COVER en boekenlegger proefschri˜ Inez Curfs.indd 2 17-4-2019 … · COVER en boekenlegger...
157
Transcript of COVER en boekenlegger proefschri˜ Inez Curfs.indd 2 17-4-2019 … · COVER en boekenlegger...

COVER en boekenlegger proefschri� Inez Curfs.indd 1 17-4-2019 09:54:06COVER en boekenlegger proefschri� Inez Curfs.indd 2 17-4-2019 09:54:08
Inez curfs cover + boekenlegger 428x240 v0.indd Alle pagina's 29-4-2019 10:45:36

© Inez Curfs, Maastricht 2019, All rights reserved
Cover: Susan Lejeune @ Lejeune Grafisch Ontwerp
Layout: Tiny Wouters Lenssen
Production: proefschriftmaken.nl
ISBN: 978‐94‐6380‐319‐9
Financial support:
Caphri – Maastricht University
FORTE – onderzoek stichting Zuyderland Orthopedie
Nederlandse Orthopedische Vereniging (NOV)
Dutch Spine Society (DSS)
Smeets Loopcomfort
Spronken Orthopedie
Penders Voetzorg

DECISION MAKING IN THE TREATMENT OF
THORACOLUMBAR FRACTURES
PROEFSCHRIFT
ter verkrijging van de graad van doctor aan de Universiteit Maastricht,
op gezag van de Rector Magnificus, Prof. dr. Rianne M. Letschert,
volgens het besluit van het College van Decanen,
in het openbaar te verdedigen
op vrijdag 28 juni om 12.00 uur
door
Inez Curfs

Promotores
Prof. dr. L.W. van Rhijn
Copromotoren
Dr. W.L.W. van Hemert
Dr. P.C.P.H. Willems
Beoordelingscommissie
Prof. dr. I. Heyligers (voorzitter)
Prof. dr. C. Öner
Prof. dr. M. Poeze
Prof. dr. B. Van Royen
Dr. H. Van Santbrink

Table of contents
Chapter 1 General introduction 7 Chapter 2 Reliability and clinical usefulness of current classification 23
methods in traumatic thoracolumbar fractures: a systematic
review of the literature.
Submitted Chapter 3 Reliability and agreement of different spine fracture 45
classification systems: an independent intra‐ and inter‐observer
study.
World Neurosurg. 2018 Jul;115:e695‐e702. Chapter 4 Radiological prediction of posttraumatic kyphosis after 59
thoracolumbar fracture.
Open Orthopaedic Journal. 2016;10:135‐42 Chapter 5 Two‐nation Comparison of Classification and Treatment of 71
Thoracolumbar Fractures: an internet‐based multicenter study
among spine surgeons
Spine 2015;40(22): 1749‐1756 Chapter 6 Evaluating the immobilization effect of spinal orthosis using 87
sensor based motion analysis.
Journal of Prosthetics & Orthotics. 2016;28(1):23‐29 Chapter 7 Multisegmental posterior only versus circumferential 103
stabilization in the surgical treatment of traumatic thoraco‐
lumbar spinal fractures: a comparison by surgeon equipoise.
Submitted Chapter 8 General discussion 115 Chapter 9 Valorisatie 127 Chapter 10 Summary 133 Chapter 11 Nederlandse samenvatting 139 Chapter 12 Dankwoord 145 Chapter 13 Curriculum vitae 151
List of publications and presentations 155


7
Chapter 1
General introduction

Chapter 1
8

General introduction
9
1
Epidemiology
Traumatic spine fractures are serious injuries, that can be devastating for patients
without appropriate treatment. The incidence of spinal trauma is increasing over the
years. Five to nine percent of all trauma patients suffer from spinal trauma.1,2 Almost
one‐third of the spinal trauma injuries is due to motor‐vehicle accidents. The incidence
of mortality however decreased over the last three decades.3 In 1996 Hu4 published a
cross section observational study of a 3‐year cohort between 1981‐1984, with a
mortality of 41%. In 2012 Oliver2 showed in his study a decrease in mortality from ±15%
in 1996 to 5‐6% in 2008. One of the reasons may be due to improved traffic safety
standards and health care, such as emergency and intensive care.
Most of thoracolumbar fractures occur at the thoracolumbar junction (Th11‐L2),
followed by the thoracic spine. The lower lumber spine is least affected.3 Spinal
fractures are most frequently observed in the young and active population, more often
in males than females.5,6 The incidence of neurological deficit varies from 22‐51%
depending on fracture type and localization.7
Fracture classification
Historical series, before the introduction of surgical stabilization, showed deleterious
results of conservative treatment.8,9 These disappointing results may partly have been
due to the inability to surgical stabilization and the limited information from imaging. In
more recent series with better selection criteria based on advanced imaging, the results
have improved drastically.10‐13 On these imaging criteria various classification systems
have been based.
In 1930 Böhler was the first who classified thoracolumbar fractures using five injury
types.14 Since then, a lot of different classification methods have been developed,
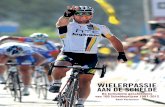
illustrated by timeline in Figure 1.1.

Chapter 1
10
Figure 1.1 Overview of the evolution in classification systems during the 20
th century.
1930
1949
1977
1982
1994
2005
2007
2013
ANATOMICAL MORPHOLOGY MECHANISM
BohlerRecognition of fracture types.Identified 5 types of injuries
NicollStable vs. unstable
WhitesidesTwo column concept
DenisThree column theory:
anterior, middle and posteriorcolumn
Magerl/AOThree main fracture types:
type A) compression, incl. burst,type B) distraction;
type C rotational type
TLISSTreatment algorithm based onthree variables: mechanism, neurology, posterior ligament
complex status
TLICSSlight modified TLISS;
changing mechanism intomorphology
New AOspine ClassificationEvolution of Magerl/AO
distinction in complete vs. incomplete burst
1930
1949
1977
1982
1994
2005
2007
2013
1930
1949
1977
1982
1994
2005
2007
2013
ANATOMICAL MORPHOLOGY MECHANISM
BohlerRecognition of fracture types.Identified 5 types of injuries
NicollStable vs. unstable
WhitesidesTwo column concept
DenisThree column theory:
anterior, middle and posteriorcolumn
Magerl/AOThree main fracture types:
type A) compression, incl. burst,type B) distraction;
type C rotational type
TLISSTreatment algorithm based onthree variables: mechanism, neurology, posterior ligament
complex status
TLICSSlight modified TLISS;
changing mechanism intomorphology
New AOspine ClassificationEvolution of Magerl/AO
distinction in complete vs. incomplete burst

General introduction
11
1
In 1949 Nicoll15 identified two basic groups of injury: stable and unstable fractures.
Whitesides16 reorganized the classification and in principle defined the two‐column
concept. In 1982 US orthopedic surgeon Francis Denis developed a new classification
(the Denis Classification) based on the three column theory: anterior‐middle‐posterior
column as assessed on CT‐scan.8 According to Denis' system, spinal traumas are
classified as minor or major injury, based on their potential risks to cause instability.
The minor injuries involve only a part of the posterior column and do not lead to acute
instability (fractures of transverse processes, articular processes, pars interarticularis,
and spinosus processes). Major spinal injuries are classified into four categories based
on fracture morphology, resulting in following types: 1) compression type; 2) burst;
3) seat belt type and 4) fracture dislocation type. As a consequence of all the previous
classification methods with their limitations, in 1994 Magerl17 developed a more
comprehensive classification from the analysis of 1445 cases. This classification is better
known as the Magerl/AO classification, and is primarily based upon the
pathomorphological characteristics of the fractures. All fracture types have a typical
underlying injury pattern which is determined by the three most important
mechanisms acting on the spine: compression, distraction, and axial torque. It
distinguishes three main fracture types: type A) compression (including burst); type B)
distraction; type C) rotational type. These fracture types are shown in Figure 1.2.
Figure 1.2 Illustration of compression (2a), burst (2b), distraction (2c) and rotational fractures (2d).
At present, the AO classification is most frequently used for fracture classification, but
the AO does not include a reliable estimation of prognosis for determination of the best
treatment.18 In 2005 the TLISS (Thoraco‐Lumbar Injury Severity Score) was developed
by Harrop et al.19 As many experts had their concerns about the reproducibility of the
trauma mechanism of the TLISS, it was slightly modified to the TLICS in 2007.20 This
classification system included a treatment algorithm, based on three objective
variables: fracture mechanism, the neurological status of the patient and the integrity
of the posterior ligament complex (Figure 1.3). Recently the new AOspine classification
has been published, which specifically distinguishes between complete and incomplete

Chapter 1
12
burst fractures, as these fractures remain subject to debate in treatment of spinal
fractures (Figure 1.4).21,22
Morphology Type Qualifier Points
Compression Compression fracture 1
Burst fracture 1 Translational/rotational 3
Distraction 4
Neurologic involvement Intact 0
Nerve Root 2
Cord, conus medullaris Incomplete 3 Complete 2
Cauda equina 3
Posterior ligamentous complex integrity Intact 0
Injury suspected/indeterminate 2
Injured 3
Figure 1.3 TLICS classification. Treatment algorithm: 0‐3 points conservative treatment; 4 points both
conservative or surgical treatment optional; >4 points surgical treatment recommended.
Figure 1.4 New AO spine classification (a), distinction between incomplete (4b) and complete (4c) burst
fractures.

General introduction
13
1
Fracture management
Commonly, treatment is based upon accurate radiological diagnosis and concomitant
use of a fracture classification system. However, the optimal treatment of traumatic
thoracolumbar fractures remains under debate. Several reviews address the
management of traumatic thoracolumbar fractures.23,24 Most thoracolumbar injuries
are stable fractures, suitable for nonoperative treatment. Clear unstable injuries
require surgical treatment, such as distraction and rotational injuries (B and C type
according to the AO classification). The optimal treatment of burst fractures is still
under investigation. Albeit these fractures are stable according to the current
classification systems (AO A‐type, TLICS 2 points), over 50% of these fractures were
operated.25 The treatment decision apparently is based on other patient and fracture
related factors, such as local kyphosis, age, localization and intervertebral disk
pathology. Current literature shows no clear benefit of surgical treatment over
conservative treatment of stable burst fractures. In a meta‐analysis, Gnanenthiran26
concluded that ‘operative management of thoracolumbar burst fractures without
neurologic deficit may improve residual kyphosis, but does not appear to improve pain
or function at an average of 4 years after injury and is associated with higher
complication rates and costs’. Bakhsheshian27 published in 2014 a review of evidence
based management of stable thoracolumbar burst fractures. He stated that no
differences were found in outcome between conservative and operative treatment of
burst fractures. However, he suggested that there should be a differentiation within
burst fractures. We need to recognize the appropriate fractures for safe conservative
management and thereby decreasing the variables that may impact the prognosis.
The main uncertainty is probably related to the integrity of the posterior‐ligamentous‐
complex (PLC). The PLC is composed of the ligamentum flavum, interspinous ligament,
facet capsule and supraspinous ligament. See Figure 1.5 for an illustration of the three
spinal columns and the PLC.
Schnake et al.28 and Leferink et al.29 showed in their studies that worse outcome may
be due to the fact that burst fractures are actually missed B‐type fractures. So, reliable
assessment of the PLC integrity is crucial. Literature regarding the reliability of MRI in
PLC status resulted in fair to moderate kappa values (kappa ± 0.4)30, and demonstrated
relatively high negative predictive values and relatively low positive predictive values
for PLC injuries.31
Clinical studies have shown contradictory evidence about the role of standard MRI in
addition to plain radiographs and CT for treatment decision making. Several studies
presented results in which MRI seemed to improve reliability and influence treatment
strategies compared to CT.32‐35 But Rajasekran36 performed a study with similar

Chapter 1
14
sensitivity for CT and MRI and reported no change in treatment decision after
additional MRI.
Figure 1.5 Illustration of three columns of the spine. The posterior ligamentous complex consists of the
ligamentum flavum, interspinous ligament, facet capsule and supraspinous ligament.
Nonoperative treatment
Simple compression or stable burst fractures without neurologic complications can be
treated non‐surgically. A recent review showed no superior conservative treatment.27
Follow up of conservative treatment is recommended to assess progression of kyphosis.
A certain degree of increasing fracture kyphosis is observed in most nonoperative
treated patients.
Typically, patients are treated with available thoracolumbar orthosis or a
hyperextension cast that permit early ambulation. Several studies have investigated the
efficiency of braces in fracture management.37,38,39 It seems that the unbraced condition
gives the same clinical and radiological results as brace treatment; however, the studies
have their limitations, mainly because of small sample sizes and poor level of evidence.
In 2009 Giele et al.40 published their results of a systematic review, in which they
included 7 retrospective studies. No differences in outcome between conservative
treatment with and without brace were found. In contrast, Karimi et al.41 showed in
2015 in a review that the use of orthosis influences the outcome of treatment in
patients with a stable fracture in the thoracolumbar spine: it reduces pain and
increases functional ability. However, the use of an orthosis does not influence the

General introduction
15
1
vertebral height and kyphotic angle. In all mentioned studies, different types of braces
were studied. Most often used were the thoracolumbar sacral orthosis (TLSO), body
cast, extension brace and 3‐point corset.
Despite the widespread use of spinal orthoses, the evidence concerning the impact on
spinal movement is poor. Several studies have investigated the impact of spinal
orthoses on physical activity.42‐46 However, an objective tool for movement analysis has
barely been used. Only a few studies have investigated the capacity of spinal orthoses
to immobilize the spine. Hashimoto et al.47 studied the effect of rotational swing in low
back pain during golf with sensor‐based movement analysis and Schmidt et al.48
investigated the effect of spinal braces in osteoporosis. Regarding the contradiction in
clinical studies and the lack of biomechanical analysis, it seems of importance to better
understand the function of the orthoses, in order to determine their position in the
conservative treatment of thoracolumbar fractures.
Operative treatment
If surgical treatment is chosen, there is no true consensus on which surgical technique
should be used.49 The main goal is to achieve spinal stability and maintain spinal
alignment. More and more new techniques are developed and used in clinical practice.
At this moment various technique systems are propagated: open pedicle screw
placements, minimal invasive percutaneous pedicle screw systems, cement augmented
screws, vertebroplasty, kyphoplasty, different types of cages and interbody support
devices. In addition, many different approaches to the spinal column are used, from a
posterior to a lateral and anterior approach. As a consequence, spine surgery is
constantly evolving, and a wide variety of possibilities are available.
In the last decades more studies are published concerning these different techniques,
but there is no superior technique over another. The decision for a certain surgical
technique is mainly based on surgeons ‘experience and country specific cultures, rather
than evidence‐based medicine.
Traditionally, spine fractures were treated by open posterior stabilization. In the last
two decades minimal invasive pedicle screw fixation is increasingly used in fracture
treatment. In this approach pedicle screws are placed by a percutaneous approach, as
shown in Figure 1.6.

Chapter 1
16
a b
Figure 1.6 a) Percutaneous pedicle screw system. b) Percutaneous surgical approach.
Advantages of this approach are less blood loss, less postoperative pain, less muscle
dissection and muscle weakness and shorter hospital stay. Several studies concerning
the minimal invasive (MIS) approach compared to the conventional open approach
have been published. MIS approach seemed to be safe and had comparable results to
the conventional open posterior stabilization with fusion.50,51 However, Dhall et al.52
concluded that it could only be used in select cases, and the role of percutaneous non‐
fusion techniques remain limited. In 2014 and 2015 two separate reviews concluded
that the results of MIS were encouraging, but level of evidence was low, and more
research was needed to ascertain how MIS could be implemented in the treatment
algorithm.53,54
An important issue of debate is the need for anterior support (circumferential
stabilization) in spine fractures. From a biomechanical point of view, it seems better to
restore the anterior column, because of the outcome of the sagittal balance. And as
known from previous studies, sagittal balance is of importance for clinical outcome, as
posttraumatic kyphosis is correlated to pain.55 On the other hand, circumferential
stabilization seems more invasive for patients. It is often performed in two stages.
Cement augmentation of the fractured vertebrae has led to new possibilities for
anterior column support in a less invasive manner. However, data on long term efficacy
and safety are not yet available.
Rationale for this thesis
With the increasing incidence of traumatic spine fractures, their influence on quality of
life, growing healthcare costs and evolving treatment possibilities, it seems of
importance to achieve consensus and optimize the treatment of traumatic
thoracolumbar spine fractures.

General introduction
17
1
The improvement of imaging possibilities, subsequently leaded to an evolution in
classification systems. The classifications aimed to create a common language with
standardization and optimization of treatment. However, until now, consensus about
treatment of thoracolumbar fractures is not reached.
Mainly the optimal treatment of (stable) burst fractures is still under debate. Several
studies have shown no difference in outcome between conservative and operative
treatment in burst fractures. However, some conservatively treated burst fractures
have poor outcome. It seems of importance to differentiate between burst fractures
and select the appropriate burst fractures for conservative treatment.
If the treatment decision is made, the type of either non‐operative and operative
treatment remains an issue. The goal of treatment is to gain fracture healing, while
maintaining alignment and function of the spinal column. While fractures occur most
frequently in the young and active population, fast recovery and return to normal daily
activities including work, is also an important issue regarding cost‐effectiveness
analysis.
In terms of the non‐operative treatment, pain control and rapid mobilization are
sought. In this perspective, the role of bracing is under discussion. Only a few studies
investigated the capacity of spinal orthoses to immobilize.
Concerning the operative treatment, many options are available. Despite functional
and radiological outcome, clinical outcome parameters such as length of hospital stay,
surgery times, blood loss and implant costs become more important. Open posterior
fusion was for years the way to stabilize a traumatic thoracolumbar fracture. However,
surgery also has negative clinical implications for the patients, like the well‐known
complications, muscle atrophy by the open posterior approach and limitations in spinal
movement. With the development of new techniques, one tries to reduce
complications and negative side effects, and to ensure alignment even better.
However, as spine surgery is constantly evolving, and new opportunities arrive rapidly,
there is limited evidence comparing the different types of surgical techniques.

Chapter 1
18
Research questions
In this thesis we enroll our search for a better understanding of how to choose the
optimal treatment of thoracolumbar fractures. Different aspects associated with
fracture management are addressed, such as classification, clinical usefulness,
conservative treatment, surgical treatment and prognosis. The following aims have
been postulated:
1. To evaluate the accuracy of the AO, TLICS/ TLISS and new AOspine classification for
traumatic thoracolumbar fractures. (Chapter 2)
2. To assess which classification could be used best for treatment decision making in
traumatic thoracolumbar spine fractures, by means of accuracy and clinical
usefulness. (Chapter 2)
3. To examine the intra‐ and interobserver reliability and agreement of different
classifications for traumatic spine fractures. (Chapter 3)
4. To determine risk factors (AO classification, age, gender, localization) that may lead
to progressive kyphosis after a thoracolumbar fracture. (Chapter 4)
5. To observer if there are nation differences in the management strategy for
traumatic thoracolumbar fractures between German and Dutch spine surgeons.
(Chapter 5)
6. To measure the movement reduction and comfortability of thoracolumbar
orthoses compared to normal spinal motion using IMA and questionnaires?
(Chapter 6)
7. To compare the functional, radiological and clinical outcome of posterior only
versus circumferential stabilization in traumatic thoracolumbar fractures?
(Chapter 7)
In chapter 2 a review of the literature was performed to assess the accuracy and clinical
usefulness of the AO, TLICS and new AOspine classification. As an accurate and clinical
applicable classification system is necessary for treatment decision making.
Some of the limitations of the current classification methods are considered to lack a
prognostic value and have no attention for kyphosis.
As there is continuously improvement in current classifications, most used
classifications were assessed for the inter‐ and intra‐observer validity in chapter 3. A
web‐based study was performed to evaluate the validity of the new AOspine
classification, the TLICS and the Load sharing classification.

General introduction
19
1
In chapter 4 a retrospective radiographic analysis of a consecutive patient cohort with a
traumatic thoracolumbar spine fracture was evaluated. Risk factors associated with
worse radiological outcome were determined.
Treatment differences are not only fracture or patient related, but they also depend on
surgeon and Nation preferences. Chapter 5 presents the results of a web‐based‐
multicenter study. Questionnaires were evaluated by German and Dutch spine
surgeons to assess and compare their management strategies of thoracolumbar
fractures.
In the next section of this thesis the focus relies on “how to do”. In chapter 6 four
different spinal orthoses were tested on their movement reduction and comfortability
compared to normal spinal motion. Ten healthy volunteers were asked to perform
several function tasks under five conditions: first without wearing an orthosis, and
subsequently while wearing four different types of orthosis. Inertia based motion
analysis (IMA) was used for objective movement measurements.
In surgical treatment a lot of different techniques are used. There is no consensus on
how to surgically treat the thoracolumbar fractures. We performed a multicentre
analysis of patients who were surgically treated for a traumatic thoracolumbar fracture
between University Hospital Aachen (Germany), Maastricht University Medical Centre
or Zuyderland Medical Centre Heerlen (Netherlands). Patients were included by surgical
equipoise. In Chapter 7 the functional, radiological and clinical outcome of posterior
only (Netherlands) versus circumferential stabilization (Germany) in traumatic
thoracolumbar fractures is compared.

Chapter 1
20
References
1. Doud AN, Weaver AA, Talton JW, et al. Has the incidence of thoracolumbar spine injuries increased in
the United States from 1998 to 2011? Clin Orthop Relat Res 2015;473:297‐304.
2. Oliver M, Inaba K, Tang A, et al. The changing epidemiology of spinal trauma: a 13‐year review from a Level I trauma centre. Injury 2012; 43(8):1296‐300.
3. Fisher CG, Noonan VK, Dvorak MF. Changing face of spine trauma care in North America. Spine (Phila Pa
1976) 2006;31(11 Suppl):S2‐8. 4. Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine
(Phila Pa 1976) 1996;21(4):492‐9.
5. Gertzbein SD. Scoliosis Research Society. Multicenter spine fracture study. Spine (Phila Pa 1976) 1992; 17(5):528‐40.
6. Gertzbein SD, Khoury D, Bullington A, et al. Thoracic and lumbar fractures associated with skiing and
snowboarding injuries according to the AO Comprehensive Classification. Am J Sports Med 2012;40(8):1750‐4.
7. Knop C, Blauth M, Bühren V, et al. Surgical treatment of injuries of the thoracolumbar transition. 1:
Epidemiology. Unfallchirurg 1999;102(12):924‐35. 8. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal
injuries. Spine (Phila Pa 1976) 1983;8(8):817‐31.
9. Willén J, Anderson J, Toomoka K, Singer K. The natural history of burst fractures at the thoracolumbar junction. J Spinal Disord 1990;3(1):39‐46.
10. de Klerk LW, Fontijne WP, Stijnen T, et al. Spontaneous remodeling of the spinal canal after conservative
management of thoracolumbar burst fractures. Spine (Phila Pa 1976) 1998;23(9):1057‐60. 11. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and
outcome of nonoperative management. Spine (Phila Pa 1976) 1993;18(8):955‐70.
12. Shen WJ, Shen YS. Nonsurgical treatment of three‐column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976) 1999;24(4):412‐5.
13. Shen WJ, Liu TJ, Shen YS. Nonoperative treatment versus posterior fixation for thoracolumbar junction
burst fractures without neurologic deficit. Spine (Phila Pa 1976) 2001;26(9):1038‐45. 14. Bohler L. Die techniek de knochenbruchbehandlung imgrieden und im kriege. Verlag von Wilhelm
Maudrich 1930.
15. Nicoll EA. Fractures of the dorso‐lumbar spine. J Bone Joint Surg [Br] 1949;31:376‐94. 16. Whitesides TE Jr. Traumatic kyphosis of the thoracolumbar spine. Clin Orthop 1977;128:78‐92.
17. Magerl F, Aebi M, Gertzbein SD, et al. A comprehensive classification of thoracic and lumbar injuries.
Eur Spine J 1994;3(4):184‐201. 18. Wood KB, Khanna G, Vaccaro AR, et al. Assessment of two thoracolumbar fracture classification systems
as used by multiple surgeons. J Bone Joint Surg Am 2005;87(7):1423‐9.
19. Harrop JS, Vaccaro AR, Hurlbert RJ, et al. Intrarater and interrater reliability and validity in the assessment of the mechanism of injury and integrity of the posterior ligamentous complex: a novel
injury severity scoring system for thoracolumbar injuries. Invited submission from the Joint Section
Meeting On Disorders of the Spine and Peripheral Nerves, March 2005. Spine Trauma Study Group. J Neurosurg Spine 2006;4(2):118‐22.
20. Whang PG, Vaccaro AR, Poelstra KA, et al. The influence of fracture mechanism and morphology on the
reliability and validity of two novel thoracolumbar injury classification systems. Spine (Phila Pa 1976) 2007;32(7):791‐5.
21. Reinhold M, Audigé L, Schnake KJ, et al. AO spine injury classification system: a revision proposal for the
thoracic and lumbar spine. Eur Spine J 2013: 22(10):2184‐201. 22. Max Aebi. AO spine classification system for thoracolumbar fractures. Eur Spine J 2013;22(10):2147‐8.
23. Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: An overview.Indian J
Orthop 2015;49(1):72–82. 24. Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J 2014;14(1):
145‐64.

General introduction
21
1
25. Joaquim AF, Daubs MD, Lawrence BD, et al. Retrospective evaluation of the validity of the Thoracolumbar Injury Classification System in 458 consecutively treated patients. Spine J 2013;13(12):
1760‐5.
26. Gnanenthiran SR, Adie S, Harris IA. Nonoperative versus operative treatment for thoracolumbar burst fractures without neurologic deficit: a meta‐analysis. Clin Orthop Relat Res 2012;470(2):567‐77.
27. Bakhsheshian J, Dahdaleh NS, Fakurnejad S, Scheer JK, Smith ZA. Evidence‐based management of
traumatic thoracolumbar burst fractures: a systematic review of nonoperative management. Neurosurg Focus 2014;37(1):E1.
28. Schnake KJ, von Scotti F, Haas NP, et al. Type B injuries of the thoracolumbar spine : misinterpretations
of the integrity of the posterior ligament complex using radiologic diagnostics. Unfallchirurg 2008;111(12):977‐84.
29. Leferink VJ, Veldhuis EF, Zimmerman KW, et al. Classificational problems in ligamentary distraction type
vertebral fractures: 30% of all B‐type fractures are initially unrecognised. Eur Spine J 2002;11(3):246‐50. 30. Lee GY, Lee JW, Choi SW, Lim HJ, Sun HY, Kang Y, Chai JW, Kim S, Kang HS. MRI Inter‐Reader and Intra‐
Reader Reliabilities for Assessing Injury Morphology and Posterior Ligamentous Complex Integrity of the
Spine According to the Thoracolumbar Injury Classification System and Severity Score. Korean J Radiol 2015;16(4):889‐98.
31. van Middendorp J, Patel A, Schuetz M, Joaquim AF. The precision, accuracy and validity of detecting
posterior ligamentous complex injuries of the thoracic and lumbar spine: a critical appraisal of the literature. Eur Spine J 2013;22(3): 461‐74.
32. Oner FC, Ramos LM, Simmermacher RK, et al. Classification of thoracic and lumbar spine fractures:
problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J. 2002 Jun;11(3):235‐45. 33. Salgado Á, Pizones J, Sánchez‐Mariscal F et al. MRI reliability in classifying thoracolumbar fractures
according to AO classification. Orthopedics 2013;36(1):e75‐8.
34. Pizones J, Izquierdo E, Alvarez P, et al. Impact of magnetic resonance imaging on decision making for thoracolumbar traumatic fracture diagnosis and treatment. Eur Spine J 2011;20 Suppl 3:390‐6.
35. Winklhofer S, Thekkumthala‐Sommer M, Schmidt D, et al. Magnetic resonance imaging frequently
changes classification of acute traumatic thoracolumbar spine injuries. Skeletal Radiol 2013;42(6): 779‐86.
36. Rajasekaran S, Vaccaro AR, Kanna RM, et al. The value of CT and MRI in the classification and surgical
decision‐making among spine surgeons in thoracolumbar spinal injuries. Eur Spine J 2017;26(5): 1463‐9. 37. Alcalá‐Cerra G, Paternina‐Caicedo AJ, Díaz‐Becerra C, et al. Orthosis for thoracolumbar burst fractures
without neurologic deficit: A systematic review of prospective randomized controlled trials.J
Craniovertebr Junction Spine 2014;5(1):25‐32. 38. Shamji MF, Roffey DM, Young DK, et al. A pilot evaluation of the role of bracing in stable thoracolumbar
burst fractures without neurological deficit.J Spinal Disord Tech 2014;27(7):370‐5.
39. Bailey CS, Urquhart JC, Dvorak MF, et al. Orthosis versus no orthosis for the treatment of thoracolumbar
burst fractures without neurologic injury: a multicenter prospective randomized equivalence trial.Spine
J 2014;14(11):2557‐64.
40. Giele BM, Wiertsema SH, Beelen A, et al. No evidence for the effectiveness of bracing in patients with thoracolumbar fractures: A systematic review. Acta Orthop 2009;80(2):226–32.
41. Karimi M. The effects of orthosis on thoracolumbar fracture healing: A review of the literature. J Orthop.
2015; 12(Suppl 2): S230–7. 42. Ryan CG, Grant PM, Dall PM, et al. Individuals with chronic low back pain have a lower level, and an
altered pattern, of physical activity compared with matched controls: an observational study. Aust J
Physiother 2009;55(1):53‐8. 43. Spenkelink CD, Hutten MMR, Hermens HJ. Assessment of activities of daily living with an ambulatory
monitoring system: a comparative study in patients with chronic low back pain and nonsymptomatic
controls. Clin Rehabil 2002;16(1):16‐26. 44. Verbunt JA, Westerterp KR, van der Heijden GJ, et al. Physical activity in daily life in patients with
chronic low back pain. Arch Phys Med Rehabil 2001;82(6):726‐30.

Chapter 1
22
45. Van Weering MGH, Vollenbroek‐Hutten MMR, Hermens HJ. The relationship between objectively and subjectively measured activity levels in people with chronic low back pain. Clin Rehabil 2011;25(3):
256‐63.
46. van den Berg‐Emons RJ, Schasfoort FC, de Vos LA, Bussmann JB, Stam HJ. Impact of chronic pain on everyday physical activity. Eur J Pain 2007;11(5):587‐93.
47. Hashimoto K, Miyamoto K, Yanagawa T, et al. Lumbar corsets can decrease lumbar motion in golf swing.
J Sports Sci Med 2013;12(1):80‐7. 48. Schmidt K, Hübscher M, Vogt L, et al. Influence of spinal orthosis on gait and physical functioning in
women with postmenopausal osteoporosis. Der Orthopade 2012;41(3):200‐5.
49. Oner FC, Wood KB, Smith JS, Shaffrey CI. Therapeutic decision making in thoracolumbar spine trauma. Spine (Phila Pa 1976) 2010;35(21 Suppl):S235‐44.
50. Lee JK, Jang JW, Kim TW, et al. Percutaneous short‐segment pedicle screw placement without fusion in
the treatment of thoracolumbar burst fractures: is it effective?: comparative study with open short‐segment pedicle screw fixation with posterolateral fusion.Acta Neurochir (Wien). 2013;155(12):2305‐12;
discussion 2312.
51. Wang H, Zhou Y, Li C, Liu J, Xiang L. Comparison of open versus percutaneous pedicle screw fixation using the sextant system in the treatment of traumatic thoracolumbar fractures. J Spinal Disord Tech
2017;30(3):E239‐46.
52. Dhall SS, Wadhwa R, Wang MY, Tien‐Smith A, Mummaneni PV. Traumatic thoracolumbar spinal injury: an algorithm for minimally invasive surgical management. Neurosurg Focus 2014;37(1):E9.
53. Koreckij T, Park DK, Fischgrund J. Minimally invasive spine surgery in the treatment of thoracolumbar
and lumbar spine trauma. Neurosurg Focus 2014;37(1):E11. 54. Oh T, Scheer JK, Fakurnejad S, Dahdaleh NS, Smith ZA. Minimally invasive spinal surgery for the
treatment of traumatic thoracolumbar burst fractures. J Clin Neurosci 2015;22(1):42‐7.
55. Buchowski JM, Kuhns CA, Bridwell KH, Lenke LG. Surgical management of posttraumatic thoracolumbar kyphosis. Spine J 2008;8(4):666‐77.

23
Chapter 2
Reliability and clinical usefulness of current classification
methods in traumatic thoracolumbar fractures:
a systematic review of the literature
I. Curfs, M. Schotanus, W. Van Hemert, M. Heymans, R. De Bie, L. Van Rhijn, P.Willems
Submitted

Chapter 2
24
Abstract
Study design
Systematic review.
Objectives
A validated classification remains the key to an appropriate treatment algorithm.
Considering the development of many classifications, it is remarkable that consensus
about treatment is still lacking. A systematic review is conducted to investigate which
classification can be used best for treatment decision making in thoracolumbar
fractures. Therefore, the reliability and clinical usefulness of currently most used
classifications (AO, TLICS/TLISS and new AOspine) are examined.
Methods
A comprehensive search is conducted using PubMed, EMBASE, Cinahl and Cochrane.
Search terms: Classification (Mesh), Spinal fractures (Mesh), and corresponding
synonyms. Of 4312 hits, 32 articles are selected for full text rating.
Results
20 articles are included; 17 to analyze reliability, 8 contain data considering clinical
usefulness. The presented kappa values indicate moderate to substantial agreement for
all three classifications. Regarding the clinical usefulness, >90% agreement between
actual treatment and classification recommendation is reported for most fractures.
However, it appears that over 50% of the patients with a stable burst fracture (TLICS 2,
AO‐A3/A4) in daily practice are operated, so in these cases treatment decision is not
primarily based on classification.
Conclusion
AO, TLICS and new AOspine classifications have acceptable accuracy regarding the
reproducibility (kappa >0.4). However, they are limited in clinical usefulness since the
treatment recommendation is not always implemented in clinical practice. The recently
validated Thoracolumbar AOspine Injury score seems promising for use in clinical
practice, because of inclusion of patient specific modifiers. Future research should
prove its definite value in treatment decision making.

