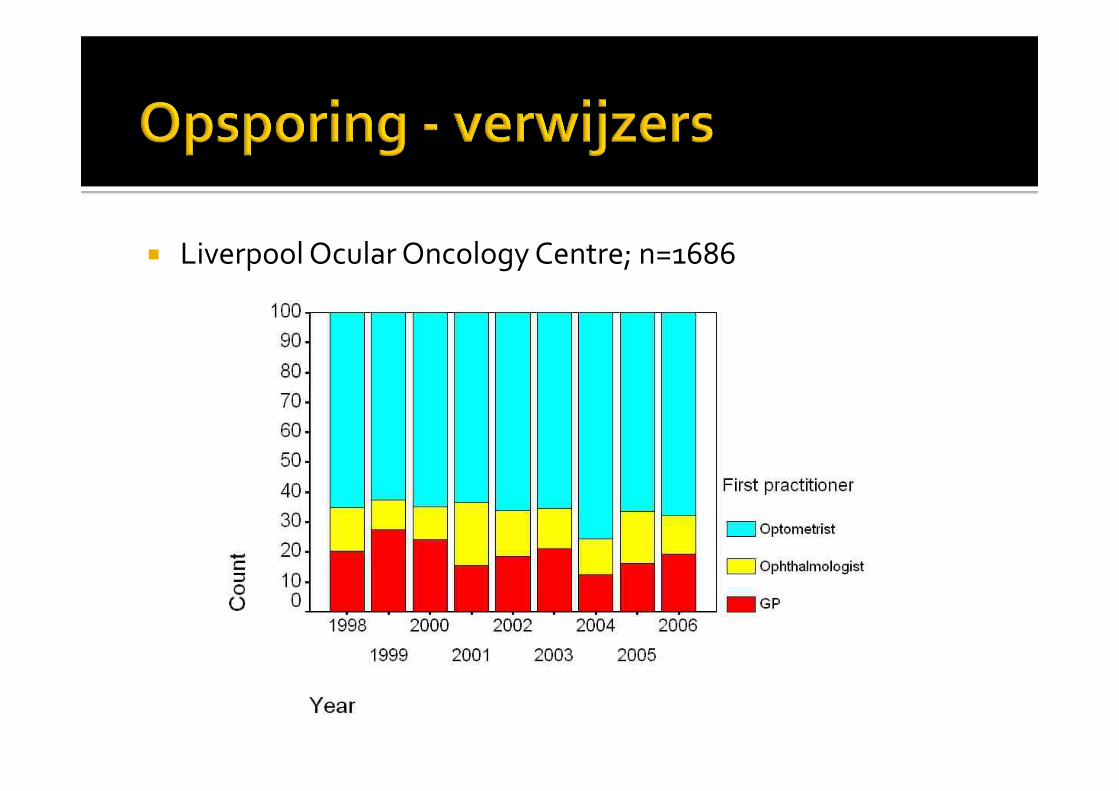
! Liverpool#Ocular#Oncology#Centre;#n=1686#
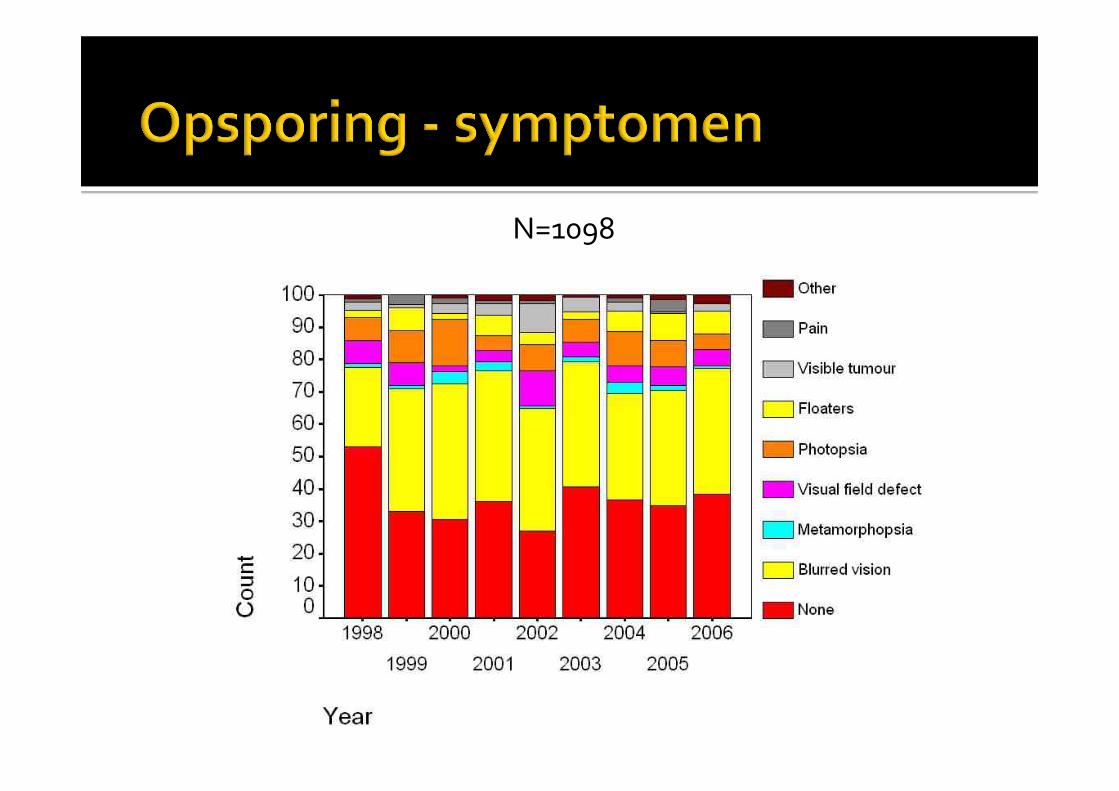
N=1098#
! Benigne)M#chorioidea:#
#naevus,#melanocytoom,#hemangioom,#osteoom#M#retina:#
#astrocytoom,#CHRPE,#angioom,#hemangioblastoom#! Maligne)
M#primair##M#melanoom##M#lymfoom,#adenocarcinoom##M#retinoblastoom,#medulloepithelioom#
M#secundair#
! Benigne#M#chorioidea:#
#naevus,#melanocytoom,#hemangioom,#osteoom#M#retina:#
#astrocytoom,#CHRPE,#angioom,#hemangioblastoom#! Maligne#
M#primair##M#melanoom##M#lymfoom,#adenocarcinoom##M#retinoblastoom,#medulloepithelioom#
M#secundair#

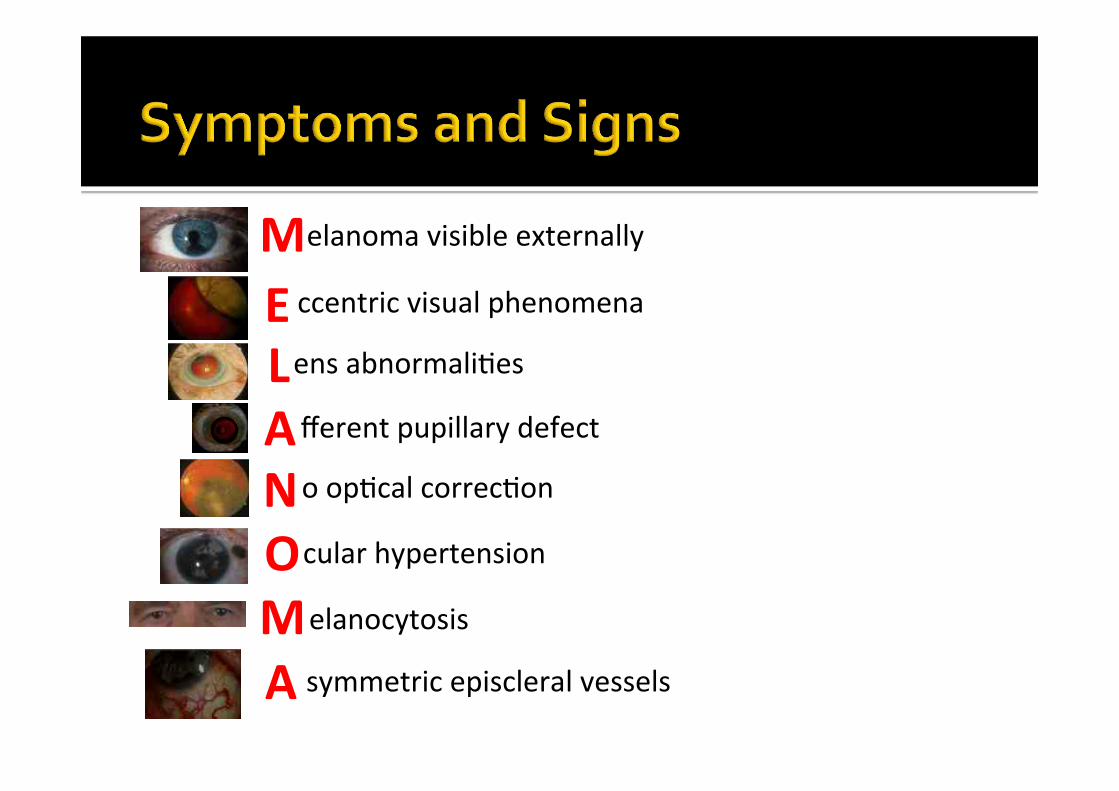
!fferent!pupillary!defect!
!o!op1cal!correc1on!
!cular!hypertension!
!elanocytosis!
!symmetric!episcleral!vessels!
!ens!abnormali1es!
!elanoma!visible!externally!
!ccentric!visual!phenomena!
M"E"L"A"N"O"M"A"
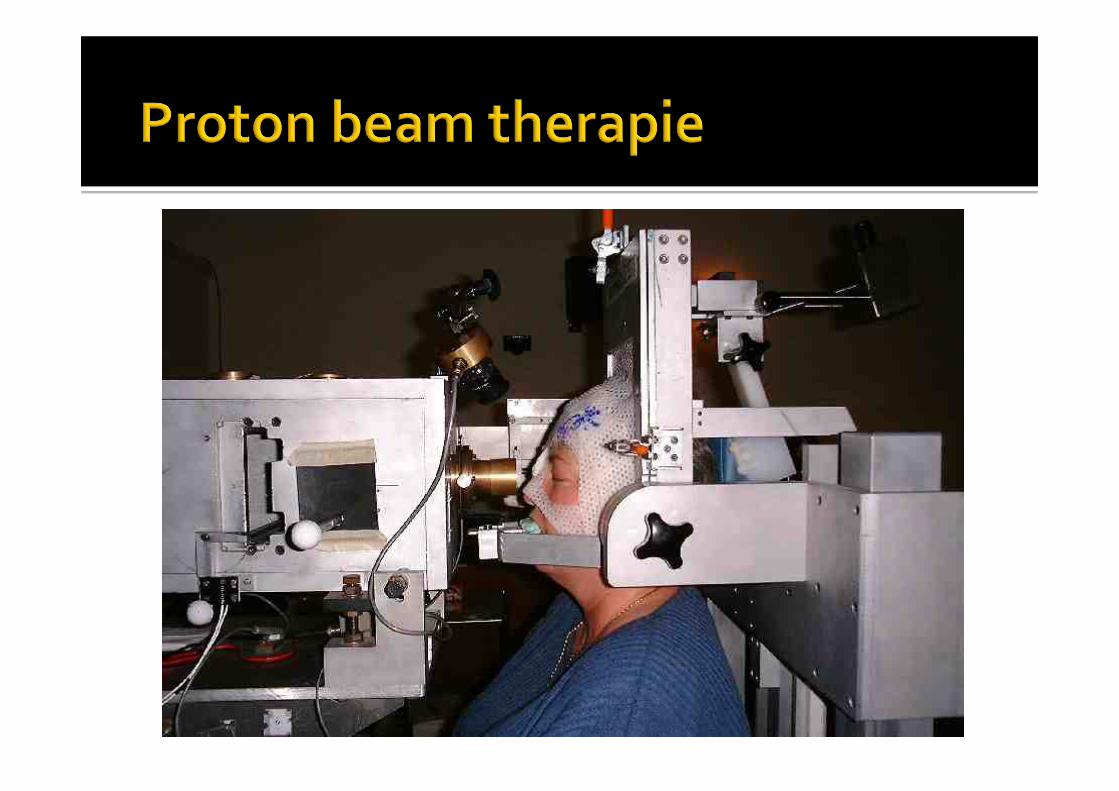
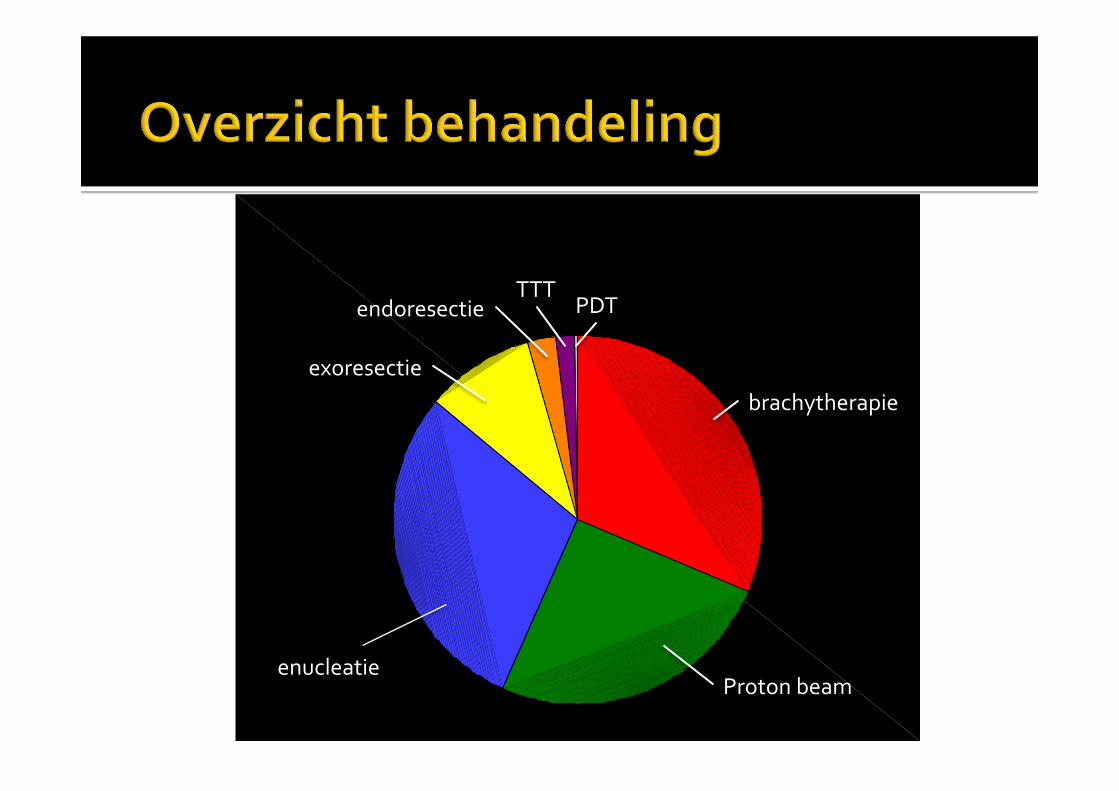
! Observa1e!als!behandeling?!! Radiotherapie:!brachytherapie!! Radiotherapie:!proton!beam!! TTT!! PDT!! Enuclea1e!! Endoresec1e,!lokale!resec1e!