Review: reliability and usefulness classifications
25
2
Introduction
Thoracolumbar fractures are common injuries. Without appropriate treatment, their
outcome can be devastating. Commonly, treatment decision is based upon accurate
radiological diagnosis and concomitant use of a fracture classification system. Several
classifications have been introduced during the past years. With the improvement of
imaging (e.g. CT, MRI), it has become possible to better understand the pathology of
the thoracolumbar spine fractures, and to recognize fracture patterns. These fracture
patterns give insight into fracture morphology, trauma mechanism and determination
of stability, and have led to various classification systems. Classifications aim to create a
common language with standardization and optimization of treatment. Currently most
used classifications are Magerl/AO and TLICS (Thoraco‐Lumbar Injury Classification and
Severity score).1‐3
AO classification is primary based on the pathomorphological characteristics of the
injury. It is often used for fracture classification, but does not include a reliable
estimation of prognosis for the determination of the best treatment.1,2 In 2005, Vaccaro
et al initially developed the TLISS (Thoraco‐Lumbar Injury Severity Score)3, which was
slightly modified to the TLICS in 2007.4 As the name already states, this classification
system includes a scoring system based on three variables, with subsequently
treatment algorithm. Recently, the new AOspine classification has been published,
which tries to simplify the comprehensive Magerl/AO classification and incorporates
features of both TLICS and Magerl/AO classifications.5,6 Table 2.1 shows a description of
the Magerl/AO, TLICS and new AOspine classification systems.
Considering the existence of various classification systems, and the quantity of research
that has been done to classify thoracolumbar fractures, it is remarkable that consensus
about treatment is still lacking. A validated classification of fractures remains the key to
an appropriate treatment algorithm. In an attempt to achieve worldwide consensus in
the treatment decision of traumatic thoracolumbar fractures, there is need for a
classification that should have two important characteristics: 1) it needs to create a
worldwide common language concerning the recognition of injury types (accuracy);
2) the treatment recommendation by the classification should be highly correlated to
the actual treatment (clinical usefulness).
For this reason, we have performed a systematic review to investigate the AO,
TLICS/TLISS and new AOspine classification concerning accuracy and clinical usefulness
in treatment decision making for traumatic thoracolumbar fractures.
The following research question is defined: ‘In traumatic thoracolumbar spine fractures,
which classification can be used best for treatment decision making?’

Chapter 2
26
Two sub questions are formulated: 1) What is the accuracy and 2) what is the clinical
usefulness of the AO, TLICS/ TLISS and new AOspine classification for traumatic
thoracolumbar fractures?
Table 2.1 Description of the Magerl/AO, TLICS and new AOspine classifications.
Magerl/AO TLICS New AOspine
Year 1994 2006 2013
Goal More comprehensive
classification, including all fracture types.
Simplified classification and
facilitate treatment decision making.
Allow for a development of a
globally accepted treatment algorithm.
Combination of Magerl/AO and
TLICS.
Concept Primarily based on the pathomorphology of the
injury pattern.
Treatment algorithm with point allocation, based on
Fracture morphology
Neurological status Posterior ligament complex
integrity
Classification based on the evaluation of three basic
parameters:
Fracture morphology Neurological status
Patient specific modifiers
Distinction Three main categories: A‐type: compressive force
which causes compression
and burst injuries B‐type: tensile force which
causes injuries with
transverse disruption C‐type: axial torque which
causes rotational injuries
Further division into 9
groups, 27 subtypes, and
over 50 specifications
Fracture morphology: Compression
Translational/rotational
Distraction
Neurological:
Intact Nerve root
Cord/conus medullaris
Cauda equina
Posterior ligament complex:
Intact Injury suspected/
indeterminate
Injured
Fracture morphology: Type A: compression
Type B: tension band injuries
Type C: translational injuries
Neurological status
N0 intact N1 transient deficit, no longer
present
N2 radiculopathy N3 incomplete spinal cord
injury
N4 complete spinal cord injury Nx not able to evaluate
Clinical modifiers M1: PLC integrity
M2: patient specific
comorbidities (rheuma, ankylosing spondylitis etc)
Treatment
management
Classification contains no
treatment recommendation. Consensus in clinical
application: conservative
treatment for A‐type (excluding burst), and
surgical treatment for B‐ and
C‐type fractures.
Treatment algorithm:
Nonoperative 0‐3points Nonoperative
or operative 4‐5points
Operative >5points
Treatment algorithm
(validated): Nonoperative 0‐3points
Nonoperative
or operative 4‐5points Operative >5points

Review: reliability and usefulness classifications
27
2
Methods
A comprehensive search of the English literature was conducted using PubMed,
EMBASE, Cinahl and the Cochrane Database. The literature was searched without any
data limitations. Search terms include: “Classification (MESH)”, with subsequent
corresponding synonyms (ao spine, ao classification, tlics, tliss, classification*,
systematics, taxonom*); AND “Spinal Fractures (MESH)” with subsequent synonyms
(spinal fracture*, spine fracture*, thoracolumbar fracture*, thoracic fracture*, lumbar
fracture *, vertebra fracture*, vertebral fracture*.) The full search process is shown in
Appendix 2.1.
All hits (PubMed 1128, EMBASE 2775, Cinahl 279, Cochrane 134; in total 4312 hits)
were imported to Refworks. Two independent researchers (IC AND MS) viewed all
references and included full text papers. In case of a different opinion, a third author
(PW) was consulted. Literature was in‐/excluded based on the following criteria.
Inclusion: thoracolumbar fractures; English language; analysis of AO, new AO spine,
TLICS or TLISS classification; measurements: intra‐ and/or inter observer validity (kappa
values,) or clinical usefulness expressed in specificity/sensitivity of an algorithm, or any
other way the applicability was scored. Exclusion: congress papers, instructional course
lectures, reviews; cadaver studies; cervical spine fractures; all other classification
methods except those mentioned in the inclusion; children; osteoporotic or other
pathological fractures; the expression of the clinical usefulness associated with
treatment related outcome.
The Prisma EBM checklist for diagnostic articles was used for the qualitative analysis.
See Table 2.2 for the qualitative analysis of the included literature.
Outcome parameters
Accuracy is defined as the inter‐ and intra‐observer reliability of the classification
systems. The reliability is expressed in kappa values, which are commonly used and
accepted for the measurement of data collection accuracy.7 For clinical usefulness, we
decide to focus on the applicability of the current classifications. This is quantified by
the agreement between classification recommendation and actual treatment, and
shows the correlation between classification recommendations and decision making.
Statistical analysis
Pooling of data could not be performed, because case cohorts and number of observers
were too variable in the included studies. As raw data were not available, it was not
possible to perform a meta‐analysis of kappa values.

Chapter 2
28
Table 2.2
Report of ‘worst case’ scenario of the 25 patients.
Study
Classification
Number
Study design
Quality
TLICS/TLISS
AO
New AO Fractures/patients Observer
Patient‐selection
Blinding
Level o
f evidence
Reliability
Oner (2002)8
x
60
5
Retrospective
+ +
4
Pishnam
az (2015)9
x
91
12
Case series
+ +
4
Kaul (2017)10
x
x 50
11
Retrospective
+ +
4
Urratia (2014)11
x 70
6
Retrospective
+ +
4
Lenarz (2009)12
x x
97
3
Retrospective
+ +
4
Cheng (2017)13
x 109
6
Retrospective
+ ?
4
Patel (2007)14
x
25
21
Prospective
+ +
3
Wood (2005)2
x
31
19
Retrospective
? +
4
Whang (2007)4
x
25
5
Prospective
+ +
3
Park (2016)15
x
134
2
Retrospective
+ +
4
Kriek (2006)16
x
150
6
Retrospective
+ +
4
Kep
ler (2016)17
x 25
100
Retrospective, validity
+ +
4
Vaccaro (2006)18
x
71
5
Validity
? +
4
Azimi (2015)19
x 56
2
Retrospective
? ‐
4
Reinhold (2013)5
x
110
5
Validity
+ ‐
4
Harrop (2006)3
x
56
30
Validity
? ?
4
Vaccaro (2013)20
x 40
9
Validity
+ ?
4
Clinical usefulness
Pishnam
az (2015)9
x
91
12
Case series
+ +
4
Vaccaro (2006)18
x
71
5
Validity
? +
4
Joaquim
(2010)21
x
49
Retrospective
+ ‐
4
Joaquim
(2013)22
x
458
Retrospective
+ ‐
4
Park (2016)15
x
134
2
Retrospective
+ +
4
Whang (2007)4
x
25
5
Prospective
+ +
3
Rajasekran
(2017)23
x 30
41
Retrospective
? +
4
Harrop (2006)3
x
56
30
Validity
? ?
4

Review: reliability and usefulness classifications
29
2
Results
Twenty‐eight articles were selected for full text rating. Four more were selected by
cross reference. After full text screening, the following 12 articles were excluded. The
full text article of Yacoub et al.24 was not available. One article by Mirza et al.25 was a
review of previous literature. Five articles were not applicable to answer the research
question of this review: Salgado26, Pizones27 and Winklhofer28 studied the influence of
the MRI on the classification system, instead of analyzing the reliability of the
classifications itself; Shen29 investigated the prognostic factors of failure of
conservatively treated burst fractures; and Pneumoticos30 compared TLICS 1‐3 and
TLICS 4 conservatively treated thoracolumbar spine fractures. Five articles contained
subgroup analysis of the same cohort published earlier (Joaquim 201431 presented the
same cohort as Joaquim 2013.22 Ratliff32 and Raja Rampersaud33 performed subgroup
analysis of the same cohort published by Harrop et al.3; and Sadiqi34 and Schroeder35
had subgroup analysis of the cohort studied by Kepler et al.17).
Seventeen papers were eligible for the first sub question regarding the inter‐ and intra‐
observer reliability. Eight articles could be used for answering the second question,
considering the clinical usefulness of the classification methods. The in‐ and exclusion
process is summarized in the PRISMA flow diagram (Figure 2.1).
Reliability
Seventeen articles described the inter‐ and/or intra‐observer validity of at least one of
the classification systems. Some studies showed different kappa values depending on
level of expertise and function of the observer. In that case we chose the kappa values
represented by the attending spine surgeons, as these were most representative for
clinical decision making. The data of the inter‐and intra‐observer kappa values are
shown in Table 2.3 and 2.4 respectively.
Regarding the proposed guidelines of Landis and Koch (1977)36, the kappa values
indicated moderate to substantial agreement (kappa >0.4) for all three classification
methods. A wide range of kappa values have been described in literature. These values
were influenced by various factors, including the number of observers, cases and
options, prevalence, blinding and work‐up bias. When taking that into account, all
current classifications had acceptable reliability. Kappa values of the new AO spine
classification seem slightly better than the Magerl/AO classification. In Figure 2.2 the
mean interobserver kappa values of the total TLICS score were expressed against the
number of observers. The larger the number of observers (and cases), the lower the
kappa value. The study of Patel et al.14 shows an outlier with a mean interobserver

Chapter 2
30
kappa value of 0.51 in 21 observers. This is higher than expected, but could be
explained by the fact that the attending observers had been involved in the
development of the TLISS system and that they had trained the remaining observers on
the use of the system. The kappa values of the validity studies were slightly higher than
the kappa values of the independent prospective cohort studies.
Figure 2.1 PRISMA flow diagram.

Review: reliability and usefulness classifications
31
2
Table 2.3
Overview interobserver kappa values.
Study
N Cases
N Observers
Diagnostics
Kap
pa values
AO classification
AO‐ABC
AO‐A
AO‐B
AO‐C
Oner (200
2)8
60
5 X, CT, M
RI
0.31 (.16‐.50)
0.61 (.47‐.86)
Pishnam
az (20
15)9
91
12
X,CT
0.45
Lenarz (2009)12
97
3 X, CT
0.71
Wood (2005
)2
31
19
X, CT
0.475 (.39‐.60)
Kriek (2006)16
150
6 X
0.403
New AOspine classification
AO‐ABC
AO‐A
AO‐B
AO‐C
Kaul (201
7)10
50
11
X, CT, M
RI
0.59
(±.01)
Vaccaro (2013)20
40
9 X, CT, M
RI
0.64
0.72
0.58
0.70
Reinhold (2013)5
110
5 X, CT
0.77
0.81
0.71
0.81
Chen
g (2017
)13
109
6 X, CT
0.362
0.38
5 0.292
0.55
2
Kep
ler (2016)
17
25
100
CT
0.74
0.80
0.68
0.72
Urratia (2014)11
70
6 X, CT
0.62
0.61
0.57
0.69
Azimi (20
15)15
74
2 X, CT, M
RI
0.88 (.8‐.94)
0.86 (.83‐.93)
0.89 (.84‐.94)
TLICS/TLISS classification
TLICS
total
TLICS
Mech
TLICS
PLC
TLICS
neu
Kaul (201
7)10
50
11
X, CT, M
RI
0.29
(±.01)
0.43 (±.01
) 0.47 (±.01)
0.85 (±.01
)
Lenarz (2009)12
97
3 X, CT
0.65
0.66
0.73
Patel (20
07)14
25
21
X, CT, M
RI
0.509 (±.006
) 0.636 (±.04)
0.534 (±.049
)
Whang (2007)4
25
5
X, CT, M
RI
0.45
5 0.626
0.447
Park (201
6)15
134
2 X, CT, M
RI
0.880 (±.033
) 0.96
6 (±.024)
0.858 (±.042
)
Vaccaro (2006)18
71
5 X, CT, M
RI
0.46
(±.03)
0.57 (±.04
) 0.48 (±.04)
0.93 (±.02
)
Harrop (2006)3
56
30
X, CT, M
RI
0.2403
0.2951
0.33
59
0.93
5

Chapter 2
32
Table 2.4
Overview intra‐observer kappa values.
Study
N Cases
N Observers
Diagnostics
Kap
pa values
AO classification
AO‐ABC
AO‐A
AO‐B
AO‐C
Oner (2002)8
60
5
X, CT, M
RI
0.35
Pishnam
az(2015)9
91
12
X, CT
‐
Lenarz (2009)12
97
3
X, CT
0.70
Wood (2005)2
31
19
X, CT
0.63
Kriek (2006
)16
150
6
X
0.334 (.18‐.49)
New AOspine classification
AO‐ABC
AO‐A
AO‐B
AO‐C
Kaul (201
7)10
50
11
X, CT, M
RI
0.61 (±.13
)
Vaccaro (2013)20
40
9
X, CT, M
RI
0.85
(.75‐.96)
0.72
0.43
Reinhold (2013)5
110
5
X, CT
‐
Chen
g (2017)13
109
6
X, CT
0.442
0.48
5 0.412
Kep
ler (201
6)17
25
100
CT
0.81
(.32‐1.0)
0.57
0.43
Urratia (2014)11
70
6
X, CT
0.77
(.72‐.83)
Azimi (20
15)15
74
2
X, CT, M
RI
0.84 (.82‐.91)
0.83 (.81‐.88
) 0.86
(.83‐.92)
TLICS/TLISS classification
TLICS
total
TLICS
Mech
TLICS
PLC
TLICS
neu
Kaul (201
7)10
50
11
X, CT, M
RI
0.44 (±.10
)
Lenarz (2009)12
97
3
X, CT
0.65
0.65
0.72
Patel (20
07)14
25
21
X, CT, M
RI
‐
Whang (2007)4
25
5
X, CT, M
RI
‐
Park (201
6)15
134
2
X, CT, M
RI
‐
Vaccaro (2006)18
71
5
X, CT, M
RI
0.29 (±.02
) 0.33 (±.03)
0.35
(±.03
) 0.91 (±.02
)
Harrop (2006)3
56
30
X, CT, M
RI
0.429
0.47
8

Review: reliability and usefulness classifications
33
2
Figure 2.2 Mean interobserver kappa TLICS total.
Clinical usefulness
Eight articles were included with data concerning the clinical usefulness of the
classification methods. Pishnamaz et al.9 used the AO classification and illustrated the
treatment strategy depending on AO fracture type. There was a large difference
between German and Dutch spine surgeons regarding treatment of burst fractures (AO
type A3). Whereas in Germany 96.2% of the A3 fractures were treated surgically, in the
Netherlands only 41.2% of these burst fractures were operated. They stated that
despite the internationally used classification systems, there is insufficient evidence to
install a standard treatment algorithm for fractures of the thoracolumbar spine.
Rajasekran et al.23 published their results concerning the usefulness of the new AO
spine classification in 2016. Forty‐one AOspine members classified 30 sets of images of
patients with thoracolumbar spine trauma of varying severity. Cases were assessed
independently and the reviewers were asked to answer questions regarding fracture
classification, type of treatment and need for further investigations. The presented
kappa values were not correlated with the observers, but with the diagnostics, as they
were measured in plain radiographs, CT and MRI. Hence, these data could not be
included in the aforementioned reliability section. However, they also looked for the
decision on fracture management. After the first assessment with plain radiographs,
72% of the patients were indicated for surgical treatment. This percentage increased
significantly to 81.7% with CT images. Additional MRI, however, did not alter treatment
strategy.

Chapter 2
34
Six papers debated the applicability of the treatment algorithm of the TLICS/TLISS
system. Vaccaro18, who proposed the TLISS, showed in his study in 2006 a >96%
agreement on the treatment recommendation of the TLISS within a group of five
observers scoring 71 clinical cases. Harrop et al.3, who were also part of the
development team for the TLISS classification, published the results of 48 observers
who assessed 56 cases. They reported an agreement of >90% among the surgeons on
the preferred management of the fracture and the TLISS graded management. In 2007,
Whang et al.4 presented validity data of the assessment of 25 cases by 5 observers.
They distinguished between TLICS and TLISS, but did not report any significant
differences between these two (almost) equal classifications. A correct prediction was
achieved in >90% of the cases, with a sensitivity of 89% and a specificity of 95%. In
2010, Joaquim et al.21 collected the data of a retrospective surgical cohort and
presented the safety and applicability of the TLICS system. Forty‐nine patients were
included. In 47 of the 49 patients (95.9%), the TLICS accurately matched surgical
decision making. There were two patients with a TLICS score of 2 points who
underwent surgical treatment. Both patients were diagnosed with a L1 burst fracture
without neurological injury. Operative treatment was recommended by the surgeon
because of concerns about the comminution and the possibility of progressive
deformity. In addition to this study, in 2013 Joaquim et al.22 performed an analysis of a
large retrospective cohort (N=458). 310 patients were treated conservatively. 99% of
these patients had a TLICS <4. There were nine failures, defined as patients that
received surgical treatment in a second stage. Three missed B‐type fractures required
surgery because of progressive deformity and severe pain. One patient needed surgery
after six months because of severe L5 radiculopathy (unknown if this was related to the
fracture). Five patients with burst fractures underwent surgery because of persistent
pain or progressive kyphosis. Only two of these had pain improvement postoperatively.
Furthermore, the author stated that of the 125 patients with burst fractures without
neurological deficit (TLICS 2), 96% were successfully treated without surgery. The
second group consisted of 148 patients who all received surgical treatment. Twenty‐
four complications (16.2%) were reported, varying from instrumental removal and
urinary infection to death (N=1). Surgical treatment matched the TLICS
recommendation only in 46.6% of the cases. The 53.4% mismatches were all stable
burst fractures (TLICS 2). No details about complications or other clinical implications in
the subgroup of surgically treated patients with stable burst fractures were described.
Recently, Park et al.15 described a modified TLICS score (mTLICS), and measured the
clinical usefulness of this mTLICS and the original TLICS classification. The analysis was
performed on 134 fractures, and images were independently interpreted by two
observers. Thirty‐one patients were treated surgically. Two of these patients had a

Review: reliability and usefulness classifications
35
2
TLICS <4 (6%). 58% (n=18) of the surgically treated patients scored a TLICS 4. Of the
103 conservatively treated patients, only one scored TLICS 5 by both observers.
In summary, literature concerning the clinical usefulness of the classification methods is
sparse. Joaquim et al.22 reported the largest series, in which it appeared that over 50%
of patients suffering a stable burst fracture (TLICS 2, AO type A3/A4) were surgically
treated, and treatment decision was based on other patient and fracture related
factors, mainly persistent pain and progressive kyphosis.
Discussion
With the available literature, we would postulate that the accuracy of all three
reviewed classifications is sufficient for use in clinical practice.2‐5,8‐20 Although kappa
values are in favor of the TLICS, we also believe that the accuracy of the AOspine
classification is sufficient for use in clinical practice. Since these classifications have a
different design, and the kappa values are calculated from different numbers of
variables (more fracture morphology options in the AOspine classification), it is difficult
to directly compare the kappa values of the TLICS versus the AO. With interobserver
kappa values of 0.36‐0.77 for the new AOspine, and 0.24‐0.88 for TLICS management,
they do not all reach the kappa value of >0.55, which is necessary for a classification
system to be clinically reliable, according to Sanders et al.37 But in answer to that
criterion, Öner et al.38 stated that this is too stringent for assessing the reliability of a
spinal fracture classification system. As kappa values depend on the number of options
(fracture types), observers and cases, one could state that in studies with many
observers and many fracture types a kappa value of <0.55 may be deemed acceptable.
Blinding of observers regarding treatment decision and outcome is important to have
the lowest risk of bias in kappa values. Therefore, study design is paramount. The
absolute kappa values found in the literature should therefore always be seen in
relation to the quality of the studies, and numbers of cases and observers.
Regarding the clinical usefulness, TLICS is the only current classification system that
contains a point allocation with treatment recommendation in practice. As an
extension of the new AOspine classification, Vaccaro et al introduced the
Thoracolumbar AOspine Injury score.20 This score contains a treatment algorithm, not
only based on the classification of the fracture morphology, but it also has a point
allocation for neurological status and patient‐specific‐modifiers (e.g. PLC status and
ankylosing spondylitis). In 2016, Kepler et al.39 and Vaccaro et al.40 presented a
validation study of this AOspine Injury score. In these studies, a worldwide surgeons’

Chapter 2
36
input was used to determine the initial treatment recommendation. However, there
are no results about the applicability of this score in clinical practice.
So, for all classifications scientific evidence of clinical usefulness is still poor. Very often,
treatment decisions are not based on the classification alone. Current literature shows
>90% agreement for the quite obvious treatment decision in simple compression
fractures (conservative) and clearly unstable B and C type fractures (surgical).3,4,18,21,22
However, in only 50% of the cases regarding stable burst fractures (AO A3/A4 and TLICS
2), treatment recommendation of the TLICS classification is followed by the surgeons,
as shown by Joaquim et al. (2013).22 Despite the evidence considering the safety of
conservative treatment41,42 and well known negative clinical implications of surgery
(e.g. complications, limitation in spinal movement), in most patients with stable burst
fractures an operation was performed.
In 2016, Bakhsheshian43 published a review of evidence based management of stable
thoracolumbar burst fractures. They concluded that a high level of evidence
demonstrated similar functional outcomes with conservative management when
compared with open surgical operative management. However, some burst fractures
treated conservatively had a poor outcome with progressive kyphosis and persistent
pain, which could be the reason for uncertainty in the clinical management of burst
fractures. For an appropriate treatment algorithm, the prognostic factors responsible
for worse outcome of these burst fractures should be elucidated.
The uncertainties concerning PLC integrity and burst fractures
Burst fractures and the Posterior‐ligament‐complex (PLC) integrity remain the most
important uncertainties. Clarification regarding these parameters would improve
uniform decision. Schnake et al.44 and Leferink et al.45 showed in their studies that
worse outcome may be due to the fact that burst fractures are actually missed B‐type
fractures. The difference between burst and B‐type fractures relies on the integrity of
the PLC. So, reliable assessment of the PLC integrity is crucial in these cases.
Unfortunately, evidence about the role of standard MRI in addition to plain radiographs
and CT is contradictory. Oner8, Salgado26, Pizones27, and Winklhofer28 presented results
in which MRI seemed to improve reliability and influence treatment strategies
compared to CT. But Rajasekaran23 performed a study with similar sensitivity for CT and
MRI, and reported no change in treatment decision after additional MRI. This would
indicate that plain radiographs and CT suffice for classification and treatment decision.
Literature regarding the reliability of MRI in PLC status resulted in fair to moderate
kappa values (kappa ± 0.4)46, and demonstrated relatively high negative predictive
values and relatively low positive predictive values for PLC injuries.47

Review: reliability and usefulness classifications
37
2
Despite the controversial evidence regarding MRI and PLC, agreement on the PLC status
is important, especially in burst fractures. We suggest in burst fractures routine MRI
could be of additional value. Without any edema in the PLC on MRI, the integrity is
established. But without an additional MRI, it is probably safer to value PLC as
undetermined in most burst fractures, leading to recommendation of surgical
treatment.
Prognostic patient and fracture related parameters
In addition to the PLC status, anterior comminution remains an important risk factor for
worse outcome in burst fractures, although definite evidence concerning its role is still
lacking. Recently, Spiegl et al.48 discussed a key role for the intervertebral disc in
determining the long‐term clinical and radiological outcome of burst fractures.
Incorporation of the intervertebral disc pathology into the existing classification
systems might be a valuable prognostic factor. Except these factors, previous studies
also stated that several other parameters might influence outcome in thoracolumbar
fractures. Shen et al.29 published results of a radiological and binary logistic regression
analysis. They showed that VAS pain scores and interpedicular distance could be
significant risk factors for failure of nonoperative treatment of burst fractures.
Furthermore, lower bone quality and bone regeneration (e.g. osteoporosis), higher age
and fracture localization at the thoracolumbar junction seem to be responsible for
worse radiological outcome.29,49
Clinical usefulness of the current classifications is still limited as outcome is influenced
by the abovementioned patient‐ and fracture related parameters. Including these
parameters in future classification systems may enhance prognostic value and thus
clinical usefulness of such classifications.
In this respect, with the addition of patient specific modifiers, the Thoracolumbar
AOspine Injury Score shows insight that other patient and fracture related parameters
are important in the search for a worldwide applicable and accepted classification and
treatment algorithm for thoracolumbar spine fractures.
Conclusion
Current TLICS and new AOspine classification have acceptable accuracy regarding their
reproducibility, but are limited in clinical usefulness since the treatment
recommendation is not always implemented in clinical practice, mainly in burst
fractures. The recently validated Thoracolumbar AOspine Injury score including patient

Chapter 2
38
specific modifiers seems promising for use in clinical practice. However, we would
suggest further evaluation of the clinical usefulness of this score, and consider adding
more relevant parameters associated with worse outcome.

Review: reliability and usefulness classifications
39
2
References
1. Magerl F, Aebi M, Gertzbein SD, et al. A comprehensive classification of thoracic and lumbar injuries.
Eur Spine J 1994;3(4):184‐201.
2. Wood KB, Khanna G, Vaccaro AR, et al. Assessment of two thoracolumbar fracture classification systems as used by multiple surgeons. J Bone Joint Surg Am 2005;87(7):1423‐9.
3. Harrop JS, Vaccaro AR, Hurlbert RJ, et al. Intrarater and interrater reliability and validity in the
assessment of the mechanism of injury and integrity of the posterior ligamentous complex: a novel injury severity scoring system for thoracolumbar injuries. Invited submission from the Joint Section
Meeting On Disorders of the Spine and Peripheral Nerves, March 2005. Spine Trauma Study Group. J
Neurosurg Spine 2006;4(2):118‐22. 4. Whang PG, Vaccaro AR, Poelstra KA, et al. The influence of fracture mechanism and morphology on the
reliability and validity of two novel thoracolumbar injury classification systems. Spine (Phila Pa 1976)
2007;32(7):791‐5. 5. Reinhold M, Audigé L, Schnake KJ, et al. AO spine injury classification system: a revision proposal for
the thoracic and lumbar spine. Eur Spine J 2013:22(10):2184‐201.
6. Max Aebi. AO spine classification system for thoracolumbar fractures. Eur Spine J 2013;22(10):2147‐8. 7. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 2012;22(3):276‐82.
8. Oner FC, Ramos LM, Simmermacher RK, et al. Classification of thoracic and lumbar spine fractures:
problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J 2002;11(3):235‐45. 9. Pishnamaz M, Curfs I, Balosu S, et al. Two‐nation comparison of classification and treatment of
thoracolumbar fractures: An internet‐based multicenter study among spine surgeons. Spine (Phila Pa
1976) 2015;40(22):1749‐56. 10. Kaul R, Chhabra HS, Vaccaro AR, et al. Reliability assessment of AOSpine thoracolumbar spine injury
classification system and Thoracolumbar Injury Classification and Severity Score (TLICS) for
thoracolumbar spine injuries: results of a multicentre study. Eur Spine J 2017;26(5):1470‐6. 11. Urrutia J, Zamora T, Yurac R, et al. An independent interobserver reliability and intraobserver
reproducibility evaluation of the new AOSpine Thoracolumbar Spine Injury Classification System. Spine
(Phila Pa 1976) 2015;40(1): E54‐8. 12. Lenarz CJ, Place HM, Lenke LG, et al. Comparative reliability of 3 thoracolumbar fracture classification
systems. J Spinal Disord Tech 2009;22(6):422‐7.
13. Cheng J, Liu P, Sun D, et al. Reliability and reproducibility analysis of the AOSpine thoracolumbar spine injury classification system by Chinese spinal surgeons. Eur Spine J 2017;26(5):1477‐82.
14. Patel AA, Whang PG, Brodke DS, et al. Evaluation of two novel thoracolumbar trauma classification
systems. Indian J Orthop 2007;41(4):322‐6. 15. Park, Lee, Park NH, et al. Modified thoracolumbar injury classification and severity score (TLICS) and its
clinical usefulness. Acta Radiol 2016;57(1):74‐81.
16. Kriek JJ, Govender S. AO‐classification of thoracic and lumbar fractures‐‐reproducibility utilizing radiographs and clinical information. Eur Spine J 2006;15(8):1239‐46.
17. Kepler CK, Vaccaro AR, Koerner JD, et al. Reliability analysis of the AOSpine thoracolumbar spine injury
classification system by a worldwide group of naïve spinal surgeons. Eur Spine J 2016;25(4):1082‐6. 18. Vaccaro AR, Baron EM, Sanfilippo J, et al. Reliability of a novel classification system for thoracolumbar
injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976) 2006;31(11 Suppl):S62‐9;
discussion S104. 19. Azimi P, Mohammadi HR, Azhari S, et al. The AOSpine thoracolumbar spine injury classification system:
A reliability and agreement study. Asian J Neurosurg 2015;10(4):282‐5.
20. Vaccaro AR, Oner C, Kepler CK, et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976) 2013;38(23):2028‐37.
21. Andrei F. Joaquim, MD, Yvens B. Fernandes, PhD, MD, Rodrigo A. C. Cavalcante, MD, et al. Evaluation of
the thoracolumbar injury classification system in thoracic and lumbar spinal trauma. Spine2011;36: 33‐6.