! Avas1n?!
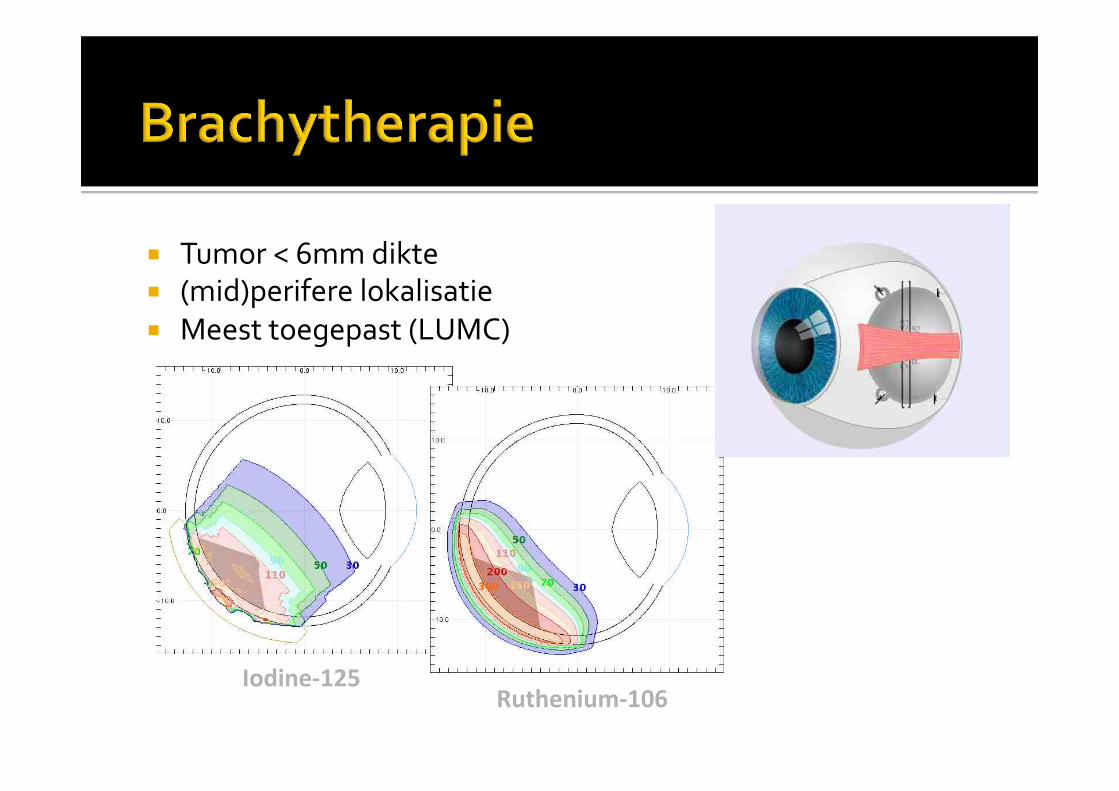
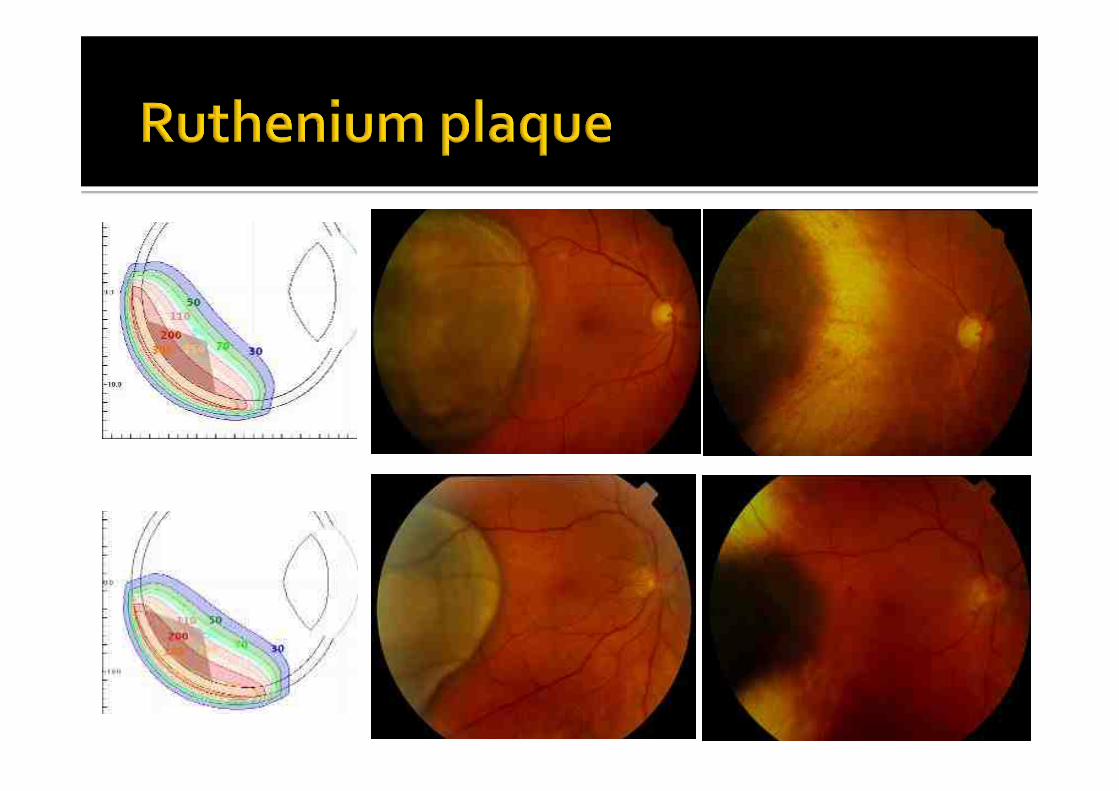
! Tumor#<#6mm#dikte#! (mid)perifere#lokalisatie#! Meest#toegepast#(LUMC)#
Iodine.125"Ruthenium.106"
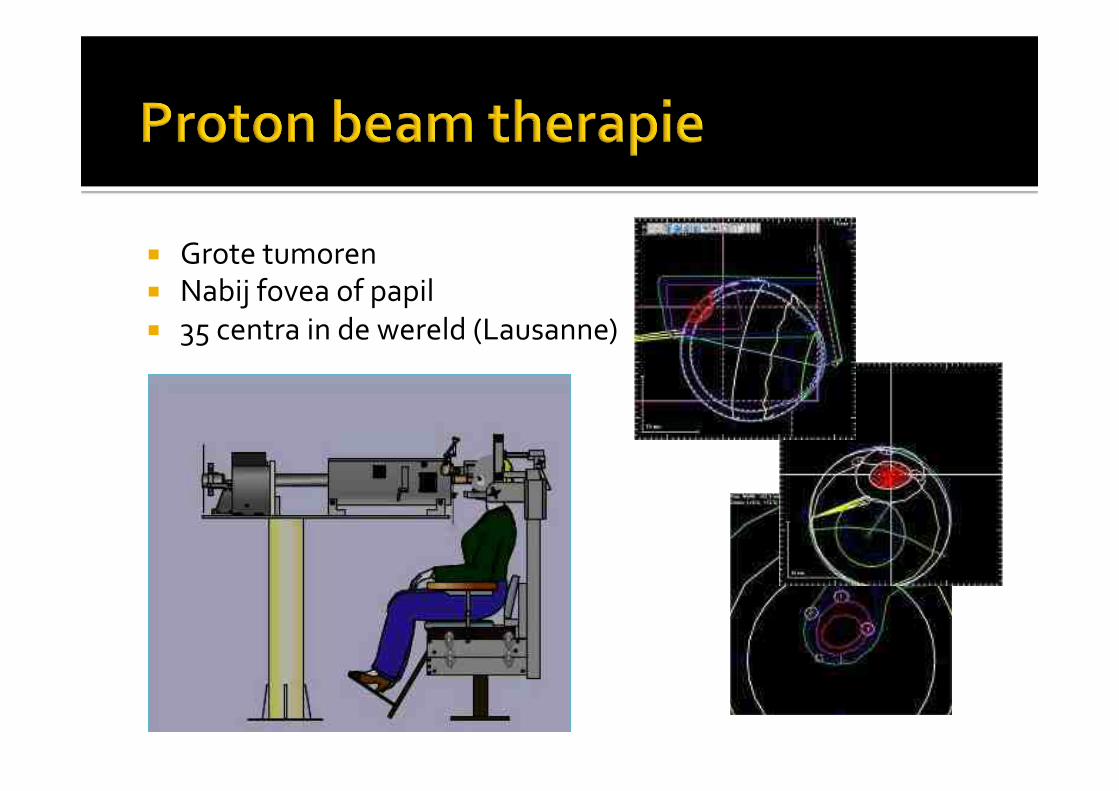
! Grote#tumoren#! Nabij#fovea#of#papil#! 35#centra#in#de#wereld#(Lausanne)#
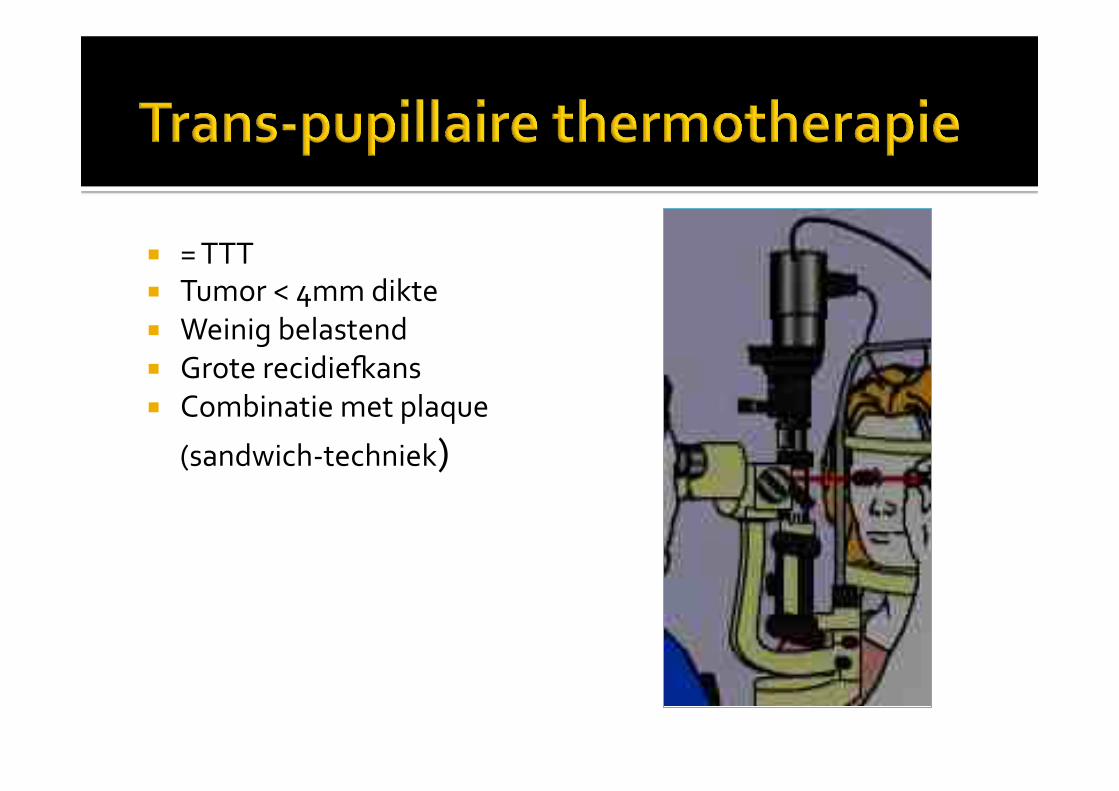
! =#TTT#! Tumor#<#4mm#dikte#! Weinig#belastend#! Grote#recidiebans#! Combinatie#met#plaque#
(sandwichMtechniek)#
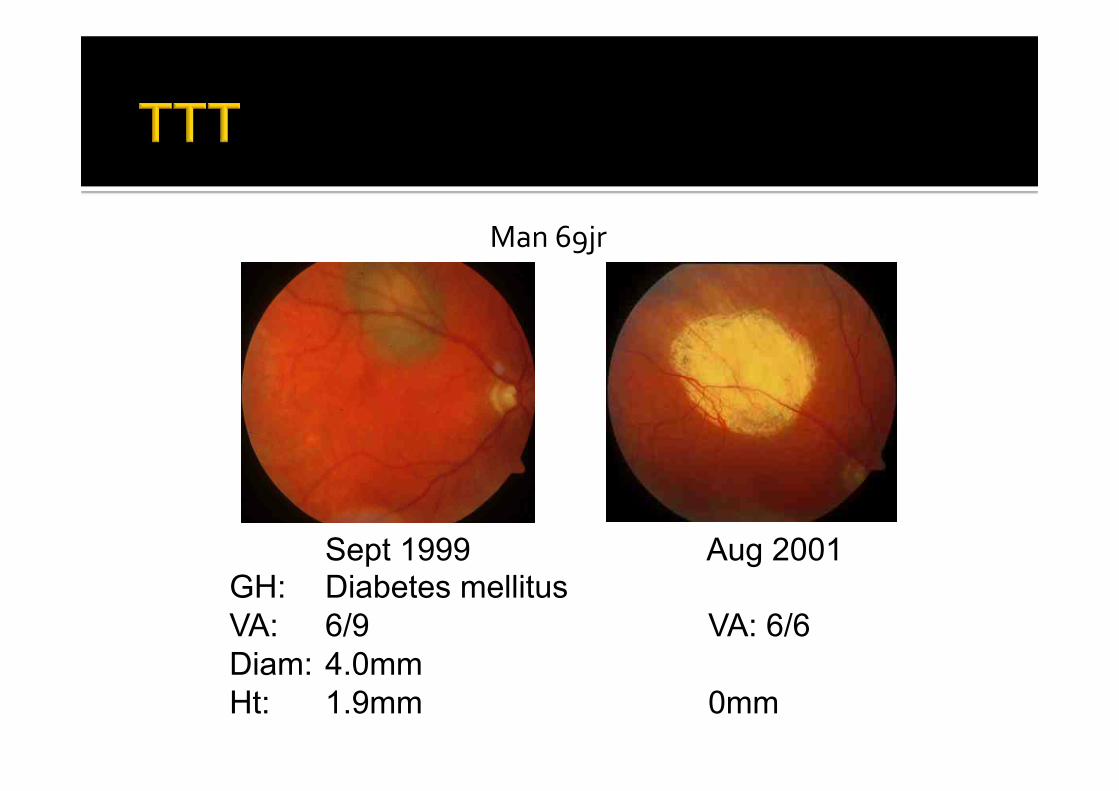
Man#69jr#