Chapter 2
40
22. Joaquim AF, Daubs MD, Lawrence BD, et al. Retrospective evaluation of the validity of the Thoracolumbar Injury Classification System in 458 consecutively treated patients. Spine J 2013;13(12):
1760‐5.
23. Rajasekaran S, Vaccaro AR, Kanna RM, et al. The value of CT and MRI in the classification and surgical decision‐making among spine surgeons in thoracolumbar spinal injuries. Eur Spine J 2017;26(5):1463‐9.
24. Yacoub AR, Joaquim AF, Ghizoni E, et al. Evaluation of the safety and reliability of the newly‐proposed
AO spine injury classification system. J Spinal Cord Med 2017;40(1):70‐5. 25. Mirza SK, Mirza AJ, Chapman JR, et al. Classifications of thoracic and lumbar fractures: rationale and
supporting data. J Am Acad Orthop Surg 2002;10(5):364‐77.
26. Salgado Á, Pizones J, Sánchez‐Mariscal F, et al. MRI reliability in classifying thoracolumbar fractures according to AO classification. Orthopedics 2013;36(1):e75‐8.
27. Pizones J, Izquierdo E, Alvarez P, et al. Impact of magnetic resonance imaging on decision making for
thoracolumbar traumatic fracture diagnosis and treatment. Eur Spine J 2011;20 Suppl 3:390‐6. 28. Winklhofer S, Thekkumthala‐Sommer M, Schmidt D, et al. Magnetic resonance imaging frequently
changes classification of acute traumatic thoracolumbar spine injuries. Skeletal Radiol 2013;42(6):
779‐86. 29. Shen J, Xu L, Zhang B,
et al. Risk factors for the failure of spinal burst fractures treated conservatively
according to the thoracolumbar injury classification and severity score (TLICS): A retrospective cohort
trial. PLoS One 2015;10(8):e0135735. 30. Pneumoticos, Karampinas PK, Triantafilopoulos G, et al. Evaluation of TLICS for thoracolumbar
fractures. Eur Spine J 2016;25(4):1123‐7.
31. Joaquim AF, Lawrence B, Daubs M, et al. Measuring the impact of the Thoracolumbar Injury Classification and Severity Score among 458 consecutively treated patients. J Spinal Cord Med
2014;37(1):101‐6.
32. Ratliff J, Anand N, Vaccaro AR, et al. Regional variability in use of a novel assessment of thoracolumbar spine fractures: United States versus international surgeons. World J Emerg Surg 2007;2:24.
33. Raja Rampersaud Y, Fisher C, Wilsey J, et al. Agreement between orthopedic surgeons and
neurosurgeons regarding a new algorithm for the treatment of thoracolumbar injuries: a multicenter reliability study. J Spinal Disord Tech 2006;19(7):477‐82.
34. Sadiqi S, Oner FC, Dvorak MF, et al. The influence of spine surgeons' experience on the classification
and intraobserver reliability of the novel AOSpine thoracolumbar spine injury classification system‐an international study. Spine (Phila Pa 1976) 2015;40(23):E1250‐6.
35. Schroeder GD, Kepler CK, Koerner JD, et al. Is there a regional difference in morphology interpretation
of A3 and A4 fractures among different cultures? J Neurosurg Spine 2015:1‐8. 36. Landis JR, Koch GC. The measurement of observer agreement for categorical data. Biometrics
1977;36:207‐16.
37. Sanders RW: Editorial. The problem with apples and oranges. J Orthop Trauma 1997;11:465‐6. 38. Oner FC, van Gils AP, Dhert WJ et al: MRI findings of thoracolumbar spine fractures: a categorization
based on MRI examinations of 100 fractures. Skeletal Radiol 1999;28:433‐43.
39. Christopher K.Kepler, Alexander R.Vaccaro, Gregory D. Schroeder et al. The Thoracolumbar AOSpine Injury Score. Global Spine J 2016;6:329‐34.
40. Vaccaro AR, Schroeder GD, Kepler CK et al. The surgical algorithm for the AOSpine thoracolumbar spine
injury classification system. Eur Spine J 2016;25(4):1087‐94. 41. Weninger P, Schultz A, Hertz H. Conservative management of thoracolumbar and lumbar spine
compression and burst fractures: functional and radiographic outcomes in 136 cases treated by closed
reduction and casting. Arch Orthop Trauma Surg 2009;129(2):207‐19. 42. Abudou M, Chen X, Kong X, Wu T. Surgical versus non‐surgical treatment for thoracolumbar burst
fractures without neurological deficit. Cochrane database, 2013;(6):CD005079.
43. Bakhsheshian J, Dahdaleh NS, Fakurnejad S, et al. Evidence‐based management of traumatic thoracolumbar burst fractures: a systematic review of nonoperative management. Neurosurg Focus.
2014;37(1):E1.

Review: reliability and usefulness classifications
41
2
44. Schnake KJ, von Scotti F, Haas NP, et al. Unfallchirurg.Type B injuries of the thoracolumbar spine : misinterpretations of the integrity of the posterior ligament complex using radiologic diagnostics.
Unfallchirurg 2008;111(12):977‐84
45. Leferink VJ, Veldhuis EF, Zimmerman KW et al. Classificational problems in ligamentary distraction type vertebral fractures: 30% of all B‐type fractures are initially unrecognised. Eur Spine J 2002;11(3):246‐50
46. Lee GY, Lee JW, Choi SW, et al. MRI inter‐reader and intra‐reader reliabilities for assessing injury
morphology and posterior ligamentous complex integrity of the spine according to the thoracolumbar injury classification system and severity score. Korean J Radiol 2015;16(4):889‐98
47. van Middendorp J, A Patel, Schuetz M, Joaquim AF. The precision, accuracy and validity of detecting
posterior ligamentous complex injuries of the thoracic and lumbar spine: a critical appraisal of the literature. Eur Spine J 2013; 22(3): 461‐74.
48. Spiegl UJ, Josten C, Devitt BM et al. Incomplete burst fractures of the thoracolumbar spine: a review of
literature. Eur Spine J. 2017;26(12):3187‐98. 49. Curfs I, Grimm B, van der Linde M, et al. Radiological Prediction of Posttraumatic Kyphosis After
Thoracolumbar Fracture. Open Orthop J 2016;10:135‐42.

Chapter 2
42
Appendix 2.1
Search process
PubMed Search date: 16‐03‐2017 Hits 1128
Search Query Items found
#15 Search #10 AND #14 1128
#14 Search #12 OR #13 17811
#13 Search spinal fracture*[tiab] OR spine fracture*[tiab] OR thoracolumbar
fracture*[tiab] OR thoracic fracture*[tiab] OR lumbar fracture*[tiab] OR vertebra fracture*[tiab] OR vertebral fracture*[tiab]
10664
#12 Search "Spinal Fractures"[Mesh] 12457
#10 Search #7 OR #8 OR #9 818927 #9 Search ao spine[tiab] OR TLICS[tiab] OR ao classification [tiab] OR
TLISS[tiab]
808
#8 Search Classification*[tiab] OR Systematics[tiab] OR Taxonom*[tiab] 303573 #7 Search "Classification"[Mesh] OR "classification" [Subheading] 606407
EMBASE date: 16‐03‐2017 Hits 2775
Cochrane date: 16‐03‐2017 Hits 134

Review: reliability and usefulness classifications
43
2
CINAHL date: 16‐03‐2017 Hits 279

Chapter 2
44

45
Chapter 3
Reliability and agreement of different spine fracture
classification systems: an independent intra‐ and
interobserver study
M. Pishnamaz, S. Balosu, I. Curfs, D. Uhing, M. Laubach, P. Willems, C. Herren,
C. Weber, F. Hildebrand, P. Kobbe
World Neurosurg 2018;115:e695‐e702

Chapter 3
46
Abstract
Objective
Currently, no spinal classification system has achieved universal acceptance. Therefore,
it is important to choose a reliable classification within clinical practice. The objective of
this study was to determine and compare the intraobserver and interobserver
agreement of the Load Sharing Classification (LSC), the Thoracolumbar Injury
Classification System (TLICS), and the AOSpine Thoracolumbar Spine Injury
Classification System.
Methods
In this web‐based intraobserver and interobserver study (www.spine.hostei.com), plain
radiographs and computed tomographic scans of traumatic thoracolumbar fractures
(T12eL2) were evaluated. By use of a questionnaire, fractures were classified according
to the LSC, the TLICS, and the AOSpine classification. Data were analyzed with SPSS
(Version 21, 76 Chicago, Illinois, USA).
Intraobserver and interobserver agreement was determined by the Cohen k. Statistical
significance was defined as P<0.05.
Results
Data from 91 patients were classified twice by 7 board‐certified spine surgeons. The
intraobserver and interobserver reliability considering the LSC total score was noted as
fair (intraobserver/interobserver reliability: k [ 0.26/0.22). Considering the resulting
TLICS total score, a moderate intraobserver agreement (k [ 0.41) was noted, whereas
the interobserver results presented only fair reliability (k [ 0.23). In contrast to the LSC
and the TLICS, the AOSpine classification showed substantial agreement considering the
fracture type (A;B;C) (intraobserver/interobserver reliability: k [ 0.71/0.61) and
moderate agreement considering the fracture subtype (e.g., A0;A1;.;B1;.)
(intraobserver/interobserver reliability: k [ 0.57/0.48).
Conclusion
In conclusion, the reliability of the AOSpine fracture classification is superior to the
TLICS and the LSC. Therefore, this classification system could best be applied within
clinical practice.

Reliability and agreement study on classifications
47
3
Introduction
Spinal fracture classifications aim to describe the morphology and the severity of an
injury in a reproducible way. An ideal classification should incorporate relevant clinical
factors to standardize the therapeutic decision‐making process.1‐3 Currently, various
classification systems are used to describe thoracolumbar fractures, but a universally
accepted classification system is still missing.4,5 To facilitate the decision‐making
process for surgical stabilization of spinal fractures, McCormack et al.6 developed a
classification system that should distinguish fractures that can be treated by short
segment stabilization from those that require additional anterior fusion.2 By the use of
plain radiographs and computed tomography (CT) they created a point system that
describes 3 different fracture site characteristics: the amount of vertebral body
comminution, the apposition of the fracture fragments, and the degree of kyphotic
deformity. Unfortunately, this classification does not address the neurologic status of
the patient, and injuries of the posterior ligamentous complex (PLC) seem to be
underestimated. The Thoracolumbar Injury Classification System (TLICS) describes the
natural history of an injury pattern but also serves to rank the degree of instability. This
system is based on 3 major characteristics: the morphology of the injury, the integrity
of the PLC, and the neurologic status of the patient.1 By including the neurologic status
and the integrity of the PLC, additional facets of instability and severity of the injury
should be considered to improve the decision‐making process within clinical
management.
Depending on the fracture type, some authors could show notable limitations with the
TLICS.7,8 The AOSpine Thoracolumbar Spine Injury Classification System was introduced
in 2013 by Vaccaro et al.8 This classification system was an improvement and
simplification of the overly complex comprehensive classification of Magerl et al.9 and
incorporates features of both the Magerl classification and the TLICS. Even though the
use of this classification is increasingly popular in many countries, none of the above‐
mentioned classifications have achieved universal acceptance.
Under consideration of the advantages and disadvantages of those classification
systems, this study aimed to determine and compare the intraobserver and
interobserver agreement of the Load Sharing Classification (LSC), the TLICS, and the
AOSpine classification by analysis of 91 clinical cases. This study was approved by the
Independent Ethics Committee of the RWTH Aachen University, Aachen, Germany
(Reference number: EK‐078/15).

Chapter 3
48
Methods and materials
This intraobserver and interobserver study was performed on the basis of online
documentation. A website (www.spine.hostei.com) provided details of patients with
traumatic fractures of the thoracolumbar junction. Plain anterior and lateral
radiographs and CT scans (1‐mm slices) in all 3 reconstructions (axial, sagittal, and
coronal)
were uploaded (Figure 3.1). For sample size planning, a precedent pilot study was
performed. Consequently, all participating surgeons were asked to classify the cases by
applying the LSC, TLICS, and AOSpine classifications. Recall bias was prevented by
applying a 3‐month time lapse after the first assessment round.
Figure 1.3 Exemplary illustration of the patients’ computed tomographic scans in all 3 reconstructions
(axial, sagittal, and coronal).

Reliability and agreement study on classifications
49
3
Participants
All participants were experienced surgeons from orthopedic or trauma departments,
specialized in spine surgery. Each participant was well versed in the LSC, the TLICS, and
the AOSpine classification schemes and received the original article of each
classification system 1 month before the start of the study. All participants stated that
they would routinely apply the new AOSpine classification at the time of the study. The
spine surgeons from Germany stated that they used the AO Magerl classification before
the implementation of the AOSpine classification in 2015, whereas the participating
surgeons from the Netherlands indicated that they had used the TLICS previous to the
AOSpine classification.
Inclusion criteria of patients
A committee of experts assembled a case series of 91 consecutive patients treated in
1 of 2 university hospitals (Aachen and Maastricht). Only patients with acute traumatic
injuries of the thoracolumbar junction (T11‐L2) were included. Patients with
osteoporotic fractures, tumors, or spondylodiscitis and patients with incomplete CT
reconstructions were excluded. The treating surgeons did not serve as observers in the
study.
Classifications
The LSC uses 3 radiologic spinal fracture characteristics and allocates 1 to 3 points to
each of those items. Consequently, this results in a scale of at least 3 to a maximum of
9 points.6 Within the LSC, k values for each of the 3 items: amount of vertebral body
comminution (LSC A), apposition of the fracture fragments (LSC B), and the correction
of kyphotic deformity (LSC C) along with the LSC total score (LSC AþBþC) were
determined.
The TLICS is an advancement of the thoracolumbar injury severity score (TLISS). Within
this classification system, 3 major elements are scored: fracture morphology
(1‐4 points), integrity of the posterior ligamentous complex (0, 2, or 3 points) and
neurologic status (0, 2, or 3 points). By summing up the scores of the 3 categories, a
total score of 1 to 10 points can be allocated.1 The k values and percentage agreement
for each category and the resulting TLICS total score were analyzed. In contrast to the
AOSpine classification, the observers were asked to determine the neurologic status
within the TLIC system. This course of action was chosen because the neurologic status
in the TLIC system is an elementary component for the calculation of the TLICS score
and the associated recommendation for therapy.

Chapter 3
50
The AOSpine classification consists of a morphologic fracture classification and a
grading system for neurologic status, and it involves patient‐specific modifiers.
Thoracolumbar fractures are classified on the basis of 3 major fracture types (type A, B,
or C) and 9 further specified subtypes (e.g., A0;A1;.;B1;.).8
Inasmuch this study focused on the reliability of the AO fracture type and subtypes, the
AO qualities of neurologic status and patient modifiers were not part of this
investigation. Analogous to the LSC and the TLICS, k values and percentage agreement
of the fracture type and the subgroups were calculated.
Statistical methods
The deidentified data were analyzed with SPSS (Version 21, 76, Chicago, Illinois, USA).
To determine interobserver agreement, the Cohen k and the percentage agreement
between the surgeons were used. As in previous studies, we used the guidelines of
Landis and Koch10 to categorize k values from 0 to 0.2 indicating slight reliability, 0.21
to 0.4 fair, 0.41 to 0.6 moderate, 0.61 to 0.8 substantial, and 0.81 to 1 almost perfect
reliability. The agreement of the first and second assessment was compared by the use
of a paired t test. Statistical significance was defined as P<0.05.
Results
The plain radiographs and CT scans of the 91 patients were classified twice by 7 board‐
certified spine surgeons. An overview of the patients’ characteristics can be found in
Table 3.1. As a result, 1274 case‐specific classifications were obtained for each of the
LSC, the TLICS, and the AOSpine classifications.
Table 3.1 Demographic data of patients.
Characteristics Number (5)
Age (years) ± SD 50.8 ± 18.1
Sex
Male 45 (49.5) Female 46 (50.5)
Fracture distribution
T11 9 (9.9) T12 27 (29.7)
L1 34 (37.4)
L2 21 (23.1)
SD, standard deviation.

Reliability and agreement study on classifications
51
3
Intraobserver reliability
Within the LSC, moderate and almost equal agreement was found between all
3 subgroups (comminution, apposition of fragments, and deformity) (k value/
percentage agreement: LSC A, k=0.46 (67%); LSC B, k=0.46 (67%); LSC C, k=0.44 (68%)).
Only fair intraobserver agreement was found in the resulting LSC total score (k=0.26;
percentage agreement: 39%) (Table 3.2). The TLICS classification showed moderate
agreement determining the variable injury pattern (k=0.51; percentage agreement,
73%) and integrity of the PLC (k=0.47; percentage agreement, 74%). Even substantial
reliability was found for the variable neurologic status (k=0.78; percentage agreement,
96%).
Table 3.2 Intraobserver reliability of the load sharing classification (LSC).
κ value/% agreement LSC A LSC B LSC C LSC total score
Observer 1 0.46 69%
0.46 66%
0.52 73%
0.24 38%
Observer 2 0.39
66%
0.47
71%
0.29
69%
0.20
38%
Observer 3 0.44 64%
0.52 69%
0.46 65%
0.21 34%
Observer 4 0.53
70%
0.42
67%
0.52
70%
0.24
36% Observer 5 0.55
70%
0.35
60%
0.39
60%
0.33
43%
Observer 6 0.42 62%
0.62 78%
0.38 63%
0.32 43%
Observer 7 0.46
68%
0.38
64%
0.54
73%
0.26
41% Mean 0.46
67%
0.46
68%
0.44
68%
0.26
39%
Considering the resulting TLICS total score, moderate agreement (k=0.41; percentage
agreement, 58%) was noted (Table 3.3). Overall, the intraobserver reliability for the
AOSpine fracture type (A;B;C) showed substantial results (k=0.71; percentage
agreement, 92%). One observer even achieved almost perfect agreement (k=0.81;
percentage agreement, 95%) (Table 3.4). The evaluation of the fracture subgroups (e.g.,
A0;A1;.;B1;.) revealed moderate results between the first and the second rounds
(k=0.57). Consequently, the percentage agreement was 68% (Table 3.4).

Chapter 3
52
Table 3.3 Intraobserver reliability of the thoracolumbar injury classification (TLIC) system.
κ value/% agreement Morphology of injury Integrety of PLC Neurologic status TLICS total score
Observer 1 0.65
79%
0.56
80%
0.93
99%
0.52
68%
Observer 2 0.41 62%
0.37 67%
0.66 95%
0.31 46%
Observer 3 0.47
70%
0.52
71%
0.85
97%
0.44
55% Observer 4 0.76
86%
0.45
74%
0.80
97%
0.52
64%
Observer 5 0.39 67%
0.25 63%
0.66 93%
0.20 413%
Observer 6 0.61
75%
0.51
74%
0.94
99%
0.51
63% Observer 7 0.30
70%
0.64
90%
0.62
95%
0.36
66%
Mean 0.51 73%
0.47 74%
0.78 96%
0.41 58%
Table 3.4 Intraobserver agreement of the AOSpine classification.
AO fracture type (A;B;C) AO fracture subgrpup (A0;A1;...;B1;...)
Observer κ % κ %
Observer 1 0.66 90 0.54 66
Observer 2 0.79 95 0.62 71 Observer 3 0.55 89 0.55 66
Observer 4 0.81 95 0.57 67
Observer 5 0.67 90 0.55 65 Observer 6 0.74 91 0.61 69
Observer 7 0.77 95 0.58 69
Mean 0.71 92 0.57 68
Interobserver reliability
The interobserver agreement of the LSC during the first assessment was fair (k=0.24),
whereas the agreement of the second assessment showed only slight reliability
(k=0.19). Interestingly, there was no significant difference in the agreement between
both assessments (percentage agreement: first assessment, 36%; second assessment,
32%; P>0.05). Overall, the interobserver agreement for the LSC total score was noted as
fair (first þ second assessment: k=0.22; percentage agreement, 34%). The TLICS total
score showed fair agreement during the first (k=0.21) and the second assessments
(k=0.26). There was no significant difference in the agreement between both rounds
(percentage agreement: first assessment, 38%; second assessment, 43%; P>0.05).
In summary, this went along with a median k value of 0.23 and a percentage agreement
of 41% for both assessments. The interobserver reliability of the AOSpine fracture type

Reliability and agreement study on classifications
53
3
(A;B;C) showed substantial reliability (k=0.61; percentage agreement, 89%). There was
no significant difference between the first and second evaluations (P>0.05). Considering
the fracture subgroups (e.g., A0;A1;.;B1;.) there was still moderate interobserver
agreement within the first (k=0.41) and second assessments (k=0.54). Interestingly, the
percentage agreement was significantly higher in the second assessment than in the
first (percentage agreement: first assessment, 54%; second assessment, 66%; P<0.05).
Overall, we found moderate agreement for the AOSpine subgroup evaluation (first þ
second assessment: k=0.48; percentage agreement, 60%) (Table 3.5).
Table 3.5 Overall (median of first and second assessments) interobserver reliability (κ) and % agreement
of the AOSpine, load sharing classifications.
AOSpine classification TLICS classification Load sharing classification
Observer κ % κ % κ %
Observer 1‐2 0.43 58 0.25 45 0.14 31
Observer 1‐3 0.35 53 0.17 33 0.30 42 Observer 1‐4 0.36 51 0.35 51 0.14 28
Observer 1‐5 0.40 54 0.17 34 0.24 30
Observer 1‐6 0.33 48 0.26 37 0.24 31 Observer 1‐7 0.43 59 0.34 62 0.25 39
Observer 2‐3 0.65 75 0.17 34 0.18 33
Observer 2‐4 0.57 66 0.24 40 0.06 19 Observer 2‐5 0.37 52 0.19 36 0.17 31
Observer 2‐6 0.53 63 0.19 34 0.16 31
Observer 2‐7 0.78 84 0.21 45 0.20 37 Observer 3‐4 0.46 58 0.31 47 0.23 34
Observer 3‐5 0.32 48 0.35 50 0.26 37
Observer 3‐6 0.41 53 0.23 40 0.29 40 Observer 3‐7 0.78 84 0.12 30 0.29 41
Observer 4‐5 0.40 54 0.29 47 0.22 33
Observer 4‐6 0.71 78 0.37 51 0.22 34 Observer 4‐7 0.49 60 0.19 41 0.16 29
Observer 5‐6 0.40 54 0.26 44 0.25 37
Observer 5‐7 0.39 54 0.11 31 0.23 36 Observer 6‐7 0.44 56 0.10 25 0.30 42
Median 0.48 60 0.23 41 0.22 34
AOSpine, Arbeitsgemeinschft für Osteosynthesefragen system; TLICS, thoracolumbar Injury classification system.
Discussion
Fracture classifications are conceptual tools for the understanding and communication
of an injury pathomechanism with, preferably, therapeutic and prognostic
consequences.11 As yet, a fully accepted and universally used spinal classification

Chapter 3
54
system is still missing.1,5,12,13 An optimal classification system should describe the
morphology and determine the severity of an injury by involving the radiologic, clinical,
and neurologic aspects as a guide through the decision‐making process, but this is
difficult to realize.5 One major problem is the poor reliability and reproducibility of
more detailed classification systems. Furthermore, the application of severity scoring
systems may not reflect global surgical preferences.8 The aim of this study was to
determine and compare the reliability of the LSC, the TLICS,
and the AOSpine classifications to identify which of those classification systems is the
most reliable within the clinical setting. In this line our main findings are as follows:
1. The interobserver agreement of the AOSpine fracture classification was superior to
the results of the TLICS and the LSC total score.
2. The intraobserver agreement for fracture subtypes (e.g., A0;A1;.;B1;.) of the
AOSpine classification and the TLICS total score were moderate, whereas the LSC
total score just achieved fair reliability.
3. The intraobserver reliability of the LSC and the TLICS showed moderate to
substantial results when the subgroup qualities were considered.
Several studies have focused on the reliability of LSC,2,14 the TLICS,1,7,13,15,16 and the
AOSpine classification,4,5,7,8,12,17‐19 but to our knowledge this is first study to compare
these 3 classifications by means of a single case series. Urrutia et al.18 performed an
independent intraobserver and interobserver study to investigate the reliability of the
AOSpine classification. They observed substantial interobserver agreement (k=0.62) for
the major fracture types (A;B;C) and moderate agreement when considering the
subtypes (k=0.55). Their intraobserver reproducibility was substantial in both the
fracture type and subtype (fracture type, k=0.77; subtype, k=0.71).1
Kaul et al.7 compared the reliability of the AOSpine classification and the TLICS. They
also found moderate interobserver reliability (k=0.45 and 0.59 with and without
fracture subtype) and substantial intraobserver reliability (k=0.61 and 0.68 with and
without fracture subtype) for the fracture subtype of the AOSpine classification. Our k
values also show substantial intraobserver and interobserver agreement considering
the major fracture type, and moderate to substantial agreement considering the
fracture subtype. Those findings are in agreement with other studies4,17 and show the
high reliability of this classification. Nonetheless, the k values of independent spine
surgeons considering the AOSpine classification are frequently slightly below the values
of its original group.7,8,18 Within this study we found moderate to substantial
intraobserver agreement for the individual TLICS elements, and moderate to fair

Reliability and agreement study on classifications
55
3
intraobserver and interobserver reliability regarding the TLICS total score. These
findings are in line with the results of Kaul et al.,7 who also noted moderate
interobserver (k=0.44) and fair interobserver reliability (k=0.29) in terms of the TLICS
total score. By contrast, Lewkonia et al.15 found higher agreement of the TLICS total
score (intraobserver reliability: Pearson product moment correlation coefficient (rxy):
0.74; interobserver reliability: (rxy): 0.73‐0.74) by grading 54 cases on 2 different
occasions, and Koh et al.16 even presented a substantial TLICS total score agreement
with almost perfect agreement in terms of the elements integrity of the PLC and
neurologic status. This discrepancy may be due to the fact that both of those studies
provided magnetic resonance imaging (MRI) scans for the grading of the fractures in
addition to CT scans and plain radiographs. Nevertheless, the availability of MRI is
difficult in many parts of the world, and, therefore, more recently proposed
classification systems are solely based on plain radiographs and CT scans.4,8 To compare
the classifications within our study, it seemed to be better to exclude additional MRI
scans to avoid confusion in the interpretation of the LSC and AOSpine classifications.
Within this study, the LSC presented the lowest agreement compared to the TLICS and
AOSpine classifications. Even though all 3 separate components of the classification
achieved moderate agreement, the intraobserver and interobserver agreement for the
total score showed only fair results. Elzinga et al.2 observed a series of 40 spinal
fractures and also found fair reliability of the LSC total score (intraobserver reliability,
k=0.29; interobserver reliability, k=0.22). By contrast, Dai et al.14 showed in their study
a substantial interobserver agreement (k=0.73‐0.92) with an almost perfect
intraobserver agreement of all participants regarding the 3 separate LSC components
(k=0.89). One possible explanation for the high reliability observed by Dai et al.14 was
brought up by Elzinga et al.,2 who assumed that Dai et al.14 included only fractures with
the highest (9) and the lowest (3) LSC scores, which would inevitably be accompanied
by a loss of variability.
This is due to the fact that the highest and lowest LSC scores are possible only if the
rating for the respective components are also rated with the highest or lowest ratings.
By contrast, a LSC score of 6 or 7 can be obtained in different ways and thus in turn
generates space for disagreement.2 However, besides the discrepancy regarding
reliability, another weakness of this classification might be identified by Radcliff et al.,20
who showed that the LSC does not uniformly correlate with PLC injuries and neurologic
status. Chhabra et al.13 performed an international survey among 42 spine surgeons.
They postulated that none of the existing classification systems were ideal and that
better classifications need to be developed to address deficits in the reliability and
guidance for treatment and to be more comprehensive in order of priority. By means of
our study we confirm this statement. On the other hand, we think it will not be possible

Chapter 3
56
to generate a unique classification system that could address all requirements for the
diversity of thoracolumbar fractures in a perfect way. Within this study the reliability of
the AOSpine fracture classification was superior to the TLICS and the LSC and therefore
is the classification that at present could best be applied within clinical practice.
Furthermore, we believe that additional consideration of the neurologic status and the
inclusion of modifiers can provide further benefits. However, on the basis of our data
the use of a scoring system does not seem to be helpful in the decision‐making process
because it has a negative impact on the reliability of the classification.
Strengths and limitations
One strength of our study is the large sample of 91 spine cases, which subsequently
leads to a high variability regarding the fracture morphology. Furthermore, the
inclusion of 3 different spine classification systems offers the possibility to compare the
reliability within a single case series. By contrast, our study has certain limitations. First,
the participating surgeons of this study may be more familiar with the AO system
because of their previous use of the Magerl classification, from which the new
classification system is derived. Furthermore, we did not consider the influence of
different fracture types on the reliability of the respective classification systems within
our study. Other studies could show that particular fracture types appear to be more or
less difficult to classify.12 Further studies are necessary to prove whether the AOSpine
classification is advantageous in all fracture subtypes. Finally, we did not provide MRI
scans for the observation of our fractures. MRI provides additional information
regarding injuries to the PLC or epidural bleeding. Therefore, its use can increase the
reliability of classifications. However, the implementation of MRI is not possible all over
the world, and, therefore, the use of MRI data should be avoided in proving the
reliability of global classification systems.
Conclusion
In conclusion, the reliability of the AOSpine fracture classification is higher than the
TLICS and the LSC. By means of our study, this classification system could best be
applied within clinical practice.

Reliability and agreement study on classifications
57
3
References
1. Vaccaro AR, Lehman RA Jr, Hurlbert RJ, Anderson PA, Harris M, Hedlund R, et al. A new classification of
thoracolumbar injuries: the importance of injury morphology, the integrity of the posterior ligamentous
complex, and neurologic status. Spine 2005;30:2325‐33. 2. Elzinga M, Segers M, Siebenga J, Heilbron E, de Lange‐de Klerk ES, Bakker F. Inter‐ and intraobserver
agreement on the Load Sharing Classification of thoracolumbar spine fractures. Injury 2012;43:416‐22.
3. Pishnamaz M, Curfs I, Balosu S, Willems P, Hemert W, Pape HC, et al. Two‐nation comparison of classification and treatment of thoracolumbar fractures: an internet‐based multicenter study among
spine surgeons. Spine 2015;40:1749‐56.
4. Kepler CK, Vaccaro AR, Koerner JD, Dvorak MF, Kandziora F, Rajasekaran S, et al. Reliability analysis of the AOSpine thoracolumbar spine injury classification system by a worldwide group of naive spinal
surgeons. Eur Spine J 2016;25: 1082‐6.
5. Schnake KJ, Schroeder GD, Vaccaro AR, Oner C. AOSpine classification systems (subaxial, thoracolumbar). J Orthop Trauma 2017;31:S14‐23.
6. McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine
1994;19:1741‐4. 7. Kaul R, Chhabra HS, Vaccaro AR, Abel R, Tuli S, Shetty AP, et al. Reliability assessment of AOSpine
thoracolumbar spine injury classification system and Thoracolumbar Injury Classification and Severity
Score (TLICS) for thoracolumbar spine injuries: results of a multicentre study. Eur Spine J 2017;26: 1470‐6.
8. Vaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, et al. AOSpine thoracolumbar spine
injury classification system: fracture description, neurological status, and key modifiers. Spine 2013; 38:2028‐37.
9. Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and
lumbar injuries. Eur Spine J 1994;3: 184‐201. 10. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics
1977;33:159‐74.
11. Oner FC, Ramos LM, Simmermacher RK, Kingma PTD, Diekerhof CH, Dhert WJA, et al. Classification of thoracic and lumbar spine fractures: problems of reproducibility: A study of 53 patients using CT and
MRI. Eur Spine J 2002;11: 235‐45.
12. Schroeder GD, Kepler CK, Koerner JD, Chapman JR, Bellabarba C, Cumhur F, et al. Is there a regional difference in morphology interpretation of A3 and A4 fractures among different cultures? J Neurosurg
Spine 2016;24(2):332‐9.
13. Chhabra HS, Kaul R, Kanagaraju V. Do we have an ideal classification system for thoracolumbar and subaxial cervical spine injuries: what is the expert’s perspective? Spinal Cord 2015;53:42‐8.
14. Dai LY, Jin WJ. Interobserver and intraobserver reliability in the load sharing classification of the
assessment of thoracolumbar burst fractures. Spine 2005;30:354‐8. 15. Lewkonia P, Paolucci EO, Thomas K. Reliability of the thoracolumbar injury classification and severity
score and comparison with the denis classification for injury to the thoracic and lumbar spine. Spin.
2012;37:2161‐7. 16. Koh YD, Kim DJ, Koh YW. Reliability and validity of Thoracolumbar Injury Classification and Severity
Score (TLICS). Asian Spine J 2010;4: 109‐17.
17. Cheng J, Liu P, Sun D, Qin T, Ma Z, Liu J. Reliability and reproducibility analysis of the AOSpine thoracolumbar spine injury classification system by Chinese spinal surgeons. Eur Spine J 2017;26:
1477‐82.
18. Urrutia J, Zamora T, Yurac R, Campos M, Palma J, Mobarec S, et al. An independent interobserver reliability and intraobserver reproducibility evaluation of the new AOSpine thoracolumbar spine injury
classification system. Spine 2015;40: E54‐8.
19. Sadiqi S, Oner FC, Dvorak MF, Aarabi B, Schroeder GD, Vaccaro AR. The influence of spine surgeons’ experience on the classification and intraobserver reliability of the novel AOSpine thoracolumbar spine
injury classification system: an international study. Spine 2015;40:E1250‐6.

Chapter 3
58
20. Radcliff K, Kepler CK, Rubin TA, Maaieh M, Hilibrand AS, Harrop J, et al. Does the loadsharing classification predict ligamentous injury, neurological injury, and the need for surgery in patients with
thoracolumbar burst fractures?: Clinical article. J Neurosurg Spine 2012;16:534‐8.

59
Chapter 4
Radiological prediction of posttraumatic kyphosis after
thoracolumbar fracture
I. Curfs, B. Grimm, M. Van Der Linde, P. Willems, W. van Hemert
Open Orthopaedic Journal 2016;10:135‐42

Chapter 4
60
Abstract
Objectives
Classification methods that are currently being used for clinical decision making in
thoracolumbar fractures, are limited by reproducibility and prognostic value.
Additionally, they do not include kyphosis. As a posttraumatic kyphosis is related to
persistent pain, it is of importance to determine a risk of posttraumatic kyphosis based
on fracture type and patient characteristics. Purpose: To determine risk factors (AO
classification, age, gender, localization) that may lead to progressive kyphosis after a
thoracolumbar fracture.
Materials and methods
Retrospective radiographic analysis of a consecutive patientcohort that presented in
our clinic with a traumatic fracture of the thoracolumbar spine between 2004 and
2011. Cobb angle, Gardner angle, vertebral compression angle and anterior vertebral
body compression were measured on plain radiographs, direct post‐trauma and at
follow‐up.
Results
Age and localization are not significant correlated, but there seems to be an increased
risk of progression of kyphosis in age > 50 years and fractures localized at Th12 or L1.
A3 type fractures are significantly more at risk for posttraumatic kyphosis compared to
A1 and A2 type fractures. 30‐50% of the A3 type fractures have an end Gardner angle
and end vertebral compression angle of more than 20 degrees.
Conclusion
AO‐type A3 fractures appear to be at risk of progression of kyphosis. Localization at
Th12‐L1 and age above 50 years seem to be risk factors for significant posttraumatic
kyphosis. These findings should be used in patient counseling and a meticulous
evaluation by weekly radiographs is recommended to determine the treatment
strategy of thoracolumbar fractures.