Sept 1999 Aug 2001 GH: Diabetes mellitus VA: 6/9 VA: 6/6 Diam: 4.0mm Ht: 1.9mm 0mm
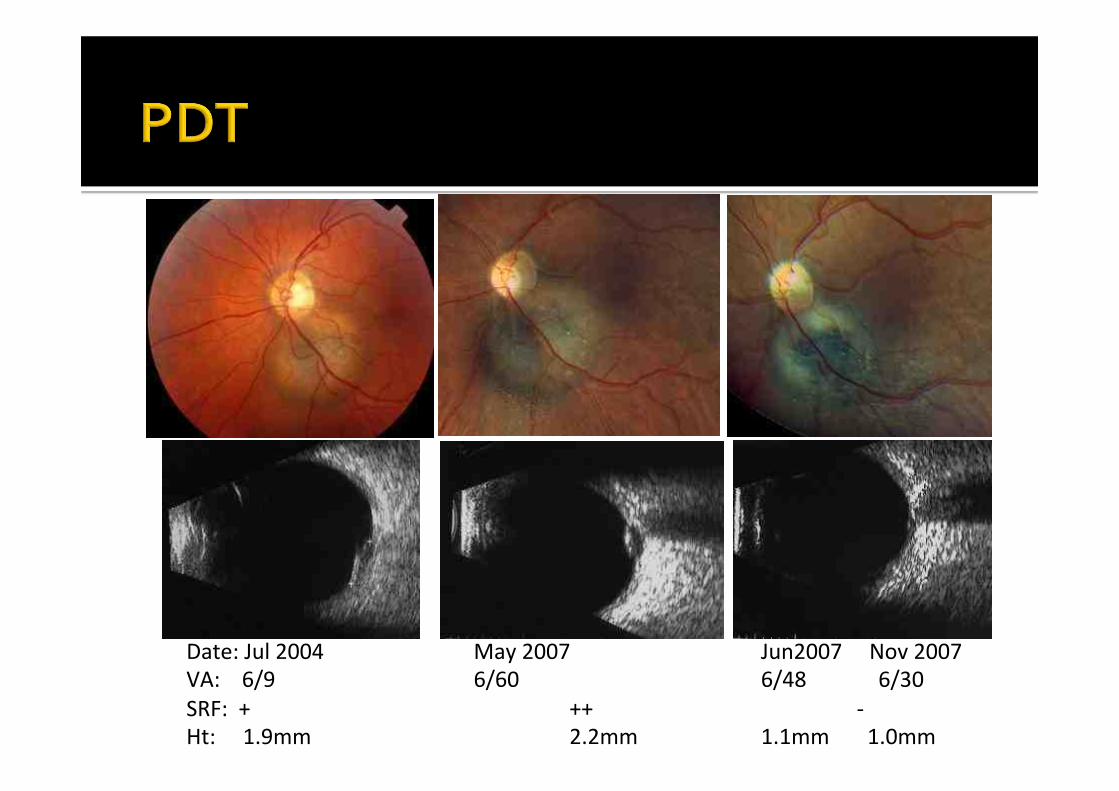
Date:!Jul!2004!!!!!!!!!!!!!!!!!!!!!!!!!!!!May!2007 ! !Jun2007!!!!!Nov!2007!VA:!!!!6/9! ! !6/60 ! ! !6/48 !!!!!6/30!SRF:!!+ ! ! ! !++ ! ! !T!Ht:!!!!!1.9mm ! ! !2.2mm!!!!! !1.1mm!!!!!!!1.0mm!
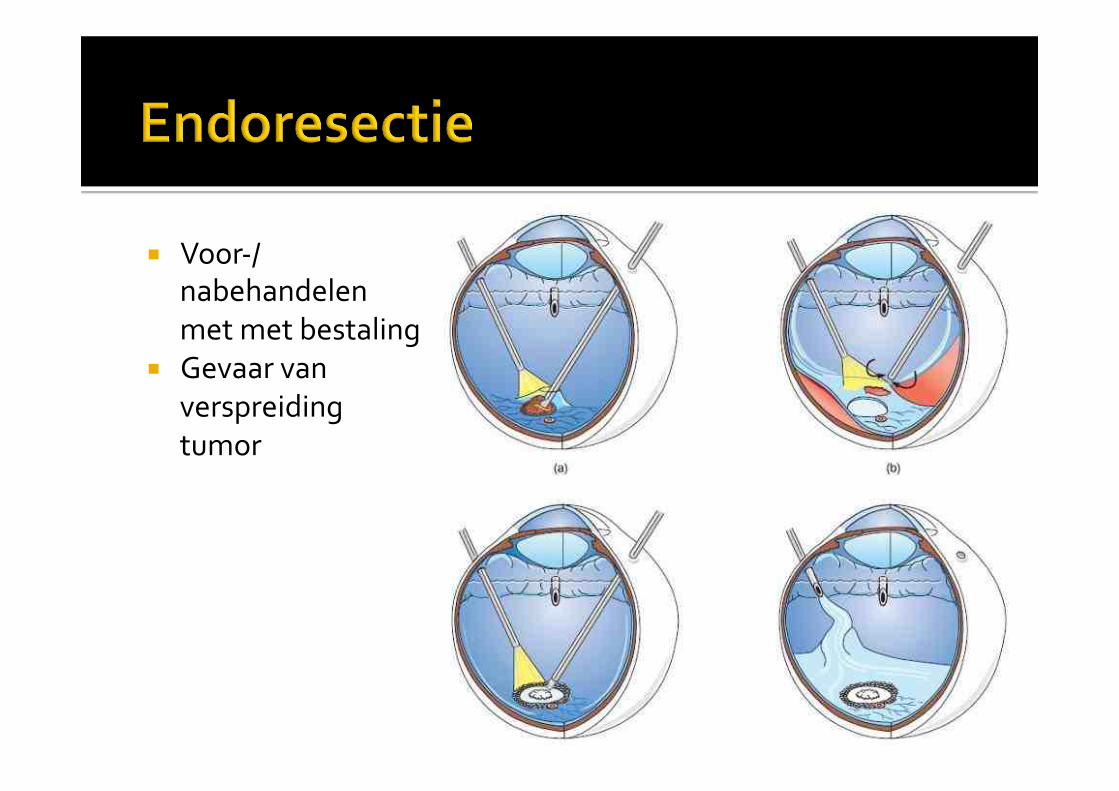
! VoorM/nabehandelen#met#met#bestaling#
! Gevaar#van#verspreiding#tumor#
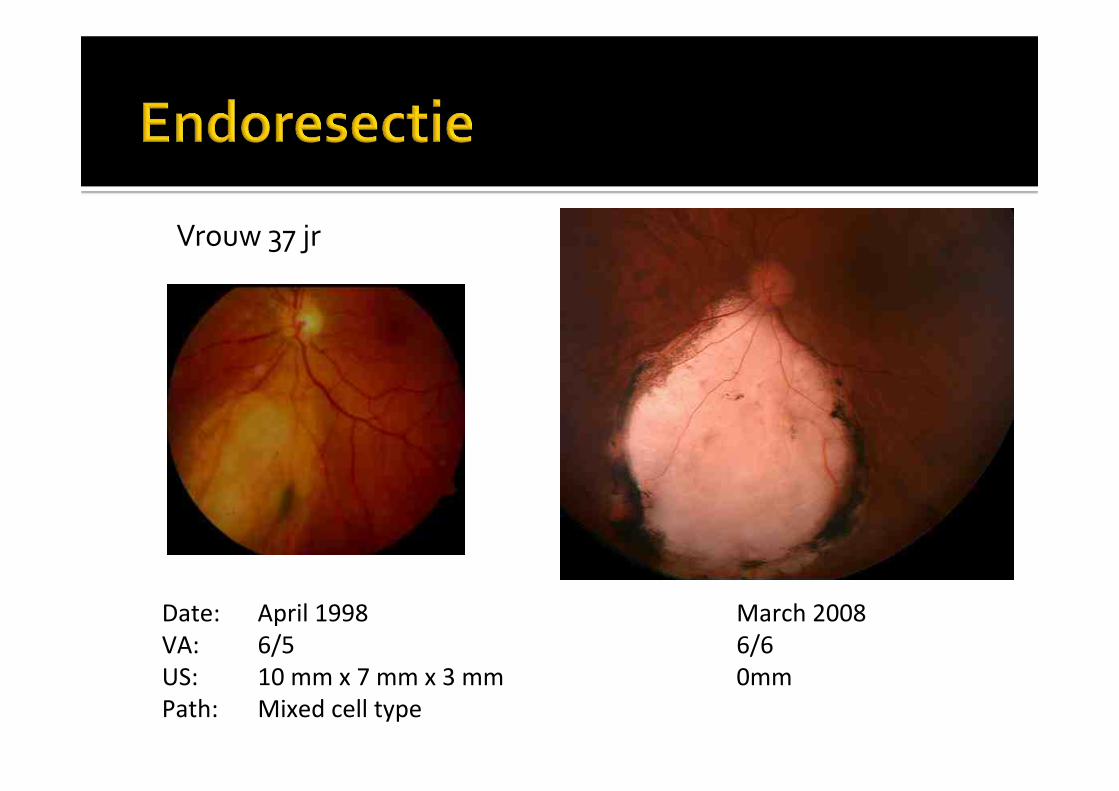
Date: !April!1998 ! ! ! !March!2008!VA: !6/5 ! ! ! ! !6/6!US: !10!mm!x!7!mm!x!3!mm ! ! !0mm!Path: !Mixed!cell!type!