Radiological prediction
61
4
Introduction
Reported incidences of traumatic fractures of the thoracolumbar spine vary from 1 in
every 150.000 in the Netherlands to 1 in 350.000 reported in United States.
Thoracolumbar fractures are debilitating and may lead to variable outcomes.1,2
Historical series, before the introduction of surgical stabilization, showed deleterious
results of conservative treatment.3,4 These disappointing results may have been due to
limited information from imaging as in more recent series with better selection criteria
based on advanced imaging the results have improved dramatically.5‐8
On these imaging criteria various classification systems have been based. Denis based
his classification on the three column theory: anterior‐middle‐posterior column as
assessed on CT‐scan. Both AO and Denis classify the fractures to their morphology,
resulting in following types: 1) compression type, including burst; 2) distraction type; 3)
rotational type.9 All currently used classification methods have variable or unknown
reproducibility (intra‐ and inter‐observer validity) and do not include a reliable
estimation of prognosis for the determination of the best treatment.10 Because of these
limitations in 2007 the ThoracoLumbar Injury Classification and Severity score (TLICS)
was developed, in which not only fracture morphology, but also fracture mechanism
has been incorporated. Furthermore, this classification pays attention to the
neurological status of the patient and the integrity of the posterior ligament complex.11
The loss of sagittal balance due to an increased kyphosis is believed to be the main
cause of posttraumatic spinal problems with concurring pain.12 Bergstrom et al.13
studied late sequelae of spinal fractures and found that there is no evidence that the
bony injury to the vertebral column itself influences the development of late scoliosis
or lordosis, however, vertebral bony injury may induce the development kyphosis.
Secondary treatment of kyphotic deformity is challenging and often disappointing.14
None of the prior mentioned classification methods have incorporated parameters to
evaluate vertebral kyphosis or height loss as possible predictors of secondary kyphotic
deformity.
Several methods are available to evaluate kyphosis on radiological exams. The Cobb
angle, Gardner angle, vertebral compression angle (VCA) and anterior vertebral body
compression (AVBC) percentage (Figure 4.1) have been described as useful and reliable
measurements in the evaluation of thoracolumbar fractures.15‐17
The purpose of this study is to investigated whether it is possible to predict the
fractures at risk for a progressive angular kyphosis, by means of radiologic features,
age, localization or classification.

Chapter 4
62
Figure 4.1 Measurements performed on plain X‐rays.
Materials and methods
A consecutive series of 104 patients who presented with a traumatic thoracolumbar
fracture between 2004 and 2011, was included for evaluation. We excluded patients
older than 70 years, and patients who received surgical treatment. Furthermore
spontaneous fractures, fractures after minor trauma or patients with proven
osteoporosis were excluded. After exclusion there were 63 patients left for evaluation.
Data was collected from patient files. We searched for age, gender, date and
mechanism of trauma, treatment, BMI and bone density. However, no information
about weight, height or BMI was available, and just in a few patients a DEXA scan was
performed.
Plain radiographs of the thoracolumbar spine directly post trauma and at a minimum
follow‐up of 6 weeks (mean 13 weeks, range of 6‐38 weeks) were compared
retrospectively. Based on the radiographs, the fractures were classified according to the
AO classification9 using available CT. Additionally, the following measurements were
performed using plain radiographs (Figure 4.1).15
1. Cobb angle (defined as the angle formed between a line drawn parallel to the
superior endplate of 1 vertebra above the fracture and a line drawn parallel to the
inferior endplate of the vertebra 1 level below the fracture)
2. Gardner angle (defined as the angle formed from lines drawn parallel to the lower
endplate of the fractured vertebra and the upper endplate of the adjacent cephalad
vertebrae)
3. Vertebral compression angle (VCA; defined as the angle between lower and upper
border of fractured vertebra) and

Radiological prediction
63
4
4. Anterior vertebral body compression percentage (AVBC; The ratio of the AVH to
PVH. AVH is measured from the anterosuperior corner of the vertebra to the
anteroinferior corner, and PVH is measured from the posterosuperior to
posteroinferior corner) .
Retrospective analysis of the radiographs (classification according to AO, as well as the
measurements) was performed by the first author, who was blinded to the patients,
primary classification and treatment decision.
Statistics
Data analysis was performed using Statistical Package for the Social Science (SPSS) 17.0
(Chicago, Illinois, USA). Subgroups were stratified for age (<50 and >50), localization
(Th10‐11, Th12, L1, L2 and L3‐5) and classification (A1, A2, A3, and B). Differences of
the mean of age, localization, and classification with the end values and the differences
between start and end values (Δ) were checked among groups using ANOVA and t‐test.
Level of significance was set at P<0.05.
Results
Thirty‐three men and thirty women, with a mean age of 46.5 years (range 14‐70 years)
were treated for 73 spinal fractures, 54 uni‐ and 9 multi‐segmental. Seventy‐three % of
the fractures were localized at L1 or T12. Demographics and fracture characteristics are
listed in Table 4.1.
Table 4.1 Baseline characteristics.
Number of patients 63
Number of fractures 73
Sex 33 M 30 F
Age (range) Mean 46.5 (14‐70) 29p <50year 34p > 50 years Segments Uni 54 Multi 9 (19 fractures)
Level Th10/11 (6) Th12 (23) L1 (30) L2 (10) L3 (4)
Classification A1 (48) A2 (9) A3 (13) B (3) C (0)
All patients received conservative treatment, consisting of analgetics, physiotherapy
(exercise) and 55 patients were immobilized with spinal cast or brace.
Seven of the 63 patients have had a DEXA scan, with normal outcome or mild
osteopenia. From one of the patients the BMD value of the lumbar spine was not

Chapter 4
64
measured because of a cast. The mean BMD value of the lumbar spine in the other six
patients is 0,985 g/m2 , with a range between 0,884 g/cm2 and 1,198g/cm2.
Age
Patients with age above 50 were compared to parameters of patients younger than
50 years of age. With age above 50 years, all angles increased more over time than
patients younger than 50 years of age, however, these findings were not significant.
Results are summarized in Table 4.2. The end anterior vertebral body compression was
significantly lower for the older patients. The mean end AVBC was 63% and 55%
respectively for the group of patients younger than 50 years and patients above
50 years of age (t‐test P=0.02). For patients above 50 years, the mean delta AVBC was
6% compared to 4% for patients <50 years.
Table 4.2 Delta values of angles and AVBC of patients <50 years compared to patients >50 years. Mean,
standard deviation and range are visible in table. As shown in the table: in patients >50 years,
all angles increased more over time.
Age >50 Age <50
RANGE RANGE Mean SD
MIN MAX
Mean SD
MIN MAX
Delta Cobb (°) 3,43 5,22 ‐4 18 1,28 4,08 ‐8 12
Delta Gardner (°) 3,78 5,71 ‐5 19 2,33 4,63 ‐7 13 Delta VCA (°) 2,68 4,37 ‐6 13 1,22 4,06 ‐12 10
Delta AVBC (%) 6 8 0 11 4 8 ‐8 27
Localization
Most of the fractures were localized at Th12 or L1. For the comparison, three groups
were made: Th12, L1 and all the other levels (Th10‐11, L2‐3‐4‐5). As Cobb angle is in
normal anatomy the highest at the thoracolumbar junction, this parameter was not
used for comparison.
There was a trend towards worse end VCA for fractures localized at Th12 or L1 (P 0.06).
Mean end VCA was 13.09 and 13.83 for Th12 and L1 respectively, compared to an end
VCA of 10.95 degrees for the other levels. Delta VCA angle seemed worse in fractures
localised at Th12.
A significant worse end gardner angle was found for fractures localized at Th12 or L1
compared to the other levels (Th12 14.9 degrees, L1 15.9 degrees, other levels 11.0
degrees). However, also gardner angle is influenced by normal anatomy already, and
the delta Gardner angle did show comparable outcome for all levels.

Radiological prediction
65
4
No differences were found concerning the anterior vertebral body compression
percentage.
See overview of the results in Table 4.3.
Table 4.3 Overview of delta and end Gardner and VCA angles and AVBC percentage associated with
localization. Mean values and standard deviation are shown.
Th12 L1 Th11, L2‐L5
Mean SD Mean SD Mean SD
Delta Gardner (°) 3,35 5,58 2,26 5,18 3,45 5,06
Delta VCA (°) 2,0 4,80 1,27 4,23 2,95 3,61
Delta AVBC (%) 4 9 5 8 5 5 End Gardner (°) 14,91 7,83 15,93 7,09 10,95 7,32
End VCA (°) 13,09 6,16 13,83 4,94 10,95 4,25
End AVBC (%) 66 13 61 12 63 0,12
Classification
Most fractures were classified as AO type A1. Three fractures were classified as B‐type
fractures. These fractures were probably misdiagnosed. However it were only three
fractures, radiological outcome was quite similar to A3 type fractures.
With regard to end kyphosis angles, AO type A1 had best outcome, followed by AO type
A2 and AO type A3/B showed worst outcome. All parameters were significantly worse
for AO type A3 compared to A1. Results are shown in Table 4.4.
Table 4.4 End values of angles and compression percentage compared to classification. Mean, standard
deviation and range are shown. (* P‐ value <0.05, ** P<0.01).
A1 A2 A3
RANGE RANGE RANGE Mean (SD)
MIN MAX
Mean (SD)
MIN MAX
Mean (SD)
MIN MAX
End Cobb (°) 10,08 (7,83) ‐20 28 11,3 (9,6) 1 30 16 * 4 30
End Gardner (°) 12,17 (5,94) ‐8 23 13,3 (5,5) 6 23 20,69 * 4 33
End VCA (°) 11,06 (3,86) 3 22 12,8 (4,0) 7 21 17,46 * 8 28 End AVBC (%) 67 (10) 45 81 65 (3) 63 67 53 ** 43 70
End Gardner angle was 12.1 degrees for A1 type fractures, compared to 20.7 degrees
for A3 type. Also the progression is higher in A3 type, shown by a delta gardner angle of
2.1 degrees for A1 and 6.2 degrees for A3. A2 type fractures had a mean end Gardner
angle of 13.3 degrees and mean delta angle of 3.9 degrees (Figure 4.2).

Chapter 4
66
Figure 4.2 Results of AO classification versus Gardner angle. A3 type fractures have worse outcome than
A1 and A2 type fractures.
The end AVBC was 67% for A1, 65% for A2 and 53% for A3 type fractures (P<0.01). The
delta AVBC was highest for AO type A3 fractures, with values of respectively 2%, 4%
and 10% for A1, A2 and A3 fractures (P<0.01).
Also VCA showed worst results for A3 type fractures. Delta VCA was 1.0 degrees for A1,
3.9 degrees for A2 and 4.2 degrees for A3 fractures. End VCA was respectively 11.1
degrees, 12.8 degrees and 17.5 degrees for A1, A2 and A3.
Cobb angles increased also with AO classification, with a mean end Cobb angle of
10.1 degrees for A1, 11.3 degrees for A2 and 16.0 degrees for A3. The increase of Cobb
angle during time was 1.8 degrees for A1, 2.9 degrees for A2 and 4.1 degrees for A3.
End Gardner, Cobb or VCA angles of more than 20 degrees or delta angles of more than
10 degrees, seem of clinical importance because of their possible influence on the
sagital balance. Therefor we measured the percentage of fractures that met these
criteria, and noticed that 30‐50% of all AO type A3 fractures had such angles. Table 4.5.
Table 4.5 Overview of angles versus AO classification. Percentage of fractures with delta angle of more
than 10 degrees or end kyphotic angle of more than 20 degrees.
AO Number Cobb (% of all fractures)
Gardner (% of all fractures
VCA (% of all fractures)
Delta (>10) End (>20) Delta (>10) End (>20) Delta (>10) End (>20)
A1 48 2.1% 10,4% 4.2% 6.3% 0% 2.1%
A2 9 22.2% 22,2% 22.2% 11.1% 11.1% 11.1%
A3 13 30.8% 30,8% 38.5% 53.8% 30.8% 30.8%
B 3 0% 33,3% 0% 66.7% 0% 66.7%

Radiological prediction
67
4
Discussion
This study was intended to predict progressive posttraumatic kyphosis after a
thoracolumbar fracture based on plain radiographs. AO‐type A3 fractures appear to be
at risk of progression of kyphosis, with 30‐50% of the fractures have end kyphotic
angles of more than 20 degrees. Localization at Th12‐L1 and age above 50 years also
seem to be risk factors for significant posttraumatic kyphosis. These findings should be
used in patient counseling and a meticulous evaluation by weekly radiographs of
progression of kyphosis is recommended to determine the treatment strategy. CT
should be used to judge the end plate comminution and vertebral body involvement.
Careful analysis of concomitant injury of the posterior ligament complex (PLC) by
means of a MRI could be advocated in these fractures.
Involvement of the posterior column in fracture morphology could also be suggested
on PA radiographs by an increased distance of the vertical pedicle or on axial CT‐images
by the separation of a facet joint. It is important to pay attention to the position of the
processes spinosi on the sagittal view, and the distance between the pedicles and
processes spinosi on the coronal view of plain radiographs and CT‐scans (Schnake et
al.).18
Misinterpretation of the integrity of the PLC may explain the higher rate of progression
to kyphotic deformity of A3 fractures. In case of involvement of the posterior ligament
complex a fracture should be classified as B type fracture, and then surgical treatment
is recommended. In figure 3 and 4 we show some X‐rays of such a A3 type fracture with
worse outcome.
Schnake et al.18 performed a study on the reliability of fracture classification, mainly for
B‐fractures. They found that initially almost 42% of the B‐type fractures were
misdiagnosed as type A. Compared to our findings Schnake et al.18 listed a vertebral
kyphotic angle of >15 degrees, a pronounced compression of vertebral cancellous bone
despite minimal reduced anterior vertebral height, and a considerably reduced anterior
vertebral height of over 50% to be considered as red flag symptoms.
Oner et al.19 suggested to integrate MRI findings into future classification schemes of
thoracolumbar spine fractures for a better diagnosis and prognosis of the fractures. In
the STIR sequences the presence of a high signal indicates injury in the PLC area. In our
study, MRI had not been performed routinely in all patients.
However, in 2002 Öner et al.20 also published a study in which conservative and
operative treatment of thoracolumbar fractures were compared, and routinely trauma
MRI was made to identify predictors for worse outcome. They concluded that an
unfavorable outcome was related to the progression of kyphosis. In the conservative
group this seemed predictable concerning the endplate comminution and vertebral

Chapter 4
68
body involvement. In the operatively treated group, recurrence of the kyphotic
deformity was predictable by the lesion of the posterior longitudinal ligamentary
complex together with endplate comminution and vertebral body involvement. So,
misinterpretation of the PLC might be one of the issues related to posttraumatic
kyphosis, but end plate comminution and vertebral body involvement also seem to be
of importance. This is shown by the AVBC parameters, and in our results this
parameters is negatively influenced by age and classification (worse outcome age
<50 years and in A3 fractures).
In our study clinical outcomes were not included, but in literature kyphotic deformity is
considered to have a positive association with chronic back pain [12, 13, and 14].
Therefore, it is considered important to investigate whether principal morphology and
patient demographics are of influence on the progression of kyphosis.
We are aware of the limitations of this study. The population is relatively small and
existed of patients with a wide range of age. Furthermore we could not analyze the
sagittal balance of the individual spinal column, since full spine radiographs were not
available. Ideally, these are also available at pre‐injury stage for optimal comparison,
although this is practically not feasible.
In conclusion however, all AO‐type A3 fractures, mainly in patients older than 50 years,
and localized at the thoracolumbar junction, appear to be at risk of progression of
kyphosis. These findings should be used in patient counseling and a meticulous
evaluation of the fracture is recommended to assess vertebral body involvement and
the integrity of the PLC. Weekly radiographs are recommended, and CT and/or a
routinely MRI should be considered in these cases, to determine the treatment
strategy.

Radiological prediction
69
4
References
1. Fisher CG, Noonan VK, Dvorak MF. Changing face of spine trauma care in North America. Spine (Phila Pa
1976) 2006;31(11 Suppl):S2‐8; discussion S36.
2. Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine (Phila Pa 1976) 1996;21(4):492‐9.
3. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal
injuries. Spine (Phila Pa 1976) 1983;8(8):817‐31. 4. Willén J, Anderson J, Toomoka K, Singer K.The natural history of burst fractures at the thoracolumbar
junction. J Spinal Disord 1990;3(1):39‐46.
5. de Klerk LW, Fontijne WP, Stijnen T, Braakman R, Tanghe HL, van Linge B. Spontaneous remodeling of the spinal canal after conservative management of thoracolumbar burst fractures. Spine (Phila Pa 1976)
1998;23(9):1057‐60.
6. Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976) 1993;18(8):955‐70.
7. Shen WJ, Shen YS. Nonsurgical treatment of three‐column thoracolumbar junction burst fractures
without neurologic deficit. Spine (Phila Pa 1976) 1999;24(4):412‐5. 8. Shen WJ, Liu TJ, Shen YS. Nonoperative treatment versus posterior fixation for thoracolumbar junction
burst fractures without neurologic deficit. Spine (Phila Pa 1976) 2001;26(9):1038‐45.
9. Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994;3(4):184‐201.
10. Wood KB, Khanna G, Vaccaro AR, Arnold PM, Harris MB, Mehbod AA. Assessment of two thoracolumbar
fracture classification systems as used by multiple surgeons. J Bone Joint Surg Am 2005;87(7):1423‐9. 11. Lenarz CJ, Place HM, Lenke LG, Alander DH, Oliver D. Comparative Reliability of 3 Thoracolumbar
Fracture Classification Systems. J Spinal Disord Tech 2009;22(6):422‐7.
12. Buchowski JM, Kuhns CA, Bridwell KH, Lenke LG. Surgical management of posttraumatic thoracolumbar kyphosis. Spine J 2008;8(4):666‐77.
13. Bergström EM, Henderson NJ, Short DJ, Frankel HL, Jones PR. The relation of thoracic and lumbar
fracture configuration to the development of late deformity in childhood spinal cord injury. Spine (Phila Pa 1976) 2003;28(2):171‐6.
14. Doo TH, Shin DA, Kim HI et al. Clinical Relevance of Pain Patterns in Osteoporotic Vertebral Compression
Fractures. J Korean Med Sci 2008;23(6):1005‐10. 15. Keynan O, Fisher CG, Vaccaro A et al. Radiographic measurement parameters in thoracolumbar
fractures: a systematic review and consensus statement of the spine trauma study group. Spine (Phila
Pa 1976) 2006;31(5):E156‐65. 16. Street J, Lenehan B, Albietz J, Bishop P, Dvorak M, Fisher C; Spine Trauma Study Group. Intraobserver
and interobserver reliabilty of measures of kyphosis in thoracolumbar fractures. Spine J 2009;9(6):
464‐9. 17. Ulmar B, Gühring M, Schmälzle T, Weise K, Badke A, Brunner A. Inter‐ and intra‐observer reliability of
the Cobb angle in the measurement of vertebral, local and segmental kyphosis of traumatic lumbar
spine fractures in the lateral X‐ray. Arch Orthop Trauma Surg 2010;130(12):1533‐8. 18. Schnake KJ, von Scotti F, Haas NP, Kandziora F. Unfallchirurg.Type B injuries of the thoracolumbar spine
: misinterpretations of the integrity of the posterior ligament complex using radiologic diagnostics.
Unfallchirurg 2008;111(12):977‐84. 19. Oner FC, van Gils AP, Dhert WJ, Verbout AJ. MRI findings of thoracolumbar spine fractures: a
categorisation based on MRI examinations of 100 fractures. Skeletal Radiol 1999;28(8): 433‐43.
20. Oner FC, van Gils AP, Faber JA, Dhert WJ, Verbout AJ. Some complications of common treatment schemes of thoracolumbar spine fractures can be predicted with magnetic resonance imaging:
prospective study of 53 patients with 71 fractures. Spine (Phila Pa 1976) 2002;27(6):629‐36.

Chapter 4
70

71
Chapter 5
Two‐nation Comparison of Classification and Treatment of
Thoracolumbar Fractures: an internet‐based multicenter
study among spine surgeons
M. Pishnamaz, I. Curfs, S. Balosu, P. Willems, W. van Hemert, H.C. Pape, P. Kobbe
Spine 2015;40(22):1749‐56

Chapter 5
72

Country specific differences
73
5
Abstract
Study Design
Web‐based‐multicenter study
Objective
To assess and compare the management strategy for traumatic thoracolumbar
fractures between German and Dutch spine surgeons.
Summary of Background Data
To date, there is no evidence‐based treatment algorithm for thoracolumbar spine
fractures. Thereby an international controversy concerning optimal treatment exists.
Methods
In this web‐based‐multicenter study (www.spine.hostei.com) CT‐scans of traumatic
thoracolumbar fractures (T12‐L2) were evaluated by German and Dutch spine surgeons.
Supplementary case‐specific information as age, gender, height, weight, neurological
status, and injury mechanism were provided.
By use of a questionnaire, fractures were classified according to the AO‐Magerl
Classification, followed by six questions concerning the treatment algorithm. Data were
analyzed using SPSS (Version 21, 76 Chicago IL, USA). The interobserver agreement was
determined by Cohens‐Kappa. Statistical significance was defined as P<0.05.
Results
Twelve surgeons (six/country) evaluated each 91 cases. The fractures were classified as
AO Type A in 82% (898 votes), Type B in 14% (150 votes) and Type C in 4% (44 votes).
No significant difference concerning the AO Classification between German and Dutch
spine surgeons was found. Overall German spine surgeons had a lower threshold
concerning the indication for surgical treatment (Ger 87% vs. NL 30%; P<0.05). There
was consensus about operative stabilization of AO Type B and C injuries and injuries
with neurologic deficit, whereas a discrepancy in the therapeutic algorithm for AO Type
A fractures was observed. This difference was most pronounced regarding the
indication for posterior (Ger 96.6%; NL 41.2%; P<0.05) and circumferential stabilization
(Ger 53.4%; NL 0%; P<0.05) for burst fractures.
Conclusion
There is consensus to stabilize AO Type B and C fractures, whereas country‐specific
differences in the treatment of Type A fractures, especially in case of burst fractures,
occur. Prospective, controlled multicenter outcome studies may provide more evidence
in optimal treatment for thoracolumbar fractures.

Chapter 5
74
Introduction
The optimal treatment strategy for fractures of the thoracolumbar spine is still under
debate1‐3, although this region is most affected by trauma.2,4 It appears that only a few
studies with a high level of evidence are available that sufficiently support either
treatment concept.2,5‐8 This leads to the fact that no generally acknowledged therapy
concept has been established. Numerous surgical treatment options have been
published in literature, but these were mainly non‐controlled studies based on
individual surgeon’s preferences or traditional local treatment concepts. In addition to
this controversy, country‐specific therapy concepts have been reported.9 One of the
main controversies concerns the treatment of burst fractures. In North America burst
fractures of the thoracolumbar junction without neurological deficit are commonly
treated by a brace or a stand‐alone posterior instrumentation. In contrast, the
treatment of this type of fracture by circumferential stabilization is more popular in
some European countries.1,10 Especially in border areas differences in national
treatment strategies can come into conflict.
The aim of this study was to assess and compare the management strategy for
thoracolumbar spine fractures between German and Dutch spine surgeons.
Materials and methods
This internet‐based‐multicenter study was performed on the basis of a web
documentation.
Presented were example cases of traumatic fractures of the thoracolumbar junction.
Radiographic data and associated case information was uploaded. For sample size
planning a precedent pilot study was performed. Consequently an anonymized
questionnaire was handed over to all participating surgeons.
Participants
All participants were experienced surgeons from orthopedic, neurosurgical, or trauma
departments, specialized in spine surgery. Each participant was well versed in the AO
classification scheme and received the original article of this system11 one month prior
to the start of the study.

Country specific differences
75
5
Development of the website
The website (www.spine.hostei.com) provided complete axial, sagittal and coronary
CT‐sequences of the fracture. Supplementary specific details as the patient’s age,
gender, height, weight, neurological status and injury mechanism were given. An
overview of the classification and a detailed manual of the website were added.
Inclusion criteria of patients
A Committee of experts assembled a case series of 91 consecutive patients treated in
the University Hospitals of Aachen (Ger) or Maastricht (NL). Included were acute
traumatic injuries of the thoracolumbar junction (T11‐L2) from 2010 to 2013. Patients
with osteoporotic fractures, tumors or spondylodiscitis and patients with incomplete
CT‐reconstructions were excluded. The treating surgeons did not serve as observers in
the study.
Questionnaire
The first part of the anonymized questionnaire was focused on the fracture assessment.
By applying the AO Classification, the surgeons were asked to assess the cases up to the
second subdivision (e.g. A3.2/ B2.1/ C1.3). Accordingly the interobserver agreement for
the AO Classification was stepwise measured from the basic level (A, B or C) to the
more precise levels (e.g. A.3.1).
The second part of the questionnaire included six questions regarding the management
and treatment of each case (Figure 5.1).
Statistical methods
The deidentified data were analyzed using SPSS (Version 21, 76 Chicago IL, USA). Data
are presented as means and standard deviation. Continuous variables were compared
using t‐test for normally distributed data or the Mann‐Whitney U‐test otherwise. To
determine interobserver agreement Cohens‐Kappa and the percentage agreement
between the surgeons were used. As in previous studies we used the guidelines of
Landis & Koch to categorize Kappa values from 0‐0.2 indicating slight reliability;
0.21‐0.4 fair; 0.41‐0.6 moderate; 0.61‐0.8 substantial and 0.81‐1 almost perfect
reliability. Statistical significance was defined as P<0.05.

Chapter 5
76
1. How would you treat? Case
If you chose a) / b) you can skip to the next case 1 2 3 4 5
a) Nonoperative (without a brace/orthosis)
b) Nonoperative (with brace/orthosis)
c) Vertebro‐ or Kyphoplasty
d) Posterior spinal stabilization (internal fixator)
e) Single stabilization from anterior (stand alone)
f) Circumferential stabilization (within one stay/ over the course)
2. If the posterior stabilization is part of your treatment, what would you prefer? Case
1 2 3 4 5
a) No part of my concept
b) Percutaneous (paraspinal approach)
c) Open (median approach)
3. How would you perform posterior stabilization? Case
1 2 3 4 5
a) Not at all
b) Instrumentation of one or two segments (mono‐/bisegmental)
c) Instrumentation of more than two segments (multisegmental)
d) Augmented pedicle screws
e) Conventional internal fixator and additional Vertebro‐ or Kyphoplasty of the fractured vertebra
f) Internal fixator with augmented pedicle screws and additional Vertebro‐ or
Kyphoplasty of the fractured vertebra
4. Would you decompress routinely in the case at hand? Case
1 2 3 4 5
a) Yes
b) No
c) Depending on the intraoperative amount of reduction
5. How would you do your anterior fusion? Case
1 2 3 4 5
a) Out of question
b) Strut graft
c) Complete vertebral body replacement
d) Strut graft and additional plate
e) Vertebral body replacement and additional plate
6. What priority would you assign regarding the urgency of operation Case
1 2 3 4 5
a) Emergency
b) High urgent 12‐24h after trauma
c) Urgent 24‐48h after trauma
d) Low priority >48h
Figure 5.1 Illustration of the 2nd part of the questionnaire: “Treatment strategy”

Country specific differences
77
5
Results
Participants and case details
Twelve board certified spine surgeons (six/country) of four trauma hospitals evaluated
data on 91 injuries of the thoracolumbar junction.
The patients’ age at the time of injury was 51±18.1 years. The neurological examination
showed in 82 of the patients (90.1%) normal findings (ASIA E), eight patients (8.8%)
showed slightly to complete neurological deficits (ASIA A‐D) and in one case (1.1%) the
neurological status preoperatively could not be evaluated.
Fracture classification and reliability
Overall 82% (898 votes) of all fractures were classified as AO Type A fractures. Type B
fractures were seen in 14% (150 votes) and Type C in 4% (44 votes). The AO System
showed the highest percentage agreement at the basic level (A, B, C) (Ger 81.03%, NL
85.57%, Ger/NL 83.33%); consecutive a moderate reliability in both countries (κ‐value:
Ger 0.41; NL 0.50; Ger/NL 0.45) was found (Table 5.1). There was no significant
difference concerning the AO Classification between German and Dutch Spine
Surgeons.
Table 5.1 Illustrating the κ‐values and the percentage agreement of the AO Classification.
Type/Subtype Ger (%) [κ‐value] NL (%) [κ‐value] Ger/NL (%) [κ‐value]
In A, B, C 81.03 [0.41] 85.57 [0.5] 83.33 [0.45]
In A 1, A2, A3,… 52.28 [0.32] 48.28 [0.28] 43.77 [0.23]
AO Classification In A 1.1, A 1.2,… 33.11 [0.25] 27.55 [0.18] 19.78 [0.11]
Surgical treatment
Nonoperative vs operative therapy
Independent from the previously used classification an operative treatment was
selected significantly more frequent in Germany than in the Netherlands (Operation:
Ger 86.8%; NL 30.22%; P<0.05) (Figure 5.2).
Considering the results of the AO Classification this difference was solely caused by the
opposing therapy of Type A fractures (Operation/Type A: Ger: 83.64%; NL: 16.45%,
P<0.05) while classified Type B and C fractures were consistently treated by a surgical
intervention in both countries.

Chapter 5
78
Figure 5.2 Illustrating the treatment of German and Dutch surgeons independently from the fracture
classification (all cases). (*P<0.05).
The results of the AO subclassifications (e.g. A.1) showed that Dutch surgeons selected
nonoperative treatment in almost all Type A.1 and A.2 fractures and in most Type A.3
fractures (Nonoperative/NL: A.1 96.61%; A.2 94.03%; A.3 58.82%). In contrast German
surgeons showed a clear trend for operative treatment for Type A.2 fractures and
chose almost solely for operation in the largest of all groups, the Type A.3 fractures
(Operative/Ger: A.1 59.12%; A.2 82.9% A.3 96.59%) (Table 5.2).
Table 5.2 Illustrating the treatment strategy of German and Dutch spine surgeons depending on the AO
Type A subclassification.
NonSurgical Surgical Treatment
Overall Stabilization (Overall) AO Type
Country/Cases In (%) [abs.] Ø Brace Brace
Vertebro/‐ Kyphoplasty Posterior Anterior Circumferential
40.88*[56] 52.56*[72] Germany (%)
[n=137] 38.69[53] 2.19[3] 6.57[9]
42.34[58] 4.38[6] 5.84[8]
96.61[228] 2.12[5] A.1
Netherlands (%)
[n=236] 15.68[37] 80.93[191] 1.27[3]
2.12[5] ‐ ‐
17.1*[7] 82.93*[34] Germany (%)
[n=41] 17.1[7] ‐ ‐
36.59[15] 4.88[2] 41.46[17]
94.03[63] 5.97[4] A.2
Netherlands (%)
[n=67] 23.88[16] 70.15[47] ‐
5.97[4] ‐ ‐
3.41*[9] 96.21*[254] Germany (%)
[n=264] 3.03[8] 0.38[1] 0.38[1]
40.15[106] 2.65[7] 53.41[141]
58.82[90] 41.18[63] A.3
Netherlands (%)
[n=153] 3.92[6] 54.90[84] ‐
41.18[63] ‐ ‐
*P<0.05

Country specific differences
79
5
Regarding the A.3 subdivisions (e.g. A.3.1) this treatment discrepancy between German
and Dutch surgeons was especially found in Type A.3.1 fractures (Operation/Type A.3.1:
Ger 95.43%; NL 32.1%; p< 0.05) (Table 5.3).
Table 5.3 Illustrating the treatment strategy of German and Dutch spine surgeons depending on the AO
Type A.3 subclassification.
Non Surgical Surgical Treatment
Overall Overall Stabilization AO
Type
Country/Cases
In (%) [abs.] Ø Brace Brace
Vertebro/‐
Kyphoplasty Posterior Anterior Circumferential
4.57*[7] 94.78*[145] Germany (%) [n=153] 3.92[6] 0.65[1]
0.65 [1] 54.25[83] 3.27[5] 37.26[57]
67.9[55] 32.1[26]
A. 3.1 Netherlands (%)
[n=81] 3.70[3] 64.20[52] ‐
32.1[26] ‐ ‐
3.51*[2] 96.48*[55] Germany (%) [n=57] 3.51[2] ‐
‐ 17.54[10] 1.75[1] 77.19[44]
65.71[23] 34.29[12]
A. 3.2 Netherlands (%)
[n=35] 5.71[2] 60[21] ‐
34.29[12] ‐ ‐
‐ 100*[54] Germany (%) [n=54] ‐ ‐
‐ 24.07[13] 1.85[1] 74.07[40]
32.43[12] 67.57[25]
A. 3.3 Netherlands (%)
[n=37] 2.70[1] 29.73[11] ‐
67.57[25] ‐ ‐
* P<0.05
Type of nonoperative Treatment
In both countries nonoperative treatment was only performed in Type A fractures
(Nonoperative/Type A: Ger 16.3%; NL 83.6%; p< 0.05). In this case, Dutch surgeons
favored the application of a supportive brace in contrast to the German surgeons
(Nonoperative/Brace: NL 84.51%; Ger 5.56%; p< 0.05) (Table 5.2, 5.3).
Vertebroplasty and Kyphoplasty
The indication for vertebro‐ or kyphoplasty as an initial treatment was rarely and only
seen in Type A fractures in elderly patients. (VB or KB/Type A: Ger 2.27%, mean age
65.7 years; NL: 0.33%, mean age 66 years; NS).
Posterior stabilization
German and Dutch surgeons preferred the percutaneous approach in case of Type A
fractures (Percutaneous/Type A: Ger 77.7%; NL 63.9%; NS), whereas Type B fractures
were treated more frequently by the open approach (Percutaneous /Type B: Ger
41.2%; NL 33.9%; NS). In case of Type C fractures the percutaneous approach was the
exception in both countries (Percutaneous /Type C: Ger 5.3%; NL 4%; NS) (Table 5.4).