Vrouw#37#jr#
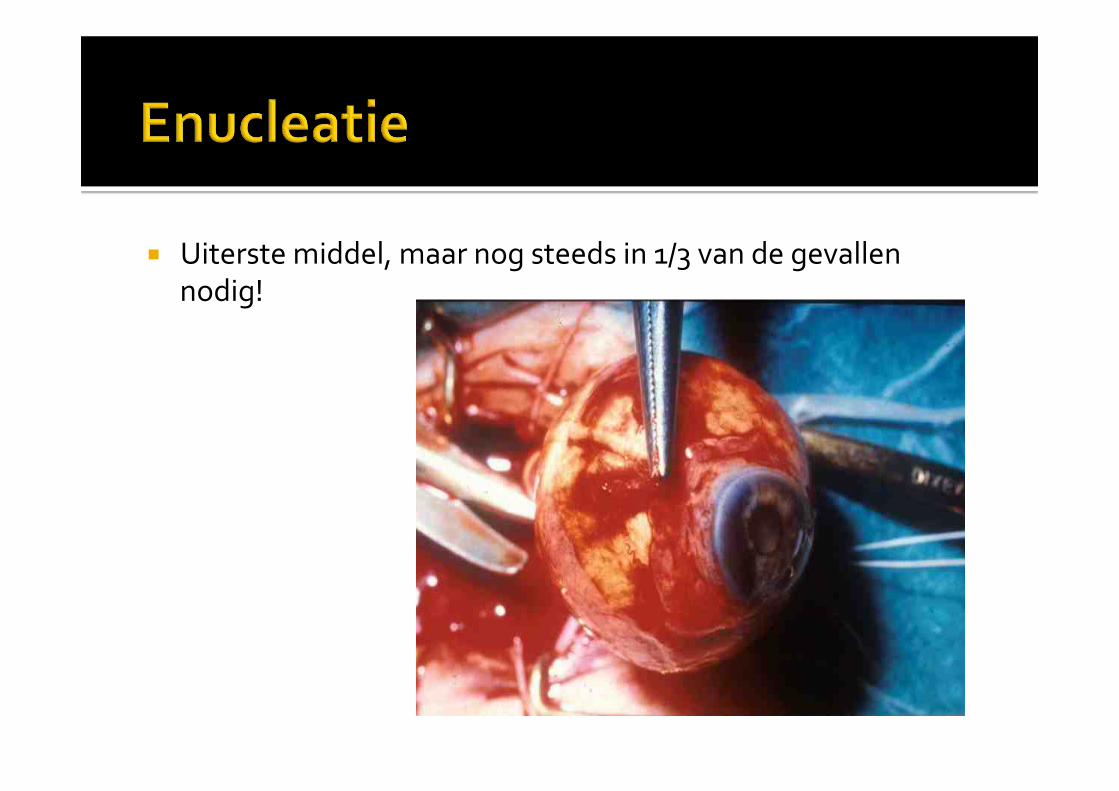
! Uiterste#middel,#maar#nog#steeds#in#1/3#van#de#gevallen#nodig!##
7
6
5
4
3
2
1brachytherapie#
Proton#beam#enucleatie#
exoresectie#
endoresectie#TTT#
PDT#
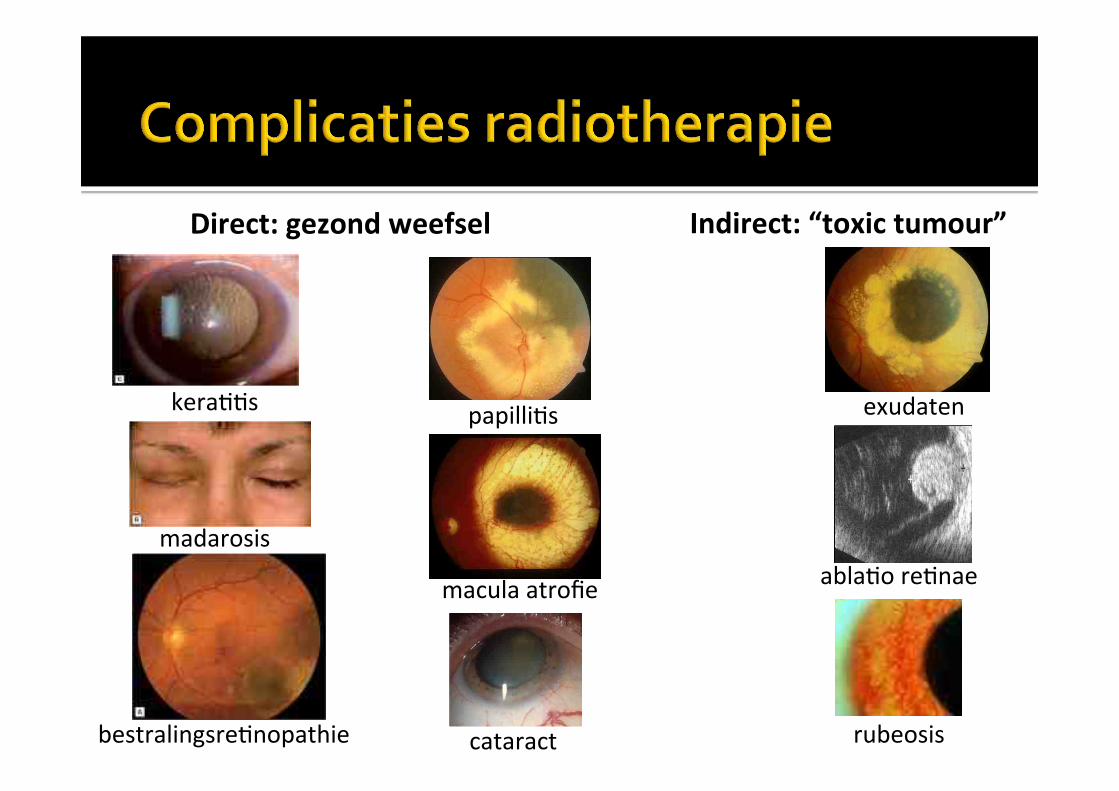
Direct:"gezond"weefselCT" Indirect:"“toxic"tumour”"
papilli1s!
macula!atrofie!
cataract!
exudaten!
abla1o!re1nae!
rubeosis!
kera11s!
madarosis!
bestralingsre1nopathie!
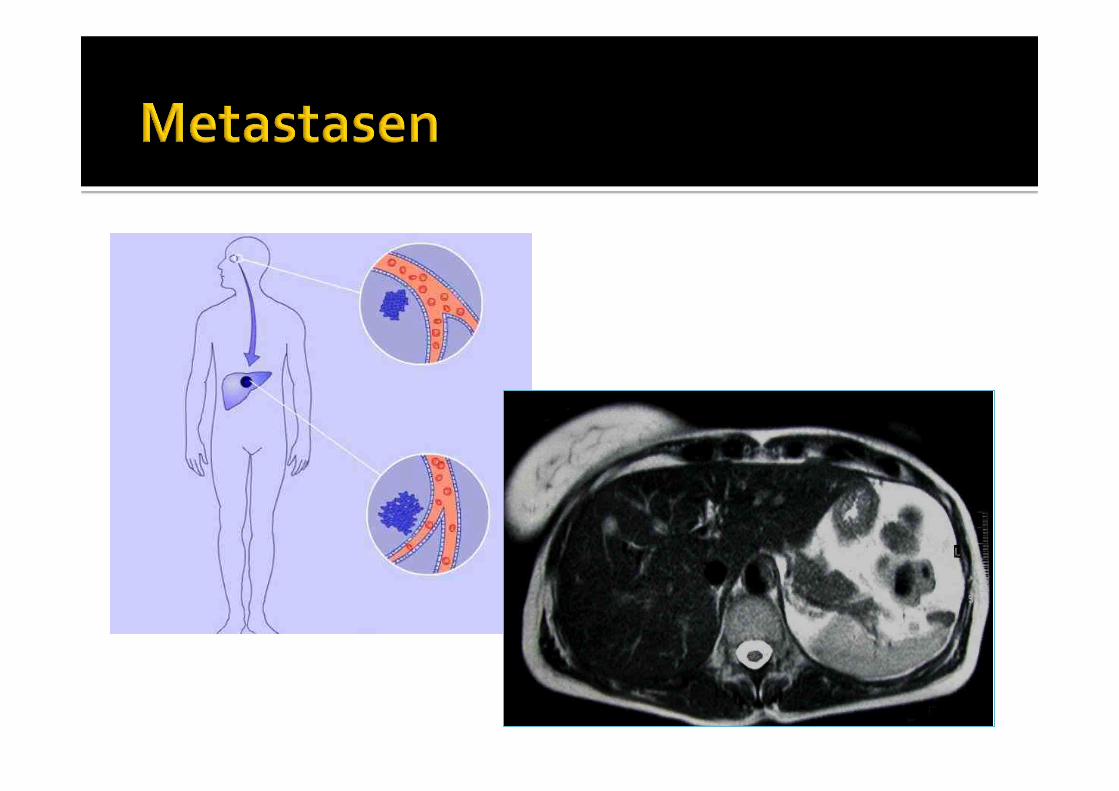

! Partiele#hepatectomie,#hepatectomie#met#transplantatie,#intraMhepatische#chemotherapie#
! Controversieel:#wel#van#belang#voor#de#prognose,#maar#niet/nauwelijks#voor#de#behandeling.#
#! Leverfuncties,#echo#en/of#MRI#bovenbuik#! 6Mmaandelijks#
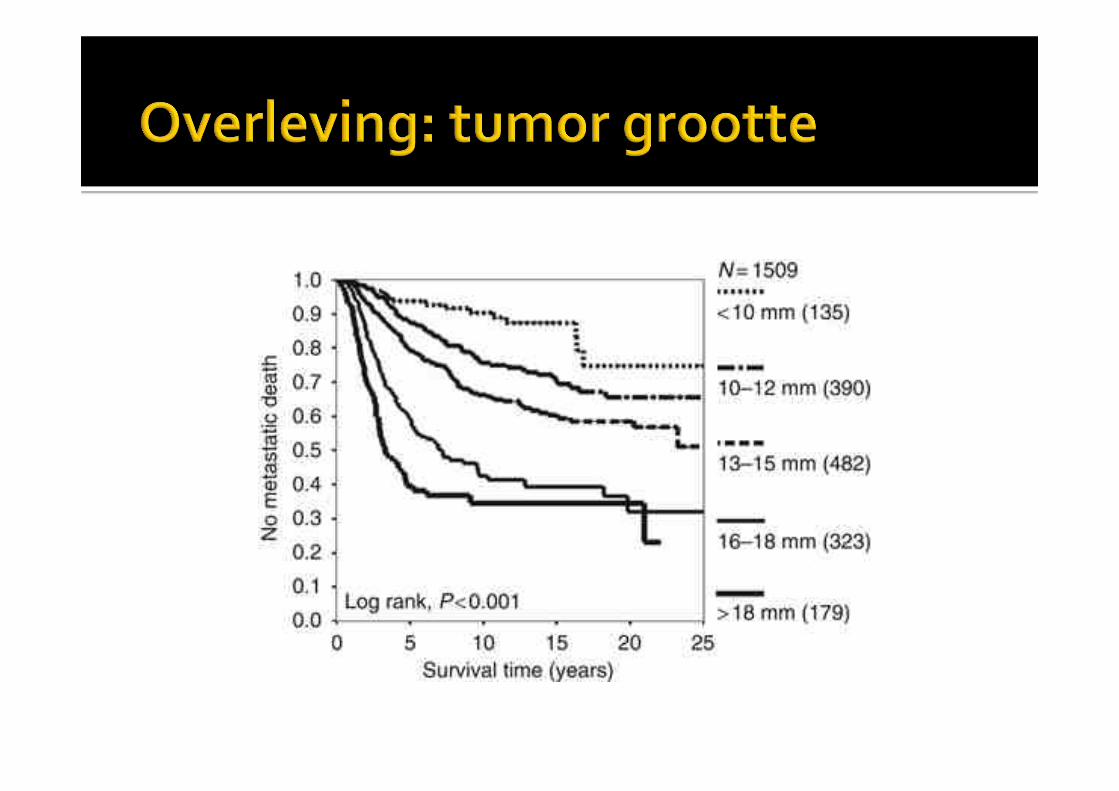
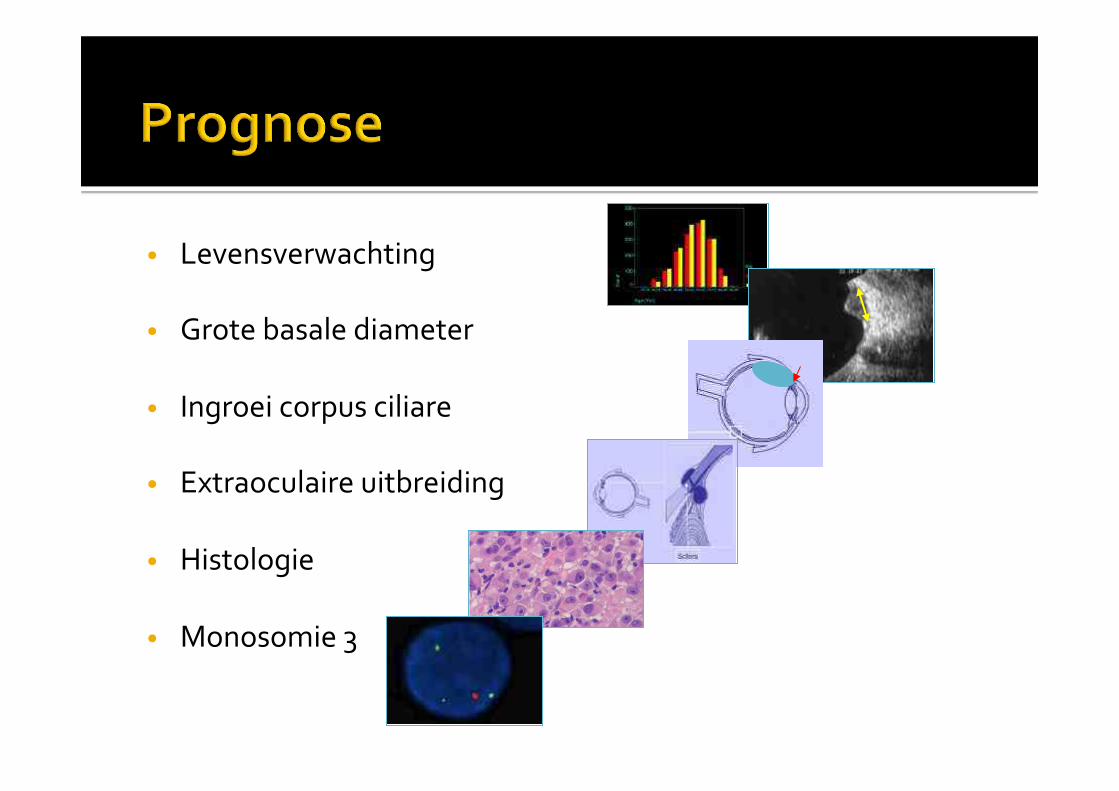
• Levensverwachting#
• Grote#basale#diameter#
• Ingroei#corpus#ciliare#
• Extraoculaire#uitbreiding#
• Histologie#
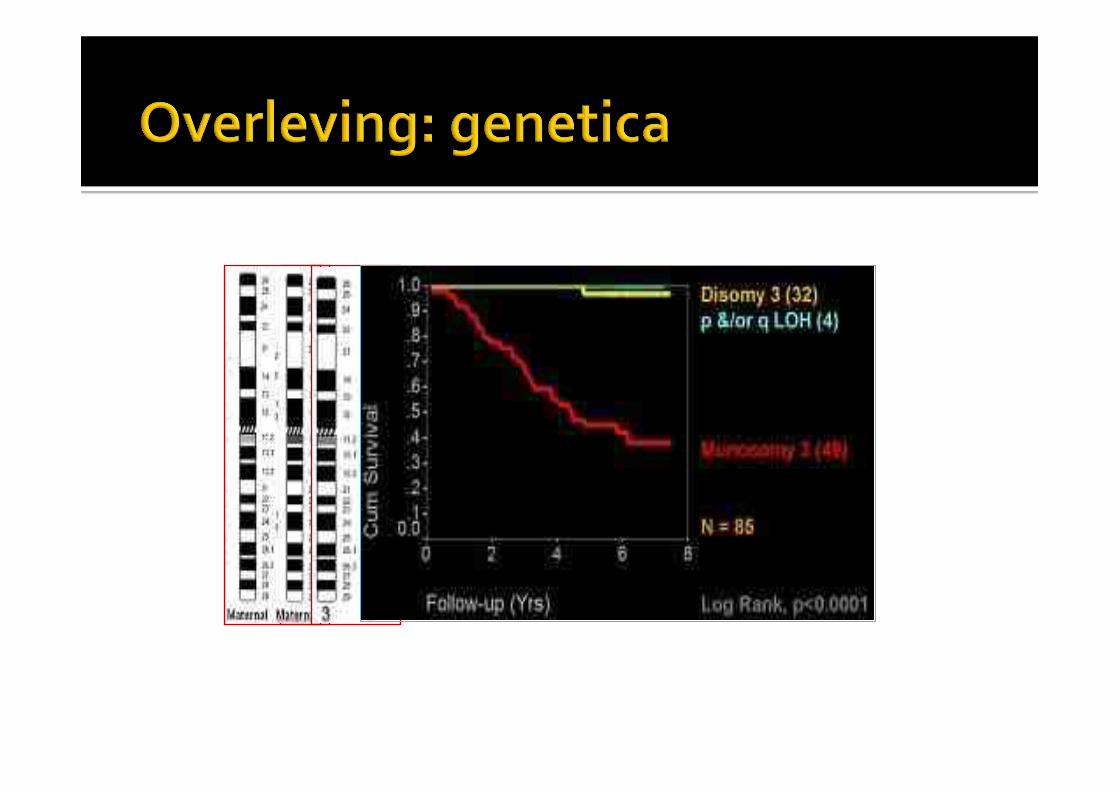
• Monosomie#3##
! 200#chorioidea#melanomen#per#jaar#in#Nederland#! Behandeling#in#een#centrum:#160#per#jaar#in#LUMC#! Informatie#patient#en#familie:#uitleg,#folders,#DVD#! Gespecialiseerde#verpleegkundigen#! Klinisch#psycholoog#
! Chorioidea#naevus#! RPE#laesies#! Metastasen#! Lymfoom#! Vasculaire#tumoren#! Overige,#zeldzame,#afwijkingen#
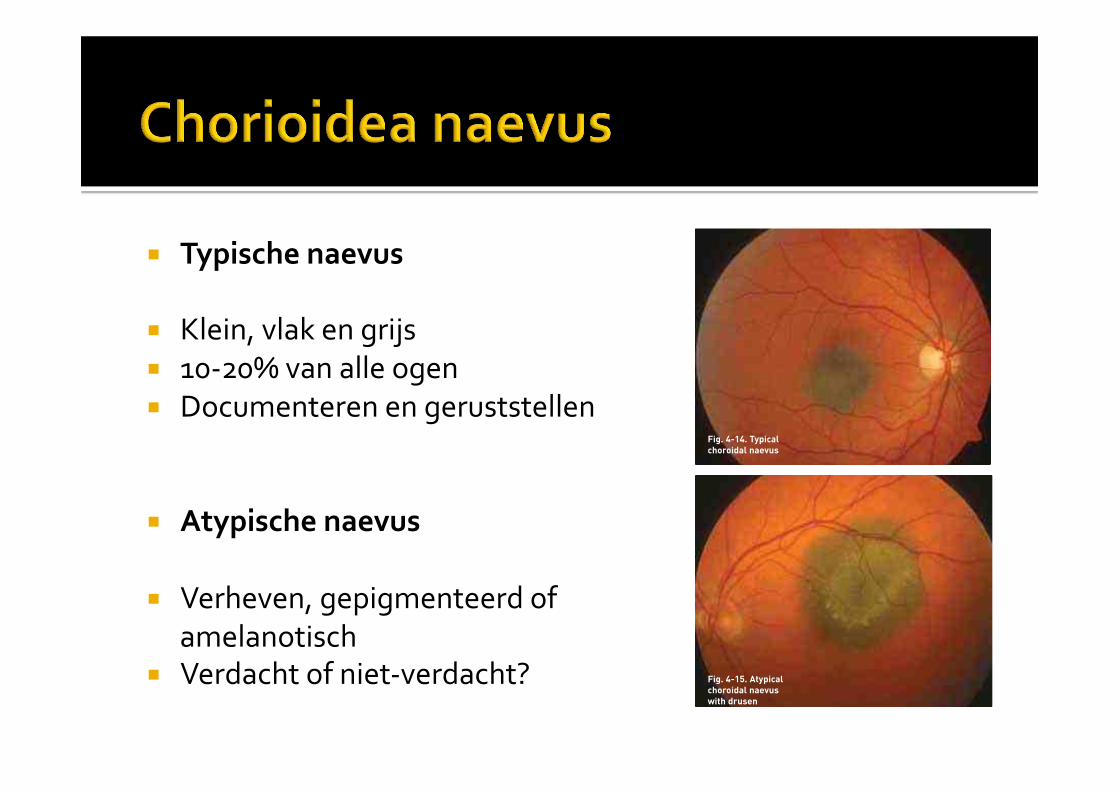
! Typische)naevus)
! Klein,#vlak#en#grijs#! 10M20%#van#alle#ogen#! Documenteren#en#geruststellen#
! Atypische)naevus)
! Verheven,#gepigmenteerd#of##amelanotisch#
! Verdacht#of#nietMverdacht?#
There is a need for adjuvant systemic therapy in high-risk patients, starting this treatment as early aspossible. Possible therapies include systemicchemotherapy, immunotherapy, anti-angiogenicagents and perhaps controversially Cox-2 inhibitors.Large, multicentre, randomised, prospective studiesare required to evaluate the efficacy and safety of suchagents.
CHOROIDAL NAEVUSChoroidal naevi are reported to occur in about 10 to 20percent of the population, with about 90 percentdeveloping posterior to the equator.
We classify pigmented choroidal tumours into twocategories: (a) typical naevi, which are small, flat and
grey; and (b) atypical naevi, which are dome shapedand pigmented or amelanotic. Atypical lesions areeither: (i) non-suspicious; or (ii) suspicious ofmalignancy. Suspicious features are: (a) thicknessgreater than 2 mm; (b) serous retinal detachment; (c)confluent orange pigment; (d) symptoms, such asphotopsia; and (e) contact with optic disc.(Shields et al.1995b)
DiagnosisSymptoms such as blurred vision, metamorphopsiaand photopsia (i.e. a ‘ball of light’) are noted. Binocularindirect ophthalmoscopy is performed, documentingthe clinical features with photography.
ManagementTypical naevusPatients are informed of any typical naevi, withreassurance that these are extremely common andinsignificant. The presence of any naevi is documentedin the casenotes.
Atypical naevusThe diameter of the lesion is documented with colourphotography and, if possible, the thickness ismeasured with ultrasonography, obtainingmeasurements from the internal scleral surface.
Surveillance of the lesion is organised, which shouldbe life-long, with review every four to six months, thenonce a year for a year or two, and then every two years.Comparison of the ophthalmoscopic appearances witha baseline colour photograph greatly enhances the
THE
LIVE
RPO
OL
OCU
LAR
ON
COLO
GYCE
NTR
E
28A GUIDE FOR PRACTITONERS
Fig. 4-14. Typicalchoroidal naevus
Fig. 4-15. Atypicalchoroidal naevuswith drusen
Fig. 4-16. Orange pigment over apigmented choroidal tumour,variously labelled as ‘suspiciousnaevus’, ‘melanoma’ and‘indeterminate melanocytic tumour’
There is a need for adjuvant systemic therapy in high-risk patients, starting this treatment as early aspossible. Possible therapies include systemicchemotherapy, immunotherapy, anti-angiogenicagents and perhaps controversially Cox-2 inhibitors.Large, multicentre, randomised, prospective studiesare required to evaluate the efficacy and safety of suchagents.
CHOROIDAL NAEVUSChoroidal naevi are reported to occur in about 10 to 20percent of the population, with about 90 percentdeveloping posterior to the equator.
We classify pigmented choroidal tumours into twocategories: (a) typical naevi, which are small, flat and
grey; and (b) atypical naevi, which are dome shapedand pigmented or amelanotic. Atypical lesions areeither: (i) non-suspicious; or (ii) suspicious ofmalignancy. Suspicious features are: (a) thicknessgreater than 2 mm; (b) serous retinal detachment; (c)confluent orange pigment; (d) symptoms, such asphotopsia; and (e) contact with optic disc.(Shields et al.1995b)
DiagnosisSymptoms such as blurred vision, metamorphopsiaand photopsia (i.e. a ‘ball of light’) are noted. Binocularindirect ophthalmoscopy is performed, documentingthe clinical features with photography.
ManagementTypical naevusPatients are informed of any typical naevi, withreassurance that these are extremely common andinsignificant. The presence of any naevi is documentedin the casenotes.
Atypical naevusThe diameter of the lesion is documented with colourphotography and, if possible, the thickness ismeasured with ultrasonography, obtainingmeasurements from the internal scleral surface.
Surveillance of the lesion is organised, which shouldbe life-long, with review every four to six months, thenonce a year for a year or two, and then every two years.Comparison of the ophthalmoscopic appearances witha baseline colour photograph greatly enhances the
THE
LIVE
RPO
OL
OCU
LAR
ON
COLO
GYCE
NTR
E
28A GUIDE FOR PRACTITONERS
Fig. 4-14. Typicalchoroidal naevus
Fig. 4-15. Atypicalchoroidal naevuswith drusen
Fig. 4-16. Orange pigment over apigmented choroidal tumour,variously labelled as ‘suspiciousnaevus’, ‘melanoma’ and‘indeterminate melanocytic tumour’
! Verdachte#of#nietMverdachte#atypische#naevus?##
! Niet-verdacht#=#géén#TFSOM#! M#documenteren#met#kleuren#fundusfoto#en#echografie#
M#6Mmaandelijkse#controle#>>#2Mjaarlijks#M#levenslang#
! Verdacht#=#TFSOM#M#keuze:#controleren#of#behandelen#M#risico#op#maligniteit?#kuur#erger#dan#de#kwaal?#levensverwachting?#
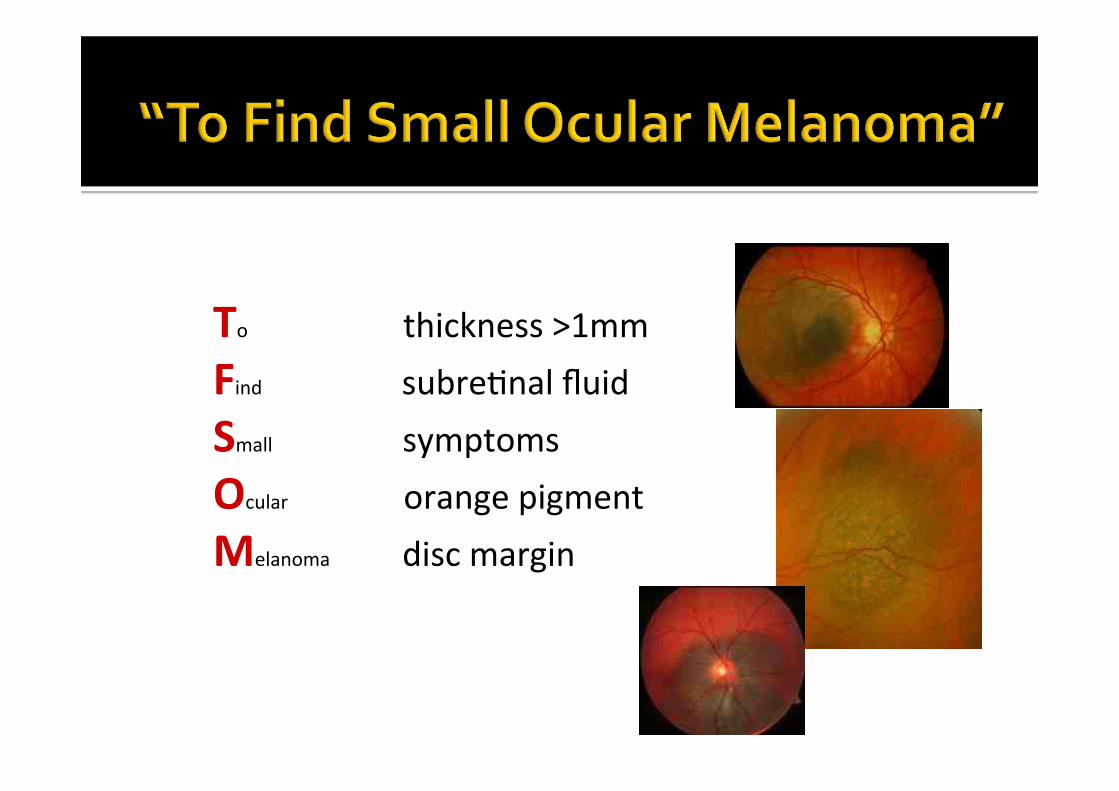
To!!"""""""""""""thickness!>1mm"Find!!!!!!!!!!!!!!!!!!!!!!!!!!!!!subre1nal!fluid"Small!!!!!!!!!!!!!!!!!!!!!!!!!!!symptoms!Ocular!!!!!!!!!!!!!!!!!!!!!!!!orange!pigment!Melanoma!!!!!!!!!!!!!!!disc!margin!