Chapter 5
80
Table 5.4 Illustrating the approach of posterior stabilization of German and Dutch surgeons depending on the AO Basic Level.
AO Type Country/cases in (%) [abs.] Median approach Percutaneous approach
Germany (%) [n=345] 22.3 [77] 77,7 [268] A
Netherlands (%) [n=72] 36.1 [26] 63.9 [46] Germany (%) [n= 85] 58.8 [50] 41.2 [35] B
Netherlands (%) [n=65] 66.2 [43] 33.9 [22]
Germany (%) [n=19] 94.7 [18] 5.3 [1] C Netherlands (%) [n=25] 96.0 [24] 4.0 [1]
Type of posterior stabilization
In our study mono‐ or bisegmental instrumentation was the treatment of choice for
German surgeons independent of the previous classified fracture type, (Mono‐
/bisegmental/Ger: Type A 79.88%, B 83.56%, C 76.47%). On the opposite,
multisegmental stabilization was the main selected procedure in all types of fractures
by Dutch surgeons (Multisegmental/NL: Type A 47.22%, B 55.38%, C 96%). Other
techniques like cement‐augmented pedicle screws or hybrid techniques were selected
rarely in both countries and were mainly seen in elderly patients (Augmented
techniques: Ger 13.71%, mean age 73.1 years; NL 3.03%, mean age 70.8 years).
Anterior fusion
Whereas in Germany circumferential fixation was frequently advocated in classified
Type A.2 and A.3 fractures (Circumferential/Ger: A.1 5.84%; A.2 41.46%; A.3 53.4%), the
indication for additional anterior fusion was never chosen by Dutch surgeons in any
Type A fracture (Table 5.2).
In Type B and C fractures circumferential fusion remained exceptional for Dutch
surgeons (Circumferential/NL: Type B 3.08%; Type C 12%), whereas German surgeons
favored the circumferential treatment with increasing severity of injury/vertebral
destruction (Circumferential/Ger: Type B 63.5%; Type C 100%).
Stand‐alone anterior fusion was only selected by German surgeons and only in case of
Type A fractures (Type A/anterior fusion Ger: 3.4%). Dutch surgeons never selected a
purely anterior approach.
Urgency and decompression
German surgeons evaluated Type B fractures more urgent as the Dutch surgeons, but
both countries chose highest priority in case of Type C fractures (Operation within
24 h/Type A fracture: Ger 41.94%; NL 59.72%; Type B: Ger 89.41%; NL 30.76%; Type C:

Country specific differences
81
5
Ger 100%; NL 68%) (Table 5.5). Equally, in both countries the indication for
decompression was selected most frequently in Type C fractures. (Indication for
decompression/Type A fracture: Ger 4.44%; NL 26.39%; Type B fracture: Ger 16.47%;
NL 13.85%; Type C fracture: Ger 94.74%; NL 44%) (Table 5.5).
Table 5.5 Illustrating the frequency of decompression and the evaluation of surgical urgency of German
and Dutch surgeons depending on the AO Basic Level (Vertebro‐ and Kyphoplasty are not
included).
Decompression Timing of Operation
AO
Type
Country/ Cases
in (%) [abs.]
yes Decision
within surgery
no Emergency <24h >24h‐<48h >48h
Germany (%)
[n=360]
4.44*
[16]
6.94*
[25]
88.61*
[319]
4.72*
[17]
37.22
[134]
39.72*
[143]
18.33
[66]
A
Netherlands
(%) [n=72]
26.39
[19]
22.22
[16]
51.39
[37]
12.5
[9]
47.22
[34]
18.06
[13]
22.22
[16] Germany (%)
[n=85]
16.47
[14]
74.12
[63]
9.41
[8]
11.76
[10]
77.65*
[66]
9.41*
[8]
1.18*
[1]
B
Netherlands (%) [n=65]
13.85 [9]
75.38 [49]
10.77 [7]
15.38 [10]
15.38 [10]
53.85 [35]
15.38 [10]
Germany (%)
[n=19]
94.74*
[18]
‐ 5.26*
[1]
100*
[19]
‐ ‐ ‐ C
Netherlands
(%) [n=25]
44
[11]
40
[10]
16
[4]
28
[7]
40
[10]
28
[7]
4
[1]
*P<0.05.
Discussion
Despite internationally used classification systems for fracture assessment there is
insufficient evidence to install a standard treatment algorithm for fractures of the
thoracolumbar spine.10,12‐14 A lack of consensus in treatment strategies may cause
variation in practice among individual surgeons or between clinics or countries, which is
not desirable for optimization of care and patient counseling.9
Our main findings are:
1. Fracture assessment between the German and Dutch surgeons was comparable
regarding the AO Classification.
2. In the Netherlands, surgeons usually recommend nonoperative treatment in Type
A fractures whereas German surgeons usually tend to surgery in case of Type A.2
and particularly A.3 fractures.
3. In Germany circumferential fusion was an often selected procedure, in Type A
fractures as well as in Type B and C fractures. In contrast, the Dutch surgeons never

Chapter 5
82
selected an additional anterior fusion in Type A fractures and rarely in Type B and C
fractures.
4. Operative treatment of Type B and C fractures was recommended in both
countries without exception.
Some authors disapprove of the AO Classification system because of its reduced
reliability and reproducibility.15,16 On the other hand, the high number of subtypes
offers a more precise categorization of the injury. Furthermore, the application of the
AO System may allow for accurate evaluation of therapy as related to this
categorization.
In the present survey we found a moderate reliability for the AO Classification at the
basic level (Type A/B/C). Consecutive the reliability decreased with further subtype
analysis. Comparable results have been described in several studies.15‐18 This decreasing
reliability in case of more accurate fracture classification may diminish comparability
between different observers. However, interobserver reliability was not the focus of
this study. The use of this classification system in our survey was rather to verify to
what extent differences in surgeons’ treatment are caused by differences in individual
fracture assessment and categorization.
In terms of this, we found a consistent treatment strategy within both countries;
however with partially opposing therapeutical strategies concerning AO Type A
fractures.
There is mainly consensus on the possible nonoperative treatment of stable
compression fractures (Type A.1).14 In our study nonoperative treatment of this type of
fracture was also predominantly performed by German and Dutch surgeons.
In the literature both nonoperative and operative therapy is recommended regarding
Type A.2 fractures.19 The background for the surgical treatment of A.2 (split) fractures is
despite the definition as stable fracture the relatively frequent development of painful
non‐unions.4 In our study German surgeons tend to the operative treatment in case of
A.2 fractures whereas this fracture type was a domain of nonoperative treatment in the
Netherlands. Burst fractures are prone to kyphotic deformity1,2,5 and spinal stenosis
may be caused by dislocation of posterior wall fragments. Besides the neurological
status and the location of the fracture, the amount of vertebral body destruction and
kyphotic deformity plays a role considering for or against surgical treatment.4,20,21
Hitchinson et al. recommended surgical stabilization in case of at least 20° kyphotic
deformity, 50% spinal stenosis, or a loss of anterior body height of more than 50%. The
few controlled studies with a high level of evidence comparing nonoperative vs
operative treatment of thoracolumbar fractures show heterogeneous results.
Stadhouder et al. included 190 patients independent of their neurological status and

Country specific differences
83
5
fracture type over a mean follow up of 6.2 years.6 This study showed comparable
results for nonoperative and operative treatment. Wood et al. found similar results in
47 neurological intact patients with burst fractures after 3.7 years.5 In contrast
Siebenga et al. found significantly better results in all functional outcome scores in the
operative group of 34 Type A.3 fractures after 4.3years.2
The results of the present survey confirm this controversy by showing that German
surgeons usually operate on Type A.3 fractures (96.6%), whereas Dutch surgeons treat
those fractures in 58.8% of cases nonoperatively.
Several studies have reported that stand‐alone posterior stabilization leads to
secondary loss of reduction in the course.1,22 The clinical consequences of this loss of
reduction, however, are unknown. Anterior stabilization can decrease the load on the
posterior fixation system significantly.23 Further, the aim of a combined anterior‐
posterior stabilization is to achieve anatomical reduction and maintain a long‐lasting
stability.10 Our study showed that the indication for an additional anterior treatment
was selected more frequently by the German surgeons with increasing degree of
instability/vertebral destruction. In contrast, independent of the fracture type,
additional anterior fusion was rarely selected by Dutch surgeons. One reason for the
more frequent indication for an anterior approach in Germany appears to be that
adjacent disc injuries are interpreted as a causal reason for the absence of vertebral
bone healing and consequent posttraumatic kyphosis. Another reason might be that
full restoration of sagittal alignment is defined as a primary goal of therapy in Germany.
However, currently it is still unclear whether improved radiological results are
associated with an improved long term outcome.1,2
The initial treatment of Type B and C fractures according to the AO Classification by
posterior stabilization is an established procedure in literature.19 Our results confirm
that this strategy is practiced by both German and Dutch surgeons. In this study
circumferential treatment was chosen more frequently by the German surgeons in case
of Type B and C fractures whereas in the Netherlands the dorsal multisegmental
approach was rather preferred. Reinhold et al. also reported a trend towards a
combined approach in B and C injuries in a study population of 865 patients.19 Among
the individual assessment of Type B and C fractures in the present study, a high grade
of vertebral body destruction was found. Regarding the indication of additional anterior
stabilization, it appeared that the amount of vertebral body destruction was the
decisive factor for the German surgeons in our study.
Concerning the timing of stabilization, more unstable fractures were rated as
increasingly urgent in both countries with a more frequent indication for open
decompression and stabilization. This is in line with current literature.4,19,22 In our study,

Chapter 5
84
the indication for decompression did not significantly differ between both countries
considering absolute numbers; however the percentage of performed decompressions
were lower in Germany due to the higher number of performed surgeries.
Techniques like vertebro‐/kyphoplasty, augmented pedicle screws or hybrid techniques
were selected rarely by all surgeons. This may be explained by the relatively young age
of the trauma cases and the exclusion of osteoporotic and pathological fractures.
This study has a number of important limitations: The participating surgeons in our
study are from orthopaedic, neurosurgical and trauma departments. Differences in
treatment strategy thus, were also influenced by the medical background and the
subspecialty‐training of the surgeons. This aspect may reduce the pure country specific
comparability. On the opposite it is necessary to reflect the opinions of spine surgeons
from different departments to consider interdisciplinary differences. Furthermore,
border‐area‐studies offer the possibility to demonstrate commonalities and differences
of local regions, but they do not necessarily represent the opinion of all spine surgeons
of the participating countries. National surveys by the respective spine societies may
provide more generalizable results. Randomized controlled studies for patient
categories with different treatment options (nonoperative vs operative, posterior vs
circumferential) may help to find the optimal treatment strategy for patients and help
to install national and international consensus based guidelines.
Conclusion
German and Dutch surgeons agree to stabilize AO Type B and C fractures, whereas
country‐specific differences in the treatment of Type A fractures, especially in case of
burst fractures occur. In the Netherlands, surgeons usually recommend nonoperative
treatment in Type A.1‐A.3 fractures whereas German surgeons have a lower threshold
concerning posterior stabilization and anterior fusion in case of Type A.2 and
particularly A.3 fractures. Prospective, controlled multicenter outcome studies may
provide more evidence in optimal treatment for thoracolumbar spine fractures.

Country specific differences
85
5
References
1. Reinhold M, Knop C, Beisse R, et al. Operative treatment of traumatic fractures of the thoracic and
lumbar spinal column: Part III: Follow up data. Unfallchirurg 2009;112:294‐316.
2. Siebenga J, Leferink VJ, Segers MJ, et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine
2006;31:2881‐90.
3. Wild MH, Glees M, Plieschnegger C, et al. Five‐year follow‐up examination after purely minimally invasive posterior stabilization of thoracolumbar fractures: a comparison of minimally invasive
percutaneously and conventionally open treated patients. Arch Orthop Trauma Surg 2007;127:335‐43.
4. Wood KB, Li W, Lebl DS, et al. Management of thoracolumbar spine fractures. Spine J 2014; 14:145‐64. 5. Wood K, Buttermann G, Mehbod A, et al. Operative compared with nonoperative treatment of a
thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone
Joint Surg Am 2003;85‐A:773‐81. 6. Stadhouder A, Buskens E, de Klerk LW, et al. Traumatic thoracic and lumbar spinal fractures: operative
or nonoperative treatment: comparison of two treatment strategies by means of surgeon equipoise.
Spine 2008;33:1006‐17. 7. Wood KB, Buttermann GR, Phukan R, et al. Operative Compared with Nonoperative Treatment of a
Thoracolumbar Burst Fracture without Neurological Deficit: A Prospective Randomized Study with
Follow‐up at Sixteen to Twenty‐Two Years. J Bone Joint Surg Am 2015;97:3‐9. 8. Lenehan B, Dvorak MF, Madrazo I,et al. Diversity and commonalities in the care of spine trauma
internationally. Spine 2010;35:S174‐9.
9. Schnake KJ, Stavridis SI, Kandziora F. Five‐year clinical and radiological results of combined anteroposterior stabilization of thoracolumbar fractures. J Neurosurg Spine 2014;20:497‐504.
10. Magerl F, Aebi M, Gertzbein SD,et al. A comprehensive classification of thoracic and lumbar injuries.
Eur Spine J 1994;3:184‐201. 11. Thomas KC, Bailey CS, Dvorak MF, et al. Comparison of operative and nonoperative treatment for
thoracolumbar burst fractures in patients without neurological deficit: a systematic review. J Neurosurg
Spine 2006;4:351‐8. 12. Schweitzer KM, Vaccaro AR, Harrop JS, et al. Interrater reliability of identifying indicators of posterior
ligamentous complex disruption when plain films are indeterminate in thoracolumbar injuries. J Orthop
Sci 2007;12:437‐42. 13. van der Roer N, de Lange ES, Bakker FC, et al. Management of traumatic thoracolumbar fractures: a
systematic review of the literature. Eur Spine J 2005;14:527‐34.
14. Wood KB, Khanna G, Vaccaro AR, et al. Assessment of two thoracolumbar fracture classification systems as used by multiple surgeons. J Bone Joint Surg Am 2005;87:1423‐9.
15. Patel AA, Vaccaro AR. Thoracolumbar spine trauma classification. J Am Acad Orthop Surg 2010;18:
63‐71. 16. Blauth M, Bastian L, Knop C, et al. Inter‐observer reliability in the classification of thoraco‐lumbar spinal
injuries. Orthopade 1999;28:662‐81.
17. Oner FC, Ramos LM, Simmermacher RK, et al. Classification of thoracic and lumbar spine fractures: problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J 2002;11:235‐45.
18. Reinhold M, Knop C, Beisse R, et al. Operative treatment of traumatic fractures of the thorax and
lumbar spine. Part II: surgical treatment and radiological findings]. Unfallchirurg 2009;112:149‐67. 19. Hitchon PW, Torner JC, Haddad SF, et al. Management options in thoracolumbar burst fractures. Surg
Neurol 1998;49:619‐626.
20. Dai LY, Jiang SD, Wang XY, et al. A review of the management of thoracolumbar burst fractures. Surg Neurol 2007;67:221‐31.
21. Vaccaro AR, Lim MR, Hurlbert RJ, et al. Surgical decision making for unstable thoracolumbar spine
injuries: results of a consensus panel review by the Spine Trauma Study Group. J Spinal Disord Tech 2006;19:1‐10.

Chapter 5
86
22. Knop C, Lange U, Bastian L, et al. Three‐dimensional motion analysis with Synex. Comparative biomechanical test series with a new vertebral body replacement for the thoracolumbar spine. Eur
Spine J 2000;9:472‐85.
23. Haiyun Y, Rui G, Shucai D et al. Three‐column reconstruction through single posterior approach for the treatment of unstable thoracolumbar fracture. Spine 2010;35:E295‐302.

87
Chapter 6
Evaluating the Immobilization Effect of Spinal Orthosis using
Sensor Based Motion Analysis
I. Curfs, W. van Rooij, R. Senden, B. Grimm, W. van Hemert
Journal of Prosthetics &Orthotics. 2016;28(1):23‐29

Chapter 6
88
Abstract
Introduction
External spinal orthoses are commonly used in treating spinal disorders. The purpose of
a spinal orthosis is to relieve pain and reduce spinal motion. Despite the widespread
use of spinal orthoses, evidence of their efficacy is lacking, and
there is no literature comparing different types of orthoses with regard to objective
measurements of the immobilization effect on the thoracolumbar spine.
Aim
The aim of this study was to evaluate and compare movement reduction and comfort
of four types of thoracolumbar orthoses on the normal motion using inertia sensor‐
based motion analysis (IMA).
Methods
Ten healthy volunteers were asked to perform five tasks of daily living without an
orthosis and with four different types of orthoses. Motion analysis was performed using
IMA. Comfort and subjective immobilization were analyzed by a questionnaire.
Results
All gait parameters were comparable in the different conditions. During the sit‐to‐stand
(STS) test, the maximum angular bending rate was significantly impaired by all orthoses
compared with the unbraced condition. During the block‐step test, significant
differences were found in pelvic obliquity for braced conditions. The bending angle was
significantly reduced during the flexion and extension test for all orthoses. Wearing an
orthosis showed significantly larger pelvic obliquity during lateroflexion compared with
the unbraced condition. In a subjective analysis using the questionnaire, the bandage
scored best, and the Jewett scored worst in comfort and movement restriction.
Conclusions
All orthoses influence spinal movement during several daily tasks as was shown by IMA.
The most rigid orthoses provided the most movement restriction, but simultaneously
scored worse in comfort. The choice for a certain brace should be based on individual
patient characteristics and diagnosis because of the experienced differences in
impairment and comfort.

Immobilization effect of spinal orthosis
89
6
Introduction
External spinal orthoses are commonly used in treating spinal disorders, such as
osteoporotic or traumatic fracture, spondylolysis, and in post‐surgical stabilization. The
main goal of a spinal orthosis is to relieve pain and reduce spinal motion. It is designed
to allow optimal restoration of the spine to a condition were it can effectively resume
its purposes, such as load transfer, protection of the spinal cord and movement in three
planes. A spinal orthosis has five main functions: to serve as a psychological reminder
and to offer total contact, three‐point pressure, end‐point control, and elevated
pressure.1
Several types of spinal orthoses are available, all of which all have special mechanical
considerations, variable prices (range of €62,00‐605,83) and differences in comfort.
Every spinal orthosis uses some degree of three‐point pressure to maintain the desired
position. Orthoses that use pads give excessive pressure on a localized part of the body
(e.g., the Jewett brace). Few orthoses achieve end‐point control, which gives a firm
grasp of the proximal (thorax) and distal (pelvis) spinal region of interest. Elevated
intra‐abdominal pressure reduces the net force applied to the spine and reduce some
of the stress placed on the spine itself.1 Total contact between the orthosis and the
wearer results in an equal distribution of pressure and good control. However, because
the spine is surrounded by skin and soft tissues, complete immobilisation will never be
achieved, especially in obese patients. Besides offering control and pressure, an
orthosis serves as a kinesthetic reminder to limit motion or adapt movements to unload
the spine. A soft and a rigid orthosis may be equally effective for this purpose.
Despite the widespread use of spinal orthoses in clinical practice, evidence of their
efficacy in the treatment of several spinal conditions is lacking. Only a few studies have
investigated the capacity of spinal orthoses to immobilize. Hashimoto et al. studied the
effect of rotational swing in low back pain during golf with sensor‐based movement
analysis and showed that lumbar extension and rotation angles are decreased in braced
condition during golf swing, whereas hip rotation is increased.2
Sato et al. evaluated the long‐term effect of a lumbar orthoses in patients with chronic
low back pain, and found that patients treated with corset had less pain and increased
muscle endurance for a short period of time. There was no difference in muscle
atrophy between patients treated with or without corset.3
Schmidt et al. investigated the effect of spinal braces by using it as a proprioceptive
kinesthetic reminder in osteoporosis and found a beneficial impact on gait stability.4
Several studies have investigated the efficiency of braces in fracture management.5,6,7 It
seems that the unbraced condition gives the same clinical and radiological results as
brace treatment; however the studies have their limitations, mainly because of small

Chapter 6
90
sample sizes. Therefore, further research with a randomized controlled trial is
necessary to objectify best conservative treatment in thoracolumbar spinal fractures.
As there is no general guideline to choose the appropriate orthosis, hospitals use their
own directives, which can be quite different. Recommendations for the use of spinal
orthoses are mainly based on literature reviews, without studies describing objective
immobilization effects.8
In our concern, there is no literature comparing the effect on spinal movement while
wearing different types of thoracolumbar spine orthoses in daily motion tasks such as
gait, stair climbing, and raising a chair.
There are several validated methods available for movement analysis. Accelerometer‐
based movement analysis is such a validated, non‐invasive, non‐time consuming,
cheap, and objective method for objective movement analysis in a 3D view.9,10 It shows
the biomechanical response to an immobilization or movement restriction caused by
pathologies of musculoskeletal origin. It is easy to use in different settings, such as an
outpatient clinic or even at home, for objective motion analysis in daily tasks.
In our clinic we use the inertia sensor‐based motion analysis (IMA) for movement
analysis in different pathologies. This method allows to objectively measure the effect
of a brace on the performance of movements, which may provide further insight into
the movement reduction of the braces.
The aim of this study is to evaluate and compare movement reduction and
comfortability of four types of thoracolumbar orthoses compared to normal spinal
motion using IMA and questionnaires.
Methods
Ten healthy volunteers (6 male, 4 female; age 18‐60years (mean 27.7 years)), without a
history of back pain, musculoskeletal problems or obesity, were included. The Atrium
Medical Center [METC Atrium‐Orbis] Ethics Committee approved the study using able‐
bodied volunteers as research subjects. The subjects were asked to perform several
function tasks under five conditions: first without wearing an orthosis and subsequently
while wearing four different types of orthosis.
Orthoses
Four commonly used orthoses (e.g., bandage, SecuTec dorso, Jewett, spinal cast) were
evaluated (Figure 6.1):

Immobilization effect of spinal orthosis
91
6
1. Lumbo‐assist (Spronken®) is a contoured elastic support with anatomical fit and
gives support to the lumbar (and low thoracic) spine. Price: €62.
2. The SecuTec Dorso (Bauerfeind®) is a modified orthosis for the support of the
lower thoracic and lumbar spine. Price: €605,84.
3. The Jewett (Spronken®) is a thoracolumbar hyperextension orthosis and is
designed to unload the anterior column. Price: €354,24.
Spinal cast, dorsal‐lumbar corset (OKM system) is a combination of polyurethane rigid
foam as a splint and the elastic stocking as bandage surface. The bandage is applied in
soft condition and hardens on the body. It is easy to modify and self‐molding, which
assures a perfect fit. In addition it is removable through the integrated zippers. Price:
€236.
Figure 6.1 Spinal orthoses (from left: Bandage, SecuTec Dorso, Jewett, spinal cast).
Function tasks
Motion analysis is performed using inertia‐based motion analysis (IMA). The sensor is a
3D accelerometer and gyroscope. It is a small (44x58x21mm) and low weight (45g)
MicroStrain Inertia Link sensor. The sensor measures acceleration (g), and angular rate
(°/sec) in three different planes, which are converted to attitudes (°).
The inertia sensor was attached on the sacrum (Figure 6.2), while the following function
tasks were performed:
1) Gait test: Subjects walked a 10m distance at preferred walking speed11
2) Sit – stand –sit test (STS): Subjects had to ascend and descend from a chair at
preferred speed without using their arms. They started in a sitting position, with
their knees flexed in 90 degrees11
3) Block stepping test: Subjects stepped up and down a 20 cm wooden block starting
first with the left leg, and subsequently repeating it with the right leg11
4) Flexion‐extension test: Subjects had to bend forward and backward as far as
possible without bending their knees.
5) Latero‐flexion test: Subjects had to bend as far as possible to the left, followed by
bending to the right. Every function task was performed three times, with a

Chapter 6
92
3‐5 seconds break in between. Averages of the three repetitions were used for
analysis.
Figure 6.2 Attachment of the sensor on the sacrum.
All tasks were performed in every condition, starting without wearing an orthosis,
followed by wearing one of the four orthosis. A fixed order was used: the bandage, the
SecuTec Dorso, the Jewett and the spinal cast.
Raw data were analysed using self‐developed, validated algorithms.10 Averages were
used for analysis. Group comparison was performed using T‐test, and the LSD as post
hoc test.
For each task, many specific parameters were derived. Relevant outcome parameters
used for analysis are mentioned below:
1. Walking speed (distance / walking time) in kilometers per hour. Used in gait
analysis.
2. Step time (time from foot contact to foot contact) in seconds. Used in gait analysis.
3. Step length (distance / number of steps) in meters. Used in gait analysis.
4. Variability step time left/right: difference between left/right step times. Used in gait
analysis.
5. (Absolute) bending angle with a forward and backward motion (flexion and
extension) in degrees. Used in block step, sit‐to‐stand, and flexion‐extension test.
6. Maximum angular rate bending (angular velocity) in degrees/second. Used in block
step, sit‐to‐stand, and flexion‐extension test.
7. Start sway (swing in anterior‐posterior direction) in degrees. Used in sit‐to‐stand
test.

Immobilization effect of spinal orthosis
93
6
Pelvic obliquity (lateral sway) in degrees. Used in block step, and sit‐to‐stand test.
Questionnaire
To analyse comfort and subjective immobilization, subjects completed a self‐designed
questionnaire for each orthosis. The questionnaire consisted of 12 questions,
concerning disability and comfort. Every question was scored from 1 to 5, with
1 representing total discomfort or total immobilization, and 5 representing no
discomfort and no immobilization experienced (Figure 6.3).
Orthosis Questionnaire
1= strongly disagree; 2= disagree; 3= neutral; 4= agree; 5= totally agree
Comment The orthosis: 1 2 3 4 5
1. ... is comfortable 1 2 3 4 5
2. ... causes no pain 1 2 3 4 5 3. ... does not pinch 1 2 3 4 5
4. ... can easily be worm under clothes 1 2 3 4 5
5. ... can easily be kept clean 1 2 3 4 5 6. ... is easy and quick to use 1 2 3 4 5
7. ... is sustainable 1 2 3 4 5
8. ... does not hinder gait 1 2 3 4 5 9. ... does not hinder standing op from a chair 1 2 3 4 5
10. ... does not hinder sitting down 1 2 3 4 5
11. ... does not hinder stair climbing 1 2 3 4 5 12. ... does not hinder forward bending 1 2 3 4 5
13. ... does not hinder backward bending 1 2 3 4 5
14. ... does not hinder lateral bending 1 2 3 4 5 15. ... does not interfering breathing 1 2 3 4 5
Figure 6.3 Questionnaire.
Results
Gait test
In the unbraced condition, subjects walked with a walking speed of 5.33 (±0.64) km/h
and a step time of 0.61 (±0.14) seconds. Mean step length was 0.95m (±0.23); and the
variability in step time left/right was 0.13 (±0.099). No effect of wearing an orthosis was
found on gait parameters.

Chapter 6
94
Sit to stand (STS) test
In the unbraced condition the mean bending angle during rising was 42.0° (±6.3), with a
maximum angular rate in forward bending of 1.9 °/s (±0.5). Wearing an orthosis had
just a small limiting effect on the absolute bending angle, with only a significant
reduced bending sway for the spinal cast compared to the unbraced condition
(Table 6.1).
The largest effect on the rising performance of the STS‐test was shown by a significantly
reduced maximum angular bending rate. The spinal cast provided the largest reduction
(‐0.55°/s), followed by the Jewett (‐0.44°/s), the SecuTec Dorso (‐0.34°/s) and finally the
bandage (‐0.16°/s) which caused the smallest reduction.
During sitting, bending angle in normal condition was 48.0 (±8.9) degrees with a
maximum angular rate of 1.1 °/s (±0.4). Only with Jewett brace the bending angle
during sitting was significantly reduced and start‐sway significantly increased in the
unbraced condition.
Normal sway was 0.063° (±0.06). In all braced conditions start sway was increased.
However this finding was only significant during rising with regard to the unbraced
condition for the Jewett (an increase of 0.98°). With sitting down the bending angle and
pelvic obliquity were significantly reduced when wearing the Jewett (‐8.3° bending
angle, P<0.01 resp. ‐1.09° pelvic obliquity, P<0.05) compared to the unbraced condition
(Figure 6.4).
Table 6.1 Averages (standard deviations) of the produced parameters during the STS test.
Unbraced Bandage Secu Tec
Dorse
Jewett Spinal Cast
Bending angle rising, degrees 42.0 (±6.3) 38.5 (±7.7) 37.8 (±5.6) 37.8 (±3.7) 35.0 (±6.5)a
Bending angle sitting, degrees 48.0 (±8.9) 44.6 (±8.6) 44.6 (±8.4) 40.8 (±4.3)a 42.0 (±8.8)
Maximum angular rate forward bending rising, degrees/s 1.9 (±0.5) 1.7 (±0.5)a 1.6 (±0.4)a 1.5 (±0.3)a 1.4 (±0.3)a,b (1)
Maximum angular rate forward bending sitting, degrees/s 1.1 (±0.4) 1.1 (±0.3) 1.2 (±0.4) 1.1 (±0.4) 1.1 (±0.4)
a significant difference (P<0.05) compared with the unbraced condition; b significant differenc (P<0.05) compared with other
orthoses: 1, bandage; 2, Secu Tec Dorso; 3, Jewett; 4, spinal cast. STS, sit‐to‐stand.
Figure 6.4 Selection of IMA STS: averages and standard deviations of start‐sway (degrees). IMA, inertia sensor‐based motion analysis; STS, sit‐to‐stand.

Immobilization effect of spinal orthosis
95
6
Block step test
During stepping up the bending angle was 9.9° (±2.7) in the unbraced condition, and
the pelvic obliquity was 11.8° (±3.0). During stepping down in the unbraced condition,
the bending angle and pelvic obliquity were respectively 12.54° (±3.08) and 9.5° (±2.6).
The pelvic obliquity was lower in stepping up when wearing an orthosis compared to
the unbraced condition (Table 6.2). A lower pelvic obliquity was also found during block
stepping down when wearing an orthosis compared to the unbraced condition. The
largest difference in pelvic obliquity was found in the Secutec Dorso, while spinal cast
showed the least decrease.
Table 6.2 IMA Block‐step: averages and standard deviations of measured parameters.
Unbraced Bandage Secu Tec
Dorse
Jewett Spinal Cast
Bending angle up, degrees 9.9 (±2.7) 8.6 (±2.5) 8.3 (±3.4) 8.5 (±3.6) 9.5 (±2.6)
Pelvic obliquity up, degrees 11.8 (±3.0) 8.3 (±1.4) a 7.7 (±1.9)
a 7.8 (±2.2)
a 8.4 (±2.0)
a
Pelvic obliquity down, degrees 9.5 (±2.6) 7.1 (±1.5)a 6.2 (±1.6)
a,b (4) 6.6 (±1.2)
a 7.0 (±1.3)
a
a significant difference (P<0.05) compared with the unbraced condition;
b significant difference (P<0.05)
compared with other orthoses: 1, bandage; 2, SecuTec Dorso; 3, Jewett; 4, spinal cast. IMA, inertia sensor‐
based motion analysis.
Flexion‐extension test
In the normal condition, forward bending was 64.5 (±11.6) degrees, with a maximum
bending rate of 1.2 (±0,3). Mean bending backward angle unbraced was 16.8 (±9.8)
degrees, with a maximum bending rate of 0.4°/s (±0.2). The mean pelvic obliquity for
left and right were respectively 4.5° (±2.5) and 2.0° (±0.7).
Every orthosis, with exception of the bandage, caused a significant reduction in the
forward and backward bending angle during the flexion and extension test (Table 6.3).
The spinal cast provided the largest decline in the forward bending angle (46.3 ±14.7
degrees), while the bandage had the least reduction in the forward bending angle (59.1
±13.5 degrees). During backward bending, the secutec dorso showed the largest
reduction (bending angle 11.3 ±5.4 degrees) and the spinal cast had the least reduction
with a bending angle of 13.4 (±6.6) degrees. Pelvic obliquity seemed to be slightly
reduced by wearing an orthosis. But only with the bandage a significant reduction of
pelvic obliquity right was measured, with a mean angle of 1.3 (± 0.6) degrees.