! Verdachte#of#nietMverdachte#atypische)naevus?##
! Niet-verdacht#=#géén#TFSOM#! M#documenteren#met#kleuren#fundusfoto#en#echografie#
M#6Mmaandelijkse#controle#>>#2Mjaarlijks#M#levenslang#
! Verdacht#=#TFSOM#M#keuze:#controleren#of#behandelen#M#risico#op#maligniteit?#kuur#erger#dan#de#kwaal?#levensverwachting?#

! Congenitale#hypertrofie#van#het#RPE#
! Vlak#! Zwart#of#bruin#! Scherp#begrensd#! Atrofische#lacunae#! Solitair#of#gegroepeerd:#1%#bevolking#
! Atypisch:#associatie#met#FPC#en#colonca:#0.001%#
! Maligne#ontaarding#tot#adenocarcinoom:#zeer#zeldzaam#
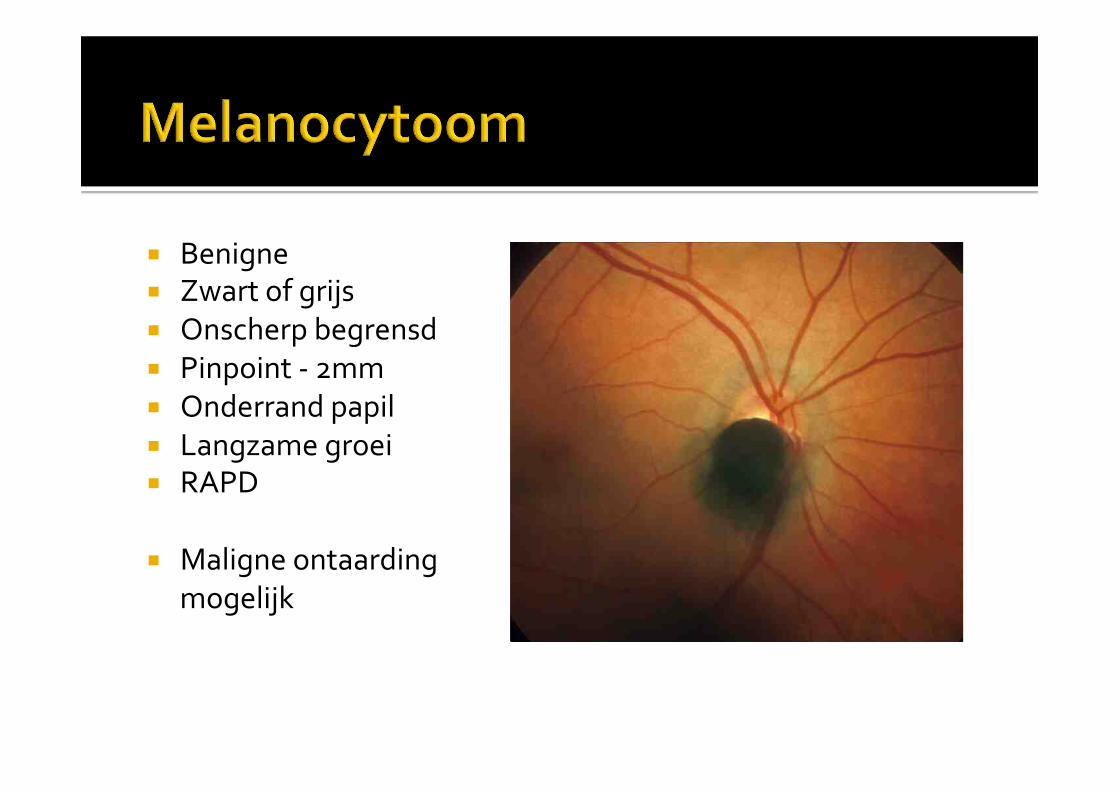
! Benigne#! Zwart#of#grijs#! Onscherp#begrensd#! Pinpoint#M#2mm#! Onderrand#papil#! Langzame#groei#! RAPD#
! Maligne#ontaarding#mogelijk#
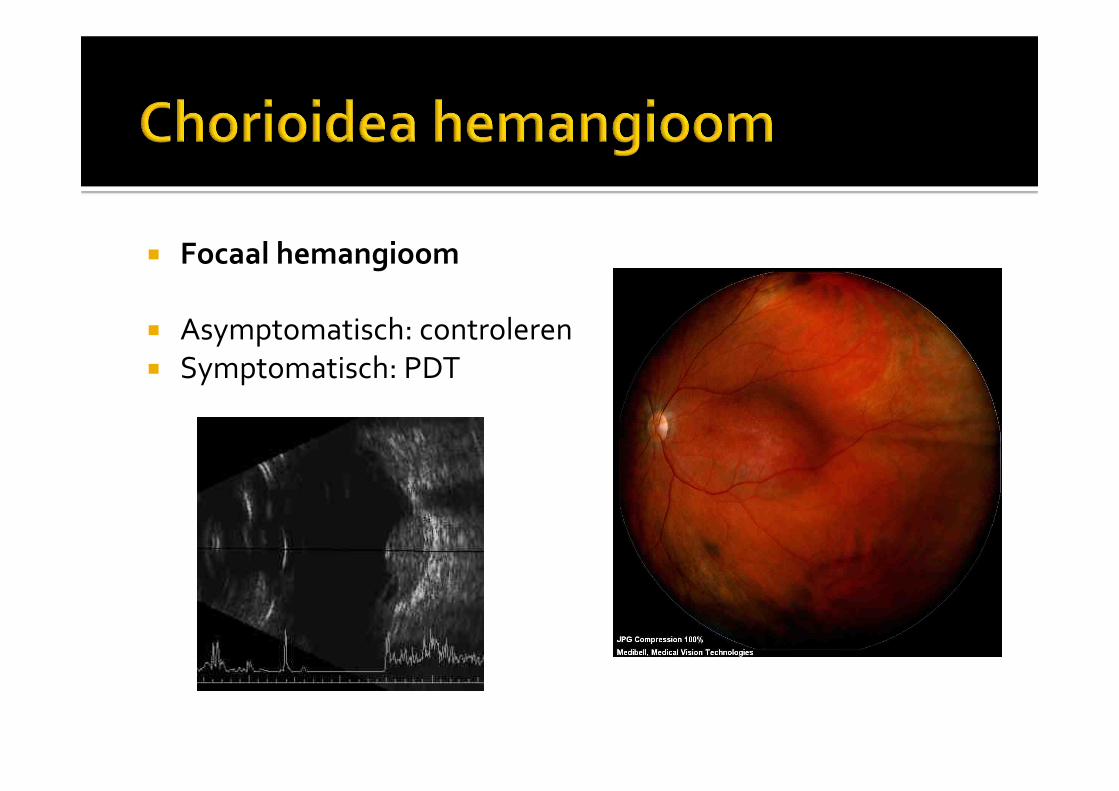
! Focaal)hemangioom)
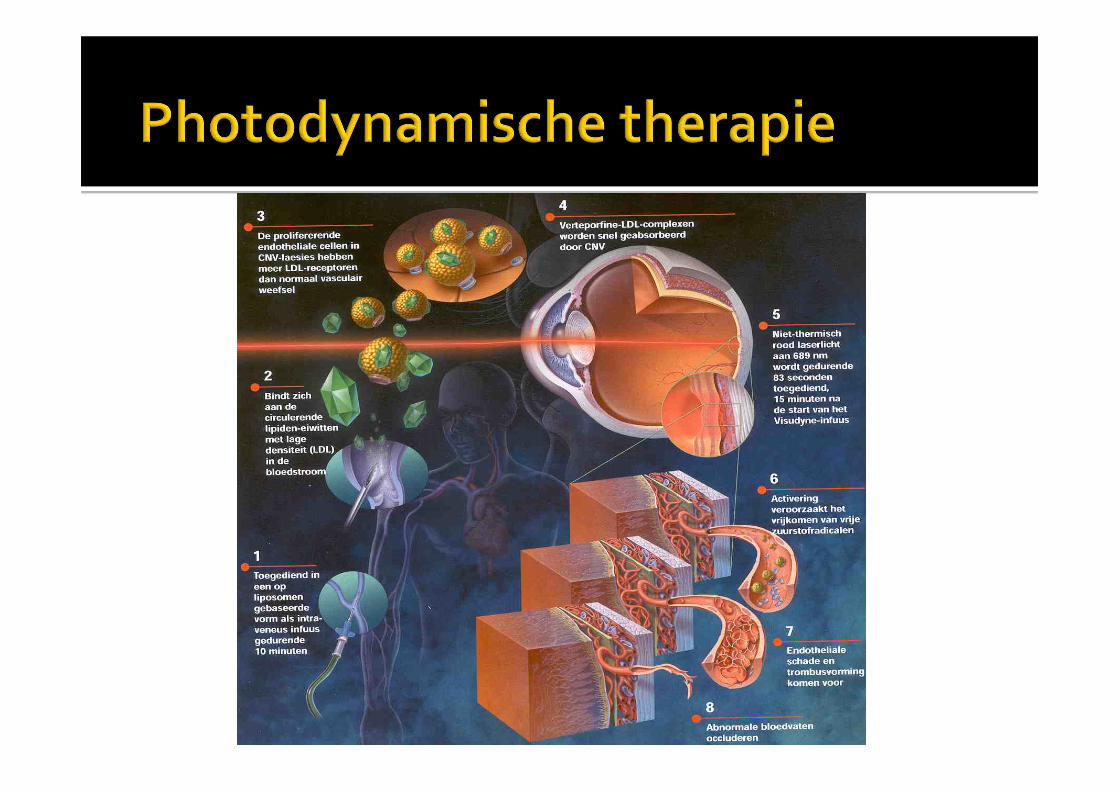
! Asymptomatisch:#controleren#! Symptomatisch:#PDT#
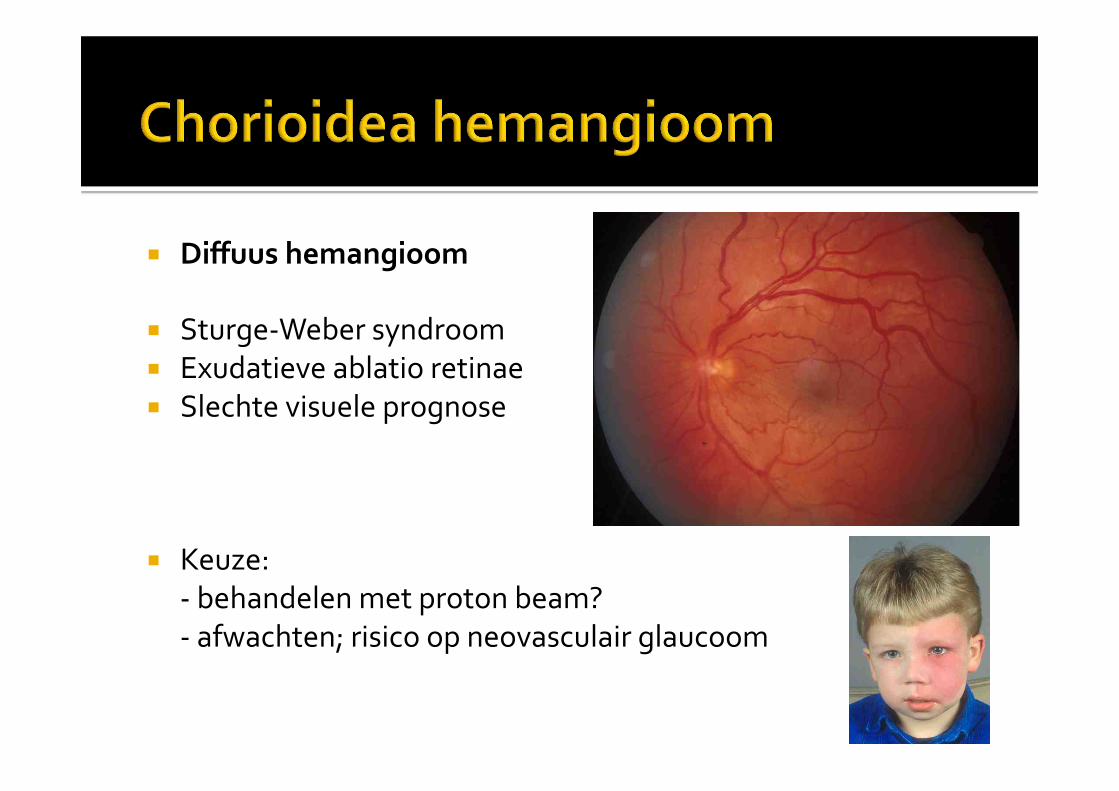
! Diffuus)hemangioom)
! SturgeMWeber#syndroom#! Exudatieve#ablatio#retinae#! Slechte#visuele#prognose#
! Keuze:#M#behandelen#met#proton#beam?#M#afwachten;#risico#op#neovasculair#glaucoom#
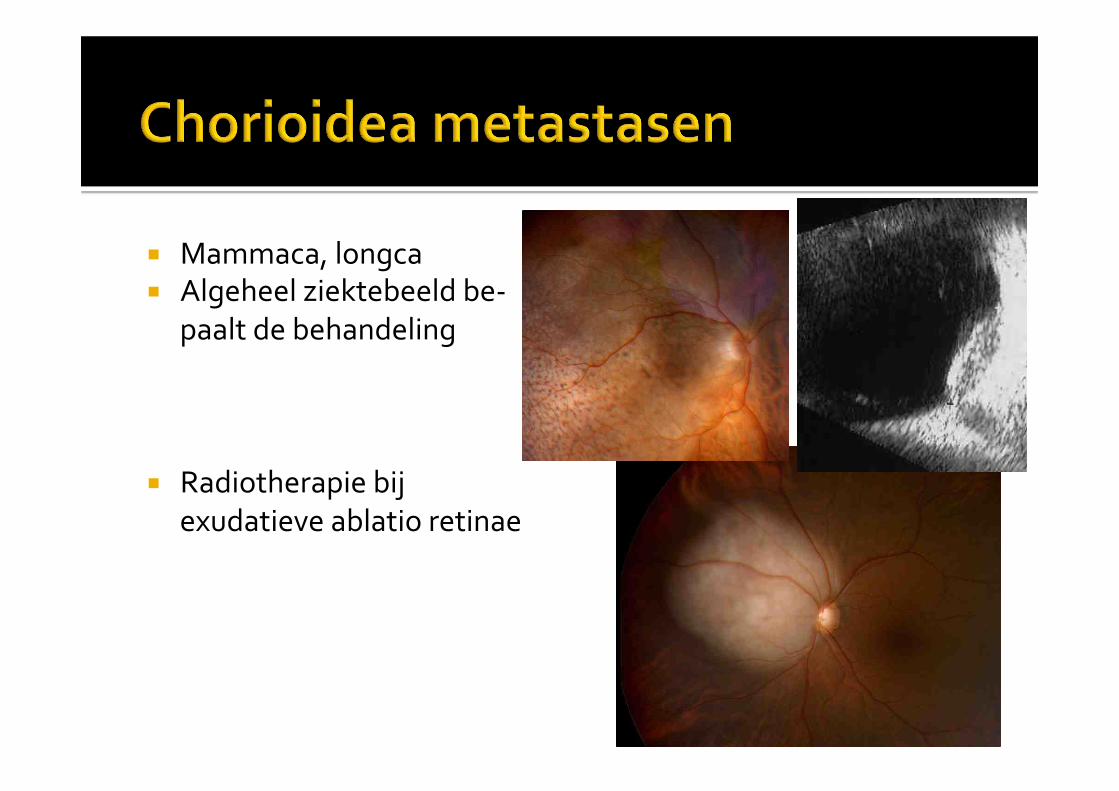
! Mammaca,#longca#! Algeheel#ziektebeeld#beM#
paalt#de#behandeling#
! Radiotherapie#bij#exudatieve#ablatio#retinae#
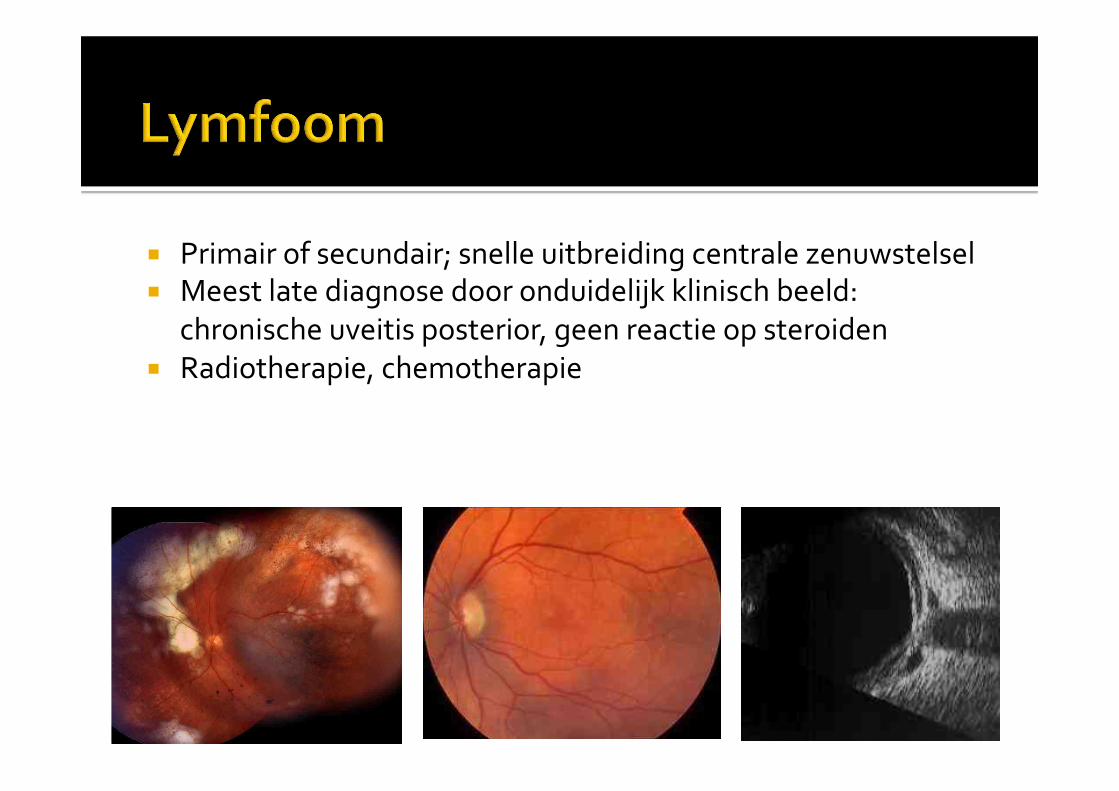
! Primair#of#secundair;#snelle#uitbreiding#centrale#zenuwstelsel#! Meest#late#diagnose#door#onduidelijk#klinisch#beeld:#
chronische#uveitis#posterior,#geen#reactie#op#steroiden#! Radiotherapie,#chemotherapie#
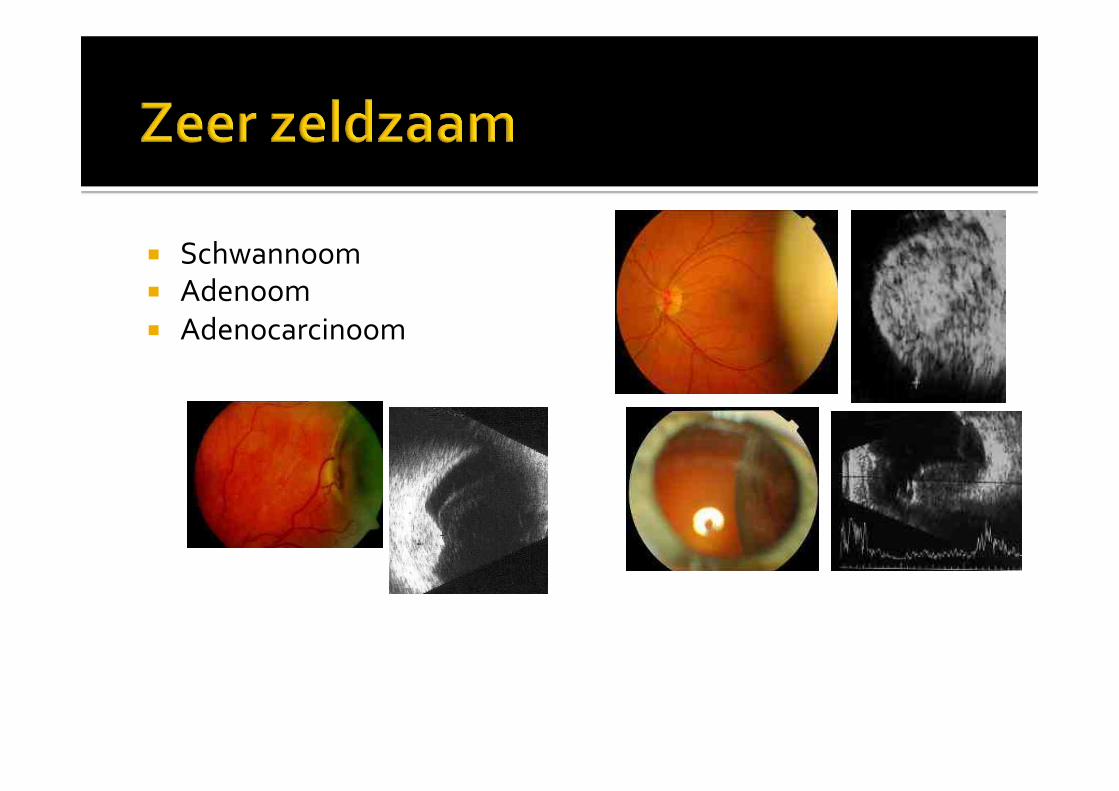
! Schwannoom#! Adenoom#! Adenocarcinoom#
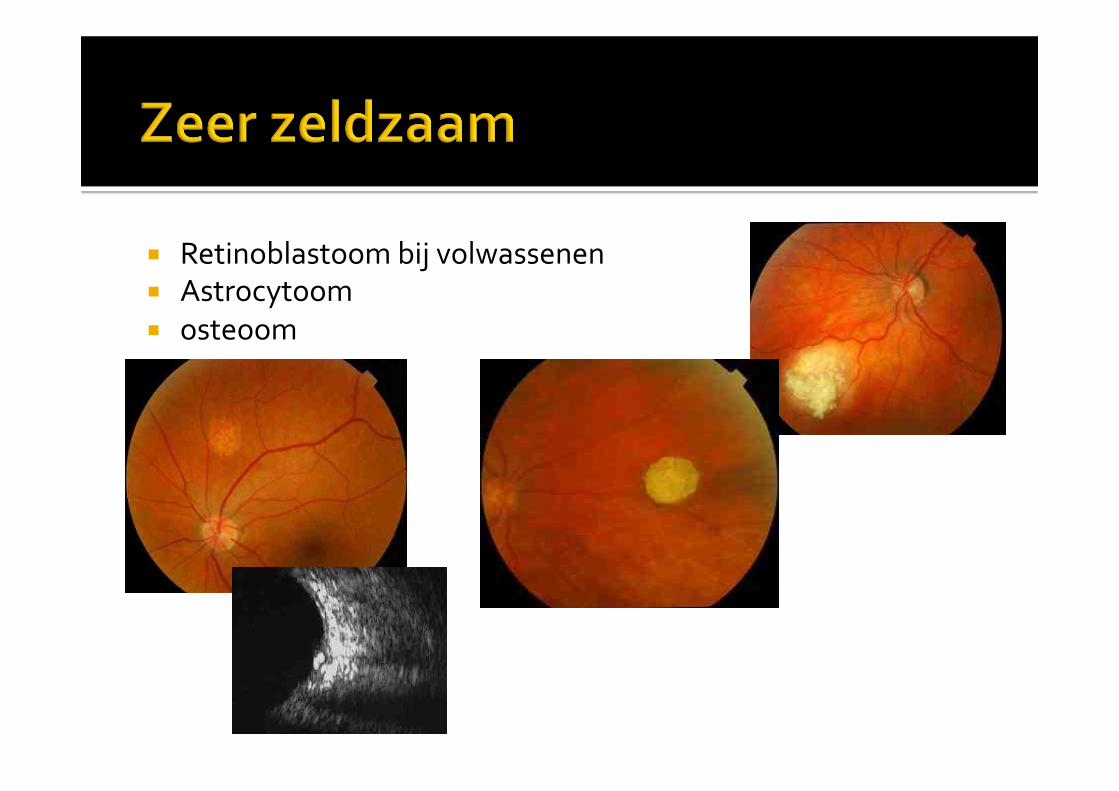
! Retinoblastoom#bij#volwassenen#! Astrocytoom#! osteoom#
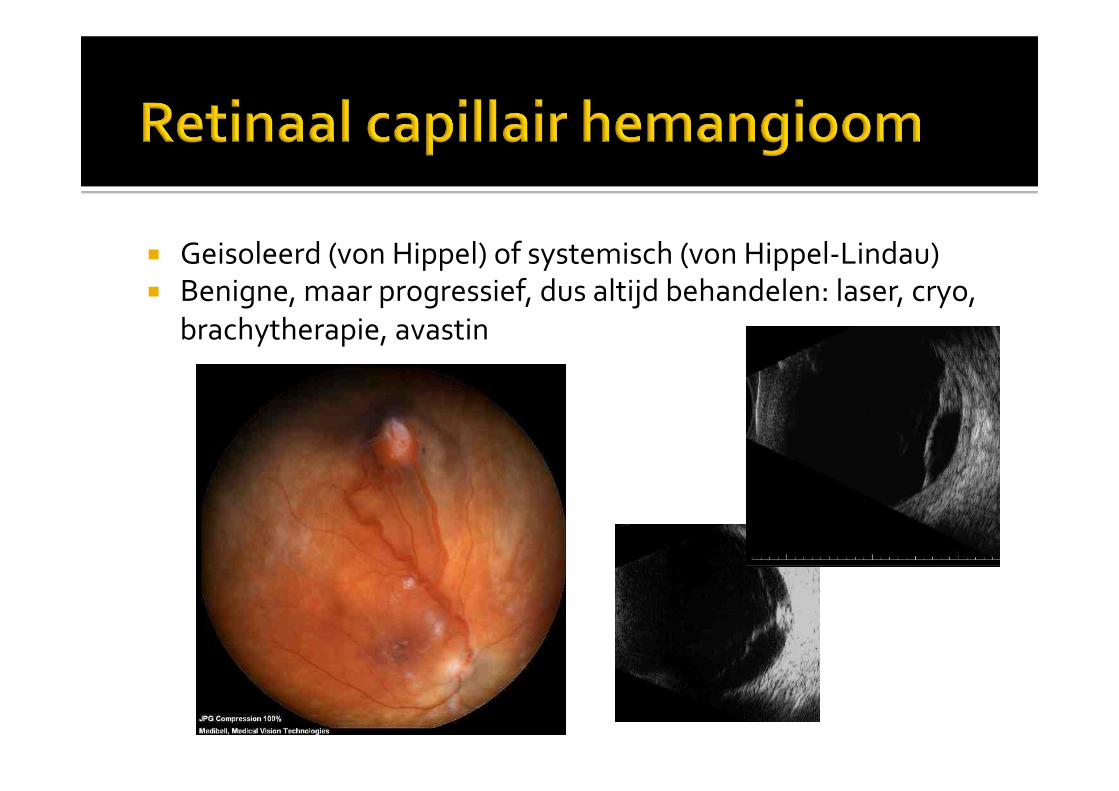
! Geisoleerd#(von#Hippel)#of#systemisch#(von#HippelMLindau)#! Benigne,#maar#progressief,#dus#altijd#behandelen:#laser,#cryo,#
brachytherapie,#avastin#