Chapter 6
96
Table 6.3 IMA flexion‐extension test: averages and standard deviations of measured parameters.
Unbraced Bandage Secu Tec
Dorse
Jewett Spinal Cast
Bending angle forward, degrees 64.5 (±11.6) 59.1 (±13.5) 56.8 (±14.2)a 50.5 (±13.4)a 46.3 (±14.7)a,b (1)
Bending angle backward, degrees 16.8 (±9.8) 12.2 (±4.1) 11.3 (±5.4)a 12.5 (±6.8)a 13.4 (±6.6)
Maximum bending rate forward, degrees/s 1.2 (±0.3) 0.6 (±0.6a,b(2) 1.0 (±0.4)a 0.8 (±0.5) 1.1 (±0.6)
Maximum bending rate backward, degrees/s 0.4 (±0.2) 0.2 (±0.2)a 0.3 (±0.1)a 0.2 (±0.1)a 0.4 (±0.2)
Pelvic obliquity left, degrees 4.5 (±2.5) 3.0 (±1.4) 3.6 (±2.1) 3.7 (±1.7) 3.9 (±2.3) Pelvic obliquity right, degrees 2.0 (±0.7) 1.3 (±0.6)a 1.9 (±0.9) 1.5 (±1.0) 1.4 (±0.6) a significant difference (P<0.05) compared with the unbraced condition;
b significant difference (P<0.05)
compared with other orthoses: 1, bandage; 2, SecuTec Dorso; 3, Jewett; 4, spinal cast. IMA, inertia sensor‐based motion analysis.
Latero‐flexion test
During normal condition, pelvic obliquity angles for left and right were respectively 7.5
(±2.5) and 7.2 (±2.3) degrees. Wearing an orthosis had a significant effect on the pelvic
obliquity during latero‐flexion, showing a significant increased pelvic obliquity when
wearing an orthosis with regard to the unbraced condition. The bandage and spinal cast
showed the largest increase in pelvic obliquity. Wearing the Jewett showed the least
increase in pelvic obliquity (Figure 6.5).
Figure 6.5 Selection of IMA latero‐flexion: averages and standard deviations of pelvic obliquity left and
right (degrees). IMA, inertia sensor‐based motion analysis.
Questionnaire
Compared to the unbraced conditions, every volunteer experienced a limitation in
movement when wearing an orthosis. However, with the bandage, limitations were not
experienced in all tasks and in the other tasks just very small. The largest obstruction in
movements was reported for the Jewett brace and the spinal cast. Concerning comfort,
the bandage scored the best, showing no difference with the unbraced condition. With
regard to pain caused by the orthoses, the bandage scored best by causing no pain. The

Immobilization effect of spinal orthosis
97
6
bandage was followed by the secutec dorso and the spinal cast. The Jewett scored
worst.
The spinal cast is scored less hygienic compared to the other orthoses (Figure 6.6).
Figure 6.6 Selection of questionnaire: averages and standard deviations.
Discussion
The purpose of this study was to evaluate and compare movement reduction and
comfortability of four types of thoracolumbar orthoses compared to normal spinal
motion using IMA and questionnaires.
As the results show, orthoses limit movements during daily activities, visualized by
decreased bending angles, reduced angular rates, differences in sway and changes in
pelvic movement.
This indicates that wearing an orthosis does influence the motion of the spinal
segments in thoracolumbar region. The most rigid orthoses provided the most
movement restriction, but simultaneously scored worse in comfort.
We objectified differences between the orthoses. Jewett was most restrictive in sit‐to‐
stand test, while secutec dorso had the highest influence of movement during block‐
step test. The spinal cast had the largest reduction of flexion test; however, it also
showed the least reduction in backward bending.
Overall spinal cast seemed most rigid but least comfortable, while the bandage was in
all tasks least restrictive, but most comfortable.
Pelvic obliquity seemed an interesting parameter. During braced conditions, in some
tasks it decreased, while in other tasks it increased. In daily tasks, as stair climbing
(block step test) and getting up from a chair (sit‐to‐stand test), pelvic obliquity

Chapter 6
98
decreased when wearing a brace, probably as a result of total movement restriction.
However, in the latero‐flexion test, where volunteers were encouraged to move as far
as possible, pelvic obliquity increased compared to the unbraced condition.
A systematic review of Van Poppel et al. in 1994 showed that there is evidence that
lumbar supports reduce trunk motion for flexion‐extension and lateral bending.12 These
findings are consistent with the findings of this study, but in addition this study showed
that the decrease of the motion in the spinal segments is compensatory increased by
movement of the sacro‐iliacal joints and pelvis, as measured by an increase of pelvic
obliquity.
Because of the compensatory increase in sacro‐iliacal, pelvic and hip movements, these
joints should be clinically investigated in patients with lower back pathologies. Pain or
stiffness in the sacro‐iliacal of hip joints, could be a relative contraindication for a
thoracolumbar orthosis.
The bending angle is the most restricted movement, mainly forward bending, as shown
in the flexion‐extension test. This restriction is caused by the mechanical impairment
due to the rigidity of the orthoses, but also because of the lumbar lordosis achieved by
the orthoses.
Barring the reduction of the bending angle, the bending angular rate was also reduced.
So, while wearing a brace, not only absolute movement restrictions were measured,
the peak velocities were also decreased. During sit‐to‐stand, or block step test, these
impairments were compensated by an increased sway, either in forward or lateral
direction.
It was shown by the smaller range of motion during sitting down that was compensated
by an increase in start sway (Jewett). Also during rising from a chair the bending angle
and bending angular rate were decreased, but start sway was increased (all braces, but
most with spinal cast). These objective results are comparable to the questionnaire
which indicates that the Jewett and the spinal cast provide more impairment in the
bending angle than the other orthoses.
Also in the other tasks, the objective outcomes provided by the sensor measurements
are comparable to results provided by the questionnaire; wherein the more rigid
orthoses (spinal cast, Jewett) provided more movement restriction. However they also
scored worse in comfort.
All braces except the bandage are evaluated as less comfortable compared to the
unbraced condition. Especially the Jewett and the spinal cast are observed as the least
comfortable orthoses, with the Jewett scoring worst as it is pinching off, not easy to
wear under clothes, and interferes with breathing; however, the spinal cast is the least
hygienic.

Immobilization effect of spinal orthosis
99
6
However, comfort reported by able‐bodied subjects may be different compared to
patients with spinal disorders. Able‐bodied subjects only experience the negative issues
of the spinal braces, while for patients with spinal disorders who experience pain and
other complaints, braces do have a certain goal of achieving pain control by movement
restriction. Furthermore, in this study there was only one size of each orthosis available
for all subjects. Therefore, optimal fit was not always achieved, which may have caused
additional discomfort.
Moreover, the questionnaire is not validated and the clinical relevance of the questions
can be discussed. However, we used the questionnaire to get information of the
comfortability of the braces, and as far as we known, there isn’t a validated
questionnaire available to analyse this.
A recent study of Morrisette et al. comparing inextensible (e.g., spinal cast) with
extensible (e.g., bandage) lumbar spine orthosis in patients with low back pain showed
better subjective results for the inextensible orthosis. Thus despite increased stiffness
and motion restriction of the inextensible orthoses, patients with low back pain
experienced these orthoses as more effective and comfortable compared to the
extensible orthosis.13
Important to mention is the sensor positioning. Before the study started, the position
of the sensor was extensively discussed regarding how to achieve the best results. It
could not be placed on the lumbar spine itself, because of the orthoses. A few options
were discussed; e.g., above the orthosis, the sternum, and the sacrum. The sacrum was
chosen because it can be easily identified in every patient, and moreover the sacrum is
the connection between the spinal column and pelvis. Spinal and pelvic movements are
very much related to each other; restriction in pelvic movement results in
compensatory increase of motion in the lumbar spine and vice versa. Therefore,
measuring sacral movement gives a good impression of the motion of the spine.
As discussed in the introduction, because of the lack of evidence, the choice for one
specific brace is often made according to the preference of the hospital or surgeon.
With the worldwide increase in health costs, the choice is probably also dependent on
price. The bandage is the cheapest orthosis (€ 62,00), subsequently followed by the
spinal cast (€ 236), the Jewett (€ 354,24), and the SecuTec Dorso (€ 605,84). However,
with regards to hygienic aspects, a spinal cast cannot be cleaned, so in many cases after
8‐12weeks a new cast has to be made, doubling the cost.

Chapter 6
100
Conclusion
In conclusion, all orthoses influence spinal movement during several daily tasks such as
rising from a chair, climbing stairs, and bending forward and backward as was shown by
IMA. There are differences in the braces regarding the degree of motion reduction,
comfort, and costs. Therefore it is important to treat patients with spinal problems as
individuals and for some indications more or less rigidity is needed to achieve the
desired immobilization.
Recommendations for clinical practice
Although, in this study we performed analysis on healthy individuals, we tried to
translate the data to recommendations for clinical practice. The spinal cast seems to be
most suitable in conservative treatment of thoracolumbar fractures in young active
patients because it is the most rigid orthosis with the highest movement restrictions,
and thus seems to achieve the best prevention for posttraumatic kyphosis. The elderly
patient with an (osteoporotic) thoracolumbar fracture, could best be treated with a
secutec dorso because it is easier to use and more comfortable. The bandage is useful
in chronic aspecific low back pain, where movement restriction is not really necessary.
Attention should be paid to the compensatory pelvic movement, wherein spinal
orthoses are relatively contraindicated in patients with sacro‐iliacal or hip pathologies.
Further research on patients with spinal disorders should be performed to confirm
these statements.

Immobilization effect of spinal orthosis
101
6
References
1. Agabegi SS, Asghar FA, Herkowitz HN. Spinal orthoses. J Am Acad Orthop Surg 2010;18(11): 657‐67.
2. Hashimoto K, Miyamoto K, Yanagawa T, et al. Lumbar corsets can decrease lumbar motion in golf
swing. J Sports Sci Med 2013;12(1):80‐7. 3. Sato N, Sekiguchi M, Kikuchi S, et al. Effects of long‐term corset wearing on chronic low back pain.
Fukushima J Med Sci 2012;58(1):60‐5.
4. Schmidt K, Hübscher M, Vogt L, et al. Influence of spinal orthosis on gait and physical functioning in women with postmenopausal osteoporosis Orthopade 2012;41(3):200‐5.
5. Alcalá‐Cerra G, Paternina‐Caicedo AJ, Díaz‐Becerra C, et al. Orthosis for thoracolumbar burst fractures
without neurologic deficit: A systematic review of prospective randomized controlled trials. J Craniovertebr Junction Spine 2014;5(1):25‐32.
6. Shamji MF, Roffey DM, Young DK, et al. A pilot evaluation of the role of bracing in stable thoracolumbar
burst fractures without neurological deficit. J Spinal Disord Tech 2014;27(7):370‐5. 7. Bailey CS, Urquhart JC, Dvorak MF, et al. Orthosis versus no orthosis for the treatment of
thoracolumbar burst fractures without neurologic injury: a multicenter prospective randomized
equivalence trial. Spine J 2014;14(11):2557‐64. 8. Calmels P, Fayolle‐Minon I. An update on orthotic devices for the lumbar spine based on a review of the
literature. Rev Rhum Engl Ed 1996;63(4):285‐91.
9. Kavanagh JJ, Menz HB. Accelerometry: a technique for quantifying movement patterns during walking. Gait Posture 2008;28(1):1‐15.
10. Mathie MJ, Coster AC, Lovell NH, Celler BG. Accelerometry: providing an integrated, practical method
for long‐term, ambulatory monitoring of human movement. Physiol Meas 2004;25(2):R1‐20. 11. Bolink SAAN, van Laarhoven SN, Lipperts M, Heyligers IC, et al. Inertial sensor motion analysis of gait,
sit‐stand transfers and step‐up transfers: differentiating knee patients from healthy controls. Physiol
Meas 2012;33(11):1947‐58. 12. van Poppel, MN. et al., Mechanisms of action of lumbar supports: a systematic review. Spine (Phila Pa
1976) 2000;25(16):2103‐13.
13. Morrisette, DC, Cholewicki J, Logan S, et al. A randomized clinical trial comparing extensible and inextensible lumbosacral orthoses and standard care alone in the management of lower back pain.
Spine (Phila Pa 1976) 2014;39(21):1733‐42.

Chapter 6
102

103
Chapter 7
Multisegmental Posterior only versus Circumferential
stabilization in the Surgical Treatment of Traumatic
Thoracolumbar Spinal Fractures:
a Comparison by Surgeon Equipoise
I. Curfs, M. Pishnamaz, M. Laubach, P. Kobbe, W. van Hemert, P. Willems
Submitted

Chapter 7
104
Abstract
Study design and objective
Retrospective cohort, surgeon equipoise. To compare the clinical, functional and
radiological outcome of multisegmental posterior versus circumferential stabilization in
traumatic thoracolumbar fractures. Summary of background data
There is an ongoing debate about optimal treatment in traumatic thoracolumbar spinal
fractures. If surgery is chosen, the most appropriate surgical technique is unknown. In
literature there is hardly any evidence whether thoracolumbar fractures are best
treated by posterior only or by circumferential stabilization. Methods
Multicentre analysis of patients who were surgically treated between 2009‐2015 for
traumatic thoracolumbar fractures either by circumferential stabilization in University
Hospital Aachen (Germany), or by posterior fixation only in Maastricht University
Hospital and Zuyderland MC Heerlen (Netherlands). Patients were included by surgeon
equipoise. Exclusion: multilevel fractures, age >65 years, ISS score >30 and neurological
deficit. Outcome measurement: regional sagittal angle (RSA), VAS pain score and
Oswestry Disability Index (ODI). Clinical data were extracted from patient files. Results
Fifty‐six patients were included for analysis (27 posterior only, 29 circumferential).
Length of stay was 16.9 days for the circumferential cohort compared to 9.3 days for
the posterior group (P<0.01). Total surgery times were longer for circumferential
surgery (264 vs. 110minutes, P<0.01). In the posterior only group a mean of
3.6 segments were fixed compared to 3.0 in the circumferential group (P<0.01).
Seventy percent completed 2‐year follow up. Radiological analysis showed no
significant differences between groups. Mean reduction of the kyphosis was 10° in both
groups, and mean rebound kyphosis at end point follow up was 9.2° in the
circumferential group versus 8.3° in the posterior group. Functional outcome
measurements showed no significant differences. In the circumferential group three
revisions were performed due to posterior hardware failure before anterior surgery. In
the posterior group two patients had a reoperation because of deep infection. Conclusions
This study showed similar radiological and functional outcome between multisegmental
posterior only and circumferential stabilization at endpoint follow up. Circumferential
stabilization was accompanied by longer surgery times and longer length of hospital
stay, but on average less segments were fixed. Further studies are necessary to
investigate the long term outcome of those patients.

Posterior only vs. circumferential stabilization
105
7
Introduction
Optimal management of traumatic thoracolumbar spinal fractures is still under debate.
If surgical treatment is chosen, there is no true consensus about the optimal surgical
technique.1 Nevertheless, various new surgical techniques have been introduced and
studied in the last decades. However, the level of evidence for these techniques is
limited and there seems to be no superior technique. There is also limited evidence
comparing circumferential versus posterior stabilization in the surgical treatment of
traumatic thoracolumbar fractures. Available literature mainly consists of retrospective
cohort studies. The largest cohort was presented in 2010 by the Spine Study Group of
the German Association of Trauma Surgery. They presented epidemiological data, and
outcome at two year follow up of 733 surgically treated patients, and showed better
functional outcome in only posteriorly stabilized patients, but radiological deformity
was better corrected in patients who had been stabilized circumferentially.2 There is
only poor evidence about the comparison of posterior versus circumferential
stabilization in thoracolumbar fractures. Been et al.3 and Mayer et al.4 published both
results of posterior only versus posterior‐anterior fusion in a retrospective cohort of
surgically treated thoracolumbar fractures, and found no significant differences.
However, Eui Gyu‐Sin et al.5 compared 25 patients treated by combined anterior‐
posterior stabilization with 86 patients treated by posterior only stabilization for
thoracolumbar fractures and found significantly better outcome regarding
posttraumatic kyphosis and pain in the circumferentially treated patients.
Worse outcome is mainly defined as a posttraumatic kyphosis, which is associated with
worse functional outcome and pain.6 It is a common potential complication of
inadequate treatment of spinal fractures, and is a challenging condition to treat.7
Combined anterior‐posterior surgery seemed to bear a lower risk for posttraumatic
spinal deformity. On the other hand, circumferential stabilization is more invasive for
patients. Additionally, it is often done two‐staged and subsequently costs are higher,
length of hospital stay increases, and recovery times are longer.2
Because of these conflicting findings it is important to perform a study to compare the
clinical and radiological outcome of patients treated for traumatic thoracolumbar spinal
fractures with posterior only stabilization compared to a circumferential stabilization.
For this kind of clinical questions, performing a randomized controlled trial to minimize
the risk of selection bias is not always feasible because inclusion and follow up may
take a long time, but mainly because of the confidence in one superior technique of
preference by many spine surgeons. In 2008 Stadhouder et al published a different
study approach to minimize risk of selection bias: the surgical equipoise.8 We used this
surgeon equipoise to perform a two nation (Germany and the Netherlands)

Chapter 7
106
comparative study in the treatment of thoracolumbar fractures, as in both countries
two different surgical techniques are used for thoracolumbar fractures.
Aim
To compare the functional, radiological and clinical outcome of posterior only versus
circumferential stabilization in traumatic thoracolumbar fractures.
Methods
Multicentre analysis of a consecutive cohort of patients who were surgically treated for
a traumatic thoracolumbar fracture between 01.01.2009‐31.12.2015 in University
Hospital Aachen (Germany), Maastricht University Hospital (Netherlands) and
Zuyderland MC Heerlen (Netherlands). Patients with multilevel fractures, age >65 years,
ISS score >30 and neurological deficit were excluded. In Germany patients were treated
by circumferential stabilization, while in Dutch patients the fractures were only
stabilized posteriorly.
Patients for analysis were included by surgeon equipoise as described by Stadhouder et
al.8. The proposed methodology was a cohort study with head‐to‐head comparison of
posterior only versus circumferential spinal stabilization/fusion. The cases were
discussed by a panel of spine surgeons representative of the medical centres from each
country. They had access to patient characteristics, trauma mechanism, neurological
state, comorbidities and pre‐operative radiological diagnostics (radiographs, CT and/or
MRI). Patients were included if there was a disagreement on the suggested treatment
method (posterior only or circumferential). Thus, remained two comparable groups
undergoing either posterior only or circumferential stabilization for thoracolumbar
spinal fractures.
Surgical approach
German patients were first stabilized posteriorly (55% treated by a percutaneous
approach and 45% by an open approach). The fixation was accomplished by
bisegemental instrumentation in the lumbar spine and bisegmental to multisegmental
instrumentation in the thoracic spine. In second stage surgery a corpectomy and cage
replacement was performed using an anterior approach by thoracoscopic or minimal
invasive lateral lumbar approach. In patients with incomplete burst fractures only
mono‐segmental anterior fusion was performed. In these cases the posterior fixation
was removed within one year, to restore spinal mobility in the non‐fused segments.

Posterior only vs. circumferential stabilization
107
7
From 2009‐2013 anterior stabilization was performed in a second stage procedure after
the patient was initially discharged (about three month after posterior stabilization).
From 2014 all circumferential treated patients received anterior stabilization within one
single hospital stay.
All patients in the Netherlands (MUMC Maastricht and Zuyderland Medical Centre)
received one stage surgery. Fractures were stabilized from posterior by pedicle screw
placement. In 56% of the cases a percutaneous stabilization was used, as in 44% an
open approach was performed. The number of levels that were fixed, depended on
fracture type and decision of the surgeon.
Radiological outcome measurements
Radiological analysis was performed using pre‐operative radiographs and computed
tomography (in supine positioning), and postoperative radiographs (standing
positioning) direct post trauma and at end point follow up with a minimum of 2 year
follow up.
Fractures were classified according to the AO spine classification.9 The Regional Sagittal
angle (RSA) was measured on lateral radiographs as shown in Figure 7.1. Other
measurements, such as the Gardner angle and vertebral body compression angle could
not be measured, because of the corpectomy and cage interposition in the
circumferential stabilized patients. All measurements were performed by the first and
second author.
Figure 7.1 Regional Sagittal Angle (RSA).

Chapter 7
108
Clinical outcome measurements
Age, gender, body mass index, comorbidities, surgical treatment, neurological state,
and complications were extracted from patient files. Outcome measures included VAS
pain score and Oswestry Disability Index. Patients were invited by letter (twice),
contacted by phone (once) or invited for outpatient contact.
Statistical analysis
Statistical Package for the Social Sciences Statistics Software version 25.0 for Windows
(SPSS, Inc., Chicago, Illinois). The Shapiro‐Wilk test showed that data were not normally
distributed. Therefore, Wilcoxon signed ranks tests were performed on significant
interactions. The Pearson Chi‐square was used to test any difference of proportions.
P‐value was considered to be statistically significant at P≤0.05 for all analyses. Results
are presented as either with mean (SD) or proportions (%).
The study was approved by the Medical Ethical Committee of the Maastricht University
Medical Centre (METC 15‐4‐144).
Results
Fifty‐six patients were selected by surgeon equipoise. Twenty‐nine patients had been
treated by two stage circumferential stabilization, and twenty‐seven patients by
posterior stabilization only as described in the methods section.
Completed two year follow up was accomplished by 21 patients in the posterior only
group and 18 patients in the circumferential group. Mean follow up was 53 months in
the circumferential group and 43 months in the posterior group (P=0.14), with a
minimum follow up of 24 months and maximum of 98 months.
Baseline characteristics are shown in Table 7.1. There was a significant difference in AO
classification. Difference in fracture type was mainly in burst and B‐type fractures, as in
the German population most fractures were burst fractures (79%) and in the Dutch
population there were 48% burst and 48% B‐type fractures (P<0.01). As most issues of
debate concern the burst fractures, a subgroup analysis was performed within these
fracture types. However, this subgroup analysis showed equal results compared to
whole group analysis.

Posterior only vs. circumferential stabilization
109
7
Table 7.1 Baseline characteristics.
Circumferential cohort, N=30
Median (range)
Posterior only cohort, N=27
Median (range)
P‐value
Age (years) 37.7 (18‐63) 41.9 (16‐64) 0.28
Gender 15 male, 14 female 18 male, 9 female 0.26 BMI 26.6 (19.8‐44.3) 24.9 (19.1‐33.0) 0.24
Localization T5‐T10 n=1
T11‐L2 n=27 L3‐L5 n=6
T5‐T10 n=2
T11‐L2 n=21 L3‐L5 n=4
0.19
AO Spine classification A1/A2 n=6
A3/A4 n=23 B n=0
C n=0
A1/A2 n=0
A3/A4 n=13 B n=13
C n=1
<0.01
Vertebral body injury A1 n=3 A2 n=3
A3 n=13
A4 n=10 Change n=0
Fracture dislocation n=0
A1 n=0 A2 n=1
A3 n=13
A4 n=13 Change n=0
Fracture dislocation n=0
0.20
ISS 12.3 (9‐19) 12.5 (9‐25) 0.96 End point follow‐up (N) N=18 N=21
Follow‐up (months) 53 (24‐83) 43 (24‐98) 0.14
Levels of significance P<0.05. ISS: Injury Severity Score.
Functional outcome
In the posterior only group 21 patients completed the questionnaires at two year follow
up. In the circumferential group 16 patients completed the questionnaires at two year
follow up. Results regarding the VAS and ODI are summarized in Table 7.2. There were
no significant differences between VAS and ODI in both groups, although there was a
trend towards better outcome scores in the posterior only group.
Table 7.2 Overview of outcome of questionnaires.
Circumferential
Mean (SD)
N=16
Posterior only
Mean (SD)
N=21
P‐value
(t‐test)
VAS 38 (27) 23 (19) 0.06
ODI 26 (22) 16 (17) 0.13
VAS scale 0‐100; zero indicates no pain and 100 worst possible pain. ODI scale 0‐100; 0‐20 = minimal disability, 21‐40 = moderate disability, 41‐60 = severe disability, 61‐80 =
crippling back pain, 81‐100 = bed bound or exaggeration of symptoms.
In subgroup analysis concerning only burst fractures (AO type A3 and A4), 11 patients in
the posterior and 12 patients in the circumferential group completed end point follow
up. There were no significant differences between patients treated posterior or

Chapter 7
110
circumferential (mean VAS in the posterior group was 26.4 [SD 22], compared to 44.2
[SD 28] in the circumferential group (P=0.15). Mean ODI score was respectively 22
versus 29 points in the posterior and the circumferential group (P=0.65)).
Radiological outcome
Pre‐operative radiographs were taken in supine position as part of the trauma
screening, while all postoperative radiographs were taken in standing position.
Eighteen patients of the circumferential group and twenty‐one patients in the posterior
group completed end point follow up. Results regarding the RSA are summarized in
Table 7.3. There were no significant differences in both groups. Subgroup analysis of
patients with burst fractures showed also no differences.
Table 7.3 Regional Sagittal angles in degrees in Dutch patients, who were only posterior stabilized, and in
German patients who were circumferentially stabilized.
RSA Circumferential mean
angle in degrees (SD) N=18
RSA Posterior only mean
angle in degrees (SD) N=21
P‐value
(t‐test)
Pre‐operative 12.6 (8.2) 10.1 (12) 0.47
Post‐operative 2.9 (6.8) ‐0.4 (11) 0.30
2 year 12.1 (9.4) 7.7 (12) 0.23
Difference pre‐operative vs. postop ‐9.7 (9.6) ‐10.5 (7) 0.77 Difference postop. vs. 2 year 9.2 (8.4) 8.3 (5.9) 0.70
Negative values indicate lordosis, positive values indicate kyphosis. P‐value was set at 0.05.
Within the circumferential cohort the treatment strategy changed since 2014 by means
of timing between the posterior and anterior surgery. We encountered loss of
reduction between posterior fixation and anterior surgery in case of longer intervals
between both surgeries. Since loss of reduction is difficult to address by the subsequent
anterior approach, this resulted in more kyphosis. We performed a subgroup analysis of
patients treated before 2014 versus patients treated since 2014. Baseline angles were
equal. At one year follow up, the mean RSA of the patients treated before 2014 was
9.4degrees (n=15), compared to 0.4degrees (n=9) in patients treated since 2014
(P=0.04). Rebound kyphosis was respectively 6.3 vs. 2.3degrees (P=0.08).
Clinical outcome
Overall length of stay was 16.9 days for the circumferential cohort compared to
9.3 days for the posterior group (P<0.01). Surgery times were significantly longer for
circumferential surgery (264 vs. 110minutes, P<0.01). There were no differences in the
duration of the posterior surgeries (respectively 107 vs. 110 minutes).

Posterior only vs. circumferential stabilization
111
7
In the posterior only group a mean of 3.6 segments were fixed compared to 3.0 in the
circumferential group (P<0.01). Results are summarized in Table 7.4.
Table 7.4 Overview of general outcome measurements: length of in hospital stay (days), total surgery
times (minutes) and length of segment fixation (number of levels).
Circumferential Posterior only P‐value
Posterior Anterior One admission Total
Lenght of hospital stay
(days)
9.01
(6.11) 10.0 (5‐17)
15.72
(8‐28) 16.9
3
(8‐28) 9.3
(4‐31)
1P=0.71 2P<0.01 3P<0.01
Total surgery
times (minutes)
1071
(38‐279)
162
(93‐329)
264
(173‐462)
110
(70‐165)
1P=0.889 2P<0.01
Number of
levels
3.0
(3)
3.6
(3‐5)
P<0.01
Levels of significance set at P<0.05.
Complications & revision rate
There were no significant differences in complications and revision. In the posterior
only group there was one superficial infection treated with oral antibiotics and two
early deep infections treated with surgical debridement and intravenous antibiotics.
There was one patient who was postoperatively diagnosed with a cauda syndrome, that
did not recover over time. This patient had suffered a L1 burst fracture, and was
treated with percutaneous stabilization T12‐L2. Postoperative MRI showed conus
contusion, without signs of compression.
In the circumferentially fused group three pulmonary problems were noticed after the
thoracic approach. Two patients suffered from re‐pneumothorax after removal of the
thoracic drain. One patient did not need re‐intervention, in the other patient a new
thoracic drain was necessary. There was one patient suffered from pleural effusion with
spontaneous remission. Two patients had numbness after surgery in the corresponding
thoracic dermatome and at the left thigh after bone grafting.
In the circumferential cohort three patients had undergone re‐operation. A revision of
the posterior stabilization was performed, because of loss of reduction before anterior
surgery . All these patients were treated before 2014.

Chapter 7
112
Discussion
Within this surgical equipoise study no significant differences in radiological and
functional outcome at minimum of two year follow up of posterior only compared to
circumferential stabilization of traumatic thoracolumbar fractures could be found.
We found equal radiological outcome with regard to kyphosis correction and rebound
kyphosis. In the posterior only group the kyphosis was initially overcorrected, as also
reported in other literature3, but subsequently showed a mean rebound kyphosis of 8
degrees at follow up. Under consideration of the fact that the circumferential
treatment was performed within two stage procedure (63 ±72 days between anterior
and posterior procedure) we also found a mean rebound kyphosis of 9 degrees at
follow up within this group. This is in line with Pishnamaz et al. who showed that the
highest amount of reduction loss is occurs within early postoperative stage.10 At this
point the authors would like to note, that in their experience anterior stabilization, if
thought necessary, should be either performed in one surgery after posterior fixation
or as soon as possible in the course to avoid rebound kyphosis. Further, the design of
cage endplates has improved in the last years in terms of larger surface contact areas
and consequently less cage subsidence. Subgroup analysis of our study clearly showed
this benefit. This is in line with other literature, as Eui Guy et al5 showed superior
radiological results of circumferential stabilization. They found a better intraoperative
correction of the kyphotic angle in the circumferential group (17 degrees compared to
12 degrees), and there was also significantly less rebound kyphosis at two year follow
up.
Indications for anterior fusion would be the lower risk of non‐union and persistent pain
due to intervertebral disk damage. Spiegl et al.11 recently described a possible key role
for intervertebral disk pathology in the treatment of (in)complete burst fractures. This
was based on studies of Öner12 and Sanders13 who both showed a correlation between
creeping of the intervertebral disk in the endplate of the fractured vertebra and worse
radiological outcome. Although these changes were seen on MRI after 18 months
follow up, probably a follow up period of two years is too short to show difference in
functional outcome caused by this intervertebral disk pathology.
Another potential benefit of circumferential would be mono‐segmental immobilization
compared to longer segment mobility loss in posterior only group. In the cases of
mono‐segmental anterior fusion, posterior hardware was removed within the first year
after surgery. In the posterior only group, hardware removal was performed in only
20% of the patients. Current literature shows clinical benefit of hardware removal
within two years after spinal surgery, as it decreases pain and disability, probably due
to restoration of segment mobility.14 However, in this study we found no correlation

Posterior only vs. circumferential stabilization
113
7
between functional outcome parameters and length of segment immobilization or
hardware removal.
This study is limited by its retrospective nature, which subsequently explains
differences in treatment within both cohorts, such as open versus percutaneous
approaches and some cases of spinal fusion versus stabilization in the posterior only
group. Although RCT would provide the highest level of evidence, the surgical equipoise
has its benefit over current available literature, as it minimizes the risk of selection bias.
There was a significant difference in AO classification, as in the posterior only group less
burst fractures and more B‐type fractures were included. However, subgroup analysis
of burst fractures only showed comparable results.
Overall this study shows comparable outcome in surgically treated thoracolumbar spine
fractures either by posterior only and circumferential stabilization. As posterior only
stabilization is less invasive, it seems justified to use this approach for the treatment of
thoracolumbar fractures. However, circumferential stabilization benefits from shorter
segment immobilisation, which may be an important reason to perform this kind of
surgery. Longer follow up is recommended to investigate the role of intervertebral disk
pathology in long term outcome, as this might be the indication for a circumferential
surgical approach. Further, multisegmental posterior stabilization may be functionally
better tolerated as long as the patients´ possess compensating mechanisms. As our
patient population is relatively young and the follow‐up relatively short, this functional
impairment may become relevant with a longer follow‐up period.
Conclusion
This comparative study shows similar radiological and functional outcome in surgically
treated thoracolumbar spinal fractures by posterior only compared to circumferential
stabilization. Although the circumferential stabilization had the advantage of shorter
segment immobilizations this was not reflected by a better clinical outcome.
Further studies are necessary to investigate the long term outcome of those patients.