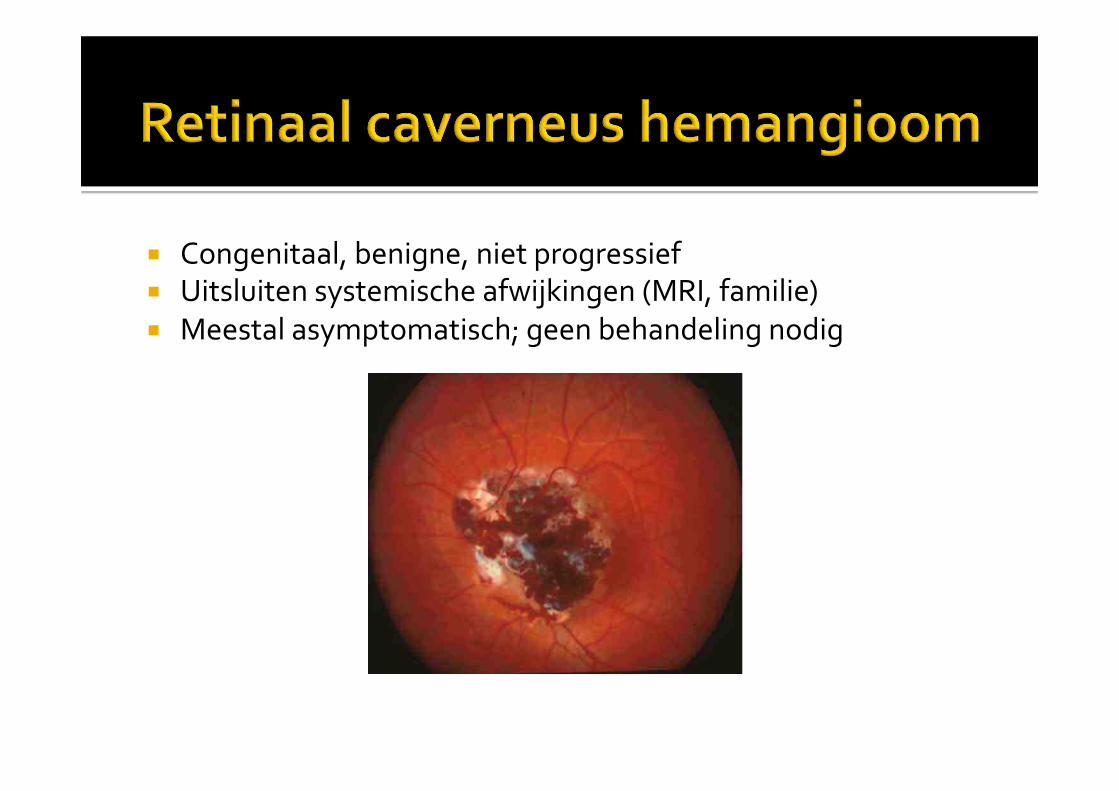
! Congenitaal,#benigne,#niet#progressief#! Uitsluiten#systemische#afwijkingen#(MRI,#familie)#! Meestal#asymptomatisch;#geen#behandeling#nodig#
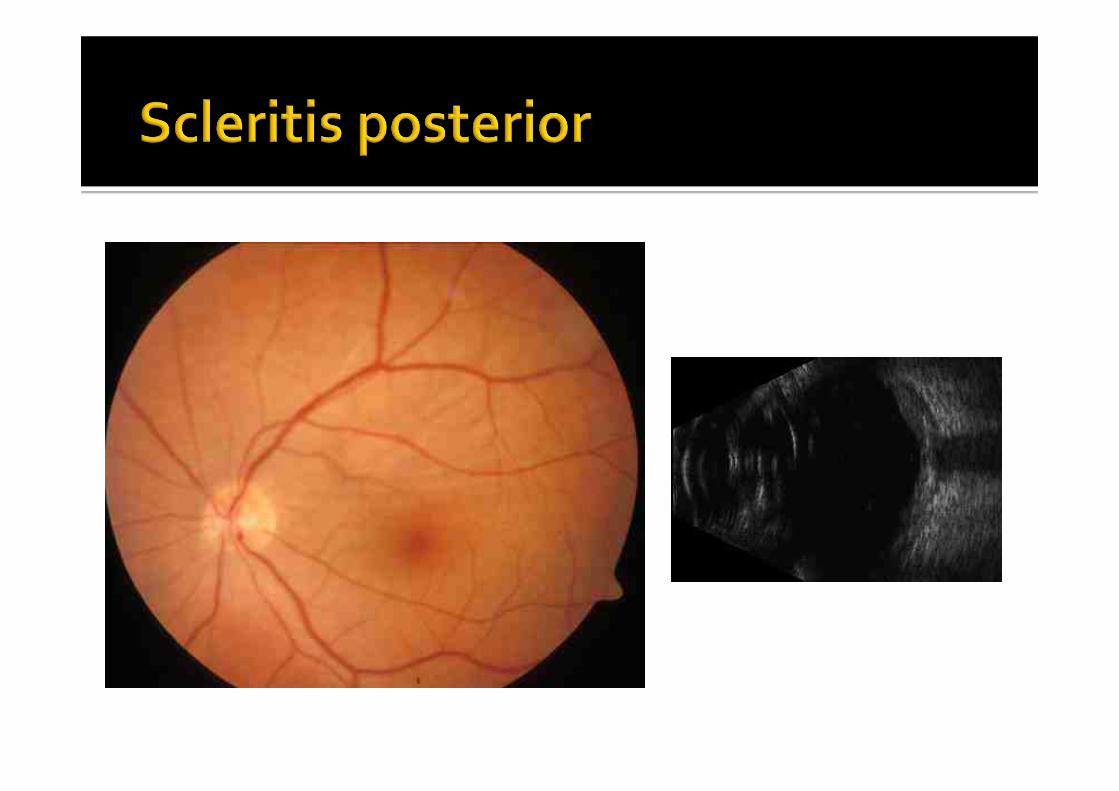
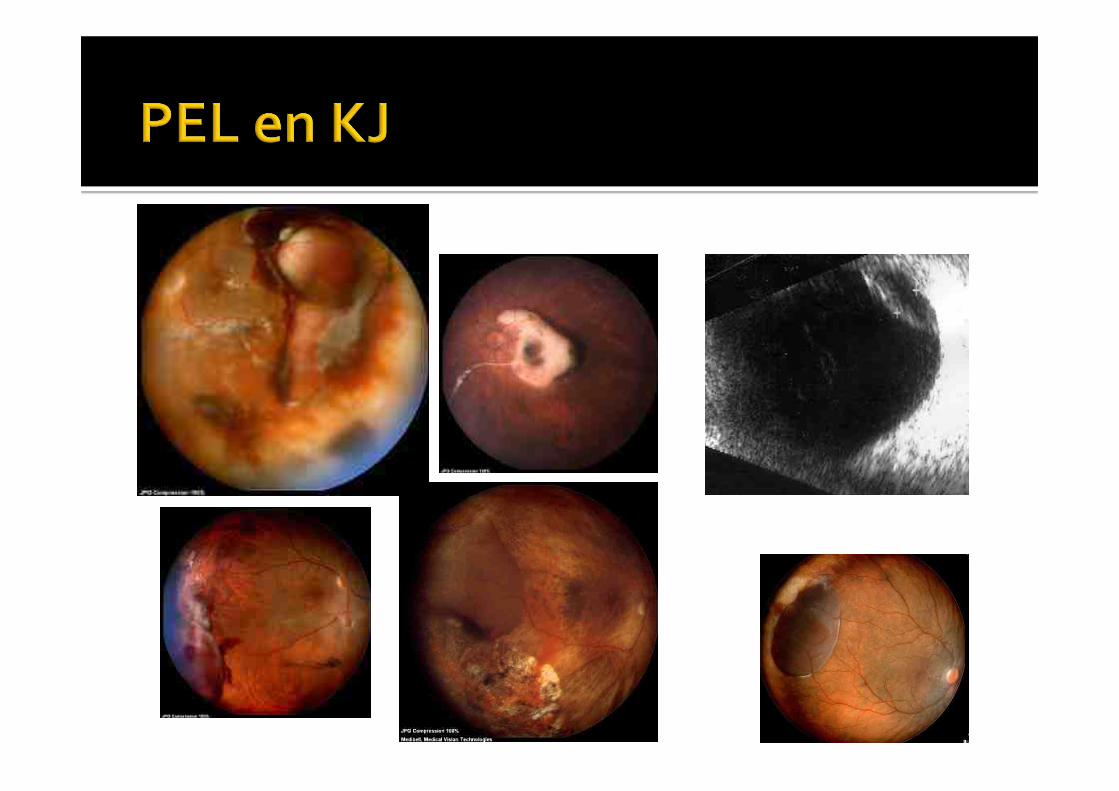
! Oedeem#M#scleritis#posterior#M#solutio#chorioideae#M#pigmentepitheelloslating#(PEL)#
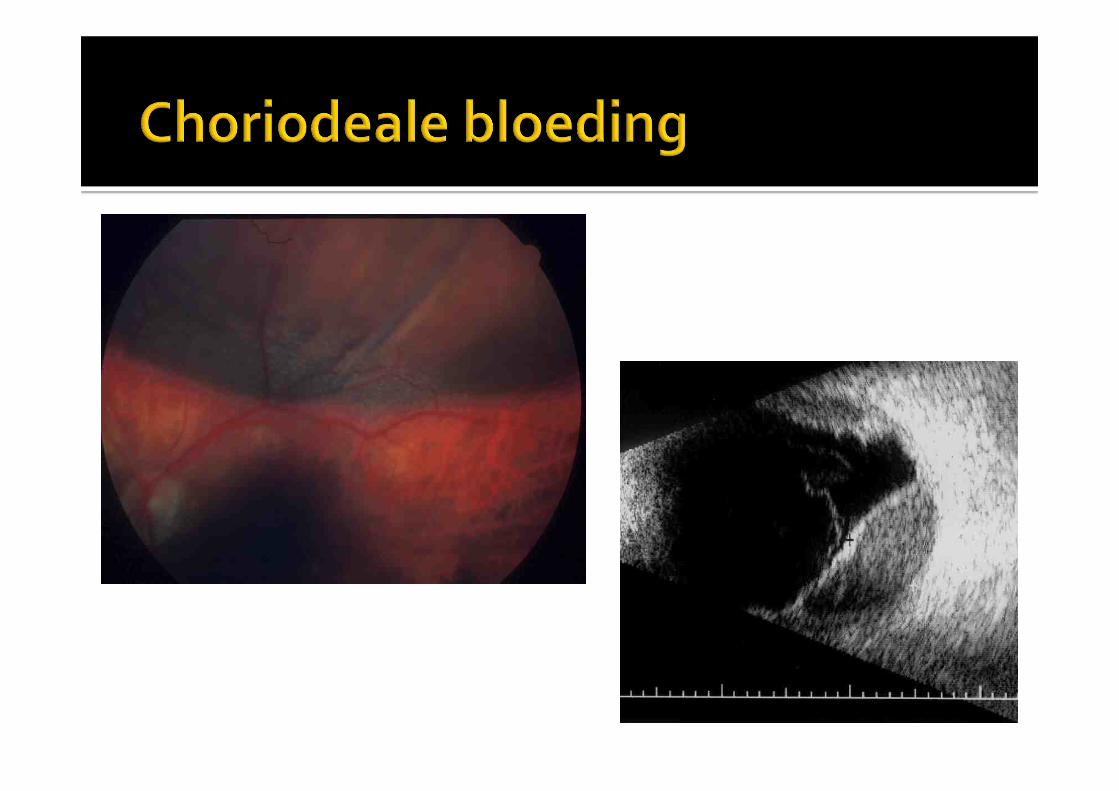
! Bloeding#M#KuhntMJunius#maculadegeneratie#M#perifere#CNV#Mchorioideale#bloeding#

! Niet#verwijzen/geruststellen:#M#CHRPE#M#Typische#naevus#
! Vervolgen:#M#Atypische#naevus#M#vereist#kleuren#fundusfotografie#en#echografie#
! Verwijzen:#M#de#rest#
! 90%#achtersegment#tumoren#=#melanoom#! Vroege#opsporing#en#behandeling#essentieel#! Soort#behandeling#apankelijk#van#grootte#en#lokalisatie#
! Snelle#verwijzing#vanuit#eerste#lijn#! Nauwkeurige##documentatie#en#followMup#bij#controle#! Behandeling#in#een#centrum#
http://www.eyetumours.com/mainpage.html)
Vragen?#