Chapter 7
114
References
1. Oner FC, Wood KB, Smith JS, Shaffrey CI. Therapeutic decision making in thoracolumbar spine trauma.
Spine (Phila Pa 1976) 2010;35(21 Suppl):S235‐44.
2. Reinhold M, Knop C, Beisse R, et al. Operative treatment of 733 patients with acute thoracolumbar spinal injuries: comprehensive results from the second, prospective, Internet‐based multicenter study of
the Spine Study Group of the German Association of Trauma Surgery. Eur Spine J 2010;19(10):1657‐76.
3. BeenHD, Bouma GJ. Comparison of two types of surgery for thoraco‐lumbar burst fractures: combined anterior and posterior stabilisation vs. posterior instrumentation only. Acta Neurochir (Wien)
1999;141:349‐57.
4. Mayer M, Ortmaier R, Koller H, et al. Impact of Sagittal Balance on Clinical Outcomes in Surgically Treated T12 and L1 Burst Fractures: Analysis of Long‐Term Outcomes after Posterior‐Only and
Combined Posteroanterior Treatment.Biomed Res Int 2017;2017:1568258.
5. Eui‐Gyu Sin, Hyun‐Woo Kim, Cheol‐Young Lee, et al. Results of combined 360‐degree fusion versus posterior fixation alone for thoracolumbar burst fractures. Korean J Neurotrauma 2013;9(2):52‐56.
6. Schoenfeld AJ, Wood KB, Fisher CF, et al. Posttraumatic kyphosis: current state of diagnosis and
treatment: results of a multinational survey of spine trauma surgeons. J Spinal Disord Tech 2010; 23(7):e1‐8.
7. Buchowski JM, Kuhns CA, Bridwell KH, Lenke LG. Surgical management of posttraumatic thoracolumbar
kyphosis. Spine J 2008;8(4):666‐77. 8. Stadhouder A, Oner FC, Wilson KW, et al. Surgeon equipoise as an inclusion criterion for the evaluation
of nonoperative versus operative treatment of thoracolumbar spinal injuries. Spine J 2008;8(6):975‐81.
9. Vaccaro AR, Oner C, Kepler CK et al. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine (Phila Pa 1976) 2013;38(23):2028‐37.
10. Pishnamaz M, Oikonomidis S, Knobe M, Horst K, Pape HC, Kobbe P. Open versus percutaneous
stabilization of thoracolumbar spine fractures: A short‐term functional and radiological follow‐up. Acta Chir Orthop Traumatol Cech 2015;82(4):274‐81.
11. Spiegl UJ, Josten C, Devitt BM, et al. Incomplete burst fractures of the thoracolumbar spine: a review of
literature. Eur Spine J 2017;26(12):3187‐98. 12. Oner FC, van der Rijt RH, Ramos LM et al. Changes in the disc space after fractures of the thoracolumbar
spine. J Bone Joint Surg Br 1998;80:833‐9.
13. Sander AL, Lehnert T, El Saman A, et al. Outcome of traumatic intervertebral disk lesions after stabilization by internal fixator.AJR Am J Roentgenol 2014;203(1):140‐5.
14. Jeon CH, Lee HD, Lee YS, Seo JH, Chung NS. Is it beneficial to remove the pedicle screw instrument after
successful posterior fusion of thoracolumbar burst fractures? Spine (Phila Pa 1976) 2015;40(11): E627‐33.

115
Chapter 8
General discussion

Chapter 8
116

General discussion
117
8
General introduction
There is no evidence‐based treatment algorithm for thoracolumbar spine fractures. A
validated classification remains key to an appropriate treatment algorithm. Currently,
no spinal classification system has achieved universal acceptance. Therefore, it is
important to search for a reliable classification to guide decision making within clinical
practice. This thesis focused on the most appropriate current classifications and
addressed contributing factors and concerns regarding decision making in treatment of
thoracolumbar spinal fractures:
1. The importance of an accurate and applicable classification system.
2. The identification of fractures associated with worse radiological outcome after
conservative treatment.
3. International differences in classification and treatment decision making.
4. The efficacy of immobilization by different spinal orthoses.
5. The comparison in functional and radiological outcome of posterior stabilization
only and circumferential stabilization of traumatic thoracolumbar spinal fractures.
A systematic review was conducted (chapter 2) to investigate which classification can
be used best for treatment decision making in thoracolumbar fractures.1 The reliability
and clinical usefulness of AO‐, TLICS‐ and new AOspine‐classification were examined.
With the available literature, it is postulated that the accuracy of all three reviewed
classifications is sufficient for use in clinical practice, as kappa values were deemed
sufficient for use in clinical practice.2‐17 In the second part of this review the clinical
usefulness of current classifications was evaluated. Regarding the clinical usefulness,
TLICS was the only current classification system that contains a point allocation with
treatment recommendation, but its use in clinical practice was limited, as only in 50%
of the burst fractures the treatment recommendation by the classification was followed
by the treating physician.18 As an extension of the new AOspine classification, Vaccaro
et al introduced the Thoracolumbar AOspine Injury score.19 This score is compiled from
the AOspine classifications and the TLICS, and contains a treatment algorithm, not only
based on the classification of the fracture morphology, but it also has a quantifiable
point allocation for neurological status and patient‐specific‐modifiers (e.g. PLC status
and ankylosing spondylitis). In 2016, Kepler et al.20 and Vaccaro et al.21 presented a
validation study of this AOspine Injury score. In these studies, a worldwide surgeons’
input was used to determine the initial treatment recommendation. However, no
results about the applicability of this score in clinical practice have been published yet.
So, until now, scientific evidence of clinical usefulness of current classifications remains
poor. Very often, treatment decisions are not based on the classification alone. Current

Chapter 8
118
literature shows >90% agreement for the quite obvious treatment decision in simple
compression fractures (conservative) and evident unstable B and C type fractures
(surgery).3,4,16,18,22 However, regarding stable burst fractures (AO A3/A4 and TLICS 2),
the treatment recommendation by the TLICS classification is followed by the surgeons
in only 50% of the cases.18
In chapter 3 results of a two nation intra‐observer and interobserver study comparing
the Load Sharing Classification (LSC), TLICS and AOspine classification were presented.23
Data from 91 patients was analyzed twice by seven board‐certified spine surgeons. In
contrast to the LSC and the TLICS, the AOSpine classification showed substantial
agreement considering the fracture type (A;B;C) (intraobserver/interobserver
reliability: κ=0.71/0.61). It was concluded that the reliability of the AOSpine fracture
classification is superior to the TLICS and the LSC. Therefore, one could postulate this
classification system could best be applied within clinical practice.
Concluding, worldwide spine surgeons aim to improve classifications in the search for
consensus in the treatment of traumatic thoracolumbar fractures. It seems that current
classifications have acceptable inter‐ and intra‐observer reliability, but their clinical
applicability remains poor. Most discussion concerns the stable burst fracture, in which
in 50% of the cases, treatment decision is not based on the recommendation by the
classification. What makes these fractures so special?
It could be explained by the supposed worse outcome in some burst fractures and the
tendency by surgeons to prefer surgical treatment to provide a definite solution in
order to avoid undertreatment. Also we found burst fractures to be more at risk for
worse outcome. In chapter 4 we presented the results of a retrospective study that was
conducted to determine risk factors associated with worse outcome.24 Since
posttraumatic kyphosis is related to persistent pain25,26, we retrospectively examined
cases of conservatively treated traumatic thoracolumbar fractures, and searched for
prognostic factors that may lead to progressive kyphosis. Recognition of these risk
factors associated with worse outcome, may influence treatment decision making.
However, current classifications fail to include these prognostic factors, such as initial
kyphosis. We identified an increased risk of progression of kyphosis in age >50 years
and in fractures localized at Th12 or L1. A3 type fractures were significantly more at risk
for posttraumatic kyphosis than A1 and A2 type fractures. 30‐50% of the A3 type
fractures have a regional (Gardner angle) and segmental (vertebral compression angle)
kyphosis of more than 20 degrees. This finding is in accordance with several other
studies, that stated that burst fractures and fracture localization at the thoracolumbar
junction are prone for progressive kyphotic deformity.27‐29 It is therefore recommended
to integrate angular kyphosis in current classifications or at least take account for when
interpreting a thoracolumbar fracture.

General discussion
119
8
The high risk of posttraumatic kyphosis in burst fractures might be explained by a
possible misinterpretation of the integrity of the PLC in these fractures. Schnake et al.30
performed a study on the reliability of fracture classification, mainly for B‐fractures.
They found that initially almost 42% of the B‐type fractures were misdiagnosed as type
A. Schnake listed a vertebral kyphotic angle of >15 degrees, a pronounced compression
of vertebral cancellous bone despite minimal reduced anterior vertebral height, and a
considerably reduced anterior vertebral height of over 50% to be considered as red flag
symptoms for worse radiological outcome. So, reliable assessment of the PLC integrity
is crucial in these cases. Unfortunately, evidence about the role of standard MRI in
addition to plain radiographs and CT is contradictory. Literature regarding the reliability
of MRI in PLC status resulted in fair to moderate kappa values (kappa ± 0.4)31, and
demonstrated relatively high negative predictive values and relatively low positive
predictive values for PLC injuries.32
In addition to the PLC status, anterior comminution is a second important risk factor for
worse outcome in burst fractures. In 2002 Öner et al.33 published a study in which
conservative and operative treatment of thoracolumbar fractures were compared, and
routinely an MRI was made to identify predictors for worse outcome. They concluded
that an unfavorable outcome was related to the progression of kyphosis. In the
conservative group this could be predicted by the endplate comminution and vertebral
body involvement. In the operatively treated group, recurrence of the kyphotic
deformity was predicted by the lesion of the posterior longitudinal ligamentary
complex together with endplate comminution and vertebral body involvement.
Other studies also reported on the role of the amount of vertebral body destruction
and kyphotic deformity in the choice for or against surgical treatment.34‐36 Hitchon et
al.35 recommended surgical treatment in case of: >20 degrees kyphosis, >50% spinal
canal encroachment, or more than 50% loss of anterior body height.
However, in 2011 Gnanenthiran performed a meta‐analysis comparing conservative
and operative treatment in burst fractures. The data of four trials (2 RCT,
1 pseudorandomized trial and 1 prospective cohort study) was included for analysis.
This meta‐analysis showed less residual kyphosis in surgical treatment (11° surgical
versus 16° in conservative treatment), but no differences in clinical outcome between
conservative treatment and surgical treatment of traumatic thoracolumbar burst
fractures37. Although radiological outcome was in favor of surgical treatment, surgery
was accompanied by higher complication rates and increased costs of treatment. This
finding was in accordance with the conclusion of a review performed by
Bakhsheshian.38
Recently, Spiegl et al.39 discussed a key role for the intervertebral disc in determining
the long‐term clinical and radiological outcome of burst fractures. It is of interest

Chapter 8
120
to investigate whether the amount of kyphosis or clinical outcome is influenced by disc
destruction and whether incorporation of the intervertebral disc pathology into the
existing classifications could be of value.
Therefore this thesis postulated that not only the PLC but also level of injury, degree of
kyphosis, comminution and disc damage should be integrated as depending
determinants of injury that were previously obviously seen as independent. Except
these factors, previous studies also stated that several other parameters might
influence outcome in thoracolumbar fractures. Shen et al.40 showed that high VAS pain
scores and large interpedicular distance could be significant risk factors for failure of
nonoperative treatment of burst fractures. Furthermore, lower bone quality and bone
regeneration (e.g. osteoporosis), higher age and fracture localization at the
thoracolumbar junction seem to be responsible for worse radiological outcome.24,40.
Concluding, it is not possible to solely lean on classifications in treatment decision
making, as the prognostic value of classifications is still limited, mainly in the grey area
of burst fractures. In the search to enroll a worldwide accepted treatment algorithm for
traumatic thoracolumbar spinal fractures, it seems necessary to add more patient and
fracture related information to the current classification systems. Including these
parameters in treatment decision making may enhance prognostic value. With the
addition of patient specific modifiers, the Thoracolumbar AOspine Injury Score
acknowledges that other patient and fracture related parameters are important in the
search for a worldwide applicable and accepted classification and treatment algorithm
for thoracolumbar spine fractures.19‐21 However, it is difficult to include all these factors
in a point allocation system.
So, we might have to look more for individual phenotypes, instead of focusing on
improving the clinical usefulness of current classifications. Phenotyping has become
more important over the past decades in several specialisms in medical care. It comes
closer to personalized medicine, often defined as ‘the right treatment for the right
person at the right time’. In the case of treating traumatic spinal fractures, we should
not only look for the radiological recognition of ‘instability’, but also look for patients
with worse outcome. Probably this approach will allow the recognition of certain
fractures phenotypes, which may lead to a worldwide accepted treatment algorithm of
traumatic thoracolumbar fractures.
A lack of consensus in treatment strategies may cause variation in practice among
individual surgeons or between clinics or countries, which is not desirable for
optimization of care and patient counseling.41 In this thesis the results of a multicenter,
two‐nation study within three hospitals (University Hospital Aachen, Maastricht
University Medical Centre, Zuyderland Medical Centre Heerlen‐Geleen), were

General discussion
121
8
presented (chapter 5).42 Wide differences between nations were observed. Fracture
assessment between the German and Dutch surgeons was comparable regarding the
AO Classification. We found a consistent treatment strategy within both countries;
however with partially opposing therapeutic strategies concerning AO Type A fractures.
Operative treatment of Type B and C fractures was recommended in both countries
without exception. In the Netherlands, surgeons usually recommend nonoperative
treatment in Type A fractures whereas German surgeons usually tend to surgery in case
of Type A.2 and particularly A.3 fractures. In Germany circumferential fusion was an
often selected procedure, in Type A fractures as well as in Type B and C fractures. In
contrast, the Dutch surgeons never selected an additional anterior fusion in Type A
fractures and rarely in Type B and C fractures. One reason for the more frequent
indication for an anterior approach in Germany appears to be that adjacent disc injuries
are interpreted as a causal reason for the absence of vertebral bone healing and
consequent posttraumatic kyphosis, and may cause long‐term persistent pain as well.
Another reason might be that full restoration of sagittal alignment is defined as a
primary goal of therapy in Germany. However, currently it is still unclear whether
improved radiological results are associated with an improved long term clinical
outcome.27,28 It is therefore of interest to initiate a discussion among experts to discuss
how to eliminate such vital differences. As classifications and findings in literature are
internationally acknowledged, the interpretation of these findings in clinical practice, is
obviously not.
In case of operative treatment, there are various ways to stabilize fractures, and
current evidence shows not one superior technique. Despite the lack of consensus in
treatment decision making, a number of papers focus on new treatment techniques.
During the last decades spinal surgery is evolving rapidly. Also in spinal trauma new
insights have led to the development of new treatment modalities. In the past years,
many new surgical techniques have been applied. Most innovations are mainly based
on expert opinions or even industry driven, sometimes supported by biomechanical
studies. Since the evolution progresses at high speed, there seems to be not enough
time to collect the data on the impact of these techniques on long‐term patient
outcome. For example, data on the need for anterior support and endplate stabilization
in order to theoretically prevent long‐term intervertebral disk pathology and retain a
better balanced spine in the sagittal plane. However, high level evidence in clinical
studies is not available. Care should be taken with the massive introduction of novel
techniques without firm evidence on their safety and efficacy. There is an increasing
demand for faster recovery by using less invasive techniques, with less complications
and better restoration of alignment. However, attention should be paid to the

Chapter 8
122
advantages and disadvantages of current and novel techniques. Recently, an article
considering the issues of implementation of new medical techniques was published in
Medisch Contact.43 Innovations are necessary to improve quality of medical care, but
there must be a right relationship between the possibility of innovation and safety. In
the past, the careless introduction of innovative techniques has led to unwanted and
disappointing results. There are currently no obligations associated with the rules
considering medical devices. Therefore, the Federation Medical Specialists
(Netherlands) has introduced a guideline, how to implement a novel technique in a
careful and safe way. Furthermore new regulations of the European Union will be in
place in 2020 to ensure that healthcare professionals can rely on the quality of a new
medical device.
One of the main issues regarding the surgical treatment of traumatic thoracolumbar
spine fractures, is the need for anterior support of the spinal column. Chapter 7
presents the results of a comparative study of posterior versus circumferential
stabilization in traumatic thoracolumbar fractures.44 We found that circumferential
stabilization was accompanied by longer operation times and longer length of hospital
stay. On average, less segments were fixed by circumferential stabilization (3.6 vs. 3.0,
respectively). End time follow up showed also no significant differences in radiological
and functional outcome between posterior only and circumferential stabilization. These
findings call for a well‐designed randomised controlled trial comparing posterior only
vs. circumferential stabilisation, which should focus on patient related outcome and
safety, but also on healthcare related costs.
Most literature describes retrospective cohort studies or prospective case series (level
of evidence 3‐4). Due to small sample sizes, and the confidence of surgeons by one
approach, it seems difficult to perform randomized controlled trials (RCT). Current
clinical practice is therefore mainly based on expert opinions and country specific
treatment decisions. However, we can use additional research techniques to achieve
more evidence. Although retrospectively, surgical equipoise seems to be a good
alternative limiting selection bias in the comparison of different treatment
techniques.45 This research design also has the advantage that it allows different
centers to collaborate and communicate with each other. With the availability of the
internet, distance does not seem to be an issue anymore considering collaboration
between nations and even continents. As there are large nation differences in daily
practice, connecting and learning from each other results in the possibility to optimize
treatment. We should use this for better prospective studies and registries.
Collaboration will lead to better future research projects, which eventually should help
to achieve consensus in the decision making for treatment of traumatic thoracolumbar
fractures.

General discussion
123
8
References
1. I. Curfs, M. Schotanus, W. Van Hemert, M. Heymans, R. De Bie, L. Van Rhijn, P. Willems. Reliability and
clinical usefulness of current classification methods in traumatic thoracolumbar fractures: a systematic
review of the literature. Submitted Injury. 2. Wood KB, Khanna G, Vaccaro AR, et al. Assessment of two thoracolumbar fracture classification systems
as used by multiple surgeons. J Bone Joint Surg Am 2005;87(7):1423‐9.
3. Harrop JS, Vaccaro AR, Hurlbert RJ, et al. Intrarater and interrater reliability and validity in the assessment of the mechanism of injury and integrity of the posterior ligamentous complex: a novel
injury severity scoring system for thoracolumbar injuries. Invited submission from the joint section
meeting on disorders of the spine and peripheral nerves, March 2005. Spine Trauma Study Group. J Neurosurg Spine 2006;4(2):118‐22.
4. Whang PG, Vaccaro AR, Poelstra KA, et al. The influence of fracture mechanism and morphology on the
reliability and validity of two novel thoracolumbar injury classification systems. Spine (Phila Pa 1976) 2007;32(7):791‐5.
5. Reinhold M, Audigé L, Schnake KJ, et al. AO spine injury classification system: a revision proposal for the
thoracic and lumbar spine. Eur Spine J 2013:22(10):2184‐201. 6. Oner FC, Ramos LM, Simmermacher RK, et al. Classification of thoracic and lumbar spine fractures:
problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J 2002;11(3):235‐45.
7. Pishnamaz M, Curfs I, Balosu S, et al. Two‐Nation Comparison of Classification and Treatment of Thoracolumbar Fractures: An Internet‐Based Multicenter Study Among Spine Surgeons. Spine (Phila Pa
1976) 2015;40(22):1749‐56.
8. Kaul R, Chhabra HS, Vaccaro AR, et al. Reliability assessment of AOSpine thoracolumbar spine injury classification system and Thoracolumbar Injury Classification and Severity Score (TLICS) for
thoracolumbar spine injuries: results of a multicentre study. Eur Spine J 2017;26(5):1470‐6.
9. Urrutia J, Zamora T, Yurac R, et al. An independent interobserver reliability and intraobserver reproducibility evaluation of the new AOSpine Thoracolumbar Spine Injury Classification System. Spine
(Phila Pa 1976) 2015;40(1): E54‐8.
10. Lenarz CJ, Place HM, Lenke LG, et al. Comparative reliability of 3 thoracolumbar fracture classification systems. J Spinal Disord Tech 2009;22(6):422‐7.
11. Cheng J, Liu P, Sun D, et al. Reliability and reproducibility analysis of the AOSpine thoracolumbar spine
injury classification system by Chinese spinal surgeons. Eur Spine J 2017;26(5):1477‐82. 12. Patel AA, Whang PG, Brodke DS, et al. Evaluation of two novel thoracolumbar trauma classification
systems. Indian J Orthop. 2007;41(4):322‐6
13. Park, Lee, Park NH, et al. Modified thoracolumbar injury classification and severity score (TLICS) and its clinical usefulness. Acta Radiol 2016;57(1):74‐81.
14. Kriek JJ, Govender S. AO‐classification of thoracic and lumbar fractures‐‐reproducibility utilizing
radiographs and clinical information. Eur Spine J 2006;15(8):1239‐46. 15. Kepler CK, Vaccaro AR, Koerner JD, et al. Reliability analysis of the AOSpine thoracolumbar spine injury
classification system by a worldwide group of naïve spinal surgeons. Eur Spine J 2016;25(4):1082‐6.
16. Vaccaro AR, Baron EM, Sanfilippo J, et al. Reliability of a novel classification system for thoracolumbar injuries: the Thoracolumbar Injury Severity Score. Spine (Phila Pa 1976) 2006;31(11 Suppl):S62‐9;
discussion S104.
17. Azimi P, Mohammadi HR, Azhari S, et al. The AOSpine thoracolumbar spine injury classification system: A reliability and agreement study. Asian J Neurosurg 2015;10(4):282‐5.
18. Joaquim AF, Daubs MD, Lawrence BD, et al. Retrospective evaluation of the validity of the
Thoracolumbar Injury Classification System in 458 consecutively treated patients. Spine J 2013;13(12):1760‐5.
19. Vaccaro AR, Oner C, Kepler CK, et al. AOSpine thoracolumbar spine injury classification system: fracture
description, neurological status, and key modifiers. Spine (Phila Pa 1976) 2013;38(23):2028‐37. 20. Kepler CK, Vaccaro AR, Schroeder GD, et al. The Thoracolumbar AOSpine Injury Score. Global Spine J
2016;6:329‐34.

Chapter 8
124
21. Vaccaro AR, Schroeder GD, Kepler CK, et al. The surgical algorithm for the AOSpine thoracolumbar spine injury classification system. Eur Spine J 2016;25(4):1087‐94.
22. Joaquim AF, Fernandes YB, Cavalcante RA, et al. Evaluation of the Thoracolumbar Injury Classification
System in Thoracic and Lumbar Spinal Trauma. Spine 2011;36:33–6. 23. Pishnamaz M, Balosu S, Curfs I, Uhing D, Laubach M, Willems P, Herren C, Weber C, Hildebrand F, Kobbe
P. Reliability and agreement of different spine fracture classification systems: an independent intra‐ and
interobserver study. World Neurosurg. 2018;115:e695‐702. 24. Curfs I, Grimm B, van der Linde M, Willems P, van Hemert W. Radiological prediction of posttraumatic
kyphosis after thoracolumbar fracture. Open Orthopaedic Journal 2016;10:135‐42.
25. Buchowski JM, Kuhns CA, Bridwell KH, Lenke LG. Surgical management of posttraumatic thoracolumbar kyphosis. Spine J 2008;8(4):666‐77.
26. Doo TH, Shin DA, Kim HI et al. Clinical Relevance of Pain Patterns in Osteoporotic Vertebral Compression
Fractures. J Korean Med Sci 2008;23(6): 1005‐10. 27. Reinhold M, Knop C, Beisse R, et al. Operative treatment of traumatic fractures of the thoracic and
lumbar spinal column: Part III: Follow up data. Unfallchirurg 2009;112:294‐316.
28. Siebenga J, Leferink VJ, Segers MJ, et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine
2006;31:2881‐90.
29. Wood K, Buttermann G, Mehbod A, et al. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone
Joint Surg Am 2003;85‐A:773‐81.
30. Schnake KJ, von Scotti F, Haas NP, Kandziora F. Unfallchirurg.Type B injuries of the thoracolumbar spine : misinterpretations of the integrity of the posterior ligament complex using radiologic diagnostics.
Unfallchirurg 2008;111(12):977‐84.
31. Lee GY, Lee JW, Choi SW, et al. MRI Inter‐Reader and Intra‐Reader Reliabilities for Assessing Injury Morphology and Posterior Ligamentous Complex Integrity of the Spine According to the Thoracolumbar
Injury Classification System and Severity Score. Korean J Radiol. 2015;16(4):889‐98
32. van Middendorp J, Patel A, Schuetz M, Joaquim AF. The precision, accuracy and validity of detecting posterior ligamentous complex injuries of the thoracic and lumbar spine: a critical appraisal of the
literature. Eur Spine J 2013; 22(3):461‐74.
33. Oner FC, Ramos LM, Simmermacher RK, et al. Classification of thoracic and lumbar spine fractures: problems of reproducibility. A study of 53 patients using CT and MRI. Eur Spine J 2002;11(3):235‐45.
34. Wood KB, Li W, Lebl DS, et al. Management of thoracolumbar spine fractures. Spine J 2014;14:145‐64.
35. Hitchon PW, Torner JC, Haddad SF, et al. Management options in thoracolumbar burst fractures. Surg Neurol 1998;49:619‐26.
36. Dai LY, Jiang SD, Wang XY, et al. A review of the management of thoracolumbar burst fractures. Surg
Neurol 2007;67:221‐31. 37. Gnanenthiran SR, Adie S, Harris IA. Nonoperative versus operative treatment for thoracolumbar burst
fractures without neurologic deficit: a meta‐analysis. Clin Orthop Relat Res 2012;470(2):567‐77.
38. Bakhsheshian J, Dahdaleh NS, Fakurnejad S, Scheer JK, Smith ZA. Evidence‐based management of traumatic thoracolumbar burst fractures: a systematic review of nonoperative management. Neurosurg
Focus 2014;37(1):E1
39. Spiegl UJ, Josten C, Devitt BM et al. Incomplete burst fractures of the thoracolumbar spine: a review of literature. Eur Spine J 2017;26(12):3187‐98.
40. Shen J, Xu L, Zhang B, et al. Risk factors for the failure of spinal burst fractures treated conservatively
according to the Thoracolumbar Injury Classification and Severity Score (TLICS): A Retrospective Cohort Trial. PLoS One 2015;10(8):e0135735.
41. Schnake KJ, Stavridis SI, Kandziora F. Five‐year clinical and radiological results of combined
anteroposterior stabilization of thoracolumbar fractures. J Neurosurg Spine 2014;20:497‐504. 42. Pishnamaz M, Curfs I, Balosu S, Willems P, van Hemert W, Pape H, Kobbe P. Country‐specific treatment
differences of thoracolumbar spine fractures: results of an internet‐based multicenter comparison
between Germany and the Netherlands. Spine 2015;40(22):1746‐56.

General discussion
125
8
43. Holewijn R, Stadhouder A, de Kleuver M. Nieuwe techniek introduceren? Weeg eerst de risico’s. Medisch Contact (36), 6 sep 2018.
44. Curfs, I; Pishnamaz, M; Laubach, M; Kobbe, P; Van Hemert, W; Willems, P. Multisegmental posterior
only versus circumferential stabilization in the surgical treatment of traumatic thoracolumbar spinal fractures: a comparison by surgeon equipoise. Submitted Spine, august 25th 2018.
45. Stadhouder A, Oner FC, Wilson KW, Vaccaro AR, Williamson OD, Verbout AJ, Verhaar JA, de Klerk LW,
Buskens E. Surgeon equipoise as an inclusion criterion for the evaluation of nonoperative versus operative treatment of thoracolumbar spinal injuries. Spine J 2008;8(6):975‐81.

Chapter 8
126

127
Chapter 9
Valorisatie

Chapter 9
128

Valorisatie
129
9
Valorisatie
Traumatische thoracolumbale wervelfracturen komen steeds vaker voor in onze
maatschappij en worden voornamelijk gezien bij mannen tussen de 20‐40 jaar als
gevolg van verkeersongevallen. Traumatische wervelfracturen hebben potentieel
ernstige consequenties, zoals overlijden in ongeveer 5% van de patiënten, en
ruggenmergletsel waarvan de incidentie wordt geschat op 22‐51%.
Er is wereldwijd grote variatie in de behandeling van traumatische thoracolumbale
wervelfracturen. Er is weinig high‐level evidence beschikbaar over wat de beste
behandeling per type fractuur is, en derhalve wordt de behandeling veelal gebaseerd
op ‘expert opinion’ of traditioneel gebruikelijke manier van werken per kliniek.
Mede gezien de stijgende incidentie, oplopende zorgkosten en de ontwikkeling van
nieuwe behandelmogelijkheden, wordt het steeds belangrijker om consensus te
bereiken in de behandeling van traumatische thoracolumbale wervelfracturen. Dit
proefschrift richt zich op de optimalisatie van behandeling van thoracolumbale
wervelfracturen. Het onderzoek is vooral van belang voor patiënten, medisch
specialisten, en beleidsbepalers in de gezondheidszorg.
Er is vooral onenigheid over de optimale behandeling van burst fracturen. Dit zijn
breuken van de wervelkolom waarbij het wervellichaam is gebroken, maar de achterste
pijler nog intact is, en dus in principe een stabiele fractuur betreft. Het merendeel van
de burst fracturen lijkt conservatief goed behandeld te kunnen worden. Echter, een
deel hiervan kent een slecht klinisch resultaat, gekenmerkt door een lokale
posttraumatische kyfose, waarvan bekend is dat deze gepaard gaat met beperkingen
en een grotere kans op chronische pijn.
Vier onderzoeken in dit proefschrift zijn internationale, multicenter studies, uitgevoerd
in een academisch ziekenhuis in Duitsland, een academisch ziekenhuis in Nederland en
een top klinisch perifeer ziekenhuis in Nederland. De beschreven studies geven inzicht
in de internationale verschillen die er bestaan qua behandeling van thoracolumbale
wervelfracturen. Vooral in het geval van de bovengenoemde burst fracturen lopen
behandelingen zeer uiteen. In Duitsland wordt hierbij vrijwel altijd voor een operatieve
behandeling gekozen, in tegenstelling tot in Nederland. De resultaten van dit onderzoek
laten zien op welke manier verschillen in behandeling tot stand komen. Dit geeft inzicht
in besluitvorming en kwaliteit van behandeling, maar vooral ook aanleiding tot meer en
beter wetenschappelijk onderzoek met meer internationale samenwerking.
Voor een uniforme behandeling is een geschikte classificatie om de fractuur te typeren
onontbeerlijk. Er zijn de laatste jaren vele verschillende classificaties ontwikkeld, die

Chapter 9
130
allen voor‐ en nadelen hebben. In dit proefschrift hebben we gepoogd de classificaties
te beoordelen op betrouwbaarheid (validiteit) en toepasbaarheid in de praktijk. Het
blijkt dat met name de klinische toepasbaarheid nog erg beperkt is, aangezien in meer
dan de helft van de burst fracturen het advies van de classificatie in de praktijk niet
wordt gevolgd. Om tot een beter toepasbaar classificatie systeem te komen,
presenteren we een aantal prognostische factoren die van invloed kunnen zijn op de
uitkomst van de fractuurbehandeling, zoals leeftijd, lokalisatie van de fractuur en
fractuurtype. Ook in de literatuur is er steeds meer aandacht voor patiënt‐ en fractuur‐
gerelateerde factoren die invloed hebben op de uitkomst, zoals osteoporse,
hoogteverlies van de wervel, comorbiditeit, lokale kyfose en beschadiging van de
tussenwervelschijf. Bij het opstellen van een beter classificatie systeem voor klinische
toepasbaarheid is het belangrijk om deze zogenaamde ‘modifiers’ te incorporeren. De
modifiers zorgen voor een meer op de individuele patiënt gericht beleid voor
behandeling, oftewel personalised medicine, met een uiteindelijk beter klinisch
resultaat.
Als we in staat zijn een betere behandelkeuze te maken, kunnen we zinnigere zorg
leveren; dus niet opereren als het niet nodig is.
Als eenmaal de indicatie voor operatieve behandeling gesteld is, kan gekozen worden
voor verschillende operatietechnieken, waarvan niet bekend is welke de beste is voor
een patiënt. Nieuwe chirurgische technieken hebben gezorgd voor een evolutie in de
operatieve behandeling van thoracolumbale wervelfracturen. Echter, er bestaat tot op
heden vooral een theoretische onderbouwing in de keuze voor een bepaalde
operatieve behandeling, want vergelijkende klinische studies zijn amper beschikbaar.
Overbehandeling leidt tot onnodige blootstelling aan risico’s en complicaties, maar
zeker ook aan hogere zorgkosten. Daarentegen kan onderbehandeling leiden tot een
slechtere uitkomst, met mogelijk chronische klachten, beperkingen en arbeids‐
ongeschiktheid in een jonge, actieve populatie tot gevolg.
In dit proefschrift hebben we een vergelijkende studie tussen twee operatieve
behandelmogelijkheden verricht. Beide behandeltechnieken worden veelvuldig in de
praktijk toegepast, waarbij de keuze van een behandeling vooral gebaseerd is op lokale
cultuur. In Duitsland wordt er vaker gekozen voor een meer invasieve behandeling
waarbij er twee operaties plaatsvinden om de fractuur zowel van anterieur als van
posterieur te stabiliseren. In Nederland wordt vrijwel uitsluitend gekozen voor één
ingreep waarbij de fractuur alleen van posterieur benaderd wordt. Beide
behandelingen hebben voor‐ en nadelen, maar de resultaten van het onderzoek laten
geen duidelijke verschillen in functionele of radiologische uitkomsten tussen beide
behandelingen zien. Op klinisch gebied zijn er wel verschillen, waarbij de minder

Valorisatie
131
9
invasieve methode gepaard gaat met een kortere operatie tijd en kortere opname duur
met dus ook minder kosten, terwijl bij de meer invasieve behandeling er minder
segmenten geïmmobiliseerd worden. Deze uitkomsten kunnen op verschillende
manieren vertaald worden naar de klinische praktijk. Echter, aangezien er tot dusver
geen klinische voordelen van de meer invasieve methode zijn aangetoond, zou met het
oog op kortere opnameduur en economische belangen momenteel de voorkeur gaan
naar de minder invasieve behandeling. Voor mogelijke voordelen van de invasievere
methode op langere termijn, is aanvullend wetenschappelijk onderzoek nodig.
De uitkomsten van de onderzoeken in dit proefschrift geven een aanzet tot een meer
patiëntgerichte benadering in de behandeling van traumatische thoracolumbale
wervelfracturen. Het inzicht in de grote internationale verschillen in de behandeling van
thoracolumbale wervelfracturen, zou moeten worden gebruikt voor betere
prospectieve studies. Als we onze kennis er ervaring internationaal met elkaar delen,
kunnen we gezamenlijk betere behandelstrategieën ontwikkelen. Hierdoor wordt de
kwaliteit van behandeling en klinische uitkomsten verbeterd, en kunnen we ook
kosteneffectiever werken; twee termen die zeer essentieel zijn in de huidige transitie
van de zorg naar value based healthcare.

Chapter 9
132

133
Chapter 10
Summary

Chapter 10
134

Summary
135
10
Summary
With the increasing incidence of traumatic thoracolumbar spine fractures, their
substantial impact on quality of life, with emerging treatment options and techniques
while growing healthcare costs, there is a rationale to achieve consensus for
optimization of treatment of these fractures.
An accurate classification system is key to a worldwide accepted treatment algorithm.
Once the decision for operative or nonoperative treatment is made, the type or
technique of either the non‐operative or operative treatment remains an issue. The
goal of treatment is to gain fracture healing, while maintaining alignment and function
of the spinal column. As traumatic thoracolumbar spinal fractures occur most
frequently in the young and active population, fast recovery and return to normal daily
activities including work, is regarding major outcome measure to consider, especially in
the light of cost‐effectiveness of treatment.
In case of non‐operative treatment, pain control, support and rapid mobilization are
sought. In this perspective, the role of bracing is under discussion. Concerning operative
treatment, many techniques of surgery are available. In addition to functional and
radiological outcome, clinical in‐hospital parameters such as length of hospital stay,
surgery times, blood loss and implant costs become more important. New techniques
aim to restore stability and alignment in order to regain function as fast as possible
while reducing complications and negative side effects. However, as spine surgery is
constantly evolving and new opportunities arrive rapidly, there is limited time to gather
evidence for the efficacy, safety and cost‐effectiveness of these different types of
surgical techniques.
In this thesis we enroll our search for a better understanding of what aspects to
consider when choosing the optimal treatment of thoracolumbar fractures. Different
aspects associated with fracture management are addressed, such as classification,
radiographic modifiers, clinical usefulness, conservative treatment, surgical treatment
and prognosis.
Classification
Despite the fact that there are many classifications available, until now, consensus
about treatment of thoracolumbar fractures has not been reached. In chapter 2 a
review of the literature was performed to assess the accuracy and clinical usefulness of
the AO, TLICS and new AOspine classification. In terms of accuracy, the presented
kappa values indicate moderate to substantial agreement for all three classifications.
Regarding the clinical usefulness, over 90% agreement between actual treatment and

Chapter 10
136
classification recommendation was reported for most fractures. However, it appears
that over 50% of the patients with a stable burst fracture (TLICS 2, AO‐A3/A4) in daily
practice are operated, so in these cases treatment decision is not primarily based on
classification.
An intra‐ and interobserver study was performed to evaluate the validity of the new
AOspine classification, the TLICS and the Load sharing classification (LSC) (chapter 3).
Plain radiographs and computed tomographic scans of traumatic thoracolumbar
fractures were evaluated. By use of a questionnaire, fractures were classified according
to the LSC, the TLICS, and the AOSpine classification. Data from 91 patients were
classified twice by 7 board‐certified spine surgeons. The intra‐observer and
interobserver reliability considering the LSC total score was noted as fair (k=0.26/0.22).
Considering the resulting TLICS total score, a moderate intra‐observer agreement (k =
0.41) was noted, whereas the interobserver results (k=0.23) presented only fair
reliability. The AOSpine classification showed substantial agreement
(intra/interobserver reliability: k=0.71/0.61) considering the fracture type (A;B;C). So, it
seems that the reliability of the AOSpine fracture classification is superior to the TLICS
and the LSC.
In addition to the AO spine classification, recently the Thoracolumbar AOspine Injury
score was validated. This score seems promising for use in clinical practice, because of
inclusion of patient specific modifiers. These modifiers are important, as there are more
parameters besides fracture type, that have been proven to influence outcome.
In chapter 4 we present the results of a retrospective analysis in which we tried to
identify risk factors associated with posttraumatic kyphosis after a thoracolumbar
fracture. There is a trend of increased risk of progression of kyphosis in age >50 years
and fractures localized at Th12 or L1, although results were not significant. A3 type
fractures are significantly more at risk for posttraumatic kyphosis compared to A1 and
A2 type fractures.
Treatment
Treatment differences are not solely fracture or patient related, but also depend on
surgeon and national or cultural preferences. In chapter 5 CT‐scans of traumatic
thoracolumbar fractures were evaluated in a two‐nation study by German and Dutch
spine surgeons. Fractures were classified according to the AO‐Magerl classification,
followed by six questions concerning the treatment algorithm. No significant difference
concerning the AO Classification between German and Dutch spine surgeons was
found. However, for some fracture types German spine surgeons had a lower threshold
concerning the indication for surgical treatment (Ger 87% vs. NL 30%; p< 0.05). There

Summary
137
10
was consensus about operative stabilization of AO Type B and C injuries and injuries
with neurologic deficit, whereas a discrepancy in the therapeutic algorithm for AO Type
A fractures was observed. This difference was most pronounced regarding the
indication for posterior (Ger 96.6%; NL 41.2%; p< 0.05) and circumferential stabilization
(Ger 53.4%; NL 0%; p< 0.05) for type A3 and A4 burst fractures.
If conservative treatment is chosen, a patient can be treated with a spinal orthosis.
Despite the widespread use of spinal orthoses, evidence of their efficacy is
contradictory and there is little literature comparing different types of orthoses with
regard to objective measurements of the immobilization effect on the thoracolumbar
spine. In chapter 6 four different spinal orthoses were evaluated on their movement
reduction and comfort compared to normal spinal motion. Ten healthy volunteers were
asked to perform several function tasks subsequently without and with four different
types of orthosis. Inertia based motion analysis (IMA) was used for objective movement
measurements. All orthoses influenced spinal movement during several daily tasks as
was shown by IMA. The most rigid orthoses provided the most movement restriction,
but simultaneously scored worse in comfort. The choice for a certain brace should be
based on individual patient characteristics, diagnosis, and aim of the treatment,
because of the experienced differences in immobilization and comfort.
If surgical treatment is chosen, many different techniques can be used. There is no
consensus on how to surgically treat thoracolumbar fractures best. Chapter 7 presents
the results of a multicentre analysis of patients who were surgically treated for a
traumatic thoracolumbar fracture in the University Hospital Aachen (Germany),
Maastricht University Medical Centre or Zuyderland Medical Center Heerlen
(Netherlands). The functional, radiological and clinical outcome of posterior only versus
circumferential stabilization was compared. Fifty‐six patients were included for analysis
(27 posterior only, 29 circumferential). This study showed similar radiological and
functional outcome between posterior only and circumferential stabilization at
endpoint follow up. Circumferential stabilization was accompanied by longer surgery
times (264 vs 110minutes, p<0.01) and longer length of hospital stay (16.9 days vs 9.3
days, p<0.01) On average, slightly less segments were fixed (3.0 vs 3.6, p<0.01) by
circumferential stabilization. Further studies are necessary to investigate the long term
outcome of patients treated by these techniques.

Chapter 10
138
Conclusion
Worldwide, spine surgeons aim to improve classifications in the search for consensus
and optimization of treatment for traumatic thoracolumbar fractures. It seems that
current classifications have acceptable inter‐ and intra‐observer reliability, but their
clinical applicability remains poor. It is not possible to solely lean on a classification in
treatment decision making, as the prognostic value of classifications is still limited,
especially in the grey area of burst fractures. With the addition of patient specific
modifiers, the Thoracolumbar AOspine Injury Score acknowledges that other patient
and fracture related parameters are important in the search for a worldwide applicable
and accepted classification and treatment algorithm for thoracolumbar spine fractures.
However, it is difficult to include all these factors in a point allocation system. So, we
may have to look more for individual phenotypes of the patient and the fracture. This
comes closer to personalized medicine, often defined as ‘the right treatment for the
right person at the right time’.
In case of operative treatment, there are various ways to stabilize fractures, and
current evidence shows not one superior technique. Care should be taken with the
massive introduction of novel techniques without firm evidence on their safety and
efficacy. As there are large nation differences in daily practice, connecting and learning
from each other results in the possibility to optimize treatment. We should use this for
better prospective studies and registries. Collaboration will lead to better future
research projects, which eventually should help to achieve consensus in the decision
making for treatment of traumatic thoracolumbar fractures.

139
Chapter 11
Nederlandse samenvatting

Chapter 11
140

Nederlandse samenvatting
141
11
Nederlandse samenvatting
Traumatische wervelfracturen komen steeds vaker voor en kunnen een grote impact
hebben op kwaliteit van leven. Mede gezien de stijgende zorgkosten en de snelle
ontwikkelingen van nieuwe behandelmogelijkheden, wordt het steeds belangrijker om
consensus te bereiken en de behandeling te optimaliseren. Classificatie van de fractuur
heeft een belangrijke rol in de behandelkeuze. Een betrouwbaar classificatie systeem
lijkt dan ook de sleutel naar een wereldwijd geaccepteerd behandelalgoritme voor
traumatische wervelfracturen.
Nadat er een keuze is gemaakt voor conservatieve danwel operatieve behandeling,
blijft de keuze van techniek en type behandeling zowel conservatief als operatieve een
issue. Het doel van de behandeling is fractuurgenezing, met behoudt van vorm en
functie van de wervelkolom. Aangezien fracturen vooral voorkomen in de jonge en
actieve bevolking, is snel herstel en terugkeer naar normale dagelijkse activiteiten,
inclusief werk, ook belangrijk met het oog op kosten‐effectiviteit. In termen van
conservatieve behandeling wordt er gezocht naar pijnbeheersing en snelle mobilisatie.
In dit perspectief komt de rol van brace behandeling ter sprake.
Ten aanzien van de operatieve behandeling zijn er veel opties beschikbaar. Naast het
functioneel en radiologisch resultaat, worden klinische uitkomstparameters zoals
opnameduur in het ziekenhuis, operatietijden, bloedverlies en implantaatkosten steeds
belangrijker. Met de ontwikkeling van nieuwe technieken probeert men de
complicaties en negatieve bijwerkingen te verminderen en de resultaten te
optimaliseren. De evolutie van nieuwe technieken gaat echter zo snel, dat
wetenschappelijk onderzoek naar de effectiviteit en vergelijking van verschillende
soorten chirurgische technieken beperkt is.
In dit proefschrift hebben we wetenschappelijk onderzoek uitgezet, met als doel om tot
een optimale behandelkeuze van thoracolumbale wervelfracturen te komen.
Verschillende aspecten komen aan bod, zoals betrouwbaarheid en klinische
toepasbaarheid van classificatie systemen, conservatieve behandeling, operatieve
behandeling en prognose.
Classificatie
Ondanks het feit dat er veel classificatie systemen beschikbaar zijn, is er tot op heden
nog altijd geen consensus bereikt over de behandeling van thoracolumbale
wervelfracturen. In hoofdstuk 2 is een overzicht van de literatuur beschreven om de
nauwkeurigheid en klinische toepasbaarheid van de AO, TLICS en de nieuwe AOspine‐

Chapter 11
142
classificatie te beoordelen. Met betrekking tot de nauwkeurigheid, kan gesteld worden
dat voor alle drie de classificaties de kappa‐waarden redelijk tot ‘voldoende tot goed’
(kappa 0.4‐0.8) zijn. Ten aanzien van de klinische toepasbaarheid, blijkt dat voor de
meeste fracturen een overeenkomst van >90% tussen de feitelijke behandeling en de
classificatie wordt bereikt. Echter, in het geval van de stabiele burst fractuur (TLICS 2 en
AO‐A3/4), wordt slechts in 50% van de patiënten het advies van de classificatie gevolgd.
In deze gevallen is de keuze voor een behandeling dus niet alleen gebaseerd op
classificatie, maar spelen ook andere factoren een rol.
We hebben zelf ook een inter‐ en intraobserver studie verricht om de betrouwbaarheid
van de AOspine classificatie, de TLICS en de Load Sharing Classification (LSC) te
evalueren (hoofdstuk 3). Hiervoor zijn röntgenfoto's en CT scans van traumatische
thoracolumbale fracturen van 91 patiënten tweemaal geclassificeerd door
7 gecertificeerde wervelkolom chirurgen. Intra‐ en interobserver betrouwbaarheid
werd bepaald door de Cohen κ (kappawaarde). De betrouwbaarheid van de LSC werd
als redelijk beoordeeld (intra‐ en interobserver betrouwbaarheid: kappa = 0.26/0.22).
Voor de TLICS score, werd een voldoende‐tot‐goed intra‐observer (kappa = 0.41)
overeenkomst genoteerd, terwijl de resultaten van de interobserver (kappa = 0.23) een
redelijke betrouwbaarheid opleverden. De AOspine‐classificatie toonde een
aanzienlijke mate van overeenstemming (intra‐ en interobserver betrouwbaarheid:
kappa = 0.71/0.61). Op basis van deze resultaten lijkt de betrouwbaarheid van de
AOspine fractuur classificatie superieur aan de TLICS en de LSC, er derhalve wordt het
gebruik van deze classificatie in de klinische praktijk geadviseerd.
In navolging op de AOspine classificatie, is recent ook de Thoracolumbar AOspine Injury
score gevalideerd. Deze score lijkt veelbelovend voor gebruik in de klinische praktijk
vanwege de opname van patiënt‐specifieke parameters, die naast de fractuur‐
classificatie ook van invloed (kunnen) zijn op de behandelkeuze. Die invloed van andere
parameters hebben we aangetoond in een retrospectief onderzoek naar de invloed van
risicofactoren de uitkomst van fracturen, waarbij er met name gekeken is naar
posttraumatische kyfose (hoofdstuk 4). Het is bekend dat posttraumatische kyfose
geassocieerd is met chronische pijn. Er lijkt een verhoogd risico te zijn op progressie van
kyfose in de leeftijd >50 jaar en fracturen gelokaliseerd op Th12 of L1, hoewel deze
verschillen niet significant waren. Burst fracturen lopen significant meer risico op
posttraumatische kyfose vergeleken met A1 en A2 compressiefracturen.
Behandeling
Behandelverschillen zijn niet alleen fractuur‐ of patiënt gerelateerd, maar zijn ook
afhankelijk van de voorkeuren van chirurg en lokale gebruiken. We hebben een aantal

Nederlandse samenvatting
143
11
studies verricht samen met onze collegae uit Duitsland. Hoofdstuk 5 presenteert de
resultaten van een internationale web‐based‐multicenter studie waarbij CT‐scans van
traumatische thoracolumbale fracturen werden geëvalueerd door Duitse en
Nederlandse wervelkolomchirurgen. Middels vragenlijsten werden behandelstrategieën
van thoracolumbale fracturen beoordeeld en vergeleken. Fracturen werden
geclassificeerd volgens de AO‐Magerl‐classificatie, gevolgd door zes vragen met
betrekking tot het behandelalgoritme. Twaalf chirurgen (zes per land) evalueerden elk
91 casussen. Er werd geen significant verschil tussen Duitse en Nederlandse
wervelkolomchirurgen gevonden met betrekking tot de AO‐classificatie.
Over het algemeen hadden Duitse wervelkolomchirurgen een lagere drempel voor
chirurgische behandeling (D 87% vs. NL 30%; p<0,05). Er was consensus over operatieve
stabilisatie van AO Type B en C letsels en fracturen met neurologisch uitval, terwijl er
een discrepantie in het therapeutisch algoritme voor AO Type A fracturen werd
waargenomen. Dit verschil was het meest uitgesproken wat betreft de indicatie voor
posterior (D 96,6%; NL 41,2%; p<0,05) en circumferentiële stabilisatie (D 53,4%; NL 0%;
p<0,05) voor burst‐fracturen.
Indien er gekozen wordt voor een conservatieve behandeling, kan de patiënt
behandeld worden met een brace. Ondanks dat spinale braces veel gebruikt worden, is
er tegengesteld bewijs over de effectiviteit en is er beperkte literatuur waarin
objectieve metingen van het immobilisatie‐effect op de wervelkolom worden gemeten.
In hoofdstuk 6 presenteren we de resultaten van een studie waarin vier verschillende
braces werden beoordeeld op bewegingsbeperking en comfort in vergelijking met
normale beweeglijkheid van de wervelkolom. Tien gezonde vrijwilligers voerden
verschillende alledaagse taken uit zonder én met vier verschillende braces. Inertia
based motion analysis (IMA) werd gebruikt voor objectieve bewegingsmetingen. Het
bleek dat alle braces invloed hebben op de beweging van de wervelkolom. De meest
stijve orthesen leverden de meeste bewegingsbeperking op, maar scoorden
tegelijkertijd slechter in comfort. De keuze voor een bepaalde brace zou derhalve
gebaseerd moeten worden op de individuele kenmerken en diagnose van de patiënt.
In het geval van een chirurgische behandeling zijn er veel verschillende typen en
technieken beschikbaar. Er is geen consensus over welke operatieve techniek het beste
is. In hoofdstuk 7 presenteren we de resultaten van een multicenter analyse van
patiënten die chirurgisch werden behandeld voor een traumatische thoracolumbale
fractuur in het Universitair Ziekenhuis Aken (Duitsland), het Universitair Medisch
Centrum Maastricht of Zuyderland Heerlen (Nederland). De functionele (Oswestry
Disability Index en VAS‐pijn), radiologische en klinische uitkomsten tussen posterieure

Chapter 11
144
en circumferentiële stabilisatie zijn vergeleken. Zesenvijftig patiënten werden
opgenomen voor analyse (27 posterieur, 29 circumferent). Radiologische en functionele
uitkomsten vertoonden geen significante verschillen. Circumferentiële stabilisatie ging
gepaard met langere operatietijden (264 vs. 110 minuten, p<0.01) en een langere
opnameduur (16.9 vs. 9.3 dagen, p<0.01), maar gemiddeld werden minder segmenten
gefixeerd (3.0 vs. 3.6, p<0.01). Verdere studies zijn nodig om de langetermijn resultaten
te onderzoeken.
Conclusie & discussie
Naar aanleiding van dit proefschrift kunnen we stellen dat er wereldwijd door
wervelkolomchirurgen wordt gestreefd naar het verbeteren van de classificaties in de
zoektocht naar consensus in de behandeling van traumatische thoracolumbale
fracturen. Het lijkt erop dat huidige classificaties een aanvaardbare betrouwbaarheid
hebben, maar hun klinische toepasbaarheid blijft matig. Het is niet mogelijk om
uitsluitend te leunen op classificaties bij de besluitvorming over de behandeling,
aangezien de prognostische waarde van classificaties nog steeds beperkt is,
voornamelijk in het grijze gebied van burst fracturen. Met de toevoeging van patiënt‐
specifieke‐modifiers erkent de Thoracolumbar AOspine Injury Score dat andere
parameters gerelateerd aan de patiënt en de fractuur belangrijk zijn. Het is echter
moeilijk om al deze factoren in een punttoewijzingssysteem op te nemen. Wellicht
moeten we meer op zoek naar individuele fenotypes, waarbij we steeds dichter in de
buurt komen van gepersonaliseerde geneeskunde, vaak gedefinieerd als 'de juiste
behandeling voor de juiste persoon op het juiste moment'.
In het geval van een operatieve behandeling zijn er verschillende manieren om breuken
te stabiliseren, en het huidige bewijs toont niet één superieure techniek. Gedurende de
laatste decennia evolueert de wervelkolomchirurgie snel. Ook bij spinale trauma's
hebben nieuwe inzichten geleid tot de ontwikkeling van nieuwe behandelings‐
mogelijkheden. Men moet voorzichtig zijn met de massale introductie van nieuwe
technieken zonder stevig bewijs van hun veiligheid en werkzaamheid. We kunnen
echter aanvullende onderzoekstechnieken gebruiken om meer bewijs te verkrijgen.
Omdat er in de dagelijkse praktijk grote nationale verschillen zijn, zouden we meer
gebruik moeten maken van de mogelijkheid om te verbinden en te leren van elkaar.
Samenwerking zal leiden tot betere toekomstige onderzoeksprojecten, die uiteindelijk
moeten leiden tot consensus in de behandeling van traumatische thoracolumbale
fracturen.

145
Chapter 12
Dankwoord

Chapter 12
146

Dankwoord
147
12
Dankwoord
Nu het einde van dit proefschrift in zicht komt, wordt het tijd om in dit dankwoord mijn
waardering uit te spreken voor collega’s, vrienden, familie en anderen die geholpen
hebben bij de totstandkoming van mijn boekje.
Allereerst wil ik mijn promotieteam bedanken. Lodewijk van Rhijn, een aantal jaren
geleden kwam ik met ideeën over een PhD‐traject bij jou terecht. Lange tijd hebben we
beiden waarschijnlijk twijfel gehad of dit proefschrift echt afgerond zou worden,
aangezien het aanvankelijk maar moeizaam op gang kwam. Ik wil je bedanken voor het
vertrouwen en alle steun op wetenschappelijk, maar zeker ook op menselijk vlak.
Paul Willems, co‐promotor en begeleider tijdens mijn fellowship wervelkolom in het
MUMC: jij hebt de connectie gelegd met onze collegae uit Aken. Dank voor je input,
vertrouwen en alle feedback. Ik heb veel van je geleerd en hoop dat we in de toekomst
nog veel zullen samenwerken.
Wouter van Hemert, toen ik tien jaar geleden als keuze‐co‐assistent bij de orthopedie
in het Atrium MC in Heerlen kwam, was jij orthopedisch chirurg in opleiding. Ik heb in
die periode een zeer gedreven en enthousiaste dokter aan het werk gezien. Iets dat mij
enorm getriggerd heeft om ook deze richting uit te gaan. Via jou heb ik kennis gemaakt
met de wervelkolomchirurgie en samen hebben we de basis gelegd voor wat
uiteindelijk mijn proefschrift is geworden. Ik wil je enorm bedanken voor je
onvoorwaardelijk vertrouwen in mij als mens en dokter en ben erg blij dat we directe
collega’s zullen blijven.
Naast mijn promotieteam zijn er nog veel andere mensen betrokken geweest bij de
wetenschappelijke output van dit proefschrift. Miguel Pishnamaz en Philip Kobbe, het
was zeer prettig om met jullie samen te werken. Martijn Schotanus, Matthijs van der
Linde, Bernd Grimm, Willemijn van Rooij, Rachel Senden, Stephan Balosu, Markus
Laubach, Hans Pape, Marion Heymans en Rob de Bie: dank voor jullie hulp bij de
totstandkoming van de publicaties in dit proefschrift.
Leescommissie, bedankt voor jullie inzet bij de beoordeling van dit proefschrift.
Ook op persoonlijk vlak heb ik steun gevonden bij een heel aantal mensen. Te beginnen
bij Lieke Amkreutz, Paulien Cornelissen en Rélana Nowacki. We zijn samen gestart aan
de studie Geneeskunde en hebben zes jaar later samen de eed afgelegd. Ondanks dat
we daarna alle vier een heel andere richting hebben gekozen, zien we elkaar nog
regelmatig. Wat ben ik blij dat ik jullie heb leren kennen!

Chapter 12
148
Sandra Prinsen, Tim Boymans, Loek Verlaan en Mark Hulsbosch, tijdens de opleiding
orthopedie heb ik met jullie het meest intensief samengewerkt. Een tijd die ik als heel
prettig heb ervaren en een periode waar de basis voor dit proefschrift werd gelegd.
De orthopedisch chirurgen uit het MUMC wil ik bedanken voor de begeleiding tijdens
mijn opleidingsperiode. Een persoonlijke noot voor Mark van den Boogaart, voor de
leuke én leerzame tijd tijdens mijn fellowship, en Adhiambo Witlox, voor de gezellige
sporturen buiten ons werk.
De wervelkolomchirurgie is een zeer multidisciplinair onderdeel van de geneeskunde,
waarin ik veel samenwerk met de neurologen en neurochirurgen. Een persoonlijk
dankwoord aan Henk van Santbrink, Kim Rijkers, Mariel Ter Laak en Toon Boselie, voor
de intensieve en prettige samenwerking in de afgelopen jaren.
Beste collega’s orthopedie Zuyderland, ik ben blij dat ik sinds 1 januari officieel deel
uitmaak van de vakgroep. Ik hoop dat we komende jaren de orthopedie in het
Zuyderland MC verder op de kaart gaan zetten. Ide Heyligers, huidige collega, opleider
tijdens mijn opleiding en voorzitter van de leescommissie, dank voor al je inzet en
begeleiding de afgelopen jaren.
Dan mijn paranimfen, die me tijdens de openbare verdediging bij zullen staan.
Steffie Klemann, we hebben een groot deel van onze opleiding tot orthopedisch chirurg
samen gedeeld en altijd was er een hele fijne samenwerking. Daarnaast zijn we al een
tijdje collega’s in het Zuyderland, inmiddels beiden met een vaste aanstelling. Wat ben
ik daar blij om. Ik hoop dat we de komende jaren op dezelfde manier mogen
samenwerken.
Anne, dank voor je input bij de totstandkoming van dit proefschrift. Je hebt me erg
bijgestaan in het wetenschappelijk Engels en vele hoofdstukken van dit proefschrift
gelezen. Maar ik doe je te kort als ik alleen je hulp bij dit proefschrift noem, want je
bent een fantastisch mens! Ik vind het dan ook heel leuk dat je op deze dag naast me
zult staan als paranimf.
Vrienden en familie mogen absoluut niet ontbreken in dit dankwoord. Ondanks dat het
voor hen af en toe on(be)grijpbaar is wat ‘dokter zijn’ en ‘een proefschrift schrijven’
inhoudt, staan ze altijd naast me als ik ze nodig heb.

Dankwoord
149
12
Beste pap en mam, wat ben ik jullie dankbaar. Jullie hebben mij (en Lars en Ties)
geleerd om te investeren in en te werken voor iets dat je graag wilt bereiken. Zonder
die input had ik hier waarschijnlijk vandaag niet gestaan. Ik ben er trots op jullie
dochter te zijn.
Lars en Ties, lieve broers, dank voor alles. Ieder doet waar hij goed in is, haalt het
maximale eruit, en het feit dat jullie dat doen, geeft mij ook de steun die nodig is
geweest om dit te bereiken. Ik ben trots op ieder van ons. Ties, bedankt voor je fijne
broer‐zus gesprekken, je kritische blik op mijn stellingen en andere hoofdstukken.
Lieve Daan, ik besef me maar al te goed dat het niet altijd gemakkelijk is geweest om
ons gezin, sport, werk, vrije tijd en promotie onderzoek goed te combineren. We zijn op
sommige vlakken erg verschillend, maar graag spreek ik hier op papier nogmaals mijn
waardering voor jou uit. Zonder jouw steun was dit veel moeilijker geweest. We
hebben samen twee prachtige kinderen, Evi en Sten: de belangrijkste mensen in mijn
leven. Ik heb veel ambities op werkgebied, maar mijn grootste doel is met mensen die
ik lief heb gelukkig te zijn. Ik hou van jullie!

Chapter 12
150

151
Chapter 13
Curriculum vitae
List of publications and presentations

Chapter 13
152

Curriculum vitae
153
13
Curriculum vitae
Inez Curfs werd geboren op 8 juni 1985 te Heerlen. Ze groeide op als middelste kind in
een sportief gezin met twee broers. Na de basisschool ging ze naar het gymnasium op
het Grotius College te Heerlen. Daar haalde ze in 2003 haar diploma. Sport had een
belangrijke plaats in haar leven; tot aan haar studie was ze 6 dagen per week bezig met
sport (atletiek en voetbal). Ze heeft korte tijd zelfs gevoetbald in nationale
jeugdselecties, tot blessureleed een einde maakte aan haar ambities op sportgebied.
Hierdoor kwam ze wel in aanraking met een nieuwe interesse: orthopedie. In 2003
startte ze met de opleiding Geneeskunde aan de Universiteit Maastricht. Keuze coschap
en semi‐arts stage werden doorlopen bij de orthopedie in het toenmalig Atrium
Medisch Centrum, waar de interesse voor dit vakgebied alleen maar toenam. In 2009
studeerde ze af en begon als ANIOS orthopedie in het Atrium Medisch Centrum te
Heerlen, waarna ze op 1 januari 2010 mocht beginnen aan de opleiding tot
orthopedisch chirurg.
De opleiding orthopedie heeft ze gevolgd in ROGO Zuid: in het Maastricht Universitair
Medisch centrum (MUMC), Atrium Medisch Centrum Heerlen en Orbis Sittard‐Geleen.
Tijdens de opleiding tot orthopedisch chirurg werd haar aandacht getriggerd door de
wervelkolompathologie. Wetenschappelijk onderzoek werd gestart, de basis voor dit
proefschrift. In mei 2016 voltooide ze de opleiding tot orthopedisch chirurg. Ze heeft
zich nadien op medisch inhoudelijk gebied verder ontwikkeld middels een fellowship
wervelkolomchirurgie in het Maastricht Universitair Medisch Centrum en als chef de
clinique in het Zuyderland MC. Gedurende deze periode werd ook de laatste hand
gelegd aan de inhoud van dit proefschrift. Daarnaast volgt ze momenteel een
managementopleiding om zich ook op organisatorisch gebied te ontwikkelen. Per 1
januari 2019 is ze toegetreden tot de vakgroep orthopedie Zuyderland Medisch
Centrum. Hier zal ze haar carrière als orthopedisch chirurg met aandachtsgebieden
wervelkolom, sport en traumatologie voortzetten.
In 2007 leerde ze Daniëlle kennen, waar ze in 2011 mee is getrouwd. Samen hebben ze
twee kinderen: Evi (6 jaar) en Sten (5 jaar).

Chapter 13
154

List of publications and presentations
155
List of publications and presentations
Publications
Two Nation Comparison of Classification and Treatment of Subaxial Cervical Spine
Fractures: An Internet‐Based Multicentre study Among Spine Surgeons. M Pishnamaz,
I. Curfs, D. Uhing, C. Herren, H. Van Santbrink, C. Mueller, M. Scholz, P. Lichte, K.
Rijkers, T. Boselie, F. Hildebrand, P. Willems, P. Kobbe. World Neurosurg. 2019;123:
e125‐e132.
Reliability and Agreement of Different Spine Fracture Classification Systems: An
Independent Intraobserver and Interobserver Study. M. Pishnamaz, S. Balosu, I. Curfs,
D. Uhing, M. Laubach, C. Herren, C. Weber, F. Hildebrand, P. Willems, P. Kobbe. World
Neurosurg. 2018;115:e695‐e702.
Radiological prediction of posttraumatic kyphosis after thoracolumbar fractures.
I. Curfs, M. vd Linde, B. Grimm, P. Willems, W. van Hemert. Open Orthopaedic Journal,
2016;10:135‐42.
Evaluating the immobilization effect of spinal orthoses using sensor based motion
analysis. I. Curfs, W. Van Rooij, R. Senden, B. Grimm, W. Van Hemert. Journal of
Prosthetics&Orthotics. 2016;28(1):23‐29.
Two nation comparison of classification and treatment of thoracolumbar fractures: An
internet‐based multicenter study among spine surgeons. M. Pishnamaz, I. Curfs,
S. Balosu, P. Willems, W van Hemert, C. Pape, P. Kobbe. Spine 2015;40(22):1749‐1756.
Complications in 223 cases of the Oxford Phase 3 Unicondylar Arthroplasty (UCA) in a
country hospital. J. Bloemsaat‐Minekus, I. Curfs, A. Lisowski, L. Lisowski. Arthroscopy
The Journal of Arthroscopic and Related Surgery. 2012;28 (9): e364.

Chapter 13
156
Presentations
EFORT Congress, may 2010 (poster)
“Thoracolumbar fractures: radiological prediction of deterioration.
I.Curfs, MD; M. van der Linde, MD; I.C. Heyligers, MD; B. Grimm, PhD ; W. van Hemert,
MD; AHORSE Foundation, Atrium MC Heerlen”.
EFORT Congress, may 2010 (poster) “Dynamic sway during gait and stair climbing as an outcome measure in orthopaedics;
I. Curfs, S. Prinsen, K. van Tilburg, R. Senden, I.C. Heyligers, B. Grimm; Atrium MC,
department of orthopedics & AHORSE.
NOF Congress, Aarhus, Denmark, may 2010 (oral) “Dynamic sway during chair raising test as an outcome measure in knee arthroplasty”;
I. Curfs, S. Prinsen, K. van Tilburg, R. Senden, I.C. Heyligers, B. Grimm; Atrium MC,
department of orthopedics & AHORSE.
Nederlands orthopedische vereniging, januari 2011 (oral) “Posttraumatisch kyfose na thoracolumbale fracturen: voorspellende factoren?”
I.Curfs, MD; M. van der Linde, MD; I.C. Heyligers, MD; B. Grimm, PhD ; W. van Hemert,
MD; AHORSE Foundation, Atrium MC Heerlen”.
Eurospine, Berlin, October 5‐7th 2016 (oral) “Posterior only versus circumferential stabilization in thoracolumbar fractures.
I. Curfs, M. Pishnamaz, P. Kobbe, W. Van Hemert, P. Willems.”
Maastricht University Spine Course, June 2018 (faculty, oral presentation)
“Trauma and tumor of thoracolumbar spine”.
I. Curfs
NASS Congress, Los Angeles, September 26th 2018 (oral) “Two Nation Comparison of Surgical Treatment of Traumatic Thoracolumbar Spinal
Fractures: Posterior only versus Circumferential Stabilization.
I. Curfs, W. van Hemert, P. Kobbe, P. Willems.”

COVER en boekenlegger proefschri� Inez Curfs.indd 1 17-4-2019 09:54:06COVER en boekenlegger proefschri� Inez Curfs.indd 2 17-4-2019 09:54:08
Inez curfs cover + boekenlegger 428x240 v0.indd Alle pagina's 29-4-2019 10:45:36